Embedded Case Manager
|
|
|
- Christian Daniel
- 5 years ago
- Views:
Transcription

1 Embedded Case Manager Joann Sciandra, RN, BSN, CCM Medical Home Summit ProvenHealth Navigator
2 Geisinger Health System An Integrated Health Service Organization Provider Facilities Managed Care Companies Geisinger Medical Center Danville Campus includes Hospital for Advanced Medicine, Janet Weis Children s Hospital, Women s Health Pavilion, Level I Trauma Center, Ambulatory Surgery Center Geisinger Shamokin Community Hospital Geisinger-Bloomsburg Hospital Geisinger Wyoming Valley Medical Center with Heart Hospital, Henry Cancer Center, and Level II Trauma Center Geisinger South Wilkes-Barre campus with Urgent Care, Ambulatory Surgery Center and Inpatient Rehabilitation Geisinger Community Medical Center with specialized medical & surgical services, including Level II Trauma and comprehensive cardiac & orthopedic services Marworth Alcohol & Chemical Trtmt Center Mountain View Care Center Bloomsburg Health Care Center >72K admissions/obs & SORUs Heal 1,593 Teach licensed Discover inpatient Serve beds Physician Practice Group Multispecialty group ~1,000 physicians ~520 advanced practitioner FTEs 65 primary & specialty clinic sites (37 Community Practice Sites) Freestanding outpatient surgery center > 2.1 million clinic outpatient visits ~360 resident & fellow FTEs ~298,000 members (including ~63,000 Medicare Advantage members) Diversified products ~30,000 contracted providers/facilities 43 PA counties PA Medicaid initiative Out of state TPA contracts Note: Numerical references based on fiscal 2012 budget plus impact of GSACH, GCMC and GBH acquisitions. 2



3 Partnership of PCP s & GHP provides 24/7 360 degree patient care and navigation 3
4 Geisinger s PHN model has Patient-centered primary care Integrated population management Medical Neighborhood five core components Patient and family engagement & education Enhanced access and scope of services PCP led team-delivered care Chronic disease and preventive care optimized with HIT Population segmentation and risk stratification Preventive care GHP employed in-office case management Disease management Micro-delivery referral systems 360 care systems SNF, ED, hospitals, HH, etc Quality outcomes Value-based reimbursement Patient satisfaction HEDIS and bundled chronic disease metrics Preventive services metrics Fee-for-service with P4P payments for quality outcomes Physician and practice transformation stipends Value-based incentive payments Payments distributed on Quality Performance 4
5 Sites PHN Expansion MA members Commercial members Medicare members Total** , ,000 31, ,300 8,500 11, , ,600 7,000 7,800 94, ,300 7,100 5,300 55, ,100 4,600 3,000 61,000 Total 46* 20,500 28,000 29, ,000 * 37 Geisinger CPSL practices & 9 non-geisinger primary care practices **Total Geisinger patients, non-geisinger patients not quantified 5
6 Case Management Identifying and Managing the Highest Risk in Your Population 6


7 Why Case Management? Fragmented care Poor care coordination Gaps in care Poor communication Health care is complex Aging population Multiple transitions of care 7
8 Medicare 30 Day Readmission Rates 30% readmitted from SNF to hospital 20% readmitted from home to hospital N Engl J Med 2009; 360:
9 Causes of Readmissions Heart Failure 37% readmitted in 30 days COPD Sepsis Pneumonia Psychoses N Engl J Med 2009; 360:
10 The Acute Care Environment Unnecessary or short stay medical admissions Pneumonia HF COPD DM UTI A-fib Dehydration Ambulatory Care Sensitive Conditions (ACSC) 10
11 Geisinger s Approach to CM High risk identification Targeted populations - HF, COPD, oncology, multiple trauma, ESRD, frail elderly - TOC Comprehensive assessment - Driving issue behind case - Frequent follow-up with patient/family Daily interaction with Provider and team 11
12 Embedded Case Managers are Key to Success Embedded Case Manager 1 CM / 800 Medicare or 5000 commercial lives High risk patient case load 15-20% for Medicare 3 to 5% of commercial Total case load pts NOT traditional disease management focus on those at most risk and what is driving issue with the care Challenge of caseload management is gauging acuity and complexity 12

13 Targeting CM at High Risk Populations High risk Post Hospital Discharge Predictive Modeling PCP referral Site team: Nurse, Ancillary staff, etc. Self referral Targeted medical management referrals Targeted conditions HF COPD 13
14 Site# Forecasted Risk Index AIS CIS Risk Rank Sex Age Total Paid Forecasted Cost Primary ETG Group Program Status C M 82 $42, $44, C M 68 $46, $43, Cerebrovascular Accident Cardiovascular Surgery MHOpen MH CL - Need met C M 67 $137, $67, Infectious Disease MHIdentified C F 75 $70, $34, C M 81 $49, $49, Degenerative Ortho disease Cerebrovascular Accident MHCL- Needs meet C F 71 $133, $110, Renal Failure, Chronic & Nephrosis MHOpen C M 81 $25, $60, Renal Failure, Chronic & Nephrosis MHIdentified C F 79 $113, $96, Renal Failure, Chronic & Nephrosis MHCL- CC 14
15 When to Refer to a Case Manager Complex chronic conditions Caregiver stress Coordination of services Psychosocial issues Home safety concerns Advancing Illness Outpatient management of an acute medical condition 15
16 Key Case Management Activities Personal patient link Transitions follow up (discharges, ER visits) Direct line access questions, exacerbation protocols Family support contact Recognized site team member Regular follow ups for high risk patients Facilitate access PCP, specialist, ancillary Facilitate special arrangements (emergency home care, hospice care) 16
17 Functions of Case Manager Transitions of care Chronic Care Exacerbation management Self management Telephonic and/or device monitoring Frequent follow up 17

