NHS Tayside. Directorate. Infection Control and Management. Annual Report 2011/12
|
|
|
- Elinor Cobb
- 5 years ago
- Views:
Transcription
 Executive Management Team NHS Tayside Board")
1 NHS Tayside Directorate of Infection Control and Management Annual Report 2011/12 Approval Record Date approved Signature Risk Health and Safety Management Committee (Operational) Executive Management Team NHS Tayside Board
2 CONTENTS Page 1. Executive Summary 3 2. Purpose of this Report 4 3. Governance 4 4. Funding for Infection Control 4 5. Infection Control Work Programme Hand Hygiene Antimicrobial Prescribing Needlestick Injuries MRSA Screening Staph aureus Bacteraemias New Acquisitions of MRSA New Acquisitions of Clostridium difficile Central Venous Catheter Bacteraemias Surveillance-Surgical Site Infection Alert Organisms Ventilator Associated Pneumonia (VAP) Education and Training Cleanliness Champions Summary Audit Legionella and water quality Decontamination Communication/Public Involvement Outbreaks/Incidents Summary Infection Control Policy and Procedures Complaints 28 Annual Work Programme Outcomes Glossary 34 Linked Documents 34 Infection Control Annual Report
3 1. Executive Summary The Directorate of Infection Control and Management provide assurance to NHS Tayside (NHST) that prevention, management, diagnosis of infection, antimicrobial stewardship, and hand hygiene remain priorities to ensure a cohesive approach from Board to Point of Care. This remains a challenge, however, is enabled by collaborative working between clinical and support services. This Annual Report covers the reporting period April 2011 to March Key activities include:- Review of governance, reporting and accountability arrangements within Infection Control by Internal Audit. (Section 3). NHS Tayside participation in the Second National Prevalence Survey: Healthcare Associated Infection (HAI) and Antimicrobial Prescribing (Section 8). Continuing efforts to meet the HEAT target 2012 to reduce the incidents of all Staphylococcus aureus bacteraemia (including MRSA) by a rate of 0.27 per 1000 AOBD by March 2012 (Section ). Achieving improvement in hand hygiene compliance continued to be a key priority at a national and local level. All healthcare staff, including medical staff have been challenged to continue to improve compliance and rates have averaged 92% nationally in 2011/2012 (Section 5.1) Engagement with a wider audience and in order to seek views from members of the public, the Infection Control team have been working proactively with NHS Tayside s Public Involvement Team to be early adopters of the new E Participation website when launched. Options include taking part in a discussion forum, completing an online survey or quick poll. Launching the Infection Prevention and Control Foundation elearning Module In November This is mandatory for all staff and recorded in their PDP as contributing towards their HAI objective. A specific medical and dental staff module is launched in April Increasing the number of staff completing the Cleanliness Champion programme concluded with a total of 2195 Cleanliness Champions in NHS Tayside with an average of 45 staff completing per month and is a marked increase from last year. Responding to HAI Inspections to NHS Tayside during the reporting period by Healthcare Environment Inspectorate (HEI):- Unannounced Ninewells Hospital April 2011 Stracathro Hospital May 2011 Ninewells Hospital November 2011 Perth Royal Infirmary February 2012 Infection Control Annual Report
4 2. PURPOSE OF THE REPORT The purpose of the report is to highlight and summarise progress and achievement throughout 2011/2012 against the broader HAI agenda and the Infection Control Annual Work Programme. 3. GOVERNANCE Reporting and governance arrangements are clearly detailed within the Infection Control and Management Reporting and Governance Document which can be accessed via the Infection Control section of Staffnet. In the autumn of 2011, the Director Infection Control and Management commissioned Internal Audit to undertake a review of Governance, Reporting and Accountability arrangements for Infection Control. The scope and objectives of the review were to ascertain whether: Governance and accountability arrangements for Infection Control are robust, appropriate and clearly defined. There is clear and effective reporting of Infection Control issues throughout the organisation and to the Board. There are adequate structures and protocols in place to manage Infection Control throughout the organisation. An appropriate monitored and reported action plan is in place to address recommendations from HEI reports. Report No. T20A/12 concluded that arrangements are robust and the Directorate met control objectives with only 4 minor weaknesses being identified. These weaknesses have now been addressed. The overall audit was graded band B. 4. FUNDING FOR INFECTION CONTROL In Financial year 2011/12 Infection Control incurred overall expenditure of 2,612k. This allowed clinical and infection control teams to support infection control targets such as surgical site infection surveillance and hand hygiene. Included within this expenditure are the following:- - 1,438k on requirements following Environmental Audits. - 1,078k on Staff costs. - 96k Miscellaneous supplies costs the majority of which relate to the implementation of the MRSA Screening project. From this 50k relates to reagents costs within the laboratories and 24k relates to clinical waste. The remaining 22k relates to general supplies/travel within the department. 5. INFECTION CONTROL WORK PROGRAMME The Annual Work Programme (AWP) is compiled by a collaborative approach with input from Public Partners, Antimicrobial Management Team, Estates, Site Services, Safety Clinical Governance and Risk, and takes cognisance of the Healthcare Associated Infection Delivery Plan, Better Health Better Care, NHS Scotland Quality Strategy, Scottish Patient Safety Programme and local strategic drivers. Infection Control Annual Report
5 Updating of the programme is co-ordinated monthly by the General Manager Infection Control & Management. A number of factors are taken into account including, emerging developments, changes in national policy, new legislation and action required as a consequence of discussion at a number of relevant senior fora e.g. NHS Tayside Board. The AWP is readily available to all staff via the Infection Control section of Staffnet and is monitored at each Infection Control Performance Review Meeting. 5.1 Hand Hygiene The Local Health Board Co-ordinator has continued to develop and implement actions to raise Hand Hygiene (HH) compliance across NHS Tayside. Hand Hygiene auditing continues to be linked with the Scottish Patient Safety Programme. This has been in accordance with the Scottish Government s Zero Tolerance expectations stated in May NHS Tayside s response to these expectations can be found on staffnet, please click here to access. Key developments in 2011/2012: Worked with Executive Management to explore the recommendations from the Scottish Government funded Social Marketing Study Following forging links with the Practice Education Facilitator for Care Homes, training was delivered in seven Care Homes, across Tayside where nursing students receive placements Focus on hand skin care throughout the year when delivering presentations in order to try and address national HH audits Targeted work with clinical areas in relation to audit findings Undertook partnership work with Special Needs School in Dunkeld Provided input to the NHS Tayside s Glove Policy Support for Volunteer staff management around key points for effective HH HH Steering Group delivered the Exit Strategy which was signed off by the Executive Management Team Provided HH education for the Medical Centre Staff at RN Condor Led on the delivery of necessary Risk Assessments for the use of Alcohol Based Hand Rubs and availability of wash hand basins Working with Clinical Governance to design Standard Operating Procedures for the use of the HH audit tool Working with the Acting Head of Health and Safety to deliver a more robust assessment and management process for staff skin health Liaised with IC nurse from the Care Inspectorate to promote collaborative working in Tayside Working with those involved with the setting up of the Clinical Dashboard to ensure compliance with Scottish Government expectations National HH audits continued bimonthly during 2011/12 with NHS Tayside sustaining compliance between 90 and 94% averaging 92% for the year. The areas audited were stipulated by Health Protection Scotland (HPS), with the actual wards being selected at random locally. NHS Tayside s confidence in their HH compliance continues to be supported locally by clinical staff undertaking monthly audits reported to both Infection Control and the Scottish Patient Safety Programme. This involves all hospital settings, including the Infection Control Annual Report
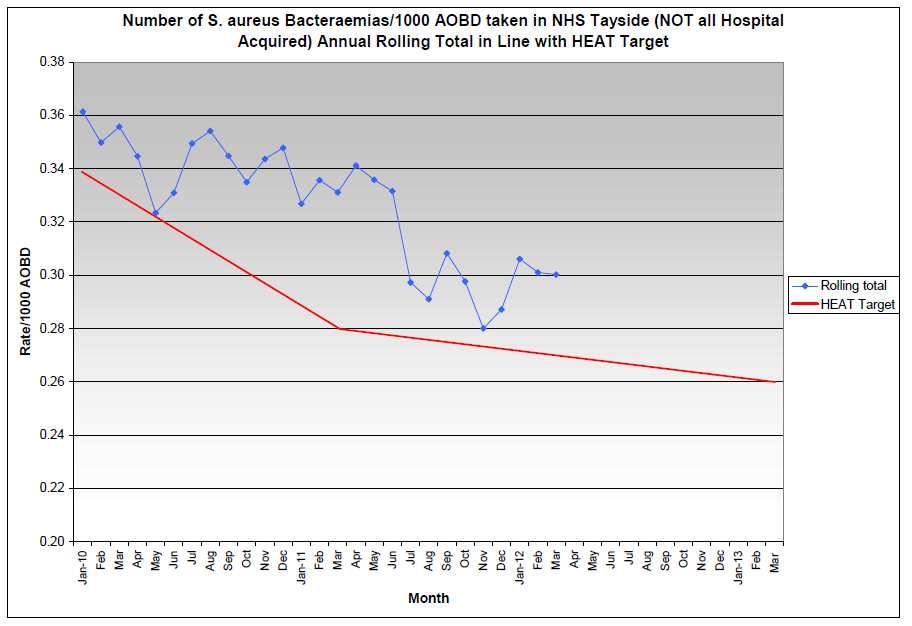
6 Integrated Dental Service. Infection Control Nurses also support the overall auditing process through their annual snapshot process. The number of clinical areas reporting their HH compliance for local analysis has continued to increase: Year Areas Antimicrobial Prescribing The Antimicrobial Management Group Annual Report for 2011/12 is attached to this report. 5.3 Needlestick injuries A Sharps Group was established to review sharps management. Membership comprises Safety, Clinical Governance & Risk, Procurement, Education, Infection Control and Health and Safety. This group will have a lead role in implementing the EU Sharps Directive Prevention from sharps injuries in the hospital and healthcare sector by May 2013 which will involve the further introduction of safety devices and awareness raising and training for staff. 5.4 MRSA Screening As part of the SGHD programme, all NHS Boards have introduced a revised MRSA Screening Protocol as from April 2011 which involves a Clinical Risk Assessment to be undertaken to identify those requiring to be screened as well as continuing with screening for all admissions to high risk specialties of Orthopaedic, Renal, vascular and cardiovascular. Non recurring funding was secured to assist with this implementation which has progressed well with NHST meeting the required milestones and being reported in the monthly SGHD return. 5.5 Staphylococcus aureus Bacteraemias (SABs) NHS Tayside missed the HEAT target 2011 by 10 episodes. The overall trend has been downwards with the major reduction being seen in the MRSA episodes. Over the past year the rate of reduction has stabilised. The 2013 target is based on the final rate and it is quite possible that NHST may not meet this target: contributory factors include the fact that 30-40% are community acquired and thus not amenable to intervention. Ninewells and PRI figures are shown below with Figure 1a showing the areas from which the episodes are acquired which does not take into account patient numbers. The chart shows a slight increase in episodes in renal areas. A SAB action group was set up December and the Board participated in a 90 day improvement plan. Work continues to focus around preventing line associated infections by continuing to increase compliance with CVC and PCV bundles in particular and a focus on reducing the number of renal unit related infections. Infection Control Annual Report


7 Infection Control Annual Report
