ASETnews Spring 2013 IN THIS ISSUE BRIEFINGS FROM THE BOARD TECHNICAL TIPS INTEREST SECTIONS GOVERNMENTAL AFFAIRS AND ADVOCACY CONNECTIONS CORNER
|
|
|
- Colin Stone
- 5 years ago
- Views:
Transcription




1 IN THIS ISSUE BRIEFINGS FROM THE BOARD TECHNICAL TIPS INTEREST SECTIONS GOVERNMENTAL AFFAIRS AND ADVOCACY CONNECTIONS CORNER NEW MEMBERS ASETnews Spring 2013



2 SPRING 2013 VOLUME 37, NUMBER 1 ASET OFFICERS PRESIDENT Judy Ahn-Ewing, R. EEG/EP T., CNIM, CLTM, FASET, BA St. John Providence Health System Detroit, MI jahnewing@tir.com PRESIDENT ELECT Brian Markley, R. EEG/EP T., R.NCS.T., BS The Neurology Center, PA Silver Spring, MD bam@neurologycenter.com SECRETARY/TREASURER Pat Smith, R. EEG T., AA Child Neurology Center of Orlando, PA Orlando, FL psmith016@yahoo.com BOARD OF TRUSTEES Susan Agostini, R. EEG/EP T., CLTM Banner Good Samaritan Medical Center Phoenix, AZ TJ Amdurs, R. EEG T., MS University of Pittsburgh Medical Center Pittsburgh, PA Sara Batson, R. EEG/EP T., RPSGT, CNIM, CLTM Neurology Mobile System Associates, Inc. Miami, FL Scott Blodgett, R. EEG T., RPSGT, RST, BBA ResMed Corporation Rochester, NY Marcia Davidson, R. EEG/EP T., RPSGT, CNIM, RET, RN St. Mary s Hospital Madison, WI Ryan Lau, R. EEG/EP T., CNIM, CLTM, MS Indiana University Health Indianapolis, IN Cheryl Plummer, R. EEG T., CLTM, BS University of Pittsburgh Medical Center Pittsburgh, PA Christine Scott, R. EEG/EP T., CLTM, BA Massachusetts General Hospital Boston, MA Cherie Young, R. EEG T., CNIM Children s Hospital New Orleans, LA 2

3 BRIEFINGS FROM THE BOARD Editor s Note: This new column replaces the President s Message and From the Executive Director s Desk newsletter columns. ASET BOARD APPROVES FIRST CHAPTER CHARTER At its March 1-2, 2013 midyear meeting, the ASET Board of Trustees voted unanimously to approve the Hawaii Pacific petition to be charted as the Hawaii Pacific (HIP) Chapter of ASET The Neurodiagnostic Society. The new chapter covers the territory of Hawaii and the Pacific Islands. HIP annual chapter dues are only $20 for individual memberships and $30 for organizations, corporations, and institutions. The chapter plans on holding monthly meetings with guest lectures that qualify for ACE credit hours, starting a lending library for distributing educational resources, developing a job resource guide for contract and coverage work in its territory, producing annual meetings, and organizing chapter trips to the ASET annual conferences. For more information and to join the chapter, contact Michelle Russo, HIPASET Chapter President, at michellelearusso@gmail.com. The Hawaii Pacific Chapter becomes the first organization to be chartered as an ASET chapter since the program was officially adopted by the ASET board at its August 2012 meeting. To learn more about the new chapter program and for helpful tools to start a chapter in your area, or to learn how your current local, state or regional neurodiagnostic society can be recognized as an ASET chapter, click here, or visit the Chapters page under the membership tab of the ASET website. Welcome H I P A S E T NEW MEMBER-GET-A-MEMBER REWARD PROGRAM Effective January 1, 2013, any Active, Associate or Student member in good standing of the Society who sponsors a new Active member for the 2013 member year will have the choice of receiving a $10 gift certificate for use in purchasing any item in the ASET store, including webinar and online course registrations, or a $10 credit toward their 2014 member dues. Any Institutional employee member who sponsors a new Active member for the 2013 member year will receive a $10 gift certificate for use in purchasing any item in the ASET store. To be credited with sponsoring a new Active member, all you need do is have him or her enter your name where it asks for the Sponsor s Name/Who Introduced You to ASET on either the hardcopy or online member application form. When ASET receives the new Active member application, you will be notified by and asked to let us know whether you would like to receive the gift certificate or dues credit. (Institutional employee members will automatically be mailed the gift certificate.) There is no limit on the amount of credit that you can earn. The more new Active members that you sponsor, the more gift certificates or dues credits you can accumulate. In addition, it does not matter what time of year the new Active member application is received. Even though the first-year dues are pro-rated, you will still receive the gift certificate or dues credit for the full $10. Click here or click on the Membership tab of the ASET website for some tips for recruiting your co-workers and colleagues. 3

4 BRIEFINGS FROM THE BOARD continued ASET BOARD ANNOUNCES NEW RECOGNITION AWARD The ASET board is pleased to announce the ASET Trustees Award. The purpose of this new award is to honor an individual, institution, neurodiagnostic program, or industry supplier who, through a body of work, has made a profound impact on the neurodiagnostic profession or advancement in the improvement of quality patient care. The nomination criteria for the new award is that the body of work for which the individual, institution, neurodiagnostic program, or industry supplier is being nominated must encompass at least two of the following six criteria: 1. Has made a profound impact on the neurodiagnostic profession 2. Contributed to the improvement of quality patient care 3. Advanced the practice, art, and science of neurodiagnostics 4. Reflects the values, ideals and ethics of the neurodiagnostic profession 5. Presents an extraordinary and heightened favorability view of the values and contributions of the neurodiagnostic profession to the general public and community at large, or within the neurodiagnostic profession 6. Represents an extraordinary commitment to the neurodiagnostic profession and/or to ASET The Neurodiagnostic Society For information on how to nominate an individual, organization, or supplier for the ASET Trustees Award, and to access the nomination form, click here, or visit the Awards page under the About tab of the ASET website. The deadline for submitting nominations is May 31, The recipient of the annual award will receive recognition and presentation of the award at the business meeting & awards luncheon held in conjunction with the ASET Annual Conference, a suitably engraved plaque, and recognition in The Neurodiagnostic Journal. BALLOTING FOR THE 2013 ELECTION IS ABOUT TO OPEN The ASET Nominating Committee is putting the finishing touches on its report and slate of candidates for the 2013 election. This year, you will be asked to cast your vote for the offices of President- Elect and Secretary/Treasurer, and for two trustees to the board. When the Nominating Committee Report is published, please carefully review each candidate s information to determine the skills, background and experience, and strategic foresight that you think will best guide ASET into the future, and then cast your vote. All Active, Associate, Student, Lifetime and Emeritus members and Institutional members voting representatives/primary billing contacts in good standing of the Society are eligible to vote. Your vote is critically important and may very well influence the outcomes of the election. As with prior year elections, voting will be electronic. Announcement of when voting is open will be posted under the Breaking News section of the ASET website and sent in a broadcast to the membership. 4

5 TECHNICAL TIPS MEDICARE UPDATES 2013 Kathryn Hansen, R. EEG T., BS, CPC Healthcare Consultant Integration Consultants Lexington, Kentucky Regulatory challenges have tested our practice profitability with the need to implement documentation and billing changes. This year there are additional factors which will impact clinical and financial practices: CPT coding guidelines updates, place of service (POS) code updates, ordering and referral edits in Provider Enrollment, Chain and Ownership System (PECOS), and implementation of ICD-10-CM code changes. A very important change in wording for 2013, as documented in the CPT Coding Guidelines and subsequent CPT Codes, is the definition of a qualified healthcare professional. This is the description noted in the 2013 CPT Manual published by the American Medical Association (AMA): When advanced practice nurses and physician assistant are working with physicians, they are considered as working in the exact same specialty and exact same subspecialties as the physician. A physician or other qualified health care professional is an individual who is qualified by education, training, licensure/regulation (when applicable), and facility privileging (when applicable) who performs a professional service within his or her scope of practice and independently reports that professional service. These professionals are distinct from clinical staff. A clinical staff member is a person who works under the supervision of a physician or other qualified health care professional..who does not individually report that professional service. For practices who bill evaluation and management codes and professional services associated with interpretation of procedures, these changes may impact subsequent credentialing for contracting with third party payers. Take time now to ensure all providers who are submitting claims for your patients are enrolled with a current profile documenting current credentials for practice. This may be impacted by the information posted in PECOS as well. Related to this is another important update on PECOS and the need for validating ordering/ referring edits. All providers who submit claims to Centers for Medicare & Medicaid Services (CMS) for services, that were ordered or referred by a provider, who has not been approved through the PECOS system, will have the claim denied. This is being introduced in two phases. At the end of the second phase, specifically: if the ordering/referring provider is not on the claim, it will be rejected; if the ordering/ referring provider is on the claim, Medicare will verify that the ordering/referring provider is in PECOS and is eligible to order/refer; and if the ordering/referring provider is not in PECOS or is in PECOS, but is not of the type/specialty allowed to order or refer, the claim will be rejected starting May 1. TECHNICAL TIPS 5
6 TECHNICAL TIPS continued Physicians with a valid opt-out affidavit on file are excused. Others must have a valid enrollment on file, either on paper via 855-O or electronically via PECOS, or claims will be rejected. (CMS mentioned in the Open Door call that practitioners with a current 885-I would also be covered.) Another factor, which will impact our practice in sleep medicine, is the documentation for Place of Service POS. Effective after April 1, 2013, POS is defined as the setting in which the beneficiary receives the face-to-face service. If the face-to-face is not completed by the physician, such as those when a physician provides the professional interpretation of a diagnostic test from a distant site, the POS is the setting in which the beneficiary received the technical component of the service. For example: a patient receives a sleep study or EEG at an outpatient hospital near his home. The hospital submits a claim for the technical component. The Physician submits a claim for the interpretation in her office. Submit POS 22 for the professional component to indicate the patient received the face-to-face portion of the procedure at the outpatient hospital facility. It is time to prepare our electronic medical records with comprehensive clinical templates to ensure more detailed documentation for the new code set. And yes, the integration of ICD-10 CM will occur October 1, According to all communication this author has received from CMS and published national coding initiatives, the implementation will occur on this date. Therefore, it is time to prepare our electronic medical records with comprehensive clinical templates to ensure more detailed documentation for the new code set. Critical to this implementation is a strong knowledge of anatomy and physiology for each coder working in your program to effectively translate the clinical documentation into the appropriate code selection. As well, clinicians will need to identify what additional clinical documentation and descriptive language needs to be added to digital templates in billing and coding systems to ensure selection of the correct code for ICD 10. Take time to identify how your practice enters key words, medical notes, and content in the medical records so the protocols are clearly communicated to the coder. If your practice and providers use a billing service or clearinghouse, take time to work with them to collaborate on the content in templates, on encounter forms, and in documentation templates to ensure they have the same information you have in updated electronic records and reports. Additional education on anatomy and physiology may be required to clearly communicate with coding and billing staff the required clinical condition(s) and associated co-morbidities which are medically indicated to define the comprehensive clinical documentation required for medical necessity supporting the procedure. This documentation is critical to reduce denials, reduce delays obtaining reimbursement for services, and reducing the time to rework a claim. All of these delays cost money. Today, efficiency and streamlined services reduce costs and subsequently increases revenue. There may be other opportunities to consider in the face of all these changes. With the changing landscape for clinical providers, there are opportunities to consider as we respond to all these changes. Integrating monitoring of testing outcomes is needed to ensure effective therapies and patient adherence with therapy. Collaboration with third party payers, the patient, your referral network, and the community will boost recognition of your services. 6
7 INTEREST SECTION BRIEFINGS WELCOME FROM THE INTEREST SECTION COORDINATOR By Margaret Hawkins, R. EEG/EP T., CNIM, CLTM Four times each year I ask the members of the Special Interest Group to compose articles for this ASET Newsletter feature. I give them a theme, pose some questions, try to tweak their imaginations, and they then do the hard part of reaching into their individual experiences, knowledge bases, current and past employment situations, etc. to come up with a pertinent and interesting written item. Because I believe that we are each a product of our past and present, I thought it would be fun to explore and share something old and/or something new as related to neurodiagnostics. As usual, these special people did not fail in their response to this challenge. I hope you enjoy (and learn from!) their submissions. Lucy has informed me that this is the Spring Issue of ASETnews Perhaps by the time it reaches your inbox, our Midwest piles of snow and sub-freezing temperatures will have given way to greening grass and sunshiny days! Acute/Critical Care Neurodiagnostics By Sara Batson, R. EEG/EP T., CNIM, CLTM, RPSGT The theme for this newsletter is Something Old, Something New. As we all know in the EEG world, continuous EEG monitoring at bedside in the ICUs has been growing over the recent years. Let s discuss some old and new methods of applying the leads in these cases. In Neurodiagnostic school, we had to obtain one glue competency per semester, either in lab class or at the clinical site. Most of the class utilized the classroom lab. I was taught then, to pre-fill my EEG cup lead with conductive paste, and then to use a little glass dish filled with collodion to dip the gauze square in. After that, I would cover the lead on the head with the saturated gauze square, and dry with an air hose pump. One of my classmates tried gluing the lead with hair crossed over the top of the lead per a suggestion. She would then proceed using a bottle with an applicator tip filled with collodion to squeeze the glue out, saturating the area, and drying it with the air hose pump. (I happened to be the lucky recipient on the other end of that glue bottle. I picked dried glue out of my long hair for over a week after that.) At the clinical site I attended, gluing was not very common. Generally, if there was a need to use collodion it was for a long-term monitoring patient. In that case, I was taught by a little older lady, (who had been a tech longer than I had been alive,) to fill the EEG cup lead with conductive paste and place it in the spot I had scrubbed with the skin prep product on the patient s scalp. Following, I would put the gauze square in the palm of my hand while wearing gloves. Once I had done that I would begin using the bottle with an applicator tip like at school or just thecollodion bottle itself, and saturate the gauze in my hand. What a mess that was! INTEREST SECTION COORDINATOR Margaret Hawkins, R. EEG/EP T., CNIM, CLTM Wausau, WI margaret.hawkins@ministryhealth.org INTEREST SECTION LEADERS ACUTE/CRITICAL CARE NEURODIAGNOSTICS Sara Batson, R. EEG/EP T., RPSGT, CNIM, CLTM Miami, FL endtech_2007@yahoo.com Erika Diaz, R. EEG T., CLTM Chicago, IL ediaz@nmh.org AMBULATORY MONITORING Jennifer Carlile, R. EEG T. Cleveland, OH carlileja@aol.com CLINICAL EEG Keith Davidson, R. EP T., BA Mankato, MN davidson.keith@mayo.edu Petra Davidson, R. EEG/EP T., BS. Mankato, MN davidson.petra@mayo.edu COMPUTERS IN THE WORKPLACE TJ Amdurs, R. EEG T., MS Pittsburgh, PA amdurstj@upmc.edu CPT CODES Lynn Bragg, R. EEG/EP T. Canton, OH lmbragg54@yahoo.com Kristina Port, R. EEG/EP T., RPSGT, MPH Novelty, OH kaport@prodigy.net DEPARTMENT MANAGERS Stephanie Jordan, R. EEG/EP T., CNIM, CLTM Seattle, WA Stephanie.Jordan@swedish.org Pat Lordeon, R. EEG T. Pittsburgh, PA patricia.lordeon@chp.edu 7
8 EPILEPSY MONITORING Susan Agostini, R. EEG/EP T., CLTM Phoenix, AZ Cheryl Plummer, R. EEG T., CLTM, BS Pittsburgh, PA INTRAOPERATIVE NEUROMONITORING Jeff Balzer, PhD, FASNM, DABNM Pittsburgh, PA Ryan Lau, R. EEG/EP T., CNIM, CLTM, BA Indianapolis, IN Justin Silverstein, CNIM, R.NCS.T., CNCT, MS Deer Park, NY MAGNETOENCEPHALOGRAPHY Hisako Fujiwara, R. EEG/EP T., CLTM, RPSGT Cincinnati, OH JP Lowe, R. EEG/EP T., CNIM, CLTM Summit, NJ NERVE CONDUCTION STUDIES Dorothy J. Gaiter, R. EEG T., R.NCS.T., CNCT, FASET, MHA Birmingham, AL Jerry Morris, R.NCS.T., CNCT, MS Shreveport, LA NEURODIAGNOSTIC EDUCATION Mary Feltman, R. EEG T., MEd Hewitt, TX Mark Ryland, R. EP T., RPSGT, R.NCS.T., CNCT, AuD Parma, OH Acute/Critical Care Neurodiagnostics...Continued The sweet little older tech had mastered the art of it, but I had it spread from me to the patient and everything in between, including the head of the bed. After graduation, I began working at a Level 1 Trauma Facility. This is where I learned to master gluing. We would glue several patients a day whether it was for a routine order or a continuous order. These patients ranged in all ages. Whether the tech decided to glue or not always depended on the patient, the situation, and the order. It was here I was taught by a tech to put the conductive paste on the back of my hand and fill the EEG cup lead one at a time. This was much more efficient for me. After filling and placing the EEG cup lead on the prepped area of the patients scalp I could then pull a collodion saturated gauze square from a frozen meal dish, such as what is used for microwavable dinners. It was wonderful! Yes, she showed me that frozen meal dinner containers could come in handy. They could be used for more than warming up your dinner. They could be used in the world of Neurodiagnostic Technology. Who would have ever thought? Utilizing these wide and shallow dishes, I could neatly lay out the amount of gauze squares I needed all at once, individually count them out, and then pour the collodion glue over the top so they were completely covered. As each square is picked up out of the dish the excess glue can be wiped off on the edge of the container and applied to the EEG cup lead on the scalp. Then it is dried with an air hose plugged into the air outlet in the wall behind the bed using a chemtron and christmas tree. (If the air supply is being utilized by the vent we have a T-bar, which is like a splitter enabling us to share the air supply with the vent. I always call the Respiratory tech to plug this in for me in this type of situation.) I was very pleased to have a good air supply and less mess; becoming more proficient with time soon followed. Afterwards, the excess glue dries nicely and neatly in the container which can then be pulled out and thrown in the trash or the whole container can be thrown away. There s typically always someone eating a frozen dinner, so as long as the container is cleaned out well, it can be ready to go glue the next patient. For instances when all I need to do is repair a lead or two, then I use a medicine cup with a gauze square in it and a little bit of collodion. A couple techs I know use collodion in a tube. It can be purchased that way and it is great for repairing just a few leads when needed. Whether utilizing an air pump or the wall outlet, I have always used a steel tip applicator to put in the EEG cup hole and twist the top to make the hole open for refilling. I refill it with conductive cream via a blunt tip needle and syringe when needed to keep impedances down. It will also allow for the recording to look good and be as artifact free as possible. Some techs have told me they use an air hose with just the open end of the hose and no applicator tip for drying. Some techs use gauze squares of various sizes and made out of various types of woven mesh. Some techs prefer to pre-fill the EEG cup leads prior to gluing them on. Some techs apply all the EEG cup leads empty and then fill the leads with conductive cream after all the leads have been applied. I prefer the paste on the back of the gloved hand method! I have tried utilizing EC2 Genuine Grass Electrode Cream for those patients in ICU that are comatose, but I personally have not found it to work very well. The patient may not be moving, but everyone else around the patient is constantly moving the patient. Rotating the patient side to side intermittently, pulling the patient up in bed, and moving the 8

