The Effect of Indian Community Health Workers: Multiple Tasks and Few Results
|
|
|
- Lindsay Vivien Reeves
- 5 years ago
- Views:
Transcription
1 The Effect of Indian Community Health Workers: Multiple Tasks and Few Results Mark Walsh 1 Undergraduate Honors Thesis Stanford University May 4, 2016 Abstract The Government of India s Accredited Social Health Activist (ASHA) program is the largest community health worker program in the world and is credited with improving the healthcare of rural Indians. However, there have been no comprehensive quantitative evaluations of this program. This paper exploits the early rollout of the ASHA program in high focus states to identify the effect of the ASHA program using a year and state fixed effects model. I find no evidence that the ASHA program had a positive effect on health inputs or health outcomes. I propose that the ASHA program s performance payment scheme may create a multitasking problem that explains this absence of a measureable effect. 1 address: mwalsh24@stanford.edu. I thank Kim Barbiarz, Nomita Divi, Garima Gupta, Charu Sharma, Rajan Singh, Rohit Mujumdar, Benita Menezes, Hadley Reid, Lina Vadlamani and Pooja Makhijani for furthering my understanding of the ASHA program and the Indian healthcare system. I especially want to thank Grant Miller for inspiring my interest in global health, helping me gather information on this project and giving advice that greatly improved this paper. I am also thankful to Marcelo Clerci-Arias for his support throughout this process. 1
2 1 Introduction By many measures, the health of rural Indians lags behind urban Indians and even populations in least developed countries. In 2009, rural India s infant mortality rate (55 per 1000 live births) far exceeded urban India s (34 per 1000 live births), and rural India s neonatal mortality (42.5 per 1000 live births) far exceeded urban India s (28.5 per 1000 live births) and even exceeded the average for least developed countries (32.5 per 1000 live births) (Saikia, 2013; Uphadyay et. al., 2012; WDI, 2016). Both supply- side and demand- side issues contribute to the poor health of rural Indians. On the supply- side, endemic staff shortages, corruption, absenteeism and shirking compromise the quality of public healthcare. On the demand- side, credit and information constraints attenuate rural Indians willingness to pay for health interventions. In 2005, the Government of India introduced the National Rural Health Mission (NRHM) in order to combat the myriad of problems facing the rural Indian healthcare system. One of the central components of the NRHM was the Accredited Social Health Activist (ASHA) program. The ASHA program sought to institute a local female health worker in every village with a population over 1,000. By July of 2015, there were 856,405 ASHAs functioning in India, which makes the ASHA program the largest community health worker program in the world (NHRSC, 2015). While ASHAs began with a relatively narrow set of tasks, they are currently relied upon to improve maternal health, child health, immunization, family planning, adolescent health, tuberculosis control, leprosy eradication, vector- borne disease control (including malaria control) and public health sector accountability. The central and 2
3 state governments of India incentivize ASHAs through a novel performance payment scheme that provides the ASHA with payments for completing a given task. In , state governments alone spent crore Rs. (approximately $134.7 million in 2013 dollars 2 ) on funding for these incentives and the rest of the ASHA program (NHRSC, 2014). Despite these wide- ranging responsibilities and substantial investments of human resources and government revenue, rigorous evidence on the effect of the ASHA program remains scarce. In theory, ASHAs could ease both supply- side and demand- side constraints. On the supply- side, ASHAs should alleviate personnel shortages and pressure the public sector to stamp out corruption, absenteeism and shirking. On the demand- side, ASHAs should ease information constraints by educating their fellow community members about health interventions and generate additional demand by encouraging their fellow community members to use public health services. Overall, ASHA s efforts should increase the number of rural Indians using the public healthcare services while also increasing the quality of these public healthcare services. This combination of higher quantity and quality of healthcare for rural Indians should significantly improve rural Indians health. In this paper, I conduct the first comprehensive quantitative evaluation of the ASHA program. The qualitative studies of the ASHA program could not rigorously investigate the counterfactual. The only quantitative study of the ASHA program looked solely at the ASHAs effect on immunizations. This narrow focus prevented the author from evaluating whether the ASHAs effectively handle all of their 2 Calculated using the Indian rupee to US dollar closing market exchange rate on January 1 st, 2013 from xe.com. 3
4 responsibilities. In addition, large community health worker programs have become increasingly popular in the developing world. For example, the United Nations Sustainable Development Network recently launched a campaign to scale up community health worker programs in ten sub- Saharan African countries. A comprehensive quantitative evaluation of the largest community health worker program could provide more reliable evidence about the effectiveness of scaling up community health worker programs. I evaluate the effect of the ASHA program on both health inputs and health outcomes by exploiting the variation in the Government of India s policies toward non- focus states and high focus states (states with poor health indicators and health infrastructure). The Government of India mandated that high focus states institute the ASHA program and directly funded these programs. In non- focus states, the Government of India only mandated that areas with a high concentration of scheduled tribes institute the ASHA program and only directly funded areas with a high concentration of scheduled tribes. As a result, high focus states had significantly higher concentrations of ASHAs in (Rao, 2013). This variation in the intensity of ASHA program implementation between high focus and non- focus states allows me to evaluate the impact of the ASHA program by looking at the differences in ASHA- related health inputs and health outcomes between high focus and non- focus states. I use a model with state- fixed effects and year- fixed effects in order to rigorously estimate the effect of the more intense implementation on ASHA- related health inputs and health outcomes. 4
5 For health inputs, I find that the ASHA program has no effect on institutional delivery rates or tubectomy rates. I also find that the ASHA program has a negative effect on household toilet usage, but this finding may be biased by significant reporting errors (refer to Table A1). For health outcomes, I find that the ASHA program has no effect on the infant mortality rate or the neonatal mortality rate. These findings remain robust to alternative specifications with state linear time trends, district fixed effects and district linear time trends. I propose that these results may be evidence of a multitasking problem. Multitasking is when rewarding performance on a subset of tasks leads to a reduction in effort in other tasks (Holmstrom and Milgrom, 1991). In the ASHA s performance payment scheme, some tasks require greater effort than others, yet the incentive payments for these tasks do not significantly vary. For example, ASHAs might have to expend a relatively high amount of effort to convince households to give institutional deliveries, undergo tubectomies or construct a household toilet because of rural Indians entrenched negative beliefs about the public healthcare system, government family planning programs and indoor sanitation. In contrast, rural Indians have relatively flexible beliefs about immunizations and there are inframarginal patients who are already planning to utilize the incentivized health inputs. Since the performance payment scheme does not differentiate between marginal and inframarginal patients and immunization sessions yield fairly high incentive payments (refer to Table 2), ASHAs are incentivized to focus upon these low effort tasks rather than more difficult tasks, like convincing individuals to give institutional deliveries, get tubectomies or construct household toilets. ASHA s 5
6 avoidance of these difficult tasks would explain why I do not find positive effects on health inputs or health outcomes. 2.1 Background In this section, I first provide background on other community health worker programs. Next, I survey the literature on performance pay to outline the possible effects of the ASHA program s novel performance pay scheme. Then, I review research on rural healthcare in India. Finally, I present the structure of the ASHA program and previous evaluations of it. 2.2 Community Health Workers Developing countries have typically used community health worker programs as a strategy to address health personnel shortages, especially in rural areas. Community health worker programs train community members to serve their own communities through a variety of low- skilled healthcare tasks. Theoretically, these programs allow for the cost- effective extension of basic healthcare services and strengthen the link between the healthcare system and the community. When used for specific and simple interventions, community health worker programs have shown significant promise. A randomized- controlled trial in Ethiopia that trained local coordinators to instruct mothers to promptly give antimalarials to their sick children led to a 40% reduction in under- 5 mortality (Kidane and Morrow, 2000). In the rural Indian context, a controlled trial that trained community health workers to identify the signs of sepsis in neonates and to provide other forms of basic neonatal care produced substantial reductions in neonatal and infant 6
7 mortality rates in the treatment areas relative to the control areas (Bang et. al, 1999). When community health workers responsibilities are expanded to more complex tasks, their efficacy appears to decrease. An assessment of the Lady Health Worker Program in Pakistan found that performance on simple tasks, such as diarrhea management and vaccination counseling, was stronger than performance on more complex tasks, such as recognizing and treating acute respiratory infections (Bhutta et. al, 2005). When Gambian community health workers were tasked with administering primary care, an even more complex task, researchers found no impact on health outcomes relative to control areas (Wang ombe, 1984). A review of community health worker programs that set them up to be change agents in their community found that community health workers typically failed at this complicated task as well (Gilroy et. al, 1989). In addition to difficulty with complex tasks, community health workers often suffer from a lack of motivation, which leads to high attrition rates. One review of community health worker programs found attrition rates of 30% over nine months in Senegal and 50% over two years in Nigeria (Parlato and Favin, 1982). High attrition raises the costs of community health worker programs by necessitating another round of selection and training (Bhattacharrya et. al, 2001). A commonly cited reason of community health workers for leaving their posts is inadequate pay (Lehmann and Sanders, 2007). While many programs have treated community health workers as volunteers, who receive little to no remuneration, these programs have not proven to be sustainable (Lehmann and Sanders, 2007). While the 7
8 literature suggests that community health workers need adequate remuneration, there has been little research on the costs and benefits of different payment schemes. In terms of large- scale community health worker programs like the ASHA program, research is mostly qualitative and the results appear to be heterogeneous. The Brazilian state of Ceará s Agentes de Saudé employed community health workers to visit households for checkups, prenatal care, vaccinations, breastfeeding promotion and oral rehydration (McGuire, 2001). The implementation of the program coincided with a 32% drop in infant mortality over a five- year period (Cufine Svitone et. al, 2000). In 1994, the national government adopted this program, and by 2007, the program covered over 50 million people (Lehmann and Sanders, 2007). On the other hand, India s attempt to establish a large national community health worker program in the late 1970s failed to be sustainable (Chatterjee, 1993; Bose, 1983). In many states, the scheme collapsed due to opposition from the medical profession and vacillating government policies (Chatterjee, 1993; Bose, 1983). In the remaining states, community health workers were seen as employees of the state and were discontent with their small honoraria (Lehmann and Sanders, 2007). As a result both communities and community health workers became disillusioned with the program and by the 1980s, few community health workers functioned effectively (Lehmann and Sanders, 2007). 2.3 Performance Pay As mentioned previously, low motivation from community health workers has been a consistent issue for community health worker programs. The ASHA 8
9 program attempts to solve this problem by providing incentive payments for certain tasks that the ASHA performs. While there is little evidence regarding the use of performance pay with community health workers, the previous literature on the effects of performance pay in general suggests that there may be benefits and drawbacks to this approach. There is some empirical evidence that performance pay can help solve community health workers incentive problems. In a context fairly similar to the ASHA program, multiple studies of performance pay for health inputs in Rwanda found that these schemes increased health provider effort and improved population health (Basinga et. al. 2011; Gertler and Vermeersch, 2012; de Walque et. al 2015). In contrast to the ASHA program, the incentivized cadres in Rwanda were licensed health providers rather than low skilled community volunteers, but these results suggest that incentives for health inputs can work with rank- and- file health workers. On the other hand, performance pay may have deleterious effects in the context of low- level health workers and health input incentives. One concern is that incentives for health inputs will discourage providers from utilizing their local knowledge to improve health (Miller and Barbiarz, 2013). A related concern is that rewarding low- level health workers will have little effect, because they are beholden to their managers and cannot innovate (Miller and Barbiarz, 2013). Additionally, low- level health workers are generally more risk- averse, so will demand to be paid more in a performance pay scheme relative to a fixed pay scheme (Miller and Barbiarz, 2013). 9
