VIRGINIA S MEDICAID EXPANSION PROGRAM
|
|
|
- Trevor Matthews
- 5 years ago
- Views:
Transcription



1 VIRGINIA S MEDICAID EXPANSION PROGRAM JENNIFER LEE, MD DIRECTOR, DEPARTMENT OF MEDICAL ASSISTANCE SERVICES
2 Medicaid Expansion Overview Agenda Coming Soon: Medicaid Expansion Vision and Goals Eligibility, Delivery System, and Covered Services Medicaid Reforms: Dual-Track Process Provider Assessments Next Steps Implementation Visit the Cover VA Website & Partner With Us 2
3 Coming Soon: Medicaid Expansion! Beginning January 1, 2019 Up to 400,000 more adults living in Virginia will have access to quality, low cost health coverage 3
4 Medicaid Expansion Vision and Goals To implement a comprehensive system of care that empowers individuals to improve their health and well-being, ensures access to high quality treatment and services, fosters personal responsibility, and maximizes the use of Federal and State dollars Provides individuals with access to high-quality, low-cost health care Provides access to services that keep people healthy so they can engage in their communities (i.e., by attending school and work) and enhances opportunities to improve their lives 3. Provides care coordination and a focus on the social determinants of health to improve outcomes for individuals with complex health conditions 4. Encourages healthy behavior and use of preventive services and promotes personal responsibility and accountability for appropriate use of health services 5. Effectively manages expenditures, encourages use of appropriate care settings such as primary care, and deters use of avoidable services 4

5 Who is Eligible Under Medicaid Expansion? Medicaid expansion will provide quality, low cost health care coverage to expansion eligible individuals Adults ages 19 64, not Medicare eligible Income from 0% to 138% Federal Poverty Level Not already eligible for a mandatory coverage group 5 *Percent income may vary by locality
6 Medicaid Expansion Uses Current Delivery Models 6 Coverage will be provided for most individuals through the Medallion 4.0 and Commonwealth Coordinated Care Plus (CCC Plus) managed care programs Expansion Populations 1. Caretaker Adult, 100% FPL, 2. Caretaker Adult, > 100% FPL 3. Childless Adults, 100% FPL, 4. Childless Adults, > 100% FPL 5. Incarcerated Adults (excluded from managed care) 6. Presumptive Eligible Adults 133% FPL (excluded from managed care) Expansion Delivery Systems Commonwealth Coordinated Care Plus (CCC Plus) will serve populations who are medically frail Medallion 4.0 will serve populations other than those who are medically frail Fee for Service will serve populations excluded from managed care, including: incarcerated adults, presumptively eligible adults, and newly eligible individuals until they are enrolled in a MCO
7 What Services are Covered? The Medicaid expansion population will receive all State Plan services and additional federally-required adult preventive services Doctor, hospital and emergency services, including primary and specialty care Prescription drugs Laboratory and X-ray services Maternity and newborn care Home health services Behavioral health services, including addiction & recovery treatment services Rehabilitative services, including physical, occupational and speech therapies Family planning services Medical equipment and supplies Preventive and wellness services, including annual wellness exams, immunizations, smoking cessation and nutritional counseling And more 7
8 Medicaid Reforms: Dual Track Process The 2018 Appropriations Act directs DMAS to: 1. Amend the State Plan for Medical Assistance, and any waivers thereof, to implement coverage for newly eligible individuals under the ACA (Track 1) 2. Begin the process of implementing a 1115 demonstration project to transform the Medicaid program for newly eligible individuals and eligible individuals enrolled in the existing Medicaid program (Track 2) Track 1: Implemented via contracts and/or other policy changes Track 2: 1115 Demonstration Waiver Early reforms for newly eligible individuals Required reforms that transform the Medicaid program for eligible individuals DMAS is working in parallel to begin the process of applying for a 1115 waiver while submitting the State Plan Amendments to CMS 8
9 Early Medicaid Reforms: Track 1 Early Medicaid reforms will be implemented through contracts and/or other policy changes Referrals to job training, education, and job placement assistance for all unemployed, able-bodied adults Health and Wellness Accounts Appropriate Utilization of ED Services Healthy Behavior Incentives Enhanced Fraud Prevention Efforts 9
10 Medicaid Reforms: Track 2 Required Track 2 reforms will be implemented through a 1115 Waiver Population earning % Federal Poverty Level Monthly Premiums, copayments and deductibles Waiting period prior to re-enrollment if premium not paid Cost-sharing to promote healthy behaviors and appropriate ED use Cost-sharing reductions for compliance with healthy behaviors 10
11 Medicaid Reforms: Track 2 Required Track 2 reforms will be implemented through a 1115 Waiver Training, Enrollment, Education, Employment and Opportunity Program (TEEOP) Gradually escalating participation in community engagement increases to at least 80 hours per month Community engagement includes employment, job skills training, job search activities, education, volunteering, and caregiving Exemptions medically frail, children < 18 y/o, individuals > 55 y/o, primary caregivers with a dependent child < 18 y/o, etc. 11
12 Provider Assessments Provider assessments help to fund the State share of the costs of Medicaid expansion Two types of provider assessments: Coverage Assessment Payment Rate Assessment Most private hospitals required to pay assessments Exempted hospitals include: Public hospitals Freestanding psychiatric or rehabilitation hospital Children s hospital Long-stay hospital Long-term care hospital Critical access hospital 12
13 Next Steps Implementation Program Authorities SPAs, 1115 Waiver Systems Changes Streamlined Enrollment Strategies Contract Modifications and Rates Communications and Outreach Education and Training Testing and Readiness Go-Live 13
14 Regular Updates About Medicaid Expansion Please visit the website regularly for updates. More information will be coming soon on the timing and process for enrollment. Outreach materials will be posted on the website so that our partners can share them in their communities. 14

15 Partner With Us On Expansion You can help support Medicaid expansion Assist with intensive marketing and outreach to educate and inform newly eligible individuals, other providers, and stakeholder groups Support enrollment efforts and access to services for newly eligible individuals Share the Cover Virginia banner and link on your website and social media pages 15

16 MEDICAID PROVIDER MANAGED CARE LIAISON COMMITTEE MEDALLION 4.0 UPDATES JUNE 14, 2018 Cheryl J. Roberts, J.D. Deputy Director of Programs & Operations


17 MEDALLION 4.0 MODEL GROWING STRONGER... TOGETHER


18 MEDALLION 4.0 Will cover approximately 740,000 Medicaid and FAMIS members effective August 1,




19 MEDALLION 4.0 HEALTH PLANS Aligned With CCC Plus 4
20 LAUNCH BY REGION Anticipated Launch Date Region of Virginia Regional Launch Population August 1, 2018 Tidewater 161,421 September 1, 2018 Central 189,438 October 1, 2018 Northern/Winchester 178,416 November 1, 2018 Charlottesville/Western 88,486 December 1, 2018 Roanoke/Alleghany 72,827 December 1, 2018 Southwest 46,558 Total 737,146 5
21 MANAGED CARE ALIGNMENT Six Managed Care Organizations with statewide service Six Regions Services Medallion 4.0 and CCC Plus Managed Care Programs Internal collaboration Are Aligned In Many Ways Provider and member engagement Strong compliance, program integrity, and reporting Streamlined processes and shared services {Common Core Formulary, ARTS, ED Care Coordination} 6

22
23 MEDALLION 4.0 PROGRAM DESIGN Will serve as the platform, along with CCC Plus, for access to health care for those enrolled under the Medicaid expansion Focus on member-centric care for pregnant women, infants, children, parents/caregivers, and expansion adults Members have a choice of six plans in each of the six regions It s the best of Medallion 3, new initiatives, and alignment with CCC Plus 8

24 MEDALLION 4.0 AND EXPANSION MEMBERS The first and foremost goal and expectation of Medallion 4.0 and the expansion is to improve the quality of life and health outcomes for enrolled individuals IT S ALL ABOUT THE MEMBER MEMBER CHOICE MEMBER FOCUS MEMBER ENGAGEMENT 9

25 POPULATION FOCUS Pregnant Women Infants Children/Teens Foster Care & Adoption Assistance Caretaker Adults Expansion Adults 10
 utilization Opioid treatment through ARTS program Targeted projects")
 babies and substance-exposed infants (SEI) Early intervention (EI) Increase immunizations Increase")
26 PREGNANT WOMEN Expanded case management Increase prenatal and postpartum utilization Increase family planning and long acting reversible contraception (LARC) utilization Opioid treatment through ARTS program Targeted projects focus on continuum of care INFANTS Newborn enrollment Promote safe sleep initiatives Decrease neonatal abstinence syndrome (NAS) babies and substance-exposed infants (SEI) Early intervention (EI) Increase immunizations Increase well visits 11



27 12 Increase CHILDREN Oral health utilization Vision screenings Early and periodic screening, diagnosis, and treatment (EPSDT) Prevent and/or reduce obesity, asthma, and other chronic conditions Children and youth with special health care needs TEENS Increase well visits Expanded vision care and access Focus on messaging to adolescents EPSDT focus



