Increasing resident incident reporting. Michelle Brooks VCU Health Ashley Duckett MUSC Winter Williams UAB Starr Steinhilber - UAB
|
|
|
- Jason Fields
- 5 years ago
- Views:
Transcription

1 Increasing resident incident reporting Michelle Brooks VCU Health Ashley Duckett MUSC Winter Williams UAB Starr Steinhilber - UAB
2 What can we help you with?

3 An Incident...





4
5 Background - Incident Reporting IOM report - To Err is Human - 98,000 deaths/year due to medical error1 New studies - 200, ,000 deaths/year2 Underreporting is common3 Recommendation from IOM - establish reporting system4 Patient Safety and Quality Improvement Act of 2005
6 Background - Incident Reporting Identify safety hazards, prioritize where to focus resources, develop interventions, evaluate5 Anonymous web-based incident reporting tool6 Tradeoff between number & quality of reports7 Trend toward baseline - lack of sustainable QI efforts to improve incident reporting in literature8 Barriers
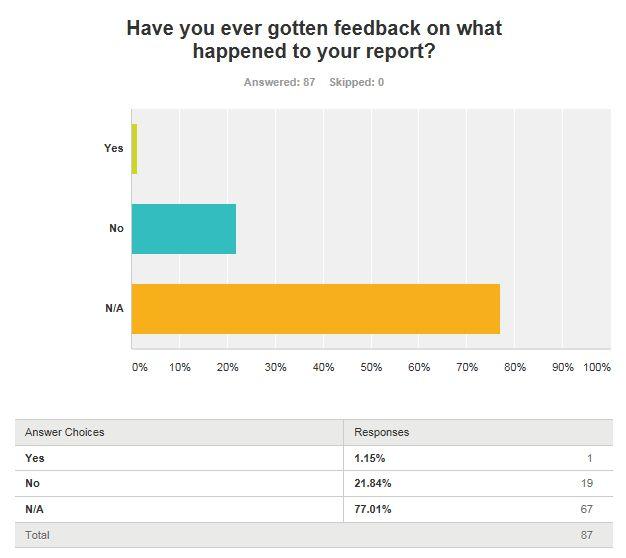
7 Background - CLER In general, residents and fellows lacked clarity and awareness of the range of conditions that define patient safety events and were unaware of how CLEs use the reporting of adverse events and near misses/close calls to improve systems of care, both broadly and at the individual departmental level. 9 Though most residents and fellows were aware of their CLE s process for reporting patient safety events, fewer of them appeared to have used it themselves to report events. When trainees did file a report, or have others file it for them, many received little or no feedback from the CLE. 9

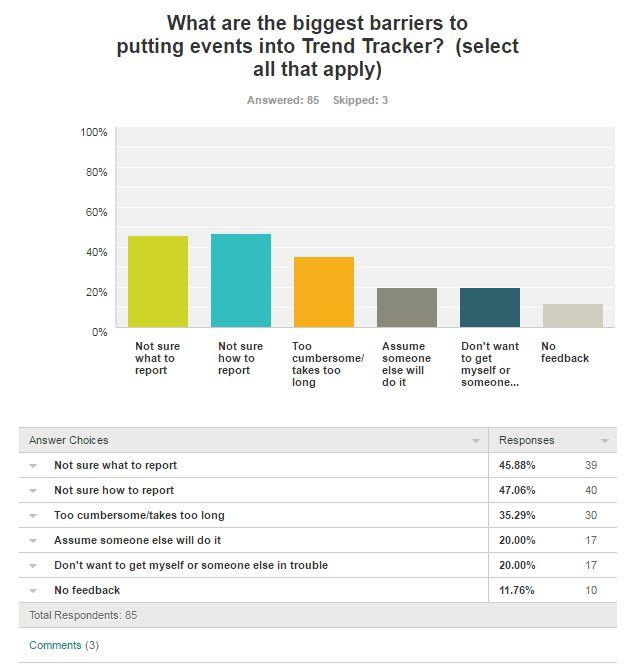
8 Barriers to Incident Reporting?
9 Incident Reporting Barriers & Challenges Individual Reporting Hutchinson et al. Qual Saf Health Care 18:5; Data Handling & Analysis
10 Data Handling & Analysis Barriers Report Volume Sampling error Input Process Lack of feedback Punitive use of information Output Lack of standardized process Lack of transparency Staffing needs
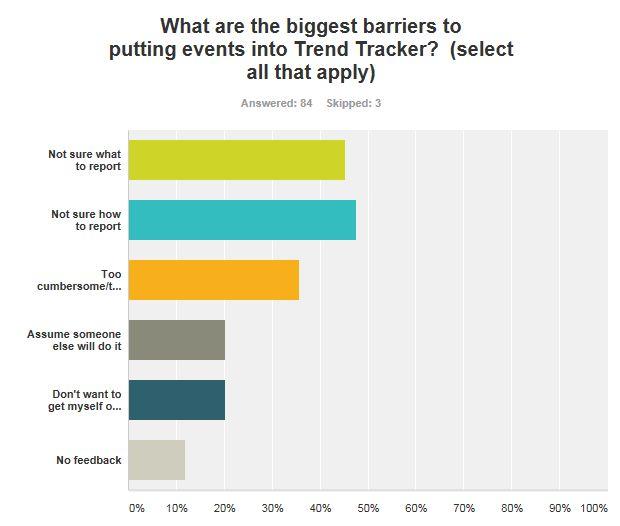
11 Individual Reporting Barriers Attitude Problem deference Shame Fear of retaliation, liability Skills Time-consuming Cumbersome Knowledge What to report How to report Who reports

12 Local Barriers
13 Different approaches
14 Experience 850 residents and fellows ACGME CLER visit < 1% of incident reports placed by trainees 129 medicine/medpeds residents QI / PS Curriculum with M&M, longitudinal projects, monthly lectures Needs Assessment

15 Experience Anecdotal: Past 4 months, 3 incidents reported into STARS
16
17
18 VA slide
19 Improvement strategies Got access to resident reports Town Hall in-service on how to put one in Patient Safety Rounds The life of a trend tracker Thank you s sent to residents Working with Incident Reporting Administration to decrease the number of fields
20 Different approaches
21 Experience 700 residents/fellows 190 residents/fellows in Dept of Medicine 90 residents (IM, Med-Peds, Med-Psych) Institutional QI/patient safety training during GME orientation Rapid cycle QI, team meetings in UIM MM and I conference
22 Incident Reporting CLER visit 2014 Baseline reporting -<2/month from physicians Pay for performance -- Resident Improvement Projects January phone hotline added July 2015 GME promotion of reporting project Access to reporting dashboard Inter-professional collaboration October 2016 EPIC button
23 Implementation Strategies Educational efforts Opportunities for reporting Monthly review at housestaff conference Quarterly review sessions with risk manager & nurse managers Quarterly submission of data MM and I cases IMPROVE project


24 PSI reporting by the numbers
25 Future Directions Individual feedback E-Value VA Faculty Development

26 Different approaches
27 Experience 750 trainees (residents/fellows) 250 trainees Department of Internal Medicine 141 Residents IM + 16 Med-Peds + 10 EM-IM Institutional QI/patient safety training during GME orientation (Walk the Walk) Institutional QI processes/initiatives; requirement for IHI modules Departmental QI curricula
28 VCU Health Incident Reporting Timeline 2013 Survey Previous APD and PD work toward encouraging patient safety reporting Gap Years Difficulties obtaining access to reports filed by residents Issues with the reporting process Reluctance to train learners in a process that was not ideal
29 CLER Report 2015 Feedback Number of reports filed by physicians = 217/10413 (2%) No feedback given to residents Feb CLER Do your residents file reports? How many? What kind of feedback do they receive? Mar Apr Residents start to receive feedback on reports via standardized . Sep Access to Reports Reports filed by residents filtered through performance improvement representative to the APD Dec
30 Intern Orientation 2016 Just-in-Time Teaching Associate Chair for QI for the department available to encourage residents to report. Jan Mar Targeted teaching on reporting during a didactic session. No practice/simulation June July Good Catch Award Requirement to Report Monthly award given at Morbidity, Mortality, & Improvement conference. Institutional requirement for residents to report with numerical goals for each department.