8 Figure 1a 60 Number of S. aureus Bacteraemias per Group (Ninewells and PRI) April 2010/11 and April 2011/ Number 30 MSSA MRSA / / / / / / / / / / / /12 Medical (N1-6,P3,P6) Surgical (N7-12/HDU,P1,P5) Orthopaedics (N16-19,P7-8) Group Renal (N22/RDU,PRDU) Ward N20/PITU Admissions (N15,NAE,P4) 5.6 New Acquisitions of MRSA Over this period there were changes to the screening programme in line with national recommendations which required to be fully implemented by end of March As a result of funding being secured to appoint a lead officer to focus on this implementation, this target was monitored and achieved within NHST by March The impact of this on the laboratory is shown in the figure below. A recent audit has shown that about half of the new MRSA positives are detected on screening with the remainder being detected from samples taken for investigation of clinical infection. Overall, 0.2% of screening swabs yielded new positives in Figures 2 and 3 show the numbers of new cases for the two acute hospital sites neither of which are outwith control parameters. Outbreaks/clusters of infection with MRSA are detailed in the outbreak section Total Number of MRSA Screening Specimens Taken NHST 2008 onwards 3000 Number of Specimens Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Month Infection Control Annual Report



9 Figure 2 Figure 3 Figure 4 Infection Control Annual Report
10 5.7 New Acquisitions Clostridium difficile Local data (which includes all new cases not just the >65 yrs) is showing a trend towards stability (Figs 5-7) in all acute sites and RVH. NHS Tayside is well in line with the HEAT target (Fig 8) due to improved compliance with antimicrobial prescribing, early detection and isolation and adherence to standard and contact infection control precautions. Outbreaks/clusters of infection are detailed in the incidents and outbreaks section. The ribotying profile has changed over the years with less 027 and 106 ribotypes and an increase in 002 and 078 apparent for those that are typed. 078 types are unable to be subtyped, but have been seen in a couple of small clusters of infection which are detailed in the Outbreaks and incidents section NB: These are only those C. Diffs sent for typing (N = 111), same time period 215 positive samples were taken Number of C. Diff Episodes by Type and Location NHST Jan Mar 2012 CAI Community Hospital RVH PRI NW Number of Episodes Type Infection Control Annual Report



11 Figure 5 Figure 6 Figure 7 Infection Control Annual Report

12 Figure Central Venous Catheter (CVCs) Bacteraemias CVC infection remains low in ICU at Ninewells. The Renal Unit continues to experience CVC related infections in these vulnerable groups with numerous risk factors and actions which contributes to the staphylococcal bacteraemia burden. Regular screening for staphylococcal carriage continues in the renal patients and each SAB event in this unit is reviewed by a multidisciplinary group. Surgical unit CVC usage in terms of line days and infections was stable and just within the locally set target of less than 3 episodes per 1000 line days. 9 CVC Infection Rate/1000 Catheter Days for Ward 20, Ninewells Hospital Jan Mar Rate/1000 Catheter Days Jan-11 Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan-12 Feb Mar Month Infection Control Annual Report
13 3 CVC Infection Rate/1000 Catheter Days for Ward 22, Ninewells Hospital Jan Mar Rate/1000 Catheter Days Jan-11 Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan-12 Feb Mar Month 600 CVC Infection Rate/1000 Catheter Days for Wards 7-12 including SHDU, Ninewells Hospital January Mar N o. o f C a th e te r D a y s R a te / C D Total CD Rate/1000 CD Target Line for Rate/1000 CD 6 per. Mov. Avg. (Rate/1000 CD ) J a n -1 0 F e b -1 0 M a r-1 0 A p r-1 0 M a y -1 0 J u n -1 0 J u l-1 0 A u g -1 0 S e p -1 0 O c t-1 0 N o v -1 0 D e c -1 0 J a n -1 1 F e b -1 1 M a r-1 1 A p r-1 1 M a y -1 1 J u n -1 1 J u l-1 1 A u g -1 1 S e p -1 1 O c t-1 1 N o v -1 1 D e c -1 1 J a n -1 2 F e b -1 2 M a r-1 2 Month 5.9 Surveillance Surgical Site Infection PRI and Ninewells operates a proactive 30-day telephone post discharge surveillance (PDS) for all primary total hip and knee joint replacements, abdominal hysterectomy and Caesarean section procedures. Mandatory 30 day PDS is occurring for all other hip procedures including fracture neck of femur, hip revisions and resurfacings, continues through passive surveillance. Infection Control Annual Report
14 Surveillance is undertaken for specific vascular and breast procedures, but over the course of the year there were no issues with SSIs in these procedures. During 2011 NHS Tayside took the option to move towards light surveillance The results of surveillance are fed back to Directorates as Statistical Process Control charts. Superficial and deep Surgical Site infection Report NHS Tayside Jan 11 to Feb 12 (latest data set available as there is a 30 day post operation surveillance period) NOF = Neck of femur TAH = Total Abdominal Hysterectomy Vasc = Vascular Month Breast no. (% infection) C section no. (% infection) NOF no. (% infection) Hip no. (% infection) Knee no. (% infection) TAH No. (% infection) Vasc no. (% infection) Jan11 24 (4) 88 (7) 73 (3) 58 (5) 42 (2) 8 (25) 21 (5) Feb 20 (5) 79 (4) 54 (0) 50 (4) 47 (6) 12 (0) 14 (0) Mar 33 (0) 96 (2) 51 (4) 57 (2) 55 (2) 22 (0) 22 (5) April 29 (0) 93 (3) 48 (4) 48 (2) 41 (0) 10 (0) 14 (0) May 25 (0) 91 (4) 63 (2) 58 (2) 37 (8) 8 (13) 20 (5) June 26 (4) 95 (5) 44 (5) 60 (2) 44 (5) 16 (0) 14 (7) July 24 (0) 104 (12) 45 (2) 45 (4) 39 (0) 8 (0) 14 (0) Aug 42 (0) 99 (9) 54 (6) 58 (7) 46 (3) 15 (20) 19 (16) Sep 33 (3) 96 (4) 38 (5) 55 (0) 47 (0) 8 (0) 22 (9) Oct 25 (4) 102 (2) 56 (0) 40 (0) 54 (0) 9 (0) 18 (0) Nov 33 (0) 94 (5) 50 (4) 97 (2) 63 (2) 11 (0) 16 (0) Dec 30 (0) 108 (12) 70 (0) 56 (4) 42 (0) 6 (0) 21 (0) Jan (0) 101(9) 61 (2) 51 (2) 41 (0) 12 (17) 25 (8) Feb 39 (0) 82 (1) 65 (0) 50 (4) 44 (0) 11 (0) 19 (0) Mar 11 (0) 107 (6) 65 (0) 53 (0) 62 (2) 15 (0) 37 (0) The SSI programme continues to identify any deviations and allow investigations to be done where required. Individual months may demonstrate high SSI rates which should be treated with caution especially when the number of operative procedures is low (e.g. Total Abdominal Hysterectomies), small numbers are annotated on the statistical process control charts when a significant deviation occurs. When a trigger of 2 SSIs is identified within 30 days of a specific procedure, Infection control is notified. Deviations are reviewed to identify any issues, evaluate practices and recommend relevant actions. Stracathro orthopaedic procedures were included in the figures in Local and national surveillance via HPS identified that the cumulative incidence of superficial and deep SSI to day 10 for C section procedures between 1 st July to 30 th September 2011 and again over December 2011 and January was higher than expected. NHS Tayside was above the national 95% confidence limits with a rate of 5.4% (14 superficial SSIs from 261 procedures). A review was carried out on both occasions but no common links were found between the cases. Several patients has risk factors which would increase the chance of infection and the infecting organisms were acquired from the patients own flora. However, several areas identified for improvements including: Infection Control Annual Report
15 Standardisation of theatre practice in relation to skin disinfection Introduction of Chlorhexidine 2% in 70% alcohol for surgical site skin preparation. Use of warming pads Change in antibiotic prophylaxis dosing to within 30 minutes of incision rather than after cord clamping Making sure dressings stayed in place for first 48 hours Development of a maternal sepsis clinical management algorithm. Patient information in terms of advice on hair removal and looking after the wound was developed Work continues to understand recording of some other infections to see how these impact on post C-section infections and the recording. An action plan was returned to HPS in response to the quarterly exception report which included the above actions. The rate returned to baseline before the interventions but these were all deemed to be significant improvements to be introduced anyway. On the second occasion the situation was discussed with HPS and other external agencies but no systematic reason was found for the clustering of infections Alert Organisms The Infection Control Team monitors the incidence of a number of organisms which have characteristics such as antibiotic resistance or the potential to cause outbreaks. These are termed alert organisms. These are reported in the HAI Scorecard format (e.g. C difficile and MRSA) and relevant reports to clinical areas as a monitoring tool and the HAI Board report. Details on breaches can be found in the outbreaks and incidents sections. In response to CEL 3 (2010) Pseudomonas aeruginosa bacteraemias and all pseudomonas isolates from NICU were added to the list of ALERTS in 2012 to allow early detection of any issues. See Legionella and Water Quality Section. 20 Number of New ESBL Patients per Month Jan 2010 onwards Number of Patients Angus CHP P & K CHP Dundee CHP STX PRI NW Jan-10 Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan-11 Feb Month Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan-12 Feb Mar Infection Control Annual Report
16 5.11 Ventilator Associated Pneumonia (VAP) The locally set target is to remain below 15 episodes per 1000 ventilator days in this unit, which accommodates trauma, medical and surgical cases. Ventilator bundles are in place but the rate will be driven but the underlying medical condition of the patients and duration of ventilation. It can be seen that this target was attained apart from one breach September. 18 VAP Rate/1000 Ventilator Days for Ward 20, Ninewells Hospital Jan Mar VAP/1000 Ventilator Days Jan-11 Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan-12 Feb Mar Month 5.12 Education and Training As part of the annual process all Infection Control education content has been reviewed during The Infection Control team continue to deliver an extensive range of face to face education sessions and have developed specific sessions for community nursing staff. All education provided is included within the HAI Training and Development Strategy and Education Spreadsheet which is available to all staff via the Infection Control page of Staffnet. As well as the continuation of the successful Cleanliness Champions programme, an HAI learnpro module has been launched as a mandatory module for all NHST staff to complete. A module specifically designed for medical and dental staff is to be launched in April NHS Tayside is one of three Boards involved in a NES national project reviewing education requirements for community staff in relation to HAI.. A report will be published in Spring 2012 making recommendations as to future delivery of education. Increasing awareness in relation to norovirus was carried out in Tayside from September 2011 onwards involving local media and internal communications as well as formal education sessions. KSF has been carried out for all members of the ICT nursing team, along with reviewing nursing posts in line with national IPS competencies. Three members of Infection Control Annual Report
17 the Dundee team continue to carry out their MSc Infection Control, with one member of the Dundee team having successfully completed their MSc. Summary of Education Attendance Summary of documented Education Ninewells, RVH, Ashludie, Carsview, Kingscross, Strathmartine All Activities Numbers Staff Groups 2010/ /12 Registered Nursing Staff Untrained Nursing Staff Student Nurses Medical Staff FY th Year Medical Students Other Medical Students GPs - 14 GP Trainees - 15 GP staff - 9 DDH Technicians - 27 Dental Staff - 87 AHP AHP Students 1 10 Radiographers Pharmacy 20 8 Phlebotomists - 16 A & C Support Services* Estates - 25 Laundry Cleanliness Champions Support Workers 3 7 Volunteers Angus (Stracathro and Community Hospitals) All Activities Numbers Staff Groups 2010/ /12 Registered Nursing Staff Untrained Nursing Staff Medical Staff 2 6 AHP Support Services* Estates - 31 Cleanliness Champions Perth & Kinross (PRI and Community Hospitals) All Activities Numbers Staff Groups 2010/ /12 Registered Nursing Staff Untrained Nursing Staff Medical Staff AHP Support Services* Estates - 45 Cleanliness Champions *Includes Domestic and Portering staff. Infection Control Annual Report
