Hamilton Niagara Haldimand Brant LHIN. PAG Service Delivery Model Reviews
|
|
|
- Rudolf Fletcher
- 5 years ago
- Views:
Transcription
1 Hamilton Niagara Haldimand Brant LHIN PAG Service Delivery Model Reviews April, 2009
2 2 Deloitte & Touche LLP and affiliated entities.
3 Table of Contents Overview of Service Delivery Models 5 Ontario s Chronic Disease Prevention and Management Framework 8 Endocrine PAG 11 Maternal/Newborn PAG 19 Neurosciences PAG 25 Orthopaedics PAG 31 Rehabilitation/Complex Continuing Care PAG 37 Urology/Renal/CKD PAG 45 Ophthalmology PAG 55 Cardiac PAG 59 Respiratory PAG 69 Ear, Nose, and Throat PAG 77 GI/Hepatobiliary PAG 83 Mental Health PAG 89 3 Deloitte & Touche LLP and affiliated entities.
4 4 Deloitte & Touche LLP and affiliated entities.
5 Introduction Overview of Service Delivery Models This document presents a summary of peer practice service delivery models researched across published sources and through first-hand knowledge of other health organizations. Although outcomes are not available in many instances, the models and considerations that are provided in this summary give insights into the options and principles other health organizations are using to coordinate clinical service delivery. They are intended to inform the Planning Advisory Group (PAG) as it designs the future model of service delivery for the Hamilton Niagara Haldimand Brant (HNHB) LHIN. To support initial planning discussions, an orientation to a common typology of service delivery models is provided below, which can be used as a foundation for discussion. An orientation to broader work underway in Ontario with respect to chronic disease prevention and management (CDPM) is also provided below. This summary document is intended as one input to the planning process. As the PAG considers future service delivery models that are LHIN-wide and result in quality care, equitable access, and efficient delivery, members will also draw on the expertise of the group and colleagues, as well as any other leading practices with which they are familiar. Summary of General Service Delivery Models In examining the type of service delivery model to consider for a specific clinical area, there are three generic models of service delivery presented for consideration at the local, district and LHIN-wide levels. Depending on the clinical focus, each option may present different benefits and challenges. Each of the models presented below is intended to depict providers across the full continuum of care and across health sectors: providers may be hospitals, long-term care facilities, community care agencies, individual physicians or others. As a frame of reference, a graphical representation of the continuum of care and patient movement across the continuum is provided below. Examples of Providers Involved Across Health Sectors Long-Term Care Meals on Wheels Physician CCAC Hospital Community Agencies Health Promotion and Prevention Public Awareness and Education Primary Care Emergency Medical Services Acute Care Rehabilitation Home Care Long Term Care Palliative Care As the generic service delivery models on the following page are reviewed, several key considerations are noted for PAG members: Critical mass volumes, technology intensity, level of specialized knowledge, availability of health human resources, and access to service availability are parameters to consider across all models. In modelling local vs. district vs. LHIN-wide care provision, multi-direction flows of providers and patients should be considered. For example, the PAG may consider a two-way flow of practitioners between a specialized hub of service delivery and local community service delivery where community-based physicians have access and opportunity to deliver specialty services in the hub, and specialist hubbased physicians are involved in care delivery in the local community. Principles from Lean service delivery in health care may be helpful for the PAG to consider as it begins its work: lean principles suggest service delivery design should focus on being patient-centered to maximize the value from the patients perspective. This includes focusing on connection points between care providers at the organization and individual levels and ensuring seamless coordination to eliminate waste in duplication of efforts across the service model. 5 Deloitte & Touche LLP and affiliated entities.
6 Common Service Delivery Models Community A Local Providers Community C Local Service Provision Local Providers Local Providers Community B Local Service Provision: Services needed by the local population are provided locally through the local hospital, community care agencies, individual physicians or others, with locally-based utilization of resources and expertise pertinent to patient needs. Although some information or best practice sharing between local communities may exist, there is limited service coordination. This model provides care close to home, but may create duplication in services and redundancies in infrastructure across hospital and community providers, and may be challenging to deliver because of the intensity of human resource and funding requirements. District Service Provision: Services are organized with a district provider institution for populations across select communities within the LHIN, supported by local providers in each community. This model effectively creates a network of large and small hospitals, community care agencies, physicians and others, where multi-directional flow of providers and patients across the continuum of care is coordinated at a sub-lhin level. The district provider will capture a large proportion of residents who may require certain types of subspecialty programs, yet do not need to travel to a regional site. This can create additional efficiencies for human resources (depending on the level of specialization of skills), technology requirements (depending on complexity of technology required to support the service), and cost effectiveness, but may create access challenges for patients who are required to travel to the district site. Community A District Provider District and Local Service Provision Community C Local Providers Local Providers Community B Local Providers Community A Local Providers Community D LHIN-Wide Centre LHIN-Wide Centre Provision Community B Local Providers Community C Local Providers District Provider Community E LHIN-Wide Centre Provision: Highly specialized services that will promote access LHIN-wide are consolidated into centralized service provider site(s). These sites will have the critical mass required to sustain quality standards of care and clinical efficiencies for specialized services. This model creates a LHIN-wide network of large and small hospitals, community care agencies, physicians and others, where multi-directional flow of providers and patients across the continuum of care is coordinated at a LHIN level. One or more district and local models may exist within this LHIN-wide model to ensure appropriate balance of LHIN-level vs. local care, all coordinated in a central manner. From a patient perspective, this will mean requiring travel to the LHIN-wide centre for select services, but the need for specialization, economies of scale for academic programs, and appropriate critical mass make this necessary. 6 Deloitte & Touche LLP and affiliated entities.
7 Applying the General Service Delivery Models To provide a tangible example of how the generic service delivery models can be applied to HNHB LHIN s clinical service planning, the table below presents a sample of different levels of sites providing services across specific points along the continuum of care (highlighted).* Health Promotion and Prevention Public Awareness and Education Primary Care Emergency Medical Services Acute Care Rehabilitation Home Care Long Term Care Palliative Care While this table only presents a sample of facility/site-based services, it provides an additional frame of reference for PAG members to consider. The integration of these site-based services with broader community-based services will also be a critical component of planning by the PAG. Service Components Level 1: Regional Centre Level 2: Area Centre Level 3: Affiliate Site Level 4: Satellite Site Level 5: Basic Care Site Screening Services Manages and participates in all screening services. Participates in all screening services. Participating in screening programs is desired, but optional. Participating in screening programs optional. Participating in screening programs optional. Assessment & Diagnostic Services Full range of assessment & diagnostic services Provides selected range of assessment and diagnostic services. Refers to Level 1 when appropriate. May have limited set of basic assessment and diagnostic services. Likely to refer to Level 2 or 1 as appropriate. Basic assessment & diagnostic services are optional. Expected to refer to Level 2 or 1 as appropriate. No assessment & diagnostic service necessary. Expected to refer to Level 2 or 1 as appropriate. Treatment Services Full range of treatment services across. May refer to another Level 1. Intervention and therapy for defined set of patient types. Provides pre & post treatment care. Intervention care Provides limited and may provide intervention and therapy for limited therapy. Provides pre set of patient types. & post treatment care. Provides pre & post treatment care. May provide pre & post treatment care. Pre/Post Treatment Care, Supportive Care, Symptom Management & Palliative Care Services Full range of Full range of specialized services available to all patients. Includes complex pre & post treatment care, symptom management & palliative care. services, for patients available in the hospital or local community. Can provide pre/post treatment care for most patients treated at Level 1. Core range of services available in hospital or local community. Able to provide routine pre/post treatment care. Essential range of services available in hospital or local community to be able to provide routine pre/post treatment care as well as basic supportive & palliative care. Services not required to be available within the hospital other than for emergent / urgent care. Specialization Provides a full range of specialized services across all of the recognized disease-related areas. Provides full range of services for the high volume and less complex patient types. Patients go to Level 1 for complex treatment. Provides specified set of services for the high volume and less complex patient types. Provides pre and post treatment care for patients from catchment area. Provides specific screening and therapy treatment along with selected pre and post treatment care for patients from catchment area. * This framework is adapted from a draft developed by Brian Orr, Regional Vice President, London Regional Cancer Program. Unscheduled urgent / emergent pain and symptom management care for patients from catchment area. Limited pre & post treatment care. 7 Deloitte & Touche LLP and affiliated entities.

8 Ontario s Chronic Disease Prevention and Management Framework Summary Ontario s Chronic Disease Prevention and Management (CDPM) framework is provided below to highlight some general principles for the PAG to consider as it approaches the task of designing an optimal future service delivery model. The purpose of the CDPM framework is to provide a common policy framework to guide efforts toward effective prevention and management of chronic diseases (e.g. diabetes, COPD). System Design Elements of the Ontario Framework for Chronic Disease Prevention and Management CDPM System Design Elements Increased interdisciplinary care teams with defined roles and responsibilities 1 Innovative patient interactions 2 Description An interdisciplinary mix of specialty care professionals, working either collaboratively or in an organized team, has been shown to improve care for the chronically ill, and provide effective prevention. One factor found to be important to interdisciplinary teams success is a shared vision and commitment among members to patient-centered care. Prevention and health promotion experts in the community extend the breadth of the primary health care team, delivering prevention, health promotion and self- management supports to a practice s individual clients as well as to the population as a whole. A variety of interventions patient reminders, outreach workers, physician reminders, or patient orientation have been shown to be effective in maintaining ongoing client contact, which can take the form of return visits, home visits, s, or telephone calls. 1 Preventing and Managing Chronic Disease: Ontario s Framework, Ontario Ministry of Health and Long-Term Care, May p18. 2 Ibid. p Deloitte & Touche LLP and affiliated entities.
9 CDPM System Design Elements Care planning, care paths and care management 3 Enhanced health promotion and prevention 4 Description Regular planned visits anchor the planning and coordination of clients care which is based on a patient-centred care plan tailored to the client s specific needs, capacities, circumstances and wishes. Activities in care plan include: risk assessment, education and skills training to prevent/manage chronic disease; screening, diagnosis, testing to detect early onset of disease or onset of co-morbidities; and treatment, rehabilitation, medication management and counselling for chronically ill patients. Effective execution of the plan requires use of care paths that plot the sequence of care, and next steps for each point in disease management. Emphasis on prevention in risk assessments (for genetic, environmental, behavioural, social factors, for example) and pro-active follow-up for screening and tests to detect disease early, and information, education, skills training, and supports to stay healthy. The prevention and health promotion services that clinical team members deliver may need to be expanded by drawing upon, or developing services with community organizations. Outreach and population-needs based care and cultural sensitivity 5 Recognition of the role of culture, income and other determinants of health in shaping individuals health and access to health care is critical. This includes ensuring equal access and sensitivity to the cultural and linguistic needs. Can also include supporting community organizations in making health services, information and education accessible to all sub-populations in their catchment area. e.g., aboriginal population, Francophones and marginalized or cultural/linguistic minority populations. The framework components include: Health Care Organizations: to make systematic efforts to improve prevention and management of chronic disease; Delivery System Design: focused on prevention and improving access, continuity of care and flow through the system; Provider Decision Support: to integrate evidence-based guidelines into daily practice; Information Systems: for enhancing information for providers to provide quality care; for clients to support them in managing their disease on a day to day basis; and for integrating services across health system; Personal Skills & Self-Management Support: to empower individuals to build skills for healthy living and coping with disease; Healthy Public Policy: to develop and implement policies to improve individual and population health and address inequities; Supportive Environments: to remove barriers to healthy living and promote safe, enjoyable living and working conditions; and, Community Action: support for activities undertaken collectively to improve the health of the residents. 3 Ibid. 4 Ibid., p Ibid. 9 Deloitte & Touche LLP and affiliated entities.
10 10 Deloitte & Touche LLP and affiliated entities.
11 Hamilton Niagara Haldimand Brant LHIN Endocrine PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
12 Endocrine Specific Models of Service Delivery A summary of research into peer practice endocrine service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within endocrine services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model enablers suggest several implications for Endocrine Services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having local service delivery because of large patient populations (making critical mass possible) and low technology requirements for clinic based services, supported by central coordination and specialized services. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms. Need to secure and maintain adequate health human resources to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. Maintenance of a central registry for select services and chronic diseases (e.g. diabetes) to support service access and population health. 12 Deloitte & Touche LLP and affiliated entities.
13 Endocrine Health Network Model of Care (Australia) The Australian Endocrine Health Network Diabetes Model of Care 6 was developed to provide a framework for comprehensive, accessible and efficient provision of coordinated diabetes prevention and management services. As noted in the in the model s documentation, the objective of the framework is to ensure that diabetes services are optimally configured to: Prevent and delay the onset of diabetes; Prevent and slow progression of diabetic complications, especially heart disease, renal failure, impaired vision and lower limb amputations; Improve the quality of life of people who have diabetes; and Reduce inequities in diabetes service provision, particularly for Aboriginal people and other disadvantaged groups. The supporting service delivery model / model of care for each stage of diabetes consists of three components: health promotion; GP-coordinated multidisciplinary prevention and management, including targeted programs for high risk and vulnerable groups; and specialist team services. The roles of each are summarized in the framework on the following page. The Diabetes Model of Care is aimed at assisting service delivery and integration of diabetes services in the following ways: Increasing the capacity of GP-coordinated multidisciplinary services to prevent and manage diabetes and its complications; Developing an efficient interface between general practice and the diversity of community-based diabetes prevention and management services at the local level, especially in under-resourced and high need locations; Improving accessibility and quality of diabetes self-management education; Enhancing service quality by increasing the use of guidelines, local protocols, service directories, registers, recall systems and patient-held management plans to ensure that all people with diabetes receive comprehensive, ongoing care; Improving local service coordination and increasing knowledge of available resources by health care providers and people with diabetes; Improving access to and effectiveness of specialist services to address specific problems and refer back to general practice for long-term management. Supporting the model is a tiered service delivery structure where urban and rural primary health care providers have ready access to specialist multi-disciplinary teams in designated tertiary and secondary care centres for advice and shared care. In addition, outreach and telehealth services are provided in accordance with community need, regional capacity and identified service gaps. 6 Diabetes Model of Care, Endocrine Health Network, 2008, 13 Deloitte & Touche LLP and affiliated entities.
14

15 Herefordshire and Newcastle Primary Care Trust Diabetes Service Models Efforts from the diabetes commissioning framework within the National Health Services in the UK drove the development of two similar initiatives across the Herefordshire and Newcastle Primary Care Trusts. Both Trusts developed an integrated local diabetes service based on the community delivery of diabetes care, supporting primary care and interfacing with specialist care. 7, 8 In both models, three levels of care were identified in a coordinated service delivery model, with region-wide guidelines, referral criteria, and integrated pathways of diabetes care. A depiction of this model and summary of each level of care is summarized on the following page. Level 1 (primary care) is supported by district-wide podiatry, digital retinal screening and health care provider education. Level 2 (community-based service) includes a pathway for newly-diagnosed type 2 diabetes encompassing structured group education and a pathway for continuing care of more complex type 2 diabetes, supported by additional community services such as weight management groups, and community-based group insulin starts. Level 3 (specialist services) provided at the Diabetes Centre include preconception care, a medical foot clinic, a young adults clinic, an insulin pump service and a diabetes renal clinic %20Model%2025'06'08.pdf

16 Kaiser Permanente Care Management Institute s Integrated Diabetes Care Program 9 Developed in the late1990 s, Kaiser Permanente s (KP) Care Management Institute s Integrated Diabetes Care (IDC) program was established to be a nationally consistent, evidence-based, process-efficient approach to delivery of health care that is customized to the individual member. The IDC model of care is depicted below, and contains four key components: population identification through a registry; stratification of patients; commitment to a team approach; and evaluation of care. Specifically with respect to the team approach, KP has designed a service delivery model that assigns responsibilities to a variety of providers across the continuum of care (e.g. a care coordinator, diabetes educator, primary care physician, or eye-care specialist). Primary care physicians play more of an oversight and management role, while direct patient contact is often delegated to other health team members. Team member roles are clarified and reinforced by position descriptions, support materials, and specially tailored training sessions. Manitoba First Nations Committee Diabetes Integration Project As noted on their website: 10 The Diabetes Integration Project (DIP) is an Integrated Diabetes Health Care Service Delivery Model that was developed to begin to address the needs for First Nations people who have been diagnosed with diabetes. The project will overcome barriers to access to a comprehensive, coordinated and integrated diabetes care and treatment service for limb, eye, cardiovascular and kidney complications. The DIP will utilize Mobile Diabetes Health Care Service Delivery Teams to provide diabetes care and treatment services in First Nation communities throughout Manitoba. The goal of the DIP is to improve the health status of First Nation individuals, families and communities through actions aimed at reducing prevalence and incidence of diabetes and its risk factors, and to prevent or delay the complications of diabetes. While this model is still in implementation, it presents additional insight to the PAG when considering the large First Nations community within HNHB LHIN. The model uses a mobile health approach, where 5 geographic nursing teams will be positioned across the health region to provide local service delivery. The Deloitte & Touche LLP and affiliated entities.

