Electronic Patient Record (EPR) and Public Reporting
|
|
|
- Julianna Allen
- 5 years ago
- Views:
Transcription
1 Electronic Patient Record (EPR) and Public Reporting Elisa L. Horbatuk, MA Data Manager, Decision Support Services Stony Brook University Medical Center MIT Information Quality Industry Symposium July, 2010
2 OVERVIEW
3 Overview About Stony Brook University Medical Center (SBUMC) EPR Implementation at SBUMC Public Reporting EPR and Public Reporting
4 ABOUT US
 33 Hospital Based Clinics/Tests Level 1 Trauma Center Level 3 NICU, Regional Perinatal Center Burn Center Renal Transplant Program Autologous/Allogenic Bone Marrow")
5 Stony Brook University Medical Center Long Island, New York Region s only tertiary care center 540 Acute Inpatient Beds 31,600 discharges in 2008 Adult / Pediatric Emergency Dept. 76,565 visits (FY 07-08) 33 Hospital Based Clinics/Tests Level 1 Trauma Center Level 3 NICU, Regional Perinatal Center Burn Center Renal Transplant Program Autologous/Allogenic Bone Marrow Transplant Program/Unit
6 Stony Brook University Medical Center Hospital is part of the State University of New York at Stony Brook Affiliated with a major academic medical center, including medical, nursing, and health technology management schools 50 accredited training programs with 447 residents 465 Full time, 506 Voluntary Physicians >4,800 Full-time Employees
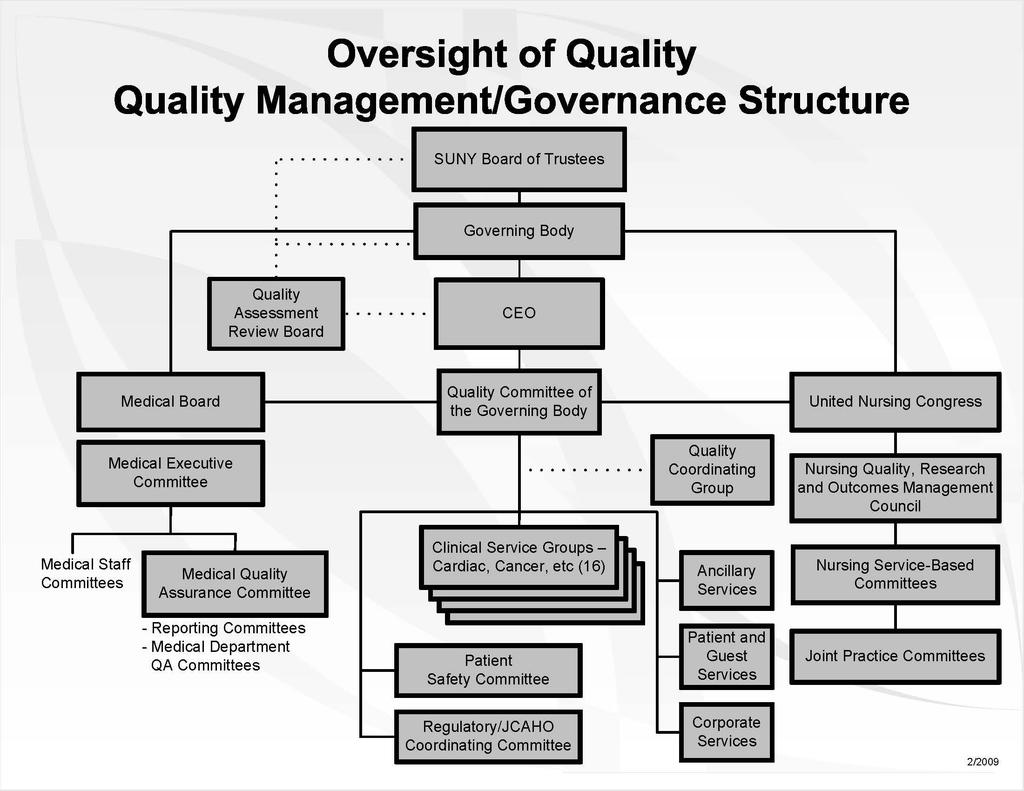
7 Quality Management Structure Hospital strategic goals are designed to achieve the outcome of becoming a high reliability organization (HRO) The Quality Committee of the Governing Body sets quality improvement (QI) priorities aligned with strategic goals High level oversight of quality priorities of the Medical Board, Patient Safety, Operating Room Committee, United Nursing Congress, and Clinical Service Groups The Quality Coordinating Group oversees QI efforts of Clinical Service Groups The Quality division facilitates QI activities for Clinical Service Groups and QI teams, and is also responsible for most public reporting requirements
8
9 Strategic Plan STONY BROOK UNIVERSITY HOSPITAL STRATEGIC GOAL: HRO INPUTS QUALITY RELATIONSHIPS GREAT PLACE TO WORK LONG TERM SUCCESS OUTPUTS Mission Vision Values: Simple Rules of Work Patient & Family Centered Care UHC 5 Star Quality & Accountability Thompson/Solucients s Top 100 Hospitals for Programs of Distinction MAGNET AWARD Modern Healthcare s Best Place to Work in Healthcare Award BALDRIGE AWARD Top 100 Hospitals for 5 consecutive years High Reliability Organization (Failure Free Operation) World Class Organization Organizational Drivers 100% DEPLOYMENT
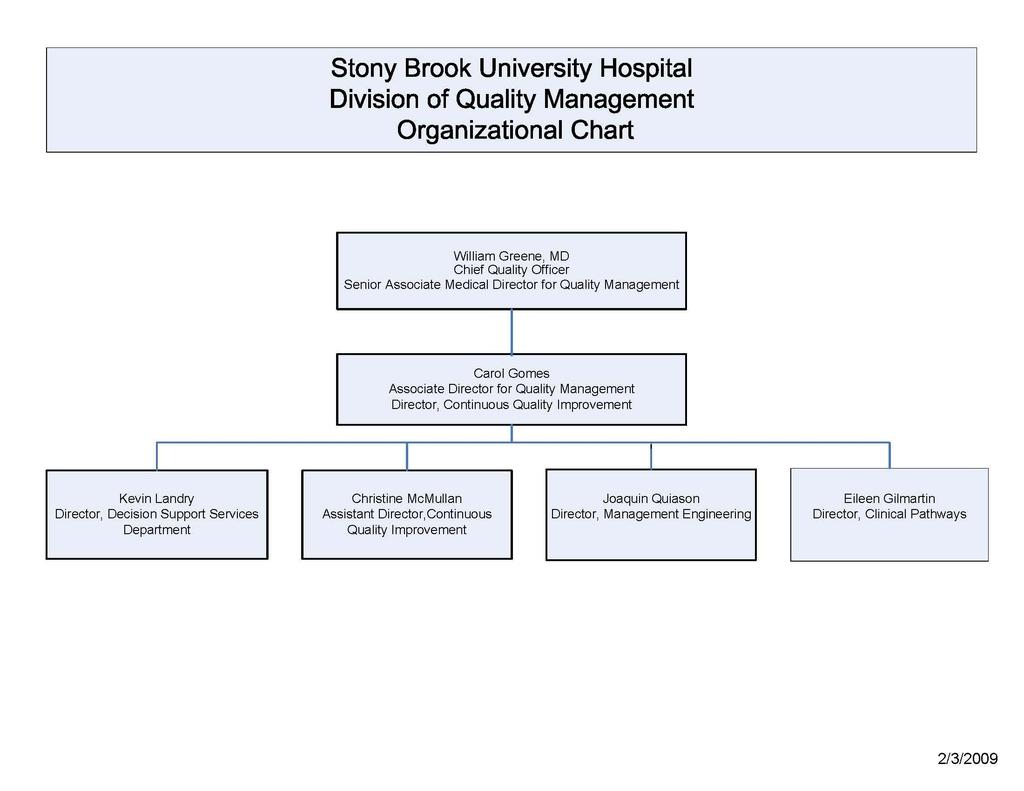
10 Decision Support Services Part of Quality division Holds much of the responsibility for public reporting Staff includes analysts and nursing staff working closely together Collaborates with Continuous Quality Improvement (CQI) department, participating in Clinical Service Group (CSG) meetings and CQI teams (e.g., door-to-balloon, heart failure)
11
12 EPR IMPLEMENTATION AT SBUMC
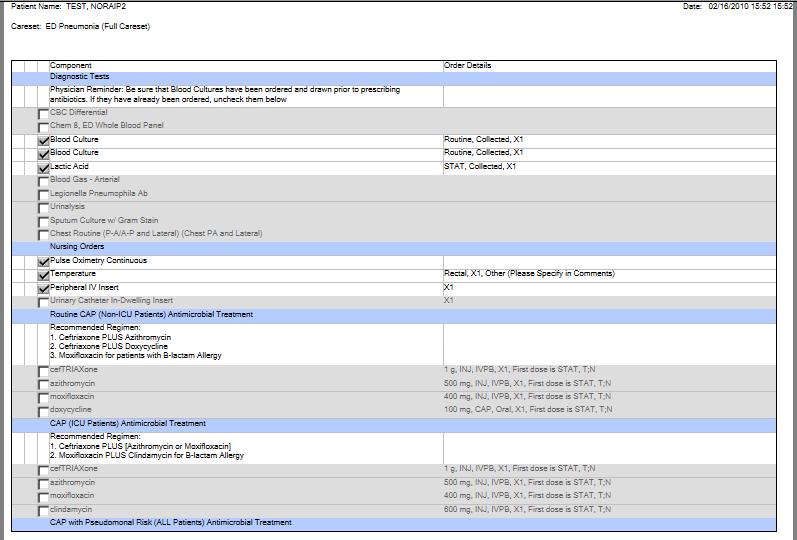
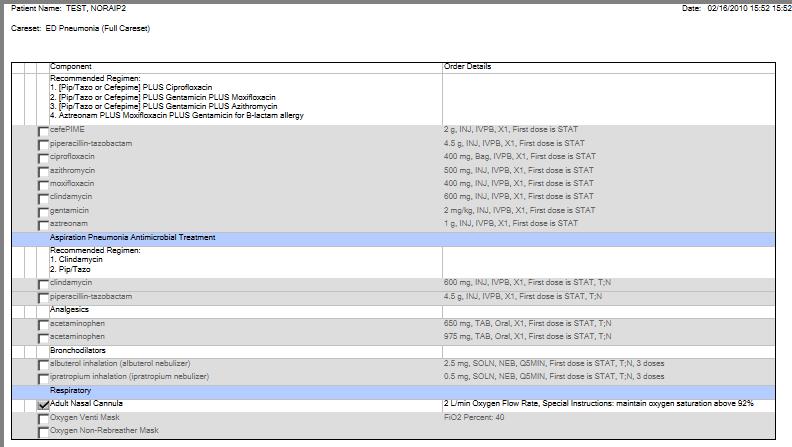
13 EPR Implementation at SBUMC During the past few years we have implemented Nursing documentation Laboratory results and flowsheets Medication administration documentation Medication reconciliation Intraoperative reporting Emergency Department documentation Computerized Physician Order Entry

