SOUTH ISLAND HEALTH SERVICES PLAN
|
|
|
- Gervase Lewis
- 5 years ago
- Views:
Transcription

1 SOUTH ISLAND HEALTH SERVICES PLAN QUARTER 4 REPORT INTRODUCTION When the South Island Alliance was established in 2011 we recognised that the challenges the five South Island DHBs faced individually and collectively required a whole of system approach to achieving sustainability and meeting the future needs of our population. With limited health resources, our region continues to be more focused on how we respond to increasing pressures and challenge traditional approaches, and boundaries, to get the best outcome for our health spend and investment. In the past 12 months, the Alliance has noticeably gained momentum as the workstreams have brought a range of activities and initiatives to fruition. The achievements of the individual programmes of work over the last twelve months are outlined in this report. This progress would not have been possible without the strong relationships and clear vision for how South Island health services should work together that has been developed over the past five years. This is also demonstrated at a strategic level through the: further embedding of the South Island Strategic Framework development of South Island Outcomes Measures to track how we are progressing development of a South Island picture encapsulating where the region is heading (see following page) commitment of CEOs to the Alliance model by travelling to each South Island DHB through the year to better understand the challenges and opportunities they face. All of these achievements are undertaken through a whole of system approach that aligns with the New Zealand Health Strategy. Key components to the success of the Alliance approach include: People powered working regionally to agree our approaches to programmes including: advance care planning, healthy weight management, and hepatitis C management. Closer to Home supporting people to spent less time in care facilities. Reducing the time people waste within our system both our patients and the health care providers. Smart System aligning our information systems. This increasingly allows our healthcare professionals access to the same information about their patients, preventing duplication, and improves the quality and timeliness of treatments. The South Island is supporting our primary care providers in the care of the population by providing clarity and information through our HealthPathways and electronic referral systems One Team addressing our workforce challenges together through education and training opportunities to ensure we have a workforce that is fit for purpose as our workforce and our population ages. Value and High Performance Improving the quality and safety of our services at all levels. Improving equity of access to services. All of this work and much more is supported through the best for people, best for system framework that facilitates the development of relationships and is resulting in a more integrated and collaborative approach to healthcare for our population. 1 P a g e
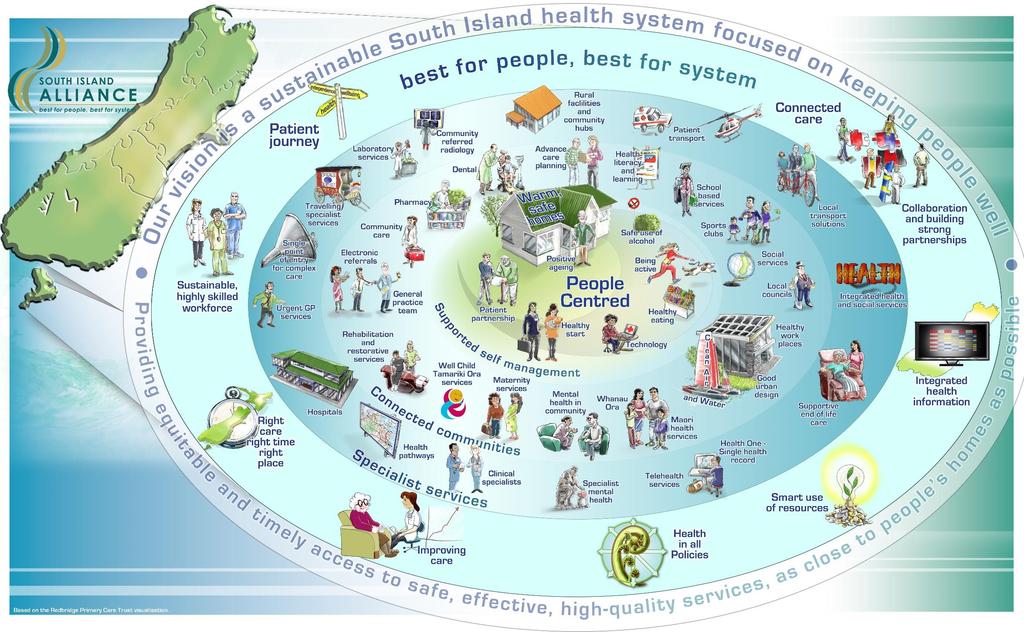
2 2 P a g e
3 Contents Introduction... 1 South Island Alliance activities supporting achieving better outcomes for people... 4 CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION SOUTHERN CANCER NETWORK CHILD HEALTH SERVICES MENTAL HEALTH SERVICES HEALTH OF OLDER PEOPLE SERVICES PALLIATIVE CARE CARDIAC SERVICES ELECTIVE SERVICES MAJOR TRAUMA SERVICES PUBLIC HEALTH STROKE SERVICES HEPATITIS C KEY ENABLERS QUALITY & SAFETY INFORMATION SERVICES THE WORKFORCE DEVELOPMENT HUB SUPPORT SERVICES Appendix One: Primary Care Dementia Education Summary Report Appendix Two: Resorative Care Flyer Appendix Three: Cardiac Data Appendix Four: Acute Rheumatic Fever reporting Requirements Appendix Five: Stroke Data P a g e

4 SOUTH ISLAND ALLIANCE ACTIVITIES SUPPORTING ACHIEVING BETTER OUTCOMES FOR PEOPLE Below are some of the activities, initiatives, changes and developments the South Island Alliance has led over the past 12 months that support achieving our vision of best for people, best for system and the eight outcomes identified in the South Island Outcomes Framework. Outcome 1: Improved environments to support health and wellbeing Why this is a priority: Health promotion and disease prevention contribute to improved health status and reduction of health inequalities, as well as reducing demand for healthcare services. Tobacco smoking, inactivity, poor nutrition and rising obesity rates are major and common contributors to a number of the most prevalent long-term conditions. These are avoidable risk factors; preventable through a supportive environment, improved awareness and personal responsibility, for health and wellbeing. Supporting people to make healthy choices will enable our population to attain a higher quality of life and avoid, delay or reduce the impact of long-term conditions. Actions have we taken in to achieve this outcomes: Support Services Sustainable health care initiatives are shared across the South Island to support more efficient and cost-effective health care delivery, including energy initatives, lighting, waste reduction, and a decrease in carbon emissions. Public Health Alcohol Harm Reduction The Public Health Partnership continues to support DHBs to implement Alcohol Harm Reduction Strategies, and has collaborated with the Child Health SLA on the Emergency Department Youth Alcohol Scoping Project. The Alcohol in Schools document was finalised and is now be used with school principals throughout the South Island. Quality and Safety A South Island consumer engagement stocktake has been completed involving the Alliance, DHBs, and various government and non-government organisations. The findings will inform further work on ensuring greater levels of consumer engagement and participation in health service planning and delivery. Public Health The Public Health Partnership has worked to strengthen their alliance and map their strategic direction. Significant progress has been made in developing a shared vision and work plan. The Public Health Partnership have partnered with Te Herenga Hauora on shared actions around smokefree initiatives, and supporting Southern Cancer Network s focus on increasing Maori cervical screening rates. 4 P a g e

5 Outcome 2: People have increased access to planned care Why this is a priority: Improving access to planned care, rather than emergency care, is important for patients. By providing planned access to services, people suffering from health conditions can get better, timelier care; allowing them to regain their quality of life sooner. This may also allow people to resume or maintain their productive contribution to the community. In personalised care planning, clinicians and patients work together using a collaborative process of shared decision-making to agree goals, identify support needs, develop and implement action plans, and monitor progress. This is a continuous process, not a one-off event. Actions have we taken in to achieve this: Cancer Services Faster Cancer Treatment Over the last 12 months, approximately 81 percent of patients in the South Island have received their first treatment within 31 days of a confirmed cancer diagnosis. SCN identified the need to provide better support to Multi-disciplinary Meeting/Team co-ordinators, as there has been high turnover in the role. SCN hosted two workshops to increase opportunities for peer support and networking, improve collaboration between DHBs and provide opportunities for learning. Feedback has been very positive, with strong support for ongoing regional engagement between co-ordinators. Staff turnover has decreased, assisting to embed MDM processes. Elective Services Regional Bariatric Surgery volumes have been met and the South Island have reviewed and amended the bariatric surgery pathway. The region has also agreed and implemented a urology pathway which has provided clarity for GPs, and ensures greater equity for patients across the South Island. Workforce Development Nurse Practitioners A national survey of nurse practitioners undertaken by SIWDH was completed and the information is now part of a toolkit for Executive Directors of Nursing to assist in developing clinical pathways for nurse practitioners in identified areas of need. Nurse Practitioner numbers have increased from 11 in 2010 to 35 in 2016 with a further 12 on identified pathways, but the information received in the survey will help inform the development of a consistent regional pathway aimed at increasing this number further. With 57 nurse practitioners taking the time to share their experiences, we were delighted with the depth of information shared. The results provided us with excellent background information for nursing leaders as they work on supporting and sustaining a nurse practitioner workforce in the South Island. Heather Gray, Chair of the South Island Nurse Practitioner Group Workforce Development Calderdale Framework Eight Allied Health staff in four DHBs have completed requirements for Calderdale Framework facilitator training since 2015, with a further one in training. Calderdale Framework is a clinically-led workforce development tool aimed at developing a more flexible and skilled allied health workforce. the Projects in each DHB have been tailored to specific services and primarily involve delegation to Allied Health Assistants and delegation/professional skill sharing between allied health practitioners. 5 P a g e
6 Information Services ereferrals The one millionth electronic referral or request for specialist advice in the South Island was received on 16 March 2016 from a GP in Dunedin. Using ERMS, general practice teams make a referral or request for specialist services via an electronic form which are securely and automatically delivered to one of over 700 community and hospital services. ERMS provides unprecedented connectedness and transparency for health services. ERMS is one of several IS initiatives we are working on at a regional level that aim to provide people with equal access to the right care when they need it. Paul Goddard, Information Services Programme Director ERMS is also making processes easier and more efficient for staff: When we turned on edelivery (electronic delivery of referrals), the BIC administrative team noticed benefits to their process immediately. Receiving ERMS referral forms directly into their practice management system, meant the manual steps of printing, scanning and importing are no longer required. I love how it works, it makes sense, our process is more streamlined. Brief Intervention Counselling Team Elective Services Inter-district patient flows The Electives Workstream began working to understand inter-district flows and the impact on DHBs, particularly Canterbury DHB s, ability to deliver elective services. This has resulted in three projects which will continue into : demand analysis including consideration of demographics and forecasting volumes; supply analysis including forecasting South Island capacity; and the development of appropriate models of care and health pathways. Feedback on the process has been very positive, particularly the availability of clear data and analytics to identify issues that need to be addressed and support decision making. 6 P a g e

7 Outcome 3: People wait less Why this is a priority: Delayed access to medical care may subject patients to increased pain, suffering, and mental anguish. Waiting for healthcare can also have broader economic consequences, such as increased absenteeism, reduced productivity, and reduced ability to work. The individual waiting is affected, as well as family members and friends who are concerned or may be called to assist them with activities of daily living. Waiting may also lead to poorer care outcomes and a requirement for more complex treatments as a result of deterioration in the patients condition while waiting for treatment. Health services must value people s time. By looking at the how, where, when and who of care provision and looking at it from the patient s perspective, we can remove barriers and make the system more integrated. This focus improves quality and efficiencies and supports our best for people, best for system approach. Actions have we taken in to achieve this outcome: Major Trauma Work has continued on implementing major trauma pathways. Good progress has been made towards developing regional destination policies with St John and Emergency Care Co-ordination Teams so that trauma patients receive the most appropriate, timely care. Three DHBs have identified and assigned trauma roles to staff and the two other DHBs are working through identifying and recruiting these resources. Data collection to better understand patient flows and is beginning to be collected and regional training has occurred. Cardiac Services The South Island Cardiac Workstream has developed and agreed to the scope of the South Island Cardiac Services Model of Care. The model aims to support equitable and sustainable services for the South Island and consists of three main projects: Access to Tests; Optimal Health Pathways; and Planning for Sustainability. Workgroups have been established with representation from across the South Island and strong links to national and other regions work programmes. These projects will continue into Stroke Services The Workstream has supported each DHB to implement a system to rapidly confirm a diagnosis of stroke and identify patients who may benefit from thrombolysis therapy, along with a thrombolysis pathway. Work towards the achieving the national standards for organised stroke services/units in all DHBs continues, with progress being made in Cardiac Services Across the South Island, over 80 percent of high-risk Acute Coronary Syndrome patients receive a coronary angiogram within three days (the national target is 70 percent). 7 P a g e

8 Outcome 4: People have prevented and/or delayed burden of long term conditions Why this is a priority: Chronic diseases are now the most common cause of death and disability. People with chronic diseases tend to be high users of healthcare resources and social care. The prevalence of long-term conditions rises with age and many older people have more than one chronic condition. The World Health Organisation (WHO) estimates more than 70 per cent of all health funding is spent on long-term conditions. As our population ages, the incidence and burden of long-term conditions increases. Long-term conditions are also more prevalent amongst Māori and Pacific people and are closely associated with significant disparities in health outcomes across population groups. It is now widely recognised that the care and support needed to live with a long-term condition requires a radical re-design of services, allowing patients to drive the care planning process. By intervening early, and with improved coordination and proactive provision of care, people, families and whānau with complex conditions have improved health outcomes. This supports people to stay well and maintain their functional independence. Actions have we taken in to achieve this outcome: Health of Older People The Alliance undertook the Primary Care Dementia Education project focused on importance of assessment, early diagnosis, intervention and ongoing support for people living with dementia and their carers/family/whanau. Progress through the year was significant, with highlights including: o education sessions attended by 457 primary care staff at locations around the South Island o all DHBs using a regionally aligned Cognitive Impairment Pathway o the development of video clips for training purposes that involve interviews with those diagnosed with dementia, their carers and health professionals. The dementia care training video clips developed by HOPSLA have been described as profound and having a tangible impact on the care given: One GP commented that they would not usually tell a person they had dementia. After viewing a video of a patient explaining the value of having a diagnosis and knowing what was causing their problems, along with a video of an example of a doctor sensitively telling a person they had dementia, the GP responded that understanding this would result in changes to their practice. Others commented that they would be more aggressive about diagnosing and informing patients about dementia; and that it was useful to have practical information that can be easily applied to their practice. Cancer Services To meet the needs of patients whose cancer diagnosis has a large psychological and/or social impact, additional support is being provided. Lead psychologists have been appointed in each of the South Island cancer services, in addition to psychologists or social workers being appointed or recruiting underway in each DHB. Regional leads are working together to plan implementation of the service, including templates for referrals, criteria, progress notes, etc. Ultimately it is envisioned that the group will work as one regional team to better support cancer patients with high and complex psychological or supportive care needs. 8 P a g e
9 Hepatitis C A South Island Workstream was established to review and assess current Hepatitis C services and assessed clinical and diagnostic capacity and capability. A proposal for an integrated approach to Hepatitis C services, in conjunction with national initiatives is now being considered. Child Health Childhood obesity South Island DHBs have agreed to a regional approach to address child obesity. Originally started in 2014, this work now supports the government s Childhood Obesity Plan and new health target. A suite of referral options will be made available to GPs to refer at-risk children and their families, ensuring equal access to high quality resources for all South Island residents. Amongst these will be Triple P Lifestyle (a cost-effective, evidence-based parenting course that focuses on behavioural change, nutrition and physical activity advice for the whole family) and BeSmarter, which was developed as a parent/child friendly way to start conversations about health and goal-setting. Consistent messages are very important. At present, a patient might visit two different health professionals and be told two completely different things. So, we have agreed on a common set of key resources so that the same messages are delivered consistently across the region. Professor Barry Taylor, Chair of the South Island Childhood Healthy Weight Clinical Advisory Group Stroke Services The Workstream arranged a very successful South Island Stroke Study Day. Fourteen speakers presented on a range of topics related to stoke that engaged all disciplines. More than 190 people attended in person and over 100 joining through video-conference from across the South Island. Participants reported that they found it beneficial for their care of stroke patients. Child Health e-growth charts E-growth charts went live as part of Health Connect South on 30 June E-growth charts enables the collection of electronic growth data, from birth to death. It provides a view of key patient information, resulting in both improved population data and availability of information across the South Island DHBs. 9 P a g e

10 Outcome 5: People have fewer and shorter episodes in care facilities Why this is a priority: Reducing the length of stay in healthcare facilities will release capacity in the system, including beds and staff time, which helps to minimise waiting times, maximise productivity and improve the patient experience. Advancements in medical and health technology have enabled the population to live longer. However, more people are living with co-morbidities and need complex care interventions. We know that investing in community services and the community workforce will help to deliver positive health outcomes and free hospitals to provide more acute and specialised care. This approach also reduces average hospital length of stay, increases patient choice and satisfaction, improves health outcomes, reduces unscheduled healthcare use, embraces prevention and health promotion models, delivers care closer to people s homes and saves money. Actions have we taken in to achieve this outcome: Health of Older People Restorative Care After wide consultation, a South Island Restorative Consensus Statement has been developed. Guides for both health professionals and consumers help support older people to live independently, care for themselves and maintain integration with the community. Mental Health and Addictions Eating Disorders The South Island continues to be strong in the provision and sustainability of Maudsley Family Based Therapy for young people with eating disorders. This year the South Island Eating Disorder Service found that young people were being admitted with increasingly embedded and complex issues, as often they have not recovered with Maudsley Family Based Therapy. Further training has been provided to services around the region to help address this and provide better support for patients and their families closer to home. Health of Older People Use of interrai data The findings of a collaboration between the Alliance and University of Canterbury to understand and improve health care needs of older people has been presented to the health care community. Data analysis reviews looking at predictors of poor outcomes in dementia; predictors of hip fractures; and end of life issues were carried out using interrai data combined with other data sets. Presentations to clinical Teams were held at nine sites throughout the South Island using videoconference. There was positive feedback from HOPSLA and DHB teams on how they can use this information to shape service delivery to frail/vulnerable populations. We achieved some really interesting results, for example, 2,800 people in New Zealand suffer from hip fractures every year, which is a very traumatic and painful experience. The data showed the predictors for those who have a higher chance of suffering from hip fractures, so they can now be targeted through the health sector. Dr Hamish Jamieson, Geriatrician and Senior Lecturer Cardiac Services Accelerated Chest Pain Pathways have now been implemented in three of five DHBs on schedule. Having the pathway in place should mean a reduction in unnecessary admissions for patients. 10 P a g e

11 Outcome 6: No wasted resource Why this is a priority: We have an obligation to provide health services in the most efficient way possible, so patients receive timely access to the most appropriate care, in the most appropriate place. It s about getting the greatest value for our people from the system, enabling evidence to inform how our scarce healthcare dollars are best invested and ensuring people receive the care they need as close to home as possible. As our population ages, so does our workforce. Alongside the other drivers of change in the health sector, the changing demographics of the workforce will require us to think differently about the way staff are utilised. We need to enable health professionals to work at the top of their scope of practice with the support of an appropriately trained unregulated workforce. We need to build an innovative and flexible workforce that will support the emerging models of healthcare. Actions have we taken in to achieve this outcome: Support Services Inter-hospital transfers South Island DHBs implemented a regional agreement with St John for inter-hospital transfers that includes regular scheduled journeys and greater clarity around administration and costs. The agreement has resulted in a significant reduction in out of schedule transfers and more efficient planning of services for clinicians and patients. Feedback from clinical staff has been very positive as the regular scheduled journeys allows greater confidence in decision making around patient care. After being in place for one year, all parties are pleased with the efficiencies and benefits and it has been agreed the agreement will be rolled over for a further year. An additional agreement for out of schedule journeys has also been negotiated with St John. Workforce Development elearning Approval has been given and work is now underway to roll out elearning across the South Island. A regionally representative group has co-designed a South Island suite of Intravenous learning packages for use across the sector. A respiratory package has also been developed. Information Services South Island Patient Information Care System (SI PICS) SI PICS went live on 30 May 2016 in Canterbury DHB with some outpatient services. The launch represents the first phase of implementation and coincided with the opening of the new Burwood facility. Staff in older person s health and rehabilitation outpatient and community services are the first users of the system. Whilst some teething problems have been experienced, the transition has been relatively smooth, with users experiencing a far richer operating environment. More than 75,000 patient records were migrated to the new system and the software was put through its paces with several rounds of testing. Super-user Niki Bailey had no problem transitioning to SI PICS and believes that, although more advanced functionality is yet to come, from day one SI PICS will still provide a better user experience: As confidence and capability grows, I m sure staff will find it much more intuitive and user-friendly than previous patient management systems Workforce Development Inter-disciplinary learning A South Island Inter-disciplinary learning workshop was held in March attended by over 50 people with whole of health and tertiary education representation. Very positive feedback about the workshop has been received. South Island principles to foster greater interdisciplinary learning have been developed and endorsed. A draft action plan is currently out for consultation. 11 P a g e