18 Transitions of Care Pt contact within hrs post discharge Telephonic outreach Medication reconciliation and optimization Ensure safe transition post discharge with appropriate services in place Home Health DME Safe to be in their home? Facilitate post hospital PCP & CM appt within 3-5 days Close follow-up for 30 days 18
19 Chronic Care Management Heart Failure Diuretic Titration Protocol Daily weights & Tele-monitoring Medication management Education Self management Outreach COPD Rescue kit Symptom monitoring Medication management Education Self management Outreach 19
* Angina Asthma")

20 Target Ambulatory Care Sensitive Conditions (ACSC)* Angina Asthma Cellulitis COPD HF Dehydration Diabetes Gastroenteritis Seizures HTN Hypoglycemia * AHRQ 20
 - Outbound calls post discharge - HF IVR Blue tooth blood pressure")
21 Tele-Monitoring Tools Blue tooth scales - Managing HF - Transmits daily weights to EHR Nurse sees weight real time - Diuretic titration protocols - Trending Interactive Voice Response (IVR) - Outbound calls post discharge - HF IVR Blue tooth blood pressure cuff 21
22 22

23 DTP Smart Set Tool Diuretic Titration Protocol 3/6/

24 COPD Smart Set Tool COPD Rescue Kit 3/6/

25 Vertical Build of Case Management Care Transitions 360 degree SNF LTC Deep dive into causes of readmissions Advanced illness management On-Call 24 / 7 Nurses linked to providers, hospitalists, inpatient case managers, patients, and community resources 25
26 Case Management Finding the Right Person for the Role 26
27 Choosing the Right Case Manager Must be a good fit for clinic Providers need to be involved in selection Prior case management experience not a must Hospital Home health nursing SNF/ LTC experience Clinic nurse Often don t t find a case manager rather you help create a case manager 27


28 Traits of a Good Case Manager Autonomous & self motivated Highly organized Good time management skills Understands and manages main driving force as well as all other complex issues Easily manages multiple tasks at one time Can shift focus easily, be pulled into different directions and still remain on task Willing to nudge the providers 28

29 Essential Skills and Competencies Strong communication skills People skills Problem solving skills Critical thinking skills Patient engagement and activation skills Negotiating and conflict resolution skills Must be able to think out of the box 29

30 Skill Set of a Case Manager Interpret clinical information and assess implication of treatment Develop and implement Plan of Care Determine appropriate level of care PCP office Hospital Assisted Living /SNF/ LTC Palliative Care, Hospice 30
31 Investment in Case Management Dedicated staff needed to drive outcomes Manager Trainer Resources to support development Dedicated clinic space Dedicated phone line Administrative support 31
32 Training for Success Considerations for the Orientation Process 32
33 Orientation Process Time frame weeks Learn basic CM/DM role; begin to understand CM/DM functions Build beginning relationships with clinic and staff Community resources, facilities - Hospitals, HH agencies, DME providers, Skilled nursing facilities, pharmacies Understand health plan activities & benefits Understand IT tools necessary to perform job role - EHR, CM platform, disease registries, etc. 33
34 Ensuring Success Right Preceptor Has accountability to provide foundation to CM functions and provide guided oversight to the new Case Manager Works under direction of the Director Structured learning environment Ensure that the is exposed to the necessary elements required to perform in the CM role Completion of the orientation checklist Reports gaps and areas of need to Director at weekly progress check points 34

35 Making Orientation Count Primary preceptor for training 2 weeks didactic training in group session with other new CM 4 weeks in clinic with preceptor - Observation - Record review - Case finding - Case review & planning - Case management 35
36 36

37 Integration into the Practice Site Key clinic activities/operations Time with front office Nursing Ancillary services Key HP departments Customer service Utilization management Provider network 37

38 As the nurse gains experience Alternate exposure with another CM Forging partnerships in the Medical Neighborhood Home health, nursing homes, hospitals Pharmacies, community agencies Disease management skills Further emphasis on EMR and other communication tools 38
39 Ready to Transition into CM Role Transition targeted referrals at week 6 of orientation while still with preceptor Assist with transition into practice meetings Practice staff meetings (nurses and front desk) Provider Site Medical Home meetings Keep buddy system with preceptor for 3 6 months 39
40 Maximizing Success of Your Staff Monthly 1:1 time with each staff - Reviewing cases/documentation - Evaluating CM s understanding of the driving force of cases - Provider/staff interaction - Troubleshooting Productivity and caseload management - Nurse visit summary sheets - Areas of opportunity Readmissions trending up - Why? - Gaps in role - Patient engagement and ongoing follow-up 40

41 Ongoing Staff Development Four CE days per year All staff come on site for training CE and CCM credits Outside speakers Topics relevant to disease and case management Learning packets Current articles pertinent to chronic condition Medications Outside CE programs 41

42 Local Team Building Regional meetings monthly Less time away from office for staff Provide updates, mini educational sessions Pharmacy integration Round table to discuss cases in more informal setting Develop staff relationships 3 nurse educators 42
43 Management Tools 43
44 Nurse Visit Summary

