Improving the HCAHPS Score for Pain Well Controlled
|
|
|
- Hubert Craig
- 6 years ago
- Views:
Transcription

1 The University of San Francisco USF Scholarship: a digital Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall Improving the HCAHPS Score for Pain Well Controlled Uwaezu J. Umeh University of San Francisco, joyumeh@gmail.com Follow this and additional works at: Part of the Medicine and Health Sciences Commons Recommended Citation Umeh, Uwaezu J., "Improving the HCAHPS Score for Pain Well Controlled" (2014). Master's Projects and Capstones This Project/Capstone is brought to you for free and open access by the Theses, Dissertations, Capstones and Projects at USF Scholarship: a digital Gleeson Library Geschke Center. It has been accepted for inclusion in Master's Projects and Capstones by an authorized administrator of USF Scholarship: a digital Gleeson Library Geschke Center. For more information, please contact repository@usfca.edu.
2 Running head: IMPROVING PAIN WELL CONTROLLED 1 Improving the HCAHPS score for pain well controlled Uwaezu J. Umeh University of San Francisco
3 2 Abstract This project took place on a Renal/Endocrine unit of a northern California Hospital. As observed on this unit, pain was not well controlled and this caused the HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score for pain well controlled to be low. Hence, this project sought to address the underlying reasons why pain was not well controlled and to proffer solutions to raise the HCAHPS score to at least 65% from an average of 55%. In order to find the root causes, the nurses were surveyed, the patients and certified nursing assistants (CNAs) were interviewed, and a 24-hour chart review was conducted on three different days. The results revealed that about 30% of the nurses had little or no knowledge of HCAHPS; 73% of the CNAs did not know when to report patients pain score to the nurses and 80% of the patients had to wait until their pain level was severe before asking for pain medication. Following the unit s policy and procedure for pain management, the goal for effective pain management was to maintain patients pain intensity at 3 or the patients stated goal. To achieve this goal and also address the above issues, it was recommended that the nurses maintain an open communication with the patient, perform an initial assessment, and reassess the patient within one hour of medication administration, offer non-pharmacological therapies such as heat/cold therapy, repositioning, and music therapy. Keyword: HCAHPS score, pain control, pain management, pain medication
4 3 The Problem This project took place in a 34 bed Endocrine/Renal unit at a Northern California hospital in the Bay Area. The purpose of this project was to address the underlying issues of why pain is not well controlled and why the HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) score for pain well controlled has been consistently low over a period of 12 months. The unit s monthly HCAHPS goal for pain well controlled is 65% but for 12 consecutive months starting July 2013 to June 2014, the unit s goal was met only four times, and this represents 33% of the time. The HCAHPS scores through those 12 consecutive months ranged from 33% to 78%, the purpose of this project is to find the underlying reasons why it has remained consistently low and try to proffer solutions to raise these scores to at least 65% which is the unit s benchmark. Studer et.al (2010) noted that 76.5 million Americans (1 in 4) struggle with pain without appropriate treatment (p. 159). These statistics are very alarming and if the issue of pain not well controlled persists, it could reduce patients quality of life, affect the hospital s reputation, and even affect their reimbursement. In the process, the hospital might lose business since it is only so natural not to return to a hospital where one s pain was poorly controlled. The issue of pain is a very important one to address because poorly controlled pain could lead to several undesired effects, including the quality of life and prolong hospital stay. Wells et al, (2008) found that patients may become depressed or anxious and want to end their lives. Patients are sometimes unable to do many of the things they did without pain, and this state of living in pain affects their relationships with others and sometimes their ability to maintain employment (p.470). Pain is highly subjective and this makes it even more difficult to be properly assessed
5 4 and treated. It is important to note that for pain to be well controlled, it should be patientcentered and tailored to meet the individual s needs. There is not a one size fits all for pain management. According to Casey (2011), pain is the primary reason why people seek medical advice (p.24). Wells et. al. (2008) found that inadequately managed pain can lead to adverse physical and psychological patient outcomes for individual patients and their families (p.465). Studer at al. (2010) found that patients perception of the type of care that they receive is based on whether or not their pain was well managed and kept under control (p. 159). Through careful observation, survey administration, chart reviews, patient and staff interviews, a few causes or obstacles were identified as some of the reasons why pain is not well controlled in this unit. These include but are not limited to longer reassessment times, knowledge deficit, infrequent use of non-pharmacological therapies, poor communication and lack of knowledge of the policy and procedures of pain management. The above-mentioned factors were identified as some of the underlying factors that led to the low HCAHPS scores on pain well controlled. Based on these issues, some solutions have been proffered to help raise the HCAHPS scores to at least 65%. Overview of HCAPHS Now, one would wonder what HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) is and why it is so important to raise the scores. According to the Centers for Medicare and Medicaid Services, the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) is the first national standardized publicly reported survey of patients perspectives of hospital care (p1). It is a tool that is used across the nation to measure patients satisfaction and experience of their hospital stay. It measures different aspects of
6 5 individuals care received while hospitalized. Some of the areas it measures are communication, staff responsiveness, cleanliness and quietness of patient care area and also pain management. It is important to note that these surveys are administered to patients randomly and they are not restricted only to Medicare patients. Following the enactment of the Deficit Reduction Act of 2005 that allowed acute care hospitals to participate in HCAHPS, there became a need for more hospitals to participate. And, hospitals that elected to join the Inpatient Prospective Payment System (IPPS) must collect and submit HCAHPS data in order to receive their complete annual IPPS payment. IPPS hospitals that fail to publicly report the required quality measures, which include the HCAHPS survey, may receive an annual payment update that is reduced by 2.0 percentage points (Centers for Medicare and Medicaid). This implies that the government is trying to reward hospitals for quality of care provided. While it makes sense to reward hospitals which provide better quality care and withhold the payment by at least 2 percent to hospitals that fall short based on the HCAHPS surveys and other determinants, research has shown that high acuity hospitals tend to have lower patient satisfaction scores (Geiger, 2012). Medicare values the perceptions of patients care and takes that into consideration while reimbursing the participating hospitals. Hence, it becomes very important to manage patients pain since it is part of Medicare s determinant for reimbursement and also a way to improve quality care and outcomes. Literature Review Pain has been said to be the primary reason why people seek medical care. Casey (2011) estimated that 20 percent of the population suffers from chronic pain (p.24). When dealing with the issue of pain management, it is important to keep in mind that different kinds of pain would
7 6 respond to therapy or treatment differently. Acute pain if not properly treated could lead to chronic pain, and research has shown that chronic pain causes personal suffering and loss of quality life, including reduced economic, career and social opportunities (Casey, 2011, p.24). Makris et. al (2014), found that persistent pain in older adults frequently develops via a multifactorial pathway, resulting in adverse sequelae that include poor self reported health, decreased quality of life, and significant disability that often occurs and is attributable to falls, depression, or anxiety, sleep impairment and decreased socialization (p.826). And Ogston-Tuck (2014), found that older people experience persistent pain and one in five adults suffers from chronic pain (p.512). Pain could be difficult and challenging to treat. It is said to be a complex experience, with many variables that can influence the patient experience and interpretation. The various factors include age, gender, cultural influences, social class, personality and emotional factors such as anxiety, fear and depression (Gregory and Waterman, 2012, p.3523). The above factors are very important to consider when managing pain because pain could be influenced by one s age, personality, gender and culture. Since pain is a very serious issue facing older adults, the lack of proper pain management can affect the older adults quality of life and general well-being (Gropeli & Sharer, 2013 p. 375). Since the measurement of pain is very subjective, it has also been said to be whatever the patient said it is. Ogston-Tuck (2014), opined that pain is personal, it is unbiased. Hence, it is whatever the experiencing person says it is, existing whenever they say it does (p. 512). There is no accurate objective way to measure a person s pain other the use of scale and faces. Yet, it is still whatever the patient said it is. Gammons and Caswell (2014) found that pain is subjective, unique to the individual and multifaceted, so it is a challenge to form the objective description
8 7 required to develop an intervention (p.274). Koch (2012) found that patient self-reporting is the most reliable indicator of the existence and intensity of pain (p.189). According to Wang & Tsai (2010), pain refers to an unpleasant sensory and emotional experience associated with actual or potential tissue damage. Since uncontrolled pain could actually lead to some kind of actual or potential tissue damage, it is important to teach patients especially adult patients to report their pain level when it is moderate and not to wait until the pain has really reached its severe stage. Gammons and Caswell (2014), found that pain in adults is common especially when associated with comorbidities. They went ahead to note that untreated pain can have a negative impact on the older person s quality of life (p.274). Even though numerous pain assessment tools have been developed to aid in the management of pain, a gold standard for the evaluation of pain is still lacking and the most reliable indicator has remained patients self report of pain which could be totally different from the nurse s evaluation of pain (Gammons & Caswell, p.275). This is where it becomes important for the nurse to put his/her biases aside and focus on what the patient actually reports as their pain score. Even though, one can try to elicit a pain score through non-verbal cues, it remains important to listen to the patient and treat them accordingly. Poor communication is a huge barrier in managing patients pain. For pain to be properly controlled; it has to be a joint effort among healthcare providers and the patient; hence it is a multidisciplinary approach. This would also mean clear communication between the patients and the healthcare providers because it is near impossible to control a patient s pain if their goal for pain is not known or clearly stated. Makris et. al (2014) were of the view that, to formulate an
9 8 effective treatment plan for older patients with persistent pain requires a clear understanding of their comorbidities, cognitive and functional status, treatment goals and expectations (p.834). Without fully understanding the above factors, it would be hard to effectively treat the patient s pain. Since nurses are at the frontline when it comes to pain management in the hospital setting, it is important for them to know the physiology of pain, myths and misconceptions about pain, and ethical issues in pain management (Wang & Tsai, 2010, p.3189). Patients sometimes do not receive much information regarding their pain management. Communication, therefore, remains an important aspect of a registered nurse s role and other healthcare team rely on the nurses to provide accurate information about their group of patients (Gregory & Waterman, 2012 p. 3528). For effective pain management to happen, effective communication among all members of the health care is highly important (Gropeli & Sharer, 2013 P. 381). Communicating with the patient as well gives them the opportunity to build a relationship with the nurse, hence Studer et.al, (2010) found hourly rounding to be the best tactics to communicate with patients about pain and to take steps to proactively manage it (p. 165). Communicating with patients is very vital because it lets the nurse understand the patient s expectation and they will both work towards achieving that goal. This would also provide an opportunity for the nurse to educate the patient if his/her pain goal is unrealistic. The nurse would then have the opportunity to reach an agreement with the patient on what would be a tolerable or an acceptable pain level for the patient (Studer et.al 2010, p. 167). Studer et. al, (2010) highly recommended the use of whiteboards to serve as a visual reminder for patients on how they are doing regarding pain.