17 teams will be supported by a core team of clinicians comprised of: dietitians, mental health providers, medical advisor, physician specialists, surveillance coordinator and administrative support. Rapid Access Multi-Disciplinary Team Thyroid and Parathyroid Clinic 11 Developed by the North West London Hospitals NHS Trust in the UK, this clinic focuses on the care of thyroid cancer patients with both malignant and non-malignant disease. General principles of the service delivery model include: Hospitals providing secondary care for patients with suspected thyroid cancer should develop well defined and streamlined pathways of referral and care; Designated diagnostic clinics with appropriate resources for patients with thyroid lumps are desirable; Patients should be referred to a surgeon, endocrinologist, clinical oncologist or nuclear medicine physician who has a specialist interest in thyroid cancer and is a member of the multi-disciplinary team (MDT); The local cancer centre or cancer unit should provide clear guidance to GPs on referral pathways to secondary care. The proposed model for a one-stop thyroid/parathyroid clinic is conceptualized below: Multi-disciplinary Thyroid / Parathyroid One Stop 11 Parathyroid_Rapid_Access_Clinic_ pdf 17 Deloitte & Touche LLP and affiliated entities.
18 Western Australia Cystic Fibrosis Model of Care 12 This model of care sets out a holistic patient-centred approach to the provision of services for people with Cystic Fibrosis (CF), with a focus on: Transition issues across the continuum of care and disease progression An increase in consumer participation A shift from an acute hospital-based approach to a wellness approach Services delivered where possible in community settings by a multi-disciplinary team. The CF model of care is designed to be a state-wide service with a centre of excellence comprising tertiary paediatric and adult hospitals with appropriate management structures to support the model Deloitte & Touche LLP and affiliated entities.
19 Hamilton Niagara Haldimand Brant LHIN Maternal/Newborn PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
20 Maternal/Newborn Specific Models of Service Delivery A summary of research into peer practice maternal/newborn service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within maternal/newborn services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model enablers suggest several implications for Maternal/Newborn Services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms. Need to secure and maintain adequate health human resources and specialization to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. National Center of Excellence in Women s Health Model 13 The University of California, San Francisco (UCSF) National Center of Excellence in Women's Health (CoE) has developed a new model to transform the traditional Academic Medical Center from a fragmented set of activities into a dynamic and multi-disciplinary health care system focused on the needs of all women Women s health matters, 2002, 20 Deloitte & Touche LLP and affiliated entities.
21 The model includes five components: Integrated clinical care to provide seamless health care services to women Research focused on women's health issues to better understand women's health needs Professional education to better educate tomorrow's women's health care providers Leadership activities to encourage women interested in this field Community outreach to expand services and the reach of the program beyond the walls of the university setting. UCSF Women s Health s One Stop Shopping model gives women the tools and the knowledge they need to be active partners in their choices for health care. The Center offers a variety of services including: The Resource Center was created to encourage women to make informed decisions about their health and to provide tools for women to become active partners in their care. Services include a lending library, classes and workshops, a mini-bookstore, referrals to UCSF and other community providers, and links to clinical trials and research on women's health. The CoE participates in community activities and regularly hosts educational events and programs for girls and women of all ages and with diverse interests. The Osher Center for Integrative Medicine looks to identify the most effective treatments for patients by combining nontraditional and traditional approaches that address all aspects of health and wellness - biological, psychological, social and spiritual. Through scientific research, the Center's faculty will document the value of non-traditional treatments. Clinical services include medical massage, acupuncture manipulation, psychotherapy, mindfulness based stress reduction support groups, yoga, and Qi Gong. The Center is the regional referral hospital for births that present a high risk for mother or baby, as well as the place where mothers come for normal childbirth with experienced nurses, doctors and midwives. The Center includes pre-natal and post-partum services including prenatal diagnosis and antenatal testing. Family-Centred Maternity and Newborn Care National Guidelines 14 (Canada) Health Canada has developed guidelines for the regionalization of maternity and newborn services. Regionalization of these services implies the development of a coordinated, cooperative system of care within a defined geographic area. The goals of such care are: Provision of quality care for all women, newborns, and their families; Appropriate use of personnel and facilities; Coordination of services; Provision of referral mechanisms; Provision of professional education; and Incorporation of research and evaluation. A region s continuum of care is provided by a variety of personnel who provide care for women and newborns during the preconception, pregnancy, labour, birth, and postpartum periods. These services can be offered in a number of settings including: primary care facilities, community-based organizations, and the places where women actually give birth. Professional education and support is provided via maternal and newborn outreach programs. A discussion of each of these settings and the care provided is provided below Deloitte & Touche LLP and affiliated entities.
22 Primary Care. Most preconception, prenatal, and postpartum/newborn services are provided in primary care settings, including office-based individual or group practices, community health centres or health department clinics, and the home. Offered are basic preventive and health promotion services. Community-based Care. Many services are provided through community-based organizations, either nongovernmental or governmental agencies. Programs include childbirth education, breastfeeding support, maternal and newborn bereavement, parent support, community-based nursing, child care, home care, family and social services, and infant development programs. As well, services are offered via health units, parent resource centres and maternity homes. Childbirth Care. The vast majority of births take place in hospital (ranging from small units to large tertiary centres) although some births also take place in the home. Primary or level I hospitals, provide care to women that are expected to have a normal healthy birth of a full term baby. These hospitals may be in smaller rural communities. Level II hospitals in addition to providing level I care are expected to have the resources to care for women with selected health conditions and babes born prematurely at greater than or equal to 32 weeks. Level III or tertiary level hospitals provide level I and II care and care for women whose pregnancies are at risk (less than 32 weeks), or have severe medical conditions. Maternal and Newborn Outreach Programs. The principal function of regional outreach programs is to assist agencies, institutions, and care providers to provide optimal care for their community through coordinated educational programs. Their responsibilities may include: Development / facilitation of continuing professional education; Provision of advice regarding practice, care, policies, procedures, problem solving and equipment purchases; Provision of collaborative assistance in the introduction of new approaches to care; Preservation of quality assurance and continuous improvement; Sharing of information, newsletters, lending libraries, and manuals; Provision of a supportive environment for ongoing maternal and newborn care in the community. 22 Deloitte & Touche LLP and affiliated entities.
23 Provincial Perinatal Health Program B.C. Perinatal Health Program 15 (BCPHP) works towards optimizing maternal, neonatal, and fetal health in the province through educational support to care providers, outcome analysis, networks and multidisciplinary perinatal guidelines. The program works with hospitals, health authorities, community agencies, academic institutions and private practitioners to effectively link perinatal health care data and research to education and professional needs of care providers across BC. A committee structure is organized to support the mandate of the BC Perinatal Health Program (BCPHP). Committees include: Interdisciplinary Support and Education Committee Perinatal Morbidity & Mortality Provincial Perinatal Advisory Provincial Specialized Perinatal Services The mandate includes: Consultation to and liaison with perinatal care providers and institutions Promotion and facilitation of inter-professional outreach education Development of guidelines for patient care and services planning Promotion of perinatal care networks within the province Assisting in the identification of appropriate perinatal care provider roles and skill levels Collection and analysis of perinatal data to evaluate provincial perinatal outcomes, and to improve health care initiatives Other provincial programs such as, Alberta Perinatal Health Program 16 and Reproductive Care Program of Nova Scotia 17 also have committee structures. Committees meet regularly and are responsible for review, critique and approve all written materials that are generated. Guidelines and clinical practices are disseminated to regional and community hospitals as well as centers within the province to ensure standardization and best practice guideline are utilized. Youth Pregnancy & Parenting Program 18 (Vancouver, British Columbia) Vancouver Coastal Health Authority and BC Women s Hospital collaborated to provide young mothers with access to medical and support services at Evergreen Community Health Centre. The benefit to the program is having all the services under one roof instead of having to visit multiple sites. The program provides youth-friendly pre and postnatal care and education programs for youth and teens up to 22 years old in a fun, casual environment. Services include: physician/specialist consultations, prenatal or parenting groups, access to counsellors, youth groups, recreational activities & special events and father s group at Collingwood Neighborhood House. MOREOB Program 19 MORE OB (Managing Obstetrical Risk Efficiently) is a comprehensive, three-year, patient safety, professional development, and performance improvement program for caregivers and administrators in hospital obstetrics Deloitte & Touche LLP and affiliated entities.
24 units. The Program structure is based on: safety as the priority, effective communication, teamwork, decreased hierarchy in emergencies, practice for emergencies, and reflective learning. The program integrates evidence-based professional practice standards and guidelines with current and evolving patient safety concepts, principles and tools. The MORE OB Program is delivered to hospitals on-site. A local, inter-professional Birthing Unit Core Team is trained, by expert facilitators, and empowered by hospital administration, to lead all unit healthcare workers in the implementation of patient care and safety processes that are adapted to the unit s needs and practice environment. Hospital teams receive ongoing support through the services of MORE OB Regional Representatives who are skilled in the Program and available to respond to the client s needs in a timely manner. Program tools to support safety, quality service delivery, effective communication, and teamwork include items such as: Annual program environmental scan where hospitals can benchmark their performance; Patient satisfaction survey; Learning tools including clinical care content, case exercises, decision trees, and audit tools; Culture assessment survey; Skills drills; Event tracking tools to identify near misses and adverse events; Root cause analysis and case analysis review toolkit; and, Communication and teamwork tools. The involvement of all front-line professionals and all levels of hospital management leads to improved team performance, alignment of safety goals throughout the organization, and a fulfilling experience for all stakeholders, including women and their babies. 24 Deloitte & Touche LLP and affiliated entities.
25 Hamilton Niagara Haldimand Brant LHIN Neurosciences PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
26 Neuroscience Specific Models of Service Delivery A summary of research into peer practice neuroscience service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within neuroscience services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Consideration of Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model key success factors suggest several implications for Neuroscience Services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having hub and spoke type service delivery to provide local access for core services with centralized centre(s) of excellence which can provide tertiary services, support for staff training, standardized resources for clients and staff, and leading practices through academic affiliations. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for integration between providers along the continuum, with engagement of clinical leaders to develop and support resource tools and communication mechanisms. This includes formalized linkages with primary care and community providers. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This may include identification of multi-directional provider flow across urban and rural centres, where appropriate. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms (e.g. exploration of telehealth opportunities for satellite clinics to provide remote consultation in rural areas and standardization of care pathways for multidisciplinary teams to deliver best practice care). Need to secure and maintain adequate health human resources to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. 26 Deloitte & Touche LLP and affiliated entities.

27 Maintenance of a central registry for select services and chronic diseases to support service access and population health. Neurosciences Service Delivery Model Scotland The Scottish Executive Health Department in collaboration with NHS Scotland is currently implementing a redesign of their Neurosurgical Services 20. The new model of care moves from current configuration of four neurosurgical centers to a model of a single, nationally organized service into three levels. This three tier model describes a pyramid of care through which patients would pass, as necessary, from level one (local clinics) through level two (more complex) and finally on to level three (most complex) where necessary 21. Level 3 - The specialist neurosurgical centre co-located with all neurosciences specialties and the major specialties of a teaching hospital. It will provide: complex medical and surgical management, CT/MRI/CTA/MRA/ang iography, interventional neuroradiology, neuro critical care, inpatient neurosurgery, emergency surgery and paediatric neurosurgery. Level 2 - Focused through District General Hospitals, this would be supported by neurologically trained emergency resuscitation staff and specialist outreach and follow-up clinics with rapid access to deal with urgent neurological emergencies. It will provide: CT/MRI, with image transfer, rehabilitation, stroke medicine, general neurology, neurophysiology, local orthopedic service, outpatient neurosurgery, post-operative care for neurosurgery and general intensive care. Level 1 - Focused through Community Health Partnerships (CHP), Minor Injury Services and GP practices, this level will promote access to neurological teams supported by nurse-led clinics and rehabilitation facilities. These services will include simple tests, referrals, decision support, pre-admission clinics and local neurology. Supporting this model will be improved communication, agreed standards for care, more co-operative and consistent working through and across the many professional groups involved in patient care, and clear guidance on where, how and when patients will be treated Deloitte & Touche LLP and affiliated entities.


; Access to state of the art diagnostic imaging (e.g.intraoperative MRI); Access to critical care units and")


.")
28 Fraser Health Authority 22 Model of Care Delivery The Fraser Health Authority in British Columbia uses a hub and spoke service delivery model similar to the proposed model of care for Scotland, where neurosurgery is performed at two of the twelve centers and specialized outpatient clinics are located in one center. Key considerations for successful service delivery of a comprehensive neurosciences program include: Access to specialised physicians and staff for the continuum of care; Access to state of the art technologies to provide the most appropriate care (e.g. guided imaging; for tumour surgery and vagal nerve stimulation equipment for epilepsy); Access to state of the art diagnostic imaging (e.g.intraoperative MRI); Access to critical care units and specialized clinics; Availability and access to telemedicine for consultations for rural and remote patients; Accepted and clear provider referral pathways; and Practice in an atmosphere of scientific inquiry, analyzing surgical practice for ways to improve through research. Ontario Stroke Strategy 23 The Ontario Stroke Strategy framework creates an integrated or coordinated system of care. Services and sectors function as a unified whole and link to the different services across the continuum of care and across the province. The supporting service delivery model / model of care for The Ontario Stroke Strategy framework has influences across the continuum of care, looking at seven components of health promotion and primary prevention, recognition of symptoms, pre-hospital, acute care, secondary prevention, rehabilitation, long-term care and community care (identified in the graphic to the right). The Ontario Stroke Strategy is aimed at assisting service delivery in the following ways: Comprehensiveness: Improve stroke services across the entire continuum of care, from prevention programs to care in a long term care or community setting. Integrated: Create an integrated or co-ordinated system of care. An integrated system is one where different services and sectors function as a unified whole. An integrated system of stroke care links the different services across the continuum of care and across Ontario Ontario Stroke Strategy, Ministry of Health and Long Term Care, November 5, Deloitte & Touche LLP and affiliated entities.
29 Evidence-based: High quality stroke care is provided, using best practice that has been supported by scientific evidence. Province-wide: Improvements to stroke care should benefit all irrespective of their geographic location. Consideration of the specific needs of geographic areas are addressed e.g. telestroke Service delivery for the acute care phase is provided in a three-tiered approach: 1. Regional Stroke Center: The Regional Stroke Centre takes a leadership role in the development, implementation and coordination of stroke care for the region. As well as offering the highest level of neurologic care (e.g. thrombolytic therapy, neurosurgery and interventional neuroradiology), the Regional Stroke Centre acts as an educational and organizational resource for all hospitals in the region. 2. District Stroke Center: Depending upon the size and population of a region, as well as hospital resources, a region may have one or more District Stroke Centers. District Stroke Centers differ from community hospitals in that they are organized to facilitate the use of tpa for acute ischemic stroke on an around-the-clock basis. They may or may not have Neurosurgical capacities. Patients transported from a District Stroke Centre to a Regional Stroke Centre may subsequently be repatriated to the District Centre or the community hospital closest to home. 3. Community Hospital: Community hospitals continue to play an important role in the treatment of stroke patients. They provide care to stroke patients in their catchment areas who neither require advanced neurosurgical/interventional radiology care nor are eligible for thrombolytic therapy. After the acute phase, patients who are treated at a District or Regional Stroke Centre may be repatriated to their community hospital for longer-term care and rehabilitation. Neuromusculoskeletal Program 24 (Vancouver Costal Health, British Columbia) Some centres look at clustering neuromusculoskeletal disorders into one comprehensive program. The Neuromusculoskeletal (NMS) program in Vancouver specializes in providing ambulatory and rehabilitation services for people with a variety of neuromusculoskeletal impairments: neuromuscular disease, polio, complex trauma, multiple sclerosis, cerebral palsy, cancer, and neurodegenerative diseases. The NMS program is based out of a dedicated rehabilitation center that provides care for both in and out patients. Services include: ALS Team: This team works closely with clients and families from referral until end of life. NMS Inpatients: Intensive rehabilitation for adults with post-acute short term rehabilitative needs. NMS Outpatients: To provide time limited outpatient assessment and intervention to people with complex neuromusculoskeletal and/or neurological conditions. The core neuromusculoskeletal program team may include: occupational therapist, physiatrist, physiotherapist, social worker, nursing and speech language pathologist Deloitte & Touche LLP and affiliated entities.
30 30 Deloitte & Touche LLP and affiliated entities.
31 Hamilton Niagara Haldimand Brant LHIN Orthopaedics PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
32 Orthopaedic Specific Models of Service Delivery A summary of research into peer practice orthopaedic service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within orthopaedic services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified in the pages that follow as well as general service delivery model enablers suggest several implications for Orthopaedic Services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having local service delivery because of large patient populations (making critical mass possible) and low technology requirements for clinic based services, supported by central coordination and specialized services. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms (e.g. exploration of telehealth opportunities for satellite clinics to provide remote consultation in rural areas and standardization of care pathways for multi-disciplinary teams to deliver best practice care). Need to secure and maintain adequate health human resources to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. For example, availability of a Case Manager to play a central role in patient s care for some models, and access to a multidisciplinary team (includes nurse clinicians, physiotherapists, occupational therapists, and dietitians) to deliver specialized care that is centrally located. Networking and information systems to help ensure efficient, effective care for bone and joint patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. 32 Deloitte & Touche LLP and affiliated entities.
33 Maintenance of a central registry for select surgical services (e.g. joint and hip replacement surgery and access to hospital beds) to support service access and population health. Alberta Bone and Joint Health Institute Hip and Knee Replacement Model 25 In this service delivery model, community-based clinics serve as the hub for services. Devoted strictly to hip and knee care for patients, the clinics are a one-stop shop providing or managing all services other than surgery including assessment of their condition, diagnosis, education and instruction, and follow-up after surgery. While services are offered in community areas, one stop clinics must be located where access to services is practical and centrally located. Access to a multi-disciplinary team within the clinic promotes a patient-centered approach. Services are fully integrated and standardized so that patients receive the same type and level of treatment regardless of where they are located in Alberta. Post surgery, all care is coordinated through the case manager at the clinics, including education. Family physicians are also updated on their patient s treatment and condition. The model for hip and knee replacements features: Fully integrated continuous services delivered in a multidisciplinary environment. Assessment, diagnosis and non-surgical treatment centralized in single-purpose clinics. A shared-case approach that puts patients at the centre of their care. Clear patient and care provider responsibilities supported by accountability mechanisms. The right care provided to the right individuals in the right way by the right provider at the right time. In surgical centre, smart operating rooms are used to minimize patient discomfort, speed recovery and reduce operating costs and waiting times throughout the province. OsteoArthritis Service Integration System - Vancouver Coastal Health 26 The OsteoArthritis Service Integration System (OASIS) is designed to support people living with osteoarthritis of the hip and knee. It s an assessment and referral program that provides people with the tools they need to take control of their osteoarthritis. It helps people with osteoarthritis self-manage their condition and access support services at any stage of the disease. The OASIS program is applied to both urban and rural settings. Applying to rural settings involves: Web-based screening and assessment tools available to primary care physicians and allied health professionals; Inventory of local services (public and private) to participate and/or partner with; Assessment Clinics staffed by multidisciplinary teams that travel on scheduled basis into rural communities. The OASIS Team spans the continuum of care. Patients have access to care in the Primary Health Care Network, the Community Care Network or the Acute Care Network. Primary care is received in the patient s doctor s office and in clinics; acute care in hospitals; and care in the community through home support and programs that promote health and wellness. Community networks may be independent organizations that work with OASIS to identify and fill gaps in care, and develop services to meet the needs of people with osteoarthritis. For example: Mary Pack Osteoarthritis - OASIS - OsteoArthritis Service Integration System - Vancouver Coastal Health 33 Deloitte & Touche LLP and affiliated entities.