9 NEUROFEEDBACK Bill Coslett, CNIM, PhD, BCIA, EEG-C Lake Worth, FL Riki Rager, R. EEG T., FASET, BS Nashville, TN NEW TECHNOLOGIES & RESEARCH Andrew Ehrenberg, R. EEG T., CNIM, BS Atlanta, GA Marco Moreno, R. EEG T., MS Fenton, MO PEDIATRICS & NEONATOLOGY Shelly Gregory, R. EEG T. Snohomish, WA Melanie Sewkarran, R. EEG T., CLTM St. Louis, MO POLYSOMNOGRAPHY/SLEEP TECHNOLOGY Scott Blodgett, R. EEG T., RPSGT, BBA Rochester, NY Kathryn Johnson, R. EEG/EP T., RPSGT, FASET Huntington, WV Acute/Critical Care Neurodiagnostics...Continued patients head pillow or pillows, etc. causes EEG leads to be tugged and pulled on which in turn can cause the leads to fall off. I have also tried the new collodion (Collodion A10) due to complaints from hospital staff, patients, and family members in our facility who do not like the smell of the collodion glue. Collodion A10 does not have the pungent odor (which I feel is better smelling than some other things in the hospital,) but I have not found it to dry very well or keep the leads adhered to the patient s head. There have been questions raised by new techs in the lab that do not find this method of gluing to be very sanitary. In that case some techs utilize the emesis basins for the method I described above in place of the frozen dinner containers. We utilize emesis basins for removing glued leads by lining the bottom with cotton balls and then pouring acetone or collodion remover over the cotton balls until they are saturated. Then we dispose of the container properly afterwards. I recommend you check with your safety officer at your facility and see what works best for you in your situation. Collodion has to be stored in a fire safe. Collodion cannot be left sitting out anywhere in its container or in any other type of container, such as the bottle with the applicator tip. This is according to our Safety Champion in our area of the facility. I hope I have given you Something Old and Something New to ponder for the next time you need to glue a continuous EEG at bedside on a patient in your facility. Thanks for reading the interest section. Ambulatory Monitoring By Jennifer Carlile, R. EEG T. The theme for this newsletter is something old and something new. I thought it would be a good time to revisit the question to glue or not to glue? For many years I have been asked the same question, is there a way to attach electrodes without using collodion? So many people complain of the strong odor and the residue it leaves in the hair. Well, I am very excited to share with you another way to attach electrodes without collodion! For the past 6 years, I personally have been using this type of adhesive tape to apply electrodes for ambulatory EEG monitoring. Okay, I know what you are thinking, I thought the same thing what, tape on patient s hair no, way! Well, I am here to tell you it works and works well. The name of the product is Cover-roll stretch adhesive gauze (Figure 1). It comes in 2 inches x 10 yards and other various sizes. As listed on the box, it is hypoallergenic, air permeable, cross elastic, nonwoven adhesive bandage. This is the only brand I have tried and I swear by it. As with anything, the more you use it, the more comfortable you become and the more efficient you will work. Your patients will be happy because there is no collodion residue left in the hair after electrode removal. And not only your patients but your 9

10 Ambulatory Monitoring...Continued co-workers will be most happy because no more collodion odor. It is always best to use on clean-product free hair. However, I have used this method successfully on a little African-American girl whose mother the night before put special oil all over her hair. There were a few electrodes that I thought might not hold up (posterior region) but I was unable to use collodion at this lab, and so I really did not have any other choice but to try. Well, I cannot begin to tell you how excited I was to see how well this method worked even with the oily hair product. How to use: the adhesive tape comes on a 10 yard roll. Cut the tape into 2 to 2½ inches in length. Just like applying electrodes with collodion, after measuring the head as normal, use a small amount of skin prepping cleanser, with the electrode, scoop a nice amount of electrode paste into the electrode, depending on how long the electrodes need to stay in place, (use a bit more if monitoring for more than two days), then place the electrode onto head. Making sure the paste is laying directly on the scalp and that the surrounding hairs are lying flat, take a 2 to 2½ inch piece of tape, peel off the backing paper cover, exposing the sticky side, lay the sticky side over top of the electrode. Making sure to center the tape over the electrode helps eliminate any potential lifting, which could cause popping artifacts. Holding that portion of the electrode and tape down, use your other hand to peel off the remaining paper covering of the tape, then press firmly over top the entire electrode (covering above tip of electrode, past the hub), again insure the entire electrode is covered. If it is not, add another piece of tape going diagonal, making sure to cover the biggest part of the electrode. As with most tapes, a little bit of heat makes the adhesive stickier, so once all electrodes are in place, I wrap the head with cotton gauze rolls. Between the head wrap and the patient s body temperature, the tape really sticks well. The most important challenge is making sure the hairs are laying as flat as possible or at least make sure once the tape is in place. If the patient has longer hair, take a strand of their hair and lay it over the piece of tape, kind of holding it down until the head wrap is in place. Because some people are active sleepers, tossing and turning all night, if the head wrap comes off, instruct the patient not to remove the entire wrap, give them extra gauze and tape to add to what is already on their head. The electrodes really should not come off without using a remover, unless the patient actually pulls them off, and they can do that even with collodion. As far as removing the electrodes, once the test is complete I use collodion remover (acetone not necessary), starting on one side, saturate a piece of tape, move to the next electrode, until you get all the way around the head. By that time, where you first started saturating the tape, that piece of tape should pull off easily without pulling any hair with it. Remove each piece of tape then peel off the actual electrodes. I then like to take a towel and really give a good head massage, absorbing the excess oil from the remover as well as any leftover paste. You should be able to easily comb through the hair. Then I instruct the patient to go home and wash as normal. There should be no residue like there is with collodion. If you have any questions and wish to discuss this application process, please feel free to either me or call me. I am so excited to share this method with everyone who has had hurdles to jump with collodion. In my opinion, collodion is still the very best way to attach electrodes; however, this tape method is a close second. I am including a few samples of the tape method that was used on a patient for 7 days (Figures 2 through 4) can you tell the difference between collodion vs. tape? 10


11 Ambulatory Monitoring...Continued 11
12 Clinical EEG By Petra Davidson, R. EEG/EP T., BS and Keith Davidson, R. EP T., BS Greetings readers, Yeah, Spring!! We are looking forward to some green grass, buds on trees, and hearing birds again. Looking forward to the things which seem new after the long winter, we are reminded of the new things that greet us at the ASET conferences, in the ASET journal, and from the colleagues we meet. Keith and I have each been performing EEGs for over 13 years. In that time we have developed a great deal of confidence in our preparation and application of electrodes. We also felt very secure with how we performed EEGs on children. While our lab has very specific policies and guidelines on how to perform an EEG in a variety of circumstances, our written policy on how to attach the electrodes is intentionally vague. The reason for this is to allow freedom to perform this action in the manner most efficient for each of our techs with some general guidelines on supplies used but nothing too specific. The great thing about keeping this policy vague is that we have the freedom to try new things out without having to rewrite a policy every time a change is made. For example, for years we used collodion on all patients that had a high risk of removing the electrodes. It successfully served its purpose and still does. However, we have had patients and staff complain about the odor, had near misses with the collodion coming into contact with patient s faces, and experienced the unpredictability of the formula of collodion. At the last ASET conference, a presentation was done on securing electrodes. EC2 Genuine Grass Electrode Cream was mentioned and methods used to secure the electrodes utilizing EC2 were explained. We brought our newly acquired information back home and after a trial period of using EC2 we found we love this stuff (after getting past the learning curve). No smell, no special remover, easier to control where it goes, formulation remains consistent, and it doesn t require special storage. We have now been using EC2 in place of collodion for many months. In the realm of pediatric EEG it was not until after our youngest son had his first seizure that we really evaluated how we performed EEGs on kids. He was 2 years old at the time (yes, we were both already EEG techs and that was strange having work show up at home in your arms that way). We had a bad experience with his first EEG at another facility. At the time we (patients parents) were the only EEG techs in our facility so we had to take him elsewhere for his test. It ended with sedation with chloral hydrate, scabs on his head that lasted over a month, and no results for six months. We promised ourselves we would make it better for those who came to our facility. We ordered televisions, DVD players, movies, and books for our patients. We banned chloral hydrate from our lab. We banned the papoose boards. Yes, we know there are labs who love them. We allow a parent to hold the child, gently swaddling the child in the parents arms with a blanket, and we turn on a movie. As the child watches the movie, we explain about the camel snot we will use to clean their head, the toothpaste that holds the little wires, and how their brain draws us pictures. We also explain to the parents that the smaller children will cry a bit and that is okay, it is the same as the breathing exercise we would ask an older child or adult to perform. We then turn down the lights, allow the movie to play while the parents and technologist talk quietly. Soon the child sleeps naturally. The children play bubbles or pinwheels with us to perform hyperventilation. When they wake up, we play with the strobe light and the child is shown how to make their fingers move in slow motion. When all is done, we wash their hair with a little warm water and give them a sticker and they are a new friend. A technologist that trained both of us once said these very wise words the moment you think you know everything there is to know about EEG, a patient will walk in the lab and turn everything on its side. He was so right and this has served as a reminder to always be open to what s new and changing, whether that is in how we prep our patients, or in how we work to calm them during the test, remember there is always something new about to walk in the door. Computers in the Workplace By TJ Amdurs, R. EEG T., MS I never envisioned that I would have a career in Neurodiagnostics. It surely never was the plan when I first began college. Life takes many different twists and turns. My life was no different. I started college as a music performance major. I continued with this path until I was injured during a summer job that changed my life forever. Due to the injury, I could no longer endure the amount of time it took for practicing, rehearsals, and performances. I did not know what I was going to do at that point until a conversation that I had with a neurologist. I was explaining that I wanted to continue on with school yet did not know what I may want to do. Music had been such a big part of my life. He told me of a program they had at one of the local colleges. It was called EEG Technology. I enrolled into the EEG Technology Certificate program at Carlow University in Pittsburgh, Pennsylvania. I figured it would at least provide me with education and training to be able to work. When the day came to start, I tried to keep an open mind and see what this EEG Technology was all about. I sat there talking to a few people not knowing what to expect. As the class started and the instructor began with the frequency ranges: alpha, theta, delta, and beta, I thought I made a huge mistake. 12



