CREATING PHYSICIAN-FOCUSED ALTERNATIVE PAYMENT MODELS
|
|
|
- Elijah Lester
- 5 years ago
- Views:
Transcription
1 CREATING PHYSICIAN-FOCUSED ALTERNATIVE PAYMENT MODELS Better Care for Patients, Lower Cost for Payers, and Financially Viable Physician Practices Harold D. Miller President and CEO Center for Healthcare Quality and Payment Reform
2 Three Doors to the Future Under MACRA MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) MACRA ALTERNATIVE PAYMENT MODELS (APMs) PHYSICIAN-FOCUSED PAYMENT MODELS 2
3 Door #1: MIPS (Pay for Performance) MIPS = PAY FOR PERFORMANCE SGR Repeal 3
4 PROBLEM The Problem That P4P Was Supposed to Solve Physicians are paid the same amount under fee-for-service regardless of the quality of care they deliver 4
5 Most P4P Solutions Have Been Worse Than the Problem PROBLEM Physicians are paid the same amount under fee-for-service regardless of the quality of care they deliver BAD P4P Requiring physicians to deliver high-quality care regardless of whether they are paid adequately to do so Penalizing physicians for quality problems they did not cause and cannot control Penalizing physicians when patients don t receive services they don t need or want 5
6 Do Physicians Need Incentives to Deliver Higher Value Care? $ Bonus Penalty P4P Based on Quality and Cost Measures FFS 6
7 The Problem Isn t Incentives But Barriers in FFS Payment $ Bonus Penalty FFS P4P Based on Quality and Cost Measures A small bonus may not be enough to pay for delivering a high-value service or for the added costs of improving quality A small bonus may not be enough to offset the costs of collecting and reporting the quality data A small penalty may be less than the loss of fee-for-service revenue from healthier patients or lower utilization Unpaid Services 7
8 Door #2: Alternative Payment Models MACRA ALTERNATIVE PAYMENT MODELS (APMs) 8
9 MACRA Encourages Use of APMs Instead of MIPS Physicians who participate in approved Alternative Payment Models (APMs) at more than a minimum level: are exempt from MIPS receive a 5% lump sum bonus receive a higher annual update (increase) in their FFS revenues receive the benefits of participating in the APM 9
10 The Need for Alternative Payment Models PROBLEM Barriers in fee-for-service prevent physicians from delivering higher-quality care at lower total cost 10
11 The Need for Alternative Payment Models PROBLEM Barriers in fee-for-service prevent physicians from delivering higher-quality care at lower total cost BARRIER #1 No payment or inadequate payment for many high-value services, e.g., Responding to patient phone calls that can avoid office or ER visits Calls among physicians to determine a diagnosis or coordinate care delivery Hiring nurses to help chronic disease patient avoid exacerbations Providing palliative care, not just hospice BARRIER #2 Loss of revenue when patients stay healthy and don t need procedures 11
12 Most APMs Are Shared Savings Programs PROBLEM ALTERNATIVE PAYMENT MODELS Barriers in fee-for-service prevent physicians from delivering higher-quality care at lower total cost? Shared Savings If the physician or health system can reduce spending below expected levels, the provider receives a share of the payer s savings 12
13 Is Shared Savings Better Than MIPS? 13
14 MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Is Shared Savings Better Than MIPS? 14
15 MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average Is Shared Savings Better Than MIPS? 15
16 Is Shared Savings Better Than MIPS? MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average SHARED SAVINGS Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates 16
17 Is Shared Savings Better Than MIPS? MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average SHARED SAVINGS Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if: spending is lower than expected and quality has improved ( Track 2 ) Impose a penalty if: spending is higher than expected 17
18 Is Shared Savings Better Than MIPS? MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average SHARED SAVINGS Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if: spending is lower than expected and quality has improved ( Track 2 ) Impose a penalty if: spending is higher than expected SHARED SAVINGS IS JUST A DIFFERENT FORM OF P4P 18
19 Medicare ACOs Aren t Succeeding Due to Flaws in Payment Model 2013 Results for Medicare Shared Savings ACOs 46% of ACOs (102/220) increased Medicare spending Only one-fourth (52/220) received shared savings payments After making shared savings payments, Medicare spent more than it saved 2014 Results for Medicare Shared Savings ACOs 45% of ACOs (152/333) increased Medicare spending Only one-fourth (86/333) received shared savings payments After making shared savings payments, Medicare spent more than it saved 19


20 Private Shared Savings ACOs Are Also Floundering 20
21 Why?? No Change in the Way Physicians Are Paid Fee-for-Service Payment MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain ACO Pregnancy Primary Care Cardiology Hematology Oncology Neurosurgery OB/GYN 21
22 Most ACOs Spend a Lot on IT and Nurse Care Managers Fee-for-Service Payment MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Expensive IT Systems ACO Nurse Care Managers Pregnancy Primary Care Cardiology Hematology Oncology Neurosurgery OB/GYN 22
23 Possible Future Shared Savings Doesn t Support Better Care Today Fee-for-Service Payment MEDICARE, MEDICAID HEALTH PLAN Shared Savings Payment??? PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Expensive IT Systems ACO Nurse Care Managers Share of Shared Savings Payment?? Pregnancy Primary Care Cardiology Hematology Oncology Neurosurgery OB/GYN 23
24 Most ACOs Today Aren t Truly Fee-for-Service Payment Redesigning Care MEDICARE, MEDICAID HEALTH PLAN Shared Savings Payment??? PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Expensive IT Systems ACO Nurse Care Managers Share of Shared Savings Payment?? Pregnancy Primary Care Cardiology Hematology Oncology Neurosurgery OB/GYN 24
25 Problems With Shared Savings Already efficient providers receive little or no additional revenue and may be forced out of business Physicians who have been practicing inefficiently or inappropriately are paid more than conservative physicians Physicians could be rewarded for denying needed care as well as by reducing overuse Physicians are placed at risk for costs they cannot control and random variation in spending Shared savings bonuses are temporary and when there are no more savings to be generated, physicians are underpaid 25
26 The Problem With ACO Payment Is It Doesn t Solve Barriers in FFS MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average APM Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if: spending is lower than expected and quality has improved ( Track 2 ) Impose a penalty if: spending is higher than expected 26
27 The Obvious Solution: Improve Physician Payment MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average APM Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Change the way physicians are paid to address FFS barriers Provide a bonus if: spending is lower than expected and quality has improved ( Track 2 ) Impose a penalty if: spending is higher than expected 27
28 Instead, Everyone Thinks the Answer is More Risk MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average APM Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if: spending is lower than expected and quality has improved ( Track 2 ) Impose a penalty if: spending is higher than expected 28
29 Or Only Pay Physicians Differently If They Accept Significant Risk MIPS/P4P Continue to pay only for what is billable under the Physician Fee Schedule at standard payment rates Provide a bonus if quality is higher than average and spending is lower than average Impose a penalty if: quality is lower than average and spending is higher than average APM Add additional payments beyond what is billable under the Physician Fee Schedule Provide a bonus if: spending is lower than expected and quality has improved ( Track 2 ) Impose a LARGE financial penalty if: spending is higher than expected 29
30 Requirements for Financial Risk What MACRA Says The APM Entity must bear financial risk for monetary losses under such alternative payment model that are in excess of a nominal amount; or be a medical home expanded by the Innovation Center in APMs 30
31 Requirements for Financial Risk in APMs What MACRA Says The APM Entity must bear financial risk for monetary losses under such alternative payment model that are in excess of a nominal amount; or be a medical home expanded by the Innovation Center What Proposed Regs Say The APM Entity is required to repay Medicare when spending on patients exceeds expected amounts, up to: 4% of total Medicare spending (except for PCP practices with <50 clinicians) 31
32 Only 16% of Medicare Spending Goes to Physicians Physicians: 16% 32

33 4% of Medicare Spending = Huge Risk for Average Physician 4% of Total Medicare Spending Physicians: 16% 25% of Physician Revenues 33
34 What CMS Definition of More Than Nominal Risk Means for Oncology Hypothetical oncology practice 500 new Medicare patients each year Average Medicare payments to the practice: $4,000/patient Projected total Medicare spending on the patients: $50,000/patient Target Medicare spending under APM: $48,000/patient (-4%) Actual Medicare spending under APM: $55,000/patient (+10%) 34
35 What CMS Definition of More Than Nominal Risk Means for Oncology Hypothetical oncology practice 500 new Medicare patients each year Average Medicare payments to the practice: $4,000/patient Projected total Medicare spending on the patients: $50,000/patient Target Medicare spending under APM: $48,000/patient (-4%) Actual Medicare spending under APM: $55,000/patient (+10%) Impact of CMS APM financial risk standards on the practice Current practice revenue from Medicare: $2 million (500 x $4,000) Total Medicare spending on patients: $27.5 million (500 x $55,000) Medicare spending above target: $3.5 million (500 x $7,000) 4% of Medicare spending = $1.1 million (500 x $55,000 x 4%) Risk: 55% of practice revenue ($1.1 million/$2 million) 35
36 Current CMS Alternative Payment Models Bundled Payments for Care Improvement (BPCI) Comprehensive Care for Joint Replacement (CJR) Comprehensive ESRD Care Large Dialysis Organization Comprehensive ESRD Care Small Dialysis Organization Comprehensive Primary Care Plus Frontier Community Health Integration Program Home Health Value Based Purchasing Model Independence at Home Demonstration Medicare Value-Based Insurance Design Model Part D Enhanced Medication Therapy Management Model Reducing Hospitalizations Among Nursing Home Residents Intravenous Immune Globulin Demonstration Maryland All-Payer Hospital Model Medicare Part B Drug Payment Model Medicare Care Choices Model Medicare Shared Savings Program (ACO) Track 1 Medicare Shared Savings Program (ACO) Track 2 Medicare Shared Savings Program (ACO) Track 3 Million Hearts Cardiovascular Risk Reduction Model Next Generation ACO Model Oncology Care Model Track 1 Oncology Care Model Track 2 36
37 APMs Meeting the Risk Standards Under Proposed Rule Bundled Payments for Care Improvement (BPCI) Comprehensive Care for Joint Replacement (CJR) Comprehensive ESRD Care Large Dialysis Organization Comprehensive ESRD Care Small Dialysis Organization Comprehensive Primary Care Plus (Only for Small Practices) Frontier Community Health Integration Program Home Health Value Based Purchasing Model Independence at Home Demonstration Medicare Value-Based Insurance Design Model Part D Enhanced Medication Therapy Management Model Reducing Hospitalizations Among Nursing Home Residents Intravenous Immune Globulin Demonstration Maryland All-Payer Hospital Model Medicare Part B Drug Payment Model Medicare Care Choices Model Medicare Shared Savings Program (ACO) Track 1 Medicare Shared Savings Program (ACO) Track 2 Medicare Shared Savings Program (ACO) Track 3 Million Hearts Cardiovascular Risk Reduction Model Next Generation ACO Model Oncology Care Model Track 1 Oncology Care Model Track 2 37
