Facilitation Interns Acquisition of
|
|
|
- Cory Moody
- 6 years ago
- Views:
Transcription

1 Facilitation Interns Acquisition of Medical Knowledge and Core Skills through Experiential Learning Raquel Belforti, DO, Kevin Hinchey, MD Reham Shaaban, DO Mihaela Stefan, MD Baystate Medical Center Tufts University School of Medicine
2 Agenda Discussion of the orientation experience Review the role of experiential learning for new interns orientation Describe the Baystate Internal Medicine Program Model
3 Objectives 1. Understand the advantage of an intensive two weeks training to improve rapid acquisition of clinical competence in early internship 2. Recognize the benefits of using scenario based simulation training during intern orientation 3. Gain the skills necessary to re-organize initial month of internship to facilitate interns acquisition of the basic skills needed to manage an unsupervised situation and reduce risks to patients
4 Discussion #1 Intern orientation content Goals for the first month

5 Intern Orientation
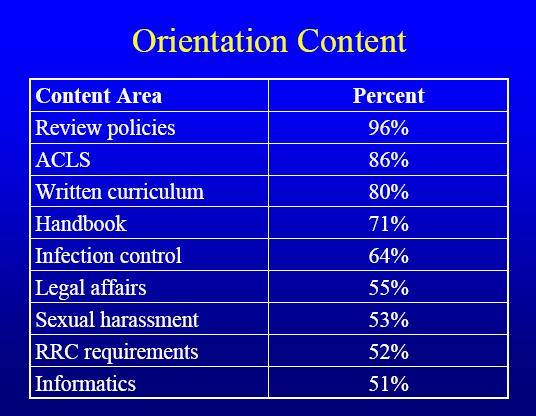
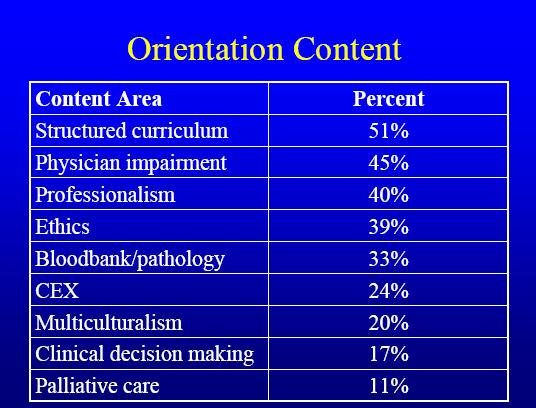
6 National Orientation Data Survey of Program Directors n= % University Affiliated
7
8
9 Discussion #2 Methods/types of teaching activities
10
11 Perfect World Medical Knowledge Professionalism Communication Practice-based Learning System-based Practice
12 Perfect World Medical Knowledge Professionalism Patient Safety Communication Practice-based Learning System-based Practice
13 Discussion #3 What is experiential learning? How is it different from the see one, do one teach one approach
14 Experiential learning Experiential Learning is the process of making meaning from direct experience, the connecting of learning to real life situations "For the things we have to learn before we can do them, we learn by doing them Aristotle
15 Patient Care Core competencies Medical Knowledge Practice-Based Learning and Improvement Interpersonal and Communication Skills Professionalism Systems-Based Practice
16 Discussion #4 Experiential learning: why simulation has become so important
17 SIMULATION
18 Discussion #5 Video Based on our video scenario, we will discuss: Simulation as an Educational Instrument Intern perspective/experience Simulation as an Evaluative Instrument Faculty/Program perspective with regards to assessment and learning: Diagnosing the learner
19 Goals of BMC Curriculum for Interns - First month To help interns to gain the necessary competencies and confidence to manage unsupervised critical situations To enforce the emergency and safe care practices and survival skills as required to begin a medical residency Simulation based training will be used to orient and guide learners through the basics of fundamental and safe medical practice for inpatient care To reduce risk to patients To allowed the educators to identify earlier the strong and the weak residents
20 Baystate Curriculum Pre-test Confidence questionnaire Boot camp binder (literature for self-study, study, pre-test for each session) 2 week simulation course of 2 hours/day 8 cases Chest pain SOB Hypotension Mental status changes Nursing and ancillary staff support Checklists Debriefing EKGs, Quizzes, progress notes, H&P, discharge summaries, handovers Post test
21 Test results Bootcamp Knowledge Assessment Test 100 % correct answers Pre 1 Test Post Test
22 Discussion #6 Costs and Benefits
23 Why use simulation for interns orientation? Enhance resident confidence Reduced risk to patients Better/more efficient training Active vs. passive learning More degrees of freedom (redo, errors ok, pause time, part tasks)
24 Simulators Come in Many Varieties Standardized patients (OSCE) Screen based simulators (virtual patients, pharmacology and physiology simulations) Electronic and non-electronic mannequins Actors: patients, staff, family members
25 Why use simulation? Safety Standardization Efficiency
26 Barriers Faculty development Implementation costs Resource support Scheduling time Not Very Efficient Must Plan Ahead Difficult to Develop Techno-phobia Status Quo is Easier
27 Conclusion Impact on Interns Impact on Program
28 Feedback from participants I I admitted a patient last night with CHF exacerbation and I knew exactly what to do We had a patient with an active GI bleed and my intern was telling me to start octreotide,, I cannot believe he knew that
29 Set Standards of our Program Pre-reading reading questions- Professionalism Be on time- Professionalism Working together- Teamwork Communication Asking for help- Patient safety Debriefing- Self reflection
30 Baystate Simulation Center Patient Development Form Clinical Service: INTERNAL MEDICINE Target Audience: R1 for management and R3 for teaching Lesson Title/ Scenario File Name in HPS6 Software: Hypotension secondary to Sepsis Type Teaching: Intern Nightfloat called to evaluate a patient with hypotension Date Built: 4/29 Date Last Revised: 6/16 Developer: Mihaela Stefan, Raquel Belforti Synopsis of Scenario: 74 y male NH resident, admitted 3 days ago for syncope, off monitor x 24 hours. Nurse calls the intern because patient is hypotensive, febrile and obtunded. It will be a case of sepsis secondary to UTI Foley catheter was left by mistake in place. Hospital course from admission: 74 y male, admitted 3 days ago after a syncopal episode, no clear cause identified. -Carotid Doppler, head CT, Hip X-Ray are negative -Echocardiogram done today- results pending -Telemetry monitor discontinued 24 hours ago. -No other episodes in the hospital, still some dizziness when standing. Past Medical History: DM COPD CAD s/p PCI to LAD many years ago BPH Medication at home: Atrovent, Lisinopril, Atenolol, Glipizide, Trazodone Soc Hx: Lives with wife. Quit Tobacco 20 years ago (40pk/hr), +Etoh 1 glass wine with dinner daily ALL: NKDA Medication: Lovenox 40 Units sc, Atrovent prn, Lisinopril 20 mg daily, Atenolol 25 mg daily, Glipizide 10 mg BID, Nexium 40 mg daily, Seroquel 25 mg QHS Current review of Systems: complains of some lower abdominal pain Current Physical Examination: BP 85/60, HR 100/min, O2S 87%, RR 22/min, T 101.8, GEN: obtunded, diaphoretic, shallow breathing HEENT: PERRL, mucous membranes dry, Jugular veins flat HEART: Tachycardic, regular rhythm, no murmur LUNGS: Clear to auscultation ABD: soft, BS positive, some tenderness in hypogastrium. EXT: warm, good peripheral pulses. No edema Foley draining cloudy urine.
