PROVIDER PARTICIPATION REQUEST FORM
|
|
|
- Alan Moore
- 6 years ago
- Views:
Transcription


 evidence that you are Medicare and Medicaid eligible; and 2) evidence of licensure to operate according to State and Federal regulations.")

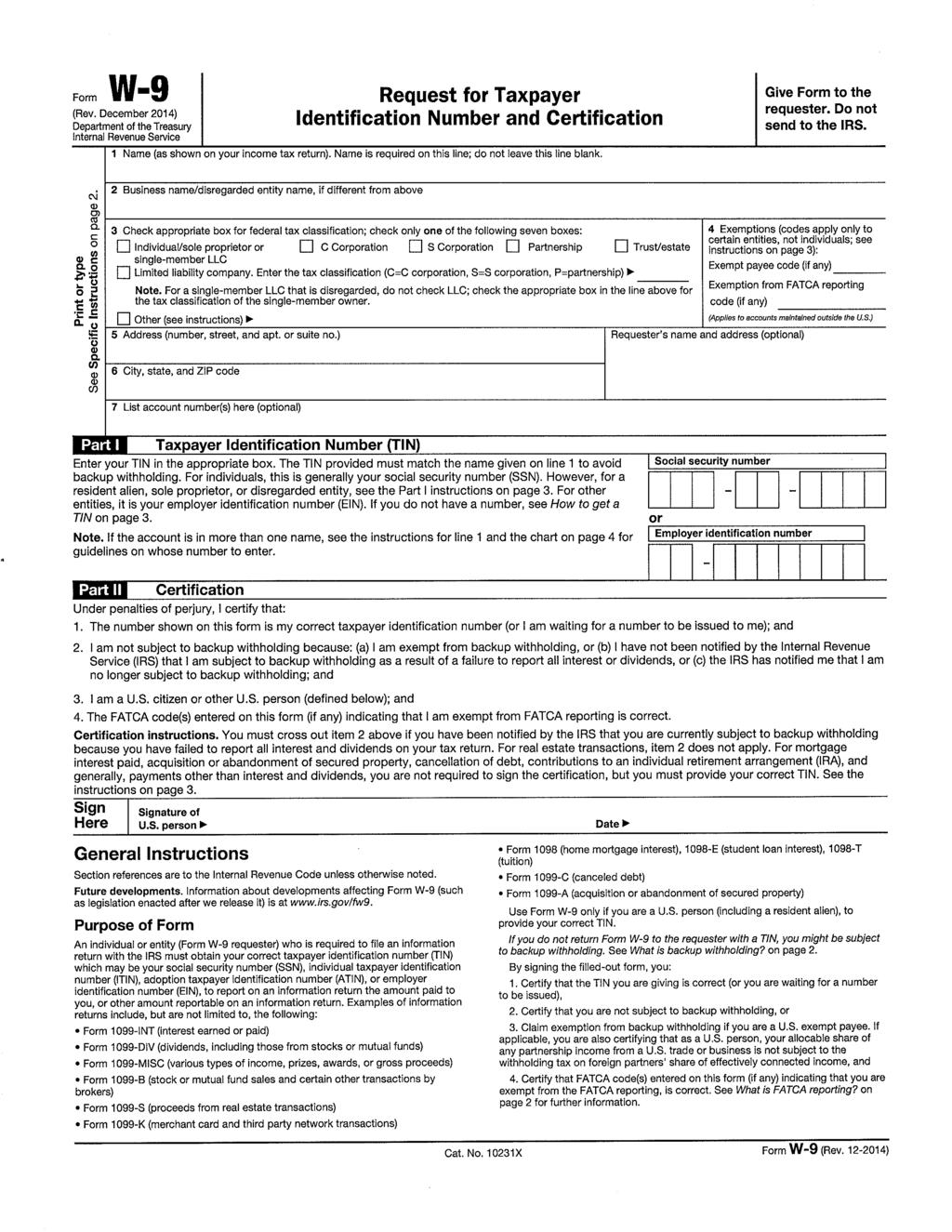
1 PROVIDER PARTICIPATION REQUEST FORM Thank you for your interest in becoming a participating provider with Quartz. Your request will be evaluated for participation in all Quartz affiliate networks. In order to expedite the processing of your application, please do the following: 1. Complete the application in full. Please print clearly or fill out electronically and attach any additional information or brochures that may help in our evaluation of your facility and the services you provide. 2. Attach a copy of your W-9 form and provide the requested information specific to all facilities, practitioners and services (a W-9 form is attached for your convenience). 3. If applicable, provide: 1) evidence that you are Medicare and Medicaid eligible; and 2) evidence of licensure to operate according to State and Federal regulations. PLEASE RETURN VIA: providercommunications@quartzbenefits.com Facsimile: (608) Mail: Quartz Health Solutions, Inc. Attn: Provider Relations Dept. 840 Carolina Street Sauk City, WI SECTION I: BILLING INFORMATION Please verify all information and complete all blank areas. Enter N/A if not applicable. Legal Entity Name: (include d/b/a if applicable) Ownership Type: (Sole Proprietor, LLC, SC, etc.) Tax ID Number: Mailing Street Address: Mailing City, State, Zip: Billing Address: Billing City, State, Zip: Phone Number: Fax Number: 2nd Phone Number: Website URL:
2 Quartz Provider Participation Request Form SECTION II: GENERAL INFORMATION Please verify all information and complete all blank areas. Enter N/A if not applicable Have you ever applied for or had a contract with Unity Health Plans Insurance Corporation, Quartz Health Solutions, Inc. (f/k/a SPWI TPA, Inc.), Gundersen Health Plan, Inc., Gundersen Health Plan Minnesota, or Physicians Plus Insurance Corporation? If yes, under what name or group? Covered Service Area (City and Counties): Please list any Quartz network providers that currently refer to your office: (Gundersen/PPIC/Unity) Please provide a brief description regarding your facility and the services you currently provide: Does your facility have a restraint policy regarding patient restraints? Is public transportation accessible to and from your facility? Does your facility accommodate for people with physical disabilities (including exam rooms and equipment)? Does your organization allow mid-level practitioners (e.g. nurse practitioners and/or physicians assistants) to be selected by patients as a Primary Care Physician? Comments: SECTION III: CONTACT INFORMATION Please verify all information and complete all blank areas. Enter N/A if not applicable Contact Type Contact Name/Title (First and Last Name) Phone Number Address Preferred Contact Method Primary Contact: Phone Contract Signature: Phone Agreement Notification: Phone Billing: Phone Provider Manual: Phone Provider Updates/CMS Verifications: Phone Compliance Representative Phone are separate legal entities. Page 2 of 13
3 Quartz Provider Participation Request Form A. Practice Type Group Individual B. For Group Practice SECTION IV: BEHAVIORAL HEALTH PROVIDER INFORMATION Please complete the following if you are applying to join our network as a behavioral health provider. 1. Does the practice have a Psychiatrist consulting on staff or referral arrangements with a Psychiatrist at another location? Yes No 2. What are these arrangements and if there aren t any, what are the means for getting patients psychiatric care? C. Provider Information Name Degree License D. After Hours/Emergency Care and General Availability Please describe your process for handling calls after hours for urgent and emergent patient situations: Number of hours/week in practice? Hours available (include evening/weekend hours): E. Treatment Information Area(s) of specialization/interest (include special populations): Conditions treated: Methods/approaches used in treatment: F. Other Information are separate legal entities. Page 3 of 13
4 Quartz Provider Participation Request Form SECTION V: FACILITY CREDENTIALING FORM Please update and/or verify the below information and complete columns to the right of each section. Facility State License Medicare Certification Medicaid Certification The Joint Commission License/Accrediting Body AAAHC - Accreditation Association for Ambulatory Health Care AAAASF - American Association for Accreditation of Ambulatory Surgical Facilities ACHC - Accreditation Commission for Health Care CARF - Commission on Accreditation of Rehabilitation Facilities CHAP - Community Health Accreditation Program COA - Council on Accreditation DNV Healthcare - Det Norske Veritas Healthcare, Inc. HFAP - Healthcare Facilities Accreditation Program Indicate Yes, No or N/A Number Effective Date Expiration Date Please attach copies of the following documents: Copy of the facility s state license Most recent State/CMS survey results and the cover letter stating acceptance of the plan of correction, if applicable Explanation regarding any loss or change of certification or accreditation status within the past three years. For facilities without accreditation, Quartz Health Solutions, Inc. reserves the right to conduct an on-site visit of your facility. are separate legal entities. Page 4 of 13
5 Quartz Provider Participation Request Form SECTION VI: SERVICES Please review each service listed and indicate the services provided by your facility. BEHAVIORAL HEALTH SERVICES Mental Illness Adult Inpatient Treatment Mental Illness Child/Adolescent Inpatient Treatment Mental Illness Adult Outpatient Treatment Mental Illness Child/Adolescent Outpatient Treatment AODA Adult Inpatient Treatment AODA Adolescent Inpatient Treatment AODA Adult Outpatient Treatment AODA Adolescent Outpatient Treatment EYE CLINICS SERVICES Ophthalmology Services Optometry Services Vision Care/Screening Vision Supplies (Eye Glasses & Contacts) DIALYSIS Inpatient Outpatient DURABLE MEDICAL EQUIPMENT SERVICES Apnea Monitors BI-Pap Bone Growth Stimulator CPAP DME/HME (standard wheelchair, hospital bed, etc.) Oxygen Concentrator Oxygen-Liquid Photo Therapy Respiratory DME TENS Unit Ventilators Wound Vac Other Specialty DME Items: HOME HEALTH SERVICES Durable Medical Equipment Home Infusion Home Health Services - Skilled Home Health Services - Aid Occupational Therapy Physical Therapy Speech Therapy are separate legal entities. Page 5 of 13
