ORANGE IS THE NEW GREEN : TRAUMA PI AND RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT: 2014
|
|
|
- Everett Murphy
- 6 years ago
- Views:
Transcription
1 ORANGE IS THE NEW GREEN : TRAUMA PI AND RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT: 2014 Glen Tinkoff MD, FACS, FCCM (gtinkoff@christianacare.org) Associate Vice Chair of Surgery Christiana Care Health System, Newark, DE 18TH ANNUAL CONFERENCE SOCIETY OF TRAUMA NURSES JACKSONVILLE, FL March 27 th, 2015
2 Delaware s Inclusive Trauma System Hospital Care 9 acute care hospitals in the state Wilmington Hospital designated Level I Trauma Center in 1984 No coordination of services for the injured or differentiation of clinical capabilities Injured routinely taken to nearest hospital
3 Delaware s Inclusive Trauma System Rate of Unintentional Injury-related Mortality (per 100,000 population) Annual Averages by County U.S. Kent Cty New Castle Cty Sussex Cty

4 HB Delaware s Trauma System Legislation 7/8/96 Amended Chapter 97, Title 16 of Delaware Code Emergency Medical Services Systems
5 Delaware s Inclusive Trauma System Christiana Hospital S. Chester Co., PA Cecil Co., MD St. Francis Hospital New Castle Co., DE DuPont Hospital for Children Wilmington Hospital Salem Co., NJ All Trauma Centers verified by ACS COT State VRC designated and Level designated I by the DE Division of Public Health State designated Level III State designated Participating Trauma Center Fully Inclusive Trauma System inaugurated 1/2000 Kent Co., DE Sussex Co., DE Nanticoke Memorial Hospital Kent General Hospital Milford Memorial Hospital Beebe Medical Center

6 Delaware Trauma Data ( ) Mortality by ISS category by year National Trauma Data Bank ( ): Mortality by ISS category by year 50.0% 45.0% 40.0% 35.0% 30.0% 25.0% 20.0% 15.0% 45.0% 40.0% 35.0% 30.0% 25.0% 20.0% 15.0% 10.0% 10.0% 5.0% 0.0% % 0.0% > > 24
7 National Trauma Data Bank vs Delaware Trauma Data (ISS > 24) 50.0% 45.0% 40.0% 35.0% 30.0% 25.0% 20.0% 15.0% 10.0% 5.0% 3%/ yr decrease in mortality 0.0% NTDB Delaw are Linear (NTDB) Linear (Delaw are)
8
9 Objectives Outline the development and current vision of the American College of Surgeons Committee on Trauma (ACS COT) PI efforts Discuss fundamental structure and processes required for an effective trauma PI program. Review changes to the PI chapter (chapter 16) in the revised edition of the Resources for Optimal Care of the Injured Patient
10 PERFORMANCE IMPROVEMENT PROBLEM SOLVING FLOWSHEET Don t mess with it YES Does the stupid thing work? NO Did you mess with it? NO NO Does anyone know? Hide it YES NO You Idiot!! You poor guy! Can you blame someone else? YES YES NO PROBLEM Will you get in trouble? NO Throw it away



11 Trauma Center Standards
12 Basic Principles of Trauma Center Performance Improvement (PI) A trauma center should provide care to the injured patient that is: Efficient (functioning in the best possible manner with the least waste of time and effort) Effective (able to produce the desired result) Safe (free from mishap or danger)
13 Basis for Trauma Center PI Theory and Practice Earnest A. Codman MD ( ) End Results Idea The common sense notion that every hospital should follow every patient it treats, long enough to determine whether or not the treatment has been successful, and then to inquire, If not, why not? with a view to preventing similar failures in the future Clin Orthop Relat Res. Nov 2009; 467(11): Basis for the hospital standardization movement founded by the American College of Surgeons, and the precursor to the Joint Commission on Accreditation of Hospitals formed in 1951
14 Basis for Trauma Center PI Theory and Practice William Edwards Deming ( ) Total Quality Management (TQM) Customer-focused Total employee involvement Process centered Integrated system-based Continual improvement Fact-based decision-making Effective communication Plan/ Do/ Study (Check)/ Act
15 Basis for Trauma Center PI Theory and Practice Avedis Donabedian MD, MPH ( ) Evaluation of Health Care Structure + Process = Outcomes Outcome measures performance, which are conditional on structure and process (which can be manipulated) System redesigns and other inputs correct deficiencies, improving quality of care Continued performance monitoring keeps quality of care high
 Multidisciplinary")
16 Basis for Trauma Center PI Theory and Practice Medical audit process consisting of: J Trauma 1987; 27(8); Systematic medical record review Precise definitions of preventability Utilization of risk-adjusted probability of survival (TRISS) Multidisciplinary review for determination of preventability
17 A Medical Culture Paradox Do No Harm & To Err is Human

18 The Patient Safety Crisis 44,000 to 98,000 deaths per year $37.6B in costs per year Preventable mistakes cost $17 to $29 billion/yr Medical errors consume 10-15% of a hospital s annual operating budget Annual Deaths Medical Errors are a Leading Cause of Death 0 Heart Disease Cancer Stroke Lung Disease Medical Errors Diabetes Pneumonia Alzhemer's Kidney Disease

19 The Patient Safety Crisis The American health care delivery system is in need of fundamental change. Patients, doctors, nurses, and health care leaders are concerned that the care delivered is not the care we should receive. Yet the problems remain. Health care today harms too frequently and routinely fails to deliver its potential benefits.
20 Basis for Trauma Center PI Theory and Practice James Reason Ph.D. Human factors engineer Risk and human error analysis Swiss Cheese model of accident causation
21 Reason s Swiss cheese model of accident causation Some holes due to active failures Hazards Losses Other holes due to latent conditions Successive layers of defences, barriers and safeguards System defences

22 Reason s - Defenses
23 Basis for Trauma Center PI Theory and Practice PI and Patient Safety (PIPS) Freedom from accidental injury Establishment of operational systems and processes that minimize the likelihood of errors and maximizes the likelihood of intercepting them when they occur