10 Furthermore, performance pay may lead to multitasking and/or a reduction of intrinsic motivation, which would lower the quality of health provision. A Kenyan school meal program became an example of multitasking when researchers found that rewarding reductions in pupil malnutrition rates caused teaching time to fall by 15% (Vermeersch and Kremer, 2005). In an experimental setting, Gneezy and Rustichini (2000) find that providing small monetary rewards for pro- social activities crowds out intrinsic motivation and may even lower overall motivation. 2.4 Rural Indian Healthcare One of the most pressing problems facing rural Indian healthcare is the underuse of cost- effective health interventions. India s immunization rates are lower than the averages for sub- Saharan Africa and least developed countries (Dreze and Sen, 2013). In 2001, only 31% of Indian households had their own toilet (Hueso and Bell, 2011). In addition, the institutional delivery rate in rural India was only 28.9% as of (Gupta, 2012). This failure to utilize health interventions is caused by a combination of demand- side and supply- side constraints. On the demand- side, the poverty and limited medical knowledge of rural Indian households attenuates their desire to employ cost- effective health interventions. While Indian public health care is technically free for most services, bribes create a price and exclude poor Indians from accessing these services. This propensity for bribery led the 2005 corruption surveys, which interviews public officials, business executives and the general public, to rank the health sector as the second most corrupt sector in India (Lewis, 2006). While, hypothetically, poor Indians should be able to save up in order to prepare for health emergencies and 10
11 invest in cost- effective medical interventions, credit constraints often prevent them from doing so. A recent study in Orissa demonstrated that providing micro- consumer loans increased uptake of insecticide- treated bednets significantly, which suggests that poor households demand for preventative health is constrained by a lack of access to credit (Tarozzi et. al, 2011). Rural Indians limited medical knowledge may cause them to underrate the benefits of health interventions. For example, only 12.8% of respondents in a study of rural Indians in Tamil Nadu villages considered water a source of diarrhea and most did not believe that there was any association between open- air defecation and diarrheal diseases (Banda et. al, 2007). Unsurprisingly, very few of these respondents chose to invest in and use household toilets (Banda et. al, 2007). A 2005 study in Kerala found that an informational campaign on hand washing produced a long lasting improvement in behavior, which indicates that information constraints were suppressing demand for this health intervention as well (Caincross et. al, 2005). On the supply- side, a dearth of medical infrastructure and personnel, paired with the absenteeism and low effort of existing personnel, hampers the efficacy of health interventions. In terms of infrastructure, a network of public sector community health centers (CHCs), primary health centers (PHCs) and sub- centers services rural populations (Pangariya, 2008). The sub- center is the first point of contact between the community and the public health care system, and is responsible for maternal health, child health, immunizations, nutrition, diarrhea control and communicable diseases. By 2005 norms, there should have been one 11
12 sub- center per 5000 people, but in reality, there was a shortfall of 21,983 relative to the 158,000 required (MOHFW, 2005). In terms of human resources, these sub- centers are supposed to have one male worker and one female auxiliary nurse midwife (ANM), but there was a shortfall of 67,261 male workers and 11,191 ANMs (MOHFW, 2005). Even if the requirements were met, the Government of India admitted that the current one ANM and one male worker per subcenter was not found to be adequate to attend to the complete needs of maternal and childcare in any village (MOHFW, 2005). PHCs and CHCs also suffer from persistent shortages (Rao et. al, 2011). In 2011, 18% of PHCs did not have a doctor, 38% did not have a laboratory technician and 16% did not have a pharmacist (Rao et. al., 2011). For CHCs, 55% of surgeon posts were vacant, 48% of obstetrician and gynecologist posts were vacant, 55% of physician posts were vacant and 47% of pediatrician posts were vacant (Rao et. al., 2011). Filling these staffing gaps is difficult, because trained medical personnel generally prefer to work in urban areas. In urban areas, medical personnel can earn more, work more effectively (because of better facilities), enjoy better living conditions and have better educational opportunities for their children (Rao et. al, 2011). Even when the posts for health personnel are technically filled, absenteeism and low effort restrict rural Indians access to quality healthcare. A nationally representative survey of public health facilities found a 43% staff absenteeism rate (Chaudhury et. al., 2006). A study of public sector doctors in Delhi found that they exerted little effort and utilized only a fraction of their knowledge (Das and Hammer, 2007). In contrast, private sector doctors exerted far more effort, 12
13 presumably because their income depends on retaining clients while public sector health employees receive fixed incomes and are nearly impossible to fire (Das and Hammer, 2007). While this study was done in an urban area, rural public sector health personnel are typically less qualified and face less competition, so shirking may be even more pronounced in these environments. The low level of healthcare resulting from these constraints leads to poor health outcomes in rural India. In 2005, the year of ASHA program roll out, India s neonatal mortality rate was 38.3 deaths per 1000, which exceeded the average among least developed countries (WDI, 2016). India s infant mortality rate was also a relatively high 55.8 deaths per 1000 (WDI, 2016). 2.5 The ASHA program In response to this poor performance, the Government of India introduced the NRHM in The NRHM created Village Health and Sanitation Committees, scaled up staff in the public health sector, provided untied grants to local institutions, provided annual maintenance grants to public health institutions, and put in place community and top- down monitoring systems in all states. In addition to these reforms, the Government of India mandated that 18 high- focus states institute an ASHA in villages with a population over In contrast, the Government only mandated that non- focus states institute the ASHA program in areas with high concentrations of scheduled tribes. The government chose the high focus states based upon their poor infrastructure and low health indicators. The government provided direct funding only to high focus states and the areas in non- focus states with high concentrations of scheduled tribes in order to support the 13
14 ASHA program. While non- focus states were allowed to rollout the ASHA program in other areas, the degree of program implementation in non- focus states lagged behind high- focus states. By , 74.02% of villages in high focus states had an ASHA, while only 33.04% of villages in non- focus states had an ASHA (Rao, 2012). Additionally, the average number of ASHAs who had completed a round of training in a given sub- center area was 4.6 in high focus states and only 1.66 in non- focus states (Rao, 2012). The NRHM imagined the ASHA as a female community member with some medical training who could link the community to the public health care system by addressing both supply and demand- side issues. ASHAs were meant to generate demand for the public health system by providing information about the benefits of preventative healthcare and facilitating referrals and transportation to public health centers. On the supply side, ASHAs constituted additional human resources and could extend basic healthcare services directly into the homes of villagers. Finally, in their role as activists, ASHAs were tasked with mobilizing the community to bring bottom- up accountability and monitoring to public health provision. In theory, this activism should have increased the quality of public health provision by stamping out absenteeism, shirking and corruption. The government compensates the ASHA through a system of performance incentives for the provision of specified health inputs. The original national guidelines for ASHA compensation reward them for institutional births, child immunizations, family planning operations, toilet construction, provision of DOTS, treatment of leprosy, treatment of malaria and facilitating community health 14
15 meetings (refer to Table 1 for more information) (Wang et. al, 2012). While many states added more activities, states generally adhered closely to these guidelines in the early years of the program. According to qualitative evaluations of the ASHA program, these incentive schemes shaped ASHAs behavior. Instead of focusing upon broad demand generation, supplying of basic healthcare or social activism, most ASHAs focused 15
16 upon the incentivized activities (Bajpai and Dholakia, 2011) (Mishra, 2012). As a result, communities viewed ASHAs as extensions of the public health sector rather than as social activists for the community (Mishra, 2012). Given this situation, it is not surprising that none of the evaluations of the ASHA program mention lower corruption, lower absenteeism or higher effort from public healthcare staff. The evaluations also do not report significant progress on demand generation or supply provision of non- incentivized health inputs (Mishra, 2012) (Singh, 2008) (Scott and Shanker, 2010) (Bajpai and Dholakia, 2011). In fact, ASHAs often received substandard training, which further reduced their usefulness as providers of basic treatment and helpful advice (Bajpai and Dholakia, 2011). On the other hand, these qualitative evaluations reported significant progress on heavily incentivized health inputs. Specifically, ASHAs appeared to focus upon institutional deliveries and immunization sessions, which were their two largest sources of income. (Mishra, 2012) (Scott and Shanker, 2010). One evaluation reported that this focus distracted ASHA s from their other responsibilities, such as Village Health and Sanitation Days and outreach to smaller hamlets and villages (Bajpai and Dholakia, 2011). While evaluations did report progress on immunizations and institutional deliveries, they also noted some significant difficulties. The corruption, poor quality and poor reputation of public healthcare facilities constrained the ASHAs ability to generate demand for immunizations and institutional deliveries (Scott and Shanker, 2010) (Gopalan et. al, 2011). ASHAs association with the public health sector also undermined trust between the ASHA and the community (Gopalan et. al, 2011). 16
17 The only quantitative study of the ASHA program looked at its effect on immunization rates. The study used a difference- in- differences framework to test whether the differential rollout of the ASHA program in high focus states and non- focus states improved the immunization rates of children in high focus states (Rao, 2012). The author found that the ASHA program increased immunization rates from 12-17% (Rao, 2012). This finding supports the qualitative studies claim that ASHAs put significant effort into raising immunization rates. 3.1 Data Estimating the effect of the ASHA program requires data on health inputs and health outcomes from each state. For health inputs, I focus on the ASHA s incentivized tasks in order to evaluate whether the ASHA s activities increased usage of the health inputs that they were responsible for promoting. I use health outcomes to see if any of the activities that the ASHA performed improved the overall health of their population. For both health inputs and health outcomes data, panel data of the years preceding and the years following program implementation would be ideal in order to establish the effect of the program and control for state linear time trends. The District Level Household & Facility Survey (DLHS) in India fills most of these criteria. The Indian Institute of Population Studies (IIPS) collects the DLHS in order to provide information on family planning, maternal health, child health, reproductive health and utilization of health services. IIPS surveys a representative sample for each district in India. Since the surveys are representative at the district- level, the district will be my unit of observation for each variable. I will use data 17
18 from the DLHS- 2 gathered from and DLHS- 3 gathered from Both rounds contain individual, household, village and public health facility questionnaires. While both rounds also contain data on numerous important health outcomes, I chose to focus upon infant and neonatal mortality, because they are areas that ASHAs were expected to improve. The NRHM explicitly states reductions in infant and neonatal mortality as one of its goals (MOHFW, 2005), and many of the health inputs the ASHAs are incentivized to promote, such as institutional deliveries and toilet construction, are expected to reduce infant and neonatal mortality. To create these infant mortality and neonatal mortality measures, I use the individual surveys administered to married women who were years old. These individual surveys contain retrospective birth histories of each woman as well as how long each of their infants survived after a given birth. These retrospective histories allow me to create panel data from of the annual infant mortality rate and neonatal mortality rate for each district. I chose to only use data going back to 1999 in order to minimize attrition and reporting bias. Another method for dealing with attrition bias and other sources of bias in the neonatal mortality and infant mortality data is to control for the mother s age. The DLHS- 2 and the DLHS- 3 both record the mother s age at each birth. By matching the mother s age to each birth and averaging these ages at the district- level, I create a retrospective measure of the average age of a mother at the time of birth in each district for each year from
19 For the health inputs, I chose institutional deliveries, tubectomies and toilet construction. Of the original eight incentivized health inputs, these three have the best available data and would contribute most to existing research. DOTS and leprosy cases are not recorded in the DLHS data. The Village Health and Sanitation Day only occurs after 2005, so I cannot establish any baseline data on this measure. The effect of the immunization sessions and Pulse Polio Days was already evaluated in Tanvi Rao s study (2012). In contrast, the DLHS has data on institutional deliveries, tubectomies and toilet construction and the ASHA s effect on them has not yet been empirically studied. In addition, a desire to lower the neonatal mortality rate motivated the Indian government s decision to incentivize institutional deliveries, and a desire to lower the infant mortality rate drove the government s decision to incentivize toilet construction, so looking at these health inputs and health outcomes jointly should help me understand the effect of these policies. For institutional deliveries, both the DLHS- 2 and the DLHS- 3 asked married women from Where did your last delivery take place? With this question, I construct panel data from for the annual institutional delivery rate in each district. For tubectomies and toilet sanitation, I do not have retrospective data. The DLHS- 2 and DLHS- 3 only ask married women from ages whether they have had a tubectomy. Using this data, I can construct the tubectomy rate among married women from ages for and For toilet sanitation, both the DLHS- 2 and DLHS- 3 measure whether a household uses a toilet and whether they 19
