INTRODUCTION TO HIGH VALUE CARE:
|
|
|
- Sophia Hancock
- 5 years ago
- Views:
Transcription
1 INTRODUCTION TO HIGH VALUE CARE: ELIMINATING HEALTHCARE WASTE Bindu Swaroop, MD Associate Clinical Professor Department of Medicine University of California, Irvine
2 Learning Objectives Understand some of the current problems with health care spending Recognize the role that residents, faculty and teaching hospitals play in the problem Introduce the five step model for delivering high value, cost conscious care Articulate strategies for bringing high value care into daily practice
3 Why Worry About Cost Now? Health Care Costs in the US in Billions of Dollars *30% of these costs are wasted care (around $765 billion in 2009)
4 What is the problem? 1 Since 1970, healthcare spending is rising 2.4% faster than GDP. Estimated $765 billion of healthcare waste annually. Physicians responsible for 87% of wasteful spending. Definition of Waste in healthcare: Healthcare spending that can be eliminated without reducing the quality of care.
5 Estimated Sources of Excess Costs in Health Care Unnecessary Services $210 Billion Excessive Administration Costs $190 Billion Inefficient Service Delivery $130 Billion Prices That Are Too High $105 Billion Fraud $75 Billion Missed Prevention $55 Billion IOM 2010
6 Ordering more services 3 Tests Imaging Two areas of greatest expenditures and most rapid growth: imaging and tests
7 Reasons Residents Over-Order Tests 9 1. Duplicating role modeled behavior 2. Desire to be complete 3. Pre-emptive ordering/rushing an evaluation/unnecessary duplication of tests 4. Discomfort with Diagnostic Uncertainty 5. Curiosity 6. Lack of knowledge of the costs and harms 7. Defensive medicine 8. Patient requests 9. Faculty demand 10. No training in weighing benefit relative to cost and harm 11. Ease of access to services when patient is hospitalized

8 .
9 What is High Value, Cost Conscious Care? Providing the best possible care to our patients and Simultaneously reducing unnecessary costs to the healthcare system
10
11
12 Steps Toward High Value, Cost Conscious Care Five-Step Framework: High-Value, Cost-Conscious Care Step 1 Understand the benefits, harms, and relative costs of the interventions that you are considering Step 2 Decrease or eliminate the use of interventions that provide no benefit and/or may be harmful Step 3 Choose interventions and care settings that maximize benefits, minimize harms, and reduce costs (using comparative-effectiveness and cost-effectiveness data) Step 4 Customize a care plan with the patient that incorporates their values and addresses their concerns Step 5 Identify system-level opportunities to improve outcomes, minimize harms, and reduce health care waste

13 Case #1 Ms. B is 57 year-old woman presenting to the ED with chest pain. She has a history of recurrent UTIs; she denies dysuria or urinary frequency. Afebrile WBC count 5.5 Should she have a routine urinalysis and urine culture?
14 Case #1 How would you manage this patient? Additional testing? Treatment? Do your recommendations change if she has an indwelling Foley catheter?
15 Step 1: Understand the benefits, harms, and costs of diagnostic testing How much do you think the following cost: Urinalysis? Urine culture? 7 days of oral ciprofloxacin? What are the potential downstream costs?
16 Case #1: Follow Up Urinalysis: cloudy, WBC, RBC, 2+ bacteria Urine culture: >100,000 E. coli Ms. B was discharged to complete 7 days of oral ciprofloxacin. She returned 10 days later with fever, abdominal pain and diarrhea. Stool Clostridium difficile assay was positive.
17 Case #1: Approximate Charges Initial episode of care: Downstream: Urinalysis $94 Urine culture $94 Ciprofloxacin 500 mg po bid x 7 days $23 C. difficile PCR assay $38 Metronidazole x 10 days $36 Vancomycin po x 10 days $2,284 (UCIMC: Urinalysis w/ microscopy = $128!) Illness and lost days of work due to C. difficile colitis
18 Steps Toward High Value, Cost-Conscious Care 4 Step one: Understand the benefits, harms, and relative costs of the interventions that you are considering. Step two: Decrease or eliminate the use of interventions that provide no benefits and/or may be harmful. Step three: Choose interventions and care settings that maximize benefits, minimize harms, and reduce costs (using comparative-effectiveness and cost-effectiveness data). Step four: Customize a care plan with the patient that incorporates their values and addresses their concerns. Step five: Identify system level opportunities to improve outcomes, minimize harms, and reduce healthcare waste.

19 Step 2: Decrease or eliminate care that provides no benefit and/or may be harmful.
20 Step 2: Decrease or eliminate care that provides no benefit and/or may be harmful.

21 Case #2 Mr. M is a 75 year-old man with OA presenting with acute-on-chronic right hip pain. He slipped out of bed this morning and is now unable to bear weight on his right leg. Exam is notable only for moderate tenderness over the right hip. Hip and pelvis x-rays were negative for fracture. Should he have further imaging? Which type?

22 Clinical Decision Support Tools American College of Radiology: Appropriateness Criteria Criteria

23 ACR Appropriateness Criteria: Acute Hip Pain Suspected Fracture
24 Case #2: Follow Up CT pelvis was performed and was non-diagnostic. Pain persisted and he remained unable to bear weight. MRI was obtained and revealed a nondisplaced femoral fracture in the setting of severe osteoarthritis. Patient underwent nonemergent repair of the fracture.