6 Quartz Provider Participation Request Form NURSING HOME SERVICES Skilled Nursing Services PATHOLOGY SERVICES Pathology Services (Professional) Pathology Services (Technical) PODIATRIC SERVICES Radiology Diagnostic & Therapeutic Podiatric Services PROSTHETICS/ORTHOTICS SERVICES Mastectomy Supplies Orthotic Supplies Prosthetic Supplies RADIOLOGY SERVICES Bone Density Measurement CT (Professional) MRI (Professional) MRI (Technical) Nuclear Medicine Nuclear Medicine (Professional) Open MRI Radiation Oncology Radiation Therapy Radiology General Services (Technical) Radiology Services Diagnostic & Therapeutic Radiology Services Mammography Ultrasound Vascular and Interventional Radiology SPORTS MEDICINE SERVICES Durable Medical Equipment (Dispensed In-house) Occupational Therapy (Outpatient) Physical Therapy (Outpatient) Orthotic Supplies Prosthetic Supplies Radiology Diagnostic & Therapeutic (In-house) Orthopedic Surgery (Adult) Orthopedic Surgery (Pediatric) OTHER SERVICES Anti-Hemophiliac Factor are separate legal entities. Page 6 of 13
7 Anesthetists ECG Interpretation Insulin Pump Therapy Cardiac Outpatient Telemetry Specialty Clinic Urgent Care Services Quartz Provider Participation Request Form CLINIC SERVICES Allergy Services Audiology Hearing Screening Audiology Hearing Aids Behavioral Health: Mental Illness Adult Outpatient Treatment Mental Illness Child/Adolescent Outpatient Treatment Alcoholism/Chemical Dependency Adult Outpatient Treatment Alcoholism/Chemical Dependency Adolescent Outpatient Treatment Cardiology Services Dental Services Dermatology Services Durable Medical Equipment Endocrinology Services Eye Glasses & Contacts Family Practice Gastroenterology Services Hematology/Oncology Services Infectious Disease Services Internal Medicine Services Laboratory Services Nephrology Services Neurology Services Neurosurgery Obstetrics & Gynecology Occupational Health Services Occupational Therapy (Outpatient) Ophthalmology Services Optometry Services Oral/Maxillofacial Surgery Orthopedics Services Otolaryngology (ENT) Pediatric Services Physical Medicine & Rehabilitation Physical Therapy (Outpatient) Plastic & Reconstructive Surgery - General Podiatric Services Orthotic Supplies Prosthetic Supplies Pulmonary Medicine Services Radiation Therapy are separate legal entities. Page 7 of 13
8 Radiology Services Diagnostic & Therapeutic Radiology Services Mammography Renal Dialysis Rheumatology Services Speech Therapy Sports Medicine Services Surgery - Outpatient or Ambulatory Urgent Care Services Urology Services Quartz Provider Participation Request Form HOSPITAL SERVICES Acute Inpatient Hospital Care Behavioral Health: Mental Illness Adult Inpatient Treatment Mental Illness Child/Adolescent Inpatient Treatment Mental Illness Adult Outpatient Treatment Mental Illness Child/Adolescent Outpatient Treatment Alcoholism/Chemical Dependency Adult Inpatient Treatment Alcoholism/Chemical Dependency Adolescent Inpatient Treatment Alcoholism/Chemical Dependency Adult Outpatient Treatment Alcoholism/Chemical Dependency Adolescent Outpatient Treatment Cardiology Services Cardiac Surgery Program Cardiac Catheterization Services Critical Care Services Intensive Care Units (ICU) Durable Medical Equipment Emergency & Trauma Center Endocrinology Services Gastroenterology Services Hematology/Oncology Services Home Health Infectious Disease Services Laboratory Services Neonatal Intensive Care Unit Neurology Services Neurosurgery Occupational Health Services Occupational Therapy (Inpatient) Occupational Therapy (Outpatient) Orthopedic Surgery (Adult) Orthopedic Surgery (Pediatric) Otolaryngology (ENT) Outpatient Infusion/Chemotherapy Pediatric Services Physical Medicine & Rehabilitation Physical Therapy (Inpatient) Physical Therapy (Outpatient) Plastic & Reconstructive Surgery - General are separate legal entities. Page 8 of 13
9 Pulmonary Medicine Services Radiation Oncology Services Radiology Services Diagnostic & Therapeutic Radiology Services - Mammography Rheumatology Services Speech Therapy (Outpatient) Surgery Outpatient or Ambulatory Surgery (General) Transplant Program: Heart Transplant Heart/Lung Transplant Kidney Transplant Liver Transplant Lung Transplant Pancreas Transplant Swing Bed (Skilled Nursing Services) Urgent Care Services Urology Vascular Surgery Quartz Provider Participation Request Form SECTION VII: LANGUAGES Please list below all languages spoken by the employees of your facility. SECTION VIII: ATTESTATION I hereby verify that the information provided herein is current, correct and complete as of the date of my signature below and that, at a minimum, the staff are legally and professionally qualified for the positions they hold and that there are no state or federal sanctions against this facility. As an administrative representative of this facility, I have the authority to sign on behalf of the organization. Signature Title Date are separate legal entities. Page 9 of 13
10 QUARTZ CONTRACT IMPLEMENTATION FORM Billing and Facility Information Contact Information (for information regarding claims, address changes, and/or practitioner changes): Contact Name: Contact Address: Contact Telephone Number: Contact Address: Contact Fax Number: Credentialing Recipient: Contact Name: Contact Address: Contact Telephone Number: Contact Address: Contact Fax Number: Service Site Locations: 1. Location/Clinic: Street Address: City: State: Zip + 4: Billing Address: City: State: Zip + 4: County: Phone Number: Fax Number: Clinic National Provider Identification (NPI) Number: Billing National Provider Identification (NPI) Number: Swing Bed Facility? Essential Community Provider Type: Total # of Beds: Federally Qualified Health Center Provider Ryan White Provider # of Certified Medicare Beds: Indian Health Provider Other ECP Provider # of ICU/CCU Beds: Family Planning Provider Hospital Provider On Call/After Hours Coverage? Regular Office Hours: 2. Location/Clinic: Street Address: City: State: Zip + 4: Billing Address: City: State: Zip + 4: County: Phone Number: Fax Number: Clinic National Provider Identification (NPI) Number: Billing National Provider Identification (NPI) Number: Swing Bed Facility? Essential Community Provider Type: Total # of Beds: Federally Qualified Health Center Provider Ryan White Provider # of Certified Medicare Beds: Indian Health Provider Other ECP Provider # of ICU/CCU Beds: Family Planning Provider Hospital Provider On Call/After Hours Coverage? Regular Office Hours:
