RESIDENT CENSUS AND CONDITIONS OF RESIDENTS
|
|
|
- Wilfrid Stevens
- 6 years ago
- Views:
Transcription
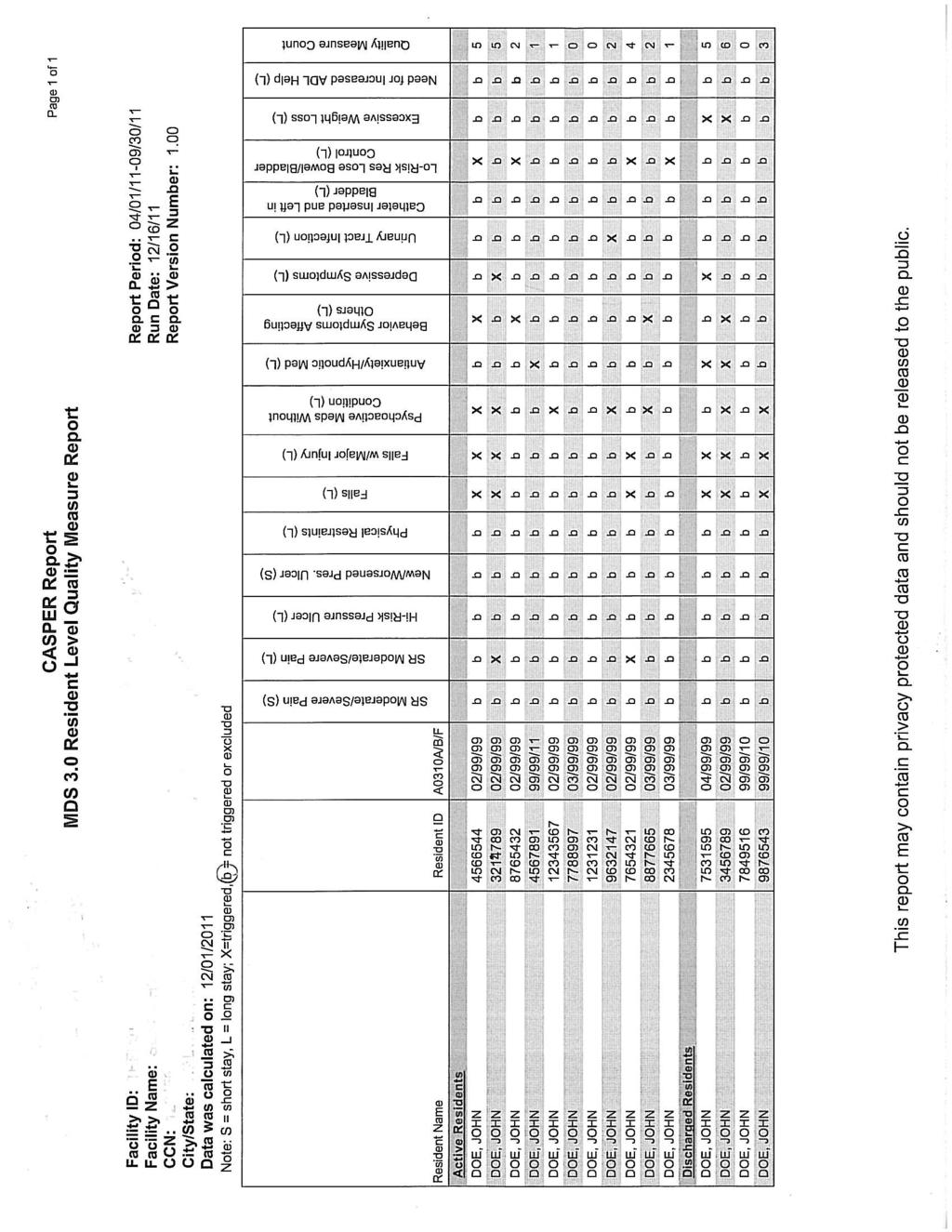
1 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES Provider No. RESIDENT CENSUS AND CONDITIONS OF RESIDENTS Medicare Medicaid Other Total Residents F75 F76 F77 ADL Independent Assist of One or Two Staff Dependent F78 Bathing F79 F80 F81 Dressing F82 F83 F84 Transferring F85 F86 F87 Toilet Use F88 F89 F90 Eating F91 F92 F93 A. Bowel/Bladder Status F94 With indwelling or external catheter F95 Of total number of residents with catheters, were present on admission. F96 Occasionally or frequently incontinent of bladder F97 Occasionally or frequently incontinent of bowel F98 On individually written bladder training program F99 On individually written bowel training program B. Mobility F100 Bedfast all or most of time F101 In chair all or most of time F102 Independently ambulatory F103 Ambulation with assistance or assistive device F104 Physically restrained F105 Of total number of residents restrained, were admitted with orders for restraints. F106 With contractures F107 Of total number of residents with contractures, had contractures on admission. C. Mental Status F108 With mental retardation F109 With documented signs and symptoms of depression F110 With documented psychiatric diagnosis (exclude dementias and depression) F111 Dementia: multi-infarct, senile, Alzheimer s type, or other than Alzheimer s type D. Skin Integrity F115 With pressure sores (exclude Stage I) F116 Of the total number of residents with pressure sores excluding Stage I, how many residents had pressure sores on admission?. F117 Receiving preventive skin care F118 With rashes F112 With behavioral symptoms F113 Of the total number of residents with behavioral symptoms, the total number receiving a behavior management program. F114 Receiving health rehabilitative services for MI/MR Form CMS-672 ( /1 ) 1
2 RESIDENT CENSUS AND CONDITIONS OF RESIDENTS E. Special Care Fl19 Receiving hospice care benefit F120 Receiving radiation therapy F121 Receiving chemotherapy F122 Receiving dialysis F123 Receiving intravenous therapy, parenteral nutrition, and/or blood transfusion F124 Receiving respiratory treatment F125 Receiving tracheostomy care F126 Receiving ostomy care F. Medications F133 Receiving any psychoactive medication F134 Receiving antipsychotic medications F135 Receiving antianxiety medications F136 Receiving antidepressant medications F137 Receiving hypnotic medications F138 Receiving antibiotics F139 On pain management program F127 Receiving suctioning F128 Receiving injections (exclude vitamin B12 injections) F129 Receiving tube feedings Fl30 Receiving mechanically altered diets including pureed and all chopped food (not only meat) F131 Receiving specialized rehabilitative services (Physical therapy, speech-language therapy, occupational therapy) F132 Assistive devices while eating G. Other F140 With unplanned significant weight loss/gain F141 Who do not communicate in the dominant language of the facility (include those who use sign language) F142 Who use non-oral communication devices F143 With advance directives F144 Received influenza immunization F145 Received pneumococcal vaccine I certify that this information is accurate to the best of my knowledge. Signature of Person Completing the Form Title Date TO BE COMPLETED BY SURVEY TEAM F146 Was ombudsman office notified prior to survey? Yes No F147 Was ombudsman present during any portion of the survey? Yes No F148 Medication error rate % Form CMS-672 ( /1 ) 2
3 GENERAL INSTRUCTIONS: RESIDENT CENSUS AND CONDITIONS OF RESIDENTS (use with Form CMS-672) THIS FORM IS TO BE COMPLETED BY THE FACILITY AND REPRESENTS THE CURRENT CONDITION OF RESIDENTS AT THE TIME OF COMPLETION There is no federal requirement to automate the 672 form. This form may and in many instances will need to be completed manually. A facility may use its MDS data to assist in completing the entry fields for the 672 form, however, facilities should ensure that the MDS information is not simply counted and copied over into the form. The Resident Census and Conditions of Residents information is designed to be a representation of the facility during survey; it does not directly correspond to the MDS data in every field. The information entered on this form must be reflective of all residents as of the day of survey; therefore all information entered must be independently verified. For the purpose of completing this form the terms: facility means certified beds (i.e., Medicare and/or Medicaid certified beds) and residents means residents in certified beds regardless of payer source. Following the definition of certain entry fields, the related MDS 3.0 item(s) is noted. Remember, that although the MDS item(s) are noted for some entry fields, the field itself may need to be completed differently to reflect the current status of all residents as of the day of survey. The MDS items below are provided only as a reference point, but the form is to be completed using the time frames and other specific instructions as noted below. Where a field refers to the admission assessment, use only the counts from the first assessment since the most recent admission/entry or reentry (OBRA or Scheduled PPS i.e., A0310A = 01; A0310B = 01 or 06; A0310E = 1; for each resident). INSTRUCTIONS AND DEFINITIONS: Complete each field by specifying the number of residents in each category. If no residents fall into a category enter a 0. Provider Number: Facility CMS certification provider number. A0100B; leave blank for initial certifications. Block F75: Residents whose primary payer is Medicare. Block F76: Residents whose primary payer is Medicaid. Block F77: Residents whose primary payer is neither Medicare nor Medicaid. Block F78: Residents for whom a bed is maintained on the day the survey begins, including those temporarily away in a hospital or on leave. This should be representative of residents in the nursing facility or those who have a bed-hold. ADLS (F79 F93): To determine resident status, unless otherwise noted, consider the resident s condition for the 7 days prior to the survey. Horizontal totals across the three columns (Independent, Assist of One or Two Staff, and Dependent) must equal the number in Block F78. The ADL categories for each resident include Bathing, Dressing, Transferring, Toilet Use and Eating. Bathing (F79 F81): This includes a full-body bath/shower, sponge bath, and transfer into and out of tub or shower. G0120A = 0; F80: G0120A = 1, 2, or 3; G0120A = 4. Facilities may provide setup assistance to residents such as drawing water for a tub bath or laying out clothes, bathing supplies/ toiletries, etc. Also, a resident may only need assistance with washing their back or shampooing their hair. If either of these are the case, and the resident requires no other assistance, count the resident as independent. Dressing (F82 F84): How the resident puts on, and takes off all items of clothing. May also include applying and/or removing elastic stockings or prostheses (e.g., braces and artificial limbs). G0110G1 = 0; G0110G1 = 1, 2, or 3; G0110G1 = 4. Facilities may set out clothes for residents. If this is the case and this is the only assistance the resident receives, count the resident as independent. However, if a resident receives assistance, such as with dressing, donning a brace, elastic stocking, a prosthesis, or securing fasteners, etc. count the resident as needing the assistance of 1 or 2 staff, as appropriate. Transferring (F85 F87): How the resident moves between surfaces, including, to/from bed, chair, wheelchair, or standing position. (EXCLUDES transfers to/from the bath/toilet). G0110B1 = 0; G0110B1 = 1, 2, or 3; G0110B1 = 4. Facilities may provide setup assistance to residents, such as handing equipment (e.g., quad cane) to the resident. If this is the case and is the only assistance required, count the resident as independent. Toilet Use (F88 F90): How the resident uses the toilet, commode, bedpan, or urinal; transfers on/off toilet; cleanses self after elimination; changes pad(s); manages ostomy or catheter, and adjusts clothing. If all that is done for the resident is to open a package (e.g., a clean incontinence pad), count the resident as independent. G0110I1 = 0; G0110I1 = 1, 2, or 3; G0110I1 = 4. Eating (F91 F93): How a resident eats and drinks, regardless of skill. Do not include eating/drinking during medication pass. Includes intake of nourishment by other means (e.g., tube feeding, total parenteral nutrition, includes IV fluids administered for nutrition or hydration). Facilities may provide setup activities, such as opening containers, buttering bread, and organizing the tray; if this is the case and is the only assistance a resident needs, count this resident as independent. G0110H1 = 0; G0110H1 = 1, 2, or 3; G0110H1 = 4. Form CMS-672 (02/12) 3
4 RESIDENT CENSUS AND CONDITIONS OF RESIDENTS (use with Form CMS-672) A. BOWEL/BLADDER STATUS (F94 F99) F94: With an indwelling or an external catheter: Residents whose urinary bladder is constantly drained by a catheter (e.g., an indwelling catheter, a suprapubic catheter or nephrostomy tube) or who wears an appliance that is applied over the penis and connected to a drainage bag to collect urine from the bladder (e.g., condom catheter or similar appliance). H0100A or B = checked. F95: Of the total number of residents with catheters: Number of residents who had a catheter present on admission/ entry or reentry. H0100A or B = checked. To complete this field use only the counts from the first assessment since the most recent admission/ entry or reentry (OBRA or Scheduled PPS), i.e., A0310A = 01, A0310B = 01 or 06; A0310E = 1 for each resident. F96: Occasionally or frequently incontinent of bladder: Residents who have an incontinent episode two or more times per week. Do not include residents with an indwelling or external catheter. H0100A and B = not checked and H0300 =1, 2, or 3. F97: Occasionally or frequently incontinent of bowel: Residents who have a loss of bowel control two or more times per week. H0400 = 2 or 3. F98: On urinary training/toileting program: Residents with a systematically implemented, individualized urinary training/ toileting program (i.e. bladder rehabilitation/ retraining, prompted voiding, habit training/scheduled voiding) to decrease or prevent urinary incontinence or minimizing or avoiding the negative consequences of incontinence (e.g., pelvic floor exercises). Count all residents on urinary training programs including those who are incontinent. H0200A = 1; H200C = 1; H0300 = 1, 2 or 3. F99: On bowel toileting program: Residents with a systematically implemented, individualized bowel toileting program to decrease or prevent bowel incontinence or minimizing or avoiding the negative consequences of incontinence (e.g., use of adequate fluid intake, fiber in the diet, exercise, and scheduled times to attempt bowel movement). Count all residents on toileting programs including those who are incontinent. H0400 = 2 or 3; H0500 = 1. B. MOBILITY (F100 F107) Total for F100 F103 should = the number in Block F78, Total Residents. Algorithm to force mutual exclusivity: Test for each resident. If F100 = 1 then add 1 to F100, and go to the next resident; If F101 = 1 then add 1 to F101 and go to the next resident; If F103 = 1 then add 1 to F103 and go to the next resident; If F102 = 1 then add 1 and go to the next resident. F100: Bedfast all or most of time: Residents who are bedfast all or most of the time (e.g., in bed or geriatric chair/recliner) includes bedfast with bathroom privileges. F101: In a chair all or most of time: Residents who depend on a chair for mobility includes those residents who can stand with assistance to pivot from bed to wheelchair or to otherwise transfer. The resident cannot take steps without extensive or constant weight-bearing support from others and is not bedfast all or most of the time. G0300A or E = 2; G0600C = checked. F102: Independently ambulatory: Residents who require no help or oversight; or help or oversight was provided only 1 or 2 times during the past 7 days. Do not include residents who use a cane, walker or crutch. G0110C1 or G0110D1 = 0 or 7 and G0110C2 or G0110D2 = 0 or 1; G0600A and G0600B = not checked. F103: Ambulation with assistance or assistive devices: Residents who require oversight, cueing, physical assistance or who use a cane, walker, or crutch. Count the use of lower leg splints, orthotics, and braces as assistive devices. G0110C1 or G0110D1 = 1, 2, or 3 and G0110C2 or G0110D2 = 1, 2 or 3; G0300B = 0; G0600A1 or G0600B1 = checked. F104: Physically restrained: Residents for whom restraints were used. Restraints include any manual or physical method or mechanical device, material or equipment attached or adjacent to the resident s body in such a way that the individual cannot remove easily and it restricts freedom of movement or normal access to one s body. Do not include devices such as braces which are used for medical/clinical reasons. P0100A through H = 1 or 2. F105: Of total number of restrained residents: Residents on admission/entry or reentry with an order for restraint(s). P0100A through H = 1 or 2. To complete this field use only the counts from the first assessment since the most recent admission/ entry or reentry (OBRA or Scheduled PPS), i.e., A0310A = 01, A0310B = 01 or 06; A0310E = 1 for each resident. F106: With contractures: Residents that have a restriction of full passive range of motion of any joint due to deformity, disuse, pain, etc., includes loss of range of motion in neck, fingers, wrists, elbows, shoulders, hips, knees and ankles. G0400A and/or B = 1 or 2. F107: Of the total of number with contractures, those who had a contracture(s) on admission: To complete this field use only the counts from the first assessment since the most recent admission/entry or reentry (OBRA or Scheduled PPS), i.e., A0310A = 01, A0310B = 01 or 06; A0310E = 1 for each resident (although neck contractures not included in MDS data note if present). Form CMS-672 (02/12) 4
5 RESIDENT CENSUS AND CONDITIONS OF RESIDENTS (use with Form CMS-672) C. MENTAL STATUS (F108 F114) F108: With intellectual disability (mental retardation as defined at (a)) or developmental disability: Residents in all of the categories of intellectual or developmental disability regardless of severity, as determined by the State Mental Health or State Mental Retardation Authorities. A1550A, B through E = checked. F109: With documented signs and symptoms of depression: Residents with documented signs and symptoms of depression. Column D02001A through D = 1 for any indicator present; D02001I = 1; column D02002A through D = 2 or 3 for symptom frequency; D0300 = or column D05001A through D = 1 for any indicator present; D05001I = 1; column D05002A through D = 2 or 3 for symptom frequency; D0600 = F110: With documented psychiatric diagnosis (exclude dementias and depression): Residents with primary or secondary psychiatric diagnosis including: Schizophrenia Schizo-affective disorder Schizophreniform disorder Delusional disorder Anxiety disorder Psychotic mood disorders (including mania and depression with psychotic features, acute psychotic episodes, brief reactive psychosis, and atypical psychosis). I5700, I5900, I5950, I6000 or I6100 = checked. F111: Dementia: Non-Alzheimer s Dementia (e.g., Lewy- Body, vascular or Multi-infarct, mixed, frontotemporal such as Pick s disease; and dementia related to Parkinson s or Creutzfeldt-Jakob diseases), or Alzheimer s Disease: Residents with a primary or secondary diagnosis of dementia or organic mental syndrome including, Non-Alzheimer s Dementia (e.g., Lewy-Body, vascular or Multi-infarct, mixed, frontotemporal such as Pick s disease; and dementia related to Parkinson s or Creutzfeldt-Jakob diseases). I4200 or I4800 = checked. F112: With behavioral health care needs: Residents with one or more of the following indicator(s): wandering, verbally abusive, physically abusive, socially inappropriate/ disruptive, and resistive to care. E0200A, B, C = 1, 2, or 3; E0500A, B, C = 1; E0600A, B, C = 1; E0300 = 1 or E0800 = 1, 2, or 3 or E0900 = 1, 2, or 3; E1000A, B = 1. F113: Of the total number with behavioral health care needs, those having an individualized care plan to support them: Residents with behavior symptoms who are receiving an individualized care plan/program designed to support and manage behavioral needs (as noted in F112). F114: Receiving health rehabilitative services for MI and/ or ID/DD: Residents for whom the facility is providing health rehabilitative services for MI and/or ID/DD (mental retardation as defined at (a)). D. SKIN INTEGRITY (F115 F118) Fl15: With pressure ulcers: Residents with localized injury to the skin and/or underlying tissue, usually over a bony prominence, as a result of pressure, or pressure in combination with shear and/or friction (exclude Stage I); M0300B1, M0300C1, or M0300D1; M0300E1, M0300F1 and/or M0300G1 > 0. To complete this field, use only the counts from the first assessment since the most recent admission/ entry or reentry (OBRA or Scheduled PPS), i.e., A0310A = 01, A0310B = 01 or 06; A0310E = 1 for each resident. F116: Of the total number of residents with pressure ulcers (excluding Stage I), those who had pressure ulcers on admission/entry or reentry: M0300B2, M0300C2, M0300D2, M0300E2, M0300F2 and/or M0300G2 > 0. F117: Receiving preventive skin care: Residents receiving non-routine skin care ordered by a physician, and/or included in the resident s comprehensive plan of care (e.g., hydrocortisone ointment to areas of dermatitis three times a day, granulex sprays, etc.) M1200A through I = checked. Fl18: With rashes: Residents who have rashes which may or may not be treated with any medication or special baths, etc. (e.g., may include but are not limited to antifungals, corticosteroids, emollients, diphenhydramines or scabicides). E. SPECIAL CARE (F119 F132) F119: Receiving hospice care: Residents who have elected or are currently receiving the hospice benefit. O0100K2= checked. F120: Receiving radiation therapy: Residents who are under a treatment plan involving radiation therapy. O0100B1 or O0100B2 = checked. F121: Receiving chemotherapy: Residents under a specific treatment plan involving chemotherapy. O0100A1 or O0100A2 = checked. F122: Receiving dialysis: Residents receiving hemodialysis or peritoneal dialysis either within the facility or offsite. O0100J1 or O0100J2 = checked. F123: Receiving intravenous therapy, IV nutrition and/or blood transfusion: Residents receiving fluids, medications, all or most of their nutritional requirements and/or blood and blood products administered intravenously. K0510A2, O0100H2, or O0100I2 = checked. F124: Receiving respiratory treatment: Residents receiving treatment by the use of respirators/ ventilators, oxygen, IPPB or other inhalation therapy, pulmonary toilet, humidifiers, and other methods to treat conditions of the respiratory tract. This does not include residents receiving tracheostomy care or respiratory suctioning. O0100C2, O0100F2, or O0100G2 = checked. Form CMS-672 (02/12) 5
6 RESIDENT CENSUS AND CONDITIONS OF RESIDENTS (use with Form CMS-672) F125: Receiving tracheotomy care: Residents receiving care involved in maintenance of the airway, the stoma and surrounding skin, and dressings/coverings for the stoma. O0100E2 = checked. F126: Receiving ostomy care: Residents receiving care for a colostomy, ileostomy, uretrostomy, or other ostomy of the intestinal and/or urinary tract. DO NOT include tracheostomy. H0100C = checked, identifies residents who use these appliances. F127: Receiving suctioning: Residents that require use of a mechanical device which provides suction to remove secretions from the respiratory tract via the oral cavity, nasal passage, or tracheostomy. O0100D2 = checked (Note: O0100D2 does not include oral suctioning, so residents who receive oral suctioning will have to be counted separately). F128: Receiving injections: Residents that have received one or more injections within the past 7 days. (Exclude injections of Vitamin B 12.) Review residents where N0300 = > 0. Omit from the count any resident whose only injection currently is B12. F129: Receiving tube feeding: Residents who receive all or most of their nutritional requirements via a feeding tube that delivers food/nutritional substances directly into the GI system (e.g., nasogastric tube, gastrostomy tube). K0510B2 = checked. F130: Receiving mechanically altered diets: Residents receiving a mechanically altered diet including pureed and/or chopped foods (not only meat). K0510C2 = checked. F131: Receiving rehabilitative services: Residents receiving care designed to improve functional ability provided by, or under the direction of a rehabilitation professional (physical therapist, occupational therapist; speech-language pathologist). Exclude health rehabilitation for MI and/or ID/DD. Minutes entered > 0 for O0400A1, 2, or 3; O0400B1, 2, or 3; or O0400C1, 2, or 3. F132: Assistive devices with eating: Residents who are using devices to maintain independence and to provide comfort when eating (i.e., plates with guards, large handled flatware, large handle mugs, extend hand flatware, etc.). O0500C or H = > 0. F. MEDICATIONS (F133 F139) F133: Receiving psychoactive medications: Residents that receive medications classified as antipsychotics, anxiolytics, antidepressants, and hypnotics. Days entered >0 for N0410A, B, C or D. Use the following lists to assist you in determining the number of residents receiving psychoactive medications. These lists are not meant to be all inclusive; therefore, a resident receiving a psychoactive medication not on this list, should be counted under F133 and any other medication category that applies: F134, F135, F136, and/or F137. F134: Receiving antipsychotic medications: N0410A = > 0 Clozapine Haloperidol Haloperiodal Deconate Droperidol Loxapine Thioridazine Molindone Theothixene Zyprexa Pimozide Fluphenazine Deconate Fluphenazine Quetiapine Risperidone Mesoridazine Promazine Trifluoperazine Chlorprothixene Chlorpromazine Acetophenazine Perphenazine F135: Receiving antianxiety medications (anxiolytics): N0410B = > 0 Lorazepam Oxazepam Prazepam Diazepam Clonazepam Hydroxyzine Chlordiazepoxide Halazepam Alprazolam F136: Receiving antidepressant medications: N0410C = > 0 Aripiprazole Amoxapine Nortriptyline Wellbutrin Trazodone Venlafaxine Amtriptyline Lithium Maprotiline Isocarboxazid Phenelzine Serzone Desipramine Tranylcypromine Paroxetine Fluoxetine Sertraline Doxepin Imipramine Protriptyline Form CMS-672 (02/12) 6
7 RESIDENT CENSUS AND CONDITIONS OF RESIDENTS (use with Form CMS-672) F137: Receiving hypnotic medications: N0410D = > 0 Flurazepam Quazepam Estazolam Temazepam Triazolam Zolpidem F138: Receiving antibiotics: Residents receiving antibacterial sulfonamides, antibiotics, etc., either for prophylaxis or treatment. N0410F = > 0. F139: On a pain management program: Residents with a specific plan for control of difficult to manage or intractable pain, which may include self medication pumps or regularly scheduled administration of medication alone or in combination with non-medication interventions (e.g., massages heat/cold, biofeedback, etc.). J0100A, B, or C = 1. G. OTHER RESIDENT CHARACTERISTICS (F140 F146) F140: With unplanned significant weight loss/gain: Residents who have experienced unplanned weight loss/gain of > 5% in one month or > 10% over six months. K0300 or K0310 = 2. F141: Who do not communicate in the dominant language at the facility? Residents who do not speak in the dominant language of the facility; for example residents who speak only Spanish, but the majority of staff that care for the residents speak only English. A1100A = 1; A1100B = alternate language identified (e.g. Spanish, French, Portuguese, etc.). F142: Who use non-oral communication? Residents who communicate via non-oral methods, including, picture boards, computers, etc. A1100B, Preferred Language (e.g. American Sign Language). F143: Who have advanced directives? Residents who have advance directives, such as Physician s Orders for Life- Sustaining Treatment (POLST), a living will or durable power of attorney for health care, recognized under state law and relating to the provisions of care when the individual is incapacitated. F144: Received influenza immunization: Residents known to have received the influenza immunization within the last 12 months. O0250A = 1. F145: Received pneumococcal vaccine: Residents known to have received the pneumococcal vaccine. O0300A = 1. LEAVE BLANK (F146-F148) To Be Completed By Survey Team F146: Ombudsman notice: Indicate whether or not the State Ombudsman was notified prior to the survey. F147: Ombudsman presence: Indicate whether or not the State Ombudsman was present at any time during the survey. F148: Medication error rate: Calculate and enter the medication error percentage of the facility. Form CMS-672 (02/12) 7
8 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES Offsite Phase I Phase 2 Provider # ROSTER/SAMPLE MATRIX Total Sample: Phase 1 Phase 2 Individual Interview (I) Family Interview (F) Closed Record (CL) Comprehensive (C) Focused Review (FO) Resident Number Resident Room Surveyor Assigned Interview: Individual/Family Closed Record/Comprehensive/Focused Privacy/Dignity Issues Social Services Self-Determination/Accommodation of Needs Abuse/Neglect Clean/Comfort/Homelike Moderate/Severe Pain (Constant or Frequent) Hi-Risk Pressure Ulcer (Stage II-IV) New/Worsened Pressure Ulcers (Stage II-IV) Physical Restraints Falls including Falls with Major Injury Psychoactive Meds with Absence of Condition Antianxiety/Hypnotic Med Use Behavior Symptoms Affecting Others/Self Depressive Symptoms Urinary Tract Infection Indwelling Urinary Catheter Lo-Risk Resident Lose Bowel/Bladder Control Excessive Weight Loss/Gain Need for Increased ADL Help Hospice Dialysis Admittance/Transfer/Discharge MI (Non-Dementia) or ID/DD Language/Communication Vision/Hearing/Other Assistive Devices Fecal Impaction ROM/Contractures/Positioning Specialty Care (Tube Feeding, Central Lines, Ventilators, ) O2 Hydration/Swallowing/Oral Health Infections Specialized Rehab Services (OT, PT, Speech) Resident Name Form CMS-802 (02/12)
9 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES ROSTER/SAMPLE MATRIX INSTRUCTIONS FOR PROVIDERS (use with Form CMS-802) The Roster/Sample Matrix form (CMS-802 ) is used to list all current residents (including residents on bed-hold) and to note pertinent care categories. The facility completes the: resident name, resident room, and columns 6 31, which are described below. Columns 1 5 and blank columns are for Surveyor Use Only. There is no federal requirement to automate the 802 form. This form may and in many instances will need to be completed manually. information is not simply copied over into the form. The Roster/Sample Matrix information is designed to be a representation of All information entered on this form by instructions noted below. The information required on the Provider Instructions is not based on the Quality Measures. For each resident mark all columns that are pertinent needs pain medication, comfort measures or is on a pain management has a stage 2, appropriate letter for all possible responses. P0100A = 1 or 2, has fallen within the past 30 days and/or has fallen within the past 180 days all possible receives any psychoactive medications but has no psychiatric mood diagnoses. receives anxiolytics has has symptoms of depression. has an infection or is on has an indwelling urinary incontinent of bladder/ 1 enter T. Form CMS-802P (02/12) 1
10 had an unintended weight had chronic insidious weight loss/gain or is at nutritional or nutritional risk. Insidious weight loss is a slow, steady, and persistent weight loss over time that when reviewed in condition. has shown a decline in ADL areas. has elected or currently receiving hospice care. is receiving hemodialysis or peritoneal dialysis either within the facility or offsite. O0100J1 or O0100J2 = checked. enter the appropriate letter in this column if the resident was admitted within the past 30 days or is scheduled to be transferred or discharged within reentry after discharge without expectation of return. if the resident has a diagnosis of mental illness or intellectual or developmental mental illness not classified as dementia. A1500 =1, language of the facility. (If a resident uses American Sign has significant impairment of vision or hearing, or uses devices to aid vision uses special devices to assist with eating or mobility (e.g., tables, utensils, hand splints, canes, has functional limitations checked. O0100F = checked. has nutrition, has infections or infectious disease. I1700 checked. uses a language other than the dominant language of the facility or exhibits difficulty communicating his/her needs. This must be individually determined. In some facilities the predominant language is Form CMS-802P (02/12) 2
11 DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES ROSTER/SAMPLE MATRIX INSTRUCTIONS FOR SURVEYORS (use with Form CMS-802) The Roster/Sample Matrix form (CMS-802) is used to list all current residents (including residents on bed-hold) and to note pertinent care categories. The facility completes the: resident name, resident room, and columns 6-31, all remaining columns are for Surveyor Use Only. The Roster/Sample Matrix is a tool for selecting the resident sample and may be used for recording information acquired during the tour. When using the form to identify the resident sample, indicate by a check whether this CMS-802 is being used for the sample from Offsite, Phase 1 or Phase 2. The horizontal rows list residents chosen for review (or residents encountered during the tour) and Operations Manual (SOM) to identify the number of residents required in the sample. In the vertical column under the heading Interview: Individual/Family mark the column with I for each resident receiving an interview or with F for any non-interviewable resident receiving a family interview and/or staff observation. Mark the Closed Record/Comprehensive/Focused column with CL for a closed record review, C for a resident chosen for a comprehensive review or FO for a resident chosen for a focused review. Use the vertical columns numbered 1 through 31 to check the characteristics for each resident, as appropriate. During each portion of the survey (Offsite, Phase I, Phase 2) highlight the vertical columns for each Resident Number: Number each line sequentially down the rows continuing the numbering sequence for any additional pages needed. Resident Name: List the name of the resident. Surveyor Assigned: List initials or surveyor number of surveyor assigned to review each resident. Resident Room: Identify room number for the resident. COLUMNS 6 31: Highlight each column that is an area of concern. For each resident entered on the roster/sample matrix, check all columns that pertain to the resident according to the Offsite and Sample Selection Tasks of the Survey. 1. Privacy/Dignity: residents right to privacy (accommodations, written and telephone communication, visitation, personal care, etc.) or concerns that the facility does not maintain or enhance residents dignity. 2. Social Services: medically related or other social services; e.g., interpersonal relationships, grief, clothing, etc. 3. Self-Determination/Accommodation of Needs: residents ability to exercise their rights as citizens; freedom from coercion, discrimination or reprisal; self-determination and participation; choice of care and schedule, etc. 4. Abuse/Neglect: resident abuse, neglect or misappropriation of resident property or how the facility responds to allegations of abuse, neglect or misappropriation of resident property. 5. Clean/Comfortable/Homelike: facility environment including cleanliness, lighting levels, temperature, comfortable sound levels, or homelike environment and the residents ability to use their personal belongings and individualize their room to the extent possible. 6. Moderate/Severe Pain (constant or frequent: timely assessment and intervention with residents needing pain medications or measures to provide comfort, including nonmedication interventions, or who are on a pain management program. 7. Hi-Risk Pressure Ulcers (Stage 2-4): risk assessment, clinical assessment, treatment, monitoring, evaluation, and prevention of pressure ulcers; or other necessary skin care. or 4 pressure ulcers or unstageable pressure ulcers. 8. New/Worsened Pressure Ulcers (Stage 2-4): risk assessment, clinical assessment, treatment, monitoring, evaluation, and prevention of pressure ulcers; or other as having new or worsened stage 2, 3, or 4 pressure ulcers. 9. Physical Restraints: as physically restrained daily, including side rails. 10. Falls and/or Falls with Major Injury: residents that have fallen within the past 30 days and/or have fallen within the past 180 days and incurred a major injury. 11. Psychoactive Medications with Absence of Condition: medications in the absence of a psychiatric or mood related diagnoses or conditions. 12. Antianxiety/Hypnotic Medications: anxiolytics and/or hypnotics. 13. Behavioral Symptoms Affecting Others or Self: residents with behavioral health care needs (e.g., verbal or physical outbursts, withdrawing/ isolation). Form CMS-802S (02/12) 1
12 14. Depressive Symptoms: residents with symptoms of depression with or without antidepressant therapy. 15. Urinary Tract Infections (UTl): having a UTI. 16. Indwelling Urinary Catheter: residents with an indwelling urinary catheter. 17. Lo-Risk Resident Lose Bowel/Bladder Control Incontinence/Toileting Programs: resident bowel and/or bladder incontinence and facility toileting programs. 18. Excessive Weight Loss/Gain: residents with an unintended weight loss/gain of >5% in one month or >10% in six months, or has had an insidious weight loss/gain or is at nutritional risk. 19. Need for Increased ADL Help: residents receive appropriate treatment and services to maintain or improve decline. 20. Hospice: residents who have elected or are receiving hospice care. 21. Dialysis: care and coordination of services for residents receiving hemo or peritoneal dialysis either in the facility or offsite. 22. Admission/Transfer/Discharge: care/treatment for residents admitted within the past 30 days or is scheduled to be transferred or discharged within the next 30 days. Including but not limited to, resident preparation and procedures for transfer or discharge, such as: to next care providers, (i.e., Home Health; Hospital, Primary Care Provider, etc.); and resident needs upon transfer and/or discharge. 23. MI (Non-Dementia) or ID/DD: care and treatment of residents with a diagnosis of mental illness, intellectual or developmental disabilities. 24. Language/Communication: facility assisting those residents with communication challenges to communicate speaking other than the dominant language of the facility, or using non-oral communication such as, picture boards, 25. Vision/Hearing/Other Assistive Devices: facility assisting those residents with visual or hearing impairments to function at their highest practicable level, including those residents who have glasses or hearing aids. Include residents needing special devises to assist with eating or mobility. 26. Fecal Impaction: management of constipation or residents having a fecal impaction. 27. ROM/Contractures/Positioning: occurrence, prevention or treatment of contractures, staff provision or lack of provision of appropriate application/use of splints, ROM exercises, or decline in ROM. 28. Special Care (Tube Feeding, Central Lines, Ventilators, O 2, etc.): residents receiving nutrition via a feeding tube. Care provided to residents with tracheostomies or ventilators, residents needing suctioning, and residents receiving oxygen, IPPB or have special care areas, (e.g., prosthesis, ostomy, injection, IV s, including total parenteral nutrition, etc.), that may be of concern. 29. Hydration/Swallowing/Oral Health: residents, who show signs or symptoms, have risk factors for, or who are swallowing problems. Provision or lack of provision for oral health care for residents. 30. Infections: presence or prevalence of resident infections, residents receiving antibiotics or have an infectious disease or residents under strict isolation precautions. 31. Specialized Rehab: facility s provision or lack of provision of specialized rehabilitative services including, but not limited to; Note any other concerns; e.g., residents who are comatose, have delirium, have special skin care needs other than pressure ulcers or observed to spend most of their time in bed or a chair, such as a geriatric chair, recliner, etc. If during offsite preparation, concerns arise about the accuracy of the MDS information, enter MDS accuracy as a concern. Form CMS-802S (02/12) 2
13 Nursing Home Discharge Planning Checklist MDS 3.0 Section Q Disclaimer: Our facility is completing this information in accordance with MDS 3.0 Section Q regarding transition back into the community. We understand that the resident has a right to receive the needed long term care services in the least restrictive and most integrated setting. This information is true and correct to the best of our knowledge based in the information received from the resident during an interview. Date Section Q Interview Conducted: Person Conducting Interview: Personal Information Resident Name: Room Number: Primary Contact Person: Relationship to Resident: Medicare # Medicaid # Has the resident been adjudicated incompetent by a court of law? Yes No Has the resident been placed in the facility by DHR? Yes No If yes, was the placement by DHR: Court Ordered/Protective Placement Yes No Please attach a copy of the Court Order Has the resident been placed in the facility by a Court Order other than from DHR? Please attach a copy of the Court Order Yes No Is the discharge medically contraindicated by a physician? Yes No The physician progress note can be located: If the discharge is medically contraindicated by a physician, please explain If yes to any of the above questions, please stop the discharge planning process with respect to MDS 3.0 Section Q because it has been determined that discharge to the community is not feasible at this time. Before automatically stopping the discharge planning process, the nursing facility must document in the resident s medical record why it has been determined that discharge is not feasible at this time. If the resident persists and can feasibly be discharged, the discharge planning process should continue and include collaboration with the physician, guardian or court system. Page 1 of 10
14 Communication Discharge Planning Start Date: Local Contact Agency Assigned: Has coordination been established with the Local Contact Agency? When did the initial conversation occur with the Local Contact Agency? Date: Time: Name of person contacted: Title of person contacted: Anticipated date and time of visit/call by Local Contact Agency: Briefly describe the initial conversation with the Local Contact Agency: Date: Time: What type of visit is expected from the Local Contact Agency. i.e., phone call, face-to-face? Dates and times of additional follow-up contact made with the Local Contact Agency: Date: Time: Date: Time: Date: Time: Signature of Facility Representative: Date Signed: Printed Name and Title of Facility Representative: Page 2 of 10
15 Housing RAI Manual Q0400 What type of residence has the resident indicated that they wish to be discharged, i.e., another nursing facility, assisted living facility, private home, etc.? Anticipated New Address: Have any barriers and/ or challenges been identified by the Local Contact Agency? List the barriers and/or challenges identified by the Local Contact Agency: Assistive Technology - RAI Manual Q0400 Does the resident require assistive technology (Hardware and software that help people who are physically impaired)? Examples include, but are not limited to: eyeglasses, hearing aids, large print books, translating devices, TDD/TYY for phone service, etc. If so, what does the resident require? List all that apply Has the facility communicated to the Local Contact Agency that the resident requires assistive technology: Date: Time: Name of person contacted: Medical Needs/Referrals - RAI Manual Q0400 Is the resident enrolled in a managed care plan? Name of managed care plan: Has the resident been referred for Hospice services? Name of Hospice Date of Referral Has the resident been referred for Home Health services? Name of Home Health Date of Referral Page 3 of 10
16 Has the resident been referred for other services? Name of Other Services Date of Referral Name of Other Services Date of Referral Name of Other Services Date of Referral Durable Medical Equipment - RAI Manual Q0400 Does the resident require any durable medical Has the facility communicated to the Local Contact equipment, i.e., hospital bed, wheelchair, walker, etc.? Agency that the resident requires durable medical If so, what does the resident require? List all that equipment: apply Date: Time: Name of person contacted: Medical Support - RAI Manual Q0400 On the day of transition, the following information has been communicated with the Local Contact Agency: Type of transportation used to transition into the community: Name of transportation Date Completed Date set up Name of person contacted Page 4 of 10
17 Are medication orders written? Medication orders requested and written Date Completed Date set up Name of physician Are treatment orders written? Treatment orders requested and written Date Completed Date set up Name of physician Are special diet orders written? Special Diet orders requested and written Date Completed Does the resident have any allergies or reactions to medications? Date set up Name of physician Known allergies or reactions to medications Date Completed Are special nursing needs required? Special nursing needs requested Date Completed Date set up Name of Provider Page 5 of 10
18 Does the resident need Mental Health support? Mental Health needs requested Date Completed Date set up Name of Provider Does the resident require assistance with Activities of Daily Living? Activity of Daily Living needs requested Date Completed Date set up Name of Provider Does the resident require therapy? Therapy needs requested Date Completed Have any medical or special appointments been pre-arranged for the resident upon discharge? Date set up Name of Provider List of pre-arranged appointments Date set up Name of Provider Date Completed Date set up Name of Provider Page 6 of 10
19 Date set up Name of Provider Date set up Name of Provider Has the resident/responsible party received medication education? Medication education provided for (list drugs): Date Completed Date medication education provided Name and signature of Educator Has the resident/responsible party received prevention and disease management education? Prevention and disease management education provided for (list diseases): Date Completed Date education provided Name and signature of Educator Page 7 of 10
20 Medical Support - RAI Manual Q0400 The following medications and/or scripts have been sent with the resident/responsible party upon discharge: Name of Medication and/or Script Dosage Instructions Amount of Medication Distributed Certification and Signature of Receiving Party Facility RN Signature Receiving Party Signature Facility RN Signature Receiving Party Signature Facility RN Signature Receiving Party Signature Facility RN Signature Receiving Party Signature Facility RN Signature Receiving Party Signature Page 8 of 10
21 Medical Support - RAI Manual Q0400 Attach a copy of the medical records release form dated and signed to this document! The following documents have been sent with the resident/responsible party upon discharge: Name of Document/Information Advance Directive Certification and Signature of Receiving Party Facility Signature and Date Receiving Party Signature and Date Brief Medical History Facility Signature and Date Receiving Party Signature and Date Medication Education Facility Signature and Date Receiving Party Signature and Date Post Discharge Plan of Care Facility Signature and Date Receiving Party Signature and Date Prevention and Disease Management Education Facility Signature and Date Receiving Party Signature and Date List of resident preferences and needs for care and supports Facility Signature and Date Receiving Party Signature and Date Name and phone number of who to call in case of an emergency or if symptoms of decline occur Facility Signature and Date Receiving Party Signature and Date Page 9 of 10
22 Facility Signature and Date Receiving Party Signature and Date Facility Signature and Date Receiving Party Signature and Date Facility Signature and Date Receiving Party Signature and Date Facility Signature and Date Receiving Party Signature and Date Facility Signature and Date Receiving Party Signature and Date Date Discharge Completed: Signature of Facility Representative: Date Signed: Printed Name and Title of Facility Representative: Signature of Local Contact Agency Representative: Date Signed: Printed Name and Title of Local Contact Agency Representative: Signature of Resident or Responsible Party: Date Signed: Page 10 of 10
23
24
25
RESIDENT CENSUS AND CONDITIONS OF RESIDENTS (use with Form CMS-672)
") GENERAL INSTRUCTIONS: RESIDENT CENSUS AND CONDITIONS OF RESIDENTS THIS FORM IS TO BE COMPLETED BY THE FACILITY AND REPRESENTS THE CURRENT CONDITION OF RESIDENTS AT THE TIME OF COMPLETION There is no federal
GENERAL INSTRUCTIONS: RESIDENT CENSUS AND CONDITIONS OF RESIDENTS THIS FORM IS TO BE COMPLETED BY THE FACILITY AND REPRESENTS THE CURRENT CONDITION OF RESIDENTS AT THE TIME OF COMPLETION There is no federal
3/12/2015. Session Objectives. RAI User s Manual. Polling Question
 Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
Michigan Medicaid Nursing Facility Level of Care Determination
 Michigan Department of Health and Human Services Michigan Medicaid Nursing Facility Level of Care Determination Applicant's Name: Medicaid ID: Field 1 (Last) (First) (M.I.) Field 2 Date of Birth: Field
Michigan Department of Health and Human Services Michigan Medicaid Nursing Facility Level of Care Determination Applicant's Name: Medicaid ID: Field 1 (Last) (First) (M.I.) Field 2 Date of Birth: Field
Initial Pool Process: Resident Interview
 Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Initial Pool Process: Resident Interview Care Area Probes Response Options Choices Are you able to make choices about your daily life that are important to you? I d like to talk to you about your choices.
Nursing Assistant
 Western Technical College 30543300 Nursing Assistant Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 The course prepares individuals for employment
Western Technical College 30543300 Nursing Assistant Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 3.00 The course prepares individuals for employment
Kentucky Medically Frail Provider Attestation v5
 P a g e 1 Kentucky Medically Frail Provider Attestation v5 This Attestation is to be completed by an enrolled Medicaid Provider whose scope of expertise qualifies them to assess the Member for medical
P a g e 1 Kentucky Medically Frail Provider Attestation v5 This Attestation is to be completed by an enrolled Medicaid Provider whose scope of expertise qualifies them to assess the Member for medical
POSITION SUMMARY. 2. Communicates: Reads, writes and speaks in English as required for taking direction and performing job-related activities.
 Department/s: Nursing Approved By: Senior Management Committee Date Approved: Mar 20 1992 Date Revised: Feb 16 2010 Page 1 of 6 POSITION SUMMARY The Personal Support Worker (PSW) at Fairhaven is responsible
Department/s: Nursing Approved By: Senior Management Committee Date Approved: Mar 20 1992 Date Revised: Feb 16 2010 Page 1 of 6 POSITION SUMMARY The Personal Support Worker (PSW) at Fairhaven is responsible
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
CNA OnSite Series Overview: Understanding Restorative Care Part 1 - Introduction to Restorative Care
 Series Overview: Understanding Restorative Care Part 1 - Introduction to Restorative Care Administering the Program Read the Guide View the Video Review the Suggested Questions Complete Post-Test Answer
Series Overview: Understanding Restorative Care Part 1 - Introduction to Restorative Care Administering the Program Read the Guide View the Video Review the Suggested Questions Complete Post-Test Answer
Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission
 Table 1. Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission Measure Description Numerator and Window Numerator Exclusions Covariates The percent of short-stay residents
Table 1. Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission Measure Description Numerator and Window Numerator Exclusions Covariates The percent of short-stay residents
Session #: R14. Robin L. Hillier. Agenda 4/9/2014. Simply Quality Measures. (330) RLH Consulting.
 RLH Consulting.") Session #: R14 Simply Quality Measures Robin L. Hillier robin@rlh-consulting.com (330) 807-2850 RLH Consulting Agenda Quality Measures How are they calculated How to read the reports How to use the reports
Session #: R14 Simply Quality Measures Robin L. Hillier robin@rlh-consulting.com (330) 807-2850 RLH Consulting Agenda Quality Measures How are they calculated How to read the reports How to use the reports
Based on the comprehensive assessment of a resident, the facility must ensure that:
 13.A. Quality of Care Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental, and psychosocial well-being,
13.A. Quality of Care Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental, and psychosocial well-being,
Kentucky Medically Frail Provider Attestation v5
 Page 1 of 8 Kentucky Medically Frail Provider Attestation v5 This Attestation is to be completed by an enrolled Medicaid Provider whose scope of expertise qualifies them to assess the Member for medical
Page 1 of 8 Kentucky Medically Frail Provider Attestation v5 This Attestation is to be completed by an enrolled Medicaid Provider whose scope of expertise qualifies them to assess the Member for medical
Listed below are additional coding tips: you think the patient can do or what the patient s potential is. your shift, even if it only occurs once.
 1 It is important to always accurately code how much assistance your patients require to perform their activities of daily living and provide assistance in the safest manner possible for you and the patient.
1 It is important to always accurately code how much assistance your patients require to perform their activities of daily living and provide assistance in the safest manner possible for you and the patient.
RAPID RUG GUIDE RUG-III, VERSION GROUPER Effective for Assessments With an ARD on or After 10/1/2013
 RAPID RUG GUIDE RUG-III, VERSION 5.20 34-GROUPER Effective for Assessments With an ARD on or After 10/1/2013 Step 1: Calculation To calculate the score of Bed Mobility (G0110A), Transfer (G0110B) and Toilet
RAPID RUG GUIDE RUG-III, VERSION 5.20 34-GROUPER Effective for Assessments With an ARD on or After 10/1/2013 Step 1: Calculation To calculate the score of Bed Mobility (G0110A), Transfer (G0110B) and Toilet
RESPITE REQUEST APPLICATION FORM: INPATIENT/OUTPATIENT
 1 RESPITE REQUEST APPLICATION FORM: INPATIENT/OUTPATIENT Please complete all sections of this form to ensure prompt processing within the requested period. NOTE: This information will be shared with Holland
1 RESPITE REQUEST APPLICATION FORM: INPATIENT/OUTPATIENT Please complete all sections of this form to ensure prompt processing within the requested period. NOTE: This information will be shared with Holland
Application form: Saturday Night Fun! program
 Application form: Saturday Night Fun! program Applications for Saturday Night Fun! will be accepted until January 12, 2018. The program will run on Saturday, February 24, 2018 from 5:30-9:30 p.m. Holland
Application form: Saturday Night Fun! program Applications for Saturday Night Fun! will be accepted until January 12, 2018. The program will run on Saturday, February 24, 2018 from 5:30-9:30 p.m. Holland
CMS Updates RAI User s Manual
 CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
CMS Updates RAI User s Manual By Rena R. Shephard, MHA, RN, RAC MT, C NE AANAC Executive Editor The Centers for Medicare & Medicaid Services (CMS) June 2 posted revisions to the Long Term Care Facility
5. Personal Care Services
 5. Personal Care Services Chapter IV - Services to Children A. Overview A child who requires personal care services is a child with a chronic medical condition or with medical needs requiring specialized
5. Personal Care Services Chapter IV - Services to Children A. Overview A child who requires personal care services is a child with a chronic medical condition or with medical needs requiring specialized
*PLEASE NOTE THAT COMPLETION OF THE PRE-ADMISSION FORM DOES NOT GUARANTEE PLACEMENT AT THIS FACILITY.
 FALLON MEDICAL COMPLEX RESIDENT PROFILE PRE-ADMISSION/ADMISSION INFORMATION SHEET This Facility is owned and operated by Fallon Medical Complex, INC. This Facility accepts residents of all backgrounds
FALLON MEDICAL COMPLEX RESIDENT PROFILE PRE-ADMISSION/ADMISSION INFORMATION SHEET This Facility is owned and operated by Fallon Medical Complex, INC. This Facility accepts residents of all backgrounds
G0110: Activities of Daily Living (ADL) Assistance
 Assistance") SECTION G: FUNCTIONAL STATUS Intent: Items in this section assess the need for assistance with activities of daily living (ADLs), altered gait and balance, and decreased range of motion. In addition, on
SECTION G: FUNCTIONAL STATUS Intent: Items in this section assess the need for assistance with activities of daily living (ADLs), altered gait and balance, and decreased range of motion. In addition, on
FH16 - Developed by Polaris Group Page 1 of 140
 FH16 - Developed by Polaris Group www.polaris-group.com Page 1 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page 2 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page
FH16 - Developed by Polaris Group www.polaris-group.com Page 1 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page 2 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page
Quality Measures Are My Friends
 s Are My Friends Advantage Home Health Services AdvantageCare Rehabilitation Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA Nurse Consultant / CMI Specialist & Medicare Reimbursement Specialist Dave Lishinsky,
s Are My Friends Advantage Home Health Services AdvantageCare Rehabilitation Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA Nurse Consultant / CMI Specialist & Medicare Reimbursement Specialist Dave Lishinsky,
(M1025) Case-Mix Diagnosis (Optional) OPTIONAL Complete only if a Z-code in Column 2 is reported in place of a resolved condition
 Case-Mix Diagnosis (Optional) OPTIONAL Complete only if a Z-code in Column 2 is reported in place of a resolved condition") HOME HEALTH 2017 PPS CALCULATION WORKSHEET PATIENT NAME: ID NUMBER: DATE: TYPE OF ASSESSMENT: Start of care Follow-up M0110 - EPISODE TIMING: Is the Medicare home health payment episode f which this assessment
HOME HEALTH 2017 PPS CALCULATION WORKSHEET PATIENT NAME: ID NUMBER: DATE: TYPE OF ASSESSMENT: Start of care Follow-up M0110 - EPISODE TIMING: Is the Medicare home health payment episode f which this assessment
NORTH DAKOTA LEVEL OF CARE FORM INSTRUCTIONS TO BE USED WITH LOC FORM ND
 For this section, select which type of LOC screen is to be reviewed Requested Screen Type NORTH DAKOTA LEVEL OF CARE FORM INSTRUCTIONS Nursing Facility Swingbed CMFN PACE MFP Provisional MFP Final Tech.
For this section, select which type of LOC screen is to be reviewed Requested Screen Type NORTH DAKOTA LEVEL OF CARE FORM INSTRUCTIONS Nursing Facility Swingbed CMFN PACE MFP Provisional MFP Final Tech.
Based on the comprehensive assessment of a resident, the facility must ensure that:
 7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
Connecticut LTC Level of Care Determination Form To be maintained in the individual s medical record.
 I. Demographics A. Individual First Name: Middle Initial: Mailing Address: City: State: Zip: Phone: Social Security #: Date of Birth: _/ / Marital Status: M S W D Gender: Male Female Connecticut LTC Level
I. Demographics A. Individual First Name: Middle Initial: Mailing Address: City: State: Zip: Phone: Social Security #: Date of Birth: _/ / Marital Status: M S W D Gender: Male Female Connecticut LTC Level
Nursing Facility 90 Day Redetermination Online Referral for Medicaid Level of Care
 12/15/2014 Nursing Facility 90 Day Redetermination Online Referral for Medicaid Level of Care Quarterly MDS Assessment Results This screen will be completed based on certain values from the first quarterly
12/15/2014 Nursing Facility 90 Day Redetermination Online Referral for Medicaid Level of Care Quarterly MDS Assessment Results This screen will be completed based on certain values from the first quarterly
11/23/2011. Identify Residents risks for decline to establish programs to stave off decline unless it is clinically unavoidable.
 Robin A. Bleier, RN, HCRM-FACDONA Clinical Risk & Operations Consultant R B Health Partners, Inc. 210 So. Pinellas Ave. Suite 260 Tarpon Springs, FL 34689 robin@rbhealthpartners.com 727-744-2021 Restorative
Robin A. Bleier, RN, HCRM-FACDONA Clinical Risk & Operations Consultant R B Health Partners, Inc. 210 So. Pinellas Ave. Suite 260 Tarpon Springs, FL 34689 robin@rbhealthpartners.com 727-744-2021 Restorative
OAR Changes. Presented by APD Medicaid LTC Policy
 OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
OAR 411-015 Changes 1 Presented by APD Medicaid LTC Policy Table of Contents 2 Service Priority OAR 411-015 Project Overview Why Are We Making These Changes Overarching Changes Changes to ADLS (each ADL
Common Course Outline for: NURS 1057 NURSING ASSISTANT
 Common Course Outline for: NURS 1057 NURSING ASSISTANT A. COURSE DESCRIPTION 1. Number of credits: 4 credits 2. Lecture hours per week: 1 hour 50 minutes per week. Lab hours per week: 3 hours 50 minutes.
Common Course Outline for: NURS 1057 NURSING ASSISTANT A. COURSE DESCRIPTION 1. Number of credits: 4 credits 2. Lecture hours per week: 1 hour 50 minutes per week. Lab hours per week: 3 hours 50 minutes.
Improving Quality Care
 Improving Quality Care Making Restorative estoat enursing us Fun FADONA 25 TH Anniversary Convention Presented by: Harmony Healthcare International, Inc. PPS & Case Mix Onsite Chart Audits MMQ Audits Seminars
Improving Quality Care Making Restorative estoat enursing us Fun FADONA 25 TH Anniversary Convention Presented by: Harmony Healthcare International, Inc. PPS & Case Mix Onsite Chart Audits MMQ Audits Seminars
Attachment C: Itemized List of OASIS Data Elements
 Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES
 COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
Restorative Nursing: The NHA s Role and Organizational Outcomes
 Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
Quality Measures (QM) & Five Star Rating System. Objectives 4/18/2016 MDS CODING FOR QUALITY MEASURES
 & Five Star Rating System. Objectives 4/18/2016 MDS CODING FOR QUALITY MEASURES") Quality Measures (QM) & Five Star Rating System Carol Hill MSN, RN, RAC-CT, DNS-CT, RAC-MT, QCP Objectives At the conclusion of this educational offering the participant will be able to: Identify MDS items
Quality Measures (QM) & Five Star Rating System Carol Hill MSN, RN, RAC-CT, DNS-CT, RAC-MT, QCP Objectives At the conclusion of this educational offering the participant will be able to: Identify MDS items
NURSING HOME PRE-ADMISSION ASSESSMENT FORM
 Clients Name: NHS No AIS No (if applicable) DOB: Home Address NOK Contact Details Telephone: Relationship: Other contact: Marital status Religion GP Details and Address Ethnic origin Date of Referral:
Clients Name: NHS No AIS No (if applicable) DOB: Home Address NOK Contact Details Telephone: Relationship: Other contact: Marital status Religion GP Details and Address Ethnic origin Date of Referral:
CMS Forms, CMS-672 and the Matrix
 CMS Forms, CMS-672 and the Matrix Contents The Matrix introduced by CMS in November 2017...2 Logic of the System...2 Links to MDS Questions...3 CMS-672...3 The MATRIX...3 Maintain Data...7 CMS-672...7
CMS Forms, CMS-672 and the Matrix Contents The Matrix introduced by CMS in November 2017...2 Logic of the System...2 Links to MDS Questions...3 CMS-672...3 The MATRIX...3 Maintain Data...7 CMS-672...7
Historical Document: Transition Occured to RUG - IV - 01/01/2012. RUG IV & MN Case Mix. Objectives. Why RUG IV? 11/21/2011
 RUG IV & MN Case Mix November 2011 James Sims, Principal Planner Marci Martinson, Case Mix Review Director Objectives O By the end of this session the participant will be able to: O State the reasons for
RUG IV & MN Case Mix November 2011 James Sims, Principal Planner Marci Martinson, Case Mix Review Director Objectives O By the end of this session the participant will be able to: O State the reasons for
Washtenaw Community College Comprehensive Report. HSC 100 Basic Nursing Assistant Skills Effective Term: Winter 2018
 Washtenaw Community College Comprehensive Report HSC 100 Basic Nursing Assistant Skills Effective Term: Winter 2018 Course Cover Division: Health Sciences Department: Nursing & Health Science Discipline:
Washtenaw Community College Comprehensive Report HSC 100 Basic Nursing Assistant Skills Effective Term: Winter 2018 Course Cover Division: Health Sciences Department: Nursing & Health Science Discipline:
REHABILITATION AND RESTORATIVE CARE UPDATE APRIL 2013
 REHABILITATION AND RESTORATIVE CARE UPDATE APRIL 2013 Rehabilitation Helping patients attain the highest possible level of functional ability Focusing on physical ability Restorative care Helping attain
REHABILITATION AND RESTORATIVE CARE UPDATE APRIL 2013 Rehabilitation Helping patients attain the highest possible level of functional ability Focusing on physical ability Restorative care Helping attain
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Skilled skin care should be provided by an agency licensed to provide home health
 8.5.D. LIMITATIONS OF PERSONAL CARE In order to delineate the types of services that can be provided by a personal care worker, the following are examples of limitations where skilled home healthcare would
8.5.D. LIMITATIONS OF PERSONAL CARE In order to delineate the types of services that can be provided by a personal care worker, the following are examples of limitations where skilled home healthcare would
RESIDENT SCREENING SHEET
 Department of County Human Services Aging, Disability & Veterans Services Adult Care Home Program RESIDENT SCREENING SHEET MCAR 023-080-200 through 023-080-225: To be completed by the operator before you
Department of County Human Services Aging, Disability & Veterans Services Adult Care Home Program RESIDENT SCREENING SHEET MCAR 023-080-200 through 023-080-225: To be completed by the operator before you
CMS RAI MANUAL ERRATA DOCUMENT
 CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
Activities of Daily Living (ADL) Critical Element Pathway
 Critical Element Pathway") Use this pathway for a resident who requires assistance with or is unable to perform ADLs (Hygiene bathing, dressing, grooming, and oral care; Elimination toileting; Dining eating, including meals and
Use this pathway for a resident who requires assistance with or is unable to perform ADLs (Hygiene bathing, dressing, grooming, and oral care; Elimination toileting; Dining eating, including meals and
Page Introduction 1. Factors to Consider When Evaluating Whether an Individual Needs to be Screened 1. Pre-Admission Screening Criteria 2
 Revision Date APPENDIX B PRE-ADMISSION SCREENING CRITERIA Revision Date i TABLE OF CONTENTS APPENDIX B Introduction 1 Factors to Consider When Evaluating Whether an Individual Needs to be Screened 1 2
Revision Date APPENDIX B PRE-ADMISSION SCREENING CRITERIA Revision Date i TABLE OF CONTENTS APPENDIX B Introduction 1 Factors to Consider When Evaluating Whether an Individual Needs to be Screened 1 2
Resident Name Medicaid # - - If Pending Medicaid, Social Security # - - Medicare # Date of Birth / / Responsible Party. Responsible Party Address
 URSIG FACILIT LEVEL OF CARE REQUEST FOR ADMISSIO Resident ame Medicaid # - - Room # Room Certified for Medicaid es o If Pending Medicaid, Social Security # - - Medicare # Date of Birth / / Marital Status
URSIG FACILIT LEVEL OF CARE REQUEST FOR ADMISSIO Resident ame Medicaid # - - Room # Room Certified for Medicaid es o If Pending Medicaid, Social Security # - - Medicare # Date of Birth / / Marital Status
MEDICAL CERTIFICATION FOR NURSING FACILITY/HOME- AND COMMUNITY-BASED SERVICES FORM (Replaces Patient Transfer and Continuity of Care Form)
") MEDICAL CERTIFICATION FOR NURSING FACILITY/HOME- AND COMMUNITY-BASED SERVICES FORM (Replaces Patient Transfer and Continuity of Care Form) (A) FACILITY INFORMATION Facility From (E) HISTORY & PHYSICAL
MEDICAL CERTIFICATION FOR NURSING FACILITY/HOME- AND COMMUNITY-BASED SERVICES FORM (Replaces Patient Transfer and Continuity of Care Form) (A) FACILITY INFORMATION Facility From (E) HISTORY & PHYSICAL
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES
 UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated February 2018 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated February 2018 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF
A Closer Look at the Revised Nursing Facility Regulations. Quality of Care
 A Closer Look at the Revised Nursing Facility Regulations Quality of Care Executive Summary The substantive requirements for quality of care are retained in the revised regulations, and the Centers for
A Closer Look at the Revised Nursing Facility Regulations Quality of Care Executive Summary The substantive requirements for quality of care are retained in the revised regulations, and the Centers for
Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2009 Through 2014
 REPORT Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2009 Through 2014 August 2015 Prepared by: Charlene Harrington, Ph.D. Helen Carrillo, M.S. University of California San Francisco
REPORT Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2009 Through 2014 August 2015 Prepared by: Charlene Harrington, Ph.D. Helen Carrillo, M.S. University of California San Francisco
Assisted Living Individualized Service Plan (ISP)
") Assisted Living Individualized Service Plan (ISP) Resident Name: Female Male Date: For: Initial Six months Other Note: Services to be provided and by whom: Any additional information or change of service
Assisted Living Individualized Service Plan (ISP) Resident Name: Female Male Date: For: Initial Six months Other Note: Services to be provided and by whom: Any additional information or change of service
Successful Restorative Program When Therapy and Nursing Collaborate
 Successful Restorative Program When Therapy and Nursing Collaborate AdvantageCare Rehabilitation / Advantage Home Health Services Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA CMI Specialist & Medicare Reimbursement
Successful Restorative Program When Therapy and Nursing Collaborate AdvantageCare Rehabilitation / Advantage Home Health Services Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA CMI Specialist & Medicare Reimbursement
Minnesota Department of Health Health Policy, Information and Compliance Monitoring Division COMMUNITY-WIDE TRANSFER AGREEMENT BETWEEN HOSPITALS AND
 Minnesota Department of Health Health Policy, Information and Compliance Monitoring Division COMMUNITY-WIDE TRANSFER AGREEMENT BETWEEN HOSPITALS AND RELATED HEALTH FACILITIES IN THE SEVEN COUNTY METROPOLITAN
Minnesota Department of Health Health Policy, Information and Compliance Monitoring Division COMMUNITY-WIDE TRANSFER AGREEMENT BETWEEN HOSPITALS AND RELATED HEALTH FACILITIES IN THE SEVEN COUNTY METROPOLITAN
Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2009 Through 2016
 April 2018 Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2009 Through 2016 Prepared by: Charlene Harrington, Ph.D. Helen Carrillo, M.S. University of California San Francisco and Rachel
April 2018 Nursing Facilities, Staffing, Residents and Facility Deficiencies, 2009 Through 2016 Prepared by: Charlene Harrington, Ph.D. Helen Carrillo, M.S. University of California San Francisco and Rachel
APD & MHA RESIDENT SCREENING SHEET
 Department of County Human Services Aging, Disability & Veterans Services Adult Care Home Program APD & MHA RESIDENT SCREENING SHEET MCAR 023-080-200 through 023-080-225: To be completed by the operator
Department of County Human Services Aging, Disability & Veterans Services Adult Care Home Program APD & MHA RESIDENT SCREENING SHEET MCAR 023-080-200 through 023-080-225: To be completed by the operator
CAP/DA Services - NEW Request
 CAP/DA Services - NEW Request * = Required Request Date * Beneficiary Demographics Beneficiary's First Name Last Name Beneficiary has Medicaid? * Yes Pending Medicaid MID Social Security Number Medicare
CAP/DA Services - NEW Request * = Required Request Date * Beneficiary Demographics Beneficiary's First Name Last Name Beneficiary has Medicaid? * Yes Pending Medicaid MID Social Security Number Medicare
RESTORATIVE NURSING SERIES OVERVIEW 1st Session
 RESTORATIVE NURSING SERIES OVERVIEW 1st Session Everything You Ever Wanted to Know But Were Afraid to Ask HealthCap RMS 1 Learner Objectives Evaluate the need for a restorative program Design a restorative
RESTORATIVE NURSING SERIES OVERVIEW 1st Session Everything You Ever Wanted to Know But Were Afraid to Ask HealthCap RMS 1 Learner Objectives Evaluate the need for a restorative program Design a restorative
Today s educational presentation is provided by. The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE
 Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
Today s educational presentation is provided by The software that powers HOME HEALTH. THERAPY. PRIVATE DUTY. HOSPICE At Kinnser, we believe post-acute care businesses need the right software solution for
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES
 UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated May 2017 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF CONTENTS
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated May 2017 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF CONTENTS
Understanding the New MDS 3.0 Quality Measures. Updated May 2017
 Understanding the New MDS 3.0 Quality Measures Updated May 2017 Contents Introduction... 3 Background History of the MDS 3.0:... 3 Percent of Short-Stay Residents Who Self-Report Moderate to Severe Pain...
Understanding the New MDS 3.0 Quality Measures Updated May 2017 Contents Introduction... 3 Background History of the MDS 3.0:... 3 Percent of Short-Stay Residents Who Self-Report Moderate to Severe Pain...
Categorization of In-Home Support Services (IHSS) Services Use only for IHSS Services
 Services Use only for IHSS Services") Table 1: Limits and Restrictions Categorization of In-Home Support Services (IHSS) Services Use only for IHSS Services Personal Care Family members that have been designated as a client s Authorized Representative
Table 1: Limits and Restrictions Categorization of In-Home Support Services (IHSS) Services Use only for IHSS Services Personal Care Family members that have been designated as a client s Authorized Representative
Skills Standards RESIDENTIAL CARE AIDE OD68604 MEETS OSDH NURSE AIDE REGISTRY CERTIFICATION REQUIREMENTS
 Skills Standards RESIDENTIAL CARE AIDE OD68604 MEETS OSDH NURSE AIDE REGISTRY CERTIFICATION REQUIREMENTS Competency-Based Education: OKLAHOMA S RECIPE FOR SUCCESS BY THE INDUSTRY FOR THE INDUSTRY Oklahoma
Skills Standards RESIDENTIAL CARE AIDE OD68604 MEETS OSDH NURSE AIDE REGISTRY CERTIFICATION REQUIREMENTS Competency-Based Education: OKLAHOMA S RECIPE FOR SUCCESS BY THE INDUSTRY FOR THE INDUSTRY Oklahoma
SKILLED NURSING & REHAB APPLICATION Name Date of Birth Age Address Street/R.R. Box No.
 SKILLED NURSING & REHAB APPLICATION Date of Birth Age Street/R.R. Box No. Town State Zip Township County Marital Status M W S D Sex Birthplace Social Security Number Two (2) persons to contact in case
SKILLED NURSING & REHAB APPLICATION Date of Birth Age Street/R.R. Box No. Town State Zip Township County Marital Status M W S D Sex Birthplace Social Security Number Two (2) persons to contact in case
DRAFT. WORKING DRAFT Nursing associate skills annexe. Part of the draft standards of proficiency for nursing associates. Page 1
 WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
WORKING Nursing associate skills annexe Part of the draft standards of proficiency for nursing associates Page 1 Working draft version of the nursing associate skills annexe, part of the draft nursing
Department of Veterans Affairs VHA DIRECTIVE Veterans Health Administration Washington, DC December 7, 2005
 Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
Department of Veterans Affairs VHA DIRECTIVE 2005-061 Veterans Health Administration Washington, DC 20420 VA NURSING HOME CARE UNIT (NHCU) ADMISSION CRITERIA, SERVICE CODES, AND DISCHARGE CRITERIA 1. PURPOSE:
LONG TERM CARE ASSISTANT Course Syllabus. Mosby's Textbook for Long Term Care Nursing Assistant 7th Ed., Mosby Evolve (2015).
