THE IMPACT OF THE PATIENT-CENTERED MEDICAL HOME MODEL ON MATERNAL & CHILD HEALTH OUTCOMES IN A COMMUNITY HEALTH CENTER SETTING IN NORTH CAROLINA
|
|
|
- Bryce Collin James
- 5 years ago
- Views:
Transcription
1 THE IMPACT OF THE PATIENT-CENTERED MEDICAL HOME MODEL ON MATERNAL & CHILD HEALTH OUTCOMES IN A COMMUNITY HEALTH CENTER SETTING IN NORTH CAROLINA by Kristina Wharton A paper presented to the faculty of The University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Public Health in the Department of Maternal and Child Health. Chapel Hill, N.C. April 20, 2015, 2015 Approved by: First Reader Second Reader
2 Table of Contents Table of Contents 2 Abstract:... 4 Introduction... 5 Background on PCMH... 7 Problem Statement Hypotheses and Relevance to Maternal & Child Health Methods: Design, Sampling, Data Collection, Data Analysis Results and Interpretation of Results Policy Implications and Recommendations and Significance for Maternal and Child Health Conclusions References Acknowledgments Appendices A. Theory and Concept Models Institute for Healthcare Improvement s Design of a Triple Aim Enterprise¹ MU Registration for Intent: Conceptual Model PCMH Conceptual Model : Organizational Learning Model and Learning Health System B. Terms & Definitions Glossary of Abbreviations and Terms Key Term and Program Descriptions C. Definition of Patient-Centered Medical Home Key Terminology² D. Health Center Data & Results⁹ List of Community Health Centers Included in Study Uniform Data System 2013 Definitions for Table 6B "Quality of Care Indicators/Health Outcomes" ¹⁰ RESULTS: All NC Community Health Centers 2013 Uniform Data System Maternal and Child Health Quality and Outcomes
3 4. RESULTS: Non-PCMH-Recognized NC Community Health Centers 2013 Uniform Data System Maternal and Child Health Quality and Outcomes RESULTS: PCMH-Recognized NC Community Health Centers 2013 Uniform Data System Maternal and Child Health Quality and Outcomes RESULTS: 2011 & 2012 Trend & Comparative Data: All NC Community Health Centers Uniform Data System Maternal and Child Health Quality and Outcomes RESULTS: 2011 & 2012 Trend & Comparative Data for PCMHs: NC Community Health Centers Uniform Data System Maternal and Child Health Quality and Outcomes RESULTS: 2011 & 2012 Trend & Comparative Data for Non-PCMHs: NC Community Health Centers Uniform Data System Maternal and Child Health Quality and Outcomes RESULTS: 2011, 2012, Year Average of Adjusted Quartile Rankings for Medical Homes RESULTS: 2011, 2012, Year Average of Adjusted Quartile Rankings for Medical Homes
4 Abstract: Objectives: Currently, the Patient-Centered Medical Home model is an important tool for primary care providers to improve quality of care and health outcomes. Its adoption at practices across the US is incentivized by enhanced reimbursement and ability to participate in Accountable Care Organizations. However, because the model is relatively new in its implementation, there is not much information available regarding its effectiveness. As more and more community health centers adopt the model to improve the health of vulnerable populations, this study addresses the question of whether PCMH is effective at achieving the goals in the context of federally qualified health centers. Specifically, we will look at performance of FQHCs in North Carolina with respect to five Maternal and Child Health indicators to assess the impact of PCMH on safety-net providers. Methods: Secondary data from the HRSA Bureau of Primary Healthcare Uniform Data System report data from UDS Table 6B: Quality of Care Indicators/Health Outcomes from were used to compare five MCH quality of care indicators. Including all 33 North Carolina FQHCs that reported UDS data since 2011, we reviewed 18 of primary care medical homes and 15 non-medical homes. No significant differences on the quality of care indicators between the medical homes and non-medical homes for the 5 MCH indicators analyzed for this study were found. However, due to small sample sizes and other factors influencing medical home transformation imact, more research is necessary to establish a confident conclusion on the model s effect on quality of care for MCH population in NC FQHCs. 4
5 Results: We did not find significant differences between NC FQHCs with and without PCMH recognition with regard to the five MCH indicators when comparing recognized medical homes to non-medical homes. Conclusions: PCMH recognition does not seem to have an impact on MCH outcomes. Given the investment of resources being allocated to medical home transformation by practices and third party payors, our results emphasize the need for additional research on the efficacy of the PCMH model to improve quality of care in FQHCs. Introduction The Patient-Centered Medical Home model is an evidence-based model of healthcare delivery implemented for the purpose of achieving the Institute for Healthcare Improvement s Triple Aim ¹ of the contemporary U.S. healthcare industry: improving the patient experience of care (including quality and satisfaction); improving the health of populations; and reducing the per capita cost of health care (Appendix A- 1).¹ Primarily implemented in primary healthcare settings,² the Patient-Centered Medical Home model and program (referred to as PCMH) offer direct service providers a concrete framework of clear and specific criteria ² from which to transform the ways they organize care around patients ² to support the national initiatives to improve patients experience, health outcomes, and cost of care (Appendices A1-3).¹ PCMH operates concurrently and collaboratively with the present federal, state and local systems that also aim to improve care quality, patient outcomes, and mitigate the rising costs of healthcare 1,2. The model employs and is advantaged by the 5
6 availability of the resources and enterprises in our current political, economic and technological landscape. For example: the passing of the ACA and HITECH Act, and other legislative investments in health systems infrastructure (see Appendix A-2 and A-3 for rich picture models explaining how PCMH and MU fit into the political landscape).³also, PCMH integrates the use of certified health information technology (CHIT) incentivized by the Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009.⁴ Furthermore, PCMH was designed intentionally designed for its Standards, Elements and Factors to align with the Centers for Medicare and Medicaid Services Meaningful Use (MU) program throughout its three Stages. The MU program is designed to assure consistent data collection that also contributes to reliable state and federal surveillance systems (Appendix A-2). 2,5 The model both reflects and supports the different systems working collectively² to meet the shared goals of generating more actionable information related to the provision of quality care and health outcomes¹ to ultimately create a national health information infrastructure (Appendix A-3).⁶ This paper seeks to evaluate the effectiveness of the PCMH model objective of enhancing actionable situation awareness⁷ at the practice-level by requiring consistent and systematic reporting and review of the practices performance with regard to meeting PCMH Standards, including population management and continuous quality improvement. Specifically, this study investigates the impact PCMH has on the IHI Triple Aim s first two goals: 1) improving the patient experience of care, and 2) improving the health of populations¹ on specified maternal and child health outcomes, which are: prenatal visits in the first trimester, low birth weight, cervical cancer screenings, 6
7 adolescent weight screening and follow-up and childhood immunizations, in the 33 Federally Qualified Health Centers in the state of North Carolina. Background on PCMH PCMH is rooted in the field of Pediatric Medicine as its origins are an initiative to address the specific care coordination essentials of care for children with special healthcare needs.² Including care coordination, the model employs a six-prong approach to improving patient health quality and outcomes by providing clear explanations and requirements associated with the six core concepts, called Standards, of PCMH which are illustrated in Table 1 (See Appendix C for detailed definitions of the PCMH model Standards).² Table 1: The Six Standards, or Goals, of PCMH PCMH Standards² Assure patient access Population management Patient care management Supporting patient self-care Coordinate and manage care Continuous quality improvement Note: 2011 NCQA PCMH Standards² Outcomes² Use practice management system and patient portal to assure patients are able to see and communicate with their care team. Assure continuity of care and cultural competency of care. Collecting key demographic and clinical data, proactive identification and recall of patients with medical needs Documented evidence-based treatment plans, goals and outcomes. Medication management and e-prescribing. Documented self-care goals and outcomes, linking patient to community resources. Diagnostic test/lab/image tracking and follow up, referral management, electronic exchange of information for care transition Clinical performance data and patient satisfaction data collected, reported, and acted upon (Plan Do Study Act model) 7
8 PCMH model structure consists of 6 Standards, each with 2-7 Elements, the most valuable of which is must pass, which means the practice must meet its criteria.² Each element is comprised of individual Factors, the most important of which are critical so that a practice would not get credit for the entire element without the critical factor.², ³ This strict model forces practices to prioritize policy and workflow change to promote situation awareness. Situation awareness can be operationally defined as the ways in which users interface with information generating systems produces a better understanding of the situation. ⁷ This enables the user to better manage the information/respond to the situation, which in this context refers to patients quality of care and health outcomes.⁷ Situation awareness is categorized into three levels of individual and organizational cognitive processes: perception, comprehension and projection (decision-making).⁷ Standard 1, assuring access to care, requires accessible hours of operation, availability of various communication methods with practice and providers (phone, secure electronic, after hours, etc.) and accessibility of care with respect to cultural competency and patient understanding of how the practice serves them as a medical home.² Standard 2, population management, requires all three levels of situation awareness through proactive care delivery models that involve systematically obtaining demographic and clinical care data and reporting on it to evaluate if patients who need specific chronic and preventive services are obtaining them.² Standards 3, 4and 5 require the practice to provide coordinated care management that engaged both the practice team (other practice staff beyond the provider), the patient and their family, as 8
9 well as referral agencies such as specialist and other community resources that could improve patient care.² Document care and services in the EMR in a manner that allows searches of the data/emr to be done efficiently so information can be shared within the practice or externally with patients or other providers as needed. This practice is believed to promote situation awareness.² Documentation and reporting requirements are used to monitor success of the organization at meeting the goals of PCMH. Lastly, Standard 6 dictates how the practice reports clinical performance measures and patient satisfaction survey results to support practice situation awareness.² Using structured plan do study act models, Standard 6 promotes systematic continuous quality improvement. All of these standards, or PCMH objectives, enhance situation awareness at the practice level for the goal of quality improvement.² Information sharing is the key PCMH s contribution to surveillance systems at state and federal levels, promoting broadened situation awareness throughout these external agencies as well as internally within the medical home. Federally Qualified Health Centers (FQHC) are required to submit Uniform Data System (UDS) reports to Health Resource and Service Administration HRSA as an accountability component³ for receiving federal funds, which include reporting clinical performance measures as are outlined in National Commission for Quality Assurance (NCQA) PCMH Standard 6 above.² HRSA and Centers for Medicare and Medicaid Services (CMS) promote the use of PCMH to improve such clinical performance measures to promote reduction of health disparities between the states amongst in vulnerable populations.³ Compared to national clinical performance on the UDS 9
10 measures at health centers across the US, North Carolina FQHCs underperformed in 2 of the 5 maternal and child health outcomes reported on the 2013 UDS. 74.9% of prenatal visits started the first trimester of pregnancy in in NC, which is better than the national average of 71.6%.⁹ While the percentage of children born with low birth weight was 7.3% in NC, compared to 7.3% nationally. ⁹ Cervical cancer screening rates in NC FQHCS were 56.7% compared to 57.8% nationally.⁹ While adolescent weight screening and follow up were 49.8% in NC and 51.8% nationally.⁹ Finally, data for childhood immunizations showed that 78.2% of children who receive pediatric care at an FQHC received all recommended vaccines by the age of 3 in NC, compared to 76.4% in all health centers in the US. Problem Statement Does increased situation awareness produced by using certified health information technology, meeting Meaningful Use requirements, and obtaining Patient- Centered Medical Home Recognition impact quality of care indicators/health outcomes related to maternal & child health in community health centers in NC? Situation Awareness is the state of organizations and individuals after going through the process of collecting information, understanding information and making projections based off of that information to perform a task or function.⁸ Situation awareness is described as: know(ing) what is going on, what led to the situation and what risk is associated to it, is certainly supported by surveillance systems unique ability to inform users of various indicator trends. ⁷ situation awareness, theoretically 10
11 produced by the collaborating fields of public health informatics and quality improvement/quality assurance, aims to improve the health of populations us(ing) a wide range of interventions to achieve its goals, and the constraints of operating in a governmental context. ⁸ The intervention of interest for this study is the primary care model, Patient-Centered Medical Home. PCMH promotes practice-level situation awareness by requiring the practice to employ multiple evidence-based strategies to improve their quality of care performance and ultimately their patient population s health. Hypotheses and Relevance to Maternal & Child Health Hypotheses: FQHCs with PCMH recognition will be more effective 1) at achieving the goals of quality of care performance improvement, and 2) ultimately patient population health with respect to five Maternal and Child Health indicators compared to FQHCs without PCMH recognition. The quality of care indicators being measured in this study are: prenatal visits conducted in the first trimester; low birth weight outcomes; cervical cancer screenings; adolescent weight screening and follow-up, and childhood immunizations.⁹ Methods: Design, Sampling, Data Collection, Data Analysis 11
12 Because the aim of this study is to evaluate the effectiveness of the PCMH model at its broad and theoretical objectives described above, the goal was to demonstrate if the model actually was effective or not for maternal and child health indicators at FQHCs in NC. An ecological study design was used to compare the two groups of interest, FQHCs with PCMH recognition and FQHCs without PCMH recognition. The data was collected from Uniform Data System (UDS) reports for all 33 NC FQHCs that submitted UDS reports for calendar year In order to receive their federal funding through the HRSA 330 Grant, FQHCs are required to submit an annual, standardized performance report to HRSA s Bureau of Primary Healthcare Uniform Data System. UDS reports include demographic, clinical performance and QI/QA performance data and can impact an FQHC s future funding. UDS reports are also publicly available online.⁹ For this evaluation, FQHC UDS data was used as reported on the public, online UDS reports and were used to compare the two FQHC groups on maternal and child health indicators of interest.⁹ The year 2013 was selected as it provides the most current publicly available data.⁹ About the Sample The study population included all 33 federally qualified health centers in North Carolina which served a total of 454,675 patients in 2013 across the state as reported in the Uniform Data System.⁹ Of the 33 health centers in this study population, 18 (54.5%) were recognized Patient-Centered Medical Homes and 15 (45.5%) were not recognized as medical homes within the calendar year The 18 recognized medical homes accounted for 75% (339,961 patients) of the patients served compared to the nonmedical homes at 25% (114,714 patients) as shown in Figure 1. Also of note 31 (94%) of 12

