Review of due diligence undertaken by PWC January 2014
|
|
|
- Marion Porter
- 5 years ago
- Views:
Transcription
 2. The findings of the original due diligence: a.")
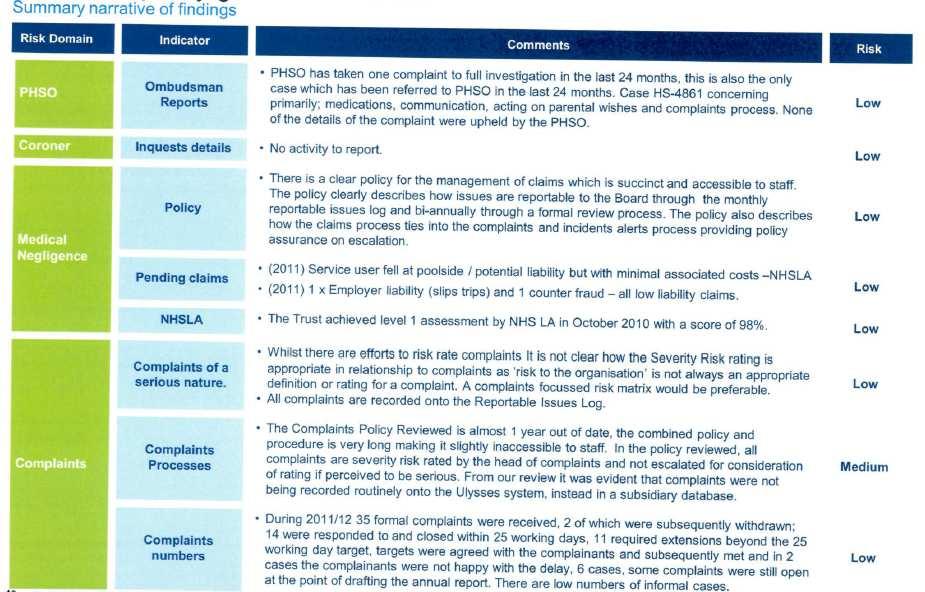
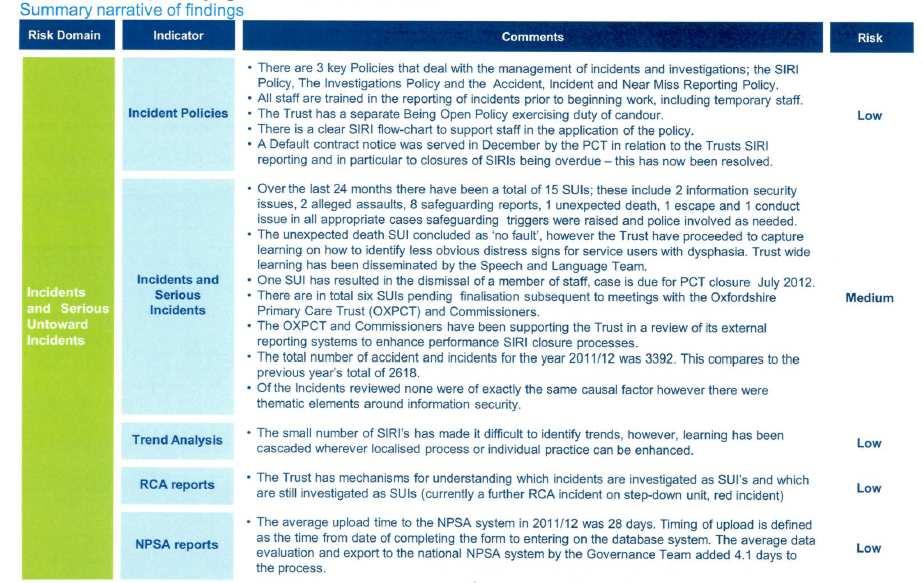
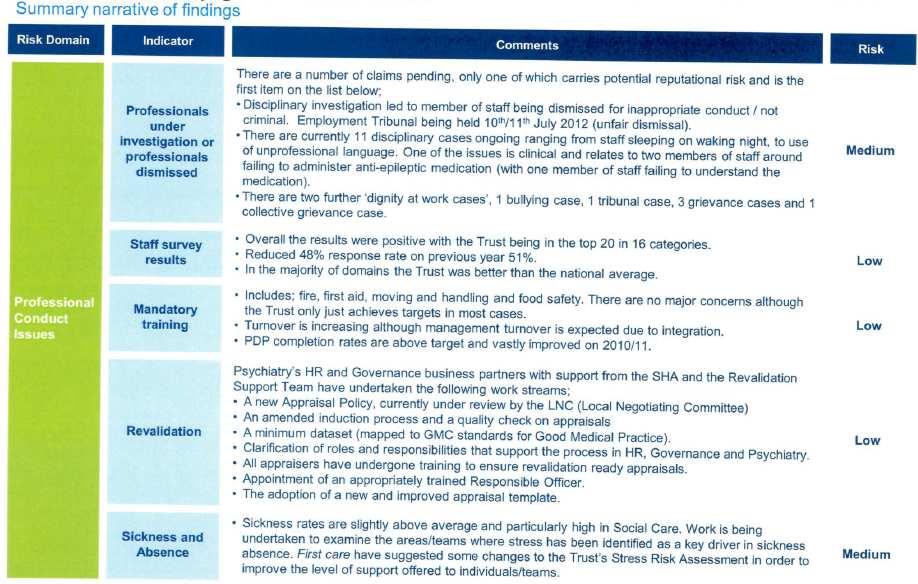
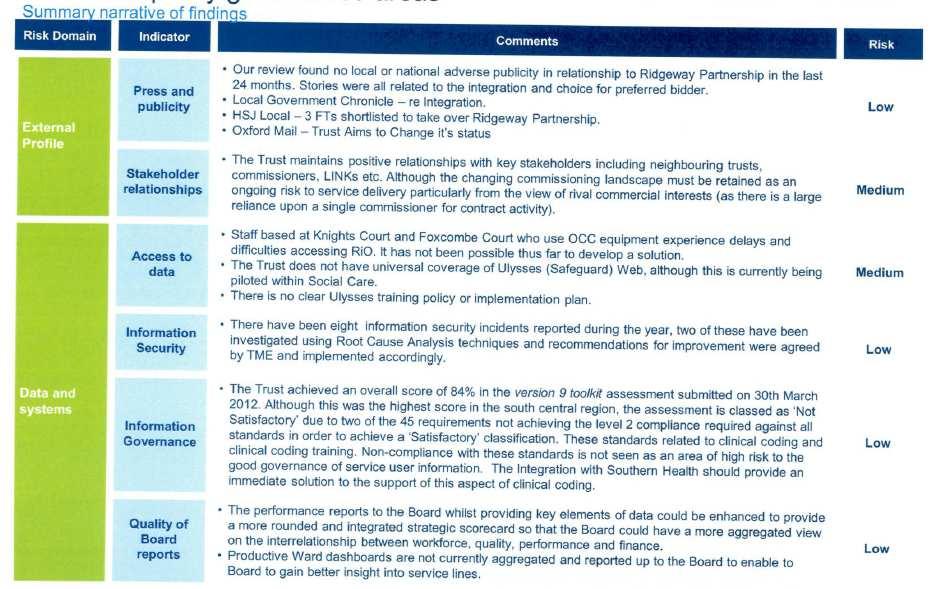
1 FOI615 FOI request concerning the due diligence undertaken on the acquisition of Oxfordshire Learning Disability Trust (OLDT) and the subsequent review of that due diligence. This response includes details of the following: 1. The review of the due diligence completed by PWC in January 2014 (pg.2) 2. The findings of the original due diligence: a. KPMG Phase 1 review completed in December 2011 before the Trust was awarded preferred bidder status (pg.6) b. KPMG Phase1b review also completed in December 2011 before the Trust was awarded preferred bidder status (pg.16) c. KPMG Phase 2 review completed in June 2012 once the Trust had been awarded preferred bidder status (pg.19) d. Deloitte review completed in May 2012 once the Trust had been awarded preferred bidder status (pg.29) e. In-house review carried out over several months and completed in November 2012 (pg.38) Details of the scope of each review and the findings and recommendations are provided under each of the different headings below. 1
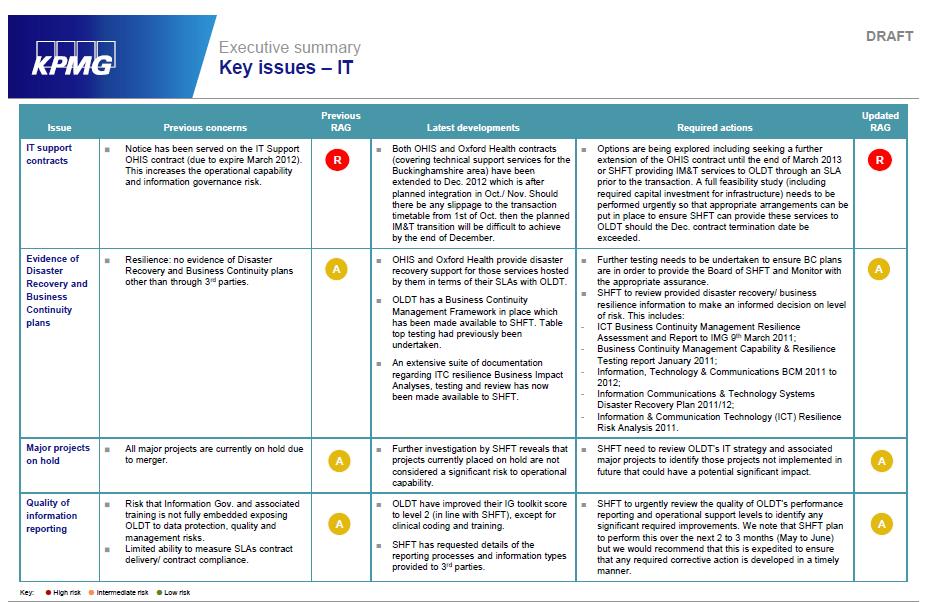
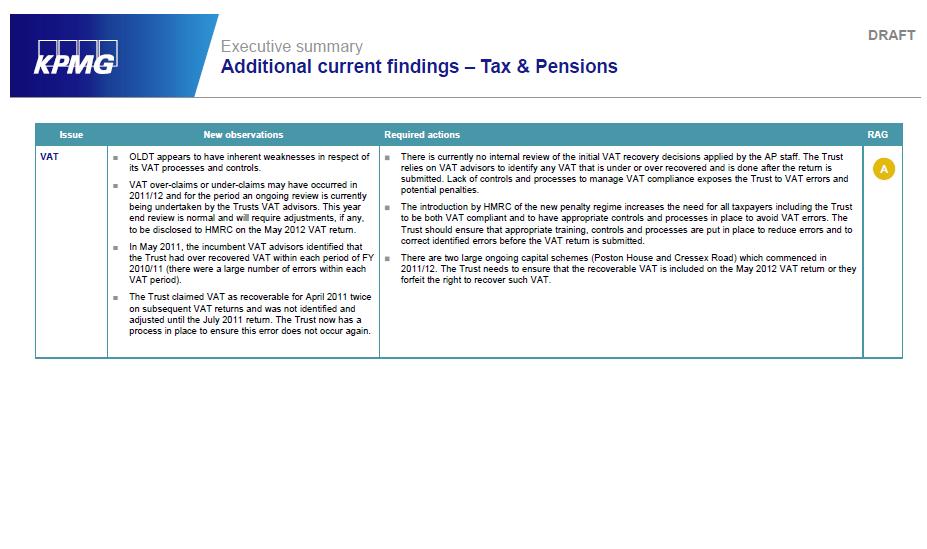
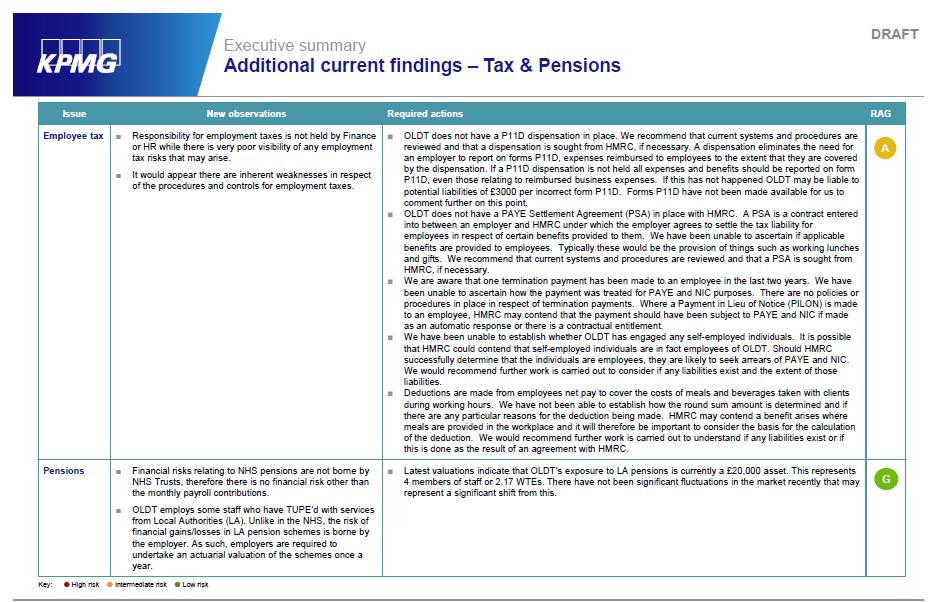
2 Review of due diligence undertaken by PWC January 2014 Scope The deliverable was intended to include the following: The planned scope of the due diligence on Ridgeway compared to the NHS Transactions Manual for providers and commissioners of NHS services (published February 2009) and the Addendum to the Transaction Manual (published October 2010); The actual scope of the due diligence on Ridgeway compared to the NHS Transactions Manual for providers and commissioners of NHS services (published February 2009) and the Addendum to the Transaction Manual (published October 2010); Whether any areas of the planned due diligence were not carried out and whether this was flagged in reports to the Board in its meetings between November 2011 to November 2012; What risks were flagged in the due diligence reports to the Board in its meetings between November 2011 to November 2012; Stakeholders (as set out above) views on the due diligence exercise; and Recommendations for future due diligence exercises. Findings Some initial due diligence was performed in December 2011 by KPMG and, following the announcement of the Trust as the preferred bidder in March 2012, more detailed due diligence was performed by KPMG, Deloitte and an in house specialist Learning Disabilities team. A number of reports were considered by the Trust Board in May and June 2012 and at other times throughout the period covered by the review. KPMG was commissioned by the Trust to provide financial, legal, estates and workforce due diligence with Deloitte being commissioned to provide a high level assessment against Monitor s Quality Governance Framework. In addition, the Trust s in-house team also undertook some due diligence procedures at Ridgeway which, although these did not directly correspond to the requirements as set out in the manual, consisted of a review to provide assurance relating to quality, safety and engagement. Since some of the due diligence process took place more than two years ago, a number of members of staff who were heavily involved in the transaction have left the Trust. The level of staff change, combined with incomplete central retention of documents by the Trust, made it difficult to establish a complete picture of events that occurred during the period covered by the review. There were 4 main findings from the review summarised below: 1. There were comprehensive project plans in place for the transaction, including due diligence, but these were not clearly linked through to the 2
3 certification that the Board made to Monitor. The Trust provided the reviewers with a number of documents which together formed an overall project plan for the transaction, including the due diligence requirements, governance and timetable. The review of Board minutes did not find evidence that the plans went, in aggregate, to the Board for approval, but it was understood from interviews with Board members that they felt fully informed in relation to the transaction governance, due diligence and timetable. The Trust mobilised nine individual project work streams to deliver the transaction and each work stream had its own set of project plans and action logs. The work stream leads met on a weekly basis to discuss progress and there were monthly programme Board meetings. The Trust s Investment Committee undertook detailed scrutiny of the transaction in the year leading up to the transaction date and made recommendations to the Board. A high level milestone plan was presented to the Board at its monthly meetings to summarise progress to date and matters arising. It was noted that the work undertaken by Deloitte and KPMG covered many of the areas of the indicative scopes included in the Manual, but it was not clear whether the Trust had consciously decided that other elements were not necessary given the scale and nature of the transaction, or whether commissioning of due diligence on these areas was omitted in error. In the course of interviews with staff and Board members the reviewers were told that the Board was comfortable that sufficient work had been undertaken for it to make the required certifications to Monitor, but the reviewers were not able to find written evidence within minutes and other documents that clearly linked the project plan, the due diligence outputs and the action plans to the certifications made by the Board to Monitor. 2. Some findings within the due diligence report, which were included in the Trust s subsequent action plans, also appear in the recent CQC report on Slade House. There were key themes within the Deloitte Quality Governance report and the in-house Quality and Safety Review report that also appear in the CQC report at Slade House. These points were captured in the action plans that were prepared by the Trust in response to the due diligence findings but the fact that these issues continued to exist at the time of recent CQC inspection indicates that the action plans were not sufficient to fully, and permanently, address the issues identified. It was noted that some of the actions, particularly around changes to service models, may have taken a longer period of time to fully implement than then interval between the transaction date and the CQC report, and would have been dependent on commissioner agreement. 3
