GREY BRUCE CHRONIC DISEASE PREVENTION AND MANAGEMENT FRAMEWORK
|
|
|
- Clemence Eaton
- 5 years ago
- Views:
Transcription
1 GREY BRUCE CHRONIC DISEASE PREVENTION AND MANAGEMENT FRAMEWORK IMPLEMENTATION TOOL KIT Bumstead, L., Goetz-Perry, C., Miller, L., Solomon, M. (2008) 1
2 WHERE DID THE CDPM FRAMEWORK COME FROM? Wagner (1999) Barr et al (2002) Ontario Ministry of Health and Long term Care The health care system transformation agenda 2
3 CDPM Framework - Purpose To provide a common policy framework to guide efforts toward effective prevention and management of chronic diseases To guide Ministry transformation initiatives such as: Local Health Integration Networks Primary Health Care Renewal, Family Health Teams Public Health Renewal - health promotion and prevention initiatives e-health strategy, HHR strategy Specific chronic disease strategies To engage ministry stakeholders in a systematic approach to addressing chronic disease 3
4 CDPM Framework: Purpose Not just a model: changes the paradigm for care A way for conceptualizing care A framework for organizing or re- organizing care Applicable to any system, organization or program 4
5 5
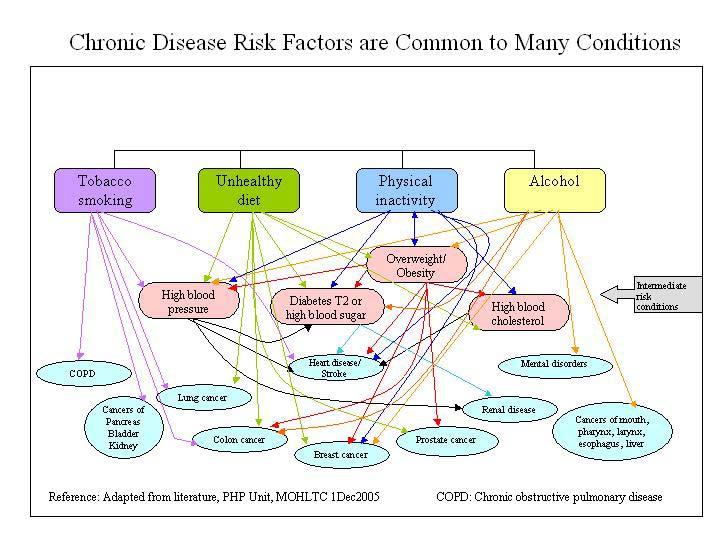
6 What Makes People Healthy / Unhealthy? Estimated Impact of Determinants of Health on the Health Status of the Population Biology and Genetic Endowment 15% Health Care System 25% Physical Environment 10% Social and Economic Environment 50% 6
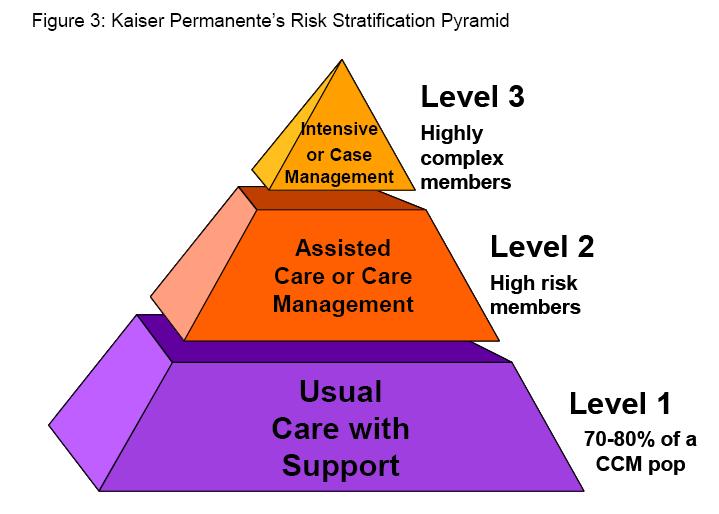
7 FROM Illness orientation The Transformation TO Wellness orientation prevention not a priority a solo provider approach Provider, disease centred reactive and episodic care limited role for individuals in self management prevention at all points of continuum an integrated, interdisciplinary care team approach patient centred proactive, complex, continuing care individuals empowered for self- management and part of care team A System Involving Health Care Organizations Individuals and Families Communities 7
8 Why does the CDPM system have that capacity? Focuses on populations Focuses on longitudinal care (creates a system of prevention and care) Supports coordination of prevention and care along a health continuum Recognizes individuals and communities as partners Offers early access to prevention and support as well as treatment Offers multi-disciplinary, multi-sectoral strategies 8
9 WHAT IS THE KIT? Written and electronic resources that help groups understand the framework, and develop practical applications for it Step-by by-step support to apply the framework to your existing programs, or build new ones A way of establishing a common perspective and language between partners when undertaking new strategies related to chronic disease prevention and management 9
10 HOW DO WE USE THE KIT? Identify the current or potential program, project or partnership initiative requiring development/reassessment/redesign Establish a core stakeholder work group Use the resources, references, and steps outlined in the tool kit as process supports for developmental activities 10
11 OVERVIEW OF FRAMEWORK APPLICATION: THE WORKFLOW 11
12 CDPM Framework Workflow Understanding the Framework Step 1 Review the Ontario Chronic Disease Prevention and Management Framework diagram. Step 2 Review the Element Definitions in CDPM Step 3 Review the Logic Models Applying the Framework Step 4 Complete Program Feasibility Checklist Step 5 Complete the Logic Model for Program Planning Step 6 Complete the Initiating a Health Program Checklist Step 7 Revise Program (Logic Model) Plan as required 12
13 Step I: REVIEW THE OCDPM FRAMEWORK DIAGRAM 13


14 Supportive Environments Ontario s CDPM Framework Healthy Public Policy INDIVIDUALS AND FAMILIES Personal Skills & Self- Management Support HEALTH CARE ORGANIZATIONS Community Action Delivery System Design Provider Decision Support Information Systems Productive interactions and relationships Activated communities & prepared, proactive community partners Informed, activated individuals & families Prepared, proactive practice teams Improved clinical, functional and population health outcomes 14
15 STEP 2: REVIEW THE ELEMENT DEFINITIONS IN THE OCDPM DIAGRAM 15
16 Individuals and Families The centre of the CDPM framework Direct involvement and self management of health and chronic diseases is key Team members in prevention and care Informed, person-centred choices for living 16
17 Health Care Organizations - make systematic efforts to improve prevention and management of chronic disease: strong leadership (e.g., CDPM champions) alignment of resources, incentives (e.g. Admin support, IT support for providers, etc.) accountability for results (e.g., set goals, measure effectiveness in improving outcomes for clients, population and system ) 17
18 Personal Skills & Self-Management Support - empower individuals to build skills for healthy living and coping with disease: emphasizing the individual s s and families central role in their health, and as a member of the care team engaging them in shared decision-making, goal-setting and care planning providing access to education programs & health information (e.g. asthma education programs, consumer information) behaviour modification programs (e.g. smoking cessation) counselling and support services (e.g. self-management support groups) integration of community resources (e.g. referral to community physical activity programs) follow-up (e.g. reminders, self-monitoring assistance) 18