13 the total 33 health centers in the sample had electronic health records that were installed at all practices and used by all providers" in In 2013, 53% of the 33 FQHCs in NC were PCMH recognized compared to 59% of the 1,202 FQHC grantees reporting to HRSA in 2013.⁹ The evidence does not clearly support the correlation between PCMH recognition and the differences found on the five above mentioned indicators. In terms of policy and practice, a correlation is implied between PCMH recognition and performance improvement. The goal for this study was to demonstrate if the PCMH model is actually effective or not for the five maternal and child health indicators at FQHCs in NC. An ecological study design was used to compare the two groups of interest, patients treated in a FQHC with PCMH recognition and patients treated in a FQHC without PCMH recognition. Figure Percentages of FQHCs with Patient-Centered Medical Home Recognition in NC 13
14 Secondary data from the HRSA Bureau of Primary Healthcare Uniform Data Reports for calendar year 2013 for HRSA 330 Grant recipients in the state of NC were accessed for this study. These data are publicly accessible online and available at the FQHC-level (compiling practice and outreach site data by grant recipient) as well as at the state level aggregating all FQHC UDS reported data.⁹ The data were accessed for five distinct types of information for all 33 of the NC FQHCs: 1. Identification of 330 Grant recipients in NC; 2. whether the FQHCs had EHR installed and whether the FQHCs were officially recognized as a PCMH; 3. percentage of eligible patients who met the 2013 UDS criteria for five performance measures; 5. adjusted quartile ranking of the FQHC for each of the five performance measures as compared nationally to other FQHCs UDS reported data. Using this decision method, 33 FQHC Grant recipients in 2013 from across NC were identified. See: Appendix D-1, List of Community Health Centers Included in the Study.⁹ The five performance measures selected for this study were: prenatal visits conducted in the first trimester, low birth weight outcomes, cervical cancer screenings, adolescent weight screening and follow-up and childhood immunizations. These were selected from the UDS Table 6B: Quality of Care Indicators/Health Outcomes measures and were chosen as they were the outcomes reflecting the care of maternal and child populations. Performance measures are reported in percentages where the numerator (the healthcare screening or service provided) is defined by ICD-9 codes defined by HRSA s BPHC annually and outlined in the UDS Reporting Instructions for Health Centers. Similarly, the denominator (patient samples selected to be eligible for the 14
15 screening or service according to clinical best practices) is also defined by HRSA. See: Appendix D-2, Uniform Data System 2013 Table 6B: Quality of Care Indicators/Health Outcomes Definitions (Appendices: D-2a, prenatal visits conducted in the first trimester; D-2a low birth weight outcomes; D-2c, cervical cancer screenings; D-2d, adolescent weight screening and follow-up and, D-2b, childhood immunizations).¹⁰ Data analysis was completed by entering the 2013 UDS data for the 33 NC FQHCs from the HRSA BPHC UDS website into Microsoft Excel and then averages (means) for the two groups of interest were calculated for each of the indicators of interest: patients treated in an NC FQHC with PCMH recognition and those treated in one without. The two groups performance in each of the UDS Table 6B: Quality of Care Indicators/Health Outcomes was compared using OpenEpi to calculate the following measures of association: risk, risk ratio, risk difference, chi square tests of association. Results and Interpretation of Results Differences Between the 2013 Groups of FQHC Medical Homes and Non-Medical Homes Before the PCMH Model is Introduced Before delving into impact the PCMH model has on FQHCs, we will first assess if the potential differences between the two groups (FQHC medical homes and FQHC nonmedical homes) before the PCMH model is introduced with the aim of changing QI/QA activities to improve patient care and clinical outcomes. We are doing this introduced in order to see if there were already differences between the FQHCs which received medical home transformation and those that did not. 15