31 Current Labs: WBC 20,000, neutrophiles 85% and 20% bands Platelets 110,000 Hb 13, Na 148, K 3.3 Chlorite 104, HCO3 16, BUN 30, Cr 1.6, Glucose 340 Trop 0.01 lactic acid 5 UA specific gravity 1024, WBC 80, nitrite pos, cloudy ABG 7.33/28/60 on RA Imaging: CXR clear ECG associated with this state: sinus tachycardia Admitting Labs: WBC 10, Hb 12, Ht 43, Platelets 240, Na 142, K 3.8, Chlorite 105, HCO3 22, BUN 17, Cr 0.9, Glucose 200 PE at admission: BP 140/60, HR76/, O2 96%, lugs clear, heart regular S1, S2, abdomen normal, alert, oriented x3 Patient Name, Age, Gender: Smith Santana, Room: S2 28A Time: 10:30 PM Chief Complaint (Nurse SBAR) S: Patient is hypotensive, febrile and lethargic. B: 74 y admitted 3 days ago with syncope A: BP 85/60, HR 100/min, O2S 87%, T 101.8, obtunded. R: I need you to come to evaluate him ASAP Patient is not on the monitor if monitor is suggested, the nurse will call telemetry charge nurse for a bed, but they will not have one. The nurse can suggest to use the crash card monitor if the patient is really sick or call RRT Roles with brief description: Interns: One working team of 2 R1 will take care of the patient, one observing team will watch from outside Nurse: Respectful, initial minimally helpful; if the residents get stuck, will give suggestions. The nurse will question fluid monitoring. If the intern order antibiotic without checking allergies, the nurse will make a specific, loud comment about the risk. Materials to be used in the debriefing: Sepsis NEJM article
32 Learning Objectives or Assessment Objectives At the end of this session the interns will be able to: 1. Recognize an unstable patient with hypotension 2. Stabilize unstable hypotensive patient 3. List differential for shock a. Distributive (septic shock) b. Cardiogenic c. Obstructive d. Hypovolemic (hemorrhagic) 4. Recognize and implement early goal directed therapy for septic patients a. IVF b. Cultures c. Appropriate antibiotics 5. Recognize medical error of Foley induced Urosepsis 6. Order set for sepsis
33 Instructor s Observations/Checklist of Critical Actions Recognition and initial work-up of hypotension Assessment of patient s instability (hypotension) Physcial exam (other signs hypoperfusion) Starts IVF Assures Adequate IV access Head of the bed down Cardiac Monitor EKG Labs, cultures Reviews history and medication list Recognizes and Management of Sepsis Continues fluids When not responsive to IVF, starts vasopressors, calls ICU Gets blood cultures Reviews possible sources of infection (urine, lungs, abdomen) Starts broad spectrum antibiotics Calls R3 for help Differential Diagnosis Differential for Hypotension Distributive- septic shock Cardiogenic Hemorrhagic Differential for possible etiologies of infection Urine Lung Abdomen Blood Teamwork With Nurse Ask R3 for help Calls ICU resident Error No recognize septic shock No recognize foley as culprit for infection Does not start broad spectrum antibiotics No ask allergies before give antibiotics
34
2016 HCPro, a division of BLR. All rights reserved. These materials may not be duplicated without express written permission.
 Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
Surviving Sepsis: How CDI Can Improve Sepsis Core Measure Compliance Sarah Jackson, RN, BSN Clinical Documentation Specialist II Rush Oak Park Hospital Oak Park, IL 1 Learning Objectives At the completion
University of South Dakota Vermillion, South Dakota Department of Nursing
 Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Title: To cite this reference: Simulation Scenario Complex Patient: Multi-System Organ Failure Part 2 (Sepsis) Multi-System Organ Failure (MSOF) Sepsis (Part 2 of 2) Overview Concept: Complex Patient Target
Provider-Payer Relations: Sample Cases. Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017
 Provider-Payer Relations: Sample Cases Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017 2017 Presenter Aetna Name Inc. May 2017 1 Documentation Apropos documentation is the vital
Provider-Payer Relations: Sample Cases Anand Nilakantan, DO, MBA Aetna Mid-Atlantic Medical Director July 20, 2017 2017 Presenter Aetna Name Inc. May 2017 1 Documentation Apropos documentation is the vital
*Your Name *Nursing Facility. radiation therapy. SECTION 2: Acute Change in Condition and Factors that Contributed to the Transfer
 Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
Gaining information about resident transfers is an important goal of the OPTIMISTC project. CMS also requires us to report these data. This form is where data relating to long stay transfers are to be
 Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
Unfolding Clinical Reasoning Case Study: STUDENT Sepsis I. Data Collection History of Present Problem: Jean Kelly is an 82 year old woman who has been feeling more fatigued for the last three days and
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Leadership: Triage/Prioritization (Part 1) Overview
 Overview") Title: To cite this reference: Triage/Prioritization (Part 1 of 2) University of South Dakota Simulation Scenario Leadership: Triage/Prioritization (Part 1) Overview Target Group: Second Year Concept:
Title: To cite this reference: Triage/Prioritization (Part 1 of 2) University of South Dakota Simulation Scenario Leadership: Triage/Prioritization (Part 1) Overview Target Group: Second Year Concept:
Sepsis Care in the ED. Graduate EBP Capstone Project
 Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Sepsis Care in the ED Graduate EBP Capstone Project University of Mary EBP Graduate Capstone Project Members Alicia Vermeulen- Operations Manager, Avera McKennan Hospital Wendy Moore, RN- Ambulatory Nurse
Brief Summary. Educational Rationale. Learning Objectives: Nurse. Learning Objectives: Doctor
 Title Simulation Scenario Gastrointestinal haemorrhage and ALD Version 1.3 Target Audience FY doctors & student nurses Run time 10-15 mins Authors J Foxlee, U Naidoo, M Loughrey, P Wilder Last review 4/7/18
Title Simulation Scenario Gastrointestinal haemorrhage and ALD Version 1.3 Target Audience FY doctors & student nurses Run time 10-15 mins Authors J Foxlee, U Naidoo, M Loughrey, P Wilder Last review 4/7/18
Student name: Section: Date: Patient initials: Time began: Time ended: Points: Faculty: Points deducted due to:
 MEDICATION ACTIVITY This is a timed medication administration check off. It is worth 6 points. It is divided into 3 points for clinical reasoning, being able to correctly identify which meds should be
MEDICATION ACTIVITY This is a timed medication administration check off. It is worth 6 points. It is divided into 3 points for clinical reasoning, being able to correctly identify which meds should be
Brief Summary. Educational Rationale. Learning Objectives: Nurse. Learning Objectives: Doctor
 Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Simulation Scenario Title Bacterial meningitis Version 10 Target Audience FY doctors & student nurses Run time 10-15 mins Authors Niamh Feely, Andrew Smith, Udesh Naidoo, Paul Wilder, Mark Loughrey Last
Documentation 101: CDI JULY 19, 2017
 Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Documentation 101: CDI THE FIFTH NATIONAL PHYSICIAN ADVISOR AND UTILIZATION REVIEW BOOT CAMP JULY 19, 2017 Infirmary Health: About Us Infirmary Health is the largest non-governmental healthcare system
Learning Objectives. Denver Health Medical Center. Complex Coding Scenarios and Resolution
 Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
Complex Coding Scenarios and Resolution Eric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC Manager of Coding Denver Health Medical Center Denver, Colo. 2 Learning Objectives Denver Health Medical Center Evaluate
CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES. Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN
 CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN NYSNA is accredited as a provider of continuing nursing education by the American Nurses
CRITICAL THINKING IN THE ICU: IMPLEMENTING BEST PRACTICES Your Presenter: Carol Lynn Esposito, Ed.D., JD, MS, RN NYSNA is accredited as a provider of continuing nursing education by the American Nurses
Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways
 For Patients not eligible for other TICKER Clinical Pathways") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: TICKER Short Stay (Expected LOS 5 days) For Patients not eligible for other TICKER Clinical Pathways Notes: (1) This pathway
Neighborhood Hospital
 Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
Physician Progress Notes Time Mon S/P HoLEP Procedure without complications; estimated blood loss < 100 ml; stable condition to recovery room. 1530 To be admitted to Urology following PACU. Dan Stein,
During the hospital medicine rotation, residents will focus on the following procedures as permitted by case mix:
 Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Educational Goals & Objectives The Inpatient Family Medicine rotation will provide the resident with an opportunity to evaluate and manage patients with common acute medical conditions. Training will focus
Unfolding Case Scenarios: A Unique Opportunity for Learners
 Unfolding Case Scenarios: A Unique Opportunity for Learners Cynthia Shum, MEd, RN, CHSE-A Nurse Educator, Simulation Center VA Palo Alto Health Care System Objectives ü Define an unfolding case scenarios.
Unfolding Case Scenarios: A Unique Opportunity for Learners Cynthia Shum, MEd, RN, CHSE-A Nurse Educator, Simulation Center VA Palo Alto Health Care System Objectives ü Define an unfolding case scenarios.
Writing RAC Appeals, RAC Denial Prevention, and Case Management Collaboration
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Writing RAC Appeals, RAC Denial Prevention, and Case Management Collaboration Kathy Shumpert, MSN, RN, CCDS Clinical
7th Annual Association for Clinical Documentation Improvement Specialists Conference Writing RAC Appeals, RAC Denial Prevention, and Case Management Collaboration Kathy Shumpert, MSN, RN, CCDS Clinical
Disclosure of Proprietary Interest. HomeTown Health HCCS
 HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 2 Clinical Documentation Program: E ssentials and Took Kits Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
Inpatient Quality Reporting Program
 SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
SEP-1 Early Management Bundle, Severe Sepsis/Septic Shock Part I: Severe Sepsis Questions & Answers Moderator: Candace Jackson, RN IQR Support Contract Lead, Hospital Inpatient Value, Incentives, and Quality
RECOMMENDATION FOR CONSIDERATION
 Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Board Meeting Date: June 15, 2016 RECOMMENDATION FOR CONSIDERATION Subject: Critical Care Transfer of Care Data Elements and Form VTR#: 0616-04 Committee/Task Force: Critical Care Transport Task Force
Learning Objectives. Compliant Strategies for Unsupported Diagnoses
 1 Compliant Strategies for Unsupported Diagnoses Patti Nemeth, BSN, RN, CCDS, CCS, AHIMA Approved ICD 10 CM/PCS Trainer CDI Manager Susan Haley, RHIT, CCS, CRC, CCDS, AHIMA Approved ICD 10 CM/PCS Trainer
1 Compliant Strategies for Unsupported Diagnoses Patti Nemeth, BSN, RN, CCDS, CCS, AHIMA Approved ICD 10 CM/PCS Trainer CDI Manager Susan Haley, RHIT, CCS, CRC, CCDS, AHIMA Approved ICD 10 CM/PCS Trainer
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT
 CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
CRITICAL CARE OUTREACH TEAM AND THE DETERIORATING PATIENT Outreach Objectives To avert or ensure more timely admission to DCCQ To ensure that patients discharged from Critical Care continue to progress
Why did we conduct a simulation day? Why should your department? How did we conduct a simulation day? How can you?