24
25 Basis for Trauma Center PI Theory and Practice Value of Care = Quality of Process + Quality of Outcome Cost
26 Trauma PI or Peer Review? Peer Review - process whereby peers evaluate the quality of work performed by their colleagues Evidence or consensus based analysis Regular intervals Expert review Produce effective corrective strategies Used in credentialing/ privileges Integrate into hospital-wide PI Provide protection from discovery
27 Trauma PI or Peer Review? Efficient Fosters standardization Self regulatory - Polices the profession Credentialing Core of trauma center PI activities
28 Trauma PIPS Program Structure Board of Directors Medical Staff Trauma Medical Director Trauma Program Manager
29 Trauma PIPS Program Structure Administrative Accountability TMD must be empowered to address multidisciplinary issues Determine the qualifications of trauma panel Recommend changes to trauma panel based on performance review
30 Trauma PIPS Program Structure Scope Defined the trauma patient population: Patients with ICD-9-CM Dx Trauma-related hospital admissions Injury-related deaths in ED or after admission

31 Trauma PIPS Program Structure Registry Foundation National Trauma Data Standard
")

32 Trauma PIPS Program Structure Trauma Registry Foundation National Trauma Data Standard Concurrent (80% cases/ 60d of discharge) Confidentiality assured Monitored for data validity Annual NTDB submission Risk-stratified benchmarking system to measure performance and outcomes (TQIP)
33 Trauma PIPS Program Structure

34 TQIP Inclusion Criteria
35 TQIP Cohort Definitions
36 TQIP Cohort Definitions

37 TQIP Cohort Definitions

38 TQIP Variables for Risk-Adjusting
39 TQIP Variables for Risk-Adjusting

40 TQIP Patient Cohorts and Chacteristics

41 TQIP Process Measures
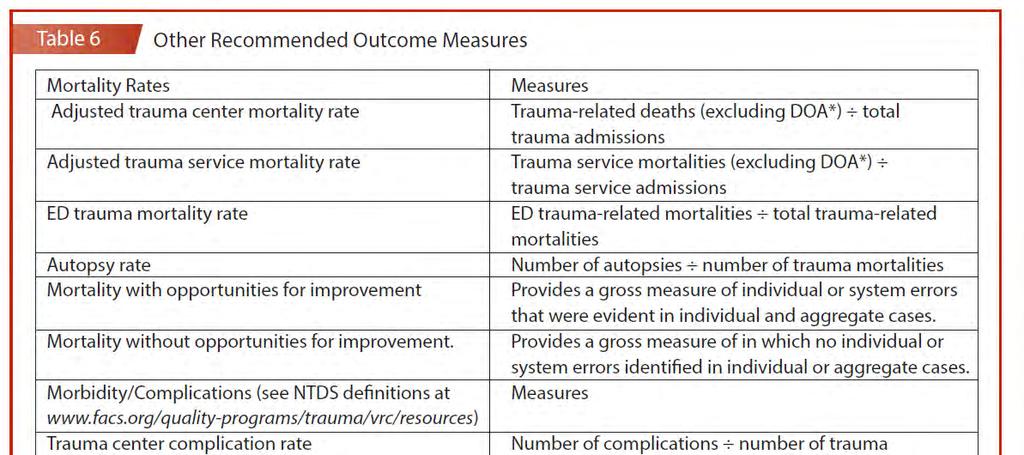
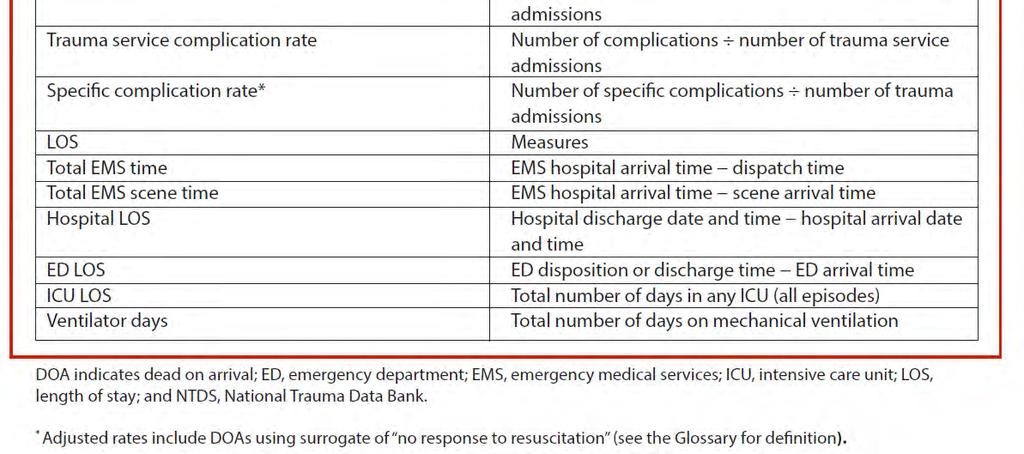
42 TQIP Outcomes Mortality* Major Complications (w & w/o death)* MOI* Resource Utilization Co-morbidites Complications Time to Death D/C Disposition * graphical inter-facility comparison by OR s and deciles

43 TQIP Reports & Inter-facility comparison March 2014 report 198 centers 160, 560 incidents

44 TQIP Reports & Inter-facility comparison

45 TQIP Reports & Inter-facility comparison

46 TQIP Model for PTSF?
47 Trauma PIPS Program Structure Personnel PI Coordinator Trauma Registrars Trauma panel, specialty liaisons, and service representatives Physician extenders, Residents, Trauma Nurses Hospital administration EMS Medical Examiner
48 Trauma PIPS Program Structure Measures of Performance ( audit filters ) Process Outcome Benchmarks
49 Trauma PIPS Program Structure Committees Executive committee Operational Process Performance Committee (Systems committee) Multidisciplinary Peer Review Committee
50 Trauma PIPS Program Process
51 Trauma PIPS Program Process LEVELS OF REVIEW 1 o Review Identification 2 o Review Delegation & Distribution 3 o Review Discussion & Determination
52 Trauma PIPS Program Process Categorization of Mortalities Old Preventable Non- Preventable Possibly Preventable New Unanticipated mortality with opportunity for improvement Mortality without opportunity for improvement Anticipated mortality with opportunity for improvement
53 Trauma PIPS Program Process System-related issues Guidelines & protocols Education Enhanced resources ($) Provider-related issues Education & mentoring Counseling Change in privileges Corrective Actions

54 Trauma PIPS Program Process
55 Trauma PIPS Program Process Problem Resolution = Closing the Loop Demonstrating a corrective action has the desired effect by continuous monitoring Improvement can not always be demonstrated; however, the PIPS process can!