14 PATIENT NAME

15 PATIENT NAME

16 PATIENT NAME MRN PATIENT NAME PATIENT NAME DATE OF BIRTH AGE SEX ENCOUNTER # ADMIT DATE/ TIME MRN INSERT SCREEN SHOT OF LAB RESULTS AND FLOW SHEETS

17 PATIENT NAME MRN PATIENT NAME PATIENT NAME DATE OF BIRTH AGE ENCOUNTER # SEX ADMIT DATE/ TIME MRN

18 PATIENT NAME DATE OF BIRTH AGE ENCOUNTER # SEX ADMIT DATE/ TIME MRN
19 NURSING STAFF ENCOUNTER # ADMIT DATE
20 NURSING STAFF SURGEON ANESTHESIOLOGIST NURSING STAFF NURSING STAFF NURSING STAFF NURSING STAFF NURSING STAFF OR TECHNICIAN ANESTHESIOLOGIST

21 PATIENT NAME MRN PATIENT NAME PATIENT NAME DATE OF BIRTH AGE ENCOUNTER # SEX ADMIT DATE/ TIME MRN NURSING STAFF NURSING STAFF ENCOUNTER # NURSING STAFF NURSING STAFF
22
23
24 EPR Implementation at SBUMC Discharge summaries, operative reports, and certain test results are also available in the EPR as free text imported from other systems

25 PATIENT NAME MRN PATIENT NAME PATIENT NAME DATE OF BIRTH AGE SEX MRN ENCOUNTER # ADMIT DATE/ DISCHARGE TIME DATE/ TIME CLINICAL STAFF ENCOUNTER # ADMIT-DISCHARGE DATES

26 PATIENT NAME PATIENT NAME PATIENT NAME DATE OF BIRTH AGE SEX MRN ENCOUNTER # ADMIT DATE/ DISCHARGE TIME DATE/ TIME SURGEON NAME ENCOUNTER # ADMIT-DISCHARGE DATES SURGEON NAME SURGEON NAME

27 PATIENT NAME MRN ENCOUNTER # ADMIT-DISCHARGE DATES RADIOLOGIST NAME RADIOLOGIST NAME
28 EPR Implementation at SBUMC Scheduled for implementation: Discharge process Physician documentation ICU flowsheets
29 EPR Implementation at SBUMC Role of Decision Support Services (DSS) Prior to the most recent phase of implementation, DSS staff assessed all required data elements for public reporting, flagging elements captured on paper tools that were scheduled for replacement by electronic tools For example, contraindications to medications were often captured on paper order sets. Since paper order sets were soon to be replaced by CPOE, it was imperative that CPOE incorporate a method for capturing contraindications

30 Electronic Patient Record Core Measure Data Elements Acute Myocardial Infarction Currently If Currently Available in Cerner If Not Currently Available in Cerner Data Element Available in Location Revisions Considerations Notes Planned? Immediate Potential Notes EPR? needed? need?* Location Contraindication to Beta Blocker on Arrival No No Yes - CPOE will replace all paper physician orders (nondischarge) by Fall CPOE/ EMAR Checklist item on AMI orders. If not selected, "contra" field becomes enabled. Entered to EMAR at time of administration. Contraindication to Both ACEI and ARB at Discharge No No No Power Form: Discharge Orders Field will be enabled by lack of selection of either ACEI or ARB on AMI discharge orders. Discharge orders may not be completed without this field, if applicable. Discharge Date Yes - Cerner, Siemens Visit List No N/A Entered by? Discharge Status Yes - Siemens Only (similar data element in Cerner but options not as inclusive) Non-Primary PCI Race Yes - Sensis Cath Lab reports Yes - Cerner, Siemens Nursing Assessment Patient Demographics Yes Process and workflow evaluation needed. May need to consider an alternate source. Entered by? No N/A Entered by Admitting No No? Sensis Cath Lab reports to be interfaced with Power Charts? * An immediate need exists if the current hard copy source for the data element will be replaced in the near future by an electronic source.
