Objectives. Scottish Mortality and Morbidity Review Programme Update and shape the next phase
|
|
|
- Cecily Joseph
- 5 years ago
- Views:
Transcription
1
2 Dr Brian Robson

3 Objectives Scottish Mortality and Morbidity Review Programme Update and shape the next phase Best Practice Guide review Develop a collaborative network for shared learning and linking M&M with organisational governance as well as other relevant national work streams Develop a Short Life Working Group to design and test a training programme to support a structured Mortality and Morbidity process across NHS Scotland
4 100 colleagues attending today 40 medics 29 Anaesthetists 14 MDs / managers 14 surgeons 3 nurses




5 11 / 14 NHS Boards represented








6
7 Dr Alex Stirling
8
9 Acknowledgements We would like to thank our colleagues for their input into this report. SMMP Operational Group Mr Manoj Kumar Scottish Mortality and Morbidity Programme Steering Group Lead and Consultant Surgeon, NHS Grampian Dr Andrew Longmate -Clinical Quality & Safety Lead, Scottish Government (until May 2016) Isobel Macleod Clinical Co-ordinator, NHS National Services Scotland (until Dec 2015) Dr Brian Robson-Executive Clinical Director, Healthcare Improvement Scotland Dr Alex Stirling, Consultant in Public Health Medicine, National Services Scotland Christine Watters- Clinical Co-ordinator, NHS National Services Scotland (from February 2016) NSS Scottish Healthcare Audits Stuart Baird, Service Manager, NHS National Services Scotland Hazel Dodds, Senior Nurse, NHS National Services Scotland Martin O Neil Principal Information Analyst, NHS National Services Scotland NHS Education for Scotland Paul Bowie Programme Director (Safety & Improvement), NHS Education for Scotland



10 Anecdotal evidence of variation in practice across Scotland Consultant grade Lime survey
11 Respondent characteristics Other Not recorded Tayside National Waiting Times Island Boards Lothian Lanarkshire Highland Greater Glasgow and Clyde Grampian Forth Valley Fife Dumfries and Galloway Borders Ayrshire and Arran ~18.4% did not record a response ~17.5% did not provide a health board 74% work with adult population Proportion of responses (%) Paediatric Adult No response

12 88.1% of respondents said their specialty had an M&M or similar peer review meeting for mortality and morbidity case discussion



13 Meeting characteristics 59% took place at least monthly Within mental health, 70% of respondents said meetings were 6 monthly or ad hoc. weekly meetings occurred most frequently in critical care only
14 Meeting structure 25% 7% 1% 2% 3% No structure 7% 11% 28% 9% 7% Pre-defined criteria PowerPoint Proforma esystem Pre-set questions Learning and action Care score Don'tknow Other The most commonly reported meeting structure: power point (28%), learning and action (25%) 7% of respondents reported no structure 35% reported using either predefined criteria, a proforma or pre-set questions Only 10% of respondents are currently using an e system.

15 Job planned activity: variation by specialty
16 Timeliness 50% 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% 9% of M&Ms are conducted within two weeks 9% reported that the M&M took place over 3 months after the death 11% were unsure of Within specialty reported timeliness of M&M the timing. Within 2 weeks > 3 months Critical Care (53%) Haematology (37.1%) General Surgery (18.8%) Mental Health (30%) Neurology (60%)
 and nurses (52%).Learning is rarely shared with other hospitals or boards (4%).")
17 Learning - WHO Where learning points are shared they are done so frequently amongst consultant colleagues (79%) and nurses (52%).Learning is rarely shared with other hospitals or boards (4%).

18 Why we do it?
19 Timeliness 50% 45% 40% 35% 30% 9% of M&Ms are conducted within two 25% 20% weeks 15% 10% 5% 0% Within 2 weeks Approximately within 1 month Between 1-3 months Over 3 months Unsure Not recorded 9% reported that the M&M took place over 3 months after the death Within specialty reported timeliness of M&M Within 2 weeks > 3 months Critical Care (53%) Haematology (37.1%) 11% were unsure of the timing. General Surgery (18.8%) Mental Health (30%) Neurology (60%)

20 Sharing learning - HOW
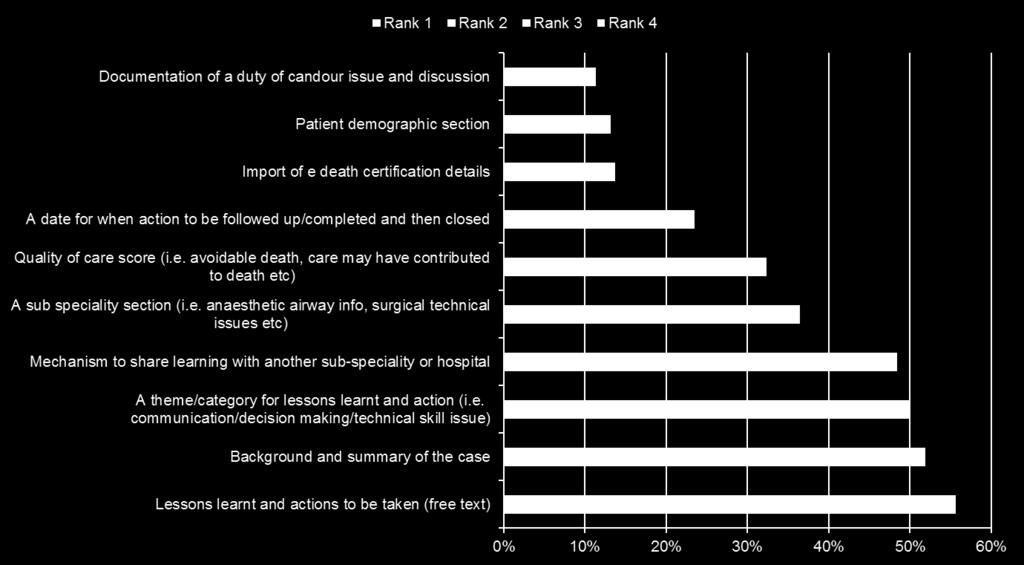
21 Recommendations for the M & M 60% Programme 50% 40% 30% 20% 10% Rank 9 Rank 8 Rank 7 Rank 6 Rank 5 Rank 4 Rank 3 Rank 2 Rank 1 0% Provision of an electronic structured M&M system in NHS Scotland Assistance with quality improvement generated from M&M Analyses, reports and support with data provision A best practice statement M&M A case selection facilitator/chair screening tool training Link with adverse event framework programme A generic paper proforma for M&M in NHS Scotland Other characteristics
22 Is the learning used? 50% of respondents reported that learning from M&Ms is used routinely/most of the time or frequently in NHS. In contrast 31% thought it was used infrequently % perceived that it was never used Routinely/most of the time Frequently Infrequently Rarely Never No repsonse
23 Learning Meetings regularly attended by consultants and senior trainees learning points so frequently amongst consultant colleagues (79%) and nurses (52%) learning is rarely shared with other hospitals or boards (4%) 50% of respondents reported that learning from M&Ms is used routinely or frequently Culture For improvement For learning (Not as and end in itself) Variations in practice by board and speciality Opportunities to improve learning within meetings Opportunities to share learning outside meetings Within departments Within hospitals and organisations Across Specialties /organisations and disciplines
24 Recommendations for the M & M Programme 60% 50% 40% 30% 20% 10% Rank 9 Rank 8 Rank 7 Rank 6 Rank 5 Rank 4 Rank 3 Rank 2 Rank 1 0% Provision of an electronic structured M&M system in NHS Scotland Assistance with quality improvement generated from M&M Analyses, reports and support with data provision A best practice statement M&M A case selection facilitator/chair screening tool training Link with adverse event framework programme A generic paper proforma for M&M in NHS Scotland Other characteristics
25 Other recommendations with over 25% support included: M&M facilitator/chair training, A case selection screening tool Link with adverse event framework programme