56
57 Chapter 15: Trauma Registry Trauma registry data must be collected and analyzed by every trauma center These data must be collected in compliance with the National Trauma Data Standard (NTDS) and submitted to the National Trauma Data Bank (NTDB ) every year in a timely fashion so that they can be aggregated and analyzed at the national level The trauma registry is essential to the performance improvement and patient safety (PIPS) program and must be used to support the PIPS process The trauma registry must be used to identify injury prevention priorities that are appropriate for local implementation All trauma centers must use a risk adjusted benchmarking system to measure performance and outcomes Trauma registries should be concurrent. At a minimum, 80 percent of cases must be entered within 60 days of discharge
58 Chapter 15: Trauma Registry Trauma registrars must attend or have previously attended two courses within 12 months of being hired: ATS s Trauma Registrar course or equivalent AAAM s injury scaling course The trauma program must ensure that appropriate measures are in place to meet the confidentiality requirements One FTE dedicated to the registry must be available to process the data capturing the NTDS data set for each admitted patients annually Strategies for monitoring data validity are essential
59 CHAPTER 16 Performance Improvement and Patient Safety This chapter describes the concept of monitoring, evaluating, and improving the performance of a trauma program. There is no precise prescription for trauma performance improvement and patient safety (PIPS). However, the American College of Surgeons Committee on Trauma (ACS- COT) calls for each trauma program to demonstrate a continuous process of monitoring, assessment, and management directed at improving care) These performance improvement activities are concordant with the Institute of Medicine s six quality aims for patient care: safe, effective, patient centered, timely, efficient, and equitable.
60 Prescriptive Basic structure & processes remains unchanged Comprehensive written PIPS plan required Integration with institutional PIPS effort - clearly defined reporting structure - method for provision of feedback Integration with regional/ state trauma system
61 No Core/ non-core trauma panel All trauma surgeons and liaisons must participate (50% attendance) Emphasis on clinical practice guidelines, protocols, and algorithms derived from evidenced-based resources Defined process and outcome measures (trauma audit filters) Levels of review required Identify OFI s Corrective actions Continuous monitoring & evaluation Problem resolution Multidisciplinary trauma peer review - variety of formats
62 Must use risk stratified benchmarking system - Maintenance of certification and pay for performance. - Commitment to improving performance through comparative analysis of outcomes across appropriately risk-stratified populations
63 Level I trauma center must meet admission volume requirement (one of the following): Admit at least 1,200 trauma patients yearly Admit at least 240 admissions with an ISS > 15 Geriatric trauma (older than 65 years) # admitted with MOI = fall from standing height # isolated hip fractures included in registry data Special considerations for geriatric patient Anticoagulation reversal Comfort/palliative care Orthopaedic surgery # pelvis and acetabular cases/yr # pelvis and acetabular cases transferred out Time to ORIF for femur fractures. Time to I&D open fractures. Appropriateness and timing of intravenous antibiotics for all open fractures.
64 Blood bank. Turnaround time for massive transfusion protocol (MTP) use/times. Turnaround time for use of goal-directed component therapy. Burn patients (if not a burn center). # burn patients admitted, transferred in, transferred out. Vertebral column injuries. # vertebral column injuries admitted, transferred in, transferred out # with neurologic deficits
65
66

