Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
|
|
|
- Rodger Cameron
- 6 years ago
- Views:
Transcription
 October 29,")
1 Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
2 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement " The Model for Improvement " Use of the Model " Using Workflows & Electronic Health Records " Case Example! Monitor QI Improvements 1
3 Quality Improvement Introduction! Federal, state and local officials, as well as other stakeholders, are all encouraging providers and practices to utilize QI continuously! Quality improvement is a central focus in health care delivery today " Preventing medical errors " Reducing readmission rates " Improving care coordination 2

4 QI Process! Evaluate measures based on data/reports! Stratify data by race and ethnicity " Assess for health equity improvement! Identify disparities for areas of improvement! Choose and define QI project " Assess workflows for potential improvements " Choose realistic, attainable and measurable goal " Establish timeline for implementation and achievement of goal! Complete QI project to implement improvement! Assess for goal achievement! Sustain improvement The QI process is cyclical and continuous, never stagnant 3
5 QI Goals! Realistic: Relevant to your practice and your patient population " e.g. implement daily huddles with staff to review patients that are scheduled to be seen that day! Attainable: Determine appropriate time frame to achieve the goal " e.g. can we increase our annual well visits for eligible patients by 5% in the next six months?! Choose one preventive service! Will implementing morning huddles and scheduling visits when patients are at the practice lead to desired result?! Measureable: Include specific measurable data " e.g. to increase annual well visits by 5% in the next six months 4
6 QI Framework Link Design Create Secure Diagnose Implement 5
7 QI Data to Reduce Disparities*! Stratify by race, ethnicity and/or language! Data should be easy to collect " Registries and practice Electronic Health Records (EHR) " Health plan data from reports on HUSKY Health Provider Portal! Determine quality gap between patient populations " Where do disparities exist? " What is the magnitude of those disparities? * Using Data to Reduce Disparities & Improve Quality from the Robert Wood Johnson Foundation; part of the Assisting Health Equity with Quality Improvement: Part Two Toolkit located on the Pathway to PCMH Health Equity page of the HUSKY Health provider website 6
8 National Performance Measures Priority Area Asthma Diabetes Heart disease Screening Prenatal care Mental health Immunization Prevention Patient experience *Click on link to see full report Use of appropriate medications Measure Description Percentage of patients with most recent A1c level >9.0% (poor control) Coronary artery disease: beta blocker treatment after a heart attack Breast cancer screening Colorectal cancer screening Prenatal screening for HIV Prenatal anti-d immune globulin Antidepressant medication management Childhood immunization status Flu shots for adults aged 50 to 64 Tobacco use assessment and cessation intervention Ambulatory Consumer Assessment of Health Care Providers and Systems (ACAHPS) National_Voluntary_Consensus_Standards_for_Ambulatory_Care %E2%80%94Measuring_Healthcare_Disparities.aspx 7
9 NCQA Standard 6: Elements! Element A: Measure Performance! Element B: Measure Resource Use and Care Coordination! Element C: Measure Patient/Family Experience! Element D: Implement Continuous Quality Improvement " Must Pass Element! Element E: Demonstrate Continuous Quality Improvement! Element F: Report Performance " Share performance data reports using measures from Elements 6A, 6B and 6C! Element G: Use Certified EHR Technology 8