28 FOSTER CARE & ADOPTION ASSISTANCE Trauma informed care and resilience Enrolling eligible members in fostering futures and former foster care Focus on transition to adulthood Collaboration with VDSS, LDSS and LCPA ADULTS Wellness and prevention Expanded chronic case management and disease management Enhanced services Behavioral health Family planning/larc Social determinants of health Decrease emergency department use Foster care and adoptive parents 13
29 EXPANSION ADULTS Provides coverage for up to 400,000 more adults Adults ages Not already in or eligible for Medicare Income from 0% to 138% Federal Poverty Level The managed care population and service exclusions will follow current Medallion and CCC Plus rules This means that the few populations and services not included in current managed care programs will be served through fee-for-service, including for new expansion populations 14
30 15 MEDICAID EXPANSION USES CURRENT DELIVERY MODELS Coverage will be provided for most individuals through the Medallion 4.0 and Commonwealth Coordinated Care Plus (CCC Plus) managed care programs Expansion Populations 1. Caretaker Adult, 100% FPL, 2. Caretaker Adult, > 100% FPL 3. Childless Adults, 100% FPL, 4. Childless Adults, > 100% FPL 5. Incarcerated Adults (excluded from managed care) 6. Presumptive Eligible Adults 133% FPL (excluded from managed care) Expansion Delivery Systems Commonwealth Coordinated Care Plus (CCC Plus) will serve populations who are medically frail Medallion 4.0 will serve populations other than those who are medically frail Fee for Service will serve populations excluded from managed care, including: incarcerated adults, presumptively eligible adults, and newly eligible individuals until they are enrolled in a MCO
31 EXPANSION POPULATIONS MEDICALLY FRAIL Per Federal regulations, medically frail includes individuals with: Disabling mental disorders (including children with serious emotional disturbances and adults with serious mental illness) Chronic substance use disorder Serious and complex medical conditions Physical, intellectual or developmental disability that significantly impairs ability to perform 1 or more activities of daily living Disability determination based on Social Security criteria Other categories of individuals as defined by the State Virginia s proposed ABP is more generous than the State Plan; therefore, opt-out provisions to medically frail individuals are not required. If our State Plan included benefits not included in the State s ABP (e.g., LTSS) then we would have to provide opt-out notice, choice counseling, etc. 16
32 MEDICALLY FRAIL BENEFIT How is a person deemed Medically Frail? 1. Member Attestation - Member response to yes/no question at time of initial Medicaid application 2. Medically Frail Screening (MFS) - To be completed by MCO 3. Deemed based upon other authorized eligibility/enrollment (e.g., GAP, LTSS); no MFS required 17
33 Integration is more than an operational change It is an investment in the whole spectrum of care 18
 Services Community Mental Health and Rehabilitation Services")
34 MEDALLION 4.0 SERVICES NEWLY IN Early Intervention (EI) Services Community Mental Health and Rehabilitation Services (CMHRS) Third Party Liability (TPL) STILL OUT Dental Services School Based Services Plan First 19
35 HOLISTIC INTEGRATION - EI 20 Full integration improves the health outcomes of eligible infants and toddlers birth to age three who are not developing as expected MCOs encouraged to designate EI Lead and assign care coordinators To assist in a smooth transition, DMAS has Developed EI Provider training to address program operations, billing, etc. Training dates being set up with DBHDS Developed MCO EI training to assist MCO staff in gaining knowledge about EI services and address previous issues. Training dates being set up. Mailed letter to the parents of EI children to explain the transition of EI services into managed care
 Residential Treatment Services consisting of Psychiatric Residential Treatment Facility (PRTF) and Therapeutic")
36 HOLISTIC INTEGRATION - CMHRS Integrated delivery model that includes medical services and the full spectrum of behavioral health services MCOs responsible for care coordination, provider management, and reimbursement of CMHRS CMHRS will go live 08/01/18 in Tidewater (Regional roll-out) Residential Treatment Services consisting of Psychiatric Residential Treatment Facility (PRTF) and Therapeutic Group Home Services (TGH) for Medallion 4.0 and CCC Plus individuals transition April 1, 2019 Dedicated M4.0-CMHRS@dmas.virginia.gov 21

37 GROWING STRONGER... TOGETHER
38 NEW INITIATIVES Member Engagement Social Media and Apps Social Determinants Of Health and Supportive Services Women s Health Family Planning/Long Acting Reversible Contraceptive (LARC) Transition Planning To Help Teens and Young Adults Trauma-informed Care ACES and Resilience Infant and Early Childhood Physical and Mental Health New Contract New Rates Enhanced Services Value-Based Purchasing Arrangements 23
39 QUALITY MORE THAN NCQA, HEDIS, CAHPS Disease Management Quality Strategy Credentialing Complaints and Appeals Over/Under Utilization EPSDT CQI Networks Gaps in Care Health Disparities Care Coordination PIPS PIA


40 COMPLIANCE Contract Deliverables and Performance Monitoring and Onsites Reporting and Technical Manual Review (Business, Compliance, Management) Collaboratives Enforcement Action and Assessment Follow-up/Corrective Action 25

41 M4.0 DATA ANALYTICS AND INFORMATICS CAPABILITIES Hired new Health Economist New data warehouse New encounter system New technical manual requirements and reporting 26

42










43 KEY IMPLEMENTATION AREAS Waiver Revisions VAC Updates Contract Development Rate Development Systems DMAS Readiness Plan Readiness Communications Enrollment Broker Early Intervention CMHRS Newborns 28
 Mailed first letter to members with information on MEDALLION 4.")
44 COMMUNICATIONS Scheduled series of on-site trainings, webinars, and conference calls to engage members, providers, and stakeholders Schedule can be found at _4-meetings.aspx (see handout) Mailed first letter to members with information on MEDALLION 4.0 and invitations to trainings Distributed blast with registration information for provider/stakeholder trainings and webinars 29

45 YOUR TURN As we move forward, we value your input Send comments or questions to 30


46 GROWING STRONGER... TOGETHER





47 UPDATES ON ARTS, COMMON CORE FORMULARY, ED CARE COORDINATION, AND BEHAVIORAL HEALTH TRANSFORMATION Katherine Neuhausen, MD, MPH Chief Medical Officer Virginia Department of Medical Assistance Services
48 Addiction and Recovery Treatment Services (ARTS) Benefit Changes to DMAS s Substance Use Disorder (SUD) Services for Medicaid and FAMIS Members approved in Spring Expand short-term SUD inpatient detox to all Medicaid /FAMIS members 2 Expand short-term SUD residential treatment to all Medicaid members 3 Increase reimbursement for existing Medicaid/FAMIS SUD treatment services 4 Add Peer Support services for individuals with SUD and/or mental health conditions 5 Require SUD Care Coordinators at DMAS contracted Managed Care Plans 6 Organize Provider Education, Training, and Recruitment Activities

49 ARTS Program: Transforming the Delivery System of Medicaid SUD Services Partial Hospitalization Intensive Outpatient Programs Opioid Treatment Program Office-Based Opioid Treatment Magellan will continue to cover community-based substance use disorder treatment services for feefor-service members Residential Treatment Inpatient Detox ARTS 4/1/17 Case Management Peer Recovery Supports Effective July 1, 2017 All ARTS Services are Covered by Managed Care Plans A fully integrated Physical and Behavioral Health Continuum of Care 3
50 Increases in Addiction Providers Due to ARTS Over 350 new Addiction Treatment Provider Organizations in Medicaid 3 Addiction Provider Type Inpatient Detox (ASAM 4.0) Residential Treatment (ASAM 3.1, 3.3, 3.5, 3.7) Partial Hospitalization Program (ASAM 2.5) Intensive Outpatient Program (ASAM 2.1) # of Providers before ARTS # of Providers after ARTS % Increase in Providers Unknown 103 NEW % 0 13 NEW % Opioid Treatment Program % Office-Based Opioid Treatment Provider 0 79 NEW
51 Highlights From the First One Year of ARTS Increase in total number of Substance Use Disorder Outpatient Providers Before ARTS (Apr 2016-Mar 2017) After ARTS (Apr 2017-Mar 2018) % Change By Provider Type Total number of SUD Outpatient Providers Physicians NP Counselors and SW Other 1,087 2, , % 502% 652% 52% 50% 5
52 Highlights From the First Nine Months of ARTS Increase in total number of Opioid Use Disorder Outpatient Providers Before ARTS (Apr 2016-Mar 2017) After ARTS (Apr 2016-Mar 2017) % Change By Provider Type Total number of OUD Outpatient Providers Physicians NP Counselors and SW Other 570 1, % 358% 408% 66% 62% 6
 After ARTS (Apr-Dec 2017) % Change Members with SUD receiving treatment 12,089 20,436 69% Members with OUD receiving treatment 8,322 12,980")
53 Highlights From the First Nine Months of ARTS More members are receiving treatment for all Substance Use Disorders (SUD) and Opioid Use Disorder (OUD) Before ARTS (Apr-Dec 2016) After ARTS (Apr-Dec 2017) % Change Members with SUD receiving treatment 12,089 20,436 69% Members with OUD receiving treatment 8,322 12,980 56% 7
 After ARTS (Apr-Dec 2017) % Change ED Visits related to OUD 4,484 3,101 31% Total Spending on ED Visits $7,950,019 5,776,221 27%")
54 Highlights From the First Nine Months of ARTS Fewer Emergency Department (ED) visits and decreased costs related to Opioid Use Disorder (OUD) Before ARTS (Apr-Dec 2016) After ARTS (Apr-Dec 2017) % Change ED Visits related to OUD 4,484 3,101 31% Total Spending on ED Visits $7,950,019 5,776,221 27% 8
55 Highlights From the First Nine Months of ARTS Effect of ARTS on the Number of ED Visits for Medicaid Members with an Opioid Use Disorder Q Q Q Q Q Q Q3 OUD Non-SUD OUD without ARTS
 After ARTS")