 Multidisciplinary Interventional Radiology Simulation Day To Improve Team Communication and Patient Safety Quality Storyboard: RSNA 2015 Noy Bassik MD PhD; Bradley B. Pua MD; Jessica Waltz; Richard H.
Multidisciplinary Interventional Radiology Simulation Day To Improve Team Communication and Patient Safety Quality Storyboard: RSNA 2015 Noy Bassik MD PhD; Bradley B. Pua MD; Jessica Waltz; Richard H.
Innovative Strategies for Coaching Residents who Struggle with Time Management, Organization and Efficiency
 Innovative Strategies for Coaching Residents who Struggle with Time Management, Organization and Efficiency Allison Dekosky, MD Eric Goren, MD Mina Sedrak MD Karen Warburton, MD University of Pennsylvania
Innovative Strategies for Coaching Residents who Struggle with Time Management, Organization and Efficiency Allison Dekosky, MD Eric Goren, MD Mina Sedrak MD Karen Warburton, MD University of Pennsylvania
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario A Postoperative Patient with Tachycardia
 Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Support Facilitator Guide: Interprofessional Team Communication Simulation Scenario The purpose of interprofessional simulation is for students to participate in a simulated interprofessional experience
Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair
 or Atrial Septal Defect (ASD) Repair") Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Project TICKER Teamwork to Improve Cardiac Kids End Results Clinical Pathway: Ventricular Septal Defect (VSD) or Atrial Septal Defect (ASD) Repair Notes: (1) This pathway is a general guideline and does
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC
 Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Rapid Response Team and Patient Safety Terrence Shenfield BS, RRT-RPFT-NPS Education Coordinator A & T respiratory Lectures LLC Objectives History of the RRT/ERT teams National Statistics Criteria of activating
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
Sepsis Screening Tools
 ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
ICU Rounds Amanda Venable MSN, RN, CCRN Case Mr. H is a 67-year-old man status post hemicolectomy four days ago. He was transferred from the ICU to a medical-surgical floor at 1700 last night. Overnight
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease
 Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
Recognising the Deteriorating Adult Simulation Scenario 3 Chronic Obstructive Pulmonary Disease Course lead Colette Laws-Chapman Faculty Course / Curriculum Recognising the Deteriorating Adult Target Delegates
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Leadership: Triage/Prioritization (Part 2) Overview
 Overview") Title: To cite this reference: Triage/Prioritization (Part 2 of 2) University of South Dakota Simulation Scenario Leadership: Triage/Prioritization (Part 2) Overview Target Group: Second Year Concept:
Title: To cite this reference: Triage/Prioritization (Part 2 of 2) University of South Dakota Simulation Scenario Leadership: Triage/Prioritization (Part 2) Overview Target Group: Second Year Concept:
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Infection: Post Anesthesia Care Unit (Part 1) Overview
 Overview") Title: To cite this reference: University of South Dakota Simulation Scenario Infection: Post Anesthesia Care Unit (Part 1) Overview Post Anesthesia Care Target Group: First Year Concept: Infection Unit
Title: To cite this reference: University of South Dakota Simulation Scenario Infection: Post Anesthesia Care Unit (Part 1) Overview Post Anesthesia Care Target Group: First Year Concept: Infection Unit
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
2 Midnight Case Examples and Documentation Tips. Ralph Wuebker, MD Executive Health Resources, Inc. All rights reserved.
 2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
2 Midnight Case Examples and Documentation Tips Ralph Wuebker, MD AHA Solutions, Inc., a subsidiary of the American Hospital Association, is compensated for the use of the AHA marks and for its assistance
St. Vincent s Health System Page 1 of 8. Nursing Administration HOSPITAL SHARED POLICY?
 St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
St. Vincent s Health System Page 1 of 8 TITLE: Rapid Response Team FACILITY: St. Vincent s East FUNCTION: ORIGINATING DEPT: Nursing Administration HOSPITAL SHARED POLICY? EFFECTIVE DATE: _X_ Yes No DOCUMENT
INTRODUCTION TO HIGH VALUE CARE:
 INTRODUCTION TO HIGH VALUE CARE: ELIMINATING HEALTHCARE WASTE Bindu Swaroop, MD Associate Clinical Professor Department of Medicine University of California, Irvine Learning Objectives Understand some
INTRODUCTION TO HIGH VALUE CARE: ELIMINATING HEALTHCARE WASTE Bindu Swaroop, MD Associate Clinical Professor Department of Medicine University of California, Irvine Learning Objectives Understand some
Accountability and Collaboration Working With A Physician Assistant
 Accountability and Collaboration Working With A Physician Assistant Anthony Derro, RN Practice Consultant Linda Levesque, RN Outreach Consultant, Acute Care Karen Riddell, Director, Professional Practice
Accountability and Collaboration Working With A Physician Assistant Anthony Derro, RN Practice Consultant Linda Levesque, RN Outreach Consultant, Acute Care Karen Riddell, Director, Professional Practice
Shock - Hypovolaemia
 Shock - Hypovolaemia Research Staff: Participants should be asked to arrive dressed as they would for clinical placement. That is, in uniform, hair and jewellery appropriate, note pad, pen, watch, stethoscope,
Shock - Hypovolaemia Research Staff: Participants should be asked to arrive dressed as they would for clinical placement. That is, in uniform, hair and jewellery appropriate, note pad, pen, watch, stethoscope,
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance?
 Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Claims Denial Management: What Are Third Party Payers Really Telling You about Your Documented Quality-of-Care and Compliance? Betty Bibbins, MD, CHC, CPEHR, CPHIT President & Chief Medical Officer Website:
Medication Reconciliation. Peggy Choye, Pharm.D., BCPS
 Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Application of Simulation to Improve Clinical Efficiency Systems Integration
 Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
Application of Simulation to Improve Clinical Efficiency Systems Integration Hyun Soo Chung, MD, PhD Professor, Department of Emergency Medicine Director, Clinical Simulation Center Yonsei University College
EMERGENCY MEDICINE CLINICAL ROTATION COMPETENCY BASED CURRICULUM
 CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
CLINICAL ROTATION COMPETENCY BASED CURRICULUM EMERGENCY MEDICINE During the third year of the curriculum, students expand their knowledge of emergent conditions and gain the ability to apply the knowledge
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Complex Patient: Acute MI. Overview
 Simulation Scenario Complex Patient: Acute MI Overview Title: Acute MI with Dysrhythmias Concept: Complex Patient To cite this reference: Target Group: Second Year Nursing Students Kisner, T. & Warren,
Simulation Scenario Complex Patient: Acute MI Overview Title: Acute MI with Dysrhythmias Concept: Complex Patient To cite this reference: Target Group: Second Year Nursing Students Kisner, T. & Warren,
Office of Compliance. Complete & Accurate Documentation Core Curriculum for GWU Residents
 Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
Office of Compliance Complete & Accurate Documentation Core Curriculum for GWU Residents December 3, 2014 Medical Record The medical record tells the story of the patient from start to finish. If the story
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Safety: Patient Safety. Overview
 Simulation Scenario Safety: Patient Safety Overview Title: Patient Safety Concept: Safety Target Course: First Year Nursing Students To cite this reference Dreke, C. (2012). Simulation scenario; Safety:
Simulation Scenario Safety: Patient Safety Overview Title: Patient Safety Concept: Safety Target Course: First Year Nursing Students To cite this reference Dreke, C. (2012). Simulation scenario; Safety:
Institutional Handbook of Operating Procedures Policy
 Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Section: Admission, Discharge, and Transfer Institutional Handbook of Operating Procedures Policy 9.1.29 Responsible Vice President: EVP & CEO Health System Subject: Admission, Discharge, and Transfer
Admission Avoidance. Scenario 1 Urinary Tract Infection
 Admission Avoidance Course Scenario 1 Urinary Tract Infection Course lead Colette Laws-Chapman Faculty Course / Curriculum Admission Avoidance Target Delegates Scenario name Urinary Tract Infection Group
Admission Avoidance Course Scenario 1 Urinary Tract Infection Course lead Colette Laws-Chapman Faculty Course / Curriculum Admission Avoidance Target Delegates Scenario name Urinary Tract Infection Group
Course Outline and Assignments
 Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Clinical Documentation Requirements
 Clinical Documentation Requirements Foundational Curriculum: Cluster 2: Clinical Process Module 2: Clinical Practice and Documentation Unit 4: Clinical Documentation Requirements Curriculum Developers:
Clinical Documentation Requirements Foundational Curriculum: Cluster 2: Clinical Process Module 2: Clinical Practice and Documentation Unit 4: Clinical Documentation Requirements Curriculum Developers:
Simulation Design Template. Date: May 7, 2008 File Name: Group 4
 Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
Simulation Design Template Date: May 7, 2008 File Name: Group 4 Discipline: Nursing, medicine, radiology, EMT, possible consultant (specialist ie neurosurgeon via conference call), possible social work/pastoral
ENVIRONMENT Preoperative evaluation clinic, Preoperative holding area. Preoperative evaluation clinic, Postoperative care unit, Operating room
 Goals and Objectives, Main Operating Room Anesthesia, VAMC, CA-3 year UCSD DEPARTMENT OF ANESTHESIOLOGY OPERATING ROOM CLINICAL ANESTHESIA AT VAMC GOALS AND OBJECTIVES, CA-3 YEAR PATIENT CARE: To provide
Goals and Objectives, Main Operating Room Anesthesia, VAMC, CA-3 year UCSD DEPARTMENT OF ANESTHESIOLOGY OPERATING ROOM CLINICAL ANESTHESIA AT VAMC GOALS AND OBJECTIVES, CA-3 YEAR PATIENT CARE: To provide
CVICU. Attending feedback in the course of patient care. Assessment of clinical decisions Observation on Rounds. Annual In-service evaluation
 ACGME Competency-based Goals and Objectives ROTATION Cardiovascular Critical Care Unit, PGY 4, 5, 6 CVICU Goal 1. Develop a comprehensive and physiology-based understanding of evolving illness in children
ACGME Competency-based Goals and Objectives ROTATION Cardiovascular Critical Care Unit, PGY 4, 5, 6 CVICU Goal 1. Develop a comprehensive and physiology-based understanding of evolving illness in children
Definitions and Regulatory Considerations
 Observation Medicine Mark G. Moseley, MD, MHA, FACEP Associate Professor of Emergency Medicine Medical Director for Emergency Services Department of Emergency Medicine The Ohio State University Medical
Observation Medicine Mark G. Moseley, MD, MHA, FACEP Associate Professor of Emergency Medicine Medical Director for Emergency Services Department of Emergency Medicine The Ohio State University Medical
Surgical H&P and Consultations Daily Progress Notes and Presentations Post-Operative Notes What should I be doing throughout the day?