10 9 They suggest writing the patient s pain score on the board, their pain goal and the frequency of their medication. This would provide a visual guide for the patient to see the schedule (p. 172). It was also found that inadequate assessment and reassessment time were factors that led to poorly controlled pain. It is important to assess a patient s pain level before commencing treatment. As a result, assessment is the first step in the process of managing pain (Gregory & Waterman, 2012 p. 3528). Subramanian et.al (2011) found that pain management must begin with pain assessment. They went ahead to recommend that pain should be assessed and treated accordingly as needed by patients (p.1258). Research shows that nurses barriers to pain management have been associated with poor assessment skills and concerns about the dangers of opioid use (Wang & Tsai, 2010, p.3189). In order to properly manage pain, care must start with assessment of need. (Ogston-Tuck 2014, p.514). As subjective as pain is, it is important to first understand what the patient is experiencing in order to manage it better (Koch, 2012, p.189). Pain assessment is very important because it could give the nurse a quick idea of what initial intervention is required to keep patients pain under control. Various tools have been created to help in pain assessment such as the verbal rating scale of 0-10, the faces scale which rates pain as mild, moderate, and severe. These tools help to guide pain treatment (Koch, 2012 p. 189). The pain scale is an important pain assessment tool that can be used to manage expectations and create agreement (Studer et al. p. 167). As important as pain assessment is, so is pain reassessment. Koch (2012) found that it is important to follow-up patients and reassess treatment efficacy and side effects (P.190). This is where busyness and interruption play a role as barriers to proper reassessment and pain management. Interruption in the provision of nursing care are disruptive and act as a major
11 10 barrier to effective pain relief by reducing the opportunities for the nurse to evaluate the effectiveness of any previous analgesia. Workload, time available, multitasking, and interruptions to the provision of nursing care reduces the opportunity for comprehensive pain assessment (Gregory & Waterman, 2012 p. 3528, 3529). All these factors were evident in the nurses surveys that were conducted for this project. They cited heavy assignments or high acuity patients, lack of time, and frequent interruptions as barriers to reassessing pain in a timely manner. The use of non-pharmacological therapies has been found to be very effective in improving pain. It is always important to check to see if patients are interested in the use of nonpharmacological therapies rather than relying solely on medication (Studer et.al. 2010, p.169). Research shows that using other non-pharmacological therapies is effective in relieving patients pain. Hence, a holistic approach to nursing is widely accepted in pain management. Selimen and Andsoy (2011), suggested that holistic nursing is based on integrating the patients physical, psychological, and emotional needs with his or her social and cultural beliefs by establishing and maintaining a healthy connection between these areas of a patients life while meeting his or her health needs (p. 483). They went ahead to suggest that a holistic approach may include music, relaxation via guided imagery, therapeutic massage and touch therapy. Music therapy and guided imagery have positive effects on the recovery process (P.484). Huth et. al, (2009) opined that guided imagery has the potential to modify pain by diverting attention to a pleasant, non-painful stimulus (p.290). Guided imagery could be said to be an alternative healing practice in which relaxation, and mental visualization are used to improve mood and physical well-being reduces pain and anxiety (p.485). It is also considered a
12 11 non-pharmacologic modality as well as complementary and alternative medicine. It uses relaxation techniques and a description of mental images (Burhenn et.al, 2014, p. 501). Casida and Lemanski (2010) defined guided imagery as a therapeutic process that facilitates working with the power of the imagination to positively affect mental attitude and potentiate positive outcomes (p.22). Guided imagery is a widely used complementary therapy and its use for pain management has increased over the past two decades ( (Posadzki, et.al, 2011, p.96). It is hypothesized to modify physiological functioning through promoting immune-mediated analgesia and attenuating the sickness response (Lewandowski & Jacobson, 2013, P.373). As much as guided imagery is important in helping to alleviate patients pain, it is even more important to make patients understand that they have the power to manage their own pain. Although guided imagery is not currently being used in this facility, it is highly important to note that research has shown the efficacy of its use and that nurses at this facility showed increased interest to use it but cited lack of knowledge of how to use it. This also supports Burhenn et al. (2014) findings that nurses knew about alternative therapies to control pain but were unaware of how to implement them (p. 501). Knowledge deficit among nurses and other healthcare professionals was also found to be one of the barriers why pain is not well controlled in adult patients. Gropeli and Sharer (2013) were of the view that nurses are key to successful pain management in older adults, hence it is important that they understand that attitudes and perceptions could pose as barriers to managing pain. They also found that educational level and years of experience impacted the attitudes and perceptions of pain (p.375, 376). It is worthy to note that nurses barriers to pain management
13 12 have been associated with their poor pain-management knowledge and skills as well as misconceptions about pain (Wang & Tsai, 2010, p.3189). Although there is no evidence to support the commonly held belief that pain is a normal component of aging, many healthcare workers continue to support the myth that pain is a part of aging and should be accepted (Ogston-Tuck 2014, p. 514). Gregory and Waterman (2012) found that the quality of pain treatment depends on the knowledge and skills of those who provide the treatment (p, 3524). They also found that, nurses with higher pain knowledge did not have patients with lower pain scores (p. 3524). It is also imperative to note that Ogston-Tuck (2014) found that as a result of poor knowledge about the nature of pain and its management, nurses feel ill prepared to care for patients suffering pain and make incorrect decisions about management of their pain (p514). Gropeli and Sharer (2013), found that education of nurses had an impact on appropriate pain management and that the expert nurse was more likely to provide more effective pain management (P.376). Subramanian et.al; (2011) suggested that since nurses play a key role in pain management, their knowledge is vital in their decision making in pain management (p. 1259). They also found that there was a positive correlation between education and pain management, and that nurses who attended pain training managed patients pain well and provided effective pain management practice (Subramanian et.al; 2011, p. 1259). As a result of these findings, it is recommended that management provide frequent training sessions to keep nurses abreast of current evidence in proper pain control. As part of this study, there was also another barrier that was identified as one of the reasons why pain was not well controlled on the unit. This study found that patients waited until
14 13 their pain was severe before asking for pain medication. Studies have also shown that patient reluctance to report pain is definitely a barrier to proper pain management (Gropeli & Sharer, 2013 p. 376). Since patients play a huge role in pain management, it is important to ensure patient understanding and educate patients about their condition (Koch, 2012, P. 189). It is also important to note that organizational structures could be one piece of the puzzle why pain is not well controlled. Organizational care systems which are in place can act as a barrier to timely administration of analgesia (Gregory & Waterman, 2012 p. 3528). For instance, two nurses are required to witness the wasting of a narcotic. This could delay care provided to the patients especially when the unit is short-staffed. Root Cause Analysis Some root causes were identified as to why pain is not well controlled leading to the low HCAHPS score (See Appendix 1 and 2). Five factors were identified as the roots of this problem. These are: longer reassessment time, lapse in communication, knowledge deficit, infrequent use of non-pharmacological therapies, and not following the policy and procedures. Cost Analysis Since pain is difficult to treat, it is also expensive to be manage. Pain generates a cost to society and its management is in competition with other areas of medicine (Ogston-Tuck 2014, p.512). Pain has also been said to be a silent epidemic with increasing prevalence and impact on its sufferers (Ogston-Tuck 2014, p.512). Pain affects about 20% of the adult population in