10 Crosswalk of DSS Child/Adolescent PCMH Performance Measures and 2014 NCQA PCMH Standard Child/Adolescent PCMH Measures Well-Child Visits in the First 15 Months of Life 1 Well-Child Visits in the Third, Fourth, Fifth and Sixth Years of Life 1 Adolescent Well-Care Visits 1 Annual Dental Visit (ages 2-21) Asthma Patients (ages 2 20) with One or More Asthma-Related Emergency Room Visits 1 Rate of ED visits per 1,000 member month. Ages 0-19 Developmental Screening In the First Three Years of Life 1 Measure Source HEDIS Measure W15 HEDIS Measure W34 HEDIS Measure AWC HEDIS Measure Retired 2013 CHIPRA Measure (#20) CHIPRA ED Measure (#18/AMB-CH) CHIPRA Measure (#8/DEV-CH) Medication Management for People (ages HEDIS 5-18) with Asthma 1 Measure ASM PCMH CAHPS Survey 2014 NCQA Crosswalk 6A1,2,4* 6D1,2** 6E1,2~ 6A1,2,4* 6D1,2** 6E1,2~ 6A1,2,4* 6D1,2** 6E1,2~ 6A2,4* 6D1,2,7**, 6E1,2~ 6A3,4* 6B2 6D3,4,7**, 6E1,3~ 6B1,2 6D3,4 6E3~ 6A2,4* 6D1,2* * 6E1,2~ 6A3,4* 6B2 6D1-4,7**, 6E1-3~ 6C2,3, 6D5,6** 6E1,4~ CHNCT Available Reports (Provider Portal) Care Analyzer: Provider Effectiveness Report and Provider Detail Report Secure Provider Portal: Child Well-Care Visits - Gaps in Care Care Analyzer: Provider Effectiveness Report and Provider Detail Report Secure Provider Portal: Child Well-Care Visits - Gaps in Care Care Analyzer: Provider Effectiveness Report and Provider Detail Report Secure Provider Portal: Child Well-Care Visits - Gaps in Care Care Analyzer: HEDIS Module - Summary Report and Detail Report Secure Provider Portal: ED Utilization Report Care Analyzer: HEDIS Module - Summary Report and Detail Report Secure Provider Portal: ED Utilization Report Care Analyzer: HEDIS Module - Summary Report and Detail Report Secure Provider Portal: Child Well-Care Visits - Gaps in Care Care Analyzer: HEDIS Module - Summary Report and Detail Report Secure Provider Portal: Pharmacy Claims Report CAHPS being sent for CY 2014 Annual Provider Profile Report 1 Health Equity Measure selected by DSS * Measure may be used once for Element 6A ** Measure may be used once for Element 6D ~ Measure demonstrates results tracked over time, assesses effects and achieves improved performance if used for Element 6A, 6B or 6C. Crosswalks are part of the Assisting Health Equity with Quality Improvement: Part Two Toolkit 9
11 Crosswalk of DSS Adult PCMH Performance Measures and 2014 NCQA PCMH Standard Adult PCMH Measures Comprehensive Diabetes Care - LDL Screening 1 Comprehensive Diabetes Care - Eye Exam 1 Cholesterol Management for Patients With Cardiovascular Conditions - LDL Screening 1 Post-Admission Follow-Up Within Seven Days of an Inpatient Discharge 1 Measure Source HEDIS Measure CDC Component HEDIS Measure CDC Component HEDIS Measure CDC Component DSS Custom Measure 2014 NCQA Crosswalk 6A3,4* 6D1,2,7** 6E1,2~ 6A3,4* 6D1,2,7** 6E1,2~ 6A2,3* 6D1,2,7** 6E1,2~ 6B1,2 6D3,4,7** 6E1,3~ ED Usage HEDIS Measure 6B1,2 6D3,4,7** 6E3~ Medication Management for People (ages 19 HEDIS Measure 64) with Asthma 1 ASM Follow-Up within 30 Days After New Behavioral Health Diagnosis and Rx 1 DSS Custom Measure 6A3,4*, 6B2 6D1-4,7** 6E1-3~ 6B1 6D3,4,7** 6E1,3~ PCMH CAHPS Survey 6C2,3 6D5,6** 6E1,4~ Readmission Rate - 30 days after discharge DSS Custom Measure 6B1,2 6D3,4,7** 6E3~ CHNCT Available Reports (Provider Portal) Care Analyzer: Provider Effectiveness Report and Provider Detail Report Secure Provider Portal: Adult Diabetes Screening Tests - Gaps in Care Care Analyzer: Provider Effectiveness Report and Provider Detail Report Care Analyzer: Provider Effectiveness Report and Provider Detail Report Secure Provider Portal: Adult Diabetes Screening Tests - Gaps in Care Secure Provider Portal: Inpatient Claims Report and Inpatient Daily Census Report Care Analyzer: HEDIS Module - Summary Report and Detail Report Online Secure Provider Portal: ED Utilization Report Care Analyzer: HEDIS Module - Summary Report and Detail Report Secure Provider Portal: Pharmacy Claims Report Annual Provider Profile Report CAHPS being sent for CY 2014 Annual Provider Profile Report Secure Provider Portal: Inpatient Claims Report and Inpatient Daily Census Report Annual Provider Profile Report 10
12 Diagnose the Disparity! Relate to health measures! Improve results! Share results! Utilize Health Information Technology (HIT)! Reduce disparities 11

13 Best Practice QI Model Plan-Do-Study-Act (PDSA)! Identify potential areas for improvement! Map out the chosen improvement and define goal! Implement a change to achieve desired outcomes! Test, evaluate and/or adapt to ongoing changes The Model for Improvement was developed by Associates in Process Improvement. Graphic provided courtesy of Cambridge, Massachusetts: Institute for Healthcare Improvement; [2015]. (Available on 12