19 Delivery System Design - focus on prevention and, improve access, continuity of care and flow through the system: interdisciplinary teams (e.g., FHTs with defined roles & responsibilities) integrated health promotion and disease prevention (e.g., nutrition and physical activity counselling) planned interactions, active follow-up (e.g., care paths, case management) adjustments, innovations in practice (e.g., group office visits, central appointment booking service) outreach and population needs-based care (e.g., Latin American Diabetes) 19
20 Provider Decision Support - integrate evidence-based guidelines into daily practice: easily accessible clinical practice guidelines (e.g. web-based, based, interactive) tools (e.g. disease/risk assessment, management flow sheets, drug interaction software) provider alerts and reminders (e.g. reminders for tests, examinations) access to specialist expertise (e.g. team social worker; cardiologist ogist at tertiary care centre) provider education (e.g. working in interdisciplinary teams, collaboratives) measurement, routine reporting/feedback, evaluation (e.g. continuous quality improvement loop for target blood glucose levels els in client population with diabetes) 20
21 Information Systems are essential for enhancing information for providers to provide quality care; for clients to support them in managing their disease on a day to day basis; and for integrating services across health system: electronic health records (e.g. personal health information, test results, prevention and treatment plans) client registries to identify and provide patient subpopulations with proactive care, monitoring, and follow-up (e.g. tracking systems, automated reminders) links (e.g. between team members, care centres) information for clients (e.g. health care advice, access to records, community resources) population health data (e.g. demographic, health status, risks) 21
22 Healthy Public Policy - develop and implement policies to improve individual and population health and address inequities: legislation, regulations (e.g. smoking by-laws) fiscal, taxation measures (e.g. lowering duty on imported fruit) guidelines (e.g. Health Canada food guidelines, screening) organizational change (e.g. flex hours, day care in the workplace) 22
23 Supportive Environments - remove barriers to healthy living and promote safe, enjoyable living and working conditions: physical environments (e.g. safe air, clean water, accessible transportation, affordable housing, walking trails, bicycle lanes) social and community environments (e.g. daily physical activity in schools, seniors programs in community centres, on-site health promotion programs in the workplace) 23
24 Community Action - encourage communities to increase control over issues affecting health: collaboration between the health care sector and community organizations (e.g. Latin American Diabetes Program, London ON) effective public participation and intersectoral collaboration (e.g.( community members, private sector and schools providing breakfast nutrition/physical activity programs) 24
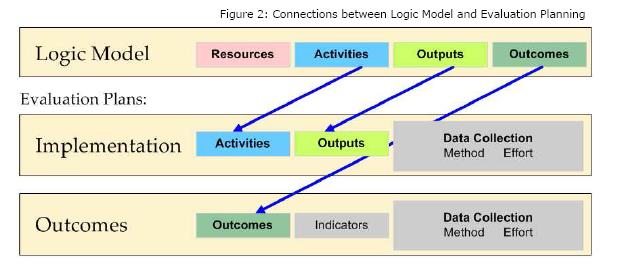
25 STEP 3:REVIEW THE LOGIC MODELS Mission A systems approach to provide integrated chronic disease prevention and management services Inputs Policy, Legislation/Regulations, Guidelines, Fiscal and Human Resources, Information Systems Components Community Capacity and Integration Individual and Family Capacity and Integration Health Care Organization (HCO) and Provider Capacity and Integration Outputs Communities collaborating with HCOs to identify and prioritize issues affecting the health of the population. Communities championing activities for healthy public policy, and supportive environments. Community collaboration with HCOs to develop, link and coordinate services and information for individuals and families. Community information and programs integrated with health care services. Education, counselling, behaviour modification programs, and information for individuals and families to build skills for healthy living and coping with disease. Care teams with individuals and families at the centre, and engaged in decision making and care planning. Self-management information and resources accessible and tailored to meet the needs of individuals and families. Community programs and resources integrated into care. Health promotion, primary, secondary, and tertiary prevention incorporated into care. Visible leadership, aligned incentives, policies, resources, measurement, and accountability for CDPM system changes. Interdisciplinary team practices, with links to specialists, where health care providers collaboratively provide patient-centred care in a seamless and coordinated manner. Integrated electronic information systems with comprehensive, accurate information for providers and individuals to share information & make the best decisions. Evidence-based tools for prevention, assessment and management incorporating planned interactions, and prompts for follow-up. Short-term outcomes Increased community collaboration with HCOs to identify and prioritize issues affecting health. Increased community action for healthy public policy, supportive environments to meet the needs of their population. Increased awareness, linkages and referral to community programs, information, and resources. Individuals and families have increased skills and knowledge for healthy behaviours. Individuals, families and providers have improved understanding of their roles as partners on care teams, and consumers are involved in care planning. More individuals and families have increased knowledge of their disease processes and role as daily self-manager. Increased knowledge and skills of consumers in selfmanagement. More individuals and families are aware of and linked to community programs and resources. Providers have increased knowledge, skills and tools to incorporate