4 3. The implementation of actions identified in response to the due diligence reviews were not monitored routinely by the Board after the transaction date. An action plan developed post implementation was reported to the Trust s Quality Improvement and Development Forum in March 2013, five months after acquisition. This was not presented to the Trust Board. A number of action plans address the findings of each of the pieces of due diligence, but it was not clear how the implementation of these plans was monitored after the transaction date and it is understood that changes in Trust staff contributed to slippage in the implementation of actions. 4. Board challenge and debate in relation to the transaction could have been more thoroughly minuted. The most cited transaction risks known at the time of the transaction, as recollected by the individuals we interviewed, were: Poor financial performance of Ridgeway; An outdated operating model at Ridgeway; The geographical distance of Ridgeway from the rest of the Trust; and The Trust s management capacity, which was under pressure due to the ongoing integration work following the acquisition on 1 April 2011 by Hampshire Partnership NHS Foundation Trust of Hampshire Community Health Care NHS Trust and also the diversity of services provided by the Trust. These risks were evidenced as being presented to the Board during its meetings between November 2011 and November 2012, however, minuted discussion was limited. Recommendations 1. when considering future transactions, the Board should determine, and clearly set out in a written record, what information and assurances it requires in order to: a) Make a decision to approve the transaction b) To sign the declarations required by Monitor c) Discharge any other related duties that arise for the specific transaction. Once the Board has determined its requirements, these should be formulated into a project plan setting out responsibilities for providing the required information and assurances and the timeframes. The project plan should be clearly mapped to the requirements of regulators, legislation and any other applicable guidance. 2. the Board (and relevant sub-committees) should consider how information is evaluated in the future. Consideration of what may be seemingly low risk or insignificant observations could, when taken in conjunction with other observations, be a signal of something more serious. In future due diligence exercises, the read-across between different elements of work by appropriately skilled individuals should be built into the project plan to ensure that appropriate triangulation takes place on a timely basis allowing a fuller identification and mitigation of risks. 4
5 3. The Trust should ensure that key decisions, processes and considerations are effectively documented to ensure that knowledge is retained within the organisation. Where action plans are developed, an Executive Lead should be assigned and for a transaction of this nature and size, consideration should also be given to whether a Non-Executive Lead also should be assigned. Action plans should be prepared on a timely basis and should cover all relevant internal and external risks. 4. There is a disconnect between the minuted discussions at Board and the recollection of Board members of the debate and challenge surrounding the transaction decision-making. This may be reflective of some gaps in the minutes of meetings and/ or the fact that some information and discussion occurred outside the Board room, for example in the Investment Committee. In the future the Trust should endeavour to ensure that good governance can be demonstrated by retaining complete and accurate evidence of Board information and debate. Note: PWC would like it noted that their report was addressed to, and prepared solely for, Southern Health NHS Foundation Trust and was not prepared with the interests of anyone other than Southern Health NHS Foundation Trust in mind. On this basis, PricewaterhouseCoopers LLP does not accept any duty or responsibility to anyone else. 5
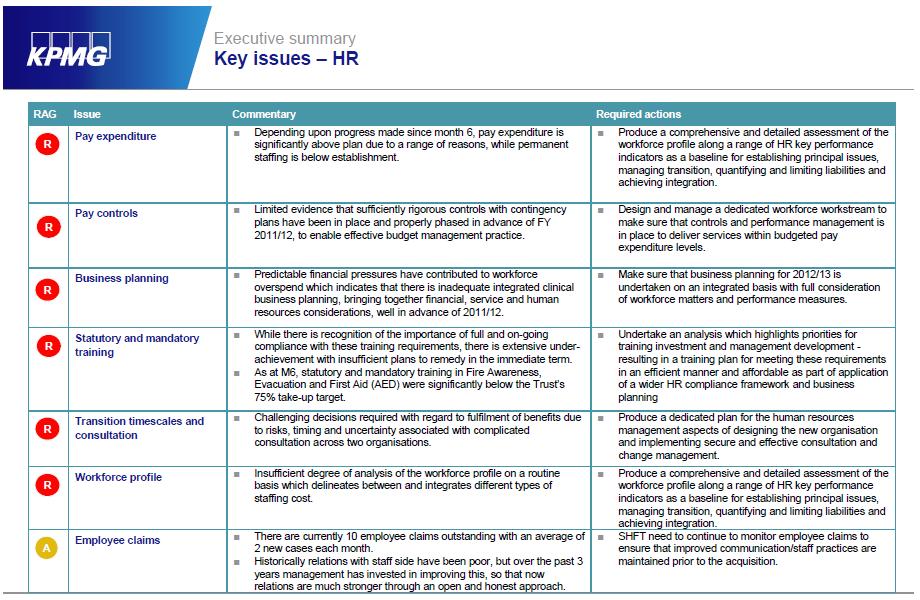
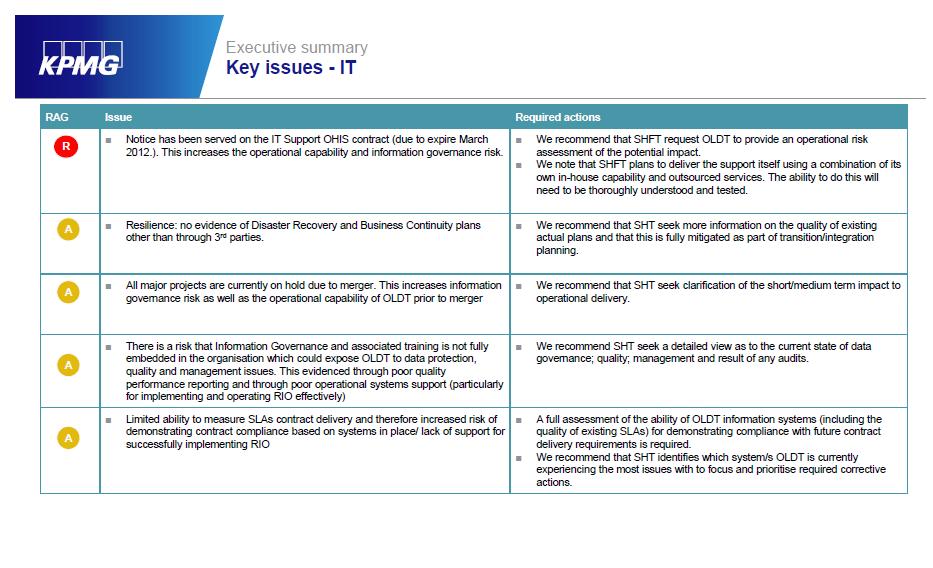
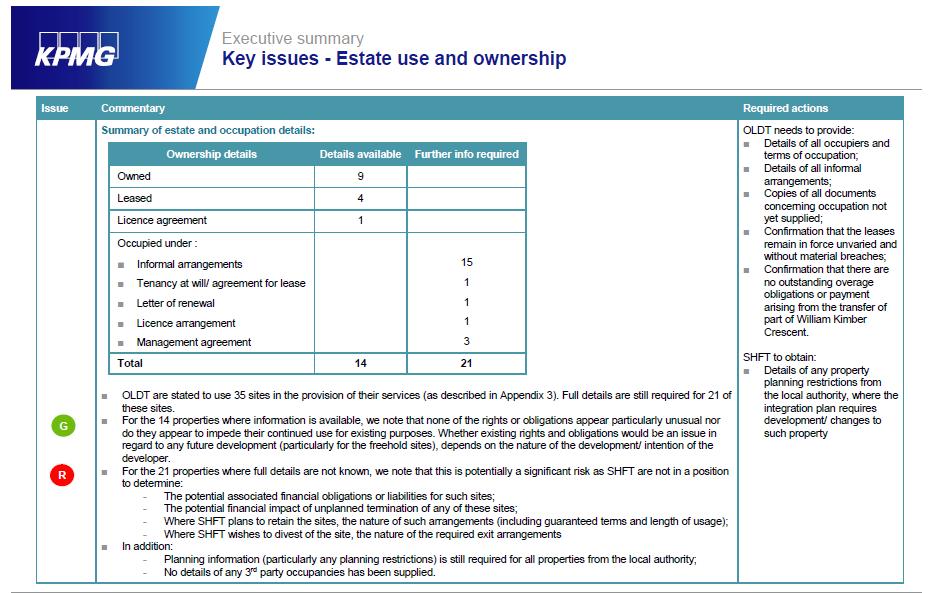
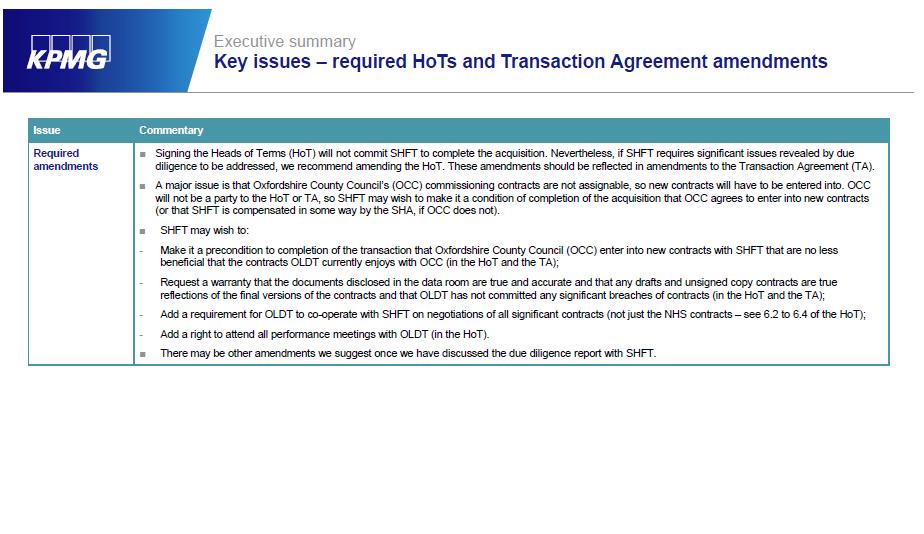
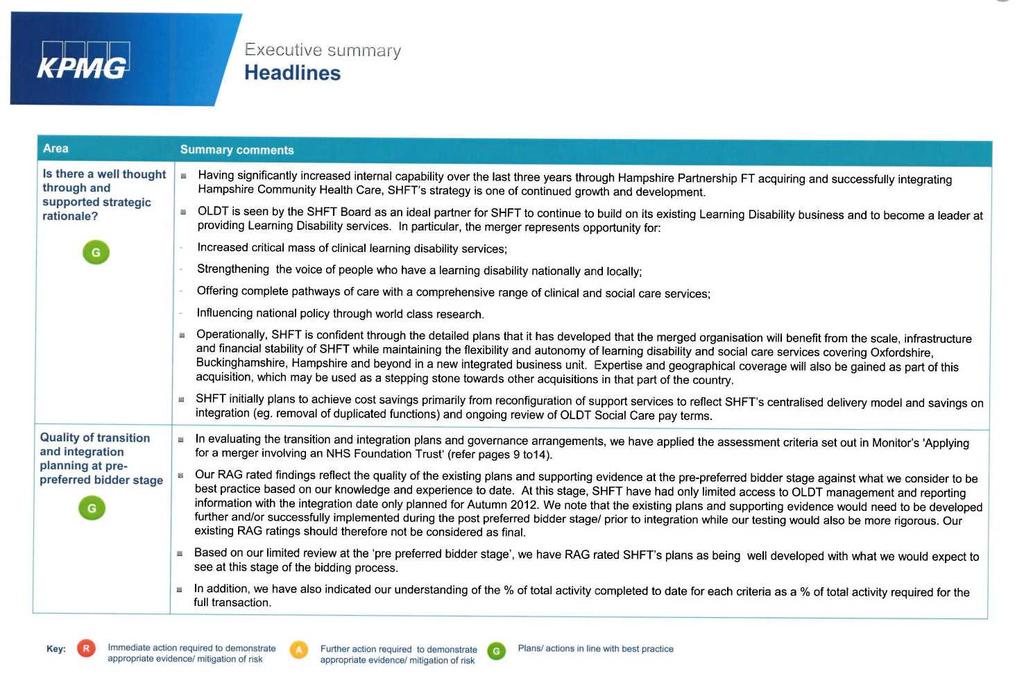
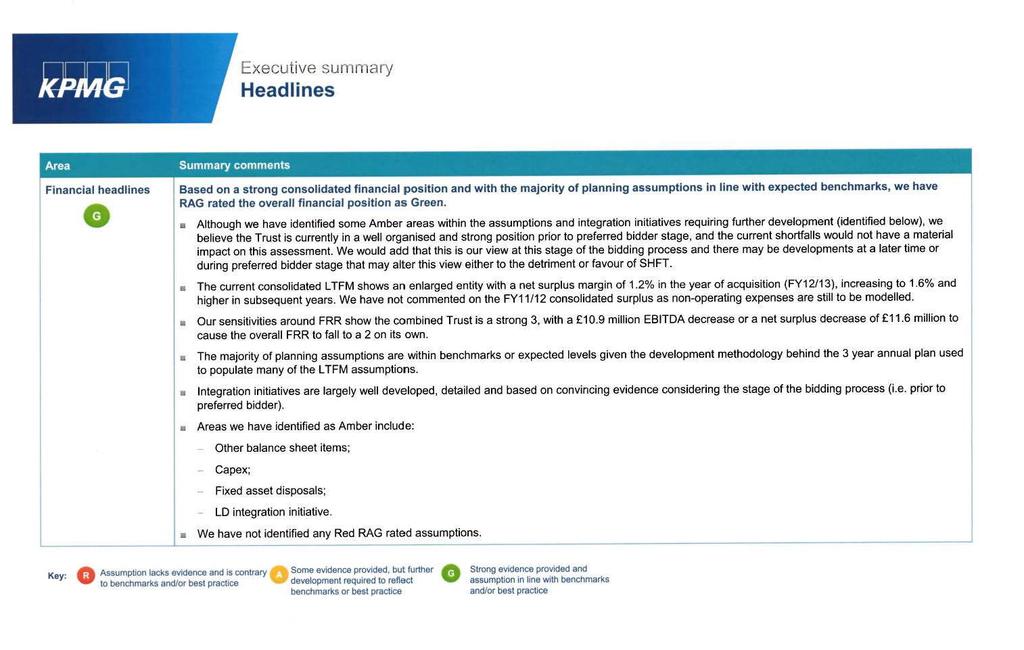
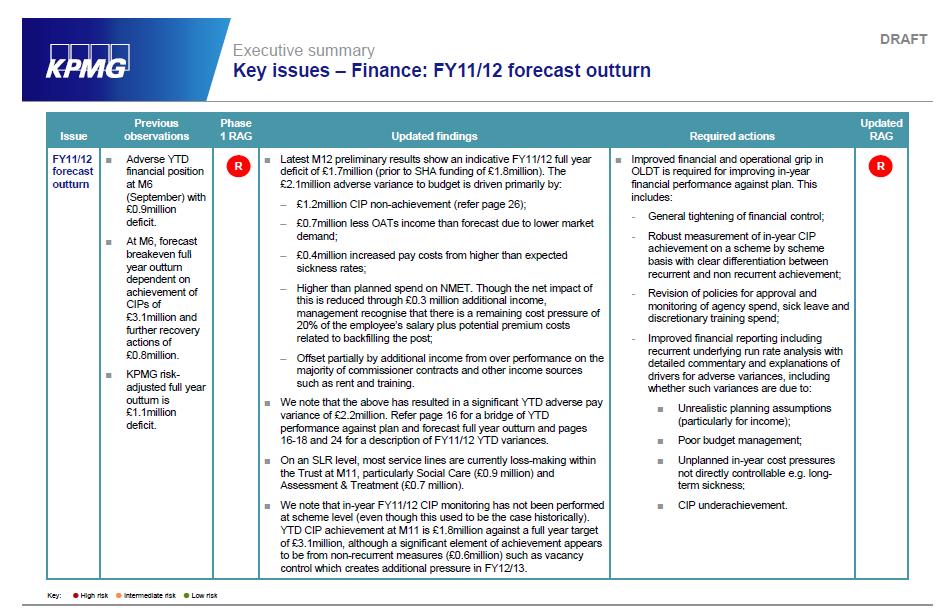
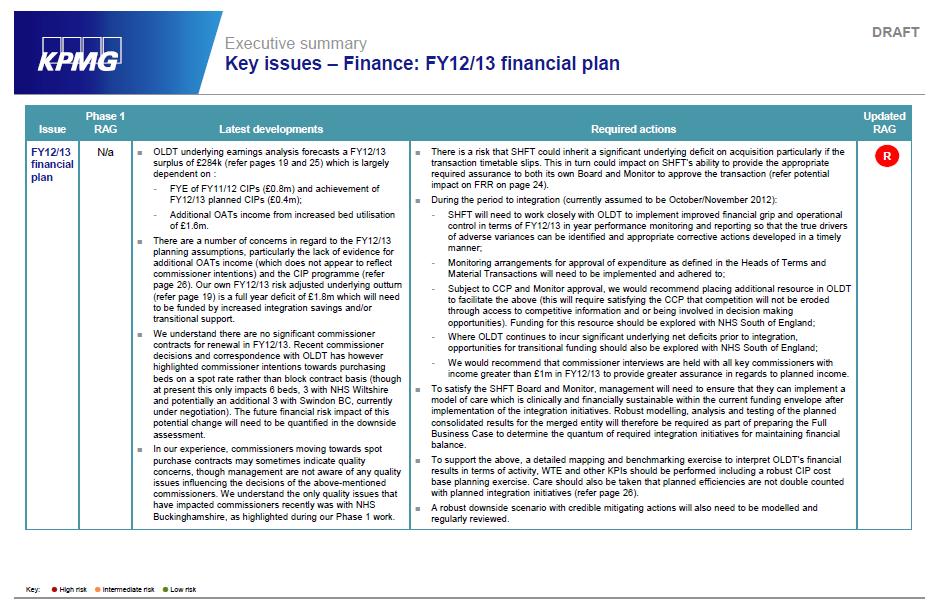
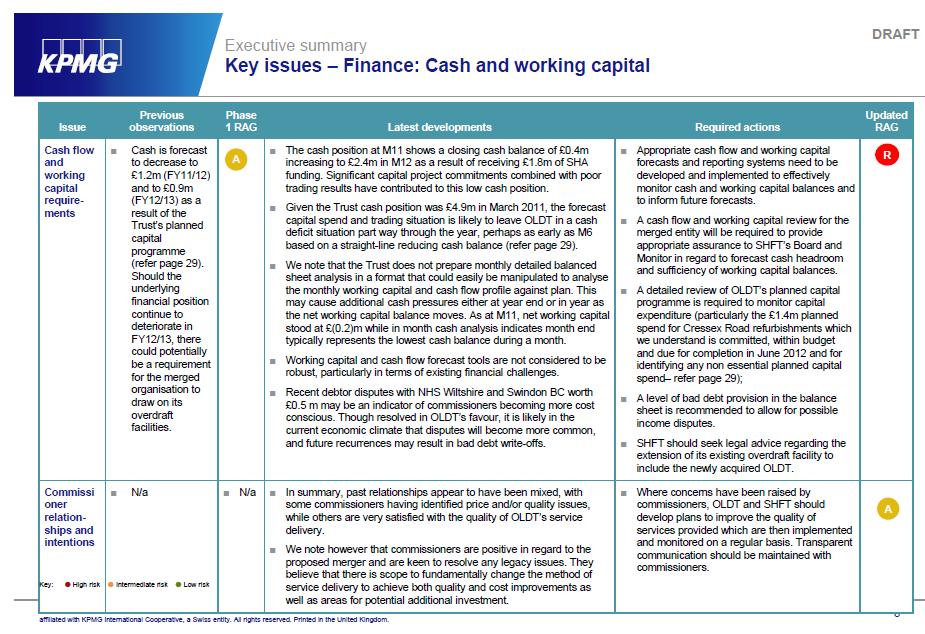
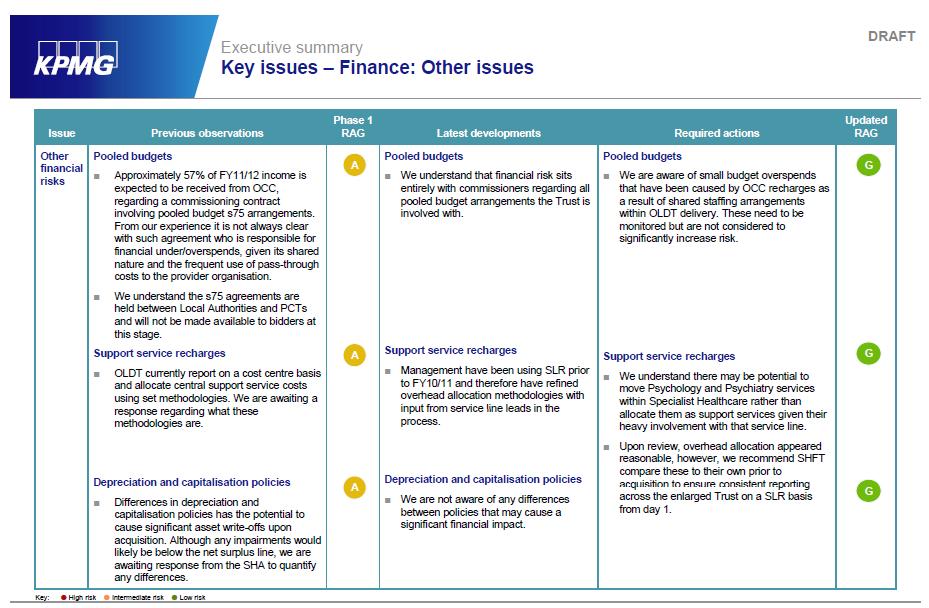
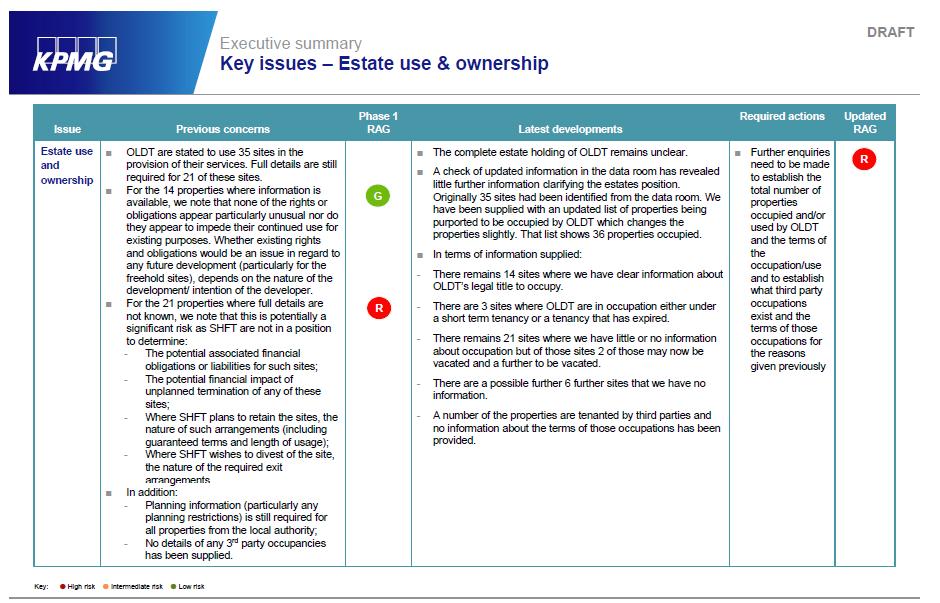
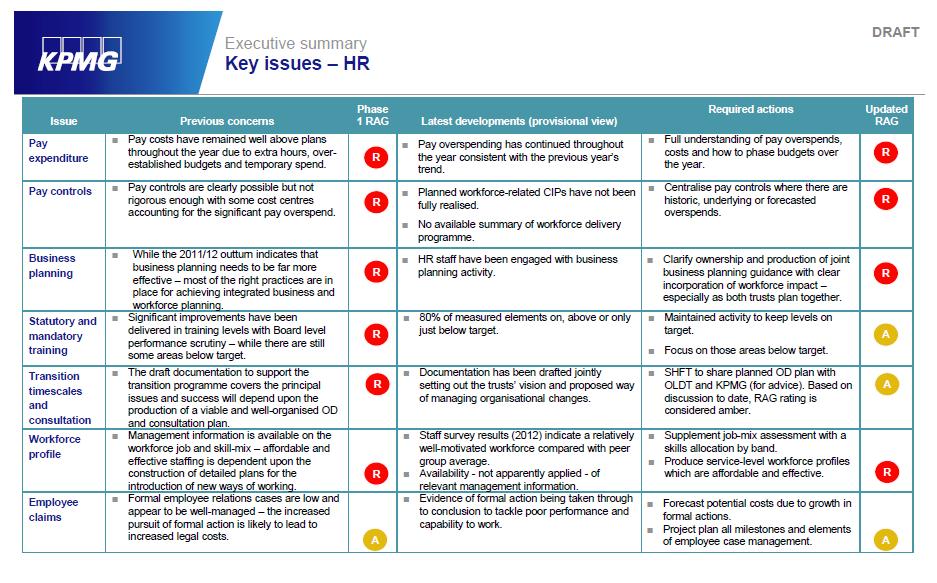
6 KPMG Phase 1 Pre-transaction due diligence Scope The scope of work was limited to high level financial due diligence of information available in the OLDT data room, publically available information and conversations with SHFT workstream leads. The primary purpose of the work was to identify significant potential risks prior to submission of the ISDP and consequent further required actions should SHFT be appointed as preferred bidder. Phase 1 work should therefore not be interpreted to constitute a historic due diligence or the provision of assurance that SHFT should enter into the transaction prior to detailed further due diligence and integration planning and testing to be performed post preferred bidder status. Findings and recommendations These are summarised on the following pages
7 7
8 8
9 9

10 10
11 11
12 12
13 13
14 14
15 15