45 Caseload Summary
46 PHN Outcomes 46


47 Medicare Risk Adjusted Acute Admissions/

48 Medicare Risk Adjusted Readmissions/


49 Medicare Risk Adjusted ER Visits/


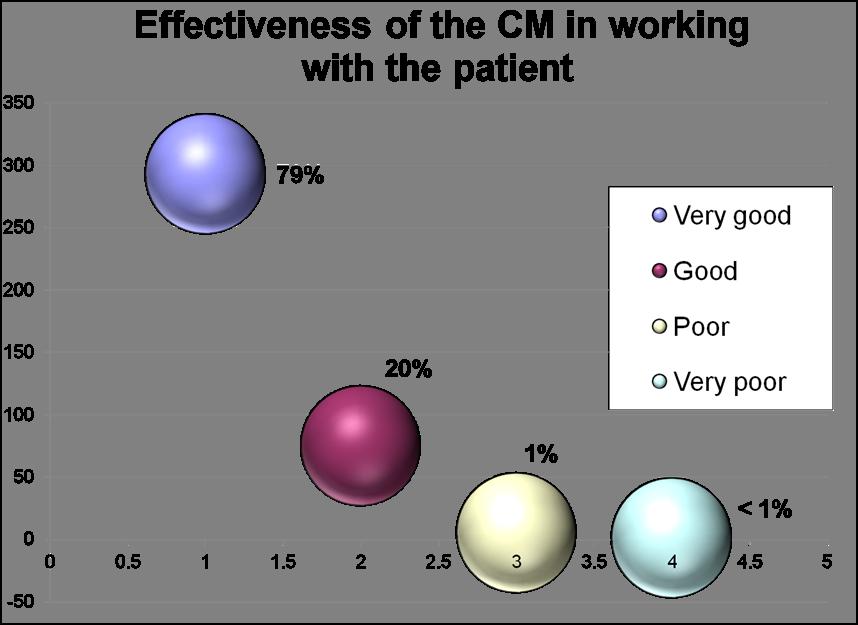
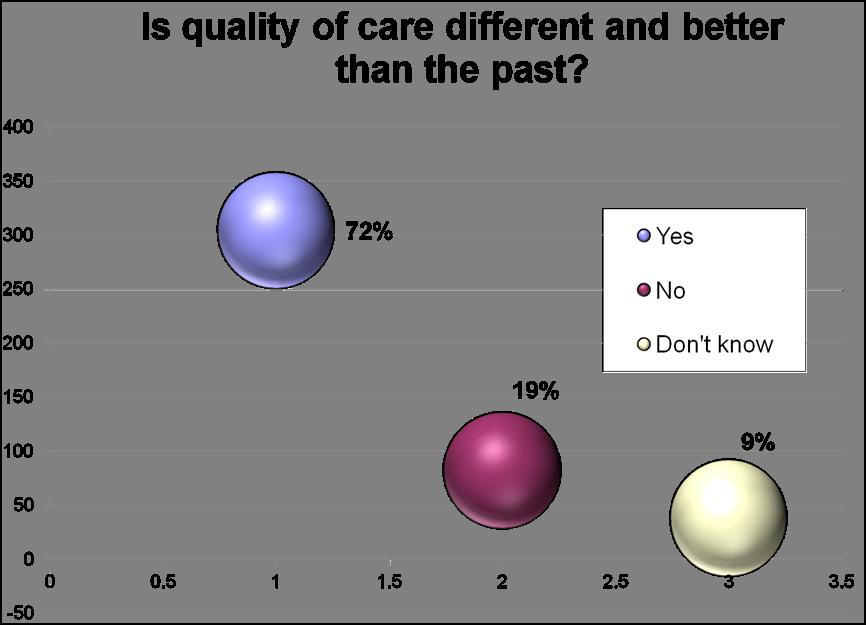