67
68
69
70
71
72
73
74
75
76

77 The methods, language, and concepts of PIPS are evolving. Trauma program staff who are interested in developing and further refining their trauma performance improvement processes should attend the Trauma Outcomes and Performance Improvement Course (TOPIC) offered by the Society of Trauma Nurses (see
78 Transforming Trauma Center PIPS: From QA to a Culture of Safety What s Next? Shift the emphasis on error and preventability to outcomes, system re-design and behavioral change Adopt uniform patient safety taxonomy Apply CRM and AHRQ s TeamSTEPPS measures Implement Just Culture methodology for peer review Aspire to be a High Reliability Organizations
79 Summary Foundational Principles - Codman - Deming - Donebidian - Reasons - Resouces Document Shackford/ Tepas/ Rhodes/ Metzger/ Cryer Trauma PIPS premise Optimal Structure + Processes = Optimal Outcomes The Orange Book Prescriptive Structure & Processes Well-defined audit filters Risk-adjusted Outcomes (TQIP)
Trauma Verification Q&A Web Conference
 Trauma Verification Q&A Web Conference November 16, 2017 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification
Trauma Verification Q&A Web Conference November 16, 2017 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification
ACS Spotlight Lecture: Update on ACS COT
 ACS Spotlight Lecture: Update on ACS COT R. Todd Maxson, MD, FACS Trauma Medical Director Arkansas Children s Hospital Vice-Chair of the American College of Surgeons Verification Review Committee of the
ACS Spotlight Lecture: Update on ACS COT R. Todd Maxson, MD, FACS Trauma Medical Director Arkansas Children s Hospital Vice-Chair of the American College of Surgeons Verification Review Committee of the
Developing a Trauma Center
 Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
Developing a Trauma Center Amy Koestner, RN, BSN, MSN Trauma Program Manager Spectrum Health Medical Center Carol Spinweber, MS, RN Trauma Program Manager St. Joseph Mercy Oakland Objectives: Describe
REVIEW AGENDA AND LOGISTICS
 REVIEW AGENDA AND LOGISTICS The purpose of the American College of Surgeons Verification, Review, & Consultation (VRC) Program is to verify a hospital s compliance with the ACS standards for a trauma center.
REVIEW AGENDA AND LOGISTICS The purpose of the American College of Surgeons Verification, Review, & Consultation (VRC) Program is to verify a hospital s compliance with the ACS standards for a trauma center.
TQIP and Risk Adjusted Benchmarking
 TQIP and Risk Adjusted Benchmarking Melanie Neal, MS Manager Trauma Quality Improvement Program TQIP Participation Adult Only Centers 278 Peds Only Centers 27 Combined Centers 46 Total 351 What s new TQIP
TQIP and Risk Adjusted Benchmarking Melanie Neal, MS Manager Trauma Quality Improvement Program TQIP Participation Adult Only Centers 278 Peds Only Centers 27 Combined Centers 46 Total 351 What s new TQIP
Trauma Quality Programs Verification, TQIP and the Future
 Trauma Quality Programs Verification, TQIP and the Future Daniel Margulies, MD FACS Cedars- Sinai Medical Center Los Angeles, California Chair of the Verification Review Committee of the American College
Trauma Quality Programs Verification, TQIP and the Future Daniel Margulies, MD FACS Cedars- Sinai Medical Center Los Angeles, California Chair of the Verification Review Committee of the American College
TRAUMA CENTER REQUIREMENTS
 California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
California Trauma Center Level III Criteria California Code of Regulations,, Chapter 7 - Trauma Care System with American College of Surgeons (Green Book) references; includes FAQ clarifications TRAUMA
Welcome New TQIP Centers! Julia McMurray Business Operations Manager Trauma Quality Improvement Program
 Welcome New TQIP Centers! Julia McMurray Business Operations Manager Trauma Quality Improvement Program What are the goals for this webinar? Recognize that the ultimate goal of the Trauma Quality Improvement
Welcome New TQIP Centers! Julia McMurray Business Operations Manager Trauma Quality Improvement Program What are the goals for this webinar? Recognize that the ultimate goal of the Trauma Quality Improvement
Trauma Verification Q&A Web Conference
 Trauma Verification Q&A Web Conference February 22, 2018 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification
Trauma Verification Q&A Web Conference February 22, 2018 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification
Ten Things that Can Improve your Trauma PI Program
 Ten Things that Can Improve your Trauma PI Program Mike Glenn, RN, Trauma QI Coordinator Harborview Medical Center 1 Trauma centers must have a PIPS program that includes a comprehensive written plan outlining
Ten Things that Can Improve your Trauma PI Program Mike Glenn, RN, Trauma QI Coordinator Harborview Medical Center 1 Trauma centers must have a PIPS program that includes a comprehensive written plan outlining
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.
 Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.") Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Trauma Verification Q&A Web Conference
 Trauma Verification Q&A Web Conference December 15, 2017 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification
Trauma Verification Q&A Web Conference December 15, 2017 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification
NEW MEXICO TRAUMA PROCESS IMPROVEMENT PLAN
 2014 NEW MEXICO TRAUMA PROCESS IMPROVEMENT PLAN TRAUMA PERFORMANCE IMPROVEMENT COMMITTEE This manual contains a descriptive overview of the PI model and emphasizes a continuous multidisciplinary effort
2014 NEW MEXICO TRAUMA PROCESS IMPROVEMENT PLAN TRAUMA PERFORMANCE IMPROVEMENT COMMITTEE This manual contains a descriptive overview of the PI model and emphasizes a continuous multidisciplinary effort
RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT
 CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical
CALIFORNIA TRAUMA REGULATIONS (Title 22) versus ACS RESOURCES FOR OPTIMAL CARE OF THE INJURED PATIENT 2006 (Green Book) (Level I/II Trauma Centers Only) Requirement TITLE 22 ACS GREEN BOOK Trauma Medical
Trauma Verification Q&A Web Conference
 Trauma Verification Q&A Web Conference July 26, 2018 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification Rachel
Trauma Verification Q&A Web Conference July 26, 2018 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification Rachel
TQIP Monthly Registry Staff Web Conference. July 31, 2014
 TQIP Monthly Registry Staff Web Conference July 31, 2014 Your TQIP Staff Tammy Morgan National TQIP Educator Julia McMurray TQIP Program Manager Announcements Registration for the 2014 TQIP conference
TQIP Monthly Registry Staff Web Conference July 31, 2014 Your TQIP Staff Tammy Morgan National TQIP Educator Julia McMurray TQIP Program Manager Announcements Registration for the 2014 TQIP conference
Trauma Verification Q&A Web Conference
 Trauma Verification Q&A Web Conference May 31, 2018 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification Rachel
Trauma Verification Q&A Web Conference May 31, 2018 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification Rachel
The following policy was adopted by the San Luis Obispo County EMS Agency and will become effective March 1, 2012 at 0800 hours.
 SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