16 KPMG Phase 1b Analysis of Southern Health integration initiatives in relation to the potential acquisition of OLDT Scope The scope of work for phase 1b was limited to attending internal SHFT challenge sessions and performing a short high level analysis of the robustness of key integration and modelling assumptions and the capability of SHFT to implement the initiatives. The primary purpose of the work was to identify significant potential risks prior to submission of the ISDP and consequent further required actions should SHFT be appointed as preferred bidder. The work should not be interpreted to constitute a detailed review or the provision of assurance that SHFT should enter into the transaction prior to detailed further due diligence and integration planning and testing to be performed post preferred bidder status. Findings and recommendations These are summarised on the following pages
17 17
18 18
19 KPMG Phase 2 due diligence on the acquisition of Oxford Learning Disability NHS Trust Scope The primary purpose of the final Phase 2 work was to identify what had changed in regards to risks identified in the Phase 1 report, to identify any further additional potential risks that may have arisen in the intervening period to May 2012, and to recommend appropriate required actions necessary to remedy such risk. KPMG were not engaged to perform any clinical due diligence review. Findings and recommendations These are summarised on the following pages
20 20
21 21
22 22
23 23
24 24
25 25
26 26
27 27
28 28
29 Deloitte Quality Governance Integration Review Scope An independent high level assurance review of quality governance at Ridgeway Partnership NHS Trust which included: An analysis of the Trust s overarching compliance with the Monitor Quality Governance Framework A detailed assessment of any adverse outcomes, compliance issues, or limited assurance issues to support due diligence processes Recommendations in relation to any perceived gaps rated in accordance with associated governance risks and prioritised accordingly. Findings: These are summarised on the following pages
30 30
31 31
32 32
33 33
34 34
35 35

36 Quality Governance Framework Summary 36
37 37
38 In-house review In addition to the above mentioned formal due diligence, the Trust also took it upon itself to carry out an additional review relating to quality, safety and engagement. This work continued right up to the point of transaction in November 2012 and as such was not part of the formal due diligence. Findings and recommendations: A number of areas of good practice were identified and a number of recommendations for improvement were made which included further explorative and developmental activity. A summary Analysis and Recommendations from the Review are included in the following pages. Action plans were subsequently developed within the division to begin addressing the identified gaps. 38
39 Summary Analysis and Recommendations from in-house Clinical Quality Review Initiated December 2012 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations 1. Record Keeping Matron Walk Round Tool High Risk Patient Review Mock CQC CQC - Multi-disciplinary team (MDT) working - Planning and delivering person centred care - Clinical governance & patient safety - Workforce & staff training - Clinical Leadership - Record Keeping - Policy Implementation - Care Planning Recommendation: It is recommended that the use of RiO and secondary files could be reviewed to ensure that all information is consistently recorded and available to all clinicians. There is an opportunity to utilise and further develop RiO guidance to ensure that its use is consistent and meaningful. In addition the use of secondary files to record information which cannot be recorded onto RiO should be standardised. The standards applied to clinical record keeping should be done consistently across the service and there is an opportunity to collaborate with staff in SHFT to develop consistent practice that supports Learning Disability clinical assessment and treatment. 2. Multi-disciplinary Working Matron Walk Round Tool High Risk Patient Review Mock CQC - Multi-disciplinary team (MDT) working - Planning and delivering person centred care - Clinical governance & patient safety - A meaningful day - Workforce & staff training - Clinical Leadership 39
40 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations - Supervision - Record Keeping - Policy Implementation - Attitudes/ Culture - Care Planning - Communication Recommendation: It is recommended that the MDT approach to practice is reviewed to ensure that the collaborative approach to assessment and treatment is clearly documented and reflected within MDT plans and CPA. In addition all clinicians should be able to access all relevant clinical records. 3. Risk Assessment & Risk Management Matron Walk Round Tool High Risk Patient Review Mock CQC - Multi-disciplinary team (MDT) working - Planning and delivering person centred care - Clinical governance & patient safety - Supervision - Record Keeping - Policy Implementation - Care Planning Recommendation: It is recommended that clinical risk assessment and management processes are reviewed to ensure consistent approaches and record keeping. The 5x5 risk assessment process although effective has not translated well across to the RiO risk assessment record. The clinical risk assessment approach in community teams needs to be improved, particularly where patients are presenting risks to themselves or others and/ or have complex needs. A collaborative approach to clinical risk assessment and management should be evidenced within records.. Care plans should be updated in line with changes to risk assessment and management plans. 4. Capacity & Consent Matron Walk Round Tool - Multi-disciplinary team (MDT) working 40
