Infection Control (F441) F Cindy Deporter DHSR
|
|
|
- Dwain Holt
- 5 years ago
- Views:
Transcription
1 Infection Control (F441) F Cindy Deporter DHSR 1
2 2
3 3
4 4
5 Federal Regulatory Language Infection Control F 880 The facility must establish and maintain an infection prevention and control program designed to provide a safe, sanitary and comfortable environment and to help prevent the development and transmission of communicable disease and infection. 5
6 483.80(a) Infection Control Program The facility must establish an Infection prevention and control program (IPCP) that must include, at a minimum, the following elements: 6
7 7
8 8
9 9
10 10
11 11
12 12
13 Program Elements: 1) A system for preventing, identifying, reporting, investigation and controlling infections and communicable diseases for all residents, staff, volunteers, visitors and other individuals providing services under a contractual arrangement based upon the facility assessment conducted according to ( e) and following accepted national standards: 13
14 Programs Elements (2) Written standards, policies, and procedures for the program, which must include, but are not limited to: (i) A system of surveillance designed to identify possible communicable diseases or infections before they can spread to other persons in the facility; (ii) When and to whom possible incidents of communicable disease or infections should be reported; (iii) Standard and transmission-based precautions to be followed to prevent spread of infections; 14
15 Program elements. (iv) When and how isolation should be used for a resident; including but not limited to: (A) The type and duration of the isolation, depending upon the infectious agent or organism involved, and (B) A requirement that the isolation should be the least restrictive possible for the resident under the circumstances. (v) The circumstances under which the facility must prohibit employees with a communicable disease or infected skin lesions from direct contact with residents or their food, if direct contact will transmit the disease; and (vi)the hand hygiene procedures to be followed by staff involved in direct resident contact. 15
16 16
17 17
18 18
19 Program Elements. (3) An antibiotic stewardship program that includes antibiotic use protocols and a system to monitor antibiotic use. (4) A system for recording incidents identified under the facility s IPCP and the corrective actions taken by the facility. 19
20 (b) Infection preventionist [ (b) and all subparts will be implemented beginning November 28, 2019 (Phase 3)] Remember in NC we have a State Law that requires that you have a designated staff to be the Infection Preventionist We already require in NC most of this under state law. 20
21 483.80(b) Infection Preventionist: all subparts implemented beginning 11/28/19 (Already required in NC) The facility must designate one or more individual(s) as the infection Preventionist(s) (IP)(s) who is responsible for the facility s IPCP. The IP must: (1) Have primary professional training in nursing, medical technology, microbiology, epidemiology, or other related field; (2) Is qualified by education, training, experience or certification; (3) Works at least part-time at the facility; and (4) Has completed specialized training in infection prevention and control. NC SPICE Program 21
22 (c) IP participation on QA and A Committee (beginning November 28, 2019 (Phase 3) The individual designated as the IP, or at least one of the individuals if there is more than one IP, must be a member of the facility s quality assessment and assurance committee and report to the committee on the IPCP on a regular basis. [ (c) will be implemented beginning November 28, 2019 (Phase 3)] 22
23 ( c) continued (e) Linens. Personnel must handle, store, process, and transport linens so as to prevent the spread of infection. (f) Annual review. The facility will conduct an annual review of its IPCP and update their program, as necessary. 23
24 24
25 Annual Review (f) Annual review. The facility will conduct an annual review of its IPCP and update their program, as necessary. 25
26 Annual Review: Intent Develops and implements an ongoing infection prevention and control program (IPCP) to prevent, recognize, and control the onset and spread of infection to the extent possible and reviews and updates the IPCP annually and as necessary. -This would include revision of the IPCP as national standards change; 26
27 Intent Establishes facility-wide systems for the prevention, identification, investigation and control of infections of residents, staff, and visitors. It must include an ongoing system of surveillance designed to identify possible communicable diseases or infections before they can spread to other persons in the facility and procedures for reporting possible incidents of communicable disease or infections; 27
28 Intent Develops and implements written policies and procedures for infection control that, at a minimum: Explain how standard precautions and when transmissionbased precautions should be utilized, including but not limited to the: type and duration of precautions for particular infections or organisms involved and that the precautions should be the least restrictive possible for the resident given the circumstances and the resident s ability to follow the precautions; 28
29 Intent Prohibit staff with a communicable disease or infected skin lesions from direct contact with residents or their food, if direct contact will transmit the disease; and Require staff follow hand hygiene practices consistent with accepted standards of practice. Requires staff handle, store, process, and transport all linens and laundry in accordance with accepted national standards in order to produce hygienically clean laundry and prevent the spread of infection to the extent possible. 29
30 Definition Cleaning: removal of visible soil (e.g., organic and inorganic material) from objects and surfaces and is normally accomplished manually or mechanically using water with detergents or enzymatic products. Cohorting: the practice of grouping residents infected or colonized with the same infectious agent together to confine their care to one area and prevent contact with susceptible residents (cohorting residents). During outbreaks, healthcare staff may be assigned to a specific cohort of residents to further limit opportunities for transmission (cohorting staff). The terms cohort or cohorting is standardized language used in the practice of infection prevention and control; the use of this terminology is not intended to offend residents or staff. 30
31 Definition Contaminated laundry: laundry which has been soiled with blood/body fluids or other potentially infectious materials or may contain sharps. Decontamination: the use of physical or chemical means to remove, inactivate, or destroy pathogenic organisms on a surface or item to the point where they are no longer capable of transmitting infectious particles and the surface or item is rendered safe for handling, use, or disposal. Disinfectant: usually a chemical agent (but sometimes a physical agent) that destroys disease-causing pathogens or other harmful microorganisms but might not kill bacterial spores. It refers to substances applied to inanimate objects. Disinfection: thermal or chemical destruction of pathogenic and other types of microorganisms. Disinfection is less lethal than sterilization because it destroys most recognized pathogenic microorganisms but not necessarily all microbial forms (e.g., bacterial spores). 31
32 Definition Infection preventionist: term used for the person(s) designated by the facility to be responsible for the infection prevention and control program. NOTE: Designation of a specific individual, detailed training, qualifications, and hourly requirements for an infection preventionist are not required until implementation of Phase 3. 32
33 Definition (Regulated) Medical waste: liquid or semi-liquid blood or other potentially infectious materials; contaminated items that would release blood or other potentially infectious materials in a liquid or semi-liquid state if compressed; items that are caked with dried blood or other potentially infectious materials and are capable of releasing these materials during handling (e.g., blood-soaked bandages); contaminated sharps. Follow state law. 33
34 Infection Control & Prevention Program Healthcare-associated infections (HAIs) can cause significant pain and discomfort for residents in nursing homes and can have significant adverse consequences. The facility must establish and maintain an IPCP designed to provide a safe, sanitary, and comfortable environment and to help prevent the development and transmission of communicable diseases and infections. This program must include, at a minimum, a system for preventing, identifying, reporting, investigating, and controlling infections and communicable diseases for all residents, staff, and visitors. The IPCP must follow national standards and guidelines. 34
35 Program requirements. For purposes of this guidance, we would expect facilities to tailor the emphasis of their IPCP for visitors. We expect facilities to work to prevent transmission of infection to the resident from the visitor using reasonable precautions and national standards. For example, passive screening through the use of signs at the entrances to alert visitors with signs and symptoms of communicable diseases not to enter the facility. 35
36 Program Requirements: If a facility has a visitor exception protocol (e.g., end-of-life care), this would need to be determined by the facility. In this case, if a symptomatic visitor/family member must enter the facility, the visitor must still follow the facility s policies for prevention of transmission (e.g., following respiratory hygiene/cough etiquette procedures). 36
37 The program must include: A system for preventing, identifying, reporting, investigating, and controlling infections and communicable diseases that: Covers all residents, staff, volunteers, visitors, and other individuals providing services under a contractual arrangement; - Is based on the individual facility assessment; - Follows accepted national standards; 37
38 Program must include: Written standards, policies and procedures in accordance with (a)(2); A system for recording incidents identified under the IPCP and corrective actions taken by the facility; and An antibiotic stewardship program (ASP) (F881). 38
