|
|
|
- Carmella Norris
- 5 years ago
- Views:
Transcription
1 New Mexico Stakeholder Summit August 19, 2015
 Tres Schnell, Director, Office of Policy and Accountability, DOH 9:40 10:40")

2 New Mexico Health System Innovation Stakeholder Summit August 19, :30 am 3:00 pm DoubleTree Hotel, Albuquerque, NM 8:30-9:00 Registration, Coffee and Informal Question/Answer Session 9:00 9:05 Welcome Sean Pearson, Deputy Secretary, Human Services Department 9:05-9:40 Framing the NM Health System Innovation (HSI) Tres Schnell, Director, Office of Policy and Accountability, DOH 9:40 10:40 Conversation About the NM HSI Design Mixed Committee Member Roundtables insights and observations 10:40 11:00 The ECHO Model: a Tool for Health System Innovation Dr. Miriam S. Komaromy, Associate Director, Project ECHO; Co-Medical Director/IAP Clinic, UNM 11:00 11:15 Break and Move into Stakeholder Committees 11:15 12:15 Stakeholder Committee Sessions Population Health (red) Health Care (light blue) Payment Models (black) Alignment & Integration of Public Health and Primary Care (yellow): Health Information Systems (orange) Tribal (navy blue) Workforce and Training Needs (green) 12:15 12:45 Box Lunch Provided Please pick up lunch and rejoin your committee 12:45 1:45 Stakeholder Committee Sessions (cont.) 1:45 2:00 Break and Rejoin the Large Group 2:00 3:00 Stakeholder Committee Reports, Wrap Up, and Next Steps THANKS! Next Summit: September 16, 2015 Lunch Sponsored by: NM Primary Care Training Consortium and Southwest Center for Health Innovation Check the website for all things related to New Mexico Health System Innovation: resources, committee work, and information on the developing design.
3
4 WELCOME HEALTH SYSTEM INNOVATION DESIGN AUGUST 19, 2015 Welcome Stakeholder Summit # 4 Sean Pearson, Deputy Cabinet Secretary Human Services Department 2 1


5 New Mexico Health System Innovation Model Tres Hunter Schnell, Director Department of Health 3 Recap Health System Innovation Design Centers for Medicare and Medicaid Innovation Award to Department of Health, in collaboration with Human Services Department $2 million Intended to achieve the triple aim: Improved Population Health and Health Outcomes Reduced health care costs and investment in health promotion Enhanced experience of care for the person, quality and satisfaction 4 2
6 A shared commitment to achieve results Alignment and integration of public health, behavioral health and primary care Reduce costs and slowing the rate of health care inflation, while increasing investments in community wellness Increase the number of New Mexicans who have health insurance and access to healthy choices Build the health system workforce and support the infrastructure Expand the use and integration of the state s health information system, including technology, personal access and transparency Health Improvement Priorities Obesity Diabetes Tobacco Use 3

7 Summit objectives To learn about next steps and timelines for finalizing New Mexico s design for health system innovation To promote cross committee dialogue, and contribute design observations and input To learn how telehealth contributes to health system innovation, and access to well being and health services To continue a dialogue with stakeholders to collaboratively design an integrated system of wellbeing and care To focus in on committee design recommendations New Mexico Health System Innovation Model Patient Centered Medical Home Integrating: Behavioral Health, Oral Health, Public Health Workforce: CHW, CEMS, Residency Programs Standards and Criteria Established Community Well Being Center Based on Community Centered Health Home Concept SDOH All sectors contribute to improve health Identified center unknown may be local public health office No established standards or The Community Criteria Established Health IT System: Information, Analysis, Sharing, Delivery 8 4
 are essential to address social")
8 What does an integrated PCMH look like in NM? First Choice Community Healthcare, South Valley Community Commons: Partnerships (Schools, farmers, county government, health council, UNM, Molina, DOH public health) are essential to address social determinants The person and community centered concept drives First Choice Residency program training, work with diverse teams Integration of Community Health Workers (CHW) into primary care using models for Medicaid reimbursement for services 9 What does integration look like for NM? First Choice Community Healthcare, South Valley Community Commons: Screen all patients (e.g., nutrition, housing, transportation, child care, employment, job training, substance use, safety) Environmental conditions WellRx prescriptions to promote healthy behaviors Respond: Food distribution and cooking classes; diabetes education; child development; walking trails in neighborhood. Increased patient engagement and satisfaction Increased health equity 10 5
9 NCQA PCMH 2014 Content (6 standards/27 elements) June Summit Dr. McGrath 1: Enhance Access and Continuity A. *Patient-Centered Appointment Access B. 24/7 Access to Clinical Advice C. Electronic Access 2: Team-Based Care A. Continuity B. Medical Home Responsibilities C. Culturally and Linguistically Appropriate Services (CLAS) D. *The Practice Team 3: Population Health Management A. Patient Information B. Clinical Data C. Comprehensive Health Assessment D. *Use Data for Population Management E. Implement Evidence-Based Decision-Support 4: Plan and Manage Care A. Identify Patients for Care Management B. *Care Planning and Self-Care Support C. Medication Management D. Use Electronic Prescribing E. Support Self-Care and Shared Decision-Making 5: Track and Coordinate Care A. Test Tracking and Follow-Up B. *Referral Tracking and Follow-Up C. Coordinate Care Transitions 6: Measure and Improve Performance A. Measure Clinical Quality Performance B. Measure Resource Use and Care Coordination C. Measure Patient/Family Experience D. *Implement Continuous Quality Improvement E. Demonstrate Continuous Quality Improvement F. Report Performance G. Use Certified EHR Technology 11 Community Centered Health (Well Being) Home No Standards and Criteria ta bu la ra sa noun: tabula rasa an absence of preconceived ideas or predetermined goals; a clean slate. stakeholders have complete freedom and a tabula rasa from which to work" 12 6
10 Our challenge We don t need to have all the answers We design how we will get the answers Community Centered Well Being is less defined than the Patient Centered Medical Home. How do we define CCWB? How does DOH public health and partners transform to serve the model? How do we formalize collective work to reach common health improvement goals? What are the criteria that would serve as the framework for CCWB? What might this look like in your community? Who are the partners that might contribute? Prevention Institute questions in your packet! 13 Public Health Accreditation Domains and Standards as a Guide Standards for how the public health discipline practices provide an excellent foundation for the work to develop a community well being centered construct for New Mexico go to: content/uploads/phab Standards Overview Version 1.0.pdf Also, many models provide guidance: Collective Impact Community Health Improvement Process Place Matters Health Equity Evidence Based Approaches: The Community Guide (CDC) 14 7
11 Our Health System Innovation Model So Far 15 New Mexico Health System Innovation Model How did we arrive at this emerging model? The Model Design is developing with the following: Stakeholder Input and Feedback Summit meetings (May July) and Workgroup meetings (May July) Human Services Department Centennial Care Innovation Waiver approved by CMS NM s Centers for Medicare and Medicaid Services (CMS) State Innovation Model (SIM) Design Proposal The original proposal is the guiding document CMS uses to evaluate all plan submissions is the plan aligned with what we said we would do? (available:
