by Melinda D. Sawyer DrPH candidate
|
|
|
- Bartholomew Jefferson
- 5 years ago
- Views:
Transcription
1 EVALUATING THE TEAM AND IMPLEMENTATION FACTORS ASSOCIATED WITH HOSPITAL- BASED COMPREHENSIVE UNIT-BASED SAFETY PROGRAM (CUSP) TEAM EFFECTIVENESS by Melinda D. Sawyer DrPH candidate A dissertation submitted to Johns Hopkins University in conformity with the requirements for the degree of Doctorate in Public Health Baltimore, MD February 2017
2 Table of Contents List of Tables... iv List of Figures... v Abstract... vi Chapter 1: Introduction... 1 Patient Safety in Healthcare... 1 Overview of CUSP... 1 Evaluating CUSP Team Processes and Outcomes: The CUSP Scorecard... 3 Theoretical Framework... 4 Conceptual Model of CUSP Team Effectiveness... 6 Study Aims and Hypotheses... 7 Significance Chapter 2: Literature Review Mindful Organizing and High Reliability Patient Safety Culture and Patient Safety Climate Evaluating Patient Safety Climate Implementation Science and The Comprehensive Unit-based Safety Program Spreading CUSP Beyond the ICU Contextual Factors Associated with CUSP Implementation Team Science: Drawing from the Science of Project Teams Chapter 3: Methods Research Question Study Aims and Hypotheses Protection of Human Subjects Study Design Inclusion Criteria Exclusion Criteria Sources of Data Study Variables Analysis Creation of the master database Exploratory data analysis ii
3 Data analysis for each study aim and hypothesis Chapter 4: Results Baseline Characteristics of CUSP teams Overview of CUSP Scorecard Data Aim 1 Hypothesis 1 Results: Provider attendance Aim 1 Hypothesis 2 Results: Executive Attendance Aim 1 Hypothesis 3 Results: CUSP Meetings Held Aim 1 Hypothesis 4 Results: Total CUSP Team Projects Additional Analyses: Provider Attendance and Total CUSP Projects Completed Aim 2 and Aim 3 Results: Safety Climate Domain Scores Mediation Chapter 5: Discussion and Implications Discussion Strengths and Limitations Implications & Conclusions References APPENDIX A: CUSP SCORECARD APPENDIX B: CURRICULUM VITAE iii
4 List of Tables Table 1: Variables Examined in Each Aim... 9 Table 2: Johns Hopkins Hospital-basd CUSP Teams by Affiliate as of July 1, Table 3: SAQ Survey Safety Climate Items Table 4: Characteristics of CUSP Teams, Scorecard and Safety Climate Survey Table 5: Factors Contributing to Provider Attendance at CUSP Meetings Table 6: Factors contributing to Executive Attendance at CUSP Meetings Table 7: Factors Contributing to CUSP Meetings Held Table 8: Goodness of Fit for Bivariate Analyses using Poisson Regression between CUSP meetings held, provider attendance and executive attendance and Total CUSP Projects completed Table 9: Model fit for total projects completed with age as a confounder compared to adding an age x process interaction term Table 10: Factors Contributing to Total CUSP Projects Completed Table 11: Factors Contributing to the Proportion of Data-driven Improvement Projects Completed Table 12: Factors Contributing to the Safety Climate Domain Score iv
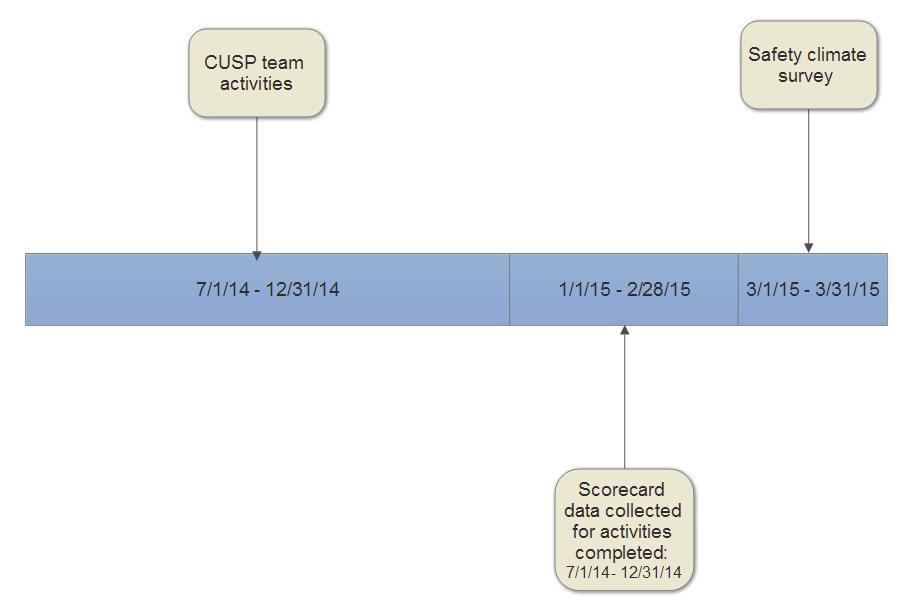
5 List of Figures Figure 1: Theoretical CUSP Framework Adapted from Donabedian and Team Science... 6 Figure 2: Conceptual Model of CUSP Team Effectiveness... 7 Figure 3: Data Collection Timeline v
6 Abstract Problem Statement: The Comprehensive Unit-based Safety Program (CUSP) has been successfully implemented in thousands of clinical areas across the United States and around the world and has demonstrated improvements in clinical outcomes, operational outcomes and safety culture. Despite its overwhelming success, some CUSP teams have been more successful than others and the factors associated with success are not well understood. Purpose: The purpose of this dissertation is to examine the team and implementation factors associated with CUSP team effectiveness using a transdisciplinary framework combining team theory and implementation science. Methods: This study used prospectively collected administrative data from CUSP teams from a large, multi-hospital health system. Multivariate linear regression, multivariate logistic regression and multivariate negative binomial regression modeling were used to examine the assocations between CUSP team structures, processes, proximal outcomes (total CUSP projects completed) and the distal outcome of unit-level patient safety climate scores. Results: A total of 88 of 106 CUSP teams had sufficient data to include in this analysis. Compared to teams with champions that received no safety training, teams whose champions received both CUSP basic training and Patient Safety Certificate training had 7.76 greater odds (p=0.07) of having high provider attendance versus low provider attendance. There were significant differences (p=0.02) among unit types (ICU, non- vi
7 ICU, other) in the odds of having high provider attendance versus low provider attendance. For CUSP teams that met regularly, there was an 8.33-fold increase (p=0.009) in the total number improvement projects completed for every one percentage point increase in the percentage of meetings held. There was a significant association between the age of the teams and total team projects completed with more projects being completed as age increased (Incidence rate ratio (IRR) = 1.003, 95% confidence interval (CI): 1.000, 1.007, p=0.03). Contrary to the hypotheseis, there was significant less improvement projects completed when provider attendance was highest (IRR= 0.59, 95% CI: 0.41, 0.84, p=0.009). There was no association detected between total projects completed (proximal outcome) and unit-level safety climate domain scores (distal outcome). Conclusion: There are several key team and implementation factors associated with CUSP team effectiveness. Unit type is associated with provider attendance, differences exist between hospitals with regard to regular meeting being held, regular meetings and the age of the team were associated with total projects completed while regular provider attendance was associated with less projects completed. More research is needed to confirm these findings and to identify the proximal team outcome(s) that are associated with the distal outcome of unit-level patient safety climate scores. vii
8 Chapter 1: Introduction Patient Safety in Healthcare Despite enormous pressure from policy makers to patients in the seventeen years since to Err is Human was published, there are few instances of success in reducing preventable harm in healthcare. 1-4 In order to achieve and sustain improvements that reduce preventable harm, healthcare must learn to become highly reliable. 5-7 One core component essential to reducing preventable harm and becoming highly reliable is to create a culture of safety. 1,7-10 The comprehensive unit-based safety program (CUSP), teamwork and communication training, and executive walk rounds are three of the interventions that are associated with improvements in patient safety culture. 8,9 Unfortunately, few studies describe the critical aspects associated with success. 9,11,12 Overview of CUSP The Comprehensive Unit-based Safety Program (CUSP), developed at Johns Hopkins, is a five step program that improves specific safety outcomes and safety culture The five steps of CUSP include 17 : 1. Training staff in the science of safety 2. Identifying defects 3. Partnering with a senior executive 4. Learning from defects 5. Implementing improvement tools 1
9 CUSP s success in reducing central line-associated blood stream infections (CLABSI) in the State of Michigan from , the Agency for Healthcare Research and Quality funded the On the CUSP: STOP BSI program in which CUSP was implemented in 1,071 ICU s in 44 states across the United States and resulted in an 43% reduction of CLABSI s. 2,13 Subsequently, CUSP, in combination with clinical interventions, reduced the risk of ventilator-associated pneumonia (VAP) and surgical site infections (SSI). 13,18-20 In addition to outcomes such as CLABSI, SSI and VAP noted above, the implementation of CUSPsuggest is the program is associated with improvements in safety climate scores as measured by the Safety Attitudes Questionnaire (SAQ). 21 In turn, improvements in safety climate are associated with downstream safety outcomes such as improvements in nurse turnover. 17,22 Although CUSP rose to prominence through the success of the national program to reduce CLABSI, it began as a program to improve patient safety generally, and implementation of CUSP has continued at Johns Hopkins since its inception in ,13,21,23 Today there are 158 CUSP teams throughout Johns Hopkins Medicine, a large health system that includes 2 large tertiary-care academic medical centers, 1 large tertiary-care academic pediatric medical center, 3 community hospitals, a large 35-site ambulatory community practice and a home care company. 24 2
10 While CUSP can improve safety outcomes and facilitate quality improvement, some CUSP teams are more successful than others. The factors associated with their success are currently not well understood. The purpose of this dissertation is to examine the team and implementation factors associated with CUSP effectiveness using a transdisciplinary framework combining team theory and implementation science. Specifically, this study aims to examine the CUSP structures, processes, and proximal outcomes associated with the distal outcome of unit-level patient safety climate. CUSP provides unit-level infrastructure for improvements in safety and quality by engaging the spectrum of stakeholders from front-line staff to institution executives. This begins with the assembly of an active and engaged team that acquires safety training, continued focus on teamwork, identification of problems and interventions to address these problems. Using the specific steps of CUSP as a guideline, experts at Johns Hopkins, including those who designed the program initially and those who continue to oversee its successful implementation locally, nationally, and internationally, defined a Scorecard to evaluate the progress and performance of CUSP teams. Evaluating CUSP Team Processes and Outcomes: The CUSP Scorecard To develop the CUSP Scorecard a group of five CUSP experts and measurement experts were brought together in 2012 to develop a set of measures that could potentially identify the team and implementation factors associated with success. These measures 3
