CASE MANAGEMENT TOOLS:
|
|
|
- Rosalind Samantha Sparks
- 6 years ago
- Views:
Transcription

1 CASE MANAGEMENT TOOLS: ENGAGING PATIENTS AS PARTNERS IN CARE September 19, 2017 Chinle Service Unit Diabetes Program Navajo Area Indian Health Service Miranda Williams Krista Haven





2 CHINLE SERVICE UNIT Canyon de Chelly, Chinle, AZ Chinle Comprehensive Healthcare Facility Pinon Health Center Tsaile Health Center
3 CHINLE SERVICE UNIT Chinle Service Unit is a federally run Indian Health Service site with 60 bed hospital and 3 ambulatory health care centers. Population: Almost 37,000 Native Americans in 17 chapters (communities) in the central part of the Navajo Nation. Approximately 180,000 outpatient visits annually.
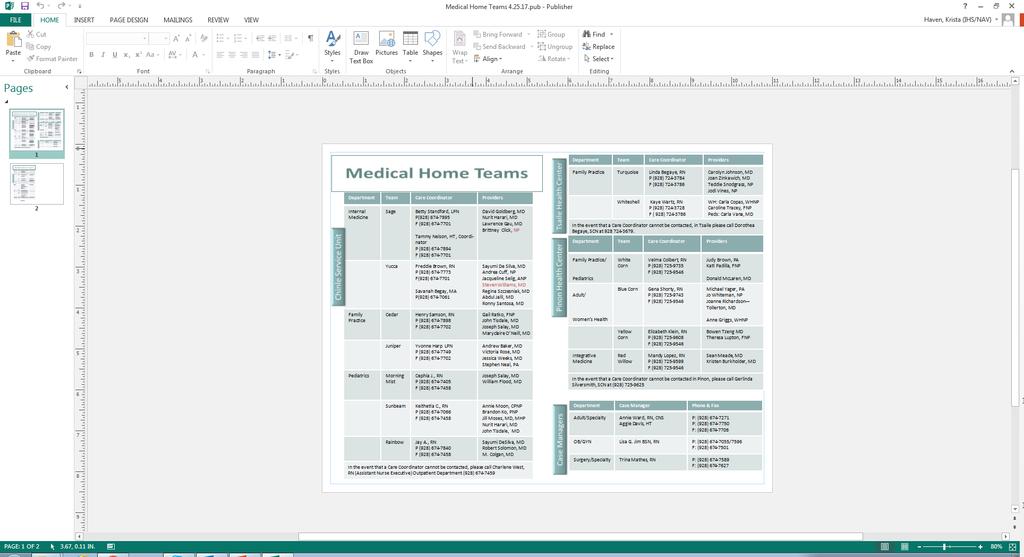
4 CHINLE SERVICE UNIT MEDICAL HOME MODEL: PRIMARY CARE BASED Chinle has embraced the Patient Centered Medical Home model, including team-based care. Teams consist of primary care providers, health techs (medical assistants), nurses, health coaches, care managers, Native Medicine, pharmacist, integrated behavioral health team, and dietitian in clinic. DM clinical interventions (4500+ DM patients) Focused on primary care with complex needs Includes consultation for in-patients, limited ED/Urgent Care
5 PROGRAM AIM STATEMENT The aim of the Chinle Diabetes Program is to support the wellbeing of our community through the introduction of education in self-management care to prevent diabetes, manage the progression of diabetes, and address other chronic diseases. Our goal is to enhance the systems of care for the patient while utilizing a consistent cultural approach.
