The Aftermath of Medical Errors: Supporting Our Second Victim Colleagues Hanan H. Edrees, DrPH, MHSA
|
|
|
- Nickolas Haynes
- 5 years ago
- Views:
Transcription

1 The Aftermath of Medical Errors: Supporting Our Second Victim Colleagues Hanan H. Edrees, DrPH, MHSA Associate Faculty, Johns Hopkins Bloomberg School of Public Health, USA Manager, Ministry of National Guard Health Affairs, Kingdom of Saudi Arabia May 2017

2 Kimberly Hiatt Nurse for 24 years Seattle Children s Hospital Medication error (September 2010): child 5 mo/patient dies dispensed 1.4 grams of CaCl instead of 140 milligrams Dismissed from job
3 What about.? What about the doctor who wrote this order? What about the pharmacist that approved this order? What about the process/system that set them up?



4 Kimberly Hiatt commits suicide after 10 months after the event


5 Second Victims Second victims: Healthcare providers who are involved with a patient-related adverse event or medical error, and as a result, they experience emotional and sometimes physical distress First victim: patients and families Term coined by Dr. Albert Wu: 2000 Second victims often Feel personally responsible for the outcome Feel as though they have failed the patient Second guess their clinical skills and knowledge Signs & symptoms Similar to Post Traumatic Stress Disorder symptoms Physical and psychological distress Negative emotional responses Impaired performance Wu, A. (2000). Medical Error: The Second Victim. British Medical Journal
6 Signs & Symptoms of Second Victims Short term: shock helplessness worry and depression guilt and inadequacy anger poor concentration and memory intrusive thoughts and nightmares sleep disturbance physical symptoms social avoidance Long term: (Indistinguishable from posttraumatic stress disorder) recurrent experience of the event avoidance emotional numbing chronic signs of hyper-arousal including sleep disturbance, irritability, poor concentration, diminished memory withdrawal and depression social functioning can be impaired, and personal and professional relationships can suffer
7 Burnout Symptoms Procrastination Chronic fatigue Cynicism Tardiness Anhedonia Pessimism Diminished future outlook Loss of life satisfaction
8 Impact of Error on Second Victims and the Organization 1. Impact on the individual Clinical conditions o Post-Traumatic Stress Disorder (> 3 months) o Acute Stress Reaction (up to 1 month) Stress Reactions & Distress 1. Impact on the organization and healthcare team 2. Management & treatment of psychological care Continuum of Care
9 Prevalence of Second Victims Study 1 Study 2 Study 3 Study 4 Prevalence 10.4% 1 30% % % 4 Population otolaryngologists sample of medical students, physicians, and nurses physicians, nurses, and pharmacists, and other healthcare professionals physicians, nurses, and pharmacists, and other healthcare professionals Feelings/sympto ms described an error they were involved in during the past 6 months personal problems related to anxiety, depression, and challenges in their ability to provide care during the past 12 months the error had a moderately severe or severe harmful effect on their personal lives experienced problems, such as anxiety, depression, or concern about their ability to perform their job 1 Lander, L. I., Connor, J. A., Shah, R. K., Kentala, E., Healy, G. B., & Roberson, D.W. (2006). Otolaryngologists responses to errors and adverse events. Laryngoscope,116, Scott, SD; Hirschinger, LE; Cox, K; et al. (2010). Caring for Our Own: Deploying A Systemwide Second Victim Rapid Response Team. Joint Commission Journal Quality Patient Safety, 36: Wolf, Z. R., Serembus, J. F., Smetzer, J., Cohen, H., & Cohen, M. (2000). Responses and concerns of healthcare providers to medication errors. Clinical Nurse Specialist,14: Edrees H, Paine LA, Feroli ER, & Wu A (2011). Healthcare workers as second victims of medical errors. Polish Archives of Internal 9 Medicine.
10 Limited studies on second victims Limited literature Prevalence of second victims: 10.4% % Studies on concept of second victims: Switzerland, Belgium, Denmark, Sweden, Italy, the United Kingdom, and the United States Descriptions of organizational support programs Little documentation of the steps involved in their development Limited resources for evaluating the feasibility and effectiveness of these programs
11 Natural History of the Second Victim (1) Initial response to incident (2) Peer response (3) Investigation (4) Complaint system/ Malpractice suit
12 Second Victim Trajectory of Recovery Scott S, et al (2009). The natural history of recovery for the healthcare provider second victim after adverse patient events. BMJ Qual Saf Health Care.

13 Doing better but feeling worse Under the Bus Good disclosure but poor follow through At expense of the feelings of health care workers? Courtesy of Dr Albert Wu
14 Making the case for peer support.
15 Assessing the Need for Second Victim Support Objective: To assess patient safety leaders perspectives on the concept of second victims and support programs Methods: In-depth, semi-structured interviews 43 patient safety representatives from 38 acute hospitals in Maryland Descriptive statistics were generated for hospital and participant characteristics Response Rate: 83%
16 PART I: Does One Size Fit All? Assessing Need for Organizational Second Victim Support Programs Objectives: To assess the extent of the second victim problem, To determine the availability of emotional support services, and To assess the need for organizational support programs. Results: All participants reported that they and their executives were aware of the second victim problem. All participants believed that hospitals should offer organizational support. There continues to be a stigma associated with speaking up and accessing support if it were offered. Edrees H & Wu A. (2016). Does One Size Fit All? Assessing the Need for Organizational Second Victim Support Programs [accepted: Journal of Patient Safety-July 2016]
17 Part II: Do Hospitals Support Second Victims? Collective Insights from Patient Safety Leaders Objectives: To describe the extent to which organizational support for second victims is perceived as desirable, and To identify existing support programs Results: All of the hospitals offered Employee Assistance Programs to their employees, but there were gaps in the services Moreover, there are no valid measures in place to assess the effectiveness of these services. Participants identified a need for peer support, both for the second victim and for individuals who provide that support. Approximately 6 Maryland hospitals offer a second victim support program, with differences in structure, accessibility, and outcomes. Edrees H, Morlock L, Wu A. (2017). Do Maryland Hospitals Support Second Victims: Collective Insights from Patient Safety Leaders in Maryland Hospitals [accepted: The Joint Commission Journal on Quality and Patient Safety]
18 Organizations that care for the caregiver Support programs for hospital workforce Medically Induced Trauma Support Services (MITSS) University of Missouri: foryou program Kaiser Permanente Program Boston Children s Hospital: The Office of Clinician Support (OCS) Brigham and Women s Hospital: The Center for Professionalism and Peer Support (CPPS) Johns Hopkins Hospital: Resilience In Stressful Events (RISE) Program Support for other psychological trauma Psychological First Aid (PFA) & RAPID-PFA Critical Incidence Stress Management (CISM) Support programs for the military
19 Schrøder K, Jørgensen JS, Lamont RF & Hvidt NC. (2016). Blame and guilt a mixed methods study of obstetricians' and midwives' experiences and existential considerations after involvement in traumatic childbirth. Acta obstetricia et gynecologica Scandinavica. The Buddy Study Odense University Hospital & Department of Public Health Department of Obstetrics and Gynecology Department of Oncology Dr. Katja Schrøder kschroeder@health.sdu.dk Schrøder K, la Cour K, Jørgensen JS, Lamont RF, & Hvidt NC. (2017). Guilt without fault: A qualitative study into the ethics of forgiveness after traumatic childbirth. Social Science & Medicine.
20 Implementing a Second Victim Peer Support Structure at The Johns Hopkins Hospital

21 RISE at The Johns Hopkins Hospital 1,075-licensed bed, urban, academic medical center in the state of Maryland, USA Medical errors and adverse patientrelated events are inevitable reported, investigated and debriefed with staff Several events occurred Hospital leadership created second victim taskforce to establish an organizational support program/service for second victims
22 Our Current Infrastructure Patient Safety & Quality Departments Risk Management Employee Assistance Program Chaplain Services Occupational Health Human Resources.. no clear pathway to help second victims cope with their emotions
23 Organizational Assessment Organizational survey was administered at 2 nd Annual Johns Hopkins Patient Safety Summit in June 2010 Results (n=140): Two-thirds reported experiencing emotional distress following an unanticipated adverse event More than half had reached out for support from a peer or colleague The need for a peer support program to benefit second victims in the Hospital Edrees HH, Paine LA, Feroli ER, Wu AW. (2011). Health care workers as second victims of medical errors. Pol Arch Med Wewn, 121(4):

24 RISE Team: Resiliency In Stressful Events Mission: To provide timely support to employees who encounter stressful, patient-related events Objectives: 1. Increase awareness of the second victim phenomenon 2. Provide multi-disciplinary, one-to-one or group, peer support in a non-judgmental environment 3. Equip managers & employees with healthy coping strategies to promote well-being 4. Reassure & guide employees to continue thriving in their role
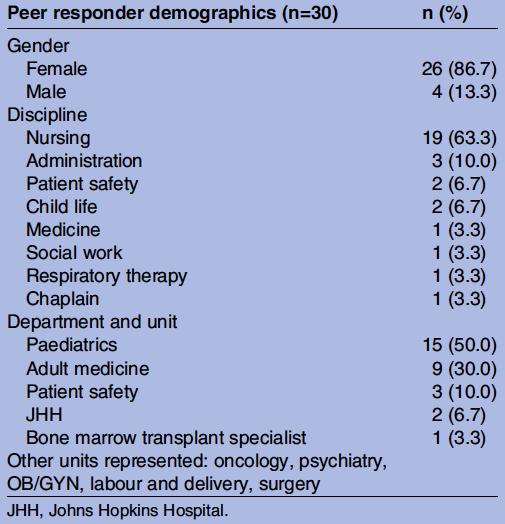
25 Developing the RISE program Phase 1: Developing the RISE Team Phase 2: Recruiting and training Peer Responders Phase 3: Launching RISE pilot in Department of Pediatrics Phase 4: Launching RISE hospital-wide Edrees H, Connors C, Paine LA, Norvell M, Taylor H, & Wu AW. (2016). Implementing the RISE second victim support programme at the Johns Hopkins Hospital: a case study. BMJ Open.




26 Contacting RISE Event happens Second victim pages RISE Referrals: self, manager, legal/risk management, peer RISE page received by Peer Responder Peer Responder meets with second victim Peer Responder activates debriefing with RISE team to discuss de-identified interaction with second victim - learning opportunity for RISE team - support for the Peer Responder

27 What does RISE do? Supportive and attentive conversation Facilitate resources within the hospital that might be helpful Provide 24/7 available support One to one or group support
28 What does RISE NOT do? We are not counselors or psychiatrists We do not investigate or report back to supervisors We do not problem solve We do not fix employment problems
29 Training Peer Responders 1. Psychological First Aid (PFA) used to describe early interventions to address emotional distress goals of PFA are similar to that of physical first aid stabilize, mitigate psychological distress, facilitate recovery, and promote access to additional resource 2. Peer Responder meetings Educational sessions: lecture presentations, Role-play, Video excerpts, Handouts, Narratives 3. Debriefings
30 Continuum of Care Psych First Aid** Crisis Intervention Counseling Psychotropic Meds & Psychotherapy Physical First Aid Basic Life Support Advanced Life Support Medicine & Surgery ** stabilize psychological and behavioral functioning, mitigate psychological distress and dysfunction, facilitate recovery and return to adaptive psychological and behavioral functioning, and promote access to additional resources
31 Financial Impact of Implementing RISE OBJECTIVE : To conduct an economic evaluation on cost-benefit of RISE for nursing staff who used the program between 2015 & 2016 METHODS: The cost of running RISE, nurse turnover, and nurse time off Data on costs and probabilities of quitting or taking time off with or without the RISE program Net monetary benefit and budget impact of RISE RESULTS: Net monetary benefit savings of US $22, per nurse who initiated a RISE call. The budget impact analysis revealed that a hospital could save US $1.81 million each year from the RISE program. Moran, D et al (2017). Cost-Benefit Analysis of a Support Program for Nursing Staff. Journal of Patient Safety.


32 Pager:


33
34 How can your organization participate Acknowledge the problem of the second victim When errors happen, encourage staff to be involved in system changes that will mitigate future errors Hold debriefings and offer training, formal organizational support and coping strategies for individuals Develop multidisciplinary second victim support programs that align with existing organizational infrastructure Communicate and collaborate with institutions that have existing or emerging programs
.")

35 Things to say and not to say to colleagues after an adverse event Edrees H, et al (2011). Healthcare workers as second victims of medical errors. Polish Archives of Internal Medicine.
36 A Medical Oncologist s Poetry: Dr. Jazieh Hospital Rounds I walked into your room and here you were Lying down there yellow skin and swollen face You peeped at me with those jaundiced eyes You were still gracious as I knew you all the times We exchanged comforting looks, I needed them too as much as you did Your weakened voice declared that you are still there: You did your best, Doc! You are still my favorite I felt my inside shivering How can I be empathetic yet not cry? Do not push more buttons, Please so they do not flood the eyes As it may not be good for the young doctors around watching the drama unfold Watching how someone would die yet be gracefully thankful How the dying comfort those who stay behind How a man who is supposed to heal let his patient say good bye How the partners in such a struggle depart from each other at last O Donnell, JF. A Medical Oncologist s Poetry: Abdul-Rahman Jazieh, MD, MPH (2005). Journal of Cancer Education, 20(4).
37 Acknowledgements Odense University Hospital & The University of Southern Denmark Dr. Kim Brixen, Dr. Kirsten Kyvik, & Dr. Katja Schrøder Johns Hopkins RISE Program Dr. Albert Wu, Dr. Lori Paine, Ms. Cheryl Connors, & Mr. Matt Norvell Dr. Henry Taylor Dr. George Everly Johns Hopkins RISE Peer Responders Johns Hopkins Second Victim Advisory Board Maryland Patient Safety Center

38 Hanan H. Edrees, DrPH, MHSA Associate Faculty, Johns Hopkins University
39 Additional Slides

40 Scott Three-Tiered Interventional Model of Second Victim Support Scott S, et al (2010).Caring for Our Own: Deploying a Systemwide Second Victim Rapid Response Team. The Joint Commission Journal on Quality and Patient Safety
41
, other: difficult situations, burnout, staff assault,")
42 Characteristics of RISE Calls (n=80) Description of calls: death of a patient (45%), involved in adverse event (21%), other: difficult situations, burnout, staff assault, conflicts, etc.
43 PFA PFA was co-developed in 2006 by the National Center for Post Traumatic Stress Disorder, a division of the United States Department of Veterans Affairs, and the National Child Traumatic Stress Network as a technique used to assist individuals in the immediate aftermath of a disaster and to reduce the occurrence of PTSD.
Enhancing Caregiver Resilience The Role of Staff Support
 Enhancing Caregiver Resilience The Role of Staff Support Albert W. Wu, MD, MPH Johns Hopkins Bloomberg School of Public Health Bonn, 29 March 2017 Wu AW 2017 Burnout When passionate, committed people become
Enhancing Caregiver Resilience The Role of Staff Support Albert W. Wu, MD, MPH Johns Hopkins Bloomberg School of Public Health Bonn, 29 March 2017 Wu AW 2017 Burnout When passionate, committed people become
Adverse Events and the Second Victim
 Adverse Events and the Second Victim Albert Wu, MD, MPH, FACP Johns Hopkins University 1 Wu AW, BMJ 2000 Definition A health care provider involved in an unanticipated adverse patient event and/or medical
Adverse Events and the Second Victim Albert Wu, MD, MPH, FACP Johns Hopkins University 1 Wu AW, BMJ 2000 Definition A health care provider involved in an unanticipated adverse patient event and/or medical
Caring For The Caregiver After Adverse Clinical Effects. Susan D. Scott, PhD, RN, CPPS University of Missouri Health Care System March 11, 2016
 Caring For The Caregiver After Adverse Clinical Effects Susan D. Scott, PhD, RN, CPPS University of Missouri Health Care System March 11, 2016 University of Missouri Health Care University of Missouri
Caring For The Caregiver After Adverse Clinical Effects Susan D. Scott, PhD, RN, CPPS University of Missouri Health Care System March 11, 2016 University of Missouri Health Care University of Missouri
Health care workers as second victims of medical errors
 ORIGINAL ARTICLE Health care workers as second victims of medical errors Hanan H. Edrees, Lori A. Paine, E. Robert Feroli, Albert W. Wu Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland,
ORIGINAL ARTICLE Health care workers as second victims of medical errors Hanan H. Edrees, Lori A. Paine, E. Robert Feroli, Albert W. Wu Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland,
Human resources. OR Manager Vol. 29 No. 5 May 2013
 Human resources Second victim rapid-response team helps fellow clinicians recover from trauma One Friday evening at University of Missouri Health System (MUHS) in Columbia, Missouri, Tony*, an RN with
Human resources Second victim rapid-response team helps fellow clinicians recover from trauma One Friday evening at University of Missouri Health System (MUHS) in Columbia, Missouri, Tony*, an RN with
Northwest Second Victim Programs
 Northwest Second Victim Programs The Washington Patient Safety Coalition September 30, 2013 www.wapatientsafety.org P a g e 2 Background The speakers at the closing session of the 2012 Washington Patient
Northwest Second Victim Programs The Washington Patient Safety Coalition September 30, 2013 www.wapatientsafety.org P a g e 2 Background The speakers at the closing session of the 2012 Washington Patient
Burnout in Palliative Care. Palliative Regional Rounds January 16, 2015 Craig Goldie
 Burnout in Palliative Care Palliative Regional Rounds January 16, 2015 Craig Goldie Overview of discussion Define burnout and compassion fatigue Review prevalence of burnout in palliative care Complete
Burnout in Palliative Care Palliative Regional Rounds January 16, 2015 Craig Goldie Overview of discussion Define burnout and compassion fatigue Review prevalence of burnout in palliative care Complete
Healing Our Own. The Second Victim Phenomenon & a New Approach to Quality Care. September, 2014 Joshua Clark, RN, CPPS
 Healing Our Own The Second Victim Phenomenon & a New Approach to Quality Care September, 2014 Joshua Clark, RN, CPPS Objectives Define the term "Second Victim Discuss how the Second Victim concept materialized
Healing Our Own The Second Victim Phenomenon & a New Approach to Quality Care September, 2014 Joshua Clark, RN, CPPS Objectives Define the term "Second Victim Discuss how the Second Victim concept materialized
Physician Support After Adverse Patient Events Women s Leadership Forum Massachusetts Medical Society September 30, 2016
 Physician Support After Adverse Patient Events Women s Leadership Forum Massachusetts Medical Society September 30, 2016 Carol Mostow LICSW Associate Director, Psychosocial Training Department of Family
Physician Support After Adverse Patient Events Women s Leadership Forum Massachusetts Medical Society September 30, 2016 Carol Mostow LICSW Associate Director, Psychosocial Training Department of Family
Page 1. Care for the Care Provider: A Second Victim Staff Support Program. PSHP Annual Assembly October 30, Our Journey
 Care for the Care Provider: A Second Victim Staff Support Program PSHP Annual Assembly October 30, 2015 Jill G. Huzinec, RPh, CPPS Director Patient Safety Hospital University of Pennsylvania Learning Objectives
Care for the Care Provider: A Second Victim Staff Support Program PSHP Annual Assembly October 30, 2015 Jill G. Huzinec, RPh, CPPS Director Patient Safety Hospital University of Pennsylvania Learning Objectives
Second Victim: Gaining A Deeper Understanding To Mitigate Suffering
 Second Victim: Gaining A Deeper Understanding To Mitigate Suffering Susan D. Scott 1, RN, MSN, Laura E. Hirschinger 1, RN, MSN, Myra McCoig 1, Julie Brandt 2, PhD, Karen R. Cox 1,2 PhD,RN, Leslie W. Hall,
Second Victim: Gaining A Deeper Understanding To Mitigate Suffering Susan D. Scott 1, RN, MSN, Laura E. Hirschinger 1, RN, MSN, Myra McCoig 1, Julie Brandt 2, PhD, Karen R. Cox 1,2 PhD,RN, Leslie W. Hall,
International Focus on Second Victim Work
 M11 This presenter has nothing to disclose International Focus on Second Victim Work Dr. Kris Vanhaecht Senior Research Fellow School of Public Health KU Leuven, University of Leuven, Belgium European
M11 This presenter has nothing to disclose International Focus on Second Victim Work Dr. Kris Vanhaecht Senior Research Fellow School of Public Health KU Leuven, University of Leuven, Belgium European
Meeting the challenge of interdisciplinary care for psychological impact of pediatric trauma
 Meeting the challenge of interdisciplinary care for psychological impact of pediatric trauma Nancy Kassam-Adams, PhD nlkaphd@upenn.edu Flaura Winston, MD, PhD Meghan Marsac, PhD Overview Quick review of
Meeting the challenge of interdisciplinary care for psychological impact of pediatric trauma Nancy Kassam-Adams, PhD nlkaphd@upenn.edu Flaura Winston, MD, PhD Meghan Marsac, PhD Overview Quick review of
4th Australasian Natural Hazards Management Conference 2010
 4th Australasian Natural Hazards Management Conference 2010 Advances in Psychological First Aid Dr Sarb Johal Massey University Department of Health, UK nzpsych.blip.tv sarb@equanimity.co.nz What is Psychological
4th Australasian Natural Hazards Management Conference 2010 Advances in Psychological First Aid Dr Sarb Johal Massey University Department of Health, UK nzpsych.blip.tv sarb@equanimity.co.nz What is Psychological
Ian Nisonson, M.D. 11/2/2017
 Ian Nisonson, M.D., FACS Conference Director President of Baptist-South Miami Medical Staff (1997-1999) Senior Active Medical Staff, Baptist Hospital of Miami Adjunct Assistant Professor, Herbert Wertheim
Ian Nisonson, M.D., FACS Conference Director President of Baptist-South Miami Medical Staff (1997-1999) Senior Active Medical Staff, Baptist Hospital of Miami Adjunct Assistant Professor, Herbert Wertheim
The second victim phenomenon is a serious
 Clinician Support: Five Years of Lessons Learned By Laura E. Hirschinger, RN, MSN; Susan D. Scott, RN, PhD; and Kristin Hahn-Cover, MD The second victim phenomenon is a serious consequence of any healthcare
Clinician Support: Five Years of Lessons Learned By Laura E. Hirschinger, RN, MSN; Susan D. Scott, RN, PhD; and Kristin Hahn-Cover, MD The second victim phenomenon is a serious consequence of any healthcare
Course Descriptions. ICISF Course Descriptions:
 ICISF Course Descriptions: http://www.icisf.org/sections/education-training/coursedescriptions/ Course Descriptions Advanced Assisting Individuals in Crisis Advanced Group Crisis Intervention Assaulted
ICISF Course Descriptions: http://www.icisf.org/sections/education-training/coursedescriptions/ Course Descriptions Advanced Assisting Individuals in Crisis Advanced Group Crisis Intervention Assaulted
Supporting Healing. Restoring Hope.
 Session Code: M22 This presenter has nothing to disclose Supporting Healing. Restoring Hope. Linda K. Kenney President, MITSS (Medically Induced Trauma Support Services) IHI Forum, December 2013 Orlando,
Session Code: M22 This presenter has nothing to disclose Supporting Healing. Restoring Hope. Linda K. Kenney President, MITSS (Medically Induced Trauma Support Services) IHI Forum, December 2013 Orlando,
VOLUME THREE / ISSUE TWO APRIL 2018
 VOLUME THREE / ISSUE TWO APRIL 2018 A just culture allows for the imperfectness of humans and the recognition that there are other factors at play when an error occurs but also allows for individual accountability.
VOLUME THREE / ISSUE TWO APRIL 2018 A just culture allows for the imperfectness of humans and the recognition that there are other factors at play when an error occurs but also allows for individual accountability.
Compassion Fatigue: Are you running on fumes?
 Compassion Fatigue: Are you running on fumes? What is compassion? Feeling deep sympathy and sorrow for another who is stricken by suffering or misfortune, accompanied by a strong desire to alleviate the
Compassion Fatigue: Are you running on fumes? What is compassion? Feeling deep sympathy and sorrow for another who is stricken by suffering or misfortune, accompanied by a strong desire to alleviate the
Agenda. Office of Clinician Support. Staff Responses to An Adverse Event. A Safe Place To Talk. Traumatic Stress Symptoms
 Office of Clinician Support: Caring for Children s Hospital Clinicians David R. DeMaso, MD Psychiatrist-in-Chief & Chairman of Psychiatry Children s Hospital Boston Professor of Psychiatry & Pediatrics
Office of Clinician Support: Caring for Children s Hospital Clinicians David R. DeMaso, MD Psychiatrist-in-Chief & Chairman of Psychiatry Children s Hospital Boston Professor of Psychiatry & Pediatrics
Beginning May 1, 2014,
 HEALTHCARE SERVICES GROUP Risk Management & Patient Safety Newsletter SPRING 2014 VOLUME 11, NO. 2 HSG INTRODUCES Healthcare Event Assistance & Lending Support Program (HEALS) ARVIDS V. PETERSONS, JD,
HEALTHCARE SERVICES GROUP Risk Management & Patient Safety Newsletter SPRING 2014 VOLUME 11, NO. 2 HSG INTRODUCES Healthcare Event Assistance & Lending Support Program (HEALS) ARVIDS V. PETERSONS, JD,
MOST EXPERIENCED NURSES, physicians,
 J Nurs Care Qual Vol. 27, No. 1, pp. 1 5 Copyright c 2012 Wolters Kluwer Health Lippincott Williams & Wilkins AHRQ Commentary This commentary on patient safety in nursing practice comes from the Agency
J Nurs Care Qual Vol. 27, No. 1, pp. 1 5 Copyright c 2012 Wolters Kluwer Health Lippincott Williams & Wilkins AHRQ Commentary This commentary on patient safety in nursing practice comes from the Agency
Involvement of healthcare professionals in an adverse event: the role of. management in supporting their work force
 Involvement of healthcare professionals in an adverse event: the role of management in supporting their work force Article ID: AOP_14_035 ISSN: 1897-9483 Authors: Eva Van Gerven, Deborah Seys, Massimiliano
Involvement of healthcare professionals in an adverse event: the role of management in supporting their work force Article ID: AOP_14_035 ISSN: 1897-9483 Authors: Eva Van Gerven, Deborah Seys, Massimiliano
PSYCHOSOCIAL ASPECTS OF PALLIATIVE CARE IN MENTAL HEALTH SETTINGS. Dawn Chaitram BSW, RSW, MA Psychosocial Specialist
 PSYCHOSOCIAL ASPECTS OF PALLIATIVE CARE IN MENTAL HEALTH SETTINGS Dawn Chaitram BSW, RSW, MA Psychosocial Specialist WRHA Palliative Care Program April 19, 2017 OUTLINE Vulnerability and Compassion Addressing
PSYCHOSOCIAL ASPECTS OF PALLIATIVE CARE IN MENTAL HEALTH SETTINGS Dawn Chaitram BSW, RSW, MA Psychosocial Specialist WRHA Palliative Care Program April 19, 2017 OUTLINE Vulnerability and Compassion Addressing
NOT PROTECTIVELY MARKED
 POLICY / PROCEDURE Security Classification Disclosable under Freedom of Information Act 2000 NOT PROTECTIVELY MARKED Yes POLICY TITLE Welfare Services REFERENCE NUMBER A114 Version 1.1 POLICY OWNERSHIP
POLICY / PROCEDURE Security Classification Disclosable under Freedom of Information Act 2000 NOT PROTECTIVELY MARKED Yes POLICY TITLE Welfare Services REFERENCE NUMBER A114 Version 1.1 POLICY OWNERSHIP
Presented by Rosalie Lo, PsyD Senior Clinical Psychologist Certified Traumatologist
 Presented by Rosalie Lo, PsyD Senior Clinical Psychologist Certified Traumatologist Corporate Clinical Psychology Services (CCPS) Hospital Authority, Hong Kong Challenges Facing HCWs They experience
Presented by Rosalie Lo, PsyD Senior Clinical Psychologist Certified Traumatologist Corporate Clinical Psychology Services (CCPS) Hospital Authority, Hong Kong Challenges Facing HCWs They experience
Section V Disaster Mental Health Services Team and Program Development
 Disaster Mental Health Services Disaster Mental Health Services Team and Program Development Section V Disaster Mental Health Services Team and Program Development TEAM FORMATION AND SELECTION Staffing
Disaster Mental Health Services Disaster Mental Health Services Team and Program Development Section V Disaster Mental Health Services Team and Program Development TEAM FORMATION AND SELECTION Staffing
Although recent publications have
 Second Victim Support: Implications for Patient Safety Attitudes and Perceptions By Susan D. Scott, PhD, RN, CPPS Although recent publications have enhanced our understanding of the second victim phenomenon,
Second Victim Support: Implications for Patient Safety Attitudes and Perceptions By Susan D. Scott, PhD, RN, CPPS Although recent publications have enhanced our understanding of the second victim phenomenon,
TRINITY HEALTH THE VALUE OF SPIRITUAL CARE
 TRINITY HEALTH THE VALUE OF SPIRITUAL CARE 2015 Trinity Health, Livonia, MI 20555 Victor Parkway Livonia, Michigan 48152?k The Good Samaritan MISSION We, Trinity Health, serve together in the spirit of
TRINITY HEALTH THE VALUE OF SPIRITUAL CARE 2015 Trinity Health, Livonia, MI 20555 Victor Parkway Livonia, Michigan 48152?k The Good Samaritan MISSION We, Trinity Health, serve together in the spirit of
Critical Incident 5/7/2018. Defining Critical Incident. Defusing. Defusing and Debriefing
 Critical Incident Defusing and Debriefing Defining Critical Incident Any event that overwhelms the normal coping abilities of an emergency worker such as EMS, Fire, Police, and Emergency room personnel.
Critical Incident Defusing and Debriefing Defining Critical Incident Any event that overwhelms the normal coping abilities of an emergency worker such as EMS, Fire, Police, and Emergency room personnel.
Outcome and Process Evaluation Report: Crisis Residential Programs
 FY216-217, Quarter 4 Outcome and Process Evaluation Report: Crisis Residential Programs April Howard, Ph.D. Erin Dowdy, Ph.D. Shereen Khatapoush, Ph.D. Kathryn Moffa, M.Ed. O c t o b e r 2 1 7 Table of
FY216-217, Quarter 4 Outcome and Process Evaluation Report: Crisis Residential Programs April Howard, Ph.D. Erin Dowdy, Ph.D. Shereen Khatapoush, Ph.D. Kathryn Moffa, M.Ed. O c t o b e r 2 1 7 Table of
Integrated Care Condolence Teams for Missing, Injured or Deceased Standards and Procedures
 Integrated Care Condolence Teams for Missing, Injured or Deceased Standards and Procedures Disaster Cycle Services Standards & Procedures DCS SP Respond January 2016 Change Log Date Page(s) Section Change
Integrated Care Condolence Teams for Missing, Injured or Deceased Standards and Procedures Disaster Cycle Services Standards & Procedures DCS SP Respond January 2016 Change Log Date Page(s) Section Change
Improving Inpatient Diabetes Management
 Improvement from Front Office to Front Line May 2012 Volume 38 Number 5 Improving Inpatient Diabetes Management Features Performance Improvement Implementing and Evaluating a Multicomponent Inpatient Diabetes
Improvement from Front Office to Front Line May 2012 Volume 38 Number 5 Improving Inpatient Diabetes Management Features Performance Improvement Implementing and Evaluating a Multicomponent Inpatient Diabetes
MICHAEL E. KILPATRICK, M.D. DEPUTY DIRECTOR, DEPLOYMENT HEALTH SUPPORT BEFORE THE VETERANS AFFAIRS COMMITTEE U.S. HOUSE OF REPRESENTATIVES
 MICHAEL E. KILPATRICK, M.D. DEPUTY DIRECTOR, DEPLOYMENT HEALTH SUPPORT BEFORE THE VETERANS AFFAIRS COMMITTEE U.S. HOUSE OF REPRESENTATIVES POST TRAUMATIC STRESS DISORDER July 27, 2005 Mr. Chainnan and
MICHAEL E. KILPATRICK, M.D. DEPUTY DIRECTOR, DEPLOYMENT HEALTH SUPPORT BEFORE THE VETERANS AFFAIRS COMMITTEE U.S. HOUSE OF REPRESENTATIVES POST TRAUMATIC STRESS DISORDER July 27, 2005 Mr. Chainnan and
Workshop Framework: Pathways
 2011 National Conference The National Association of Catholic Chaplains One Day at a time: Companioning Caregivers in Perinatal Loss Judy Friedrichs, MS, RN, CT Rush University Medical Center Workshop
2011 National Conference The National Association of Catholic Chaplains One Day at a time: Companioning Caregivers in Perinatal Loss Judy Friedrichs, MS, RN, CT Rush University Medical Center Workshop
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
To disclose, or not to disclose (a medication error) that is the question
 that is the question") To disclose, or not to disclose (a medication error) that is the question Jennifer L. Mazan, Pharm.D., Associate Professor of Pharmacy Practice Ana C. Quiñones-Boex, Ph.D., Associate Professor of Pharmacy
To disclose, or not to disclose (a medication error) that is the question Jennifer L. Mazan, Pharm.D., Associate Professor of Pharmacy Practice Ana C. Quiñones-Boex, Ph.D., Associate Professor of Pharmacy
Action Timeline, Training, and Support for Psychosocial/Disaster Mental Health Responders
 Action Timeline, Training, and Support for Psychosocial/Disaster Mental Health Responders IPRED Psychosocial Working Group The Timeline depends in part on the type of disaster; moreover, the phases of
Action Timeline, Training, and Support for Psychosocial/Disaster Mental Health Responders IPRED Psychosocial Working Group The Timeline depends in part on the type of disaster; moreover, the phases of
Leader Guide and Postvention Checklist
 3 Leader Guide and Postvention Checklist 1 Leaders Guide to Suicide and Postvention Checklist June 2016 Leaders Guide and Suicide Postvention Checklist Purpose: This checklist is designed to assist leaders
3 Leader Guide and Postvention Checklist 1 Leaders Guide to Suicide and Postvention Checklist June 2016 Leaders Guide and Suicide Postvention Checklist Purpose: This checklist is designed to assist leaders
Collaborative Care in Pediatric Mental Health: A Qualitative Case Study
 Collaborative Care in Pediatric Mental Health: A Qualitative Case Study Megan McLeod, M.D. Supervised by Sourav Sengupta, M.D., M.P.H. March 3 rd, 2017 Acknowledgements Thank you Dr. Sengupta Outline 1.
Collaborative Care in Pediatric Mental Health: A Qualitative Case Study Megan McLeod, M.D. Supervised by Sourav Sengupta, M.D., M.P.H. March 3 rd, 2017 Acknowledgements Thank you Dr. Sengupta Outline 1.
Disclosure of Adverse Events and Medical Errors. Albert W. Wu, MD, MPH
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Adult Apgar Test. 1. I am satisfied with the ACCESS I have to my emotions -- to laugh, to be sad, to feel pleasure or even anger.
 Adult Apgar Test Score 0=hardly ever 1=sometimes 2=almost always 1. I am satisfied with the ACCESS I have to my emotions -- to laugh, to be sad, to feel pleasure or even anger. 2. I am satisfied that my
Adult Apgar Test Score 0=hardly ever 1=sometimes 2=almost always 1. I am satisfied with the ACCESS I have to my emotions -- to laugh, to be sad, to feel pleasure or even anger. 2. I am satisfied that my
Traumatic Brain Injury in the Defense Department
 Defense and Veterans Brain Injury Center Recovery Care Coordinator Training Traumatic Brain Injury in the Defense Department Elizabeth Pletcher, MSW, LSW Recovery Support Specialist Defense and Veterans
Defense and Veterans Brain Injury Center Recovery Care Coordinator Training Traumatic Brain Injury in the Defense Department Elizabeth Pletcher, MSW, LSW Recovery Support Specialist Defense and Veterans
Children s Senior Psychotherapist. Therapeutic Services GRADE: 05. Context and Purpose of the Job
 JOB TITLE: TEAM: GROUP: LOCATION: REPORTS TO: Children s Psychotherapist Therapeutic Services Operations Luton Children s Senior Psychotherapist GRADE: 05 HOURS: 21 hours per week Context and Purpose of
JOB TITLE: TEAM: GROUP: LOCATION: REPORTS TO: Children s Psychotherapist Therapeutic Services Operations Luton Children s Senior Psychotherapist GRADE: 05 HOURS: 21 hours per week Context and Purpose of
ANATOMY OF AN OBSTETRIC LOSS HEALING THE FAMILIES AND OURSELVES
 ANATOMY OF AN OBSTETRIC LOSS HEALING THE FAMILIES AND OURSELVES Cynthia Chazotte, MD, FACOG Montefiore Medical Center Albert Einstein College of Medicine CONFLICT OF INTEREST DISCLOSURE STATEMENT I have
ANATOMY OF AN OBSTETRIC LOSS HEALING THE FAMILIES AND OURSELVES Cynthia Chazotte, MD, FACOG Montefiore Medical Center Albert Einstein College of Medicine CONFLICT OF INTEREST DISCLOSURE STATEMENT I have
Psychiatric Intensive Care for Acutely Suicidal Adolescent Patients A Shift from Observation to Engagement
 Psychiatric Intensive Care for Acutely Suicidal Adolescent Patients A Shift from Observation to Engagement Joanne Bartlett MS RN NPP Mary Lou Heinrich RN-BC, BA, MPS Kay Bogren BSN University of Rochester
Psychiatric Intensive Care for Acutely Suicidal Adolescent Patients A Shift from Observation to Engagement Joanne Bartlett MS RN NPP Mary Lou Heinrich RN-BC, BA, MPS Kay Bogren BSN University of Rochester
The Impact of Patient Suicide on Mental Health Nurses THESIS SUMMARY KERRY CROSS RN MN 2017
 The Impact of Patient Suicide on Mental Health Nurses THESIS SUMMARY KERRY CROSS RN MN 2017 Overview Thesis origin Aim, Purpose, Objectives Research Methodology Questionnaire Impact of Event Scale Revised
The Impact of Patient Suicide on Mental Health Nurses THESIS SUMMARY KERRY CROSS RN MN 2017 Overview Thesis origin Aim, Purpose, Objectives Research Methodology Questionnaire Impact of Event Scale Revised
EVIDENCE-BASED SPIRITUAL CARE FOR CHAPLAINS: Desirable? Feasible? How do we get there?
 EVIDENCE-BASED SPIRITUAL CARE FOR CHAPLAINS: Desirable? Feasible? How do we get there? George Fitchett, DMin, PhD Department of Religion, Health and Human Values Rush University Medical Center, Chicago,
EVIDENCE-BASED SPIRITUAL CARE FOR CHAPLAINS: Desirable? Feasible? How do we get there? George Fitchett, DMin, PhD Department of Religion, Health and Human Values Rush University Medical Center, Chicago,
Reporting and Disclosing Adverse Events
 Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Any nurse can become involved in an. Creating Healthy Work Environments for Second Victims of Adverse Events ABSTRACT
 AACN d Critical Care Volume 28, Number 4, pp. 366-374 2017 AACN Creating Healthy Work Environments for Second Victims of Adverse Events Linda M. Tamburri, RN, MS, APN, CCRN ABSTRACT Adverse events may
AACN d Critical Care Volume 28, Number 4, pp. 366-374 2017 AACN Creating Healthy Work Environments for Second Victims of Adverse Events Linda M. Tamburri, RN, MS, APN, CCRN ABSTRACT Adverse events may
Provider Orientation Training Webinar 2017_01
 Provider Orientation Training Webinar 2017_01 Training Topics Administrative Orientation Welcome and Introductions Overview of ValueOptions/Beacon Health Options Military OneSource Program Participant
Provider Orientation Training Webinar 2017_01 Training Topics Administrative Orientation Welcome and Introductions Overview of ValueOptions/Beacon Health Options Military OneSource Program Participant
Self-care and burnout
 Self-care and burnout Karen Brouhard, LICSW Faculty and Staff Assistance Office Boston University Resilience and Mindfulness Program for Physicians Bringing Intention, Attention and Reflection to Clinical
Self-care and burnout Karen Brouhard, LICSW Faculty and Staff Assistance Office Boston University Resilience and Mindfulness Program for Physicians Bringing Intention, Attention and Reflection to Clinical
Reference Understanding and Addressing Moral Distress, Epstein & Delgado, Nursing World, Sept. 30, 2010
 Moral Distress and Moral Resilience Nurses encounter many situations in their work place that can cause moral distress. Moral distress is defined by an inability to act in alignment with one s moral values
Moral Distress and Moral Resilience Nurses encounter many situations in their work place that can cause moral distress. Moral distress is defined by an inability to act in alignment with one s moral values
NOT PROTECTIVELY MARKED
 POLICY / PROCEDURE Security Classification Disclosable under Freedom of Information Act 2000 NOT PROTECTIVELY MARKED Yes POLICY TITLE Services REFERENCE NUMBER A114 Version 1.2 POLICY OWNERSHIP DIRECTORATE
POLICY / PROCEDURE Security Classification Disclosable under Freedom of Information Act 2000 NOT PROTECTIVELY MARKED Yes POLICY TITLE Services REFERENCE NUMBER A114 Version 1.2 POLICY OWNERSHIP DIRECTORATE
Prevalence of Stress and Coping Mechanism Among Staff Nurses of Intensive Care Unit in a Selected Hospital
 International Journal of Neurosurgery 2018; 2(1): 8-12 http://www.sciencepublishinggroup.com/j/ijn doi: 10.11648/j.ijn.20180201.12 Prevalence of Stress and Coping Mechanism Among Staff Nurses of Intensive
International Journal of Neurosurgery 2018; 2(1): 8-12 http://www.sciencepublishinggroup.com/j/ijn doi: 10.11648/j.ijn.20180201.12 Prevalence of Stress and Coping Mechanism Among Staff Nurses of Intensive
Nothing to disclose. Learning Objectives 4/10/2014. Caring for the Caregiver: Taking Care of You (first) and Your Staff (second)
 and Your Staff (second)") Caring for the Caregiver: Taking Care of You (first) and Your Staff (second) Judith S. Gooding VP Signature Programs March of Dimes NICU Leadership Forum: April 30, 2014 Nothing to disclose Neither I nor
Caring for the Caregiver: Taking Care of You (first) and Your Staff (second) Judith S. Gooding VP Signature Programs March of Dimes NICU Leadership Forum: April 30, 2014 Nothing to disclose Neither I nor
10/3/2014. Problem Identification: Practice Gap. Increasing Satisfaction With the Birth Experience Through a Focused Postpartum Debriefing Session
 Increasing Satisfaction With the Birth Experience Through a Focused Postpartum Debriefing Session Jennifer A. Johnson, DNP, RN, ANP-C, WHNP-BC Dr. Melissa D. Avery, PhD, RN, CNM, FACNM, FAAN, Faculty Advisor
Increasing Satisfaction With the Birth Experience Through a Focused Postpartum Debriefing Session Jennifer A. Johnson, DNP, RN, ANP-C, WHNP-BC Dr. Melissa D. Avery, PhD, RN, CNM, FACNM, FAAN, Faculty Advisor
Predicting the Risk of Compassion Fatigue: An Empirical Study of Hospice Nurses By Maryann Abendroth, MSN, RN Executive Summary September 1, 2005
 Predicting the Risk of Compassion Fatigue: An Empirical Study of Hospice Nurses By Maryann Abendroth, MSN, RN Executive Summary September 1, 2005 Compassion fatigue (CF), is a secondary traumatic stress
Predicting the Risk of Compassion Fatigue: An Empirical Study of Hospice Nurses By Maryann Abendroth, MSN, RN Executive Summary September 1, 2005 Compassion fatigue (CF), is a secondary traumatic stress
Workplace Bullying/Critical Adverse Events
 Workplace Bullying/Critical Adverse Events October 25, 2014 Lynn Reede, CRNA, DNP, MBA AANA Senior Director, Professional Practice Explore Discuss the impact and how to mitigate vertical and lateral violence
Workplace Bullying/Critical Adverse Events October 25, 2014 Lynn Reede, CRNA, DNP, MBA AANA Senior Director, Professional Practice Explore Discuss the impact and how to mitigate vertical and lateral violence
Hospice 101. Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati
 Hospice 101 Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati Hospice of Cincinnati Hospice of Cincinnati creates the best possible and most meaningful EOL experience for all who
Hospice 101 Janet Montgomery, BSN, MBA Chief Marketing Officer, Hospice of Cincinnati Hospice of Cincinnati Hospice of Cincinnati creates the best possible and most meaningful EOL experience for all who
Mitigating Disputes in Healthcare Using Assertive Honoring TM. Doron Pely, PhD*
 Mitigating Disputes in Healthcare Using Assertive Honoring TM Doron Pely, PhD* Table of Content The Problem... 3 The Impact on Employees... 3 The Cost for Employers... 3 Searching for a Solution... 4 The
Mitigating Disputes in Healthcare Using Assertive Honoring TM Doron Pely, PhD* Table of Content The Problem... 3 The Impact on Employees... 3 The Cost for Employers... 3 Searching for a Solution... 4 The
Leader Guide and Postvention Checklist
 Leader Guide and Postvention Checklist 1 DoD Leader Guide and Postvention Checklist Purpose: This checklist is designed to assist leaders in guiding their response to suicides and suicide attempts. Research
Leader Guide and Postvention Checklist 1 DoD Leader Guide and Postvention Checklist Purpose: This checklist is designed to assist leaders in guiding their response to suicides and suicide attempts. Research
NOTE: The first appearance of terms in bold in the body of this document (except titles) are defined terms please refer to the Definitions section.
 are defined terms please refer to the Definitions section.") TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
TITLE DISCLOSURE OF HARM SCOPE Provincial APPROVAL AUTHORITY Quality Safety and Outcomes Improvement Executive Committee SPONSOR Quality and Healthcare Improvement PARENT DOCUMENT TITLE, TYPE AND NUMBER
Battlemind Training: Building Soldier Resiliency
 Carl Andrew Castro Walter Reed Army Institute of Research Department of Military Psychiatry 503 Robert Grant Avenue Silver Spring, MD 20910 USA Telephone: (301) 319-9174 Fax: (301) 319-9484 carl.castro@us.army.mil
Carl Andrew Castro Walter Reed Army Institute of Research Department of Military Psychiatry 503 Robert Grant Avenue Silver Spring, MD 20910 USA Telephone: (301) 319-9174 Fax: (301) 319-9484 carl.castro@us.army.mil
Nebraska Lifespan Respite Caregiver Survey
 Nebraska Lifespan Respite Caregiver Survey Welcome to the Nebraska Lifespan Caregiver Survey! Respite is planned or emergency care provided to a child or adult with special needs in order to provide temporary
Nebraska Lifespan Respite Caregiver Survey Welcome to the Nebraska Lifespan Caregiver Survey! Respite is planned or emergency care provided to a child or adult with special needs in order to provide temporary
Collaboration to Address Compassion Fatigue in Hospital Staff
 Collaboration to Address Compassion Fatigue in Hospital Staff Presenters Sabrina Derrington, MD Jim Manzardo, STB, BCC Kristi Thime, RN, CNML Objectives Understand risk factors for compassion fatigue and
Collaboration to Address Compassion Fatigue in Hospital Staff Presenters Sabrina Derrington, MD Jim Manzardo, STB, BCC Kristi Thime, RN, CNML Objectives Understand risk factors for compassion fatigue and
A story of resilience: being a pediatrician in Spain
 A story of resilience: being a pediatrician in Spain Health, lifestyles and working conditions of pediatricians in Spain Working team Director: Lucía Baranda Supported by: Galatea Foundation: Anna Mitjans
A story of resilience: being a pediatrician in Spain Health, lifestyles and working conditions of pediatricians in Spain Working team Director: Lucía Baranda Supported by: Galatea Foundation: Anna Mitjans
Family & Children s Services. Center
 Family & Children s Services CrisisCare Center When severe psychiatric crisis makes daily life seem impossible, Family & Children s Services new CrisisCare Center can help. Services are available around
Family & Children s Services CrisisCare Center When severe psychiatric crisis makes daily life seem impossible, Family & Children s Services new CrisisCare Center can help. Services are available around
Ethical Pain Management: Have the Tides Changed? Conflict of Interest Disclosure. Objectives 9/4/2014
 Ethical Pain Management: Have the Tides Changed? Helen N Turner, DNP, RN BC, PCNS BC, FAAN Clinical Nurse Specialist, Pediatric Pain Management ASPMN President Elect turnerh@ohsu.edu Conflict of Interest
Ethical Pain Management: Have the Tides Changed? Helen N Turner, DNP, RN BC, PCNS BC, FAAN Clinical Nurse Specialist, Pediatric Pain Management ASPMN President Elect turnerh@ohsu.edu Conflict of Interest
Training Doctors to Manage Their
 This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues, clients or customers visit http://www.djreprints.com. http://www.wsj.com/articles/training-doctors-to-manage-their-feelings-1462808283
This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues, clients or customers visit http://www.djreprints.com. http://www.wsj.com/articles/training-doctors-to-manage-their-feelings-1462808283
Transforming Care for Older Adults AGE DIFFERENT. Jann Dorman, Alen Vartan, Faye Sahai, and Estee Neuwirth, Phd
 Transforming Care for Older Adults AGE DIFFERENT Jann Dorman, Alen Vartan, Faye Sahai, and Estee Neuwirth, Phd Minicourse 16 Annual IHI National Forum on Quality Improvement in Health Care Dec. 8, 2014
Transforming Care for Older Adults AGE DIFFERENT Jann Dorman, Alen Vartan, Faye Sahai, and Estee Neuwirth, Phd Minicourse 16 Annual IHI National Forum on Quality Improvement in Health Care Dec. 8, 2014
PHYSICIAN BURNOUT DISCLOSURES... A BURNING EPIDEMIC I HAVE NO DISCLOSURES TO REPORT.
 PHYSICIAN BURNOUT A BURNING EPIDEMIC I HAVE NO DISCLOSURES TO REPORT. DISCLOSURES... HISTORICAL DEFINITION. FREUDENBERGER..1974 coined the term Burnout. PROCESS One Year Progression Historical term used
PHYSICIAN BURNOUT A BURNING EPIDEMIC I HAVE NO DISCLOSURES TO REPORT. DISCLOSURES... HISTORICAL DEFINITION. FREUDENBERGER..1974 coined the term Burnout. PROCESS One Year Progression Historical term used
Note: This is a guide, not a policy. This document should be used as a guide for supervisors to use all the tools at their disposal.
 Note: This is a guide, not a policy. This document should be used as a guide for supervisors to use all the tools at their disposal. As always, when addressing employee issues, it is strongly recommended
Note: This is a guide, not a policy. This document should be used as a guide for supervisors to use all the tools at their disposal. As always, when addressing employee issues, it is strongly recommended
Symptoms and stress in family caregivers of ICU patients. Hanne Birgit Alfheim RN, CCN, PhD student Photo:
 Symptoms and stress in family caregivers of ICU patients Hanne Birgit Alfheim RN, CCN, PhD student Photo: oystein.horgmo@medisin.uio.no Why are the family caregivers so important for the patients? Family
Symptoms and stress in family caregivers of ICU patients Hanne Birgit Alfheim RN, CCN, PhD student Photo: oystein.horgmo@medisin.uio.no Why are the family caregivers so important for the patients? Family
POLICE Seeking help for a mental health problem. Blue Light Programme
 POLICE Seeking help for a mental health problem Blue Light Programme Seeking help for a mental health problem This is a guide for police service staff and volunteers on how to seek professional help for
POLICE Seeking help for a mental health problem Blue Light Programme Seeking help for a mental health problem This is a guide for police service staff and volunteers on how to seek professional help for
Core Domain You will be able to: You will know and understand: Leadership, Management and Team Working
 DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
DEGREE APPRENTICESHIP - REGISTERED NURSE 1 ST0293/01 Occupational Profile: A career in nursing is dynamic and exciting with opportunities to work in a range of different roles as a Registered Nurse. Your
Palliative Care Competencies for Occupational Therapists
 Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
Principles of Palliative Care Demonstrates an understanding of the philosophy of palliative care Demonstrates an understanding that a palliative approach to care starts early in the trajectory of a progressive
CARERS WELCOME PACK COMMUNITY MENTAL HEALTH DIVISION
 CARERS WELCOME PACK COMMUNITY MENTAL HEALTH DIVISION Contents WELCOME CARE, TREATMENT AND SUPPORT FOR SERVICE USERS CARER S SUPPORT NATIONAL AND LOCAL CARERS SERVICES CARING IN A CRISIS INFORMATION SHARING
CARERS WELCOME PACK COMMUNITY MENTAL HEALTH DIVISION Contents WELCOME CARE, TREATMENT AND SUPPORT FOR SERVICE USERS CARER S SUPPORT NATIONAL AND LOCAL CARERS SERVICES CARING IN A CRISIS INFORMATION SHARING
Measuring Pastoral Care Performance
 PASTORAL CARE Measuring Pastoral Care Performance RABBI NADIA SIRITSKY, DMin, MSSW, BCC; CYNTHIA L. CONLEY, PhD, MSW; and BEN MILLER, BSSW BACKGROUND OF THE PROBLEM There is a profusion of research in
PASTORAL CARE Measuring Pastoral Care Performance RABBI NADIA SIRITSKY, DMin, MSSW, BCC; CYNTHIA L. CONLEY, PhD, MSW; and BEN MILLER, BSSW BACKGROUND OF THE PROBLEM There is a profusion of research in
Walking the Walk Individual Creative Tools for Transforming Compassion Fatigue & Vicarious Trauma
 Walking the Walk Individual Creative Tools for Transforming Compassion Fatigue & Vicarious Trauma Kay Glidden, M.S., Certified Compassion Fatigue Specialist & Trainer Beth Reynolds-Lewis, B.S., Certified
Walking the Walk Individual Creative Tools for Transforming Compassion Fatigue & Vicarious Trauma Kay Glidden, M.S., Certified Compassion Fatigue Specialist & Trainer Beth Reynolds-Lewis, B.S., Certified
Physician Burnout: What Is It and What Causes It?