11 Quartz Provider Participation Request Form QUARTZ CONTRACT IMPLEMENTATION FORM Billing and Facility Information Service Site Locations Cont d: 3. Location/Clinic: Street Address: City: State: Zip + 4: Billing Address: City: State: Zip + 4: County: Phone Number: Fax Number: Clinic National Provider Identification (NPI) Number: Billing National Provider Identification (NPI) Number: Swing Bed Facility? Essential Community Provider Type: Total # of Beds: Federally Qualified Health Center Provider Ryan White Provider # of Certified Medicare Beds: Indian Health Provider Other ECP Provider # of ICU/CCU Beds: Family Planning Provider Hospital Provider On Call/After Hours Coverage? Regular Office Hours: 4. Location/Clinic: Street Address: City: State: Zip + 4: Billing Address: City: State: Zip + 4: County: Phone Number: Fax Number: Clinic National Provider Identification (NPI) Number: Billing National Provider Identification (NPI) Number: Swing Bed Facility? Essential Community Provider Type: Total # of Beds: Federally Qualified Health Center Provider Ryan White Provider # of Certified Medicare Beds: Indian Health Provider Other ECP Provider # of ICU/CCU Beds: Family Planning Provider Hospital Provider On Call/After Hours Coverage? Regular Office Hours: 5. Location/Clinic: Street Address: City: State: Zip + 4: Billing Address: City: State: Zip + 4: County: Phone Number: Fax Number: Clinic National Provider Identification (NPI) Number: Billing National Provider Identification (NPI) Number: Swing Bed Facility? Essential Community Provider Type: Total # of Beds: Federally Qualified Health Center Provider Ryan White Provider # of Certified Medicare Beds: Indian Health Provider Other ECP Provider # of ICU/CCU Beds: Family Planning Provider Hospital Provider On Call/After Hours Coverage? Regular Office Hours: are separate legal entities. Page 11 of 13
12 Practitioner Name (First, MI, Last): Quartz Provider Participation Request Form QUARTZ CONTRACT IMPLEMENTATION FORM Practitioner Information Individual NPI: Accepting New Patients? Taxonomy: Has Practitioner completed Cultural Competency Training? Practitioner Is this provider employed by your organization? Yes Available for patients to choose as their PCP? No Area(s) of Specialty: Gender: Male Female Race: African American American Indian Asian Caucasian Hispanic/Latino Native Hawaiian or Other Pacific Islander Languages Spoken: American Sign Language: In-Training/Non-Licensed? Credentials/Degree: Please List Hospital Affiliations: Medicare #: Medicaid #: Comments: DOB: Participating? Yes No Accepting Assignment? Certified? Yes No Please list the Service Site numbers for this practitioner (from the previous page(s)) and answer the following for each site: Practitioner Name (First, MI, Last): Individual NPI: Accepting New Patients? Taxonomy: Has Practitioner completed Cultural Competency Training? Practitioner Available for patients to choose as their PCP? Is this provider employed by your organization? Area(s) of Specialty: Gender: Male Female Race: African American American Indian Asian Caucasian Hispanic/Latino Native Hawaiian or Other Pacific Islander Credentials/Degree: Languages Spoken: American Sign Language: In-Training/Non-Licensed? Please List Hospital Affiliations: Medicare #: Participating? Accepting Assignment? Medicaid #: Certified? Comments: Please list the Service Site numbers for this practitioner (from the previous page(s)) and answer the following for each site: DOB: are separate legal entities. Page 12 of 13
13 Practitioner Name (First, MI, Last): Quartz Provider Participation Request Form Individual NPI: Accepting New Patients? Taxonomy: Has Practitioner completed Cultural Competency Training? Practitioner Available for patients to choose as their PCP? Is this provider employed by your organization? Area(s) of Specialty: Gender: Male Female Race: African American American Indian Asian Caucasian Hispanic/Latino Native Hawaiian or Other Pacific Islander Credentials/Degree: Languages Spoken: American Sign Language: In-Training/Non-Licensed? Please List Hospital Affiliations: Medicare #: Participating? Accepting Assignment? Medicaid #: Certified? Comments: Please list the Service Site numbers for this practitioner (from the previous page(s)) and answer the following for each site: Hospitalist? Can this Practitioner be selected as a PCP at this location: DOB: Can an appointment be scheduled at this location Practitioner Name (First, MI, Last): Individual NPI: Accepting New Patients? Taxonomy: Has Practitioner completed Cultural Competency Training? Practitioner Available for patients to choose as their PCP? Is this provider employed by your organization? Area(s) of Specialty: Gender: Male Female Race: African American American Indian Asian Caucasian Hispanic/Latino Native Hawaiian or Other Pacific Islander Credentials/Degree: Languages Spoken: American Sign Language: In-Training/Non-Licensed? Please List Hospital Affiliations: Medicare #: Participating? Accepting Assignment? Medicaid #: Certified? Comments: Please list the Service Site numbers for this practitioner (from the previous page(s)) and answer the following for each site: *This page may be copied if you have additional practitioner information to provide. DOB: are separate legal entities. Page 13 of 13
14
Hospital Credentialing Application
 Hospital Credentialing Application Thank you for your interest in Superior HealthPlan. Please use this checklist to ensure you have all necessary contract and credentialing items to avoid processing delays.
Hospital Credentialing Application Thank you for your interest in Superior HealthPlan. Please use this checklist to ensure you have all necessary contract and credentialing items to avoid processing delays.