34 Arthritis Centre measures the impact of programs offered and increases access to services; local community centres offer education sessions. Within the clinics, patients have access to a multi-disciplinary team made up of physiotherapists, occupational therapists, nurse clinicians and dietitians offering a one stop shop assessment for patients. The Regional Office supports the clinics and works closely with community networks to identify and fill gaps in care and develop services. Education specialists develop and run education sessions and administrators monitor and evaluate programs and services. Features of the program include: Focus on continuum of care from prevention through medical supports to surgical intervention and post-operative care Multidisciplinary needs assessment teams Use of on-line database to help patients access programs and support services within their communities. Personalized action and referral plans Timely education and information Patient navigation through the system Focus on needs of individuals, families, care-givers and communities Complex and long-term partnerships Builds on related initiatives Focus on assessment, triage and education 34 Deloitte & Touche LLP and affiliated entities.
35 Orthogeriatric Model of Care 27 Australia The orthogeriatric model addresses gaps in service delivery, while also incorporating planned infrastructure changes and adjustments for demographic forecasts and other challenges. The focus of the model is the care of older people presenting with fragility fractures to the tertiary care environment. The model is a collaborative approach between orthopaedic and aged care services in the care of older people with fractures. Examples of configuration of services are: Orthopaedic Surgical Services: Surgery for hip and other fractures will continue to be mainly performed at the regional hospitals where acute care is supported. However, some trauma surgery may be supported at other urban hospitals where the appropriate level of resource is available. Orthogeriatric Services: An orthogeriatric service will be available on a 9 hour, daily basis at those urban hospitals with an emergency department, enabling coverage of the acute hospital wards and the EDs. Geriatric-led Multi-disciplinary Rehabilitation Services: Orthogeriatric rehabilitation services will continue to be concentrated within larger organizations as well as tertiary rehab centers until sufficient beds are available to allow the current service to decentralize to the Acute Care Rehabilitation Unit s (ACRU). Regional ACRUs should be established making close to home rehabilitation also available for rural patients. There will be a degree of coverage by geriatricians in these rural rehabilitation units. There will be a reliance on formal partnerships with metropolitan area ACRUs for visiting geriatric consultation supported also through the use of tele-health. The use of PACS should also provide support and improve the capacity of orthopaedic services. Outpatient Services: Outpatient osteoporosis or fragile bone clinics will be conducted at urban hospitals with an ED where all appropriate specialist services are available. In rural regions, such clinics may again be supported by tele-health and visiting geriatric and other specialist services Deloitte & Touche LLP and affiliated entities.
36 Sunnybrook Holland Orthopaedic & Arthritic Centre Model 28 The Sunnybrook Holland Orthopaedic & Arthritic Centre model framework is being implemented in the Toronto Central LHIN and includes: Process & Role Redesign, Collaboration/Consensus/Communication, Assigning Champions, Human Resource Strategy, Information Systems/Technology, Physical Facilities, and Evaluation. New roles are developed for Advanced Practice Physiotherapists, Anaesthesia Assistants, Nurse Practitioners (Acute Pain Service), Post-op Medical Management, RN First Assistants, and a Critical Care Rapid Response Team in to adopt partnerships for a multidisciplinary approach for the continuum of care along the patient flow diagrammed below. Examples of change include: Surgery, where an RN First Assistant provides technical assistance at surgery and support the perioperative care process. Anaesthesia Assistants (RN s & RT s) work collaboratively with Anaesthetists to improve efficiency and quality of care. Post-op Management changes, where a Nurse Practitioner provides timely post-operative assessment and treatment for medical problems, and the Critical Care Rapid Response Team is available Monday to Friday during working hours to respond to urgent patient management concerns. Pain Management Acute Pain Service, where an Anaesthetist and Nurse Practitioner work collaboratively to supervise post-operative pain management. Follow-Up After Discharge, where Advanced Practice Physiotherapists manage routine follow-up visits after discharge from Hospital. The Sunnybrook Centre Model of Care is aimed at assisting service delivery in the following ways: Improved access, shorter wait times Shorter hospital stays Reduced time spent by specialist physicians in routine care (i.e. surgeons, anaesthetists) High patient satisfaction System savings vs. costs Core and Specialized Services When planning for a service delivery model in orthopaedics, there are some components of service that are considered to be core and offered in local communities while other components of service are highly specialized and thus provided as more regional or tertiary services. Some examples to consider for orthopaedics include: Consideration for a district approach for orthopaedic trauma services by accumulating critical mass from nearby hospitals. Focused practitioner expertise in the specialty of upper extremity care within a district. Consideration for spinal services through a tertiary centre, recognizing the high cost and specialization of this area. 28 Evolving New Practices in Hip & Knee Arthroplasty: It Takes A Team!, CCHSE National Healthcare Leadership Conference, 2007; es%20in%20hip%20&%20knee%20arthroplasty.pdf 36 Deloitte & Touche LLP and affiliated entities.
37 Hamilton Niagara Haldimand Brant LHIN Rehabilitation/ Complex Continuing Care PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
38 Rehabilitation/Complex Continuing Care Specific Models of Service Delivery A summary of research into peer practice rehabilitation/complex continuing care service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within rehabilitation/complex continuing care services that are not included in the models provided; particularly as there are many patient population specific rehab streams to consider (i.e. stroke, cardiac, neuro, etc) however the models presented share common elements to what is demonstrated in these other areas. For these reasons PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model enablers suggest several implications for Rehabilitation / Complex Continuing Care Services that can serve as an input into PAG planning. Recognition for the need to plan for services (i.e. appropriate type of services, associated support serves such to support cognitive and behavioural issues, and location of rehab and CCC resources) using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). Being mindful of equitable access to high quality services and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points including standardized admission and discharge processes and individualized care plans. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms. Need to secure and maintain adequate health human resources to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery (e.g. specialized psychiatrists and interprofessional teams). Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. Maintenance of a central registry for select services and chronic diseases (e.g. diabetes) to support service access and population health. 38 Deloitte & Touche LLP and affiliated entities.
39 Delivery Framework for Adult Rehabilitation 29 NHS Scotland The delivery framework for adult rehabilitation in Scotland identifies early intervention for the selfmanagement group where emphasis is placed on self management and health promotion utilizing community culture and leisure centers, lifelong learning opportunities and voluntary agencies services. The framework for adult rehabilitation is organized into four phases: The condition management phase into which an individual can self refer when appropriate to a rehabilitation team via a single point of access to enable specific needs, either social or health, to be addressed. In the acute phase vital specialist interventions are undertaken by hospital rehabilitation teams with the aim of stabilizing the patient and ensuring a timely, seamless discharge process. The longer-term rehabilitation phase calls for community rehabilitation teams to work in partnership not only with acute rehabilitation teams, but also across all health, local authority, independent and voluntary sectors and, crucially, with individuals, carers and communities. The vocational rehabilitation phase outlines the support structures that should be available to individuals in workplaces to promote health and well-being at work. It then identifies a rapid access referral process through which individuals should be able to secure support and specialist advice from a dedicated vocational rehabilitation team consisting of a range of professionals using case management approaches. Settings in which rehabilitation teams work include GP practice, care homes, client homes, day hospitals/centres, community hospitals, community pharmacies, mental health services, specialist outreach services, community nursing services, sheltered housing, community resource centres, job centres, etc. The highlights of the model satisfy the need to: Develop person and carer-centred rehabilitation services; Create direct access to rehabilitation services, where appropriate; Create a single point of access to rehabilitation services, where appropriate; Promote a focus on maximizing individuals autonomy and enablement; Provide rehabilitation services closer to individuals homes, when appropriate; Encourage multi-disciplinary, multi-agency teams genuinely to work together in whole-systems approaches; Adopt a holistic model of rehabilitation encompassing physical, psychological, emotional and social needs; Strengthen the Single Shared Assessment system (streamlining the assessment process to reduce duplication of activity in the area of needs assessment).on accessing services; Provide the same quality of treatment for all, regardless of class, age, culture or geographical location; Review and analyze outcomes on an ongoing basis, with a particular focus on feedback from individuals and carers. 29 A Delivery Framework for Adult Rehabilitation in Scotland, Scottish Executive, Deloitte & Touche LLP and affiliated entities.


40 Delivery Framework for Adult Rehabilitation
41 Acquired Brain Injury Service Pathway 30 (HNHB LHIN) The HNHB LHIN Acquired Brain Injury Service Pathway was developed to provide a pathway for expanded, accessible and efficient provision of coordinated Acquired Brain Injury (ABI) management services. As noted in the in the model s documentation 31, the guiding principles of the ABI Network are used in planning the provision of care to ensure that ABI services are optimally configured to: Provide client centered services that are responsive to individual needs; Provide equitable and timely access to services regardless of location; Provide universal accessibility of environment and language; Provide seamless transition across the health continuum; Provide specialized services; Establish specific discharge and admission guidelines for all services that direct where people go to ensure access for those who cannot advocate for themselves; To maximize existing technology to offer training and consultation opportunities through videoconferencing or telemedicine; and Establish a common evaluation tool to measure outcomes The supporting service delivery model / model of care for ABI looks at the continuum of care from the patient being ready for discharge from an acute care setting to discharge in a private or public residence. The model takes into account: bed availability, long term care needs, availability of community supports, crisis management, funding and ongoing outreach services. The ABI Service Pathway is aimed at assisting service delivery and integration of ABI patients into the community. Key components of the model are: A transfer process from hospital to community and vice versa; A transition process from paediatric to adult services; Navigational supports for the individual to facilitate access to services; Community supports to minimise hospitalization; Coordinate services among sectors to address multiple issues e.g. ABI, mental health and addictions; Long term facilities that are willing to admit individuals with ABI and behavioural challenges; Age appropriate services in long term care facilities for younger adults; Community transitional services to facilitate return to independent living and allow earlier discharge from acute and specialized rehabilitation beds; Transportation services; Affordable housing; Timely access to acute care mental health beds for crisis or medication review; Specialized supports for rehabilitation or behavioural programming for individuals transferred to local hospitals; An on call system to support individuals in the community; Respite opportunities; and Discharge planning started while in acute care to facilitate timely access to funding, equipment, services and to start the application to long term care if appropriate. 30 The HNHB LIHN ABI Service Pathway, March Clinical Planning and Integration, HNHB Community Support Services Network and the HNHB ABI Network
42 ABI Service Pathway 42 Deloitte & Touche LLP and affiliated entities.
43 Bruyère Continuing Care 32 (Ottawa, Ontario) The Complex Continuing Care (CCC) program is a goal-oriented program for people who require medical management, skilled nursing care and a range of interdisciplinary diagnostic and therapeutic services and technologies either for a continuous or an extended period of time. The inter-professional health care team work closely with patients and families to develop an individualized care plan. Complex Continuing Care has three major care streams: Specialized Complex Care. Patients in the Specialized Complex Care stream have a progressive disease and multiple medical conditions requiring ongoing monitoring by an interdisciplinary team. Restorative Care. Patients in the Restorative Stream may require inpatient treatment by an interdisciplinary team for functional improvement over an extended period of time, with the goal to be discharged to another program, home or to the community. Supportive Care. Patients in the supportive stream have severe functional impairment requiring care above what can be provided from community agencies or long-term care facilities or an improved condition, or are maintaining their health status, or are good candidates to be transitioned to the community. Patients will be moved from stream to stream as their care requirement improves or changes. Once a patient no longer needs Complex Continuing Care, the inter-professional team will ensure efficient and appropriate discharge into the community Deloitte & Touche LLP and affiliated entities.
44 44 Deloitte & Touche LLP and affiliated entities.
45 Hamilton Niagara Haldimand Brant LHIN Urology/Renal/CKD PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
46 Urology/Renal/CKD Specific Models of Service Delivery A summary of research into peer practice urology/renal/ckd service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within urology/renal/ckd services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the pages that follow as well as general service delivery model enablers suggest several implications for Urology/Renal/CKD Services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having hub and spoke type service delivery to provide concentrated centres for screening and treatment with centralized centre of excellence which can provide tertiary services, support for staff training, standardized resources for clients and staff, and leading practices through academic affiliations. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for integration between providers along the continuum, with engagement of clinical leaders to develop and support resource tools and communication mechanisms. This includes formalized linkages with primary care and community providers. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms. Opportunity to explore alternate provider delivery models for less specialized care and interventions (urology nurse specialists for cystoscopy and consideration of RN/RPN skill mix for dialysis care). Need to secure and maintain adequate health human resources to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. Maintenance of a central registry for select services and chronic diseases to support service access and population health. 46 Deloitte & Touche LLP and affiliated entities.

47 Nova Scotia Urology Model 33 Nova Scotia identified a need to develop a provincial multiple-site shared service model for urology with an implementation plan for the Northern Area. To build this model, they engaged various stakeholders, a steering committee, and senior leaders of the District Health Authority and government in consultation sessions. The driver of change was to allow new services to fit the definition of quality care in terms of standard of care, accessibility, fiscal responsibility, and a positive environment (i.e. recruitment and retention). The service delivery model design included health human resource considerations and equipment requirements. The outcome of the model has been more patient focus with improved accessibility for patients and referring physicians. Travel to consult with specialists, workup, or minor surgery now takes less than 30 minutes. Travel for major surgery and care take less than 1.25 hours. Outreach Urology Model (UK) 34 The objective was to convert experience in delivering outreach urology by 5 urology nurse specialists (UNSs) into a truly primary care based office urology service delivered entirely by UNSs and ultrasonographers for 2 Primary Care Trusts serving a population of 300,000. The driver for change was an inability of specialist care teams at secondary care hospitals being able to meet increasing demands for capacity and local care. The transfer of UNSs from secondary to primary care offered an opportunity to provide a new model of care in a primary care setting. A UNS was trained to perform flexible cystoscopy on patients with bladder cancer considered to be at low-risk for recurrence. Training was supervised by a urological associate specialist and after undertaking in excess of 100 supervised flexible cystoscopies, clinical competencies were assessed and approved by a urological consultant. The outcomes of the shift in model included: Shortened wait lists across the board in Urology through increasing the availability of middle grade urology staff. New capacity was generated by freeing up the staff grade urologist s time. This enabled them to focus on meeting other waiting list targets which would be equivalent to two sessions per week. These patients were able to have their procedure performed at their local community hospital, thus saving them a 40 mile trip to an alternate centre 33 Evidence Based Approach to Provincial Urology Services, Healthcare Leadership Conference Deloitte & Touche LLP and affiliated entities.
48 Shared Care Prostate Clinic In the UK a model for a shared care specialist nursing prostate assessment clinic was developed that has since been adopted for benign prostate hyperplasia, prostate cancer, and continence 35. The model started in primary care, involving the GP in the service delivery model. Key components of the model include: A structured referral protocol for use by local GPs A structured interview guide for use in the clinic Nurse-led clinics Specialist nurse sees the patient and completes a full assessment including necessary investigations Results of the assessment are discussed with the urologist and a patient management plan is developed Results of the assessment and plan are shared with the GP After uncomplicated endoscopic prostate surgeries, a nurse-led telephone service follows-up with patients 4-6 weeks after surgery (there is no outpatient clinic visit for these patients. This follow-up is protocol based and designed to assess residual symptoms using a scoring system. The feedback from this change in model has been favourable. GPs are pleased with the access and information sharing and patients are satisfied with the thoroughness of the assessment Deloitte & Touche LLP and affiliated entities.
, BCPRA coordinates all aspects of kidney care related to service delivery, funding, research and education, patient")
49 BC Provincial Renal Agency (BC PRA) The BC PRA is a virtual agency that oversees renal services in the province of British Columbia. Through linkages to other organizations (including the involvement of primary care), BCPRA coordinates all aspects of kidney care related to service delivery, funding, research and education, patient support, and government liaison. A network of committees supports this work. These committees ensure consistency of service delivery standards, use of best practices, and review of outcomes across the province. BC PRA works closely with the five regional Health Authority Renal Programs (HARPs) to coordinate services delivered to patients in eleven hospitals and 24 community dialysis units throughout the province. In addition, provincial guidelines for each HARP have been established to identify the structure and guidelines for establishing renal services 36. As an example, the Fraser Valley Health Authority, with a population of approximately 1.5 million people, provides the following distribution of services for their area: Chronic Kidney Disease Care Centre (non-hospital based offering clinics for patients who have kidney disease but do not require dialysis); Two in-hospital hemodialysis units; Several community hemodialysis units (approximately 4 units); Both peritoneal dialysis (3 sites) and home hemodialysis (1 site) independent programs Deloitte & Touche LLP and affiliated entities.

50 Chronic Kidney Disease Model of Care Western Australia 37 Western Australia issued a model of care for CKD in December The model was developed to address the significant health burden of CKD in Australia. The CKD Model of Care identifies gaps in the current delivery of renal services and provides strategies to improve and integrate service provision for the different stages of the disease. The model emphasises the importance of partnership and collaboration with primary care, community health workers, nephrologists and renal professionals in the management of CKD. Key objectives of the CKD Model of Care are to ensure that renal services are optimally configured to: Prevent or delay the onset of CKD Prevent and slow progression of CKD and its complications, especially end-stage renal disease, heart disease, stroke and peripheral vascular disease Improve the quality of life of people who have CKD Reduce CKD-related presentations to tertiary hospitals An overview of the CKD Model of Care is provided on the right whereby each level of care is supported by a targeted strategy (i.e. primary prevention strategy, early detection strategy, secondary prevention strategy, specialist nephrology services strategy, and dialysis and transplantation services strategy). The model also proposes an approach for integrating primary care and multidisciplinary team CKD clinics which is shown on the following page: Deloitte & Touche LLP and affiliated entities.

51 51 Deloitte & Touche LLP and affiliated entities.