26 Characteristics of a national electronic system


27 Benefits of a national approach (N=856) Improvements Shared learning from M&M Governance Quality of care Staff engagement Variation Reassurance No Benefits Don t know Other Not recorded

28 In summary 88.1% of respondents said their specialty had an M&M or similar peer review meeting for mortality and morbidity case discussion 59% said meetings took place at least monthly Variable methods used to structure, report and disseminate findings 58.4% of respondents said that their time to attend M&M was protected. Variation between specialties and boards for job planned activity
29 Prof Craig White
30 Duty of Candour Procedure Professor Craig White FRCP FBPsS Scottish
31

32

33

34

35

36
:1001-8 Copyright BMJ Publishing Group Ltd")
37 BMJ Qual Saf Dec;21(12): Copyright BMJ Publishing Group Ltd and the Health Foundation. All rights reserved.

38
39

40








41 National Implementation Guidance Raise Awareness Section 22 Regulations Organisational Duty of Candour Support Leadership


42 Effectiveness is key





43 Keep focused on peoples needs Recognise pain & distress Listen & respond honestly Support with matters to them Communication of the learning and change

44 @craigwhitephd
45 Norma Shippin

46 Litigation A sign of the times? Norma A Shippin
47 NHS (Clinical Negligence and Other Risks Indemnity Scheme (Scotland) Regs 2000 The Scheme was launched on 1 April 2000 Membership - mandatory for Boards Expanded from 1 April 2015 to assist health and social care integration Clinical and non-clinical claims and risks
48 Clinical - CNORIS Medical and Dental including provision to prison service Nurses Midwives PAMs Ambulance and Laboratory staff Forensic service
49 Non-clinical - Employers liability CNORIS Public liability ( including directors) Product liability Professional indemnity Income generation (but only in respect of NHS to NHS activity)
50 Payments under the scheme TRENDS SCOTLAND 2009/ m 2010/ m 2011/ m 2012/13 35m 2013/ m 2014/15 42m 2015/16 52m
51 Claims Accident and Emergency General Surgery Obstetrics and Gynaecology Value of Claims in last 3 years 10,350,830 3,368,549 2,439,815 52,595,640 6,300,169 2,355,949 1,152,201 20,779, , ,421 1,207,435 Non-clinical Accident and Emergency Anaesthetics Clinical (unclassified) Gynaecology Healthcare Acquired Infection Medication Error (excl anaesthetics) Obstetrics Oncology (excl Radiology and Surgery) Radiological Investigation Surgery (excl obstetrics)
52 CNORIS Claims New clinical claims in Scotland - 1 April March (669) New non- clinical claims in same period 457 (495) (Figures in brackets are for 1 April March 2014)
53 NHS in Scotland Existing clinical claims /actions 1684 (1573)
54 Prescription of claims Normally 3 years from date of incident proposed change to 5 years Discretion of court Position of children/incapax
55 Voluntary pre Action protocol for PI cases based on clinical negligence Benefits Avoid need for litigation Speed up case handling Early and full disclosure of information Narrowing of issues in dispute Enables us to have a trial and see how it works in practice
56 Voluntary pre Action protocol for PI cases based on clinical negligence Challenges Time scales could be tight where information from Boards is not forthcoming New approach always takes time to establish

57 Questions?? Norma Shippin
58 Dr Andrew Gibson

59 National Mortality Case Record Review Programme Andrew Gibson June 2016
60 Retrospective case record review (RCRR): structured judgement review (SJR) SJR methodology Implementing SJR in hospitals SJR in action
61 SJR methodology Hutchinson A, et al. A structured judgement method to enhance mortality case note review: development and evaluation. BMJ Quality and Safety 2013 doi: /bmjqs Explicit judgements Phases of care Analysis
62 What is the purpose of SJR? It is not just about counting numbers. It is about gathering quantitative and qualitative information about what goes well, or not so well, in a care system. The review system can be used for individual cases (eg morbidity and mortality M&M ) and for groups of cases. The information allows units or organisations to ask why questions about things that happen, to enable learning and action where required.
63 SJR: unique selling points It examines both interventions and holistic care. Reviewers give written explicit judgements on safety and quality of phases of care much more readily than with other commonly used tools (eg GGT). Reviewers give overall care and phase of care scores to accompany judgements. the scores are Results show good care as well as poor care (and good care is much more frequent). It is an internal review process usually based on one reviewer, with a second stage where there is cause for concern.
64 Phases of care Admission and initial care first 24 hours approximately Care during a procedure Perioperative/procedure care Ongoing care up to end of life or discharge of the patient (this phase may cover a prolonged period) End-of-life care or discharge care Care overall
65 Scoring phases of care 1 Very poor care 2 Poor care 3 Adequate care 4 Good care 5 Excellent care
66 Case selection is your choice High case fatality disorders All end-of-life care All elective deaths All learning disability deaths All borders deaths A random sample of all deaths A directorate by directorate analysis
67 Low scores in phases of care All scores of 1 or 2 have second stage review Independent of first stage review 1 or 2 does not mean avoidable death
68 SJR: implementing in hospital setting Trained reviewers National case record review can support this Mature, robust and transparent governance structures Action on process failure Action on person failure Mechanisms for selecting case notes for review (eg national Hospital Standardised Mortality Ratio (HSMR) data for high case fatality disorders) Timeliness of reviews
69 SJR: the regional experience Study site / cohort (n) Percentage with scores <2 Sheffield Teaching Hospitals Foundation Trust (STHFT) cardiac arrest (80) 11% STHFT weekend data (80) 18% MYHNT (24) 16% Hogan et al 2016 Avoidable death ~3%
70 SJR in action: cardiac arrest as a harm event Admission 48 hours pre cardiac arrest During Post arrest


71 SJR: thematic analysis and PDSA cycles


72 SJR: second stage review of low scores
73 Summary SJR methodology is a validated tool to review mortality. SJR methodology includes robust governance. SJR methodology can reveal themes and poor or excellent practice.
74 Dr Paul Bowie
75 Enhancing Mortality and Morbidity Meetings: Incorporating Human Factors Principles and Approaches Paul Bowie PhD MIEHF FRCPE (Hon.) Programme Director (Safety & Improvement)
76 Content NES role in Scottish M&M Programme What is Human Factors? Correcting HF misunderstandings Incorporating key HF principles into M&M Taking a Systems Approach to enhancing M&M
77 What is Human Factors (or is it Ergonomics)?