16 The data displayed in Table 2, comparing three-year (2011, 2012 and 2013) averages of the two groups, 2013 medical homes and non-medical homes, demonstrates the differences existing between the two groups before the medical homes model is introduced. Table 2. Three-Year Comparison of Adjusted Quartile Rankings of 2013 Medical Homes and Non-Medical Homes for 5 MCH Indicators Figures 2-6 graphically depict that there are not extreme differences between these two groups in 2011, before the medical home model is introduced, in the comparison of the five MCH indicators by adjusted quartile rankings. In Figure 7, we see that while there are not major differences between the two groups, the majority (4 out 16
17 of 5) of the MCH indicators adjusted quartile rankings average demonstrate that the 2013-recognized medical home group performs better than the FQHCs that did not receive their recognition by Figures 2-6: Adjusted Quartile Rankings for 5 MCH Indicators over Period for 2013 Recognized Medical Homes Versus 2013 Non-Medical Homes 17
18 Difference in 3-Avg. Adjusted Quartile Rankins THE IMPACT OF THE PATIENT-CENTERED MEDICAL HOME MODEL ON MATERNAL & CHILD HEALTH OUTCOMES Figure 7. The Difference Between the Group of FQHCs with PCMH Recognition in 2013 and the Group of FQHCs with No PCMH Recognition in 2013 by 3-Year Average Adjusted Quartile Rankings Differences Differences Between 2013 Medical Homes and Non-Medical Homes by 3-Year Avg. Adjusted Quartile Rankings st Trimester Prenatal Visit Low Birth Weight Cervical Cancer Screening 0.17 Adolescent Weight Screen/Follow Up Childhood Immunizations st Trimester Prenatal Visit Low Birth Weight Cervical Cancer Screening Adolescent Weight Screen/Follow Up Childhood Immunizations Despite these being relatively small differences between the two groups of FQHCs (the largest difference is less than half of a quartile ranking), it should still be considered that perhaps the 2013-recognized medical homes were already performing better on clinical performance measures and self-selected /were more prepared to undergo PCMH transformation in the years following Differences Between the 2013 Groups of FQHC Medical Homes and Non-Medical Homes After the PCMH Model is Introduced Averages (in means) of performance, as a percentage of patients who met UDS criteria for the Table 6B Quality of Care Indicators, was also explored to compare the two groups of patients served by PCMH and non-pcmh health centers for each of the five MCH quality of care measures in Figure8. The same comparison was made for 18
19 adjusted quartile rankings in Figure 9. The charts depict that there is no obvious difference between the medical homes and the non-medical homes in performance on the said five quality indicators. In fact, descriptive analysis 2 illustrates that non-medical homes out-performed the recognized medical homes on two measures when looking at percentage of patients who met criteria: 1. Low birth weight by 10 percentage points and, 2. adolescent weight screening and follow-up by 18 percentage points. Likewise in Figure 9, when comparing adjusted quartiles, non-medical homes out-performed the recognized medical homes on two measures when looking at adjusted quartile ranking: 1.cervical cancer screenings, and 2. childhood immunizations. Figure 8. Performance Uniform Data System 2013 Table 6B: Quality of Care Indicators Related to Maternal and Child Health: Recognized Medical Homes Compared to Non- PCMH Recognized FQHCs by Percentage of Patients who Meet Measure Criteria 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 69% 67% 1st Trimester Prenatal Visit 8% 18% 52% 49% Low Birth Weight Cervical Cancer Screening 40% 58% Adolescent Weight Screen/Follow Up 77% 61% Childhood Immunizations PCMH Non-PCMH Figure 9. Performance Uniform Data System 2013 Table 6B: Quality of Care Indicators Related to Maternal and Child Health: Recognized Medical Homes Compared to Non- PCMH Recognized FQHCs by Adjusted Quartile Ranking 19
20 PCMH 1.0 Non-PCMH 0.0 1st Trimester Prenatal Visit Low Birth Weight Cervical Cancer Screening Adolescent Weight Screen/Follow Up Childhood Immunizations The study also investigated how the PCMH Model might impact quality of care indicators over time by looking at the previous year s (2012) UDS data. The UDS Reports include adjusted quartile rankings (AQR) which compare national FQHC performance by ranking quality indicator performance by quartiles. Figure 3 compares the 2012 AQR for the MCH performance indicators to the 2013 AQR that this study investigated to assess whether the presence of PCMH recognition in 2013 improved performance over the course of one year. The results demonstrated that only one performance measure s 2013 AQR, adolescent weight screening and follow-up, was improved for PCMHrecognized FQHCs. Figure 11 assesses the same measures, but for non-pcmh recognized FQHCs, where three indicators improved over 2012 to This suggests that PCMH recognition does not help improve AQR categorization for the quality indicators. Unfortunately, information regarding the important variable of when the medical home recognition was awarded is unavailable, which is discussed in greater detail in the limitations section below. 20
21 Figure 10.Comparison of Adjusted Quartile Rankings from 2012 to 2013 for Medical Homes PCMH PCMH 0.0 1st Trimester Prenatal Visit Low Birth Weight Cervical Cancer Screening Adolescent Weight Screen/Follow Up Childhood Immunizations Figure 11.Comparison of Adjusted Quartile Rankings from 2012 to 2013 for Non- Medical Homes Non-PCMH Non-PCMH 0.0 1st Trimester Prenatal Visit Low Birth Weight Cervical Cancer Screening Adolescent Childhood Weight Immunizations Screen/Follow Up Lastly, the study analyzed measures of association between the two groups: NC FQHCs with and without PCMH recognition for each of the MCH quality indicators over the course of two years. UDS report data demonstrating the percent change in performance on the quality indicator between the UDS Report data for 2011 to


22 was used to assess progress over time. The percent change was classified as positive if it was >0% and negative (or unchanged) if it was reported to be <=0%. The data was entered into 2x2 tables by each MCH quality indicator and then aggregated into a combined outcome category to assess the overall impact on outcomes as displayed in Table 2. Note that Child Immunizations data was very minimally available as the measure changed and not many FQHCs reported on it in Table 2. Positive or Negative Percent Change from 2011 UDS Report Data to 2013 for MCH Quality Outcomes by PCMH-Recognized and non-pcmh Recognized FQHCs Table 3. Measures of Association for Positive or Negative Percent Change from 2011 UDS Report Data to 2013 for MCH Quality Outcomes by PCMH-Recognized and non- PCMH Recognized FQHCs The measures of association in Table 7 can be interpreted to suggest there is not a relationship between PCMH recognition and the improvement of MCH UDS quality indicators. PCMH-recognized FQHCs were times as likely to improve the percentage change of performance on the MCH quality indicators compared to non- PCMH-recognized FQHCs over the 2-year timeframe. Among those FQHCs with
23 PCMH recognition, the risk of improving performance in MCH quality indicators was 22.17% higher than among non-pcmh-recognized FQHCs over the two-year time period. However, the Chi Square tests results of p-values of greater than 0.05 suggest that there is not a statistically significant relationship between PCMH recognition and improvement of UDS Table 6B: Quality of Care Indicators Related to Maternal and Child Health over two years. Policy Implications and Recommendations and Significance for Maternal and Child Health These results could have implications for federal funding considerations related to promoting PCMH recognition in FQHCs as a mean to support health centers in achieving improved performance in quality of care and health outcome indicators. As practice PCMH transformation efforts are costly and time consuming, direct service providers are given financial incentives by these systems such as: per member/per month payments for PCMH activities and or recognition; pay for performance; enhanced fee-for-service compensation and accountable care organization (ACO) membership based on recognition.⁴ Acknowledging the importance of creating a health information infrastructure that includes medically underserved populations, especially for assessing health disparities, federal agencies such as HRSA and CMS have funded/incentivized FQHCs medical home transformation efforts in the ways mentioned above.⁴ As more FQHCs obtain PCMH recognition, more evaluations of the impact of the model on its goals of improving quality of care should be investigated. 23
24 Limitations Consideration should be given to the limitations of the study. Notably, the sample size of 33 health centers in NC is small and the sub-samples of medical homes versus non-medical-homes (18 and 15, respectively) are even smaller creating a bias that makes it difficult to draw confident conclusions regarding the questions of this evaluation.⁹ Another limitation of the study was the missing data on the health centers UDS reports, especially on childhood immunization measure and the adolescent weight screening and follow-up measures.⁹ It should also be considered that UDS Table 6 reporting requirements change slightly each year, making the results of a comparison such as this study less reliable.¹⁰ Three limiting factors discovered in this evaluation, 1. small sample size, 2. lack of available data and, 3. short period of time that the model has been implemented in FQHCs, require that further research must be conducted to draw conclusions regarding the effectiveness of the PCMH model in health centers. Another key limitation to this evaluation is the lack of available information regarding when each of the 18 health center medical homes received their recognition. According to Fixsen, a prominent researcher on implementation science of evidencebased programs, there are six stages of implementation through which organizations must go to fully implement new models and programs: exploration, installation, initial implementation, full implementation, innovation, and sustainability.¹² These stages are not linear and different organizations are going to progress through them differently, suggesting that there is a sincere limitation to evaluating and comparing PCMHs to non- PCMHs, or even medical homes to other medical homes, because the health centers are 24
25 likely at different stages of implementation since the model is still relatively new (current model was published in 2011). 2,12 Also according to Fixsen, each stage is associated with different levels of development towards meeting the goals of the evidence-based program. 12 This is a consideration and limitation for this evaluation because during Fixsen s middle stages of implementation, installation and initial implementation, performance may actually decrease due to changes the organization is experiencing and learning curve associated with them. 12 This certainly applies to implementing the PCMH model because it requires extensive workflow reconfiguration and electronic health record modification and utilization change to be fully implemented. 2 While this study suggests that perhaps PCMH recognition does not positively correlate with improvement of MCH health outcomes of prenatal visits conducted in the first trimester, low birth weight outcomes, cervical cancer screenings, adolescent weight screening and follow-up and childhood immunizations in an FQHC setting in the state of NC, it is highly probable that more information is needed to better assess the relationship before making recommendations for the significance of the primary care model for MCH for the above mentioned reasons. Although, this evaluation aims to lay the foundation for further research on the impact of PCMH models to achieve the goals of improved quality of care and health outcomes for MCH. This could better inform funding decisions for HRSA and CMS in financially supporting FQHCs to obtain PCMH recognition if more substantial evidence was collected and analyzed with a larger sample size, fewer missing data, and with a longer duration in which the PCMH model 25
26 has been implemented to address the concerns related to applying Fixsen s implementation science theory.¹² Conclusions This study investigated the impact Patient-Centered Medical Home recognition on the Institute for Healthcare Improvement Triple Aim s first two goals: improving the patient experience of care and improving the health of populations¹ as applied to maternal and child health outcomes in a Federally Qualified Health Center setting in the state of North Carolina. While the results suggested that PCMH recognition does not impact the performance on MCH quality of care and health outcome indicators as reported in the Uniform Data System, it could be argued that more data may be necessary to more fully understand the impact the PCMH model has on quality performance and improvement of MCH health outcomes. More data on FQHCs performance in relation to PCMH recognition will be available as more FQHCs obtain the recognition and employ the PCMH standards as a part of their standard practices over time. References 1. The Institute for Healthcare Improvement. Initiatives: The IHI Triple Aim. Cambridge, MA: 2015 [updated 2015, cited 2015 Mar 20]. Available from: 2. National Commission on Quality Assurance. Standards and Guidelines for NCQA s Patient-Centered Medical Home (PCMH) Washington, DC: NCQA; 2011 Nov p. Accessible from: HomePCMH.aspx 26
27 3. Agency for Healthcare Research and Quality. Patient-Centered Medical Home Resource Center: Evidence and Evaluation. Rockville, MD: US DHHS, AHRQ; Accessible from: 4. HITECH Act Enforcement Interim Final Rule. Washington, DC: US DHHS; Accessible from: nforcementifr.html 5. Agency for Healthcare Research and Quality. Closing the Quality Gap: Revisiting the State of the Science Series Overview. 23 June Accessible from: 6. Friedman C, Wong A, Blumenthal D. Achieving the Nationwide Learning Health System [Internet]. Science Translational Medicine: 2010 Nov 10. Vol 2 Issue 5757, cm29. Accessible from: 7. Denecke, K. Event-Driven Surveillance: Possibilities and Challenges. New York, NY: Springer Science & Business Media; DOI: / _1. 8. Yasnoff W, O'Carroll P, Koo D., Linkins R, Kilbourne E. Informatics Perspectives- Public Health Informatics: Improving and Transforming Public Health in the Information Age. Topics in Health Information Management: (3), p. 9. Uniform Data System: 2013 Health Center Profile Program Grantee Health Center Profiles. Health Services and Resource Administration: Bureau of Primary Care. Accessible from: UNIFORM DATA SYSTEM (UDS) Calendar Year 2013: UDS Reporting Instructions for Health Centers: CARE BPHC UNIFORM DATA SYSTEM MANUAL. Health Services and Resource Administration: Bureau of Primary Care. Rockville,MD: 2013 Dec 19. Accessible from: Alliance of Chicago Health Centers and Health IT. A Site Visit for the Assistant Secretary for Planning and Evaluation [Internet]. Chigaco, IL; 2010 [updated 2010 Aug 20; cited 2014, Mar 1]. Available from: Fixsen, D. L., Blase, K. A., Naoom, S. F., & Wallace, F. Core implementation components [Internet]. Research on Social Work Practice, 19(5), [2009]. Available from: %20Implementation%20Components.pdf 27
28 Acknowledgments Mary Kristina Wharton would like to deferentially acknowledge all of her professional and academic mentors, to whom the author concedes she owes her knowledge, skills, development, direction and ability to manifest her personal and professional goals to contribute to the improvement of access to health systems and health outcomes for the medically underserved by implementing evidence-based, patient-centered primary care models, cultural competency and quality assurance initiatives in nonprofit healthcare settings. The author would like to express distinctive gratitude to her professional mentor, Penella Washington, CEO of Wake Health Services, and her advisor and first reader, Dr. Tamar Ringel-kulka and second reader, Dr. Sherri Green. 28