52 Central North Adelaide Health Service (Australia) Renal Model of Care 38 A new model is being designed for the Central North Adelaide Health Service (CNAHS) in Australia that will see the implementation of an integrated hub and spoke approach to the delivery of renal services. The model of care is focused on patient-centered approach including: Healing environment (characteristics such as natural light, controls on noise and temperature); Patient journey (care that is patient-centred, safe, evidenced-based and multidisciplinary in its approach); Clinical teaching and research; Safe environments and safe care; Fostering innovation and best practice; Sustainability. Patients will experience a streamlined service from a highly skilled multidisciplinary team of renal clinical staff, who may attend at any of the sites to meet patient needs. Medical and nursing staff, with allied health staff from some disciplines, will be dedicated to the renal service, working in partnership with other clinical units to meet the range of patients needs. The model has identified a hub site that will provide the most complex services including transplantation service, in-centre haemodialysis, acute inpatient services and a day renal service. Spoke centres will include services for dialysis (including training for home haemodialysis and peritoneal dialysis), hospitalisation for less complex medical conditions and minor or elective procedures, and outpatient clinics. The hub and spoke sites will support a number of community and rural services to provide local support and care for renal patients within and outside the CNAHS region. Services offered in community and rural sites will include post transplantation care, satellite haemodialysis, and outpatient care. 38
53 British Renal Society Workforce Ratios The British Renal Society (BRS), the society that represents all branches of the collective workforce, published a workforce confederation document in The document analyzed the requirement of various professional group requirements (physicians, surgeons, renal nurses etc) and recommended the following workforce ratios for various dialysis treatments. Professional Group Renal Physicians Transplant Surgeons Recommended Workforce Ratios 1 physician per 75 RRT patients (1 FTE per 100 RRT patients) 2 surgeons PMP ( FTE PMP) Donor Transplant Coordinators 1 FTE PMP and 1 FTE per 20 live donor transplants Renal Nurses and Health Care Assistants (HCA) Hemodialysis: 1 FTE per 4.5 patients Skill mix: 1.5 nurses:1 HCA Peritoneal dialysis: 1 FTE per 20 patients Skill mix: 5 nurses:1 HCA Ward based: 1.4 FTE per bed Skill mix: 2.5 nurses:1 HCA Dieticians Hemodialysis: 1 FTE per 135 patients; Peritoneal dialysis: 1 FTE per 270 patients; Transplant patients: 1 FTE per 540 Renal Social Workers 1 FTE per 140 RRT patients Renal Clinical Psychologists 1 FTE per 1000 RRT patients Renal Clinical Technologists Maintenance Hemodialysis: 1 FTE per 50 patients; Home Hemodialysis: 1 FTE per 20 patients Renal Pharmacists 1 FTE per 250 RRT patients Renal Admin & Managers 1 FTE per 150 dialysis patients RRT = Renal Replacement Therapy PMP = Per Million Population Deloitte & Touche LLP and affiliated entities.
54 54 Deloitte & Touche LLP and affiliated entities.
55 Hamilton Niagara Haldimand Brant LHIN Ophthalmology PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
56 Ophthalmology Specific Models of Service Delivery A summary of research into peer practice ophthalmology service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within ophthalmology services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Consideration of Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model enablers suggest several implications for ophthalmology services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having local service delivery because of large patient populations (making critical mass possible) and low technology complexity requirements for clinic based services, supported by central coordination and specialized services. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms. Need to secure and maintain adequate health human resources to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. 56 Deloitte & Touche LLP and affiliated entities.
57 Victorian Ophthalmology Service Planning Framework 40 (Australia) The Victorian ophthalmology service planning framework provides a planning framework for the delivery of public ophthalmology services in Victoria. The framework aims to guide the future provision of care, both in the design of the service system and the development of an appropriate workforce to support it. The service system was conceptualized according to primary, secondary and tertiary service delivery. Primary care is characterized as care provided following self-referral. It includes care provided by community ophthalmologists, general practitioners and hospital emergency departments for conditions such as refractive error, screening for eye health, monitoring of chronic eye conditions, removing foreign bodies and managing conjunctivitis. Secondary care is characterized as specialist care provided following referral from another practitioner, not including highly specialized care which, because of cost, quality or technical issues, is best provided from a small number of service sites. It includes most ophthalmic surgical and medical services, including monitoring and management of cataract, glaucoma, diabetic eye disease and macular degeneration, management of most eye trauma and optometry services provided on referral from another practitioner. Tertiary care is characterized as highly specialized care provided in a limited number of locations following referral from another practitioner. It includes monitoring and managing complicated glaucoma, diabetic eye disease, trauma and complicated and or rare viteo-retinal or other conditions. Smaller hospitals that do not provide ophthalmology services should have access to ophthalmology support and linkages. Elective surgery may be provided in alternate settings to the tertiary site or regional hospital, such as in same day and elective surgery centers or rural hospitals. This framework focuses on the provision of services funded and/or provided by the public sector, although the public sector as a component of an overall service system that has a substantial private component. Innovative Eye Care Centres in Ontario 41 Kensington Eye Institute 42 (Ontario) The Kensington Eye Institute is an ambulatory cataract surgery centre, not-for-profit, corporation licensed under the Ministry of Health and Long Term Care as an Independent Health Facility (IHF). Independent Health Facilities are community-based facilities that provide insured diagnostic and surgical/treatment procedures as part of the publicly funded health care system. Cataract surgery is a relatively simple surgery well-suited to being performed in an outpatient care facility such as Kensington. The Kensington Eye Institute will perform 5,000 new, routine cataract surgeries annually. In addition, another 1,700 annual procedures will be moved to Kensington from Toronto's four acute-care teaching hospitals - University Health Network, Mount Sinai Hospital, St. Michael's Hospital and Sunnybrook and Women's Hospital. Kensington s downtown location will help to meet the needs of the Greater Toronto Area community for improved cataract services. North York Cataract High Volume Centre 43 The Cataract High Volume Centre, a partnership of Markham Stouffville, North York General and Humber River Regional Hospitals, is improving the vision of people in those communities waiting for cataract surgery. Two operating rooms at North York General s Branson site are shared by 17 ophthalmologists from the three hospitals. This collaboration meant standardizing procedures and processes, such as surgical equipment and medication, to enhance patient safety and patient flow Deloitte & Touche LLP and affiliated entities.
58 Perth/Smiths Falls District Hospital Cataract Surgery Model 44 (South East LHIN) This centralized single intake high volume center is intended to increase capacity, reduce wait times, as well as improve efficiencies and patient outcomes. It will reduce the number of patients that need to travel to Kingston for surgery, increasing access to health services for patients living in this area Deloitte & Touche LLP and affiliated entities.
59 Hamilton Niagara Haldimand Brant LHIN Cardiac PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
60 Cardiac Specific Models of Service Delivery A summary of research into peer practice cardiac service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within cardiac services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Consideration of Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model key success factors suggest several implications for Cardiac Services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points, and including linkages with primary care. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms (e.g. exploration of telehealth opportunities for satellite clinics to provide remote consultation in rural areas and standardization of care pathways for multidisciplinary teams to deliver best practice care). Need to secure and maintain adequate health human resources and specialization to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. Maintenance of a central registry for select services (e.g. triaging and monitoring referrals for treatment and rehab) to support service access and population health. 60 Deloitte & Touche LLP and affiliated entities.
61 Australian Resource Centre for Healthcare Innovations Cardiology Model of Care 45 The model of care has been developed by New South Wales Health and seeks to fundamentally redesign major health care systems to ensure that each patient journey is safe and of the highest quality. There are four components to the Cardiology Model of Care 46 : 1. Chest Pain Evaluation: Providing a dedicated area for the evaluation of chest pain patients to provide both better patient diagnosis and management and reduces overcrowding in the Emergency Department. Use of good practice chest pain processes Dedicated staff skilled in cardiac care 12 lead ECG machine and exercise stress test equipment available seven days a week Outpatient chest pain clinics 2. Bed Management (various options) 23-Hr Beds: Dedicated or virtual 23-hour bed availability ensures that there is a continual focus on coordinating the discharge of patients who only need to be in hospital overnight. High-turnover 23- hour beds also free low-turnover inpatient beds for patients who will have a longer length of stay. Hot Beds: Dedicated or virtual hot beds ensure that patients receive immediate and high quality care in order of clinical priority. When high acuity patients can be directly admitted to a Hot Bed under a clearly defined escalation plan this improves the outcome for the patient and reduces stress on both the ward staff and other patients who may need to be moved to create room for the incoming patient. Flex Beds: Flex beds can accommodate patients for a short period of time during peaks in demand. These beds are usually located in close proximity to the cardiology ward or in other wards and are made available during periods of high cardiology activity. Ward by-pass for urban hospital patients transferring between facilitites Co-locating cardiology related beds (i.e. CCU, cardiology inpatient, and cath lab) 3. Innovative Care Practices Some patients receive angioplasty on a day-only basis. This reduces the number of bed days from the traditional 2-3 days and increases the number of available beds. Only patients that fit the guidelines will be eligible for day-only procedures and patients recover in recovery bed for a minimum of 4 hours. Medi-hotels are designed to help people who need to be close to a hospital, but don't necessarily need to stay in a hospital bed. They offer inexpensive accommodation in close proximity to a hospital, with a nurse on-call at all times. These facilities offer patients appropriate communication devices to establish immediate contact with hospital staff in case of emergency. Examples of patient who would access this service include: People who are travelling from rural areas and have appointments at the hospital on consecutive days). Patient recovery in a less clinical atmosphere while freeing up beds within the main hospital for patients who really need them. This has a positive effect on both patient recovery and waiting times. 4. Integrated Chest Pain Management: Details not publicly available.overview of ARCHI Patient Pathways for Cardiology Models of Care Deloitte & Touche LLP and affiliated entities.
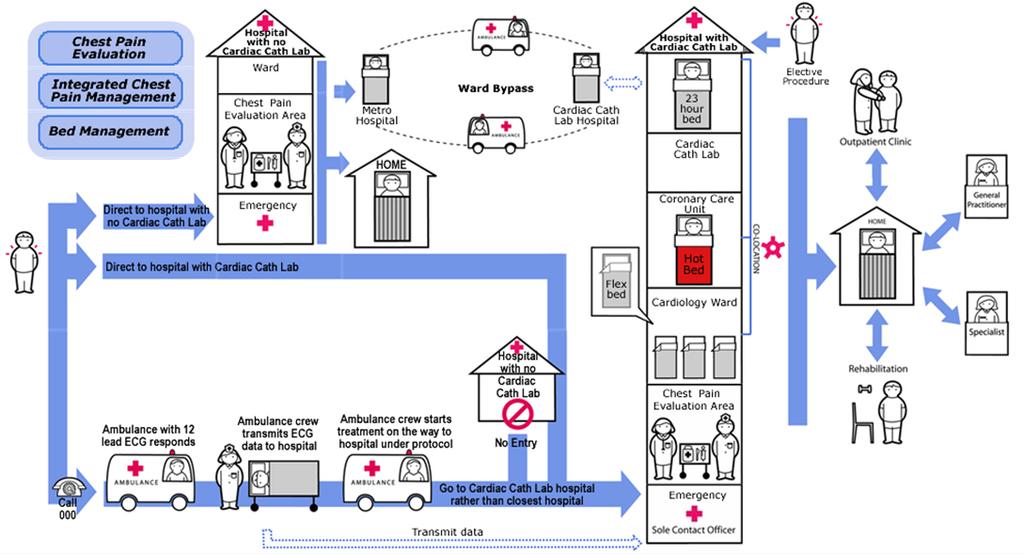
62

63 National Health Service Initiatives (UK) The UK has undertaken a heart improvement initiative to improve cardiac patient pathways and access. Some of the highlights of this work are provided below for review and reference. Referral to Treatment Map The National Health Service (NHS) has developed a care map to identify the flow from referral to diagnosis, intervention, care, and follow-up and rehabilitation 47. The map and the relationships between care points is provided below. Following the map are case study examples of changes that have been made to improve patient access. Introduction to Case Studies Key enablers for all of the case examples was access to and analysis/understanding of data supply, demand, wait-times as well as reviewing of processes to identify redundancies and inefficiencies. As well, in each case patients were involved as part of the review team either directly or through survey feedback to ensure that the process changes were focused on patient needs. One-Stop Cardiology Clinics 48,49 Findings from the implementation of a one-stop clinic from two Health Trusts are provided. The implementation of a one-stop clinic has seen improvements in access to care where wait times for assessment have fallen from 9 weeks to 2-3 weeks. The clinic provides diagnostics, clinical opinion and management plan (with time for the patient to understand and discuss the diagnosis, medication, and treatment options) in one visit. Following the visit, a report is faxed to patients GP within 24 hours. Some of the key learnings from instituting this system include: Primary care will use a specialist referral form if this clearly results in a better service; eader=true& =true&moduletype=forum 49
64 GPs with Special Interest (GPwSIs) trained by their local Cardiologist can manage 50% or more of cardiology referrals (directly - with access to tests - by advising the referrer) and ensure that those who need to see the Cardiologist have rapid access; Systematic triage at the front end of the process can reduce unnecessary appointments leading to reduced waiting times for all patients; Changing the management of referrals from a central system to one where the department administers their own referrals was an essential step in developing triage systems to manage demand and cut waiting times; Triage of referrals by a cardiac technician identifies more than one in four referrals as suitable for test only (this is endorsed by experience of GPwSIs in the community); Triage of referrals by lead nurse for rapid access chest pain clinic (RACPC) can identify all referrals that meet the criteria for RACPC (approximately one in three referrals); Diagnostic tests are arranged for on the same day as the clinic visit (or in advance for 7 day event monitoring, etc.); Reducing follow-up appointments (from having care plans developed in the initial visit) has reduced the number of no-show appointments; Addressing letters containing management plan to patients (copied to GP) is both doable and popular with patients and GPs. Reduction of Waiting Times from Referral to Cardiac Surgery 50 The South West London Cardiac and Stoke Network undertook a project to reduce the average time from referral to treatment from 32 weeks to 11 weeks. The key components of this reduction related to better access to diagnostic tests and clinic appointments (as outlined in the section above). Process changes that were put in place to impact this change include: Introduction of an electronic elective cardiac referral form with a defined minimum data set; Improvements in access to diagnostics and clinic assessments (as identified in the section above); Sharing of electronic clinical data across institutions; Patient education materials were developed to inform patients of the process and involve them in care; Multi-disciplinary team meetings were revised to increase information sharing and thereby reducing the need for patient follow-up visits. Introduction of a 24/7 Cardiology Service 51 In one of the NHS Trusts (East Lancashire Hospitals) cardiology service was shifted from two sites to one in order to increase efficiency and overall coverage. Before the change there were 3 cardiologists (2 who did not participate in call rotation), 45 cardiology beds, and 12 CCU beds. With the reorganization of services, 3 new interventional cardiologists were recruited for a total complement of 6 cardiologists, and beds were reduced to 26 inpatient beds and 10 CCU beds. To support more timely patient care, 24/7 coverage was implemented (with daily ward rounds), with all 6 cardiologists providing call coverage. The trust considers the change a success. The average length of stay has decreased from 9 days to 6, creating more system capacity eader=true& =true&moduletype=forum 64 Deloitte & Touche LLP and affiliated entities.
65 Connected Cardiac Care for Heart Failure Patients 52 Massachusetts General Hospital has implemented a care model to reduce hospital re-admissions by heart failure patients. This program uses tele-monitoring to monitor patients heart rate, blood pressure, blood oximetry, weight and symptoms on a daily basis. Using this information, each patient's physician establishes parameters for which alert levels are set and a tele-monitoring nurse reviews the information with interventions as necessary. Overall the system serves to better educate and engage patients in their health care. Patients better understand the links between their daily life and their disease, and they are enabled to coordinate care with their physician when necessary. Cardiac Care Network (Ontario) Cardiac Surgery Perspectives 53 The Cardiac Care Network (CCN) believes that cardiac services in Ontario needs to be viewed and organized as not only a network of independent clinical programs, but also as a single integrated virtual program, with a greater degree of province-wide planning and management. The CCN s proposed large virtual program, would retain the mandate and ability to respond to local needs (as well as the benefits of healthy competition between programs), but would allow the system as a whole to deal more effectively with many of the current challenges. In particular, greater overall capacity within this integrated model provides more flexibility to deal with rapid shifts in the nature and volume of clinical activity. The chart below shows the current distribution of centres and services throughout the province 54. The virtual program vision would work to establish further integration and standardization across these programs. LHIN Centre Catheterization Angioplasty Surgery Erie St. Clair Hotel-Dieu Grace Hospital (Windsor) Development South West London Health Sciences Centre Waterloo Wellington St. Mary s General Hospital (Kitchener) Hamilton Niagara Haldimand Brant Hamilton Health Sciences Corporation General Campus Central West William Osler Health Centre Mississauga Halton Toronto Central Trillium Health Centre Toronto East General Hospital St. Michael s Hospital Sunnybrook Health Sciences Centre University Health Network Deloitte & Touche LLP and affiliated entities.
66 LHIN Centre Catheterization Angioplasty Surgery Central Southlake Regional Health Centre (Newmarket) Central East Rouge Valley Health System Centenary (Toronto) Peterborough Regional Health Centre South East Kingston General Hospital Champlain University of Ottawa Heart Institute North Simcoe Muskoka North East North West None Sault Area Hospital Sudbury Regional Hospital Memorial Site Thunder Bay Regional Health Sciences Centre The CCN has highlighted a series of issues and policy options for further consideration, some of which have relevance to the service delivery planning process of the HNHB LHIN and have been provided below for consideration. Enhance integrated provincial planning and monitoring Coordinate volume planning for interventions and practitioners to ensure quality outcomes Collaboration between centres for technology evaluation and adoption Coordinated administrative structures at the hospital and LHIN level including cardiology, cardiac surgery, and vascular surgery to better promote share responsibility in patient care Coordinated human resource planning across organizations and disciplines including ICU, ORs, perfusion, anaesthesia, surgeons, and interventionists Calgary Health Region Approach to Cardiac Services The Calgary Health Region (CHR) has a mix of centralized and decentralized services in their cardiac program. Key highlights on the service delivery model include: Centralization of quaternary services at one site. Plan to consolidate CCUs from three sites to one. At those sites where the CCU will be closed, units will be converted to chest pain units with specialized training provided for staff. Increased delivery of ambulatory care services over the past three years. Plans to implement a shared care model linking congestive heart failure and primary care. Initial work indicates that such a shared care model will decrease hospital admissions. Organizational structure includes the division of imaging in the cardiac services program. 66 Deloitte & Touche LLP and affiliated entities.
67 Central East LHIN Future Cardiac Service Model 55 The Central East LHIN has recently undergone a clinical services planning exercise and selected a cardiac services model that will see services provided in two clusters (districts). At the district sites, interventional cardiology services will be provided while at local facilities core emergency-related and non-interventional diagnostics will be offered. Cardiac rehab services will be provided using a hub and spoke approach. The intended outcomes of these shifts include: Equitable, timely access; Increased collaboration within a LHIN-wide network and strengthened relationships between clinicians; Enhanced quality of care and adoption of evidence-based practice; Sharing of expertise throughout the LHIN; Clear definition of each hospital s role as part of an overall LHIN-wide cardiac program; enables sites other than PRHC and RVHS-Centenary, to define their niche role within the cardiac service model; As rehabilitation services are not physician-based programs, clusters are able to lead program through multi-disciplinary rehabilitation roles equitably distributed across the LHIN. Primary Care Model of Cardiac Rehabilitation (Australia) 56 Given the low uptake of conventional rehabilitation programs and the inaccessibility of programs in rural and remote areas the Northern Queensland Rural Division of General Practice and the Townsville Division of General Practice in Australia have developed a primary care cardiac rehabilitation program. Under this model, the patient s rehabilitation is supervised by their GP, delivered on a one-to-one basis. The program incorporates a home-based walking/exercise program, with educational support delivered through written patient education modules. For the first two months post discharge patients visit their GPs every 1-2 weeks to monitor progress. After the two months, ongoing review intervals are determined by the patient and GP. To support GPs in this model, the following steps were taken: Information sessions for GPs outlining the benefits of cardiac rehabilitation, structure of the primary care program, and guidelines for management. GP prompt card outlining CVD risk factors and guidelines for management; and Development and production of patient education resources addressing recovery issues, exercise, and medication. Outcomes of the program have been positive with a higher level of participation in cardiac rehab programs and noted changes in lifestyle risk factors MHA_Posted_March_27_2009.pdf Deloitte & Touche LLP and affiliated entities.
68 68 Deloitte & Touche LLP and affiliated entities.
69 Hamilton Niagara Haldimand Brant LHIN Respiratory PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
70 Respiratory Specific Models of Service Delivery A summary of research into peer practice respiratory service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within respiratory services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Consideration of Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model key success factors suggest several implications for respiratory services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having local service delivery because of large patient populations (making critical mass possible) and low technology requirements for clinic based services, supported by central coordination and specialized services. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points and with primary care. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms. Need to secure and maintain adequate health human resources to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. 70 Deloitte & Touche LLP and affiliated entities.
71 Chronic Obstructive Pulmonary Disease (COPD) Model of Care (Western Australia) 57 The COPD Working Group was formed to review the implementation of the Western Australia Chronic Respiratory Disease Clinical Services Improvement Framework 58 which sets out standards for COPD service provision in Western Australia. This working group built on the initial review to develop a model of care for COPD, including the following key recommendations. Develop a statewide coordinated prevention plan to reduce smoking prevalence Increase access to spirometry Improve access to appropriate services with a focus on self management, exercise training and COPD action plans by: expanding the range of community-based ambulatory services developing integrated referral pathways and protocols to guide access to appropriate service delivery Build on ambulatory care services to reduce the risk of acute exacerbations and avoidable hospitalizations Develop a model of service delivery for end of life and palliation Enhance the capacity of the community-based health workforce through the expansion of multidisciplinary teams Support the development of information and communication technology including clinical support services, telehealth and database sharing An Integrated Model of Care for COPD (Australia) 59 A group from the Prince Charles Hospital Health Services District (PCHHSD) reviewed the ideal features of an effective model of care for chronic conditions through the COPD and chronic disease management literature to develop an integrated model of care for COPD. Key findings of this work included: Core interventions offered in integrated COPD services include pulmonary rehabilitation, smoking cessation clinics, individual COPD education and self-management plans; Common additional services include hospital in the home (HITH), respiratory outreach services, maintenance pulmonary rehabilitation and case management; Rapid access to specialist outpatient clinics can successfully reduce avoidable admissions, particularly in conjunction with outreach services, HITH or case management; Tools and strategies that enable timely communication of patient information between all health team members are vital to the success of an integrated care service; Importance of self-management plans; All successful respiratory services with an integrated model of care have a clinical champion - a physician with clinical and research expertise in COPD leading change in service delivery. The integrated model of care developed comprises three phases: 1. Establishment This phase may last between one and eight weeks and aims to: f Deloitte & Touche LLP and affiliated entities.
72 Complete a detailed assessment of the patient's disease severity, complications, functional status and their ability to manage their condition; Enable access to all COPDX-recommended interventions as appropriate to the patient's current needs and preferences. 2. Maintenance For the majority of patients, the maintenance phase is where they will spend most of the time. The aim of this phase is for prospectively planned and integrated reviews of the patient's progress towards their goals and clear communication of assessments, interventions and outcomes to all members of the care team including the patient. Appointments with different members of the care team are timed strategically to maximize support, minimize duplication and enable the implementation of an integrated ongoing plan of care. Aspects to be reviewed regularly include: Spirometry, complications, quit status of current and recent ex-smokers, and functional status; Actions taken by patient as part of a care plan (exercise, diet, medication, oxygen); Coping skills, knowledge, quality-of-life and self-management skills; Self-management plan; Patient's progress towards their goals. All patients are expected to have a GP as their primary medical care provider, but in addition, those with higher disease impact will have some or all of the following in their maintenance care team: community health nurse, community or acute care-based allied health professional, respiratory specialist, respiratory nurse. Patients who have been referred to the community health nurse COPD program receive structured home visits post discharge from hospital and ongoing maintenance visits or phone support as required. For those with severe COPD who frequently use inpatient or emergency department services, the community-based respiratory nurse will function in the role of care coordinator with the aim of providing regular and as-needed access to intensive support to improve quality of life and promote more appropriate resource usage. 3. Transition The transition phase describes the period of time where the patient experiences an increase in the intensity of care required due to an exacerbation of COPD. The emphasis of this phase is on the recognition of the early signs of exacerbation by the patient/carer and prompt action as described in the self-management plan. Rapid access to the appropriate level of assessment, interventions and support quickly follows patient-initiated changes to medications as per the plan. Assessment may take the form of GP review, community health nurse home visit, rapid access to respiratory specialist obstructive pulmonary disorder clinic or emergency department and review depending on the previous plan and the severity of current symptoms. Supportive interventions may include one of the following: Community care - more frequent community health nurse visits, GP review and extra medications; Hospital admission - usually 6-7 days; Hospital in the home service - daily to second daily respiratory nurse home visits; Brief hospital admission of 2-3 days with supported early discharge. Patients with COPD who are admitted for hospital-based acute care are referred to the community health nurse COPD program before discharge. They receive structured home visits post discharge with the aim of assessing progress and reinforcing the education provided while in hospital. The transition phase continues through to recovery (2-6 weeks later), where the patient re-enters the maintenance phase after baseline care requirements are reassessed and their self-management plan is re-established. 72 Deloitte & Touche LLP and affiliated entities.
73 Somerset Integrated COPD Service (UK) 60 The vision of the integrated COPD service in Somerset is to establish a model of care built around the needs of patients with a focus on: Improving the patient experience in terms of access and convenience Seamless care pathways based on best evidence Steering the correct patient towards pulmonary rehabilitation, oxygen therapy or exacerbation care as appropriate Reducing unplanned admissions to hospital wherever possible Enabling planned early discharge Measurability in terms of patient outcomes and value for money Working within the wider health and social care environment, as well as with the patients, their carers and support groups Building on the relationships and expertise of the local Acute Trusts, the Hospice, South Western Ambulance Service, Social Services, the Acute Care GP service and Somerset Primary Link. In order to achieve the vision the patient will need to access different elements of service whenever and wherever needed. The following table aims to describe the key themes of each of the elements of the management program. Service Element Key Features Availability (opening hours) Assessment Clinics Pulmonary Rehabilitation Urgent Response Unscheduled Rapid Support Case Management Routine assessments of chronically stable patients Therapy review Management plans Oxygen assessment and management Nebuliser assessment and management Structured programme of exercise and education 2 x 2 hour sessions per week Venues selected according to patient need Combination of group and 1:1 support Rapid response service, based in the community for those patients who become unwell. Telephone access 24 hours per day Triage and urgent assessment Home visits Therapy maximisation Admission avoidance Flexible service that enables an unscheduled response for: Unplanned assessment Early discharge assessment and management Home visits Monday to Friday, 8 hours per day (between 8:00 and 20:00) Alternating between a range of venues across the country Monday to Friday with occasional Saturday access Concurrent programs to cover both East and West 24 hours a day, 365 days a year Initially available Monday to Friday, 8 hours per day (between 8:00 and 20:00) Deloitte & Touche LLP and affiliated entities.
74 This new team, which will consist of a combination of Respiratory Nurse Specialists, Community Respiratory Nursing, Physiotherapy, and, where appropriate, Respiratory Technicians and will be community based and work in conjunction with the existing program teams. Manchester Primary Care Trust COPD Services in the Community 61 The Manchester Primary Trust is looking to expand COPD services in the community in order to address gaps that were identified through the development of a Level of Care model. The main objectives of the community services for COPD are to: Deliver improved services and health outcomes for patients ensuring an integrated approach to both acute and chronic disease management across Central Manchester s health community. Avoid admissions to hospital Improve service consistency, delivery and access for patients with COPD in a cost-effective manner. Assist with the current secondary care early discharge programs for patients with COPD who can be managed in a community setting with the assistance of a professional multidisciplinary care team. The key foci for community services to support the model include: A nurse-led COPD clinic / outreach service including acute exacerbation assessment and management and clinical governance of diagnostic testing in primary care Pulmonary rehabilitation (8 week rolling program) Community oxygen assessment clinics Intermediate care programs Active case management Pharmacy support Smoking cessation and dietary support Palliative and end-of-life care services Support groups and expert patient groups St. Mary s Chest Program (Kitchener) 62 The Chest Program s Activation/Reactivation approach has been recognized provincially as an innovative approach to the care of patients with COPD. The intensive 3 week outpatient program provides education, smoking cessation, nutrition counselling and exercise to patients with COPD. Patients are also provided with an action plan that will help them maintain or improve their quality of life. The program also offers: An Airway Clinic an outpatient education and rehabilitation service for patients with asthma or chronic obstructive pulmonary disease (COPD). The Short-Term Rehabilitation Unit (STRU) for patients who no longer require the care of an acute setting Deloitte & Touche LLP and affiliated entities.
75 Adult Asthma Care Management Program 63 The Asthma Care Management Program is a special Kaiser Permanente program designed to provide patients with the highest quality of care. The program identifies a personal care manager for each patient (a specially trained nurse, respiratory therapist, or clinical pharmacist) who works in partnership with the patient and GP to optimally manage asthma care. The asthma care manager works with patients for up to six months. Initial visits are in person and follow-up visits, in most cases, can be done by telephone. At each visit, the patient and care manager will assess asthma control. Patients work with care managers to better manage symptoms; monitoring peak flows and asthma symptoms; making the best use of medications; and managing asthma flare-ups. This approach has produced positive results reducing health care costs and emergent needs for health services. Asthma Management in Australia 64 In Australia the Asthma Management Service (AMS) has developed a model of care where nurse provide education and doctors oversee review in order to improve patient outcomes. Patients are referred to AMS by their GP or from an inpatient admission. The initial visits includes a one hour review with a nurse educator. Following the initial visit there are follow-up visits with the nurse educator (30 minute sessions) and physician for 2-3 more visits. After completing the program patients are discharged to the care of their primary provider. Nurse Role in Clinic Physician Role in Clinic Provision of Education Assess Control: Symptoms, FEV1 and Peak Flows Assess patients willingness and ability to self manage and provide self management support Assess and Correct Skills o Inhaler Technique o Self Monitoring o Written Action Plans o Adherence o Knowledge of Medications o Trigger Avoidance and Management Optimize medical management Assess control and change treatment according to response Prescription of written action plan Paediatric Asthma Care Models The website details the efforts of 14 research teams across the United States who are working to change the outlook for children with asthma through programs that range from communitybased coalitions to new reimbursement models in Medicaid managed care and provocative emergency department interventions. Summaries of three case studies are provided below to highlight some of the key components included in the models of care delivery. Medicaid Managed Care Deloitte & Touche LLP and affiliated entities.
76 The Affinity Health Plan program in the Bronx focused on early detection of asthma and prompt intervention. To reduce inpatient services and emergency department visits, strategies were implemented to identify and stratify children with asthma at key times: when they first enrolled in Affinity or after receiving inpatient or emergency department services. After identifying the patients, case managers taught them self-management techniques. Primary care providers were trained using a case-based interactive program entitled The Asthma Dialogues. Results of this initiative showed a significant reduction in costs for paediatric asthma care services, a decrease in inpatient utilization, and a drop in emergency room visits by 400%. Community Coalitions 66 The Fight Asthma Milwaukee Allies (FAM Allies) is a US wide group that brings together community-based agencies and individuals to work as a coalition to improve quality of life for children with asthma and their families. Strategies and programs the group has implemented include: Care coordination and case management: Developed a standardized protocol to assess the needs of children with asthma in their homes. Programs include the Milwaukee Healthy Homes Demonstration Project and Emergency Department Allies research study. Clinical quality improvement: Designed programs for health care providers who diagnose and treat asthma. Programs include Physician Asthma Care Education (PACE) seminars for primary care physicians and nurses treating asthma. Family and community education (some programs provided in Spanish and English): Provided programs and training sessions to help people in the community and schools understand and manage asthma. Programs include Asthma Basics for Schools, Asthma Care at Childcare and Asthma 101 for community members. Emergency Department Models 67 Improving Paediatric Asthma Care in the District of Columbia (IMPACT DC) uses families familiarity with the emergency department (ED) as a site of care to recruit them into a program that provides asthma education and encourages families to seek a long-term relationship with their primary care provider. Within two weeks after an asthma-related ED visit, patients return to the IMPACT DC Asthma Clinic where they are taught both medical and environmental management of asthma. The follow-up clinic operates within the ED itself and also at a community site within an area of high pediatric asthma prevalence. IMPACT DC also works with school nurses and local organizations to provide necessary equipment, smoking cessation education, tenant advocacy, outreach and home visits. The program showed results in changes to lifestyle behaviours and awareness for environmental triggers that cause asthma flare-ups as well as a reduction in unplanned visits to the ED Deloitte & Touche LLP and affiliated entities.
77 Hamilton Niagara Haldimand Brant LHIN Ear, Nose, and Throat PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
78 Ear, Nose, and Throat Specific Models of Service Delivery A summary of research into peer practice ear, nose, and throat service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within ear, nose, and throat services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Consideration of Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model key success factors suggest several implications for ear, nose, and throat services that can serve as an input into PAG planning. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points. This may be enabled by shared patient information where feasible (e.g. from ENT surgery to oncology services). Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms (e.g. implementing standardized clinical assessment tools and care plans that can be individualized). Need to secure and maintain adequate health human resources and specialization to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. 78 Deloitte & Touche LLP and affiliated entities.