78
79 Definition of Human Factors Ergonomics (or human factors) is the scientific discipline concerned with the understanding of interactions among humans and other elements of a system, and the profession that applies theory, principles, data and methods to design in order to optimize human well-being and overall system performance... (IEA, 2000) The settled will of the international Human Factors community! In other words, ergonomics/human factors is designing for people.
80 Wide ranging discipline focused on the evaluation and improvement of all aspects of human work HF can benefit a diverse range of important healthcare problems where performance and wellbeing are often compromised e.g. the introduction of new information technology reducing work-related musculoskeletal disorders amongst clinicians decision-making to inform NHS procurement of products and services the design of physical care environments staff wellbeing e.g. addressing job stress, fatigue and burnout reflecting on and learning from the prevailing safety culture supporting the needs of the ageing clinical workforce the design and usability of medical equipment Patient safety and Quality improvement interventions ** Key differences between healthcare and other industries need to be appreciated to ensure HF Integration reflects care complexity and uncertainty
81 Twin Aims of Human Factors 1. To enhance the well-being of employees and consumers (patients and clients) 2. To enhance the well-being of the organisation. Individual wellbeing = personal health, safety, comfort, convenience, satisfaction, interest and enjoyment; Organisational wellbeing = performance (in terms of safety, productivity, efficiency, quality, flexibility, responsiveness) and competitiveness (where appropriate). Twin Aims not mutually exclusive but are interdependent known as joint optimisation (Atkinson, 2014)

82 HF System Components and Interactions - Onion Model (Grey, Wilson, 2003)


83 Human Factors Misunderstandings in Healthcare

84

85

86
87
88 Some Perspective and Understanding - The HF Profession Building HF capacity and capability QI model? Chartered profession in the UK highly specialist, 6-years of training Knowledge and evidence across: Anatomy, anthropometry and physiology in human activities; Environmental stressors (performance shaping factors), psychophysiology; Socio-technical systems; general and organisational psychology; Survey and research methods Expertise in principles, standards, legislation and methods NOT on how work is actually done, experienced and impacts on performance and wellbeing healthcare workforce, patients Some HF principles and approaches are transferable to frontline care professionals and staff group
89 Distinguishing Features of Human Factors/Ergonomics (Dul et al, 2012) 1. It takes a systems approach (holistic) 2. It is design driven (to take account of human characteristics, needs and capabilities) 3. It focuses on two closely related outcomes: Performance and Well-being ( of people and organisations joint optimisation )
90 Integrating Human Factors Principles into the M&M Process
91 For example: Understand healthcare as a complex sociotechnical system Why things go wrong (and right) How to respond to when things go wrong Incorporating systems thinking Taking a participatory approach (i.e. speak to people who do the work and co-design) Simplification and standardisation (where judged appropriate)
92 Healthcare as a Complex System? A system characterised by multiple interactions between various components, both human and technological: Decisions often made with imprecise information Actions vary dependent on conditions to ensure successful and safe outcomes. Systems conditions are dynamic and can change rapidly - not always predictable. Demand may increase e.g. due to holidays or influx of emergency cases. Capacity can change e.g. due to staff absence or resource cuts Wishes and health of patients can change e.g. influencing our understanding and how we clinically manage
93 FIRST PRINCIPLE (No.1) Understanding Why Things go Wrong e.g. The Human Error problem (misnomer, not a cause ) System complexity and interactions (contributory factors) Goal conflicts (e.g. increase productivity Vs decreased resource) Trade-offs (e.g. safety Vs efficiency) Performance variability (e.g. adapting to context to get job done) Organisational constraints (e.g. resources, priorities, culture) Local rationality (e.g. makes sense based on available info/context) (Compensating for complexity and system deficiencies)
94 FIRST PRINCIPLE (No.2) Response to When Things go Wrong e.g. We don t got to work to do a bad job - axiomatic Blame (self and colleagues) psychological need and counterproductive to learning and improvement Human biases need to manage these esp. The Hindsight bias & Attribution bias Emotional impacts on staff 2 nd victim, frequent, inhibits openness, barrier to engagement and learning Professional Accountability report, apologise, commit to learn Organisational Accountability create and sustain the conditions Egregious or reckless behaviours/actions PM issue Openness, transparency, no-blame, learning, but accountability = Just Culture
95 Taking a Systems Approach (to understanding safety and implementing change) Characteristic of a safe and just culture Don t need to be an expert in systems thinking : key principles to consider: 1. Understand interactions and relationships between system components i.e. How these contributed to the problem or safety incident; Change is implemented by considering these interactions when improving overall system performance. 2. Multiple perspectives are necessary - How the system works appears different to different people as interactions change frequently. Speak to people who do the job, they re the experts in everyday work! 3. Define your boundaries - Systems are subjected to many influences and it is not possible to consider all of these, need to agree upon a boundary done on a case-by-case basis. 4. Anticipate what can go wrong - designing suitable defence or coping mechanisms to minimising the risks and impacts of error 5. Limitations of linear cause and effect methods
96 Standardise and Simplify? Problematic given the complexity and diversity of clinical needs/systems in healthcare Standardising common work procedures may make it easier (e.g. less mental effort, workload and stress) communication tools, checklists, etc Proposed M&M process e.g. data collection, documentation, use of tools, systems approach
97 Thank You! Any Questions?
98 Jenny Long
99 LEARNING FROM ADVERSE EVENTS: A national framework for Scotland Because human error is normal and, by definition, is unintended, well-intentioned people who make errors or are involved in systems that have failed around them need to be supported, not punished, so they will report their mistakes and the system defects they observe, such that all can learn from them. The best way to reduce harm is for the NHS to embrace wholeheartedly a culture of learning. A promise to learn a commitment to act, The National Advisory Group on the Safety of Patients in England, chaired by Don Berwick, August 2013 Jenny Long jennifer.long1@nhs.net hcis.adverseevents@nhs.net


100 Sharing learning for improvement As part of the learning from adverse events programme, a learning summary template has been developed as a way to ensure: a consistent approach for sharing key learning points to improve services, and we are open and transparent with findings from significant adverse event reviews with staff, patients, families and carers. This mechanism for sharing learning can be used for any form of learning, not just from adverse events and we would like to encourage the use of these across the organisation and all other care providers. Examples of the learning summaries can be found on the adverse events community of practice ( support can be provided by the team (hcis.adverseevents@nhs.net) Jan-15 Mar-15 Learning summaries shared May-15 Jul-15 Sep-15 Nov-15 Jan-16 Mar-16 Total Cumulative total 0 Page views Jan-15 Mar-15 May-15 Jul-15 Sep-15 Nov-15 Jan-16 Mar-16 Unique page views Baseline median page views
Using the structured judgement review method
 National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
National Mortality Case Record Review Programme Using the structured judgement review method A clinical governance guide to mortality case record reviews Supported by: Commissioned by: Dr Andrew Gibson
Learning from adverse events. Learning and improvement summary
 Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report. Results for July Dec 2016
 NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report Results for July Dec 2016 March 2017 National Catering and Nutritional Services Specification: Half Yearly
NHSScotland National Catering and Nutritional Services Specification: Half Yearly Compliance Report Results for July Dec 2016 March 2017 National Catering and Nutritional Services Specification: Half Yearly
Findings from the Balance of Care / NHS Continuing Health Care Census
 Publication Report Findings from the Balance of Care / NHS Continuing Health Care Census Census held 31 Publication date 23 June 2015 A National Statistics Publication for Scotland Contents Findings from
Publication Report Findings from the Balance of Care / NHS Continuing Health Care Census Census held 31 Publication date 23 June 2015 A National Statistics Publication for Scotland Contents Findings from
Findings from the Balance of Care / Continuing Care Census
 Publication Report Findings from the Balance of Care / Continuing Care Census Census held 31 March 2013 Publication date 25 June 2013 A National Statistics Publication for Scotland Contents Introduction...
Publication Report Findings from the Balance of Care / Continuing Care Census Census held 31 March 2013 Publication date 25 June 2013 A National Statistics Publication for Scotland Contents Introduction...
Findings from the 6 th Balance of Care / Continuing Care Census
 Publication Report Findings from the 6 th Balance of Care / Continuing Care Census Census held 31 March Publication date 28 June A National Statistics Publication for Scotland Contents Contents... 1 About
Publication Report Findings from the 6 th Balance of Care / Continuing Care Census Census held 31 March Publication date 28 June A National Statistics Publication for Scotland Contents Contents... 1 About
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 30 th September 2013 26 th November 2013 A National Statistics Publication for Scotland Contents
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 30 th September 2013 26 th November 2013 A National Statistics Publication for Scotland Contents
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st December 2014 24 th February 2015 A National Statistics Publication for Scotland Contents
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st December 2014 24 th February 2015 A National Statistics Publication for Scotland Contents
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st March 2015 26 th May 2015 A National Statistics Publication for Scotland Contents Contents...
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31 st March 2015 26 th May 2015 A National Statistics Publication for Scotland Contents Contents...
Child & Adolescent Mental Health Services in NHSScotland
 Publication Report Child & Adolescent Mental Health Services in NHSScotland Workforce Information as at 31 December 2015 23 February 2016 A National Statistics Publication for Scotland Contents Contents...
Publication Report Child & Adolescent Mental Health Services in NHSScotland Workforce Information as at 31 December 2015 23 February 2016 A National Statistics Publication for Scotland Contents Contents...
Prescribing and Medicines: Minor Ailments Service (MAS)
") Publication Report Prescribing and Medicines: Minor Ailments Service (MAS) April 2010 March 2011 Publication date 28 June 2011 Contents Contents... 1 About ISD... 2 Official Statistics... 2 Introduction...
Publication Report Prescribing and Medicines: Minor Ailments Service (MAS) April 2010 March 2011 Publication date 28 June 2011 Contents Contents... 1 About ISD... 2 Official Statistics... 2 Introduction...
GUIDANCE ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY
 ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
ON SUPPORTING INFORMATION FOR REVALIDATION FOR SURGERY Based on the Academy of Medical Royal Colleges and Faculties Core Guidance for all doctors GENERAL INTRODUCTION JUNE 2012 The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for Supporting information for appraisal and revalidation: guidance for ophthalmology
 FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
FOREWORD As part of revalidation, doctors will need to collect and bring to their appraisal six types of supporting information to show how they are keeping up to date and fit to practise. The GMC has
Child and Adolescent Mental Health Services Waiting Times in NHSScotland
 Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2016 Publication date 6 December 2016 An Official Statistics Publication for Scotland
Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2016 Publication date 6 December 2016 An Official Statistics Publication for Scotland
Child and Adolescent Mental Health Services Waiting Times in NHSScotland
 Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2017 Publication date 12 December 2017 A National Statistics Publication for Scotland
Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 September 2017 Publication date 12 December 2017 A National Statistics Publication for Scotland
Child & Adolescent Mental Health Services in NHS Scotland
 Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31st December 2012 26th February 2013 A National Statistics Publication for Scotland Contents Introduction...
Publication Report Child & Adolescent Mental Health Services in NHS Scotland Workforce Information as at 31st December 2012 26th February 2013 A National Statistics Publication for Scotland Contents Introduction...
Systemic Anti-Cancer Therapy Delivery. June 2017 National External Review
 Systemic Anti-Cancer Therapy Delivery June 2017 National External Review Healthcare Improvement Scotland is committed to equality. We have assessed the review process for likely impact on equality protected
Systemic Anti-Cancer Therapy Delivery June 2017 National External Review Healthcare Improvement Scotland is committed to equality. We have assessed the review process for likely impact on equality protected
Child and Adolescent Mental Health Services Waiting Times in NHSScotland
 Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 June 2017 Publication date 5 September 2017 A National Statistics Publication for Scotland
Publication Report Child and Adolescent Mental Health Services Waiting Times in NHSScotland Quarter ending 30 June 2017 Publication date 5 September 2017 A National Statistics Publication for Scotland