6 SELF-MANAGEMENT Patient s health largely depends on their own behaviors Lifestyle issues (diet, exercise, and sleep), taking medications, checking home blood sugars, getting preventive screenings, foot and eye exams, immunizations, and tobacco/alcohol cessation Ultimately, patients have to take care of themselves: SELF-MANAGEMENT Health care personnel can provide support (SMS), education (SME) In our program we have added health coaching which supports lifelong learning
7 AADE SELF-CARE BEHAVIORS Being Active Healthy Coping Healthy Eating Monitoring Problem Solving Reducing Risks Taking medications
8 TOOLS Provide diabetes education using motivational interviewing strategies: Ask Tell Ask, Brainstorming, Teach Back, Brief Action planning Enhance understanding by addressing language and health literacy barriers Provide culturally sensitive communication Certified Navajo interpreters Promote shared decision making and collaborative relationship with providers
9 DIABETES HEALTH COACHES: PRIMARY ROLES Help patients change behavior (SMS and SME) Understanding readiness for change Recognizing and addressing behavioral barriers Teaching skills of problem solving, realistic goal setting and action planning Utilizing Healthy Heart, Balancing Your Life in Diabetes, Lifestyle Balance curriculum Provide care coordination and follow-up
10 CASE MANAGEMENT Case Management: Pre-DM Patients Newly Diagnosed DM patients Primary Care DM patients with an A1C, B/P, or Statin Use Inpatient - DM Patients ER/UC DM patients Case Management of High risk, High cost patients (eg, A1C>11, alcohol abuse, frequent hospitalizations) Goal: Educate pre-dm patients with handouts and Wellness Center and nutrition referrals Engage new DM patients in care, support their personal journey with DM, educate them about DM and its management (AADE self-care behaviors), and treat with lifestyle interventions and medications Goals: A1C below 8 Blood pressure below 140/90 StatinUse for patients that have risk factors and/or >40 To decrease cardiovascular risk Influence patients to use their care teams for follow-up and introduce Diabetes team Influence patients to us their care teams for care and introductions to DM team Determine what are the behavior barriers/drivers that cause patients to be high risk, then intervene, utilizing intensive case management for 3 months. Bahozhoo care model
 Presents with new dizziness that he thinks is medication related Provider")
11 PATIENT STORY 83 year old male with diabetes and recent hospitalization and skilled nursing facility Admission for NSTEMI and new systolic heart failure (both high risk conditions for readmission) Discharge on 11 daily meds, most new to patient, three not on Chinle formulary Has a new medical equipment need (nebulizer) Presents with new dizziness that he thinks is medication related Provider playing catch up, risk for patient being confused, many unanswered questions regarding what the patient needs What can we do differently to improve care to complex patients?

12 THIS CARE IS DIFFERENT HOW WE HOPE PATIENTS TALK ABOUT THEIR EXPERIENCE There is a team helping me and they all seem to know what they re doing They care about me and what I want They are easy to get a hold of My appointments are better things really get done They ve taught me so that I can now really take care of myself They helped me get through one of the hardest periods of my life I am on more meds but I understand them better They listen I feel better
13 13 TOOLS FOR CASE MANAGEMENT OF COMPLEX HIGH RISK PATIENTS Scale-up Challenges Staff Space Training Risk/need assessment forms Care coordination with outside hospital Case management documentation Ideas to Overcome the Challenges Identified case manager and coach to develop and test enhanced care model new roles Identified a room in which to provide enhanced care model Identified case management and coaching training for team Identifying assessment tools for risk stratification and to identify needs/barriers Partnering with inpatient case managers to develop process for assessment and care planning before discharge Building templates for assessment and care plans to assure consistency
14 INTERVENTION Key principles: Use of Patient Activation Measure (PAM) concept/measurement of increasing activation in self-managed care Patient centeredness challenge always! Broad view of health beyond medical (biopsychosocial) and with attention to traumatic life experiences/lifecycle, home assessment Team care coordination, training up of staff (not traditional assembly line), physical space critical (team rooms) Complex care with excellent primary care access and stronger coordination of specialty input, availability to patient Fast appointments and ID card for patients Flag in the EHR if the patient is in the hospital call the BHLC team Risk stratification of patients with assessment tool
15 INTERVENTION Activity/ Staff Member Hospital Home Visit Visit #1 4-6 weeks * Contact with hospital staff for risk assessment nurse case manager * Contact with patient to introduce our awareness of hospitalization and the program Public Health Nurse /Health Coach Health coach to coordinate care with the case manager and update care plan * PAM Score (low PAM consider ACE) * PHQ/GAD (consider, may add ACE with high scores) * DOMAINS assessment (team) Medical neighborhood Medical trajectory Social support Self-management and mental health Clinical Assessment and activity * Severity and appropriateness for BHLC * Key elements of medical record to PCP (admit, specialist consultation, key tests, discharge summary) Assess home environment, self-management, introduce the program, identify key questions or issues for Visit #1, and build rapport * Update medication list * Order medical equipment * Internal and external referrals * Assess patient goals and barriers Select primary DOMAINS area Identify patient goal
16 BAA HÓZHǪa PROCESS Patient admitted to outside hospital Nurse care coordinator and hospital case manager learn patient needs Care plan made with patient before discharge Early contact with team after discharge through home visit or clinic visit Follow up by phone call, clinic visit or home visit by patient preference and complexity Motivational interviewing and brief action planning used to help patient reach goals Patient priorities determine care plan at each visit and documented in EHR Holistic assessment of patient needs and barriers using standard tools Patient has regular appointments as frequent/seldom as needed Coach and case manager are accessible to patients between visits Referrals to additional needed services coordinated Care plan tracked to assure goals are met
17
18

19 ASSESSMENT TOOL FOR RISK

20 NEMT PROVIDERS
21
22 CLINIC HANDOUT

23 LIST OF COMMUNITY RESOURCES
24 ASSESSMENT FOR PATIENT ACTIVATION
25 EUROQUAL VISUAL ANALOG SCALE Scale measuring patient s perception of today s health from worst to best on a continuous 0 to 100 point scale.