25 Case #2: Approximate Charges This hospitalization: Femur x-ray: $700 Pelvis x-ray: $800 CT hip/pelvis: $3000 MRI hip: $ nights in the hospital: $12,000 Femur fracture repair: $12, 415 Downstream: Delay in therapy, leading to increased morbidity/mortality Radiation exposure
26 Value, Cost and Health Care Cost Value Cost Cost of Test Cost includes cost of test and downstream costs, benefits and harms High-cost interventions may provide good value because they are highly beneficial Low-cost interventions may have little or no value if they provide little benefit or increase downstream costs
27 Clinical Case #3: Syncope Mr. P., a 42 year-old man with hypertension treated with HCTZ, presents to the emergency department after passing out. He was outside working in his garden on a hot afternoon when he started to feel ill and then suddenly lost consciousness. His wife witnessed the event and noticed that he fell to the ground and was unresponsive for about 10 seconds. He did not hit his head. He then woke up and returned to his baseline mental status. T 37.5 o C BP 110/70, HR 95, RR 12, 0 2 sat 98% on ambient air Exam notable for: dry mucus membranes, no cardiac murmurs, normal neurologic exam

28 Step 1: Benefits, harms, costs Evaluation and Management of Syncope What is your workup for a patient with syncope? Which labs or initial studies do you want to order? What are the benefits, harms, and costs of each test or intervention?
29 Hospital Course Mr. P. was admitted for 2 days during which time: ECG was normal; TTE was also obtained and revealed mild LVH Head CT revealed no abnormalities. Carotid duplex ultrasound revealed 10-50% stenosis, bilaterally. Lab evaluation with CBC, BMP, troponin were all within normal limits. He was monitored on telemetry, which revealed occasional PVCs. He was given 1 liter of normal saline and discharged on hospital day 2.
30 Case #3: Approximate Charges* One night on telemetry $7,000 Electrolyte panel: $175 CBC: $170 CXR: $500 Head CT: $3,000 TTE: $3,000 Carotid ultrasound:$1900 IV fluid bolus: $150 *Charges from CA Chargemaster website and patient bills; actual charges vary by institution (
31 Approximate Cost? What is the total charge for this patient s 2-day admission? Approximately $19,000 In addition to financial costs, what are some harms and potential downstream costs of this patient s management? Examples: Repeated phlebotomy, IV catheter-related phlebitis or infection, days of work lost, etc.
32 Discussion When does a patient with syncope require a limited workup versus an extensive evaluation? When does a patient with syncope require inpatient admission? Key: When managing a patient with syncope, risk stratify your patient to assist in the decision to admit or treat as an outpatient.


33 Step 2: Decrease or eliminate care that provides no benefit and/or may be harmful.
34 Step 2: Decrease or eliminate care that provides no benefit and/or may be harmful.
35 Case Presentation 70 y/o female POD#3 from laparoscopic cholecystectomy Patient recovering well with plan for discharge While ambulating became acutely SOB with tachycardia Complained of right shoulder and chest pain associated with diaphoresis
36 Step 1: Benefits, Harms, Costs What is your work-up? What factors lead us to make these orders or recommendations? How much does this cost?
37 Benefits, Harms, Costs Test Benefit Harm Costs CT Angio TTE EKG D-dimer BNP Troponin (serial) ABG LE U/S Doppler Hypercoagulable work up
38 Benefits, Harms, Costs Test Benefit Harm Costs CT Angio TTE EKG D-dimer BNP Troponin (serial) Best sensitivity for identifying PE Assess RV strain Identify arrythmia, non-invasive Easy to obtain, helpful in ruling out PE if negative ABG LE U/S Doppler Hypercoagulable work up no contrast, noninvasive
39 Benefits, Harm, Costs Test Benefit Harm Costs CT Angio Best sensitivity for identifying PE Contrast, radiation, incidental findings TTE Assess RV strain Low specificity EKG D-dimer BNP Troponin (serial) ABG LE U/S Doppler Hypercoagulable work up Identify arrythmia, non-invasive Easy to obtain, helpful in ruling out PE if negative no contrast, noninvasive Low specificity Repeated phlebotomy Arterial Stick Low yield in patient with clear risk factor for PE
40 Benefits, Test Harms, Benefit Costs Harm Costs CT Angio Best sensitivity for identifying PE Contrast, radiation, incidental findings $ TTE $ EKG D-dimer Identify arrythmia, non-invasive Easy to obtain, helpful in ruling out PE if negative $79.18 Low specificity $65.88 BNP $18.75 Troponin (serial) Repeated phlebotomy $26.01 (x 1) ABG Arterial Stick $35.94 LE U/S Doppler Hypercoagulable work up no contrast, noninvasive Low yield in patient with clear risk factor for PE $ $79.18


41 Step 2: Decrease or eliminate care that provides no benefit and/or may be harmful Which tests had the potential to change management? -CT Angio -D-dimer -Fibrinogen -BNP -Serial Troponin -Hypercoagulable panel -TTE -LE Ultrasound -ABG

42 Step 2: Decrease or eliminate care that provides no benefit and/or may be harmful