12 The NM HSI Model Stakeholders say the model needs to be: Community centered, focused on prevention and built environments, health in all policies, well being, and personal responsibility for health; Team based and patient centered care; coordination of care, built on blended model of practices that have achieved certification (NCQA, AAHC, Joint Commission, NM model); Flexible for adaptation in all communities; Addresses social determinants of health and improved health equity; Phased in over time starting in underserved areas and populations; Integration of tribal health systems; Multiple entry points/"no wrong door" approach; Focus on coordination of care and seamless transition between services and providers; "Well being Coordinator" who helps navigate and improve the system for patients/communities; CHWs/CHRs within the clinic and in the community; EMS personnel with enhanced primary care roles; and, Networks of multi disciplinary provider teams and services that integrate primary care, behavioral health, public health, and oral health across the lifespan. 17 The NM HSI Model Centennial Care: Comprehensive care coordination system; health literacy; inclusive of individual, cultural, and community needs; whole person philosophy; utilization of CHWs PCMH vision for NM: Team based and patient centered care; coordination of care; built on blended model of practices that have achieved certification (NCQA, AAHC and Joint Commission) workgroup over past 4 years DOH/HSD Proposal: Focus on quality of services; patient centered care; multi disciplinary health teams (CHWs and EMS personnel); integration of lay Health Leads model to connect patients to basic resources; strategies to improve recruitment & retention of healthcare professionals; leverage Centennial Rewards program across other payers; robust HIE that enables data sharing among providers, payers, and patients 18 9
13 Payment Models Stakeholders say: Use of value based payment with shared savings model; incentivize providers to provide "whole person" services that improve population health outcomes; consistent payment structure throughout State; reimbursement for nontraditional services; i.e., social services; expanded CHW and EMS services. Centennial Care: Stratification of recipients by risk and capitation payment; tiered reimbursement with incentives tied to target measures for PCMHs; pay for performance, outcome based reimbursement and bundled payments. PCMH Vision for NM: Model is uniform across payers; provide financial support to move practices towards national PCMH certification; standardized, based on level of PCMH achievement and evidence of quality care to patients; provide incentives for patient proactive healthcare DOH/HSD Proposal: Payment for health outcomes; implement promising and evidence based payment models; complement PCMH initiative and aligned with Centennial Care (bundled payments, pay forperformance, shared savings) 19 PCMH Requirements Stakeholders say: One certifying organization; built on existing successful state programs; improved access to care through flexible scheduling, including same day appointments, accommodating walk ins, after hours and weekend office hours; sustained recruitment and training of IT and data input staff Centennial Care: Incentivizing proliferation of PCMHs; incorporation of health homes (management of chronic conditions Medicaid only) PCMH Vision for NM: Develop a "Glide Path" open to all practices seeking PCMH status; certification is based on nationally vetted standards; commitment to use of EHRs and MU; data integration and information sharing in real time; integration of PH, BH, OH; provide support to tribal 638 clinics to become FQHCs DOH/HSD Proposal: PCMH quality improvement collaborative; TA center for a uniform state approach; integration of behavioral health and oral health services, including Screening, Brief Intervention, and Referral to Treatment (SBIRT); increased utilization of SBHCs 20 10
14 Performance Metrics (Measures) Stakeholders say: Focus on clinical and population health outcomes including overall health, race/ethnicity, behavioral health, quality of care, social determinants of health, cost of care, and effectiveness of PCMH model interventions Centennial Care: Measures of process, health outcomes, quality of life, recipient choice, recipient and provider satisfaction and performance PCMH Vision for NM: Measures are aligned with identified State level health priorities along the lifespan; health equity is foundational lens DOH/HSD Proposal: Standardized quality clinical and population health metrics, based upon nationally vetted measures, i.e., HP2020, NQF, AHRQ, developed via a collaborative process of statewide stakeholders and utilized by providers and payers; measures to evaluation performance of NM PCMH model 21 Key Infrastructure, Policies Required Stakeholders say: Need state level oversight entity; data sharing infrastructure to connect all payers, providers, and patients; technical assistance for providers; development of tribal data exchange; incentivized recruitment of primary care providers, CHWS, and EMS personnel, and IT staff; improved reciprocity laws to enable licensed health care professionals to quickly practice in New Mexico; increased collaboration among payers and providers and shared vision of innovation PCMH Vision for NM: Use of APCD, HIE, and evidence based interventions; real time data exchange; develop policies to improve data collection and utilization DOH/HSD Proposal: Expanded options for delivery and payment of services via Centennial Care; expanded and more robust HIE ; coordination with NMHIX to further ACA implementation and establish criteria for qualified health plans; development of a standardized set of statewide metrics 22 11
15 23 We are grateful for your continued contributions and commitment to this work. QUESTIONS? More information:
16 What s Next? Stakeholder Summit Schedule: September 16, 2015 December 15, 2015 Final Presentation of HSI Model to Stakeholders October and November: Stakeholder Summits are cancelled and replaced with committee and workgroup for Health System Innovation Plan finalization 25 Roundtable Conversations 9:40 AM 10:40 AM Mixed committee member groups What are the strengths of the model What is missing from the model Committee members take notes to capture recommendations, questions, and observations from colleagues Deliver key points back to the committee for consideration Staff available to support the conversation, answer questions 19 13
17 Roundtable Jump Start Questions Do you have a clear understanding of the draft NM Health System Innovation design after the framing presentation? What are any specific questions you have? (Any further information you need to better understand the design?) Many of you contribute to different committees: What questions do you have for a member of a different committee? What suggestions, information, insights, observations or helpful comments about committee work would you like to pass on to Roundtable colleagues for specific design recommendations? 20 Project ECHO (Extension for Community Health Outcomes) Miriam Komaromy, MD, FACP Associate Professor of Medicine Associate Director of Project ECHO Department of Medicine University of New Mexico Health Sciences Center Tel: miriamk1@salud.unm.edu 14

18 At ECHO, our mission is to democratize medical knowledge and get best practice care to underserved people all over the world. Our goal is to touch the lives of 1 billion people by Supported by New Mexico Department of Health, Agency for Health Research and Quality, New Mexico Legislature, the Robert Wood Johnson Foundation, the GE Foundation and Helmsley Trust Copyright 2013 Project ECHO NEJM : 364: 23, June , Arora S, Thornton K, Murata G 15
19 Goals of Project ECHO Develop capacity to safely and effectively treat common, complex diseases such as HCV in all areas of New Mexico and to monitor outcomes. Develop a model to treat common, complex diseases in underserved locations in the US and around the world. Copyright 2013 Project ECHO Methods Use Technology to leverage scare resources Sharing best practices Case based learning Web based database to monitor outcomes Arora S, Geppert CM, Kalishman S, et al: Acad Med Feb;82(2): Copyright 2013 Project ECHO 16
20 Benefits to Rural Clinicians No cost CMEs and Nursing CEUs Professional interaction with colleagues with similar interest Less isolation with improved recruitment and retention A mix of work and learning Access to specialty consultation with GI, hepatology, psychiatry, infectious diseases, addiction specialist, pharmacist, patient educator Copyright 2013 Project ECHO Project ECHO Clinicians HCV Knowledge Skills and Abilities (Self Efficacy) scale: 1 = none or no skill at all 7= expert can teach others Community Clinicians N=25 BEFORE Participation MEAN (SD) TODAY MEAN (SD) Paired Difference (p value) MEAN (SD) Effect Size for the change 1. Ability to identify suitable candidates for treatment for HCV. 2.8 (1.2) 5.6 (0.8) 2.8 (1.2) (<0.0001) Ability to assess severity of liver disease in patients with HCV. 3.2 (1.2) 5.5 (0.9) 2.3 (1.1) (< ) Ability to treat HCV patients and manage side effects. 2.0 (1.1) 5.2 (0.8) 3.2 (1.2) (<0.0001) 2.6 Copyright 2013 Project ECHO (continued) 17
 2.8* (0.9) 5.5* (0.6) 2.7 (0.9) (<0.0001) 2.9 Cronbach s alpha for the BEFORE ratings = 0.")
:1124 33 Copyright 2013 Project ECHO Outcomes of Treatment for Hepatitis C Virus Infection by Primary Care Providers Results of the HCV Outcomes Study Arora S, Thornton K, et al.")