31 EPR Implementation at SBUMC Role of Decision Support Services (DSS) As electronic copies of order sets became available, DSS staff reviewed the order sets to identify data elements that would potentially go uncaptured
32 PowerPlan Builds Review Order Sets Affecting Core Measure Data Capture Order Set Name Reviewer Status Notes Initials Acute Coronary Syndrome Admission PowerPlan CI/LAW Reviewed in Cerner Build - Needs 1.No order sets found NSTEMI/STEMI Edits 2. Currently SUGGESTS to order ASA, BB, ACE/ARB,etc.--doesn't clearly indicate that these must be ordered and if not you must provide a contraindication. (should clearly state this is a requirement for CMS/JCACHO) 3. There is no space provided to write contraindications and has no prompts to be alerted. 4.found to have too much reading required for MD's. An example was the suggestive source or the recent documentation re:studies of uses of medication. 5. There was no space provided to write in for delay of PCI ( requirement for CMS/JCACHO) Cardiothoracic Surgery Post-Operative PowerPlan (Adult) LCW/SV Reviewed in Cerner Build - Needs No where to document contra's to betablockers (LCW). Edits Remove SCIP Hysterectomy Surgery Quality Measures Subphase (JM/SV). See table below for SCIP compliant antibiotic adminstration (JM/SV). Heart Failure PowerPlan (Adult) LCW Reviewed in Cerner Build - Needs Edits No where to document contra's to ace, arb or Betablockers under the medication section; on the original paper on page one, there is a prompt to document the EF--THIS DOES NOT APPEAR IN THE ELECTRONIC VERSION Pneumonia PowerPlan (Adult) jm Reviewed in Cerner Build - OK all the elements for the core measures are present however if the plan is not selected in the ED then cultures before ABX will be missed.
33 EPR Implementation at SBUMC Role of Decision Support Services (DSS) Now that implementation of a public reporting application is planned, DSS is working with Clinical Informatics (CI) and Information Technology (IT) to identify any gaps in data capture
34 PUBLIC REPORTING
35 Public Reporting The Joint Commission(TJC)/Centers for Medicare and Medicaid Services (CMS) Core Measures (inpatient and outpatient) New York State Department of Health (NYSDOH requirements) Professional Society Registries
36 Public Reporting Current State Primarily retroactive, manual abstraction Use of applications such as Lumedx Apollo and Cerner PowerInsight Different registry modules in Apollo can share data fields Data elements such as laboratory results and height/weight can be queried from our EPR and imported to Apollo
37 EPR AND PUBLIC REPORTING
38 Ways EPR Facilitates Data Capture More data can be captured at the point of care Inclusion of queriable data fields in EPR reduces burden of chart abstraction and decreases human error from abstraction and entry Automatic feeds from EPR components comprising the legal medical record import required data elements to reporting applications Real-time feedback for certain elements from our vendor s public reporting application or from queries
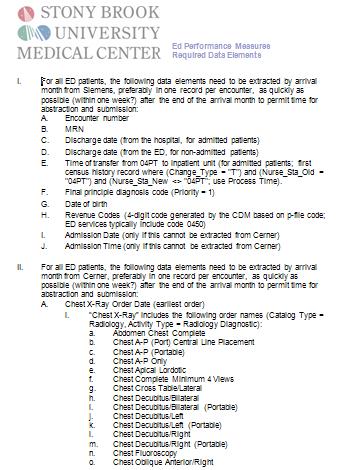
39 Maximizing Benefits to Public Reporting A cooperative effort among DSS, Clinical Informatics, and Information Technology staff has begun to translate core measure specifications into query specifications to extract required data elements from the EPR, replacing manual abstraction This process began with the upcoming Emergency Department core measures, as these contain the most data elements amenable to electronic data abstraction at SBUMC. The process has continued with all inpatient core measures
40 Data Element in Specifications Field name in merged file Source Notes ENCOUNTER Both Need for merging purposes MRN Both Need for merging purposes Arrival Date INPATIENTARRIVEDT Cerner Arrival Time INPATIENTARRIVETM Cerner Arrival Date OUTPATIENTARRIVEDT Cerner Arrival Time OUTPATIENTARRIVETM Cerner These fields are split by Inpatient and Outpatient just because of the collaborative requirements for separate fields. The source is the same, ED Arrival Date/Time. As we discussed, there are multiple potential sources for ED Arrival Date/Time*. Note that even after this field is electronically available for all cases, ED and CQI staff will still need to review manually, as occasionally earlier dates/times are documented on paper tools. Admission Date; Decision To Admit Date ADMITDATE Cerner Date of physician order to admit. Admission Time; Decision To Admit Time ADMITTIME Cerner Time of physician order to admit. Chest X-Ray Order Date ORIGORDERDT Cerner Will be blank for patients who did not receive a chest x-ray Chest X-Ray Order Time ORIGORDERTM Cerner Will be blank for patients who did not receive a chest x-ray Chest X-Ray Exam Date CLINICALEVENTPERFORMEDDT Cerner Will be blank for patients who did not receive a chest x-ray Chest X-Ray Exam Time CLINICALEVENTPERFORMEDTM Cerner Will be blank for patients who did not receive a chest x-ray INP/OUTP Cerner Flag indicating whether patient was admitted as inpatient or discharged from ED Pain Medication Administration Date Not currently included Cerner The earliest date that any pain medication (based on list sent separately) is administered (not ordered!) to the patient Pain Medication Administration Time Not currently included Cerner The earliest time that any pain medication (based on list sent separately) is administered (not ordered!) to the patient Birthdate PT BIRTH DT Siemens Not sent to collaborative; used for age-based exclusion-criteria. May now be possible to obtain from Cerner. ICD-9-CM Principal diagnosis Code DF1 DX CODE Siemens Principal final diganosis code. May now be possible to obtain from Cerner. ED Departure Date ERDISCHARGEDT Siemens Not sent to collaborative; used for age calculation. May now be possible to obtain from Cerner. ED Departure Time ERDISCHARGETM Siemens No longer needed INADMITDISCHARGEDT Siemens Not sent to collaborative; used for LOS calculation. May now be possible to obtain from Cerner. ED Departure Date PROCESS DT IP Siemens Date patient transferred from 04PT to inpatient unit. May now be possible to obtain from Cerner ED Departure Time PROCESS TM IP Siemens Time patient transferred from 04PT to inpatient unit. May now be possible to obtain from Cerner Admission Date PROCESS DT 04PT Siemens Originally used when date of admission order was not available electronically. Also used for LOS and age calculation. Can be replaced by ADMITDATE from Cerner. Admission Time PROCESS TM 04PT Siemens Originally used when time of admission order was not available electronically. Can be replaced by ADMITTIME from Cerner. Observation - we don't have this N/A N/A All patients will be set for no Observation, since we do not have an Observation Unit at this time Revenue Codes N/A N/A Not used by collaborative Discharge Status N/A N/A Not used by collaborative * These potential sources include the following: "ED Triage Time" (appearing on the ED Patient Education Sheet) "ED Triage Time" (appearing on the ED Triage Form) The earliest "Performed" time on all Procedure Notes. Note that in the future we will be required by CMS to exclude Procedure Notes by Respiratory Therapy describing an intubation. However, that exclusion is not required by the current collaborative and need not be addressed at this time.