18 5.13 Cleanliness Champions 2011 concluded with a total of 2195 Cleanliness Champions in NHS Tayside. This resulted in an average of 45 staff completing per month which continues to be a pleasing upward trend. The first Cleanliness Champion Study day took place in October 2011 and this proved to be very successful with 38 staff from various disciplines attending. There was a range of speakers from NHS Tayside, some of whom were showcasing the work undertaken within their clinical area. Topics included: The Cleanliness Champion Journey Topical issues in Mental Health Influencing the Elderly in Hand Hygiene Challenges for Cleanliness Champions in Physiotherapy Bugs and Drugs Seasonal issues and screening MRSA, VRE and Norovirus What s new in Education As this event was a resounding success it is envisaged that this will now become an annual event. Along with the study day the Cleanliness Champion annual updates were well attended in February, May and September. A variety of topics were included, some of which were requested by the Cleanliness Champions. These sessions received positive evaluations from the participants. The annual updates will continue throughout 2012/13 and will be delivered at different locations throughout NHS Tayside, including a dedicated event for dental staff held at Dundee Dental Hospital. During 2011 NES visited Boards throughout Scotland advising of the introduction of a time limit of six months for completion of a revised Cleanliness Champion programme and the move towards e learning from April This has been communicated to members of staff who are undertaking the programme. Final year medical students continue to complete this programme which is mostly mentored by NHS Tayside infection control and microbiology staff Audit General Currently there are several different levels of audit related to HAI being undertaken within NHS Tayside. The audit tool that is utilised during a Healthcare Environment Inspection (HEI) process was adapted to inform the production of a HAI Quality Assurance Monitoring Tool (QAMT) that both the ICT and clinical staff are utilising. All clinical areas audit their environment on a regular basis utilising this tool and report via their own management structure. A summary of the overall findings are incorporated within the HAI Report which is presented at each NHS Tayside board meeting. As from September 2011 a spot audit tool was also introduced which mirrors main themes from the external HEI inspection process. The ICT have carried out spot audits on a rolling programme basis with summarised reports being shared with clinical managers and the Executive Team. Infection Control Annual Report
19 Each of the Directorates/CHPs undertake a programme of walkrounds within each of their areas of responsibility. Infection Control are involved in these walkrounds with non executives invited to attend. A self-assessment audit tool was produced for GP practices to carry out their own audit with Infection Control staff providing advice and support on request. This has been monitored as part of the Primary Care contract and has highlighted a few minor issues and one main issue of concern within a particular practice which has been addressed. Utilisation of the GP self audit tool also highlighted potential gaps as this may not include areas within Health Centres where other community staff are located and working clinically e.g. Health visitors, anti-coagulation clinics, AHPs, etc. As a result of this, a small team has been visiting Health Centres and a decision has been taken to review the self assessment audit tool. Discussions are ongoing within the Senior Management Team of Infection Control to agree an audit process which fulfils HAI requirements without duplicating audits already carried out by Clinical and Domestic Services. A proposal describing a revised process will be presented to the Executive Management Team for consideration in March NHS Tayside continued to be monitored against the national cleaning specification and consistently scored green (compliance of 90% and above). The cleanliness of our hospitals continues to be a priority for 2011/ Planned audit programme Infection Control Team The Infection Control Teams have continued with a planned programme of audits, snapshots and observational studies as detailed below. This enabled Infection Control staff to look at general activities and work patterns in a variety of clinical areas over a 1 1½ hour period in order to identify any areas where Infection Control practices could be improved. Audits Undertaken - Dundee 106 audits in Ninewells 50 audits in Dundee Community Hospitals 14 audits in GP Surgeries (podiatry/dental) 10 audits in DDH Audits Undertaken Angus 9 Improvement Objectives completed in Stracathro 3 audits in Dental and Podiatry Practices 16 Improvement Objectives completed in Community Hospitals Audits Undertaken Perth & Kinross 31 Improvement Objectives completed in Perth Royal Infirmary 20 audits in Dental and Podiatry Practices 27 Improvement Objectives completed in Perth & Kinross Community Hospitals 9 Improvement Objectives completed in Perth & Kinross Community Bases 3 audits in Prison Services During the autumn of the Infection Control team carried out monthly spot audits within all wards in Ninewells Hospital, PRI and Stracathro Hospital. The results Infection Control Annual Report
20 of the spot audits were presented at the Executive Team. In addition, the following snapshots were also undertaken:- 21 snapshots in Perth Royal Infirmary 9 snapshots in Angus community 6 snapshots in Stracathro Hospital 10 snapshots in Perth & Kinross community There were 3 main areas of non-compliance highlighted during the snapshots, these were:- Use of temporary closures on sharps bins. Full implementation of Patient Equipment Cleaning Schedules Over ordering of stock leading to clutter and storage issues. Subsequent auditing has demonstrated a marked increase in compliance External Inspections and Audits Healthcare Environment Inspectorate (HEI) The Healthcare Environment Inspectorate (HEI) are now in year 3 of their programme which focuses on unannounced inspections to acute hospitals. HAI Inspections to NHS Tayside to date by Healthcare Environment Inspectorate (HEI):- Announced Ninewells Hospital - November 2009 Perth Royal Infirmary - May 2010 Unannounced Ninewells Hospital November 2010 Ninewells Hospital April 2011 Stracathro Hospital May 2011 Ninewells Hospital November 2011 Perth Royal Infirmary February 2012 NHS Tayside submitted a revised on-line HAI Self Assessment in September To ensure that governance and accountability arrangements are robust and appropriate, reports are provided at a number of senior fora in relation to requirements and recommendations assigned as a result of each Inspection. Progress being made is detailed within inspection specific Improvement Action Plans which are also shared at senior fora and reported at each NHST Board. To date there are 3 outstanding requirements, one which is being progressed nationally in relation to NHST not fully meeting the requirements of HDL (2005)8 and HDL (2001)10 which requires the ICM to have full accountability for domestic services and decontamination. This is a similar position for most other Boards in Scotland hence the HDLs are currently being reviewed nationally. The outcome of this review is not expected before summer One relates to the implementation of NHST policy tracker which is undergoing testing. The third outstanding requirement is from the latest report which relates to PVC/CVC bundle compliance, the expected completion date is June These reports and Improvement Action Plans can be accessed on the Infection Control Section of Staffnet. Infection Control Annual Report
21 Health Protection Scotland (HPS) The Infection Control Team invited review from Health Protection Scotland (HPS) relating to VRE incident 2010/2011 and also discussed the C section SSI issue. No further actions were required as a result of these visits. NHS Tayside was involved in the Scottish Prevalence Survey of HAI & Antimicrobial Prescribing. This survey involved a resource intensive collection of data from 6 acute and community hospital settings throughout Tayside during September and October The data was collected by staff from Microbiology, Infection Control, Safety, Clinical Governance & Risk, Infectious Diseases, Pharmacy and Antimicrobial. Local reports were made available in February 2012 with restricted circulation until the national report was published in Spring The results will inform future national policy and also provide NHS Boards with an epidemiological evidence base for local priority setting and will be used as the NHSScotland Healthcare Quality Strategy HAI Outcome Measures. External Sharps Audit As a result of a change in the National Contract for supplier of sharps commodities, a decision was taken by Procurement in discussion with Infection Control and clinical services to run a trial of sharps bins provided by the new supplier. This trial took place on the Stracathro site during January March The evaluation of the trial will be complete by the middle of April Daniels Healthcare undertook a sharps audit covering Angus and Perth & Kinross in May The outcome of the audit was positive with improvements seen from the previous year. Daniels completed an external audit within Dundee of all clinical areas within hospital settings in relation to sharps management. Findings noted were that areas ranged from 75% to 100% compliance with most areas showing a compliance level of over 95%. Issues related to temporary closure mechanism not being in situ, non matching lids and containers, inappropriate contents e.g. non-sharps and number of containers unlabelled whilst in use. There was no protruding sharps noted and all bins were assembled correctly Legionella and water quality The Legionella (and latterly Water Quality) Group met during this year and the Chair was handed back to Estates. The group was set up to oversee surveillance, sampling and response requirements in accordance with current Scottish Health Technical Memorandum (SHTM) 2040 and HSE Approved Code of Practice and Guidance Document (L8). The current external Water Management consultancy has expired and a tender exercise is currently under-way to appoint a new consultancy which is expected to be in place in The existing risk assessments of the water systems across NHS Tayside are still extant and recommendations from these are being worked through which includes regular testing for Legionella across the Delivery Unit and actions as required. There is an ongoing programme of expanding the testing regime across NHS Tayside and numerous smaller sites within the previous primary care umbrella are now part of this regimen. Currently the sampling regimen is carried out quarterly as a Infection Control Annual Report