21 Project ECHO Clinicians HCV Knowledge Skills and Abilities (Self Efficacy) Community Clinicians N=25 BEFORE Participation MEAN (SD) TODAY MEAN (SD) Paired Difference (p value) MEAN (SD) Effect Size for the change Overall Competence (average of 9 items) 2.8* (0.9) 5.5* (0.6) 2.7 (0.9) (<0.0001) 2.9 Cronbach s alpha for the BEFORE ratings = 0.92 and Cronbach s alpha for the TODAY ratings = 0.86 indicating a high degree of consistency in the ratings on the 9 items Arora S, Kalishman S, Thornton K, Dion D et al: Hepatology Sept;52(3): Copyright 2013 Project ECHO Outcomes of Treatment for Hepatitis C Virus Infection by Primary Care Providers Results of the HCV Outcomes Study Arora S, Thornton K, et al. N Engl J Med Jun; 364: Copyright 2013 Project ECHO 18
22 Treatment Outcomes Outcome ECHO UNMH P value N=261 N=146 SVR* (Cure) Genotype 1 50% 46% NS SVR* (Cure) Genotype 2/3 70% 71% NS Minority 68% 49% P<0.01 *SVR=sustained viral response NEJM : 364: 23, June , Arora S, Thornton K, Murata G Copyright 2013 Project ECHO Disease Selection Common diseases Management is complex Evolving treatments and medicines High societal impact (health and economic) Serious outcomes of untreated disease Improved outcomes with disease management Copyright 2013 Project ECHO 19
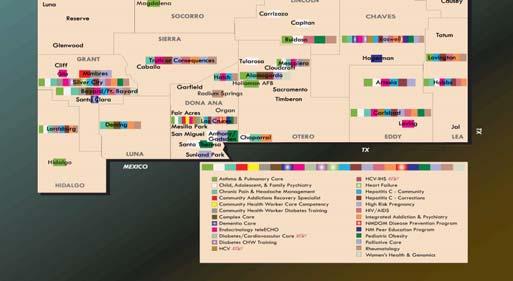
23 Successful Expansion into Multiple Diseases Mon Tue Wed Thurs Fri 8 10 a.m. Hepatitis C Arora Thornton Diabetes & Endocrinology Bouchonville Geriatrics/ Dementia Herman Palliative Care Neale a.m. Rheumatology Bankhurst Chronic Pain Katzman Integrated Addictions & Psychiatry Komaromy Complex Care Neale Komaromy 2 4 p.m. HIV Iandiorio Thornton Prison Peer Educator Training Thornton Women s Health & Genomics Curet Copyright 2013 Project ECHO 20
24 Expanding the concept of the primary care team: Community Health Workers and ECHO Copyright 2013 Project ECHO ECHO CHW Training Multiple Tracks CHW Specialist Training CREW: Diabetes, Obesity, Hypertension, Cholesterol, Smoking Cessation, Exercise Physiology CARS: Substance Use Disorders ECHO Care : Complex Multiple Diagnoses Endo ECHO: Diabetes and other endocrine disorders Family Obesity Intervention: DOH funded collaboration Prison Peer Educator Training Copyright 2013 Project ECHO 21
25 Specialty CHW Program Narrow Focus Deep Knowledge Standardized Curriculum 3 Day Onsite Webcam/Weekly Video Based Clinics Health coaching Diet Exercise Smoking Cessation Motivational Interviewing Finger Stick Foot Exam Ongoing support via CHW teleecho clinics Part of Disease Management Team Copyright 2013 Project ECHO Community Health Workers in Prison The New Mexico Peer Education Program Pilot training cohort, CNMCF Level II, July 27 30, 2009 First day of peer educator training Photo consents on file with Project ECHO and CNMCF Copyright 2013 Project ECHO 22

 Integration of Public Health into treatment paradigm to Copyright 2013 Project ECHO Copyright 2013 Project")
26 Potential Benefits of ECHO Model Health System Quality and Safety Rapid Learning and best practice dissemination Reduce variations in care Access for Rural and Underserved Patients, reduced disparities Workforce Training and Force Multiplier Democratize Knowledge Improving Professional Satisfaction/Retention Supporting the Medical Home Model Cost Effective Care Avoid Excessive Testing and Travel Prevent Cost of Untreated Disease (e.g.: liver transplant or dialysis) Integration of Public Health into treatment paradigm to Copyright 2013 Project ECHO Copyright 2013 Project ECHO 23



27 Copyright 2013 Project ECHO Copyright 2013 Project ECHO 24




28 Copyright 2013 Project ECHO ECHO Care is a special health care program designed to support Medicaid patients who have complex health care needs 25

29 5% of Medicaid patients account for almost 60% of Medicaid dollars Alittlereality.blogspot.com Goals of ECHO Care Improve quality and access to care Decrease cost of care Improve patient satisfaction 26
30 Collaboration Federal CMMI grant Partnerships with: NM state Medicaid office (HSD) All of the Medicaid managed care organizations (MCOs) Numerous Community Health Centers (CHCs) MCOs jointly provide salaries for the ECHO Care teams CHCs provide the clinic locations Multidisciplinary, Integrated RN CHW NP Patient Coun selor Cardiology CHW Endocrinology Psychiatry ECHO Complex Care Specialists Addiction Infectious Disease Pharmacy Clinical Social Work Etc. 27
31 Survey of patients enrolled in ECHO Care, a teambased intervention for Medicaid Superutilizers In the past 6 months. Baseline 6 months 12 months My primary healthcare teams always spends enough time with me My primary healthcare team always shows respect for me My primary healthcare team cares about me as a person My primary healthcare team talked with me about my health goals My primary healthcare team provides the best possible care I am very satisfied with the care I receive Copyright 2013 Project ECHO PRELIMINARY Results: Non OB Admissions/1, Admissions/1, Post enrollment hospitalization rates were 37% of Pre enrollment rates (12 mo) Months Before/After ECHO Enrollment First Full Month Of ECHO Enrollment
32 PRELIMINARY Results: Total Cost per Member per Month Cost/Month 5,000 4,500 4,000 3,500 3,000 2,500 2,000 1,500 1, Post enrollment costs were 60% of Pre enrollment rates (12 mo): $1850 vs $3050 PMPM Months Before/After ECHO Enrollment First Full Month Of ECHO Enrollment ECHO provides a flexible model that can be adapted to expand access to high quality care for a variety of common complex diseases in high need communities Copyright 2013 Project ECHO 29

 Copyright 2013 Project ECHO Thank you Charlie Alfero and Staff!")
33 Potential value of the ECHO model for the SIM initiative Level of impact Patient Care Improve Quality and Safety of care Reduce variations/disparities in care Cost Effective Care: Avoid Excessive Testing and Travel Triage only highest need patients to specialists Access Improve Access for Rural and Underserved Patients Healthcare Workforce Workforce Training and Force Multiplier Improve Professional Satisfaction/Retention Rapid Learning and best practice dissemination Public Health/ Population Health Integration of Public Health with the treatment arm of the health system Prevent Cost of Untreated Disease (e.g.: liver transplant or dialysis) Copyright 2013 Project ECHO Thank you Charlie Alfero and Staff!! Lunch generously provided by: Southwest Center for Health Innovation New Mexico Primary Care Training Consortium 60 30
34 THANK YOU! HEALTH SYSTEM INNOVATION DESIGN AUGUST 19,
35 First DRAFT: NM Model Design New Mexico Model Design: Overview Population Health Improvement (Insert content) New Mexico plans an innovative version of the patient centered medical home (PCMH) approach that focuses on the quality of services and moves prevention into the community setting. This communitycentered approach incorporates networks of multi disciplinary provider teams and services that integrate primary care, behavioral health, public health, and oral health across the lifespan and includes community health workers (CHWs)/tribal community health representatives (CHRs) who work within the clinic and in the community to enhance the patient experience of care. Emergency Medical Service (EMS) personnel will also have enhanced roles within the community. Strategies will be identified to improve recruitment and retention of healthcare professionals, and utilize successful lay models to support this model. Comprehensive care coordination and seamless transition between services and providers are cornerstones of the model. All patients will be able to enter the healthcare system through a portal that regards their health holistically, treats them as individuals (knowledge of risk factors, concerns, and specific perspectives), and provides the highest quality care efficiently (both prevention and treatment). This access will be a no wrong door approach that includes multiple entry points with the help of a Wellbeing Coordinator and others to assist them with navigation of the healthcare system and connect with basic resources that may be needed. Care must be coordinated within the PCMH practice, but also between it and community settings, labs, specialists and hospitals. The responsibility of the PCMH is not just to be informed by community providers and resources, but to reach out and connect in meaningful ways with other sources of service and link with them, so that information is communicated appropriately, consistently and without delay. concepts/care coordination This will require a multi disciplinary team approach with smooth connections and communications among providers, tribal governments and organizations, a Well being Coordinator trained to coordinate care and collaborate with providers, patients, and partners, a health information system that captures all relevant information to be exchanged, and payment that incentivizes this type of work. Population Health Community Centered Well Being (Expand here concepts and strategies) No Wrong Door Multiple entry points to the system will be established for those needing healthcare or other services. A patient may enter from a PCMH, Indian Health Service, tribal 638 clinic, or other clinical service, another service area such as SNAP, WIC, or due to personal needs such as lack of access to transportation or a healthy food supply. Well being Coordinators at each entry point will have a standardized intake form including an assessment with core questions to help guide patients in referring them to the right services. Health Information Technology will assist in this process of being able to make automatic referrals based on the answers that are provided (developing concept). 8/18/2015
36 First DRAFT: NM Model Design The Model will be focused on prevention, well being, and personal responsibility for health and take a whole person philosophy. In the Centennial Care rewards program, there is a focus on helping Medicaid patients to be active participants in their health through rewards for healthy behaviors. This approach will be reviewed and may be leveraged across other payers. Social determinants of health (i.e., education, food, neighborhood and built environment, social and community context, and economic stability, etc.) will be addressed within this inclusive model of individual, cultural and community perspectives. Improved health equity and health literacy will be cornerstones, as culturally sensitive, relevant, and accessible materials and education are developed, and, based on the premises of Centennial Care, will focus on using the healthcare system wisely and effectively. The roll out of this Model will be phased in over time balancing underserved areas and populations with quick win opportunities, and demand by high volume regions. The unique need and recommendations of the 23 American Indian tribes, pueblos and nations, and urban off reservation population is essential. In order for the Model to be successful statewide, it must be flexible for adaptation in all communities and be responsive to community needs. It will be necessary for the Model to include a mechanism for communication and collaborations across governments so that tribes, pueblos and nations may consider the value and benefit of participating in this initiative. A first step is consideration of a robust health information exchange that enables data sharing across tribal and state health systems, and among providers, payers, and patients will need to be instituted. Due to the wide service disparities across New Mexico s urban, frontier, rural areas, multiple Information technology methodologies such as telehealth, and Mobile (health) Services will be incorporated as alternative health delivery systems. A robust workforce will be necessary to carry out core components of this model. Resources will be invested in the workforce that currently exists in the State, with policy levers examined to further enable recruitment and expansion beyond current numbers. Project ECHO may be utilized to enhance the skills of the current workforce, including CHWs and Community EMS personnel, and others via telehealth technology. Work Force Recruitment and Retention of Health care professionals [Developing concept] Well Being Coordinator (needs to be clearly defined. What type of professional is the WB Coordinator and what are the credentials/training that would be required for this position, a public health staff member, public health nurse, etc.?) Some of the responsibilities of this position may be: Coordination of services among the providers and staff who interact with a client Linkage of clients to community resources that respond to their social service needs. Integration of behavioral health and specialty care into care delivery through co location or referral agreements. Tracking and support of patients when they obtain services outside the practice. Follow up with patients within a few days of an emergency room visit or hospital discharge. Communication of test results and care plans to patients, families, and care givers. 8/18/2015
37 First DRAFT: NM Model Design The Well being Coordinator will also coordinate services provided by CHWs and EMS personnel, and align them with the services provided by the primary care physician. For example, a prescription for diabetes self care instruction to be provided by a CHW will be monitored and tracked to ensure alignment with the patient s overall treatment and wellness regimen. Coordination with services of EMS personnel may include scheduling and tracking non emergency medical transports, or coordination of basic primary care services provided by EMTs with the primary care physician. Community Health Workers/Community Health Representatives (expand here) EMS Personnel (expand here) Public Health Staff (expand here) Health Leads The Health Leads model facilitates prescriptions for basic resources like food, heat, and physical exercise, and referral of patients to the resource. Health Leads Advocates, college students who recruited and trained to fulfill prescriptions, work side by side with patients to connect them with the basic resources they need to be healthy. When clients visit a clinic, they are screened for basic needs that can affect their health. Healthcare providers prescribe resources to meet these needs, [often using the electronic medical record????] to refer patients to a Health Leads Advocate who navigate the complexity of the resource landscape including tracking down phone numbers, printing maps, securing transportation, and completing applications. Advocates follow up with clients regularly by phone, , or during clinic visits. Relationships may be long term or short term based on clients needs and preferences. As part of the clinic team, Advocates also provide ongoing updates on an individual s progress in securing basic resources to other team members. [NOTE: It is important not to blur role identities here the WB coordinator may be a high level position who will be overseeing the entire spectrum of clinical and social services of clients. And EMS personnel may best serve the system by conforming to their own scope of practice. The Health Lead Advocate should be faithful to the original model, i.e., health or social services, college students, retired persons, etc. so as to augment the workforce] Payment Model The payment model to support the Model Design will incentivize providers to provide whole person services that improve population health outcomes. With the expansion of the multi disciplinary provider teams, reimbursement mechanisms will be explored for the non traditional services provided (e.g., social services, expanded CHW and EMS services, prevention/wellness programs, indigenous traditional healers, etc.). This payment model complements the PCMH initiative and will be aligned with Centennial Care s payment mechanisms, which include pay for performance, outcome based reimbursement, and bundled payments to providers for episodes of care. Promising and evidence based payment models will be explored, including a tiered reimbursement with incentives that are tied to targeted PCMH measures. 8/18/2015
38 First DRAFT: NM Model Design Incentives may also be used to promote wellness and patient proactive healthcare, while high cost medical care and procedures may be de incentivized. Pay for performance will be explored as providers are charged with influencing population health outcomes, and improvement in their patients outcomes may result in reward through compensation. For instance, a provider, who improves low birth weight of patients through referrals to home visiting programs, would be rewarded. A plan to re evaluate CPT (spell out) codes to de incentivize high cost medical procedures and place additional value on lower cost items will be explored. As the expansion of PCMHs in the State moves forward, financial support will be provided to move practices towards achievement of national PCMH certification. Upon certification, payment will be standardized based on level of PCMH achievement and evidence of quality care to patients. Movement towards a shared savings model may be examined including using a portion of the shared savings to support the community through funding education and prevention in schools, or other community activities. Plan costs and cost drivers will need to be understood in order to be able to identify opportunities for cost savings. Care coordination among primary care, behavioral, oral, and public health will be included in the payment model, with the patient having the ability to decide where to go based on available metrics of provider performance. PCMH Requirements With the statewide expansion of the PCMH, a Technical Assistance Center (TAC) will be developed to promote best practices, facilitate education, and encourage a uniform state approach to PCMH. One certifying organization will be established for the State, and a Glide Path to certification will be offered to all practices. The Glide Path will be modeled on the process successfully implemented by the State of Connecticut to support practices that may be less resourced or those that are just beginning the PCMH transformation process. Support will also be provided to tribal 638 clinics to become PCMHs via the TAC. The development of PCMHs will be incentivized by certification that is based on nationally vetted standards. The PCMH model will be built on successful state programs that integrate primary care, behavioral, oral, and public health, including the use of Screening, Brief Intervention, and Referral to Treatment (SBIRT) for patients with substance use and abuse disorders. The Medicaid health home model, as set forth in Centennial Care, will also be incorporated into the State s PCMH approach. Improved access to care is an important part of the PCMH approach with flexible scheduling including same day appointments, walk in accommodations, and after hours and weekend office hours to ensure that the patients needs are met. Health Homes Centennial Care provides for a comprehensive care coordination system with the objective of achieving cost effective care and improved quality outcomes. The Centennial Care Health Homes will benefit the most vulnerable members of the State s population and provide integrated and coordinated care for members with complex chronic conditions, specifically those with serious mental illness (SMI) or severe emotional disturbance (SED). The Health Homes focus on these members due to their high personal physical and emotional risk as well the financial risk the pose to the State. This Health Home model will be integrated to address physical and behavioral needs, along with existing comorbidities, and focus on 8/18/2015



![[Expand HIT here] Performance Metrics (Measures) Performance metrics will be standardized across quality clinical and population health metrics that focus on outcomes including overall health,](/docs-images/87/95249150/images/39-3.jpg "race/ethnicity, behavioral health, social determinants of health, and quality of life.")
39 First DRAFT: NM Model Design conditions more successfully ameliorated through intensive care coordination. The model will be implemented using providers in the community who are experienced and skilled at addressing member needs through a whole person philosophy. The PCMHs must be committed to the use of electronic health records (EHRs) and adherence to meaningful use (MU) requirements of the Office of the National Coordinator (ONC) for Health Information Technology. To better ensure effective care coordination, data integration and information sharing will move towards real time transmission. For all the necessary requirements of health information technology to occur in a PCMH, an emphasis on recruitment and training of IT and data input staff will be a requirement. A health information technology plan will be developed to incorporate these concepts and develop a three year road map for implementation. [Expand HIT here] Performance Metrics (Measures) Performance metrics will be standardized across quality clinical and population health metrics that focus on outcomes including overall health, race/ethnicity, behavioral health, social determinants of health, and quality of life. Metrics will also be inclusive of process, performance of the PCMH model, quality and cost of care, recipient choice and satisfaction, and provider satisfaction and performance. The metrics will be developed via a collaborative process of statewide stakeholders and utilized by providers and payers. The measures will be based off of nationally vetted measures and will be aligned with state level health priorities across the lifespan with health equity being the foundational lens, and with Centennial Care metrics. It will be inherent that any of the metrics chosen should have reliable, available, and agreeable data for both clinical and population health metrics. 8/18/2015
40




41 Assessing & Promoting Adoption of the Community-Centered Health Home Model FINDINGS FROM CALIFORNIA THIS DOCUMENT WAS PREPARED BY PREVENTION INSTITUTE Prevention Prevention and equity nstitute at the center of community well-being PRINCIPAL AUTHORS: Rea Pañares Dalila Butler Leslie Mikkelsen September 2014
42 APPENDIX II Sample Interview Questions for Site Visits I. Leadership Support and Organizational Capacity 1. When you hear the term community prevention, what does it mean to you? 2. How, from your perspective, does your health center address community prevention? 3. How is community prevention institutionalized within the clinic? Can you describe any systems, programs, and/ or personnel in place that work directly with community prevention efforts? 4. How do you assign roles or provide sufficient staff to support your community prevention work? How are staffed trained and supported to engage in community change efforts? 5. How does your mission, along with other internal policies and practices, align with your commitment to community prevention? 6. How would a change in leadership influence the clinic s commitment to community prevention as a priority? 7. How do you set your organizational direction? 8. Is there time and space for community conditions discussions at staff meetings? 9. How are community prevention related programs developed? 10. How do you define health equity? How is health equity embedded in the clinic s internal practices and mission? How does health equity relate to the clinic s programs and community prevention activities? II. Data & Analysis 1. How do you monitor the health of your patient population? How do you recognize and understand emerging health trends among your patients? 2. Do you use any additional data sources beyond clinic data to enhance the understanding of the health status of the population your clinic serves? 3. What are the implications of health information technology implementation on your clinic s operations? Are you utilizing health information technology to collect information that focuses on the social determinants of health or asks about community conditions? If so, how? 4. How does information get recorded, compiled, and analyzed? 5. How is data used to make decisions about new initiatives, programs, or practice changes to improve population health? 28