41
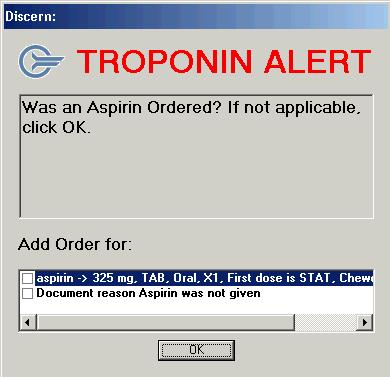
42 EPR and Public Reporting Identification of All Electronic and Paper (Imaged) Data Sources Measure Set: Acute Myocardial Infarction Arrival Time Data Element Aspirin Received Within 24 Hours Before or After Hospital Arrival Electronic - Queriable For ED Patients: earliest of Registration Time on ED Pat Edu form; Triage Time on ED Triage form. For Direct Admits: Siemens Admission Time Electronic - Non-Queriable ("blob") None at this time Paper (Imaged) ED documents, Nsg. Admission Assessment/admitting note, Observation record, procedural notes, VS graphic record; Cardiac flowsheet. If a direct admit may also utilize face sheet emar, Medication Reconciliation None at this time Ambulance record, ER document, H&P, Med. Administration record, Med. Rec. form, Nsg. Admission assessment, transfer sheet Birthdate Birthdate None at this time N/A Comfort Measures Only "Comfort Measures Only" order (available as individual order or on Discharge summary MICU preprinted order sheet, Progress Notes, Consultation Notes, H&P, Comfort Care Form Comfort Care Power Plan, MICU Comfort Care Power Plan) Clinical Trial None at this time None at this time signed consent as well as protocol documentation First PCI Date None at this time Operative reports Diagnostic test reports, procedure notes First PCI Time None at this time Operative reports Diagnostic test reports, procedure notes
43

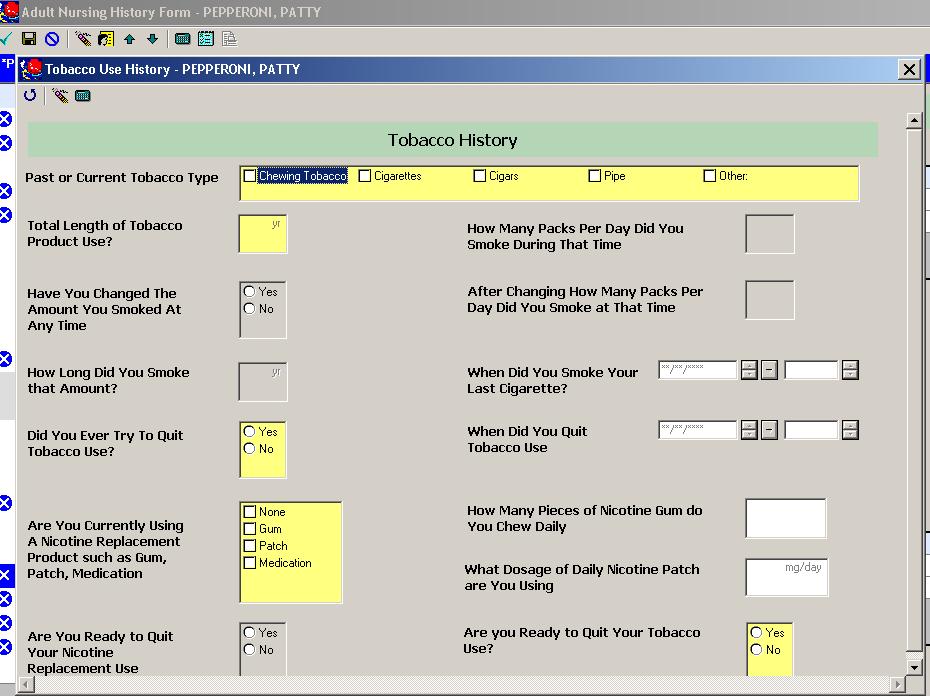
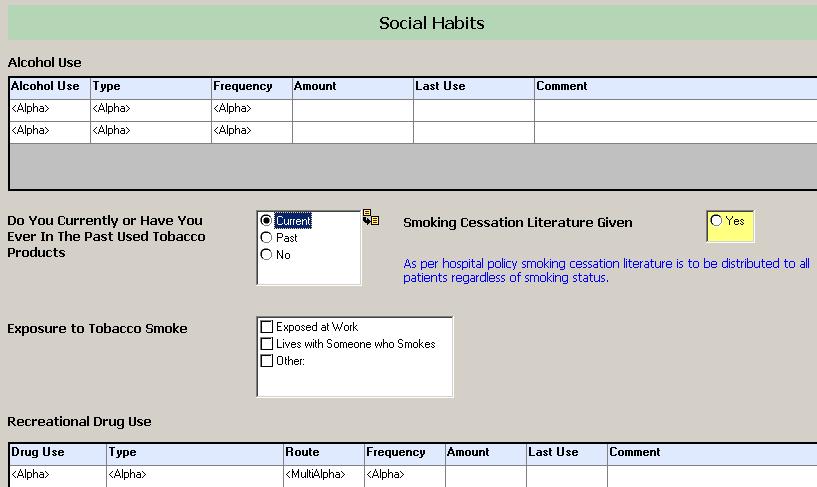
44 SCREENSHOT OF NEW SMOKING CESSATION HISTORY SCREENS, IF AVAILABLE IN TIME
45
46
47 Challenges Met A hybrid medical record consisting of paper tools and multiple electronic systems results in several possible sources for certain data elements. DSS, CI, and IT have collaborated to identify these many sources
48 Challenges Met Public reporting specifications are not yet always oriented to the electronic world, and there are cases in which application of rules that were logical in the paper world result in a misleading picture of care documented electronically DSS staff have submitted numerous questions to Quest, the forum for core measure specification clarifications Specifications are gradually changing
49 Challenges Met Desire to exploit decision support tools must be balanced with avoidance of alert fatigue Alerts are used very sparingly Care sets must be updated as specifications change Part of the routine when new specs are released is to review care sets for necessary changes
50 Outstanding Challenges A potential benefit of EPR is the possibility of data capture at the point of care, resulting in real-time feedback to providers. However, reports designed for real-time feedback on public reporting indicators are dependent on the point-of-care providers fully understanding the specifications, which requires extensive training
51 Outstanding Challenges Data may be captured in an electronic source that is not part of the legal medical record and not transferred to a location in the legal medical record DSS is working with CI, Nursing, and service staff to find ways to capture vital data in the legal medical record Until such time as a local regional health information exchange is fully operational, all documentation from transferring hospitals is received on paper and must be manually reviewed
52 Outstanding Challenges Many data elements are still found in free text fields, or blobs, rather than discrete data fields, which means they cannot currently be queried Different registries define similar elements differently, which limits the ability to collect such elements via simple checklists/drop-downs External validators must interpret the printed medical record without benefit of background knowledge possessed by hospital staff
53 Outstanding Challenges Inconsistent use of care sets Start content is not always sufficient when you have a hybrid system Customization is possible, but must be repeated whenever applications are upgraded Dynamic environment, so some data are not preserved after subsequent encounters
54 Discussion What is your current stage of EPR implementation? What are some benefits related to public reporting requirements that your organization has reaped from EPR implementation? What are the biggest challenges solved or unsolved that EPR implementation has posed to public reporting at your organization? What advice do you have for hospitals in earlier stages of EPR implementation? What do you wish someone had told you earlier in the implementation process?