29 Appendices A. Theory and Concept Models 1. Institute for Healthcare Improvement s Design of a Triple Aim Enterprise¹ 2. MU Registration for Intent: Conceptual Model 29

30 Wharton, M. K. Conceptual Model for PCMH [Rich Picture Model for INLS600, Dr. Ryan Urquhart]. The University of North Carolina. Chapel Hill, NC: Unpublished;

31 3. PCMH Conceptual Model : Organizational Learning Model and Learning Health System Wharton, M. K. Conceptual Model for PCMH [Conceptual Model for HPM625, Dr. Timothy Carney]. The University of North Carolina. Chapel Hill, NC: Unpublished; B. Terms & Definitions 1. Glossary of Abbreviations and Terms Commonly Used Abbreviations and Terms 31
32 ACA - Patient Protection & Affordable Care Act, 2010 ARRA - American Recovery & Reinvestment Act, 2009 CCNC Community Care of North Carolina (Medicaid MCO in NC) CHERT - Certified Electronic Health Record Technology (CHIT) CHIT - Certified Health Information Technology: referring to electronic health records (CHERT) CMS - Centers for Medicaid & Medicare Services, a federal agency CQI Continuous Quality Improvement DPH - Division of Public Health within the NC Department of Health & Human Services EHR - Electronic health records used to securely collect and transmit PHI FQHC Federally Qualified Health Center HIPAA - Health Insurance Portability & Accountability Act, 1996 HITECH - Health Information Technology for Economic and Clinical Health Act, 2010 HRSA - Health Resources and Services Administration (federal agency: branch of US DHHS) HRSA 330 Grant Competitive federal funding for FQHCs IHI Institute for Healthcare Improvement (independent, nonprofit promoting QI/QA) MCO Managed Care Organization (an organization delivering the model for healthcare service including insurance, care provision and administration) MU - Meaningful Use: may refer to any of the three stages of MU (1, 2, or 3) NC North Carolina (the state of, may refer to the state-level government) NCCCR - North Carolina Central Cancer Registry NC DETECT - NC Disease Event Tracking and Epidemiologic Collection Tool NC DHHS - NC Department of Health & Human Services, including the Div. of Public Health NCEDSS - North Carolina Electronic Disease Surveillance System NCID - North Carolina Identification for MU Registration of Intent Step 1 32
33 NCIR - North Carolina Immunization Registry, a public health system benefited by MU NCQA - National Commission for Quality Assurance NPI - National Provider Index, gives individual providers a national ID number PCMH - Patient-Centered Medical Home PDSA Plan > Do > Study > Act (CQI Model) PHI - Patient Health Information, always secure in accordance with HIPAA PPACA - Patient Protection & Affordable Care Act, 2010 (Also referred to as ACA) QA - Quality Assurance QI - Quality Improvement UDS - Uniform Data System (reporting system required of FQHCs from HRSA) 2. Key Term and Program Descriptions Situation Awareness⁸ Situation Awareness is the state of organizations and individuals after going through the process of collecting information, understanding information and making projections based off of that information to perform a task or function.⁸ Meaningful Use⁴ In an effort to use electronic health records (EHRs) to increase the quality of health care in United States, the Health Information Technology for Economic and Clinical Health Act (HITECH) of 2009 provides incentive payments through Medicare and Medicaid to clinicians and hospitals when they use EHRs and demonstrate meaningful use of the EHRs to improve care. In order to demonstrate meaningful use, clinicians and hospitals must register their intent to use EHRs meaningfully, and then report data on the quality of their care to their designated state agency. Providers and hospitals in the State of North Carolina complete registration of intent to report this data on the North Carolina Department of Public Health Registration of Intent Site.⁴ 33
34 C. Definition of Patient-Centered Medical Home Key Terminology² 34
35 PCMH Term Advance Care Planning Advance Directive Adverse Reaction Allergy Alternative Type Of Clinical Encounter Appointment Wait Times Care Coordination Measure Clinical Summary NCQA Definition & Examples Practice guidance and documentation of patient/family preferences for care at the end of life or for patients who are unable to speak for themselves. A document in which members can explain the type and extent of health care services they prefer if they become unable to make medical decisions. The document may identify another person who can make those decisions on behalf of the individual (e.g., about routine treatments and life-saving methods). Advance directives are frequently called living wills. A noxious or unintended reaction to a drug that is administered in standard doses by the proper route for the purpose of prophylaxis, diagnosis or treatment. An adverse reaction to a substance. A scheduled meeting between the patient and a clinician, using a mode of real-time communication in lieu of an in-person office visit; for example, standalone communication or a combination of telephone, video chat and secure instant messaging. The period between the date/time a patient makes an initial request for an appointment and the actual appointment date/time) for both urgent and routine care. Note: Cycle times (i.e., time from scheduled appointment to the patient actually being seen by the clinician) are not considered appointment wait times in these standards. A metric that uses an aspect of clinical performance or patient experience to identify better performance or worse performance, with respect to the deliberate organization of patient care activities between two or more participants (including the patient) involved in a patient's care to facilitate the appropriate delivery of health care services. A summary of a visit that can be provided to patients/families/caregivers through a personal health record, a patient portal on the practice s web site, secure , electronic media (e.g., a cd or usb fob [electronic memory stick/flash drive]) or a printed copy. The summary, as defined by cms, contains: 1. The patient s name. 2. The provider's name and office contact information. 3. The date and location of the office visit. 4. The reason for the office visit. 5. A list of current problems. 6. A list of current medications. 7. A list of current medications the patient is allergic to. 8. Procedures performed during the visit. 9. Immunizations or medications administered during the visit. 10. Vital signs taken during the visit (or other recent vital signs). 11. Laboratory test results. 12. A list of diagnostic tests pending. 13. Clinical instructions. 14. Future appointments. 15. Referrals to other providers. 16. Future scheduled tests. 17. Demographic information o Maintained in certified electronic health record technology (CEHRT) (sex, race, ethnicity, date of birth, preferred language). 18. Smoking status. 19. Care plan fields, including goals and instructions.
36 Critical Factor Care Plan De-Identify Demographic Information Diversity Documented Process Electronic Clinical Summary Emergency Admission Evidence Based Guidelines Example Factor Legal Guardian Or Health Care Proxy Materials Meaningful Use Requirements A factor identified as central to the concept being assessed within particular elements and is required for practices to receive more than minimal or, for some elements, any points. Critical factors are identified in the scoring section of the element. A plan for day-to-day medical care and services. The plan can include: 1. A summary of medical information (e.g., history of hospitalizations, procedures, tests). 2. A list of providers, medical equipment and medications for patients with special health care needs. 3. Obstacles to transitioning to an adult care clinician. Arrangements for release and transfer of medical records to the adult care clinician. Removal of individual identifiers. Under the HIPAA Privacy Rule, protected health information is de-identified if all individual identifiers are removed. There are 18 categories of identifiers that include name; street address and zip code; telephone and fax number; dates (except year) directly related to a person, including date of birth and dates of service; address and Web URL; Social Security Number; medical record number and account number; vehicle identifiers, including license plate number; device identifiers and serial number; and any other unique identifying number, characteristic or code. Information that includes at least ethnicity, gender, marital status, date of birth, type of work, hours of work and preferred language. A meaningful characteristic of comparison for managing population health that accurately identifies individuals within a non-dominant social system who are underserved. These characteristics of a group may include, but are not limited to, race, ethnicity, gender identity, sexual orientation and disability. Written statements describing procedures. Statements may include protocols or other documents that describe actual processes or blank forms the practice uses in work flow (e.g., referral forms, checklists, flow sheets). Documented processes include an effective date. A summary of a visit that includes, when appropriate, diagnoses, medications, recommended treatment and follow-up. An unscheduled medical or behavioral healthcare event that results in either an emergency room visit or in hospital admission. Clinical practice guidelines based on scientific evidence; or in the absence of scientific evidence, professional standards; or in the absence of professional standards, expert opinion. See practice guidelines. A document, report or prepared material that illustrates implementation of systems or processes by the practice. A scored item in an element. For example, an element may require the organization to demonstrate that a specific document includes four items. Each item is a factor. An individual designated by the patient or family or by the courts to make health care decisions for the patient if the patient is unable to do so. Prepared information that the practice provides to patients, including clinical guidelines and self-management and educational resources such as brochures, Web sites, videos and pamphlets. The CMS implementation of the American Recovery and Reinvestment Act (ARRA) of 2009 (Recovery Act) provides incentive payments to eligible professionals for adopting and demonstrating meaningful use of certified EHR technology. Criteria for meaningful use are electronically capturing health information in a coded format, using the information to track key clinical conditions, communicating the information for care coordination and reporting clinical quality measures and public
37 health information. 1. Stage 1 has 13 Core Requirements that must be met and 9 Menu Requirements, 5 must be met. 2. Stage 2 has 17 Core Requirements that must be met and 6 Menu Requirements, 3 must be met. Multi-Site Group Must Pass Elements No Show Appointments No Show Rates PHI Population Management Practice Guidelines Practice Team Primary Caregiver Records Or Files Registry Reports Risk Factors Sample Three or more practice sites using the same systems and processes, including an electronic medical record system shared across all practice sites. For a multi-site group, NCQA reviews some elements once and applies the results to all practice sites in the group. Designated elements that a practice must pass at a score of 50% to achieve NCQA Recognition. A scheduled appointment that is not kept, unexpectedly and without notification. A specific ratio that compares the number of appointments scheduled versus no-show appointments. Number of patients who did not keep their pre-scheduled appointments during a specific period of time (i.e. a session or a day) divided by the number of patients who were pre-scheduled to come to the center for appointments during the same period of time Protected health information. PHI is associated with an individual s past, present or future physical or mental health or condition, or with the provision of or payment for health care to a person, and identifies the individual. Under the HIPAA Privacy Rule, there are 18 categories of identifiers (e.g., name, street address, address, telephone number, social security number, medical record number, health plan beneficiary or account number, birth date, dates of service and five-digit zip code). Age is not PHI, except for individuals older than 89 years; HIPAA allows the age for these individuals to be aggregated into a single category of age 90 or above. Assessing and managing the health needs of a patient population rather than individual patients, such as defined groups of patients (e.g., patients with specific clinical conditions such as hypertension or diabetes, patients needing tests such as mammograms or immunizations). Systematically developed descriptive tools or standardized protocols for care to support clinician and patient decisions about appropriate health care for specific clinical circumstances. Practice guidelines are typically developed through a formal process and are based on authoritative sources that include clinical literature and expert consensus. A group of clinical and nonclinical staff (e.g., physicians, nurse practitioners, physician assistants, nurses, medical assistants, educators, schedulers) who manage patient care and population health by interacting with patients and working to achieve stated objectives. An individual who provides day-to-day care for a patient and must receive instructions about the patient s care. Actual patient medical files or registry entries that document an action taken. The files are a source for estimating the extent of performance against an element. A searchable list of patient data that the practice proactively uses to assist in patient care. Aggregated data showing evidence of action; may include manual and computerized reports. Behaviors, habits, age, family history or other factors that may increase the likelihood of poor health outcomes. A statistically valid representation of the whole.