2015 Physician Licensure Survey
 2015 Physician Licensure Survey 1. What is your racial background? Please select all that apply. White American Indian or Alaska Native Native Hawaiian/Pacific Islander Black or African American Asian
2015 Physician Licensure Survey 1. What is your racial background? Please select all that apply. White American Indian or Alaska Native Native Hawaiian/Pacific Islander Black or African American Asian
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION
 VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Please choose facility type (check all that apply):
VANTAGE HEALTH PLAN FACILITY CREDENTIALING APPLICATION GENERAL INFORMATION Primary Practice Facility Location The type of application being submitted: Please choose facility type (check all that apply):
Provider Profile GENERAL DETAILS STATE/ PROVINCE: OTHERS (PLEASE SPECIFY): CONTACT DETAILS DESIGNATION NAME PHONE MOBILE
: CONTACT DETAILS DESIGNATION NAME PHONE MOBILE") Provider Profile Dear Valued Provider, Kindly fill up this form with the information requested below. Availability of accurate and detailed information about your facility will definitely help QLM staff
Provider Profile Dear Valued Provider, Kindly fill up this form with the information requested below. Availability of accurate and detailed information about your facility will definitely help QLM staff
2014 Accreditation Report The University of Kansas Medical Center
 2014 Report s current of Degree and Certificate Programs Audiology - AUD GR Council on Academic in Audiology and Speech-Language Pathology (CAA) Cont. Accred. 2009 8 years 2016 Clinical Laboratory Sciences
2014 Report s current of Degree and Certificate Programs Audiology - AUD GR Council on Academic in Audiology and Speech-Language Pathology (CAA) Cont. Accred. 2009 8 years 2016 Clinical Laboratory Sciences
BCBSNC Provider Application for Participation
 BCBSNC Provider Application for Participation This application is to be used if you wish to become a participating provider facility with BCBSNC. This application is not a contract. Please follow the applicable
BCBSNC Provider Application for Participation This application is to be used if you wish to become a participating provider facility with BCBSNC. This application is not a contract. Please follow the applicable
AmeriHealth Caritas North Carolina Provider Data Intake Form
 AmeriHealth Caritas North Carolina Provider Data Intake Form Section 1 instructions: Please complete all fields below for the provider. Entity name (as written on W9): IPA name (if applicable): Category:
AmeriHealth Caritas North Carolina Provider Data Intake Form Section 1 instructions: Please complete all fields below for the provider. Entity name (as written on W9): IPA name (if applicable): Category:
Molina Healthcare of Washington, Inc. Health Delivery Organization (HDO) Application
 Application") INSTRUCTIONS: If your organization has multiple physical locations/businesses, include a separate full application for any facility grouping for which there is an independent facility survey and/or facility
INSTRUCTIONS: If your organization has multiple physical locations/businesses, include a separate full application for any facility grouping for which there is an independent facility survey and/or facility
AgeWell New York Provider Relations 1991 Marcus Avenue Suite M201 Lake Success, NY 11042
 Dear Provider/Facility: Thank you for your interest in becoming a network provider/facility for AgeWell New York, LLC. In accordance with our commitment to the quality of health care services delivered
Dear Provider/Facility: Thank you for your interest in becoming a network provider/facility for AgeWell New York, LLC. In accordance with our commitment to the quality of health care services delivered
PROVIDER NETWORK ADEQUACY INSTRUCTIONS
 Revised 5/21/2018 PROVIDER NETWORK ADEQUACY INSTRUCTIONS MANAGED CARE SYSTEMS PROVIDER NETWORK ADEQUACY INSTRUCTIONS Minnesota Department of Health Managed Care Systems PO Box 64882 St. Paul, MN 55164-0882
Revised 5/21/2018 PROVIDER NETWORK ADEQUACY INSTRUCTIONS MANAGED CARE SYSTEMS PROVIDER NETWORK ADEQUACY INSTRUCTIONS Minnesota Department of Health Managed Care Systems PO Box 64882 St. Paul, MN 55164-0882
PROVIDER NETWORK ADEQUACY INSTRUCTIONS
 PROVIDER NETWORK ADEQUACY INSTRUCTIONS MANAGED CARE SYSTEMS PROVIDER NETWORK ADEQUACY INSTRUCTIONS Minnesota Department of Health Managed Care Systems PO Box 64882, St. Paul, MN 55164-0882 651-201-5100
PROVIDER NETWORK ADEQUACY INSTRUCTIONS MANAGED CARE SYSTEMS PROVIDER NETWORK ADEQUACY INSTRUCTIONS Minnesota Department of Health Managed Care Systems PO Box 64882, St. Paul, MN 55164-0882 651-201-5100
HEALTH CARE FACILITY APPLICATION FOR NETWORK PARTICIPATION
 HEALTH CARE FACILITY APPLICATION FOR NETWORK PARTICIPATION NAME OF FACILITY/AGENCY: INFORMATION COMPILED BY: Print Name: Title: Date: NOTE: After we receive your completed application, we will credential
HEALTH CARE FACILITY APPLICATION FOR NETWORK PARTICIPATION NAME OF FACILITY/AGENCY: INFORMATION COMPILED BY: Print Name: Title: Date: NOTE: After we receive your completed application, we will credential
ANCILLARY/FACILITY APPLICATION CREDENTIALING / RE-CREDENTIALING
 ANCILLARY/FACILITY APPLICATION CREDENTIALING / RE-CREDENTIALING Please attach copies of all applicable documents to the application: Copy of all Federal, State and/or local licenses required to operate
ANCILLARY/FACILITY APPLICATION CREDENTIALING / RE-CREDENTIALING Please attach copies of all applicable documents to the application: Copy of all Federal, State and/or local licenses required to operate
Denver Health Medical Plan, Inc Access Plan for Large Group and Exchange Plans
 Denver Health Medical Plan, Inc. 2016 Access Plan for Large Group and Exchange Plans Table of Contents Page INTRODUCTION 3 I. DHMP NETWORKS OF PRIMARY CARE, SPECIALISTS, BEHAVIORAL HEALTH, HOSPITALS AND
Denver Health Medical Plan, Inc. 2016 Access Plan for Large Group and Exchange Plans Table of Contents Page INTRODUCTION 3 I. DHMP NETWORKS OF PRIMARY CARE, SPECIALISTS, BEHAVIORAL HEALTH, HOSPITALS AND
Descriptions: Provider Type and Specialty
 Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Your Out-of-Pocket Type of Service
 Calendar Year Deductible (CYD) 1 $0 single/ 3x family Out-of-Pocket Maximum - Deductibles, coinsurance and copays all accrue toward the outof-pocket maximum. With respect to family plans, an individual
Calendar Year Deductible (CYD) 1 $0 single/ 3x family Out-of-Pocket Maximum - Deductibles, coinsurance and copays all accrue toward the outof-pocket maximum. With respect to family plans, an individual
Your Out-of-Pocket Type of Service
 Calendar Year Deductible (CYD) 1 $3,000 single/ 3x family Out-of-Pocket Maximum - Deductibles and copays all accrue towards the out-of-pocket $6,200 single/ 2x family maximum. With respect to family plans,
Calendar Year Deductible (CYD) 1 $3,000 single/ 3x family Out-of-Pocket Maximum - Deductibles and copays all accrue towards the out-of-pocket $6,200 single/ 2x family maximum. With respect to family plans,
Required documentation. Application submission
 https://providers.amerigroup.com Washington Organizational Credentialing Streamline Application Application to be used for location, specialty and market additions for facilities, ancillaries, and supportive
https://providers.amerigroup.com Washington Organizational Credentialing Streamline Application Application to be used for location, specialty and market additions for facilities, ancillaries, and supportive
Facility Credentialing Application
 Facility Credentialing Application Thank you for your interest in Sanford Health Plan. This application will need to accompany a signed and dated Participating Provider Agreement (not required for re-credentialing).
Facility Credentialing Application Thank you for your interest in Sanford Health Plan. This application will need to accompany a signed and dated Participating Provider Agreement (not required for re-credentialing).
Table 4.2c: Hours Worked per Week for Primary Clinical Employer by Respondents Who Worked at Least
 CONTENTS INTRODUCTION HIGHLIGHTS OF NATIONAL STATISTICS SECTION 1: CHARACTERISTICS OF 2009 AAPA CENSUS RESPONDENTS Table 1.1: Number and Percent Distribution of Census Respondents by State Where Employed...
CONTENTS INTRODUCTION HIGHLIGHTS OF NATIONAL STATISTICS SECTION 1: CHARACTERISTICS OF 2009 AAPA CENSUS RESPONDENTS Table 1.1: Number and Percent Distribution of Census Respondents by State Where Employed...
CUSTODIAL NURSING HOME CARE
 CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
REQUEST FOR MEMBERSHIP AND CLINICAL PRIVILEGES
 REQUEST FOR MEMBERSHIP AND CLINICAL PRIVILEGES *Applicant Printed Name: *Denotes required fields (Last) (First) (M.I) (Degree) Maiden Name (Alias): (Last) (First) *DOB: *SSN Sex: Male Female *Applicant
REQUEST FOR MEMBERSHIP AND CLINICAL PRIVILEGES *Applicant Printed Name: *Denotes required fields (Last) (First) (M.I) (Degree) Maiden Name (Alias): (Last) (First) *DOB: *SSN Sex: Male Female *Applicant
NEIGHBORHOOD HEALTH PARTNERSHIP POS SUMMARY OF BENEFITS
 XV-2 $30/$60/$200/$1,000/80% R NEIGHBORHOOD HEALTH PARTNERSHIP POS SUMMARY OF BENEFITS A quick glance at this Summary of Benefits will introduce you to the Point of Service (POS) Plan you have with Neighborhood
XV-2 $30/$60/$200/$1,000/80% R NEIGHBORHOOD HEALTH PARTNERSHIP POS SUMMARY OF BENEFITS A quick glance at this Summary of Benefits will introduce you to the Point of Service (POS) Plan you have with Neighborhood
FACILITY BASED SERVICES
 CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
CUSTODIAL NURSING HOME CARE Chiropratic Services Custodial Nursing Home Care DME Equipment and Supplies Incontinence Supplies: Diapers, briefs, wipes, gloves, pads Infusion (IV, Enteral) Services Outpatient
KERN HEALTH SYSTEMS PARTICIPATING HOSPITAL/FACILITY APPLICATION
 KERN HEALTH SYSTEMS PARTICIPATING HOSPITAL/FACILITY APPLICATION Facility Name: Chief Administrative Officer: Chief Financial Officer: Chief Medical Officer: Corporate Tax Status: If Facility Medi-cal Certified?
KERN HEALTH SYSTEMS PARTICIPATING HOSPITAL/FACILITY APPLICATION Facility Name: Chief Administrative Officer: Chief Financial Officer: Chief Medical Officer: Corporate Tax Status: If Facility Medi-cal Certified?
FACILITY BASED SERVICES
 FACILITY BASED SERVICES Inpatient Hospital Care Elective Inpatient Admission or Elective Inpatient Surgery Inpatient Rehabilitation Care Skilled Nursing Facility Admission Non-Custodial Nursing Home Care
FACILITY BASED SERVICES Inpatient Hospital Care Elective Inpatient Admission or Elective Inpatient Surgery Inpatient Rehabilitation Care Skilled Nursing Facility Admission Non-Custodial Nursing Home Care
Application Checklist for Facilities
 Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for the facility to participate with
Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for the facility to participate with
Summary of Benefits CCPOA (Basic) Custom Access+ HMO
 Custom Access+ HMO") Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits CCPOA (Basic) Custom Access+ HMO CCPOA Effective January 1, 2019 HMO Benefit Plan This Summary of Benefits
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits CCPOA (Basic) Custom Access+ HMO CCPOA Effective January 1, 2019 HMO Benefit Plan This Summary of Benefits
Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx]
![Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx]](/thumbs/86/94175655.jpg "Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx]") Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx] Group Plan HMO Benefit
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits [Silver Access+ HMO 1750/55 OffEx] [Silver Local Access+ HMO 1750/55 OffEx] Group Plan HMO Benefit
Summary of Benefits Platinum Full PPO 0/10 OffEx
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Full PPO 0/10 OffEx Group Plan PPO Benefit Plan This Summary of Benefits shows the amount
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Full PPO 0/10 OffEx Group Plan PPO Benefit Plan This Summary of Benefits shows the amount
Our Providers and Locations. The island of Molokai and Lanai
 Our Providers and Locations The island of Molokai and Lanai Your Medical Care Primary Care Providers This directory shows you where our primary care physicians and providers are located. We strongly encourage
Our Providers and Locations The island of Molokai and Lanai Your Medical Care Primary Care Providers This directory shows you where our primary care physicians and providers are located. We strongly encourage
MMA Benefits at a Glance
 MMA Benefits at a Glance You must get covered services by providers that are part of the Molina plan. You must also make sure that approval is obtained if needed. Ambulance Art Therapy Assistive Care Services
MMA Benefits at a Glance You must get covered services by providers that are part of the Molina plan. You must also make sure that approval is obtained if needed. Ambulance Art Therapy Assistive Care Services
WHAT DOES MEDICALLY NECESSARY MEAN?
 WHAT DOES MEDICALLY NECESSARY MEAN? Your Primary Care Provider (PCP) will help you get the services you need that are medically necessary as defined below. Medically Necessary means appropriate and necessary
WHAT DOES MEDICALLY NECESSARY MEAN? Your Primary Care Provider (PCP) will help you get the services you need that are medically necessary as defined below. Medically Necessary means appropriate and necessary
Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members
 Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members DEDUCTIBLE (per calendar year) Annual in-network deductible must be paid first for the following services: Imaging, hospital
Choice PPO Retired Employees Health Program Non-Medicare Eligible Retired Members DEDUCTIBLE (per calendar year) Annual in-network deductible must be paid first for the following services: Imaging, hospital
1998 AAPA Census Report
 Section I. General Information about Respondents Table 1. Distribution of Respondents by Sex Respondents... 15716 100.0% Male... 7413 47.2% Female... 8303 52.8% Table 2. Distribution of Respondents by
Section I. General Information about Respondents Table 1. Distribution of Respondents by Sex Respondents... 15716 100.0% Male... 7413 47.2% Female... 8303 52.8% Table 2. Distribution of Respondents by
The Green Valley Hospital: Looking Forward
 The Green Valley Hospital: Looking Forward Community Forum hosted by: The Green Valley Council Your Community Voice Introduction: Green Valley Hospital Citizen Advisory Committee Green valley Council Health
The Green Valley Hospital: Looking Forward Community Forum hosted by: The Green Valley Council Your Community Voice Introduction: Green Valley Hospital Citizen Advisory Committee Green valley Council Health
UB-82 AND UB-92 CONVERSION TABLE - TO BE USED FOR REPORTING NON-INSTITUTIONAL HCSRS
 6010.50-M, MAY 1999 DATA REQUIREMENTS CHAPTER 2 ADDENDUM H UB-82 AND UB-92 CONVERSION TABLE - TO BE USED FOR REPORTING NON-INSTITUTIONAL HCSRS The revenue codes listed below are authorized by the National
6010.50-M, MAY 1999 DATA REQUIREMENTS CHAPTER 2 ADDENDUM H UB-82 AND UB-92 CONVERSION TABLE - TO BE USED FOR REPORTING NON-INSTITUTIONAL HCSRS The revenue codes listed below are authorized by the National
2017 Comparison of the State of Iowa Medicaid Enterprise Basic Benefits Based on Eligibility Determination
 General Plan Provisions Benefits Available from Out-of-Network Providers 2017 Comparison of the State of Iowa Enterprise Cost Sharing: A variety of methods are used to share expenses between the state
General Plan Provisions Benefits Available from Out-of-Network Providers 2017 Comparison of the State of Iowa Enterprise Cost Sharing: A variety of methods are used to share expenses between the state
Summary of Benefits Platinum Trio HMO 0/25 OffEx
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Trio HMO 0/25 OffEx Group Plan HMO Benefit Plan This Summary of Benefits shows the amount
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum Trio HMO 0/25 OffEx Group Plan HMO Benefit Plan This Summary of Benefits shows the amount
A BETTER WAY. to invest in employee health
 A BETTER WAY to invest in employee health A BETTER WAY to take care of business Rely on A BETTER WAY Manage costs Invest in employee health Build the future 2 May 9, 2013 Kaiser Permanente 2012. All Rights
A BETTER WAY to invest in employee health A BETTER WAY to take care of business Rely on A BETTER WAY Manage costs Invest in employee health Build the future 2 May 9, 2013 Kaiser Permanente 2012. All Rights
Medicare Advantage 2014 Precertification Requirements
 Medicare Advantage 2014 Precertification Requirements (Effective for Jan 1, 2014 to June 30, 2014) The precertification requirements filed with the Centers for Medicare & Medicaid Services remain in effect
Medicare Advantage 2014 Precertification Requirements (Effective for Jan 1, 2014 to June 30, 2014) The precertification requirements filed with the Centers for Medicare & Medicaid Services remain in effect
2016 ANNUAL PHYSICIAN COMPENSATION SURVEY
 2016 ANNUAL PHYSICIAN COMPENSATION SURVEY Pinnacle Health Group s compensation data is based on mean compensation and/or base salary for 175 surveyed physicians and 160 healthcare organizations, covering
2016 ANNUAL PHYSICIAN COMPENSATION SURVEY Pinnacle Health Group s compensation data is based on mean compensation and/or base salary for 175 surveyed physicians and 160 healthcare organizations, covering
Organizational Provider Credentialing Application
 Organizational Provider Credentialing Application New Mexico Organizational provider identification Legal business name (as reported to the IRS): Medicaid number: Doing Business As (DBA) name (if applicable):
Organizational Provider Credentialing Application New Mexico Organizational provider identification Legal business name (as reported to the IRS): Medicaid number: Doing Business As (DBA) name (if applicable):
Services That Require Prior Authorization
 Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
2017 SPECIALTY REPORT ANNUAL REPORT
 2017 SPECIALTY REPORT ANNUAL REPORT National Commission on Certification of Physician Assistants Table of Contents Message from the President... 3 About the Data Collection and Methodology...4 All Specialties....
2017 SPECIALTY REPORT ANNUAL REPORT National Commission on Certification of Physician Assistants Table of Contents Message from the President... 3 About the Data Collection and Methodology...4 All Specialties....
2001 AAPA Physician Assistant Census Report 1. Respondents % Male % Female %
 1 Section I. Personal Characteristics of Respondents* Table 1. Distribution of Respondents by Sex Respondents... 19786 100.0% Male... 8603 43.5% Female... 11183 56.5% Table 2. Distribution of Respondents
1 Section I. Personal Characteristics of Respondents* Table 1. Distribution of Respondents by Sex Respondents... 19786 100.0% Male... 8603 43.5% Female... 11183 56.5% Table 2. Distribution of Respondents
2009 AAPA Physician Assistant Census National Report
 Report # CENS2009-01 January 2010 2009 AAPA Physician Assistant Census National Report Introduction The American Academy of Physician Assistants (AAPA) was founded in 1968 and is the only national organization
Report # CENS2009-01 January 2010 2009 AAPA Physician Assistant Census National Report Introduction The American Academy of Physician Assistants (AAPA) was founded in 1968 and is the only national organization
Organizational Provider Credentialing Application
 Prior to completing this credentialing application, please read and observe the following: INSTRUCTIONS This form should be typed (using a different font than the form) or legibly printed in black or blue
Prior to completing this credentialing application, please read and observe the following: INSTRUCTIONS This form should be typed (using a different font than the form) or legibly printed in black or blue
Medicaid Benefits at a Glance
 Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
HPHC Insurance Company, Inc. THE HPHC INSURANCE COMPANY DEDUCTIBLE TIERED COPAYMENT PPO PLAN MAINE
 ID: MD0000003250 X Schedule of s HPHC Insurance Company, Inc. THE HPHC INSURANCE COMPANY DEDUCTIBLE TIERED COPAYMENT PPO PLAN MAINE This Schedule of s summarizes your benefits under the The HPHC Insurance
ID: MD0000003250 X Schedule of s HPHC Insurance Company, Inc. THE HPHC INSURANCE COMPANY DEDUCTIBLE TIERED COPAYMENT PPO PLAN MAINE This Schedule of s summarizes your benefits under the The HPHC Insurance
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION
 INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must be completed in its entirety 3. Must be signed and dated 4.
INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must be completed in its entirety 3. Must be signed and dated 4.
Kaiser Permanente Group Plan 301 Benefit and Payment Chart
 301 Kaiser Permanente Group Plan 301 Benefit and Payment Chart 10119 CITY AND COUNTY OF SAN FRANCISCO About this chart This benefit and payment chart: Is a summary of covered services and other benefits.
301 Kaiser Permanente Group Plan 301 Benefit and Payment Chart 10119 CITY AND COUNTY OF SAN FRANCISCO About this chart This benefit and payment chart: Is a summary of covered services and other benefits.
HEALTH CARE DELIVERY ORGANIZATION/ANCILLARY/LONG TERM CARE PROVIDER APPLICATION
 HEALTH CARE DELIVERY ORGANIZATION/ANCILLARY/LONG TERM CARE PROVIDER APPLICATION **Please note: Submission of a completed application does not guarantee approval as a participating provider as additional
HEALTH CARE DELIVERY ORGANIZATION/ANCILLARY/LONG TERM CARE PROVIDER APPLICATION **Please note: Submission of a completed application does not guarantee approval as a participating provider as additional
AMGA Webinar: MSSP Final Rule. Scott Hines, MD Chief Quality Officer Crystal Run Healthcare July 16, 2015
 AMGA Webinar: MSSP Final Rule Scott Hines, MD Chief Quality Officer Crystal Run Healthcare July 16, 2015 Crystal Run Healthcare Physician owned MSG in NY State, founded 1996 >350 providers, >30 locations
AMGA Webinar: MSSP Final Rule Scott Hines, MD Chief Quality Officer Crystal Run Healthcare July 16, 2015 Crystal Run Healthcare Physician owned MSG in NY State, founded 1996 >350 providers, >30 locations
CLASSIC BLUE SECURE/BLUE CROSS BLUE SHIELD COMPLEMENTARY Monroe County Benefit Summary/Comparison (Over 65 Retirees)
") WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
WHO IS COVERED Enrollment Requirement Members must be enrolled in both Medicare Parts A and B Members must be enrolled in both Medicare Parts A and B Type of Tier Single only Single only Dependent/Student
Cigna Summary of Benefits Open Access Plus Copay Plan (OAP10)
") Cigna Care Network (CCN) Cigna Summary of Benefits Open Access Plus Copay Plan (OAP10) Cigna Care Network (CCN) Your employer has selected a Cigna Care Network (CCN) plan. When you need specialty care,
Cigna Care Network (CCN) Cigna Summary of Benefits Open Access Plus Copay Plan (OAP10) Cigna Care Network (CCN) Your employer has selected a Cigna Care Network (CCN) plan. When you need specialty care,
APPLICATION For PRE ACCREDITATION ENTRY LEVEL FOR HOSPITAL
 APPLICATION For PRE ACCREDITATION ENTRY LEVEL FOR HOSPITAL Issue No.: 01 Issue Date: July 2014 1 TIOL ACCREDITATION BOARD FOR HOSPITALS and HEALTHCARE PROVIDERS TIOL ACCREDITATION BOARD FOR HOSPITALS and
APPLICATION For PRE ACCREDITATION ENTRY LEVEL FOR HOSPITAL Issue No.: 01 Issue Date: July 2014 1 TIOL ACCREDITATION BOARD FOR HOSPITALS and HEALTHCARE PROVIDERS TIOL ACCREDITATION BOARD FOR HOSPITALS and
KY Medicaid Co-pays. Acute admissions medical Per admission diagnoses $0 Acute health care related to. Per admission substance abuse and/or for
 This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
UB-92 CONVERSION TABLE - TO BE USED FOR REPORTING NON-INSTITUTIONAL HCSRS
 6010.50-M, MAY 1999 DATA REQUIREMENTS CHAPTER 2 ADDENDUM H UB-92 CONVERSION TABLE - TO BE USED FOR REPORTING NON-INSTITUTIONAL HCSRS The revenue codes listed below are authorized by the National Uniform
6010.50-M, MAY 1999 DATA REQUIREMENTS CHAPTER 2 ADDENDUM H UB-92 CONVERSION TABLE - TO BE USED FOR REPORTING NON-INSTITUTIONAL HCSRS The revenue codes listed below are authorized by the National Uniform
Kaiser Foundation Health Plan, Inc. A NONPROFIT HEALTH PLAN - HAWAII REGION
 Kaiser Foundation Health Plan, Inc. A NONPROFIT HEALTH PLAN - HAWAII REGION 2019 Summary of Important Changes for Contract Renewals for the Kaiser Permanente Group Plan (These changes are subject to regulatory
Kaiser Foundation Health Plan, Inc. A NONPROFIT HEALTH PLAN - HAWAII REGION 2019 Summary of Important Changes for Contract Renewals for the Kaiser Permanente Group Plan (These changes are subject to regulatory
All Out-of-Network hospitalizations, surgeries, procedures, referrals, evaluations, services and treatment require prior authorization.
