A Layered Learning Medication Reconciliation Program
|
|
|
- Leon Ball
- 5 years ago
- Views:
Transcription
1 A Layered Learning Medication Reconciliation Program Brittany Bates, PharmD, BCPS Clinical Pharmacist, Lima Memorial Health System Clinical Assistant Professor, Ohio Northern University Jana Randolph, PharmD Candidate 2018 Ohio Northern University
2 Objectives Pharmacist Learning Objectives: Describe a medication reconciliation independent study course utilizing pharmacy students in an institutional setting Review drug classes and patient factors associated with a high risk of medication reconciliation errors Technician Learning Objective: Review drug classes and patient factors associated with a high risk of medication reconciliation errors
3 Medication Reconciliation Definition: the process of preventing unintended discrepancies in medication profiles by reviewing each patient s full medication regimen at every care transition, including admission, transfer, and discharge Strategy for minimizing adverse drug events (ADEs) In an observational study, errors in medication history were the most common cause of unintended medication discrepancies (186/257, 72%) Included in The Joint Commission s National Patient Safety Goals Agency for Healthcare Research and Quality [Internet] The Joint Commission [Internet] Pippins JR, et al. J Gen Intern Med. 2008
4 Impact of ADEs Retrospective study in Australia found a 5.5% risk of experiencing an adverse drug reaction (ADR) while hospitalized In a meta-analysis of 24,128 patients, 1.6% of inpatients experienced a preventable adverse drug reaction 45% of inpatient ADRs were preventable In a retrospective analysis, among 596 patients with ADEs, estimated direct cost per patient: $ Hauck K, Zhao X. Med Care Hakkarainen KM, et al. PLoS One Gyllensten H, et al. PLoS One
5 Who Can Perform Medication Reconciliation Nurses Physicians Pharmacists Pharmacy technicians Students One study found that pharmacy students identified significantly more preadmission medications per patient than did nurses or physicians Lancaster JW, Grgurich PE. Am J Pharm Educ
6 Layered Learning A core group of clinicians leading a team which may include pharmacy residents and students Advantages include: Supporting Practice Advancement Initiatives (PAI) Partnerships between institutions and pharmacy schools may result in the success of each party Students are low-cost resources Improved patient satisfaction Pinelli NR et al. Am J Health-Syst Pharm Soric MM et al. Am J Health-Syst Pharm 2016.
7 Layered Learning: The LMHS Med Rec Model Pharmacists Shared Faculty Member (course coordinator) Pharmacy Residents, Staff Pharmacists Students (P4-P5 year) Students (P2-P3 year)
8 Medication Reconciliation Course Started in Fall 2015 as a semester-long independent study course at Ohio Northern University (0-6 program) Fall Semester: P2 and P4 students Spring Semester: P3 and P5 students Why? Layered Learning Additional hands-on experience with patients Assist LMHS in correctly identifying home medications and preventing ADRs
9 Medication Reconciliation Course Week 1: Overview/Background on Course and Med Rec Weeks 2-4: On-site Training Students paired with a pharmacist, resident, and/or APPE student Computer training Shadow ER med rec technician Putting it all together Weeks 5 and After Independent portion begins Pharmacists available 24/7 if questions arise
10 Medication Reconciliation Course Expectations of students: A pair of students assigned each weekday Spend 1-3 hours at the site, typically in the afternoon/evening Identify patients, complete medication history, and update home medication list within the EMR Document interventions in EMR and give forms to pharmacist for review Urgent changes addressed by evening pharmacist(s) Non-urgent changes addressed by clinical pharmacist the following day
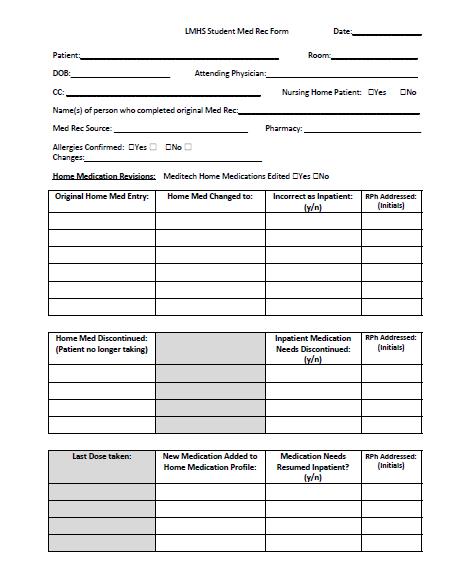
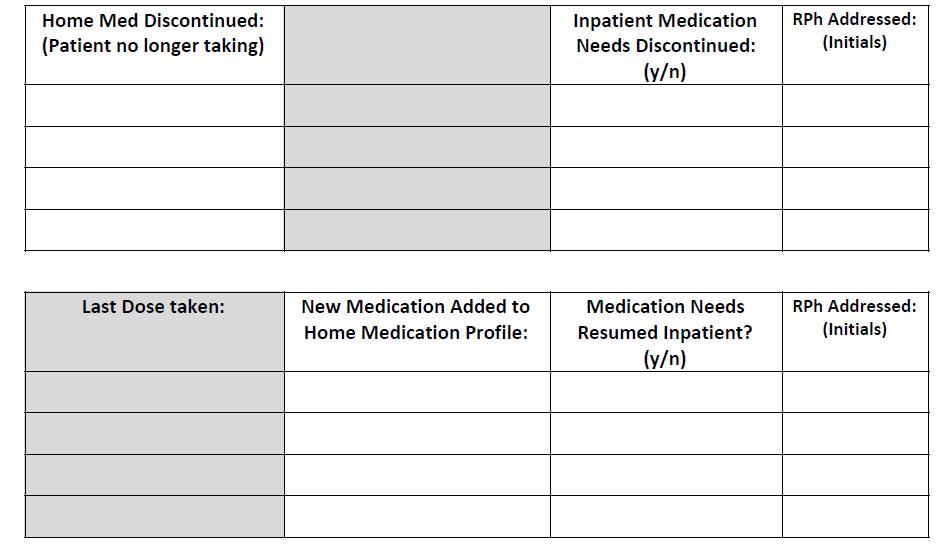
11
12 High-Risk Disease State Home Medication Review DATA COLLECTED DURING SPRING SEMESTER 2017
13 Patient Demographics Location of admission Admission Location n (%) Emergency department 51 (68.9%) Transfer from another facility 12 (16.2%) Direct admission 7 (9.5%) Internal transfer 4 (5.4%) Person who gathered initial medication history Title n (%) Pharmacy technician 44 (59.5%) Other hospital staff 27 (36.5%) APPE student 1 (1.4%) Pharmacy intern 1 (1.4%) Unknown 1 (1.4%)
14 Number of Discrepancies Identified Students identified at least one error in home medication list in 50 of 74 patients (67.6%) Overall average 2.01 ± 2.6 discrepancies per patient Female: Male: 2.6 ± 2.9 discrepancies 1.6 ± 2.3 discrepancies