43 Step 3: Choose interventions and care settings that maximize benefits, minimize harms, and reduce costs Use comparative-effectiveness and cost-effectiveness data In this case: Well s or Geneva Score to determine pre test probability Mini Lectures Residency Program Residency Program Department of Medicine School of Medicine University of California, Irvine
44 Wells Score Clinical symptoms of DVT (leg swelling, pain with palpation) 3.0 Traditional clinical probability assessment (Wells criteria) Other diagnosis less likely than pulmonary embolism 3.0 Heart rate > Immobilization ( 3 days) or surgery in the previous four weeks 1.5 Previous DVT/PE 1.5 Hemoptysis 1.0 Malignancy 1.0 High >6.0 Moderate 2.0 to 6.0 Low <2.0 Simplified clinical probability assessment (Modified Wells criteria) PE likely >4.0 PE unlikely 4.0
45 Simplified Geneva Score Variable Score Age >65 1 Previous DVT or PE 1 Surgery or fracture within 1 month 1 Active malignancy 1 Unilateral lower limb pain 1 Hemoptysis 1 Pain on deep vein palpation of lower limb and unilateral edema Heart rate 75 to 94 bpm 1 Heart rate greater than 94 bpm 2 Score of less than 2 is low probablility for PE, score of less than 2 plus a negative D-dimer results in a likelihood of PE of 3% 1
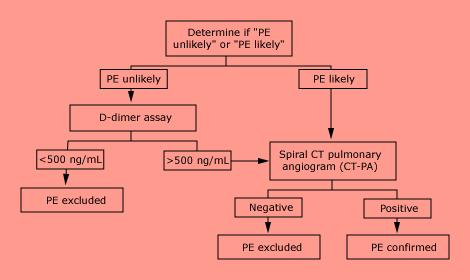
46 Diagnostic Algorithm

47 Start with the H+P! The first step is to perform a good history and physical examination Cost = $0 Risk = Zero Yield = Priceless
48
49 Cost of an ED Visit Community hospital in Southern California Patient fell, seen in ED for evaluation Clinically stable
50 Quiz: What is the patient charged? One bag of normal saline given IV: Actual bill: $158.55
51 Quiz: What does is the patient charged? A comprehensive metabolic panel: Actual bill: $1, (UCIMC Outpatient Charge: $115)
52 Quiz: What is the patient charged? One set of blood cultures: Actual bill: $510 (remember, we usually order 2 sets)
53 Quiz: What is the patient charged? Electrocardiogram: Actual bill: $706
54 What is the patient charged? Troponin (x 1): Actual bill: $402 (remember, we usually order x 3)
55 Quiz: What is the patient charged? CT Head w/o contrast: Actual bill: $2930 (At UCIMC: $3,939)
56 ED Bill Community hospital in Southern California Patient fell, seen in ED for evaluation Clinically stable Discharged from ED Total cost billed to patient (not including physician fees): $10,
57 Disclaimer Cost of test and charge to patient is complex and involves many factors, and is not just monetary Clinical reasoning and individualized care are very important Cost-conscious care is not about discouraging appropriate care, nor denying beneficial services
58 Steps Toward High Value, Cost Conscious Care Five-Step Framework: High-Value, Cost-Conscious Care Step 1 Understand the benefits, harms, and relative costs of the interventions that you are considering Step 2 Decrease or eliminate the use of interventions that provide no benefit and/or may be harmful Step 3 Choose interventions and care settings that maximize benefits, minimize harms, and reduce costs (using comparative-effectiveness and cost-effectiveness data) Step 4 Customize a care plan with the patient that incorporates their values and addresses their concerns Step 5 Identify system-level opportunities to improve outcomes, minimize harms, and reduce health care waste
59 Questions to Ask Before Ordering a Test 8 Did the patient have this test previously? Will the result of this test change the care of the patient? What are the probability and potential adverse consequences of a false positive result? Is the patient in potential danger in the short term if I do not perform this test? Am I ordering the test primarily because the patient wants it or to reassure the patient?
60
61 Summary START: Using validated clinical tools and follow diagnostic algorithms to avoid overuse of tests Asking yourself before you order the test if the results will change what you do for the patient STOP: routinely obtaining studies if results will not alter your management
62 References 1) ABIM Foundation, Choosing Wisely Campaign. (accessed 5/1/12). 2) Kaniecki R. Headache assessment and management. JAMA.2003;289: ) Sager A, Socolar D. Health Costs Absorb One-Quarter of Economic Growth, Boston: Health Reform Program, Boston University School of Public Health; ) Cooke M. Cost consciousness in patient care--what is medical education s responsibility? NEJM. 2010;362: ) Thomas Reuters. Where can $700 billion in waste be cut annually from the U.S Health Care system? October, ) Uwe E. Reinhardt blog, NY Times, 12/24/ ) Laine C. High-value testing begins with a few simple questions. Ann Intern Med. 2012;156: ) Adapted from Neel Shah. Commonhealth. Accessed 10/ ) Qaseem, A. Appropriate Use of Screening and Diagnostic Tests to Foster High-Value, Cost- Conscious Care. Ann Intern Med. 2012;156:
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Guidelines for the Oral Presentation
 Guidelines for the Oral Presentation Nersi Nikakhtar, M.D. University of Minnesota Medical School 1 Table of Contents The Oral Presentation: An Introduction... 3 Why Worry About the Oral Presentation?...
Guidelines for the Oral Presentation Nersi Nikakhtar, M.D. University of Minnesota Medical School 1 Table of Contents The Oral Presentation: An Introduction... 3 Why Worry About the Oral Presentation?...