15 14 Europe and USA, it is a common problem that affects people of all ages, socioeconomic groups and ethnicities (Ogston-Tuck 2014, p.514). Pain if left untreated could be very costly and could cost hospitals millions of dollars in the long run. It could cost patients their happiness, and quality of life. Cost could be both direct and indirect. While direct costs are derived from patients report of their use of health care resources such as inpatient and outpatient care, indirect cost included lost productivity, and lost leisure time (Gannon et.al. p. 1519). Pain well controlled is one of the tools that Medicare use as a yardstick to reimburse hospitals who meet their goals, hence if this component is not met, the hospital could lose about 2% of its annual income from the Centers for Medicare and Medicaid. One of the recommendations for better pain control was to implement guided imagery and the use of other non-pharmacological therapies such as heat/cold therapy. The cost for implementing guided imagery would be $50 for a compact disc player, $10 for the compact disc and $5 a piece for the disposable headset. This would bring the cost for each set to $65. Since this would be the very first time guided imagery would be used on this unit, it was recommended that only 3 compact disc players be purchased at this time bringing the total cost to $195. Heat and cold therapy is already available on the unit and will come at no additional cost. Education has been provided to the nurses to offer more of this therapy to patients. As research has already shown, the cost of implementing guided imagery is almost nothing compared to what the positive outcome of reducing pain would be. Methodology and Pre-implementation Several methodologies were used in conducting this study. Over 300 hours were equally spent in gathering and analyzing these data. Data were collected through surveys of Registered
16 15 Nurses (RN), patients interviews, Certified Nurse Assistants (CNA) interview, chart review and observation. For the RNs surveys, all three shifts were covered: day shift, PM shift and night shift. Twenty five RN surveys were administered, but 20 were returned. Fifteen CNAs among all three shifts (AM, PM, and night) were interviewed one on one. Fifteen patients who at some point during their hospital stay had received pain medication or were currently on pain medications were equally interviewed. There was also a random chart audit on twenty patients done on three different days. Based on these data collection methods, there were identifiable causes as to why pain is not well controlled on the unit where this study was conducted. Findings/Results of the RNs Survey A total of 20 completed surveys were received from the RNs, The results of the surveys showed that 40% of the nurses were not familiar with HCAHPS (See Appendix 3). It was interesting to find that the nurses believed that the HCAHPS score for pain well controlled was low for various reasons (See Appendix 4). Thirty five percent of the nurses had no idea why HCAHPS score was low, 20% believed that it was as a result of longer reassessment time and 10% believed that pain is subjective and therefore difficult to control. Twenty percent believed that the physicians were either not ordering the right medication or reluctant to order more medications. Fifteen percent believed that it was as a result of miscommunication between staff and patients, 20% believed that it was as a result of patients goal being unrealistic, 5% believed understaffed or short-staffed to be the issue, and finally 5% believed that the patients do not ask for pain medication at the right time. Another question was raised on what could be done to improve the HCAHPS score for pain well controlled ; various answers were obtained from this question (See Appendix 5).
17 16 Twenty five percent believed that frequent reassessment would play a major role, while another 20% believed that better staffing would improve the HCAHPS scores. Ten percent believed that teaching patients about non-pharmacological therapies would improve the HCAHPS score. Five percent believed that administering medication on time, having a preset pain order, updating the whiteboard, and discussing patients goal would help address patients pain. Another ten percent expressed no idea as to what would improve the HCAHPS scores. Thirty five percent believed that educating patients about different types of pain and what to expect would improve HCAHPS scores. Finally, ten percent believed that better communication among the healthcare team members would improve the HCAHPS scores. Various responses were also obtained from the question on what nurses can do to control patients pain (See Appendix 6). Five percent suggested better communication with the health care team, 45% suggested that administering medication on time would help control patients pain. Another ten percent believed that emotional support, and position changes would help. Twenty percent believed that offering heat/ice therapy would be helpful. Twenty five percent believed that educating patients about their PRN pain medication (as needed medication) and also teaching them not to wait until pain level is severe before calling for pain medication. Finally, fifteen percent stated that they were not sure what would help control patients pain. Results from these surveys (see Appendix 7) showed that 40% of RNs were teaching patients heat/ice therapy, 35% taught deep breathing, position changes, and relaxation, 10% taught music therapy and distraction, 5% taught range of motion exercises, and another 10% did not utilize any non-pharmacological methods.
18 17 When the question of how often pain was reassessed was asked, 55% percent said they reassessed pain most times, 35% answered always and 10% answered usually (See Appendix 8). There were also identified barriers as to what was preventing RNs from reassessing pain in a timely manner (See Appendix 9). Thirty five percent cited been busy with other patients as a barrier. Five percent believed it was language barrier, 10% believed it was as a result of heavy assignment, 10% believed it was as a result of interruption, 10% believed it was due to under staffed, and 10% believed it was because the patient was sleeping. Twenty percent cited that it was because the patients were off the unit for other procedures. When asked of the changes that would make pain reassessment easier (see appendix 10), 30% cited having less work load, 45% stated having more staff, and 25% stated informing CNAs and patients to call for pain medication. Findings/Results from patients Survey During this process, 15 patients were surveyed and sked series of questions to gain insights into how well their pain was well controlled. When asked to what extent their pain was well controlled using a scale of 1(extremely controlled) to 5(not controlled at all), 33% circled 2, 53% circled 4 and 13% circled 3 (See appendix 11). This correlates with the other findings that pain is not well controlled on the unit. When asked how much pain relief the patients were currently receiving using a scale of 1 (a great deal of relief) to 5 (no relief at all), 40 % circled 3, 33% circled 4, 13% circled 5, and another 13% circled 2 (see appendix 12). This also represents that the patients are not getting adequate pain relief. When asked how much pain relief they expect to receive while hospitalized, using the same scale of 1 (a great deal of relief) to 5 (no relief), 40% circled 2, 33% circled 1 and 27% circled 3 (Appendix 13). This indicates that the
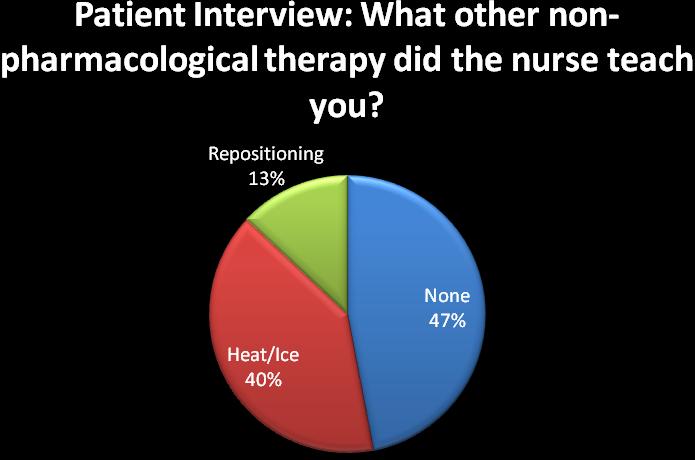
19 18 patients expected a great deal of relief and this should provide an opportunity for the nurses to educate the patients concerning the type of pain that they have. Unfortunately, depending on the patients diagnosis, some type of pain would never go away completely and patients need to understand this. Patients were also asked when they usually asked their nurse for pain medicine, using mild, moderate and severe as the options (see appendix 14). Eighty percent stated severe and 20% stated moderate. This is another opportunity to educate the patients not to wait until pain is severe before calling for pain medicine. When asked the patients what other nonpharmacological therapy other than medications that the nurses taught them, 47% stated none, 40% stated heat/ice therapy, and 13% stated repositioning (see appendix 15). Findings/Results from CNAs Interviews A total number of 15 CNAs were interviewed regarding when they called the nurses to report patients pain score. The policy and procedure for this facility stated that the CNA should call the RN if patients pain was 4 or not tolerable as stated by the patient (see appendix 16). Only 27% of the CNAs stated that they needed to report pain to the RN when pain was at 4. Seven percent said they would call the nurse when pain was at 8, and 13% stated to call the RN when pain was at 6. Twenty percent stated that the RN needed to be called when pain was at 5 or greater, 13% stated that they would call the RN when pain was at 3, 7% stated to call RN when pain is 2 and 13% stated to call the nurse when pain is at 1. Findings/Results from chart review A 24-hours chart review was done to see if patients pain was reassessed within one hour after medication administration (Appendix 17). Twenty random patients charts were reviewed