12 Outcome 7: People are protected from harm or needless death Why this is a priority: It is fundamental to health service provision that people receive high quality, safe care and are protected from harm. This is implicit in the high trust relationship between patients and health professionals and is regulated through legislation and professional oversight. As well as the negative impact on patients, adverse events and delays in treatment drive unnecessary costs and redirect resources away from other services. Quality improvement in systems and processes increase patient safety, reduce the number of events causing injury or harm and improve health outcomes. Our focus on best for people, best for system places an emphasis on the system of care delivery that prevents errors; learns from the errors that do occur; and is built on a culture of safety that involves healthcare professionals, organisations, and patients. Actions have we taken in to achieve this: Information Services HealthOne HealthOne was successfully implemented in November 2015 in South Canterbury DHB, the third South Island DHB. HealthOne gives South Island primary and community healthcare providers with access to patient information at the point of patient care. It extracts information from a number of sources (such as GP records, community pharmacy and care coordination referrals), and displays this as a combined single view alongside the patient s hospital record. HealthOne is viewed nearly 60,000 times each month: 45,000 from secondary users and 15,000 from GP users. In CDHB usage has increased by 33 percent among secondary users and 52 percent among GPs in the past year. Across the three DHBs there are nearly 1500 GP users and 450 pharmacy users. HealthOne has data relating to 580,000 people amounting to more than 57 million patient data items in HealthOne. 1.7million data items are received every month from primary and community providers. Quality and Safety The Alliance facilitates a fortnightly meeting with Quality Managers from each DHB and the Health Quality and Safety Commission. The progress on implementing the Open for Better Care campaign is discussed, along with sharing ideas and innovations, and discussing any challenges. Participants in the meetings have found the regional collaboration useful to support quality improvement initiatives. Information Services HealthOne continued Preparation also began to bring St John, private hospitals and home-based care providers into HealthOne, along with the business case for implementing HealthOne in Southern DHB being approved (expected to go-live in September 2016). There have been some extremely positive reports of the value of this system in terms of practices being able to access medication lists for people travelling through the district from other areas, as well as community pharmacy being able to check dispensing from other pharmacies. The system has also made a positive difference for hospital pharmacists, as it is saving them significant time reconciling medicine for those admitted to hospital, as they previously had to wait for information from primary care providers. Ruth Kibble, General Manager Primary and Community Services, SCDHB Workforce Development Lippencott Procedures There have been over 76,000 hits on Lippincott across the South Island. In the community it has been rolled out to 69 organisations so far, including six Maori NGOs in Canterbury. Eighteen clinical nurse specialist/educator expert groups have been established across the South Island and Midland regions to collaboratively review and develop clinical procedures. 12 P a g e
13 Information Services emedicines Electronic prescribing and administration is available in over 1300 beds in the South Island. When CDHB 3 rd Cluster goes live on 29 August they will have 1340 beds, for a total of 2,107 beds live on epa across the South Island DHBs. Beds In Use Total Beds Ratio Completion CDHB 550 1, % NMDHB % SCDHB % SDHB % WCDHB % Southern DHB have completed the implementation of electronic prescribing and administration (MedChart) into the targeted adult inpatient beds in Southern DHB s core hospitals. This will substantially improve the patients medication experience as each patient now has an electronic medication record which is current, up to date and accessible for treatment. Canterbury DHB have migrated their implementation of electronic prescribing and administration (MedChart) to using the New Zealand Universal List of Medicines as its source of medication information. This is a first in New Zealand and is a significant achievement for CDHB s emedicines programme. Targeted implementation sites for eprescribing and Administration in CDHB have transitioned to NZULM, meaning as a patient moves between these sites, the chart is available electronically to the clinician, improving both the patient experience and safety of care provided. 13 P a g e

14 Outcome 8: People die with dignity Why this is a priority: For many people, end of life is a time of increased interaction with health services and can be a frightening and stressful time for patients and their whānau. While preventing pain and suffering underlies all healthcare and treatment, different people will have different views on what this means in terms of level of medical intervention and what setting they want to be in at the end of their life. It is important that health services support patients to die with dignity by enabling them to understand their options and respecting their needs. Actions have we taken in to achieve this outcome: Palliative Care The Palliative Care Workstream carried out the first comprehensive survey of palliative care services within 14 hospitals and eight hospices across the South Island. The survey provided insight into the how services are currently being managed and have prompted significant discussion about how the South Island can support better palliative care services for patients and their families. To complete our understanding of palliative care services, a survey of palliative care in primary care is planned for early , including PHOs, planning and funding, and aged residential care. Health of Older People Advance Care Planning Level 2 Advance Care Planning education continued with eight workshops held around the South Island to equip senior health professionals to enhance their communication skills needed to ensure appropriate discussions regarding care choices at end of life. Health of Older People Conversations that Count HOPSLA supported the many and varied activities that took place around the South Island for Conversations that Count day in April. Examples included morning teas arranged to get people having conversations that count, posters and postcards, and media stories. People who live in the South Island were encouraged to have a Conversation that Counts with their family to talk about their choices for their own life. Having a conversation that counts gives us the opportunity to talk about who we are, our values and beliefs, and our choices for future treatment. The next step is having an advance care plan written and lodged with the health services to guide health staff, family and caregivers, if we are unable to speak for ourselves. I am really happy with how the day went this year and how many people were interested in starting a conversation that counts. Val Fletcher, geriatrician and Chair of HOPSLA 14 P a g e
15 PROGRESS AGAINST LEGEND REASON FOR DEVIATION CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION SOUTHERN CANCER NETWORK SOUTH ISLAND FASTER CANCER TREATMENT People get timely services across the whole cancer pathway (screening, detection, diagnosis, treatment and management, palliative care) Achieving the Faster Cancer Treatment Health Target Support the delivery of the FCTs targets by DHBs At least 85% of patients receive their first treatment within 62 days of being referred with a high suspicion of cancer and a need to be seen within 2 weeks by July The focus for SCN over the last 12 months has been to support the South Island DHBs with their delivery of the FCT Targets. Due to a change in SCN staffing, a new member of the team with extensive service improvement skills has been working with all DHBs since last October. The DHB FCT Teams are very committed to the Health Target, however progress has been variable due to the amount of manual intervention required to identify patients and prospectively manage them along the pathways. The encouraging progress seen in Q2 was not sustained in Q3, in line with many other NZ DHBs due to Christmas and summer breaks. Preliminary data for, is cautiously optimistic for many of the South Island DHBs. The DHBs face challenges with surgical capacity which is the first treatment for many patients. All DHBs recognise that to make progress towards delivering and sustaining the target, prospective case identification and active patient management by clinical and service teams are now a priority. Support for this by SCN will continue through 2016/17. 1a The region has also had a focus on the reasons for delays in pathways and to understand the proportion of patients not treated within 62-days due to patient choice or clinical complexity. This work is not completed at this stage, but with the expectation that the reporting delay codes will become mandated in 2016/17 this is an important area to support the DHBs in. The SCN continue to hold fortnightly FCT Leads meetings and to provide quarterly South Island FCT dashboards, along with more focused reviews relating to tumour streams or treatment modalities to help the DHBs to understand where some of their more challenging areas might be. This is difficult for the smaller DHBs where 1 or 2 patients can have a big impact on their performance. Finally, SCN continue to support all DHBs with the additionally funded FCT projects and, despite a few challenges with recruitment, all projects are now up and running and will be back on track by the end of Q1 2016/17. Improved or maintained performance against the Policy Priority (PP30) Faster Cancer Treatment Indicators 2a Support the maintenance or improvement of the 31 day Indicator proportion of patients with a confirmed diagnosis of Q2,4 Over the last 12 months, all DHBs have reported over 75 percent of patients receiving their first treatment within 31-days (approximately 81 percent for 15 P a g e CANCER SERVICES
16 cancer who receive their first cancer treatment within 31 days. PROGRESS AGAINST LEGEND REASON FOR DEVIATION the South Island). The main challenges to improving this are access to surgery. The SCN provide quarterly dashboards to support and help the DHBs. 2b 3a 3b Support DHBs with sustaining the National radiotherapy and chemotherapy waiting time targets all patients, ready for treatment, wait less than 4 weeks for radiotherapy and chemotherapy. Q2,4 Disseminate findings of audits (Head & Neck, Thyroid and Bowel) undertaken in Support the South Island-wide review of further services against national tumour standard. In addition, whilst the performance has been steady across the last 4 quarters, approximately 81% for the region for the year, the number of cases reported each month by most DHBs continue to be as expected based on NZ CR registrations This has been shared with the FCT Leads and will be a continued area of focus in 2016/17. A greater understanding of the number of patients who are treated privately, especially in the CDHB area has also being made to enable their ascertainment model to be reviewed. It had been the aim of the SCN to include the quarterly data submitted to the MoH in the FCT Quarterly Dashboard as this will help to support the FCT findings. This has not happened, but regular reviews of the FCT performance against the knowledge that both cancer centres achieve the national radiotherapy and chemotherapy waiting times targets does assist with understanding pathway delays along the FCT pathways. The national tumour standards of service provision are implemented Q1 Q2,4 During 15/16 the DHB and Regional reports of findings were disseminated across the South Island for the Head & Neck, thyroid and bowel audits. The data collection and analysis parts of the Review of South Island Gynae Services has been completed. The team are now preparing a regional report which will be circulated in Q1 2016/17. This has been delayed due to each stage taking longer than planned. SOUTH ISLAND CANCER SERVICE COORDINATION AND QUALITY IMPROVEMENT Going into 2016/17 SCN and DHBs will be more realistic of the time it takes to extract the required data manually from local systems. People have access to services that maintain good health and independence and receive excellent services wherever they are. Services make the best use of available resources 4a Establish the (revised) SCN Working Groups Structure. All SCN network groups are provided with ongoing support to progress actions in their respective work plans Q1 Whilst progress has been made with the engagement of non-oncology clinical leads, this has been an area of frustration for SCN. Due to the many claims on clinical and service managers time, getting groups together is challenging, coupled with changes within the SCN Team in the early part of 2015/16. The proposals agreed with the SI ALT to develop a cancer clinical leads group that is broader than oncology is still seen as a priority. However in the interim the SCN Manager is engaging with cancer and oncology clinical teams and SMOs to CANCER SERVICES 16 P a g e
17 4b 5a 6 Identify Cancer Clinical Priorities, through the South Island/SCN Cancer Clinical Leads Group. Support the South Island DHBs to improve the functionality and coverage of MDTs by implementing regionally agreed MDT priorities. Understand radiation oncology requirements and agree implementation plan for future linac capacity, usage and location. Q1 PROGRESS AGAINST LEGEND REASON FOR DEVIATION gain a greater understanding of priority areas for the SI going forward. The SI Blood and Cancer Group have met & identified radiotherapy services as a priority areas for oncology, with regard to capacity, workforce and variation in clinical practice. These has been factored into the work plans, with a focus on radiation oncology which will commence with a shared meeting between both cancer centres in July. Further areas of priority have been identified through FCT work such as provision of sustainable colorectal pathways in preparation for the introduction of a Bowel screening Programme in 2017/18. Improved functionality and coverage of MDMs across the region Q1, Q2, All projects are now moving forward Southern MDM/FCT Management Tool Following the SI-wide agreement to give all SI DHBs access to the SDHB tool/system to support their MDMs the required funding has been identified and agreed for release from the SIA/SCN underspend. This work will begin in 2016/17 with a view to a 12 month rollout across the SI led by SCN. SCN are also working closely with the MoH as part of the implementation process for the Cancer Health Information Strategy. SI-Wide MDM Activity Review: All MDMs have been reviewed by SCN and the review was widely supported by them all. The findings will be available by the end of Q1 2016/17. Supporting MDM Coordinators: A second well supported Workshop for the regions MDT Coordinators was held, these will continue with a view to reducing staff turnover and support those in post. Initiatives to understand and harmonise medical and radiation oncology services Q1 There have been many ongoing discussions on this topic both regionally and nationally. All centres providing radiation oncology services have submitted data about services to a MoH project in conjunction with Ernst & Young. Based on these findings both of the public cancer centres have suggested a joint awayday to consider the findings and commence discussions towards more close alignment of services across the South Island. CANCER SERVICES 17 P a g e
18 6b 7a 7b 7c 7d Progress towards harmonisation of services through regular activity reporting for medical and radiation oncology. Initiatives that support patient, family and whānau access to cancer services and reduce inequalities are identified and implemented across all equality groups. Run a Maori Awareness Wananga in Invercargill (TBC, dependent on access to resources). Identify needs for Pacifica and Asian communities and modes of engagement. Support rollout of a regional psychosocial and supportive care service. Q2,4 PROGRESS AGAINST LEGEND REASON FOR DEVIATION Unfortunately limited progress has been made due to changes in staff roles within SCN to support FCT. However as mentioned above the two public radiation oncology centres will be meeting in Q1 2016/17 to consider closer alignment of services across the South Island. Initiatives that reduce inequalities and support access to cancer services Q2 SCN & NMDHB were successful in a bid through the FCT RFP initiative to run a region wide project to improve cancer pathways for Maori. Recruitment for the project has now been successful and the project has commenced. SCN in collaboration with the GMs Maori and Te Waipounamu Maori Leadership Group for Cancer have agreed to undertake a shared piece of work across all DHBs for 2016/17 with a focus on improving the uptake of cervical screening across the Maori Community. Recruitment to take this forward will commence shortly. In May SCN ran an Equity Workshop in Dunedin, using the HEAT Tool. This was well attended by four DHBs and the feedback was that the day was valuable in understanding in equities, especially with regard accessing cancer services. Whilst planning was on track and resources identified in the early part of 2015/16, due to the loss of a member of the team this event was postponed. Since then TWMLG has been discussing its role and remit with SCN and David Meates and a much clearer alignment of values and aspirations has been attained. This will be built upon during 2016/17. Preliminary work in this area commenced with a new Pacifica Consumer joining the South Island Cancer Consumer Group. Sadly, she felt unable to commit to the group and has since left. This will be revisited again in 2016/17. Both the Lower & Upper South Cancer Centre Clinical Psychology Leads are in post along with many of the support psychologists and social workers. The South Island-wide Steering Group has been reconvened to oversee and lead this initiative. The group has met twice to date and have agreed an outline work plan and identified priority areas for the immediate future. CANCER SERVICES 18 P a g e
19 PROGRESS AGAINST LEGEND REASON FOR DEVIATION SOUTH ISLAND CLINICAL CANCER INFORMATION SYSTEM Implementation of the South Island Clinical Cancer Information System (SICCIS): Robust cancer data and information sources are developed and shared that enable informed service development & planning decision-making 8a 8b 8c 8d 9 10 Implement the proposed Cancer Informatics Working Groups Structure (in collaboration with the SI Information Services SLA). Support DHBs with further alignment of MOSAIQ across the Cancer Centres. Support integration and expansion of Metriq (AKA SICCIS). Produce a Quarterly Cancer Dashboard to understand progress against cancer standards and targets. SICCIS, the regional clinical data repository for cancer implementation continues Q1 Q1,4 Q2,4 With the introduction of the NZ Cancer Health Information Strategy (CHIS) and the extended leave of a SCN team member, further progress in this area will be deferred until 2016/17. However, the plans for implementing CHIS are now clearer and will form the basis of a new programme of work going forward. Continuing to align and rollout MOSAIQ across the South Island is important, but the implementation of PICS within CDHB & NM DHB are of a more immediate priority. Consideration will be given in 2016/17 to the role of SCN in this work or whether it is better sited within the DHBs to take forward. The findings from a review of METRIQ by an MBA Student was reported to the SCN Steering Group, whose advice was to refrain from taking the project any further forward until Ursula Jewell has returned to the team and there is more clarity regarding the implementation of the NZ CHIS. The SI/SCN FCT Quarterly Dashboard is now operational and shared with the South Island DHB Operational and Exec Teams, and cascaded across all clinical groups. SOUTHERN CANCER NETWORK SUPPORT FOR NATIONAL PROJECTS To ensure that the tumour standards continue to promote quality of care and guide uniform standards of service provision across DHBs To deliver Stage B & C of the Tumour standards project by supporting the MoH Tumour Stream Working Groups. Supporting the MoH Tumour Standards Working Groups (in collaboration with the Sapere Research Group) Host and support the NZ National Lead. TE: this may not now be going ahead Supporting National Lead for the Psychological and Social Support Workforce Initiative The relationship between SCN and the National Clinical Lead has gone well and all parties have benefitted from the relationship. CANCER SERVICES 19 P a g e
20 PROGRESS AGAINST LEGEND REASON FOR DEVIATION CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION CHILD HEALTH SERVICES GROWING UP HEALTHY responding to national strategies for improving children's health outcomes and preventing child abuse a 4b South Island Children's Action Plan (Government strategy) Healthy Families New Zealand aims to improve people s health where they live, learn, work and play in order to prevent chronic disease Identify and monitor the implementation of agreed South Island regional interventions to better manage safety, reduce family violence and childhood poverty. Implement the findings of the audit of the South Island sudden death in infancy policy. Evaluate and implement an e-tool that would meet the needs of youth, in particular Māori and Pacific Island, health outcomes. E-prosafe is one of the tools being used to help protect vulnerable children and deter family violence. The Child Protection Coordinator, CDHB and a lead paediatrician are working to understand changes required to provide useful e- prosafe data. The South Island regional group of Violence Intervention Coordinators have been consulted and feedback to CH SLA will occur in August. Regional Sudden and Unexpected Death in Infants (SUDI) rates continue to trend downwards Q2 Following considerable work and consultation, the audit tools and supporting information were developed. The audit package has been distributed to all South Island DHBs and the audits are underway. The audit is expected to be complete by July August YOUNG PERSONS HEALTH responding to the Prime Ministers youth Mental Health project Pathway to improve health outcomes for Māori and Pacific Island youth with mental health conditions The review of costs involved to implement BRAVE regionally were found to be excessive. For now, BRAVE will not be taken up regionally. CH SLA have undertaken discussions with Mental Health SLA to see if work using e-tools, in particular SPARK, could be aligned to work they are undertaking. CH SLA have increased the awareness of SPARK amongst clinical communities as far as they can. This project has been reliant on an external person to progress. Her competing demands have at times rightfully taken precedence. It has also been dependent on the scheduling of external meetings. This project will continue into This work was delayed as we determined the most appropriate channels and identified who needed to be consulted prior to the audit occurring. The practicality of the CH SLA progressing this item is not achievable. It will not be carried into the plan. Support programmes which reduce youth risk taking resulting in injury/disease from smoking, alcohol, drug and sexual diseases In partnership with the Health Promotion Agency, South Island Public Health Partnership and Mental Health Service Level Alliance implement findings of South Island Emergency Department scoping exercise. Explore options and identify solutions to reduce teen pregnancy and referrals to Sexual health. Q3 Q3 The final South Island Youth Alcohol Emergency Department Presentations Scoping Project Report was received in March from Dr Paul Quigley. The Report findings and recommendations were considered by the Child Health SLA, SPaIT and ALT in April/May. SPaIT have requested feedback on the recommendations on the report from the SI DHBs. Once this is known there will be ongoing discussions for future direction. Dr Edward Coughlan, Clinical Director Christchurch Sexual Health, presented to CH SLA on this topic in May. South Island data on rates of infection and referrals to CYFS and Public Health s role were discussed. This prompted discussion on what a model of care and services could look like. Due to the late delivery of the report and subsequent additions this has impacted on the project timeline. HPA has had some personnel turnover which has also delayed the project. The templates required to complete Ashburton and Timaru ED surveys are needed and have proved very challenging to get. The work will continue within the plan. The project has been reviewed and rescoped. The new focus will be reflected in the plan. CHILD HEALTH SERVICES 20 P a g e
