Sierra Health Foundation Getting Ready for Pay for Performance and the Future of CHCs
|
|
|
- Isabella Wood
- 5 years ago
- Views:
Transcription
1 Sierra Health Foundation Getting Ready for Pay for Performance and the Future of CHCs June 22, 2016 Curt Degenfelder
2 Today s Agenda Understand what pay for performance is Dig into health center operations Look at key reporting metrics 1
3 The Triple Aim Total Cost of Care Improving Health of Populations Improving Patient Experience 2
4 Thinking About Pay For Performance (P4P) Pay = revenue Current P4P revenue is typically a small portion of a health center s revenue. How much does P4P need to be to move the needle? Current payments from managed care organizations and IPAs seem to be arbitrary and capricious 3
5 Identifying Timing of P4P Revenue HRSA quality bonus announced broadly before paid out; based on historical (CY UDS) data Managed care/ipa usually after a quarter/fical year for the managed care organization. Often based on total managed care organization profit, total cost care for health center patients, and/or quality Process based rewards: - Engagement for new patients - Follow up on inpatient - Appointment availability standards 4
6 Earning P4P Changing operations to earn performance based rewards Infrastructure - Personnel for quality and data management - EHR - IT infrastructure 5
7 Quality 6
8 HMO PROVIDES RECOMMENDED CARE What is HEDIS? PATIENTS RATE THEIR EXPERIENCE RATE THEIR HMO GETTING CARE EASILY HMO HELPS MEMBERS GET ANSWERS Click on plan name for plan s star ratings and information: Aetna Health of California, Inc. HMO PROVIDES RECOMMENDED CARE PATIENTS RATE HMO PATIENTS RATE ACCESS PATIENTS RATE SERVICE Two stars Three stars One star Three stars Anthem Blue Cross - HMO Three stars Three stars One star Three stars Blue Shield of California - HMO Three stars Three stars Two stars Three stars Cigna HMO Three stars Two stars One star Two stars Health Net of California, Inc. Three stars Three stars One star One star Kaiser Permanente - Northern California Four stars Three stars Three stars Two stars Kaiser Permanente - Southern California Four stars Three stars One star Three stars Sharp Health Plan Three stars Four stars One star Three stars UnitedHealthcare of California Three stars Three stars One star Two stars Western Health Advantage Three stars Three stars One star 7

9 8

10 9
11 What is HEDIS? The Health Effectiveness Data and Information Set (HEDIS) is a measurement system developed by the National Committee for Quality Assurance (NCQA) used by health plans nationwide HEDIS focuses on process measures for an assigned patient population Generally, the source of data for Medicaid HEDIS is the MCO claims system. Thus MCO quality payments are likely to be based on HEDIS (not UDS) 10
12 HEDIS Medicaid Quality Measures Children immunization Adolescent immunization HPV for female adolescents Lead screening in children Breast cancer screening Cervical cancer screening Chlamydia screening Pharyngitis testing for children URI treatment for children Antibiotic avoidance adlt bronchitis Spirometry testing for COPD Pharmacotherapy mgmt of COPD Initiation & engagement for AOD Timeliness of prenatal & postpartum Frequency of adolescent care ED visits Follow up on ADHD meds Use of asthma meds Asthma med mgt Asthma medication ratio Cholesterol mgmt for CV conditions Beta blocker after heart attack Comprehensive diabetes care DMARD therapy Imaging studies for low back pain Antidepressant med mgmt MH hospitalization f/u Monitoring for persistent meds Adult access to preventive/ambulatory Child access to PCP Frequency of prenatal care Frequency of well child visits Annual dental visits Developmental screening
13 Methodology Numerator services from claims database. HEDIS criteria looks for specific CPT and ICD codes Denominator attributed patients (see explanation next page) meeting criteria for each measure Measures are not use rates, i.e. services per patient, but rather a measure of % of patients who received indicated service. Calculation is called administrative measure MCO may calculate hybrid measures, using chart reviews for certain measures. Hybrid measure performance is usually better than the administrative measure. However sampling methodology allows for limited chart review Not outcomes measures such as diabetic or hypertension control 12
14 UDS vs. HEDIS Sample Attributed Not Seen Timely Entry Into Prenatal Care Childhood Immunzation* UDS HEDIS UDS HEDIS Health Center A 11% 74% 48% 68% 1% Health Center B 11% 85% 66% 93% 0% Health Center C 12% 86% 60% 84% 0% Health Center D 9% 56% 53% 97% 1% Statewide Administrative 59% 4.7% Statewide Hybrid 64.7% *Combination of Dtap, IPV, MMR, HiB, HepB, VZV, PCV 13
15 UDS vs. HEDIS Sample Cervical Cancer Screening Asthma Pharm Therapy UDS HEDIS UDS HEDIS Health Center A 61% 47% 79% 84% Health Center B 43% 72% 90% 84% Health Center C 60% 66% 75% 86% Health Center D 70% 69% 91% 92% Statewide Administrative 66% 87%
16 Potential Points of Data Failure Provider not recording the service Provider not recording the service with code (chart only) Provider not using code required by HEDIS Provider not recording code in PM/EHR FQHC not billing/recording code on claims (for example PAP immunizations) Reported code not making it into MCO s system 15
17 Total Cost of Care
18 What Drives Total Cost of Care? SumOfPaid_Amount Cumulative Cost % of Total Count of Pts $ 1,536,800 $ 1,536, % 1 $ 585,072 $ 2,121, % 2 $ 564,305 $ 2,686, % 3 $ 502,359 $ 3,188, % 4 $ 480,759 $ 3,669, % 5 $ 461,517 $ 4,130, % 6 $ 441,076 $ 4,571, % 7 17
19 What Drives Total Cost of Care? SumOfPaid_Amount Cumulative Cost % of Total Count of Pts $ 3 $ 893,869, % 115,291 $ 2 $ 893,869, % 115,292 $ 2 $ 893,869, % 115,293 $ 2 $ 893,869, % 115,294 $ 1 $ 893,869, % 115,295 $ 1 $ 893,869, % 115,296 $ 1 $ 893,869, % 115,297 18
20 What Drives Total Cost of Care? Top (Costs): 10% 20% 30% $ 89,386,928 $ 178,773,855 $ 268,160,783 # of Pts: 422 1,234 2,570 % of Total Patients: 0.37% 1.07% 2.23% Range (High): $ 1,536,800 $ 151,691 $ 84,269 Range (Low): $ 151,777 $ 84,342 $ 54,665
21 What Drives Total Cost of Care? Top (Costly Pts): 10% 20% Everyone Else # of Pts: 11,539 23,078 92,311 % of Total Costs: 59.3% 75.1% 24.9% 20