20 share the toilet they use. Unfortunately, the structure of the questions in the DLHS- 2 differs significantly from the structure in the DLHS- 3 (refer to Table A1 for the exact questions from each survey). Despite these differences, I can still use the questions in each survey to extract the percentage of households that have their own toilet in and in a given district. I also construct a measure of the percentage of households that use any type of toilet in and for a given district, just in case the household toilet rate misses some shared toilets that the ASHA s efforts helped create. 3.2 Summary Statistics Table 2 provides the summary statistics for the high- focus and non- focus states. Column 1.) provides sample means for the high focus before ASHA program implementation; column 2.) for the non- focus states before ASHA program implementation; column 3.) for the high- focus states after ASHA program implementation; column 4.) for the non- focus states after ASHA program implementation. In column 1.) and column 2.), we see that non- focus states have higher institutional delivery rates, tubectomy rates, household toilet rates and toilet usage rates, and lower infant mortality rates and neonatal mortality rates. These differences persist into the after implementation period as column 3.) and column 4.) show. From before to after implementation, health input usage rates tend to rise and mortality rates fall in both high focus and non- focus states. The only exceptions are household toilet rates and toilet usage rates in high- focus states. However, this exception may be due to reporting bias (refer to Section 5.3). 20

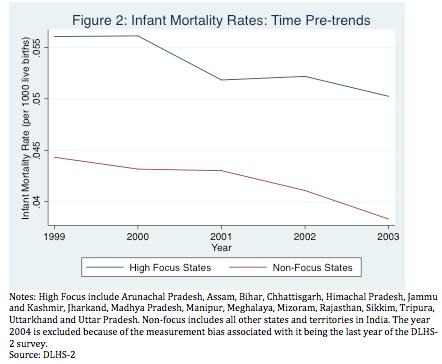
21 Figure 1 plots the sample mean institutional delivery rates by year for high focus and non- focus states before program implementation; Figure 2 for the sample mean infant mortality rates; Figure 3 for the sample mean neonatal mortality rates. There does not appear to be clear and significant linear time trend leading up to implementation for institutional delivery rates, infant mortality rates or neonatal mortality rates. 21

22 22

23 4.1 Empirical Strategy To estimate the effect of the ASHA program on health inputs and health outcomes in high- focus states, I exploit the fact that high focus states rolled out the ASHA program more intensely than non- focus states. Thus, high focus states should experience the effects of the ASHA program to a greater degree than non- focus states. In order to isolate the effect of this more intense rollout of the ASHA program on health inputs and health outcomes, I use the following equation: 1. ) DVdt = B0 + B1ASHAit + B2yt + B3si + eit with the dependent variable (DVdt) representing either the institutional delivery rate, the tubectomy rate, the household toilet rate, toilet usage rate, the infant mortality rate or the neonatal mortality for a district d in year t. ASHAit is a dummy variable equal to one if the state i is a high- focus state and the year t is after
24 (when the ASHA program was rolled out in high- focus states), and otherwise is equal to 0. yt represents year fixed effects. These variables ensure that my regression is not biased by a general trend toward increasing health inputs and improving health outcomes over time that occur regardless of whether or not a district has the ASHA program. si represents state fixed effects. These variables control for the level differences in the dependent variables before the implementation of the ASHA program, so that even though Table 2 shows large differences between high focus and non- focus states prior to implementation, these differentials should not bias my regression. Finally, I cluster standard errors by state to account for any arbitrary correlations in the error term, eit,, in a given state i in a given year t. The coefficient of interest is B1. B1 estimates the average difference in the changes in the dependent variable after the rollout of the ASHA program between high- focus districts and the non- focus districts. If I assume that the year and state fixed effects capture all other sources of variation in the dependent variable between high focus and non- focus districts, then B1 estimates the effect of the more intense rollout of the ASHA program. The assumption underlying my estimate could be wrong if there are ASHA program- independent factors that affect the rate of change of my dependent variables and affect high- focus states and non- focus states to different degrees. This situation could occur if high- focus states poor infrastructure and health indicators prevented them from increasing health input usage and improving health outcomes as fast as non- focus states. This variation would downwardly bias my estimate of 24
25 the ASHA program s effect. On the other hand, high- focus states could experience catch- up, because they are going after the low- hanging fruit in terms of increasing health inputs and improving health outcomes. For example, a high- focus state can focus on improving health inputs in more densely populated areas, while a non- focus state might have to focus on less densely populated areas in order to find populations who are not using the health input already. This scenario would upwardly bias my estimates of the effect of the ASHA program. In order to control for these trend differences, I add state- specific linear time trends to equation 1.). State- specific linear time trends should strip out the differences in the rate of change of the dependent variable that exist before and after the implementation of the ASHA program, which should isolate the effect of the ASHA program. However, this approach cannot account for factors that may affect the dependent variables, but do not precede the implementation of the ASHA program. One possible factor that could affect the dependent variable in this way is the age of the birth mother for neonatal deaths, infant deaths and institutional deliveries. The demographics of high focus and non- focus states could be changing differently during the period in which the ASHA program is implemented. For example, generally poorer high- focus states fertility rates may be decreasing slower, so they may have a younger population. This means that they will have more young mothers giving births, which will affect neo- natal deaths, infant deaths and institutional deliveries. Because of these possible differences between the mother s age in high- focus and non- focus states, I include a specification with a control for 25
26 mother s age for the neonatal mortality, infant mortality and institutional delivery estimates. Unfortunately, other sources of bias may be unobservable. These biases will be further discussed in section 5.3. Lastly, I use district fixed effects and district linear time trends to check the robustness of my estimates. Since dependent variables are measured at the district- level, district fixed effects could control for heterogeneity within a state. This specification will have the same weakness in terms of differences in the rate of change of dependent variable and mother s age, so I also include district linear time trends and mother s age (for neonatal mortality, infant mortality and institutional delivery) in a specification to reduce these biases. 5.1 Results Table 3 presents my estimates of the effect of the more intense rollout of the ASHA program on district institutional delivery rates. Column 1.) only controls for state fixed effects. The coefficient on ASHA indicates that the more intense rollout of the ASHA program is associated with a 9.8 percentage point rise in the institutional delivery rate for a given district (p<.01). Column 2.) controls for state fixed effects and year fixed effects. The ASHA coefficient becomes negative and statistically insignificant. When I add state linear time trends in Column 4.), the ASHA coefficient remains negative and statistically insignificant. Finally in Column 5.), I add mother s age to the regression and again find a negative and statistically insignificant ASHA coefficient. 26
27 Column 1.) and Column 2.) in Table 4 estimate the effect of the more intense rollout of the ASHA program on district household toilet rates. When I control for only state fixed effects in Column 1.), I estimate that the more intense rollout of the ASHA program is associated with a 6.7 percentage point decrease in the district household toilet rate (p<.10). When I add controls for year fixed effects in Column 2.), the effect size increases to a 7.2 percentage point decrease in the district household toilet rate (p<.01). Since the mean household toilet rate is 41.5%, the estimated decrease accounts for an economically significant 17.3% reduction of the sample mean. In Table A2, I run a robustness check for these results by performing 27
28 the same analysis on the toilet usage rate. I again find negative ASHA coefficients and the magnitude of the coefficients increases. Column 3.) and Column 4.) in Table 4 estimate the effect of the more intense rollout of the ASHA program on district tubectomy rates. With only state fixed effects in Column 3.), the ASHA coefficient indicates that the more intense rollout of the ASHA program is associated with a 6.1 percentage point increase in a district s tubectomy rate (p<.01). When I add year fixed effects in Column 4.), the coefficient remains positive, but the effect size becomes statistically insignificant. Table 5 presents the estimates of the effect of the more intense rollout of the ASHA program on district infant mortality rates. Column 1.) with state fixed effects estimates a 1.7 percentage point decrease (p<.01) in the infant mortality rate from 28
29 a district implementing the ASHA program. Column 2.) with year and state fixed effects finds no statistically significant relationship between the ASHA program and district infant mortality rate. Column 3.) with year fixed effects, state fixed effects and state linear time trends also finds no statistically significant relationship between the ASHA program and district infant mortality rates. Column 4.) adds a control for mother s age and once again finds no statistically significant relationship between the ASHA program and district infant mortality rates. Table 6 presents the estimates of the effect of the more intense rollout of the ASHA program on district neonatal mortality rates. With just state fixed effects in Column 1.), I estimate that the implementation of the ASHA program is followed by a 1.2 percentage point decrease in the neonatal mortality rate (p<.01). When I add 29
30 year fixed effects in Column 2.), the coefficient becomes statistically insignificant. When I add state linear time trends in Column 3.), the coefficient remains statistically insignificant. With the addition of a control for the mother s age in Column 4.), I still find a negative and statistically insignificant coefficient. Table A3- A6 test the robustness of these results when using district fixed effects instead of state fixed effects and district linear time trends rather than state linear time trends. Table A3 presents the robustness check for institutional deliveries, Table A4 presents the robustness check for household toilets and tubectomies, Table A5 presents the robustness check for infant mortality rates and Table A6 presents the robustness check for neonatal mortality rates. While there are 30
31 minor variations in the size of the ASHA coefficient, the significance and direction of my estimates do not change. 5.2 Multitasking When combined with Rao s (2012) finding (which I confirm using my empirical strategy; refer to Table A7) that the ASHA program strongly and positively affected immunization rates, my finding that the ASHA program has no significant positive effects suggests that the ASHA program had heterogeneous effects. In this section, I propose that the incentives created by the ASHA s performance pay scheme led to these heterogeneous outcomes. The performance pay scheme incentivized ASHAs to provide the services that reaped the largest return in terms of the incentive payments and required the least amount of effort to accomplish. These incentives may have created a multitasking problem where the ASHAs directed effort towards low- effort, high- reward activities, such as immunizations and infra- marginal institutional deliveries and tubectomies, while neglecting lower reward or higher cost activities such as toilet construction and the promotion of borderline institutional deliveries or tubectomies. In terms of institutional deliveries, the performance pay scheme creates incentives for ASHAs to transport infra- marginal patients. ASHAs can expend the lowest amount of effort by transporting patients who already are planning to give an institutional delivery. Patients who did not plan to give an institutional delivery might live far away from health facilities, which would require increased transportation costs for the ASHA, or might hold strong negative beliefs about 31
32 institutional deliveries, which would require that the ASHA spend time changing those beliefs. The qualitative evaluations of the ASHA program show how transportation costs drew ASHAs away from borderline institutional deliveries. Bajpai and Dholakia (2011) note that ASHAs rarely performed outreach to smaller hamlets or villages, because of the higher cost of traveling to these villages. ASHAs also complained that the costs of transporting patients who lived far away from health facilities exceeded the benefits from their incentive payment (Scott and Shanker, 2010). The failure of past institutional delivery programs demonstrates that many rural Indians hold strong beliefs about the inefficacy of institutional deliveries. In Gujurat, the government introduced the Chiranjeevi Yojani program in 2006, which covered the cost of delivery for below poverty line women at designated hospitals (Mohonan et. al, 2013). A recent evaluation of this program that controlled for time- invariant differences between Gujurati districts found that the program did not have an effect on institutional delivery rates, maternal mortality rates or delivery- related household expenditure (Mohonan et. al, 2013). The authors propose that perceptions of poor service and corruption may have prevented this program from increasing institutional delivery rates and lowering delivery- related household expenditure (Mohonan et. al., 2013). In the high focus states, perceptions of poor service are likely to be an even greater problem since these states were chosen because of their poor health infrastructure. In a qualitative evaluation of the ASHA program in Uttarakhand, ASHAs repeatedly claimed that absenteeism, resource 32