22 minimum, with notifications of results passed back from the water consultant to the relevant microbiologist as well as the Responsible person and Deputy Responsible persons. These results are also trended over several periods in order that relevant action can be carried out to areas where it appears a common or regular occurrence of higher than normal counts appears. The Logbook system is working well with all work carried out on water systems recorded as a matter of course. These logbooks will be externally audited by our external water consultant to ensure accuracy and governance once appointed. Investigations are still ongoing to look at the possibility of introducing an electronic logbook in the near future. In line with guidance, showerhead cleaning is in place across Tayside with an external contractor cleaning all shower heads on a quarterly basis. In line with guidance for Thermostatic Mixing Valves (TMVs), an external contractor carries out 6 monthly and annual checking and testing of these at Ninewells Hospital and in-house estates staff carry out the same function elsewhere. Tank cleaning has been carried out locally on each site with the intention being that a pan Tayside contract will be put in place in the near future. Responsible Person training is planned for June and August 2012, after this training the Responsible Persons, deputies and Authorised Persons will be appointed. Estates staff have been trained in Legionella awareness and investigations are being carried out into the introduction of e-training for clinical groups which would be staffed and managed by the Infection Control Team as part of any other updates. The majority of work carried out in 2012/13 will be driven by the risk assessments carried out and the risks identified as part of this process. Following the release of CEL 03 (2012), which related to Pseudomonas in water outlets in high risk areas in hospitals, guidance was issued and pending further SGHD advice, flushing in high risk areas has been enhanced. Stracathro Borewell Following water quality issues, a working group met which included representation from the Infection Control Team, Estates, Health Protection Team, Environmental Health and a Scottish Government (SG) Regulation Manager, on behalf of the Drinking Water Quality Regulator. Following discussion it was agreed that an external consultant would be appointed. The external consultant:- Has overseen an upgrade of the Stracathro borewell and also the water treatment plant, both of which are now complete. Is currently in the process of producing a set of maintenance instructions for directly employed maintenance staff. Is advising on a final version of a Water Safety Plan which will then be agreed by the SG Regulation Manager. Work is now ongoing to identify and develop a back-up borewell supply for resilience and business continuity planning. Infection Control Annual Report
23 5.16 Decontamination Overview Primary care decontamination compliance for GDPs is almost complete with only one practice still to develop compliant LDU facilities. Broxden Dental Centre, LDU is now undertaking all Perth & Kinross NHS dental and podiatry decontamination. The decontamination solution for Dundee and Angus community dental and podiatry sites will consist of a combination of CDU provision and increased LDU utilisation at Kings Cross. This has required the purchase of further instruments for completion of the Podiatry move to a central service and re-costing of instrumentation for procurement and separate consultation exercises to move the Community Dental solution forward. Following completion of the new PRI endoscopy unit in August 2011, NHS Tayside now has three sites providing endoscopy decontamination services from compliant facilities using Wassenburg washers and Labcaire HEPA cabinets. ENT decontamination guidance recommendations although advising an automated process as best practice has recognised that a manual decontamination process is acceptable. HFS are undertaking further evidence based work to support a manual process. Risk assessment undertaken re manual decontamination of nasendoscopes using Tristel wipes and this practice continues SBAR completed following Medical Device Alert for laryngoscope handles. NHS Tayside already use single use blades, however now looking at a trial of single use handles and blades for Theatres with most other areas using a combination of single use or reprocessing handles in CDU. There is ongoing work looking at how NHS Tayside can achieve compliance with National CJD guidance recommendations for Ophthalmology decontamination for front of eye instruments. Posterior eye instruments are single use. Outstanding Decontamination Issues Replacement Reverse Osmosis plant required for Stracathro, Endoscopy Unit. SBAR completed and added to Risk Register as no funding identified. This plant is requiring additional maintenance and deteriorating function. The current LDU at Kings Cross Dental Unit is non compliant with national guidance and SHPN 13 part 2. There is a medium term outline business case for a potential new site for Dundee being progressed. Scotland wide, Ophthalmology is unable to comply with decontamination guidelines for Phacoemulsification handpieces. HFS alerted and have now escalated the issue to Professor Sir Kent Woods, Chief Executive, Medicines and Healthcare Products Regulatory Agency (MHRA) to obtain national UK wide guidance. Other Ophthalmology issues are currently under review as manufacturers guidance and national requirements are giving rise to practical difficulties in terms of implementation A server is required to enable activation of independent monitoring software as per UK and European guidance for automated endoscope washer decontamination processes on the PRI and Stracathro sites. Infection Control Annual Report
24 6. Communication Public Involvement NHS Tayside has an active Public Partners HAI Forum which meets regularly. The group has University representation. At each meeting, the group discusses the most recent HAI Board Report and the Infection Control AWP. The Public Partners HAI Forum met 5 times during 2011/12. Members continue to be involved in a variety of infection prevention and control activities, with the aim of promoting public engagement. These include:- Involvement in the development of the Infection Control Annual Work Programme Participation in cleanliness monitoring Involvement in the development, review of and display of patient/public information Participation in Public Awareness Events on Infection Control and Hand Hygiene, e.g. Blairgowrie event in May Attendance at information sharing sessions, e.g. MRSA Screening Protocol update. Members of the HAI Forum were asked to complete an online survey using the E Participation website to help evaluate the forum with the aim of ensuring that it continues to meet the needs of participants. They were also asked for their views on how NHS Tayside could involve the wider public in HAI. Results were analysed and the findings discussed with forum members in November As a result, the forum will be adopting a variety of new avenues to engage more widely with the public in relation to HAI and Infection Control will be participating in the two planned Public Involvement Events in April and October In addition, an online participation website has been piloted within NHS Tayside which will give the wider public the opportunity to share suggestions, comments and opinions on NHS Tayside services by accessing consultation, discussion and feedback online forums. As HAI is a key priority within NHS Tayside it was agreed to utilise the consultation forum to seek public opinion in relation to promoting hand hygiene amongst visitors to healthcare facilities when the E Participation website is launched in Spring Staff In order to heighten awareness and to increase staff engagement in relation to achieving HEI standards on a more consistent basis, a series of meetings were held with Heads of Nursing and SCNs during June/July 2011.These meetings allowed constructive input to implementation of revised systems and processes. Since the meetings a number of communication bulletins have been issued widely to keep staff updated on progress of the various systems and processes. Communications department issue a communication following the Board meeting which includes any particular HAI issues as a consequence of the HAI Board report. The annual pre norovirus season reminder was released via Vital Signs to highlight the key points of control of this infection in hospitals. Infection Control Annual Report

25 General Information Banners, as below, have been purchased to assist with alerting public and staff to important events and situations leading to a ward or department closure within NHS Tayside. To gain most coverage the banners will be placed at the main entrance to the relevant hospital involved in the event/situation. Infection Control Annual Report
26 7. INCIDENTS/OUTBREAKS Summary Table TYPE DATE RISK SCORE Clostridium Oct 11 Green difficile (CDI) AREA Surgical NW ACTIONS 4 patients. 3 were. 078 and infections clustered around a 3 week period and resolved. Ward not required to close Nov 11- Apr Green RVH 4 patients with CDI 078 all found after discharge from the ward. However, all patients had been in other wards as well. There is no subtyping procedure to assess if these were all the same strain. The period over which these 4 cases were identified was quite long which again can make pinpointing acquisition difficult 078 is the 2nd commonest ribotype we are seeing at the moment. Ward not required to close Oct 11 Jan 12 Green Renal NW 6 cases of CDI, 3 of which were 015 a relatively common strain locally. Rest were unrelated strains. Ward not required to close Infection Control Annual Report
27 TYPE DATE RISK SCORE MRSA Sept to Dec Green 2011 AREA Medical NW ACTIONS 8 patients : 4 were of the same strain over a 12 week period. Review of practice and enhanced screening put in place for this period. Ward did not require to be closed. these were identified post discharge in 6 cases. One patient was an infection the other patients were detected through standard or enhanced screening. Nov 2011 Green SCABIES Various Not required Surgical NW Various (3 areas) 3 patients all same type. Ward not closed and no further cases noted. Several episodes whereby staff and other patients needed preventative treatment. In all cases these were imported form the community and no spread within hospitals was noted Hepatitis B September Green Orthopaedics 36 patients contacted for hepatitis B screening after a new case came to light within a ward. This was lead by Health Protection Team Norovirus update 22 wards affected on different occasions across NHST for this year Green but amber on 2 occasions when there was an impact on admission s due to number of wards closed in a particular site/ specialty Several sites including acute and community hospitals 284 patients with suspected or confirmed norovirus 1 st episode was in late October 2011 and season lasted into May The peak month was February 2011 with 92 cases and 6 ward closures. Infection Control Annual Report
28 8. INFECTION CONTROL POLICY AND PROCEDURES The Infection Control Policy is available on the Safe & Effective Working Section of Staffnet and is updated regularly to reflect developments and changes to current practice. As the policy is a large document, individual sections of the policy have been hyperlinked to improve ease of access and aid navigation. Paper copies are regarded as uncontrolled if printed. In recognition of the need for staff to easily access Infection Control information, resources and tools, the Infection Control section of Staffnet was reorganised. This included creating a dedicated Resource section, a dedicated HEI section and initially featuring those items most readily accessed. Updating the policies is an ongoing process and with the introduction of HPS national policies links to these are added as they become available and these will supersede local policy. 9. COMPLAINTS There were 7 complaints reported to Infection Control for Tayside between the months of April 2011 until March The complaints were received from patients/relatives/visitors. Every complaint was treated individually and full detailed explanations were given back to the complaints office. In summary the complaint themes were related to the following: Hand Hygiene Compliance (2) General Infection Control Practice (1) Complaints in relation to clinical services in which Infection Control was highlighted (4) Appropriate action was taken by the Infection Control Team liaising with all appropriate services. Infection Control Annual Report