39 F 881: (a)(3) An antibiotic stewardship program that includes antibiotic use protocols and a system to monitor antibiotic use. Intent: Develops and implements protocols to optimize the treatment of infections by ensuring that residents who require an antibiotic, are prescribed the appropriate antibiotic; Reduces the risk of adverse events, including the development of antibiotic-resistant organisms, from unnecessary or inappropriate antibiotic use; and Develops, promotes, and implements a facility-wide system to monitor the use of antibiotics. 39
40 Antibiotic Stewardship Antibiotic Stewardship As part of their IPCP programs, facilities must develop an antibiotic stewardship program that promotes the appropriate use of antibiotics and includes a system of monitoring to improve resident outcomes and reduce antibiotic resistance. -This means that the antibiotic is prescribed for the correct indication, dose, and duration to appropriately treat the resident while also attempting to reduce the development of antibioticresistant organisms. 40
41 Program requirements: The facility must develop an antibiotic stewardship program which includes the development of protocols and a system to monitor antibiotic use. This development should include leadership support and accountability via the participation of the medical director, consulting pharmacist, nursing and administrative leadership, and individual with designated responsibility for the infection control program if different. 41
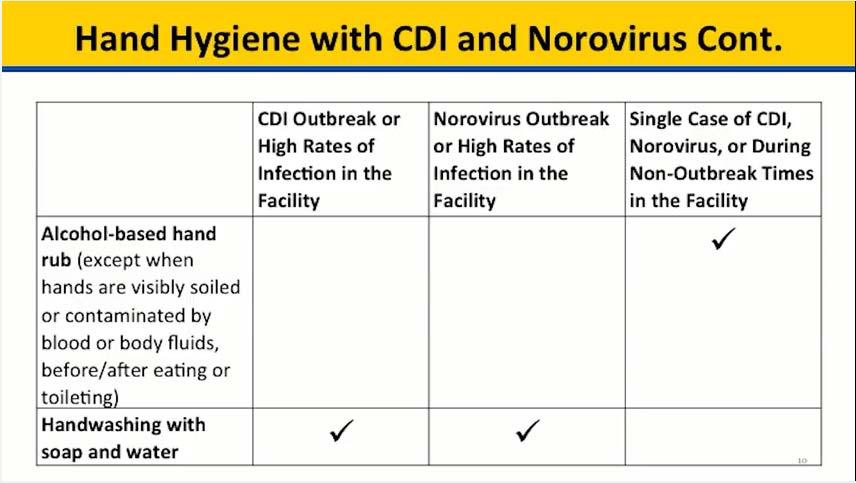
42 Program The Antibiotic Stewardship Program in Relation to Pharmacy Services The assessment, monitoring, and communication of antibiotic use shall occur by a licensed pharmacist in accordance with (c), F756, Drug Regimen Review. A pharmacist must perform a medication regimen review (MRR) at least monthly, including review of the medical record and identify any irregularities, including unnecessary drugs. 42
43 43
44 44
45 Facility Assessment (F838): The facility must conduct and document a facility-wide assessment to determine what resources are necessary to care for its residents competently during both day-to-day operations and emergencies. The facility must review and update that assessment, as necessary, and at least annually. The facility must also review and update this assessment whenever there is, or the facility plans for, any change that would require a substantial modification to any part of this assessment. 45
46 Facility Assessment F 883 continued: The facility assessment must address or include a facility-based and community-based risk assessment, utilizing an all-hazards approach. See (e) (F838) for guidance on the facility assessment. -The results of the facility assessment must be used, in part, to establish and update the IPCP, its policies and/or protocols to include a system for preventing, identifying, reporting, investigating, and controlling infections and communicable diseases for residents, staff, and visitors. 46
47 Facility Assessment NOTE: A community-based risk assessment should include review for risk of infections (e.g., multidrug-resistant organisms- MDROs) and communicable diseases such as tuberculosis and influenza. Appropriate resident tuberculosis screening should be performed based on state requirements. 47
48 Policies and Procedures The facility must develop and implement written policies and procedures for the provision of infection prevention and control. The facility administration and medical director should ensure that current standards of practice based on recognized guidelines are incorporated in the resident care policies and procedures. These IPCP policies and procedures must include, at a minimum: As necessary, and at least annually, review and revision of the IPCP based upon the facility assessment (according to (e)) which includes any facility and community risk; An ongoing system of surveillance designed to identify possible communicable diseases or infections before they can spread to other persons in the facility; When and to whom possible incidents of communicable disease or infections should be reported within the facility; 48
49 Policies and Procedures How to use standard precautions and how and when to use transmission-based precautions (i.e., contact precautions, droplet precautions, airborne isolation precautions). The areas described below are part of standard and transmission-based precautions 40 which are further described under their respective sections. For example: Hand hygiene (HH) (e.g., hand washing and/or ABHR): consistent with accepted standards of practice such as the use of ABHR instead of soap and water in all clinical situations except when hands are visibly soiled (e.g., blood, body fluids), or after caring for a resident with known or suspected Clostridium (C.) difficile or norovirus infection during an outbreak, or if infection rates of C. difficile infection (CDI) are high; in these circumstances, soap and water should be used. 49
50 Link ml NOTE: According to the CDC, strict adherence to glove use is the most effective means of preventing hand contamination with C. difficile spores as spores are not killed by ABHR and may be difficult to remove even with thorough hand washing. For further information on appropriate hand hygiene practices see the following CDC website: 50
51 Policies and Procedures The selection and use of PPE (e.g., indications, donning/doffing procedures) and the clinical conditions for which specific PPE should be used (e.g., CDI, influenza); Addressing the provision of facemasks for residents with new respiratory symptoms; Addressing the provision of facemasks for residents with new respiratory symptoms; Addressing resident room assignment (e.g. single/private room/cohorted) as appropriate and/or available, based on a case by case analysis of the presence of risk factors for increased likelihood of transmission (e.g., uncontained drainage, stool incontinence); 40 The process to manage a resident on transmission-based precautions when a single/private room is not available; Limiting the movement of a resident with a highly infectious disease (e.g., norovirus, CDI) who is on transmission-based precautions with active symptoms (e.g., resident has diarrhea, vomiting, draining wounds, or other uncontained excretions or secretions) while outside of his/her room for medically necessary purposes only; 40 and 51
52 Policies and Procedures Respiratory Hygiene/Cough Etiquette: Implementing policies and procedures would include providing resources and instructions for performing HH in or near lobby areas or entrances; provide conveniently-located dispensers of ABHR and supplies for hand washing where sinks are available. During times of increased prevalence of respiratory infections in the community, facilities must have facemasks available and should offer facemasks to coughing or sneezing visitors and other symptomatic persons (e.g., family who accompany ill residents upon entry to the facility). Symptomatic (e.g., coughing) visitors should wear a facemask or maintain at least a three foot separation from others in common areas (e.g., admitting office 52
53 Posting of Signs In addition, the facility should consider posting signs in the facility with instructions to family/visitors with symptoms of respiratory infection to cover their mouth/nose when coughing or sneezing; use and dispose of tissues; perform hand hygiene after contact with respiratory secretions; and to take appropriate precautions if they are having symptoms of respiratory infection or other communicable diseases. 53
54 Resident Care Activities Urinary catheters, which must include a written rationale for the use, consistent with evidence-based guidelines (e.g., acute urinary retention, bladder outlet obstruction, neurogenic bladder or terminally ill for comfort measures) (Refer to (e)(2)(i)(ii)&(iii) Incontinence, F690, for further information.); Wound care, fecal/urinary incontinence care, and skin care. Since the IPCP must be based on the facility assessment, the presence of certain resident conditions would require that the facility have policies and procedures related to other specific services such as mechanical ventilation, infusion therapy, and/or dialysis either onsite or at an offsite dialysis facility; Performing fingersticks and point-of-care testing (e.g., assisted blood glucose monitoring) to the extent identified as a resident need based on the facility assessment; Preparation, administration, and care for medications administered by injection or peripheral and central venous catheters, if performed by the facility; and Use and care of peripheral and central venous catheters, if performed by the facility. 54
55 55
56 Environmental Cleaning and Disinfection Environmental cleaning/disinfection: Routine cleaning and disinfection of high-touch surfaces in common areas, resident rooms, and at the time of discharge; and NOTE: Privacy curtains in the resident s room should be changed when visibly dirty by laundering or cleaning with an Environmental Protection Agency (EPA)-registered disinfectant per manufacturer s instructions. Cleaning/disinfection of resident care equipment including equipment shared among residents (e.g., blood pressure cuffs, rehabilitation therapy equipment, blood glucose meters, etc.). 56
57 Surveyors Next slides go over areas that surveyors review about your policy and procedures to assure that they meet the intent of the regulation. 57
58 Written Health Occupational Policies that must cover Reporting of staff illnesses and following work restrictions per nationally recognized standards and guidelines; Prohibiting contact with residents or their food when staff have potentially communicable diseases or infected skin lesions Assessing risks for tuberculosis (TB) based on regional/community data and screening staff to the extent permitted under applicable federal guidelines and state law; Monitoring and evaluating for clusters or outbreaks of illness among staff; Implementing an exposure control plan in order to address potential hazards posed by blood and body fluids, from dialysis, glucose monitoring or any other point of care testing; and 58
59 Written Health Occupational Education and competency assessment: Facilities must ensure staff follow the IPCP s standards, policies and procedures. Therefore, staff must be informed and competent. Knowledge and skills pertaining to the IPCP s standards, policies and procedures are needed by all staff in order to follow proper infection control practices (e.g., hand hygiene and appropriate use of personal protective equipment) while other needs are specific to particular roles, responsibilities, and situations (e.g., injection safety and point of care testing). 59
60 Written Health Occupational. Furthermore, residents and their representatives should receive education on the facility s IPCP as it relates to them (e.g., hand hygiene, cough etiquette) and to the degree possible/consistent with the resident s capacity. For example, residents should be advised of the IPCP s standards, policies and procedures regarding hand hygiene before eating and after using the restroom. 60
61 Surveillance The facility must establish a system for surveillance based upon national standards of practice and the facility assessment, including the resident population and the services and care provided. The facility must establish routine, ongoing, and systematic collection, analysis, interpretation, and dissemination of surveillance data to identify infections (i.e., HAI and community-acquired), infection risks, communicable disease outbreaks, and to maintain or improve resident health status. As part of the system of surveillance, identification and prevention, the facility should determine how it will track the extent to which staff are following the facility s IPCP policies and procedures, and facilities would want to particularly address any areas that are related to a corrective action. 61
62 Surveillance The facility s surveillance system must include a data collection tool and the use of nationally-recognized surveillance criteria such as but not limited to CDC s National Healthcare Safety Network (NHSN) Long Term Care Criteria to define infections or updated McGeer criteria 50. -Furthermore, the facility must know when and to whom to report communicable diseases, healthcare-associated infections (as appropriate), and potential outbreaks (e.g., list of communicable diseases which are reportable to local/state public health authorities). The facility must document follow-up activity in response to important surveillance findings (e.g., outbreaks). 62
63 Surveillance In addition, the facility must establish and implement a system, including who to notify (e.g. infection preventionist), for early detection and management of a potentially infectious, symptomatic resident at the time of admission. This includes the identification and use of appropriate transmissionbased precautions. This is important to incorporate into the resident s baseline care plan that must be developed within 48 hours of admission and include the minimum healthcare information necessary to properly care for a resident, including physician orders (e.g., medication orders). See , Comprehensive Person- Centered Care Planning for further information. 63
64 Surveillance Furthermore, the facility must have a process for communicating information at the time of transfer (e.g., CDC, state, or other standardized inter-facility infection transfer form) when a resident has an infection or is colonized. When a resident is transferred, the information provided to the receiving provider must include special instructions or precautions for ongoing care and other necessary information including a discharge summary. When a resident is discharged, the discharge summary must include the resident s disease diagnoses and health conditions, course of illness/treatment or therapy, medications, and pertinent lab, radiology, consultation results, and instructions or precautions for ongoing care. See (c)(2), Discharge Summary (F661) and (c)(2)(iii), Transfer and Discharge (F622) for further information on these requirements. 64
65 Process Surveillance Process surveillance is the review of practices by staff directly related to resident care. The purpose is to identify whether staff implement and comply with the facility s IPCP policies and procedures. Some areas that facilities may want to consider for process surveillance are the following: 65
66 Process Hand hygiene; Appropriate use of personal protective equipment (e.g., gowns, gloves, facemask); Injection safety; Point-of-care testing (e.g., during assisted blood glucose monitoring); Implementation of infection control practices for resident care such as but not limited to urinary catheter care, wound care, injection/iv care, fecal/urinary incontinence care, skin care, respiratory care, dialysis care, and other invasive treatments; Managing a bloodborne pathogen exposure. NOTE: This may not lend itself to monitoring and feedback; Cleaning and disinfection products and procedures for environmental surfaces and equipment; Appropriate use of transmission-based precautions; and Handling, storing, processing, and transporting linens so as to prevent the spread of infection. 66
67 Process Another component of a system of identification is outcome surveillance. For example, this addresses the criteria that staff would use to identify and report evidence of a suspected or confirmed HAI or communicable disease. This process consists of collecting/documenting data on individual resident cases and comparing the collected data to standard written definitions (criteria) of infections. NOTE: Refer to the CDC/SHEA Position Statement: Surveillance Definitions of Infections in Long-Term Care Facilities: Revisiting the McGeer Criteriahttps:// for examples of nationally accepted surveillance definitions. 67
68 System Surveillance Data DATA ANALYSIS, DOCUMENTATION AND REPORTING The facility s policies and procedures for a system of surveillance must include data to properly identify communicable diseases or infections before they spread. Therefore, the policies and procedures would include identifying: Data to be collected, including how often and the type of data to be documented, including: 68
69 System Surveillance Data The infection site (i.e., type of infection), pathogen (if available), signs and symptoms, and resident location, including summary and analysis of the number of residents (and staff, if applicable) who developed infections; Observations of staff including the identification of ineffective practices (e.g., not practicing hand hygiene and/or using PPE when indicated as well as practices that do not follow the facility s IPCP policies and procedures), if any; and The identification of unusual or unexpected outcomes (e.g. foodborne outbreak), infection trends and patterns. 69
70 Surveillance Data includes How the data will be used and shared with appropriate individuals (e.g., staff, medical director, director of nursing, quality assessment and assurance committee- QAA), when applicable, to ensure that staff minimize spread of the infection or disease (e.g., require revision of staff education and competency assessment). The facility must identify how reports will be provided to staff and/or prescribing practitioners in order to revise interventions/approaches and/or re-evaluate medical interventions related to the infection rates and outcomes. 70
71 RECOGNIZING, CONTAINING AND REPORTING COMMUNICABLE DISEASE OUTBREAKS The facility must know how to recognize and contain infectious disease outbreaks. An outbreak is the occurrence of more cases than expected in a given area or among a specific group of people over a particular period of time. If a condition is rare or has serious health implications, an outbreak may involve only one case. While a single case of a rare infectious condition or one that has serious health implications may or may not constitute an outbreak, facilities should not wait for the definition of an outbreak to act. 71
72 Outbreaks Take the appropriate steps to diagnose and manage cases, implement appropriate precautions, and prevent further transmission of the disease as well as documentation of follow-up activity in response; and Comply with state and local public health authority requirements for identification, reporting, and containing communicable diseases and outbreaks. 72
73 Prevention and Controlling Transmission -Direct Contact Transmission (Person-to-Person) occurs when microorganisms such as methicillinresistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), carbapenemresistant Enterobacteriaceae (CRE), influenza, or mites from a scabies-infected resident are transferred from an infected or colonized person to another person. In nursing homes, resident-toresident direct contact transmission may occur in common areas of the facility such as the recreation room, rehabilitation area, and/or dining room. -Indirect Contact Transmission: involves the transfer of an infectious agent through a contaminated inanimate object or person. The following are examples of opportunities for indirect contact transmission: Clothing, uniforms, laboratory coats, or isolation gowns used as PPE may become contaminated with potential pathogens after care of a resident colonized or infected with an infectious agent, (e.g., MRSA, VRE, and C. difficile); and -Contamination of high touch environmental surfaces (e.g., bedside table, bed rails, toilets, sinks, and handrails), contributes to transmission of pathogens including C. difficile and norovirus. 73
74 General Survey Information SAFE INJECTION PRACTICES 74
75 MEDICAL DEVICE SAFETY Medical devices may be used for administration of medications, pointof-care testing, or for other medical uses. Point-of-Care Testing Point-of-care testing is diagnostic testing that is performed at or near the site of resident care. This may be accomplished through use of portable, handheld instruments such as blood glucose meters or prothrombin time meters. This testing may involve obtaining a blood specimen from the resident using a fingerstick device. 75
76 Fingerstick Devices CDC recommends the use of single-use, autodisabling fingerstick devices in settings where assisted blood glucose monitoring is performed. This practice prevents inadvertent reuse of fingerstick devices for more than one person. Additionally, the use of single-use, auto-disabling fingerstick devices protects healthcare staff from needlestick injuries. If reusable fingerstick devices are used for assisted monitoring of blood glucose, then they must never be used for more than one resident. 76
77 Fingerstick. NOTE: If fingerstick devices are used on more than one resident, surveyors must cite at this tag and utilize the guidelines in Appendix Q for immediate jeopardy. Furthermore, the state survey agency (SA) must notify the appropriate state public health authority of the deficient practice. NOTE: For information on fingerstick safety, please refer to:
78 Blood Glucose Meters Blood glucose meters, can become contaminated with blood and, if used for multiple residents, must be cleaned and disinfected after each use according to manufacturer s instructions for multi-patient use. Additionally, staff must not carry blood glucose meters in pockets. The FDA has released guidance for manufacturers regarding appropriate products and procedures for cleaning and disinfection of blood glucose meters. nostics/ucm htm NOTE: If the facility failed to clean and disinfect, per device manufacturer s instructions, and blood glucose meters are used for more than one resident, surveyors must cite this tag and utilize the guidelines in Appendix Q as it may constitute immediate jeopardy. 78
79 Safe Medication Administration All injectable medications must be prepared and administered in accordance with safe injection practices NOTE: If it is identified that needles or syringes are used for more than one resident, surveyors must cite noncompliance at this tag and utilize the guidelines in Appendix Q for immediate jeopardy. The SA must notify the appropriate state public health authority of the deficient practice; 79
80 Other devices. Single dose (single-use) medication vials, ampules, and bags or bottles of intravenous solution are used for only one resident; Medication administration tubing and connectors are used for only one resident. NOTE: Surveyors must cite at this tag if noncompliance is identified and utilize the guidelines in Appendix Q for immediate jeopardy. The SA must notify the appropriate state public health authority of the deficient practice; 80
81 Investigative Summary Surveyors would use the Infection Control Facility Task to determine compliance with the infection control part of the survey. One surveyor should coordinate the review of the facility s overall infection prevention and control program (IPCP), however, each member of the survey team should assess for compliance throughout the entire survey when observing his/her assigned areas and tasks. The IPCP must be facility-wide and include all departments and contracted services. The surveyor should corroborate any concerns observed through interviews and record and/or document review. 81
82 F (d) Influenza and pneumococcal immunizations Influenza. The facility must develop policies and procedures to ensure that- (i) Before offering the influenza immunization, each resident or the resident s representative receives education regarding the benefits and potential side effects of the immunization; (ii) Each resident is offered an influenza immunization October 1 through March 31 annually, unless the immunization is medically contraindicated or the resident has already been immunized during this time period; 82
83 F 883 (iii) The resident or the resident s representative has the opportunity to refuse immunization; and (iv)the resident s medical record includes documentation that indicates, at a minimum, the following: (A) That the resident or resident s representative was provided education regarding the benefits and potential side effects of influenza immunization; and (B) That the resident either received the influenza immunization or did not receive the influenza immunization due to medical contraindications or refusal. 83
84 483.80(d)(2) Pneumococcal disease. The facility must develop policies and procedures to ensure that- (i) Before offering the pneumococcal immunization, each resident or the resident s representative receives education regarding the benefits and potential side effects of the immunization; (ii) Each resident is offered a pneumococcal immunization, unless the immunization is medically contraindicated or the resident has already been immunized; (iii) The resident or the resident s representative has the opportunity to refuse immunization; and (iv)the resident s medical record includes documentation that indicates, at a minimum, the following: (A) That the resident or resident s representative was provided education regarding the benefits and potential side effects of pneumococcal immunization; and 84
85 Pneumococcal. (B) That the resident either received the pneumococcal immunization or did not receive the pneumococcal immunization due to medical contraindication or refusal. 85
86 General Information NOTE: A nursing home may encounter residents who do not have adequate documentation of vaccinations. With the exception of influenza vaccine and pneumococcal polysaccharide vaccine (PPSV), providers should only accept written, dated records as evidence of vaccination. Self-reported doses of influenza vaccine and PPSV are acceptable. A resident representative can report on behalf of the resident if he/she is unable to self-report and the representative has knowledge of the resident s medical care. State laws may have more stringent requirements related to documentation. 86
87 NOTE NOTE: As of the date of publication of this guidance, ACIP recommends that both 23-valent pneumococcal polysaccharide vaccine (PPSV23) and 13-valent pneumococcal conjugate vaccine (PCV13) vaccines should be administered routinely in series to all adults aged 65 years. 65 years so they should be vaccinated based on the ACIP recommendations for their age group. For more up-to-date information on timing and intervals between vaccines, please refer to ACIP vaccine recommendations located at and 71 ACIP explained that PPSV23 is effective in preventing invasive pneumococcal disease (IPD) but the effectiveness of PPSV23 in preventing non-bacteremic pneumococcal pneumonia has been inconsistent. ACIP expects administration of both PCV13 and PPSV23 will provide optimal protection against pneumococcal infections. The recommendations for adults aged <65 years are different than for adults aged The recommendations for adults aged <65 years are different than for adults age For more up-to-date information on timing and intervals between vaccines, please refer to ACIP vaccine recommendations located at and 87
88 Questions? 88

89 YAY We are done! 89
Infection Prevention, Control & Immunizations
 Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Infection Control: This facility task must be used to investigate compliance at F880, F881, and F883. For the purpose of this task, staff includes employees, consultants, contractors, volunteers, and others
Infection Control. Regulatory Changes and Interpretive Guidance Surveyor Training
 Infection Control Regulatory Changes and Interpretive Guidance Surveyor Training 1 F Tags Regulatory Group: Infection Control F880: Infection Prevention and Control ( Old F441 ) 483.80 (a)(1-2)(4)(e-f)
Infection Control Regulatory Changes and Interpretive Guidance Surveyor Training 1 F Tags Regulatory Group: Infection Control F880: Infection Prevention and Control ( Old F441 ) 483.80 (a)(1-2)(4)(e-f)
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care
 Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care Melissa Schaefer, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Infection Prevention and Control in Ambulatory Care Settings: Minimum Expectations for Safe Care Melissa Schaefer, MD Division of Healthcare Quality Promotion Centers for Disease Control and Prevention
Infection Control (F441) Surveyor Training Interpretive Guidance Investigative Protocol Cindy Deporter Updated 1/17
 Surveyor Training Interpretive Guidance Investigative Protocol Cindy Deporter Updated 1/17") 483.80 Infection Control (F441) Surveyor Training Interpretive Guidance Investigative Protocol Cindy Deporter Updated 1/17 1 Federal Regulatory Language 483.80 Infection Control The facility must establish
483.80 Infection Control (F441) Surveyor Training Interpretive Guidance Investigative Protocol Cindy Deporter Updated 1/17 1 Federal Regulatory Language 483.80 Infection Control The facility must establish
Infection Control and Prevention On-site Review Tool Hospitals
 Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Infection Control and Prevention On-site Review Tool Hospitals Section 1.C. Systems to Prevent Transmission of MDROs Ask these questions of the IP. 1.C.2 Systems are in place to designate patients known
Self-Instructional Packet (SIP)
") Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
Self-Instructional Packet (SIP) Advanced Infection Prevention and Control Training Module 4 Transmission Based Precautions February 11, 2013 Page 1 Learning Objectives Module One Introduction to Infection
Infection Prevention and Control and Isolation Authored by: Infection Prevention and Control Department
 Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention and Control and Isolation 2015 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL
 NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
NEW EMPLOYEE ORIENTATION INFECTION PREVENTION AND CONTROL Infection Control Rev. 3/2018 Hand Hygiene Standard Precautions TOPICS Transmission-Based Precautions Personal Protective Equipment (PPE) Multiple
Isolation Categories of Transmission-Based Precautions
 Isolation Categories of Transmission-Based Highlights Policy Statement Standard shall be used when caring for residents at all times regardless of their suspected or confirmed infection status. Transmission-Based
Isolation Categories of Transmission-Based Highlights Policy Statement Standard shall be used when caring for residents at all times regardless of their suspected or confirmed infection status. Transmission-Based
Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases
 Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Infection Prevention Infection Prevention Implementation and adherence to infection prevention practices are the keys to preventing the transmission of infectious diseases to yourself, family members,
Infection Prevention and Control Program
 Infection Prevention and Control Program UNDERSTANDING AND MANAGING THE REGULATORY CHANGES IN YOUR PROGRAM Melissa J. Mitchell, R.N., B.S.N F Tag 880 According to F Tag 880 the Infection Prevention and
Infection Prevention and Control Program UNDERSTANDING AND MANAGING THE REGULATORY CHANGES IN YOUR PROGRAM Melissa J. Mitchell, R.N., B.S.N F Tag 880 According to F Tag 880 the Infection Prevention and
Vancomycin-Resistant Enterococcus (VRE)
") Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
Approved by: Vancomycin-Resistant Enterococcus (VRE) Vice President & Chief Medical Officer Corporate Policy & Procedures Manual VI-40 Date Approved July 14, 2016 August 12, 2016 Next Review (3 years from
Lightning Overview: Infection Control
 Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
STANDARD PRECAUTIONS POLICY Page 1 of 8 Reviewed: May 2017
 Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
Page 1 of 8 Policy Applies to: All Mercy Staff, Credentialed Specialists, Allied Health Professionals, students, patients, visitors and contractors will be supported to meet policy requirements Related
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 CONTACT PRECAUTIONS... 4 DROPLET PRECAUTIONS... 6 ISOLATION PROCEDURES... 7
 ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
ISOLATION TABLE OF CONTENTS STANDARD PRECAUTIONS... 2 BARRIERS INDICATED IN STANDARD PRECAUTIONS... 2 PERSONAL PROTECTIVE EQUIPMENT... 3 CONTACT PRECAUTIONS... 4 RESIDENT PLACEMENT... 4 RESIDENT TRANSPORT...