Alcohol Brief Interventions 2015/16
 Publication Report Alcohol Brief Interventions 2015/16 Publication date 14 June 2016 An Official Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Publication Report Alcohol Brief Interventions 2015/16 Publication date 14 June 2016 An Official Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Audiology Waiting Times
 Publication Report Audiology Waiting Times Quarter ending 30 September 2012 Publication date 27 November 2012 An Official Statistics Publication for Scotland Contents Introduction... 2 Key points... 3
Publication Report Audiology Waiting Times Quarter ending 30 September 2012 Publication date 27 November 2012 An Official Statistics Publication for Scotland Contents Introduction... 2 Key points... 3
Diagnostic Waiting Times
 Publication Report Diagnostic Waiting Times Quarter Ending 31 December 2015 Publication date 23 February 2016 A National Statistics Publication for Scotland Contents Introduction... 2 Key points... 3 Results
Publication Report Diagnostic Waiting Times Quarter Ending 31 December 2015 Publication date 23 February 2016 A National Statistics Publication for Scotland Contents Introduction... 2 Key points... 3 Results
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Audiology Waiting Times
 Publication Report Audiology Waiting Times Quarter ending 30 June 2012 Publication date 28 August 2012 Contents Contents... 1 Introduction... 2 Key points... 3 Results and Commentary... 4 Current waiting
Publication Report Audiology Waiting Times Quarter ending 30 June 2012 Publication date 28 August 2012 Contents Contents... 1 Introduction... 2 Key points... 3 Results and Commentary... 4 Current waiting
Child & Adolescent Mental Health Services Workforce in NHSScotland
 Publication Report Child & Adolescent Mental Health Services Workforce in NHSScotland Workforce Information as at 31 March 2016 Publication date: 07 June 2016 A National Statistics Publication for Scotland
Publication Report Child & Adolescent Mental Health Services Workforce in NHSScotland Workforce Information as at 31 March 2016 Publication date: 07 June 2016 A National Statistics Publication for Scotland
NHSScotland Child & Adolescent Mental Health Services
 Publication Report NHSScotland Child & Adolescent Mental Health Services Workforce Information as at 31st December 2011 27th March 2012 A National Statistics Publication for Scotland Contents About ISD...
Publication Report NHSScotland Child & Adolescent Mental Health Services Workforce Information as at 31st December 2011 27th March 2012 A National Statistics Publication for Scotland Contents About ISD...
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, June 2014 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for psychiatry
 Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for psychiatry Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose of revalidation
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013
 Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for Occupational Medicine, April 2013 Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine
 Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Supporting information for appraisal and revalidation: guidance for pharmaceutical medicine Based on the Academy of Medical Royal Colleges and Faculties Core for all doctors. General Introduction The purpose
Alcohol Brief Interventions 2016/17
 Publication Report Alcohol Brief Interventions 2016/17 Publication date 27 June 2017 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Publication Report Alcohol Brief Interventions 2016/17 Publication date 27 June 2017 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points... 3 Results and
Scottish Patient Safety Programme Reducing Pressure Ulcers in Care Homes Improvement Programme (SPSP-RPUCH) Induction Event June 2016
 Induction Event June 2016") Scottish Patient Safety Programme Reducing Pressure Ulcers in Care Homes Improvement Programme (SPSP-RPUCH) Induction Event 27-28 June 2016 Health and Social Care Partnerships Argyll and Bute and Highland
Scottish Patient Safety Programme Reducing Pressure Ulcers in Care Homes Improvement Programme (SPSP-RPUCH) Induction Event 27-28 June 2016 Health and Social Care Partnerships Argyll and Bute and Highland
Indicator 5c Mortality Survey
 Indicator 5c Mortality Survey Undertaken by NCEPOD on behalf of NHS England Dr Neil Smith - Clinical Researcher and Deputy CEO Dr Hannah Shotton - Clinical Researcher Dr Marisa Mason - Chief Executive
Indicator 5c Mortality Survey Undertaken by NCEPOD on behalf of NHS England Dr Neil Smith - Clinical Researcher and Deputy CEO Dr Hannah Shotton - Clinical Researcher Dr Marisa Mason - Chief Executive
SPSP: Sepsis in Primary Care Collaborative. Dr Paul Davidson Associate Medical Director Primary Care NHS Highland
 SPSP: Sepsis in Primary Care Collaborative Dr Paul Davidson Associate Medical Director Primary Care NHS Highland Collaborative Ambition Improve early recognition and timely delivery of evidence-based interventions,
SPSP: Sepsis in Primary Care Collaborative Dr Paul Davidson Associate Medical Director Primary Care NHS Highland Collaborative Ambition Improve early recognition and timely delivery of evidence-based interventions,
Child & Adolescent Mental Health Services Workforce in NHSScotland
 Publication Report Child & Adolescent Mental Health Services Workforce in NHSScotland Workforce Information as at 30 June 2016 Publication date: 06 September 2016 A National Statistics Publication for
Publication Report Child & Adolescent Mental Health Services Workforce in NHSScotland Workforce Information as at 30 June 2016 Publication date: 06 September 2016 A National Statistics Publication for
Child Healthy Weight Interventions
 Publication Report Child Healthy Weight Interventions 2012/13 Publication date 27 August 2013 An Official Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Key points... 3 Results
Publication Report Child Healthy Weight Interventions 2012/13 Publication date 27 August 2013 An Official Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Key points... 3 Results
Improving ethnic data collection for equality and diversity monitoring
 Publication Report Improving ethnic data collection for equality and diversity monitoring October 2010 September 2012 Publication date 26 th February 2013 Contents Contents... 1 Introduction... 2 Key points...
Publication Report Improving ethnic data collection for equality and diversity monitoring October 2010 September 2012 Publication date 26 th February 2013 Contents Contents... 1 Introduction... 2 Key points...
Child & Adolescent Mental Health Services Workforce in NHSScotland
 Publication Report Child & Adolescent Mental Health Services Workforce in NHSScotland Workforce Information as at 30 September 2016 Publication date: 06 December 2016 A National Statistics Publication
Publication Report Child & Adolescent Mental Health Services Workforce in NHSScotland Workforce Information as at 30 September 2016 Publication date: 06 December 2016 A National Statistics Publication
Improving ethnic data collection for equality and diversity monitoring
 Publication Report Improving ethnic data collection for equality and diversity monitoring April 2010 March 2012 Publication date 28 th August 2012 Contents Contents... 1 Introduction... 2 Key points...
Publication Report Improving ethnic data collection for equality and diversity monitoring April 2010 March 2012 Publication date 28 th August 2012 Contents Contents... 1 Introduction... 2 Key points...
NES Patient Safety Programme. Human Factors in Healthcare. NES Educational Developments and Resources
