Using the CDC framework for program evaluation in public health to assess tuberculosis contact investigation programs
|
|
|
- Debra Carroll
- 5 years ago
- Views:
Transcription
1 INT J TUBERC LUNG DIS 7(12):S375 S IUATLD Using the CDC framework for program evaluation in public health to assess tuberculosis contact investigation programs S. Logan,* J. Boutotte,* M. Wilce, S. Etkind* * Division of Tuberculosis Prevention and Control, Massachusetts Department of Public Health, Jamaica Plain, Massachusetts, Division of Tuberculosis Elimination, Centers for Disease Control and Prevention, Atlanta, Georgia, USA SUMMARY SETTING: In Massachusetts, despite the efforts of state and local health department tuberculosis (TB) programs, the rates of contact testing and follow-up remain below the state and national objectives. Changes in contact investigation practices are therefore needed to achieve these objectives. OBJECTIVE: To develop contact investigation selfevaluation tools in accordance with the Centers for Disease Control and Prevention s (CDC) Framework for Program Evaluation in Public Health. These tools will be used to assess state and local level contact investigation practices. DESIGN: The self-evaluation tools were developed using the CDC s framework and pilot-tested by public health nurse case managers in five city health departments. The tools were revised according to feedback received from the nurses. RESULTS: The Massachusetts TB Division conducted three of the six steps of the CDC s framework. Stakeholders of the evaluation were identified and engaged, logic models were created describing state and local TB program components, and self-evaluation tools were developed. CONCLUSION: The CDC s framework provided a useful methodology for beginning the assessment process for evaluating TB contact investigation programs. When the contact investigation self-evaluation tools are implemented statewide, the findings will be used to target areas in need of improvement and develop strategies to make noteworthy changes. KEY WORDS: program evaluation; tuberculosis; contact investigation ACCOUNTABILITY is a key issue for public health agencies, and one way to justify program operations and expenditures is through evaluation. Program evaluation identifies practices that are successful and worth funding, as well as areas in need of improvement. However, in many cases, proper program assessments are not done because staff may lack the necessary tools and expertise. The Centers for Disease Control and Prevention (CDC), in collaboration with evaluation experts, developed an organizational framework for program evaluation of public health practices in According to the framework, well-designed, credible program evaluations adhere to the following standards: 1 3 1) utility ensuring that the user s information needs are satisfied; 2) feasibility ensuring that the evaluation is viable and pragmatic; 3) propriety ensuring that the evaluation is ethical; and 4) accuracy ensuring that the evaluation produces findings that are considered correct. In addition, program evaluations should be practical, done on a routine and ongoing basis, and involve all program staff. 1,2 Tuberculosis (TB) contact investigation procedures vary widely, 4 as do program operations, 5 7 sometimes leading to ineffective programs. Recent studies show that contact investigations may not be achieving optimal outcomes, 8,9 Contact investigations often fail to identify the most at-risk contacts in a timely manner, 10 and systematic failures in processes for conducting contact investigations result in missed opportunities for TB prevention. 11 Recently, the Advisory Council for the Elimination of Tuberculosis recommended enhancing the effectiveness of contact investigations. 12 Program enhancements, such as clarifying screening and monitoring policies 13 and improving training, 14 can positively impact on contact investigation outcomes. An evaluation of these program enhancements is needed to provide data on their effectiveness. This evaluation project focuses on contact investigation programs in the state and local health departments in Massachusetts. Although contact investigation outcomes have recently improved due to initiatives by the Massachusetts Department of Public Health Division of Tuberculosis Prevention and Control (TB Correspondence to: Janice Boutotte, Division of Tuberculosis Prevention and Control, Massachusetts Department of Public Health, 305 South Street, Jamaica Plain, MA 02130, USA. Tel: ( 1) Fax: ( 1) janice. boutotte@ state.ma.us
2 S376 The International Journal of Tuberculosis and Lung Disease Division), they still fall short of state and national objectives. For example, the evaluation rate for contacts of acid-fast bacilli (AFB) smear-positive cases in 1999 was 60.5%, rising to 73.2% in 2000 (the national objective is 95%), 15 and the latent TB infection (LTBI) treatment completion rates in 1999 and 2000 were 60.0% and 59.2%, respectively (the national objective is 85%). Thus, further changes in the contact investigation program appear to be warranted. One of the purposes of this project was to use the CDC s framework for program evaluation and adapt it for application by local level program managers and staff. The process of working through the framework s six steps can result in a set of self-evaluation tools that meet the established standards for contact investigations. 16 Once the tools are designed, pilottested, and validated, the TB Division will provide training and guidance at the local level on the appropriate use of the tools. STUDY SAMPLE Public health nurse case managers in five city health departments in Massachusetts agreed to participate in this evaluation project. Nurse case managers manage TB cases and suspects who reside in their local communities, and conduct the contact investigations. These health departments were selected because they 1) were located in a higher-risk city, defined as those cities with: a) a 7-year average incidence of four or more cases and b) a 7-year mean TB case rate above the state average, 2) represented each of the five TB geographical regions of the state, and 3) had experienced staff and well-developed contact investigation policies and procedures in place. Each health department received $200 and signed a statement of commitment to the project. APPLYING THE CDC S FRAMEWORK FOR PROGRAM EVALUATION Contact investigation self-evaluation tools for use by local public health agencies were developed in accordance with the CDC s Framework for Program Evaluation in Public Health. 1 There are six main steps to the CDC s framework: 1) engage stakeholders; 2) describe the program; 3) focus the evaluation design; 4) gather credible evidence; 5) justify conclusions; and 6) ensure use and share lessons learned. The first three steps of the framework were conducted for this evaluation and are described as they were applied to the local and state contact investigation programs. Step one: engage stakeholders Step one of the framework engages stakeholders, persons or organizations having an investment in what will be learned [by the evaluation] and what will be done with the knowledge. 1 There are three principal groups of stakeholders: 1) those involved in program operations; 2) those served or affected by the program; and 3) primary users of the evaluation. Nurse case managers were identified as key stakeholders and primary users of the program evaluation. Other important stakeholders are the state public health nurses from the TB Division who advise local nurse case managers and the TB Division s contact program staff. TB cases, suspects, and their close contacts are stakeholders because the program serves them and they are affected by the findings. Others affected by the evaluation are workers in congregate settings (e.g., jails, shelters, and schools) or in private businesses. Community members served by the local TB programs are also stakeholders because they make decisions on funding for public health resources. Finally, the CDC Division of TB Elimination is an important stakeholder because not only is it a major funding source for a large portion of the TB Division s staff and activities, it also provides the TB Division with guidance, sets standards and objectives, and works closely with the TB Division in many research and program activities. For this project, the local and state level public health nurses were the only stakeholders invited to plan and pilot test the evaluation. In the planning stage, important values and standards about the contact investigation program were elicited. They discussed values such as building a trusting relationship with the TB case, counseling and educating contacts, and providing interpretation services for non-english speaking contacts. The nurses also indicated that interpersonal and communication skills are vital to success in contact investigations. The local and state public health nurses wanted the self-evaluation tools to exemplify high standards for contact investigation. It was important that the evaluation materials gathered data that would accurately assess the programs. The tools should also be useful for training purposes, especially for new or inexperienced nurse case managers. Other ideal values they placed on the self-evaluation tools were that they be kept as simple as possible and be universal, to fit almost every case/suspect investigation. Step two: describe the program Step two of the framework describes the state and local level contact investigation programs to convey the mission and objectives of the program being evaluated. 1 This includes explaining the need for the program and what it aims to accomplish, the activities of all persons involved, the resources, the program s stage of development, and the setting and environment in which the program operates. In step two, the project staff described the state and local contact investigation programs. Information about the state program was gathered from a variety of sources: state TB Division written policies,
3 Assessing TB contact investigation programs S377 procedures, reports, and recommendations; daily activities of staff involved in patient management and contact investigations; budget documents; and aggregate reports of contact follow-up and treatment of LTBI. Information about local TB programs was obtained by interviewing nurse case managers at the pilot sites. Within a week after the initial interviews, the research assistant made phone contact with the nurse case managers and, using a standardized data collection tool, gathered information on their resources and capacity to conduct contact investigations. They were asked about the health departments infrastructure and resources, such as staff time and experience, equipment, foreign language capabilities, methods for documenting contact information, and funding sources. Selected data on health department staff and resources were organized into a chart for comparison (see Table 1). Case rates, averaged over a 7-year period from 1994 to 2000, varied among the five health departments, ranging from 6.30 to 14.9 per Staff time was proportionate to the rate of cases: the cities with the higher case rates had more available staff. The availability of office equipment varied among the five health departments. Administrative support also varied among the five health departments, with the program with the greatest morbidity reporting no administrative support and only one full-time outreach worker. Finally, three of the five health departments collected contact investigation data only on the state forms, which record simple demographics, TB skin tests, chest X-rays, and treatment of LTBI; no additional data were collected that might help the nurse case managers to prioritize contacts and more effectively manage their cases. A major task of step two was the construction of logic models, graphic representations that illustrate and summarize the contact investigation program. In evaluation, logic models are used to provide a documented description of the rationale behind program activities and the cause-and-effect relationships between specific activities and expected outcomes. 17,18 In addition to their uses during an evaluation, logic models can also serve as valuable communication tools by visually summarizing a program for administrators, funders, and new staff members. 19 Table 1 TB case statistics and resources in five city health departments in Massachusetts 7-year mean caseload (case rate)* Staff time and experience in TB Office equipment HD 1 HD 2 HD 3 HD 4 HD 5 88 (14.9) 9 (9.2) 8 (8.76) 14 (13.3) 11 (6.30) 5 FT public health nurses; 1 nurse supervisor; 4 20 years in TB Voice mail, , fax machines, copiers, computers, printers and direct connection to the state network via high-speed modems 3.5 FT public health nurses; 1 nurse supervisor; 7 20 years in TB Voice mail, , fax machines, computers, printers, highspeed internet access, and access to laboratory and radiology reports 2 FT public health nurses; 1 nurse supervisor; 1 30 years in TB 1 centrally-located fax machine and an inadequate computer 3.5 FT public health nurses; 1 nurse supervisor; years in TB , fax machines, copiers, computers, and printers, but no personal voice mail Administrative Inadequate Inadequate ND Excellent Excellent support Outreach 1 FT outreach Available from an outside source as needed Nursing staff language capability Access to interpreters Record-keeping other than using state forms Chinese, Vietnamese and Spanish Excellent; through hospital staff A separate chart is used Haitian Creole, Cape Verde Creole, Portuguese and Spanish Excellent No additional data collected; use MS Access database None Available as needed 2 FT public health nurses, but only 1 does CI; 3 FT nurses help with DOT as needed; 1 2 years in TB Fax machines, phones (direct lines and a long distance line), and copiers Available from an outside source as needed English only ND Office staff speak Spanish Adequate; one Asian interpreter once/week; also phone interviews No additional data collected Excellent Additional data collected Adequate; Albanian and Vietnamese interpreters through outside source No additional data collected * Data are averaged over a 7-year period, Case rates are number of cases per population, based on 2000 census information. Described on the scale: excellent, adequate, and inadequate. HD health department; TB tuberculosis; FT full time; DOT directly observed treatment; CI contact investigation; ND not determined.