31 2016 Patient Safety Rounds Proactive patient safety rounding by QI resident with encouragement to report, peer coaching. July QI Pager Introduced a QI resident consult pager, with flyers in team rooms to have residents call with any questions about reporting. Aug Sep Structured Feedback Patient safety report on-demand assessment developed for entry into New Innovations. Intern re-training Oct Nov Integration into MMI 5 potential incidents in one MMI
32 Results Patient Safety Rounds Proactive patient safety rounding by QI resident with encouragement to report, peer coaching.
33 Implementation Strategies Intern training session Routine reminders and website demonstration Structured feedback on every report entered Incorporation of feedback/assessment into milestones Institutional and departmental establishment of requirements to report Patient safety rounds with peer coaching*
34 Future Directions Faculty education and support with similar feedback methods VA - eper system - difficulties with access to resident reports Upcoming CLER site visit GME training
35 Reaction to approaches
36 Assessment Tool Event Description Summary of Event Type of Event 1. Timeliness 2. Clarity 3. Objectivity 4. Language/Professionalism Reviewed By Outcome Adverse reaction Behavioral event Care coordination/communication Complication of procedure Equipment/device problem Fall Healthcare-associated infection Lab test Medication-related Omission/error in assessment, diagnosis, monitoring Other Radiology/imaging test Quality of Report Within 24 hours of event > 24 hours of event Succinct/simple Complex/difficult to understand Facts only Subjective comments No direct blame placed on Finger pointing/blaming other parties language used in report Adapted from Boike et. al. 2013
37 Assessment in New Innovations
38 The Incident Oscar got it wrong, wrong, sooooo wrong. The presenters announced the wrong Best Picture; Moonlight was the winner, not La La Land. It was the biggest, most embarrassing, most awkward mistake in the history of the Academy Awards Warren Beatty and Faye Dunaway were presenting but looked lost. When he opened the envelope, he paused for a long few seconds. He looked at Dunaway, puzzled. She took the envelope, read it, paused, and said La La Land.

39 The Incident...the accountant from PriceWaterhouseCoopers jumped and said, He took the wrong envelope! and goes running onstage. No one knows how Beatty got the best actress envelope instead of the best picture envelope.
40 The Incident Award announcer opens envelope and paused. Announcer checks envelope. The audience laughs. The announcer states, And the Academy Award for best picture goes to, and again pauses. The announcer showed the contents of the envelope to the co-announcer, who reported La La Land. The recipients take the stage. Someone then locates another envelope with contents that state that Moonlight won best picture.
41 Small group cases

42 How was using the tool?
43 Today we have: Discussed barriers to incident reporting Shared differing approaches to the process Practiced with an assessment tool that can be used to overcome the barrier to feedback and help residents improve their reporting What is one Incident Reporting task you want to do when you get home?

44 Conclusion
45 References 1. Kohn, L. T., Corrigan, J., & Donaldson, M. S. (2000). To err is human: Building a safer health system. Washington, D.C: National Academy Press. 2. James JT. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf. 2013;9: Noble DJ, Pronovost PJ. Underreporting of patient safety incidents reduces health care's ability to quantify and accurately measure harm reduction. J Patient Saf. 2010;6: Elkin PL, Johnson HC, Callahan MR, Classen DC. Improving Patient Safety Reporting with the Common Formats: Common Data Representation for Patient Safety Organizations. J Biomed Inform Pronovost PJ, Morlock LL, Sexton JB, et al. Improving the value of patient safety reporting systems. In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 1: Assessment). Rockville (MD): ; Conlon P, Havlisch R, Kini N, Porter C. Using an anonymous web-based incident reporting tool to embed the principles of a high-reliability organization. In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 1: Assessment). Rockville (MD): ; Clarke JR, Johnston J, Davis M, et al. Mapping a large patient safety database to the 2005 patient safety event taxonomy. In: Henriksen K, Battles JB, Keyes MA, Grady ML, eds. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 1: Assessment). Rockville (MD): ; Boike JR, Bortman JS, Radosta JM, et al. Patient safety event reporting expectation: does it influence residents' attitudes and reporting behaviors? J Patient Saf. 2013;9: Weiss KB, Bagian JP, CLER Evaluation Committee. Challenges and Opportunities in the Six Focus Areas: CLER National Report of Findings J Grad Med Educ. 2016;8:25-34.