33 shortages and poor quality service at sub- centers hindered their ability to generate demand (Scott and Shanker, 2010). The corruption in institutional delivery programs could also engender distrust between the public healthcare sector and the community, which might undermine the ASHA s efforts to convince borderline patients. In addition to the possible corruption in the Chiranjeevi Yojani, the Janani Suraksha Yojana (JSY), a national program that gives cash to women for giving institutional deliveries, also suffered from corruption. A recent evaluation of the JSY found that most of the cash transfer went to health providers through bribes (Coffey, 2014). This corruption could create distrust between the community and public healthcare sector. Since the ASHA is associated with the government, this distrust could cause community members to discount ASHA s advice regarding institutional deliveries. A survey of 386 ASHAs in Orissa found that community distrust hampered the efficacy of the ASHA (Gopalan et. al, 2012). In some cases, this distrust may be justified. Mishra (2012) reported that ASHAs in South Orissa pushed for institutional deliveries without regard for the safety of the mother. In terms of tubectomies, distrust of public family planning programs increase the effort costs of convincing marginal women. During the Emergency period from , the Indian government undertook a mass sterilization campaign that used coercive techniques on poor Indians (Connelly, 2006). Understandably, poor Indians have been particularly wary of government programs promoting sterilization ever since. The ASHA s association with the public health 33
34 sector might trigger some Indian women to extend their suspicion to the ASHA s advice as well. In addition, a tubectomy is a high- stakes decision for the patient, and Indians are fairly well informed about female sterilizations. Since a tubectomy procedure precludes the woman from having future children and poses significant health risks, a woman s opposition to a tubectomy may be difficult for an ASHA to alter. Even prior to the ASHA program, the DLHS- 2 data shows that female sterilization was the most popular and most well known form of contraception in India. Using the DLHS- 2 data, I found that 95.6% of married women from the ages of were already aware that female sterilization as a family planning method. The high- stakes of the tubectomy decision and lack of trust in ASHAs may have made it too costly for ASHAs to convince borderline patients to get tubectomies. Similar to institutional deliveries, ASHAs might only focus upon infra- marginal cases, which would not impact the overall tubectomy rate. Toilet construction would be most exposed to the multitasking problem, because ASHAs received relatively low incentives and would have to expend high effort costs. As Table 1 shows, ASHAs received only 75 rupees for motivating toilet construction. This compensation is the lowest for any activity in the national guidelines and is half as much as the incentive for immunizations or tubectomies. Information and cultural barriers increase the effort costs ASHAs must expend in order to convince households to construct toilets. As mentioned previously, Banda et. al (2007) found that households in South Orissa were generally unaware of the benefits of toilet usage. Additionally, Banda et. al. (2007) 34
35 noted that open defecation was a traditional practice, so there was no stigma associated with it. These barriers have prevented the success of other sanitation programs. In 1985, the Government of India launched the Centrally Sponsored Rural Sanitation Program (CRSP). The CRSP took a supply- side approach by subsidizing up to 2,000 of the 2,500 Rs. cost of toilet construction for poor households (Gunyon, 1998). Despite this large subsidy, only limited progress was made, because the program did not address the informational and cultural barriers restricting demand (Hueso and Bell, 2011). In 1999, the Government of India admitted failure and restructured the program as the Total Sanitation Campaign (TSC) (Hueso and Bell, 2011). With these low incentives and high effort costs, it is unsurprising that ASHAs did not focus upon toilet sanitation. While the original national ASHA guidelines estimated caseload for toilet construction was 12, the average annual caseload for ASHAs in Bihar was 2 and the average annual caseload in Rajasthan was 0 (Bajpai and Dholakia, 2011). This lack of focus explains why I did not find any evidence that ASHA s increased toilet construction. It is even possible that implementing the ASHA program decreased the rate of toilet construction in high focus states. When the TSC was introduced in 1999, it offered local governments a large ex- post monetary incentive to reduce open defecation (Spears, 2012). This scheme gave local governments a large degree of autonomy in deciding how to reduce open defecation. In high focus states, local governments may have assigned ASHAs to lead this effort. In non- focus states, local governments would need to rely upon other methods and community leaders. Since 35
36 the ASHAs were generally not focused upon toilet construction, the other methods employed by non- focus states would likely yield superior results. In the existing literature on the effect of the TSC, I find some supporting evidence for this hypothesis. Two empirical studies that examine the ASHA program in high focus states (Orissa and Madhya Pradesh) found little or no effect of the TSC (Patil et. al, 2014; Barnard et. al, 2013). Spears (2012) examined the effects of the TSC on infant mortality and child s height across the entire country and found a significant reduction in infant mortality and significant increase in child s height. Together these three results suggest that the ASHA program may have hindered the effect of the TSC in high focus states relative to non- focus states. In contrast, immunization sessions were rewarded well and rural Indians beliefs about them are more flexible. ASHAs were paid twice as much for immunization sessions than for toilet construction (refer to Table 1). Evidence from other immunization interventions implies that rural Indians do not have a strong aversion to immunizations even in areas where immunization rates are low. A randomized control trial in rural Rajasthan provided a once monthly reliable immunization camp to control villages and provided a once monthly reliable immunization camp with small incentives (raw lentils and metal plates) for households if their child became fully immunized to treatment villages (Banerjee et. al, 2010). In the control villages, 75% of children received the first immunization, but only 18% of children became fully immunized. In the treatment villages, 40% of children became fully immunized (Banerjee et. al, 2010). The fact that 75% of children got the first immunization indicates that most households intended to get 36
37 their children fully immunized. The ultimate failure of most households to achieve this goal suggests that these households are facing a commitment problem. The small nudge offered by the raw lentils and metal plates allowed them to overcome this commitment problem. Similarly, a small nudge from the ASHA in the form of a reminder or piece of advice could be enough for borderline households to overcome this commitment problem. This small nudge would require low effort from the ASHA relative to the effort required for borderline cases of institutions deliveries, tubectomies or household toilets. 5.3 Threats to Validity The validity of my regression analysis results could be threatened by factors that vary over time and across districts. NRHM implementation is an example of a possible source of bias. Since the NRHM was implemented concurrently with the ASHA program, the state or district linear time trends will not be able to control for it. While the NRHM technically should have been implemented uniformly across districts, high focus states may be less effective in implementing the NRHM because of their worse governance. This less effective implementation of the NRHM would downwardly bias my estimates of ASHA s effect on health inputs and health outcomes, which is an alternative explanation for why I did not find any significant positive effects. Even if they are unbiased, my estimates will only be a lower bound on the effect of the ASHA program. Since the ASHA program was partially rolled out in non- focus states, my estimates only show the effect of the more intense roll out in high focus states rather the full effect of the ASHA program. Additionally, my data only 37
38 captures the first 3-4 years after the implementation of the ASHA program. After this 3-4 year period, the ASHAs received more training and gained more experience, which may have made them more effective. This systematic underestimation may have obscured the ASHA s positive effects on health inputs and outcomes. For institutional delivery rates, infant mortality rates and neonatal mortality rates, my data may be vulnerable to reporting or attrition bias. Since mothers report births and deaths from their memory, they may underreport deaths of children that they have forgotten or may get the date of their death incorrect. However, this bias should not affect my main results unless it varies across states and over time. Attrition bias may occur because our sample will exclude women who gave birth but died before the survey date. This bias might affect high- focus states that have higher mortality rates more than non- focus states. While I should be able to control for these differences if they are time- invariant, the ASHA program might reduce the mortality of women in high focus states, which would decrease attrition bias over time. I would expect attrition bias to downwardly bias the estimates of infant mortality and neonatal mortality, because the deceased mothers would be more likely to have had deceased infants or neonates that would be unrecorded. If the ASHA program reduced this bias, then my estimates of the decreases in the infant mortality rate and neonatal mortality rate in high focus states would be artificially smaller. This underestimation of the ASHA s effect could explain why I did not find an effect on infant mortality and neonatal mortality. However, there is no evidence that the ASHA program significantly changed the mortality rates of women, so attrition bias may not have affected my results. 38
39 For household toilet rates, toilet usage rates and tubectomy rates, state or district time pre- trends could confound my estimates. Because I only have two data points for each measure, I cannot control for state or district linear time trends. If these rates were already increasing at a slower rate in high focus states relative to non- focus states prior to ASHA program implementation, then it would downwardly bias my estimates. This downward bias could explain why I found that the ASHA program had no effect on the tubectomy rate and a negative effect on the household toilet rate and the toilet usage rate. For my measures of the household toilet rate and toilet usage rate, reporting bias may vary across districts and over time. As mentioned previously, the DLHS- 2 asked about toilets in a different manner than the DLHS- 3 (Table A1). As Table A1 shows, the DLHS- 2 includes no toilet, but the DLHS- 3 includes an option for no facility/uses open space or field. Some individuals answering the DLHS- 2 may have interpreted using an open space or field as using a type of own pit toilet, shared toilet or public- community toilet. In this case, the DLHS- 2 would overestimate the household toilet rate and the toilet usage rate. Table 1 supports this interpretation, because high focus states have falling household toilet and toilet usage rates, while non- focus states only experience a small rise. This pattern does not cohere with past research, which finds progress in toilet sanitation across India during this period (Hueso and Bell, 2011). This discrepancy would be explained by overestimates of the household toilet and toilet usage rate in the DLHS- 2. While year fixed effects should adjust for uniform discrepancies between reporting in the DLHS- 2 and DLHS- 3, the validity of my toilet sanitation results is threatened if the reporting bias 39
40 varies across districts. Unfortunately, reporting bias may be higher in high focus states because individuals in these states are poorer and thus, may use open space or field defecation more often. This higher reporting bias would downwardly bias my estimates of the ASHA program s effect on household toilet rates and toilet usage rates, which could explain why I found negative effects. 6 Conclusions In this paper, I exploit the variation in the Government of India s support for the ASHA program in high focus and non- focus states to test the effect of the ASHA program on health inputs and health outcomes. I find no evidence that the ASHA program increased institutional deliveries, tubectomies or toilet construction and no evidence that the ASHA program reduced the infant mortality rate or the neonatal mortality rate. In addition, I estimate that the ASHA program had a negative effect on household toilet rates, but reporting bias (refer to section 5.3) prevents me from drawing any strong conclusions from these estimates. At the least, my analysis provides no evidence that the ASHA program had a positive effect on household toilet rates. I interpret these results as evidence that the performance payment structure for ASHAs may have created a multitasking problem. These findings contradict the qualitative evaluations of the ASHA program, which often report that ASHAs improved the healthcare in their communities. These qualitative evaluations relied upon a comparison between healthcare before and after the implementation of the ASHA program. In my regression specifications with only state fixed effects, I find positive effects of the ASHA program on institutional delivery rates, tubectomy rates, infant mortality rates and neonatal mortality rates. 40
41 These findings confirm the qualitative evaluations assertion that healthcare improved with the arrival of the ASHAs. However, the regression specifications with state fixed effects and year fixed effects find no positive effects. These findings show that the improvements in healthcare in high focus states were not significantly greater than the improvements in healthcare in non- focus states, which indicates that other factors (for example, the other NRHM components that were implemented concurrently and across all of India) drove the improvements in healthcare. These qualitative studies also confuse ASHA activity with ASHA impact. Even if ASHAs are facilitating institutional deliveries, tubectomies and toilet construction, it does not mean that they are causing more of these activities to occur than would have occurred in their absence. ASHAs may be serving infra- marginal patients that would have accessed these health inputs even if the ASHAs were not there. If my multitasking interpretation of the results is correct, then the Government of India needs to rethink its payment of ASHAs. Over the past decade, the range of activities for which ASHAs can receive incentive payments has been greatly expanded. My research implies that incentivizing these new activities will only be successful if the remuneration exceeds the effort costs. Even then, the expanding range of activities will still lead to a multitasking problem. To combat these issues, I would propose that the range of activities is limited only to low effort activities. For example, simple activities such as immunizations, follow- up visits to mothers and children, delivering condoms and distributing sanitary napkins, could be kept, while more complex activities, such as motivating institutional deliveries, 41