29 1. GOVERNANCE Infection Control and Management Directorate - Annual Work Programme 2011/12 Part Two: Specific Activities / Developments Objective Action Required Timescales Provide assurance that there is awareness of HAI Driver Diagrams Monitor elective admission receipt of Patient HAI Information Leaflet prior to admission Actions plans for external and internal reviews Provide assurance that there is full compliance with governance arrangements around Infection Control and Management 2. PREVENTION AND CONTROL OF INFECTION Audit awareness of ICMD HAI Driver Diagrams Audit to include different staff groups. Audit the admission process undertaken by Waiting List Secretaries to confirm that the HAI leaflet is included within admission documentation. Monitor progress with external and internal audit reports e.g. HEI, internal audit, SGHD template report, HFS visits Clinical Quality Forum and Senior Management Team meetings incorporate Infection Control and Management elements within their terms of reference By March 2012 By March audits March 2012 September 2011 Responsible person GM ICM Performance Indicator/ Outcome High awareness of HAI Driver Diagrams GM IC&M Audits completed 100% compliance demonstrated. GM ICM DICM GM ICM Progress monitored by various Infection Control and management forums Satisfies internal audit requirements and external assessment Progress Nov NHS Tayside Internal Audit team are currently assisting with audit process. Documents reviewed and now available on IC Staffnet page. Further supplies regularly requested and supplied to all localities through IC Admin Team. Spot checks undertaken by GM IC&M. 100% compliance HEI Paper submitted to August & Nov. Board Meeting. Action Plans updated frequently with progress against actions being detailed within the HAI Board template. IC&M included within NHS Tayside Internal Audit programme for 2011/12. Report issued December Complete. i.) HAI Strategy Ensure HAI is prioritised and addressed in clinical and non-clinical areas ii.) Reduce intravascular device associated infections Work with JCBs and CHPs to embed HAI learning and pro-active action. Review corporate HAI risks identified on SMART system Short Life SAB Action Group established in partnership with SP predominantly focussing on Ward 15, NWs and A&E NWs in conjunction with 90 day rapid cycle initiative. March 2012 August 2011 February 2012 March 2012 GM ICM/ DICM/GMs Clinical Team ownership. Performance monitored via a number of forums Minutes of a variety of fora record IC attendance and relevant interaction. GM ICM / RM Reviewed 6 monthly. Reviewed August & November NC HAI / SP Reduced device related sepsis as contributory factor in SABs CVC policy nearing completion. Improvement in the blood culture contamination rates in A&E and Ward 15 have shown sustained improvement. Infection Control Annual Report
NHS Tayside. Directorate. Infection Control and Management. Annual Report 2010/11
 NHS Tayside Directorate of Infection Control and Management Annual Report 2010/11 Approval Record Date approved Signature Executive Management Team NHS Tayside Board Risk Health and Safety Management Committee
NHS Tayside Directorate of Infection Control and Management Annual Report 2010/11 Approval Record Date approved Signature Executive Management Team NHS Tayside Board Risk Health and Safety Management Committee
NHS Tayside. Infection Prevention and Control Programme 2009/2010
 NHS Tayside Infection Prevention and Control Programme 2009/2010 Approval Record HAI Network Chief Executive Officer Medical Director Improvement and Quality Committee Risk Management/ Health and Safety
NHS Tayside Infection Prevention and Control Programme 2009/2010 Approval Record HAI Network Chief Executive Officer Medical Director Improvement and Quality Committee Risk Management/ Health and Safety
NHS Tayside INFECTION CONTROL. Infection Prevention and Control Scorecard Strategy 2009/10. Information for Clinical Groupings including CHPs
 NHS Tayside INFECTION CONTROL Infection Prevention and Control Scorecard Strategy 29/ Information for Clinical Groupings including CHPs Author: Gabby Phillips Review Group: Infection Control SMT Review
NHS Tayside INFECTION CONTROL Infection Prevention and Control Scorecard Strategy 29/ Information for Clinical Groupings including CHPs Author: Gabby Phillips Review Group: Infection Control SMT Review
HEI self-assessment. Completing the self-assessment - Guidance to NHS boards
 HEI self-assessment Completing the self-assessment - Guidance to NHS boards INTRODUCTION This document should be read in conjunction Healthcare Improvement Scotland healthcare associated infection (HAI)
HEI self-assessment Completing the self-assessment - Guidance to NHS boards INTRODUCTION This document should be read in conjunction Healthcare Improvement Scotland healthcare associated infection (HAI)
HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE 2016
 Appendix--75 Borders NHS Board HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE Aim The purpose of this paper is to update Board members of the current status of Healthcare Associated
Appendix--75 Borders NHS Board HEALTHCARE ASSOCIATED INFECTION PREVENTION AND CONTROL REPORT JUNE Aim The purpose of this paper is to update Board members of the current status of Healthcare Associated
NHS Highland Infection Prevention & Control Annual Work Plan End of Year
 NHS Highland Board 5 April Item 5.7 NHS Highland & Control Annual Work Plan End of Year Update for COIC Prepared by Catherine Stokoe and Jonty Mills (as of 01/03/) Objective Activity Time Scale Lead Officer
NHS Highland Board 5 April Item 5.7 NHS Highland & Control Annual Work Plan End of Year Update for COIC Prepared by Catherine Stokoe and Jonty Mills (as of 01/03/) Objective Activity Time Scale Lead Officer
Unannounced Theatre Inspection Report
 Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
Unannounced Theatre Inspection Report Perth Royal Infirmary NHS Tayside 12 13 July 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is
Report by Liz McClurg, Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive Lead, Infection Prevention & Control
 INFECTION PREVENTION & CONTROL ANNUAL WORK PLAN (2013 2014) Highland NHS Board 4 June 2013 Item 5.5(c) Report by Liz McClurg, Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive
INFECTION PREVENTION & CONTROL ANNUAL WORK PLAN (2013 2014) Highland NHS Board 4 June 2013 Item 5.5(c) Report by Liz McClurg, Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Announced Inspection Report
 Announced Inspection Report Udston Hospital NHS Lanarkshire 20 21 September 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is part
Announced Inspection Report Udston Hospital NHS Lanarkshire 20 21 September 2017 www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April 2009 and is part
Board Meeting 01/12/16 Open Session Item 10. Performance and Quality Report to the Board December 2016
 Board Meeting 01/12/16 Open Session Item 10 Performance and Quality Report to the Board ember Introduction This report summarises key areas of performance which includes, but is not limited to, Local Delivery
Board Meeting 01/12/16 Open Session Item 10 Performance and Quality Report to the Board ember Introduction This report summarises key areas of performance which includes, but is not limited to, Local Delivery
Checklists for Preventing and Controlling
 Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Checklists for Preventing and Controlling Clostridium difficile Infection (CDI) This document has been developed to specifically assist senior management and all ward staff to take appropriate actions,
Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36
 Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
Healthcare-associated infections: prevention ention and control Public health guideline Published: 11 November 2011 nice.org.uk/guidance/ph36 NICE 2017. All rights reserved. Subject to Notice of rights
BOARD CLINICAL GOVERNANCE & QUALITY UPDATE MARCH 2013
 Borders NHS Board BOARD CLINICAL GOVERNANCE & QUALITY UPDATE MARCH 2013 Aim The aim of this report is to provide the Board with an overview of progress in the areas of: Patient Safety Person Centred Health
Borders NHS Board BOARD CLINICAL GOVERNANCE & QUALITY UPDATE MARCH 2013 Aim The aim of this report is to provide the Board with an overview of progress in the areas of: Patient Safety Person Centred Health
MRSA: National developments, Progress, Challenges and Targets
 MRSA: National developments, Progress, Challenges and Targets Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London The MRSA challenge - 2007 Bacteraemia
MRSA: National developments, Progress, Challenges and Targets Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London The MRSA challenge - 2007 Bacteraemia
Inspection Report. Royal Infirmary of Edinburgh. NHS Lothian 18 and 19 January February 2010
 Inspection Report Royal Infirmary of Edinburgh NHS Lothian 18 and 19 January 2010 2 February 2010 qüé=eé~äíüå~êé=båîáêçåãéåí=fåëééåíçê~íé=áë=~=é~êí=çñ=kep=nì~äáíó=fãéêçîéãéåí=påçíä~åç= The Healthcare Environment
Inspection Report Royal Infirmary of Edinburgh NHS Lothian 18 and 19 January 2010 2 February 2010 qüé=eé~äíüå~êé=båîáêçåãéåí=fåëééåíçê~íé=áë=~=é~êí=çñ=kep=nì~äáíó=fãéêçîéãéåí=påçíä~åç= The Healthcare Environment
Infection Prevention and Control Strategy (NHSCT/11/379)
") Infection Prevention and Control Strategy (NHSCT/11/379) September 2010 September 2010 Contents Page No. 1. Foreword 1 2. Introduction 2-3 3. Key Principles 4-5 4. Objectives 6-13 5. Organisational Arrangements
Infection Prevention and Control Strategy (NHSCT/11/379) September 2010 September 2010 Contents Page No. 1. Foreword 1 2. Introduction 2-3 3. Key Principles 4-5 4. Objectives 6-13 5. Organisational Arrangements
Ayrshire and Arran NHS Board
 Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
Paper 6 Ayrshire and Arran NHS Board Monday 11 December 2017 SPSP Update: Acute Adult Programme Author: Laura Harvey, QI Lead for Acute Services, Person Centred & Customer Care Sponsoring Director: Liz
The safety of every patient we care for is our number one priority
 HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
HUMBER NHS FOUNDATION TRUST INFECTION PREVENTION AND CONTROL STRATEGY 2015-2017 1. Introduction Healthcare associated infections (HCAI) continue to be a major cause of patient harm and although nationally
Infection Prevention. & Control. Report
 Infection Prevention & Control Report April 2012 March 2013 Author Joanne Raper, Infection Prevention & Control Nurse Manager Page 1 of 10 1.0 Purpose of the Paper The purpose of this report is to provide
Infection Prevention & Control Report April 2012 March 2013 Author Joanne Raper, Infection Prevention & Control Nurse Manager Page 1 of 10 1.0 Purpose of the Paper The purpose of this report is to provide
Tom Walsh Infection Control Manager May 2008 ANNUAL INFECTION CONTROL REPORT 2007/08
 Tom Walsh Infection Control Manager May 2008 ANNUAL INFECTION CONTROL REPORT 2007/08 CONTENTS 1. INTRODUCTION... 1 2. ACCOUNTABILITY ARRANGEMENTS FOR PREVENTION & CONTROL OF INFECTION WITHIN NHSGGC...