26 PATIENT SATISFACTION QUESTION

27 PATIENT STORY Patient admitted to outside hospital with foot infection needing urgent amputation Patient was upset with plan of care and intended to leave hospital against medical advice Hospital case manager called Chinle care coordinator Had prior relationship with health coach Care coordinator arranged for patient to talk by phone with health coach and then staff native healer Patient decided to stay in the hospital and continue health care Baa Hózhǫ team and hospital continued to collaborate on care


28 Chinle Comprehensive Healthcare Facility PO Drawer PH Hwy 191, Hospital Way Chinle, AZ Miranda Williams, BS CSU Diabetes Program Coordinator Office #: Krista Haven, RN, BSN, CDE CSU Diabetes Improvement Specialist Office #:
Standard #1: Internal Structure
 Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Standard #1: Internal Structure
 Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
EVOLENT HEALTH, LLC Diabetes Program Description 2018
 EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
EVOLENT HEALTH, LLC Diabetes Program Description 2018 1 Evolent Health Diabetes Program Description 2018 Table of Contents Section Page Number I. Introduction... 3 II. Program Scope... 3 III. Program Goals...
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
Using the Patient Activation Measure (PAM) to Promote Patient Engagement
 to Promote Patient Engagement") Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
Using the Patient Activation Measure (PAM) to Promote Patient Engagement Mary Jo Muscolino, RN, MPA, CCM, CASAC Director, Behavioral Health Services YourCare Health Plan Objectives Discuss patient engagement
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Advanced Medical Homes: Bending the Trend. Alan Glaseroff, MD Co-Director Stanford Coordinated Care
 Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Advanced Medical Homes: Bending the Trend Alan Glaseroff, MD Co-Director Stanford Coordinated Care aglasero@stanford.edu 1 Hot Spotting in Employed Populations 1. Humboldt County, CA : Priority Care Partnered
Maternity Management. The best part? These are available to you at no additional cost. Intro
 Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
Telligen provides the following services for Connecticut Carpenters members to help you better manage your health and enjoy a good quality of life. The programs include both Maternity Management and Condition
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Commonwealth Regional Specialty Hospital Community Health Needs Assessment & Strategic Implementation Plan for
 Commonwealth Regional Specialty Hospital Community Health Needs Assessment & Strategic Implementation Plan for 2016-2018 Executive Summary The Patient Protection and Affordable Care Act of 2010 included
Commonwealth Regional Specialty Hospital Community Health Needs Assessment & Strategic Implementation Plan for 2016-2018 Executive Summary The Patient Protection and Affordable Care Act of 2010 included
CDR Chad Deegala, PharmD., NCPS-PP Pharmacist Practitioner/Educator Health Education Center for Wellness Northern Navajo Medical Center, Shiprock NM
 CDR Chad Deegala, PharmD., NCPS-PP Pharmacist Practitioner/Educator Health Education Center for Wellness Northern Navajo Medical Center, Shiprock NM Review 3 models of Diabetes management offered at the
CDR Chad Deegala, PharmD., NCPS-PP Pharmacist Practitioner/Educator Health Education Center for Wellness Northern Navajo Medical Center, Shiprock NM Review 3 models of Diabetes management offered at the
Introducing. UPMC Community Care. UPMC Community Care. Your choice for wellness and recovery. at a glance
 Introducing UPMC Community Care Your choice for wellness and recovery There are two parts to good health behavioral and physical. You ve already taken a step toward good health by accessing behavioral
Introducing UPMC Community Care Your choice for wellness and recovery There are two parts to good health behavioral and physical. You ve already taken a step toward good health by accessing behavioral
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA
 Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
Clinical Integration and P4P: Using Pay for Performance to Build Clinical Integration within a Physician-Hospital IPA March 9, 2010 Presented by: Michael Edbauer, DO, Vice President, Medical Affairs CIPA
