Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
|
|
|
- Silas Perry
- 5 years ago
- Views:
Transcription

1 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School of Nursing 28 th International Nursing Research Congress July 28, 2017

2 Ronald Reagan UCLA Medical Center Los Angeles, CA, USA
3 Introduction Heart disease is the leading cause of death for both men and women in most ethnicities in the United States. Heart failure (HF) is the final common pathway for heart disease. About half of people who develop HF die within 5 years of diagnosis. HF continues to be a major burden in healthcare system despite the advances in medical knowledge and technology. High rates of morbidity, mortality, and cost

4 Background Most of the cost associated with the care of HF patients is attributable to patient rehospitalizations. Nearly one in four patients hospitalized with HF is rehospitalized within 30 days of discharge. 30 day rates of rehospitalizations in HF have risen over the past 2 decades. HF rehospitalizations may be preventable, but effective strategies to prevent rehospitalizations were traditionally underutilized due to lack of incentives.



5 Traditional Heart Failure Admission Tune up with diuretics A little bit of education List of discharge prescriptions Push patient out the door and wave good-bye Bye-bye...Don t come back within 30 days!!
6
7 All-Cause Mortality After Each Subsequent Rehospitalization for HF The risk of death is greatest in the early period after hospital discharge and is directly related to the frequency of HF hospitalizations. Setoguchi S, Stevenson, LW et al. Am Heart J. 2007;154:







8 What Causes Hospital Readmissions? Fragility on discharge Lack of understanding of discharge instructions Stresses within the hospital Readmissions Inability to carry out discharge instructions
9

10 30-Day HF and AMI Readmission Rate Ronald Reagan UCLA Medical Center Data Source: UHC 2015 Risk Model

11 30-Readmission Rates by Unit Heart Failure Service Line Ronald Reagan UCLA Medical Center Data Source: UHC 2015 Risk Model

12 How Does It Work? 35 hospitals recruited over 3 years Established administrator and physician champions as well as Navigator team members American College of Cardiology (ACC) provided onsite training, toolkits, assessments, and webinars Hospitals required to report back on metrics
13 HF/AMI Readmission Committee ACC Patient Navigator Program Team Charter Charge Guiding Principles Goals Navigator Identified Opportunities for Improvement To reduce avoidable hospital readmissions by providing personalized support to patients diagnosed with: Acute Myocardial Infarction Heart Failure Use data to understand all causes of AMI and HF readmissions at Ronald Regan Medical Center The data will drive our interventions and improvements in quality Develop and apply patient-centered solutions that address functional disabilities, stressors, and other challenges confronting AMI and HF patients that increases these patients risk of readmission. Risk Model to identify high risk of readmissions prior to discharge Verifying follow-up appointments are documented in the medical record 7-day follow-up appointments for all patients Follow-up visit for cardiac rehab (MI patients) Identify AMI and CHF patients to be part of our committee and give us timely feedback Education (e.g. teach-back) and documentation Treatment regimen (self-care plan) and when to call their health provider Documentation of all prescribed medications and instructions on when and how they should be taken, and about any changes to medications Community resources for patients Performance and documentation of medication reconciliation
14 Risk Prediction Models Risk scores allow a prediction to be made to assist in clinical decision making. Use factors to calculate or predict an outcome. Models are usually developed from large data sets using logistic regression with a combination of categorical and continuous variables. Aim to determine the likelihood of the future event occurring within a given population. Risk can be assessed in either relative or absolute conditions. Relative risk is the risk of the endpoint, such as disease, death, readmission, among those exposed versus the risk of the endpoint among the unexposed. Absolute risk, is the probability of an event in a population under study, as contrasted with the relative risk. Betihavas, V., Davidson, P. M., et al. Australian critical care. 2012;25(1):31-40.
15 Clinical risk models CMS Risk Model Risk Tools OPTIMIZE-HF Post Discharge Risk Model GWTG-HF Post Discharge Risk Model Lace/Lace+ Index Biomarkers BNP / NT-BNP Galectin-3 Time limited disease management First 30 days of discharge Am Heart J 2012;164:365-72
16 LACE Index Used to predict the risk of unplanned readmission within 30 days after hospital discharge in both medical and surgical patients. The LACE high risk index may have utility as a screening tool to predict high risk ED revisits after hospital discharge. The LACE index may not accurately predict unplanned readmissions within 30 days from hospital discharge in CHF patients.
17 The tool scores patients from 0 to 19 on the basis of all the following parameters: Length of stay (L) of the index admission. Acuity of admission (A) - specifically if the patient is admitted through the Emergency Department vs. an elective admission. Comorbidity (C) - incorporates the Charlson Co-Morbidity Index. Emergency department visits in the preceding 6 months (E).
18 Reliability and Validity Of all the various tools available, LACE has been studied most extensively. Moderate to high predictive value in identifying those patients at risk for readmission. High predictive value in identifying those patients at risk to return the Emergency Department. The LACE index was very discriminative for early death (C statistic 0.793, 95% CI ) and well calibrated (Hosmer Lemeshow statistic 4.7, p = 0.79).