Tom Walsh Infection Control Manager May 2008 ANNUAL INFECTION CONTROL REPORT 2007/08 CONTENTS 1. INTRODUCTION... 1 2. ACCOUNTABILITY ARRANGEMENTS FOR PREVENTION & CONTROL OF INFECTION WITHIN NHSGGC...
Clostridium difficile Infection (CDI) Trigger Tool
 Trigger Tool") Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland March 2014 Version 3.0 A CDI trigger is the number of new CDI
Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland March 2014 Version 3.0 A CDI trigger is the number of new CDI
Healthcare quality lessons from the best small country in the world
 Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Healthcare quality lessons from the best small country in the world Scotland and Canada Scotland 5.5 Million people Scottish Politics Scottish Politics Devolution - 1997 Scottish National Party minority
Antimicrobial stewardship in Scotland: quality improvement agenda
 Antimicrobial stewardship in Scotland: quality improvement agenda Dr Jacqueline Sneddon Project Lead Scottish Antimicrobial Prescribing Group Background Scottish Antimicrobial Prescribing Group (SAPG)
Antimicrobial stewardship in Scotland: quality improvement agenda Dr Jacqueline Sneddon Project Lead Scottish Antimicrobial Prescribing Group Background Scottish Antimicrobial Prescribing Group (SAPG)
WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT
 WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT 2006-2007 Author(s) Gill Harris, Director of Infection Prevention and Control EXECUTIVE
WRIGHTINGTON, WIGAN AND LEIGH HEALTH SERVICES NHS TRUST DIRECTOR OF INFECTION PREVENTION AND CONTROL ANNUAL REPORT 2006-2007 Author(s) Gill Harris, Director of Infection Prevention and Control EXECUTIVE
Healthcare Associated Infection Reporting Template (HAIRT) The NHS Board is asked to note the latest 2 monthly report on HAI within NHSGGC
 The NHS Board is asked to note the latest 2 monthly report on HAI within NHSGGC") NHS Meeting 17 th ruary 2015 Medical Director Paper No.15/04 Recommendation: Healthcare Associated Infection Reporting Template (HAIRT) The NHS is asked to note the latest 2 monthly report on HAI within
NHS Meeting 17 th ruary 2015 Medical Director Paper No.15/04 Recommendation: Healthcare Associated Infection Reporting Template (HAIRT) The NHS is asked to note the latest 2 monthly report on HAI within
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS 22 FEBRUARY 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST EXECUTIVE SUMMARY: BOARD OF DIRECTORS C 22 FEBRUARY 2012 Subject: Supporting : Author: Status (see footnote): Update on the Clostridium difficile (C.diff)
REPORT SUMMARY SHEET
 Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 27 th October 2016 Infection Prevention and Control
Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 27 th October 2016 Infection Prevention and Control
abc INFECTION CONTROL STRATEGY
 abc INFECTION CONTROL STRATEGY 1. INTRODUCTION East and North Hertfordshire NHS Trust (ENHT) considers the reduction of Healthcare Associated infections (HCAI) a key component of patient safety systems
abc INFECTION CONTROL STRATEGY 1. INTRODUCTION East and North Hertfordshire NHS Trust (ENHT) considers the reduction of Healthcare Associated infections (HCAI) a key component of patient safety systems
Public Services Reform (Scotland) Bill. Scottish Independent Hospitals Association
 Bill. Scottish Independent Hospitals Association") Public Services Reform (Scotland) Bill Scottish Independent Hospitals Association The following submission is presented to the Health and Sport Committee of the Scottish Government as an outline of the
Public Services Reform (Scotland) Bill Scottish Independent Hospitals Association The following submission is presented to the Health and Sport Committee of the Scottish Government as an outline of the
TRUST BOARD. Date of Meeting: 05/10/2010
 TRUST BOARD Date of Meeting: 05//20 Enclosure: 7 Agenda Item No: 8.3 Title of Report: Interim Report for Infection Prevention and Control 20-2011 Aims: To inform the Board of the work of the Trust in controlling
TRUST BOARD Date of Meeting: 05//20 Enclosure: 7 Agenda Item No: 8.3 Title of Report: Interim Report for Infection Prevention and Control 20-2011 Aims: To inform the Board of the work of the Trust in controlling
Board of Directors Infection Prevention and Control Report. Dr Claire Thomas, DIPC
 Board of Directors 25 November Report to: Title: Author: Sponsoring Director Purpose: Decision Sought: Board of Directors Infection Prevention and Control Report Dr Claire Thomas, DIPC Donna Green 6 monthly
Board of Directors 25 November Report to: Title: Author: Sponsoring Director Purpose: Decision Sought: Board of Directors Infection Prevention and Control Report Dr Claire Thomas, DIPC Donna Green 6 monthly
National Hand Hygiene NHS Campaign
 National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
Unannounced Inspection Report
 Unannounced Inspection Report Stobhill Hospital Glasgow Royal Infirmary NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April
Unannounced Inspection Report Stobhill Hospital Glasgow Royal Infirmary NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in April
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
NHS LANARKSHIRE QUALITY DASHBOARD Board Report October 2011 (Data available as at end August 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with
Provincial Surveillance
 Provincial Surveillance Provincial Surveillance 2011/12 Launched first provincial surveillance protocols Establishment of provincial data entry & start of formal surveillance reports Partnership with AB
Provincial Surveillance Provincial Surveillance 2011/12 Launched first provincial surveillance protocols Establishment of provincial data entry & start of formal surveillance reports Partnership with AB
NHS GREATER GLASGOW & CLYDE STANDARD OPERATING PROCEDURE (SOP)
") This SOP applies to all staff employed by NHS Greater Glasgow & Clyde and locum staff on fixed term contracts and volunteer staff. SOP Objective To minimise the risk of Pseudomonas aeruginosa infection
This SOP applies to all staff employed by NHS Greater Glasgow & Clyde and locum staff on fixed term contracts and volunteer staff. SOP Objective To minimise the risk of Pseudomonas aeruginosa infection
Clostridium difficile Infection (CDI) Trigger Tool
 Trigger Tool") Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland V2.0 November 2011 A CDI Trigger is the point at which the Infection
Hospital ward/clinical Area Date Trigger Tool Commenced Date Trigger Tool Closed Person closing the CDI Trigger Health Protection Scotland V2.0 November 2011 A CDI Trigger is the point at which the Infection
Healthcare Associated Infection (HAI) inspection tool
 inspection tool") Healthcare Associated Infection (HAI) inspection tool Hospital: Ward/Department: Inspector: Date: Guidance note: This tool is designed to assist HEI inspectors assess NHS boards compliance with NHS Quality
Healthcare Associated Infection (HAI) inspection tool Hospital: Ward/Department: Inspector: Date: Guidance note: This tool is designed to assist HEI inspectors assess NHS boards compliance with NHS Quality
Healthcare infection incidents and outbreaks in Scotland
 Healthcare infection incidents and outbreaks in Scotland Version: 1.0 Date: March 2017 Owner/Author: Infection Control Team DOCUMENT CONTROL SHEET Key Information: Literature Review: Title: Literature
Healthcare infection incidents and outbreaks in Scotland Version: 1.0 Date: March 2017 Owner/Author: Infection Control Team DOCUMENT CONTROL SHEET Key Information: Literature Review: Title: Literature
Quality and Safety Committee. Prevention and Control of Healthcare Acquired Infections performance to February 2012
 Betsi Cadwaladr University Health Board Committee Paper 05.04.12 Item QS12/37.5 Name of Committee: Subject: Summary or Issues of Significance National / Local Objectives Addressed: Legislation or Healthcare
Betsi Cadwaladr University Health Board Committee Paper 05.04.12 Item QS12/37.5 Name of Committee: Subject: Summary or Issues of Significance National / Local Objectives Addressed: Legislation or Healthcare
HCAI Local implementation team action plan
 HCAI Local implementation team action plan Item Type Report Authors New Governance HCAI Group Publisher New Governance HCAI Group Download date 16/09/2018 18:12:09 Link to Item http://hdl.handle.net/10147/110814
HCAI Local implementation team action plan Item Type Report Authors New Governance HCAI Group Publisher New Governance HCAI Group Download date 16/09/2018 18:12:09 Link to Item http://hdl.handle.net/10147/110814
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
REPORT SUMMARY SHEET
 Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 29 th September 2016 Infection Prevention and Control
Quality care for you, with you REPORT SUMMARY SHEET Meeting: Date: Title: Lead Director: Corporate Objective: Purpose: High level context: Trust Board 29 th September 2016 Infection Prevention and Control
National Hand Hygiene NHS Campaign
 National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
Shetland NHS Board. Control of Infection Committee Annual Report
 Shetland NHS Board Control of Infection Committee Annual Report April 20- March 2009 1 Acronyms and Abbreviations ARI AOBD CDU CoIC CSBS HAI HAI SCRIBE HDL HEAT targets HPS ICT NES MMR PFPI PPE MRSA MSSA
Shetland NHS Board Control of Infection Committee Annual Report April 20- March 2009 1 Acronyms and Abbreviations ARI AOBD CDU CoIC CSBS HAI HAI SCRIBE HDL HEAT targets HPS ICT NES MMR PFPI PPE MRSA MSSA
National Standards for the prevention and control of healthcare-associated infections in acute healthcare services.