21 PROGRESS AGAINST LEGEND REASON FOR DEVIATION ACCESS TO CHILD HEALTH SERVICES Supporting innovation, good practice and equity. 5a 5b 5c 5d 6a Review and regionalise the Canterbury DHB Dermatitis and Eczema HealthPathway. Increase GP training on Dermatitis and Eczema. Improve systems across South Island for young people with Diabetes in particular Type 1. Establish triage criteria and tool for referral to Children s Outpatient Department. Develop a regional integrated obesity management programme. Interventions to reduce hospital admission with emphasis on at risk children and families, Māori and Pacific Q3 Q3 Healthpathways for dermatitis and eczema in each region have been regionalised from the existing Canterbury DHB pathway in South Canterbury, West Coast and Nelson Marlborough. HPW are referred to in a number of clinical resources including the National Eczema clinical network. Most Primary Health Organisations in SI have provided Dermatitis and Eczema education in their GP annual training. CDHB has run a large group session for GPs with the PHO Pegasus (2013) with Diana Purvis, Paediatric dermatologist. The Health pathway and all the resources attached provide the ongoing education. WCDHB video link into Canterbury Initiative and can access Health Learn which provides on- line education. It is challenging for WC to have dermatologists attend CME to provide training. Their education is multidisciplinary. NMDHB have recently included Dermatitis in their CME and Wairau to follow soon. Southern have undertaken CME training this year. Model of Care is in development. A scoping exercise has been undertaken looking at regional resourcing. A minimum standard for workforce is being developed by the working group. Staffing recommendation for Diabetes Nurse Specialist is completed and will be put forward to CH SLA for comment. This will be considered within the context of the model of care and resourcing in other DHBs. Following the discussions around ERMs, the SDHB presented to the CH SLA their model for refining triage from GP to OPD. Ongoing work is required A regional integrated obesity management programme The South Island Childhood Healthy Weight Program Clinical Advisory Group has built on the work completed to date in the CH SLA Work Plan , along with the South Island DHB individual action plans. Each DHB has, or is in the process of establishing a Local Implementation Group (LIG). The key deliverables of LIG are to work with the CH SLA, to implement the aims in the South Island Child Obesity Action Plan at a local/district level by sharing ideas, information and by providing support to each other and strengthening the sector s working relationships. The LIGs vary from DHB to DHB, but it is planned that they This work will carry on into This work will carry on into Progression of this has been delayed due to resourcing and other priorities. It will be continued in the plan. The resourcing of this project will be linked to Item 9. CHILD HEALTH SERVICES 21 P a g e
22 6b 6c 7 Enhance collaboration with child dental health services. Share learnings healthy family initiatives in Heathcote Spreydon (Christchurch) and Invercargill. PROGRESS AGAINST LEGEND REASON FOR DEVIATION will made up of representatives from across the child health sector, which may include paediatricians, Planning and Funding, Maori managers, Maori and Pacific health provider groups, local iwi groups, B4SC deliverers, Healthy Families, sports trusts, and the oral health sector. A strategic Plan is due for submission to CH SLA in July. Evaluation is a key area of work as is IS systems. Individual data will need to be able to be transferred to repositories so analysis can take place. Healthy eating & good oral health are linked. The SICAG intend to optimise/link these through the following: liaise locally and nationally with education sector; send healthy eating/ good oral health messages out; liaise nationally with oral health groups; and for CH SLA members to liaise with their local oral health groups. Information and learnings are being shared through a number of mechanisms: Healthy Families manager Invercargill is on South Island Clinical Advisory Group Healthy Weight Childhood Healthy Family Newsletter circulated to CH SLA Healthy Families personnel included and attending forums in Christchurch and Invercargill for Healthy Weight in Childhood A regional electronic growth chart that will become part of a National solution to recording growth from birth. Implement a South Island e growth chart. Q1 E-growth charts went live through HCS on 30 June This solution enables the collection of electronic growth data, which is essential for clinicians. It provides a view of key patient information which results in both improved population data and availability of information across the five South Island District Health Boards capturing patients who access healthcare across the SI DHBs. The graphs are plotted against World Health Organisation (WHO) Child Growth Standards This work will continue into SUCCESSFUL TRANSITION INTO HEALTHY ADULTHOOD FOR CHILDREN WITH LIFELONG HEALTH CONDITIONS (for example, implementation of cystic fibrous pathway) 8 Implement agreed transition pathway for young people with complex disability and with lifelong health conditions. To provide youth specific services and transition planning/clinics to young people with a range of diseases Canterbury transition model has been presented to the CH SLA. Regional roll out is being considered. Some areas identified for development are: a resource for health professionals working with adolescents; activity packs distributed to adult wards; boredom buster activities; information about face book page etc.; adolescent specific welcome book in the peadiatric wards. Delays due to lead person who was informing this work has left the group. CHILD HEALTH SERVICES 22 P a g e
23 PROGRESS AGAINST LEGEND REASON FOR DEVIATION TO ADEQUATELY ADDRESS THE CHALLENGES OF BEHAVIOURAL PROBLEMS IN CHILDREN AND YOUNG PEOPLE. CHILD DEVELOPMENT AND DISABILITY CHILD AND YOUTH HEALTH COMPASS REPORT Develop a South Island under 5 years old behavioural pathway. Strengthen models of care within primary care Right place Right time Right Service Scoping of activity in regions underway. Initial focus in regions is developing a referral form that promotes good quality referral information to allow triage into the appropriate service to best meet the need as perceived by the referrer. CONSUMER CONSULTATION This project has been delayed due to resourcing. CDHB Service Manager has agreed to progress the work on coordinating a regional HPW in To include children, young people and whānau in the planning, delivery and evaluation of health services 10 Develop a parent/care giver survey. Q3,4 Awaiting report from Q&S SLA and their stocktake of consumer groups in South Island DHBs. 23 P a g e CHILD HEALTH SERVICES
24 CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION MENTAL HEALTH SERVICES PROGRESS AGAINST LEGEND REASON FOR DEVIATION EATING DISORDERS 1a 1b 2a Continued regional provision of eating disorder inpatient services, being cognisant of the needs of Maori and Pacifica in all activity. Develop and review reports from the regional service including access, trends, key performance indicators and quality improvement activities. Identify and support change process as required. Q1,2,3,4 Q1,2,3,4 Specialists from regional Eating Disorders services (SIEDS) have visited and advised colleagues in district services again this quarter. Extra clinicians have been sent to respond flexibly to the needs of each district, for example, two clinicians met with the Nelson Child and Adolescent MHS and paediatric team to discuss collaborative systems. Consumers admitted from districts who are under 18 have increasingly embedded and complex issues, as often they have not recovered with Maudsley Family- Based Therapy (MFBT). Therefore SIEDs has delivered further successful MFBT training. The region continues to be strong in MFBT and the model is working in a sustainable fashion. The regional service is hosting the Australian and NZ Academy of Eating Disorders Conference in August this year. This conference is seen as an excellent opportunity for workforce development for the region. We are pleased to note that clinicians from both SIEDs and the districts have submitted work to present at the conference. Work is being done on improving engagement with Maori consumers and their whanau in the Canterbury district. The EDT team has joined with the MBT working group to improve processes and relationships. Increased liaison between senior nurses on the inpatient ward and DHB case managers is occurring by video conferencing and phone. For Canterbury region the pathway for binge eating disorder is now embedded into SIEDS. We will continue to work with each district on strengthening their pathways. ADULT FORENSIC SERVICES Improved adult forensic service capacity and responsiveness, being cognisant of the needs of Maori and Pacifica in all activity Robust regional contribution to the national network of forensic inpatient services. Clinical Leads of Adult Forensic Services continue to contribute to the national network of forensic inpatient services through the national key performance indicator forum and with MoH at the New Zealand Forensic Psychiatry Advisory Group (NZFPAG). The NZFPAG March meeting saw discussion of forensic KPI benchmarking, outcome measures and proposed seclusion indicator definition MENTAL HEALTH & ADDICTION SERVICES 24 P a g e
25 2b 3a 4a 4b Prison screening occur with agreed timeframes with 80% of prisoners referred seen within 7 days of receipt of referral. Review the community youth forensic hub and spoke model. Q1,2,3,4 PROGRESS AGAINST LEGEND REASON FOR DEVIATION and test data. This was expanded and refined at the June meeting. For the period Feb 2016-Apr 2016, SDHB report that 71% of prison screening occurs within 7 days and 83% within 14 days. CDHB report that 46% of prison screening occurs within 7 days and 84% within 14 days. YOUTH FORENSIC SERVICE CAPACITY AND RESPONSIVENESS Development of Community Youth Forensic Services which are cognisant of the needs of Maori and Pacifica. The working group continues to work on drafts of the pathway document and is consulting with DHB teams on the content. This is nearly complete and should be finalised in early August. PERINATAL AND MATERNAL MENTAL HEALTH SERVICE OPTIONS AS PART OF A SERVICE CONTINUUM Continued regional provision of regional mothers and babies services, being cognisant of the needs of Maori and Pacifica in all activity Develop and review reports from the regional service including access, trends, key performance indicators and quality improvement activities. Identify and support change process as required. Q1,2,3,4 Q1,2,3,4 Work continues to be done on improving engagement with Maori consumers and their whanau in the Canterbury district. Working group has been set up to improve processes and relationships, and a Hui was held with a wide range of Maori services in February. This work will continue this year, and likely into Planning is underway to hold hui with service providers and establish links to improve access. A process has been developed to ensure contacts with DHBs are recorded on the Healthlinks computer based clinical records. We continue to have an increased use of video conferencing on specific inpatients, to plan treatment and transitions from and to the districts, which has been very helpful, especially in complex cases. Regional cases can involve a lot of additional work around liaising with district services such as CYFS. Our local CYFS liaison SW has been actively involved in supporting Mothers and babies with this. The admission processes for regional admissions has been improved with a pathway developed to guide clinicians. A policy for companions on the unit was developed, detailing process for when partners or family stay with consumer. This now operational. Training in use of tool for rating infant distress has been completed. Work is underway on post course evaluation and learning. Monthly video conferencing with all DHBs now includes a regular education component. This involves more preparation work by MBT for each session. In addition the education part of regional video conferencing to be revamped, with the expectation that each MENTAL HEALTH & ADDICTION SERVICES 25 P a g e
26 5 A stocktake and analysis of the range of models and activities in primary and community provision of Maternal Mental Health. PROGRESS AGAINST LEGEND REASON FOR DEVIATION DHB will more actively contribute to their own learning through a journal club. Documentation was developed to ensure consistency of information obtained for case consultations was introduced and is now being used. This is yet to be formally evaluated by the team. Primary and Community A generalized stocktake to establish the types of service offered was completed. The mental health pathways reported in each DHB Maternity Quality and Safety Programme was also used. Overall there is good coverage for services across the South Island. There are wait lists for services in Canterbury only. However, client experience and health pathways are currently unknown. ALCOHOL AND OTHER DRUG SERVICES 6a 6b Continued regional provision of alcohol and other drug services, being cognisant of the needs of Maori and Pacifica in all activity Develop and review reports from the regional service including access, trends, key performance indicators and quality improvement activities. Identify and support change process as required. Q1,2,3,4 Q1,2,3,4 There has been ongoing consolidation of regional medical inpatient withdrawal management service and social withdrawal management service to provide packages of care for people with very complex issues. Services working together to look at being able to transfer clients within the medical and social withdrawal management services to free up medical beds. South Island Withdrawal Management meetings with services to look at regional capability for clients requiring withdrawal management without the client having to travel out of their communities and away from their families remains an ongoing process Work being done on the required training packages to enable nurses and AOD workers in regional services to up skill in withdrawal management at SIWM meeting remains ongoing. The Kennedy referral pack has recently been updated and will be ed out to all services that refer clients to Kennedy. This will include a What to expect on arrival to Kennedy pack for clients to take away and read. Regional discussion looking at the availability of appropriate supported accommodation and or possibility of use of hospital beds in local communities remains ongoing. The issue of lack of consistency in travel support for clients remains under review. MENTAL HEALTH AND ADDICTION SERVICE CAPACITY FOR PEOPLE WITH HIGH AND COMPLEX NEEDS. 7 Understand the challenges DHBs face in providing individualised care Mental Health and Intellectual Disability Dual Diagnosis The working group is working on the challenges Mental Health Services face MENTAL HEALTH & ADDICTION SERVICES 26 P a g e
27 8 for people with high and complex needs. Report on the impact of the new behaviour support arrangements on the South Island. Q3 PROGRESS AGAINST LEGEND REASON FOR DEVIATION with people with an intellectual disability where there may or may not be a major mental illness present. Otago is seeing increasing referrals for personality disorder, pushing ID and challenging behaviour into the MH field. Explore staff develop behaviour support plans with clients, carers and NGOs however the need is often more one of support rather than behaviour. Behaviour Support The MHASLA working group has met with MoH Disability Support Services (DSS) and Explore to discuss progress. Explore are still recruiting to the SI roles and putting the new arrangements in place. Consequently, the focus of this work shifted to finding ways to assist DSS and Explore to establish the new behaviour support arrangements. An update report was requested from Explore however DSS have pointed out that Explore are not in a position to provide reports to organisations other than the Ministry (22/12/15). At DSS suggestion, MHASLA drafted specific questions about developments. A response has been received from MoH with limited information included. MĀORI MENTAL HEALTH Priority focus on Maori health equity Alternative avenues for gathering information are being tried. Seclusion 9 Collaborate on seclusion and restraint across South Island DHBs with a specific focus on Māori. Q1 A regional collegial support group has been established for this item. Opportunities for collegial support have been taken up to share information on seclusion reduction strategies with a specific focus on Māori. PACIFICA MENTAL HEALTH Consultation on advice regarding responsiveness to Pacifica need 10 Seek feedback from the sector on the 2015 South Island Pacifica report Reducing Inequity and Embracing Cultural Competencies. Q2 Feedback on this report has been received and shared with MHASLA. The feedback indicates that the recommendations are admirable but it is unclear how progress will be resourced and sustained. There may be an opportunity to support South Island DHB engagement with Le Va (the national hub for Pasifika mental health and addiction workforce development) to determine the next steps. MHASLA meeting with Le Va and Te Pou occurred in June. WORKFORCE 11a Workforce development recommendations and integrated plan for primary and NGO sector inclusive of the needs of Maori and Pacifica Develop recommendations and integrated plan for South Island DHBs, primary and NGO sector inclusive of the needs of Maori and Pacifica. South Island workforce plan has been drafted, currently being modified prior to circulating it for wider consultation. A small working group has been established to progress this work and to organise a regional strategy meeting. 27 P a g e MENTAL HEALTH & ADDICTION SERVICES
28 11b Mental Health Core Education Group identify and prioritise a regional suite of elearning packages. PROGRESS AGAINST LEGEND REASON FOR DEVIATION A number of focus groups across the South Island have been held to receive feedback on the recommendations. South Island Mental Health and Addiction Education and Training Workgroup established a 12 month workplan based on recommendations. The stocktake of regional training resources was completed, including elearning. INFORMATION SERVICES 12 Agree South Island functionality and delivery of the overall solution for the Health Connect South (HCS) Mental Health module. A number of workshops to confirm requirements have been held with South Island representation from both Clinical and IT specialities. The original requirements gathered to develop the incumbent West Coast DHB Mental Health Solution have been reviewed and updated to reflect changes and additional requirements. All participants were in agreement in regards to the desired direction of the project and that the key requirement is around user experience and seamless integration. To address the required functionality the South Island proposes, where practical, to leverage off our existing tool kit and approach the market to address the outstanding functionality. Two key gaps identified in functionality are access to a community medication system and a tool to support workflow. It is proposed that the delivery of the South Island Mental Health system will occur over three phases: Paper-lite; Integrated systems; and workflow. A readiness assessment is currently being completed with each of the DHBs and will form the basis for the development of an implementation roadmap. Next steps include issuing a Registration of Interest (ROI) to ascertain what products are available to address the identified gaps. Work is underway with South Island procurement teams to develop the ROI. Work supported by the Mental Health and Addiction Service Level Alliance: Regional projects supported by the Mental Health and Addiction Service Level Alliance but led by other SLAs and Workstreams Pathway to improve health outcomes for Māori and Pacific Island youth with mental health conditions (page 20, item 3) Owner: Child Health SLA Support programmes which reduce youth risk taking resulting in injury/disease from alcohol (page 20, item 4a) Owner: Child Health SLA MENTAL HEALTH & ADDICTION SERVICES 28 P a g e
29 CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION HEALTH OF OLDER PEOPLE SERVICES PROGRESS AGAINST LEGEND REASON FOR DEVIATION DEMENTIA SERVICES 1 2 3a 3b 4 Improved services for people with dementia by implementing the New Zealand Framework for Dementia Care in the South Island Embed a Person Centred Care approach to services that enables people with dementia, their family and whānau to be valued partners in an integrated health and support system. Agree a South Island Regional Cognitive Impairment Pathway. Dementia education supporting the use of CIP is available in a variety of modalities suitable for GPs, Practice Nurses and other community staff across the health care continuum including NGOs. Encourage uptake of Dementia Education in South Island districts. Q1,2,3 South Island Dementia Video Conferences are held with participation from each DHB. This facilitates progress in embedding the Dementia Framework in a consistent manner in each South Island DHB. In addition to Matthew Croucher (South Island Clinical Leader for Dementia), 3 members of the South Island Alliance attended the first NZ Dementia Summit held Wellington in November The direct referral to Alzheimer s Organisations in South Island has been added into ERMS improving direct access and reducing time delays for Primary Care All planned activities have been achieved this year. TO FURTHER DEVELOP THE PRIMARY CARE WORKFORCE AND IMPROVE THE TIMELINESS FOR A DIAGSIS A Cognitive Impairment Pathway (CIP) will be promoted for adoption across all South Island DHBs All South Island DHBs now have a Cognitive Impairment pathway that has regional consistencies with local variation. Develop appropriate education/ training materials for South Island primary health care dementia Q1,2,3,4 The nationally consistent education modules developed in conjunction with, and for use by, Primary Care Teams are being finalised. A report outlining all of the achievements in developing Primary Care Dementia Education is included in Appendix 1. All planned activities have been achieved this year. A Primary Care Dementia Education Calendar has been developed with PHO hosting sessions in each South Island district. Whilst there has been a delay with completion of the final national education package, South Island Alliance has developed video clips of patients experience. These are brief (2-3 minutes) and provide the Persons Voice about the value to them of receiving a diagnosis. These have been well received by GPs and Practice nurses. Walking in Another s Shoes (WiAS) programme (person centred care) to reach a wider range of staff working with people with dementia WiAS programme is further developed and enables South Island DHBs to become Dementia Friendly where integration occurs across the health, support and community sectors. Q3 South Island DHBs are continuing to offer master classes to those who have attended a WiAS programme in the past. This help graduates to refresh and reinforce skills developed to deliver person centred care to those who have dementia. 6 courses have been delivered in the SI to date. HEALTH OF OLDER PEOPLE SERVICES 29 P a g e
30 PROGRESS AGAINST LEGEND REASON FOR DEVIATION RESTORATIVE MODEL OF CARE These activities are best achieved at a regional level 5 A Web Based Toolkit that is evidence based and guides service providers to deliver restorative, person centred care Promote the use of South Island approved principles for restorative care by all services in the South Island. Q3,4 The final version of the South Island Restorative Consensus Statement Health Service Guide & South Island Restorative Consensus Statement Consumer Guide are on the Alliance website and printed versions will be circulated to Consumer agencies as soon as they arrive from the printer. Consumer guide: umer Health professional guide: ssional A flyer about the Consensus Statement is included in Appendix 2. COMPREHENSIVE CLINICAL ASSESSMENT (interrai) 6a 6b 7 Comprehensive Clinical Assessment using a standardised assessment tool (interrai) facilitating a system wide approach to common assessment Advocate to use the information from comprehensive clinical assessment (interrai) proactively in the South Island DHBs. Advocate to encourage use of the information from comprehensive clinical assessment (interrai) proactively in plan of care. Monitor interrai reports to identify equity, population and service trends data to influence changes in service through advocacy. Q2,3,4 The data analysis reviews using interrai data combined with other data sets was completed in February Presentations to clinical teams were held at 9 sites throughout the South Island using VC. The report is for wide circulation. DHB teams (from around New Zealand) have responded that the report adds useful information. Monitor population and service data trend to influence changes in service through advocacy Q1,2,3,4 The South Island Summary interrai Home Care Report is now on hold replaced with a national report available from TAS National InterRAI Data Service. This is being discussed each quarter to improve the presentation of the report. There is no trend emerging at present as the report has only been available for a short duration. FALLS PREVENTION & FRACTURE LIAISON SERVICE 8a 8b South Island DHBs are supported to develop evidence based Fracture Liaison Service A South Island Policy on Community Based Falls Prevention Programmes based on the evidence of the Otago Exercise Programme Facilitate South Island DHBs to share information and ideas to progress falls prevention and embed Fracture Liaison Services. Q2,4 Encourage development of Fracture Liaison Services in each South Island DHB Q3 All DHBs participate and share ideas when attending South Island Regional Falls- Prevention teleconference. Participants express how useful it is to have this discussion. A South Island report using Atlas of Variation data is being developed to help inform a South Island metric. A South Island Regional Falls- Prevention/FLS teleconference meeting is planned to be held mid The meeting is planned for Q when the Atlas of Variation report is available. HEALTH OF OLDER PEOPLE SERVICES 30 P a g e

31 PROGRESS AGAINST LEGEND REASON FOR DEVIATION A practical South Island metric that DHBs are able to consistently report on is being investigated. ADVANCE CARE PLANNING 9a 9b 9c South Island DHBs are supported to develop Advance Care Plan (ACP systems and processes to embed ACP as standard practice for those who will benefit Support DHBs to develop ACP system implementation with processes to embed ACP as standard practice for those who will benefit. ACP L 2 Training is available in a planned manner for staff in each DHB district in South Island. Support South Island DHBs to develop regionally consistent systems, processes and policies to embed ACP as standard practice for. Q2,4 Q1,3 Q1,2,3,4 South Island ACP Steering group meetings are held each quarter. This helps DHBs to plan development in line with the South Island and National ACP Programme. A South Island L2 ACP Education calendar was agreed with training being undertaken in each DHB as planned. Extensive advertising took place and a system for selection utilised to ensure staff from across the continuum were able to participate. HOPSLA and South Island members participate in regular National ACP format review discussion, scoping and planning meetings. 3 national ACP Surveys held to collect feedback closed mid-march The SI was well represented: 9 focus groups - 6 held in the South Island 70 members of the public approx.. 65% from South Island 166 healthcare staff approx. 50% from South Island A revised and improved national ACP resource is now available for use. 10a Support South Island DHBs to participate and support National Conversations that Count Day. This will encourage individuals, communities and health staff to have conversations useful for a person to document their ACP and develop a shared understanding of an individual s choice. South Island DHB are supported to participate in Conversations that Count (CtC) awareness raising day April 2015 Q2,3 South Island DHBs used posters, postcard and activities to raise awareness for people in our communities to have A Conversation that Counts. Activities commenced in each DHB 11 April through to 16 April the national awareness day. South Island DHBs held Morning Tea with ACP, Stalls at markets, sessions at libraries and many community events to Get them Talking. 10b CtC education (Peer education for the public delivered by the public ) is available in each South Island DHB. Q3 Plans to run a SI CtC education course were brought forward from Q3 to Q1 to enable the candidates CtC graduates to be confident in their roles prior to the April 2016 CtC day. A course was run 2 & 3 HEALTH OF OLDER PEOPLE SERVICES 31 P a g e
32 PROGRESS AGAINST LEGEND REASON FOR DEVIATION September with candidates from Hokitika, Nelson, Blenheim, Dunedin and Christchurch. The system for selection mirrored the Auckland process and each potential candidate was interviewed. 11 Develop and implement an electronic ACP accessible to all health care clinicans. Q1,2,3,4 ACPs incorporated into the regional IS system/plan Discussion continued to ensure that a single version of ACP document is endorsed for electronic use in the South Island. The final version NZ ACP document is to be release in the n 32 P a g e HEALTH OF OLDER PEOPLE SERVICES
33 CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION PALLIATIVE CARE PROGRESS AGAINST LEGEND REASON FOR DEVIATION INFORMATION TECHLOGY AND SERVICES By using new electronic systems and tools health professionals are able to securely share and gather relevant patient information that will result in safer, better and timely palliative care to patients 1a 1b 2a 2b To inform and influence information systems to support the delivery of more efficient and safer transfer of patient information between Palliative Care Providers (including Hospice services) across the South Island while reducing costs and risk. Support the development of a business case and pilot for the implementation of the Palliative Care tool of InterRAI by Canterbury DHB (in partnership with Mid Central and Hawke s Bay DHBs) Palliative Care Workstream continue to monitor uptake of e-prescribing in Hospices and sharing the learnings. Information Services (IS) across South Island Hospices has been assessed through the surveying that was undertaken in August IS appears from the survey results to be an area requiring further development for all but one hospice. Information Service (IS) across South Island Hospitals has also been assessed through the surveying undertaken in June SPaIT and ALT are considering the findings of these surveys. The data will be reviewed in conjunction with the results of surveying that will be undertaken in primary community setting. The pilot project has been completed that tested the use of the interrai Palliative Care assessment and care planning tools in three District Health Boards (Hawkes Bay, Mid Central and Canterbury) in the home based community setting. Recommendations to InterRai NZ was that the tool be introduced in NZ. No decision has been made on this. HOSPICE AND HOSPITAL PALLIATIVE CARE SERVICES To provide all people who are dying and their family /whānau access to an equitable and quality palliative care service wherever that service may be located in the South Island Understand the current models of care and how hospital and hospice palliative care services. Benchmark against the Resource and Capability Framework for Integrated Adult Palliative Care Services in New Zealand MOH 2013 and the Guidance for Integrated Paediatric Palliative Care Services in New Zealand 2012). Findings have been included in the Hospice and Hospital reports that are being considered by SPaIT and ALT. A report has been completed and submitted to SPaIT and ALT on findings from the survey of palliative care services within 14 hospitals across the region and eight hospices across the South Island. A Survey of Palliative Care Services Primary care is planned and will include PHOs, Planning and Funding, and ARC PALLIATIVE CARE SERVICES 33 P a g e
34 PROGRESS AGAINST LEGEND REASON FOR DEVIATION PRIMARY AND COMMUNITY CARE 3a 3b 3c 4 To explore the provision of Primary Palliative Care and support services to consumers and communities (Including St John, Maori, Allied Health, NGOS, Private). Understand the current workforce delivering Palliative Care in the community(s) and identify any workforce development opportunities. Support HWNZ initiative to create Specialist Nurse and Educator roles to support primary care and ARC. To demonstrate communication with Consumers and Maori on their experience of End of life and PC services in the South Island based on information obtained from the patients and their family/whānau s experience. To include key socio-demographic variables, including ethnicity and age. To provide the expertise and resources to enable patients to die in their preferred place of care. Q3 Q2 Primary palliative care surveys are being developed for PHOs, planning and funding teams and aged residential care facilities across the South Island. The aim of these surveys is to help us evaluate the current scope of palliative care provision in nonspecialist areas. PCW are consulting with national groups, for example NZed Care Association, to provide insight to the quality and direction of the surveying. PCW has provided expert subject matter input St John into the training and education of St John personnel on Palliative Care Workforce information is contained within the Hospice and Hospital reports that have gone to SPaIT and ALT. NETWORKING AND ENGAGEMENT Funding support has been confirmed to undertake the VOICES survey across the South Island. Planning is underway. It is intended that University of Canterbury will partner with the Alliance to deliver the survey and results. School of Nursing Faculty of Medical and Health Sciences University of Auckland will be a key stakeholder to the project. The mechanism through which workforce initiatives are being developed has changed. Improving Palliative Care support to Primary Care and ARC is now being progressed through Ministry funding to Hospices around new initiatives - proposals due Feb 2016 and worked up in collaboration with DHBs. PALLIATIVE CARE SERVICES 34 P a g e
35 PROGRESS AGAINST LEGEND REASON FOR DEVIATION CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION CARDIAC SERVICES MEETING NATIONAL INDICATORS Improved outcomes for people with suspected Acute Coronary Syndrome 1a 1b >70% of high-risk ACS patients accepted for coronary angiography having it within 3 days of admission. ( Day of Admission being Day 0 ). >95% of patients presenting with ACS who undergo coronary angiography have completion of ANZACS QI ACS & Cath/Percutaneous Coronary Intervention (PCI) registry data collection, within 30 days. Q1,2,3,4 Q1,2,3,4 Standardised intervention rates for ACS patients Consistently achieved across the region during the year. See Appendix 3. There has been a real commitment to completing the forms as shown by the accompanying graph in Appendix 3, particularly from December onward when the gradual decline in completion of forms was pointed out to DHBs. The region has exceeded the target at times and is almost touching the target at 94.3% For the March, April, May period. 1c 1d 2a 2b 2c 2d 2e Achieve Percutaneous revascularisation target rate of at least 12.5 per 10,000 of population. Achieve Coronary angiography target rate of at least 34.7 per 10,000 of population. Q1,2,3,4 Q1,2,3,4 Generally achieved as a region as per the most up to date figures from MoH to 31 March The South Island has consistently performed well as a region. West Coast is the only SI district which is significantly behind. See Appendix 3. Generally achieved as a region as per the most up to date figures from MoH to 31 March The South Island has consistently performed well as a region. West Coast is the only SI district which is significantly behind. See Appendix 3. Cardiac surgery targets achieved which will improve equity of access as identified and agreed by The National Cardiac Network Maintain standardised intervention rates: Cardiac surgery: 6.5 per 10,000 of population. Achieve agreed proportion of patients scored using the national cardiac surgery Clinical Priority Access (CPAC) tool, and of patients treated within assigned urgency timeframe. The waiting list for cardiac surgery remains between 5% and 7.5% of planned annual cardiac throughput, and does not exceed 10% of annual throughput. Patients wait no longer than four months for a cardiology first specialist assessment, or for cardiac surgery. >95% of patients undergoing cardiac surgery will have completion of Cardiac Surgery Q1,2,3,4 Achieved as a region as per the most up to date figures from MoH to 31 March All South Island districts are rated Not significantly different than expected rates. See Appendix 3. This has been achieved across the South Island and work to maintain it continues. This has been achieved across the South Island and work to maintain it continues. This has been achieved across the South Island and work to maintain it continues. Work on this is ongoing. Data is recorded on Dendrite registry and submitted to MoH. CARDIAC SERVICES 35 P a g e
36 3 4a 4b 5a 5b 5c registry data collection within 30 days of discharge. Monitor access rates for high risk population groups. PROGRESS AGAINST LEGEND REASON FOR DEVIATION EQUITY OF ACCESS Ensure access to angiography for high risk populations group such as Māori, Pacific and South Asian people Strategies to support access to angiography for Māori, and other high risk population groups Q1,2,3,4 HEALTH PATHWAYS Health pathway are agreed and utilised Awaiting National ANZACS QI charts for work looking at this to begin. Percutaneous Coronary Intervention (PCI) regional health pathways for acute coronary syndrome patients across the South Island Agree PCI regional HealthPathway PCI HealthPathway live and accessible on the Regional HealthPathways site. Completed accelerated chest pain pathway workshops across the South Island DHBs Agree processes and protocols for accelerated chest pain pathway Implement accelerated chest pain pathway in 3 South Island DHBs Q1 Q3 A regional pathway was agreed and submitted to pathway site. Completed and awaiting official final approval before regarded as go live. CHEST PAIN PATHWAY An agreed accelerated chest pain pathway which will reduce unnecessary admissions Q1 Q2 Q3 Workshops conducted by Martin Than. Agreement reached in the South Island for implementation of the ACPP. Pathways have been implemented in Invercargill, Dunedin, Christchurch and Nelson. 5d Implement accelerated chest pain pathway in remaining South Island DHBs Martin Than is in the process of starting a pilot chest pain pathway in the Midlands region. Completing this pilot will provide a model on which to plan future services in Southern and rural sites GUIDELINES FOR THE ARRANGED TRANSPORTING OF CARDIAC PATIENTS 6 7 Review agreed 2013 guidelines and update if required (2 year cycle). Report developed and endorsed by key stakeholders, based on meeting the less than 90 minute transport/retrieval time. Regionally agreed guidelines for the arranged transportation of cardiac patients This work has now been incorporated into Project B HealthPathways of the South Island Cardiac Model of Care. A project group has been established and draft scope is under consideration. GUIDELINES FOR THE TRANSPORTING/RETRIEVING OF EMERGENCY/ACUTE CARDIAC PATIENTS Regionally agreed guidelines for the transporting/retrieving of emergency/acute cardiac patients This work has now been incorporated into Project B HealthPathways of the South Island Cardiac Model of Care. A project group has been established and draft scope is under consideration. MINIMUM FACILITIES GUIDELINES 8 Prepare current status document of regional and rural South Island Hospitals financial and time requirements to meet minimum guidelines for cardiac facilities Review agreed 2013 guidelines and update if required (2 year cycle). This work has now been incorporated into Project B HealthPathways of the South Island Cardiac Model of Care. A project group has been established and draft scope is under consideration for the CARDIAC SERVICES 36 P a g e
37 PROGRESS AGAINST LEGEND REASON FOR DEVIATION project, but work specifically on the guidelines review has not yet started. WORKFORCE TRAINING Workforce training maintained A regional approach to cardiology nurse training developed in collaboration with the South Island Regional Training Hub. Initial focus to include: -increased exposure to cardiology during nursing training -training opportunities in New Zealand for Clinical Nurse Specialists in Cardiology Agree and implement a draft plan developed by CDHB staff. Develop and implement an action plan. Q1,2,3,4 Q3 South Island Cardiac Nurse Educators in limited rather than regular contact now due to availability of staff time. CDHB continues to develop and deliver a range of education opportunities from community to hospitals in its district and intends to extend these opportunities regionally in the future. Opportunities for training in echocardiography identified This has become a nationally led matter but will also be addressed during the project work for the SI Cardiac Model of Care. Investigate the feasibility of establishing a National Registrar training rotation that would be regionally based in line with other specialties Determine feasibility of establishing a National Registrar training rotation that would be regionally based in line with other specialties. Q3 This matter has been raised and discussed with the National Network. The logistics involved are likely to mean this matter is on hold especially as the National Network has other projects of higher priority. ECG STORAGE AND SHARING Contact maintained with National Network a 13b 13c Implement a South Island Clinical Electrocardiogram data repository and software. A common regional method of storing and sharing Electrocardiogram (ECGs) HEART FAILURE The project extended to a wider SI Cardiac Tests Repository (including ECGs). The Business Case has been approved by the Alliance and the project is expected to begin in August 2016 as one of the key projects of the SI Cardiac Model of Care. This will be reflected in the workplan. Implement locally, regionally and nationally agreed protocols, guidance, processes and systems to ensure optimal management of patients with heart failure. Determine current clinical situation of the management of patients with heart failure across South Island DHBs. Identify resources required and barriers to the management of patients with heart failure in the South Island. Utilise primary pathways for the management of patients with heart failure in all South Island DHBs. Q1 Q2 Q3 A stocktake of services and initiatives around the SI is currently underway. This has been included in the workplan and will be part of the SI Cardiac Model of Care. This has been included in the workplan and will be part of the SI Cardiac Model of Care. CARDIAC SERVICES 37 P a g e
38 PROGRESS AGAINST LEGEND REASON FOR DEVIATION FIRST SPECIALIST ASSESSMENT Assist the National Network in developing a nationally agreed standard of patient referrals for the first assessment. 14 Implement agreed standard of patient referrals for the first assessment. The National Network has begun some initial work on this and SI Workstream members are contributing to the National Network initiative where required. New work: the South Island Model of Care was developed by the Cardiac Workstream in 2015 and approved by the South Island Alliance Alliance Leadership Team in October Work is underway on the three main projects Access to Tests, Optimal HealthPathways, and Planning for Sustainability. A number of existing priorities on the 2015/16 workplan have been rolled into the Model of Care work along with new deliverables. These will be fully articulated in the 2016/17 South Island Health Services Plan. CARDIAC SERVICES 38 P a g e
39 CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION ELECTIVE SERVICES 1 2a 2b 2c 3a 3b 4 5a 5b 6a Improve equity of access, system quality and practice in selected elective service areas through the establishment of project teams. Implement South Island urology HealthPathways. Agree and implement consistent triage and prioritisation processes for urology referrals. Urology nursing practice & service delivery supports clinical consistency, equity of access and improved patient outcomes via Lippincott Procedures Manual implementation. Evaluate the first year of the service, and the local and South Island HealthPathways. Provide evaluation to the MOH. Develop South Island Model of Care and engage with key stakeholders. Agree the process for a single South Island waiting list. Fully operationalize the service across the South Island. Establish process and criteria for access to plastic surgery to bariatric patients (Body contouring following massive weight loss HealthPathway). Q1 Q2 Q2 Q1 Q2 Q2 Q2 Q2 PROGRESS AGAINST LEGEND REASON FOR DEVIATION IMPROVE EQUITY OF ACCESS TO ELECTIVE SERVICES Project teams have been established for: Urology, Vascular (national); Sustainable Cardiac Services; Colonoscopy; and Inter District Flows. Project teams are to be established for Plastics & Ophthalmology. Urology Pathways implemented. Consistent triage of patients. Protocols are in test before full adoption. Consistent nursing practice and service delivery is being supported via nursing meetings and implementation of Lippincott Procedures Manual. Bariatric Surgery Evaluation completed. HealthPathways reviewed and amended. The evaluation has been accepted by MOH. Cardiac Interventions The South Island Cardiac Model of Care was accepted by ALT in October Implementation projects underway, including Sustainable SI Cardiac Services further detail in Cardiac Services Workstream report, page 30. Infertility A single waiting list has been agreed. The service has been operationalised. Plastics The South Island will participate in the MOH-announced process for plastic surgery for bariatric patients. A national prioritisation tool has been developed. 6b Support South Island DHBs to meet ESPI targets. Q1,2,3,4 A national process is in place that has developed tools that are now being implemented. A South Island stocktake has been completed. While this and the national processes, have been underway, it was appropriate to postpone the establishment of a South Island group. This work will also link to South Island Inter-district Flows projects. Timing and readiness: national process continues; South Island Plastics will be established after full peer review of the stocktake. 39 P a g e ELECTIVE SERVICES
40 6c 6d 7 8a 8b Prepare for implementation of 3 Plastics national prioritization tools (currently in testing phase): Appearance related deformity (Breast & Body); Plastics Other; Skin Lesions, sharing learnings. Localise Plastics HealthPathways across 5 South Island DHBs. Assess the benefits of developing a sustainable Model of Care for the South Island. Assess the benefits of consistent SI preparation for implementation of the national cataracts tool (due 2016) across the South Island. Assess the benefits of consistent macular degeneration service protocols and thresholds across the South Island (NB Midland region has done similar work which may be useful). Identify requirements for a sustainable Maxillofacial workforce for the South Island. Identify baseline for Maori access (current and evidence) in selected priority areas. Collate and share innovations in the selected service areas via best practice documents and use of HealthPathways. Provide Ministry of Health with South Island Electives Programme Stage 6 final evaluation report. Q2 Q3 Q2 Q2 Q3 Q1,2,3,4 Q1,2,3,4 Q3 PROGRESS AGAINST LEGEND REASON FOR DEVIATION Prioritisation tools in test and review in South Island DHBs Plastics services. HealthPathways localisation underway, but not yet complete. Vascular South Island Vascular group yet to be established Ophthalmology South Island DHBs implementing national cataracts tool South Island Eye Health group is yet to be established. A stocktake of Eye Health services has been completed which will help inform future decisions on consistent protocols and thresholds, along with models of care. Maxillofacial This has been included in South Island Inter-district Flows Projects; a South Island group is yet to be established. Selected Elective Services Consideration of Maori access is included in selected priority areas. Innovations in selected service areas are shared between DHBs through the various working groups and stocktakes. Programme evaluation accepted by MOH. Timing and readiness Timing and readiness: South Island focus has been on service delivery and national processes South Island focus has been on Cataracts tool implementation. New work: The Electives Workstream recently began working to understand inter-district flows and the impact on DHBs, particularly Canterbury DHB s, ability to deliver elective services. This will be reflected in the 2016/17 South Island Health Services Plan. ELECTIVE SERVICES 40 P a g e
41 Work supported by the Electives Workstream: Project: National Patient Flow Owner: Nationally led The Electives Workstream will support the delivery of the following national projects: The Electives Workstream will support the delivery of the following regional initiatives: Improve access to elective services The Electives Workstream will support the South Island DHBs, individually and collectively, to achieve the Government s Health Targets and targets for EPSIs Two and Five updates on the progress against the Health Targets and EPSI s can be found in individual DHB quarterly reports. Owner: Individual South Island DHBs Reported: Individually by the South Island DHBs quarterly Maintain reduced waiting times for elective first specialist assessment and treatment Elective Services Patient Flow Indicators expectations are met, and patients wait no longer than four months for first specialist assessment and treatment, and all patients are prioritised using the most recent national tool available. Owner: Individual South Island DHBs Reported: Individually by the South Island DHBs quarterly Lippincott Procedures Manual (page 61; item 2b) Agree South Island localisation of Lippincott nursing procedures for Urology Services Owner: South Island Workforce Development Hub ELECTIVE SERVICES 41 P a g e