4 S378 The International Journal of Tuberculosis and Lung Disease (continues) * Outreach educators are employed by MDPH TB Division and Refugee and Immigrant Health Program; they work on the local level with TB cases and their families. The TB clinics are funded by the MDPH TB Division, but clinic personnel (physicians, nurses, office administrators) are employed by the local hospital or health department. A systematic approach, recommended by the MDPH TB Division, to identify, prioritize, and test contacts (see ref 15). Figure 1 Logic model of the contact investigation process: state and local level interactions. Text in bold highlights necessary services/interventions provided by the Contact Program. Note that these activities are linked to resulting outputs and outcomes. If federal funding was no longer available, the capacity to maintain these activities would be greatly compromised. VNA Visiting Nurse Association; BOH Board of Health; LTBI latent tuberculosis infection; AFB acid-fast bacilli; TST tuberculin skin test.

5 Assessing TB contact investigation programs S379

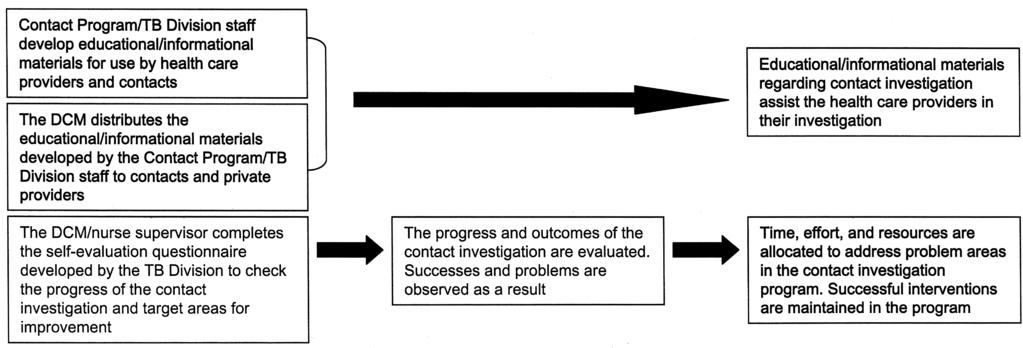
6 S380 The International Journal of Tuberculosis and Lung Disease Figure 2 Summary logic model of the contact investigation process: state and local level interactions. BOH Board of Health; VNA Visiting Nurse Association; CI contact investigation; AFB acid-fast bacilli; LTBI latent tuberculosis infection. Three logic models were constructed: the first model depicts the interactions between the state and local level contact investigation programs (Figure 1), the second summarizes the previous model (Figure 2), and the third is an illustration of the local program only (not shown). The third model is a duplicate of the first model, except that it does not contain state-dependent resources and responsibilities. Each model lists current resources, activities, intermediate outputs, and expected outcomes. The activities and outputs are essential elements in Massachusetts TB case and contact management and are outlined in the state nursing protocols. The expected short-term outcomes are national and state contact investigation objectives. Finally, the expected long-term outcome, to prevent TB cases from occurring, depends on the fulfillment of the short-term outcomes. The complexity of the models necessitates some explanation. The models are arranged in sequential order, from notifying public health officials about the infectious case to generating contact reports and conducting a self-evaluation at the conclusion of the investigation. Arrows link each column with the next, portraying how the activities are involved in cause-and-effect relationships with the intermediate outputs. Also, certain boxes within the same column are grouped. For example, in Figure 1, the sixth and seventh activities are grouped under contact identification. These activities are related to the intermediate outputs of identifying contacts, such as contacts were identified within 3 working days. Finally, the intermediate outputs lead to the expected short-term outcome, which is the national objective that contacts are identified for at least 90% of highly infectious TB cases. Step three: focus the evaluation design Step three of the framework focuses the evaluation design to assess the issues of greatest concern to stakeholders while using time and resources as efficiently as possible. 1 Four basic elements of focusing the evaluation design were addressed: 1) the purpose of the evaluation plan (to change contact investigation program practices that were not working well and to motivate the nurse case managers to utilize program evaluation and build it into the framework of their contact investigation programs); 2) the intended users, particularly the state and local public health nurses; 3) the potential uses of the evaluation findings; and 4) evaluation questions to measure the contact investigation program s quality and effectiveness. Table 2 provides a sample list of questions developed by project staff and key stakeholders.
7 Assessing TB contact investigation programs S381 Table 2 Selected evaluation questions for step 3 of the CDC s framework: focusing on the evaluation design Sample questions Did the nurse case manager identify the initial contacts within 3 working days of TB case notification? Was the nurse case manager able to retrieve results from private providers? Did the contacts with newly acquired LTBI receive chest X-rays and were they evaluated for treatment? Did the nurse case manager send the contact report to the state nurse after the first round of TB skin testing? If so, within how many days was it sent? Did the nurse case manager use/distribute the following materials to other health care providers and contacts during this contact investigation, when appropriate: the TB Contact Investigation Fact Sheet and the contact educational pamphlet, Someone I Know Has TB? CDC Centers for Disease Control and Prevention; TB tuberculosis; LTBI latent tuberculosis infection. Developing and pilot-testing contact investigation self-assessment materials Information obtained from working through steps 1 3 of the CDC s framework laid the groundwork for creating self-assessment materials. Three tools were created: 1) the self-evaluation questionnaire, 2) the transmission risk assessment checklist, and 3) the contact investigation decision tree. Each tool was pilot-tested in the participating cities. The latter two tools were not designed to evaluate contact investigations, but to improve the investigators performance in conducting contact investigations. First, the self-evaluation questionnaire was created by formulating evaluation questions based on program activities and outputs depicted in the logic models. The questionnaire form was organized into four parts: 1) identification of contacts, 2) medical evaluation, 3) treatment of LTBI, and 4) administrative (e.g., timeliness of reporting and utilizing educational materials developed by the TB Division). Where appropriate, TB Division recommendations were inserted into the questionnaire as a reminder to the nurse case managers conducting the evaluation. The nurse case managers at the pilot sites were instructed to complete a minimum of two self-evaluation questionnaires on previously conducted contact investigations. Eleven questionnaires were received from four of the five pilot sites and entered into the database. The results were inspected for missing data, unanswered questions, inserted answers, and side notes that might indicate confusion about a question or that a question was unnecessary. In the post pilot test meetings with the nurse case managers, more was learned about the usefulness and feasibility of the questionnaire. One question was particularly problematic: Did the close contacts the nurse case manager identified have a higher than expected rate of infection? They had difficulty determining what was higher than expected, especially for non-us-born contacts who came from countries with a high TB incidence. Another question the nurse case managers had difficulty answering was, Were the contacts of the infectious case identified within 3 working days of TB case notification? They felt it was unrealistic to expect the TB case/suspect to disclose names of close family and friends at their first encounter; sometimes it takes 1 or 2 months to build a trusting relationship with the patients. Reasons for not cooperating were anger about the diagnosis, mistrust of public officials, and fear of being kicked out of the home. A nurse who used the questionnaire suggested that space be provided to explain the difficulty in identifying contacts. Other general comments made were that the questionnaire be universal to fit most types of cases, simplified, flexible enough to be used during and after the contact investigation, and should not include redundant information recorded on other forms. The second component of the self-assessment materials was the transmission risk assessment checklist, which is to be used at initial visits to the TB case/ suspect s home, work or school, and other places where they spent a lot of time. The checklist provides details centered on the TB case/suspect: the degree of infectiousness, type of housing, work environment, and amount of time spent with friends or in other social settings. The nurse case managers were instructed to complete a minimum of three risk assessment checklists on current contact investigations. However, no new cases/suspects occurred in the 1-month period given them to use the tools. Six checklists completed on previous cases were received from two pilot sites, two other sites did not complete the forms because they had no new cases/suspects, and the fifth site did not submit the forms. The nurse case managers felt that the checklist, which contains check-off items regarding the size of the room, ventilation, etc., would be helpful to inexperienced investigators. Finally, the third component of the self-evaluation tools was the decision tree. It illustrates the contact investigation process at the patient level, from determining the infectiousness of the TB case/suspect to screening close contacts for TB infection and disease. The nurse case managers were to use the decision tree as a guide in their current investigations, but due to a lack of current cases, they were not able to use it as instructed. However, most of the nurses said that they liked the decision tree and would use it in their investigations. LESSONS LEARNED The Framework for Program Evaluation in Public Health was found to be a useful methodology to plan a TB contact investigation program self-assessment. By working through the first three steps of the framework, a rather complex and detailed process was