11 needed to be specific to the CUSP program and feasible to collect by an organization regardless of the number of CUSP teams. Eight measures were ultimately selected that were believed to achieve both of these goals. The CUSP Scorecard was pilot tested across 14 CUSP teams in one department in 2013, feedback was obtained and adjustments were made to the Scorecard. The final CUSP Scorecard was then implemented across Johns Hopkins Medicine starting in July, 2014 (Appendix A). The development of the CUSP scorecard underscored the need to understand the team and implementation factors associated with CUSP team effectiveness and provided a mechanism to start to investigate some of these important questions. Theoretical Framework Understanding the factors associated with CUSP team success is rooted in multiple fields of science. First, team science from the perspective of organizational psychology and organizational behavior offers important insights into the characteristics of highly functional teams. As healthcare becomes increasingly complex and reliant on individuals working within teams to deliver care an understanding of the drivers of team performance and effectiveness are also critical. 8 Next, the science of project management offers critical knowledge regarding the relationship between project teams and project performance. 25 Finally, the classic Donabedian model of structure, process, and outcomes to evaluate quality in medical care, from implementation and improvement science, provides critical insights into factors associated with health outcomes. 26 Donabedian s model emphasized that health care structures were driving 4
12 forces for care processes that ultimately lead to health outcomes. 26 By drawing on the knowledge across all three fields I propose a theoretical framework designed to articulate some of the team and implementation factors associated with CUSP effectiveness (Figure 1). Teams theory differentiates intra vs. inter team processing in examining CUSP team processes. 27 Intra-team structures such as team knowledge, team leader knowledge, and the amount of dedicated time given to the team leader are critical drivers for teams. 26,27 Intra-team processes, including communication processes and the functional diversity of the team, are important to achieve the proximal CUSP team outcomes and may be effected by how long the team has been working together. 25,27 In this framework, functional diversity of the team is included as an intrateam process rather than an intra-team structure because the degree of functional diversity within the team (as measured by attendance) represents a proxy indicator of interdisciplinary discussion and collective problem solving during a team meeting. The primary goal, or proximal outcome, of CUSP teams has been to learn from defects. 17,25 Learning from defects, as defined in the CUSP program, represents the impactful products (projects) of the CUSP team processes. These can include projects associated with either rate-based preventable harm or non-rate based preventable harm. 15 Together these projects are called total CUSP team projects. Project management science differentiates proximal team outcomes from distal team outcomes. Distal team outcomes, like safety culture, are the value the output creates for the organization. 25 Proximal outcomes are more closely related contextually to their antecedents and correlations should be stronger than for more distal outcomes. 25 Finally, organizational 5
13
14
15 Hypothesis 2: Teams reporting more (a) protected time for the team CUSP Champion, (b) training for CUSP champion, and (c) SOS training for staff will also report greater executive attendance than those reporting less protected time and training for their CUSP Champion and less training of their staff. Hypothesis 3: Teams reporting more (a) protected time for the team CUSP Champion and (b) training for the champion and (c) SOS training for staff will also report more meetings held than those reporting less protected time and training for their CUSP Champion and less training of their staff. Hypothesis 4: Teams reporting greater (a) provider and (b) executive attendance and (c) meetings held will also report higher number of CUSP team projects than those reporting less attendance and meetings held. Aim 2: Examine the association between proximal CUSP team outcomes (total CUSP team projects completed) and unit-level safety climate, a distal CUSP team outcome. Hypothesis 1: Teams reporting more total CUSP team projects will also report higher unit-level safety climate scores than those reporting fewer total team projects. Aim 3: Examine the association between the CUSP processes and unit-level safety climate. Hypothesis 1: The relationship between CUSP processes (a) provider and (b) executive attendance and (c) meetings held rates and unit-level safety climate is partially mediated by the proximal team outcomes. 8
16 Table 1: Variables Examined in Each Aim Aim/ Theory Dependent Variables (Type) Independent Variables (Type) Covariates/ potential confounders Variables (Type) A1 H1 <80% of meetings with provider in attendance, 80% of meetings with provider in attendance (dichotomous) % of staff with SOS training (continuous) CUSP champion training (ordinal) Protected time for champion (continuous) Affiliate ID (nominal) Unit type (nominal) A1 H2 % executive attendance (continuous) % of staff with SOS training (continuous) CUSP champion training (ordinal) Protected time for champion (continuous) Affiliate ID (nominal) Unit type (nominal) A1 H3 <80% of meetings held, 80% of meetings held (dichotomous) % of staff with SOS training (continuous) CUSP champion training (ordinal) Protected time for champion (continuous) Affiliate ID (nominal) Unit type (nominal) A1 H4 # of total CUSP team projects (count) % of CUSP meetings held (continuous), spline knot at 80% % provider attendance (continuous) % executive attendance (continuous) % of staff with SOS training (continuous) CUSP champion training (ordinal) Protected time for champion (continuous) Affiliate ID (nominal) Unit type (nominal) Age of CUSP team (continuous) A2 H1 Safety climate domain score (continuous) # of total CUSP team projects (count) % of CUSP team meetings held (continuous) % provider attendance (continuous) % executive attendance (continuous) Affiliate ID (nominal) Unit type (nominal) A3 H1 a Mediator Safety climate domain score (continuous) % of CUSP meetings held (continuous) % executive attendance (continuous) % provider attendance (continuous) Affiliate ID (nominal) Unit type (nominal) # of total CUSP team projects (count) a 9
17 Significance There is a growing demand from patients to policy makers that healthcare organizations must deliver the best quality care, every single time, at the lowest possible cost. 5,28 Healthcare organizations are far from achieving this goal. In order to achieve these goals healthcare organizations must work toward becoming highly reliable, in other words, mindful. Organizations that engage in mindful organizing commit to safety at all levels, which creates a culture of safety. 5,7 CUSP is one intervention in healthcare that promotes a culture of safety. 8 Despite spreading CUSP across thousands of teams in the United States and around the world it is not yet know what team and implementation factors are associated with CUSP success. This leaves organization leaders in the dark regarding the critical elements that must be in place to truly spread CUSP across their organization in order to create organizational mindfulness. As the CUSP program continues to proliferate across the United States and beyond, there is a growing need to understand which CUSP team structures and processes are associated with proximal CUSP team outcomes. And to understand what, if any, associations exist between these and distant CUSP team outcomes like improvements in unit-level safety climate domain scores. This will allow for organizational leaders to appropriately invest in the CUSP program and will allow teams to drive performance on the critically important steps associated with improving a culture of safety. This dissertation begins to answer some of these important questions. For example, are teams more successful when specific organizational structures are in place, for instance, 10
18 when a CUSP champion has dedicated time for improvement related work? If so, how much dedicated time is necessary? Providing dedicated time to do this work may be an expensive but necessary step to achieving CUSP outcomes and ultimately achieving organizational mindfulness. Chapter 2: Literature Review Mindful Organizing and High Reliability The hypotheses examined in this study draw together several theoretical schools of thought, including (1) high reliability theory, (2) implementation science and (3) team science from the perspectives of organizational psychology and project management science. Each is briefly summarized and synthesized in order to describe the theoretical landscape that serves as a foundation for the specific hypotheses examined in this study. Findings from previous studies of CUSP and safety climate measurement are also examined and summarized. Since the 1999 Institute of Medicine report, To Err is Human, healthcare has sought to eliminate preventable harm and create a learning culture in which errors are investigated and responses to mistakes are just. 1,29 Arguably few organizations in healthcare have achieved this level of quality so healthcare has looked to other industries to identify the very characteristics that help them achieve high reliability. Previous research by Vogus and Sutcliffe identified five characteristics that all members 11
19 of an organization must commit to in order to become highly reliable. 30 These include sensitivity to operations, preoccupation with failure, deference to expertise, resilience, and a reluctance to simplify. 5,30 Collectively these are referred to as organizational mindfulness. 5,6,31 In order to approach organizational mindfulness, organizations must start on a path to engage everyone, especially frontline staff in mindful organizing. 30 Mindful organizing represents a dynamic process comprising specific ongoing actions rather than enduring organizational characteristic (p.724). 30 It relies on continuous real-time communication and interactions, results from bottom-up processes, and engages the front line in thinking and action within an organization. 6,32,33 Highly reliable organizations demonstrate a preoccupation with failure. 6 People within resilient organizations are constantly looking for small cues that systems are not acting as they should, are resistant to normalizing unexpected findings, are wary even when there are signs of success, and are able to maintain a spirit of contradiction or doubt as opposed to a spirit of accord (p.52 ). 7 Highly reliable organizations demonstrate a reluctance to simplify. 6 People within mindful organizations are reluctant to simplify because doing so hides signals and details which leads to unreliable performance. 7 These threats to performance can have subtle, but important, distinctions and oversimplifying them may mean the difference between early and late detection. 5 Highly reliable organizations demonstrate a sensitivity to operations. 6 People within these organizations are acutely aware that early threats to organizational performance are often seen in the daily operations. 5 As a result, early signal of deviations of 12
20 performance within a system must be reported and acted upon. Failures to detect these early warnings can be a result of ignorance, casualness and distractions. 7 In order to avoid these, Todd LA Porte (p. 224) describes the need for operators to engage in the state of cognitive integration and collective mind that allows the integration of tightly coupled interactive complexity as a dynamic operational process. 7,34 Highly reliable organizations demonstrate resilience. 6 They are not error-free but they are also not disabled when errors do occur. 7 People within resilient organizations recognize errors quickly and contain them before causing harm. To achieve organizational resilience, the organization must learn from error and implement learning swiftly. 7 Highly reliable organizations demonstrate a deference to those with the most expertise. 6 When a situation arises, people within these organizations must have an understanding of the limits of their own knowledge and experience and have mechanisms in place to quickly identify the individuals who do. 7 These mechanisms are indifferent to hierarchy and rank. In summary, healthcare organizations must work toward becoming highly reliable. In order to move the organization in this direction all members of the organization must commit to practicing these five characteristics. Collectively these are what moves an organizational into mindfulness. Mindful organizations commit to safety at all levels, which creates a culture of safety. Patient Safety Culture and Patient Safety Climate A hallmark of highly reliable organizations is an organizational commitment to safety throughout all levels of the organization. 5 It is through this commitment that the 13
21 organization creates a culture of safety. 5 The term safety culture was first used in the investigational report following the Chernobyl disaster and stated, safety culture is that assembly of characteristics and attitudes in organizations and individuals which establishes that, as an overriding priority, nuclear plant safety issues receive the attention warranted by their significance (p.89). 35,36 In 2004, the Agency for Healthcare Research and Quality (AHRQ) funded the development of a hospital survey to measure safety attitudes called the Hospital Survey of Patient Safety Culture. 37 AHRQ adopted the following definition of safety culture stating (p.1) : The safety culture of an organization is the product of individual and group values, attitudes, perceptions, competencies, and patterns of behavior that determine the commitment to, and the style and proficiency of, an organization s health and safety management. Organizations with a positive safety culture are characterized by communications founded on mutual trust, by shared perceptions of the importance of safety, and by confidence in the efficacy of preventive measures. 37 Patient safety culture and safety climate are often used interchangeably in healthcare practice. While patient safety culture is described above, patient safety climate refers to the shared perceptions about the norms, policies, and procedures related to patient safety. 8 Specifically, climate is measured using a questionnaire and provides information from a moment in time from clinician s and staff of the observable attributes of safety culture. 8 Evaluating Patient Safety Climate The airline industry began measuring pilot attitudes about safety and interpersonal interactions through surveys including the Flight Management Attitude Questionnaire 14
22 (FMAQ) and Cockpit Management Attitudes Questionnaire (CMAQ). 38,39 This early work found that these attitudes were responsive to training interventions and could predict performance. 40 In 2006, Sexton and colleagues, developed the Safety Attitudes Questionnaire (SAQ), a healthcare-specific survey to measure the attitudes of healthcare workers toward patient safety. 22 Since safety climate is a more readily measurable aspect of safety culture, Sexton s SAQ survey measured 6 domains of safety including safety climate, teamwork climate, job satisfaction, perceptions of management, stress recognition and working conditions. 22 The SAQ is a valid and psychometrically sound instrument for assessing these 6 safety-related domains. 22 Over time it has been found to be sensitive to interventions, including CUSP. 2,21,41,42 After recognizing the potential association between culture and outcomes, the Joint Commission began requiring that all hospitals regularly evaluate their culture of patient safety beginning in ,44 Implementation Science and The Comprehensive Unit-based Safety Program The comprehensive unit-based safety program started in 2001 in two surgical intensive care units (ICU), the Weinberg intensive care unit (WICU) and the surgical intensive care unit (SICU), at Johns Hopkins Hospital. 21 CUSP began as an eight step program to engage and empower staff to identify and eliminate hazards and ultimately improve the climate of safety. 21 This study was a quasi-experimental design with one unit receiving the intervention, CUSP, immediately and the other unit serving as a control for 6 months prior to receiving the intervention. Safety climate was measured in both units before 15
23 and six months after the implementation of CUSP. A medical version of aviation s Safety Climate Scale was used to assess culture. Compared to the pre-intervention survey, the WICU and SICU achieved statistically significant improvements (p<0.05) in the postintervention period with regard to three statements: 1) The physician and nurse leaders in my area listen to me and care about my concerns, 42% relative improvement in the WICU and 121% relative improvements in the SICU, 2) My suggestions about safety would be acted upon if I expressed them to management, 53% relative improvement in the WICU and 51% relative improvement in the SICU, 3) I am aware that patient safety has become a major area for improvement in my institution, 41% relative improvement in the WICU and 46% relative improvement in the SICU. Interestingly, the WICU also saw statistically significant improvements in the following 5 items: 1) I am encouraged by my supervisors and coworkers to report any unsafe conditions I observe, 2) I know the proper channels to report my safety concerns, 3) I am satisfied with availability of clinical leadership, 4) Leadership is driving us to be a safety-centered institution, and 5) I believe that most adverse events occur as a result of multiple system failures, and are not attributable to one individual s actions. Overall, the SICU s percent of staff reporting a positive safety climate improved from 34.6% to 52.2% and the WICU s improved from 40% to 67.7%. In addition, both ICU s saw statistically significant reductions (p<0.05) in their length of stay from 2.2 to 1.1 in the WICU and from 3.0 to 2.3 in the SICU. 16
24 From March 2004 to September 2005, 108 ICUs across 67 Michigan hospitals began a multifaceted evidence-based intervention to reduce catheter-associated bloodstream infections (CLABSI) in the Michigan Keystone ICU collaborative. 2 A CUSP team was the first of the interventions that was implemented in order to activate the team for subsequent interventions. Within three months of implementation the median rate of CLABSI s improved to zero from 2.7 CLABSI s per 1000 central line days (p<0.002). 2 Improvements were seen in hospitals regardless of teaching status and number of beds. In this collaborative CUSP was reduced to 6 steps. 45 Safety climate was measured using the SAQ before CUSP was implemented and again 1 year after CUSP. Seventy-two of the 99 ICUs participated in both the baseline and post-cusp SAQ administration. Response rates were high for both, 75% and 65% respectively. Teamwork climate significantly improved from 46.5% to 50.5%, p< However, improvements varied with 19 ICU s increasing teamwork climate by ³ 10 points while 6 ICU s had decreasing teamwork climate by ³ 10 points. Within the Michigan Keystone Collaborate, in an effort to try to quantify the impact of CUSP on safety climate, team progress barriers and CLABSI, a team checkup tool was created in an attempt to differentiate teams that had implemented CUSP compared to teams that had not implemented CUSP within the Keystone CLABSI Collaborative. 12,46 ICUs were asked to self-administer the team checkup tool monthly starting 1 year after CUSP implementation and included information on team activities and progress barriers. Monthly reporting rates for the team checkup tool ranged from 51% to 70% in 17
25 the first year and declined to 32% to 53% in the second year and 19% to 37% for the last year. 12 Analysis revealed that 60 ICUs used CUSP activities, 17 ICUs did not use CUSP, and 26 ICUs did not have sufficient data to determine the use of CUSP. Safety climate was measured before and after implementation of CUSP among all ICUs, changes in SAQ domains were analyzed and an adjusted difference-in-difference analysis was performed to compare ICUs with and without CUSP. Compared to the non-cusp ICUs, ICUs that implemented CUSP had statistically significantly greater improvements in safety climate (9.6%, p=0.023), job satisfaction (9.6%, p=0.037), and working conditions domains (9.8%, p=0.032). 12 This represented the first published study to examine the association between successful versus unsuccessful CUSP teams and safety climate. Long-term follow up for this collaborative revealed that participating ICUs maintained a median CLABSI rate of zero from months after implementation. 47 Further study found evidence that this state-wide initiative had an impact on hospital mortality among patients ³ 65 years old when comparing Keystone participating ICU s (n=95) to the patients admitted to nearby hospital ICUs in the Midwest region (n=354). 48 Reductions in mortality were greater among Keystone participating ICUs at 12 months (OR 0.83, p=0.041) and at 22 months (OR 0.76, p=0.007) highlighting that CUSP, an intervention to improve safety climate, could contribute to long-term improvements in patient safety and mortality
26 From October 2007 to September 2008, a multicenter, phased, cluster-randomized control trial was completed to determine the causal effects of an intervention to reduce CLABSIs in the ICU. 42 This study sought to replicate the interventions in the Michigan Keystone Collaborative and was implemented in 45 ICUs within 35 hospitals and included a further refined 5-step CUSP program. At baseline, mean CLABSI rates were 4.48 and 2.71 (p=0.28) for the intervention and control group, respectively. 42 After 9 months the intervention group CLABSI rate declined to 1.33 compared to 2.16 in the control group (adjusted IRR 0.19, p=0.003, 95% CI ). 42 Similar projects have been attempted with an aim to improve ventilator associated pneumonia (VAP). The Rhode Island ICU collaborative implemented CUSP within a multifaceted set of interventions and achieved a 15% reduction in VAP state-wide which was not significantly different than from baseline. 49 Meanwhile another Keystone ICU Collaborative focusing on VAP including 112 ICU s reduced the median rate of VAP from 5.5 at baseline to 0 at months following the intervention (IRR 0.29, p<0.001, 95% CI ). 50 In an effort to match the results of CUSP and CLABSI reductions in Michigan, multiple countries have replicated the multifaceted intervention including CUSP at a national level. From April 2008 to June 2010, Spain conducted a prospective time series study including a similar multifaceted set of interventions, including CUSP, across 192 ICUs
27 CLABSI rates statistically significantly decreased to a median incidence rate of 1.12 from 3.07 (IRR 0.50, p<0.001, 95% CI ( ). From May 2009 to December 2010, the United Kingdom conducted a four-cluster, stepped, non-randomized study of the same multifaceted intervention, including CUSP, that was similar to the study completed in Michigan. 52 This Matching Michigan project adult ICUs mean CLABSI rate statistically significantly decreased from 3.7 at baseline to 1.48 (p<0.0001) at 20 months postimplementation. 52 Pediatric ICUs in the same program mean CLABSI rate decreased from 5.65 to 2.89 (p=0.625). The pediatric ICU s represented the first published largescale implementation of this set of interventions that did not achieve statistically significant decreases in CLABSI rates leaving many to wonder why it didn t work. Finally, from 2009 to 2013, the United States conducted a cohort study using a multifaceted set of interventions, including CUSP, across 1,564 ICUs in 986 hospitals in 44 states, the District of Columbia, and Puerto Rico. 13 CLABSI rates decreased from 1.96 at baseline to 1.15 after months after intervention (adjusted IRR 0.57, 95% CI ), representing a 43% decreased incidence of CLABSIs. 13 Spreading CUSP Beyond the ICU Johns Hopkins Hospital launched its first CUSP teams outside of an ICU in 2003 in the Emergency Department and the medical progressive care unit. 16 The impact of CUSP on safety climate outside of an ICU was not evaluated until 2008 in an inpatient surgical unit. 16,17 SAQ teamwork climate and safety climate domain scores were measured using the SAQ before and after implementation of the CUSP program. Both teamwork and 20
28 safety domain scores in 2008 had statistically significant (p<0.001) improvements compared to This provided evidence that CUSP could impact safety climate outside the confines of an ICU. In 2008, Johns Hopkins Hospital sought to evaluate the impact their safety program was having on the hospital s safety culture. 23 Their safety program included rolling out CUSP in more than 30 units, web-based event reporting, a lessons learned newsletter, patient safety grand rounds, quality and safety journal club, departmental quality and safety dashboards, infrastructure investments, a patient safety budget process, a safety star recognition program, development and implementation of a code of conduct policy and Board of Trustee engagement in patient safety. 23 Safety climate was measured using the SAQ in 2006 and 2008 and showed statistically significant improvements in all domain scores except stress recognition highlighting that a robust patient safety program across an organization, that included CUSP, can be associated with improved safety climate. Between July 2009 and July 2011, a peri-operative CUSP team started as part of a multifaceted bundle to improve surgical site infections among the colorectal surgical population. 18 This represented the first published evidence that CUSP was effective in the peri-operative setting. Surgical site infections were significantly reduced when comparing the one year before CUSP to the one year after CUSP implementation 18.2% 21
29 vs. 27.3% respectively, representing a 33.3% decrease (p<0.05, 95% CI 9-58%). 18 Addition evaluation revealed a variable direct cost reduction of $955 per case among surgeons participating in CUSP compared to surgeons not participating in CUSP. 53 Cost savings were found in laboratory work by $191 (p=0.009), operating room utilization by $149 (p=0.05) and supplies by $615 (p=0.003). 53 Contextual Factors Associated with CUSP Implementation In an effort to understand the contextual factors associated with success of a quality improvement intervention, the Team Check-up Tool (TCT) was created. 12,46 This tool was found to be reliable and valid for monitoring team progress using CUSP to improve CLABSI in ICU s. 12 The TCT has the potential to serve as a model for developing comparable measures for other team-based interventions. 12 The TCT is a short instrument that measures participation in intervention components, perceptions of unit performance on infection prevention behaviors and key barriers to team progress including lack of leadership support and physician engagement. Unfortunately, the barriers to team progress did not predict time to zero CLABSI rate but this may have been limited by the variance in CLABSI among the ICU s included in the study. 12 Response rate of ICU teams for the monthly TCT was found to be highly variable and low (median= 4 across all ICU-months, min=1, max=15). 12 Overwhelmingly CUSP, in combination with technical interventions, has led to significant improvements in clinical outcomes like CLABSI, SSI, VAP and significant improvements in 22
30 safety culture including all domains except stress recognition. Unfortunately, not all teams are able to achieve similar improvements and some teams are not able to improve at all. It is not yet understood which team and implementation factors are associated with CUSP success. These factors are important for operational quality and safety leaders who have provided an initial investment in CUSP and are considering spreading this program throughout their organization. Team Science: Drawing from the Science of Project Teams The CUSP program is designed to bring together a multidisciplinary group of healthcare staff, from frontline staff to senior leaders, in order to identify and learn from defects. CUSP is an intervention to improve safety climate by training staff in the science of safety then allowing them to tackle projects aimed at eliminating preventable harm and improving quality. In essence CUSP is an organizational initiative to implement and sustain unit-level, safety-focused project teams. The fields of project management and of organizational psychology are both interested in the science of teams and together can help us understand factors associated with CUSP team success. 25 There is an increasing prevalence of teams in all types of modern organizations, not just in healthcare. 54 Teams have been used to achieve higher levels of process efficiency and outcome efficacy. 55 Meanwhile, projects are the means by which change is brought forth in organizations. 25 As such healthcare generally, and CUSP teams specifically, 23
31 could benefit tremendously by incorporating this knowledge in the implementation and sustainability of project teams. Training all staff in the science of safety is the first critical step in CUSP. Since project teams generally, and CUSP teams specifically, are multidisciplinary, having a shared understanding is critical to success. 25 Team learning results in the change of the status quo, changes behaviors, and causes the team to share knowledge which improves productivity and efficiency. 25,56 One issue identified with managing project teams is the need to plan for and measure team member churn as team churn can affect project performance. 25 If a CUSP team only trains staff in the science of safety once, just prior to CUSP team kick-off, natural turnover of team members, including the addition of new team members, that are not exposed to this training can dilute team performance and efficiency. As a result, CUSP teams should have a plan in place to train new team members as they are hired and ensure concepts and knowledge are regularly refreshed for experienced team members. These same concepts apply to the project team leader. An initial investment in learning for the CUSP champion is believed to be critical to CUSP team success. Additional opportunities to learn about patient safety and quality improvement methodologies over time should further improve the CUSP champion s effectiveness. Finally, investing in these learning opportunities any time there is CUSP champion churn will be critical to the sustained success of the team. 24
32 Engaging a senior executive is another critical element of CUSP. The presence of a senior executive offers functional diversity to the unit-based team which comprises multiple types of frontline staff. Bunderson and Sutcliffe define functional diversity as a multidimensional construct embracing a variety of differences in individual functional expertise, experience, and knowledge. 57 The CUSP Scorecard includes senior executive and provider or designee attendance as these two roles are identified as important roles that add to the functional diversity of the CUSP team. In particular, these two roles add to the interpersonal functional diversity that adds the breadth of functional diversity at the team level. Interpersonal functional diversity facilitates project team performance because it is associated with increased task conflict and expanding communication and boundaries of project teams. 25,57 A moderate level of task conflict can improve the quality of team performance by generating ideas, evaluating alternatives, and encouraging constructive criticism. 25,58,59 Compared to homogenous teams, task conflict created by functionally diverse teams stimulate creativity and innovation and can enhance the depth of problem evaluation and assessment of options. 25,60-62 Functionally diverse teams are more efficient at crossing boundaries to facilitate information transfer and intersect inter- and intra-organizational boundaries. 25 Finally, functionally diverse teams offer a unique advantage to teams by providing multiple sources of communication and networks that enhance project outcomes. 25 In summary, functionally diverse teams demonstrate improved communication, are efficient boundary spanners, and have increased task conflict which are all positively associated with team performance. Collectively, the fields of project management and of 25
33 organizational psychology help us understand factors associated with CUSP team success. Chapter 3: Methods Research Question The primary research question guiding this dissertation is: What team and implementation factors are associated with CUSP effectiveness? Study Aims and Hypotheses Using the CUSP Scorecard data, we examined the association between the elements of CUSP and safety climate through the following specific aims. Aim 1: Examine the CUSP team structures and processes that are associated with proximal CUSP team outcomes (total CUSP team projects). Hypothesis 1: Teams reporting more (a) protected time and (b) training for the team CUSP Champion, and (c) SOS training for staff will report greater provider attendance than those reporting less protected time and training for their CUSP Champion and less training of their staff. Hypothesis 2: Teams reporting more (a) protected time for the team CUSP Champion, (b) training for CUSP champion, and (c) SOS training for staff will also report greater executive attendance than those reporting less protected time and training for their CUSP Champion and less training of their staff. Hypothesis 3: Teams reporting more (a) protected time for the team CUSP Champion and (b) training for the champion and (c) SOS training for staff will also 26
34 report more meetings held than those reporting less protected time and training for their CUSP Champion and less training of their staff. Hypothesis 4: Teams reporting greater (a) provider and (b) executive attendance and (c) meetings held will also report higher number of CUSP team projects than those reporting less attendance and meetings held. Aim 2: Examine the association between proximal CUSP team outcomes (total CUSP team projects completed) and unit-level safety climate, a distal CUSP team outcome. Hypothesis 1: Teams reporting more total CUSP team projects will also report higher unit-level safety climate scores than those reporting fewer total team projects. Aim 3: Examine the association between the CUSP processes and unit-level safety climate. Hypothesis 1: The relationship between CUSP processes (a) provider and (b) executive attendance and (c) meetings held and unit-level safety climate is partially mediated by the proximal team outcomes. Protection of Human Subjects This study received approval by the Johns Hopkins University School of Medicine Institutional Review Board on June 10, 2016 (IRB # ). To protect the identity of CUSP team members no information on individual member names were included in the database and results were reported in aggregate only. 27
35
36 and initiated for all teams that are in place for more than 6 months. All active hospitalbased CUSP teams in place prior to July 1, 2014 were included in this analysis. This is due to the fact that the CUSP team activities for this scorecard include all activities that occurred between July1, 2014 December 31, Inclusion Criteria The study population included all active hospital-based CUSP teams throughout Johns Hopkins Medicine as of July 1, Using this inclusion criterion, this study included 106 CUSP teams across 2 academic medical centers and 2 community hospitals (see Table 2). Table 2: Johns Hopkins Hospital-basd CUSP Teams by Affiliate as of July 1, 2014 Organization Name Type # of Beds # of CUSP Teams The Johns Hopkins Hospital Academic 1, Sibley Hospital Community Johns Hopkins Bayview Medical Academic Center Howard County General Hospital Community Exclusion Criteria Units were excluded if they did not have an active CUSP team in place by July 1, For example, units that had formally discontinued their CUSP team by notifying their hospital CUSP coordinator of such by July 1, 2014 and teams that had not yet had their 1 st CUSP team meeting called their kick-off meeting by July 1, 2014 were excluded. CUSP teams were also excluded if they were not hospital-based. For example, if the 29
37 clinic or ambulatory surgery center was associated with a community practice or as a stand-alone center rather than explicitly associated with a hospital. Sources of Data The data included in these analyses were collected for operational purposes. Data on the number and names of active CUSP teams and their characteristics (ex. kick-off date, CUSP champion name) were collected in an Excel spreadsheet that is maintained in the Armstrong Institute for Patient Safety and Quality s Patient Safety Department. The CUSP coordinator, who oversees the CUSP program for each affiliate organization, regularly updates this file as new teams are added or in the rare circumstance that teams are discontinued. The date the CUSP team started is defined as the date of the 1 st CUSP meeting, what is known as the kick-off meeting. Second, Scorecard data were collected by each CUSP team s facilitator or the affiliate organization s CUSP coordinator with each team s assistance. CUSP coordinators and facilitators have advanced skills and knowledge of CUSP and are external to the individual teams. Verbal and written instructions were provided for all Scorecard measures including a contact person for questions. Data was collected and submitted to the Armstrong Institute for Patient Safety and Quality Patient Safety Department. 30
38 As described in chapter one, the CUSP Scorecard was developed to evaluate the progress of CUSP teams in order to help them improve their team performance. Specifically, the Scorecard consists of eight measures, all of which were used in this analysis: The measures include three CUSP team structures (% of staff with Science of Safety training, CUSP champion training and protected time for CUSP champion), three CUSP team processes (% of CUSP meetings held, % of provider attendance and % of executive attendance) and two proximal CUSP team outcomes (# of data-specific improvement projects and # of projects with defects leading to a systems change). Finally, the safety climate domain data of the Safety Attitudes Questionnaire was collected through online or paper surveys. Specifically, this survey has 7 questions which form the Safety Climate Domain (Table 3). The Armstrong Institute for Patient Safety and Quality contracted with Pascal Metricsâ to manage all aspects of the survey administration including the survey creation (paper and online), the database and a web-based platform to conduct basic survey analytics. The Armstrong Institute for Patient Safety and Quality s Patient Safety Department is the organizational coordinator for all aspects of the safety climate survey and has access to the results for all clinical areas surveyed across Johns Hopkins Medicine. Study Variables Unit-level safety climate domain score 31
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
The significance of staffing and work environment for quality of care and. the recruitment and retention of care workers. Perspectives from the Swiss
 The significance of staffing and work environment for quality of care and the recruitment and retention of care workers. Perspectives from the Swiss Nursing Homes Human Resources Project (SHURP) Inauguraldissertation
The significance of staffing and work environment for quality of care and the recruitment and retention of care workers. Perspectives from the Swiss Nursing Homes Human Resources Project (SHURP) Inauguraldissertation
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus
 University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen The attitude of nurses towards inpatient aggression in psychiatric care Jansen, Gradus IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
The Determinants of Patient Satisfaction in the United States
 The Determinants of Patient Satisfaction in the United States Nikhil Porecha The College of New Jersey 5 April 2016 Dr. Donka Mirtcheva Abstract Hospitals and other healthcare facilities face a problem
The Determinants of Patient Satisfaction in the United States Nikhil Porecha The College of New Jersey 5 April 2016 Dr. Donka Mirtcheva Abstract Hospitals and other healthcare facilities face a problem
Targeted Solutions Tools
 TARGETED SOLUTIONS TOOL NOW AVAILABLE FOR OUR INTERNATIONAL CUSTOMERS! Joint Commission Center for Transforming Healthcare Targeted Solutions Tools Hand Hygiene Safe Surgery Hand-off Communications Preventing
TARGETED SOLUTIONS TOOL NOW AVAILABLE FOR OUR INTERNATIONAL CUSTOMERS! Joint Commission Center for Transforming Healthcare Targeted Solutions Tools Hand Hygiene Safe Surgery Hand-off Communications Preventing
Addressing Cost Barriers to Medications: A Survey of Patients Requesting Financial Assistance
 http://www.ajmc.com/journals/issue/2014/2014 vol20 n12/addressing cost barriers to medications asurvey of patients requesting financial assistance Addressing Cost Barriers to Medications: A Survey of Patients
http://www.ajmc.com/journals/issue/2014/2014 vol20 n12/addressing cost barriers to medications asurvey of patients requesting financial assistance Addressing Cost Barriers to Medications: A Survey of Patients
Measuring Patient Safety Culture Manual, Part I: Getting Started & Planning Your Survey Process
 The Armstrong Institute for Patient Safety and Quality Measuring Patient Safety Culture Manual, Part I: Getting Started & Planning Your Survey Process This manual has been adapted from the publically available
The Armstrong Institute for Patient Safety and Quality Measuring Patient Safety Culture Manual, Part I: Getting Started & Planning Your Survey Process This manual has been adapted from the publically available
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations
 ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
ABMS Organizational QI Forum Links QI, Research and Policy Highlights of Keynote Speakers Presentations When quality improvement (QI) is done well, it can improve patient outcomes and inform public policy.
From Value to High-Reliability Organization
 From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
From Value to High-Reliability Organization William R Mayfield MD, FACS Chief Surgical Officer WellStar Health System ACS NSQIP Chicago July 2015 No disclosures Outline Origins of the High-Reliability
You have joined the CUSP Communication & Teamwork Tools Informational Session!
 You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
You have joined the CUSP Communication & Teamwork Tools Informational Session! The session will begin shortly. To access the audio for the session, Dial: 800-977-8002, Participant code 083842# Registrants
A Comprehensive Framework for Patient Safety
 These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
These presenters have nothing to disclose A Comprehensive Framework for Patient Safety Allan Frankel, MD and Carol Haraden, PhD 8 October 2015 A Framework for a System of Safety Objectives 1. Link safety
HIMSS Davies Award Enterprise Application. --- Cover Page --- IT Projects and Operations Consultant Submitter s Address: and whenever possible
 HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
HIMSS Davies Award Enterprise Application --- Cover Page --- Name of Applicant Organization: Truman Medical Centers Organization s Address: 2301 Holmes Street, Kansas City, MO 64108 Submitter s Name: Angie
USE OF NURSING DIAGNOSIS IN CALIFORNIA NURSING SCHOOLS AND HOSPITALS
 USE OF NURSING DIAGNOSIS IN CALIFORNIA NURSING SCHOOLS AND HOSPITALS January 2018 Funded by generous support from the California Hospital Association (CHA) Copyright 2018 by HealthImpact. All rights reserved.
USE OF NURSING DIAGNOSIS IN CALIFORNIA NURSING SCHOOLS AND HOSPITALS January 2018 Funded by generous support from the California Hospital Association (CHA) Copyright 2018 by HealthImpact. All rights reserved.
Creating a Highly Reliable Health System: the Leadership Challenge. 6 th Annual Patient Safety Symposium Rick Foster, MD
 Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Creating a Highly Reliable Health System: the Leadership Challenge 6 th Annual Patient Safety Symposium Rick Foster, MD April 18, 2013 Moving Toward Zero It may seem a strange principle to enunciate as
Identifying Solutions / Implementation
 Patient Safety Research Introductory Course Session 5 Identifying Solutions / Implementation Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Patient Safety Research Introductory Course Session 5 Identifying Solutions / Implementation Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
School of Public Health and Health Services Department of Prevention and Community Health
 School of Public Health and Health Services Department of Prevention and Community Health Master of Public Health and Graduate Certificate Community Oriented Primary Care (COPC) 2009-2010 Note: All curriculum
School of Public Health and Health Services Department of Prevention and Community Health Master of Public Health and Graduate Certificate Community Oriented Primary Care (COPC) 2009-2010 Note: All curriculum
SURGEONS ATTITUDES TO TEAMWORK AND SAFETY
 SURGEONS ATTITUDES TO TEAMWORK AND SAFETY Steven Yule 1, Rhona Flin 1, Simon Paterson-Brown 2 & Nikki Maran 3 1 Industrial Psychology Research Centre, University of Aberdeen, Aberdeen, Scotland, UK Departments
SURGEONS ATTITUDES TO TEAMWORK AND SAFETY Steven Yule 1, Rhona Flin 1, Simon Paterson-Brown 2 & Nikki Maran 3 1 Industrial Psychology Research Centre, University of Aberdeen, Aberdeen, Scotland, UK Departments
EXECUTIVE SUMMARY. The Military Health System. Military Health System Review Final Report August 29, 2014
 EXECUTIVE SUMMARY On May 28, 2014, the Secretary of Defense ordered a comprehensive review of the Military Health System (MHS). The review was directed to assess whether: 1) access to medical care in the
EXECUTIVE SUMMARY On May 28, 2014, the Secretary of Defense ordered a comprehensive review of the Military Health System (MHS). The review was directed to assess whether: 1) access to medical care in the
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN
 UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
UNIVERSITY OF MISSISSIPPI MEDICAL CENTER PATIENT SAFETY PLAN 2014 1 PATIENT SAFETY PLAN 2014 PROGRAM GOALS The goal of the Patient Safety Program at University of Mississippi Medical Center (UMMC) is to
Healthcare- Associated Infections in North Carolina
 2018 Healthcare- Associated Infections in North Carolina Reference Document Revised June 2018 NC Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program NC Department of Health
2018 Healthcare- Associated Infections in North Carolina Reference Document Revised June 2018 NC Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program NC Department of Health
2017/18 Quality Improvement Plan Improvement Targets and Initiatives
 2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
2017/18 Quality Improvement Plan Improvement Targets and Initiatives AIM Measure Change Effective Effective Care for Patients with Sepsis % Eligible Nurses who have Completed the Sepsis Education Bundle
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
STUDY PLAN Master Degree In Clinical Nursing/Critical Care (Thesis )
") STUDY PLAN Master Degree In Clinical Nursing/Critical Care (Thesis ) I. GENERAL RULES AND CONDITIONS:- 1. This plan conforms to the valid regulations of the programs of graduate studies. 2. Areas of specialty
STUDY PLAN Master Degree In Clinical Nursing/Critical Care (Thesis ) I. GENERAL RULES AND CONDITIONS:- 1. This plan conforms to the valid regulations of the programs of graduate studies. 2. Areas of specialty
Scoring Methodology FALL 2016
 Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Scoring Methodology FALL 2016 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 7 Process/Structural Measures... 7 Computerized Physician Order
Baptist Health Nurse Leader Competency Model
 Baptist Health Nurse Leader Competency Model Strategic Visionary Systems Thinking Quality Care and Performance Improvement Fiscal and Management Excellence Management of Self and Others 1 - Strategic,
Baptist Health Nurse Leader Competency Model Strategic Visionary Systems Thinking Quality Care and Performance Improvement Fiscal and Management Excellence Management of Self and Others 1 - Strategic,
Rutgers School of Nursing-Camden
 Rutgers School of Nursing-Camden Rutgers University School of Nursing-Camden Doctor of Nursing Practice (DNP) Student Capstone Handbook 2014/2015 1 1. Introduction: The DNP capstone project should demonstrate
Rutgers School of Nursing-Camden Rutgers University School of Nursing-Camden Doctor of Nursing Practice (DNP) Student Capstone Handbook 2014/2015 1 1. Introduction: The DNP capstone project should demonstrate
Learning Activity: 1. Discuss identified gaps in the body of nurse work environment research.
 Learning Activity: LEARNING OBJECTIVES 1. Discuss identified gaps in the body of nurse work environment research. EXPANDED CONTENT OUTLINE I. Nurse Work Environment Research a. Magnet Hospital Concept
Learning Activity: LEARNING OBJECTIVES 1. Discuss identified gaps in the body of nurse work environment research. EXPANDED CONTENT OUTLINE I. Nurse Work Environment Research a. Magnet Hospital Concept
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
U.H. Maui College Allied Health Career Ladder Nursing Program
 U.H. Maui College Allied Health Career Ladder Nursing Program Progress toward level benchmarks is expected in each course of the curriculum. In their clinical practice students are expected to: 1. Provide
U.H. Maui College Allied Health Career Ladder Nursing Program Progress toward level benchmarks is expected in each course of the curriculum. In their clinical practice students are expected to: 1. Provide
Collaborative. Decision-making Framework: Quality Nursing Practice
 Collaborative Decision-making Framework: Quality Nursing Practice SALPN, SRNA and RPNAS Councils Approval Effective Sept. 9, 2017 Please note: For consistency, when more than one regulatory body is being
Collaborative Decision-making Framework: Quality Nursing Practice SALPN, SRNA and RPNAS Councils Approval Effective Sept. 9, 2017 Please note: For consistency, when more than one regulatory body is being
Global Health Evidence Summit. Community and Formal Health System Support for Enhanced Community Health Worker Performance
 Global Health Evidence Summit Community and Formal Health System Support for Enhanced Community Health Worker Performance I. Global Health Evidence Summits President Obama s Global Health Initiative (GHI)
Global Health Evidence Summit Community and Formal Health System Support for Enhanced Community Health Worker Performance I. Global Health Evidence Summits President Obama s Global Health Initiative (GHI)
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model
 Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
Report on Feasibility, Costs, and Potential Benefits of Scaling the Military Acuity Model June 2017 Requested by: House Report 114-139, page 280, which accompanies H.R. 2685, the Department of Defense
Fee: The fee for the 12-month renewal is $10,000.
 CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
CHILDHOOD CANCER AND BLOOD DISORDERS NETWORK 2017 RENEWAL TOOLS HOW TO Renew To renew, simply submit a completed Childhood Cancer & Blood Disorders Network Renewal Form to Gena Paulk via email at gena.paulk@childrenshospitals.org.
Missed Nursing Care: Errors of Omission
 Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
Missed Nursing Care: Errors of Omission Beatrice Kalisch, PhD, RN, FAAN Titus Professor of Nursing and Chair University of Michigan Nursing Business and Health Systems Presented at the NDNQI annual meeting
Assess the individual, community, organizational and societal needs of the general public and at-risk populations.
 School of Public Health and Health Services Department of Prevention and Community Health Master of Public Health and Graduate Certificate Health Promotion 2011 2012 Note: All curriculum revisions will
School of Public Health and Health Services Department of Prevention and Community Health Master of Public Health and Graduate Certificate Health Promotion 2011 2012 Note: All curriculum revisions will
How Data-Driven Safety Culture Changes Can Lower HAC Rates
 How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
How Data-Driven Safety Culture Changes Can Lower HAC Rates Session #226, February 23, 2017 Holly O Brien & Abby Dexter Children s Hospital of Wisconsin 1 Speaker Introduction Holly O Brien, MSN RN Safety
Scoring Methodology SPRING 2018
 Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
Scoring Methodology SPRING 2018 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 6 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician
SPC Case Studies Answers
 SPC Case Studies Answers Ref: JC Benneyan, RC Lloyd, PE Plsek, Statistical process control as a tool for research and healthcare improvement, Qual. Saf. Health Care 2003; 12:458 464 doi:10.1136/qhc.12.6.458
SPC Case Studies Answers Ref: JC Benneyan, RC Lloyd, PE Plsek, Statistical process control as a tool for research and healthcare improvement, Qual. Saf. Health Care 2003; 12:458 464 doi:10.1136/qhc.12.6.458
SCORING METHODOLOGY APRIL 2014
 SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
Improving teams in healthcare
 Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Mary Baum President & CEO BA&T September 18, 2015
 Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
Mary Baum President & CEO BA&T September 18, 2015 Objective Why patient safety is so difficult to solve? The problem remains Advances in clinical workflow A collaborative approach Metrics matter Just start.
American Board of Dental Examiners (ADEX) Clinical Licensure Examinations in Dental Hygiene. Technical Report Summary
 Clinical Licensure Examinations in Dental Hygiene. Technical Report Summary") American Board of Dental Examiners (ADEX) Clinical Licensure Examinations in Dental Hygiene Technical Report Summary October 16, 2017 Introduction Clinical examination programs serve a critical role in
American Board of Dental Examiners (ADEX) Clinical Licensure Examinations in Dental Hygiene Technical Report Summary October 16, 2017 Introduction Clinical examination programs serve a critical role in
Alberta Health Services. Strategic Direction
 Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Collaborative. Decision-making Framework: Quality Nursing Practice
 Collaborative Decision-making Framework: Quality Nursing Practice December 7, 2016 Please note: For consistency, when more than one regulatory body is being discussed in this document, the regulatory bodies
Collaborative Decision-making Framework: Quality Nursing Practice December 7, 2016 Please note: For consistency, when more than one regulatory body is being discussed in this document, the regulatory bodies
Michael Andrew Basinger University of Nevada, Las Vegas, UNLV Theses, Dissertations, Professional Papers, and Capstones
 UNLV Theses, Dissertations, Professional Papers, and Capstones 5-1-2014 The Reduction of Central Line-Associated Bloodstream Infections in Intensive Care Units through the Implementation of the Comprehensive
UNLV Theses, Dissertations, Professional Papers, and Capstones 5-1-2014 The Reduction of Central Line-Associated Bloodstream Infections in Intensive Care Units through the Implementation of the Comprehensive
Critique of a Nurse Driven Mobility Study. Heather Nowak, Wendy Szymoniak, Sueann Unger, Sofia Warren. Ferris State University
 Running head: CRITIQUE OF A NURSE 1 Critique of a Nurse Driven Mobility Study Heather Nowak, Wendy Szymoniak, Sueann Unger, Sofia Warren Ferris State University CRITIQUE OF A NURSE 2 Abstract This is a
Running head: CRITIQUE OF A NURSE 1 Critique of a Nurse Driven Mobility Study Heather Nowak, Wendy Szymoniak, Sueann Unger, Sofia Warren Ferris State University CRITIQUE OF A NURSE 2 Abstract This is a
Standards of Practice for Professional Ambulatory Care Nursing... 17
 Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
CLINICAL PREDICTORS OF DURATION OF MECHANICAL VENTILATION IN THE ICU. Jessica Spence, BMR(OT), BSc(Med), MD PGY2 Anesthesia
, BSc(Med), MD PGY2 Anesthesia") CLINICAL PREDICTORS OF DURATION OF MECHANICAL VENTILATION IN THE ICU Jessica Spence, BMR(OT), BSc(Med), MD PGY2 Anesthesia OBJECTIVES To discuss some of the factors that may predict duration of invasive
CLINICAL PREDICTORS OF DURATION OF MECHANICAL VENTILATION IN THE ICU Jessica Spence, BMR(OT), BSc(Med), MD PGY2 Anesthesia OBJECTIVES To discuss some of the factors that may predict duration of invasive
High Reliability and Robust Process Improvement
 High Reliability and Robust Process Improvement Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission July 26, 2016 3000 patients over 6 years 1 2 Current State of Quality Routine
High Reliability and Robust Process Improvement Mark R. Chassin, MD, FACP, MPP, MPH President and CEO, The Joint Commission July 26, 2016 3000 patients over 6 years 1 2 Current State of Quality Routine
COOK COUNTY HEALTH & HOSPITALS SYSTEM
 COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
COOK COUNTY HEALTH & HOSPITALS SYSTEM CCHHS Board of Directors Quality and Patient Safety Committee Quality and Reliability in Health Care Krishna Das, MD, Chief Quality Officer 15 March 2016 Quality:
Creating a Culture in Support of Patient Safety
 Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Session: L11 Ms. Ching has nothing to disclose Ms. Derheimer is an employee of the Virginia Mason Institute; a not-for-profit organization that provides education and training in the Virginia Mason Production
Reducing the Risk of Wrong Site Surgery
 Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Joint Commission Center for Transforming Healthcare Reducing the Risk of Wrong Site Surgery Wrong Site Surgery Project Participants The Joint Commission s Center for Transforming Healthcare aims to solve
Supplementary Online Content
 Supplementary Online Content Harris AD, Pineles L, Belton B, Benefits of Universal Glove and Gown (BUGG) investigators. Universal Glove and Gown Use and Acquisition of Antibiotic Resistant Bacteria in
Supplementary Online Content Harris AD, Pineles L, Belton B, Benefits of Universal Glove and Gown (BUGG) investigators. Universal Glove and Gown Use and Acquisition of Antibiotic Resistant Bacteria in
Higher Degree by Research Confirmation of Candidature- Guidelines
 Higher Degree by Research Confirmation of Candidature- Guidelines Introduction These Guidelines document Faculty, School or discipline specific requirements that are in addition to the information provided
Higher Degree by Research Confirmation of Candidature- Guidelines Introduction These Guidelines document Faculty, School or discipline specific requirements that are in addition to the information provided
Hospitals Face Challenges Implementing Evidence-Based Practices
 United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
United States Government Accountability Office Report to Congressional Requesters February 2016 PATIENT SAFETY Hospitals Face Challenges Implementing Evidence-Based Practices GAO-16-308 February 2016 PATIENT
DOD INSTRUCTION AVIATION HAZARD IDENTIFICATION AND RISK ASSESSMENT PROGRAMS (AHIRAPS)
") DOD INSTRUCTION 6055.19 AVIATION HAZARD IDENTIFICATION AND RISK ASSESSMENT PROGRAMS (AHIRAPS) Originating Component: Office of the Under Secretary of Defense for Acquisition, Technology, and Logistics
DOD INSTRUCTION 6055.19 AVIATION HAZARD IDENTIFICATION AND RISK ASSESSMENT PROGRAMS (AHIRAPS) Originating Component: Office of the Under Secretary of Defense for Acquisition, Technology, and Logistics
NURSING SPECIAL REPORT
 2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Nursing skill mix and staffing levels for safe patient care
 EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
EVIDENCE SERVICE Providing the best available knowledge about effective care Nursing skill mix and staffing levels for safe patient care RAPID APPRAISAL OF EVIDENCE, 19 March 2015 (Style 2, v1.0) Contents
2013, Vol. 2, Release 1 (October 21, 2013), /10/$3.00
, /10/$3.00") Assessing Technician, Nurse, and Doctor Ratings as Predictors of Overall Satisfaction of Emergency Room Patients: A Maximum-Accuracy Multiple Regression Analysis Paul R. Yarnold, Ph.D. Optimal Data Analysis,
Assessing Technician, Nurse, and Doctor Ratings as Predictors of Overall Satisfaction of Emergency Room Patients: A Maximum-Accuracy Multiple Regression Analysis Paul R. Yarnold, Ph.D. Optimal Data Analysis,
Chapter 39. Nurse Staffing, Models of Care Delivery, and Interventions
 Chapter 39. Nurse Staffing, Models of Care Delivery, and Interventions Jean Ann Seago, Ph.D., RN University of California, San Francisco School of Nursing Background Unlike the work of physicians, the
Chapter 39. Nurse Staffing, Models of Care Delivery, and Interventions Jean Ann Seago, Ph.D., RN University of California, San Francisco School of Nursing Background Unlike the work of physicians, the
Healthcare- Associated Infections in North Carolina
 2012 Healthcare- Associated Infections in North Carolina Reference Document Revised May 2016 N.C. Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program N.C. Department of
2012 Healthcare- Associated Infections in North Carolina Reference Document Revised May 2016 N.C. Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program N.C. Department of
An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU. A thesis presented by. Shelby L. Holden
 Shelby Holden 1 An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU A thesis presented by Shelby L. Holden Presented to the College of Education and Health Professions in partial
Shelby Holden 1 An Educational Intervention to Increase CLABSI Bundle Compliance in the ICU A thesis presented by Shelby L. Holden Presented to the College of Education and Health Professions in partial
USING AGILE IMPLEMENTATION TO CREATE A LEARNING HEALTHCARE SYSTEM
 INDIANA UNIVERSITY HEALTH ACADEMIC HEALTH CENTER USING AGILE IMPLEMENTATION TO CREATE A LEARNING HEALTHCARE SYSTEM Center for Health Innovation & Implementation Science TABLE OF CONTENTS Executive Summary...4
INDIANA UNIVERSITY HEALTH ACADEMIC HEALTH CENTER USING AGILE IMPLEMENTATION TO CREATE A LEARNING HEALTHCARE SYSTEM Center for Health Innovation & Implementation Science TABLE OF CONTENTS Executive Summary...4
What Every Patient Safety Officer Must Know:
 What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
What Every Patient Safety Officer Must Know: Tapping into the Best Resources in the Country John R. Combes, MD Senior Medical Advisor Hospital and Healthsystem Association of Pennsylvania Harrisburg, PA
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health
 The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health 2. Title Of Initiative Implementation of a Patient Blood Management
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Jefferson Health 2. Title Of Initiative Implementation of a Patient Blood Management
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients
 Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
Analysis of 340B Disproportionate Share Hospital Services to Low- Income Patients March 12, 2018 Prepared for: 340B Health Prepared by: L&M Policy Research, LLC 1743 Connecticut Ave NW, Suite 200 Washington,
Analysis of Nursing Workload in Primary Care
 Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
Analysis of Nursing Workload in Primary Care University of Michigan Health System Final Report Client: Candia B. Laughlin, MS, RN Director of Nursing Ambulatory Care Coordinator: Laura Mittendorf Management
2. Title Of Initiative Quality Improvement Project
 The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Einstein Medical Center Montgomery 2. Title Of Initiative Quality Improvement Project
The Health Care Improvement Foundation 2017 Delaware Valley Patient Safety and Quality Award Entry Form 1. Hospital Name Einstein Medical Center Montgomery 2. Title Of Initiative Quality Improvement Project
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall. Total. Application Analysis 1.
 Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
Cognitive Level Certified Professional in Patient Safety Detailed Content Outline Recall Application Analysis Total 1. CULTURE 2 12 4 18 A. Assessment of Patient Safety Culture 1. Identify work settings
2013 Workplace and Equal Opportunity Survey of Active Duty Members. Nonresponse Bias Analysis Report
 2013 Workplace and Equal Opportunity Survey of Active Duty Members Nonresponse Bias Analysis Report Additional copies of this report may be obtained from: Defense Technical Information Center ATTN: DTIC-BRR
2013 Workplace and Equal Opportunity Survey of Active Duty Members Nonresponse Bias Analysis Report Additional copies of this report may be obtained from: Defense Technical Information Center ATTN: DTIC-BRR
Scoring Methodology FALL 2017
 Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
Scoring Methodology FALL 2017 CONTENTS What is the Hospital Safety Grade?... 4 Eligible Hospitals... 4 Measures... 5 Measure Descriptions... 9 Process/Structural Measures... 9 Computerized Physician Order
HOLYANGELUNIVERSITY GRADUATE SCHOOL OF NURSING AngelesCity. DOCTOR OF PHILOSOPHY IN NURSING EDUCATION Major in Educational Leadership and Management
 HOLYANGELUNIVERSITY GRADUATE SCHOOL OF NURSING AngelesCity DOCTOR OF PHILOSOPHY IN NURSING EDUCATION Major in Educational Leadership and Management Mission and Vision The primary mission of HAU PhD in
HOLYANGELUNIVERSITY GRADUATE SCHOOL OF NURSING AngelesCity DOCTOR OF PHILOSOPHY IN NURSING EDUCATION Major in Educational Leadership and Management Mission and Vision The primary mission of HAU PhD in
Reliability of Evaluating Hospital Quality by Surgical Site Infection Type. ACS NSQIP Conference July 22, 2012
 Reliability of Evaluating Hospital Quality by Surgical Site Infection Type ACS NSQIP Conference July, 01 Surgical Site Infection Common cause of patient morbidity 5%-6% for colorectal procedures Significant
Reliability of Evaluating Hospital Quality by Surgical Site Infection Type ACS NSQIP Conference July, 01 Surgical Site Infection Common cause of patient morbidity 5%-6% for colorectal procedures Significant
CAPE/COP Educational Outcomes (approved 2016)
") CAPE/COP Educational Outcomes (approved 2016) Educational Outcomes Domain 1 Foundational Knowledge 1.1. Learner (Learner) - Develop, integrate, and apply knowledge from the foundational sciences (i.e.,
CAPE/COP Educational Outcomes (approved 2016) Educational Outcomes Domain 1 Foundational Knowledge 1.1. Learner (Learner) - Develop, integrate, and apply knowledge from the foundational sciences (i.e.,
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations.
 ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
ZERO It s powerful. It s controversial. And it s the cornerstone of high reliability organizations. 1 Thornton Kirby, President & CEO South Carolina Hospital Association Lorri Gibbons, RN, MSHL Vice President
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages. This SPSRN work is funded by
 Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Reviewing Methods Used in Patient Safety Research: Advantages and Disadvantages Dr Jeanette Jackson (j.jackson@abdn.ac.uk) This SPSRN work is funded by Introduction Effective management of patient safety
Critical Review: What effect do group intervention programs have on the quality of life of caregivers of survivors of stroke?
 Critical Review: What effect do group intervention programs have on the quality of life of caregivers of survivors of stroke? Stephanie Yallin M.Cl.Sc (SLP) Candidate University of Western Ontario: School
Critical Review: What effect do group intervention programs have on the quality of life of caregivers of survivors of stroke? Stephanie Yallin M.Cl.Sc (SLP) Candidate University of Western Ontario: School
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
19th Annual. Challenges. in Critical Care
 19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
19th Annual Challenges in Critical Care A Multidisciplinary Approach Friday August 22, 2014 The Hotel Hershey 100 Hotel Road Hershey, Pennsylvania 17033 A continuing education service of Penn State College
A critical evaluation of healthcare quality improvement and how organizational context drives performance
 University of Iowa Iowa Research Online Theses and Dissertations Spring 2013 A critical evaluation of healthcare quality improvement and how organizational context drives performance Justin Mathew Glasgow
University of Iowa Iowa Research Online Theses and Dissertations Spring 2013 A critical evaluation of healthcare quality improvement and how organizational context drives performance Justin Mathew Glasgow
Effectively implementing multidisciplinary. population segments. A rapid review of existing evidence
 Effectively implementing multidisciplinary teams focused on population segments A rapid review of existing evidence October 2016 Francesca White, Daniel Heller, Cait Kielty-Adey Overview This review was
Effectively implementing multidisciplinary teams focused on population segments A rapid review of existing evidence October 2016 Francesca White, Daniel Heller, Cait Kielty-Adey Overview This review was
Implementing and Validating a Comprehensive Unit-Based Safety Program
 JOBNAME: jops 1#1 2005 PAGE: 1 OUTPUT: Tue March 15 15:21:54 2005 ORIGINAL ARTICLE Implementing and Validating a Comprehensive Unit-Based Safety Program Peter Pronovost, MD, PhD,* Brad Weast, MHA, Beryl
JOBNAME: jops 1#1 2005 PAGE: 1 OUTPUT: Tue March 15 15:21:54 2005 ORIGINAL ARTICLE Implementing and Validating a Comprehensive Unit-Based Safety Program Peter Pronovost, MD, PhD,* Brad Weast, MHA, Beryl
Quality Standards. Process and Methods Guide. October Quality Standards: Process and Methods Guide 0
 Quality Standards Process and Methods Guide October 2016 Quality Standards: Process and Methods Guide 0 About This Guide This guide describes the principles, process, methods, and roles involved in selecting,
Quality Standards Process and Methods Guide October 2016 Quality Standards: Process and Methods Guide 0 About This Guide This guide describes the principles, process, methods, and roles involved in selecting,
HIMSS Submission Leveraging HIT, Improving Quality & Safety
 HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
HIMSS Submission Leveraging HIT, Improving Quality & Safety Title: Making the Electronic Health Record Do the Heavy Lifting: Reducing Hospital Acquired Urinary Tract Infections at NorthShore University
Hospital-Acquired Infections Prevention is in Your Hands. Rachel L. Stricof
 Hospital-Acquired Infections Prevention is in Your Hands Rachel L. Stricof rstricof@gmail.com Morbidity 1.7 Million infections per year (estimate 2002) Mortality 99,000 deaths per year (estimate 2002)
Hospital-Acquired Infections Prevention is in Your Hands Rachel L. Stricof rstricof@gmail.com Morbidity 1.7 Million infections per year (estimate 2002) Mortality 99,000 deaths per year (estimate 2002)
Introduction. Singapore. Singapore and its Quality and Patient Safety Position 11/9/2012. National Healthcare Group, SIN
 Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
Introduction Singapore and its Quality and Patient Safety Position Singapore 1 Singapore 2004: Top 5 Key Risk Factors High Body Mass (11.1%; 45,000) Physical Inactivity (3.8%; 15,000) Cigarette Smoking
A Comparison of Job Responsibility and Activities between Registered Dietitians with a Bachelor's Degree and Those with a Master's Degree
 Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 11-17-2010 A Comparison of Job Responsibility and Activities between Registered Dietitians
Florida International University FIU Digital Commons FIU Electronic Theses and Dissertations University Graduate School 11-17-2010 A Comparison of Job Responsibility and Activities between Registered Dietitians
Supplementary Online Content
 Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
Supplementary Online Content Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012.
TC911 SERVICE COORDINATION PROGRAM
 TC911 SERVICE COORDINATION PROGRAM ANALYSIS OF PROGRAM IMPACTS & SUSTAINABILITY CONDUCTED BY: Bill Wright, PhD Sarah Tran, MPH Jennifer Matson, MPH The Center for Outcomes Research & Education Providence
TC911 SERVICE COORDINATION PROGRAM ANALYSIS OF PROGRAM IMPACTS & SUSTAINABILITY CONDUCTED BY: Bill Wright, PhD Sarah Tran, MPH Jennifer Matson, MPH The Center for Outcomes Research & Education Providence
Engaging Students Using Mastery Level Assignments Leads To Positive Student Outcomes
 Lippincott NCLEX-RN PassPoint NCLEX SUCCESS L I P P I N C O T T F O R L I F E Case Study Engaging Students Using Mastery Level Assignments Leads To Positive Student Outcomes Senior BSN Students PassPoint
Lippincott NCLEX-RN PassPoint NCLEX SUCCESS L I P P I N C O T T F O R L I F E Case Study Engaging Students Using Mastery Level Assignments Leads To Positive Student Outcomes Senior BSN Students PassPoint
International Journal of Nursing Studies
 International Journal of Nursing Studies 50 (2013) 240 252 Contents lists available at SciVerse ScienceDirect International Journal of Nursing Studies journal homepage: www.elsevier.com/ijns The association
International Journal of Nursing Studies 50 (2013) 240 252 Contents lists available at SciVerse ScienceDirect International Journal of Nursing Studies journal homepage: www.elsevier.com/ijns The association
Profiles in CSP Insourcing: Tufts Medical Center
 Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
Profiles in CSP Insourcing: Tufts Medical Center Melissa A. Ortega, Pharm.D., M.S. Director, Pediatrics and Inpatient Pharmacy Operations Tufts Medical Center Hospital Profile Tufts Medical Center (TMC)
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes
 Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Lessons From Infection Prevention Research in Emergency Medicine: Methods and Outcomes Patricia W. Stone, PhD, RN FAAN Centennial Professor in Health Policy Director PhD Program and Director Center for
Phase I Study: A longitudinal analysis of nursing specialty certification by Magnet status and patient unit type.
 Report on NDNQI Certification Research Studies Diane K. Boyle, PhD, RN, FAAN June 2015 Phase I Study: A longitudinal analysis of nursing specialty certification by Magnet status and patient unit type.
Report on NDNQI Certification Research Studies Diane K. Boyle, PhD, RN, FAAN June 2015 Phase I Study: A longitudinal analysis of nursing specialty certification by Magnet status and patient unit type.
A Comprehensive Framework for Patient Safety
 A Comprehensive Framework for Patient Safety A Framework for a System of Safety Objectives 1. Link safety to organizational strategy and resources 2. Define a culture of safety 3. Apply improvement methods
A Comprehensive Framework for Patient Safety A Framework for a System of Safety Objectives 1. Link safety to organizational strategy and resources 2. Define a culture of safety 3. Apply improvement methods
CASE STUDY The Safer Patients Initiative
 CSE STUDY The Safer Patients Initiative Critical care in practice: Royal ree Hospital and the University Hospital of Wales 1. INTRODUCTION In late 4, the Health oundation funded the Institute for Healthcare
CSE STUDY The Safer Patients Initiative Critical care in practice: Royal ree Hospital and the University Hospital of Wales 1. INTRODUCTION In late 4, the Health oundation funded the Institute for Healthcare
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
D.N.P. Program in Nursing. Handbook for Students. Rutgers College of Nursing
 1 D.N.P. Program in Nursing Handbook for Students Rutgers College of Nursing 1-2010 2 Table of Contents Welcome..3 Goal, Curriculum and Progression of Students Enrolled in the DNP Program in Nursing...
1 D.N.P. Program in Nursing Handbook for Students Rutgers College of Nursing 1-2010 2 Table of Contents Welcome..3 Goal, Curriculum and Progression of Students Enrolled in the DNP Program in Nursing...