19 The LACE+ Index (score 0-90) is a modified version of the LACE Index in which each patient receives a score based on all the same parameters used by LACE, as well as the following: Age Gender Teaching status of the hospital Number of days on alternative level of care during admission Number of elective admissions in previous year Number of urgent admissions in previous year.
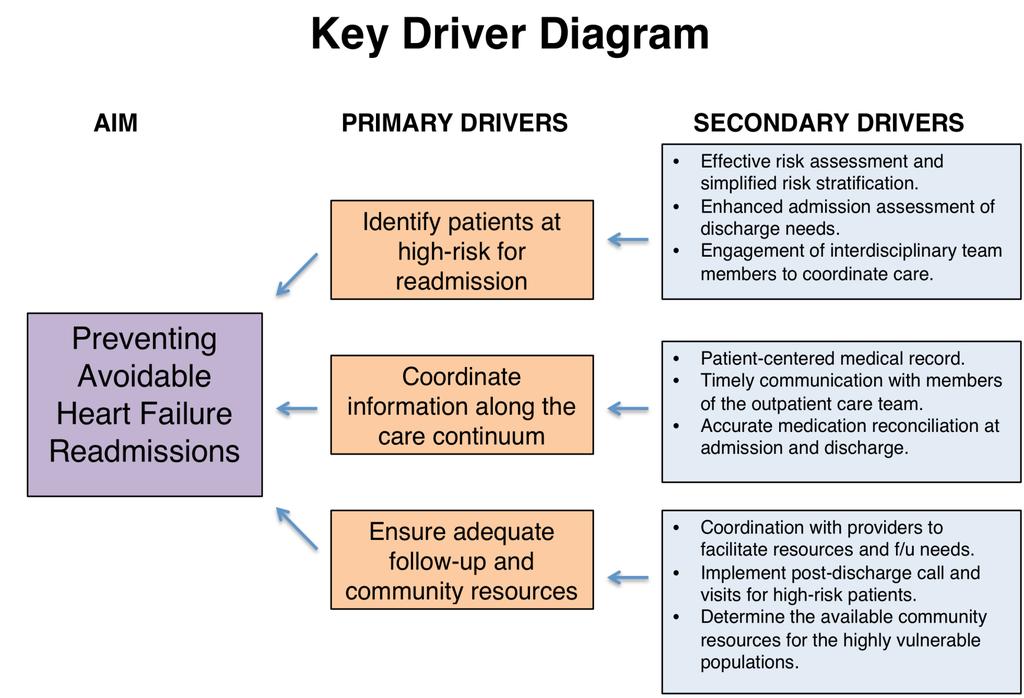
20 Strategies in Response to LACE Score Identify patients At Risk for Readmission Improve self-management skills Coordination of care along the care continuum Adequate follow-up and community resources 20
21 LACE Risk Stratification Score & Bundled Interventions LACE Score Intervention Needed and Responsible Provider Low (0 6) Med (7 10) High ( 11) Standardized D/C summary (after-visit summary) X X X Medication reconciliation (MD/pharmacist) X X X Update medication list (RN) X X X Physical therapy consultation X X Pharmacy 1:1 teaching X X Social work (psychosocial issues/complex cases) Care coordination: home health, communitybased care transition program (case management) Nutrition 1:1 teaching (dietician) Post hospital follow-up visit with physician (Department of Medicine staff) Palliative care (PRN) 5 days 5 days 3 days/home Health RN X X X Abbreviations: D/C, discharge; LACE, length of stay, acuity of admission, comorbid conditions, and emergency department visits; MD, physician; PRN, as needed; RN, registered nurse.

22 LACE Interventions: 9/15/15-11/30/15 96 Cases
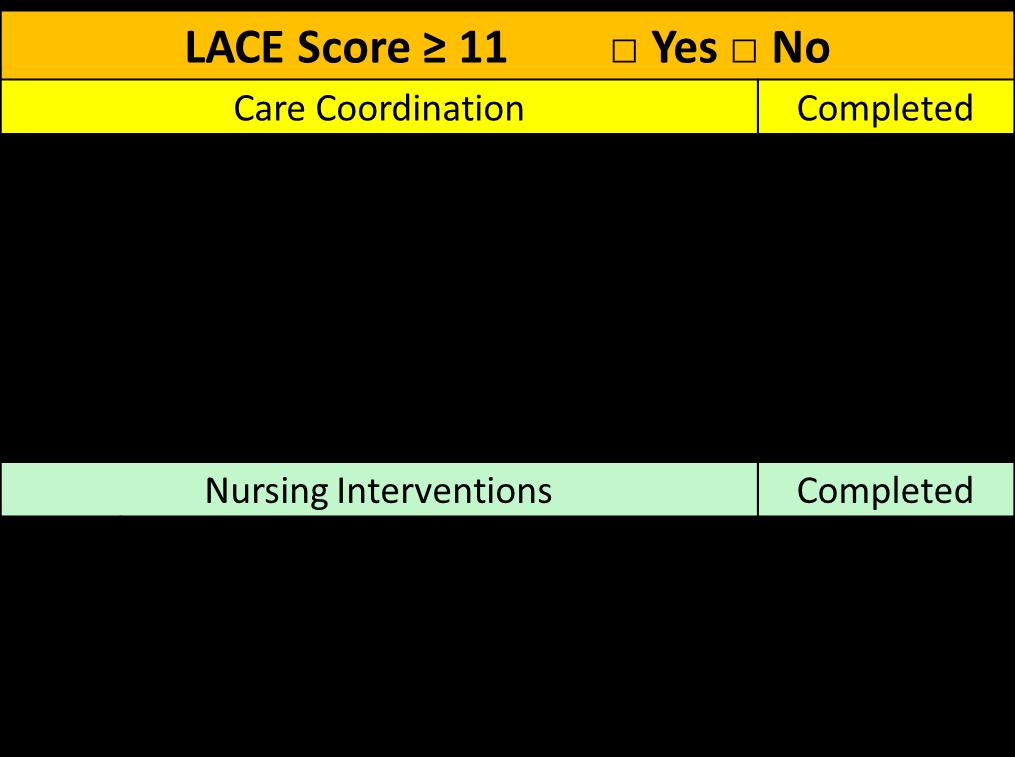
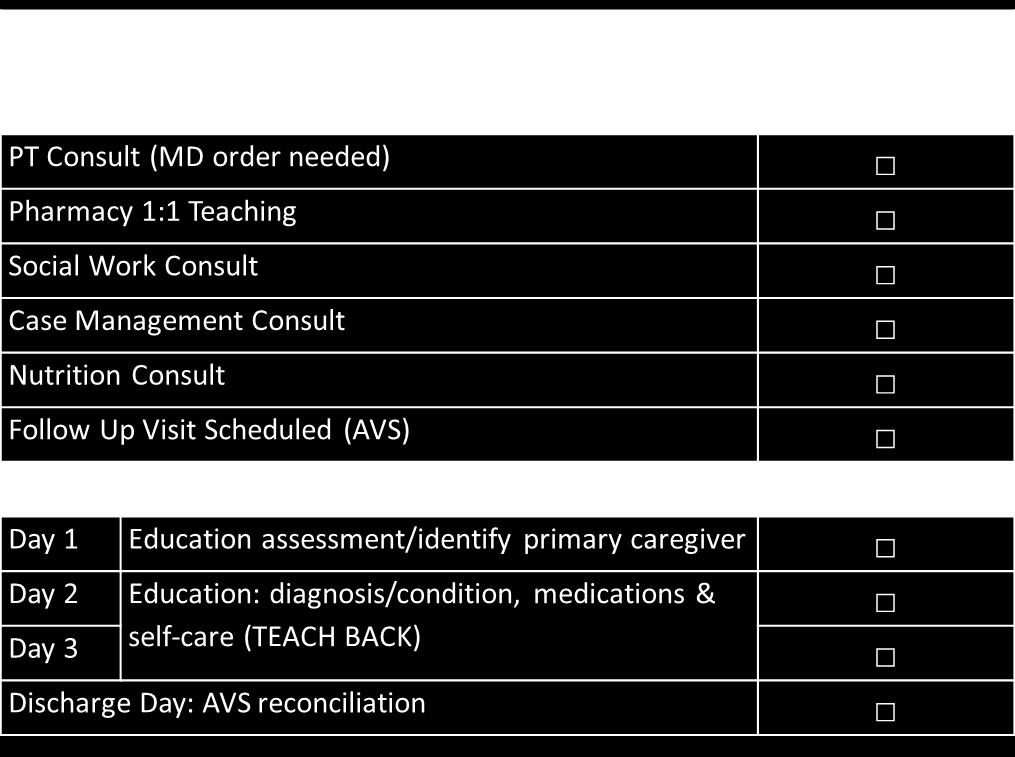
23 Visual Management

