An 8-Step Approach to Involving Your Team in Performance Improvement. James E. Tcheng, MD, FACC Duke University Medical Center, Durham, NC
|
|
|
- Donald Newman
- 5 years ago
- Views:
Transcription

1 An 8-Step Approach to Involving Your Team in Performance Improvement James E. Tcheng, MD, FACC Duke University Medical Center, Durham, NC
2 Faculty & Commercial Disclosures Course Director: James E. Tcheng, MD, FACC Professor of Medicine Professor of Community & Family Medicine (Informatics) Director, Performance Improvement, Duke Heart Center Duke University Medical Center, Durham NC Commercial Interest : Nothing to Disclose Faculty: Deepak Bhakta, MD, FACC Associate Professor of Clinical Medicine Krannert Institute of Cardiology Indiana University School of Medicine, Indianapolis, IN Indiana University Health Physicians Commercial Interest : Nothing to Disclose
3 Faculty & Commercial Disclosures Sunil V. Rao, MD, FACC Associate Professor of Medicine Duke University Medical Center Duke Clinical Research Institute Commercial Interest : Nothing to Disclose Frederick G. Welt, MD, MSc, FACC Assistant Professor Harvard University, Boston, MA Director, Interventional Cardiology Director, Invasive Cardiologic Experimental Laboratory Brigham and Women's Hospital Commercial Interest : Nothing to Disclose
4 ARS Question 1 How would you describe yourself relative to performance improvement (PI) in your organization? 1. Physician leader, (potentially) responsible for organizational PI 2. Individual physician looking for the best way to accomplish PI 3. QA/PI expert / resource (non-md/do) 4. Clinical care staff, contributing in other ways to QA/PI efforts 5. Curious bystander
5 ARS Question 2 For Physicians The last time I received credit for MOC Part IV: 1. I completed an ACC PIM product 2. I completed an ABIM PIM product 3. I completed a Completed Project PIM 4. I completed a Self-Directed PIM 5. I ve never done this before 6. I have no idea what you are talking about
6 8 Steps for Groups to Obtain MOC Part IV Overview of the (new) ABIM Maintenance of Certification (MOC) requirements Options for obtaining MOC Part IV (performance improvement project) credit Walk through 8 step approach for groups to follow to obtain MOC Part IV credit Synopsis

7 Maintenance of Certification Parts I - IV Part I Licensure & Professional Standing Part II Self-Evaluation of Medical Knowledge Part III Cognitive Expertise & Examination Part IV Self Evaluation of Practice Performance






8 MOC 2014: Points and Cycle Changes Complete an MOC activity every 2 years Earn total of 100 points every 5 years 20 points Part II 20 points Part IV 20 points Either Part II, III or IV 20 points Either Part II, III or IV 20 points Either Part II, III or IV Patient Safety Module every 5 years Patient Survey Module every 5 years Part II = Self-Evaluation of Medical Knowledge modules Part III = MOC secure Boards exam (20 points for 1 st exam) Part IV = Self-Evaluation of Practice Performance modules
9 Options for Obtaining MOC Part IV Credit Documentation of Part IV MOC is via the Practice Improvement Module (PIM) In ABIM parlance, these modules are products that you order (on your ABIM personal page) Structured ABIM products Generic, disease-specific internal medicine PIMs Structured ACC products Afib (TEAM-A), Imaging (FOCUS) PIMs ABIM framework products Completed Project PIM, Self-Directed PIM
10 Options for Obtaining MOC Part IV Credit Original PIM concept products designed for individual MD to complete on own time highly prescriptive largely designed for the individual MD have proven difficult for MDs to address individually most PIM submissions do not leverage group PI activities, hospital-organized PI work PI is best accomplished as a team team-based clinical improvement projects eligible for Part IV MOC 8 Step Approach
11 Performance Improvement Process Activity: Measurement Identify Benchmarks Gap Analysis Action Planning Implement Change Re-Measure Addressing the Question: What is the current state? What is the desired state? Where is the difference between current and desired states? How can we change to meet the desired state? Will the change plan work? What is the new current state?

12 8 Step Process for Team-Based PI How to Organize Your PI Activity to Obtain MOC Part IV Credit for Multiple Team Participants - while keeping the work of the individual physician to a minimum The Easy Button is a registered trademark of Staples the Office Superstore LLC.
13 8 Step Process for Team-Based PI 1. Create the PI leadership team 2. Champions learn PI principles, MOC process specifics 3. Champions identify potential opportunities for PI (environmental scan, data analysis, etc.) 4. Inaugural team meeting (everyone) 5. Begin ABIM Self-Directed PIM ( order product ) 6. Action planning meeting (everyone) 7. Implement action plan 8. Re-measure and analyze MOC Part IV credit!