8 S382 The International Journal of Tuberculosis and Lung Disease pulled apart and scaled down to focus on local programs and their interaction with the state program in conducting contact investigations. It was also found that keeping a project log and documenting lessons learnt along the way were important to maintain perspective, review procedures, and record unsuccessful strategies. The state and local public health nurses, as well as the CDC, were key stakeholders and played an essential part in laying the groundwork for the evaluation. They were involved in each step of the process: affirming their commitment to program evaluation, reviewing drafts of the program descriptions and logic models, and providing input into the development of the selfassessment materials. Using stakeholders to assist in planning the evaluation, as recommended by the CDC s framework, produced evaluation questions that were based on their value systems. More importantly, the product of this collaboration was an instrument they would use. For example, the self-evaluation questionnaire was designed to accommodate most of the investigators needs. It can be used as an analytic tool (to calculate rates and timeliness of their investigations) and a form to take notes on cases when necessary. The process of developing logic models, step two of the CDC s framework, required discussion and consensus among stakeholders, thus elucidating assumptions and expectations. 20 Multiple logic models are often needed to meet the needs of the different stakeholder groups. 21 For this evaluation project, three models were developed, each highlighting different aspects of the contact investigation program. The first, developed for staff directly involved in the program, showed the details of how the state and local programs coordinate activities related to contact investigations (see Figure 1). The summary model (see Figure 2) explained this complex network to managers, clients, and others who needed an overview of operations. The local model enabled nurse case managers and program managers to see the positive effects of their activities on program goals and objectives. This effort (creating logic models) was the first attempt to systematically document how contact investigation programs achieve patient and cohort level outcomes. As indicated previously, the local nurse case managers pilot-tested the self-evaluation materials for a 1-month period. This exercise provided valuable information and insight into each of the next steps of the CDC s framework. Regarding their future use, the Massachusetts TB Division recently started a 3-year project to study intervention strategies for contact evaluation, one of which is utilizing the transmission risk assessment checklist. The Division proposes to focus on the evaluation phase of contact investigations (initial and repeat skin testing and medical evaluations) in several higher risk cities and on large worksite investigations to observe whether interventions such as the checklist affect rates. In conclusion, the goals of contact investigation program evaluation, using the CDC s framework as a guide, are to improve contact outcomes and achieve state and national objectives. The means of reaching these goals include: 1) using the validated selfevaluation tools, as well as the logic models, as: i) guidelines for recommended contact investigation program activities and ii) training tools for new and inexperienced nurses, 2) assessing each contact investigation conducted, 3) using the evaluation findings to target problem areas for change, and 4) making recommendations based on valid and credible evidence, which will help garner political support and funding to sustain successful program activities and provide resources for new strategies. It is hoped that through the utilization of these evaluation instruments and findings in Massachusetts, and by conducting similar self-evaluation projects elsewhere, the rates of contact medical evaluation and treatment completion will improve. Acknowledgements The authors would like to thank Heather Miller, Kathryn Hendricks, MDPH Division of Tuberculosis Prevention and Control Patient Management Services Unit, and the public health nursing staff of the Boston, Cambridge, Lowell, Quincy, and Worcester, MA Health Departments. Supported by a grant from the Division of Tuberculosis Elimination, Centers for Disease Control and Prevention, Atlanta, GA. References 1 Centers for Disease Control and Prevention. Framework for program evaluation in public health. MMWR 1999; 48(RR- 11): Patton M Q. Utilization-focused evaluation: the new century text. 3rd ed. Thousand Oaks, CA: Sage Publications, Joint Committee on Standards for Educational Evaluation. Program evaluation standards: how to assess evaluations of educational programs. 2nd ed. Thousand Oaks, CA: Sage Publications, Wilce M, Shrestha-Kuwahara R, Taylor Z, Qualls N, Marks S. Tuberculosis contact investigation policies, practices, and challenges in 11 US communities. J Public Health Manag Pract 2002; 8: Glaser T, Simmons C. Contact investigation in New York City. Investigation of Contacts to Tuberculosis Cases Symposium Summary. New York, NY: New York City Department of Health, Bureau of Tuberculosis Control, 1996: Holcombe J M. Contact investigation in a rural setting: a state perspective. Investigation of Contacts to Tuberculosis Cases Symposium Summary. New York, NY: New York City Department of Health, Bureau of Tuberculosis Control, 1996: Ruben F L, Lynch D C. Tuberculosis control through contact investigation. PA Med 1996; 99: Marks S, Taylor Z, Qualls N, Shrestha-Kuwahara R, Wilce M, Nguyen C. Outcomes of contact investigations of infectious tuberculosis patients. Am J Respir Crit Care Med 2000; 162: Reichler M R, Reves R, Bur S, et al. Evaluation of investiga-
9 Assessing TB contact investigation programs S383 tions conducted to detect and prevent transmission of tuberculosis. JAMA 2002; 287: Chin D P, Crane C M, Ya D M, et al. Spread of Mycobacterium tuberculosis in a community implementing recommended elements of tuberculosis control. JAMA 2000; 283: McAnulty J M, Fleming D W, Hawley M A, Barron R C. Missed opportunities for tuberculosis prevention. Arch Intern Med 1995; 155: Centers for Disease Control and Prevention. Tuberculosis elimination revisited: obstacles, opportunities, and a renewed commitment. Advisory Council for the Elimination of Tuberculosis (ACET). MMWR 1999; 48(RR-9): MacIntyre C R, Plant A J. Impact of policy and practice on effectiveness of contact screening for tuberculosis. Prev Med 1998; 27: Jasmer R M, Hahn J, Small P, et al. A molecular epidemiologic analysis of tuberculosis trends in San Francisco, Ann Intern Med 1999; 130: Massachusetts Department of Health, Division of Tuberculosis Prevention and Control. Aggregate Reports for Tuberculosis Program Evaluation: follow-up and treatment for contacts to tuberculosis cases. Jamaica Plain, MA: MA Dept of Health, data reports. 16 Etkind S, Veen J. Contact follow-up in high- and low-prevalence countries. In: Reichman L, Hershfield E S, eds. TB: a comprehensive international approach. New York, NY: Marcel Dekker, 2000: pp United Way of America. Measuring program outcomes: a practical approach. Arlington, VA: United Way of America, Weiss C. Evaluation. 2nd ed. Upper Saddle River, NJ: Prentice Hall, Porteous N, Sheldrick B J, Stewart P J. A blueprint for public health management: a program evaluation tool kit. Ottawa: University of Ottawa, Wholey J S. Evaluability assessment: developing program theory. In: Bickman L, ed. Using program theory in evaluation. new directions for program evaluation, 33. San Francisco, CA: Jossey-Bass, Harris J. Logic model basics. The Evaluation Exchange, 2001; 2(VII) 2: 14.
Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
 and cure individuals with active TB disease") Tuberculosis (TB) Control and Prevention Program Program Purpose Program Information PHD/CHPB Evelyn Poppell, x5600 Nga Nguyen, x5663 Prevent the transmission of tuberculosis (TB) and cure individuals
Tuberculosis (TB) Control and Prevention Program Program Purpose Program Information PHD/CHPB Evelyn Poppell, x5600 Nga Nguyen, x5663 Prevent the transmission of tuberculosis (TB) and cure individuals
TB Elimination. Respiratory Protection in Health-Care Settings
 TB Elimination Respiratory Protection in Health-Care Settings Introduction All health-care settings need an infection-control program designed to ensure prompt detection, airborne precautions, and treatment
TB Elimination Respiratory Protection in Health-Care Settings Introduction All health-care settings need an infection-control program designed to ensure prompt detection, airborne precautions, and treatment
Overview: TB Case Management and Contact Investigation
 Overview: TB Case Management and Contact Investigation Karen A Martinek, RN, MPH Alaska DHSS, DPH, Section of Epidemiology Overview Define tuberculosis (TB) case management Describe the roles and responsibilities
Overview: TB Case Management and Contact Investigation Karen A Martinek, RN, MPH Alaska DHSS, DPH, Section of Epidemiology Overview Define tuberculosis (TB) case management Describe the roles and responsibilities
Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
 and cure individuals with active TB disease") Tuberculosis (TB) Control and Prevention Program Program Purpose PHD/CHPB Evelyn Poppell, x5600 Rachel Kidanne, x5605 Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
Tuberculosis (TB) Control and Prevention Program Program Purpose PHD/CHPB Evelyn Poppell, x5600 Rachel Kidanne, x5605 Prevent the transmission of tuberculosis (TB) and cure individuals with active TB disease
Tuberculosis (TB) risk assessment worksheet
 risk assessment worksheet") 128 Tuberculosis (TB) Risk MMWR Assessment Worksheet December 30, 2005 Tuberculosis (TB) risk assessment worksheet This model worksheet should be considered for use in performing TB risk assessments for
128 Tuberculosis (TB) Risk MMWR Assessment Worksheet December 30, 2005 Tuberculosis (TB) risk assessment worksheet This model worksheet should be considered for use in performing TB risk assessments for
KEY ACTIVITIES IN TB CONTROL. Using Epidemiology for Data-Driven Decision-Making in Tuberculosis Programs February 24, 2016
 BROADENING THE APPLICATION OF EPIDEMIOLOGY IN TUBERCULOSIS CONTROL Shama Desai Ahuja, PhD, MPH Director, Office of Sur veillance and Epidemiology Bureau of Tuberculosis Control New York City Depar tment
BROADENING THE APPLICATION OF EPIDEMIOLOGY IN TUBERCULOSIS CONTROL Shama Desai Ahuja, PhD, MPH Director, Office of Sur veillance and Epidemiology Bureau of Tuberculosis Control New York City Depar tment
Tuberculosis Prevention and Control Protocol, 2018
 Ministry of Health and Long-Term Care Tuberculosis Prevention and Control Protocol, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective: January 1, 2018 or upon
Ministry of Health and Long-Term Care Tuberculosis Prevention and Control Protocol, 2018 Population and Public Health Division, Ministry of Health and Long-Term Care Effective: January 1, 2018 or upon
Attitudes Toward Managing Latent TB Infection in Primary Care
 Attitudes Toward Managing Latent TB Infection in Primary Care Jonathan Carey Jackson, M.D. Harborview Medical Center, WA Attitudes Toward Managing Latent TB Infection in Primary Care Investigators Carey
Attitudes Toward Managing Latent TB Infection in Primary Care Jonathan Carey Jackson, M.D. Harborview Medical Center, WA Attitudes Toward Managing Latent TB Infection in Primary Care Investigators Carey
Administrative Without, TB control fails. TB Infection Control What s New? Early disease prevention Modern cough etiquette
 Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
Early disease prevention Modern cough etiquette TB Infection Control What s New? Mark Lobato, MD Division of TB Elimination CDC TB Intensive Workshop Global TB Institute, Newark, NJ September 16, 2010
Facility Tuberculosis (TB) Risk Assessment for Correctional Facilities
 Risk Assessment for Correctional Facilities") Facility Tuberculosis (TB) Risk Assessment for Correctional Facilities The various areas within correctional facilities have different levels of risk for TB transmission. Apply this worksheet to assess
Facility Tuberculosis (TB) Risk Assessment for Correctional Facilities The various areas within correctional facilities have different levels of risk for TB transmission. Apply this worksheet to assess
Practical Aspects of TB Infection Control
 Practical Aspects of TB Infection Control Sundari Mase, MD Division of TB Elimination, CDC TB Intensive Workshop October 1, 2014 National Center for HIV/AIDS, Viral Hepatitis, STD & TB Prevention Division
Practical Aspects of TB Infection Control Sundari Mase, MD Division of TB Elimination, CDC TB Intensive Workshop October 1, 2014 National Center for HIV/AIDS, Viral Hepatitis, STD & TB Prevention Division
FAST. A Tuberculosis Infection Control Strategy. cough
 FAST A Tuberculosis Infection Control Strategy FIRST EDITION: MARCH 2013 This handbook is made possible by the support of the American people through the United States Agency for International Development
FAST A Tuberculosis Infection Control Strategy FIRST EDITION: MARCH 2013 This handbook is made possible by the support of the American people through the United States Agency for International Development
APNS and Program Planning: An Example of a Primary Care Provider Educational Program on TB in the US Foreign Born
 St. John Fisher College Fisher Digital Publications Nursing Doctoral Wegmans School of Nursing 2011 APNS and Program Planning: An Example of a Primary Care Provider Educational Program on TB in the US
St. John Fisher College Fisher Digital Publications Nursing Doctoral Wegmans School of Nursing 2011 APNS and Program Planning: An Example of a Primary Care Provider Educational Program on TB in the US
Initiating a Contact Investigation
 Initiating a Contact Investigation Jessica Quintero, M.Ed. September 14, 2017 TB Nurse Case Management September 12 14, 2017 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed. has
Initiating a Contact Investigation Jessica Quintero, M.Ed. September 14, 2017 TB Nurse Case Management September 12 14, 2017 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Jessica Quintero, M.Ed. has
Tuberculosis Case Management for Removable Alien Inmates/Detainees in Federal Custody
 Background Tuberculosis Case Management for Removable Alien Inmates/Detainees in Federal Custody Federal Bureau of Prisons (Department of Justice) United States Marshals Service (Department of Justice)
Background Tuberculosis Case Management for Removable Alien Inmates/Detainees in Federal Custody Federal Bureau of Prisons (Department of Justice) United States Marshals Service (Department of Justice)
Florida Tuberculosis System of Care
 Table of Contents I. Introduction... 4 II. Florida s Charge... 5 III. Florida Tuberculosis System of Care... 5 IV. Florida Department of Health Tuberculosis Program... 7 V. Florida Department of Health
Table of Contents I. Introduction... 4 II. Florida s Charge... 5 III. Florida Tuberculosis System of Care... 5 IV. Florida Department of Health Tuberculosis Program... 7 V. Florida Department of Health
Frequently Asked Questions about TB Protocols at Duke Hospital and Clinics ( Revision)
") Frequently Asked Questions about TB Protocols at Duke Hospital and Clinics (7-2018 Revision) A. PAPRs B. Portable HEPAs C. N95 Respirator Masks D. Tuberculin Skin Testing (TST) E. Negative Pressure Isolation
Frequently Asked Questions about TB Protocols at Duke Hospital and Clinics (7-2018 Revision) A. PAPRs B. Portable HEPAs C. N95 Respirator Masks D. Tuberculin Skin Testing (TST) E. Negative Pressure Isolation
New Jersey Administrative Code Department of Health and Senior Services Title 8, Chapter 57, Communicable Disease
 New Jersey Administrative Code Department of Health and Senior Services Title 8, Chapter 57, Communicable Disease SUBCHAPTER 5: MANAGEMENT OF TUBERCULOSIS 8:57-5.1: Purpose and Scope The principle purpose
New Jersey Administrative Code Department of Health and Senior Services Title 8, Chapter 57, Communicable Disease SUBCHAPTER 5: MANAGEMENT OF TUBERCULOSIS 8:57-5.1: Purpose and Scope The principle purpose
Risk of TB infection among HCWs in the era of HIV and MDR-TB. Madhukar Pai, MD, PhD Assistant Professor of Epidemiology McGill University Montreal
 Risk of TB infection among HCWs in the era of HIV and MDR-TB Madhukar Pai, MD, PhD Assistant Professor of Epidemiology McGill University Montreal TB exposure: a fact of life for health care workers in
Risk of TB infection among HCWs in the era of HIV and MDR-TB Madhukar Pai, MD, PhD Assistant Professor of Epidemiology McGill University Montreal TB exposure: a fact of life for health care workers in
WHO policy on TB infection control in health care facilities, congregate settings and households.
