Richard E. Wild, MD,JD,MBA, FACEP
|
|
|
- Madlyn Thompson
- 5 years ago
- Views:
Transcription

1 CMS Incentive Program for Meaningful Use of HIT and Reporting Quality of Care Measures Healthcare Transparency & Patient Advocacy Conference Lexington, KY November 19, 2010 Richard E. Wild, MD,JD,MBA, FACEP Chief Medical Officer CMS Region 4, Atlanta
2 Disclaimers This presentation was current at the time it was published or uploaded onto the web. Medicare policy changes frequently so links to the source documents have been provided within the document for your reference. This presentation was prepared as a tool to assist providers and is not intended to grant rights or impose obligations. Although every reasonable effort has been made to assure the accuracy of the information within these pages, the ultimate responsibility for the correct submission of claims and response to any remittance advice lies with the provider of services. The Centers for Medicare & Medicaid Services (CMS) employees, agents, and staff make no representation, warranty, or guarantee that this compilation of Medicare information is error-free and will bear no responsibility or liability for the results or consequences of the use of this guide. This publication is a general summary that explains certain aspects of the Medicare Program, but is not a legal document. The official Medicare Program provisions are contained in the relevant laws, regulations, and rulings. (CPT only, copyright 2008 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS\DFARS Restrictions Apply to Government Use. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for data contained or not contained herein.)
3 Presentation Overview Problems with US Healthcare Today, Quality and Cost HIT and Congressional Initiatives to address Quality and Cost CMS E.HR Incentive Program for Meaningful Use of HIT
4 CMS Quality Improvement Roadmap Vision: The right care for every person every time Institute of Medicine: Crossing the Quality Chasm: A New Health System for the 21st Century, March, Make care: Safe Effective Efficient: absence of waste, overuse, misuse, and errors Patient-centered Timely Equitable
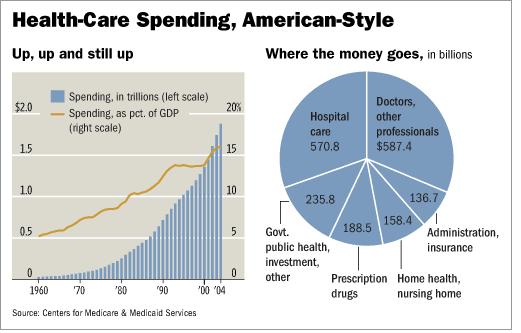
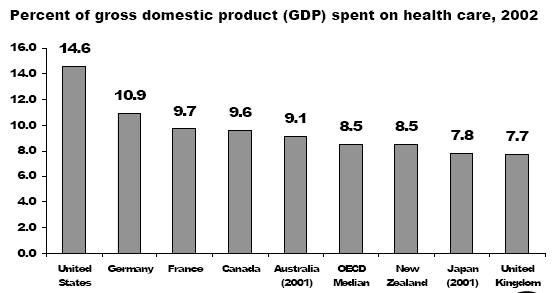
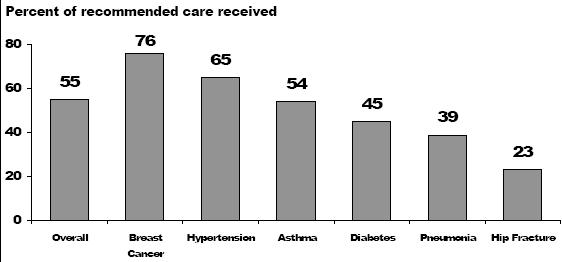
5 What s Wrong with US Healthcare Today? Too Costly? Inefficient? Disparities in Access and Quality? Evidence Base foundation often lacking? Lack of Prevention focus? Fragmentation of care, between providers and sites of care? (Silos, care transitions) Poor information and data sharing and transfer? Patient safety and quality? (Compare to aviation industry?) A payment system that rewards providing services rather than outcomes? Coordinated, accountable or Uncoordinated, Unaccountable care?

6 Aviation or Health Care?
7
8 Increasing Expenditures Medicare Expenditures $ billions Total Expenditures Physican and Clinical Services
9 Table 3.6 Number of Medicare serves Beneficiaries, The number of people Medicare serves will nearly double by Medicare Enrollment (millions) Disabled & ESRD Elderly * * * * Numbers may not sum due to rounding. Source: CMS, Office of the Actuary. Calendar Year
10 Workers per Medicare Beneficiary 200 Selected Years 150 in millions Covered Workers Part A enrollment Worker to Beneficiary Ratio Source: OACT CMS and SSA
11 Medicare Will Place An Unprecedented Strain on the Federal Budget in the Future if Spending increases not slowed 12% Historical Estimated 9% Total expenditures HI deficit Percentage of GDP 6% 3% State transfers General revenue transfers Premiums 0% Tax on benefits Payroll taxes Calendar year Source: 2008 Trustees Report
12
13 Higher Per Capita Spending in the U.S. does not Translate into Longer Life Expectancy Average Life Expectancy (years) Japan San Marino Monaco Switzerland Australia Sweden Iceland Andorra Canada France Italy Austria Spain Norway Singapore Israel Luxembourg Source: 2006 CIA FACT BOOK United States New Zealand Netherlands Germany Greece Malta Belgium Finland United Kingdom Denmark United States Cuba Cyprus Ireland Portugal Life Expectancy Per Capita Spending Per Capita Spending in USD
14
15
16

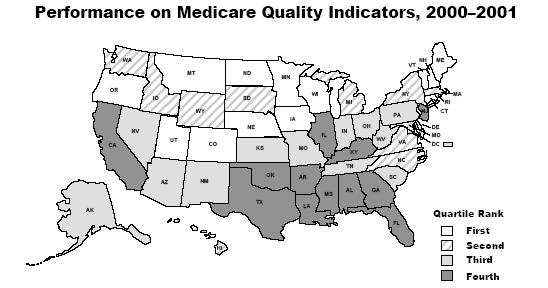
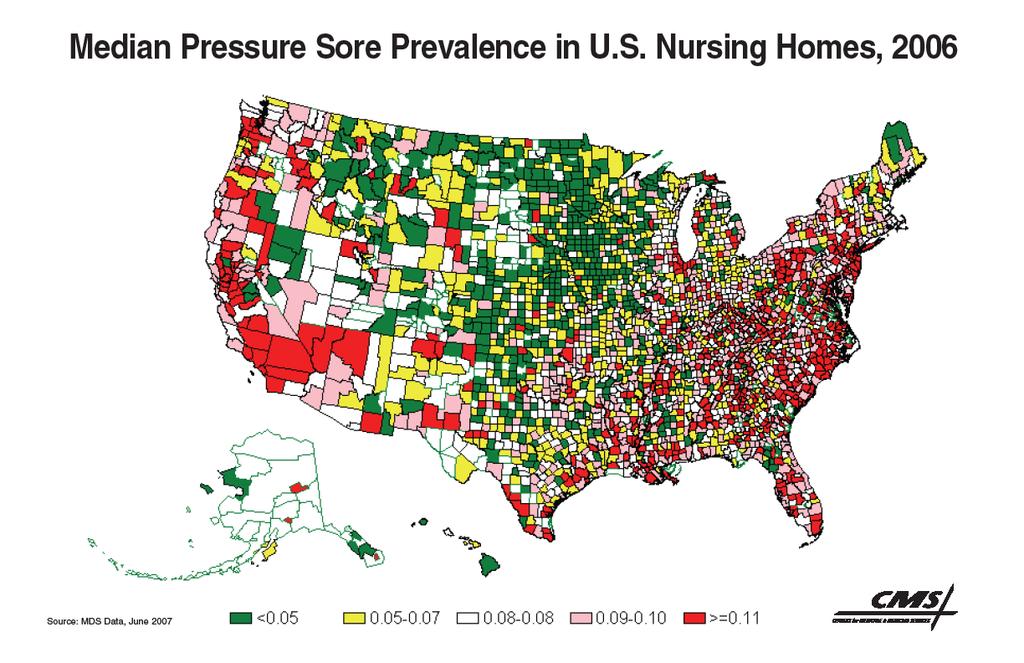
17 A Variation Problem Dartmouth Atlas of Healthcare
18 HIT Overview HIT and Congressional Initiatives ARRA of 2009, HITECH ACT, established CMS E.HR incentive program for Meaningful Use of HIT Recent Studies: Archives of Internal Medicine, Jan , Amarasingham, et.al, Clinical Information Technologies and Inpatient Outcomes, a Multiple Hospital Study -Hospitals with automated notes and records, order entry and clinical decision support had fewer complications, lower mortality rates, and lower costs.