.") Course Syllabus Course Number: THRP-000A OHLAP Credit: OCAS Code: 9324 Course Length: 75 Hours Career Cluster: Health Science Career Pathway: Therapeutic Services Career Major(s): Practical Nurse No Pre-requisite(s):
Course Syllabus Course Number: THRP-000A OHLAP Credit: OCAS Code: 9324 Course Length: 75 Hours Career Cluster: Health Science Career Pathway: Therapeutic Services Career Major(s): Practical Nurse No Pre-requisite(s):
Navigating the New CMS Quality Measures
 Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 PAGE 1 of 8 PURPOSE To provide guidelines on: 1. rating offenders using patient acuity, 2. how to properly handle offenders who are housed in facilities with conflicting acuity levels, 3. how to properly
PAGE 1 of 8 PURPOSE To provide guidelines on: 1. rating offenders using patient acuity, 2. how to properly handle offenders who are housed in facilities with conflicting acuity levels, 3. how to properly
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Nurse Assistant (Certified) OUTLINE
 OUTLINE") Nurse Assistant (Certified) OUTLINE DESCRIPTION: Nurse Assistant - Certified is designed to prepare students for employment as a Nurse Assistant in a variety of settings. Students will learn patient care,
Nurse Assistant (Certified) OUTLINE DESCRIPTION: Nurse Assistant - Certified is designed to prepare students for employment as a Nurse Assistant in a variety of settings. Students will learn patient care,
RUG-III V ERSION 5.20 CALCULATION WORKSH E E T 34 GROUP MOD E L F OR MDS 3.0
 RUG-III V ERSION 5.20 CALCULATION WORKSH E E T 34 GROUP MOD E L F OR MDS 3.0 This RUG-III Version 5.20 calculation worksheet is a step-by-step walk through to manually determine the appropriate RUG-III
RUG-III V ERSION 5.20 CALCULATION WORKSH E E T 34 GROUP MOD E L F OR MDS 3.0 This RUG-III Version 5.20 calculation worksheet is a step-by-step walk through to manually determine the appropriate RUG-III
NM DDSD Intensive Medical Living Services Eligibility Parameter Tool A. MEDICATION ADMINISTRATION SEVERE 4 SIGNIFICANT 3 MODERATE 2 LOW 1 NONE - 0
 FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
FACT Scheduled Medications: Note: Any injections provided by Home Health, Hospice or other clinical providers may not be included in these totals for the agency nursing time. Do not include delivery of
Current Medication List
 Current Medication List As of: Patient Name: DOB: Medication Dose Route Frequency STANDARD ADMISSIONS RECORD AND AGREEMENT Print Form Resident's Last Name First Middle/Maiden Medical Record No. Social
Current Medication List As of: Patient Name: DOB: Medication Dose Route Frequency STANDARD ADMISSIONS RECORD AND AGREEMENT Print Form Resident's Last Name First Middle/Maiden Medical Record No. Social
SECTION P: RESTRAINTS
 SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
SECTION P: RESTRAINTS Intent: The intent of this section is to record the frequency over the 7-day look-back period that the resident was restrained by any of the listed devices at any time during the
Conflict of Interest Statement
 Conflict of Interest Statement RESTORATIVE NURSING: A WIN WIN for Everyone Involved! (Almost) Everything You Ever Wanted to Know About Restorative Nursing But Were Afraid to Ask! HealthCap s educational
Conflict of Interest Statement RESTORATIVE NURSING: A WIN WIN for Everyone Involved! (Almost) Everything You Ever Wanted to Know About Restorative Nursing But Were Afraid to Ask! HealthCap s educational
ADMISSION CARE PLAN. Orient PRN to person, place, & time
 ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
ADMISSION DATE: CODE STATUS: ADMISSION CARE PLAN ADMISSION DIAGNOSIS: 1. DELIRIUM 2. COGNITIVE LOSS Resident will be as alert and oriented as possible Resident will be as alert and oriented as comfortable
Chances are.. Based on my experience MDS 3.0 Update for Long Term Care PRESENTED BY 2/13/2017. New focus on Data by CMS and Regulatory Agencies
 PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
SCOPE OF SERVICES. Services Allowed by Home Instead Senior Care. CAREGivers cannot. Charlotte County, Collier County, and Lee County areas.
 Services Allowed by Home Instead Senior Care Givers in Charlotte County, Collier County, and Lee County areas. TYPE OF SERVICE BATHING -SKIN - -HAIR - -AL ARE- Givers can Assist with bathing when the client
Services Allowed by Home Instead Senior Care Givers in Charlotte County, Collier County, and Lee County areas. TYPE OF SERVICE BATHING -SKIN - -HAIR - -AL ARE- Givers can Assist with bathing when the client
Acute Care to Rehab & Complex Continuing Care (CCC) Referral
 Referral") o General Rehabilitation Low Intensity Rehabilitation (GRH, SJHCG) o (CMH, GRH, SJHCG) o Chronic Assisted Ventilator (GRH only) o o Ischemic o Hemorrhagic Stroke Rehab: Program Readiness Date: Complex
o General Rehabilitation Low Intensity Rehabilitation (GRH, SJHCG) o (CMH, GRH, SJHCG) o Chronic Assisted Ventilator (GRH only) o o Ischemic o Hemorrhagic Stroke Rehab: Program Readiness Date: Complex
OASIS ITEM ITEM INTENT
 (M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
(M2400) Intervention Synopsis: (Check only one box in each row.) At the time of or at any time since the previous OASIS assessment, were the following interventions BOTH included in the physician-ordered
ON THE JOB LEARNING OUTLINE
 ON THE JOB LEARNING OUTLINE 1. Occupational Title: Certified Nursing Assistant, Geriatric Specialty 2. DOT Code: 355.674-014 3. O*NET Code: 31-1012.00 4. RAIS Code: 0824-G 5. Occupational Description:
ON THE JOB LEARNING OUTLINE 1. Occupational Title: Certified Nursing Assistant, Geriatric Specialty 2. DOT Code: 355.674-014 3. O*NET Code: 31-1012.00 4. RAIS Code: 0824-G 5. Occupational Description:
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SKILLED NURSING SERVICES
 DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
Discharge to Community Measure
 The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM
 RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM Day 5 DAY 5 1) Physical Needs Monitoring residents for changes in condition Health-related services Allowable, restricted, and prohibited conditions Diabetes
RCFE ADMINISTRATOR INITIAL CERTIFICATION PROGRAM Day 5 DAY 5 1) Physical Needs Monitoring residents for changes in condition Health-related services Allowable, restricted, and prohibited conditions Diabetes
PERSONAL CARE WORKER (PCW) - Job Description
 - Job Description") PERSONAL CARE WORKER (PCW) - Job Description Definition Provides unskilled personal care and household services for stable, maintenance clients in their homes in compliance with a service plan. Level of
PERSONAL CARE WORKER (PCW) - Job Description Definition Provides unskilled personal care and household services for stable, maintenance clients in their homes in compliance with a service plan. Level of
PERSONAL CARE/RESPITE SERVICE SPECIFICATIONS (These rules are subject to change with each new contract cycle.)
") PERSONAL CARE/RESPITE SERVICE SPECIFICATIONS (These rules are subject to change with each new contract cycle.) 1.0 Definition Personal Care/Respite (PC/R) services enable a client to achieve optimal function
PERSONAL CARE/RESPITE SERVICE SPECIFICATIONS (These rules are subject to change with each new contract cycle.) 1.0 Definition Personal Care/Respite (PC/R) services enable a client to achieve optimal function
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Hospice and End of Life Care and Services Critical Element Pathway
 Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
Use this pathway for a resident identified as receiving end of life care (e.g., palliative care, comfort care, or terminal care) or receiving hospice care from a Medicare-certified hospice. Review the
MDS 3.0: What Leadership Needs to Know
 MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
Quality Measures and the Five-Star Rating
 Quality Measures and the Five-Star Rating Pennsylvania Health Care Association Presented by Reinsel Kuntz Lesher LLP Senior Living Services Consulting October 23, 2014 Disclaimer The information contained
Quality Measures and the Five-Star Rating Pennsylvania Health Care Association Presented by Reinsel Kuntz Lesher LLP Senior Living Services Consulting October 23, 2014 Disclaimer The information contained
Centralized Intake and Referral Application to Specialty Hospitals
 Centralized Intake and Referral Application to Specialty Hospitals CLIENT INFORMATION **** upon completion of referral please fax to 416-506-0439 **** Client Name: Gender: Male Female Other Client Preferred
Centralized Intake and Referral Application to Specialty Hospitals CLIENT INFORMATION **** upon completion of referral please fax to 416-506-0439 **** Client Name: Gender: Male Female Other Client Preferred
Should you have any questions or concerns during the application process, we are available to assist you; please do not hesitate to contact us.
 Dear Prospective Resident: We thank you for choosing Santa Teresita s Assisted Living as your choice of residence and care. Our Admission s Department would like to assist you in gathering all the needed
Dear Prospective Resident: We thank you for choosing Santa Teresita s Assisted Living as your choice of residence and care. Our Admission s Department would like to assist you in gathering all the needed
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES CHAPTER 411 DIVISION 34 PERSONAL CARE SERVICES
 DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES 411-034-0000 Purpose (Amended 10/5/2007) CHAPTER 411 DIVISION 34 PERSONAL CARE SERVICES (1) These
DEPARTMENT OF HUMAN SERVICES SENIORS AND PEOPLE WITH DISABILITIES DIVISION OREGON ADMINISTRATIVE RULES 411-034-0000 Purpose (Amended 10/5/2007) CHAPTER 411 DIVISION 34 PERSONAL CARE SERVICES (1) These
E: Nursing Practice. Alberta Licensed Practical Nurses Competency Profile 51
 E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
KENTUCKY LTC FACILITIES EVACUATION TRANSPORTATION ASSESSMENT TOOL
 KENTUCKY LTC FACILITIES EVACUATION TRANSPORTATION ASSESSMENT TOOL 1 Dear Nursing Facility Administrator: INSTRUCTIONS The attached tool will assist in determining the necessary transportation resources
KENTUCKY LTC FACILITIES EVACUATION TRANSPORTATION ASSESSMENT TOOL 1 Dear Nursing Facility Administrator: INSTRUCTIONS The attached tool will assist in determining the necessary transportation resources
Request for Information Documenting Patient s Functional Limitations (Form Attached)
") Request for Information Documenting Patient s Functional Limitations (Form Attached) Your patient applied for, or is a recipient of, In-Home Supportive Services (IHSS). The IHSS program provides attendant
Request for Information Documenting Patient s Functional Limitations (Form Attached) Your patient applied for, or is a recipient of, In-Home Supportive Services (IHSS). The IHSS program provides attendant
ADULT LONG-TERM CARE SERVICES
 ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period
ADULT LONG-TERM CARE SERVICES Long-term care is a broad range of supportive medical, personal, and social services needed by people who are unable to meet their basic living needs for an extended period