2 Midnight Case Examples and Documentation Tips. Ralph Wuebker, MD Executive Health Resources, Inc. All rights reserved.
 2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures. Today s Presenters
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
AHRQ Safety Program for Long-term Care: HAIs/CAUTI The Culture of Culturing: The Importance of Knowing When to Order Urine Cultures National Content Webinar Series October 15, 2015 Today s Presenters Barbara
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
LABORATORY-IDENTIFIED (LABID) EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE. National Healthcare Safety Network (NHSN)
 EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE. National Healthcare Safety Network (NHSN)") LABORATORY-IDENTIFIED (LABID) EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE National Healthcare Safety Network (NHSN) CMS PARTICIPATION Acute care hospitals, Long Term Acute Care (LTACs),IP Rehabilitation
LABORATORY-IDENTIFIED (LABID) EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE National Healthcare Safety Network (NHSN) CMS PARTICIPATION Acute care hospitals, Long Term Acute Care (LTACs),IP Rehabilitation
Learning Objectives. Denver Health Medical Center. Complex Coding Scenarios and Resolution
 Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
Writing RAC Appeals, RAC Denial Prevention, and Case Management Collaboration
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Writing RAC Appeals, RAC Denial Prevention, and Case Management Collaboration Kathy Shumpert, MSN, RN, CCDS Clinical
7th Annual Association for Clinical Documentation Improvement Specialists Conference Writing RAC Appeals, RAC Denial Prevention, and Case Management Collaboration Kathy Shumpert, MSN, RN, CCDS Clinical
 Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES. Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN
 CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN NYSNA is accredited as a provider of continuing nursing education by the American Nurses
CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN NYSNA is accredited as a provider of continuing nursing education by the American Nurses
University of South Dakota Vermillion, South Dakota Department of Nursing
 Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
Section: Emergency Department Application: Medical Center. Contact Person: Director, Emergency Services. Approved:
 Subject: Triage of Patients Core X General Recommended: Section: Emergency Department Application: Medical Center Contact Person: Director, Emergency Services Approved: Policy Number: ED 101 Date of Issue:
Subject: Triage of Patients Core X General Recommended: Section: Emergency Department Application: Medical Center Contact Person: Director, Emergency Services Approved: Policy Number: ED 101 Date of Issue:
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model
 CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
CMS Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Phase 2--Payment Model The Revolving Door One fourth of all nursing home resident go the hospital each year - Some many
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare
 Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Valorie Sweigart, DNP g, Samuel Shartar, RN, CEN Emory Healthcare Why build Principles of observational medicine ROI ED Hospital Clinical implications Define intended d use Open, closed or mixed use Impact
Facilitation Interns Acquisition of
 Facilitation Interns Acquisition of Medical Knowledge and Core Skills through Experiential Learning Raquel Belforti, DO, Kevin Hinchey, MD Reham Shaaban, DO Mihaela Stefan, MD Baystate Medical Center Tufts
Facilitation Interns Acquisition of Medical Knowledge and Core Skills through Experiential Learning Raquel Belforti, DO, Kevin Hinchey, MD Reham Shaaban, DO Mihaela Stefan, MD Baystate Medical Center Tufts
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Medical Necessity verses Medical Decision Making. Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC
 Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Medical Necessity verses Medical Decision Making Presented Kevin Solinsky,CPC, CPC-I, CEDC, CEMC of Healthcare Coding Consultants, LLC Objectives We will first look at Medical Decision Making in detail.
Parsimonious Practice: Ideas for Implementing a High Value Care Curriculum
 Parsimonious Practice: Ideas for Implementing a High Value Care Curriculum Anna K. Donovan, MD Maggie K. Benson, MD Thomas D. Painter, MD Peggy B. Hasley, MD, MHSc Definition High Value Care (HVC): Care
Parsimonious Practice: Ideas for Implementing a High Value Care Curriculum Anna K. Donovan, MD Maggie K. Benson, MD Thomas D. Painter, MD Peggy B. Hasley, MD, MHSc Definition High Value Care (HVC): Care
Diagnostics for Patient Safety and Quality of Care. Vulnerable System Syndrome
 Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
Diagnostics for Patient Safety and Quality of Care Carol Haraden, PhD APAC Forum This presenter has nothing to disclose. Vulnerable System Syndrome Three core pathologies - Blame - Denial - And the pursuit
LABORATORY IDENTIFIED (LABID) EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE. National Healthcare Safety Network (NHSN)
 EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE. National Healthcare Safety Network (NHSN)") LABORATORY IDENTIFIED (LABID) EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE National Healthcare Safety Network (NHSN) CMS PARTICIPATION Acute care hospitals, Long Term Acute Care (LTACs),IP Rehabilitation
LABORATORY IDENTIFIED (LABID) EVENT REPORTING MRSA BACTEREMIA AND C. DIFFICILE National Healthcare Safety Network (NHSN) CMS PARTICIPATION Acute care hospitals, Long Term Acute Care (LTACs),IP Rehabilitation
How does one report the performance of both a screening mammogram on the right breast and a diagnostic on the left breast at the same encounter?