42 motivating tubectomies, motivating toilet construction, ensuring spacing of children after marriage and organizing monthly meetings with adolescent girls pertaining to menstrual hygiene, could be passed on to more specialized health personnel. While more research is needed to confirm my results, reforming the ASHA program should be a priority for the Government of India. If my results are valid, then the majority of the ASHA program is a waste of human resources and government revenue. However, my results imply that simply altering the payment structure could transform this waste into an effective program. Experimenting with different payment structures and rigorously testing their effects will be crucial to ensuring that this transformation occurs. 8 References Bajpai, Nirupam, and Ravindra H. Dholakia. "Improving the performance of accredited social health activists in India." (2011) Banda, Kalyan, et al. "Water handling, sanitation and defecation practices in rural southern India: a knowledge, attitudes and practices study." Transactions of the royal society of tropical medicine and hygiene (2007): Bang, Abhay T., et al. "Effect of home- based neonatal care and management of sepsis on neonatal mortality: field trial in rural India." The lancet (1999): Banerjee, Abhijit Vinayak, et al. "Improving immunisation coverage in rural India: clustered randomised controlled evaluation of immunisation campaigns with and without incentives." Bmj 340 (2010): c2220. Barnard, Sharmani, et al. "Impact of Indian Total Sanitation Campaign on latrine coverage and use: a cross- sectional study in Orissa three years following programme implementation." PloS one 8.8 (2013): e Basinga, Paulin, et al. "Effect on maternal and child health services in Rwanda of payment to primary health- care providers for performance: an impact evaluation." The Lancet (2011):
43 Bhattacharyya, K. "Community Health Worker Incentives and Disincentives: How They Affect Motivation, Retention and Sustainability." (2001). Bhutta, Zulfiqar A., et al. "Community- based interventions for improving perinatal and neonatal health outcomes in developing countries: a review of the evidence." Pediatrics 115.Supplement 2 (2005): Bose, Ashish. "The Community Health Worker Scheme: an Indian experiment." (1983): Cairncross, Sandy, et al. "What causes sustainable changes in hygiene behaviour? A cross- sectional study from Kerala, India." Social Science & Medicine (2005): Chatterjee, Meera. "Health for too many: Indias experiments with truth." (1993): Chaudhury, Nazmul, et al. "Missing in action: teacher and health worker absence in developing countries." The Journal of Economic Perspectives 20.1 (2006): Connelly, Matthew. "Population control in India: Prologue to the emergency period." Population and Development Review 32.4 (2006): Das, Jishnu, and Jeffrey Hammer. "Money for nothing: The dire straits of medical practice in Delhi, India." Journal of Development Economics 83.1 (2007): De Walque, Damien, et al. "Using provider performance incentives to increase HIV testing and counseling services in Rwanda." Journal of health economics 40 (2015): 1-9. Drèze, Jean, and Amartya Sen. An uncertain glory: India and its contradictions. Princeton University Press, Gertler, Paul J., and Christel Vermeersch. "Using performance incentives to improve health outcomes." World Bank Policy Research Working Paper 6100 (2012). Gilson, Lucy, et al. "National community health worker programs: how can they be strengthened?." Journal of public health policy (1989): Gneezy, Uri, and Aldo Rustichini. "Pay enough or don't pay at all." Quarterly journal of economics (2000): Gopalan, Saji Saraswathy, Satyanarayan Mohanty, and Ashis Das. "Assessing community health workers performance motivation: a mixed- methods approach on India's Accredited Social Health Activists (ASHA) programme." BMJ open 2.5 (2012): e
44 Gunyon, William. "India: making government funding work harder." A WaterAid Report (1998). Holmstrom, Bengt, and Paul Milgrom. "Multitask principal- agent analyses: Incentive contracts, asset ownership, and job design." Journal of Law, Economics, & Organization 7 (1991): Hueso, Andrés, and Brian Bell. "An untold story of policy failure: the Total Sanitation Campaign in India." Water policy 15.6 (2013): Kidane, Gebreyesus, and Richard H. Morrow. "Teaching mothers to provide home treatment of malaria in Tigray, Ethiopia: a randomised trial." The lancet (2000): Lehmann, Uta, and David Sanders. "Community health workers: what do we know about them." The state of the evidence on programmes, activities, costs and impact on health outcomes of using community health workers. Geneva: World Health Organization (2007): Lewis, Maureen. "Governance and corruption in public health care systems." Center for Global Development working paper 78 (2006). McGuire, James W. "Democracy, social policy, and mortality decline in Brazil." Department of Government, Wesleyan University, Middleton, Conn. Processed (2001). Miller, Grant, and Kimberly Singer Babiarz. Pay- for- performance incentives in low- and middle- income country health programs. No. w National Bureau of Economic Research, Mishra, Arima. "The role of the Accredited Social Health Activists in effective health care delivery: evidence from a study in South Orissa." BMC proceedings. Vol. 6. No. Suppl 1. BioMed Central (2012). Ministry of Health and Family Welfare (MOHFW). National Rural Health Mission: Framework for Implementation (2005). Mohanan, Manoj, et al. "Effect of Chiranjeevi Yojana on institutional deliveries and neonatal and maternal outcomes in Gujarat, India: a difference- in- differences analysis." Bulletin of the World Health Organization 92.3 (2014): National Health Resource Systems Resource Centre (NHRSRC). Update on ASHA Programme July 2014 (2014). National Health Resource Systems Resource Centre (NHRSRC). Update on ASHA Programme July 2015 (2015). 44
45 Panagriya, Arvind. India: The Crisis in Rural Healthcare The Brookings Institute (2008). Parlato, Margaret Burns, and Michael Neil Favin. "Primary health care: progress and problems. An analysis of 52 AID- assisted projects." (1982). Patil, Sumeet R., et al. "The effect of India's total sanitation campaign on defecation behaviors and child health in rural Madhya Pradesh: a cluster randomized controlled trial." PLoS Med 11.8 (2014): e Rao, Tanvi. "The Impact Of Community Health Workers On Childhood Immunization: Evidence From India's Asha Worker Program." (2013). Rao, Mohan, et al. "Human resources for health in India." The Lancet (2011): Scott, Kerry, and Shobhit Shanker. "Tying their hands? Institutional obstacles to the success of the ASHA community health worker programme in rural north India." AIDS care 22.S2 (2010): Singh, Nirvikar. "Decentralization and public delivery of health care services in India." Health Affairs 27.4 (2008): Spears, Dean. "Effects of rural sanitation on infant mortality and human capital: Evidence from india s total sanitation campaign." Washington, DC: Princeton University (2012). Svitone, Ennio Cufino, et al. "Primary health care lessons from the Northeast of Brazil: the Agentes de Saúde Program." Revista Panamericana de Salud Pública 7.5 (2000): Saikia, Nandita, et al. "Explaining the rural- urban gap in infant mortality in India." Demographic Research 29 (2013): Tarozzi, Alessandro, et al. "Micro- loans, Insecticide- Treated Bednets and Malaria: Evidence from a randomized controlled trial in Orissa (India)." Economic Research Initiatives at Duke (ERID) Working Paper 104 (2011). Upadhyay, Ravi Prakash, et al. "High neonatal mortality rates in rural India: what options to explore?." ISRN pediatrics 2012 (2012). Vermeersch, Christel, and Michael Kremer. School meals, educational achievement, and school competition: evidence from a randomized evaluation. Vol World Bank Publications,
46 Wang, H., et al. "Performance- based payment system for ASHAs in India: what does international experience tell us." Bethesda, MD: The Vistaar Project, IntraHealth International Inc., Abt Associates Inc (2012). Wang'ombe, Joseph K. "Economic evaluation in primary health care: the case of Western Kenya community based health care project." Social science & medicine 18.5 (1984): Databases: The Indian Institute of Population Studies (IIPS). District Level Household & Facility Survey (DLHS- 2). (2005). The Indian Institute of Population Studies (IIPS). District Level Household & Facility Survey (DLHS- 3). (2009). World Bank Group, ed. World Development Indicators World Bank Publications,
47 9 Appendix 47
48 48

49 49


50 50

51 51
Work-time analysis of ANM and ASHA: A Priority for Strengthening Health Systems
 Work-time analysis of ANM and ASHA: A Priority for Strengthening Health Systems Anu-Raga Mahalingashetty, Master of Public Health Candidate, Department of Population & Family Health, Global Health Track
Work-time analysis of ANM and ASHA: A Priority for Strengthening Health Systems Anu-Raga Mahalingashetty, Master of Public Health Candidate, Department of Population & Family Health, Global Health Track
Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh
 Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh 1 CHAPTER Deepak Kumar,* Manisha* and Archana Dwivedi** INTRODUCTION Himachal Pradesh (HP) is one
Has Janani Suraksha Yojana Stimulated Institutional Delivery? A Study in Una District of Himachal Pradesh 1 CHAPTER Deepak Kumar,* Manisha* and Archana Dwivedi** INTRODUCTION Himachal Pradesh (HP) is one
CHAPTER 30 HEALTH AND FAMILY WELFARE
 CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
CHAPTER 30 HEALTH AND FAMILY WELFARE The health of the population is a matter of serious national concern. It is highly correlated with the overall development of the country. An efficient Health Information
Appendix. We used matched-pair cluster-randomization to assign the. twenty-eight towns to intervention and control. Each cluster,
 Yip W, Powell-Jackson T, Chen W, Hu M, Fe E, Hu M, et al. Capitation combined with payfor-performance improves antibiotic prescribing practices in rural China. Health Aff (Millwood). 2014;33(3). Published
Yip W, Powell-Jackson T, Chen W, Hu M, Fe E, Hu M, et al. Capitation combined with payfor-performance improves antibiotic prescribing practices in rural China. Health Aff (Millwood). 2014;33(3). Published
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur
 State Institute of Health & Family Welfare, Jaipur") Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Janani Suraksha Yojana (JSY) State Institute of Health & Family Welfare, Jaipur JSY A safe motherhood intervention, replacing the National Maternity Benefit Scheme, under NRHM 100 % centrally sponsored
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012
 Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
Dr. Ajay Khera Deputy Commissioner Ministry of Health and Family Welfare, Government of India February 17 th, 2012 1 What has India achieved so far? Goals Achievements National Rural Health Mission (By
INTRODUCTION. 76 MCHIP End-of-Project Report. (accessed May 8, 2014).
.") Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
Redacted INTRODUCTION Between 1990 and 2012, India s mortality rate in children less than five years of age declined by more than half (from 126 to 56/1,000 live births). The infant mortality rate also
MEETING THE NEONATAL CHALLENGE. Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009
, GoI New Delhi November 14, 2009") MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
MEETING THE NEONATAL CHALLENGE Dr.B.Kishore Assistant Commissioner (CH), GoI New Delhi November 14, 2009 Presentation Outline 1. Background 2. Key Initiatives of GoI 3. Progress 4. Major challenges & way
Growth of Primary Health Care System in Kerala-A comparison with India
 Growth of Primary Health Care System in Kerala-A comparison with India Dr. Suby Elizabeth Oommen Assistant Professor Department of Economics, Christian College, Chengannur, Alappuzha, Kerala, INDIA, 689121
Growth of Primary Health Care System in Kerala-A comparison with India Dr. Suby Elizabeth Oommen Assistant Professor Department of Economics, Christian College, Chengannur, Alappuzha, Kerala, INDIA, 689121
Sources for Sick Child Care in India
 Sources for Sick Child Care in India Jessica Scranton The private sector is the dominant source of care in India. Understanding if and where sick children are taken for care is critical to improve case
Sources for Sick Child Care in India Jessica Scranton The private sector is the dominant source of care in India. Understanding if and where sick children are taken for care is critical to improve case
Development of Policy Conference Nay Pi Taw 15 th February
 Development of Policy Conference Nay Pi Taw 15 th February To outline some Country Examples of the Role of Community Volunteers in Health from the region To indicate success factors in improvements to
Development of Policy Conference Nay Pi Taw 15 th February To outline some Country Examples of the Role of Community Volunteers in Health from the region To indicate success factors in improvements to
Growing microenterprises: How gender and family can impact outcomes evidence from Uganda. What Works in SME Development. 1.
 Issue Brief No 2, March 2017 Growing microenterprises: How gender and family can impact outcomes evidence from Uganda 1. Key findings Lack of access to finance and management ability are important constraints
Issue Brief No 2, March 2017 Growing microenterprises: How gender and family can impact outcomes evidence from Uganda 1. Key findings Lack of access to finance and management ability are important constraints
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care. Harold D. Miller
 Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
Creating a Patient-Centered Payment System to Support Higher-Quality, More Affordable Health Care Harold D. Miller First Edition October 2017 CONTENTS EXECUTIVE SUMMARY... i I. THE QUEST TO PAY FOR VALUE
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r
 RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
RWANDA S COMMUNITY HEALTH WORKER PROGRAM r Summary Background The Rwanda CHW Program was established in 1995, aiming at increasing uptake of essential maternal and child clinical services through education
Kingdom of Saudi Arabia Ministry of Defense General Staff Command Medical Services Directorate King Fahad Armed Forces Hospital, Jeddah
 Kingdom of Saudi Arabia Ministry of Defense General Staff Command Medical Services Directorate King Fahad Armed Forces Hospital, Jeddah Aim: To share with the participants the development of the health
Kingdom of Saudi Arabia Ministry of Defense General Staff Command Medical Services Directorate King Fahad Armed Forces Hospital, Jeddah Aim: To share with the participants the development of the health
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA.
 UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
UNIVERSAL HEALTH COVERAGE AND INNOVATIONS IN HEALTH SECTOR OF TRIPURA. Date : 20 th January, 2014 OBJECTIVES 1. Equity in access to health. 2. Social Health Protection (Non-exclusion and non-discrimination).