43 III. Advocacy Efforts and Partnerships 1. What do you see as your clinic s role in advocacy and policy change? And how do you staff that role? 2. How do you decide which coalitions you are involved with? 3. Are you involved with or connected to any advocacy organizations? If so, which ones? (i.e., CPCA, NACHC, Health Access, housing coalition, food and farm coalition, etc.)? 4. Are you also involved in efforts around policy change or changes to community environments? Are there policies (local, state, federal) that the clinic has helped champion or changes to specific community conditions that support health? 5. How do you pay for staff time to do advocacy work? 6. What partners do you work with outside the health care sector? How do these partnerships inform you work? 7. What is the nature of your partnerships with surrounding or local health care organizations? IV. Payment and Funding for Primary Prevention 1. What are your major sources of funding, in general? How do the funds break down? 2. How are efforts that focus on changing community conditions currently funded? If you have found any limitations that exist with current funding streams, how do you work through/around those limitations? 3. What are you able to accomplish with current funding streams (Medicaid, Medicare, etc.)? 4. Do you see opportunities within the ACA for paying for community prevention? Do you see any opportunity for intersection with the CDC s Community Transformation Grants (CTG) or other federal funds? 5. How are philanthropic (or other) dollars leveraged? V. Clinician Perspective 1. What information are you collecting during the appointment? How are you recording your information? 2. How often are patients asked about other factors (housing, environment) that may contribute to their health conditions during the clinical encounter? For the Medical Director 3. How are you standardizing information that is collected by different clinicians? Is data on social, economic, and community conditions collected from individual patients on the patient intake form? 29
44 VI. Final Overarching Questions 1. Who are you connected to that would promote changes at the local, state, and federal level to support this work? 2. Who do you look to for leadership around issues related to population health or community prevention? 3. How can we be helpful to you? 30
45 Triple Aims Primary Drivers Secondary Drivers New health system models and policies Improve educational infrastructure to prepare support health access for underserved populations public health/health care professionals Improve Population Health Outcomes by 2020 Public health, behavioral health, and primary care functions integrated and co-located Provide appropriate access to essential, quality, consistent, seamless patient-centered services statewide Health system addresses adverse social determinants, emphasizes prevention and healthy lifestyle choices, and reduces Promote healthy eating/active lifestyles (obesity), diabetes prevention/management, prevent/control tobacco use Driver Diagram health disparities Address sub-populations that can produce ROI (e.g. ED frequent users, small areas with disparities). Health system is patient centered, culturally sensitive, Address social determinants of health affecting health NM Department of Health NM Human Services Department June 1, 2015 Improve Patient Experience and Quality of Care by 2020 meets local needs Primary care, public health, and behavioral health services are integrated & managed for quality Acute and long-term care managed for quality Involve consumers in decision making about their own health and well being options Expand use of PCMH to engage patients (assessments, wellness activities and technology) Develop a payment model that supports PCMH and Value-based care provided by a multidisciplinary, diverse, community centered wellness geographically distributed health system workforce reflecting NM demographics Train and integrate health professionals and paraprofessionals (e.g. community health workers and community EMS.) Develop inclusive recruitment and retention policies and processes Slow the Rate of Growth in Health Care Costs by 2020 Multi-payer strategy and/or value-based reimbursement for care policies Develop sustainable pricing and payment models to support innovation design Functional, interoperable health information system Improve care coordination, medication management, EHR interoperability, evaluation of health system performance Draft Version #3 June 1, 2015
46 SIM Timeline OPA will combine Business, workforce, HIT and Sustainability plans into a final document. 8/30/2015 Model HSI Design 1st Draft 10/21/2015 Oct Summit - Cancelled 11/18/ /30/2015 Final HSI Design Draft Nov Summit - Cancelled 9/1/ /1/ /1/ /1/2015 1/1/2016 8/1/2015 1/15/2016 8/19/2015 Aug Summit - Design Validation 9/16/2015 Sept Summit - Project Status 9/30/2015 Gap Assessment Report Input from sustainability, workforce and HIT plans are given to OPA for integration into the Business Plan 10/15/2015 Scale & Scope Roll Out Plan HIT, Workforce roll-out plans to be integrated in over-all roll out 12/2/2015 Present Final HSI Draft to Steering Committee 12/16/2015 Present Final HSI Draft to Public At Dec Summit (final) 1/15/2016 Submit Final HSI Draft to CMS 12/5/2015 Present Final HSI Draft to Governor The Governor will make the final decision on Governance for the Health System July 28, 2015 Version 1.0 Page 1
47 NM Health System Innovation Committee Member Organizations Aging and Long Term Services Department Alliance of Health Councils Board of Nursing Chronic Disease Prevention Council Children, Youth, and Families Department Department of Information Technology General Services Department Indian Affairs Department Legislators (Democrat and Republican) New Mexico Economic Development Department New Mexico Hospital Association New Mexico Medical Board New Mexico Primary Care Association New Mexico State University Office of the Governor Office of the Superintendent of Insurance Representative of people with Disabilities Presbyterian Healthcare Services Public Education Department Tribal Representative University of New Mexico
48 August 19, 2015 Health System Innovation Summit Registration List Last Name First Name Company Committee Acosta Susan Department of Health- PHD Population Health Acosta-Fresquez Jeanette Project ECHO Payment Models Adams Freida NMDOH Workforce and Training Needs Adams Nicole NM HED Workforce and Training Needs Ahner Tamera Gila Regional Medical Center Health Care Alamo Ashley Na Payment Models Allocco Scott SJA Healthcare Strategies Payment Models Alverson Dale UNM Center for Telehealth Health Information Systems Amezquita Denise UNM nursing student Population Health Antle David Pueblo of Isleta Tribal Armijo Kari HSD/Medical Assistance Division Payment Models Armistad Amy Project ECHO Tribal Atcitty Janelle Presbyterian Tribal Atkinson Bill Molina Healthcare New Mexico Health Information Systems Avery Catherine NMDOH Population Health Avery Alexis NMDOHPHD Population Health Baum Susan NMDOH Integration of Public Health and Primary Care Beato Cristina UNMHSC Workforce and Training Needs Berna Joannie State of NM Health Information Systems Bonner Gloria DOH/Family Health Bureau Population Health Brown Coffee UNM SOM EMS Academy Workforce and Training Needs Bryan Lupe Jemez Pueblo Health Board Tribal Burkhart Ruth New Mexico State University Integration of Public Health and Primary Care Burmeister Ina RMCHCS Health Care Camden Kelly New Mexico Breastfeeding Task Force Population Health Campbell Kristina New Mexico Medical Insurance Pool Health Care Canfield Suzanne NMNA Population Health Carver Adrian N NM Forum for Youth in Community adrian@nmforumforyouth.org Population Health Caverly Priscilla HUMAN SERVICES DEPARTMENT priscilla.caverly@state.nm.us Tribal Chacon Susan DOH/CMS susan.chacon@state.nm.us Population Health Chavez Francisco DOH-OSAH francisco.chavez@state.nm.us Population Health Chavez Shirley University of New Mexico shirl3868@gmail.com Population Health Chavez Rosemary Sandoval County Community Health rochavez@sandovalcountynm.gov Population Health Chenier Eric Legislative Finance Committee eric.chenier@nmlegis.gov Population Health Ciesielski Bette Jo NM Community Health Worker Association bjciesielski@centurylink.net Workforce and Training Needs Conejo David RMCHCS dconejo@rmchcs.org Tribal Crist-Ruiz Shawna HSD shawna.crist-ruiz@state.nm.us Health Care Crossey Michael J. Tricore Reference Laboratory michael.crossey@tricore.org Population Health DeBolt Chris Gila Regional Medical Center cdebolt@wildblue.net Population Health Dugas Karen NM Dept of Health, Office of Injury Preventionkaren.dugas@state.nm.us Population Health Dunlap Taylor HealthInsight New Mexico tdunlap@healthinsight.org Payment Models Duran Jacqueline UNMH jduran2@unm.edu Health Care Dye Jeff New Mexico Hospital Association jdye@nmhsc.com Health Care East Thomas D. LCF Research (NMHIC) thomas.east@lcfresearch.org Health Information Systems Edwards Rick Iatric Systems rick.edwards@iatric.com Health Information Systems Falcon Rodriguez Tatiana Presbyterian Healthcare Services: Healthy Hetfalconro@phs.org Integration of Public Health and Primary Care Falconer Gail BHPC gailfalconer@gmail.com Population Health
Sanjeev Arora MD. New Mexico 3/6/2014
 Sanjeev Arora MD Distinguished Professor of Medicine (Gastroenterology/Hepatology) Director of Project ECHO Department of Medicine University of New Mexico Health Sciences Center The mission of Project
Sanjeev Arora MD Distinguished Professor of Medicine (Gastroenterology/Hepatology) Director of Project ECHO Department of Medicine University of New Mexico Health Sciences Center The mission of Project
Project ECHO (Extension for Community Health Outcomes)
") Project ECHO (Extension for Community Health Outcomes) SanjeevArora MD Distinguished Professor of Medicine (Gastroenterology/Hepatology) Director of Project ECHO Department of Medicine University of New
Project ECHO (Extension for Community Health Outcomes) SanjeevArora MD Distinguished Professor of Medicine (Gastroenterology/Hepatology) Director of Project ECHO Department of Medicine University of New
Project ECHO New Mexico
 Mission Project ECHO New Mexico Michelle Iandiorio, MD Medical Director, HIV ECHO Associate Professor, UNM DOIM, Div ID Democratize medical knowledge and get best practice care to underserved people all
Mission Project ECHO New Mexico Michelle Iandiorio, MD Medical Director, HIV ECHO Associate Professor, UNM DOIM, Div ID Democratize medical knowledge and get best practice care to underserved people all
THE TRANSFORMATIVE MODEL IN EDUCATION AND CARE DELIVERY
 THE TRANSFORMATIVE MODEL IN EDUCATION AND CARE DELIVERY ECHO Colorado (Extension for Community Health Outcomes) helps democratize knowledge and develops capacity in rural and underserved communities. Using
THE TRANSFORMATIVE MODEL IN EDUCATION AND CARE DELIVERY ECHO Colorado (Extension for Community Health Outcomes) helps democratize knowledge and develops capacity in rural and underserved communities. Using
Only 5% of New Mexicans infected with hepatitis C were able to access treatment.