20 19 on three different days and the results showed that 90% of the time, pain was not reassessed within an hour of medication administration. This was more noticeable during the night and could also support the fact that the RNs surveys cited patients sleeping as a barrier to pain reassessment. It is important to keep in mind that it is possible that the nurses were probably reassessing pain within an hour as 55% of them noted on the surveys, but were not always documenting that pain has been reassessed. Intervention/Implementation Several issues were identified as reasons why pain is not well controlled thereby leading to low HCAHPS score. These include knowledge deficit and lack of knowledge of the policy and procedure, this was addressed by providing education to the CNAs on the need to call the RN and at what pain score RN should be notified of patients pain. And also to educate patients to call nurses for pain medication when their pain is moderate instead of waiting for when pain is severe before calling the RNs. RNs were equally educated on the importance of HCAHPS and how the scores are tied to the hospital s reimbursement. Huddles were conducted during a two weeks period with the RNs, sharing with them the findings of the surveys and what could be done to improve pain control thereby raising the HCAHPS scores. A pain management brochure was designed for both the nurses and the patients. The purpose of the brochure on the one hand was to educate the patients on the need to call the nurses when their pain score is moderate and not to wait until it is severe; and on the other hand, to serve as a visual reminder for the nurses on pain management tips. Longer reassessment time was also found to be one of the causes why pain is not well controlled. Nurses did agree that they did not simply forget to reassess but were constantly busy
21 20 or getting interrupted throughout the day. To address this issue, teamwork was encouraged among the nurses and other staff. Since this unit is very busy and has high acuity patients, team work would be a way to work around this issue of longer reassessment times. Communication was also an identified issue, communication between nurses and patients, and communication between nurses and CNAs. To address this issue, reinforcement on the use of whiteboard was encouraged. The whiteboard would be used to communicate patients stated goal, patients pain level as of the time pain medication was given, the frequency of pain medication and also when the next dose of medication would be due. The CNAs were educated one on one and reminded on the need to call the RN when patients pain score is 4. This also would mean complying with the policy and procedure which stated for the nursing assistant to notify the RN when pain is 4. Infrequent use of alternative therapies was also found to be one of the issues affecting pain control. To address this issue, the use of heat/ice therapy was reinforced. The use of guided imagery was also encouraged and information on implementing it was left with the unit supervisors. Music therapy the use of CARE channel (channel 93) should frequently be used. This music channel would depict a healing environment for patients. Post Intervention/post implementation After implementing the use of alternative therapies such as heat/ice and music therapy, it was observed that 8 out of 12 patients who were receiving pain medication were also offered ice/heat therapy, 4 patients out of 12 patients receiving pain medication reported having been offered music therapy. The use of whiteboard was reinforced during staff teaching, it was observed that the whiteboard was updated in 12 rooms out of 16 rooms of patients who were
22 21 receiving pain medication (See Appendix 18). The whiteboard was updated with patients pain goal, pain score and time medication was administered. The CNAs were interviewed again to see if they have understood at what pain score the RN should be notified of patients' pain, 10 out of 12 CNAs were able to identify that the RN should be notified when a patient's pain score is 4 (See Appendix 19). A post-implementation chart review showed that pain was reassessed within one hour of medication administration 50% of the time. This represents a 40% increase from the pre-implementation phase (See Appendix 20). These observations seem encouraging but this is where the issue of sustainability comes into play. It would be observed if these improvements made any changes in the HCAHPS scores within the next quarter in about 3 months from now. Sustainability When a new idea was implemented, sustainability often became a huge issue. How would that idea remain alive and not be forgotten like many others that were previously implemented. It has been brought to the attention of management that about 30% of the nurses who were surveyed had no idea what HCAHPS was all about. This however, affected the staff who worked only weekends more than any other shift. If an organization is trying to push for a change and the staff is not made aware of the goals of the unit, it would be hard for them to accomplish their goal. Hence, the recommendation to hold staff meeting on weekends at least two times a year. This idea would help keep the weekend staff abreast of what is going on in the unit and the hospital as a whole. Since part of reimbursement is tied to the HCAHPS score, it is highly important that all staff be made aware of what it is and how to accomplish the goals. To sustain the idea of heat/cold therapy and the use of whiteboard, discussion with the unit supervisors revealed that
23 22 they would be willing to hold weekly huddles with the staff with the teaching pamphlet that was made for staff. They would also be responsible for educating the CNAs annually to ensure that they comply with the policy and procedure of calling the nurses when patients pain is 4. Discussion The purpose of this study was to investigate the underlying reasons why pain was not well controlled in the older adult population of the Endocrine/Renal unit at a hospital in the Bay Area. A Few barriers were identified, such as longer reassessment times, heavy workload, knowledge deficit, infrequent use of alternative therapies, and not following the policy and procedures. Studies have shown that there is a need for standardized pain management to guide nurses in decision making (Subramanian et.al; 2011, p. 1258). Based on observations and research conducted on the unit s need assessment, it was found that pain management is a top priority that needs prompt attention. Even though nurses have the obligations to provide effective pain relief to patients, they often struggled to fulfil this obligation due to institutional regulations or limited coordination with other healthcare providers (Subramanian et.al; 2011, p. 1258). The results of the surveys, interviews and chart reviews showed that a big part of the problem lies in knowledge deficit. Educating patients, CNAs, and the nurses was a big component to this project. Closing the gap that the knowledge deficit created would go a long way to accomplish the goal of raising the HCAHPS score and hopefully bringing it up to 65%. Conclusion
24 23 This project has identified an issue with pain control on a medical unit. As a result, the HCAHPS score has consistently been low for the past 12 consecutive months except for 4 times out of those 12 months. After over 300 hours that were committed toward this project, it was found that some of the underlying reasons why pain was not well controlled on the unit were as a result of longer reassessment times, knowledge deficit, poor communication, policy and procedure not followed and infrequent use of non-pharmacological therapies. Some solutions were proffered to help improve pain management and also raise the HCAHPS score. Teamwork was recommended to deal with the issue of longer reassessment time; the use of whiteboard was reinforced as a communication tool between the nurses and patients. To address knowledge deficit, education was provided to the patients, CNAs and the RNs. To address the issue of not following policies and procedures, education was provided and team work was also recommended. In the case of infrequent use of alternative therapies, music therapy was implemented and the use of CARE channel was recommended. Also, the use of heat/ice therapy was recommended. Due to time constraints, guided imagery could not be implemented, but information to implement it was made available to the unit supervisors. Over a course of three to six months, the goal would be for the HCAHPS score for pain well controlled to increase to at least 65% every month.
25 24 Appendix 1: The Unit's HCAHPS Scores HCAHPS Scores : Pain Well Controlled Percent Jul-13 Aug- 13 Sep- 13 Oct- 13 Nov- 13 Dec- 13 jan- 14 Feb- 14 Mar- 14 Apr- 14 May- 14 Goal Score Jun- 14

26 25 Appendix 2: Root Cause Analysis
27 26 Appendix 3: RN Knowledge of HCAHPS 40% 60% Yes No
28 27 Appendix 4:
29 28 Appendix 5:
30 29 Appendix 6:
31 30 Appendix 7: Appendix 8:
32 31 Appendix 9: RN Survey: Barriers preventing pain Reassessment 18% 32% Busy with other patients Language barrier Heavy assignment 18% 9% 9% 9% 5% Understaffed Patient sleeping Patient off unit Interruption
33 32 Appendix 10: Appendix 11:
34 33 Appendix 12: Appendix 13:
35 34 Appendix 14: Appendix 15:
36 35
37 36 Appendix 16: The goal is to notify the RN when pain is 4 Appendix 17:

38 37 Chart Review: Pain reassessment within 1 hour of medication administration Reassessment within 1 hour Reassessmet after 1 hour Appendix 18: Post Intervention Results 43% 38% Heat/ Ice Music therapy Whiteboard 19%
39 38 Appendix 19: Appendix 20:
40 39 Survey Questions for Patients 1. To what extent is your pain well controlled? Extremely not at all 2. How much pain relief are you currently receiving? A great deal no relief 3. How much pain relief did you expect to have while hospitalized? A great deal no relief 4. When do you usually ask your nurse for pain medicine? When pain is: Mild Moderate Severe 5. How often did you receive pain medication when you needed it? Never Sometimes Usually Most times Always 6. How often were the nurses reassessing your pain within one hour after medicating you? Never Sometimes Usually Most times Always 7. What other non-pharmacological therapy (such as massage, heat, ice, relaxation, music) do you use for pain relief? 8. What other non-pharmacological therapy did your nurse teach you? 9. If you received pain medication and it did not help, what did you do about it? 10. When in pain, what keeps you from asking the nurse for pain medication?