 2018 OptumCare Utah Contracted Provider Prior Authorization List Items listed below require prior authorization. Out-of-Network All Out-of-Network hospitalizations, surgeries, procedures, referrals, evaluations,
2018 OptumCare Utah Contracted Provider Prior Authorization List Items listed below require prior authorization. Out-of-Network All Out-of-Network hospitalizations, surgeries, procedures, referrals, evaluations,
Covered Services List and Referrals and Prior Authorizations for MassHealth Members enrolled in Partners HealthCare Choice
 Covered Services Covered Services List and s and Prior Authorizations for MassHealth Members enrolled in Partners HealthCare Choice This chart tells you two things: 1. the covered services and benefits
Covered Services Covered Services List and s and Prior Authorizations for MassHealth Members enrolled in Partners HealthCare Choice This chart tells you two things: 1. the covered services and benefits
Your gateway to 300+ associations in the National Healthcare Career Network
 Your gateway to 300+ associations in the National Healthcare Career Network ACADEMIA & RESEARCH AdvaMed American Association for the Study of Liver Diseases American Association of Colleges of Osteopathic
Your gateway to 300+ associations in the National Healthcare Career Network ACADEMIA & RESEARCH AdvaMed American Association for the Study of Liver Diseases American Association of Colleges of Osteopathic
NEVADA HEALTH CO-OP SOUTHERN STAR/ESTRELLA GOLD 100% 34996NV
 NEVADA HEALTH CO-OP SOUTHERN STAR/ESTRELLA GOLD 100% 34996NV003 0002 Attachment A Benefit Schedule Lifetime Maximum: Unlimited. Benefits apply when you obtain or arrange for Covered through a Nevada Health
NEVADA HEALTH CO-OP SOUTHERN STAR/ESTRELLA GOLD 100% 34996NV003 0002 Attachment A Benefit Schedule Lifetime Maximum: Unlimited. Benefits apply when you obtain or arrange for Covered through a Nevada Health
Benefit Explanation And Limitations
 Benefit Explanation And Limitations SFHP providers supply many medical benefits and services, some of which are itemized on the following pages. For specific information not covered in this table, please
Benefit Explanation And Limitations SFHP providers supply many medical benefits and services, some of which are itemized on the following pages. For specific information not covered in this table, please
Benefit Name In Network Out of Network Limits and Additional Information. N/A Pharmacy. N/A Pharmacy
 Excellus BluePPO Drug Coverage Excluded Benefit Time Period: 01/01/2018-12/31/2018 HOBART & WILLIAM SMITH COLLEGES General Information Cost Sharing Expenses Deductible - Single $0 $500 Deductible - Family
Excellus BluePPO Drug Coverage Excluded Benefit Time Period: 01/01/2018-12/31/2018 HOBART & WILLIAM SMITH COLLEGES General Information Cost Sharing Expenses Deductible - Single $0 $500 Deductible - Family
Basic Covered Benefits and Services
 Basic Covered Benefits and A prior authorization is when UnitedHealthcare Community Plan gives the doctor permission to perform certain services. Bed Liners Coverage Covered for members age 4 and up; Prior
Basic Covered Benefits and A prior authorization is when UnitedHealthcare Community Plan gives the doctor permission to perform certain services. Bed Liners Coverage Covered for members age 4 and up; Prior
This document contains the format of each file that is exported by AHS and prepared for each Health Plan.
 Florida Health Plan Export File Formats This document contains the format of each file that is exported by AHS and prepared for each Health Plan. Contents Health Plan Export File Formats... 1 Revision
Florida Health Plan Export File Formats This document contains the format of each file that is exported by AHS and prepared for each Health Plan. Contents Health Plan Export File Formats... 1 Revision
Summary of Benefits Full PPO Savings Two-Tier Embedded Deductible 1500/2700/3000
 Summary of Benefits Full PPO Savings Two-Tier Embedded Deductible 1500/2700/3000 Group Plan PPO Savings Benefit Plan This Summary of Benefits shows the amount you will pay for Covered Services under this
Summary of Benefits Full PPO Savings Two-Tier Embedded Deductible 1500/2700/3000 Group Plan PPO Savings Benefit Plan This Summary of Benefits shows the amount you will pay for Covered Services under this
Caldwell Medical Center Departments
 Caldwell Medical Center Departments Surgery Medical / Surgery Same Day Surgery Lab Education Administration Special Care Unit Women s Center Admission Emergency Services Radiology Cardiac Rehab Admission
Caldwell Medical Center Departments Surgery Medical / Surgery Same Day Surgery Lab Education Administration Special Care Unit Women s Center Admission Emergency Services Radiology Cardiac Rehab Admission
GIC Employees/Retirees without Medicare
 GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
GIC Active Employees & Retirees without Medicare 7/1/18 GIC Employees/Retirees without Medicare HMO Summary of Benefits Chart This chart provides a summary of key services offered by your Health New England
Application Checklist for Facilities
 Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for each facility to participate with
Application Checklist for Facilities Please use the following checklist to complete the credentialing process. Current copies of all items listed below are required for each facility to participate with
Welcome to Kaiser Permanente: NAME (Please Print):
:") Welcome to Kaiser Permanente: NAME (Please Print): You have made a great choice for your health! We value each and every member and aim to make your transition from your prior insurance company to Kaiser
Welcome to Kaiser Permanente: NAME (Please Print): You have made a great choice for your health! We value each and every member and aim to make your transition from your prior insurance company to Kaiser
KY Medicaid Co-pays Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following:
 This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
This is a list of current covered services and co-pays. Except for the Pharmacy Non-Preferred co-pay, co-pays do not apply to the following: Non-KCHIP children Children under 19 in foster care Pregnant
Telemedicine services $0 copay Not applicable Primary care provider (PCP) CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance
 CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance CYD/Coinsurance") Calendar Year Deductible (CYD) 2 Plan includes an embedded individual deductible provision. An embedded deductible combines individual and family deductibles in $4,000 Single / $8,000 Family $12,000 Single
Calendar Year Deductible (CYD) 2 Plan includes an embedded individual deductible provision. An embedded deductible combines individual and family deductibles in $4,000 Single / $8,000 Family $12,000 Single
Summary of Benefits Silver 70 HMO Trio
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Silver 70 HMO Trio Individual and Family Plan HMO Benefit Plan This Summary of Benefits shows the amount
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Silver 70 HMO Trio Individual and Family Plan HMO Benefit Plan This Summary of Benefits shows the amount
Benefits. Benefits Covered by UnitedHealthcare Community Plan
 Benefits Covered by UnitedHealthcare Community Plan As a member of UnitedHealthcare Community Plan, you are covered for the following MO HealthNet Managed Care services. (Remember to always show your current
Benefits Covered by UnitedHealthcare Community Plan As a member of UnitedHealthcare Community Plan, you are covered for the following MO HealthNet Managed Care services. (Remember to always show your current
Summary of Benefits Platinum 90 HMO Trio
 Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum 90 HMO Trio Individual and Family Plan HMO Benefit Plan This Summary of Benefits shows the
Blue Shield of California is an independent member of the Blue Shield Association Summary of Benefits Platinum 90 HMO Trio Individual and Family Plan HMO Benefit Plan This Summary of Benefits shows the
CAMC Health System SNAPSHOT 2018
 CAMC Health System SNAPSHOT 2018 Special designations Southern West Virginia s largest medical center Only kidney transplant center in WV Level I (highest ranking) Trauma Center Level I pediatric intensive
CAMC Health System SNAPSHOT 2018 Special designations Southern West Virginia s largest medical center Only kidney transplant center in WV Level I (highest ranking) Trauma Center Level I pediatric intensive
PacificSource Community Solutions Referral Frequently Asked Questions
 PacificSource Community Solutions Referral Frequently Asked Questions **For Provider Use Only** 1. What is the difference between a referral and a preapproval? A referral is the process by which the member
PacificSource Community Solutions Referral Frequently Asked Questions **For Provider Use Only** 1. What is the difference between a referral and a preapproval? A referral is the process by which the member
Member s Responsibility: Deductible, Copays, Coinsurance and Maximums
 Benefits-at-a-Glance for GradCare 2018 This is intended as an easy-to-read summary. It is not a contract. Refer to the Your Benefits chapter in the Certificate for an official description of benefits.
Benefits-at-a-Glance for GradCare 2018 This is intended as an easy-to-read summary. It is not a contract. Refer to the Your Benefits chapter in the Certificate for an official description of benefits.
GOLD 80 HMO NETWORK 1 MIRROR
 GOLD 80 HMO NETWORK 1 MIRROR Summary of Benefits Group An independent member of the Blue Shield Association (Intentionally left blank) Gold 80 HMO Network 1 Mirror Summary of Benefits The Summary of Benefits
GOLD 80 HMO NETWORK 1 MIRROR Summary of Benefits Group An independent member of the Blue Shield Association (Intentionally left blank) Gold 80 HMO Network 1 Mirror Summary of Benefits The Summary of Benefits
Summary of Benefits Prominence HealthFirst Small Group Health Plan
 POS Triple Choice 3000 Summary of Benefits Calendar Year Deductible (CYD) $3,000 Single / $9,000 Family $7,000 Single / $21,000 Family $21,000 Single / $63,000 Family Coinsurance 40% coinsurance 50% coinsurance
POS Triple Choice 3000 Summary of Benefits Calendar Year Deductible (CYD) $3,000 Single / $9,000 Family $7,000 Single / $21,000 Family $21,000 Single / $63,000 Family Coinsurance 40% coinsurance 50% coinsurance
MyHPN Solutions HMO Gold 7
 MyHPN Solutions HMO Gold 7 HIOS ID: 95865NV0030074 Attachment A Benefit Schedule Calendar Year Deductible (CYD): $3,000 of EME per Member and $6,000 of EME per family. The Calendar Year Out of Pocket Maximum
MyHPN Solutions HMO Gold 7 HIOS ID: 95865NV0030074 Attachment A Benefit Schedule Calendar Year Deductible (CYD): $3,000 of EME per Member and $6,000 of EME per family. The Calendar Year Out of Pocket Maximum
CURRICULUM ON PATIENT CARE MSU INTERNAL MEDICINE RESIDENCY PROGRAM
 CURRICULUM ON PATIENT CARE MSU INTERNAL MEDICINE RESIDENCY PROGRAM Faculty representative: Venu Chennamaneni, MD Original document by: Davoren Chick, MD, Kelly Morgan, MD Resident Representative: None
CURRICULUM ON PATIENT CARE MSU INTERNAL MEDICINE RESIDENCY PROGRAM Faculty representative: Venu Chennamaneni, MD Original document by: Davoren Chick, MD, Kelly Morgan, MD Resident Representative: None
Inpatient Rehabilitation. Scope of Services
 Inpatient Rehabilitation Scope of Services Inpatient Rehabilitation is a 12-bed inpatient unit located within Nationwide Children s Hospital. Nationwide Children s is a 451-bed, Level I Trauma Center.
Inpatient Rehabilitation Scope of Services Inpatient Rehabilitation is a 12-bed inpatient unit located within Nationwide Children s Hospital. Nationwide Children s is a 451-bed, Level I Trauma Center.
MEDICARE By Peter G. Pan
 Wendell K. Kimura Acting Director Research (808) 587-0666 Revisor (808) 587-0670 Fax (808) 587-0681 LEGISLATIVE REFERENCE BUREAU State of Hawaii State Capitol Honolulu, Hawaii 96813 No. 02-13 October 7,
Wendell K. Kimura Acting Director Research (808) 587-0666 Revisor (808) 587-0670 Fax (808) 587-0681 LEGISLATIVE REFERENCE BUREAU State of Hawaii State Capitol Honolulu, Hawaii 96813 No. 02-13 October 7,
Must meet specific criteria. Prior authorization required. Must meet specific criteria
 MIDWEST HEALTH Acupuncture NOT A BENEFIT NOT A BENEFIT NOT A BENEFIT Acute Care Observation Post Operative Emergency Room Allergy Testing/Allergy Injections Ambulance-Emergency Land Plan Notification Not
MIDWEST HEALTH Acupuncture NOT A BENEFIT NOT A BENEFIT NOT A BENEFIT Acute Care Observation Post Operative Emergency Room Allergy Testing/Allergy Injections Ambulance-Emergency Land Plan Notification Not
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION
 HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
HOSPITAL-ANCILLARY-CLINIC PROVIDER CREDENTIALING APPLICATION INSTRUCTIONS: In order to be considered complete: 1. All information must be legible. Please print or type all information 2. Application must
STATEMENT OF PURPOSE
 STATEMENT OF PURPOSE This is the Statement of Purpose for Hull and East Yorkshire Hospitals NHS Trust as required by the Health and Social Care Act 2008 (regulated Activities) Regulations 2014 Schedule
STATEMENT OF PURPOSE This is the Statement of Purpose for Hull and East Yorkshire Hospitals NHS Trust as required by the Health and Social Care Act 2008 (regulated Activities) Regulations 2014 Schedule
Summary of Benefits Prominence Preferred Health Insurance Small Group Health Plan
 Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family $3,000 Single / $9,000 Family Coinsurance - Member responsibility 20% coinsurance 50% coinsurance Out-of-Pocket Maximum 3 - Deductibles, coinsurance
Calendar Year Deductible (CYD) 2 $1,000 Single / $3,000 Family $3,000 Single / $9,000 Family Coinsurance - Member responsibility 20% coinsurance 50% coinsurance Out-of-Pocket Maximum 3 - Deductibles, coinsurance
First Look: Plan Benefit Filings
 July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
July 30, 2014 First Look: Plan Filings Maryland and Washington, D.C. 1 Disclaimers MedStar does not currently have a contract with CMS for the State of MD nor any special needs plans in Washington, D.C.
interchange Provider Important Message
 HUSKY Health Primary Care Increased Payments Policy In accordance with Provider Bulletin PB14-75, certain primary care providers are eligible to receive increased Medicaid payments for primary care services
HUSKY Health Primary Care Increased Payments Policy In accordance with Provider Bulletin PB14-75, certain primary care providers are eligible to receive increased Medicaid payments for primary care services
Freedom Blue PPO SM Summary of Benefits
 Freedom Blue PPO SM Summary of Benefits R9943-206-CO-308 10/05 Introduction to the Summary of Benefits for Freedom Blue PPO Plan January 1, 2006 - December 31, 2006 California YOU HAVE CHOICES IN YOUR
Freedom Blue PPO SM Summary of Benefits R9943-206-CO-308 10/05 Introduction to the Summary of Benefits for Freedom Blue PPO Plan January 1, 2006 - December 31, 2006 California YOU HAVE CHOICES IN YOUR
Blue Cross Premier Bronze
 An individual PPO health plan from Blue Cross Blue Shield of Michigan. You will have a broad choice of doctors and hospitals within BCBSM s unsurpassed statewide PPO network including nationwide coverage.
An individual PPO health plan from Blue Cross Blue Shield of Michigan. You will have a broad choice of doctors and hospitals within BCBSM s unsurpassed statewide PPO network including nationwide coverage.
Benefit Explanation And Limitations
 Benefit Explanation And Limitations SFHP providers supply many medical benefits and services, some of which are itemized on the following pages. For specific information not covered in this table, please
Benefit Explanation And Limitations SFHP providers supply many medical benefits and services, some of which are itemized on the following pages. For specific information not covered in this table, please
IMPORTANT INFORMATION:
 Schedule of Benefits ElevateHealth Options HMO NEW HAMPSHIRE ID: MD0000018209_A13 X Coverage under this Plan is under the jurisdiction of the New Hampshire Insurance Commissioner. IMPORTANT INFORMATION:
Schedule of Benefits ElevateHealth Options HMO NEW HAMPSHIRE ID: MD0000018209_A13 X Coverage under this Plan is under the jurisdiction of the New Hampshire Insurance Commissioner. IMPORTANT INFORMATION:
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File
 North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
North Carolina Ambulatory Surgery Visit Data - Data Dictionary FY2011 Alphabetic List of Variables and Attributes Standard Research File One of these three variables must be suppressed (Diag1, fac, ptzip)
(2) A renewal certificate of registration as specified in Form 17 shall be valid for one year.
 A renewal certificate of registration as specified in Form 17 shall be valid for one year.") 11. Registration and functions of recognized medical institution or hospital.- (1) An application for registration shall be made to the Monitoring Authority as specified in Form 11. The application shall
11. Registration and functions of recognized medical institution or hospital.- (1) An application for registration shall be made to the Monitoring Authority as specified in Form 11. The application shall
HomeHospital (Rambam) Database Tables and Fields
 Database Tables and Fields") TECHNION - Israel Institute of Technology The William Davidson Faculty of Industrial Engineering and Management Center for Service Enterprise Engineering (SEE) http://ie.technion.ac.il/labs/serveng/ HomeHospital
TECHNION - Israel Institute of Technology The William Davidson Faculty of Industrial Engineering and Management Center for Service Enterprise Engineering (SEE) http://ie.technion.ac.il/labs/serveng/ HomeHospital