UNIVERSITY OF CHICAGO MEDICINE & INSTITUTE FOR TRANSLATIONAL MEDICINE COMMUNITY BENEFIT FY2018 DIABETES GRANT GUIDELINES
 UNIVERSITY OF CHICAGO MEDICINE & INSTITUTE FOR TRANSLATIONAL MEDICINE COMMUNITY BENEFIT FY2018 DIABETES GRANT GUIDELINES The following grant guidelines will help you prepare your grant proposal and assemble
UNIVERSITY OF CHICAGO MEDICINE & INSTITUTE FOR TRANSLATIONAL MEDICINE COMMUNITY BENEFIT FY2018 DIABETES GRANT GUIDELINES The following grant guidelines will help you prepare your grant proposal and assemble
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
Saint Francis University. Health and Wellness Program
 2015 Saint Francis University www.francis.edu/disepio Health and Wellness Program ABOUT THE WELLNESS PROGRAM Saint Francis University is committed to being a University where employee health and wellness
2015 Saint Francis University www.francis.edu/disepio Health and Wellness Program ABOUT THE WELLNESS PROGRAM Saint Francis University is committed to being a University where employee health and wellness
TO BE RESCINDED Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
RE Sutton and Associates
 RE Sutton and Associates It has been our pleasure to work with Carmel Clay Schools for the last 25 + year as your Benefit Advisor. RE Sutton and Associates is a benefit consulting firm that specializes
RE Sutton and Associates It has been our pleasure to work with Carmel Clay Schools for the last 25 + year as your Benefit Advisor. RE Sutton and Associates is a benefit consulting firm that specializes
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Community Health Improvement Plan
 Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM
 ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
ABBEVILLE COUNTY EMERGENCY SERVICES COMMUNITY PARAMEDIC PROGRAM Objectives Understand the needs/goals that the Community Paramedic program was designed to address Understand how Abbeville County implemented
Benefits are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
PLAN FEATURES Annual Deductible The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Hearing aid reimbursement does not apply to the out-of-pocket
DISEASE MANAGEMENT PROGRAMS. Procedural Manual. CMPCN Policy #5710
 DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
DISEASE MANAGEMENT PROGRAMS Procedural Manual CMPCN Policy #5710 Effective Date: 01/01/2012 Revision Date(s) 11/18/2012; 10/01/13 ; 01/07/14 Approval Date(s) 12/18/2012 ; 10/23/13, 05/27,14 Annotated to
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Coordinated Veterans Care (CVC) Toolkit Questionnaires for use in a comprehensive needs assessment
 Toolkit Questionnaires for use in a comprehensive needs assessment") Coordinated Veterans Care (CVC) Toolkit Questionnaires for use in a comprehensive needs assessment This resource is a guide to conducting a comprehensive needs assessment for the Coordinated Veterans Care
Coordinated Veterans Care (CVC) Toolkit Questionnaires for use in a comprehensive needs assessment This resource is a guide to conducting a comprehensive needs assessment for the Coordinated Veterans Care
The Health Integration Collaborative A Year in the Making
 The Health Integration Collaborative A Year in the Making Mary Jo Whitfield, VP of Behavioral Health Cheri DeBree, Director of Integrated Health Presentation Objectives An overall look at integrated health
The Health Integration Collaborative A Year in the Making Mary Jo Whitfield, VP of Behavioral Health Cheri DeBree, Director of Integrated Health Presentation Objectives An overall look at integrated health
Mental Health at Mercy Health: Treating the Whole Person. David E. Blair, MD Mercy Health Physician Partners President and CMO
 Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Mental Health at Mercy Health: Treating the Whole Person David E. Blair, MD Mercy Health Physician Partners President and CMO Trinity Health s 22-state diversified system today $17.6B In Revenue 1.3M Attributed
Blending Behavioral Health and Primary Care. Applying the Model. Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist
 Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Blending Behavioral Health and Primary Care Applying the Model Brittany Tenbarge, Ph.D. Behavioral Health Consultant Licensed Clinical Psychologist Overview Introducing the Model to Patients Key Components
Community-based Care Coordination (CCC) Maturity Assessment RidgePointe Healthcare District
 Maturity Assessment RidgePointe Healthcare District") Who/What Program Elements Level 1. Beginning Level 2. Progressing Level 3. Intermediate Level 4. Advanced Organization(s) sponsoring CCC Providers Community services Patients (pts) Payers A. LEADERSHIP
Who/What Program Elements Level 1. Beginning Level 2. Progressing Level 3. Intermediate Level 4. Advanced Organization(s) sponsoring CCC Providers Community services Patients (pts) Payers A. LEADERSHIP
Community Health Needs Assessment IMPLEMENTATION STRATEGY. and
 2015-2018 Community Health Needs Assessment IMPLEMENTATION STRATEGY and Collaborative Health Improvement Plan Palisades Medical Center Implementation Strategy - 1- Introduction: Palisades Medical Center
2015-2018 Community Health Needs Assessment IMPLEMENTATION STRATEGY and Collaborative Health Improvement Plan Palisades Medical Center Implementation Strategy - 1- Introduction: Palisades Medical Center
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
HealthPartners and the Triple Aim. IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners
 HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
HealthPartners and the Triple Aim IHI Open School August 23, 2012 Beth Waterman, RN MBA Chief Improvement Officer HealthPartners HealthPartners Not for profit, consumer governed Integrated care and financing
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network & Out-of- Annual Deductible This is the amount you have to pay out of pocket before the plan will pay
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN FEATURES Network & Out-of- Annual Deductible This is the amount you have to pay out of pocket before the plan will pay
2015 IHS PUBLIC HEALTH NURSING, COMMUNITY BASED PHN CASE MANAGEMENT SERVICE
 2015 IHS PUBLIC HEALTH NURSING, COMMUNITY BASED PHN CASE MANAGEMENT SERVICE PHN PROGRAM AWARDS (COMMUNITY SUICIDE PREVENTION PINE RIDGE SERVICE UNIT AND THE GREAT PLAINS AREA) PHN Rodney R. Sahr RN, BSN
2015 IHS PUBLIC HEALTH NURSING, COMMUNITY BASED PHN CASE MANAGEMENT SERVICE PHN PROGRAM AWARDS (COMMUNITY SUICIDE PREVENTION PINE RIDGE SERVICE UNIT AND THE GREAT PLAINS AREA) PHN Rodney R. Sahr RN, BSN
Burns & McDonnell On-Site Clinic
 Burns & McDonnell On-Site Clinic A Prescription for Financial and Productivity Success Fall 2013 Lockton Companies Company P r ofi le Engineering, architecture, construction, environmental and consulting
Burns & McDonnell On-Site Clinic A Prescription for Financial and Productivity Success Fall 2013 Lockton Companies Company P r ofi le Engineering, architecture, construction, environmental and consulting
Managing Patients with Multiple Chronic Conditions
 Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Managing Patients with Multiple Chronic Conditions Sponsored by AMGA and Merck & Co., Inc. 1 Group Pre-work Affinity Medical Group Heart, Lung & Vascular Center COURAGE Clinic 2 Medical Group Profile Affinity
Big Rapids Hospital Community Health Needs Assessment (CHNA) Implementation Plan July 2015 June 2018
 Implementation Plan July 2015 June 2018") Big Rapids Hospital Community Health Needs Assessment (CHNA) Implementation Plan July 2015 June 2018 Attachment A Spectrum Health Big Rapids Hospital Community Health Needs Assessment Summary of Significant
Big Rapids Hospital Community Health Needs Assessment (CHNA) Implementation Plan July 2015 June 2018 Attachment A Spectrum Health Big Rapids Hospital Community Health Needs Assessment Summary of Significant
Benefits are effective January 01, 2017 through December 31, 2017
 Benefits are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of- Annual Deductible $0 This is the amount
Benefits are effective January 01, 2017 through December 31, 2017 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY PLAN FEATURES Network & Out-of- Annual Deductible $0 This is the amount
Integration Workgroup: Bi-Directional Integration Behavioral Health Settings
 The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
The Accountable Community for Health of King County Integration Workgroup: Bi-Directional Integration Behavioral Health Settings May 7, 2018 1 Integrated Whole Person Care in Community Behavioral Health
VHA Transformation to a Patient Centered Medical Home Model of Care
 VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
VHA Transformation to a Patient Centered Medical Home Model of Care Joanne M. Shear MS, FNP-BC VHA Primary Care Clinical Program Manager Office of Primary Care Operations & Policy Washington, DC Joanne.shear@va.gov