24 Physician Reminders LACE Score > 11 Document comorbidities in CareConnect Problem List Place an order for Physical Therapy and Home Health Place discharge medication orders to the UCLA outpatient pharmacy 24 hours prior to discharge This ensures 1:1 pharmacy teaching for patients. Post hospital follow up visit with a Cardiologist or PCP within 3 days Request appointment on Friday if the patient will be d/c on the weekend. STAT request: appointment will be scheduled prior to patient discharge or within 24 hours of patient discharge on business day.
25 Three Specific Goals 1. To ensure seamless transition of high-risk HF patients to community by optimizing utilization of Home Health, Communitybased Care Transitions Program (CCTP), and Interdisciplinary Rounds (IDR) by 80% by June 30, To ensure timely and high-quality follow-up with cardiologist and/or primary-care physician for all HF patients within 3-5 days, with an initial target of 80% of patients by June 30, Increase nutrition consult for all high risk HF/AMI LACE patients (score 11) by his/her discharge date to 80% by June 30, 2016.





26 Key Strategies: LACE Implementation Optimization of the LACE score Partners in Care Relationship Medicine Resident champion Daily IDR Education on home health services
27 Care Coordination: LACE Implementation Where have we been? No risk assessment tool used routinely No interventions associated with risk assessment score Delayed referrals to home health Unstructured IDR Where are we today? During IDR, case management informs team on the patient s LACE score The score is also communicated during the discharge planning meeting If a patient is in-house 4 days EPIC automatically triggers a consult to nutrition and pharmacy Where are we going? Roll out LACE plus system wide Review data for patients who have a high LACE score






28 Key Strategies: Follow-up Appointments Education to residents and attending physicians EHR Tip Sheet for physicians to make f/u appointment request STAT requests for high risk patients Loop- back appointments
29 Post-Discharge Follow-Up Appointments Where have we been? Inconsistent follow-up clinic appointments Follow-up orders written for the wrong time frames Limited patient transportation options Where are we today? House staff triggers follow-up system and navigators call patients to schedule appointments Navigators understand the urgency of followup appointments for HF patients and places order as STAT Navigators help to identify patient barriers for appointments Where are we going? Looking into using UberHealth for transportation barriers