13 Computers in the Workplace...Continued It was as if he was speaking a foreign language or in tongues. I am not a physicist! Everyone started asking questions right away with a lost and confused look. At the very least, I am not alone. I slowed myself down and remembered to keep an open mind. I went home and started reading and talking to others in the class. I ended up doing very well in the program and came to love EEG. I tried to learn as much as possible and still continue to learn today. As the program progressed into the final semester, I enrolled into a Health Science bachelor s degree program at Carlow University. Around the same time, I began my first job in EEG. I began working at Children s Hospital of Pittsburgh in the Epilepsy Monitoring Unit. There were many special people who worked I moved to a smaller community hospital where I was the only technologist. I gained valuable experience and built some great bonds with people there. there and I was very proud of my first job in my Neurodiagnostic career. After working nights for a few years, I moved to a smaller community hospital where I was the only technologist. I gained valuable experience and built some great bonds with people there. One of them was a neurologist who asked me to come and work at my next job at a large city hospital. It was the Chief Technologist position where I held management responsibility as well. As I worked here, I went back to school and completed my Master s Degree in Health Services/Professional Leadership. I soon after wanted more responsibility in management. I moved to Boise, Idaho and worked at a great health system there. I was responsible for Neurodiagnostics, an epilepsy monitoring unit and intraoperative monitoring. While I was here, I was on the Board of Directors for the Epilepsy Foundation of Idaho. It was a great experience. Following this, we ultimately moved back home to Pittsburgh to work at the University of Pittsburgh Medical Center where I am currently the Coordinator for MEG Services. I remain active in ASET and am on the Membership Committee and I am on the Board of Trustees for ASET. The work for ASET has been some of the most rewarding work I have done. It has been an awesome career and I have met many incredible people along the way. I can t wait to see where the road takes me next! CPT Coding By Lynn Bragg, R. EEG/EP T. Ahh!! The good old days. Remember when you could have a kidney stone and the doctors would order an EEG because you happen to mention you had a headache a week ago? So much has changed through the years and I have my suspicions that billing and coding will be high on the list of most changes for some time. Just in the past year or so, look at how coding and billing for EMGs has changed. In past years for EEG, billing for portable studies was permitted. Now it is based on awake, drowsy, sleep, or length of recording, regardless of how much tech time is needed for a study. Accepted diagnoses are now a major part of reimbursement. As mentioned at the beginning of my article, years ago kidney stones would not have been questioned, today probably not so much. Most of the studies done today regardless of the modality should be billed from the interpreted report. Electronic Medical Records (EMR) is the future of medical records. Interpretations are being done by completing templates that have been specifically formatted for the modality tested. My office has been using EMR for several years and we have been using templates for all the testing done in the 13 office. For the technologist it is a bit more work, filling out the demographic information and patient history. For me personally, it is double the work since I complete a patient history for the EEG recording in the EEG acquisition process as well. The changes in reimbursement and requirements for billing purposes have made changes in our field a global change. It most likely will be a continuing force for us as well as many other fields of medicine. Unfortunately, with these changes, if it doesn t work well for your lab you can t change it like you could if you had changed your brand of paste or gauze. SAVE THE DATE SATURDAY, AUGUST 3, 2013 ASET ANNUAL CONFERENCE RENO, NV CPT CODING WORKSHOP
14 Department Managers By Pat Lordeon, R. EEG T. When I look back and compare how our labs operate now compared to how they operated years ago, some changes seem very dramatic, and others more subtle. Some changes were implemented with a firm start date: today we do this, but tomorrow and every day afterwards we will do that. Other changes evolved over time, gradually and unobtrusively becoming part of our everyday routine until we can t remember a time we didn t do it this way! If asked to detail the most substantial change we have experienced over time, I would have to say that the change in our workflow due to the increase in our volume is the most obvious. When I started working in the EMU years ago, we were a four bed unit; our hours were Monday to Friday 7am to 4 pm; we had a staff of four techs and two RNs; and only performed an occasional depth electrode monitoring. Now we are a Level IV eight bed EMU; open 24/7; responsible for all emergent/on call EEGs (thus eliminating the need to have a tech on call for the hospital); we implant and monitor grid electrodes; provide ceeg for ICU patients; and have a staff of 16 techs, 16 RNs, and 1 Physician Assistant. Our work flow is more regulated and systematic, with the techs adopting and following many nursing policies. The tech I was would be dazzled with the way things work in the unit today! The other dramatic change is in the way we train our techs. I was trained in an on the job training manner. We were fortunate to have a physician in our department who was quite invested in tech education. He taught classes in Instrumentation, Neuroanatomy, Seizure Disorders, Metabolic Disorders, and many more topics to both our lab techs as well as to techs from neighboring hospitals, one to two hours per week. During the other 38 to 39 hours of the week you worked in the lab. The only pre-requisite for the job was a high school diploma. Currently, we operate a formal tech education program for our tech trainees, with a dedicated staff of tech and physician educators; a diverse curriculum consisting of several half days of didactic classroom experience (plus a brain cutting); graded tests; Neurodiagnostic area rotations; and established pre-requisites for entry into the program (including possessing at least an associate degree). Very different from the days of old! However, the something new in both of these examples has its roots in the something old. The workflow changes evolved from the addition of new tasks to our basic job structure. We still do EEGs we just do more of them, in more diverse situations and in a more complex manner. We still train techs.we just increased the amount of classroom time and varied the types of experience. Lest we begin to think that everything new is good, keep in mind that the best and most acceptable changes are usually those with a familiar base or starting point. Radical 14 changes are the most likely to meet pushback, or to not be implemented successfully. Change for the sake of change is never a good idea. The successful manager keeps one foot in the past, and one in the future. By Stephanie Jordan, R. EEG/EP T., CNIM, CLTM Here is something very old taken from: The American Board of Registration of Electroencephalographic and Evoked Potential Technologists (ABRET) Code of Ethics and Standards of Practice: Principle Number Seven: 7. Refuse primary responsibility for interpretation of testing or monitoring of Electroencephalograms, Evoked Potentials, or Neurophysiologic Intraoperative Monitoring for purposes of clinical diagnosis and treatment. Individuals who are licensed or otherwise authorized by practice standards to provide interpretation are excluded. The ABRET code of ethics and standards of practice have been around as long as I have, yet seem to remain new. This is something that Managers and Supervisors should go over with students and new hires during their orientation; the students and new hires are so eager to share what they have learned or know. It can also be refreshed with staff at department meetings under the umbrella of patient safety; what if a medicine was withheld or given due to technologist interpretation? There have been many times I have been pressured by an attending physician to give EEG results at the bedside that could possibly influence diagnosis and treatment. I have always relied on the code of ethics that comes with your ABRET registration certificate. There is always a distressed family member that asks for the results or an anxiety ridden patient who pleads and begs. Use Principle Number 7. When evoked potentials moved into the operating room and surgeons came to rely on intraoperative monitoring to guide their surgery, the pressure to give interpretation became palpably higher. But you can stand your ground on Principle Number 7. Do not enter the operating room without a licensed or authorized interpreter. As registered technologists we are responsible to have an impression of the recording that we can share with the interpreting physician. We must analyze what we are recording to best document the clinical neurophysiologic events occurring for the patient at the time of our recordings but our responsibility stops there. Don t forget Principle Number 7; it is like the Rock of Gibraltar.
15 Epilepsy Monitoring By Susan Agostini, R. EEG/EP T., CLTM Something old, something new made me think about our Epilepsy Monitoring Unit (EMU) and how easily we tend to become comfortable with the way we do things every day. The staff is familiarized with the equipment. The procedures, and the overall daily workflows and operations are clear and smooth. I am going to share our own experience when we had to deal with changes to our EMU environment that shook the floor beneath us! Change is inevitable, and specifically in the healthcare arena we have been hit pretty hard in the recent years as a result of the economy downturn. Medical insurances coverage, optimization projects, re-engineering projects, patient volumes changes, and staffing changes are only a few of the many challenges that we are currently facing. When we opened our EMU doors in 2011, I chose to create a culture that embraces and fosters change, turning them into opportunities to tap into our creative juices coming up with possible ideas and solutions! Change is not easy, and it certainly creates a sense of instability in the staff that has to be addressed in order to successfully transition from the something old to the something new. I think that one of the most important details when faced with what could seem as a drastic change is to maintain patient safety as our #1 priority in every action we take and every decision we make. Our most recent change in the Epilepsy Monitoring Unit was the possibility of utilizing available EMU beds in situations when the hospital is faced with patient overflow. The first time I heard of this idea I became very anxious as we had created a culture of ownership and accountability within the core staff that now would be tested by opening our doors to a different type of patient population and to staff that have not been in the unit before. For most, this idea seemed most logical and feasible; however, the reason why it also raised some concern was because our unit is not located in the main inpatient tower. We are located in an adjacent tower connected by a spine with the main tower. Some of the questions and concerns were What kind of medical problems will these non-emu patients have, and are we fully equipped for this?, Will float staff take care of our unit the way we do?, Will things disappear from the unit?, We have been a self-contained unit since we opened, and now we have to share our unit (the protective in us)?... Will our EMU patients continue to be safe when we have other patients to take care of? The first step was to meet with all parties involved (patient placement, nursing managers, pharmacy) in order to identify the type of patients that we could manage in our unit, and the areas that we would have to modify in order to 15 accommodate the care of our new guests! We communicated the change to the staff that would be affected and reassured them that all processes would be in place before initiating this new workflow. EMU core staff gave many ideas, suggestions, and recommendations that were taken in consideration during the planning phase. The day came when we had to put into practice our new workflows. There were two patients transferred to our unit as a pilot. These two patients were hand-picked by the nursing director. Needleless to say, it was an anxious and stressful situation, but it did not take too long for the staff to continue providing the same excellent patient care that we have always provided. Management debriefed the experience and it has been decided that the option of transferring non- EMU patients to the EMU will be entertained when the need to facilitate patient flow is absolutely imminent, and of course if there are EMU beds available. The patients that will be selected for this will be pending discharge, or neurological conditions such as stable post-stroke patients. So, our epilepsy patients continue to be our priority and our passion! Every day that goes by is one more day that we prove to ourselves that we can manage changes, and that we can be team players! So, during times when I am faced with a challenging situation such as the one that I shared with you today, I remind myself of the unofficial Marine Corps motto shared by my husband and other retired military personnel, a long time ago Improvise, Adapt, and Overcome. So true! By Cheryl Plummer, R. EEG T., CLTM, BS Well speaking of new, there are two new anticonvulsants that I wanted to be sure that all of you are aware of. One of the new medications is called Oxtellar XR (oxcarbazepine extended release). This medication is used as adjunct therapy for partial seizures in adults and in children 6 years to 17 years of age. It comes in three size tables: 150 mg, 300 mg, and 600 mg tablets. To read more about this medication and its side effects visit pro/oxtellar-xr.html. The other drug is called Fycompa (perampanel) which is used for adjunct treatment of partial onset seizures with and without secondary generalization. This is used in patients who are 12 and older. Fycompa is a once a day dose medication and the first FDA approved noncompetitive AMPA (alpha-amino-3-hydroxy-5-methyl-4- isoxazolepropionic acid) glutamate receptor antagonist. This medication has interactions with other anticonvulsants in that it can reduce their benefits. To read more about this drug and its side effects, visit fycompa.html. Wishing you all a happy Spring.
16 Intraoperative Neuromonitoring By Justin Silverstein, R. EP T., CNIM, R.NCS.T., CNCT, MS Adding Specificity to the Neurophysiological Monitoring Paradigm by Adding More SSEPs About a year and a half ago I decided after starting my own practice that I wanted to offer better monitoring to my patients by being more specific with the neurophysiological monitoring. I implemented median nerve and deep peroneal nerve SSEPs in addition to ulnar nerve and posterior tibial nerve (PTN) SSEPs during every surgery. When I first began in IONM I was taught to run ulnar nerve SSEPs almost exclusively for monitoring of upper extremities and PTN SSEPs for monitoring of lower extremities. There was always the option to run other nerves such as the median or peroneal; however, this was presented as use for very specific procedures for example, median nerve SSEPs during carotid endarterectomy. I want to stress that we stimulate the deep peroneal nerve superior to the medial malleolus, as opposed to the deep peroneal at the fibular neck or the common peroneal at the lateral popliteal fossa. The reason for this is that the deep peroneal innervates the muscles for dorsiflexion of the foot (tibialis anterior muscle and extensor digitorum brevis muscle). Which in turn are the muscles that are affected when a patient has a foot drop. We feel we can be more predictive of injury to these innervations if we stimulate distal to them. By stimulating the deep peroneal distally at the ankle, we are able to better monitor for foot drop, which could be missed if stimulated at the fibular neck, especially if the issue is caused by leg positioning and not nerve root injury. It is really nice to have a more global view of the nervous system and with more specificity I am able to trouble shoot better. For example, not too long ago I was monitoring an ACDF where the right upper extremity ulnar cortical SSEP became attenuated. To rule out technical issues I ran the median SSEP to learn that the right median cortical SSEP was also attenuated. This allowed me to deduce that it was most likely a carotid artery occlusion caused by the surgeon s retractors. When I informed the surgeons and they removed the retractors, the responses from both nerves came back (Figures 1A, 1B, 1C, 1D). It gives you a nice feeling when you do not have to second-guess yourself because you are double checking yourself electrophysiologically. In another example, I was unable to obtain the right ulnar SSEP response at baseline for a posterior cervical decompression and fusion likely due to a technical issue. I could have fixed the technical issue, but the surgeon would have had to undo the entire patient positioning and taping. The surgeon felt comfortable enough to move forward just monitoring the right upper extremity with the median nerve because it allowed us to monitor spinal cord function without being inhibited by not having the ulnar SSEPs (Figures 2A and 2B). 16
17 Intraoperative Neuromonitoring...Continued 17

 during an ALIF.")
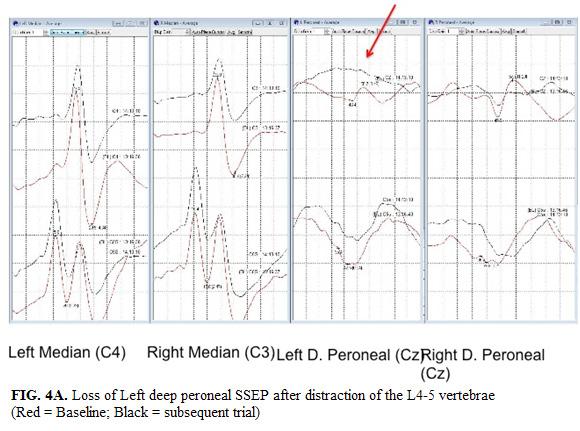
18 Intraoperative Neuromonitoring...Continued I have my entire group monitoring all these nerves and we have seen isolated deep peroneal SSEP losses that were attributed to retraction of the L5 nerve root during a laminectomy (Figures 3A, 3B, and 3C) and distraction of the L4-L5 disc space (Figures 4A, 4B, and 4C) during an ALIF. We feel our intervention in both cases prevented post-operative foot drop and upon initial follow up learned that the patients were neurologically intact. 18