 WHO policy on TB infection control in health care facilities, congregate settings and households. Rose Pray Stop TB, WHO Why should we develop a policy on TB infection control? To guide countries on what
WHO policy on TB infection control in health care facilities, congregate settings and households. Rose Pray Stop TB, WHO Why should we develop a policy on TB infection control? To guide countries on what
TB PREVENTION AND CONTROL: WORKING WITH THE HOMELESS
 CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TB PREVENTION AND CONTROL: WORKING WITH THE HOMELESS OBJECTIVES Upon completion of this session, participants will be able to: 1. Explain the responsibilities
CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TB PREVENTION AND CONTROL: WORKING WITH THE HOMELESS OBJECTIVES Upon completion of this session, participants will be able to: 1. Explain the responsibilities
Terms of Reference Kazakhstan Health Review of TB Control Program
 1 Terms of Reference Kazakhstan Health Review of TB Control Program Objectives 1. In the context of the ongoing policy dialogue and collaboration between the World Bank and the Government of Kazakhstan
1 Terms of Reference Kazakhstan Health Review of TB Control Program Objectives 1. In the context of the ongoing policy dialogue and collaboration between the World Bank and the Government of Kazakhstan
Financial impact of TB illness
 Summary report Costs faced by (multidrug resistant) tuberculosis patients during diagnosis and treatment: report from a pilot study in Ethiopia, Indonesia and Kazakhstan Edine W. Tiemersma 1, David Collins
Summary report Costs faced by (multidrug resistant) tuberculosis patients during diagnosis and treatment: report from a pilot study in Ethiopia, Indonesia and Kazakhstan Edine W. Tiemersma 1, David Collins
Fundamentals of Nursing Case Management
 Fundamentals of Nursing Case Management Shea Rabley, RN, MN TB Nurse Educator Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures No relevant financial relationships No off-label investigational
Fundamentals of Nursing Case Management Shea Rabley, RN, MN TB Nurse Educator Mayo Clinic Center for Tuberculosis 2014 MFMER slide-1 Disclosures No relevant financial relationships No off-label investigational
Catalina Navarro, RN, BSN March 17, TB Nurse Case Management March 17 19, 2015 San Antonio, Texas
 Principles of TB Nurse Case Management: Why are We Here? Catalina Navarro, RN, BSN March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Catalina
Principles of TB Nurse Case Management: Why are We Here? Catalina Navarro, RN, BSN March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Catalina
Key elements of the program discussed in the following pages include: Appropriate use of data with community leaders and local politicians
 CASE STUDY 3 COMMUNITY PARTNERSHIP PROJECT: SAN DIEGO COUNTY Key elements of the program discussed in the following pages include: Co-location of services Decentralization of LTBI therapy Cost and reimbursement
CASE STUDY 3 COMMUNITY PARTNERSHIP PROJECT: SAN DIEGO COUNTY Key elements of the program discussed in the following pages include: Co-location of services Decentralization of LTBI therapy Cost and reimbursement
BIOSTATISTICS CASE STUDY 2: Tests of Association for Categorical Data STUDENT VERSION
 STUDENT VERSION July 28, 2009 BIOSTAT Case Study 2: Time to Complete Exercise: 45 minutes LEARNING OBJECTIVES At the completion of this Case Study, participants should be able to: Compare two or more proportions
STUDENT VERSION July 28, 2009 BIOSTAT Case Study 2: Time to Complete Exercise: 45 minutes LEARNING OBJECTIVES At the completion of this Case Study, participants should be able to: Compare two or more proportions
Education Specialist Credential Program Application Full or Part Time. Student Information. Program Information. Field Placement (EHD 178)
") Item 1 Education Specialist Credential Program Application Full or Part Time Semester of Application Semester/Year Student Information Last Name First Name Former Name (If applicable) Student ID Undergraduate
Item 1 Education Specialist Credential Program Application Full or Part Time Semester of Application Semester/Year Student Information Last Name First Name Former Name (If applicable) Student ID Undergraduate
Diana Fortune, RN, BSN has the following disclosures to make:
 Community TB Prevention Diana Fortune, RN, BSN Barbarah Martinez, RN, BSN September 23, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Diana Fortune,
Community TB Prevention Diana Fortune, RN, BSN Barbarah Martinez, RN, BSN September 23, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Diana Fortune,
NTNC: TB Program Core Competencies for PH Nurses 2008 and Future Challenges
 NTNC: TB Program Core Competencies for PH Nurses 2008 and Future Challenges Kathleen Hursen, RN, MS MPD Division of TB Prevention and Control TB Control Priorities by 2015 1. 93% complete treatment
NTNC: TB Program Core Competencies for PH Nurses 2008 and Future Challenges Kathleen Hursen, RN, MS MPD Division of TB Prevention and Control TB Control Priorities by 2015 1. 93% complete treatment
INTRODUCTION: TB CONTROL TOOLBOXES
 INTRODUCTION: TB CONTROL TOOLBOXES The TB Control Toolboxes have been developed to help tuberculosis (TB) control programs take advantage of tested strategies and innovations. The Model TB Centers and
INTRODUCTION: TB CONTROL TOOLBOXES The TB Control Toolboxes have been developed to help tuberculosis (TB) control programs take advantage of tested strategies and innovations. The Model TB Centers and
Massachusetts Department of Fire Services
 Massachusetts Department of Fire Services Language Access Plan (January, 2013) I. Introduction The Department of Fire Services, (hereinafter referred to as DFS has prepared this revised and updated (January,
Massachusetts Department of Fire Services Language Access Plan (January, 2013) I. Introduction The Department of Fire Services, (hereinafter referred to as DFS has prepared this revised and updated (January,
Objectives. Clinic Scenario. Addressing TB in Our Communities November 19, 2015 Curry International Tuberculosis Center
 Addressing TB Infection Prevention in our Healthcare Settings Lana Kay Tyer, RN MSN TB Nurse Consultant WA State DOH Objectives Describe droplet precautions and circumstances when personal N95 respirators
Addressing TB Infection Prevention in our Healthcare Settings Lana Kay Tyer, RN MSN TB Nurse Consultant WA State DOH Objectives Describe droplet precautions and circumstances when personal N95 respirators
California TB Controller Association Conference. 4/21/15 Time
 California TB Controller Association Conference 4/21/15 Time HISTORIC LESSONS LEARNED IN SANTA CLARA COUNTY SANTA CLARA COUNTY TB STATUS 1996 Tuberculosis epidemiology TB Status in Santa Clara County 1996
California TB Controller Association Conference 4/21/15 Time HISTORIC LESSONS LEARNED IN SANTA CLARA COUNTY SANTA CLARA COUNTY TB STATUS 1996 Tuberculosis epidemiology TB Status in Santa Clara County 1996
Tuberculosis Indicators Project (TIP) Overview
 Overview") Tuberculosis Indicators Project (TIP) Overview Anne Cass, MPH TIP Coordinator Melissa Ehman, MPH Lead TIP Epidemiologist California Department of Public Health Tuberculosis Control Branch (TBCB) Careful
Tuberculosis Indicators Project (TIP) Overview Anne Cass, MPH TIP Coordinator Melissa Ehman, MPH Lead TIP Epidemiologist California Department of Public Health Tuberculosis Control Branch (TBCB) Careful
The Role of Public Health in the Management of Tuberculosis
 The Role of Public Health in the Management of Tuberculosis Lorna Will, RN, MA TB Nurse Consultant Wisconsin TB Program Ann Steele, RN Public Health Nurse Appleton Health Dept November 2016 2014 MFMER
The Role of Public Health in the Management of Tuberculosis Lorna Will, RN, MA TB Nurse Consultant Wisconsin TB Program Ann Steele, RN Public Health Nurse Appleton Health Dept November 2016 2014 MFMER
PROJECT GRANTS AND COOPERATIVE AGREEMENTS FOR TUBERCULOSIS CONTROL PROGRAMS TUBERCULOSIS CONTROL PROGRAMS
 APRIL 2011 93.116 PROJECT GRANTS AND COOPERATIVE AGREEMENTS FOR TUBERCULOSIS CONTROL State Project/Program: PROJECT GRANTS AND COOPERATIVE AGREEMENTS FOR TUBERCULOSIS CONTROL Federal Authorization: U.
APRIL 2011 93.116 PROJECT GRANTS AND COOPERATIVE AGREEMENTS FOR TUBERCULOSIS CONTROL State Project/Program: PROJECT GRANTS AND COOPERATIVE AGREEMENTS FOR TUBERCULOSIS CONTROL Federal Authorization: U.
Hello. Welcome to this webinar titled Preventing and Controlling Tuberculosis in Correctional Settings.