41 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations High Risk Patient Review Mock CQC CQC - Planning and delivering person centred care - Record Keeping - Policy Implementation Recommendation: It is recommended that the actions to ensure that capacity and consent is recorded for all patients should be rolled out across all services to ensure a consistent approach where this applied particularly where patients are subject to the MHA. 5. Physical Health Monitoring Matron Walk Round Tool High Risk Patient Review Mock CQC - Multi-disciplinary team (MDT) working - Planning and delivering person centred care - Workforce & staff training - Clinical Leadership - Re cord Keeping - Policy Implementation - Care Planning Recommendation: It is recommended that the Physical Assessment and Monitoring policy recently launched within SHFT is rolled out across all OLDT services. This would also link to other relevant policies such as the Slips Trips & Falls Policy. This would ensure that physical assessment is clinically recorded in a consistent way and that when monitoring is required this is also recorded in a more appropriate way. Appropriate care plans should be devised in relation to physical health care. LD staff within SHFT have benefitted from more focussed training in relation to physical assessment and monitoring and training needs should be considered for OLDT staff accordingly. 6. Nutrition Matron Walk Round Tool - Multi-disciplinary team (MDT) working - Planning and delivering person centred care - Workforce & staff training - Clinical Leadership 41
42 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations - Re cord Keeping - Policy Implementation - Care Planning Recommendation: It is recommended that nutrition focussed assessments are completed for all in-patients and appropriate application of nutrition assessment should be considered for community patients. The use of the MUST tool should be used consistently across services. 7. Clinical Pathways/ Evidence Base Matron Walk Round Tool High Risk Patient Review Mock CQC SHA Review - Multi-disciplinary team (MDT) working - Planning and delivering person centred care - A meaningful day - Environment and facilities - Workforce & staff training - Organisational structure and culture - Commissioning - Clinical governance & patient safety - Clinical Leadership - Supervision - Record Keeping - Policy Implementation - Attitudes/ Culture - Care Planning Recommendation: It is recommended that the ongoing work related to clinical pathways continues and that clinical pathways or maps are developed to provide a consistent approach to assessment and treatment. This would also help to inform focussed training development in line with appropriate expectations of competence for professionals and ensure consistent recording of assessment and treatment processes. The evidence base exists in both SHFT and OLDT and a consistent approach would help to identify the packages of care/ 42
43 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations assessment and treatment made available to patients which will help inform commissioners/ partners of what assessment and treatment is being purchased, expected outcomes and time frames. 8. Measuring Patient Experience Matron Walk Round Tool - Organisational structure and culture - Commissioning - Clinical governance & patient safety - Policy Implementation - Attitudes/ Culture Recommendation: It is recommended that the patient experience is evaluated in a consistent and meaningful way. There was evidence of good practice which could be further developed in partnership with SHFT colleagues to ensure that the experiences of service users are gathered regularly and help to inform the agenda of continuous improvement. 9. Clinical Supervision & Management Supervision Matron Walk Round Tool High Risk Patient Review Mock CQC - Multi-disciplinary team (MDT) working - Workforce & staff training - Organisational structure and culture - Clinical governance & patient safety - Clinical Leadership - Supervision - Policy Implementation - Attitudes/ Culture Recommendation: It is recommended that arrangements for both clinical and management supervision are reviewed to ensure that both can occur on a regular basis every month. The review could include the different models and formats of supervision which could be available. 10. Mental Health Act/ Mental Matron Walk Round Tool - Multi-disciplinary team (MDT) working 43
44 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations Health Care High Risk Patient Review Mock CQC CQC - Planning and delivering person centred care - A meaningful day - Environment and facilities - Workforce & staff training - Organisational structure and culture - Commissioning - Clinical governance & patient safety Recommendation: It is recommended that a review of policies related to observation, section 17 leave and locked doors is undertaken with regard to the responsibilities of nurses in caring for patients detained under the MHA. Areas of good practice should be modelled consistently across the service. 11. Environment Matron Walk Round Tool High Risk Patient Review Mock CQC CQC Recommendation: - Environment and facilities - Clinical governance & patient safety It is recommended that a review for the management of the environment is undertaken which includes regular safety reviews and ligature assessments with appropriate development or management plans put into place. 12. Medical Devices Matron Walk Round Tool Mock CQC - Environment and facilities - Workforce & staff training - Clinical governance & patient safety - Policy Implementation Recommendation: It is recommended that the medical devices policy is reviewed to ensure that appropriate inventory, maintenance and calibration occurs of medical devices. The practice at Postern House could be replicated in each service with a member of staff designated as the lead for medical devices. 44