 NES Patient Safety Programme Human Factors in Healthcare NES Educational Developments and Resources Introduction The three Quality Ambitions articulated in the Healthcare Quality Strategy include a focus
NES Patient Safety Programme Human Factors in Healthcare NES Educational Developments and Resources Introduction The three Quality Ambitions articulated in the Healthcare Quality Strategy include a focus
Child & Adolescent Mental Health Services (CAMHS) Benchmarking Balanced Scorecard
 Benchmarking Balanced Scorecard") Publication Report Child & Adolescent Mental Health Services (CAMHS) Benchmarking Balanced Scorecard Quarter ending 31 st December 2013 Publication date 25 th March 2014 An Official Statistics Publication
Publication Report Child & Adolescent Mental Health Services (CAMHS) Benchmarking Balanced Scorecard Quarter ending 31 st December 2013 Publication date 25 th March 2014 An Official Statistics Publication
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB)
") Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
WORKING DRAFT. Standards of proficiency for nursing associates. Release 1. Page 1
 WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
WORKING DRAFT Standards of proficiency for nursing associates Page 1 Release 1 1. Introduction This document outlines the way that we have developed the standards of proficiency for the new role of nursing
UKMi PDS Tuesday 27 th September 2016
 Implications of the Carter report for MI, what we can learn from colleagues in Scotland? Yvonne Semple Lead Pharmacist, MI Services NHS GGC UKMi PDS Tuesday 27 th September 2016 What can we learn from
Implications of the Carter report for MI, what we can learn from colleagues in Scotland? Yvonne Semple Lead Pharmacist, MI Services NHS GGC UKMi PDS Tuesday 27 th September 2016 What can we learn from
High level guidance to support a shared view of quality in general practice
 Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Regulation of General Practice Programme Board High level guidance to support a shared view of quality in general practice March 2018 Publications Gateway Reference: 07811 This document was produced with
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
LIVING & DYING WELL AN ACTION PLAN FOR PALLIATIVE AND END OF LIFE CARE IN HIGHLAND PROGRESS REPORT
 Highland NHS Board 4 October 2011 Item 5.3 LIVING & DYING WELL AN ACTION PLAN FOR PALLIATIVE AND END OF LIFE CARE IN HIGHLAND PROGRESS REPORT Report by Chrissie Lane, Cancer Nurse Consultant/Project Lead
Highland NHS Board 4 October 2011 Item 5.3 LIVING & DYING WELL AN ACTION PLAN FOR PALLIATIVE AND END OF LIFE CARE IN HIGHLAND PROGRESS REPORT Report by Chrissie Lane, Cancer Nurse Consultant/Project Lead
PAUL GRAY, DIRECTOR-GENERAL HEALTH & SOCIAL CARE, SCOTTISH GOVERNMENT AND CHIEF EXECUTIVE NHSSCOTLAND, 26 OCTOBER 2017
 PAUL GRAY, DIRECTOR-GENERAL HEALTH & SOCIAL CARE, SCOTTISH GOVERNMENT AND CHIEF EXECUTIVE NHSSCOTLAND, 26 OCTOBER 2017 1. Agency Staff Spend and Data Annexe C NHSScotland spends around 6.5 billion a year
PAUL GRAY, DIRECTOR-GENERAL HEALTH & SOCIAL CARE, SCOTTISH GOVERNMENT AND CHIEF EXECUTIVE NHSSCOTLAND, 26 OCTOBER 2017 1. Agency Staff Spend and Data Annexe C NHSScotland spends around 6.5 billion a year
Public Health Skills and Career Framework Multidisciplinary/multi-agency/multi-professional. April 2008 (updated March 2009)
") Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
Public Health Skills and Multidisciplinary/multi-agency/multi-professional April 2008 (updated March 2009) Welcome to the Public Health Skills and I am delighted to launch the UK-wide Public Health Skills
NPSA Alert 03: Reducing the harm caused by oral Methotrexate. Implementation Progress Report July Learning and Sharing
 NPSA Alert 03: Reducing the harm caused by oral Methotrexate Implementation Progress Report July 2006 Learning and Sharing CONTENTS Page 1 Background 3 2 Findings 4 Appendix 1 Summary of responses 6 Appendix
NPSA Alert 03: Reducing the harm caused by oral Methotrexate Implementation Progress Report July 2006 Learning and Sharing CONTENTS Page 1 Background 3 2 Findings 4 Appendix 1 Summary of responses 6 Appendix
Diagnostic Waiting Times
 Publication Report Diagnostic Waiting Times Quarter Ending 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points...
Publication Report Diagnostic Waiting Times Quarter Ending 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main points...
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
M16 Is there a perfect system?
 M16 Is there a perfect system? Scotland s Quality Journey 1 NHSScotland 5 million people 12 billion 14 Health Boards 8 Support Boards Integrated delivery Moving towards social care integration Public Finances
M16 Is there a perfect system? Scotland s Quality Journey 1 NHSScotland 5 million people 12 billion 14 Health Boards 8 Support Boards Integrated delivery Moving towards social care integration Public Finances
NHS Education for Scotland (NES) Information Services Division (ISD) Workforce Planning for Psychology Services in NHS Scotland
 Information Services Division (ISD) Workforce Planning for Psychology Services in NHS Scotland") NHS Education for Scotland (NES) Information Services Division (ISD) Workforce Planning for Psychology Services in NHS Scotland Characteristics of the Workforce Supply in 2005 Contents Page Summary...
NHS Education for Scotland (NES) Information Services Division (ISD) Workforce Planning for Psychology Services in NHS Scotland Characteristics of the Workforce Supply in 2005 Contents Page Summary...
Healthcare Improvement Scotland. NHS Tayside
 Faculty Site Visit Report Healthcare Improvement Scotland NHS Tayside 8 th June 2011 FINAL VERSION 19 July 2011 CONTENTS 1. Key Contacts... 2 NHS Tayside... 2 Site Visit Team... 2 2. SPSP Programme Key
Faculty Site Visit Report Healthcare Improvement Scotland NHS Tayside 8 th June 2011 FINAL VERSION 19 July 2011 CONTENTS 1. Key Contacts... 2 NHS Tayside... 2 Site Visit Team... 2 2. SPSP Programme Key
Psychology Services Workforce in NHSScotland
 Publication Report Psychology Services Workforce in NHSScotland Workforce Information at 31 December 2015 23 February 2016 A National Statistics Publication for Scotland Contents Introduction... 2 Key
Publication Report Psychology Services Workforce in NHSScotland Workforce Information at 31 December 2015 23 February 2016 A National Statistics Publication for Scotland Contents Introduction... 2 Key
NHS Research Scotland Permissions Coordinating Centre
 permissions NHS Research Scotland Permissions Coordinating Centre (NRS Permissions CC) Coordinating faster permissions for Scotland A guide to who we are and what we do nrs c c Foreword from Professor
permissions NHS Research Scotland Permissions Coordinating Centre (NRS Permissions CC) Coordinating faster permissions for Scotland A guide to who we are and what we do nrs c c Foreword from Professor
Primary Care Workforce Survey 2013
 Experimental Report Primary Care Workforce Survey 2013 Out of Hours GP Services Strand Sections 1,2,3 and 6 Publication Date 19 November 2013 Contents Introduction... 2 Method of completing the survey...
Experimental Report Primary Care Workforce Survey 2013 Out of Hours GP Services Strand Sections 1,2,3 and 6 Publication Date 19 November 2013 Contents Introduction... 2 Method of completing the survey...
Diagnostic Waiting Times
 Publication Report Diagnostic Waiting Times Quarter Ending 30 September 2017 Publication date 28 November 2017 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main
Publication Report Diagnostic Waiting Times Quarter Ending 30 September 2017 Publication date 28 November 2017 A National Statistics Publication for Scotland Contents Contents... 1 Introduction... 2 Main
Facilities Shared Services Programme Transport & Fleet Management Short Life Working Group
 Facilities Shared Services Programme Short Life Working Group Terms of Reference Author: Michael Jackson, Chair Contact: michaeledwinjackson@nhs.net Date Published: 2013-12-10 Version: 1.1 Page 1 of 6
Facilities Shared Services Programme Short Life Working Group Terms of Reference Author: Michael Jackson, Chair Contact: michaeledwinjackson@nhs.net Date Published: 2013-12-10 Version: 1.1 Page 1 of 6
National Mortality Case Record Review Programme. Using the structured judgement review method A guide for reviewers (England)
") National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
National Mortality Case Record Review Programme Using the structured judgement review method A guide for reviewers (England) Supported by: Commissioned by: Dr Allen Hutchinson Emeritus professor in public
Mortality Policy. Learning from Deaths
 Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Mortality Policy Learning from Deaths Name of Author and Job Title: Frank Jacobs, Datix project manager Ian Brandon, Head of governance and risk Name of Review/ Development Body: Ratification Body: Mortality
Sharing to improve. Sharing Intelligence for Health & Care Group Summary report for National Services Scotland
 Sharing to improve Sharing Intelligence for Health & Care Group Summary report for 2016 2017 National Services Scotland Published August 2017 Produced in partnership with: Audit Scotland, Care Inspectorate,
Sharing to improve Sharing Intelligence for Health & Care Group Summary report for 2016 2017 National Services Scotland Published August 2017 Produced in partnership with: Audit Scotland, Care Inspectorate,
Patient Safety. At the heart of all we do
 Patient Safety At the heart of all we do Introduction from our Medical Director Over the last 15 years it has been recognised that patient safety problems exist throughout the NHS as they do in every health
Patient Safety At the heart of all we do Introduction from our Medical Director Over the last 15 years it has been recognised that patient safety problems exist throughout the NHS as they do in every health
Guidance on supporting information for revalidation
 Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Guidance on supporting information for revalidation Including specialty-specific information for medical examiners (of the cause of death) General introduction The purpose of revalidation is to assure
Transporting Patients to and from the Dialysis Unit A National Audit
 Transporting Patients to and from the Dialysis Unit A National Audit Introduction Patients receiving hospital haemodialysis commonly identify travelling time to the dialysis unit as an important factor
Transporting Patients to and from the Dialysis Unit A National Audit Introduction Patients receiving hospital haemodialysis commonly identify travelling time to the dialysis unit as an important factor
Standards for the initial education and training of pharmacy technicians. October 2017
 Standards for the initial education and training of pharmacy technicians October 2017 The text of this document (but not the logo and branding) may be reproduced free of charge in any format or medium,
Standards for the initial education and training of pharmacy technicians October 2017 The text of this document (but not the logo and branding) may be reproduced free of charge in any format or medium,
Draft Practice Guide for Mortality and Morbidity Meetings
 Draft Practice Guide for Mortality and Morbidity Meetings Scottish Mortality and Morbidity Programme November 2016 Healthcare Improvement Scotland 2016 Published November 2016 This document is licensed
Draft Practice Guide for Mortality and Morbidity Meetings Scottish Mortality and Morbidity Programme November 2016 Healthcare Improvement Scotland 2016 Published November 2016 This document is licensed
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
The New Queen s Nurse Title 2018 Guidance for Applicants
 The New Queen s Nurse Title 2018 Guidance for Applicants Promoting excellence in community nursing to improve the health and well-being of the people of Scotland Contents About QNIS... 3 What is a Queen
The New Queen s Nurse Title 2018 Guidance for Applicants Promoting excellence in community nursing to improve the health and well-being of the people of Scotland Contents About QNIS... 3 What is a Queen
NHS 24 SCTT Strategy
 NHS 24 SCTT Strategy 2010-12 Background SCTT est 2006 following publication of Delivering For Health Provide a centre of expertise to define and disseminate best practice Provide practical and informed
NHS 24 SCTT Strategy 2010-12 Background SCTT est 2006 following publication of Delivering For Health Provide a centre of expertise to define and disseminate best practice Provide practical and informed
SCOTTISH AMBULANCE SERVICE JOB DESCRIPTION
 SCOTTISH AMBULANCE SERVICE JOB DESCRIPTION Job Title: Reporting To: Department(s)/Location: Lead Consultant Paramedic Medical Director Clinical Directorate Job Reference number (coded): The Scottish Ambulance
SCOTTISH AMBULANCE SERVICE JOB DESCRIPTION Job Title: Reporting To: Department(s)/Location: Lead Consultant Paramedic Medical Director Clinical Directorate Job Reference number (coded): The Scottish Ambulance
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Emergency Department Waiting Times
 Publication Report Emergency Department Waiting Times (formerly Accident & Emergency Waiting Times) Quarter ending 30 June 2011 Publication date 30 August 2011 A National Statistics Publication for Scotland
Publication Report Emergency Department Waiting Times (formerly Accident & Emergency Waiting Times) Quarter ending 30 June 2011 Publication date 30 August 2011 A National Statistics Publication for Scotland
Initial education and training of pharmacy technicians: draft evidence framework
 Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
Initial education and training of pharmacy technicians: draft evidence framework October 2017 About this document This document should be read alongside the standards for the initial education and training
Facilities Shared Services Programme Car Leasing Short Life Working Group
 Facilities Shared Services Programme Car Leasing Short Life Working Group Terms of Reference Author: Douglas Seago, Programme Director Contact: Douglas.Seago@nhs.net Date Published: 2014-02-17 Version:
Facilities Shared Services Programme Car Leasing Short Life Working Group Terms of Reference Author: Douglas Seago, Programme Director Contact: Douglas.Seago@nhs.net Date Published: 2014-02-17 Version:
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Improving teams in healthcare
 Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
Improving teams in healthcare Resource 1: Building effective teams Developed with support from Health Education England NHS Improvement Background In December 2016, the Royal College of Physicians (RCP)
SPSP Maternity and Children
 Healthcare Improvement Scotland s Improvement Hub SPSP Maternity and Children End of phase report August 2016 Healthcare Improvement Scotland 2016 First published August 2016 The contents of this document
Healthcare Improvement Scotland s Improvement Hub SPSP Maternity and Children End of phase report August 2016 Healthcare Improvement Scotland 2016 First published August 2016 The contents of this document
Prescribing & Medicines: Minor Ailments Service (MAS)
") Publication Report Prescribing & Medicines: Minor Ailments Service (MAS) Financial Year 2012/13 Publication date 25 June 2013 A National Statistics Publication for Scotland Contents Introduction... 2 Background...