38 A Better Way to Define More Than Nominal Financial Risk What MACRA Says The APM Entity must bear financial risk for monetary losses under such alternative payment model that are in excess of a nominal amount; or be a medical home expanded by the Innovation Center What Proposed Regs Say The APM Entity is required to repay Medicare when spending on patients exceeds expected amounts, up to: 4% of total Medicare spending (except for PCP practices with <50 clinicians) 5% of the entity s total revenue 38
39 More Reasonable Risk Standard Should Be Used for All Practices What MACRA Says The APM Entity must bear financial risk for monetary losses under such alternative payment model that are in excess of a nominal amount; or be a medical home expanded by the Innovation Center What Proposed Regs Say The APM Entity is required to repay Medicare when spending on patients exceeds expected amounts, up to: 4% of total Medicare spending (except for PCP practices with <50 clinicians) 5% of the entity s total revenue, if the entity is a primary care practice with 50 or fewer clinicians (2.5% of revenue in 2017, 3% in 2018, 4% in 2019) 39
40 Excessive Risk Is Not the Only Problem with CMS APMs 40

41 Excessive Risk Is Not the Only Problem with CMS APMs 41
42 EM E&M E&M E&M E&M E&M E&M E&M E M E M E M E M E M Infusion Infusion Infusion Infusion Infusion Infusion Starting with Current Payments for an Oncology Practice HOW ONCOLOGY PRACTICE IS PAID TODAY $1200 $900 $600 $300 $ Dx TREATMENT MONTHS POST-TREATMENT CARE 42
43 EM E&M E&M E&M E&M E&M E&M E&M E M E M E M E M E M Infusion Infusion Infusion Infusion Infusion Infusion How Does the CMS Oncology Care Model Improve Payments? HOW ONCOLOGY PRACTICE IS PAID IN CMMI OCM PROGRAM $1200 $900?????? $600 $300?????????? $ Dx TREATMENT MONTHS POST-TREATMENT CARE 43
44 EM E&M E&M E&M E&M E&M E&M E&M E M E M E M E M E M Infusion Infusion Infusion Infusion Infusion $ $ $ $ Infusion $ $ Higher Payments When Chemotherapy is Given HOW ONCOLOGY PRACTICE IS PAID IN CMMI OCM PROGRAM $1200 $900 $600 $960 in New Payment (6 x $160) for each 6 Month Episode $300 $ Dx TREATMENT MONTHS POST-TREATMENT CARE 44
45 EM E&M E&M E&M E&M E&M E&M E&M E M E M E M E M E M Infusion Infusion Infusion Infusion Infusion $ $ $ $ Infusion $ $ Practice is at Risk for Total Spending on Patients HOW ONCOLOGY PRACTICE IS PAID IN CMMI OCM PROGRAM $1200 Performance-Based Payment Risk-Sharing on Total Spending $900 $600 $960 in New Payment (6 x $160) for each 6 Month Episode $300 $ Dx TREATMENT MONTHS POST-TREATMENT CARE 45
46 Problems with OCM Structure $160 Monthly Enhanced Oncology Services (MEOS) MEOS only paid if a patient receives chemotherapy, so it penalizes the practice even more than today for avoiding fruitless treatment Practice is required to significantly increase services, and it s not clear the payment is adequate to cover the higher costs of those services The MEOS payment will be recouped if patient is not attributed to the practice later based on the number of face-to-face office visits in claims data, even though the payment doesn t require face-to-face services 46
47 Problems with OCM Structure $160 Monthly Enhanced Oncology Services (MEOS) MEOS only paid if a patient receives chemotherapy, so it penalizes the practice even more than today for avoiding fruitless treatment Practice is required to significantly increase services, and it s not clear the payment is adequate to cover the higher costs of those services The MEOS payment will be recouped if patient is not attributed to the practice later based on the number of face-to-face office visits in claims data, even though the payment doesn t require face-to-face services Performance-Based Payment (Risk-Sharing) Practices would receive bonuses for delivering cheaper, less effective treatments to patients and for avoiding important surveillance testing Practices would be penalized for higher-cost types of cancer and for health problems the patient has that are unrelated to cancer Practices that are currently overusing services could be rewarded because target spending is based on the practice s own historical costs Practices could be penalized for treating higher-risk patients because risk adjustment does not capture major factors affecting spending 47
48 OCM Also Blindly Uses Episodes Where They Don t Make Sense An episode starts when chemotherapy starts and lasts 6 months even if chemotherapy ends sooner 48
49 What Happens If One of the Patient s Treatments is Delayed? Many patients have to delay a treatment because of side effects 49
50 Logic Would Say That It s Now a Longer (7 Month) Episode 50


51 But CMMI Says It s a New Episode With $960 More in Payments 51
52 And Shared Savings Is More Likely With Same Spending in 2 Episodes 52

53 Undesirable New Incentives for Oncology Practices Penalty for Helping Patients Avoid Side Effects? Incentive to Stretch Out Treatment? 53
54 Physicians Must Design Payments to Support Good Care for Patients THE RIGHT WAY TO DESIGN PAYMENT REFORMS Physicians Redesign Care and Identify Payment Barriers Payers Change Payment to Support Redesigned Care Patients Get Better Care and Physicians Stay Financially Viable 54
55 The Third Door Under MACRA MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) MACRA ALTERNATIVE PAYMENT MODELS (APMs) PHYSICIAN-FOCUSED PAYMENT MODELS 55
56 How Do You Define a Physician-Focused Alternative Payment Model?
57 Step 1: Identify Opportunities to Reduce Related Spending $ Total Spending Relevant to the Physician s Services Physician Practice Revenue Fee-for-Service Payment (FFS) Avoidable Spending Payments to Other Providers for Related Services FFS Payments to Physician Practice OPPORTUNITIES TO REDUCE SPENDING THAT PHYSICIANS CAN CONTROL Reduce Avoidable Hospital Admissions Reduce Unnecessary Tests and Treatments Use Lower-Cost Tests and Treatments Deliver Services More Efficiently Use Lower-Cost Sites of Service Reduce Preventable Complications Prevent Serious Conditions From Occurring 57
58 $ Total Spending Relevant to the Physician s Services Step 2: Identify Barriers in Current Payments That Need to Be Fixed Fee-for-Service Payment (FFS) Avoidable Spending Payments to Other Providers for Related Services OPPORTUNITIES TO REDUCE SPENDING THAT PHYSICIANS CAN CONTROL Reduce Avoidable Hospital Admissions Reduce Unnecessary Tests and Treatments Use Lower-Cost Tests and Treatments Deliver Services More Efficiently Use Lower-Cost Sites of Service Reduce Preventable Complications Prevent Serious Conditions From Occurring Physician Practice Revenue FFS Payments to Physician Practice Unpaid Services BARRIERS IN CURRENT FFS SYSTEM No Payment for Many High-Value Services Insufficient Revenue to Cover Costs When Using Fewer or Lower-Cost Services 58
59 $ Total Spending Relevant to the Physician s Services Physician Practice Revenue Step 3: Design an APM That Removes the Payment Barriers Fee-for-Service Payment (FFS) Avoidable Spending Payments to Other Providers for Related Services FFS Payments to Physician Practice Unpaid Services Physician-Focused Alternative Payment Model Flexible, Adequate Payment for Physician s Services 59
60 $ Total Spending Relevant to the Physician s Services Physician Practice Revenue Step 4: Include Provisions to Assure Control of Cost & Quality Fee-for-Service Payment (FFS) Avoidable Spending Payments to Other Providers for Related Services FFS Payments to Physician Practice Unpaid Services Physician-Focused Alternative Payment Model Savings Avoidable Spending Payments to Other Providers for Related Services Flexible, Adequate Payment for Physician s Services Accountability for Controlling Avoidable Spending 60
61 The CMS Models Are NOT the Only Way to Define APMs CMS APM Models Primary Care Medical Home Episode Payment to Hospital Upside-Only Shared Savings Two-Sided Risk Shared Savings Full-Risk Capitation 61
62 There are More & Better Ways to Create Physician-Focused APMs Primary Care Medical Home Episode Payment to Hospital Upside-Only Shared Savings Two-Sided Risk Shared Savings Full-Risk Capitation APM #1: Payment for a High-Value Service APM #2: Condition-Based Payment for a Physician s Services APM #3: Multi-Physician Bundled Payment APM #4: Physician-Facility Procedure Bundle APM #5: Warrantied Payment for Physician Services APM #6: Episode Payment for a Procedure APM #7: Condition-Based Payment 62
63 How Would You Design APMs for Hematology/Oncology? 63
64 Look at Each Condition Separately Conditions Treated Cancer Sickle Cell Disease Hemophilia Other Conditions & Procedures 64
65 Step 1: Identify the Opportunities to Improve Care & Reduce Cost Conditions Treated Cancer Opportunities to Improve Care and Reduce Cost Reduce avoidable ED visits, admits Reduce avoidable spending on drugs Reduce avoidable testing/imaging Reduce fruitless end-of-life care Sickle Cell Disease Hemophilia Other Conditions & Procedures 65
66 Step 2: Identify the Barriers in the Current Payment System Conditions Treated Cancer Opportunities to Improve Care and Reduce Cost Reduce avoidable ED visits, admits Reduce avoidable spending on drugs Reduce avoidable testing/imaging Reduce fruitless end-of-life care Barriers in Current Payment System Inadequate payment for diagnosis & treatment planning Most revenues come from treatment No payment for care management svcs Sickle Cell Disease Hemophilia Other Conditions & Procedures 66
67 Step 3: Design Solutions to Overcome the Barriers Conditions Treated Opportunities to Improve Care and Reduce Cost Barriers in Current Payment System Solutions via Alternative Payment Models Cancer Reduce avoidable ED visits, admits Reduce avoidable spending on drugs Reduce avoidable testing/imaging Reduce fruitless end-of-life care Inadequate payment for diagnosis & treatment planning Most revenues come from treatment No payment for care management svcs Additional payment for tx planning and care management with accountability for utilization Condition-based payment for controllable spending Sickle Cell Disease Hemophilia Other Conditions & Procedures 67
68 Opportunities, Barriers, and Solutions Will Differ by Condition Conditions Treated Opportunities to Improve Care and Reduce Cost Barriers in Current Payment System Solutions via Alternative Payment Models Cancer Reduce avoidable ED visits, admits Reduce avoidable spending on drugs Reduce avoidable testing/imaging Reduce fruitless end-of-life care Inadequate payment for diagnosis & treatment planning Most revenues come from treatment No payment for care management svcs Additional payment for tx planning and care management with accountability for utilization Condition-based payment for controllable spending Sickle Cell Disease Reduce ED visits and hospitalizations due to pain and other complications Reduce unnecessary transfusions No payment for care management No payment for phone & consultations with specialists Care management payment with accountability for utilization Specialty medical home payment Hemophilia Other Conditions & Procedures 68
69 Different Payment Models for Different Hem/Onc Conditions Conditions Treated Opportunities to Improve Care and Reduce Cost Barriers in Current Payment System Solutions via Alternative Payment Models Cancer Reduce avoidable ED visits, admits Reduce avoidable spending on drugs Reduce avoidable testing/imaging Reduce fruitless end-of-life care Inadequate payment for diagnosis & treatment planning Most revenues come from treatment No payment for care management svcs Additional payment for tx planning and care management with accountability for utilization Condition-based payment for controllable spending Sickle Cell Disease Reduce ED visits and hospitalizations due to pain and other complications Reduce unnecessary transfusions No payment for care management No payment for phone & consultations with specialists Care management payment with accountability for utilization Specialty medical home payment Hemophilia Manage clotting factor doses Prevent & managing joint bleeding Inadequate payment for management of drug administration No payment for care management svcs Additional payment for enhanced svcs Condition-based payment for management Other Conditions & Procedures 69
70 Not Every Condition Needs an Alternative Payment Model Conditions Treated Opportunities to Improve Care and Reduce Cost Barriers in Current Payment System Solutions via Alternative Payment Models Cancer Sickle Cell Disease Hemophilia Other Conditions & Procedures Reduce avoidable ED visits, admits Reduce avoidable spending on drugs Reduce avoidable testing/imaging Reduce fruitless end-of-life care Reduce ED visits and hospitalizations due to pain and other complications Reduce unnecessary transfusions Manage clotting factor doses Prevent & managing joint bleeding Inadequate payment for diagnosis & treatment planning Most revenues come from treatment No payment for care management svcs No payment for care management No payment for phone & consultations with specialists Inadequate payment for management of drug administration No payment for care management svcs Additional payment for tx planning and care management with accountability for utilization Condition-based payment for controllable spending Care management payment with accountability for utilization Specialty medical home payment Additional payment for enhanced svcs Condition-based payment for management FFS APM 70
71 Creating a Better Oncology APM 71
72 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 Opportunities to Reduce Cancer Spending w/o Harming Patients Current Spending Per Patient ER/Hospital Admissions Other Services Testing Avoidable $ Drugs E&M Infusions ED visits and hospital admissions for chemotherapy-related complications Unnecessarily expensive tests Unnecessary testing Unnecessarily expensive drugs Unnecessary drugs Unnecessary end-of-life treatment 72

73 ASCO Choosing Wisely List Targets Areas of High Spending 73

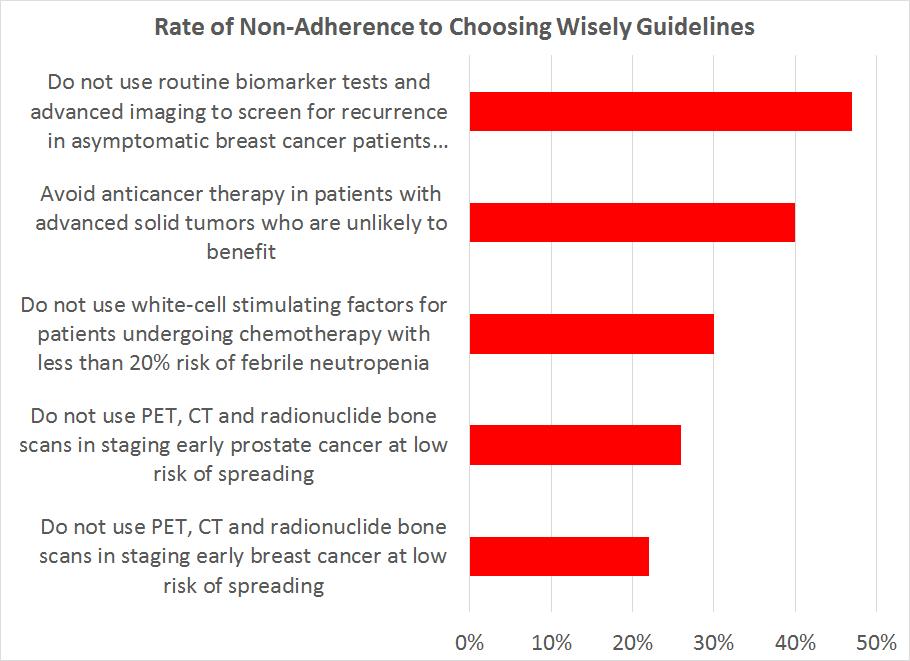
74 20-50% Non-Adherence to Choosing Wisely Criteria 74
75 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 No Payment For Many Services Essential to Quality Cancer Care Current Spending Per Patient ER/Hospital Admissions Other Services Testing Avoidable $ Drugs E&M Infusions Non-E&M No payment for physician time outside of face-to-face visits with patients No payment for time spent with patients by non-physician staff (nurses, social workers, financial counselors, etc.) 75
76 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 Inadequate Time for Effective Diagnosis & Treatment Planning Current Spending Per Patient ER/Hospital Admissions Other Services Testing Avoidable $ Drugs E&M Infusions Non-E&M With inadequate time: Easier to order multiple tests than to figure out which ones are most appropriate Easier to order the usual drugs rather than determine what s exactly right for this patient Easier to order drugs that patients want than to help them understand the tradeoffs between length of life and quality of life Easier to continue treatment than to have a difficult end-of-life discussion No payment for physician time outside of face-to-face visits with patients No payment for time spent with patients by non-physician staff (nurses, social workers, financial counselors, etc.) 76
77 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 No Payment For Services Needed to Improve Outcomes of Care Current Spending Per Patient ER/Hospital Admissions Other Services Testing Avoidable $ Drugs E&M Infusions Non-E&M ED visits and hospital admissions for chemotherapy-related complications 77
78 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 No Payment For Services Needed to Improve Outcomes of Care Current Spending Per Patient ER/Hospital Admissions Other Services Testing Avoidable $ Drugs E&M Infusions Non-E&M Care Mgt No payment for 24/7 hotline and triage services needed by patients experiencing complications No payment for extended hours or open schedule slots for urgent care 78
79 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 Inability to Address Problems in the Practice High Use of ED Current Spending Per Patient ER/Hospital Admissions Other Services Testing Avoidable $ Drugs Drug Margin E&M Infusions Non-E&M Care Mgt Lack of practice resources to help patients: No choice for patients but to visit ED Delay in seeking treatment may cause more severe complications requiring hospitalization No payment for 24/7 hotline and triage services needed by patients experiencing complications No payment for extended hours or open schedule slots for urgent care 79

80 Large Reductions in Avoidable Hospitalizations Are Possible Source: Sprandio JD. Oncology patientcentered medical home and accountable cancer care. Community Oncology, December
81 Failure to Pay for Good Care Leads to Costly, Low-Value Services $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 Current Spending Per Patient ER/Hospital Admissions Other Services Testing Avoidable $ Drugs Drug Margin E&M Infusions Non-E&M Care Mgt ED visits and hospital admissions for chemotherapy-related complications Unnecessarily expensive tests Unnecessary testing Unnecessarily expensive drugs Unnecessary drugs Unnecessary end-of-life treatment No payment for physician time outside of face-to-face visits with patients No payment for time spent with patients by non-physician staff (nurses, social workers, financial counselors, etc.) No payment for 24/7 hotline and triage services needed by patients experiencing complications No payment for extended hours or open schedule slots for urgent care 81
82 ASCO Payment Reform Developed by Oncologists & Practice Managers Christian Thomas, MD, New England Cancer Specialists Dan Zuckerman, MD, Mountain States Tumor Institute Tammy Chambers, Center for Cancer and Blood Disorders James Frame, MD, CAMC Cancer Center Bruce Gould, MD, Northwest Georgia Oncology Center Ann Kaley, Mountain States Tumor Institute Justin Klamerus, MD, Karmanos Cancer Institute Lauren Lawrence, Karmanos Cancer Institute Barbara McAneny, MD, New Mexico Cancer Center Roscoe Morton, MD, Cancer Center of Iowa Julie Moran, Seidman Cancer Center Ray Page, DO, PhD, Center for Cancer and Blood Disorders Scott Parker, Northwest Georgia Oncology Center Charles Penley, MD, Tennessee Oncology Gabrielle Rocque, MD, University of Alabama at Birmingham Barry Russo, Center for Cancer and Blood Disorders Joel Saltzman, MD, Seidman Cancer Center Laura Stevens, Innovative Oncology Business Solutions Jeffery Ward, MD, Swedish Cancer Institute Kim Woofter, Michiana Hematology Oncology Robin Zon, MD, Michiana Hematology Oncology 82
83 $45,000 $40,000 $35,000 PCOP Part 1: More Payment to Practices Where It s Needed Current FFS Payment Patient- Centered Oncology Payment $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 Drug Margin E&M Infusions Non-E&M Care Mgt Better Payment for Practices Drug Margin PCOP Pmts E&M Infusions Oncology Practice Receives Higher Payments Than Today 83
84 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 PCOP Part 2: Implement ASCO Guidelines & Control Hospital Use Current FFS Payment ER/Hospital Admissions Other Services Testing Avoidable $ Drugs Drug Margin E&M Infusions Non-E&M Care Mgt Lower Spending without Rationing Better Payment for Practices Patient- Centered Oncology Payment ER/Admissions Other Services Testing Drugs Drug Margin PCOP Pmts E&M Infusions Oncology Practice Helps Patients Avoid Use of ED/Hospital for Complications of Treatment Oncology Practice Follows ASCO Guidelines for Use of Chemotherapy, Supportive Drugs, Testing/Imaging, and End-of-Life Care Oncology Practice Receives Higher Payments Than Today 84
85 $45,000 $40,000 $35,000 $30,000 $25,000 $20,000 $15,000 $10,000 $5,000 $0 PCOP Result: Better Care, Better Payment, Payer Savings Current FFS Payment ER/Hospital Admissions Other Services Testing Avoidable $ Drugs Drug Margin E&M Infusions Non-E&M Care Mgt Lower Spending without Rationing Better Payment for Practices Patient- Centered Oncology Payment SAVINGS ER/Admissions Other Services Testing Drugs Drug Margin PCOP Pmts E&M Infusions Payer Spends Less in Total Oncology Practice Helps Patients Avoid Use of ED/Hospital for Complications of Treatment Oncology Practice Follows ASCO Guidelines for Use of Chemotherapy, Supportive Drugs, Testing/Imaging, and End-of-Life Care Oncology Practice Receives Higher Payments Than Today 85
86 Analysis of PCOP Shows Large Net Savings from Better Payment 86
87 New Billing Codes Will Be Easy for Payers & Practices to Implement New Billing Code for New Patient Treatment Planning The oncology practice would bill the payer for a $750 payment for each new oncology patient who begins treatment or active management with the practice. New Billing Code for Care Management During Treatment The oncology practice would bill the payer for a $200 payment for each month in which an oncology patient is receiving parenteral or oral anti-cancer treatment prescribed by the practice. This payment would also be made for patients who are in hospice if the oncologist is the hospice physician. New Billing Code for Care Management During Active Monitoring The oncology practice would bill the payer for a $50 per month payment when an oncology patient was not receiving anti-cancer treatment but was being actively monitored by the practice. This would include any months in which treatment was not received before a treatment regimen was completed and up to six months after the completion of treatment. Continuation of Current Billing Codes for Services The practice would continue to bill the payer for all existing CPT and HCPCS codes (e.g., E&M services, infusions, drugs administered in the practice, etc.) 87
88 What Do Payers Need to Know and Do to Implement APMs? 88
89 Five Key Elements of an APM KEY ELEMENTS OF AN APM Trigger for Payment of Service? Services Included In a Single Payment? Amount of Payment for Service? Adjustment for Differences in Patient Needs? Physician Who Is Accountable for Cost & Quality? Current RBRVS Submission of claim with CPT and ICD codes CPT code defines services included; coding rules avoid double billing Defined in advance by standard RVU weight and annual conversion factor More billable services delivered to higher-need pts Physician who bills using the CPT code Physician-Defined APMs Submission of claim with bundled service or condition mgt code Bundled service code defines services included and excluded & time period involved Defined in advance based on expected cost of delivering services in bundle Multiple levels defined based on patient characteristics Physician who bills as the manager of the bundle of services Payer-Administered APMs Trigger formula based on retrospective pattern of CPT and ICD codes Claims retrospectively grouped into bundle using formula based on CPT and ICD codes Determined after services delivered by comparison to FFS billings by non-bundled providers + discount Adjusted using risk score based on (some) prior ICD codes Physician is attributed responsibility after care is delivered using CPTs 89
90 Implementation of These Elements in the Physician Fee Schedule KEY ELEMENTS OF AN APM Trigger for Payment of Service? Services Included In a Single Payment? Amount of Payment for Service? Adjustment for Differences in Patient Needs? Physician Who Is Accountable for Cost & Quality? Current RBRVS Submission of claim with CPT and ICD codes CPT code defines services included; coding rules avoid double billing Defined in advance by standard RVU weight and annual conversion factor More billable services delivered to higher-need pts Physician who bills using the CPT code Physician-Defined APMs Submission of claim with bundled service or condition mgt code Bundled service code defines services included and excluded & time period involved Defined in advance based on expected cost of delivering services in bundle Multiple levels defined based on patient characteristics Physician who bills as the manager of the bundle of services Payer-Administered APMs Trigger formula based on retrospective pattern of CPT and ICD codes Claims retrospectively grouped into bundle using formula based on CPT and ICD codes Determined after services delivered by comparison to FFS billings by non-bundled providers + discount Adjusted using risk score based on (some) prior ICD codes Physician is attributed responsibility after care is delivered using CPTs 90