42 CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION MAJOR TRAUMA SERVICES PROGRESS AGAINST LEGEND REASON FOR DEVIATION SOUTH ISLAND MAJOR TRAUMA SERVICES 1a 1b 2a 2b 2c Systems and processes agreed to support people surviving major trauma and recovering with a good quality of life Agree and progress the requirements for systems and process to support the people of the South Island surviving and recovering from major trauma. Agree and develop regional clinical guidelines for the management of trauma Agree data collection systems/processes for the NZ Major Trauma Minimum Dataset Confirm required data fields for the NZ Major Trauma Minimum Dataset Commence capturing and recording data for the NZ Major Trauma Minimum Dataset A wide range of expertise across the South Island is represented on the workstream which meets regularly to consider and prepare appropriate systems and processes in conjunction with the National Network also. This is being done in conjunction with the National Network, on which the South Island is well represented. NZ MAJOR TRAUMA MINIMUM DATASET System established for South Island region major trauma data collection Q1 Q2 Q2 It has been agreed data will be collected on Midland s Collector system for an interim two years pending implementation of South Island PICS Agreement has been reached, including using National generic form. Identification of trauma nurse coordinators has enabled training, followed by collecting and entering some major cases into the national registry in four of the five DHBs, albeit very limited at this stage. 3 4a 4b 4c 5 Establish regional oversight role to ensure any actions required to contribute to NZMYMD collection are implemented Establish regional oversight role to ensure any actions required to contribute to NZMYMD collection are implemented. Identify options for clinical lead and coordinator roles across South Island DHBs within current resources. Confirm staffing configuration of the 2 South Island Clinical Hubs (Dunedin, Christchurch) Confirm staffing configuration for the remaining South Island DHBs Q2 South Island Major Trauma Workstream is established and meeting on a regular basis. CE and COO level sponsors for the workstream have been appointed. CLINICAL LEADERSHIP South Island DHBs major trauma clinical leaders; co-ordinators; and administrators appointed Q1 Q1 Q1 WORKFORCE DHBs have made a commitment to assigning trauma roles within their respective current resources, noting that they may not all act within the same timeframes. Three of the five DHBs have identified and assigned trauma roles to staff and the others are working through the process. As above. As above. Regions and DHBs are encouraged to explore opportunities for additional experience to be provided to trauma care providers at centres with more exposure to major trauma management. Develop a training plan to ensure relevant clinical staff are appropriately trained in trauma care. Q2 Subject to appointment of clinical staff as in Item 4a, 4b, 4c. Discussions have been held with National Network regarding potential training opportunities for South Island MAJOR TRAUMA 42 P a g e
43 PROGRESS AGAINST LEGEND REASON FOR DEVIATION personnel. National and Midland personnel arranged and delivered a data capture and entry training day on 5 April in Christchurch and South Island staff also attended further training in May in the Waikato. DESTINATION POLICIES Implementation of Regional Destination Policies in collaboration with DHBs, Ambulance and Air Transport providers 6 Implement Regional Destination Policies in collaboration with DHBs, Ambulance and Air Transport providers Q2 Further progress has been made between ECCT Committees and St John. Draft documents are now with the workstream for consideration. INTER HOSPITAL TRANSFER PROTOCOLS Development and implementation of inter-hospital transfer protocols. 7 Develop and implement Interhospital transfer protocols. Q2 This is being progressed in parallel with and subject to the above work ECCT committees are doing in conjunction with St John. SPINAL CORD IMPAIRMENT ACTION PLAN Acknowledge South Island DHBs intentions regarding MoH requirements as outlined in the New Zealand Spinal Cord Impairment Action Plan Recognise the development of acute supra regional spinal services and early rehabilitation pathways, (Canterbury DHB) and support as required. Links have been maintained with the CDHB coordinator, who has also attended meetings of the workstream. MAJOR TRAUMA 43 P a g e
44 MILESTONE DASHBOARD CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION PUBLIC HEALTH PROGRESS AGAINST LEGEND REASON FOR DEVIATION ALCOHOL 1a 1b 1c 1d 1e 2a 2b Monitor alcohol harm reduction efforts (e.g. Strategy development and implementation) across South Island DHBs and identifying outcome trends for DHBs and South Island communities. Agree plan for production of annual indicator reports. Identify plan for data development projects. DHB Alcohol Harm Reduction Strategy (AHRS) promotion (South Island PHP responsible). Strategies in place and implemented by all South Island DHBs (South Island DHBs responsible). Coordinated health promotion and health protection activity demonstrated South Island-wide where joint South Island activity adds value e.g. development of school policies and legal responses as needed. South Island DHBs Alcohol Position Statement and DHB Alcohol Harm Reduction Strategies (AHRS) Q2,4 Q2,4 Q2,4 Q2,4 Q2 The South Island Alcohol Working Group continues to monitor alcohol harm reduction efforts in concert with individual DHBs and is actively identifying strategies for across the South Island. Collaborative work continues with the Child Health SLA re the Emergency Department Youth Alcohol Scoping Project. Massey University has picked up the work, and has advised that they are now focusing on rolling out several SI PHP AHR indicators throughout NZ. Acknowledgement will be given to the South Island PHP. The indicator sets are now in use in each South Island PHU and are informing the AHRs. The working group continues to be ready to respond to any requests for further work in this area. Data re the Emergency Department presentations has been identified as the top priority. Meeting with ED medial staff involved in developing data system held in NM. The DHBs continue to hold responsibility for utilisation and development of their indicators to help leverage strategic development. The Alcohol in Schools document has been finalised by the SI Public Health Alcohol Network and is being used with school principals. Further coordinated activity is being identified by the SI Alcohol Work Group. TOBACCO South Island DHBs Tobacco Position Statement and joint South Island wide smokefree initiatives implemented and evaluated according to National Smokefree Coalition Action Plan. Ongoing focus on collation and review of needs analyses data to help inform process to achieve Smokefree Q2,4 Focus will be on creating joinedup process for the development of DHBs Smokefree Control Plans and seeking collaborative communication opportunities. Q2,4 Information continued to be shared between SI PHUs. Progress was significantly delayed in this area due to prolonged uncertainty due to the national realignment of Smokefree services. Te Herenga Hauora were encouraged and supported to prioritise Smokefree and subsequently endorsed a joint statement supporting World Smokefree Day on 31 May While there have been so many changes around funding and contracting for Smokefree services at national level, there has been little value in expending significant resources developing more joined up ways of operating locally. Once we have a better feel for what these proposed changes mean and what infrastructure will then exist, we will PUBLIC HEALTH 44 P a g e
45 MILESTONE DASHBOARD a 3b 3c 3d PROGRESS AGAINST LEGEND REASON FOR DEVIATION SUSTAINABILITY develop a more SI- centric approach to this area. Increased awareness around environmental sustainability and the co-benefits of action in this area for population health. Project plans implemented & monitored. Short-term: Number and quality of new initiatives Long-term: Measures of environmental sustainability with public health co-benefits. Prepare sustainability Policy / Position Statement. All South Island DHBs are members of the Green and Healthy Hospital Initiative (GGHI). Promotion of consistent environmental / sustainability monitoring systems. 1 Identify projects where specific synergies occur with public health and environmental benefit (co-benefits approach) e.g. relevant to other regional priority areas. Q3 Q2,4 Public health analysts have been allocated to work on this in 2016/2017. DHBs are at different stages regarding work on sustainability. CDHB is the most advanced but has not yet signed up to the GGHI. A stocktake of sustainability initiatives across South Island DHBs by the Sustainability Work Group is underway. This will inform subsequent promotion of consistent systems. Work is underway on this, with the stocktake of sustainability initiatives across South Island DHBs poised to make a significant contribution. RHEUMATIC FEVER South Island Rheumatic fever cases monitored The Partnership supports DHBs to have mechanisms in place to ensure the Rheumatic Fever Prevention and Management Plan is implemented as intended 4 Ongoing monitoring and collective South Island public health response to results. Q2,4 The South Island monitoring system continues for the reporting of new and recurrent cases. See Appendix 4. MĀORI 5 Public health services in the priority areas and through workforce development are responsive to Māori health issues and improve equity Work in partnership with Te Herenga Hauora to develop key messages on South Island priority public health issues as they pertain to Māori. Q2,4 Te Herenga Hauora were encouraged and supported to develop and issue a joint statement endorsing World Smokefree Day and smokefree initiatives in general. Partnered with Te Herenga Hauora supporting a focus on cervical screening for Māori as a priority for the Southern Cancer Network. OTHER HEALTH DETERMINANTS Housing 6 Support for DHB efforts to address housing where it impacts health outcomes, including multistakeholder and intersectoral engagement. Q2,4 Public health analysts have been allocated to develop position statements on air quality and warm homes. Obesity and obesogenic environments 7a Explore the impact and learnings from the two Healthy Families NZ Communities to contribute to wider South Island PHU/DHB efforts Q2,4 Meetings were held with the two Healthy Families NZ Communities, including the Well Child Project Manager. This continues to be monitored. 1 Note, public health can seek to influence here but the outcome is highly dependent on wider DHB commitment and support. PUBLIC HEALTH 45 P a g e
46 MILESTONE DASHBOARD b Review opportunities for a coordinated South Island response to obesity and obesogenic environments PROGRESS AGAINST LEGEND REASON FOR DEVIATION Q2,4 The PHP has reviewed its contribution to the South Island Healthy Weight Action Plan. Links have been strengthened between the CH SLA and SIPHP. A meeting between the Healthy Weight Clinical Advisory Group and the PHP to further discuss will take place on 8 July Contribution includes position statement work and may also include mapping of evidence based solutions. DHB position statements 8 Stocktake of South Island DHB Position statements and identification of opportunities for development of similar position statements on key public health issues e.g. Housing and Fluoridation. Fluoridation Position Statement to be rolled out in South Canterbury and Nelson Marlborough DHB first. Q2,4 The stocktake was completed. Public health analysts have been allocated to develop position statements on identified, ranked public health issues. The water fluoridation position statement is now part of a national process. Nelson Marlborough DHB adopted a Fluoridation Position Statement in August The South Canterbury DHB did likewise in March Work supported by the Public Health Partnership: Regional projects supported by the Public Health Partnership but led by other SLAs and Workstreams South Island Children s Action plan (page 20; item 1) Identify and monitor the implementation of agreed South Island regional interventions to better manage safety, reduce family violence and childhood poverty Owner: Child Health SLA Support programmes which reduce youth risk taking resulting in injury/disease from alcohol (page 20, item 4a) In partnership with the Health Promotion Agency, Child Health and Mental Health Service Level Alliances implement findings of South Island Emergency Department scoping exercise Owner: Child Health SLA Child Health Obesity Prevention programmes (page 22, item 6a) The Public Health Partnership will keep abreast of Child Health-led programmes and seek opportunities to link with a public health approach. Owner: Child Health SLA Child Health Obesity Prevention programmes (page 22, item 6b) Owner: Child Health SLA Enhance collaboration with child health dental services. PUBLIC HEALTH 46 P a g e
47 PROGRESS AGAINST LEGEND REASON FOR DEVIATION CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION STROKE SERVICES EQUITABLE ACCESS TO ACUTE STROKE SERVICES FOR THE SOUTH ISLAND POPULATION Ensure rapid access to treatment for potential thrombolysis candidates 1 2a 2b Agree and implement a system to rapidly confirm a diagnosis of stroke and identify patients who may benefit from thrombolysis therapy. Each SI DHB has a system to rapidly confirm a diagnosis of stroke and identify patients who may benefit from thrombolysis therapy and this system is implemented in each South Island DHB. Achieve 6% compliance for thrombolysis of eligible stroke clients. Q2,4 Each South Island DHB has a system to rapidly confirm a diagnosis of stroke and identify patients who may benefit from thrombolysis therapy. The South Island dashboard has had the addition of Ambulance prenotification added. Support all South Island DHBs to have stroke thrombolysis pathways Q2,4 Thrombolysis register is used in a consistent manner in South Island DHBs and reported regionally. Q2,4 Achieve 80% compliance for stroke patients to be cared for in organised stroke unit (for smaller DHBs with demonstrated stroke pathway as defined by lead Stroke Clinician). Monitor stroke access data by ethnicity and report regionally. Q2,4 South Island DHBs use standardised audit tools which are specific to delivery of Organised Stroke Services to regularly undertake quality assurance activities to inform continued improvement. Q2,4 See Appendix 5. The Stroke Workstream is jointly discussing the result in each DHB. The national data is discussed each quarter. Local stroke teams are encouraged to raise profile where able to improve the response time. Organised stroke services /units The South Island dashboard has had the addition of Ambulance prenotification added. Definitions have been developed. Two South Island DHBs are still working towards achieving the minimum standard: WCDHB has made progress and now appointed a Lead Stoke Nurse however the Lead Stroke Physician (LSP) is on leave until September with no cover for the LSP role in his absence. Whilst NMDHB has made some progress with staff appointments, gaps in service remain with limited ability for any allied health assessment in the acute medical service and no Lead Stroke Nurse. Organised stroke services are accessible and appropriate for Māori and Pacific people Q1,2,3,4, Data is being reviewed each quarter. No trends are evident as numbers are very small. Support Participation in Stroke Audit The Stroke Workstream has developed an audit Position Statement that recommends all South Island DHB Stroke teams have goals for audit of stroke service for each year and document their priorities for audit. 47 P a g e STROKE SERVICES
48 PROGRESS AGAINST LEGEND REASON FOR DEVIATION 6 South Island DHB are supported to develop policies and protocols - utilising technology /distance expertise /transport to support isolated communities to deliver best practice stroke care. All South Island DHBs now have access to a web-hosted stroke audit tool that is based on the Australian National Stroke Foundation Acute Stroke Audit (2013). A plan for each DHB to use this tool is being finalised. CDHB has completed an audit of stroke acute and rehabilitation service using this tool. Learnings and opportunities for improvement are to be shared with other DHBs. NMDHB has done a charts review of last 150 stroke discharges. Findings and opportunities for learning were shared with other South Island DHBs in April SCDHB has completed an audit of part of the service. Learnings and opportunities for improvement are to be shared with other South Island DHBs. Risks and mitigation strategies for geographic isolation Q3 Modification of the CDHB TIA protocol for appropriate use in WCDHB is being progressed. SCDHB has modified and adopted a CDHB protocol. INTEGRATED STROKE REHABILITATION SERVICES FOR THE SOUTH ISLAND POPULATION System used to measure agreed stroke rehabilitation targets / indicators. 7 South Island DHBs deliver inpatient and community stroke rehabilitation services which reflect best practice and are regionally consistent. Q2,4 DHBs are able to measure the proportion of all stroke admissions who are referred to community rehabilitation. However there is no known process to measure the percentage of above who receive a face to face community rehabilitation session within 5 working days after in-patient discharge. This measure is needed for and resolution to this issue is being explored. WORKFORCE PLANNING AND DEVELOPMENT Named stroke specialist/s within the inter-disciplinary team Each South Island DHB has a named lead rehabilitation clinician for stroke rehabilitation. A contact list has been developed. Named lead stroke physician & nurse in each DHB with specific remit to develop and improve Stroke Services for that DHB Each South Island DHB has a named lead stroke physician with specific remit to develop and improve Stroke Services for that DHB There is currently a Lead Stroke Physician in each SI DHB. Name lead stroke nurse in each DHB with specific remit to develop and improve Stroke Services for that DHB Each South Island DHB has a designated Lead Stroke Nurse who has assigned non clinical hours to South Island DHBs are continuing to work towards achieving this: 48 P a g e STROKE SERVICES
49 11 achieve the Stroke Nurse role. Including developing and improving the Stroke Service. (In small centres it may not be a fulltime position). PROGRESS AGAINST LEGEND REASON FOR DEVIATION SCDHB and CDHB have Lead Stroke Nurses in place. WCDHB has now appointed a Lead Stroke Nurse. NMDHB has no Lead Stroke Nurse. SDHB - Dunedin has a Lead Stroke Nurse, but not Southland. Health professionals have access to continuing education for acute, rehabilitation and long-term/chronic stroke management South Island Stroke teams have access to a range of educational opportunities to support continued development of knowledge and skill in delivering best practice stroke services. Q1,4 South Island Stroke Study Day was held on 26 November 2015 organised jointly by the Alliance and Southern Stroke Foundation. 290 people attended in person or by VC. This provided 6.5 hours of stroke specific education. Local teams are organising further sessions. STROKE SERVICES 49 P a g e
50 PROGRESS AGAINST LEGEND REASON FOR DEVIATION CLINICAL SERVICES: SUSTAINABILITY & CLINICAL INTEGRATION HEPATITIS C EQUITABLE ACCESS TO INTEGRATED HEPATITIS C SERVICES FOR THE SOUTH ISLAND POPULATION Review and assess the current state of hepatitis C services and the current service delivery model across the South Island Compare the review with the learning and developments from Central and Midland regions Establishment of clinical care pathways and their inclusion in electronic health pathways Assessment of clinical and diagnostic capacity and capability requirements Development and delivery of an implementation plan for the region Understand and agree options to support the development of an Integrated Hepatitis C service Q1 Q3 Q3 (amended to ) (amended to Q1 2016/17) Current hepatitis C services on the South Island have been reviewed and assessed South Island Alliance has been in regular contact and continue to liaise with Central and Midland regions. The approach in the South Island will be different as there has been no pilot programme here. A current state analysis has been completed. This has informed the development of a draft business case which is undergoing approval within the South Island Alliance before being offered to MoH for agreement. Further advice has been provided by PHARMAC and the national advisory group on 1st July In accordance with MoH advice, SIA will and Update the clinical hepatitis C pathway to reflect PHARMAC s new access criteria for direct acting antiviral treatments Complete preparations for implementation of the clinical hepatitis C pathway across the region Assessment has been completed. MoH have been informed of diagnostic capacity and capability requirements, especially the need for portable liver elastography scanning facilities if the South Island is to address the deliverables in the draft 2016/17 service specifications. An implementation plan and business case will be agreed with MoH. HEPATITIS C 50 P a g e
51 KEY ENABLERS QUALITY & SAFETY PROGRESS AGAINST LEGEND REASON FOR DEVIATION OPEN FOR BETTER CARE Reducing Perioperative Harm 1a 1b Support South Island DHBs to participate in the HQSC roll-out of the team work and communication interventions. Support South Island DHBs to prepare for the implementation of the new national Quality & Safety marker. NMDHB and CDHB are both in Cohort 2. Cohort 2 is in implementation phase. SDHB, SCDHB and WCDHB are cohort 3. Their auditor training was held in May. From 1 July the trained auditor teams in each DHB will start collecting the quality and safety marker data. PROMOTING SAFETY FRAMEWORK Safety 1 st 2a Provide governance to the implementation of Safety 1 st including: identifying quality & system improvements; future planning & extension to primary and community care. The incident management component of Safety1st is in use in all five South Island DHBs. The Feedback Module is in various stages of roll out. The Risk Module is currently in the testing phase. Each South Island DHB will roll this out into their DHB themselves, it will not be a regional rollout. A regional change procedure and regional change request forms have been developed Changes to Safety1st taxonomy continues following recommendations from the Safety1st Health Check. The Safety1st Board met on 14 June 2016 and have recommended the project close. Additional modules can be released as business as usual and undertaken as projects. It has been identified that a project manager will be required to develop a business case and framework for the roll out of Safety 1st into Primary and Community Organisations. A resource request application for this has been submitted to the South Island Alliance. The resource request is for 2016/2017 therefore this action has been transferred to the 2016/2017 work plan. 2b 2c Capture learnings from implementation and utilise to inform ongoing quality and service improvement. Inform and develop system capability and improvement by robust review & analysis. The Safety 1 st Post Implementation work shop was held on 4 December A report on this has been written. The Health Check of the Incident reporting component of Safety1st is complete. The Health Check involved a survey of South Island District Health Boards staff, analysis undertaken by the vendor, review of the Safety1st data and a Safety1st Health Check Workshop. A key outcome of this health check is the changes identified as required to be made to a number of the forms. These changes are in progress. PARTNERS IN CARE Consumer involvement 3 Consumer involvement in South Island Alliance. Consumer Engagement stocktake for South Island Alliance has been completed. 51 P a g e QUALITY & SAFETY
52 PROGRESS AGAINST LEGEND REASON FOR DEVIATION Stock take for the South Island has been completed. HQSC and NMDHB models for consumer engagement have been reviewed. The Q&S SLA has made recommendations for consumer engagement in the South Island Alliance. The recommendations will be discussed with SPaIT and others within the Alliance in Q CLINICAL GOVERNANCE 4a 4b South Island DHBs, working together, support the HQSC Clinical Governance Framework development. Agree South Island approach to implementation, with tailored localisation as appropriate. Work on this has not yet commenced See Item 4a. The HQSC are finalising a draft document which has not yet been circulated for consultation. This has been carried over to the 2016/2017 Quality and Safety SLA Work plan. Work supported by the Quality and Safety Service Level Alliance: REGIONAL INITATIVES Open for Better Care campaign Implement and support the Open for Better Care national patient safety including: falls, hand hygiene, SSI and Medication Safety Owner: Individual South Island DHBs Reported: Individually by the South Island DHBs quarterly 52 P a g e QUALITY & SAFETY
53 PROGRESS AGAINST LEGEND REASON FOR DEVIATION KEY ENABLERS INFORMATION SERVICES 1 IS SLA Portfolio Management Further establish the IS SLA s Portfolio Management framework to enable the successful delivery of the Health Service Plan. Agree and implement the IS SLA portfolio management framework The IS SLA has devoted time and energy to developing the Portfolio management tool. An initial meeting, organised by the IS SLA, has been held with SI CFO s. CFO s have endorsed the value of these meetings and it has been agreed that these will occur on a regular basis, with IS becoming a standing agenda item. A Regional Hosting Agreement framework has been developed and is currently being progressed amongst key stakeholders for sign-off. The framework provides the SI DHBs with a generic set of principles that will sit over all regionally hosted solutions, each solution will have its own Service Level Schedule attached to the framework. The IS SLA have developed a regional costing/support model for HCS, this model has been endorsed by all key stakeholder groups and will be adopted for use in the 2016/17 financial year by the SI DHBs. Scoping and feasibility and Business case approval frameworks have been developed and endorsed by the IS SLA. The IS SLA have endorsed the standardisation of a number of key portfolio management aspects. These include: Reporting template Risk/issues registers Standardised Steering Commitment (structure, ToR) Decision making matrix The IS SLA have hosted a number of workshops with the SI CIOs to formalise the SI informatics strategy. These included: BAU/Support models Operationalising the IS work programme, through workforce maximisation. A number of key actions have been identified from this workshops and will be progressed over the 2016/17 financial year with the CIOs and IS SLA, as the SI DHBs look to maximise workforce utilisation and agree BAU/Support models for the regional portfolio. The IS SLA have collated a single view of South Island IT projects INFORMATION SERVICES 53 P a g e
54 PROGRESS AGAINST LEGEND REASON FOR DEVIATION REGIONAL PROJECTS HealthOne HealthOne enables pharmacists and other authorised clinicians to view patient information that is shared between multiple healthcare providers, including test results, allergies, prescribed and dispensed medications together with hospital information. Progress HealthOne Business Case and Financial Model for South Island. Progress implementation planning for SDHB Progress implementation planning for NMDHB Progress roll-out of HealthOne across the Region Establish a South Island TeleHealth Strategy Progress with defining requirements and scope for a regional ED solution. Q1,3 Q3 Q3 Each South Island District Health Board (SI DHB s), with the exception of Nelson Marlborough District Health Board, has progressed business cases and implementations locally with approval being given from either their respective local DHB Board or as part of local Chief Executive delegated authority. On the advice of the Technology and Digital Services division of the Ministry of Health (formerly the National Health IT Board) the SI DHB s will proceed with a local business cases to support the implementation of HealthOne The Technology and Digital Services division of the Ministry of Health have requested that the SI DHBs provide an overview of DHB investment for HealthOne as the regional product including any future investment profile of the product working on the assumption that all DHBs will at some stage in the future implement the regional instance of HealthOne. SDHB HealthOne implementation planning in progress. Dependency on HCS delivery date. HealthOne implemented in SCDHB in November TeleHealth To scope and define a TeleHealth regional direction for the South Island Q1,3,4 (carried over to ) ED Whiteboard Provide a regional solution to support visibility of ED activity. Q2,3,4 Requirements have been defined. It has been agreed that the scope of SI PICS is limited to the delivery the administration component of an ED Information System, this functionality will be available for CDHB Phase 2. The IS SLA will develop a position statement on how it intends to address the At this stage NMDHB will not be progressing a local HealthOne implementation. NMDHB implementation planning will proceed when the local business case approval has been received and funding is available to support the implementation. The IS SLA have reprioritised the focus on this work plan item and will not be in the position to achieve this deliverable for 2015/16 due to resourcing availability. The deliverable has been rebased and included in the 2016/17 IS SLA work plan. 54 P a g e INFORMATION SERVICES
55 PROGRESS AGAINST LEGEND REASON FOR DEVIATION requirements associated with clinical functionality in 2016/17. Patient Portal To implement a Patient Portal that helps patients be involved in their care. It also ensures clear communication resulting in a better patient experience and improved patient outcomes. The IS SLA to agree a regional patient portal solution for the South Island. Project scoping and agreement of regional direction. Project scoping and agreement of regional direction. Scope regional mobility strategy. Q2,3,4 eordering of Laboratory Tests To implement a fully electronic laboratory ordering process. (carried over to ) eordering of Radiology Tests To implement a fully electronic radiology ordering process. (carried over to ) Q3 (carried over to ) Mobility Strategy To define the South Island regional mobility strategy Initial Data Store to address SI PICS Requirements The IS SLA continue to support the PHO s to progress patient portals, with the understanding that the requirement exists to connect to or integrate with existing portals to realise the vision of providing patients with access to patient scheduling, through PICS. At this stage this piece of work is being progressed individually by the SI PHOs and is not a current focus for the IS region programme of work. Due to the complexity of this piece of work and a number of existing dependencies (i.e. RPI, HCS, licencing, resourcing, Business Case, Standardising ordering processes across the SI, confirming operational costs, regional contract) that need to be completed/achieved prior to commencing this project the timeframe for delivery will be carried over to 2016/17 First steps will include defining readiness for regional deployment. CDHB Radiology are currently using eordering. A regional process is being developed to support the implementation of eorders across the remaining SI DHB s. This deliverable will be rolled-over into 2016/17. RPI needs to be implemented before we implement this. The IS SLA have reprioritised the focus on this work plan item and will not be in the position to achieve this deliverable for 2015/16 due to resourcing availability. The deliverable has been rebased and included in the 2016/17 IS SLA work plan. An initial warehousing solution for CDHB and NMDHB for future SI PICS requirements, which has potential to form the foundation for a future regional warehouse approach To consolidate basic warehouse requirements for CDHB and NMDHB into a single solution that can be used to meet the Q1,2,4 NMDHB and CDHB have agreed to adopt a single data source to address reporting requirements from within SI PICS. The Project Initiation Document to outline the INFORMATION SERVICES 55 P a g e
56 warehousing requirements for the South Island PICS solution. PROGRESS AGAINST LEGEND REASON FOR DEVIATION overall approach, scope, timeframe and financial impact has been developed and circulated to the IS SLA for review. Reporting capability is to be developed out of existing data warehouse solution. The build will provide a platform for other DHBs to utilise with the implementation of SI PICS. emedicines PROGRAMME eprescribing and Administration (epa) Implementing epa into inpatient wards across the South Island DHBs (incorporating NZULM & NZ Formulary when sources are available) with the aim of improving medication safety for patients whilst an inpatient 10a 10b 10c 10d 10e Southern DHB eprescribing and Administration project complete. Canterbury DHB eprescribing and Administration project progressed. 2 South Canterbury eprescribing and Administration DHB project complete. West Coast DHB eprescribing and Administration progressed. 3 Nelson Marlborough DHB eprescribing and Administration project progressed. 4 (amended to Q ) The SDHB roll-out to adult beds has been completed. CDHB have experienced delays to their rollout of MedChart, with completion due in September this year. Plan to implement Paeds when bugs fixed for SDHB. ED will follow after next MedChart upgrade which enables mobility functionality. Costing phase for implementation planning has commenced. WCDHB implementation to follow on from CDHB implementation utilising the core project resources from to expedite the implementation. Costing phase for implementation planning has commenced. Implementation to be completed by end of 2016/17. emedicine Reconciliation (emr) The Paediatric implementation will be progressed when SDHB have recruited to the vacant Pharmacist role. Slight deviation to plan caused by App issues, and the Mobile Device Management (MDM) solution not being ready to be implemented. Implementing electronic Medication Reconciliation across South Island DHBs. emr helps health professionals create the most accurate and up-to-date list available of a patient s medicines on presentation to hospital (incorporating NZULM & NZ Formulary when sources are available) Complete the implementation of emedicines Reconciliation within Canterbury DHB and commence implementation planning for remaining South Island DHBs CDHB are currently rebasing the project planning to determine implementation progression order following the Burwood implementation. epharmacy Management (epm) Due to resource issues CDHB have had to down scale the implementation of emeds Rec in order to attain implementation of epa. Implement epharmacy into South Island DHBs using a single Regional instance (incorporating NZULM & NZ Formulary when sources are available) to enable the management of medications from a shared South Island perspective Define requirements, scope and progress Regional Business Case for an epharmacy Management Solution for the South Island. CDHB epharmacy upgrade is progressing. The epm requires the CDHB instance to be multi-campus; it is anticipated that this functionality will be available Q3 2015/16. The Regional defining of requirements, scope and development of a business case has not started as the SI have decided to complete a review of the model of service delivery for hospital pharmacy services. This item is on hold until this review has been completed and recommendations agreed. Due to resource issues CDHB have had to down scale the implementation of epm in order to attain implementation of epa. 2 Dependency on release on NZULM from vendor 3 Dependency on release on NZULM from vendor 4 Dependency on release on NZULM from vendor INFORMATION SERVICES 56 P a g e
57 PROGRESS AGAINST LEGEND REASON FOR DEVIATION A potential delay to completing the epa and emr rollouts has been identified, as both projects are currently utilising the same resource pool. erefferals PROGRAMME Complete regional Stage One implementation of ereferrals for SDHB and NMDHB. Complete regional Stage Two implementation of ereferrals for SDHB and NMDHB Stage 1 Regional implementation of Stage 1. ereferrals received by ERMS via fax. Q1,2,3 SDHB - The 59 WellSouth MedTech practices have ERMS installed. The 8 remaining MedTech practices are with South Link Health and use the BPAC solution. NMDHB - 100% complete Profile Integration work expected to be completed by December and roll out in Feb/March Stage 2 ereferrals received through the RMS module in Health Connect South. Q3,4 Stage 3 Stage 2 implementation of ereferrals into SDHB and NMDHB is dependent on the Regional instance of HCS to be implemented first. SDHB and NMDHB will not be completed in 2015/16. There is high likelihood, SDHB and NMDHB will skip Stage 2 and go directly to Stage 3. Implementation etriage - ereferrals received through the RMS module in Health Connect South with triage functionality. Pilot implementation of Stage 3 with Canterbury DHB. Once pilot is complete progress with regional implement.ation Q2 Pilot complete in CDHB, second part of Pilot kicked off with WCDHB. Regional business case approved, all DHB s on the Roadmap for implementation to be completed by Feb HEALTH CONNECT SOUTH PROGRAMME Regional Programme 16 Functional development and enhancements for the regional Health Connect South instance. Release 41 delivered in December Release 42 delivered in February Release 43 delivered in March Release 44 delivered in April Southern HCS Implementation 17 Complete Southern DHB s Health Connect South implementation. 5. Q3,4 (Q1 2016/17) The SDHB project has been re-planned into a phased approach. Demographics are live, and encounters due to be introduced in the next 4 weeks. Radiology and laboratory results are now live feeding, with backloads in progress. Cardiology reports live feeding. Alerts functionality in progress. Document templates being created in SMT and SMTr/Meddocs The re-planned phased schedule is progressing well. Nelson Marlborough HCS Implementation 18 Complete Nelson Marlborough DHB s Health Connect South implementation. Q2,3 (Q2 2016/17) Waitlist, Referrals and Outpatients still to be developed and loaded. Issues identified with Waitlist messages, requiring some rework. Re planning required. 5 Dependency on SMT solution 57 P a g e INFORMATION SERVICES
58 PROGRESS AGAINST LEGEND REASON FOR DEVIATION 19 To fully implement fedischarge for all South Island DHBs. edischarges (National Transfer of Care) To implement the National Transfer of Care template to create standardisation. SOUTH ISLAND PATIENT INFORMATION CARE SYSTEM (PICS) The IS SLA propose to move this to operational delivery within the HCS programme, and rather than implementing a standardised template would look to ensure that all existing electronic discharge summaries have the required information and aligns to the National Standard. Regional Programme 20 Supporting the first implementation of SI PICS and define the Second Phase of the solution. Q1,2,3,4 Software delivery schedule has been updated by Orion. The programme has undertaken a re-planning exercise. Canterbury DHB Implementation Go-live Phase I and prepare for implementation into the balance of Canterbury DHB sites. Go live with Outpatient functionality at the Burwood facility Software was received from Orion Health in April covering the outpatient functionality needed for the Burwood facility. This software was extensively tested, data was migrated, users trained and the software was taken live in June. 21 Along with the new software, staff were moved into a new facility, with new processes and ways of working. Whilst some teething problems have been experienced, the transition has been relatively smooth, with users experiencing a far richer operating environment, with much more efficient transaction processing capabilities. Go live with Inpatient functionality at the Burwood facility This has not been achieved and has been rescheduled as part of the programme replanning. Software delivery timeframes were not able to be met by the vendor Nelson Marlborough DHB Implementations 22 Project go-live for Nelson Marlborough DHB. This has not been achieved and has been rescheduled as part of the programme replanning. Software delivery timeframes were not able to be met by the vendor. South Canterbury DHB Implementation 23 Prepare for SI PICS Implementation. West Coast Implementation 24 Prepare for SI PICS Implementation. Southern DHB Implementation 25 Prepare for SI PICS Implementation. Work supported by the Information Services, Service Level Alliance: National projects enabled by the IS SLA but led nationally or by DHBs or by other South Island Workstreams: INFORMATION SERVICES 58 P a g e
59 Project: National Trauma Minimum Dataset (page 43, item 3) Owner: South Island Major Trauma Workstream Project: National Infrastructure Programme Owner: Nationally led Project: National Patient Flow Owner: Nationally led Project: National Maternity Solution Owner: Nationally led and implemented by individual DHBs Regional projects enabled by the IS SLA but led by other SLAs and Workstreams: Project: elearning (page 61, item 1) Support the regional elearning implementation led by South Island Workforce Development Hub. Owner/Lead: South Island Workforce Development Hub Project: Safety First (Risk Management Project (RL6) (page 52, item 2a) To implement a regional Risk Management solution. This will include reporting of incidents, risks and enables shared clinical learnings from outcome reviews. Owner: Quality and Safety SLA Project: Advance Care Plan (page 33, item 11) Implement an electronic Advance Care Plan accessible to all health care clinicians. Owner: Health of Older Peoples SLA Project: Growth Charts (page 23, item 7) To implement a growth chart solution to replace paper-based forms. Owner: Child Health SLA Project: South Island Clinical Cancer Information System (page 19, item 8a) Implement proposed cancer informatics working group structure. Owner: Southern Cancer Network Project: Mental Health Module (HCS) (page 29, item 12) To standardise Mental Health workflow to create a trusted source of patient care information. (HCS) Owner: Mental Health and Addiction SLA Project: South Island Electrocardiogram Clinical Data Repository (page 38, item 12) To implement a South Island Clinical Electrocardiogram data repository and software to allow all five South Island DHBs to upload clinical data regardless of the end devices Owner: Cardiac Workstream INFORMATION SERVICES 59 P a g e
60 MILESTONES DASHBOARD PROGRESS AGAINST LEGEND REASON FOR DEVIATION KEY ENABLERS THE WORKFORCE DEVELOPMENT HUB 1 2a 2b 3 4 A common elearning platform is available to all DHB staff. Nursing Nursing Community of Practice has identified and prioritised a regional suite of 2 elearning packages. Nursing Lippincott on-line evidenced based clinical procedures has been introduced to all South Island DHBs. Interprofessional A coordinated clinical simulation network for the South Island is established. Interprofessional The opportunities for interprofessional learning in a clinical environment are increased. An elearning platform and eportfolio is accessible to the health workforce across the South Island. Resources have been approved to roll out elearning platform across the South Island. This will commence 4 th July and work will continue under the 16/17 RSP. e-learning packages and teaching resources across the South Island A regionally representative group has been developing a South Island suite of Intravenous learning packages. Final drafts were reviewed at the November meeting for some of the modules. There are national guidelines for independent vaccinators and approval is required by the Medical Officer of Health in each Public Health Unit. The South Island is adapting CDHBs Speaking Up education resource content into their education programmes. This has now been made available across the South Island. Respiratory Clinical Nurse Specialists have completed the respiratory elearning package. Work has commenced on a regional cardiac long term condition elearning resource. Agreement has been reached for this to be extended to an interdisciplinary group. To date there have been over 76,207 hits on the Lippincott site across the South Island. In the community it has been rolled out to 69 organisations so far, including six Māori NGOs in Canterbury. The national discussion around a Memorandum of Understanding and a national Lippincott contract continues. Clinical simulation is accessible to staff working in the smaller centres and rural areas of the South Island. The working group and the SIWDH Steering Group are determining the next steps and the development of an action plan. Work will continue in the 16/17 RSP. Regional coordination and development of Interprofessional learning As a follow up from the workshop in March, an action plan and South Island principles have been developed. Work will continue in the 16/17 RSP. 60 P a g e WORKFORCE DEVELOPMENT
61 MILESTONES DASHBOARD PROGRESS AGAINST LEGEND REASON FOR DEVIATION 5a 5b 6a 6b 6c 6d 6e Career Events All HWNZ funded trainees have access to career guidance and a career plan aligned to individual aspirations and future workforce needs. Medicine Support the DHBs to integrate the increased number of PGY1s (NZ citizens and permanent residents) into the workforce. Nursing Specialist Nurses are available to perform colonoscopies as required. Nursing The role of the Clinical Nurse Specialist is expanded as identified by the Nursing leaders in the South Island. Nursing Nursing sustainability Strategy and planning supports older nurses in the workforce to maximise their contribution. Nursing The Aged Residential Care Gerontology Acceleration Nursing Programme (GAP) has been implemented in a further South Island site (currently operating in Canterbury). Kaiawhina workforce Allied Health Assistants (AHAs): Implement a delegation model for AHAs (Calderdale framework). 6 Support all South Island HWNZ funded trainees to make appropriate career choices Q1,2,3,4 Q2 Careers fairs for post grad education have been held in Nelson, Marlborough Canterbury and South Canterbury. Southern has hosted a career fest for high schools. The November 2015 intake has achieved the South Island share of the national pool of PGY1s. Planning has commenced for the November 2016 intake. South Island vulnerable workforces are identified and plans established to mitigate these A Clinical Nurse Specialist from Southern DHB has commenced Nurse Endoscopy training. Work will continue in the 16/17 RSP. Legislation for this extended scope of practice for registered nurse prescribing is currently being drafted. Lippincott has provided the opportunity to establish 18 Clinical Nurse Specialist/Educator Expert Groups across South Island and Midland regions to collaboratively review and develop clinical procedures. A suite of regional tools to support the nursing workforce are being developed. Roster guidelines have been completed. A guide for Handling health concerns (nursing and midwifery) eg physical disability and cognitive impairment, has been drafted and circulated for comment. Work will continue in the 16/127 RSP. Child Health in Canterbury DHB is about to commence a child health programme mirrored on the GAP programme. Nelson Marlborough DHB is also investigating the possibility of a GAP programme. Also refer to 10b. Calderdale Framework (CF) 6 projects underway in a variety of clinical settings include delegation to AHAs. Development of 33 Clinical Task Instructions for AHAs & related workplace training resources has begun alongside current CF projects. AHAs have attended Awareness Raising & Foundation training where appropriate. 6 Subject to funding approval WORKFORCE DEVELOPMENT 61 P a g e
62 MILESTONES DASHBOARD PROGRESS AGAINST LEGEND REASON FOR DEVIATION 6f Kaiawhina workforce Allied Health Assistants (AHAs): AHAs have access to appropriate NZQA level 3 training. Regionally 52 AHAs have completed their Level 3 training since October 2013 with a further 22 in training, using the new Health Assistant strand of the new Health & Wellbeing Level 3 qualification. Level 4: initial discussion underway for scoping delivery of Level 4 regionally. 6g Sonography The number of Sonography trainees has increased to meet the identified South Island need from 2 to 4. South Island representation on the national Sonography group. Trainee numbers continue to be monitored. Currently 4.5 trainees in public and 6 in private. 6h Midwifery Midwives are recruited into hard to staff areas in the South Island. There is now one South Island recruitment process for new grad midwives. Will continue to monitor midwifery recruitment issues. 6i Rural Health The opportunity of a regional rural health medicine training programme is explored. Ashburton and the West Coast are currently reviewing their medical model of care with the aim of increasing rural hospital medicine specialists. A regional meeting has been held and a stocktake of current RHM specialists and trainees is about to commence. 6j Medical Physicists The South Island has sufficient Medical physicists to meet its clinical need and this will continue to be monitored. Ongoing monitoring of medical physicist numbers in the South Island. No workforce issues currently in the South Island. Participating in the national discussion. 6k Cardiac Physiologists Training, recruitment and retention of cardiac physiologists is supported. Ongoing monitoring of cardiac physiologist numbers in the South Island. No workforce issues currently identified in the South Island. Participating in the national discussion. 7a 7b Development of primary and secondary care health workforce to support shift in care to be more community based PGY 2 rotation into general practice & community to meet the new pre vocational curriculum criteria has commenced. Nurse Practitioner (NP): NP roles have increased across the South Island in identified areas of need. Q1,2,3,4 Canterbury, South Canterbury, Nelson Marlborough and West Coast DHBs have commenced community placements. Evaluation of CDHBs pilot projects is about to be published. Southern DHB are planning their first placement to commence August 2016 and further placements are planned. National nurse practitioner survey undertaken by SIWDH complete. This information is now part of a toolkit for Executive Directors of Nursing for developing clinical pathways for nurse practitioners in identified areas of need. 62 P a g e WORKFORCE DEVELOPMENT