Improvements & Sustained Change through the Implementation of High Reliability Units
 Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Improvements & Sustained Change through the Implementation of High Reliability Units Tammy Van Dyk, MSN, RN, CPEN Quality Management & Patient Safety Manager Objective Describe how high reliability principles
Text-based Document. The Culture of Incident Reporting Among Filipino Nurses. de Guzman, Barbara Michelle. Downloaded 28-Apr :54:41
 The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
The Henderson Repository is a free resource of the Honor Society of Nursing, Sigma Theta Tau International. It is dedicated to the dissemination of nursing research, researchrelated, and evidence-based
Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center
 Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Engaging the team: Steps to Reduce Complications Susan Moffatt-Bruce, MD, PhD Chief Quality and Patient Safety Officer Associate Professor of Surgery The Ohio State University s Wexner Medical Center Safety
Patient Safety Culture: Sample of a University Hospital in Turkey
 Original Article INTRODUCTION Medical errors or patient safety is an important issue in healthcare quality. A report from Institute 1. Ozgur Ugurluoglu, PhD, Hacettepe University, Department of Health
Original Article INTRODUCTION Medical errors or patient safety is an important issue in healthcare quality. A report from Institute 1. Ozgur Ugurluoglu, PhD, Hacettepe University, Department of Health
Ambulatory Patient Safety
 We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
We Harm Patients Too: Ambulatory Patient Safety James Park, MD Associate Medical Director Primary & Urgent Care Jeri Craine, RN, MN Health Promotions Program Manager UW Medicine Valley Medical Center Clinic
Quality Improvement/Systems-based Practice. Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery
 Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
Quality Improvement/Systems-based Practice Erica L. Mitchell, M.D., MEd Professor Surgery Vice-Chair Quality, Department of Surgery Objectives Define and understand the importance of Systems Based Practice
IM Residency Curriculum Quality Improvement and Patient Safety. Program Director s Retreat January 23, 2018
 IM Residency Curriculum Quality Improvement and Patient Safety Program Director s Retreat January 23, 2018 IM residency QI and PS curriculum Goals and Objectives Key Concepts Mapping to ACGME goals Overview
IM Residency Curriculum Quality Improvement and Patient Safety Program Director s Retreat January 23, 2018 IM residency QI and PS curriculum Goals and Objectives Key Concepts Mapping to ACGME goals Overview
Translating Evidence to Safer Care
 Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Translating Evidence to Safer Care Patient Safety Research Introductory Course Session 7 Albert W Wu, MD, MPH Former Senior Adviser, WHO Professor of Health Policy & Management, Johns Hopkins Bloomberg
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship
 Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Developing a Curriculum in Patient Safety and Quality Improvement for Your Clerkship Diane Levine, Wayne State University Allison Heacock, The Ohio State University Amy Shaheen, University of North Carolina
Building and Sustaining a Culture of Safety
 Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
Building and Sustaining a Culture of Safety Ann Shimek, MSN, RN, CASC Senior Vice President, Clinical Operations United Surgical Partners International 028 Session Objectives q Describe organizational
A Quiz. I am comfortable going to any healthcare provider or hospital in my city/town.
 A Quiz I am comfortable going to any healthcare provider or hospital anywhere in the country. I am comfortable going to any healthcare provider or hospital in my city/town. I am comfortable going to my
A Quiz I am comfortable going to any healthcare provider or hospital anywhere in the country. I am comfortable going to any healthcare provider or hospital in my city/town. I am comfortable going to my
Strategies for Good Communication of the Medical Laboratory Staff with the TB Program and Healthcare Providers
 Strategies for Good Communication of the Medical Laboratory Staff with the TB Program and Healthcare Providers Vasiti Uluiviti Regional Laboratory Coordinator PIHOA 2017 PITCA Meeting Sept 11 th 15 th
Strategies for Good Communication of the Medical Laboratory Staff with the TB Program and Healthcare Providers Vasiti Uluiviti Regional Laboratory Coordinator PIHOA 2017 PITCA Meeting Sept 11 th 15 th
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital
 Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
Robert J. Welsh, MD Vice Chief of Surgical Services for Patient Safety, Quality, and Outcomes Chief of Thoracic Surgery William Beaumont Hospital Royal Oak, Michigan, USA 1 ARE OUR OPERATING ROOMS SAFE?
PREPARING FOR THE CLER SITE VISIT FOR BEN TAUB GENERAL HOSPITAL
 PREPARING FOR THE CLER SITE VISIT FOR BEN TAUB GENERAL HOSPITAL 1 Goals and Objectives Overview the Clinical Learning Environment Review (CLER) program Discuss the concept of maintaining a culture of readiness
PREPARING FOR THE CLER SITE VISIT FOR BEN TAUB GENERAL HOSPITAL 1 Goals and Objectives Overview the Clinical Learning Environment Review (CLER) program Discuss the concept of maintaining a culture of readiness
Assessment of patient safety culture in a rural tertiary health care hospital of Central India
 International Journal of Community Medicine and Public Health Goyal RC et al. Int J Community Med Public Health. 2018 Jul;5(7):2791-2796 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original Research
International Journal of Community Medicine and Public Health Goyal RC et al. Int J Community Med Public Health. 2018 Jul;5(7):2791-2796 http://www.ijcmph.com pissn 2394-6032 eissn 2394-6040 Original Research
A Blueprint for Alignment
 A Blueprint for Alignment Engaging Residents in the Quality and Safety Mission of Penn Medicine PJ Brennan, MD Chief Medical Officer, UPHS Jennifer S. Myers, MD Director of Quality and Safety Education
A Blueprint for Alignment Engaging Residents in the Quality and Safety Mission of Penn Medicine PJ Brennan, MD Chief Medical Officer, UPHS Jennifer S. Myers, MD Director of Quality and Safety Education
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009
 The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
The Medication Safety Journey Natasha Nicol, Pharm. D., FASHP Director of Medication Safety June 4, 2009 About me I am someone s mother, wife, daughter, granddaughter, sister, aunt, cousin and niece. I
Nexus of Patient Safety and Worker Safety
 Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Nexus of Patient Safety and Worker Safety Jeffrey Brady, MD, MPH & James Battles, PhD Agency for Healthcare Research and Quality October 25, 2012 Diagnosing the Safety Problem is One Challenge The fundamental
Ensuring Patient Safety and Quality Measures for RRT in AKI 2. Eileen Lischer MA, BSN, RN, CNN University of California, San Diego
 Ensuring Patient Safety and Quality Measures for RRT in AKI 2 Eileen Lischer MA, BSN, RN, CNN University of California, San Diego Today we may be doing what we can, but tomorrow we can improve Hughes,
Ensuring Patient Safety and Quality Measures for RRT in AKI 2 Eileen Lischer MA, BSN, RN, CNN University of California, San Diego Today we may be doing what we can, but tomorrow we can improve Hughes,
The Clinical Learning Environment Review (CLER) Program Update
 Program Update") Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program Update October 10, 2013 Updates CLER program development Early observations CLER Evaluation
Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program Update October 10, 2013 Updates CLER program development Early observations CLER Evaluation
QI Quarterly. In the Journal. Safety First. Kudos: Resident experience. Stop & Resolve when questions arise. Validate and verify.