91 How Do You Build an APM on the FFS Architecture? KEY ELEMENTS OF AN APM Trigger for Payment of Service? Services Included In a Single Payment? Amount of Payment for Service? Adjustment for Differences in Patient Needs? Physician Who Is Accountable for Cost & Quality? Current RBRVS Submission of claim with CPT and ICD codes CPT code defines services included; coding rules avoid double billing Defined in advance by standard RVU weight and annual conversion factor More billable services delivered to higher-need pts Physician who bills using the CPT code Physician-Defined APMs Submission of claim with bundled service or condition mgt code Bundled service code defines services included and excluded & time period involved Defined in advance based on expected cost of delivering services in bundle Multiple levels defined based on patient characteristics Physician who bills as the manager of the bundle of services Payer-Administered APMs Trigger formula based on retrospective pattern of CPT and ICD codes Claims retrospectively grouped into bundle using formula based on CPT and ICD codes Determined after services delivered by comparison to FFS billings by non-bundled providers + discount Adjusted using risk score based on (some) prior ICD codes Physician is attributed responsibility after care is delivered using CPTs 91
92 Physicians Find Out What They ll Be Paid After Care is Delivered KEY ELEMENTS OF AN APM Trigger for Payment of Service? Services Included In a Single Payment? Amount of Payment for Service? Adjustment for Differences in Patient Needs? Physician Who Is Accountable for Cost & Quality? Current RBRVS Submission of claim with CPT and ICD codes CPT code defines services included; coding rules avoid double billing Defined in advance by standard RVU weight and annual conversion factor More billable services delivered to higher-need pts Physician who bills using the CPT code Physician-Defined APMs Submission of claim with bundled service or condition mgt code Bundled service code defines services included and excluded & time period involved Defined in advance based on expected cost of delivering services in bundle Multiple levels defined based on patient characteristics Physician who bills as the manager of the bundle of services Payer-Administered APMs Trigger formula based on retrospective pattern of CPT and ICD codes Claims retrospectively grouped into bundle using formula based on CPT and ICD codes Determined after services delivered by comparison to FFS billings by non-bundled providers + discount Adjusted using risk score based on (some) prior ICD codes Physician is attributed responsibility after care is delivered using CPTs 92
93 Payments Are Tied to What Is Coded Using CPT & ICD Codes KEY ELEMENTS OF AN APM Trigger for Payment of Service? Services Included In a Single Payment? Amount of Payment for Service? Adjustment for Differences in Patient Needs? Physician Who Is Accountable for Cost & Quality? Current RBRVS Submission of claim with CPT and ICD codes CPT code defines services included; coding rules avoid double billing Defined in advance by standard RVU weight and annual conversion factor More billable services delivered to higher-need pts Physician who bills using the CPT code Physician-Defined APMs Submission of claim with bundled service or condition mgt code Bundled service code defines services included and excluded & time period involved Defined in advance based on expected cost of delivering services in bundle Multiple levels defined based on patient characteristics Physician who bills as the manager of the bundle of services Payer-Administered APMs Trigger formula based on retrospective pattern of CPT and ICD codes Claims retrospectively grouped into bundle using formula based on CPT and ICD codes Determined after services delivered by comparison to FFS billings by non-bundled providers + discount Adjusted using risk score based on (some) prior ICD codes Physician is attributed responsibility after care is delivered using CPTs 93
94 Example #1 of Problems w/ APMs Built on (Current) FFS Structure Patient-Centered Medical Home (PCMH) programs (e.g., CMS Comprehensive Primary Care Initiative and private health plan programs) pay PCPs a monthly payment per patient (PMPM) in addition to E&M payments for face-to-face visits Good: PMPM gives PCP flexibility to deliver a wide range of services beyond what is possible through E&M visits; PMPM provides resources to manage patient care without the need for face-to-face visits Bad: PMPM is only paid for patients attributed to the PCP, and the attribution formula is based on the number of E&M visits the physician had with the patient, so if the physician doesn t bring the patient in for office visits, they could lose the payment needed to support the non-office-visitbased care What s Missing: A way for the physician to indicate that they are managing the patient s care for one or more conditions during the month 94
95 Example #2 of Problems w/ APMs Built on (Current) FFS Structure CMS and private health plans are using episode groupers to determine which services are related to a patient s condition or treatment and they are using episode attribution rules to determine which physician is responsible for the episode Good: Most physicians can only influence the services patients receive for the conditions they are treating, not the total cost of care for all of the patient s health problems Bad: Episode groupers guess at which services are inter-related based on their proximity in time and based on the presence or absence of diagnosis codes, and the groupers make a lot of mistakes Bad: Attribution rules assign episodes to physicians based on who had the most expensive services or who saw the patient the most, not based on who was actually in charge, and the attribution formula can make mistakes What s Missing: A way for a physician to indicate that they are managing the patient s care during an episode and a way to determine the clinical rationale for a service and whether it s related to previous services 95
96 Example #3 of Problems w/ APMs Built on (Current) FFS Structure CMS uses the Hierarchical Condition Category (HCC) system to risk adjust payments to physicians under various APMs Good: Risk adjustment is needed to ensure that physicians receive higher payments for patients who have more health problems that require more services and increase the likelihood of poor outcomes Bad: HCCs were designed to predict total spending by Medicare Advantage plans (and do not do that very well), they were not designed to predict patient needs for services related to specific health problems Bad: HCCs are based on ICD diagnosis codes, and even ICD-10 codes do not capture many important differences in disease severity or other patient characteristics that can significantly affect service needs and outcomes Bad: HCCs weight diagnoses codes the same way for all patients, even though different diagnoses have different impacts on the types of care delivered by different physicians What s Missing: A way for the physician to indicate that a patient has the specific characteristics that affect their need for the services delivered by that physician and/or their risk of complications and poor outcomes 96
97 Trigger for Payment of Service A Better Way to Define APMs: An Expanded FFS Architecture Services Included In Single Payment Amount of Payment for Service Adjustment for Differences in Patient Needs Physician Accountable for Cost & Quality Current RBRVS Submission of claim with CPT and ICD codes CPT code defines services included; coding rules avoid double billing Defined in advance by standard RVU weight and annual conversion factor More billable services delivered to higher-need pts Physician who bills using the CPT code Physician-Focused APMs Submission of claim with bundled service or condition mgt code Bundled service code defines services included and excluded & time period involved Defined in advance based on expected cost of delivering services in bundle Multiple levels defined based on patient characteristics Physician who bills as the manager of the bundle of services Payer-Administered APMs Trigger formula based on retrospective pattern of CPT and ICD codes Claims retrospectively grouped into bundle using formula based on CPT and ICD codes Determined after services delivered by comparison to FFS billings by non-bundled providers + discount Adjusted using risk score based on (some) prior ICD codes Physician is attributed responsibility after care is delivered using CPTs 97
98 MACRA Requires Development of Three New Types of Codes Care Episode Groups (and associated codes) Patient Condition Groups (and associated codes) Patient Relationship Categories (and associated codes) 98
99 Care Episode & Patient Condition Groups Under MACRA DEVELOPMENT OF CARE EPISODE AND PATIENT CONDITION GROUPS The Secretary shall establish care episode groups and patient condition groups, which account for a target of an estimated 1/2 of expenditures under parts A and B (with such target increasing over time as appropriate); and assign codes to such groups. CARE EPISODE GROUPS. In establishing care episode groups, the Secretary shall take into account the patient s clinical problems at the time items and services are furnished during an episode of care, such as the clinical conditions or diagnoses, whether or not inpatient hospitalization occurs, and the principal procedures or services furnished; and other factors determined appropriate by the Secretary. PATIENT CONDITION GROUPS. In establishing patient condition groups, the Secretary shall take into account the patient s clinical history at the time of a medical visit, such as the patient s combination of chronic conditions, current health status, and recent significant history (such as hospitalization and major surgery during a previous period, such as 3 months); and other factors determined appropriate by the Secretary. 99
100 Patient Relationship Categories Under MACRA DEVELOPMENT OF PATIENT RELATIONSHIP CATEGORIES AND CODES The Secretary shall develop patient relationship categories and codes that define and distinguish the relationship and responsibility of a physician or applicable practitioner with a patient at the time of furnishing an item or service. Patient relationship categories shall include different relationships of the physician or applicable practitioner to the patient (and the codes may reflect combinations of such categories), such as a physician or applicable practitioner who (i) considers themself to have the primary responsibility for the general and ongoing care for the patient over extended periods of time; (ii) considers themself to be the lead physician or practitioner and who furnishes items and services and coordinates care furnished by other physicians or practitioners for the patient during an acute episode; (iii) furnishes items and services to the patient on a continuing basis during an acute episode of care, but in a supportive rather than a lead role; (iv) furnishes items and services to the patient on an occasional basis, usually at the request of another physician or practitioner; or (v) furnishes items and services only as ordered by another physician or practitioner. 100