 1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
1 of 6 05/27/2008 4:21 PM FAQ Wisconsin Medical Society FAQ If you have any questions regarding the following, please direct all your questions to: efaq@wismed.org. Medicare / Medicaid Medicare does not
TITLE CLIN_189 CRITICAL RESULT NOTIFICATION. APPLICABILITY Edward Hospital, Linden Oaks Hospital
 Policies and procedures are guidelines and are not a substitute for the exercise of individual judgment. If you are reading a printed copy of this policy, make sure it is the most current by checking the
Policies and procedures are guidelines and are not a substitute for the exercise of individual judgment. If you are reading a printed copy of this policy, make sure it is the most current by checking the
Consultation in Academic Medicine
 Consultation in Academic Medicine John W. Gnann, Jr., M.D. Professor of Medicine Division of Infectious Diseases Alan M. Stamm, M.D. Professor of Medicine Division of General Internal Medicine Outline
Consultation in Academic Medicine John W. Gnann, Jr., M.D. Professor of Medicine Division of Infectious Diseases Alan M. Stamm, M.D. Professor of Medicine Division of General Internal Medicine Outline
Patient Diary. Vascular Surgery Enhanced Recovery Programme
 2-3 days following discharge, someone from the vascular team will contact you at home. If you have any problems please do not hesitate to contact the ward. We are here to help. Please contact us on the
2-3 days following discharge, someone from the vascular team will contact you at home. If you have any problems please do not hesitate to contact the ward. We are here to help. Please contact us on the
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
POLICY FOR X RAY REFERRAL BY QUALIFIED NURSE PRACTITIONERS WORKING IN GENERAL PRACTICE
 POLICY FOR X RAY REFERRAL BY QUALIFIED NURSE PRACTITIONERS WORKING IN GENERAL PRACTICE APPROVED BY: Chief Nurse May 2016 EFFECTIVE FROM: May 2016 REVIEW DATE: May 2018 Version Control Policy Category:
POLICY FOR X RAY REFERRAL BY QUALIFIED NURSE PRACTITIONERS WORKING IN GENERAL PRACTICE APPROVED BY: Chief Nurse May 2016 EFFECTIVE FROM: May 2016 REVIEW DATE: May 2018 Version Control Policy Category:
Patient Charge Disclosure List
 Patient Charge Disclosure List In compliance with state law, Union Hospital is providing this price list containing our charges for room and board, emergency department, operating room, delivery, physical
Patient Charge Disclosure List In compliance with state law, Union Hospital is providing this price list containing our charges for room and board, emergency department, operating room, delivery, physical
Patient Price Information List
 Caring for the Health of Our Community Patient Price Information List In compliance with state law, Wyandot Memorial Hospital is providing this price list containing our charges for room and board, emergency
Caring for the Health of Our Community Patient Price Information List In compliance with state law, Wyandot Memorial Hospital is providing this price list containing our charges for room and board, emergency
Patient Price Information List
 Patient Price Information List In compliance with state law, OhioHealth is providing this price list for O'Bleness Memorial Hospital that contains our charges for room and board, emergency department,
Patient Price Information List In compliance with state law, OhioHealth is providing this price list for O'Bleness Memorial Hospital that contains our charges for room and board, emergency department,
Iowa Healthcare Collaborative - HEN 2.0 Measures
 Iowa Healthcare Collaborative - HEN 2.0 Measures Yellow Pink Purple Green Blue Legend Readmissions and Care Transitions Healthcare-associated Infections Hospital Acquired Conditions Safety Across the Board
Iowa Healthcare Collaborative - HEN 2.0 Measures Yellow Pink Purple Green Blue Legend Readmissions and Care Transitions Healthcare-associated Infections Hospital Acquired Conditions Safety Across the Board
Patient Diary. Enhanced Recovery After Surgery (ERAS) Total Knee Replacement. Helping patients get better sooner after surgery.
 Total Knee Replacement. Helping patients get better sooner after surgery.") Contact numbers If you need any support or advice before or after surgery please do not hesitate to call us. Claire Ward enhanced recovery nurse (Monday Friday 8-4) 07816448518 Ward 12B 01494426398 How
Contact numbers If you need any support or advice before or after surgery please do not hesitate to call us. Claire Ward enhanced recovery nurse (Monday Friday 8-4) 07816448518 Ward 12B 01494426398 How
E-Learning Module M: Assessment Review
 E-Learning Module M: Assessment Review This Module requires the learner to have read Chapter 12 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised: August
E-Learning Module M: Assessment Review This Module requires the learner to have read Chapter 12 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised: August
The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012
 The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012 Objectives Discuss what is a Urinary Tract Infection (UTI) Reflect on current practices
The Urine Dipstick: A Quick Way To Over-Treat! Ann McFeeters, RN Infection Control Practitioner September 26, 2012 Objectives Discuss what is a Urinary Tract Infection (UTI) Reflect on current practices
Case Presentation. Cindy Felty MSN, RN, CNP, FCCWS Assistant Professor of Medicine Mayo Clinic March 27, 2008
 Case Presentation Cindy Felty MSN, RN, CNP, FCCWS Assistant Professor of Medicine Mayo Clinic March 27, 2008 Acute DVT Case 1- Day 1 68 year old male admitted overnight to hospital for painful acute DVT
Case Presentation Cindy Felty MSN, RN, CNP, FCCWS Assistant Professor of Medicine Mayo Clinic March 27, 2008 Acute DVT Case 1- Day 1 68 year old male admitted overnight to hospital for painful acute DVT
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Establishing an Emergency Department Sepsis Screen
 Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Establishing an Emergency Department Sepsis Screen Phelan Bailey, RN, CEN Emergency Department Nurse Manager St. Claire Regional Medical Center Kentucky 2 About Us St. Claire Regional Medical Center is
Definitions and Regulatory Considerations
 Observation Medicine Mark G. Moseley, MD, MHA, FACEP Associate Professor of Emergency Medicine Medical Director for Emergency Services Department of Emergency Medicine The Ohio State University Medical
Observation Medicine Mark G. Moseley, MD, MHA, FACEP Associate Professor of Emergency Medicine Medical Director for Emergency Services Department of Emergency Medicine The Ohio State University Medical
Quarterly CERT Error Findings Report WPS GHA Part A J8 MAC ~ Indiana and Michigan ~
 Quarterly CERT Error Findings Report WPS GHA Part A J8 MAC ~ Indiana and Michigan ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed April 1, 2017, through June 30,