22 Reducing Total Cost of Care 21
23 CHC Provider s Take on High Cost Patients There were 101 high cost patients. Of these, 25 are "not currently attributed" to this CHC. Of the 76 attributed patients, 14 were children, 62 adults. All of the 14 children were high need/intrinsically high cost - 2 with hemophilia (one with physical and sexual abuse), 5 complicated preemies, 2 cancers (malignancies), 2 severe autism/developmental delay, 1 cystic fibrosis with liver transplant, 1 severe ulcerative colitis with colectomy. The only one with asthma also has psychosis. We can identify the 62 adults by the clusters of conditions which are the highest cost: HIV, Hep C, Substance Abuse Cancer Advanced Age with multiple conditions Severe mental illness plus or minus other health conditions Neurodegenerative disorders Dialysis, transplants I find it hard to imagine how to impact their costs. There are about 2-3 adults who have problem lists and medication lists that are not huge, and for whom it is not totally evident why their costs are high. Each of these has home care services, which may be a major contributor to their cost. 22
24 Risk Adjustment of Total Cost of Care Predicted Risk Score Predicted Total Cost PMPY Actual Total Cost PMPY Actual % of Predicted Actual Total Cost PMPY Health Center A 1.52 $ 7,894 $ 7,700 98% $ 6,860 Health Center B 1.21 $ 6,307 $ 5,419 86% $ 5,026 Health Center C 1.59 $ 8,276 $ 8,233 99% $ 7,420 Health Center D 1.03 $ 5,370 $ 5,318 99% $ 4,775 Health Center E 1.54 $ 8,007 $ 7,417 93% $ 6,781 Health Center F 1.08 $ 5,605 $ 5, % $ 5,167 Health Center G 1.21 $ 6,267 $ 5,654 90% $ 5,052 Health Center H 1.37 $ 7,101 $ 6,810 96% $ 6,393 Health Center I 1.30 $ 6,756 $ 6,299 93% $ 5,496 Health Center J 0.98 $ 5,086 $ 5, % $ 5,160 Health Center K 1.78 $ 9,245 $ 8,784 95% $ 8,275 Health Center L 1.25 $ 6,471 $ 6,004 93% $ 5,121 Health Center M 1.94 $ 10,099 $ 9,583 95% $ 8,683 Health Center N 0.99 $ 5,137 $ 4,758 93% $ 4,593 FQHC Average $ 6,663 Statewide Average 1.00 $ 5,197 23
25 Patients With High Cost To Health Center Medical 2013 Medical 2012 # of Visits Patients Visits # of Visits Patients Visits 1 4,585 4, ,988 5, ,313 6, ,723 7, ,472 7, ,641 7, ,386 9, ,242 8, ,945 9, ,581 7, ,325 7, , , , , , , , , , , Total: 18,637 69,855 Total 18,755 58,367 Single Visits 2013 Single Visits 2012 Est 39.72% Est 31.53% New 60.28% New 68.47% 24
26 Driving The Health Center Towards Triple AIM Goals
27 FQHC Revenue Today & In The Future TODAY PPS BASED ON VOLUME NONE SERVICE PAYMENT TRIPLE AIM PAYMENT APM BASED ON PATIENTS PCMH/CASE MANAGEMENT ADD-ON SHARED SAVINGS QUALITY BONUS PATIENT ENGAGEMENT BONUS FUTURE 26
28 IMPACT OF PROVIDER MARKET ON TODAY S REIMBURSEMENT MODEL Provider Vacancies Current Provider FTEs 10 8 Visits/FTE 3,900 3,900 Total Visits 39,000 31,200 Net Revenue/Visit $ $ Patient Service Revenue $ 4,680,000 $ 3,744,000 Grant & Other Revenue $ 1,300,000 $ 1,300,000 Total Revenue $ 5,980,000 $ 5,044,000 Provider Compensation $ 1,750,000 $ 1,400,000 Variable Staff Compensation $ 1,200,000 $ 960,000 Fixed Staff Compensation $ 1,600,000 $ 1,600,000 Total Compensation $ 4,550,000 $ 3,960,000 Variable OTPS $ 600, ,000 Fixed OTPS $ 780,000 $ 780,000 Total OTPS $ 1,380,000 $ 1,260,000 Total Expense $ 5,930,000 $ 5,220,000 Note: Need to define what full provider staffing means Will a larger CHC always have provider vacancies? Net Income $ 50,000 $ (176,000) 27
29 IMPACT OF PROVIDER MARKET ON TODAY S REIMBURSEMENT MODEL Future (Current?) Market Current Provider FTEs Visits/FTE 3,900 3,650 Total Visits 39,000 36,500 Net Revenue/Visit $ $ Patient Service Revenue $ 4,680,000 $ 4,380,000 Provider Salary $ 1,750,000 $ 2,220,000 Fringe $ 350,000 $ 350,000 Total COGS $ 2,100,000 $ 2,570,000 Gross Margin $ 2,580,000 $ 1,810,000 Variable Staff Compensation $ 1,200,000 $ 1,200,000 Fixed Staff Compensation $ 1,600,000 $ 1,600,000 Total Compensation $ 2,800,000 $ 2,800,000 Variable OTPS $ 600, ,000 Fixed OTPS $ 780,000 $ 780,000 Total OTPS $ 1,380,000 $ 1,380,000 Total Other Expense $ 4,180,000 $ 4,180,000 Grant & Other Revenue $ 1,600,000 $ 1,600,000 Net Income $ - $ (770,000) 28
30 COST OF TURNOVER Recruitment Cost $ 10,000 Length of Vacancy 3.5 Months Annual Productivity 3,600 Visits Lost Visits 1,050 Net Revenue/visit $ Lost Revenue $ 126,000 Provider Comp $ 54,900 $180K, 22% fringe Marginal Cost Coverage $ 71,100 Months to Full Rampup 6 Lost Visit % 10% Lost Visits 180 Lost Revenue $ 21,600 Total Financial Impact $ 102,700 29
31 Patient Centered Health Home Metrics
32 The Ongoing Economics of the EHR New licenses/depreciation of license cost Maintenance fees IT infrastructure Provider productivity hit Staff productivity/work Meaningful use $ Using integrated EHR/PM to make practice more efficient PPS change in scope 31
33 PCHH Metrics/Performance Standards Panel Size per Provider FTE - Top down: current number of patients served by provider. Address issues such as patients seen by multiple providers, patients who came in once and haven t returned. etc. - Bottom up: total visit slots divided by visits per patient per year (acuity adjusted?) is the word on the street, but it is rarely seen (maybe because of unassigned patients) - What happens to a panel when a provider leaves? - Who s in charge of all this the CMO or the person who does scheduling? 32
34 PCHH Metrics/Performance Standards Physical capacity How many patients/visits can be handled with the current facilities Division of clinical vs. administrative space - Is the current space configured appropriately to support PCHH? Will appropriate configuration require more or less space? Visits per patient per year Are patients coming in on clinically indicated intervals? - How many patients came in once? How many new patients (esp in second half of year)? How many patients came in more than 10 times? How does OB drive this number? - Is access denied/delayed because of long 3 rd next available appointment? What are variations based on diagnoses? - What are variations based on payor? Will this change in 2014? 33