 National Standards for the prevention and control of healthcare-associated infections in 2017 1 Safer Better Care Note on terms and abbreviations used in these standards A full range of terms and abbreviations
National Standards for the prevention and control of healthcare-associated infections in 2017 1 Safer Better Care Note on terms and abbreviations used in these standards A full range of terms and abbreviations
National Hand Hygiene NHS Campaign
 National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
National Hand Hygiene NHS Campaign
 National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
National Hand Hygiene NHS Campaign Compliance with Hand Hygiene - Audit Report Your Questions Answered Germs. Wash your hands of them Prepared for the Scottish Government Health Directorate HAI Task Force
IQC/2013/48 Improvement and Quality Committee October 2013
 Item 9.4 IQC/2013/48 Improvement and Quality Committee October 2013 Pressure Ulcer Prevalence Improvement Plan 1. SITUATION AND BACKGROUND This paper is to update the Improvement and Quality Committee
Item 9.4 IQC/2013/48 Improvement and Quality Committee October 2013 Pressure Ulcer Prevalence Improvement Plan 1. SITUATION AND BACKGROUND This paper is to update the Improvement and Quality Committee
Healthcare associated infections across the health and social care community
 Healthcare associated infections across the health and social care community Professor Brian Duerden CBE Inspector of Microbiology and Infection Control, Department of Health, London Infection is different..it
Healthcare associated infections across the health and social care community Professor Brian Duerden CBE Inspector of Microbiology and Infection Control, Department of Health, London Infection is different..it
North East Ambulance Service NHS Trust Infection Prevention and Control Annual Work Plan April 2009 March 2010 October review (2)
") North East Ambulance Service NHS Trust Infection Prevention and Control Annual Work Plan April 2009 March 2010 October review (2) No. Objective Actions Lead Date of 1 Leadership throughout Accountability
North East Ambulance Service NHS Trust Infection Prevention and Control Annual Work Plan April 2009 March 2010 October review (2) No. Objective Actions Lead Date of 1 Leadership throughout Accountability
The National Standards for the Prevention and Control of Healthcare Associated Infection
 The National Standards for the Prevention and Control of Healthcare Associated Infection The View of the Regulator Sean Egan Inspector Manager, HIQA Presentation Overview The role and function of the Health
The National Standards for the Prevention and Control of Healthcare Associated Infection The View of the Regulator Sean Egan Inspector Manager, HIQA Presentation Overview The role and function of the Health
Prevention and Control of Infection Annual Report 2014/15
 Golden Jubilee Foundation Prevention and Control of Infection Annual Report 20/ Approval record Date approved Board Prevention and Control of Infection Committee 11 September 20 Clinical Governance Risk
Golden Jubilee Foundation Prevention and Control of Infection Annual Report 20/ Approval record Date approved Board Prevention and Control of Infection Committee 11 September 20 Clinical Governance Risk
The prevention and control of infections North Cumbria University Hospitals NHS Trust
 The prevention and control of infections North Cumbria University Hospitals NHS Trust Region: North West Provider s code: RNL Type of organisation: Acute trust Type of inspection: Enhanced Sites we visited:
The prevention and control of infections North Cumbria University Hospitals NHS Trust Region: North West Provider s code: RNL Type of organisation: Acute trust Type of inspection: Enhanced Sites we visited:
Progress Report on C.Diff Action Plan
 NHS GREATER GLASGOW AND CLYDE NHS Board Meeting 16 December 2008 Paper No. 08/55 Board Medical Director Progress Report on C.Diff Action Plan Recommendation The NHS Board is asked to receive this further
NHS GREATER GLASGOW AND CLYDE NHS Board Meeting 16 December 2008 Paper No. 08/55 Board Medical Director Progress Report on C.Diff Action Plan Recommendation The NHS Board is asked to receive this further
Infection Prevention and Control. Quarterly Report
 Infection Prevention and Control Quarterly Report 1 st July 2009 30 th September 2009 Dr Nick Harper Director of Infection Prevention and Control Mrs Johanne Lickiss Nurse Consultant Infection Prevention
Infection Prevention and Control Quarterly Report 1 st July 2009 30 th September 2009 Dr Nick Harper Director of Infection Prevention and Control Mrs Johanne Lickiss Nurse Consultant Infection Prevention
Establishing an infection control accreditation programme to control infection
 International Journal of Infection Control www.ijic.info ISSN 1996-9783 Establishing an infection control accreditation programme to control infection Julie Parker Sheffield Teaching Hospitals NHS Foundation
International Journal of Infection Control www.ijic.info ISSN 1996-9783 Establishing an infection control accreditation programme to control infection Julie Parker Sheffield Teaching Hospitals NHS Foundation
Report by Liz McClurg, Interim Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive Lead for Infection Control
 INFECTION CONTROL REPORT Highland NHS Board 1 June 2 Item 4.5 Report by Liz McClurg, Interim Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive Lead for Infection Control
INFECTION CONTROL REPORT Highland NHS Board 1 June 2 Item 4.5 Report by Liz McClurg, Interim Infection Control Manager on behalf of Heidi May, Board Nurse Director & Executive Lead for Infection Control
Shetland NHS Board Communicable Disease Control Policy
 Shetland NHS Board Communicable Disease Control Policy Version Version 4 Completion date May 2015 Review date May 2017 Approved by Control of Infection Committee Clinical Governance Committee NHS SHETLAND
Shetland NHS Board Communicable Disease Control Policy Version Version 4 Completion date May 2015 Review date May 2017 Approved by Control of Infection Committee Clinical Governance Committee NHS SHETLAND
INFECTION CONTROL SURVEILLANCE POLICY
 INFECTION CONTROL SURVEILLANCE POLICY Version: 3 Ratified by: Date ratified: July 2016 Title of originator/author: Title of responsible committee/group: Senior Managers Operational Group Head of Infection
INFECTION CONTROL SURVEILLANCE POLICY Version: 3 Ratified by: Date ratified: July 2016 Title of originator/author: Title of responsible committee/group: Senior Managers Operational Group Head of Infection
Infection Prevention and Control (IPC) Annual Programme 20010/11
 Annual Programme 20010/11") Infection Prevention and Control (IPC) Annual Programme 20010/11 1. Introduction The Code of Practice for the Prevention and Control of Healthcare Associated Infections (DH, 2009) otherwise known as the
Infection Prevention and Control (IPC) Annual Programme 20010/11 1. Introduction The Code of Practice for the Prevention and Control of Healthcare Associated Infections (DH, 2009) otherwise known as the
Inspecting Informing Improving. Hygiene code inspection report: West Hertfordshire Hospitals NHS Trust
 Inspecting Informing Improving Hygiene code inspection report: West Hertfordshire Hospitals NHS Trust December 2008 Outcome of inspection for: Hospital(s) visited: West Hertfordshire Hospitals NHS Trust
Inspecting Informing Improving Hygiene code inspection report: West Hertfordshire Hospitals NHS Trust December 2008 Outcome of inspection for: Hospital(s) visited: West Hertfordshire Hospitals NHS Trust
Unannounced Inspection Report: Independent Healthcare
 Unannounced Inspection Report: Independent Healthcare Marie Curie Hospice - Edinburgh Marie Curie Cancer Care Edinburgh 22 May 2013 Healthcare Improvement Scotland is committed to equality. We have assessed
Unannounced Inspection Report: Independent Healthcare Marie Curie Hospice - Edinburgh Marie Curie Cancer Care Edinburgh 22 May 2013 Healthcare Improvement Scotland is committed to equality. We have assessed
Infection Control. Annual Report 2014 / 15
 Infection Control Annual Report 2014 / 15 July 2015 Report 1. Introduction and Background 1.1 The Trust supports the principle that healthcare acquired infections should be prevented wherever possible
Infection Control Annual Report 2014 / 15 July 2015 Report 1. Introduction and Background 1.1 The Trust supports the principle that healthcare acquired infections should be prevented wherever possible
NHS Greater Glasgow and Clyde Health Board response to allegations concerning Vale of Leven c.diff outbreak
 NHS Greater Glasgow and Clyde Health Board response to allegations concerning Vale of Leven c.diff outbreak 1. Infection-free patients placed into rooms which contain those infected with c.diff It has
NHS Greater Glasgow and Clyde Health Board response to allegations concerning Vale of Leven c.diff outbreak 1. Infection-free patients placed into rooms which contain those infected with c.diff It has
Infection Prevention & Control Annual Report 2011/2012
 Infection Prevention & Control Annual Report 2011/2012 Board of Directors Approval date: 1 November 2012 Infection Prevention & Control Committee Submission date: 1 August 2012 Position at 31 March 2012
Infection Prevention & Control Annual Report 2011/2012 Board of Directors Approval date: 1 November 2012 Infection Prevention & Control Committee Submission date: 1 August 2012 Position at 31 March 2012
Shetland NHS Board Control of Infection Committee Annual Report April March 2010 FINAL VERSION
 Shetland NHS Board Control of Infection Committee Annual Report April 2009 - March 2010 FINAL VERSION NHS Shetland Control of Infection Committee Annual Report 2009-2010 Acronyms and Abbreviations ARI
Shetland NHS Board Control of Infection Committee Annual Report April 2009 - March 2010 FINAL VERSION NHS Shetland Control of Infection Committee Annual Report 2009-2010 Acronyms and Abbreviations ARI
Healthcare Acquired Infections
 Healthcare Acquired Infections Emerging Trends in Hospital Administration 9 th & 10 th May 2014 Prof. Hannah Priya HICC In charge What is healthcare acquired infection? An infection occurring in a patient
Healthcare Acquired Infections Emerging Trends in Hospital Administration 9 th & 10 th May 2014 Prof. Hannah Priya HICC In charge What is healthcare acquired infection? An infection occurring in a patient
Internal Audit. Health and Safety Governance. November Report Assessment
 November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
November 2015 Report Assessment G G G A G This report has been prepared solely for internal use as part of NHS Lothian s internal audit service. No part of this report should be made available, quoted
Reducing Mortality and Harm in ABMU Local Health Board
 10 th June 2011 Reducing Mortality and Harm in ABMU Local Health Board Insert name of presentation on Master Slide Programme Driver Diagram Aims/Outcome Measure Reduce Mortality Reduce RAMI to
10 th June 2011 Reducing Mortality and Harm in ABMU Local Health Board Insert name of presentation on Master Slide Programme Driver Diagram Aims/Outcome Measure Reduce Mortality Reduce RAMI to
Control of Infection Committee: Overarching Work Programme
 Control of Infection Committee: Overarching Work Programme 2015 16 To be updated as required, at least on a quarterly basis. Action Responsibility Timescale / progress 1 1.1 SURVEILLANCE Healthcare Associated
Control of Infection Committee: Overarching Work Programme 2015 16 To be updated as required, at least on a quarterly basis. Action Responsibility Timescale / progress 1 1.1 SURVEILLANCE Healthcare Associated
Improvement Action Plan NHS Tayside, Perth Royal Infirmary Healthcare associated infection inspection Inspection date: July 2017
 Improvement Action Plan Declaration It is the responsibility of the NHS board Chief Executive and NHS board Chair to ensure the improvement plan is accurate and complete and that the s are measurable,
Improvement Action Plan Declaration It is the responsibility of the NHS board Chief Executive and NHS board Chair to ensure the improvement plan is accurate and complete and that the s are measurable,
Key prevention strategies for MRSA bacteraemia: a case study. Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta
 Key prevention strategies for MRSA bacteraemia: a case study Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta 1 Mortality following Staphylococcus aureus bacteraemia
Key prevention strategies for MRSA bacteraemia: a case study Dr. Michael A. Borg Director of Infection Prevention & Control Mater Dei Hospital Malta 1 Mortality following Staphylococcus aureus bacteraemia
SUBJECT: Healthcare Associated Infection (HCAI) Reporting Template
 Reporting Template") Meeting of Lanarkshire NHS Board: 31 uary 2018 Lanarkshire NHS Board Kirklands Bothwell G71 8BB Telephone: 098 855500 www.nhslanarkshire.org.uk SUBJECT: Healthcare Associated Infection (HCAI) Reporting
Meeting of Lanarkshire NHS Board: 31 uary 2018 Lanarkshire NHS Board Kirklands Bothwell G71 8BB Telephone: 098 855500 www.nhslanarkshire.org.uk SUBJECT: Healthcare Associated Infection (HCAI) Reporting
Report of the unannounced inspection at the Mater Misericordiae University Hospital, Dublin.