56 Highlights From the First Nine Months of ARTS Decrease in total number of prescriptions and members with prescriptions for Opioid pain medications Before ARTS (Apr-Dec 2016) After ARTS (Apr-Dec 2017) % Change Total number of prescriptions for opioid pain medication 420, ,598 29% Number of members with prescriptions for Opioid pain medications 116,286 97,529 16% 10
57 Why ARTS is Achieving These Outcomes Critical Elements for Successful ARTS Implementation Intensive stakeholder engagement collaborated with MCOs, agencies, and providers to design and implement ARTS System transformation using national ASAM criteria Increased provider qualifications Payment for evidence-based treatment Innovative delivery models for Medication Assisted Treatment Office-Based Opioid Treatment providers Implementation of CDC Opioid Prescribing Guidelines collaborated with MCO pharmacy directors, MSV, DHP, VDH Extensive provider training by DBHDS and VDH Education and recruitment of providers by DMAS Enhanced reimbursement 11
58 Next Steps 12 DMAS Addiction Treatment Priorities Increase ARTS provider networks before expansion Project ECHO for Preferred OBOTs and Buprenorphine Waiver trainings (with VDH) Implement CMS requirement that all ASAM levels of care ensure access to MAT, especially residential Integrated behavioral health and primary care SBIRT (Screening, Brief Intervention, Referral to Treatment) Buprenorphine initiation in EDs Transitions from jails and prisons Coverage of non-pharmacologic, evidence-based treatments for chronic pain (e.g. acupuncture, chiropractice) Opioid dashboard and data sharing with sister agencies
59 COMMON CORE FORMULARY
60 What is the Common Core Formulary The Common Core Formulary (CCF) is a list of preferred drugs on DMAS Preferred Drug List (PDL) Medallion 4.0 and CCC Plus Health plans are contractually required to cover all drugs on the CCF The CCF includes 90 common drug classes Some drugs are not on the CCF and health plans will decide which drugs to include on their formularies For example, drugs used to treat HIV, hemophilia & cancer are not on the CCF Health plans cannot require additional prior authorizations (PAs) or added restrictions (e.g., step edits) on CCF drugs Plans can add drugs to the CCF but cannot remove Advantages Increased continuity of care No additional PAs or switching drugs Less administrative burden Providers can spend more time with patients The CCF does not apply to Medicare Part D plans 14
61 CCF Implementation Timeline 15 CCC Plus Health Plans started regional implementation of CCF beginning August 1, 2017 with full implementation on January 1, 2018 for all ABDs and complex populations Medallion 4.0 Health Plans will be required to comply with CCF effective August 1, 2018 with regional implementation and full implementation on December 1, CCF will also apply to new Medicaid Expansion population Consistent drug coverage for member transitioning from FFS or between MCOs for drugs
62 Stakeholders Response Medical Society of Virginia Survey: Physicians overwhelmingly cited prior authorizations (PAs) as the primary reason for not accepting Medicaid. 47% cite prescription PAs as a reason to not accept Medicaid. Respondents also cited services PAs, the time involved in PAs, reimbursement, and inconsistent administrative requirements Physicians who accept Medicaid cited prior authorizations (52%) as the biggest problem they face in treating Medicaid patients; 40% identified inconsistent requirements for medications. The Common Core Formulary will reduce the PA burden for prescribers. 16
63 Contact Info for Prior Authorization Issues Health Plan Pharmacy PA Coordinator Direct Line Anthem HealthKeepers (Medallion & CCC Plus) Debbie Stephens (804) Aetna Better Health (Medallion & CCC Plus) Bob Coalson (717) Optima Family (Medallion) Theresa Carpenter (757) Optima Family (CCC Plus) Kevin White (757) Virginia Premier (Medallion & CCC Plus) Tinikki Jackson (804) , x United Health (CCC Plus) Pharmacy PA Help Line (800) Magellan Complete Care (CCC Plus) Gabrielle Williams (800) Kasier Permanente (Medallion) MedImpact (800) INTotal Health (Medallion) Kristi Fowler (703)
64 Resources Common Core Formulary/DMAS PDL link Please questions regarding the Common Core formulary to 18
65 ED CARE COORDINATION Lead Agency: VDH Partner Agencies: DMAS, DHP, DBHDS



66 EDCC Program Dashboard IT Implementation Progress As of June 13th
67 Hospital IT Implementation Status As of 6/13/18 Pre-Implementation (1) Implementing (1) Testing (18) Go Live (3) Virginia Hospital Center Buchanan General Hospital Augusta Health Bath County Community Hospital Bon Secours Health System, Inc. Carilion Clinic Centra Health, Inc. Chesapeake Regional Medical Center Children's Hospital of the Kings Daughters Health System Community Health Systems, Inc. Mountain States Health Alliance (Ballad Health) UVA Health System HCA Healthcare Inova Health System LifePoint Health Mary Washington Healthcare Novant Health Riverside Healthcare Association, Inc. Sentara Health System University of Virginia VCU Health System Valley Health System Wellmont Health System (Ballad Health)
68 Medicaid MCOs IT Implementation Status All 6 currently in implementation: Aetna Anthem Magellan Complete Care of Virginia, LLC As of 6/13/18 Optima Health (DBA Sentara Family Care) United Health Group (UnitedHealthcare Insurance Company) Virginia Premier Health Plan, Inc.
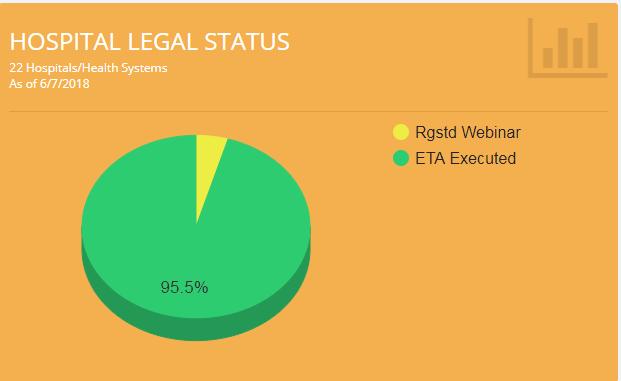
69 Legal Update As of 6/13/18 Novant Health is the last System that needs to sign the ETA for its 3 entities. Executed EXCHANGE Trust Agreements Hospitals/Health Systems (20/21) Health Plans (6/6) Augusta Health Inova Health System Aetna Better Health of Virginia Bath County LifePoint Health (5/5 entities) Ballad Health (MSHA and Wellmont) Bon Secours Health System Mary Washington Healthcare Anthem Health Keepers (Medicaid MCO) Magellan Complete Care of Virginia, LLC Optima Health Buchanan General Hospital Riverside Health System UnitedHealthcare Carilion Clinic Sentara Healthcare Virginia Premier (Medicaid MCO) Centra Health (3/3 entities) Valley Health System Chesapeake Regional Medical UVA Healthcare Center Children s Hospital of the King s VCU (2/2 entities) Daughters CHS (3/3 entities) Virginia Hospital Center HCA 23

70 EDCC Program Dashboard Training Progress As of June 13th
71 BEHAVIORAL HEALTH TRANSFORMATION Partner Agencies: DBHDS, VDSS, Office of Children s Services, Department of Education
72 Expenditures on Community-Based Mental Health Services $300.0 $250.0 $200.0 Millions of Dollars $150.0 $100.0 $50.0 $ Intensive In-Home $55.4 $75.2 $112.1 $148.0 $176.5 $129.3 $94.4 $87.1 $99.3 $108.3 $108.3 $127.6 Therapeutic Day Treatment $30.8 $45.0 $66.8 $112.7 $144.9 $166.1 $139.2 $144.9 $151.6 $171.8 $176.5 $186.0 Mental Health Skill Building $23.4 $30.7 $46.4 $65.8 $92.6 $138.2 $185.3 $224.5 $239.1 $191.4 $204.6 $251.0 Other Behavioral Health Services $33.9 $36.2 $42.8 $46.5 $47.4 $52.4 $57.3 $59.6 $59.9 $58.1 $60.0 $


73 Vision DMAS and DBHDS vision for the future of behavioral health is that there is no wrong door for access that any person seeking care will have a pathway to receive care. 27
74 Next Steps DMAS and DBHDS Partnership with Farley Center University of Colorado Farley Center for Health Policy will support DMAS and DBHDS in developing a comprehensive system reform plan including a continuum of evidence-based and trauma-informed mental health services. Redesigned continuum will provide those receiving services with a more seamless healthcare experience starting with early intervention services at the beginning of life. Continuum will also include: Integrated behavioral heath in primary care School-based health centers Early intervention services Supportive housing and employment benefit targeted to high risk Medicaid members with behavioral health conditions 28
75 Opportunities to Collaborate with Virginia Department of Health Shannon Pursell, MPH Maternal & Infant Health Coordinator Virginia Department of Health 1
: Substance Exposed Infants (SEI), Antibiotic Stewardship, Infant Mortality, Oral Health, Safe Sleep,")
76 MCH Initiatives by Population Women: Decrease unintended pregnancy, LARC initiative Pregnant Women: Maternal mental health screening, Substance Use Disorder (SUD), Decrease Preterm Birth, Obstetric Hemorrhage, Oral Health, Breastfeeding Infants (up to 1yr): Substance Exposed Infants (SEI), Antibiotic Stewardship, Infant Mortality, Oral Health, Safe Sleep, Breastfeeding 2
77 MCH Initiatives by Population Children (1-9yr): Development screening, Homevisiting (Early Impact Virginia, Healthy Start, MIECHV), Immunizations Adolescent (10-21yr): Physical Activity, Obesity, Suicide, prev. tobacco, Sexual Risk Avoidance Education, Immunization CYSHCN: Medical Home, Transition (CDC, CCC) 3
78 Challenges/Opportunities for Collaboration 1. Access to Care a) Maldistribution of Programs/Services b) Transportation c) Number of providers 2. Health Literacy a) Preferred language b) Reading level c) Culturally appropriate d) Format/how is it presented 4
79 Virginia Neonatal Perinatal Collaborative Vision Ensure the best perinatal care and the best start for infants Data-driven collaborative Create a stronger, healthier Virginia Goals Decrease maternal mortality by 50% through QI Enhance the quality of state-wide perinatal data Improve neonatal outcomes through QI Inform and involve the community Achieve health equity in pregnancy and neonatal outcomes Legislative Charge Improve pregnancy outcomes for women and newborns through QI Focus on pregnant women with SUD and infants with NAS 5
80 VNPC Structure and Projects Steering Committee (6 Members) Executive Committee (15 Members) Advisory Committees Improving Perinatal Outcomes Improving Neonatal Outcomes Data Acquisition and Management Community Engagement Advocacy and Sustainability Project Workgroups Neonatal Abstinence Syndrome (NAS) Maternal Opioid Use Disorder (OUD) Antibiotic Stewardship in the NICU and Newborn Nursery Obstetric Hemorrhage 17OH-Progesterone 6
 Acceptance Pilot State")
81 VNPC Wins General Assembly Funding for SFY19, SFY20 Received March of Dimes community grant CDC Grant: Approved (Not Funded) CDC & NICHQ Recognition as State Perinatal Quality Collaborative Vermont Oxford Network Contract for NAS QI Project, first data collection will be July 9-13, 2018, 38 hospitals will be participating Alliance for Innovation on Maternal Health (AIM) Acceptance Pilot State for Maternal OUD bundle Partnership with Virginia s Maternal Mortality Review Team 2 nd Annual Summit will be Oct 29, 2018 in Charlottesville Website in development: 7
82 How to Collaborate to Achieve Shared Goals? 1. Participate in the VNPC 2. Coordinate efforts to increase health literacy across all MCH populations Media Campaigns: 3Rs, Right time, Right service, Right location; Translation services 3. Active Engagement and participation in the implementation of HB1157 through participation in the environmental scan and/or commitment to address gaps in services. 8
83 Questions My VNPC Website: VNPC 9
84 DBHDS Initiatives for Pregnant and Parenting Women and their Children: Opportunities for Collaboration presented to the Medicaid Provider Managed Care Liaison Committee June 14, 2018 Mellie Randall Substance Use Disorder Policy Director DBHDS Vision: A life of possibilities for all Virginians
85 Community System Overview 39 Community services boards (CSBs) and one behavioral health authority (BHA) Independent entities of local government Code of Virginia requires Emergency Services Case management where resources are available STEP Va Significant variability in capacity, types of services Funded by General Funds, Federal Block Grants, fees (including Medicaid), local taxes, other grants and revenues Slide 2
 Child")
86 Substance Abuse Prevention and Treatment (SAPT) Block Grant SAPT BG requires MOE (base $) for Pregnant Women and Women with Dependent Children Preferential admission for pregnant women. Service requirements include: Primary medical care/referral for prenatal care Primary pediatric care, including immunizations Gender-specific substance abuse treatment (trauma and parenting) Child care while women are receiving services Therapeutic interventions for children in the custody of women in treatment that address developmental needs and issues of sexual/physical abuse and neglect Case management and transportation to ensure access to care Slide 3
87 Residential Services for Pregnant and Parenting Women with SUDs Four residential programs for mothers that include young dependent children Southeastern Family Center (Hampton-Newport News) PPW only Rubicon East Women s Campus (Richmond Behavioral Health Authority) PPW and Mothers Bethany Hall (private nonprofit Roanoke very limited space)ppw and Mothers Demeter House (Phoenix) private Arlington PPW and Mothers Slide 4
88 Project Link Model Goal: Create a coordinated system of care for pregnant and parenting women with or at risk of SUDs that supports access to services and supports for the women and their children Objectives: Coordinate and connect women to existing services within the community Educate and train existing service providers about the needs of these women and their families Enhance communication between and among service providers Provide a no wrong door approach to services, including SUD treatment, health care, income supports and other services that support and enhance the family towards health and well being Slide 5
89 SAMHSA PPW Project Link 2017 $1+ million for 3 years ( ) Nine sites Goals: Reduce abuse of alcohol and other drugs Increase engagement in treatment services Increase retention in the appropriate level and duration of treatment Ensure that women with opioid use disorder have access to a range of MAT and appropriate support services Enhance parenting and family functioning Slide 6
90 Federal State Targeted Response (STR) to the Opioid Crisis Opioid Prevention, Treatment and Recovery in Virginia (OPT-R Va) = $9.7 million (May 2017) and continued one additional year Year 1: MOU with James Madison University to develop online training modules (video) for CPS workers MOU with VDH to develop online video training modules (video) for Early Impact Virginia (home visiting) Slide 7

91 Prevention Adverse Childhood Experiences (ACEs) Prepared Communities Initiative 9 ACE Prepared Communities have been funded and have created a community ACEs Advisory Council to develop a comprehensive approach to address ACEs. First cohort of ACE Interface Master Trainers in Virginia completed training December Slide 8
92 Children and Adolescents SAMHSA System of Care Grant $2.8 million X 4 years ( ) - statewide Coordinates a network of community-based services and supports for children and youth (up to 21) with mental health or other BH challenges and their families to improve functioning at home, school and community. EBP High Fidelity Wraparound Services- Youth-guided and family-driven planning process Services to Youth in Detention Centers through 5 CSBs Child Psychiatry and Children s Crisis Services Services for Children with SED not mandated for CSA Slide 9
93 SAMHSA Grant-Transition Age Youth Substance Abuse Treatment $3.2 million X 4 years ( ) Utilizes EBP assessment (GAIN) and intervention (A-CRA) 4 CSB Demonstration sites Goals: Improve Substance Use and Mental Health treatment services for transition age youth (ages 16-25) with SUD and/or co-occurring disorders Increase state-wide access to evidence-based assessments, treatment models and recovery services by strengthening the existing infrastructure system. Increase use of EBPs Increase collaboration among treatment providers, policy agencies, and youth and family members. Slide 10
 Primary Care Integration Targeted")
94 STEP-VA Next Steps Detoxification Care Coordination Peer and Family Support Psychosocial Rehab/Skill Building Possible Development for the 2018 Session Same Day Access (Remaining CSBs) Primary Care Integration Targeted Case Management for Children Outpatient Services Permanent Supportive Housing 2017 General Assembly Session Same Day Access (Partial Implementation) MAT (Partial Implementation new Federal Grant Funding) Permanent Supportive Housing Funds Future Sessions Targeted Case Management for Adults Veterans (included in each service) Person-Centered Treatment Mobile Crisis Services Future Sessions Slide 11
95 Part C of IDEA Early Intervention Services Infant & Toddler Connection of Virginia June 14, 2018 Catherine Hancock MS, RN, PMHCNS, BC Early Intervention Administrator Dept. of Behavioral Health and Developmental Services
96 What is Early Intervention Part C Early Intervention provides supports and services to infants and toddlers from birth through age two who are not developing as expected or who have a medical condition that can delay normal development. Early intervention supports and services focus on increasing the child's participation in family and community activities that are important to the family. Slide 13
 to ensure that all children with disabilities from birth through age two would receive")
.")
97 Federal Law 1986: Congress enacted early intervention (EI) legislation as an amendment to the Education of Handicapped Children s Act (1975) to ensure that all children with disabilities from birth through age two would receive appropriate EI services, forming Part H of the Act. 1991: The Act was re-authorized and renamed the Individuals with Disabilities Education Act (IDEA). 1998: IDEA was re-authorized and Part H became Part C of the Act. 2004: Re-authorized Slide 14

.")
98 Virginia State Law Since 1987, the Department of Behavioral Health and Developmental Services (DBHDS) has served as the State Lead Agency in Virginia for Part C Early Intervention Services. Virginia s Part C System is called the Infant & Toddler Connection of Virginia (ITCVA) There are 40 Local Lead Agencies, including 30 CSBs and 10 other entities (local government, universities). The local systems are called the Infant & Toddler Connection of Slide 15

99 Who is eligible? In Virginia, children from birth to age three are eligible for Part C early intervention services if: The are functioning 25% or more below their chronological age or adjusted age in one or more areas of development (i.e., cognitive, physical, communication, social-emotional, or adaptive development); They show atypical development (e.g., behavioral disorders, affective disorders, abnormal sensory-motor responses); and/or They have a diagnosed physical or mental condition that has a high probability of resulting in a developmental delay. Autism is one of the conditions in this category. Slide 16
100 Annual Number of Infants & Toddlers Served 30,000 25,000 22,453 24,699 20,000 15,000 14,069 15,676 15,523 16,272 17,022 17,839 19,085 20,412 11,766 12,234 10,000 5,

101 Slide Local ITC Systems Organized by Regions
 for eligible children are provided according to federal and state regulations, including employing and/or contracting with certified EI service providers; System and fiscal management, data")
102 Local Infant & Toddler Connection Systems Each of the 40 local ITCs, led by a local system manager (LSM) is responsible for: Ensuring that EI services listed on the Individual Family Services Plan (IFSP) for eligible children are provided according to federal and state regulations, including employing and/or contracting with certified EI service providers; System and fiscal management, data collection, public awareness, child find, training and local lead agency administration; etc. Connect with your Local System Managers (LSM). Slide 19


103 Part C Early Intervention Services May Include: Assistive technology Audiology Developmental Services Family training, counseling and home visits Health services Medical services (for diagnostic and evaluation purposes only) Nursing Services Nutrition services Occupational therapy Physical therapy Psychological services Social work services Speech-language pathology Transportation Vision services Slide 20
104 Who Can Provide Early Intervention Services? Audiologist Developmental Services Assistant Behavior Analyst Developmental Services Behavior Analyst Licensed Certified Therapeutic Recreation Specialist Assistive Technology Services Counselor Licensed Professional Counselor Early Intervention Service Coordinator 21 Early Intervention Assistant Educators Family & Consumer Science Professional Family Therapist Music Therapist Nurse- RN and Nurse Practitioner Occupational Therapist Occupational Therapy Assistant Physical Therapist Physical Therapy Assistant Physician Psychologist Registered Dietician Certified Nurse s Aide

.")

105 Natural Environments, Routines, Coaching & Functional Outcomes Some Key Principles: Early intervention services are to be provided in natural environments to the maximum extent appropriate. Infants and toddlers learn best through everyday experiences and interactions with familiar people in familiar contexts (routines). All families, with the necessary supports and resources, can enhance their children s learning and development (coaching). The primary role of the service provider in EI is to work with and support family members and caregivers in children s lives (coaching). IFSP outcomes (goals) must be functional and based on children s and families needs and family-identified priorities (functional outcomes). Slide 22

106 Funding Part C Early Intervention Services Federal Part C funds are allocated to local system lead agencies and are available as payor of last resort. Many private insurance plans pay for some early intervention services. Medicaid covers all Part C early intervention services. A sliding fee scale is available to families. No child and family will be denied services due to an inability to pay. Slide 23
107 Early Intervention Works Early intervention (EI) services reduce costs for education (special education, grade retention), crime, welfare Early social interventions reported a $7 return on $1 investment Sources: Rand research brief, the Brookings Institution Research briefs, Perry Preschool Project, Harvard University Slide 24