prevention into their practices. More HCOs promote system change and provide incentives, align policies, resources, measurement, and accountability. Increased number of interdisciplinary teams, with links to specialists working collaboratively and providing coordinated, patient-centred care. More providers using electronic information systems and sharing information among team members, their clients, other health providers and settings. More providers using evidence-based tools, and quality improvement approaches for prevention, assessment and management. Intermediate outcomes Improved healthy public policies and supportive environments. More community information and programs integrated with health care services. More people exhibiting healthy behaviours Individuals and families at the centre of the care team, actively engaged in decision-making, and daily managers of their wellness. More individuals and families gaining benefits through involvement in self-management Increased participation in community programs and resources Increased overall satisfaction of individuals and families with the responsiveness of the health care system to meet their needs Health promotion and prevention integrated across continuum of care. Health care coordinated across the continuum of care, providers and settings. The appropriate type and number of health care providers working in collaboration to meet the needs of the individual and family. Care is evidence based and meets the diverse needs of consumers. Care is proactive, and provides for complex and continuing care, with follow-up and ease of navigation. Integrated information systems with consumer, decision support and community information. Long-term outcomes Activated communities and prepared, proactive partners Informed, engaged individuals and families Prepared, proactive practice teams Vision An integrated, coordinated system for the prevention and management of chronic diseases that is proactive, individual and family-centred, and that provides access to quality care by the right provider at the right time in the right place, resulting in improved clinical, functional and population health outcomes 25
26 Mission A systems approach to provide integrated chronic disease prevention and management services Roles and Responsibilities Components Health Promotion Primary Prevention Community Capacity and Integration Roles Responsibility Individual and Family Capacity Roles Responsibility Health Care Organization Roles Responsibility Secondary Prevention Tertiary Prevention 26
27 27
28 STEPS 4-7: 4 BUILDING YOUR PROGRAM 28
29 29

30 Developing Logic Models 30
31 31
32 32
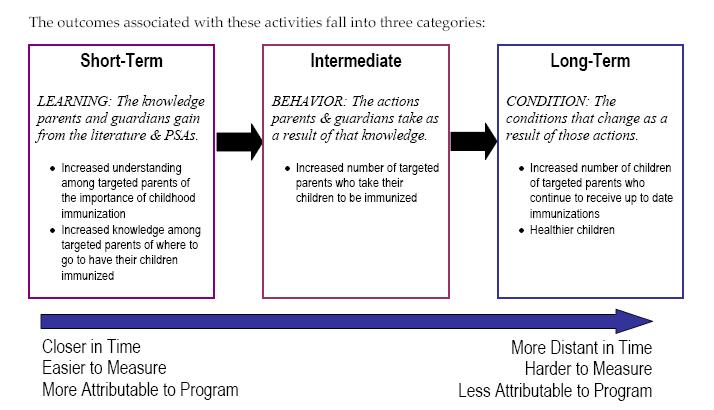
33 Program Name Problem Statement: Program Goal (s): Logic Model Activities What happens in our organization? Resources What resources do we have to work with? Outputs What are the tangible products of our activities? Short-term Outcomes What changes do we expect to occur within the short term? Intermediate Outcomes What changes do we want to see occur after that? Long-term Outcomes What changes do we hope to see over time? Rationale (s): The explanation of a set of beliefs, based on a body of knowledge, about how change occurs in your field and with your specific clients (or audience). Assumptions: Facts or conditions you assume to be true. External Factors: 33
34 A VALUABLE REFERENCE FOR PROGRAM PLANNING USING THE LOGIC MODEL APPROACH: Innovation Network, Inc. (2005) Logic model workbook 34
35 35
36 GB-CDPM FRAMEWORK TOOLKIT PLANNING GROUP Lynda Bumstead Grey Bruce Health Unit Nancy Dool-Kontio Southwest Community Care Access Centre Cathy Goetz-Perry Grey Bruce Victorian Order of Nurses Carolyn Grace Owen Sound Family health Team Jessica Meleskie Grey Bruce Health Network Lisa Miller Grey Bruce Diabetes Program Susan Pouget Closing The Gap Health Care Group Grey Bruce Mary Solomon Grey Bruce District Stroke Centre Michelle Walter Brockton and Area Family Health Team 36
East Gippsland Primary Care Partnership. Assessment of Chronic Illness Care (ACIC) Resource Kit 2014
 Resource Kit 2014") East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
East Gippsland Primary Care Partnership Assessment of Chronic Illness Care (ACIC) Resource Kit 2014 1 Contents. 1. Introduction 2. The Assessment of Chronic Illness Care 2.1 What is the ACIC? 2.2 What's
Preventing and Managing Chronic Disease: Ontario s Framework
 Preventing and Managing Chronic Disease: Ontario s Framework "This document has been developed to inform planning for chronic disease prevention and management (CDPM) in Ontario. It provides the evidence
Preventing and Managing Chronic Disease: Ontario s Framework "This document has been developed to inform planning for chronic disease prevention and management (CDPM) in Ontario. It provides the evidence
Hanover and District Hospital Strategic Plan
 Hanover and District Hospital 2012 Strategic Plan Prepared By: the President/CEO and the Board of Directors With input from Senior Staff, Employees, Physicians, and the Community Created June 2011- February
Hanover and District Hospital 2012 Strategic Plan Prepared By: the President/CEO and the Board of Directors With input from Senior Staff, Employees, Physicians, and the Community Created June 2011- February
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
All 28 items with minimal wording changes to reflect prenatal tobacco screening and treatment instead of chronic illness
 Assessing Chronic Illness Care Source: Bonomi AE, Wagner EH, Glasgow RE, VonKorff M. Assessment of Chronic Illness Care (ACIC): A practical tool to measure quality improvement. Health Services Research