 Hello. Welcome to this webinar titled Preventing and Controlling Tuberculosis in Correctional Settings. This webinar was produced by the Minnesota Department of Health Tuberculosis Program. This is the
Hello. Welcome to this webinar titled Preventing and Controlling Tuberculosis in Correctional Settings. This webinar was produced by the Minnesota Department of Health Tuberculosis Program. This is the
Required Local Public Health Activities
 Required Local Public Health Activities This document is intended to respond to requests for clarity about the mandated activities that community health boards must undertake in order to meet statutory
Required Local Public Health Activities This document is intended to respond to requests for clarity about the mandated activities that community health boards must undertake in order to meet statutory
Global Health Electives Curriculum Overview Internal Medicine Residency University of Colorado Health Sciences Center January 2007
 Global Health Electives Curriculum Overview Internal Medicine Residency University of Colorado Health Sciences Center January 2007 I. Educational Purpose and Goals Students and residents often participate
Global Health Electives Curriculum Overview Internal Medicine Residency University of Colorado Health Sciences Center January 2007 I. Educational Purpose and Goals Students and residents often participate
Strategy of TB laboratories for TB Control Program in Developing Countries
 Strategy of TB laboratories for TB Control Program in Developing Countries Borann SAR, MD, PhD, Institut Pasteur du Cambodge Phnom Penh, Cambodia TB Control Program Structure of TB Control Establish the
Strategy of TB laboratories for TB Control Program in Developing Countries Borann SAR, MD, PhD, Institut Pasteur du Cambodge Phnom Penh, Cambodia TB Control Program Structure of TB Control Establish the
Partnerships for Success: Laboratories and Programs Meeting the Challenge. Partnerships During a TB Outbreak
 Partnerships for Success: Laboratories and Programs Meeting the Challenge Partnerships During a TB Outbreak 2015 National TB Conference Atlanta, GA David Warshauer, PhD., D(ABMM), Deputy Director, Communicable
Partnerships for Success: Laboratories and Programs Meeting the Challenge Partnerships During a TB Outbreak 2015 National TB Conference Atlanta, GA David Warshauer, PhD., D(ABMM), Deputy Director, Communicable
Staffing Your TB Program
 TB Program Management San Antonio, Texas November 5-7, 2008 Staffing Your TB Program Lynelle Phillips, RN, MPH November 6, 2008 Staffing Your TB Program Lynelle Phillips RN MPH Program Manager s Course
TB Program Management San Antonio, Texas November 5-7, 2008 Staffing Your TB Program Lynelle Phillips, RN, MPH November 6, 2008 Staffing Your TB Program Lynelle Phillips RN MPH Program Manager s Course
Kentucky TB Prevention & Control Program. Special Edition
 Kentucky TB Prevention & Control Program Welcome... To our Special Edition 2016. - Kentucky TB Program staff Special Edition In this issue TB Regulations: Highlights p.1 Fact Sheet: LTC Regulation p.2-4
Kentucky TB Prevention & Control Program Welcome... To our Special Edition 2016. - Kentucky TB Program staff Special Edition In this issue TB Regulations: Highlights p.1 Fact Sheet: LTC Regulation p.2-4
TUBERCULOSIS INFECTION CONTROL PROGRAM
 TUBERCULOSIS INFECTION CONTROL PROGRAM TB Infection Control Program for (Health Department Name) I. Assignment of Responsibility. A. (PersonIPosition) has overall responsibility for TB infection control
TUBERCULOSIS INFECTION CONTROL PROGRAM TB Infection Control Program for (Health Department Name) I. Assignment of Responsibility. A. (PersonIPosition) has overall responsibility for TB infection control
Los Angeles County (LAC) at a glance
 at a glance") TB Cohort Review in Los Angeles County It was the best of times, it was the worst of times, it was the age of wisdom, it was the age of foolishness, it was the epoch of belief, it was the epoch of incredulity
TB Cohort Review in Los Angeles County It was the best of times, it was the worst of times, it was the age of wisdom, it was the age of foolishness, it was the epoch of belief, it was the epoch of incredulity
Public Health/Primary Care Collaboration: Success Strategies in Denver
 Public Health/Primary Care Collaboration: Success Strategies in Denver Randall Reves, M.D., M.Sc. Carolyn Bargman, R.N.-C., M.A. Denver Metro Tuberculosis Control Program Denver Public Health Department
Public Health/Primary Care Collaboration: Success Strategies in Denver Randall Reves, M.D., M.Sc. Carolyn Bargman, R.N.-C., M.A. Denver Metro Tuberculosis Control Program Denver Public Health Department
Number: Ratio of the airflow to the space volume per unit time, usually expressed as the number of air changes per hour.
 POLICIES & PROCEDURES Number: 40 175 Title: Tuberculosis (TB) Management Program Authorization: [X] SHR Infection Control Committee [ ] Facility Board of Directors Source: Infection Prevention & Control
POLICIES & PROCEDURES Number: 40 175 Title: Tuberculosis (TB) Management Program Authorization: [X] SHR Infection Control Committee [ ] Facility Board of Directors Source: Infection Prevention & Control
Tricks of the Trade: Strategies for Pediatric TB Case Management
 Tricks of the Trade: Strategies for Pediatric TB Case Management Lillian Pirog, RN, BSN, PNP Nurse Manager, Global Tuberculosis Institute Suzanne Tortoriello, RN, MSN, APN Advanced Practice Nurse, Global
Tricks of the Trade: Strategies for Pediatric TB Case Management Lillian Pirog, RN, BSN, PNP Nurse Manager, Global Tuberculosis Institute Suzanne Tortoriello, RN, MSN, APN Advanced Practice Nurse, Global
Yale New Haven Health System Center for Healthcare Solutions
 Table of Contents Yale New Haven Health System Center for Healthcare Solutions 2012 Winter/Spring Course Guide TOPICS center@ynhh.org www.ynhhs.org/chs Pages www.ynhhs.org/chs Page 0 Solutions for Healthcare
Table of Contents Yale New Haven Health System Center for Healthcare Solutions 2012 Winter/Spring Course Guide TOPICS center@ynhh.org www.ynhhs.org/chs Pages www.ynhhs.org/chs Page 0 Solutions for Healthcare
SOCIAL AND BEHAVIORAL SCIENCES EXERCISE 1: Explaining Health Behavior with the Health Belief Model- Screening for Latent Tuberculosis Infection
 SBS Exercise 1: Explaining Health Behavior with the Health Belief Model (HBM) Estimated time to complete this exercise: 35 minutes LEARNING OBJECTIVES At the completion of this exercise, participants should
SBS Exercise 1: Explaining Health Behavior with the Health Belief Model (HBM) Estimated time to complete this exercise: 35 minutes LEARNING OBJECTIVES At the completion of this exercise, participants should
Role of National TB Program in LTBI Reseach. Dr Hung, Vietnam
 Role of National TB Program in LTBI Reseach Dr Hung, Vietnam 1 TB Epidemiology in Viet Nam 12 th / 22 of the TB HBCs 14th / 27 MDR HBC. 2 Nguồn: Báo cáo WHO 2012 WHO 2014 TB RESEARCH IN VIET NAM Level
Role of National TB Program in LTBI Reseach Dr Hung, Vietnam 1 TB Epidemiology in Viet Nam 12 th / 22 of the TB HBCs 14th / 27 MDR HBC. 2 Nguồn: Báo cáo WHO 2012 WHO 2014 TB RESEARCH IN VIET NAM Level
CDPH - CTCA Joint Guidelines Guidelines for the Follow-Up and Assessment of Persons with Class A/B Tuberculosis
 CDPH - CTCA Joint Guidelines Guidelines for the Follow-Up and Assessment of Persons with Class A/B Tuberculosis These guidelines are intended to be used as an educational aid to help clinicians make informed
CDPH - CTCA Joint Guidelines Guidelines for the Follow-Up and Assessment of Persons with Class A/B Tuberculosis These guidelines are intended to be used as an educational aid to help clinicians make informed
TB in Alameda County & Zika Update
 Alameda County BOS Health Committee TB in Alameda County & Zika Update Monday, January 9, 2017 Erica Pan, MD MPH FAAP Deputy Health Officer Director, Division of Communicable Disease Control & Prevention
Alameda County BOS Health Committee TB in Alameda County & Zika Update Monday, January 9, 2017 Erica Pan, MD MPH FAAP Deputy Health Officer Director, Division of Communicable Disease Control & Prevention
Mahoning County. TUBERCULOSIS ELIMINATION PLAN Mahoning County General Health District Board of Health Edition
 Mahoning County TUBERCULOSIS ELIMINATION PLAN Mahoning County General Health District Board of Health 1997 Edition CONTENTS Purpose of Document... 3 Background Information... 4 Problems with TB Control
Mahoning County TUBERCULOSIS ELIMINATION PLAN Mahoning County General Health District Board of Health 1997 Edition CONTENTS Purpose of Document... 3 Background Information... 4 Problems with TB Control
Directly Observed Therapy for Active TB Disease and Latent TB Infection
 Directly Observed Therapy for Active TB Disease and Latent TB Infection Policy Number TB-5001 Effective Date (original issue) September 6, 1995 Revision Date (most recent) June 26, 2008 Subject Matter
Directly Observed Therapy for Active TB Disease and Latent TB Infection Policy Number TB-5001 Effective Date (original issue) September 6, 1995 Revision Date (most recent) June 26, 2008 Subject Matter
TUBERCULOSIS INFECTION CONTROL
 OBJECTIVES TUBERCULOSIS INFECTION CONTROL At the end of this presentation, you will be able to: List infection control approaches to TB prevention and control Describe the type of protective equipment
OBJECTIVES TUBERCULOSIS INFECTION CONTROL At the end of this presentation, you will be able to: List infection control approaches to TB prevention and control Describe the type of protective equipment
HEALTH WORKFORCE SUPPLY AND REQUIREMENTS PROJECTION MODELS. World Health Organization Div. of Health Systems 1211 Geneva 27, Switzerland
 HEALTH WORKFORCE SUPPLY AND REQUIREMENTS PROJECTION MODELS World Health Organization Div. of Health Systems 1211 Geneva 27, Switzerland The World Health Organization has long given priority to the careful
HEALTH WORKFORCE SUPPLY AND REQUIREMENTS PROJECTION MODELS World Health Organization Div. of Health Systems 1211 Geneva 27, Switzerland The World Health Organization has long given priority to the careful
Copy. RECORDS RETENTION SCHEDULE Department of Public Health- Infectious Disease RECORDS RETENTION SCHEDULE#
 SCHEDULE 1. SCOPE: This schedule lists records unique to Department of Public Health and is used in conjunction with the General Records Retention Schedules and other relevant Records Retention Schedules.
SCHEDULE 1. SCOPE: This schedule lists records unique to Department of Public Health and is used in conjunction with the General Records Retention Schedules and other relevant Records Retention Schedules.