14 AMA s PI CME Process Stage A Stage B Stage C MEASURE Identify evidence-based measure(s) and assess practice CHANGE Intervention RE- MEASURE Document Improvement Effective January 2005 AMA PRA, AAFP, and AOA
15 Step 1. Create the PI Leadership Team Identify Champions: Physician Champion This needs to be an extra credit job PI/QI expert (where one exists) Data / performance measures expert (again, where one exists) MOC office / czar? (strongly recommended) And the logical group of aligned physicians who can work together on a MOC Part IV PI project
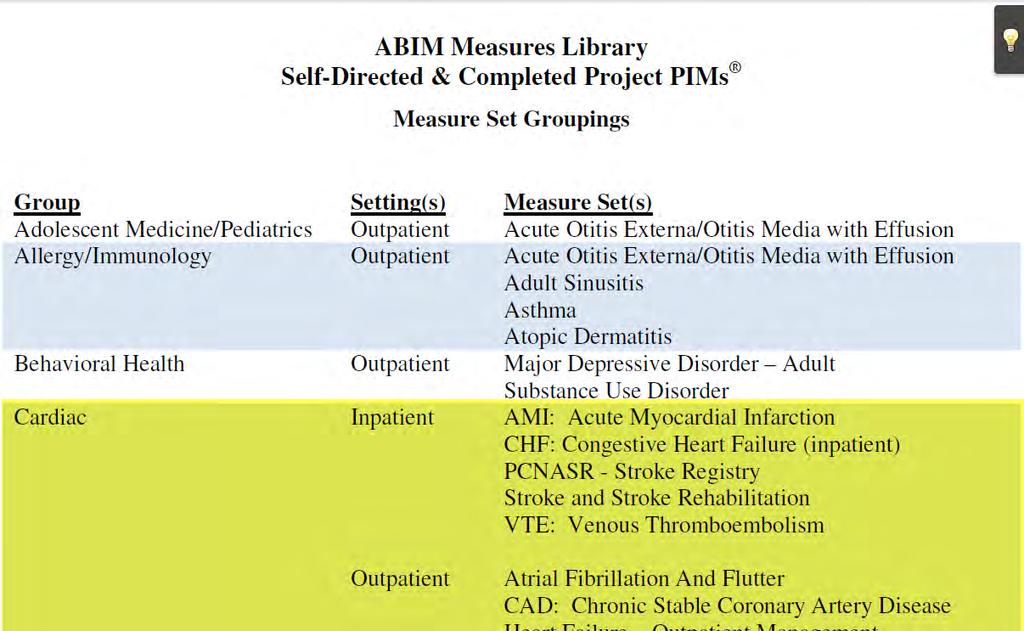
16 Step 2. Education of the PI Leader Team PI Leadership Team must become informed about: PI theory and practice choosing an approach, being able to teach PI to the rest of the group MOC specifics ABIM MOC requirements, Web site Self-Directed PIM process ordering the product, being a logistical resource Concepts of measurement measure sets, the ABIM Measures Library 500 clinical measures compiled by ABIM in Measures Library, structured in groups by setting and specialty
17
 AF & Flutter (3) CAD (12) HF (13) VTE - Outpatient Management (6) Chronic Illness HF - Outpatient Management (13) Outpatient IVD (9) Patient Experience /Satisfaction ABIM Locum")
18 Structure of ABIM s Measures Library SETTING CONDITION MEASURE SET (# measures) AMI (29) Inpatient Cardiac Patient Experience /Satisfaction Cardiac CHF (10) Stroke & Stroke Rehab (17) VTE (11) H-CAHPS Survey (10) AF & Flutter (3) CAD (12) HF (13) VTE - Outpatient Management (6) Chronic Illness HF - Outpatient Management (13) Outpatient IVD (9) Patient Experience /Satisfaction ABIM Locum Tenens Survey (10) CAHPS Clinical & Group Survey (28) Prevention Primary Prevention of Cardiovascular Disease (13)
19 Step 3. Environmental Scan PI Leadership Team: Evaluates existing sources of data and analyses Identifies candidate clinical practice areas / questions for potential performance improvement Evaluates ABIM performance measures library with respect to candidate areas / questions Puts together teaching materials about PI, MOC to present to the group Compiles all of the above to present to the first allinclusive team meeting
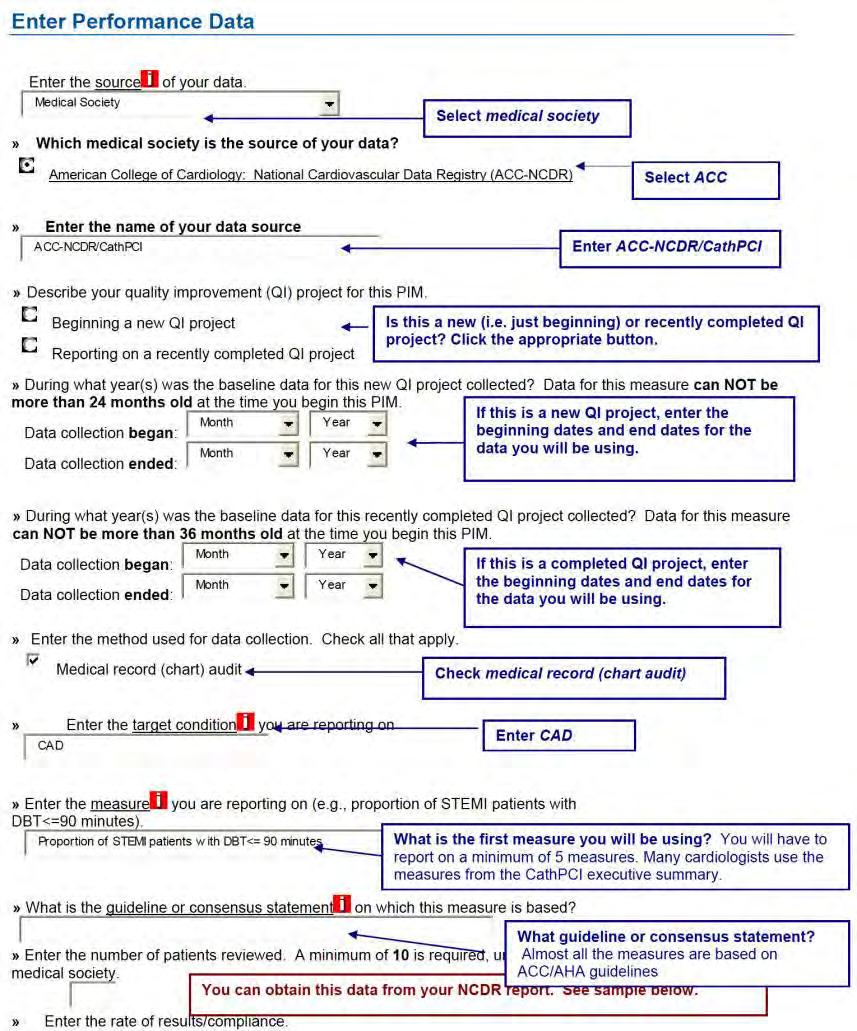
20 Performance Data Comes From Data sources for a Self-Directed PIM: National payment systems (e.g. PQRS) Local, regional or national registries (e.g. NCDR ) Large reputable quality initiatives (e.g. Bridges to Excellence) Chart abstraction (paper records or EHR abstraction)
21 Performance Measures Must Be PI principles require measures to be: SMART: o Specific, Measurable, Actionable, Relevant, Time-bound ABIM requires measures to be: From ABIM s Measures Library OR: Evidence-based, rooted in practice guidelines, nationally endorsed ACC Performance Measures The Joint Commission National Committee for Quality Assurance
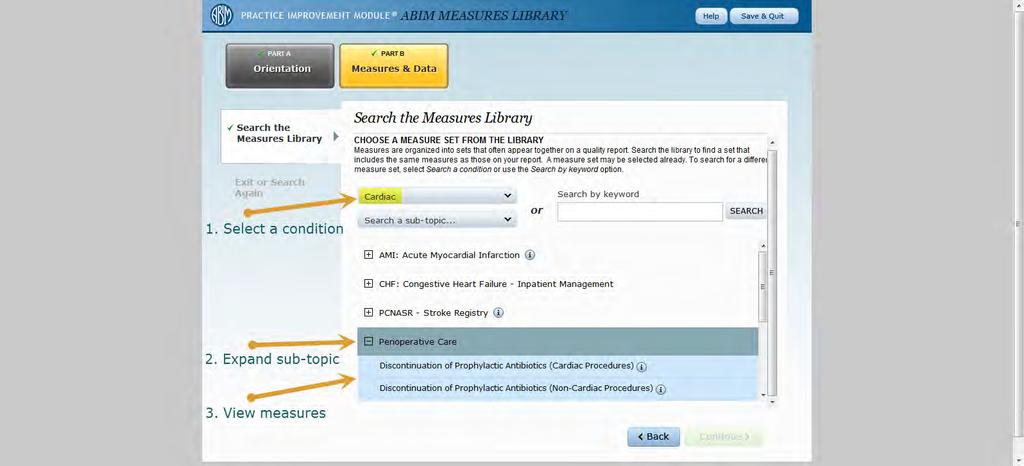
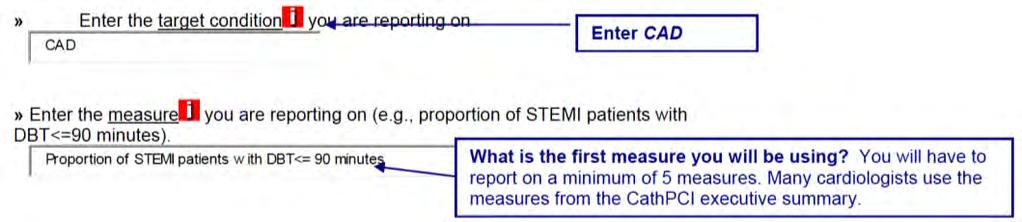
22 Choosing Performance Measures from ABIM s Measures Library Do the following: Search for relevant conditions or groups in the library (including Cardiac, Chronic Illness, Patient Satisfaction, Prevention) Click + to expand group and show names of performance measures Click i to review the measure definitions Select two or three measures from one group or if there are no applicable measures, then author your own
23
24
25 Variation in Measure Definition - Minor ACEI or ARB for LVSD ABIM Measures Library (Cardiac; Inpatient; AMI) Definition: Percentage of AMI patients with Left Ventricular Systolic Dysfunction who are prescribed an Angiotensin Converting Enzyme Inhibitor (ACEI) or Angiotensin Receptor Blockers (ARB) at discharge. ICD Registry National Outcomes Report (Executive Summary) Definition: Proportion of patients with left ventricular systolic dysfunction who were prescribed ACE-I or ARB therapy.
26 Variation in Measure Definition - Significant Chronic Anticoagulation Therapy ABIM Measures Library (Cardiac; Outpatient; AF & Flutter) Definition: Percentage of patients aged 18 years and older with a diagnosis of nonvalvular AF or atrial flutter at high risk for thromboembolism who were prescribed warfarin during the 12 month reporting period. PINNACLE Registry National Outcomes Report (Executive Summary) Definition: Prescription of warfarin, or another oral anticoagulant drug that is FDA-approved for the prevention of thromboembolism, for all patients with nonvalvular AF or atrial flutter at high risk of thromboembolism according to CHADS 2 risk stratification.
27 Measurement Questions Do you collect this information systematically as data? Will the abstraction of the data be manual (i.e., FTE to manually perform chart abstraction) or electronic (i.e., FTE to write code to export the data) Will you need to complete and submit one of ABIM s Non-Approved Measures Application Forms?