 Wrong dosage 24 (16%) Unnecessary medication 60 (40%) Medication omission 44")
15 Types of Discrepancies (N=151) Wrong drug 8 (5%) Wrong frequency 14 (9%) Wrong dosage form 1 (1%) Wrong dosage 24 (16%) Unnecessary medication 60 (40%) Medication omission 44 (29%)
16 Discrepancies by Drug Class N/A Antiparasitic Agents Sensory Organs Genitourinary Agents Dermatological Agents Musculoskeletal System Antiinfectives Systemic Hormonal Preparations Respiratory System Nervous System Alimentary Tract & Metabolism Cardiovascular System Number of Discrepancies 39 43
 1.3 ± 1.5 Acute renal failure 3 (3.7%) 1.3 ± 2.3 Hyperglycemia 2 (2.5%) 0.5 ± 0.7 End-stage renal disease 1 (1.2%) 4 Other 6 (7.4%) 1.")
17 Mean Number of Discrepancies By Reason for Admission Disease State # Patients (%) Mean Discrepancies ± SD Heart failure 36 (44.4%) 1.8 ± 2.4 COPD 26 (32.1%) 2.7 ± 3.1 Myocardial infarction 7 (8.6%) 1.3 ± 1.5 Acute renal failure 3 (3.7%) 1.3 ± 2.3 Hyperglycemia 2 (2.5%) 0.5 ± 0.7 End-stage renal disease 1 (1.2%) 4 Other 6 (7.4%) 1.5 ± 1.6
18 Mean Number of Discrepancies by Person Who Gathered Initial Medication History Title # of Patients (%) Mean Discrepancies ± SD Pharmacy technician 44 (59.5%) 1.9 ± 2.1 Other hospital staff 27 (36.5%) 2.3 ± 3.4 APPE student 1 (1.4%) 1 P6 student 1 (1.4%) 0 Unknown 1 (1.4%) 0
19 Medication Reconciliation Course Evolved to meet the needs of the college/students and the hospital site Fall 2017 Patients without completed home medication lists + targeted review for COPD patients Spring 2018 Changed from an Independent Study to an IPPE Elective and offered at several other local institutions
20 Key Points Medication reconciliation is a complex, multi-faceted tool with the ultimate goal of preventing patient harm Layered learning models beyond traditional IPPE/APPE experiences provide benefit to students, institutions, and patients


21 Questions
22 References Agency for Healthcare Research and Quality [Internet]. Rockville (MD): U.S. Department of Health and Human Services. Medication Reconciliation; [updated 2017 Jun; cited 2018 Mar 27]; [about 5 screens]. Available from: Gyllensten H, Hakkarainen KM, Hägg S, Carlsten A, Petzold M, Rehnberg C, Jönsson AK. Economic impact of adverse drug events: a retrospective population-based cohort study of 4970 adults. PLoS One Mar;9(3):e Hakkarainen KM, Hedna K, Petzold M, Hägg S. Percentage of patients with preventable adverse drug reactions and preventability of adverse drug reactions: a meta-analysis. PLoS One Mar;7(3):e Hauck K, Zhao X. How dangerous is a day in hospital? A model of adverse events and length of stay for medical inpatients. Med Care Dec;49(12): The Joint Commission [Internet]. The Joint Commission; c2018. National Patient Safety Goals effective January 2018; 2017 Nov 15 [cited 2018 Mar 27]; [17 p.]. Available from: Lancaster JW, Grgurich PE. Impact of students pharmacists on the medication reconciliation process in high-risk hospitalized general medicine patients. Am J Pharm Educ Mar 12;78(2):34. Pippins JR, Gandhi TK, Hamann C, Ndumele CD, Labonville SA, Diedrichsen EK, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med Sep;23(9): Pinelli NR, Eckel SF, Vu MB, Weinberger M, Roth MT. The layered learning practice model: lessons learned from implementation. Am J Health-Syst Pharm. 2016; 73(24) Soric MM, Glowczewski JE, LermanRM. Economic and patient satisfaction outcomes of a layered learning model in a small community hospital. Am J Health-Syst Pharm 2016: 73 (7) Buckley MS, Harinstein LM, Clark CS, et al. Impact of a clinical pharmacy admission medication reconciliation program on medication errors in highrisk patients. Ann Pharmacother. 2013; 47(12):
Pharmacy Technicians and Interns: Charting New Territory
 Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
Pharmacy Technicians and Interns: Charting New Territory Peter Dippel Pharm.D, BCPS Clinical Pharmacist II Baptist Health Medical Center NLR Objectives Understand what Pharmacist Extenders are and why
Impact of a Pharmacy-Led Medication Reconciliation Program
 Impact of a Pharmacy-Led Medication Reconciliation Program Naomi Digiantonio, PharmD, BCPS; Jeremy Lund, PharmD, MS, BCCCP, BCPS; and Samantha Bastow, PharmD, BCPS ABSTRACT Objective: To determine the
Impact of a Pharmacy-Led Medication Reconciliation Program Naomi Digiantonio, PharmD, BCPS; Jeremy Lund, PharmD, MS, BCCCP, BCPS; and Samantha Bastow, PharmD, BCPS ABSTRACT Objective: To determine the
Medication Reconciliation
 Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation Where are we now? Angie Powell, PharmD Director of Pharmacy Baxter Regional Medical Center Disclosures I, Angie Powell, have no relevant financial relationships to disclose. Learning
Medication Reconciliation in Transitions of Care
 Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
Medication Reconciliation in Transitions of Care Jeff West, RN MPH June 18th, 2015 Adverse Drug Events & Readmissions For every 1,000 hospital admissions, medication reconciliation could prevent 14 adverse
H2H Mind Your Meds "Challenge. Webinar #3- Lessons Learned Wednesday, April 18, :00 pm 3:00 pm ET. Welcome
 H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
H2H Mind Your Meds "Challenge Webinar #3- Lessons Learned Wednesday, April 18, 2012 2:00 pm 3:00 pm ET 1 Welcome Take Home Messages Understand how to implement the Mind Your Meds strategies and tools in
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals
 Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
Medication Challenges in Care Transitions: Issues Faced by Patients, Providers & Community Professionals Joshua Akers, PharmD Geoffrey Meer, PharmD Shanna O Connor, PharmD, BCPS Introductions GROUP WORK
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
4/26/2017. Emergency Department Pharmacist Interventions in a Small, Rural Hospital. Disclosure Statement. Learning Objectives
 Emergency Department Pharmacist Interventions in a Small, Rural Hospital Chaundra Sewell, PharmD PGY1 Pharmacy Practice Resident Community Medical Center Missoula, MT Disclosure Statement This presenter
Emergency Department Pharmacist Interventions in a Small, Rural Hospital Chaundra Sewell, PharmD PGY1 Pharmacy Practice Resident Community Medical Center Missoula, MT Disclosure Statement This presenter
Pharmacists Role in Care Transitions
 Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
Pharmacists Role in Care Transitions SHE A FA NNING, PHA RMD, PGY 1 PHA RMA C Y RE SIDENT ST. PETER S HOSPITAL HE LE NA, MT Disclosures Co-investigators: Thomas Richardson, PharmD, BCPS AQ-ID; Brad Hornung,
A Comparison of Medication Histories Obtained by a Pharmacy Technician Versus Nurses in the Emergency Department
 A Comparison of Medication Histories Obtained by a Pharmacy Technician Versus Nurses in the Emergency Department Marija Markovic, PharmD; A. Scott Mathis, PharmD; Hoytin Lee Ghin, PharmD, BCPS; Michelle
A Comparison of Medication Histories Obtained by a Pharmacy Technician Versus Nurses in the Emergency Department Marija Markovic, PharmD; A. Scott Mathis, PharmD; Hoytin Lee Ghin, PharmD, BCPS; Michelle
EMR Adoption: Benefits Realization
 EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
EMR Adoption: Benefits Realization John H. Daniels, CNM, FACHE, FHIMSS, CPHIMS Global Vice President, HIMSS Analytics Pressurring / Overload Automate to optimize clinical decision making Medical Knowledge
Avoiding Errors During Transitions of Care: Medication Reconciliation
 in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
in in Practice Avoiding Errors During Transitions of Care: Medication Reconciliation When medication errors occur, they often are the result of discrepancies in medication information during transitions
10/2/2017. Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative. Problem. Problem
 Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
Bozeman Health Deaconess Hospital Transition of Care Pharmacist Initiative KRISTAL BARKER, PHARMD EMILY STEED, PHARMD Problem Medical Error is the 3 rd leading cause of death in the United States http://www.bmj.com/content/353/bmj.i2139
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016
 COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
COMPASS Phase II Incident Analysis Report Prepared by ISMP CANADA February 2016 INTRODUCTION Incidents as part of COMPASS (Community Pharmacists Advancing Safety in Saskatchewan) Phase II reported by 87
Who Cares About Medication Reconciliation? American Pharmacists Association American Society of Health-system Pharmacists The Joint Commission Agency
 The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
The Impact of Medication Reconciliation Jeffrey W. Gower Pharmacy Resident Saint Alphonsus Regional Medical Center Objectives Understand the definition and components of effective medication reconciliation
A Framework for the Evaluation of Medication Errors in the Inpatient Setting
 University of Connecticut DigitalCommons@UConn Master's Theses University of Connecticut Graduate School 5-5-2015 A Framework for the Evaluation of Medication Errors in the Inpatient Setting Alaina J.
University of Connecticut DigitalCommons@UConn Master's Theses University of Connecticut Graduate School 5-5-2015 A Framework for the Evaluation of Medication Errors in the Inpatient Setting Alaina J.
Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
 Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Journal of Pharmacy and Pharmacology 2 (2014) 731-738 doi: 10.17265/2328-2150/2014.12.006 D DAVID PUBLISHING Reducing Readmission Rates in Heart Failure and Acute Myocardial Infarction by Pharmacy Intervention
Adverse Drug Events and Readmissions: The Global Picture
 Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Adverse Drug Events and Readmissions: The Global Picture Kyle E. Hultgren, PharmD Managing Director Center for Medication Safety Advancement Purdue University College of Pharmacy Indianapolis, IN 4 Learning
Background and Methodology
 Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Study Sites and Investigators Emergency Department Pharmacists Improve Patient Safety: Results of a Multicenter Study Supported by the ASHP Foundation Jeffrey Rothschild, MD, MPH-Principal Investigator
Disclosure. SwedishAmerican Hospital A Division of UW Health. Learning Objectives. Medication History. Medication History 2/2/2017
 Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Disclosure Pharmacy Technician- Acquired Medication Histories in the ED: A Path to Higher Quality of Care David Huhtelin, PharmD Emergency Medicine Clinical Pharmacist SwedishAmerican Hospital A Division
Identifying Errors: A Case for Medication Reconciliation Technicians
 Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Organization: Solution Title: Calvert Memorial Hospital Identifying Errors: A Case for Medication Reconciliation Technicians Program/Project Description and Goals: What was the problem to be solved? To
Original Research PRACTICE-BASED RESEARCH. University Wexner Medical Center
 Evaluation of provider documentation of medication management in a Patient-Centered Medical Home (PCMH) Trang T. Nguyen, PharmD 1 ; Bella H Mehta, PharmD, FAPhA 2 ; Jennifer L. Rodis, PharmD, BCPS 2 ;
Evaluation of provider documentation of medication management in a Patient-Centered Medical Home (PCMH) Trang T. Nguyen, PharmD 1 ; Bella H Mehta, PharmD, FAPhA 2 ; Jennifer L. Rodis, PharmD, BCPS 2 ;
A comparison of educational interventions to improve prescribing by junior doctors
 Q J Med 2015; 108:369 377 doi:10.1093/qjmed/hcu213 Advance Access Publication 16 October 2014 A comparison of educational interventions to improve prescribing by junior doctors J.S. THOMAS 1, D. GILLARD
Q J Med 2015; 108:369 377 doi:10.1093/qjmed/hcu213 Advance Access Publication 16 October 2014 A comparison of educational interventions to improve prescribing by junior doctors J.S. THOMAS 1, D. GILLARD
Pharmacists in Transitions of Care: We Can All Make a Difference
 Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Pharmacists in Transitions of Care: We Can All Make a Difference Disclosure The speakers of this panel have no actual or potential conflict of interest in relation to this program to disclose. Kenda Germain,
Safe Medication Reconciliation: An Intervention to Improve Residents Medication Reconciliation Skills
 Safe Medication Reconciliation: An Intervention to Improve Residents Medication Reconciliation Skills Cherinne Arundel, MD Jessica Logan, MD Ribka Ayana, MD Jacqueline Gannuscio, DNP, ACNP, AACC Jennifer
Safe Medication Reconciliation: An Intervention to Improve Residents Medication Reconciliation Skills Cherinne Arundel, MD Jessica Logan, MD Ribka Ayana, MD Jacqueline Gannuscio, DNP, ACNP, AACC Jennifer
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting
 Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
Medication Reconciliation Project Edmonton Zone Steps To MedRec Success Across Multiple Programs and Sites in a Large Urban Setting Natalie McMurtry, BSc Pharm, Sr. Medication Consultant; Vanessa Moorgen,
3/16/2017. A Tale of Two Specialty Pharmacies: Novel Models for Technician Incorporation. Objectives. What is Specialty Pharmacy?
 A Tale of Two Specialty Pharmacies: Novel Models for Technician Incorporation Disclosures The speakers have no actual or potential conflict of interest to the content of this presentation. Renee Advincula,
A Tale of Two Specialty Pharmacies: Novel Models for Technician Incorporation Disclosures The speakers have no actual or potential conflict of interest to the content of this presentation. Renee Advincula,
Improving Medication Safety
 Improving Medication Safety Authors: Samantha Hoekenga, Pharm.D. Candidate, Harrison School of Pharmacy, Auburn University; Jena Barrow, Pharm.D. Candidate, Harrison School of Pharmacy, Auburn University;
Improving Medication Safety Authors: Samantha Hoekenga, Pharm.D. Candidate, Harrison School of Pharmacy, Auburn University; Jena Barrow, Pharm.D. Candidate, Harrison School of Pharmacy, Auburn University;
Medication Reconciliation
 Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Medication Reconciliation Wendy Jordan, Pharm.D. Inpatient Pharmacy Manager St. Bernards Medical Center Jonesboro, AR Disclosure The speaker does not have anything to disclose Objectives Describe pharmacy
Brittany Turner, 2015 PharmD Candidate 1 Justin Campbell, PharmD 2 Katie McKinney, PharmD, MS, BCPS 2
 Discharge Medication Concierge Program: A pilot project in heart failure to reduce readmission rates, improve patient satisfaction, and increase pharmacy business metrics Brittany Turner, 2015 PharmD Candidate
Discharge Medication Concierge Program: A pilot project in heart failure to reduce readmission rates, improve patient satisfaction, and increase pharmacy business metrics Brittany Turner, 2015 PharmD Candidate
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
All Wales Multidisciplinary Medicines Reconciliation Policy
 All Wales Multidisciplinary Medicines Reconciliation Policy June 2017 This document has been prepared by the Quality and Patient Safety Delivery Group of the All Wales Chief Pharmacists Group, with support
All Wales Multidisciplinary Medicines Reconciliation Policy June 2017 This document has been prepared by the Quality and Patient Safety Delivery Group of the All Wales Chief Pharmacists Group, with support
Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service
 Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Hospital Pharmacy Volume 36, Number 11, pp 1164 1169 2001 Facts and Comparisons PEER-REVIEWED ARTICLE Performance Measurement of a Pharmacist-Directed Anticoagulation Management Service Jon C. Schommer,
Key Words: Transitions of care, care coordination, medication management, drug therapy problem
 Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Implementing a Pharmacist-Led Medication Management Pilot to Improve Care Transitions Rachel Root, PharmD, MS* 1, Pamela Phelps, PharmD, FASHP 2, Amanda Brummel, PharmD 2, and Craig Else, PharmD, MBA 3
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME
 Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
Medicine Reconciliation FREQUENTLY ASKED QUESTIONS NATIONAL MEDICATION SAFETY PROGRAMME The Process What is medicine reconciliation? Medicine reconciliation is an evidence-based process, which has been
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate
 TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
TransitionRx: Impact of a Community Pharmacy Post-Discharge Medication Therapy Management Program on Hospital Readmission Rate Heidi Luder, PharmD, MS, BCACP Assistant Professor of Pharmacy Practice University
Experiential Education
 Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Experiential Education Experiential Education Page 1 Experiential Education Contents Introduction to Experiential Education... 3 Experiential Education Calendar... 4 Selected ACPE Standards 2007... 5 Standard
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Objectives
 Objectives") Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Administrative Update: How to Implement Discharge Pharmacy Services (DPS) Morgan Pendleton, PharmD, BCOP Hematology/Oncology Clinical Pharmacist Wake Forest Baptist Health Objectives Evaluate the need
Pharmacy Services in the Emergency Department
 Pharmacy Services in the Emergency Department Targeting the Highest Risk Patients Kunal Gohil Specialist Clinical Pharmacist Emergency Department Nottingham University Hospitals NHS Trust When all else
Pharmacy Services in the Emergency Department Targeting the Highest Risk Patients Kunal Gohil Specialist Clinical Pharmacist Emergency Department Nottingham University Hospitals NHS Trust When all else
Medication Therapy Management
 Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Medication Therapy Management Presented by Sylvia Saade, PharmD Ghada Khoury, Pharm D, BCACP Objectives Describe the components of medication therapy management (MTM) programs Discuss the needs of MTM
Study of Medication Error in Hospitalised Patients in Tertiary Care Hospital
 Original Article Study of Medication Error in Hospitalised Patients in Tertiary Care Hospital Sandip Patel 1*, Ashita Patel 1, Varsha Patel 2, Nilay Solanki 1 1 Department of Pharmacology, Ramanbhai Patel
Original Article Study of Medication Error in Hospitalised Patients in Tertiary Care Hospital Sandip Patel 1*, Ashita Patel 1, Varsha Patel 2, Nilay Solanki 1 1 Department of Pharmacology, Ramanbhai Patel
Medication Reconciliation Review
 The Medication Reconciliation Review tool provides step-by-step instructions for conducting a review of closed patient records to identify errors related to unreconciled medications. Organizations that
The Medication Reconciliation Review tool provides step-by-step instructions for conducting a review of closed patient records to identify errors related to unreconciled medications. Organizations that
STANDARDIZING MEDICATION RECONCILIATION
 STANDARDIZING MEDICATION RECONCILIATION PRINCIPAL INVESTIGATORS: DR. JOHN SWEGLE, PHARMD, BCPS, BCACP DR. DIANE REIST, PHARMD, RPH CO-INVESTIGATORS: STEVEN HONG, KAYLEE KACMARYNSKI, KELBY KWOK, JESSICA
STANDARDIZING MEDICATION RECONCILIATION PRINCIPAL INVESTIGATORS: DR. JOHN SWEGLE, PHARMD, BCPS, BCACP DR. DIANE REIST, PHARMD, RPH CO-INVESTIGATORS: STEVEN HONG, KAYLEE KACMARYNSKI, KELBY KWOK, JESSICA
Saint Agnes Hospital. Pharmacist utilization of the LACE tool to prevent hospital readmissions. Program/Project Description, including Goals:
 Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Saint Agnes Hospital Pharmacist utilization of the LACE tool to prevent hospital readmissions Program/Project Description, including Goals: Safe transitions of care have always been a frontline patient
Pharmacy Technicians: Improving Patient Care through Medication Reconciliation
 Pharmacy Technicians: Improving Patient Care through Medication Reconciliation Disclosure I, Holly Katayama, have no financial relationships to disclose. Objectives Describe how to fully utilize pharmacy
Pharmacy Technicians: Improving Patient Care through Medication Reconciliation Disclosure I, Holly Katayama, have no financial relationships to disclose. Objectives Describe how to fully utilize pharmacy
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration
 One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
One or More Errors in 67% of the IV Infusions: Insights from a Study of IV Medication Administration Presented by: Marla Husch Northwestern Memorial Hospital Northwestern Memorial Hospital Chicago, Illinois
Practice Transformation Research Informing the Future Delivery of Healthcare: Insights from IHARP
 Practice Transformation Research Informing the Future Delivery of Healthcare: Insights from IHARP William T. Lee, BSPharm, MPA, FASCP Pharmacy System Director, Carilion Medical Center Gary R. Matzke, BS
Practice Transformation Research Informing the Future Delivery of Healthcare: Insights from IHARP William T. Lee, BSPharm, MPA, FASCP Pharmacy System Director, Carilion Medical Center Gary R. Matzke, BS
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 8, 2013 Presenter Disclosure MaryAnne Elma, MPH Quality Implementation and Innovations Director
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center
 Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Maryland Patient Safety Center s Annual MEDSAFE Conference: Taking Charge of Your Medication Safety Challenges November 3, 2011 The Conference Center at the Maritime Institute Reducing Hospital Readmissions
Shaping the Workforce of Tomorrow: Preparing Technicians for Advanced Roles
 Shaping the Workforce of Tomorrow: Preparing Technicians for Advanced Roles ASHLEE MATTINGLY, PHARMD, BCPS & SARAH LAWRENCE, PHARMD, MA, BCGP Speaker Contact Ashlee Mattingly, PharmD, BCPS Lab Pharmacist
Shaping the Workforce of Tomorrow: Preparing Technicians for Advanced Roles ASHLEE MATTINGLY, PHARMD, BCPS & SARAH LAWRENCE, PHARMD, MA, BCGP Speaker Contact Ashlee Mattingly, PharmD, BCPS Lab Pharmacist
PPI Deprescribing: Ascension
 PPI Deprescribing: Ascension Tonya Thomas, PharmD Clinical Pharmacist Saint Thomas West Hospital Nashville, TN, USA #derx2018 Session resources will be available at deprescribing.org/resources Learning
PPI Deprescribing: Ascension Tonya Thomas, PharmD Clinical Pharmacist Saint Thomas West Hospital Nashville, TN, USA #derx2018 Session resources will be available at deprescribing.org/resources Learning
Medication Reconciliation with Pharmacy Technicians
 Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
Technician Education Day March 29, 2014 Jacksonville, FL Outline with Pharmacy Technicians Roma Merrick RPhT., CPhT. Pharmacy Technician Coordinator St. Vincent s Medical Center Southside Jacksonville,
W e were aware that optimising medication management
 207 QUALITY IMPROVEMENT REPORT Improving medication management for patients: the effect of a pharmacist on post-admission ward rounds M Fertleman, N Barnett, T Patel... See end of article for authors affiliations...
207 QUALITY IMPROVEMENT REPORT Improving medication management for patients: the effect of a pharmacist on post-admission ward rounds M Fertleman, N Barnett, T Patel... See end of article for authors affiliations...
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care. Objectives THE BASICS AND USING TECHNICIANS 3/22/2017
 Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Medication Reconciliation: Using Pharmacy Technicians to Improve Care Becky Johnson, CPhT Megan Ohrlund, PharmD Steve Finch, RPh Objectives Evaluate the medication reconciliation process and evidence for
Disclosures. Learning Objectives 4/26/2017. Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic
 Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Impact of a Pilot Ambulatory Care Pharmacist in a Family Practice Clinic Taylor Sandvick, PharmD, PGY1 Pharmacy Resident St. Peter s Hospital, Helena, MT April 29, 2017 Disclosures 2 Financial: Nothing
Learning Objectives. Putting Patient Safety First: Trends in Adverse Drug Event
 Learning Objectives Putting Patient Safety First: Trends in Adverse Drug Event Screening and Reporting Charlene A. Hope, PharmD, BCPS Izabella Wentz, PharmD, FASCP Moderator PHARMACISTS 1. Differentiate
Learning Objectives Putting Patient Safety First: Trends in Adverse Drug Event Screening and Reporting Charlene A. Hope, PharmD, BCPS Izabella Wentz, PharmD, FASCP Moderator PHARMACISTS 1. Differentiate
Adverse Drug Events in Wyoming
 Adverse Drug Events in Wyoming Where We Are and Where We Need to Go Stevi Sy, PharmD, RPh Adverse Drug Event Task Lead Mountain-Pacific Quality Health August 2017 Objectives Upon completion of this program
Adverse Drug Events in Wyoming Where We Are and Where We Need to Go Stevi Sy, PharmD, RPh Adverse Drug Event Task Lead Mountain-Pacific Quality Health August 2017 Objectives Upon completion of this program
Disease State Management Clinics: A Pharmacist Perspective
 Disease State Management Clinics: A Pharmacist Perspective Eva Berrios Colon, Pharm.D, MPH, BCPS Associate Professor, Touro College of Pharmacy Email: evb9001@nyp.org 5/12/11 The Brooklyn Hospital Center
Disease State Management Clinics: A Pharmacist Perspective Eva Berrios Colon, Pharm.D, MPH, BCPS Associate Professor, Touro College of Pharmacy Email: evb9001@nyp.org 5/12/11 The Brooklyn Hospital Center
Transitions of Care. Objectives 1/6/2016. Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital. The author has nothing to disclose.
 Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Transitions of Care Roman Digilio, PharmD PGY1 Resident West Kendall Baptist Hospital 1 The author has nothing to disclose. 2 Objectives Discuss current healthcare trends and the need for pharmacists in
Implementation of Student Pharmacist-Led Anticoagulation Counseling
 Implementation of Student Pharmacist-Led Anticoagulation Counseling Jamie Sebaaly, PharmD Candidate Class of 2013 UNC Eshelman School of Pharmacy Co-Investigator: Jenna M. Huggins, PharmD, BCPS Clinical
Implementation of Student Pharmacist-Led Anticoagulation Counseling Jamie Sebaaly, PharmD Candidate Class of 2013 UNC Eshelman School of Pharmacy Co-Investigator: Jenna M. Huggins, PharmD, BCPS Clinical
Medication Management: Is It in Your Toolbox?
 Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
Medication Management: Is It in Your Toolbox? Brian K. Esterly, MBA, SVP, Corporate Development, excellerx, Inc. O: 215.282.1676, besterly@excellerx.com What has been your Medication Management experience?