Marianne Henry PHASE Practicum Presentation Johns Hopkins Bloomberg School of Public Health May 12, 2017
 Requiring Reporting of Latent Tuberculosis Infection in Maryland: Process and Challenges Marianne Henry PHASE Practicum Presentation Johns Hopkins Bloomberg School of Public Health May 12, 2017 PRECEPTORS
Requiring Reporting of Latent Tuberculosis Infection in Maryland: Process and Challenges Marianne Henry PHASE Practicum Presentation Johns Hopkins Bloomberg School of Public Health May 12, 2017 PRECEPTORS
2/8/2017 TB RISK ASSESSMENT OVERVIEW. To identify adults with infectious tuberculosis (TB) to prevent from spreading TB HISTORY
 to prevent from spreading TB HISTORY") RISK ASSESSMENT PURPOSE TB RISK ASSESSMENT OVERVIEW Tuberculosis Control and Refugee Health County of San Diego Health and Human Services Agency To identify adults with infectious tuberculosis (TB) to
RISK ASSESSMENT PURPOSE TB RISK ASSESSMENT OVERVIEW Tuberculosis Control and Refugee Health County of San Diego Health and Human Services Agency To identify adults with infectious tuberculosis (TB) to
CHAPTER 1. Documentation is a vital part of nursing practice.
 CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
902 KAR 20:200. Tuberculosis (TB) testing for residents in long-term care settings.
 testing for residents in long-term care settings.") 0 KAR :0. Tuberculosis (TB) testing for residents in long-term care settings. The final version was copied on April, from the Kentucky Legislative Commission Website, http://www.lrc.ky.gov/kar/0/0/0.htm.
0 KAR :0. Tuberculosis (TB) testing for residents in long-term care settings. The final version was copied on April, from the Kentucky Legislative Commission Website, http://www.lrc.ky.gov/kar/0/0/0.htm.
Quality Management Program
 Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Ryan White Part A HIV/AIDS Program Las Vegas TGA Quality Management Program Team Work is Our Attitude, Excellence is Our Goal Page 1 Inputs Processes Outputs Outcomes QUALITY MANAGEMENT Ryan White Part
Re: Rewarding Provider Performance: Aligning Incentives in Medicare
 September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
September 25, 2006 Institute of Medicine 500 Fifth Street NW Washington DC 20001 Re: Rewarding Provider Performance: Aligning Incentives in Medicare The American College of Physicians (ACP), representing
Late-Breaker Abstract Session Submission Guidelines Deadline: Online submission 25 June 3 August 2018
 Late-Breaker Abstract Session Submission Guidelines Deadline: Online submission 25 June 3 August 2018 GENERAL INFORMATION: The 49 th Union World Conference on Lung Health is pleased to offer three late-breaker
Late-Breaker Abstract Session Submission Guidelines Deadline: Online submission 25 June 3 August 2018 GENERAL INFORMATION: The 49 th Union World Conference on Lung Health is pleased to offer three late-breaker
Checklists for screening for active tuberculosis in high-risk groups
 Checklists for screening for active tuberculosis in high-risk groups General screening program considerations The following are aspects of design and implementation that should be considered before planning
Checklists for screening for active tuberculosis in high-risk groups General screening program considerations The following are aspects of design and implementation that should be considered before planning
FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH. National Tuberculosis and Leprosy Control Programme. A Tuberculosis Infection Control Strategy
 FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH National Tuberculosis and Leprosy Control Programme FAST A Tuberculosis Infection Control Strategy 1 Acknowledgements This FAST Guide is developed
FEDERAL MINISTRY OF HEALTH DEPARTMENT OF PUBLIC HEALTH National Tuberculosis and Leprosy Control Programme FAST A Tuberculosis Infection Control Strategy 1 Acknowledgements This FAST Guide is developed
CureTB Binational Tuberculosis Referral Training
 CureTB Binational Tuberculosis Referral Training (CureTB Enhancement Project) CureTB Kathleen Moser, MD, MPH Alberto Colorado Carlos Vera Training Objectives By the end of the training, participants will:
CureTB Binational Tuberculosis Referral Training (CureTB Enhancement Project) CureTB Kathleen Moser, MD, MPH Alberto Colorado Carlos Vera Training Objectives By the end of the training, participants will:
Data Management Benita Cook, RN, BS
 TB Contact Investigation Albuquerque, New Mexico April 22-23, 23 2010 Data Management Benita Cook, RN, BS April 23, 2010 Contact Investigation Data Management Benita Cook, RN, BS Region 5 TB Nurse Coordinator
TB Contact Investigation Albuquerque, New Mexico April 22-23, 23 2010 Data Management Benita Cook, RN, BS April 23, 2010 Contact Investigation Data Management Benita Cook, RN, BS Region 5 TB Nurse Coordinator
MEDICAL SURVEILLANCE MONTHLY REPORT
 MAY 213 Volume 2 Number 5 msmr MEDICAL SURVEILLANCE MONTHLY REPORT PAGE 2 Editorial: Can the active component U.S. military achieve tuberculosis elimination? James D. Mancuso, Naomi E. Aronson, Lisa W.
MAY 213 Volume 2 Number 5 msmr MEDICAL SURVEILLANCE MONTHLY REPORT PAGE 2 Editorial: Can the active component U.S. military achieve tuberculosis elimination? James D. Mancuso, Naomi E. Aronson, Lisa W.
The local health department shall maintain annually reviewed policies and procedures.
 MPR 1 The local health department must have a system in place that allows for the referral of disease incidence and reporting information from physicians, laboratories, and other reporting entities to
MPR 1 The local health department must have a system in place that allows for the referral of disease incidence and reporting information from physicians, laboratories, and other reporting entities to
Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test 2 Select the correct response and jot down your rationale for choosing the answer. 1. If data are plotted over time, the resulting chart will be a (A) Run chart (B) Histogram (C) Pareto
UNC2 Practice Test 2 Select the correct response and jot down your rationale for choosing the answer. 1. If data are plotted over time, the resulting chart will be a (A) Run chart (B) Histogram (C) Pareto
Regulations on Tuberculosis Control
 Regulations on Tuberculosis Control Date 13.02.2009, No. 205 Ministry Department Published Ministry of Health and Care Services Department of Public Health In 2009, Booklet 2 (Comments) Entry into force
Regulations on Tuberculosis Control Date 13.02.2009, No. 205 Ministry Department Published Ministry of Health and Care Services Department of Public Health In 2009, Booklet 2 (Comments) Entry into force
Quality Standards. Process and Methods Guide. October Quality Standards: Process and Methods Guide 0
 Quality Standards Process and Methods Guide October 2016 Quality Standards: Process and Methods Guide 0 About This Guide This guide describes the principles, process, methods, and roles involved in selecting,
Quality Standards Process and Methods Guide October 2016 Quality Standards: Process and Methods Guide 0 About This Guide This guide describes the principles, process, methods, and roles involved in selecting,
UNC2 Practice Test. Select the correct response and jot down your rationale for choosing the answer.
 UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
UNC2 Practice Test Select the correct response and jot down your rationale for choosing the answer. 1. An MSN needs to assign a staff member to assist a medical director in the development of a quality
The presentation of the 5th Nationwide Tuberculosis Epidemiological Sampling Survey in China
 The presentation of the 5th Nationwide Tuberculosis Epidemiological Sampling Survey in China National Center for TB Control and Prevention, China CDC Shiwen Jiang 2010.10.05 Contents Overview Preparation
The presentation of the 5th Nationwide Tuberculosis Epidemiological Sampling Survey in China National Center for TB Control and Prevention, China CDC Shiwen Jiang 2010.10.05 Contents Overview Preparation
AFMRD Guidelines for Individual Areas of Concentration
 AFMRD Guidelines for Individual Areas of Concentration Background Many family medicine residents have specific areas of interest within the breadth of family medicine. At present there is no uniform framework
AFMRD Guidelines for Individual Areas of Concentration Background Many family medicine residents have specific areas of interest within the breadth of family medicine. At present there is no uniform framework
Guidelines for Coordination of TB Prevention and Control by Local and State Health Departments and California Correctional Health Care Services 2015
 Guidelines for Coordination of TB Prevention and Control by Local and State Health Departments and California Correctional Health Care Services 2015 These guidelines are intended to be used as an educational
Guidelines for Coordination of TB Prevention and Control by Local and State Health Departments and California Correctional Health Care Services 2015 These guidelines are intended to be used as an educational
Applied Research, Community Health Epidemiology, and Surveillance (ARCHES) Update
 Update") Applied Research, Community Health Epidemiology, and Surveillance (ARCHES) Update Wayne Enanoria, PhD, MPH Health Commission Meeting March 20, 2018 Overview 1 2 3 A3 Overview Maven Electronic Health Record
Applied Research, Community Health Epidemiology, and Surveillance (ARCHES) Update Wayne Enanoria, PhD, MPH Health Commission Meeting March 20, 2018 Overview 1 2 3 A3 Overview Maven Electronic Health Record
Communicable Disease Control Manual Chapter 4: Tuberculosis
 Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual July, 2018 Page 1 TABLE OF CONTENTS APPENDIX B: INFECTION PREVENTION AND CONTROL... 2
Provincial TB Services 655 West 12th Avenue Vancouver, BC V5Z 4R4 www.bccdc.ca Communicable Disease Control Manual July, 2018 Page 1 TABLE OF CONTENTS APPENDIX B: INFECTION PREVENTION AND CONTROL... 2
NICU CI. Tools For TB Elimination April 22, 2015 Curry International Tuberculosis Center. CI in Healthcare Facilities 1. Case Summary.