EXIT STRATEGIES STUDY: INDIA BEATRICE LORGE ROGERS, CARISA KLEMEYER, AMEYA BRONDRE
 EXIT STRATEGIES STUDY: INDIA 1 BEATRICE LORGE ROGERS, CARISA KLEMEYER, AMEYA BRONDRE Overview of India Study 2 One program (CARE); one sector (health) Four states: AP, Orissa, Chhattisgarh, UP India contrasts
EXIT STRATEGIES STUDY: INDIA 1 BEATRICE LORGE ROGERS, CARISA KLEMEYER, AMEYA BRONDRE Overview of India Study 2 One program (CARE); one sector (health) Four states: AP, Orissa, Chhattisgarh, UP India contrasts
Fertility Response to the Tax Treatment of Children
 Fertility Response to the Tax Treatment of Children Kevin J. Mumford Purdue University Paul Thomas Purdue University April 2016 Abstract This paper uses variation in the child tax subsidy implicit in US
Fertility Response to the Tax Treatment of Children Kevin J. Mumford Purdue University Paul Thomas Purdue University April 2016 Abstract This paper uses variation in the child tax subsidy implicit in US
Executive Summary. Rouselle Flores Lavado (ID03P001)
") Executive Summary Rouselle Flores Lavado (ID03P001) The dissertation analyzes barriers to health care utilization in the Philippines. It starts with a review of the Philippine health sector and an analysis
Executive Summary Rouselle Flores Lavado (ID03P001) The dissertation analyzes barriers to health care utilization in the Philippines. It starts with a review of the Philippine health sector and an analysis
Chapter II. Health Care System in India
 Chapter II Health Care System in India Chapter II HEALTHCARE SYSTEM IN INDIA 2.1- Introduction: Healthy citizens are the greatest assets any country can have Winston S. Churchill Health is a state subject
Chapter II Health Care System in India Chapter II HEALTHCARE SYSTEM IN INDIA 2.1- Introduction: Healthy citizens are the greatest assets any country can have Winston S. Churchill Health is a state subject
Impact of caregiver incentives on child health: Evidence from an experiment with Anganwadi workers in India
 Impact of caregiver incentives on child health: Evidence from an experiment with Anganwadi workers in India Prakarsh Singh and William Masters Amherst College and Tufts University World Bank Workshop January
Impact of caregiver incentives on child health: Evidence from an experiment with Anganwadi workers in India Prakarsh Singh and William Masters Amherst College and Tufts University World Bank Workshop January
Introduction: Statement of the problem:
 Introduction: The fundamental truth that human well-being is revolving round the fulcrum of health is receiving increasing acceptance in the world scenario. This fact can be perceived if one cares to look
Introduction: The fundamental truth that human well-being is revolving round the fulcrum of health is receiving increasing acceptance in the world scenario. This fact can be perceived if one cares to look
A STUDY OF HEALTH CARE SERVICES IN TRIBAL AREA. Dr. Tukaram Vaijanathrao Powale
 A STUDY OF HEALTH CARE SERVICES IN TRIBAL AREA Research Paper : Dr. Tukaram Vaijanathrao Powale Assistant Professor of Economics Late Babasaheb Deshmukh Gorthekar Mahavidyalaya, Umri, Dist. Nanded - 431807
A STUDY OF HEALTH CARE SERVICES IN TRIBAL AREA Research Paper : Dr. Tukaram Vaijanathrao Powale Assistant Professor of Economics Late Babasaheb Deshmukh Gorthekar Mahavidyalaya, Umri, Dist. Nanded - 431807
Indian Healthcare System: Issues and Challenges
 Indian Healthcare System: Issues and Challenges Dr. Bimal Jaiswal1, Ms. Noor Us Saba1 1Department of Applied Economics, Faculty of Commerce, University of Lucknow, Lucknow, U.P. 2Visiting Faculty, Institute
Indian Healthcare System: Issues and Challenges Dr. Bimal Jaiswal1, Ms. Noor Us Saba1 1Department of Applied Economics, Faculty of Commerce, University of Lucknow, Lucknow, U.P. 2Visiting Faculty, Institute
Improving Health Outcomes Incentives for Immunization and Reliable Services
 Session 1, Part A: 9:30am 10:15am Improving Health Outcomes Incentives for Immunization and Reliable Services Rachel Glennerster & Neelima Khetan The poor in rural Rajasthan spend a lot on health care
Session 1, Part A: 9:30am 10:15am Improving Health Outcomes Incentives for Immunization and Reliable Services Rachel Glennerster & Neelima Khetan The poor in rural Rajasthan spend a lot on health care
DISTRICT BASED NORMATIVE COSTING MODEL
 DISTRICT BASED NORMATIVE COSTING MODEL Oxford Policy Management, University Gadjah Mada and GTZ Team 17 th April 2009 Contents Contents... 1 1 Introduction... 2 2 Part A: Need and Demand... 3 2.1 Epidemiology
DISTRICT BASED NORMATIVE COSTING MODEL Oxford Policy Management, University Gadjah Mada and GTZ Team 17 th April 2009 Contents Contents... 1 1 Introduction... 2 2 Part A: Need and Demand... 3 2.1 Epidemiology
Health and Nutrition Public Investment Programme
 Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Government of Afghanistan Health and Nutrition Public Investment Programme Submission for the SY 1383-1385 National Development Budget. Ministry of Health Submitted to MoF January 22, 2004 PIP Health and
Impact Evaluation Concept Note HEALTH MILLENNIUM DEVELOPMENT GOALS PROGRAM-FOR-RESULTS (P4 R) ETHIOPIA
 ETHIOPIA") Impact Evaluation Concept Note HEALTH MILLENNIUM DEVELOPMENT GOALS PROGRAM-FOR-RESULTS (P4 R) ETHIOPIA Development Impact Evaluation Initiative Innovating in Design: Evidence for Impact in Health Cape
Impact Evaluation Concept Note HEALTH MILLENNIUM DEVELOPMENT GOALS PROGRAM-FOR-RESULTS (P4 R) ETHIOPIA Development Impact Evaluation Initiative Innovating in Design: Evidence for Impact in Health Cape
EFFECTIVENESS OF VIDEO ASSISTED TEACHING (VAT) ON KNOWLEDGE AND PRACTICE REGARDING PERSONAL HYGIENE AMONG SCHOOL CHILDREN
 ON KNOWLEDGE AND PRACTICE REGARDING PERSONAL HYGIENE AMONG SCHOOL CHILDREN") Original Research Article Nursing International Journal of Pharma and Bio Sciences ISSN 0975-6299 EFFECTIVENESS OF VIDEO ASSISTED TEACHING (VAT) ON KNOWLEDGE AND PRACTICE REGARDING PERSONAL HYGIENE AMONG
Original Research Article Nursing International Journal of Pharma and Bio Sciences ISSN 0975-6299 EFFECTIVENESS OF VIDEO ASSISTED TEACHING (VAT) ON KNOWLEDGE AND PRACTICE REGARDING PERSONAL HYGIENE AMONG
Barriers & Incentives to Obtaining a Bachelor of Science Degree in Nursing
 Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 4-2011 Barriers & Incentives to Obtaining a Bachelor of Science Degree in Nursing Tiffany Boring Brianna Burnette
Southern Adventist Univeristy KnowledgeExchange@Southern Graduate Research Projects Nursing 4-2011 Barriers & Incentives to Obtaining a Bachelor of Science Degree in Nursing Tiffany Boring Brianna Burnette
Utilization of health facilities at primary health centre. Utilization of health facilities at primary health centre by rural community of Pondicherry
 Utilization of health facilities at primary health centre Original Research Article ISSN: 2394-0026 (P) Utilization of health facilities at primary health centre by rural community of Pondicherry K N Prasad
Utilization of health facilities at primary health centre Original Research Article ISSN: 2394-0026 (P) Utilization of health facilities at primary health centre by rural community of Pondicherry K N Prasad
Child Survival among Urban Poor- Challenges and Approaches for Involving Pediatricians
 Child Survival among Urban Poor- Challenges and Approaches for Involving Pediatricians IAP Central Zone Workshop February 9th, 2006 Shreemaya Residency, Indore Dr. Siddharth Agarwal Urban Health Resource
Child Survival among Urban Poor- Challenges and Approaches for Involving Pediatricians IAP Central Zone Workshop February 9th, 2006 Shreemaya Residency, Indore Dr. Siddharth Agarwal Urban Health Resource
Models of Supportive Supervision for IMNCI Implementation in Selected Districts of Bihar, Orissa and Rajasthan in India
 224 Indian Journal of Public Health Research & Development. January-March 2013, Vol. 4, No. 1 Models of Supportive Supervision for IMNCI Implementation in Selected Districts of Bihar, Orissa and Rajasthan
224 Indian Journal of Public Health Research & Development. January-March 2013, Vol. 4, No. 1 Models of Supportive Supervision for IMNCI Implementation in Selected Districts of Bihar, Orissa and Rajasthan
Health Manpower Planning
 Health Manpower and Management 10.5005/jp-journals-10055-0013 1 Rajoo S Chhina, 2 Rajdeep S Chhina, 3 Ananat Sidhu, 4 Amit Bansal ABSTRACT Manpower is the most crucial resource toward delivery of health
Health Manpower and Management 10.5005/jp-journals-10055-0013 1 Rajoo S Chhina, 2 Rajdeep S Chhina, 3 Ananat Sidhu, 4 Amit Bansal ABSTRACT Manpower is the most crucial resource toward delivery of health
PROGRAM BRIEF UGANDA. Integrated Case Management of Pneumonia, Diarrhea & Malaria through the Five & Alive Franchise Network
 PROGRAM BRIEF UGANDA Integrated Case Management of Pneumonia, Diarrhea & Malaria through the Five & Alive Franchise Network I ntegrated case management (ICM) is a strategy to reduce child morbidity and
PROGRAM BRIEF UGANDA Integrated Case Management of Pneumonia, Diarrhea & Malaria through the Five & Alive Franchise Network I ntegrated case management (ICM) is a strategy to reduce child morbidity and
Case Study HEUTOWN DISTRICT: PLANNING AND RESOURCE ALLOCATION
 Case Study HEUTOWN DISTRICT: PLANNING AND RESOURCE ALLOCATION Di McIntyre Health Economics Unit, University of Cape Town, Cape Town, South Africa This case study may be copied and used in any formal academic
Case Study HEUTOWN DISTRICT: PLANNING AND RESOURCE ALLOCATION Di McIntyre Health Economics Unit, University of Cape Town, Cape Town, South Africa This case study may be copied and used in any formal academic
8 November, RMNCAH Country Case-Studies: Summary of Findings from Six Countries
 8 November, 2012 RMNCAH Country Case-Studies: Summary of Findings from Six Countries Country Case-Studies: September October 2012 6 countries Bangladesh, India, Indonesia, Nepal, Papua New Guinea and Solomon
8 November, 2012 RMNCAH Country Case-Studies: Summary of Findings from Six Countries Country Case-Studies: September October 2012 6 countries Bangladesh, India, Indonesia, Nepal, Papua New Guinea and Solomon
Conclusion: what works?
 Chapter 7 Conclusion: what works? Fishermen (Abdel Inoua) 7. Conclusion: what works? It is a convenient untruth that there has been no progress in health in the Region. This report has used a wide range
Chapter 7 Conclusion: what works? Fishermen (Abdel Inoua) 7. Conclusion: what works? It is a convenient untruth that there has been no progress in health in the Region. This report has used a wide range
Research Design: Other Examples. Lynda Burton, ScD Johns Hopkins University
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Continuum of Care Services: A Holistic Approach to Using MOTECH Suite for Community Workers
 CASE STUDY Continuum of Care Services: A Holistic Approach to Using MOTECH Suite for Community Workers Providing coordinated care across the continuum of maternal and child health in Bihar, India PROJECT
CASE STUDY Continuum of Care Services: A Holistic Approach to Using MOTECH Suite for Community Workers Providing coordinated care across the continuum of maternal and child health in Bihar, India PROJECT
Task shifting to optimise the roles of health workers to improve the delivery of maternal and child healthcare
 An Evidence Brief for Policy Task shifting to optimise the roles of health workers to improve the delivery of maternal and child healthcare Executive Summary This policy brief was prepared by the Uganda
An Evidence Brief for Policy Task shifting to optimise the roles of health workers to improve the delivery of maternal and child healthcare Executive Summary This policy brief was prepared by the Uganda
DOI: /jemds/2014/1887 ORIGINAL ARTICLE
 EVALUATION OF ASHA PROGRAMME IN SELECTED BLOCK OF RAISEN DISTRICT OF MADHYA PRADESH UNDER THE NATIONAL RURAL HEALTH MISSION Bhagwan Waskel 1, Sanjay Dixit 2, Rama Singodia 3, D.K. Pal 4, Manju Toppo 5,
EVALUATION OF ASHA PROGRAMME IN SELECTED BLOCK OF RAISEN DISTRICT OF MADHYA PRADESH UNDER THE NATIONAL RURAL HEALTH MISSION Bhagwan Waskel 1, Sanjay Dixit 2, Rama Singodia 3, D.K. Pal 4, Manju Toppo 5,
Making the Business Case
 Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
Making the Business Case for Payment and Delivery Reform Harold D. Miller Center for Healthcare Quality and Payment Reform To learn more about RWJFsupported payment reform activities, visit RWJF s Payment
UHC. Moving toward. Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES. Public Disclosure Authorized
 Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
Public Disclosure Authorized Public Disclosure Authorized Moving toward UHC Sudan NATIONAL INITIATIVES, KEY CHALLENGES, AND THE ROLE OF COLLABORATIVE ACTIVITIES re Authorized Public Disclosure Authorized