Assessing Chronic Illness Care Source: Bonomi AE, Wagner EH, Glasgow RE, VonKorff M. Assessment of Chronic Illness Care (ACIC): A practical tool to measure quality improvement. Health Services Research
Building Coordinated, Patient Centered Care Management Teams
 Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Building Coordinated, Patient Centered Care Management Teams Jim Barr, MD CMO/VP Physician Network Development Optimus Healthcare Partners ACO & VP of Medical Services Aveta Health Solutions MSO Patient
Table of Contents for CCC Toolkit
 Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
Section 0.2 Overview Table of Contents for CCC Toolkit This document lists and briefly describes all the tools in the CCC Toolkit in alphabetic order. Time needed: As needed Suggested other tools: How
Michigan Primary Care Transformation Project. HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care
 Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
Michigan Primary Care Transformation Project HEDIS, Quality and the Care Manager s Role in Closing Gaps in Care 7.22.15 Topics for Today s Webinar Healthcare Effectiveness Data and Information Set (HEDIS)
CROSSWALK FOR AADE S DIABETES EDUCATION ACCREDITATION PROGRAM
 Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
Standard 1 Internal Structure: The provider(s) of DSME will document an organizational structure, mission statement, and goals. For those providers working within a larger organization, that organization
The LHIN s role in creating integrated health service delivery systems
 PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
Chapter 2. At a glance. What is health coaching? How is health coaching defined?
 Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
Chapter 2 What is health coaching? This chapter describes: What health coaching is and it s applications How health coaching relates to wider systems and programmes of care How health coaching relates
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Four Game-Changing Strategies for Transforming the Patient Experience
 Four Game-Changing Strategies for Transforming the Patient Experience Reaching and engaging your population is one of the most challenging components of patient-centered care. Despite the challenges, there
Four Game-Changing Strategies for Transforming the Patient Experience Reaching and engaging your population is one of the most challenging components of patient-centered care. Despite the challenges, there
NATIONAL STANDARDS, ESSENTIAL ELEMENTS AND INTERPRETIVE GUIDANCE
 Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
Standard 1. Organizational Structure The DSME entity will have documentation of its organizational structure, mission statement & goals and will recognize and support quality DSME as an integral component
California Academy of Family Physicians Diabetes Initiative Care Model Change Package
 California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
California Academy of Family Physicians Diabetes Initiative Care Model Change Package Introduction The Care Model (CM) is a unique and proven approach for implementing proactive strategies that are responsive
2017 National Standards for Diabetes Self-Management Education and Support INTERPRETIVE GUIDANCE
 2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
2017 National Standards for Diabetes Self-Management Education and Support The provider(s) of DSMES services will define and document a mission statement and goals. The DSMES services are incorporated
Peripheral Arterial Disease: Application of the Chronic Care Model. Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario
 Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
Peripheral Arterial Disease: Application of the Chronic Care Model Marge Lovell RN CCRC BEd MEd London Health Sciences Centre London, Ontario Objectives Provide brief overview of PAD Describe the Chronic
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
ONTARIO PUBLIC HEALTH STANDARDS
 ONTARIO PUBLIC HEALTH STANDARDS DRAFT April 30, 2007 The following document, Ontario Public Health Standards, has been produced by the Technical Review Committee. This document is subject to change. Prior
ONTARIO PUBLIC HEALTH STANDARDS DRAFT April 30, 2007 The following document, Ontario Public Health Standards, has been produced by the Technical Review Committee. This document is subject to change. Prior
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Adopting a Care Coordination Strategy
 Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Assessment of Chronic Illness Care Version 3.5
 Assessment of Chronic Illness Care Version 3.5 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the Learning Collaborative
Assessment of Chronic Illness Care Version 3.5 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the Learning Collaborative
The Burden of Diabetes
 The Burden of Diabetes Cost-Effectiveness of Interventions for Preventing & Treating Diabetes Priority Level 1 Glycemic control in people with A1c>9 Blood pressure control in people with BP>160/95 Foot
The Burden of Diabetes Cost-Effectiveness of Interventions for Preventing & Treating Diabetes Priority Level 1 Glycemic control in people with A1c>9 Blood pressure control in people with BP>160/95 Foot
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS) 1,2,3
 1,2,3") Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
Assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS),2,3 Individuals interested in using the PCRS in quality improvement work or research are free to do so. We request
PCFHC STRATEGIC PLAN
 PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
PCFHC 2016-2019 STRATEGIC PLAN A community partner growing to improve your family s well-being ABSTRACT Petawawa Centennial Family Health Centre (PCFHC) was established in 2005. PCFHC was one of the first
Promoting Interoperability Performance Category Fact Sheet
 Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Promoting Interoperability Fact Sheet Health Services Advisory Group (HSAG) provides this eight-page fact sheet to help providers with understanding Activities that are eligible for the Promoting Interoperability
Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network
 Healthcare Quarterly ONLINE CASE STUDY Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network Jessica Meleskie and Katrina Wilson 1 Abstract The Grey Bruce Health
Healthcare Quarterly ONLINE CASE STUDY Development of a Regional Clinical Pathway for Total Hip Replacement in a Rural Health Network Jessica Meleskie and Katrina Wilson 1 Abstract The Grey Bruce Health
bestpath Evidence Informed Improvement Package Chronic Disease Management Person-centred Appropriate Timely Healthcare
 Evidence Informed Improvement Package bestpath Person-centred Appropriate Timely Healthcare Chronic Disease Management Introduction & Overview ACKNOWLEDGEMENTS This workbook is the result of the efforts
Evidence Informed Improvement Package bestpath Person-centred Appropriate Timely Healthcare Chronic Disease Management Introduction & Overview ACKNOWLEDGEMENTS This workbook is the result of the efforts
The Chronic Care Model (Katherine Gibbs and Melanie Taylor)
") The Chronic Care Model (Katherine Gibbs and Melanie Taylor) INTRODUCTION A large proportion of time spent by those working currently within the field of primary health care revolves around short consultations
The Chronic Care Model (Katherine Gibbs and Melanie Taylor) INTRODUCTION A large proportion of time spent by those working currently within the field of primary health care revolves around short consultations
Provider Information Guide Complex Care and Condition Care Overview
 Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
Complex and Overview Introduction Complex and are essential components of Passport Health Plan s (Passport) Coordination services, which are used to support the practitioner-patient relationship and plan
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Keenan Pharmacy Care Management (KPCM)
") Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Keenan Pharmacy Care Management (KPCM) This program is an exclusive to KPS clients as an additional layer of pharmacy benefit management by engaging physicians and members directly to ensure that the best
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans
 Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Fast-Track PCMH Recognition
 Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
Fast-Track PCMH Recognition i2i Systems integrated package of Population Health Management and reporting technology, documented processes and consulting services aligned with NCQA guidelines supports and
RNAO International Affairs and Best Practice Guidelines Program
 RNAO International Affairs and Best Practice Guidelines Program Dr. Doris Grinspun, RN, MSN, PhD, LLD(hon), O.ONT Chief Executive Officer Dr. Irmajean Bajnok, RN, MScN, PhD Director, RNAO International
RNAO International Affairs and Best Practice Guidelines Program Dr. Doris Grinspun, RN, MSN, PhD, LLD(hon), O.ONT Chief Executive Officer Dr. Irmajean Bajnok, RN, MScN, PhD Director, RNAO International
Developed by members of the Public Health and Community Nutrition Interest Group
 Adopted: February 2015 To be reviewed: February 2018 Public Health and Community Nutrition Role Statement Role Statement for Accredited Practising Dietitians practising in the area of public health and
Adopted: February 2015 To be reviewed: February 2018 Public Health and Community Nutrition Role Statement Role Statement for Accredited Practising Dietitians practising in the area of public health and
Assessment of Chronic Illness Care Version 3
 Assessment of Chronic Illness Care Version 3 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the ICIC/IHI team. We would
Assessment of Chronic Illness Care Version 3 Please complete the following information about you and your organization. This information will not be disclosed to anyone besides the ICIC/IHI team. We would
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure
 Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
Improvement Activities for ACI Bonus Measures
 Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Improvement Activity Performance Category Subcategory Expanded Practice Activity Name Activity Improvement Activity Performance Category Weight Provide 24/7 access to eligible clinicians or groups, who
Chronic Disease Management & Prevention System Level Logic Model
 Chronic Disease Management & Prevention System Level Logic Model Prepared by : Planning Subcommittee Members: Dr. Louis Balogh, Regional Vice President, Southlake Regional Health Centre Ms. Kathy Condie,
Chronic Disease Management & Prevention System Level Logic Model Prepared by : Planning Subcommittee Members: Dr. Louis Balogh, Regional Vice President, Southlake Regional Health Centre Ms. Kathy Condie,
Staying Connected with Patient-Generated Health Data
 Staying Connected with Patient-Generated Health Data April 14, 2015 Dr. Danny Sands, Chief Medical Officer Dr. Philip Marshall, Chief Product Officer DISCLAIMER: The views and opinions expressed in this
Staying Connected with Patient-Generated Health Data April 14, 2015 Dr. Danny Sands, Chief Medical Officer Dr. Philip Marshall, Chief Product Officer DISCLAIMER: The views and opinions expressed in this
At EmblemHealth, we believe in helping people stay healthy, get well and live better.