Quarterly CERT Error Findings Report WPS GHA Part A J8 MAC ~ Indiana and Michigan ~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed April 1, 2017, through June 30,
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry
 TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
TITLE/DESCRIPTION: Admission and Discharge Criteria for Telemetry DEPARTMENT: PERSONNEL: Telemetry Telemetry Personnel EFFECTIVE DATE: 6/86 REVISED: 02/00, 4/10, 12/14 Admission Procedure: 1. The admitting
Polling Question #1. Denials and CDI: A Recovery Auditor s Perspective
 1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
Running head: ADULT HEALTH 1 CASE STUDY 1
 Running head: ADULT HEALTH 1 CASE STUDY 1 Adult Health 1 Case Study Jian Salcedo California State University, Stanislaus September 20 th, 2010 ADULT HEALTH 1 CASE STUDY 2 Mrs. Smith is an 89-year-old white
Running head: ADULT HEALTH 1 CASE STUDY 1 Adult Health 1 Case Study Jian Salcedo California State University, Stanislaus September 20 th, 2010 ADULT HEALTH 1 CASE STUDY 2 Mrs. Smith is an 89-year-old white
Guidelines for the Preoperative Process
 Guidelines for the Preoperative Process Preparation of Patients for Procedural Sedation and Anesthesia. Department of Anesthesiology Thomas May, MD Witold Waberski, MD Department of Internal Medicine Aized
Guidelines for the Preoperative Process Preparation of Patients for Procedural Sedation and Anesthesia. Department of Anesthesiology Thomas May, MD Witold Waberski, MD Department of Internal Medicine Aized
Clostridium difficile
 Clostridium difficile Michelle Luscombe & Karly Herberholz Hagel 5/14/2012 1 Outline What is clostridium difficile infection (CDI)? Symptoms & Complications Risk Factors Transmission Prevention and Control
Clostridium difficile Michelle Luscombe & Karly Herberholz Hagel 5/14/2012 1 Outline What is clostridium difficile infection (CDI)? Symptoms & Complications Risk Factors Transmission Prevention and Control
HOSPITAL ACQUIRED COMPLICATIONS. Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program
 HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
Room and Board -- Per Day Charges
 Patient Price Information List Mansfield Hospital In compliance with state law, OhioHealth is providing this price list for Mansfield Hospital that contains our charges for room and board, emergency department,
Patient Price Information List Mansfield Hospital In compliance with state law, OhioHealth is providing this price list for Mansfield Hospital that contains our charges for room and board, emergency department,
EC OR ADULT OUTPATIENT SURGERY PLAN - Phase: PACU Orders
 - Phase: PACU Orders DETAILS Admit/Discharge/Transfer This plan should only be placed on a patient that is being discharged from outpatient surgery. If patient is being admitted, this plan should not be
- Phase: PACU Orders DETAILS Admit/Discharge/Transfer This plan should only be placed on a patient that is being discharged from outpatient surgery. If patient is being admitted, this plan should not be
Rural-Relevant Quality Measures for Critical Access Hospitals
 Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
STANDARDIZED PROCEDURE LUMBAR DRAIN INSERTION (Adults, Peds)
") I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
I. Definition The purpose of this standardized procedure is for the Advanced Health Practitioner to safely place a lumbar drain. II. Background Information A. Setting: The setting (inpatient vs outpatient)
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
? Prehab, immunonutrition. Safe surgical principles. Optimizing Preoperative Evaluation
 Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Optimizing Preoperative Evaluation Timothy Geiger, MD, MMHC Associate Professor of Surgery Executive Medical Director, Surgery Patient Care Center Chief, Division of General Surgery Director, Colon and
Antimicrobial Stewardship in Continuing Care. Nursing Home Acquired Pneumonia Clinical Checklist
 Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Antimicrobial Stewardship in Continuing Care Nursing Home Acquired Pneumonia Clinical Checklist March 2015 What is Antimicrobial Stewardship? Using the: right antimicrobial agent for a given diagnosis
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient)
") Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition
 Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Chapter 01: Professional Nursing Practice Lewis: Medical-Surgical Nursing, 10th Edition MULTIPLE CHOICE 1. The nurse completes an admission database and explains that the plan of care and discharge goals
Are you at risk of blood clots?
 Are you at risk of blood clots? DVT (deep vein thrombosis) & PE (pulmonary embolism) Information for patients in hospital or going home from hospital Are you at risk of blood clots? (DVT & PE) This leaflet
Are you at risk of blood clots? DVT (deep vein thrombosis) & PE (pulmonary embolism) Information for patients in hospital or going home from hospital Are you at risk of blood clots? (DVT & PE) This leaflet
Surgical Technology Patient Care Skills Preop Routine Objectives:
 Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
General information. Hospital type : Acute Care Hospitals. Provides emergency services : Yes. electronically between visits : Yes
 General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
How to Write a Medical Note for the. Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note
 Note") How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
How to Write a Medical Note for the Foundations of Doctoring Course and Beyond: Demystifying the Focused (SOAP) Note and the Comprehensive (H&P) Note by Todd Guth, MD Overview of the Medical Note Medical
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
Accountability and Collaboration Working With A Physician Assistant
 Accountability and Collaboration Working With A Physician Assistant Anthony Derro, RN Practice Consultant Linda Levesque, RN Outreach Consultant, Acute Care Karen Riddell, Director, Professional Practice
Accountability and Collaboration Working With A Physician Assistant Anthony Derro, RN Practice Consultant Linda Levesque, RN Outreach Consultant, Acute Care Karen Riddell, Director, Professional Practice
Observation Unit. Romil Chadha
 Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Observation Unit Romil Chadha Observation vs Inpatient Whenever in doubt please call 3-3070 to get assistance from Utilization Review (UR) Randy A. Rosen, MD, reviews cases and usually emails about patients
Provider-Payer Relations: Sample Cases. Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017
 Provider-Payer Relations: Sample Cases Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017 2017 Presenter Aetna Name Inc. May 2017 1 Documentation Apropos documentation is the vital