TITLE: Medication Reconciliation at Discharge: A Review of the Clinical Evidence and Guidelines
 TITLE: Medication Reconciliation at Discharge: A Review of the Clinical Evidence and Guidelines DATE: 09 April 2012 CONTEXT AND POLICY ISSUES Medication accuracy at transitions in care represents one of
TITLE: Medication Reconciliation at Discharge: A Review of the Clinical Evidence and Guidelines DATE: 09 April 2012 CONTEXT AND POLICY ISSUES Medication accuracy at transitions in care represents one of
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues
 Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
Improving Primary Care Medication Patient Safety: System-level Medication Adherence Issues Marie Smith, PharmD Professor and Asst. Dean, Practice and Public Policy Partnerships Meg Mello Moniz, PharmD
MEDICINES RECONCILIATION GUIDELINE Document Reference
 MEDICINES RECONCILIATION GUIDELINE Document Reference G358 Version Number 1.01 Author/Lead Job Title Jackie Stark Principle Pharmacist Clinical Services Date last reviewed, (this version) 29 November 2012
MEDICINES RECONCILIATION GUIDELINE Document Reference G358 Version Number 1.01 Author/Lead Job Title Jackie Stark Principle Pharmacist Clinical Services Date last reviewed, (this version) 29 November 2012
Transition from Hospital to Home: Importance of Medication Education and Reconciliation
 Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
Transition from Hospital to Home: Importance of Medication Education and Reconciliation Julie Baron, PharmD, CGP, BCACP/Clinical Pharmacy Specialist/Kaiser Permanente Lindsay Salsburg, PharmD, BCACP/Clinical
4/28/2017. Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC Presenter. Overview
 Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC 2017 Presenter Debra Demar, MS is the Community Liaison for White Cross Pharmacy, serving RI, MA and CT. She has
Medication Management for Improved Compliance & Home Care Satisfaction PREPARED FOR NEHCC 2017 Presenter Debra Demar, MS is the Community Liaison for White Cross Pharmacy, serving RI, MA and CT. She has
Utilization of pharmacy technicians for accurate and timely medication histories. Brenda Asplund, PharmD, CPPS March 11, 2018
 Utilization of pharmacy technicians for accurate and timely medication histories Brenda Asplund, PharmD, CPPS March 11, 2018 Disclosure The content of this presentation does not relate to any product of
Utilization of pharmacy technicians for accurate and timely medication histories Brenda Asplund, PharmD, CPPS March 11, 2018 Disclosure The content of this presentation does not relate to any product of
Prescription audit in outpatient department of multispecialty hospital in western India: an observational study
 International Journal of Clinical Trials Solanki ND et al. Int J Clin Trials. 215 Feb;2(1):14-19 http://www.ijclinicaltrials.com pissn 2349-324 eissn 2349-3259 Research Article DOI: 1.5455/2349-3259.ijct21523
International Journal of Clinical Trials Solanki ND et al. Int J Clin Trials. 215 Feb;2(1):14-19 http://www.ijclinicaltrials.com pissn 2349-324 eissn 2349-3259 Research Article DOI: 1.5455/2349-3259.ijct21523
Pharmacy s Role in Decreasing Hospital Readmissions
 Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Pharmacy s Role in Decreasing Hospital Readmissions ACPE UAN 107-000-11-004-L04-P & 107-000-11-004-L04-T Activity Type: Knowledge-Based 0.15 CEU/1.5 Hr Program Objectives for Pharmacists: Upon completion
Measuring Harm. Objectives and Overview
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3. Measuring Harm
 Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Patient Safety Research Introductory Course Session 3 Measuring Harm Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg School of Public Health
Medication Safety Dashboard
 How Safe Are Your Patients? Creating a Meaningful & Actionable Medication Safety Dashboard By: Helga Brake, PharmD, CPHQ Patient Safety Leader Northwestern Memorial Hospital No Conflicts of Interest to
How Safe Are Your Patients? Creating a Meaningful & Actionable Medication Safety Dashboard By: Helga Brake, PharmD, CPHQ Patient Safety Leader Northwestern Memorial Hospital No Conflicts of Interest to
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING
 Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Ensuring our safeguarding arrangements act to help and protect adults PRACTICE GUIDANCE FOR REPORTING MEDICATION INCIDENTS INTO SAFEGUARDING Contents Page 1.0 Purpose 2 2.0 Definition of medication error
Impact of a Pharmacist-managed, Studentsupported Inpatient Warfarin Education Program on HCAHPS Scores in a Community Teaching Hospital
 Impact of a Pharmacist-managed, Studentsupported Inpatient Warfarin Education Program on HCAHPS Scores in a Community Teaching Hospital Submitted by: Daniel T. Abazia, Pharm.D., BCPS, Clinical Pharmacist
Impact of a Pharmacist-managed, Studentsupported Inpatient Warfarin Education Program on HCAHPS Scores in a Community Teaching Hospital Submitted by: Daniel T. Abazia, Pharm.D., BCPS, Clinical Pharmacist
Medication Reconciliation. Peggy Choye, Pharm.D., BCPS
 Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Medication Reconciliation Peggy Choye, Pharm.D., BCPS What is it? Medication reconciliation The process of identifying the most accurate list of all medications that a patient is taking including name,
Medicines Reconciliation Policy
 Medicines Reconciliation Policy Lead executive Medical Director Authors details Senior Clinical Pharmacy Technician - 01244 39 7494 Document level: Trustwide (TW) Code: MP19 Issue number: 3 Type of document
Medicines Reconciliation Policy Lead executive Medical Director Authors details Senior Clinical Pharmacy Technician - 01244 39 7494 Document level: Trustwide (TW) Code: MP19 Issue number: 3 Type of document
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
How to Improve the Discharge Process. Michelle Mourad, MD Ryan Greysen, MD
 How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
How to Improve the Discharge Process Michelle Mourad, MD Ryan Greysen, MD Who are we? Why are we here? I mean BOB is the reason we are all really here. Do you have a BOB where you are? Or perhaps you like
Pharmaceutical Services Report to Joint Conference Committee September 2010
 Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmaceutical Services Report to Joint Conference Committee September 21 Background: Pharmaceutical Services staffing has increased by 31 FTE from 26 due to program changes and to comply with regulatory
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02
 Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Pharmacological Therapy Practice Guidance Note Medicine Reconciliation on Admission to Hospital for Adults in all Clinical Areas within NTW V02 V02 issued Issue 1 May 11 Issue 2 Dec 11 Planned review May
Transition of Care Practices. Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI
 Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
Transition of Care Practices Nancy MacDonald, PharmD, BCPS, FASHP Henry Ford Hospital Detroit, MI Objectives Pharmacist 1. Describe transition of care opportunities 2. Explain ways to use pharmacist extenders
D DAVID PUBLISHING. 1. Introduction. Sumana Alex, Jennifer C. Kerns, Ayne B. Adenew, Cherinne Arundel
 Journal of Pharmacy and Pharmacology 2 (2014) 722-730 doi: 10.17265/2328-2150/2014.12.005 D DAVID PUBLISHING Clinical Pharmacist and Physician Team Collaboration to Improve Medication Safety and Cost Savings
Journal of Pharmacy and Pharmacology 2 (2014) 722-730 doi: 10.17265/2328-2150/2014.12.005 D DAVID PUBLISHING Clinical Pharmacist and Physician Team Collaboration to Improve Medication Safety and Cost Savings
University of Mississippi Medical Center University of Mississippi Health Care. Pharmacy and Therapeutics Committee Medication Use Evaluation
 University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
University of Mississippi Medical Center University of Mississippi Health Care Pharmacy and Therapeutics Committee Medication Use Evaluation TJC Standards for Medication Management March 2012 Purpose The
Code Sepsis: Wake Forest Baptist Medical Center Experience
 Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Code Sepsis: Wake Forest Baptist Medical Center Experience James R. Beardsley, PharmD, BCPS Manager, Graduate and Post-Graduate Education Department of Pharmacy Wake Forest Baptist Health Assistant Professor
Presentation Outline
 Pharmacist Practice Expectations Weighing Value and Setting Priorities Nick Honcharik, Pharm. D. Presentation Outline Pharmacist Practice Expectations Background/rationale Development Selective examples
Pharmacist Practice Expectations Weighing Value and Setting Priorities Nick Honcharik, Pharm. D. Presentation Outline Pharmacist Practice Expectations Background/rationale Development Selective examples
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge
 Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
Evaluation of a Pharmacist-Led Bedside Medication Delivery Service for Cardiology Patients at Hospital Discharge Julianna Burton, Pharm.D., BCPS, BCACP, FCSHP Assistant Chief, Ambulatory Clinical Services
Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology
 Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology Healthcare Information and Management Systems Society Electronic Poster Session CPR System Planning The
Maimonides Medical Center Makes a Quantum Leap with Advanced Computerized Patient Record Technology Healthcare Information and Management Systems Society Electronic Poster Session CPR System Planning The
Chapter 13. Documenting Clinical Activities
 Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Chapter 13. Documenting Clinical Activities INTRODUCTION Documenting clinical activities is required for one or more of the following: clinical care of individual patients -sharing information with other
Medication Reconciliation in the Era of Telepharmacy: An Innovator s Tale
 Medication Reconciliation in the Era of Telepharmacy: An Innovator s Tale Christopher A. Keeys, Pharm.D., BCPS, R.Ph. President, Clinical Pharmacy Associates, Inc. CEO, MedNovations, Inc. 5/20/2018 CPA/MedNovations
Medication Reconciliation in the Era of Telepharmacy: An Innovator s Tale Christopher A. Keeys, Pharm.D., BCPS, R.Ph. President, Clinical Pharmacy Associates, Inc. CEO, MedNovations, Inc. 5/20/2018 CPA/MedNovations
Objectives. Prevalence of Non-Adherence. Medications and Care Transitions. The Cost of Readmissions. The Pharmacist s Role in Improving Care 4/22/2015
 MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
MEDS TO BEDS: DELIVERING REDUCED READMISSIONS, LOWER COSTS, AND IMPROVED QUALITY Laura S. Carr PharmD, Senior Attending Pharmacist, Transitional Care Massachusetts General Hospital Ed Cohen, PharmD, FAPhA
Poor admission medication reconciliation can follow
 Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
Importance of Medication Reconciliation in the Continuum of Care Cynthia R. Hennen, BS, RPh; and James A. Jorgenson, RPh, MS, FASHP Specialty Healthcare Benefits Council Poor admission medication reconciliation
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Constant Pursuit of Medication Safety. Geraldine Koh Chief Pharmacist
 Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
Constant Pursuit of Medication Safety Geraldine Koh Chief Pharmacist 1 Alexandra Hospital 400 beds Multi discipline except Paeds & ObGyn Restructured in Oct 2000 Transformation Creating A Safety Culture
National Quality Strategy (NQS) Domain: Communication and Care Coordination. Measure Type: Composite; Process
 Domain: Communication and Care Coordination. Measure Type: Composite; Process") Surgical Phase of Care Measure 6 ACS20 Optimal Postoperative Communication Plan and Patient Care Coordination Composite National Quality Strategy (NQS) Domain: Communication and Care Coordination Measure
Surgical Phase of Care Measure 6 ACS20 Optimal Postoperative Communication Plan and Patient Care Coordination Composite National Quality Strategy (NQS) Domain: Communication and Care Coordination Measure
Medication Reconciliation: Preventing Errors and Improving Patient Outcomes
 Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
Murray State's Digital Commons Scholars Week 2016 - Spring Scholars Week Apr 18th, 12:00 PM - 2:00 PM Medication Reconciliation: Preventing Errors and Improving Patient Outcomes Amanda S. Boren Murray
PHARMACY SERVICES/MEDICATION USE
 25.01. 10 Drug Reactions & Administration Errors & Incompatibilities. Drug administration errors, adverse drug reactions and incompatibilities must be immediately reported to the attending physician and
25.01. 10 Drug Reactions & Administration Errors & Incompatibilities. Drug administration errors, adverse drug reactions and incompatibilities must be immediately reported to the attending physician and
St. Michael s Hospital Medication Reconciliation Learning Package
 St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications
St. Michael s Hospital Medication Reconciliation Learning Package What is Medication Reconciliation? A formal process which begins with obtaining a complete and accurate list of each patient s home medications