TERMS OF REFERENCE: PRIMARY HEALTH CARE
 TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
TERMS OF REFERENCE: PRIMARY HEALTH CARE A. BACKGROUND Health Status. The health status of the approximately 21 million Citizens of Country Y is among the worst in the world. The infant mortality rate is
Evidence Based Practice: Strengthening Maternal and Newborn Health
 Evidence Based Practice: Strengthening Maternal and Newborn Health Address Mauakowa Malata PhD RNM FAAN Kamuzu College of Nursing International Confederation of Midwives 1 University of Malawi Kamuzu College
Evidence Based Practice: Strengthening Maternal and Newborn Health Address Mauakowa Malata PhD RNM FAAN Kamuzu College of Nursing International Confederation of Midwives 1 University of Malawi Kamuzu College
Water, sanitation and hygiene in health care facilities in Asia and the Pacific
 Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
Water, sanitation and hygiene in health care facilities in Asia and the Pacific A necessary step to achieving universal health coverage and improving health outcomes This note sets out the crucial role
National Rural Health Mission (NRHM) State Institute of Health & Family Welfare, Jaipur
 State Institute of Health & Family Welfare, Jaipur") National Rural Health Mission (NRHM) State Institute of Health & Family Welfare, Jaipur NRHM N Newer Initiatives. R Rural Poor Population H Holistic Holistic Health Package. M Monitoring mechanisms To
National Rural Health Mission (NRHM) State Institute of Health & Family Welfare, Jaipur NRHM N Newer Initiatives. R Rural Poor Population H Holistic Holistic Health Package. M Monitoring mechanisms To
IMPLEMENTATION OF THE WARD BASED PRIMARY HEALTH CARE OUTREACH TEAMS IN THE EKURHULENI HEALTH DISTRICT: A PROCESS EVALUATION
 IMPLEMENTATION OF THE WARD BASED PRIMARY HEALTH CARE OUTREACH TEAMS IN THE EKURHULENI HEALTH DISTRICT: A PROCESS EVALUATION Carmen Whyte A research report submitted to the Faculty of Health Sciences, University
IMPLEMENTATION OF THE WARD BASED PRIMARY HEALTH CARE OUTREACH TEAMS IN THE EKURHULENI HEALTH DISTRICT: A PROCESS EVALUATION Carmen Whyte A research report submitted to the Faculty of Health Sciences, University
Scaling Up Public-Private Partnerships to Achieve Family Planning Equity Goals in India
 Scaling Up Public-Private Partnerships to Achieve Family Planning Equity Goals in India Suneeta Sharma, PhD MHA, Managing Director, Futures Group India Tanya Liberham, MA, Knowledge Management Officer,
Scaling Up Public-Private Partnerships to Achieve Family Planning Equity Goals in India Suneeta Sharma, PhD MHA, Managing Director, Futures Group India Tanya Liberham, MA, Knowledge Management Officer,
National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year
 National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year 2010-11 District :-Sriganganagar A RCH - TECHNICAL STRATEGIES & ACTIVITIES (RCH Flexible Pool) A.1 MATERNAL
National Rural Health Mission District Sriganganagar Proposed NRHM PIP for the Financial Year 2010-11 District :-Sriganganagar A RCH - TECHNICAL STRATEGIES & ACTIVITIES (RCH Flexible Pool) A.1 MATERNAL
Workload and perceived constraints of Anganwadi workers
 Workload and perceived constraints of Anganwadi workers Damanpreet Kaur, Manjula Thakur, Amarjeet Singh, Sushma Kumari Saini Abstract : Integrated Child Development Service scheme is most important nutritional
Workload and perceived constraints of Anganwadi workers Damanpreet Kaur, Manjula Thakur, Amarjeet Singh, Sushma Kumari Saini Abstract : Integrated Child Development Service scheme is most important nutritional
Supplementary Material Economies of Scale and Scope in Hospitals
 Supplementary Material Economies of Scale and Scope in Hospitals Michael Freeman Judge Business School, University of Cambridge, Cambridge CB2 1AG, United Kingdom mef35@cam.ac.uk Nicos Savva London Business
Supplementary Material Economies of Scale and Scope in Hospitals Michael Freeman Judge Business School, University of Cambridge, Cambridge CB2 1AG, United Kingdom mef35@cam.ac.uk Nicos Savva London Business
Global Health Evidence Summit. Community and Formal Health System Support for Enhanced Community Health Worker Performance
 Global Health Evidence Summit Community and Formal Health System Support for Enhanced Community Health Worker Performance I. Global Health Evidence Summits President Obama s Global Health Initiative (GHI)
Global Health Evidence Summit Community and Formal Health System Support for Enhanced Community Health Worker Performance I. Global Health Evidence Summits President Obama s Global Health Initiative (GHI)
GLOBAL GRANT MONITORING AND EVALUATION PLAN SUPPLEMENT
 ENGLISH (EN) GLOBAL GRANT MONITORING AND EVALUATION PLAN SUPPLEMENT Global grant sponsors for humanitarian projects and vocational training teams must incorporate monitoring and evaluation measures within
ENGLISH (EN) GLOBAL GRANT MONITORING AND EVALUATION PLAN SUPPLEMENT Global grant sponsors for humanitarian projects and vocational training teams must incorporate monitoring and evaluation measures within
The Internet as a General-Purpose Technology
 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Policy Research Working Paper 7192 The Internet as a General-Purpose Technology Firm-Level
Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Policy Research Working Paper 7192 The Internet as a General-Purpose Technology Firm-Level
0 MODEL DISTRICTS AS A ROADMAP FOR PUBLIC HEALTH SCALE UP IN INDIA
 MODEL DISTRICTS AS A ROADMAP FOR PUBLIC HEALTH SCALE UP IN INDIA Nirupam Bajpai, Megan Towle, and Jyothi Vynatheya Working Paper No. 4 July 2011 WORKING PAPERS SERIES Columbia Global Centers South Asia,
MODEL DISTRICTS AS A ROADMAP FOR PUBLIC HEALTH SCALE UP IN INDIA Nirupam Bajpai, Megan Towle, and Jyothi Vynatheya Working Paper No. 4 July 2011 WORKING PAPERS SERIES Columbia Global Centers South Asia,
Evaluation Of Immunization Coverage By Lot Quality Assurance Sampling In A Primary Health Center Area
 ISPUB.COM The Internet Journal of Public Health Volume 1 Number 1 Evaluation Of Immunization Coverage By Lot Quality Assurance Sampling In A Primary Health Center P BS, Gangaboraiah, U S Citation P BS,
ISPUB.COM The Internet Journal of Public Health Volume 1 Number 1 Evaluation Of Immunization Coverage By Lot Quality Assurance Sampling In A Primary Health Center P BS, Gangaboraiah, U S Citation P BS,
Call for expressions of interest: impact evaluations in environment, governance, infrastructure and public finance sectors
 Development Priorities Window Call for expressions of interest: impact evaluations in environment, governance, infrastructure and public finance sectors Issue date: 2 December 2015 Deadline for questions:
Development Priorities Window Call for expressions of interest: impact evaluations in environment, governance, infrastructure and public finance sectors Issue date: 2 December 2015 Deadline for questions:
Communicating Research Findings to Policymakers
 Communicating Research Findings to Policymakers Increasing the Chances of Success Satellite Session: Strengthening Research on Policy Implementation and Why it Matters to Health Outcomes Suneeta Sharma,
Communicating Research Findings to Policymakers Increasing the Chances of Success Satellite Session: Strengthening Research on Policy Implementation and Why it Matters to Health Outcomes Suneeta Sharma,
USAID/Philippines Health Project
 USAID/Philippines Health Project 2017-2021 Redacted Concept Paper As of January 24, 2017 A. Introduction This Concept Paper is a key step in the process for designing a sector-wide USAID/Philippines Project
USAID/Philippines Health Project 2017-2021 Redacted Concept Paper As of January 24, 2017 A. Introduction This Concept Paper is a key step in the process for designing a sector-wide USAID/Philippines Project
Chapter 6 PROBLEMS OF THE WOMEN ENTREPRENEURS IN KERALA AND TAMIL NADU
 Chapter 6 PROBLEMS OF THE WOMEN ENTREPRENEURS IN KERALA AND TAMIL NADU Several barriers and constraints, viz. cultural, educational, technological, financial and legal lie in the way of women entrepreneurs
Chapter 6 PROBLEMS OF THE WOMEN ENTREPRENEURS IN KERALA AND TAMIL NADU Several barriers and constraints, viz. cultural, educational, technological, financial and legal lie in the way of women entrepreneurs
IMPACT OF DEMOGRAPHIC AND WORK VARIABLES ON WORK LIFE BALANCE-A STUDY CONDUCTED FOR NURSES IN BANGALORE
 IMPACT OF DEMOGRAPHIC AND WORK VARIABLES ON WORK LIFE BALANCE-A STUDY CONDUCTED FOR NURSES IN BANGALORE Puja Roshani, Assistant Professor and Ph.D. scholar, Jain University, Bangalore, India Dr. Chaya
IMPACT OF DEMOGRAPHIC AND WORK VARIABLES ON WORK LIFE BALANCE-A STUDY CONDUCTED FOR NURSES IN BANGALORE Puja Roshani, Assistant Professor and Ph.D. scholar, Jain University, Bangalore, India Dr. Chaya
How to evaluate the impact of poverty programs. Rachel Glennerster Abdul Latif Jameel Poverty Action Lab at MIT povertyactionlab.
 How to evaluate the impact of poverty programs Rachel Glennerster Abdul Latif Jameel Poverty Action Lab at MIT povertyactionlab.org Presentation to MIT DLab III Class Thursday, April 19, 2007 1 Overview
How to evaluate the impact of poverty programs Rachel Glennerster Abdul Latif Jameel Poverty Action Lab at MIT povertyactionlab.org Presentation to MIT DLab III Class Thursday, April 19, 2007 1 Overview
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region. Community IMCI. Community IMCI
 Implementation in the Western Pacific Region. Community IMCI. Community IMCI") Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Integrated Management of Childhood Illness (IMCI) Implementation in the Western Pacific Region 5 What is community IMCI? is one of three elements of the IMCI strategy. Action at the level of the home and
Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor
 Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor Overview- What gets measured, gets done Operation ASHA -serving more than 54 Lakh people in
Empowering States & Districts & using biometric technology to deliver healthcare to the doorsteps of the poor Overview- What gets measured, gets done Operation ASHA -serving more than 54 Lakh people in
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
REQUEST FOR LETTERS OF INTEREST
 REQUEST FOR LETTERS OF INTEREST February 7, 2018 potentially high-impact, scalable interventions to be funded, implemented and evaluated through the Bengaluru Innovation Challenge. The purpose of this
REQUEST FOR LETTERS OF INTEREST February 7, 2018 potentially high-impact, scalable interventions to be funded, implemented and evaluated through the Bengaluru Innovation Challenge. The purpose of this
Enhancing Sustainability: Building Modeling Through Text Analytics. Jessica N. Terman, George Mason University
 Enhancing Sustainability: Building Modeling Through Text Analytics Tony Kassekert, The George Washington University Jessica N. Terman, George Mason University Research Background Recent work by Terman
Enhancing Sustainability: Building Modeling Through Text Analytics Tony Kassekert, The George Washington University Jessica N. Terman, George Mason University Research Background Recent work by Terman
Impact Evaluation Design for Community Midwife Technicians in Malawi
 Impact Evaluation Design for Community Midwife Technicians in Malawi Nathan B.W. Chimbatata, ( Msc. Epi, BscN, Dip Opth), Mzuzu University, Mzuzu, Malawi Chikondi M. Chimbatata, (BscN, pgucm) Kamuzu College
Impact Evaluation Design for Community Midwife Technicians in Malawi Nathan B.W. Chimbatata, ( Msc. Epi, BscN, Dip Opth), Mzuzu University, Mzuzu, Malawi Chikondi M. Chimbatata, (BscN, pgucm) Kamuzu College
Guidelines for Performance based Payment for ASHA under National Leprosy Eradication Programme
 Guidelines for Performance based Payment for ASHA under National Leprosy Eradication Programme Introduction: Under Health System, Multi-purpose Workers (MPW- Male & Female) at the sub- centre act as the
Guidelines for Performance based Payment for ASHA under National Leprosy Eradication Programme Introduction: Under Health System, Multi-purpose Workers (MPW- Male & Female) at the sub- centre act as the
Kiva Labs Impact Study
 TYPE: Call for Expression of Interest EMPLOYER: Kiva Microfunds LOCATION OF JOB: Remote POSTED DATE : 20 June 2017 CLOSING DAT E: 7 July 2017 Kiva Labs Impact Study Kiva is seeking Expressions of Interest
TYPE: Call for Expression of Interest EMPLOYER: Kiva Microfunds LOCATION OF JOB: Remote POSTED DATE : 20 June 2017 CLOSING DAT E: 7 July 2017 Kiva Labs Impact Study Kiva is seeking Expressions of Interest
UNICEF WCARO October 2012
 UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