38 Shared Decision- Making Aid Social Determinants of Health Standardized Tool Vulnerable Populations Walk-In Access Provides detailed information without advising the audience to choose one decision over another and helps prepare patients to make informed, values-based decisions with their care team. Note: More information and resources can be found through the International Patient Decision Aid Standards Collaboration (IPDASC). Conditions in the environment that affect a wide range of health, functioning and quality-of-life outcomes and risks. Examples of social determinants include: 1. Availability of resources to meet daily needs (e.g., safe housing and local food markets). 2. Access to educational, economic, and job opportunities. 3. Access to health care services. 4. Quality of education and job training. 5. Availability of community-based resources in support of community living and opportunities for recreational and leisure-time activities. 6. Transportation options. 7. Public safety. 8. Social support. 9. Social norms and attitudes (e.g., discrimination, racism, and distrust of government). 10. Exposure to crime, violence, and social disorder (e.g., presence of trash and lack of cooperation in a community). 11. Socioeconomic conditions (e.g., concentrated poverty and the stressful conditions that accompany it). 12. Residential segregation. 13. Language/literacy. 14. Access to mass media and emerging technologies (e.g., cell phones, the Internet, and social media). 15. Culture. More information on social determinants of health can be found on the Healthy People 2020 Web site at A means of collecting information, using a current, evidence-based approach, that has been developed, field-tested and endorsed by a national or regional organization. People who are made vulnerable by their financial circumstances or place of residence, health, age, personal characteristics, functional or developmental status, ability to communicate effectively, and presence of chronic illness or disability (AHRQ definition). An approach to patient appointment scheduling that allows established patients to be seen by a member of the care team during regular office hours, without prior notice. D. Health Center Data & Results⁹ 1. List of Community Health Centers Included in Study
39 Community Health Center City State ALBEMARLE HOSPITAL AUTHORITY Elizabeth City North Carolina ANSON REGIONAL MEDICAL SERVICES Wadesboro North Carolina BAKERSVILLE COMMUNITY MEDICAL CLINIC, INC. Bakersville North Carolina BERTIE COUNTY RURAL HEALTH ASSOCIATION Windsor North Carolina BLUE RIDGE COMMUNITY HEALTH SERVICES, INC. Hendersonville North Carolina CABARRUS ROWAN COMMUNITY HEALTH CENTERS, INC Concord North Carolina CAROLINA FAMILY HEALTH CENTERS, INC. Wilson North Carolina CASWELL FAMILY MEDICAL CENTER Yanceyville North Carolina FIRST CHOICE COMMUNITY HEALTH CENTERS Mamers North Carolina GASTON FAMILY HEALTH SERVICES, INC. Gastonia North Carolina GOSHEN MEDICAL CENTER, INC. Faison North Carolina GREENE COUNTY HEALTH CARE INCORPORATED Snow Hill North Carolina HIGH COUNTRY COMMUNITY HEALTH Boone North Carolina KINSTON COMMUNITY HEALTH CENTER, INC. Kinston North Carolina LINCOLN COMMUNITY HEALTH CENTER, INC Durham North Carolina MEDICAL RESOURCE CENTER FOR RANDOLPH COUNTY, INC Asheboro North Carolina
40 METROPOLITAN COMMUNITY HEALTH SERVICES, INC. Washington North Carolina NC DEPARTMENT OF HEALTH AND HUMAN SERVICES Raleigh North Carolina NEW HANOVER CHC Wilmington North Carolina OPPORTUNITIES INDUSTRIALIZATION CENTER, INC. Rocky Mount North Carolina PERSON FAMILY MEDICAL CENTER, INC. Roxboro North Carolina PIEDMONT HEALTH SERVICES, INC. Carrboro North Carolina ROANOKE CHOWAN COMMUNITY HEALTH CENTER INC Ahoskie North Carolina ROBESON HEALTH CARE CORPORATION Pembroke North Carolina RURAL HEALTH GROUP, INC. Roanoke Rapids North Carolina SOUTHSIDE UNITED HEALTH CENTER Winston Salem North Carolina STEDMAN-WADE HEALTH SERVICES, INC. Wade North Carolina THE C.W. WILLIAMS COMMUNITY HEALTH CENTER, INC. Charlotte North Carolina TRI COUNTY COMMUNITY HEALTH COUNCIL, INC Newton Grove North Carolina TRIAD ADULT AND PEDIATRIC MEDICINE, INC. Greensboro North Carolina WAKE HEALTH SERVICES, INC. Raleigh North Carolina WEST CALDWELL HEALTH COUNCIL, INC Collettsville North Carolina WESTERN NC COMMUNITY HEALTH SERVICES INC Asheville North Carolina
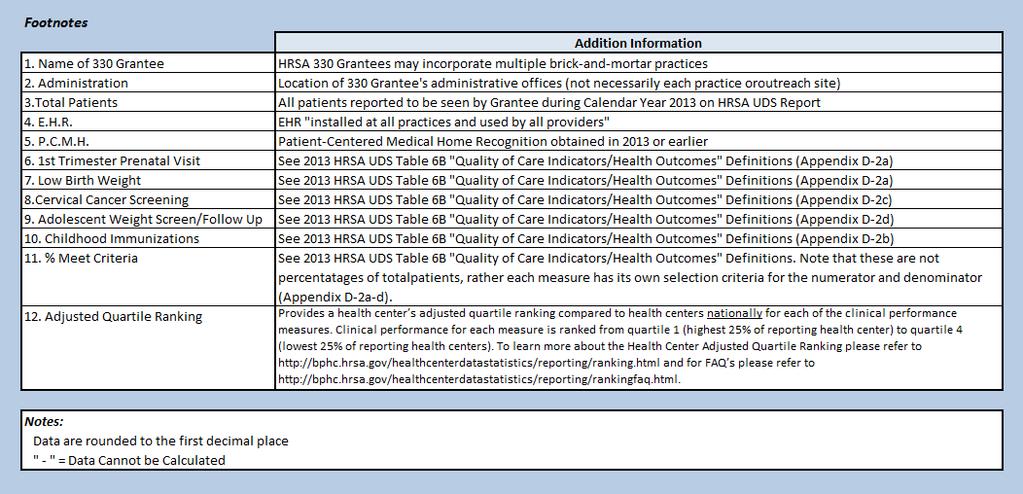
41 2. Uniform Data System 2013 Definitions for Table 6B "Quality of Care Indicators/Health Outcomes" ¹⁰ INSTRUCTIONS FOR TABLE 6B QUALITY OF CARE MEASURES Table 6B is included only in the Universal report. It is completed by all health centers. This table reports data on selected quality of care measures. The quality of care measures have historically been seen in the health care community as indicators of overall community health. More recently, they have become critical elements in the implementation of the national drive to implement Electronic Health Records (EHRs). BPHC first implemented these measures in 2008 and has been updating and adding to them since then. As health centers continue to implement their EHRs, BPHC will continue to revise and expand these measures consistent with the National Quality Strategy and other national quality initiatives. These qualities of care measures are process measures which means that they document services which are thought to be correlated with and serve as a proxy for good long term health outcomes. We know that individuals who receive timely routine and preventive care are more likely to have improved health status. Thus, by increasing the proportion of health center patients who receive timely preventive care and routine acute and chronic care, we can expect improved health status of the patient population in the future. Specifically: Early entry into prenatal care: If women enter care in their first trimester then the probability of adverse birth outcome will be reduced. Childhood immunizations: If children receive their vaccinations in a timely fashion then they will be less likely to contract vaccine preventable diseases or to suffer from the sequela of these diseases. Pap tests: If women receive Pap tests as recommended then they can be treated earlier and will be less likely to suffer adverse outcomes from HPV and cervical cancer. Weight assessment and counseling for children and adolescents: If clinicians ensure that their patients body mass indicator (BMI) percentile is recorded, and if patients (and parents) are counseled on nutrition and physical activity (regardless of the patient s weight) then the likelihood of obesity and its sequela will be reduced. Adult Weight screening and follow-up: If clinicians routinely calculate and record the BMI for their adult patients, and IF they identify patients with weight problems and develop a follow-up plan for overweight and underweight patients, then the likelihood of the debilitating sequela of serious weight problems can be reduced.
42 Tobacco use assessment: If patients are routinely queried about their tobacco use (including smokeless tobacco) then providers will be able to intervene more quickly and effectively and reduce the incidence of cancer, asthma, emphysema, and other tobacco related illnesses. Tobacco use intervention: If tobacco users are provided with an effective mix of counseling and pharmacologic intervention then tobacco users will be more likely to quit smoking and will therefore have a lower incidence of cancer, asthma, emphysema, and other tobacco related illnesses. Pharmacologic treatment of asthmatics: If patients identified with persistent asthma are provided with appropriate pharmacological intervention then they will be less likely to have asthma attacks, they will require fewer emergency room visits, and be less likely to develop complications related to asthma including death. Coronary artery disease (CAD) and lipid lowering therapy: If clinicians ensure that patients with established coronary artery disease receive lipid lowering therapy then the likelihood of CAD related clinical events will be reduced. Ischemic Vascular Disease (IVD) and antithrombotic therapy: If clinicians ensure that patients with established ischemic vascular disease (IVD) use aspirin or another antithrombotic drug, then the likelihood of myocardial infarctions, and other vascular events can be reduced. Colorectal cancer screening: If patients 50 to 75 years old receive appropriate colorectal screening then early intervention is possible and premature death can be averted. UDS Manual December 19, 2013 Version Source: a. Prenatal Care Measure SECTIONS A AND B: DEMOGRAPHIC CHARACTERISTICS OF PRENATAL CARE PATIENTS Only health centers that provide or assume primary responsibility for some or all of a patient's prenatal care, whether or not the health center does the delivery, are required to complete Sections A and B. Health centers who do not provide prenatal care will indicate this by checking a box at the beginning of the table. SECTION A: AGE OF PRENATAL CARE PATIENTS (Lines 1-6) Report the total number of patients who received prenatal care services at any time during the reporting period by age group. Be sure to include all women receiving any
43 prenatal care during the reporting year, including the delivery of her child, regardless of when that care was initiated, including women who: began prenatal care during the previous reporting period and continued into this reporting period began care and delivered during the reporting year began their care in this reporting period, but will not/did not deliver until the next year. Total prenatal patients includes patients who: receive all their perinatal care from the health center began prenatal care with another provider but transferred to the health center began prenatal care with the health center, but were transferred to another provider at some point during their prenatal care were provided with all their prenatal care by a health center provider, but were delivered by another provider. To determine the appropriate age group, use the woman's age on June 30 of the reporting period. As many as half of all patients reported will usually have been reported in the prior year or will be reported in the next year. The total number of women reported in Section A on line 6 must be equal to the total women reported in section B Trimester of Entry into Prenatal Care. SECTION B: ENTRY INTO PRENATAL CARE MEASURE (Lines 7-9) PERFORMANCE MEASURE: The performance measure is Proportion of prenatal care patients who entered treatment during their first trimester. The measure itself, which is not dependent on which category of performance measurement achievement a woman might fall into, is calculated as follows: Numerator: Number of women entering prenatal care during their first trimester (Line 7, Columns A+B) Denominator: Total number of women seen for prenatal care during the year (Line 7 + Line 8 + Line 9, Columns A+B) UDS Manual December 19, 2013 Version b. Childhood Immunization Measure SECTION C: CHILDHOOD IMMUNIZATION (Line 10) Children with at least one medical visit during the reporting period, who had their third birthday during the reporting period or on the following January 1, and who were first seen ever by the health center prior to their third birthday are reported on Line 10. For the purposes of this year's reporting this includes children whose date of birth is between January 2, 2010 and January 1, These dates are the result of the criteria reading before their third birthday as opposed to the old criteria which was by their second birthday.
44 c. Cervical Cancer Screening Measure SECTION D: PAP TESTS (Line 11) Women aged 21 through 64 with at least one medical visit during the reporting period, who were first seen by the health center at some point prior to their 65th birthday are reported on Line 11. For the purposes of this year's reporting this includes women whose date of birth is between January 1, 1949 and December 31, (NOTE: This is the same measure that had been previously called Women 24 through 64 for clarity purposes. No women aged 21, 22, or 23 in the reporting period should be included in the calculation of this measure.) d. Weight Assessment and Counseling for Children and Adolescents SECTION E: WEIGHT ASSESSMENT AND COUNSELING FOR CHILDREN AND ADOLESCENTS (Line 12) Children and adolescents aged 3 until 17 with at least one medical visit during the reporting period, who had their third birthday during or prior to the reporting period, and who were first seen ever by the health center prior to their 17th birthday are reported on Line 12. For the purposes of this year's reporting this includes children and adolescents whose date of birth is between January 1, 1996 and December 31, UDS Manual December 19, 2013 Version