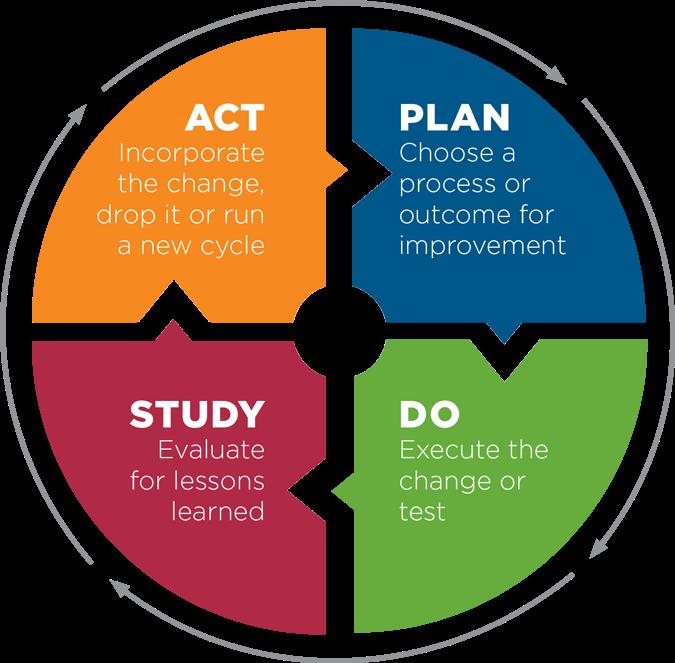
14 Plan-Do-Study-Act (PDSA) 13
15 Using Workflows for QI! Workflows consist of connected steps to accomplish a collective action or goal! EHR information can be used to: " Measure workflow effectiveness and accomplish the goal! Identify and prioritize quality issues and efficiency gains 14
16 QI Process Sample Workflow Map Workflow Shape Key Terminator start or stop a workflow Internet Citation: Figure 5.1. Sample workflow map: lab result followup. In: Practice Facilitation Handbook. Module 5. Mapping and redesigning workflow. (May 2013.) Agency for Healthcare Research and Quality, Rockville, MD. improve/system/pfhandbook/fig5.1.html. Process step - action/work Decision point workflow branch 15
17 Utilization of HIT! Implements quality improvement within your entire patient population! Allows you to track the referral process! Improves administrative process efficiency in support of care delivery! Strengthens communication and coordination among health care providers managing a patient s continuum of care 16
18 QI Process Example: Evaluate a Measure! Adult Quality Measure! Link quality and equity " Adult ages18-75 with diagnosis of Type 1 or Type 2 diabetes who received at least one HgA1c screening during the measurement year! Report baseline " Electronic Health Records! White Males vs. Hispanic Males! Ages who have received at least one HgA1c screening during the measurement year! Run a previous 6-12 months report, stratified by race and ethnicity, what does the data show? 17
19 QI Process Example: Identify Disparities! Stratify data obtained for measure by race and ethnicity! Example data disparity results: " 55% compliance with this measure for White Males " 45% compliance with this measure for Hispanic Males " There is a 10% disparity gap between White Males and Hispanic Males 18
20 QI Process Example: Identify a Goal! Use identified disparities to choose and set a goal " The data indicates a 10% disparity gap between two of the practice population groups " Goal is to improve compliance of annual HgA1c screening in all Adult Males ages and reduce disparity 19
21 QI Process Example: Project Definition Increase compliance by 25% among all adult males and reduce disparity between White and Hispanic males by 50% within 6 months by assessing and addressing barriers to care for target population! Realistic " Develop and implement new assessment beginning November 2015 " Establish individualized patient plans for compliance " Establish follow up program to assess for and reinforce compliance! Attainable " Reasonable for practice to implement in defined timeframe " Estimate impacts and expected results for defined timeframe! Measurable " Evaluate reports beginning May 2016 and compare to baseline " 68.75% target compliance for White Males " 65.31% target compliance for Hispanic Males 20
22 Sustainability! Ability to maintain and hold the gains! Ensure continuity in improvement Graphic provided courtesy of Cambridge, Massachusetts: Institute for Healthcare Improvement; [2015]. (Available on 21
23 Monitoring QI Improvements through Benchmarking Baseline performance standards for benchmarking:! Data Reports for Federal Requirements " Early and Periodic Screening, Diagnosis and Treatment (EPSDT)! NCQA-HEDIS " NCQA created Healthcare Effectiveness Data & Information Set (HEDIS) to set standardized performance measures! CT Department of Social Services Measure Requirements " 4 custom measures defined by DSS 22
24 Quality Performance Measures! The defined set of measures are a combination of: " Nationally recognized measures from Healthcare Effectiveness Data and Information Set (HEDIS) " Children's Health Insurance Program Reauthorization Act (CHIPRA) " Custom measures approved by Department of Social Services (DSS)! Key quality measures were selected by DSS and include: " Preventive care, treatment of chronic diseases and utilization of services 23