 Report of the unannounced inspection of the prevention and control of healthcare associated infection at X Hospital Report of the unannounced inspection at the Mater Misericordiae University Hospital,
Report of the unannounced inspection of the prevention and control of healthcare associated infection at X Hospital Report of the unannounced inspection at the Mater Misericordiae University Hospital,
REPORT SUMMARY SHEET
 REPORT SUMMARY SHEET Meeting: Trust Board 27 th November 2014 Date: Title: Environmental Cleanliness Annual Report 2013/14 Lead Director: Corporate Objectives: Purpose: Director of Acute Services Provide
REPORT SUMMARY SHEET Meeting: Trust Board 27 th November 2014 Date: Title: Environmental Cleanliness Annual Report 2013/14 Lead Director: Corporate Objectives: Purpose: Director of Acute Services Provide
HEALTH & SAFETY. Management of Health & Safety Policy
 NHS TAYSIDE HEALTH & SAFETY Management of Health & Safety Policy Author: Chief Executive Review Group: Strategic Risk/ Management Group Review Date: January 2014 Last Update: January 2013 Document : HS/03
NHS TAYSIDE HEALTH & SAFETY Management of Health & Safety Policy Author: Chief Executive Review Group: Strategic Risk/ Management Group Review Date: January 2014 Last Update: January 2013 Document : HS/03
NHS Borders Feedback and Complaints Annual Report
 NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
NHS Borders Feedback and Complaints Annual Report 2016-17 1 Introduction NHS Borders Feedback and Complaints Annual Report 2016-17 is a summary of the feedback provided by the complaints, comments, concerns
Quality Assurance Accreditation Scheme Assignment Report 2016/17. University Hospitals of Morecambe Bay NHS Foundation Trust
 Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
Quality Assurance Accreditation Scheme Assignment Report 2016/17 Contents 1. Introduction 2. Executive Summary 3. Findings, Recommendations and Action Plan Appendix A: Terms of Reference Appendix B: Assurance
SUBJECT: CLINICAL GOVERNANCE
 Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
Meeting of Lanarkshire NHS Board Lanarkshire NHS Board Kirklands 25 September 2013 Fallside Road Bothwell G71 8BB Telephone: 01698 855500 www.nhslanarkshire.org.uk 1. PURPOSE SUBJECT: CLINICAL GOVERNANCE
The State Hospital Clinical Effectiveness Strategy & Delivery Plan January 2011 December 2013
 The State Hospital Strategy & Delivery Plan January 2011 December 2013 NATIONAL STANDARDS NATIONAL GUIDELINES CLINICAL AUDIT CLINICAL EFFECTIVENESS INTEGRATED CARE PATHWAYS MANAGING CHANGE EDUCATION AND
The State Hospital Strategy & Delivery Plan January 2011 December 2013 NATIONAL STANDARDS NATIONAL GUIDELINES CLINICAL AUDIT CLINICAL EFFECTIVENESS INTEGRATED CARE PATHWAYS MANAGING CHANGE EDUCATION AND
Phoenix Therapy and Care Ltd - Care at Home Support Service Care at Home 1 Lodge Street Haddington EH41 3DX Telephone:
 Phoenix Therapy and Care Ltd - Care at Home Support Service Care at Home 1 Lodge Street Haddington EH41 3DX Telephone: 01620 828 566 Inspected by: Michelle Deans Type of inspection: Announced (Short Notice)
Phoenix Therapy and Care Ltd - Care at Home Support Service Care at Home 1 Lodge Street Haddington EH41 3DX Telephone: 01620 828 566 Inspected by: Michelle Deans Type of inspection: Announced (Short Notice)
Open and Honest Care in your Local Hospital
 Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Open and Honest Care in your Local Hospital Report for: Royal Wolverhampton NHS Trust January 2016 The Open and Honest Care: Driving Improvement Programme aims to support organisations to become more transparent
Quality Assurance Framework
 Quality Assurance Framework NHS Bromley Clinical Commissioning Group Quality Assurance Framework was developed to support the commissioning, contract monitoring and procurement processes. NAME OF ORGANISATION/SERVICE
Quality Assurance Framework NHS Bromley Clinical Commissioning Group Quality Assurance Framework was developed to support the commissioning, contract monitoring and procurement processes. NAME OF ORGANISATION/SERVICE
INFECTION PREVENTION & CONTROL. ANNUAL REPORT Northern Devon Healthcare NHS Trust
 INFECTION PREVENTION & CONTROL ANNUAL REPORT 2013-14 Northern Devon Healthcare NHS Trust incorporating community services in Exeter, East and Mid Devon 1 Kevin Marsh David Richards Joint Directors of Infection
INFECTION PREVENTION & CONTROL ANNUAL REPORT 2013-14 Northern Devon Healthcare NHS Trust incorporating community services in Exeter, East and Mid Devon 1 Kevin Marsh David Richards Joint Directors of Infection
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Infection Prevention and Control Assurance
 Infection Prevention and Control Assurance Who Should Read This Policy Target Audience All Clinical Staff Version 1.0 November 2015 Infection Prevention and Control Assurance Policy Ref. Contents Page
Infection Prevention and Control Assurance Who Should Read This Policy Target Audience All Clinical Staff Version 1.0 November 2015 Infection Prevention and Control Assurance Policy Ref. Contents Page
Director of Infection Prevention and Control Annual Report 01 April March 2013
 Director of Infection Prevention and Control Annual Report 01 April 2012 31 March 2013 Agenda Item: Reference: Meeting Name: Board Meeting Meeting Date: 3 rd June 2013 Lead Director: Lisa Cooper Job Title:
Director of Infection Prevention and Control Annual Report 01 April 2012 31 March 2013 Agenda Item: Reference: Meeting Name: Board Meeting Meeting Date: 3 rd June 2013 Lead Director: Lisa Cooper Job Title:
Mandatory Surveillance of Healthcare Associated Infections Report 2006
 Mandatory Surveillance of Healthcare Associated Infections Report 2006 Contents 1. Introduction...2 2. Key Points...3 3. Results of the fifth year of mandatory surveillance of MRSA bacteraemia, including
Mandatory Surveillance of Healthcare Associated Infections Report 2006 Contents 1. Introduction...2 2. Key Points...3 3. Results of the fifth year of mandatory surveillance of MRSA bacteraemia, including
Unannounced Follow-up Inspection Report
 Unannounced Follow-up Inspection Report Queen Elizabeth University Hospital NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in
Unannounced Follow-up Inspection Report Queen Elizabeth University Hospital NHS Greater Glasgow and Clyde www.healthcareimprovementscotland.org The Healthcare Environment Inspectorate was established in
EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT
 EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT Agenda Item No. 7 23 rd January 2008 1. Christmas Day Visit From Mayor of Stevenage and General Secretary, Royal College of Nursing Alison
EAST AND NORTH HERTFORDSHIRE NHS TRUST CHIEF EXECUTIVE S REPORT Agenda Item No. 7 23 rd January 2008 1. Christmas Day Visit From Mayor of Stevenage and General Secretary, Royal College of Nursing Alison
Infection Prevention and Control Annual Report 2012/13
 Infection Prevention and Control Annual Report 2012/13 Infection Prevention and Control Annual Report 2012/13 1 Contents 1. Executive Overview 2. Key Achievements 3. Infection Prevention and Control Team
Infection Prevention and Control Annual Report 2012/13 Infection Prevention and Control Annual Report 2012/13 1 Contents 1. Executive Overview 2. Key Achievements 3. Infection Prevention and Control Team
Director of Infection Prevention and Control
 Director of Infection Prevention and Control 2016-17 2 Contents Page 1. Executive Summary 4 2. Infection prevention and control arrangements 5 3. Healthcare Associated Infection Performance 6 3.1. Mandatory
Director of Infection Prevention and Control 2016-17 2 Contents Page 1. Executive Summary 4 2. Infection prevention and control arrangements 5 3. Healthcare Associated Infection Performance 6 3.1. Mandatory
General Ward Driver Diagram and Change Package
 General Ward Driver Diagram and Change Package The Institute for Healthcare Improvement A driver diagram is used to conceptualise an issue and to determine its system components which will then create
General Ward Driver Diagram and Change Package The Institute for Healthcare Improvement A driver diagram is used to conceptualise an issue and to determine its system components which will then create
Sepsis Collaborative May 2015 Report
 Report Table of Contents Background... 3 Collaborative set up... 3 Impact... 4 Process measures... 4 Outcome measures... 4 1. Coding... 4 2. Mortality in patients undergoing a blood culture... 5 Sustainability...
Report Table of Contents Background... 3 Collaborative set up... 3 Impact... 4 Process measures... 4 Outcome measures... 4 1. Coding... 4 2. Mortality in patients undergoing a blood culture... 5 Sustainability...
Infection Prevention and Control Strategy
 Infection Prevention and Control Strategy 2015 2018 Foreword This three year plan has been produced to support the work which has been taken forward in previous years across the organisation to reduce
Infection Prevention and Control Strategy 2015 2018 Foreword This three year plan has been produced to support the work which has been taken forward in previous years across the organisation to reduce
HAI Prevention. Beyond the Bundle. March 18, 2016
 HAI Prevention Beyond the Bundle March 18, 2016 Krystyna Strozewski Director of Quality Lake Health System Karen Mrazik Infection Preventionist Tripoint Medical Center Elizabeth Reed Infection Preventionist
HAI Prevention Beyond the Bundle March 18, 2016 Krystyna Strozewski Director of Quality Lake Health System Karen Mrazik Infection Preventionist Tripoint Medical Center Elizabeth Reed Infection Preventionist
Combating Healthcare Associated Infections in the NHS. Inspector of Microbiology and Infection Control, Department of Health, London
 Combating Healthcare Associated Infections in the NHS Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London 2007 -The challenge of HCAI MRSA bacteraemia
Combating Healthcare Associated Infections in the NHS Professor Brian Duerden Inspector of Microbiology and Infection Control, Department of Health, London 2007 -The challenge of HCAI MRSA bacteraemia