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Foreign Service Benefit Plan
 Simple Steps to Living Well Together Foreign Service Benefit Plan 2018 Wellness Benefits and Incentive Rewards Health Plan Accredited by The FOREIGN SERVICE BENEFIT PLAN has Health Plan Accreditation from
Simple Steps to Living Well Together Foreign Service Benefit Plan 2018 Wellness Benefits and Incentive Rewards Health Plan Accredited by The FOREIGN SERVICE BENEFIT PLAN has Health Plan Accreditation from
TEXAS CHILDREN S EMPLOYEE MEDICAL CLINIC
 DEPARTMENT NAME TEXAS CHILDREN S EMPLOYEE MEDICAL CLINIC THE NEW VALUE IN EMPLOYER HEALTH CENTERS & SERVICES Julie Griffith, Manager, Employee Medical Clinic and Wellness Houston Business Coalition on
DEPARTMENT NAME TEXAS CHILDREN S EMPLOYEE MEDICAL CLINIC THE NEW VALUE IN EMPLOYER HEALTH CENTERS & SERVICES Julie Griffith, Manager, Employee Medical Clinic and Wellness Houston Business Coalition on
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc.
 Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Hypertension Best Practices Symposium Sponsored by AMGA and Daiichi Sankyo, Inc. October 13-15, 15, 2010 Scottsdale, AZ Kaiser Permanente of the Mid-Atlantic States (KPMAS) 1 KPMAS Medical Group Profile
Benefits and Premiums are effective January 01, 2018 through December 31, 2018 PLAN DESIGN AND BENEFITS PROVIDED BY AETNA LIFE INSURANCE COMPANY
 The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
The maximum out-of-pocket limit applies to all covered Medicare Part A and B benefits including deductible. Primary Care Physician Selection Optional There is no requirement for member pre-certification.
Using EHRs and Case Management to Improve Patient Care and Population Health
 Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
Using EHRs and Case Management to Improve Patient Care and Population Health Session #211, February 22, 2017 Thomas Schiller, MD and Jennifer Kuroda, SwedishAmerican Health System A Division of UW 1 Speaker
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
This product was developed by the Robert Wood Johnson Foundation Diabetes Initiative. Support for this product was provided by a grant from the
 This product was developed by the Robert Wood Johnson Foundation Diabetes Initiative. Support for this product was provided by a grant from the Robert Wood Johnson Foundation in Princeton, New Jersey.
This product was developed by the Robert Wood Johnson Foundation Diabetes Initiative. Support for this product was provided by a grant from the Robert Wood Johnson Foundation in Princeton, New Jersey.
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Connected Care Connected Car Program Connected Care
 Connected Care Program Connected Care Initiative to improve the connection and coordination of care for those with Serious Mental Illness among health plans, PCPs, and behavioral health providers in outpatient,
Connected Care Program Connected Care Initiative to improve the connection and coordination of care for those with Serious Mental Illness among health plans, PCPs, and behavioral health providers in outpatient,
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
When preparing for an ACE certification exam,
 Introduction to Coaching CHAPTER 1 APPENDIX B Exam Content Outline For the most up-todate version of the Exam Content Outline, please go to www.acefitness.org/ HealthCoachexamcontent and download a free
Introduction to Coaching CHAPTER 1 APPENDIX B Exam Content Outline For the most up-todate version of the Exam Content Outline, please go to www.acefitness.org/ HealthCoachexamcontent and download a free
diabetes care and quality improvement in our practice
 The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
The Multidisciplinary Team: The key to successful planned diabetes care and quality improvement in our practice Robb Malone, PharmD UNC General Internal Medicine January 20, 2009 Objectives Review the
Health Home Flow Hypothetical Patient Scenario
 Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Health Home Flow Hypothetical Patient Scenario Client Background: Soozie SoonerCare Soozie is a single female, age 42, 5'6" tall 215 pounds. She smokes 2 packs of cigarettes a day. At age 24, Soozie was
Understanding Health Literacy Skills in Patients With Cardiovascular Disease and Diabetes Patrick Dunn, Ph.D. Vasileios Margaritis, Ph.D.