Publication Report Prescribing & Medicines: Minor Ailments Service (MAS) Financial Year 2012/13 Publication date 25 June 2013 A National Statistics Publication for Scotland Contents Introduction... 2 Background...
A Resident-led PICU Morbidity and Mortality Conference
 A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
A Resident-led PICU Morbidity and Mortality Conference James Moses, MD, MPH Associate Program Director Boston Combined Residency Program Director of Patient Safety and Quality Department of Pediatrics
NHS TAYSIDE MORTALITY REVIEW PROGRAMME
 NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
NHS TAYSIDE MORTALITY REVIEW PROGRAMME Aim Primary Drivers Processes, Rules of Conduct, Structure MEASUREMENT Secondary Drivers Components, Activities Understand how mortality rates/ratios are measured
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance
 Directorate for Health Workforce and Performance") Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Quality and Efficiency Support Team (QuEST) Directorate for Health Workforce and Performance A Whole System Approach to Patient Flow for Scotland Our Quality Improvement Approach Jane Murkin Programme
Summary of recommendations
 Summary of recommendations Improving Safety Through Education and Training Report by the Commission on Education and Training for Patient Safety www.hee.nhs.uk/the-commission-on-education-and-training-for-patient-safety
Summary of recommendations Improving Safety Through Education and Training Report by the Commission on Education and Training for Patient Safety www.hee.nhs.uk/the-commission-on-education-and-training-for-patient-safety
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
A summary of: Five years of cerebral palsy claims
 A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
A summary of: Five years of cerebral palsy claims A thematic review of NHS Resolution data September 2017 Advise / Resolve / Learn Our report Five years of cerebral palsy claims, provides an in-depth examination
Volume 15 - Issue 2, Management Matrix
 Volume 15 - Issue 2, 2015 - Management Matrix Leadership in Healthcare: A Review of the Evidence Prof. Michael West ******@***lancaster.ac.uk Professor - Lancaster University Thomas West ******@***aston.ac.uk
Volume 15 - Issue 2, 2015 - Management Matrix Leadership in Healthcare: A Review of the Evidence Prof. Michael West ******@***lancaster.ac.uk Professor - Lancaster University Thomas West ******@***aston.ac.uk
Disability and Work Division. Jobcentre Plus Pathways to Work: Official Statistics
 Disability and Work Division Jobcentre Plus Pathways to Work: Official Statistics October 2009 Jobcentre Plus Pathways to Work 2 of 21 Executive summary This is the official statistics publication of Jobcentre
Disability and Work Division Jobcentre Plus Pathways to Work: Official Statistics October 2009 Jobcentre Plus Pathways to Work 2 of 21 Executive summary This is the official statistics publication of Jobcentre
NHS Research Scotland Permissions Coordinating Centre
 permissions NHS Research Scotland Permissions Coordinating Centre (NRS Permissions CC) Coordinating faster permissions for Scotland A guide to who we are and what we do nrs c c Foreword from Sir John Savill,
permissions NHS Research Scotland Permissions Coordinating Centre (NRS Permissions CC) Coordinating faster permissions for Scotland A guide to who we are and what we do nrs c c Foreword from Sir John Savill,
British Association of Dermatologists
 Guidance producer: British Association of Dermatologists Guidance product: Service Guidance and Standards Date: 13 March 2017 Version: 1.2 Final Accreditation Report Page 1 of 26 Contents Introduction...
Guidance producer: British Association of Dermatologists Guidance product: Service Guidance and Standards Date: 13 March 2017 Version: 1.2 Final Accreditation Report Page 1 of 26 Contents Introduction...
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
!!!!!!!!!!!!!!!!!!!!!!!!!!! For Physician Assistant Practitioners in Australia !!!!!!!!!!!!!!!!!! !!! Effective from September 2011 Version 1
 For Physician Assistant Practitioners in Australia Effective from September 2011 Version 1 "ASPA Incorporated 2011 Published by The Australian Society of Physician Assistants Incorporated (ASPA), September
For Physician Assistant Practitioners in Australia Effective from September 2011 Version 1 "ASPA Incorporated 2011 Published by The Australian Society of Physician Assistants Incorporated (ASPA), September
Care of Burns in Scotland ANNUAL REPORT 2015/16. Care of Burns in Scotland (COBIS): Annual report
: Annual report") Care of Burns in Scotland ANNUAL REPORT 2015/16 Lead Clinician: John Kinsella Programme Manager: Alison Gilhooly Contents Care of Burns in Scotland... i ANNUAL REPORT 2015/16... i Contents... ii Executive
Care of Burns in Scotland ANNUAL REPORT 2015/16 Lead Clinician: John Kinsella Programme Manager: Alison Gilhooly Contents Care of Burns in Scotland... i ANNUAL REPORT 2015/16... i Contents... ii Executive
Integration Scheme. Between. Glasgow City Council. and. NHS Greater Glasgow and Clyde
 Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
Integration Scheme Between Glasgow City Council and NHS Greater Glasgow and Clyde December 2015 Page 1 of 60 1. Introduction 1.1 The Public Bodies (Joint Working) (Scotland) Act 2014 (the Act) requires
FORTH VALLEY CLINICAL AND CARE GOVERNANCE FRAMEWORK
 HEALTH AND SOCIAL CARE INTEGRATION: FORTH VALLEY CLINICAL AND CARE GOVERNANCE FRAMEWORK The Scottish Government, National Health and Wellbeing Outcomes: A framework for improving the planning and delivery
HEALTH AND SOCIAL CARE INTEGRATION: FORTH VALLEY CLINICAL AND CARE GOVERNANCE FRAMEWORK The Scottish Government, National Health and Wellbeing Outcomes: A framework for improving the planning and delivery
PG snapshot Nursing Special Report. The Role of Workplace Safety and Surveillance Capacity in Driving Nurse and Patient Outcomes
 PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
PG snapshot news, views & ideas from the leader in healthcare experience & satisfaction measurement The Press Ganey snapshot is a monthly electronic bulletin freely available to all those involved or interested
NES NHS Life Sciences: Healthcare Science (HCS) Support Worker (SW) and Assistant Practitioner (AP) education and training group.
 Support Worker (SW) and Assistant Practitioner (AP) education and training group.") NES NHS Life Sciences: Healthcare Science (HCS) Support Worker (SW) and Assistant Practitioner (AP) education and training group. SUMMARY Remit of NES NHS Life Sciences The NES NHS Life Sciences: Healthcare
NES NHS Life Sciences: Healthcare Science (HCS) Support Worker (SW) and Assistant Practitioner (AP) education and training group. SUMMARY Remit of NES NHS Life Sciences The NES NHS Life Sciences: Healthcare
Final Accreditation Report
 Guidance producer: The Royal College of Physicians of London Guidance product: National Clinical Guideline for Stroke Date: 19 September 2016 Version: 1.2 Final Accreditation Report Report Page 1 of 21
Guidance producer: The Royal College of Physicians of London Guidance product: National Clinical Guideline for Stroke Date: 19 September 2016 Version: 1.2 Final Accreditation Report Report Page 1 of 21
Diagnostic Waiting Times
 Publication Report Diagnostic Waiting Times Monthly Data to 31 December 2014 Publication date 24 February 2015 A National Statistics Publication for Scotland Contents Introduction... 2 Key points... 3
Publication Report Diagnostic Waiting Times Monthly Data to 31 December 2014 Publication date 24 February 2015 A National Statistics Publication for Scotland Contents Introduction... 2 Key points... 3