45 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations 13. Dress Code Matron Walk Round Tool Mock CQC - Environment and facilities - Workforce & staff training - Organisational structure and culture - Clinical governance & patient safety - Clinical Leadership - Supervision - Policy Implementation - Attitudes/ Culture Recommendation: It is recommended that the policy related to dress code is reviewed to ensure that it is appropriate to the clinical environments and that staff are aware of the various rationales related to the implementation of a dress code policy. 14. Learning Out of Concerns Matron Walk Round Tool Mock CQC CQC SHA Review - Workforce & staff training - Organisational structure and culture - Commissioning - Clinical governance & patient safety - Clinical Leadership - Supervision - Policy Implementation - Attitudes/ Culture - Communication Recommendation: It is recommended that regular internal reviews and checks are undertaken which involve staff at the ward level e.g. Conducting the monthly Matron Walk Round Tool, undertaking care plan audit etc which engages staff and allows them to develop improvements as a team within their own clinical environments. Learning from investigations, audit and reviews should be shared regularly in both formal and informal ways which 45
46 Theme Evidenced In External Review/ OLDT Potential SIRI Themes/ Winterbourne View Recommendations involve staff and patients at the ward/ team level so they may be engaged in team led development and improvement with appropriate facilitation and support. 46
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
Report. Leigh House, Specialised Services Winchester
 Report Leigh House, Specialised Services Winchester Thursday 23 rd February 2012 Overall Impression Leigh house appeared to have a calm and relaxed atmosphere with a non-clinical feel, a nice environment
Report Leigh House, Specialised Services Winchester Thursday 23 rd February 2012 Overall Impression Leigh house appeared to have a calm and relaxed atmosphere with a non-clinical feel, a nice environment
Level 2: Exceptional LEP Review Visit by School Level 3: Exceptional LEP Trigger Visit by Deanery with Externality... 18
 Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
Postgraduate Training Ongoing Quality Review and Enhancement Framework Version 1: 2010 Contents Contents... 2 PMET Quality Review Framework Introduction... 3 Introduction... 3 Postgraduate Training Quality
The Care Values Framework
 The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
PATIENT AND SERVICE USER EXPERIENCE STRATEGY
 PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
PATIENT AND SERVICE USER EXPERIENCE STRATEGY APRIL 2017 TO MARCH 2020 Date 24 March 2017 Version Final Version Previously considered by The Patient Experience Group version 0.1 draft The Executive Management
NHS 111 Clinical Governance Information Pack
 NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
NHS 111 Clinical Governance Information Pack This pack is designed to help you develop your local NHS 111 clinical governance framework and explain how it fits in to the wider context. It takes you through
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
REQUIREMENT. Identify a minimum of 4 theme areas which are considered to have caused concern for patients during 2012/13
 2012/13 SSOTP CQUIN INDICATOR TARGETS INDICATOR REQUIREMENT 1. Patient Experience Milestone 1 (15th working day of April 2012) Identify a minimum of 4 theme areas which are considered to have caused concern
2012/13 SSOTP CQUIN INDICATOR TARGETS INDICATOR REQUIREMENT 1. Patient Experience Milestone 1 (15th working day of April 2012) Identify a minimum of 4 theme areas which are considered to have caused concern
Quality Assurance Accreditation Scheme Assignment Report 2016/17. University Hospitals of Morecambe Bay NHS Foundation Trust
 Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Special Measures Action Plan. Norfolk and Suffolk NHS Foundation Trust
 Special Measures Action Plan Norfolk and Suffolk NHS Foundation Trust June 2015 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver 1 Norfolk and Suffolk NHS Foundation
Special Measures Action Plan Norfolk and Suffolk NHS Foundation Trust June 2015 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver 1 Norfolk and Suffolk NHS Foundation
Northumberland, Tyne and Wear NHS Foundation Trust. Board of Directors Meeting. Meeting Date: 25 October Executive Lead: Rajesh Nadkarni
 Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
Agenda item 9 ii) Northumberland, Tyne and Wear NHS Foundation Trust Board of Directors Meeting Meeting Date: 25 October 2017 Title and Author of Paper: Clinical Effectiveness (CE) Strategy update Simon
DR KUMAR CQC INSPECTION ACTION PLAN
 DR KUMAR CQC INSPECTION ACTION PLAN REVIEWED: 28 TH DECEMBER 2015 RED NOT COMPLETED AMBER STARTED TO COMPLETE or SUPPORT AGREED WITH OTHER PARTNERS/ AGENCIES GREEEN COMPLETED GENERAL CQC CONCERNS ASSURANCE
DR KUMAR CQC INSPECTION ACTION PLAN REVIEWED: 28 TH DECEMBER 2015 RED NOT COMPLETED AMBER STARTED TO COMPLETE or SUPPORT AGREED WITH OTHER PARTNERS/ AGENCIES GREEEN COMPLETED GENERAL CQC CONCERNS ASSURANCE
Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome:
 TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
TRUST BOARD Date of Meeting: Agenda Item No: 6.2 Enclosure: 4 17/1/02012 Intended Outcome: For noting For information For decision Title of Report: Update on Clinical Strategy Aims: To brief Trust Board
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Transforming Mental Health Services Formal Consultation Process
 Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
Project Plan for the Transforming Mental Health Services Formal Consultation Process June 2017 TMHS Project Plan v6 21.06.17 NOS This document can be made available in different languages and formats on
Mental Health Act Policy. Board library reference Document author Assured by Review cycle. Introduction Purpose or aim Scope...
 Mental Health Act Policy Board library reference Document author Assured by Review cycle P041 Associate Director of Governance, Quality and Regulatory Compliance Quality and Standards Committee 1 Year
Mental Health Act Policy Board library reference Document author Assured by Review cycle P041 Associate Director of Governance, Quality and Regulatory Compliance Quality and Standards Committee 1 Year
North Cumbria University Hospitals NHS Trust Proposed Acquisition by a Foundation Trust. Stakeholder Event Wednesday, 12 October 2011
 North Cumbria University Hospitals NHS Trust Proposed Acquisition by a Foundation Trust Stakeholder Event Wednesday, 12 October 2011 Stakeholder and Foundation Trust Briefing Information 1 1. Contents