 Physician Burnout: What Is It and What Causes It? By Michael Baron, MD, MPH, FASAM Editor's Note: This is part two in a four-part series on physician burnout. Part one was published in the January 2018
Physician Burnout: What Is It and What Causes It? By Michael Baron, MD, MPH, FASAM Editor's Note: This is part two in a four-part series on physician burnout. Part one was published in the January 2018
Common Questions Asked by Patients Seeking Hospice Care
 Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
Common Questions Asked by Patients Seeking Hospice Care C o m i n g t o t e r m s w i t h the fact that a loved one may need hospice care to manage his or her pain and get additional social and psychological
"Me Time": Investing in Self Care to Stay Centered during Stressful Times
 Annual Conference- Atlanta, Georgia - August 23, 2016 "Me Time": Investing in Self Care to Stay Centered during Stressful Times Sandra Edmonds Crewe, Ph.D., ACSW Dean and Professor of Social Work 1. Understand
Annual Conference- Atlanta, Georgia - August 23, 2016 "Me Time": Investing in Self Care to Stay Centered during Stressful Times Sandra Edmonds Crewe, Ph.D., ACSW Dean and Professor of Social Work 1. Understand
Self-Care for Nurses: Staying in Balance
 Self-Care for Nurses: Staying in Balance Lisa Rosenzweig, PhD Psychologist MJHS Bereavement Coordinator May 10, 2016 Financial Disclosures Lisa Rosenzweig, PhD has no financial arrangements or affiliations
Self-Care for Nurses: Staying in Balance Lisa Rosenzweig, PhD Psychologist MJHS Bereavement Coordinator May 10, 2016 Financial Disclosures Lisa Rosenzweig, PhD has no financial arrangements or affiliations
Using Innovation to Maximize Behavioral Health Accommodations. Regions Hospital Case Study
 Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
Using Innovation to Maximize Behavioral Health Accommodations Regions Hospital Case Study DISCLAIMER The following slides are provided for informational purposes only and do not constitute legal advice.
The natural history of recovery for the healthcare provider second victim after adverse patient events
 University of Missouri Health System, University of Missouri- Columbia, Columbia, Missouri, USA Correspondence to: S D Scott, Office of Clinical Effectiveness, University of Missouri Health System, One
University of Missouri Health System, University of Missouri- Columbia, Columbia, Missouri, USA Correspondence to: S D Scott, Office of Clinical Effectiveness, University of Missouri Health System, One
TBI and the Caregiver. TBI and the Caregiver. The Role of the Caregiver after Traumatic Brain Injury TBI TBI DR. CHIARAVALLOTI HAS NO
 The Role of the Caregiver after Traumatic Brain Injury Nancy D. Chiaravalloti, Ph.D. Director of Neuroscience and Neuropsychology Director of Traumatic Brain Injury Research DR. CHIARAVALLOTI HAS NO DISCLOSURES
The Role of the Caregiver after Traumatic Brain Injury Nancy D. Chiaravalloti, Ph.D. Director of Neuroscience and Neuropsychology Director of Traumatic Brain Injury Research DR. CHIARAVALLOTI HAS NO DISCLOSURES
Moral Distress and Burnout: Clinicians
 Moral Distress and Burnout: Clinicians Sean M Bagshaw, MD, MSc Department of Critical Care Medicine, University of Alberta, Edmonton, Canada CCCF, Toronto, Canada October 2, 2017 13:30 13:50 2017 Disclosures
Moral Distress and Burnout: Clinicians Sean M Bagshaw, MD, MSc Department of Critical Care Medicine, University of Alberta, Edmonton, Canada CCCF, Toronto, Canada October 2, 2017 13:30 13:50 2017 Disclosures
Clinician burnout 3/28/ Allina Health System. Decreased effectiveness at work. Disclosure. Objectives. Why caring for the healer matters
 Who heals the healers? March 28, 2016 Disclosure There are no conflicts of interest or relevant financial interests in making this presentation and have indicated that my presentation does not include
Who heals the healers? March 28, 2016 Disclosure There are no conflicts of interest or relevant financial interests in making this presentation and have indicated that my presentation does not include
R2 - Research presentations
 R2 - Research presentations A randomized controlled trial evaluating the effect of facilitated small group sessions on physician well-being and job satisfaction (C. West, L. Dyrbye, J. Sloan, T. Shanafelt)
R2 - Research presentations A randomized controlled trial evaluating the effect of facilitated small group sessions on physician well-being and job satisfaction (C. West, L. Dyrbye, J. Sloan, T. Shanafelt)
Caring for Carers. Includes Caregiver Health Checklists
 Caring for Carers Includes Caregiver Health Checklists The role of carer can provide great satisfaction, but being a caregiver can also be very emotionally stressful between a third and a half of carers
Caring for Carers Includes Caregiver Health Checklists The role of carer can provide great satisfaction, but being a caregiver can also be very emotionally stressful between a third and a half of carers
Physician Margin, Overload and Burnout
 Physician Margin, Overload and Burnout Black Hills Pediatric Symposium June 23, 2017 Craig J. Uthe, MD AAFP ASAM Sanford Family Physician, Internal Locum Tenens Sanford Medical Director of Clinic Services,
Physician Margin, Overload and Burnout Black Hills Pediatric Symposium June 23, 2017 Craig J. Uthe, MD AAFP ASAM Sanford Family Physician, Internal Locum Tenens Sanford Medical Director of Clinic Services,
Advance Care Planning: Goals of Care - Calgary Zone
 Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Advance Care Planning: Goals of Care - Calgary Zone LOOKING BACK AND MOVING FORWARD PRESENTERS: BEV BERG, COORDINATOR CHANDRA VIG, EDUCATION CONSULTANT TRACY LYNN WITYK-MARTIN, QUALITY IMPROVEMENT SPECIALIST
Emergency & Critical Incident Policy
 Emergency & Critical Incident Policy 1. Preamble Emergency and Critical Incident Management is the management of emergencies and critical incidents from a human, hazard identification, and risk assessment
Emergency & Critical Incident Policy 1. Preamble Emergency and Critical Incident Management is the management of emergencies and critical incidents from a human, hazard identification, and risk assessment
NURSING SPECIAL REPORT
 2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
2017 Press Ganey Nursing Special Report The Influence of Nurse Manager Leadership on Patient and Nurse Outcomes and the Mediating Effects of the Nurse Work Environment Nurse managers exert substantial
Perceptions of the role of the hospital palliative care team
 NTResearch Perceptions of the role of the hospital palliative care team Authors Catherine Oakley, BSc, RGN, is Macmillan lead cancer nurse, St George s Hospital NHS Trust, London; Kim Pennington, BSc,
NTResearch Perceptions of the role of the hospital palliative care team Authors Catherine Oakley, BSc, RGN, is Macmillan lead cancer nurse, St George s Hospital NHS Trust, London; Kim Pennington, BSc,
Resilience Rules the Day!
 Resilience Rules the Day! Assistant Professor of Pediatrics Director of Perinatal Health Systems Research, Perinatal Epidemiology and Health Outcomes Research Unit Division of Neonatal and Developmental
Resilience Rules the Day! Assistant Professor of Pediatrics Director of Perinatal Health Systems Research, Perinatal Epidemiology and Health Outcomes Research Unit Division of Neonatal and Developmental
Pediatric Psychology
 Pediatric Psychology Welcome to Pediatric Psychology at CHOC Children's. Please read this information carefully and write down any questions that you might have, so that we can discuss them. PSYCHOLOGICAL
Pediatric Psychology Welcome to Pediatric Psychology at CHOC Children's. Please read this information carefully and write down any questions that you might have, so that we can discuss them. PSYCHOLOGICAL
To err is human. When things go wrong: apology and communication. Apology and communication position statement
 When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the
When things go wrong: apology and communication Kristi Eldredge R.N., J.D., CPHRM Senior Risk and Safety Consultant Fresident To err is human position statement To err is human. Mistakes are part of the