35 PCHH Metrics/Performance Standards Integrated medical, dental & behavioral health - % of OB, dental and behavioral health patients receiving primary care at CHC - % of medical patients receiving dental & behavioral health Continuity - Patient centered: percent of visits with your PCP (or touches with team) - Provider (team) centered: % of visits (touches) with your own patients % of chronic care patients receiving care within clinically indicated timeframe Next and 3 rd next available appointment (within 48 or 72 hours) 34
36 PCHH Metrics/Performance Standards Urgent care only for low acuity issues No ER visits for non-emergent conditions No visits to other PCPs New patients less than 20% Existing patient walk-in less than 10% No show rate less than 15% Assurance that ordered ancillaries & specialty are received Retention of 90% of aged-in Medicare eligibles Non-visit means for patient access to information (portal, /text, telephonic, staff) 35
37 PCHH Metrics Actual Access Standards (from Managed Care Organization) Appointment Type Non-urgent appointment with Primary Care physician Urgent care appointment that do not require prior auth. Urgent care appointment that require prior auth. Non-urgent appointment for ancillary services Non-urgent appointment with non-physician mental health providers Offer the Appointment within 10 bus. days of request 48 hours of request 96 hours of request 15 bus. Days of request 10 bus. days of request Initial health assessment (complete history and physical examination) 120 days of enrollment 36
38 PCHH Metrics Actual Access Standards (from CHC) CHC - 3rd Next Available Dental Visit by Clinic Dental Patient Type New November Established New December Established New January Established Eastside Westside CHC - 3rd Next Available Medical Visit by Clinic Medical November December January Patient Type New Established New Established New Established Eastsiide Westside Downtown
39 PCHH Metrics - Actual Why is it important? In a system with assigned members, patients utilizing other providers may be reassigned, reducing capitated revenue. Patient movement will impact the accuracy of quality scores. If there is a large amount of patient leakage, are we really a health home? Reattributed Member Months Total Member Months % Lost To Attribution Health Center A , % Health Center B 1, , % Health Center C , % 38
40 PCHH Metrics Actual Short Tenure Patients Overview of CHC patients: > For period: 7/1/11-6/30/12 New patients = 10,527 All patients = 21,909 Percentage = 10,527 / 21,909 = 48% > For period: 7/1/12-6/30/13 New patients = 9,709 All patients = 21,416 Percentage = 9,709 / 21,416 = 43.3% 39
41 PCHH Metrics Actual Employee Tenure Median All employees: 2 years, 3 months and 15 days Non-providers: 2 years, 6 months and 26 days Providers: 1 year, 8 months Mean (Average) All employees: 4 years, 5 months and 18 days Non-providers: 4 years, 7 months and 22 days Providers: 3 years, 7 months and 8 days 40
42 PCHH Metrics Actual Touches Quarter # of Patients Office Visits Referral Updates Screenings Updates Letter Count Interpreter Services Problem List Updates Telephone Encounter Interim Notes Home Care Visit March Q2/ Q3/ Q4/ No data No data Pre-Visit Planning Individual and Family Support Referral to Community Services Ancillary Services Goal Updates Health Promotion Comprehensive Care Planning Care Coordination Comprehensive Transitional Care Total Touches
43 PCHH Metrics Actual Visits to Touches Health Center Health Center Health Center A B C Visits 31,219 60,315 25,107 Engagement Touches 7,743 13,557 7,073 Visits & Engagement Touches 38,962 73,872 32,180 Ratio of Visits to Touches PPS Rate $ $ $ Equivalent PPS Earned $8,855,283 $13,927,088 $7,306,147 Total Payments $ 7,640,004 $ 14,057,474 $ 6,518,592 Earned - Payments $1,215,280 ($130,386) $787,555 16% -1% 12% 42


44 PCHH Metrics Moving Visits 43
45 Calculations for PCHH/UDS Patient Target 1 Redistributed Visits 3,947 New Patient Visits* 1,800 Established Patient Visits 347 Total Visits Available 2,147 *Take twice as long as established 3 2 New Medical Patients # of Visits Patients Visits 1 1,500 1, Total: 1,800 2,147 Total Patients After Practice Transformation 20,437 Total Visits 68,055 Visits PPPY 3.33 Old Panel Size (20 FTEs) 932 New Panel Size 1,022 44
46 Calculations for Closing Panel 1 Medical Visits # of Visits Patients Visits 1 6,585 6, ,313 6, ,472 7, ,386 9, ,879 9, ,225 7, ,439 Total: 18,637 52,355 Visits PPPY Foregone New Patients 2,000 New Patient Visits* 2,000 Incremental Established Patient Visits 2,000 Revised Total Visits 54,355 Revised Total Patients 16,637 Visits PPPY 3.27 *Take twice as long as established Should also look at 3rd next available appointment 45
47 How Do We Pay For The Patient Centered Health Home?
48 Practice Restructuring PCHH How Do We Pay For It? Basic systems envision an add-on to current per visit rates, more advanced systems envision paying for additional cost through capitation To get appropriately compensated, may need to record services of all staff (especially for patients who receive service from a non-billable provider) Health center may be assigned management of a population (either in an ACO or PCMH model) Note the savings from PCMH are downstream, so we must start working with payors to look at the total costs of our patients. Don t just look at: 1) individual indicators such as ER utilization (will miss diabetics who don t need dialysis) or 2) incremental savings (since you are already saving money!) 47
49 Practice Restructuring PCHH How Do We Pay For It? PCMH Gradual Implementation Budget what is affordable over time One-time (practice redesign) vs. ongoing (staff, IT, EHR modules & portal) cost Redefining roles of existing positions/staff Sample short term goals - Hire call center RN - Move Discharge from Operational to Clinical to better coordinate scheduling of follow-up visits - Evaluate data management & referral processes
50 Cost Savings From Patient Retention (Eliminating Costs of Non-Retention) Health Center Cost Per RVU $ $ RVU for CPT Code Cost per Procedure $ $ Addl Registration/Enrollment Effort $ (3 $20/hr comp cost) Total Cost Per Service $ $
51 Shifting Work Physician - $170,000 $210,000 RN - $65,000 (is shortage easing?) Medical assistant 1 - $12/hr Medical assistant 2 - $14/hr Medical assistant 3 - $20/hr Care coordinator - $20/hr Front desk - $13/hr Scribe 50
52 Work, and Does It Work?
53 The Daily Priority of Work 1 Keeping the Doors Open 2 External Relations ACTIVITIES 3 Improvement Scheduling patients Processing patients Billing & collections Staff management Fixing problems Board Regulatory reporting Community partners Provider management Growth Quality Customer service Meaningful use PCHH 52
54 Continuum of CHC Performance Best Practice Many Good Attributes Average Not So Good Train Wreck 12% 27% 37% 18% 6% OK in 2016 OK in
55 Work in a Community Health Center Clinical staff in CHCs almost universally say there is too much work in a day. Some of this is driven by the EHR and increased requirements (Meaningful use and PCMH certification) Clinic administrative staff also report too many tasks/too much work 54
56 Performance Improvement Seeks to identify and remove the causes of defects and errors Based on concept that sustained quality improvement requires a reduction in process variation Focuses on achieving measurable and quantifiable results, based on verifiable data One system, Six Sigma, has a goal of 3.4 defects per million transactions; applying the Six Sigma methodology moves an organization towards that goal Also tied into people management Jack Welch 10% rule 55
57 Sample Performance Improvement Process Define process improvement goals Measure key aspects of current processes and collect relevant data Analyze the data to verify cause and effect Improve the process based on data analysis Control deviations from target performance 56

58 Sample of Data 57
59 Distribution of Productivity 4 3 # Staff <60% 60-69% 70-79% 80+ % Efficiency 58
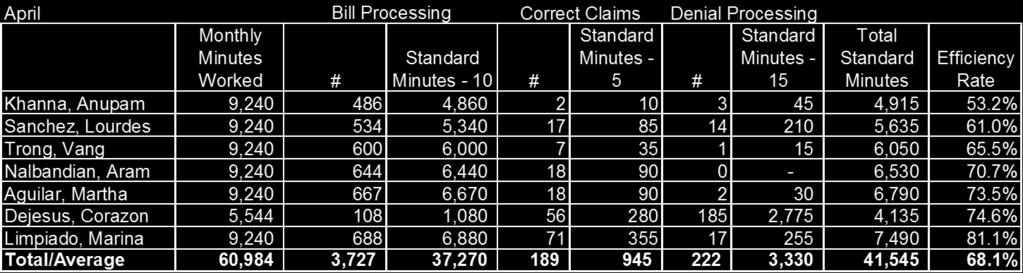
60 Picture of Improvement April Bill Processing Correct Claims Denial Processing Monthly Minutes Worked # Standard Minutes - 10 # Standard Minutes - 5 # Standard Minutes - 15 Total Standard Minutes Efficiency Rate Average 9,240 6, % Sanchez, Lourdes 9, , , % Trong, Vang 9, , , % Nalbandian, Aram 9, , , % Aguilar, Martha 9, , , % Dejesus, Corazon 5, , ,775 4, % Limpiado, Marina 9, , , % Old Performance 60,984 3,727 37, ,330 41, % New Performance 60,984 42, % By getting the worst performer to average performance, or by replacing the worst performer with an average performer, the health center could increase overall efficiency from 68% to over 70%, and get over 22 hours (1,380 minutes or.15 of an FTE) of service activity from the same number of staff. 59
61 Sample Performance Improvement Implementation Plan Activity #1: Develop Performance Improvement Team (PIT) Activity #2: Develop DMAIC process management Define what process CHC is trying to improve Measure the process, by identifying the steps in the process, and measurements used determine if the process is working Analyze the data, to understand where the process is/isn t working Improve develop solutions to improve the process, and determine if those solutions are effective Control put in standard policies, procedures, and workflows that capture the improvement solutions. Monitor performance using data. Activity #3: Implement Define & Measurement for the revenue cycle currently the Billing Department is correcting a large number of errors up to 250 per day, or 60% of all bills. The revenue cycle includes scheduling, registration, and billing (this effort will not include the recording of clinical data, which is also included on bills). CHC will define the measurement variables and collect the data 60
62 Sample Performance Improvement Implementation Plan Activity #4: Hire Coder to Audit Billing Activity #5: Implement Analyze, Improve and Control for the revenue cycle Activity #6: Implement Define & Measurement for the UDS clinical quality measures CHC reports 16 clinical quality measures HRSA on an annual basis via the Uniform Data System (UDS) report. This timing will allow CHC to understand data issues in advance of preparing the UDS for calendar year
Sierra Health Foundation Tales From the Front: Dealing With Today s Financial Issues November 19, 2015
 Sierra Health Foundation Tales From the Front: Dealing With Today s Financial Issues November 19, 2015 Curt Degenfelder curt@degenfelderhealth.com 310-740-0960 Today s Agenda Discuss the current dynamics
Sierra Health Foundation Tales From the Front: Dealing With Today s Financial Issues November 19, 2015 Curt Degenfelder curt@degenfelderhealth.com 310-740-0960 Today s Agenda Discuss the current dynamics
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives. Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018
 Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
Medi-Cal Performance Measurement: Making the Leap to Value-Based Incentives Dolores Yanagihara IHA Stakeholders Meeting October 3, 2018 Why Standardization? MEDI-CAL CROSS PRODUCT San Francisco Health
California Pay for Performance: A Case Study with First Year Results. Tom Williams Integrated Healthcare Association (IHA) March 17, 2005
 March 17, 2005") California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
California Pay for Performance: A Case Study with First Year Results Tom Williams Integrated Healthcare Association (IHA) March 17, 2005 Agenda National Perspective California Program Overview Data Collection
Piloting Performance Measurement of Physician Organizations in Medi-Cal Managed Care: Findings and Implications
 Issue Brief No. 13 January 2015 Piloting Performance Measurement of Physician Organizations in Medi-Cal Managed Care: Findings and Implications Ann Hardesty, Project Manager Jill Yegian, Senior Vice President,
Issue Brief No. 13 January 2015 Piloting Performance Measurement of Physician Organizations in Medi-Cal Managed Care: Findings and Implications Ann Hardesty, Project Manager Jill Yegian, Senior Vice President,
Florida Medicaid: Performance Measures (HEDIS)
") Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
Florida Medicaid: Performance Measures (HEDIS) Justin M. Senior Florida Medicaid Director Agency for Health Care Administration Senate Health Policy October 20, 2015 Statewide Medicaid Managed Care (SMMC)
California Community Health Centers
 California Community Health Centers Financial & Operational Performance Analysis, 2011-2014 Prepared by Sponsored by Blue Shield of California Foundation Introduction This report, prepared by Capital Link
California Community Health Centers Financial & Operational Performance Analysis, 2011-2014 Prepared by Sponsored by Blue Shield of California Foundation Introduction This report, prepared by Capital Link
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care
 An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
An Introduction to MPCA and Federally Qualified Health Centers~ Partners for Quality Care AIM Partnership Forum June 5, 2014 Lynda C. Meade, MPA Director of Clinical Services Michigan Primary Care Association
Ohio Department of Medicaid
 Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
Ohio Department of Medicaid Joint Medicaid Oversight Committee March 19, 2015 John McCarthy, Medicaid Director 1 Payment Reform Care Management Quality Strategy Today s Topics Managed Care Performance
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM
 IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
IMPROVING THE QUALITY OF CARE IN SOUTH CAROLINA S MEDICAID PROGRAM VICE PRESIDENT, PUBLIC POLICY & EXTERNAL RELATIONS October 16, 2008 Who is NCQA? TODAY Why measure quality? What is the state of health
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015