25 PCMH Quality Measures Pediatric Quality Measures! Well-child visits in the first 15 months of life! Well-child visits in the third, fourth, fifth and sixth years of life! Adolescent well-care visits! Percentage of eligible beneficiaries ages 1-21 with at least one dental visit during the measurement year! Annual percentage of asthma patients (ages 2-20) with one or more asthma-related emergency department visits (Custom measure based on CHIPRA)! Use of appropriate medications for people with asthma, with several age ranges 5-11, and total 5-18! Rate of emergency department visits per 1,000 member months (ages birth-19)! Developmental screening in the first three years of life; three age breakouts: ages 1, 2, and 3 (CHIPRA measure)! PCMH Consumer Assessment of Healthcare Providers and Systems (CAHPS) Survey 24
26 Adult Quality Measures PCMH Quality Measures! Adults ages with a diagnosis of Type I or Type II diabetes who received at least one LDL-C screening during the measurement year! Adults ages with a diagnosis of Type I or Type II diabetes who received at least one eye screening for diabetic retinal disease in a two year period! Cholesterol Management for Patients With Cardiovascular Conditions - LDL Screening! Post-Admission Follow-Up Within Seven Days of an Inpatient Discharge! Use of appropriate medications for people with asthma, with several age ranges 19-50, and total 19-64! Percentage of adults given a new psychiatric diagnoses, and medication, by a PCP who received a follow-up visit within 30 days (Custom measure)! Readmission rate within 30 days after discharge (Custom measure)! Emergency department usage! PCMH Consumer Assessment of Healthcare Providers and Systems (CAHPS) Survey 25
27 Enhanced Fee-for-Service Payments! The department shall make enhanced fee-for-service payments to a practice " Enhancements are to the current base Medicaid fee schedule, visit rate or other fee applicable to the practice! The enhanced fee-for-service will be limited to primary care practices! The primary care codes for which enhanced fee-forservice payments are available shall be posted on the department s website or by other means accessible to providers For more information on the PCMH Participation Fee Differential Payments and Code List, go to PCMH_Participation_Fee_Differential_Payments.pdf 26
28 Performance-Based Supplemental Payments! The two types of Per Member Per Month (PMPM) performance-based supplemental payments to eligible PCMH practices or providers are: " Performance Incentive Supplemental Payment " Performance Improvement Supplemental Payment For more information on the methodology for calculating the performance payments, go to Based_Payment_Program.pdf 27
29 Next Webinar! Using Provider Portal Reports to Manage HUSKY Members " Learn to access and use reports available on the Provider Portal " Member data specific to your practice! The data foundation for identifying opportunities for QI! Join us on Thursday, November 19 th at noon 28
30 Questions? Thank you! 29
Medical Assistance Program Oversight Council. January 10, 2014
 Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
Medical Assistance Program Oversight Council January 10, 2014 Presentation Outline Ø Ø Ø Ø Ø Ø Ø Ø Ø Ø Evolution of the Concept of Patient-Centered Medical Home A New Model of HealthCare Delivery PCMH
TO BE RESCINDED Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
and HEDIS Measures
 1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
=======================================================================
 ======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers
: Strategies to Overcome Implementation Barriers") Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers March 23, 2017 A Department of Social Services PCMH Presentation Hosted by Community Health Network of CT,
Physical & Behavioral Health Integration (BHI): Strategies to Overcome Implementation Barriers March 23, 2017 A Department of Social Services PCMH Presentation Hosted by Community Health Network of CT,
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Communicator. the JUST A THOUGHT. Ensuring HEDIS-Compliant Preventive Health Services. Provider Portal Features. Peer-to-Peer Review BY DR.
 WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
PCMH 2017 Performance Measurement and Quality Improvement
 PCMH 2017 Performance Measurement and Quality Improvement Performance Measurement and Quality Improvement If you are PCMH 2011 practice or PCMH 2014 Level 1: you are not eligible for annual reporting If
PCMH 2017 Performance Measurement and Quality Improvement Performance Measurement and Quality Improvement If you are PCMH 2011 practice or PCMH 2014 Level 1: you are not eligible for annual reporting If
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Quality Management Utilization Management
 Aetna Better Health Aetna Better Health Kids Quality Management Utilization Management 2015 Program Evaluation EXECUTIVE SUMMARY Aetna Better Health, a Medicaid Physical Health-Managed Care Organization
Aetna Better Health Aetna Better Health Kids Quality Management Utilization Management 2015 Program Evaluation EXECUTIVE SUMMARY Aetna Better Health, a Medicaid Physical Health-Managed Care Organization
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
HEDIS TOOLKIT FOR PROVIDER OFFICES. A Guide to Understanding Medicaid Measure Compliance
 HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
CHNCT Provider Collaborative Program
 CHNCT Provider Collaborative Program Community Health Network of Connecticut, Inc. (CHNCT), on behalf of the Department of Social Services (DSS) and the HUSKY Health program, offers a comprehensive program
CHNCT Provider Collaborative Program Community Health Network of Connecticut, Inc. (CHNCT), on behalf of the Department of Social Services (DSS) and the HUSKY Health program, offers a comprehensive program
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
ENGAGED LEADERSHIP. TC-02 (Core): Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.
: Defines practice organizations structure and staff responsibilities/skills to support key PCMH functions.") Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
Change Concepts for Practice Transformation AND 2014 NCQA PCMH Standards Crosswalk to 2017 NCQA Standards Change Concept Element 2014 NCQA PCMH Standards 2014 --> 2017 2017 NCQA Standards ENGAGED LEADERSHIP
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
2014 PCMH STANDARDS. Renewals & Annual Data Requirements
 2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
2014 PCMH STANDARDS Renewals & Annual Data Requirements PCMH Renewal Process Streamlined process for renewal through reduced documentation requirements. Even though some elements do not require documentation,
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
2012 HEDIS/CAHPS Effectiveness of Care Report for 2011 Measures Oregon Commercial Business
 2012 HEDIS/CAHPS Effectiveness of Care Report for 2011 Measures Oregon Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely used set of performance
2012 HEDIS/CAHPS Effectiveness of Care Report for 2011 Measures Oregon Commercial Business About HEDIS The Healthcare Effectiveness Data and Information Set (HEDIS 1 ) is a widely used set of performance
Practice Implications for Accountable Care Organizations
 Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Meaningful Use: a Primer
 Health Information Technology Extension Center of Los Angeles Meaningful Use: a Primer Mary Mitchell Director of Meaningful Use Defined as: What is Meaningful Use? A. Use of a certified EHR in a meaningful
Health Information Technology Extension Center of Los Angeles Meaningful Use: a Primer Mary Mitchell Director of Meaningful Use Defined as: What is Meaningful Use? A. Use of a certified EHR in a meaningful
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Best Practices Managing Patients with Multiple Chronic Conditions Dartmouth-Hitchcock Physicians Case Study Organization Profile Headquartered in Bedford, New Hampshire, Dartmouth-Hitchcock is a large
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
QUALITY IMPROVEMENT. Articles of Importance to Read: Quality Improvement Program. Winter Pages 1, 2, 3, 4 and 5 Quality Improvement
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Florida Medicaid: Performance Measures (HEDIS)
") Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Quality Measurement and Reporting Kickoff
 Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Quality Measurement and Reporting Kickoff All Shared Savings Program ACOs April 11, 2017 Sandra Adams, RN; Rabia Khan, MPH Division of Shared Savings Program Medicare Shared Savings Program DISCLAIMER
Medicare Advantage Star Ratings
 Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
Medicare Advantage Star Ratings December 2017 The Star Rating System measures how well Medicare Advantage (MA) and its prescription drug plans perform for consumers. As an integrated health system, Presbyterian
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Health Care Home Benchmarking. Marie Maes-Voreis MDH Director, Health Care Homes Nathan Hunkins MNCM Account/Program Manger
 Health Care Home Benchmarking Marie Maes-Voreis MDH Director, Health Care Homes Nathan Hunkins MNCM Account/Program Manger Presentation Objectives Background: HCH Measurement & Benchmarks (Marie Maes-Voreis)
Health Care Home Benchmarking Marie Maes-Voreis MDH Director, Health Care Homes Nathan Hunkins MNCM Account/Program Manger Presentation Objectives Background: HCH Measurement & Benchmarks (Marie Maes-Voreis)
Section IX Special Needs & Case Management
 Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
A. DIABETES AND HEART/STROKE Data Detail
 A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
A. DIABETES AND HEART/STROKE Data Detail Under the category of Effective Care, MHMC currently reports practices who have achieved national recognition for any of the Bridges to Excellence (BTE) clinical
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
PATIENT CENTERED. Medical Home. Attestation. Facility Compliance
 2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Chapter 7. Unit 2: Quality Performance Measures
 Chapter 7 Unit 2: Quality Performance Measures In This Unit Topic See Page Unit 2: QualityBLUE Physician Pay-for-Performance Program Clinical Quality 2 Acute Pharyngitis Testing 10 Adolescent Well Care
Chapter 7 Unit 2: Quality Performance Measures In This Unit Topic See Page Unit 2: QualityBLUE Physician Pay-for-Performance Program Clinical Quality 2 Acute Pharyngitis Testing 10 Adolescent Well Care
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training
 Model of Care (MOC) Initial and Annual Training") Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Special Needs Plans (SNP) Model of Care (MOC) Initial and Annual Training 2018 Learning Objectives Program participants will be able to: List the three overall goals of the SNP Model of Care Describe the
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff
 Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
McLaren Health Plan Quality Improvement Update 2014
 McLaren Health Plan Quality Improvement Update 2014 Since the incorporation of McLaren Health Plan (MHP) in November 1997, the staff has continued to utilize their extensive clinical and administrative
McLaren Health Plan Quality Improvement Update 2014 Since the incorporation of McLaren Health Plan (MHP) in November 1997, the staff has continued to utilize their extensive clinical and administrative
HEDIS 101 for Providers
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions HEDIS 101 for Providers Aetna Better Health of Kentucky 2017 HEDIS 101 for Providers Aetna Better Health 2 HEDIS
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions HEDIS 101 for Providers Aetna Better Health of Kentucky 2017 HEDIS 101 for Providers Aetna Better Health 2 HEDIS
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Oregon's Health System Transformation
 Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
Weaving Expanded Roles of the RN into Population Management
 Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
Weaving Expanded Roles of the RN into Population Management Lois K. Andrews, DNP, RN-BC, CNS, ACNS-BC, CCRN Sentara Quality Care Network (SQCN), Norfolk, Va. Objectives: Explore the evolution of healthcare
National Conference NFPRHA Lorrie Gavin, Senior Health Scientist, CDC Mytri Singh, MPH, Director Clinical Quality Improvement, PPFA
 National Conference NFPRHA 2014 Lorrie Gavin, Senior Health Scientist, CDC Mytri Singh, MPH, Director Clinical Quality Improvement, PPFA Agenda 1. Quality in family planning services What it is? and Why
National Conference NFPRHA 2014 Lorrie Gavin, Senior Health Scientist, CDC Mytri Singh, MPH, Director Clinical Quality Improvement, PPFA Agenda 1. Quality in family planning services What it is? and Why
Fast-Track NCQA-PCMH Recognition. Using i2i Systems NCQA Pre-Validated PCMH Solution
 Fast-Track NCQA-PCMH Recognition Using i2i Systems NCQA Pre-Validated PCMH Solution Goal of Today s Webinar Share Why NCQA-PCMH Pre-Validation Matters Learn How to Fast-Track to NCQA-PCMH Recognition Hear
Fast-Track NCQA-PCMH Recognition Using i2i Systems NCQA Pre-Validated PCMH Solution Goal of Today s Webinar Share Why NCQA-PCMH Pre-Validation Matters Learn How to Fast-Track to NCQA-PCMH Recognition Hear
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
June Thank you for attending today s Webinar. We will begin shortly. June Brian Clark. Diana Charlton. Debbie Barkley Aetna Inc.