63 MILESTONES DASHBOARD PROGRESS AGAINST LEGEND REASON FOR DEVIATION Practitioners Nurse Practitioner numbers have grown from 11 in 2010 to 35 in 2016 with a further 12 on identified pathways. The increase in numbers has been to the identified priority areas of mental health, primary care, palliative care and aged residential care. Increase participation of Māori in the clinical workforce Māori Increased number of Māori working in health. Te Herenga Hauora are currently updating their Maori Workforce Strategy and SIWDH will support their action. Slow progress for this year however we expect this to gather momentum in 2016/17. 8 We continue to liaise with the South Island Kia Ora Hauora Programme Director to help support Kia Ora Hauora health graduates into new graduate positions in the South Island. Increase participation of Pacific People in the clinical workforce 9 Pacific Increased number of Pacific working in health. A clear pathway for Pacific workforce data and development has not yet been identified. Pacific Lead in the Ministry has provided some South Island Pacific contacts which are currently being followed up. South Island contact follow up has been hampered by the resignation of the CEO of Pacific Trust. Awaiting new appointment. Regional collaboration to further strengthen clinical leadership 10a Midwifery A pathway has been developed for future clinical Midwifery Leaders. SI Midwifery leaders have agreed to support development of a pathway for future clinical midwifery leaders. This has been escalated to the National DHB Midwifery Leaders for further development. Further review of programmes already underway and established overseas, specific to Midwifery, has commenced. 10b Allied Health Scientific & Technical A model of professional skill sharing and delegation across AH professions has been implemented. Q2 Also Refer to 6 e. 8 Calderdale Framework Facilitators completed all Facilitator training requirements in April further Facilitator is in training. Planning for training a further cohort of Facilitators underway and budget approved. Interim reports for 5 projects in 4 DHBs delivered in April projects active in 5 DHBs. 10c Allied Health Scientific & Technical A regional clinical/professional leadership role is identified and Regional DHB Speech Language Therapy Leaders network meets monthly. Initial Action Plan included the identification of 63 P a g e WORKFORCE DEVELOPMENT
64 MILESTONES DASHBOARD PROGRESS AGAINST LEGEND REASON FOR DEVIATION implemented for an Allied Health profession. highest risk clinical areas regionally. Regional SLT clinical working group is meeting to ensure the delivery of a regional paediatric dysphagia service. Dysphagia service which in the future may include the establishment of a regional clinical leadership role. Audiology has been identified as the second AH profession to consider. Stakeholder consultation and a regional Audiology Leaders network established with the first meeting scheduled for late July. 11 Registered Nurses South Island new graduate nurses have participated in a NetP (New entry to practice) programme. Provision of 1 year internship for nursing graduates Review is underway of the content of the NetP programme to meet the broader needs of the South Island health sector. Development of South Island Health Library Services 12 SIWDH explore the development of a South Island wide consortium to provide access to learning resources. Stock take of current South Island resources, staffing, costs and duplication has been completed and is currently being reviewed. Work supported by the South Island Workforce Development Hub: Regional projects enabled by SIWDH but led by other SLAs and Workstreams South Island vulnerable workforces (Mental Health & Addiction)are identified and plans established to mitigate these (page 28, item 11a) Mental Health & Addictions workforce meets the identified health needs and is fiscally responsible. Owner: Mental Health and Addiction SLA Mental Health e-learning packages and resources across the South Island (page 28, item 11b) Mental Health Core Education Group have identified and prioritised a regional suite of elearning packages. Owner: Mental Health and Addictions SLA Understanding the Palliative Care workforce requirements (page 35, item 3c) Understand the current PC workforce delivering PC in the community(s)and identify any workforce development opportunities Owner: Palliative Care Workstream A regional approach to cardiology nurse training developed (page 38 item 9) Agree and implement a draft plan developed by CDHB staff Owner: Cardiac Workstream Opportunities for training in echocardiography identified (page 38, item 10) Action plan developed and implemented. Owner: Cardiac Workstream Investigate the feasibility of establishing a National Registrar training rotation that would be regionally based in line with other specialties (page 38, item 11) Determine feasibility of establishing a National Registrar training rotation that would be regionally based in line with other specialties Owner: Cardiac Workstream WORKFORCE DEVELOPMENT 64 P a g e
65 MILESTONES DASHBOARD PROGRESS AGAINST LEGEND REASON FOR DEVIATION KEY ENABLERS SUPPORT SERVICES PROCUREMENT AND SAVINGS Achieve and report savings in line with nationally agreed methodology 1a 1b 2 Aggregate procurement requirements and improve purchasing power (using nationally agreed methodology) Develop and adhere to the regional procurement plan and policy (for non-health Alliance out of scope). Savings of $3 million (using nationally agreed methodology) reported during the year through the South Island Procurement and Supply Chain workstream. Agree and implement opportunities where appropriate. Q1,2,3,4 Q1,2,3,4 Procurement teams have adapted to working with new agencies but there has been limited regional work. Procurement teams are reporting savings using agreed national methodology and have met savings targets. SI Procurement managers have expressed concerns to ALT regarding healthalliance s significant under performance against their expected outcomes. HPL has acknowledged healthalliance s underperformance and is now working with DHBs to return procurement work to the DHB teams. Opportunities for joint ventures with providers of services Q3 Ongoing work through the procurement sector. The workstream has established a formal relationship with HPL to enhance its work. Chris Marandola, General Manager of Commercial Services, has been appointed HPL s representative on the South Island workstream. PROJECT AND SAVINGS COLLABORATION WITH OTHER WORKSTREAMS OF THE SLA 3 4 Increase rationalisation and standardisation of products and services. Projects active and achieved through collaboration with other agencies for example DHBs, health Alliance, Pharmac, MOBIE. Align with the target of collective procurement driven by national agencies Q1,2,3,4 Achieved but see note under Item 1b. MANAGE CHANGE IN CONJUNCTION WITH NATIONAL AGENCIES FOR LOCAL AND REGIONAL BENEFITS Q3 Achieved but see note under Item 1b. INCORPORATE SUSTAINABILTY PRACTICES 5 Sustainability practices acknowledged in workstreams. Q1 Workstreams incorporate sustainability practices Facilities Maintenance Workstream has shared, encouraged and practiced sustainable health care initiatives including energy initiatives, lighting, waste reduction and a decrease in carbon emissions. 65 P a g e
66 MILESTONES DASHBOARD PROGRESS AGAINST LEGEND REASON FOR DEVIATION ST JOHN REGIONAL AGREEMENT FOR PATIENT TRANFSER SERVICE (PTS) Assistance given to develop and implement a new Regional PTS agreement between South Island DHBs and St John 6 Facilitate the annual review of the regional PTS agreement negotiated between the South Island DHBs and St John. Complete annual review of the regionally co-ordinated PTS agreement. Q2 The regional agreement commenced on 1 May 2015 with the first review due on 30 June Adjustments and variations to the terms have been agreed by both parties to roll over for the next 12 month period. 66 P a g e
67 APPENDIX ONE: PRIMARY CARE DEMENTIA EDUCATION SUMMARY REPORT SOUTH ISLAND ALLIANCE Primary Care Dementia Education Summary Report Subject Authors Chair Primary Care Dementia Education Summary Report Rebecca Winsor Carole Kerr Chair Health of Older Persons Service Level Alliance (South Island Alliance) Reporting Period May June 2016 Purpose Information only Decision Required The Primary Care Dementia Education project has been funded directly by the Ministry of Health in order to progress the New Zealand Dementia Care Framework (MoH 2013). This project focusses on the part of the framework that identifies the importance of assessment, early diagnosis, intervention and ongoing support for people living with dementia and their carers/family/ whanau. Dementia Services To further develop the primary care workforce and improve the timeliness for a diagnosis A Cognitive Impairment Pathway will be promoted for adoption across all South Island DHBs Develop appropriate dementia education/ training materials for South Island primary health care Milestones Dashboard Deliverable Activities to achieve deliverable Outputs Progress to date Implement Dementia education supporting the use of the Cognitive Impairment Pathway which is available in a variety of modalities suitable for General Practitioners, Practice Nurses and other community staff Communicate with all South Island Health of Older People and Primary Care Portfolio Managers an outline of the business case and the programme for education that will need to be undertaken. Collate the information provided by DHBs and utilise these to develop reports and inform the training resources All five South Island DHB s visited May to September 2015 and information gathered for implementation into training resources, including how care for people with dementia was currently occurring in their DHBs. In each SI DHB during this period met with Health of Older People portfolio managers who identified further key contacts within their areas who were also contacted. May to September 2015 Met also with each PHO manager within the SI as well as some PHO education facilitators 67 P a g e
68 Deliverable Activities to achieve deliverable Outputs Progress to date across the health care continuum including NGOs. Set up meetings with Portfolio Managers, Primary Health Organisation Representatives, Alzheimer s Society representatives and Older Person s Health specialist staff. May to September met up with all Alzheimers organisations managers from across the South Island as well as field workers of rural areas such as the West Coast. Stakeholder contact list set up with all key contacts across the South Island from different disciplines and specialties across primary, specialist and NGO sectors. An aim of these initial meeting was to seek ways to improve collaboration. One way in which this occurred was to include Electronic referral links direct from the each SI DHB cognitive impairment pathway on HealthPathways (used by Primary care settings to provide consistent care and processes) to Electronic Referral Management Service (ERMS) referral process. This has reduced duplications and delays in referral processes between Primary Care and Alzheimer s Organisations Develop training online and DVD of the MoCA that can be utilised across the Region and Nationally. Trial the effectiveness of these with a demonstration group and then review and revise. Expand circulation. Regular feedback and input into the online training package to be hosted by Goodfellow Unit. Further development of a package to be hosted by healthlearn.ac.nz, which provides e-learning opportunities for people in Canterbury and West Coast DHBs. This to be further collated with elearning platforms available in Southern DHB and Nelson Marlborough DHB as able. Video clips have been filmed for training purposes; these include insights from the person diagnosed with dementia and their carers. Filming of healthcare professionals has also been undertaken, particularly around the considerations of cognitive testing and providing a diagnosis for someone. Additional filming has also been undertaken including information from healthcare professionals around pain and nutrition in relation to dementia. Key people to provide informal education sessions around the MoCA have been identified to provide education to select groups in DHBs/ PHOs around how to complete a MoCA. Develop pre and Post questionnaires for General Practice for completion before and after education sessions Trial these with a demonstration group to gain feedback and then act on results from these, reviewing the effectiveness of education offered Pre and post questionnaire has been developed and finalised. Has been circulated to resource group and national group. Survey has been translated into survey monkey and link to be made available once people have completed the online training. Develop a feasibility study of a Regional Cognitive Impairment pathway and information for support services in each Report completed on similarities and differences between each DHB s Cognitive Impairment pathway Report circulated to South Island Health of Older People Service Level Alliance (HOPSLA) and the Resource group. Discussion around localised cognitive impairment HealthPathway integration held with South Island regional dementia framework group. HealthPathways clinical editors are currently reviewing the regional cognitive impairment pathways Take a lead role in the National Dementia Education Collaboration Primary Care Dementia Education meeting. Write and circulate the minutes of these meetings and review the appropriate action and follow up points in line with national initiatives Meetings chaired and minutes circulated. Also provided regular input into a meeting chaired by Alzheimers New Zealand regarding the development of resources for people living with dementia and their families. 68 P a g e
69 Deliverable Activities to achieve deliverable Outputs Progress to date Encourage uptake of Dementia Education in South Island districts. Education resources with training manuals are available (DVD or online) for implementation in DHB/PHO. Develop an expert group to support the implementation of training resources and to provide feedback to their relevant organisations. The group will be representative of all South Island DHB s and include PHO representation, Specialist services, Alzheimer s Society and consumer input. Feedback gained from the expert group and their representative groups will inform training materials. Arrange regular meetings to enable enhanced communication and collaboration across sectors. A resource group was established which included representation from: Two different Alzheimers organisations, Practice Nurse, General Practitioners, Nurse Practitioners, Portfolio Manager, Pharmacist, Maori health representative, Needs Assessment Coordinator, Geriatricians, PHO Manager, Nurse manager representatives from HBSS, Psychiatrists of Old Age, Registered Nurse from the memory clinic, Walking in another shoes dementia educators, as well as the two PCDE Coordinators who chair and minute. Monthly meetings are held with Terms of Reference set. This resource group has been instrumental in reviewing resources so far and will be assisting in reviewing the information on a continuing basis with regular meetings set and facilitated by HOPSLA. Collect the number of referrals being generated to Alzheimer s from General Practice. Over the 12 months referral numbers to Alzheimer s organisations from Primary care have increased Referral numbers collected and submitted to the Ministry of Health as required- see Appendices 1 and 2. Develop a report from DHB pharmacies that capture the prescribing and use of acetyl cholinesterase inhibitors Collect information from regional pharmacies that can be used to assist this data collection Report developed from data warehouse and completed for the five DHB s by Canterbury DHB- see Appendix 3. Develop a co-ordinated timetable for education being offered throughout DHBs and establish opportunities for shared resources and education across the South Island Review different education being offered regionally and the effectiveness of these in each respective setting. Evaluate how these could be utilised effectively regionally where appropriate All South Island PHOs and DHB s have arranged face-to-face education dates around timely diagnosis and management of people with dementia. These sessions are each facilitated by the two Primary Care Dementia Education Co-ordinators with 24 sessions booked between February and June 2016 across the South island, including areas such as Greymouth, Cromwell, Invercargill, Kaikoura, as well as other rural areas such as Darfield and Oxford in Canterbury. 457 people have attended the educations to date, with most of those being practice nurses and GPs (see Appendix Four). In order to promote collaboration, Alzheimers organisation and specialist services representation has been present at most education sessions. Face to face education was arranged through PHO managers and educators and with information provided to portfolio managers. Education sessions each 1 ½ hrs long (except in select cases). Content includes updates around dementia and MCI, local statistics as well as national over 65 census and PHO data, information around training that will soon be available and information around why a timely diagnosis of dementia is important. Integration of video resources included in sessions. Sample of comments received: Good practical information that will be helpful in practice I am going to be more aggressive about diagnosing and informing patients 69 P a g e
70 Deliverable Activities to achieve deliverable Outputs Progress to date Good to know what resources available, is a growing problem/increasing number in our community. Develop other training materials to assist health care professionals support people to live well with dementia Create and circulate a flyer to be distributed amongst PHOs Around Primary care Dementia Education Flyer circulated to raise the profile of Alzheimers organisations, the cognitive Impairment pathway and the New Zealand Framework for Dementia Care (2013) 5 different flyers created, each specific to a SI DHB. The flyers contain the contact details for the relevant Alzheimers organisation, as well as providing the flowchart outlined for each SI DHB respectively. Principles of the national Framework for Dementia care are outlined also. Flyers distributed at each education session attended, and also given in bulk to PHOs for distribution amongst practices. Update and circulate a poster created by NMDHB in conjunction with Alzheimer s Nelson Marlborough: I have dementia, try walking in my shoes Health care Professionals will be aware of resources that have been developed and these will be distributed around the South Island. This provides standardised information that reflects the principles of personcentred care It has also proven to be a good resource for families. Poster updated to reflect South island Alliance branding and distributed around the South Island. A draft model of care document for the South Island will be presented on project completion to HOPSLA for their consideration Create a discussion document outlining recommendations and principles to guide a dementia model of care for the South Island. Discussion document developed regarding different recommendations for a model of care across the South Island, including recommendations for Primary care and specialist services, as well as the community sector against the New Zealand framework for Dementia Care. International research undertaken with particular attention given to recent research and models of care developed in other countries and areas. Discussion document created which outlines principles and recommendations for a dementia model of care for the South Island. Also includes information regarding the current ways f of working and challenges that may be present. Presented to HOPSLA for feedback 8 th June 2016 with feedback incorporated accordingly. 70 P a g e
71 Jan-14 Feb-14 Mar-14 Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Attachment One: Cognitive Impairment Pathway 'Hits' May June July August September October November Nelson Marlborough Canterbury West Coast Aoraki Southern Attachment Two- Referrals to Alzheimers Organisation Alzheimers referrals Nelson Marlborough Canterbury West Coast South Canterbury Southern Jul- Sep 2014 Oct- Dec 2014 Jan- Mar 2015 Apr- Jun 2015 Jul- Sep 2015 Attachment Three- Use of cholinesterase inhibitors across the South Island South Island Donepezil Usage 71 P a g e
72 Attachment Four: Primary Care Dementia Education Sessions May June 2016 Other (lawyer/ admin staff/ Community support workers/ St Johns) Students- Medical / Nursing / Pharmacist 2 6 Allied Health- Physiotherapists / OT / SW / CA Aged residential care staff/ Heath care assistants Primary care educators / coordinators / Dementia educator 6 Pharmacists 42 Other RN / EN (incl. ARC RN) 75 Practice Nurses 192 Nurse Practitioner / CNS / CNM / NE 13 GP / medical director Series1 72 P a g e

73 APPENDIX TWO: RESORATIVE CARE FLYER 73 P a g e


74 APPENDIX THREE: CARDIAC DATA 74 P a g e
A N N U A L P R O G R E S S R E P O R T
 A N N U A L P R O G R E S S R E P O R T 2 0 1 5-2 0 1 6 When the South Island Alliance was established in 2011, the five South Island district health boards (DHBs) recognised the challenges they faced
A N N U A L P R O G R E S S R E P O R T 2 0 1 5-2 0 1 6 When the South Island Alliance was established in 2011, the five South Island district health boards (DHBs) recognised the challenges they faced
Te Wai Pounamu South Island Health Services Plan
 Te Wai Pounamu South Island Health Services Plan 2016-19 South Island Health Services Plan 2016-19 Produced in May 2016 By the South Island Alliance Programme Office On behalf of the five South Island
Te Wai Pounamu South Island Health Services Plan 2016-19 South Island Health Services Plan 2016-19 Produced in May 2016 By the South Island Alliance Programme Office On behalf of the five South Island
SOUTH ISLAND HEALTH SERVICES PLAN
 SOUTH ISLAND HEALTH SERVICES PLAN QUARTER ONE REPORT 2014-2015 Introduction The South Island Alliance continues to build on the outcomes from the previous year in the first quarter of 2014 2015. We are
SOUTH ISLAND HEALTH SERVICES PLAN QUARTER ONE REPORT 2014-2015 Introduction The South Island Alliance continues to build on the outcomes from the previous year in the first quarter of 2014 2015. We are
Te Waipounamu South Island Health Services Plan
 Te Waipounamu South Island Health Services Plan 2017-2020 South Island Health Services Plan 2017-20 Produced in May 2017 By the South Island Alliance Programme Office On behalf of the five South Island
Te Waipounamu South Island Health Services Plan 2017-2020 South Island Health Services Plan 2017-20 Produced in May 2017 By the South Island Alliance Programme Office On behalf of the five South Island
Auckland DHB Strategy to 2020
 Our Vision Healthy communities World-class healthcare Achieved together Kia kotahi te oranga mo te iti me te rahi o te hāpori Our Strategic Themes Community, family/whānau and patientcentric model of healthcare
Our Vision Healthy communities World-class healthcare Achieved together Kia kotahi te oranga mo te iti me te rahi o te hāpori Our Strategic Themes Community, family/whānau and patientcentric model of healthcare
NHS GRAMPIAN. Clinical Strategy
 NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
NHS GRAMPIAN Clinical Strategy Board Meeting 02/06/2016 Open Session Item 9.1 1. Actions Recommended The Board is asked to: 1. Note the progress with the engagement process for the development of the clinical
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Strategic Plan
 Strategic Plan 2013-2025 Toi Te Ora Public Health Service (Toi Te Ora) is one of 12 public health units funded by the Ministry of Health and is the public health unit for the Bay of Plenty and Lakes District
Strategic Plan 2013-2025 Toi Te Ora Public Health Service (Toi Te Ora) is one of 12 public health units funded by the Ministry of Health and is the public health unit for the Bay of Plenty and Lakes District
Monthly Update. An Update from the G.M. May Staff Get Cooking to Help Families at Ronald McDonald House
 Monthly Update May 2015 An Update from the G.M. As we head towards the end of this financial year, I would like to acknowledge the ongoing efforts that the South Island Alliance Service Level Alliance
Monthly Update May 2015 An Update from the G.M. As we head towards the end of this financial year, I would like to acknowledge the ongoing efforts that the South Island Alliance Service Level Alliance
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Bristol CCG North Somerset CGG South Gloucestershire CCG. Draft Commissioning Intentions for 2017/2018 and 2018/2019
 Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Bristol CCG North Somerset CGG South Gloucestershire CCG Draft Commissioning Intentions for 2017/2018 and 2018/2019 Programme Area Key intention Primary and community care Sustainable primary care Implement
Policy Health. Policy highlights. Delivering a healthy NZ
 Delivering a healthy NZ The National-led Government is helping New Zealanders to stay healthy, as well as delivering world class health services. is our top funding priority, with a record $16.8b to be
Delivering a healthy NZ The National-led Government is helping New Zealanders to stay healthy, as well as delivering world class health services. is our top funding priority, with a record $16.8b to be
Te Ao Māramatanga New Zealand College of Mental Health Nurses
 Te Ao Māramatanga New Zealand College of Mental Health Nurses Mental Health and Addictions Credential in Primary Care (Nursing) Monitoring and Evaluation Handbook - ABRIDGED 19 April 2013 Jointly prepared
Te Ao Māramatanga New Zealand College of Mental Health Nurses Mental Health and Addictions Credential in Primary Care (Nursing) Monitoring and Evaluation Handbook - ABRIDGED 19 April 2013 Jointly prepared
SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN
 Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
Appendix-2016-59 Borders NHS Board SCOTTISH BORDERS HEALTH & SOCIAL CARE INTEGRATED JOINT BOARD UPDATE ON THE DRAFT COMMISSIONING & IMPLEMENTATION PLAN Aim To bring to the Board s attention the Scottish
In this edition we will showcase the work of the development of a model for GP- Paediatric Hubs
 Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Focusing on the principle of home first and designing the Perfect Locality from the lens of the community Issue 7 June 2017 Welcome to the seventh issue of Our Future Wellbeing, a regular update on the
Designated Title: Clinical Nurse Specialist. Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery
 Designated Title: Clinical Nurse Specialist Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery This role is considered a non-core children s worker and will be subject to safety checking
Designated Title: Clinical Nurse Specialist Position Title: Clinical Nurse Specialist Reconstructive Breast Surgery This role is considered a non-core children s worker and will be subject to safety checking
Capital & Coast DHB System Level Measures Improvement Plan 2016/17
 Capital & Coast DHB System Level Measures Improvement Plan 2016/17 Written by: Astuti Balram, ICC Programme Manager, on behalf of the CCDHB Integrated Care Collaborative (ICC) Alliance Version 4 Released
Capital & Coast DHB System Level Measures Improvement Plan 2016/17 Written by: Astuti Balram, ICC Programme Manager, on behalf of the CCDHB Integrated Care Collaborative (ICC) Alliance Version 4 Released
Living With Long Term Conditions A Policy Framework
 April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
April 2012 Living With Long Term Conditions A Policy Framework Living with Long Term Conditions Contents Page Number Minister s Foreword 3 Introduction 4 Principles 13 Chapter 1 Working in partnership
NHS GRAMPIAN. Local Delivery Plan - Section 2 Elective Care
 NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
NHS GRAMPIAN Local Delivery Plan - Section 2 Elective Care Board Meeting 01/12/2016 Open Session Item 7 1. Actions Recommended The NHS Board is asked to: Consider the context in which planning for future
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
17. Updates on Progress from Last Year s JSNA
 17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
17. Updates on Progress from Last Year s JSNA 3. The Health of People in Bromley NHS Health Checks The previous JSNA reported that 35 (0.5%) patients were identified through NHS Health Checks with non-diabetic
NHS Bradford Districts CCG Commissioning Intentions 2016/17
 NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
NHS Bradford Districts CCG Commissioning Intentions 2016/17 Introduction This document sets out the high level commissioning intentions of NHS Bradford Districts Clinical Commissioning Group (BDCCG) for
Our five year plan to improve health and wellbeing in Portsmouth
 Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
Our five year plan to improve health and wellbeing in Portsmouth Contents Page 3 Page 4 Page 5 A Message from Dr Jim Hogan Who we are What we do Page 6 Page 7 Page 10 Who we work with Why do we need a
DRAFT. Rehabilitation and Enablement Services Redesign
 DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
DRAFT Rehabilitation and Enablement Services Redesign Services Vision Statement Inverclyde CHP is committed to deliver Adult rehabilitation services that are easily accessible, individually tailored to
End of Life Care Strategy
 End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
End of Life Care Strategy 2016-2020 Foreword Southern Health NHS Foundation Trust is committed to providing the highest quality care for patients, their families and carers. Therefore, I am pleased to
North Central London Sustainability and Transformation Plan. A summary
 Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Sustainability and Transformation Plan A summary N C L Introduction Hospitals, local authorities, GPs, commissioners, and mental health trusts across north central London have all come together to transform
Solent. NHS Trust. Allied Health Professionals (AHPs) Strategic Framework
 Strategic Framework") Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
Solent NHS Trust Allied Health Professionals (AHPs) Strategic Framework 2016-2019 Introduction from Chief Nurse, Mandy Rayani As the executive responsible for providing professional leadership for the
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
Draft Commissioning Intentions
 The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
The future for Luton s primary care services Draft Commissioning Intentions 2013-14 The NHS will have less money to spend over the next three years. Overall, it has to make 20 billion of efficiency savings
EMPLOYEE HEALTH AND WELLBEING STRATEGY
 EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
EMPLOYEE HEALTH AND WELLBEING STRATEGY 2015-2018 Our community, we care, you matter... Document prepared by: Head of HR Services Version Number: Review Date: September 2018 Employee Health and Wellbeing
TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE
 TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE Summary Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV) adapted the model line concept from industry
TEES, ESK & WEAR VALLEYS NHS FOUNDATION TRUST: DEVELOPING A MODEL LINE FOR RECOVERY- FOCUSED CARE Summary Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV) adapted the model line concept from industry
South Canterbury District Health Board Annual Plan 2016/17
 Crown copyright. This copyright work is licensed under the Creative Commons Attribution 4.0 International licence. In essence, you are free to copy, distribute and adapt the work, as long as you attribute
Crown copyright. This copyright work is licensed under the Creative Commons Attribution 4.0 International licence. In essence, you are free to copy, distribute and adapt the work, as long as you attribute
Medicines New Zealand
 Implementing Medicines New Zealand 2015 to 2020 Medicines New Zealand Access Quality Optimal use Released 2015 health.govt.nz Citation: Ministry of Health. 2015. Implementing Medicines New Zealand 2015
Implementing Medicines New Zealand 2015 to 2020 Medicines New Zealand Access Quality Optimal use Released 2015 health.govt.nz Citation: Ministry of Health. 2015. Implementing Medicines New Zealand 2015
Wolverhampton CCG Commissioning Intentions
 Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Wolverhampton CCG Commissioning Intentions 2015-16 * Areas of particular focus and priority CI Ref Contract Provider Brief CI001 CI002 CI003 Child Protection Information Sharing Implement the new Child
Milton Keynes CCG Strategic Plan
 Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
Milton Keynes CCG Strategic Plan 2012-2015 Introduction Milton Keynes CCG is responsible for planning the delivery of health care for its population and this document sets out our goals over the next three
grampian clinical strategy
 healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
healthfit caring listening improving consultation grampian clinical strategy 2016 to 2021 1 summary version NHS Grampian Clinical Strategy 2016 to 2021 Purpose and aims 5 Partnership working and the changing
C A N T E R B U R Y H E A L T H S Y S T E M. System Level Measures Improvement Plan
 C A N T E R B U R Y H E A L T H S Y S T E M System Level Measures Improvement Plan 2018-19 1 INTRODUCTION The Canterbury Health System places a high priority on implementing the System Level Measures Framework
C A N T E R B U R Y H E A L T H S Y S T E M System Level Measures Improvement Plan 2018-19 1 INTRODUCTION The Canterbury Health System places a high priority on implementing the System Level Measures Framework
grampian clinical strategy
 healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
healthfit caring listening improving grampian clinical strategy 2016 to 2021 1 summary version For full version of the Grampian Clinical Strategy, please go to www.nhsgrampian.org/clinicalstrategy Document
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014
 MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
MEETING OF THE GOVERNING BODY IN PUBLIC 7 January 2014 Title: Bedfordshire and Milton Keynes Healthcare Review: The way forward Agenda Item: 4 From: Jane Meggitt, Director of Communications and Engagement
Strategic Plan for Fife ( )
") www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
www.fifehealthandsocialcare.org Strategic Plan for Fife (2016-2019) Summary Document Supporting the people of Fife together Foreword NHS Fife and Fife Council are working together in a new Integrated Health
Delivering Local Health Care
 Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
Delivering Local Health Care Accelerating the pace of change Contents Joint foreword by the Minister for Health and Social Services and the Deputy Minister for Children and Social Services Foreword by
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
POPULATION HEALTH. Outcome Strategy. Outcome 1. Outcome I 01
 Section 2 Department Outcomes 1 Population Health Outcome 1 POPULATION HEALTH A reduction in the incidence of preventable mortality and morbidity, including through national public health initiatives,
Section 2 Department Outcomes 1 Population Health Outcome 1 POPULATION HEALTH A reduction in the incidence of preventable mortality and morbidity, including through national public health initiatives,
GOULBURN VALLEY HEALTH Strategic Plan
 GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
GOULBURN VALLEY HEALTH Strategic Plan 2014-2018 VISION Healthy communities VALUES Compassion Respect Excellence Accountability Teamwork Ethical Behaviour PRIORITIES Empowering Your Health Strengthening
Child Health 2020 A Strategic Framework for Children and Young People s Health
 Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
Child Health 2020 A Strategic Framework for Children and Young People s Health Consultation Paper Please Give Us Your Views Consultation: 10 September 2013 21 October 2013 Our Child Health 2020 Vision
A Prudent Approach to Health: Prudent Health Principles
 A Prudent Approach to Health: Prudent Health Principles 1. Summary The following paper sets out the Bevan Commission s final advice on the Prudent Health Principles to the Minister for Health and Social
A Prudent Approach to Health: Prudent Health Principles 1. Summary The following paper sets out the Bevan Commission s final advice on the Prudent Health Principles to the Minister for Health and Social
IQ Action Plan: Supporting the Improving Quality Approach
 IQ Action Plan: Supporting the Improving Quality Approach i ii Citation: Minister of Health. 2003.. Wellington:. Published in September 2003 by the PO Box 5013, Wellington, New Zealand ISBN 0-478-25800-3
IQ Action Plan: Supporting the Improving Quality Approach i ii Citation: Minister of Health. 2003.. Wellington:. Published in September 2003 by the PO Box 5013, Wellington, New Zealand ISBN 0-478-25800-3
DRAFT Optimal Care Pathway
 DRAFT Optimal Care Pathway 1. Introduction... 3 1.1 Background... 3 1.2 Intent of the Optimal Care Pathways... 3 1.3 Key principles of care... 3 2. Steps in the care of patients with x cancer... 4 Step
DRAFT Optimal Care Pathway 1. Introduction... 3 1.1 Background... 3 1.2 Intent of the Optimal Care Pathways... 3 1.3 Key principles of care... 3 2. Steps in the care of patients with x cancer... 4 Step
Guideline scope Intermediate care - including reablement
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Intermediate care - including reablement Topic The Department of Health in England has asked NICE to produce a guideline on intermediate
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report
 Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Welsh Government Response to the Report of the National Assembly for Wales Public Accounts Committee Report on Unscheduled Care: Committee Report We welcome the findings of the report and offer the following
Dietitian - Community
 Dietitian - Community Position Description Date: October 13 Job Title : Dietitian - Community Department Location Reporting To Direct Reports Functional Relationships with : Medicine and Health of Older
Dietitian - Community Position Description Date: October 13 Job Title : Dietitian - Community Department Location Reporting To Direct Reports Functional Relationships with : Medicine and Health of Older
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
National Primary Care Cluster Event ABMU Health Board 13 th October 2016
 National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Primary Care Cluster Event ABMU Health Board 13 th October 2016 1 National Primary Care Cluster Event - ABMU Health Board Introduction The development of primary and community services is a fundamental
National Perinatal Pathology Services
 Service Model for National Perinatal Pathology Services Prepared by: Jane Potiki Date: December 2016 Version: v 5.0 Status: Final Draft Contents Figures... 3 Tables... 3 Executive Summary... 4 Recommendations...
Service Model for National Perinatal Pathology Services Prepared by: Jane Potiki Date: December 2016 Version: v 5.0 Status: Final Draft Contents Figures... 3 Tables... 3 Executive Summary... 4 Recommendations...
Powys Teaching Health Board. Respiratory Delivery Plan
 Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
Powys Teaching Health Board Respiratory Delivery Plan 2016-17 CONTENTS 1. BACKGROUD AND CONTEXT 1.1 The Vision 1.2 The Drivers 1.3 What do we want to achieve? 2. ORGANISATIONAL PROFILE 2.1 Overview 3.
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Norfolk Island Central and Eastern Sydney PHN
 Norfolk Island Central and Eastern Sydney PHN Activity Work Plan 2016-2018: Norfolk Island Coordinated and Integrated Primary Health Care Services Mental Health and Suicide Prevention Drug and Alcohol
Norfolk Island Central and Eastern Sydney PHN Activity Work Plan 2016-2018: Norfolk Island Coordinated and Integrated Primary Health Care Services Mental Health and Suicide Prevention Drug and Alcohol
Annual Report. WellSouth. Primary Health Network Hauora Matua Ki Te Tonga
 2015 Annual Report WellSouth Primary Health Network Hauora Matua Ki Te Tonga Chair and CE Report - Kia ora koutou We take pleasure in presenting the Annual Report and Financial Statements for WellSouth
2015 Annual Report WellSouth Primary Health Network Hauora Matua Ki Te Tonga Chair and CE Report - Kia ora koutou We take pleasure in presenting the Annual Report and Financial Statements for WellSouth
Healthy London Partnership. Transforming London s health and care together
 Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
Healthy London Partnership Transforming London s health and care together London-wide transformation In 2014, two publications set out London s transformation priorities NHS Five Year Forward View Better
London Councils: Diabetes Integrated Care Research
 London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
London Councils: Diabetes Integrated Care Research SUMMARY REPORT Date: 13 th September 2011 In partnership with Contents 1 Introduction... 4 2 Opportunities within the context of health & social care
Stockport Strategic Vision. for. Palliative Care and End of Life Care Services. Final Version. Ratified by the End of Life Care Programme Board
 Stockport Strategic Vision for Palliative Care and End of Life Care Services Final Version Ratified by the End of Life Care Programme Board on 8 th February 2012 Clinical Commissioning Pathfinder Contents
Stockport Strategic Vision for Palliative Care and End of Life Care Services Final Version Ratified by the End of Life Care Programme Board on 8 th February 2012 Clinical Commissioning Pathfinder Contents
Commissioning Intentions 2019 / 20
 Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Commissioning Intentions 2019 / 20 September 2018 Version 1.1 Final version. Approved at JCC on 26th September (by Jon Singfield - 24/09/18) 1) Introduction Introduction The development of commissioning
Collaborative Commissioning in NHS Tayside
 Collaborative Commissioning in NHS Tayside 1 CONTEXT 1.1 National Context Delivering for Health was the Minister for Health and Community Care s response to A National Framework for Service Change in the
Collaborative Commissioning in NHS Tayside 1 CONTEXT 1.1 National Context Delivering for Health was the Minister for Health and Community Care s response to A National Framework for Service Change in the
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Aintree University Hospital NHS Foundation Trust Corporate Strategy
 Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
Aintree University Hospital NHS Foundation Trust Corporate Strategy 2015 2020 Aintree University Hospital NHS Foundation Trust 1 SECTION ONE: BACKGROUND AND CONTEXT 1 Introduction Aintree University Hospital
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Our Health & Care Strategy
 MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
MO Our Health & Care Strategy 2015-2020 Norfolk Community Health and Care NHS Trust Final September 2015 Version control Date Changes 1 19 th July 2015 Initial document 2 29 th July 2015 Following feedback
The LHIN s role in creating integrated health service delivery systems
 PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
PATIENTS FIRST UPDATE The LHIN s role in creating integrated health service delivery systems February 7, 2018 Overview 1. Review of five goals of Patients First 2. South West LHIN committees, alliances
AMP Health and Social Care Professional Implementation Group Update
 AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
AMP Health and Social Care Professional Implementation Group Update November 2016 Welcome to another update from the National Acute Medicine Programme s Health and Social Care Professionals Implementation
Transforming Cancer Services In South East Wales
 Transforming Cancer Services In South East Wales Clinical Service Model January 2016 Cancer survival rates are increasing. But the number of people getting cancer is increasing too. At Velindre NHS Trust
Transforming Cancer Services In South East Wales Clinical Service Model January 2016 Cancer survival rates are increasing. But the number of people getting cancer is increasing too. At Velindre NHS Trust
Integrated heart failure service working across the hospital and the community
 Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
Integrated heart failure service working across the hospital and the community Lynne Ruddick Professional Lead (South) British Heart Foundation 31st October 2017 Heart Failure is an epidemic. NICE has
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Plans for urgent care in west Kent:
 Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Plans for urgent care in west Kent: Introduction and background A summary of our draft strategy NHS West Kent Clinical Commissioning Group (CCG) is working to improve urgent care services and we would
Primary Health Networks
 Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Drug and Alcohol Treatment Budget Northern Sydney PHN The Activity Work Plan will be lodged to Alexandra Loudon
Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 Drug and Alcohol Treatment Budget Northern Sydney PHN The Activity Work Plan will be lodged to Alexandra Loudon
NHS Ayrshire and Arran. 1. Which of the following performance frameworks has the most influence on your budget decisions:
 A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
A: Budget setting process Performance budgeting 1. Which of the following performance frameworks has the most influence on your budget decisions: National Performance Framework Quality Measurement Framework
Alberta Health Services. Strategic Direction
 Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Alberta Health Services Strategic Direction 2009 2012 PLEASE GO TO WWW.AHS-STRATEGY.COM TO PROVIDE FEEDBACK ON THIS DOCUMENT Defining Our Focus / Measuring Our Progress CONSULTATION DOCUMENT Introduction
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
West Wandsworth Locality Update - July 2014
 Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Attach 5 West Wandsworth Locality Update - July 2014 1) Introduction The West Wandsworth Locality covers the areas of Roehampton and Putney, and the nine practices that lie in these areas. The 2013 GP
Equality and Health Inequalities Strategy
 Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Equality and Health Inequalities Strategy 1 Schematic of the Equality and Health Inequality Strategy Improving Lives: People and Patients Listening and Learning Gaining Knowledge Making the System Work
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
WORKFORCE DEVELOPMENT ACTION PLAN
 Hāpai te Tūmanako - Raise HOPE Implementation Plan WORKFORCE DEVELOPMENT ACTION PLAN 2016-2019 Our Vision To have a sustainable, experienced and highly skilled workforce delivering quality mental health
Hāpai te Tūmanako - Raise HOPE Implementation Plan WORKFORCE DEVELOPMENT ACTION PLAN 2016-2019 Our Vision To have a sustainable, experienced and highly skilled workforce delivering quality mental health
WORKING DRAFT. Standards of proficiency for nursing associates. Release 1. Page 1
 WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
ALBERTA HEALTH SERVICES. Action Plan Supplement to Health Plan and Business Plan Amended February 2014
 ALBERTA HEALTH SERVICES Action Plan 2013-14 Supplement to Health Plan and Business Plan 2013-2016 Amended February 2014 AHS Action Plan 2013-14 (This document was amended in February 2014, to include the
ALBERTA HEALTH SERVICES Action Plan 2013-14 Supplement to Health Plan and Business Plan 2013-2016 Amended February 2014 AHS Action Plan 2013-14 (This document was amended in February 2014, to include the
Inpatient and Community Mental Health Patient Surveys Report written by:
 2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
2.2 Report to: Board of Directors Date of Meeting: 30 September 2014 Section: Patient Experience and Quality Report title: Inpatient and Community Mental Health Patient Surveys Report written by: Jane
Health and Care Framework
 Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
Annex 1 Health and Care Framework The NHS Grampian 2020 A Possible Future 1. NHS Grampian has agreed its Health Plan and has embarked on its Health and Care Framework (H&CF) process to determine in detail
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Finance Committee. Draft Budget Submission from North Ayrshire Community Planning Partnership
 Finance Committee Draft Budget 2012-13 Submission from North Ayrshire Community Planning Partnership 1. To what extent has preventative spending been embedded within the CPP s work so that it focuses on
Finance Committee Draft Budget 2012-13 Submission from North Ayrshire Community Planning Partnership 1. To what extent has preventative spending been embedded within the CPP s work so that it focuses on
End of Life Care. LONDON: The Stationery Office Ordered by the House of Commons to be printed on 24 November 2008
 End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
End of Life Care LONDON: The Stationery Office 14.35 Ordered by the House of Commons to be printed on 24 November 2008 REPORT BY THE COMPTROLLER AND AUDITOR GENERAL HC 1043 Session 2007-2008 26 November
GOVERNING BODY REPORT
 GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
GOVERNING BODY REPORT Date of Governing Body Meeting: Title of Report: Key Messages: Finance, Performance and Commissioning Committee Report At the end of September 2017 we have reported an inyear deficit
Staff Health, Safety and Wellbeing Strategy
 Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
Staff Health, Safety and Wellbeing Strategy 2013-16 Prepared by: Effective From: Review Date: Lead Reviewer: Hugh Currie Head of Occupational Health and Safety 31 st January 2013 01 st April 2014 Patricia
South Canterbury District Health Board
 South Canterbury District Health Board - Timaru Hospital Introduction This report records the results of a Surveillance Audit of a provider of hospital services against the Health and Disability Services
South Canterbury District Health Board - Timaru Hospital Introduction This report records the results of a Surveillance Audit of a provider of hospital services against the Health and Disability Services
WAITING TIMES 1. PURPOSE
 Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
REPORT 1 FRAIL OLDER PEOPLE
 REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
REPORT 1 FRAIL OLDER PEOPLE Contents Vision f-3 Principles / Parameters f-4 Objectives f-6 Current Frail Older People Model f-8 ABMU Model for Frail and Older People f-11 Universal / Enabling f-12 Specialist
2020 Objectives July 2016
 ... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
... 2020 Objectives July 2016 1 About NHS Improvement NHS Improvement is responsible for overseeing NHS foundation trusts, NHS trusts and independent providers. We offer the support these providers need
2018 Optional Special Interest Groups
 2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
2018 Optional Special Interest Groups Why Participate in Optional Roundtable Meetings? Focus on key improvement opportunities Identify exemplars across Australia and New Zealand Work with peers to improve
Trust Strategy
 Trust Strategy 2012 2022 Approved November 2012 Contents Introduction 3 Overview of St George s Healthcare NHS Trust 4 The drivers for change 6 Our mission, vision and values 7 Our guiding principles (values
Trust Strategy 2012 2022 Approved November 2012 Contents Introduction 3 Overview of St George s Healthcare NHS Trust 4 The drivers for change 6 Our mission, vision and values 7 Our guiding principles (values
Report to Governing Body 19 September 2018
 Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Report to Governing Body 19 September 2018 Report Title Author(s) Governing Body/Clinical Lead(s) Management Lead(s) CCG Programme Purpose of Report Summary NHS Lambeth Clinical Commissioning Group (CCG)
Your Care, Your Future
 Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts
Your Care, Your Future Update report for partner Boards April 2016 Introduction The following paper has been prepared for the Board members of all Your Care, Your Future partner organisations: NHS Herts