 Understanding Health Literacy Skills in Patients With Cardiovascular Disease and Diabetes Patrick Dunn, Ph.D. Vasileios Margaritis, Ph.D., & Cheryl Anderson, Ph.D. January 13, 2017 Prose Print Diabetes
Understanding Health Literacy Skills in Patients With Cardiovascular Disease and Diabetes Patrick Dunn, Ph.D. Vasileios Margaritis, Ph.D., & Cheryl Anderson, Ph.D. January 13, 2017 Prose Print Diabetes
WPS Integrated Care Management Improving health, one member at a time
 WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
WPS Integrated Care Management Improving health, one member at a time Integrated Care Management supports and promotes member health Looking for more from your group health insurance for your employees?
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Duration of study: November 4-25, 2016 (three weeks) Total participants: 98
 Total participants: 98") Attachment D Standardized Nursing Assessment of the Social Determinants of Health Among Ohio s Hospital and Health Department CNOs & DONs, and Among Ohio s Deans of Colleges & Schools of Nursing: Baseline
Attachment D Standardized Nursing Assessment of the Social Determinants of Health Among Ohio s Hospital and Health Department CNOs & DONs, and Among Ohio s Deans of Colleges & Schools of Nursing: Baseline
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement
 Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Provider Network Management & Clinical Performance Optimization In Population Health Management: Preparing For Value-Based Reimbursement #OMPerformance The 2017 OPEN MINDS Performance Management Institute
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Chronic Disease Management Resources & Services
 Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
2017 Summary of Benefits
 H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
H5209 004_DSB9 23 16 File & Use 10/14/2016 DHS Approved 10 7 2016 This is a summary of drug and health services covered by Care Wisconsin Medicare Dual Advantage Plan (HMO SNP) January 1, 2017 to December
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Medicare Coverage That Works for You
 Medicare Coverage That Works for You A simple guide to your University of California benefits Health Net Seniority Plus (Employer HMO) CA_19_8249EGBROC_C 08132018 Helping You Make the Right Choice For
Medicare Coverage That Works for You A simple guide to your University of California benefits Health Net Seniority Plus (Employer HMO) CA_19_8249EGBROC_C 08132018 Helping You Make the Right Choice For
Expanding PCMH: Beyond the Practice to the Community
 Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
Expanding PCMH: Beyond the Practice to the Community Project Leader Tracy Callahan, RN, MSN, CDE Email: callat@mmc.org Phone: 207.482.7053 The MMC Physician-Hospital Organization is located at 110 Free
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Classic Plan (HMO-POS) Value Plan (HMO) Rewards Plan (HMO)
 Value Plan (HMO) Rewards Plan (HMO)") January 1, 2016 December 31, 2016 Classic Plan Value Plan Rewards Plan SECTION I INTRODUCTION This booklet gives you a summary of what we cover and what you pay. It doesn't list every service that we cover
January 1, 2016 December 31, 2016 Classic Plan Value Plan Rewards Plan SECTION I INTRODUCTION This booklet gives you a summary of what we cover and what you pay. It doesn't list every service that we cover
Your Choice. 3-Tier Network Option Plan
 Your Choice 3-Tier Network Option Plan What is Your Choice? Click Here to Watch Video Your Top Questions What is Your Choice? Are my doctors in the plan? Are my medications covered by the plan? If I get
Your Choice 3-Tier Network Option Plan What is Your Choice? Click Here to Watch Video Your Top Questions What is Your Choice? Are my doctors in the plan? Are my medications covered by the plan? If I get
Commercial. Health Net. Group Retiree Plans. PPO Medicare Coordination of Benefits (COB) Pam White, We help members make informed decisions.