19 Post The Affordable Care Act Strategic Value of Meaningful Use
20 The Triple Aim Goals of CMS Better Care Patient Safety Quality Patient Experience Reduce Per Capita Cost Reduce unnecessary and unjustified medical cost Reduce administrative cost thru process simplification Improve Population Health Decrease health disparities Improve chronic care management and outcome Improve community health status

21 Better Care Closing the Quality Chasm CMS Specific Aims for Health System Improvement Safety Effectiveness Patient-centeredness Timeliness Efficiency Equity 21


22 Essential Elements of The Patient Experience Transformed Healthcare System Informed, Activated Patient Productive Interactions Prepared Clinical Team Requires new web based Health E-Learning, Electronic Care Planning and Self Care Management Tools Common Set of Patient Health Information Electronic Health Records and Exchange of Health Information
23 The CMS Vision of Leveraging Meaningful Use of HIT
24 A Strategic System Approach to Healthcare Delivery Transformation Strategic Planning Logic Map Strategic HIT Focus Areas Cost Containment Quality Improvement Administrative Efficiency Population Health & Research Meaningful USE Barrier HIT Strategic Performance Metrics Meaningful Use of EHR to reduce Duplication, Errors and improve care Cost Effectiveness Meaningful Use of EHR to better coordinate care and Quality Performance Meaningful use of EHR to Reduce Admin. Process Cycle Times Meaningful Use of EHR to build Population Health Mgmt. & Research Quality and Cost Performance Outcomes Reduced Unnecessary Cost/Utilization = Reduced PMPM & Lower % Admin Cost Improved Quality HEDIS & Patient Wellness Benchmarks Higher Provider Satisfaction & Reduction in Admin. Cost Improve health status Reduction in Health Disparities PERFORMANCE Management Barrier







25 Health Care Delivery System Transformation Adoption of Health Information Technology Infrastructure Barrier Enhancing Health System Performance Competencies Clinical Care Knowledge Barrier Transformation Barrier Integrated Care Episodic/ Uncoordinated Accountable Care Personalized Health Care Management

26 Medical Home 1.0 E- Prescribing Electronic Health Record Medical Home 1.0 Individual Patient Care Plans Care Coordination Capable





27 Medical Home 2.0 Integrate e-prescribing and COEs Advance Chronic Disease Management Patient Registries HIE Connected Population Health Bio Surveillance Medical Home 2.0 E-Clinical Decision Making Electronic Patient Access and Communication Two Way Quality Report Electronic Eligibility System Interface

28 Medical Home 3.0 Fully e-health Capable Advanced Care Management Capable Clinical Practice Translational Research Remote Bio Metrics Monitoring and Tele health Capable Medical Home 3..0 Connected to Community Resource Databases Integrated Electronic Clinical Network Interfaces Patient E-Learning Center Community Health Surveillance Network Psycho/Social Evaluation and Intervention
29 Health Plans Data Sharing Partners Medicaid The Relationships Development for Meaningful Use of Health Information Exchange and EHR Data Partners are organizations that share or exchange data through the HIE-EHR Infrastructure e.g. Health Plans Hospitals Physicians Labs Imaging Labs Other HIEs Dept of Health Services Public Health Medicare Indian Health Services (IHS) etc. Providers With HIT Hospitals Small/ Medium Practices Physicians Utility Users (business partners) HIE/EHR Infrastructure Medicaid Members Analysis Users Business Partners are organizations that expose web content and applications through the Utility web portal, for gain or mutual benefit; in other words, transact business through the Utility. e.g. Laboratories Imaging Suppliers Durable Medical Equipment Pharmacies SureScripts RX Hub Other HIEs etc Laboratories Imaging Business Partners Suppliers Other vendors Operations Admin Monitoring HIE-EHR Management & Support Training and Education Maintenance Help Desk Utility Users are persons who use the functionality of the portal. e.g. Physicians Small/medium Practices Analysis users (TBD) Emergency Depts Dept of Public Safety Department of Health Services etc Administrative and management users use the portal to access administrative and management applications supported by the portal.

30 Health Care System Transformation Maturity Initial Level of Health System Transformation Maturity Episodic Non Integrated Care Episodic Health Care Sick care focus Uncoordinated care High Use of Emergency Care Multiple clinical records Fragmentation of care Lack integrated care networks Lack quality & cost performance transparency Poorly Coordinate Chronic Care Management Managed Performance Level of Health System Transformation Maturity Accountable Care Transparent Cost Quality Performance Results oriented Access and coverage Accountable Provider Networks Designed Around the patient Focus on care management and preventive care Primary Care Medical Home Utilization management Medical Management Optimize Care Level of Health System Transformation Maturity Integrated Health Patient Care Centered Patient centered Health Care Productive and informed interactions between Family and Provider Cost and Quality Transparency Accessible Health Care Choices Aligned Incentives for wellness Integrated networks with community resources wrap around Aligned reimbursement/cost Rapid deployment of best practices Patient and provider interaction Aligned care management E-health capable E-Learning resources

31 Return on Investment from HIT Wide Spread Adoption of Electronic Health Information (EHI) Technologies for Better Outcomes, Lower Cost, Improve Population Health Improving Health Care Quality, Cost Performance, Population Health ROI of EHI at Point of Care: Improved Patient Safety Reduced Complications Rates Reduced Cost per Patient Episode of Care Enhanced cost & quality performance accountability Improved Quality Performance Improve Community Health Surveillance Better Outcomes Lower Costs Population Health

32 Timeline for Delivery System Reform and Transformation MU Stage 2 MU Stage 3 MU Stage 1 Successful Payment and Service Model Innovation Program and Policy Redesign Healthcare Delivery System Reform and Transformation
33 Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009
34
35 What the Final Rule Does Harmonizes MU criteria across CMS programs as much as possible Closely links with the ONC Certification and Standards final rules Builds on the recommendations of the HIT Policy Committee and Public Commenters Coordinates with existing CMS quality initiatives Provides a platform that allows for a staged implementation of EHRs over time 35
36 Eligibility Overview for the E.HR Incentive Program Medicare Fee-For-Service (FFS) Eligible Professionals (EPs) Eligible hospitals and critical access hospitals (CAHs) Medicare Advantage (MA) MA EPs MA-affiliated eligible hospitals Medicaid EPs Eligible hospitals 36
37 Who is a Medicare Eligible Provider? Eligible Providers in Medicare FFS Eligible Professionals (EPs) Doctor of Medicine or Osteopathy Doctor of Dental Surgery or Dental Medicine Doctor of Podiatric Medicine Doctor of Optometry Chiropractor Eligible Hospitals Acute Care Hospitals* Critical Access Hospitals (CAHs) *Subsection (d) hospitals that are paid under the PPS and are located in the 50 States or Washington, DC (including Maryland) 37
38 Who is a Medicaid Eligible Provider? Physicians Eligible Providers in Medicaid Eligible Professionals (EPs) Nurse Practitioners (NPs) Certified Nurse-Midwives (CNMs) Dentists Physician Assistants (PAs) working in a Federally Qualified Health Center (FQHC) or rural health clinic (RHC) that is so led by a PA Eligible Hospitals Acute Care Hospitals (now including CAHs) Children s Hospitals 38
39 Meaningful Use: HITECH Act Description The Recovery Act specifies the following 3 components of Meaningful Use: 1. Use of certified EHR in a meaningful manner (e.g., e-prescribing) 2. Use of certified EHR technology for electronic exchange of health information to improve quality of health care 3. Use of certified EHR technology to submit clinical quality measures (CQM) and other such measures selected by the Secretary 39
40 Meaningful Use Stage 1 Health Outcome Priorities* Improve quality, safety, efficiency, and reduce health disparities Engage patients and families in their health care Improve care coordination Improve population and public health Ensure adequate privacy and security protections for personal health information *Adapted from National Priorities Partnership. National Priorities and Goals: Aligning Our Efforts to Transform America s Healthcare. Washington, DC: National Quality Forum;