UNICEF WCARO October 2012 Case Study on Narrowing the Gaps for Equity Benin Equity in access to health care for the most vulnerable children through Performance- based Financing of Community Health Workers
The challenge of delivering healthcare to the poor: Udaipur Example. Improving Health Status
 The challenge of delivering healthcare to the poor: Udaipur Example. Esther Duflo, 14.73, October 28, 2009 povertyactionlab.org Improving Health Status Seva Mandir was keen to find new interventions for
The challenge of delivering healthcare to the poor: Udaipur Example. Esther Duflo, 14.73, October 28, 2009 povertyactionlab.org Improving Health Status Seva Mandir was keen to find new interventions for
Rural Health Care System in India
 Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
Rural Health Care System in India Rural Health Care System the structure and current scenario The health care infrastructure in rural areas has been developed as a three tier system (see Chart 1) and is
Citizen s Engagement in Health Service Provision in Kenya
 Citizen s Engagement in Health Service Provision in Kenya Hon. (Prof) Peter Anyang Nyong o, EGH, MP Minister for Medical Services, Kenya Abstract Kenya s form of governance has moved gradually from centralized
Citizen s Engagement in Health Service Provision in Kenya Hon. (Prof) Peter Anyang Nyong o, EGH, MP Minister for Medical Services, Kenya Abstract Kenya s form of governance has moved gradually from centralized
2018 Visiting Fellowship Application
 East Africa Social Science Translation (EASST) Collaborative 2018 Visiting Fellowship Application Release Date: 22 January 2018 The East Africa Social Science Translation (EASST) Collaborative invites
East Africa Social Science Translation (EASST) Collaborative 2018 Visiting Fellowship Application Release Date: 22 January 2018 The East Africa Social Science Translation (EASST) Collaborative invites
Minister. Secretaries of State. Department of Planning and Health Information. Department of Human Resources Development
 KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
KINGDOM OF CAMBODIA NATION RELIGION KING 1 Minister Secretaries of State Cabinet Under Secretaries of State Directorate General for Admin. & Finance Directorate General for Health Directorate General for
Splash. Goldilocks Toolkit Innovations for Poverty Action poverty-action.org/goldilocks
 Splash Goldilocks Toolkit Innovations for Poverty Action poverty-action.org/goldilocks Right-fit monitoring and evaluation (M&E) systems embody the principles of Credible, Actionable, Responsible, and
Splash Goldilocks Toolkit Innovations for Poverty Action poverty-action.org/goldilocks Right-fit monitoring and evaluation (M&E) systems embody the principles of Credible, Actionable, Responsible, and
Janani Suraksha Yojana ( JSY )
") Concurrent Assessment of Janani Suraksha Yojana ( JSY ) in Selected States Bihar, Madhya, Orissa, Rajasthan, Uttar United Nations Population Fund - India Concurrent Assessment of Janani Suraksha Yojana
Concurrent Assessment of Janani Suraksha Yojana ( JSY ) in Selected States Bihar, Madhya, Orissa, Rajasthan, Uttar United Nations Population Fund - India Concurrent Assessment of Janani Suraksha Yojana
Quality and access to family planning services in select urban cities of Uttar Pradesh, India
 Quality and access to family planning services in select urban cities of Uttar Pradesh, India Pranita Achyut, Sushmita Mukherjee, Laili Irani, Anurag Mishra, Ilene Speizer, and Priya Nanda Abstract Improving
Quality and access to family planning services in select urban cities of Uttar Pradesh, India Pranita Achyut, Sushmita Mukherjee, Laili Irani, Anurag Mishra, Ilene Speizer, and Priya Nanda Abstract Improving
Minutes of Meeting Subject
 Minutes of Meeting Subject APPROVED: Generasi Impact Evaluation Proposal Host Joint Management Committee (JMC) Date August 04, 2015 Participants JMC, PSF Portfolio, PSF Cluster, PSF Generasi Agenda Confirmation
Minutes of Meeting Subject APPROVED: Generasi Impact Evaluation Proposal Host Joint Management Committee (JMC) Date August 04, 2015 Participants JMC, PSF Portfolio, PSF Cluster, PSF Generasi Agenda Confirmation
Table 1. State-Wise Area, Districts and Villages in India 14. State-Wise Rural and Urban Population as per 1991 and 2001 Census
 CONTENTS Page Part 1. Rural Health Care System in India 1 Part 2. Detailed Statistics Chapter I. Demographic Indicators Table 1. State-Wise Area, Districts and Villages in India 14 Table 2. State-Wise
CONTENTS Page Part 1. Rural Health Care System in India 1 Part 2. Detailed Statistics Chapter I. Demographic Indicators Table 1. State-Wise Area, Districts and Villages in India 14 Table 2. State-Wise
FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO
 FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO Mariana López-Ortega National Institute of Geriatrics, Mexico Flavia C. D. Andrade Dept. of Kinesiology and Community Health, University
FUNCTIONAL DISABILITY AND INFORMAL CARE FOR OLDER ADULTS IN MEXICO Mariana López-Ortega National Institute of Geriatrics, Mexico Flavia C. D. Andrade Dept. of Kinesiology and Community Health, University
To evaluate the impact of NRHM interventions, by Agencies outside the Government, and make recommendations on:
 TOT OF ZONAL AGENCIES To evaluate the impact of NRHM interventions, by Agencies outside the Government, and make recommendations on: The institutional mechanisms and monitoring systems that have been put
TOT OF ZONAL AGENCIES To evaluate the impact of NRHM interventions, by Agencies outside the Government, and make recommendations on: The institutional mechanisms and monitoring systems that have been put
How can the township health system be strengthened in Myanmar?
 How can the township health system be strengthened in Myanmar? Policy Note #3 Myanmar Health Systems in Transition No. 3 A WPR/2015/DHS/003 World Health Organization (on behalf of the Asia Pacific Observatory
How can the township health system be strengthened in Myanmar? Policy Note #3 Myanmar Health Systems in Transition No. 3 A WPR/2015/DHS/003 World Health Organization (on behalf of the Asia Pacific Observatory
Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial
 Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial 24 April 2018 Katherine Semrau, PhD, MPH Health Systems Global Webinar Introductions Bejoy Nambiar Chair,
Improving Quality of Care during Childbirth: Learnings & Next Steps from the BetterBirth Trial 24 April 2018 Katherine Semrau, PhD, MPH Health Systems Global Webinar Introductions Bejoy Nambiar Chair,
INDONESIA S COUNTRY REPORT
 The 4 th ASEAN & Japan High Level Officials Meeting on Caring Societies: Support to Vulnerable People in Welfare and Medical Services Collaboration of Social Welfare and Health Services, and Development
The 4 th ASEAN & Japan High Level Officials Meeting on Caring Societies: Support to Vulnerable People in Welfare and Medical Services Collaboration of Social Welfare and Health Services, and Development
4 September 2011 PROVINCIAL GUIDELINES FOR THE IMPLEMENTATION OF THE THREE STREAMS OF PHC RE-ENGINEERING
 4 September 2011 PROVINCIAL GUIDELINES FOR THE IMPLEMENTATION OF THE THREE STREAMS OF PHC RE-ENGINEERING 1. Introduction 1.1. The National Health Council has mandated that in order to improve health outcomes
4 September 2011 PROVINCIAL GUIDELINES FOR THE IMPLEMENTATION OF THE THREE STREAMS OF PHC RE-ENGINEERING 1. Introduction 1.1. The National Health Council has mandated that in order to improve health outcomes
Part 1. Rural Health Care System in India 1. Table 1. State-Wise Area, Districts and Villages in India 28
 CONTENTS Page List of Abbreviations Highlights ii vii-x Part 1. Rural Health Care System in India 1 Part 2. Detailed Statistics Section I. Demographic Indicators Table 1. State-Wise Area, Districts and
CONTENTS Page List of Abbreviations Highlights ii vii-x Part 1. Rural Health Care System in India 1 Part 2. Detailed Statistics Section I. Demographic Indicators Table 1. State-Wise Area, Districts and
Factors associated with disease outcome in children at Kenyatta National Hospital.
 Factors associated with disease outcome in children at Kenyatta National Hospital. Magu D 1,Wanzala P 2, Mwangi M 2, Kamweya A 3!"!# $%&'(($($ ) * +, - - $. */ 0 ' 0!"!# $(12$'(($(() * 3 4 5*!"!#$%&'(($($)
Factors associated with disease outcome in children at Kenyatta National Hospital. Magu D 1,Wanzala P 2, Mwangi M 2, Kamweya A 3!"!# $%&'(($($ ) * +, - - $. */ 0 ' 0!"!# $(12$'(($(() * 3 4 5*!"!#$%&'(($($)
Building a Reliable, Accurate and Efficient Hand Hygiene Measurement System
 Building a Reliable, Accurate and Efficient Hand Hygiene Measurement System Growing concern about the frequency of healthcare-associated infections (HAIs) has made hand hygiene an increasingly important
Building a Reliable, Accurate and Efficient Hand Hygiene Measurement System Growing concern about the frequency of healthcare-associated infections (HAIs) has made hand hygiene an increasingly important
CASE STUDY 4: COUNSELING THE UNEMPLOYED
 CASE STUDY 4: COUNSELING THE UNEMPLOYED Addressing Threats to Experimental Integrity This case study is based on Sample Attrition Bias in Randomized Experiments: A Tale of Two Surveys By Luc Behaghel,
CASE STUDY 4: COUNSELING THE UNEMPLOYED Addressing Threats to Experimental Integrity This case study is based on Sample Attrition Bias in Randomized Experiments: A Tale of Two Surveys By Luc Behaghel,
Module 3 Identifying Health Problems
 Slide 1: Title Slide Module 3 Thank you for joining us for Module 3:. Now that we have defined our community, it s time to identify its priority health problems. Slide 2: Disclosures for Continuing Medical
Slide 1: Title Slide Module 3 Thank you for joining us for Module 3:. Now that we have defined our community, it s time to identify its priority health problems. Slide 2: Disclosures for Continuing Medical
Hospital Staffing and Inpatient Mortality
 Hospital Staffing and Inpatient Mortality Carlos Dobkin * University of California, Berkeley This version: June 21, 2003 Abstract Staff-to-patient ratios are a current policy concern in hospitals nationwide.
Hospital Staffing and Inpatient Mortality Carlos Dobkin * University of California, Berkeley This version: June 21, 2003 Abstract Staff-to-patient ratios are a current policy concern in hospitals nationwide.
A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH
 EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
EXECUTIVE SUMMARY THE STATE OF THE WORLD S MIDWIFERY 2014 A UNIVERSAL PATHWAY. A WOMAN S RIGHT TO HEALTH REPRODUCTIVE HEALTH PREGNANCY CHILDBIRTH POSTNATAL Executive Summary The State of the World s Midwifery
Study Team. Bella Patel Uttekar Sandhya Barge Yashwant Deshpande Vasant Uttekar Jashoda Sharma Shweta Shahane
 Study Team Bella Patel Uttekar Sandhya Barge Yashwant Deshpande Vasant Uttekar Jashoda Sharma Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component of the National Rural Health Mission,
Study Team Bella Patel Uttekar Sandhya Barge Yashwant Deshpande Vasant Uttekar Jashoda Sharma Shweta Shahane PREFACE JSY, Janani Suraksha Yojana, is an integral component of the National Rural Health Mission,
AVAILABILITY AND UTILIZATION OF SOCIAL SERVICES (EDUCATION AND HEALTH) BY RURAL COMMUNITY IN DISTRICT CHARSADDA
 BY RURAL COMMUNITY IN DISTRICT CHARSADDA") Sarhad J. Agric. Vol.25, No.1, 2009 AVAILABILITY AND UTILIZATION OF SOCIAL SERVICES (EDUCATION AND HEALTH) BY RURAL COMMUNITY IN DISTRICT CHARSADDA MUHAMMAD ISRAR*, MALIK MUHAMMAD SHAFI* and NAFEES AHMAD**
Sarhad J. Agric. Vol.25, No.1, 2009 AVAILABILITY AND UTILIZATION OF SOCIAL SERVICES (EDUCATION AND HEALTH) BY RURAL COMMUNITY IN DISTRICT CHARSADDA MUHAMMAD ISRAR*, MALIK MUHAMMAD SHAFI* and NAFEES AHMAD**
Using Vouchers for Paying for Performance and Reaching the Poor: the Kenyan Safe Motherhood Initiative
 Using Vouchers for Paying for Performance and Reaching the Poor: the Kenyan Safe Motherhood Initiative Ben Bellows 1, Francis Kundu 2, Richard Muga 2, Julia Walsh 1, Malcolm Potts 1, Claus Janisch 3 1
Using Vouchers for Paying for Performance and Reaching the Poor: the Kenyan Safe Motherhood Initiative Ben Bellows 1, Francis Kundu 2, Richard Muga 2, Julia Walsh 1, Malcolm Potts 1, Claus Janisch 3 1
NBER WORKING PAPER SERIES USING PERFORMANCE INCENTIVES TO IMPROVE MEDICAL CARE PRODUCTIVITY AND HEALTH OUTCOMES. Paul Gertler Christel Vermeersch
 NBER WORKING PAPER SERIES USING PERFORMANCE INCENTIVES TO IMPROVE MEDICAL CARE PRODUCTIVITY AND HEALTH OUTCOMES Paul Gertler Christel Vermeersch Working Paper 19046 http://www.nber.org/papers/w19046 NATIONAL
NBER WORKING PAPER SERIES USING PERFORMANCE INCENTIVES TO IMPROVE MEDICAL CARE PRODUCTIVITY AND HEALTH OUTCOMES Paul Gertler Christel Vermeersch Working Paper 19046 http://www.nber.org/papers/w19046 NATIONAL