Profit = Price - Cost. TAKT Time Map Capacity Tables. Morale. Total Productive Maintenance. Visual Control. Poka-yoke (mistake proofing) Kanban.
|
|
|
- Kevin Wilson
- 6 years ago
- Views:
Transcription
 Setup Reduction Changeover Multi-process Operations Quality Cost Delivery Safety Measures Standard Operations Heijunka (Leveling) Continuous Flow Morale TAKT Time Map Capacity Tables")
1 GPS Mod 22 7 Flows of Medicine MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t Jidoka (human automation) Setup Reduction Changeover Multi-process Operations Quality Cost Delivery Safety Measures Standard Operations Heijunka (Leveling) Continuous Flow Morale TAKT Time Map Capacity Tables Total Productive Maintenance Poka-yoke (mistake proofing) Kanban Visual Control Andon 7 Flows of Medicine Module 22 RPIW Kaizen Kaikuku 3P Prod Prep 7 Flows Factory Product/Patient Quantity Analysis 7 Flows Medicine 4 No s Sorting Simplifying 5S Sweeping Standardizing Self Discipline 7 Wastes Value Stream Mapping ONE PIECE FLOW TAKT TIME PULL PRODUCTION Global Production System , John Black and Associates LLC (modified from Hiroyuki Hirano, Productivity Press). Committed Leaders 1
2 7 Flows of Medicine 1. Flow of Patients 2. Flow of Family 3. Flow of Providers 4. Flow of Medications 5. Flow of Supplies 6. Flow of Information 7. Flow of Equipment Mod 22 7 Flows of Medicine v
3 1. Flow of Patients A. No patient waits. 3 Mod 22 7 Flows of Medicine B. Minimize patient walking; bring the services to the patient. C. Problems must force the process to stop. D. Patient flow is in only one direction with successive steps in order of processing. E. Incorporate quality checks at each step of the process with mistake-proofing methods. F. If there is single-piece flow, schedulers/planners are not needed for the process. G. Understand Takt Time meeting the demand. H. Use between processes time to complete indirect patient care tasks.
4 Questions to ask about Patient Flow: How many patients does your unit treat in a day? In a week? What do you treat them for? How much time per patient is allotted? Is this time too little or too much, based on the patient load and the severity of cases? Where do waits occur? When and where do clinicians wait for patients? Where are opportunities to optimize patient flow? If unavoidable waits exist between processes, can other value-added work be done? Can the service be brought closer to the patient? (e.g., can lab work be performed near the patient rather than sending the patient to a central lab?) v

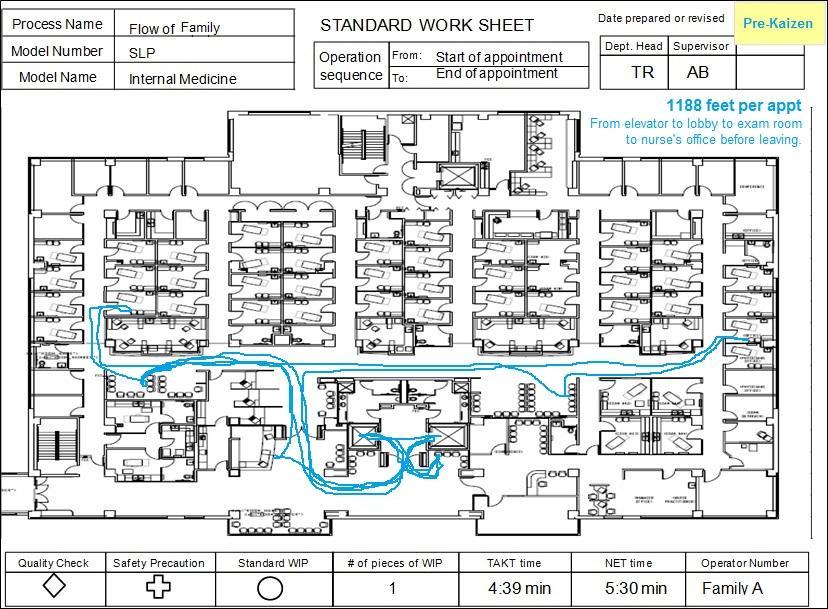
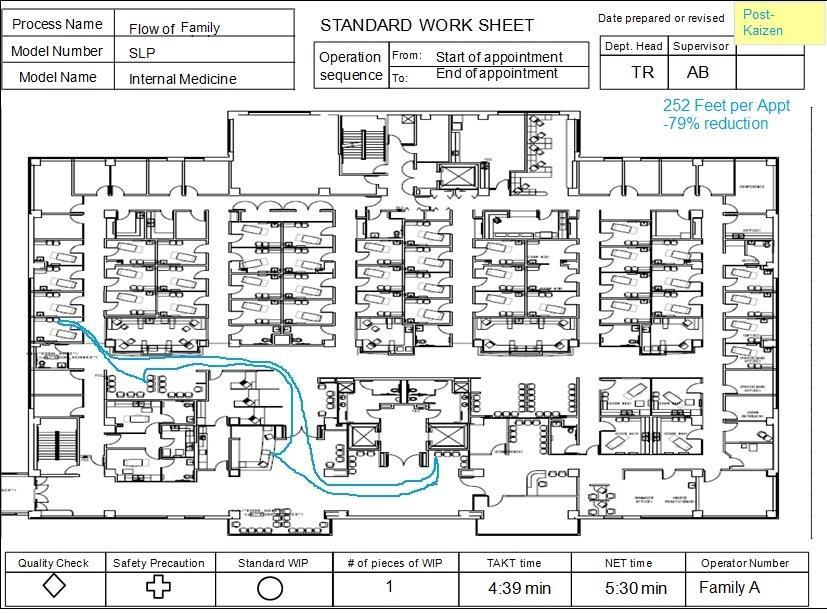
5 2. Flow of Family A. Family and important relationships are defined by the patient. B. Family travels with the patient where appropriate and as the patient desires. C. Family is a respected part of the patient care team. D. Family concerns stop the process until addressed. E. Family is a respected source of information about the patient. F. Information should flow to the family throughout the process as desired by the patient. 5
6 Questions to ask about Family/Relationships Flow Mod 22 7 Flows of Medicine How does the patient define their family or important relationships and how does the patient want them involved? When and where can the family be included in the process to improve care for the patient? Where are the opportunities to optimize information flow between care team, patient, and family? What unique information might they have that would enhance the care of the patient? v



7 3. Flow of Providers A. Understand Takt Time and cycle times of the work. B. Look for standard work it is critical to people flow. C. Do not isolate people in islands. D. Understand people movement, especially if across several process steps. E. Providers are part of the process when they stop, the process should stop. F. All supplies, instruments and materials should be as close to the provider as possible. G. Examine motion of hands, feet, and eyes. H. Stand when possible do not use chairs! I. Do not tolerate rework! J. Avoid unreasonableness (i.e., Muri). 7
8 Healthcare clinicians are the people most instrumental in providing value-added work to healthcare processes. The flow of clinicians between the clinic, the hospital, and other patient-care delivery centers should be quick, easy, and stress-free for both clinicians and patients. Doctors, nurses, and other practitioners are often stressed when forced to scramble around, traveling from one appointment to another. This situation sometimes results in a curt demeanor and poor patient relations. Studies show that physicians who are known for a good bedside manner and for taking time to know their patients are less likely to be sued for malpractice. 8
9 Questions to ask about Clinician Flow: How many patients does your unit treat in a day? In a week? What do you treat them for? What is the average length of time required to process and treat one patient? Where can you better arrange work cells? How easy would it be to reconfigure the work space? Is it possible to set up satellite labs or pharmacies for smaller, less invasive treatments, reducing the time a patient or a clinician takes to travel to a central site. Can you reduce interruptions to the provider? v

10 4. Flow of Medications A. Single-piece flow with signal/pull from provider. B. Introduce point-of-use. Get as close as possible to the point of use. C. Kit medications where possible. D. Make smaller, specialized satellite pharmacies where possible. Mod 22 7 Flows of Medicine E. Bring medications to the patient, no patient walking. F. No waiting for medications. 10
11 Optimally, the medications flow through the system JIT only in the amount needed, at the place and time needed, at the appropriate cost. Here are some ways to improve flow of medications. Provide single-piece flow with signal/pull from clinician. Locate medications as close as possible to the point of use. Combine medications (kit) commonly used together in one container where possible. Add to the kits any additional medications prescribed by the physician. For example, kitting medications the night before discharge enables a patient and family to exit the system more quickly. Create smaller, specialized satellite pharmacies where possible. Satellite pharmacies bring pharmacy staff closer to high patient population locations and make it easier to eliminate backlogs and long queues. 11
12 Questions to ask about Medication Flow Can a satellite pharmacy be placed at each service delivery center so that medications are delivered quickly and effectively? Where can you pre-kit medications and stimulate flow? Can medications be kitted the night before patients are to be discharged? How often are medications being ordered? Are you stocking medications not used regularly, just in case? Are some of them reaching their expiration dates before use? Are you increasing costs by being overly cautious? v

13 5. Flow of Supplies A. Do the supplies flow to point of use? B. Just in Time only material on-hand needed at the right place and at the right time. C. Make the flow visual for simple control. D. Introduce min/max, or 2 bin strategies to resupply point of use. E. Presentation of materials and sequencing is key. F. Quality is critical. G. Inventory reduction strategies use kanban for total inventory reduction. H. Think of flow upstream to suppliers is it Just In Time? (JIT) 13
14 Questions to Ask Regarding Supply Flow How can you create systems to bring supplies into the medical center in a quick and efficient way? Is there pull from patient service delivery centers to central supply and out to suppliers? Where can you make it visual so that patients or employees can scan supplies or the process at a glance and tell what is happening and what action to take next? Is safety stock necessary? If so, where? v

15 6. Flow of Information A. Information travels with patient. 15 Mod 22 7 Flows of Medicine B. When information flow stops, the process stops. C. When designing the process, consider how information flows. D. Only the minimum information necessary to perform the process should be released. E. Introduce mistake proofing and go/no go gauges to ensure the flow of correct information. F. Information can come in many forms signals, lights, sounds, music, spaces, etc. G. Information must facilitate pull processes, not push. H. Open room arrangements facilitate the flow of information between providers and staff.
16 The efficient and effective flow of information enables timely, high-quality patient care, and enhanced safety. You don t want a stop in information flow for example, a missing chart or lab results to interrupt patient flow. Do not have incorrect or missing information (e.g., allergies to medications) that can endanger the patient. Consider how many times hospital clinicians take time to verify patient identification. This is a quality check to ensure that the correct person receives the correct treatment. Value-stream mapping can tell you: How information flows through the system. Where redundancy and rework exist. How many data systems exist that all ask the same questions and keep the same data. 16
17 Questions to ask about Information Flow: Where and how can you make information travel with the patient? Are you providing information clinicians don t use? Where do you find redundancy and rework in information flow? Can we put all the vital patient information on an electronic card that can simply be swiped upon arrival at the medical center? What is your process for flow of information? How can you improve this flow to better serve your patients? How do you ensure that information is correct every time? v

18 7. Flow of Equipment A. Arrange equipment in a sequence that facilitates the flow of patients, providers and information. B. Separate people from machine work (i.e., Jidoka). C. Use equipment with narrow frontage. Think townhouse not ranch house. D. Operation in front maintenance in back. E. Right-sized, small, economical equipment on wheels that is home-made. F. No money and no time are just excuses. G. Use of small, single-purpose machines with in-process checks. H. No roots, no ivy, no anchors. I. Equipment must facilitate flexible arrangements as demand and processes change. J. Is there wasted machine movement? 18
19 Whenever possible, use right-sized, small, home-made economical equipment on wheels that s easy to move and light enough for one person to manage. This approach limits walls and monuments (immovable equipment or furnishings), so the space available can be configured in the most effective and efficient way possible. Optimize equipment use. Machines can operate 24 hours a day, seven days a week. Are you optimizing the use of your equipment? For example, you could offer MRI services in two or three shifts. Be flexible in your equipment use. Explore adding or subtracting equipment as demand varies. Can equipment that is not currently needed be easily dismantled or folded up and stored nearby for future use? 19
20 Questions to ask about Flow of Equipment How will a piece of equipment improve patient flow, quality of care, and safety? Is it the most cost-efficient solution? How often will the equipment be used? Can it be used more if demand increases? Is the equipment located where it makes the most sense in terms of patient flow? Can it easily be moved to the point of service delivery? Does every piece of equipment have a preventive maintenance schedule? Is it being followed? v
21 Summary and Key Learnings Studying the seven flows in your facility and identifying the waste within the processes can lead to creative ways of improving both the facility and patient care. Improved flow creates greater patient satisfaction and greater staff satisfaction. It also reduces the chance for errors and increases the percentage of value-added work. If you want to improve flow, go to the place of action and see what the clinicians are doing. Look for long wait times or clutter piling up in the system. The seven flows work together and complement each other. An existing facility can be redesigned to enhance and streamline all those flows. The seven flows also can and should be applied in the preliminary design of a new facility or site. This will optimize the new design and improve all seven flows of healthcare. v
22 A Few Other Thoughts: Takt Time is a crucial measure of the seven flows in your medical center. It is the primary tool to measure demand for the medical center s rooms, equipment, and patient delivery services. There is no room for complacency. If you find yourself becoming complacent, that s a sure sign that something needs to be improved. Eliminate preconceived notions. If necessary, take a walk through the facility as a patient would and try to see it through their eyes. Kaizen is everybody s responsibility in the medical center. v
23 Process Name Model Number Model Name Date prepared or revised Pre-Kaizen / / Flow of Patient STANDARD WORK SHEET Dept. Head Supervisor SLP Operation From: Start of appointment Internal Medicine sequence To: End of appointment TR AB 1188 feet per appt From elevator to lobby to exam room to nurse s office to leaving Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 1 4:39 min N/A Patient A 23
24 Process Name Model Number Model Name Date prepared or revised Post- / / Flow of Patient STANDARD WORK SHEET Kaizen Dept. Head Supervisor SLP Operation From: Start of appointment Internal Medicine sequence To: End of appointment TR AB 252 feet per appt -79% reduction Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 1 4:39 min N/A Patient A 24
25 25
26 26
27 Process Name Model Number Model Name Date prepared or revised Pre-Kaizen / / Flow of Clinician STANDARD WORK SHEET Dept. Head Supervisor SLP Operation From: Start of clinic day Internal Medicine sequence To: End of clinic day TR AB 7920 feet per day From office to exam room to nurse s station to dictation Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 28:14 min 20:02 min Clinician A 27
28 Process Name Model Number Model Name Date prepared or revised Post- / / Flow of Clinician STANDARD WORK SHEET Kaizen Dept. Head Supervisor SLP Operation From: Start of clinic day Internal Medicine sequence To: End of clinic day TR AB 3960 feet per day -50% reduction Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 28:14 min 20:02 min Clinician A 28
29 Process Name Model Number Model Name Date prepared or revised Pre-Kaizen / / Flow of Nurse STANDARD WORK SHEET Dept. Head Supervisor SLP Operation From: Start of clinic day Internal Medicine sequence To: End of clinic day TR AB 3775 feet per day From lobby to exam room to triage office Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 15:29 min 30:07 min Nurse A 29
30 Process Name Model Number Model Name Date prepared or revised Post- / / Flow of Nurse STANDARD WORK SHEET Kaizen Dept. Head Supervisor SLP Operation From: Start of clinic day Internal Medicine sequence To: End of clinic day TR AB 203 feet per day -95% reduction Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 15:29 min 30:07 min Nurse A 30
31 Process Name Model Number Model Name Date prepared or revised Pre-Kaizen / / Flow of Technician STANDARD WORK SHEET Dept. Head Supervisor SLP Operation From: Start of appointment Internal Medicine sequence To: End of appointment TR AB 540 feet per day From supply room to exam room to supply room Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 4:39 min 11:00 min Technician A 31
32 Process Name Model Number Model Name Date prepared or revised Post- / / Flow of Technician STANDARD WORK SHEET Kaizen Dept. Head Supervisor SLP Operation From: Start of appointment Internal Medicine sequence To: End of appointment TR AB 21 feet per day -96% reduction Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 4:39 min 11:00 min Technician A 32
33 Process Name Model Number Model Name Date prepared or revised Pre-Kaizen / / Flow of Equipment STANDARD WORK SHEET Dept. Head Supervisor SLP Operation From: Start of appointment Internal Medicine sequence To: End of appointment TR AB 270 feet per day From storage to exam room to storage Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 4:39 min 5:30 min EKG Cart 33

34 Process Name Model Number Model Name Date prepared or revised Post- / / Flow of Equipment STANDARD WORK SHEET Kaizen Dept. Head Supervisor SLP Operation From: Start of appointment Internal Medicine sequence To: End of appointment TR AB 15 feet per day -94% reduction Quality Check Safety Precaution Standard WIP # of pieces of WIP TAKT time NET time Operator Number 4 4:39 min 5:30 min EKG Cart 34
35 Measures Baseline Final Walking Distance (ft) Overall average per day. Clinician A Nurse A Technician A Patient A Family A Part Travel Distance (ft) EKG cart moved to exam room and back to storage. Leadtime (mm:ss) Overall average per day Patient visit VA time (non wait) NVA time (wait) Cycle Time(mm:ss) Daily weighted average cycle time by operator Clinician A Nurse A Technician A Percent Change -50% -95% -96% -79% -79% % 46:24 56% 44% 20:02 15:42 30:07 31:02 93% 7% 17:15 10:56 24:12-33% 66% -84% -14% -30% -20% Summary of Impact Daily Impact: 2 more patients seen per day. Monthly Impact: 40 more patients seen per month. Yearly Impact: 480 more patients seen per year. For 1 clinician! 35
Standard Operations Module 11
 GPS Mod 11 Standard Ops MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t RPIW Jidoka (human automation) Setup
GPS Mod 11 Standard Ops MUDA MUDA Cost Reduction By Eliminating Waste Just-in-Time Profit = Price - Cost GPS Depth Study NVA/VA- Functions/Mgrs R e d e p l o y m e n t RPIW Jidoka (human automation) Setup
LEAN Transformation Storyboard 2015 to present
 LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
LEAN Transformation Storyboard 2015 to present Rapid Improvement Event Med-Surg January 2015 Access to Supply Rooms Problem: Many staff do not have access to supply areas needed to complete their work,
Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA
 These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
These presenters have nothing to disclose. Applying Critical ED Improvement Principles Jody Crane, MD, MBA Kevin Nolan, MStat, MA April 28, 2015 Cambridge, MA Session Objectives After this session, participants
Lean Six Sigma in Healthcare. 4 Simple BFO s s that Change Everything
 Lean Six Sigma in Healthcare 4 Simple BFO s s that Change Everything Presented By: Joseph Duhig Senior Vice President Juran Institute, Inc. February 23, 2008 BFO s = Blinding Flashes of the Obvious 8005
Lean Six Sigma in Healthcare 4 Simple BFO s s that Change Everything Presented By: Joseph Duhig Senior Vice President Juran Institute, Inc. February 23, 2008 BFO s = Blinding Flashes of the Obvious 8005
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health
 REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
REDESIGNING ALLIED HEALTH OUTPATIENTS - Lean Thinking Applications to Allied Health Josephine Kitch, Director, Allied Health Division,Flinders Medical Centre, SA Brenda Crane, RDC Clinical Facilitator,
When going Lean, Waste is the Enemy
 When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
When going Lean, Waste is the Enemy Eric S. Kastango, MBA, RPh, FASHP Clinical IQ, LLC March 31, 2009 Objectives Review the definition, elements and wastes of Lean Review the difference between Six Sigma
Partnerships- Cooperation with other care providers that is guided by open communication, trust, and shared decision-making.
 1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
1 E P 7: Describe and demonstrate the structure(s) and process(es) used to engage internal experts and external consultants to improve care in the practice setting. When Riverside nurses from any level
WHITE PAPER. Transforming the Healthcare Organization through Process Improvement
 WHITE PAPER Transforming the Healthcare Organization through Process Improvement The movement towards value-based purchasing models has made the concept of process improvement and its methodologies an
WHITE PAPER Transforming the Healthcare Organization through Process Improvement The movement towards value-based purchasing models has made the concept of process improvement and its methodologies an
Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust Tel
 Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
Lean Thinking Neil Westwood Associate Service Transformation and Hereford Hospitals NHS Trust neil.westwood@institute.nhs.uk Tel 07747794976 NHS Institute for Innovation and Improvement Plan for today
3sHealth Supports the Flow of Services to the Patient
 report Summer 2013 card The seven flows of medicine centred around the flow of the patient. 3sHealth Supports the Flow of Services to the Patient When most people think of patient care in a medical setting,
report Summer 2013 card The seven flows of medicine centred around the flow of the patient. 3sHealth Supports the Flow of Services to the Patient When most people think of patient care in a medical setting,
Building a Lean Team. Using Lean Methodology to Develop a Collaborative Rounding Model. April 28 th, 2010
 Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
Building a Lean Team Using Lean Methodology to Develop a Collaborative Rounding Model April 28 th, 2010 Faculty APD, Internal Medicine Residency Program Co-Sponsor, LEAN Improvement Team APD, Internal
The Quality Journey of
 The Quality Journey of New Territories West Cluster, Hong Kong Dr. T W Lee Hospital chief Executive Pok Oi Hospital New Territories West Cluster Hong Kong The Sick Hospital Medical treatment improves with
The Quality Journey of New Territories West Cluster, Hong Kong Dr. T W Lee Hospital chief Executive Pok Oi Hospital New Territories West Cluster Hong Kong The Sick Hospital Medical treatment improves with
Continuous Quality Improvement Made Possible
 Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Continuous Quality Improvement Made Possible 3 methods that can work when you have limited time and resources Sponsored by TABLE OF CONTENTS INTRODUCTION: SMALL CHANGES. BIG EFFECTS. Page 03 METHOD ONE:
Improving the Safety, Efficiency & Effectiveness of the Medication Administration Process
 Improving the Safety, Efficiency & Effectiveness of the Medication Administration Process Northwest Patient Safety Conference May 19, 2011 Joan Ching RN, MN, CPHQ Administrative Director, Hospital Quality
Improving the Safety, Efficiency & Effectiveness of the Medication Administration Process Northwest Patient Safety Conference May 19, 2011 Joan Ching RN, MN, CPHQ Administrative Director, Hospital Quality
Pursuit of the Perfect Patient Experience: How Virginia Mason Became a High Performing Healthcare System
 Pursuit of the Perfect Patient Experience: How Virginia Mason Became a High Performing Healthcare System Sarah Patterson, Executive VP & COO The King s Fund Annual Conference November 13, 2014 Virginia
Pursuit of the Perfect Patient Experience: How Virginia Mason Became a High Performing Healthcare System Sarah Patterson, Executive VP & COO The King s Fund Annual Conference November 13, 2014 Virginia
(Muda) Objectives. Determine what is Value added vs. Non-Value added. Identify the eight types of waste. Understand the Barriers to.
 Objectives. Determine what is Value added vs. Non-Value added. Identify the eight types of waste. Understand the Barriers to.") Identifying Waste (Muda) Erika Sundrud, MA AVP Quality, Safety & Performance Improvement 1 Objectives Determine what is Value added vs. Non-Value added Identify the eight types of waste Understand the
Identifying Waste (Muda) Erika Sundrud, MA AVP Quality, Safety & Performance Improvement 1 Objectives Determine what is Value added vs. Non-Value added Identify the eight types of waste Understand the
Quick Guide to A3 Problem Solving
 Quick Guide to A3 Problem Solving What is it? Toyota Motor Corporation is famed for its ability to relentlessly improve operational performance. Central to this ability is the training of engineers, supervisors
Quick Guide to A3 Problem Solving What is it? Toyota Motor Corporation is famed for its ability to relentlessly improve operational performance. Central to this ability is the training of engineers, supervisors
HOW 5S ORGANIZING BOOSTS MONEY, TIME, AND PATIENT OUTCOMES
 HOW 5S ORGANIZING BOOSTS MONEY, TIME, AND PATIENT OUTCOMES WHAT IS 5S? THE CORE OF LEAN PHILOSOPHY Lean concepts have revolutionized the industrial world. Originating in Japan, and popularized by Toyota,
HOW 5S ORGANIZING BOOSTS MONEY, TIME, AND PATIENT OUTCOMES WHAT IS 5S? THE CORE OF LEAN PHILOSOPHY Lean concepts have revolutionized the industrial world. Originating in Japan, and popularized by Toyota,
Academy of Architecture for Health On-line Professional Development. Health Care 101 Series
 Academy of Architecture for Health On-line Professional Development LEAN Concepts Drive Healthcare Architecture Planning and Design Health Care 101 Series 10, October, 2017 2:00 pm 3:00 pm ET 1:00 pm 2:00
Academy of Architecture for Health On-line Professional Development LEAN Concepts Drive Healthcare Architecture Planning and Design Health Care 101 Series 10, October, 2017 2:00 pm 3:00 pm ET 1:00 pm 2:00
System redesign in Primary Care
 System redesign in Primary Care A focus on Lean Anthony Behm, D.O. Chief of Staff, Erie VAMC Primary care(pc) satisfaction: up and down Satisfaction rates for PC s started dropping in the late 90 s. Physicians
System redesign in Primary Care A focus on Lean Anthony Behm, D.O. Chief of Staff, Erie VAMC Primary care(pc) satisfaction: up and down Satisfaction rates for PC s started dropping in the late 90 s. Physicians
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Eliminating Waste Will Transform American Healthcare
 Reprinted from The Toyota Way to Healthcare Excellence by John Black with David Miller (Health Administration Press 2008) C H A P T E R 2 Eliminating Waste Will Transform American Healthcare OVERVIEW:
Reprinted from The Toyota Way to Healthcare Excellence by John Black with David Miller (Health Administration Press 2008) C H A P T E R 2 Eliminating Waste Will Transform American Healthcare OVERVIEW:
How Pharmacy Informatics and Technology are Evolving to Improve Patient Care
 How Pharmacy Informatics and Technology are Evolving to Improve Patient Care HealthcareIS.com 2 Table of Contents 3 Impact of Emerging Technologies 3 CPOE 5 Automated Dispensing Machines 6 Barcode Medication
How Pharmacy Informatics and Technology are Evolving to Improve Patient Care HealthcareIS.com 2 Table of Contents 3 Impact of Emerging Technologies 3 CPOE 5 Automated Dispensing Machines 6 Barcode Medication
Discharge Before Noon DH32
 Discharge Before Noon DH32 Green Belts: Champion: Susan Christensen, RN Eric Belen Hai Tran Alice Issai Date: March 21, 2012 1 DEFINE Problem Statement 1. Baseline data shows only 18% of patient discharges*
Discharge Before Noon DH32 Green Belts: Champion: Susan Christensen, RN Eric Belen Hai Tran Alice Issai Date: March 21, 2012 1 DEFINE Problem Statement 1. Baseline data shows only 18% of patient discharges*
Applying Toyota Production System Principles And Tools At The Ghent University Hospital
 Proceedings of the 2012 Industrial and Systems Engineering Research Conference G. Lim and J.W. Herrmann, eds. Applying Toyota Production System Principles And Tools At The Ghent University Hospital Dirk
Proceedings of the 2012 Industrial and Systems Engineering Research Conference G. Lim and J.W. Herrmann, eds. Applying Toyota Production System Principles And Tools At The Ghent University Hospital Dirk
Practical Applications on Efficiency
 Practical Applications on Efficiency Maryland MGMA September 19, 214 Owen J. Dahl, FACHE, LSSMBB Objectives To offer practical scenarios for the application of Lean Tools in YOUR practice To discuss and
Practical Applications on Efficiency Maryland MGMA September 19, 214 Owen J. Dahl, FACHE, LSSMBB Objectives To offer practical scenarios for the application of Lean Tools in YOUR practice To discuss and
Emergency Department Throughput
 Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
Emergency Department Throughput Patient Safety Quality Improvement Patient Experience Affordability Hoag Memorial Hospital Presbyterian One Hoag Drive Newport Beach, CA 92663 www.hoag.org Program Managers:
INSERIRE LOGO CLIENTE GRANDE SERVICE FACTORY. A real office where to learn from experience
 INSERIRE LOGO CLIENTE GRANDE SERVICE FACTORY A real office where to learn from experience WHAT IS THE SERVICE FACTORY? The Service Factory is a training workshop where you can learn how to improve efficiency
INSERIRE LOGO CLIENTE GRANDE SERVICE FACTORY A real office where to learn from experience WHAT IS THE SERVICE FACTORY? The Service Factory is a training workshop where you can learn how to improve efficiency
Bluewater Health. Sarnia/Lambton, Ontario, Canada. Case Study
 Sarnia/Lambton, Ontario, Canada When began planning for a major renovation that combined two facilities under one roof and added five floors, they wanted maximum flexibility because they knew change was
Sarnia/Lambton, Ontario, Canada When began planning for a major renovation that combined two facilities under one roof and added five floors, they wanted maximum flexibility because they knew change was
Lean Six Sigma DMAIC Project (Example)
") Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Lean Six Sigma DMAIC Project (Example) Green Belt Project Objective: To Reduce Clinic Cycle Time (Intake & Service Delivery) Last Updated: 1 15 14 Team: The Speeders Tom Jones (Team Leader) Steve Martin
Laguna Honda Lean Transformation. Laguna Honda Strategic Performance Management November 2017
 Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
Laguna Honda Lean Transformation Laguna Honda Strategic Performance Management November 2017 Background MAKE IT BETTER 4. 1. Performance Improvement FIX IT Do the work and make it happen 3. Create best
University of Michigan Emergency Department
 University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
University of Michigan Emergency Department Efficient Patient Placement in the Emergency Department Final Report To: Jon Fairchild, M.S., R.N. C.E.N, Nurse Manager, fairchil@med.umich.edu Samuel Clark,
What Does a Pharmacist Do?
 What Does a Pharmacist Do? KYLE LYONS BRIANA NEGAARD CORBIN NICHOL Poll Everywhere: https://pollev.com/briananegaar863 Outline Background Objectives Methods Results Discussion Conclusion/References Questions
What Does a Pharmacist Do? KYLE LYONS BRIANA NEGAARD CORBIN NICHOL Poll Everywhere: https://pollev.com/briananegaar863 Outline Background Objectives Methods Results Discussion Conclusion/References Questions
The Introduction of Automated Medication Management and Dispensing System with Omnicell
 The Introduction of Automated Medication Management and Dispensing System with Omnicell The Introduction of Automated Medication Management and Dispensing System with Omnicell Sinead Fisher Clinical Nurse
The Introduction of Automated Medication Management and Dispensing System with Omnicell The Introduction of Automated Medication Management and Dispensing System with Omnicell Sinead Fisher Clinical Nurse
GENERAL DENTIST. Dental Receptionist Manual
 GENERAL DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
GENERAL DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
H ospital Voice. Oregon Community Hospitals. Lean Methods and Mindsets. The CEO Perspective. Taking Aim at Health Care Reform
 H ospital Voice A magazine for and about Oregon Community Hospitals A magazine for and about Oregon Community Hospitals Taking Aim at Health Care Reform Triple Aim to change health care for good The CEO
H ospital Voice A magazine for and about Oregon Community Hospitals A magazine for and about Oregon Community Hospitals Taking Aim at Health Care Reform Triple Aim to change health care for good The CEO
PEDIATRIC DENTIST. Dental Receptionist Manual
 PEDIATRIC DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
PEDIATRIC DENTIST Dental Receptionist Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing your
Eliminating Common PACU Delays
 Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
Eliminating Common PACU Delays Jamie Jenkins, MBA A B S T R A C T This article discusses how one hospital identified patient flow delays in its PACU. By using lean methods focused on eliminating waste,
An academic medical center is practicing wasteology to pare time, expense,
 Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Quality improvement Practicing wasteology in the OR An academic medical center is practicing wasteology to pare time, expense, and hassle from its OR processes. Using lean thinking, the center is streamlining
Using Lean Principles to Decrease Outpatient Registration Wait Times. It s a Journey not a Destination
 Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Using Lean Principles to Decrease Wait Times It s a Journey not a Destination 533 Bed Acute Care System 461 Beds at AnMed Health Medical Center 72 Beds at AnMed Health Women s and Children's Hospital 45
Lab Quality Confab Process Improvement Institute. New Orleans, LA. John Waugh 11/3/2015
 Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
Implementing a Single Quality Management System Across Multiple Hospitals of the Henry Ford Health System: Combining ISO 15189 with Lean to Deliver More Value Lab Quality Confab Process Improvement Institute
ResearcH JournaL 2012 / VOL
 ResearcH JournaL 2012 / VOL 04.02 www.perkinswill.com The Impact of an Operational Process on Space 05. THE IMPACT OF AN OPERATIONAL PROCESS ON SPACE: Improving the Efficiency of Patient Wait Times Amanda
ResearcH JournaL 2012 / VOL 04.02 www.perkinswill.com The Impact of an Operational Process on Space 05. THE IMPACT OF AN OPERATIONAL PROCESS ON SPACE: Improving the Efficiency of Patient Wait Times Amanda
SHRI GURU RAM RAI INSTITUTE OF TECHNOLOGY AND SCIENCE MEDICATION ERRORS
 MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
MEDICATION ERRORS Patients depend on health systems and health professionals to help them stay healthy. As a result, frequently patients receive drug therapy with the belief that these medications will
University of Michigan Health System. Final Report
 University of Michigan Health System Program and Operations Analysis Analysis of Medication Turnaround in the 6 th Floor University Hospital Pharmacy Satellite Final Report To: Dr. Phil Brummond, Pharm.D,
University of Michigan Health System Program and Operations Analysis Analysis of Medication Turnaround in the 6 th Floor University Hospital Pharmacy Satellite Final Report To: Dr. Phil Brummond, Pharm.D,
Enhancing the Patient Experience. Disclosures 3/13/2015. Jill Maher, MA, COE Senior Eye Care Business Advisor, Allergan, Inc Allergan Access
 Enhancing the Patient Experience EXCELLENCE IN PRACTICE MANAGEMENT Embracing the Process of Effective and Patient Flow Jill Maher, MA, COE Senior Eye Care Business Advisor Disclosures Jill Maher, MA, COE
Enhancing the Patient Experience EXCELLENCE IN PRACTICE MANAGEMENT Embracing the Process of Effective and Patient Flow Jill Maher, MA, COE Senior Eye Care Business Advisor Disclosures Jill Maher, MA, COE
PERIOPERATIVE CONSULTING SERVICES
 SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
SPT Sourcing PERIOPERATIVE CONSULTING SERVICES Improve efficiency and financial savings. Surgical Supply Management Solutions Keep everyone in-sync and in control with THE RIGHT SUPPLIES AT THE RIGHT TIME.
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Admissions and Planned Discharge
 Releasing Time to Care The Productive Mental Health Ward Admissions and Planned Discharge Version 1 This document is for ward leaders, lead nurses, matrons, nursing directors and directors with responsibility
Releasing Time to Care The Productive Mental Health Ward Admissions and Planned Discharge Version 1 This document is for ward leaders, lead nurses, matrons, nursing directors and directors with responsibility
Healthcare Finance Management Association: Continuous Improvement Foundations
 Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
Like us on Facebook and enjoy some helpful downloads and connections Continuous Improvement Solutions, LLC 8801 Bethnal Rd., Bella Vista, AR 72714 479.685.8380 cisolutionsllp@gmail.com Chad Smith: Trainer,
ATTACKING WASTE AND VARIATION HOSPITAL-WIDE: A COMPREHENSIVE LEAN SIGMA DEPLOYMENT
 ATTACKING WASTE AND VARIATION HOSPITAL-WIDE: A COMPREHENSIVE LEAN SIGMA DEPLOYMENT Charles Johnson, Ph.D., Richard H. Allen, Dr.P.H., Thomas A. Sonderman, M.D., and Ian D. Wedgwood, Ph.D. Abstract Columbus
ATTACKING WASTE AND VARIATION HOSPITAL-WIDE: A COMPREHENSIVE LEAN SIGMA DEPLOYMENT Charles Johnson, Ph.D., Richard H. Allen, Dr.P.H., Thomas A. Sonderman, M.D., and Ian D. Wedgwood, Ph.D. Abstract Columbus
Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology
 Organization: Anne Arundel Medical Center Solution Title: Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology Program/Project Description, Including Goals: What
Organization: Anne Arundel Medical Center Solution Title: Improving the Delivery of Troponin Results to the Emergency Department using Lean Methodology Program/Project Description, Including Goals: What
Patient Centric Model (PCM)
") Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
Patient Centric Model (PCM) Operations Manual A product of your state pharmacy association For more information, contact: PCM Project Manager 804-285-4431 PCM@naspa.us Background The typical pharmacy model
Oregon Medical Group Team Medicine 3 April 2014
 Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Oregon Medical Group Team Medicine 3 April 2014 Joshua P. Kimball Chief Operating Officer Oregon Medical Group Oregon Medical Group Oregon Medical Group is a physician owned, primary care heavy, multispecialty
Goals of System Modeling:
 Goals of System Modeling: 1. To focus on important system features while downplaying less important features, 2. To verify that we understand the user s environment, 3. To discuss changes and corrections
Goals of System Modeling: 1. To focus on important system features while downplaying less important features, 2. To verify that we understand the user s environment, 3. To discuss changes and corrections
Final Report. Karen Keast Director of Clinical Operations. Jacquelynn Lapinski Senior Management Engineer
 Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Assessment of Room Utilization of the Interventional Radiology Division at the University of Michigan Hospital Final Report University of Michigan Health Systems Karen Keast Director of Clinical Operations
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1)
 Medication Chart implementation and training guide (version 1.1)") Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Aged residential care (ARC) Medication Chart implementation and training guide (version 1.1) May 2018 Prepared by and the Health Quality & Safety Commission Version 1, March 2018; version 1.1, May 2018
Built with a singular goal: to help solve your most complex challenges.
 [ STANLEY Healthcare Experience Center ] Built with a singular goal: to help solve your most complex challenges. 4 Emergency Department/ Post-Anesthesia Care Unit 6 Operating Room/Cardiac Catheter Lab
[ STANLEY Healthcare Experience Center ] Built with a singular goal: to help solve your most complex challenges. 4 Emergency Department/ Post-Anesthesia Care Unit 6 Operating Room/Cardiac Catheter Lab
Emergency Department Strategic Design Considerations
 Emergency Department Strategic Design Considerations James Augustine, MD Director of Clinical Operations, EMP Associate Clinical Professor, Wright State University Department of Emergency Medicine. ED
Emergency Department Strategic Design Considerations James Augustine, MD Director of Clinical Operations, EMP Associate Clinical Professor, Wright State University Department of Emergency Medicine. ED
National Rural Health Resource Center. Introduction to Lean Thinking February 27, Presented by: John L. Roberts, MA Lean Healthcare Black Belt
 National Rural Health Resource Center Introduction to Lean Thinking February 27, 2015 Presented by: John L. Roberts, MA Lean Healthcare Black Belt Today s Agenda Introduction into Lean Thinking The Challenge
National Rural Health Resource Center Introduction to Lean Thinking February 27, 2015 Presented by: John L. Roberts, MA Lean Healthcare Black Belt Today s Agenda Introduction into Lean Thinking The Challenge
SCHEDULING COORDINATOR MANUAL GENERAL DENTIST. Scheduling Coordinator Manual
 GENERAL DENTIST Scheduling Coordinator Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing
GENERAL DENTIST Scheduling Coordinator Manual Note: The following policies and procedures comprise general information and guidelines only. The purpose of these policies is to assist you in performing
I. Description. Triage Counseling is an individual level intervention that establishes a direct link between primary. Rural
 Rural triage Counseling 2 Triage Counseling is an individual level intervention that establishes a direct link between primary medical care and mental health services for patients living with HIV. The
Rural triage Counseling 2 Triage Counseling is an individual level intervention that establishes a direct link between primary medical care and mental health services for patients living with HIV. The
Part 4. Change Concepts for Improving Adult Cardiac Surgery. In this section, you will learn a group. of change concepts that can be applied in
 Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Change Concepts for Improving Adult Cardiac Surgery Part 4 In this section, you will learn a group of change concepts that can be applied in different ways throughout the system of adult cardiac surgery.
Alvin S. Calderon, MD, PhD Roger W. Bush, MD Virginia Mason Medical Center. LeeAnn Cox, MD Noelle Sinex, MD Indiana University School of Medicine
 How Lean Concepts can improve your Residency by addressing the competencies of PBLI and SBP. 2011 APDIM Fall Meeting Workshop Session II, Workshop 209 Saturday October 22, 2011 Alvin S. Calderon, MD, PhD
How Lean Concepts can improve your Residency by addressing the competencies of PBLI and SBP. 2011 APDIM Fall Meeting Workshop Session II, Workshop 209 Saturday October 22, 2011 Alvin S. Calderon, MD, PhD
From Big Data to Big Knowledge Optimizing Medication Management
 From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
From Big Data to Big Knowledge Optimizing Medication Management Session 157, March 7, 2018 Dave Webster, RPh MSBA, Associate Director of Pharmacy Operations, URMC Strong Maria Schutt, EdD, Director Education
JOB DESCRIPTION. Revised:1/24/2018
 JOB DESCRIPTION TITLE: DEPARTMENT: REPORTS TO: FLSA: Nurse Resident Emergency Department Director ED Non-Exempt SUMMARY OF JOB: To provide critical care assessment, intervention and care, including emotional
JOB DESCRIPTION TITLE: DEPARTMENT: REPORTS TO: FLSA: Nurse Resident Emergency Department Director ED Non-Exempt SUMMARY OF JOB: To provide critical care assessment, intervention and care, including emotional
Nursing Notes Best Practices. Anna Rivera, Senior Application Specialist Vanessa Sampedro, Application Specialist
 Anna Rivera, Senior Application Specialist Vanessa Sampedro, Application Specialist Topics Configurations Templates Template Sets Questionnaires ROS Coding (ASC Codes) Interview Forms Scheduler: Areas
Anna Rivera, Senior Application Specialist Vanessa Sampedro, Application Specialist Topics Configurations Templates Template Sets Questionnaires ROS Coding (ASC Codes) Interview Forms Scheduler: Areas
UCLA Health DEPARTMENT SPECIFIC ORIENTATION
 Department of Nursing Employee Name: Classification: Supervisor: UCLA Health DEPARTMENT SPECIFIC ORIENTATION Form Department Hire : Dept. of Nursing Orientation : Department/Unit: Please complete all sections
Department of Nursing Employee Name: Classification: Supervisor: UCLA Health DEPARTMENT SPECIFIC ORIENTATION Form Department Hire : Dept. of Nursing Orientation : Department/Unit: Please complete all sections
Surgical Instrumentation: Eliminating Chaos. The Complex Process of Surgical Instrument Maintenance and Improving the Healthcare Environment
 Surgical Instrumentation: Eliminating Chaos The Complex Process of Surgical Instrument Maintenance and Improving the Healthcare Environment 1 Knowledge of Surgical Instrument Procedures Individuals considering
Surgical Instrumentation: Eliminating Chaos The Complex Process of Surgical Instrument Maintenance and Improving the Healthcare Environment 1 Knowledge of Surgical Instrument Procedures Individuals considering
How can oncology practices deliver better care? It starts with staying connected.
 How can oncology practices deliver better care? It starts with staying connected. A system rooted in oncology Compared to other EHRs that I ve used, iknowmed is the best EHR for medical oncology. Physician
How can oncology practices deliver better care? It starts with staying connected. A system rooted in oncology Compared to other EHRs that I ve used, iknowmed is the best EHR for medical oncology. Physician
Lean: the implications for information management and IM & T
 Lean: the implications for information management and IM & T Paul Brady, Principal Facilitator, Lean Healthcare Academy Andrew Ruck, Director, HealthSystems Group Ltd Contents 1. Introduction to Lean 2.
Lean: the implications for information management and IM & T Paul Brady, Principal Facilitator, Lean Healthcare Academy Andrew Ruck, Director, HealthSystems Group Ltd Contents 1. Introduction to Lean 2.
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS
 APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
APPENDIX 8-2 CHECKLISTS TO ASSIST IN PREVENTING MEDICATION ERRORS Use the following checklists in the appropriate areas of your office, facility or practice to assist in preventing medications errors:
Managing Queues: Door-2-Exam Room Process Mid-Term Proposal Assignment
 Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
Concept/Objectives Managing Queues: Door--Exam Process Mid-Term Proposal ssignment Children s Healthcare of tlanta (CHO has plans to build a new facility that will be over 00,000 sq. ft., and they are
The Cost of a Misfiled Medical Document
 : The Cost of a Misfiled Medical Document INTRODUCTION Misfiling of medical documents is a common problem in all types of medical practices. A document may be misfiled for a number of reasons, and each
: The Cost of a Misfiled Medical Document INTRODUCTION Misfiling of medical documents is a common problem in all types of medical practices. A document may be misfiled for a number of reasons, and each
Standard operating procedures for the conduct of outreach training and supportive supervision
 The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Standard operating procedures for the conduct of outreach training and supportive supervision Download all the
The MalariaCare Toolkit Tools for maintaining high-quality malaria case management services Standard operating procedures for the conduct of outreach training and supportive supervision Download all the
Data Capture at the Point of Care Guide For Resellers
 Data Capture at the Point of Care Guide For Resellers Todays Topics What s Driving Healthcare? Hospital Applications Differentiators & Alternative Solutions Healthcare Certifications / Partners Wrap up
Data Capture at the Point of Care Guide For Resellers Todays Topics What s Driving Healthcare? Hospital Applications Differentiators & Alternative Solutions Healthcare Certifications / Partners Wrap up
A Step-by-Step Guide to Tackling your Challenges
 Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
Institute for Innovation and Improvement A Step-by-Step to Tackling your Challenges Click to continue Introduction This book is your step-by-step to tackling your challenges using the appropriate service
TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE
 Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
Publication Year: 2011 TEAM ASSESSMENT PULL PROCESS CHILDREN S HEALTHCARE OF ATLANTA AT SCOTTISH RITE Summary: The Team Assessment Pull Process (TAPP) is a technique to redesign emergency department patient
Development and Implementation of a New Process for Handling Add-On Lab Orders at Duluth Clinic Ashland
 Development and Implementation of a New Process for Handling Add-On Lab Orders at Duluth Clinic Ashland Submitted by Pam Helgeson-Britton Director of Process Excellence & Organizational Productivity SMDC
Development and Implementation of a New Process for Handling Add-On Lab Orders at Duluth Clinic Ashland Submitted by Pam Helgeson-Britton Director of Process Excellence & Organizational Productivity SMDC
Healthcare Competency Skills/Evaluation (Page 1 of 5)
") (Page 1 of 5) COMPETENCY SKILLS 1 of 5 1 = Cannot Perform Skills Independently EVS Tech 2 = Requires Some Assistance to Perform Skills EVS OR Tech 3 = Can Perform Independently EVS Floor Tech NA = Not
(Page 1 of 5) COMPETENCY SKILLS 1 of 5 1 = Cannot Perform Skills Independently EVS Tech 2 = Requires Some Assistance to Perform Skills EVS OR Tech 3 = Can Perform Independently EVS Floor Tech NA = Not
A Case Study in Primary Care Access: Clinica Family Health. Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services
 A Case Study in Primary Care Access: Clinica Family Health Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services IHI s 26 th Annual National Forum on Quality Improvement in Health Care Orlando, Florida
A Case Study in Primary Care Access: Clinica Family Health Dr. Karen A. Funk, MD, MPP Vice-President Clinical Services IHI s 26 th Annual National Forum on Quality Improvement in Health Care Orlando, Florida
Building a Lean healthcare machine
 Building a Lean healthcare machine PULSE Summer 2016 We re using Lean as a cultural transformation. We want to empower every member of our organization, particularly those at the frontlines and the bedside,
Building a Lean healthcare machine PULSE Summer 2016 We re using Lean as a cultural transformation. We want to empower every member of our organization, particularly those at the frontlines and the bedside,
Lean Method, a Solution to Problem in Hospital
 Lean Method, a Solution to Problem in Hospital Sfandyarifard, E. The University of Salford, UK (email: e.sfandyarifard@pgr.salford.ac.uk) Abstract It is becoming increasingly difficult to ignore the importance
Lean Method, a Solution to Problem in Hospital Sfandyarifard, E. The University of Salford, UK (email: e.sfandyarifard@pgr.salford.ac.uk) Abstract It is becoming increasingly difficult to ignore the importance
Standard Work for the Shopfloor Standard Work for Lean Healthcare
 Standard Work for Lean Healthcare Lean Tools for Healthcare Series Series Editor: Thomas L. Jackson PubLiSHed 5S for Healthcare Standard Work for Lean Healthcare forthcoming Just-in-Time for Healthcare
Standard Work for Lean Healthcare Lean Tools for Healthcare Series Series Editor: Thomas L. Jackson PubLiSHed 5S for Healthcare Standard Work for Lean Healthcare forthcoming Just-in-Time for Healthcare
SAMPLE REPORTS: A SPECIAL INSIDE LOOK FOR MORE COST-EFFICIENT OPERATIONS
 HOSPICE Increase your profitability with up-to-date, industry-specific benchmarks SAMPLE REPORTS: A SPECIAL INSIDE LOOK FOR MORE COST-EFFICIENT OPERATIONS 1 Financial Monitor is the culmination of a 50-yearold
HOSPICE Increase your profitability with up-to-date, industry-specific benchmarks SAMPLE REPORTS: A SPECIAL INSIDE LOOK FOR MORE COST-EFFICIENT OPERATIONS 1 Financial Monitor is the culmination of a 50-yearold
Hospital of the Future Planning a new Medicine/Telemetry Unit with confidence
 GE Healthcare Infrastructure Solutions Hospital of the Future Planning a new Medicine/Telemetry Unit with confidence Humber River Regional Hospital The Background Humber River Regional Hospital (HRRH)
GE Healthcare Infrastructure Solutions Hospital of the Future Planning a new Medicine/Telemetry Unit with confidence Humber River Regional Hospital The Background Humber River Regional Hospital (HRRH)
Activity 3: TRANSFER TO A WHEELCHAIR Future tense
 Contextualized Grammar I-BEST SUN Path Curriculum Unit for Nursing Assistant with ESL Support - Page 1 of 10 Activity 3: TRANSFER TO A WHEELCHAIR Future tense Learning Goal(s) Demonstrate the indirect
Contextualized Grammar I-BEST SUN Path Curriculum Unit for Nursing Assistant with ESL Support - Page 1 of 10 Activity 3: TRANSFER TO A WHEELCHAIR Future tense Learning Goal(s) Demonstrate the indirect
Dental Hygiene Quality Assurance Manual and Protocol Portland Campus 716 Stevens Avenue Portland, Maine (207)
") Dental Hygiene Quality Assurance Manual and Protocol 2017-2018 Portland Campus 716 Stevens Avenue Portland, Maine 04103 (207)-221-4900 UNE/Dental Hygiene Quality Assurance Manual and Protocol The UNE Dental
Dental Hygiene Quality Assurance Manual and Protocol 2017-2018 Portland Campus 716 Stevens Avenue Portland, Maine 04103 (207)-221-4900 UNE/Dental Hygiene Quality Assurance Manual and Protocol The UNE Dental
The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites
 The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites By Abdul N. Mansour, MHA, DBA, Scottsdale Healthcare August 2011 One of Arizona s largest health
The Benefits of Standardization: Anesthesia Cart Standardization in 62 Operating Rooms Over 5 Surgical Sites By Abdul N. Mansour, MHA, DBA, Scottsdale Healthcare August 2011 One of Arizona s largest health
2. What is the main similarity between quality assurance and quality improvement?
 Chapter 6 Review Questions 1. Quality improvement focuses on: a. Individual clinicians or system users b. Routine measurement of performance c. Information technology issues d. Constant training 2. What
Chapter 6 Review Questions 1. Quality improvement focuses on: a. Individual clinicians or system users b. Routine measurement of performance c. Information technology issues d. Constant training 2. What
Demand and capacity models High complexity model user guidance
 Demand and capacity models High complexity model user guidance August 2018 Published by NHS Improvement and NHS England Contents 1. What is the demand and capacity high complexity model?... 2 2. Methodology...
Demand and capacity models High complexity model user guidance August 2018 Published by NHS Improvement and NHS England Contents 1. What is the demand and capacity high complexity model?... 2 2. Methodology...
PREPARATION AND ADMINISTRATION
 LESSON PLAN: 12 COURSE TITLE: UNIT: IV MEDICATION TECHNICIAN PREPARATION AND ADMINISTRATION SCOPE OF UNIT: Guidelines and procedures for preparation, administration, reporting, and recording of oral, ophthalmic,
LESSON PLAN: 12 COURSE TITLE: UNIT: IV MEDICATION TECHNICIAN PREPARATION AND ADMINISTRATION SCOPE OF UNIT: Guidelines and procedures for preparation, administration, reporting, and recording of oral, ophthalmic,
Excellence in Healthcare Delivery
 The Performance Management Group LLC Excellence in Healthcare Delivery Lean Transformation in Healthcare: Improving patient outcomes while driving down the cost of patient care Helping You Make It Happen!
The Performance Management Group LLC Excellence in Healthcare Delivery Lean Transformation in Healthcare: Improving patient outcomes while driving down the cost of patient care Helping You Make It Happen!
How CHRISTUS Spohn Health System uses automation to improve standardization and re-deploy pharmacists to clinical functions
 A culture of medication safety: How CHRISTUS Spohn Health System uses automation to improve standardization and re-deploy pharmacists to clinical functions Authored and produced by CareFusion, August 2013
A culture of medication safety: How CHRISTUS Spohn Health System uses automation to improve standardization and re-deploy pharmacists to clinical functions Authored and produced by CareFusion, August 2013
Submitted electronically via: May 20, 2015
 Submitted electronically via: http://www.regulations.gov May 20, 2015 Jane Axelrad, JD Associate Director for Policy, CDER Division of Dockets Management (HFA-305) Food and Drug Administration 5630 Fishers
Submitted electronically via: http://www.regulations.gov May 20, 2015 Jane Axelrad, JD Associate Director for Policy, CDER Division of Dockets Management (HFA-305) Food and Drug Administration 5630 Fishers
ABOUT REVEAL LINQ DURING
 TALKING ABOUT REVEAL LINQ DURING CONSULT INTRODUCE THE SYSTEM o Help patients understand how the components work together Two primary components: Reveal LINQ ICM a small device that is inserted just under
TALKING ABOUT REVEAL LINQ DURING CONSULT INTRODUCE THE SYSTEM o Help patients understand how the components work together Two primary components: Reveal LINQ ICM a small device that is inserted just under
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow
 The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
The Impact of CPOE and CDS on the Medication Use Process and Pharmacist Workflow Conflict of Interest Disclosure The speaker has no real or apparent conflicts of interest to report. Anne M. Bobb, R.Ph.,
Applying Lean Principles to a Continuing Care Patient Discharge Process
 Applying Lean Principles to a Continuing Care Patient Discharge Process Presenter: Valerie Maier-Speredelozzi Assistant Professor, Industrial and Manufacturing Engineering Graduate Students: Amy Thompson
Applying Lean Principles to a Continuing Care Patient Discharge Process Presenter: Valerie Maier-Speredelozzi Assistant Professor, Industrial and Manufacturing Engineering Graduate Students: Amy Thompson
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing
 AHA Leadership Summit Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing Presented by: Patty Toney, VP/Chief Nurse Executive,
AHA Leadership Summit Critical Success Factors for Becoming a High Reliability Organization: Lean, Six Sigma, Change Leadership and Value-based Purchasing Presented by: Patty Toney, VP/Chief Nurse Executive,
Collaborative Progress Where are We Now?
 Collaborative Progress Where are We Now? Traci Treasure, MS, CPHQ, LNHA Quality Improvement Consultant May 30 th, 2013 Learning Session 2, Part 1 Qualis Health is one of the nation s leading healthcare
Collaborative Progress Where are We Now? Traci Treasure, MS, CPHQ, LNHA Quality Improvement Consultant May 30 th, 2013 Learning Session 2, Part 1 Qualis Health is one of the nation s leading healthcare