 June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,
June 2018 Brian Clark Diana Charlton Debbie Barkley Thank you for attending today s Webinar. We will begin shortly. June 2018 1 Brian Clark Diana Charlton Debbie Barkley Welcome Illinois, New Jersey, Florida,
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
In This Issue. Issue: 8. Codes Utilization FAQs Harry s Health Highlights. Who s Harry? HEDIS News
 Issue: 8 Who s Harry? Born from the mists of success, and integrated into the core of our measures; Harry forges forward in an undying quest to bring H knowledge to Cenpatico s provider network. In This
Issue: 8 Who s Harry? Born from the mists of success, and integrated into the core of our measures; Harry forges forward in an undying quest to bring H knowledge to Cenpatico s provider network. In This
Meaningful Use Final Rule:
 Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary
 2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
Medicare Physician Group Practice Demonstration
 Medicare Physician Group Practice Demonstration Disease Management Colloquium Philadelphia, Pennsylvania June 23, 2005 John Pilotte Senior Research Analyst Medicare Demonstrations Program Group Centers
Medicare Physician Group Practice Demonstration Disease Management Colloquium Philadelphia, Pennsylvania June 23, 2005 John Pilotte Senior Research Analyst Medicare Demonstrations Program Group Centers
Quality Improvement Program
 How we measure up At HealthKeepers, Inc., we focus on helping our Anthem HealthKeepers Plus members get healthy and stay healthy. To help us serve you the best we can, each year we look closely at the
How we measure up At HealthKeepers, Inc., we focus on helping our Anthem HealthKeepers Plus members get healthy and stay healthy. To help us serve you the best we can, each year we look closely at the
HouseCalls Objectives
 Overview Agenda Overview Objectives Background Case studies Member Experience Primary Care Provider Experience Referrals and Follow-up Influence on Centers for Medicare & Medicaid Services (CMS) Star Ratings
Overview Agenda Overview Objectives Background Case studies Member Experience Primary Care Provider Experience Referrals and Follow-up Influence on Centers for Medicare & Medicaid Services (CMS) Star Ratings
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
Using Quality Improvement to Reduce Racial and Ethnic Disparities in Medicaid Managed Care: Lessons from Oregon
 Using Quality Improvement to Reduce Racial and Ethnic Disparities in Medicaid Managed Care: Lessons from Oregon Matthew Carlson, Ph.D. Assistant Professor of Sociology Portland State University Charles
Using Quality Improvement to Reduce Racial and Ethnic Disparities in Medicaid Managed Care: Lessons from Oregon Matthew Carlson, Ph.D. Assistant Professor of Sociology Portland State University Charles
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER
 PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
ACO GPRO 2016 Ready to Report Basics GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017
 ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
Assistance. Improving. Consumer Health. Strategies for
 Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
Assistance Strategies for Improving Consumer Health A resource to help educate consumers about available preventive health incentives and eliminating barriers to receiving care www.bhpi.org www.healthsharesolutions.org
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin