Social Innovation Fund (SIF) Training. Seattle, Washington October 10, 2016
|
|
|
- Kerry Hines
- 6 years ago
- Views:
Transcription
1 Social Innovation Fund (SIF) Training Seattle, Washington October 10, 2016

2 Welcome & Introductions University of Washington AIMS Center

3 Welcome & Introductions John A. Hartford Foundation Mary Jane Koren, MD Program Consultant

4 Clinic Introductions
5 Agenda Time Topic Location 8:30 Welcome, Introductions, Updates Cedar 9:45 Break 10:00 Overcoming Challenges Cedar 11:45 Lunch 12:45 Engaging Men in Depression Care Cedar 1:30 Break 1:45 Breakout A: Group PST Cedar 1:45 Breakout B: Roundtable Q&A Alder 3:00 Break 5:00 Adjourn
6 Facilities & Materials Bathrooms Lunch location Folder Name Tags Sign in sheets Evaluations
7 Social Innovation Fund We ve Come a Long Way Together Diane Powers, MA Jürgen Unützer, MD, MA, MPH
8 Timeline Nov 2011 Mar 2012 July 2012 Nov 2012 June 2013 Sept 2013 Oct 2013 June 2014 Sept 2014 Sept 2015 June 2016 Sept 2016 JAHF and UW began collaboration on grant application Grant submitted to CNCS Grant awarded RFA published by JAHF Cohort 1 clinics receive grants from JAHF First In person Training; Cohort 1 clinics launch Second RFA published by JAHF Cohort 2 clinics receive grants from JAHF Second In person Training; Cohort 2 clinics launch Third In person Training Cohort 1 completes initial 3 year grant period Final In person Training
9 SIF Initiative Overview CNCS Corporation for National and Community Service SIF Social Innovation Fund GRANTEE The John A. Hartford Foundation Contractor: University of Washington AIMS Center SUB GRANTEE WWAMI Rural Primary Care Clinics

10 Why WWAMI? Why Rural? Source County Health Rankings, Robert Wood Johnson Foundation and University of Wisconsin Population Health Institute

11 FQHCs nation s largest and fastest growing primary care network 8,000 clinics 20 million patients FQHCs are safety net 72% FQHC patients live in poverty 49% live in rural areas 36% uninsured 67% from racial/ethnic minority populations
12 Mental Health in FQHCs Mental health most commonly reported reason for visit Only 5.5% of visits include on site mental health specialist Counselor / therapist Clinical social worker Psychologist Psychiatric nurse practitioner Psychiatrist Rare in rural areas
13 Collaborative Care (aka IMPACT) Evidence based model for treating behavioral health conditions in primary care
14 Evidence based Treatments Individualized tx plan includes one or both Medications Consultant helps PCPs expand capacity Psychotherapy Modalities appropriate for primary care Brief Structured Strong evidence

15 IMPACT Summary Less depression IMPACT more than doubles effectiveness of usual care Less physical pain Better functioning Higher quality of life Greater patient and provider satisfaction More cost effective TRIPLE AIM I got my life back
16 Paradigm Shift Evidence based integrated care NOT simply specialty BH services grafted onto primary care PRIMARY CARE behavioral health Requires all providers to actively collaborate with a shared care plan, not simply practice in parallel

17 Co Location Is NOT Enough 50% or greater improvement in depression at 12 months % Participating Organizations





18 Principles of Collaborative Care Patient Centered Collaboration. Primary care and mental health providers collaborate effectively using shared care plans. Population Based Care. A defined group of patients is tracked in a registry so that no one falls through the cracks. Treatment to Target. Progress is measured regularly and treatments are actively changed until clinical goals are achieved. Evidence Based Care. Providers use treatments that have research evidence for effectiveness. Accountable Care. Providers are accountable and reimbursed for quality of care and clinical outcomes, not just volume of care.
19 Patients Treated: 4,155 As of 7/19/16 SITE Total Patients Treated CHCCW 594 Mat Su 382 Partnership 1308 Peninsula 652 Valley View 474 Bighorn 144 KANA 223 SWMCHC 378 TOTAL 4155
20 Depression Severity at Baseline Patient outcomes as of 5/1/16 Valley Cohort 1 Cohort 2 CHCCW Mat Su Partnership Peninsula Bighorn KANA SMCHC TOTAL View Sub total Sub total Baseline PHQ 9 score n=562 n=367 n=1247 n=575 n=442 n=3193 n=131 n=190 n=325 n=646 n=3839 None or Mild (0 to 9) 7% 13% 14% 7% 11% 11% 21% 27% 5% 18% 14% Moderate (10 to 14) 32% 26% 27% 27% 22% 27% 41% 32% 27% 34% 30% Moderately severe (15 to 19) 33% 31% 29% 33% 31% 31% 20% 29% 34% 28% 30% Severe (20 to 27) 28% 31% 31% 33% 36% 31% 18% 12% 33% 21% 26% Baseline PHQ 9 score (mean) % No PHQ 9 at Intake 7% 3% 5% 4% 1% 4% 14% 13% 4% 10% 7% Most recent PHQ 9 score n=560 n=367 n=1244 n=574 n=442 n=3187 n=129 n=190 n=324 n=643 n=3830 None or Mild (0 to 9) 49% 50% 42% 51% 48% 47% 63% 58% 42% 54% 40% Moderate (10 to 14) 22% 21% 24% 21% 22% 22% 20% 18% 23% 20% 21% Moderately severe (15 to 19) 18% 16% 18% 15% 17% 17% 12% 18% 17% 16% 17% Severe (20 to 27) 11% 13% 16% 14% 13% 14% 5% 6% 18% 10% 12% Most recent PHQ 9 score (mean) Average reduction in PHQ 9 from baseline to last/most recent Level of Depression at Intake among IMPACT Patients* 61% 63% 72% 63% 63% 64% 62% 73% 68% 68% 66% % 50% decrease or PHQ 9 <10* 47% 46% 36% 50% 45% 45% 50% 42% 41% 44% 45% % w/phq 9<5* 33% 32% 20% 25% 22% 26% 30% 29% 23% 27% 27% **Excludes patients with PHQ 9<10 at baseline
21 Depression Severity After Treatment Patient outcomes as of 5/1/16 Valley Cohort 1 Cohort 2 CHCCW Mat Su Partnership Peninsula Bighorn KANA SMCHC TOTAL View Sub total Sub total Baseline PHQ 9 score n=562 n=367 n=1247 n=575 n=442 n=3193 n=131 n=190 n=325 n=646 n=3839 None or Mild (0 to 9) 7% 13% 14% 7% 11% 11% 21% 27% 5% 18% 14% Moderate (10 to 14) 32% 26% 27% 27% 22% 27% 41% 32% 27% 34% 30% Moderately severe (15 to 19) 33% 31% 29% 33% 31% 31% 20% 29% 34% 28% 30% Severe (20 to 27) 28% 31% 31% 33% 36% 31% 18% 12% 33% 21% 26% Baseline PHQ 9 score (mean) % No PHQ 9 at Intake 7% 3% 5% 4% 1% 4% 14% 13% 4% 10% 7% Most recent PHQ 9 score n=560 n=367 n=1244 n=574 n=442 n=3187 n=129 n=190 n=324 n=643 n=3830 None or Mild (0 to 9) 49% 50% 42% 51% 48% 47% 63% 58% 42% 54% 40% Moderate (10 to 14) 22% 21% 24% 21% 22% 22% 20% 18% 23% 20% 21% Moderately severe (15 to 19) 18% 16% 18% 15% 17% 17% 12% 18% 17% 16% 17% Severe (20 to 27) 11% 13% 16% 14% 13% 14% 5% 6% 18% 10% 12% Most recent PHQ 9 score (mean) Average reduction in PHQ 9 from baseline to last/most recent Level of Depression at Intake among IMPACT Patients* 61% 63% 72% 63% 63% 64% 62% 73% 68% 68% 66% % 50% decrease or PHQ 9 <10* 47% 46% 36% 50% 45% 45% 50% 42% 41% 44% 45% % w/phq 9<5* 33% 32% 20% 25% 22% 26% 30% 29% 23% 27% 27% **Excludes patients with PHQ 9<10 at baseline
22 Response More than Double Usual Care Patient outcomes as of 5/1/16 Valley Cohort 1 Cohort 2 CHCCW Mat Su Partnership Peninsula Bighorn KANA SMCHC TOTAL View Sub total Sub total Baseline PHQ 9 score n=562 n=367 n=1247 n=575 n=442 n=3193 n=131 n=190 n=325 n=646 n=3839 None or Mild (0 to 9) 7% 13% 14% 7% 11% 11% 21% 27% 5% 18% 14% Moderate (10 to 14) 32% 26% 27% 27% 22% 27% 41% 32% 27% 34% 30% Moderately severe (15 to 19) 33% 31% 29% 33% 31% 31% 20% 29% 34% 28% 30% Severe (20 to 27) 28% 31% 31% 33% 36% 31% 18% 12% 33% 21% 26% Baseline PHQ 9 score (mean) % No PHQ 9 at Intake 7% 3% 5% 4% 1% 4% 14% 13% 4% 10% 7% Most recent PHQ 9 score n=560 n=367 n=1244 n=574 n=442 n=3187 n=129 n=190 n=324 n=643 n=3830 None or Mild (0 to 9) 49% 50% 42% 51% 48% 47% 63% 58% 42% 54% 40% Moderate (10 to 14) 22% 21% 24% 21% 22% 22% 20% 18% 23% 20% 21% Moderately severe (15 to 19) 18% 16% 18% 15% 17% 17% 12% 18% 17% 16% 17% Severe (20 to 27) 11% 13% 16% 14% 13% 14% 5% 6% 18% 10% 12% Most recent PHQ 9 score (mean) Average reduction in PHQ 9 from baseline to last/most recent Level of Depression at Intake among IMPACT Patients* 61% 63% 72% 63% 63% 64% 62% 73% 68% 68% 66% % 50% decrease or PHQ 9 <10* 47% 46% 36% 50% 45% 45% 50% 42% 41% 44% 45% % w/phq 9<5* 33% 32% 20% 25% 22% 26% 30% 29% 23% 27% 27% **Excludes patients with PHQ 9<10 at baseline
23 Remission Rate VERY Impressive 5 points higher than last year Patient outcomes as of 5/1/16 Valley Cohort 1 Cohort 2 CHCCW Mat Su Partnership Peninsula Bighorn KANA SMCHC TOTAL View Sub total Sub total Baseline PHQ 9 score n=562 n=367 n=1247 n=575 n=442 n=3193 n=131 n=190 n=325 n=646 n=3839 None or Mild (0 to 9) 7% 13% 14% 7% 11% 11% 21% 27% 5% 18% 14% Moderate (10 to 14) 32% 26% 27% 27% 22% 27% 41% 32% 27% 34% 30% Moderately severe (15 to 19) 33% 31% 29% 33% 31% 31% 20% 29% 34% 28% 30% Severe (20 to 27) 28% 31% 31% 33% 36% 31% 18% 12% 33% 21% 26% Baseline PHQ 9 score (mean) % No PHQ 9 at Intake 7% 3% 5% 4% 1% 4% 14% 13% 4% 10% 7% Most recent PHQ 9 score n=560 n=367 n=1244 n=574 n=442 n=3187 n=129 n=190 n=324 n=643 n=3830 None or Mild (0 to 9) 49% 50% 42% 51% 48% 47% 63% 58% 42% 54% 40% Moderate (10 to 14) 22% 21% 24% 21% 22% 22% 20% 18% 23% 20% 21% Moderately severe (15 to 19) 18% 16% 18% 15% 17% 17% 12% 18% 17% 16% 17% Severe (20 to 27) 11% 13% 16% 14% 13% 14% 5% 6% 18% 10% 12% Most recent PHQ 9 score (mean) Average reduction in PHQ 9 from baseline to last/most recent Level of Depression at Intake among IMPACT Patients* 61% 63% 72% 63% 63% 64% 62% 73% 68% 68% 66% % 50% decrease or PHQ 9 <10* 47% 46% 36% 50% 45% 45% 50% 42% 41% 44% 45% % w/phq 9<5* 33% 32% 20% 25% 22% 26% 30% 29% 23% 27% 27% **Excludes patients with PHQ 9<10 at baseline
 Fewer call attempts to reach patients")
24 Augmenting Collaborative Care Engagement Patient education In-app interventions Automated reminders for self-monitoring and medication taking Patient satisfaction Convenient patients can check in remotely at the time they prefer Secure and private communication Provider efficiency Less provider documentation (patients enter their own symptom scores) Fewer call attempts to reach patients Enhancing treatment-to-target Current information on patient status







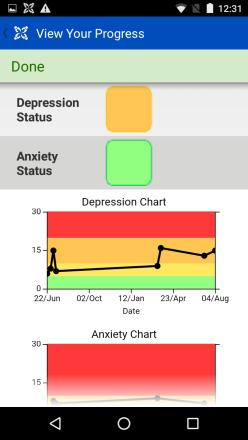
25 Smartphone App Design Check In Outcomes Monitoring Progress Graph Scores Learn More Educational Content Call for Help Personalized Contacts Your Info Customizable Reminders, Content


26 Patient Generated Data integrated into Clinical Registry
27 CHCCW Pilot Patient Feedback The reminders were wonderful, had forgotten and when the reminder popped up, immediately took PHQ 9. [PHQ 9] took only a minute is discreet enough even if you were in a public setting. Great idea, especially for people who live far from a doctor.
28 SIF Evaluation Requirement CNCS requires evaluation as part of SIF Meeting intended outcomes and impacts Understanding how program is successful How program can be improved Building on lessons learned for future projects 28
29 Evaluation Purpose Understand Effect on Clinics Effect on Providers Effect on Patients Use information to help other rural clinics with implementation 29
30 Effect on Clinics Clinic experience implementing IMPACT Information about the organization (survey) Organizational information about their efforts to implement IMPACT (interview) Leadership surveys Pre Launch 18 months Post Launch Cohort 1 End of Grant Cohort 2 End of Grant (June 2017)
31 Effect on Providers Provider experience implementing IMPACT Primary care providers, psychiatric consultants, care managers, behavioral health providers, clinical supervisors and others Provider surveys 18 months Post Launch Survey Interview (optional)
32 Patient Demographics CHCCW Mat Su Partnership Peninsula Valley View Bighorn KANA SWMCHC All Organizations % n % n % n % n % n % n % n % n % n Total* Gender Women 72% % % % % % 83 68% % % 2607 Age group Men 28% % % % % % 48 32% 60 28% 92 32% 1218 <18 2% 10 1% 5 1% 13 2% 10 <1% 3 2% 3 12% 22 <1% 1 2% to 34 46% % % % % % 42 39% 74 38% % to 54 37% % % % % % 55 34% 65 36% % to 74 14% 80 21% 76 21% % 73 24% % 28 11% 21 19% 63 18% and older 1% 7 2% 8 1% 17 0% 0 % 3 2% 3 4% 8 6% 21 2% 67 Race American Indian / Alaska Native 1% 5 1% 5 3% 38 <1% 5 3% 12 48% 63 81% 153 3% 9 8% 290 Asian <1% 3 <1% 3 <1% 2 2% 11 <1% 3 0% 0 1% 2 0% 0 <1% 24 African American 2% 12 2% 7 <1% 6 3% 20 <1% 2 0% 0 1% 2 <1% 2 1% 51 Pacific Islander 0% 0 0% 0 <1% 6 2% 9 1% 4 0% 0 0% 0 <1% 1 <1 20 White 89% % % % % % 65 11% 22 91% % 3201 Mixed Race / Other 3% 14 <1% 1 <1% 9 3% 15 2% 7 0% 0 2% 3 <1% 2 1% 51 Unknown/Not reported 5% 29 5% 17 <1% 4 2% 9 12% 50 2% 3 4% 7 5% 14 4% 133 *Excludes patients without an initial PHQ 9
33 Effect on Patients Patient experience Symptoms, Quality of life, Economic well being Data Primary: Online care management registry (CMTS) Secondary: Clinic administrative data systems Secondary: Patient survey Cohort 1 & 2 33
34 Progress to Date: Economic Outcomes Clinic Administrative Data UDS data Cohort 1 complete Cohort 2 June 2017
35 Questions?
36 BREAK
37 Overcoming Common Challenges: Maintaining Caseload and Engagement Issues CHCCW KANA Bighorn
38 Overcoming Common Challenges: CHCCW Social Innovation Fund October 2016
39 Challenges Identified High turn over rates: providers, CMAs and dental assistants. Direct correlation with patients volume.
40 How Did We Know? Decrease in warm connections calls Drop in number of referrals Decrease in number of appointments Inconsistent screening Change in Care manager FTE, from 1.75 to 1.5 (October 2015)
41 Retention/Recruitment of Providers Recruitment to a rural place like Wyoming can be difficult. We definitely have shortages in the state, said Joe Steiner, dean of health sciences at the University of Wyoming. A lot of physicians are reaching retirement age. There s a pretty high demand for medical care across the state.
42 Recruitment Challenges in the Region The most often identified challenging position to recruit was Physician Family Practice without OB Clinical positions are much more difficult to fill than administrative positions The most often identified position with challenging turnover was Medical Assistant 2014 CHAMPS Region VIII Health Centers
43 Casper, Wyoming Industry Wyoming s economy is vulnerable to swings in commodities prices and global price competition. When the U.S. is doing well, Wyoming has more economic difficulties. Wyoming Department of Employment, Occupational Outlook 2010
44 Current Economic Environment Unemployment rates have increased with the decline in oil prices: statewide average in June was 5.7%, Natrona county 7.8%. Some individuals retained employment with a decrease in pay as high as 70%.
45 Weather Annual high temperature 59.2,low is 31.3 Average rainfall of inches Average snowfall of 75 inches We have the most wind in the US: average of 12.9 mph, but can reach 65 mph or higher.
46 The Challenge CHCCW s turn over rates between 2015 and 2016: 10 providers 8 dental assistants 20 Certified Medical Assistants OB/GYN department closed February 2016 Providers rotating between Quick Care and Family medicine Employees leaving town with spouses who lost jobs in the energy industry Employees leaving for other opportunities with higher pay/working multiple jobs to support families during difficult economic time


47 Turnover Last Day Job Title 1/2/ /25/ /31/ /30/ /9/ /18/ /27/ /11/ /30/ /8/201 5 Physicians Assistant Physicians Assistant Physician Physician Physician Nurse Practitioner Nurse Practitioner Nurse Practitioner Dentist Dentist
48 How the Challenge Looks in the Registry March 2015
49 Active Caseload 2015 April patients May June July August September PCP, NP left October 2015 November December IMPACT Champion PCP left OB/GYN left
50 Active Caseload 2016 January February 2016 March 2016 April 2016 May 2016 June July 2016 August 81 September OB/GYN department closed down 71 OB/GYN, CMO and PCP, NP left 71 RN Coordinator left 72 Hired MD, new CMO, Champion PCP 75 Hired NP, PCP
51 Addressing the Challenge Orientation to the IMPACT Model New Champion Provider Radke, MD (May 2016) New Primary Care Providers Quick Care Providers as PCPs Acclimating to the collaborative model Identifying schedule for consultation The cost benefit of collaborative care, 6:1 ratio Medical Assistants The importance of the MA role in identifying depression On going training Screening for depression is the 5th vital sign Communication with provider Not assuming the role of a mental health provider


52 Current Active Caseload
53 Discussion Is retention/recruitment a challenge in your clinic? What are some strategies you have used to minimize turn over?

54 IMPACT Challenges: Year 1 Kodiak Area Native Association SIF and John E Hartford Subgrantee Cohort 2 Year 2


55 Clinic Setting Kodiak Area Native Association is a non profit serving Alaska Natives, veterans and, since 2015, other community members in the Koniag region. KANA provides medical, dental, behavioral health and community services to citizens of Kodiak and the six rural communities on the island. In 2015, HRSA grant facilitated the opening of the new Mill Bay, which provides clinical services primarily to non Native patients. Total Patients at KANA 2789 Uninsured 45% Medicaid/Medicare 30% Commercial Insurance 25%
56 A Challenge We ve Identified Lower than expected enrollment numbers Anticipation that Mill Bay Clinic opening would increase enrollment. Monthly reports are not showing an increase. Today s Presentation Ongoing efforts to identify solutions Hypotheses moving forward Possible future solutions
57 How the Challenge Looks in the Registry SITE Care Mgr FTE Care Mgr Type Total Patients Treated Active Caseload Goal Minimum 1 Active Caseload 2 Contact >2months Active Caseload: % of Minimum 5+ Point Decrease 50%+ Decrease After at Least 10 Weeks Psychiatric Consultation 3 KANA June 2015 KANA Jan 2016 KANA April All in one % 46% 76% 83% 1 All in one % 36% 69% 69% 1.5 All in one % 47% 69% 63% Expectation that the opening of the Mill Bay clinic (October, 2015) would increase enrollment is not reflected in data. Note: data pulled from months when low enrollment could not be accredited to recent Care Manager turnover


58 Addressing the Challenge Hypothesis no.1: Low PHQ 9 completion rate: we aren t identifying clients in need of treatment. Solutions put into place: incorporate program information in to PHQ 9 so patients understand the purpose of the survey Remove patient name, use MRN to increase privacy Care managers will collect ALL PH 9s and count them against clinic visits to tabulate actual completion rate Re train front desk staff with script for delivering the PHQ 9 to patients
59 Data Obtained from PHQ 9 Collection May June July August Lost in the Workflow: Main 49% 61% 72% 65% Lost in the Workflow: MB 36% 45% 54% 52% These percents represent the proportion of PHQ 9s that don't get returned to the Care Manager. Reasons could include Patient leaves in waiting room, patient discardes, stuffed in pocket/bag, nurse doesn't get to review due to pressing medical issue, etc. Refused: Main 11% 15% 17% 20% Refused: MB 15% 15% 14% 20%
60 Addressing the Challenge cont. Hypothesis 2: Lack of collaborative approach Solution: Review workflow with front desk staff, ensure PHQ 9s are handed out every time. Ensure nurse staff gives patient PHQ 9 if is hasn t been completed in waiting room. Review language used by medical staff eliminate referral language and review team language
61 How it Looks Now in the Registry SITE Care Mgr FTE Care Mgr Type Total Patients Treated Active Caseload Goal Minimum 1 Active Caseload 2 Contact >2months Active Caseload: % of Minimum 5+ Point Decrease 50%+ Decrease After at Least 10 Weeks Psychiatric Consultation 3 KANA present 1.5 All in one % 42% 62% 65% Why no improvement? What we learned: While front desk staff and medical staff are all playing their part in the work flow, we have a high number of surveys that are not making it all the way through the workflow, and a number of clients declining to complete the survey which is limiting our new referrals. Hypotheses moving forward: 1. With a geographically limited population, do we have a limited number of people who will respond to our current approach 2. New cultural demographics added (military, Phillipino) means we have to explore cultural significance of reporting depression symptoms 3. Need to re examine program material may be too dense for patients
62 Continued Challenges, Questions, Concerns Work we plan to continue: Re examine IMPACT literature for maximum clarity and increased completion rates. Continue to hone teamwork efforts to unify all staff working on patients team. Work we plan to start: Take a deeper look at cultural and practical barriers that may be preventing patients from filling out the PHQ 9 and determine resolutions.
63 Discussion Interested in other clinics experience/success using PHQ 2 vs PHQ 9 Interested in other clinics experience with patients declining to fill out the PHQ 9 and solutions

64 Overcoming Common Challenges Social Innovation Fund October 2016
65 Clinic Setting Located In: Ashland, Montana Hardin, Montana Clinic serves 70% BVHC patients are Tribal Members 10% BVHC patients are 65 years and over 13% BVHC patients on Medicaid
66 Program Specifics 1 full time care manager/therapist 1 psych consultant 6 full time Primary Care Providers 3 part time Primary Care Providers
67 A Challenge We ve Identified Low Retention rates of patients IMACT program not reaching goal of minimum active case load Losing pt. in the IMACT program process Majority of pt. with high PHQ 9 also have chronic pain as chief complaint and were not returning to address depression symptoms
68 How it Looked in the Registry SITE Care Mgr FTE Care Mgr Type Total Patients Treated Active Caseload Goal Minimum 1 September 2015 Active Caseload 2 Contact >2months Active Caseload: % of Minimum 5+ Point Decrease 50%+ Decrease After at Least 10 Weeks Psychiatric Consultation 3 Bighorn 0.5 Shared % 64% 89% 88%
69 Addressing the Challenge Failures Wait for pt. to contact us after missing apt. Mail reminders Have only one contact phone number
70 Addressing the Challenge Successes Combined Care manger and Therapist one full time position Get everyone on board of understanding program Competition with PCP to see their referral stats Meet with team to identify trends (Chronic Pain and Depression) Large number of chronic pain patents not returning but the care manger gives the pt. their script after meeting with them. This has improved treatment outcomes!

71 How it Looks Now in the Registry
72 Chronic Pain and Depression in Registry Patient 1 Patient 2 DATE OF CONTACT CONTACT TYPE WEEKS IN TX PHQ- 9 DATE OF CONTACT CONTACT TYPE WEEKS IN TX PHQ- 9 12/2/2015 Initial Visit /31/2015 Psychiatric Consultation Note 4 1/11/2016 Follow Up /20/2016 Follow Up /25/2016 Psychiatric Consultation Note 7 2/29/2016 Follow Up /17/2016 Follow Up /25/2016 Follow Up /25/2016 Psychiatric Consultation Note 20 5/10/2016 Follow Up 22 5/17/2016 Follow Up /24/2016 Follow Up /14/2016 Follow Up /10/2015 Initial Visit /30/2015 Follow Up /7/2015 Follow Up /21/2015 Follow Up /31/2015 Psychiatric Consultation Note 7 1/4/2016 Follow Up /26/2016 Follow Up /2/2016 Follow Up /14/2016 Psychiatric Consultation Note 17 3/22/2016 Follow Up /20/2016 Follow Up 23 5/12/2016 Relapse Prevention Plan /7/2016 Discharge 30 6/15/2016 Relapse Prevention Plan 28 1
73 Chronic Pain and Depression in Registry Patient 3 Patient 4 Date of Contact Type Contact DATE OF CONTACT CONTACT TYPE WEEKS IN TX PHQ-9 7/31/2015 Initial Visit 0 9 8/6/2015 Follow Up 0 8 9/10/2015 Follow Up /19/2015 Follow Up /30/2015 Psychiatric Consultation Note 13 11/2/2015 Psychiatric Consultation Note 13 11/13/2015 Follow Up /20/2015 Follow Up /14/2015 Psychiatric Consultation Note 19 12/14/2015 Psychiatric Consultation Note 19 12/15/2015 Follow Up /22/2015 Follow Up /31/2015 Follow Up 21 1/20/2016 Follow Up /25/2016 Psychiatric Consultation Note 25 2/3/2016 Follow Up /17/2016 Follow Up /22/2016 Psychiatric Consultation Note 29 2/24/2016 Follow Up /23/2016 Follow Up 33 4/20/2016 Relapse Prevention Plan /11/2016 Follow Up /7/2016 Discharge 44 Weeks in Tx 6/4/2015 Initial Visit /25/2015 Psychiatric Consultation Note 3 10/20/2015 Follow Up /20/2015 Psychiatric Consultation Note 19 11/6/2015 Follow Up /9/2015 Follow Up 22 11/30/2015 Follow Up 25 12/4/2015 Follow Up /14/2015 Psychiatric Consultation Note 27 1/26/2016 Follow Up /22/2016 Psychiatric Consultation Note 37 2/29/2016 Follow Up /7/2016 Follow Up 39 3/15/2016 Follow Up /22/2016 Follow Up /5/2016 Follow Up /20/2016 Follow Up /2/2016 Psychiatric Consultation Note 47 6/7/2016 Relapse Prevention Plan /7/2016 Follow Up /28/2016 Discharge 60 PHQ 9
74 Continued Challenges, Questions, Concerns High Nomadic Population Chronic pain Depression or pill seeking? Poverty Phone coverage Internet access Mail Dispersed Population No Public Transportation Family Dynamics
75 Continue to Improve Continue to look at trends Continue to be flexible and make changes accordingly Continue to communicate with team and pt. to strive for improvement
76 Overcoming Common Challenges: Maintaining the Model of Care Issues SWMCHC Peninsula Partnership
77 Overcoming Common Challenges Social Innovation Fund October 2016
 Depression/Mood disorder Visits (2015) 5,742 Depression is the highest diagnosis in our clinic, close to half of all patients we")
78 Clinic Setting Organization FQHC established 1986 Serves approximately 13,000 unique patients/yr Locations Butte, MT Dillon, MT Sheridan, MT (Pharmacy) Patients (2015 # s) 24% Medicaid 13% Medicare 31% Uninsured 32% Private Insurance (Increase ACA) Depression/Mood disorder Visits (2015) 5,742 Depression is the highest diagnosis in our clinic, close to half of all patients we see
79 A Challenge We ve Identified Reluctance to discharge patients with 2 months of no contact High need patients that we want to track but have not been able to successfully contact Many contacts attempts are made, but for a variety of reasons, we are unable to have that positive contact Due to busy schedules, multiple responsibilities, wanting to track patients this occasionally does not happen

80 How the Challenge Looks in the Registry
81 Addressing the Challenge Our Shared Care Managers have worked hard to manage their caseloads Implemented policy of 30 days and 3 contact attempts At 30 days from first contact attempt, if we are unable to contact the patient, then we will discharge them from IMPACT Always willing to re admit them into IMPACT

82 How it Looks Now in the Registry
83 Continued Challenges, Questions, Concerns Staff turnover Burnout
84 Discussion

85 Overcoming Common Challenges Peninsula Community Health Services October 2016
86 Clinic Setting PCHS opened its doors in 1987 In 1988 we had 11 staff Serving over 2,211 patients 87% of patients had a household income of less than $1,000 a month In 1993 became FQHC Fast forward to 2015: Nearly 200 staff Serving over 24,000 patients
87 A Challenge We ve Identified Maintaining a more even distribution of 2 contacts per month 1 via in person 1 via phone Phone contacts are difficult due to: Transient nature of patients Patients with limited phone minutes Time for Care Manager to make calls
88 How the Challenge Looks in the Registry
89 Addressing the Challenge Hired administrative staff to assist with other BH programs to free up Care Manager time Focus on schedule optimization Designated admin time for phone contacts
90 How it Looks Now in the Registry
91 Continued Challenges, Questions, Concerns Inaccurate contact numbers Challenge with connecting with patients in timely manner Access issues Continue scheduling optimization Consider expanding roles and responsibilities of non clinical staff to assist with contacts
92 Discussion How are you, as Care Managers, able to complete 2 contacts per month with one via in person and one via phone?
93 Overcoming Common Challenges: Partnership Social Innovation Fund October 2016

94 Partnership Health Center

95 Clinic Setting Location Missoula, MT Organization Established in 1989 FQHC established in ,092 unique patients in ,395 unique patients in 2015 Patients in 2012: 62% Self pay 19% Medicare 11% Medicaid 9% Private Pay Patients in 2015: 39% Self pay 14% Medicare 20% Medicaid 27% Private Pay
96 A Challenge We ve Identified PHQ9 completion rates lower in Behavioral Health compared to the medical clinic. Medical clinic completion rate 76.1% in Tracked using the depression screening UDS measure.

97 How the Challenge Looks in the Registry Completion of PHQ9 with Patients
98 Addressing the Current Challenge Discussing in staff meetings how care managers and therapists introduce the PHQ9 to patients. Identifying successful strategies for completing PHQ9 during follow up calls. Ex.: mailing patient a copy of the PHQ9.

99 How it Looks Now in the Registry
100 Continued Challenges, Questions, Concerns Continued Challenge Decreasing completion rates of PHQ9. Trying to identify what changed between the spring to now. Was the previous workflow more effective?
101 Discussion Have other clinics set goals for PHQ9 completion? Strategies used to engage patient in completing PHQ9 when they express screener burnout.
102 LUNCH
Overcoming Common Challenges: Maintaining Caseload and Engagement Issues. CHCCW KANA Bighorn
 Overcoming Common Challenges: Maintaining Caseload and Engagement Issues CHCCW KANA Bighorn Overcoming Common Challenges: CHCCW Social Innovation Fund October 2016 Challenges Identified High turn over
Overcoming Common Challenges: Maintaining Caseload and Engagement Issues CHCCW KANA Bighorn Overcoming Common Challenges: CHCCW Social Innovation Fund October 2016 Challenges Identified High turn over
Social Innovation Fund (SIF) Training. Welcome & Introductions. Welcome & Introductions. Seattle, Washington September 27-28
 Training. Welcome & Introductions. Welcome & Introductions. Seattle, Washington September 27-28") Social Innovation Fund (SIF) Training Seattle, Washington September 27-28 Welcome & Introductions John A. Hartford Foundation Welcome & Introductions University of Washington AIMS Center 1 Implementing
Social Innovation Fund (SIF) Training Seattle, Washington September 27-28 Welcome & Introductions John A. Hartford Foundation Welcome & Introductions University of Washington AIMS Center 1 Implementing
Social Innovation Fund (SIF)
") Welcome & Social Innovation Fund (SIF) Pre-Launch Training John A. Hartford Foundation Seattle, Washington September 14-15, 2013 Welcome & Implementing IMPACT University of Washington AIMS Center 1. Lay
Welcome & Social Innovation Fund (SIF) Pre-Launch Training John A. Hartford Foundation Seattle, Washington September 14-15, 2013 Welcome & Implementing IMPACT University of Washington AIMS Center 1. Lay
Creating the Collaborative Care Team
 Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
Creating the Collaborative Care Team Social Innovation Fund July 10, 2013 Social Innovation Fund Corporation for National & Community Service Federal Funder The John A. Hartford Foundation Philanthropic
RPC and OMH Collaborative Care Webinar. February 1, pm
 RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
RPC and OMH Collaborative Care Webinar February 1, 2018 1 2pm AGENDA Welcome & Introductions OMH Care Collaborative Overview Q&A Cathy Hoehn, LMHC RPC Initiative Director CH@clmhd.org 518 396 0788 www.clmhd.org/rpc
Integrated Mental Health Care. Questions
 Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Integrated Mental Health Care Closing the gap between what we know and what we do. Jürgen Unützer, MD, MPH, MA Questions Due to the large number of participants, it is not practical to take questions over
Overview Report Context. Getting Started with Monthly Overview Reports. Materials Needed. Metrics Captured In Overview Report
 SIF Webinar: Overview Reporting and Organizational Relapse Prevention Planning Overview Report Context Getting Started with Monthly Overview Reports Juliann Salisbury Program Assistant, UW AIMS Center
SIF Webinar: Overview Reporting and Organizational Relapse Prevention Planning Overview Report Context Getting Started with Monthly Overview Reports Juliann Salisbury Program Assistant, UW AIMS Center
Best Management Practices In Integrated Behavioral Health/Primary Care Programs
 Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Community Care of North Carolina
 Community Care of North Carolina 2007 Community Care of North Carolina Mail Service Center 2009 Raleigh, NC 27699-2009 (919) 715-1453 www.communitycarenc.com Background Several networks in the Community
Community Care of North Carolina 2007 Community Care of North Carolina Mail Service Center 2009 Raleigh, NC 27699-2009 (919) 715-1453 www.communitycarenc.com Background Several networks in the Community
Physician Workforce Fact Sheet 2016
 Introduction It is important to fully understand the characteristics of the physician workforce as they serve as the backbone of the system. Supply data on the physician workforce are routinely collected
Introduction It is important to fully understand the characteristics of the physician workforce as they serve as the backbone of the system. Supply data on the physician workforce are routinely collected
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers. Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW
 Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Behavioral Health Billing and Coding Guide for Montana FQHCs & Primary Care Providers Virna Little, PsyD, LCSW-R, SAP, CCM Laura Leone, MSSW, LMSW Objectives Answer questions specific to FQHC and Primary
Health Center Program Update
 Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE
 9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
9/26/213 REPORTING METRICS FOR INTEGRATION OF PHYSICAL-BEHAVIORAL HEALTH CARE MARISA DERMAN, MD, MSC (OMH) M. ASHLEY HEALD, MA (UW) OBJECTIVES FOR THIS WEBINAR Review goals/ standards Review mandatory
Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center
 Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center Advancing Integrated Mental Health Solutions The Healthier
Financing and Sustainability Strategies for Behavioral Health Integration Anna Ratzliff, MD, PhD Associate Director for Education AIMS Center Advancing Integrated Mental Health Solutions The Healthier
INVESTING IN INTEGRATED CARE
 INVESTING IN INTEGRATED CARE The Maine Health Access Foundation s 12 year journey (2005 2016) to improve patient centered care in Maine through the Integrated Care Initiative. Table of Contents The MeHAF
INVESTING IN INTEGRATED CARE The Maine Health Access Foundation s 12 year journey (2005 2016) to improve patient centered care in Maine through the Integrated Care Initiative. Table of Contents The MeHAF
Collaborative Care (IMPACT)- An Overview June 11, 2015
- An Overview June 11, 2015") Collaborative Care (IMPACT)- An Overview June 11, 2015 1 2 Mental Health in the US Depression is the leading cause of disability worldwide ~7% of US adults experienced major depression at least once during
Collaborative Care (IMPACT)- An Overview June 11, 2015 1 2 Mental Health in the US Depression is the leading cause of disability worldwide ~7% of US adults experienced major depression at least once during
Fostering Effective Integration of Behavioral Health and Primary Care in Massachusetts Guidelines. Program Overview and Goal.
 Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
RN Behavioral Health Care Manager in Primary Care Settings
 RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
RN Behavioral Health Care Manager in Primary Care Settings Integrated Care and the Expanding Role of Nurses Seattle Airport Marriott, SeaTac, WA Tuesday, January 9, 2018 The Healthier Washington Practice
Not to be completed by paper. Please complete online.
 2018 Survey of Community Health Centers Experiences and Activities under the Affordable Consent Form and Information Sheet about the Research Study (IRB #: 101705) Not to be completed by paper. Please
2018 Survey of Community Health Centers Experiences and Activities under the Affordable Consent Form and Information Sheet about the Research Study (IRB #: 101705) Not to be completed by paper. Please
Selected State Background Characteristics
 State Profile: Florida Selected State Background Characteristics Population Total Pop. (millions) 17.4 293.7 Pop. 60+ (thousands) 3,787.4 48,883.4 % 60+ 21.8 16.6 National Ranking 60+ 1 % White (60+) 79.3
State Profile: Florida Selected State Background Characteristics Population Total Pop. (millions) 17.4 293.7 Pop. 60+ (thousands) 3,787.4 48,883.4 % 60+ 21.8 16.6 National Ranking 60+ 1 % White (60+) 79.3
Integrated Behavioral Health Services
 Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Integrated Behavioral Health Services Anitra Walker, LCSW Liz Frye, MD, MPH Integrated Behavioral Health Background SHLI Integrated Care Initiative started in July 2011 2 initial demonstration sites; Focus
Transforming Healthcare Delivery, the Challenges for Behavioral Health
 Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Selected State Background Characteristics
 State Profile: Louisiana Selected State Background Characteristics Population Total Pop. (millions) 4.5 293.7 Pop. 60+ (thousands) 719.0 48,883.4 % 60+ 15.9 16.6 National Ranking 60+ 40 % White (60+) 73.3
State Profile: Louisiana Selected State Background Characteristics Population Total Pop. (millions) 4.5 293.7 Pop. 60+ (thousands) 719.0 48,883.4 % 60+ 15.9 16.6 National Ranking 60+ 40 % White (60+) 73.3
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Behavioral Health Integration in the Primary Care Setting
 Behavioral Health Integration in the Primary Care Setting Rajvee Vora, MD,MS Director, Ambulatory Behavioral Health for DSRIP Implementation Health Solutions, Northwell Health Assistant Professor, Department
Behavioral Health Integration in the Primary Care Setting Rajvee Vora, MD,MS Director, Ambulatory Behavioral Health for DSRIP Implementation Health Solutions, Northwell Health Assistant Professor, Department
THE UTILIZATION OF MEDICAL ASSISTANTS IN CALIFORNIA S LICENSED COMMUNITY CLINICS
 THE UTILIZATION OF MEDICAL ASSISTANTS IN CALIFORNIA S LICENSED COMMUNITY CLINICS Tim Bates and Susan Chapman UCSF Center for the Health Professions Overview Medical Assistants (MAs) play a key role as
THE UTILIZATION OF MEDICAL ASSISTANTS IN CALIFORNIA S LICENSED COMMUNITY CLINICS Tim Bates and Susan Chapman UCSF Center for the Health Professions Overview Medical Assistants (MAs) play a key role as
THE NYS COLLABORATIVE CARE INITIATIVE:
 THE NYS COLLABORATIVE CARE INITIATIVE: RAISING THE STANDARDS FOR DEPRESSION CARE Jay Carruthers, MD Project Manager August 27, 2014 NYS CCI: OVERVIEW How far have we come in advancing implementation of
THE NYS COLLABORATIVE CARE INITIATIVE: RAISING THE STANDARDS FOR DEPRESSION CARE Jay Carruthers, MD Project Manager August 27, 2014 NYS CCI: OVERVIEW How far have we come in advancing implementation of
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion. All Ohio Institute on Community Psychiatry March 25, 2017
 Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Implementation of Ohio SBIRT in an Integrated Health Center: Panel Discussion All Ohio Institute on Community Psychiatry March 25, 2017 SBIRT Panelists: Introduction Ellen Augsperger Director of Ohio SBIRT
Psychiatric Consultant Guide CMTS. Care Management Tracking System. University of Washington aims.uw.edu
 Psychiatric Consultant Guide CMTS Care Management Tracking System University of Washington aims.uw.edu rev. 8/13/2018 Table of Contents TOP TIPS & TRICKS... 1 INTRODUCTION... 2 PSYCHIATRIC CONSULTANT ACCOUNT
Psychiatric Consultant Guide CMTS Care Management Tracking System University of Washington aims.uw.edu rev. 8/13/2018 Table of Contents TOP TIPS & TRICKS... 1 INTRODUCTION... 2 PSYCHIATRIC CONSULTANT ACCOUNT
Selected State Background Characteristics
 State Profile: Nevada Selected State Background Characteristics Population Total Pop. (millions) 2.3 293.7 Pop. 60+ (thousands) 369.0 48,883.4 % 60+ 15.8 16.6 National Ranking 60+ 42 N/A % White (60+)
State Profile: Nevada Selected State Background Characteristics Population Total Pop. (millions) 2.3 293.7 Pop. 60+ (thousands) 369.0 48,883.4 % 60+ 15.8 16.6 National Ranking 60+ 42 N/A % White (60+)
Selected State Background Characteristics
 State Profile: Alabama Selected State Background Characteristics Population Total Pop. (millions) 4.5 293.7 Pop. 60+ (thousands) 810.1 48,883.4 % 60+ 17.9 16.6 National Ranking 60+ 15 % White (60+) 79.8
State Profile: Alabama Selected State Background Characteristics Population Total Pop. (millions) 4.5 293.7 Pop. 60+ (thousands) 810.1 48,883.4 % 60+ 17.9 16.6 National Ranking 60+ 15 % White (60+) 79.8
Site Manager Guide CMTS. Care Management Tracking System. University of Washington aims.uw.edu
 Site Manager Guide CMTS Care Management Tracking System University of Washington aims.uw.edu rev. 8/13/2018 Table of Contents INTRODUCTION... 1 SITE MANAGER ACCOUNT ROLE... 1 ACCESSING CMTS... 2 SITE NAVIGATION
Site Manager Guide CMTS Care Management Tracking System University of Washington aims.uw.edu rev. 8/13/2018 Table of Contents INTRODUCTION... 1 SITE MANAGER ACCOUNT ROLE... 1 ACCESSING CMTS... 2 SITE NAVIGATION
A Collaborative Approach to Integrating Mental Health Services with Pediatrics and Obstetrics for an Urban Population
 Mercy St. Vincent Medical Center Healthy Connections A Collaborative Approach to Integrating Mental Health Services with Pediatrics and Obstetrics for an Urban Population Healthy Connections: Multi-disciplinary
Mercy St. Vincent Medical Center Healthy Connections A Collaborative Approach to Integrating Mental Health Services with Pediatrics and Obstetrics for an Urban Population Healthy Connections: Multi-disciplinary
Module 1 Program Description
 Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Module 1 Program Description Palliative Care Program Description 1. What type(s) of communities does your palliative care program serve? Check all that apply. Urban Suburban Rural 2. Which counties does
Change is Good: You Go First
 Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
Change is Good: You Go First Judith Schaefer Better Self Management of Diabetes Missouri Foundation for Health St. Louis, Missouri December 2 nd, 2009 Foundation s goals Support organizations that: Strengthen
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
Selected State Background Characteristics
 State Profile: Colorado Selected State Background Characteristics Population Total Pop. (millions) 4.6 293.7 Pop. 60+ (thousands) 622.9 48,883.4 % 60+ 13.5 16.6 National Ranking 60+ 48 N/A % White (60+)
State Profile: Colorado Selected State Background Characteristics Population Total Pop. (millions) 4.6 293.7 Pop. 60+ (thousands) 622.9 48,883.4 % 60+ 13.5 16.6 National Ranking 60+ 48 N/A % White (60+)
Project Inception 4/5/2018
 The Periscope Project: An Approach to Improving Access to Specialized Psychiatric Care in the Perinatal Period CHRISTINA L. WICHMAN, D.O., F.A.P.M. M E D I C A L D I R E C T O R, T H E P E R I S C O P
The Periscope Project: An Approach to Improving Access to Specialized Psychiatric Care in the Perinatal Period CHRISTINA L. WICHMAN, D.O., F.A.P.M. M E D I C A L D I R E C T O R, T H E P E R I S C O P
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Psychiatric Consultant Guide SPIRIT CMTS. Care Management Tracking System. University of Washington aims.uw.edu
 Psychiatric Consultant Guide SPIRIT CMTS Care Management Tracking System University of Washington aims.uw.edu rev. 9/20/2016 Table of Contents TOP TIPS & TRICKS... 1 INTRODUCTION... 2 PSYCHIATRIC CONSULTANT
Psychiatric Consultant Guide SPIRIT CMTS Care Management Tracking System University of Washington aims.uw.edu rev. 9/20/2016 Table of Contents TOP TIPS & TRICKS... 1 INTRODUCTION... 2 PSYCHIATRIC CONSULTANT
Shana Scott, JD, MPH, Health Systems Team Lead Tuesday, October 3, 2017
 Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
Health Systems Transformation & Health System Interventions: Innovative Public Health Approaches to Improve Quality of Care for Georgians with Chronic Conditions Presentation at 2017 Southern Obesity Summit
The State of Health in Rural C olorado
 Snapshot of Rural Health 2016 Edition The State of Health in Rural C olorado COLORADO ADDRESSING RURAL THE HEALTH ISSUES CENTER COLORADO S RURAL POPULATION RURAL WORKFORCE ACCESS TO CARE ADDRESSING THE
Snapshot of Rural Health 2016 Edition The State of Health in Rural C olorado COLORADO ADDRESSING RURAL THE HEALTH ISSUES CENTER COLORADO S RURAL POPULATION RURAL WORKFORCE ACCESS TO CARE ADDRESSING THE
Selected State Background Characteristics
 State of the States in Support State Profile: Oregon Selected State Background Characteristics Population Total Pop. (millions) 3.6 293.7 Pop. 60+ (thousands) 619.8 48,883.4 % 60+ 17.2 16.6 National Ranking
State of the States in Support State Profile: Oregon Selected State Background Characteristics Population Total Pop. (millions) 3.6 293.7 Pop. 60+ (thousands) 619.8 48,883.4 % 60+ 17.2 16.6 National Ranking
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care
 Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Care Transitions Engaging Psychiatric Inpatients in Outpatient Care Mark Olfson, MD, MPH Columbia University New York State Psychiatric Institute New York, NY A physician is obligated to consider more
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Changes in health workforce needs How health workforce planning happens What works and the available policy levers Information needed for health
 August 11, 2015 Bianca Frogner, PhD, Director Center for Health Workforce Studies Sue Skillman, Deputy Director, Center for Health Workforce Studies Associate Director, WWAMI Area Health Education Center
August 11, 2015 Bianca Frogner, PhD, Director Center for Health Workforce Studies Sue Skillman, Deputy Director, Center for Health Workforce Studies Associate Director, WWAMI Area Health Education Center
Practice Report Out. Western Slope CPC Practices
 Practice Report Out Western Slope CPC Practices Aspen Internal Medicine Consultants Ricci Bickling, Quality Improvement Specialist 2 Providers 8 Staff EMR: GE Centricity 1755 Active Patients Aspen Area
Practice Report Out Western Slope CPC Practices Aspen Internal Medicine Consultants Ricci Bickling, Quality Improvement Specialist 2 Providers 8 Staff EMR: GE Centricity 1755 Active Patients Aspen Area
Selected State Background Characteristics
 State Profile: Missouri Selected State Background Characteristics Population Total Pop. (millions) 5.8 293.7 Pop. 60+ (thousands) 1,029.2 48,883.4 % 60+ 17.9 16.6 National Ranking 60+ 14 % White (60+)
State Profile: Missouri Selected State Background Characteristics Population Total Pop. (millions) 5.8 293.7 Pop. 60+ (thousands) 1,029.2 48,883.4 % 60+ 17.9 16.6 National Ranking 60+ 14 % White (60+)
Integrating Primary Medical Care and Behavioral Health Services: The New Mexico SBIRT Experience
 Integrating Primary Medical Care and Behavioral Health Services: The New Mexico SBIRT Experience Ana Moseley, LISW, ACSW, Clinical Director Tom Peterson, Ph.D., Associate Clinical Director Arturo Gonzales,
Integrating Primary Medical Care and Behavioral Health Services: The New Mexico SBIRT Experience Ana Moseley, LISW, ACSW, Clinical Director Tom Peterson, Ph.D., Associate Clinical Director Arturo Gonzales,
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
Health Resources & Services Administration and the Affordable Care Act: Strategies for Increasing Provider Capacity & Retention
 Health Resources & Services Administration and the Affordable Care Act: Strategies for Increasing Provider Capacity & Retention Hal Zawacki, San Francisco Regional Office Health Resources and Services
Health Resources & Services Administration and the Affordable Care Act: Strategies for Increasing Provider Capacity & Retention Hal Zawacki, San Francisco Regional Office Health Resources and Services
HRSA & Health Workforce: National Health Service Corps...and so much more
 HRSA & Health Workforce: National Health Service Corps...and so much more U.S. Department of Health and Human Services (HHS) Health Resources and Services Administration (HRSA) Office of Regional Operations
HRSA & Health Workforce: National Health Service Corps...and so much more U.S. Department of Health and Human Services (HHS) Health Resources and Services Administration (HRSA) Office of Regional Operations
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
The Nursing Workforce: Challenges for Community Health Centers and the Nation s Well-being
 The Nursing Workforce: Challenges for Community Health Centers and the Nation s Well-being Jane K Kadohiro, DrPH, APRN, CDE University of Hawaii at Manoa Overview Today s nursing workforce Determinants
The Nursing Workforce: Challenges for Community Health Centers and the Nation s Well-being Jane K Kadohiro, DrPH, APRN, CDE University of Hawaii at Manoa Overview Today s nursing workforce Determinants
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Specialty Behavioral Health and Integrated Services
 Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Introduction Behavioral health services that are provided within primary care clinics are important to meeting our members needs. Health Share of Oregon supports the integration of behavioral health and
Health Professions Workforce
 Health Professions Workforce For the Health of Texas February 28, 2011 Ben G. Raimer, MD, MA, FAAP Past Chairman (1997-2010), Statewide Health Coordinating Council Senior Vice President, Health Policy
Health Professions Workforce For the Health of Texas February 28, 2011 Ben G. Raimer, MD, MA, FAAP Past Chairman (1997-2010), Statewide Health Coordinating Council Senior Vice President, Health Policy
10/21/2012. Healthcare in Very Rural and Frontier Communities: Balancing Equity, Effectiveness and Efficiency.
 www.frontierus.org Healthcare in Very Rural and Frontier Communities: Balancing Equity, Effectiveness and Efficiency Susan Wilger, MPAff National Center for Frontier Communities American Public Health
www.frontierus.org Healthcare in Very Rural and Frontier Communities: Balancing Equity, Effectiveness and Efficiency Susan Wilger, MPAff National Center for Frontier Communities American Public Health
COMMUNITY CLINIC GRANT PROGRAM
 COMMUNITY CLINIC GRANT PROGRAM FINAL GRANT APPLICATION GUIDANCE Grant Project Period: April 1, 2015 March 31, 2016 Application Due: December 22, 2014 MINNESOTA DEPARTMENT OF HEALTH OFFICE OF RURAL HEALTH
COMMUNITY CLINIC GRANT PROGRAM FINAL GRANT APPLICATION GUIDANCE Grant Project Period: April 1, 2015 March 31, 2016 Application Due: December 22, 2014 MINNESOTA DEPARTMENT OF HEALTH OFFICE OF RURAL HEALTH
Blending Behavioral Health and Primary Care. Cherokee Health Systems Clinical Model
 Blending Behavioral Health and Primary Care Cherokee Health Systems Clinical Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Our Mission To improve the quality
Blending Behavioral Health and Primary Care Cherokee Health Systems Clinical Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Our Mission To improve the quality
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System
 Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Innovative Ways of Achieving The Triple Aim: Lessons from a Rural Community Health System Roxanne Elliott, MS Policy Director FirstHealth of the Carolinas Goals For Today Review scope of project Integrate
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
Cancer Screening in Primary Care: Lessons from Community Health Centers
 Cancer Screening in Primary Care: Lessons from Community Health Centers Dialogue for Action Washington, DC April 11, 2018 Durado Brooks, MD, MPH Managing Director, Cancer Control Intervention American
Cancer Screening in Primary Care: Lessons from Community Health Centers Dialogue for Action Washington, DC April 11, 2018 Durado Brooks, MD, MPH Managing Director, Cancer Control Intervention American
Selected State Background Characteristics
 State Profile: Tennessee Selected State Background Characteristics Population Total Pop. (millions) 5.9 293.7 Pop. 60+ (thousands) 1,013.5 48,883.4 % 60+ 17.2 16.6 National Ranking 60+ 25 % White (60+)
State Profile: Tennessee Selected State Background Characteristics Population Total Pop. (millions) 5.9 293.7 Pop. 60+ (thousands) 1,013.5 48,883.4 % 60+ 17.2 16.6 National Ranking 60+ 25 % White (60+)
Selected State Background Characteristics
 State Profile: New York Selected State Background Characteristics Population Total Pop. (millions) 19.2 293.7 Pop. 60+ (thousands) 3,347.4 48,883.4 % 60+ 17.4 16.6 National Ranking 60+ 20 % White (60+)
State Profile: New York Selected State Background Characteristics Population Total Pop. (millions) 19.2 293.7 Pop. 60+ (thousands) 3,347.4 48,883.4 % 60+ 17.4 16.6 National Ranking 60+ 20 % White (60+)
Rhode Island Primary Care Providers Implications of Health Reform
 Rhode Island Primary Care Providers Implications of Health Reform Working Paper October 31, 2013 (Updated) Cindy J Wong, PhD Research & Evaluation Consultant cindy@cindyjwongresearch.net (831) 531-2661
Rhode Island Primary Care Providers Implications of Health Reform Working Paper October 31, 2013 (Updated) Cindy J Wong, PhD Research & Evaluation Consultant cindy@cindyjwongresearch.net (831) 531-2661
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care
 Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Value-Based Payment Model Designs for Behavioral Health Services in Primary Care Using collaborative depression care management as a case study due to existing evidence, experience, and measures Robert
Primary Care Setting Behavioral Health Billing Codes
 Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Primary Care Setting s Medicaid Medicare Third Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though
Northern Neck-Middlesex Free Health Clinic Inc.
 Northern Neck-Middlesex Free Health Clinic Inc. General Information Contact Information Nonprofit Northern Neck-Middlesex Free Health Clinic Inc. Address P.O. Box 1694 Kilmarnock, VA 22482 Phone 804 435-0575
Northern Neck-Middlesex Free Health Clinic Inc. General Information Contact Information Nonprofit Northern Neck-Middlesex Free Health Clinic Inc. Address P.O. Box 1694 Kilmarnock, VA 22482 Phone 804 435-0575
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective
 Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
Three World Concept of Behavioral Health and Primary Care Integration Part 3 The Clinician Perspective Colorado Behavioral Health Association October 3, 2010 Three World Model C. J. Peek suggests that
8 / 1 9 / 2. Factors Supporting Critical Access Hospital Turnaround. Muskie School of Public Service
 Factors Supporting Critical Access Hospital Turnaround NOSORH Region C Grantee Meeting Omaha, NE August, Maine Rural Health Research Center Flex Monitoring Team Contact Information John A. Gale Maine Rural
Factors Supporting Critical Access Hospital Turnaround NOSORH Region C Grantee Meeting Omaha, NE August, Maine Rural Health Research Center Flex Monitoring Team Contact Information John A. Gale Maine Rural
Trends, Tasks, and Teamwork
 Nurses in the Behavioral Health Workforce: Trends, Tasks, and Teamwork National Forum of State Nursing Workforce Centers Conference June 8, 2017 Angela J. Beck, PhD, MPH, Director Clinical Assistant Professor
Nurses in the Behavioral Health Workforce: Trends, Tasks, and Teamwork National Forum of State Nursing Workforce Centers Conference June 8, 2017 Angela J. Beck, PhD, MPH, Director Clinical Assistant Professor
Discussion Board in Learning Community Site
 Discussion Board in Learning Community Site The Discussion Board feature allows you to start discussion threads, share resources, and ask questions or seek input from the Care Partners community. Make
Discussion Board in Learning Community Site The Discussion Board feature allows you to start discussion threads, share resources, and ask questions or seek input from the Care Partners community. Make
s n a p s h o t Medi-Cal at a Crossroads: What Enrollees Say About the Program
 s n a p s h o t Medi-Cal at a Crossroads: What Enrollees Say About the Program May 2012 Introduction Medi-Cal, which currently provides health and long term care coverage for more than 7.5 million Californians,
s n a p s h o t Medi-Cal at a Crossroads: What Enrollees Say About the Program May 2012 Introduction Medi-Cal, which currently provides health and long term care coverage for more than 7.5 million Californians,
11/10/2015. Workforce Shortages and Maldistribution. Health Care Workforce Shortages/Maldistribution: Why? Access to Health Care Services
 Workforce Shortages and Maldistribution DEVELOPING NEW STATE LEGISLATIVE HEALTH LEADERS Access to Health Care Services Health Professional Shortage Areas (HPSAs) are geographic areas, or populations within
Workforce Shortages and Maldistribution DEVELOPING NEW STATE LEGISLATIVE HEALTH LEADERS Access to Health Care Services Health Professional Shortage Areas (HPSAs) are geographic areas, or populations within
A Case Study in Primary Care Access: Clinica Family Health. Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services
 A Case Study in Primary Care Access: Clinica Family Health Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services IHI s 26 th Annual National Forum on Quality Improvement in Health Care Orlando, Florida
A Case Study in Primary Care Access: Clinica Family Health Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services IHI s 26 th Annual National Forum on Quality Improvement in Health Care Orlando, Florida
Minnesota s Physician Assistant Workforce, 2016
 OFFICE OF RURAL HEALTH AND PRIMARY CARE Minnesota s Physician Assistant Workforce, 2016 HIGHLIGHTS FROM THE 2016 PHYSICIAN ASSISTANT SURVEY Table of Contents Minnesota s Physician Assistant Workforce,
OFFICE OF RURAL HEALTH AND PRIMARY CARE Minnesota s Physician Assistant Workforce, 2016 HIGHLIGHTS FROM THE 2016 PHYSICIAN ASSISTANT SURVEY Table of Contents Minnesota s Physician Assistant Workforce,
Improving Behavioral Health Services in Pediatric Primary Care: Collaboration and Integration
 Improving Behavioral Health Services in Pediatric Primary Care: Collaboration and Integration A B I G A I L S C H L E S I N G E R, M D M E D I C A L D I R E C T O R, C H I L D R E N S H O S P I T A L C
Improving Behavioral Health Services in Pediatric Primary Care: Collaboration and Integration A B I G A I L S C H L E S I N G E R, M D M E D I C A L D I R E C T O R, C H I L D R E N S H O S P I T A L C
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18
 Health Care Homes (HCH) Initial Certification. Reviewed: 03/15/18") Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Minnesota Department of Health (MDH) Health Care Homes (HCH) Initial Certification Reviewed: 03/15/18 1 Learning Objectives 1. Describe the HCH legislative rule subpart criteria required for initial certification.
Prenatal Care Webinar. Luz Jimenez, RN, BSN VP Clinical Operations Erie Family Health Center
 Prenatal Care Webinar Luz Jimenez, RN, BSN VP Clinical Operations Erie Family Health Center National Center for Health in Public Housing The National Center for Health in Public Housing (NCHPH), a project
Prenatal Care Webinar Luz Jimenez, RN, BSN VP Clinical Operations Erie Family Health Center National Center for Health in Public Housing The National Center for Health in Public Housing (NCHPH), a project
Continuity: Why It Matters and How to Build It
 Summit 2011 LEARN SHARE TRANSFORM Continuity: Why It Matters and How to Build It Clinica Family Health Services-Pecos Clinic Judy Troyer, Clinic Director Session 1B March 7,11:00 AM -12:30 PM Safety Net
Summit 2011 LEARN SHARE TRANSFORM Continuity: Why It Matters and How to Build It Clinica Family Health Services-Pecos Clinic Judy Troyer, Clinic Director Session 1B March 7,11:00 AM -12:30 PM Safety Net
Expanding Mental Health Services in the Face of Workforce Shortage
 Expanding Mental Health Services in the Face of Workforce Shortage Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital
Expanding Mental Health Services in the Face of Workforce Shortage Please note that the views expressed are those of the conference speakers and do not necessarily reflect the views of the American Hospital
FQHC Behavioral Health Billing Codes
 FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
FQHC s Eligible Documentation Assessment 90792 Psychiatric Prescribers only (MD, NP, PA, APRN) Psychiatric diagnostic evaluation with medical services. Medical though process clearly reflected in assessment
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
Resident Rotation: Collaborative Care Consultation Psychiatry
 Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD James Basinski, MD With contributions from: Jurgen Unutzer, MD, MPH, MA Jennifer Sexton, MD, Catherine Howe, MD, PhD
Resident Rotation: Collaborative Care Consultation Psychiatry Anna Ratzliff, MD, PhD James Basinski, MD With contributions from: Jurgen Unutzer, MD, MPH, MA Jennifer Sexton, MD, Catherine Howe, MD, PhD
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes
 Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
Designing & Delivering Whole-Person Transitional Care Coordinating care across settings and over time to drive outcomes Amy E. Boutwell, MD, MPP CNYCC Annual Meeting November 6, 2017 Agenda Design data,
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE
 THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
THE CENTER FOR POLICY, ADVOCACY, AND EDUCATION OF THE MENTAL HEALTH ASSOCIATION OF NEW YORK CITY INTEGRATION AND COORDINATION OF BEHAVIORAL HEALTH SERVICES IN PRIMARY CARE A Presentation at The Community
Alaska s Behavioral Health Workforce: Identifying occupations that are hardest for employers to fill and assessing what can be done to help
 Alaska s Behavioral Health Workforce: Identifying occupations that are hardest for employers to fill and assessing what can be done to help UA Behavioral Health Workforce Development Meeting October 25,
Alaska s Behavioral Health Workforce: Identifying occupations that are hardest for employers to fill and assessing what can be done to help UA Behavioral Health Workforce Development Meeting October 25,
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services
 The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services Indiana Council of Community Mental Health Centers Ft. Wayne, Indiana May 19, 2011 David B. Bingaman, LCSW, ACSW U.S. Department
The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services Indiana Council of Community Mental Health Centers Ft. Wayne, Indiana May 19, 2011 David B. Bingaman, LCSW, ACSW U.S. Department
Illinois Child-Parent Psychotherapy Learning Collaborative Agency Application: Cohort V:
 Illinois Child-Parent Psychotherapy Learning Collaborative Agency Application: Cohort V: 2018-2019 About this application This application is for agencies that wish to participate in the Learning Collaborative
Illinois Child-Parent Psychotherapy Learning Collaborative Agency Application: Cohort V: 2018-2019 About this application This application is for agencies that wish to participate in the Learning Collaborative
Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers
 Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers November 30, 2015 Joshua Rubin HealthManagement.com Plan CCBHC basics NYS Health Reform
Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers November 30, 2015 Joshua Rubin HealthManagement.com Plan CCBHC basics NYS Health Reform
Selected State Background Characteristics
 State Profile: South Carolina Selected State Background Characteristics Population Total Pop. (millions) 4.2 293.7 Pop. 60+ (thousands) 718.4 48,883.4 % 60+ 17.1 16.6 National Ranking 60+ 27 N/A % White
State Profile: South Carolina Selected State Background Characteristics Population Total Pop. (millions) 4.2 293.7 Pop. 60+ (thousands) 718.4 48,883.4 % 60+ 17.1 16.6 National Ranking 60+ 27 N/A % White
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it
 Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
The National Study of Nursing Home Social Services
 The National Study of Nursing Home Services The University of Iowa School of Work Contact information on back cover. START HERE Are you thesocialservicedirectororleadsocial services person on-site most
The National Study of Nursing Home Services The University of Iowa School of Work Contact information on back cover. START HERE Are you thesocialservicedirectororleadsocial services person on-site most
california C A LIFORNIA HEALTHCARE FOUNDATION Health Care Almanac Financial Health of Community Clinics
 california Health Care Almanac C A LIFORNIA HEALTHCARE FOUNDATION Financial Health of Community Clinics March 2009 Introduction Community clinics are a vital part of California s health care safety net
california Health Care Almanac C A LIFORNIA HEALTHCARE FOUNDATION Financial Health of Community Clinics March 2009 Introduction Community clinics are a vital part of California s health care safety net
What is Mental Health Integration?
 What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
What is Mental Health Integration? Quality Experience Cost A standardized clinical and operational team process that incorporates mental health as a complementary component of wellness & healing * Mental
Southern California Regional Implementation & Improvement Science Webinar Series Welcome to the Webinar
 Southern California Regional Implementation & Improvement Science Webinar Series Welcome to the Webinar Karen Coleman, PhD Research Scientist II Southern California Permanente Medical Group Thoughts about
Southern California Regional Implementation & Improvement Science Webinar Series Welcome to the Webinar Karen Coleman, PhD Research Scientist II Southern California Permanente Medical Group Thoughts about