30 Key Strategies: Nutrition Standardize education for HF Have LACE score available during rounds MD/RN refer high risk pt to nutritionist
31 Nutrition Where have we been? Delayed referrals to nutrition services High risk patients were defined different by nutritionist Lack of standardized nutrition education Where are we today? LACE Score available during rounds Standardized referral process Where are we going? Continue to look into auto referrals in EPIC for nutrition consult Continue to refine educational resources
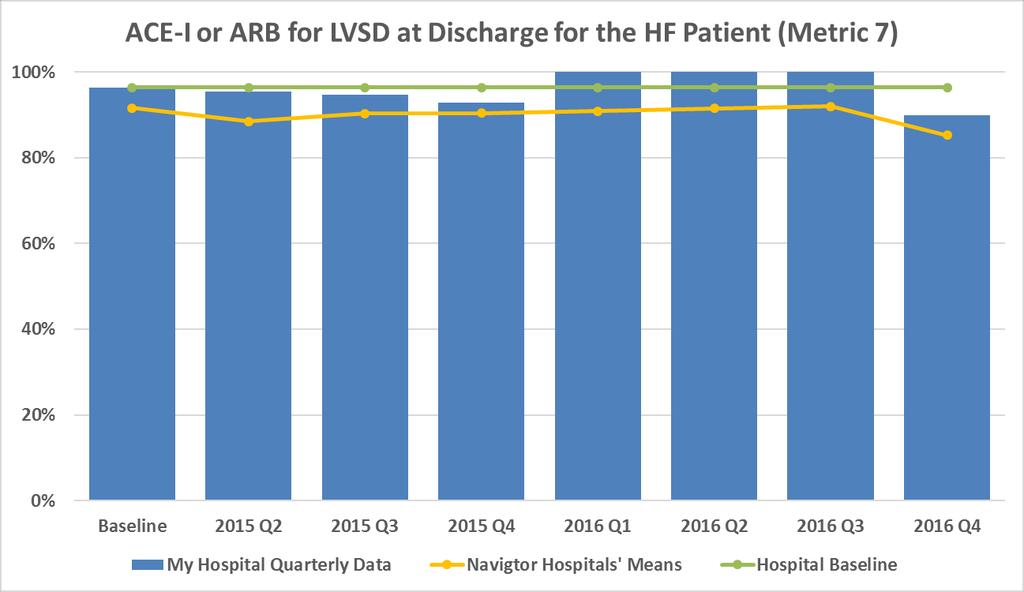
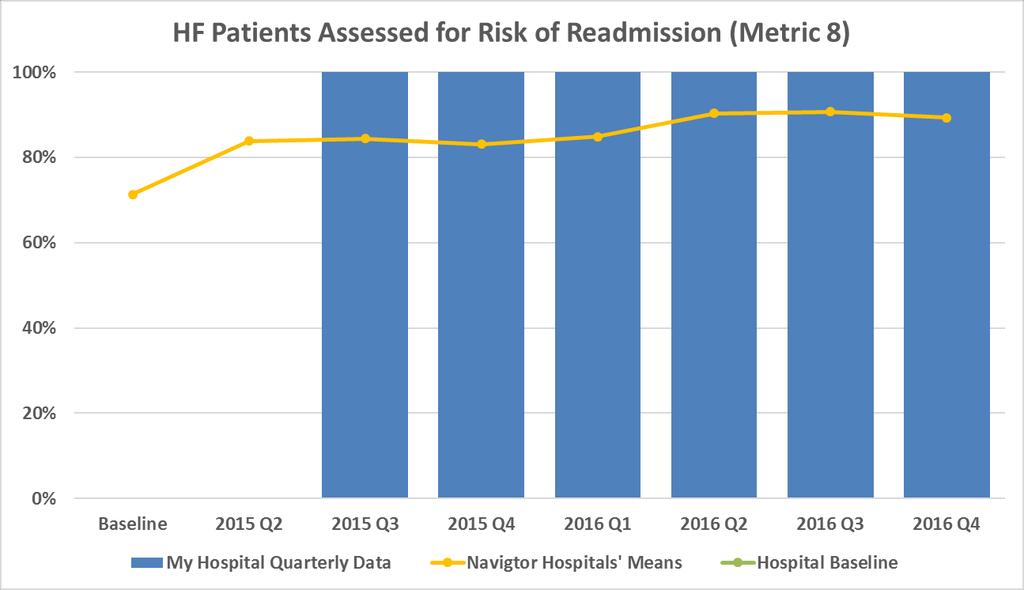
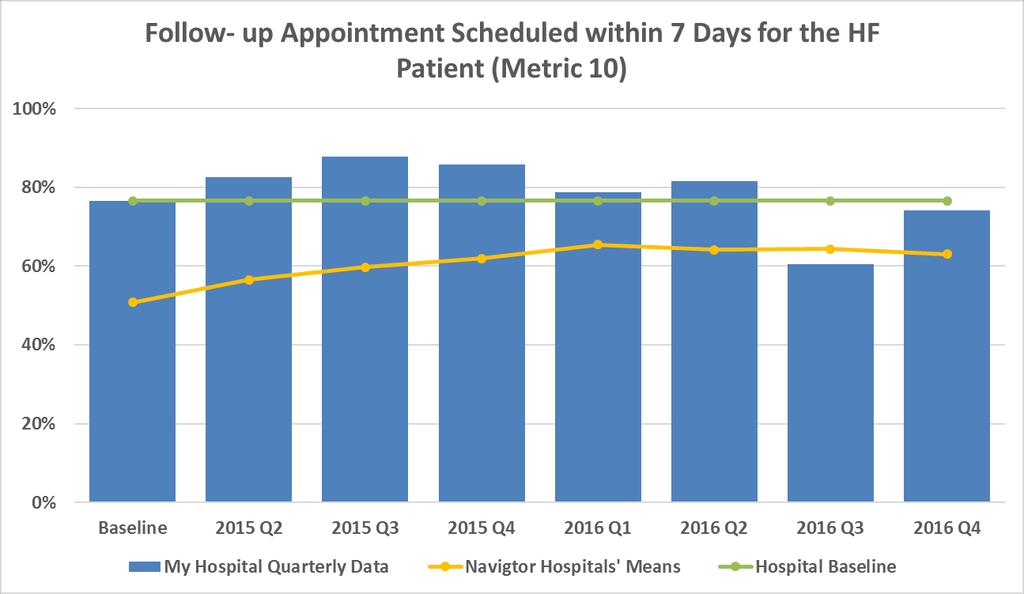
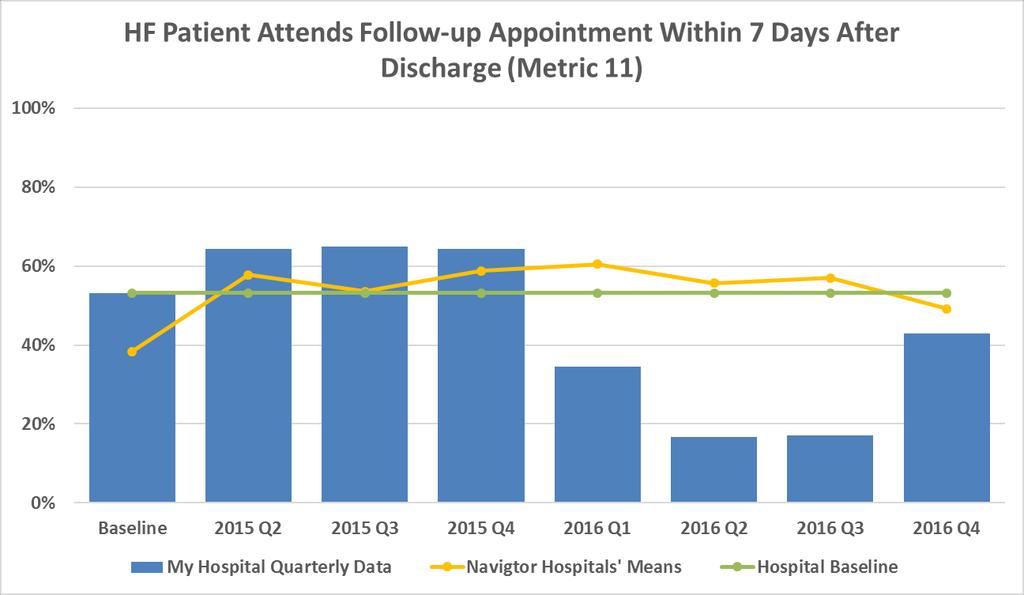
32 Results 32
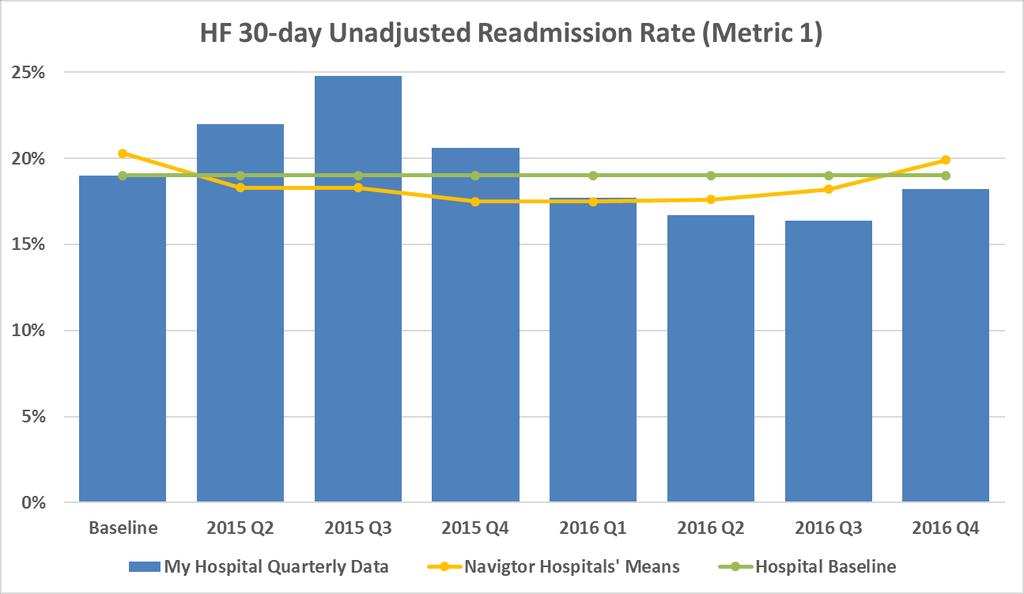
33
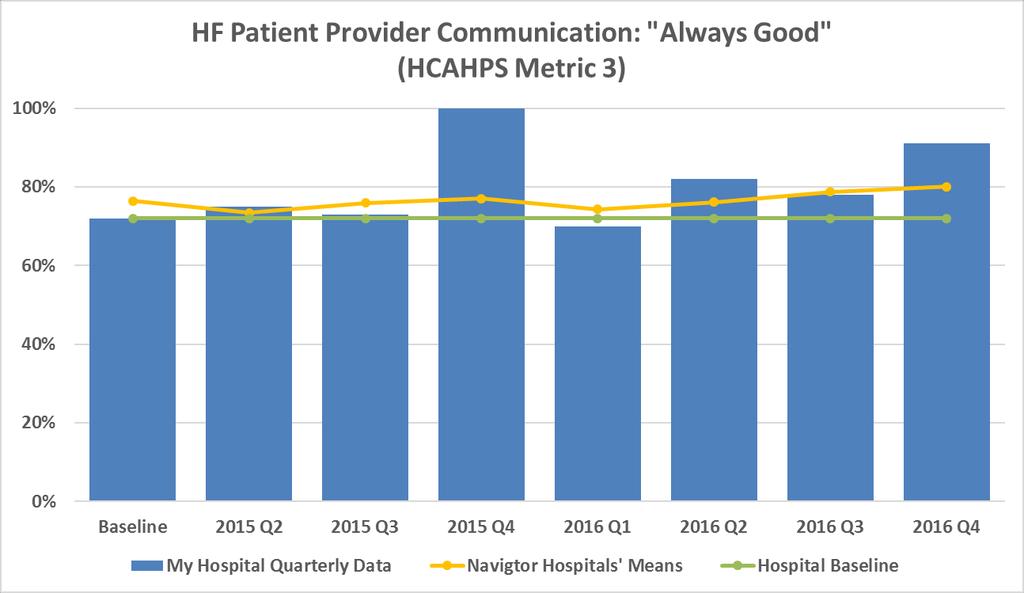
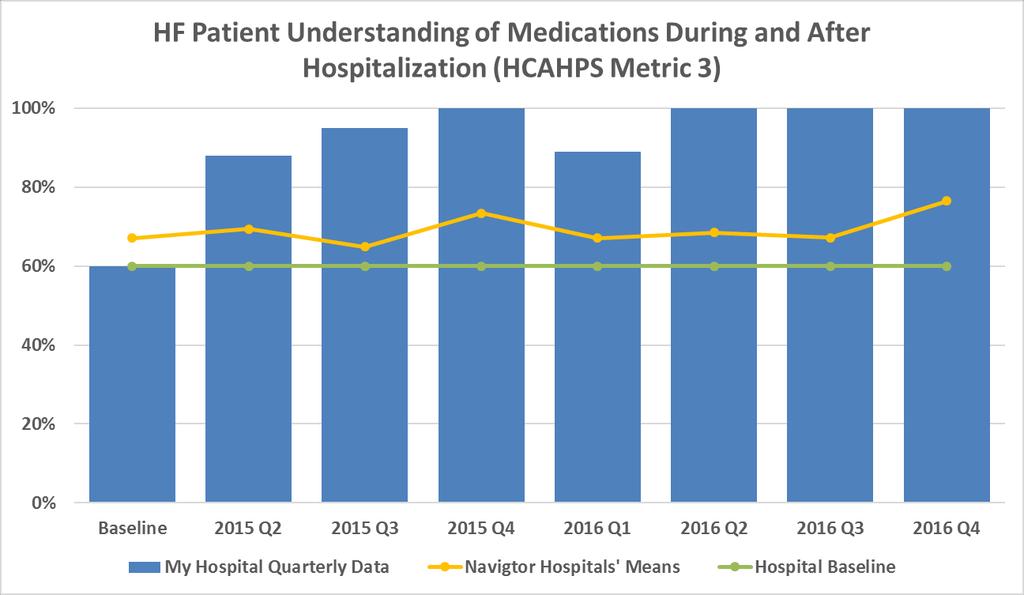
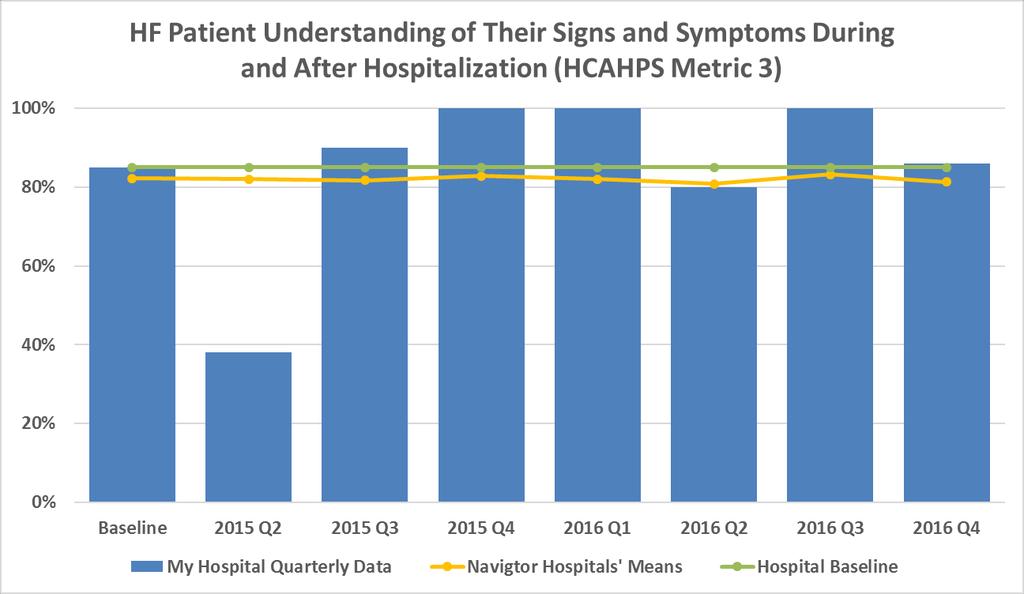
34
35
36
37
38
39
40
41 Summary: Strategies to Improve Readmissions Readmissions Risk Assessment Tool is now in the EHR Ability to identify patients at higher risk using LACE+ Develop plan of care based on the results of the risk assessment Stratify intervention by patient risk level Low risk: focus on prevention and wellness Moderate risk: Work on symptom management, good follow-up, literacy appropriate teaching strategies with strong teach back emphasis High risk: Identify any physiological determinants that would continue to send patient back and in those cases address quality of life, advance directives, and palliative care with the patient and family/caregiver