 Pam White, We help members make informed decisions.") Commercial Health Net Group Retiree Plans PPO Medicare Coordination of Benefits (COB) Pam White, Health Net We help members make informed decisions. Health Net PPO Medicare Coordination of Benefits At
Commercial Health Net Group Retiree Plans PPO Medicare Coordination of Benefits (COB) Pam White, Health Net We help members make informed decisions. Health Net PPO Medicare Coordination of Benefits At
THE CAREER SUPPORT NETWORK
 THE CAREER SUPPORT NETWORK Workforce Programming through a New Lens Rickie Brawer, PhD, MPH, MCHES James Plumb, MD, MPH Stephen Kern, Ph.D., OTR/L, FAOTA Department of Family and Community Medicine Center
THE CAREER SUPPORT NETWORK Workforce Programming through a New Lens Rickie Brawer, PhD, MPH, MCHES James Plumb, MD, MPH Stephen Kern, Ph.D., OTR/L, FAOTA Department of Family and Community Medicine Center
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Explorer Plan (HMO-POS) SunSaver Plan (HMO-POS)
 SunSaver Plan (HMO-POS)") January 1, 2016 December 31, 2016 Explorer Plan SunSaver Plan SECTION I INTRODUCTION This booklet gives you a summary of what we cover and what you pay. It doesn't list every service that we cover or list
January 1, 2016 December 31, 2016 Explorer Plan SunSaver Plan SECTION I INTRODUCTION This booklet gives you a summary of what we cover and what you pay. It doesn't list every service that we cover or list
Provider Guide. Medi-Cal Health Homes Program
 Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Medi-Cal Health Provider Guide This provider guide provides information on the California Medi-Cal Health (HHP) for Community-Based Care Management Entities (CB-CMEs), providers, community-based organizations,
Recognition, Publications, & Activities
 Recognition, Publications, & Activities Research Publications Hammond, Barba. A Toolkit for Primary Care Specialty Care Integration. Medical Home News v3 no.2. Feb 2011. McDoniel, Hammond, A Comprehensive
Recognition, Publications, & Activities Research Publications Hammond, Barba. A Toolkit for Primary Care Specialty Care Integration. Medical Home News v3 no.2. Feb 2011. McDoniel, Hammond, A Comprehensive
How to Register and Setup Your Practice with HowsYourHealth. Go to the main start page of HowsYourHealth:
 How to Register and Setup Your Practice with HowsYourHealth Go to the main start page of HowsYourHealth: After you have registered you will receive a practice code and password. Save this information!
How to Register and Setup Your Practice with HowsYourHealth Go to the main start page of HowsYourHealth: After you have registered you will receive a practice code and password. Save this information!
Improving Western NY s Population Health Using Patient Centered Medical Home
 Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Improving Western NY s Population Health Using Patient Centered Medical Home Presented by: Dr. Riffat Sadiq Western NY Medical Center Jeanette Ball, RN BSN PCMH CCE CTG Health Solutions Session C7 IHI
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015
 Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
Nevada County Health and Human Services FY14 Rural Health Care Services Outreach Grant Project Evaluation Report June 30, 2015 I. Executive Summary The vision of Nevada County Behavioral Health (NCBH)
COMMUNITY HEALTH IMPLEMENTATION PLAN
 COMMUNITY HEALTH IMPLEMENTATION PLAN 2017 2017-2020 Table of Contents Letter from Jeff Feasel, President & CEO 1 About Halifax Health 3 Executive Summary 6 Halifax Health Community Health Plan 2017-2020
COMMUNITY HEALTH IMPLEMENTATION PLAN 2017 2017-2020 Table of Contents Letter from Jeff Feasel, President & CEO 1 About Halifax Health 3 Executive Summary 6 Halifax Health Community Health Plan 2017-2020
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Measureable Goals and Outcomes. Collaborative Care Plan. SMART Goals
 Measureable Goals and Outcomes Collaborative Care Plan SMART Goals SMART Goals Specific Specifically define the goal for the member using action verbs what member will do or maintain, and how. What exactly
Measureable Goals and Outcomes Collaborative Care Plan SMART Goals SMART Goals Specific Specifically define the goal for the member using action verbs what member will do or maintain, and how. What exactly
Complex Care Coordination A new line of business
 Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,
Ho okele Health Navigators Complex Care Coordination A new line of business 2013 NAHC Annual Meeting and Exposition 10/31/13 "Medicine used to be simple, ineffective, and relatively safe. It is now complex,