Quality Account London North West University Healthcare NHS Trust
|
|
|
- Roland O’Neal’
- 5 years ago
- Views:
Transcription


1 Quality Account London North West University Healthcare NHS Trust
2 QUALITY ACCOUNT 4 PART 1: 6 INTRODUCING OUR QUALITY ACCOUNT 6 Welcome by the Chief Executive 7 Statement of directors responsibilities 9 Key Achievements for 2017/18 10 PART 2: 13 REVIEW OF OUR QUALITY ACHIEVEMENTS 13 Sign up to Safety Campaign 14 Review of 2017/18 Performance against Priorities 15 Priority one: Safer Care 15 Priority two: Better Outcomes 21 Priority three: Improved Experience 26 PART 3: 31 REVIEW OF OUR QUALITY PERFORMANCE 31 The NHS Outcomes Framework: Quality Indicators 32 What is the NHS Outcome Framework 32 SUS Data Quality 35 Information Governance 35 Patient Safety Incidents 36 Serious Incidents and Never Events 40 Patient Safety Alert Compliance 42 Ward/Service to Board- Excellence Assessment Tool (EAT)- Perfect Ward 44 Safe Staffing Levels 46 Duty of Candour 47 Patient-led assessments of the care environment (PLACE) 47 2
3 PART 4 : 49 STATEMENTS OF ASSURANCE 49 Statements of assurance from the Board include: Review of Services 50 Clinical Audit and Effectiveness 51 National Audits Reports received during National Confidential Enquiries 61 Research and Development 63 Commissioning for Quality and Innovation (CQUIN) 63 Access to seven day services 70 What others say about the Trust? 72 Information Governance toolkit 73 STAFF SURVEY 2017: Summary of Results 74 PART 5: 78 LOOKING FORWARD - OUR PLANS FOR THE FUTURE 78 Proposed Quality and Safety Improvement Priorities for Priority one: Safer Care (Safe, Caring, Responsive and Well Led) 79 Priority two: Better Outcomes- (Effective Safe and Caring) 82 Priority three: Improved Experience (Caring, Responsive and Well Led) 85 PART 6: 89 ANNEX 89 Amendments made following consultation 90 Statements on the content of the Quality Account from our stakeholders 91 Abbreviations 97 AUDITOR S OPINION 100 3
4 Quality Account What is a Quality Account? The Quality Account is an annual report published to the public from providers of NHS healthcare about the quality of the services it provides. The report provides details on progress and achievements against the Trust s quality and safety priorities for the previous year and what the Trust will focus on in the next year. What should a Quality Account look like? Some parts of the Quality Account are mandatory and are set out in regulations (NHS Quality Account Regulations 2010 and Department of Health Quality Accounts Toolkit 2010/2011). This toolkit can be accessed via The Quality Account must include: Part 1 (Introduction) A statement from the Board (or equivalent) of the organisations summarising the quality of NHS services provided. Part 2 (Looking back at the previous financial year performance) Organisations priorities for the quality improvement for the previous financial year A series of statements from the Board for which the format and information required is prescribed and set out in the regulations and the toolkit. Part 3 (Looking forward at the priorities for the coming financial year) A review of the quality of services in the organisation for the coming financial year. This must be presented under three domains; patient safety, clinical effectiveness and patient experience A series of statements from Stakeholders on the content of the Quality Account. Providers are able to add additional sections and information; however the Quality Account must have an introduction, it must then look back at previous performance and then look forward at the priorities for the coming financial year. What does it mean for London North West University Healthcare NHS Trust? The Quality Account allows NHS healthcare organisations such as London North West University Healthcare NHS Trust to demonstrate their commitment to continuous, evidencebased quality improvement and to explain its progress against agreed quality and safety priorities, how the organisation performed in other quality areas e.g. service delivery, and to inform the public of its future plans and priorities. 4
5 What does it mean for patients, members of the public and stakeholders? By putting information about the quality of services in an organisation into the public domain, NHS healthcare organisations are offering their approach to quality for scrutiny, debate and reflection. The Quality Account should assure patients, members of the public and its stakeholders that as an NHS healthcare organisation we are scrutinising each and every one of our services, providing particular focus on those areas that require the most attention. How will the Quality Account be published? In line with legal requirements all NHS Healthcare providers are required to publish their Quality Account electronically on the NHS Choices website by 30th June London North West University Healthcare NHS Trust also makes its Quality Account available on its website. 5

6 Part 1: Introducing our Quality account This section includes A statement on Quality from the Chief Executive, Dame Jaqueline Docherty DBE Statement of Directors responsibilities An overview of some of our success stories and highlights from 2017/18 6

7 Welcome by the Chief Executive I am delighted to present our Quality Account for 2017/18, which examines how we performed on our quality indicators and priorities over the last year, and outlines our vision and aspirations for providing high quality care in the year ahead. The Quality Account sits beside our Annual Report, which provides a comprehensive overview not only of our financial position, but also of our progress and future plans. In May 2017, we were proud to launch our HEART values (Honesty, Equality, Accountability, Respect, and Teamwork), which were chosen by our staff after significant discussion and engagement with both staff and patient groups. 95% of our staff now tell us that they are familiar with the values, demonstrating how closely we are working as a cohesive unit with shared goals. Over the last year, our services have worked to develop a range of innovative quality initiatives which are having a significant impact for our patients. Introducing the Perfect Ward mobile app has supported our matrons with smart quality walkabouts, where they use observation of care and documentation, and discussion with patients, staff, and the nurse in charge to make real time improvements for patients. Meanwhile, our pharmacy teams have become the first in the country to introduce bilingual labelling for our medicines, so that patients can receive instructions on how to take their medication in their preferred language. Our commitment to education and research continues to be a vital component of improving the quality of our services. In a year when we were awarded University Hospital status, our radiology department also launched the first Ultrasound Training Academy in the UK, furthering the careers of staff across the sector, and helping us to develop our own, highly skilled sonographers. This focused approach to quality improvement has shown some extraordinary results: Trust-attributable pressure ulcers at Grades 3 and 4, for instance, have dropped by 60%, while the percentage of our patients with sepsis who receive IV antibiotics within one hour increased to 95% last year. We are committed to a programme of continuous insight, reflection and improvement, and our Quality Priorities set out our areas of focus for the year ahead. They have been developed following extensive consultation with our patients, our local Healthwatch organisations (who represent our patients), our commissioners (who purchase our services on behalf of our patients), local authorities, NHS England, NHS Improvement, and of course our staff. Our thanks are owed to everyone who contributed their thoughts and ideas: working closely with our community is an essential part of being able to offer our patients and service users the standard of care we want to provide. 7
8 Like other NHS Trusts, we have seen an increase in demand for our services over the last year. This has presented us with a challenge, and our staff have demonstrated real commitment to not only providing high quality care in the face of rising activity but to improving that care wherever possible. On behalf of the Board, I would like to thank our all staff and volunteers for their continued dedication to improving the quality and safety of our services. Finally, I can confirm, in accordance with my statutory duty, that to the best of my knowledge, the information provided in this Quality Account is accurate. Jacqueline Docherty DBE Chief Executive 8
9 9




10 Key Achievements for 2017/18 Safer Care Better Outcomes 10




11 Better Patient Experience 11




12 Workforce 12

13 Part 2: Review of our Quality Achievements This section includes Information on Sign up to Safety campaign An overview of performance against 2017/18 A detailed update on the performance, achievements and further improvements against the 2017/18 quality improvements 13

14 Sign up to Safety Campaign The Sign up to Safety campaign is a national patient safety campaign with a mission to strengthen patient safety in the NHS and make it the safest healthcare system in the world through continuous learning and improvement. It is supported by NHS England, NHS Resolution, NHS Improvement, Care Quality Commission, and the Department of Health. The Trust has signed up to the campaign and made the following safety core pledges in 2016/17 which we aim to continue in : Put Patient Safety First Commit to reduce avoidable harm in the NHS by half and to make public the goals and plans developed locally. Continually learn Review incident reporting and investigation processes to make sure that the Trust learns from them and using these lessons to make the organisation more resilient to risks. Listen, learn and act on the feedback from patients and staff and by constantly measuring and monitoring how safe services are. Honest Being open and transparent. Support staff to be open and honest with patients and their relatives when things go wrong. Collaborative Take a leading role and actively collaborating with other organisations in sharing work, ideas and learning so that improvements are made across all of the local services that patients use. Support Helping staff to bring joy and pride to their work. Give staff the time and support to improve and to celebrate success. The Trust decided to align the Sign up to Safety campaign with the Quality Account improvement plan and the Care Quality Commission (CQC) five key domains of quality and safety: safe, effective, caring, responsive and well-led. The Trust continues to monitor the Sign up to Safety campaign pledges through a quality and safety programme. A bespoke dashboard has been developed to monitor the progress and action plans in relation to the campaign pledges and this is reported monthly to the Clinical Quality and Risk Executive Committee. The Trust sub-board committee is attended by members of the Executive Team and Divisional triumvirates. 14
15 Review of 2017/18 Performance against Priorities At the heart of everything we do, is a strong focus on quality to make sure that our patients receive the optimum and safe care. In , we have made a significant progress against our three main quality improvement priorities which were: 1. Safer care 2. Better outcomes 3. Better patient experience We have developed a quality and safety dashboard which monitors the quality account improvement plan and various sets of local improvement priorities. We also have introduced a mobile app for the weekly quality inspection walkabout of Matrons and the wards quarterly assessment based on CQC five domains. The following section provides an overview of performance against all targets during 2017/18 and the improvements made. Most of our targets were achieved or on track for achievement. We also recognise that some changes have been difficult to implement and we will be learning from this experience. Key Goal achieved Improvement made compared to previous year Goal not achieved Priority 1: Safer Care 1. Safer Care (Safe, Caring, Responsive and Well Led) 1.1 Pressure Ulcer (PU) Significant progress was made to reduce pressure ulcers both within the acute and community settings. The Trust achieved over 45% reduction in 2016/17 and further 60% reduction in 2017/18 for Trust attributed grade 3& 4 pressure ulcers serious incidents (SI). Nil grade 3 &4 hospital acquired pressure ulcers serious incidents were reported in bedded units since July We also achieved a reduction in Trust acquired grade 2 PU and have introduced a local investigation checklist. The Trust participated in the national Stop the Pressure Campaign and has been a member of the North West London Pressure Ulcer Steering Group. 15
16 What did we set out to achieve? Zero incident Trust attributed avoidable grade 3 & 4 PU in acute hospitals 50% reduction in Trust attributed avoidable grade 3 & 4 PU in community services 50% reduction in Trust attributed avoidable grade 2 PU in the acute hospitals Increase staff compliance on PU prevention and management training Introduce a local investigation checklist for all Trust attributed PU (grade 2, 3 & 4) Continued participation in the National Stop the Pressure campaign Actual outcome: ACHIEVED Outcome Measures Zero incident Trust attributed avoidable grade 3 & 4 PU in acute hospitals *The Trust had two attributed grade 3/4 PU in the beginning of the year (April & June 2017). Nil attributed grade 3&4 PU in the acute hospitals since July Achieved 60% reduction in the Trust attributed grade 3 and 4 PU serious incidents (SI) in comparison to previous year 50% reduction in Trust attributed avoidable grade 3 & 4 PU in community services 50% reduction in Trust attributed avoidable grade 2 PU in the acute hospitals Increase staff compliance on PU prevention and management training Introduce a local investigation checklist for all Trust attributed PU (grade 2, 3 & 4) Continued participation in the National Stop the Pressure campaign Outcome Improvements achieved: Achieved 60% reduction in the Trust attributed grade 3 and 4 PU serious incidents (SI) Nil Trust attributed grade 3 and 4 PU in the acute hospitals since July 2017 Reduction in the Trust attributed grade 2 PU compared to last year Pressure ulcers learning sessions conducted across different sites Stop the Pressure events and awareness conducted in line with the National Stop the Pressure campaign Implementation of an integrated tissue viability service to streamline reporting arrangements for tissue viability nurses across community and acute hospitals. In addition to face to face training, a new online refresher training module on PU prevention and management was launched in Replacement of the old mattresses (Pentaflex) with a new hybrid mattresses and pumps across trust bedded units. 16