108 Who can make a referral? Anyone can make a referral. Any child who is suspected of being eligible can be referred to Virginia s Part C system. Anyone can make a referral, including parents and/or family members, social workers, physicians and others with whom the child and family have contact. *Referral sources do not need parental permission to refer, but Part C does need parental permission to share information with anyone (FERPA=Family Educational Rights & Privacy Act). Central Point of Entry -COUNTIES-all.pdf Or Slide 25
109 Reference Manuals Virginia Medicaid Early Intervention Services Provider Manual rtal/providermanual Virginia Early Intervention Practice Manual Slide 26
COMMONWEALTH COORDINATED CARE PLUS. A Managed Long Term Services and Supports Program
 COMMONWEALTH COORDINATED CARE PLUS A Managed Long Term Services and Supports Program Agenda Background and Key Facts Populations Services Regional Launch CCC Plus Enrollment 2 Overview of Commonwealth
COMMONWEALTH COORDINATED CARE PLUS A Managed Long Term Services and Supports Program Agenda Background and Key Facts Populations Services Regional Launch CCC Plus Enrollment 2 Overview of Commonwealth
VDH and Neonatal Abstinence Syndrome. May 12, 2017 Vanessa Walker Harris, MD Director, Office of Family Health Services Virginia Department of Health
 VDH and Neonatal Abstinence Syndrome May 12, 2017 Vanessa Walker Harris, MD Director, Office of Family Health Services Virginia Department of Health Neonatal Abstinence Syndrome Discharges per 1,000
VDH and Neonatal Abstinence Syndrome May 12, 2017 Vanessa Walker Harris, MD Director, Office of Family Health Services Virginia Department of Health Neonatal Abstinence Syndrome Discharges per 1,000
Michigan Council for Maternal and Child Health 2018 Policy Agenda
 Michigan Council for Maternal and Child Health 2018 Policy Agenda MCMCH Purpose! MCMCH s purpose is to advocate for public policy that will improve maternal and child health and optimal development outcomes
Michigan Council for Maternal and Child Health 2018 Policy Agenda MCMCH Purpose! MCMCH s purpose is to advocate for public policy that will improve maternal and child health and optimal development outcomes
Federal Legislation to Address the Opioid Crisis: Medicaid Provisions in the SUPPORT Act
 October 2018 Issue Brief Federal Legislation to Address the Opioid Crisis: Medicaid Provisions in the SUPPORT Act MaryBeth Musumeci and Jennifer Tolbert On October 3, 2018, the Senate overwhelmingly passed
October 2018 Issue Brief Federal Legislation to Address the Opioid Crisis: Medicaid Provisions in the SUPPORT Act MaryBeth Musumeci and Jennifer Tolbert On October 3, 2018, the Senate overwhelmingly passed
Residential Treatment Services. Covered Services 6/30/2017 CHAPTER IV COVERED SERVICES AND LIMITATIONS. Manual Title. Page. Chapter.
 Revision Date Covered Services CHAPTER COVERED SERVICES AND LIMITATIONS Revision Date 1 CHAPTER TABLE OF CONTENTS PAGE General Information... 4 Medallion 3.0... 5 Coverage for FAMIS MCO Enrollees*... 6
Revision Date Covered Services CHAPTER COVERED SERVICES AND LIMITATIONS Revision Date 1 CHAPTER TABLE OF CONTENTS PAGE General Information... 4 Medallion 3.0... 5 Coverage for FAMIS MCO Enrollees*... 6
Drug Medi-Cal Organized Delivery System
 Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
Drug Medi-Cal Organized Delivery System Presented by Elizabeth Stanley-Salazar, MPH CMS Approval of DMC-ODS Waiver under ACA August 13, 2015 Pathway to Parity 2010 President Obama Signs the Affordable
Maryland Medicaid Program. Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 31, 2012
 Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 31, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Maryland Medicaid Program Aaron Larrimore Medicaid Department of Health and Mental Hygiene May 31, 2012 1 Maryland Medicaid In Maryland, Medicaid is also called Medical Assistance or MA. MA is a joint
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014
 Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014 NM Title V MCH Block Grant 2016 Application/2014 Report Executive Summary
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2016 Annual Report for 2014 NM Title V MCH Block Grant 2016 Application/2014 Report Executive Summary
Coverage of Behavioral Health Services for Children, Youth, and Young Adults with Significant Mental Health Conditions
 Coverage of Behavioral Health Services for Children, Youth, and Young Adults with Significant Mental Health Conditions Webinar Website: http://gucchdtacenter.georgetown.edu/resources/tawebinars.html Coverage
Coverage of Behavioral Health Services for Children, Youth, and Young Adults with Significant Mental Health Conditions Webinar Website: http://gucchdtacenter.georgetown.edu/resources/tawebinars.html Coverage
ILLINOIS 1115 WAIVER BRIEF
 ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
ILLINOIS 1115 WAIVER BRIEF STATE TESTING FOR THE FOLLOWING ACHIEVED RESULTS: 1. Increased rates of identification, initiation, and engagement in treatment 2. Increased adherence to and retention in treatment
Draft Children s Managed Care Transition MCO Requirements
 Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
Draft Children s Managed Care Transition MCO Requirements OVERVIEW On February 1 st, New York State released for stakeholder feedback a draft version of the Medicaid Managed Care Organization (MCO) Children
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction
 Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Minnesota s Plan for the Prevention, Treatment and Recovery of Addiction Background Beginning in June 2016, the Alcohol and Drug Abuse Division (ADAD) of the Minnesota Department of Human Services convened
Section IX Special Needs & Case Management
 Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
Section IX Special Needs & Case Management Special Needs and Case Management 181 Integrated Health Care Management (IHCM) The Integrated Health Care Management (IHCM) program is a population-based health
Service Array: Mental Health Medicaid Specialty Supports and Services Descriptions Note:
 Service Array: Mental Health Medicaid Specialty Supports and Services Descriptions Note: If you are a Medicaid beneficiary and have a serious mental illness, or serious emotional disturbance, or developmental
Service Array: Mental Health Medicaid Specialty Supports and Services Descriptions Note: If you are a Medicaid beneficiary and have a serious mental illness, or serious emotional disturbance, or developmental
Maternal and Child Health Services Title V Block Grant for New Mexico. Executive Summary. Application for Annual Report for 2015
 Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2017 Annual Report for 2015 Title V Block Grant History and Requirements Enacted in 1935 as a part
Maternal and Child Health Services Title V Block Grant for New Mexico Executive Summary Application for 2017 Annual Report for 2015 Title V Block Grant History and Requirements Enacted in 1935 as a part
MEDICAID MANAGED LONG-TERM SERVICES AND SUPPORTS OPPORTUNITIES FOR INNOVATIVE PROGRAM DESIGN
 Louisiana Behavioral Health Partnership MEDICAID MANAGED LONG-TERM SERVICES AND SUPPORTS OPPORTUNITIES FOR INNOVATIVE PROGRAM DESIGN Rosanne Mahaney - Delaware Lou Ann Owen - Louisiana Brenda Jackson,
Louisiana Behavioral Health Partnership MEDICAID MANAGED LONG-TERM SERVICES AND SUPPORTS OPPORTUNITIES FOR INNOVATIVE PROGRAM DESIGN Rosanne Mahaney - Delaware Lou Ann Owen - Louisiana Brenda Jackson,
The Mommies Program An Integrated Model of Care. Karen Palombo, LCSW, LCDC Texas Women s SUD Intervention Specialist
 The Mommies Program An Integrated Model of Care Karen Palombo, LCSW, LCDC Texas Women s SUD Intervention Specialist Objectives Discuss the effects of opioid epidemic on pregnant women Recognize the importance
The Mommies Program An Integrated Model of Care Karen Palombo, LCSW, LCDC Texas Women s SUD Intervention Specialist Objectives Discuss the effects of opioid epidemic on pregnant women Recognize the importance
THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL
 PROVIDER MANUAL") THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL SUPPLEMENTAL INFORMATION This Supplement to the Optima Health Provider Manual is available for Providers who provide services
THE ADDICTION AND RECOVERY TREATMENT SERVICES PROGRAM (ARTS) PROVIDER MANUAL SUPPLEMENTAL INFORMATION This Supplement to the Optima Health Provider Manual is available for Providers who provide services
1115 Waiver Renewal Tribal Consultation June 23, New Mexico Human Services Department
 1115 Waiver Renewal Tribal Consultation June 23, 2017 New Mexico Human Services Department 1 Centennial Care 2.0 Concepts Public Comments Wrap Up Provide information about Centennial Care: overview, goals,
1115 Waiver Renewal Tribal Consultation June 23, 2017 New Mexico Human Services Department 1 Centennial Care 2.0 Concepts Public Comments Wrap Up Provide information about Centennial Care: overview, goals,
Section V: To be completed by the PIHP contract manager as applicable. Section VI: To be completed by the PIHP Credentialing Committee as applicable.
 Sections I-IV: To be completed by the organizational provider at the time of initial network application for enrollment and credentialing; or at the time of the biennial re-credentialing. Section I. Agency
Sections I-IV: To be completed by the organizational provider at the time of initial network application for enrollment and credentialing; or at the time of the biennial re-credentialing. Section I. Agency
MassHealth Restructuring Overview
 1 MassHealth Restructuring Overview State of the State, Assuring Access, Equity and Integrated Care Massachusetts League of Community Health Centers Marylou Sudders, Secretary Executive Office of Health
1 MassHealth Restructuring Overview State of the State, Assuring Access, Equity and Integrated Care Massachusetts League of Community Health Centers Marylou Sudders, Secretary Executive Office of Health
VIRGINIA NICU EARLY INTERVENTION COLLABORATIVE AN INITIATIVE FUNDED BY THE VIRGINIA BOARD FOR PEOPLE WITH DISABILITIES (VBPD)
") VIRGINIA NICU EARLY INTERVENTION COLLABORATIVE AN INITIATIVE FUNDED BY THE VIRGINIA BOARD FOR PEOPLE WITH DISABILITIES (VBPD) Wanda Clevenger BSN, RN, MBA VHHA, Director of Performance Improvement Catherine
VIRGINIA NICU EARLY INTERVENTION COLLABORATIVE AN INITIATIVE FUNDED BY THE VIRGINIA BOARD FOR PEOPLE WITH DISABILITIES (VBPD) Wanda Clevenger BSN, RN, MBA VHHA, Director of Performance Improvement Catherine
Presentation Overview. Overview of Medicaid Coverage Policies for Perinatal Care. Medicaid Births. Medicaid Births.
 Presentation Overview Overview of Medicaid Coverage Policies for Perinatal Care Rachel Currans-Henry, MPP Director, Bureau of Benefits Management Division of Medicaid Services April 23, 2018 1. Importance
Presentation Overview Overview of Medicaid Coverage Policies for Perinatal Care Rachel Currans-Henry, MPP Director, Bureau of Benefits Management Division of Medicaid Services April 23, 2018 1. Importance
Covered Services List and Referrals and Prior Authorizations for MassHealth Members enrolled in Partners HealthCare Choice
 Covered Services Covered Services List and s and Prior Authorizations for MassHealth Members enrolled in Partners HealthCare Choice This chart tells you two things: 1. the covered services and benefits
Covered Services Covered Services List and s and Prior Authorizations for MassHealth Members enrolled in Partners HealthCare Choice This chart tells you two things: 1. the covered services and benefits
Medicaid Fundamentals. John O Brien Senior Advisor SAMHSA
 Medicaid Fundamentals John O Brien Senior Advisor SAMHSA Medicaid Fundamentals Provides medical benefits to groups of low-income people with no medical insurance or inadequate medical insurance. Federally
Medicaid Fundamentals John O Brien Senior Advisor SAMHSA Medicaid Fundamentals Provides medical benefits to groups of low-income people with no medical insurance or inadequate medical insurance. Federally
FIDA. Care Management for ALL
 Care Management for ALL In 2011, Governor Andrew M. Cuomo established a Medicaid Redesign Team (MRT), which initiated significant reforms to the state s Medicaid program. This included a critical initiative
Care Management for ALL In 2011, Governor Andrew M. Cuomo established a Medicaid Redesign Team (MRT), which initiated significant reforms to the state s Medicaid program. This included a critical initiative
The CCBHC: An Innovative Model of Care for Behavioral Health
 The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
The CCBHC: An Innovative Model of Care for Behavioral Health B R E N D A G O G G I N S, J D V I C E P R E S I D E N T O A K S I N T E G R A T E D C A R E M I C H A E L D A M I C O, L C S W D I R E C T
RFS-7-62 ATTACHMENT E INDIANA CARE SELECT PROGRAM DESCRIPTION AND COVERED BENEFITS
 The following services are covered by the Indiana Care Select Program. Dual-eligible members, those members eligible for both IHCP and Medicare, will not receive any benefits under Indiana Care Select,
The following services are covered by the Indiana Care Select Program. Dual-eligible members, those members eligible for both IHCP and Medicare, will not receive any benefits under Indiana Care Select,
Residential Treatment Services Manual 6/30/2017. Provider Participation Requirements PROVIDER PARTICIPATION REQUIREMENTS CHAPTER II. Chapter.
 Subject 1 PROVIDER PARTICIPATION REQUIREMENTS CHAPTER Subject 2 CHAPTER TABLE OF CONTENTS PAGE Managed Care Enrolled Members... 4... 5 Provider Qualifications... 7 Psychiatric Residential Treatment Facilities...
Subject 1 PROVIDER PARTICIPATION REQUIREMENTS CHAPTER Subject 2 CHAPTER TABLE OF CONTENTS PAGE Managed Care Enrolled Members... 4... 5 Provider Qualifications... 7 Psychiatric Residential Treatment Facilities...
Widespread prescribing, distribution and availability of naloxone for high risk individuals and as rescue medication 2
 Co Occurring Collaborative Serving Maine Expanding Medication Assisted Recovery Services & Building a Stronger Recovery Oriented System for SUD Treatment in Maine April 2018 Introduction: With support
Co Occurring Collaborative Serving Maine Expanding Medication Assisted Recovery Services & Building a Stronger Recovery Oriented System for SUD Treatment in Maine April 2018 Introduction: With support
Clinical Utilization Management Guideline
 Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
DMC-ODS. System Transformation. Presented at DHCS 2017 Annual Conference. Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW
 DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
CCBHCs 101: Opportunities and Strategic Decisions Ahead
 CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
CCBHCs 101: Opportunities and Strategic Decisions Ahead Rebecca C. Farley, MPH National Council for Behavioral Health Speaker Name Title Organization It Passed! The largest federal investment in mental
Bright Futures: An Essential Resource for Advancing the Title V National Performance Measures
 A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
A S S O C I A T I O N O F M A T E R N A L & C H I L D H E A L T H P R O G R A MS April 2018 Issue Brief An Essential Resource for Advancing the Title V National Performance Measures Background Children
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS
 UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
UPDATE ON MANAGED CARE IN NY STATE: IMPLICATIONS FOR PROVIDERS November 18, 2013 NYS OMH Behavioral Health Transition 2 Key MRT initiative to move fee-for-service populations and services into managed
NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA)
") NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA) The Affordable Care Act (ACA) The Affordable Care Act 3 Officially called the Patient Protection and Affordable Care Act (PPACA)
NEW YORK STATE MEDICAID REDESIGN TEAM AND THE AFFORDABLE CARE ACT (MRT & ACA) The Affordable Care Act (ACA) The Affordable Care Act 3 Officially called the Patient Protection and Affordable Care Act (PPACA)
SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery. o--,-.m-a----,laa~-d-c~~~~~~~~~~-
 Page 11 of 8 SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery Departmental Policy and Procedure Section Sub-section Alcohol and Drug Program (ADP) Policy Drug Medi-Cal
Page 11 of 8 SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery Departmental Policy and Procedure Section Sub-section Alcohol and Drug Program (ADP) Policy Drug Medi-Cal
WHAT DOES MEDICALLY NECESSARY MEAN?
 WHAT DOES MEDICALLY NECESSARY MEAN? Your Primary Care Provider (PCP) will help you get the services you need that are medically necessary as defined below. Medically Necessary means appropriate and necessary
WHAT DOES MEDICALLY NECESSARY MEAN? Your Primary Care Provider (PCP) will help you get the services you need that are medically necessary as defined below. Medically Necessary means appropriate and necessary
Early and Periodic Screening, Diagnosis, and Treatment Program EPSDT Florida - Sunshine Health Annual Training
 Early and Periodic Screening, Diagnosis, and Treatment Program EPSDT Florida - Sunshine Health Annual Training EPSDT Overview EPSDT purpose and requirements mandated by the Agency for Health Care Administration
Early and Periodic Screening, Diagnosis, and Treatment Program EPSDT Florida - Sunshine Health Annual Training EPSDT Overview EPSDT purpose and requirements mandated by the Agency for Health Care Administration
DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM (DMC-ODS) PERFORMANCE METRICS. (version 6/23/17)
 PERFORMANCE METRICS. (version 6/23/17)") 1 Access Enrollment information to include the number of DMC-ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
1 Access Enrollment information to include the number of DMC-ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
TABLE OF CONTENTS. Primary Care 3. Child Health Services. 10. Women s Health Services. 13. Specialist Health Services 16. Mental Health Services.
 TABLE OF CONTENTS Primary Care 3 Child Health Services. 10 Women s Health Services. 13 Specialist Health Services 16 Mental Health Services. 24 2 PRIMARY CARE What is it? Primary care is a patient's first
TABLE OF CONTENTS Primary Care 3 Child Health Services. 10 Women s Health Services. 13 Specialist Health Services 16 Mental Health Services. 24 2 PRIMARY CARE What is it? Primary care is a patient's first
o Recipients must coordinate these testing services with other HIV prevention and testing programs to avoid duplication of efforts.
 E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
E. GENERAL SERVICE DEFINITIONS & SERVICE DELIVERY The following section provides specific service definitions, service delivery and any special reporting requirements for each of the services funded in
An Overview of the Health Home Serving Children
 An Overview of the Health Home Serving Children Webinar Logistics All attendees will be automatically muted and in listen-only mode for the duration of the presentation Participation is highly encouraged!
An Overview of the Health Home Serving Children Webinar Logistics All attendees will be automatically muted and in listen-only mode for the duration of the presentation Participation is highly encouraged!
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Medicaid 101: The Basics for Homeless Advocates
 Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Medicaid 101: The Basics for Homeless Advocates July 29, 2014 The Source for Housing Solutions Peggy Bailey CSH Senior Policy Advisor Getting Started Things to Remember: Medicaid Agency 1. Medicaid is
Summer Optima Health News. Industry News. Provider Resources. Authorizations and Medical Policies. Billing and Reimbursement.
 providernews Optima Health News Medallion 4.0 Optima Community Complete (HMO SNP) Industry News Reminder Complete Your Cultural Competency Training Provider Resources Credentialing Application Questions
providernews Optima Health News Medallion 4.0 Optima Community Complete (HMO SNP) Industry News Reminder Complete Your Cultural Competency Training Provider Resources Credentialing Application Questions
Community Health Needs Assessment July 2015
 Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
Community Health Needs Assessment July 2015 1 Executive Summary UNM Hospitals is committed to meeting the healthcare needs of our community. As a part of this commitment, UNM Hospitals has attended forums
SUBSTANCE EXPOSED NEWBORNS CPS ALTERNATIVE RESPONSE AND. Marlys Baker September, 2017
 SUBSTANCE EXPOSED NEWBORNS AND CPS ALTERNATIVE RESPONSE Marlys Baker September, 2017 How did we get here? Three elements combined: Casey Family Programs (2014) Substance Exposed Newborn Task Force (2016)
SUBSTANCE EXPOSED NEWBORNS AND CPS ALTERNATIVE RESPONSE Marlys Baker September, 2017 How did we get here? Three elements combined: Casey Family Programs (2014) Substance Exposed Newborn Task Force (2016)
Medicaid Covered Services Not Provided by Managed Medical Assistance Plans
 Medicaid Covered Services Not Provided by Managed Medical Assistance Plans This document outlines services not provided by MMA plans, but are available to Medicaid recipients through Medicaid fee-for-service.
Medicaid Covered Services Not Provided by Managed Medical Assistance Plans This document outlines services not provided by MMA plans, but are available to Medicaid recipients through Medicaid fee-for-service.
10 State Strategies for Improving Medicaid: Quality, Outcomes and The Bottom Line JUNE 2018
 10 State Strategies for Improving Medicaid: Quality, Outcomes and The Bottom Line JUNE 2018 10 State Strategies for Improving Medicaid: Quality, Outcomes and The Bottom Line By Kristine B. Goodwin The
10 State Strategies for Improving Medicaid: Quality, Outcomes and The Bottom Line JUNE 2018 10 State Strategies for Improving Medicaid: Quality, Outcomes and The Bottom Line By Kristine B. Goodwin The
Behavioral health provider overview
 Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
Behavioral health provider overview KSPEC-1890-18 February 2018 Agenda Provider manual and provider website Behavioral Health (BH) program goals Access and availability standards Care coordination and
Quality Management Plan Fiscal Year
 Quality Management Plan Fiscal Year 2016-2017 Mental Health and Substance Abuse Division Contractor Services Section Quality Management and Compliance Unit Contents Introduction... 3 Purpose... 4 QM Committee...
Quality Management Plan Fiscal Year 2016-2017 Mental Health and Substance Abuse Division Contractor Services Section Quality Management and Compliance Unit Contents Introduction... 3 Purpose... 4 QM Committee...
DRUG MEDI-CALWAIVER STAKEHOLDER FORUM
 October 27, 2015 DRUG MEDI-CALWAIVER STAKEHOLDER FORUM Patrick Zarate Division Manager, Alcohol & Drug Programs Objectives for Today Learn About the Drug Medi-Cal Organized Delivery System waiver Gain
October 27, 2015 DRUG MEDI-CALWAIVER STAKEHOLDER FORUM Patrick Zarate Division Manager, Alcohol & Drug Programs Objectives for Today Learn About the Drug Medi-Cal Organized Delivery System waiver Gain
Covered Services and Limitations 07/31/2015 CHAPTER IV COVERED SERVICES AND LIMITATIONS. Manual Title Community Mental Health Rehabilitative Services
 Community Mental Health Rehabilitative Services Revision Date CHAPTER COVERED SERVICES AND LIMITATIONS Revision Date i CHAPTER TABLE OF CONTENTS PAGE BEHAVIORAL HEALTH SERVICES ADMINISTRATOR 1 MEDALLION
Community Mental Health Rehabilitative Services Revision Date CHAPTER COVERED SERVICES AND LIMITATIONS Revision Date i CHAPTER TABLE OF CONTENTS PAGE BEHAVIORAL HEALTH SERVICES ADMINISTRATOR 1 MEDALLION
Florida Medicaid. Early Intervention Services Coverage Policy. Agency for Health Care Administration August 2017
 + Florida Medicaid Early Intervention Services Coverage Policy Agency for Health Care Administration August 2017 Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal
+ Florida Medicaid Early Intervention Services Coverage Policy Agency for Health Care Administration August 2017 Table of Contents Florida Medicaid 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives
 Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
Adult Behavioral Health Home and Community Based Services Quality and Infrastructure Program: Improving Lives April 30, 2018 2 Agenda for the Day Vision and Overview: HARP and BH HCBS Recovery Coordination
The Money Follows the Person Demonstration in Massachusetts
 The Money Follows the Person Demonstration in Massachusetts Use of Concurrent 1915(b)(c) Waivers to Serve Elders and Adults with Disabilities Transitioning from Long-Stay Facilities HCBS Conference Arlington,
The Money Follows the Person Demonstration in Massachusetts Use of Concurrent 1915(b)(c) Waivers to Serve Elders and Adults with Disabilities Transitioning from Long-Stay Facilities HCBS Conference Arlington,
Weekly Provider Q&A Session 3 rd Quarter 2017
 Weekly Provider Q&A Session 3 rd Quarter 2017 Type Issue/Agenda Item Response/Outcome/Updates Are providers allowed to bill for the MHSS service while a member is in hospital/acute care? It is important
Weekly Provider Q&A Session 3 rd Quarter 2017 Type Issue/Agenda Item Response/Outcome/Updates Are providers allowed to bill for the MHSS service while a member is in hospital/acute care? It is important
General Frequently Asked Questions (FAQs)
") General Frequently Asked Questions (FAQs) Revision Date: 10/1/2017 Phone Numbers for Medicaid Enrolled Pharmacies Provider Information Telephone Number(s) Information Provided Magellan Medicaid Administration
General Frequently Asked Questions (FAQs) Revision Date: 10/1/2017 Phone Numbers for Medicaid Enrolled Pharmacies Provider Information Telephone Number(s) Information Provided Magellan Medicaid Administration
Medicaid Transformation
 JOINT LEGISLATIVE COMMITTEE ON MEDICAID AND NC HEALTH CHOICE Medicaid Transformation Dr. Mandy Cohen, Dave Richard, Jay Ludlam Department of Health and Human Services Nov. 14, 2017 Recap: Where We Are
JOINT LEGISLATIVE COMMITTEE ON MEDICAID AND NC HEALTH CHOICE Medicaid Transformation Dr. Mandy Cohen, Dave Richard, Jay Ludlam Department of Health and Human Services Nov. 14, 2017 Recap: Where We Are
Drug Medi-Cal Organized Delivery System Demonstration Waiver
 Drug Medi-Cal Organized Delivery System Demonstration Waiver All County Orientation to Standard Terms and Conditions & Fiscal Provisions Presentation by DHCS and Harbage September 28, 2015 Overview of
Drug Medi-Cal Organized Delivery System Demonstration Waiver All County Orientation to Standard Terms and Conditions & Fiscal Provisions Presentation by DHCS and Harbage September 28, 2015 Overview of
SMMC: LTC and MMA. Linda R. Chamberlain, P.A. Member Firm Florida Elder Lawyers PLLC
 SMMC: LTC and MMA Linda R. Chamberlain, P.A. Member Firm Florida Elder Lawyers PLLC 727.443.7898 Why should you care about SMMC Florida has 7M+ people 50 y/o + 4M+ Social Security beneficiaries 3.5M+ Medicare
SMMC: LTC and MMA Linda R. Chamberlain, P.A. Member Firm Florida Elder Lawyers PLLC 727.443.7898 Why should you care about SMMC Florida has 7M+ people 50 y/o + 4M+ Social Security beneficiaries 3.5M+ Medicare
Medicaid & Global Commitment
 Medicaid & Global Commitment Nolan Langweil, Joint Fiscal Office, Lindsay Parker, Vermont Agency of Human Services Updated January 13, 2017 1 PART ONE Medicaid Background 2 What is Medicaid? Created in
Medicaid & Global Commitment Nolan Langweil, Joint Fiscal Office, Lindsay Parker, Vermont Agency of Human Services Updated January 13, 2017 1 PART ONE Medicaid Background 2 What is Medicaid? Created in
Welcome to the Webinar!
 Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
Welcome to the Webinar! We will begin the presentation shortly. Thank you for your patience. Attendees can access the presentation slides now at: http://www.mctac.org/page/events A recording of the event
Healthy Kids Connecticut. Insuring All The Children
 Healthy Kids Connecticut Insuring All The Children Goals & Objectives Provide affordable and accessible health care to the 71,000 uninsured children Eliminate waste in the system Develop better ways to
Healthy Kids Connecticut Insuring All The Children Goals & Objectives Provide affordable and accessible health care to the 71,000 uninsured children Eliminate waste in the system Develop better ways to
COVERED SERVICES LIST FOR HNE BE HEALTHY MEMBERS WITH MASSHEALTH STANDARD OR COMMONHEALTH COVERAGE
 COVERED SERVICES LIST FOR HNE BE HEALTHY MEMBERS WITH MASSHEALTH STANDARD OR COMMONHEALTH COVERAGE This is a list of all covered services and benefits for MassHealth Standard and CommonHealth members enrolled
COVERED SERVICES LIST FOR HNE BE HEALTHY MEMBERS WITH MASSHEALTH STANDARD OR COMMONHEALTH COVERAGE This is a list of all covered services and benefits for MassHealth Standard and CommonHealth members enrolled
Healthfirst NY Medicaid Managed Care (MMC) and Child Health Plus (CHP) Benefit Grid
 and Child Health Plus (CHP) Benefit Grid") BENEFITS (Subject to policies and procedures) Healthfirst NY Medicaid Managed Care (MMC) and Child Health Plus (CHP) Benefit Grid **Benefit Changes are subjected to NYSDOH/CMS changes MMC Non-SSI/Non-
BENEFITS (Subject to policies and procedures) Healthfirst NY Medicaid Managed Care (MMC) and Child Health Plus (CHP) Benefit Grid **Benefit Changes are subjected to NYSDOH/CMS changes MMC Non-SSI/Non-
The Budget: Maximizing Federal Reimbursement For Parolee Mental Health Care Summary
 The 2013-14 Budget: Maximizing Federal Reimbursement For Parolee Mental Health Care MAC Taylor Legislative Analyst MAY 6, 2013 Summary Historically, the state has spent tens of millions of dollars annually
The 2013-14 Budget: Maximizing Federal Reimbursement For Parolee Mental Health Care MAC Taylor Legislative Analyst MAY 6, 2013 Summary Historically, the state has spent tens of millions of dollars annually
Executive, Legislative & Regulatory 2018 AGENDA. unitypoint.org/govaffairs
 Executive, Legislative & Regulatory 2018 AGENDA unitypoint.org/govaffairs Dear Policy Makers and Community Stakeholders, In the midst of tumultuous times, we bring you our 2018 State Legislative Agenda.
Executive, Legislative & Regulatory 2018 AGENDA unitypoint.org/govaffairs Dear Policy Makers and Community Stakeholders, In the midst of tumultuous times, we bring you our 2018 State Legislative Agenda.
THIS INFORMATION IS NOT LEGAL ADVICE
 Medicaid Medicaid is a federal/state program that gives certain groups of people a card that can be used to get free medical care, nursing home care, and prescription drugs at reduced prices. In general,
Medicaid Medicaid is a federal/state program that gives certain groups of people a card that can be used to get free medical care, nursing home care, and prescription drugs at reduced prices. In general,
WV Bureau for Medical Services & Molina Medicaid Solutions
 WV Bureau for Medical Services & Molina Medicaid Solutions On January 1, 2014, Medicaid eligibility was expanded to qualified individuals ages 19 to 64 making 138% of the Federal Poverty Level. 112,464
WV Bureau for Medical Services & Molina Medicaid Solutions On January 1, 2014, Medicaid eligibility was expanded to qualified individuals ages 19 to 64 making 138% of the Federal Poverty Level. 112,464
Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver
 Waiver") Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Medi-Cal Managed Care Advisory Committee Uma K. Zykofsky, LCSW Director, Behavioral Health Services Alcohol & Drug Administrator Waiver Authority
Drug Medi-Cal Organized Delivery System (DMC-ODS) Waiver Medi-Cal Managed Care Advisory Committee Uma K. Zykofsky, LCSW Director, Behavioral Health Services Alcohol & Drug Administrator Waiver Authority
The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services
 The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services Indiana Council of Community Mental Health Centers Ft. Wayne, Indiana May 19, 2011 David B. Bingaman, LCSW, ACSW U.S. Department
The Affordable Care Act, HRSA, and the Integration of Behavioral Health Services Indiana Council of Community Mental Health Centers Ft. Wayne, Indiana May 19, 2011 David B. Bingaman, LCSW, ACSW U.S. Department
RYAN WHITE HIV/AIDS PROGRAM SERVICES Definitions for Eligible Services
 RYAN WHITE HIV/AIDS PROGRAM SERVICES Definitions for Eligible Services (Last Updated: July 15, 2013) Ryan White HIV/AIDS Program funds are intended to support only the HIV-related needs of clients. All
RYAN WHITE HIV/AIDS PROGRAM SERVICES Definitions for Eligible Services (Last Updated: July 15, 2013) Ryan White HIV/AIDS Program funds are intended to support only the HIV-related needs of clients. All
SERVICES COVERAGE LIMITS/ EXCLUSIONS Alcohol, Drug, and Substance Abuse Services
 SERVICES COVERAGE LIMITS/ EXCLUSIONS Alcohol, Drug, and Substance Abuse Services Alcohol, drug, and substance abuse treatment services are provided by the Department of Alcohol and Other Drug Abuse Services
SERVICES COVERAGE LIMITS/ EXCLUSIONS Alcohol, Drug, and Substance Abuse Services Alcohol, drug, and substance abuse treatment services are provided by the Department of Alcohol and Other Drug Abuse Services
approved Nevada s State Innovation Model (SIM) Round October 2015 Division of Health Care Financing and Policy Introduction to SIM
 Round October 2015 Division of Health Care Financing and Policy Introduction to SIM") Nevada State Innovation Model (SIM) October 2015 1 Introduction to SIM The Center for Medicare and Medicaid Services (CMS) approved Nevada s State Innovation Model (SIM) Round Two application to improve
Nevada State Innovation Model (SIM) October 2015 1 Introduction to SIM The Center for Medicare and Medicaid Services (CMS) approved Nevada s State Innovation Model (SIM) Round Two application to improve
Medicaid Managed Care Managed Long Term Care and Fully Integrated Dual Advantage Plans. August 2, 2012
 Medicaid Managed Care Managed Long Term Care and Fully Integrated Dual Advantage Plans August 2, 2012 Community Health Advocates Community Health Advocates (CHA) is a network of 31 organizations that assist
Medicaid Managed Care Managed Long Term Care and Fully Integrated Dual Advantage Plans August 2, 2012 Community Health Advocates Community Health Advocates (CHA) is a network of 31 organizations that assist
Provider Evaluation of Performance. Plan. Tennessee
 Provider Evaluation of Performance Plan Tennessee 2018 Executive Summary UnitedHealthcare Community Plan is committed to ensuring the services members receive from network providers meet the requirements
Provider Evaluation of Performance Plan Tennessee 2018 Executive Summary UnitedHealthcare Community Plan is committed to ensuring the services members receive from network providers meet the requirements
Continuing Certain Medicaid Options Will Increase Costs, But Benefit Recipients and the State
 January 2005 Report No. 05-03 Continuing Certain Medicaid Options Will Increase Costs, But Benefit Recipients and the State at a glance Florida provides Medicaid services to several optional groups of
January 2005 Report No. 05-03 Continuing Certain Medicaid Options Will Increase Costs, But Benefit Recipients and the State at a glance Florida provides Medicaid services to several optional groups of
SUMMARY OF FAMIS COVERED SERVICES No cost sharing will be charged to American Indians and Alaska Native
 SUMMARY OF COVERED SERVICES No cost sharing will be charged to American Indians and Alaska Native Service Inpatient Hospital Outpatient Hospital $15 per $2 per visit (waived if admitted) $25 per $5 per
SUMMARY OF COVERED SERVICES No cost sharing will be charged to American Indians and Alaska Native Service Inpatient Hospital Outpatient Hospital $15 per $2 per visit (waived if admitted) $25 per $5 per
DRUG MEDI-CAL ORGANIZED DELIVERY SYSTEM (DMC-ODS) YEAR 1 PERFORMANCE METRICS (version 10/24/17)
 YEAR 1 PERFORMANCE METRICS (version 10/24/17)") 1 Access Enrollment information to include the number of DMC- ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
1 Access Enrollment information to include the number of DMC- ODS beneficiaries served in the DMC-ODS program Clients Served: 1. Number of DMC-ODS beneficiaries served (admissions) by the DMC- ODS County
Medicaid Simplification
 Medicaid Simplification This Act authorizes the director of the state department of health and welfare to restructure the state Medicaid program in order to achieve improved health outcomes for Medicaid
Medicaid Simplification This Act authorizes the director of the state department of health and welfare to restructure the state Medicaid program in order to achieve improved health outcomes for Medicaid
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
CHILDREN'S MENTAL HEALTH ACT
 40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION
 -OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
-OPTUM PIERCE BEHAVIORAL HEALTH ORGANIZATION CARE MANAGEMENT AND SERVICE PLANNING POLICY Policy: CM-10 Section: Care Management and Service Planning Approved by Bea Dixon, Executive Director Effective
MassHealth Delivery System Restructuring Provider Overview
 MassHealth Delivery System Restructuring Provider Overview Executive Office of Health & Human Services Spring 2017 Agenda I. Background and Timeline II. Strategy for Reform III. Introduction to ACO Models
MassHealth Delivery System Restructuring Provider Overview Executive Office of Health & Human Services Spring 2017 Agenda I. Background and Timeline II. Strategy for Reform III. Introduction to ACO Models
SUMMARY OF THE STATE GRANT OPPORTUNITIES IN THE PATIENT PROTECTION AND AFFORDABLE CARE ACT: H.R (May 24, 2010)
") National Conference of State Legislatures 444 North Capitol Street, N.W., Suite 515 Washington, D.C. 20001 SUMMARY OF THE STATE GRANT OPPORTUNITIES IN THE PATIENT PROTECTION AND AFFORDABLE CARE ACT: H.R.
National Conference of State Legislatures 444 North Capitol Street, N.W., Suite 515 Washington, D.C. 20001 SUMMARY OF THE STATE GRANT OPPORTUNITIES IN THE PATIENT PROTECTION AND AFFORDABLE CARE ACT: H.R.
MassHealth Accountable Care Update
 MassHealth Accountable Care Update Marylou Sudders Secretary Executive Office of Health & Human Services May 16, 2018 Partnering with CHCs: In it together! Community health centers have been providing
MassHealth Accountable Care Update Marylou Sudders Secretary Executive Office of Health & Human Services May 16, 2018 Partnering with CHCs: In it together! Community health centers have been providing
KyHealth Choices. Presentation to Medicaid Congress June 15, Mark D. Birdwhistell Secretary, Cabinet for Health and Family Services
 KyHealth Choices Presentation to Medicaid Congress June 15, 2007 Mark D. Birdwhistell Secretary, Cabinet for Health and Family Services Agenda Background & Vision for Kentucky Medicaid Comprehensive Medicaid
KyHealth Choices Presentation to Medicaid Congress June 15, 2007 Mark D. Birdwhistell Secretary, Cabinet for Health and Family Services Agenda Background & Vision for Kentucky Medicaid Comprehensive Medicaid
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo.
 This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
This report is a summary of the November 2015 Behavioral Health Stakeholder s Summit that was held in Fargo. February 10, 2016 ADULT BEHAVIORAL HEALTH November 2015 Summary Report Exchange of information
Maternal and Child Health Oregon Health Authority, Public Health Division. Portland, Oregon. Assignment Description
 Maternal and Child Health Oregon Health Authority, Public Health Division Portland, Oregon Assignment Description Overview of the Fellow's assignment including description of fellow's placement in division
Maternal and Child Health Oregon Health Authority, Public Health Division Portland, Oregon Assignment Description Overview of the Fellow's assignment including description of fellow's placement in division
HHW-HIPP0314 (9/13) MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.
 MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.") HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
HEALTH PLAN BENEFITS AND COVERAGE MATRIX
 HEALTH PLAN BENEFITS AND COVERAGE MATRIX THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
HEALTH PLAN BENEFITS AND COVERAGE MATRIX THIS MATRIX IS INTENDED TO BE USED TO HELP YOU COMPARE COVERAGE BENEFITS AND IS A SUMMARY ONLY. THE EVIDENCE OF COVERAGE AND PLAN CONTRACT SHOULD BE CONSULTED FOR
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
STAR+PLUS through UnitedHealthcare Community Plan
 STAR+PLUS through UnitedHealthcare Community Plan Optum 06012014 Who We Are United Behavioral Health (UBH) was created February 2, 1997, through a merger of U.S. Behavioral Health, Inc. (USBH) and United
STAR+PLUS through UnitedHealthcare Community Plan Optum 06012014 Who We Are United Behavioral Health (UBH) was created February 2, 1997, through a merger of U.S. Behavioral Health, Inc. (USBH) and United
Kentucky Rural Health Summit June 8, 2018
 Kentucky Rural Health Summit June 8, 2018 Kentucky Health Program Overview Kentucky HEALTH is the Commonwealth s new program for certain low-income adults and their families. The program gets its name
Kentucky Rural Health Summit June 8, 2018 Kentucky Health Program Overview Kentucky HEALTH is the Commonwealth s new program for certain low-income adults and their families. The program gets its name
2017 Comparison of the State of Iowa Medicaid Enterprise Basic Benefits Based on Eligibility Determination
 General Plan Provisions Benefits Available from Out-of-Network Providers 2017 Comparison of the State of Iowa Enterprise Cost Sharing: A variety of methods are used to share expenses between the state
General Plan Provisions Benefits Available from Out-of-Network Providers 2017 Comparison of the State of Iowa Enterprise Cost Sharing: A variety of methods are used to share expenses between the state
HHSC Value-Based Purchasing Roadmap Texas Policy Summit
 HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10
 Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March
Health Care Reform Provisions Affecting Older Adults and Persons with Special Needs 3/30/10 On March 23, 2010, President Obama signed a comprehensive health care reform bill (H.R. 3590) into law. On March