Provider-Payer Relations: Sample Cases Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017 2017 Presenter Aetna Name Inc. May 2017 1 Documentation Apropos documentation is the vital
The Case for Home Care Medicine: Access, Quality, Cost
 The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
The Case for Home Care Medicine: Access, Quality, Cost 1. Background Long term care: community models vs. institutional care Compared with most industrialized nations the US relies more on institutional
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Payment Model
 Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents Payment Model Payment Model Six Enhanced Care and Coordination Providers (ECCPs) entered into cooperative agreements with
Inferior Vena Cava (IVC) Filter Placement
 Filter Placement") If you have any questions, ask your doctor or nurse. Filters may also be used. Inferior Vena Cava (IVC) Filter Placement An IVC filter is used to prevent blood clots from moving from the lower part of
If you have any questions, ask your doctor or nurse. Filters may also be used. Inferior Vena Cava (IVC) Filter Placement An IVC filter is used to prevent blood clots from moving from the lower part of
STROKE PATIENT PATHWAY
 STROKE PATIENT PATHWAY My Stroke Team Health Care Team Member Acute Stroke Unit Rehabilitation Unit Community Dietitian(s) Doctor(s) Nurse(s) Occupational Therapist(s) Psychologist(s) Physiotherapist(s)
STROKE PATIENT PATHWAY My Stroke Team Health Care Team Member Acute Stroke Unit Rehabilitation Unit Community Dietitian(s) Doctor(s) Nurse(s) Occupational Therapist(s) Psychologist(s) Physiotherapist(s)
Neighborhood Hospital
 Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
eclinicalworks integrates with CommonWell and MEDITECH XCA, CCDA MEDITECH integrates with HIMSS Interoperability Showcase 2018 Page 1 of 12
 Use Case Title: Nationwide Care Transitions Overview: Cynthia, 66, is admitted, treated, and discharged at home in Florida for pulmonary embolism. While visiting her daughter in Colorado, she suffers a
Use Case Title: Nationwide Care Transitions Overview: Cynthia, 66, is admitted, treated, and discharged at home in Florida for pulmonary embolism. While visiting her daughter in Colorado, she suffers a
Patient Price Information List
 Patient Price Information List In compliance with state law, OhioHealth is providing this price list for Riverside Methodist Hospital, Grant Medical Center, Doctors Hospital, and Dublin Methodist Hospital
Patient Price Information List In compliance with state law, OhioHealth is providing this price list for Riverside Methodist Hospital, Grant Medical Center, Doctors Hospital, and Dublin Methodist Hospital
Proactive Care Team Contingency Plan Original completed: Patient Details. Frameworki Number: First Name: Margaret Lives Alone: Yes No
 Proactive Care Team Contingency Plan Original completed: Patient Details Surname: Jones NHS Number: Frameworki Number: First Name: Margaret Lives Alone: Yes No Known As: Maggie Key safe: Yes No Number
Proactive Care Team Contingency Plan Original completed: Patient Details Surname: Jones NHS Number: Frameworki Number: First Name: Margaret Lives Alone: Yes No Known As: Maggie Key safe: Yes No Number
UI Health Hospital Dashboard September 7, 2017
 UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
UI Health Hospital Dashboard September 20 September 7, 20 UI Health Metrics FY Q4 Actual FY Q4 Target FY Q4 Actual 4th Quarter % change FY vs FY Discharges 4,558 4,680 4,720 Combined Observation Cases
Final Report. January 12, Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek
 Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
Final Report Evaluation of the Parma D.A.Y. (Designed Around You) Program January 12, 2010 Evaluation Team: Katherine Jones Susan Tullai McGuinness Mary Dolansky Amany Farag Mary Jo Krivanek Project Supported
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD
 UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
UNIVERSITY OF ILLINOIS HOSPITAL & HEALTH SCIENCES SYSTEM HOSPITAL DASHBOARD January 19, 2017 UI Health Metrics FY17 Q1 Actual FY17 Q1 Target FY Q1 Actual Ist Quarter % change FY17 vs FY Discharges 4,836
National Blood Clot Alliance
 National Blood Clot Alliance National Survey About Deep Vein Thrombosis and Pulmonary Embolism Awareness, Information, Prevention, Adherence Gaps in Hospital VTE Prophylaxis Demonstrate Need for Technology
National Blood Clot Alliance National Survey About Deep Vein Thrombosis and Pulmonary Embolism Awareness, Information, Prevention, Adherence Gaps in Hospital VTE Prophylaxis Demonstrate Need for Technology
When is it really a UTI?
 When is it really a UTI? Adrienne Mims, MD, MPH, FAAFP, AGSF VP, Chief Medical Officer Adrienne.Mims@AlliantQuality.org 2/19/2016 1 Disclosure This educational activity does not have commercial support
When is it really a UTI? Adrienne Mims, MD, MPH, FAAFP, AGSF VP, Chief Medical Officer Adrienne.Mims@AlliantQuality.org 2/19/2016 1 Disclosure This educational activity does not have commercial support
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Unit 8 Med Surg Nursing Quiz
 Unit 8 Med Surg Nursing Quiz 1. How will the nurse assess the flank area of a patient with pyelonephritis for tenderness? a. Push gently into the two lowest intercostal spaces. b. Palpate along both sides
Unit 8 Med Surg Nursing Quiz 1. How will the nurse assess the flank area of a patient with pyelonephritis for tenderness? a. Push gently into the two lowest intercostal spaces. b. Palpate along both sides
Peripherally Inserted Central Catheter
 UW MEDICINE PATIENT EDUCATION Peripherally Inserted Central Catheter Understanding your PICC procedure and consent form Please read this handout before reading and signing the form Special Consent for
UW MEDICINE PATIENT EDUCATION Peripherally Inserted Central Catheter Understanding your PICC procedure and consent form Please read this handout before reading and signing the form Special Consent for
Increase Your Bottom Line by Eliminating Physician Driven Denials. Olakunle Olaniyan MD President Case Management Covenants
 Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Increase Your Bottom Line by Eliminating Physician Driven Denials Olakunle Olaniyan MD President Case Management Covenants Escalating cost of care Physician Driven Denials Denial drivers Working with physicians
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
Hospital Outpatient Quality Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: January, 2018
 Hospital Outpatient Quality Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: January, 2018 Background Hospitals have separate quality measures for the outpatient population. These measures
Hospital Outpatient Quality Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: January, 2018 Background Hospitals have separate quality measures for the outpatient population. These measures
End Of Life Decision Making - Who s Decision Is It Anyway?