Principles of Infection Prevention and Control
 Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
Principles of Infection Prevention and Control Liz Van Horne Manager, Core Competencies Senior Infection Prevention & Control Professional OAHPP Outbreak Management Workshop September 15, 2010 Objectives
Objectives. IPC Open calls - bi-weekly series. Introduction to Infection Prevention & Control (IPC) Open Call Series
 Open Call Series") Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
Introduction to Infection Prevention & Control (IPC) Open Call Series #4 Transmission Precautions Isolate the Organism and Not the Resident Diane Dohm MT, IP, CIC, CPHQ MetaStar Anne Haddad, MPH MPRO March
TRANSMISSION-BASED PRECAUTIONS
 TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
TRANSMISSION-BASED PRECAUTIONS PRECAUTIONS Standard Precautions infection prevention practices used with all patients regardless of suspected or confirmed diagnosis. Based on the principle that all blood,
INFECTION C ONTROL CONTROL CONTROL EDUCATION PROGRAM
 INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
INFECTION CONTROL EDUCATION PROGRAM Isolation Precautions Isolating the disease not the patient The Purpose is To protect compromised patient from environment To prevent the spread of communicable diseases.
Infection Control Policy and Procedure Manual. Post-Anesthesia Care Unit (Recovery Room) Page 1 of 6
 Page 1 of 6") (Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
(Recovery Room) Page 1 of 6 Purpose: The purpose of this policy is to establish infection prevention guidelines to prevent or minimize transmission of infections in the. Policy: All personnel will adhere
Objectives. Industry Landscape. Infection Prevention and Control Changes, Updates and Quality Results!
 Infection Prevention and Control Changes, Updates and Quality Results! Sue LaGrange, RN, BSN, NHA, CDONA, FACDONA, CIMT Director of Education Pathway Health 1 Objectives 1.Describe the recent industry
Infection Prevention and Control Changes, Updates and Quality Results! Sue LaGrange, RN, BSN, NHA, CDONA, FACDONA, CIMT Director of Education Pathway Health 1 Objectives 1.Describe the recent industry
Infection Control, Still the Most Commonly Cited Tag in Texas
 July 2016 Commitment to Care Quality Topic Infection Control, Still the Most Commonly Cited Tag in Texas F -441 continues to show up on the list of top 10 deficiencies every quarter here in Texas. During
July 2016 Commitment to Care Quality Topic Infection Control, Still the Most Commonly Cited Tag in Texas F -441 continues to show up on the list of top 10 deficiencies every quarter here in Texas. During
THE INFECTION CONTROL STAFF
 INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
INFECTION CONTROL THE INFECTION CONTROL STAFF INTEGRIS BAPTIST V. Ramgopal, M.D., Hospital Epidemiologist Gwen Harington, RN, BSN, CIC, Infection Control Specialist Kathy Knecht, RN, Surveillance Coordinator
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
2014 Annual Continuing Education Module. Contents
 This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
This self-directed learning module contains information you are expected to know to protect yourself, our patients, and our guests. Content Experts: Infection Prevention Target Audience: All Teammates
Investigating Clostridium difficile Infections
 CALIFORNIA DEPARTMENT OF PUBLIC HEALTH Investigating Clostridium difficile Infections Erin P. Garcia, MPH, CPH Healthcare-Associated Infections (HAI) Program Center for Health Care Quality California Department
CALIFORNIA DEPARTMENT OF PUBLIC HEALTH Investigating Clostridium difficile Infections Erin P. Garcia, MPH, CPH Healthcare-Associated Infections (HAI) Program Center for Health Care Quality California Department
Approval Signature: Date of Approval: December 6, 2007 Review Date:
 Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
Personal Care Home/Long Term Care Facility Infection Prevention and Control Program Operational Directive Management of Methicillin-Resistant Staphylococcus Aureus (MRSA) Approval Signature: Supercedes:
Infection Prevention and Control Annual Education Authored by: Infection Prevention and Control Department
 Infection Prevention and Control Annual Education 2013 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Prevention and Control Annual Education 2013 Authored by: Infection Prevention and Control Department Objectives After you complete this Computer-Based Learning (CBL) module, you should be able
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator
 Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator F282- Comprehensive Care Plans Regulatory language (SOM): 483.21(b)(3) Comprehensive
Reviewing regulatory requirements for top ten federal Nursing Home Tags issued in Minnesota. Eva Loch, MDH Nursing Evaluator F282- Comprehensive Care Plans Regulatory language (SOM): 483.21(b)(3) Comprehensive
Routine Practices. Infection Prevention and Control
 Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
Routine Practices Infection Prevention and Control Routine Practices Elements of Routine Practices: Risk assessment + hand hygiene + personal protective equipment Environmental controls (patient placement,
Safe Care Is in YOUR HANDS
 Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
Safe Care Is in YOUR HANDS 1 in25 patients has a Healthcare-Associated Infection Would you like to be part of prevention? It s EASY and we can start TODAY! STOP the spread of germs! Hand Hygiene Before
INFECTION CONTROL POLICY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT
 Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
Of, INFECTION CONTROL POLICY DEPARTMENT OF RADIOLOGY DATE: 03/01/01 REVISED: 7/15/09 STATEMENT GENERAL The Department of Radiology adheres to the Duke Infection Control policies and the DUMC Exposure Control
PRECAUTIONS IN INFECTION CONTROL
 PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
PRECAUTIONS IN INFECTION CONTROL Standard precautions Transmission-based precautions Contact precautions Airborne precautions Droplet precautions 1 2/25/2015 WHO HAVE TO PROTECT IN HOSPITALS? Patients
Department of Infection Control and Hospital Epidemiology. New Employee Orientation
 Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
Department of Infection Control and Hospital Epidemiology New Employee Orientation Infection Control Contact Information Office 350 Parnassus Ave, Suite 510 Main Office Phone: 353-4343 Practitioner On-Call:
8. Droplet/Contact Precautions. 8.1 Introduction
 8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
8. Droplet/Contact Precautions 8.1 Introduction Droplet/Contact Precautions are required for patients diagnosed with, or suspected of having infectious microorganisms transmitted by the droplet route and
DEVELOPMENT OF AN INFECTION CONTROL PROGRAM FOR LONG-TERM CARE FACILITIES. Evelyn Cook, RN, CIC Associate Director
 DEVELOPMENT OF AN INFECTION CONTROL PROGRAM FOR LONG-TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director Understanding Long-Term Care Varying terms and degrees of inclusiveness Difficult to have
DEVELOPMENT OF AN INFECTION CONTROL PROGRAM FOR LONG-TERM CARE FACILITIES Evelyn Cook, RN, CIC Associate Director Understanding Long-Term Care Varying terms and degrees of inclusiveness Difficult to have
Infection Prevention and Control
 Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
Infection Prevention and Control Infection Prevention and Control Program IPAC program consists of three healthcare professionals IPAC department is located on the 9 th floor and is available Monday to
Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures
 Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures Facility name:... Completed by:... Date:... A. Written infection prevention policies and procedures specific
Infection Prevention Checklist Section I: Policies and Practices I.1 Administrative Measures Facility name:... Completed by:... Date:... A. Written infection prevention policies and procedures specific
Single room with negative pressure ventilation in relation to surrounding areas
 7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
7. Airborne/Contact Precautions 7.1 Introduction Airborne/Contact Precautions are required for patients diagnosed with, or suspected of having an infectious microorganism transmitted by the airborne and
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Neurology (Hemby Lane) Date Originated: 2/20/14 Date Reviewed: 6.5.18 Date Approved: 6/3/14 Page 1 of 7 Approved by: Department Chairman Administrator/Manager
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Neurology (Hemby Lane) Date Originated: 2/20/14 Date Reviewed: 6.5.18 Date Approved: 6/3/14 Page 1 of 7 Approved by: Department Chairman Administrator/Manager
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings
 in Healthcare Settings") Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
Guidance for the Selection and Use of Personal Protective Equipment (PPE) in Healthcare Settings : Program Goal Improve personnel safety in the healthcare environment through appropriate use of PPE. :
Background of Initiative
 Outline 2 Background of Initiative 3 Development of Recommendations 4 5 6 Development and Recommendations 7 Routine Practices Based on the premise that: All patients are potentially infectious (even if
Outline 2 Background of Initiative 3 Development of Recommendations 4 5 6 Development and Recommendations 7 Routine Practices Based on the premise that: All patients are potentially infectious (even if
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance
 Open Call Series #1 Surveillance") Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Introduction to Infection Prevention and Control (IPC) Open Call Series #1 Surveillance Diane Dohm MT, IP, CIC, CPHQ MetaStar February 6, 2018 IPC Open calls: Bi-weekly Series Surveillance What data should
Infection Control Prevention Strategies. For Clinical Personnel
 Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
Infection Control Prevention Strategies For Clinical Personnel What is Infection Control? Infection Control is EVERYONE s responsibility It protects patients, employees and visitors by preventing and controlling
The revisions to F441 were made to provide definition, education, explanation, and examples for the surveyors to reference
 Slide 1 483.65 Infection Control (F441) Surveyor Training of Trainers: Interpretive Guidance Investigative Protocol Objectives: Identify compliance with the regulation as it relates to infection prevention
Slide 1 483.65 Infection Control (F441) Surveyor Training of Trainers: Interpretive Guidance Investigative Protocol Objectives: Identify compliance with the regulation as it relates to infection prevention
Learning Objectives. Successful Antibiotic Stewardship. Byron Health Center & GrandView Pharmacy
 Successful Antibiotic Stewardship Byron Health Center & GrandView Pharmacy Learning Objectives Understand the core requirements of an antibiotic stewardship program as defined by the CMS Requirements of
Successful Antibiotic Stewardship Byron Health Center & GrandView Pharmacy Learning Objectives Understand the core requirements of an antibiotic stewardship program as defined by the CMS Requirements of
Five Top Tips to Prevent Infections in Long-term Care Settings
 Five Top Tips to Prevent Infections in Long-term Care Settings Tip No. 1 Vigilance Open Your Eyes Staff Education Reduce Risks Be Proactive Know the Signs and Symptoms of Infection Tip No. 2 Hand Hygiene
Five Top Tips to Prevent Infections in Long-term Care Settings Tip No. 1 Vigilance Open Your Eyes Staff Education Reduce Risks Be Proactive Know the Signs and Symptoms of Infection Tip No. 2 Hand Hygiene
Objectives. Hot Topics in Infection Prevention and Control in Post Acute Care Settings. NADONA Infection Prevention and Control Webinar Series
 Hot Topics in Infection Prevention and Control in Post Acute Care Settings J. Hudson Garrett Jr., PhD, MSN, MPH, FNP BC, PLNC, CDONA, VA BC, FACDONA PRESENTS Hot Topics in Infection Prevention and Control
Hot Topics in Infection Prevention and Control in Post Acute Care Settings J. Hudson Garrett Jr., PhD, MSN, MPH, FNP BC, PLNC, CDONA, VA BC, FACDONA PRESENTS Hot Topics in Infection Prevention and Control
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards. Infection Prevention and Control: Personal Protective Equipment
 PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards : Personal Protective Equipment PHYSICIAN PRACTICE ENHANCEMENT PROGRAM Assessment Standards 2016 PERSONAL PROTECTIVE EQUIPMENT Personal protective
Oregon Health & Science University Department of Surgery Standard Precautions Policy
 Standard Precautions Policy 1. Policy Standard Precautions are to be followed by all employees for all patients within and entering the OHSU system. Standard Precautions are designed to reduce the risk
Standard Precautions Policy 1. Policy Standard Precautions are to be followed by all employees for all patients within and entering the OHSU system. Standard Precautions are designed to reduce the risk
ISOLATION PRECAUTIONS INTRODUCTION. Standard Precautions are used for all patient care situations, but they
 ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
ISOLATION PRECAUTIONS INTRODUCTION Standard Precautions are used for all patient care situations, but they may not always be sufficient. If a patient is known or suspected to be infected with certain pathogens
IC CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017
 IC.04.03 CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017 Standard In addition to Routine Practices, Contact Precautions or Contact Plus Precautions will be used for patients known or suspected to have
IC.04.03 CONTACT and CONTACT PLUS PRECAUTIONS REV. JULY 2017 Standard In addition to Routine Practices, Contact Precautions or Contact Plus Precautions will be used for patients known or suspected to have
Guidelines for the Management of C. difficile Infections in. Healthcare Settings. Saskatchewan Infection Prevention and Control Program November 2015
 Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
Guidelines for the Management of C. difficile Infections in Healthcare Settings Saskatchewan Infection Prevention and Control Program November 2015 Agenda What is C. difficile infection (CDI)? How do we
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE)
") DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others
DISEASE TRANSMISSION PRECAUTIONS AND PERSONAL PROTECTIVE EQUIPMENT (PPE) Course Health Science Unit VII Infection Control Essential Question What must health care workers do to protect themselves and others
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
Infection Prevention and Control Guidelines for Cystic Fibrosis Patients
 AU Medical Center Policy Library Infection Prevention and Control Guidelines for Cystic Fibrosis Patients Policy Owner: Epidemiology POLICY STATEMENT Based upon best practices for the care of cystic fibrosis
AU Medical Center Policy Library Infection Prevention and Control Guidelines for Cystic Fibrosis Patients Policy Owner: Epidemiology POLICY STATEMENT Based upon best practices for the care of cystic fibrosis
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent
 Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
Taking Action to Prevent and Manage Multidrug-resistant Organisms and C. difficile in the Nursing Home: Part 3 Strategies to prevent Nimalie D. Stone, MD,MS Division of Healthcare Quality Promotion National
Preventing Infection in Care
 Infection Prevention and Control: Older Person Care Homes & Home Environment Learning Programme Workbook NHS Education for Scotland 2011. You can copy or reproduce the information in this document for
Infection Prevention and Control: Older Person Care Homes & Home Environment Learning Programme Workbook NHS Education for Scotland 2011. You can copy or reproduce the information in this document for
Emergency Department Isolation Precautions
 Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
Carolinas HealthCare System Department of Infection Prevention I. SCOPE Emergency Department Isolation Precautions This policy applies to all Carolinas HealthCare System Emergency Department (ED) locations
BEHAVIORAL HEALTH & LTC. Mary Ann Kellar, RN, MA, CHES, IC March 2011
 BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
BEHAVIORAL HEALTH & LTC Mary Ann Kellar, RN, MA, CHES, IC March 2011 CDC Isolation Guidelines-adapting to special environments MDRO s CMS-F 441 C.difficile Norovirus Federal (CMS), State & Joint Commission
Fall HOLLY ALEXANDER Academic Coordinator of Clinical Education MS157
 Fall 2010 HOLLY ALEXANDER Academic Coordinator of Clinical Education 609-570-3478 AlexandH@mccc.edu MS157 To reduce infection & prevent disease transmission Nosocomial Infection: an infection acquired
Fall 2010 HOLLY ALEXANDER Academic Coordinator of Clinical Education 609-570-3478 AlexandH@mccc.edu MS157 To reduce infection & prevent disease transmission Nosocomial Infection: an infection acquired
Infection Control OVERVIEW
 Infection Control OVERVIEW Infections are a significant source of illness and death for nursing home residents and account for up to half of all nursing home resident transfers to hospitals. Infections
Infection Control OVERVIEW Infections are a significant source of illness and death for nursing home residents and account for up to half of all nursing home resident transfers to hospitals. Infections
Infection Control: You are the Expert
 Infection Control: You are the Expert The engaged participant will be able to: List Recognize Identify Three most frequently cited deficiencies Two ways to make hand washing safer Most important practice
Infection Control: You are the Expert The engaged participant will be able to: List Recognize Identify Three most frequently cited deficiencies Two ways to make hand washing safer Most important practice
Personal Hygiene & Protective Equipment. NEO111 M. Jorgenson, RN BSN
 Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
Personal Hygiene & Protective Equipment NEO111 M. Jorgenson, RN BSN Hand Hygiene the single most effective way to help prevent the spread of infections agents. (CDC, 2002.) Consistency & Compliancy 50%
Name of Assessor Unit Date. Element Yes No Action Needed
 Figure 10.5 Checklist: Contact Precautions Name of Assessor Unit Date Element Yes No Action Needed CONTACT PRECAUTIONS GENERAL Contact Precautions are used for patients with known or suspected infections
Figure 10.5 Checklist: Contact Precautions Name of Assessor Unit Date Element Yes No Action Needed CONTACT PRECAUTIONS GENERAL Contact Precautions are used for patients with known or suspected infections
Standard Precautions (SP) & Transmission-Based Isolation Policies
 & Transmission-Based Isolation Policies") SJMHS Infection Control Policy Standard Precautions (SP) & Transmission-Based Isolation Policies Control of Communicable Disease Section Number 3 Policy Number 1.1 Effective Date: 11/63 Revised Date: 9/96,
SJMHS Infection Control Policy Standard Precautions (SP) & Transmission-Based Isolation Policies Control of Communicable Disease Section Number 3 Policy Number 1.1 Effective Date: 11/63 Revised Date: 9/96,
Infection prevention & control
 Infection control in Australian medical practice: Current practice and future developments John Ferguson Infectious Diseases & Microbiology Director, Infection Prevention & Control, Hunter New England
Infection control in Australian medical practice: Current practice and future developments John Ferguson Infectious Diseases & Microbiology Director, Infection Prevention & Control, Hunter New England
Guidelines on Infection Prevention and Control for Cork Kerry Community Healthcare 06: Transmission Based Precautions
 Guidelines on Infection Prevention and Control for Cork Kerry Community Healthcare 06: Transmission Based Precautions This guidance document has been adopted as the policy document by: Organisation:...
Guidelines on Infection Prevention and Control for Cork Kerry Community Healthcare 06: Transmission Based Precautions This guidance document has been adopted as the policy document by: Organisation:...
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY
 EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Pediatrics-Hem/Onc-Module F Date Originated: 03/6/2012 Date Reviewed: 6/14, 9/12/17 Date Approved: 6/5/12 Page 1 of 8 Approved by: Department
EAST CAROLINA UNIVERSITY INFECTION CONTROL POLICY Department: Pediatrics-Hem/Onc-Module F Date Originated: 03/6/2012 Date Reviewed: 6/14, 9/12/17 Date Approved: 6/5/12 Page 1 of 8 Approved by: Department
Infection Prevention and Control for Phlebotomy
 Page 1 of 10 POLICY STATEMENT: It is Sunnybrook s Policy to prevent the spread of infection within the health care institution from patient to patient, patient to staff, staff to patient by: a) providing
Page 1 of 10 POLICY STATEMENT: It is Sunnybrook s Policy to prevent the spread of infection within the health care institution from patient to patient, patient to staff, staff to patient by: a) providing
Healthcare Associated Infections Know No Boundaries: A View Across the Continuum of Care
 Healthcare Associated Infections Know No Boundaries: A View Across the Continuum of Care J. Hudson Garrett Jr., PhD, MSN, MPH, FNP, CSRN, VA-BC Vice President Clinical Affairs, PDI Healthcare Healthcare
Healthcare Associated Infections Know No Boundaries: A View Across the Continuum of Care J. Hudson Garrett Jr., PhD, MSN, MPH, FNP, CSRN, VA-BC Vice President Clinical Affairs, PDI Healthcare Healthcare
Infection Prevention and Control Annual Education 2010
 Infection Prevention and Control Annual Education 2010 Authored by: Cathy Clark, RN MPH CIC Mary Whitaker, RN CIC Bola Ogundimu, RN MPH Marie Commiskey, RN CCRN CIC Modified for affiliated schools students
Infection Prevention and Control Annual Education 2010 Authored by: Cathy Clark, RN MPH CIC Mary Whitaker, RN CIC Bola Ogundimu, RN MPH Marie Commiskey, RN CCRN CIC Modified for affiliated schools students
08/09/ elements required for Infection to occur. Chain of Infection. Evolution of Standard & Transmission Based Precautions
 Helen Murphy, Infection Prevention & Control Nurse Manager, Health Protection Surveillance Centre HPSC/RCPI 2017 Safe Patient Care Course Chain of Infection Evolution of Standard & Transmission Based Precautions
Helen Murphy, Infection Prevention & Control Nurse Manager, Health Protection Surveillance Centre HPSC/RCPI 2017 Safe Patient Care Course Chain of Infection Evolution of Standard & Transmission Based Precautions
Standard Precautions must always be used in addition to Transmission Based Precautions.
 4. Airborne Precautions Airborne Precautions are recommended in addition to Standard Precautions to prevent the transmission of infections spread by very small respiratory particles which are expelled
4. Airborne Precautions Airborne Precautions are recommended in addition to Standard Precautions to prevent the transmission of infections spread by very small respiratory particles which are expelled
Antibiotics - Are they OVERUSED? 4/6/2018. Antibiotic Stewardship Key Clinical Strategies for Successful Outcomes. Pathway Health 1.
 Antibiotic Stewardship Key Clinical Strategies for Successful Outcomes Louann Lawson, BA, RN, RAC-CT, CIMT Nurse Consultant Clinical Reimbursement Team Leader/Clinical Education Manager Pathway Health
Antibiotic Stewardship Key Clinical Strategies for Successful Outcomes Louann Lawson, BA, RN, RAC-CT, CIMT Nurse Consultant Clinical Reimbursement Team Leader/Clinical Education Manager Pathway Health
Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas
 Prevention and Management Toolkit for Inpatient Areas") Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas This toolkit includes examples advice leaflets and forms which may be helpful for use by teams or
Carbapenemase Producing Enterobacteriaceae (CPE) Prevention and Management Toolkit for Inpatient Areas This toolkit includes examples advice leaflets and forms which may be helpful for use by teams or
Prevention and Control of Infection in Care Homes. Infection Prevention and Control Team Public Health Norfolk County Council January 2015
 Prevention and Control of Infection in Care Homes Infection Prevention and Control Team Public Health Norfolk County Council January 2015 Content for today Importance of IPAC -refresher IPAC audits in
Prevention and Control of Infection in Care Homes Infection Prevention and Control Team Public Health Norfolk County Council January 2015 Content for today Importance of IPAC -refresher IPAC audits in
August 22, Dear Sir or Madam:
 August 22, 2012 Office of Disease Prevention and Health Promotion 1101 Wootton Parkway Suite LL100 Rockville, MD 20852 Attention: Draft Phase 3 Long-Term Care Facilities Module Dear Sir or Madam: The Society
August 22, 2012 Office of Disease Prevention and Health Promotion 1101 Wootton Parkway Suite LL100 Rockville, MD 20852 Attention: Draft Phase 3 Long-Term Care Facilities Module Dear Sir or Madam: The Society
Welcome to the Cooper Infection Prevention Team
 Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
Welcome to the Cooper Infection Prevention Team We Need YOU on the Team Healthcare Associated Infections Increase Morbidity & Mortality (Pain, Suffering and Death) CDC estimates that each year about 2
F441 F445. Infection Control. CMS DRAFT Infection Control Guidance.
 F441 F445 Infection Control CMS DRAFT Infection Control Guidance www.cpl-store.com Regulatory information contained in this document is in the public domain and no copyright is claimed. However, all shading,
F441 F445 Infection Control CMS DRAFT Infection Control Guidance www.cpl-store.com Regulatory information contained in this document is in the public domain and no copyright is claimed. However, all shading,
Development of an Infection Control Program for Nursing Homes. Objective of Lecture. Epidemiology of Infections in the Elderly
 Development of an Infection Control Program for Nursing Homes Karen K. Hoffmann, RN, MS, CIC khoffman@med.unc.edu Statewide Program for Infection Control and Epidemiology (SPICE) http://www.unc.edu/depts/spice/
Development of an Infection Control Program for Nursing Homes Karen K. Hoffmann, RN, MS, CIC khoffman@med.unc.edu Statewide Program for Infection Control and Epidemiology (SPICE) http://www.unc.edu/depts/spice/
Welcome and Introduction
 Welcome and Introduction 1 Webinar Speakers Lynn Tabor, MS, RN, WCC, IP-BC, ASCOM Director of Education and Training, American Medical Technologies Jan Ruhl, BSN, RN, IPCO Golden Age Nursing Home, Guthrie
Welcome and Introduction 1 Webinar Speakers Lynn Tabor, MS, RN, WCC, IP-BC, ASCOM Director of Education and Training, American Medical Technologies Jan Ruhl, BSN, RN, IPCO Golden Age Nursing Home, Guthrie
Isolation Care of Patients in Isolation due to Infection or Disease
 Infection Prevention and Control Assurance - Standard Operating Procedure 6 (IPC SOP 6) Isolation Care of Patients in Isolation due to Infection or Disease Why we have a procedure? The spread of infection
Infection Prevention and Control Assurance - Standard Operating Procedure 6 (IPC SOP 6) Isolation Care of Patients in Isolation due to Infection or Disease Why we have a procedure? The spread of infection
Infection Prevention and Control
 Infection Prevention and Control University Hospital Infection Prevention and Control Department Information Melissa Widman ULH Infection Prevention & Control Data Specialist Sarah Bishop Manager of Infection
Infection Prevention and Control University Hospital Infection Prevention and Control Department Information Melissa Widman ULH Infection Prevention & Control Data Specialist Sarah Bishop Manager of Infection
Infection Control Manual. Table of Contents
 This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
This policy has been adopted by UNC Health Care for its use in infection control. It is provided to you as information only. Infection Control Manual Policy Name Patients with Cystic Fibrosis Policy Number
DEPARTMENTAL POLICY. Northwestern Memorial Hospital
 Northwestern Memorial Hospital DEPARTMENTAL POLICY Subject: INFECTION CONTROL AND PREVENTION Title: ISOLATION PRECAUTIONS 1 of 8 Revision of: 04/2004 Policy # Effective Date: 01/2007 I. PURPOSE: Appropriate
Northwestern Memorial Hospital DEPARTMENTAL POLICY Subject: INFECTION CONTROL AND PREVENTION Title: ISOLATION PRECAUTIONS 1 of 8 Revision of: 04/2004 Policy # Effective Date: 01/2007 I. PURPOSE: Appropriate
CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION
 22nd edition CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION Infection Control Module No part of this publication may be reproduced or distributed in any form or by any means, or stored in a database
22nd edition CPNE CLINICAL PERFORMANCE IN NURSING EXAMINATION Infection Control Module No part of this publication may be reproduced or distributed in any form or by any means, or stored in a database
Center for Medicaid and State Operations/Survey and Certification Group
 DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-12-25 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations/Survey
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services 7500 Security Boulevard, Mail Stop S2-12-25 Baltimore, Maryland 21244-1850 Center for Medicaid and State Operations/Survey
Standard Precautions & Managing High risk cases. Tuminah Binti Jantan (SRN)
") Standard Precautions & Managing High risk cases Tuminah Binti Jantan (SRN) Outline 1. Infection risk 2. Infection control in dental practice 3. Standard precautions 4. The element of SP (sharps injury)
Standard Precautions & Managing High risk cases Tuminah Binti Jantan (SRN) Outline 1. Infection risk 2. Infection control in dental practice 3. Standard precautions 4. The element of SP (sharps injury)
Chapter 10. medical and Surgical Asepsis. safe, effective Care environment. Practices that Promote Medical Asepsis
 chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis
chapter 10 Unit 1 Section Chapter 10 safe, effective Care environment safety and Infection Control medical and Surgical Asepsis Overview Asepsis The absence of illness-producing micro-organisms. Asepsis
Welcome to Risk Management
 Welcome to Risk Management Risk Management is the Safety Net Report, Report, Report! Keeping Your Back Safe Follow the guidelines Associates are responsible and will be held accountable Use proper lift
Welcome to Risk Management Risk Management is the Safety Net Report, Report, Report! Keeping Your Back Safe Follow the guidelines Associates are responsible and will be held accountable Use proper lift
Infection Prevention and Control Training
 National Center for Emerging and Zoonotic Infectious Diseases Infection Prevention and Control Training Abimbola (Bola) Ogundimu, DrPH, RN, CIC Infection Preventionist for LTC CDC Division of Healthcare
National Center for Emerging and Zoonotic Infectious Diseases Infection Prevention and Control Training Abimbola (Bola) Ogundimu, DrPH, RN, CIC Infection Preventionist for LTC CDC Division of Healthcare
Developed in response to: Best Practice Infection Prevention and Control
 Transfer of patients within MEHT Clinical Guideline Developed in response to: Best Practice Infection Prevention and Control Version Number 1.0 Issuing Directorate Corporate Governance Approved by Clinical
Transfer of patients within MEHT Clinical Guideline Developed in response to: Best Practice Infection Prevention and Control Version Number 1.0 Issuing Directorate Corporate Governance Approved by Clinical
ACG GI Practice Toolbox. Developing an Infection Control Plan for Your Office
 ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
ACG GI Practice Toolbox Developing an Infection Control Plan for Your Office AUTHOR: Louis J. Wilson, MD, FACG, Wichita Falls Gastroenterology Associates, Wichita Falls, Texas INTRODUCTION: Preventing
Infection Control in Healthcare. Facilities
 Infection Control in Healthcare Basic Principles Facilities Hand Hygiene / Respiratory Etiquette Exclusion of ill staff and visitors Standard and droplet precautions Facility-specific measures Hospitals
Infection Control in Healthcare Basic Principles Facilities Hand Hygiene / Respiratory Etiquette Exclusion of ill staff and visitors Standard and droplet precautions Facility-specific measures Hospitals
Standard Precautions
 Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
Standard Precautions Speciality: Infection Control 1. Indications 1.1 Background Standard Precautions This definition broadens the coverage of the previously known Universal Precautions by recognizing
Policy - Infection Control, Safety and Personal Security
 Policy - Infection Control, Safety and Personal Security Origin Date: October 28, 2013 Last Evaluated: April 2018 Responsible Party: Program Director Minimum Review Frequency: Annually Approving Body:
Policy - Infection Control, Safety and Personal Security Origin Date: October 28, 2013 Last Evaluated: April 2018 Responsible Party: Program Director Minimum Review Frequency: Annually Approving Body:
Tag Description Page. F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125. F622 Transfer & Discharge 155
 Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans
Tag Description Page F607 Policies to Prohibit and Prevent Abuse, Neglect, Exploitation 125 F622 Transfer & Discharge 155 F626 Permitting Residents to Return to Facility 170 F656 Comprehensive Care Plans