 October 29, 2015") Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Enhancing Outcomes with Quality Improvement (QI) October 29, 2015 Learning Objectives! Introduce Quality Improvement (QI)! Explain Clinical Performance Person-Centered Medical Home (PCMH) Measures! Implement
Total Cost of Care Technical Appendix April 2015
 Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Total Cost of Care Technical Appendix April 2015 This technical appendix supplements the Spring 2015 adult and pediatric Clinic Comparison Reports released by the Oregon Health Care Quality Corporation
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
QUALITY IMPROVEMENT. Articles of Importance to Read: Quality Improvement Program. Winter Pages 1, 2, 3, 4 and 5 Quality Improvement
 Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Important information for physicians and other health care professionals and facilities serving UnitedHealthcare Medicaid members Winter 2009 QUALITY IMPROVEMENT Quality Improvement Program The Quality
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Tennessee Health Care Innovation Initiative
 March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
March 8, 2016 1 Tennessee Health Care Innovation Initiative It s my hope that we can provide quality health care for more Tennesseans while transforming the relationship among health care users, providers
Health Center Strong:
 Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
Health Center Strong: Developing and Expressing Health Center Value Jonathan Chapman Director, CHC Advisory Services, Capital Link NHCHC National Conference and Policy Symposium May 18, 2018 1 Capital
2018 MGMA Practice Operations Survey Guide
 2018 MGMA Practice Operations Survey Guide Due Date: April 13, 2018 This document is intended to serve as a guide for completing the 2018 MGMA Practice Operations Survey. An explanation of each survey
2018 MGMA Practice Operations Survey Guide Due Date: April 13, 2018 This document is intended to serve as a guide for completing the 2018 MGMA Practice Operations Survey. An explanation of each survey
HHW-HIPP0314 (9/13) MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.
 MDwise Annual IHCP Seminar. Exclusively serving Indiana families since 1994.") HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
HHW-HIPP0314 (9/13) MDwise 101 2013 Annual IHCP Seminar Exclusively serving Indiana families since 1994. Agenda Indiana Health Coverage Overview MDwise Overview MDwise Hoosier Healthwise MDwise Healthy
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare
 Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
Gateway to Practitioner Excellence GPE 2017 Medicaid & Medicare Recognizing and Rewarding Excellent Practices Improving the Health of Gateway Members PRACTICE ELIGIBILITY (see PCMH slide #27 for separate
HEDIS TOOLKIT FOR PROVIDER OFFICES. A Guide to Understanding Medicaid Measure Compliance
 HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
HEDIS TOOLKIT FOR PROVIDER OFFICES A Guide to Understanding Medicaid Measure Compliance TABLE OF CONTENTS WHAT IS HEDIS 1?... 1 ANNUAL HEDIS TIMELINE... 2 HEDIS MEDICAL RECORD REQUEST PROCESS:... 2 TIPS
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Communicator. the JUST A THOUGHT. Ensuring HEDIS-Compliant Preventive Health Services. Provider Portal Features. Peer-to-Peer Review BY DR.
 WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
WINTER 2016 MHS NEWSLETTER FOR PHYSICIANS Ensuring HEDIS-Compliant Preventive Health Services Here are a few best practice strategies for raising HEDIS and EPSDT onsite review scores, as demonstrated by
Value Based P4P Program Updates MY 2017 & MY 2018
 Value Based P4P Program Updates MY 2017 & MY 2018 January 31, 2018 Lindsay Erickson, Director Ginamarie Gianandrea, Senior Program Coordinator Thien Nguyen, Project Manager Brandi Melville, Health Care
Value Based P4P Program Updates MY 2017 & MY 2018 January 31, 2018 Lindsay Erickson, Director Ginamarie Gianandrea, Senior Program Coordinator Thien Nguyen, Project Manager Brandi Melville, Health Care
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
State Policy Report #47. October Health Center Payment Reform: State Initiatives to Meet the Triple Aim. Introduction
 Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
Health Center Payment Reform: State Initiatives to Meet the Triple Aim State Policy Report #47 October 2013 Introduction Policymakers at both the federal and state levels are focusing on how best to structure
and HEDIS Measures
 1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
1 SC Medicaid Managed Care Initiative and HEDIS Measures - 2009 Ana Lòpez De Fede, PhD Institute for Families in Society University of South Carolina Regina Young, RNC SC Department of Health and Human
Central Ohio Primary Care (COPC) Spotlight on Innovation
 Spotlight on Innovation") Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Central Ohio Primary Care (COPC) Spotlight on Innovation BY BETTER MEDICARE ALLIANCE MARCH 2017 Central Ohio Primary Care Spotlight on Innovation 1 Central Ohio Primary Care (COPC) Spotlight on Innovation
Analysis and Use of UDS Data
 Analysis and Use of UDS Data Welcome and thanks for dropping by to learn about how to analyze and use the valuable UDS data you are reporting! Please click START to begin. Welcome If you have attended
Analysis and Use of UDS Data Welcome and thanks for dropping by to learn about how to analyze and use the valuable UDS data you are reporting! Please click START to begin. Welcome If you have attended
2018 Practice Improvement Program (PIP) Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)
 Orientation. January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP)") 2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
2018 Practice Improvement Program (PIP) Orientation January 4 th, 2018 San Francisco Health Plan Practice Improvement Program (PIP) Practice Improvement Program (PIP) Leadership Team James Glauber, Chief
HEDIS 101 for Providers 2018
 HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
HEDIS 101 for Providers 2018 Improving Quality of Care HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). Author: Commercial & GBD Communication HEDIS Team Document
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
Federally Qualified Health Centers Rural Health Clinics. February Interim. Pay for. Quality
 Federally Qualified Health Centers Rural Health Clinics February 2018 2018 Interim Pay for Quality P R O G R A M G U I D E Table of Contents Introduction to the 2018 Primary Care Pay-for-Quality Program....2
Federally Qualified Health Centers Rural Health Clinics February 2018 2018 Interim Pay for Quality P R O G R A M G U I D E Table of Contents Introduction to the 2018 Primary Care Pay-for-Quality Program....2
Money and Members: Pay for Performance in a Medicaid Program
 Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Money and Members: Pay for Performance in a Medicaid Program IHA National Pay for Performance Summit March 9, 2010 Greg Buchert, MD, MPH Chief Operating Officer 1 AGENDA CalOptima Overview CalOptima P4P
Table of Contents. ii 2016 New Jersey HMO & PPO Performance Report
 Table of Contents Commissioner s Letter... 1 Introduction... 2 Quality Matters... 3 Staying Healthy... 4 Breast Cancer Screening... 5 Cervical Cancer Screening... 6 Colorectal Cancer Screening... 7 Childhood
Table of Contents Commissioner s Letter... 1 Introduction... 2 Quality Matters... 3 Staying Healthy... 4 Breast Cancer Screening... 5 Cervical Cancer Screening... 6 Colorectal Cancer Screening... 7 Childhood
ProviderReport. Managing complex care. Supporting member health.
 ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
ProviderReport Supporting member health Managing complex care Do you have patients whose conditions need complex, coordinated care they may not be able to facilitate on their own? A care manager may be
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
Pay for Performance and the Integrated Healthcare Association. Tom Williams Dolores Yanagihara April 23, 2007
 Pay for Performance and the Integrated Healthcare Association Tom Williams Dolores Yanagihara April 23, 2007 Agenda Why Community Collaboration? Case Study: California P4P Program Structure Program Governance
Pay for Performance and the Integrated Healthcare Association Tom Williams Dolores Yanagihara April 23, 2007 Agenda Why Community Collaboration? Case Study: California P4P Program Structure Program Governance
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator
 Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
Post Acute Continuum Lessons Learned from Geisinger s ProvenHealth Navigator Janet Tomcavage, RN, MSN VP Health Services, Geisinger Health Plan Danville, PA February 3, 2012 Patient-centered primary care
How to Approach Data Collection and Evaluation in SBHCs
 How to Approach Data Collection and Evaluation in SBHCs California School Health Centers Association Annual Conference March 15, 2013 Presenters: Serena Clayton PhD, Executive Director, California School
How to Approach Data Collection and Evaluation in SBHCs California School Health Centers Association Annual Conference March 15, 2013 Presenters: Serena Clayton PhD, Executive Director, California School
Meaningful Use and PCC EHR
 Meaningful Use and PCC EHR (tim@pcc.com) Users Conference 2016 Agenda MU basics and eligibility How to participate in MU Meeting MU measures in PCC EHR Understanding CQM reporting in PCC EHR Takeaways
Meaningful Use and PCC EHR (tim@pcc.com) Users Conference 2016 Agenda MU basics and eligibility How to participate in MU Meeting MU measures in PCC EHR Understanding CQM reporting in PCC EHR Takeaways
Medicaid 101: The Basics
 Medicaid 101: The Basics April 9, 2018 Miranda Motter President and CEO Gretchen Blazer Thompson Director of Govt. Affairs Angela Weaver Director of Regulatory Affairs OAHP Overview Who We Are: The Ohio
Medicaid 101: The Basics April 9, 2018 Miranda Motter President and CEO Gretchen Blazer Thompson Director of Govt. Affairs Angela Weaver Director of Regulatory Affairs OAHP Overview Who We Are: The Ohio
HEDIS Updates to quality ratings, measures & reporting. Wilhelmina Delostrinos, Director of Quality Improvement & Accreditation
 HEDIS 2018 Updates to quality ratings, measures & reporting Wilhelmina Delostrinos, Director of Quality Improvement & Accreditation Agenda HEDIS Overview HEDIS 2018 Changes to Existing Measures HEDIS 2018
HEDIS 2018 Updates to quality ratings, measures & reporting Wilhelmina Delostrinos, Director of Quality Improvement & Accreditation Agenda HEDIS Overview HEDIS 2018 Changes to Existing Measures HEDIS 2018
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association 1 Agenda Incentives in PPS: what does
10/6/2017. FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction. Agenda. Incentives in PPS: what does excludable mean?
 FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
FQHC Incentive Payments: A Critical Practice for Quality and Patient Satisfaction Meaghan McCamman Assistant Director of Policy California Primary Care Association Agenda Incentives in PPS: what does excludable
Developmental Screening Focus Study Results
 Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Developmental Screening Focus Study Results February 28, 2018 Lisa Albers, MD, MC II Medical Quality Improvement Unit, Supervisor Managed Care Quality and Monitoring Division Objectives Review performance
Medical Management. G.2 At a Glance. G.3 Procedures Requiring Prior Authorization. G.5 How to Contact or Notify Medical Management
 G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
G.2 At a Glance G.3 Procedures Requiring Prior Authorization G.5 How to Contact or Notify Medical Management G.6 When to Notify Medical Management G.11 Case Management Services G.14 Special Needs Services
Thought Leadership Series White Paper The Journey to Population Health and Risk
 AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
AMGA Consulting Thought Leadership Series White Paper The Journey to Population Health and Risk The Journey to Population Health and Risk Howard B. Graman, M.D., FACP White Paper, January 2016 While the
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
Alternative Managed Care Reimbursement Models
 Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
Alternative Managed Care Reimbursement Models David R. Swann, MA, LCSA, CCS, LPC, NCC Senior Healthcare Integration Consultant MTM Services Healthcare Reform Trends in 2015 Moving from carve out Medicaid
2017 Quality Rewards Program
 2017 Quality Rewards Program Overview High-level Program Description and Guidelines What Is Changing in 2017 Bonus Payments Description Payment Timing 2 Doc #: PCA-1-005014-02032017_03092017 Updated 06262017
2017 Quality Rewards Program Overview High-level Program Description and Guidelines What Is Changing in 2017 Bonus Payments Description Payment Timing 2 Doc #: PCA-1-005014-02032017_03092017 Updated 06262017
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff
 Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Payment Transformation: Essentials of Patient Attribution An Introduction for Internal Staff May 6, 2016 Payment Transformation Will Address Key Goals In Pursuit of Māhie 2020 - Maximize Value to Members,
Iowa Medicaid: Innovations & Initiatives
 Iowa Medicaid: Innovations & Initiatives ICD-10 ACA Expansion Presumptive Eligibility Health Information Technology PERM DHS Initiatives Adult Quality Measures SIM CDAC Topics 2 ICD-10 3 1 ICD-10 Background
Iowa Medicaid: Innovations & Initiatives ICD-10 ACA Expansion Presumptive Eligibility Health Information Technology PERM DHS Initiatives Adult Quality Measures SIM CDAC Topics 2 ICD-10 3 1 ICD-10 Background
XYZ Community Health Center