19 Intraoperative Neuromonitoring...Continued 19


20 Intraoperative Neuromonitoring...Continued 20

21 Intraoperative Neuromonitoring...Continued The method of monitoring multiple nerves also has great benefit when troubleshooting a change in the evoked potential caused by patient positioning. We are able to differentiate distal injuries vs. proximal or ischemic injuries in the upper extremities by using median and ulnar SSEPs. If the ulnar nerve attenuates or has a prolonged latency from initial baseline and the median nerve does not change, we know the event is occurring distal to the brachial plexus, most likely at or about the elbow and the cubital tunnel (Figures 5A and 5B). If both the median and ulnar attenuate, we know the injury is most likely occurring at the brachial plexus or the limb has become ischemic (Figure 6). By monitoring multiple nerves with SSEPs, we have made our monitoring paradigm more specific and less sensitive. We are more specific because we have become more focal in determining the source of a potential injury or technical issue. For example, if I were monitoring only ulnar SSEPs for a positional injury during a lumbar surgery and had a positive event occur where a change in the ulnar nerve is detected, I know that there is an issue affecting the limb in question; however, I cannot pinpoint where the injury is occurring (i.e. brachial plexus, cubital tunnel or ischemic event) therefore, the modality is highly sensitive but not specific. Whereas, if I am also running median SSEPs and they are also changed, we have now taken a sensitive modality and made it specific, because I know this is either a brachial plexus injury or an ischemic event, and definitely not an event occurring due to pressure or entrapment of the cubital tunnel. Another example would be a loss of the peroneal nerve SSEP due to the belt that straps the patient to the Jackson table impinging the peroneal nerve at the fibular neck. This again, is a specific injury, which would not have been seen if I were only running PTN SSEPs. Therefore, by adding multiple nerves to our SSEPs we are able to predict and prevent injuries from occurring that may have gone unnoticed. Surgeons and anesthesiologists like the fact that we are able to monitor more of the nervous system and we are able to give them better feedback regarding the neurological status of their patient during surgery. 21

22 Intraoperative Neuromonitoring...Continued Magnetoencephalography By Hisako Fujiwara, R. EEG/EP T., CLTM, RPSGT Brain network On February 18th 2013, it was revealed that the U.S. government is planning a large-scale project that seeks to create the most comprehensive map of the human brain assembled so far. It is called The Brain Activity Map. Scientists likened the Brain Activity Map effort to the Human Genome Project, the government-led initiative that helped decipher the human genetic code and provided a huge boost for the genetics industry. According to Dr. John Donoghue, a neuroscientist at Brown University, the idea of this project is to organize a national effort to crack the problem of how the brain functions at its deepest levels, and how various neurological ailments might be better treated. Advocates for the project hope that exhaustive research into the brain s neurons would produce insights that could be used to understand mental illness (i.e., schizophrenia) help treat diseases such as Parkinson s and Alzheimer s and even enable advances in artificial intelligence. A comprehensive map of brain activity has similar scope to the Human Genome Project, which recorded all the genes in human DNA and was completed in 2003 at a cost of $3.8 billion. This would be a great opportunity for the MEG world to be part of this project. In recent years, the interest has grown in the study of connectivity between spatially separate, functionally specific brain regions. The default network is a network of brain regions that are active when the individual is not focused on the outside of the world and the brain is at wakeful rest. It is also called resting state networks or task-negative network. The ways in which separate areas synchronize to form networks is integral to information processing. Abnormal communication between regions is thought to be the basis for a number of neurological pathologies (i.e., Alzheimer s, autism, schizophrenia). If we are to generate a complete understanding of brain function, then elucidation of the role of brain networks will be critical. All the same requirements apply to brain dysfunction. (Well, it is a basic principle of neuroscience. If you do not know what the normal function is and what it looks like, than you cannot tell what the abnormal looks like, right?) 22
 signals originating in spatially separate brain regions are correlated in time.")
23 Magnetoencephalography...Continued The majority of research on this default, or resting state, network has been conducted using functional magnetic resonance imaging (fmri). During the resting state, bloodoxygenation level dependent (BOLD) signals originating in spatially separate brain regions are correlated in time. More recently, there have also been studies investigating resting state networks using noninvasive measurements of electrophysiology, including MEG. MEG has an advantage in that it offers a useful way to measure connectivity between brain regions and does not rely on a delayed hemodynamic response, such as BOLD signals in fmri, which is an indirect measure of brain activity. By comparison MEG measures directly the electrophysiological basis of brain activity by measuring the magnetic fields associated with the synchronized current flow in neuronal assemblies. Unlike EEG, magnetic fields are not distorted by inhomogeneous conductivity in the head. With higher sensor density and complex source reconstruction algorithms, MEG provides improved spatial resolution compared to standard EEG topography. With its excellent temporal resolution MEG has become the most attractive noninvasive technique for measurement of electrodynamic connectivity in the human brain. However, there are still challenges and unanswered questions in the MEG field, especially the projection of sensor space data to its source level. MEGers have been working hard on this task worldwide. So we already see progress on solving this task each and every day. Would you like to be a part of this national project The Brain Activity Map? Nerve Conduction Studies By Jerry Morris, R.NCS.T., CNCT, MS Hey all you nerve stimulators out there! I m baaaack!! Dorothy was so gracious and kind to write the last couple of newsletter articles while I recouped from a knee injury and surgery. Weren t her articles terrific? Here in Louisiana Spring is here, not just around the corner the jonquils and tulip trees and redbuds and plum trees are already budding and blooming..and the crawfish are cookin maybe the old groundhog got it right, at least for this part of the south. Margaret, the only white stuff I ve seen is the white blossoms on the Bradford pear trees that are so abundant around here. Here in our area the EMG/NCS coding changes have been very noticeable. The EMG coding changes that took place for 2013 took away a good bit of revenue from the needle exam portion of the study. Several of the physicians affiliated with our hospital have been affected by these coding changes. There is less reimbursement coming in from the insurance company pay outs; on top of that the price of needles has either increased or remained the same with no decrease in price. Pay more to make less, so to speak plus the 23 time frame to do the test is still the same. With other aspects of their neurology or rehab practice requiring as much if not more time, it is difficult to add a patient or two or three to compensate for the loss of revenue. From what I understand, the specifics of this part of the study is never compromised by these physicians, so what do you do, work longer hours to squeeze in a few more patients?? In our hospital setting, we do a lot fewer EMGs than NCVs. With the new NCV codes put in for 2013 it is hard to tell yet how it will affect our reimbursement. I would guess we would have decreased revenues from our NCV studies but time and the end of the fiscal year will tell. The same would hold true for the physician NCV studies as well. In my lab we still have the same protocols for CTS, neuropathies, radiculopathies. You get the idea. the only time there is deviation from these protocols, is when I see something during the exam that shows me that some other study or studies need to be done. Fortunately I have the leeway to do that. I still do the same nerves the same way using the necessary time and then bill them by a different name than I did in To me the quality and thoroughness of my NCS exam is absolutely essential in order to help the physician with the patient s diagnosis. Other coding changes in all aspects of electrodiagnosis may be just around the corner. From what I understand, a lot of the changes were to prevent billing abuse from individuals, offices, or companies that were simply doing lots and lots of unnecessary studies. They do bad we all suffer! Who would have thought 3 to 5 or even 10 years ago we would be where we are now. As healthcare changes these next few years we may see more changes, some good; some bad. Have a wonderful summer. Reno will be here before you know it a great program, great friends, terrific networking, and a fun city with Lake Tahoe only an hour away. See you there!
24 Neurodiagnostic Education By Mark Ryland, R. EP T., RPSGT, R.NCS.T., CNCT, AuD When it comes to the latest and greatest technology I must definitely put myself in the category of Pterodactyl. My cell phone has an IQ of about -3; I can actually call people with it, and have proudly acquired the ability to text (not easy on a device developed in the late Jurassic Period). Last year my wife and I purchased our first flat screen TV, and there is nothing automatic in the 2006 Mazda 3 I drive. My notion of new may be skewed a bit. So my new topic is not really all that new, but it is new to me. In 2010, I completed my AuD degree through a distance learning Audiology Program. That was an absolute leap for me. I had some basic computer skills from teaching for four years, but the notion of not being in classroom was new. I now find myself on the other end of the computer, teaching several courses for the UNC BA Distance END Program as well as my brick and mortar END/Poly Program at Tri-C. The adaptations for online learning have been interesting. I think one of the most compelling differences boils down to human nature. I tend to make many off-thewall references/comments during lectures at Tri-C, which occasionally sends students into a tail spin or just makes their heads explode. When you make off-the-wall comments to an online student, the miscommunication is compounded and can be amusing at times. I recently made a comment to a UNC student that her lab assignment was so well done, that she could present with it. Her interpretation was that this was going to be requirement! After assuring her it was merely a compliment, I assume she had a reduction in blood pressure which averted a significant CVA. My assumption is that online learning is not going away, and indeed more programs will be developed as our field moves forward. If a dinosaur like me can adapt to online learning from both a student and instructor standpoint, then there is nothing we can t do. Neurofeedback By Bill Coslett, CNIM, BCIA, EEG-C, PhD The theme of this article is the changes that you have witnessed in your field. Perhaps things that we used to do and no longer do or things that we are now doing that we did not do early in our careers. I am working in the field of intraoperative neuromonitoring (IONM). I first came into the field in 2003, and have witnessed many changes in the way that IONM is done. I must be the first to admit that I am not always one to welcome change. It seems like once I develop a comfort zone, I have a tendency to stay within that zone. I am sure that I am not the only one with this tendency!! 24 When I first entered the IONM field, I was very obsessive compulsive. I would have individual packs of supplies for each patient including tape measure and marking pen to mark for precise measurement for cortical electrodes. It seems like after the first 1,000 patients I was more comfortable in localizing placement for cortical leads and stopped marking each patient s head. I have talked to many of my co-workers who experienced the same process. Cortical electrodes were placed through anatomical markers. I have been thinking that maybe I will go back to marking individual heads! Early in my career, I was encouraged to used cup style electrodes rather than subdermal needle electrodes. Today I almost exclusively use subdermal needle electrodes. My father used to tell me that the more things change, the more things stay the same. I find that this holds particular truth in the field of IONM. Many of the modalities that I used early in my career have changed. I started out using very basic modalities such as SSEP and EMG monitoring. Today, we have added TCMEP to ensure motor function as well as specific nerve root function. EEG has been added to ACDF as well as laryngeal monitoring to ensure patient safety during cervical procedure. Additional channels of EMG have been created to more complete monitoring abilities. Even though technology has created fast computers for real time monitoring, the basic assumption that we are truly patient advocates during their procedure hold true as the day I first entered this field. Early in my career, it seemed as if there was no real consensus as to what montages should be used. Asking ten different technologists what montages they used would produce as many as ten different responses. I distinctly remember how amazed I was to realize when talking with other professionals that there were different montages that were being used. I know the company that I work for has spent a lot of time and effort to standardize montages to be used in our data collection. I remember my first introduction to intraoperative neuromonitoring. I wondered if I was qualified to be in the field. I remembered how amazed I was to find out that the only requirement was a high school degree. Why, anyone could sit in front of a computer and do monitoring. As the profession changed so did the expectation for those monitoring. The field strove to increase their professional image. Soon entrance requirements increased. Professional schools opened teaching the needed skills to enter the field of IONM. Although still a shortage of skilled professionals, employers are no longer looking for any warm body to fill a seat behind the computer!! Companies are looking for professionals who possess the needed skills to do their monitoring.
25 Neurofeedback...Continued One of the most enjoyable changes for me has been the addition of a neurologist online to help watch and answer questions that may arise. The neurologist is also available to speak directly to the surgeon if need be. When I first started monitoring, I was one of three techs in a mom and pop monitoring company. There was a reading physician, although he was not online with me. I was instructed to use my cell phone camera to take a picture of the screen if I needed his help or opinion and then text it to him! Talk about feeling out on a limb. Today, we have much better and faster technology that allows neurologist to be online and monitoring the case with you. It is reassuring to me to have them online and available to input into the case. Well I have rambled on long enough about how things were then and how they are now. Times have changed. Technology has improved. Our understanding of neurophysiology has improved. But the most important thing has not changed and that is the protection of the patient. We need to continue to be proactive for our patients. Be safe out there!! By Riki Rager, R. EEG T., FASET, BS This article is the Neurofeedback Section because I used to do neurofeedback. However, this time I am writing about something old from EEG that could be something new for today s EEG technologists. Since becoming an educational program director, I have learned that electrocerebral inactivity (ECI) recordings are ordered very infrequently now. The physicians tell me it is because interpretable EEGs are hard to obtain and are full of artifacts. In addition, the use of other testing is becoming more widely accepted. New technologies always present a challenge for EEG. However, we shouldn t let new technologies replace what we do due to poor techniques. There are still times when ECI is needed and interpretable recordings are indeed possible. During the past week, we spent a lot of time in the classroom talking about artifacts and how to eliminate or monitor them. Because we are starting a new long-term monitoring program in the ICU and artifacts are so prevalent in that setting, we felt a real need to make sure everyone is educated on artifact recognition and control. For my part, I would like to resurrect a technique for monitoring ventilator artifact on the EEG. This technique was published in the Delta Recorder many years ago. Unfortunately, I cannot remember the author s name or date of publication. There are many techniques for monitoring ventilator generated artifact. Respiration belts that use strain gauges are often employed. Trying to get the belts on an ICU patient can be challenging. Some techs place electrodes on the abdomen or on the ventilator itself. These often introduce another type of artifact and often do not show the true respiratory pattern. The following method works extremely well but requires seeking assistance from respiratory therapists initially. With training from the respiratory therapists, the EEG techs become competent and can do this on their own. A bronchoscopy adaptor (Figure 1) is placed in-line between the patient s mouthpiece and the ventilator tubing. The adaptor has a plastic tab that can be opened to insert a bronchoscopy. Using that opening, place a single airflow thermocouple (Figure 2) into the tubing and close the tab. The thermocouple is then plugged into any available channel. The resulting recording is a very smooth, artifact free oscillating waveform Figure 3, bottom channel). With each inspiration and expiration, the waves rise and fall. This is due to the change in the temperature of the cooler air being inhaled and the warmer air being exhaled. I used this technique for many years in the hospital environment and never encountered any problems with insertion of the adaptor or with introducing unwanted artifacts. Here is an old paper recording obtained before reformatting was possible (Figure 3). We often used combinations of montages to localize abnormalities. In this example, the referential portion clearly shows a generalized spike and wave while the bipolar circumferential portion shows equipotential at Fp1 and Fp2. On the referential portion, highest amplitude appears to be at F3 and F4. The next montage used might have been a combination of referential and transverse bipolar going through F3 and F4. Having the freedom to play around with montages often produced some unexpected findings. Creativity was encouraged as long as the combined montages followed the American Clinical Neurophysiology Society (ACNS) recommendations of anterior to posterior, left over right, etc. See Figure 3 on next page... 25
26 Neurofeedback...Continued New Technologies and Research By Andrew Ehrenberg, R. EEG T, CNIM, BS The following is in a form inspired by the 1993 commencement address at Harvard University, commonly known as Wear Sunscreen. The content, opinions and advice contained here though, no one else bears responsibility for except my own self. Ladies and Gentlemen of the field of neurophysiology; If I could offer you only one piece of advice, head measuring would be it. The proper placement of electrodes ensures recording from specific and comparable neuroanatomical locations. The correlation of the International System to these locations has been verified by neuro-imaging and literature and is the key to a technically accurate EEG;...Whereas the rest of my advice has no basis more reliable than my own opinions and experience. I will dispense this advice now -Realize the opportunities to grow you are afforded; oh never mind, you probably won t even realize the opportunities until after they have passed, and you either took it and grew or just nodded your head and let it pass you by. Trust me, you will look back in years to come and laugh at how much you thought you knew now. -There is no perfect anything in neurophysiology. No perfect montage, or technique, paper versus digital, one vendor or another... The only way to use anything is to know both its strengths and its weaknesses. -Know your own strengths and weaknesses. -Ask questions -Don t be stingy with your knowledge; don t put up with people who are. 26

