Session #: R14. Robin L. Hillier. Agenda 4/9/2014. Simply Quality Measures. (330) RLH Consulting.
|
|
|
- Marion Cox
- 6 years ago
- Views:
Transcription
1 Session #: R14 Simply Quality Measures Robin L. Hillier (330) RLH Consulting Agenda Quality Measures How are they calculated How to read the reports How to use the reports Case Studies 1
2 Uses of Quality Measures Public Reporting Consumer Use Nursing Home Compare Medicaid Quality Incentive Program Pain(L), Restraints (L), UTI (L), Pressure Ulcer (L), Pneumococcal Vaccine (L), Flu Vaccine (L) 5 Star (see next slide) ACO s, Hospitals, MCO s Survey Process Quality Assurance RLH Consulting 4 Quality Measures in 5 Star Only uses 9 of the QMs on Nursing Home Compare site 7 Long Stay ADL decline High-risk residents with pressure ulcers Indwelling catheter Physically restrained UTI Self-report moderate to severe pain Fall with major injury 2Short Stay New or worsened pressure ulcers Self-report moderate to severe pain 5 Public Quality Measures Part of Nursing Home Quality Initiative -the CMS effort to improve quality of care in nursing homes QMs for 12 clinical care areas, plus pneumococcal and flu vaccination Recalculated and reposted quarterly Facilities receive preview in Folder in MDS system Not current data RLH Consulting 6 2
3 Quality Measures for Survey Process and Quality Assurance Indicators of possible problems Must be validated onsite via record review, interviews, direct observation Includes the same clinical measures that are publicly reported plus three additional measures 7 How Assessments are Used to Generate QMs Software uses assessments in several different ways to calculate the QMs: For most QMs, looks for specific information on the target assessment For example: UTI (L) For one short stay measure, compares initial and a subsequent assessment Antipsychotic present, not on initial assessment (S) RLH Consulting 8 How Assessments are Used to Generate QMs Software uses assessments in several different ways to calculate the QMs: For one long stay measure, compares target assessment with a prior assessment ADL Decline (L) The other method is to look at all assessments in the entire episode* known as the look-back scan New or Worse Pressure Ulcer (S) Antipsychotic Present, Not on Initial (S) Falls With Major Injury (L) Falls (L) RLH Consulting 9 3
4 Key Concepts Admission vs. Reentry Discharge Return Anticipated vs. Discharge Return Not Anticipated Understanding MDS manual definitions vs. billing, facility policy, etc. is key Bed hold status is irrelevant Stay vs. Episode Is Resident Short Stay or Long Stay? Case Study#1 Resident Admitted 10/12/13 Discharged Return Anticipated 12/28/13 Reentered 1/3/14 Still in facility today Resident has had one episode, which included 2 stays; current episode = 164 days as of 3/31/14 Stay #1 = 76 days, Stay #2 = 88 days as of 3/31 12/31/13 QM = Short stay, 3/31/14 QM = Long Stay Case Study #2 Resident Admitted 10/12/13 Discharged Return Not Anticipated 12/28/13 Admitted again 1/3/14 Still in facility today Resident has had two separate episodes Episode #1 = 76 days, Episode #2 = 88 days as of 3/31/14 12/31/13 QM = Short stay, 3/31/14 QM = Short Stay 4
5 Look Back Scan Scenario Resident in previous case study has a fall with a major injury captured on an MDS in November 2013 In case study #1, the FWMI will appear on QM report on 3/31/14 because she is still in the same episode. In case study #2, the FWMI will not appear on any QM because she was short stay on 12/31/13 QM and now she is in a new episode and look back scans only scan the current episode. QM Definitions: Admission Any time an admission entry record (A0310F = 01 and A1700 = 1) is completed; when the resident: Has never been admitted before OR Has been in this facility previously and is returning after a discharge return not anticipated OR Has been in this facility previously and was discharged return anticipated and is returning more than 30 days after discharge RLH Consulting 14 QM Definitions: Reentry Any time a reentry record (A0310F = 01 and A1700 = 2) is completed; when the resident was: Discharged return anticipated AND Returned to the facility within 30 days of discharge RLH Consulting 15 5
6 QM Definitions: Stay A set of contiguous days in a facility The period of time between a resident s entry into a facility and either a discharge of any type or the end of the target period, whichever comes first RLH Consulting 16 QM Definitions: Episode A period of time spanning one or more stays An episode begins with an admission Entry record (A0310F = 01 and A1700 = 1) RLH Consulting 17 QM Definitions: Cumulative Days in Facility (CDIF) Total number of days within an episode during which the resident was in the facility Sum of the number of days within each stay included in an episode If more than one stay is involved, only the days as a resident in the facility count RLH Consulting 18 6
7 QM Definitions: Target Date The event date for an MDS record The A1600 Entry date for an Entry Record (A0310F = 01) The A2000 Discharge date for a Discharge record (A0310F= 10 or 11) or Death-in-facility record (A0310F = 12) The A2300 Assessment Reference Date for all other records RLH Consulting 19 QM Definitions: Target Period The span of time that defines the QM reporting period (e.g., a calendar quarter) RLH Consulting 20 QM Definitions: Short Stay vs Long Stay All residents whose latest episode either ends during the target period or is ongoing at the end of the target period are selected for computing the QMs Short Stay: CDIF is less than or equal to 100 days as of the end of the target period Long Stay: CDIF is greater than or equal to 101 days at the end of the target period RLH Consulting 21 7
8 QM Record Definitions For Short Stay Measures: Look-Back Scan.A scan of all assessments within the episode to see if certain QM events or conditions occurred Includes target assessment and earlier assessment that are: OBRA scheduled assessment (A0310A = 01-06) OR PPS scheduled assessment (A0310B = 01-06) OR Discharge assessment (A0310F= 10 or 11) RLH Consulting 22 QM Record Definition For Long Stay Measures: Prior Assessment(used for ADL Decline-L): Latest assessment within the episode that is 46 to 165 days prior to the target assessment Must be OBRA scheduled assessment (A0310A = 01-06) OR PPS scheduled assessment (A0310B = 01-06) OR Discharge assessment (A0310F= 10 or 11) See example, next slide RLH Consulting 23 Prior Assessment Scenario MDS 1/15 ARD shows resident requiring supervision in late loss ADLs Second week in March, resident has a decline, begins needing extensive assistance in bed mobility, transfers and toilet use Part B therapy initiated and sig change ARD set for 3/17 Resident still on therapy in April, Quarterly ARD set for 4/7 ADLS still extensive assist 8
9 Prior Assessment Scenario On 3/31 QMs, resident will trigger for ADL decline, as 3/17 MDS will be compared to 1/15 MDS On 4/30 QMs, resident will trigger for ADL decline, because 4/7 MDS will be compared to 1/15 MDS because 3/17 MDS was not 46 days prior Resident will continue to trigger until another MDS is done with ARD at least 46 days after 4/7 (5/22 or later) QM Record Definitions For Long Stay Measures: Look-Back Scan.Evaluates all assessments in current episode with target dates no more than 275 days prior to the target assessment Must be OBRA scheduled assessment (A0310A = 01-06) OR PPS scheduled assessment (A0310B = 01-06) OR Discharge assessment (A0310F= 10 or 11) RLH Consulting 26 QMs: The Basic Calculation Each QM is calculated based on specific MDS items When resident s MDS responses indicate resident has the QM condition, that assessment increases the facility score Higher scores indicate possible problems, except scores related to vaccinations Lower scores indicate less occurrence of the QM condition, considered to reflect better care (except vaccination QMs) For vaccination QMs, higher scores reflect better care, because they indicate that a higher proportion of residents received the vaccine RLH Consulting 27 9
10 QMs: The Basic Calculation Basic calculation is a simple ratio expressed as a percentage that results in an indication of a facility s performance relative to each indicator at a given point in time RLH Consulting 28 QMs: The Basic Calculation Numerator: The top number of the fraction; the actual number of residents who had the QM condition Divided by Denominator: Bottom number of the fraction; the number of facility residents with assessments X 100 Equals percentage of residents with the QM condition RLH Consulting 29 Antipsychotic Medication Use This QM identifies short-stay residents who newly started on antipsychotic medication after the initial assessment and who do not have any of the exclusion diagnoses. Does this by capturing the percentage of shortstay residents whoreceived apsychoactive medication ona target assessment but not on the initial assessment
11 Some QMs are Risk Adjusted Use of Exclusions Use of Covariates Stratification of sample based on risk Risk Adjustments: Exclusions Residents who are not included in the numerator or denominator due to a certain diagnosis or condition. Example: Long-stay QM Percent of Low Risk Residents who Lose Control of their Bowel or Bladderexcludes any resident who is comatose (B0100=1) or who has an indwelling catheter (H0100A=1) or who has an ostomy (H0100C=1) on the target assessment RLH Consulting 32 Risk Adjustments: Covariates Adjust for individual resident characteristics or health conditions that are essentially out of the facility s control that may contribute to worse outcomes for a particular QM The residents with those conditions are not excluded, levels the playing field when a facility has more residents with the covariate conditions that other facilities have RLH Consulting 33 11
12 Risk Adjustments: Covariates Three QMs utilize a Covariate New or Worse Pressure Ulcer (S) On initial assessment: impaired bed mobility, occasional bowel incontinence, diabetes, PVD, low BMI Self Reported Pain (L) Independent or modified independence in daily decision making, BIMS Indwelling Catheter (L) On prior assessment: frequent bowel incontinence or stage 2,3 or 4 PU RLH Consulting 34 Risk Adjustments: Stratification Divides residents into high-risk and low-risk Low Risk Residents who Lose Control of Bladder or Bowel (L) High Risk Residents who Get a Pressure Ulcer (L) RLH Consulting 35 THE CASPER REPORTS RLH Consulting 36 12
13 CASPER QM Reports Available through the national analytic reporting system, the Certification and Survey Provider Enhance Reporting (CASPER) system RLH Consulting 37 QM CASPER Reports Access via CMS Welcome screen same screen through which assessments are transmitted to QIES ASAP national database Click MDS link, then Click CASPER Reporting Online Reports link RLH Consulting 38 QM CASPER Reports Two reports Facility Quality Measure Report Resident Level Quality Measure Report Reports default to a 6-month reporting period ending with the most recently ended month You can change the dates of the reporting period manually RLH Consulting 39 13
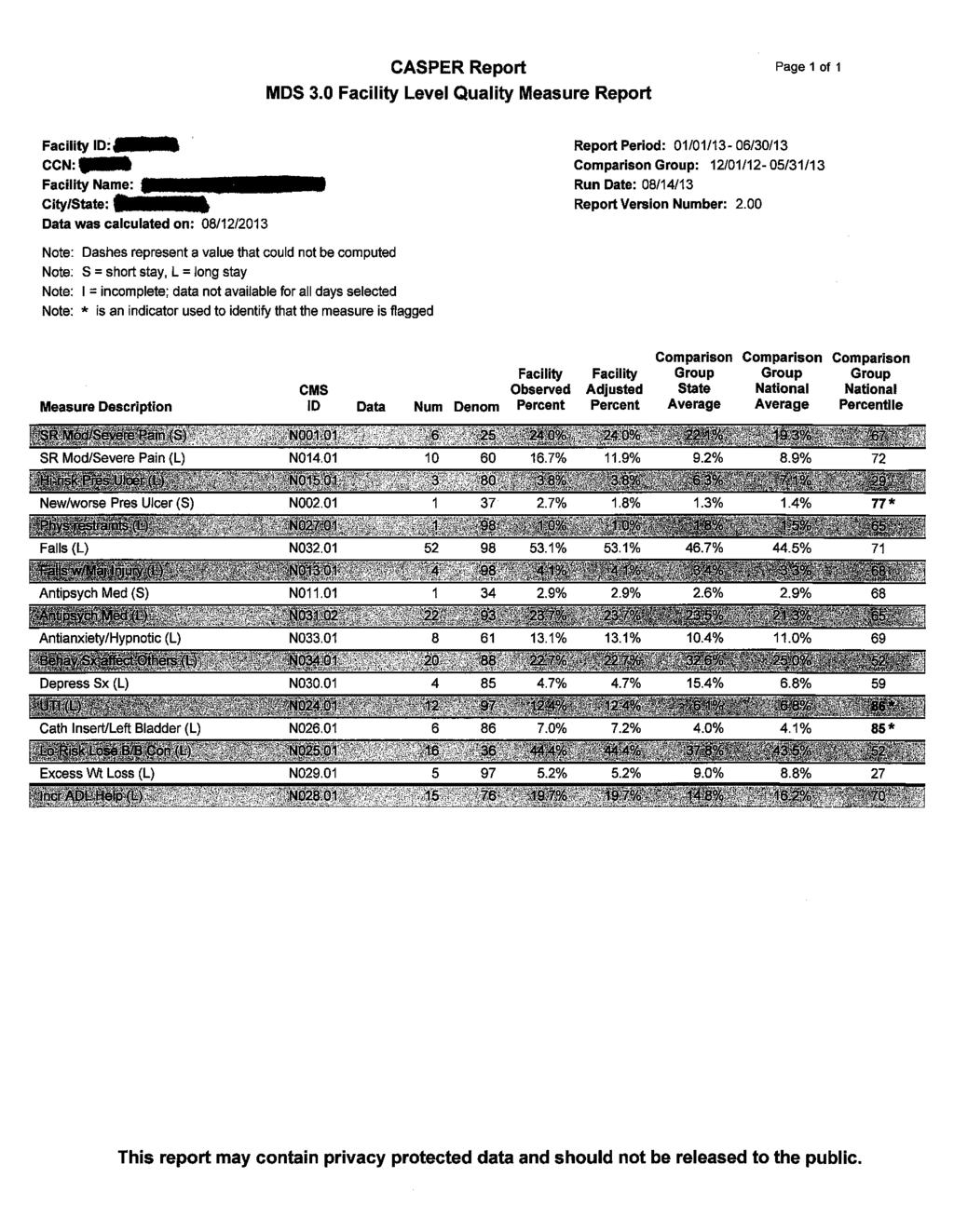
14 CASPER QM Reports Facility Quality Measure Report Lists Each QM Numerator and denominator used for the calculation Facility percentage of occurrence Comparison of facility score with all facilities in state and nation Percentile ranking of facility score Identifies potential areas for further emphasis in facility quality improvement activities or investigation during the survey process RLH Consulting 40 CASPER QM Reports Facility Quality Measure Report Identifying Info Facility ID information Date data was calculated Data is calculated or updated weekly Report Period covered Comparison Group Data calculated monthly with two-month delay Run Date Date the report was accessed by the facility RLH Consulting 41 CASPER QM Reports Facility Quality Measure Report Num Numerator; top number of the fraction The number of residents who have the QM condition in the reporting period Denom Denominator; number of residents who have assessments and were evaluated for the QM condition (no dashes), and Had a stay during the timeframe of the reporting period RLH Consulting 42 14
15 CASPER QM Reports Facility Quality Measure Report Observed Percent Numerator denominator x 100 For QMs not risk adjusted, this is the final score the percentage of residents with the QM condition Adjusted Percent Results after a covariate is applied to the observed percent as risk adjustment This is the final QM score for the three measures that use a covariate to risk adjust RLH Consulting 43 CASPER QM Reports Facility Quality Measure Report Comparison Group State Average Comparison Group National Average Comparison Group National Percentile Facility-specific rank relative to all facilities in the nation Represents percentage of facilities scoring betteron the QM than your facility scored Higher percentile rank means greater likelihood the care captured by the measure warrants review Asterisk appears next to any ranking of 75 th percentile i.e., Flagged RLH Consulting 44 CASPER QM Reports Facility Quality Measure Report State and national percentages should not be used as benchmarks Percentile rankings below the 75 th or scores better the state or national averages are not necessarily indicative of satisfactory performance RLH Consulting 45 15
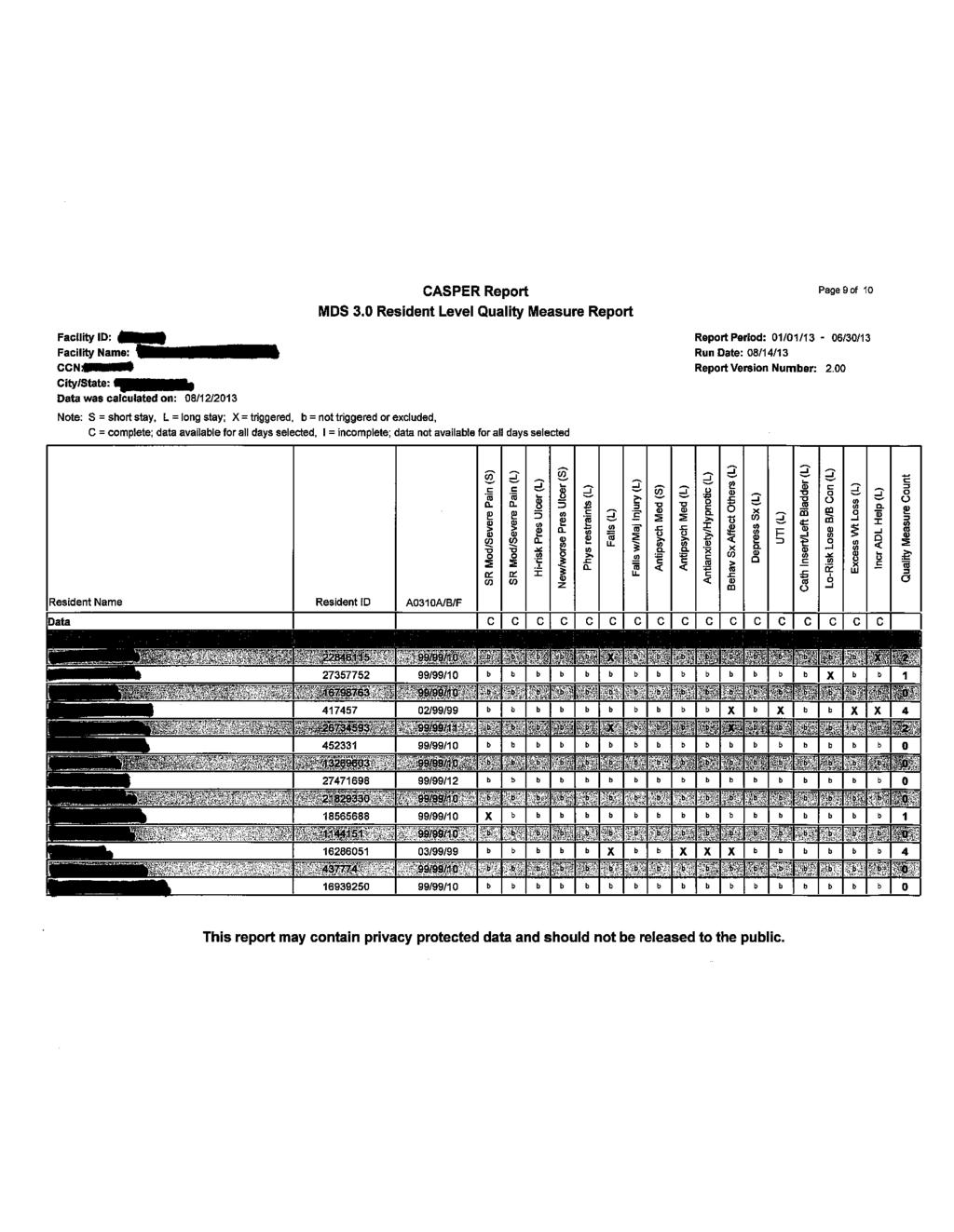
16 CASPER QM Reports Resident Level Quality Measure Report Identifies all residents, active and discharged, included in the QM calculations They are the residents in the numerator of the calculations Also indicates which QMs triggered for each resident Important tool that facilitates detailed record reviews of residents in the numerator of a QM for use in QA/QI activities and survey process RLH Consulting 46 SELECTED SHORT STAY QUALITY MEASURES RLH Consulting 47 New or Worsened Pressure Ulcers Captures any new or worsening Stage 2-4 pressure ulcers coded on any qualifying assessment since the beginning of the episode RLH Consulting 48 16
17 New or Worsened Pressure Ulcers Numerator Short-stay residents for which a look-back scan indicates one or more new or worsening Stage 2-4 pressure ulcers Where on any assessment in the look-back scan: 1. Stage 2 (M0800A) > [0] and M0800A < = M0300B1 OR 2. Stage 3 (M0800B) > [0] and M0800B < = M0300C1 OR 3. Stage 4 (M0800C) > [0] and M0800C < = M0300D1 (The number of new or worsened pressure ulcers in M0800 for a particular stage can t be greater than the number of pressure ulcers present at that stage as indicated in M0300.) RLH Consulting 49 New or Worsened Pressure Ulcers Denominator All residents with one or more assessments that are eligible for a look-back scan, except those with exclusions Exclusions Residents are excluded if none of the assessments included in the look-back scan has a usable response for M0800A, M0800B, or M0800C Usable assessment: One in which the number of new or worsening pressure ulcers at a particular stage is not greater than the total number of pressure ulcers present at that stage in M0300 or in which both items, M0300 and M0800, at a particular stage are skipped RLH Consulting 50 New or Worsened Pressure Ulcers Covariates 1. Requiring limited or more assistance in bed mobility self-performance dependence on the initial assessment: 2. Bowel incontinence at least occasionally on the initial assessment: 3. Diabetes or peripheral vascular disease on initial assessment: 4. Low Body Mass Index on the initial assessment with range (BMI = (weight * 703 / height2) = ((K0200B) * 703) / (K0200A2)]) 5. All covariates are missing if no initial assessment is available RLH Consulting 51 17
18 Antipsychotic Medication Use Numerator Short-stay residents for whom one or more assessments in a look-back scan (not including the initial assessment) indicates that an antipsychotic medication was received: N0410A, Antipsychotic medication, coded Antipsychotic Medication Use Denominator All short-stay residents who do not have exclusions and who have both a target assessment and an initial assessment. The target assessment and the initial assessment cannot be the same 53 Antipsychotic Medication Use Exclusions The target assessment does not have psychoactive medications checked [-] Any of the following are checked on any assessment in the look-back scan: a.schizophrenia (I6000 = 1) b.tourette s Syndrome (I5350 = 1) c. Huntington s Disease (I5250 = 1) The initial assessment indicates antipsychotic medication use or use is unkown(n0410a = 1 7, or - ) 54 18
19 SELECTED LONG STAY QUALITY MEASURES RLH Consulting 55 Falls with Major Injury Identifies residents with at least one fall with an injury classified as a major Includes bone fracture, joint dislocation, closed head injury with altered consciousness, subdural hematoma RLH Consulting 56 Falls with Major Injury Numerator Long-stay residents with one or more look-back scan assessments that indicate one or more falls that resulted in major injury (J1900C=[1,2]) Denominator All long-stay residents with one or more look-back scan assessments except those with exclusions Exclusions Missing MDS responses RLH Consulting 57 19
20 Residents Who Self-Report Moderate to Severe Pain Identifies long-stay residents who selfreported High frequency of daily pain with at least one episode of at least moderate intensity pain or Severe/horrible pain at any frequency Admission, 5-day, and Readmission/Return assessments are not included RLH Consulting 58 Residents Who Self-Report Moderate to Severe Pain Numerator Target assessment meets either or both of the following conditions: 1. Resident report almost constant or frequent moderate to severe pain in the last 5 days. Both of the following conditions must be met: a. Almost constant or frequent pain (J0400=[1,2]) and b. At least one episode of moderate to severe pain: (J0600A=[05,06,07,08,09] OR J600B=[2,3]) 2. Resident reports very severe/horrible pain of any frequency (J0600A=[10] OR J0600B=[4]) RLH Consulting 59 Residents Who Self-Report Moderate to Severe Pain Denominator All long-stay residents with a selected target assessment, except those with exclusions Exclusions 1. Target assessment is an Admission assessment, a PPS 5-day assessment, or a PPS Readmission/Return assessment (A0310A=[01] or A0310B=[01, 06] 2. Key pain self-report items were not completed RLH Consulting 60 20
21 Residents Who Self-Report Moderate to Severe Pain Covariates Independence or modified independence in daily decision making on the prior assessment C1000, cognitive skills for daily decision-making = 0-1 or BIMS Summary Score (C0500) = Compensates for decreased self-report of pain in facilities with more cognitively impaired residents RLH Consulting 61 Urinary Tract Infection Numerator Long-stay residents with a selected target assessment that indicates urinary tract infection within the last 30 days (I2300 = checked) Denominator All long-stay residents with a selected target assessment, except those with exclusions Exclusions Target assessment is an admission assessment (A0310A = [01]) or a PPS 5-day or readmission/return assessment (A0310B = [01, 06]) Missing data RLH Consulting 62 Low Risk Residents who Lose Control of Bowel or Bladder Identifies low risk residents by excluding high risk Then calculates proportion of remaining residents with frequent or always incontinent coded on the last qualifying assessment in the three-month reporting period RLH Consulting 63 21
22 Low Risk Residents who Lose Control of Bowel or Bladder High risk: Severe cognitive impairment on the target assessment as indicated by (C1000 = [3] and C0700 = [1]) OR (C0500 [7]). Totally dependent in bed mobility selfperformance (G0110A1 = [4, 7, 8]). Totally dependent in transfer self-performance (G0110B1 = [4, 7, 8]). Totally dependent in locomotion on unit selfperformance (G0110E1 = [4, 7, 8]) RLH Consulting 64 Low Risk Residents who Lose Control of Bowel or Bladder Numerator Target assessment that indicates frequently or always incontinence of the bladder (H0300 = [2,3]) or bowel (H0400 = [2, 3]) Denominator All long-stay residents with a selected target assessment, except those with exclusions RLH Consulting 65 Low Risk Residents who Lose Control of Bowel or Bladder Exclusions Admission (A0310A = [01]) or a PPS 5-day or readmission/return assessment (A0310B = [01, 06]) Resident is not in numerator and H0300 = [-] OR H0400 = [-]. Residents who have any of the high risk conditions Resident does not qualify as high risk and cognitive status items are blank or skipped Resident does not qualify as high risk and ADL items are dashed Resident is comatose (B0100 = [1]) or comatose status is missing Resident has indwelling catheter (H0100A = [1]) or indwelling catheter status is missing Resident has an ostomy (H0100C = [1]) or ostomystatus is missing RLH Consulting 66 22
23 Increased Need for ADL Help 1 Compares late-loss ADLs on the target assessment and the most recent MDS prior to that one Increase in need for help with ADLs is defined as: An increase in two or more coding points, such as from supervision to extensive, in one late-loss ADL item, or One point increase, such as from limited to extensive, in two or more late-loss ADL items RLH Consulting 67 Increased Need for ADL Help Compares late-loss ADLs on the target assessment and the most recent MDS prior to that one Increase in need for help with ADLs is defined as: An increase in two or more coding points, such as from supervision to extensive, in one late-loss ADL item, or One point increase, such as from limited to extensive, in two or more late-loss ADL items RLH Consulting 68 Increased Need for ADL Help Numerator Residents meet the definition of increased need of help with late-loss ADLs Denominator All residents with a selected target and prior assessment except those with exclusions RLH Consulting 69 23
24 Increased Need for ADL Help Exclusions 1. All four of the late-loss ADL items indicate total dependence (coded 4,7, or 8) on prior assessment 2. 3 late-loss ADLs indicate total dependence on prior assessment AND the 4th indicates extensive assistance (3) on prior assessment 3. Comatose (B0100 = [1, -] ) on target assessment 4. Life expectancy less than 6 month (J1400 = [1, -] ) on target assessment 5. Hospice care (O0100K2 = [1, -]) on the target assessment 6. Resident is not in the numerator AND at least one of the four ADLs was dashed on prior or target assessment RLH Consulting 70 Residents with Depressive Symptoms Considering all long-stay residents with a target assessment except those coded as comatose, the proportion of residents with: Little interest or pleasure in doing things 7-14 days OR Feeling or appearing down, depressed, or hopeless 7-14 days AND Total Severity Score 10 RLH Consulting 71 Residents with Depressive Symptoms Numerator CONDITION A (The resident mood interview must meet Part 1 and Part 2 below) PART 1: Little interest or pleasure in doing things half or more of the days over the last two weeks is equal or greater than two (D0200A2 = [2, 3]) OR Feeling down, depressed, or hopeless half or more of the days over the last two weeks (D0200B2 = [2, 3]) PART 2: The resident interview total severity score indicates the presence of depression (D0300 [10] and D0300 [27]). RLH Consulting 72 24
25 Residents with Depressive Symptoms Numerator CONDITION B: (The staff assessment of resident mood must meet Part 1 and Part 2 below) PART 1: Little interest or pleasure in doing things half or more of the days over the last two weeks is equal or greater than two (D0500A2 = [2, 3]) OR Feeling or appearing down, depressed, or hopeless half or more of the days over the last two weeks (D0500B2 = [2, 3]) PART 2: The staff assessment total severity score indicates the presence of depression (D0600 [10] and D0600 [30]). RLH Consulting 73 Residents with Depressive Symptoms Denominator All long-stay residents with a selected target assessment, except those with exclusions Exclusions 1. Resident is comatose or comatose status is missing (B0100 = [1, -]) 2. Resident is not included in the numerator (the resident did not meet the depression symptom conditions for the numerator) AND both of the following are true: a. D0200A2 = [^, -] OR D0200B2 = [^, -] OR D0300=[99, -, ^] b. D0500A2 = [^, -] OR D0500B2 = [^, -] OR D0600=[-, ^] RLH Consulting 74 Antipsychotic Medication Use Captures the percentage of long-stay residents who are receiving a antipsychotic medication in the target period
26 Antipsychotic Medication Use Numerator Long-stay residents who qualify for the denominator and for whom the selected target assessment indicates that antipsychotic medication was received. N0400A, Antipsychotic medication, coded 1 (checked) (for assessments with target dates on or before March 31, 2012) N0410A, Antipsychotic medication, coded 1-7 (for assessments with target date on or after April 1, 2012) Denominator All long-stay residents who do not have a qualifying exclusion and who have a selected target assessment. 76 Antipsychotic Medication Use Exclusions Any of the following related conditions are present on the target assessment (unless otherwise indicated): Schizophrenia (I6000 = [1]) Tourette ssyndrome (I5350 = [1]) Tourette ssyndrome (I5350 = [1]) on the prior assessment if this item is not active on the target assessment and if a prior assessment is available Huntington s Disease (I5250 = [1]) 77 Prevalence of Falls Percentage of long-stay residents with a fall on any assessment in the look-back scan RLH Consulting 78 26
27 Prevalence of Falls Numerator Long-stay residents with one or more look-back scanassessments that indicate the occurrence of a fall (J1800 = [1] Denominator All long-stay residents with one or more look-back scan assessments except those with exclusions Exclusions The occurrence of falls was not assessed (J1800 = [-]) for all look-back scan assessments RLH Consulting 79 Antianxiety & Hypnotic Meds Long-stay residents with a target assessment, except those with exclusions 80 Antianxiety & Hypnotic Meds Numerator Long-stay residents with a selected target assessment where either of the following conditions are true: Antianxiety medications received (N0410B = 1-7), or Hypnotic medications received (N0410D = 1 7) Denominator Long-stay residents with a selected target assessment, except those with exclusions 81 27
28 Antianxiety & Hypnotic Meds Exclusions Schizophrenia (I6000 = 1) Psychotic disorder (I5950 = 1) Manic depression (bipolar disease) (I5900 = 1) Tourette s Syndrome (I5350 = 1) Huntington s Disease (I5250 = 1) Hallucinations (E0100A = 1) Delusions (E0100B = 1) Anxiety disorder (I5700 = 1) Post traumatic stress disorder (I6100 = 1) 82 Behavior Symptoms Affecting Others All residents in the target period who were coded with physical, verbal, or other behavioral symptoms directed toward others as a proportion of all facility residents with a target assessment (except exclusions) RLH Consulting 83 Behavior Symptoms Affecting Others Numerator Target assessments with any of the following coded 1, 2, or 3, indicating the behavior occurred at least once E0200A, physical behavioral symptoms directed at others E0200B, verbal behavioral symptoms directed toward others E0200C, other behavioral symptoms not directed toward others E0800, rejection of care E0900, wandering RLH Consulting 84 28
29 Behavior Symptoms Affecting Others Denominator All residents with a selected target assessment, except those with exclusions Exclusions The resident is not in the numerator and The target assessment is a discharge assessment (A0310F = 10 or 11) OR Any of the five numerator MDS items is coded with a dash indicating information not available or is skipped RLH Consulting 85 IMPROVING YOUR QUALITY MEASURES 86 Quality Improvement Identify measure(s) to work on Identify MDS items impacting that measure Verify MDS coding accuracy Evaluate process issues with MDS coding Interview, documentation, Steps for Assessment Examine Care delivery Using Root Cause Analysis Evaluate resident detail report, review records, identify trends 29
30 MDS Accuracy Misunderstandings about coding definitions is a problem QM scores are derived from MDS data Inaccurate coding can result in misleading Quality Measure scores Inaccurate MDS coding can result in inappropriate resident care Inaccurate MDS coding can result in inappropriate reimbursement 88 MDS Accuracy: Common Coding Problems Impacting QMs ADLs (Section G) Rule of 3, ADL algorithm, inconsistent documentation, failure to use all available sources of information Pressure Ulcers (Section M) No back-staging, definition of worsening pressure ulcer ( bigger vs. staging, new PU on 1 st assessment) Influenza Vaccine (Section O) Capturing vaccine from season just ended when new season hasn t started yet, not capturing vaccine given in late September 89 MDS Accuracy: Common Coding Problems Impacting QMs Restraints (Section P) QM is only if the device meets the definition of daily restraint Urinary Tract Infection (Section I) Definition is very specific; code only if all 4 criteria are present Interview process (Mood, Pain) Who is being interviewed? Are you using cue cards? Are you rewording the questions or responses to make it easier for the resident to respond? How do you follow up on interview responses? 90 30
31 MDS Accuracy: Common Coding Problems Impacting QMs Use the most current version of the RAI User s Manual Use it thoroughly Use it OFTEN Resources for Quality Care QIO resources Advancing Excellence AHCA Quality Initiative website, OHCA Quality Commission, Leadership and supervision are the keys to success 92 Quality Improvement Be proactive Perform root cause analysis Monitor key systems and assign accountability Work in teams, not individually Looks for interrelationship between QM scores 93 31
32 Quality Improvement Use all information available to you, such as: QIs and QMs Internal tracking reports (skin, weight, falls, etc.) Survey history Resident and family satisfaction surveys Safety committee issues Resident, family, staff, physician feedback 94 Case Study #1 Self Reported Moderate or Severe Pain (L) Numerator = 19, Denominator = 73, Observed % = 26%, Adjusted % = 19%, 83 rd %ile Denominator for Falls (L) = 123 Case Study #1 Self Report Moderate or Severe Pain (L) Began attempting interview for pain on all residents. Next QM Shows Numerator = 20, denominator = 119, observed % = 16.8%, adjusted % = 15% Some residents are reporting moderate or severe pain, but nurses documentation states no complaints of pain. Many are on the same unit 32
33 Case Study #1 Self Report Moderate or Severe Pain (L) Talked with residents whose interview results conflicted with nurse s documentation. Identified one nurse who was never asking about pain or offering PRN meds; she thought residents would peak up if they were really in pain Are we done? What else could we do? Case Study #1 Self Report Moderate or Severe Pain (L) Is there a trend with many residents complaining of pain having the same doc? Is there a trend with many residents being newly long stay, or very long stay? When are pain interviews being done relative to timing of pain med administration? Do residents think they have to report moderate or severe pains in order to keep their pain management regimen in place? Case Study #2 UTIs MDS coding accurate? 30 day lookback:symptomatic, Dr. diagnosis, abnormal labs, treatment Do we get labs on too many people? How do we define abnormal labs? Are many UTIs on the same unit? Do many residents with UTI have the same Dr? Do we utilize appropriate prevention? 33
34 Case Study #3 Decline in ADLs MDS Coding Accurate? Rule of three, algorithm, quality of documentation, talk to residents, steps for assessment Who is declining? Is therapy willing to screen and do nurses provide appropriate information? Is restorative nursing appropriate? Case Study #4 Related QMs Facility flagged for Pain Falls Falls with major injury Behavior symptoms affecting others Antipsychotics Resources CMS MDS 3.0 Training Materials, including RAI User s Manual NHQIMDS30TrainingMaterials.asp#TopOfPage MDS 3.0 Quality Measures User s Manual Patient-Assessment- Instruments/NursingHomeQualityInits/Downloads/ MDS-30-QM-Users-Manual-V60.pdf
35 Questions? 35
36
37
38
39
40
41
42
43
44
45
46
47
FH16 - Developed by Polaris Group Page 1 of 140
 FH16 - Developed by Polaris Group www.polaris-group.com Page 1 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page 2 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page
FH16 - Developed by Polaris Group www.polaris-group.com Page 1 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page 2 of 140 FH16 - Developed by Polaris Group www.polaris-group.com Page
Quality Measures Are My Friends
 s Are My Friends Advantage Home Health Services AdvantageCare Rehabilitation Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA Nurse Consultant / CMI Specialist & Medicare Reimbursement Specialist Dave Lishinsky,
s Are My Friends Advantage Home Health Services AdvantageCare Rehabilitation Kathy Kemmerer, NAC, RAC-CT 3.0, CPRA Nurse Consultant / CMI Specialist & Medicare Reimbursement Specialist Dave Lishinsky,
Quality Measures (QM) & Five Star Rating System. Objectives 4/18/2016 MDS CODING FOR QUALITY MEASURES
 & Five Star Rating System. Objectives 4/18/2016 MDS CODING FOR QUALITY MEASURES") Quality Measures (QM) & Five Star Rating System Carol Hill MSN, RN, RAC-CT, DNS-CT, RAC-MT, QCP Objectives At the conclusion of this educational offering the participant will be able to: Identify MDS items
Quality Measures (QM) & Five Star Rating System Carol Hill MSN, RN, RAC-CT, DNS-CT, RAC-MT, QCP Objectives At the conclusion of this educational offering the participant will be able to: Identify MDS items
Leveraging Your Facility s 5 Star Analysis to Improve Quality
 Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
Leveraging Your Facility s 5 Star Analysis to Improve Quality DNS/DSW Conference November, 2016 Presented by: Kathy Pellatt, Senior Quality Improvement Analyst, LeadingAge NY Susan Chenail, Senior Quality
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES
 UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated May 2017 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF CONTENTS
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated May 2017 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF CONTENTS
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES
 UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated February 2018 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF
UNDERSTANDING THE NEW MDS 3.0 QUALITY MEASURES Updated February 2018 235 Promenade Street, Suite 500, Box 18, Providence, RI 02908 T 401.528.3200 F 401.528.3279 www.healthcarefornewengland.org TABLE OF
Understanding the New MDS 3.0 Quality Measures. Updated May 2017
 Understanding the New MDS 3.0 Quality Measures Updated May 2017 Contents Introduction... 3 Background History of the MDS 3.0:... 3 Percent of Short-Stay Residents Who Self-Report Moderate to Severe Pain...
Understanding the New MDS 3.0 Quality Measures Updated May 2017 Contents Introduction... 3 Background History of the MDS 3.0:... 3 Percent of Short-Stay Residents Who Self-Report Moderate to Severe Pain...
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know
 New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
New Quality Measures Will Soon Impact Nursing Home Compare and the 5-Star Rating System: What providers need to know Presented by: Kathy Pellatt, Senior Quality Improvement Analyst LeadingAge New York
MDS Coding. Antipsychotic Quality Measure
 MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
MDS Coding Antipsychotic Quality Measure The information in this presentation may be subject to copyright and may not be reproduced without permission of the presenter. Introduction Jessica Mirabal, RN
Quality Measures and the Five-Star Rating
 Quality Measures and the Five-Star Rating Pennsylvania Health Care Association Presented by Reinsel Kuntz Lesher LLP Senior Living Services Consulting October 23, 2014 Disclaimer The information contained
Quality Measures and the Five-Star Rating Pennsylvania Health Care Association Presented by Reinsel Kuntz Lesher LLP Senior Living Services Consulting October 23, 2014 Disclaimer The information contained
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT
 Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
Maggie Turner RN RAC-CT Kara Schilling RN RAC-CT Lisa Gourley RN RAC-CT We do not have any financial relationships to disclose We do not have any conflicts of interest to disclose We will not promote any
11/23/2011. Proactive vs. Reactive Relationship
 Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
Overview Focus on Resident Voice Assessment Schedule EOT OMRA and New Resumption Items New PPS Assessment: COT OMRA CMS Clarifications Coding New Quality Measures Draft MDS and Care Planning as Risk Management
WHAT S IN THE STARS FOR YOUR FACILITY
 WHAT S IN THE STARS FOR YOUR FACILITY LIBBY YOUSE, BS, LNHA LEADERSHIP COACH CRYSTAL PLANK, BSN, RN QIPMO CLINICAL EDUCATOR BACKGROUND December 18, 2008-5-Star Quality Rating System was added to the Nursing
WHAT S IN THE STARS FOR YOUR FACILITY LIBBY YOUSE, BS, LNHA LEADERSHIP COACH CRYSTAL PLANK, BSN, RN QIPMO CLINICAL EDUCATOR BACKGROUND December 18, 2008-5-Star Quality Rating System was added to the Nursing
Navigating the New CMS Quality Measures
 Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Navigating the New CMS Quality Measures Dawn Murr-Davidson RN, BSN Director of Quality Initiatives Pennsylvania Health Care Association 1 Objectives Discuss the CMS Nursing Home Compare new quality measures
Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission
 Table 1. Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission Measure Description Numerator and Window Numerator Exclusions Covariates The percent of short-stay residents
Table 1. Percentage of Short-Stay Residents who were Re-hospitalized after a Nursing Home Admission Measure Description Numerator and Window Numerator Exclusions Covariates The percent of short-stay residents
Welcome and thank you for viewing What s your number? Understanding the Long- Stay Urinary Tract Infection Quality Measure. This presentation is one
 Welcome and thank you for viewing What s your number? Understanding the Long- Stay Urinary Tract Infection Quality Measure. This presentation is one in a series of videos explaining the 13 quality measures
Welcome and thank you for viewing What s your number? Understanding the Long- Stay Urinary Tract Infection Quality Measure. This presentation is one in a series of videos explaining the 13 quality measures
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide
 Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide April 2018 April 2018 Revisions Beginning with the April 2018 update of the Nursing Home Compare website and the Five-Star
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide April 2018 April 2018 Revisions Beginning with the April 2018 update of the Nursing Home Compare website and the Five-Star
US Health Health Policy
 Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
Memorandum US Health Health Policy Date January 22, 2015 To From Subject CMS Abt Associates MDS 3.0 Focused Survey Pilot Results Executive Summary This memo describes the results of the MDS 3.0 Focused
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide
 Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide February 2018 Note: On November 28, 2017 the Centers for Medicare and Medicaid Services (CMS) instituted a new Health
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide February 2018 Note: On November 28, 2017 the Centers for Medicare and Medicaid Services (CMS) instituted a new Health
CMS s RAI Version 3.0 Manual October 2016
 Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Presented by: CMS s RAI Version 3.0 Manual October 2016 RAI SOM CAAs MDS Resident Assessment Instrument Utilization Guidelines from the State Operations Manual Care Area Assessments Minimum Data Set Affinity
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide
 Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide July 2016 Note: In July 2016, the Centers for Medicare & Medicaid Services (CMS) is making several changes to the
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide July 2016 Note: In July 2016, the Centers for Medicare & Medicaid Services (CMS) is making several changes to the
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES
 COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
COMMONWEALTH OF KENTUCKY OFFICE OF INSPECTOR GENERAL AND MYERS AND STAUFFER LC PRESENT MDS CODING AND INTERPRETATION ANSWER SLIDES WOULD YOU COMPLETE A SIGNIFICANT CHANGE IN STATUS ASSESSMENT? Example
5/26/2016. What's New? What's Changed? Urgent Updates QM Manual v10. Faculty Disclosure. Requirements for Successful Completion
 What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
What's New? What's Changed? Urgent Updates QM Manual v10 Presented by: Judi Kulus, MSN, MAT, RN, NHA, RAC-MT, DNS-CT VP of Curriculum Development jkulus@aanac.org Faculty Disclosure I have no financial
Discharge to Community Measure
 The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
The Discharge to Community Measure determines the percentage of all new admissions from a hospital who are discharged back to the community and remain out of any skilled nursing center for the next 30
QM, 5 Star, VBP: Taking the Confusion Out of All the Reports and the Impact of QMs on Reimbursement Presented for WHCA
 QM, 5 Star, VBP: Taking the Confusion Out of All the Reports and the Impact of QMs on Reimbursement 414 476 1112 fax 414 476 6118 www.specializedmed.com The materials contained herein include information
QM, 5 Star, VBP: Taking the Confusion Out of All the Reports and the Impact of QMs on Reimbursement 414 476 1112 fax 414 476 6118 www.specializedmed.com The materials contained herein include information
Quality Outcomes and Data Collection
 Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Quality Outcomes and Data Collection Presented By: Joanne Jones Director, Clinical Consulting Services August 30, 2016 Quality Measurement in LTC CMS Nursing Home Compare 5 Star Rating System New measures
Disclaimer. Learning Objectives
 Data Analysis in Today s Skilled Nursing Facilities: How Data is Driving Reimbursement and 5-Star Ratings Presented by: Reinsel Kuntz Lesher Senior Living Services Consulting 0 Disclaimer The information
Data Analysis in Today s Skilled Nursing Facilities: How Data is Driving Reimbursement and 5-Star Ratings Presented by: Reinsel Kuntz Lesher Senior Living Services Consulting 0 Disclaimer The information
Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report
 Overall Quality Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report Incorporating data reported through 11/30/2017 Ratings for Saint Anthony Rehab And Nursing Center (155604)
Overall Quality Nursing Home Compare Five-Star Ratings of Nursing Homes Provider Rating Report Incorporating data reported through 11/30/2017 Ratings for Saint Anthony Rehab And Nursing Center (155604)
OASIS QUALITY IMPROVEMENT REPORTS
 6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
6 OASIS QUALITY REPORTS GENERAL INFORMATION... 2 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) REPORT... 4 AGENCY PATIENT-RELATED CHARACTERISTICS (CASE MIX) TALLY REPORT 9 HHA REVIEW AND CORRECT REPORT...13
AANAC Education Advancement. MDS Essentials: An Introduction. Learning Objectives 3/22/2017. Education Advancement
 AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
AANAC Education Advancement MDS Essentials: An Introduction to MDS 3.0 We want to provide you with the right education at the right time in your career path Consider the following to identify your needs:
QAPI: Driving Quality or Just Driving You Crazy
 QAPI: Driving Quality or Just Driving You Crazy Julie Kueker, MBA, MT(ASCP) Nursing Home QIN-QIO Task Lead Objectives Review the Final Rule Changes and Updates for QAPI Describe the format of QAPI methodology
QAPI: Driving Quality or Just Driving You Crazy Julie Kueker, MBA, MT(ASCP) Nursing Home QIN-QIO Task Lead Objectives Review the Final Rule Changes and Updates for QAPI Describe the format of QAPI methodology
MDS 3.0/RUG IV OVERVIEW
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
MDS 3.0/RUG IV Distance Learning Series January - May 2016 OVERVIEW In keeping with the success of their previous highly-rated distance learning education offerings, LeadingAge state affiliates and Plante
Understanding the Five Star Quality Rating System Design For Nursing Home Compare
 Understanding the Five Star Quality Rating System Design For Nursing Home Compare Nathan Shaw RN, BSN, MBA, LHRM, RAC CT 3.0 Director of Clinical Reimbursement March 23rd, 2015 Objectives Objectives Provide
Understanding the Five Star Quality Rating System Design For Nursing Home Compare Nathan Shaw RN, BSN, MBA, LHRM, RAC CT 3.0 Director of Clinical Reimbursement March 23rd, 2015 Objectives Objectives Provide
6/29/2015. Focused Survey for MDS Assessment. Objectives: Review the results of the MDS pilot study.
 Focused Survey for MDS Assessment Idaho Health Care Association July 21, 1015 1:45 P.M. 3:15 P.M. Louann Lawson, BA, RN, RAC-CT AHIMA Approved ICD-10-CM/PCS Trainer Nurse Consultant, Clinical Reimbursement
Focused Survey for MDS Assessment Idaho Health Care Association July 21, 1015 1:45 P.M. 3:15 P.M. Louann Lawson, BA, RN, RAC-CT AHIMA Approved ICD-10-CM/PCS Trainer Nurse Consultant, Clinical Reimbursement
CMS Announced Changes On Feb 12 th CMS s Open Door Forum conference call
 SUMMARY OF THE CHANGES TO FIVE STAR ANNOUNCED BY CMS Mark Parkinson AHCA/NCAL President & CEO All member call February 13 th, 2015 CMS Announced Changes On Feb 12 th CMS s Open Door Forum conference call
SUMMARY OF THE CHANGES TO FIVE STAR ANNOUNCED BY CMS Mark Parkinson AHCA/NCAL President & CEO All member call February 13 th, 2015 CMS Announced Changes On Feb 12 th CMS s Open Door Forum conference call
SUMMARY OF THE CHANGES TO FIVE STAR ANNOUNCED BY CMS. Mark Parkinson AHCA/NCAL President & CEO All member call February 13 th, 2015
 SUMMARY OF THE CHANGES TO FIVE STAR ANNOUNCED BY CMS Mark Parkinson AHCA/NCAL President & CEO All member call February 13 th, 2015 AHCA Requests to CMS Do not go back to a curve Phase in any changes Rebasing
SUMMARY OF THE CHANGES TO FIVE STAR ANNOUNCED BY CMS Mark Parkinson AHCA/NCAL President & CEO All member call February 13 th, 2015 AHCA Requests to CMS Do not go back to a curve Phase in any changes Rebasing
LTCH Lay of the Land: Reporting the LTCH CARE Data Set (2 of 3) August 21, 2012
 August 21, 2012") LTCH Lay of the Land: Reporting the LTCH CARE Data Set (2 of 3) August 21, 2012 Purpose: What s New? In Brief LTCH Quality Reporting Program New developments Updated CMS LTCH QRP Manual Final FY13 rule:
LTCH Lay of the Land: Reporting the LTCH CARE Data Set (2 of 3) August 21, 2012 Purpose: What s New? In Brief LTCH Quality Reporting Program New developments Updated CMS LTCH QRP Manual Final FY13 rule:
MDS 3.0: What Leadership Needs to Know
 MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
MDS 3.0: What Leadership Needs to Know especially prepared for CANPFA Ann Spenard RN, MSN History of the MDS and RAI Process The Resident Assessment Instrument (RAI) was part of a set of reforms enacted
LSSCC Action Period 1: Composite Score Reports June 25, 2015
 LSSCC Action Period 1: Composite Score Reports June 25, 2015 The National Nursing Home Quality Care Collaborative (NNHQCC) Composite Measure! Composite Measure tool used to help monitor NNHQCC progress
LSSCC Action Period 1: Composite Score Reports June 25, 2015 The National Nursing Home Quality Care Collaborative (NNHQCC) Composite Measure! Composite Measure tool used to help monitor NNHQCC progress
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs
 What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
What s Happening in the Nursing Home? Cherry Meier, RN, MSN, NHA Vice President of Public Affairs Objectives Describe the benefits of partnering with hospice Explain the regulations for the interface between
AHCA Requests to CMS
 SUMMARY OF THE CHANGES TO FIVE STAR ANNOUNCED BY CMS Mark Parkinson AHCA/NCAL President & CEO All member call February 13 th, 2015 AHCA Requests to CMS Do not go back to a curve Phase in any changes Rebasing
SUMMARY OF THE CHANGES TO FIVE STAR ANNOUNCED BY CMS Mark Parkinson AHCA/NCAL President & CEO All member call February 13 th, 2015 AHCA Requests to CMS Do not go back to a curve Phase in any changes Rebasing
Wilhide Consulting, Inc. (c) 1
 1") Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Required by the Omnibus Reconciliation Act of 1987 Correction OBRA Scheduling January 2017 NC
Quality Measurement in Skilled Nursing Facilities Five Star Rating System
 Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Quality Measurement in Skilled Nursing Facilities Five Star Rating System January 2018 NC & VA
Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Quality Measurement in Skilled Nursing Facilities Five Star Rating System January 2018 NC & VA
HSAG the QIN-QIO NHQCC II and CDI Initiative Kick-off
 (HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
(HSAG) the Quality Innovation Network-Quality Improvement Organization Ohio National Nursing Home Quality Care Collaborative II (NHQCC II) Introduction James H. Barnhart III, BSH, LNHA Quality Improvement
New York State Department of Health 2016 Nursing Home Quality Initiative Methodology
 New York State Department of Health 206 Nursing Home Quality Initiative Methodology Updated March 206 The 206 Nursing Home Quality Initiative (NHQI) is comprised of three components: [] the Quality Component
New York State Department of Health 206 Nursing Home Quality Initiative Methodology Updated March 206 The 206 Nursing Home Quality Initiative (NHQI) is comprised of three components: [] the Quality Component
JudyWilhide.com (c) 1
 1") Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Overview Quality Measures Quality Measurement in Skilled Nursing Facilities Five Star Rating
Judy Wilhide Brandt, RN, BA, RAC-MT, QCP, CPC, DNS-CT judy@judywilhide.com 909-800-9124 www.judywilhide.com Overview Quality Measures Quality Measurement in Skilled Nursing Facilities Five Star Rating
Learning Session 2 for the Ohio Nursing Home Quality Care Collaborative II (NHQCC II) and the Clostridium difficile Infection (CDI) Initiative
 and the Clostridium difficile Infection (CDI) Initiative") Learning Session 2 for the Ohio Nursing Home Quality Care Collaborative II (NHQCC II) and the Clostridium difficile Infection (CDI) Initiative National Nursing Home Quality Care Collaborative (NNHQCC)
Learning Session 2 for the Ohio Nursing Home Quality Care Collaborative II (NHQCC II) and the Clostridium difficile Infection (CDI) Initiative National Nursing Home Quality Care Collaborative (NNHQCC)
2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications
 Program Description & Measurement Specifications") 2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications Developed by: The QIP Team QIP@partnershiphp.org Released December 15, 2016 Updated July 12, 2017
2017 Long-Term Care Quality Improvement Program (QIP) Program Description & Measurement Specifications Developed by: The QIP Team QIP@partnershiphp.org Released December 15, 2016 Updated July 12, 2017
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert-
 New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
New Survey Focus MDS Accuracy and Staffing -Compliance Risk Alert- Rodney Farley, CHC Terry Raser, RN, RAC-CT, C-NE LW Consulting, Inc. LW Consulting, Inc. 5925 Stevenson Ave, Suite G 5925 Stevenson Ave,
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide. February 2015
 Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide February 2015 Introduction In December 2008, The Centers for Medicare & Medicaid Services (CMS) enhanced its Nursing
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide February 2015 Introduction In December 2008, The Centers for Medicare & Medicaid Services (CMS) enhanced its Nursing
New SNF Quality Measures
 New SNF Quality Measures Strategies to Boost your Facility Performance Dr. Kathleen Weissberg, OTD, OTR/L Education Director Select Rehabilitation kweissberg@selectrehab.com Objectives Understand the measure
New SNF Quality Measures Strategies to Boost your Facility Performance Dr. Kathleen Weissberg, OTD, OTR/L Education Director Select Rehabilitation kweissberg@selectrehab.com Objectives Understand the measure
QIES Help Desk. Objectives. Nursing Home Quality Initiatives and Five-Star Quality Rating System
 Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
Nursing Home Quality Initiatives and Five-Star Quality Rating System Diane Henry, RN, LHHA State RAI Coordinator Quality Improvement & Evaluation Service Oklahoma State Department of Health QIES Help Desk
HOSPICE QUALITY REPORTING PROGRAM
 4 HOSPICE QUALITY REPORTING PROGRAM GENERAL INFORMATION... 3 HOSPICE PATIENT STAY-LEVEL QUALITY MEASURE REPORT... 5 HOSPICE-LEVEL QUALITY MEASURE REPORT... 9 12/2016 v1.00 Certification And Survey Provider
4 HOSPICE QUALITY REPORTING PROGRAM GENERAL INFORMATION... 3 HOSPICE PATIENT STAY-LEVEL QUALITY MEASURE REPORT... 5 HOSPICE-LEVEL QUALITY MEASURE REPORT... 9 12/2016 v1.00 Certification And Survey Provider
OASIS-B1 and OASIS-C Items Unchanged, Items Modified, Items Dropped, and New Items Added.
 Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Items Added. OASIS-B1 Items UNCHANGED on OASIS-C OASIS-C Item # M0014 M0016 M0020 M0030 M0032 M0040 M0050 M0060 M0063 M0064 M0065 M0066 M0069 M0080 M0090 M0100 M0110 M0220 M1005 M1030 M1200 M1230 M1324
Session Objectives. Long Term Care Luncheon: The CMS Five-Star Quality Rating System. Quality Ratings of U.S. Nursing Homes on Nursing Home Compare
 April 12, 2018 Long Term Care Luncheon: The CMS Five-Star Quality Rating System Quality Ratings of U.S. Nursing Homes on Nursing Home Compare Jennifer Pettis, MS, RN, WCC Nurse Researcher / Associate Abt
April 12, 2018 Long Term Care Luncheon: The CMS Five-Star Quality Rating System Quality Ratings of U.S. Nursing Homes on Nursing Home Compare Jennifer Pettis, MS, RN, WCC Nurse Researcher / Associate Abt
CASPER Reports. Objectives: What is Casper? 4/27/2012. Certification And Survey Provider Enhanced Reports
 CASPER Reports By Cindy Skogen, RN Oasis Education Coordinator at MDH Contact #: 651-201-4314 E-mail: Health.OASIS@state.mn.us Source: Center for Medicare/Medicaid Services (CMS). Objectives: Following
CASPER Reports By Cindy Skogen, RN Oasis Education Coordinator at MDH Contact #: 651-201-4314 E-mail: Health.OASIS@state.mn.us Source: Center for Medicare/Medicaid Services (CMS). Objectives: Following
Data Stewardship: Essential Skills for Long Term Care Facility Managers
 Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Data Stewardship: Essential Skills for Long Term Care Facility Managers PRESENTED BY LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@sbcglobal.net Data
Sneak Peak: MDS 3.0 Changes & New QRP s. Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma
 Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
Sneak Peak: MDS 3.0 Changes & New QRP s Effective October 1, 2018 Natashia Mason, RN Director of Professional Development Care Providers Oklahoma Disclaimer These materials, including any medical literature
3/12/2015. Session Objectives. RAI User s Manual. Polling Question
 Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
Session Objectives MDS 3.0 Coding Challenges: Questions, Answers, and Explanations Jen Pettis, BS, RN, WCC Associate March 19, 2015 Upon completion of the program, the participate will: Describe the four
AHCA NURSING HOME PROSPECTIVE PAYMENT SYSTEM STUDY
 AHCA NURSING HOME PROSPECTIVE PAYMENT SYSTEM STUDY PUBLIC HEARING JUNE 30, 2016 1:00 P.M. 4:00 P.M. 1 AGENDA Welcome Project Overview Stakeholder Engagement Payment Methodology Options Quality Incentive
AHCA NURSING HOME PROSPECTIVE PAYMENT SYSTEM STUDY PUBLIC HEARING JUNE 30, 2016 1:00 P.M. 4:00 P.M. 1 AGENDA Welcome Project Overview Stakeholder Engagement Payment Methodology Options Quality Incentive
Preparing for the 2015 QIS Changes in abaqis
 Preparing for the 2015 QIS Changes in abaqis Resident Interview 2 Changed Question for QP210 Participation in Care Plan Before After RESIDENT INTERVIEW 3 CMS Removed Food Quality from Stage 1 Moved from
Preparing for the 2015 QIS Changes in abaqis Resident Interview 2 Changed Question for QP210 Participation in Care Plan Before After RESIDENT INTERVIEW 3 CMS Removed Food Quality from Stage 1 Moved from
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING
 MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
MEDICARE UPDATES: VBP, SNF QRP, BUNDLING PRESENTED BY: ROBIN L. HILLIER, CPA, STNA, LNHA, RAC-MT ROBIN@RLH-CONSULTING.COM (330)807-2850 MEDICARE VALUE BASED PURCHASING 1 PROTECTING ACCESS TO MEDICARE ACT
Any Willing Qualified Provider Appeal Request and Quality Performance Plan (QPP) Report Webinar
 Report Webinar") Any Willing Qualified Provider Appeal Request and Quality Performance Plan (QPP) Report Webinar Division of Aging Services (DoAS) and Division of Medical Assistance and Health Services (DMAHS) 1 Agenda
Any Willing Qualified Provider Appeal Request and Quality Performance Plan (QPP) Report Webinar Division of Aging Services (DoAS) and Division of Medical Assistance and Health Services (DMAHS) 1 Agenda
Methodology Report U.S. News & World Report Nursing Home Finder
 Methodology Report U.S. News & World Report 2017-18 Nursing Home Finder Avery Comarow Anna George, M.A. Greta Martin, M.S. Geoff Dougherty Ben Harder October 31, 2017 U.S. News & World Report s Nursing
Methodology Report U.S. News & World Report 2017-18 Nursing Home Finder Avery Comarow Anna George, M.A. Greta Martin, M.S. Geoff Dougherty Ben Harder October 31, 2017 U.S. News & World Report s Nursing
2014 AANAC 9_30_ AANA C AANA
 2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
2013 2014 AANAC AANAC 9_30_14 Expert Advisory Panel Guests Deb Myhre, RN, RAC-MT, C-NE Mark McDavid, OTR, RAC-CT Requirements for Successful Completion 1 Contact hour will be awarded for this continuing
Reporter. MDS 3.0: A More Objective Resident Assessment Tool for Nursing Home Use 2010 ISSUE
 FALL MIM Reporter The Review of Medical Information Management for Litigation Published as an educational service to the Corporate, Insurance and Defense Legal Community by Litigation Management, Inc.
FALL MIM Reporter The Review of Medical Information Management for Litigation Published as an educational service to the Corporate, Insurance and Defense Legal Community by Litigation Management, Inc.
Agenda: Noon Overview of the regulatory sections affected by the Reform of RoP in Phase 2
 Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Webinar: Driving Five Star & RoP Implementation Through a QAPI Approach: Final Rule: Integrating Phase 2 New Requirements of Participation into Practice (Part 1) Presentation Date: 02/15/17 Live Webinar
Quality Indicators: FY 2015 July 8, Kristen Smith, MHA, PT
 Quality Indicators: FY 2015 July 8, 2014 Kristen Smith, MHA, PT Objectives Review upcoming IRF-PAI changes effective October 1, 2014 Discuss the new quality reporting items as part of the Medicare Quality
Quality Indicators: FY 2015 July 8, 2014 Kristen Smith, MHA, PT Objectives Review upcoming IRF-PAI changes effective October 1, 2014 Discuss the new quality reporting items as part of the Medicare Quality
Attachment C: Itemized List of OASIS Data Elements
 Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
Attachment C: Itemized List of OASIS Data Item Description Number of Data SOC ROC FU TOC DTH DIS M0010 CMS Certification Number 1 1 M0014 Branch State 1 1 M0016 Branch ID Number 1 1 M0018 National Provider
2. D Mood E Behavior F Preferences for Customary Routine and Activities G Functional Status H Bladder and Bowel
 Newslet ter Title R A I C o o r d i n a t or 1-7 1 7-7 8 7-1 8 1 6 q a - m d s @ s t a t e. p a. u s RAI Spotlight MDS 3.0 Training R AI C o o r d i n a t o r 1-7 1 7-7 8 7-1 8 1 6 q a -m ds @ state.p
Newslet ter Title R A I C o o r d i n a t or 1-7 1 7-7 8 7-1 8 1 6 q a - m d s @ s t a t e. p a. u s RAI Spotlight MDS 3.0 Training R AI C o o r d i n a t o r 1-7 1 7-7 8 7-1 8 1 6 q a -m ds @ state.p
Transitioning to the New IRF-PAI
 Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
Transitioning to the New IRF-PAI 2014. FIM, UDS-PROi, UDSMR, and the UDSMR logo are trademarks of, a division of UB Foundation Activities, Inc. Agenda August 2014 final rule summary Discuss IRF PPS changes
HOW PROCESS MEASURES ARE CALCULATED
 HOW PROCESS MEASURES ARE CALCULATED 1) Timely initiation in care (check at SOC and ROC) (5-star) Percentage of home health episodes of care in which the start or resumption of care date was either on the
HOW PROCESS MEASURES ARE CALCULATED 1) Timely initiation in care (check at SOC and ROC) (5-star) Percentage of home health episodes of care in which the start or resumption of care date was either on the
DATA ACCURACY A KEY FACTOR FOR SUCCESSFUL OPERATIONS
 Disclosure of Commercial Interests List the Name of Your Employer: -Executive Director -The Alliance Training Center -Providing Solutions in Health Care If consultant for organizations, only list the names
Disclosure of Commercial Interests List the Name of Your Employer: -Executive Director -The Alliance Training Center -Providing Solutions in Health Care If consultant for organizations, only list the names
Restorative Nursing: The NHA s Role and Organizational Outcomes
 Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
Restorative Nursing: The NHA s Role and Organizational Outcomes SUE LAGRANGE, RN, BSN, NHA, CDONA, CIMT DIRECTOR OF EDUCATION PATHWAY HEALTH 1 Objectives Upon completion of this program, attendees should
CMS Forms, CMS-672 and the Matrix
 CMS Forms, CMS-672 and the Matrix Contents The Matrix introduced by CMS in November 2017...2 Logic of the System...2 Links to MDS Questions...3 CMS-672...3 The MATRIX...3 Maintain Data...7 CMS-672...7
CMS Forms, CMS-672 and the Matrix Contents The Matrix introduced by CMS in November 2017...2 Logic of the System...2 Links to MDS Questions...3 CMS-672...3 The MATRIX...3 Maintain Data...7 CMS-672...7
RAPID RUG GUIDE RUG-III, VERSION GROUPER Effective for Assessments With an ARD on or After 10/1/2013
 RAPID RUG GUIDE RUG-III, VERSION 5.20 34-GROUPER Effective for Assessments With an ARD on or After 10/1/2013 Step 1: Calculation To calculate the score of Bed Mobility (G0110A), Transfer (G0110B) and Toilet
RAPID RUG GUIDE RUG-III, VERSION 5.20 34-GROUPER Effective for Assessments With an ARD on or After 10/1/2013 Step 1: Calculation To calculate the score of Bed Mobility (G0110A), Transfer (G0110B) and Toilet
Contents [1] This document has been edited for spelling and punctuation errors.
![Contents [1] This document has been edited for spelling and punctuation errors.](/thumbs/72/67584533.jpg "Contents [1] This document has been edited for spelling and punctuation errors.") Centers for Medicare & Medicaid Services SNF Quality Reporting Program Call MLN Connects National Provider Call Moderator: Leah Nguyen July 12, 2016 1:30 pm ET Contents Announcements and Introduction...
Centers for Medicare & Medicaid Services SNF Quality Reporting Program Call MLN Connects National Provider Call Moderator: Leah Nguyen July 12, 2016 1:30 pm ET Contents Announcements and Introduction...
Attachment A - Comparison of OASIS-C (Current Version) to OASIS-C1 (Proposed Data Collection)
 to OASIS-C1 (Proposed Data Collection)") Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Attachment A - Comparison of OASIS-C (Current Version) to (Proposed Data Collection) OASIS-C M0010 CMS Certification Number S M0010 CMS Certification Number M0014 Branch State S M0014 Branch State S M0016
Results from the Green House Evaluation in Tupelo, MS
 Results from the Green House Evaluation in Tupelo, MS Rosalie A. Kane, Lois J. Cutler, Terry Lum & Amanda Yu University of Minnesota, funded by the Commonwealth Fund. Academy Health Annual Meeting, June
Results from the Green House Evaluation in Tupelo, MS Rosalie A. Kane, Lois J. Cutler, Terry Lum & Amanda Yu University of Minnesota, funded by the Commonwealth Fund. Academy Health Annual Meeting, June
OASIS-C Home Health Outcome Measures
 OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
OASIS-C Home Measures 1 End Result Grooming groom self. (M1800) Grooming 2 End Result Grooming same in ability to groom self. (M1800) Grooming 3 End Result Upper Body Dressing dress upper body. (M1810)
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide
 Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide July 2012 Introduction In December 2008, The Centers for Medicare & Medicaid Services (CMS) enhanced its Nursing Home
Design for Nursing Home Compare Five-Star Quality Rating System: Technical Users Guide July 2012 Introduction In December 2008, The Centers for Medicare & Medicaid Services (CMS) enhanced its Nursing Home
Dazed and Confused: Initial Results from the IRF QRP Data
 Dazed and Confused: Initial Results from the IRF QRP Data Troy Hillman Manager, Analytical Services Uniform Data System for Medical Rehabilitation 2017 Uniform Data System for Medical Rehabilitation, a
Dazed and Confused: Initial Results from the IRF QRP Data Troy Hillman Manager, Analytical Services Uniform Data System for Medical Rehabilitation 2017 Uniform Data System for Medical Rehabilitation, a
Improving Nursing Home Compare for Consumers. Five-Star Quality Rating System
 Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
Improving Nursing Home Compare for Consumers Five-Star Quality Rating System Improving Nursing Home Compare Major Revision to Nursing Home Compare Mid-December Improved Navigation - Similar to Hospital
MDS 3.0/RUG IV Distance Learning Series January-June 2014
 MDS 3.0/RUG IV Distance Learning Series January-June 2014 ROUTE TO: Administrator; MDS Coordinator; Director of Nursing; Director of Social Services; Director of Activities; Director of Rehabilitation
MDS 3.0/RUG IV Distance Learning Series January-June 2014 ROUTE TO: Administrator; MDS Coordinator; Director of Nursing; Director of Social Services; Director of Activities; Director of Rehabilitation
Why is the Five Star Rating Important in Today s LTPAC Reimbursement World?
 Payers and Billing: Opportunities with Managed Care and Other Entities Section 3.2: Understanding LTPAC Five Star Ratings and How the Pharmacist Can Help The introduction to the User s Guide for Five Star
Payers and Billing: Opportunities with Managed Care and Other Entities Section 3.2: Understanding LTPAC Five Star Ratings and How the Pharmacist Can Help The introduction to the User s Guide for Five Star
Policy Brief. Nurse Staffing Levels and Quality of Care in Rural Nursing Homes. rhrc.umn.edu. January 2015
 Policy Brief January 2015 Nurse Staffing Levels and Quality of Care in Rural Nursing Homes Peiyin Hung, MSPH; Michelle Casey, MS; Ira Moscovice, PhD Key Findings Hospital-owned nursing homes in rural areas
Policy Brief January 2015 Nurse Staffing Levels and Quality of Care in Rural Nursing Homes Peiyin Hung, MSPH; Michelle Casey, MS; Ira Moscovice, PhD Key Findings Hospital-owned nursing homes in rural areas
Nursing Home Walk of Fame Visiting What Really Works. Call in Number
 Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
Nursing Home Walk of Fame Visiting What Really Works Call in Number 877.442.2859 Enter to Win Book Giveaways! Type in a successful practice (one or two sentences) from your nursing home in the chat box.
CMS RAI MANUAL ERRATA DOCUMENT
 CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
CMS RAI MANUAL ERRATA DOCUMENT SECTION I UTI S In Chapter 3, page I-9, under Coding Tips in I: Active Diagnoses in the Last 7 Days, a third bullet has been added: If the diagnosis of UTI was made prior
MDS 3.0 Questions. Significant change criteria - Resident's incontinence pattern changes - Does this include both bowel and bladder? Yes.
 Section A MDS 3.0 Questions Following are questions raised during OHCA s MDS 3.0 training programs. The reference information provided is based on the CMS Long-Term Care Resident Assessment Instrument
Section A MDS 3.0 Questions Following are questions raised during OHCA s MDS 3.0 training programs. The reference information provided is based on the CMS Long-Term Care Resident Assessment Instrument
QAPI Quality Assurance Process Improvement
 QAPI Quality Assurance Process Improvement Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC 2017 Final Rule in the Federal Register of January 13, 2017
QAPI Quality Assurance Process Improvement Presented by: Sharon M. Litwin, RN, BSHS, MHA, HCS D Senior Managing Partner 5 Star Consultants, LLC 2017 Final Rule in the Federal Register of January 13, 2017
On-Time Quality Improvement Manual for Long-Term Care Facilities Tools
 On-Time Quality Improvement Manual for Long-Term Care Facilities Tools Prepared for: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services 540 Gaither Road Rockville,
On-Time Quality Improvement Manual for Long-Term Care Facilities Tools Prepared for: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services 540 Gaither Road Rockville,
AVOID FINANCIAL PENALTIES BY PREPARING FOR MDS 3.0 UPDATE
 AVOID FINANCIAL PENALTIES BY PREPARING FOR MDS 3.0 UPDATE SNF QRP Quality Measures or Not? August 25, 2016 Carol Smith, RN,BSN, RAC-CT Managing Consultant csmith@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing
AVOID FINANCIAL PENALTIES BY PREPARING FOR MDS 3.0 UPDATE SNF QRP Quality Measures or Not? August 25, 2016 Carol Smith, RN,BSN, RAC-CT Managing Consultant csmith@bkd.com Suzy Harvey, RN-BC, RAC-CT Managing
5DAY = 1 AND
 July 2008 Revision Table CH. Sect. Pg. July 2008 Revision NA Title Page NA Change the revised date to July 2008 CH 2 2.2 2-11 Revise as follows: Delete the second sentence of the second paragraph, The
July 2008 Revision Table CH. Sect. Pg. July 2008 Revision NA Title Page NA Change the revised date to July 2008 CH 2 2.2 2-11 Revise as follows: Delete the second sentence of the second paragraph, The
MEASURING POST ACUTE CARE OUTCOMES IN SNFS. David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015
 MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MEASURING POST ACUTE CARE OUTCOMES IN SNFS David Gifford MD MPH American Health Care Association Atlantic City, NJ Mar 17 th, 2015 Principles Guiding Measure Selection PAC quality measures need to Reflect
MDS Training for Social Services Directors
 MDS Training for Social Services Directors Kathy Sanders RN, RAC-CT, DNSCT Sanders Consulting 630 N. 3 rd St. Tecumseh, NE 68450 Hm: (402) 335-2736 Cell: (402) 921-0250 kathy@mdshelp.com Disclaimer The
MDS Training for Social Services Directors Kathy Sanders RN, RAC-CT, DNSCT Sanders Consulting 630 N. 3 rd St. Tecumseh, NE 68450 Hm: (402) 335-2736 Cell: (402) 921-0250 kathy@mdshelp.com Disclaimer The
Chances are.. Based on my experience MDS 3.0 Update for Long Term Care PRESENTED BY 2/13/2017. New focus on Data by CMS and Regulatory Agencies
 PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
PRESENTED BY 2017 MDS 3.0 Update for Long Term Care LEAH KLUSCH EXECUTIVE DIRECTOR THE ALLIANCE TRAINING CENTER ALLIANCE, OHIO 330-821-7616 leahklusch@tatci.com New focus on Data by CMS and Regulatory
Shifting from PPS to Quality & Value
 Shifting from PPS to Quality & Value Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Celtic Consulting www.celticconsulting.org 1 Objectives Review CMS initiatives for healthcare reform based on
Shifting from PPS to Quality & Value Maureen McCarthy, RN, BS, RAC-MT, QCP-MT President/CEO Celtic Consulting www.celticconsulting.org 1 Objectives Review CMS initiatives for healthcare reform based on
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
MDS 3.0/RUG IV Distance Learning Series January - May 2016
 MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;
MDS 3.0/RUG IV Distance Learning Series January - May 2016 ROUTE TO: _Administrator; _MDS Coordinator; _Director of Nursing; _Director of Accounting; _Director of Social Services; _Director of Activities;