 Federally Qualified Health Centers and other safety-net clinics such as [XYZ Community Health Center] provide tremendous value and impacts to their communities from JOBS and ECONOMIC STIMULUS to local
Federally Qualified Health Centers and other safety-net clinics such as [XYZ Community Health Center] provide tremendous value and impacts to their communities from JOBS and ECONOMIC STIMULUS to local
N.E.W.T. Level Measurement:
 N.E.W.T. Level Measurement: Voldemort or Dumbledore? Nathan Spell, MD, FACP Chief Quality Officer, Emory University Hospital Georgia Chapter Scientific Meeting American College of Physicians Savannah,
N.E.W.T. Level Measurement: Voldemort or Dumbledore? Nathan Spell, MD, FACP Chief Quality Officer, Emory University Hospital Georgia Chapter Scientific Meeting American College of Physicians Savannah,
Commonwealth of Puerto Rico Puerto Rico Health Insurance Administration
 ANNUAL EXTERNAL QUALITY REVIEW TECHNICAL REPORT UNITED HEALTHCARE OF THE MIDLANDS, INC. Prepared on Behalf of Nebraska Department of Health and Human Services Division of Medicaid and Long Term Care Reporting
ANNUAL EXTERNAL QUALITY REVIEW TECHNICAL REPORT UNITED HEALTHCARE OF THE MIDLANDS, INC. Prepared on Behalf of Nebraska Department of Health and Human Services Division of Medicaid and Long Term Care Reporting
Chapter 2 Provider Responsibilities Unit 5: Specialist Basics
 Chapter 2 Provider Responsibilities Unit 5: Specialist Basics In This Unit Topic See Page Unit 5: Specialist Basics Participation in the Highmark s Networks as a Specialist 2 Specialist and Personal Physician
Chapter 2 Provider Responsibilities Unit 5: Specialist Basics In This Unit Topic See Page Unit 5: Specialist Basics Participation in the Highmark s Networks as a Specialist 2 Specialist and Personal Physician
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Describe the process for implementing an OP CDI program
 1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
1 Outpatient CDI: The Marriage of MACRA and HCCs Marion Kruse, RN, MBA Founding Partner LYM Consulting Columbus, OH Learning Objectives At the completion of this educational activity, the learner will
HEDIS Measures and the Family Physician Office. Pablo J Calzada DO, MPH, FAAFP, FACOFP
 HEDIS Measures and the Family Physician Office Pablo J Calzada DO, MPH, FAAFP, FACOFP Disclaimer HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). NCQA and payers
HEDIS Measures and the Family Physician Office Pablo J Calzada DO, MPH, FAAFP, FACOFP Disclaimer HEDIS is a registered trademark of the National Committee for Quality Assurance (NCQA). NCQA and payers
Medical Management. G.2 At a Glance. G.2 Procedures Requiring Prior Authorization. G.3 How to Contact or Notify Medical Management
 G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
G.2 At a Glance G.2 Procedures Requiring Prior Authorization G.3 How to Contact or Notify G.4 When to Notify G.7 Case Management Services G.10 Special Needs Services G.12 Health Management Programs G.14
Quality Improvement Program
 How we measure up At HealthKeepers, Inc., we focus on helping our Anthem HealthKeepers Plus members get healthy and stay healthy. To help us serve you the best we can, each year we look closely at the
How we measure up At HealthKeepers, Inc., we focus on helping our Anthem HealthKeepers Plus members get healthy and stay healthy. To help us serve you the best we can, each year we look closely at the
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease
 Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
Guidance for Developing Payment Models for COMPASS Collaborative Care Management for Depression and Diabetes and/or Cardiovascular Disease Introduction Within the COMPASS (Care Of Mental, Physical, And
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary
 2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
2012 QUALITY ASSURANCE ANNUAL REPORT Executive Summary Jai Medical Systems Managed Care Organization, Inc. (JMS) and its providers have closed out their fifteenth full year in the Maryland Medicaid HealthChoice
Emerging Models of Care Delivery Christy Mokrohisky Ex. Dir. of PI & Emerging Models
 Emerging Models of Care Delivery Christy Mokrohisky Ex. Dir. of PI & Emerging Models 1 Sacred Encounters Perfect Care Healthiest Communities St. Joseph Heritage Healthcare Founded in 1994 Manage 7 Medical
Emerging Models of Care Delivery Christy Mokrohisky Ex. Dir. of PI & Emerging Models 1 Sacred Encounters Perfect Care Healthiest Communities St. Joseph Heritage Healthcare Founded in 1994 Manage 7 Medical
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Minnesota Perspective: Fairview Health Services. National Accountable Care Organization Congress October 25, 2010
 Minnesota Perspective: Fairview Health Services National Accountable Care Organization Congress October 25, 2010 Fairview Overview Not-for-profit organization established in 1906 Partner with the University
Minnesota Perspective: Fairview Health Services National Accountable Care Organization Congress October 25, 2010 Fairview Overview Not-for-profit organization established in 1906 Partner with the University
THE BEST OF TIMES: PHARMACY IN AN ERA OF
 OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
OBJECTIVES THE BEST OF TIMES: PHARMACY IN AN ERA OF ACCOUNTABLE CARE Toni Fera, BS, PharmD October 17, 2014 1. Describe the role of pharmacists in accountable care organizations (ACO). 2. List four key
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
Chapter 7. Unit 2: Quality Performance Measures
 Chapter 7 Unit 2: Quality Performance Measures In This Unit Topic See Page Unit 2: QualityBLUE Physician Pay-for-Performance Program Clinical Quality 2 Acute Pharyngitis Testing 10 Adolescent Well Care
Chapter 7 Unit 2: Quality Performance Measures In This Unit Topic See Page Unit 2: QualityBLUE Physician Pay-for-Performance Program Clinical Quality 2 Acute Pharyngitis Testing 10 Adolescent Well Care
Patient-centered medical homes (PCMH): eligible providers.
: eligible providers.") ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
ACTION: Final DATE: 09/21/2018 3:40 PM 5160-1-71 Patient-centered medical homes (PCMH): eligible providers. (A) A Patient-centered medical home (PCMH) is a team-based care delivery model led by primary
MEMBER REQUIREMENT: None.