101 Timetable for CMS Adoption and Use of New Codes Under MACRA Estimated Date April 16, 2016 (Completed) November 25, 2016 April 20, 2017 December 20, 2017 January 1, 2018 Care Episode Groups and Codes Draft list of care episode codes Operational list of care episode codes Include care episode codes on claim forms Patient Condition Groups and Codes Draft list of patient condition codes Operational list of patient condition codes Include patient condition codes on claim forms Patient Relationship Categories & Codes Draft patient relationship categories and codes Operational list of patient relationship categories and codes Include patient relationship category codes on claim forms 101
102 Potential Patient Characteristics for Stratifying Chemo Payment Amounts 1. Comorbidities, measured using the Charlson Comorbidity Scale but with no points assigned to cancer diagnoses 2. Performance status, measured using the ECOG scale 3. Toxicity of the patient s drug regimen 4. Complexity of administration of the drug regimen for both the practice and patient 102
103 Examples of a Stratification Structure 103
104 What Happens to ACOs with Physician-Focused APMs? 104
105 Each Patient Should Have a Good Primary Care Practice PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Primary Care Practice 105
106 With Payment That Enables Delivery of Good Primary Care MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice 106
107 And PCPs Take Accountability for Costs They Can Control/Influence MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice Accountability for: Avoidable ER Visits Avoidable Hospitalizations Unnecessary Tests Unnecessary Referrals Adequate Preventive Care 107
108 Give PCPs a Medical Neighborhood to Consult With on Difficult Cases MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice Cardiology, Hem/Onc, Physiatry 108
109 Pay the Medical Neighbors to Support the PCPs MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice Cardiology, Hem/Onc, Physiatry Payment That Supports Diagnostic & Care Management Help From Specialists 109
110 Ask the Medical Neighbors to Be Accountable for Costs They Control MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice Cardiology, Hem/Onc, Physiatry Accountability for: Appropriate Use of Testing and Interventions Improving Chronic Disease Management Payment That Supports Diagnostic & Care Management Help From Specialists 110
111 Have Good Specialists Ready to Manage Serious Conditions MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice Cardiology, Hem/Onc, Physiatry Cardiology Group Neurosurg. Group Hem/Onc Group Payment That Supports Diagnostic & Care Management Help From Specialists 111
112 Pay Them To Deliver Quality Care at the Most Affordable Cost MEDICARE, MEDICAID HEALTH PLAN PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice Cardiology, Hem/Onc, Physiatry Cardiology Group Neurosurg. Group Hem/Onc Group Payment That Supports Diagnostic & Care Management Help From Specialists Payment That Supports Good Management of Heart Disease Payment That Supports Good Care for Back Pain Payment That Supports Good Care for Cancer & Blood Disorders 112
113 PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Ask Specialists to Be Accountable for Costs They Can Control Payment That Supports Good Primary Care MEDICARE, MEDICAID HEALTH PLAN Primary Care Practice Cardiology, Hem/Onc, Physiatry Cardiology Group Neurosurg. Group Hem/Onc Group Payment That Supports Diagnostic & Care Management Help From Specialists Accountability for: Using Appropriate Procedures Avoiding Complications of Procedures Payment That Supports Good Management of Heart Disease Payment That Supports Good Care for Back Pain Payment That Supports Good Care for Cancer & Blood Disorders 113
114 That s an ACO, But Built from the Bottom Up, Not the Top Down MEDICARE, MEDICAID HEALTH PLAN Alternative Payment Models PATIENTS Heart Disease Cancer & Blood Disorders Back Pain Payment That Supports Good Primary Care Primary Care Practice Cardiology, Hem/Onc, Physiatry Cardiology Group Neurosurg. Group Hem/Onc Group Payment That Supports Diagnostic & Care Management Help From Specialists Payment That Supports Good Management of Heart Disease Payment That Supports Good Care for Back Pain Payment That Supports Good Care for Cancer & Blood Disorders ACO 114
115 PATIENTS Heart Disease Cancer & Blood Disorders Back Pain A True ACO Can Take a Global Payment And Make It Work Payment That Supports Good Primary Care MEDICARE, MEDICAID HEALTH PLAN, EMPLOYER Primary Care Practice Cardiology, Hem/Onc, Physiatry ACO Risk-Adjusted Global Payment Cardiology Group Neurosurg. Group Hem/Onc Group Payment That Supports Diagnostic & Care Management Help From Specialists Payment That Supports Good Management of Heart Disease Payment That Supports Good Care for Back Pain Payment That Supports Good Care for Cancer & Blood Disorders 115
116 Instead of a Vision That Won t Work and Patients Don t Want 116
117 Instead of a Vision That Won t Work and Patients Don t Want Primary Care from a Medical Home PATIENT 117
118 Instead of a Vision That Won t Work and Patients Don t Want Primary Care from a Medical Home PATIENT Joint Replacement from a Hospital 118
119 Instead of a Vision That Won t Work and Patients Don t Want Primary Care from a Medical Home PATIENT Everything Else from an ACO Coordinated Low Quality High-Priced Health Care Joint Replacement from a Hospital 119
120 Pursue a Vision That Will Benefit Patients, Providers & Payers 120
121 HEALTHY PATIENTS Pursue a Vision That Will Benefit Patients, Providers & Payers A Better Vision Primary Care from a Medical Home Accountable Medical Home Payment 121
122 HEALTHY PATIENTS Pursue a Vision That Will Benefit Patients, Providers & Payers A Better Vision Primary Care from a Medical Home Accountable Medical Home Payment PATIENTS WITH A HEALTH PROBLEM PCP Specialist Condition- Based Payment 122
123 HEALTHY PATIENTS Pursue a Vision That Will Benefit Patients, Providers & Payers A Better Vision Primary Care from a Medical Home Accountable Medical Home Payment PATIENTS WITH A HEALTH PROBLEM PATIENTS WITH A SERIOUS CONDITION PCP Specialist Treatment & Management by a Specialist Condition- Based Payment Specialty Medical Home Payment 123
124 HEALTHY PATIENTS Pursue a Vision That Will Benefit Patients, Providers & Payers A Better Vision Primary Care from a Medical Home Accountable Medical Home Payment PATIENTS WITH A HEALTH PROBLEM PATIENTS WITH A SERIOUS CONDITION PCP Specialist Treatment & Management by a Specialist Condition- Based Payment Specialty Medical Home Payment PATIENTS WITH MULTIPLE HEALTH PROBLEMS Accountable Care Team PCP Specialist Specialist Specialist Multi- Condition Payment or Risk-Adjusted Global Payment 124
125 Physician-Focused APMs Can Create Win-Win-Win Solutions MERIT-BASED INCENTIVE PAYMENT SYSTEM (MIPS) MACRA ALTERNATIVE PAYMENT MODELS (APMs) PHYSICIAN-FOCUSED PAYMENT MODELS 125





126 Learn More About Win-Win-Win Payment and Delivery Reform 126
MACRA for Critical Access Hospitals. Tuesday, July 26, 2016 Webinar
 MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
MACRA for Critical Access Hospitals Tuesday, July 26, 2016 Webinar MACRA presenters Harold D. Miller, President & CEO CHQPR Claudia Sanders, Sr. Vice President, Policy Development Andrew Busz, Policy Director,
CREATING A PATIENT-CENTERED PAYMENT SYSTEM
 CREATING A PATIENT-CENTERED PAYMENT SYSTEM Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices & Hospitals Harold D. Miller President and CEO Center for Healthcare
CREATING A PATIENT-CENTERED PAYMENT SYSTEM Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices & Hospitals Harold D. Miller President and CEO Center for Healthcare
REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN
 REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN Supporting Collaborative Regional Approaches to Sustainable High-Value Healthcare Harold D. Miller President and CEO Center for Healthcare
REDESIGNING HEALTH CARE FROM THE BOTTOM UP INSTEAD OF FROM THE TOP DOWN Supporting Collaborative Regional Approaches to Sustainable High-Value Healthcare Harold D. Miller President and CEO Center for Healthcare
WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Physicians, Hospitals, Patients, and
 WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Physicians, Hospitals, Patients, and Payers Can All Benefit from Better Healthcare Payment Systems Harold D. Miller President and CEO Center for Healthcare
WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Physicians, Hospitals, Patients, and Payers Can All Benefit from Better Healthcare Payment Systems Harold D. Miller President and CEO Center for Healthcare
CREATING A PHYSICIAN-LED HEALTHCARE FUTURE Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices & Hospitals
 CREATING A PHYSICIAN-LED HEALTHCARE FUTURE Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices & Hospitals Harold D. Miller President and CEO Center for Healthcare
CREATING A PHYSICIAN-LED HEALTHCARE FUTURE Better Care for Patients, Lower Healthcare Spending, & Financially Viable Physician Practices & Hospitals Harold D. Miller President and CEO Center for Healthcare
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care. Harold D. Miller
 Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
Quality Payment Program and Alternative Payment Models. Brian R. Bourbeau, MBA COA Administrators Network April 11, 2018
 Quality Payment Program and Alternative Payment Models Brian R. Bourbeau, MBA COA Administrators Network April 11, 2018 Speaker Background Associate Director, Business Metrics & Analysis Clinical Affairs
Quality Payment Program and Alternative Payment Models Brian R. Bourbeau, MBA COA Administrators Network April 11, 2018 Speaker Background Associate Director, Business Metrics & Analysis Clinical Affairs
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Alternative Payment Models and Health IT
 Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
Alternative Payment Models and Health IT Health DataPalooza Preconference May 8, 2016 Kelly Cronin, MS, MPH, Director, Office of Care Transformation, ONC/HHS HHS Goals for Medicare Payment Reform In January
WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE
 WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Providers, Hospitals, Employers, and Patients Can All Benefit from Healthcare Payment and Delivery Reform Harold D. Miller President and CEO Center for Healthcare
WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Providers, Hospitals, Employers, and Patients Can All Benefit from Healthcare Payment and Delivery Reform Harold D. Miller President and CEO Center for Healthcare
The Quality Payment Program Overview Fact Sheet
 Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
Quality Payment Program The Quality Payment Program Overview Background On October 14, 2016, the Department of Health and Human Services (HHS) issued its final rule with comment period implementing the
MIPS, MACRA, & CJR: Medicare Payment Transformation. Presenter: Thomas Barber, M.D. May 31, 2016
 MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
MIPS, MACRA, & CJR: Medicare Payment Transformation Presenter: Thomas Barber, M.D. May 31, 2016 Michael Porter- Value Based Care Delivery, Annals of Surgery 2008 Principals: Define Value as a Goal Care
WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Physicians, Hospitals, Patients, and Payers Can All Benefit From Healthcare Payment & Delivery Reform
 WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Physicians, Hospitals, Patients, and Payers Can All Benefit From Healthcare Payment & Delivery Reform Harold D. Miller President and CEO Center for Healthcare
WIN-WIN-WIN APPROACHES TO ACCOUNTABLE CARE How Physicians, Hospitals, Patients, and Payers Can All Benefit From Healthcare Payment & Delivery Reform Harold D. Miller President and CEO Center for Healthcare
Medicare Physician Payment Reform:
 Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Medicare Physician Payment Reform: Implications and Options for Physicians and Hospitals Background The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) was signed into law on April 14, 2015.