 NICU CI Michael Stacey MD, MPH CMO/Dep Health Officer/TB Controller Solano County Public Health Case Summary Index Case: Pregnant 34 yo Filipino descent sent to Sacramento County hospital from a Solano
NICU CI Michael Stacey MD, MPH CMO/Dep Health Officer/TB Controller Solano County Public Health Case Summary Index Case: Pregnant 34 yo Filipino descent sent to Sacramento County hospital from a Solano
MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH POLICY ON THE RETENTION, STORAGE, AND USE OF NEWBORN SCREENING DATA AND RESIDUAL SPECIMENS DECEMBER 2015
 MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH POLICY ON THE RETENTION, STORAGE, AND USE OF NEWBORN SCREENING DATA AND RESIDUAL SPECIMENS DECEMBER 2015 I. Introduction II. Background III. Definitions IV. Rationale
MASSACHUSETTS DEPARTMENT OF PUBLIC HEALTH POLICY ON THE RETENTION, STORAGE, AND USE OF NEWBORN SCREENING DATA AND RESIDUAL SPECIMENS DECEMBER 2015 I. Introduction II. Background III. Definitions IV. Rationale
The Coordinating Council of Broward (CCB) Broward County's Health, Education and Human Service Resources 2000
 Broward County's Health, Education and Human Service Resources 2000") The Coordinating Council of Broward (CCB) Broward County's Health, Education and Human Service Resources 2000 This document was produced with financial support from the Healthy Communities Initiative of
The Coordinating Council of Broward (CCB) Broward County's Health, Education and Human Service Resources 2000 This document was produced with financial support from the Healthy Communities Initiative of
CLINIC Outline for CIR/Legalization Preparation and Implementation Plans
 CLINIC Outline for CIR/Legalization Preparation and Implementation Plans Parent agency name: Program name: Contact person: (include e-mail and phone number) Size of service area: (Number of counties served)
CLINIC Outline for CIR/Legalization Preparation and Implementation Plans Parent agency name: Program name: Contact person: (include e-mail and phone number) Size of service area: (Number of counties served)
Correctional Tuberculosis Screening Plan Instructions
 Correctional Tuberculosis Screening Plan Instructions The Correctional Tuberculosis (TB) Screening Plan (Publication # TB-805) is designed for jails and community corrections facilities which meet Texas
Correctional Tuberculosis Screening Plan Instructions The Correctional Tuberculosis (TB) Screening Plan (Publication # TB-805) is designed for jails and community corrections facilities which meet Texas
Experiences from Peru; What have we learned? Dr. Martin Yagui Moscoso
 Experiences from Peru; What have we learned? Dr. Martin Yagui Moscoso 1. PERU Area: 1,285,215 Km Total population: 28 millions Average life expectancy:69years Population living in poverty: 54% TB incidence:
Experiences from Peru; What have we learned? Dr. Martin Yagui Moscoso 1. PERU Area: 1,285,215 Km Total population: 28 millions Average life expectancy:69years Population living in poverty: 54% TB incidence:
The local health department shall maintain annually reviewed policies and procedures.
 MPR 1 The local health department must have a system in place that allows for the referral of disease incidence and reporting information from physicians, laboratories, and other reporting entities to
MPR 1 The local health department must have a system in place that allows for the referral of disease incidence and reporting information from physicians, laboratories, and other reporting entities to
Public Health Accreditation Board STANDARDS. Measures VERSION 1.0 APPLICATION PERIOD 2011-JULY 2014 APPROVED MAY 2011
 Public Health Accreditation Board STANDARDS & Measures VERSION 1.0 APPLICATION PERIOD 2011-JULY 2014 APPROVED MAY 2011 Introduction The Public Health Accreditation Board (PHAB) Standards and Measures document
Public Health Accreditation Board STANDARDS & Measures VERSION 1.0 APPLICATION PERIOD 2011-JULY 2014 APPROVED MAY 2011 Introduction The Public Health Accreditation Board (PHAB) Standards and Measures document
SESSION 1: INTRODUCTION TO DOT
 FRANCIS J. CURRY NATIONAL TUBERCULOSIS CENTER SESSION 1: INTRODUCTION TO DOT INTRODUCTION In this 2-hour session, participants will learn the current scope of TB in the United States and in their own states
FRANCIS J. CURRY NATIONAL TUBERCULOSIS CENTER SESSION 1: INTRODUCTION TO DOT INTRODUCTION In this 2-hour session, participants will learn the current scope of TB in the United States and in their own states
Assessing the Quality of Facility-Level Family Planning Services in Malawi
 QUALITY ASSURANCE PROJECT QUALITY ASSESSMENT CASE STUDY Assessing the Quality of Facility-Level Family Planning Services in Malawi Center for Human Services 7200 Wisconsin Avenue, Suite 600 Bethesda, MD
QUALITY ASSURANCE PROJECT QUALITY ASSESSMENT CASE STUDY Assessing the Quality of Facility-Level Family Planning Services in Malawi Center for Human Services 7200 Wisconsin Avenue, Suite 600 Bethesda, MD
INFECTION CONTROL TRAINING CENTERS
 INFECTION CONTROL TRAINING CENTERS ASSESSMENT of TRAINING IMPACT on HOSPITAL INFECTION CONTROL PRACTICES REPORT for TBILISI, GEORGIA AMERICAN INTERNATIONAL HEALTH ALLIANCE December 2003 Evaluation funded
INFECTION CONTROL TRAINING CENTERS ASSESSMENT of TRAINING IMPACT on HOSPITAL INFECTION CONTROL PRACTICES REPORT for TBILISI, GEORGIA AMERICAN INTERNATIONAL HEALTH ALLIANCE December 2003 Evaluation funded
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Northern Kentucky Independent District Health Department, KY. Accreditation Preparation and Quality Improvement Demonstration Sites Project
 Northern Kentucky Independent District Health Department, KY Accreditation Preparation and Quality Improvement Demonstration Sites Project Final Report May 30, 2008 Summary Northern Kentucky utilized an
Northern Kentucky Independent District Health Department, KY Accreditation Preparation and Quality Improvement Demonstration Sites Project Final Report May 30, 2008 Summary Northern Kentucky utilized an
AIRBORNE PATHOGENS. Airborne Pathogens: Microorganisms that may be present in the air and can cause diseases in exposed humans.
 MARICOPA COUNTY SHERIFF S OFFICE POLICY AND PROCEDURES Subject Related Information CRITICAL POLICY PURPOSE AIRBORNE PATHOGENS Supersedes CP-7 (8-14-15) Policy Number CP-7 Effective Date 01-04-17 The Office
MARICOPA COUNTY SHERIFF S OFFICE POLICY AND PROCEDURES Subject Related Information CRITICAL POLICY PURPOSE AIRBORNE PATHOGENS Supersedes CP-7 (8-14-15) Policy Number CP-7 Effective Date 01-04-17 The Office
Implementation Guide for Central Line Associated Blood Stream Infection
 Implementation Guide for Central Line Associated Blood Stream Infection March 27, 2013 Contents 1. Introduction... 3 2. Central Line Associated Blood Stream Infection Prevention Evidence-Based Practices...
Implementation Guide for Central Line Associated Blood Stream Infection March 27, 2013 Contents 1. Introduction... 3 2. Central Line Associated Blood Stream Infection Prevention Evidence-Based Practices...
902 KAR 20:205. Tuberculosis (TB) testing for health care workers.
 testing for health care workers.") 0 KAR :. Tuberculosis (TB) testing for health care workers. The final version was copied on April, from the Kentucky Legislative Commission Website, http://www.lrc.ky.gov/kar/0/0/.htm. 0 0 0 KAR :. Tuberculosis
0 KAR :. Tuberculosis (TB) testing for health care workers. The final version was copied on April, from the Kentucky Legislative Commission Website, http://www.lrc.ky.gov/kar/0/0/.htm. 0 0 0 KAR :. Tuberculosis
Tuberculosis: Surveillance and the Health Care Worker
 Tuberculosis: Surveillance and the Health Care Jo Fagan Director Public Health PHAC Delivering a Healthy WA Overview 1. Pre-employment assessment 2. Post-exposure follow-up 3. Routine follow up testing
Tuberculosis: Surveillance and the Health Care Jo Fagan Director Public Health PHAC Delivering a Healthy WA Overview 1. Pre-employment assessment 2. Post-exposure follow-up 3. Routine follow up testing
3HP A WAY TO DO IT INITIATION OF 3HP IN A STATEWIDE TB PROGRAM MISSISSIPPI STATE DEPARTMENT OF HEALTH
 3HP A WAY TO DO IT INITIATION OF 3HP IN A STATEWIDE TB PROGRAM MISSISSIPPI STATE DEPARTMENT OF HEALTH NTCA April 2017, Atlanta GA TB Education and Training Projects: Updates from the Field August 10, 2017
3HP A WAY TO DO IT INITIATION OF 3HP IN A STATEWIDE TB PROGRAM MISSISSIPPI STATE DEPARTMENT OF HEALTH NTCA April 2017, Atlanta GA TB Education and Training Projects: Updates from the Field August 10, 2017
PATIENT CENTERED APPROACH
 BCARE I PATIENT CENTERED APPROACH Providing patient-centered care is crucial to achieving universal access to quality TB services for all people. TB CARE I responded to this need with the patient-centered
BCARE I PATIENT CENTERED APPROACH Providing patient-centered care is crucial to achieving universal access to quality TB services for all people. TB CARE I responded to this need with the patient-centered