Human Factors and Patient Safety
|
|
|
- Justin Bryant
- 6 years ago
- Views:
Transcription


1 Human Factors and Patient Safety Frank Federico, RPh This presenter has nothing to disclose. 8 October 2015
2 Objectives List three factors that degrade human performance Describe three error reduction strategies that take into consideration human factors principles Explain how to assess the work environment for human factors violations
3 Discussion What are some key features of a good design? What is it about a design that makes a piece of equipment or a process easy or difficult to use? If not easy to use, how would you modify the design? Insert some examples of poor or good design.
4 Human Error 4 1. Errors are common 2. The causes of errors are known 3. Many errors are caused by activities that rely on weak aspects of cognition 4. Systems failures are the root causes of most errors Lucian Leape, Error in Medicine JAMA, 1994
5 Human Factors Human Factors Engineering: Examines a particular activity in terms of its component tasks and then considers each task in terms of: physical demands, adequate lighting, skill demands, mental workload, and other such factors limited noise, or other distractions device design, and team dynamics
6 Human Factors 6 Human Factors focuses on human beings and their interaction with each other, products, equipment, procedures, and the environment Human Factors leverages what we know about human behavior, abilities, limitations, and other characteristics to ensure safer, more reliable outcomes
7 What is the study of Human Factors? Human factors, human factors engineering and ergonomics are often used interchangeably Human factors seeks to understand and design systems that take human limitations into account, supporting people in areas we know to be challenging and capitalizing on human strengths. Poor design is in the eye of the beholder such as human factors professionals
8 Our Focus Understanding the violations of human factors principles that set us up for errors Determining what to do to address these violations (building a better bus!) 8
9 Think of Systems People tend to spend time looking at individual problems without stepping back to see how all the individual pieces fit together in the larger scheme of things.
10 Case Nurse administers incorrect medication Root Causes Analysis completed. Nurse read label incorrectly Deeper investigation Short staffed Nurse caring for three very sick and intense patients Nurse interrupted repeatedly while on medication rounds Changes: Training and education on 6 rights Font on medication label increased. Did this solve the problem?
11 Case Parenteral solutions administered via wrong route Changes Training and education Labels on tubing Be more vigilant
12 Case Jim Taylor Immediately scheduled for surgery to repair the femur Night shift Focus on his agitation Change in vital signs Changes Focus on DVT prophylaxis process only Retraining of nurses on DVT issues
13 What did the proposed changes miss?
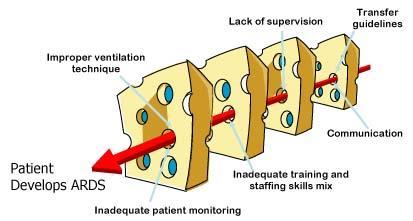
14

15 Interruptions Fatigue Poor Design Overconfidence FAILURES
16 What Impacts Our Performance? Overestimate abilities Underestimate limitations External stimuli Noise Distractions Environmental conditions Internal response to stress Release of stress hormones Anxiety Increased heart rate
17 Error-Producing Conditions Unfamiliarity with task x17 Shortage of time x11 Poor communication x10 Information overload x 6 Misperception of risk (drift) x 4 Inadequate procedures / workflow x 3 These are compounded by human factors violations such as fatigue, stress, work environment (e.g., psychologically unsafe environment), interruptions and distractions, and ambiguity regarding roles and responsibilities. Handbook of Human Factors and Ergonomics Gavriel Salvendy
18 Capacity or Complexity Human factors engineering research shows that what is important is not the number of tasks but the nature of the tasks being attempted. An example: A doctor may be able to tell a student the steps in a simple operation while he is doing one but if it was a complicated case he may not be able to do that because she/he has to concentrate.
19 Human Factors Violations: Drivers of Human Error Fatigue Lack of sleep Illness Drugs or alcohol Boredom, frustration Cognitive shortcuts Fear Stress Shift work Reliance on memory Reliance on vigilance Interruptions & distractions Noise Heat Clutter Motion Lighting Too many handoffs Unnatural workflow Procedures or devices designed in an accident prone fashion 19
20 Fatigue Two factors with the most impact are fatigue and stress. Prolonged work has been shown to produce the same deterioration in performance as a person with a blood alcohol level of 0.05 mmol/l, which would make it illegal to drive a car in many countries
21 Shift Work Truck drivers are typically allowed to work no more than 10 hours at a time and no more than 60 hours in one week. Airline pilots and air traffic controllers work regulated hours and some data suggest waning performance as work-hours increase. No studies that evaluated direction of shift work rotation among medical personnel Sleep deprivation and disturbances of circadian rhythm lead to fatigue, decreased alertness, and poor performance on standardized testing. No testing in healthcare workers
22 Shift Work The direction of shift rotation may impact worker fatigue. A forward rotation of shift work (morning shifts followed by evening shifts followed by night shifts) may lead to less fatigue on the job than backward rotation (day shift to night shift to evening shift).
23 Stress While high stress is something that everyone can relate to, it is important to recognize that low levels of stress are also counterproductive, as this can lead to boredom and failure to attend to a task with appropriate vigilance.
24 Reliance on Memory Working memory is limited, and when attention is drawn elsewhere, it can be especially vulnerable
25 Short Term Memory Do you easily remember things like medical record numbers or verbal orders? What do you think would happen if you were interrupted or distracted while remembering these things? Why do you think you forget this information?
26 Long Term Memory Long term memory is where people store facts about the world and how to do things. Mental models are used to store this information and it can be retrieved either by recalling it or recognizing it A phone number A song Directions Recipe
27 Attention Attention describes the ability to concentrate on someone or something. Attention is limited and so those stimuli that are ignored will never get processed by the brain. Instead what is ignored will go unnoticed and will not be remembered.
28
29

30
31 Attention Multitasking Interruptions Adverse events can occur when the available cognitive resources such as memory are insufficient for the task at hand. IT Current generation clinical ITs are designed with the implicit assumption that their users are carrying out a single task and that their attention is devoted entirely to the interaction with the technology.
32 Error Reduction Overview: Hierarchy of Controls 32 Facilitate Mitigate Policies, Training, Inspection Minimize consequences of errors Make errors visible Make it easy to do the right thing Human Factors Make it hard to do the wrong thing Eliminate Eliminate the opportunity for error Standardization & Simplification Doug Bonacum
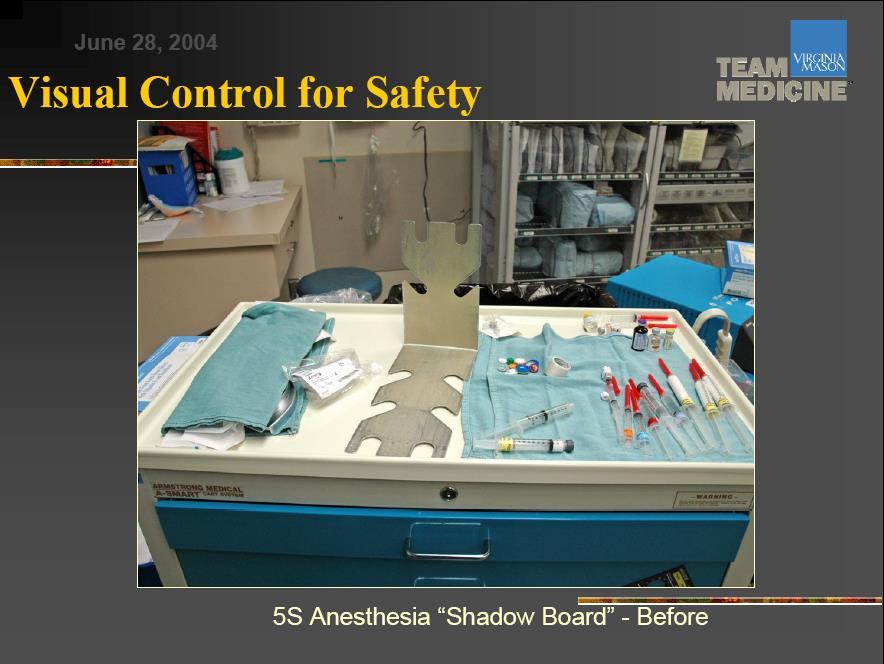
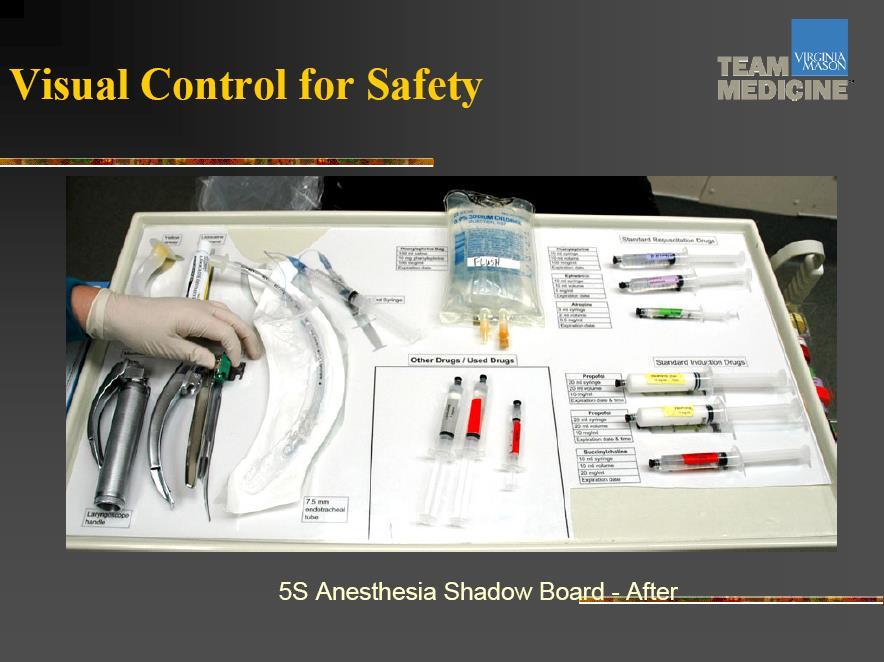
33 Specific Error Reduction Strategies 33 Use visual controls Avoid reliance on memory Simplify and Standardize Use constraints/forcing functions Use protocols and checklists Improve access to information Reduce handoffs Decrease look-alike / sound-alikes Automate carefully Reduce interruptions and distractions Take advantage of habits and patterns Promote effective team functioning
34 Usability Testing Usability testing is also essential for identifying workarounds the consistent bypassing of policies or safety procedures by frontline workers. Workarounds frequently arise because of flawed or poorly designed systems that actually increase the time necessary for workers to complete a task. As a result, frontline personnel work around the system in order to get work done efficiently.
35 Ease of Use The design of a process or device should provide visual clues as to how the process should flow or the piece of equipment is to be used The environment should give clues about how to interact with the process or equipment. 1. Norman, The Design of Everyday Things

36




37
38
39 Forcing functions An aspect of a design that prevents an unintended or undesirable action from being performed or allows its performance only if another specific action is performed first. For example, automobiles are now designed so that the driver cannot shift into reverse without first putting his or her foot on the brake pedal.
40 Anesthesia Mix up of gases Changed connectors for different gases Mix up of gases no longer a problem.

41 Tubing Connections Figure 1. Tube delivering oxygen fell off nebulizer Figure 2. The oxygen tubing was connected to a Baxter Clearlink needleless port.
42 Affordances Perceived and actual properties of technologies that determine how they might be used. For example, if someone sees a button, he/she assumes it must be pressed rather than trying to slide or turn a button to get it to work.

43

44
45 Standardization An axiom of human factors engineering is that equipment and processes should be standardized whenever possible, in order to increase reliability, improve information flow, and minimize cross-training needs. Standardized equipment across clinical settings as in the defibrillator Standardized processes such as the use of checklists
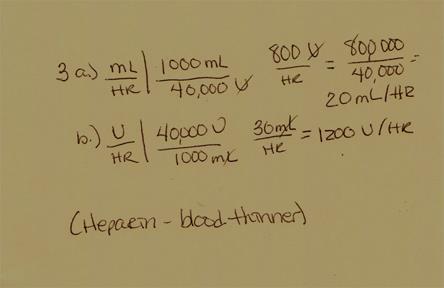
46 Environmental Cues Enhance an individual s capacity to recover from interruption. When calculating a drug dose on paper, The paper acts as a cue to help a clinician re-engage with the task after an interruption, Recalling their position in the task sequence and recording intermediate calculations and initial data.


47 The Case of Nifedipine Gel

48 Simplicity of Design


49 Use Visual Controls 49 Which dial turns on the burner? Stove A Stove B
50 50
51 51
52 Avoid Reliance on Memory Computerized drug-drug interaction checking Drug information databases Customized drug rules Preprinted orders Chemotherapy order form Pain management order forms 52
53 Simplify Formulary restrictions Remove items Eliminate therapeutic duplications Limit availability Heparin weight based protocol Simplifies ordering process Provides comprehensive orders 53
54 Why Simplify Workflow? STEP 1 STEP 2 STEP 3 STEP 4 90% 90% 90% 90% First step = 90% Process reliability = 90% * 90% * 90% * 90% = 66% 54
55 Standardize Who, what, with what, when, where, how Example from Reliability Session Win / Win - Less work, better care Standard solutions Ease of ordering Ease of preparation Ease of administration 55
56 Use Protocols and Checklists Checklists Reminders of every step in the process NOT rigid molds for non-thinking behavior Pilot checklists: includes method to designate where stopped if interrupted Anesthesia Machine Checklist 56
57 Improve Access to Information Include Indication with orders/prescriptions Drug information sources Determine ease of use Location of medication list/problem list 57
58 Reduce Handovers Pharmacists on rounds MD and Pharmacist interact directly Increases likelihood of the correct order Reduces delays caused by problematic orders Communicating critical test results Communicate directly with ordering provider 58
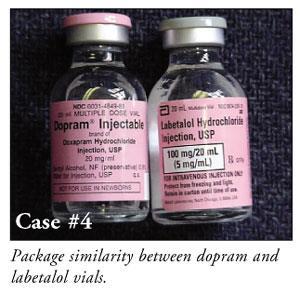
59 Strategy: Avoid Look-alike/Sound-alike Drug Names Display lists of easily confused drug names How effective? Strongly encourage Writing prescriptions more clearly Printing in block letters rather than writing in cursive Avoiding the use of abbreviations Indicating the reason for the drug 59
60 Automate Carefully Errors multiply if input is incorrect Automated dispensing machines Computerized physician order entry 60

61 Reduce Interruptions and Distractions 61
62 Reduce Interruptions and Distractions Ask: What are critical alarms? Are personal phones best way to help nurses? Have you thought about patient comfort? How many alerts pop-up in a computer system during order entry? Is there a quiet zone for medication administration? (e.g. Green Vest at KP) 62

63 Take Advantage of Habits and Patterns Identifying high risk patients in the office setting Engage patients while waiting Hand hygiene Must become part of behaviors Habit 63

64 Habits and Patterns (Continued) Patient medication list Sleeve to hold insurance card and medication list 64
65 Hand Hygiene 65 Using a nudge instead of a rule Nudge theory is mainly concerned with the design of choices, which influences the decisions we make. Nudge theory proposes that the designing of choices should be based on how people actually think and decide (instinctively and rather irrationally), rather than how leaders and authorities traditionally (and typically incorrectly) believe people think and decide (logically and rationally).

66 Promote Effective Team Functioning 66
67 Listening Exercise 67
68 Please decide if the following statements are true, false or? (unable to determine with the information given) 68 A man appeared after the owner had True /False /? turned off his store lights The robber was a man. The robber did not demand money. The owner opened the cash register. True /False/? True/False/? True /False/? After the man who demanded the money scooped up the contents of the cash register, he ran away. True /False/? While the cash register contained money, the story does not state how much. True /False/? Steve Kerr, GE
69 Technology 69

70 What are the technologies employed at your hospital? Computerized prescriber order entry Electronic medication administration records SMART Pumps Robotic dispensing Ventilators Defibrillators Anesthesia machine Bar code technology Radio Frequency Devices Automated dispensing machines Diagnostic equipment And..
71 Global Problems with Technology Magical thinking It starts something like this: Let s have technology do that. What does this type of thinking miss? Can you think of examples of magical thinking?
72 The Problem Sometimes it is in the design Sometimes it is in the interface with users Sometimes it is in the implementation Sometimes it is in how applied Sometimes it is in our expectations Sometimes it is a mismatches between system workflow and clinical workflow
73 Implementation Failure to understand the adaptive nature of implementation is no doubt one of the main reasons health IT systems flounder post-installation. The implementation work required when new information systems are installed also provides an opportunity for redesign and optimization of existing clinical processes Clinical processes, work practices and their supporting technologies probably need to be designed with a useby date.
74 Automation Bias When humans delegate tasks to a computer system they may also shed task responsibility Computer users may then take themselves out of the decision loop
75 Automation Bias Automation bias or automation-induced complacency is a very specific bias associated with computerized decision support and monitoring technologies A user can make either errors of omission (they miss events because the system did not prompt them to take notice) or A user can make errors of commission (they did what the decision system told them to do, even when it contradicts their training and available data)
76 Socio-technical Aspect The socio-technical nature of IT means that the technology and the context within which it is used cannot be separated


77 The Impact of the Automated Automobile
78 The Monk and the Help Desk
79 Tendency to underestimate the complexity embedded in paper The problem with making the transition from the paper world to the electronic world is that in the paper world a lot of things happen by convention & understanding implementing the electronic tools to make that happen is a bigger deal than I think anybody expects. Chair, Medical Informatics Committee Evanston Northwestern Healthcare
80

81

82
83 Alarm-related Deaths According to The Joint Commission, there were 80 alarm-related deaths in the U.S. between January 2009 and June 2012.
84
85 MGH Death Spurs Review of Patient Monitors A Massachusetts General Hospital patient died last month after the alarm on a heart monitor was inadvertently left off, delaying the response of nurses and doctors to the patient s medical crisis.

86 Hospitals don t turn up the volume, lower the noise. Noise in health care facilities has increased by multiples in past decades, and it has a negative effect on health in several ways, not only through missed alarms. These include increased stress and disrupted sleep for patients, lost privacy, communication errors, and clinician burn-out. SoundEar _turn_up_the_volume_lower_the_noise/

87
88 In order to achieve effective alarm management Must deal with culture Must use a multidisciplinary approach Develop appropriate processes One size does not fit all
89 What Can You Do? Include human factors analysis in incident investigations Conduct human factors review of organization Are processes standardized? Is there ready access to information? Are redundancies and reminders in place? Conduct a human factors task analysis How many interruptions are there during the work shift? How complex are the tasks or instructions? 89
90 Usability testing Human factors engineers test new systems and equipment under real-world conditions as much as possible, in order to identify unintended consequences of new technology. Example of the clinical applicability of usability testing involves electronic medical records and computerized provider order entry (CPOE). A seminal study found increased mortality in a pediatric intensive care unit after implementation of a commercial CPOE system, attributable in part to an unnecessarily cumbersome order entry process that reduced clinicians' availability at the bedside
91 What Can You Do? Conduct human factors audits Noise levels; distractions; design of workspace; label format; work hours review; shift reviews Train staff: Self-awareness of human factors issues Staff in position to monitor ongoing situations Information overload Back to back shifts or only short breaks between shifts 91
92 Role of Leaders Proper review of new technology for usability Encourage reporting of technology-related errors and defects Include examination of human factors and technology design after an adverse event Obtain feedback from users Look for workarounds that may indicate technology or processes not easy to use
93 Recommendation You can play an integral role in ensuring that the organization has a plan to evaluate where to dedicate resources Done by including technology as part of strategy Important because technology is part of structure Technology can introduce a whole new set of problems Think of unintended consequences
94 VA National Patient Safety Center 94
95 We can t change the human condition, but we can change the conditions under which humans work. James Reason 95
96 Take a moment to reflect on your own work. What will you incorporate from this session into your plans?
Human Factors. Frank Federico, RPh. This presenter has nothing to disclose.
 Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Human Factors Frank Federico, RPh This presenter has nothing to disclose. 25 February 2015 Culture Learning System Improvement and Measurement Transparency Continuous Learning Accountability Teamwork &
Medication Safety in LTC. Objectives. About ISMP Canada
 Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
Medication Safety in LTC Part II -Vulnerabilities in the Medication Use Process and Strategies to Enhance Medication Safety Lynn Riley, RN ISMP Canada Thursday, October 20, 2011 Objectives At the end of
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Human Factors Engineering in Health Care. Awatef O. Ergai, PhD Post-Doctoral Research Associate Healthcare Systems Engineering Institute
 Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
Human Factors Engineering in Health Care Awatef O. Ergai, PhD Post-Doctoral Research Associate Outline 1. What s human factors engineering (HFE) 2. Why is human factors engineering important in health
Objectives. Key Elements. ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management 5/20/2014
 ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
ICAHN Targeted Focus Areas: Staff Competency and Education Quality Processes and Risk Management Matthew Fricker, RPh, MS, FASHP Program Director, ISMP Rebecca Lamis, PharmD, FISMP Medication Safety Analyst,
Medication Safety Technology The Good, the Bad and the Unintended Consequences
 Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
Medication Safety Technology The Good, the Bad and the Unintended Consequences Michelle Mandrack RN, MSN Director of Consulting Services Matthew Fricker, RPh, MS Program Director 1 Objectives Consider
(10+ years since IOM)
") Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Medication Errors We're Looking Down the Tunnel and Seeing Light (10+ years since IOM) Michael R. Cohen, RPh, MS, ScD Institute for Safe Medication Practices mcohen@ismp.org 1 Disclosure Information Michael
Preventing Medical Errors
 Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
Presents Preventing Medical Errors Contact Hours: 2 First Published: March 31, 2017 This Course Expires on: March 31, 2019 Course Objectives Upon completion of this course, the nurse will be able to: 1.
2. Why Applying Human Factors Is Important For Patient Safety
 PATIENT SAFETY 436 TEAM 2. Why Applying Human Factors Is Important For Patient Safety Objectives: Understand Human Factors And Its Relationship To Patient Safety Define The Meaning Of The Term Human Factors
PATIENT SAFETY 436 TEAM 2. Why Applying Human Factors Is Important For Patient Safety Objectives: Understand Human Factors And Its Relationship To Patient Safety Define The Meaning Of The Term Human Factors
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
Example of a Health Care Failure Mode and Effects Analysis for IV Patient Controlled Analgesia (PCA) Failure Modes (what might happen)
 Failure Modes (what might happen)") Prescribing Assess patient Choose analgesic/mode of delivery Prescribe analgesic Institute for Safe Medication Practices Example of a Health Care and Effects Analysis for IV Patient Controlled Analgesia
Prescribing Assess patient Choose analgesic/mode of delivery Prescribe analgesic Institute for Safe Medication Practices Example of a Health Care and Effects Analysis for IV Patient Controlled Analgesia
How BPOC Reduces Bedside Medication Errors White Paper
 How BPOC Reduces Bedside Medication Errors White Paper July 2008 Brad Blackwell, M.S., R.Ph. Eloise Keeler, R.N., B.S.N. Abstract Medication errors are a significant source of harm to patients in U.S hospitals,
How BPOC Reduces Bedside Medication Errors White Paper July 2008 Brad Blackwell, M.S., R.Ph. Eloise Keeler, R.N., B.S.N. Abstract Medication errors are a significant source of harm to patients in U.S hospitals,
Just Culture Toolkit Scenarios
 Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
Just Culture Toolkit Scenarios In order to promote a just culture where staff is comfortable in reporting errors or near misses, healthcare organizations must adopt a disciplinary system theory approach.
9/15/2017. Nursing Management Congress 2017 Interruptions in Clinical Practice. Interruptions in Clinical Practice. Review of the Literature
 Nursing Management Congress 2017 Interruptions in Clinical Practice Elizabeth A. Duthie, RN, Ph.D., CPPS Director of Patient Safety at Montefiore Health System Interruptions in Clinical Practice The speaker
Nursing Management Congress 2017 Interruptions in Clinical Practice Elizabeth A. Duthie, RN, Ph.D., CPPS Director of Patient Safety at Montefiore Health System Interruptions in Clinical Practice The speaker
Anatomy of a Fatal Medication Error
 Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Anatomy of a Fatal Medication Error Pamela A. Brown, RN, CCRN, PhD Nurse Manager Pediatric Intensive Care Unit Doernbecher Children s Hospital Objectives Discuss the components of a root cause analysis
Objectives. Demographics: Type and Services 1/22/2014. ICAHN Aggregate Results. ISMP Medication Safety Self Assessment for Hospitals
 ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
ICAHN Aggregate Results ISMP Medication Safety Self Assessment for Hospitals Matthew Fricker, RPH, MS, FASHP Rebecca Lamis, PharmD, FISMP January 23, 2014 1 Objectives Report the demographic characteristics
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Encouraging pharmacy involvement in pharmacovigilance; an international perspective.
 Encouraging pharmacy involvement in pharmacovigilance; an international perspective. Michael R. Cohen, RPh, MS, ScD (hon) DPS (hon) Chairperson, International Medication Safety Network and President, Institute
Encouraging pharmacy involvement in pharmacovigilance; an international perspective. Michael R. Cohen, RPh, MS, ScD (hon) DPS (hon) Chairperson, International Medication Safety Network and President, Institute
Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L
 Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L Principles of Medication Administration Talk with the patient and explain what you are doing
Medication Administration & Preventing Errors M E A G A N R A Y, R N A M G S P E C I A L T Y H O S P I T A L Principles of Medication Administration Talk with the patient and explain what you are doing
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER
 Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
Sandra Trotter, MBA, MPHA, CPHQ PATIENT SAFETY PROGRAM LUCILE PACKARD CHILDREN S HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER LUCILE PACKARD CHILDRENS HOSPITAL STANFORD UNIVERSITY MEDICAL CENTER PALO ALTO,
OHTAC Recommendation. Implementation and Use of Smart Medication Delivery Systems
 OHTAC Recommendation Implementation and Use of Smart Medication Delivery Systems July 2009 Background The Ontario Health Technology Advisory Committee (OHTAC) engaged the University Health Network s (UHN)
OHTAC Recommendation Implementation and Use of Smart Medication Delivery Systems July 2009 Background The Ontario Health Technology Advisory Committee (OHTAC) engaged the University Health Network s (UHN)
Management of Reported Medication Errors Policy
 Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
Management of Reported Medication Errors Policy Approved By: Policy & Guideline Committee Date of Original 6 October 2008 Approval: Trust Reference: B45/2008 Version: 4 Supersedes: 3 February 2015 Trust
WHAT are medication errors?
 Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Healthcare Case Study: Errors Cause Mapping Problem Solving Incident Investigation Root Cause Analysis Errors Angela Griffith, P.E. webinars@thinkreliability.com www.thinkreliability.com Office 281-412-7766
Prepared for Institute for Safe Medication Practices Canada 2075 Bayview Avenue E226 Toronto ON, M4N 3M5
 Prepared for Institute for Safe Medication Practices Canada 2075 Bayview Avenue E226 Toronto ON, M4N 3M5 by Laura Lin Gosbee, MASc Human Factors Engineering Consultant Red Forest Consulting, LLC First
Prepared for Institute for Safe Medication Practices Canada 2075 Bayview Avenue E226 Toronto ON, M4N 3M5 by Laura Lin Gosbee, MASc Human Factors Engineering Consultant Red Forest Consulting, LLC First
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety
 All High-Risk Medication Safety") Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Medication Safety Action Bundle Adverse Drug Events (ADE) All High-Risk Medication Safety Background The Institute of medicine (IOM) estimates that 1.5 million preventable Adverse Drug Events (ADE) occur
Ghalib Abbasi, RPh, MS, PharmD Pharmacy Technology Consultant Florida, USA
 Ghalib Abbasi, RPh, MS, PharmD Pharmacy Technology Consultant Florida, USA Disclosure Information Let s Fly! IV Medication Errors in the Hospital Pharmacy Ghalib Abbasi I have no financial relationship
Ghalib Abbasi, RPh, MS, PharmD Pharmacy Technology Consultant Florida, USA Disclosure Information Let s Fly! IV Medication Errors in the Hospital Pharmacy Ghalib Abbasi I have no financial relationship
Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company of Allied World
 Slide 1 Human Factors: The Science of Reliability MSHRM February 2015 Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company
Slide 1 Human Factors: The Science of Reliability MSHRM February 2015 Anne Huben-Kearney, RN, BSN, MPA, CPHQ, CPHRM Assistant Vice President, Healthcare Risk Management AWAC Services, a member company
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY
 REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
REVISED FIP BASEL STATEMENTS ON THE FUTURE OF HOSPITAL PHARMACY Approved September 2014, Bangkok, Thailand, as revisions of the initial 2008 version. Overarching and Governance Statements 1. The overarching
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Lesson 9: Medication Errors
 Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Lesson 9: Medication Errors Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow, Medical Director for the Office of Developmental Programs. I will be your narrator for this webcast.
Resilience in Health Care
 Resilience in Health Care Erik Hollnagel, Ph.D. Professor, University of Southern Denmark Chief Consultant, Center for Kvalitet, Region of Southern Denmark E-mail: erik.hollnagel@rsyd.dk There is something
Resilience in Health Care Erik Hollnagel, Ph.D. Professor, University of Southern Denmark Chief Consultant, Center for Kvalitet, Region of Southern Denmark E-mail: erik.hollnagel@rsyd.dk There is something
How Pharmacy Informatics and Technology are Evolving to Improve Patient Care
 How Pharmacy Informatics and Technology are Evolving to Improve Patient Care HealthcareIS.com 2 Table of Contents 3 Impact of Emerging Technologies 3 CPOE 5 Automated Dispensing Machines 6 Barcode Medication
How Pharmacy Informatics and Technology are Evolving to Improve Patient Care HealthcareIS.com 2 Table of Contents 3 Impact of Emerging Technologies 3 CPOE 5 Automated Dispensing Machines 6 Barcode Medication
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
Patient Care Coordination Variance Reporting
 Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Section 4.8 Implement Patient Care Coordination Variance Reporting This tool provides an overview of patient care coordination (CC) variances, suggestions for documenting and reporting on variances, and
Improving teams in healthcare
 Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Improving teams in healthcare Resource 3: Team communication Developed with support from Background In December 2016, the Royal College of Physicians (RCP) published Being a junior doctor: Experiences
Guidance for Medication Reconciliation and System Integration Process
 Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
Guidance for Medication Reconciliation and System Integration Process Identifying points of failure within the medication reconciliation process and determining systematic approaches (via health IT) to
MEDICATION USE EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014
 TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
TITLE / DESCRIPTION: SAFETY PROCEDURES FOR MEDICATION USE DEPARTMENT: Pharmacy PERSONNEL: All Pharmacy Personnel EFFECTIVE DATE: 06/2003 REVISED: 2/2005, 04/2008, 06/2014 Leadership and Culture A culture
Medication Safety Way Beyond the 5 Rights
 Safety Way Beyond the 5 Rights JoAnne Phillips, MSN, RN, CCRN, CCNS, CPPS The University of Pennsylvania Health System Philadelphia, PA Current State. Of Chaos Prescriptions 12 per /person / year 4 BILLION
Safety Way Beyond the 5 Rights JoAnne Phillips, MSN, RN, CCRN, CCNS, CPPS The University of Pennsylvania Health System Philadelphia, PA Current State. Of Chaos Prescriptions 12 per /person / year 4 BILLION
On the CUSP: Stop BSI
 On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
On the CUSP: Stop BSI Learning From Defects December 6, 2011 Comprehensive Unit-based Safety Program (CUSP) 1. Educate staff on science of safety (www.safercare.net) 2. Identify defects 3. Assign executive
In-Patient Medication Order Entry System - contribution of pharmacy informatics
 In-Patient Medication Order Entry System - contribution of pharmacy informatics Ms S C Chiang BPharm, MRPS, MHA, FACHSE, FHKCHSE, FCPP Senior Pharmacist Chief Pharmacist s Office In-Patient Medication
In-Patient Medication Order Entry System - contribution of pharmacy informatics Ms S C Chiang BPharm, MRPS, MHA, FACHSE, FHKCHSE, FCPP Senior Pharmacist Chief Pharmacist s Office In-Patient Medication
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS
 APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Improving Staff Education
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Improving Staff Education
Guidelines for Managing Pharmacy Systems for Quality and Safety November 2002
 November 2002 Guidelines for Managing Pharmacy Systems for Quality and Safety Background The Australian Council for Safety and Quality in Health Care (ACSQHC) was established by Australian Health Ministers
November 2002 Guidelines for Managing Pharmacy Systems for Quality and Safety Background The Australian Council for Safety and Quality in Health Care (ACSQHC) was established by Australian Health Ministers
VAE PROJECT MASTER ACTION PLAN. Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies
 VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
VAE PROJECT MASTER ACTION PLAN Note: Please be aware that these areas overlap to reduce duplication and optimize the synergies Practice NHSN Surveillance Data Collection Is VAE NHSN Surveillance data collection
Appendix G: The LFD Tool
 Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Appendix G: The LFD Tool What is a defect? A defect is any event or situation that you don t want to repeat. This could include an incident that caused patient harm or put patients at risk for harm, like
Overview. Diane Cousins, R.Ph U.S. Pharmacopeia. 1 Pharmacy Labeling with Color
 As more medications are approved and become available to Americans, the opportunity for potentially dangerous or even deadly errors due to drug mix-ups from look alike or sound alike names becomes increasingly
As more medications are approved and become available to Americans, the opportunity for potentially dangerous or even deadly errors due to drug mix-ups from look alike or sound alike names becomes increasingly
Safety Innovations FOUNDATIONHTSI. Healthcare Alarm Safety What We Can Learn From Military Alarm Management Strategies
 FOUNDATIONHTSI Healthcare Technology Safety Institute Safety Innovations Healthcare Alarm Safety What We Can Learn From Military Alarm Management Strategies Lockheed Martin (LM) Advanced Technology Laboratories
FOUNDATIONHTSI Healthcare Technology Safety Institute Safety Innovations Healthcare Alarm Safety What We Can Learn From Military Alarm Management Strategies Lockheed Martin (LM) Advanced Technology Laboratories
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Accreditation Program: Long Term Care
 ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
ccreditation Program: Long Term are National Patient Safety Goals indicates scoring category ; indicates scoring category ; indicates situational decision rules apply; indicates 2009 The Joint ommission
THE ROLE OF HUMAN FACTORS FOR INFECTION PREVENTION IN THE EMERGENCY DEPARTMENT
 THE ROLE OF HUMAN FACTORS FOR INFECTION PREVENTION IN THE EMERGENCY DEPARTMENT Connie Savor Price, MD Director, Infection Prevention and Chief, Division of Infectious Diseases Denver Health and Hospital
THE ROLE OF HUMAN FACTORS FOR INFECTION PREVENTION IN THE EMERGENCY DEPARTMENT Connie Savor Price, MD Director, Infection Prevention and Chief, Division of Infectious Diseases Denver Health and Hospital
Uses a standard template but may have errors of omission
 Evaluation Form Printed on Apr 19, 2014 MILESTONE- BASED FELLOW EVALUATION Evaluator: Evaluation of: Date: This is a new milestone-based evaluation. To achieve a level, the fellow must satisfy ALL the
Evaluation Form Printed on Apr 19, 2014 MILESTONE- BASED FELLOW EVALUATION Evaluator: Evaluation of: Date: This is a new milestone-based evaluation. To achieve a level, the fellow must satisfy ALL the
SafetyFirst Alert. Improving Prescription/Order Writing. Illegible handwriting
 SafetyFirst Alert Massachusetts Coalition for the Prevention of Medical Errors January 2000 This issue of Safety First Alert is a publication of the Massachusetts Coalition for the Prevention of Medical
SafetyFirst Alert Massachusetts Coalition for the Prevention of Medical Errors January 2000 This issue of Safety First Alert is a publication of the Massachusetts Coalition for the Prevention of Medical
Top Ten Health Technology Hazards
 Top Ten Health Technology Hazards MASHMM July 19, 2013 James P. Keller, M.S. Vice President, Health Technology Evaluation and Safety jkeller@ecri.org (610) 825-6000, ext. 5279 Presentation Overview ECRI
Top Ten Health Technology Hazards MASHMM July 19, 2013 James P. Keller, M.S. Vice President, Health Technology Evaluation and Safety jkeller@ecri.org (610) 825-6000, ext. 5279 Presentation Overview ECRI
9/29/2014. Disclosure: I, Amber Sanders have no financial relationship to disclose. Objectives. Medication Safety in Pediatric Populations
 Medication Safety in Pediatric Populations By: Amber Sanders Disclosure: I, Amber Sanders have no financial relationship to disclose Objectives Identify Pediatric Medication Safety Guidelines Institute
Medication Safety in Pediatric Populations By: Amber Sanders Disclosure: I, Amber Sanders have no financial relationship to disclose Objectives Identify Pediatric Medication Safety Guidelines Institute
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS
 PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
PATIENT SAFETY ORGANIZATION TERMINOLOGY AND ACRONYMS Active Error An error that occurs at the point of contact. Active errors are generally readily apparent (e.g., pushing an incorrect button, ignoring
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
TITLE MEDICATION ORDERS SCOPE Provincial APPROVAL AUTHORITY Clinical Operations Executive Committee SPONSOR Provincial Medication Management Committee PARENT DOCUMENT TITLE, TYPE AND NUMBER Not applicable
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Just Culture. The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes.
 Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Just Culture November 2016 Just Culture The single greatest impediment to error prevention in the medical industry is that we punish people for making mistakes. Dr Lucian Leape Harvard School of Public
Ensuring Safe & Efficient Communication of Medication Prescriptions
 Ensuring Safe & Efficient Communication of Medication Prescriptions in Community and Ambulatory Settings (September 2007) Joint publication of the: Alberta College of Pharmacists (ACP) College and Association
Ensuring Safe & Efficient Communication of Medication Prescriptions in Community and Ambulatory Settings (September 2007) Joint publication of the: Alberta College of Pharmacists (ACP) College and Association
THE INSTITUTE FOR SAFE MEDICATION PRACTICES: THE EXPERT WITNESS
 THE INSTITUTE FOR SAFE MEDICATION PRACTICES: THE EXPERT WITNESS Judy L. Smetzer, BSN, RN, FISMP jsmetzer@ismp.org 215-947-7797 2 Objectives Explain the mission and function of the Institute for Safe Medication
THE INSTITUTE FOR SAFE MEDICATION PRACTICES: THE EXPERT WITNESS Judy L. Smetzer, BSN, RN, FISMP jsmetzer@ismp.org 215-947-7797 2 Objectives Explain the mission and function of the Institute for Safe Medication
Daily Summary from Workshop 1 Day 3 (Wednesday 2 May 2018) Access to Community Mental Health Services
 Access to Community Mental Health Services") Daily Summary from Workshop 1 Day 3 (Wednesday 2 May 2018) Access to Community Mental Health Services Context The group summarised the work carried out throughout the last couple of days and reflected
Daily Summary from Workshop 1 Day 3 (Wednesday 2 May 2018) Access to Community Mental Health Services Context The group summarised the work carried out throughout the last couple of days and reflected
Human Factors and Ergonomics in Health Care and Patient Safety
 Human Factors and Ergonomics in Health Care and Patient Safety Pascale Carayon, Ph.D. Procter & Gamble Bascom Professor in Total Quality Department of Industrial and Systems Engineering Director of the
Human Factors and Ergonomics in Health Care and Patient Safety Pascale Carayon, Ph.D. Procter & Gamble Bascom Professor in Total Quality Department of Industrial and Systems Engineering Director of the
Medication Safety & Electrolyte Administration. Objectives. High Alert Medications. *Med Safety Electrolyte Administration
 Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Medication Safety & Electrolyte Administration Jennifer Doughty, PharmD PGY2 Pharmacy Resident Emergency Medicine Stormont Vail Health, Topeka, KS Objectives Define and identify high alert medications
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Overview of Root Cause Analysis
 Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Overview of Root Cause Analysis Brian Harmon Quality Consultant Performance Improvement University of Minnesota Medical Center February 25, 2006 What is a Sentinel Event? A sentinel event is an unexpected
Chapter 2: Admitting, Transfer, and Discharge
 Chapter 2: Admitting, Transfer, and Discharge MULTIPLE CHOICE 1. The patient is scheduled to go home after having coronary angioplasty. What would be the most effective way to provide discharge teaching
Chapter 2: Admitting, Transfer, and Discharge MULTIPLE CHOICE 1. The patient is scheduled to go home after having coronary angioplasty. What would be the most effective way to provide discharge teaching
Nursing Documentation 101
 Nursing Documentation 101 Module 5: Applying Knowledge Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 5: Applying Knowledge Part
Nursing Documentation 101 Module 5: Applying Knowledge Part I Handout 2014 College of Licensed Practical Nurses of Alberta. All Rights Reserved. Nursing Documentation 101 Module 5: Applying Knowledge Part
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN
 Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Adverse Drug Events: A Focus on Anticoagulation Steve Meisel, Pharm.D., CPPS Director of Patient Safety Fairview Health Services, Minneapolis, MN Fairview Health Services 6 hospitals, ranging from rural
Tip Sheet Promoting Mobility, Reducing Falls and Alarms
 Tip Sheet Promoting Mobility, Reducing Falls and Alarms WHAT IT IS: Promoting mobility means building and maintaining core strength, endurance and balance, and providing supports to enable residents to
Tip Sheet Promoting Mobility, Reducing Falls and Alarms WHAT IT IS: Promoting mobility means building and maintaining core strength, endurance and balance, and providing supports to enable residents to
Sentinel Event Data. Root Causes by Event Type Copyright, The Joint Commission
 Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
Sentinel Event Data Root Causes by Event Type 2004 2014 Joint Commission Root Cause Information www.jointcommission.org/sentinel_event_policy_and_procedures/ Sentinel Events are reported to The Joint Commission
SPOK MESSENGER. Improving Staff Efficiency and Patient Care With Timely Communications and Critical Connectivity
 SM SPOK MESSENGER Improving Staff Efficiency and Patient Care With Timely Communications and Critical Connectivity THE CHALLENGE OF PROVIDING PATIENT CARE WHILE MAINTAINING EFFICIENCY Many hospitals today
SM SPOK MESSENGER Improving Staff Efficiency and Patient Care With Timely Communications and Critical Connectivity THE CHALLENGE OF PROVIDING PATIENT CARE WHILE MAINTAINING EFFICIENCY Many hospitals today
Elisa 800. Rediscover ventilation!
 p-elisa800-e Stand: 05/2014 Heinen + Löwenstein Arzbacher Straße 80 D - 56130 Bad Ems Phone: +49 26 03/96 00 0 Fax: +49 26 03/96 00 50 www.hul.de Elisa 800 Rediscover ventilation! Homecare Pneumology Neonatology
p-elisa800-e Stand: 05/2014 Heinen + Löwenstein Arzbacher Straße 80 D - 56130 Bad Ems Phone: +49 26 03/96 00 0 Fax: +49 26 03/96 00 50 www.hul.de Elisa 800 Rediscover ventilation! Homecare Pneumology Neonatology
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
10/4/2012. Disclosure. Leading a Meaningful Event Investigation. Just Culture definition. Objectives. What we all have in common
 Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
Leading a Meaningful Event Investigation Natasha Nicol, Pharm D, FASHP Director, Medication Safety Cardinal Health Disclosure I do not have a vested interest in or affiliation with any corporate organization
End-to-end infusion safety. Safely manage infusions from order to administration
 End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
End-to-end infusion safety Safely manage infusions from order to administration New demands and concerns 56% 7% of medication errors are IV-related. 1 of high-risk IVs are compounded in error. 2 $3.5B
A Discussion of Medication Error Reduction Strategies
 A Discussion of Medication Error Reduction Strategies By: Donald L. Sullivan, R.Ph., Ph.D. Program Number: 071067-011-01-H05 C.E.U.s: 0.1 Contact Hours: 1 hour Release Date: 4/1/11 Expiration Date: 4/1/14
A Discussion of Medication Error Reduction Strategies By: Donald L. Sullivan, R.Ph., Ph.D. Program Number: 071067-011-01-H05 C.E.U.s: 0.1 Contact Hours: 1 hour Release Date: 4/1/11 Expiration Date: 4/1/14
IMPACT OF TECHNOLOGY ON MEDICATION SAFETY
 Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
03/24/2017. Measuring What Matters to Improve the Patient Experience. Building Compassion Into Everyday Practice
 Building Compassion Into Everyday Practice Christy Dempsey, MSN MBA CNOR CENP FAAN Chief Nursing Officer First OUR GOAL: OUR GOAL: Prevent suffering by optimizing care delivery Alleviate by responding
Building Compassion Into Everyday Practice Christy Dempsey, MSN MBA CNOR CENP FAAN Chief Nursing Officer First OUR GOAL: OUR GOAL: Prevent suffering by optimizing care delivery Alleviate by responding
Running head: MEDICATION ERRORS 1. Medications Errors and Their Impact on Nurses. Kristi R. Rittenhouse. Kent State University College of Nursing
 Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
Running head: MEDICATION ERRORS 1 Medications Errors and Their Impact on Nurses Kristi R. Rittenhouse Kent State University College of Nursing MEDICATION ERRORS 2 Abstract One in five medication dosages
Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist
 Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist CPSI Safe Surgery Saves Lives Workshop Montréal, QC 29Mar2011 Julie Greenall, RPh, BScPhm, MHSc, FISMPC Institute
Medication Safety in the Operating Room: Using the Operating Room Medication Safety Checklist CPSI Safe Surgery Saves Lives Workshop Montréal, QC 29Mar2011 Julie Greenall, RPh, BScPhm, MHSc, FISMPC Institute
Usability Evaluation of a Computerized Physician Order Entry for Medication Ordering
 5 Medical Informatics in a United and Healthy Europe K.-P. Adlassnig et al. (Eds.) IOS Press, 009 009 European Federation for Medical Informatics. All rights reserved. doi:0./978--60750-0-5-5 Usability
5 Medical Informatics in a United and Healthy Europe K.-P. Adlassnig et al. (Eds.) IOS Press, 009 009 European Federation for Medical Informatics. All rights reserved. doi:0./978--60750-0-5-5 Usability
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU. Change Package.
 Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Reducing Harm Improving Healthcare Protecting Canadians MEDICATION RECONCILIATION IN THE ICU Change Package January 2012 Background The ultimate goal of medication reconciliation is to prevent adverse
Objectives MEDICATION SAFETY & TECHNOLOGY. Disclosure. How has technology improved the way we dispense and compound medications AdminRx AcuDose Rx
 MEDICATION SAFETY & TECHNOLOGY Objectives Identify technology that can improve medication safety and decrease medication errors Identify ways that technology can cause medication errors if used inappropriately
MEDICATION SAFETY & TECHNOLOGY Objectives Identify technology that can improve medication safety and decrease medication errors Identify ways that technology can cause medication errors if used inappropriately
HealthStream Ambulatory Regulatory Course Descriptions
 This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Pedi-CSI: Pediatric Clinical Safety Investigation Through Virtual Patient Safety Rounds
 Pedi-CSI: Pediatric Clinical Safety Investigation Through Virtual Patient Safety Rounds Training Manual Boston Children s Hospital Medicine Patient Services and Boston College William F. Connell School
Pedi-CSI: Pediatric Clinical Safety Investigation Through Virtual Patient Safety Rounds Training Manual Boston Children s Hospital Medicine Patient Services and Boston College William F. Connell School
Social care guideline Published: 14 March 2014 nice.org.uk/guidance/sc1
 Managing medicines in care homes Social care guideline Published: 14 March 2014 nice.org.uk/guidance/sc1 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Managing medicines in care homes Social care guideline Published: 14 March 2014 nice.org.uk/guidance/sc1 NICE 2018. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
D Pure possibilities. Dräger perseus A500
 D-91730-2013 Pure possibilities Dräger perseus A500 02 How about more workspace? D-91310-2013 D-91554-2013 Great expectations Today s perioperative environment presents new challenges. As caseloads increase
D-91730-2013 Pure possibilities Dräger perseus A500 02 How about more workspace? D-91310-2013 D-91554-2013 Great expectations Today s perioperative environment presents new challenges. As caseloads increase
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Session 2 Improving Narcotics and Opiate Management
 Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
Session 2 Improving Narcotics and Opiate Management Frank Federico, RPh, IHI Executive Director Steve Meisel, Pharm.D., IHI Faculty January 31,2012 12:00-1:00pm ET Beth O Donnell, MPH Beth O Donnell, MPH,
To prevent harm to patients from adverse medication events involving high-alert medications.
 TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
TITLE MANAGEMENT OF HIGH-ALERT MEDICATIONS DOCUMENT # PS-46-01 PARENT DOCUMENT LEVEL LEVEL 1 PARENT DOCUMENT TITLE Management of High-alert Medications Policy APPROVAL LEVEL Alberta Health Services Executive
#104 - Prevention of Medical Errors [1]
![#104 - Prevention of Medical Errors [1]](/thumbs/74/70423609.jpg "#104 - Prevention of Medical Errors [1]") Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
Published on Excellence In Learning (https://excellenceinlearning.net) Home > #104 - Prevention of Medical Errors #104 - Prevention of Medical Errors [1] Please login [2] or register [3] to take this course.
Assessing Non-Technical Skills. A Guide to the NOTSS Tool Adapted for the Labour Ward
 Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Assessing Non-Technical Skills A Guide to the NOTSS Tool Adapted for the Labour Ward Acknowledgements The original NOTSS system was developed and evaluated in a multi-disciplinary project comprising surgeons,
Best Practices and Performance Measures for Systemic Treatment Computerized Prescriber Order Entry Systems (ST CPOE) in Chemotherapy Delivery
 in Chemotherapy Delivery") Best Practices and Performance Measures for Systemic Treatment Computerized Prescriber Order Entry Systems (ST CPOE) in Chemotherapy Delivery Dr. Vishal Kukreti, MD, FRCPC, MSc Clinical Lead, Systemic
Best Practices and Performance Measures for Systemic Treatment Computerized Prescriber Order Entry Systems (ST CPOE) in Chemotherapy Delivery Dr. Vishal Kukreti, MD, FRCPC, MSc Clinical Lead, Systemic
Patient Safety. If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator Updated:
 Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Patient Safety If you have any questions, contact: Sheila Henssler Performance Improvement/Patient Safety Coordinator 615-7018 Updated: 2013-05-03 Learning Objectives In this presentation, you will learn:
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm
 Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Making it safe for acutely ill patients - a whistlestop tour of medical error & patient harm Sara Barton Acute Physician Salford Royal NHS Foundation Trust What is medical error? Medical errors can be
Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels. Nick Snyder, Esq.
 Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels Nick Snyder, Esq. How Can We Impact Inappropriate Over-Prescribing of Opioids in Maine? What have other States or Organizations
Steps Taken to Combat the Opiate Epidemic Through Legal And Technological Channels Nick Snyder, Esq. How Can We Impact Inappropriate Over-Prescribing of Opioids in Maine? What have other States or Organizations
Practice Spotlight. Baystate Health - Baystate Medical Center Springfield, Massachusetts
 Practice Spotlight Baystate Health - Baystate Medical Center Springfield, Massachusetts www.baystatehealth.org Erin Taylor, PharmD Clinical Pharmacy Supervisor Gary Kerr, PharmD, MBA Director, Pharmacy
Practice Spotlight Baystate Health - Baystate Medical Center Springfield, Massachusetts www.baystatehealth.org Erin Taylor, PharmD Clinical Pharmacy Supervisor Gary Kerr, PharmD, MBA Director, Pharmacy