27 New Technologies and Research...Continued -Don t waste your time on regret; Sometimes you do a perfect test, sometimes you don t. Sometimes you do a perfect test on the wrong patient. Own it and make it right. People will respect you for it. -Praise in public, criticize in private. -Feel good about the patients you help; Don t feel bad about the ones you can t. If you succeed in doing this please tell me how. -Never stop learning. -Actually, this is brain science. -Remember Ars Longa, Vita Brevis, Our search for knowledge is an endless, ever branching road with an ever expanding horizon, but never forget Carpe Diem, Seize each day and what it has to offer. -Pay attention to detail; but know that at some point you will step away from your patient for one second and that s when they will seize. -Don t feel embarrassed about the things you don t know. Some of the smartest people I know will be the first to tell you all about how much they don t know. In fact, I d be wary of those who say they have nothing left to learn. -Work in the OR at some point, it teaches you to be confident. Work with pediatrics at some point, it teaches you to be tender. -Be confident with what you know, be honest about what you don t. -Maybe you ll get registered, maybe you won t. Maybe you ll get published, maybe you won t. Maybe one day you will be speaking at a conference on something you are struggling to learn now, because you have become THE expert in it. -Be intentional. In your work, relationships, learning, managing... -Get involved in research. Don t ask to get paid and you will be surprised how many people will want the free labor. Seeing your name in print, being published, realize how much more valuable that is than money. -Network with your peers. You never know when it will come in handy And really, fellow neuro-nerds are the only people who will understand half of what you are talking about when you are excited by your first craniotomy. -Learn the system. -Where you work employs you but does not own your professional name. Always maintain your integrity as a professional, for your patients, with coworkers and peers, and especially for yourself. -Be deserving of the sacred trust that is the responsibility of patient care. Remember anywhere else, a seizure would result in 911 or a code blue being called; we see them all the time and try to make them happen. -Care...even if it s not your patient, or not a patient at all but a visitor who looks lost. Treat them how you would want your loved ones treated, because they are someone s loved one And one day you too will be a patient or a visitor somewhere and be scared or lost. -Don t limit yourself. You can achieve greatness. Know that the only person who can keep you from learning or achieving everything you want is yourself. -Remember that you stand upon the shoulders of giants. Those great clinicians who pioneered this field and know that, one day, someone will be standing on the shoulders of giants of which you might be one. -Accept certain inalienable truths; healthcare will change, new procedures and technology will come, some of your knowledge and experience will become outdated, and people will have their own opinions and experiences. Always take other people s opinions and experience with a grain of salt. But trust me on the head measuring... 27
28 Pediatrics and Neonatology By Shelley Gregory, R. EEG T. Something old, Something new, that s the theme for this edition. As I am sure most hospitals around the country have done or are doing is to standardize whatever lab processes they can. Seattle Children s Neurodiagnostics was recently asked to be part of a group of similar Seattle Children s Diagnostic Departments (Echo, Radiology, MRI/CT, etc.) and have a production dashboard. This is the term that administration gives for a board that reflects our daily inpatient/outpatient EEG schedule as well as EEG reader of the day and staff vacations that allows us to track patient and interpreter no shows or late arrivals. For the patient and interpreter no shows or late arrivals, we can see if there are any commonalities or trends to improve on in those areas. As an example, we have interpreters that show up late for an EEG and we have already applied the electrodes. We really don t need to have them start the introduction period as we already have used the telephone interpreter to communicate with the parent. We have different buttons that reflect if a patient is in isolation, if there is an alert on a parent, or an interpreter is ordered for the study. If cancellations occur during the day and the Neurology clinic has an add-on patient, it gives a great quick visual of where to put them in. We also have the Reader of the Day, Emergency Reader, and Telemetry Attending on it as well. This is helpful when you are going to do a portable in the NICU so you know whom to page for an emergent read. We have been using this for two weeks now and really haven t had any issues arise. For us it was a culmination of various lists and schedules all put into one place making it very visual for anyone that needs to know. It is definitely a step up from the former EEG schedule that was one single paper hidden under a coversheet so we were HIPPA compliant. It also gives us a chance to work with other departments in the hospital and exchange ideas. Polysomnography/Sleep Technologies By Kathy Johnson, R. EEG/EP T., RPSGT, FASET The theme of something old, something new really hit home with me right now. My sleep center recently got capital funds approved to replace our sleep study equipment and I found myself giving the purchase even more than usual thought and debate. In the distant past (I am giving away my age here), I considered things like how easy it was to switch out tubes in the EEG machine or fill the ink wells or load the paper. When we moved into the future with computer recordings, we had to think about different criteria, like sampling rates and monitor resolution. More recently, commercially available computerized systems have become pretty standardized with respect to the capabilities of the PC but we have had to think about how recordings can be accessed over the internet from a remote location and stored on a server or the cloud. So I finally gained a basic understanding of computers and felt comfortable that we had it all covered..and then here comes home sleep testing! Of course, home sleep testing (HST) did not appear overnight but many of us tried to ignore it for a long time. We knew it was out there but CMS previously did not recognize it as an appropriate diagnostic tool. Many labs did not think HST would have any effect on them some sleep specialists had no interest in home testing, declared that they would not use it, and would not read those studies so many of us believed that ended it for our labs. Well, we were wrong. As most of us now know, the insurance payers have become the primary decision maker in determination of the type of testing they will cover for their subscribers. This is where it becomes challenging. Many insurance companies are now using HST as a way to reduce the cost of sleep evaluations and they frequently utilize sleep management companies and/or require pre-authorization for sleep studies, which can be an arduous process. Some payers will only approve home sleep testing instead of in-lab tests. So, most sleep labs have incorporated HST into their procedures. If you have not, you probably will in the near future. Keep in mind, however, that many insurance companies use outside contractors to provide the home sleep testing rather than their local sleep centers/labs. So, what did I do with my recent equipment purchase? For my six bed sleep lab, we kept our old (but still functional) equipment for two beds. We will replace parts with the extra equipment from the other rooms as these devices die off. We replaced four beds with new equipment which is capable of performing not only PSG but also clinical EEG, including continuous EEG in ICUs. We also purchased two HST devices in hopes that we can capture some of this market for payers who do not have a contracted service. We also plan to use the HST equipment for inpatient studies when needed and hope to be able to use it for pre-operative screening studies in the near future. We believe this will give us flexibility to meet the foreseeable changes in the world of sleep medicine (until the next new thing comes along). 28
29 GOVERNMENTAL AFFAIRS AND ADVOCACY By Bradley A. Hix, Governmental & Grassroots Advocacy Manager Legislative Update: Currently the majority of State legislative bodies are in session, only Louisiana has yet to convene this year. A few State legislative bodies have adjourned for the year. The Governmental Advocacy Committee has been busy reviewing hundreds of bills and regulations and has identified a few that directly impact the neurodiagnostic profession. The bills we are tracking have been posted in our Neurodiagnostic Legislative & Regulatory Action Center website, accessible under the Advocacy tab of the ASET website. Details on the legislation and the actions we have taken to address our concerns are below: Indiana: House Bill 1383 would license polysomnographic technologists. The legislation would establish licensing requirements to practice polysomnography. The bill seeks to establish the polysomnography standards committee under the medical licensing board. It provides that, beginning July 1, 2015, a person must have a license to practice polysomnography or use certain titles. The bill has been referred to be considered for study by an Interim Study Committee and will not see further action this year. The Indiana Legislative Council will determine after the session has adjourned whether or not the topics related to the practice of polysomnography will be officially assigned to a study committee. We will monitor the study committee to make sure that Neurodiagnostic Technologists performing EEG studies are not inadvertently prohibited from practice if any legislation is proposed by the committee. Iowa: House Study Bill 59 and Senate Study Bill 1091 are identical study bills which would license polysomnographic technologists. The legislation would establish licensing requirements to practice polysomnography. The bills are proposing to add the practice of polysomnography to the respiratory therapy board and add members to that board who practice polysomnography. The bills provide that, beginning January 1, 2014, a person must have a license to practice polysomnography or use certain titles. The bills have been introduced at the request of the Iowa Sleep Society. We held a conference call with the President of the Iowa Sleep Society to discuss our concern that Neurodiagnostic Technologists performing EEG studies may be inadvertently prohibited from practice. In addition, we sent a letter requesting exemption language be included in the bill to clarify that regulations which might result from this legislation do not adversely affect the Neurodiagnostic Technologists ability to practice their profession. Both bills have been assigned to a subcommittee of their respective State Government Committee. At this time neither bill has been scheduled for a hearing. Nevada: Assembly Bill 73 is a bill which revises provisions governing chiropractic practice. Specifically, it would allow a chiropractor to use a needle for diagnostic purposes. If enacted, the bill would change the scope of chiropractic practice and allow them to perform diagnostic procedures, including presumably Needle Electromyography (EMG). We sent a letter to the committee requesting that language be added to the bill which would make sure that needle electromyography is only performed by practitioners who are specifically educated, trained, skilled, and licensed to perform the procedure. The bill has been referred to the Assembly Commerce and Labor Committee but has not been scheduled for a hearing. We worked with the American Association of Neuromuscular & Electrodiagnostic Medicine, the Physical Medicine and Rehabilitation Society of Nevada and the American Academy of Neurology to coordinate our opposition to the bill. The lobbying effort was successful as it has been reported that the bill will not see further action this year. New Hampshire: House Bill 326 is a bill which would require persons practicing polysomnography to be licensed by the board of respiratory care practitioners. Included in the legislation s definition of practice of polysomnography are (1) sleep staging, including surface electroencephalography, surface electrooculography, and surface submental electromyography, and (2) surface electromyography. We sent a letter requesting exemption language be included in the bill to clarify that regulations which might result from this legislation do not adversely affect the Neurodiagnostic Technologists ability to practice their profession. The bill has been referred to a summer study committee by the House Executive Departments and Administration Committee. We will monitor the study committee and make sure they are aware of our concerns with the bill. 29

30 GOVERNMENTAL AFFAIRS AND ADVOCACY continued Pennsylvania: SB 137 is the Speech-Language Pathologists and Audiologists Licensure Act. Areas of audiology practice proposed in the legislation include administration of electrophysiologic measures of neural function, including, but not limited to, sensory and motor-evoked potentials, tests of nerve conduction velocity and electromyography, plus preoperative and postoperative evaluation of neural function, neurophysiologic intraoperative monitoring of the central nervous system, spinal cord and cranial nerve function. SB 137 is the reintroduction of SB 1352 from last session. SB 1352 passed the Senate and was referred to the House Professional Licensure Committee but was not heard before the Pennsylvania General Assembly adjourned for the year. SB 137 has been referred to the Senate Consumer Protection and Professional Licensure Committee but has not been scheduled for a hearing at this time. ASET has requested that the language which would allow Audiologists to expand their scope of practice into Intraoperative Neuromonitoring be stricken from the bill. We are working with a coalition of interest groups to tighten up the language if Audiologists are ultimately allowed to perform IONM. Point of Contact Handbook: The ASET Point of Contact program is ASET s coordinated legislative grassroots effort. Its aim is to promote the best possible patient care while protecting the neurodiagnostic profession. To achieve this aim the program seeks to utilize and strengthen existing relationships between neurodiagnostic technologists and state legislators to make certain our message and point of view are heard and considered in the public policy arena. A handbook has been created to provide details on how to best develop personal relationships with elected officials. Development of these personal relationships is critical to making sure the voice of neurodiagnostic technology is heard by elected officials. When an issue that impacts neurodiagnostic technology is being debated in committee or on the floor of the House or the Senate, members of the Point of Contact Team are activated to communicate ASET s position to their legislators and ask them to support our position. Click here, or visit the Advocacy tab of the ASET website to download a copy of the handbook. 30

31 CONNECTIONS CORNER Interviews Connecting Members Technologist, Teacher, Advocate, Volunteer, ASET Member By Sarah Dolezilek, Marketing & Communications Manager Susan Denise Agostini, R. EEG/EP T., CLTM Incoming Manager for Epilepsy Monitoring Unit and Neurodiagnostic Manager Banner Good Samaritan Medical Center Phoenix, AZ Technologist, teacher, advocate, volunteer, passionate, mentee, mentor; all these things describe one, Susan Denise Agostini, ASET member. I first met Susan in Atlanta, GA at ASET s Annual Conference in 2011, where she was installed as a Board of Trustee. I remember reading her biography for the board nomination packet and hoping that she would get elected. You could tell just by reading it that she had a special interest in the neurodiagnostic field and would make a terrific board member. Since joining the ASET board in 2011 she has been on numerous committees and taskforces, never shying away from leading a committee or discussion on topics close to her heart. Currently, she serves as the Chair of the Standards and Practices Committee, Special Interest Section Leader for the Epilepsy Monitoring Interest Section, and on the Marketing Committee. My interview with Susan was done on March 27, 2013 via a phone conversation. My intention with this interview and the ones to follow in this new section of the newsletter is for you to learn more about the amazing individuals who make up the neurodiagnostic profession, who live and breathe it every day. The profession would not be where it is today without these remarkable, hard-working, intelligent believers. ASET: How did you first learn of the field of neurodiagnostics and what drew you to it? Susan: My mother passed away from brain cancer in 1984, from then I began developing a very strong interest in the brain. In 1988 I moved to Tampa, Florida, found a job at the University of South Florida Medical Clinic, which is where I met an EEG technologist, Lydia, who became my mentor, and role model. She was very passionate about EEG and the brain, and I wanted to be just like her. Lydia was willing to share her knowledge with me and she provided me with the information to pursue a career in Neurodiagnostics. Now I am a passionate technologist, just like her. I would be so happy to see Lydia again. I recently met the physician who worked with her at a meeting. She had the same fondness for Lydia. I think Lydia saw something in me that she thought would be good for the field. She would leave little notes of encouragement on my desk saying I was right for this field, and she was totally right, this is my field. ASET: Tell me how you first got involved with ASET Susan: Lydia was an ASET member and she always said ASET takes care of us. She showed me that it was important to be involved. I joined as a student member in 1989, then after school, transitioned into an Active member and eventually became an Institutional member. When I ran for the Board of Trustees I upgraded to the Active class of membership again. I encourage my students to join ASET. When I was a tech on my own, just starting out, ASET became my home, held my hand and was my virtual educator. 31 Susan Agostini (left) with her mentor Lydia (1990)