28 Step 4. Inaugural Team Meeting (Everyone) Champion convenes all members of PI Project Team: Physicians who need MOC Part IV points PI/QI resource Data and measures expert Other members of the multi-disciplinary team familiar with potential areas for improvement
29 Step 4. Inaugural Team Meeting (cont.) Meeting Actions: Share ABIM s MOC requirements Educate about basics of PI process Review findings of environmental scan / analyses (baseline data) Review applicable performance measures Instruct MDs on logistics of navigating ABIM site and signing up for Self-Directed PIM Assign homework study the candidate performance measures, identify / prioritize the ones that would be suitable for the actual PI project
30 Step 5. Begin ABIM s Self-Directed PIM Direct all physicians to ABIM s website to: Register as an MOC diplomate Order the Self-Directed PIM product All physicians review: Part A Orientation All Physicians review (but do not complete): Part B Measures and Data (review of ABIM Measures Library)
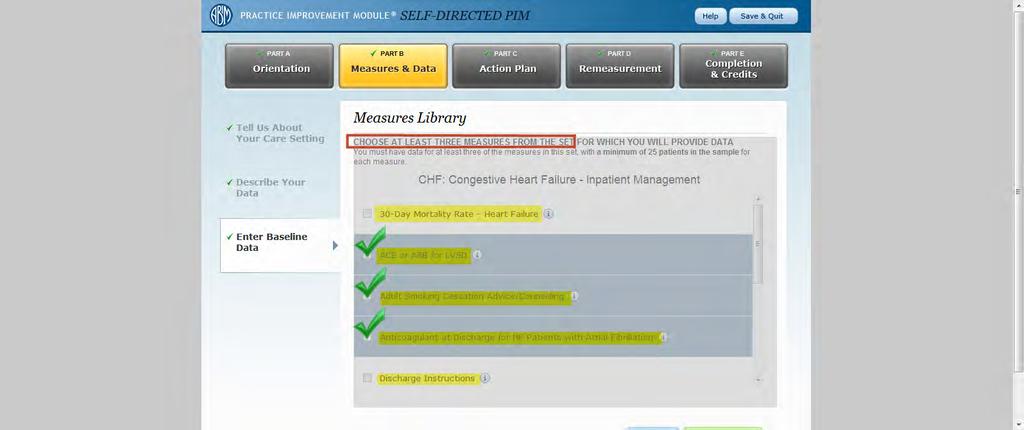
31 6. Action Planning Meeting(s) Meeting Action: Discuss the homework, finalize the selection of three measures to be addressed in the PI project, distribute relevant data for input onto the ABIM site Discuss / create the plan to change / improve the selected measures, assigning responsibilities for executing the components of the plan Assign responsibility for completing the Action Planning document (to redistribute back to the group) All physicians complete: Part B Measures and Data Part C Action Plan
32
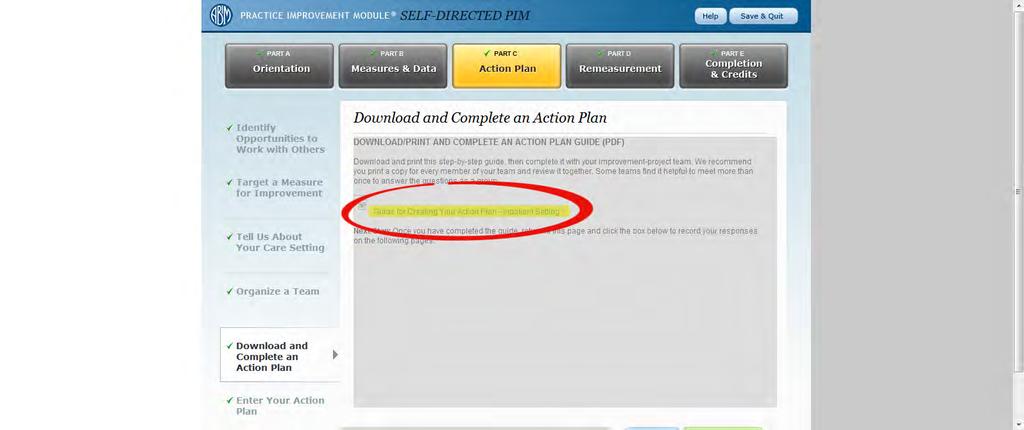
33 Requesting Use of Other Performance Measures If you do not see all three of the performance measures you wish to use in the same group, or you want to use measures which do not appear in the library: You must request approval from ABIM o Click on Submit your measures for approval o Complete and submit one of ABIM s Non-Approved Measures Application Forms

34 Example of one of ABIM s four Non- Approved Measures Application Forms (Page 1 of up to 5)
35 Non-Approved Measures Application Form The following information may be required: Title of each measure Description of each measure Name of clinical practice guideline from which each measure was derived Guideline citations Grade or level of evidence Sample size Baseline performance rate
36 Step 7. Implement Action Plan Implement intervention over three to six months where data available quarterly ACC NCDR Executive Summary Implement over one to three months where data available monthly NCDR dashboards EHR abstraction or data export Allow time for action plan implementation to affect data
37 Step 8. Re-Measurement and Credit Reassess performance Use same performance measure data used in the measurement phase Discuss results Codify new processes into policies and procedures Reflect on what has been learned All physicians complete: Part D Completion and Credits Physicians claim 20 MOC Part IV credits

38
39 Resources MOC czar if you don t have one, you need one Most likely hospital-based Patient experience surveys qualifying surveys (e.g., Press Ganey) are already being done by your hospital no need to repeat! Patient safety activity options being developed
40 Frederick Welt MD FACC QA/PI PRINCIPLES AND METHODOLOGIES WHAT DO I NEED TO KNOW?
41 QA/PI Not a New Concept The ultimate goal is to manage quality. But you cannot manage it until you have a way to measure it, and you cannot measure it until you are able to monitor it. -Florence Nightingale
42 Continuous Process Improvement Borrowed from Business and Industry Kaoru Ishikawa and the fishbone diagram Lean Six Sigma Defects, Overproduction, Waiting, Non-Utilized Talent, Transportation, Inventory, Motion, Extra-Processing Pareto principle 80/20 or principle of factor sparsity. 80% of effects come from 20% of causes.
43 Principles in Healthcare Settings Emphasis on systems and processes Focus on patients Focus on teamwork Focus on collection and use of data
44 Principles in Healthcare Settings Emphasis on systems and processes Focus on patients Focus on teamwork Focus on collection and use of data
45 Emphasis on Systems and Processes Resources People Infrastructure Materials Information Technology Activities What is done How is it done Outcomes Health services delivered Change in health status Patient satisfaction Understand your organization
46 Principles in Healthcare Settings Emphasis on systems and processes Focus on patients Focus on teamwork Focus on collection and use of data
47 Focus on Patients Patient access Evidence based practice Patient safety Care coordination Patient participation
48 Principles in Healthcare Settings Emphasis on systems and processes Focus on patients Focus on teamwork Focus on collection and use of data
49 Focus on Teamwork Complex systems rarely involve one person in care delivery Cross-discipline needs Reliance on staff requires commitment across team Identify stakeholders and leaders of the team
50 Principles in Healthcare Settings Emphasis on systems and processes Focus on patients Focus on teamwork Focus on collection and use of data
51 Focus on Collection and Use of Data Distinguish between what is thought to be happening and what is actually happening Establish a baseline (starting low is okay) Put in place monitoring Value in both quantitative and qualitative data
52 Putting It All Together Analysis 1 Stakeholder involvement 2 Situational analysis 3 Health goals Strategy 4 Quality goals 5 Choose interventions Implementation 6 Implementation 7 Monitoring
53 Sunil V. Rao MD CQI PROJECT: SCAI QIT AS A TEMPLATE
54 ARS Question 3 Quality is defined as: A. The degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge B. Prevention of recurrent MI C. < 20% residual stenosis, TIMI 3 flow after coronary stenting D. Something intangible, but I know it when I see it
55 CQI Project What is quality? SCAI QIT Proposed projects
56 Domains of Quality The degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge Structure Process Outcomes
57 Domains of Quality Structure relates to having the ingredients necessary to deliver quality care Process measures refer to the application of evidence based diagnostic and therapeutic measures Outcomes are consequences of the applied measures Markers of disease progression (e.g. mortality) Health status (e.g. QOL) Costs Appropriate use
58 Performance Measures Represent a meaningful outcome to patients and society Be valid, reliable, and readily measured Have the ability to be adjusted for patient variability Be modifiable through improvements in care processes Be practical to measure Krumholz HM, et. al. Circulation 2000

59 SCAI Quality Improvement Toolkit







60 What s In This for Me? Yes Are You an Invasive Cardiologist? No Learn about Tools to Help You Improve the Quality of Care Provided in your Cardiac Cath Lab Learn about Tools to Help You Improve the Quality of Care for Patients That You re Thinking About Referring to the Cardiac Cath Lab Slide courtesy of Kalon Ho MD cb /winniethepooh/images/2/2f/pooh_and_piglet,_thinking.jpg
 features several tools focused on: Guidelines; Peer review conferences; Random case selection; National database participation; Pre-procedure checklists;")
61 SCAI is inviting you to join the interventional cardiology community in tackling continuous quality improvement (CQI) in the cardiac cath lab. SCAI's Quality Improvement Toolkit (SCAI-QIT) features several tools focused on: Guidelines; Peer review conferences; Random case selection; National database participation; Pre-procedure checklists; Data collection; and Inventory management The beauty of SCAI-QIT is that it is flexible and can be customized for each user. Even better, you will lead the way at your own institution, using its practical tools to document your strengths, identify opportunities for improvement, and prepare for governmentmandated "Pay-for-Quality" initiatives. Slide courtesy of Kalon Ho MD


62 Aims of the SCAI-QIT Syllabus Develop QI programs in catheterization laboratories Maintain existing QI programs Allow labs to tailor QI programs to local environments Slide courtesy of Kalon Ho MD








63 Outline Defining Quality in the Cath Lab Operator and Staff Requirements Procedural Quality Benchmarking Key conferences Cath Lab Best Practices Facility and Environmental Issues Care Coordination with Referring Physicians


64 Slide courtesy of Kalon Ho MD Sign Up to be a SCAI Quality Champion Benefits include: Listserv Receive guidelines, standards and position papers when published Receive Monthly SCAI-QIT Tips of the Month Notification of webinars and educational opportunities Venue for questions to the QI Committee with personalized or published answers Opportunities to participate in development of new SCAI-QIT tools, comment on new data standards and guidelines Public recognition of your commitment to Continuous Quality Improvement


65 Webinar Archives Navigating the New 2012 Appropriate Use Criteria for Diagnostic Cardiac Catheterization What the 2012 Cath Lab Standards Update Has to Offer for Quality Improvement Navigating the New 2012 Revascularization Appropriate Use Criteria Navigating the Revised 2011 Guidelines to PCI SCAI-QIT: Defining Quality in the Cath Lab, Facility and Environmental Issues Tools, and Accreditation for Cardiovascular Excellence SCAI-QIT: Operator and Staff Requirements SCAI-QIT: Procedural Quality and Cath Lab Best Practices Upcoming Webinars PCI without Surgical Backup, with Greg Dehmer, 18 Mar 2014 CathPCI Registry Tools That Work, with Skip Anderson, 21 Mar 2014 Documentation Module, with Kirk Garratt Care Coordination, with Hank Jennings Slide courtesy of Kalon Ho MD
66
67 Potential CQI Projects* Documentation of radiation exposure during angiography and PCI Reduction in contrast use during angiography and PCI Documentation of appropriateness of procedures *Measures other than those listed by the ABIM need approval
68 Deepak Bhakta MD FACC FACP FAHA FHRS CCDS ACTION PLAN DEVELOPMENT
69 ARS Question 4 Which one of the following is most closely associated with your clinical practice? A. Percutaneous coronary intervention B. Peripheral arterial angioplasty C. ICD implantation D. Inpatient cardiovascular management E. Outpatient cardiovascular management
70 Performance Improvement: Action Plan: Development Patient #: Aspirin? Beta-blocker? ACE-inhibitor? ARB? CAD? CHF? NYHA class LV assessment? 1 Yes Yes Yes No Yes Yes III Yes 10 2 No Yes Yes No Yes Yes II Yes 44 3 No Yes No No No No I Yes 50 4 Yes Yes Yes No Yes No I Yes 60 5 No No Yes No No Yes II Yes 33 Drug therapy: 6 Yes Yes Yes No Yes Yes II Yes 30 7 Yes Yes Yes No Yes Yes II Yes 35 8 Yes No Yes No Yes Yes II Yes 24 1) Aspirin use in CAD patients 2) ACE-I/ARB use in patients with LVEF <0.40 3) Beta-blocker use in patients with LVEF < Yes Yes Yes No Yes Yes II Yes Yes Yes Yes No No Yes II Yes Yes Yes Yes No Yes Yes II Yes Yes Yes Yes No Yes Yes III Yes Yes Contraindicated Yes No No Yes III Yes No Yes Yes No No Yes II Yes Yes Yes Yes No No Yes II Yes Yes Contraindicated Contraindicated Contraindicated Yes Yes III Yes Yes Yes Yes No Yes Yes III Yes No Yes No Yes No Yes III Yes Yes Yes Contraindicated Contraindicated Yes Yes II Yes 35 LVEF (%) ACE = angiotensin converting enzyme ARB = angiotensin receptor blocker CAD = coronary artery disease CHF = congestive heart failure LV = left ventricular LVEF = left ventricular ejection fraction NYHA = New York Heart Association Source: National Cardiovascular Data Registry - ICD Registry (Individual data)
71 Performance Improvement: Action Plan: Development Drug therapy 1) Aspirin use in CAD patients 2) ACE-I/ARB use in patients with LVEF <0.40 3) Beta-blocker use in patients with LVEF <0.40 Patient CAD? #: Aspirin? Beta-blocker? ACE-inhibitor? ARB? CAD? CHF? NYHA class LV assessment? Yes 1 Yes Yes Yes No Yes Yes III Yes 10 Yes 2 No Yes Yes No Yes Yes II Yes 44 No 3 No Yes No No No No I Yes 50 Yes 4 Yes Yes Yes No Yes No I Yes 60 Baseline data: 11/12 (91.7%) No 5 No No Yes No No Yes II Yes 33 Yes 6 Yes Yes Yes No Yes Yes II Yes 30 Yes 7 Yes Yes Yes No Yes Yes II Yes 35 Yes 8 Yes No Yes No Yes Yes II Yes 24 Yes 9 Yes Yes Yes No Yes Yes II Yes No Yes Yes Yes No No Yes II Yes 20 Yes 11 Yes Yes Yes No Yes Yes II Yes 34 Yes 12 Yes Yes Yes No Yes Yes III Yes No Yes Contraindicated Yes No No Yes III Yes No No Yes Yes No No Yes II Yes No Yes Yes Yes No No Yes II Yes 33 Yes 16 Yes Contraindicated Contraindicated Contraindicated Yes Yes Not recorded Yes 25 Yes 17 Yes Yes Yes No Yes Yes III Yes No No Yes No No No Yes III Yes 25 Yes 19 Yes Yes Contraindicated Contraindicated Yes Yes II Yes 35 LVEF (%)
72 Performance Improvement: Action Plan: Development LVEF (%) Beta-blocker? ACEinhibitor/ARB? 10 Yes Yes 44 Yes Yes 50 Yes No 60 Yes Yes 33 No Yes 30 Yes Yes 35 Yes Yes 24 No Yes 33 Yes Yes Drug therapy 1) Aspirin use in CAD patients 2) ACE-I/ARB use in patients with LVEF <0.40 3) Beta-blocker use in patients with LVEF <0.40 Baseline data (ACE-I/ARB) : 15/16 (93.8%) Baseline data (beta-blocker): 14/16 (87.5%) 20 Yes Yes 34 Yes Yes 36 Yes Yes 15 Contraindicated Yes 21 Yes Yes 33 Yes Yes 25 Contraindicated Contraindicated 34 Yes Yes 25 Yes No 35 Yes Contraindicated
73 Performance Improvement: Action Plan: Implementation Metric Baseline performance Target performance Aspirin use in CAD patients 11/12 (91.7%) >95% ACE-I/ARB use in patients with LVEF <0.40 Beta-blocker use in patients with LVEF < /16 (93.8%) >95% 14/16 (87.5%) >95% Action plan: 1) Review, documentation and initiation of pharmacotherapy in outpatient ICD referral patients (including drug contraindications/intolerance) at the time of visit or implantation 2) Review, documentation, and initiation of appropriate drug therapy in inpatient ICD recipients (including drug contraindications/intolerance) 3) Communication with primary cardiovascular caregiver regarding details of pharmacotherapy 4) Re-measurement of selected metrics using above action plan


74 Performance Improvement: Action Plan: Implementation
75 Performance Improvement: Action Plan: Implementation Process/Out come Metric Q Q Q Q Q Q Q All Hospitals 50 th Percentile (2013 Q1) All Hospitals 90 th Percentile (2012 Q4) LVEF <0.40, ACE-I/ARB? LVEF <0.40, betablocker? Prior MI, betablocker? Suggested metrics: Evidence-based, guideline-directed Collected by registry Multi-purpose metrics Capable of process improvement/intervention 91.6% 99.3% 98.9% 100% 100% 100% 99.2% 82.8% 99.1% 98.4% 97.9% 100% 100% 100% 100% 100% 94.2% 100% 88.4% 97.5% 99.3% 100% 100% 100% 100% 93.9% 100% Antibiotics prior to procedure? Class I, IIa and Iib indications? Suggested interventions: Improved documentation Improved chart review Communication with all caregivers Involvement of all care team elements 99.0% 99.5% 100% 100% 100% 100% 100% 100% 100% 88.6% 96.1% 97.2% 96.9% 100% 95.9% 100% 91.1% 100% Mortality 0.3% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.2% N/A Failure to place CS/LV lead 8.1% 6.9% 8.4% 4.5% 6.6% 7.3% 4.5% 8.4% 2.3% Source: National Cardiovascular Data Registry - ICD Registry (Institutional data)
76 ARS Question 5 Which one of the following is most closely associated with your clinical practice? A. Percutaneous coronary intervention Cath PCI Registry B. Peripheral arterial angioplasty PVI Registry C. ICD implantation ICD Registry D. Inpatient cardiovascular management ACTION Registry (ACS/NSTEMI) E. Outpatient cardiovascular management PINNACLE Registry
77 Performance Improvement: Action Plan: Available Registries Registry benefits Systematic data collection Standardized variables Comparison within and between practices/institutions Applicable in multiple arenas
MOC Part IV: Your Guide to Making it Happen.
 MOC Part IV: Your Guide to Making it Happen. Joseph P. Drozda, Jr., MD, F.A.C.C. Mercy, MO Paul D. Varosy, MD, F.A.C.C., FAHA, FHRS University of Colorado Denver School of Medicine, CO Disclosures Course
MOC Part IV: Your Guide to Making it Happen. Joseph P. Drozda, Jr., MD, F.A.C.C. Mercy, MO Paul D. Varosy, MD, F.A.C.C., FAHA, FHRS University of Colorado Denver School of Medicine, CO Disclosures Course
SIMPLE SOLUTIONS. BIG IMPACT.
 SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
SIMPLE SOLUTIONS. BIG IMPACT. SIMPLE SOLUTIONS. BIG IMPACT. QUALITY IMPROVEMENT FOR INSTITUTIONS combines the American College of Cardiology s (ACC) proven quality improvement service solutions and its
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2012 DATA PUBLISHED 2015 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
Improving Quality of Care for Medicare Patients: Accountable Care Organizations
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Improving Quality of Care for Medicare Patients: FACT SHEET Overview http://www.cms.gov/sharedsavingsprogram On October
Benchmark Data Sources
 Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
Medicare Shared Savings Program Quality Measure Benchmarks for the 2016 and 2017 Reporting Years Introduction This document describes methods for calculating the quality performance benchmarks for Accountable
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule
 HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
HIT Incentives: Issues of Concern to Hospitals in the CMS Proposed Meaningful Use Stage 2 Rule Lori Mihalich-Levin, J.D. lmlevin@aamc.org; 202-828-0599 Jennifer Faerberg jfaerberg@aamc.org; 202-862-6221
Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA
 Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA Introduce the methods of using core measures to compare quality of health care US hospitals provide Have
Olutoyin Abitoye, MD Attending, Department of Internal Medicine Virtua Medical Group New Jersey,USA Introduce the methods of using core measures to compare quality of health care US hospitals provide Have
ACC State Chapters Best Practice Guide. Working with States on Clinical Data Requests
 ACC State Chapters Best Practice Guide Working with States on Clinical Data Requests Prepared by: Science, Education and Quality Division As of: 3/16/2016 Contents 1. Introduction... 1 2. NCDR Registries
ACC State Chapters Best Practice Guide Working with States on Clinical Data Requests Prepared by: Science, Education and Quality Division As of: 3/16/2016 Contents 1. Introduction... 1 2. NCDR Registries
General Ward Driver Diagram and Change Package
 General Ward Driver Diagram and Change Package The Institute for Healthcare Improvement A driver diagram is used to conceptualise an issue and to determine its system components which will then create
General Ward Driver Diagram and Change Package The Institute for Healthcare Improvement A driver diagram is used to conceptualise an issue and to determine its system components which will then create
Implementing AHA Quality Improvement Programs: Get With the Guidelines
 Implementing AHA Quality Improvement Programs: Get With the Guidelines Sidney C. Smith, Jr. MD FAHA, FACC, FESC Professor of Medicine/Cardiology University of North Carolina Past President, American Heart
Implementing AHA Quality Improvement Programs: Get With the Guidelines Sidney C. Smith, Jr. MD FAHA, FACC, FESC Professor of Medicine/Cardiology University of North Carolina Past President, American Heart
WebEx Quick Reference
 IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
IHI Expedition: Effective Implementation of Heart Failure Core Processes Peg Bradke, RN, MA, Faculty Christine McMullan, MPA, Director December 15, 2011 These presenters have nothing to disclose WebEx
ACO GPRO 2016 Ready to Report Basics GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017
 ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
ACO GPRO 2016 Ready to Report Basics 2016 GPRO ACO Random Sample Reporting January 17, 2017 to March 17, 2017 ACO GPRO 2016 Ready to Report Basics What is an Accountable Care Organization (ACO)? Which
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES
 MEASURES") NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
NEW JERSEY HOSPITAL PERFORMANCE REPORT 2014 DATA PUBLISHED 2016 TECHNICAL REPORT: METHODOLOGY RECOMMENDED CARE (PROCESS OF CARE) MEASURES New Jersey Department of Health Health Care Quality Assessment
War on Warfarin: Integrating DOACs into your Anticoagulation Service
 War on Warfarin: Integrating DOACs into your Anticoagulation Service David DeiCicchi, Pharm.D, CACP Brigham and Women s Hospital September 30 th, 2016 Disclosures I have no financial conflict of interest
War on Warfarin: Integrating DOACs into your Anticoagulation Service David DeiCicchi, Pharm.D, CACP Brigham and Women s Hospital September 30 th, 2016 Disclosures I have no financial conflict of interest
It s All About Revenue MIPS & Cardiology Best Practices JUSTIN T. BARNES
 It s All About Revenue MIPS & Cardiology Best Practices JUSTIN T. BARNES PARTNER, IHEALTH INNOVATIONS CO-CHAIR, ACCOUNTABLE CARE COMMUNITY OF PRACTICE About Justin T. Barnes Justin is a nationally recognized
It s All About Revenue MIPS & Cardiology Best Practices JUSTIN T. BARNES PARTNER, IHEALTH INNOVATIONS CO-CHAIR, ACCOUNTABLE CARE COMMUNITY OF PRACTICE About Justin T. Barnes Justin is a nationally recognized
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL
 CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
CHAPTER 9 PERFORMANCE IMPROVEMENT HOSPITAL PERFORMANCE IMPROVEMENT Introduction to terminology and requirements Performance Improvement Required (Board of Pharmacy CQI program, The Joint Commission, CMS
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond)
") Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
Meaningful Use Measures: Quick Reference Guide Stage 2 (2014 and Beyond) Core Measures Required: All 17 objectives Objective: Requirement: Exclusions: Accomplish in Clinical 1. Computerized - Documenting
SBAR: NCDR Registries Initiation and Feedback Phase
 SBAR: NCDR Registries Initiation and Feedback Phase Title: NCDR Registries CECCV-36 Situation: Less than ~76% of TH procedure sites belong to NCDR Registries. Background: Registries ensure evidenced-based
SBAR: NCDR Registries Initiation and Feedback Phase Title: NCDR Registries CECCV-36 Situation: Less than ~76% of TH procedure sites belong to NCDR Registries. Background: Registries ensure evidenced-based
The SCAI Cardiovascular Professional (CVP) Quality Improvement Toolkit was developed with support from Daiichi Sankyo and Lilly.
 Quality Improvement Toolkit was developed with support from Daiichi Sankyo and Lilly.") The SCAI Cardiovascular Professional (CVP) Quality Improvement Toolkit was developed with support from Daiichi Sankyo and Lilly. The Society gratefully acknowledges this support, while taking sole responsibility
The SCAI Cardiovascular Professional (CVP) Quality Improvement Toolkit was developed with support from Daiichi Sankyo and Lilly. The Society gratefully acknowledges this support, while taking sole responsibility
ACO Name and Location. ACO Primary Contact. Organizational Information
 ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
2018 Collaborative Quality Initiative Fact Sheet
 2018 Collaborative Quality Initiative Fact Sheet Blue Cross Blue Shield of Michigan Cardiovascular Consortium Overview The Blue Cross Blue Shield of Michigan Cardiovascular Consortium, commonly called
2018 Collaborative Quality Initiative Fact Sheet Blue Cross Blue Shield of Michigan Cardiovascular Consortium Overview The Blue Cross Blue Shield of Michigan Cardiovascular Consortium, commonly called
Best Practices for emeasure Implementation. Breakout Session #2: Implementation in Office-Based Practice Settings
 Best Practices for emeasure Implementation Breakout Session #2: Implementation in Office-Based Practice Settings Track Leaders: Kendra Hanley John Maese, MD Michael Mirro, MD April 26, 2012 emeasure Learning
Best Practices for emeasure Implementation Breakout Session #2: Implementation in Office-Based Practice Settings Track Leaders: Kendra Hanley John Maese, MD Michael Mirro, MD April 26, 2012 emeasure Learning
CHF Readmission Initiative. Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana
 CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
CHF Readmission Initiative Mary Fischer MSN, CCRN, PCCN, CHFN Cardiology Clinical Nurse Specialist St. Vincent Hospital Indianapolis, Indiana St. Vincent 86 th Street Campus Heart Failure Program History
ACO Name and Location. ACO Primary Contact. Organizational Information
 ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
ACO ame and Location Ascension Care Management Health Partners Indianapolis, LLC Previous Legal Business Entity ame: MissionPoint Indianapolis, LLC 523 Mainstream Dr ashville, Tennessee 37228-1238 ACO
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
Slide 1. Slide 2 Rural Princeton. Slide 3 Agenda Rural ACO RURAL ACOS CAN WORK AND LEAD THE WAY
 Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
Slide 1 RURAL ACOS CAN WORK AND LEAD THE WAY Nebraska Rural Health Association September 20, 2017 Slide 2 Rural Princeton Slide 3 Agenda Rural ACO Illinois Rural Community Care Organization (IRCCO)/Statewide
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Shared Savings Program ACO Public Reporting Instructions. with Pre-Populated Template
 Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
Shared Savings Program ACO Public Reporting Instructions Introduction with Pre-Populated Template The purpose of this document is to provide ACOs participating in the Shared Savings Program with a public
Presenter Disclosure
 Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Improving Transitions from the Hospital to Community Settings IHI National Forum Learning Lab Sunday, December 9, 2012 Session L20 Presenter Disclosure Leora Horwitz, MD Assistant Professor of medicine
Assuring Data Integrity for Healthcare Public Reporting and Using Results to Evaluate Patient Care Quality
 Assuring Data Integrity for Healthcare Public Reporting and Using Results to Evaluate Patient Care Quality ABSTRACT This presentation describes (1) steps insuring data integrity for public reporting; (2)
Assuring Data Integrity for Healthcare Public Reporting and Using Results to Evaluate Patient Care Quality ABSTRACT This presentation describes (1) steps insuring data integrity for public reporting; (2)
3/29/2013. Effective ACO Compliance. Objectives THE HEALTH CARE DILEMMA: ARE ACOS THE ANSWER? HCCA Compliance Institute April 21, 2013
 Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
Effective ACO Compliance HCCA Compliance Institute April 21, 2013 Margaret Hambleton, MBA, CHC, CHPC Sr. Vice President, Chief Compliance Officer St. Joseph Health System 1 Objectives Understand Accountable
United Medical ACO Participation Criteria
 United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
United Medical ACO Participation Criteria Items Requiring Practice Reporting 1) Submission of Reports: Practices must report A,B, and C to UMACO A. Thirty-four ACO Quality Measures -See Appendix A B. Average
Managing Your Patient Population: How do you measure up?
 Managing Your Patient Population: How do you measure up? Paul M. Palevsky, M.D. Chief, Renal Section VA Pittsburgh Healthcare System Professor of Medicine University of Pittsburgh School of Medicine Ben
Managing Your Patient Population: How do you measure up? Paul M. Palevsky, M.D. Chief, Renal Section VA Pittsburgh Healthcare System Professor of Medicine University of Pittsburgh School of Medicine Ben
INSERT ORGANIZATION NAME
 INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
INSERT ORGANIZATION NAME Quality Management Program Description Insert Year SAMPLE-QMProgramDescriptionTemplate Page 1 of 13 Table of Contents I. Overview... Purpose Values Guiding Principles II. III.
Case Study High-Performing Health Care Organization December 2008
 Case Study High-Performing Health Care Organization December 2008 Luther Midelfort Mayo Health System: Laying Tracks for Success Jen n i f e r Ed w a r d s, Dr.P.H. Health Management Associates The mission
Case Study High-Performing Health Care Organization December 2008 Luther Midelfort Mayo Health System: Laying Tracks for Success Jen n i f e r Ed w a r d s, Dr.P.H. Health Management Associates The mission
National Hospital Inpatient Quality Reporting Measures Specifications Manual
 National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.4a Release Notes Completed: October 21, 2014 Guidelines for Using Release Notes Release Notes 4.4a
National Hospital Inpatient Quality Reporting Measures Specifications Manual Release Notes Version: 4.4a Release Notes Completed: October 21, 2014 Guidelines for Using Release Notes Release Notes 4.4a
ACTION Registry-GWTG. NCDR13 Updates 3/22/2013. ACTION Cumulative Records Submitted Q Q Q Q Q3 Records Submitted
 ACTION Registry-GWTG NCDR13 Updates 500000 450000 400000 350000 300000 250000 200000 150000 100000 50000 0 ACTION Cumulative Records Submitted 457970 327168 219151 138117 83446 2008 Q3 2009 Q3 2010 Q3
ACTION Registry-GWTG NCDR13 Updates 500000 450000 400000 350000 300000 250000 200000 150000 100000 50000 0 ACTION Cumulative Records Submitted 457970 327168 219151 138117 83446 2008 Q3 2009 Q3 2010 Q3
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals
 Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Proposed Meaningful Use Incentives, Criteria and Quality Measures Affecting Critical Access Hospitals Paul Kleeberg, MD, FAAFP, FHIMSS Clinical Director Regional Extension Assistance Center for HIT (REACH)
Rural-Relevant Quality Measures for Critical Access Hospitals
 Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
Rural-Relevant Quality Measures for Critical Access Hospitals Ira Moscovice PhD Michelle Casey MS University of Minnesota Rural Health Research Center Minnesota Rural Health Conference Duluth, Minnesota
EHR Enablement for Data Capture
 EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
EHR Enablement for Data Capture Baylor Scott & White (15 min) Bonnie Hodges, RN University of Chicago Medicine(15 min) Susan M. Sullivan, RHIA, CPHQ Kaiser Permanente (15 min) Molly P. Clopp, RN Tammy
National Patient Safety Goals & Quality Measures CY 2017
 National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
National Patient Safety Goals & Quality Measures CY 2017 General Clinical Orientation 2017 January National Patient Safety Goals 1. Identify Patients Correctly 2. Improve Staff Communication 3. Use Medications
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model. Rome H. Walker MD February 28, 2008
 Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Aligning Hospital and Physician P4P The Q-HIP SM /QP-3 SM Model Rome H. Walker MD February 28, 2008 A Concerted Effort Because the rewards are based on shared performance, the program is intended to create
Objective Measurement
 STEMI Designation Contract HOSPITAL SERVICES A. Current license to provide Basic Emergency Services in Contra Costa County Copy of License B. Cardiac Catheterization Laboratory services Copy of License.
STEMI Designation Contract HOSPITAL SERVICES A. Current license to provide Basic Emergency Services in Contra Costa County Copy of License B. Cardiac Catheterization Laboratory services Copy of License.
ACO Update. LVHN Scholarly Works. Lehigh Valley Health Network. Lehigh Valley Health Network. Spring 2017
 Lehigh Valley Health Network LVHN Scholarly Works ACO Update Newsletters Spring 2017 ACO Update Lehigh Valley Health Network Follow this and additional works at: https://scholarlyworks.lvhn.org/acoupdate
Lehigh Valley Health Network LVHN Scholarly Works ACO Update Newsletters Spring 2017 ACO Update Lehigh Valley Health Network Follow this and additional works at: https://scholarlyworks.lvhn.org/acoupdate
Achilles Heel for PI Programs
 Achilles Heel for PI Programs Engaging Physicians in All 3 Stages Alliance for Continuing Education in the Health Professions FEBRUARY 1, 2013 2013 Annenberg Center for Health Sciences at Eisenhower Medical
Achilles Heel for PI Programs Engaging Physicians in All 3 Stages Alliance for Continuing Education in the Health Professions FEBRUARY 1, 2013 2013 Annenberg Center for Health Sciences at Eisenhower Medical
NCDR 13 Annual Conference. ACTION Registry-GWTG Workshop #1. Disclosures Dr. Fonarow, MD, FACC, FAHA. Objectives 2/28/2013.
 NCDR 13 Annual Conference ACTION Registry-GWTG Workshop #1 Disclosures Dr. Fonarow, MD, FACC, FAHA Boston Scientific, Takeda, Amgen, Johnson&Johnson, Medtronic, Gambro, NIH/NIAID, Novartis, NHLBI Kim Hustler
NCDR 13 Annual Conference ACTION Registry-GWTG Workshop #1 Disclosures Dr. Fonarow, MD, FACC, FAHA Boston Scientific, Takeda, Amgen, Johnson&Johnson, Medtronic, Gambro, NIH/NIAID, Novartis, NHLBI Kim Hustler
Working to Improve the Patient Experience
 Arizona Critical Access Hospital Quality Network Working to Improve the Patient Experience March 12, 2013 2 3:30pm Arizona Rural Hospital Flexibility Program AZ-CAH Quality Network CAH Participants Benson
Arizona Critical Access Hospital Quality Network Working to Improve the Patient Experience March 12, 2013 2 3:30pm Arizona Rural Hospital Flexibility Program AZ-CAH Quality Network CAH Participants Benson
MEANINGFUL DIPLOMATE PARTICIPATION IN MOC- DEVELOP YOUR TOOLKIT. Lindsey Safford Marshfield Clinic Health Systems, Inc.