79 Victorian Ear, Nose and Throat Service Planning Framework 68 (Australia) The Victorian ear, nose and throat service planning framework provides a planning framework for the delivery of public ear, nose and throat (ENT) services in Victoria. The framework aims to guide the future provision of care, both in the design of the service system and the development of an appropriate workforce to support it. The service system was conceptualized according to primary, secondary and tertiary service delivery. Primary care is provided by general practitioners, hospitals emergency departments, audiologists and other allied health care professionals following patient self-referral. Secondary care is specialized care following referral from another health care practitioner. It does not include highly specialized care, which, because of cost quality or technical issues is best provided at a smaller number of service sites (i.e. tonsillectomy requires secondary care). Tertiary care is highly specialized care provided in a limited number of locations, because of cost or quality reasons. Tertiary care follows referral from another health care practitioner (i.e. cochlear implants). Smaller hospitals that do not provide ENT services should have access to ENT support and linkages. Elective surgery may be provided in alternate settings to the tertiary site or regional hospital, such as in same day and elective surgery centers or rural hospitals. Fraser Health Authority 69 Model of Care Delivery The Fraser Health Authority in British Columbia uses a hub and spoke service delivery model where ENT is performed at four of the twelve centers and specialized outpatient clinics are located in one center. Elective day care surgery is performed in community hospital in the Fraser Health region. Based on both the Fraser Health experience and the Australian experience above, key considerations for successful service delivery of a comprehensive ENT surgical program include: For tertiary level services: (1) Access to specialised physicians and staff for the continuum of care; (2) Designated diagnostic clinics with appropriate resources and access to state of the art diagnostic imaging (e.g. MRI and Nuclear Medicine); (3) Access to critical care units and specialized clinics; (4) Availability and access to telemedicine for consultations for rural and remote patients; (5) Practice in an atmosphere of scientific inquiry, analyzing surgical practice for ways to improve through research. In addition, core ENT services considerations include: (1) Access to specialized secondary services such as oncologists; (2) Accepted and clear provider referral pathways; and (3) Provisions for airway management and other core services Deloitte & Touche LLP and affiliated entities.
80 ENT Care Model Development (UK) 70 The Hartlepool Primary Care Trust and the South Tees Acute Hospitals worked to develop a multi-disciplinary model of care focusing on services delivered in a community or primary care setting. The main areas of focus for the model include a clinical assessment / triage approach and strong partnership approach with local service providers. Specialist Care Primary/Community Service First Contact Self Care Patient with symptoms Patient presents with symptoms Patient referred to primary care ENT service Referral assessed by multidisciplinary team Self care Diagnostics MDT decision about suitable service Audiology led clinic Nurse clinic Consultant clinic Diagnostic procedure at clinic Treatment delivered/ prescribed at clinic Patient requires follow up Admission for treatment required Patient attends specialist care outpatient appointment Choice offered Patient placed direct on theatre list 70
81 Audiology Service Provision (Surrey, UK) 71 Within Surrey (UK) audiology services are provided by hospitals, community providers, health units, and independent providers. Across these groups a range of services including: GP direct referrals generally for people over the age of 60 who have age related hearing loss. Patients are provided with hearing aid assessment and fittings GP referrals to an ENT specialist, including the following: (1) Hearing aid referrals (2) Vestibular assessments and rehabilitation (3) Tinnitus support (4) Otoacoustic emissions (very faint sounds inside the ear) (5) Speech tests (6) Hearing assessments within an ENT outpatient clinic Referrals from other healthcare professionals e.g. Neurology, physiotherapy, speech and language therapy. Paediatric service, including onward support following new born hearing screening program m%206%20-%20audiology%20update.pdf
82 82 Deloitte & Touche LLP and affiliated entities.
83 Hamilton Niagara Haldimand Brant LHIN GI/Hepatobiliary PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
84 GI/Hepatobiliary Specific Models of Service Delivery A summary of research into peer practice GI/hepatobiliary service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. oncology or paediatrics). We recognize that there are other areas within GI/hepatobiliary services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Consideration of Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model key success factors suggest several implications for GI/hepatobiliary services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having local service delivery focusing on patient self-care where applicable supported by central coordination and specialized services. Benefit in having one or more centre(s) of excellence which can provide tertiary services, support for staff training, resources for clients and staff, and leading practices through academic affiliations and new technologies. Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points, and including linkages with primary care. This may be enabled by shared patient information where feasible. Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms (e.g. standardization of care pathways for multi-disciplinary teams to deliver best practice care). Need to secure and maintain adequate health human resources and specialization to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery. Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. Maintenance of a central registry for select services (e.g. triaging and monitoring referrals for treatment) to support service access and population health. 84 Deloitte & Touche LLP and affiliated entities.
85 Care of Patients with Gastrointestinal Disorders in the UK 72 In 2006, the British Society of Gastroenterology issued a report that defined a strategy for the future of GI related services in the UK. Some of the overarching perspectives shared with regards to service delivery included: Keeping Care Close to the Patient There is good evidence that patients with chronic diseases such as inflammatory bowel disease or irritable bowel syndrome can manage themselves with fewer hospital or General Practitioner appointments if they are given enough education about their condition, including how to cope with the physical, emotional and social implications, and are supported by expert services that they can easily access. High quality gastrointestinal services should be delivered locally wherever possible. There should be closer integration between primary and secondary care with the development of care pathways and models of care for chronic diseases. Centralization of Complex Services Centralization of some services is essential, (e.g. complex liver disease, liver transplantation, complex hepato-biliary and pancreatic disease and home TPN). However, in other areas there is a need to balance the loss of surgical expertise (from managing care centrally) with the need to maintain surgical skills to manage non cancer surgery. It is crucial that the required levels of skill and expertise are maintained at a secondary level to provide the optimal care required in management of emergency gut, liver and pancreatic problems. As part of this report a number of service model recommendations were made for specific clinical areas including: Functional Gastrointestinal Disorders (FGID) The vast majority of patients with FGID are managed in primary care. A smaller number are referred to secondary and tertiary care. Thus, the report recommends integrated service provision at the level of primary care with emphasis on a multidisciplinary approach to management of patients with FGID. Referral to secondary/tertiary care might be for clarification of diagnosis and formulation of a management plan or for management of rare complex disorders As in other specialties (including Inflammatory Bowel Disease in gastroenterology), there is emerging evidence that self management of patients with FGID has distinct advantages. Inflammatory Bowel Disease (IBD) Patient-centered care for IBD needs different approaches at different times within the life-long disease. No single model is appropriate for all patients all the time. Choice between three approaches is appropriate: hospital care, shared-care with primary care and assisted self-managed care. Close liaison between primary and secondary care is facilitated by General Practitioners with a Special Interest (GPwSIs) if these independent practitioners have formal links (such as joint meetings, endoscopy session, or parallel clinics) with secondary care. Within secondary care, parallel clinics between medical gastroenterology, dietetics and colorectal surgery that focus care on patients with IBD should be the norm. An IBD multi-disciplinary team meeting should have similar priority to the cancer MDT but should take place separately. Tertiary provision for an adolescent transition clinic should be established, to facilitate management of adolescent IBD and transfer of patients from paediatric to adult gastroenterology services at the age of 15-17years old Deloitte & Touche LLP and affiliated entities.
86 Hepato-Pancreato-Biliary Surgery (HPB) There are four groups of hospitals providing services for disease. All hospitals including district general and university-associated hospitals treat common conditions such as gallstone disease, uncomplicated acute pancreatitis, and are involved in the initial assessment of patients with HPB disease. A few hospitals have more expertise and undertake some HPB surgery in addition to the above but are not specialized pancreatic centres and may not be associated with a Hepatology Centre. Teaching hospitals with a major interest in HPB disease, but who do not undertake liver transplantation (approximately 8-10 such units in the UK). Each of the units will be a designated HPB or Pancreatic Centre. The teaching hospitals who also undertake liver transplantation in addition to the above. Endoscopy To improve service delivery, the report recommends: Implementing communal waiting lists across centres Use of non-medical, trained endoscopists to deliver basic diagnostic services. Use of Global Rating Scale to assess the quality of the service being offered. The UK Global Rating Scale (GRS) has several appropriateness indicators requiring locally agreed written referral guidelines for all diagnostic, therapeutic and recall (surveillance) procedures performed in the unit, including open access 73 Endoscopy Global Rating Scale P 1 2 The patient experience 2 dimensions: clinical quality & quality of the patient experience patient centred items Each item has four levels A-D (descriptors) D C B A Each level is underpinned with 1-5 measures Clinical Quality 1. Appropriateness 2. Information / consent 3. Safety 4. Comfort 5. Quality of the procedure 6. Timely results Quality of Patient Experience 7. Equality of access 8. Timeliness 9. Choice 10.Privacy and dignity 11.Aftercare 12.Ability to provide feedback to the service Deloitte & Touche LLP and affiliated entities.
87 Areas for Specialization in Hepatology, Hepatobiliary and Pancreatic Surgery The Department of Health in the UK has undertaken work to define specialized services for hepatology, hepatobiliary and pancreatic surgery 74. In their definitions they include the following four areas: 1. Specialized services for the treatment of patients with viral hepatitis The focus in this area is to provide diagnosis, treatment and structured follow-up of patients with acute and chronic hepatitis due to hepatitis viruses A, B, C, D and E. Essential elements of the service will include hepatologists or in some centres infectious diseases specialists, specialist hepatitis nurses/nurse consultants, dedicated liver histopathology services and appropriate virology services. 2. Specialized services for patients with acute liver failure and advanced complications of cirrhosis Most early complications of chronic liver disease will be managed by locally commissioned services, however, more advanced or complex cases require specialist multidisciplinary expertise involving hepatologists, HPB surgeons, pathologists and radiologists. Care for these patients should be provided in coordination with specialist liver centres. 3. Specialized services for patients with benign and malignant liver tumours and cancer of the intra and extra hepatic biliary tree (including pancreas) The overall aim of a specialized service for the management of patients with HPB tumours is to provide accurate diagnosis and staging and appropriate individually tailored treatment. Ideally this should be delivered by an integrated multidisciplinary team consisting of HPB surgeons, hepatologist(s), radiologists, oncologists, radiotherapists, anaesthetists, intensivists and dedicated liver pathologists experienced in the management of these patients. 4. Specialized hepatobiliary and pancreatic surgery services The other major area of specialist hepatobiliary surgery (outside of those identified above) is the interventional management of bile duct strictures including iatrogenic. The complex reconstructive surgery required for these patients requires extensive specialist experience and should only be undertaken in designated centres. The management of severe acute pancreatitis, which requires a multidisciplinary approach, and to the surgery of chronic pancreatitis (e.g. total pancreatectomy, radical lymph node dissection, and Whipple procedure) should also be designated to specialized centres. Even though each unit should be clear about the conditions it is recognized to treat, each service should function as part of a clinical network to achieve maximum effectiveness. In many cases advice from a specialist centre will be sufficient to enable local treatment to be progressed. Unless a robust clinical network is in place scarce skills and resources will not be used to maximum effect and patients will not receive optimal care. This will need to be taken into account in future service planning. Colorectal Screening in Ontario The ColonCancerCheck program is the first province-wide, organized screening program designed to raise screening rates and reduce deaths from colorectal cancer 75. The program provides funding to screen all average risk adults 50 years and older for colorectal cancer using the Fecal Occult Blood Test (FOBT) every two years, and to screen those at increased risk with colonoscopy. The introduction of this program also has implications for service delivery models and resourcing. Recognizing the increase in referrals, and increased capacity for endoscopy, HealthForce Ontario has introduced a new nurse endoscopist role to provide additional capacity for the system H_ Deloitte & Touche LLP and affiliated entities.
88 Dedicated Gastrointestinal Cancer and Wellness Centre The Jay Monahan Center for Gastrointestinal Health at the New York Presbyterian Hospital is one of only a few comprehensive cancer and wellness centers in the U.S. exclusively dedicated to gastrointestinal health 77. The Center offers an array of services, from prevention and early detection to treatment, research, education and community outreach. Unique aspects of this program include: Gastroenterologists, oncologists, and surgeons meet with patients in one single setting to coordinate all aspects of patient care and patients and families have access to social workers, genetic counsellors, and nutritionists. There is no waiting room. Instead patients and families wait for their appointments in the education center, where they can access the internet, books, brochures, and videos for the latest information on gastrointestinal health, prevention, and treatment. An on-site education coordinator is available for patients and families to provide one-on-one assistance with accessing information on screening, treatment, clinical trials, and education and support programs. The Center promotes education on prevention, screening, and the latest advances in cancer treatment for its patients and families, the general public, and other health professionals, both locally and globally. Through its education and outreach initiatives, the Center focuses on the promotion of early screening, knowledge of the latest in cancer treatment, and access to clinical trials. The Center offers a comprehensive website and video library dedicated to the promotion of gastrointestinal health and gastrointestinal cancer treatment, care, and support Integrating Gastrointestinal and Endocrine Clinical Networks (Australia) 78 In Western Australia, there is an initiative to establish a Gastrointestinal and Endocrine Clinical Network. While it is recognized that there is minimal overlap between the gastrointestinal and endocrine areas in terms of tasks and procedures that clinicians undertake, there is however significant overlap in terms of what is happening for patients and community issues and concerns. There is also synergy in terms of shared lifestyle risk factors and the methods and strategies that are employed to modify them. This model emphasizes the growing trend to examine health care service delivery from a patient-focused perspective scussion.pdf 88 Deloitte & Touche LLP and affiliated entities.
89 Hamilton Niagara Haldimand Brant LHIN Mental Health PAG Service Delivery Model Review April, Deloitte & Touche LLP and affiliated entities.
90 Mental Health Specific Models of Service Delivery A summary of research into peer practice mental health service delivery models is presented below. Models have been selected based on a review of forward-looking service delivery practices in other jurisdictions and models identified by advisory groups. The models presented below provide an overview of areas where service delivery models have been developed and documented, and are not intended to limit the PAG in terms of focus. In some instances, models also highlight where there are linkages to other PAGs (i.e. paediatrics). We recognize that there are other areas within mental health services that are not included in the models provided; for these areas PAG members will be asked to provide insight into the most appropriate service delivery models for the LHIN. Models presented are intended to give insights into the options and principles other health organizations are using to coordinate clinical service delivery. For each model, a summary of the key attributes of service delivery along the continuum of care and outcomes achieved is provided as available. Literature or web-based references are also provided, so that PAG members may obtain additional information. Consideration of Key Success Factors As the PAG plans future service delivery models for the HNHB LHIN, it will need to reflect on several inputs including items outlined in the PAG guide, in addition to the enablers and barriers to service delivery that must be considered for implementation. Insights gained from the peer practice service delivery models identified on the following pages as well as general service delivery model key success factors suggest several implications for mental health services that can serve as an input into PAG planning. Recognition for the need to plan for services from health promotion and prevention through to management in acute care using a coordinated system of access across providers. Services are most successful when they are focused on the patients needs and adding value from a patient s perspective (and not being provider focused). This may be facilitated through shared care relationships where the patient / family is a recognized member of the care delivery team. Benefit to having local service delivery with specialized support services. Need for accountability agreements between sites regarding acceptance/transfer of patients and repatriation, not only within between regions, but amongst all hospitals Being mindful of equitable access and locating services strategically to minimize the impact of distance on patient access to services. Need for adequate community resources to support clients in their communities. Access to tele-health for rural and remote patients for education and consultations. (e.g. tele-visiting for families who have to be separated). Need for standards of practice and role clarity in provider responsibilities within the service model to help improve care coordination across the continuum, improves the patient experience, and provides accountability. This includes identification of multi-directional provider flow across urban and rural centres, where appropriate and establishing effective relationships between adult and paediatric psychiatrists to manage paediatric and adolescent population Need to develop standardized assessments, protocols, order sets and terminology consistently applied throughout the LHIN Benefit in having one or more centre(s) of excellence which can provide support for staff training, resources for clients and staff, and leading practices through academic affiliations and new approaches. Establishment of communications and feedback loops for program evaluation and information sharing across the LHIN. Need to enhance communication between providers across the continuum of care particularly at transition points, and including linkages with primary care. This may be supported by infrastructure, such as E-Health records for consistent care between healthcare providers (e.g. drug regimes for patients). Need for integration between health professionals along the continuum, with support for resource tools and communication mechanisms (e.g. implementing standardized clinical assessment tools and care plans that can be individualized). 90 Deloitte & Touche LLP and affiliated entities.
91 Need to secure and maintain adequate health human resources and specialization to meet the needs for the LHIN, balancing local, district and LHIN-wide service delivery (mental health caregivers). Networking and information systems to help ensure efficient, effective care for patients and creating an up-to-date inventory of resources/community supports for the LHIN, opening the information loop and support services further for rural and remote patients. Mental Health Reform 79 (Ontario) The Ontario Ministry of Health and Long-Term Care has developed an implementation plan that outlines a strategy to increase the capacity of the system for comprehensive and integrated treatment, rehabilitative and support services of citizens with mental health needs, while focusing on community alternatives wherever possible. This implementation plan will guide planning and service delivery at the local, regional and provincial levels. Best practice literature has identified that at the service delivery level, a reformed mental health system should include: Case management; Assertive community treatment teams; Crisis response and emergency services; Assessment; Community and housing supports; Inpatient and outpatient care; Treatment; Vocational and educational services; Consumer self-help and consumer initiatives; and Family self-help. Three levels of need have been identified in the reformed mental health system, First Line: refers to prevention, assessment and treatment provided by frontline health care providers including general practitioners, mental health services, social services, hospital emergency services and hospital primary care clinics. Intensive: refers to mental health assessment, treatment and support services which are provided in community or hospital settings and are focused on people with serious mental illness. Specialized: refers to highly specialized mental health programs provided in community or hospital settings and which focus on serving people with serious mental illness who have complex, rare, and unstable mental disorders. Long term care is not synonymous with specialized care. Treatment, rehabilitation and support services are integrated within each program/service type and provided through a multi-disciplinary team approach Deloitte & Touche LLP and affiliated entities.
92 Characteristics of the levels of need 80 are provided for consideration in the tabled below: Levels of Need First Line Intensive Specialized Definition Refers to prevention, assessment and treatment by front line healthcare providers. This includes general practitioners, mental health services, social services, hospital emergency services and hospital primary care clinics. Refers to mental health assessment, treatment and support services which are provided in community or hospital settings and are focused on people with serious mental illness. Refers to highly specialized mental health programs provided in community or hospital settings and which focus on serving people with serious mental illness who have complex, rare and unstable mental disorders. Long term care is not synonymous with specialized care. Treatment, rehabilitation and support services are integrated within each program/service type and provided through a multidisciplinary team approach. Populations to be Served People with serious mental illness. First line emergency crisis services must be acceptable to all people with symptoms of mental health. People with serious mental illness who do not have an on-going need for services provided within the specialized level of need. E.g. the client with multiple and complex needs who is at risk of repeated or prolonged institutionalizations in healthcare or correctional facilities. People with serious mental illness that cannot be managed within the existing array of first line or intensive services. These people require ongoing support, more structured and intensive treatment or a higher level of coordination, security and support. Services Information and referral Crisis telephone lines Mobile crisis teams Schedule 1 hospital emergency services Holding/safe beds Primary care physicians Mental health counseling Community health centers Health service organizations Intensive care management/housing supports Skill development and psycho-social rehabilitation programs Medication clinics Schedule 1 psychiatric inpatient and outpatient service, including triage to inpatient care, day hospital and home treatment and ambulatory outpatient services. Assertive community treatment teams Specialized mobile outreach teams Residential treatment facilities Specialized inpatient and outpatient services Regional forensic services Deloitte & Touche LLP and affiliated entities.
93 Models of Care for Treatment of Adult Drug Mis-Users 81 (NHS, England) This framework, in use in England, supports drug action teams (DATs), joint commissioners and treatment providers in the development of an efficient and effective treatment and care system for drug mis-users. The models of care also provides specific guidance to support the co-ordination of drug and alcohol treatment and the effective management of care across drug misuse treatment services and general health, social and other care. The framework is grouped into four tiers. Tier 1, Drug Interventions and Generic Service: Tier 1 consists of a range of drug-related interventions that can be provided by generic providers depending on their competence and partnership arrangements with specialized drug services. E.g. care provided in inpatient hepatology units for drug users suffering from problems caused by hepatitis C infection. Tier 2, Drug Interventions: Tier 2 interventions include, interventions to engage people into drug treatment, interventions to support people prior to structured treatment, interventions to help retain people in the treatment system, a range of drug misuse harm reduction interventions and interventions to support active drug users who may not want or need intensive structured drug treatment at that point in their lives. Tier 2 interventions focus on those who are still actively using illegal drugs and those who are drug-free and wish to remain so. Tier 2 interventions can be a component of aftercare. Aftercare includes, drug-related supports, such as relapse prevention, support groups and individual support for those wishing to remain drug-free, and access to user groups and advocacy mechanisms (such as Narcotics Anonymous or equivalent).non-drug-related support are included, such as access to education or training, support from advisory services, helping develop social networks and employment support. Community-Based Tier 2 and Tier 3 Interventions: Providers can and do provide a range of interventions at different tiers. This tier allows flexibility for providers to use services within both Tier 2 and Tier 3 for their clients. The most appropriate guide to deciding whether interventions are Tier 2 or Tier 3 is whether interventions are provided in the context of a comprehensive care plan, following a comprehensive assessment. Tier 3 All Substitute Prescribing Interventions: all substitute prescribing interventions, including those delivered by prison healthcare. These interventions require comprehensive assessment, should be care planned and carry a high duty of care for the clinician prescribing controlled drugs. Framework for Action (Northwest Territories Health and Social Services) 82 The Framework for Action for Mental Health and Addiction Services provides a framework for improving wellness services. The framework addresses: addictions, mental health and family violence using an Integrated Service Delivery Model (ISDM) approach. The component of the framework include, prevention, healing and treatment, education and training, community and family development and system management. The ISDM is a team based, client focused approach to provide health and social services. The ISDM combines 3 key elements: 1. Use of primary community care approach, bringing together people who need help with people who provide help. Services are as close to the client as possible. Community service providers will function as members of the Primary Community Care (PCC) Team who link with supports to strengthen community culture (e.g. counseling, education and specialized treatment) Deloitte & Touche LLP and affiliated entities.