41 Do you have any suggestions about how your pain management could be improved? Survey Questions for Nurses 1. Are you familiar with HCAPHS scores and why they are important? 2. Why is the HCAHPs score for 'pain well controlled' low? 3. What can be done to improve the HCAHPS score for 'pain well controlled'? 4. What do you think nurses can do to control patients' pain? 5. What other non-pharmacological therapy (such as massage, heat, ice, relaxation, music) do you teach your patients? 6. Overall, whom do you think is responsible for ensuring that pain is well controlled? 7. How often do you reassess your patients pain within an hour after medicating them? Never Sometimes Usually Most times Always 8. What are the barriers that prevent you from reassessing patients pain as often as you would like? 9. What changes would make it easier for you to reassess pain as often as you would like?
42 Has there been a time when pain medication was necessary but you were uncomfortable contacting the physician? If so what happened?
43 42 References Burhenn, P., Olausson, J., Villegas, G., & Kravits, K. (2014). Guided Imagery for Pain Control. Clinical Journal of Oncology Nursing, 18(5), Doi: /14.CJON Casey, G. (2011). Pain- the fifth vital sign. Continuing professional development. Kai Tiaki Nursing New Zealand, 17(5), Retrieved from &site=eds-live&scope=site Casida, J., Lemanski, S. (2010). An evidence-based review on guided imagery utilization in adult cardiac surgery. Clinical scholars review, 3(1), Doi:10.189/ Centers for Medicare and Medicaid. (2014). HCAHPS: Patients Perspective of Care Survey. Retrieved from Instruments/HospitalQualityInits/HospitalHCAHPS.html Gammons, V., & Caswell, G. (2014). Older people and barriers to self-reporting of chronic pain. British Journal of Nursing, 23(5), Retrieved from eds.a.ebscohost.com.ignacio.usfca.edu/eds/pdfviewer/pdfviewer?vid=30&sid=5fddde6d- 6dc4-4d21-b8cc-deaa4abd012a%40sessionmgr4003&hid=4202 Geiger, N. F. (2012). On Tying Medicare Reimbursement to Patient Satisfaction Surveys. AJN, American Journal of Nursing, volume 112-Issue 7-p 11 doi: /01.NAJ a. Retrieved from ment_to_patient.2.aspx Gregory, J., & Waterman, H. (2012). Observing pain management practice on a medical unit
44 43 following changes arising from an action research study. Journal Of Clinical Nursing, 21(23/24), doi: /j x. Retrieved from eds.a.ebscohost.com.ignacio.usfca.edu/eds/pdfviewer/pdfviewer?sid=5fddde6d-6dc4-4d21-b8cc-deaa4abd012a%40sessionmgr4003&vid=17&hid=4202 Gropelli, T., & Sharer, J. (2013). Nurses' Perceptions of Pain Management in Older Adults. MEDSURG Nursing, 22(6), Retrieved from eds.a.ebscohost.com.ignacio.usfca.edu/eds/pdfviewer/pdfviewer?sid=5fddde6d-6dc4-4d21-b8cc-deaa4abd012a%40sessionmgr4003&vid=4&hid=4202 Huth, M.M., Daraiseh, N.M., Henson, M.A., & McLeod, S.M. (2009). Evaluation of the magic island: Relaxation for kids compact disc. Pediatric Nursing, 35(5), Retrieved from Koch, K. K. (2013). Acute pain management in general practice: steps to effective pain control: review article. South African Practice, (6), 520. Retrieved from Lewandowski, W., & Jacobson, A. (2013). Bridging the Gap Between Mind and Body: A Biobehavioral Model of the Effects of Guided Imagery and Pain, Pain Disability, and Depression. Pain Management Nursing, 14(4), Doi: /j.pmn Makris UE, Abrams RC, Gurland B, Reid M. Management of Persistent Pain in the Older Patient: A Clinical Review. JAMA. 2014;312(8): doi: /jama Retrieved from Ogston-Tuck, S. (2014). A silent epidemic: effective pain management in the community. British
45 44 JournalOf Healthcare Management, 20(6), Retrieved from eds.a.ebscohost.com.ignacio.usfca.edu/eds/pdfviewer/pdfviewer?sid=5fddde6d-6dc4-4d21-b8cc-deaa4abd012a%40sessionmgr4003&vid=15&hid=4202 Posadzki, P; Lewandowski, W; Terry, R; Ernst, E; & Sterns, A. (2012). Guided Imagery for nonmusculoskeletal pain: a systematic review of randomized clinical trials. Journal of Pain and Sympom Management, 44(1), Doi: /j.jpainsymman Selimen, D; & Andsoy, I. I. (2011). The importance of a holistic approach during the perioperative period. Association of operating room nurses. AORN Journal, 93(4), 482-7; quiz Doi: Wang, H., & Tsai, Y. (2010). Nurses' knowledge and barriers regarding pain management in intensive care units. Journal of Clinical Nursing, 19(21/22), doi: /j x. Retrieved from eds.a.ebscohost.com.ignacio.usfca.edu/eds/pdfviewer/pdfviewer?sid=5fddde6d-6dc4-4d21-b8cc-deaa4abd012a%40sessionmgr4003&vid=23&hid=4202 Wells, N., Pasero, C., McCaffery, M. (2008). Improving the Quality of Care Through Pain Assessment and Management. In: Hughes RG, editor. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. Rockville (MD): Agency for Healthcare research and Quality (US); 2008 Apr. Chapter 17. Retrieved from Studer, Q., Robinson, B.C., & Cook, K. (2010). The HCAHPS Handbook: Hardwire your
46 45 Hospital for Pay-for-Performance Success. Florida: Fire Starter Publishing.