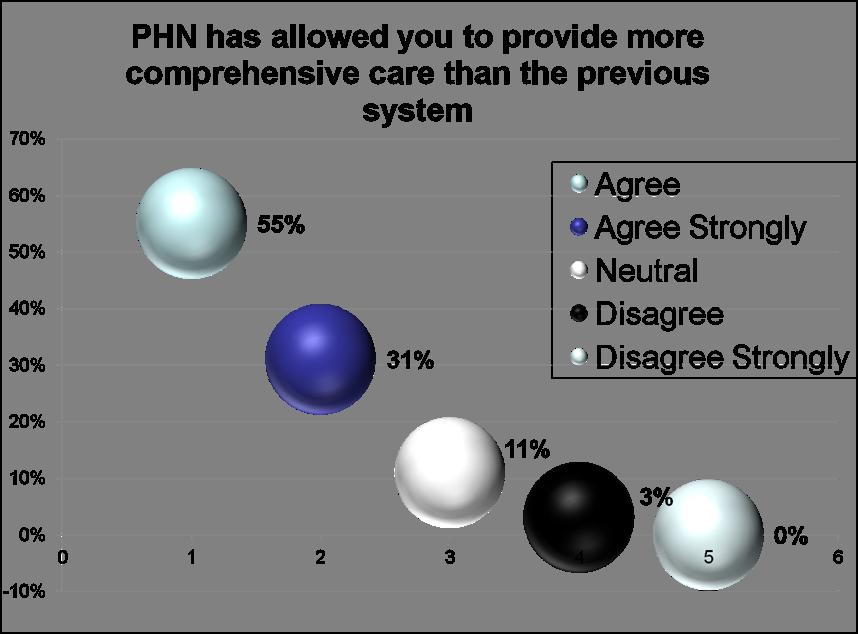
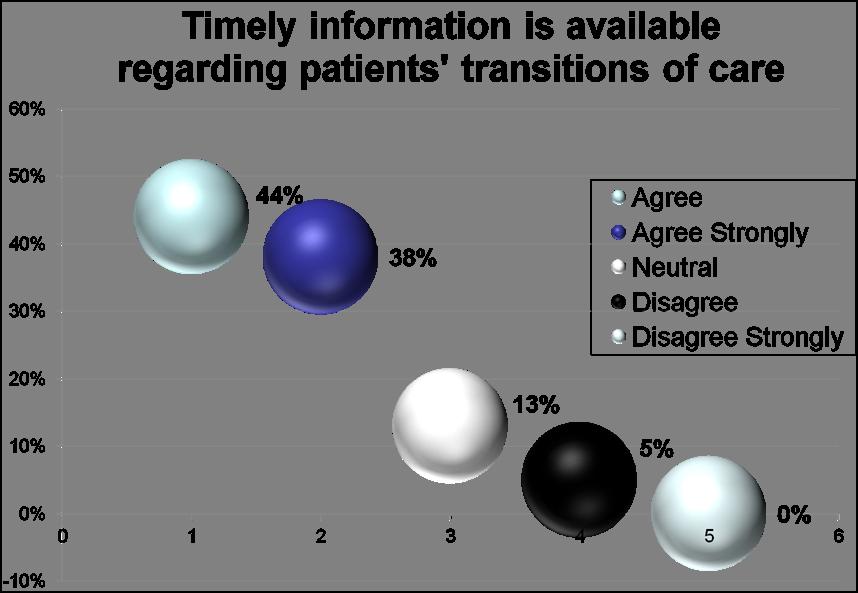
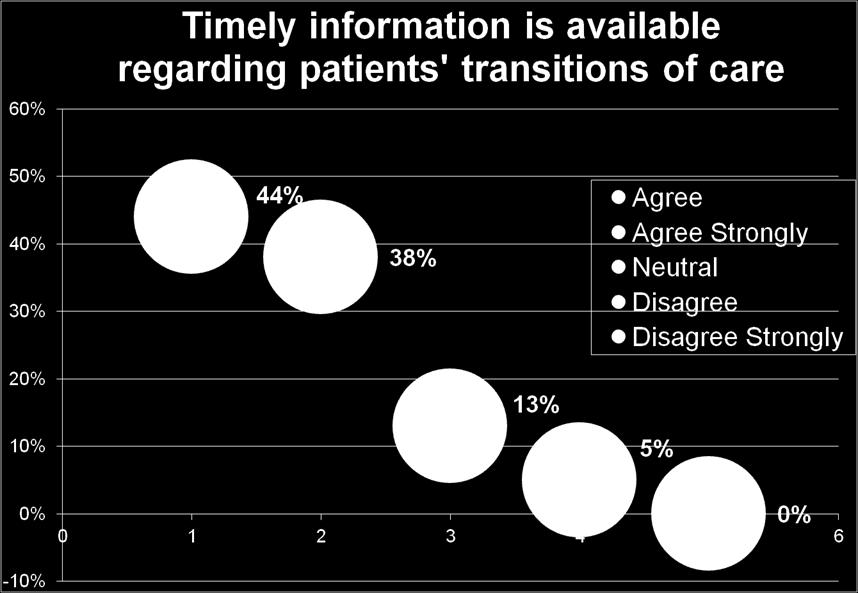
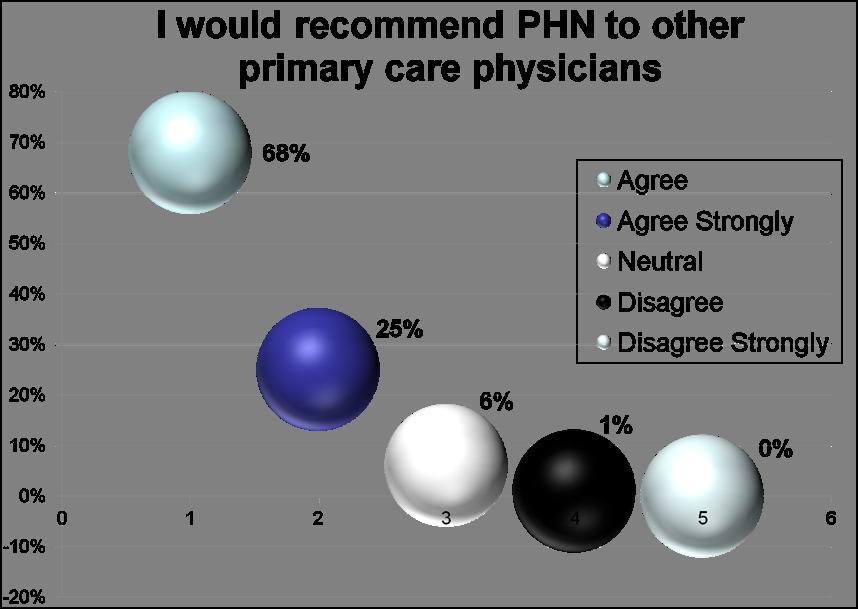
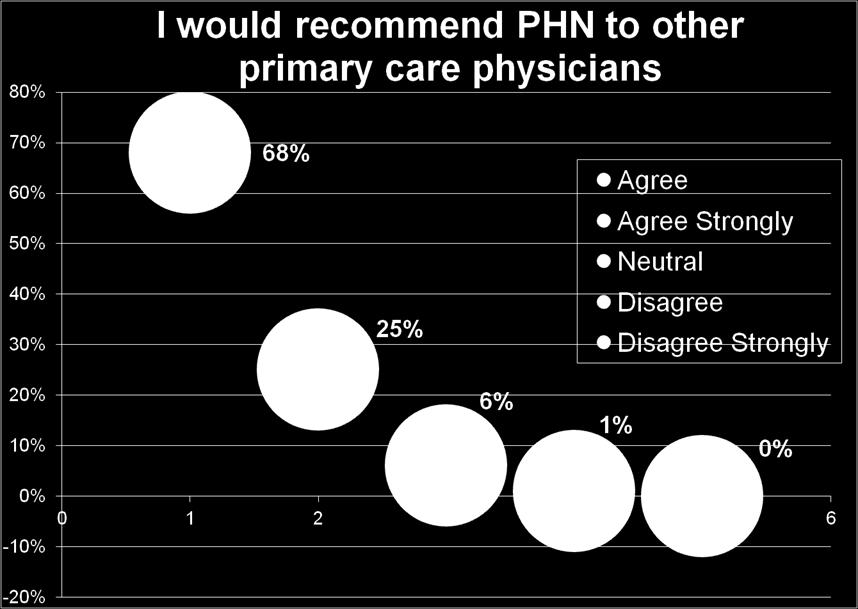
50 Provider and Patient Satisfaction Survey Results 50
51 51