94 2. Mechanisms to ensure all caregivers and their organizations are connected and work together; and 3. Approaches to describe and strengthen core services. The family and individual are at the center of services and programs, people can enter services at any point in their care. The continuum of care includes crisis services, community supported housing, prevention and promotion initiatives, community counseling programs, case management, acute care and community treatment programs. The continuum is circular and can be entered and/or exited at any point. The model of care is graphical picture below. Psychogeriatric Care (Australia) 83 Australia has issued a report of the residential care of people with psychogeriatric disorders. The report highlights that the best care outcomes for people with psychogeriatric disorders are achieved where there is effective integration and cooperation across sectors. Collaborative networks across the primary health, mental health and aged care service sectors are critical. A useful representation of the spectrum of care needs for psychogeriatric disorders and modalities of care is provided by the seven tiered Brodaty-Draper triangle of interventions and service delivery (shown below), which ranges from no dementia or mental disorder through tiers of increasingly severe behavioural and psychological symptoms associated with extreme mental disorders and/or dementia Deloitte & Touche LLP and affiliated entities.
95 Seven Tiered Brodaty-Draper Triangle of Interventions and Service Delivery in Old Age
96 It is important to note that care recipients may not remain in a single tier throughout an episode of care. In some people, the behavioural and psychological symptoms may become increasingly severe over time, with the care recipient moving to a higher tier in the Brodaty-Draper triangle. In other cases, a care recipient s behavioural and psychological symptoms may be stabilised, so that they move to a lower tier in the Brodaty- Draper triangle. People with either extreme mental disorders or behavioural and psychological symptoms of dementia, as represented by Tier 7, require either acute or specialist mental health services. However, older people whose behaviours are in the moderate to severe range (Tiers 4-6) do not need services of this intensity, but may still require access to specialist expertise, including tailored behavioural management strategies and higher levels of care. Working within the current care framework in Australia, the report recommends the following supports to ensure the most effective care delivery model: Mainstream aged care homes capacity to care for people with behavioural problems is important not only to facilitate step-down care but also, to contain growth in the number of clients requiring high dependency services by preventing escalation of behavioural problems. For this to occur, mainstream aged care homes also need to incorporate dementia sympathetic design, with committed management and staff with the necessary skills. GPs are often the first point of contact in the system and need to ensure that conditions are properly diagnosed, that early signs of behavioural problems or onset of dementia are identified, and that timely referrals to old age psychiatrists are made. Accurate and expert diagnosis is essential to distinguish those conditions which are treatable from those with symptoms which can only be managed and to ensure appropriate pharmacological regimens as well as behavioural management strategies are in place. Access to expert assessment, diagnosis and treatment can prevent unnecessary admission to acute care, or, admission to acute care can be facilitated when escalating behaviours need more intensive specialist intervention than is provided in the high dependency units. Clear eligibility criteria for admission should be based on factors such as the current client mix (the potential impact of the new client on the existing residents and the existing residents on the new client), and the ability of the facility to provide appropriate care. For example, residential aged care facilities need to be able to ensure that frail non-ambulant residents can be protected from potential aggression of ambulant residents. Skills in managing clients with aggressive behaviours are important in all service areas. While it is essential that high dependency units have some staff with mental health nursing qualifications, it was also evident that on-going in-service training and support for staff are necessary to ensure the continuing development of staff skills and a stable workforce. Deloitte, one of Canada's leading professional services firms, provides audit, tax, consulting, and financial advisory services through more than 7,700 people in 57 offices. Deloitte operates in Québec as Samson Bélair/Deloitte & Touche s.e.n.c.r.l. Deloitte is the Canadian member firm of Deloitte Touche Tohmatsu. Deloitte refers to one or more of Deloitte Touche Tohmatsu, a Swiss Verein, and its network of member firms, each of which is a legally separate and independent entity. Please see for a detailed description of the legal structure of Deloitte Touche Tohmatsu and its member firms. Deloitte & Touche LLP and affiliated entities. TM 2006, VANOC.