Payment Reforms to Improve Care for Patients with Serious Illness
 Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
Payment Reforms to Improve Care for Patients with Serious Illness Discussion Draft March 2017 Payment Reforms to Improve Care for Patients with Serious Illness Page 2 PAYMENT REFORMS TO IMPROVE CARE FOR
PALLIATIVE CARE: CHARTING A COURSE MEETING OF THE PATIENT QUALITY OF LIFE COALITION FEBRUARY 18, 2015
 PALLIATIVE CARE: CHARTING A COURSE MEETING OF THE PATIENT QUALITY OF LIFE COALITION FEBRUARY 18, 2015 HENRY R. DESMARAIS, MD, MPA HEALTH POLICY ALTERNATIVES, INC. A POSSIBLE OPTION MENU QUALITY Ø Add palliative
PALLIATIVE CARE: CHARTING A COURSE MEETING OF THE PATIENT QUALITY OF LIFE COALITION FEBRUARY 18, 2015 HENRY R. DESMARAIS, MD, MPA HEALTH POLICY ALTERNATIVES, INC. A POSSIBLE OPTION MENU QUALITY Ø Add palliative
BETTER CARE AT LOWER COST THROUGH PHYSICIAN LEADERSHIP
 BETTER CARE AT LOWER COST THROUGH PHYSICIAN LEADERSHIP Redesigning Care Delivery, Payment Systems, & Benefit Designs so Physicians, Hospitals, Patients, & Purchasers All Benefit Harold D. Miller President
BETTER CARE AT LOWER COST THROUGH PHYSICIAN LEADERSHIP Redesigning Care Delivery, Payment Systems, & Benefit Designs so Physicians, Hospitals, Patients, & Purchasers All Benefit Harold D. Miller President
Overview of Quality Payment Program
 Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
Overview of Quality Payment Program Policies for 2017 & 2018 Performance Years The Medicare program has transformed how it reimburses psychiatrists and other clinicians for providing services, under the
CMS Priorities, MACRA and The Quality Payment Program
 CMS Priorities, MACRA and The Quality Payment Program Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services Presentation on behalf of HSAG November 16, 2016
CMS Priorities, MACRA and The Quality Payment Program Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services Presentation on behalf of HSAG November 16, 2016
Making the Business Case
 Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
WELCOME. Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association
 WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
WHAT IS MACRA? WELCOME Kate Gainer, PharmD Executive Vice President and CEO Iowa Pharmacy Association WELCOME Anthony Pudlo, PharmD, MBA, BCACP Vice President of Professional Affairs Iowa Pharmacy Association
The Pain or the Gain?
 The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
The Pain or the Gain? Comprehensive Care Joint Replacement (CJR) Model DRG 469 (Major joint replacement with major complications) DRG 470 (Major joint without major complications or comorbidities) Actual
QUALITY PAYMENT PROGRAM
 NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
NOTICE OF PROPOSED RULE MAKING Medicare Access and CHIP Reauthorization Act of 2015 QUALITY PAYMENT PROGRAM Executive Summary On April 27, 2016, the Department of Health and Human Services issued a Notice
Submitted electronically:
 Mr. Andy Slavitt Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-5517-FC P.O. Box 8013 7500 Security Boulevard Baltimore, MD 21244-8013
Mr. Andy Slavitt Acting Administrator Centers for Medicare and Medicaid Services Department of Health and Human Services Attention: CMS-5517-FC P.O. Box 8013 7500 Security Boulevard Baltimore, MD 21244-8013
The Role of Pharmacy in Alternative Payment Models
 The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
The Role of Pharmacy in Alternative Payment Models July 15, 2015 Disclaimer Organizations may not re use material presented at this AMCP webinar for commercial purposes without the written consent of the
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement. Craig J. Wilson
 Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
Population Health and the Accelerating Leap to Outcomes-Based Reimbursement Craig J. Wilson Agenda / Goals Define Population Health Management Review emerging reimbursement landscape eg MACRA Review why
ASCO s Payment Reform Model
 ASCO s Payment Reform Model Washington State Medical Oncology Society November 7, 2014 Presenter Andrew Hertler, MD, FACP Conflict of Interest Information Dr. Hertler is employed by and has stock options
ASCO s Payment Reform Model Washington State Medical Oncology Society November 7, 2014 Presenter Andrew Hertler, MD, FACP Conflict of Interest Information Dr. Hertler is employed by and has stock options
MACRA & Implications for Telemedicine. June 20, 2016
 MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
MACRA & Implications for Telemedicine June 20, 2016 Presentation Overview Introductions Deep Dive Into MACRA Implications for Telemedicine Questions Growth in Value-Based Care Over Next Two Years Growth
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
MACRA Fall into Place. By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof
 MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
MACRA Fall into Place By Stephanie Cecchini, CPC, CEMC, CHISP, AAPC Fellow, AAPC MACRA Prof About the Presenter https://www.linkedin.com/in/stephaniececchini 2 Introduction Love it Hate it Don t know a
Getting Ready for the Post-SGR World. Presented by: Sybil R. Green, JD, RPh, MHA. West Virginia Oncology Society Spring Meeting May 5, 2016
 Getting Ready for the Post-SGR World Presented by: Sybil R. Green, JD, RPh, MHA West Virginia Oncology Society Spring Meeting May 5, 2016 CME/CE Information For Physicians: This activity has been planned
Getting Ready for the Post-SGR World Presented by: Sybil R. Green, JD, RPh, MHA West Virginia Oncology Society Spring Meeting May 5, 2016 CME/CE Information For Physicians: This activity has been planned
Understanding Medicare s New Quality Payment Program
 Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
Understanding Medicare s New Quality Payment Program Your introduction to MACRA and getting started with MIPS 1 Understanding Medicare s New Quality Payment Program 2016 Mingle Analytics. All Rights Reserved.