17 Review and merger of the legacy Trusts PU guidelines which includes standardisation of documentations and PU incident notification process. Multidisciplinary development and rollout of the Pressure Ulcer Life Cycle 1.2 Nutrition and Hydration Malnutrition and dehydration have substantial adverse effects on health, disease and wellbeing. Good nutrition and hydration is imperative for both the physiological and psychological health of our patients. It is important that all inpatients in the Trust are monitored for risk of malnutrition and dehydration and any deterioration is escalated in a timely manner. Nutrition Study Day What did we set out to achieve? Standardised food chart across the Trust bedded units and compliance monitored through walkabouts and Matrons audit Promote Patient Protected Mealtime and Beverages and monitor through regular audit Introduction of bell in the wards for patients protected mealtime Invite peer/external review (Health Watch) with regards to nutrition and hydration in the wards Standardised nutritional screening tool Trust wide (acute and community) Improve staff compliance on conduct of patient nutritional screening assessment on admission i.e. weight and height Introduce Weigh-Day Weekend across bedded units Standardised food chart across the Trust bedded units and compliance monitored through walkabouts and Matrons audit 17
18 Actual outcome: ACHIEVED Outcome Measures Standardised food chart across the Trust bedded units and compliance monitored through walkabouts and Matrons audit Promote Patient Protected Mealtime and Beverages and monitor through regular audit Introduction of bell in the wards for patients protected mealtime Invite peer/external review (Health Watch) with regards to nutrition and hydration in the wards Standardised nutritional screening tool Trust wide (acute and community Improve staff compliance on conduct of patient nutritional screening assessment on admission i.e. weight and height Introduce Weigh-Day Weekend across bedded units Standardised food chart across the Trust bedded units and compliance monitored through walkabouts and Matrons audit Outcome Improvements achieved: Throughout 2017/18, there was a Trust wide focus on Nutrition and Hydration. A nutrition and hydration event was held in September 2017 attended by over 80 members of staff from different specialties from acute and community services. We have launched the meal time check list and guidelines for nurses and AHPs regarding their role at patient s meal time which includes a protected mealtime bell ringing process. A Trust Nutrition and Hydration website page was introduced which includes the following new initiatives: Nutrition and Hydration video involving nurses, catering and AHP staff demonstrating a gold standard meal time process Trust wide standardisation of nutritional screening through implementation of the Malnutrition Universal Screening Tool (MUST) Standardised Food and Drinks chart across bedded units Weigh in weekend Diet board completion guideline 18
19 1.3 Medicine Optimisation Medicines are the most common therapeutic intervention and it is imperative that the Trust has assurance about the impact medicines have on the quality of care, patient safety and patient experience. The Trust has undertaken a range of initiatives to improve medicines optimisation in 2017/18. We have achieved reduction in total antibiotic consumption per 1,000 admissions compared to previous year. What did we set out to achieve? Increase in the number of medication incidents and near misses reported during 2017/18 compared to 2016/17 by improving the reporting culture within the Trust in line with the HEART values Increase the range of methods used to feedback the lessons learned from reported medication incidents Improve the level of patient satisfaction with the local medicine related patient experience measures during 2017/18 compared to 2016/17 Revise the local medication safety dashboard to reflect current medication related priorities, improve compliance with these standards during 2017/18 and provide feedback to clinical staff Reduction in antibiotic consumption per 1000 admissions compared to 2016/17 median values measured quarterly Actual outcome: ACHIEVED Outcome Measures Increase in the number of medication incidents and near misses reported during 2017/18 compared to 2016/17 by improving the reporting culture within the Trust in line with the HEART values Increase the range of methods used to feedback the lessons learned from reported medication incidents Improve the level of patient satisfaction with the local medicine related patient experience measures during 2017/18 compared to 2016/17 Revise the local medication safety dashboard to reflect current medication related priorities, improve compliance with these standards during 2017/18 and provide feedback to clinical staff Reduction in antibiotic consumption per 1000 admissions compared to 2013/14 median values measured quarterly Outcome Improvements achieved: The pharmacy team has developed a local medication safety dashboard reflecting current medication related priorities and to provide feedback to clinical staff compliance. In 2017/18, the Trust had one medication incidents declared as SI. This is about a reduction of 75% in comparison to previous year total of four incidents. In , the 19
20 Trust achieved significant reduction in total antibiotics consumption per 1000 admissions in comparison to previous year. Reduction of 10.7% in Q3 and 4.1% in Q4 of WHO Checklist The introduction of the WHO Safer Surgery Checklist was a great step forward in the delivery of safer care for patients undergoing surgical operations and invasive procedures. Experience with its use has suggested that the benefits of a checklist approach can be extended beyond surgery to all invasive procedures performed in hospitals. Continuous safety improvement depends on continuous audit of outcome and compliance with safety standards What did we set out to achieve? Monitor compliance on WHO Surgical Safety Checklist across hospitals sites Improve compliance on WHO Surgical Safety Checklist Development and monitoring of surgical safety checklist compliance in the maternity services Development and monitoring of surgical safety checklist compliance in: Endoscopy Ophthalmology Interventional radiology Inpatient wards Cardiology (cath lab) Actual outcome: ACHIEVED Outcome Measures Monitor compliance on WHO Surgical Safety Checklist across hospitals sites Improve compliance on WHO Surgical Safety Checklist * Development and monitoring of surgical safety checklist compliance in the maternity services * Development and monitoring of surgical safety checklist compliance in Endoscopy -achieved Ophthalmology-achieved interventional radiology -achieved inpatient wards safety checklist template developed and awaiting audit results Cardiology (cath lab) - achieved Outcome The Trust reported two Never Events in 2017/18 related to retained foreign object post procedure 20
21 Improvements achieved: In 2017/18, the Trust has developed a quality and safety dashboard of monitoring services compliance on safety standards for invasive procedures. Audit compliance on safety standards is now presented by the Divisions to the Clinical Quality and Risk Committee. The Trust has collaborated with the Perfect ward in the development of safety checklist through a mobile app. The project has been funded by Innovate UK and aimed to be piloted in the acute Trust in July-August Safety checklist developed and results of audits are reported monthly to the Clinical Quality and Risk Committee for the following service: Endoscopy Ophthalmology Interventional radiology Cardiology (cath lab) Inpatient wards template developed awaiting implementation and audit results A safety checklist for chest drain insertion has been developed for the inpatient wards and emergency department. Audit results on compliance in this local safety checklist will be reported monthly in Priority two: Better Outcomes (Effective Safe and Caring) 2.1. Deteriorating Patient Patients who are admitted to hospital expect that should their condition deteriorate then they are in the best place for prompt and effective treatment. However, there is evidence that patients who are, or become acutely unwell in hospital may receive suboptimal care. This may be because their deterioration is not recognised, or because despite indications of clinical deterioration, it is not appreciated, or not acted upon quickly enough. Early recognition of a patient s deterioration through the use of observations will enable appropriate planning and escalation of care. The Trust has participated in the World Sepsis day campaign in 2017/18, with information stalls, ward based teaching and a staff quiz on sepsis. The percentage of patients receiving IV antibiotics within one hour of presenting with Sepsis, also known as the Golden Hour, has increased from 88% in 16/17 to 95% in 17/18. The 24 hour Fluid Balance Chart has also been standardised across the Trust. This was launched during the acute kidney injury (AKI) awareness week. The Trust has also launched the New Adult Admission and Assessment Booklet in March 2018 which incorporates forms that are completed daily by the doctors, nurses, support workers and allied health professionals. 21
22 What did we set out to achieve? Review cardiac arrest calls outside critical care and identify themes and areas for improvement Reduction in number of cardiac arrest calls Improve Sepsis bundle compliance Review acute kidney injury (AKI) bundle and monitor compliance improvement Monitor number of patients admitted to ITU/ICU for hemofiltration as a result of AKI and identify themes and areas for improvement Actual outcome: PARTIALLY ACHIEVED Outcome Measures Review cardiac arrest calls outside critical care and identify themes and areas for improvement Reduction in number of cardiac arrest calls Improve Sepsis bundle compliance Improve acute kidney injury (AKI) bundle compliance Monitor number of patients admitted to ITU/ICU for hemofiltration as a result of AKI and identify themes and areas for improvement Outcome Improvements achieved: The Deteriorating Patient Group (DPG) was launched in 2017 chaired by the Deputy Medical Director. The DPG received regular updates and monitors improvement plans with regards to sepsis, acute kidney injuries, cardiac arrest and emergency calls within the organisation. The group recommended that the AKI bundle needs to be reviewed in light of emerging evidence and the data collection and format updated to ensure ease of use by frontline staff.. A new clinical lead has been appointed to lead the AKI group and will be reporting regularly to the DPG. Cardiac arrest calls are now reported on DATIX. Number of cardiac arrests calls and medical emergency calls by site and ward are presented in the DPG. Learning and themes on cardiac arrest calls are discussed in the DPG as part of its work plan. 2.2 Baby Friendly Initiative Infant and young child feeding practices have a strong impact on the nutrition status of children under 2 years of age as well as on their risk for infectious diseases and mortality There are several research studies demonstrating breastfeeding health benefits to the children and the mother. 22
23 What did we set out to achieve? NPH Baby Friendly Hospital Initiative accreditation Increase the breastfeeding initiation rates by 2% from previous year Achieve 80% training compliance for eligible staff Reduction in the incidence of re-admissions of new-born babies and mothers with breastfeeding related issues Develop user friendly public website with adequate information for new mothers and families Actual outcome: ACHIEVED Outcome Measures NPH Baby Friendly Hospital Initiative accreditation Increase the breastfeeding initiation rates by 2% from previous year Achieve 80% training compliance for eligible staff Reduction in the incidence of re-admissions of new-born babies and mothers with breastfeeding related issues Outcome Develop user friendly public website with adequate information for new mothers and families Improvements achieved: In 2017/18, breastfeeding initiation rates increased in NPH maternity services. Northwick Park Hospital achieved Baby Friendly Hospital re-accreditation from UNICEF. This is internationally recognised mark of quality, showing that we are committed to providing parents with the best possible care to build close and loving relationships with their baby and feed their baby in ways which will support optimum health and development. 2.3 Continence Care Robert Francis referred to continence as this most basic of needs, in his report highlighting significant concerns in this area of care (Department of Health, 2010). An ageing population, greater prevalence of bladder and bowel problems and the wide range of care groups affected, mean that continence services require a higher priority. Effective community-based continence services can save valuable NHS resources whilst restoring dignity to people and improving quality of life. 23
24 What did we set out to achieve? Monitor number of monthly new referrals to the Bladder and Bowel Service and identify trends Improve the response time of the service Development of care pathway between primary community and secondary care Standardised continence care products across hospital sites and community Actual outcome: ACHIEVED Outcome Measures Monitor number of monthly new referrals to the Bladder and Bowel Service and identify trends Improve response time of the service Development of care pathway between primary community and secondary care Standardised continence care products across hospital sites and community Outcome Improvements achieved: The Trust has achieved its contractual target with regards to the continence service response time for home visits in Brent and Ealing. However, there is slight deterioration on its performance in comparison to the beginning of the financial year which was attributed to vacancies and staff sickness. Active recruitment for substantive post and bank is ongoing to fill the current vacancies in the service. Care pathway between primary care and secondary care is under development. 2.4 Allied Health Professionals Allied Health Professionals (AHPs) are the next biggest clinical workforce in the Trust after nursing and midwifery. AHPs expertise and contribution in the management of patient care is vital in the speedy recovery of patients, reducing length of stay, and unnecessary care costs which are required to ensure affordable and sustainable NHS service in the future. AHP interventions can significantly reduce unnecessary hospital stay and diminish dependency on care services, resulting in significant savings. 24
25 What did we set out to achieve? Monitor therapist productivity (allocated and actual patient seen) and triangulate with staffing and workforce data 95% compliance on response time for therapy input within 24 hours from time of referral (bedded units) Improve waiting time for therapy input in community services Improve staff turnover rates and vacancy rates of therapist by March 2018 Maintain Ealing MSK interface Surgical Conversion Rates at 80% and onward referral into secondary care at 20% Address service historical service boundaries and reduce duplication and fragmentation Continue monitoring of dietetics activity (new referrals and total contacts received from inpatient wards/units) Actual outcome: PARTIALLY ACHIEVED Outcome Measures Monitor therapist productivity (allocated and actual patient seen) and triangulate with staffing and workforce data 95% compliance on response time for therapy input to bedded units within 24 hours from time of referral Improve waiting time for therapy input in community services Improve staff turnover rates and vacancy rates of therapists by March 2018 Maintain Ealing MSK interface Surgical Conversion Rates at 80% and onward referral into secondary care at 20% Address service historical service boundaries and reduce duplication and fragmentation Continue monitoring of dietetics activity (new referrals and total contacts received from inpatient wards/units) Outcome 25
26 Improvements achieved: In 2017/18 we have developed a bespoke safer staffing template for the AHP. This is completed daily to assess staffing against the demand of the service. The AHPs staffing levels in the acute sites are now included in the Safer Staffing report presented monthly by the Chief Nurse to the Trust Board. The level of AHP demand exceeds the level of current resource capacity. Collaboration and discussion with external partners and commissioners is ongoing whilst active recruitment and retention campaign continues. The Trust participated in the NHSI 90 days retention programme in 2017 to learn and share good practice among NHS organisations. Priority three: Improved Experience (Caring, Responsive and Well led) 3.1 Dementia Dementia is a syndrome associated with an ongoing decline of the brain and its functions. The risk of developing dementia increases as you get older especially in people over the age of 65. Dementia is a significant challenge for the NHS with an estimated 25% of acute beds occupied by patients with dementia. Their length of stay is longer than patients without dementia and they are often subject to delays in discharge when leaving hospital. Patients with dementia are also more likely to come to harm than patients without dementia. What did we set out to achieve? Increase staff training compliance on dementia Monitor usage of carer s passport/agreement in the bedded units through the daily safety brief Confusion Care Pathway (CCP) embedded in the wards for staff guidance in using best practice in caring for people with dementia, cognitive impairment and/or delirium Conduct of Carers experience survey to identify themes and areas for improvement Digital Reminiscence Therapy (DRT) for elderly care patients Monitor number of activities conducted Monitor number of participants 26
27 Actual outcome: ACHIEVED Outcome Measures Increase staff training compliance on dementia Monitor usage of carer s passport/agreement in the bedded units through the daily safety brief Confusion Care Pathway (CCP) embedded in the wards for staff guidance in using best practice in caring for people with dementia, cognitive impairment and/or delirium Conduct of Carers experience survey to identify themes and areas for improvement Digital Reminiscence Therapy (DRT) for elderly care patients Monitor number of activities conducted Monitor number of participants Outcome Improvements achieved: There was achievement of significant increase in staff training compliance on dementia in 2017/18 resulting in the set target. We have included in the daily safety brief the usage of carer s passport/agreement in the bedded units and number of patients on Confusion Care Pathway (CCP). Although CCP compliance has increased in 2017/18, there is still room for improvement with regards to its full utilisation in the bedded units. Compliance on CCP completion is monitored through the Matrons weekly walkabout via the Perfect ward app. We have refurbished our Care of the Elderly wards to make them dementia friendly (Hardy and Fielding ward, NPH) We have invested in activity coordinators in the elderly wards resulting in a significant increase in activities utilising the Reminiscence Interactive Therapy Activity (RITA) in NPH. RITA therapy software is aimed at offering support for older people as a means of supporting them and reducing their agitation, isolation, depression and delirium. It provides stimulation for activities and engagement that helps improve health, wellbeing and the quality of care received by the patients in the acute elderly wards and provides a positive patient experience. We aimed to roll out the usage of RITA in other acute sites as part of next year quality improvement plan. 27
28 3.2 End of Life Care How we care for the dying is an indicator of how we care for all sick and vulnerable people. End of life care helps people with advanced, progressive and incurable illness to live as well as possible until the moment of death. What did we set out to achieve? Improved compliance with usage of Last Days of Life Care Agreement (LDLCA) in the acute hospitals Improved compliance of matrons and ward managers on syringe pump, SAGE & THYME and Recognising Dying training Conduct of bereavement survey twice a year End of life complaints collated and themes reported to the End of Life Group for development of action plans Actual outcome: ACHIEVED Outcome Measures Improved compliance with usage of Last Days of Life Care Agreement (LDLCA) in the acute hospitals Improved compliance of matrons and ward managers on syringe pump, SAGE & THYME and Recognising Dying training Conduct of bereavement survey twice a year End of life complaints collated and themes reported to the End of Life Group for development of action plans Outcome Improvements achieved: In 2017/18, we achieved 15% increase in staff compliance on training in comparison to previous year but acknowledged that further improvement is still needed. We have recruited additional staff in palliative care and rolled out train the trainers to further increase training compliance. The Trust has launched the Last Day of Life Care Agreement (LDLCA) booklet across bedded units for staff guidance on caring for the dying patient. Completion of the LDLCA is monitored through the Matrons weekly walkabout using the Perfect ward app. 28

29 3.3 End Pyjama Paralysis Campaign We know that if patients stay in their pyjamas or gowns for longer than they need to, they have a higher risk of infection, lose mobility, fitness and strength, and stay in hospital longer. But if we can help patients get back to their normal routine as quickly as possible, including getting dressed, we can support a quicker recovery, help patients maintain their independence and help get them home sooner. What did we set out to achieve? Promote End Pyjama Paralysis Campaign in the bedded units Trial the campaign in the pilot wards and monitor patient length of stay Actual outcome: ACHIEVED Outcome Measures Promote End Pyjama Paralysis Campaign in the bedded units Trial the campaign in the pilot wards and monitor patient length of stay Outcome Improvements achieved: The Trust has signed up to the EndPJ paralysis campaign and piloted this initiative onto selected wards across bedded units: Northwick Park Hospital o Hardy and Fielding wards Care of Elderly (COE) o Regional Rehabilitation Unit o Evelyn ward - Surgery o Frederick Salmon and IFU St Mark s Hospital Ealing Hospital o 5 South- Care of Elderly (COE) o 7 North Surgery Community Hospitals - Willesden and Clayponds sites 29

30 We have participated in the 70 days challenge to get 1 million patients dressed and mobilised in line with NHS 70 year s anniversary. The Trust envisage that the campaign will be rolled out trust wide as part of next year quality improvement plan. 30

31 PART 3: REVIEW OF OUR QUALITY PERFORMANCE This section includes Trust Performance for 2016/17 and 2017/18 against the NHS OUTCOMES. SUS Data Quality An overview of the patient safety incidents reporting rates and actions taken to improve incident reporting across the organisation. An overview of Serious Incidents and Never Events and actions taken to learn lessons. Trust compliance with National Patient Safety Alerts. Information on the Ward/Service Accreditation Assessment Tool - Excellence Assessment Tool (EAT) Information on what actions the Trust has and will continue to take to provide safe staffing levels. Staff Survey Duty of Candour Patient-led assessments of the care environment (PLACE) 31
32 The NHS Outcomes Framework: Quality Indicators What is the NHS Outcome Framework Measuring and publishing information on health outcomes is important for encouraging improvements in quality. The White Paper: Liberating the NHS outlined the Government s intention to move the NHS away from focusing on process targets to measuring health outcomes. The NHS Outcomes Framework reflects the vision set out in the White Paper and contains a number of indicators selected to provide a balanced coverage of NHS activity. The NHS Outcomes Framework is grouped around five domains that set out the high level national outcomes that the NHS should be aiming to improve. Performance against the quality indicators that are relevant to London North West University Healthcare Trust are detailed below. They relate to: The Summary Hospital-level Mortality Indicator (SHMI). Patient Reported Outcome Measures (PROMs). Readmission rate with 28 days of discharge. Trust s responsiveness Patient Experience Performance against Friends and Family Test for staff. Performance against Clostridium difficile infection (C. diff) Performance against Meticillin Resistant Staphylococcus aureus (MRSA) bloodstream infection (BSI) Summary Hospital Mortality Indicator (SMHI) Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available standardised data for the Trust is supplied by NHS Digital for the period October 2016 to September Trust SHMI Value Trust SHMI Banding The percentage of patient deaths receiving palliative care Better than Expected Better than expected As Expected Better than Expected Worse than expected 28.9% 32.0% 31.5% 59.8% 11.5% The trust performs better compared to previous period and national average. Action includes improvement in the management and learning from mortality review data with a DATIX module to capture all information and lessons arising from the Divisions. Performance on mortality indicator including improvement plans is monitored by the Clinical Excellence Committee. 32
33 Patient Reported Outcome Measure (PROM) adjusted average health gain Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available standardised data for the Trust is provisionally supplied by NHS Digital for the period April 2016 to March 2017 for the adjusted average health gain based on the EQ-5D Index Groin hernia (Negative Oulier) (Not an Oulier) Varicose veins (Not an outlier) (Not an outlier) Hip replacement (Not an outlier) (Not an outlier) Knee replacement (Negative Oulier) (Not an Oulier) The trust is not an outlier and performs better compared to previous period except in varicose veins. Patient related outcome measures (PROMS) are included in 2018/19 improvement priorities and this will be monitored in the Clinical Quality and Risk Committee. Readmission rate within 28 days of discharge Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available standardised data for the Trust has been analysed using the Healthcare Intelligence Portal from Dr Foster Intelligence for the period November 2016 to October Patients aged % 6.6% 10.3% 3.9% 17.4% Patients aged 16 or over 8.0% 11.8% 13.0% 9.7% 16.1% The trust performs better compared to national average. The trust collaborates with local partners to provide a full health economy approach through the local A&E delivery board. This includes provision of pre-crisis support such as Harrow Rapid Response Team, Home ward and Brent STARRS. Trust's Responsiveness (Patient experience of hospital care) Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available data for the Trust has been supplied by NHS England for the 2016 Adult Inpatient survey completed in July Overall Patient Experience Score The trust launched the HEART values putting patient at the heart of everything that we do. Divisions encourage all staff to give FFT survey forms to all patients to increase response rate. Continue working with the Matrons, ward managers to review and improve results. Divisional action plans to improve performance are monitored by the Patient Experience Committee. Continue recruitment of volunteers for A&E to support promotion of FFT survey completion. 33
34 Friends and Family Test for Staff Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available data for the Trust has been supplied by NHS England for the period July 2017 to September Staff who would recommend the Trust as a provider of care to family and friends 69.4% 71.6% 80.0% 100% 42.9% There is an improvement in comparison to previous period. New values launched (known as HEART) and adopted by staff (95% of staff aware of values). Improvement action includes roll out of a new suite of leadership and management development programmes to support and equip managers to undertake operational management more effectively VTE Risk Assessment Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available data for the Trust has been supplied by NHS England for the period October 2017 to December Adult inpatients who have been risk assessed for VTE on admission 94.3% 94.3% 95.4% 100.0% 76.1% Improvement on VTE assessment compliance to be led by the Medical Director and this will be reported on Clinical Excellence Committee. Continue usage of safety thermometer monthly survey for monitoring of VTE assessment compliance in the bedded units by the Matrons. C. Difficile Infection Rate Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available data for the Trust has been supplied by Public Health England for the period April 2016 to March 2017* Clostridium difficile (C. diff) infection rate per 100,000 bed-days (patients aged 2 or over) Performance is better in comparison to previous period and national average. Continue antibiotic stewardship and monitoring by the Trust Infection Control Committee. MRSAb Infection Rate Prescribed Information Trust Values Comparators Previous Period Current Period National Average Best Performer Worst Performer The most recent available data for the Trust has been supplied by Public Health England for the period April 2016 to March 2017 Methicillin Resistant Staphylococcus aureus
35 (MRSA) bloodstream infection (BSI) rate per 100,000 bed-days Trust Infection Prevention and Control work plan reported to the Clinical Excellence Committee. MRSA screening compliance in bedded units is included in the wards monthly key performance indicators (KPI). Wards KPI performance and action plans are discussed in the Matrons and Head of Nursing monthly meeting. SUS Quality Data London North West Healthcare NHS Trust submitted records during 2017/18 to the Secondary Uses Service (SUS) for inclusion in the Hospital Episode Statistics (HES) which are included in the latest published data. The percentage of records in the published provisional data for the period April 2017 to January 2018 which included the patient s valid NHS Number was: 98.6% for admitted patient care; 98.9% for outpatient care; and 96.0% for accident and emergency care The percentage of records in the published data which included the patient s valid General Medical Practice Code was: 99.98% for admitted patient care; 99.99% for outpatient care; and 99.96% for accident and emergency care The Trust carried out an audit using version 10 of the Clinical Coding Audit Methodology of its clinical coded data in line with the Information Governance Toolkit (IGT) Requirement 505. The Trust attained level 2 and is working towards achieving level 3. The Trust improves data quality through: Regular review of compliance with the Trust Data Quality Policy through cleansing, audit and feedback to clinical and non-clinical teams. Ensuring compliance with the Information Governance Toolkit minimum Level 2 for data quality standards. Working closely with clinicians to ensure the accuracy of coded data through regular and ad hoc joint reviews and through an education programme. Reviewing the level of risk associated with data quality through the Data Quality Management Group and the Corporate Quality and Risk Committee. Continuing the data quality assurance programme ensuring key elements of information reporting including data assurance, presentation and validation are delivered within national guidance and standards. Validation of 18 week referral to treatment time (RTT) and cancer pathways through audit, validation and education of both clinical and non-clinical teams. Information Governance The Information Governance Toolkit Assessment Report overall score for 2017/18 was 74%, an improvement of 3% in comparison to last year. 35