97 National Program for Improving Mental Health and Wellbeing 84 (Scotland) The National Program for Improving Mental Health and Wellbeing was developed to provide a framework to support a series of key initiatives and partnerships that are focused on different aspects of improving Scotland's Mental Health. The National Program works alongside other Scottish Government departments and policies. These include those on health improvement, social justice and social inclusion, education and young people, arts and culture, enterprise, and life-long learning. The following areas have been identified as priorities in need of action: Improving infant mental health (the early years) Improving the mental health of children and young people Improving mental health and wellbeing in employment and working life Improving mental health and wellbeing in later life Improving community mental health and wellbeing Improving the ability of public services to act in support of the promotion of mental health and the prevention of mental illness. One of the main tasks of the National Program is to engage with, and support groups of agencies and those with interests in taking forward the aims and priorities of the program. Some of these agencies include: Scottish Executive Departments, NHS Health Scotland, Scottish Prison Service, a range of local Community Planning Partners (Local Authorities, Health Boards, Enterprise Councils, Police, Voluntary Agencies and others), Local Authorities (especially Social Work, Education, Housing, Social, Leisure and Cultural activities), Health (especially Public Health, Health Promotion, Mental Health, Primary Care), Professionals and practitioners in health, social care, education, housing, social inclusion, community learning and development and employment 85. Both the priorities of this program and the inter-connectedness with other areas highlights the importance of a network of groups working together towards a common objective. As the Scottish program continues to evolve and make progress towards their priorities, there will be a clear network of providers working in collaboration with one another Deloitte & Touche LLP and affiliated entities.
A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services
 A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services Clinical Strategy and Programmes Division Vision for Paediatric Health Services Introduction
A National Model of Care for Paediatric Healthcare Services in Ireland Chapter 4: Vision for Paediatric Health Services Clinical Strategy and Programmes Division Vision for Paediatric Health Services Introduction
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM
 Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
Kingston Health Sciences Centre EXECUTIVE COMPENSATION PROGRAM Background In 2010, the Province of Ontario legislated a two-year compensation freeze for all non-unionized employees in the Broader Public
James Meloche, Executive Director. Healthy Human Development Table Meeting January 14, 2015
 James Meloche, Executive Director Healthy Human Development Table Meeting January 14, 2015 2 1. Introduction to PCMCH 2. Overview of Perinatal Mental Health 3. Perinatal Mental Health Initiatives at PCMCH
James Meloche, Executive Director Healthy Human Development Table Meeting January 14, 2015 2 1. Introduction to PCMCH 2. Overview of Perinatal Mental Health 3. Perinatal Mental Health Initiatives at PCMCH
DRAFT Optimal Care Pathway
 DRAFT Optimal Care Pathway 1. Introduction... 3 1.1 Background... 3 1.2 Intent of the Optimal Care Pathways... 3 1.3 Key principles of care... 3 2. Steps in the care of patients with x cancer... 4 Step
DRAFT Optimal Care Pathway 1. Introduction... 3 1.1 Background... 3 1.2 Intent of the Optimal Care Pathways... 3 1.3 Key principles of care... 3 2. Steps in the care of patients with x cancer... 4 Step
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans
 Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
End-of-Life Care Action Plan
 The Provincial End-of-Life Care Action Plan for British Columbia Priorities and Actions for Health System and Service Redesign Ministry of Health March 2013 ii The Provincial End-of-Life Care Action Plan
The Provincial End-of-Life Care Action Plan for British Columbia Priorities and Actions for Health System and Service Redesign Ministry of Health March 2013 ii The Provincial End-of-Life Care Action Plan
The LHIN s role in creating integrated health service delivery systems
 PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
Community Health and Hospital Services Integration Planning Process DRAFT Integrated Service Delivery Model for Northumberland County December 2013
 Overview The Central East Local Health Integration Network is one of 14 Local Health Integration Networks (LHINs) established by the Government of Ontario in 2006. LHINs are community-based organizations
Overview The Central East Local Health Integration Network is one of 14 Local Health Integration Networks (LHINs) established by the Government of Ontario in 2006. LHINs are community-based organizations
Recommendations for Adoption: Diabetic Foot Ulcer. Recommendations to enable widespread adoption of this quality standard
 Recommendations for Adoption: Diabetic Foot Ulcer Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
Recommendations for Adoption: Diabetic Foot Ulcer Recommendations to enable widespread adoption of this quality standard About this Document This document summarizes recommendations at local practice and
NATIONAL HEALTHCARE AGREEMENT 2011
 NATIONAL HEALTHCARE AGREEMENT 2011 Council of Australian Governments An agreement between the Commonwealth of Australia and the States and Territories, being: the State of New South Wales; the State of
NATIONAL HEALTHCARE AGREEMENT 2011 Council of Australian Governments An agreement between the Commonwealth of Australia and the States and Territories, being: the State of New South Wales; the State of
Health. Business Plan to Accountability Statement
 Health Business Plan 1997-1998 to 1999-2000 Accountability Statement This Business Plan for the three years commencing April 1, 1997 was prepared under my direction in accordance with the Government Accountability
Health Business Plan 1997-1998 to 1999-2000 Accountability Statement This Business Plan for the three years commencing April 1, 1997 was prepared under my direction in accordance with the Government Accountability
Preventing and Managing Chronic Disease: Ontario s Framework
 Preventing and Managing Chronic Disease: Ontario s Framework "This document has been developed to inform planning for chronic disease prevention and management (CDPM) in Ontario. It provides the evidence
Preventing and Managing Chronic Disease: Ontario s Framework "This document has been developed to inform planning for chronic disease prevention and management (CDPM) in Ontario. It provides the evidence
PRIMARY HEALTH CARE TRANSFORMATION FAMILY CARE CLINIC APPLICATION KIT WAVE 1
 PRIMARY HEALTH CARE TRANSFORMATION FAMILY CARE CLINIC APPLICATION KIT WAVE 1 DRAFT FOR STAKEHOLDER ENGAGEMENT DECEMBER 20, 2012 FOREWORD Primary Health Care in Alberta Our Changing Society Alberta is changing
PRIMARY HEALTH CARE TRANSFORMATION FAMILY CARE CLINIC APPLICATION KIT WAVE 1 DRAFT FOR STAKEHOLDER ENGAGEMENT DECEMBER 20, 2012 FOREWORD Primary Health Care in Alberta Our Changing Society Alberta is changing
Catherine Hughson Kathryn Kearney Number of supervisors relinquishing role since last report:
 Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Name of Local Supervising Authority: Western Isles Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising Authority
Quality Surveillance Team. Neonatal Critical Care (NCC) Quality Indicators
 Quality Indicators") Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Joint Position Paper on Rural Maternity Care
 Joint Position Paper on Rural Maternity Care Katherine Miller Carol Couchie William Ehman, Lisa Graves Stefan Grzybowski Jennifer Medves JPP Working Group Kaitlin Dupuis Lynn Dunikowski Patricia Marturano
Joint Position Paper on Rural Maternity Care Katherine Miller Carol Couchie William Ehman, Lisa Graves Stefan Grzybowski Jennifer Medves JPP Working Group Kaitlin Dupuis Lynn Dunikowski Patricia Marturano
Primary Health Care The foundation of our health care system
 Primary Health Care The foundation of our health care system October, 2015 Lynn Edwards Dr. Tara Sampalli National and Local Context PRIMARY HEALTH CARE How PHC has Evolved in Canada Late 1990s Recognition
Primary Health Care The foundation of our health care system October, 2015 Lynn Edwards Dr. Tara Sampalli National and Local Context PRIMARY HEALTH CARE How PHC has Evolved in Canada Late 1990s Recognition
Hanover and District Hospital Strategic Plan
 Hanover and District Hospital 2012 Strategic Plan Prepared By: the President/CEO and the Board of Directors With input from Senior Staff, Employees, Physicians, and the Community Created June 2011- February
Hanover and District Hospital 2012 Strategic Plan Prepared By: the President/CEO and the Board of Directors With input from Senior Staff, Employees, Physicians, and the Community Created June 2011- February
NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY
 PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
PLEASE NOTE POLICY IS UNDER REVIEW NORTH EAST ESSEX CLINICAL COMMISSIONING GROUP CONSULTANT TO CONSULTANT REFERRAL POLICY Target Audience Brief Description (max 50 words) Action Required Providers, Commissioners
Advisory Panel on Health System Structure Saskatchewan Ministry of Health 3475 Albert St. Regina, Saskatchewan S4S 6X6
 Saskatchewan Registered Nurses' Association 2066 Retallack Street Regina, Saskatchewan, S4T 7X5 Advisory Panel on Health System Structure Saskatchewan Ministry of Health 3475 Albert St. Regina, Saskatchewan
Saskatchewan Registered Nurses' Association 2066 Retallack Street Regina, Saskatchewan, S4T 7X5 Advisory Panel on Health System Structure Saskatchewan Ministry of Health 3475 Albert St. Regina, Saskatchewan
South East Local Health Integration Network Integrated Health Services Plan EXECUTIVE SUMMARY
 South East Local Health Integration Network Integrated Health Services Plan DISCUSSION DRAFT July, 2006 1.0 Background and Objectives The Government of Ontario has established the South East Local Health
South East Local Health Integration Network Integrated Health Services Plan DISCUSSION DRAFT July, 2006 1.0 Background and Objectives The Government of Ontario has established the South East Local Health
DRAFT 2. Specialised Paediatric Services in Scotland. 1 Specialised Services Definition
 Specialised Paediatric Services in Scotland 1 Specialised Services Definition Services provided for low numbers of patients. They require a critical mass of staff, facilities and equipment and are delivered
Specialised Paediatric Services in Scotland 1 Specialised Services Definition Services provided for low numbers of patients. They require a critical mass of staff, facilities and equipment and are delivered
Template #1: Maternal Newborn: Strengths and Challenges within the Current System in Addressing Population Needs. Whither the continuum?
 Template #1: Maternal Newborn: Strengths and Challenges within the Current System in Addressing Population Needs Strengths Challenges Full spectrum of (hospital?) care within maternal newborn care continuum
Template #1: Maternal Newborn: Strengths and Challenges within the Current System in Addressing Population Needs Strengths Challenges Full spectrum of (hospital?) care within maternal newborn care continuum
Specialised Services Service Specification: Inherited Bleeding Disorders
 Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
Specialised Services Service Specification: Inherited Bleeding Disorders Document Author: Assistant Specialised Services Planner Cardiac and Cancer Specialised Services Planner Cancer and Blood Executive
NATIONAL ASSOCIATION OF BOARDS OF PHARMACY (NAPB) / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011
 / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011") NATIONAL ASSOCIATION OF BOARDS OF PHARMACY (NAPB) / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011 7:30-8:30 PM SHERATON CAVALIER HOTEL SASKATOON SPEAKING
NATIONAL ASSOCIATION OF BOARDS OF PHARMACY (NAPB) / AMERICAN ASSOCIATION OF COLLEGES OF PHARMACY (AACP) DISTRICT V MEETING THURSDAY, AUGUST 4, 2011 7:30-8:30 PM SHERATON CAVALIER HOTEL SASKATOON SPEAKING
Ministry of Health Patients as Partners Provincial Dialogue Report
 Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
Ministry of Health Patients as Partners 2017 Provincial Dialogue Report Contents Executive Summary 4 Introduction 6 Balanced Participation: Demographics and Representation at the Dialogue 8 Engagement
#NeuroDis
 Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
Inequalities Sensitive Practice Initiative
 Inequalities Sensitive Practice Initiative Maternity Unit Report - 2008 Royal Alexandria Hospital 1 Acknowledgment I would like to take this opportunity to thank the staff from the maternity services in
Inequalities Sensitive Practice Initiative Maternity Unit Report - 2008 Royal Alexandria Hospital 1 Acknowledgment I would like to take this opportunity to thank the staff from the maternity services in
Framework for Cancer CNS Development (Band 7)
") Framework for Cancer CNS Development (Band 7) Opening Statement This framework provides a common understanding of the CNS role across the London Cancer Alliance and will be used to support the development
Framework for Cancer CNS Development (Band 7) Opening Statement This framework provides a common understanding of the CNS role across the London Cancer Alliance and will be used to support the development
ERN Assessment Manual for Applicants
 Share. Care. Cure. ERN Assessment Manual for Applicants 3.- Operational Criteria for the Assessment of Networks An initiative of the Version 1.1 April 2016 History of changes Version Date Change Page 1.0
Share. Care. Cure. ERN Assessment Manual for Applicants 3.- Operational Criteria for the Assessment of Networks An initiative of the Version 1.1 April 2016 History of changes Version Date Change Page 1.0
Central Zone Healthcare Plan. For Placement Only. Strategy Overview
 Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Alberta Health Services Central Zone Healthcare Plan For Placement Only Strategy Overview A plan for us Alberta Health Services (AHS) recognizes every community in Alberta is unique. That s why health
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
GOULBURN VALLEY HEALTH Strategic Plan
 GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
THE FUTURE OF YOUR HOSPITALS: Planned Care site
 THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
THE FUTURE OF YOUR HOSPITALS: Planned Care site We have a real opportunity to shape healthcare in Shropshire for future generations. Care Centres. Doctors, nurses and other healthcare professionals are
Our Shared Purpose: Advancing the Health of Our Patients and Our Urban Communities
 Our Shared Purpose: Advancing the Health of Our Patients and Our Urban Communities Proposal for Voluntary Integration An Integration Proposal Submitted to the Toronto Central Local Health Integration Network
Our Shared Purpose: Advancing the Health of Our Patients and Our Urban Communities Proposal for Voluntary Integration An Integration Proposal Submitted to the Toronto Central Local Health Integration Network
Neurocritical Care Fellowship Program Requirements
 Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
Neurocritical Care Fellowship Program Requirements I. Introduction A. Definition The medical subspecialty of Neurocritical Care is devoted to the comprehensive, multisystem care of the critically-ill neurological
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
September Sub-Region Collaborative Meeting: Bramalea. September 13, 2018
 September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
September Sub-Region Collaborative Meeting: Bramalea September 13, 2018 Agenda Item # Agenda Item Action Lead Time 1.0 Welcome Call to Order, Introductions, Objectives Co-Chairs 5 min 2.0 Integrated Health
GUIDE TO BAYFRONT.
 GUIDE TO BAYFRONT www.bayfront.org MISSION Quality healthcare for all we serve VALUES Trust, respect and dignity reflecting our responsibility to achieve healthcare excellence for our community VISION
GUIDE TO BAYFRONT www.bayfront.org MISSION Quality healthcare for all we serve VALUES Trust, respect and dignity reflecting our responsibility to achieve healthcare excellence for our community VISION
PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification. 12 months
 E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
E09/S(HSS)/b 2013/14 NHS STANDARD CONTRACT FOR VEIN OF GALEN MALFORMATION SERVICE (ALL AGES) PARTICULARS, SCHEDULE 2 THE SERVICES, A Service Specification Service Specification No. Service Commissioner
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA
 COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
COLLEGE OF MIDWIVES OF BRITISH COLUMBIA DEFINITION OF A MIDWIFE MIDWIFERY MODEL OF PRACTICE A midwife is a person who, having been regularly admitted to a midwifery educational programme duly recognised
Descriptions: Provider Type and Specialty
 Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Descriptions: Provider Type and Specialty PROVIDER TYPE/SPECIALTY ADULT PRIMARY CARE Provides care for adults by treating common health problems, performing check-ups and providing prevention services.
Community Health Improvement Plan
 Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016
 Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016 Introduction The Ministry of Health and Long Term Care s (MOHLTC) Patients First: Action Plan for Health Care exemplifies
Palliative Care Community Teams: Supporting a Central East LHIN Model of Care June 2016 Introduction The Ministry of Health and Long Term Care s (MOHLTC) Patients First: Action Plan for Health Care exemplifies
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation
 Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Specialised Services Commissioning Policy: CP160 Specialised Paediatric Neurological Rehabilitation April 2018 Version 4.0 Document information Document purpose Document name Author Policy Specialised
Supporting Best Practice for COPD Care Across the System
 Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
Supporting Best Practice for COPD Care Across the System May 3, 2017 Health Quality Ontario The provincial advisor on the quality of health care in Ontario Overview Health Quality Ontario background QBP
Community and. Patti-Ann Allen Manager of Community & Population Health Services
 Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Community and Population Health Services Patti-Ann Allen Manager of Community & Population Health Services October 2017 Community and Population Health Services-HHS ALC Corporate Planning Site Admin Managers
Visiting Professional Programme: Obstetric Medicine
 Visiting Professional Programme: Obstetric Medicine Visiting Professional Programme Obstetric Medicine 1 Introduction The Guy s and St Thomas NHS Foundation Trust Obstetric Medicine Visiting Professional
Visiting Professional Programme: Obstetric Medicine Visiting Professional Programme Obstetric Medicine 1 Introduction The Guy s and St Thomas NHS Foundation Trust Obstetric Medicine Visiting Professional
South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017
 South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017 Overview of today s presentation Provide background on
South West LHIN Initiatives and Priorities Presentation to the Grey County Warden s Forum Michael Barrett, CEO, South West LHIN April 20 th, 2017 Overview of today s presentation Provide background on
The Movement Towards Integrated Funding Models
 The Movement Towards Integrated Funding Models Financial Models and Fiscal Incentives in Health Conference Board of Canada Toronto, December 1, 2015 Jason M. Sutherland Associate Prof, Centre for Health
The Movement Towards Integrated Funding Models Financial Models and Fiscal Incentives in Health Conference Board of Canada Toronto, December 1, 2015 Jason M. Sutherland Associate Prof, Centre for Health
Victorian Labor election platform 2014
 Victorian Labor election platform 2014 July 2014 1. Background The Victorian Labor Party election platform provides positions on key elements of State Government policy. The platform offers a broad insight
Victorian Labor election platform 2014 July 2014 1. Background The Victorian Labor Party election platform provides positions on key elements of State Government policy. The platform offers a broad insight
PCFHC STRATEGIC PLAN
 PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario
 Narrative for Health Care Organizations in Ontario") Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
Quality Improvement Plan (QIP) Narrative for Health Care Organizations in Ontario 3/29/2017 This document is intended to provide health care organizations in Ontario with guidance as to how they can develop
STRATEGIC PLAN Prepared by: Approved by the Board of Directors: June 25, June 2014 Page 1 of 12
 STRATEGIC PLAN 2014-2019 Prepared by: Approved by the Board of Directors: June 25, 2014 June 2014 Page 1 of 12 Section 1 Introduction Espanola General Hospital (EGH) was incorporated as a hospital in 1948.
STRATEGIC PLAN 2014-2019 Prepared by: Approved by the Board of Directors: June 25, 2014 June 2014 Page 1 of 12 Section 1 Introduction Espanola General Hospital (EGH) was incorporated as a hospital in 1948.
Ontario s Digital Health Assets CCO Response. October 2016
 Ontario s Digital Health Assets CCO Response October 2016 EXECUTIVE SUMMARY Since 2004, CCO has played an expanding role in Ontario s healthcare system, using digital assets (data, information and technology)
Ontario s Digital Health Assets CCO Response October 2016 EXECUTIVE SUMMARY Since 2004, CCO has played an expanding role in Ontario s healthcare system, using digital assets (data, information and technology)
SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS
 SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS About The Chartis Group The Chartis Group is an advisory services firm that provides management consulting and applied research to
SEPTEMBER 2011 CREATING SUCCESSFUL MATERNAL FETAL MEDICINE PARTNERSHIPS About The Chartis Group The Chartis Group is an advisory services firm that provides management consulting and applied research to
Transforming Clinical Services. Our developing clinical strategy
 Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
Transforming Clinical Services Our developing clinical strategy Transforming clinical services A developing clinical strategy for the new Foundation Trust Since 1 April 2011, County Durham and Darlington
GREY BRUCE CHRONIC DISEASE PREVENTION AND MANAGEMENT FRAMEWORK
 GREY BRUCE CHRONIC DISEASE PREVENTION AND MANAGEMENT FRAMEWORK IMPLEMENTATION TOOL KIT Bumstead, L., Goetz-Perry, C., Miller, L., Solomon, M. (2008) 1 WHERE DID THE CDPM FRAMEWORK COME FROM? Wagner (1999)
GREY BRUCE CHRONIC DISEASE PREVENTION AND MANAGEMENT FRAMEWORK IMPLEMENTATION TOOL KIT Bumstead, L., Goetz-Perry, C., Miller, L., Solomon, M. (2008) 1 WHERE DID THE CDPM FRAMEWORK COME FROM? Wagner (1999)
A Collection of Referral and Consultation Process Improvement Projects
 A Collection of Referral and Consultation Process Improvement Projects Volume 3: ~Physician Directories~ Selected project summaries originally prepared for CMA: The Referral and Consultation Process Making
A Collection of Referral and Consultation Process Improvement Projects Volume 3: ~Physician Directories~ Selected project summaries originally prepared for CMA: The Referral and Consultation Process Making
Standards for competence for registered midwives
 Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
Standards for competence for registered midwives The Nursing and Midwifery Council (NMC) is the nursing and midwifery regulator for England, Wales, Scotland and Northern Ireland. We exist to protect the
Perinatal Designation Matrix 3/21/07
 Codes: N = Neonatal Criteria M= Maternal Criteria P= Perinatal Criteria (both N & P) Perinatal Designation Matrix 3/21/07 Service/ 1. (N) Minimum NICU bed capacity Minimum of 10 NICU beds. Minimum of 15
Codes: N = Neonatal Criteria M= Maternal Criteria P= Perinatal Criteria (both N & P) Perinatal Designation Matrix 3/21/07 Service/ 1. (N) Minimum NICU bed capacity Minimum of 10 NICU beds. Minimum of 15
RECOMMENDATION STATUS OVERVIEW
 Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Chapter 2 Section 2.01 Community Care Access Centres Financial Operations and Service Delivery Follow-Up on September 2015 Special Report RECOMMENDATION STATUS OVERVIEW # of Status of Actions Recommended
Quality Improvement Plan (QIP) Narrative: Markham Stouffville Hospital Last updated: March 2017
 Narrative: Markham Stouffville Hospital Last updated: March 2017") Overview The Quality Improvement Plan (QIP) is an integral part of the quality framework at (MSH). This QIP, our seventh, was developed in partnership with patients, families, and the community we serve.
Overview The Quality Improvement Plan (QIP) is an integral part of the quality framework at (MSH). This QIP, our seventh, was developed in partnership with patients, families, and the community we serve.
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Vanguard Programme: Acute Care Collaboration Value Proposition
 Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
Vanguard Programme: Acute Care Collaboration Value Proposition 2015-16 November 2015 Version: 1 30 November 2015 ACC Vanguard: Moorfields Eye Hospital Value Proposition 1 Contents Section Page Section
2.0 APPLICABILITY OF THIS PROTOCOL AGREEMENT FRAMEWORK
 Roles and Responsibilities of the Director (Child, Family and Community Service Act) and the Ministry Of Health: For Collaborative Practice Relating to Pregnant Women At-Risk and Infants At-Risk in Vulnerable
Roles and Responsibilities of the Director (Child, Family and Community Service Act) and the Ministry Of Health: For Collaborative Practice Relating to Pregnant Women At-Risk and Infants At-Risk in Vulnerable
Corporate Partners Program
 Mercy Health Foundation St. Louis Mercy Health Foundation 615 S. New Ballas Road St. Louis, MO 63141 Office: 314-251-1800 Fax: 314-251-1801 mercyhealthfoundation.stl@mercy.net Corporate Partners Program
Mercy Health Foundation St. Louis Mercy Health Foundation 615 S. New Ballas Road St. Louis, MO 63141 Office: 314-251-1800 Fax: 314-251-1801 mercyhealthfoundation.stl@mercy.net Corporate Partners Program
Hamilton Niagara Haldimand Brant LHIN. Strategic Health System Plan: Survey Report
 Hamilton Niagara Haldimand Brant LHIN Strategic Health System Plan: Survey Report April 2012 Table of Contents Survey: Approach 4 Survey Design 4 Survey Launch 5 Survey Response 5 Survey Results 7 Demographic
Hamilton Niagara Haldimand Brant LHIN Strategic Health System Plan: Survey Report April 2012 Table of Contents Survey: Approach 4 Survey Design 4 Survey Launch 5 Survey Response 5 Survey Results 7 Demographic
Standards of Practice for Professional Ambulatory Care Nursing... 17
 Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Toolkit to Support Effective Collaboration within an Integrated Care Team
 Toolkit to Support Effective Collaboration within an Integrated Care Team January 2015 1 P a g e PCMCH Toolkit to Support Integrated Care Team Members The Provincial Council for Maternal and Child Health
Toolkit to Support Effective Collaboration within an Integrated Care Team January 2015 1 P a g e PCMCH Toolkit to Support Integrated Care Team Members The Provincial Council for Maternal and Child Health
Healthy Babies Healthy Children Service Levels and Update on Provincial Review
 HL27.02 REPORT FOR ACTION Healthy Babies Healthy Children Service Levels and Update on Provincial Review Date: June 4, 2018 To: Board of Health From: Medical Officer of Health Wards: All SUMMARY Healthy
HL27.02 REPORT FOR ACTION Healthy Babies Healthy Children Service Levels and Update on Provincial Review Date: June 4, 2018 To: Board of Health From: Medical Officer of Health Wards: All SUMMARY Healthy
At EmblemHealth, we believe in helping people stay healthy, get well and live better.
 At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
Indian Council of Medical Research
 Indian Council of Medical Research Call for Letters of Intent Grants Programme for Implementation Research on Maternal and Child Health Deadline: 31 May 2017 India has made significant progress in reducing
Indian Council of Medical Research Call for Letters of Intent Grants Programme for Implementation Research on Maternal and Child Health Deadline: 31 May 2017 India has made significant progress in reducing
Community and Mental Health Services High Level Market Research PROSPECTUS
 and Mental Health Services High Level Market Research PROSPECTUS February 2014 Supporting people in Dorset to lead healthier lives NHS DORSET CLINICAL COMMISSIONING GROUP PROSPECTUS FOR COMMUNITY AND MENTAL
and Mental Health Services High Level Market Research PROSPECTUS February 2014 Supporting people in Dorset to lead healthier lives NHS DORSET CLINICAL COMMISSIONING GROUP PROSPECTUS FOR COMMUNITY AND MENTAL
SCHEDULE 2 THE SERVICES
 SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
SCHEDULE 2 THE SERVICES A. Service Specifications Mandatory headings 1 4. Mandatory but detail for local determination and agreement Optional headings 5-7.Optional to use, detail for local determination
Alberta Health Services. Strategic Direction
 Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Michigan Council for Maternal and Child Health 2018 Policy Agenda
 Michigan Council for Maternal and Child Health 2018 Policy Agenda MCMCH Purpose! MCMCH s purpose is to advocate for public policy that will improve maternal and child health and optimal development outcomes
Michigan Council for Maternal and Child Health 2018 Policy Agenda MCMCH Purpose! MCMCH s purpose is to advocate for public policy that will improve maternal and child health and optimal development outcomes
Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience.
 Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience. Jo Maitland Perinatal Mental Health Training & Service Development Lead 5 Year Forward View Community
Perinatal Mental Health Clinical Networks : The national picture and lessons from the London experience. Jo Maitland Perinatal Mental Health Training & Service Development Lead 5 Year Forward View Community
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
GRADUATE NURSING AND MIDWIFERY PROGRAMS. MonashHealth. One place, a world of healthcare.
 GRADUATE NURSING AND MIDWIFERY PROGRAMS MonashHealth One place, a world of healthcare. About us Monash Health is Victoria s most integrated public health service. As one of Victoria s leading teaching
GRADUATE NURSING AND MIDWIFERY PROGRAMS MonashHealth One place, a world of healthcare. About us Monash Health is Victoria s most integrated public health service. As one of Victoria s leading teaching
Healthy Start Initiative: Provincial Perinatal, Child and Family Public Health Services. April 2013
 Healthy Start Initiative: Provincial Perinatal, Child and Family Public Health Services April 2013 Provincial Public Health Perinatal, Child and Family Health Services Introduction - Advancing the Health
Healthy Start Initiative: Provincial Perinatal, Child and Family Public Health Services April 2013 Provincial Public Health Perinatal, Child and Family Health Services Introduction - Advancing the Health
Health and Wellness. Business Plan to restated. Accountability Statement
 Health and Wellness Business Plan 1999-2000 to 2001-02 - restated Accountability Statement As a result of government re-organization announced on May 25, 1999, the Ministry Business Plans included in Budget
Health and Wellness Business Plan 1999-2000 to 2001-02 - restated Accountability Statement As a result of government re-organization announced on May 25, 1999, the Ministry Business Plans included in Budget
Oxford Condition Management Programs:
 Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
Oxford Condition Management Programs: Helping your employees learn, be encouraged and get support. Committed to helping improve the health and well-being of those we serve and improve the health care
City and Hackney Clinical Commissioning Group Prospectus May 2013
 City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
City and Hackney Clinical Commissioning Group Prospectus May 2013 Foreword We are excited to be finally live as a CCG, picking up our responsibilities as commissioners for the bulk of the NHS. The changeover
Board of Health and Local Health Integration Network Engagement Guideline, 2018
 Ministry of Health and Long-Term Care Board of Health and Local Health Integration Network Engagement Guideline, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective:
Ministry of Health and Long-Term Care Board of Health and Local Health Integration Network Engagement Guideline, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective:
Appendix D Francophone Population Profile
 Appendix D Profile 1 Appendix D: Profile The in the South West LHIN According to the 2006 Census, the Francophone population in the South West LHIN is approximately 11,000 people, representing 1.3% of
Appendix D Profile 1 Appendix D: Profile The in the South West LHIN According to the 2006 Census, the Francophone population in the South West LHIN is approximately 11,000 people, representing 1.3% of
Referral Guidance DIRECT REFERRAL SERVICE FOR THE ELDERLY DEAF
 Referral Guidance A & E GPs are strongly requested to contact the specialty teams DIRECTLY WHEN APPROPRIATE to avoid unnecessary delays for their patients in A & E. Relevant non-urgent conditions can be
Referral Guidance A & E GPs are strongly requested to contact the specialty teams DIRECTLY WHEN APPROPRIATE to avoid unnecessary delays for their patients in A & E. Relevant non-urgent conditions can be
Section IX Special Needs & Case Management
 Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
NWT Primary Community Care Framework
 NWT Primary Community Care Framework August 2002 Table of Contents Introduction... 1 National Perspective... 2 NWT Vision for Primary Community Care... 2 Principles... 3 The NWT Approach to Primary Community
NWT Primary Community Care Framework August 2002 Table of Contents Introduction... 1 National Perspective... 2 NWT Vision for Primary Community Care... 2 Principles... 3 The NWT Approach to Primary Community
Regional Hospice Palliative Care Model Action Plan
 ITEM 11.1 Regional Hospice Palliative Care Model Action Plan Central LHIN Board of Directors October 28, 2014 1 Agenda Background Declaration A Vision for Palliative Care in Ontario Central LHIN Approach
ITEM 11.1 Regional Hospice Palliative Care Model Action Plan Central LHIN Board of Directors October 28, 2014 1 Agenda Background Declaration A Vision for Palliative Care in Ontario Central LHIN Approach
Primary and Community Care in B.C.: A Strategic Policy Framework Executive Summary
 Primary and Community Care in B.C.: A Strategic Policy Framework Executive Summary Strategic Context This is the first time that the Ministry of Health has attempted to capture the significant and sometimes
Primary and Community Care in B.C.: A Strategic Policy Framework Executive Summary Strategic Context This is the first time that the Ministry of Health has attempted to capture the significant and sometimes
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Child Health 2020 A Strategic Framework for Children and Young People s Health
 Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Karen King (Link) Kathleen Hamblin Carole McBurnie Frances Wright Joyce Linton Catriona Thomson
 Kathleen Hamblin Carole McBurnie Frances Wright Joyce Linton Catriona Thomson") Name of Local Supervising Authority: Dumfries and Galloway Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising
Name of Local Supervising Authority: Dumfries and Galloway Health Board Period of report: 2005/2006 Date: September 2006 1. Supervision of Midwives and Midwifery Practice 1.1 Designated Local Supervising
Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives
 NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect
NHS Dorset Clinical Commissioning Group Hospital Generated Inter-Speciality Referral Policy Supporting people in Dorset to lead healthier lives PREFACE This Document outlines the CCG s policy in respect
Health Quality Ontario Business Plan
 Health Quality Ontario Business Plan 2017-20 October 2016 Table of Contents 1 Executive Summary...1 2 Mandate and Strategy...2 3 Environmental Scan...4 4 Programs and Activities...5 5 Risks... 18 6 Resources...
Health Quality Ontario Business Plan 2017-20 October 2016 Table of Contents 1 Executive Summary...1 2 Mandate and Strategy...2 3 Environmental Scan...4 4 Programs and Activities...5 5 Risks... 18 6 Resources...
Understanding Monash Health s environment
 Understanding Monash Health s environment Context for developing our 2018-2023 Strategic Plan Working draft September 2017 Introduction Monash Health is a health care, teaching and research institution
Understanding Monash Health s environment Context for developing our 2018-2023 Strategic Plan Working draft September 2017 Introduction Monash Health is a health care, teaching and research institution