 PERFORMANCE TARGET MEASURES FORMULARY ADHERENCE This measure seeks to maintain quality of care while reducing costs of prescription drugs. The CBI Program encourages PCPs to reduce the number of costly
PERFORMANCE TARGET MEASURES FORMULARY ADHERENCE This measure seeks to maintain quality of care while reducing costs of prescription drugs. The CBI Program encourages PCPs to reduce the number of costly
producing an ROI with a PCMH
 REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
REPRINT April 2016 Emma Mandell Gray Rachel Aronovich healthcare financial management association hfma.org producing an ROI with a PCMH Patient-centered medical homes can deliver high-quality care and
Examining the Differences Between Commercial and Medicare ACO Models
 Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Examining the Differences Between Commercial and Medicare ACO Models Michelle Copenhaver December 10, 2015 Agenda 1 Understanding Accountable Care Organizations 2 Moving to Accountable Care: Enhancing
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Disclosures. Platforms for Performance: Clinical Dashboards to Improve Quality and Safety. Learning Objectives
 Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
Platforms for Performance: Clinical Dashboards to Improve Quality and Safety Disclosures The program chair and presenters for this continuing pharmacy education activity report no relevant financial relationships.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM. Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017
 ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
ESSENTIAL STRATEGIES IN MEDI-CAL PAYMENT REFORM Richard Popper, Director, Medicaid & Duals Strategy August 3, 2017 1 DISCLAIMER The enclosed materials are highly sensitive, proprietary and confidential.
Emerging Outpatient CDI Drivers and Technologies
 7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
7th Annual Association for Clinical Documentation Improvement Specialists Conference Emerging Outpatient CDI Drivers and Technologies Elaine King, MHS, RHIA, CHP, CHDA, CDIP, FAHIMA Outpatient Payment
Standardizing Medi-Cal Pay for Performance Advisory Committee Meeting. November 3, 2016
 Standardizing Medi-Cal Pay for Performance Advisory Committee Meeting November 3, 2016 Agenda Welcome & Introductions Core Measure Set MY 2017 EAS Measure Set Update Benchmarks Core Measure Set Adoption
Standardizing Medi-Cal Pay for Performance Advisory Committee Meeting November 3, 2016 Agenda Welcome & Introductions Core Measure Set MY 2017 EAS Measure Set Update Benchmarks Core Measure Set Adoption
2016 EPSDT. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2016 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2016 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2016 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Clinical Webinar: Integrated Pharmacy
 Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Clinical Webinar: Integrated Pharmacy Benjamin Gross, Pharm D, MBA, BCPS, BCACP, CDE, BC ADM, ASH CHC Associate Professor Director of Residency Programs Lipscomb University College of Pharmacy Objectives
Beyond RVUs: Changing Your Primary Care Compensation Plan from Volume to Value
 Beyond RVUs: Changing Your Primary Care Compensation Plan from Volume to Value Objectives Compare different primary care compensation models Identify keys to success and best methods for transitioning
Beyond RVUs: Changing Your Primary Care Compensation Plan from Volume to Value Objectives Compare different primary care compensation models Identify keys to success and best methods for transitioning
Quality Measures for HMO s: Understanding HEDIS
 Quality Measures for HMO s: Understanding HEDIS DANE COUNTY IMMUNIZATION COALITION MEMBERSHIP MEETING November 29, 2011 Elaine Rosenblatt MSN, FNP-BC Director, Quality and Care Management UW Medical Foundation/
Quality Measures for HMO s: Understanding HEDIS DANE COUNTY IMMUNIZATION COALITION MEMBERSHIP MEETING November 29, 2011 Elaine Rosenblatt MSN, FNP-BC Director, Quality and Care Management UW Medical Foundation/
10/10/2017. Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP
 Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP") Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Mythbusters: Primary Care Edition (Expanding Opportunities) Amina Abubakar, PharmD, AAHIVP Olivia bentley, PharmD, CFts, AAHIVP 1 Disclosures Amina Abubakar, PharmD, AAHIVP, RX Clinic Pharmacy and Olivia
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
2017 EPSDT. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
2017 EPSDT Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Early and Periodic Screening, Diagnosis, and Treatment Program Evaluation Program Title: Early
The Oklahoma Public Health Network & Billing for Services November AIM/CDC Program Manager Meeting Atlanta, Georgia
 The Oklahoma Public Health Network & Billing for Services 2012 November AIM/CDC Program Manager Meeting Atlanta, Georgia Oklahoma State Department of Health 68 Counties with Health Departments under the
The Oklahoma Public Health Network & Billing for Services 2012 November AIM/CDC Program Manager Meeting Atlanta, Georgia Oklahoma State Department of Health 68 Counties with Health Departments under the
Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management
 Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management Christopher T. Olivia, MD, President Michael Renzi, DO, Chief Medical Officer March 18, 2014 2014, Continuum Health
Ambulatory Care Delivery Strategy: The Key to Successful Population Health Management Christopher T. Olivia, MD, President Michael Renzi, DO, Chief Medical Officer March 18, 2014 2014, Continuum Health
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
PATIENT CENTERED. Medical Home. Attestation. Facility Compliance
 2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
2 0 1 7 Attestation PATIENT CENTERED Medical Home of Facility Compliance State of Wyoming, Department of Health, Division of Healthcare Financing Check the Patient Centered Medical Home (PCMH) Programs
Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim
 Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim Christopher T. Olivia, MD, President June 11, 2014, All Rights Reserved and CONTINUUM HEALTH
Building an Ambulatory System of Care: Using Population Health to Combat Secular Trends & Achieve the Triple Aim Christopher T. Olivia, MD, President June 11, 2014, All Rights Reserved and CONTINUUM HEALTH
Safety Net Success: Evaluation of the Illinois Medicaid Medical Home Program. Fourth National Medical Home Summit, February 27 29, 2012
 Safety Net Success: Evaluation of the Illinois Medicaid Medical Home Program Fourth National Medical Home Summit, February 27 29, 2012 History of Illinois Health Connect Implemented in 2006; driven by
Safety Net Success: Evaluation of the Illinois Medicaid Medical Home Program Fourth National Medical Home Summit, February 27 29, 2012 History of Illinois Health Connect Implemented in 2006; driven by
CHCANYS NYS HCCN ecw Webinar
 CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
CHCANYS NYS HCCN ecw Webinar Meaningful Use, V10 and UDS January 30, 2013 Stephanie Rose, Project Director Desiree Railine, HIT Implementation Specialist/Trainer Agenda Meaningful Use Stage 1 2014 Review
Behavioral Health Providers: The Key Element of Value Based Payment Success
 Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
Behavioral Health Providers: The Key Element of Value Based Payment Success December 6, 2017 Presented by: Andrew Cleek, Psy.D. Meaghan Baier, LMSW Goals of the Presentation Understand the intersect between
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for