 THE TRANSFORMATIVE MODEL IN MEDICAL EDUCATION AND CARE DELIVERY Project ECHO (Extension for Community Healthcare Outcomes) helps democratize medical knowledge and develops specialty care capacity in underserved
THE TRANSFORMATIVE MODEL IN MEDICAL EDUCATION AND CARE DELIVERY Project ECHO (Extension for Community Healthcare Outcomes) helps democratize medical knowledge and develops specialty care capacity in underserved
THE TRANSFORMATIVE MODEL IN MEDICAL EDUCATION AND CARE DELIVERY
 THE TRANSFORMATIVE MODEL IN MEDICAL EDUCATION AND CARE DELIVERY Project ECHO (Extension for Community Healthcare Outcomes) helps democratize medical knowledge and develops specialty care capacity in underserved
THE TRANSFORMATIVE MODEL IN MEDICAL EDUCATION AND CARE DELIVERY Project ECHO (Extension for Community Healthcare Outcomes) helps democratize medical knowledge and develops specialty care capacity in underserved
Report on Project ECHO A Great Investment for the State of New Mexico
 Report on Project ECHO A Great Investment for the State of New Mexico The University of New Mexico Health Sciences (UNMHSC) serves as New Mexico s flagship institution of higher learning through demonstrated
Report on Project ECHO A Great Investment for the State of New Mexico The University of New Mexico Health Sciences (UNMHSC) serves as New Mexico s flagship institution of higher learning through demonstrated
approved Nevada s State Innovation Model (SIM) Round October 2015 Division of Health Care Financing and Policy Introduction to SIM
 Round October 2015 Division of Health Care Financing and Policy Introduction to SIM") Nevada State Innovation Model (SIM) October 2015 1 Introduction to SIM The Center for Medicare and Medicaid Services (CMS) approved Nevada s State Innovation Model (SIM) Round Two application to improve
Nevada State Innovation Model (SIM) October 2015 1 Introduction to SIM The Center for Medicare and Medicaid Services (CMS) approved Nevada s State Innovation Model (SIM) Round Two application to improve
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Click to edit Master title style. ECHO Care: a program to care for complex patients
 ECHO Care: a program to care for complex patients Miriam Komaromy, MD Associate Director, Project ECHO miriamk1@salud.unm.edu ECHO Care is a special health care program designed to support patients insured
ECHO Care: a program to care for complex patients Miriam Komaromy, MD Associate Director, Project ECHO miriamk1@salud.unm.edu ECHO Care is a special health care program designed to support patients insured
Project ECHO: Enhancing Health Outcomes Through Democratization of Knowledge
 Project ECHO: Enhancing Health Outcomes Through Democratization of Knowledge MeHAF Advancing Rural Health Transformation Conference November 10, 2016 Danielle Louder, Program Director Northeast Telehealth
Project ECHO: Enhancing Health Outcomes Through Democratization of Knowledge MeHAF Advancing Rural Health Transformation Conference November 10, 2016 Danielle Louder, Program Director Northeast Telehealth
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Community Health Needs Assessment July 2015
 Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
1115 Waiver Renewal Tribal Consultation June 23, New Mexico Human Services Department
 1115 Waiver Renewal Tribal Consultation June 23, 2017 New Mexico Human Services Department 1 Centennial Care 2.0 Concepts Public Comments Wrap Up Provide information about Centennial Care: overview, goals,
1115 Waiver Renewal Tribal Consultation June 23, 2017 New Mexico Human Services Department 1 Centennial Care 2.0 Concepts Public Comments Wrap Up Provide information about Centennial Care: overview, goals,
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Patient-Centered Medical Home 101: General Overview
 Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Patient-Centered Medical Home 101: General Overview Publicly Available Slide Deck Last Updated: January 2015 Suggested Citation: PCPCC Map Tools. (2015). Patient-Centered Medical Home 101: General Overview.
Minnesota Accountable Health Model Accountable Communities for Health Grant Program
 Request for Proposals Minnesota Accountable Health Model Accountable Communities for Health Grant Program September 2, 2014 Page 1 of 79 Contents: 1. Overview... 3 2. Available Funding and Estimated Awards...
Request for Proposals Minnesota Accountable Health Model Accountable Communities for Health Grant Program September 2, 2014 Page 1 of 79 Contents: 1. Overview... 3 2. Available Funding and Estimated Awards...
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships
 States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
States of Change: Expanding the Health Care Workforce and Creating Community-Clinical Partnerships Thursday, November 7, 2013 12:00 1:30 pm ET Sponsored by Merck Foundation www.alliancefordiabetes.org
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE. Tennessee Primary Care Association Annual Conference October 25 26, 2012.
 IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
IMPLEMENTATION OF INTEGRATED CARE FROM A LEADERSHIP PERSPECTIVE Tennessee Primary Care Association Annual Conference October 25 26, 2012 Outline I. Brief Overview of Cherokee (Who are we?) II. The Integrated
A CDC REACH, NIH, OPHS and HRSA CHC grantee applies lessons learned to create a new paradigm for community health care financing and delivery
 A CDC REACH, NIH, OPHS and HRSA CHC grantee applies lessons learned to create a new paradigm for community health care financing and delivery Census 2010 Population / % served: Grant County: 29,514 / 55.4%
A CDC REACH, NIH, OPHS and HRSA CHC grantee applies lessons learned to create a new paradigm for community health care financing and delivery Census 2010 Population / % served: Grant County: 29,514 / 55.4%
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care
 Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Value-Based Payments 101: Moving from Volume to Value in Behavioral Health Care Nina Marshall, MSW Senior Director, Policy and Practice Improvement NinaM@TheNationalCouncil.org Bill Hudock Senior Public
Introduction for New Mexico Providers. Corporate Provider Network Management
 Introduction for New Mexico Providers Corporate Provider Network Management Overview New Mexico snapshot. Who we are. Why Medicaid managed care? Why AmeriHealth Caritas? Why partner with us? Medical Management
Introduction for New Mexico Providers Corporate Provider Network Management Overview New Mexico snapshot. Who we are. Why Medicaid managed care? Why AmeriHealth Caritas? Why partner with us? Medical Management
Fostering Effective Integration of Behavioral Health and Primary Care in Massachusetts Guidelines. Program Overview and Goal.
 Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Person Centered Agenda
 1 Person Centered Agenda Initial Confusion Overwhelmed by Statistics and Acronyms Dramatic Engagement of Issue Extreme Interest and Curiosity Deep Sense of Relief SAMHSA S STRATEGIC INITIATIVES Leading
1 Person Centered Agenda Initial Confusion Overwhelmed by Statistics and Acronyms Dramatic Engagement of Issue Extreme Interest and Curiosity Deep Sense of Relief SAMHSA S STRATEGIC INITIATIVES Leading
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Working Together for a Healthier Washington
 Working Together for a Healthier Washington Laura Kate Zaichkin, Administrator, Office of Health Innovation & Reform Health Care Authority April 29, 2015 Why do we need health system transformation? Because
Working Together for a Healthier Washington Laura Kate Zaichkin, Administrator, Office of Health Innovation & Reform Health Care Authority April 29, 2015 Why do we need health system transformation? Because
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Mary L. Blankson DNP, APRN, FNP-C Bernadette Thomas DNP, APRN, FNP-C, MPH My Phuong Tong, BA
 Translation of the Primary Care Provider-centered Project ECHO Model into a Tool to Support Frontline Nurses in Complex Care Management Using the Knowledge to Action Framework Mary L. Blankson DNP, APRN,
Translation of the Primary Care Provider-centered Project ECHO Model into a Tool to Support Frontline Nurses in Complex Care Management Using the Knowledge to Action Framework Mary L. Blankson DNP, APRN,
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs. September 20, 2017
 Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
HHSC Value-Based Purchasing Roadmap Texas Policy Summit
 HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017
 D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
D21/E21 These presenters have nothing to disclose Project ECHO: Action for Improvement Elizabeth Clewett, PhD, MBA Cory Sevin, RN, MSN December 13, 2017 Session Objectives P2 Describe how Project ECHO
UC Davis Pain Management Telehealth Academy
 UC Davis Pain Management Telehealth Academy Project ECHO Pain Management Telementoring Train the Trainers: Primary Care Pain Management Fellowship David J. Copenhaver, MD, MPH Associate Professor, Anesthesiology
UC Davis Pain Management Telehealth Academy Project ECHO Pain Management Telementoring Train the Trainers: Primary Care Pain Management Fellowship David J. Copenhaver, MD, MPH Associate Professor, Anesthesiology
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare
: Billing, Codes and Need at Adelante Healthcare") Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Medical Nutrition Therapy (MNT): Billing, Codes and Need at Adelante Healthcare An investigation of Medical Nutrition Therapy (MNT) billing requirements and handling By Melissa Brito Phillips Beth Israel
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it
 Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Financing SBIRT in Primary Care: The Alphabet Soup and Making Sense of it CAPT Hernan Reyes, MD Deputy Regional Administrator, HRSA Region 6 July 13, 2016 Objectives Understand the role of HRSA within
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL
 PROGRAM DESIGN AND BUDGET PROPOSAL") LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL SESSION LAW 2015-245, SECTION 8 FINAL REPORT State of North Carolina
LEGISLATIVE REPORT NORTH CAROLINA HEALTH TRANSFORMATION CENTER (TRANSFORMATION INNOVATIONS CENTER) PROGRAM DESIGN AND BUDGET PROPOSAL SESSION LAW 2015-245, SECTION 8 FINAL REPORT State of North Carolina
HIT Glossary and Acronym List
 HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
Michigan s Vision for Health Information Technology and Exchange
 Michigan s Vision for Health Information Technology and Exchange Health information exchange or HIE is the mobilization of health care information electronically across organizations within a region, community
Michigan s Vision for Health Information Technology and Exchange Health information exchange or HIE is the mobilization of health care information electronically across organizations within a region, community
Integrating Population Health into Delivery System Reform
 Integrating Population Health into Delivery System Reform Population Health Roundtable IOM Jim Hester Washington DC June 13, 2013 Theme The health care system is transitioning from payment rewarding volume
Integrating Population Health into Delivery System Reform Population Health Roundtable IOM Jim Hester Washington DC June 13, 2013 Theme The health care system is transitioning from payment rewarding volume
Center for Community Health Navigation at NewYork-Presbyterian Hospital
 Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
Center for Community Health Navigation at NewYork-Presbyterian Hospital CENTER MISSION Mission: To support the health and wellbeing of patients through the delivery of culturallysensitive, peer-based support
Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012
 Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012 Joan Cleary, Interim Executive Director Minnesota Community Health Worker Alliance
Community Health Workers & Rural Health: Increasing Access, Improving Care Minnesota Rural Health Conference June 26, 2012 Joan Cleary, Interim Executive Director Minnesota Community Health Worker Alliance
Financing of Community Health Workers: Issues and Options for State Health Departments
 Financing of Community Health Workers: Issues and Options for State Health Departments ASTHO Technical Assistance Presentation Terry Mason, PhD Carl Rush, MRP Geoff Wilkinson, MSW This webinar is supported
Financing of Community Health Workers: Issues and Options for State Health Departments ASTHO Technical Assistance Presentation Terry Mason, PhD Carl Rush, MRP Geoff Wilkinson, MSW This webinar is supported
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs. September 20, 2017
 Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Bridging to Preventive Care: The Roadmap to Medicaid Coverage of Community Based Chronic Disease Prevention & Management Programs September 20, 2017 Introductions & Agenda Introduce Panelists Overview
Project ECHO- Nevada Extension for Community Health Outcomes
 Project ECHO- Nevada Extension for Community Health Outcomes Evan Klass, M.D. Associate Dean, Statewide Initiatives Project Director, Project ECHO- Nevada The Mission of Project ECHO Nevada To improve
Project ECHO- Nevada Extension for Community Health Outcomes Evan Klass, M.D. Associate Dean, Statewide Initiatives Project Director, Project ECHO- Nevada The Mission of Project ECHO Nevada To improve
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process
 Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process November 16, 2017 1:00-2:00 PM, ET For audio: 888-757-2790 Passcode: 105799 Press *6 to mute/unmute your line. Please
Serving CYSHCN in Medicaid Managed Care: Contract Language and the Contracting Process November 16, 2017 1:00-2:00 PM, ET For audio: 888-757-2790 Passcode: 105799 Press *6 to mute/unmute your line. Please
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Welcome to. Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes
 Welcome to ASTHO s Delivery and Payment Reform Technical Assistance Call Series Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes Presented by ASTHO and
Welcome to ASTHO s Delivery and Payment Reform Technical Assistance Call Series Primary Care and Public Health: Linking Public Health and Advanced Primary Care to Improve Outcomes Presented by ASTHO and
Oregon s Health System Transformation & The Innovator Agent Role
 Oregon s Health System Transformation & The Innovator Agent Role Joell E. Archibald, RN, BSN, MBA Estela Gomez, MSW Belle Shepherd, MPH OHA Transformation Center Innovator Agents Background: Oregon s Health
Oregon s Health System Transformation & The Innovator Agent Role Joell E. Archibald, RN, BSN, MBA Estela Gomez, MSW Belle Shepherd, MPH OHA Transformation Center Innovator Agents Background: Oregon s Health
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers
 Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers November 30, 2015 Joshua Rubin HealthManagement.com Plan CCBHC basics NYS Health Reform
Certified Community Behavioral Health Centers and New York State s Healthcare Reform: Considerations for Providers November 30, 2015 Joshua Rubin HealthManagement.com Plan CCBHC basics NYS Health Reform
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
State Levers to Advance Accountable Communities for Health
 A PUBLICATION OF THE NATIONAL ACADEMY FOR STATE HEALTH POLICY May 2016 State Levers to Advance Accountable Communities for Health Felicia Heider, Taylor Kniffin, and Jill Rosenthal Introduction In an era
A PUBLICATION OF THE NATIONAL ACADEMY FOR STATE HEALTH POLICY May 2016 State Levers to Advance Accountable Communities for Health Felicia Heider, Taylor Kniffin, and Jill Rosenthal Introduction In an era
Partner with Health Services Advisory Group
 Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Partner with Health Services Advisory Group Bonnie Hollopeter, LPN, CPHQ, CPEHR Health Services Advisory Group (HSAG) Quality Improvement Lead Rosalie McGinnis, MS, RN HSAG Quality Improvement Lead November
Albany Medical Center. AMCH PPS Clinical & Quality Affairs Committee
 Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Tara Foster, MS, RN Mingie Kang, MPH Mark Quail, MEd Brendon Smith, PhD Susan Kopp MBA, BSN, RN January
Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Tara Foster, MS, RN Mingie Kang, MPH Mark Quail, MEd Brendon Smith, PhD Susan Kopp MBA, BSN, RN January
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Draft Covered California Delivery Reform Contract Provisions Comments Welcome and Encouraged
 TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
Reforming Health Care with Savings to Pay for Better Health
 Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Reforming Health Care with Savings to Pay for Better Health Mark McClellan, MD PhD Director, Initiative on Health Care Value and Innovation Senior Fellow, Economic Studies October 2014 National Forum on
Health Center Program Update
 Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Health Center Program Update NACHC Policy & Issues Forum March 14, 2018 Jim Macrae Associate Administrator, Bureau of Primary Health Care (BPHC) Health Resources and Services Administration (HRSA) 3/22/2018
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination
 Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Community Needs Assessment for Albany Medical PPS Stage 1 Summary Results. HCDI Assessment Team 9/29/14
 Community Needs Assessment for Albany Medical PPS Stage 1 Summary Results 1 HCDI Assessment Team 9/29/14 HCDI Assessment Team Healthy Capital District Initiative Project Management Kevin Jobin-Davis, Executive
Community Needs Assessment for Albany Medical PPS Stage 1 Summary Results 1 HCDI Assessment Team 9/29/14 HCDI Assessment Team Healthy Capital District Initiative Project Management Kevin Jobin-Davis, Executive
LegalNotes. Disparities Reduction and Minority Health Improvement under the ACA. Introduction. Highlights. Volume3 Issue1
 Volume3 Issue1 is a regular online Aligning Forces for Quality (AF4Q) publication that provides readers with short, readable summaries of developments in the law that collectively shape the broader legal
Volume3 Issue1 is a regular online Aligning Forces for Quality (AF4Q) publication that provides readers with short, readable summaries of developments in the law that collectively shape the broader legal
Navigating an Enhanced Rural Health Model for Maryland
 Executive Summary HEALTH MATTERS: Navigating an Enhanced Rural Health Model for Maryland LESSONS LEARNED FROM THE MID-SHORE COUNTIES To access the Report and Accompanied Technical Reports go to: go.umd.edu/ruralhealth
Executive Summary HEALTH MATTERS: Navigating an Enhanced Rural Health Model for Maryland LESSONS LEARNED FROM THE MID-SHORE COUNTIES To access the Report and Accompanied Technical Reports go to: go.umd.edu/ruralhealth
New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature
 New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature November 2012 Division of Medical Assistance and Health Services NJ Department of Human Services Introduction In September,
New Jersey Medicaid Medical Home Demonstration Project Report to the Legislature November 2012 Division of Medical Assistance and Health Services NJ Department of Human Services Introduction In September,
Integration of Clinical Care and Public Health Systems: The need as reflected in the work of the Alliance to Reduce Disparities in Diabetes
 Integration of Clinical Care and Public Health Systems: The need as reflected in the work of the Alliance to Reduce Disparities in Diabetes Moderator and Presenter Belinda W. Nelson, PhD Center for Managing
Integration of Clinical Care and Public Health Systems: The need as reflected in the work of the Alliance to Reduce Disparities in Diabetes Moderator and Presenter Belinda W. Nelson, PhD Center for Managing
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Primary Care 101: A Glossary for Prevention Practitioners
 PREVENTION COLLABORATION IN ACTION Engaging the Right Partners Primary Care 101: A Glossary for Prevention Practitioners As the U.S. healthcare landscape continues to change under the Affordable Care Act
PREVENTION COLLABORATION IN ACTION Engaging the Right Partners Primary Care 101: A Glossary for Prevention Practitioners As the U.S. healthcare landscape continues to change under the Affordable Care Act
WPCC Workgroup. 2/20/2018 Meeting
 WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
WPCC Workgroup 2/20/2018 Meeting Today s Agenda 1. Introductions 2. Medicaid Transformation Overview 3. WPCC in the Transformation 4. Change Plan Overview 5. Review of Supporting Data 6. Change Plan Deep
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
PCA/HCCN Health Center Program Update
 PCA/HCCN Health Center Program Update National Association of Community Health Centers Community Health Institute August 30, 2016 Tonya Bowers, MHS Acting Associate Administrator Bureau of Primary Health
PCA/HCCN Health Center Program Update National Association of Community Health Centers Community Health Institute August 30, 2016 Tonya Bowers, MHS Acting Associate Administrator Bureau of Primary Health
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Checklist for Ocean County Community Health Improvement Plan Implementation of Strategies- Activities for Ocean County Health Centers: CHEMED & OHI
 Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
Checklist for Community Health Improvement Plan Implementation of Strategies- Activities for Lead Organizations Activities Target Date Progress to Date Childhood Obesity (4 Health Centers 1-Educate on
1:00pm EST Webinar will begin shortly.
 Community Health Workers: Part of the Solution for Advancing Health Equity; Perspectives and Initiatives from the New England Regional Health Equity Council 1:00pm EST Webinar will begin shortly. Community
Community Health Workers: Part of the Solution for Advancing Health Equity; Perspectives and Initiatives from the New England Regional Health Equity Council 1:00pm EST Webinar will begin shortly. Community
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts
 Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Effective Care for High-Need, High-Cost Patients: How to Maximize Prevention and Population Health Efforts May 9, 2018 www.hcttf.org 1 Speakers Jeff Micklos Executive Director HCTTF Kelly McCracken National
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014
 Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014 NM Title V MCH Block Grant 2016 Application/2014 Report Executive Summary
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014 NM Title V MCH Block Grant 2016 Application/2014 Report Executive Summary
Payment Reform Strategies. Ann Thomas Burnett BlueCross BlueShield of South Carolina
 Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
Payment Reform Strategies Ann Thomas Burnett BlueCross BlueShield of South Carolina Disclosure I have no relevant financial relationships with commercial interests to disclose. The Current Market Landscape
The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure
 The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure Marci Nielsen, PhD, MPH Executive Director Amy Gibson, MS, RN Chief Operating Officer Patient-Centered
The Patient-Centered Primary Care Collaborative: New Vision, New Strategic Plan, New Organizational Structure Marci Nielsen, PhD, MPH Executive Director Amy Gibson, MS, RN Chief Operating Officer Patient-Centered
Opportunities to Leverage Telehealth Within Your ACO Strategy
 Opportunities to Leverage Telehealth Within Your ACO Strategy Shawn Valenta RRT, MHA Administrator of Telehealth Center for Telehealth Phillip Warr, MD Interim Chief Medical Officer Case Management and
Opportunities to Leverage Telehealth Within Your ACO Strategy Shawn Valenta RRT, MHA Administrator of Telehealth Center for Telehealth Phillip Warr, MD Interim Chief Medical Officer Case Management and
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
The Integration of Behavioral Health and Primary Care: A Leadership Perspective
 The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Integration of Behavioral Health and Primary Care: A Leadership Perspective Eboni Winford, Ph.D. Behavioral Health Consultant Cherokee Health Systems Our Mission To improve the quality of life for
The Influence of Health Policy on Clinical Practice. Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center
 The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
The Influence of Health Policy on Clinical Practice Dr. Kim Kuebler, DNP, APRN, ANP-BC Multiple Chronic Conditions Resource Center Disclaimer Director: Multiple Chronic Conditions Resource Center www.multiplechronicconditions.org
Recovery Homes: Recovery and Health Homes under Health Care Reform
 Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Recovery Homes: Recovery and Health Homes under Health Care Reform 4/27/11 Richard H. Dougherty, Ph.D. DMA Health Strategies Challenges of health reform Increasing coverage Reducing costs of coverage Reducing
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
State Health Department Support for CHW Workforce Development and Engagement
 State Health Department Support for CHW Workforce Development and Engagement Geoff Wilkinson, Senior Policy Advisor Office of the Commissioner Massachusetts Department of Public Health New England Regional
State Health Department Support for CHW Workforce Development and Engagement Geoff Wilkinson, Senior Policy Advisor Office of the Commissioner Massachusetts Department of Public Health New England Regional
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Health Care Evolution
 Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Health Care Evolution Patient-Centered Medical Home to Clinical Integration & Accountable Care Ken Bertka, MD bertka@mindspring.com 419-346-8719 Agenda Top 3 Challenges of Health Care Reform PCMH & ACO
Certified Community Behavioral Health Clinic (CCHBC) 101
 101") Certified Community Behavioral Health Clinic (CCHBC) 101 On April 1, 2014, the President signed the Protecting Access to Medicare Act (PAMA) into law, which included a provision authorizing a two part
Certified Community Behavioral Health Clinic (CCHBC) 101 On April 1, 2014, the President signed the Protecting Access to Medicare Act (PAMA) into law, which included a provision authorizing a two part
Promoting Mental Health and Preventing Substance Abuse as part of NY s Prevention Agenda Taking Action November 12, 2014
 Promoting Mental Health and Preventing Substance Abuse as part of NY s Prevention Agenda 013-017 Taking Action November 1, 014 Guthrie Birkhead, MD, MPH Deputy Commissioner New York State Department of
Promoting Mental Health and Preventing Substance Abuse as part of NY s Prevention Agenda 013-017 Taking Action November 1, 014 Guthrie Birkhead, MD, MPH Deputy Commissioner New York State Department of
NEW MEXICO ACTION COALITION
 1 NEW MEXICO ACTION COALITION OUR MISSION: The New Mexico Action Coalition strives to provide strategic direction through community collaboration and grassroots efforts with key stakeholders to transform
1 NEW MEXICO ACTION COALITION OUR MISSION: The New Mexico Action Coalition strives to provide strategic direction through community collaboration and grassroots efforts with key stakeholders to transform