42 Thank You! Anna Dermenchyan Twitter: Adermenchyan
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned
 A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
A Regional Payer/Provider Partnership to Reduce Readmissions The Bronx Collaborative Care Transitions Program: Outcomes and Lessons Learned Stephen Rosenthal, MBA President and COO, Montefiore Care Management
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
CMS AMI and CABG Bundled Payment Initiative AMGA HF Collaborative December 13, 2016
 CMS AMI and CABG Bundled Payment Initiative AMGA HF Collaborative December 13, 2016 Agenda Collaborative Learnings HF Correlation to AMI and CABG Bundled Payments CMS AMI & CABG Bundled Payment Programs
CMS AMI and CABG Bundled Payment Initiative AMGA HF Collaborative December 13, 2016 Agenda Collaborative Learnings HF Correlation to AMI and CABG Bundled Payments CMS AMI & CABG Bundled Payment Programs
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
University Cincinnati Medical Center
 University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
University Cincinnati Medical Center Best Practice: The Journey to an Advanced Heart Failure Program Dr. Stephanie H. Dunlap, DO Medical Director of the Advanced Heart Failure program and the Advanced
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Passport Advantage Provider Manual Section 10.0 Care Management
 Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management Page 1 of 9 10.0
Passport Advantage Provider Manual Section 10.0 Care Management Table of Contents 10.1 Model of Care 10.2 Medication Therapy Management 10.3 Care Coordination 10.4 Complex Case Management Page 1 of 9 10.0
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Program Development. Completion of Gap Analysis. Review of Data. Multi-disciplinary team
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke
 These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
These presenters have nothing to disclose Developing Post- Hospital Follow-Up Care Plans and Real-time Handover Communications Peg Bradke September 28, 2015 Session Objectives Participants will be able
CMS Proposed Rule. The IMPACT Act. 3 Overhaul Discharge Planning Processes to Comply With New CoPs. Arlene Maxim VP of Program Development, QIRT
 Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Overhaul Discharge Planning Processes to Comply With New CoPs Arlene Maxim VP of Program Development, QIRT 1 CMS Proposed Rule Included discharge planning specifics However, when the CoPs were finalized,
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle.
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Systems serving as alpha sites committed to implementation
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Systems serving as alpha sites committed to implementation
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION
 PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
PACT AS A READMISSION REDUCTION STRATEGY KAISER PERMANENTE - COLORADO REGION Jodi Smith, MSN, CCMC, ANP-BC, ND Director of Hospital Operations, Specialty Services and Care Coordination Kaiser Permanente,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Admissions, Readmissions & Transitions Core Functions & Recommended Actions
 How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
How to use this resource An important single component of COMPASS for accomplishing the goals promised to CMS is the reduction of avoidable hospital admissions and readmissions as well as emergency room
The Community Care Navigator Program At Lawrence Memorial Hospital
 The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
The Community Care Navigator Program At Lawrence Memorial Hospital Presented By: Linda Gall, MSN, RN, ACM Director of Care Coordination October 21, 2011 Learning Objectives: 1. Describe the vision and
Yo Entiendo: I Understand
 Yo Entiendo: I Understand Anna Dermenchyan, BSN, RN, CCRN-K Senior Clinical Quality Specialist, UCLA Health PhD Student, UCLA School of Nursing 27th International Nursing Research Congress July 22, 2016
Yo Entiendo: I Understand Anna Dermenchyan, BSN, RN, CCRN-K Senior Clinical Quality Specialist, UCLA Health PhD Student, UCLA School of Nursing 27th International Nursing Research Congress July 22, 2016
REDUCING READMISSIONS through TRANSITIONS IN CARE
 REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
REDUCING READMISSIONS through TRANSITIONS IN CARE Christina R. Whitehouse, PhD, CRNP, CDE Postdoctoral Research Fellow NewCourtland Center for Transitions and Health University of Pennsylvania School of
Best Practices in Managing Patients with Heart Failure Collaborative
 Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Best Practices in Managing Patients with Heart Failure Collaborative Improving Care for HF Patients in a Primary Care Setting University of Utah Community Physicians Group September 1, 2016 Re-cap of Original
Expansion of Pharmacy Services within Patient Centered Medical Homes. Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice
 Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Expansion of Pharmacy Services within Patient Centered Medical Homes Jeremy Thomas, PharmD Associate Professor Department Pharmacy Practice What is a Patient Centered Medical Home (PCMH)? "an approach
Reducing Readmission Case Stories Discussion of Successes
 Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Reducing Readmission Case Stories Discussion of Successes University of California, San Francisco Maureen Carroll RN, CHFN Transitional Care Manager Heart Failure Program Coordinator UnityPoint Cedar Rapids
Analyzing Readmissions Patterns: Assessment of the LACE Tool Impact
 Health Informatics Meets ehealth G. Schreier et al. (Eds.) 2016 The authors and IOS Press. This article is published online with Open Access by IOS Press and distributed under the terms of the Creative
Health Informatics Meets ehealth G. Schreier et al. (Eds.) 2016 The authors and IOS Press. This article is published online with Open Access by IOS Press and distributed under the terms of the Creative
Care Integration and Network Models: How to Become a Player
 Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Care Integration and Network Models: How to Become a Player Hany Abdelaal, DO, BS, Chief Medical Officer, VNSNY Health Plans Samuel Heller, BA, MBA, Senior Vice President, CFO, VNSNY November 1, 2013 Table
Embedded Case Manager
 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies
Mission Health Care Network. April 2017
 Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
Mission Health Care Network April 2017 WHAT IS MISSION HEALTH CARE NETWORK? Mission Health Care Network is a Clinically Integrated Network including groups of doctors, the hospital and other health care
The impact of the heart failure health enhancement program: A retrospective pilot study
 ORIGINAL ARTICLE The impact of the heart failure health enhancement program: A retrospective pilot study Cynthia J. Hadenfeldt, Marilee Aufdenkamp, Caprice A. Lueth, Jane M. Parks Creighton University
ORIGINAL ARTICLE The impact of the heart failure health enhancement program: A retrospective pilot study Cynthia J. Hadenfeldt, Marilee Aufdenkamp, Caprice A. Lueth, Jane M. Parks Creighton University
Heart Failure Clinic a Multidisciplinary approach. Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM
 Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING
 HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
HOSPITAL READMISSION REDUCTION STRATEGIC PLANNING HOSPITAL READMISSIONS REDUCTION PROGRAM In October 2012, CMS began reducing Medicare payments for Inpatient Prospective Payment System (IPPS) hospitals
American College of Cardiology Patient Navigator Program Focus MI National PROGRAM REQUIREMENTS
 American College of Cardiology Patient Navigator Program Focus MI National 1. Participant Responsibilities PROGRAM REQUIREMENTS 1.1. Program Management 1.1.1. Upon opting-in to the Patient Navigator Program
American College of Cardiology Patient Navigator Program Focus MI National 1. Participant Responsibilities PROGRAM REQUIREMENTS 1.1. Program Management 1.1.1. Upon opting-in to the Patient Navigator Program
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
The Role of the Pharmacist in Value Based Health Care Systems. Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine
 The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
The Role of the Pharmacist in Value Based Health Care Systems Len Fromer, M.D., FAAFP Assistant Clinical Professor UCLA School of Medicine It is not the strongest of the species that survives, nor the
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
The Glasgow Admission Prediction Score. Allan Cameron Consultant Physician, Glasgow Royal Infirmary
 The Glasgow Admission Prediction Score Allan Cameron Consultant Physician, Glasgow Royal Infirmary Outline The need for an admission prediction score What is GAPS? GAPS versus human judgment and Amb Score
The Glasgow Admission Prediction Score Allan Cameron Consultant Physician, Glasgow Royal Infirmary Outline The need for an admission prediction score What is GAPS? GAPS versus human judgment and Amb Score
Minicourse Objectives
 Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Session M1 This presenter has nothing to disclose SINAI-GRACE HOSPITAL Vanguard Health Systems/Detroit Medical Center Peggy Segura RN, MSN, FNP-BC Nurse Practitioner, Quality & Safety/Clinical Effectiveness
Hospital Readmissions
 Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