North Cumbria University Hospitals NHS Trust Proposed Acquisition by a Foundation Trust Stakeholder Event Wednesday, 12 October 2011 Stakeholder and Foundation Trust Briefing Information 1 1. Contents
Report to NHS Greater Glasgow & Clyde
 www.pwc.co.uk Report to NHS Greater Glasgow & Clyde Internal Audit Report Waiting Times November 2012 FINAL REPORT Contents This report has been prepared solely for NHSGGC in accordance with the terms
www.pwc.co.uk Report to NHS Greater Glasgow & Clyde Internal Audit Report Waiting Times November 2012 FINAL REPORT Contents This report has been prepared solely for NHSGGC in accordance with the terms
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE
 POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
POLICY ON THE IMPLEMENTATION OF NICE GUID ANCE Document Type Corporate Policy Unique Identifier CO-019 Document Purpose To outline the process for the implementation and compliance with NICE guidance and
(Committee Chair) Chair) Asst. Lead Director for Children & Strategic Lead for Mental Health. Head of Estates and Property (MHSA/16/01-08 only)
 Chair) Asst. Lead Director for Children & Strategic Lead for Mental Health. Head of Estates and Property (MHSA/16/01-08 only)") POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 07 JANUARY 2016, AT 09.30AM, HAFREN TRAINING ROOM, HAFREN WARD, BRONLLYS HOSPITAL
POWYS TEACHING HEALTH BOARD MENTAL HEALTH SERVICES ASSURANCE COMMITTEE CONFIRMED MINUTES OF THE MEETING HELD ON THURSDAY 07 JANUARY 2016, AT 09.30AM, HAFREN TRAINING ROOM, HAFREN WARD, BRONLLYS HOSPITAL
QUALITY & SAFETY COMMITTEE WORKPLAN 2013/14
 QUALITY & SAFETY COMMITTEE WORKPLAN 2013/14 Introduction The role of the Quality and Safety (Q&S) Committee is to provide: evidence-based and timely advice to the Board to assist it in discharging its
QUALITY & SAFETY COMMITTEE WORKPLAN 2013/14 Introduction The role of the Quality and Safety (Q&S) Committee is to provide: evidence-based and timely advice to the Board to assist it in discharging its
Mental Health Crisis Care: Barnsley Summary Report
 Mental Health Crisis Care: Barnsley Summary Report Date of local area inspection: 17 & 18 February 2015 Date of publication: June 2015 This inspection was carried out under section 48 of the Health and
Mental Health Crisis Care: Barnsley Summary Report Date of local area inspection: 17 & 18 February 2015 Date of publication: June 2015 This inspection was carried out under section 48 of the Health and
Appendix 1: Integrated Urgent Care Service Update. 1. Purpose
 Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Appendix 1: Integrated Urgent Care Service Update 1. Purpose The purpose of this paper is to provide Governing Body members across the collaborative CCGs with an update on the progress of the Integrated
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Standard Operating Procedure Discharge/Transfer of Patients from St John s Hospice In-Patient Unit
 Standard Operating Procedure Discharge/Transfer of Patients from St John s Hospice In-Patient Unit DOCUMENT CONTROL: Version: 1.1 Ratified by: Quality Assurance Sub Committee Date ratified: 2 February
Standard Operating Procedure Discharge/Transfer of Patients from St John s Hospice In-Patient Unit DOCUMENT CONTROL: Version: 1.1 Ratified by: Quality Assurance Sub Committee Date ratified: 2 February
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Halton. Local system review report Health and Wellbeing Board. Background and scope of the local system review. The review team
 Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
Halton Local system review report Health and Wellbeing Board Date of review: 21-25 August 2017 Background and scope of the local system review This review has been carried out following a request from
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
Quality Strategy
 Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
North School of Pharmacy and Medicines Optimisation Strategic Plan
 North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
North School of Pharmacy and Medicines Optimisation Strategic Plan 2018-2021 Published 9 February 2018 Professor Christopher Cutts Pharmacy Dean christopher.cutts@hee.nhs.uk HEE North School of Pharmacy
Clinical Supervision Policy
 Clinical Supervision Policy Version: 3.2 Bodies consulted: Professional Advisory Committee Approved by: PASC Date Approved: 13.8.15 Lead Manager: Jessica Yakeley Responsible Director: Medical Director
Clinical Supervision Policy Version: 3.2 Bodies consulted: Professional Advisory Committee Approved by: PASC Date Approved: 13.8.15 Lead Manager: Jessica Yakeley Responsible Director: Medical Director
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Clinical Advisory Forum DRAFT Terms of Reference
 Clinical Advisory Forum DRAFT Terms of Reference 1. Constitution 1.1. The Trust Executive Committee (TEC) hereby resolves to establish a Forum to be known as the Clinical Advisory Forum (the Forum). The
Clinical Advisory Forum DRAFT Terms of Reference 1. Constitution 1.1. The Trust Executive Committee (TEC) hereby resolves to establish a Forum to be known as the Clinical Advisory Forum (the Forum). The
EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION. Medical Education Leads Clinical Directors (professional leadership) Director of Clinical Audit
 Director of Clinical Audit") EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION Job Title: Accountable to: Responsible for: Executive Medical Director Chief Executive Director of Research & Development Medical Education Leads Clinical Directors
EXECUTIVE MEDICAL DIRECTOR JOB DESCRIPTION Job Title: Accountable to: Responsible for: Executive Medical Director Chief Executive Director of Research & Development Medical Education Leads Clinical Directors
TRUST BOARD, 26 NOVEMBER 2009 LEARNING FROM THE CQC INVESTIGATION INTO WEST LONDON MENTAL HEALTH NHS TRUST (WLMHT)
") TRUST BOARD, 26 NOVEMBER 2009 L LEARNING FROM THE CQC INVESTIGATION INTO WEST LONDON MENTAL HEALTH NHS TRUST (WLMHT) Summary In July 2009, the Care Quality Commission (CQC) published the above report.