 Surgical H&P and Consultations Daily Progress Notes and Presentations Post-Operative Notes What should I be doing throughout the day? Surgical H&P s and Consultations For this and all other clerkships,
Surgical H&P and Consultations Daily Progress Notes and Presentations Post-Operative Notes What should I be doing throughout the day? Surgical H&P s and Consultations For this and all other clerkships,
Lunch and Learn. Clinical Documentation Excellence Understanding Those Magic Words August 20, 2014
 Lunch and Learn Clinical Documentation Excellence Understanding Those Magic Words August 20, 2014 Andrew Wilhelm, D.O. Dr. Wilhelm earned a B.S. from University of Notre Dame in 1999 and spent the following
Lunch and Learn Clinical Documentation Excellence Understanding Those Magic Words August 20, 2014 Andrew Wilhelm, D.O. Dr. Wilhelm earned a B.S. from University of Notre Dame in 1999 and spent the following
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Evaluation of an Experiential Learning and Simulation Based Clinical Orientation at UVMHN-CVPH
 The heart and science of medicine. UVMHealth.org/CVPH Evaluation of an Experiential Learning and Simulation Based Clinical Orientation at UVMHN-CVPH Tracy Coleman, RN, BS, BSN, Stephanie Drown, RN, BS,
The heart and science of medicine. UVMHealth.org/CVPH Evaluation of an Experiential Learning and Simulation Based Clinical Orientation at UVMHN-CVPH Tracy Coleman, RN, BS, BSN, Stephanie Drown, RN, BS,
Intermediate Coronary Care Unit Rotation
 1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
1 Intermediate Coronary Care Unit Rotation Section of Cardiology Dartmouth-Hitchcock Medical Center (2008-2009) I. Overview of Rotation The cardiology-specific critical care experience is in the Intermediate
Simulation Design Template
 Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
Simulation Design Template Date: May 7/8, 2008 File Name: Discipline: RN, Charge nurse, medical radiology, pharmacy tech, social work, medicine (whatever is available at the institution) Student Level:
Admission Avoidance Course Scenario 6 Infected Pressure Ulcer
 Admission Avoidance Course Scenario 6 Infected Pressure Ulcer Course lead Colette Chapman-Laws Faculty Course / Admission Avoidance Target Curriculum Delegates Scenario name Infected Pressure Ulcer Group
Admission Avoidance Course Scenario 6 Infected Pressure Ulcer Course lead Colette Chapman-Laws Faculty Course / Admission Avoidance Target Curriculum Delegates Scenario name Infected Pressure Ulcer Group
ACGME Institutional Requirements
 Graduate Medical Education : Focusing on Quality and Safety in a Clinical Learning Environment Developing a Standardized and Sustainable Resident Sign Out Process Better Hand Off = Safer Care Ron Amedee,
Graduate Medical Education : Focusing on Quality and Safety in a Clinical Learning Environment Developing a Standardized and Sustainable Resident Sign Out Process Better Hand Off = Safer Care Ron Amedee,
Alphabetical Data Dictionary
 Last Updated: Version 5.1 Alphabetical Data Dictionary The General Abstraction Guidelines explain the different sections of the data element definitions and provide direction for common questions and issues
Last Updated: Version 5.1 Alphabetical Data Dictionary The General Abstraction Guidelines explain the different sections of the data element definitions and provide direction for common questions and issues
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings
 For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
For Immediate Release: 05/11/18 Written By: Scott Whitaker Telemedicine: Solving the Root Causes for Preventable 30-day Readmissions in SNF Settings Outlining the Problem: Reducing preventable 30-day hospital
TASCS 2017 Annual Conference 3/2/2017
 Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
Texas Ambulatory Surgery Center Society 2017 Annual Conference Emergency Protocols for Ambulatory Surgery Centers Laura Schneider, RN, CGRN, CASC Objectives 1. Evaluate the level of emergency preparedness
INCLUSION CRITERIA. REMINDER: Please ensure all stroke and TIA patients admitted to hospital are designated as "Stroke Service" in Cerner.
 ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
ACUTE STROKE CLINICAL PATHWAY The clinical pathway is based on evidence informed practice and is designed to promote timely treatment, enhance quality of care, optimize patient outcomes and support effective
Montgomery College Nursing Simulation Scenario Library
 Montgomery College Nursing Simulation Scenario Library Scenario File: End of Life Discipline: Nursing Student Level: Intermediate-Advanced Expected Simulation Run Time: 15-20 minutes Guided Reflection
Montgomery College Nursing Simulation Scenario Library Scenario File: End of Life Discipline: Nursing Student Level: Intermediate-Advanced Expected Simulation Run Time: 15-20 minutes Guided Reflection
Cyclophosphamide INFUSION Infusion 4 Plus
 Cyclophosphamide Infusion Day DEPARTMENT OF RHEUMATOLOGY DAY CASE ADMISSION RECORD PATIENT DAY CASE BOOKING REQUEST To be completed by Consultant, Registrar requesting day case Admission Hospital No. Forename
Cyclophosphamide Infusion Day DEPARTMENT OF RHEUMATOLOGY DAY CASE ADMISSION RECORD PATIENT DAY CASE BOOKING REQUEST To be completed by Consultant, Registrar requesting day case Admission Hospital No. Forename
Some Practical Tips on Being a Senior Pediatric Resident at McMaster
 Some Practical Tips on Being a Senior Pediatric Resident at McMaster This document is meant to provide practical information to help Junior pediatric residents transition to the Senior pediatric resident
Some Practical Tips on Being a Senior Pediatric Resident at McMaster This document is meant to provide practical information to help Junior pediatric residents transition to the Senior pediatric resident
30 min Small group activity solving case based scenarios and questions. 30 min Case and answers for each group are discussed in combined classroom