 At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
At EmblemHealth, we believe in helping people stay healthy, get well and live better. Welcome to the 2017 course on Special Needs Plan Model of Care. This year s course is focused on how we can successfully
Standard #1: Internal Structure
 Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
TABLE H: Finalized Improvement Activities Inventory
 TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
TABLE H: Finalized Improvement Activities Inventory [We invited comments on the reassignment of improvement activities under alternate subcategories, and on the scoring weights assigned to improvement
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016
 Care Model May 12, 2016") update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
update An Inside Look Into the EHR Intersections of the Updated Patient-Centered Medical Home (PCMH) Care Model May 12, 2016 Agenda PCMH: 360 o PCMH to date o Evidence based results o Updated Standards:
Patient Centered Medical Home. History of PCMH concept. What does a PCMH look like? 10/1/2013. What is a Patient Centered Medical Home (PCMH)?
?") What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
What is a Patient Centered Medical Home (PCMH)? Patient Centered Medical Home Jeremy Thomas, PharmD, CDE UAMS Department of Pharmacy "an approach to providing comprehensive primary care that facilitates
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI
 COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
COMMUNITY HEALTH NEEDS ASSESSMENT HINDS, RANKIN, MADISON COUNTIES STATE OF MISSISSIPPI Sample CHNA. This document is intended to be used as a reference only. Some information and data has been altered
Meaningful Use Stages 1 & 2
 Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Model of Health and Wellbeing Evaluation Framework & Data Entry Manual. Presented by: CHC Regional Decision Support June 2015
 Model of Health and Wellbeing Evaluation Framework & Data Entry Manual Presented by: CHC Regional Decision Support June 2015 Topics Model Evaluation Framework: Role of Model Attributes Results Based Logic
Model of Health and Wellbeing Evaluation Framework & Data Entry Manual Presented by: CHC Regional Decision Support June 2015 Topics Model Evaluation Framework: Role of Model Attributes Results Based Logic
Improving Patient Care by Building Capacity Using an Integrated Approach to Chronic Disease Management
 Improving Patient Care by Building Capacity Using an Integrated Approach to Chronic Disease Management Jo-Anne Oake-Vecchiato RN, BScN, MHSc. National Healthcare Leadership Conference Saskatoon, June 2-3,
Improving Patient Care by Building Capacity Using an Integrated Approach to Chronic Disease Management Jo-Anne Oake-Vecchiato RN, BScN, MHSc. National Healthcare Leadership Conference Saskatoon, June 2-3,
Primary Care Development in Hong Kong: Future Directions
 Primary Care Development in Hong Kong: Future Directions HA Convention 2014 8 May 2014 Professor Sophia CHAN PhD, MPH, MEd, RN, RSCN, FAAN, FFPH, JP Under Secretary for Food and Health, Government of the
Primary Care Development in Hong Kong: Future Directions HA Convention 2014 8 May 2014 Professor Sophia CHAN PhD, MPH, MEd, RN, RSCN, FAAN, FFPH, JP Under Secretary for Food and Health, Government of the
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Draft. Public Health Strategic Plan. Douglas County, Oregon
 Public Health Strategic Plan Douglas County, Oregon Douglas County 2014 Letter from the Director Dear Colleagues It is with great enthusiasm that I present the Public Health Strategic Plan for 2014-2015.
Public Health Strategic Plan Douglas County, Oregon Douglas County 2014 Letter from the Director Dear Colleagues It is with great enthusiasm that I present the Public Health Strategic Plan for 2014-2015.
MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE. Purpose of Report: For Note
 Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Date of Meeting: 23 rd March 2017 MERTON CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMISSIONING COMMITTEE Agenda No: 7 Attachment: 6 Title of Document: Primary Care Strategy Update Purpose of Report:
Evaluation of State Public Health Actions: Overview and Progress to Date Rachel Davis, MPH
 Evaluation of State Public Health Actions: Overview and Progress to Date Rachel Davis, MPH Division for Heart Disease and Stroke Prevention Evaluation and Program Effectiveness Team Presentation Overview
Evaluation of State Public Health Actions: Overview and Progress to Date Rachel Davis, MPH Division for Heart Disease and Stroke Prevention Evaluation and Program Effectiveness Team Presentation Overview
Pathways to Diabetes Prevention
 Pathways to Diabetes Prevention How Colorado Organizations are Creating Healthcare Referral Systems that Work Introduction It is estimated that 35% of Colorado adults and half of all adults aged 65 years
Pathways to Diabetes Prevention How Colorado Organizations are Creating Healthcare Referral Systems that Work Introduction It is estimated that 35% of Colorado adults and half of all adults aged 65 years
PCMH: Recognition to Impact
 PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
PCMH: Recognition to Impact 3.1.16 Prepared by: Shannon Nielson, MHA, PCMH CCE Prepared for: OACHC 2016 Annual Conference Centerprise, Inc Objectives Defining a Patient Centered Medical Home Translating
Working at Top of License How do you reallocate work among a team? January 28, 2015
 Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Working at Top of License How do you reallocate work among a team? January 28, 2015 We Want To Hear From You! Type questions into the Questions Pane at any time during this presentation Patient-Centered
Peer Review Example: Clinician 4 (Meets Expectations)
") Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Peer Review Example: Clinician 4 (Meets Expectations) RBC- Self and Colleagues: I have observed Jane consistently role modeling team member safety through use of PPE/Goggles/safe patient handling practices,
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
ISAAC. Improving Sickle Cell Care for Adolescents and Adults in Chicago
 ISAAC Improving Sickle Cell Care for Adolescents and Adults in Chicago Improving Sickle Cell Care for Adolescents and Adults in Chicago (ISAAC) nal tools for sickle PROJECT BRIEF: ISAAC is a 6-year NIH/NHLBI-funded
ISAAC Improving Sickle Cell Care for Adolescents and Adults in Chicago Improving Sickle Cell Care for Adolescents and Adults in Chicago (ISAAC) nal tools for sickle PROJECT BRIEF: ISAAC is a 6-year NIH/NHLBI-funded
NWT Primary Community Care Framework
 NWT Primary Community Care Framework August 2002 Table of Contents Introduction... 1 National Perspective... 2 NWT Vision for Primary Community Care... 2 Principles... 3 The NWT Approach to Primary Community
NWT Primary Community Care Framework August 2002 Table of Contents Introduction... 1 National Perspective... 2 NWT Vision for Primary Community Care... 2 Principles... 3 The NWT Approach to Primary Community
ehealth to Disseminate Lay Health Coaching
 ehealth to Disseminate Lay Health Coaching Patrick Yao Tang, MPH Program Manager, Peers for Progress yptang@email.unc.edu www.peersforprogress.org Society of Behavioral Medicine Annual Meeting April 1,
ehealth to Disseminate Lay Health Coaching Patrick Yao Tang, MPH Program Manager, Peers for Progress yptang@email.unc.edu www.peersforprogress.org Society of Behavioral Medicine Annual Meeting April 1,
Health and Well-Being Grant Program Guidelines
 Ministry of Health and Long-Term Care Health and Well-Being Grant Program Guidelines 2017-18 Population and Public Health Division, Ministry of Health and Long-Term Care November 2017 Table of Contents
Ministry of Health and Long-Term Care Health and Well-Being Grant Program Guidelines 2017-18 Population and Public Health Division, Ministry of Health and Long-Term Care November 2017 Table of Contents
Mental Health Engagement Network (MHEN): Facilitating Mobile Patient Centric Care
: Facilitating Mobile Patient Centric Care") Mental Health Engagement Network (MHEN): Facilitating Mobile Patient Centric Care Presentation Outline MHEN Project Context MHEN Project Results and Findings Lessons Learned and Implications Sandbox Mental
Mental Health Engagement Network (MHEN): Facilitating Mobile Patient Centric Care Presentation Outline MHEN Project Context MHEN Project Results and Findings Lessons Learned and Implications Sandbox Mental
Integrating prevention into health care
 Integrating prevention into health care Due to public health successes, populations are ageing and increasingly, people are living with one or more chronic conditions for decades. This places new, long-term
Integrating prevention into health care Due to public health successes, populations are ageing and increasingly, people are living with one or more chronic conditions for decades. This places new, long-term
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Standard #1: Internal Structure
 Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Site/Location: Standard #1: Internal Structure The provider(s) of Diabetes Self-Management Education and Support (DSMES) will define and document a mission statement and goals. The DSMES services are incorporated
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Quality Improvement Plan (QIP) Narrative: Markham Stouffville Hospital Last updated: March 2017
 Narrative: Markham Stouffville Hospital Last updated: March 2017") Overview The Quality Improvement Plan (QIP) is an integral part of the quality framework at (MSH). This QIP, our seventh, was developed in partnership with patients, families, and the community we serve.
Overview The Quality Improvement Plan (QIP) is an integral part of the quality framework at (MSH). This QIP, our seventh, was developed in partnership with patients, families, and the community we serve.
Using Updox to Succeed with MIPS
 Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
Using Updox to Succeed with MIPS Who is Updox? A Communications Platform built by physicians, for physicians 56,000+ providers and more than 300,000 users--and growing 100+ EMR integrations 72 million
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Discuss and analyse approaches to health and health promotion, and describe Australia s health system and the different roles of government and
 Outcome 2 Pt 2 Discuss and analyse approaches to health and health promotion, and describe Australia s health system and the different roles of government and non-government organisations in promoting
Outcome 2 Pt 2 Discuss and analyse approaches to health and health promotion, and describe Australia s health system and the different roles of government and non-government organisations in promoting
Working with GPs to help deliver the NHS Health Checks Programme
 Working with GPs to help deliver the NHS Health Checks Programme Dr Matt Kearney GP Castlefields, Runcorn National Clinical Advisor Public Health England and NHS England Why do we need GP engagement? 1.
Working with GPs to help deliver the NHS Health Checks Programme Dr Matt Kearney GP Castlefields, Runcorn National Clinical Advisor Public Health England and NHS England Why do we need GP engagement? 1.
Peninsula Health Strategic Plan Page 1
 Peninsula Health Strategic Plan 2013-2018 Page 1 Peninsula Health Strategic Plan 2013-2018 The Peninsula Health Strategic Plan for 2013-2018 sets out the future directions for Peninsula Health over this
Peninsula Health Strategic Plan 2013-2018 Page 1 Peninsula Health Strategic Plan 2013-2018 The Peninsula Health Strategic Plan for 2013-2018 sets out the future directions for Peninsula Health over this
Onsite Clinic and Wellness Programs 2010 VACo Achievement Awards. Montgomery County, VA
 Onsite Clinic and Wellness Programs 2010 VACo Achievement Awards Montgomery County, VA 1. Brief overview Montgomery County implemented a fully integrated on site disease management Clinic and Wellness
Onsite Clinic and Wellness Programs 2010 VACo Achievement Awards Montgomery County, VA 1. Brief overview Montgomery County implemented a fully integrated on site disease management Clinic and Wellness
COF WEBINAR 6 AUGUST 29, 2013 HOSTED BY THE REGISTERED NURSES ASSOCIATION OF ONTARIO
 EVALUATING NURSING AND CLIENT OUTCOMES THROUGH GUIDELINE-BASED INDICATORS: THE RNAO NQUIRE INITIATIVE COF WEBINAR 6 AUGUST 29, 2013 HOSTED BY THE REGISTERED NURSES ASSOCIATION OF ONTARIO Welcome from Dr.
EVALUATING NURSING AND CLIENT OUTCOMES THROUGH GUIDELINE-BASED INDICATORS: THE RNAO NQUIRE INITIATIVE COF WEBINAR 6 AUGUST 29, 2013 HOSTED BY THE REGISTERED NURSES ASSOCIATION OF ONTARIO Welcome from Dr.
Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente
 Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente Association for Community Health Improvement (ACHI) 2015 Conference What We
Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente Association for Community Health Improvement (ACHI) 2015 Conference What We
Improvement Activities Data Validation Criteria
 Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
Activity ID Subcategory Activity Name Activity Description Activity Validation Suggested Documentation (inclusive of dates during the selected continuous 90-day or year Name Weighting long reporting period)
General Pathways Education Workshop (click t o to g o go t o to t he the desired section)
") General Pathways Education Workshop (click to go to the desired section) Introduction to Workshop/Instructions Why Care Pathways? Components of the Care Pathway Care Pathway Simulation Implementing Care
General Pathways Education Workshop (click to go to the desired section) Introduction to Workshop/Instructions Why Care Pathways? Components of the Care Pathway Care Pathway Simulation Implementing Care
Co-creating Care with Ethnic Communities
 Co-creating Care with Ethnic Communities Helen Leung, MSW Chief Executive Officer Carefirst Seniors and Community Services Association Carefirst Family Health Team February 17, 2010 Agenda 1. About Carefirst
Co-creating Care with Ethnic Communities Helen Leung, MSW Chief Executive Officer Carefirst Seniors and Community Services Association Carefirst Family Health Team February 17, 2010 Agenda 1. About Carefirst
Registered Nurse - Quality Improvement Coordinator, West Auckland Locality
 Date: December 2013 Job Title : Registered Nurse Quality Improvement Coordinator West Department Location Reporting To Direct Reports : Primary Health Care Nursing Development Team : Waitemata District
Date: December 2013 Job Title : Registered Nurse Quality Improvement Coordinator West Department Location Reporting To Direct Reports : Primary Health Care Nursing Development Team : Waitemata District
Quality Management Program
 Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
WRHA Vision: Healthy People, Vibrant Communities, Care for All
 Winnipeg Regional Health Authority Mental Health Promotion Program - Strategic Planning Conceptual Framework WRHA Vision: Healthy People, Vibrant Communities, Care for All Mental Health Promotion Program
Winnipeg Regional Health Authority Mental Health Promotion Program - Strategic Planning Conceptual Framework WRHA Vision: Healthy People, Vibrant Communities, Care for All Mental Health Promotion Program
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices
 Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
Milestones and Indicators of Progress: A Reference for Patient-Centered Primary Care Participating Practices How to Use This Guide The following Program Milestones and Indicators of Progress are drawn
South West LHIN Primary Health Care Capacity Report Final Recommendations
 South West LHIN Primary Health Care Capacity Report Final Recommendations West Elgin Community Health Centre and the South West LHIN jointly sponsored a study called Understanding Health Inequities and
South West LHIN Primary Health Care Capacity Report Final Recommendations West Elgin Community Health Centre and the South West LHIN jointly sponsored a study called Understanding Health Inequities and
MENTAL HEALTH 2018 REQUEST FOR PROPOSAL
 MENTAL HEALTH 2018 REQUEST FOR PROPOSAL HCF Providing leadership, advocacy, and resources to eliminate barriers and promote quality health for the uninsured and underserved VISION: Healthy People, Healthy
MENTAL HEALTH 2018 REQUEST FOR PROPOSAL HCF Providing leadership, advocacy, and resources to eliminate barriers and promote quality health for the uninsured and underserved VISION: Healthy People, Healthy
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs
 NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
NYSPFP- Readmission Collaborative Domain II - Kick-off Webinar Improving Care Transitions Between Hospitals and SNFs February 28, 2017 A partnership of the Healthcare Association of New York State and
PPC2: Patient Tracking and Registry Functions
 PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
PPC2: Patient Tracking and Registry Functions Element F: Use of System for Population Management At we use our EMR, clinical event manager, and the ad hoc reporting system (Business Objects) for a multi-pronged
LEARNING ABOUT CAREERS USING AND ADAPTING TEXTS FROM THE OCCUPATIONAL OUTLOOK HANDBOOK
 LEARNING ABOUT CAREERS USING AND ADAPTING TEXTS FROM THE OCCUPATIONAL OUTLOOK HANDBOOK 1. SELECT THE MATERIAL FOR YOUR LEARNERS LEVEL 2. REFLECT: Would this material be relevant to your learners? Why or
LEARNING ABOUT CAREERS USING AND ADAPTING TEXTS FROM THE OCCUPATIONAL OUTLOOK HANDBOOK 1. SELECT THE MATERIAL FOR YOUR LEARNERS LEVEL 2. REFLECT: Would this material be relevant to your learners? Why or