 QI Quarterly 1 In the Journal Creighton Quality Improvement: Internal Medicine The Delivery of true early mobilization March 2017 in an [Edition 1, Volume 1] intensive care unit. Willigen et al. BMJ Qual
QI Quarterly 1 In the Journal Creighton Quality Improvement: Internal Medicine The Delivery of true early mobilization March 2017 in an [Edition 1, Volume 1] intensive care unit. Willigen et al. BMJ Qual
Patient Safety in the Ambulatory Setting No News is Not Always Good News Tracey L. Henry, MD, MPH NPA 2015 Copello Fellow
 Patient Safety in the Ambulatory Setting No News is Not Always Good News Tracey L. Henry, MD, MPH NPA 2015 Copello Fellow July 20, 2016 Background Background Patient safety was brought to the forefront
Patient Safety in the Ambulatory Setting No News is Not Always Good News Tracey L. Henry, MD, MPH NPA 2015 Copello Fellow July 20, 2016 Background Background Patient safety was brought to the forefront
Imprinting Safety and Quality Practices on Residents and Fellows. John Szymusiak, MD Gregory M. Bump, MD
 Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
Imprinting Safety and Quality Practices on Residents and Fellows John Szymusiak, MD Gregory M. Bump, MD Introductions 2 Gregory M. Bump, MD Associate Professor of General Internal Medicine UPMC Montefiore
Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD
 Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
Presented by: Suchita Pancholi, MD Letitia Cameron, MD Aniel Rao, MD Michael Hill, MD I. Introductions II. III. IV. Marshmallow Challenge Why Teach Patient Safety? Barriers to Teaching Patient Safety V.
POLICY BRIEF. Identifying Adverse Drug Events in Rural Hospitals: An Eight-State Study. May rhrc.umn.edu. Background.
 POLICY BRIEF Identifying Adverse Drug Events in Rural Hospitals: An Eight-State Study Michelle Casey, MS Peiyin Hung, MSPH Emma Distel, MPH Shailendra Prasad, MBBS, MPH Key Findings In 2013, Critical Access
POLICY BRIEF Identifying Adverse Drug Events in Rural Hospitals: An Eight-State Study Michelle Casey, MS Peiyin Hung, MSPH Emma Distel, MPH Shailendra Prasad, MBBS, MPH Key Findings In 2013, Critical Access
Medication Errors and Safety. Educating for Quality Improvement & Patient Safety
 Medication Errors and Safety Educating for Quality Improvement & Patient Safety 1 Mandie Tiball Svatek, MD has no relevant financial relationships with commercial interests to disclose. Rayanne Wilson,
Medication Errors and Safety Educating for Quality Improvement & Patient Safety 1 Mandie Tiball Svatek, MD has no relevant financial relationships with commercial interests to disclose. Rayanne Wilson,
Journal Club. Medical Education Interest Group. Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety.
 Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journal Club Medical Education Interest Group Topic: Format of Morbidity and Mortality Conference to Optimize Learning, Assessment and Patient Safety. References: 1. Szostek JH, Wieland ML, Loertscher
Journey to an Effective Safety Culture Part I of III Exploring the Role of Culture in Safety Outcomes. Embracing Patient Safety Culture
 White Paper Journey to an Effective Safety Culture Part I of III Exploring the Role of Culture in Safety Outcomes Embracing Patient Safety Culture What is the Purpose of this Series? The purpose of this
White Paper Journey to an Effective Safety Culture Part I of III Exploring the Role of Culture in Safety Outcomes Embracing Patient Safety Culture What is the Purpose of this Series? The purpose of this
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017
 HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
HIMSS Nicholas E. Davies Award of Excellence Case Study Nebraska Medicine October 10, 2017 Nebraska Medicine $1.2 billion academic health system 8,000 employees More than 1,000 affiliated physicians Primary
Incorporating Patient Safety & Quality Improvement into GME
 Incorporating Patient Safety & Quality Improvement into GME Frederick M Schiavone MD FACEP Professor of Emergency Medicine DIO and Vice Dean for GME Director of the Center for Clinical Simulation and Patient
Incorporating Patient Safety & Quality Improvement into GME Frederick M Schiavone MD FACEP Professor of Emergency Medicine DIO and Vice Dean for GME Director of the Center for Clinical Simulation and Patient
Promoting lifelong learning in health care
 Promoting lifelong learning in health care IOM presentation 12/11/08 Dave Davis, MD, FCFP, Association of American Medical Colleges, Washington DC Adjunct Professor, Health Policy, and Family and Community
Promoting lifelong learning in health care IOM presentation 12/11/08 Dave Davis, MD, FCFP, Association of American Medical Colleges, Washington DC Adjunct Professor, Health Policy, and Family and Community
Enhancing Patient Quality and Safety with Compliance
 Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
Enhancing Patient Quality and Safety with Compliance April 23, 2013 John Kalb, JD, CCEP, CHPC Operational Excellence Executive/ Compliance Officer Kootenai Health Content A successful compliance program
The Clinical Learning Environment Review (CLER) Program. Background
 Program. Background") Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program November 2013 Background 2009-2010 ACGME Task Force Linked adherence to duty hours policies
Accreditation Council for Graduate Medical Education The Clinical Learning Environment Review (CLER) Program November 2013 Background 2009-2010 ACGME Task Force Linked adherence to duty hours policies
HPV Vaccination Quality Improvement: Physician Perspective
 HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB)
") Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
Patient safety in the NHS in England and the development of the Healthcare Safety Investigation Branch (HSIB) Dr Mike Durkin NHS National Director of Patient Safety 11 May 2016 The NHS is big! Great potential
Barriers to a Positive Safety Culture. Donna Zankowski MPH RN
 Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
Barriers to a Positive Safety Culture Donna Zankowski MPH RN What we ll talk about: 1. The Importance of Institutional Leadership 2. The Issue of Underreporting 3. Incident Reporting Tools 4. Employee
SES B38 Integrating the Health Care Matrix into your Transitional Year Quality and Safety Curriculum
 SES B38 Integrating the Health Care Matrix into your Transitional Year Quality and Safety Curriculum AHME Institute May 15, 2015 Objectives At the conclusion of this session, the learner should be able
SES B38 Integrating the Health Care Matrix into your Transitional Year Quality and Safety Curriculum AHME Institute May 15, 2015 Objectives At the conclusion of this session, the learner should be able
IMPACT OF TECHNOLOGY ON MEDICATION SAFETY
 Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
Continuous Quality Improvement IMPACT OF Steven R. Abel, PharmD, FASHP TECHNOLOGY ON Nital Patel, PharmD. MBA MEDICATION SAFETY Sheri Helms, PharmD Candidate Brian Heckman, PharmD Candidate Ismaila D Badjie
Mission Statement We improve health care by assessing and advancing the quality of resident physicians' education through accreditation.
 ACGME Mission Statement We improve health care by assessing and advancing the quality of resident physicians' education through accreditation. Vision We imagine a world characterized by: a structured approach
ACGME Mission Statement We improve health care by assessing and advancing the quality of resident physicians' education through accreditation. Vision We imagine a world characterized by: a structured approach
Adverse Events in Hospitals: How Many and Why Not Reported. Fran Griffin Senior Manager Clinical Programs, BD
 Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Adverse Events in Hospitals: How Many and Why Not Reported Fran Griffin Senior Manager Clinical Programs, BD Disclosure Currently full time employed at BD and faculty at The Institute for Healthcare Improvement
Are We a Team of Experts or an Expert Team?
 Are We a Team of Experts or an Expert Team? BEST PRACTICES: Care for the Complex Community Dwelling Older Adult July 11 12, 2008 NEBGEC Annual Conference Katherine Jones, PT, PhD kjonesj@unmc.edu Objectives
Are We a Team of Experts or an Expert Team? BEST PRACTICES: Care for the Complex Community Dwelling Older Adult July 11 12, 2008 NEBGEC Annual Conference Katherine Jones, PT, PhD kjonesj@unmc.edu Objectives
Building from the Blueprint for Patient Safety at the Hospital for Sick Children
 Designing an Agenda for Change Building from the Blueprint for Patient Safety at the Hospital for Sick Children Polly Stevens, Anne Matlow and Ronald Laxer INTRODUCTION The Hospital for Sick Children (Sick
Designing an Agenda for Change Building from the Blueprint for Patient Safety at the Hospital for Sick Children Polly Stevens, Anne Matlow and Ronald Laxer INTRODUCTION The Hospital for Sick Children (Sick
Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment
 Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment Andrew R. Buchert, MD Dept. of Pediatrics Gregory M. Bump, MD Dept. of Medicine Associate Medical Directors for GME
Facilitating Change in the Patient Safety Culture of the Clinical Learning Environment Andrew R. Buchert, MD Dept. of Pediatrics Gregory M. Bump, MD Dept. of Medicine Associate Medical Directors for GME
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE)
") COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
COMPUTERIZED PHYSICIAN ORDER ENTRY (CPOE) Ahmed Albarrak 301 Medical Informatics albarrak@ksu.edu.sa 1 Outline Definition and context Why CPOE? Advantages of CPOE Disadvantages of CPOE Outcome measures
Creating High Reliability Organizations. Enhancing the Culture of Safety for Our Patients & Our Organizations
 Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Creating High Reliability Organizations Enhancing the Culture of Safety for Our Patients & Our Organizations OUR TRUST by Dr. Don Berwick Reliability from the Patient s Perspective Don't kill me (no needless
Reporting and Disclosing Adverse Events
 Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
Reporting and Disclosing Adverse Events Objectives 2 Review definition of errors and adverse events. Examine the difference between disclosure and apology. Discuss the recognition of and care for second
NHS Borders Feedback and Complaints Annual Report
 NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
Quality Improvement: Essential Leadership
 Quality Improvement: Essential Leadership Anne Matlow, September 30, 2016 I do not have an affiliation (financial or otherwise) with a pharmaceutical, medical device or communications organization. Je
Quality Improvement: Essential Leadership Anne Matlow, September 30, 2016 I do not have an affiliation (financial or otherwise) with a pharmaceutical, medical device or communications organization. Je
Improving Nursing Home Patient Safety in Maine: A Review of the AHRQ Patient Safety Culture survey Implementation Process
 University of Southern Maine USM Digital Commons Muskie School Capstones Student Scholarship 5-1-2012 Improving Nursing Home Patient Safety in Maine: A Review of the AHRQ Patient Safety Culture survey
University of Southern Maine USM Digital Commons Muskie School Capstones Student Scholarship 5-1-2012 Improving Nursing Home Patient Safety in Maine: A Review of the AHRQ Patient Safety Culture survey
Patient Safety: Where are we and where do we want to go?
 Patient Safety: Where are we and where do we want to go? Denice Stewart, DDS, MHSA Senior Associate Dean, Clinical Affairs Professor, Community Dentistry We re moving! Occupancy July 1, 2014 As of October,
Patient Safety: Where are we and where do we want to go? Denice Stewart, DDS, MHSA Senior Associate Dean, Clinical Affairs Professor, Community Dentistry We re moving! Occupancy July 1, 2014 As of October,
TeamSTEPPS Introductory Webinar. July 19, 2018
 TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
TeamSTEPPS Introductory July 19, 2018 Agenda Welcome & HIIN Update TeamSTEPPS Master Trainer Course Presentation --Duke University Health System Master Trainers Next Steps Questions / Discussion Pre-Meeting
9/9/2016. How Respiratory Therapist Enhance Patient Safety. Introduction. Raise your hand. Tawana Shaffer CPHRM, MBA, BSc, CRT
 How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
How Respiratory Therapist Enhance Patient Safety Tawana Shaffer CPHRM, MBA, BSc, CRT Introduction Raise your hand 1 How do you define Patient Safety? What is Patient Safety? Communication Care Falls Outcomes
Preventable Adverse Event (PAE) Reporting Vickie Gillespie, PAE Clinical Analyst Bobbiejean Garcia, Epidemiologist 2014
 Reporting Vickie Gillespie, PAE Clinical Analyst Bobbiejean Garcia, Epidemiologist 2014") Preventable Adverse Event (PAE) Reporting--101 Vickie Gillespie, PAE Clinical Analyst Bobbiejean Garcia, Epidemiologist 2014 1 Preventable Adverse Event (PAE) Reporting--101 Objectives: Review the background
Preventable Adverse Event (PAE) Reporting--101 Vickie Gillespie, PAE Clinical Analyst Bobbiejean Garcia, Epidemiologist 2014 1 Preventable Adverse Event (PAE) Reporting--101 Objectives: Review the background
THE BUSINESS CASE. for. A Standardized Continuous Quality Assurance Program in Saskatchewan Pharmacies - COMPASS. by the
 THE BUSINESS CASE for A Standardized Continuous Quality Assurance Program in Saskatchewan Pharmacies - COMPASS by the Saskatchewan College of Pharmacy Professionals Submitted to the Council of the Saskatchewan
THE BUSINESS CASE for A Standardized Continuous Quality Assurance Program in Saskatchewan Pharmacies - COMPASS by the Saskatchewan College of Pharmacy Professionals Submitted to the Council of the Saskatchewan
Greetings from Michelle & Katie QUALITY IMPROVEMENT DIVISION OF HOSPITAL MEDICINE
 IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
IN THIS ISSUE: Create Raving Fans of Your Idea P. 1 Where is our waste? P. 1 Sepsis Update P. 3 Quality Updates P. 4 APeX quality tips P.5 Division Incentive Metrics P. 6 Focus Group Findings P. 2 The
LEADERSHIP CHALLENGES IN PATIENT SAFETY
 LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
LEADERSHIP CHALLENGES IN PATIENT SAFETY Kenneth W. Kizer, MD, MPH. California Hospital Patient Safety Organization Annual Meeting Sacramento, CA April 8, 2013 Presentation Charge Discuss some of the challenges
Working with trainees to turn quality improvement into scholarship and dissemination
 Working with trainees to turn quality improvement into scholarship and dissemination James Moses, MD, MPH Chief Quality Officer, Boston Medical Center Academic Advisor, Institute for Healthcare Improvement
Working with trainees to turn quality improvement into scholarship and dissemination James Moses, MD, MPH Chief Quality Officer, Boston Medical Center Academic Advisor, Institute for Healthcare Improvement
FACT SHEET. The Launch of the World Alliance For Patient Safety " Please do me no Harm " 27 October 2004 Washington, DC
 FACT SHEET The Launch of the World Alliance For Patient Safety " Please do me no Harm " 27 October 2004 Washington, DC 1. This unique and essential Alliance is set up by the World Health Organization (WHO)
FACT SHEET The Launch of the World Alliance For Patient Safety " Please do me no Harm " 27 October 2004 Washington, DC 1. This unique and essential Alliance is set up by the World Health Organization (WHO)
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Health Management Information Systems: Computerized Provider Order Entry
 Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
Health Management Information Systems: Computerized Provider Order Entry Lecture 2 Audio Transcript Slide 1 Welcome to Health Management Information Systems: Computerized Provider Order Entry. The component,
NAS in a Community Hospital
 NAS in a Community Hospital Best Practices with Limited Resources Presented By: Susan Greenwood-Clark, RN, MBA, FACHE Director, Medical Education St. Mary Mercy Hospital Date: May 13, 2015 Goals At the
NAS in a Community Hospital Best Practices with Limited Resources Presented By: Susan Greenwood-Clark, RN, MBA, FACHE Director, Medical Education St. Mary Mercy Hospital Date: May 13, 2015 Goals At the
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION
 THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
THE AMERICAN BOARD OF PATHOLOGY PATIENT SAFETY COURSE APPLICATION Requirements: Component I Patient Safety Self-Assessment Program Programs must meet the following criteria to be an ABP approved Patient
Safety in Mental Health Collaborative
 NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
NHS Tayside Safety in Mental Health Collaborative Improving Safety in Mental Health Programme Aims supported by an Improvement Advisor: Dr Noeleen Devaney Support 4 UK organisations to: reduce harm improving
Patient Safety in Ambulatory Care: Why Reporting Counts. August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH
 Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Patient Safety in Ambulatory Care: Why Reporting Counts August 11, 2010 Diane Schultz, RPh and Sheila Yates, MPH Group Health Group Health provides medical coverage and care to more than 628,000 residents
Patient Safety: 10 Years Later Why is Improvement So Hard? Patient Safety: Strong Beginnings
 Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Patient Safety: 10 Years Later Why is Improvement So Hard? G. Ross Baker, Ph.D. Institute of Health Policy, Management & Evaluation University of Toronto 3 November 2014 Patient Safety: Strong Beginnings
Frontline Improvement Using Defect Analysis March 9, 2012 R Resar, MD; N Romanoff, MD, MPH; A Majka, MD; J Kautz, MD; D Kashiwagi, MD; K Luther, RN
 Frontline Improvement Using Defect Analysis March 9, 2012 R Resar, MD; N Romanoff, MD, MPH; A Majka, MD; J Kautz, MD; D Kashiwagi, MD; K Luther, RN Introduction More than a decade ago, the Institute of
Frontline Improvement Using Defect Analysis March 9, 2012 R Resar, MD; N Romanoff, MD, MPH; A Majka, MD; J Kautz, MD; D Kashiwagi, MD; K Luther, RN Introduction More than a decade ago, the Institute of
Healthcare Solutions Nuance Clintegrity Quality Management Solutions. Quality. The Discipline to Win.
 Quality. The Discipline to Win. Brochure 2 It s not wanting to win that makes you a winner; it s refusing to fail. Peyton Manning, the first NFL quarterback to achieve 200 career wins (regular and post-season)
Quality. The Discipline to Win. Brochure 2 It s not wanting to win that makes you a winner; it s refusing to fail. Peyton Manning, the first NFL quarterback to achieve 200 career wins (regular and post-season)
Improving HPV Vaccination Rates in a Large Pediatric Practice: Implementing Effective Quality Improvement
 Improving HPV Vaccination Rates in a Large Pediatric Practice: Implementing Effective Quality Improvement Alix Casler, M.D., F.A.A.P. Chief of Pediatrics, Medical Director of Pediatrics Orlando Health
Improving HPV Vaccination Rates in a Large Pediatric Practice: Implementing Effective Quality Improvement Alix Casler, M.D., F.A.A.P. Chief of Pediatrics, Medical Director of Pediatrics Orlando Health
A Study to Assess Patient Safety Culture amongst a Category of Hospital Staff of a Teaching Hospital
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 13, Issue 3 Ver. IV. (Mar. 2014), PP 16-22 A Study to Assess Patient Safety Culture amongst a Category
SPSP Medicines. Prepared by: NHS Ayrshire and Arran
 SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
SPSP Medicines Prepared by: NHS Ayrshire and Arran Medication Reconciliation: Story so far MR happening in primary care, acute adult, paediatrics and mental health Started in acute then mental health,
Patient and Family Engagement Strategy. April 10, 2013
 Patient and Family Engagement Strategy April 10, 2013 1 Webinar Agenda Overview & Introductions Kathy Wallace Why is Patient & Family Engagement the Right Thing to do? Carrie Brady Patient & Family Advisor
Patient and Family Engagement Strategy April 10, 2013 1 Webinar Agenda Overview & Introductions Kathy Wallace Why is Patient & Family Engagement the Right Thing to do? Carrie Brady Patient & Family Advisor
Improving Safety Practices Anticoagulation Therapy
 Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Improving Safety Practices Anticoagulation Therapy Katie Cinnamon, PharmD, BCPS Clinical Pharmacist Genesis Medical Center - Davenport Objectives Review background information on medication errors and
Year in Review ro ils RO ILS
 RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
RO ILS RADIATION ONCOLOGY INCIDENT LEARNING SYSTEM Sponsored by ASTRO and AAPM Year in Review 2015 1 ro ils noun \ˈro i(-ə)ls\ Radiation Oncology Incident Learning System; a system to facilitate safer
Multi disciplinary Team Communication and Effective Handoffs
 Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
Multi disciplinary Team Communication and Effective Handoffs Lauren Destino, MD Clinical Associate Professor Associate Medical Director of the Pediatric Hospital Medicine Division Stanford University,
Culture. Safety. Process. Culture of Safety and Improvement
 Culture Safety Process Culture of Safety and Improvement Objectives Define key elements in a Culture of Safety Describe your role in the culture and process of safety Identify three personal actions to
Culture Safety Process Culture of Safety and Improvement Objectives Define key elements in a Culture of Safety Describe your role in the culture and process of safety Identify three personal actions to
Improving the Chemotherapy Appointment Experience at the BC Cancer Agency
 Improving the Chemotherapy Appointment Experience at the BC Cancer Agency Ruben Aristizabal Martin Puterman Pablo Santibáñez Kevin Huang Vincent Chow www.orincancercare.org/cihrteam Acknowledgements BC
Improving the Chemotherapy Appointment Experience at the BC Cancer Agency Ruben Aristizabal Martin Puterman Pablo Santibáñez Kevin Huang Vincent Chow www.orincancercare.org/cihrteam Acknowledgements BC
Kate Beaumont. Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign.
 Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Why Safety Matters Kate Beaumont Strategy Advisor, NPSA Head of Clinical Interventions, National Patient Safety Campaign Catherine.beaumont@npsa.nhs.uk www.npsa.nhs.uk About the NPSA What we are: Arm s
Project ENABLE - Alameda County Community Capacity Fund. Project Blueprint. March 2015
 Project ENABLE - Alameda County Community Capacity Fund Project Blueprint March 2015 Table of Contents Project Highlights Project Objectives Project Goal Current Challenges of Organizations Serving the
Project ENABLE - Alameda County Community Capacity Fund Project Blueprint March 2015 Table of Contents Project Highlights Project Objectives Project Goal Current Challenges of Organizations Serving the
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability
 Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Leveraging the Accountable Care Unit Model to create a culture of Shared Accountability How we improved Patient Safety and Quality Outcomes at Northwest Hospital Our Journey to Shared Accountability Implementation
Maryland Patient Safety Center s Call for Solutions 2017
 Maryland Patient Safety Center s Call for Solutions 7 The Neonatal Intensive Care Unit at The Herman & Walter Samuelson Children s Hospital at Sinai Hospital of Baltimore Drawing Placental Blood for Admission
Maryland Patient Safety Center s Call for Solutions 7 The Neonatal Intensive Care Unit at The Herman & Walter Samuelson Children s Hospital at Sinai Hospital of Baltimore Drawing Placental Blood for Admission
Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care
 Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care IHI Workshop 12/6/16 Gordon Schiff, MD, Associate Dir Brigham & Women s Ctr for Patient Safety Research
Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care IHI Workshop 12/6/16 Gordon Schiff, MD, Associate Dir Brigham & Women s Ctr for Patient Safety Research
The Importance of Transfusion Error Surveillance This is step #1 in error management. Jeannie Callum, BA, MD, FRCPC, CTBS
 The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
The Importance of Transfusion Error Surveillance This is step #1 in error management Jeannie Callum, BA, MD, FRCPC, CTBS 6051 Clinical Errors 9083 Laboratory Errors 15134 Errors over 6 years I don t want
Care of the Caregiver STARTS and ENDS with full leadership support and involvement!
 Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
Care of the Caregiver STARTS and ENDS with full leadership support and involvement! Care of the caregiver following an unintentional error or near miss should ideally incorporate: Unsafe Acts Algorithm
From Implementation to Optimization: Moving Beyond Operations
 From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
From Implementation to Optimization: Moving Beyond Operations Session 260, March 8, 2018 Scott Aikey, Sr. Director, Core Clinical Applications Children s Hospital of Philadelphia 1 Conflict of Interest
PERFORMANCE IMPROVEMENT REPORT
 PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
PERFORMANCE IMPROVEMENT REPORT First Quarter Fiscal Year 214 October-December, 213 Daniel Coffey, CEO 1 Executive Summary The Quarterly Performance Improvement Report summarizes the measures used to monitor
Communication Surrounding Adverse Events: A Simulation Education Program for Resident Physicians
 Communication Surrounding Adverse Events: A Simulation Education Program for Resident Physicians, Washington, DC 1 Investigators Laura J. Sigman, MD, JD, FAAP Dr. Sigman is a physician and manages legal
Communication Surrounding Adverse Events: A Simulation Education Program for Resident Physicians, Washington, DC 1 Investigators Laura J. Sigman, MD, JD, FAAP Dr. Sigman is a physician and manages legal
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Overview of a new study to assess the impact of hospice led interventions on acute use. Jonathan Ellis, Director of Policy & Advocacy
 Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
Overview of a new study to assess the impact of hospice led interventions on acute use Jonathan Ellis, Director of Policy & Advocacy The problem Almost 600,000 people die each year Half will die in a hospital
Quality, Safety and the Physician Handoff
 Quality, Safety and the Physician Handoff John M. McGregor, M.D. Department of Neurological Surgery Co-Chairman - Neuroscience Clinical Quality Management Committee Ohio State University Wexner Medical
Quality, Safety and the Physician Handoff John M. McGregor, M.D. Department of Neurological Surgery Co-Chairman - Neuroscience Clinical Quality Management Committee Ohio State University Wexner Medical
Systems approach to Patient Safety and Experience
 Systems approach to Patient Safety and Experience Dr Alex Sia Chief Executive Officer KK Women s and Children s Hospital Professor, Duke NUS Medical School Clinical Professor, YLL School of Medicine Adjunct
Systems approach to Patient Safety and Experience Dr Alex Sia Chief Executive Officer KK Women s and Children s Hospital Professor, Duke NUS Medical School Clinical Professor, YLL School of Medicine Adjunct
Hypertension. Collaborating to Control Blood Pressure: Knowing Your Numbers is Just the Beginning
 Hypertension Collaborating to Control Blood Pressure: Knowing Your Numbers is Just the Beginning Al Bradley Senior Program Manager Director, High Blood Pressure Collaborative Finger Lakes Health Systems
Hypertension Collaborating to Control Blood Pressure: Knowing Your Numbers is Just the Beginning Al Bradley Senior Program Manager Director, High Blood Pressure Collaborative Finger Lakes Health Systems
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care
 A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
A17/B17: Addressing Diagnostic Error: Creating Reliable Systems for Diagnosis and Tracking in Primary Care Gordy Schiff, MD, Associate Director of Brigham and Women s Center for Patient Safety Research
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018
 FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
FHA Call to Action: Eliminating Infection-Related Ventilator-Associated Complications IVAC Bi-Monthly Webinar #2 May 3, 2018 Agenda FHA MTC Call to Action for IVAC Data Review HRET HIIN Hospital Peer Sharing
Trends in Medical Error Education: Are We Failing Our Residents?
 Trends in Medical Error Education: Are We Failing Our Residents? Corey K. Bradley, BA; Melissa A. Fischer, MD, MEd; Kathleen E. Walsh, MD, MSc From the Davidson College, Davidson, NC (Ms Bradley); Department
Trends in Medical Error Education: Are We Failing Our Residents? Corey K. Bradley, BA; Melissa A. Fischer, MD, MEd; Kathleen E. Walsh, MD, MSc From the Davidson College, Davidson, NC (Ms Bradley); Department
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions
 National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
National Readmissions Summit Safe and Reliable Transitions: An Integrated Approach Reducing Heart Failure Readmissions Michael Kanter, MD, Medical Director Quality and Clinical Analysis Patti Harvey, RN,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT)
") Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Decreasing the Unplanned Readmission Rate of Patients receiving Outpatient Antibiotic Therapy(OPAT) Dr. Jose Cadena Dr. Amruta Parekh University of Texas Health Science Center at San Antonio San Antonio,
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/43550 holds various files of this Leiden University dissertation. Author: Brunsveld-Reinders, A.H. Title: Communication in critical care : measuring and
Cover Page The handle http://hdl.handle.net/1887/43550 holds various files of this Leiden University dissertation. Author: Brunsveld-Reinders, A.H. Title: Communication in critical care : measuring and
Pfizer Independent Grants for Learning & Change Request for Proposals (RFP) Antimicrobial Stewardship in the Asia-Pacific Region
 Antimicrobial Stewardship in the Asia-Pacific Region") Pfizer Independent Grants for Learning & Change Request for Proposals (RFP) Antimicrobial Stewardship in the Asia-Pacific Region I. Background The Joint Commission, in collaboration with Pfizer Independent
Pfizer Independent Grants for Learning & Change Request for Proposals (RFP) Antimicrobial Stewardship in the Asia-Pacific Region I. Background The Joint Commission, in collaboration with Pfizer Independent
Establishing a Culture of Quality and Safety and the Journey to High Reliability
 Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
Establishing a Culture of Quality and Safety and the Journey to High Reliability Becker s Hospital Review May 9, 2013 Charles D. Stokes System Chief Operating Officer M. Michael Shabot, M.D. System Chief
The Health Literacy Framework will focus on people with chronic conditions and complex care needs, including people with mental illness.
 Northern NSW Health Literacy Framework June 2016 Background The Northern NSW Local Health District (NNSW LHD) and North Coast Primary Health Network (NCPHN) have a shared commitment to creating an integrated
Northern NSW Health Literacy Framework June 2016 Background The Northern NSW Local Health District (NNSW LHD) and North Coast Primary Health Network (NCPHN) have a shared commitment to creating an integrated