SLO County Emergency Medical Services Agency Bulletin 2012-02 PLEASE POST New Trauma System Policies and Procedures February 9, 2012 To All SLO County EMS Providers and Training Institutions: The following
The Culture of Safety Event Taxonomy: Overview
 The Culture of Safety Event Taxonomy: Overview The Patient Safety Taxonomy Discloser: This presentation is based on the work of Donald Jenkins, MD & Carol Immermann, RN Content from the TOPIC program is
The Culture of Safety Event Taxonomy: Overview The Patient Safety Taxonomy Discloser: This presentation is based on the work of Donald Jenkins, MD & Carol Immermann, RN Content from the TOPIC program is
Trauma Verification Q&A Web Conference
 Trauma Verification Q&A Web Conference August 23, 2016 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Verification Manager Trauma Verification
Trauma Verification Q&A Web Conference August 23, 2016 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Verification Manager Trauma Verification
Quality Assessment and Performance Improvement in the Ophthalmic ASC
 Quality Assessment and Performance Improvement in the Ophthalmic ASC ELETHIA DEAN RN,BSN, MBA, PHD Regulatory Requirements QAPI Program required by: Medicare Most states ASC licensing regulations Accrediting
Quality Assessment and Performance Improvement in the Ophthalmic ASC ELETHIA DEAN RN,BSN, MBA, PHD Regulatory Requirements QAPI Program required by: Medicare Most states ASC licensing regulations Accrediting
Surgical Performance Tracking in a Multisource Data Environment
 Surgical Performance Tracking in a Multisource Data Environment Kiley B. Vander Wyst, MPH Jorge I. Arango, MD Madison Carmichael, BS Shelley Flecky, PA P. David Adelson, MD, FACS, FAAP Disclosures No conflicts
Surgical Performance Tracking in a Multisource Data Environment Kiley B. Vander Wyst, MPH Jorge I. Arango, MD Madison Carmichael, BS Shelley Flecky, PA P. David Adelson, MD, FACS, FAAP Disclosures No conflicts
Level 4 Trauma Hospital Criteria
 Level 4 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
Level 4 Trauma Hospital Criteria Hospital Commitment The board of directors, administration, and medical, nursing and ancillary staff shall make a commitment to providing trauma care commensurate to the
8/31/2015. Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success. Vanderbilt University Medical Center
 Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
Session C719 Outcomes of a Study Addressing Challenges in APRN Practice and Strategies for Success Marilyn A. Dubree, MSN, RN, NE-BC Executive Chief Nursing Officer Vanderbilt University Medical Center
The Trauma System. Prevention Pre-hospital care and transport Acute hospital care Rehab Research
 An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
An Overview The Trauma System The Office of Emergency Medical Services & Trauma System (OEMSTS) is responsible for oversight of the trauma system. The ideal trauma system includes; Prevention Pre-hospital
Support (Level III) Stroke Facility Criteria Guidance
 Stroke Facility Criteria Guidance") Support (Level III) Stroke Facilities ( SSFs ) - provides resuscitation, stabilization and assessment of the stroke victim and either provides the treatment or arranges for immediate transfer to a higher
Support (Level III) Stroke Facilities ( SSFs ) - provides resuscitation, stabilization and assessment of the stroke victim and either provides the treatment or arranges for immediate transfer to a higher
VERIFICATION SURGEON The American College of Surgeons Children s Surgery Verification Program
 VERIFICATION SURGEON The American College of Surgeons Children s Surgery Verification Program R. Lawrence Moss, MD Surgeon-in-Chief Nationwide Children's Hospital E. Thomas Boles Jr., Professor of Surgery
VERIFICATION SURGEON The American College of Surgeons Children s Surgery Verification Program R. Lawrence Moss, MD Surgeon-in-Chief Nationwide Children's Hospital E. Thomas Boles Jr., Professor of Surgery
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES BUREAU OF EMS, TRAUMA AND PREPAREDNESS EMS AND TRAUMA SERVICES SECTION STATEWIDE TRAUMA SYSTEM
 MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES BUREAU OF EMS, TRAUMA AND PREPAREDNESS EMS AND TRAUMA SERVICES SECTION STATEWIDE TRAUMA SYSTEM (By authority conferred on the department of health and human
MICHIGAN DEPARTMENT OF HEALTH AND HUMAN SERVICES BUREAU OF EMS, TRAUMA AND PREPAREDNESS EMS AND TRAUMA SERVICES SECTION STATEWIDE TRAUMA SYSTEM (By authority conferred on the department of health and human
Trauma Verification Q&A Web Conference
 Trauma Verification Q&A Web Conference August 30, 2017 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification Rachel
Trauma Verification Q&A Web Conference August 30, 2017 COTVRC@facs.org Your Trauma Quality Programs Staff Tammy Morgan Manager Trauma Center Programs Molly Lozada Program Manager Trauma Verification Rachel
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR)
") Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
Trauma Center Pre-Review Questionnaire Notes Title 22
 This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
This Pre-Review Questionnaire is designed to accompany the spread sheet appropriate for the Trauma Center being reviewed For use with review of Level III Trauma Center with American College of Surgeons'
Preventing Medical Errors : A Call to Action. Definitions of Quality. Quality of Care. Objectives. Background of the Quality Movement
 Quality Assessment, Quality Assurance and Quality Improvement in Dentistry November 18, 2003 With thanks to Drs. Georgina Zabos and James Crall Objectives Become familiar with the social, economic and
Quality Assessment, Quality Assurance and Quality Improvement in Dentistry November 18, 2003 With thanks to Drs. Georgina Zabos and James Crall Objectives Become familiar with the social, economic and
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
Decreasing Mortality in Head Strike Patients on Anticoagulants with a Head Strike Protocol
 Decreasing Mortality in Head Strike Patients on Anticoagulants with a Head Strike Protocol TraumaCon 2017 Society of Trauma Nurses April 5-8, 2017 St. Louis, MO 2.0 hours after onset 6.5 hours after onset
Decreasing Mortality in Head Strike Patients on Anticoagulants with a Head Strike Protocol TraumaCon 2017 Society of Trauma Nurses April 5-8, 2017 St. Louis, MO 2.0 hours after onset 6.5 hours after onset
Quality Management and Accreditation
 Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
Quality Management and Accreditation Lina Mekawi, RPh, MS Epidemiology, CPHQ, Senior Quality Analyst, Quality, Accreditation and Risk Management Department, AUBMC November 2017 Disclosure Slide I, Lina
Risk Adjustment Methods in Value-Based Reimbursement Strategies
 Paper 10621-2016 Risk Adjustment Methods in Value-Based Reimbursement Strategies ABSTRACT Daryl Wansink, PhD, Conifer Health Solutions, Inc. With the move to value-based benefit and reimbursement models,
Paper 10621-2016 Risk Adjustment Methods in Value-Based Reimbursement Strategies ABSTRACT Daryl Wansink, PhD, Conifer Health Solutions, Inc. With the move to value-based benefit and reimbursement models,
Objectives. Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004
 Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
2015 TQIP Data Submission Web Conference. February 11, 2015
 2015 TQIP Data Submission Web Conference February 11, 2015 Instructor Tammy Morgan, National TQIP Educator Let s talk about CE! Presenters Chris Hoeft, Technical Analyst Julia McMurray, Business Operations
2015 TQIP Data Submission Web Conference February 11, 2015 Instructor Tammy Morgan, National TQIP Educator Let s talk about CE! Presenters Chris Hoeft, Technical Analyst Julia McMurray, Business Operations
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study
 Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
Study Title: Optimal resuscitation in pediatric trauma an EAST multicenter study PI/senior researcher: Richard Falcone Jr. MD, MPH Co-primary investigator: Stephanie Polites MD, MPH; Juan Gurria MD My
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
8/10/2015. Module 1. A Fundamental Understanding of Quality. Management and its Application to Health Care
 Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Module 1 A Fundamental Understanding of Quality Management and its Application to Health Care Addressing Physician Uncertainty about Payment Reform: Skills for Success in Value-Based Delivery Systems The
Tammy Morgan Terri Swiencicki Michelle Pomphrey. Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2012
 Annual Scientific Meeting and Training 2012") TQIP Abstractor Workshop Tammy Morgan Terri Swiencicki Michelle Pomphrey Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2012 You are important to TQIP, and we want to
TQIP Abstractor Workshop Tammy Morgan Terri Swiencicki Michelle Pomphrey Trauma Quality Improvement Program (TQIP) Annual Scientific Meeting and Training 2012 You are important to TQIP, and we want to
UW HEALTH JOB DESCRIPTION
 NURSE CASE MANAGER - ED Job Code: 801009 FLSA Status: Mgt. Approval: B Liegel Date: 6-18 Department: Coordinated Care Department 93070 HR Approval: M Buenger Date: 6-18 JOB SUMMARY The Nurse Case Manager,
NURSE CASE MANAGER - ED Job Code: 801009 FLSA Status: Mgt. Approval: B Liegel Date: 6-18 Department: Coordinated Care Department 93070 HR Approval: M Buenger Date: 6-18 JOB SUMMARY The Nurse Case Manager,
Incident Reporting Systems
 Patient Safety in Radiation Oncology, Melbourne 4-54 5 October 2012 Incident Reporting Systems Ola Holmberg, PhD Head, Radiation Protection of Patients Unit Radiation Safety and Monitoring Section NSRW
Patient Safety in Radiation Oncology, Melbourne 4-54 5 October 2012 Incident Reporting Systems Ola Holmberg, PhD Head, Radiation Protection of Patients Unit Radiation Safety and Monitoring Section NSRW
Battlefield Trauma Systems
 Battlefield Trauma Systems Chapter 35 Battlefield Trauma Systems Introduction A trauma system is an organized, coordinated effort in a defined geographic area that delivers the full range of care to all
Battlefield Trauma Systems Chapter 35 Battlefield Trauma Systems Introduction A trauma system is an organized, coordinated effort in a defined geographic area that delivers the full range of care to all
Surgeon Champion: Getting Started, What You Need to Know
 Surgeon Champion: Getting Started, What You Need to Know Ninh T. Nguyen, MD, FACS Professor of Surgery Surgeon Champion Vice-Chair, Dept Surgery University of California, Irvine, Medical Center, Orange,
Surgeon Champion: Getting Started, What You Need to Know Ninh T. Nguyen, MD, FACS Professor of Surgery Surgeon Champion Vice-Chair, Dept Surgery University of California, Irvine, Medical Center, Orange,
National Priorities for Improvement:
 National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
Sue Brown Clinical Audit and Effectiveness Manager. Safety and Quality Committee
 Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient Safety
NATIONAL ASSOCIATION OF BOARDS OF PHARMACY (NAPB) / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011
 / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011") NATIONAL ASSOCIATION OF BOARDS OF PHARMACY (NAPB) / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011 7:30-8:30 PM SHERATON CAVALIER HOTEL SASKATOON SPEAKING
NATIONAL ASSOCIATION OF BOARDS OF PHARMACY (NAPB) / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011 7:30-8:30 PM SHERATON CAVALIER HOTEL SASKATOON SPEAKING
Practice Advancement Initiative (PAI) Using the ASHP PAI Ambulatory Care Self-Assessment Survey
 Using the ASHP PAI Ambulatory Care Self-Assessment Survey") Practice Advancement Initiative (PAI) Using the ASHP PAI Ambulatory Care Self-Assessment Survey Jodie Elder, PharmD, BCPS September 14, 2017 Objectives List the key components of the Practice Advancement
Practice Advancement Initiative (PAI) Using the ASHP PAI Ambulatory Care Self-Assessment Survey Jodie Elder, PharmD, BCPS September 14, 2017 Objectives List the key components of the Practice Advancement
Adverse Events: Thorough Analysis
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Adverse Events: Thorough Analysis James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Welcome New TQIP Centers! Julia McMurray Program Administrator Trauma Quality Improvement Program
 Welcome New TQIP Centers! Julia McMurray Program Administrator Trauma Quality Improvement Program Meet your TQIP staff! Melanie Neal - Manager, TQIP & NTDB Tammy Morgan National TQIP Educator Amy Svestka
Welcome New TQIP Centers! Julia McMurray Program Administrator Trauma Quality Improvement Program Meet your TQIP staff! Melanie Neal - Manager, TQIP & NTDB Tammy Morgan National TQIP Educator Amy Svestka
Health Care Quality Indicators in the Irish Health System:
 Health Care Quality Indicators in the Irish Health System Examining the Potential of Hospital Discharge Data using the Hospital Inpatient Enquiry System - i - Health Care Quality Indicators in the Irish
Health Care Quality Indicators in the Irish Health System Examining the Potential of Hospital Discharge Data using the Hospital Inpatient Enquiry System - i - Health Care Quality Indicators in the Irish
NATIONAL STANDARDS, ESSENTIAL ELEMENTS AND INTERPRETIVE GUIDANCE
 Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
Background and Context:
 Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
Session Objectives: Practice Transformation: Preparing for a Value Based Purchasing Environment Susan Brown, MPH, CPHIMS May 2, 2016 Understand the timeline and impact of MACRA/MIPS on health care payment
July 2018 TRAUMA REGISTRY UPDATE. Excellence, Innovation, Integrity & Teamwork
 Trauma Program Registrars, Trauma Program Managers/Coordinators & Trauma Performance Improvement Coordinators: Please review the below information for multiple trauma registry-related updates. If you have
Trauma Program Registrars, Trauma Program Managers/Coordinators & Trauma Performance Improvement Coordinators: Please review the below information for multiple trauma registry-related updates. If you have
POLICIES AND PROCEDURES
 POLICIES AND PROCEDURES POLICY: 535.10 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 14 I. AUTHORITY Division 2.5, California Health and Safety
POLICIES AND PROCEDURES POLICY: 535.10 TITLE: EFFECTIVE: 4/13/17 REVIEW: 4/2022 SUPERCEDES: APPROVAL SIGNATURES ON FILE IN EMS OFFICE PAGE: 1 of 14 I. AUTHORITY Division 2.5, California Health and Safety
COUNTY OF SAN DIEGO TRAUMA SYSTEM
 COUNTY OF SAN DIEGO TRAUMA SYSTEM Thirty plus years of MAC..and still going strong! Candy Schoenheit, RN, BSN, PHN, MICN QA Specialist/Trauma/EMSC System Coordinator DISCLAIMER No conflicts and nothing
COUNTY OF SAN DIEGO TRAUMA SYSTEM Thirty plus years of MAC..and still going strong! Candy Schoenheit, RN, BSN, PHN, MICN QA Specialist/Trauma/EMSC System Coordinator DISCLAIMER No conflicts and nothing
N ATIONAL Q UALITY F ORUM. Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT
 N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
N ATIONAL Q UALITY F ORUM Safe Practices for Better Healthcare 2006 Update A CONSENSUS REPORT NATIONAL QUALITY FORUM Foreword Every person who seeks care in a healthcare facility should expect to receive
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria)
") AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
AMERICAN COLLEGE OF SURGEONS 1999 TRAUMA FACILITIES CRITERIA (minus the Level IV criteria) Note: In the table below, (E) represents essential while (D) represents desirable criteria. INSTITUTIONAL ORGANIZATION
National Patient Safety Agency Root Cause Analysis (RCA) Investigation
 Investigation") National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
National Patient Safety Agency Root Cause Analysis (RCA) Investigation Margaret O Donovan Assistant Director for Acute Services Types of failure Active failures - slips, lapses, fumbles, mistakes, procedural
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Health Quality Management
 Western Technical College 10530161 Health Quality Management Course Outcome Summary Course Information Description Career Cluster Instructional Level Core Abilities Total Credits 3.00 Explores the programs
Western Technical College 10530161 Health Quality Management Course Outcome Summary Course Information Description Career Cluster Instructional Level Core Abilities Total Credits 3.00 Explores the programs
FLORIDA CENTER FOR HEALTH INFORMATION AND TRANSPARENCY
 FLORIDA CENTER FOR HEALTH INFORMATION AND TRANSPARENCY DATA CATALOG Rick Scott, Governor Justin M. Senior, Secretary Visit AHCA online at: www.floridahealthfinder.gov Revised 2017 TABLE OF CONTENTS PAGE
FLORIDA CENTER FOR HEALTH INFORMATION AND TRANSPARENCY DATA CATALOG Rick Scott, Governor Justin M. Senior, Secretary Visit AHCA online at: www.floridahealthfinder.gov Revised 2017 TABLE OF CONTENTS PAGE
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Patient Safety Overview
 Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
Patient Safety Overview Muhammad H. Islam, MBBS, MS, MCH, LSSBB Director of Patient Safety & Patient Safety Officer SUNY Downstate Medical Center, UHB www.downstate.edu/patientsafety Definitions Patient
Hospital Crosswalk. Medicare Hospital Requirements to 2012 Joint Commission Hospital Standards & EPs
 Hospital Crosswalk CFR Number Standards and Elements of Performance 482.11 TAG: A-0020 482.11 Condition of Participation: Compliance with Federal, State and Local Laws 482.11(a) TAG: A-0021 LD.04.01.01
Hospital Crosswalk CFR Number Standards and Elements of Performance 482.11 TAG: A-0020 482.11 Condition of Participation: Compliance with Federal, State and Local Laws 482.11(a) TAG: A-0021 LD.04.01.01
AHRQ Quality Indicators. Maryland Health Services Cost Review Commission October 21, 2005 Marybeth Farquhar, AHRQ
 AHRQ Quality Indicators Maryland Health Services Cost Review Commission October 21, 2005 Marybeth Farquhar, AHRQ Overview AHRQ Quality Indicators Current Uses of the Quality Indicators Case Studies of
AHRQ Quality Indicators Maryland Health Services Cost Review Commission October 21, 2005 Marybeth Farquhar, AHRQ Overview AHRQ Quality Indicators Current Uses of the Quality Indicators Case Studies of
Bariatric Surgery Registry Outlier Policy
 Bariatric Surgery Registry Outlier Policy 1 Revision History Version Date Author Reason for version change 1.0 10/07/2014 Wendy Brown First release 1.1 01/09/2014 Wendy Brown Review after steering committee
Bariatric Surgery Registry Outlier Policy 1 Revision History Version Date Author Reason for version change 1.0 10/07/2014 Wendy Brown First release 1.1 01/09/2014 Wendy Brown Review after steering committee
Data Collection and Reporting: Why and How
 Data Collection and Reporting: Why and How Disclosure Douglas C. Barnhart, MD MSPH FACS I do not have any relevant financial relationships with any commercial interest that pertains to the content of my
Data Collection and Reporting: Why and How Disclosure Douglas C. Barnhart, MD MSPH FACS I do not have any relevant financial relationships with any commercial interest that pertains to the content of my
General Eligibility Requirements
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
5D QAPI from an Operational Approach. Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Pathway Health 2013
 5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
5D QAPI from an Operational Approach Christine M. Osterberg RN BSN Senior Nursing Consultant Pathway Health Objectives Review the post-acute care data agenda. Explain QAPI principles Describe leadership
Quality and Safe Respiratory Care: Does it Work in a Productivity Model?
 Quality and Safe Respiratory Care: Does it Work in a Productivity Model? Timothy R. Myers MBA, RRT-NPS, FAARC Associate Executive Director, Brands Management American Association for Respiratory Care Adjunct
Quality and Safe Respiratory Care: Does it Work in a Productivity Model? Timothy R. Myers MBA, RRT-NPS, FAARC Associate Executive Director, Brands Management American Association for Respiratory Care Adjunct
UW HEALTH JOB DESCRIPTION
 Job Code: 801008 UW HEALTH JOB DESCRIPTION Outcomes Manager- Medicine FLSA Status: Exempt Mgt. Approval: Barbara Liegel Date: 9-16 HR Approval: R. Temple Date: 9-16 JOB SUMMARY The Outcomes Manager is
Job Code: 801008 UW HEALTH JOB DESCRIPTION Outcomes Manager- Medicine FLSA Status: Exempt Mgt. Approval: Barbara Liegel Date: 9-16 HR Approval: R. Temple Date: 9-16 JOB SUMMARY The Outcomes Manager is
Utilizing FPPE and OPPE Effectively OPPE & FPPE. Joint Commission FAQs. Utilizing FPPE and OPPE Effectively. Susan Mellott PhD, RN.
 Utilizing FPPE and OPPE Effectively Susan Mellott PhD, RN, CPHQ, FNAHQ OPPE & FPPE For the sake of this presentation, OPPE and FPPE will be discussed as it pertains to physicians. However, all information
Utilizing FPPE and OPPE Effectively Susan Mellott PhD, RN, CPHQ, FNAHQ OPPE & FPPE For the sake of this presentation, OPPE and FPPE will be discussed as it pertains to physicians. However, all information
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health
 Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Creating a Culture of Quality and Safety Gordon C. Hunt, MD, MBA Sr. Vice President & Chief Medical Officer, Sutter Health M2 This presenter has nothing to disclose December 2012 Blue Ribbon I & II In
Risk Management in the ASC
 1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
1 Risk Management in the ASC Sandra Jones CASC, LHRM, CHCQM, FHFMA sjones@aboutascs.com IMPROVING HEALTH CARE QUALITY THROUGH ACCREDITATION 2014 Accreditation Association for Conflict of Interest Disclosure
CHAPTER 12 -QUALITY MANAGEMENT AND PERFORMANCE IMPROVEMENT
 CHAPTER 12 -QUALITY MANAGEMENT AND PERFORMANCE IMPROVEMENT 12.0 QUALITY MANAGEMENT REQUIREMENTS Health Choice Integrated Care works in partnership with providers to continuously monitor and improve the
CHAPTER 12 -QUALITY MANAGEMENT AND PERFORMANCE IMPROVEMENT 12.0 QUALITY MANAGEMENT REQUIREMENTS Health Choice Integrated Care works in partnership with providers to continuously monitor and improve the
Inland Empire Health Plan Quality Management Program Description Date: April, 2017
 Inland Empire Health Plan Quality Management Program Description Date: April, 2017 Page 1 of 35 Table of Contents Introduction.....3 Mission and Vision........3 Section 1: QM Program Overview........4
Inland Empire Health Plan Quality Management Program Description Date: April, 2017 Page 1 of 35 Table of Contents Introduction.....3 Mission and Vision........3 Section 1: QM Program Overview........4
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
DOCUMENT E FOR COMMENT
 DOCUMENT E FOR COMMENT TABLE 4. Alignment of Competencies, s and Curricular Recommendations Definitions Patient Represents patient, family, health care surrogate, community, and population. Direct Care
DOCUMENT E FOR COMMENT TABLE 4. Alignment of Competencies, s and Curricular Recommendations Definitions Patient Represents patient, family, health care surrogate, community, and population. Direct Care
Quality Management (QM) Program AmeriHealth Pennsylvania
 Program AmeriHealth Pennsylvania") Quality Management (QM) Program AmeriHealth Pennsylvania Goals and Objectives The goals and objectives of the Quality Management (QM) Program are to promote the quality and safety of medical and behavioral
Quality Management (QM) Program AmeriHealth Pennsylvania Goals and Objectives The goals and objectives of the Quality Management (QM) Program are to promote the quality and safety of medical and behavioral
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
4. Hospital and community pharmacies
 4. Hospital and community pharmacies As FIP is the international professional organisation of pharmacists, this paper emphasises the role of the pharmacist in ensuring and increasing patient safety. The
4. Hospital and community pharmacies As FIP is the international professional organisation of pharmacists, this paper emphasises the role of the pharmacist in ensuring and increasing patient safety. The
EMSC s Pediatric Readiness: Improving the Lives of All Children
 EMSC s Pediatric Readiness: Improving the Lives of All Children Elizabeth A. Edgerton, MD, MPH, FAAP Director, Division of Child, Adolescent and Family Health Maternal Child Health Bureau Health Resources
EMSC s Pediatric Readiness: Improving the Lives of All Children Elizabeth A. Edgerton, MD, MPH, FAAP Director, Division of Child, Adolescent and Family Health Maternal Child Health Bureau Health Resources
MEDICAL STAFF ORGANIZATION MANUAL OF THE BYLAWS OF THE MEDICAL STAFF UNIVERSITY OF NORTH CAROLINA HOSPITALS
 MEDICAL STAFF ORGANIZATION MANUAL OF THE BYLAWS OF THE MEDICAL STAFF UNIVERSITY OF NORTH CAROLINA HOSPITALS Approved by the Executive Committee of the Medical Staff, November 5, 2001. Approved and adopted
MEDICAL STAFF ORGANIZATION MANUAL OF THE BYLAWS OF THE MEDICAL STAFF UNIVERSITY OF NORTH CAROLINA HOSPITALS Approved by the Executive Committee of the Medical Staff, November 5, 2001. Approved and adopted
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Trauma Service Area - B (BRAC) Regional Stroke Plan
 Regional Stroke Plan") Trauma Service Area - B (BRAC) Regional Stroke Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, TX 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran, Cottle,
Trauma Service Area - B (BRAC) Regional Stroke Plan Trauma Service Area- B (BRAC) P.O. Box 53597 Lubbock, TX 79453 806.791.2582 (office) BRAC serves the counties of Bailey, Borden, Castro, Cochran, Cottle,
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
The History of the development of the Prometheus Payment model defined Potentially Avoidable Complications.
 The History of the development of the Prometheus Payment model defined Potentially Avoidable Complications. In 2006 the Prometheus Payment Design Team convened a series of meetings with physicians that
The History of the development of the Prometheus Payment model defined Potentially Avoidable Complications. In 2006 the Prometheus Payment Design Team convened a series of meetings with physicians that
Catherine Porto, MPA, RHIA, CHP Executive Director HIM. Madelyn Horn Noble 3M HIM Data Analyst
 1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
1 Catherine Porto, MPA, RHIA, CHP Executive Director HIM Madelyn Horn Noble 3M HIM Data Analyst University of New Mexico Hospitals» The state s only academic medical center» The primary teaching hospital
THE MODEL OF QUALITY INCENTIVES
 1 THE MODEL OF QUALITY INCENTIVES 19 YEARS OF JOINT EFFORTS FHL-CNS Visit from Prof. Hirobumi Kawakita 6th October 2017 Presentation plan 2 History of the Inciting Quality model The EFQM Quality / performance
1 THE MODEL OF QUALITY INCENTIVES 19 YEARS OF JOINT EFFORTS FHL-CNS Visit from Prof. Hirobumi Kawakita 6th October 2017 Presentation plan 2 History of the Inciting Quality model The EFQM Quality / performance
Trauma Managers Council. Goals and Strategic Directions 2013
 Trauma Managers Council Goals and Strategic Directions 2013 Goals and Strategic Directions The Trauma Managers Council of the National Association of State EMS Officials is committed to the following vision,
Trauma Managers Council Goals and Strategic Directions 2013 Goals and Strategic Directions The Trauma Managers Council of the National Association of State EMS Officials is committed to the following vision,
How Data-Driven Safety Culture Changes Can Lower HAC Rates
 How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
Hong Kong College of Medical Nursing
 Hong Kong College of Medical Nursing Advanced Practice Nursing (Diabetes) Certification Program Clinical Log Book Name: (Email: ) Mentor s name Clinical Practice Site Period Mentor s name Clinical Practice
Hong Kong College of Medical Nursing Advanced Practice Nursing (Diabetes) Certification Program Clinical Log Book Name: (Email: ) Mentor s name Clinical Practice Site Period Mentor s name Clinical Practice
The Joint Commission:
 The Joint Commission: Over a century of quality and safety 1910-1913 Ernest Codman, M.D. proposes the end result system of hospital standardization. American College of Surgeons is founded. The end result
The Joint Commission: Over a century of quality and safety 1910-1913 Ernest Codman, M.D. proposes the end result system of hospital standardization. American College of Surgeons is founded. The end result
The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures
 The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures June 21, 2017 Caroline Isbey, RN, MSN, CDE Associate Director, Certification David Eickemeyer, MBA
The Basics: Disease-Specific Care Certification Clinical Practice Guidelines and Performance Measures June 21, 2017 Caroline Isbey, RN, MSN, CDE Associate Director, Certification David Eickemeyer, MBA
TITLE: The impact of surgical timing in acute traumatic spinal cord injury
 AWARD NUMBER: W81XWH-13-1-0396 TITLE: The impact of surgical timing in acute traumatic spinal cord injury PRINCIPAL INVESTIGATOR: Jean-Marc Mac-Thiong, MD, PhD CONTRACTING ORGANIZATION: Hopital du Sacre-Coeur
AWARD NUMBER: W81XWH-13-1-0396 TITLE: The impact of surgical timing in acute traumatic spinal cord injury PRINCIPAL INVESTIGATOR: Jean-Marc Mac-Thiong, MD, PhD CONTRACTING ORGANIZATION: Hopital du Sacre-Coeur