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Pain: Facility Assessment Checklists This is a series of self-assessment checklists for nursing home staff to use to assess processes related to pain management in the facility, in order to identify areas
Improving Nurse-patient Communication about New Medicines
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Improving
Brenda M. Nordstrom MSN, RN-BC, CHPN Baker College School of Nursing. Brenda Nordstrom MSN, RN-BC, CHPN No Conflict of Interest
 Brenda M. Nordstrom MSN, RN-BC, CHPN Baker College School of Nursing Brenda Nordstrom MSN, RN-BC, CHPN No Conflict of Interest Analyze the gap between evidence and current practice of pain management education
Brenda M. Nordstrom MSN, RN-BC, CHPN Baker College School of Nursing Brenda Nordstrom MSN, RN-BC, CHPN No Conflict of Interest Analyze the gap between evidence and current practice of pain management education
IMPROVING COMMUNICATION AND SATISFACTION THROUGH HOURLY ROUNDS
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 IMPROVING
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 IMPROVING
Optimizing Electronic Healthcare Records and Improving Process in the Healthcare Clinic
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Optimizing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Optimizing
Improving Staff Responsiveness to Patient-Initiated Call Lights
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
Reducing Avoidable Interruptions During the Medication Administration Process
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Reducing
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Reducing
Pain: Facility Assessment Checklists
 Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Pain: Facility Assessment Checklists A facility system assessment is a starting point for a quality improvement project. The checklists included in this booklet will be most useful if you take a critical
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Improving Pain Reassessment within One Hour Following the Administration of Pain Medication
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
The Clinical Nurse Leader as Risk Anticipator: Optimizing the Completion and Accuracy of the Code Blue Recorder Sheet
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-9-2017 The
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-9-2017 The
December 16, Thoracostomy Tube Removal Procedural Pain Practice Guideline Implementation Lisa M. Ring, DNP, CPNP, AC-PC
 Thoracostomy Tube Removal Procedural Pain Practice Guideline Implementation Lisa M. Ring, DNP, CPNP, AC-PC Objectives Nature and scope of the project Literature review and analysis Project methods Results
Thoracostomy Tube Removal Procedural Pain Practice Guideline Implementation Lisa M. Ring, DNP, CPNP, AC-PC Objectives Nature and scope of the project Literature review and analysis Project methods Results
Advancing Accountability for Improving HCAHPS at Ingalls
 iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
iround for Patient Experience Advancing Accountability for Improving HCAHPS at Ingalls A Case Study Webconference 2 Managing your audio Use Telephone If you select the use telephone option please dial
Improving Hand Hygiene Compliance to Reduce CLABSI Rate in Oncology ICU
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22- Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-22- Improving
Improving Nurse Education on Research Informed Consent
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
Theory Application: Theory of Comfort. RobERT Pinkston. Old Dominion University
 Running head: THEORY OF COMFORT 1 Theory Application: Theory of Comfort RobERT Pinkston Old Dominion University THEORY OF COMFORT 2 THEORY APPLICATION: THEORY OF COMFORT The Theory of Comfort was developed
Running head: THEORY OF COMFORT 1 Theory Application: Theory of Comfort RobERT Pinkston Old Dominion University THEORY OF COMFORT 2 THEORY APPLICATION: THEORY OF COMFORT The Theory of Comfort was developed
The Significance of Timing of Patient Daily Weights and the Barriers
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 The
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 The
A Roadmap for the Journey Home - A Supplemental Tool Guiding Patients from Hospital to Home
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Roadmap
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Roadmap
Chronic Pain Management in the Inpatient Care Setting
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Chronic
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Chronic
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care. Recommendation Comparison Chart
 RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
RNAO Delirium, Dementia, and Depression in Older Adults: Assessment and Care Recommendation Comparison Chart RECOMMENDATIONS FROM SCREENING FOR DELIRIUM, DEMENTIA AND DEPRESSION IN THE OLDER ADULT (2010)
Project Title: Improving Pain Management at Hospital Admission and Discharge: Implementing an Interdisciplinary Evidence-Based Approach
 Project Title: Improving Pain Management at Hospital Admission and Discharge: Implementing an Interdisciplinary Evidence-Based Approach Principal Investigators: Wendy Anderson, MD, MS University of California,
Project Title: Improving Pain Management at Hospital Admission and Discharge: Implementing an Interdisciplinary Evidence-Based Approach Principal Investigators: Wendy Anderson, MD, MS University of California,
Patient Satisfaction Related to Noise in the Coronary Care Unit
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Patient
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Patient
Follow Up on Bedside Reporting. IHI Expedition Improving Your HCAHPS Scores Through Patient Centered Care. Today s Topics
 Follow Up on Bedside Reporting The call content prompted us to: Make concrete plans to move shift report to the bedside Actually run a test of doing shift report at the bedside Make revisions to the way
Follow Up on Bedside Reporting The call content prompted us to: Make concrete plans to move shift report to the bedside Actually run a test of doing shift report at the bedside Make revisions to the way
Fall Reduction with Nursing Interventions
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Fall
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Fall
More than 60% of elective surgery
 Benefits of Preoperative Education for Adult Elective Surgery Patients NANCY KRUZIK, MSN, RN, CNOR More than 60% of elective surgery procedures in the United States were being performed as outpatient procedures
Benefits of Preoperative Education for Adult Elective Surgery Patients NANCY KRUZIK, MSN, RN, CNOR More than 60% of elective surgery procedures in the United States were being performed as outpatient procedures
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
Improving Interdisciplinary Communication to Improve Patient Satisfaction
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Improving
Proposed Standards Revisions Related to Pain Assessment and Management
 Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
Leadership (LD) Chapter LD.0001 Proposed Standards Revisions Related to Pain Assessment and Management 1 2 Leaders establish priorities for performance improvement. (Refer to the "Performance Improvement"
REDUCTION OF PSYCHIATRIC PATIENT BOARDING IN THE ED
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 REDUCTION
Implementation of a Debrief Takeaway board
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Implementation
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Summer 8-17-2015 Implementation
Obstetric Triage Improvement
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Obstetric
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Obstetric
A Multi-Prong Fall Awareness Program to Reduce the Occurrence of Falls in a Skilled Nursing Unit
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Multi-Prong
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-15-2017 A Multi-Prong
Improving Patient Safety: Reducing Medication Errors in the Microsystem
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-21-2015 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-21-2015 Improving
APPENDIX B. Physician Assistant Competencies: A Self-Evaluation Tool
 APPENDIX B Physician Assistant Competencies: A Self-Evaluation Tool Rate your strength in each of the competencies using the following scale: 1 = Needs Improvement 2 = Adequate 3 = Strong 4 = Very Strong
APPENDIX B Physician Assistant Competencies: A Self-Evaluation Tool Rate your strength in each of the competencies using the following scale: 1 = Needs Improvement 2 = Adequate 3 = Strong 4 = Very Strong
The Patient Experience at Florida Hospital Learning Module for Students
 The Patient Experience at Florida Hospital Learning Module for Students 1 Introduction Adventist Health System and its East Florida Region hospitals welcome the privilege to provide a wellrounded learning
The Patient Experience at Florida Hospital Learning Module for Students 1 Introduction Adventist Health System and its East Florida Region hospitals welcome the privilege to provide a wellrounded learning
The Triple Aim. Productivity: Digging Deep Enough 11/4/2013. quality and satisfaction); Improving the health of populations; and
; Improving the health of populations; and") NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
NAHC Annual Conference October, 2013 Cindy Campbell, BSN, RN Associate Director Operational Consulting Fazzi Jeanie Stoker, BSN, RN, MPA, BC Director AnMed Health Home Care Context AnMed Health Home Health
Improving Pain Center Processes utilizing a Lean Team Approach
 Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Center Processes utilizing a Lean Team Approach Organization Name: St. Joseph Medical Center Type: Acute Care Hospital Contact Person: Sue Mitchell Title: Nurse Mgr Pain Mgmt Center E-Mail:
Improving Pain Reassessment and Documentation Through Nurse Education
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-16-2016 Improving
Running head: IMPROVING QUALITY OF LIFE 1
 Running head: IMPROVING QUALITY OF LIFE 1 Music Therapy: Improving Quality of Life for Dementia Residents in Nursing Homes Keltie P. Keir, B.N., R.N University of New Brunswick IMPROVING QUALITY OF LIFE
Running head: IMPROVING QUALITY OF LIFE 1 Music Therapy: Improving Quality of Life for Dementia Residents in Nursing Homes Keltie P. Keir, B.N., R.N University of New Brunswick IMPROVING QUALITY OF LIFE
Nurses' Attitudes towards Drug-Seekers in the Emergency Room
 Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 1-1-2013 Nurses'
Rhode Island College Digital Commons @ RIC Master's Theses, Dissertations, Graduate Research and Major Papers Overview Master's Theses, Dissertations, Graduate Research and Major Papers 1-1-2013 Nurses'
Development and Implementation of a Patient Education Tool to Increase Fall Risk Awareness
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Development
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-12-2014 Development
DEVELOPING A CULTURE OF NURSE LED PARTNERSHIP ROUNDING
 DEVELOPING A CULTURE OF NURSE LED PARTNERSHIP ROUNDING Jenny Gilmore, BSN, RN, CMSRN Jana Jacobs, BSN, RN, CMSRN Maine Medical Center Portland, ME Objectives Describe Partnership Rounding for the staff
DEVELOPING A CULTURE OF NURSE LED PARTNERSHIP ROUNDING Jenny Gilmore, BSN, RN, CMSRN Jana Jacobs, BSN, RN, CMSRN Maine Medical Center Portland, ME Objectives Describe Partnership Rounding for the staff
Evaluating the Impact of Pain Management (PM) Education on Physician Practice Patterns A Continuing Medical Education (CME) Outcomes Study
 Education on Physician Practice Patterns A Continuing Medical Education (CME) Outcomes Study") J Canc Educ (2010) 25:224 228 DOI 10.1007/s13187-010-0040-y Evaluating the Impact of Pain Management (PM) Education on Physician Practice Patterns A Continuing Medical Education (CME) Outcomes Study L.
J Canc Educ (2010) 25:224 228 DOI 10.1007/s13187-010-0040-y Evaluating the Impact of Pain Management (PM) Education on Physician Practice Patterns A Continuing Medical Education (CME) Outcomes Study L.
Infection Control: Reducing Hospital Acquired Central Line Bloodstream Infections
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Infection
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2017 Infection
snapshot SATISFACTION Trust Your Staff But Check Validation The Key to Hardwiring Change is the problem the tactic? - or is it the execution?
 SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
State and federal regulations supersede any information provided in this toolkit.