 IPE TOC Session Overview 5 min Pre-Session SPICE-R survey 20-30 min Didactic Transitions of care lecture 20 min Review of CHF evidence based medications 30 min Small group activity solving case based scenarios
IPE TOC Session Overview 5 min Pre-Session SPICE-R survey 20-30 min Didactic Transitions of care lecture 20 min Review of CHF evidence based medications 30 min Small group activity solving case based scenarios
SENTARA HEALTHCARE. Norfolk, VA
 SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
SENTARA HEALTHCARE Norfolk, VA 1 Sentara Healthcare Overview 11 Acute Care Hospitals in Virginia with a total of 2572 licensed beds 1E Extended dstay hospital 9 Ambulatory Care Campuses; 5 with freestanding
Early Progressive Mobility- Letting Go of Bedrest
 Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Early Progressive Mobility- Letting Go of Bedrest Jacqueline Clapp BSN, RN Lehigh Valley Health Network Holly Leighton
Lehigh Valley Health Network LVHN Scholarly Works Patient Care Services / Nursing Early Progressive Mobility- Letting Go of Bedrest Jacqueline Clapp BSN, RN Lehigh Valley Health Network Holly Leighton
Student Objectives for the Integrated Curriculum Evaluation Exercise
 Student Objectives for the Integrated Curriculum Evaluation Exercise (1) Perform organized problem focused medical interviews and physical examinations, and conduct appropriate counseling for patients
Student Objectives for the Integrated Curriculum Evaluation Exercise (1) Perform organized problem focused medical interviews and physical examinations, and conduct appropriate counseling for patients
DCHARTE - A DOCUMENTATION PRESENTATION BY: JON R BOUFFARD, BS, NREMT-P, FP-C, CCP-C. Sunday, January 22, 12
 DCHARTE - A DOCUMENTATION PRESENTATION BY: JON R BOUFFARD, BS, NREMT-P, FP-C, CCP-C Objectives: At the conclusion of this lecture the student shall be able to: Describe why to document, Describe when to
DCHARTE - A DOCUMENTATION PRESENTATION BY: JON R BOUFFARD, BS, NREMT-P, FP-C, CCP-C Objectives: At the conclusion of this lecture the student shall be able to: Describe why to document, Describe when to
Inferior Vena Cava (IVC) Filter Insertion
 Filter Insertion") Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Inferior Vena Cava (IVC) Filter Insertion Radiology This leaflet informs you about the procedure known as an Inferior Vena
Patient information leaflet Royal Surrey County Hospital NHS Foundation Trust Inferior Vena Cava (IVC) Filter Insertion Radiology This leaflet informs you about the procedure known as an Inferior Vena
Northwell Sepsis Collaborative Evidence Based Best Practice
 Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Northwell Sepsis Collaborative Evidence Based Best Practice M. Isabel Friedman, DNP, MPA, RN, BC, CCRN, CNN, CHSE Director of Clinical Initiatives Department of Clinical Transformation Nicholas DaCosta,
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU)
") Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Sepsis Screening & Code Sepsis in Critical Care Units (Medical, Surgical, & CCU) Kim McDonough BSN, Teresa Jackson BSN, Ryan LeFebvre MBA and Margaret Currie-Coyoy MBA Last Revision: October 2013 Course
Saving Lives: EWS & CODE SEPSIS. Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013
 Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
Saving Lives: EWS & CODE SEPSIS Kim McDonough RN and Margaret Currie-Coyoy MBA Last Revision: August 2013 Course Objectives At the conclusion of this training, you will be able to Explain the importance
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #501: Hospital Radio Reports HOSPITAL RADIO REPORTS Effective: February 12, 2015 Replaces: January 22, 2008 Review: November 12, 2018 Resources:
County of Santa Clara Emergency Medical Services System Policy #501: Hospital Radio Reports HOSPITAL RADIO REPORTS Effective: February 12, 2015 Replaces: January 22, 2008 Review: November 12, 2018 Resources:
OUTPATIENT ENDOSCOPY (PULM) PROCEDURE PLAN - Phase: Diagnostic/Pre-Op Orders
 PROCEDURE PLAN - Phase: Diagnostic/Pre-Op Orders") - Phase: Diagnostic/Pre-Op Orders PHYSICIAN S Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Request Endoscopy Services-GI Patient Care Obtain Consent Vital Signs Per Unit Standards Insert
- Phase: Diagnostic/Pre-Op Orders PHYSICIAN S Diagnosis Weight Allergies DETAILS Admit/Discharge/Transfer Request Endoscopy Services-GI Patient Care Obtain Consent Vital Signs Per Unit Standards Insert
Polling Question #1. Denials and CDI: A Recovery Auditor s Perspective
 1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
1 Denials and CDI: A Recovery Auditor s Perspective Tim Garrett, MD Medical Director Barb Brant, RN, CCDS, CDIP, CCS Sr. Clinical Trainer/DRG Auditors Cotiviti, Atlanta, GA 2 Polling Question #1 Does inpatient
Protocol: Name of supervising ED provider: Name of RDTC Faculty: Disposition: Date: / / Time: : (military)
") RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
RDTC TRACKING SHEET Record patient information in top right corner When completed, place in RDTC binder at A-pod Faculty desk Name: MR# Stamp OR write patient information above ED provider (i.e. faculty/pa/resident
Surgical Technology Patient Care Skills Preop Routine Objectives:
 Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
Surgical Technology 8-Jul-09 Patient Care Skills Preop Routine Objectives: 1) Discuss why preop preparation of the patient is important a) Preparing the patient decreases impact and potential risks of
Chapter 4. Objectives. Objectives 01/08/2013. Documentation
 Chapter 4 Documentation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
Chapter 4 Documentation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define key terms introduced
About the Critical Care Center
 Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Patient and Family Education Section 2 About the Critical Care Center The 5-Southeast and 5-East units 5-Southeast and 5-East When You Arrive for a Visit Patient Services Specialist Waiting Rooms Patient
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Rapid Response Team Building
 Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Nicole Sardinas BSN, RN, CCRN Clinical Educator- Critical Care Ext.2703 Mabel LaForgia MSN, RN, CCRN, CNL Clinical Nurse Leader- Critical Care Ext.4149 201-978- 6423 355 Grand Street «AddressBlock», NJ
Physician Partners for CDI: Strategies for Goal Alignment. 7th Annual Association for Clinical Documentation Improvement Specialists Conference
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Physician Partners for CDI: Strategies for Goal Alignment Larry Weems II, MD Medical Director Novant Health Huntersville
7th Annual Association for Clinical Documentation Improvement Specialists Conference Physician Partners for CDI: Strategies for Goal Alignment Larry Weems II, MD Medical Director Novant Health Huntersville
Introducing Emergency Medicine to Medical Students
 Introducing Emergency Medicine to Medical Students Lecture Objectives: 1. Describe a curriculum for medical students on an emergency medicine rotation. 2. Review methods of assessment for differentiating
Introducing Emergency Medicine to Medical Students Lecture Objectives: 1. Describe a curriculum for medical students on an emergency medicine rotation. 2. Review methods of assessment for differentiating
London s Urgent and Emergency Care Collaborative
 London s Urgent and Emergency Care Collaborative Katy Millard London Community Services Director Claire Eves Operational Head of Hillingdon Health Care Partnership Thomas Dowle Clinical & Operational Lead,
London s Urgent and Emergency Care Collaborative Katy Millard London Community Services Director Claire Eves Operational Head of Hillingdon Health Care Partnership Thomas Dowle Clinical & Operational Lead,
Sec Disconnect Go to End Forward Sec Next Report Go To
 Effective 3/15/04 escription DICTATION SYSTEM FOR INPATIENT HISTORY & PHYSICALS, DISCHARGE SUMMARIES, DELIVERY (NORMAL) NOTES OPERATIVE REPORTS DIAL 3-4000 LISTEN FOR VERBAL PROMPTS. ENTER: First 5 digits
Effective 3/15/04 escription DICTATION SYSTEM FOR INPATIENT HISTORY & PHYSICALS, DISCHARGE SUMMARIES, DELIVERY (NORMAL) NOTES OPERATIVE REPORTS DIAL 3-4000 LISTEN FOR VERBAL PROMPTS. ENTER: First 5 digits
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management
 SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
SEPSIS MANAGEMENT Using Simulation to Accelerate Adoption of Evidence-Based Sepsis Management Medical Simulation Corporation is a healthcare performance improvement company, advancing clinical quality
Medical Necessity: Not just LCD. Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC
 Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
Medical Necessity: Not just LCD Debra L. Patterson, M.D. Medicare Medical Director TrailBlazer Health Enterprises, LLC Medical Necessity In The Law Social Security Act, Title XVIII Section 1862 (a) (1)
GEORGE MASON UNIVERSITY ACADEMIC OUTREACH
 1 GEORGE MASON UNIVERSITY ACADEMIC OUTREACH Return to Nursing Practice Spring 2018 Class Location: Mason Fairfax Campus Room: TBA Susan M. Senko, BSN, RN Email: ssenko@gmu.edu Office Hours: By appointment
1 GEORGE MASON UNIVERSITY ACADEMIC OUTREACH Return to Nursing Practice Spring 2018 Class Location: Mason Fairfax Campus Room: TBA Susan M. Senko, BSN, RN Email: ssenko@gmu.edu Office Hours: By appointment
University of South Dakota Vermillion, South Dakota Department of Nursing. Simulation Scenario Neural Transmission: Spinal Cord Injury (Part 2)
") Title: To cite this reference: Spinal Cord Injury (Part 2 of 2) University of South Dakota Simulation Scenario Neural Transmission: Spinal Cord Injury (Part 2) Overview Concept: Neural Target Group: Second
Title: To cite this reference: Spinal Cord Injury (Part 2 of 2) University of South Dakota Simulation Scenario Neural Transmission: Spinal Cord Injury (Part 2) Overview Concept: Neural Target Group: Second
Guidelines for the Oral Presentation
 Guidelines for the Oral Presentation Nersi Nikakhtar, M.D. University of Minnesota Medical School 1 Table of Contents The Oral Presentation: An Introduction... 3 Why Worry About the Oral Presentation?...
Guidelines for the Oral Presentation Nersi Nikakhtar, M.D. University of Minnesota Medical School 1 Table of Contents The Oral Presentation: An Introduction... 3 Why Worry About the Oral Presentation?...
Simulation Design Template. Location for Reflection:
 Simulation Design Template Date: Discipline: Expected Simulation Run Time: Location: Admission Date: Today s Date: Brief Description of Client Name: Gender: Age: Race: File Name: Student Level: Guided
Simulation Design Template Date: Discipline: Expected Simulation Run Time: Location: Admission Date: Today s Date: Brief Description of Client Name: Gender: Age: Race: File Name: Student Level: Guided
INTERN BOOT CAMP 2017
 Sign Out INTERN BOOT CAMP 2017 Objectives Review importance of sign outs Touch on less than ideal examples of verbal and written sign outs Review the IPASS system of sign outs Review disease-specific details
Sign Out INTERN BOOT CAMP 2017 Objectives Review importance of sign outs Touch on less than ideal examples of verbal and written sign outs Review the IPASS system of sign outs Review disease-specific details
Karen M. Mathias, MSN, RN, APRN-BC Director Barbara J. Peterson, RN Simulation Specialist
 On the Rural Roads with Pediatric Simulation Training Karen M. Mathias, MSN, RN, APRN-BC Director Barbara J. Peterson, RN Simulation Specialist Objectives Identify key patient safety issues that make simulation
On the Rural Roads with Pediatric Simulation Training Karen M. Mathias, MSN, RN, APRN-BC Director Barbara J. Peterson, RN Simulation Specialist Objectives Identify key patient safety issues that make simulation