Hospital Readmissions The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT TM Into Health Information Technology (HIT) In this survival guide, we ll give you the tips you need
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Health System Performance and Accountability Division MOHLTC. Transitional Care Program Framework
 Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Transitional Care Program Framework August, 2010 1 Table of Contents 1. Context... 3 2. Transitional Care Program Framework... 4 3. Transitional Care Program in the Hospital Setting... 5 4. Summary of
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Chronic Disease Management Resources & Services
 Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ. A Catholic healthcare ministry serving Ohio and Kentucky
 Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Readmission Project 2017 Janice M. Maupin, RN, MSN, CPHQ A Catholic healthcare ministry serving Ohio and Kentucky 1 Mission, Values and Promise Our Mission We extend the healing ministry of Jesus by improving
Improving Transitions of Care
 Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Improving Transitions of Care Mark V. Williams, MD, FACP, FHM Professor & Chief, Division of Hospital Medicine Northwestern University Feinberg School of Medicine Principal Investigator, Project BOOST
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management
 Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
Reducing Readmissions One-caseat-a-time Using Midas+ Community Case Management John Playford, Senior Midas+ Solutions Advisor Barb Craig, Midas+ SaaS Advisor The Problem Historically, up to 25% of patients
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
The Prevalence and Impact of Malnutrition in Hospitalized Adults: The Nutrition Care Process
 The Prevalence and Impact of Malnutrition in Hospitalized Adults: The Nutrition Care Process Donald R Duerksen Associate Professor of Medicine University of Manitoba Outline Why are hospitalized patients
The Prevalence and Impact of Malnutrition in Hospitalized Adults: The Nutrition Care Process Donald R Duerksen Associate Professor of Medicine University of Manitoba Outline Why are hospitalized patients
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
Get A Seat at the Table
 Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Get A Seat at the Table Develop Cross-Continuum Networks in the Competitive, Performance-Driven Senior Living Industry Hilary Forman, PT, RAC-CT Senior VP, Clinical Strategies Division, HealthPRO Heritage
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar. Thursday, December 13 at 8 am
 Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Southeast Michigan See You in 7 Hospital Collaborative: Session 8 Webinar Thursday, December 13 at 8 am Agenda Welcome and Introductions Hospital/Nursing Home Collaboration to Improve Early Follow-Up for
Stroke Patients: Transition From Hospital to Home
 Stroke Patients: Transition From Hospital to Home Lauren Pond RN CCM Administrative Director, Case Management Jennifer Thiesen RNP CCRN Director, Care Transitions Presenter Disclosure Information Lauren
Stroke Patients: Transition From Hospital to Home Lauren Pond RN CCM Administrative Director, Case Management Jennifer Thiesen RNP CCRN Director, Care Transitions Presenter Disclosure Information Lauren
A Care Transitions Project
 Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Hospital to Home: A Care Transitions Project Ann Roemen, MBA, CMPE Readmissions 1 in 5 elderly patients Resultsin23million 2.3 re-hospitalizations Annual cost to Medicare - $17 billion + Jencks SF,Williams
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Transitions of Care: From Hospital to Home
 Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
Transitions of Care: From Hospital to Home Danielle Hansen, DO, MS (Med Ed) Associate Director, LECOM VP Acute Care Services & Quality/Performance Improvement, Millcreek Community Hospital Objectives Discuss
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
General Eligibility Requirements
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 Overview General Eligibility Requirements Clinical Care Program Certification (CCPC)
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
Hospital Readmissions Survival Guide
 WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
WHITE PAPER Hospital Readmissions Survival Guide The Long-Term Care Provider s Ultimate Survival Guide to Incorporating INTERACT into Health Information Technology (HIT) March 2017 In this survival guide,
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS
 December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
December 2016 MODEL SCORE CARD ELEMENTS FOR LEADINGAGE POST-ACUTE AND LONG TERM SERVICES AND SUPPORTS BACKGROUND The purpose of this scorecard is threefold: 1. To help organize quality measures into internal
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System
 Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
Case-mix Analysis Across Patient Populations and Boundaries: A Refined Classification System Designed Specifically for International Quality and Performance Use A white paper by: Marc Berlinguet, MD, MPH
MALNUTRITION QUALITY IMPROVEMENT INITIATIVE (MQii) FREQUENTLY ASKED QUESTIONS (FAQs)
 FREQUENTLY ASKED QUESTIONS (FAQs)") MALNUTRITION QUALITY IMPROVEMENT INITIATIVE (MQii) FREQUENTLY ASKED QUESTIONS (FAQs) What is the MQii? The Malnutrition Quality Improvement Initiative (MQii) aims to advance evidence-based, high-quality
MALNUTRITION QUALITY IMPROVEMENT INITIATIVE (MQii) FREQUENTLY ASKED QUESTIONS (FAQs) What is the MQii? The Malnutrition Quality Improvement Initiative (MQii) aims to advance evidence-based, high-quality
HMSA Physical and Occupational Therapy Utilization Management Guide
 HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical and Occupational Therapy Utilization Management Guide Published November 1, 2010 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
A Virtual Ward to prevent readmissions after hospital discharge
 A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
A Virtual Ward to prevent readmissions after hospital discharge Irfan Dhalla MD MSc FRCPC Departments of Medicine and Health Policy, Management and Evaluation, University of Toronto Keenan Research Centre,
Post-Acute Care COMM UN I CATING T HE VA LU E L ES L IE MA RSH, CEO, L E X INGTON R EG I ONAL HEA LT H CE N T ER L E X I NGTON, N E BR ASKA
 Post-Acute Care COMMUNICATING THE VALUE LESLIE MARSH, CEO, LEXINGTON REGIONAL HEALTH CENTER LEXINGTON, NEBRASKA Swingbed CMS Definition Initially communicated to patients as a way to avoid a premature
Post-Acute Care COMMUNICATING THE VALUE LESLIE MARSH, CEO, LEXINGTON REGIONAL HEALTH CENTER LEXINGTON, NEBRASKA Swingbed CMS Definition Initially communicated to patients as a way to avoid a premature
Value Based Care An ACO Perspective
 Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Value Based Care An ACO Perspective NCIOM Task Force on Accountable Care Communities January 24, 2018 Steve Neorr Chief Administrative Officer 2 3 4 5 Source: Banthin, Jessica. Healthcare Spending Today
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure
 Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
Cost-Effective Management of a High- Risk Population Using Analytics: Care Processes That Make A Difference for Patients With Heart Failure November 16, 2016 Panelists Corinne Bott-Silverman, M.D., Cardiologist,
Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care
 Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care Robert D. Rondinelli, MD, PhD Medical Director Rehabilitation Services Unity Point Health, Des Moines Paulette
Tracking Functional Outcomes throughout the Continuum of Acute and Postacute Rehabilitative Care Robert D. Rondinelli, MD, PhD Medical Director Rehabilitation Services Unity Point Health, Des Moines Paulette
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
CHF Education March Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN
 CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
CHF Education March 2015 Courtney Reaves, BSN, RN-BC Amy Taylor, BSN, RN Corey Paris, BSN, RN, CCRN Objectives To improve patient outcomes Decrease CHF readmissions Improve patient and family compliance
The STAAR Initiative
 The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
The STAAR Initiative Getting Started Kit for the STAAR Collaborative September 2010 Institute for Healthcare Improvement, 2010 Page 1 Table of Contents STAAR Collaborative Charter... 3 Statement of Need...
Patient Activation Using Technology- Supported Navigators
 Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
Patient Activation Using Technology- Supported Navigators March 2, 2016 1PM Sands Expo: Lando 4205 Merrily Evdokimoff, RN, PhD Kinergy Health LLC Conflict of Interest Merrily Evdokimoff, RN. PhD Consulting
The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions
 1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
1 The Effect of an Interprofessional Heart Failure Education Program on Hospital Readmissions Julia N. Clarkson, Susan D. Schaffer, Joshua J. Clarkson Heart failure (HF) is a pressing concern to public
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
Optimizing Care for Complex Patients with COPD
 Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System
Optimizing Care for Complex Patients with COPD Janice Gasaway, RN, MN, Director Quality & Safety Elvin Perkins, MBA, Chronic Disease Project Manager 1 Cone Health System: Who We Are Regional Health System