 DPA Associates, Inc Toolkit author: Diane Atchinson, RN-BC, MSN, ANP, RAC-CT President, DPA Associates, Inc, Kansas City, MO E mail: diane@dpaassociates.com Clinical editor: Kathy Newman, MSW, LSCW, Consultant
DPA Associates, Inc Toolkit author: Diane Atchinson, RN-BC, MSN, ANP, RAC-CT President, DPA Associates, Inc, Kansas City, MO E mail: diane@dpaassociates.com Clinical editor: Kathy Newman, MSW, LSCW, Consultant
Pastoral Interventions and the Influence of Self-Reporting: A Preliminary Analysis
 Journal of Health Care Chaplaincy, 16:65 73, 2010 Copyright # Taylor & Francis Group, LLC ISSN: 0885-4726 print=1528-6916 online DOI: 10.1080/08854720903519976 Pastoral Interventions and the Influence
Journal of Health Care Chaplaincy, 16:65 73, 2010 Copyright # Taylor & Francis Group, LLC ISSN: 0885-4726 print=1528-6916 online DOI: 10.1080/08854720903519976 Pastoral Interventions and the Influence
Focus Group results RN Perspective
 Focus Group results RN Perspective Category Themes Communication Patient Condition Communicate Expectations and plan of care Early 1. Communicate to patient at beginning of shift and throughout shift (pain
Focus Group results RN Perspective Category Themes Communication Patient Condition Communicate Expectations and plan of care Early 1. Communicate to patient at beginning of shift and throughout shift (pain
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016
 Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Preventing Medical Errors Presented by Debra Chasanoff, MEd, OTR/L FOTA Annual Conference, November 4-5, 2016 This program was designed to meet the criteria in section 456.013(7), Florida Statutes, which
Running head: CLINICAL LADDER 1. Advancing the Nursing Profession Through the Clinical Ladder. Amy Rehm. Kent State University
 Running head: CLINICAL LADDER 1 Advancing the Nursing Profession Through the Clinical Ladder Amy Rehm Kent State University CLINICAL LADDER 2 Abstract As healthcare continues to advance clinical practices,
Running head: CLINICAL LADDER 1 Advancing the Nursing Profession Through the Clinical Ladder Amy Rehm Kent State University CLINICAL LADDER 2 Abstract As healthcare continues to advance clinical practices,
Christy Rose, MSN, RN, CCRN Denver Health Medical Center. 7th Annual Nursing Quality Conference: Reaching the Core of Quality
 Christy Rose, MSN, RN, CCRN Denver Health Medical Center 7th Annual Nursing Quality Conference: Reaching the Core of Quality Partnered with the National Database of Nursing Quality Indicators (NDNQI )
Christy Rose, MSN, RN, CCRN Denver Health Medical Center 7th Annual Nursing Quality Conference: Reaching the Core of Quality Partnered with the National Database of Nursing Quality Indicators (NDNQI )
CAHPS Focus on Improvement The Changing Landscape of Health Care. Ann H. Corba Patient Experience Advisor Press Ganey Associates
 CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
CAHPS Focus on Improvement The Changing Landscape of Health Care Ann H. Corba Patient Experience Advisor Press Ganey Associates How we will spend our time together Current CAHPS Surveys New CAHPS Surveys
Bond University Medical Program. Oncology Rotation Clinician Guide
 Bond University Medical Program Oncology Rotation Clinician Guide YEAR 5 2018 Introduction Students in the final year of the Bond University Medical Program have 6 rotations to train in a broad array of
Bond University Medical Program Oncology Rotation Clinician Guide YEAR 5 2018 Introduction Students in the final year of the Bond University Medical Program have 6 rotations to train in a broad array of
Using HCAHPS Survey Custom Questions to Drive Staff Engagement
 Using HCAHPS Survey Custom Questions to Drive Staff Engagement Diana Topjian, RN, MSN, D.M., C-ENP Account Lead/Coach Studer Group Outcome Goals Verbalize the value of adding HCAHPS custom questions to
Using HCAHPS Survey Custom Questions to Drive Staff Engagement Diana Topjian, RN, MSN, D.M., C-ENP Account Lead/Coach Studer Group Outcome Goals Verbalize the value of adding HCAHPS custom questions to
Test Content Outline Effective Date: February 6, Gerontological Nursing Board Certification Examination
 Board Certification Examination There are 175 questions on this examination. Of these, 150 are scored questions and 25 are pretest questions that are not scored. Pretest questions are used to determine
Board Certification Examination There are 175 questions on this examination. Of these, 150 are scored questions and 25 are pretest questions that are not scored. Pretest questions are used to determine
Scholars Week Spring Scholars Week 2016
 Murray State's Digital Commons Scholars Week Spring Scholars Week 2016 Apr 18th, 12:00 PM - 2:00 PM Fall prevention Cody Durbin Murray State University Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Murray State's Digital Commons Scholars Week Spring Scholars Week 2016 Apr 18th, 12:00 PM - 2:00 PM Fall prevention Cody Durbin Murray State University Follow this and additional works at: http://digitalcommons.murraystate.edu/scholarsweek
Nurse Shift Handoff Report at the Patient's Bedside: Improving Nurse-to-Nurse Communication
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Nurse
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-16-2016 Nurse
Using Innovation to Maximize Behavioral Health Accommodations. Regions Hospital Case Study
 Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing
 The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
The Reduction of Seclusion & Restraint in the University of Michigan Psychiatric Emergency Services with the Introduction of 24/7 Nurse Staffing Sharon P. Stetz MSN Marvella M. Muzik, MS PMHNP, BC Objectives
Implementing a Pain Toolkit to Improve Pain Management
 Illinois State University ISU ReD: Research and edata Theses and Dissertations Summer 8-5-2016 Implementing a Pain Toolkit to Improve Pain Management Kathleen R. Atkins DNP Illinois State University, kratki2@ilstu.edu
Illinois State University ISU ReD: Research and edata Theses and Dissertations Summer 8-5-2016 Implementing a Pain Toolkit to Improve Pain Management Kathleen R. Atkins DNP Illinois State University, kratki2@ilstu.edu
Reduce the Rooming Time
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Reduce
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Spring 5-19-2016 Reduce
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
QAPI Making An Improvement
 Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
Preparing for the Future QAPI Making An Improvement Charlene Ross, MSN, MBA, RN Objectives Describe how to use lessons learned from implementing the comfortable dying measure to improve your care Use the
HCAHPS: Background and Significance Evidenced Based Recommendations
 HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
HCAHPS: Background and Significance Evidenced Based Recommendations Susan T. Bionat, APRN, CNS, ACNP-BC, CCRN Education Leader, Nurse Practitioner Program Objectives Discuss the background of HCAHPS. Discuss
Project Description: Page Memorial Hospital (PMH) identified a need for patient care coordination and continuity for post discharge care.
 identified a need for patient care coordination and continuity for post discharge care.") Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
Title: Improving Care Transitions by Utilizing a Multidisciplinary Approach Including a Transition Coach and Primary Care Model Hospital: Valley Health Page Memorial Contacts: Portia Brown Vice President
TeamSTEPPS TM National Implementation
 TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
TeamSTEPPS TM National Implementation Implementing TeamSTEPPS in Critical Access Hospitals Katherine Jones, PT, PhD University of Nebraska Medical Center Implementing TeamSTEPPS in Critical Access Hospitals
HealthStream Regulatory Script
 HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
HealthStream Regulatory Script Advance Directives Version: [May 2006] Lesson 1: Introduction Lesson 2: Advance Directives Lesson 3: Living Wills Lesson 4: Medical Power of Attorney Lesson 5: Other Advance
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS) 1,2,3
 1,2,3") Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound)
") Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
Improving HCAHPS with a Culture of Quiet St. Francis Hospital (Puget Sound) Problem: Surveys showed that the noise level made it difficult for patients to rest. Innovation: Implemented a culture of quiet.
LOYOLA UNIVERSITY CHICAGO STRITCH SCHOOL OF MEDICINE OFFICE OF STUDENT AFFAIRS CENTER FOR COMMUNITY AND GLOBAL HEALTH
 LOYOLA UNIVERSITY CHICAGO STRITCH SCHOOL OF MEDICINE OFFICE OF STUDENT AFFAIRS CENTER FOR COMMUNITY AND GLOBAL HEALTH DATE: June TO: Class of 2014/2015 SUBJECT: Enrollment Open THIRD YEAR GLOBAL HEALTH
LOYOLA UNIVERSITY CHICAGO STRITCH SCHOOL OF MEDICINE OFFICE OF STUDENT AFFAIRS CENTER FOR COMMUNITY AND GLOBAL HEALTH DATE: June TO: Class of 2014/2015 SUBJECT: Enrollment Open THIRD YEAR GLOBAL HEALTH
Chapter 21. List two ways in which the nurse can lessen the stress of hospitalization for the child s parents.