36 Patient Safety Incidents The Trust aims to provide care that is safe, effective and high quality for all patients and service users. The Trust s risk management system is designed to support this aim and is based on an open, honest, transparent culture of learning from experience underpinned by a systematic approach to managing Patient Safety Incidents. This cultural approach fully adheres to national guidance from a staff and patient perspective, including the Management of Health and Safety at Work Regulations (1974) and the Sign up to Safety campaign. Serious incidents in healthcare are relatively uncommon but when they do occur the NHS has a responsibility to ensure that there are systemic measures in place for safeguarding people, property, NHS resources, and reputation. This includes responsibility to learn from these Patient Safety Incidents in order to minimise the risk of them happening again. The trust takes this responsibility very seriously. It continues to build its safety culture (i.e. a high level of incident reporting); and improve its reporting culture, which stresses the significance of effective incident management. Incident reporting is a fundamental tool of risk management, the aim of which is to collect information about adverse incidents, including near misses, ill health and hazards, which will help us to facilitate wider learning across the organisation. Figure 1 is taken from the latest National Reporting and Learning Service (NRLS) data report published in September 2017 for the period October March 2017 and shows the Trust to be above average for reporting of patient safety incidents. The latest report covers the 6 months between October 2016 and March Figure 1: Patient safety incidents per 1000 admissions for the period of 01 October 2016 to 31 March 2017 Trust London North West University Healthcare NHS Average 36
37 Previously the Trust was reporting in the bottom 25% of Trusts but has significantly improved its position over the past 24 months. Training is provided at induction and at each annual mandatory update. In addition, training is now targeted at those departments and services with low reporting or falling trends in reporting. Figure 1.1: Patient safety incidents reported onto the Trust s incident reporting system for the period of 01 April 2017 to 28 February 2018 London North West University Healthcare Trust Apr 2017 May 2017 Jun 2017 Jul 2017 Aug 2017 Sep 2017 Oct 2017 Nov 2017 Dec 2017 Jan 2018 Feb 2018 Figure 2 shows the incidents reported by degree of harm, comparing Trust performance with that of Acute (non-specialist) organisations and is taken from the latest National Reporting and Learning Service (NRLS) data report published September Figure 2: Incidents reported by degree of harm for Acute Teaching organisations for the period of 01 October 2016 to 31 March % 80% 70% 60% 50% 40% 30% 20% 10% 0% 76% 77% 21% 20% 2% 3% 0.3% 0.3% 0.1% 0.2% None Low Moderate Severe Death All Acute (non specialist) trusts LONDON NORTH WEST HEALTHCARE NHS TRUST As per best practice, the Trust uploads all relevant clinical incidents reported from its incident reporting system (Datix) to the NRLS system once a month. Recent analysis shows the Trust has been an outlier compared to the cluster for taking longer to upload the data to NRLS. Work has been undertaken to improve the Trusts reporting times and the next NRLS report will be analysed to determine the effectiveness of these actions. 37
38 If an incident is reported that, based on the initial information, appears to have resulted in Serious Harm or Death, the Trust will upload this incident to the NRLS earlier than the date of the next batch upload. This supports shared learning and an open and honest management of incidents and risk. Those incidents which resulted in Serious Harm or Death will be the subject of a detailed Root Cause Analysis investigation. It is not unusual to establish during the gathering of information for the investigation, or at a later stage that the harm suffered or the patient s death was not as a result of an untoward incident, but was as a result of the patient s condition or disease. At this point the incident record on Datix will be updated to reflect this new information, however, this update will not change the original record on the NRLS system and as a result there will be an over-reporting discrepancy between the number of incidents with Serious Harm or Death on the NRLS system compared to the more up to date information maintained by the Trust on Datix. There were a total of 7823 (increase from 7638 last year) incidents that occurred between 1 st October 2017 to 31 st March 2017 that were uploaded to the NRLS between 1st October 2016 and 31 st May Of these, 27 resulted in Severe Harm (down from 34 last year) and 19 contributed to the patient s death (up from 12 last year) as the result of an untoward incident. A monthly newsletter has been launched in 2018 with regards to safety incidents and learning that are published and disseminated to frontline staff. Figure 3 shows the top 5 types of incidents reported within our reporting cluster compared with the number reported by the Trust. The Trust profile does appear different from the cluster but the variance is attributed to a greater number of pressure ulcers reported due to the inclusion of community services in our acute organisation categorisation. It is worth noting that measures have been implemented over the past 2 years to reduce the number pressure ulcers developed, this has seen a general decrease in the number of pressure ulcers developed and with greater decrease in the most severe grades of pressure ulcers. There has been increased awareness and assessment for patients at risk of falling and such incidents have been reported under the category of patient accidents. This has resulted in a decrease in the number of falls patients bringing the Trust in line with the cluster with a significant reduction in the number of patient falls that have resulted in severe harm to them. The Trust has reported higher than the cluster for Access, Admission etc., and Infrastructure incidents. For the former category the highest reported issues have been the need to admit patients to beds that have breached the mixed sex accommodation requirements, delay in admitting and discharging patients and delay in transport services to discharge patients. 38
39 Figure 3: Top six patient safety incidents reported by % 20.0% 18.0% 16.0% 14.0% 12.0% 10.0% 8.0% 6.0% 4.0% 2.0% 0.0% 14.3% Implementation of care and ongoing monitoring / review 17.7% 17.2% 17.3% Patient accident 11.2% 14.4% Access, admission, transfer, discharge (including missing patient) 6.8% 13.4% Infrastructure (including staffing, facilities, environment) 10.7% 10.5% Medication All Acute (non specialist) trusts LONDON NORTH WEST HEALTHCARE NHS TRUST A number of actions were developed and undertaken resulting in increased incident reporting. There are ongoing efforts to improve staff awareness of incident reporting procedures, openness of reporting and to increase the number of incidents reported including: Reviewing areas of poor incident reporting as part of the Divisional Governance Deep Dive reports. Work is underway to upgrade the server supporting the Trust s incident reporting system (Datix) as increased capacity and responsiveness is required. Review of the incident and risk management training to further meet the demands of teams. Work with individual teams to review themes and trends of incidents reported and identification of lessons to learn e.g. patient s falls and pressure ulcers. The reporting of real-time data and learning from incidents reported to groups and committees with the responsibility for oversight of patient safety. In partnership with the Communications team, the publication of the lessons learned information. Development and implementation of a module within the Datix system to meet the requirements of Learning from all patient Deaths and developing procedures to share and learn from this information not just within patient safety, but also, audit and effectiveness and clinical claims. Further work planned: Focusing the work with Divisions to support specific groups of incident handlers to review and approve incident forms in a timely manner. Development of patient safety information dashboards within Datix to enable handlers and managers instant and real-time snapshots of incident activity within their areas of responsibility. 39
40 Building on the monthly publication of lessons learned information, developing web resources for all staff to access incident investigation reports, action plans and learning. Including updated resources for the Duty of Candour and Serious Incident management. Serious Incidents and Never Events A Serious Incident (SI) is an incident or accident involving a patient, a member of NHS staff (including those working in the community), or member of the public who face either the risk of, or experience actual, serious injury, major permanent harm or unexpected death on hospital, other health service premises or other premises where health care is provided. It may also include incidents where the actions of health service staff are likely to cause significant public concern. Not all SI will result in harm to a patient; consideration is given to the level of potential harm or disruption to service. These can include near misses, as well as looking at cluster events where a pattern of lower harm events are occurring. Clusters may become apparent during the management of individual incidents or whilst incident reporting is being reviewed at Divisional and Trust level. These are all events that the Trust believes to be worthy of investigation by an Independent Panel and/or falls into the category of an incident that must be reported to the local Commissioning agencies. Table 1 below shows the number of Never Events and SIs declared in April 2017 to March 2018 in comparison to April 2016 to March Table 1: Total number of Never Events and Serious Incidents declared in each year: Total Serious Incidents declared Of which the following number were Never Events April 15 to March 16 April 16 to March 17 April 17 to March 18 (MA to validate)
41 Table 2: Types of Serious Incident and Never Events declared during 2016/17: Serious Incidents Of the 93 SI s the following 4 were Type of Incident N o also Never Events Pressure Ulcers 22 Never Events Unexpected Death 12 Type of Incident N o Missed Diagnosis 10 Retained foreign object post Surgical &/or Treatment 10 procedure Error 2 Delayed Treatment 9 Unintentional connection of Unexpected Outcome 9 a patient requiring oxygen to 1 Delayed Diagnosis 8 an air flowmeter Other 4 Misplaced naso-gastric or Patient Fall 3 oro-gastric tubes 1 Breach of Confidentiality 2 Sub-optimal Care 2 Medication 1 Failure to Follow-up 1 The Trust has seen a reduction in most categories of Serious Incident over the past year with the biggest reductions in Pressure Ulcers and Patient Falls, however there has been increases in the categories of Missed Diagnosis, Delayed Diagnosis and very small increases in Surgical &/or Treatment Error, Unexpected Death, Breach of Patient Confidentiality. Work is underway on a Thematic Review of cases that come under Missed Diagnosis and Delayed Diagnosis, the aim of the review is to identify any common themes emerging from the investigations into these incidents that can be used to improve quality and safety of our services for patients. Last year a key theme in investigations into Serious Incidents was a failure to monitor patients appropriately and escalate signs of deterioration for the correct clinical assessment and treatment. As a result, the Trust s Deteriorating Patients Group reviews all SIs where this is identified as contributing to the incident. New policies and guidance, such as the introduction and standardisation of a single Early Warning Score, were developed and launched across the organisation and audits are undertaken to identify the impact on the quality of care in this area. There has been a reduction in the number of serious incidents reported as a result of a failure to monitor patients appropriately. In line with the recent publication by NHS Improvement (NHSI) of Reducing harm leading to avoidable admission of full-term babies into neonatal units, the Division of Women and Children s Services has reviewed the publication and their current guidance and practice against that published by NHSI. In response to the guidance the neonatal, obstetrician and midwifery and risk teams developed a weekly MDT meeting to review all of the term admissions in line with NHSI guidance, this MDT is now well established. 41
42 The team have undertaken regular audits and implemented changes in their practice as an outcome of these meetings: New Additional Postnatal Care and Transitional Care (TC) criteria established and appointing Nursery Nurses on the Post-Natal Ward. Establishing TC - Building work recently finalised. BAPM hypoglycaemia guidelines implemented. New NAS guidance developed and implemented. The Trust continues to review the Serious Incident reporting and management process to improve the timely management of these investigations. Although the Trust has not achieved the target of 100% of reports being submitted within 60 days there has been an improvement with the monthly total of overdue reports decreasing from 20 in March 2016 to 11 in March 2017 and 6 in March 2018*. The number of Serious Incidents reported has decreased. Work continues to support the shared learning with the launch of the monthly learning from our mistakes information. An audit will be carried out later in the year to analyse the quality of actions put into place as a result of investigations undertaken into Serious Incidents. *For comparison, data was taken from the point at the 1 st of each month. Patient Safety Alert Compliance Patient safety alerts are used to inform the healthcare system of recognised safety risks and offer appropriate guidance for the prevention of incidents that may result in severe harm or death to patients. These alerts are issued through the Central Alerting System (CAS) which is a web-based cascade tool utilised for issuing alerts, public health messages and useful safety information to the NHS and other healthcare organisations. Patient safety alerts can be issued for a number of reasons. Alerts can be issued for newly recognised patient safety issues, potentially where incidents have resulted in death or severe harm to a patient and where many healthcare providers will have limited knowledge or experience of the risk. Alerts can also be issued where there is a common problem occurring throughout the NHS and can be an important part of a wider programme of work. Systems and equipment are commonly subject to patient safety alerts where there are recognised errors or faults and would therefore require action to be taken to reduce the risk to patient safety. Coordination of patient safety alerts is carried out by the Corporate Governance Team who work with various Trust departments to facilitate compliance and monitor ongoing work or action plans used to address the issues raised. 42
43 NHS England Patient Safety alerts issued 2017/18 and the Trust s progress (as at 9 May 2018) Reference Title Date issued Response Deadline NHS/PSA/D/2017/006 NHS/PSA/RE/2017/004 NHS/PSA/RE/2017/002 NHS/PSA/W/2018/001 NHS/PSA/W/2017/003 NHS/PSA/W/2017/005 Confirming removal or flushing of lines and cannulae after procedures Resources to support safe transition from the Luer connector to NRFit for intrathecal and epidural procedures, and delivery of regional blocks Resources to support the safety of girls and women who are being treated with valproate. Risk of death and severe harm from failure to obtain and continue flow from oxygen cylinders Risk of death and severe harm from ingestion of superabsorbent polymer gel granules Risk of severe harm and death from infusing total parenteral nutrition too rapidly in babies 09/11/2017 Assessing Relevance 09/08/ /08/2017 Action Completed 11/12/ /04/2017 Action Completed 06/10/ /01/2018 Action Completed 20/02/ /07/2017 Action Completed 16/08/ /09/2017 Action Completed 08/11/

 and incorporated into the five CQC domains, assessing if the ward is safe, caring, effective, responsive and well-led")
44 Ward/Service to Board- Excellence Assessment Tool Delivering safe, effective and high quality care to patients is of paramount importance, and is one of the Trust s most important and key strategic objectives. The Trust must account for the quality of care it delivers to patients and ensure that care is both evidencebased, where possible, and appropriate to the needs of each individual patient. The Trust has been using the Perfect Ward App, a smart mobile application for conducting the Wards Excellence Assessment (EAT) and the Matron s Weekly Quality Walkabout since July The EAT questions have been aligned with the CQC key lines of enquiries (KLOEs) and incorporated into the five CQC domains, assessing if the ward is safe, caring, effective, responsive and well-led and given ratings if outstanding, good, requires improvement and inadequate. The methodology used during the assessment process includes the following: Observation of care given and patients documentation Discussion with patients and staff members Discussion with the Department Senior Sister/Charge nurse In order for the process of accreditation to be seen as objective, reviewers should not be operational in the areas they are assessing. To ensure the process is both robust and reflects clearly the standard of care being delivered within a clinical setting, performance and outcome data is also used alongside these audits and is triangulated with the information obtained during the assessment process. The first EAT Assessment via the Perfect Ward App was completed in October 2017 with action plans developed by the Ward Sister/Charge Nurse in conjunction with the Matron. The Head of Nursing and The Divisional Head of Nursing for the area have involvement with approval and monitoring of the performance against each action. In addition, it is a requirement that each action plan is discussed and progress reported and documented at monthly ward/unit meetings. Any area which achieved a red rating for any domain was asked to take immediate action to put improvement plans in place and re-assess the domain. In an endeavor to strengthen further the Ward to Board concept, the Chief Nurse and additional panels chaired by the Deputy Chief Nurse met with the ward managers and matrons to review progress with the action plans to ensure: Good practice is disseminated and areas of concern are reviewed and addressed from a corporate perspective. 44

45 Identification of themes across the clinical services, which require an organisational approach to resolve, for example issues relating to the nursing documentation. Provide the Chief Nurse with independent assurance in relation to the level of delivery, understanding, consistency and ownership of each of the fundamental standards at ward/department level. To ensure transparency each ward / department displays its individual results on the Quality Board. These are for patients, relatives and visitors to view as part of our drive to be more transparent and accountable for the standards on that ward. All the wards are currently being reviewed again to ensure that they meet the expected standards and continue with improvement plans as required. It is envisaged that this process will be continued quarterly to ensure expected standards are maintained. All Ward areas and Community Services also have a weekly Matrons Quality Walkabout inspection undertaken by their respective matrons which includes talking to staff and patients as well as observations and reviewing documentation. Work is in progress to roll out the Matrons Quality Walkabout and the EAT Assessment to all the Outpatient Areas within the Trust. 45
46 Safe Staffing Levels The Trust is compliant with regards to the National Quality Board (NQB) Guidance (July 2016) by ensuring that the Right staff, with the right skills, in the right place at the right time. Through the implementation of Daily Safety Brief, the Trust are able to review staffing, skill mix, patient acuity & dependency and caseload on daily basis. The Carter Report (February 2016), in which productivity and efficiency is an important element in improving standard of care, hence Care Hours per Patient Day (CHPPD) was introduced. Since May 2016, submission of care hours has become a national requirement in which the Trust is compliant. We now use the care hours to benchmark the wards within the hospitals and also against selected regional peers and national average. The Daily Safety Brief template is used cross site to include Bedded Units, Community Services and Allied Healthcare Professionals (AHPs). The organisation reviews comparative data on actual staffing alongside data that provides context for differences in staffing requirements, such as case mix (occupancy rates, caseload), patient movement and patient acuity and dependency. Systems are in place for managing and deploying staff across a range of care settings, ensuring flexible working to meet patient needs and making best use of available resources. It also allows frontline staff to escalate to senior managers of any concerns/issues in relation to staffing levels, demand and capacity impacting patient and staff safety. 46
47 The Patient and Staff Committee and the Trust Board receive a regular report on Safe Staffing levels from the Chief Nurse as part of the monthly Nursing, Midwifery and AHP Workforce Report. This report triangulates the staffing levels with quality and safety indicators including patient experiences and finance. Duty of Candour (DoC) The Trust has a contractual duty under the NHS Standard Contract to inform patients/relatives/cares if a safety incident occurs under NHS funded care that results in moderate harm, severe harm or death. The incident must be reported onto the incident management system (Datix). The patient or their family/carer must be informed within 10 working days of the incident being reported onto Datix and the initial notification must be a verbal apology. How do we measure compliance? Weekly audit of compliance against the DoC requirements is undertaken, the process involves identification of all incidents that may require DoC (graded moderate harm or above and all SI s), cleansing the data to confirm DoC is required. Datix is then checked to ensure that the DoC section has been completed as required. If this has not been done and the letter for evidence is not available Handlers and the Division are followed up to provide this. Fortnightly follow up continues with the Division until the DoC section in Datix is completed and the DoC letter is provided (DoC letter is uploaded to Datix). Out of a potential 379 incidents that required a DoC the Trust has breached the requirements on 16 occasions. Although these incidents did not meet the required timescale for providing an apology, the Duty of Candour was eventually fulfilled. How will we continue to improve? A repeat audit on DoC compliance, using the Datix system where the information is stored, has been undertaken by the Trust and conducted by the Quality and Safety Team for Brent, Harrow and Hillingdon Clinical Commissioning Group in December The results and recommendations from this will be reviewed and acted on by the Trust in Patient-led assessments of the care environment (PLACE) Patient Led Assessments of the Care Environment (PLACE) are self-assessments of a range of non-clinical services which contribute to the environment in which healthcare is delivered. They are carried out on an annual basis between February and June and NHS Digital oversees the process. The assessments are unannounced and the assessment team makes their decisions based entirely on the observations made at the actual time of the assessment. Patient Assessors make up at least 50% of the assessment team, thus providing us with an effective and independent patient voice. PLACE is also an integral part of the Trust s Quality Account, which demonstrates the Trust s commitment to continuous, evidence-based quality improvement. In addition, each year the 47