 End Of Life Decision Making - Who s Decision Is It Anyway? Kara Livy RN MN NP Critical Care Nurse Practitioner Royal Alexandra Hospital Edmonton, Alberta Kara.livy@albertahealthservices.ca End-Of-Life
End Of Life Decision Making - Who s Decision Is It Anyway? Kara Livy RN MN NP Critical Care Nurse Practitioner Royal Alexandra Hospital Edmonton, Alberta Kara.livy@albertahealthservices.ca End-Of-Life
STANDARDIZED PROCEDURE INTRAVENTRICULAR CHEMOTHERAPY VIA OMMAYA RESERVOIR (Adult, Peds)
") I. Definition The administration of chemotherapy via Ommaya Reservoir into cerebrospinal fluid (CSF) for treatment of previously diagnosed central nervous system (CNS) involvement by leukemia and lymphoma
I. Definition The administration of chemotherapy via Ommaya Reservoir into cerebrospinal fluid (CSF) for treatment of previously diagnosed central nervous system (CNS) involvement by leukemia and lymphoma
Determining the Appropriate Inpatient Rehabilitation Candidate
 Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Determining the Appropriate Inpatient Rehabilitation Candidate Brandi Damron, OTR/L, MBA Program Director Norton Community Hospital Inpatient Rehab Unit Objectives Discuss the preadmission process limitations
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications
 Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
Implementing an Outpatient CDI Program L EONTA (L EE) WIL L IAMS, R HIT, CPCO, CPC, CCS, CCD S
 WIL L IAMS, R HIT, CPCO, CPC, CCS, CCD S") Implementing an Outpatient CDI Program PR ES ENTED BY: L EONTA (L EE) WIL L IAMS, R HIT, CPCO, CPC, CCS, CCD S Disclaimer This information is meant to be simply a guide for implementation based on the
Implementing an Outpatient CDI Program PR ES ENTED BY: L EONTA (L EE) WIL L IAMS, R HIT, CPCO, CPC, CCS, CCD S Disclaimer This information is meant to be simply a guide for implementation based on the
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility
 Team to the Rescue. The Development and Implementation of a Rapid Response Program at a Regional Facility") Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
Rapid Assessment and Treatment (R.A.T.) Team to the Rescue The Development and Implementation of a Rapid Response Program at a Regional Facility Dynamics 2013 Lethbridge Chinook Regional Hospital 276 Bed
CARDIAC DISORDERS COMPREHENSIVE EXAMINATION
 2504_Ch03_073-112.qxd 102 11/4/10 9:45 PM Page 102 MED-SURG SUCCESS CARDIAC DISORDERS COMPREHENSIVE EXAMINATION 1. Which population is at a higher risk for dying from a myocardial infarction? 1. Caucasian
2504_Ch03_073-112.qxd 102 11/4/10 9:45 PM Page 102 MED-SURG SUCCESS CARDIAC DISORDERS COMPREHENSIVE EXAMINATION 1. Which population is at a higher risk for dying from a myocardial infarction? 1. Caucasian
WPS Medicare Part A - Quarterly CERT Error Findings Report ~ J5 National Providers~
 WPS Medicare Part A - Quarterly CERT Error Findings Report ~ J5 National Providers~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed July 2014 through September 2014
WPS Medicare Part A - Quarterly CERT Error Findings Report ~ J5 National Providers~ This report provides details of Comprehensive Error Rate Testing (CERT) errors assessed July 2014 through September 2014
Diagnostics: Step Outside the Box Instead of Just Checking It Off!
 Diagnostics: Step Outside the Box Instead of Just Checking It Off! http://www.publicdomainpictures.net/view image.php?image=19960 Lorelei Schmidt, MT (ASCP) Director of Training TridentUSA Health Services
Diagnostics: Step Outside the Box Instead of Just Checking It Off! http://www.publicdomainpictures.net/view image.php?image=19960 Lorelei Schmidt, MT (ASCP) Director of Training TridentUSA Health Services
Piedmont Access to Health Services. Standing Orders for Patient Work-ups
 Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Piedmont Access to Health Services Policy Number: 01-09-014 SUBJECT: Standing Orders for Patient Work-ups EFFECTIVE DATE: 8/3/09 REVIEWED/REVISED : 4/10/2012 POLICY: PATHS is committed to allowing each
Administrative Without, TB control fails. TB Infection Control What s New? Early disease prevention Modern cough etiquette
 Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
Direct Messaging is live! Enroll for your mailbox today! Are you attesting for Meaningful Use 2 for Transitions of Care?
 Direct Messaging is live! Enroll for your mailbox today! Please click HERE for more information and to enroll Are you attesting for Meaningful Use 2 for Transitions of Care? Now you can electronically
Direct Messaging is live! Enroll for your mailbox today! Please click HERE for more information and to enroll Are you attesting for Meaningful Use 2 for Transitions of Care? Now you can electronically