 MEANINGFUL DIPLOMATE PARTICIPATION IN MOC- DEVELOP YOUR TOOLKIT Lindsey Safford Marshfield Clinic Health Systems, Inc. Marshfield, WI Overview Supported by the Division of Education at Marshfield Clinic
MEANINGFUL DIPLOMATE PARTICIPATION IN MOC- DEVELOP YOUR TOOLKIT Lindsey Safford Marshfield Clinic Health Systems, Inc. Marshfield, WI Overview Supported by the Division of Education at Marshfield Clinic
March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan
 BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
BRIEFING NOTE March 28, 2018 For Decision Board of Directors Item 9.0 Comprehensive Regional Cardiac Program Plan PURPOSE To provide the WWLHIN Board of Directors with a recommendation to endorse the proposed
ACO Name and Location ACO Primary Contact
 ACO ame and Location Chrysalis Medical Services, LLC 4888 Loop Central Drive Suite 700 Houston, Texas 77081 ACO Primary Contact Primary Contact ame Adrienne Opalka Primary Contact Phone umber 914-281-0827
ACO ame and Location Chrysalis Medical Services, LLC 4888 Loop Central Drive Suite 700 Houston, Texas 77081 ACO Primary Contact Primary Contact ame Adrienne Opalka Primary Contact Phone umber 914-281-0827
2017 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2017 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2017 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
1.01 Government Programs: CMS and Pay for Performance: Current Issues. CMS Regional Administrator March 2009
 1.01 Government Programs: CMS and Pay for Performance: Current Issues David Saÿen CMS Regional Administrator March 2009 Overview Why value-based purchasing? What demonstrations are underway? Hospital demonstrations
1.01 Government Programs: CMS and Pay for Performance: Current Issues David Saÿen CMS Regional Administrator March 2009 Overview Why value-based purchasing? What demonstrations are underway? Hospital demonstrations
IMPROVING HCAHPS, PATIENT MORTALITY AND READMISSION: MAXIMIZING REIMBURSEMENTS IN THE AGE OF HEALTHCARE REFORM
 IMPROVING HCAHPS, PATIENT MORTALITY AND READMISSION: MAXIMIZING REIMBURSEMENTS IN THE AGE OF HEALTHCARE REFORM OVERVIEW Using data from 1,879 healthcare organizations across the United States, we examined
IMPROVING HCAHPS, PATIENT MORTALITY AND READMISSION: MAXIMIZING REIMBURSEMENTS IN THE AGE OF HEALTHCARE REFORM OVERVIEW Using data from 1,879 healthcare organizations across the United States, we examined
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
EVOLENT HEALTH, LLC. Heart Failure Program Description 2017
 EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
EVOLENT HEALTH, LLC Heart Failure Program Description 2017 1 Evolent Health Heart Failure Program Description 2017 Table of Contents Section Page Number I. Introduction. 3 II. Program Scope. 3 III. Program
STEMI SYSTEM RECEIVING CENTER STANDARDS AND DESIGNATION
 POLICY NO: FAC - 9 DATE ISSUED: 11/2016 DATE TO BE REVIEWED: 11/2019 STEMI SYSTEM RECEIVING CENTER STANDARDS AND DESIGNATION Purpose: To define the criteria for designation as a STEMI Receiving Center
POLICY NO: FAC - 9 DATE ISSUED: 11/2016 DATE TO BE REVIEWED: 11/2019 STEMI SYSTEM RECEIVING CENTER STANDARDS AND DESIGNATION Purpose: To define the criteria for designation as a STEMI Receiving Center
An Integrated Approach to Heart Failure Care. Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN
 An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
An Integrated Approach to Heart Failure Care Paul C. Freiman, MD, FACC and Donna A. Smith, RN, BSN Disclosure Neither presenter has an actual or potential conflict of interest, financial interest/ arrangement,
Hospital Compare Quality Measures: 2008 National and Florida Results for Critical Access Hospitals
 Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Hospital Compare Quality Measures: National and Results for Critical Access Hospitals Michelle Casey, MS, Michele Burlew, MS, Ira Moscovice, PhD University of Minnesota Rural Health Research Center Introduction
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring
 Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
Improving Clinical Outcomes The Case for Electronic ED Door to EKG Time Monitoring 2014 Distinguished Achievement Award for Clinical Excellence TM Competition October 22, 2014 St. Dominic-Jackson Memorial
MBQIP Quality Measure Trends, Data Summary Report #20 November 2016
 MBQIP Quality Measure Trends, 2011-2016 Data Summary Report #20 November 2016 Tami Swenson, PhD Michelle Casey, MS University of Minnesota Rural Health Research Center ABOUT This project was supported
MBQIP Quality Measure Trends, 2011-2016 Data Summary Report #20 November 2016 Tami Swenson, PhD Michelle Casey, MS University of Minnesota Rural Health Research Center ABOUT This project was supported
PGY 1 Pharmacy Residency Cardiology Experience Description Truman Medical Center Hospital Hill
 Experience Title: Cardiology (PGY1) PGY 1 Pharmacy Residency Cardiology Experience Description Truman Medical Center Hospital Hill Preceptor: Andrew Smith, Pharm.D., BCPS (AQ Cardiology) Cardiology Clinical
Experience Title: Cardiology (PGY1) PGY 1 Pharmacy Residency Cardiology Experience Description Truman Medical Center Hospital Hill Preceptor: Andrew Smith, Pharm.D., BCPS (AQ Cardiology) Cardiology Clinical
2017 Edition. MIPS Guide. The rule is in and Medicare physician payments are changing. What does that mean for you?
 2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
2017 Edition MIPS Guide The rule is in and Medicare physician payments are changing. What does that mean for you? MERIT-BASED INCENTIVE payment system The Merit-based Incentive Payment System (MIPS) combines
CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW
 Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Diplomate: CLINICAL PRACTICE EVALUATION II: CLINICAL SYSTEMS REVIEW A. INFORMATION MANAGEMENT 1. Does your practice currently use an electronic medical record system? Yes No 2. If Yes, how long has the
Dianne Feeney, Associate Director of Quality Initiatives. Measurement
 HSCRC Quality Based Reimbursement Program Dianne Feeney, Associate Director of Quality Initiatives Sule Calikoglu, Associate Director of Performance Measurement 1 Quality Initiative Timeline Phase I: Quality
HSCRC Quality Based Reimbursement Program Dianne Feeney, Associate Director of Quality Initiatives Sule Calikoglu, Associate Director of Performance Measurement 1 Quality Initiative Timeline Phase I: Quality
STEMI RECEIVING CENTER
 Monterey County EMS System Policy Policy Number: 5150 Effective Date: 5/1/2012 Review Date: 12/31/2016 STEMI RECEIVING CENTER I. PURPOSE To define requirements for designation as a Monterey County STEMI
Monterey County EMS System Policy Policy Number: 5150 Effective Date: 5/1/2012 Review Date: 12/31/2016 STEMI RECEIVING CENTER I. PURPOSE To define requirements for designation as a Monterey County STEMI
Cardiac Certification. Achieving excellence beyond accreditation
 Cardiac Certification Achieving excellence beyond accreditation Accreditation is just the beginning. 2 When it comes to accreditation, no organization can match The Joint Commission s experience and knowledge.
Cardiac Certification Achieving excellence beyond accreditation Accreditation is just the beginning. 2 When it comes to accreditation, no organization can match The Joint Commission s experience and knowledge.
Heart Failure Clinic a Multidisciplinary approach. Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM
 Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Heart Failure Clinic a Multidisciplinary approach Amy Benson, PA-C, MSPAS Presbyterian Heart Group Albuquerque, NM Disclosure I have no actual or potential conflict of interest in relation to this program/presentation.
Fast Facts 2018 Clinical Integration Performance Measures
 IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
IMPORTANT: LHP providers who do not achieve a minimum CI Score in 2018 will not be eligible for incentive distribution and will be placed on a monitoring plan for the 2019 performance year. For additional
DoubleTree Hotel, 100 City Drive, Orange, CA Jan. 20, :30 a.m. 3 p.m.
 2018 Cath Lab Essentials CME Conference DoubleTree Hotel, 100 City Drive, Orange, CA 92868 Jan. 20, 2018 7:30 a.m. 3 p.m. ENDORSED BY Presented by the Division of Cardiology, Department of Medicine, UC
2018 Cath Lab Essentials CME Conference DoubleTree Hotel, 100 City Drive, Orange, CA 92868 Jan. 20, 2018 7:30 a.m. 3 p.m. ENDORSED BY Presented by the Division of Cardiology, Department of Medicine, UC
2015 Congestive Heart Failure. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
2015 Congestive Heart Failure Program Evaluation Our mission is to improve the health and quality of life of our members 2015 Congestive Heart Failure Program Evaluation Program Title: Congestive Heart
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
FSMB Maintenance of Licensure (MOL) Task Force on Continuous Professional Development (CPD) Activities Draft Report January 28, 2014
 Task Force on Continuous Professional Development (CPD) Activities Draft Report January 28, 2014") 1 2 3 4 5 6 7 8 9 10 FSMB Maintenance of Licensure (MOL) Task Force on Continuous Professional Development (CPD) Activities 11 12 13 14 15 16 17 Draft Report January 28, 2014 18 19 20 21 Page 1 of 17 22
1 2 3 4 5 6 7 8 9 10 FSMB Maintenance of Licensure (MOL) Task Force on Continuous Professional Development (CPD) Activities 11 12 13 14 15 16 17 Draft Report January 28, 2014 18 19 20 21 Page 1 of 17 22
State of the State: Hospital Performance in Pennsylvania October 2015
 State of the State: Hospital Performance in Pennsylvania October 2015 1 Measuring Hospital Performance Progress in Pennsylvania: Process Measures 2 PA Hospital Performance: Process Measures We examined
State of the State: Hospital Performance in Pennsylvania October 2015 1 Measuring Hospital Performance Progress in Pennsylvania: Process Measures 2 PA Hospital Performance: Process Measures We examined
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience
 Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
Same Day Vascular Interventions in an Office or Freestanding Facility: The US Experience Jeffrey G. Carr, MD, FACC, FSCAI Founding and Immediate Past President- Outpatient Endovascular and Interventional
Cardiovascular Center of Excellence Program Overview and Eligibility v1.3
 Cardiovascular Center of Excellence Program Overview and Eligibility v1.3 Accreditation provided by American Heart Association in collaboration with American College of Cardiology Table of Contents Introduction...