 Chapter 21 The Child s Experience of Hospitalization Objectives Identify various health care delivery settings. Describe three phases of separation anxiety. List two ways in which the nurse can lessen
Chapter 21 The Child s Experience of Hospitalization Objectives Identify various health care delivery settings. Describe three phases of separation anxiety. List two ways in which the nurse can lessen
Instrument Author: Ferrell, B. R., Eberts, M. T., McCaffery, M., Grant, M. Ferrell, B. R., Eberts, M. T., McCaffery, M., Grant, M..
 Instrument Title: The Clinical Decision Making Survey (CDMS) Instrument Author: Ferrell, B. R., Eberts, M. T., McCaffery, M., Grant, M. Cite instrument as: Ferrell, B. R., Eberts, M. T., McCaffery, M.,
Instrument Title: The Clinical Decision Making Survey (CDMS) Instrument Author: Ferrell, B. R., Eberts, M. T., McCaffery, M., Grant, M. Cite instrument as: Ferrell, B. R., Eberts, M. T., McCaffery, M.,
The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus
 University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
HALF YEAR REPORT ON SENTINEL EVENTS
 HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
HALF YEAR REPORT ON SENTINEL EVENTS 1 October 2008-31 March 2009 Jul 2009-0 - TABLE OF CONTENTS Chapter Page 1. Executive Summary...... 2 2. Introduction 5 3. Sentinel Events Reported... 6 From 1 October
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Practice Problems. Managing Registered Nurses with Significant PRACTICE GUIDELINE
 PRACTICE GUIDELINE Managing Registered Nurses with Significant Practice Problems Practice Problems May 2012 (1/17) Mission The Nurses Association of New Brunswick is a professional regulatory organization
PRACTICE GUIDELINE Managing Registered Nurses with Significant Practice Problems Practice Problems May 2012 (1/17) Mission The Nurses Association of New Brunswick is a professional regulatory organization
Improving Intimate Partner Violence Screening in the Emergency Department Setting
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
IHI Expedition. Reducing Readmissions by Improving Care Transitions Session 2. Expedition Coordinator
 Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
Thursday, June 20, 2013 These presenters have nothing to disclose IHI Expedition Reducing Readmissions by Improving Care Transitions Session 2 Peg Bradke, RN, MA Saranya Loehrer, MD, MPH Expedition Coordinator
School of Nursing Applying Evidence to Improve Quality
 Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
Applying Evidence to Improve Quality Linda A Dudjak PhD RN Associate Professor University of Pittsburgh School of Nursing Compare Two Alternatives Implement a Test of Change (Experiment) to Fix a Broken
Definitions/Glossary of Terms
 Definitions/Glossary of Terms Submitted by: Evelyn Gallego, MBA EgH Consulting Owner, Health IT Consultant Bethesda, MD Date Posted: 8/30/2010 The following glossary is based on the Health Care Quality
Definitions/Glossary of Terms Submitted by: Evelyn Gallego, MBA EgH Consulting Owner, Health IT Consultant Bethesda, MD Date Posted: 8/30/2010 The following glossary is based on the Health Care Quality
NURSES KNOWLEDGE REGARDING PAIN MANAGEMENT IN HAIL REGION HOSPITALS, SAUDI ARABIA.
 NURSES KNOWLEDGE REGARDING PAIN MANAGEMENT IN HAIL REGION HOSPITALS, SAUDI ARABIA. Hamdan Albaqawi Bcs, RN, MSN, PhD candidate (School of Health Sciences), RMIT University, Australia Wesaam_2003@hotmail.com
NURSES KNOWLEDGE REGARDING PAIN MANAGEMENT IN HAIL REGION HOSPITALS, SAUDI ARABIA. Hamdan Albaqawi Bcs, RN, MSN, PhD candidate (School of Health Sciences), RMIT University, Australia Wesaam_2003@hotmail.com
Falls Program on an Acute Psychiatric Unit
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-15-2016 Falls
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-15-2016 Falls
Title & Subtitle can. accc-cancer.org March April 2017 OI
 Spiritual Care Title & Subtitle can of Cancer Patients knockout of image 30 accc-cancer.org March April 2017 OI BY REV. LORI A. MCKINLEY, MDIV, BCC A pilot study of integrated multidisciplinary care planning
Spiritual Care Title & Subtitle can of Cancer Patients knockout of image 30 accc-cancer.org March April 2017 OI BY REV. LORI A. MCKINLEY, MDIV, BCC A pilot study of integrated multidisciplinary care planning
NURSING SPECIAL REPORT
 2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
CNA Training Advisor
 CNA Training Advisor Volume 14 Issue No. 4 APRIL 2016 Teamwork is the foundation for success in any healthcare system. Because teamwork allows individuals to combine their knowledge and skill sets to do
CNA Training Advisor Volume 14 Issue No. 4 APRIL 2016 Teamwork is the foundation for success in any healthcare system. Because teamwork allows individuals to combine their knowledge and skill sets to do
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure
 Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality
 And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality Leisha Buller, MSN, ACNP-BC Lindsey Canon, MSN, RNC Ashley Hodo, MSN, RN Using The Joint Commission s Certification
And the Evidence Shows Using Specialty Certification from The Joint Commission Improves Quality Leisha Buller, MSN, ACNP-BC Lindsey Canon, MSN, RNC Ashley Hodo, MSN, RN Using The Joint Commission s Certification
snapshot Improving Experience of Care Scores Alone is NOT the Answer: Hospitals Need a Patient-Centric Foundation
 SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
This document was created and is owned by St. Michael s Hospital (the Hospital ). The Hospital hereby authorizes non-profit organizations to use and
. The Hospital hereby authorizes non-profit organizations to use and") This document was created and is owned by St. Michael s Hospital (the Hospital ). The Hospital hereby authorizes non-profit organizations to use and reproduce this document (the Document ) solely for their
This document was created and is owned by St. Michael s Hospital (the Hospital ). The Hospital hereby authorizes non-profit organizations to use and reproduce this document (the Document ) solely for their
Model of Care Scoring Guidelines CY October 8, 2015
 Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Model of Care Guidelines CY 2017 October 8, 2015 Table of Contents Model of Care Guidelines Table of Contents MOC 1: Description of SNP Population (General Population)... 1 MOC 2: Care Coordination...
Quality Improvement Program Evaluation
 Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Quality Improvement Program Evaluation 2013 Care Wisconsin 2013 Quality Improvement Program Evaluation INTRODUCTION Care Wisconsin s Quality Management Program uses the Home and Community-Based Quality
Text-based Document. Building a Culture of Safety: Aligning innovative leadership rounding and staff driven hourly rounding strategies
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
INCREASED COMMUNICATION BETWEEN NURSES AND DOCTORS ON AN ACUTE MEDICAL UNIT
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-12-2014 INCREASED
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Winter 12-12-2014 INCREASED
Barriers Encountered by Nurses and Nursing Assistants that Prevent Purposeful Rounding
 The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Barriers
The University of San Francisco USF Scholarship: a digital repository @ Gleeson Library Geschke Center Master's Projects and Capstones Theses, Dissertations, Capstones and Projects Fall 12-18-2015 Barriers
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
10/14/2014 COMMON MDS CODING ERRORS OVERVIEW OF SS/ACT SECTIONS SECTION B
 COMMON MDS CODING ERRORS K AT H Y Y O S T E N, L C S W, P I P OVERVIEW OF SS/ACT SECTIONS Section B Vision, Speech, Hearing Section C Cognitive Patterns Section D Mood Section E Behaviors Section F Preferences
COMMON MDS CODING ERRORS K AT H Y Y O S T E N, L C S W, P I P OVERVIEW OF SS/ACT SECTIONS Section B Vision, Speech, Hearing Section C Cognitive Patterns Section D Mood Section E Behaviors Section F Preferences
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress
 Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Tip Sheet Reducing Off Label Use of Antipsychotic Medications by Engaging Staff in Individualizing Care to Alleviate Resident Distress WHAT IT IS Off label use of antipsychotic medications means uses the
Unit 301 Understand how to provide support when working in end of life care Supporting information
 Unit 301 Understand how to provide support when working in end of life care Supporting information Guidance This unit must be assessed in accordance with Skills for Care and Development s QCF Assessment
Unit 301 Understand how to provide support when working in end of life care Supporting information Guidance This unit must be assessed in accordance with Skills for Care and Development s QCF Assessment