55 Elisa L. Horbatuk, MA Data Manager, Decision Support Services Stony Brook University Medical Center
Assuring Data Integrity for Healthcare Public Reporting and Using Results to Evaluate Patient Care Quality
 Assuring Data Integrity for Healthcare Public Reporting and Using Results to Evaluate Patient Care Quality ABSTRACT This presentation describes (1) steps insuring data integrity for public reporting; (2)
Assuring Data Integrity for Healthcare Public Reporting and Using Results to Evaluate Patient Care Quality ABSTRACT This presentation describes (1) steps insuring data integrity for public reporting; (2)
FACT SHEET Summary of Acute Myocardial Infarction (AMI) and Heart Failure (HF) Changes for 1/1/12+ Discharges
 and Heart Failure (HF) Changes for 1/1/12+ Discharges") FACT SHEET Summary of Acute Myocardial Infarction (AMI) and Heart Failure (HF) Changes for 1/1/12+ Discharges AMI-1, AMI-3, and AMI-5: Submission to the CMS clinical data warehouse is now optional. This
FACT SHEET Summary of Acute Myocardial Infarction (AMI) and Heart Failure (HF) Changes for 1/1/12+ Discharges AMI-1, AMI-3, and AMI-5: Submission to the CMS clinical data warehouse is now optional. This
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule
 HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
Abstraction Tricks and Tips for the Hospital Outpatient Quality Reporting (OQR) Program
 Program") Abstraction Tricks and Tips for the Hospital Outpatient Quality Reporting (OQR) Program Audio for this event is available via internet streaming. No telephone line is required. Computer speakers or headphones
Abstraction Tricks and Tips for the Hospital Outpatient Quality Reporting (OQR) Program Audio for this event is available via internet streaming. No telephone line is required. Computer speakers or headphones
Abstraction Tricks and Tips for the Hospital Outpatient Quality Reporting (OQR) Program
 Program") Abstraction Tricks and Tips for the Hospital Outpatient Quality Reporting (OQR) Program Audio for this event is available via internet streaming. No telephone line is required. Computer speakers or headphones
Abstraction Tricks and Tips for the Hospital Outpatient Quality Reporting (OQR) Program Audio for this event is available via internet streaming. No telephone line is required. Computer speakers or headphones
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Hospital Outpatient Quality Reporting Program
 Hospital Outpatient Quality Reporting Program Support Contractor OQR 2016 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN Speakers: Nina Rose, MA Samantha Berns, MSPH Bob Dickerson,
Hospital Outpatient Quality Reporting Program Support Contractor OQR 2016 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN Speakers: Nina Rose, MA Samantha Berns, MSPH Bob Dickerson,
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
Rural-Relevant Quality Measures for Critical Access Hospitals
 Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Hospital Compare Quality Measures: 2008 National and Florida Results for Critical Access Hospitals
 Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model. Rome H. Walker MD February 28, 2008
 Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Administrative Billing Data
 Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
Administrative Billing Data Patient Identification and Demographic Information: From UB-04 Data or Medical Record Face Sheet. Note: When you go to enter data on this case, the information below will already
SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER
 SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER 1 WHY IS SAN FRANCISCO GENERAL HOSPITAL IMPORTANT? and Trauma Center (SFGH) is a licensed general acute care hospital which is owned and operated by the
SAN FRANCISCO GENERAL HOSPITAL and TRAUMA CENTER 1 WHY IS SAN FRANCISCO GENERAL HOSPITAL IMPORTANT? and Trauma Center (SFGH) is a licensed general acute care hospital which is owned and operated by the
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
Outpatient Quality Reporting Program
 OQR 2016 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN Speakers: Nina Rose, MA Samantha Berns, MSPH Bob Dickerson, HSHSA, RRT Angela Merrill, PhD Colleen McKiernan, MSPH,
OQR 2016 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN Speakers: Nina Rose, MA Samantha Berns, MSPH Bob Dickerson, HSHSA, RRT Angela Merrill, PhD Colleen McKiernan, MSPH,
An Overview of the. Measures. Reporting Initiative. bwinkle 11/12
 An Overview of the National Hospital Quality Measures A National Voluntary Hospital Reporting Initiative bwinkle 11/12 What Are Hospital Quality Measures? The Joint Commission (TJC) and the Centers for
An Overview of the National Hospital Quality Measures A National Voluntary Hospital Reporting Initiative bwinkle 11/12 What Are Hospital Quality Measures? The Joint Commission (TJC) and the Centers for
News SEPTEMBER. Hospital Outpatient Quality Reporting Program. Support Contractor
 Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
Volume 1, Issue 4 Hospital Outpatient Quality Reporting Program Support Contractor News SEPTEMBER 2011 In This Issue... Emergency Department Arrival and Departure Times Page 2 Hospital OQR Benchmarks Page
National Hospital Inpatient Quality Reporting Measures Specifications Manual
 National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.4a Release Notes Completed: October 21, 2014 Guidelines for Using Release Notes Release Notes 4.4a
National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.4a Release Notes Completed: October 21, 2014 Guidelines for Using Release Notes Release Notes 4.4a
Meaningful Use Stage 2 Clinical Quality Measures Are You Ready?
 22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Meaningful Use Stage 2 Clinical Quality Measures Are You Ready? Tuesday, June 4, 1:00 pm The transition from chart-abstracted legacy core
22nd Annual Midas+ User Symposium June 2 5, 2013 Tucson, Arizona Meaningful Use Stage 2 Clinical Quality Measures Are You Ready? Tuesday, June 4, 1:00 pm The transition from chart-abstracted legacy core
Enhanced Clinical Workflow Adherence Through Real-Time Alerts and Escalations for P4P
 Enhanced Clinical Workflow Adherence Through Real-Time Alerts and Escalations for P4P Real-time alerts and escalations in hospitals can lead to forecasting, detecting and correcting adverse developments
Enhanced Clinical Workflow Adherence Through Real-Time Alerts and Escalations for P4P Real-time alerts and escalations in hospitals can lead to forecasting, detecting and correcting adverse developments
SNOMED CT AND ICD-10-BE: TWO OF A KIND?
 Federal Public Service of Health, Food Chain Safety and Environment Directorate-General Health Care Department Datamanagement Arabella D Havé, chief of Terminology, Classification, Grouping & Audit arabella.dhave@health.belgium.be
Federal Public Service of Health, Food Chain Safety and Environment Directorate-General Health Care Department Datamanagement Arabella D Havé, chief of Terminology, Classification, Grouping & Audit arabella.dhave@health.belgium.be
QI and DUE in Pharmacy Practice
 Pharmacy 483: QI and DUE in Pharmacy Practice Steve Riddle, BS Pharm, BCPS QI and Medication Utilization Lead HMC Pharmacy February 24, 2004 Acute Myocardial Infarction HA, 52yo male admitted via ER with
Pharmacy 483: QI and DUE in Pharmacy Practice Steve Riddle, BS Pharm, BCPS QI and Medication Utilization Lead HMC Pharmacy February 24, 2004 Acute Myocardial Infarction HA, 52yo male admitted via ER with
The Medicare Beneficiary Quality Improvement Project (MBQIP) Monthly Performance Improvement Call
 Monthly Performance Improvement Call") The Medicare Beneficiary Quality Improvement Project (MBQIP) Monthly Performance Improvement Call April 16, 2015 Amber Theel, Executive Director Patient Safety Susan Rivera-Lee, WSHA Consultant MBQIP MBQIP
The Medicare Beneficiary Quality Improvement Project (MBQIP) Monthly Performance Improvement Call April 16, 2015 Amber Theel, Executive Director Patient Safety Susan Rivera-Lee, WSHA Consultant MBQIP MBQIP
State of the State: Hospital Performance in Pennsylvania October 2015
 State of the State: Hospital Performance in Pennsylvania October 2015 1 Measuring Hospital Performance Progress in Pennsylvania: Process Measures 2 PA Hospital Performance: Process Measures We examined
State of the State: Hospital Performance in Pennsylvania October 2015 1 Measuring Hospital Performance Progress in Pennsylvania: Process Measures 2 PA Hospital Performance: Process Measures We examined
Note: Every encounter type must have at least one value designated under the MU Details frame.
 Meaningful Use Eligible Professionals Eligible Providers (EPs) who are participating in the EHR Incentive Program either under Medicare or Medicaid must complete at least 2 years under Stage 1 before they
Meaningful Use Eligible Professionals Eligible Providers (EPs) who are participating in the EHR Incentive Program either under Medicare or Medicaid must complete at least 2 years under Stage 1 before they
Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA
 Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA Introduce the methods of using core measures to compare quality of health care US hospitals provide Have
Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA Introduce the methods of using core measures to compare quality of health care US hospitals provide Have
Electronic Physician Documentation: Increased Satisfaction
 Electronic Physician Documentation: Increased Satisfaction Session 222, February 23, 2017 Robert (Bob) Diamond, Sr. Vice President / CIO, Health Quest Kshitij (Tij) Saxena, MD, CMIO, Health Quest 1 Speaker
Electronic Physician Documentation: Increased Satisfaction Session 222, February 23, 2017 Robert (Bob) Diamond, Sr. Vice President / CIO, Health Quest Kshitij (Tij) Saxena, MD, CMIO, Health Quest 1 Speaker
Stage 2 Meaningful Use Objectives and Measures
 Stage 2 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
Stage 2 Meaningful Use Objectives and Measures Author: Mia Evans About Technosoft Solutions: Technosoft Solutions is a healthcare technology consulting, dedicated to providing software development services
2011 Summer Institute in Nursing Informatics The Tenet Story
 2011 Summer Institute in Nursing Informatics The Tenet Story Liz Johnson, MS, FHIMSS, CPHIMS, RN-BC VP of Applied Clinical Informatics HHS Health Information Technology Standards Committee Member Modern
2011 Summer Institute in Nursing Informatics The Tenet Story Liz Johnson, MS, FHIMSS, CPHIMS, RN-BC VP of Applied Clinical Informatics HHS Health Information Technology Standards Committee Member Modern
Meaningful Use Modified Stage 2 Roadmap Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Medicare and Medicaid EHR Incentive Program. Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment
 Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
CHCANYS NYS HCCN ecw Webinar
 CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
Outpatient Quality Reporting Program
 Outpatient Quality Reporting Program Hospital Outpatient Quality Reporting (OQR) Program 2018 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN, RN Speaker: Melissa Thompson,
Outpatient Quality Reporting Program Hospital Outpatient Quality Reporting (OQR) Program 2018 Specifications Manual Update Questions & Answers Moderator: Pam Harris, BSN, RN Speaker: Melissa Thompson,
EPIC-Midas+ Integration
 EPIC-Midas+ Integration Marie C. Geraci Midas+ Integration Analyst Medical Record Number (MRN): The MRN is a unique identifier assigned to each patient record. Hospital Account (HAR): The hospital account
EPIC-Midas+ Integration Marie C. Geraci Midas+ Integration Analyst Medical Record Number (MRN): The MRN is a unique identifier assigned to each patient record. Hospital Account (HAR): The hospital account
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Meaningful Use FAQs for Behavioral Health
 Netsmart is your Meaningful Use technology partner with all the solutions you need to meet all Stage 1 Meaningful Use criteria so you don t have to integrate products from multiple vendors. For more information,
Netsmart is your Meaningful Use technology partner with all the solutions you need to meet all Stage 1 Meaningful Use criteria so you don t have to integrate products from multiple vendors. For more information,
HITECH* Update Meaningful Use Regulations Eligible Professionals
 HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
HIE Implications in Meaningful Use Stage 1 Requirements
 s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
Quality Data Model (QDM) Style Guide. QDM (version MAT) for Meaningful Use Stage 2
 Style Guide. QDM (version MAT) for Meaningful Use Stage 2") Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals. August 11, 2010
 Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
Meaningful Use Stage 2
 Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Best Practices to Improve Your Hospital Outpatient Quality Reporting. March 20, 2013
 Best Practices to Improve Your Hospital Outpatient Quality Reporting March 20, 2013 Announcements This program has been approved for 1.0 continuing education unit (CEU) given by Continuing Education (CE)
Best Practices to Improve Your Hospital Outpatient Quality Reporting March 20, 2013 Announcements This program has been approved for 1.0 continuing education unit (CEU) given by Continuing Education (CE)
MBQIP Measures Fact Sheets December 2017
 December 2017 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U1RRH29052, Rural Quality
December 2017 This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U1RRH29052, Rural Quality
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Optum Anesthesia. Completely integrated anesthesia information management system
 Optum Anesthesia Completely integrated anesthesia information management system 2 Completely integrated anesthesia information management system Optum Anesthesia Information Management System (AIMS) helps
Optum Anesthesia Completely integrated anesthesia information management system 2 Completely integrated anesthesia information management system Optum Anesthesia Information Management System (AIMS) helps
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA
 REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
REQUIREMENTS GUIDE: How to Qualify for EHR Stimulus Funds under ARRA Meaningful Use & Certified EHR Technology The American Recovery and Reinvestment Act (ARRA) set aside nearly $20 billion in incentive
Outpatient Quality Reporting Program
 The Question and Answer Show Moderator: Karen VanBourgondien, BSN, RN Speaker(s): Pam Harris, BSN, RN June 21, 2017 10:00 am Isn't Q2 submission due August 1, 2017? August 1, 2017 deadline is for Quarter
The Question and Answer Show Moderator: Karen VanBourgondien, BSN, RN Speaker(s): Pam Harris, BSN, RN June 21, 2017 10:00 am Isn't Q2 submission due August 1, 2017? August 1, 2017 deadline is for Quarter
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
Goals and Objectives for Fiscal Year 2012
 Goals and Objectives for Fiscal Year 2012 UPMC St. Margaret Teresa G. Petrick July 8, 2011 UPMC St. Margaret: Major Goals and Objectives for FY 2012 Deliver Financial Results and Operational Metrics Established
Goals and Objectives for Fiscal Year 2012 UPMC St. Margaret Teresa G. Petrick July 8, 2011 UPMC St. Margaret: Major Goals and Objectives for FY 2012 Deliver Financial Results and Operational Metrics Established
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Inpatient orders and Physician Certification MUST BE authenticated PRIOR to discharge No EXCEPTIONS.