Cardiovascular Center of Excellence Program Overview and Eligibility v1.3 Accreditation provided by American Heart Association in collaboration with American College of Cardiology Table of Contents Introduction...
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654 Minnesota Department of Health October 2011 Division of Health Policy Health Economics
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654 Minnesota Department of Health October 2011 Division of Health Policy Health Economics
Avoidable Imaging Wave II. How MIPS, CPIA, CEDR metrics relate to E-QUAL Clinician Engagement in Avoidable Imaging Initiatives
 Avoidable Imaging Wave II How MIPS, CPIA, CEDR metrics relate to E-QUAL Clinician Engagement in Avoidable Imaging Initiatives Presenters Dr. Jay Schuur Dr. John Sverha Disclaimer The project described
Avoidable Imaging Wave II How MIPS, CPIA, CEDR metrics relate to E-QUAL Clinician Engagement in Avoidable Imaging Initiatives Presenters Dr. Jay Schuur Dr. John Sverha Disclaimer The project described
How to Establish a Multi Hospital STEMI Transfer System
 How to Establish a Multi Hospital STEMI Transfer System Dr. Greg Mishkel for the Doctors of Prairie Cardiovascular and in collaboration with our Community & Springfield Hospitals MI: Evolution of care
How to Establish a Multi Hospital STEMI Transfer System Dr. Greg Mishkel for the Doctors of Prairie Cardiovascular and in collaboration with our Community & Springfield Hospitals MI: Evolution of care
Improving Clinical Outcomes
 Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
Improving clinical outcomes and reducing health care costs under the Affordable Care Act - are enhanced medication management strategies part of the solution? Sandra L. Baldinger, Pharm.D., M.S. Kenneth
INTERMACS has a Key Role in Reporting on Quality Metrics
 INTERMACS has a Key Role in Reporting on Quality Metrics Robert L Kormos MD FACS, FAHA FRCS(C) Director Artificial Heart Program University of Pittsburgh Medical Center The Patient Protection and Affordable
INTERMACS has a Key Role in Reporting on Quality Metrics Robert L Kormos MD FACS, FAHA FRCS(C) Director Artificial Heart Program University of Pittsburgh Medical Center The Patient Protection and Affordable
Practice Implications for Accountable Care Organizations
 Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
Practice Implications for Accountable Care Organizations An Overview following the Final Rule Gregory M. Marsh, MPH, PMP December 14, 2011 Why CCME? Effective EHR/HIE Implementation will: Improve patient
CME Disclosure. HCAHPS- Hardwiring Your Hospital for Pay-for-Performance Success. Accreditation Statement. Designation of Credit.
 CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
CME Disclosure Accreditation Statement Studer Group is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. Designation
St. Vincent s Health Partners
 St. Vincent s Health Partners St. Vincent s Health Partners is now working with your doctor to offer: Care Coordination Among All our Healthcare Providers St. Vincent s will work with all your providers
St. Vincent s Health Partners St. Vincent s Health Partners is now working with your doctor to offer: Care Coordination Among All our Healthcare Providers St. Vincent s will work with all your providers
Presentation Outline
 Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Chronic Disease Toolkits: Spreading Quality Outcomes Simply Gerald H. Angoff, MD, FACC, MBA Steve Sarette, BA Presentation Outline It Introduction ti Setting the scene Quality Improvement Project Details
Minnesota Statewide Quality Reporting and Measurement System: Appendices to Minnesota Administrative Rules, Chapter 4654
 This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
This document is made available electronically by the Minnesota Legislative Reference Library as part of an ongoing digital archiving project. http://www.leg.state.mn.us/lrl/lrl.asp Minnesota Statewide
Objectives. Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004
 Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Integrating Performance Improvement with Publicly Reported Quality Metrics, Value-Based Purchasing Incentives and ISO 9001/9004 Session: C658 2013 ANCC National Magnet Conference Thursday, October 3, 2013
Managing Patients with Multiple Chronic Conditions
 Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
Best Practices Managing Patients with Multiple Chronic Conditions Arch Health Partners Case Study Organization Profile Palomar Pomerado Health, a public hospital system that includes 2 hospital campuses
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
ACO Information Required to be Published on ACO Website per CMS Regulations
 ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
ACO Name and Location SJFI, LLC dba Oklahoma Health Initiatives St. John Administration 1923 S. Utica Ave Tulsa, OK 74104 ACO Primary Contact Ann Paul, MPH ACO President OKHI@sjmc.org 918.744.2180 Organizational
Heart Failure Order Sets. Standardizing Care for the Heart Failure Patient 2012
 Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Heart Failure Order Sets Standardizing Care for the Heart Failure Patient 2012 Objectives: Standardize care for all heart failure patients in Legacy Base Practice on American Heart Association Guidelines
Mission: Lifeline Hospital Accreditation Webinar. June 21, :00PM 3:00PM CST
 Mission: Lifeline Hospital Accreditation Webinar June 21, 2012 2:00PM 3:00PM CST Speaker Introductions Deb Koeppen, RN Society of Chest Pain Centers Director of Business Development Larry Brown, RN, BSN
Mission: Lifeline Hospital Accreditation Webinar June 21, 2012 2:00PM 3:00PM CST Speaker Introductions Deb Koeppen, RN Society of Chest Pain Centers Director of Business Development Larry Brown, RN, BSN
The CART Transactional Approach
 June 23 rd, 2010 FDA Headquarters The CART Transactional Approach High quality, Prospective Registry Design: Issues and Answers for TREAT Thomas T. Tsai, MD, MSc Director of Interventional Cardiology Clinical
June 23 rd, 2010 FDA Headquarters The CART Transactional Approach High quality, Prospective Registry Design: Issues and Answers for TREAT Thomas T. Tsai, MD, MSc Director of Interventional Cardiology Clinical
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management
 PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
PRISM Collaborative: Transforming the Future of Pharmacy PeRformance Improvement for Safe Medication Management Mission: To improve the health of the people of Connecticut through safe and effective medication
UNDERSTANDING THE CONTENT OUTLINE/CLASSIFICATION SYSTEM
 BOARD OF PHARMACY SPECIALTIES CRITICAL CARE PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED SEPTEMBER 2017/FOR USE ON FALL 2018 EXAMINATION AND FORWARD UNDERSTANDING THE
BOARD OF PHARMACY SPECIALTIES CRITICAL CARE PHARMACY SPECIALIST CERTIFICATION CONTENT OUTLINE/CLASSIFICATION SYSTEM FINALIZED SEPTEMBER 2017/FOR USE ON FALL 2018 EXAMINATION AND FORWARD UNDERSTANDING THE
Clinical Program Cost Leadership Improvement
 Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
Clinical Program Cost Leadership Improvement December 2017 Presbyterian recently developed a rapid-cycle process for integrating sustainable cost and quality improvements within clinical programs. Population
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Veterans Health Administration: Surveillance of Cardiovascular Disease, Diabetes Mellitus, and Chronic Obstructive Pulmonary Disease
 Veterans Health Administration: Surveillance of Cardiovascular Disease, Diabetes Mellitus, and Chronic Obstructive Pulmonary Disease Paul D. Varosy, MD Director of Cardiac Electrophysiology VA Eastern
Veterans Health Administration: Surveillance of Cardiovascular Disease, Diabetes Mellitus, and Chronic Obstructive Pulmonary Disease Paul D. Varosy, MD Director of Cardiac Electrophysiology VA Eastern
PURPOSE: The purpose of this policy is to establish requirements for designation as a STEMI Receiving Center (SRC) in San Joaquin County.
 in San Joaquin County.") PURPOSE: The purpose of this policy is to establish requirements for designation as a STEMI Receiving Center (SRC) in San Joaquin County. AUTHORITY: Health and Safety Code, Division 2.5, Sections 1797.67,
PURPOSE: The purpose of this policy is to establish requirements for designation as a STEMI Receiving Center (SRC) in San Joaquin County. AUTHORITY: Health and Safety Code, Division 2.5, Sections 1797.67,
The Veterans Health Administration CART Program: Integration of Real-Time Data Collection into the Process of Clinical Care
 The Veterans Health Administration CART Program: Integration of Real-Time Data Collection into the Process of Clinical Care Paul D. Varosy, MD Director of Cardiac Electrophysiology VA Eastern Colorado
The Veterans Health Administration CART Program: Integration of Real-Time Data Collection into the Process of Clinical Care Paul D. Varosy, MD Director of Cardiac Electrophysiology VA Eastern Colorado
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts