Northeast Cambodia Child Survival Program ANNUAL REPORT
|
|
|
- Evelyn Stevenson
- 5 years ago
- Views:
Transcription
1 Partners for Development No. 24, Street 294, P.O. Box 551 Phnom Penh, Kingdom of Cambodia PARTNERS Tel: ; Fax: DEVELOPMENT Internet: Northeast Cambodia Child Survival Program ANNUAL REPORT October 1999
2 TABLE OF CONTENTS I. Accomplishments and Constraints....1 A. Accomplishments In-country Technical and Administrative Support for NCCSP NCCSP Office Start-up Health Facility Resource Survey Child Survival Pre-implementation Workshop Staff Recruitment Staff Training Knowledge, Practice, and Coverage (KPC) Survey Qualitative Data Collection Collaboration with Other Child Survival Programs in Cambodia Developing Partnerships Collection of Cambodia-specific Data and Other Resource Materials DIP Birth Spacing Activities Community Development Activities Related to Child Survival..11 B. Constraints..12 II. Substantial Changes in Program Design...13
3 I. ACCOMPLISHMENTS AND CONSTRAINTS A. ACCOMPLISHMENTS Partners for Development (PFD) is implementing its two-year entry-level Child Survival Program, the Northeast Cambodia Child Survival Program (NCCSP), in four phases. During its first year of operation, NCCSP completed phase one, program start-up and pre-- implementation planning and coordination, and phase two, quantitative and qualitative data collection and analysis. The program has now entered into phase three, intervention planning and implementation. PFD's Cooperative Agreement for its Child Survival Program in Cambodia lists seven measurable outputs. As the table below indicates, the program has made good progress toward the achievement of six out of seven of the outputs. Output Literature review of studies done in Cambodia and elsewhere on communitybased approaches to child survival interventions Formal and informal partnerships developed with interested local agencies and communities Number of individuals trained in quantitative and qualitative research methodology Completion of the Detailed Implementation Plan DIP Number of intervention planning sessions held Direct beneficiaries from intervention Monitoring and evaluation exercises conducted Progress Achieved Completed literature review of existing sources. Continuing collection of new survey reports, qualitative data reports, resources on child survival topics, and resources on community-based approaches. Initiated collaboration with World Vision and World Relief Child Survival Programs in Cambodia. Established partnership with Helen Keller International/Cambodia. Developing partnership with Ministry of Health and Provincial Health Department. Developing partnerships with World Food Program, ADRA, and SCF/UK Reaffirmed partnerships with provincial and district Offices of Rural Development and Women's Affairs. Reaffirmed partnerships with Village Development Committees. Trained 42 individuals in quantitative survey methodology. Trained five individuals in qualitative research methodology. Completed several sections of the DIP. Held five planning sessions with the Kratie Provincial Health Department and Chhlong Operational District. Held two planning sessions with SCF/UK in Kratie. Facilitated 11 planning sessions in villages throughout the program area. Interventions not yet initiated. Conducted evaluations related to some staff training workshops (e.g., Facilitation Skills Workshop). Monitoring and evaluation of intervention activities not yet initiated. The following sections (1-14) describe in detail the accomplishments achieved by NCCSP during its first year of funding. 1. In-country Technical and Administrative Support for NCCSP PFD has provided emergency and development assistance to communities in northeast Cambodia since PFD's current wide-ranging, participatory community development project is called the Northeast Cambodia Community Development Program (NCCDP), a USAID/Cambodia-funded project initiated in Thanks to PFD's long presence in both
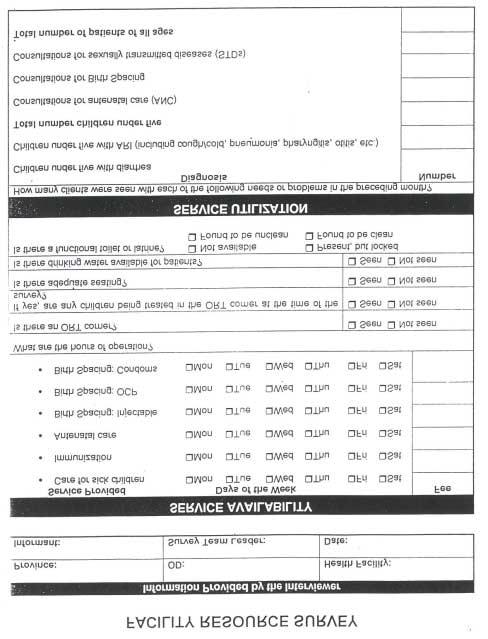
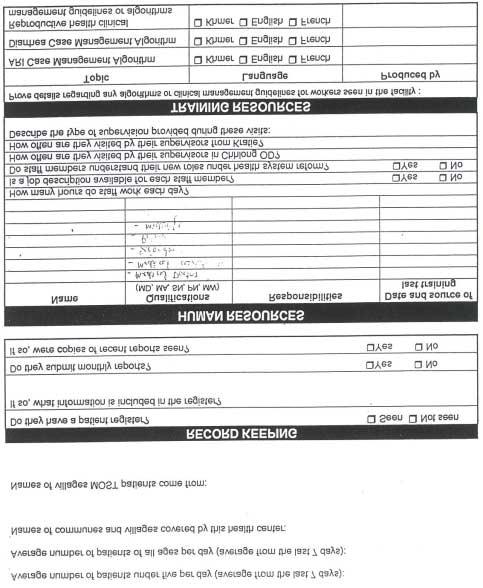
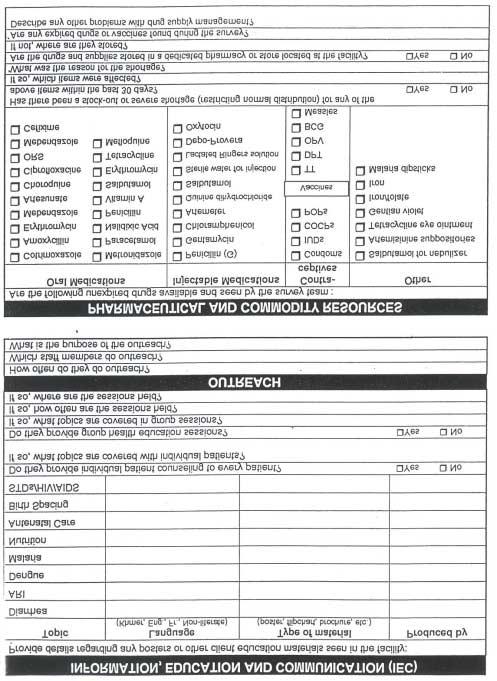
4 Cambodia and Kratie province, the Child Survival Program has benefited from existing administrative and logistical support systems. NCCSP regularly receives support from PFD's country office in Phnom Penh. PFD's country office is staffed by an expatriate Country Representative, an expatriate Program Manager, a Cambodian Finance Officer, and a Cambodian Logistics Officer. Each of these staff members provides support to NCCSP. The Country Representative, Finance Officer, and Logistics Officer assist the program with administrative and financial matters. The Program Manager helps the Child Survival Program by providing technical support, maintaining contact with NGOs and government ministries at the national level, and facilitating the search for program-related data and other materials. NCCSP also has the benefit of operating in the same province and receiving support from the NCCDP office in Kratie province. On practical, financial, and logistical levels, NCCDP staff has provided an enormous amount of assistance to NCCSP during this first year. The Cambodian Administrative Officer and Administrative Assistant help NCCSP with administrative and financial procedures as well as local procurement and logistics. PFD's Kratie office helps NCCSP stay in contact with provincial authorities and other NGOs based in the province. The two expatriate staff for the NCCDP project in Kratie have supported NCCSP in many ways. For example, they provided logistics to set up the NCCSP office; made suggestions about staffing; brainstormed ideas for implementing the Child Survival Program; and collaborated closely with NCCSP staff to ensure that the activities of the two programs are integrated. PFD's country and Kratie offices have also helped NCCSP by ensuring that appropriate child survival staff was trained in administrative and financial procedures. The Cambodian Administrative Officer for NCCSP received one week of initial training from PFD's Financial Officer in Phnom Penh on issues such as the preparation of vouchers, per diem worksheets, receipts, local staff timesheets, and monthly financial reports. The Administrative Officer was also trained in the use of Microsoft Excel software. During his first several months in Chhlong, he regularly received on-the-job training from PFD's Financial Officer in Phnom Penh and from NCCDP's Administrative Officer in Kratie on both financial procedures and administrative procedures, such as procurement. This training was necessary in order to have the program run smoothly, and also has the benefit of improving the skills of a national staff member and preparing him for the administration of such programs without NGO support in the future. Thanks to this help, NCCSP now has effective administration for the Child Survival Program and is also able to provide administrative support for NCCDP field teams working in the southern portion of Kratie province. 2. NCCSP Office Start-up Prior to the initiation of the NCCSP, the office currently used by the program was already in use as a base of operations for PFD's NCCDP activities in the Chhlong and Prek Prasap districts of Kratie province. The office is shared with government staff of the Chhlong District Offices of Rural Development and Women's Affairs. Office space is provided to PFD free of charge as a community contribution to both the NCCSP and NCCDP programs. A new 5KVA generator was donated to the program by Sam Ling International, a Malaysian logging company with a base camp located in Chhlong. 3. Health Facility Resource Survey PFD conducted a Health Facility Resource Survey from December 28-31, The purpose of the survey was to collect information on service availability, service utilization, record keeping, human resources, training resources, IEC (Information, Education and Communication) resources, outreach activities, pharmaceutical and commodity resources, and equipment resources. The survey also provided program staff with a chance to meet health center staff and see the physical structures.
5 The survey was conducted by the Child Survival Coordinator and the Deputy Director of the Provincial Health Department with assistance from NCCSP's Administrative Officer. The survey questionnaire was adapted from a similar questionnaire developed by the Reproductive and Child Health Alliance (RACHA), a USAID-funded maternal and child health program in Cambodia. (See Appendix A for NCCSP's Facility Resource Survey questionnaire.) The team visited six out of ten health centers in the Chhlong Operational District. The other four health centers were not included in the survey because the health center buildings had not been constructed and these "health centers" were functioning out of commune offices with a skeleton staff. Some of the key findings from the survey are outlined in the table below: Service Availability Health centers are only open for a few hours in the morning. No health center has a place to mix ORT or an ORT comer. Service Utilization Utilization of health centers is generally low (e.g., in the last month, average number of patients per day under five years ranged from one to four). Fees Prices for services are not standardized across health centers. Record Keeping Record keeping systems are in lace. Human Resources Adequate numbers of staff are available at existing health centers. Former district hospitals (Prek Prasap and Snoul) have more staff than needed. Supervision Supervision by the Operational District and Provincial Health Department is not standardized across health centers. Training Resources Standard case management algorithms and case management guidelines are available at all health centers. IEC Most health centers need additional IEC materials. Equipment Some key equipment is unavailable at most health centers (e.g-, I,, Resources transportation, cold chain equipment, microscope). Pharmaceutical and Some key drugs are not available at most health centers (e.g., Commodity erythromycin, mefloquine, quinine, chloramphenical, depo-provera, Resources oxytocin). There are problems with the transport of drugs and receiving drugs that are close to the expiry date. NCCSP is using information from the Health Facility Survey to assist in planning and designing interventions for the DIP. The program plans to replicate the Health Facility Survey in January 1999 and include three newly constructed health centers. 4. Child Survival Pre-implementation Workshop NCCSP held a Child Survival Pre-implementation Workshop at the Governor of Kratie province's compound in Kratie town on January 12-13, The workshop was designed to inform stakeholders about the NCCSP program, explain how NCCSP activities will be integrated with PFD's NCCDP program, and begin the process of building local participation, cooperation, and ownership. During the workshop, participants had the opportunity to formulate and present their ideas about how the program can work together with health centers and community members, and to identify problems in health centers and brainstorm possible solutions. In addition, PFD presented the results of the Health Facility Survey. Four PFD staff and two staff of the Provincial Health Department facilitated the workshop. A total of 49 participants attended the workshop. Participants included health center staff, Chhlong Operational District staff, Provincial Health Department staff, district and commune chiefs, Provincial Department of Rural Development staff, and representatives from Medicins Sans Frontieres/Kratie and UNICEF/Phnom Penh.
6 5. Staff Recruitment At this time, NCCSP has all key Child Survival Program and support staff in place for the entry-level grant. The NCCSP field team includes one expatriate Child Survival Coordinator, two Child Survival Program Officers, one Administrative Officer, one Office Guard, and one Driver/Mechanic. In addition to field-based staff, PFD headquarters has hired a Public Health Technical Advisor to provide technical assistance and backstop its Cambodia Child Survival Program. As part of the matching funding for the NCCSP grant, PFD is also implementing a birth spacing program using community-based promoters in the Chhlong Operational District. (This project is described in more detail in section 13.) Within the last year, PFD hired a Cambodian Community-Based Distribution (CBD) Program Manager to start and manage the birth spacing program. As the recently retired Chief of Maternal and Child Health of the Provincial Health Department, the CBD Program Manager has a great deal of experience with child health issues, and she spends about one week per month assisting the Program Officers with Child Survival Program activities. Utilizing and building on local capabilities, the program has been able to use some district based staff from government line ministries (Ministries of Health, Rural Development, and Women's Affairs) to assist with surveys, qualitative data collection, and community organizing work. A total of ten individuals from the three line ministries listed above have worked with the program so far. Three of them have assisted the program on a regular basis. The use of line ministry staff benefits both the program and the ministries. The program gets extra staff, on an as-needed basis, who are already experienced in facilitation and community organizing. By using staff from line ministries, the program also has the advantage of additional people to advocate for and promote the program at the provincial, district, and village level. The line ministries and staff themselves benefit because NCCSP provides them with training that helps them in their day-to-day work. In addition, participation by line ministry staff in planning and supervising child survival activities strengthens the institutional capabilities within the Operational District as well as the District Offices of Rural Development and Women's Affairs. 6. Staff Training NCCSP's Cambodian staff and district and provincial-level staff from the Ministries of Health, Rural Development, and Women's Affairs participated in a variety of training workshops throughout the first year of the program. The type and purpose of each training, name of program or organization responsible, and number of staff who attended are listed in the table below: Type of Training Program/Org. Responsible KPC survey training PFD/NCCSP 2 CS Program Officers World Vision Number/Type of NCCSP Staff Trained 7 Ministry of Health Staff 1 Ministry of Women's Affrs Staff 1 Ministry of Rural Dev Staff 3 World Vision Field Staff, 22 Interviewers Knowledge, Attitudes, and Practices PFD/NCCSP 2 CS Program Officers (KAP) survey training (for CBD 7 Ministry of Health Staff Program) 1 Ministry of Women's Affrs Staff 1 Ministry of Rural Dev Staff 22 Interviewers
7 Type of Training Program/Org. Number/Type of NCCSP Staff Responsible Trained Training on entering and checking PFD/NCCSP 2 CS Program Officers data entry in Epilnfo 1 Administrative Officer 3 PFD Staff 1 PFD Expatriate Intern Field training on Participatory Rural PFD/NCCDP 2 CS Program Officers Appraisal (PRA) 1 Ministry of Women's Affrs Staff 1 Minist of Rural Dev Staff Facilitation Skills Workshop PFD/NCCDP 2 CS Program Officers PFD/NCCSP 1 Ministry of Women's Affrs Staff 1 Minist of Rural Dev Staff Focus Group Training PFD/NCCSP 2 CS Program Officers 2 Minist of Women's Affrs Staff Field training on qualitative data PFD/NCCSP 2 CS Program Officers collection 2 Ministry of Women's Affrs Staff 1 Ministry of Rural Dev Staff Nutrition training Helen Keller 1 CS Program Officer International Workshop on the integration of family Initiatives Inc. 1 CBD Program Manager planning into other NGO/PVO programs Each of these training activities is described in detail below. 1 Ministry of Health Staff KPC and KAP Survey Trainings PFD conducted a four-day workshop prior to each survey to prepare supervisors and interviewers to conduct the surveys. Each training included sessions on the overview and purpose of the survey, roles of supervisors and interviewers, discussion of questionnaire (question by question), household selection, determining age of child, interviewing techniques, and supervision strategies. Epilnfo Training NCCSP conducted training on the use of Epilnfo before each of the two surveys. Training was provided to staff in small groups or on an individual basis. Each training session lasted about two hours. The training focused on data entry and rechecking data entry. Field Training on Participatory Rural Appraisal In June 1999, PFD/NCCDP staff decided there was a need to revise its Participatory Rural Appraisal (PRA) process. Staff in Steung Treng province initiated some revisions, and staff from NCCDP and NCCSP in Kratie province went to Steung Treng to discuss the changes and to conduct two practice PRAs in villages. Following this field test, the NCCDP/NCCSP staff returned to Kratie where they discussed their experiences with the other community organizing staff in the province. Then two teams each did an additional two practice PRAs in different villages. After the second field test, the teams met in Kratie again to discuss how well the changes worked. At this point, small changes are still being made in the PRA process, but NCCDP expects to finalize the changes and produce a revised and improved PRA manual in the coming months. Training on PRA techniques was important for child survival staff because it provided them with a chance to practice their facilitation skills, to understand the community organizing process, and to help them think how the PRA can be used within NCCSP.
8 Facilitation Skills Workshop PFD conducted this four-day workshop which was designed to teach NCCDP and NCCSP staff good techniques for facilitating meetings and activities at the village-level. The workshop included sessions on: principles of adult learning, role of a facilitator, giving and receiving feedback, verbal and non-verbal communication, how to ask questions, how to remain neutral, how to facilitate a large group, how to work with shy people, and how to conduct focus groups. Following the "teaching sessions," participants were divided into groups and given facilitation situations that they were asked to develop into a role play. The role plays were videotaped and participants provided feedback to each other about how to improve their facilitation skills. Whenever necessary, groups repeated their role plays using the feedback. Focus Group Training NCCSP conducted a one-day training on focus groups for staff involved in qualitative data collection for the Child Survival Program. This training focused on skills for facilitating focus groups and note taking. Field Training for Qualitative Data Collection In order to give staff a chance to practice and fine tune their qualitative data collection skills, the first village where the child survival qualitative data collection was conducted served as a field test The CS Coordinator observed the activities and provided feedback to the staff on their facilitation skills. Following the two days of data collection, the team met with the CS Coordinator to discuss how to improve the schedule and data collection activities. Nutrition Training HKI has provided two training workshops to NCCSP and NCCDP staff. The first training was five days and covered the food groups, micronutrients, protein-energy malnutrition, growth monitoring, breastfeeding/colostrum, supplementary/weaning foods, nutrition of adolescent girls and pregnant and lactating women, and food preparation. The second training was three days and covered skills for facilitating nutrition education sessions at the village-level. A third training will be provided in November and will focus on how to use IEC materials related to nutrition. Workshop on the integration of Family Planning into Other NGO/PVO Programs The CBD Program Manager and one Provincial Health Department staff attended two consecutive training workshops in Bangladesh from February 14-25, Both workshops were conducted by Initiatives Inc. for The SEATS Project. The first workshop lasted 4 1/2 days and focused on the integration of family planning into other NGO programs. The second workshop lasted 5 1/2 days and was a training of trainers (TOT) workshop intended to reinforce the knowledge gained during the first workshop and prepare participants to design and implement Integration Workshops in their home countries. 7. Knowledge, Practice, and Coverage (KPC) Survey NCCSP conducted its baseline KPC survey in May Prior to conducting the actual interviews, a core group (including CS Coordinator, CBD Program Manager, and one Provincial Health Department staff) reviewed the objectives of the survey, revised the standard CSTS KPC questionnaire, selected survey clusters, identified interviewers and supervisors, mobilized local officials and village chiefs, and planned for survey logistics. As these activities were carried out by the core group, they were also discussed with and reviewed by Dr. Kyi Minn, World Vision/Cambodia's Health Advisor, who provided technical assistance for the survey. With the help of Dr. Kyi Minn and his Cambodian assistant, NCCSP conducted the training of supervisors and interviewers on May 24-27, The 300 interviews were conducted on May 28-30, The day following the completion of the interviews, all supervisors and
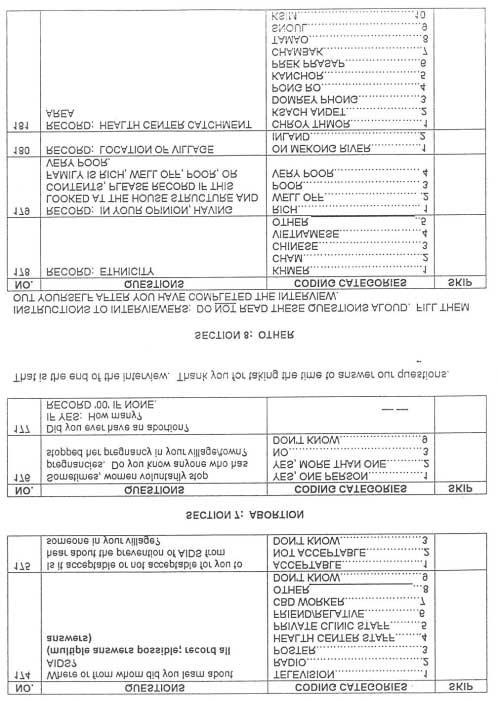
9 interviewers met back at the NCCSP office to process their field experiences, and to hand tabulate and discuss some of the key results. The results of the interviews were also entered into the Epilnfo statistical program by three PFD staff. Once the data entry was rechecked by the two CS Program Officers, the CS Coordinator analyzed the data using Epilnfo, and worked with the Program Officers to write both a short summary of the KPC results (See Appendix B) and a full-length report. The full-length report is now finalized and has been distributed to interested agencies in Phnom Penh and Kratie province. A copy of the final report will be included in the DIP proposal, which PFD will submit in December. In addition to the reports, PFD staff made the following presentations of the KPC results: The CS Coordinator made a brief presentation at the monthly PROCOCOM (Provincial Coordinating Committee) meeting in Kratie. PROCOCOM includes Provincial Health Department and Operational District staff as well as international and local NGOs involved in health in Kratie province. A copy of the KPC summary was translated to Khmer and distributed at this meeting. The CS Coordinator made a complete presentation of the KPC results to representatives of USAID, UNICEF, World Relief, Marie Stopes International, Voluntary Services Overseas, Veterans International, and Ministry of Rural Development at the PFD office in Phnom Penh. PFD/Cambodia's Program Manager presented the results of the KPC at the monthly meeting of Medicam, an organization based in Phnom Penh that provides a forum for NGOs-and government agencies involved in health to meet and exchange information. The CS Program Officers made presentations of the results of the KPC survey to community members who participated in the qualitative data collection activities. They also developed a simplified version of the KPC summary in Khmer for distribution during the village presentations. 8. Qualitative Data Collection In August and September 1999, NCCSP collected qualitative data on key child survival topics. The purpose of collecting this information was to answer the "why" questions identified by the KPC survey. In other words, the program sought to understand the reasons why parents take certain actions related to their children's health, and to understand how parents make decisions about treating their children's health problems. NCCSP's qualitative data collection activity also gave program staff the chance to present the results of the KPC survey back to members of some of the communities where it was conducted. In addition, it allowed NCCSP to get input from community members on how they would like the program to assist them in improving their children's health. The data collection activity was conducted in 11 villages. Villages were chosen on the basis of two criteria: (1) they participated in the KPC survey and (2) they have completed a Participatory Rural Appraisal and/or they have a Village Development Committee. In order to ensure that program staff heard opinions from various geographical zones within the program area, two to three villages were selected from each of the three administrative districts that are included in the Chhlong Operational District. The data collection process took about two days to complete in each village. It included the following activities: an introductory village meeting, village mapping, identification of important childhood diseases, focus groups (on nutrition, breastfeeding, immunization, and diarrhea), interviews on health-seeking behavior, and a final village meeting. A description of the methods used for qualitative data collection and a list of questions for focus groups and interviews on health-seeking behavior are included in Appendix C.
10 NCCSP plans to produce a report of the methods used and results obtained from these qualitative data collection activities. In addition, the program hopes to refine its questions on its four key child survival interventions in order to collect more information to fill in the remaining gaps in the program's understanding of people's beliefs and behaviors related to child health. NCCSP also plans to conduct some qualitative data collection on the beliefs and practices of drug sellers in the program area. 9. Collaboration with Other Child Survival Programs in Cambodia During the first year of the program, NCCSP has developed good relationships with both of the other organizations that have USAID-funded Child Survival Programs in Cambodia. The program collaborated closely with World Vision on the preparations for the KPC survey, and received technical assistance from World Vision for the training of supervisors and interviewers for the KPC baseline survey. Both the PFD Program Manager and the CS Coordinator have visited World Vision's Child Survival Program to learn more about the practical details of the implementation of their program in Kean Svay. During the CS Coordinator's visit, she was given copies of educational materials and monitoring forms produced by World Vision's program. In exchange, NCCSP has sent copies of materials produced by the program to World Vision's CS Coordinator. NCCSP and World Relief s Child Survival Programs have also exchanged materials. NCCSP and World Relief staff have been present at each other's presentation of KPC baseline survey results. The CS Coordinator and Program Officers plan to visit World Relief's Child Survival Program in November. 10. Developing Partnerships In addition to collaboration with World Vision and World Relief, NCCSP has developed or is exploring partnerships with several other organizations on the national level. Most importantly, PFD is in the process of working out a Memorandum of Understanding (MOU) with the Ministry of Health. A draft MOU has been written, and we expect it to be finalized and signed before the end of PFD already has an MOU with Helen Keller International (HKI). In this agreement, HKI is providing NCCSP and NCCDP staff with training on nutrition and gardening, and PFD is working with villages to establish village model gardens and household gardens and to provide nutrition education. HKI will assist NCCSP with nutrition posters and other IEC materials. Also on the national level, PFD has been exploring the possibility of serving as an implementing partner for the World Food Program's (WFP) supplementary feeding program. The details still need to be worked out, but NCCSP would like WFP to assist the program with rice and oil for food preparation demonstrations and/or supplementary feeding of underweight children. PFD staff have held meetings with RACHA to discuss how our programs can collaborate. NCCSP used RACHA's facility survey questionnaire as a guide in the development of our own. NCCSP will also receive copies of RACHA's training and IEC materials as they become available. In exchange, RACHA plans to send some staff to visit NCCSP and NCCDP in Kratie province to learn more about the community organizing techniques used by PFD's two programs. NCCSP recently started a collaboration with ADRA's health program in Kampong Thom province. Two NCCSP staff visited the program to attend their soy product-making (tofu, soy milk, soy cookies) and nutrition education activity. NCCSP is interested in using a similar
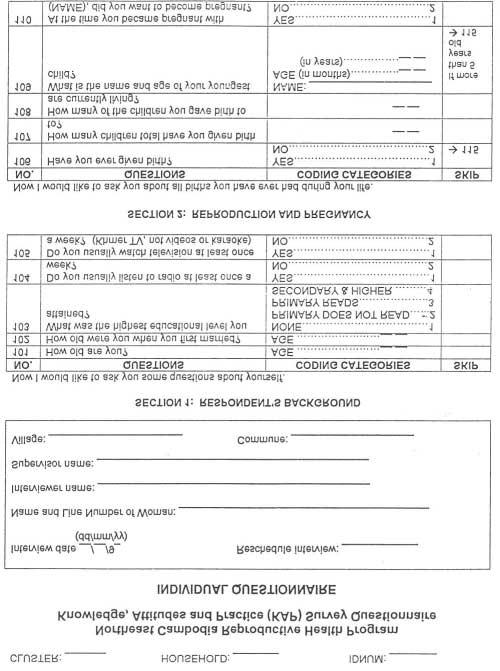
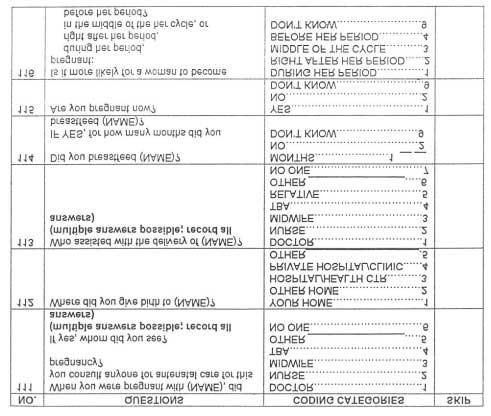
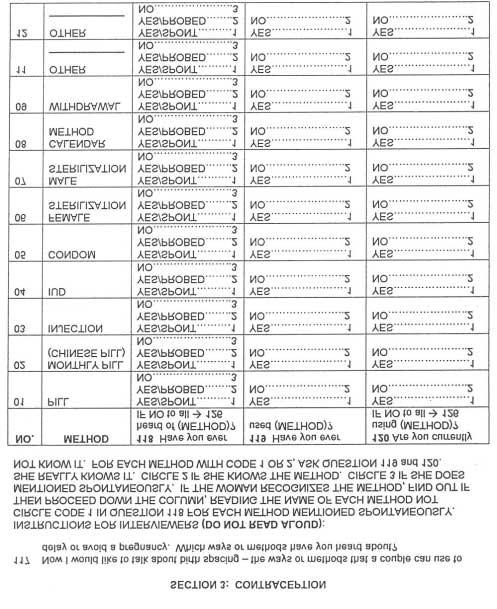
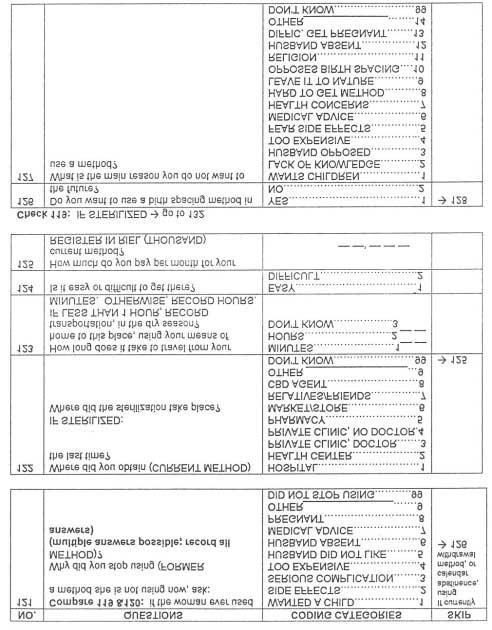
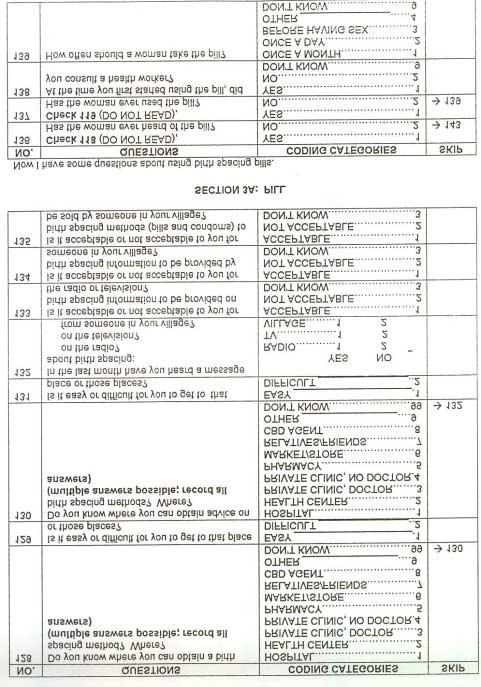
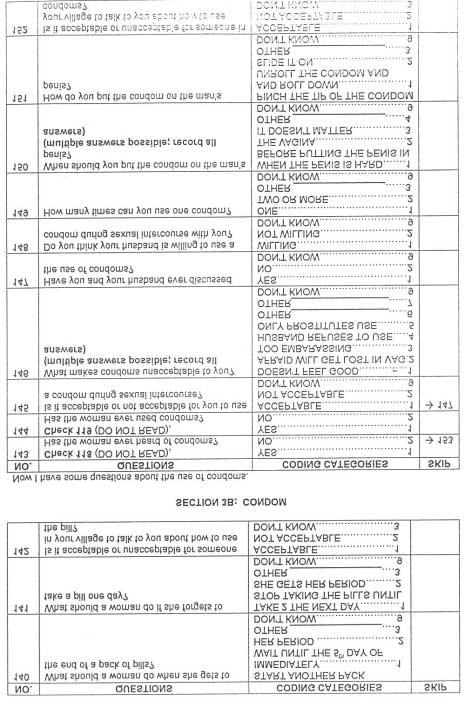
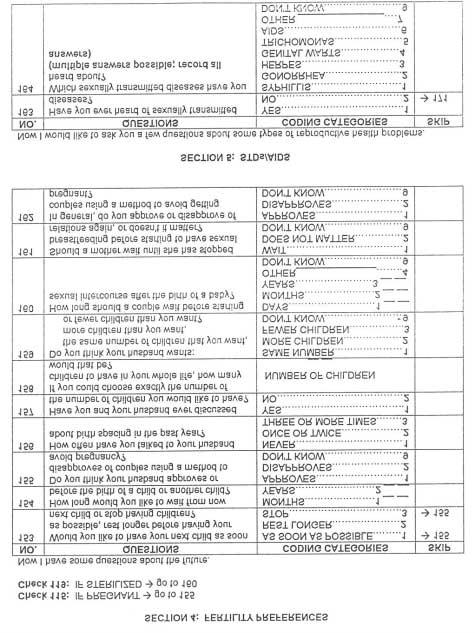
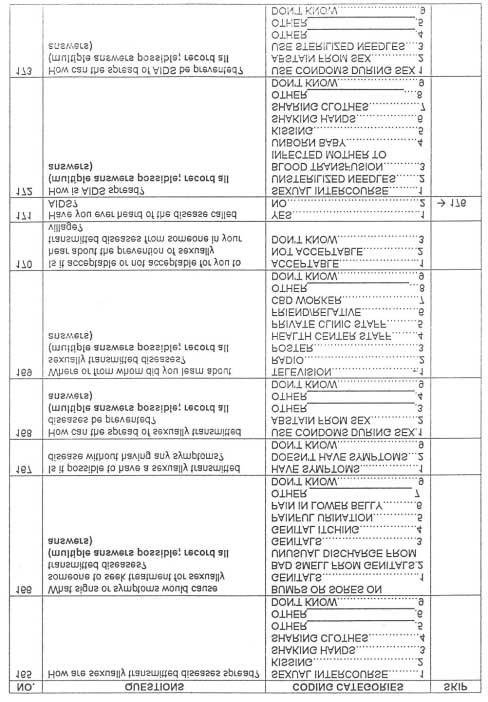
11 type of activity as part of its nutrition intervention. ADRA has offered to send one staff member to Chhlong to train NCCSP program staff on how to make soy products. On the provincial level, NCCSP has developed a close working relationship with both the Provincial Health Department and the Chhlong Operational District. Staff from the province and the Operational District attended the pre-implementation workshop. Since that time, NCCSP has held numerous meetings Health Department staff for the purpose of clarifying program goals and objectives, and planning for future activities. NCCSP staff have also met on several occasions with the staff of Save the Children/UK (SCF/UK) based in Kratie. SCF/UK has primary health care, reproductive health, and food security programs in part of Prek Prasap district, which is located in the NCCSP program area. NCCSP is in the process of working out an MOU with SCF/UK in order to coordinate the activities of both organizations and ensure that there is no duplication of efforts. Finally, during surveys, qualitative data collection, and other visits to villages, NCCSP has worked through Village Development Committees (VDCs) whenever possible. The program is committed to using existing village structures and has provided administrative support to NCCDP's community organizing teams when they hold VDC elections and conduct VDC training. 11. Collection of Cambodia-specific Data and Other Resource Materials Throughout the first year of the program, NCCSP has collected national and local survey reports that include data related to child health issues as well as other qualitative research conducted in Cambodia on child health topics. NCCSP obtained copies of relevant MOH policies, guidelines, and protocols. Program staff have checked with World Health Organization (WHO) and UNICEF staff to find out whether and/or when changes to current policies are expected. NCCSP also began making a collection of existing IEC materials on child health topics produced in Cambodia. In addition to Cambodia-specific information and materials, NCCSP obtained copies of important reference materials on data collection techniques and key child survival topics. A complete list of relevant materials will be included in the DIP. 12. DIP Using the results of the KPC survey and qualitative data collection together with input from community members, the Provincial Health Department, and other partners, NCCSP staff conceptualized an overall plan for the implementation of the Child Survival Program and began writing sections of the DIP. PFD's Public Health Technical Advisor will come to Cambodia in November to assist with the DIP, and it will be finalized in December. 13. Birth Spacing Activities As described earlier, the birth spacing activities conducted by PFD in the Chhlong Operational District are part of the matching funds for NCCSP, and the two programs are closely integrated. PFD's birth spacing program, the Northeast Cambodia Reproductive Health Program (NCRHP), is a two-year pilot Community-Based Distribution (CBD) program funded by Marie Stopes International (MSI)/UNFPA from April 1, 1999 to March 31, The objectives of the program are to increase access to contraceptives, strengthen the quality of reproductive health services, and increase knowledge of reproductive health issues (e.g., STDs and AIDS). These objectives are being met by training volunteer CBD agents to work in their own villages selling oral contraceptives and condoms, providing education and counseling on the use of contraceptives, and educating community members about other reproductive health issues. NCRHP plans to have a total of 72 CBD workers to cover the 100 villages in the program area. CBD workers will be selected and trained in three groups or phases. In addition, the program is working to strengthen the quality of
12 reproductive health services in the Operational District by sending one midwife from each health center for technical and practical training on reproductive health from the Reproductive Health Association of Cambodia, a local NOO based in Phnom Penh. NCCSP and NCRHP have collaborated closely in several different ways. First, staff from the two programs participated in both the KPC and KAP baseline surveys. The CBD Program Manager served as a member of the core team for the KPC baseline survey.. NCCSP staff assisted with the KAP survey as supervisors during the interviews and with data entry and data checking. Second, NCRHP and NCCSP have worked together in villages to hold village meetings to explain the two programs to community members. Third, NCRHP CBD workers are helping to make the Child Survival Program known in their villages and they assist the NCCSP Program Officers with child survival activities in their villages (e.g., qualitative data collection). Fourth, the CBD Program Manager spends about 25% of her time on child survival activities and issues. Implementing NCCSP and NCRHP side-by-side provides other important benefits to the Child Survival Program. Because NCRHP is slightly ahead of NCCSP in terms of implementation, it serves as a testing ground for proposed child survival activities. For example, selecting, training, and supervising CBD workers has given PFD experience within the NCCSP program area with managing volunteers, and has given the national staff a sense of the commitments and needs involved in using volunteers. The NCRHP program has also provided NCCSP staff with the opportunity to see how collaboration with the Provincial Health Department works, and has provided insight on the importance of clear communication between all players. Because NCCSP and NCRHP are integrated, it is important to review briefly the activities conducted under the birth spacing program. To date, NCRHP has completed the following activities: CBD Pre-implementation Workshop -- A pre-implementation workshop for the CBD program was held in Chhlong on May 10-11, Its purpose was to inform participants about the goals and objectives of the program, provide them with details about program implementation, and get their input on their roles in the implementation process. Fifty-three participants, mainly Provincial Health Department and Operational District staff and district and commune chiefs, attended the workshop. Baseline survey of reproductive health Knowledge, Attitudes, and Practices (KAP) - This survey was conducted in June 1999, and used the same type of cluster sampling methodology as the KPC survey. For the KAP survey, a total of 600 married women between the ages of 15 and 45 years were interviewed; 15 women were interviewed in each of 40 villages. The KAP survey asked questions about the following issues: reproduction and pregnancy, contraception, knowledge and attitudes related to condoms and oral contraceptives, fertility preferences, and STDs/AIDS. (The questionnaire is included in Appendix D.) The results of the KAP survey have been analyzed, and preliminary results are being used to develop health education messages and IEC materials. Some KAP survey results are also relevant for NCCSP, and they are being used to help plan child survival interventions and write the DIP. The final report of the KAP survey will be completed by the end of Selection and training of CBD workers - Twenty-one CBD workers were selected for the phase #1 training of the CBD program held in July The workshop lasted for five days and was facilitated by staff from the Reproductive Health Association of Cambodia. Four Team Leaders were selected from among the CBD workers and they received an additional '/Z day of training. The CBD Program Manager is currently in the process of selecting CBD workers for phase #2. About 30 CBD workers will participate in the second workshop, which will be held in October 1999.
13 Monitoring CBD workers - Following the phase #1 training, the CBD Program Manager made at least one visit to each CBD worker. CBD workers and Health Center midwives met for their first bi-monthly meeting in early September 1999, This meeting provides an opportunity for CBD workers to get together to discuss the problems they have encountered and brainstorm possible solutions. Training of Health Center Midwives - All ten midwives have already completed the technical training course on reproductive health. Four of the ten midwives have also completed the practical course and three additional midwives will attend the practical course in October Collection of IEC materials - NCRHP has collected IEC materials on birth spacing, STDs, and AIDs currently available in Cambodia. The project is using existing materials that are appropriate to its goals and target population, and plans to design new materials to fill in the gaps where needed. Design of IEC materials - The project has designed t-shirts for CBD workers and flags for them to hang at their homes to indicate that they sell contraceptives. 14. Community Development Activities Related to Child Survival As stated earlier, PFD's current development program is the Northeast Cambodia Community Development Program (NCCDP). In collaboration with staff of various government line ministries, NCCDP coordinates a wide range of activities including: Village Development Committee elections and training; Participatory Rural Appraisal; drilling and installation of handpumps; construction of home water filters; community and school-based water-use and hygiene education; construction of family latrines, schools, and health centers; distribution of impregnated bednets; school nutrition education; and family gardens. As discussed earlier, NCCSP and NCCDP have collaborated closely on administrative and logistics issues. In addition, the projects have worked to coordinate program activities. This has been a pleasure because NCCDP activities complement nicely the activities NCCSP has planned for the Chhlong Operational District. A summary of NCCDP activities directly or indirectly related to child health conducted during the first year of the Child Survival Program in Chhlong Operational District is as follows: 36 successful wells constructed 22 PRAs, 16 VDC elections, and four VDC trainings. 47 community water use and hygiene education sessions. Eight school nutrition education TOT workshops for 37 primary school teachers. Distribution of 13,324 impregnated bednets in 37 villages. Re-impregnation of 8,361 previously distributed bednets. In collaboration with HKI, the owners of four village model gardens have been trained and these gardens are in the process of being set up. Village model gardens will supply seedlings and seeds to household gardens at a small cost. Weighing and measuring of children less than five years old and women of reproductive age has been completed two times in the five villages of Ksach Andet commune in Chhlong Operational District. This activity (known as Child Woman Assessment) has been conducted as a part of UNICEF's Community Action for Social Development program for which PFD was the implementing partner in Kratie and Steung Treng provinces. Factors that Contributed the Most Toward the Achievement of Progress: As the sections above indicate, considerable progress has been made toward the implementation of the NCCSP program. The key factors that have contributed toward the achievement of progress are as follows:
14 NCCDP presence in the NCCSP program area NCCDP's presence in the Chhlong Operational District has provided a boost to the NCCSP program in several ways. First, even before NCCSP started any activities, there was already recognition of PFD as a community development organization at the community-level and among district and commune officials. Second, NCCDP's community organizing work has helped to ensure that village-based groups (VDCs) exist to assist government agencies and other programs (such as NCCSP) in the implementation of development projects and has laid the foundation for villages to take charge of their own development. Third, NCCDP assisted NCCSP staff to set up the new office in Chhlong and provided staff training and logistical support. NCHRP taking place in same program area as NCCSP As described earlier, community-based activities of the NCRHP are already being implemented. This is assisting NCCSP because CBD workers are helping to make PFD known in communities as an organization that has programs related to maternal and child health. It has also provided the opportunity for NCRHP and NCCSP staff to collaborate in the promotion of the two programs. Motivated staff All of the NCCSP staff are highly motivated. The two Program Officers and staff from the District Offices of Rural Development and Women's Affairs have shown their motivation through their willingness to work long hours and weekends, when necessary, and to make the extra effort that it takes to get to rural villages during the rainy season. The Administrative Officer and the Program Officers are also willing to learn new skills, to learn from their mistakes, and to accept constructive feedback. Experienced staff The CS Program Officers and most staff from line ministries have several years of experience in facilitating group meetings and activities, and with working on the community-level. In addition, one CS Program Officer has several of experience with EPI, and the CBD Program Manager has a great deal of experience with maternal and child health issues, as the former Chief of MCH for Kratie province. Location of NCCSP office on Mekong River Thanks to its location on the Mekong River, the flow of materials and staff from Phnom Penh and Kratie to the NCCSP office in Chhlong has been uninterrupted. B. CONSTRAINTS Although NCCSP has made good progress during its first year, there are some factors that have slowed or impeded progress. The major constraints and the program's actions to overcome them are as follows: Medecins Sans Frontieres (MSF) pull out from Chhlong In March 1999, MSF unexpectedly decided to close their operations in Chhlong. This affects the Chhlong Operational District because there is no longer an NGO providing direct assistance and support to the operation and supervision of health centers in the area. It also affects NCCSP because the program was planning to develop a partnership with MSF wherein MSF provided the necessary training, supervision, and support related to child survival interventions to the health centers in the Chhlong Operational District. As a result of MSF's decision to leave Chhlong, NCCSP has had to rethink how the program can provide assistance with training and supervision to health centers both within the current grant and for purposes of planning for the DIP.
15 NCCSP is also trying to identify other ways to assist the health centers through community-based organizations or local NGOs. Difficulty finding qualified staff NCCSP had some difficulty finding qualified national staff. Because Chhlong is a small town and the pool of trained personnel already living there is quite small, the program tried recruiting staff from Phnom Penh and Kratie. Candidates from Phnom Penh were generally not qualified and most did not want to live in the provinces. A few qualified candidates were identified in Kratie town, and the program made an effort to ensure that it did not "poach" staff from the Provincial Health Department or other NGOs. In the end, the two Program Officers and the Driver/Mechanic (as well as the CBD Program Manager) were all hired from Kratie. Although it took slightly longer than expected, NCCSP now has a good team in place. Delay in KPC survey NCCSP had originally planned to conduct the KPC baseline survey in March 1999 with the assistance of Mary Lou Rorabaugh, the Child Survival Coordinator for World Vision/Cambodia. However, Ms. Rorabaugh accepted a new position with World Vision/US and was unable to assist NCCSP. Because NCCSP wanted technical assistance for this first KPC survey, Ms. Rorabaugh suggested the program get help from Dr. Kyi Minn from World Vision/Cambodia (also trained in KPC methodology). Due to his busy schedule, NCCSP had to delay the KPC survey until May This put the program a little bit behind schedule in terms of data collection; however, NCCSP has now completed the KPC and initial qualitative data collection as planned. Change in expatriate Child Survival Coordinator There was a change in the expatriate Child Survival Coordinator during the second quarter of the program. The first Child Survival Coordinator left the program after three months. She was replaced internally by the expatriate Community Health Officer, who was working with NCCDP in Steung Treng province, Cambodia. Difficult access to inland villages About 40% of the villages in NCCSP's program area are located in the inland areas of the Chhlong Operational District. Access to these villages is difficult at the best of times and is extremely difficult during the rainy season. To date, program staff have made some heroic efforts to reach rural villages. NCCSP will continue to try to reach these under-served villages, but the program will also make sure that new interventions are phased in so that the majority of travel to these villages is carried out during the dry season. II. SUBSTANTIAL CHANGES IN PROGRAM DESIGN There are three important changes in program design from the original Program Description for this program. First, the program area has been modified to fit with the national health reform plan and now covers the Chhlong Operational District. At the time the original Program Description was prepared, the Cambodian health care system was based on administrative districts. Each district had a district hospital and a few health centers. Under the health reform plan, services are based on population size rather than administrative divisions. Each province is divided into Operational Districts, which cover a population of approximately 100,000. An Operational District has a referral hospital and several health centers. Each health center provides services to about 10,000 people. Kratie province is now divided into two Operational Districts. The Chhlong Operational District covers all or part of three administrative districts (Chhlong (all), Snoul (all except one commune), and
16 part of three administrative districts (Chhlong (all), Snout (all except one commune), and Prek Prasap (half)). This is a change from the original program area, which planned to cover Chhlong and Snout districts. See Appendix E for a map of the new program area. Second, the size of the beneficiary population has increased substantially since the original Program Description was submitted. This change is due mainly to the increased size of the program area. The increase in the beneficiary population is also related to the collection of more recent population census data. The census data used for the NCCSP's original Program Description was collected by the United Nations Transitional Authority in Cambodia (UNTAC) in The Cambodian government has recently published information from its 1998 census. Based on the 1992 data, the total population living in Chhlong and Snout districts was 69,544. The new census data indicate that there are 109,509 people living in the Chhlong Operational District. Third, NCCSP has decided that it is important to add nutrition/micronutrients as a fourth area of intervention. Since the original Program Description was submitted, it has become clear that malnutrition is an on-going and serious problem in Cambodia. Surveys conducted by UNICEF-WFP, HKI, PFD (KPC baseline survey) and others indicate that an extremely large percentage of children are underweight, wasted, and stunted, and that few children receive adequate amounts of food containing Vitamin A, iron, iodine and other important nutrients. In addition, the Cambodian government has begun to recognize nutrition as an important problem. In 1997, the National Assembly adopted the National Plan of Action for Nutrition as national policy. The plan elaborates the government's strategy to promote a community based approach to malnutrition with an emphasis on actions at the household and community level. This policy was reaffirmed in April 1999 during the National Seminar on Food Security and Nutrition. Considering the data from the field indicating the level of childhood malnutrition together with the commitment by the government to address the problem, PFD feels that an intervention on nutrition/micronutrients may be key to improving child survival in northeast Cambodia. A more detailed rationale for this addition to the program's objectives will be included in the DIP.
17 APPENDIX A: Facility Resource Survey Questionnaire
18
19
20

21 Any other observations: Description of the health center structure:
22 APPENDIX B: Baseline KPC Summary


 are")
23 Northeast Cambodia Child Survival Program Chhlong Office c/o PFD, No. 24, Street 294, P.o Box 551, Phnom Penh, Cambodia Tel./Fax: X13.335, Internet: BigPorid.com.kh Baseline Knowledge, Practice, and Coverage Survey Chhlong Operational District, Kratie Province May 1999 Objectives of the Survey For NCCSP to gain information about the following issues: Knowledge and practices of mothers of children < 2 years related to breastfeeding, nutrition, diarrhea) disease, respiratory infection, immunization, and maternal health care EPI coverage and drop-out rates for children months Target groups for health education messages Background on KPC Survey 30-cluster sample methodology 10 interviews per cluster Total of 300 interviews of mothers of children < 2 years old 3 ½ days of training provided to supervisors and interviewers Interviews conducted on May 28-30, teams conducted interviews; each team had 1 supervisor and 2 interviewers No women refused to complete the interview PFD's questionnaire contained 48 questions adapted from a standardized questionnaire KPC Results Breastfeeding Nearly all mothers (97%) are currently breastfeeding and most breastfeed for an extended period of time. Most mothers (87%) waited for more than 8 hours after delivery to start breastfeeding. Very few mothers (12%) of children age 0-5 months exclusively breastfeed them; most give the child water (73%) or sugar water in addition to breastmilk.


.")
24 Nutrition - About 1/3 of mothers know the age when a child should start eating food and the types of food to give. - About 1/2 of children in the 6-11 month age group are receiving a variety of nutritious foods. - Fewer than 10% of ` ` "~ ~~'~' 0~ mothers know that o' vitamin A helps prevent night blindness or could name foods that contain vitamin A. Diarrheal Disease - About 1/2 of mothers surveyed reported that their child had diarrhea in the last 2 weeks. - Mothers have limited knowledge of the danger signs of diarrhea and actions to take during diarrhea. - Only 15 /a of mothers of children with diarrhea in the last 2 weeks gave their child ORT (including ORS, SSS, rice soup, or home available fluids). - - Most mothers (66%) of children with diarrhea in the last 2 weeks purchased medicine or antibiotics for the child. Respiratory Illness - 42% of mothers surveyed reported that their child was ill with rapid and difficult breathing in the last 2 weeks. - 69% of mothers sought treatment for children with these symptoms - Of those who sought treatment, 72% went to a trained health worker (at hospital, health center, or private clinic). - Mothers generally do not recognize the signs of serious respiratory illness. For example, only 15% mentioned chest indrawing and 27% mentioned fast or difficult breathing. Immunizations - 38% of children age months have yellow cards. - 17% of children age months are fully immunized. - DPT drop-out rate = 44% - OPV drop-out rate = 41 10% of all mothers know the correct timing for measles immunization. - No children in the survey have a

25 record of receiving vitamin A capsules. Growth Monitoring - 1% of children in the survey were weighed in the last 4 months. Maternal Care - 21% of mothers reported that they received antenatal care. - 8% of mothers surveyed have maternal health cards. - Only about 1/4 of mothers ate more than usual during their pregnancy. - About 2/3 of mothers do not know what types of foods to eat to prevent anemia during Birth Spacing Most non-pregnant mothers (80%) do not want another child in the next 2 years. 11% of women who do not want another child in the next 2 years are using a modern birth spacing method. Key Issues to be Addressed by NCCSP - Long delay for initiation of breastfeeding - Small percentage of mothers exclusively breastfeeding - Timing of introduction of complementary foods - Types of foods given to children, especially in 6-11 month age group - Mothers' knowledge of vitamin A and the foods that contain it - Importance of giving extra liquids and food during diarrhea - Usefulness of ORT rather than medicine for treating most diarrhea - Signs of pneumonia and actions to be taken - Low rates of EPI coverage - Mothers' knowledge of the importance, timing, and side effects of immunizations Vitamin A capsule distribution - Growth monitoring - Low rates of tetanus toxoid coverage - Mothers' knowledge of the purpose and number of tetanus toxoid shots - Mothers' knowledge of the amounts and types of foods to eat during pregnancy - Low usage rates of modern contraceptive methods
26 APPENDIX C: Qualitative Data Collection Plan and Focus Group Questions
27
28
29 Breastfeeding Focus Group - When did you start giving your newborn baby breastmilk? What did you give the baby to drink/eat before giving it breastmilk? What were the reasons for giving those drinks/foods? Who advised you to give them? - Have you heard of colostrum (or first milk)? Can someone please explain what colostrum is? Did you feed your babies colostrum? Why/why not? Who advised you to give/not give colostrum to your babies? Why is colostrum considered bad? - What other liquids/foods do you give babies during the first three months? During the first six months? Why do you give these foods/liquids? Who advises you to give these liquids/foods? - At what age do women in this village stop breastfeeding their children? Why? Are you breastfeeding/did you breastfeed your youngest child? Do women continue to breastfeed when they are sick? Why/why not? When the baby is sick? Why/why not? - What types of problems have you had with breastfeeding? If you have problems with breastfeeding, who do you go to for advice? - Who would you want to give you advice or support related to breastfeeding? Whose advice would you believe most?
30 Nutrition Focus Group - Describe food preparation in your household. Who usually prepares food for the family? How is it prepared? Is food prepared separately for babies and young children? Who decides what to prepare? - What are the eating arrangements in your family? Who eats together? How many times a day do you usually eat? Where is the youngest child during meals? Who helps the youngest child eat? - What types of food do you think are most important to give to young children? To children who are just starting to eat? What makes these foods good/appropriate for young children? Who tells you that they are good? Are these foods readily available to your family? If they are not, what do you use instead? Are there any types of food that are not good for young children? Which Winds? Why are they bad? Who tells you that they are bad? - How do you know when to start giving a child food? How do you know what foods to give at a certain age? What types of foods do you usually give to children age 6-9 months? What types of foods do you usually give to children age months? To children 1-2 years? To children 2-5 years? - Who gives you advice on what foods to give or not to give children? Who do you believe most? What kinds of problems have you had with feeding your baby/child? When you have problems feeding your baby/child, who do you ask for advice? - What do you want to know more about feeding your baby to help him/her stay healthy or get healthier? Who would you like to give you this information? - Do you feel that you are able to feed your baby/children adequately - enough food and enough variety? Why/why not? Would could be done to improve the feeding of your children?
31 Immunization Focus Group - What good things have you heard about immunizations? Who did you hear this from? What bad things have you heard about immunizations? Who did you hear this from? - What are your own opinions about immunizations for children? For mothers? - For mothers: Have you received vaccinations? Why/why not? For all participants: Have your children received vaccinations? Why/why not? Where? - For participants who took children to HC or got TT shots at HC: Can you explain what happened during your visit to the HC for immunizations? What did you like ieast/most about the visit? - Can you explain what happened the last time the EPI team came to the village? What did you like least about their activities? What did you like most about their activities? How did the members of the EPI team act towards people in this community? Did the EPI team provide education about immunizations during their visit? - How did the immunizations affect the children? What are your feelings about the side effects? - What are the vaccinations given by the EPI team? What diseases do the vaccinations prevent? - How would you like to change or improve the immunization program?
32
33 Diarrhea Focus Group - What are the different names for children's illnesses with "stools that are looser, more watery, or more frequent than usual"? What are the signs and symptoms of these different types of diarrhea? What are the causes? What type of treatment is needed for the different kinds of diarrhea? What results do you expect from the different types of treatment? Are there any types of diarrhea that don't need treatment? Which kinds and why? - If your child has diarrhea, what signs or symptoms make you worry? What signs or symptoms would cause you to seek treatment or advice? Where would you go for advice? Where would you go for treatment? Are there different people/places for treatment depending on the type of diarrhea? If so, who are the different people/places and what are the different types of treatment they offer? If your child has been given drugs or IV fluids for diarrhea, what types of drugs or IV fluids were given? - Who in your family decides when to take the child for treatment for diarrhea? Who in your family decides where to take the child for treatment? If one type of treatment doesn't work, how do you decide what type of treatment to try next? - What kinds of fluids do you give a baby during diarrhea? What kinds of fluids do you give a child during diarrhea? How much fluid do you give a baby/child during diarrhea? Have any of you ever given your child ORS during diarrhea? If yes, can you explain what you did when you gave your child ORS - how did you make it, how often did you give it, what was the effect? What kinds of food do you give a child during diarrhea? How much food do you give? What kinds of food do you give a child after diarrhea? How much food do you give after diarrhea? - What happens to food and water when they are taken into the body? What goes wrong or happens differently during diarrhea? - How can diarrhea be prevented? What actions would you be willing to take in your family to prevent diarrhea?
34
35 Interview Guide on Health-seeking Behavior Identify families in the village with a child less than five years old who was ill in the last two weeks. Probe to find out the parent's thoughts and actions at each step. You should get a global view of their perceptions of the illness, their decision-making process, the health resources that are available in the community, costs and distances to these health providers. How old is the child? What type of illness did the child have? What were the first symptoms? What caused those symptoms? What did you think when you noticed those symptoms? What did you do? Probe for details about how the parents reacted to the illness/what actions they took. From whom did you seek advice or treatment? Please name all the different people you went to for advice or treatment and explain the order you went to them. Please explain how you decided who to go to first, second, etc. Probe to find out who made the decisions at each step. Probe about distance to different health practitioners and cost of treatment to see if these issues played a role in the decision-making process. How did you feel about the treatment that was provided? Wiry? (Find out the answer to these questions for each different person they went to for treatment.) Would you make the same decisions about treatment for the same illness next time? Why or why not? Probe to find out how the decision-making process is different/same for different types of illness.
36 KAP Survey Questionnaire APPENDIX D
37
38
39
40
41
42
43
44
45
46
NUTRITION BULLETIN. Ways to improve Vitamin A Capsule Distribution in Cambodia HELEN KELLER INTERNATIONAL. Vol. 2, Issue 5 April 2001
 C A M B O D I A HELEN KELLER INTERNATIONAL Vol. 2, Issue 5 April 2001 NUTRITION BULLETIN Ways to improve Vitamin A Capsule Distribution in Cambodia Vitamin A capsule (VAC) distribution programs are considered
C A M B O D I A HELEN KELLER INTERNATIONAL Vol. 2, Issue 5 April 2001 NUTRITION BULLETIN Ways to improve Vitamin A Capsule Distribution in Cambodia Vitamin A capsule (VAC) distribution programs are considered
Contracting Out Health Service Delivery in Afghanistan
 Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
Contracting Out Health Service Delivery in Afghanistan Dr M.Nazir Rasuli General director Care of Afghan Families,CAF. Kathmando Nepal 12 Jun,2012 Outline 1. Background 2. BPHS 3. Contracting with NGOs,
Risks/Assumptions Activities planned to meet results
 Communitybased health services Specific objective : Through promotion of communitybased health care and first aid activities in line with the ARCHI 2010 principles, the general health situation in four
Communitybased health services Specific objective : Through promotion of communitybased health care and first aid activities in line with the ARCHI 2010 principles, the general health situation in four
CONCEPT NOTE Community Maternal and Child Health Project Relevance of the Action Final direct beneficiaries
 CONCEPT NOTE Project Title: Community Maternal and Child Health Project Location: Koh Kong, Kep and Kampot province, Cambodia Project Period: 24 months 1 Relevance of the Action 1.1 General analysis of
CONCEPT NOTE Project Title: Community Maternal and Child Health Project Location: Koh Kong, Kep and Kampot province, Cambodia Project Period: 24 months 1 Relevance of the Action 1.1 General analysis of
Egypt, Arab Rep. - Demographic and Health Survey 2008
 Microdata Library Egypt, Arab Rep. - Demographic and Health Survey 2008 Ministry of Health (MOH) and implemented by El-Zanaty and Associates Report generated on: June 16, 2017 Visit our data catalog at:
Microdata Library Egypt, Arab Rep. - Demographic and Health Survey 2008 Ministry of Health (MOH) and implemented by El-Zanaty and Associates Report generated on: June 16, 2017 Visit our data catalog at:
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r
 RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
Community Mobilization
 Community Mobilization Objectives Target Group A capacity-building process through which community members, groups, or organizations plan, carry out, and evaluate activities on a participatory and sustained
Community Mobilization Objectives Target Group A capacity-building process through which community members, groups, or organizations plan, carry out, and evaluate activities on a participatory and sustained
Position Title: Consultant to Assess the RWANDA Thousand Days in the Land of a Thousand Hills Communication Campaign. Level: Institutional contract
 Terms of Reference for a Special Service Agreement- Institutional Contract Position Title: Level: Location: Duration: Start Date: Consultant to Assess the RWANDA Thousand Days in the Land of a Thousand
Terms of Reference for a Special Service Agreement- Institutional Contract Position Title: Level: Location: Duration: Start Date: Consultant to Assess the RWANDA Thousand Days in the Land of a Thousand
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION
 COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION") UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
UNICEF LAO PDR TERMS OF REFERENCE OF NATIONAL CONSULTANT (NOC) COMMUNICATION FOR DEVELOPMENT (C4D) IN IMPROVING ROUTINE IMMUNIZATION UNICEF H&NH Outcome: UNICEF H&N OP #: 3 UNICEF Work Plan Activity: Objective:
THe liga InAn PRoJeCT TIMOR-LESTE
 spotlight MAY 2013 THe liga InAn PRoJeCT TIMOR-LESTE BACKgRoUnd Putting health into the hands of mothers The Liga Inan project, TimorLeste s first mhealth project, is changing the way mothers and midwives
spotlight MAY 2013 THe liga InAn PRoJeCT TIMOR-LESTE BACKgRoUnd Putting health into the hands of mothers The Liga Inan project, TimorLeste s first mhealth project, is changing the way mothers and midwives
MINISTRY OF HEALTH ON INFANT AND YOUNG CHILD FEEDING
 MINISTRY OF HEALTH CONTINUOUS TRAINING PROGRAM ON INFANT AND YOUNG CHILD FEEDING Manuals for Health Workers on maternal and child health care at all levels Hanoi, January 2015 INTRODUCTION The United
MINISTRY OF HEALTH CONTINUOUS TRAINING PROGRAM ON INFANT AND YOUNG CHILD FEEDING Manuals for Health Workers on maternal and child health care at all levels Hanoi, January 2015 INTRODUCTION The United
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004
 UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
UNICEF HUMANITARIAN ACTION DPR KOREA DONOR UPDATE 12 MARCH 2004 CHILDREN IN DPRK STILL IN GREAT NEED OF HUMANITRIAN ASSISTANCE UNICEF appeals for US$ 12.7 million for action in 2004 Government and UNICEF
UNICEF WCARO October 2012
 UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. Community IMCI. Community IMCI
 Implementation in the Western Pacific Region. Community IMCI. Community IMCI") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan
 Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: Prepared by: February 7, 2017 Dr. Taban Martin Vitale I. Demographic Information
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: Prepared by: February 7, 2017 Dr. Taban Martin Vitale I. Demographic Information
Policy Guidelines and Service Delivery Standards for Community Based Provision of Injectable Contraception in Uganda
 Policy and Service Delivery Standards for Community Based Provision of Injectable Contraception in Uganda Addendum to Uganda National Policy and Service Standards for Sexual and Reproductive Health December
Policy and Service Delivery Standards for Community Based Provision of Injectable Contraception in Uganda Addendum to Uganda National Policy and Service Standards for Sexual and Reproductive Health December
Overview of good practices on safe delivery
 Overview of good practices on safe delivery Excerpt from Tata Kelola Persalinan Aman (Kinerja 2014) Kinerja 2015 http://www.kinerja.or.id 1 Introduction Kinerja has worked in the field of safe delivery
Overview of good practices on safe delivery Excerpt from Tata Kelola Persalinan Aman (Kinerja 2014) Kinerja 2015 http://www.kinerja.or.id 1 Introduction Kinerja has worked in the field of safe delivery
Positive Deviance/Hearth Consultant s Guide. Guidance for the Effective Use of Consultants to Start up PD/Hearth Initiatives.
 Positive Deviance/Hearth Consultant s Guide Guidance for the Effective Use of Consultants to Start up PD/Hearth Initiatives. The Child Survival Collaborations and Resource Group Nutrition Working Group
Positive Deviance/Hearth Consultant s Guide Guidance for the Effective Use of Consultants to Start up PD/Hearth Initiatives. The Child Survival Collaborations and Resource Group Nutrition Working Group
EXIT STRATEGIES STUDY: INDIA BEATRICE LORGE ROGERS, CARISA KLEMEYER, AMEYA BRONDRE
 EXIT STRATEGIES STUDY: INDIA 1 BEATRICE LORGE ROGERS, CARISA KLEMEYER, AMEYA BRONDRE Overview of India Study 2 One program (CARE); one sector (health) Four states: AP, Orissa, Chhattisgarh, UP India contrasts
EXIT STRATEGIES STUDY: INDIA 1 BEATRICE LORGE ROGERS, CARISA KLEMEYER, AMEYA BRONDRE Overview of India Study 2 One program (CARE); one sector (health) Four states: AP, Orissa, Chhattisgarh, UP India contrasts
Sudan High priority 2b - The principal purpose of the project is to advance gender equality Gemta Birhanu,
 Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
Sudan 2017 Appealing Agency Project Title Project Code Sector/Cluster Refugee project Objectives WORLD RELIEF (WORLD RELIEF) Comprehensive Primary Health Care Services For Vulnerable Communities in West
Improving blanket supplementary feeding programme (BSFP) efficiency in Sudan
 efficiency in Sudan") Improving blanket supplementary feeding programme (BSFP) efficiency in Sudan By Pushpa Acharya and Eric Kenefick Pushpa Acharya is currently working as Head of Nutrition for the World Food Programme in
Improving blanket supplementary feeding programme (BSFP) efficiency in Sudan By Pushpa Acharya and Eric Kenefick Pushpa Acharya is currently working as Head of Nutrition for the World Food Programme in
Ballia Rural Integrated Child Survival (BRICS) Project World Vision of India Dr. Beulah Jayakumar
 Project World Vision of India Dr. Beulah Jayakumar") Ballia Rural Integrated Child Survival (BRICS) Project World Vision of India Dr. Beulah Jayakumar Email: ballia_india_adp@wvi.org The Ballia Rural Integrated Child Survival (BRICS) Project was implemented
Ballia Rural Integrated Child Survival (BRICS) Project World Vision of India Dr. Beulah Jayakumar Email: ballia_india_adp@wvi.org The Ballia Rural Integrated Child Survival (BRICS) Project was implemented
REPORT ON THE SITUATION OF INFANT AND YOUNG CHILD FEEDING IN KUWAIT
 THE CONVENTION ON THE RIGHTS OF THE CHILD 64 th Session September/October 2013 REPORT ON THE SITUATION OF INFANT AND YOUNG CHILD FEEDING IN KUWAIT September 2013 Prepared by: Dr Mona Alsumaie (National
THE CONVENTION ON THE RIGHTS OF THE CHILD 64 th Session September/October 2013 REPORT ON THE SITUATION OF INFANT AND YOUNG CHILD FEEDING IN KUWAIT September 2013 Prepared by: Dr Mona Alsumaie (National
COUNTRY PROFILE: LIBERIA LIBERIA COMMUNITY HEALTH PROGRAMS JANUARY 2014
 COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
COUNTRY PROFILE: LIBERIA JANUARY 2014 Advancing Partners & Communities Advancing Partners & Communities (APC) is a five-year cooperative agreement funded by the U.S. Agency for International Development
Provision of Integrated MNCH and PMTCT in Ayod County of Fangak State and Pibor County of Boma State
 Provision of Integrated MNCH and PMTCT in Ayod County of Fangak State and Pibor County of Boma State Date: Prepared by: February 13, 2017 Dr. Taban Martin Vitale I. Demographic Information 1. City & State
Provision of Integrated MNCH and PMTCT in Ayod County of Fangak State and Pibor County of Boma State Date: Prepared by: February 13, 2017 Dr. Taban Martin Vitale I. Demographic Information 1. City & State
THE FUNCTIONING OF COMMUNE COMITTEE FOR WOMEN AND CHILDREN
 Royal Government of Cambodia National Committee for the Management of Decentralization and Deconcentration Reform THE FUNCTIONING OF COMMUNE COMITTEE FOR WOMEN AND CHILDREN August, 2008 Preface Content
Royal Government of Cambodia National Committee for the Management of Decentralization and Deconcentration Reform THE FUNCTIONING OF COMMUNE COMITTEE FOR WOMEN AND CHILDREN August, 2008 Preface Content
Using a Quality Improvement Approach in Facilities and Communities in Ghana:
 Using a Quality Improvement Approach in Facilities and Communities in Ghana: Enhancing Nutrition within the First 1,000 Days Photos: SPRING Introduction Since 2014, USAID s flagship multi-sectoral nutrition
Using a Quality Improvement Approach in Facilities and Communities in Ghana: Enhancing Nutrition within the First 1,000 Days Photos: SPRING Introduction Since 2014, USAID s flagship multi-sectoral nutrition
CHILD-E. Child Health Initiatives for Lasting Development in Ethiopia. Mid Term Evaluation August 2005
 CHILD-E Child Health Initiatives for Lasting Development in Ethiopia Farta Woreda, Amhara Region, Ethiopia Child Survival and Health Grants Program CSXVIII Cooperative Agreement No: HFP-A-00-02-00046-00
CHILD-E Child Health Initiatives for Lasting Development in Ethiopia Farta Woreda, Amhara Region, Ethiopia Child Survival and Health Grants Program CSXVIII Cooperative Agreement No: HFP-A-00-02-00046-00
Microbicides Readiness Assessment Tool A tool for diagnosing and planning for the introduction of microbicides in public-sector health facilities
 Microbicides Readiness Assessment Tool A tool for diagnosing and planning for the introduction of microbicides in public-sector health facilities BACKGROUND This tool is intended to help evaluate the extent
Microbicides Readiness Assessment Tool A tool for diagnosing and planning for the introduction of microbicides in public-sector health facilities BACKGROUND This tool is intended to help evaluate the extent
Mauritania Red Crescent Programme Support Plan
 Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Mauritania Red Crescent Programme Support Plan 2008-2009 National Society: Mauritania Red Crescent Programme name and duration: Appeal 2008-2009 Contact Person: Mouhamed Ould RABY: Secretary General Email:
Two Community Nutrition Projects in Africa. Interim Findings
 Findings reports on ongoing operational, economic and sector work carried out by the World Bank and its member governments in the Africa Region. It is published periodically by the Knowledge Networks,
Findings reports on ongoing operational, economic and sector work carried out by the World Bank and its member governments in the Africa Region. It is published periodically by the Knowledge Networks,
IMCI and Health Systems Strengthening
 Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI and Health Systems Strengthening 7 IMCI and Health Systems Strengthening What components of the health
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. IMCI Monitoring and Evaluation
 Implementation in the Western Pacific Region. IMCI Monitoring and Evaluation") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI Monitoring and Evaluation 8 IMCI Monitoring and Evaluation Why is monitoring and evaluation of IMCI important?
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region IMCI Monitoring and Evaluation 8 IMCI Monitoring and Evaluation Why is monitoring and evaluation of IMCI important?
The World Breastfeeding Trends Initiative (WBTi)
") The World Breastfeeding Trends Initiative (WBTi) MALAWI ASSESSMENT REPORT MINISTRY OF HEALTH NUTRITION UNIT 1 Acronyms: AIDS BFHI GIMS HIV HTC IBFAN IEC ILO IYCF MDHS M & E MOH MPC MTCT NGO PMTCT UNICEF
The World Breastfeeding Trends Initiative (WBTi) MALAWI ASSESSMENT REPORT MINISTRY OF HEALTH NUTRITION UNIT 1 Acronyms: AIDS BFHI GIMS HIV HTC IBFAN IEC ILO IYCF MDHS M & E MOH MPC MTCT NGO PMTCT UNICEF
UNICEF Baby Friendly Hospital Initiative Hong Kong Association. Baby-Friendly Hospital Designation. Hong Kong
 UNICEF Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Hospital Designation In Hong Kong Revised June 2018 www.babyfriendly.org.hk Content Page Introduction to Baby-Friendly Hospital
UNICEF Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Hospital Designation In Hong Kong Revised June 2018 www.babyfriendly.org.hk Content Page Introduction to Baby-Friendly Hospital
TERMS OF REFERENCE: PRIMARY HEALTH CARE
 TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
 -DDA-3485-726-2334-Proposal 1 of 7 3/13/2015 9:46 AM Project Proposal Organization Project Title Code WFP (World Food Programme) Targeted Life Saving Supplementary Feeding Programme for Children 6-59 s,
-DDA-3485-726-2334-Proposal 1 of 7 3/13/2015 9:46 AM Project Proposal Organization Project Title Code WFP (World Food Programme) Targeted Life Saving Supplementary Feeding Programme for Children 6-59 s,
Adapting a Health Systems Strengthening Model to Improve Access to Health Services in a Factory A Pilot Project in Haiti
 DECEMBER 2016 BRIEF Adapting a Health Systems Strengthening Model to Improve Access to Health Services in a Factory A Pilot Project in Haiti The pilot intervention described in this brief took place at
DECEMBER 2016 BRIEF Adapting a Health Systems Strengthening Model to Improve Access to Health Services in a Factory A Pilot Project in Haiti The pilot intervention described in this brief took place at
Solomon Islands experience Final 5 June 2004
 Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
Solomon Islands experience Final 5 June 2004 1. Background Information Solomon Islands is a Pacific island nation with a total population of 409,042, an annual growth rate of 2.8% and a life expectancy
Project Proposal. Sumbmitted to H & M Concious Foundation. Submitted by Plan Sweden
 Project Proposal Promoting access to water and sanitation for children and their families through Community-Led Water, Sanitation and Hygiene Improvement Sumbmitted to H & M Concious Foundation Submitted
Project Proposal Promoting access to water and sanitation for children and their families through Community-Led Water, Sanitation and Hygiene Improvement Sumbmitted to H & M Concious Foundation Submitted
Terms of Reference for Institutional Consultancy
 Terms of Reference for Institutional Consultancy Handwashing with Soap Programme-HWWS in Myanmar Section in Charge: YCSD section, WASH Unit 1. Purpose of the Assignment: 1.1. Background: Handwashing with
Terms of Reference for Institutional Consultancy Handwashing with Soap Programme-HWWS in Myanmar Section in Charge: YCSD section, WASH Unit 1. Purpose of the Assignment: 1.1. Background: Handwashing with
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL
 DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
DEMOCRATIC REPUBLIC OF CONGO NUTRITION EMERGENCY POOL MODEL The fight against malnutrition and hunger in the Democratic Republic of Congo (DRC) is a challenge that Action Against Hunger has worked to address
TFN Impact Report. MAITS (Multi-Agency International Training and Support)
") Name of your Organisation: Name of the project TFN funded: Date Funded by TFN: 6 July 2017 Were you able to undertake your project as planned? Can you describe and/or demonstrate the specific impact that
Name of your Organisation: Name of the project TFN funded: Date Funded by TFN: 6 July 2017 Were you able to undertake your project as planned? Can you describe and/or demonstrate the specific impact that
Assessing the Quality of Facility-Level Family Planning Services in Malawi
 QUALITY ASSURANCE PROJECT QUALITY ASSESSMENT CASE STUDY Assessing the Quality of Facility-Level Family Planning Services in Malawi Center for Human Services 7200 Wisconsin Avenue, Suite 600 Bethesda, MD
QUALITY ASSURANCE PROJECT QUALITY ASSESSMENT CASE STUDY Assessing the Quality of Facility-Level Family Planning Services in Malawi Center for Human Services 7200 Wisconsin Avenue, Suite 600 Bethesda, MD
MCH Programme in Vietnam Experiences for post Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam
 MCH Programme in Vietnam Experiences for post - 2015 Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam Current status: Under five mortality 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0 58,0 45,8 26,8 24,4 24,1 22,5
MCH Programme in Vietnam Experiences for post - 2015 Dinh Anh Tuan, MD, MPh MCH Dept. MOH, Vietnam Current status: Under five mortality 70,0 60,0 50,0 40,0 30,0 20,0 10,0 0,0 58,0 45,8 26,8 24,4 24,1 22,5
REPORT SHORT PROGRAMME REVIEW FOR CHILD HEALTH. Convened by: WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR THE WESTERN PACIFIC
 (WP)CAH/CAM/CAH/2.2/001-A Report series number: RS/2008/GE/56(CAM) English only REPORT SHORT PROGRAMME REVIEW FOR CHILD HEALTH Convened by: WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR THE WESTERN PACIFIC
(WP)CAH/CAM/CAH/2.2/001-A Report series number: RS/2008/GE/56(CAM) English only REPORT SHORT PROGRAMME REVIEW FOR CHILD HEALTH Convened by: WORLD HEALTH ORGANIZATION REGIONAL OFFICE FOR THE WESTERN PACIFIC
STAFF REPORT ACTION REQUIRED. Supporting Breastfeeding in Toronto SUMMARY. Date: January 15, Board of Health. To: Medical Officer of Health
 STAFF REPORT ACTION REQUIRED Supporting Breastfeeding in Toronto Date: January 15, 2007 To: From: Wards: Board of Health Medical Officer of Health All Reference Number: SUMMARY As a recognized leader in
STAFF REPORT ACTION REQUIRED Supporting Breastfeeding in Toronto Date: January 15, 2007 To: From: Wards: Board of Health Medical Officer of Health All Reference Number: SUMMARY As a recognized leader in
WFP Support to Wajir County s Emergency Preparedness and Response, 2016
 4 WFP Support to Wajir County s Emergency Preparedness and Response, 2016 OCTOBER 2016 Emergency preparedness and response programmes are now a shared function between Wajir County Government and the national
4 WFP Support to Wajir County s Emergency Preparedness and Response, 2016 OCTOBER 2016 Emergency preparedness and response programmes are now a shared function between Wajir County Government and the national
Illinois Birth to Three Institute Best Practice Standards PTS-Doula
 Illinois Birth to Three Institute Best Practice Standards PTS-Doula The Ounce recognizes that there are numerous strategies that can be employed to effectively serve pregnant and parenting teens and their
Illinois Birth to Three Institute Best Practice Standards PTS-Doula The Ounce recognizes that there are numerous strategies that can be employed to effectively serve pregnant and parenting teens and their
SNNP REGIONAL HEALTH BUREAU L10K BASELINE SURVEY HEALTH EXTENSION WORKER INTERVIEW. Q1. Location: Region Zone Woreda Kebele
 Community Questionnaire SNNP REGIONAL HEALTH BUREAU L10K BASELINE SURVEY HEALTH EXTENSION WORKER INTERVIEW Section 1: Identification and consent (to be completed before interview) Serial number: Q1. Location:
Community Questionnaire SNNP REGIONAL HEALTH BUREAU L10K BASELINE SURVEY HEALTH EXTENSION WORKER INTERVIEW Section 1: Identification and consent (to be completed before interview) Serial number: Q1. Location:
Community CCT in Indonesia The Generasi Project
 Community CCT in Indonesia The Generasi Project November 12 th, 2008 Junko Onishi jonishi@jhsph.edu Two Pilot Projects In 2007 GoI started two pilot projects: Household CCT the traditional model Quarterly
Community CCT in Indonesia The Generasi Project November 12 th, 2008 Junko Onishi jonishi@jhsph.edu Two Pilot Projects In 2007 GoI started two pilot projects: Household CCT the traditional model Quarterly
Minister. Secretaries of State. Department of Planning and Health Information. Department of Human Resources Development
 KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
Evaluation of Nigeria s Community Infant and Young Child Feeding Counselling Package
 Evaluation of Nigeria s Community Infant and Young Child Feeding Counselling Package Progress Report #4 January June 2016 Introduction This progress report is part of the evaluation of Nigeria s Community
Evaluation of Nigeria s Community Infant and Young Child Feeding Counselling Package Progress Report #4 January June 2016 Introduction This progress report is part of the evaluation of Nigeria s Community
Designing and Integrating Quality Family Health Services at the Salt Model Center in Jordan
 WARNING NO PART OF THIS TRANSMISSION MAY BE COPIED, DOWNLOADED, STORED, FURTHER TRANSMITTED, TRANSFERRED, DISTRIBUTED, ALTERED OR OTHERWISE USED IN ANY FORM OR BY ANY MEANS. HOWEVER, THERE ARE TWO EXCEPTIONS:
WARNING NO PART OF THIS TRANSMISSION MAY BE COPIED, DOWNLOADED, STORED, FURTHER TRANSMITTED, TRANSFERRED, DISTRIBUTED, ALTERED OR OTHERWISE USED IN ANY FORM OR BY ANY MEANS. HOWEVER, THERE ARE TWO EXCEPTIONS:
NUTRITION. UNICEF Meeting Myanmar/2014/Myo the Humanitarian Needs Thame of Children in Myanmar Fundraising Concept Note 5
 NUTRITION Improving Equitable Access to Essential Nutrition Interventions for Conflict-Affected Populations in Rakhine, Kachin and Northern Shan States 1 UNICEF Meeting Myanmar/2014/Myo the Humanitarian
NUTRITION Improving Equitable Access to Essential Nutrition Interventions for Conflict-Affected Populations in Rakhine, Kachin and Northern Shan States 1 UNICEF Meeting Myanmar/2014/Myo the Humanitarian
GUIDELINES FOR HEALTH SYSTEM ASSESSMENT
 GUIDELINES FOR HEALTH SYSTEM ASSESSMENT Myanmar June 13 2009 Map: Planned Priority Townships for Health System Strengthening 2008-2011 1 TABLE OF CONTENTS BOOK 1 SURVEYOR GUIDELINES List of Figures...
GUIDELINES FOR HEALTH SYSTEM ASSESSMENT Myanmar June 13 2009 Map: Planned Priority Townships for Health System Strengthening 2008-2011 1 TABLE OF CONTENTS BOOK 1 SURVEYOR GUIDELINES List of Figures...
How Do Community Health Workers Contribute to Better Nutrition? Haiti
 How Do Community Health Workers Contribute to Better Nutrition? Haiti About SPRING The Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project is a five-year USAID-funded
How Do Community Health Workers Contribute to Better Nutrition? Haiti About SPRING The Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project is a five-year USAID-funded
GENDER ACTION PLAN REVISED AT MIDTERM
 Component 1: Safe Blood Transfusion Output 1 Voluntary Non- The new national Remunerated transfusio-logy Blood Donation center is established KAP survey in Ulaanbaatar and includes gender internationally
Component 1: Safe Blood Transfusion Output 1 Voluntary Non- The new national Remunerated transfusio-logy Blood Donation center is established KAP survey in Ulaanbaatar and includes gender internationally
WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE
 DATABASE QUESTIONNAIRE") WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE Part I (1) Percentage of babies breastfed within one hour of birth (26.3%) (2) Percentage of babies 0
WORLD BREASTFEEDING TRENDS INITIATIVE (WBTi) DATABASE QUESTIONNAIRE Part I (1) Percentage of babies breastfed within one hour of birth (26.3%) (2) Percentage of babies 0
Final Technical Report Summary
 Final Technical Report Summary Development of Township Health Plans in Falam and Tedim Townships of Chin State, Myanmar Photo credit: Uzaib Saya Uzaib Saya, Than Naing Oo, David Collins, San San Min Management
Final Technical Report Summary Development of Township Health Plans in Falam and Tedim Townships of Chin State, Myanmar Photo credit: Uzaib Saya Uzaib Saya, Than Naing Oo, David Collins, San San Min Management
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health
 Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
Using lay health workers to improve access to key maternal and newborn health interventions in sexual and reproductive health improve access to key maternal and newborn health interventions A lay health
2013 CASE STUDY: Building leadership skills in Tonga
 2013 CASE STUDY: Building leadership skills in Tonga Clinical nurse supervisors attain this position with little or no formal preparation in management skills. In order to manage staff well leadership
2013 CASE STUDY: Building leadership skills in Tonga Clinical nurse supervisors attain this position with little or no formal preparation in management skills. In order to manage staff well leadership
Kingdom of Cambodia Nation King Religion
 Kingdom of Cambodia Nation King Religion 6 STANDARD OPERATING PROCEDURE (SOP) FOR THE OUTREACH/PEER EDUCATION AND 100% CONDOM USE PROGRAMME TO SEX WORKERS IN CAMBODIA June 2006 Prepared by: Technical Working
Kingdom of Cambodia Nation King Religion 6 STANDARD OPERATING PROCEDURE (SOP) FOR THE OUTREACH/PEER EDUCATION AND 100% CONDOM USE PROGRAMME TO SEX WORKERS IN CAMBODIA June 2006 Prepared by: Technical Working
upscale: A digital health platform for effective health systems
 República de Moçambique Ministério da Saúde Direcção Nacional de Saúde Pública upscale: A digital health platform for effective health systems From 2009 to 2016, Malaria Consortium tested a number of interventions
República de Moçambique Ministério da Saúde Direcção Nacional de Saúde Pública upscale: A digital health platform for effective health systems From 2009 to 2016, Malaria Consortium tested a number of interventions
Health Sector Reform in Cambodia
 Technical Report No. 2 Health Sector Reform in Cambodia February 1996 Prepared by: James Knowles, Ph.D. Abt Associates Inc. Partnerships for Health Reform Abt Associates Inc. # 4800 Montgomery Lane, Suite
Technical Report No. 2 Health Sector Reform in Cambodia February 1996 Prepared by: James Knowles, Ph.D. Abt Associates Inc. Partnerships for Health Reform Abt Associates Inc. # 4800 Montgomery Lane, Suite
Reducing Malnutrition and Child Deaths Using Care Groups
 Reducing Malnutrition and Child Deaths Using Care Groups Thomas P. Davis Jr., MPH Chief Program Officer Feed the Children November 2014 2005-2010 FH Care Group Project October 1, 2005 September 30, 2010.
Reducing Malnutrition and Child Deaths Using Care Groups Thomas P. Davis Jr., MPH Chief Program Officer Feed the Children November 2014 2005-2010 FH Care Group Project October 1, 2005 September 30, 2010.
Baby-Friendly Initiative Assessment Process & Costs for Hospitals, Maternity Facilities and Community Health Services
 The National Authority for the Baby-Friendly Initiative (BFI) Baby-Friendly Initiative Assessment Process & Costs for Hospitals, Maternity Facilities and Community Health Services The process for a hospital,
The National Authority for the Baby-Friendly Initiative (BFI) Baby-Friendly Initiative Assessment Process & Costs for Hospitals, Maternity Facilities and Community Health Services The process for a hospital,
Program to Support At Scale Implementation of the National Hygiene and Sanitation Strategy through Learning by Doing in the Amhara Region
 FINAL PROPOSAL SUMMARY Program to Support At Scale Implementation of the National Hygiene and Sanitation Strategy through Learning by Doing in the Amhara Region Ministry of Health ж Amhara Regional State
FINAL PROPOSAL SUMMARY Program to Support At Scale Implementation of the National Hygiene and Sanitation Strategy through Learning by Doing in the Amhara Region Ministry of Health ж Amhara Regional State
TERMS OF REFERENCE. East Jerusalem with travel to Gaza and West Bank. June 2012 (flexible depending on consultant availability between June-July 2012)
") TERMS OF REFERENCE THE DEVELOPMENT OF TRAINING FOR WASH CLUSTER PARTNERS IN THE DEVELOPMENT & DESIGN OF KNOWLEDGE, ATTITUDE, PRACTICE SURVEYS IN THE OCCUPIED PALESTINIAN TERRITORY. Summary Title Purpose
TERMS OF REFERENCE THE DEVELOPMENT OF TRAINING FOR WASH CLUSTER PARTNERS IN THE DEVELOPMENT & DESIGN OF KNOWLEDGE, ATTITUDE, PRACTICE SURVEYS IN THE OCCUPIED PALESTINIAN TERRITORY. Summary Title Purpose
ALIVE & THRIVE. Request for Proposals (RFP) Formative Research on Improved Infant and Young Child Feeding (IYCF) Practices in Burkina Faso
 Formative Research on Improved Infant and Young Child Feeding (IYCF) Practices in Burkina Faso") ALIVE & THRIVE Issued on: 31 July 2014 For: Request for Proposals (RFP) Formative Research on Improved Infant and Young Child Feeding (IYCF) Practices in Burkina Faso Anticipated Period of Performance:
ALIVE & THRIVE Issued on: 31 July 2014 For: Request for Proposals (RFP) Formative Research on Improved Infant and Young Child Feeding (IYCF) Practices in Burkina Faso Anticipated Period of Performance:
Faith-Based Communities in Africa: An Integral Part of Improving Family Planning and Reproductive Health February 23, 2015
 Faith-Based Communities in Africa: An Integral Part of Improving Family Planning and Reproductive Health February 23, 2015 Country-Kenya Grantee -Christian Health Association of Kenya -CHAK Presenter-
Faith-Based Communities in Africa: An Integral Part of Improving Family Planning and Reproductive Health February 23, 2015 Country-Kenya Grantee -Christian Health Association of Kenya -CHAK Presenter-
Faith-Based Communities in Africa: An Integral Part of Improving Family Planning and Reproductive Health February 23, 2015
 Faith-Based Communities in Africa: An Integral Part of Improving Family Planning and Reproductive Health February 23, 2015 Country-Kenya Grantee name- CHAK Presenter Jane Kishoyian, MPH Project Coordinator-CHAK
Faith-Based Communities in Africa: An Integral Part of Improving Family Planning and Reproductive Health February 23, 2015 Country-Kenya Grantee name- CHAK Presenter Jane Kishoyian, MPH Project Coordinator-CHAK
The World Breastfeeding Trends Initiative (WBTi)
") The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
The World Breastfeeding Trends Initiative (WBTi) Name of the Country: Swaziland Year: 2009 MINISTRY OF HEALTH KINGDOM OF SWAZILAND 1 Acronyms AIDS ART CBO DHS EGPAF FBO MICS NGO AFASS ANC CHS CSO EPI HIV
Aahar sprovision of Supplemental Readyto-Use Foods, Vitamins, and Medications
 Aahar sprovision of Supplemental Readyto-Use Foods, Vitamins, and Medications Processes and Electronic Data Collection as part of a Community-Based Management of Acute Malnutrition (CMAM) Program T he
Aahar sprovision of Supplemental Readyto-Use Foods, Vitamins, and Medications Processes and Electronic Data Collection as part of a Community-Based Management of Acute Malnutrition (CMAM) Program T he
How Do Community Health Workers Contribute to Better Nutrition? Mali
 How Do Community Health Workers Contribute to Better Nutrition? Mali About SPRING The Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project is a five-year USAID-funded
How Do Community Health Workers Contribute to Better Nutrition? Mali About SPRING The Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project is a five-year USAID-funded
Maternal and Child Health Services Title V Block Grant for New Mexico. Executive Summary. Application for Annual Report for 2015
 Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2017 Annual Report for 2015 Title V Block Grant History and Requirements Enacted in 1935 as a part
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2017 Annual Report for 2015 Title V Block Grant History and Requirements Enacted in 1935 as a part
MALAWI Humanitarian Situation Report
 MALAWI Humanitarian Situation Report HIGHLIGHTS SITUATION IN NUMBERS The Education cluster administered a situation analysis of the most affected schools over a period of 4 days via the Real Time Monitoring
MALAWI Humanitarian Situation Report HIGHLIGHTS SITUATION IN NUMBERS The Education cluster administered a situation analysis of the most affected schools over a period of 4 days via the Real Time Monitoring
How Do Community Health Workers Contribute to Better Nutrition? Philippines
 How Do Community Health Workers Contribute to Better Nutrition? Philippines About SPRING The Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project is a five-year USAID-funded
How Do Community Health Workers Contribute to Better Nutrition? Philippines About SPRING The Strengthening Partnerships, Results, and Innovations in Nutrition Globally (SPRING) project is a five-year USAID-funded
GRANT AGREEMENT (ADB Strategic Climate Fund) (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing)
 (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing)") GRANT NUMBER 0426-CAM (SCF) GRANT AGREEMENT (ADB Strategic Climate Fund) (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing) (Cambodia Component) between KINGDOM
GRANT NUMBER 0426-CAM (SCF) GRANT AGREEMENT (ADB Strategic Climate Fund) (Greater Mekong Subregion Biodiversity Conservation Corridors Project Additional Financing) (Cambodia Component) between KINGDOM
Minutes of Meeting Subject
 Minutes of Meeting Subject APPROVED: Generasi Impact Evaluation Proposal Host Joint Management Committee (JMC) Date August 04, 2015 Participants JMC, PSF Portfolio, PSF Cluster, PSF Generasi Agenda Confirmation
Minutes of Meeting Subject APPROVED: Generasi Impact Evaluation Proposal Host Joint Management Committee (JMC) Date August 04, 2015 Participants JMC, PSF Portfolio, PSF Cluster, PSF Generasi Agenda Confirmation
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan
 Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: June 13, 2016 Prepared by: Dr. Taban Martin Vitale 1. City & State Bor, Jonglei
Treatment and Prevention of Acute Malnutrition in Jonglei & Greater Pibor Administrative Area, Republic of South Sudan Date: June 13, 2016 Prepared by: Dr. Taban Martin Vitale 1. City & State Bor, Jonglei
Juba Teaching Hospital, South Sudan Health Systems Strengthening Project
 Juba Teaching Hospital, South Sudan Health Systems Strengthening Project Date: Prepared by: June 14, 2016 Dr. Taban Martin Vitale I. Demographic Information 1. City & State Juba, Central Equatoria, Republic
Juba Teaching Hospital, South Sudan Health Systems Strengthening Project Date: Prepared by: June 14, 2016 Dr. Taban Martin Vitale I. Demographic Information 1. City & State Juba, Central Equatoria, Republic
Summary of UNICEF Emergency Needs for 2009*
 UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
UNICEF Humanitarian Action in 2009 Core Country Data Population under 18 (thousands) 11,729 U5 mortality rate 73 Infant mortality rate 55 Maternal mortality ratio (2000 2007, reported) Primary school enrolment
Baby Friendly Hospital Initiative Hong Kong Association. Baby-Friendly Maternal and Child Health Centres. Hong Kong
 Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Maternal and Child Health Centres In Hong Kong March 2016 www.babyfriendly.org.hk Content Introduction to Baby-Friendly Hospital Initiative
Baby Friendly Hospital Initiative Hong Kong Association Baby-Friendly Maternal and Child Health Centres In Hong Kong March 2016 www.babyfriendly.org.hk Content Introduction to Baby-Friendly Hospital Initiative
Juba Teaching Hospital, South Sudan Health Systems Strengthening Project
 Juba Teaching Hospital, South Sudan Health Systems Strengthening Project Date: Prepared by: May 26, 2017 Dr. Taban Martin Vitale and Richard Anyama I. Demographic Information 1. City & State: Juba, Central
Juba Teaching Hospital, South Sudan Health Systems Strengthening Project Date: Prepared by: May 26, 2017 Dr. Taban Martin Vitale and Richard Anyama I. Demographic Information 1. City & State: Juba, Central
Republic of South Sudan 2011
 Republic of South Sudan 2011 Appealing Agency Project Title Project Code Sector/Cluster Refugee project VOLUNTEER ORGANIZATION FOR THE INTERNATIONAL CO-OPERATION LA NOSTRA NOTRA FAMIGLIA) Strengthening
Republic of South Sudan 2011 Appealing Agency Project Title Project Code Sector/Cluster Refugee project VOLUNTEER ORGANIZATION FOR THE INTERNATIONAL CO-OPERATION LA NOSTRA NOTRA FAMIGLIA) Strengthening
Approaches and Lessons from Rapidly Scaling-Up Nutrition Assessment, Counseling and Support (NACS) Services
 Services") Approaches and Lessons from Rapidly Scaling-Up Nutrition Assessment, Counseling and Support (NACS) Services AED - Academy for Educational Development NASCOP - Ministry of Medical Services/Public Health
Approaches and Lessons from Rapidly Scaling-Up Nutrition Assessment, Counseling and Support (NACS) Services AED - Academy for Educational Development NASCOP - Ministry of Medical Services/Public Health
Mozambique Country Report FY14
 USAID ASSIST Project Mozambique Country Report FY14 Cooperative Agreement Number: AID-OAA-A-12-00101 Performance Period: October 1, 2013 September 30, 2014 DECEMBER 2014 This annual country report was
USAID ASSIST Project Mozambique Country Report FY14 Cooperative Agreement Number: AID-OAA-A-12-00101 Performance Period: October 1, 2013 September 30, 2014 DECEMBER 2014 This annual country report was
GOAL ETHIOPIA Sidama Child Survival Program MID-TERM EVALUATION REPORT. Awassa Zuria and Boricha Woredas of the SNNP Region of Ethiopia
 GOAL ETHIOPIA Sidama Child Survival Program MID-TERM EVALUATION REPORT Awassa Zuria and Boricha Woredas of the SNNP Region of Ethiopia COOPERATIVE AGREEMENT # GHN-A-00-07-00010-00 START DATE September
GOAL ETHIOPIA Sidama Child Survival Program MID-TERM EVALUATION REPORT Awassa Zuria and Boricha Woredas of the SNNP Region of Ethiopia COOPERATIVE AGREEMENT # GHN-A-00-07-00010-00 START DATE September
Integrating Maternal, Infant and Young Child Nutrition (MIYCN) and Family Planning (FP) Services in Kenya
 and Family Planning (FP) Services in Kenya") Integrating Maternal, Infant and Young Child Nutrition (MIYCN) and Family Planning (FP) Services in Kenya Presentation by: Evelyn Matiri Nutrition Associate MCHIP, Kenya Women Deliver Conference May 27-30,
Integrating Maternal, Infant and Young Child Nutrition (MIYCN) and Family Planning (FP) Services in Kenya Presentation by: Evelyn Matiri Nutrition Associate MCHIP, Kenya Women Deliver Conference May 27-30,
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder
 Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
Newborn Health in Humanitarian Settings CORE Group Webinar 16 February 2017 Elaine Scudder Newborn Health in Humanitarian Settings: Background Newborn Health in Humanitarian Settings 16 February 2017 An
1) What type of personnel need to be a part of this assessment team? (2 min)
 What type of personnel need to be a part of this assessment team? (2 min)") Student Guide Module 2: Preventive Medicine in Humanitarian Emergencies Civil War Scenario Problem based learning exercise objectives Identify the key elements for the assessment of a population following
Student Guide Module 2: Preventive Medicine in Humanitarian Emergencies Civil War Scenario Problem based learning exercise objectives Identify the key elements for the assessment of a population following
The Rang-Din Nutrition Study in Bangladesh
 The Rang-Din Nutrition Study in Bangladesh Implementation science- The Food And Nutrition Technical Assistance (FANTA) project s experience Zeina Maalouf-Manasseh September 4, 2014 Longitudinal RCT Measuring
The Rang-Din Nutrition Study in Bangladesh Implementation science- The Food And Nutrition Technical Assistance (FANTA) project s experience Zeina Maalouf-Manasseh September 4, 2014 Longitudinal RCT Measuring
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES. Tajikistan
 CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
CENTRAL AND EASTERN EUROPE AND THE COMMONWEALTH OF INDEPENDENT STATES Tajikistan In 2010, a string of emergencies caused by natural disasters and epidemics affected thousands of children and women in Tajikistan,
Background report. Cambodian Health System. Health Status of the Cambodian Population Health Service Delivery. Public Disclosure Authorized
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Background report Cambodian Health System Health Status of the Cambodian Population Health
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Background report Cambodian Health System Health Status of the Cambodian Population Health
Juba College of Nursing and Midwifery, Republic of South Sudan
 Juba College of Nursing and Midwifery, Republic of South Sudan Date: Prepared by: July 31, 2017 Dr. Taban Martin Vitale I. Demographic Information 1. City & State Juba, Central Equatoria State, Republic
Juba College of Nursing and Midwifery, Republic of South Sudan Date: Prepared by: July 31, 2017 Dr. Taban Martin Vitale I. Demographic Information 1. City & State Juba, Central Equatoria State, Republic
HEALTH & NUTRITION Kenya Programme
 HEALTH & NUTRITION Kenya Programme 2016-2018 About Us Save the Children has been operational in Kenya since the 1950s, providing support to children through developmental and humanitarian relief programmes
HEALTH & NUTRITION Kenya Programme 2016-2018 About Us Save the Children has been operational in Kenya since the 1950s, providing support to children through developmental and humanitarian relief programmes
SCALING UP SDM IN JHARKHAND, INDIA: LEARNINGS, EXPERIENCES AND RELEVANCE FOR COMMUNITY HEALTH WORKERS. Ragini Sinha
 SCALING UP SDM IN JHARKHAND, INDIA: LEARNINGS, EXPERIENCES AND RELEVANCE FOR COMMUNITY HEALTH WORKERS Ragini Sinha Jharkhand profile: Population Population of 33 million in 24 districts with 260 blocks
SCALING UP SDM IN JHARKHAND, INDIA: LEARNINGS, EXPERIENCES AND RELEVANCE FOR COMMUNITY HEALTH WORKERS Ragini Sinha Jharkhand profile: Population Population of 33 million in 24 districts with 260 blocks
IMCI. information. IMCI training course for first-level health workers: Linking integrated care and prevention. Introduction.
 WHO/CHS/CAH/98.1E REV.1 1999 ORIGINAL: ENGLISH DISTR.: GENERAL IMCI information INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS (IMCI) DEPARTMENT OF CHILD AND ADOLESCENT HEALTH AND DEVELOPMENT (CAH) HEALTH
WHO/CHS/CAH/98.1E REV.1 1999 ORIGINAL: ENGLISH DISTR.: GENERAL IMCI information INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS (IMCI) DEPARTMENT OF CHILD AND ADOLESCENT HEALTH AND DEVELOPMENT (CAH) HEALTH