52 52

53 53
54 54
55 55


56 Questions 56
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study
 Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Geisinger s Use of Technology in Case Management and the Medical Home: A Heart Failure Study JOANN SCIANDRA, RN, BSN, CCM DOREEN SALEK, BS, RN, CCS/CPC DANIEL MAENG, PHD February 18, 2015 Geisinger at
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost
 Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost Thomas Graf, MD Chief Medical Officer Population Health and Longitudinal Care Service Lines Let us
Geisinger s Bundled Payments Experience for Better Clinical Integration to Drive Quality to Lower Cost Thomas Graf, MD Chief Medical Officer Population Health and Longitudinal Care Service Lines Let us
Geisinger Model 75% RVU, 17% Quality, 8% Population Based
 Geisinger Model 75% RVU, 17% Quality, 8% Population Based Thomas R Graf, MD Agenda What is Geisinger? What is the ProvenHealth Navigator program? How are we compensating physicians for PHN? What is the
Geisinger Model 75% RVU, 17% Quality, 8% Population Based Thomas R Graf, MD Agenda What is Geisinger? What is the ProvenHealth Navigator program? How are we compensating physicians for PHN? What is the
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention
 Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Designing Reliable Value-based Systems of Care for Chronic Disease and Prevention Frederick J. Bloom, Jr. MD MMM President, Guthrie Medical Group 1/23/15 Where We Want to Be 1. Affordable coverage for
Reducing Costs and Improving Outcomes: Strategies That Work and How to Get There
 Institute of Medicine July 16, 2009 Reducing Costs and Improving Outcomes: Strategies That Work and How to Get There Glenn Steele Jr., MD, PhD President and CEO Geisinger Health System Geisinger Health
Institute of Medicine July 16, 2009 Reducing Costs and Improving Outcomes: Strategies That Work and How to Get There Glenn Steele Jr., MD, PhD President and CEO Geisinger Health System Geisinger Health
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Dual-eligible SNPs should complete and submit Attachment A and, if serving beneficiaries with end-stage renal disease (ESRD), Attachment D.
, Attachment D.") Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Attachment A: Model of Care for Dual-eligible SNPs MA Contract Name: Geisinger Health Plan MA Contract Number: H3954-097 Type of Dual-eligible SNP: Full The model of care describes the MAO's approach to
Transitions of Care. ACOI Clinical Challenges in Inpatient Care. March 31, 2016 John B. Bulger, DO, MBA
 Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Transitions of Care ACOI Clinical Challenges in Inpatient Care March 31, 2016 John B. Bulger, DO, MBA Disclosure I have not accepted any honoraria, additional payments of reimbursements related to the
Care Management in the Patient Centered Medical Home. Self Study Module
 Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
Care Management in the Patient Centered Medical Home Self Study Module Objectives Describe the goals of care management Identify elements of successful care management Recognize the 5 step Care Management
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Transitioning Care to Reduce Admissions and Readmissions. Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH
 Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Transitioning Care to Reduce Admissions and Readmissions Sven T. Berg, MD, MPH Julie Mobayed RN, BSN, MPH Disclaimer: Potential for Error Type One Error Rejecting the null hypothesis when it is true
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Topics for Today s Discussion
 MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
MICAH Quality Network Population Insights Reporting and 2017 2018 PG5 P4P Program Year Updates Blue Cross Blue Shield of Michigan Hospital Incentive Programs August 18 th, 2017 Topics for Today s Discussion
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
Succeeding in a New Era of Health Care Delivery
 March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
March 14, 2012 Succeeding in a New Era of Health Care Delivery Building Value-Based Partnerships LeadingAge Pennsylvania Kathleen Griffin, PhD, National Director Post-Acute and Senior Services 1 Your Presenter
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process
 Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Discharge checklist and follow-up phone calls: the foundation to an effective discharge process Shari Aman, BSN, RN, MBA, CPHQ Denise Andrews, MBA Stephanie Storie, BSN, RN, CMSRN Deb Nation, RN, CMSRN
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting
 Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
Managing Congestive Heart Failure as a Business September 13, 2010 Session M30 Society for Healthcare Strategy and Market Development annual meeting Chris Kane SVP, Strategic Business Development WellStar
The Michigan Primary Care Transformation (MiPCT) Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting
 Project: An Overview. Medicaid Health Plan- MiPCT Coordination Meeting") The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
The Michigan Primary Care Transformation (MiPCT) Project: An Overview Medicaid Health Plan- MiPCT Coordination Meeting April 14, 2016 2 Welcome and Goals for the Day 3 Welcome! Our Goals for the Day Create
Transitions of Care: Primary Care Perspective. Patrick Noonan, DO
 Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Transitions of Care: Primary Care Perspective Patrick Noonan, DO Disclosures None Bio Outpatient primary care internist at New Pueblo Medicine Completed residency at the University of Iowa Graduated from
Sandra Robinson, RN, MSN, ACM, CEN
 Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
Developing and Measuring Care Coordination Outcome Goals and Objectives ACMA National Conference April 28, 2015 Cleveland Clinic Care Management Sandra Robinson, RN, MSN, ACM, CEN (robinss12@ccf.org) Joan
L8: Care Management for Complex Patients: Strategies, Tools and Outcomes
 The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
The Triple Aim 16 th Annual Summit: Institutes for Healthcare Improvement - Improving Patient Care in the Office Practice and the Community March 16, 2015 Dallas, Texas L8: Care Management for Complex
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Learning Objectives
 for Heart Failure Learning Objectives") Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Coordinated Outreach Achieving Community Health (COACH) for Heart Failure Session C917 October 9, 2015 Colleen Cameron, DNP, FNP-BC Rochelle Eggleton, MBA, BS, RN Susan Spink, BSN, RN-BC Linda Griffin,