 2 Midnight Rule for InPatient Admission On August 2, 2013 the Centers for Medicare & Medicaid Services (CMS) issued a final rule (CMS- 1599-F) updating Medicare payment policies which modifies and clarifies
2 Midnight Rule for InPatient Admission On August 2, 2013 the Centers for Medicare & Medicaid Services (CMS) issued a final rule (CMS- 1599-F) updating Medicare payment policies which modifies and clarifies
Hospital Inpatient Quality Reporting (IQR) Program Measures (Calendar Year 2012 Discharges - Revised)
 Program Measures (Calendar Year 2012 Discharges - Revised)") The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
The purpose of this document is to provide a reference guide on submission and Hospital details for Quality Improvement Organizations (QIOs) and hospitals for the Hospital Inpatient Quality Reporting (IQR)
Paragon Clinician Hub for Physicians (PCH) Reference
 Reference") Paragon Clinician Hub for Physicians (PCH) Reference Logging in to the Clinician Hub Paragon Clinician Hub (PCH) is available on any Carroll Hospital Network. VMWare View must be utilized to open the application.
Paragon Clinician Hub for Physicians (PCH) Reference Logging in to the Clinician Hub Paragon Clinician Hub (PCH) is available on any Carroll Hospital Network. VMWare View must be utilized to open the application.
TITLE: Processing Provider Orders: Inpatient and Outpatient
 POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.10 Type: Patient Care Author: Carol Vanetti; Provider Order Policy Committee Effective Date:
POLICY and PROCEDURE TITLE: Processing Provider Orders: Inpatient and Outpatient Number: 13211 Version: 13211.10 Type: Patient Care Author: Carol Vanetti; Provider Order Policy Committee Effective Date:
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage
 PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
PBSI-EHR Off the Charts Meaningful Use in 2016 The Patient Engagement Stage Please note that this document is intended to supplement the information available on the CMS website for Meaningful Use for
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal. Lori Hack & Val Tuerk, Object Health
 Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal Lori Hack & Val Tuerk, Object Health 2 3 Agenda Who Qualifies for the EHR Incentive Funds? EHR Incentive Registration Process
Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal Lori Hack & Val Tuerk, Object Health 2 3 Agenda Who Qualifies for the EHR Incentive Funds? EHR Incentive Registration Process
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE. Angel L. Moore, MAEd, RHIA Eastern AHEC REC
 THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
American Recovery & Reinvestment Act
 American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
Chronic Care Taking Disease Management Beyond Hospital Walls
 Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
Chronic Care Taking Disease Management Beyond Hospital Walls Sandra Garrison BSN MBA Director Chronic Heart Failure Initiative The Chester County Hospital Alan Barbell MBA Product Manager, Siemens Medical
The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients
 The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients Updated March 2012 Netsmart Note: The Health Information Technology for Economic
The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients Updated March 2012 Netsmart Note: The Health Information Technology for Economic
APPLICATION. Thank you for your interest in applying for the APIC Program of Distinction.
 APPLICATION Thank you for your interest in applying for the APIC Program of Distinction. This application has three parts: u PART 1: u PART 2: Personnel Information u PART 3: Required Documents Facilities
APPLICATION Thank you for your interest in applying for the APIC Program of Distinction. This application has three parts: u PART 1: u PART 2: Personnel Information u PART 3: Required Documents Facilities
Stage 1. Meaningful Use 2014 Edition User Manual
 Stage 1 Meaningful Use 2014 Edition User Manual This document, as well as the software described in it, is provided under a software license agreement with STI Computer Services, Inc. Use of this software
Stage 1 Meaningful Use 2014 Edition User Manual This document, as well as the software described in it, is provided under a software license agreement with STI Computer Services, Inc. Use of this software
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT (MBQIP)
") MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT (MBQIP) Began in September 2011 Key quality improvement activity within the Medicare Rural Hospital Flexibility grant program Goal of MBQIP: to improve
MEDICARE BENEFICIARY QUALITY IMPROVEMENT PROJECT (MBQIP) Began in September 2011 Key quality improvement activity within the Medicare Rural Hospital Flexibility grant program Goal of MBQIP: to improve
Objectives. Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004
 Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
Meaningful Use Participation Basics for the Small Provider
 Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Objective Measurement
 STEMI Designation Contract HOSPITAL SERVICES A. Current license to provide Basic Emergency Services in Contra Costa County Copy of License B. Cardiac Catheterization Laboratory services Copy of License.
STEMI Designation Contract HOSPITAL SERVICES A. Current license to provide Basic Emergency Services in Contra Costa County Copy of License B. Cardiac Catheterization Laboratory services Copy of License.
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
PASSPORT ecare NEXT AND THE AFFORDABLE CARE ACT
 REVENUE CYCLE INSIGHTS PATIENT ACCESS PASSPORT ecare NEXT AND THE AFFORDABLE CARE ACT Maximizing Reimbursements For Acute Care Hospitals Executive Summary The Affordable Care Act (ACA) authorizes several
REVENUE CYCLE INSIGHTS PATIENT ACCESS PASSPORT ecare NEXT AND THE AFFORDABLE CARE ACT Maximizing Reimbursements For Acute Care Hospitals Executive Summary The Affordable Care Act (ACA) authorizes several
Information Technology Report to Medical Executive Committee
 May 8, 2012 Information Technology Report to Medical Executive Committee Contents 1 2012 Cerner Code Upgrade Update 2 Radiology and Cardiology PACS RFP and Demos 2 Update on NHIQM Projects 2 Update on
May 8, 2012 Information Technology Report to Medical Executive Committee Contents 1 2012 Cerner Code Upgrade Update 2 Radiology and Cardiology PACS RFP and Demos 2 Update on NHIQM Projects 2 Update on
Information Technology Report to Medical Executive Committee
 November 13, 2012 Information Technology Report to Medical Executive Committee Contents 1 Meaningful Use Stage 1 Attestation Results 1 Med Rec Optimization Task Force Update 1 2012.01.07 Cerner Code Upgrade
November 13, 2012 Information Technology Report to Medical Executive Committee Contents 1 Meaningful Use Stage 1 Attestation Results 1 Med Rec Optimization Task Force Update 1 2012.01.07 Cerner Code Upgrade
PGY-1 Pharmacy Practice
 Lutheran Health Network PGY-1 Pharmacy Practice Residency Program LHN Pharmacy Residency Program Mission Statement The mission of the LHN Pharmacy Residency Program is to empower pharmacy residents to
Lutheran Health Network PGY-1 Pharmacy Practice Residency Program LHN Pharmacy Residency Program Mission Statement The mission of the LHN Pharmacy Residency Program is to empower pharmacy residents to
Emergency Department Update 2010 Outpatient Payment System
 Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Figure 1: Heat map showing zip codes and countries of residence for patients in STARR
 1 / 5 STARR Data Synopsis We operate STARR, a research data repository with 20 years of fully identified clinical data. STARR includes, but is not limited to, nightly clinical data, Epic Clarity, from
1 / 5 STARR Data Synopsis We operate STARR, a research data repository with 20 years of fully identified clinical data. STARR includes, but is not limited to, nightly clinical data, Epic Clarity, from
Journey Towards Automated. Core Measures at NYP. Scott W. Possley, PA-C, MPAS
 Journey Towards Automated Click Data to Abstraction edit Master title of CMS style Core Measures at NYP Scott W. Possley, PA-C, MPAS Objectives Describe our hospital Discuss rationale behind automation
Journey Towards Automated Click Data to Abstraction edit Master title of CMS style Core Measures at NYP Scott W. Possley, PA-C, MPAS Objectives Describe our hospital Discuss rationale behind automation
STEMI SYSTEM RECEIVING CENTER STANDARDS AND DESIGNATION
 POLICY NO: FAC - 9 DATE ISSUED: 11/2016 DATE TO BE REVIEWED: 11/2019 STEMI SYSTEM RECEIVING CENTER STANDARDS AND DESIGNATION Purpose: To define the criteria for designation as a STEMI Receiving Center
POLICY NO: FAC - 9 DATE ISSUED: 11/2016 DATE TO BE REVIEWED: 11/2019 STEMI SYSTEM RECEIVING CENTER STANDARDS AND DESIGNATION Purpose: To define the criteria for designation as a STEMI Receiving Center
Population and Sampling Specifications
 Mat erial inside brac ket s ( [ and ] ) is new to t his Specific ati ons Manual versi on. Introduction Population Population and Sampling Specifications Defining the population is the first step to estimate
Mat erial inside brac ket s ( [ and ] ) is new to t his Specific ati ons Manual versi on. Introduction Population Population and Sampling Specifications Defining the population is the first step to estimate
Ontario Shores Journey to EMRAM Stage 7. October 21, 2015
 Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
Ontario Shores Journey to EMRAM Stage 7 October 21, 2015 ICE BREAKER Agenda System overview & pervasiveness of use Review Clinical Practice Guideline implementation Discuss Patient Portal implementation
MBQIP Quality Measure Trends, Data Summary Report #20 November 2016
 MBQIP Quality Measure Trends, 2011-2016 Data Summary Report #20 November 2016 Tami Swenson, PhD Michelle Casey, MS University of Minnesota Rural Health Research Center ABOUT This project was supported
MBQIP Quality Measure Trends, 2011-2016 Data Summary Report #20 November 2016 Tami Swenson, PhD Michelle Casey, MS University of Minnesota Rural Health Research Center ABOUT This project was supported
Meaningful Use and PCC EHR. Tim Proctor Users Conference 2017
 Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
9/28/2011. Learning Agenda. Meaningful Use and why it s here. Meaningful Use Rules of Participation. Categories, Objectives and Thresholds
 Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL
 CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
Meaningful Use Final Rule:
 Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Release Notes 3.3 October 1, Specifications Manual for National Hospital Inpatient Quality Measures
 October 1, 2010 Guidelines for Using Release Notes Release Notes 3.3 provide modifications to the Specifications Manual for National Hospital Inpatient Quality Measures. The Release Notes are provided
October 1, 2010 Guidelines for Using Release Notes Release Notes 3.3 provide modifications to the Specifications Manual for National Hospital Inpatient Quality Measures. The Release Notes are provided
Connecting the Revenue and Reimbursement Cycles
 Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
Connecting the Revenue and Reimbursement Cycles Tuesday, August 19 th, 2014 Toni G. Cesta, Ph.D., RN, FAAN Consultant and Partner Case Management Concepts New York Office And Bev Cunningham, MS, RN Vice
REDUCING MEDICAL AND MEDICATION ERRORS THROUGH INFORMATION TECHNOLOGY AND PROCESS CHANGE. M. Patricia Maher Johns Hopkins Bayview Medical Center
 REDUCING MEDICAL AND MEDICATION ERRORS THROUGH INFORMATION TECHNOLOGY AND PROCESS CHANGE M. Patricia Maher Johns Hopkins Bayview Medical Center Background Acute Care Hospital- 355 beds Trauma center NICU-
REDUCING MEDICAL AND MEDICATION ERRORS THROUGH INFORMATION TECHNOLOGY AND PROCESS CHANGE M. Patricia Maher Johns Hopkins Bayview Medical Center Background Acute Care Hospital- 355 beds Trauma center NICU-
CME Disclosure. HCAHPS- Hardwiring Your Hospital for Pay-for-Performance Success. Accreditation Statement. Designation of Credit.
 CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
Procedure. Applies To: UNM Hospitals Responsible Department: HIM / Admitting/ Blood Bank Revised: 8/2015
 Title: Patient Re-identification, Information Correction, and Duplicate Medical Record Number Removal Applies To: UNM Hospitals Responsible Department: HIM / Admitting/ Blood Bank Revised: 8/2015 Procedure
Title: Patient Re-identification, Information Correction, and Duplicate Medical Record Number Removal Applies To: UNM Hospitals Responsible Department: HIM / Admitting/ Blood Bank Revised: 8/2015 Procedure