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act
 Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
Health System Transformation, CMS Priorities, and the Medicare Access and CHIP Reauthorization Act Ashby Wolfe, MD, MPP, MPH Chief Medical Officer, Region IX Centers for Medicare and Medicaid Services
MACRA Implementation: A Review of the Quality Payment Program
 MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
MACRA Implementation: A Review of the Quality Payment Program Neal Logue, Kirk Sadur Centers for Medicare and Medicaid Services, Region IX, September 15, 2017 Disclaimer This presentation was prepared
ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT
 ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT The Centers for Medicare and Medicaid Services Kate Goodrich, MD MHS Director, Clinical Standards & Quality Chief Medical Officer 1 DISCLAIMERS
ACCOUNTABLE CARE ORGANIZATION & ALTERNATIVE PAYMENT MODEL SUMMIT The Centers for Medicare and Medicaid Services Kate Goodrich, MD MHS Director, Clinical Standards & Quality Chief Medical Officer 1 DISCLAIMERS
MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the
 published in the Federal Register the") MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed criteria for the Quality Payment Program as prescribed
MIPS/APM Proposed Rule Summary On Monday, May 9, 2016 the Centers for Medicare and Medicaid Services (CMS) published in the Federal Register the proposed criteria for the Quality Payment Program as prescribed
Kate Goodrich, MD MHS. Director, Center for Clinical Standards & Quality. Center for Medicare and Medicaid Services (CMS) May 6, 2016
 May 6, 2016") Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
Kate Goodrich, MD MHS Director, Center for Clinical Standards & Quality Center for Medicare and Medicaid Services (CMS) May 6, 2016 THE MEDICARE ACCESS & CHIP REAUTHORIZATION ACT OF 2015 Quality Payment
CMS Quality Payment Program: Performance and Reporting Requirements
 CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
CMS Quality Payment Program: Performance and Reporting Requirements Session #QU1, February 19, 2017 Kristine Martin Anderson, Executive Vice President, Booz Allen Hamilton Colleen Bruce, Lead Associate,
Prior to implementation of the episode groups for use in resource measurement under MACRA, CMS should:
 Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov
Via Electronic Submission (www.regulations.gov) March 1, 2016 Andrew M. Slavitt Acting Administrator Centers for Medicare and Medicaid Services 7500 Security Boulevard Baltimore, MD episodegroups@cms.hhs.gov
Redesigning Post-Acute Care: Value Based Payment Models
 Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
Redesigning Post-Acute Care: Value Based Payment Models Liz Almeida-Sanborn, MS, PT President Preferred Therapy Solutions This session will address: Discussion of the emergence of voluntary and mandatory
The New World of Value Driven Cardiac Care
 1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
1 The New World of Value Driven Cardiac Care Disclosures MPA Healthcare Solutions is an analytic health care consultancy that provides clients with insight into clinical performance; aids them in the evaluation,
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR)
") Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
Summary and Analysis of CMS Proposed and Final Rules versus AAOS Comments: Comprehensive Care for Joint Replacement Model (CJR) The table below summarizes the specific provisions noted in the Medicare
Advancing Care Coordination Proposed Rule
 Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
Advancing Care Coordination Proposed Rule Released July 25, 2016 Erin Smith, JD VP and Executive Director, PACCR Jourdan Meltzer Research Associate, PACCR August 4, 2016 1 Presentation Overview Three new
The Urgent Need for Better Claims Data to Support Value-Based Payment
 320 Ft. Duquesne Boulevard Suite 20-J Pittsburgh, PA 15222 Voice: (412) 803-3650 Fax: (412) 803-3651 www.chqpr.org Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of
320 Ft. Duquesne Boulevard Suite 20-J Pittsburgh, PA 15222 Voice: (412) 803-3650 Fax: (412) 803-3651 www.chqpr.org Seema Verma Administrator Centers for Medicare & Medicaid Services U.S. Department of
Culture Change. Bryan J. Weiner, Ph.D.
 Culture Change Bryan J. Weiner, Ph.D. bjweiner@uw.edu WHAT IS ORGANIZATIONAL CULTURE? The way things are done around here. WHAT KIND OF CULTURE SUPPORTS PERFORMANCE IMPROVEMENT? Learning Organization:
Culture Change Bryan J. Weiner, Ph.D. bjweiner@uw.edu WHAT IS ORGANIZATIONAL CULTURE? The way things are done around here. WHAT KIND OF CULTURE SUPPORTS PERFORMANCE IMPROVEMENT? Learning Organization:
Objectives. Preparing for Value-Based Reimbursement 3/28/2016
 Preparing for Value-Based Reimbursement Tracy Bird, FACMPE, CPC, CPMA, CPC-I, CEMC Sr. Advisor Education and Consulting KaMMCO April 12, 2016 1 2 Objectives A look back - how did we get here Existing and
Preparing for Value-Based Reimbursement Tracy Bird, FACMPE, CPC, CPMA, CPC-I, CEMC Sr. Advisor Education and Consulting KaMMCO April 12, 2016 1 2 Objectives A look back - how did we get here Existing and
TKG Health Systems Advisory Panel Meeting. Healthcare in 2017: Trends & Hot Topics. Tuesday, March 24 th, 2017 Gaylord Texan Resort, Grapevine, TX
 TKG Health Systems Advisory Panel Meeting Healthcare in 2017: Trends & Hot Topics Tuesday, March 24 th, 2017 Gaylord Texan Resort, Grapevine, TX Executive Summary Key Trends The transition to value-based
TKG Health Systems Advisory Panel Meeting Healthcare in 2017: Trends & Hot Topics Tuesday, March 24 th, 2017 Gaylord Texan Resort, Grapevine, TX Executive Summary Key Trends The transition to value-based
Perspectives on Primary Care Transformation: Measurement, MACRA, Medical Homes, and Payment Reform
 Perspectives on Primary Care Transformation: Measurement, MACRA, Medical Homes, and Payment Reform Robert A. Berenson, MD Institute Fellow, the Urban Institute rberenson@urban.org Covered California Stakeholder
Perspectives on Primary Care Transformation: Measurement, MACRA, Medical Homes, and Payment Reform Robert A. Berenson, MD Institute Fellow, the Urban Institute rberenson@urban.org Covered California Stakeholder
Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference
 Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference June 22, 2017 Michael J. Sexton, MD Catherine I. Hanson, JD COI Disclosure To assure the highest quality of CME programming, the OMA
Maximizing Your Potential Under MIPS Oregon MACRA Playbook Conference June 22, 2017 Michael J. Sexton, MD Catherine I. Hanson, JD COI Disclosure To assure the highest quality of CME programming, the OMA
INTRODUCTION TO POPULATION HEALTH. Kathy Whitmire, Vice President
 INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
INTRODUCTION TO POPULATION HEALTH Kathy Whitmire, Vice President 1 Learning Objectives 1. Provide an overall framework for population health 2. Allow clinics to understand why population health is important
Community Oncology Town Hall. Moderator John Cox, DO, FASCO
 Community Oncology Town Hall Moderator John Cox, DO, FASCO Rough Waters for Practices Economic pressures Political turbulence General disruption across medicine Sequestration ICD-10 PQRS, Meaningful Use
Community Oncology Town Hall Moderator John Cox, DO, FASCO Rough Waters for Practices Economic pressures Political turbulence General disruption across medicine Sequestration ICD-10 PQRS, Meaningful Use
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS 4/19/2016. April 20, 2016
 HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
HOSPITALS & HEALTH SYSTEMS: DATA-DRIVEN STRATEGY FOR BUNDLED PAYMENT SUCCESS April 20, 2016 Eddie Marmouget National Industry Partner emarmouget@bkd.com Eric Rogers Managing Consultant erogers@bkd.com
Steps toward Sustainability with the second year of the Quality Payment Program
 Steps toward Sustainability with the second year of the Quality Payment Program Deanna Graham, QI Consultant, Qualis Health March 27, 2018 Speaker Deanna Graham QI Principal Qualis Health 2 Qualis Health
Steps toward Sustainability with the second year of the Quality Payment Program Deanna Graham, QI Consultant, Qualis Health March 27, 2018 Speaker Deanna Graham QI Principal Qualis Health 2 Qualis Health
MACRA-Impacts on Primary
 MACRA-Impacts on Primary Care Providers and Practices Jennifer Bell, MS, Chamber Hill Strategies Mara McDermott, JD, CAPG Shari Erickson, MPH (Moderator), American College of Physicians Macaran Baird,
MACRA-Impacts on Primary Care Providers and Practices Jennifer Bell, MS, Chamber Hill Strategies Mara McDermott, JD, CAPG Shari Erickson, MPH (Moderator), American College of Physicians Macaran Baird,
Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021
 Policy for Rate Year 2021") Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021 October 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410)
Draft for the Medicare Performance Adjustment (MPA) Policy for Rate Year 2021 October 2018 Health Services Cost Review Commission 4160 Patterson Avenue Baltimore, Maryland 21215 (410) 764-2605 FAX: (410)
Glossary of Acronyms for the Quality Payment Program
 The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Glossary of Acronyms for the Quality Payment Program 1 P a g e MEDICARE QPP PHYSICIAN EDUCATION
The Physicians Advocacy Institute s Medicare Quality Payment Program (QPP) Physician Education Initiative Glossary of Acronyms for the Quality Payment Program 1 P a g e MEDICARE QPP PHYSICIAN EDUCATION
Comparison of Bundled Payment Models. Model 1 Model 2 Model 3 Model 4. hospitals, physicians, and post-acute care where
 Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
Comparison of Bundled Payment Models General Description Eligible awardees Retrospective bundled Retrospective bundled payment models for payment models for hospitals, physicians, and post-acute care where
MACRA The shift to Value Based Care and Payment. Michael Munger, M.D., FAAFP
 MACRA The shift to Value Based Care and Payment Michael Munger, M.D., FAAFP Current State Silos of Care Over Utilization Volume over Value Push Towards Value and Quality 85% Medicare Payments tied to quality
MACRA The shift to Value Based Care and Payment Michael Munger, M.D., FAAFP Current State Silos of Care Over Utilization Volume over Value Push Towards Value and Quality 85% Medicare Payments tied to quality
Alternative Payment Model Environment Implications for Specialty Providers and their Partners
 Alternative Payment Model Environment Implications for Specialty Providers and their Partners Bob Dowling MD Vice President Medical Affairs and Policy ION Solutions/IntrinsiQ Specialty Solutions June 20,
Alternative Payment Model Environment Implications for Specialty Providers and their Partners Bob Dowling MD Vice President Medical Affairs and Policy ION Solutions/IntrinsiQ Specialty Solutions June 20,
The Official Definition FROM VOLUME TO VALUE: and How to Get There. What is an Accountable Care Organization?
 FROM VOLUME TO VALUE: Better Ways to Pay for Health Care, and How to Get There Harold D. Miller Executive Director Center for Healthcare Quality and Reform and President and CEO Network for Regional Healthcare
FROM VOLUME TO VALUE: Better Ways to Pay for Health Care, and How to Get There Harold D. Miller Executive Director Center for Healthcare Quality and Reform and President and CEO Network for Regional Healthcare
Centers for Medicare & Medicaid Services: Innovation Center New Direction
 Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
Centers for Medicare & Medicaid Services: Innovation Center New Direction I. Background One of the most important goals at CMS is fostering an affordable, accessible healthcare system that puts patients
MACRA, MIPS, and APMs What to Expect from all these Acronyms?!
 MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
MACRA, MIPS, and APMs What to Expect from all these Acronyms?! ACP Pennsylvania Council Meeting Saturday, December 5, 2015 Shari M. Erickson, MPH Vice President, Governmental Affairs & Medical Practice
ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods
 A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
A unique vision for an ever-changing healthcare environment ACOs the Medicare Shared Savings Program And Other Healthcare Reform Payment Methods Presented by Joe Laden, President, ORVA, LLC The Environment
The New Frontier: Value- Based Payment Models
 The New Frontier: Value- Based Payment Models Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-026-L04-P/T Activity Type: Knowledge-based Target Audience: ACPE#: Activity Type:
The New Frontier: Value- Based Payment Models Target Audience: Pharmacists and Pharmacy Technicians ACPE#: 0202-0000-18-026-L04-P/T Activity Type: Knowledge-based Target Audience: ACPE#: Activity Type:
MACRA and the Quality Payment Program. Frequently Asked Questions Edition
 MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MACRA and the Quality Payment Program Frequently Asked Questions 2018 Edition What is MACRA?...3 What is the Quality Payment Program?...3 How do payments work under the QPP?...3 What is at risk under
MACRA MACRA MACRA 9/30/2015. From the Congress: A New Medicare Payment System. The Future of Medicare: A Move Toward Value Driven Healthcare W20.