45 3. RESULTS: All NC Community Health Centers 2013 Uniform Data System Maternal and Child Health Quality and Outcomes

46 4. RESULTS: Non-PCMH-Recognized NC Community Health Centers 2013 Uniform Data System Maternal and Child Health Quality and Outcomes

47 5. RESULTS: PCMH-Recognized NC Community Health Centers 2013 Uniform Data System Maternal and Child Health Quality and Outcomes

48 6. RESULTS: 2011 & 2012 Trend & Comparative Data: All NC Community Health Centers Uniform Data System Maternal and Child Health Quality and Outcomes

49 7. RESULTS: 2011 & 2012 Trend & Comparative Data for PCMHs: NC Community Health Centers Uniform Data System Maternal and Child Health Quality and Outcomes

50 8. RESULTS: 2011 & 2012 Trend & Comparative Data for Non-PCMHs: NC Community Health Centers Uniform Data System Maternal and Child Health Quality and Outcomes

51 9. RESULTS: 2011, 2012, Year Average of Adjusted Quartile Rankings for Medical Homes

52 10.RESULTS: 2011, 2012, Year Average of Adjusted Quartile Rankings for Medical Homes
53
54 3. Theory and Concept Models 4. Crosson, Lane, White model for Organizational Learning Framework Crossan, M. M., Lane, H. W. and White, R. E. An organizational learning framework: From intuition to institution, Academy of Management Review, Vol 24, No. 3, pp
![5. PCMH Decision Support Application Model ¹¹ Wharton, M. K. Decision Support Application Model for PCMH [Model for HPM625, Dr. Timothy Carney].](/docs-images/86/94874868/images/55-0.jpg "The University of North Carolina. Chapel Hill, NC: Unpublished; 2014.")
55 5. PCMH Decision Support Application Model ¹¹ Wharton, M. K. Decision Support Application Model for PCMH [Model for HPM625, Dr. Timothy Carney]. The University of North Carolina. Chapel Hill, NC: Unpublished; Example 1: Clinical (Micro-Level) Decision Support in EHR Disease Management Template