48 Trust identifies a PLACE Improvement Plan concentrating on the areas where improvement can be implemented and, where possible supported by investment. Cleaning services are provided across the Trust by Medirest, as part of a new Soft FM Contract, which commenced on 24 March Specific PLACE responsibilities have been included in this new Contract and there are KPIs within the Contract which concentrate on the achievement of the required cleaning standards. Supervisors have designated areas of responsibility and carry out joint technical cleaning audits with Matrons, Ward Managers and service heads in line with the NHS National Cleaning Standards. Independent and unannounced audits are undertaken by the Trust s Infection Prevention and Control and Facilities Teams. In addition the Trust s Excellence Assessment Tool (ward accreditation) and the Perfect Ward Application include modules on cleaning. The PLACE scores have demonstrated a steady upward improvement since Patient Catering services are also provided by Medirest as part of a new Soft FM Contract. It was disappointing to experience a fall in PLACE scores at Northwick Park & St Mark s Hospital in 2017, but the causes were clearly identified at the time of the assessment which related to conformance with Protected Mealtimes. As a consequence a Task and Finish Group, led by the Chief Nurse, initiated a structured development plan which has been instrumental in achieving changes relating to nutrition and hydration: A new Patient Protected Mealtimes and Beverages Policy has been launched, including the introduction of bells in the wards to support the process; The nutritional screening tool and food charts have been standardised across the Trust and compliance is now monitored through walkabouts and Matrons audits; Weigh-Day Weekends have been introduced across the bedded units; The first Trust Nutrition and Hydration Study Day was held in September 2017, which will now be held annually; Peer/external reviews (Healthwatch) relating to nutrition and hydration have been undertaken in some wards. 48
 What other says about the Trust Care Quality Commission Data Quality, information governance and Clinical Coding Staff Survey")
49 Part 4: Statements of Assurance Statements of assurance from the Board include: Review of Services Participation in Clinical Audit Participation in Clinical research Goals agreed with commissioners (CQUINS) What other says about the Trust Care Quality Commission Data Quality, information governance and Clinical Coding Staff Survey 49
50 Review of Services During 2017/18, London North West University Healthcare NHS Trust (LNWUHT) provided and / or subcontracted five services for adults and children: Emergency Department admitted patient care for planned and emergency treatment critical care non-admitted patient care Integrated Community Services The LNWUHT has reviewed all the data available to them on the quality of care in these NHS services. The total income generated from services listed below in 2017/18, represents 98.5% of the total income from patient care activities. These services covered the following specialties: emergency department anaesthetics (op only) anticoagulant service audiological medicine audiology breast surgery cardiology clinical genetics clinical haematology clinical oncology (previously radiotherapy) colorectal surgery community dental community paediatric Community TB Service critical care medicine diabetic medicine district nursing service endocrinology endoscopy ear nose and throat gastroenterology general medicine general surgery genito-urinary medicine geriatric medicine GUM & iintegrated sexual & reproductive health services gynaecology health visiting infectious diseases integrated dermatology integrated respiratory intestinal failure unit maxillofacial surgery medical oncology midwife episode neonatology nephrology neurology nutrition and dietetics obstetrics occupational therapy ophthalmology orthodontics paediatric audiological medicine paediatric cardiology paediatric clinical immunology and allergy paediatric diabetic medicine paediatric ear nose and throat paediatric endocrinology paediatric gastroenterology paediatric gastrointestinal surgery paediatric infectious diseases paediatric maxillofacial surgery paediatric medical oncology paediatric nephrology paediatric neuro-disability paediatric neurology paediatric ophthalmology paediatric respiratory medicine paediatric rheumatology paediatric surgery paediatric trauma and orthopaedics paediatric urology paediatrics pain management palliative medicine physiotherapy podiatry psychotherapy restorative dentistry rheumatology speech and language therapy stroke and rehabilitation service tissue viability trauma and orthopaedics trustplus urology vascular surgery 50
51 Clinical Audit and Effectiveness Clinical audit is an essential activity for all healthcare organisations, as it is used to evaluate clinical practice and identify areas for improvement. As an organisation we encourage all services to review the care they deliver by undertaking local clinical audits. During 2017 / 18 the Trust has conducted 272 local audits. In addition to the local audits, the Trust has participated in all relevant national clinical audits, as these audits allow services to compare their practice with other similar Trusts and to benchmark their services. Each year, the Healthcare Quality Improvement Partnership (HQIP) publishes a Quality Accounts List on behalf of NHS England detailing the National Clinical Audits, Clinical Outcomes Review Program s and registries that NHS England would like each health service provider to report on. During , a list of 65 national audits was published, of which 48 national clinical audits were applicable to the services provided by the Trust. During the period of April 1, 2017, to March 2018, the Trust participated in all 48 national clinical audits and all 7 national Confidential Enquiry. Not all of the national audits were applicable to each site; therefore participation has been broken down by site for the period: Central Middlesex Hospital participated in 96% (22/23) national clinical audits and 100% of national confidential enquiries which it was eligible to participate in Ealing Hospital participated in 100% (36/36) of national clinical audits and 100% of national confidential enquiries which it was eligible to participate in Northwick Park / St Mark s Hospital participated in 100% (47/47) of national national clinical audits and 100% of national confidential enquiries which it was eligible to participate in Below is a list of the Quality Account and National clinical audits that the Trust was eligible to participate in during : Table 1: The national clinical audits that Trust participated in are listed alongside the number of cases submitted and the percentage of cases required nationally Name of National Audit / Clinical Outcome Review Programme Acute Coronary Syndrome or Acute Myocardial Infarction (MINAP) Eligible to Participate Yes Central Middlesex 7/8 (88%) ( ) Ealing 324/378 (86%) ( ) Northwick Park/St Marks 804/1069 (75%) ( ) Adult Cardiac Surgery N/A N/A N/A N/A Adult Community Acquired No longer running in Pneumonia BAUS Urology Audits: Data to be Yes N/A N/A Cystectomy validated BAUS Urology Audits: Data to be Yes N/A N/A Nephrectomy validated BAUS Urology Audits: Data to be Yes N/A N/A Percutaneous nephrolithotomy validated 51
52 Name of National Audit / Clinical Outcome Review Programme BAUS Urology Audits: Radical prostatectomy BAUS Urology Audits: Urethroplasty BAUS Urology Audits: Female stress urinary incontinence Bowel Cancer (NBOCAP) Cardiac Rhythm Management Eligible to Participate Central Middlesex Ealing Yes N/A N/A Northwick Park/St Marks Data to be validated N/A N/A N/A N/A Yes Yes Yes N/A Data to be validated Data to be validated Submitted as one Trust Information not available 75/75 (100%) Case Mix Programme Yes N/A Child Health Clinical Outcome Review Programme Congenital Heart Disease Coronary Angioplasty/National Audit of Percutaneous Coronary Interventions Diabetes (Paediatric) (NPDA) Elective Surgery (National PROMs Programme) Endocrine and Thyroid National Audit Falls and Fragility Fractures Audit programme Fractured Neck of Femur CEM Audit Head and Neck Cancer Audit (HANA) Inflammatory Bowel Disease programme Learning Disability Mortality Review Programme Major Trauma Audit (TARN) Maternal, Newborn and Infant Clinical Outcome Review Programme Medical and Surgical Clinical Outcome Review Programme Mental Health Clinical Outcome Review Programme 57/57 (100%) 447/447 (100%) 280/280 (100%) 878/878 (100%) Yes N/A See NCEPOD information below N/A N/A N/A N/A Yes N/A 196/196 (100%) Yes Yes Yes Yes Yes Yes Yes Yes N/A N/A N/A N/A 128/128 (100%) 1388/1851 (75%) Data to be validated 30/30 (100%) 50/50 (100%) Submitted as one Trust Ongoing 699/699 (100%) 279/279 (100%) Data to be validated 30/30 (100%) 125/125 (100%) Trust-wide IBD Registry Submissions are continuous Trust-wide, audit in progress Yes N/A 185/185 (100%) Yes N/A N/A Yes Yes See NCEPOD information below See NCEPOD information below National Audit of Anxiety and To be nationally commissioned in (100%) 46/46 (100%)Perinat al 1/1 (100%) Maternal 52
53 Name of National Audit / Clinical Outcome Review Programme Depression National Audit of Breast Cancer in Older Patients National Audit of Dementia Eligible to Participate Yes Yes Central Middlesex Ealing Northwick Park/St Marks Submitted as one Trust Information not available 27/27 (100%) 47/50 (94%) Willesden 51/51 (100%) 19/19 (100%) National Audit of Intermediate Care (NAIC) Yes 47/50 (94%) Denham 23/23 (100%) Rehabilitation 43/43 (100%) Clayponds 1/1 (100%) STARRS 45 /45 (100%) Re-ablement National Audit of Psychosis N/A N/A N/A N/A National Audit of Rheumatoid & Early Inflammatory Arthritis To be nationally commissioned in National Audit of Seizures & Epilepsies in Children & Young To be nationally commissioned in People National Bariatric Surgery Registry N/A N/A N/A N/A National Cardiac Arrest Audit National Chronic Obstructive Pulmonary Disease Audit programme National Clinical Audit of Specialist Rehabilitation for Patients with Complex Needs following Major Injury (NCASRI) National Comparative Audit of Blood Transfusion programme: Red Cell Platelet transfusion in adult Haematology Patients Serious Hazards of Transfusion UK National haemovigilance National Diabetes Audit Adults: Foot Care, Inpatient, Pregnancy, Transfusion & Core Data National Emergency Laparotomy Audit National End of Life care audit National Heart Failure Audit Yes Yes Yes Yes Yes Yes Yes Not Participated Local Audit Only N/A N/A Combined with NP N/A 72/72 (100%) (Q ) 97/97 (100%) Data to be validated Trust-wide audit 37/37 (100%) 5/5 (100%) 1917/1917 (100%) 32/32 (100%) Yes N/A Ongoing Audit Yes 42/48 (88%) ( ) 283/387 (73%) ( ) 212/212 (100%) (Q ) 228/228 (100%) Data to be validated 31/31 (100%) 168/168 (100%) Ongoing Audit 641/789 (81%) 53
54 Name of National Audit / Clinical Outcome Review Programme National Joint Registry (NJR) National Lung Cancer Audit National Maternity and Perinatal Audit National Neonatal Audit Programme: Neonatal Intensive & Special Care National Ophthalmology Audit Eligible to Participate Yes Yes Central Middlesex 724/728 (99%) Ongoing Audit Ealing 8/8 (100%) Ongoing Audit Northwick Park/St Marks ( ) 22/41 (54%) Ongoing Audit Submitted as one Trust Information not available Yes N/A N/A 4678(100%) Yes N/A N/A Yes 580/denominator not available ( ) N/A 534/534 (100%) National Prostate Cancer Information Yes N/A N/A not available 435 / National Vascular Registry denominator Yes N/A N/A not available ( ) Neurosurgical National Audit Programme N/A N/A N/A N/A Non-Invasive Ventilation - Adults No longer Running In Oesophago-gastric Cancer (NAOGC) Yes Submitted as one Trust Information not available Paediatric Asthma No longer Running In Paediatric Intensive Care (PICANet) N/A N/A N/A N/A Paediatric Pneumonia No longer Running In Pain in Children (care in 34/34 emergency departments) CEM Yes N/A N/A (100%) Audit Pleural Procedures No longer Running In Prescribing Observatory for Mental Health N/A N/A N/A N/A Procedural Sedation in Adults Yes N/A 31/31 (100%) 51/51 CEM Audit Sentinel Stroke National Audit programme (SSNAP) Serious Hazards of Transfusion (SHOT): UK National haemovigilance scheme Yes N/A N/A Yes Combined with NP 5/5 (100%) Smoking Cessation No longer Running In /20 20/20 (100%) Cases (100%) Cases UK Parkinson s Audit Yes 38/50 16/50 (76%) PREMS (32%) PREMS N/A (100%) 227/227 (100%) 31/31 (100%) 44/44 (100%) Cases 17/50 (34%) PREMS 54
55 National Audits Reports received during National Clinical Audit Reports were published and put into action by the Trust during the period. Below is a summary of the main changes made as a result of these national audits to improve the quality of care Quality Accounts / National Audits Emergency and Ambulatory Care Division Date National Changes or improvements made to Service Site Audit Title Report clinical care: Published A&E Ealing National Severe Trauma Audit & Reporting Network (TARN) Dec-16 Training has been delivered to medical and nursing staff in the handling and assessment of spinal injury patients. The Trust now holds regular Trauma Steering Board Meetings and has worked to improve data entry compliance to this rolling national audit. Quality Accounts / National Audits Integrated Medicine Division Date Service Site Audit Title National Report Published National Comparative Audit of Blood Transfusion audit programme: Blood Trust-wide Patient Blood Transfusion management in Jul-17 adults undergoing scheduled surgery Physiotherapy Acute Adult Cardiology Northwick Park Central Middlesex National UK Parkinson s Audit National Myocardial Ischaemia National Audit Project Apr-16 Jan-17 Changes or improvements made to clinical care: Patients are now identified at Preoperative Assessment Clinics to ensure that one PBM measurement has been taken where appropriate, surgical teams have been given education with regards to low Hb transfusion thresholds and encouraging Hb checks between transfusions. The Trust has developed Induction Packs for patients with Parkinson s, which are accessible to all Physiotherapists. The Induction packs include areas on pathophysiology, progression, management and care, outcome measurements, physiotherapy intervention for Parkinson s patients. To improve the submission of data for this national audit, administrative staff have been appointed 55
56 Quality Accounts / National Audits Integrated Medicine Division Date Service Site Audit Title National Report Published Cardiology Central Middlesex Ealing National Cardiac Arrest Audit (NCAA) and National MINAP 2014 data Validation - REPORT National - MINAP- Myocardial Ischaemia National Audit Project National Cardiac Arrest Audit (NCAA) and National Coronary Angioplasty/National Audit of Percutaneous Coronary Interventions (PCI) Jan-Dec 2014 Jun-17 Jun-15 Jan-17 Jun-17 Apr-16 Changes or improvements made to clinical care: The service has now increase resuscitation training for staff and more staff now have exposure to simulation training on the Central Middlesex site. These changes are in line with other strategies being implemented to ensure patient safety post the closure of Intensive Care unit at the site. An additional 16 courses were run on the CMH and all targeted staff were trained. The Central Middlesex site achieved better than national results with 100% achieved overall in this audit. Catheter laboratory has appropriate staffing levels at the Ealing site, to enable timely angiography within 72 hours of a patients admission (where clinically indicated) and this access is monitored via monthly reporting. Both action plans completed in tandem as the recommendations were similar. As a result of a review of the quality of the data being collection, the service has updated the Data Forms. The findings of the review were communicated to staff to raise the standard of data collection. The service now reports all Cardiac Arrests within the Risk reporting system on Datix. All ward cardiac arrests incident information is used by ward teams identify areas of learning. Ward data for the incidences of cardiac arrest is reported back to deteriorating patient group for Trustwide learning. To reduce complications with these interventions, right and left radial artery access is advocated as the default access. Access is reviewed and discussed in Clinical Governance meetings to ensure service wide learning. 56
57 Quality Accounts / National Audits Integrated Medicine Division Date Service Site Audit Title National Report Published Cardiology Northwick Park Endocrinology Neurology Central Middlesex Ealing Central Middlesex National - MINAP- Myocardial Ischaemia National Audit Project National Cardiac Arrest Audit (NCAA) and National Coronary Angioplasty / National Audit of Percutaneous Coronary Interventions 2014 National MINAP Data Validation 2014 Data National Diabetes Audit Adult bedside and hospital Characteristics NADIA 2015 National Diabetes Foot Care Audit 2015 National UK Parkinson s Audit Dec-15 Jun-17 Apr-16 Dec-16 Mar-17 Apr-16 Apr-16 Changes or improvements made to clinical care: An additional Catheter laboratory has been established at the Northwick Park site, to enable timely angiography within 72 hours of a patient's admission (where clinically indicated) and this access is monitored via monthly reporting. Both action plans completed in tandem as the recommendations were similar. The service now conducts regular paediatric simulations at Ealing ED post the paediatric service closure. PILS training continues to be provided on the Ealing site on an on-going monthly basis for all relevant staff. To improve the data being submitted to this audit, a new database has been created and notes are now scrutinized to ensure that entries are not missed. To improve data completeness and the quality of the information being submitted to this audit, Nurse practitioners now enter the data, rather than administrative staff. As a result of this audit a new electronic prescribing system has been implemented to reduce the possibility of errors and the service continues to train clinical staff in medication use for Diabetes and insulin management. The Diabetic Foot Care Services is to operate all year round, new staff have been recruited to run this service and a long term business case has been developed for additional staffing. The Trust has employed a Nurse Specialist to work across the three acute sites to allow Parkinson's patients to access additional care. New standardised assessment tools have been agreed for use with Parkinson s Patients across the Trust. 57
58 Quality Accounts / National Audits Integrated Medicine Division Date Service Site Audit Title National Report Published Cardiology Northwick Park Endocrinology Central Middlesex Ealing Northwick Park National - MINAP- Myocardial Ischaemia National Audit Project National Cardiac Arrest Audit (NCAA) and National Coronary Angioplasty / National Audit of Percutaneous Coronary Interventions 2014 National MINAP Data Validation 2014 Data National Diabetes Audit Adult bedside and hospital Characteristics NADIA 2015 National Diabetes Foot Care Audit 2015 National UK Parkinson s Audit Dec-15 Jun-17 Apr-16 Dec-16 Mar-17 Apr-16 Dec-16 Changes or improvements made to clinical care: An additional Catheter laboratory has been established at the Northwick Park site, to enable timely angiography within 72 hours of a patient's admission (where clinically indicated) and this access is monitored via monthly reporting. Both action plans completed in tandem as the recommendations were similar. The service now conducts regular paediatric simulations at Ealing ED post the paediatric service closure. PILS training continues to be provided on the Ealing site on an on-going monthly basis for all relevant staff. To improve the data being submitted to this audit, a new database has been created and notes are now scrutinized to ensure that entries are not missed. To improve data completeness and the quality of the information being submitted to this audit, Nurse practitioners now enter the data, rather than administrative staff. As a result of this audit a new electronic prescribing system has been implemented to reduce the possibility of errors and the service continues to train clinical staff in medication use for Diabetes and insulin management. The Diabetic Foot Care Services is to operate all year round, new staff have been recruited to run this service and a long term business case has been developed for additional staffing. The Trust has employed a Nurse Specialist to work across the three acute sites to allow Parkinson's patients to assess additional care. New standardised assessment tools have been agreed for use with Parkinson s Patients across the Trust. 58
59 Quality Accounts / National Audits Integrated Medicine Division Date Service Site Audit Title National Report Published Respiratory Medicine (Acute) Trust-wide National Lung Cancer Audit - NCLA 2014 and 2015 Jan-17 Changes or improvements made to clinical care: Since the reporting of this audit, the Trust-wide compliance for Stage recorded has increased in 2016 to 89.1%. Cases are now discussed within the all-site Multi-disciplinary Team Meetings. Compliance across standards has increased in 2016 and proportion of patients seen by Nurse Specialist has risen to 61.7% in 2016 and this is continuing to grow. Work has been undertaken to improve data quality being entered for this audit. Care is being individualised to patients needs and this is being accurately recorded. Additional clinics now running and a new service to undertake EBUS (Endobronchial Ultrasound) has been established locally, which is more convenient for elderly and frail patients. Quality Accounts / National Audits Surgery Division Service Site Audit Title Date National Report Published Colorectal Surgery Gastroenterology Trust-wide Northwick Park National Bowel Cancer Audit Programme (NBOCAP) National Inflammatory Bowel Disease (IBD) programme (Biologics) Dec-16 Sep-16 Changes or improvements made to clinical care: The service now runs regular audits to ensure data completeness as there have been issues with the quality of data submitted for this audit. Regular spot checks are undertaken to ensure information is being populated correctly. A review of compliance with NICE Guidance found that the population presents with Stage 3 and 4 cancers and this has been raised with Primary Care providers. The service has now moved patients to biosimilars, following a huge project that took over a year to complete and resulted in a saving of 375k over 6 months. New biological multidisciplinary clinic started and pre-treatment screening rates are now 100%, with post-induction reviews and follow-up appointments being offered to patients. The service has purchases the Registry patient management system 59
60 Quality Accounts / National Audits Surgery Division Service Site Audit Title Date National Report Published General Surgery Ophthalmology Trust-wide Central Middlesex National Elective Surgery - PROMs - Varicose Veins National Ophthalmology Audit Sep-16 Jul-17 Changes or improvements made to clinical care: (PMS) and extensive staff training undertaken to track patients effectively. Quality of Life assessments now given via a patient questionnaire and is now a standard agenda item to review findings at IBD business meetings. To increase the participation rate, patients are now given questionnaires at preassessment as well as on admission. A new One-Stop-Varicose Vein Clinic is being initiated As a result of this audit the service now ensure that new trainees understand the importance of ensuring that all data is included and accurately recorded for this audit. The service now extracts data to the new nationally agreed format and is in the process of purchasing a new system to ease the submission of data for this audit. Quality Accounts / National Audits Women and Children Division Date Service Site Audit Title National Report Published Maternity Northwick Park Northwick Park MBRRACE-UK Saving Lives, Improving mothers Care report data National Pregnancy in Diabetes Audit (NPID) Jan-17 Dec-16 Changes or improvements made to clinical care: As a result of this audit joint Obstetric and Cardiology clinics have been set up and the clinics now use joint Care Plans for an integrated approach to the delivery of care and letters are now copied to all clinicians involved in a patients care to enhance communication between the teams. The Antenatal Care guide now has specific information on immunizations added to the document. An Immunization Clinic has been established at the Ealing site, so that all three acute sites now host these clinics. As a result of the Pregnancy in Diabetes audit, the Trust has sent written to GP's to support changes in practice at the Primary Care level. 60
61 Quality Accounts / National Audits Women and Children Division Date Service Site Audit Title National Report Published Paediatrics Ealing Northwick Park National Paediatric Asthma - BTS Audit National Paediatric Diabetes Audit Nov-16 Feb-17 Changes or improvements made to clinical care: Services have reduced the use of Chest X-Ray in suspected cases of Paediatric Asthma and changes have been made to patient information documents. Paediatric Diabetes patient documentation has been improved and new electronic systems have been used to engage adolescent patients. National Confidential Enquiries There were seven national confidential enquiries that the Trust was eligible to participate in during the period 1st April 2017 to 31st March 2018, as below: Table 2: NCEPOD studies that the Trust participated in and for which data was collected within the period are listed below. National Confidential Enquiries into Perioperative Deaths (NCEPOD) Studies Cancer in Teens and young adults (0-25) Heart Failure Perioperative management of surgical patients with diabetes Submissions Central Middlesex Ealing Northwick Park/ St Mark s Case list 0/0 (0%) 24/24 (100%) 44/44 (100%) Notes 0/0 (0%) 1/1 (100%) 0/0 (0%) Clinician questionnaire 0/0 (0%) 1/1 (100%) 0/0 (0%) Organisational 1/1 (100%) 1/1 (100%) 1/1 (100%) Initial information admissions / deaths and 3/3 (100%) 132/132 (100%) 348/348 (100%) further breakdown Case list 1/1 (100%) 30/30 (100%) 42/42 (100%) Notes 0/0 (0%) 5/5 (100%) 5/5 (100%) Clinician questionnaire 0/0 (0%) 5/5 (100%) 5/5 (100%) Organisational 1/1 (100%) 1/1 (100%) 1/1 (100%) Case list 50/50 (100%) 48/48 (100%) 165/165 (100%) Notes 6/6 (100%) 4/4 (100%) 4/4 (100%) Anaesthetic 6/6 (100%) 4/4 (100%) 4/4 (100%) questionnaire Surgical questionnaire 6/6 (100%) 4/4 (100%) 4/4 (100%) Organisational 1/1 (100%) 1/1 (100%) 1/1 (100%) Bowel Obstruction List of cases for Pilot 5/5 (100%) 119/119 (100%) 372/372 (100%) Pulmonary Embolism List of cases 2/2 (100%) 24/24 (100%) 57/57 (100%) 61
62 Table 3: Child Health Studies that the Trust participated in during National Confidential Enquiries Child Health Studies Mental Health in Young People Chronic Neurodisablity Study - Cerebral Palsy Submissions List of concurrent cases from A&E List of Concurrent cases from Urgent Care Retrospective Inpatient cases Case notes Clinician Questionnaires Organisational Central Middlesex NA NA 0/0 (0%) 0/0 (0%) 0/0 (0%) Ealing 14 (100%) NA 13/13 (100%) 2/2 (100%) 2/2 (100%) Adult 1/1 (100%) Child 1/1 (100%) Northwick Park/ St Mark s 40 (100%) 3 (100%) 43/43 (100%) 2/2 (100%) 3/3 (100%) Case list 2/2 (100%) 3/3 (100%) 13/13 (100%) Notes 1/1 (100%) 1/1 (100%) 7/7 (100%) Clinician questionnaire On-going clinician Questionnaires On-going clinician Questionnaires for patient admitted to another hospital Organisational 1/1 (100%) 0/0 (0%) 1/1 (100%) 0/0 (0%) 1/1 (100%) 10/10 (100%) 7/7 (100%) 3/3 (100%) Hillingdon Urgent Care Centre NA 10 (100%) N/A N/A 62
63 Research and Development (R&D) The Trust continues to exceed expectations with both patient recruitment targets and contribution to research in 2017/18. The number of patients receiving NHS services provided by the Trust in 2017/18 that were recruited to participate in research approved by a research ethics committee and Health Research Authority was 5,309. The Trust was involved in 103 research studies. Of these 71 (69%) were adopted onto the CRN portfolio and 32 (31%) not adopted. Twenty two (21%) of the total were commercially sponsored studies that brought in an income of 706,923. Fifty nine (57%) of the studies were given approval during the 2017/18. Research and Development also supported 30 service Evaluations and 26 Quality Improvement projects which include outputs from CQUINS. Quality Improvement projects and Service Evaluations have further demonstrated the enthusiasm of staff to improve the care we provide to our patients through implementation of improvements from these projects. We continue to work with our partners and grow our research portfolio in other specialties and new diseases areas across the Trust e.g Ophthalmology where the commercial activity has increased coupled with offering more choice to our patients for treatment. Commissioning for Quality and Innovation (CQUIN) A proportion of the Trust income is linked directly to Quality Improvement and Innovation Goals under the Clinical Quality and Innovation payment framework. The CQUIN programme for 2017/2019 included a two year programme identifying key priorities for national implementation. This was in conjunction with a proportion of funding being attributed to working collaboratively on Sustainable Transformation Programmes. Below are the programmes that have been implemented in 2017/18 and the improvement criteria for 2018/ Improving staff health and wellbeing Improve staff wellbeing through offer of occupational support for health initiatives. Make a positive change to staff survey results for well-being. 2017/18 Outcomes The Trust has seen a significant improvement in the number of staff responding to surveys and reported better outcomes for staff satisfaction this year. There have been extensive changes to the offer of interventions to improve staff wellbeing as well as instinctiveness to develop the culture and behaviour we want to see sustained through the HEART values. 63
, but below the national set target of 75% 2017/18 Outcomes The Trust has seen an improvement in outcomes for 2017/18 with over 50% of staff receiving a flu vaccination.")
64 Increase staff uptake on flu vaccine, 53.4% (March 2018), in comparison to previous year, 43.5% (March 2017), but below the national set target of 75% 2017/18 Outcomes The Trust has seen an improvement in outcomes for 2017/18 with over 50% of staff receiving a flu vaccination. This was teamed with the offer of 10 vaccines for tetanus to third world countries for every flu vaccine given which proved popular with our staff. Improving catering offers to staff and visitors to support healthy eating. 2017/18 Outcomes The Trust has worked with their leading catering providers to maintain and improve on this CQUIN and has met all requirements identified by lead commissioners 2. Reducing the impact of serious infections (Sepsis and Antimicrobial Resistance) This CQUIN aims to improve the number of patients receiving appropriate management for sepsis and monitor the use of antibiotic therapy through antibiotic stewardship Sepsis The target for 2017/18 programme is to sustain 90% of patients receiving screening for sepsis in both emergency and in-patient care, and administration of antibiotic therapy within 1 hour of assessment. The Trust has met the trajectory set for the year. Sepsis Screening Emergency Care 94% Antibiotic Administration 93% This is a great achievement given the pressure on both our emergency departments. Inpatient sepsis management also met the trajectory for 90% of patients being screened and administration of antibiotic therapy. 64
65 Antibiotic Stewardship The programme set a target for improved reduction in overall use of antibiotics and empiric review of patients drug charts to promote antibiotic appropriateness. The Trust achieved the trajectory for 100% of clinical notes being empirically reviewed. There was a reduction in overall antibiotic usage of 9% against a trajectory of 2%. The Trust has also reduced the usage of specific antibiotics within the programme by 3% against a trajectory of 1%. This has been achieved due to our antibiotic stewardship team comprising Microbiologists and Pharmacists who give expert advice to all consultants. 3. Improving Health Care for Patients with Mental Health Conditions The Trust has worked closely with Mental Health Partner Trusts to develop new ways of identifying and monitoring patients who attend emergency departments on a frequent basis. This process has seen the implementation of joint frequent attenders meetings with multi-agency representatives to plan and manage patient care and expectations. The programme of work has seen a reduction of attendance in the cohort identified within the pilot programme Programme Outcomes The result has been a review of processes to enable electronic identification of patients with Mental Health attendances which are used to discuss at the frequent attendance meeting. Since embedding regular meetings and care planning in September 2017, we have seen a sustained reduction in the total number of frequent attenders coming to Northwick Park Hospital ED (<10 attendees in the last 6 months, Sept 17 March 18)). We have also achieved a reduction in ED attendances for the specific mental health CQUIN cohort of 2%. 65
66 4. NHS Digital Programme Implementation of Electronic Referral Services (e- RS) This programme has the aim to improve patient access to outpatient services and with a target that from October 2018 there will be a paper free referral process in place. Achievements 2017/18 98% of clinics have been linked to enable e-referral processes Appointment slot issues have been identified on a weekly basis and reduction identified from baseline 43% to 20% at March Collaborative working has evolved with commissioners to support the implementation of E-Referral processes. We have identified the first services to go paperless from June 2018 and there is a communication process in place Reduction of appointment slot issues (ASI) and the increased use of e-rs by GP s 57% increase in bookings using e-referral system from 3529 in July 2017 to 6173 in March Advice and Guidance This programme incorporates the linking of services to enable GP s to receive advice and guidance. The Trust has linked all clinical services to enable the use of this service and will work in the coming year on the detailed information which can be uploaded to support referral pathways. Improving Safer Discharge This programme aims to improve the number of patients over 65 being discharged within 7 days of admission. The target was a 2.5% improvement from baseline data for Q3-Q4 2016/17 to Q3-Q4 2017/18. As part of this process the trust has implemented Discharge to Assess programme or Home First. Outcomes Baseline percentage of 68% of patients discharged within 7 days. Q3-Q4 Data shows an improvement to 72.5% of patients discharged within 7 days This is a 4.5% improvement from Baseline. CQUIN Programmes 2018/19 The Trust will continue to monitor stretched targets for 2018/19 for all of the CQUIN programmes for 2018/19 with the added improvement of reporting and monitoring Smoking Cessation and Screening of Alcohol Use There will be a continued proportion of CQUIN funding for Sustainability and Transformation Programmes with the remainder of funding for the schemes below 1a 1b Improve staff health & wellbeing Healthy food for NHS staff, visitors and patients 5% improvement in 2 of 3 Staff Survey questions on H&W, MSK & Stress (Qs 9a, 9b and 9c) from 2015 baseline. Maintain the 4 changes required in 16/17 plus introduce 3 new changes to food and drink 66
67 provision from c Improve Flu vaccination uptake Improve the uptake of the flu vaccine amongst staff 2a 2b 2c Timely identification of sepsis Timely treatment of sepsis Antibiotic review of patients with sepsis 2d Reduce antibiotic consumption per 1,000 admissions (AMR) 4 Improve services for people with MH needs presenting in A&E Reduce the impact of serious infections (antimicrobial resistance and sepsis) Reduce the impact of serious infections (antimicrobial resistance and sepsis) Measure % of antibiotic prescriptions documented and reviewed by a competent clinician within 72 hrs. Reduce antibiotic consumption per 1,000 admissions by measuring total antibiotic usage, carbapenem & pip-taz usage. Reduce attendances at ED by patients with a primary mental health need 6 Advice and Guidance (A&G) Work with commissioners to set up and operate A&G services for non-urgent GP referrals using ERS or alternative platform. 7 E-Referrals Increase proportion of GP referrals made via E- referrals and reduces slot issues to no more than 4%. Implement paperless referrals by Oct a Supporting Proactive and Safe Discharge Acute Providers Increase proportion of >65 year old emergency inpatients who are discharged to their usual place of residence within 7 days. Also incorporates Electronic CDS submissions for ED. 9a Tobacco screening Record the smoking status of inpatients 9b Tobacco brief advice Record whether brief advice given to inpatients who have been recorded as being smokers. 9c Tobacco referral and medication offer Record whether inpatients are referred to smoking cessation services and which are offered smoking cessation medication. 9d Alcohol screening Record whether inpatients have been screened for drinking risk levels and whose results are recorded in local data systems. 9e Alcohol brief advice or referral Record whether inpatients with high risk levels have been provided with advice or referral to support services. 67
68 Sustainability and Spread The Trust has evidenced sustained change in the management of patients with Heart Failure which has led to improvements in mortality and readmission rates for patients. This has also led to an improvement in National Audit outcomes and has led to the Trust being invited onto regional programme boards to enable spread of best practice. Patient involvement has enabled the Trust to engage, discuss and develop training programmes to support staff in understanding self- management programmes. 68
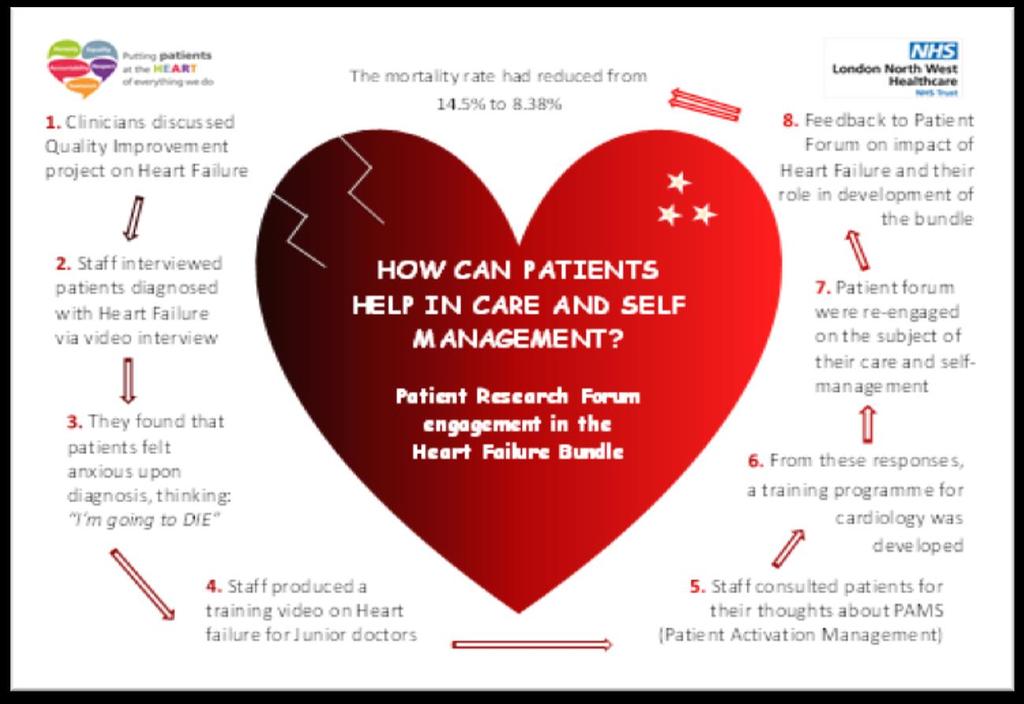

69 69
70 Access to seven day services This is a national programme of work which was undertaken following the Academy of Royal College recommendations of the implementation of four clinical standards which should be implemented as a priority to improve access to patient care. The Trust completes the National Audit for seven day services twice a year and reports findings through the governance process to the executive board. The standards are: Standard 2. Time to Consultant review Standard 5 Access to diagnostics Standard 6. Access to Consultant directed interventions Standard 8 Ongoing review. The Trust completed both audits for the year 2017/18, the first taking place in March This reviewed all 4 standards. The National Audit in September 2017 asked for Standard 2 to be audited only. Time to Consultant Review This standard identifies the need for 90% of patients to be reviewed by a consultant within 14 hours of admission. The Trust met the standard in September 2016 and March 2017 but reported that 89% of patients received a consultant review within 14 hours of admission. This was analysed and work plans reviewed to enable improvement ahead of the next audit in April- June When these results are benchmarked against the National reported data and London Commissioning Regional mean, the Trust is performing better than other Trusts and is seen as an exemplar site. Access to diagnostics The Trust has identified that there is access to diagnostic interventions week days and weekends covering the key areas for intervention within the standard. Access to Consultant directed interventions and Ongoing Review The data for March 2017 when this was last audited showed a 100% of patients had received a review by one of the designated clinicians as part of a consultant led team. It was noted that provision for those specialties where there was not seven day provision was delegated to the Acute Medical or Surgical Teams. This follows the seven day model of care signed up to by the London Region. The overall proportion of patients who required twice daily consultant reviews and were reviewed by a consultant was 100%. 70
71 Seven day service audit The Trust has identified a deterioration in the percentage of patients receiving consultant review within 14 hours of admission reported in September 2017 audit meeting 89% against a 90% standard. There has been a change to work plans to support improvement in meeting this standard and will be a focus of the April audit All other standards were fully met. The Trust will continue to audit patient care using the National Audit timeframe for audit and reporting in 2018/19. The next audit is due to be completed in April 2018 and uploaded in June This will be a full audit of all standards. The report outcomes will be released in August 2018 and a further audit will be completed in September 2018 and March
72 What others say about the Trust? LNWUH NHS Trust is fully registered with the Care Quality Commission (CQC), and there are no conditions attached to the CQC registration. The full report of the CQC formal inspection of LNWUH NHS Trust undertaken in October 2015 was published and provided to the Trust in June The table below outlines the overall report outlined below. Overall rating SAFE EFFECTIVE CARING RESPONSIVE WELL LED Requires Improvement Requires Improvement Requires Improvement Good Requires Improvement Requires Improvement In January 2016, the Trust responded to the following issues raised in a letter by the CQC which included (1) the provision of expert support for consultant radiologists at weekends, (2) sufficient trained and experienced medical and nursing cover on the High Dependency Unit all times and (3) ensuring that reportable incidents are reported within the Surgical division. The Trust immediately responded to take action to resolve these issues as a priority and has continued to monitor all of these areas of practice within the relevant divisional and board committee meetings. The Trust has made significant improvement in many areas in response to the LNWUH CQC inspection full report publication in June The Trust monitors the progress of the CQC action plan within the appropriate Trust Board Committees which meet monthly/bimonthly to ensure due diligence and progression. In addition, the Trust had a regular meeting with the Clinical Commissioning Groups (CCGs) and NHSI to provide information on the progress with the action plan, to ensure that all stakeholders are informed and engaged appropriately. The CQC Insight for acute provider was launched in 2017 and the Trust has utilised the information for monitoring performance on CQC key lines of enquiry (KLOE) and five domains. Trust data in the CQC Insight is now discussed in the Clinical Quality & Risk Committee including improvement plan from the relevant Divisions and services. The Trust received a Provider Information Request (PIR) in March 2018 in advance of the CQC inspection in June The PIR were composed of a Universal PIR, acute and community PIR which were completed and together with requested documents were uploaded on time through a secured CQC portal. Following submission of requested PIR, the Trust has responded to all CQC queries and submitted further requested additional information. The Trust was visited by CQC inspectors in June Approximately 60 inspectors visited the acute sites, community bedded units and community dental services. A well led interview is scheduled in July

73 Friends and Family Test The Friends and Family Test allows the patient s voice to be heard promptly and at volume: 70,114 patients completed the survey this year with 94 per cent saying they would recommend our services to their friends and families. What is more important is to understand the reasons and the feelings under the ratings and the patient perspective on a range of areas of their experience. This valuable data has been analysed and is now reported monthly to the divisions to inform and motivate service improvements. Not all patients are asked every question, but overall those contributing gave a 95 per cent rating for feeling safe, being treated with dignity and respect and with kindness and compassion. Less positively, patients report that they would like to feel more involved in decisions about their care and have more information, which are two areas we will now address. Patient Involvement and Engagement Strategy The Trust is committed to ensuring that patients are at the HEART of everything we do and to engaging them not only in decisions about their treatment and care but also to developing and improving Trust services. This year we plan to engage with patients, relatives, carers and other stakeholders to co-design a Patient Involvement and Engagement Strategy. This will be a practical plan for true partnership working. Always Event The Trust will continue to work with staff and patients to identify what really matters to patients and families at discharge and to work towards delivering this every time. Information Governance toolkit The Information Governance Toolkit draws together the legal rules and central guidance set out by the Department of Health Policy and presents them as a single standard containing a set of Information Governance requirements. The assessment measures compliance, and provides commissioners and the public assurance that the organisation handles information correctly, protects against unauthorised access, loss damage and destruction of data. This is measured as satisfactory with a score of 66% or above. In 2017/18 the Trust improved the score by 3% to 74%. 73

74 STAFF SURVEY 2017: Summary of Results Annually the Trust collects the views and experiences of staff working in the organisation. In 2017, more than 8000 staff were invited to take part in the survey, with more than 3800 staff responding. Consequently, the Trust saw a 12% increase in its response rate when compared to the previous year and other organisations. The survey results indicate increased engagement levels when compared to the previous year and improved staff motivation when compared to other organisations. This is important as high levels of staff engagement and motivation correlate to better-quality patient care. The most notable area of improvement since the last staff survey is in the number of staff recommending the organisation as a place to work and receive treatment. The survey also tells us that more of our staff report satisfaction with the quality of work and care they are able to deliver. Additionally, there is also an increasing trend in staff reporting experiencing high quality of appraisals and training when compared with other Trusts. As in previous years, more of our staff are reporting experiencing violence and bullying when compared with other trusts. This is important as it enables the organisation to know this is taking place and take action. A year on from the launch of our HEART values (underpinned by core the NHS Constitution) 95% of our staff say they are aware of our values. This awareness further supports a positive culture in the work place which promotes improved patient care. Top five ranking scores in 2017 Trust LNWUH Combined acute and community Trust National Median KF2 Staff satisfaction with the quality of work and care they deliver KF4 Staff motivation at work KF12 Quality of appraisal K13 K24 Quality of non-mandatory training learning and development % of staff/colleagues reporting recent experience of violence % 67% Improvements since Q3a Always know what work responsibilities are 87% 89% + Q3b Feel trusted to do my job 91% 93% + Q4a Opportunities to show initiative frequent in my role 72% 74% + 74
75 Q8b Communication between senior management 38% 41% + and staff is effective Q8d Senior managers action on staff feedback 29% 32% + Q10c Don't work any additional unpaid hours per 34% 37% + week for this organisation, over and above contracted hours Q13c Would feel confident that organisation would 50% 54% + address concerns about unsafe clinical practice Q20e Appraisal/performance review: organisational 28% 32% + values definitely discussed Q21a Care of patients/service users is organisation's 68% 71% + top priority Q21b Organisation acts on concerns raised by 66% 70% + patients/service users Q21d If friend/relative needed treatment would be happy with standard of care provided by organisation 56% 60% + Bottom five ranking scores 2017 The results were not all good news as when compared with other trusts more of our staff said they had experienced harassment and bullying from patients and the public, were witnessing potentially harmful errors and near misses and were working extra hours. In addition, there was an increase in the number of staff who said they were experiencing discrimination at work. The results also indicated that the Trust needs to take more action around staff health and wellbeing. Combined acute LNWUH &community trusts (National Median) KF16 Staff working extra hours 76% 71% K19 Organisation and management interest in and action on health and wellbeing KF20 Staff experiencing discrimination at work 22% 10% K25 K28 Staff experiencing harassment, bullying or abuse from patients, relatives or the public Staff witnessing potentially harmful errors, near misses or incidents 33% 27% 34% 29% Corporate Action Plan for Improvement An organisational wide action plan has been developed to address our five bottom findings. Nevertheless, each division/directorate/care group has been charged with developing local action plans for their own areas. A separate action plan has been developed to address negative findings from the Workforce Race Equality Standards (WRES). 75
76 Corporate Action Plan for Improvement Key themes Staff experiencing harassment, bullying or abuse from patients, relatives or the public Target zero tolerance campaign targeted at patients and the public around violence in hotspots Disseminate information and provide local training to staff on how to deescalate violence and aggression Set up a task and finish group to scope the problem, review incidents and agree on actions to reduce incidents. Systematically monitor incidents and work with hotspot areas to develop local action plans Success Criteria 5% reduction (over baseline) in the number of staff experiencing harassment, bullying or abuse from patients, relatives or the public Increase in appropriate reported incidents to allow targeted interventions within Divisions as appropriate Greater ability to triangulate findings from the staff survey to better target and further improve results Staff working extra hours Implement and continually review/ refresh a comprehensive recruitment plan for each of the Divisions Monitor working hours locally to avoid excessive hours being worked, and take action to remedy staffing issues locally Continue to reduce vacancies and time to hire Develop a retention initiative targeted at hard to recruit areas Reduction in the number of staff reporting working extra hours over current staff survey baseline Staff witnessing potentially harmful errors, near misses or incidents Care groups to regularly monitor and review DATX submissions and undertake root cause analysis to ensure where near misses incidents or errors occur, and put in place training for all staff to minimise recurrence Care groups to share learning from incidents and best practice and lessons learned at meetings Continue to run Schwartz rounds to encourage learning A reduction in the number of patient and/or carer complaints associated with errors A reduction in the number of staff witnessing potentially harmful errors, near misses or incidents over current staff survey baseline Staff more confident and empowered to report incidents through understanding of how this is used for learning 76
77 Organisation and management interest in and action on health and wellbeing Refresh and relaunch of the Trust Health and Well-being strategy and steering group to include achievement of the Health and Well-being CQIN Raise the profile of Trust health and wellbeing group Roll out Mindfulness workshops to staff and develop an in-house mindfulness coach. Continue to run staff H&W initiatives including the Virgin Global Challenge based on its success of last year. Increase in staff perception of organisational interest in health and wellbeing in next survey. Reduction in staff absences due to work related stress Improvements in results of stress audits Increase in staff participation in physical and mental well-being activities Staff experiencing discrimination at work Launch BAME positive action development initiatives for Senior roles Implement mandatory recruitment training for recruitment and selection panels Introduce requirement for visible BME on recruitment and selection panels Roll out career clinics targeted at staff at bands 2-4 Deliver WRES Action plan 2018/2019 2% reduction in BME staff believing staff does not offer career progression or promotion Identification of ten BME individuals to participate in the Trust talent management programme. 40% increase in the number of BAME staff at band 8 and above 77

78 Part 5: Looking forward - our plans for the future This section includes: Information on how the Trust consulted on the 2017/18 quality and safety priorities An overview of the Quality and Safety priorities for 2018/19 78
79 Proposed Quality and Safety Improvement Priorities for In 2017/18, the Trust reviewed its Quality Improvement Plans and continued monthly monitoring of the key indicators through the Clinical Quality and Risk Committee and Integrated Quality and Performance Report to the Trust Board and its committees. Priorities in the Trust s Quality and Safety Improvement Plan have been developed and consulted on internally, with external stakeholders including patient representatives and at a strategic level with commissioners. Workshops were conducted on different hospital sites and external stakeholders were invited together with LNWH staff from different specialties, services and sites. Below are the proposed quality and safety priorities for and this is divided under three categories; safer care, better outcomes and better patient experience. Priority one: Safer Care (Safe, Caring, Responsive and Well Led) CONTINUED FROM 2017/ Pressure Ulcer (PU) Why is it important? Pressure ulcers (PU) can develop when a large amount of pressure is applied to an area of skin over a short period of time. They can also occur when less pressure is applied over a longer period of time. The extra pressure disrupts the flow of blood through the skin. Without a blood supply, the affected skin becomes starved of oxygen and nutrients, and begins to break down, leading to an ulcer forming. Pressure ulcers tend to affect people with health conditions that make it difficult to move; especially those connected to lying in a bed or sitting for prolonged periods of time A large proportion of pressure ulcers are preventable and every effort needs to be made to ensure that they do not occur. What we aim to achieve in 2018/19 Zero incident Trust attributed avoidable grade 3 & 4 PU in acute hospitals 50% reduction in Trust attributed avoidable grade 3 & 4 PU in community services 50% reduction in Trust attributed avoidable grade 2 PU in the acute hospitals Increase staff compliance on PU prevention and management training Continued participation in the National Stop the Pressure campaign Review and implement the DH Safeguarding Adults and Pressure Ulcer Protocol Continued daily monitoring of PU incidents in the wards through the daily safety brief 79

80 1.2. Nutrition and Hydration Why is it important? Adequate nutrition and hydration is imperative for both the physiological and psychological health of our patients. It is vital we address potential barriers and obstacles that may restrict or prevent our patients receiving optimum nutrition and hydration. Up to 40% of adults have signs of malnutrition on admission to hospital and often their hospital stay makes this worse. Certain groups of patients, such as older people and those with certain physical health conditions, have particular dietary and eating requirements that need to be met to prevent malnutrition and dehydration and to aid recovery. NICE has shown that better nutritional care reduces complications and length of stay. NICE cost calculations show that better nutritional care is achievable with financial savings for the NHS What we aim to achieve in 2018/19 Promote Patient Protected Mealtime and Beverages and monitor through regular audit Invite peer/external review (Health Watch) with regards to nutrition and hydration 80
81 in the wards Standardise nutritional screening tool trust wide Improve staff compliance on conduct of patient nutritional screening assessment on admission i.e. weight and height Standardise food chart across the Trust bedded units and compliance monitored through walkabouts and Matrons audit Increase compliance on food and drink chart and monitored through the Matrons weekly quality walkabout CONTINUED FROM 2017/ Medicine Optimisation: Why is it important? Medicines are the most common therapeutic intervention and it is imperative that the Trust has assurance of the impact medicines have on the quality of care, patient safety and patient experience. The Trust will undertake a range of initiatives to improve medicines optimisation over the coming year. What we aim to achieve in 2018/19 Increase in the number of medication incidents and near misses reported during 2018/19 compared to 2017/18 by improving the reporting culture within the Trust in line with the HEART values Increase the range of methods used to feedback the lessons learned from reported medication incidents. Improve the level of patient satisfaction with the local medicine related patient experience measures during 2018/19 compared to 2017/18. Promote the local medication safety dashboard to reflect current medication related priorities, improve compliance with these standards during 2018/19 and provide feedback to clinical staff Reduction in antibiotic consumption per 1000 admissions median values measured quarterly compared to 2017/18 CONTINUED FROM 2017/ WHO checklist Why is it important? The introduction of the WHO Safer Surgery Checklist was a great step forward in the delivery of safer care for patients undergoing operations. Experience with its use has suggested that the benefits of a checklist approach can be extended beyond surgery towards all invasive procedures performed in hospitals. The aim of this priority is to strengthen the commitment of clinical staff to address safety issues within clinical settings that conduct invasive procedures. This includes improving 81
82 anaesthetic safety practices, ensuring correct site surgery, avoiding surgical site infections and improving communication within the team. Continuous safety improvement depends on continuous audit of outcome and compliance with safety standards, and on the collection and analysis of data on adverse patient events and near misses. What we aim to achieve in 2018/19 Monitor compliance on WHO Surgical Safety Checklist across hospitals sites Improve compliance on WHO Surgical Safety Checklist Development and monitoring of surgical safety checklist compliance in the maternity services Development and monitoring of surgical safety checklist compliance in o Endoscopy o Ophthalmology o Interventional radiology o Inpatient wards o Cardiology (cath lab) o Emergency Department Priority two: Better Outcomes - (Effective Safe and Caring) CONTINUED FROM 2017/ Deteriorating Patient Adult Why is it important? Patients who are admitted to hospital expect that should their condition deteriorate; they are in the best place for prompt and effective treatment. However, there are evidences that patients who are, or become acutely unwell in hospital may receive suboptimal care. This may be because their deterioration is not recognised, or because despite indications of clinical deterioration, it is not appreciated, or not acted upon sufficiently rapidly. Communication and documentation are often poor, experience might be lacking and provision of critical care expertise and including admission to critical care areas are delayed. Early recognition of a patient s deterioration through the use of observations will enable appropriate planning and escalation of care. The aim of this priority is to ensure early identification of a patient s deterioration through the use of observations to identify which patients require end of life support and to ensure end of life care plans are documented. 82
83 What we aim to achieve in 2018/19 Monitor number of Cardiac arrest calls and MET calls Review cardiac arrest calls outside critical care and identify themes and areas for improvement Reduction in number of cardiac arrest call (positive cardiac arrest call) Launched NEWS elearning module and monitor staff compliance uptake Review and implement NEWS2 trust wide in line with national guidance Improve Sepsis bundle compliance Review Acute Kidney Injury (AKI) bundle and improve compliance Monitor number of patients admitted to ITU/ICU for haemofiltration as a result of AKI and identify themes and areas for improvement Improve staff compliance on completion of the standardised LNWUH fluid chart CONTINUED FROM 2017/ Baby Friendly Initiative Why is it important? Infant and young child feeding practices have a strong impact on the nutrition status of children under 2 years of age as well as on their risk for infectious diseases and mortality The World Health Organisation (WHO) recommends that breastfeeding be initiated within 1 hour after birth, that breastfeeding be practised exclusively for the first 6 months of life followed by the introduction of safe nutritious complementary foods and that breastfeeding be continued until the child is at least 2 years old (WHO 2002). The WHO guidelines are backed up by a strong body of evidence indicating that optimal breastfeeding behaviours are strongly associated with lower incidence of gastrointestinal and respiratory tract infections as well as with child survival. There are several research studies demonstrating breastfeeding health benefits to the children and the mother. Baby Friendly Initiatives (BFI) are designed to provide parents with the best possible care to build close and loving relationships with their baby and to feed their baby in ways which will support optimum health and development. It s a unique programme designed to support breastfeeding and parent infant relations, therefore making the BFI accreditation status a nationally recognised mark of quality care. The overall goal for Northwick Park Hospital is to achieve a standalone accreditation BFI status in 2018/2019. What we aim to achieve in 2018/19 Maintain NPH Baby Friendly Hospital accreditation by UNICEF Increase the breastfeeding initiation rates by 2% from previous year Achieve 80% training compliance for eligible staff 83
84 Monitor and aim to reduce the incidence of re-admissions of new-born babies and mothers with breastfeeding related issues Promote user friendly public website with adequate information for new mothers and families CONTINUED FROM 2017/ Continence Care Why is it important? An ageing population, greater prevalence of bladder and bowel problems and the wide range of care groups affected, mean that continence services require a higher priority. Effective community-based continence services can save valuable NHS resources whilst restoring dignity to people and improving quality of life. Not all costs are financial and there is a large body of evidence about the effect of continence problems not just on the system but on people s lives. There can be considerable psychological impact and physical harm related to complications and treatments for continence problems which can lead to admission to hospital and care facilities for extended lengths of stay. What we aim to achieve in 2018/19 Monitor number of monthly new referrals to the Bladder and Bowel Service and identify trends Improve response time of the service in comparison to previous year Development of care pathway between primary community and secondary care Promote standardisation of continence care products across hospital sites and community CONTINUED FROM 2017/ Allied Health Professionals Why is it important? Allied Health Professionals (AHPs) are the next biggest clinical workforce in the Trust after nursing and midwifery. AHPs expertise and contribution in the management of patient care is vital in the speedy recovery of patients, reducing length of stay, inappropriate admissions and unnecessary care costs which are necessary to ensure affordable and sustainable NHS service in the future. AHP interventions can significantly reduce unnecessary hospital stay and diminish dependency on care services, resulting in significant savings. 84
85 What we aim to achieve in 2018/2019 Monitor therapist productivity (allocated and actual patient seen) and triangulate with staffing and workforce data 95% compliance on response time for therapy input within 24 hours from time of referral (bedded units) Improve waiting time for therapy input in community services Improve staff turnover rates and vacancy rates of therapist by March 2018 Maintain Ealing MSK interface Surgical Conversion Rates at 80% and onward referral into secondary care at 20% Address service historical service boundaries and reduce duplication and fragmentation Continue monitoring of dietetics activity (new referrals and total contacts received from inpatient wards/units) Priority three: Improved Experience (Caring, Responsive and Well Led) CONTINUED FROM 2017/ Dementia Why is it important? Dementia is a common condition that affects about 800,000 people in the UK. The risk of developing dementia increases as you get older and the condition usually occurs in people over the age of 65. Dementia is a syndrome (a group of related symptoms) associated with an ongoing decline of the brain and its functionality. Dementia is a significant challenge for the NHS with an estimated 25% of acute beds occupied by people with dementia. Their length of stay is longer than patients without dementia and they are often subject to delays in discharge when leaving hospital. Patients with dementia are also more likely to come to harm than patients without dementia. What we aim to achieve in 2018/2019 Increase staff training compliance on dementia Continue to monitor usage of carer s passport/agreement in the bedded units through the daily safety brief Increase staff compliance Confusion Care Pathway (CCP) implementation in bedded units Conduct of Carers experience survey to identify themes and areas for improvement Additional Reminiscence Interactive Therapy Activities (RITA) for elderly care patients in bedded units Monitor number of activities conducted 85
86 Monitor number of participants Development and implementation of Always Event incorporating standards that really matters to patients and families at patient admission and discharge CONTINUED FROM 2017/ End of Life Care Why is it important? Around 500,000 people die each year in the UK. Of these deaths, 75% are not sudden, but expected (NICE 2015). How we care for the dying is an indicator of how we care for all sick and vulnerable people. It is a measure of society as a whole and it is a litmus test for Health and Social Care services (DoH, 2008). End of life care helps people with advanced, progressive and incurable illness to live as well as possible until the moment of death. It facilitates the identification of the supportive and palliative care needs of the patient and his or her family and carers, and delivers the care required throughout the last phase of life and (for those left behind) into bereavement. The Trust has a duty to deliver high quality, equitable and compassionate end of life care to all patients. What we aim to achieve in 2018/2019 Increase percentage of patients who have died in acute setting for whom the Last Days of Life Care Agreement (LDLCA) was used to guide care Improved compliance with usage of Last Days of Life Care Agreement (LDLCA) in the acute hospitals Increase percentage of patients on pilot wards who have with completed ReSPECT/TEP documentation Increase percentage of patients known to Specialist Palliative Care Team who had a CMC record at the point of discharge Learning form rolling Survey of Bereaved fed back to the End of Life Care (EoLC) group End of life complaints collated, thematically analysed and reported to the End of Life Group every two months CONTINUED FROM 2017/ End Pyjama Paralysis Campaign Why is it important? We know that if patients stay in their pyjamas or gowns for longer than they need to, they have a higher risk of infection, lose mobility, fitness and strength, and stay 86
87 in hospital longer. But if we can help patients get back to their normal routine as quickly as possible, including getting dressed, we can support a quicker recovery, help patients maintain their independence and help get them home sooner. Ensuring patients get into their own clothes not only helps them to recover more quickly and changes how they are viewed by staff and the patient s family; it also has benefits for staff on the front line. It can help to build system capacity by improving patient flow, enabling more timely discharges, reducing the patient s length of stay, and enable more timely admissions for other patients. By getting patients into their own clothes and building their strength, as well as improving their mental outlook on the reason for their stay, it enhances the mental wellbeing of patients as they are encouraged to take greater responsibility for their own health and become active participants in their personal health journey. However, we do acknowledge that this is not always applicable to all inpatients in the acute hospital. What we aim to achieve in 2018/2019 Promote End Pyjama Paralysis Campaign in the bedded units trust wide Monitor the campaign through patients feedback captured by Matrons weekly quality walkabout Develop and implement monitoring of the number of patients dressed on their own clothes and had been mobilized in bedded units NEW IN 2018/ Patient Reported Outcome Measures (PROMs) Patient Reported Outcome Measures (PROMs) assess the quality of care delivered to NHS patients from the patient perspective. Currently covering four clinical procedures, PROMs calculate the health gains after surgical treatment using preand post-operative surveys. The four procedures are: hip replacements knee replacements groin hernia varicose veins PROMs have been collected by all providers of NHS-funded care since April PROMs measure a patient s health status or health-related quality of life at a single point in time, and are collected through short, self-completed questionnaires. This health status information is collected before and after a procedure and provides an indication of the outcomes or quality of care delivered to NHS patients. 87
88 What we aim to achieve in 2018/2019 Monitor Trust data with regards to the PROMs four procedures and reported to the relevant-board committee Improve performance with regards to PROMs indicators on the four procedures Development of improvement plan as result of the PROMs data by the relevant service and monitored by the Division NEW IN 2018/ Saving Babies Lives Care Bundle In November 2014, Secretary of State for Health announced a new ambition to reduce the rate of stillbirths by 50 percent in England by 2030, with a 20 percent reduction by Despite falling to its lowest rate in 20 years, one in every 200 babies is stillborn in the UK; this is more than double the rate of nations with the lowest rates. While the majority of women receive high quality care, there is around a 25 percent variation in the stillbirth rates across England. This presents us with opportunities to make improvements spanning both public health and maternity care services in order to make an overall improvement. The Saving Babies Lives Care Bundle addresses this variation by bringing together four key elements of care based on best available evidence and practice in order to help reduce stillbirth rates. It will support commissioners, providers and professionals in making care safer for women and babies. What we aim to achieve in 2018/2019 Review Saving Babies Lives care Bundle with an aim of adopting in the Trust Monitor compliance with regards to Saving Babies Lives a care bundle for reducing stillbirth compliance and performance Monitor Maternity service performance on Emergency caesarian section and benchmarked against national median/peers. 88

89 Part 6: Annex This section includes Amendments made and consultation Statements on the content of the Quality Account from our stakeholders. Trust response to the Stakeholders statements. 89
90 Amendments made following consultation The Trust would like to thank all stakeholders for their comments on the 2017/18 Quality Account. We are pleased that the statements from our stakeholders demonstrate the collaborative commitment we share in improving the quality of services we provide and the outcomes for our patients and that stakeholders are in agreement that the quality and safety improvement priorities for 2018/19 are the right ones. As a result of the formal stakeholder statements and additional comments and suggestions received to further improve the information in the Quality Account, the Trust has made the following amendments since the first draft sent to the stakeholders: Quality Account presentation on 2017/18 priorities performance reformatted to make it clear what we did aim to achieve, the actual performance and improvements delivered Inclusion of numbers and percentage to demonstrate measurable outcomes Removed duplications of table with regards to the quality improvement priorities performance Narrative with regards to NHS Outcomes Framework: Quality Indicators added The Quality and Safety priorities achievement in 2017/18 have been further updated Seven day service access have been added The priorities rolled over from last year are now indicated New priorities for this year are now clearly indicated As noted for next year we will: Solicit opinions and comments from the external stakeholders on the early stage of Quality Account development Reference to the areas that are mandated 90

91 Statements on the content of the Quality Account from our stakeholders 91
92 92

93 Healthwatch Brent s response to London Northwest Healthcare NHS Trust Quality Account for This is the response to London Northwest Healthcare NHS Trust (LNWH) Quality Account from Local Healthwatch Brent. We welcome the opportunity to comment on the quality of the services provided by the Trust. London North West Healthcare NHS Trust is one of the largest Trusts in the country. It includes Northwick Park, Central Middlesex and Ealing hospitals. As one of the largest integrated acute and community care Trusts in the country, it employs 1,300 doctors, 4,000 nurses as well as therapists, scientists and support staff to serve a diverse population of approximately 850,000. Its catchment area covers a range of vibrant and diverse communities, with over 100 first languages spoken, containing areas of great affluence as well as areas of much deprivation. The comments contained in this paper are the views of Healthwatch Brent and reflect our understanding of the needs and experiences of Brent residents, patients and service users. General comments We note the key achievements of the Trust over the past 12 months summarised including pioneering bilingual medicine labelling reflecting the diverse linguistic community the Trust delivers services to; Project Dayton with funding secured from Innovate UK to develop and pilot the WHO surgical safety checklist (WHO checklist) through a mobile app in partnership with Perfect Ward; an information booklet for new mothers leaving hospital with their babies to mention a few. Last year, we had suggested the Trust produce an Executive Summary against its priorities to make information about its performance more accessible to patients. We were disappointed to see that this was not done. It is always useful read the Trust s self-assessment. We note the Trust has reported on 57 targets of which they are working towards achieving 10 and have failed to meet one target and welcome its growing confidence. We note that it has been awarded the contract to provide a One-stop-shop for sexual and reproductive health in Brent, Ealing and Harrow and of course delighted that the Stoke Unit at Northwick Park Hospital scored 10/10 in its 2016 Acute Organisational Audit produced by the Royal College of Physicians which is reassuring given the population profile of the boroughs it serves. Last year we commented on the food and hydration and are pleased with the progress that has been achieved. The Nutrition and Hydration Day had been informed by the recommendations made by Healthwatch Brent in its Enter and View report on hospital mealtimes at Northwick Park and we anticipate that the Patient Led Assessments of the Care Environment scores to be published later in the year will confirm the improved direction of travel of the Trust in this instance. 93
94 As part of our recommendations last year Healthwatch Brent had suggested that it would have it would have been helpful if the Trust s data had been segmented into localities to better understand how it is performing in local area. The data presented is collated at its most strategic level which makes it difficult to interrogate with confidence. This recommendation was highlighted at Brent Council s Community and Wellbeing Scrutiny Committee in March Last year s priorities for We note the Trust s priority summarised in last year s Quality Account was to eliminate 90% of grade 3 and 4 pressure ulcers. It achieved the following: 60% reduction in the Trust attributed grade 3 and 4 PU and Nil Trust attributed grade 3 and 4 PU in the acute hospitals since July We note the concern raised by the Deteriorating Patient Group (DPG) to review the Assisted Kidney Injury (AKI) Bundle compliance against the latest evidence and format to improve usage in and are confident that the appointment of a new clinical lead to lead the AKI group will result in improvements. Last year, we expressed concern about the Trust s work on dementia but were heartened to read about the significant increase in staff training 2017/18 thereby achieving the set target and the measures that have been taken including the daily safety brief, monitoring the usage of carer s passport/agreement in the bedded units and increased compliance on the Confusion Care Pathway (CCP). The investment in an Activity Coordinator in the elderly wards has resulted in a significant increase in activities utilising the Reminiscence Interactive Therapy Activity (RITA) in NPH which has supported older people by reducing their agitation, isolation, depression and delirium. We note that End-of Life care has become a priority and targets achieved. Proposed priorities for The Trust is maintaining the same quality and safety categories but are focussing on Pressure Ulcers, Nutrition and Hydration, medicine optimisation, the WHO checklist, deteriorating patient adult, baby-friendly initiative, workforce development and improving care in relation to dementia, end of life care and the end pyjama paralysis campaign. We will view progress against these priorities with interest in the next Quality Accounts. Julie Pal, CEO, Community Barnet, Tel: Ext. 204, julie.pal@communitybarnet.org.uk Ian Niven, Manager, HealthWatch Brent, Tel: , ian.niven@helthwatchbrent.co.uk 94
95 Healthwatch Ealing Statement on London North West University Healthcare NHS Trust Quality Account Healthwatch Ealing is pleased to be able to respond to the London North West University Healthcare NHS Trust (LNWUH) Quality Account for The document demonstrates that the Trust is learning from feedback, incidents and complaints and is sharing the learning across the organisation to improve the quality of patient care. We enclose for consideration Healthwatch Ealing s recommendations for continued improvement and transparency: MRSA: MRSA reporting utilises orange ticks to signify improvement achieved but a comparative percentage with last year would have been useful. There appears no explanation about why the number of MRSA cases has doubled over the previous year [1.5 to 3.2] per 100,000 or why this figure is way above the national average of 0.9 per 100,000. What is the Trust strategy going forward to improve this situation as this subject appears to have not been addressed? NHS Outcomes framework: Use of a traffic light system (rather than using all blue) to show, at a glance, where improvement is required would be beneficial to improve accessibility. Perhaps a column outlining a clear performance target would be helpful. Safe staffing levels: Although compliant with data submission, there are no indications if the staffing levels were adequate. Staff survey results on page 73 indicate otherwise. For example issues of communication with management coupled with a high percentage of staff working extra hours and a low percentage of appraisal/performance reviews. PLACE Assessment results: Dignity and wellbeing targets require improvement across most sites. There is also some confusion on page 47 about the PLACE inspections concerning the food as they present three different scores for food [Food/Organisational Food/Ward Food] without any explanation about what each category means and which is the significant score to follow. Clarification around this would be hugely beneficial, making the accounts more accessible. Falls and Pressure ulcers: There does not appear to be much discussion about the number of falls that have been recorded and the fact that there has been a steady decline over the years, it is mentioned in passing along with pressure ulcers which have likewise improved, however to understand that this has happened you need to look at previous reports. Like areas of concern areas of positive practice and service improvement need to be highlighted for explanation and discussion. Readmission: There is no explanation why the "within 28 days readmission rate" for over 16 has increased from 8.0% to 11.8% even if this is well below the national average standing at 13.0%. Patient experience: There is no explanation of why the patient experience has dropped from 73.4% to 71.3% which now takes the Trust very close to the worst 95
96 performing Trust at 70.7% [0.6%]. What remedial measures are in place and has the trust engaged with their local Healthwatch to better understand this? Winter pressure: It would be interesting to have some analysis to see how the Trust performed during 2017/18 "winter pressure or how they intend to plan for the 2018/19 period. A&E delays: There appears to be no mention about the number of people that are experiencing long delays in A&E caused by breaches of the 30 minute ambulance handover times or the number of patients whose treatment/admission exceeds the 4 hour rule. Surely how A&E performs is an important issue particularly as long waiting times in A&E for treatment or admission can reflect on how well the rest of the hospital is functioning and leaves the question about number of beds available or sufficient staff on duty to be able to cope. In sections where is states partially achieved/not achieved, it would be useful to know when it is anticipated that these targets will be achieved. Feedback from patients and carers about the Trust s services During , Healthwatch Ealing collected feedback from local people about Ealing Hospital. It is helpful that the Quality Account contains information about the methods that the Trust uses to collect feedback from patients, carers and service users and examples of patient feedback and stories. The feedback collected by the Trust mirrors the positive experiences collected by Healthwatch Ealing and it is helpful to see what happens as a result of the feedback the Trust receives from patient experiences, complaints and compliments. It is not clear whether patient experience has influenced the areas chosen for the Quality Priorities for and we would like to see how feedback collected from patients, carers, service users and the public over the year is reflected in the final choice of priorities. During we hope to increase the amount of feedback we collect from local people about the services they receive from LNWUH to contribute to the delivery and review of care services, and we look forward to working more closely with the Trust to achieve this. 96
97 Abbreviations A&E Accident & Emergency A&D Acuity and Dependency ACAD Ambulatory Care and Diagnostic centre AHP Allied Health Professional AECU ambulatory emergency care unit AMU Acute Medical Unit AQuA Advancing Quality Alliance BADBIR British Association of Dermatologist s Biological Interventions Register BRCA National Breast Cancer Audit BSCN British Society for Clinical Neurophysiology BTS British Thoracic Society CCG Clinical Commissioning Groups CEM College of Emergency Medicine CEO Chief Executive Officer CHD Congenital heart disease CHPPD Care Hours per Patient Day CIP Cost Improvement Plans CLAHRC Collaboration for Leadership in Applied Health Research and Care CMP Case Mix Programme CMR Cardiovascular Magnetic Resonance COPD Chronic Obstructive Pulmonary Disease CPAU Chest Pain Assessment Unit CQC Care Quality Commission CQUIN Commissioning for Quality and Innovation CRM Cardiac Rhythm Management CSCNS Community Specialist Children Nursing Service CT Computed Tomography CT2 Core Medical Trainee Year 2 DAHNO Data for Head and Neck oncology DNA Did Not Attend DoLS Deprivation of Liberty Safeguards DTOC Delayed Transfer of Care DVT Deep Vein Thrombosis EAT Excellence Assessment Tool ECG Electrocardiogram ECHO Echocardiogram ED Emergency Department EDD Estimated Discharge Date EICO Ealing Integrated Care Organisation ERICE Education, Research, Innovation and Clinical Excellence FAIR Find, Assess, Investigate and Refer FFFAP Falls and Fragility Fractures Audit Programme FFT Friends and Family Test FY1 Foundation Year 1 (medical training) FY2 Foundation Year 2 97
98 GAS GP HCAI HES HMB HPV HSCIC IBD ICE ihv IMT IRP KPI LAS LDLCA LNWH LOLIPOP LVEF MBRRACE-UK MCAP MDT MHI MINAP MOCHA MRSA NAOGC NBOCAP NCAA NCEPOD NCISH NDIA NELA NEWS NHFD NHS NHSI NICE NIHR NIV NJR NLCA NOF NPDA NPH NPSA NQB OD Goal Attainment Scores General Practitioner Healthcare-acquired infections Hospital Episode Statistics Heavy Menstrual Bleeding Human Papilloma Virus Health & Social Care Information Centre Inflammatory Bowel Disease Intermediate Care Ealing Institute of Health Visiting Information Management Technology Independent Reconfiguration Panel Key Performance Indicator London Ambulance Service Last Day of Life Care Agreement London North West University Healthcare NHS Trust London Life Sciences Prospective Population Study Left Ventricular Ejection Fraction Mothers and Babies: Reducing Risk through Audit and Confidential Enquiries across the UK Managed Care Appropriateness Protocol Multi-disciplinary Team McKinsey Hospital Institute Myocardial Infarction National Audit Project Models of Child Health Appraised Methicillin Resistant Staphylococcus aureus National Oesophago-Gastric Cancer Audit National Bowel Cancer Audit Project National Cardiac Arrest Audit National Confidential Enquiries into Perioperative Deaths National Confidential Inquiry into Suicide and Homicide National Diabetes Inpatient Audit National Emergency Laparotomy Audit National Early Warning System National Hip Fracture Database National Health Service National Health Service Improvement National Institute for Clinical Excellence National Institute for Health Research Non-Invasive Ventilation National Joint Registry National Lung Cancer Audit Neck of Femur National Paediatric Diabetes Audit Northwick Park Hospital National Patient Safety Agency National Quality Board Organisational Development 98
99 PALS PBM PE PEWS PHSO PHE PICANet PICC PLACE PND POMH PROMS PTL R&D RTT SaHF SBAR SCBU SCPT SHMI SOAP SpR SSNAP STARRS TARN TB UCC UTI VTE WTE Patient Advice and Liaison Service Patient Blood Management Pulmonary embolism Paediatric Early Warning System Parliamentary and Health Service Ombudsman Public Health England Paediatric Intensive Care Audit Network peripherally inserted central catheter Patient Led Assessment of Care Environment Post-natal Depression Prescribing Observatory for Mental Health Patient Reported Outcome Measures Patient Tracking List Research & Development Referral To Treatment Shaping a Healthier Future situation, background, assessment, recommendation Special Care Baby Unit specialist community practice teacher Summary Hospital Mortality Indicator subjective, objective, assessment and plan Specialty Registrar Sentinel Stroke National Audit Programme Short Term Assessment, Rehabilitation and Reablement Services Trauma Audit & Research Network Tuberculosis Urgent Care Centre Urinary tract infection Venous Thromboembolism Whole Time Equivalent 99

100 Auditor s Opinion 100
101 101
102 102
Whittington Health Quality Strategy
 Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
Whittington Health Quality Strategy 2012-2017 Safe care Effective care Excellent patient experience...caring for you Quality Strategy for Whittington Health Introduction The purpose of this quality strategy
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
Quality Strategy and Improvement Plan
 Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Quality Strategy and Improvement Plan 2015-2018 STRATEGY DOCUMENT DETAILS Status: FINAL Originating Date: October 2015 Date Ratified: Next Review Date: April 2018 Accountable Director: Strategy Authors:
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Improvement Strategy
 / Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
/ Colchester Hospital University NHS Foundation Trust Quality Improvement Strategy 2015-2018 Including our four Quality goals Strategy Author Angela Tillett, Medical Director Version 1 Date of Issue -
FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 HOW WE MEASURE QUALITY 16
 Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Contents FOREWORD Introduction from the Chief Executive 2 BACKGROUND 3 OUR TRUST VALUES 4 OUR AIMS FOR QUALITY 5 - Our achievements so far - Our aims for quality 2017 2020 AIM 1: AIM 2: AIM 3: AIM 4: Reducing
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
QUALITY REPORT. Part A Patient Experience
 QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY REPORT Part A Patient Experience 1 Number of complaints Complaints and Patient Advice and Liaison Report 40 Total number of complaints received 30 20 10 Number of complaints received Trendline
QUALITY STRATEGY
 QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
QUALITY STRATEGY 2012-2016 SPONSOR: Sue Hardy Director of Nursing Signature: AUTHORS: Sue Hardy Director of Nursing Denise Flowers Associate Director Clinical Effectiveness APPROVED BY: Southend University
SUMMARY OF INDICATOR CHANGES FOR VERSION 3 INTELLIGENT MONITORING REPORTS Acute and Specialist NHS Trusts 23 June Final Draft, Subject to Change
 Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Never Event incidence Yes: 01 May 2013-30 Apr 2014 Incidence of Clostridium difficile (C.difficile) Incidence of Meticillin-resistant Staphylococcus aureus (MRSA) Dr Foster Intelligence: Mortality rates
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Quality and Safety Strategy
 Quality and Safety Strategy 2017-2020 Vision statement ESHT combines community and hospital services to provide safe, compassionate, and high quality care to improve the health and wellbeing of the people
Quality and Safety Strategy 2017-2020 Vision statement ESHT combines community and hospital services to provide safe, compassionate, and high quality care to improve the health and wellbeing of the people
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER
 Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
Quality Account 2016/17 & 2017/18 Quality Priorities
 Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
Quality Account 2016/17 & 2017/18 Quality Priorities Trust Board Item: 12 Date: 25 th January 2017 Enclosure: H Purpose of the Report: To provide the Board with the timeline for the creation of the 2016/17
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
The Care Values Framework
 The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
The Care Values Framework 2017-2020 1 States of Guernsey An electronic version of the framework can be found at gov.gg/carevaluesframework Contents Foreword from the Chief Secretary Page 05 Chief Nurse
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Our Achievements. CQC Inspection 2016
 Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
Our Achievements CQC Inspection 2016 Issued February 2017 HOW FAR WE VE COME SAFE Last year, we set out our achievements in a document for staff and patients. It was extremely well received, and as a result,
DIGITAL REMINISCENCE THERAPY (DRT) SOFTWARE PROJECT. Northwick Park Hospital Care of Elderly Wards
 SOFTWARE PROJECT. Northwick Park Hospital Care of Elderly Wards") DIGITAL REMINISCENCE THERAPY (DRT) SOFTWARE PROJECT Northwick Park Hospital Care of Elderly Wards Emily Fernandez Modern Matron Care of Elderly London Northwest Health care NHS Trust Northwick Park Hospital
DIGITAL REMINISCENCE THERAPY (DRT) SOFTWARE PROJECT Northwick Park Hospital Care of Elderly Wards Emily Fernandez Modern Matron Care of Elderly London Northwest Health care NHS Trust Northwick Park Hospital
QUALITY STRATEGY
 NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
NHS Nene and NHS Corby Clinical Commissioning Groups QUALITY STRATEGY 2017-2021 Approved: By the Joint Quality Committee on 11 April 2017 Ratified: By the NHS Corby Clinical Commissioning Group on 25 April
Patient Experience Strategy
 Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
Patient Experience Strategy 2013 2018 V1.0 May 2013 Graham Nice Chief Nurse Putting excellent community care at the heart of the NHS Page 1 of 26 CONTENTS INTRODUCTION 3 PURPOSE, BACKGROUND AND NATIONAL
We plan. We achieve.
 We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
We plan. We achieve. Salford Royal NHS Foundation Trust has a lot to tell you... l Achievements of 2008/09 l Our plans for 2009/10 l Our commitments for the next five years. We are committed to providing
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY
 Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Affiliated Teaching Hospital PATIENT EXPERIENCE AND INVOLVEMENT STRATEGY 2015 2018 Building on our We Will Together and I Will campaigns FOREWORD Patient Experience is the responsibility of everyone at
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Clinical Strategy
 Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Clinical Strategy 2012-2017 www.hacw.nhs.uk CLINICAL STRATEGY 2012-2017 Our Clinical Strategy describes how we are going to deliver high quality care in response to patient and carer feedback and commissioner
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Sustainable & Accessible Services. Strong Partnerships X X X
 SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item: 5.1 Report Title Prepared by Approved and Presented by ABMU Older Persons Assurance
SUMMARY REPORT ABM University Health Board Quality and Safety Committee Date of Meeting: 23 rd February 2017 Agenda item: 5.1 Report Title Prepared by Approved and Presented by ABMU Older Persons Assurance
Improving Patient Outcomes Strategy
 Improving Patient Outcomes Strategy 2015-2018 Hertford County I Lister I Mount Vernon Cancer Centre I QEII Improving Patient Outcomes Strategy 2015-2018 Page 1. Executive Summary 1 2. Introduction 2 3.
Improving Patient Outcomes Strategy 2015-2018 Hertford County I Lister I Mount Vernon Cancer Centre I QEII Improving Patient Outcomes Strategy 2015-2018 Page 1. Executive Summary 1 2. Introduction 2 3.
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Agenda Item: REPORT TO PUBLIC BOARD MEETING 31 May 2012
 Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
Agenda Item: 5.1.1 REPORT TO PUBLIC BOARD MEETING 31 May 2012 Title Lead Director Author(s) Purpose Previously considered by Ratification of the Strategy for the Care of Older People Siobhan Jordan, Director
Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36
 Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
Agenda Item number: 9.1. Maggie Bayley, Director of Nursing and Quality
 Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
Board meeting date: 15 December, 2011 Agenda Item number: 9.1 Enclosure: 6 Title Quality report Accountable Director: Authors(name & title): Maggie Bayley, Director of Nursing and Quality Maggie Bayley,
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Utilisation Management
 Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
Utilisation Management The Utilisation Management team has developed a reputation over a number of years as an authentic and clinically credible support team assisting providers and commissioners in generating
THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST QUALITY ACCOUNTS 2011/12
 THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST Quality Narrative QUALITY ACCOUNTS 2011/12 (WORKING DRAFT OF CONTENT) 1. Statement from the Chief Executive, and summary of the quality of NHS services
THE ROYAL NATIONAL ORTHOPAEDIC HOSPITAL NHS TRUST Quality Narrative QUALITY ACCOUNTS 2011/12 (WORKING DRAFT OF CONTENT) 1. Statement from the Chief Executive, and summary of the quality of NHS services
Whittington Health Trust Board
 Executive Offices Direct Line: 020 7288 3939/5959 www.whittington.nhs.uk The Whittington Hospital NHS Trust Magdala Avenue London N19 5NF Whittington Health Trust Board Title: 4 th March 2015 Sign up to
Executive Offices Direct Line: 020 7288 3939/5959 www.whittington.nhs.uk The Whittington Hospital NHS Trust Magdala Avenue London N19 5NF Whittington Health Trust Board Title: 4 th March 2015 Sign up to
ESHT Our ambition to be outstanding by 2020
 ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
You said We did. Care Closer to home Acute and Community Care services. Commissioning Intentions Engagement for 2017/18
 Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Commissioning Intentions Engagement for 2017/18 You said We did Care Closer to home Acute and Community Care services Top three priorities were: Shifting hospital services into the community Community
Presentation to the Care Quality Commission. Dr. Lucy Moore, CEO 15 September 2015
 Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Presentation to the Care Quality Commission Dr. Lucy Moore, CEO 15 September 2015 Our Improvement Journey- Key Messages We have Board, Executive and Divisional leadership teams now in place with serious
Improvement and assessment framework for children and young people s health services
 Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
Improvement and assessment framework for children and young people s health services To support challenged children and young people s health services achieve a good or outstanding CQC rating February
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
NHS Wales Delivery Framework 2011/12 1
 1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
1. Introduction NHS Wales Delivery Framework for 2011/12 NHS Wales has made significant improvements in targeted performance areas over recent years. This must continue and be associated with a greater
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR:
 MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
MINDING THE GAP COMMUNITY AND OLDER PEOPLE S MENTAL HEALTH SERVICE FRAMEWORK FOR: GOVERNANCE ASSURANCE AND PERFORMANCE. 1. INTRODUCTION AND CONTEXT Providing, delivering and developing the highest standards
INFECTION CONTROL SURVEILLANCE POLICY
 INFECTION CONTROL SURVEILLANCE POLICY Version: 3 Ratified by: Date ratified: July 2016 Title of originator/author: Title of responsible committee/group: Senior Managers Operational Group Head of Infection
INFECTION CONTROL SURVEILLANCE POLICY Version: 3 Ratified by: Date ratified: July 2016 Title of originator/author: Title of responsible committee/group: Senior Managers Operational Group Head of Infection
Quality Accounts April 2015 to March 2016
 Quality Accounts April 2015 to March 2016 Group Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2016. Our 2016 Quality Accounts provide a transparent picture of BMI Healthcare
Quality Accounts April 2015 to March 2016 Group Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2016. Our 2016 Quality Accounts provide a transparent picture of BMI Healthcare
Quality Account 2016/17. Best care by the best people
 Best care by the best people Quality Account 2016/17 NELFT NHS Foundation Trust Quality Account 2016/17 Contents Foreword from the chief executive Pages 4-5 Statement from the chief nurse 6 and executive
Best care by the best people Quality Account 2016/17 NELFT NHS Foundation Trust Quality Account 2016/17 Contents Foreword from the chief executive Pages 4-5 Statement from the chief nurse 6 and executive
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
OPERATIONAL PERFORMANCE REPORT: March Swindon Community Health Services Overview
 OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
OPERATIONAL PERFORMANCE REPORT: March 2018 Swindon Community Health Services Overview 1.0 Introduction This overview brings to the attention of committee members the key areas of Community Health Service
HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE 2016
 Appendix--75 Borders NHS Board HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE Aim The purpose of this paper is to update Board members of the current status of Healthcare Associated
Appendix--75 Borders NHS Board HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE Aim The purpose of this paper is to update Board members of the current status of Healthcare Associated
Quality Strategy (Refreshed March 2015)
") Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
Quality Strategy 2012-2017 (Refreshed March 2015) 1 Table of Contents 1. Executive Summary... 3 2. Drivers for improvement... 4 2.1 The Trust s ambition - vision and mission... 4 2.2 Corporate Strategy...
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
Eat, Drink, Move! Supporting people to keep well, in and out of hospital
 Eat, Drink, Move! Supporting people to keep well, in and out of hospital Helen Reilly, Therapy Lead and Professional Lead for Dietetics On behalf of HEFT Therapies Team Eat, Drink Move! Simple and transferable
Eat, Drink, Move! Supporting people to keep well, in and out of hospital Helen Reilly, Therapy Lead and Professional Lead for Dietetics On behalf of HEFT Therapies Team Eat, Drink Move! Simple and transferable
Announced Inspection Report care for older people in acute hospitals
 Announced Inspection Report care for older people in acute hospitals Hairmyres Hospital NHS Lanarkshire Healthcare Improvement Scotland is committed to equality. We have assessed the inspection function
Announced Inspection Report care for older people in acute hospitals Hairmyres Hospital NHS Lanarkshire Healthcare Improvement Scotland is committed to equality. We have assessed the inspection function
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
The Newcastle upon Tyne Hospitals NHS Foundation Trust. Clinical Assurance Toolkit (CAT) Strategy
 Strategy") The Newcastle upon Tyne Hospitals NHS Foundation Trust Clinical Assurance Toolkit (CAT) Strategy Effective: January 2014 Review: January 2015 1. Introduction The Trust s Nursing and Midwifery Strategy,
The Newcastle upon Tyne Hospitals NHS Foundation Trust Clinical Assurance Toolkit (CAT) Strategy Effective: January 2014 Review: January 2015 1. Introduction The Trust s Nursing and Midwifery Strategy,
Hip fracture Quality Improvement Programme. Update on progress one year on
 Hip fracture Quality Improvement Programme Update on progress one year on Mike Reed on behalf HIPQIP Steering Group March 2011 Introduction Hip fracture is a common condition in a frail and elderly group.
Hip fracture Quality Improvement Programme Update on progress one year on Mike Reed on behalf HIPQIP Steering Group March 2011 Introduction Hip fracture is a common condition in a frail and elderly group.
5 Boroughs Partnership NHS Foundation Trust. Quality Account Version: QA FINAL
 5 Boroughs Partnership NHS Foundation Trust Quality Account 2016-2017 Version: QA FINAL 1 Contents Part 1- Our Commitment to Quality 1.1 Our Quality Report / Quality Account 2016-17...5 1.2 Chief Executive
5 Boroughs Partnership NHS Foundation Trust Quality Account 2016-2017 Version: QA FINAL 1 Contents Part 1- Our Commitment to Quality 1.1 Our Quality Report / Quality Account 2016-17...5 1.2 Chief Executive
Learning from adverse events. Learning and improvement summary
 Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
Learning from adverse events Learning and improvement summary November 2014 Healthcare Improvement Scotland 2014 Published November 2014 You can copy or reproduce the information in this document for use
TRUST BOARD. Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director. Jo Hunter, Deputy Chief Nurse. Mary Heritage, Assistant Director of Quality
 TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
TRUST BOARD Document Title: Presenter: Quality Report Jo Hunter, Deputy Chief Nurse Authors: Contact details for further information: Jo Furley, Interim Chief Nurse Dr Ben Lobo, Medical Director Jo Hunter,
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16
 Schemes for 2015/16") Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Commissioning for Quality and Innovation (CQUIN) Schemes for 2015/16 Goal No. Indicator Name Contract 1 Acute Kidney Injury CWS CCG Contract - National CQUIN 2a Sepsis Screening CWS CCG Contract - National
Framework for NHS provider and commissioner involvement in: Maximising the appropriate use of care homes
 Publications Gateway reference number: 07483 Framework for NHS provider and commissioner involvement in: Maximising the appropriate use of care homes Cohort caring in Therapy-Led Units for inpatients ready/safe
Publications Gateway reference number: 07483 Framework for NHS provider and commissioner involvement in: Maximising the appropriate use of care homes Cohort caring in Therapy-Led Units for inpatients ready/safe
Changing for the Better 5 Year Strategic Plan
 Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Quality Care - for you, with you 5 Year Strategic Plan Contents: Section 1: Vision and Priorities for Change 3 Section 2: About the Trust 5 Section 3: Promoting Health & Wellbeing and Primary Care 6 Section
Group Chief Executive s Statement
 Group Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2016. Our 2016 Quality Accounts provide a transparent picture of BMI Healthcare s performance over the period covered
Group Chief Executive s Statement I am pleased to welcome you to our Quality Accounts 2016. Our 2016 Quality Accounts provide a transparent picture of BMI Healthcare s performance over the period covered
Claremont Private Hospital. Quality Account April March 2015
 Claremont Private Hospital Quality Account April 2014 - March 2015 Contents Welcome to Aspen Healthcare 2 Statement on Quality from the Chief Executive Aspen Healthcare 4 Introduction to Claremont Hospital
Claremont Private Hospital Quality Account April 2014 - March 2015 Contents Welcome to Aspen Healthcare 2 Statement on Quality from the Chief Executive Aspen Healthcare 4 Introduction to Claremont Hospital
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Quality Surveillance Team. Neonatal Critical Care (NCC) Quality Indicators
 Quality Indicators") Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
Quality Surveillance Team Neonatal Critical Care (NCC) Quality Indicators Neonatal Critical Care Quality Indicators Introduction These neonatal critical care quality indicators have been developed using
PAHT strategy for End of Life Care for adults
 PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
PAHT strategy for End of Life Care for adults 2017-2020 End of Life Care encompasses all care given to patients who are approaching the end of their life and following death, and may be delivered on any
Quality Strategy: Liverpool Women s NHS Foundation Trust
 Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
Quality Strategy: 2017-2020 Liverpool Women s NHS Foundation Trust Contents Foreword... 3 Our Trust... 4 Trust Board... 4 What is our Vision and what are our Aims and Values?... 5 The drivers in developing
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Open and Honest Care in your Local Hospital The Open and Honest Care: Driving Improvement programme aims to support organisations to become more transparent and consistent in publishing safety, experience
Specialist mental health services
 How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
Richard Wilson, Quality Insight and Intelligence Director
 To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
To: Board For meeting: 24 May 2018 Agenda item: 8 Report by: Richard Wilson, Quality Insight and Intelligence Director Report on: Quality Dashboard Purpose 1. This paper highlights the key observations
East Lancashire Clinical Commissioning Group. Quality Strategy
 East Lancashire Clinical Commissioning Group Quality Strategy 2016 21 1 CONTENTS Foreword 3 Executive Summary 4 Introduction 6 Local Context 7 National Context 8 What is Quality? 9 The Five Dimensions
East Lancashire Clinical Commissioning Group Quality Strategy 2016 21 1 CONTENTS Foreword 3 Executive Summary 4 Introduction 6 Local Context 7 National Context 8 What is Quality? 9 The Five Dimensions
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
Learning from Deaths Policy. This policy applies Trust wide
 Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Learning from Deaths Policy This policy applies Trust wide Document control page Name of policy Learning from Deaths Policy Names of linked Learning from Deaths Procedure procedures Accountable Medical
Quality Strategy
 Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
Quality Strategy 2017-2020 Contents 05 Foreword 06 Introduction 06 Equality & Diversity 07 Context for this Strategy 08 Definition of Quality 10 Quality Objectives 10 Strategic Quality Objectives 16 Quality
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT
 KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
KEY AREAS OF LEARNING FROM THE FRANCIS REPORT The public inquiry provided detailed and systematic analysis of what contributed to the failings in care at Mid Staffordshire NHS Foundation Trust. It identified
Quality and Leadership: Improving outcomes
 Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
Quality and Leadership: Improving outcomes Podiatry Managers/Allied Health Managers and Leaders 5 March 2014 Shelagh Morris OBE Acting Chief Allied Health Professions Officer 2 http://www.nhsemployers.org/aboutus/latest-news/pages/the-new-nhs-in-2013-infographic.aspx
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Strategy for Delivery of Clinical Quality and Patient Safety. North Norfolk Clinical Commissioning Group
 Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
Strategy for Delivery of Clinical Quality and Patient Safety North Norfolk Clinical Commissioning Group V5 Document Control Sheet Name of document: Quality Strategy 2016-18 Version: 5 Owner: Head of Clinical
GOVERNING BODY REPORT
 GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
GOVERNING BODY REPORT 1. Date of Governing Body Meeting 16 th November 2017 2. Title of Report: 3. Key Messages: BUPA ceased to be the registered provider of Crawfords Walk Nursing Home in October. The
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Date of publication:june Date of inspection visit:18 March 2014
 Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Jubilee House Quality Report Medina Road, Portsmouth PO63NH Tel: 02392324034 Date of publication:june 2014 www.solent.nhs.uk Date of inspection visit:18 March 2014 This report describes our judgement of
Sue Brown Clinical Audit and Effectiveness Manager. Safety and Quality Committee
 Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
Report to Trust Board of Directors Date of Meeting: 24 June 2014 Enclosure Number: 11 Title of Report: Clinical Audit Plan for 2014/15 Author: Executive Lead: Responsible Sub- Committee (if appropriate):
This SLA covers an enhanced service for care homes for older people and not any other care category of home.
 Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
Care Homes for Older People Service Level Agreement 2016-2019 All practices are expected to provide essential and those additional services they are contracted to provide to all their patients. This service
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT. 24 th July Dear Daniel, Fiona and Louise. Re: CCG Annual Assurance
 NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS England London Southside 4th Floor 105 Victoria Street London SW1E 6QT 24 th July 2014 Dear Daniel, Fiona and Louise Re: CCG Annual Assurance Many thanks for meeting with us on 6 th June 2014 to discuss
NHS Trafford Clinical Commissioning Group Quality and Performance Strategy S T rafford Clinical Commissioning Group
 De ce m be r 20 14 NHS Trafford Clinical Commissioning Group Quality and Performance Strategy N H 2015-2020 S T rafford Clinical Commissioning Group Version 2.0 Page 1 of 28 APRIL 2015 (RM) POLICY DOCUMENT
De ce m be r 20 14 NHS Trafford Clinical Commissioning Group Quality and Performance Strategy N H 2015-2020 S T rafford Clinical Commissioning Group Version 2.0 Page 1 of 28 APRIL 2015 (RM) POLICY DOCUMENT
St Gemma s Hospice Quality Account 2016/17
 St Gemma s Hospice Quality Account 2016/17 Part one I Overview 1 Contents Part One I Overview Statement on Quality from the Chief Executive Our Hospice Vision, Purpose and Values Our Services, Funding
St Gemma s Hospice Quality Account 2016/17 Part one I Overview 1 Contents Part One I Overview Statement on Quality from the Chief Executive Our Hospice Vision, Purpose and Values Our Services, Funding
Wolverhampton Clinical Commissioning Group - Care Home Document
 Wolverhampton Clinical Commissioning Group - Care Home Document 1 Contents Page 1. Purpose 2. Workstreams Completed 3. 2014/15 Workstreams 4. Future Workstreams 2 1. Purpose 1.1. Introduction 1.1.1. This
Wolverhampton Clinical Commissioning Group - Care Home Document 1 Contents Page 1. Purpose 2. Workstreams Completed 3. 2014/15 Workstreams 4. Future Workstreams 2 1. Purpose 1.1. Introduction 1.1.1. This