 W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
W20.8XXA The Future of Medicare: A Move Toward Value Driven Healthcare Emily L. Graham, RHIA, CCS-P VP, Regulatory Affairs, Hart Health Strategies Consultant, Coalition of State Rheumatology Organizations
Physician Compensation in an Era of New Reimbursement Models
 2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
2014 IHA Annual Membership Meeting Physician Compensation in an Era of New Reimbursement Models Taryn E. Stone Ice Miller LLP (317) 236-5872 taryn.stone@ Agenda Background New Reimbursement Models Trends
Here is what we know. Here is what you can do. Here is what we are doing.
 With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
With the repeal of the sustainable growth rate (SGR) behind us, we are moving into a new era of Medicare physician payment under the Medicare Access and CHIP Reauthorization Act (MACRA). Introducing the
ASCO s Payment Reform Model. Presenter John Hennessy Sarah Cannon
 ASCO s Payment Reform Model Presenter John Hennessy Sarah Cannon Consolidated Payments for Oncology Care Payment Reform to Support Patient-Centered Care for Cancer ASCO s Clinical Practice Committee Payment
ASCO s Payment Reform Model Presenter John Hennessy Sarah Cannon Consolidated Payments for Oncology Care Payment Reform to Support Patient-Centered Care for Cancer ASCO s Clinical Practice Committee Payment
Volume to Value Transition in the USA
 Volume to Value Transition in the USA Lee A. Fleisher, M.D. Robert D. Dripps Professor and Chair of Anesthesiology Perelman School of Medicine at the University of Pennsylvania Email: lee.fleisher@uphs.upenn.edu
Volume to Value Transition in the USA Lee A. Fleisher, M.D. Robert D. Dripps Professor and Chair of Anesthesiology Perelman School of Medicine at the University of Pennsylvania Email: lee.fleisher@uphs.upenn.edu
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
What s Next for CMS Innovation Center?
 What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
What s Next for CMS Innovation Center? A Guide to Building Successful Value-Based Payment Models Given CMMI s New Focus on Voluntary, Home-Grown Initiatives W W W. H E A L T H M A N A G E M E N T. C O
CPAs & ADVISORS. experience support // ADVANCED PAYMENT MODELS: CJR
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Andy M. Williams Partner BKD Eric M. Rogers Managing Consultant BKD Will McLeod VP of Patient Services McLeod Health Emily Adams Associate
Session V. The Numbers Game: Coding and Billing Applying MACRA to Cardio-Oncology Anita Arnold and Cathie Biga
 Session V The Numbers Game: Coding and Billing Applying MACRA to Cardio-Oncology Anita Arnold and Cathie Biga The Numbers Game Anita M. Arnold, DO FACC FSCAI MBA Medical Director: Cardio-Oncology Lee Health
Session V The Numbers Game: Coding and Billing Applying MACRA to Cardio-Oncology Anita Arnold and Cathie Biga The Numbers Game Anita M. Arnold, DO FACC FSCAI MBA Medical Director: Cardio-Oncology Lee Health
4/9/2016. The changing health care market THE CHANGING HEALTH CARE MARKET. CPAs & ADVISORS
 CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
CPAs & ADVISORS experience support // ADVANCED PAYMENT MODELS: CJR Eric. M. Rogers MEd. RT(R) Managing Consultant The changing health care market THE CHANGING HEALTH CARE MARKET HHS goal of 30% of traditional
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
Thank You to Our Sponsor!
 AMCP Webinar Emerging Physician Payment Models: What Does it Mean for AMCP Members and Medication Management? April 19, 2017 Thank You to Our Sponsor! 1 Disclaimer Organizations may not re use material
AMCP Webinar Emerging Physician Payment Models: What Does it Mean for AMCP Members and Medication Management? April 19, 2017 Thank You to Our Sponsor! 1 Disclaimer Organizations may not re use material
REPORT OF THE BOARD OF TRUSTEES
 REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
REPORT OF THE BOARD OF TRUSTEES B of T Report 21-A-17 Subject: Presented by: Risk Adjustment Refinement in Accountable Care Organization (ACO) Settings and Medicare Shared Savings Programs (MSSP) Patrice
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
The Healthcare Roundtable
 The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
The Healthcare Roundtable MACRA Update Jayme R. Matchinski Greensfelder, Hemker & Gale, P.C. April 7, 2017 New Orleans, Louisiana This presentation and outline are limited to a discussion of general principles
Statement for the Record. American College of Physicians. Hearing before the House Energy & Commerce Subcommittee on Health
 Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Statement for the Record American College of Physicians Hearing before the House Energy & Commerce Subcommittee on Health A Permanent Solution to the SGR: The Time Is Now January 21-22, 2015 The American
Legislative Update Wipfli CAH/RHC Conference
 Legislative Update Wipfli CAH/RHC Conference Nathan Baugh Director, Government Relations (202) 543-0348 Baughn@capitolassociates.org www.narhc.org Overview NARHC Washington Update MACRA Overview and Update
Legislative Update Wipfli CAH/RHC Conference Nathan Baugh Director, Government Relations (202) 543-0348 Baughn@capitolassociates.org www.narhc.org Overview NARHC Washington Update MACRA Overview and Update
May 25, SUBMITTED ELECTRONICALLY VIA Adam Boehler Deputy Administrator and Director
 May 25, 2018 SUBMITTED ELECTRONICALLY VIA DPC@cms.hhs.gov Adam Boehler Deputy Administrator and Director Center for Medicare and Medicaid Innovation ATTN: CMMI RFI on Direct Provider Contracting Models
May 25, 2018 SUBMITTED ELECTRONICALLY VIA DPC@cms.hhs.gov Adam Boehler Deputy Administrator and Director Center for Medicare and Medicaid Innovation ATTN: CMMI RFI on Direct Provider Contracting Models
Alternative Payment Models: Trends and Tactics for Success
 Alternative Payment Models: Trends and Tactics for Success James Michel Senior Director, Medicare Reimbursement & Policy American Health Care Association November 15, 2016 Discussion Review CMS priorities
Alternative Payment Models: Trends and Tactics for Success James Michel Senior Director, Medicare Reimbursement & Policy American Health Care Association November 15, 2016 Discussion Review CMS priorities
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
Specialty Payment Model Opportunities Assessment and Design
 Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Approved for Public Release. Distribution Unlimited.14.2286. CMS Alliance to Modernize Healthcare (CAMH) Specialty Model Opportunities Assessment and Design Cardiology Technical Expert Panel April 8, 2014
Paying for Outcomes not Performance
 Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Paying for Outcomes not Performance 1 3M. All Rights Reserved. Norbert Goldfield, M.D. Medical Director 3M Health Information Systems, Inc. #Health Information Systems- Clinical Research Group Created
Episode Payment Models:
 Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
Episode Payment Models: Cardiac Bundle Initiative HFMA Florida Chapter (North Florida) October 25, 2016 Robert Howey MBA, MHA, CPA Revenue Cycle Manager 2016 MFMER slide-1 Objective After the session,
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
CMS Oncology Care Model s Standards for Patient Navigation
 CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
CMS Oncology Care Model s Standards for Patient Navigation Nikolas Buescher Executive Director of Cancer Services Penn Medicine, Lancaster November 13, 2017 Ann B Barshinger Health Cancer Institute scale
Value-Based Reimbursements are Here: Are you Ready?
 Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
Value-Based Reimbursements are Here: Are you Ready? White Paper ELLIS MAC KNIGHT, MD Senior Vice President/CMO Published by Becker s Hospital Review April 2016 White Paper Value-Based Reimbursements are
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation
 New Member Orientation") SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
SVS QUALITY AND PERFORMANCE MEASURES COMMITTEE (QPMC) New Member Orientation 2017-2018 SVS QPMC Quality and Performance Measures Committee Policy and Advocacy Council (Chair Sean Roddy) Chair: Brad Johnson,
Pathways for Physician Success in Accountable Care Organizations
 Pathways for Physician Success in Accountable Care Organizations and Healthcare Reform Harold D. Miller Executive Director Center for Healthcare Quality and Reform July 16, 2011 Everybody s Talking About
Pathways for Physician Success in Accountable Care Organizations and Healthcare Reform Harold D. Miller Executive Director Center for Healthcare Quality and Reform July 16, 2011 Everybody s Talking About
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model
 Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
Questions and Answers on the CMS Comprehensive Care for Joint Replacement Model MEGGAN BUSHEE, ESQ. 704.343.2360 mbushee@mcguirewoods.com 201 North Tryon Street, Suite 3000 Charlotte, North Carolina 28202-2146
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM
 THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
THE ALPHABET SOUP OF MEDICAL PAYMENTS: WHAT IS MACRA, VBP AND MORE! Lisa Scheppers MD FACP Margo Ferguson MT MSOM THE REASON FOR CHANGE VOLUME TO VALUE Fee-for-service PAYMENT Bundled, Shared Patient FOCUS
Moving to VBP through MACRA and Other Policies May 18, Cynthia Brown VP, Government Affairs
 Moving to VBP through MACRA and Other Policies May 18, 2017 Cynthia Brown VP, Government Affairs Overview State of play for practices and payments Physicians perspective on today s value-based payment
Moving to VBP through MACRA and Other Policies May 18, 2017 Cynthia Brown VP, Government Affairs Overview State of play for practices and payments Physicians perspective on today s value-based payment
Telemedicine and Health Reform. Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center
 Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Telemedicine and Health Reform Jonathan Neufeld, PhD Clinical Director Upper Midwest Telehealth Resource Center 1 telehealthresourcecenters.org Links to all TRCs National Webinar Series Reimbursement,
Surviving and thriving in the time of MACRA: What you need to know now to optimize your future.
 Surviving and thriving in the time of MACRA: What you need to know now to optimize your future. Risk Adjustment in the Resource Use Performance Measures 2017 SGIM Annual Meeting Thursday, April 20, 2017
Surviving and thriving in the time of MACRA: What you need to know now to optimize your future. Risk Adjustment in the Resource Use Performance Measures 2017 SGIM Annual Meeting Thursday, April 20, 2017