41 Meaningful Use: Basic Overview of Final Rule Stage 1 (2011 and 2012) To meet certain objectives/measures, 80% of patients must have records in the certified EHR technology EPs have to report on 20 of 25 MU objectives (15 Core and choose 5 of 10 from menu set.) Eligible hospitals have to report on 19 of 24 MU (14 Core and 5 of 10 menu) objectives Reporting Period 90 days for first year; one year subsequently 41
42 Meaningful Use: Core Set Objectives EPs 15 Core Objectives 1. Computerized physician order entry (CPOE) 2. E-Prescribing (erx) 3. Report ambulatory clinical quality measures to CMS/States (CQMs) 4. Implement one clinical decision support rule 5. Provide patients with an electronic copy of their health information, upon request 6. Provide clinical summaries for patients for each office visit 7. Drug-drug and drug-allergy interaction checks 8. Record demographics 9. Maintain an up-to-date problem list of current and active diagnoses 10. Maintain active medication list 11. Maintain active medication allergy list 12. Record and chart changes in vital signs 13. Record smoking status for patients 13 years or older 14. Capability to exchange key clinical information among providers of care and patient-authorized entities electronically 15. Protect electronic health information 42
43 Meaningful Use: Core Set Objectives Eligible Hospitals 14 Core Objectives 1. CPOE 2. Drug-drug and drug-allergy interaction checks 3. Record demographics 4. Implement one clinical decision support rule 5. Maintain up-to-date problem list of current and active diagnoses 6. Maintain active medication list 7. Maintain active medication allergy list 8. Record and chart changes in vital signs 9. Record smoking status for patients 13 years or older 10. Report hospital clinical quality measures to CMS or States 11. Provide patients with an electronic copy of their health information, upon request 12. Provide patients with an electronic copy of their discharge instructions at time of discharge, upon request 13. Capability to exchange key clinical information among providers of care and patient-authorized entities electronically 14. Protect electronic health information 43
44 Meaningful Use: Menu Set Objectives* Eligible Professionals Drug-formulary checks Incorporate clinical lab test results as structured data Generate lists of patients by specific conditions Send reminders to patients per patient preference for preventive/follow up care Provide patients with timely electronic access to their health information Use certified EHR technology to identify patient-specific education resources and provide to patient, if appropriate Medication reconciliation Summary of care record for each transition of care/referrals Capability to submit electronic data to immunization registries/systems* Capability to provide electronic syndromic surveillance data to public health agencies* *At least 1 public health objective must be selected 44
45 Meaningful Use: Menu Set Objectives* Eligible Hospitals Drug-formulary checks Record advanced directives for patients 65 years or older Incorporate clinical lab test results as structured data Generate lists of patients by specific conditions Use certified EHR technology to identify patient-specific education resources and provide to patient, if appropriate Medication reconciliation Summary of care record for each transition of care/referrals Capability to submit electronic data to immunization registries/systems* Capability to provide electronic submission of reportable lab results to public health agencies* Capability to provide electronic syndromic surveillance data to public health agencies* *At least 1 public health objective must be selected 45
46 Meaningful Use: Applicability of Objectives and Measures Some MU objectives are not applicable to every provider s clinical practice, thus they would not have any eligible patients or actions for the measure denominator. Exclusions do not count against the 5 deferred measures In these cases, the EP, eligible hospital, or CAH would be excluded from having to meet that measure E.g., Dentists who do not perform immunizations; Chiropractors do not e-prescribe 46
47 Clinical Quality Measures (CQM) Overview 2011 EPs, eligible hospitals, and CAHs seeking to demonstrate Meaningful Use are required to submit aggregate CQM numerator, denominator, and exclusion data to CMS or the States by attestation EPs, eligible hospitals, and CAHs seeking to demonstrate Meaningful Use are required to electronically submit aggregate CQM numerator, denominator, and exclusion data to CMS or the States. 47
48 CQM: Eligible Professionals Core, Alternate Core, and Additional CQM sets for EPs EPs must report on 3 required core CQM, and if the denominator of 1 or more of the required core measures is 0, then EPs are required to report results for up to 3 alternate core measures EPs also must select 3 additional CQM from a set of 38 CQM (other than the core/alternate core measures) In sum, EPs must report on 6 total measures: 3 required core measures (substituting alternate core measures where necessary) and 3 additional measures 48
49 CQM: Core Set for EPs NQF Measure Number & PQRI Implementation Number NQF 0013 NQF 0028 NQF 0421 PQRI 128 Clinical Quality Measure Title Hypertension: Blood Pressure Measurement Preventive Care and Screening Measure Pair: a) Tobacco Use Assessment, b) Tobacco Cessation Intervention Adult Weight Screening and Follow-up 49
50 CQM: Alternate Core Set for EPs NQF Measure Number & PQRI Implementation Number NQF 0024 NQF 0041 PQRI 110 NQF 0038 Clinical Quality Measure Title Weight Assessment and Counseling for Children and Adolescents Preventive Care and Screening: Influenza Immunization for Patients 50 Years Old or Older Childhood Immunization Status 50
51 CQM: Additional Set for EPs 1. Diabetes: Hemoglobin A1c Poor Control 2. Diabetes: Low Density Lipoprotein (LDL) Management and Control 3. Diabetes: Blood Pressure Management 4. Heart Failure (HF): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD) 5. Coronary Artery Disease (CAD): Beta-Blocker Therapy for CAD Patients with Prior Myocardial Infarction (MI) 6. Pneumonia Vaccination Status for Older Adults 7. Breast Cancer Screening 8. Colorectal Cancer Screening 9. Coronary Artery Disease (CAD): Oral Antiplatelet Therapy Prescribed for Patients with CAD 10. Heart Failure (HF): Beta-Blocker Therapy for Left Ventricular Systolic Dysfunction (LVSD) 11. Anti-depressant medication management: (a) Effective Acute Phase Treatment, (b)effective Continuation Phase Treatment 12. Primary Open Angle Glaucoma (POAG): Optic Nerve Evaluation 13. Diabetic Retinopathy: Documentation of Presence or Absence of Macular Edema and Level of Severity of Retinopathy 14. Diabetic Retinopathy: Communication with the Physician Managing Ongoing Diabetes Care 15. Asthma Pharmacologic Therapy 16. Asthma Assessment 17. Appropriate Testing for Children with Pharyngitis 18. Oncology Breast Cancer: Hormonal Therapy for Stage IC-IIIC Estrogen Receptor/Progesterone Receptor (ER/PR) Positive Breast Cancer 19. Oncology Colon Cancer: Chemotherapy for Stage III Colon Cancer Patients 51
52 CQM: Additional Set for EPs, cont d 20. Prostate Cancer: Avoidance of Overuse of Bone Scan for Staging Low Risk Prostate Cancer Patients 21. Smoking and Tobacco Use Cessation, Medical Assistance: a) Advising Smokers and Tobacco Users to Quit, b) Discussing Smoking and Tobacco Use Cessation Medications, c) Discussing Smoking and Tobacco Use Cessation Strategies 22. Diabetes: Eye Exam 23. Diabetes: Urine Screening 24. Diabetes: Foot Exam 25. Coronary Artery Disease (CAD): Drug Therapy for Lowering LDL-Cholesterol 26. Heart Failure (HF): Warfarin Therapy Patients with Atrial Fibrillation 27. Ischemic Vascular Disease (IVD): Blood Pressure Management 28. Ischemic Vascular Disease (IVD): Use of Aspirin or Another Antithrombotic 29. Initiation and Engagement of Alcohol and Other Drug Dependence Treatment: a) Initiation, b) Engagement 30. Prenatal Care: Screening for Human Immunodeficiency Virus (HIV) 31. Prenatal Care: Anti-D Immune Globulin 32. Controlling High Blood Pressure 33. Cervical Cancer Screening 34. Chlamydia Screening for Women 35. Use of Appropriate Medications for Asthma 36. Low Back Pain: Use of Imaging Studies 37. Ischemic Vascular Disease (IVD): Complete Lipid Panel and LDL Control 38. Diabetes: Hemoglobin A1c Control (<8.0%) 52
53 CQM: Eligible Hospitals and CAHs 1. Emergency Department Throughput admitted patients Median time from ED arrival to ED departure for admitted patients 2. Emergency Department Throughput admitted patients Admission decision time to ED departure time for admitted patients 3. Ischemic stroke Discharge on anti-thrombotics 4. Ischemic stroke Anticoagulation for A-fib/flutter 5. Ischemic stroke Thrombolytic therapy for patients arriving within 2 hours of symptom onset 6. Ischemic or hemorrhagic stroke Antithrombotic therapy by day 2 7. Ischemic stroke Discharge on statins 8. Ischemic or hemorrhagic stroke Stroke education 9. Ischemic or hemorrhagic stroke Rehabilitation assessment 10. VTE prophylaxis within 24 hours of arrival 11. Intensive Care Unit VTE prophylaxis 12. Anticoagulation overlap therapy 13. Platelet monitoring on unfractionated heparin 14. VTE discharge instructions 15. Incidence of potentially preventable VTE 53
54 Alignment with Other Quality Programs / Initiatives CMS goals: Coordinate CQM development and reporting with implementation of the Patient Protection and Affordable Care Act (ACA) - e.g., pilot programs and State-based programs and infrastructure Align Physician Quality Reporting (PQRI/PQRS) and Hospital Inpatient Quality Reporting System (formerly known as RHQDAPU) 54
55 States Flexibility to Revise Meaningful Use for Medicaid Providers States can seek CMS prior approval to require 4 MU public health objectives be core for their Medicaid providers: Generate lists of patients by specific conditions for quality improvement, reduction of disparities, research, or outreach (can specify particular conditions) Reporting to immunization registries, reportable lab results, and syndromic surveillance (can specify for their providers how to test the data submission and to which specific destination) 55
56 Incentive Payments for Medicare EPs First Calendar Year (CY) for which the EP Receives an Incentive Payment CY 2011 $18,000 CY 2011 CY 2012 CY 2013 CY2014 CY 2015 and later CY 2012 $12,000 $18,000 CY 2013 $8,000 $12,000 $15,000 CY 2014 $4,000 $8,000 $12,000 $12,000 CY 2015 $2,000 $4,000 $8,000 $8,000 $0 CY 2016 $2,000 $4,000 $4,000 $0 TOTAL $44,000 $44,000 $39,000 $24,000 $0 56
57 Additional Incentive Payments for Medicare EPs Practicing in HPSAs First Calendar Year (CY) for which the EP Receives an Incentive Payment CY 2011 $1,800 CY 2011 CY 2012 CY 2013 CY2014 CY 2015 and later CY 2012 $1,200 $1,800 CY 2013 $800 $1,200 $1,500 CY 2014 $400 $800 $1,200 $1,200 CY 2015 $200 $400 $800 $800 $0 CY 2016 $200 $400 $400 $0 TOTAL $4,400 $4,400 $3,900 $2,400 $0 57
58 Incentive Payments for Medicaid EPs First Calendar Year (CY) for which the EP Receives an Incentive Payment CY 2011 $21,250 CY 2011 CY 2012 CY 2013 CY 2014 CY 2015 CY 2016 CY 2012 $8,500 $21,250 CY 2013 $8,500 $8,500 $21,250 CY 2014 $8,500 $8,500 $8,500 $21,250 CY 2015 $8,500 $8,500 $8,500 $8,500 $21,250 CY 2016 $8,500 $8,500 $8,500 $8,500 $8,500 $21,250 CY 2017 $8,500 $8,500 $8,500 $8,500 $8,500 CY 2018 $8,500 $8,500 $8,500 $8,500 CY 2019 $8,500 $8,500 $8,500 CY 2020 $8,500 $8,500 CY 2021 $8,500 TOTAL $63,750 $63,750 $63,750 $63,750 $63,750 $63,750 58
59 Incentive Payments for Eligible Hospitals Federal Fiscal Year $2M base + per discharge amount (based on Medicare/Medicaid share) There is no maximum incentive amount Hospitals meeting Medicare MU requirements may be deemed eligible for Medicaid payments Payment adjustments for Medicare begin in 2015 No Federal Medicaid payment adjustments Medicare hospitals: No payments after 2016 Medicaid hospitals: Cannot initiate payments after
60 Notable Differences Between the Medicare & Medicaid EHR Programs Medicare Federal Government will implement (will be an option nationally) Payment reductions begin in 2015 for providers that do not demonstrate Meaningful Use Must demonstrate MU in Year 1 Maximum incentive is $44,000 for EPs (bonus for EPs in HPSAs) MU definition is common for Medicare Last year a provider may initiate program is 2014; Last year to register is 2016; Payment adjustments begin in 2015 Only physicians, subsection (d) hospitals and CAHs Medicaid Voluntary for States to implement (may not be an option in every State) No Medicaid payment reductions A/I/U option for 1 st participation year Maximum incentive is $63,750 for EPs States can adopt certain additional requirements for MU Last year a provider may initiate program is 2016; Last year to register is types of EPs, acute care hospitals (including CAHs) and children s hospitals 60
61 EHR Incentive Program Timeline January 2011 Registration for the EHR Incentive Programs begins January 2011 For Medicaid providers, States may launch their programs if they so choose April 2011 Attestation for the Medicare EHR Incentive Program begins May 2011 EHR incentive payments begin November 30, 2011 Last day for eligible hospitals and CAHs to register and attest to receive an incentive payment for FFY 2011 February 29, 2012 Last day for EPs to register and attest to receive an incentive payment for CY Medicare payment adjustments begin for EPs and eligible hospitals that are not meaningful users of EHR technology 2016 Last year to receive a Medicare EHR incentive payment; Last year to initiate participation in Medicaid EHR Incentive Program 2021 Last year to receive Medicaid EHR incentive payment 61
62 What Providers Need to Participate All providers must: Register via the EHR Incentive Program website Be enrolled in Medicare FFS, MA, or Medicaid (FFS or managed care) Have a National Provider Identifier (NPI) Use certified EHR technology Medicaid providers may adopt, implement, or upgrade in their first year All Medicare providers and Medicaid eligible hospitals must be enrolled in PECOS 62
63 What Providers Need to Participate Certified EHR Technology: Required in order to achieve meaningful use Standards and certification criteria announced on July 13, See for more information ONC in process of authorizing testing and certification bodies for temporary certification program Certified products are expected to be available in the Fall List of certified EHRs and EHR modules will be posted on ONC web site (CHPL) Visit for more information with questions
64 Resources to Get Help and Learn More Get information, tip sheets and more at CMS official website for the EHR incentive programs: Learn about certification and certified EHRs, as well as other ONC programs designed to support providers as they make the transition: 64
65 More information: Questions? THANK YOU 65
Medicare & Medicaid EHR Incentive Program Final Rule. Implementing the American Recovery & Reinvestment Act of 2009
 Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Conceptual Approach to Meaningful Use Improved Data capture and sharing Advanced Clinical
Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Conceptual Approach to Meaningful Use Improved Data capture and sharing Advanced Clinical
Medicare & Medicaid. William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA
 Medicare & Medicaid EHR Incentive Program William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA Overview Background / Policy Context EHR Incentive Program basics
Medicare & Medicaid EHR Incentive Program William Kassler, MD Chief Medical Officer Centers for Medicare & Medicaid Services Boston, MA Overview Background / Policy Context EHR Incentive Program basics
Medicare & Medicaid EHR Incentive Program Final Rule. Implementing the American Recovery & Reinvestment Act of 2009
 Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Purpose of this Presentation To give an overview of the CMS final rule on the EHR Incentive
Medicare & Medicaid EHR Incentive Program Final Rule Implementing the American Recovery & Reinvestment Act of 2009 Purpose of this Presentation To give an overview of the CMS final rule on the EHR Incentive
Meaningful Use: a Primer
 Health Information Technology Extension Center of Los Angeles Meaningful Use: a Primer Mary Mitchell Director of Meaningful Use Defined as: What is Meaningful Use? A. Use of a certified EHR in a meaningful
Health Information Technology Extension Center of Los Angeles Meaningful Use: a Primer Mary Mitchell Director of Meaningful Use Defined as: What is Meaningful Use? A. Use of a certified EHR in a meaningful
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals. August 11, 2010
 Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
Medicare & Medicaid EHR Incentive Program Specifics of the Program for Hospitals August 11, 2010 Today s Session This training will cover the following topics: EHR Incentive Programs a Background Who Is
The Incentive Roadmap
 The Incentive Roadmap The Meaningful Use of Certified Technology: Stage 1 A Manual for Medical Practices Jim Tate jimtate@emradvocate.com www.emradvocate.com 2010 by EMRAdvocate.com All rights reserved.
The Incentive Roadmap The Meaningful Use of Certified Technology: Stage 1 A Manual for Medical Practices Jim Tate jimtate@emradvocate.com www.emradvocate.com 2010 by EMRAdvocate.com All rights reserved.
EHR Incentives for Professionals and Hospitals. Paul Forlenza, VP Policy, VITL updated October 1, 2010 v.8.1
 EHR Incentives for Professionals and Hospitals Paul Forlenza, VP Policy, VITL updated October 1, 2010 v.8.1 Disclaimer Not legal analysis or advice Analysis based on reviewing Centers for Medicare and
EHR Incentives for Professionals and Hospitals Paul Forlenza, VP Policy, VITL updated October 1, 2010 v.8.1 Disclaimer Not legal analysis or advice Analysis based on reviewing Centers for Medicare and
Provide an understanding of what comprises "meaningful use" of EHR technology
 1 Provide background on federal electronic health record (EHR) incentives Overview of Health IT Incentives Medicare/Medicaid EHR incentives Provide an understanding of what comprises "meaningful use" of
1 Provide background on federal electronic health record (EHR) incentives Overview of Health IT Incentives Medicare/Medicaid EHR incentives Provide an understanding of what comprises "meaningful use" of
Medicare & Medicaid EHR Incentive Program. Betsy L. Thompson, MD, DrPH EHR Summit October 4, 2010
 Medicare & Medicaid EHR Incentive Program Betsy L. Thompson, MD, DrPH EHR Summit October 4, 2010 1 Overview Background and Policy Context EHR Incentive Program Basics Who is Eligible to Participate How
Medicare & Medicaid EHR Incentive Program Betsy L. Thompson, MD, DrPH EHR Summit October 4, 2010 1 Overview Background and Policy Context EHR Incentive Program Basics Who is Eligible to Participate How
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
2013 EHR INCENTIVE PROGRAM MANUAL
 0 EHR INCENTIVE PROGRAM MANUAL Billing Technology Results ahsrcm.com info@ahsrcm.com 877 50 6 Table of Contents INTRODUCTION TO EHR & MEANINGFUL USE... CMS EHR INCENTIVE PROGRAM - PARTICIPATION... COMPARISON
0 EHR INCENTIVE PROGRAM MANUAL Billing Technology Results ahsrcm.com info@ahsrcm.com 877 50 6 Table of Contents INTRODUCTION TO EHR & MEANINGFUL USE... CMS EHR INCENTIVE PROGRAM - PARTICIPATION... COMPARISON
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
California Medical Association
 David Ford Medical and Regulatory Policy Think Back a Bit What if we had all just stopped there? Making the Switch Unfortunately, many physician practices that make the switch to EHR use their system as
David Ford Medical and Regulatory Policy Think Back a Bit What if we had all just stopped there? Making the Switch Unfortunately, many physician practices that make the switch to EHR use their system as
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Relevance of Meaningful Use Requirements for Pathologists and Laboratories Pathology Informatics 2011 October 5, 2011
 Relevance of Meaningful Use Requirements for Pathologists and Laboratories Pathology Informatics 2011 October 5, 2011 Walter H. Henricks, M.D. Cleveland Clinic Meaningful Use and the Laboratory Outline
Relevance of Meaningful Use Requirements for Pathologists and Laboratories Pathology Informatics 2011 October 5, 2011 Walter H. Henricks, M.D. Cleveland Clinic Meaningful Use and the Laboratory Outline
Meaningful Use: Introduction to Meaningful Use Eligible Providers
 Meaningful Use: Introduction to Meaningful Use Eligible Providers Introduction to Meaningful Use: Webinar Overview Define Meaningful Use Review Meaningful Use Key Dates & Program Incentives Discuss the
Meaningful Use: Introduction to Meaningful Use Eligible Providers Introduction to Meaningful Use: Webinar Overview Define Meaningful Use Review Meaningful Use Key Dates & Program Incentives Discuss the
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals
 The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals The HITECH EHR "Meaningful Use" Requirements for Hospitals and Eligible Professionals September 1, 2010 Presented and
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule
 HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
EHR Incentives. Profit by using LOGO a certified EHR. EHR vs. EMR. PQRI Incentives. Incentives available
 EHR vs. EMR EHR Incentives Company Profit by using LOGO a certified EHR EMR - Electronic records of health-related information on an individual that can be created, gathered, managed, and consulted by
EHR vs. EMR EHR Incentives Company Profit by using LOGO a certified EHR EMR - Electronic records of health-related information on an individual that can be created, gathered, managed, and consulted by
Understanding CQM MU Requirements for Hospitals. Phil Deering Sarah Tupper, MS, RN-BC, LHIT-HP 3/27/2012
 Understanding CQM MU Requirements for Hospitals Phil Deering Sarah Tupper, MS, RN-BC, LHIT-HP 3/27/2012 REACH - Achieving - Achieving meaningful meaningful use of your use EHR of your EHR Let s Hear Your
Understanding CQM MU Requirements for Hospitals Phil Deering Sarah Tupper, MS, RN-BC, LHIT-HP 3/27/2012 REACH - Achieving - Achieving meaningful meaningful use of your use EHR of your EHR Let s Hear Your
Meaningful Use of EHR in Dental School Clinics: How to Benefit from the U.S. HITECH Act s Financial and Quality Improvement Incentives
 Milieu in Dental School and Practice Meaningful Use of EHR in Dental School Clinics: How to Benefit from the U.S. HITECH Act s Financial and Quality Improvement Incentives Elsbeth Kalenderian, D.D.S.,
Milieu in Dental School and Practice Meaningful Use of EHR in Dental School Clinics: How to Benefit from the U.S. HITECH Act s Financial and Quality Improvement Incentives Elsbeth Kalenderian, D.D.S.,
Meaningful Use: A Brief Overview for Society of Health Systems
 Meaningful Use: A Brief Overview for Society of Health Systems Kevin Martin May 20, 2011 2011 Maestro Strategies LLC all rights reserved The Evolving Health Care Environment Multiple regulatory changes
Meaningful Use: A Brief Overview for Society of Health Systems Kevin Martin May 20, 2011 2011 Maestro Strategies LLC all rights reserved The Evolving Health Care Environment Multiple regulatory changes
Meaningful Use May, 2012
 Meaningful Use May, 2012 Shehnaz Scheyer New Jersey Institute of Technology 211 Warren Street, Newark, NJ 07103 Phone: 973-557-4571 x716 Fax: 973-846-4634 Email: sscheyer@csicorp.net www.njhitec.org Eligible
Meaningful Use May, 2012 Shehnaz Scheyer New Jersey Institute of Technology 211 Warren Street, Newark, NJ 07103 Phone: 973-557-4571 x716 Fax: 973-846-4634 Email: sscheyer@csicorp.net www.njhitec.org Eligible
HITECH Act American Recovery and Reinvestment Act (ARRA) Stimulus Package. HITECH Act Meaningful Use (MU)
 Stimulus Package. HITECH Act Meaningful Use (MU)") Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
Presents Presents: Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com Speaker: Elizabeth Woodcock, MBA, FACMPE, CPC www.elizabethwoodcock.com HITECH Act Meaningful Use (MU) Definition
ASCs and Meaningful Use. Patrick Doyle, Vice President Sales Jessica McBrayer, RN, Business Analyst Ron Pelletier, Vice President Market Strategy
 ASCs and Meaningful Use Patrick Doyle, Vice President Sales Jessica McBrayer, RN, Business Analyst Ron Pelletier, Vice President Market Strategy Today s Discussion Review of Meaningful Use and implications
ASCs and Meaningful Use Patrick Doyle, Vice President Sales Jessica McBrayer, RN, Business Analyst Ron Pelletier, Vice President Market Strategy Today s Discussion Review of Meaningful Use and implications
Medicare & Medicaid EHR Incentive Programs
 Medicare & Medicaid EHR Incentive Programs Southwest Regional Health Care Compliance Association Conference February 18, 2011 Travis Broome, Special Assistant for Quality Improvement and Survey & Certification
Medicare & Medicaid EHR Incentive Programs Southwest Regional Health Care Compliance Association Conference February 18, 2011 Travis Broome, Special Assistant for Quality Improvement and Survey & Certification
HITECH* Update Meaningful Use Regulations Eligible Professionals
 HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
HITECH* Update Meaningful Use Regulations Eligible Professionals October 2010 * Health Information Technology for Economic and Clinical Health, a component of the ARRA of 2009 McDowell Lecture December
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Meaningful Use: Stage 1 and Beyond
 Meaningful Use: Stage 1 and Beyond Rural Wisconsin Health Cooperative Paul Kleeberg, MD Clinical Director Regional Extension Assistance Center for HIT (REACH) Louis Wenzlow Director of HIT Rural Wisconsin
Meaningful Use: Stage 1 and Beyond Rural Wisconsin Health Cooperative Paul Kleeberg, MD Clinical Director Regional Extension Assistance Center for HIT (REACH) Louis Wenzlow Director of HIT Rural Wisconsin
Summary. Centers for Medicare and Medicaid Services Medicare and Medicaid Programs
 Summary Centers for Medicare and Medicaid Services Medicare and Medicaid Programs Electronic Health Record Incentive Program Proposed Rule (CMS-0033-P) Updated January 15, 2010 Prepared by Chantal Worzala,
Summary Centers for Medicare and Medicaid Services Medicare and Medicaid Programs Electronic Health Record Incentive Program Proposed Rule (CMS-0033-P) Updated January 15, 2010 Prepared by Chantal Worzala,
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
2015 MEANINGFUL USE STAGE 2 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives EPs must meet 3 of the 6 menu measures.
Moving HIT and Meaningful Use
 Moving HIT and Meaningful Use Tim Gutshall, MD March 30, 2011 EHR Adoption in Iowa Less than 50 percent of Iowa physicians have adopted EHRs As late as 2009, 89 percent of Iowa s hospitals still used some
Moving HIT and Meaningful Use Tim Gutshall, MD March 30, 2011 EHR Adoption in Iowa Less than 50 percent of Iowa physicians have adopted EHRs As late as 2009, 89 percent of Iowa s hospitals still used some
CMS Incentive Programs: Timeline And Reporting Requirements. Webcast Association of Northern California Oncologists May 21, 2013
 CMS Incentive Programs: Timeline And Reporting Requirements Webcast Association of Northern California Oncologists May 21, 2013 Objective This webcast will address CMS s Incentive Program reporting requirements
CMS Incentive Programs: Timeline And Reporting Requirements Webcast Association of Northern California Oncologists May 21, 2013 Objective This webcast will address CMS s Incentive Program reporting requirements
MEANINGFUL USE STAGE FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
MEANINGFUL USE STAGE 2 2014 FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY STAGE 2 REQUIREMENTS EPs must meet or qualify for an exclusion to 17 core objectives. EPs must meet 3 of the 6 menu measures.
Meaningful Use of an EHR System
 Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Meaningful Use of an EHR System Slide content by: David Ford of CMA CalHIPSO Meaningful Use Consultant & Reena Samantaray Director of Outreach & Education, CalHIPSO July 2010 Presented by Dr. Sherellen
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Legal Issues in Medicare/Medicaid Incentive Programss
 Meaningful Use Legal Issues in Medicare/Medicaid Incentive Programss Jane Eckels, Esq. Partner, Health Information Technology Group Deputy Chair, Technology, ebusiness and Digital Media Group Overview
Meaningful Use Legal Issues in Medicare/Medicaid Incentive Programss Jane Eckels, Esq. Partner, Health Information Technology Group Deputy Chair, Technology, ebusiness and Digital Media Group Overview
Through the 2009 HITECH (Health Information
 Milieu in Dental School and Practice Meaningful Use of EHR in Dental School Clinics: How to Benefit from the U.S. HITECH Act s Financial and Quality Improvement Incentives Elsbeth Kalenderian, D.D.S.,
Milieu in Dental School and Practice Meaningful Use of EHR in Dental School Clinics: How to Benefit from the U.S. HITECH Act s Financial and Quality Improvement Incentives Elsbeth Kalenderian, D.D.S.,
Meaningful Use Final Rule:
 Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Meaningful Use Final Rule: Safety and Quality of Care Jonathan Teich, FACMI, FHIMSS, MD, PhD CMIO, Elsevier Health Sciences August 4, 2010 Today s webinar is sponsored by History HITECH Feb. 2009 Initial
Eligibility. Program Structure and Process for Receiving Incentives
 Overview of Medicare Incentives in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use of Certified Electronic Health Records 1 Eligibility Medicare Eligibility: For Medicare
Overview of Medicare Incentives in the Centers for Medicare & Medicaid Services (CMS) Final Rule on Meaningful Use of Certified Electronic Health Records 1 Eligibility Medicare Eligibility: For Medicare
Meaningful Use Certification Details
 May 2, 2016 TRIARQ Health 1050 Wilshire, Suite 300 Troy, MI 48084 Meaningful Use Certification Details CHPL Practice Date CERTIFICATION Product Version Classification PRODUCT Type Certified EDITION NUMBER
May 2, 2016 TRIARQ Health 1050 Wilshire, Suite 300 Troy, MI 48084 Meaningful Use Certification Details CHPL Practice Date CERTIFICATION Product Version Classification PRODUCT Type Certified EDITION NUMBER
Using Telemedicine to Enhance Meaningful Use Qualification
 Beth DeStasio Director, Regulatory Affairs & Strategy, REACH Health September 2014 Copyright 2014 REACH Health, Inc. All rights Reserved Key Takeaways 1. As of September 4, 2014, the Center for Medicare
Beth DeStasio Director, Regulatory Affairs & Strategy, REACH Health September 2014 Copyright 2014 REACH Health, Inc. All rights Reserved Key Takeaways 1. As of September 4, 2014, the Center for Medicare
Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal. Lori Hack & Val Tuerk, Object Health
 Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal Lori Hack & Val Tuerk, Object Health 2 3 Agenda Who Qualifies for the EHR Incentive Funds? EHR Incentive Registration Process
Meaningful Use Basics and Attestation Process Guide for Medicare and Medi-Cal Lori Hack & Val Tuerk, Object Health 2 3 Agenda Who Qualifies for the EHR Incentive Funds? EHR Incentive Registration Process
Medicare & Medicaid EHR Incentive Programs HIT Policy Committee May 6, 2014
 Medicare & Medicaid EHR Incentive Programs HIT Policy Committee May 6, 2014 Registration and Payment Data 2 Active Registrations March 2014 March-14 Program-to-Date Medicare Eligible Professionals 8,361
Medicare & Medicaid EHR Incentive Programs HIT Policy Committee May 6, 2014 Registration and Payment Data 2 Active Registrations March 2014 March-14 Program-to-Date Medicare Eligible Professionals 8,361
3/29/2013. Effective ACO Compliance. Objectives THE HEALTH CARE DILEMMA: ARE ACOS THE ANSWER? HCCA Compliance Institute April 21, 2013
 Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
ARRA New Opportunities for Community Mental Health
 ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
ARRA New Opportunities for Community Mental Health Presented to: The Indiana Council of Community Behavioral Health Kevin Scalia Executive Vice-President, Corporate Development February 11, 2010 Overview
Meaningful Use Stages 1 & 2
 Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Meaningful Use Stages 1 & 2 Making Sure You Get the Most Out of Your EHR Tracy McDonald Medicaid EHR Incentive Program Coordinator Agenda Meaningful Use Stages & Incentive Program Timing 2014 Changes to
Medicare and Medicaid EHR Incentive Payment Basics
 Medicare and Medicaid EHR Incentive Payment Basics PPS Hospitals and CAHs, along with physicians providing care in OPDs, hospital clinics, and private practices are eligible for the program. These providers
Medicare and Medicaid EHR Incentive Payment Basics PPS Hospitals and CAHs, along with physicians providing care in OPDs, hospital clinics, and private practices are eligible for the program. These providers
9/28/2011. Learning Agenda. Meaningful Use and why it s here. Meaningful Use Rules of Participation. Categories, Objectives and Thresholds
 Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
Coding on the River 10/01/2011 Christina Catalano University of Florida Jacksonville Healthcare Inc. Director, EHR Compliance and Meaningful Use Learning Agenda Meaningful Use and why it s here Meaningful
Texas Medicaid Electronic Health Record (EHR) Incentive Program: Federally Qualified Health Centers (FQHCs)
 Incentive Program: Federally Qualified Health Centers (FQHCs)") Texas Medicaid Electronic Health Record (EHR) Incentive Program: Federally Qualified Health Centers (FQHCs) Julia Alejandre, Medicaid / CHIP Health IT Jason Phipps, Medicaid / CHIP Health IT July 20, 2012
Texas Medicaid Electronic Health Record (EHR) Incentive Program: Federally Qualified Health Centers (FQHCs) Julia Alejandre, Medicaid / CHIP Health IT Jason Phipps, Medicaid / CHIP Health IT July 20, 2012
Meaningful Use FAQs for Public Health
 Netsmart is your Meaningful Use technology partner with all the solutions you need to meet all Stage 1 Meaningful Use criteria so you don t have to integrate products from multiple vendors. For more information,
Netsmart is your Meaningful Use technology partner with all the solutions you need to meet all Stage 1 Meaningful Use criteria so you don t have to integrate products from multiple vendors. For more information,
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Alaska Medicaid Program
 Alaska Medicaid Program ALASKA ELECTRONIC HEALTH RECORDS Incentive Program Updated January 2018 Provider Manual 1 Background... 4 2 How Do I use this manual?... 6 3 How do I get help?... 7 4 Eligible provider
Alaska Medicaid Program ALASKA ELECTRONIC HEALTH RECORDS Incentive Program Updated January 2018 Provider Manual 1 Background... 4 2 How Do I use this manual?... 6 3 How do I get help?... 7 4 Eligible provider
Agenda 2. EHR Incentive Programs 3/5/2015. Overview EHR incentive programs Meaningful Use Differences between Stage 1 and Stage 2
 Meaningful Use and the Electronic Health Record Presented by: Susan Reehill CPC, CEMC, CHONC, CPMA Certified Professional Medical Auditor AHIMA Approved ICD-10 CM/PCS Trainer Overview EHR incentive programs
Meaningful Use and the Electronic Health Record Presented by: Susan Reehill CPC, CEMC, CHONC, CPMA Certified Professional Medical Auditor AHIMA Approved ICD-10 CM/PCS Trainer Overview EHR incentive programs
ACO GPRO 2016 Ready to Report Basics GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017
 ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
American Recovery & Reinvestment Act
 American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
American Recovery & Reinvestment Act Meaningful Use Dawn Ross, Clinical Informatics Director Linda Wilson, Meaningful Use Coordinator 10/26/2015 Overview American Recovery and Reinvestment Act of 2009
Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP)
") Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP) 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois
Updated 2017 Medicaid EHR Incentive Program Requirements For Eligible Providers (EP) 1 Illinois Health Information Technology Regional Extension Center (ILHITREC) SUPPORT PROVIDED BY ILHITREC: The Illinois
Exchange 9/30/2010. Hawai i Health Information
 The Hawai i Health Information Exchange Hawai i Health Information 1 Mission To facilitate the exchange of health information that enables high quality and affordable health care statewide Core Values
The Hawai i Health Information Exchange Hawai i Health Information 1 Mission To facilitate the exchange of health information that enables high quality and affordable health care statewide Core Values
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Medicaid Provider Incentive Program
 Medicaid Provider Incentive Program The Road to Meaningful Use Ohio Association of Community Health Centers 2013 Spring Conference March 6, 2013 Presenters: Elbony McIntyre, Project Manager Emma Esmont,
Medicaid Provider Incentive Program The Road to Meaningful Use Ohio Association of Community Health Centers 2013 Spring Conference March 6, 2013 Presenters: Elbony McIntyre, Project Manager Emma Esmont,
Meaningful Use of EHR Technology:
 Meaningful Use of EHR Technology: What Do the New Standards and Certification Criteria Mean for Your Organization? January 20, 2010 Mitchell J. Olejko Ropes & Gray LLP mitchell.olejko@ropesgray.com 415-315-6328
Meaningful Use of EHR Technology: What Do the New Standards and Certification Criteria Mean for Your Organization? January 20, 2010 Mitchell J. Olejko Ropes & Gray LLP mitchell.olejko@ropesgray.com 415-315-6328
CMS Quality Initiatives: Past, Present, and Future
 CMS Quality Initiatives: Past, Present, and Future Jeff Flick Regional Administrator CMS, Region IX June 29, 2007 Slide -1 Learning Objectives Value Driven Health Care CMS Quality Initiatives Premiere
CMS Quality Initiatives: Past, Present, and Future Jeff Flick Regional Administrator CMS, Region IX June 29, 2007 Slide -1 Learning Objectives Value Driven Health Care CMS Quality Initiatives Premiere
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016
 Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
Ophthalmology Meaningful Use Attestation Guide 2016 Edition Updated July 2016 Provided by the American Academy of Ophthalmology and the American Academy of Ophthalmic Executives (AAOE), the Academy's practice
Proposed Meaningful Use Content and Comment Period. What the American Recovery and Reinvestment Act Means to Medical Practices
 Proposed Meaningful Use Content and Comment Period What the American Recovery and Reinvestment Act Means to Medical Practices Session Objectives Gain a basic understanding of CMS EHR Incentive Program.
Proposed Meaningful Use Content and Comment Period What the American Recovery and Reinvestment Act Means to Medical Practices Session Objectives Gain a basic understanding of CMS EHR Incentive Program.
The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients
 The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients Updated March 2012 Netsmart Note: The Health Information Technology for Economic
The American Recovery and Reinvestment Act of 2009, Meaningful Use and the Impact on Netsmart s Behavioral Health Clients Updated March 2012 Netsmart Note: The Health Information Technology for Economic
Accelerating the Impact of Performance Measures: Role of Core Measures
 Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Accelerating the Impact of Performance Measures: Role of Core Measures Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair
Meaningful Use FAQs for Behavioral Health
 Netsmart is your Meaningful Use technology partner with all the solutions you need to meet all Stage 1 Meaningful Use criteria so you don t have to integrate products from multiple vendors. For more information,
Netsmart is your Meaningful Use technology partner with all the solutions you need to meet all Stage 1 Meaningful Use criteria so you don t have to integrate products from multiple vendors. For more information,
MEANINGFUL USE STAGE 2
 MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
MEANINGFUL USE STAGE 2 PHASED-IN IMPLEMENTATION PROCESS DECEMBER 2014 - PREPARATION MONTH Start this process as early as possible WATCH VIDEO TRAINING SESSIONS: (Sessions available starting December 1,
Practice Implications for Accountable Care Organizations
 Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Part I of the HITECH Webinar Series
 Part I of the HITECH Webinar Series August 18, 2010 The HITECH EHR Incentives and Certification Requirements Presented by Kathie McDonald-McClure, Esq. Moderators Carole Christian, Esq. Erin McMahon, Esq.
Part I of the HITECH Webinar Series August 18, 2010 The HITECH EHR Incentives and Certification Requirements Presented by Kathie McDonald-McClure, Esq. Moderators Carole Christian, Esq. Erin McMahon, Esq.
MEANINGFUL USE FOR THE OB/GYN. Steven L. Zielke, MD 6/13/2014
 MEANINGFUL USE FOR THE OB/GYN Steven L. Zielke, MD 6/13/2014 Disclosures: I have no conflicts of interest I am not being paid by CMS to present this talk I am not endorsing any EHR I cannot guarantee attestation
MEANINGFUL USE FOR THE OB/GYN Steven L. Zielke, MD 6/13/2014 Disclosures: I have no conflicts of interest I am not being paid by CMS to present this talk I am not endorsing any EHR I cannot guarantee attestation
Roll Out of the HIT Meaningful Use Standards and Certification Criteria
 Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
Roll Out of the HIT Meaningful Use Standards and Certification Criteria Chuck Ingoglia, Vice President, Public Policy National Council for Community Behavioral Healthcare February 19, 2010 Purpose of Today
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY
 PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
PROPOSED MEANINGFUL USE STAGE 2 REQUIREMENTS FOR ELIGIBLE PROVIDERS USING CERTIFIED EMR TECHNOLOGY On February 23, the Centers for Medicare & Medicaid Services (CMS) posted the much anticipated proposed
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Travis Broome AMIA
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Travis Broome AMIA 9-20-2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New clinical quality measures
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Travis Broome AMIA 9-20-2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New clinical quality measures
Meaningful Use Stage 1 Guide for 2013
 Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
Meaningful Use Stage 1 Guide for 2013 Aprima PRM 2011 December 20, 2013 2013 Aprima Medical Software. All rights reserved. Aprima is a registered trademark of Aprima Medical Software. All other trademarks
Electronic Health Records and Meaningful Use - A Year in Review
 Electronic Health Records and Meaningful Use - A Year in Review Charlene Underwood, MBA, FHIMSS Senior Director, Government & Industry Affairs HIMSS Board Chair Member, HIT Policy Meaningful Use WG July
Electronic Health Records and Meaningful Use - A Year in Review Charlene Underwood, MBA, FHIMSS Senior Director, Government & Industry Affairs HIMSS Board Chair Member, HIT Policy Meaningful Use WG July
Meaningful Use for 2014 Stag St e ag 1 Or Or Stag St e ag e 2 For Fo r 2014? Meaningful Meaningful Use: Stag St e ag e 1 1 Fo r Fo 2014
 Meaningful Use for 2014 Gerald E. Meltzer MD MSHA Medical Director imedicware Stage 1 Or Stage 2 For 2014? Meaningful Use: Stage 1 For 2014 1 Key Changes for 2014 Patient Electronic Access Clinical Quality
Meaningful Use for 2014 Gerald E. Meltzer MD MSHA Medical Director imedicware Stage 1 Or Stage 2 For 2014? Meaningful Use: Stage 1 For 2014 1 Key Changes for 2014 Patient Electronic Access Clinical Quality
Measures Reporting for Eligible Providers
 Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5a: Measures Reporting for Eligible Providers Published September 4, 2010 Measures Reporting for Eligible Providers The fourth paper in this series reviewed
Meaningful Use Participation Basics for the Small Provider
 Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Meaningful Use Participation Basics for the Small Provider Vidya Sellappan Centers for Medicare & Medicaid Services Office of E-Health Standards and Services HIT Initiatives Group July 30, 2014 EHR INCENTIVE
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Pennsylvania ehealth Initiative All Committee Meeting November 14, 2012 What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of
Transforming Health Care with Health IT
 Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Transforming Health Care with Health IT Meaningful Use Stage 2 and Beyond Mat Kendall, Director of the Office of Provider Adoption Support (OPAS) March 19 th 2014 The Big Picture Better Healthcare Better
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013 What is in the Rule Changes to Stage 1 of meaningful use Stage
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Jason McNamara Technical Director for Health IT HIMSS Meeting April 25, 2013 What is in the Rule Changes to Stage 1 of meaningful use Stage
Improving Clinical Outcomes
 Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Measures Reporting for Eligible Hospitals
 Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
Meaningful Use White Paper Series Paper no. 5b: Measures Reporting for Eligible Hospitals Published September 5, 2010 Measures Reporting for Eligible Hospitals The fourth paper in this series reviewed
American Recovery and Reinvestment Act (ARRA) of 2009
 of 2009") American Recovery and Reinvestment Act (ARRA) of 2009 An In-Depth Look into the Revolution of Health IT Colin Konschak, MBA, FHIMSS Managing Partner Scott Kizer, Esq., MIS Senior Legal Consultant Ernie
American Recovery and Reinvestment Act (ARRA) of 2009 An In-Depth Look into the Revolution of Health IT Colin Konschak, MBA, FHIMSS Managing Partner Scott Kizer, Esq., MIS Senior Legal Consultant Ernie
Stage 1. Meaningful Use 2014 Edition User Manual
 Stage 1 Meaningful Use 2014 Edition User Manual This document, as well as the software described in it, is provided under a software license agreement with STI Computer Services, Inc. Use of this software
Stage 1 Meaningful Use 2014 Edition User Manual This document, as well as the software described in it, is provided under a software license agreement with STI Computer Services, Inc. Use of this software
What Will Stage I Mean for Consumers and Purchasers
 Meaningful Use of Health IT What Will Stage I Mean for Consumers and Purchasers Christine Bechtel Vice-President National Partnership for Women & Families David Lansky President and CEO, Pacific Business
Meaningful Use of Health IT What Will Stage I Mean for Consumers and Purchasers Christine Bechtel Vice-President National Partnership for Women & Families David Lansky President and CEO, Pacific Business
Qualifying for Medicare Incentive Payments with Crystal Practice Management. Version 1.0
 Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
Qualifying for Medicare Incentive Payments with Crystal Practice Management Version 1.0 July 18, Table of Contents Qualifying for Medicare Incentive Payments with... 1 General Information... 3 Links to
Meaningful Use Is It Worth It?
 University of Tennessee Health Science Center UTHSC Digital Commons Applied Research Projects Department of Health Informatics and Information Management 2014 Meaningful Use Is It Worth It? Karen Perry
University of Tennessee Health Science Center UTHSC Digital Commons Applied Research Projects Department of Health Informatics and Information Management 2014 Meaningful Use Is It Worth It? Karen Perry
AHA Survey on Hospitals Ability to Meet Meaningful Use Requirements of the Medicare and Medicaid Electronic Health Records Incentive Programs
 AHA Survey on Hospitals Ability to Meet Meaningful Use Requirements of the Medicare and Medicaid Electronic Health Records Incentive Programs February 7, 2011 Executive Summary The vast majority of hospitals
AHA Survey on Hospitals Ability to Meet Meaningful Use Requirements of the Medicare and Medicaid Electronic Health Records Incentive Programs February 7, 2011 Executive Summary The vast majority of hospitals
Proposed 2015 PFS: Quality Updates
 SCGX1423 08/14 Proposed 2015 PFS: Quality Updates Johnson & Johnson Health Care Systems Inc. Providing services for: Janssen Biotech, Inc. Janssen Pharmaceuticals, Inc August, 2014 This document is presented
SCGX1423 08/14 Proposed 2015 PFS: Quality Updates Johnson & Johnson Health Care Systems Inc. Providing services for: Janssen Biotech, Inc. Janssen Pharmaceuticals, Inc August, 2014 This document is presented
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule
 Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Meaningful Use: Review of Changes to Objectives and Measures in Final Rule The proposed rule on meaningful use established 27 objectives that participants would meet in stage 1 of the program. The final
Medicare & Medicaid EHR Incentive Programs. Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan
 Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New
Medicare & Medicaid EHR Incentive Programs Stage 2 Final Rule Updates October 2, 2012 Rick Hoover & Andy Finnegan What is in the Rule Changes to Stage 1 of meaningful use Stage 2 of meaningful use New
A Lawyer s Take on Meaningful Use. By Steven J. Fox & Vadim Schick
 A Lawyer s Take on Meaningful Use By Steven J. Fox & Vadim Schick Overview American Reinvestment & Recovery Act (ARRA) February 2009 HITECH Act provides incentives for EHR adoption EHR Incentive NPRM issued
A Lawyer s Take on Meaningful Use By Steven J. Fox & Vadim Schick Overview American Reinvestment & Recovery Act (ARRA) February 2009 HITECH Act provides incentives for EHR adoption EHR Incentive NPRM issued
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE. Angel L. Moore, MAEd, RHIA Eastern AHEC REC
 THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
THE MEANING OF MEANINGFUL USE CHANGES IN THE STAGE 2 MU FINAL RULE Angel L. Moore, MAEd, RHIA Eastern AHEC REC WE WILL BRIEFLY DISCUSS Meaningful Use (MU) Incentive Programs, Eligibility & Timelines WE
Quality Measurement, Population Health and Payment Reform
 Quality Measurement, Population Health and Payment Reform The Move from Volume to Value Dale W. Bratzler, DO, MPH, FACOI, FIDSA Professor, Colleges of Medicine and Public Health Associate Dean, College
Quality Measurement, Population Health and Payment Reform The Move from Volume to Value Dale W. Bratzler, DO, MPH, FACOI, FIDSA Professor, Colleges of Medicine and Public Health Associate Dean, College
Overview of the EHR Incentive Program Stage 2 Final Rule published August, 2012
 I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
I. Executive Summary and Overview (Pre-Publication Page 12) A. Executive Summary (Page 12) 1. Purpose of Regulatory Action (Page 12) a. Need for the Regulatory Action (Page 12) b. Legal Authority for the
Achieving Meaningful Use with Centricity Electronic Medical Record
 GE Healthcare Achieving Meaningful Use with Centricity Electronic Medical Record Version 9.8 Revised July 2015 Centricity EMR DOC1620430 2015 General Electric Company All information is subject to change
GE Healthcare Achieving Meaningful Use with Centricity Electronic Medical Record Version 9.8 Revised July 2015 Centricity EMR DOC1620430 2015 General Electric Company All information is subject to change
GE Healthcare. Going beyond Meaningful Use with GE Healthcare
 1 GE Healthcare Going beyond Meaningful Use with GE Healthcare 1 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 0 1 0 1 1 0 1 1 0 1 0 1 1 1 0 1 1 1
1 GE Healthcare Going beyond Meaningful Use with GE Healthcare 1 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 1 0 1 0 1 0 1 0 1 0 1 0 1 0 1 1 0 1 1 0 1 0 1 1 1 0 1 1 1