")
56 Example 2: Population Management (Macro-Level) Decision Support
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
PCMH 2014 Standards and Guidelines 28 2014 PCMH Recognition November 21, 2016 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based care for both
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11
 2011 Standards 11/21/11") NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
NCQA s Patient-Centered Medical Home (PCMH) 2011 Standards 11/21/11 28 PCMH 1: Enhance Access and Continuity PCMH 1: Enhance Access and Continuity 20 points provides access to culturally and linguistically
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Appendix 6. PCMH 2014 Summary of Changes
 Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
Appendix 6 PCMH 2014 Summary of Changes 2014 PCMH Recognition July 25, 2016 Appendix 6 Summary of Changes 6-1 APPENDIX 6 SUMMARY OF CHANGES QI Worksheet Policies & Procedures Standards & Guidelines Factor
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
Version 11.5 Patient-Centered Medical Home (PCMH) 2014 Reference Guide for Sevocity Users
 2014 Reference Guide for Sevocity Users") Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
Version 11.5 Reference Guide for Sevocity Users Table of Contents Product Support Services... 3 Introduction to PCMH 2014... 4 PCMH 2014 Scoring... 5 PCMH 2014 Meaningful Use Alignment... 7 PCMH 2014 Summary
during the EHR reporting period.
 CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
CMS Stage 2 MU Proposed Objectives and Measures for EPs Objective Measure Notes and Queries PUT YOUR COMMENTS HERE CORE SET (EP must meet all 17 Core Set objectives) Exclusion: Any EP who writes fewer
2014 PCMH Standards: How CPCI Can Help with Transformation. CHCANYS Quality Improvement Program November 20, 2014
 2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
2014 PCMH Standards: How CPCI Can Help with Transformation CHCANYS Quality Improvement Program November 20, 2014 Agenda Review of PCMH 2014 Standards and Stage II MU Crosswalk PCMH Transformation and the
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017
 Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
Medicaid EHR Incentive Program Health Information Exchange Objective Stage 3 Updated: February 2017 The Health Information Exchange (HIE) objective (formerly known as Summary of Care ) is required for
CMS Incentive Programs: Timeline And Reporting Requirements. Webcast Association of Northern California Oncologists May 21, 2013
 CMS Incentive Programs: Timeline And Reporting Requirements Webcast Association of Northern California Oncologists May 21, 2013 Objective This webcast will address CMS s Incentive Program reporting requirements
CMS Incentive Programs: Timeline And Reporting Requirements Webcast Association of Northern California Oncologists May 21, 2013 Objective This webcast will address CMS s Incentive Program reporting requirements
HIT Glossary and Acronym List
 HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
HIT Glossary and Acronym List November 2011 FACT SHEET ACA Patient Protection and Affordable Care Act (see PPACA). ACO Accountable Care Organization: A group of health care providers (e.g. primary care,
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
HITECH* Update Meaningful Use Regulations Eligible Professionals
 HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
PCMH 2014 Record Review Workbook (RRWB)
") PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
STAGE 2 PROPOSED REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1
 STAGE 2 PROPOSED REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1 Requirement CPOE Use CPOE for medication orders directly entered by any licensed health care professional who can enter orders into the
STAGE 2 PROPOSED REQUIREMENTS FOR MEETING MEANINGFUL USE OF EHRs 1 Requirement CPOE Use CPOE for medication orders directly entered by any licensed health care professional who can enter orders into the
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE. Angel L. Moore, MAEd, RHIA Eastern AHEC REC
 THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
Patient-Centered Connected Care 2015 Recognition Program Overview. All materials 2016, National Committee for Quality Assurance
 Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient-Centered Connected Care 2015 Recognition Program Overview All materials 2016, National Committee for Quality Assurance Learning Objectives Introduction to Patient-Centered Connected Care and Eligibility
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
American Recovery and Reinvestment Act (ARRA) of 2009
 of 2009") American Recovery and Reinvestment Act (ARRA) of 2009 An In-Depth Look into the Revolution of Health IT Colin Konschak, MBA, FHIMSS Managing Partner Scott Kizer, Esq., MIS Senior Legal Consultant Ernie
American Recovery and Reinvestment Act (ARRA) of 2009 An In-Depth Look into the Revolution of Health IT Colin Konschak, MBA, FHIMSS Managing Partner Scott Kizer, Esq., MIS Senior Legal Consultant Ernie
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 2
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 2 Table of Contents Introduction 3 Meaningful Use 3 Terminology 4 Computerized Provider Order Entry (CPOE) for Medication, Laboratory
HIE Implications in Meaningful Use Stage 1 Requirements
 HIE Implications in Meaningful Use Stage 1 Requirements HIMSS 2010-2011 Health Information Exchange Committee November 2010 The inclusion of an organization name, product or service in this publication
HIE Implications in Meaningful Use Stage 1 Requirements HIMSS 2010-2011 Health Information Exchange Committee November 2010 The inclusion of an organization name, product or service in this publication
Part 3: NCQA PCMH 2014 Standards
 Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Part 3: NCQA PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health PCMH Standard 4: Care What s New? Management and Support Combined 2011 Standards
Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12
 New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
New York State-Health Centered Controlled Network (NYS HCCN) Webinar #5 Meaningful Use: Looking Ahead to Stage 2 and CPS 12 December 10, 2013 Ekem Merchant-Bleiberg, Director of Implementation Services
Abstract. Are eligible providers participating? AdvancedMD EHR features streamline meaningful use processes: Complete & accurate information
 Abstract As part of the American Recovery and Reinvestment Act of 2009, the Federal Government laid the groundwork for the nationwide implementation of electronic health records (EHR) systems as a measure
Abstract As part of the American Recovery and Reinvestment Act of 2009, the Federal Government laid the groundwork for the nationwide implementation of electronic health records (EHR) systems as a measure
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
The History of Meaningful Use
 A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
A Guide to Modified Meaningful Use Stage 2 for Wound Care Practitioners for 2015 The History of Meaningful Use During the first term of the Obama administration in 2009, Congress passed the Health Information
PCMH 1A Patient Centered Access
 PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
PCMH 1A Patient Centered Access The practice has a written process and defined standards for providing access to appointments, and regularly assesses its performance on: Providing same day appointments
Tips for PCMH Application Submission
 Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Tips for PCMH Application Submission Remain calm. The certification process is not as complicated as it looks. You will probably find you are already doing many of the required processes, and these are
Computer Provider Order Entry (CPOE)
") Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Computer Provider Order Entry (CPOE) Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record
Meaningful Use Hello Health v7 Guide for Eligible Professionals. Stage 1
 Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
Meaningful Use Hello Health v7 Guide for Eligible Professionals Stage 1 Table of Contents Introduction 3 Meaningful Use 3 Terminology 5 Computerized Provider Order Entry (CPOE) for Medication Orders [Core]
Indianapolis Transitional Grant Area Quality Management Plan (Revised)
") Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
Indianapolis Transitional Grant Area Quality Management Plan 2017 2018 (Revised) Serving 10 counties: Boone, Brown, Hamilton, Hancock, Hendricks, Johnson, Marion, Morgan, Putnam and Shelby 1 TABLE OF CONTENTS
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
Meaningful Use Stages 1 & 2
 Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011
 Meaningful Use Final Objectives and Measures for Stage 1, 2011") Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011 1 On demand webinars are best heard through a headset or earphones (ipod for example) that can be plugged into
Eligible Professionals (EP) Meaningful Use Final Objectives and Measures for Stage 1, 2011 1 On demand webinars are best heard through a headset or earphones (ipod for example) that can be plugged into
AHA Survey on Hospitals Ability to Meet Meaningful Use Requirements of the Medicare and Medicaid Electronic Health Records Incentive Programs
 AHA Survey on Hospitals Ability to Meet Meaningful Use Requirements of the Medicare and Medicaid Electronic Health Records Incentive Programs February 7, 2011 Executive Summary The vast majority of hospitals
AHA Survey on Hospitals Ability to Meet Meaningful Use Requirements of the Medicare and Medicaid Electronic Health Records Incentive Programs February 7, 2011 Executive Summary The vast majority of hospitals
Meaningful Use of an EHR System
 Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
HITECH Act American Recovery and Reinvestment Act (ARRA) Stimulus Package. HITECH Act Meaningful Use (MU)
 Stimulus Package. HITECH Act Meaningful Use (MU)") Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
Medicare and Medicaid EHR Incentive Program. Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment
 Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
Medicare and Medicaid EHR Incentive Program Stage 3 and Modifications to Meaningful Use in 2015 through 2017 Final Rule with Comment Measures, and Proposed Alternative Measures with Select Proposed 1 Protect
CHCANYS NYS HCCN ecw Webinar
 CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
American Recovery & Reinvestment Act
 American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
WHITE PAPER. Taking Meaningful Use to the Next Level: What You Need to Know about the MACRA Advancing Care Information Component
 Taking Meaningful Use to the Next Level: What You Need to Know Table of Contents Introduction 1 1. ACI Versus Meaningful Use 2 EHR Certification 2 Reporting Periods 2 Reporting Methods 3 Group Reporting
Taking Meaningful Use to the Next Level: What You Need to Know Table of Contents Introduction 1 1. ACI Versus Meaningful Use 2 EHR Certification 2 Reporting Periods 2 Reporting Methods 3 Group Reporting
WHITE PAPER. Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice
 WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
WHITE PAPER Maximizing Pay-for-Performance Opportunities Proven Steps to Making P4P a Proactive, Successful and Sustainable Part of Your Practice Maximizing Pay-for-Performance Opportunities In today s
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
Bureau of Primary Health Care Update
 Bureau of Primary Health Care Update February 6, 2014 Angela R. Powell, MPH, CPH Director, Southwest Division U.S. Department of Health and Human Services Health Resources and Services Administration Bureau
Bureau of Primary Health Care Update February 6, 2014 Angela R. Powell, MPH, CPH Director, Southwest Division U.S. Department of Health and Human Services Health Resources and Services Administration Bureau
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Merit-Based Incentive Payment System (MIPS) Advancing Care Information Performance Category Transition Measure 2018 Performance Period
 Advancing Care Information Performance Category Transition Measure 2018 Performance Period") Merit-Based Incentive Payment System (MIPS) Advancing Care Information Performance Category Transition Measure 2018 Performance Period Objective: Measure: Measure ID: Exclusion: Measure Exclusion ID: Health
Merit-Based Incentive Payment System (MIPS) Advancing Care Information Performance Category Transition Measure 2018 Performance Period Objective: Measure: Measure ID: Exclusion: Measure Exclusion ID: Health
Qualifying for Medicare Incentive Payments with Crystal Practice Management. Version 1.0
 Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals
 The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
Practice Transformation: Patient Centered Medical Home Overview
 Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Practice Transformation: Patient Centered Medical Home Overview Megan A. Housley, MBA Business Development Director Kentucky Regional Extension Center The Triple Aim Population Health TRIPLE AIM Per Capita
Meaningful Use Modified Stage 2 Roadmap Eligible Hospitals
 Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
Evident is dedicated to making your transition to Meaningful Use as seamless as possible. In an effort to assist our customers with implementation of the software conducive to meeting Meaningful Use requirements,
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals. August 11, 2010
 Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
Accountable Care Atlas
 Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Accountable Care Atlas MEDICAL PRODUCT MANUFACTURERS SERVICE CONTRACRS Accountable Care Atlas Overview Map Competency List by Phase Detailed Map Example Checklist What is the Accountable Care Atlas? The
Meaningful Use: Introduction to Meaningful Use Eligible Providers
 Meaningful Use: Introduction to Meaningful Use Eligible Providers Introduction to Meaningful Use: Webinar Overview Define Meaningful Use Review Meaningful Use Key Dates & Program Incentives Discuss the
Meaningful Use: Introduction to Meaningful Use Eligible Providers Introduction to Meaningful Use: Webinar Overview Define Meaningful Use Review Meaningful Use Key Dates & Program Incentives Discuss the
Measure: Patient name. Referring or transitioning healthcare provider's name and office contact information (MIPS eligible clinician only) Procedures
 Procedures") Objective: Measure: Health Information Exchange Health Information Exchange The MIPS eligible clinician that transitions or refers their patient to another setting of care or health care clinician (1)
Objective: Measure: Health Information Exchange Health Information Exchange The MIPS eligible clinician that transitions or refers their patient to another setting of care or health care clinician (1)
Meaningful Use and PCC EHR. Tim Proctor Users Conference 2017
 Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Meaningful Use and PCC EHR Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda MU basics and eligibility How to participate in MU What s Next for MU? Meeting MU measures in PCC EHR Takeaways An understanding
Quality Data Model (QDM) Style Guide. QDM (version MAT) for Meaningful Use Stage 2
 Style Guide. QDM (version MAT) for Meaningful Use Stage 2") Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Quality Data Model (QDM) Style Guide QDM (version MAT) for Meaningful Use Stage 2 Introduction to the QDM Style Guide The QDM Style Guide provides guidance as to which QDM categories, datatypes, and attributes
Meaningful Use Stage 2
 Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Meaningful Use Stage 2 Presented by: Deb Anderson, HTS Consultant HTS, a division of Mountain Pacific Quality Health Foundation 1 HTS Who We Are Stage 2 MU Overview Learning Objectives 2014 CEHRT Certification
Provision of Telemedicine Services by Community Health Centers
 Provision of Telemedicine Services by Community Health Centers Peter Shin 1, Jessica Sharac 1, and Feygele Jacobs 2 1. Department of Health Policy, The Milken School of Public Health, George Washington
Provision of Telemedicine Services by Community Health Centers Peter Shin 1, Jessica Sharac 1, and Feygele Jacobs 2 1. Department of Health Policy, The Milken School of Public Health, George Washington
STATE OF CONNECTICUT
 I. PURPOSE STATE OF CONNECTICUT MEMORANDUM OF UNDERSTANDING BETWEEN THE DEPARTMENT OF PUBLIC HEALTH AND THE DEPARTMENT OF SOCIAL SERVICES REGARDING DATA EXCHANGES Pursuant to section 19a-45a of the Connecticut
I. PURPOSE STATE OF CONNECTICUT MEMORANDUM OF UNDERSTANDING BETWEEN THE DEPARTMENT OF PUBLIC HEALTH AND THE DEPARTMENT OF SOCIAL SERVICES REGARDING DATA EXCHANGES Pursuant to section 19a-45a of the Connecticut
Patient-Centered Specialty Practice (PCSP) Recognition Program
 Recognition Program") Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
Patient-Centered Specialty Practice (PCSP) Recognition Program Standards Workshop Part 2 2013 All materials 2013, National Committee for Quality Assurance Agenda Part 1 Content of PCSP Standards and Guidelines
MEANINGFUL USE STAGE FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
9/28/2011. Learning Agenda. Meaningful Use and why it s here. Meaningful Use Rules of Participation. Categories, Objectives and Thresholds
 Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11
 Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
Meaningful Use of EHRs to Improve Patient Care Session Code: A11 & B11 Janice Magno, MPA, Project Manager, NYC REACH Liraiza Diaz, Clinical Quality Specialist, NYC REACH IHI Summit 2014, Washington DC
Note: Every encounter type must have at least one value designated under the MU Details frame.
 Meaningful Use Eligible Professionals Eligible Providers (EPs) who are participating in the EHR Incentive Program either under Medicare or Medicaid must complete at least 2 years under Stage 1 before they
Meaningful Use Eligible Professionals Eligible Providers (EPs) who are participating in the EHR Incentive Program either under Medicare or Medicaid must complete at least 2 years under Stage 1 before they
Meaningful use glossary and requirements table
 Meaningful use glossary and requirements table 2011 2012 Glossary...2 Requirements table...3. Exclusions...12 Meaningful use glossary The following spreadsheet describes the requirements an eligible professional
Meaningful use glossary and requirements table 2011 2012 Glossary...2 Requirements table...3. Exclusions...12 Meaningful use glossary The following spreadsheet describes the requirements an eligible professional
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
Begin Implementation. Train Your Team and Take Action
 Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Begin Implementation Train Your Team and Take Action These materials were developed by the Malnutrition Quality Improvement Initiative (MQii), a project of the Academy of Nutrition and Dietetics, Avalere
Meaningful Use Stage 2
 Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
Meaningful Use Stage 2 Objectives Gain understanding of the changes Focus on Transitions in Care and Patient Engagement Recognize the increasing HIE role Who Are You? What is YOUR Need Today? A. Office
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS)
") The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
The Minnesota Statewide Quality Reporting and Measurement System (SQRMS) Denise McCabe Quality Reform Implementation Supervisor Health Economics Program June 22, 2015 Overview Context Objectives and goals
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018
 September 12, 2018") Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Putting PCMH into Practice: A Transformation Series Care Coordination & Care Transitions (CC) September 12, 2018 WEBINAR FACILITATOR Hannah Stanfield NCQA PCMH CCE Practice Transformation Coordinator WACMHC
Health Centers Overview. Health Centers Overview. Health Care Safety-Net Toolkit for Legislators
 Health Centers Overview Health Centers Overview Health Care Safety-Net Toolkit for Legislators Health Centers Overview Introduction Federally Qualified Health Centers (FQHCs), also known as health centers,
Health Centers Overview Health Centers Overview Health Care Safety-Net Toolkit for Legislators Health Centers Overview Introduction Federally Qualified Health Centers (FQHCs), also known as health centers,
Request for Proposals (RFP) for CenteringPregnancy
 for CenteringPregnancy") March of Dimes State Community Grants Program Request for Proposals (RFP) for CenteringPregnancy March of Dimes Illinois 111 W. Jackson Blvd., Suite 1650 Chicago, IL 60604 (312) 765-9044 1 I. MARCH OF
March of Dimes State Community Grants Program Request for Proposals (RFP) for CenteringPregnancy March of Dimes Illinois 111 W. Jackson Blvd., Suite 1650 Chicago, IL 60604 (312) 765-9044 1 I. MARCH OF
Care Management Policies
 POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
POLICY: Category: Care Management Policies Care Management 2.1 Patient Tracking and Registry Functions Effective Date: Est. 12/1/2010 Revised Date: Purpose: To ensure management and monitoring of patient
HIE Implications in Meaningful Use Stage 1 Requirements
 s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
s in Meaningful Use Stage 1 Requirements HIMSS Health Information Exchange Steering Committee March 2010 2010 Healthcare Information and Management Systems Society (HIMSS). 1 An HIE Overview Health Information
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Maternal and Child Health North Carolina Division of Public Health, Women's and Children's Health Section
 Maternal and Child Health North Carolina Division of Public Health, Women's and Children's Health Section Raleigh, North Carolina Assignment Description The WCHS is one of seven sections/centers that compose
Maternal and Child Health North Carolina Division of Public Health, Women's and Children's Health Section Raleigh, North Carolina Assignment Description The WCHS is one of seven sections/centers that compose
Agenda 2. EHR Incentive Programs 3/5/2015. Overview EHR incentive programs Meaningful Use Differences between Stage 1 and Stage 2
 Meaningful Use and the Electronic Health Record Presented by: Susan Reehill CPC, CEMC, CHONC, CPMA Certified Professional Medical Auditor AHIMA Approved ICD-10 CM/PCS Trainer Overview EHR incentive programs
Meaningful Use and the Electronic Health Record Presented by: Susan Reehill CPC, CEMC, CHONC, CPMA Certified Professional Medical Auditor AHIMA Approved ICD-10 CM/PCS Trainer Overview EHR incentive programs
NCQA PCMH 2017 Standard Two 4/11/18. 6 PCMH Concepts within the standards
 Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
Candace Chitty RN, MBA, CPHQ, PCMH-CCE 1 6 PCMH Concepts within the standards 1. Team-Based Care and Practice Organization (TC). 2. Knowing and Managing Your Patients (KM). 3. Patient-Centered Access and
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10
 UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
UW MEDICINE ICD-10 Program UW MEDICINE ICD-10 There and back again INTEGRATION OF MANDATES ACO Quality Based Reimbursement Meaningful Use, P4P, etc. ICD-10 HIPAA, 5010 2 STRATEGIC OPPORTUNITIES Significant
Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018
 Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018 NOTE: These policies have only been proposed. No policies are final
Overview of the Changes to the Meaningful Use Program Called for in the Proposed Inpatient Prospective Payment System Rule April 27, 2018 NOTE: These policies have only been proposed. No policies are final
Meaningful Use Stage 1 Guide for 2013
 Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
CCHN Clinical Quality Improvement Plan
 CCHN Clinical Quality Improvement Plan This Document is a Collaborative Work By HIT Sub Committee Clinical Advisory Work Group Colorado Clinical Advisory Network Colorado Dental Health Network CODAN Colorado
CCHN Clinical Quality Improvement Plan This Document is a Collaborative Work By HIT Sub Committee Clinical Advisory Work Group Colorado Clinical Advisory Network Colorado Dental Health Network CODAN Colorado
How to Participate Today 4/28/2015. HealthFusion.com 2015 HealthFusion, Inc. 1. Meaningful Use Stage 3: What the Future Holds
 Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented by We ll begin momentarily Meaningful Use Stage 3: What the Future Holds Dr. Seth Flam CEO, HealthFusion Presented
The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients
 The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients Updated March 2012 Netsmart Note: The Health Information Technology for Economic
The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients Updated March 2012 Netsmart Note: The Health Information Technology for Economic
CHIME Concordance Analysis of Stage 2 Meaningful Use Final Rule - Objectives & Measures
 CHIME Concordance Analysis of Stage 2 Meaningful Use Final Rule - Objectives & Measures Stage 2 MU Objectives and Measures for EHs - Core More than 60 percent of medication, 1. Use CPOE for medication,
CHIME Concordance Analysis of Stage 2 Meaningful Use Final Rule - Objectives & Measures Stage 2 MU Objectives and Measures for EHs - Core More than 60 percent of medication, 1. Use CPOE for medication,
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement