Clinician Pay for Performance. October 31, 2016
|
|
|
- Steven Jones
- 5 years ago
- Views:
Transcription
1 Clinician Pay for Performance October 31, 2016
2 Open Door Family Medical Centers Founded in the basement of a church in 1972 We ve grown a bit since then 5 Primary Care Sites 7 School-based Health Centers Family Medicine Residency program Dental Residency program
3 Open Door Family Medical Centers By the end of 2015, we had: Over 100 Medical, Behavioral, and Dental clinicians providing care to 47,000 patients in 265,000 visits
4 Open Door PCP panel sizes Primary care panel size: 1,400/1.0 FTE PCP over 12 months 1,650/1/0 FTE PCP over 18 months 2,100/1.0 FTE PCP over 36 months
 (65 & Up) After childhood, we see a considerable")

5 Patients by Age and Sex (Under age 1) (1-19) (20-49) (50-64) (65 & Up) After childhood, we see a considerable difference between the number of men and women that we see. We attribute this trend to the high number of women that we see during child-bearing age.
6 Insurance Coverage of Our Patients % 4% 8% Uninsured Medicaid 50% CHIP 32% Medicare Private
7 Pay for Performance in Focus Salary Armageddon NP/PA incentive eclinicalworks implementation Clinical report cards introduced Pay for Performance implemented Human Resources strengthened Tableau database rolled out Relevant database rolled out AZARA PVP rolled out
8 Paying for clinical quality Clinicians of all stripes want to also be judged by the quality of care they give, not just by how many patients they can see. Clinicians are more concerned about how well they are taking care of patients much more than how fast they are moving from patient to patient.
9 Volume counts, but it s not everything Yes, volume-based reimbursement still reigns supreme. BUT. As healthcare organizations that employ clinicians, shouldn t their quality of care matter more than it currently is represented? We are all patients at some point isn t a clinician who gives good care what matters most?
10 Pay For Performance 2010 plan devised to incorporate clinical quality metrics as a compensation component 2011 plan rolled-out, first P4P payments HTN bonus trigger set at 60% control rate 2015 metric goals revised HTN bonus trigger set at 66% control rate
11 P4P magnifies need to define the PCG Using Hypertension control as an example, we only assign the quality of patient s care to the PCG if: 1) Patient is assigned to that PCG 2) Has been diagnosed with Hypertension > 12 months (eliminates concerns about newly diagnosed conditions) 3) Has seen the PCG at least twice in the past 12 months (eliminates the very common and valid concern about not having sufficient face-time with some patients on one s panel)
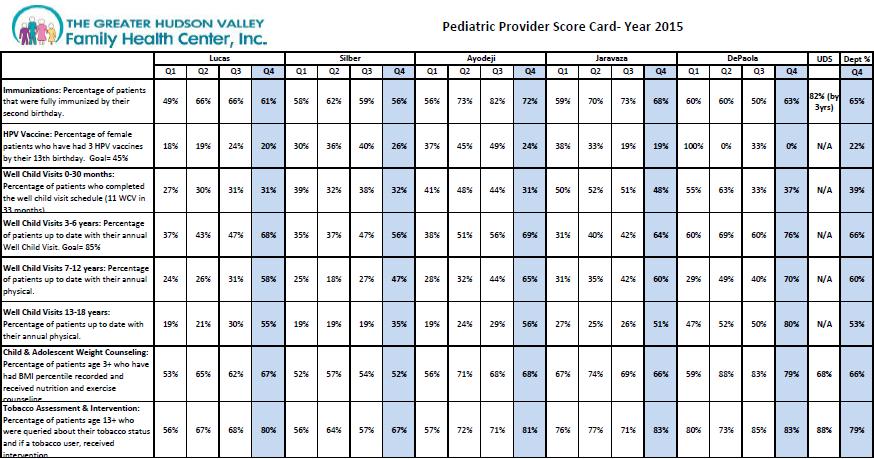
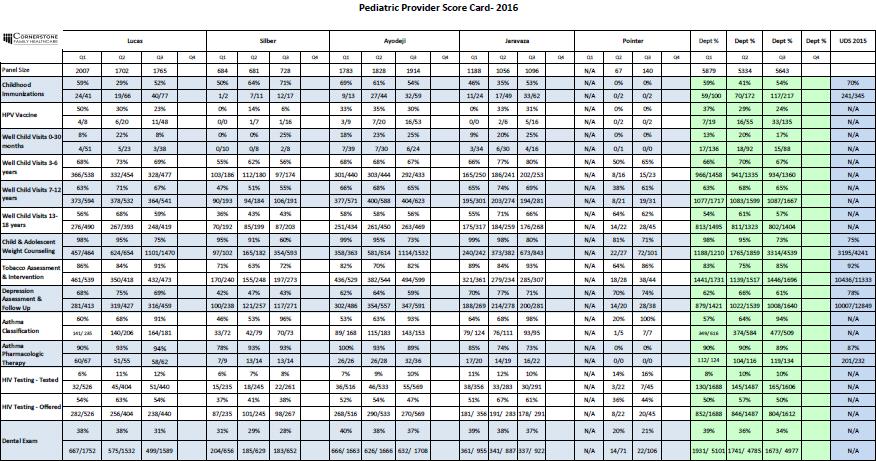
12 Open Door P4P Primary Care metrics, 1-6 (of 12) Primary Care P4P 2016 "N" needed Baseline 2016 P4P Hypertension 1 BP < 140/90, adults % 66% Diabetes 2 A1c < % 83% Asthma 3 Persistent classes with ICS 10 82% 88% or montelukast Immunizations UTD thru 2 yrs 4 % UTD 25 92% 90% tracks kids 2-4 years of age Immunizations UTD at 15 years 5 % UTD 5 67% 66% 3 HPV, 1 TDaP, 2 Varicella Paps, in last 3 years 6 % done, > 21 yo % 77% Women age HP2020 goal is 66% HP2020 goal is 80% ODFMC goal is 90% HP2020 goal is 50% ODFMC goal is 66%
13 Open Door P4P Primary Care metrics, 7-12 (of 12) Primary Care P4P 2016 "N" needed Baseline 2016 P4P Mammo, in last 2 years 7 % done, > 50 yo % 70% Women age CRC 8 % done > 50 yo 50 42% 50% Adults age Adult Pneumo 9 % done 50 79% 81% Adults age 65 and older Adult Tdap in last 10 years 10 % done 50 64% 65% Age 18 and older Depression screening/treatment 11 Age 12 and older % 60% Tobacco assessment/cessation 12 Age 13 and older % 90%
 4) Clinician s data from the most recent 2 quarters He is on track to: Hit P4P metric Miss P4P")
14 A typical Clinician Report Card A clinician s report card, showing data: 1) By Goal 2) Open Door overall 3) Clinician s site (Mount Kisco) 4) Clinician s data from the most recent 2 quarters He is on track to: Hit P4P metric Miss P4P metric
15 Pay for Performance breakdown 2016 (2017 breakdown is being revised) Bonus potential is 10% of salary for a clinician who is not in a leadership/managerial position 50% - clinician hits productivity target 25% - clinician site hits productivity 15% - clinician s clinical quality rating (1-4) 10% - individual goals set with clinician s site medical director
16 Determining Clinical Quality Rating We rate clinical quality on a scale of 1-4. Dr. XXX is on track to hit 10 of 12 P4P metrics. Metrics achieved: Clinical rating:
17 Summary Clinicians are hard to find, highly-trained, independentminded professionals that you want to nurture, support, and cultivate. Compensation strategies can help or hurt your chances at retention and recruitment. Incentivize what you want to influence (productivity, quality, panel size, satisfaction, camaraderie/citizenship, etc) Make the system as fair and transparent as possible And if at first you don t succeed, try and try again!

18 Questions???


19
, Goshen and newest site co-located in")
20 Who we are Federally Qualified Health Center 24,000 patients with 200,000 units of service in clinical sites plus 3 mobile vans including a health care for the homeless site, dedicated dental, urgent care Joint Commission Accredited PCMH Level Standards Locations in Hudson Valley include Newburgh, New Windsor, Highland Falls (West Point area), Goshen and newest site co-located in housing project in Binghamton
21 Our Services Primary Care: Internal Medicine, Pediatrics, Ob/Gyn Urgent Care Dental Specialties: Cardiology, Podiatry, ID Behavioral Health Services Care Coordination Audiology Optometry Positive Choices (HIV/AIDS Care) Women, Infants, and Children (WIC) Services Enabling Services Center For Recovery (Methadone and Day Rehab)
 6 Dentists 6 Dental Hygienists 2 Psych NP and 4 CSW 1 Optometrist 1")
22 Clinical Staff 44 clinicians overall 13 physicians 11 physician extenders (NP/PA) 6 Dentists 6 Dental Hygienists 2 Psych NP and 4 CSW 1 Optometrist 1 Nutritionist
23 History of Incentive Plan First year of incentive plan 2015; Discussions and Planning began May 2014 Why we started the program: Reflect pay for performance changes in medicine Reward high performing providers, incentivize middle of the road providers, align poor performers Recruitment and retention? Helps align goals of the providers with the practice Previous bonuses were not timely or objective enough to change behavior Guiding principles: Awarding of bonuses is objective & predictable Compensation is timely and reflective of performance Supports the goals of organization Enough skin in the game to change behavior Transparency Getting it off the ground: CEO buy in Provider workgroup meets three to four times per year to define objectives and provide feedback Ongoing meetings with CMO, COO, CFO ( three legged stool meeting) Communication and feedback from Providers
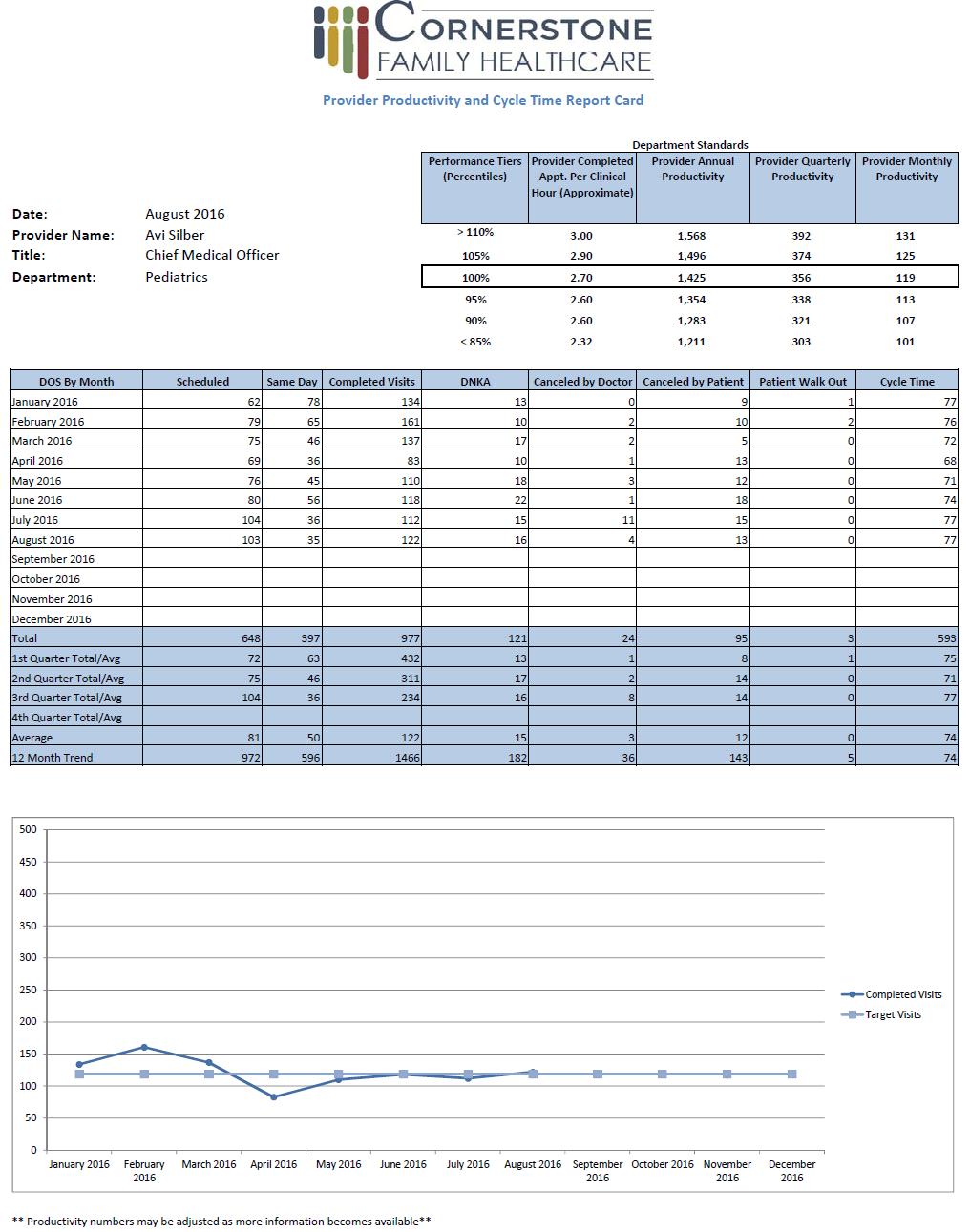
24 2015 Incentive Plan Focused on 3 elements: productivity (70%) clinical metrics (20%) and cycle time (10%) Two Phases to allow new providers time to build panel Phase 1: 5% Bonus Potential for Physicians; 6.5% for Mid-Level Providers of annual base salary; enter phase I after minimum of 6 months to a year of employment Phase 2: 10% Bonus Potential for Physicians and 11.5% for Mid-Level - with potential of 5% annual withholding; automatic enrollment in Phase 2 after one year. (may elect to enter early) Productivity based on 3 patients per hour and a 32 hour work week ( the 4200 number) Clinical Performance Measures UDS/QARR - agreed upon by CMO and Chief of Dept Cycle Time baseline was 80 minutes goal of 65 minutes
25 Internal Medicine / Pediatrics / Urgent Care and OBGYN (In Office Providers) Performance Tiers (Percentiles) PRODUCTIVITY STANDARDS Provider Completed Appt. Per Clinical Hour (Approximate) Provider Annual Productivity Provider Quarterly Productivity >110% % % % % % <80% ** Pediatric providers nursery / newborn hospital encounters are calculated on a 1:1 ratio, inpatient admission on a 3:1 ratio ** Performance Tiers (Percentiles) Phase I: Total Bonus % of Annual Salary Phase II: Total Bonus % of Annual Salary >110% 4.20% 8.40% 105% 3.50% 7.00% 100% 2.80% 5.60% 95% 2.10% 4.20% 90% 1.40% 2.80% 85% 0.70% 1.40% <80% -5%
26 Clinical Outcomes Clinical Outcomes Percent of Annual Salary: Phase I Providers Percent of Annual Salary: Phase II Providers 105% 1.0% 2.0% 100%.75% 1.5% 95%.50% 1.0% 90%.25%.50% Internal Medicine Standard Percentage of patients 18 to 85 years of age with diagnosed hypertension (HTN) whose blood pressure (BP) was less than 140/90 at the time of the last reading 70% Percentage of patients aged 50 to 75 who had appropriate screening for colorectal cancer 40% Family Practice/Highland Falls Percentage of patients 18 to 85 years of age with diagnosed hypertension (HTN) whose blood pressure (BP) was less than 140/90 at the time of the last reading ( UDS) Percentage of patients 3-6 years old who completed an annual well child visit (QARR) Standard 70% 85% OBGYN *( measure of success based on department )* Percentage of women who delivered during the measurement period that were given Tdap (Tetanus, Diphtheria, Pertussis) during their pregnancy. Standard 60% Percentage of woman between the ages of seen in the department who had a mammography in the previous 2 years. 62% Pediatrics Standard Percentage of female patients that have three HPV vaccines by age thirteen (QARR) 45% Percentage of patients 3-6 years old who completed an annual well child visit (QARR) 85%
27 Cycle Time Performance Standards Percent of Achievement 2014 Cycle Time Standard (Minutes) Percent of Annual Salary: Phase I Providers Percent of Annual Salary: Phase II Providers 105% % 1.00% 100% 65.38% 0.75% 95% % 0.50% 90% % 0.25% Percent of Achievement 2015 Cycle Time Standard (Minutes) Percent of Annual Salary: Phase I Providers Percent of Annual Salary: Phase II Providers 105% 57.50% 1.00% 100% 60.38%.75% 95% 63.25%.50% 90% 66.13%.25%
28
29
30
31
32 Administrative / Qualifying Metrics: In order to qualify for a bonus all the following standards must be met. If the criteria are not met the provider cannot benefit from quality or productivity bonus, but are still at risk for salary holdback if they do not meet 90% productivity. 1. On the 4 th Friday of every month a report will be generated. All providers must have signed off on any office visit that is more than 48 hours old. 1. Participation in one community event, health screening, health fair or lecture for medical students approval by CMO 1. Peer Review: 5 Peer Review forms will be distributed quarterly. Peer Reviews need to be completed and submitted within 2 weeks of distribution. 1. Provider must write 2 blogs for the health center on a topic of their choice first one due by 6/1/16 and 2 nd one due no later than 12/31/16.
33 What we learned from 2015? Previous issues with coverage resolved itself departments covered themselves Overall increase in productivity. Some providers respond, some not so much. Not all clinical sites and departments should be held to same standard. Difficult to reconcile this and still appear to be objective and fair. Providers made more money Have not figured out a way to include Ob s who deliver in hospital in plan Cycle Time Improved
34 2016 Plan Updates Increased weighting of clinical outcomes from 20% to 35% to reflect the shift to Value Based Compensation. Included plan to get to a 50% bonus based on clinical outcomes by 2018 Urgent Care performance tier moved up No more differentiation between mid levels and physicians This was first year providers required to have downside risk (5% holdback for productivity performance < 85%) 3 providers had money held back; 1 recently left organization and cited dissatisfaction with downside risk in exit interview Eliminated Bonus for 90%; Shifted more bonus to high performers ( >100%). Plan included to only bonus for >100% by Clinical Performance measures based on departmental performance
35 Value Based Incentives Bronx Lebanon Primary Care Isaac Dapkins MD Outgoing CMO Bronx Lebanon Integrated Services Systems Inc.
36 Background of BLISS Impetus for Change Measure Alignment Challenges Dashboarding
37 Background of Bronx Lebanon Integrated Services Systems Inc. YEAR ORGANIZATION Current MLK Jr Health Center opened its doors the first urban and largest community health center funded by the Office of Economic Opportunity. Bronx-Lebanon Hospital Center (BLHC) was directly funded by a grant from the Bureau of Community Health Services. Bronx Ambulatory Care Network (BACN), a freestanding, not-for-profit corporation, was funded by PHS under the Section 330 Grant Program. BACN contracted with BLHC and Montefiore Hospital Medical Center, as sub-recipients, to provide comprehensive primary care to the residents of the South Bronx. Bronx-Lebanon Integrated Services System Inc. (BLISS) was formed as one of two successor entities to the Bronx Ambulatory Care Network (BACN), and funded as a direct recipient of section-330 funding. 11/4/2016 3
38 Current status of Bronx-Lebanon Integrated Services Systems Inc. Two subrecipients: MLK Jr HC and Bronx Lebanon Hospital Centers 22 clinical programs at 9 different sites. All 9 sites are PCMH Level 3 (2011 Standards, 2014 application pending) Allscripts Sunrise Clinical Manager since acute care beds Over 1 million ambulatory care visits, 120,000 FQHC patients 330 long-term care beds Part owner of Healthfirst Lead of Bronx Health Access PPS


39 * Managed Medicaid PCMH Level 3 Healthfirst P4P DSRIP Go Live Click Fees Proposed VBP incentive 1 Year Incentive Review Period Key: Incentive Changes Programs impacting decision to go to value based 5
40 Impetus for Change Healthfirst Full- Risk Contract Medicare Access and CHIP Reauthorization Act of 2015 Multiple P4P Programs (DSRIP, UDS, HQIP) Decision to reduce Volume Based incentive for physicians

41 Measure Alignment Revenue flows based on Number of months patients assigned to a PCP Better quality increases the PMPM value of each client Better documentation increases the PMPM value of each client
42 PCMH Establishes a core understanding of population level healthcare Requires provider engagement on a population level Does not take into account cost of care

43 Healthfirst Quality Incentive Program (HQIP/Medicaid)
44 DSRIP DSRIP Guaranteed Funds were funneled through Equity Performance Program Revenue flows via Pay for Performance metrics through contracts with Managed Medicaid Companies DSRIP Performance Payments are shifting from Process and Reporting to Performance measures (Domains 2&3) MY3 (July 1, 2016-June 30, 2017) is the highest value year for bonus payments related to performance
45 DSRIP EPP Measures Children s Access to Primary Care 12 to 24 months Children s Access to Primary Care 7 to 11 years Prenatal and Postpartum Care Postpartum Visits EPP Measures** Children s Access to Primary Care 25 months to 6 years Children s Access to Primary Care 12 to 19 years Prenatal and Postpartum Care Timeliness of Prenatal Care Well Care Visits in the first 15 months (5 or more Visits) Childhood Immunization Status (Combination ) Frequency of Ongoing Prenatal Care (81% or more) Follow-up care for Children Prescribed ADHD Medications Continuation Phase Follow-up care for Children Prescribed ADHD Medications Initiation Phase Lead Screening in Children Med. Assist. w/ Smoking & Tobacco Use Cessation Discussed Cessation Strategies Controlling high blood pressure Comprehensive Diabetes screening All Three Tests Diabetes monitoring for persons with schizophrenia Initiation and Engagement in Alcohol and Other Drug Dependence Treatment (IET) within 14 days of substance abuse episode Behavioral Health follow up after hospitalization for mental illness (7 day) Chlamydia Screening (16 24 Years) Med. Assist. w/ Smoking & Tobacco Use Cessation Discussed Cessation Medication Comprehensive Diabetes Care Diabetes screening for persons with schizophrenia or Bipolar Disease who are using Antipsychotic Medication Adherence to anti-psychotic medications for individuals with schizophrenia Behavioral Health follow up after hospitalization for mental illness (30 day) Follow-up on Alcohol and Other Drug Dependence Treatment (IET) within 44 days of initial engagement
46 Challenges Behavioral Economics Empanelment Measuring Patient Satisfaction Tools for effectuating change in population health


47 Ann Intern Med. 2016;164(2):
48 Empanelment Patients seen in the past 15 months + Patients on Managed Medicaid Panel + Patients are asked to agree on Primary Provider ( Preferred PCP ) as part of the PCMH.
49 Telephone Survey Questions When visiting your primary care physician or specialist, how long do you usually spend in the waiting room before you see the doctor? Overall, how would you rate the quality of care you received from this doctor? How would you rate this doctor on giving you a clear explanation of tests and treatment options?
50 Tools for effectuating change How can we increase our panel? How can we get patients to come in to be seen if they need a measure? How can we see what our progress has been?
51 Bronx Lebanon Incentive Plan Total incentive could result in an increase of reimbursement of approximately 30% Data aggregated for quality across multiple HEDIS measures using RHIO data Patient satisfaction data collected on a daily basis through telephone surveys (Cipher Health) Visit volume will be a component that is phased out over time Panel size based on empanelment
52 Final Incentive Breakdown Values MEDICINE PEDIATRICS Panel 21% 35% Quality 26% 11% Visit 41% 50% Satisfaction 7% 4% Documentation 6% 0%
53 Panel Size Providers incentivized to have more 1800 patients in care: Patients seen in the past 15 months + Patients on Managed Medicaid Panel + Patients are asked to agree on Primary Provider ( Preferred PCP )
54 Quality Component Standard measures that are based on the UDS, EPP and HQIP. Each measure has a threshold above which incentive $ begin to be available and a benchmark when the maximum dollar amount is achieved. We only pay to the benchmark so doing better than benchmark does not benefit provider
55 Patient Satisfaction Provider specific patient satisfaction responses on a modified CAHPS survey Baseline threshold of >20% positive topline answers Target >55% topline answers
56 Visit Volume Incentive is a per/visit dollar value for each visit.
57 Documentation Improvement Providers receive real time alerts at time of visit Provider achieves incentive based on their response to documentation improvement alerts
58 Dashboarding!

59 Data Mall


60 Provider Action List
61 * Managed Medicaid PCMH Level 3 Healthfirst P4P DSRIP Go Live Click Fees Proposed VBP incentive 1 Year Incentive Review Period Key: Incentive Changes Programs impacting decision to go to value based 27
62 Questions Isaac Dapkins MD CMO Lutheran Family Health Center
Meeting Title. Facilitators. Conference Line
 DSRIP Meeting Agenda Date and Time 4/8/16, 3:00-4:00PM Meeting Title NYP PPS Finance Committee Location Heart Center Room 3 Facilitators Jay Gormley, Brian Kurz Go to Meeting https://global.gotomeeting.com/
DSRIP Meeting Agenda Date and Time 4/8/16, 3:00-4:00PM Meeting Title NYP PPS Finance Committee Location Heart Center Room 3 Facilitators Jay Gormley, Brian Kurz Go to Meeting https://global.gotomeeting.com/
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program
 March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
March Data Jam: Using Data to Prepare for the MACRA Quality Payment Program Elizabeth Arend, MPH Quality Improvement Advisor National Council for Behavioral Health CMS Change Package: Primary and Secondary
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Performance Incentives in the Southern California Permanente Medical Group (SCPMG):
:") Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Brian Sheitman MD
 Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Collaborative Care: Case Study of Integrating Primary Care in a Mental Health Setting Beat Steiner MD MPH Professor of Family Medicine UNC School of Medicine & Associate Medical Director Primary Care Services
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
2017 Quality Rewards Program
 2017 Quality Rewards Program Overview High-level Program Description and Guidelines What Is Changing in 2017 Bonus Payments Description Payment Timing 2 Doc #: PCA-1-005014-02032017_03092017 Updated 06262017
2017 Quality Rewards Program Overview High-level Program Description and Guidelines What Is Changing in 2017 Bonus Payments Description Payment Timing 2 Doc #: PCA-1-005014-02032017_03092017 Updated 06262017
Behavioral Health Providers: The Key Element of Value Based Payment Success
 Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
Quality: Finish Strong in Get Ready for October 28, 2016
 Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
Quality: Finish Strong in 2016. Get Ready for 2017 October 28, 2016 Agenda Stars: Medicare Advantage Quality Changes for 2017 Pay for Quality and PCMH Programs Important Announcements! 7 Stars: Medicare
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
The Florida KidCare Program Evaluation
 The Florida KidCare Program Evaluation Calendar Year 2015 MED147 Deliverable # 59 12/6/16 Prepared by the Institute for Child Health Policy University of Florida Under Contract to the Agency for Health
The Florida KidCare Program Evaluation Calendar Year 2015 MED147 Deliverable # 59 12/6/16 Prepared by the Institute for Child Health Policy University of Florida Under Contract to the Agency for Health
Florida Medicaid: Performance Measures (HEDIS)
") Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives. Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018
 Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
and HEDIS Measures
 1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
Oregon's Health System Transformation
 Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
Oregon's Health System Transformation MEASUREMENT PERIOD Baseline Year 2011 and Calendar Year 2013 JUNE 24, 2014 TABLE OF CONTENTS Executive Summary...iii 2013 CCO Performance and Quality Pool Distribution...1
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
HEDIS 101 for Providers 2018
 HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
Anthem Blue Cross and Blue Shield Serving Hoosier Healthwise, Healthy Indiana Plan and Hoosier Care Connect. Quality improvement strategies
 Serving Hoosier Healthwise, Healthy Indiana Plan Quality improvement strategies Learning objectives At the conclusion of this session, participants will be able to describe: Managed care products and eligible
Serving Hoosier Healthwise, Healthy Indiana Plan Quality improvement strategies Learning objectives At the conclusion of this session, participants will be able to describe: Managed care products and eligible
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
National Survey of Physician Organizations and the Management of Chronic Illness II (Independent Practice Associations)
") If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
If you want to use all or part of this questionnaire, please contact Patty Ramsay (email: pramsay@berkeley.edu; phone: 510/643-8063; mail: Patty Ramsay, University of California, SPH/HPM, 50 University
Patient Centered Medical Home 2011
 Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Patient Centered Medical Home 2011 NCQA Standards Rand David, MD, FACP Associate Professor of Medicine Director, Dept. of Ambulatory Care Mount Sinai School of Medicine Elmhurst Hospital Center I have
Goals & Challenges for Outpatient Quality Directors. Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE
 Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
Goals & Challenges for Outpatient Quality Directors Quality HealthCare Consulting, LLC CEO: Jennifer O'Donnell, MHA, PCMH-CCE Objectives Learn a practical way for Quality Directors to align Quality Measures
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
10/6/2017. FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction. Agenda. Incentives in PPS: what does excludable mean?
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
Overview of Six Texas Demonstrations
 Texas Case Study: Document 2 Overview of Six Texas Demonstrations The chart below provides an overview of six Texas demonstrations. Where possible, the chart indicates the purpose of the demonstration,
Texas Case Study: Document 2 Overview of Six Texas Demonstrations The chart below provides an overview of six Texas demonstrations. Where possible, the chart indicates the purpose of the demonstration,
MD, MBA, FACHE, FAAPL
 Washington Association of Medical Staff Services Vancouver, Washington Ambulatory Credentialing and Privileging Jon Burroughs, MD, MBA, FACHE, FAAPL April 20, 2018 The Healthcare Transformation Journey:
Washington Association of Medical Staff Services Vancouver, Washington Ambulatory Credentialing and Privileging Jon Burroughs, MD, MBA, FACHE, FAAPL April 20, 2018 The Healthcare Transformation Journey:
QUALITY IMPROVEMENT. Articles of Importance to Read: Quality Improvement Program. Winter Pages 1, 2, 3, 4 and 5 Quality Improvement
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
=======================================================================
 ======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the Secretary
The Patient-Centered Medical Home Model of Care
 The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
The Patient-Centered Medical Home Model of Care May 11, 2017 Louise Bryde Principal Presentation Outline Imperatives for Change Overview: What Is a Patient-Centered Medical Home? The Medical Neighborhood
Payment Transformation 2018 Measure Changes and Updates. April 4, 2018
 Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
Payment Transformation 2018 Measure Changes and Updates April 4, 2018 1. 2018 Performance Measures 2. 2018 Engagement Measures 3. Patient Attribution & Panel Management Cozeva 4. Coreo 1. Effectively Manage
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
approved Nevada s State Innovation Model (SIM) Round October 2015 Division of Health Care Financing and Policy Introduction to SIM
 Round October 2015 Division of Health Care Financing and Policy Introduction to SIM") Nevada State Innovation Model (SIM) October 2015 1 Introduction to SIM The Center for Medicare and Medicaid Services (CMS) approved Nevada s State Innovation Model (SIM) Round Two application to improve
Nevada State Innovation Model (SIM) October 2015 1 Introduction to SIM The Center for Medicare and Medicaid Services (CMS) approved Nevada s State Innovation Model (SIM) Round Two application to improve
HHW-HIPP0314 (9/13) MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.
 MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.") HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM
 IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Developing and Implementing Alternative Payment Models. Presented by AllCare Health APM Team
 Developing and Implementing Alternative Payment Models Presented by AllCare Health APM Team AllCare Service Area and Membership County Members Jackson 28,449 Josephine 19,016 Curry/Douglas 2,871 Total
Developing and Implementing Alternative Payment Models Presented by AllCare Health APM Team AllCare Service Area and Membership County Members Jackson 28,449 Josephine 19,016 Curry/Douglas 2,871 Total
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH 2014 Recognition Checklist
 1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
1 PCMH1: Patient Centered Access 10.00 points Element A - Patient-Centered Appointment Access ~~ MUST PASS 4.50 points 1 Providing same-day appointments for routine and urgent care (Critical Factor) Policy
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff
 Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
TO BE RESCINDED Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
ACTION: Final DATE: 09/21/2018 3:40 PM TO BE RESCINDED 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model
Meaningful Use and PCC EHR
 Meaningful Use and PCC EHR (tim@pcc.com) Users Conference 2016 Agenda MU basics and eligibility How to participate in MU Meeting MU measures in PCC EHR Understanding CQM reporting in PCC EHR Takeaways
Meaningful Use and PCC EHR (tim@pcc.com) Users Conference 2016 Agenda MU basics and eligibility How to participate in MU Meeting MU measures in PCC EHR Understanding CQM reporting in PCC EHR Takeaways
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
HHSC Value-Based Purchasing Roadmap Texas Policy Summit
 HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
Medicaid Benefits at a Glance
 Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
Medicaid Benefits at a Glance Mountain Health Trust Benefits Children (0 up to 21 years) Ambulatory Surgical Center Services Any distinct entity that operates exclusively for the purpose of providing surgical
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Tennessee Health Care Innovation Initiative
 March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013)
") Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
Exhibit 1. Medicare Shared Savings Program: Year 1 Performance of Participating Accountable Care Organizations (2013) 24 percent (52 ACOs) earned shared savings bonus 27 percent (60 ACOs) reduced spending,
2018 Practice Improvement Program (PIP) Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)
 Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)") 2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
IHCP Annual Workshop October 2017
 IHCP Annual Workshop October 2017 Pay for Performance (HEDIS) HHW-HIPP0519( 10/17) Exclusively serving Indiana families since 1994. Agenda Who is MDwise MDwise Delivery Systems HEDIS Overview Pay for Outcome
IHCP Annual Workshop October 2017 Pay for Performance (HEDIS) HHW-HIPP0519( 10/17) Exclusively serving Indiana families since 1994. Agenda Who is MDwise MDwise Delivery Systems HEDIS Overview Pay for Outcome
COMPREHENSIVE QUALITY STRATEGY REPORT (CQS) 2017 Report Draft
 2017 Report Draft") COMPREHENSIVE QUALITY STRATEGY REPORT (CQS) 2017 Report Draft CQS Report--Purpose Florida Medicaid is required to furnish a written quality strategy to the federal Centers for Medicare and Medicaid Services
COMPREHENSIVE QUALITY STRATEGY REPORT (CQS) 2017 Report Draft CQS Report--Purpose Florida Medicaid is required to furnish a written quality strategy to the federal Centers for Medicare and Medicaid Services
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Exhibit A.11.DY3. DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements
 Requirements") Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary
 2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER
 PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT
 SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
SUCCESS IN A VALUE - BASED PAYMENT ARRANGMENT October 3 rd, 2017 David Evangelista MediSys Health Network 1 Who is MediSys? Jamaica Hospital is a 431-bed not-for profit teaching hospital. Jamaica is a
Getting Ready for the Maryland Primary Care Program
 Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Getting Ready for the Maryland Primary Care Program Presentation to Maryland Academy of Nutrition and Dietetics March 19, 2018 Maryland Department of Health All-Payer Model: Performance to Date Performance
Note: Accredited is the highest rating an exchange product can have for 2015.
 Quality Overview Accreditation Exchange Product Accrediting Organization: NCQA HMO (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product can have for 215.
Quality Overview Accreditation Exchange Product Accrediting Organization: NCQA HMO (Exchange) Accreditation Status: Accredited Note: Accredited is the highest rating an exchange product can have for 215.
Patient-centered medical homes (PCMH): Eligible providers.
: Eligible providers.") ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/20/2016 8:11 AM 5160-1-71 Patient-centered medical homes (PCMH): Eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Advancing Care Information Performance Category Fact Sheet
 Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
Fact Sheet The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) replaced three quality programs (the Medicare Electronic Health Record (EHR) Incentive program, the Physician Quality Reporting
PCC Resources For PCMH. Tim Proctor Users Conference 2017
 PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
PCC Resources For PCMH Tim Proctor (tim@pcc.com) Users Conference 2017 Agenda Current state of PCMH and what s coming Exploration of how PCC functionality applies to new 2017 PCMH factors PCC Resources
South Dakota Health Homes Care Coordination Innovation
 South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
South Dakota Health Homes Care Coordination Innovation Senator Deb Soholt NCSL Health Innovation Task Force December 6, 2016 South Dakota Health Homes Health Homes (HH)- provide enhanced health care services
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
CMHC Healthcare Homes. The Natural Next Step
 CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
CMHC Healthcare Homes The Natural Next Step Partners in Planning A collaborative effort involving Dept. of Social Services (Mo HealthNet) Dept. of Mental Health Primary Care Association (FQHCs) Coalition
Advancing Primary Care Delivery
 Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
Advancing Primary Care Delivery Tenth National Pay for Performance Summit March 3, 2015 Simeon Schwartz, MD CEO, WESTMED Medical Group, P.C. WESTMED Medical Group Established 1996 by 16 physicians 300
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH
 INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
INTEGRATION OF PRIMARY CARE AND BEHAVIORAL HEALTH Integrating silos of care Goal of integration: no wrong door to quality health care Moving From Moving Toward Primary Care Mental Health Services Substance
Appendix 5. PCSP PCMH 2014 Crosswalk
 Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
Appendix 5 Crosswalk NCQA Patient-Centered Medical Home 2014 July 28, 2014 Appendix 5 Crosswalk 5-1 APPENDIX 5 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice () standards with
HEALTH CARE REFORM IN THE U.S.
 HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
HEALTH CARE REFORM IN THE U.S. A LOOK AT THE PAST, PRESENT AND FUTURE Carolyn Belk January 11, 2016 0 HEALTH CARE REFORM BIRTH OF THE AFFORDABLE CARE ACT Health care reform in the U.S. has been an ongoing
April L. Lyons, MSN, RN Director of Clinical Operations Westside Family Healthcare
 April L. Lyons, MSN, RN Director of Clinical Operations Westside Family Healthcare U.S. Incarceration Rates The incarceration rate of the United States is the highest in the world, at 716 per 100,00 of
April L. Lyons, MSN, RN Director of Clinical Operations Westside Family Healthcare U.S. Incarceration Rates The incarceration rate of the United States is the highest in the world, at 716 per 100,00 of
Communicator. the JUST A THOUGHT. Ensuring HEDIS-Compliant Preventive Health Services. Provider Portal Features. Peer-to-Peer Review BY DR.
 WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
A legacy of primary care support underscores Priority Health s leadership in accountable care
 Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Priority Health has been at the forefront of supporting primary care, driving accountability, improving quality and improving care for patients. A legacy of primary care support underscores Priority Health
Quality Peer Group UDS Best Practices and Data Sharing 9/9/16. ohiochc.org
 1 Quality Peer Group UDS Best Practices and Data Sharing 9/9/16 ohiochc.org Presenters 2 Ashley Ballard Director of Clinical Quality Tiffany Blair Quality Improvement Coordinator Dr. Wymyslo Chief Medical
1 Quality Peer Group UDS Best Practices and Data Sharing 9/9/16 ohiochc.org Presenters 2 Ashley Ballard Director of Clinical Quality Tiffany Blair Quality Improvement Coordinator Dr. Wymyslo Chief Medical
Medicaid 101: The Basics
 Medicaid 101: The Basics April 9, 2018 Miranda Motter President and CEO Gretchen Blazer Thompson Director of Govt. Affairs Angela Weaver Director of Regulatory Affairs OAHP Overview Who We Are: The Ohio
Medicaid 101: The Basics April 9, 2018 Miranda Motter President and CEO Gretchen Blazer Thompson Director of Govt. Affairs Angela Weaver Director of Regulatory Affairs OAHP Overview Who We Are: The Ohio
Early and Periodic Screening, Diagnosis and Treatment (EPSDT)
") Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Florida FLORIDA (FL) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Early and Periodic Screening, Diagnosis and Treatment (EPSDT) EPSDT and Bright Futures: Florida FLORIDA (FL) Medicaid s EPSDT benefit provides comprehensive health care services to children under age 21,
Analysis and Use of UDS Data
 Analysis and Use of UDS Data Welcome and thanks for dropping by to learn about how to analyze and use the valuable UDS data you are reporting! Please click START to begin. Welcome If you have attended
Analysis and Use of UDS Data Welcome and thanks for dropping by to learn about how to analyze and use the valuable UDS data you are reporting! Please click START to begin. Welcome If you have attended
State Leadership for Health Care Reform
 State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
State Leadership for Health Care Reform Mark McClellan, MD, PhD Director, Engelberg Center for Health Care Reform Senior Fellow, Economic Studies Leonard D. Schaeffer Chair in Health Policy Studies Brookings
Physician Compensation Trends and Models. Boyd P. Murayama, MBA CPC CPC-I
 Physician Compensation Trends and Models Boyd P. Murayama, MBA CPC CPC-I 1 Road Map OUR WORLD IS CHANGING EMPLOYMENT TRENDS EXPLORE COMPENSATION MODELS KEY TAKEAWAYS 2 Road Map OUR WORLD IS CHANGING 3
Physician Compensation Trends and Models Boyd P. Murayama, MBA CPC CPC-I 1 Road Map OUR WORLD IS CHANGING EMPLOYMENT TRENDS EXPLORE COMPENSATION MODELS KEY TAKEAWAYS 2 Road Map OUR WORLD IS CHANGING 3