TRUST BOARD, 26 NOVEMBER 2009 L LEARNING FROM THE CQC INVESTIGATION INTO WEST LONDON MENTAL HEALTH NHS TRUST (WLMHT) Summary In July 2009, the Care Quality Commission (CQC) published the above report.
Improving Mental Health Services in Bath & North East Somerset
 Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Improving Mental Health Services in Bath & North East Somerset Andy Sylvester Executive Director of Operations Welcome & Introductions Housekeeping Format of the day Presentations Questions and answers
Quality and Safety Committee Terms of Reference
 Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Approved May 2016 Quality and Safety Committee Terms of Reference 1. Constitution The Quality and Safety Committee is established as a sub-committee of The Hillingdon Hospitals NHS Foundation Trust (THH)
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Report of the Care Quality Commission. May 2017
 Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement
 Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
Job Description Job Title: Head of Patient &Public Engagement and Patient Services Directorate: Corporate Affairs Department: Patient and Public Engagement Grade 8b Tenure: Permanent Location of Post:
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Liverpool Heart & Chest Hospital NHS Foundation Trust Thomas
COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR:
 MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
HERTFORDSHIRE COMMUNITY NHS TRUST INTERMEDIATE CARE SERVICE UPDATE WINDMILL HOUSE MAY 2011
 HERTFORDSHIRE COMMUNITY NHS TRUST INTERMEDIATE CARE SERVICE UPDATE WINDMILL HOUSE MAY 2011 1. Purpose This paper provides an update on the outcome of the consultation to re-provide Intermediate Care Services
HERTFORDSHIRE COMMUNITY NHS TRUST INTERMEDIATE CARE SERVICE UPDATE WINDMILL HOUSE MAY 2011 1. Purpose This paper provides an update on the outcome of the consultation to re-provide Intermediate Care Services
Overall rating for this location Requires improvement
 Riverdale Grange Clinic Quality Report 93 Riverdale Road Ranmoor Sheffield South Yorkshire S10 3FE Tel:0114 230 2140 Website:http://www.riverdalegrange.co.uk Date of inspection visit: 9 August 2017 Date
Riverdale Grange Clinic Quality Report 93 Riverdale Road Ranmoor Sheffield South Yorkshire S10 3FE Tel:0114 230 2140 Website:http://www.riverdalegrange.co.uk Date of inspection visit: 9 August 2017 Date
Decision-Making Business Case
 Clinical Services Review Decision-Making Business Case Volume 2 September 2017 version 1.4 Clinical Services Review Decision-Making Business Case Volume 2 September 2017 version 1.4 DMBC CONTENTS CONTENTS
Clinical Services Review Decision-Making Business Case Volume 2 September 2017 version 1.4 Clinical Services Review Decision-Making Business Case Volume 2 September 2017 version 1.4 DMBC CONTENTS CONTENTS
Avon & Wiltshire Mental Health Partnership NHS Trust. Extract from NHS STANDARD MULTILATERAL MENTAL HEALTH AND LEARNING DISABILITY SERVICES CONTRACT
 SCHEDULE 4 QUALITY PERFORMANCE INCENTIVE SCHEMES 2011/12 Schedule 4 Part 1: Nationally Mandated Incentive Schemes Schedule 4 Part 2: National Incentive Framework for Commissioning for Quality and Innovation
SCHEDULE 4 QUALITY PERFORMANCE INCENTIVE SCHEMES 2011/12 Schedule 4 Part 1: Nationally Mandated Incentive Schemes Schedule 4 Part 2: National Incentive Framework for Commissioning for Quality and Innovation
Learning from Deaths Policy
 Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Learning from Deaths Policy The Learning from Deaths Policy sets out the minimum acceptable standards of the national learning from deaths programme. Policy group General Document Detail Version 1 Approved
Date ratified November Review Date November This Policy supersedes the following document which must now be destroyed:
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Cleaning Policy NTW(O)71 James Duncan Deputy Chief Executive / Executive Director of Finance Steve Blackburn Deputy
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Cleaning Policy NTW(O)71 James Duncan Deputy Chief Executive / Executive Director of Finance Steve Blackburn Deputy
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
NHS England (London) Assurance of the BEH Clinical Strategy
 Assurance of the BEH Clinical Strategy") NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
NHS England (London) Assurance of the BEH Clinical Strategy NHS England (London) Assurance of the BEH Clinical Strategy Status Report 8 th September 203 - Version.0 2 Contents. Overview & Executive Summary
Positive and Safe Management of Post incident Support and Debrief. Ron Weddle Deputy Director, Positive and Safe Care
 Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Positive and Safe Management of Post incident Support and Debrief NTW(C)13 Ron Weddle Deputy Director, Positive
Document Title Reference Number Lead Officer Author(s) (name and designation) Ratified by Positive and Safe Management of Post incident Support and Debrief NTW(C)13 Ron Weddle Deputy Director, Positive
Quality Assurance Committee Annual Report April 2017 March 2018
 Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Quality Assurance Committee Annual Report April 2017 March 2018 Quality Assurance Committee Annual Report April 2017 March 2018 1. Introduction The role of the quality assurance committee is to provide
Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse
 TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
TRUST BOARD IN PUBLIC REPORT TITLE: Date: 28 March 2013 Agenda Item: 2.4 Joint Chief Nurse and Medical Director s Report Susan Aitkenhead, Chief Nurse EXECUTIVE SPONSOR: Dr. Des Holden, Medical Director
CLINICAL AND CARE GOVERNANCE STRATEGY
 CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
CLINICAL AND CARE GOVERNANCE STRATEGY Clinical and Care Governance is the corporate responsibility for the quality of care Date: April 2016 2020 Next Formal Review: April 2020 Draft version: April 2016
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust
 Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Surrey Downs Clinical Commissioning Group Governing Body Part 1 Paper Acute Sustainability at Epsom & St Helier University Hospitals NHS Trust 1. Strategic Context 1.1. It has long been recognised that
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Mental Health Social Work: Community Support. Summary
 Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
Adults and Safeguarding Commitee 8 th June 2015 Title Mental Health Social Work: Community Support Report of Dawn Wakeling Adults and Health Commissioning Director Wards All Status Public Enclosures Appendix
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Engaging clinicians in improving data quality in the NHS
 Engaging clinicians in improving data quality in the NHS Key findings and recommendations from research conducted by the Royal College of Physicians ilab September 2006 Summary This document summarises
Engaging clinicians in improving data quality in the NHS Key findings and recommendations from research conducted by the Royal College of Physicians ilab September 2006 Summary This document summarises
Health Board Report SOCIAL SERVICES AND WELL-BEING ACT (WALES) 2014: REVISED REGIONAL IMPLEMENTATION PLAN
 2014: REVISED REGIONAL IMPLEMENTATION PLAN") Agenda Item 3.3 27 JANUARY 2016 Health Board Report SOCIAL SERVICES AND WELL-BEING ACT (WALES) 2014: REVISED REGIONAL IMPLEMENTATION PLAN Executive Lead: Director of Planning & Performance Author: Assistant
Agenda Item 3.3 27 JANUARY 2016 Health Board Report SOCIAL SERVICES AND WELL-BEING ACT (WALES) 2014: REVISED REGIONAL IMPLEMENTATION PLAN Executive Lead: Director of Planning & Performance Author: Assistant
Wales Psychological Therapies Plan for the delivery of Matrics Cymru The National Plan 2018
 Wales Psychological Therapies Plan for the delivery of Matrics Cymru The National Plan 2018 Written by the National Psychological Therapies Management Committee, supported by 1000 Lives Improvement, Public
Wales Psychological Therapies Plan for the delivery of Matrics Cymru The National Plan 2018 Written by the National Psychological Therapies Management Committee, supported by 1000 Lives Improvement, Public
ANEURIN BEVAN HEALTH BOARD & CAERPHILLY COUNTY BOROUGH COUNCIL ACTION PLAN
 ANEURIN BEVAN HEALTH BOARD & CAERPHILLY COUNTY BOROUGH COUNCIL RESPONSE TO THE REPORT BY HEALTH INSPECTORATE WALES REVIEW IN RESPECT OF: MR H AND THE PROVISION OF MENTAL HEALTH SERVICES, FOLLOWING THE
ANEURIN BEVAN HEALTH BOARD & CAERPHILLY COUNTY BOROUGH COUNCIL RESPONSE TO THE REPORT BY HEALTH INSPECTORATE WALES REVIEW IN RESPECT OF: MR H AND THE PROVISION OF MENTAL HEALTH SERVICES, FOLLOWING THE
Kathy McLean, Executive Medical Director and Chief Operating Officer
 To: The Board For meeting on: 24 May 2018 Agenda item: 6 Report by: Kathy McLean, Executive Medical Director and Chief Operating Officer Report on: Update on actions taken in response to Independent review
To: The Board For meeting on: 24 May 2018 Agenda item: 6 Report by: Kathy McLean, Executive Medical Director and Chief Operating Officer Report on: Update on actions taken in response to Independent review
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC
 Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
Sussex Community NHS Trust Action Plan in Response to Recommendations Made by CQC England s chief inspector of hospitals has rated the overall quality of services provided by Sussex Community NHS Trust
Overall rating for this trust Requires improvement. Inspection report. Ratings. Are services safe? Requires improvement
 Bradford District Care NHS Foundation Trust Inspection report SBS New Mill Victoria Road, Saltaire Shipley West Yorkshire BD18 3LD Tel: 01274228300 www.bdct.nhs.uk Date of inspection visit: October 4th
Bradford District Care NHS Foundation Trust Inspection report SBS New Mill Victoria Road, Saltaire Shipley West Yorkshire BD18 3LD Tel: 01274228300 www.bdct.nhs.uk Date of inspection visit: October 4th
Complaints, Compliments and Concerns (CCC) Policy
 Policy") Complaints, Compliments and Concerns (CCC) Policy Central and North West London NHS Foundation Trust (CNWL) is committed to providing quality NHS services and adopting best practice in listening and responding
Complaints, Compliments and Concerns (CCC) Policy Central and North West London NHS Foundation Trust (CNWL) is committed to providing quality NHS services and adopting best practice in listening and responding
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Strategic Risk Report 4 July 2016
 Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Strategic Report 4 July 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Group s control over the delivery of
Sheffield Learning Disability Service Review Quality Assurance Assessment
 Sheffield Learning Disability Service Review Quality Assurance Assessment "Commissioning services for people with learning disabilities is a substantial test of working together in effective partnerships
Sheffield Learning Disability Service Review Quality Assurance Assessment "Commissioning services for people with learning disabilities is a substantial test of working together in effective partnerships
abcdefghijklmnopqrstu
 Directorate for Chief Medical Officer, Public Health and Sport Sir Harry Burns, MPH FRCS (Glas) FRCP(Ed) FFPH Health and Social Care Directorate Pharmacy and Medicines Division Professor Bill Scott, MSc,
Directorate for Chief Medical Officer, Public Health and Sport Sir Harry Burns, MPH FRCS (Glas) FRCP(Ed) FFPH Health and Social Care Directorate Pharmacy and Medicines Division Professor Bill Scott, MSc,
CQC ENF , ENF , ENF
 This Action Plan is responding to the following requirement notice and enforcement action, as detailed in the CQC inspection report of 13 th February. It is also in response to the accompanying warning
This Action Plan is responding to the following requirement notice and enforcement action, as detailed in the CQC inspection report of 13 th February. It is also in response to the accompanying warning
JOB DESCRIPTION. Pharmacy Technician
 JOB DESCRIPTION Pharmacy Technician Issued by AT Medics Primary Care Pharmacy Technician Job Description Job Title: Reporting to: Location: Salary: Job status: Contract: Notice Period: Primary care pharmacy
JOB DESCRIPTION Pharmacy Technician Issued by AT Medics Primary Care Pharmacy Technician Job Description Job Title: Reporting to: Location: Salary: Job status: Contract: Notice Period: Primary care pharmacy
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Health and Social Care Directorate Quality standards Process guide
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Health and Social Care Directorate Quality standards Process guide December 2014 Quality standards process guide Page 1 of 44 About this guide This guide
Safeguarding Annual Assurance Self-assessment Tool. Sheffield Health and Social Care NHS Foundation Trust
 Safeguarding Annual Assurance Self-assessment Tool Sheffield Health and Social Care Foundation Trust Introduction - About this Self-assessment This self-assessment is an assessment of your own internal
Safeguarding Annual Assurance Self-assessment Tool Sheffield Health and Social Care Foundation Trust Introduction - About this Self-assessment This self-assessment is an assessment of your own internal
Workforce Development Fund
 Workforce Development Fund 2018 19 Partnership application form guidance January 2018 (v1.0) Contents Introduction... 2 The application process and timetable... 2 Qualifications and learning programmes
Workforce Development Fund 2018 19 Partnership application form guidance January 2018 (v1.0) Contents Introduction... 2 The application process and timetable... 2 Qualifications and learning programmes
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD
 BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD") INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
INTEGRATION SCHEME (BODY CORPORATE) BETWEEN WEST DUNBARTONSHIRE COUNCIL AND GREATER GLASGOW HEALTH BOARD This integration scheme is to be used in conjunction with the Public Bodies (Joint Working) (Integration
Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations
 No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
NHS GRAMPIAN. Grampian Clinical Strategy - Planned Care
 NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
NHS GRAMPIAN Grampian Clinical Strategy - Planned Care Board Meeting 03/08/17 Open Session Item 8 1. Actions Recommended In October 2016 the Grampian NHS Board approved the Grampian Clinical Strategy which
Quality Strategy. CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July Head of Clinical Quality & Patient Safety
 Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Quality Strategy Document Document Status Equality Impact Assessment Draft None Document Ratified/ CCG Executive, Quality Safety and Risk Committee Approved by Date Issued July 2016 Review Date September
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk. Service Model Version 1.0
 Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Integrated Health and Care in Ipswich and East Suffolk and West Suffolk Service Model Version 1.0 This document describes an integrated health and care service model and system for Ipswich and East and
Primary Care Quality Assurance Framework (Medical Services)
") PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
PCC/15/021 Primary Care Quality Assurance Framework (Medical Services) 1.0 Introduction: From the 1 April 2015 the responsibility for monitoring quality and responding to concerns arising from General
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
GOVERNING BODY REPORT 1. Date of Governing Body Meeting: 2. Title of Report: Finance, Performance and Commissioning Committee Report 3. Key Messages: At the end of March 2017 the clinical commissioning
Date 4 th September 2015 Dr Ruth Charlton, Joint Medical Director / Jill Down, Associate Director of Quality Laura Rowe, Compliance Manager
 TB 099/15 Meeting title Report title Trust Board Risk Management Strategy Date 4 th September 2015 Lead director Report author FOI status Dr Ruth Charlton, Joint Medical Director / Jill Down, Associate
TB 099/15 Meeting title Report title Trust Board Risk Management Strategy Date 4 th September 2015 Lead director Report author FOI status Dr Ruth Charlton, Joint Medical Director / Jill Down, Associate
Mortality Policy. Learning from Deaths
 Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Sustainable & Accessible Services. Strong Partnerships X X X
 SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item: 5.1 Report Title Prepared by Approved and Presented by ABMU Older Persons Assurance
SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item: 5.1 Report Title Prepared by Approved and Presented by ABMU Older Persons Assurance
Royal Care Health Recruitment & Training
 REYMC 247 (PVT) Limited Royal Care Health Recruitment & Training Inspection report Wellgate Business 149 Wellgate Rotherham S60 2NN Date of inspection visit: 29 April 2016 Date of publication: 02 June
REYMC 247 (PVT) Limited Royal Care Health Recruitment & Training Inspection report Wellgate Business 149 Wellgate Rotherham S60 2NN Date of inspection visit: 29 April 2016 Date of publication: 02 June
Quality Assurance Framework Adults Services. Framework. Version: 1.2 Effective from: August 2016 Review date: June 2017
 Quality Assurance Framework Adults Services Framework Version: 1.2 Effective from: August 2016 Review date: June 2017 Signed off by: Sharon Gogan Title: Head of Adult Social Care Date: 20 th May 2014 Quality
Quality Assurance Framework Adults Services Framework Version: 1.2 Effective from: August 2016 Review date: June 2017 Signed off by: Sharon Gogan Title: Head of Adult Social Care Date: 20 th May 2014 Quality
Overall rating for this location Requires improvement
 Oak Tree Forest Ltd. t/a Ellern Mede Ridgeway Quality Report Holcombe Hill, The Ridgeway, London, NW7 4HX Tel: 020 8959 7774 Website:http://www.ellernmede.org Date of inspection visit: 22 to 24 March 2016
Oak Tree Forest Ltd. t/a Ellern Mede Ridgeway Quality Report Holcombe Hill, The Ridgeway, London, NW7 4HX Tel: 020 8959 7774 Website:http://www.ellernmede.org Date of inspection visit: 22 to 24 March 2016
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. John Greenwood Shipman Centre 1 Farmbrook Court, Billing Brook
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. John Greenwood Shipman Centre 1 Farmbrook Court, Billing Brook
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 25 th January 2018 Agenda No: 7.2 Attachment: 7 Title of Document: Acute Sustainability at Epsom & St Helier University Hospitals NHS
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service
 Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
Inspections of Mental Health Hospitals and Mental Health Hospitals for People with a Learning Disability Indicators for the Delivery of Safe, Effective and Compassionate Person Centred Service 1 Our Vision,
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Clinical Assurance Toolkit (CAT) Strategy
 Strategy") The Newcastle upon Tyne Hospitals NHS Foundation Trust Clinical Assurance Toolkit (CAT) Strategy Effective: January 2014 Review: January 2015 1. Introduction The Trust s Nursing and Midwifery Strategy,
The Newcastle upon Tyne Hospitals NHS Foundation Trust Clinical Assurance Toolkit (CAT) Strategy Effective: January 2014 Review: January 2015 1. Introduction The Trust s Nursing and Midwifery Strategy,
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
A fresh start for registration. Improving how we register providers of all health and adult social care services
 A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care
A fresh start for registration Improving how we register providers of all health and adult social care services The Care Quality Commission is the independent regulator of health and adult social care