32 CONNECTIONS CORNER continued ASET: What was your first impression of the Society? Susan: Very good experience with ASET. I graduated from the EEG program in Tampa and went to my home island of Puerto Rico to share my knowledge. I was very scared; I needed the emotional and educational support of ASET, and their continuing education. ASET held my hand through all that. I believe in ASET, I believe in the mission, I believe that they hold true to their mission. It has been a great learning experience. ASET: Looking back at where you were when you started this journey, where did you think it was going to lead you? Susan: I never thought I would be in the position to influence others in the field of neurodiagnostics. My mother s favorite quote is you find a job that you love and you will never work a day in your life. That imprinted in my brain, I have been so lucky and blessed to find a job that I love. I share this now with my own daughter and my students. I never regret the choice I made back in 1989 when I decided to become a neurodiagnostic technologist. I believe things happen for a reason and losing my mother to brain cancer was tough, but it pushed me to where I am today. It made me be a better person and a better care provider for my patients. Susan Agostini (circa ) ASET: What accomplishments are you most proud of in your professional life? Susan: The opportunity that this whole profession has given me to give back, share my knowledge and most importantly, change people s lives. Our patients depend on us to help give them a better quality of life. That fact that we, as technologists, can change people s lives in the ways that we do, makes me most proud. ASET: What do you find most challenging about the Neurodiagnostic field? Susan: A couple of things. My definition of challenge is the opportunity to prove what seems impossible, possible. One of the challenges I see is the misconceptions of epilepsy and increasing awareness for epilepsy. [Susan is an advocate for Epilepsy in her community and with the Epilepsy Foundation]. Also, there are not enough We are not just EEG Technologists anymore, we are Neurodiagnostic Technologists. schools in the country to train technologists. As we go forward, we need more formally trained technologists out there. ASET is an amazing resource for this. ASET: What do you think will change in neurodiagnostics over the next five years? Susan: Changes in healthcare and changes overall. I think that all the new Neurodiagnostic Technologists and seasoned techs need to buckle up, continue our education, broaden our knowledge, learn all the modalities, etc I think the degree requirements will change, and I would like to see licensure. There are lots of changes to come. We have come a long way, a long way. We are not just EEG Technologists anymore, we are Neurodiagnostic Technologists. ASET: What is it like to be a volunteer for ASET? Susan: Giving back to the Neurodiagnostic Community. ASET gave me so much when I was a student and still gives me so much and see and feel like I am giving back. Volunteering is also my way of being heard. If you want to make a difference, there is only one way to do that and there is a place for you, there is a place for everyone. Volunteering is an amazing opportunity to contribute to the future of the field, our field. 32
ASETnews Summer 2013 IN THIS ISSUE BRIEFINGS FROM THE BOARD TECHNICAL TIPS INTEREST SECTIONS GOVERNMENTAL AFFAIRS AND ADVOCACY CONNECTIONS CORNER
 IN THIS ISSUE BRIEFINGS FROM THE BOARD TECHNICAL TIPS INTEREST SECTIONS GOVERNMENTAL AFFAIRS AND ADVOCACY CONNECTIONS CORNER NEW MEMBERS 3 6 8 24 25 28 ASETnews Summer 2013 SUMMER 2013 VOLUME 37, NUMBER
IN THIS ISSUE BRIEFINGS FROM THE BOARD TECHNICAL TIPS INTEREST SECTIONS GOVERNMENTAL AFFAIRS AND ADVOCACY CONNECTIONS CORNER NEW MEMBERS 3 6 8 24 25 28 ASETnews Summer 2013 SUMMER 2013 VOLUME 37, NUMBER
Strong Medicine Interview with Cheryl Webber, 20 June ILACQUA: This is Joan Ilacqua and today is June 20th, 2014.
 Strong Medicine Interview with Cheryl Webber, 20 June 2014 ILACQUA: This is Joan Ilacqua and today is June 20th, 2014. I m here with Cheryl Weber at Tufts Medical Center. We re going to record an interview
Strong Medicine Interview with Cheryl Webber, 20 June 2014 ILACQUA: This is Joan Ilacqua and today is June 20th, 2014. I m here with Cheryl Weber at Tufts Medical Center. We re going to record an interview
Marriott Newport Beach Hotel & Spa 900 Newport Center Drive Newport Beach California
 2018 ANNUAL MEETING & COURSES Friday - Sunday April 27-29, 2018 Marriott Newport Beach Hotel & Spa 900 Newport Center Drive Newport Beach California With Special Board Prep Courses By Rebecca Clark-Bash,
2018 ANNUAL MEETING & COURSES Friday - Sunday April 27-29, 2018 Marriott Newport Beach Hotel & Spa 900 Newport Center Drive Newport Beach California With Special Board Prep Courses By Rebecca Clark-Bash,
Analytics in Action. Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY
 Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
Analytics in Action Using Data to Improve Care and Reduce Costs CUSTOM MEDIA SPONSORED BY Imagine an 82-year-old gentleman walks in to your emergency department. He presents with a productive cough and
HAWAII 2015 Mid-Year Meeting & Courses Advanced EEG & cceeg Bedside Intraoperative Neurophysiologic Monitoring
 HAWAII 2015 Mid-Year Meeting & Courses Advanced EEG & cceeg Bedside Intraoperative Neurophysiologic Monitoring 37 Saturday and Sunday Oct 31 & Nov 1, 2015 Wailea Beach Marriott Resort & Spa 3700 Wailea
HAWAII 2015 Mid-Year Meeting & Courses Advanced EEG & cceeg Bedside Intraoperative Neurophysiologic Monitoring 37 Saturday and Sunday Oct 31 & Nov 1, 2015 Wailea Beach Marriott Resort & Spa 3700 Wailea
Long Term Monitoring EEG. Boy Version
 Long Term Monitoring EEG Boy Version I am getting ready for my visit to Boston Children's Hospital. When I get there with my parent, we will walk through the lobby, take a left up the stairs, and down
Long Term Monitoring EEG Boy Version I am getting ready for my visit to Boston Children's Hospital. When I get there with my parent, we will walk through the lobby, take a left up the stairs, and down
Peabody Cardiology Visit. September 2016
 Peabody Cardiology Visit September 2016 I am going to Boston Children s at Peabody to visit a heart Doctor. I will come into the lobby. I can take the elevators or the stairs to the 2 nd floor. I will
Peabody Cardiology Visit September 2016 I am going to Boston Children s at Peabody to visit a heart Doctor. I will come into the lobby. I can take the elevators or the stairs to the 2 nd floor. I will
NURS 6051: Transforming Nursing and Healthcare through Information Technology Electronic Health Records Program Transcript
 NURS 6051: Transforming Nursing and Healthcare through Information Technology Electronic Health Records Program Transcript [MUSIC PLAYING] NARRATOR: Because patient data, research evidence, and best practices
NURS 6051: Transforming Nursing and Healthcare through Information Technology Electronic Health Records Program Transcript [MUSIC PLAYING] NARRATOR: Because patient data, research evidence, and best practices
The MetLife Market Survey of Nursing Home & Home Care Costs September 2004
 The MetLife Market Survey of Nursing Home & Home Care Costs September 2004 Mature Market Institute The MetLife Mature Market Institute is the company s information and policy resource center on issues
The MetLife Market Survey of Nursing Home & Home Care Costs September 2004 Mature Market Institute The MetLife Mature Market Institute is the company s information and policy resource center on issues
Blake 13. Lori Pugsley RN MEd Massachusetts General Hospital March 6, 2012
 Blake 13 Lori Pugsley RN MEd Massachusetts General Hospital March 6, 2012 1 Newborn Family Unit Thank you for allowing me to show you all what we will be doing on Blake 13 for Innovation. I will share
Blake 13 Lori Pugsley RN MEd Massachusetts General Hospital March 6, 2012 1 Newborn Family Unit Thank you for allowing me to show you all what we will be doing on Blake 13 for Innovation. I will share
A Journal of Rhetoric in Society. Interview: Transplant Deliberations and Patient Advocacy. Staff
 Present Tense A Journal of Rhetoric in Society Interview: Transplant Deliberations and Patient Advocacy Staff Present Tense, Vol. 2, Issue 2, 2012. www.presenttensejournal.org editors@presenttensejournal.org
Present Tense A Journal of Rhetoric in Society Interview: Transplant Deliberations and Patient Advocacy Staff Present Tense, Vol. 2, Issue 2, 2012. www.presenttensejournal.org editors@presenttensejournal.org
Patient Visit Tracking Toolkit
 Dramatic Performance Improvement Patient Visit Tracking Toolkit A Bird s Eye View of Patient Experience Summary Instructions for Tracking Patient Visits. In redesign, it s imperative to truly understand
Dramatic Performance Improvement Patient Visit Tracking Toolkit A Bird s Eye View of Patient Experience Summary Instructions for Tracking Patient Visits. In redesign, it s imperative to truly understand
Hospital Admission: How to Plan and What to Expect During the Stay
 Family Caregiver Guide Hospital Admission: How to Plan and What to Expect During the Stay Admission to the hospital can happen in various ways. You family member may be treated in the Emergency Room (ER)
Family Caregiver Guide Hospital Admission: How to Plan and What to Expect During the Stay Admission to the hospital can happen in various ways. You family member may be treated in the Emergency Room (ER)
A Guide to Your Child s Hospital Stay
 A Guide to Your Child s Hospital Stay Thank you for choosing Blank Children s Hospital for your child s care. Our mission is to provide the Best Outcome, Every Patient, Every Time. As a parent or caregiver
A Guide to Your Child s Hospital Stay Thank you for choosing Blank Children s Hospital for your child s care. Our mission is to provide the Best Outcome, Every Patient, Every Time. As a parent or caregiver
National Provider Identifier (NPI)
") National Provider Identifier (NPI) Importance to the Athletic Training Profession? By Clark E. Simpson, MBA, MED, LAT, ATC National Manager, Strategic Business Development National Athletic Trainers Association
National Provider Identifier (NPI) Importance to the Athletic Training Profession? By Clark E. Simpson, MBA, MED, LAT, ATC National Manager, Strategic Business Development National Athletic Trainers Association
MAGNAGHI, M. RUSSELL (RMM): Okay Dr. Brish, my first question for everybody is: what is your birthday?
: Okay Dr. Brish, my first question for everybody is: what is your birthday?") 1 INTERVIEW WITH DR. ADAM BRISH MARQUETTE, MI OCTOBER 16, 2009 Subject: Marquette General Hospital MAGNAGHI, M. RUSSELL (RMM): Okay Dr. Brish, my first question for everybody is: what is your birthday?
1 INTERVIEW WITH DR. ADAM BRISH MARQUETTE, MI OCTOBER 16, 2009 Subject: Marquette General Hospital MAGNAGHI, M. RUSSELL (RMM): Okay Dr. Brish, my first question for everybody is: what is your birthday?
The Most Common Billing Mistakes for PA Services
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/the-most-common-billing-mistakes-for-paservices/3518/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/the-most-common-billing-mistakes-for-paservices/3518/
FUNDRAISING GUIDE. Fundraising to fight MS! Mailing Address. . Website. Bike the US for MS Fundraising Guide 2018
 FUNDRAISING GUIDE Bike the US for MS Fundraising Guide 2018 Mailing Address You and your donors can mail check donations to: Bike the US for MS P.O. Box 10001 Blacksburg, VA 24062 Don t forget to have
FUNDRAISING GUIDE Bike the US for MS Fundraising Guide 2018 Mailing Address You and your donors can mail check donations to: Bike the US for MS P.O. Box 10001 Blacksburg, VA 24062 Don t forget to have
Community Hospital Uses Mobile App to Improve Communications, Accelerate Throughput
 Community Hospital Uses Mobile App to Improve Communications, Accelerate Throughput April 1, 2018 New tool allows EMS providers to relay critical information about incoming patients to the ED EXECUTIVE
Community Hospital Uses Mobile App to Improve Communications, Accelerate Throughput April 1, 2018 New tool allows EMS providers to relay critical information about incoming patients to the ED EXECUTIVE
Transitioning to ICD-10: An Action Plan for Practices
 Transitioning to ICD-10: An Action Plan for Practices By Nancy M Enos, FACMPE, CPMA, CPC-I, CEMC 1 viterahealthcare.com/icd10 The Four T s of Transition to ICD-10: Timing, Training, Testing and Technology
Transitioning to ICD-10: An Action Plan for Practices By Nancy M Enos, FACMPE, CPMA, CPC-I, CEMC 1 viterahealthcare.com/icd10 The Four T s of Transition to ICD-10: Timing, Training, Testing and Technology
OBQI for Improvement in Pain Interfering with Activity
 CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
CASE SUMMARY OBQI for Improvement in Pain Interfering with Activity Following is the story of one home health agency that used the outcome-based quality improvement (OBQI) process to enhance outcomes for
Case managers are consummate team players, working with. IssueBrief
 IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
IssueBrief May 2016 Making hospital care management an organizational priority: Dartmouth-Hitchcock deploys case managers so patients are at the right place at the right time Case managers are consummate
Managing Population Health in Northeast Georgia: One Medical Group's Experience
 September 21, 2013 Managing Population Health in Northeast Georgia: One Medical Group's Experience By Mark Hagland Northeast Georgia Physicians Group (NGPG), based in Gainesville, Georgia, a suburb of
September 21, 2013 Managing Population Health in Northeast Georgia: One Medical Group's Experience By Mark Hagland Northeast Georgia Physicians Group (NGPG), based in Gainesville, Georgia, a suburb of
Drivers of HCAHPS Performance from the Front Lines of Healthcare
 Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Drivers of HCAHPS Performance from the Front Lines of Healthcare White Paper by Baptist Leadership Group 2011 Organizations that are successful with the HCAHPS survey are highly focused on engaging their
Ambulatory Emergency Care The Logical Way to Go
 Ambulatory Emergency Care The Logical Way to Go Ambulatory Emergency Care The Logical Way to Go The Queens Medical Centre (QMC) is part of the Nottingham University Hospitals NHS Trust, one of the largest
Ambulatory Emergency Care The Logical Way to Go Ambulatory Emergency Care The Logical Way to Go The Queens Medical Centre (QMC) is part of the Nottingham University Hospitals NHS Trust, one of the largest
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty
 Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Scenario Planning: Optimizing your inpatient capacity glide path in an age of uncertainty Examining a range of
Auckland Pediatric Surgery Journal
 Auckland Pediatric Surgery Journal Journal 2/9/2017: I ve been at the hospital for over a week now and continue to be surprised by the familiarity of it all. The day to day workings of the hospital are
Auckland Pediatric Surgery Journal Journal 2/9/2017: I ve been at the hospital for over a week now and continue to be surprised by the familiarity of it all. The day to day workings of the hospital are
STANDARDIZED PROCEDURE BONE MARROW ASPIRATION (Adult,Peds)
") I. Definition: This protocol covers the task of bone marrow aspiration by an Advanced Health Practitioner. The purpose of this standardized procedure is to allow the Advanced Health Practitioner to safely
I. Definition: This protocol covers the task of bone marrow aspiration by an Advanced Health Practitioner. The purpose of this standardized procedure is to allow the Advanced Health Practitioner to safely
Toward the Electronic Patient Record:
 June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
June 2007 Toward the Electronic Denise Henderson Director, Consulting Services MedSynergies, Inc. Toward the Electronic The TEPR (Toward the Electronic Patient Record) conference held by the Medical Records
ACG GI Practice Toolbox
 ACG GI Practice Toolbox Setting Up an Ambulatory Infusion Center in Your Practice AUTHOR: David L. Limauro, MD, University of Pittsburgh Medical Center, Pittsburgh, PA INTRODUCTION: Private practices in
ACG GI Practice Toolbox Setting Up an Ambulatory Infusion Center in Your Practice AUTHOR: David L. Limauro, MD, University of Pittsburgh Medical Center, Pittsburgh, PA INTRODUCTION: Private practices in
m/training-modules.html.
 A Publication of the Quillen EHR Team August 2013 New Resident Training Training Techniques The Green Team took a slightly different approach to new resident training this year one which we hope will give
A Publication of the Quillen EHR Team August 2013 New Resident Training Training Techniques The Green Team took a slightly different approach to new resident training this year one which we hope will give
The role of pharmacy in clinical trials it s not just counting pills. Michelle Donnison, Senior Pharmacy Technician, York Hospital
 The role of pharmacy in clinical trials it s not just counting pills Michelle Donnison, Senior Pharmacy Technician, York Hospital I am currently employed as a Senior Pharmacy Technician working at York
The role of pharmacy in clinical trials it s not just counting pills Michelle Donnison, Senior Pharmacy Technician, York Hospital I am currently employed as a Senior Pharmacy Technician working at York
WOW! Kathy s. Words of Wisdom. The Compliance Corner. In this issue: December 2013 Theme: Collections. Kathy s Opening Message. The Compliance Corner
 Kathy s WOW! Words of Wisdom December 2013 Theme: Collections In this issue: Kathy s Opening Message The Compliance Corner KMC University s Q&As Upcoming AnswerCall and Live Webinar Information ICD-10
Kathy s WOW! Words of Wisdom December 2013 Theme: Collections In this issue: Kathy s Opening Message The Compliance Corner KMC University s Q&As Upcoming AnswerCall and Live Webinar Information ICD-10
4. Which of the following support staff is typically not found in an outpatient physician practice?
 CPPM Chapter 1 Intro to Health Care Business Processes and Workflow 1. What percentage of communication occurs through body language? a. 55 b. 35 c. 15 d. 85 2. The physician who owns the practice approaches
CPPM Chapter 1 Intro to Health Care Business Processes and Workflow 1. What percentage of communication occurs through body language? a. 55 b. 35 c. 15 d. 85 2. The physician who owns the practice approaches
10 Things to Consider When Choosing a Home Care Agency
 10 Things to Consider When Choosing a Home Care Agency Introduction Diminishing health and frailty are not popular topics of conversation for obvious reasons. But then these are not areas of life we can
10 Things to Consider When Choosing a Home Care Agency Introduction Diminishing health and frailty are not popular topics of conversation for obvious reasons. But then these are not areas of life we can
Activity 3: TRANSFER TO A WHEELCHAIR Future tense
 Contextualized Grammar I-BEST SUN Path Curriculum Unit for Nursing Assistant with ESL Support - Page 1 of 10 Activity 3: TRANSFER TO A WHEELCHAIR Future tense Learning Goal(s) Demonstrate the indirect
Contextualized Grammar I-BEST SUN Path Curriculum Unit for Nursing Assistant with ESL Support - Page 1 of 10 Activity 3: TRANSFER TO A WHEELCHAIR Future tense Learning Goal(s) Demonstrate the indirect
10 Things To Know About
 10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
10 Things To Know About Nurse Call 100% Nurse Approved 10 Things to Know About Nurse Call in 2016 Nurse call systems have evolved. Today s nurse call systems provide front-line nurses with critical communications
North East LHIN HELPING YOU HEAL. Your Guide to Wound Care. Pilonidal Cysts
 North East LHIN HELPING YOU HEAL Your Guide to Wound Care Pilonidal Cysts 310-2222 www.nelhin.on.ca WOUND SELF MANAGEMENT PROGRAM THE PROGRAM This booklet will help you: Manage your wound at home Improve
North East LHIN HELPING YOU HEAL Your Guide to Wound Care Pilonidal Cysts 310-2222 www.nelhin.on.ca WOUND SELF MANAGEMENT PROGRAM THE PROGRAM This booklet will help you: Manage your wound at home Improve
How to Conduct a Medication Administration Observation
 How to Conduct a Medication Administration Observation Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow and I am the Medical Director for the Office of Developmental Programs.
How to Conduct a Medication Administration Observation Transcript Title Slide (no narration) Welcome Hello. My name is Jill Morrow and I am the Medical Director for the Office of Developmental Programs.
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
10: Beyond the caring role
 10: Beyond the caring role This section provides support if you no longer need to give the same level of care to a person with MND or your caring role has come to an end. The following information is a
10: Beyond the caring role This section provides support if you no longer need to give the same level of care to a person with MND or your caring role has come to an end. The following information is a
Hillside Medical Office
 EHR Case Study Hillside Medical Office Hillside Medical Partners with Pulse to Quickly Achieve Meaningful Use pulseinc.com Pulse Complete EHR 8 board-certified physicians. 40 employees. Over 65 years of
EHR Case Study Hillside Medical Office Hillside Medical Partners with Pulse to Quickly Achieve Meaningful Use pulseinc.com Pulse Complete EHR 8 board-certified physicians. 40 employees. Over 65 years of
Presented to you by The Cooperative of American Physicians, Inc.
 ICD-10 Action Guide for Medical Practices PAGE 1 Presented to you by The Cooperative of American Physicians, Inc. Table of Contents Introduction... 3 What Is Changing and Why?... 4 What Are the Main Provisions
ICD-10 Action Guide for Medical Practices PAGE 1 Presented to you by The Cooperative of American Physicians, Inc. Table of Contents Introduction... 3 What Is Changing and Why?... 4 What Are the Main Provisions
Neurological Technicians. in Southern California
 Neurological Technicians in Southern California October 2016 Prepared by Center of Excellence for Labor Market Research San Diego & Imperial Counties Region Job in Southern California (Los Angeles, Orange,
Neurological Technicians in Southern California October 2016 Prepared by Center of Excellence for Labor Market Research San Diego & Imperial Counties Region Job in Southern California (Los Angeles, Orange,
Implementation Issues of the Physician Practice. for ICD-10-CM
 Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
Implementation Issues of the Physician Practice for ICD-10-CM What are ICD-10-CM and the Version 5010? The Centers for Medicare & Medicaid Services (CMS) is driving the industry to upgrade core HIPAA transactions
Internships - Student Assessment of Clinical Experiences. Facility: Health South in Tempe. Clinical Instructors: Dan Angulo PT
 Internships - Student Assessment of Clinical Experiences Student Name: Aja Evertsen Facility: Health South in Tempe Clinical Instructors: Dan Angulo PT Please complete this form and provide a copy to your
Internships - Student Assessment of Clinical Experiences Student Name: Aja Evertsen Facility: Health South in Tempe Clinical Instructors: Dan Angulo PT Please complete this form and provide a copy to your
Certification Examination in Neurophysiologic Intraoperative Monitoring (CNIM) Application Form. Telephone Number: Address:
 Application Form. Telephone Number: Address:") Certification Examination in Neurophysiologic Intraoperative Monitoring (CNIM) Application Form Please read the directions in the HANDBOOK for CANDIDATES carefully before completing this Application. Name
Certification Examination in Neurophysiologic Intraoperative Monitoring (CNIM) Application Form Please read the directions in the HANDBOOK for CANDIDATES carefully before completing this Application. Name
The CVICU or Cardiovascular Intensive Care Unit
 The CVICU or Cardiovascular Intensive Care Unit #1216 (2012) The Emily Center, Phoenix Children s Hospital 1 2 (2012) The Emily Center, Phoenix Children s Hospital The CVICU or Cardiovascular Intensive
The CVICU or Cardiovascular Intensive Care Unit #1216 (2012) The Emily Center, Phoenix Children s Hospital 1 2 (2012) The Emily Center, Phoenix Children s Hospital The CVICU or Cardiovascular Intensive
Transitional Care Management Services: New Codes, New Requirements
 Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Transitional Care Management Services: New Codes, New Requirements hospital 99496 99495 99496 family practice o n Jan. 1, 2013, the much anticipated transitional care management (TCM) Two new codes will
Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the
 once again has extended the") Ambulatory Surgery Centers Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the deadline to begin using
Ambulatory Surgery Centers Sharpen coding skills and reimbursement strategies during ICD-10 delay The Centers for Medicare & Medicaid Services (CMS) once again has extended the deadline to begin using
Elizabeth Woodcock, MBA, FACMPE, CPC
 Elizabeth Woodcock, MBA, FACMPE, CPC Presentation Topics The Patient-Centered Practice: Creating the Practice of the Future Today Optimizing the workflow of your medical practice operations is difficult
Elizabeth Woodcock, MBA, FACMPE, CPC Presentation Topics The Patient-Centered Practice: Creating the Practice of the Future Today Optimizing the workflow of your medical practice operations is difficult
What is ICD10 and how will it affect me?
 What is ICD10 and how will it affect me? Vikki Lindemuth Blue Cross and Blue Shield of Kansas Statewide Specialty Provider Representative Nancy Ratzlaff Billing Director - LifeTeam Critical Care Ambulance
What is ICD10 and how will it affect me? Vikki Lindemuth Blue Cross and Blue Shield of Kansas Statewide Specialty Provider Representative Nancy Ratzlaff Billing Director - LifeTeam Critical Care Ambulance
Read Valuable Advice For Best Results Of Any Cosmetic Procedure You Want.
 SAM SPERON, M.D., F.A.C.S. Plastic & Reconstructive Surgeon MEMBER M OF THE AMERICAN A S SOCIETY FOR AESTHETIC PLASTIC SURGERY AMERICAN SOCIETY OF PLASTIC SURGEONS Learn 7 Critical Questions To Ask Any
SAM SPERON, M.D., F.A.C.S. Plastic & Reconstructive Surgeon MEMBER M OF THE AMERICAN A S SOCIETY FOR AESTHETIC PLASTIC SURGERY AMERICAN SOCIETY OF PLASTIC SURGEONS Learn 7 Critical Questions To Ask Any
Care on a hospital ward
 Care on a hospital ward People with dementia may be admitted to general hospital wards either as part of a planned procedure such as a cataract operation or following an accident such as a fall. Carers
Care on a hospital ward People with dementia may be admitted to general hospital wards either as part of a planned procedure such as a cataract operation or following an accident such as a fall. Carers
Prescription for Healthy Communities: CARRYING OUT SUCCESSFUL MEDICATION MANAGEMENT SERVICES IN COMMUNITY PHARMACIES
 Prescription for Healthy Communities: CARRYING OUT SUCCESSFUL MEDICATION MANAGEMENT SERVICES IN COMMUNITY PHARMACIES Deborah Pestka, PharmD Caitlin Frail, PharmD, MS, BCACP Laura Palombi, PharmD, MPH,
Prescription for Healthy Communities: CARRYING OUT SUCCESSFUL MEDICATION MANAGEMENT SERVICES IN COMMUNITY PHARMACIES Deborah Pestka, PharmD Caitlin Frail, PharmD, MS, BCACP Laura Palombi, PharmD, MPH,
MEASURING YOUR BLOOD PRESSURE AT HOME
 MEASURING YOUR BLOOD PRESSURE AT HOME Helping you to lower your blood pressure BLOOD PRESSURE UK About this booklet This is one of a series of booklets produced by Blood Pressure UK, to help people with
MEASURING YOUR BLOOD PRESSURE AT HOME Helping you to lower your blood pressure BLOOD PRESSURE UK About this booklet This is one of a series of booklets produced by Blood Pressure UK, to help people with
A1 Home Care. A1 Home Care Ltd. Overall rating for this service. Inspection report. Ratings. Good
 A1 Home Care Ltd A1 Home Care Inspection report Units 16-19 Robjohns House, Navigation Road Chelmsford Essex CM2 6ND Date of inspection visit: 06 April 2017 Date of publication: 08 June 2017 Tel: 01245354774
A1 Home Care Ltd A1 Home Care Inspection report Units 16-19 Robjohns House, Navigation Road Chelmsford Essex CM2 6ND Date of inspection visit: 06 April 2017 Date of publication: 08 June 2017 Tel: 01245354774
snapshot SATISFACTION Trust Your Staff But Check Validation The Key to Hardwiring Change is the problem the tactic? - or is it the execution?
 SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
SATISFACTION snapshot news, views & ideas from the leader in healthcare satisfaction measurement The Satisfaction Snapshot is a monthly electronic bulletin freely available to all those involved or interested
ICD-10: The Good, Bad and Ugly
 1 ICD-10: The Good, Bad and Ugly Presented by Ken Bradley Vice President of Strategic Planning and Regulatory Compliance Navicure 2 Navicure Learn more or request a demo at www.navicure.com 3 Follow Navicure
1 ICD-10: The Good, Bad and Ugly Presented by Ken Bradley Vice President of Strategic Planning and Regulatory Compliance Navicure 2 Navicure Learn more or request a demo at www.navicure.com 3 Follow Navicure
A National Role Delineation Study of the Pediatric Emergency Nurse. Executive Summary
 A National Role Delineation Study of the Pediatric Emergency Nurse Executive Summary Conducted for the Board of Certification for Emergency Nursing Prepared by Lawrence J. Fabrey, PhD, Sr. Vice President,
A National Role Delineation Study of the Pediatric Emergency Nurse Executive Summary Conducted for the Board of Certification for Emergency Nursing Prepared by Lawrence J. Fabrey, PhD, Sr. Vice President,
Advanced Nurse Practitioner Supervision Policy
 Advanced Nurse Practitioner Supervision Policy Supervision requirements for nurse practitioners (NP) fall into two basic categories: Full practice and collaborative practice, which requires a Collaborative
Advanced Nurse Practitioner Supervision Policy Supervision requirements for nurse practitioners (NP) fall into two basic categories: Full practice and collaborative practice, which requires a Collaborative
North East LHIN HELPING YOU HEAL. Your Guide to Wound Care. Surgical Wounds
 North East LHIN HELPING YOU HEAL Your Guide to Wound Care Surgical Wounds 310-2222 www.nelhin.on.ca WOUND SELF MANAGEMENT PROGRAM THE PROGRAM This booklet will help you: Manage your wound at home Improve
North East LHIN HELPING YOU HEAL Your Guide to Wound Care Surgical Wounds 310-2222 www.nelhin.on.ca WOUND SELF MANAGEMENT PROGRAM THE PROGRAM This booklet will help you: Manage your wound at home Improve
What to Expect on. Your Surgery Day. at Seattle Children s Bellevue Clinic and Surgery Center
 What to Expect on Your Surgery Day at Seattle Children s Bellevue Clinic and Surgery Center A note for parents/caregivers: This book was written for patients of different ages. Patients also have different
What to Expect on Your Surgery Day at Seattle Children s Bellevue Clinic and Surgery Center A note for parents/caregivers: This book was written for patients of different ages. Patients also have different
GUIDELINES FOR PROVIDING PERSONAL CARE: TEACHING PLAN
 GUIDELINES FOR PROVIDING PERSONAL CARE: TEACHING PLAN Lesson overview Time: One hour This session covers the essential elements of providing or assisting with a resident s personal care. Facility policies
GUIDELINES FOR PROVIDING PERSONAL CARE: TEACHING PLAN Lesson overview Time: One hour This session covers the essential elements of providing or assisting with a resident s personal care. Facility policies
Heart Homecare Ltd. Heart Homecare Ltd. Overall rating for this service. Inspection report. Ratings. Good
 Heart Homecare Ltd Heart Homecare Ltd Inspection report Unit G2 Wises Oast Business Centre Wises Lane Sittingbourne Kent ME9 8LR Date of inspection visit: 07 March 2017 Date of publication: 30 March 2017
Heart Homecare Ltd Heart Homecare Ltd Inspection report Unit G2 Wises Oast Business Centre Wises Lane Sittingbourne Kent ME9 8LR Date of inspection visit: 07 March 2017 Date of publication: 30 March 2017
GUIDELINES FOR PROVIDING PERSONAL CARE: TEACHING PLAN
 GUIDELINES FOR PROVIDING PERSONAL CARE: TEACHING PLAN Lesson overview Time: One hour This session covers the essential elements of providing or assisting with a resident s personal care. Facility policies
GUIDELINES FOR PROVIDING PERSONAL CARE: TEACHING PLAN Lesson overview Time: One hour This session covers the essential elements of providing or assisting with a resident s personal care. Facility policies
Martin Nesbitt Tape 36. Q: You ve been NCNA s legislator of the year 3 times?
 Martin Nesbitt Tape 36 Q: You ve been NCNA s legislator of the year 3 times? A: Well, it kinda fell upon me. I was named the chair of the study commission back in the 80s when we had the first nursing
Martin Nesbitt Tape 36 Q: You ve been NCNA s legislator of the year 3 times? A: Well, it kinda fell upon me. I was named the chair of the study commission back in the 80s when we had the first nursing
Bright Spots in primary care
 Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
Bright Spots in primary care A High- Performing Teaching Practice: Site Visit to Oregon Health & Science University s (OHSU) Family Medicine Clinic at Gabriel Park General information Tom Bodenheimer MD
HSC 360b Move and position the individual
 CASE STUDY: Planning a move Shireen is the care worker for Mrs Gold, who is 80. Shireen needs to move Mrs Gold from a bed into a chair. Mrs Gold is only able to assist a little as she has very painful
CASE STUDY: Planning a move Shireen is the care worker for Mrs Gold, who is 80. Shireen needs to move Mrs Gold from a bed into a chair. Mrs Gold is only able to assist a little as she has very painful
Quality Insights Quality Innovation Network August Care Coordination Open Office Hours Call August 27, 2015
 Quality Insights Quality Innovation Network August Care Coordination Open Office Hours Call August 27, 2015 Well, good afternoon everyone, and thanks so much for joining us. I would like to welcome you
Quality Insights Quality Innovation Network August Care Coordination Open Office Hours Call August 27, 2015 Well, good afternoon everyone, and thanks so much for joining us. I would like to welcome you
Installation Planning Guide
 Installation Planning Guide Master Checklist Installation Planning After Your Installation as Senior Councilor Confirm the date of the next installation with the Advisory Council Reserve the Masonic Hall
Installation Planning Guide Master Checklist Installation Planning After Your Installation as Senior Councilor Confirm the date of the next installation with the Advisory Council Reserve the Masonic Hall
Maidstone Home Care Limited
 Maidstone Home Care Limited Maidstone Home Care Limited Inspection report Home Care House 61-63 Rochester Road Aylesford Kent ME20 7BS Date of inspection visit: 19 July 2016 Date of publication: 15 August
Maidstone Home Care Limited Maidstone Home Care Limited Inspection report Home Care House 61-63 Rochester Road Aylesford Kent ME20 7BS Date of inspection visit: 19 July 2016 Date of publication: 15 August
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012
 HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
HMSA Physical & Occupational Therapy Utilization Management Guide Published 10/17/2012 An Independent Licensee of the Blue Cross and Blue Shield Association Landmark's provider materials are available
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS)
") PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
PROCESS FOR HANDLING ELASTOMERIC PAIN RELIEF BALLS (ON-Q PAINBUSTER AND OTHERS) REQUIRES SAFETY IMPROVEMENTS From the July 16, 2009 issue Problem: In our May 21, 2009, newsletter we noted an association
HOW TO PROTECT YOUR ORGANIZATION WITH SANCTION SCREENING WEBINAR QUESTION AND ANSWER SESSION. Q: Is it necessary to search SAM and LEIE or only LEIE?
 HOW TO PROTECT YOUR ORGANIZATION WITH SANCTION SCREENING WEBINAR QUESTION AND ANSWER SESSION Q: Is it necessary to search SAM and LEIE or only LEIE? A: Yes. As you are aware of, OIG LEIE must be screened
HOW TO PROTECT YOUR ORGANIZATION WITH SANCTION SCREENING WEBINAR QUESTION AND ANSWER SESSION Q: Is it necessary to search SAM and LEIE or only LEIE? A: Yes. As you are aware of, OIG LEIE must be screened
Acceptance Speech. Writing Sample - Write. By K Turner
 Acceptance Speech Thank you so much. Thank you to the committee for this recognition, thank you to the Texas Tech Administrators, and many thanks to my peer and friend who nominated me Jennifer Barnett.
Acceptance Speech Thank you so much. Thank you to the committee for this recognition, thank you to the Texas Tech Administrators, and many thanks to my peer and friend who nominated me Jennifer Barnett.
University College London Hospital
 University College London Hospital and Poole District General Hospital University College London Hospital Monday 23 rd June 2008 We visited the University College London Hospital on Monday 23 rd June 2008
University College London Hospital and Poole District General Hospital University College London Hospital Monday 23 rd June 2008 We visited the University College London Hospital on Monday 23 rd June 2008
Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims
 March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
March 8, 2018 Top Audit Finding: Discrepancies in Secondary Diagnosis Assignment on Outpatient and Pro-Fee Claims By Kristi Pollard, RHIT, CCS, CPC, CIRCC, AHIMA-approved ICD-10- CM/PCS trainer There is
Medication Administration Using the Home Pump (Eclipse)
") Medication Administration Using the Home Pump (Eclipse) Phone Number: Nurse/Contact: Receiving IV Therapy in the Home Your doctor has ordered for you to receive your IV medication at home. Receiving IV
Medication Administration Using the Home Pump (Eclipse) Phone Number: Nurse/Contact: Receiving IV Therapy in the Home Your doctor has ordered for you to receive your IV medication at home. Receiving IV
CDx ANNUAL PHYSICIAN CLIENT NOTICE
 CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
MLK MACC Organizational Structure (Deliverable #3)
") MLK MACC Organizational Structure (Deliverable #3) February 29, 2008 Introduction The complexity of the transition from a fully functioning hospital to an ambulatory care center should not be under-estimated.
MLK MACC Organizational Structure (Deliverable #3) February 29, 2008 Introduction The complexity of the transition from a fully functioning hospital to an ambulatory care center should not be under-estimated.
gifts for refugees a holiday fundraising guide
 gifts for refugees a holiday fundraising guide thank you for fundraising for gifts for refugees! Dear compassionate supporter, The contributions we ll receive from your fundraising campaign will allow
gifts for refugees a holiday fundraising guide thank you for fundraising for gifts for refugees! Dear compassionate supporter, The contributions we ll receive from your fundraising campaign will allow
Introduction to the Parking Lot
 Introduction to the Parking Lot In ARK Epic training sessions, The Parking Lot" is used to capture all questions for which your trainer may not have an immediate answer during session. Your ARK Epic Training
Introduction to the Parking Lot In ARK Epic training sessions, The Parking Lot" is used to capture all questions for which your trainer may not have an immediate answer during session. Your ARK Epic Training
Pediatric Surgery. What you need to know. Norton Children s Medical Center
 Pediatric Surgery What you need to know Norton Children s Medical Center Welcome to the surgical services department Norton Children s Medical Center Our staff of pediatric health care professionals understands
Pediatric Surgery What you need to know Norton Children s Medical Center Welcome to the surgical services department Norton Children s Medical Center Our staff of pediatric health care professionals understands
A CHANGE OF HEART. By Cody Moree. Performance Rights
 A CHANGE OF HEART By Cody Moree Performance Rights It is an infringement of the federal copyright law to copy this script in any way or to perform this play without royalty payment. All rights are controlled
A CHANGE OF HEART By Cody Moree Performance Rights It is an infringement of the federal copyright law to copy this script in any way or to perform this play without royalty payment. All rights are controlled
All About Your Peripherally Inserted Central Catheter (PICC)
") All About Your Peripherally Inserted Central Catheter (PICC) General Information Intravenous (IV) therapy is the delivery of fluid directly into a vein. An intravenous catheter is a hollow tube that is
All About Your Peripherally Inserted Central Catheter (PICC) General Information Intravenous (IV) therapy is the delivery of fluid directly into a vein. An intravenous catheter is a hollow tube that is
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Angel Care Tamworth Limited
 Angel Care Tamworth Limited Angel Care Tamworth Limited Inspection report Unit 4, Anker Court Bonehill Road Tamworth Staffordshire B78 3HP Date of inspection visit: 14 August 2017 Date of publication:
Angel Care Tamworth Limited Angel Care Tamworth Limited Inspection report Unit 4, Anker Court Bonehill Road Tamworth Staffordshire B78 3HP Date of inspection visit: 14 August 2017 Date of publication:
Tendercare Home Ltd. Tendercare Home Limited. Overall rating for this service. Inspection report. Ratings. Good
 Tendercare Home Limited Tendercare Home Ltd Inspection report 237-239 Oldbury Road Rowley Regis West Midlands B65 0PP Tel: 01215614984 Date of inspection visit: 20 January 2016 21 January 2016 Date of
Tendercare Home Limited Tendercare Home Ltd Inspection report 237-239 Oldbury Road Rowley Regis West Midlands B65 0PP Tel: 01215614984 Date of inspection visit: 20 January 2016 21 January 2016 Date of
Certification Examination in Long Term Monitoring (CLTM) Application Form
 Application Form") Certification Examination in Long Term Monitoring (CLTM) Application Form Please read the directions in the HANDBOOK for CANDIDATES carefully before completing this Application. Name (exactly as it appears
Certification Examination in Long Term Monitoring (CLTM) Application Form Please read the directions in the HANDBOOK for CANDIDATES carefully before completing this Application. Name (exactly as it appears
A PROMISE MADE, A PROMISE KEPT. Cape Fear Valley s New Hospital Finally Delivers
 A PROMISE MADE, A PROMISE KEPT Cape Fear Valley s New Hospital Finally Delivers It wasn t long after his arrival that Cape Fear Valley CEO Mike Nagowski began turning his attention westward toward Hoke
A PROMISE MADE, A PROMISE KEPT Cape Fear Valley s New Hospital Finally Delivers It wasn t long after his arrival that Cape Fear Valley CEO Mike Nagowski began turning his attention westward toward Hoke
A Pharmacist's Role in the Relief Efforts in Haiti
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/voices-from-american-medicine/a-pharmacists-role-in-the-relief-effortsin-haiti/6992/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/voices-from-american-medicine/a-pharmacists-role-in-the-relief-effortsin-haiti/6992/
Glengarry Rest Home and Hospital Resident Satisfaction Survey Results 2013
 Glengarry Rest Home and Hospital Resident Satisfaction Survey Results 2013 Overall Satisfaction 2013 2013 2012 10 8 6 4 84% Date of Survey Aug 2013 Aug 2012 Date Results sent to Care Home Aug 2013 Aug
Glengarry Rest Home and Hospital Resident Satisfaction Survey Results 2013 Overall Satisfaction 2013 2013 2012 10 8 6 4 84% Date of Survey Aug 2013 Aug 2012 Date Results sent to Care Home Aug 2013 Aug
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
EHR Implementation Best Practices. EHR White Paper
 EHR White Paper EHR Implementation Best Practices An EHR implementation that increases efficiencies versus an EHR that is underutilized, abandoned or replaced. pulseinc.com EHR Implementation Best Practices
EHR White Paper EHR Implementation Best Practices An EHR implementation that increases efficiencies versus an EHR that is underutilized, abandoned or replaced. pulseinc.com EHR Implementation Best Practices
Faculty of Health Staff Meeting: Health and Safety Refresher. March 23, 2012
 Faculty of Health Staff Meeting: Health and Safety Refresher March 23, 2012 Agenda 9:10 9:20 Welcome 9:20 10:00 Emergency Preparedness Plan (Randy Diceman) 10:00 10:10 Occupational Health and Safety Policy
Faculty of Health Staff Meeting: Health and Safety Refresher March 23, 2012 Agenda 9:10 9:20 Welcome 9:20 10:00 Emergency Preparedness Plan (Randy Diceman) 10:00 10:10 Occupational Health and Safety Policy
What's New February 24, Susanne Quallich, Ph.D.
 The University of Michigan Department of Urology 3875 Taubman Center, 1500 E. Medical Center Drive, SPC 5330, Ann Arbor, Michigan 48109-5330 Academic Office: (734) 232-4943 FAX: (734) 936-8037 www.medicine.umich.edu/dept/urology
The University of Michigan Department of Urology 3875 Taubman Center, 1500 E. Medical Center Drive, SPC 5330, Ann Arbor, Michigan 48109-5330 Academic Office: (734) 232-4943 FAX: (734) 936-8037 www.medicine.umich.edu/dept/urology
Kurt A. Patton, MS, RPh with a foreword by Thanasekaran Sinnathamby, MD Handoff Communication Handoff Handoff Communication, Global Edition:
 Handoff Contents About the author......................................... v Foreword............................................... vii Introduction............................................. xii Chapter
Handoff Contents About the author......................................... v Foreword............................................... vii Introduction............................................. xii Chapter
Introduction: About the Author:
 Introduction: Welcome to CUGH s bi-weekly clinical case-series, Reasoning without Resources, by Prof. Gerald Paccione of the Albert Einstein College of Medicine. These teaching cases are based on Prof.
Introduction: Welcome to CUGH s bi-weekly clinical case-series, Reasoning without Resources, by Prof. Gerald Paccione of the Albert Einstein College of Medicine. These teaching cases are based on Prof.
Saint Francis Cancer Center Combines MOSAIQ, Epic and Palabra for a Perfect Documentation Workflow ONCOLOGISTS PALABRA: THE SOFTWARE ACTUALLY LOVE
 PALABRA: THE SOFTWARE ONCOLOGISTS ACTUALLY LOVE CASE STUDY CONTRIBUTORS Dr. Stephen Z. Sack, MD, Radiation Oncologist Tyleen A. Smith, BSN, RN, Clinical Manager Dr. Charles Stewart, MD, PhD, Radiation
PALABRA: THE SOFTWARE ONCOLOGISTS ACTUALLY LOVE CASE STUDY CONTRIBUTORS Dr. Stephen Z. Sack, MD, Radiation Oncologist Tyleen A. Smith, BSN, RN, Clinical Manager Dr. Charles Stewart, MD, PhD, Radiation