Bundled Payments to Align Providers and Increase Value to Patients
 Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
Bundled Payments to Align Providers and Increase Value to Patients Stephanie Calcasola, MSN, RN-BC Director of Quality and Medical Management Baystate Health Baystate Medical Center Baystate Health Is
2016 Medical Home Summit. Reducing Hospital. Innovative Model of Care
 2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
2016 Medical Home Summit Reducing Hospital Readmissions An Innovative Model of Care June 2016 Scott Clemens, MD Who We Are Since our inception in 1994, New West Physicians has grown to become the largest
Beyond the Hospital Walls: Impact of a SNFist Practice Model
 Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Beyond the Hospital Walls: Impact of a SNFist Practice Model Aaron Snyder, MD Vice President, US Acute Care Solutions Kim Repac Chief Financial Officer, WMHS Aging Population 50 Million Distribution
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Managing Risk Through Population Health Initiatives
 Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
Managing Risk Through Health Initiatives Vicki DeBaca, DNS, RN Vice President, Health & Provider Services Sharp Rees-Stealy Medical Centers 1 Sharp Rees-Stealy Medical Centers San Diego s Multi-Specialty
EXECUTIVE SUMMARY: briefopinion: Hospital Readmissions Survey. Purpose & Methods. Results
 briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
briefopinion: Hospital Readmissions Survey EXECUTIVE SUMMARY: Purpose & Methods The purpose of this survey was to collect information about hospital readmission rates and practices. The survey was available
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN
 Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Reducing Preventable Hospital Readmissions in Post Acute Care Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history of hospital readmission
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination
 Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Innovating Predictive Analytics Strengthening Data and Transfer Information at Point of Care to Improve Care Coordination November 15, 2017 RRHA Healthcare Innovations Conference Agenda Arnot Health Overview
Healthcare Leadership Council: John Perticone Golden Living 3/9/2016
 Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Healthcare Leadership Council: Care Transitions in Post Acute Care John Perticone Golden Living 3/9/2016 Golden Living Profile Golden Living Centers and Communities 296 skilled nursing facilities 15 assisted
Consumer ehealth Affinity Group
 Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Consumer ehealth Affinity Group Embracing Barriers in the Delivery of IVR Technology for Older, Chronically ll Patients Jeremy Rich HealthCare Partners Institute and HealthCare Partners Medical Group Janelle
Presenter Disclosure Information
 The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
The following program is co-provided by the American Heart Association and Health Care Excel, the Medicare Quality Improvement Organization for Kentucky. 3/1/2013 2010, American Heart Association 1 1 2
2017 Quality Improvement Work Plan Summary
 Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Project Member Service and Satisfaction Commercial Products: Commercial Project Description: To improve member service and satisfaction and increase member understanding of how the member s plan works.
Model of Care Training
 Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Medicare Advantage Special Needs Plan Chronic Care Program Model of Care Training 2012-2013 Course Overview This course will describe: PHP s Model of Care Chronic Care Program Health Homes Interdisciplinary
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum
 Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Advanced Illness Management Leveraging Person Centered Care and Reengineering the Care Team Across the Continuum Betsy Gornet, FACHE Chief Advanced Illness Management Executive Sutter Health / Sutter Care
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Red Carpet Care: Intensive Case Management Program for Super-Utilizers
 Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Red Carpet Care: Intensive Case Management Program for Super-Utilizers Alice Stollenwerk Petrulis, MD Linda C. Stokes, PhD The MetroHealth System Picture of MH MetroHealth 750 bed facility includes Rehab,
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Model of Care Heritage Provider Network & Arizona Priority Care Model of Care 2018
 Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Model of Care Model of Care 2018 Learning Objectives Program participants will be able to: List two differences between the Complex Care Management (CCM), and Special Needs Program (SNP) programs. Identify
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Chronic Disease Management Resources & Services
 Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
Chronic Disease Management Resources & Services Michelle Nelson, RN, BSN Director of Ambulatory Services & Chronic Disease Management Gidgett Bates, RN, BSN Manager of Palliative Care, Diabetes Education,
Impact of Patient Navigation in an Integrated Care Delivery System
 Impact of Patient Navigation in an Integrated Care Delivery System Chrissy Valania, MSW, LCSW Social Worker/Patient Navigator Geisinger Cancer Institute 1 Geisinger at a Glance 9 Hospitals in Pennsylvania
Impact of Patient Navigation in an Integrated Care Delivery System Chrissy Valania, MSW, LCSW Social Worker/Patient Navigator Geisinger Cancer Institute 1 Geisinger at a Glance 9 Hospitals in Pennsylvania
Advocate Cerner Partnership Creates Big Data Analytics for Population Health
 Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Advocate Cerner Partnership Creates Big Data Analytics for Population Health Tina Esposito, VP Center for Health Information Services Rishi Sikka, MD, Senior VP Clinical Operations Scottsdale Institute
Session Objectives 10/27/2014. How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN
 How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
How Can I get Beyond the Basics of Hospital Readmission and Become a Preferred Provider? Kim Barrows RN BSN Session Objectives At the end of the session the learner will be able to: 1. Discuss the history
Program Development. Completion of Gap Analysis. Review of Data. Multi-disciplinary team
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Ministries serving as alpha sites committed to
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks
 Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
BreakThrough Care Center: A New Care Model for High Risk Patients. Dr. Richard Krouse Dr. Paul Merrick
 BreakThrough Care Center: A New Care Model for High Risk Patients Dr. Richard Krouse Dr. Paul Merrick About DMG Why Population Health About BreakThrough Care Center Patient Stories Questions? About DuPage
BreakThrough Care Center: A New Care Model for High Risk Patients Dr. Richard Krouse Dr. Paul Merrick About DMG Why Population Health About BreakThrough Care Center Patient Stories Questions? About DuPage
Chapter VII. Health Data Warehouse
 Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
Broward County Health Plan Chapter VII Health Data Warehouse CHAPTER VII: THE HEALTH DATA WAREHOUSE Table of Contents INTRODUCTION... 3 ICD-9-CM to ICD-10-CM TRANSITION... 3 PREVENTION QUALITY INDICATORS...
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE. Training Slides
 VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
VNAA BLUEPRINT FOR EXCELLENCE BEST PRACTICES TO REDUCE HOSPITAL ADMISSIONS FROM HOME CARE Training Slides 061015 Why Take Action to Prevent Readmissions? Better patient care and patient experience Home
Retrospective Bundles
 Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
Bundled Payment for Care Improvement (BPCI) Overview Shawn Matheson MBA, LNHA, FACHCA Market Manager Idaho Health Care Association Annual Convention Boise, ID July 13, 2017 Retrospective Bundles Surgeon
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015
 MODEL OF CARE TRAINING 2015") SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
SPECIAL NEEDS PLAN (SNP) MODEL OF CARE TRAINING 2015 Introduction This course is offered to meet the CMS regulatory requirements for Model of Care Training for our Special Needs Plan at Care Wisconsin.
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care
 Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Aligning Health IT with Delivery System Reform: Technology Gaps in Coordinating Patient Care Peggi M. Czinger MPH Director, Network Care Management COE The Care Management Company of Montefiore The Bronx:
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care
 Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
Structural Heart Program Staffing Considerations- Effective Models for Clinic, Procedure and Post Procedure Care Deborah Campbell Inova Fairfax Medical Campus Edwards Healthcare Leadership Series September
The Geisinger Model: A Systematic Approach to Quality and Value
 The Geisinger Model: A Systematic Approach to Quality and Value National Health Policy Forum Washington, DC October 14, 2011 Glenn Steele, Jr., MD, PhD President & CEO Geisinger Health System 2011 by Geisinger
The Geisinger Model: A Systematic Approach to Quality and Value National Health Policy Forum Washington, DC October 14, 2011 Glenn Steele, Jr., MD, PhD President & CEO Geisinger Health System 2011 by Geisinger
Leveraging Nurses in Health Transformation: Population Health and Care Management Models
 Leveraging Nurses in Health Transformation: Population Health and Care Management Models OCN Annual Conference Judy Tatman, MSHA, BSN, RN October 20, 2016 0 Population Health & the Triple Quadruple Aim
Leveraging Nurses in Health Transformation: Population Health and Care Management Models OCN Annual Conference Judy Tatman, MSHA, BSN, RN October 20, 2016 0 Population Health & the Triple Quadruple Aim
Breathing Easy: A Case Study on Asthma Prevention
 Breathing Easy: A Case Study on Asthma Prevention Bob Morrow, MD, MBA Market President, Houston & Southeast Texas Blue Cross and Blue Shield of Texas @DrBobMorrow A Division of Health Care Service Corporation,
Breathing Easy: A Case Study on Asthma Prevention Bob Morrow, MD, MBA Market President, Houston & Southeast Texas Blue Cross and Blue Shield of Texas @DrBobMorrow A Division of Health Care Service Corporation,
HOME IS THE HUB. An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017
 HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
HOME IS THE HUB An Initiative to Accelerate Progress to Reduce Readmissions in Virginia Deep Dive: Post-Acute Care Strategies May 17, 2017 HOUSEKEEPING Slides were sent this morning Webinar is being recorded
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
NGA and Center for Health Care Strategies Summit: High Utilizers
 Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Medicaid Chronic Care Initiative: Strategies for High Utilizers NGA and Center for Health Care Strategies Summit: High Utilizers February 12, 2013 Eileen Girling, MPH, RN, CAMS Director, VCCI Department
Molina Healthcare Michigan Health Care Services Department Phone: (855) Fax: (800)
 Fax: (800)") Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Utilization Management Program Molina Healthcare of Michigan s Utilization Management (UM) program utilizes a care management approach based upon empirically validated best practices, where experience
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital
 Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Population Health Management in the Safety Net Elaine Batchlor, MD, MPH CEO, Martin Luther King, Jr. Community Hospital November 5, 2013 Martin Luther King, Jr. Community Hospital Page 1 11/05/2013 Agenda
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Domain 1 Patient Engagement Speed Data Reports & Schedule
 Domain 1 Patient Engagement Speed Data Reports & Schedule Suffolk Care Collaborative (SCC) Suffolk County Performing Provider System (PPS) Delivery System Reform Incentive Payment (DSRIP) Program 2 PRESENTATION
Domain 1 Patient Engagement Speed Data Reports & Schedule Suffolk Care Collaborative (SCC) Suffolk County Performing Provider System (PPS) Delivery System Reform Incentive Payment (DSRIP) Program 2 PRESENTATION
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow
 One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
One Medicine: Incorporating Population Health Principles and Best Practices into Clinical Workflow March 5, 2018 Jayne Bassler President, Population Health Services Organization Senior Vice President,
Patient Interview/Readmission Chart Review. Hospital Review:
 Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Appendix: Readmission Review Form Patient Interview/Readmission Chart Review Patient Name: Previous Hospital Admission Date Account Number Previous Hospital D/C Date: D/C MD: Previous Hospital Discharge
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool
 Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Preventing Heart Failure Readmissions by Using a Risk Stratification Tool Anna Dermenchyan, MSN, RN, CCRN-K Senior Clinical Quality Specialist Department of Medicine, UCLA Health PhD Student, UCLA School
Ambulatory Care Practice Trends and Opportunities in Pharmacy
 Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
Ambulatory Care Practice Trends and Opportunities in Pharmacy David Chen, R.Ph., M.B.A. Senior Director Section of Pharmacy Practice Managers ASHP Objectives Describe trends in health system pharmacy reported
An Integrated Approach to Heart Failure Care. Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN
 An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
Innovations in Community- Based Advanced Illness Care: A Population Health Approach
 Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Innovations in Community- Based Advanced Illness Care: A Population Health Approach LORI YOSICK, LISW -S, CHPCA DIRECTOR COMMUNITY PALLIATIVE CARE TRINITY HEALTH TERRI MAXWELL PHD, APRN CHIEF CLINICAL
Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle.
 Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Systems serving as alpha sites committed to implementation
Background Clinical Integration and Clinical Excellence Committee at the Ascension level developed the Preventing Readmissions Bundle. Six Ascension Health Systems serving as alpha sites committed to implementation
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
February 2007 ACP, AAFP, AAP, AOA joint statement
 Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Patient Centered Medical Home in a Safety Net Community Health Clinic: The T Transformation f i off Eastside Adult Clinic Nicole Joseph, MD Denver Health GIM Grand G dr Rounds d February 7, 2012 OBJECTIVES
Transitions of Care from a Community Perspective
 Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Transitions of Care from a Community Perspective ACMA Utah Chapter 2nd Annual Education Session Dr. Larry Garrett, PhD, MPH, BSN Sr. Project Manager, HealthInsight Presenting with the 5 I s Interactive
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director
 Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Cultural Transformation and the Road to an ACO Lee Sacks, M.D. CEO Mark Shields, M.D., MBA Senior Medical Director AMGA Pre-conference Workshop 1 April 14, 2011 Washington, D.C. Disclosure Nothing in Today
Referrals, Prior Authorizations, Medical Management, and Appeals
 Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
Referrals, Prior Authorizations, Medical Management, and Appeals 1 An Independent Licensee of the Blue Cross Blue Shield Association 044506 (12-21-2017) 2017 Premera. Proprietary and Confidential. Referrals
COPD & Pneumonia Readmission Reduction Program. October 25, 2017
 COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
COPD & Pneumonia Readmission Reduction Program October 25, 2017 Susan J. Bowers, MBA, BSN, RN Chief Quality Officer Mercy Health - Lorain 2 Locations Mercy Health Lorain Hospital Lorain, Ohio 250 bed community
Community Paramedicine: Lessons Learned from South Carolina
 Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Community Paramedicine: Lessons Learned from South Carolina Dr. Chris Oxendine, CP Medical Director Abbeville Area Medical Center Will Blackwell Abbeville County EMS Sarah M. Craig, MHA South Carolina
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients
 Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Bridging the Gap: Discharge Clinics Providing Safe Transitions for High Risk Patients Northwest Patient Safety Conference May 15, 2012 Dr. Shay Martinez Medical Director, Aftercare Clinic Harborview Medical
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready. Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting
 Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
Re-Hospitalizations and the Bottom Line: What SNFs Can Do to Get Ready Maureen McCarthy, RN, BS, RAC-CT, CPRA President & CEO Celtic Consulting OBJECTIVES Define Rehospitalization and discuss current statistics
2017 Catastrophic Care. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
2017 Catastrophic Care Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Catastrophic Care Program Evaluation Table of Contents Program Purpose Page 1 Goals
Chronic Care Management. Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky
 Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Chronic Care Management Sharon A. Shover, CPC, CEMC 2650 Eastpoint Parkway, Suite 300 Louisville, Kentucky 40223 502.992.3511 sshover@blueandco.com Agenda Chronic Care Management (CCM) History Define Requirements
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Chronic Care Management Services: Advantages for Your Practices
 Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Chronic Care Management Services: Advantages for Your Practices Rachel S. Eichenbaum, RN, MSN Yvonne La-Garde, M.ED Susan Whittaker, CPC, CPMA This material was prepared by the New England Quality Innovation
Advocate Health Care. PURPOSE: Describe briefly the overall purpose of this position, i.e., Why does it exist?
 http://corp2371.ahc-ad.advocatehealth.com/jobdescriptions/printpreview.aspx?jdid=40442 4/24/2012 Advocate Health Care Title: Practice Operations Coach PURPOSE: Describe briefly the overall purpose of this
http://corp2371.ahc-ad.advocatehealth.com/jobdescriptions/printpreview.aspx?jdid=40442 4/24/2012 Advocate Health Care Title: Practice Operations Coach PURPOSE: Describe briefly the overall purpose of this
EmblemHealth Advocate for Quality
 EmblemHealth Advocate for Quality 2013 Average Health Care Spending per Capita, 1980 2009 Adjusted for differences in cost of living 1 Dollars Source: OECD Health Data 2011 (June 2011). THE COMMONWEALTH
EmblemHealth Advocate for Quality 2013 Average Health Care Spending per Capita, 1980 2009 Adjusted for differences in cost of living 1 Dollars Source: OECD Health Data 2011 (June 2011). THE COMMONWEALTH
TRANSITIONS of CARE. Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine
 TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
TRANSITIONS of CARE Francis A. Komara, D.O. Michigan State University College of Osteopathic Medicine 5-15-15 Objectives At the conclusion of the presentation, the participant will be able to: 1. Improve
New Models of Care: Diabetes and the Triple Aim
 Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
Robert Gabbay MD, PhD, FACP Chief Medical Officer Joslin Diabetes Center Harvard Medical School Boston, MA The Triple Aim New Models of Care: Diabetes and the Triple Aim Healthcare is changing, what does
How Does This Fit into the Provisions of the Affordable Care Act? The goals are aligned
 Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable
Background April 2012 The Federal Centers for Medicare and Medicaid Services (CMS) approved 3 NJ Accountable Care Organizations (ACOs) to participate in the Medicare Shared Savings Program Accountable