Nutritional Care Tool Report 2017
|
|
|
- Stewart Clifford Roberts
- 6 years ago
- Views:
Transcription
1 Nutritional Care Tool Report 2017 A Report by the BAPEN Quality and Safety Committee Dr Ailsa Brotherton, Kate Cheema, Anne Holdoway, Vera Todorovic and Professor Mike Stroud On behalf of the Quality and Safety Committee
2 BAPEN 2017 Published on BAPEN (British Association for Parenteral and Enteral Nutrition) website ISBN All enquiries to the editor, Dr Ailsa Brotherton, or to BAPEN office, Seven Elms, Dark Lane, Astwood Bank, Redditch, Worcestershire, B96 6HB. Tel: BAPEN is a Registered Charity No All rights reserved. No part of this publication may be reproduced for publication without the prior written permission of the publishers. This publication may not be lent, resold, hired out or otherwise disposed of by way of trade in any form, binding or cover other than that in which it is published, without the prior consent of the publishers. This report was produced on behalf of BAPEN by members of the Quality and Safety Committee: Ailsa Brotherton (former Chair), Kate Cheema, Anne Holdoway, Vera Todorovic and Professor Mike Stroud, on behalf of the Committee. The Nutritional Care Tool report will be published annually and will be incorporated into the work of the MAG committee. BAPEN disclaims any liability to any healthcare provider, patient or other person affected by this report. Every attempt has been made to ensure the accuracy of the data in this report.
3 Contents Page Section 1: Definitions of Terms and Registration Instructions... 4 Section 2: Executive Summary... 6 Section 3: Background and Context Section 4: Organisational measures Section 5: Nutritional Care Core dashboard Section 6: Demographics dashboard: Section 7: MUST Screening dashboard: Section 8: Conclusion Appendices
4 Section 1: Definitions of Terms and Registration Instructions Data Collection and Definition of Terms A full description of each of the demographic, organisational and clinical data collected in the BAPEN Nutritional Care Tool is fully outlined in Appendix 1, together with an explanation of the rationale for inclusion of the measure and instructions for data entry. Exclusions The following groups are excluded from the BAPEN Nutritional Care Tool data collection: Patients being cared for in their own homes Patients being cared for in an outpatient (clinic) only setting Patients under the age of 18 or under the care of paediatric team Registration Instructions Details of the registration process for the tool are available to download from: User Guides A user guide is available to download from: A data analytics user e-learning guide is available to download from: 4
5 5
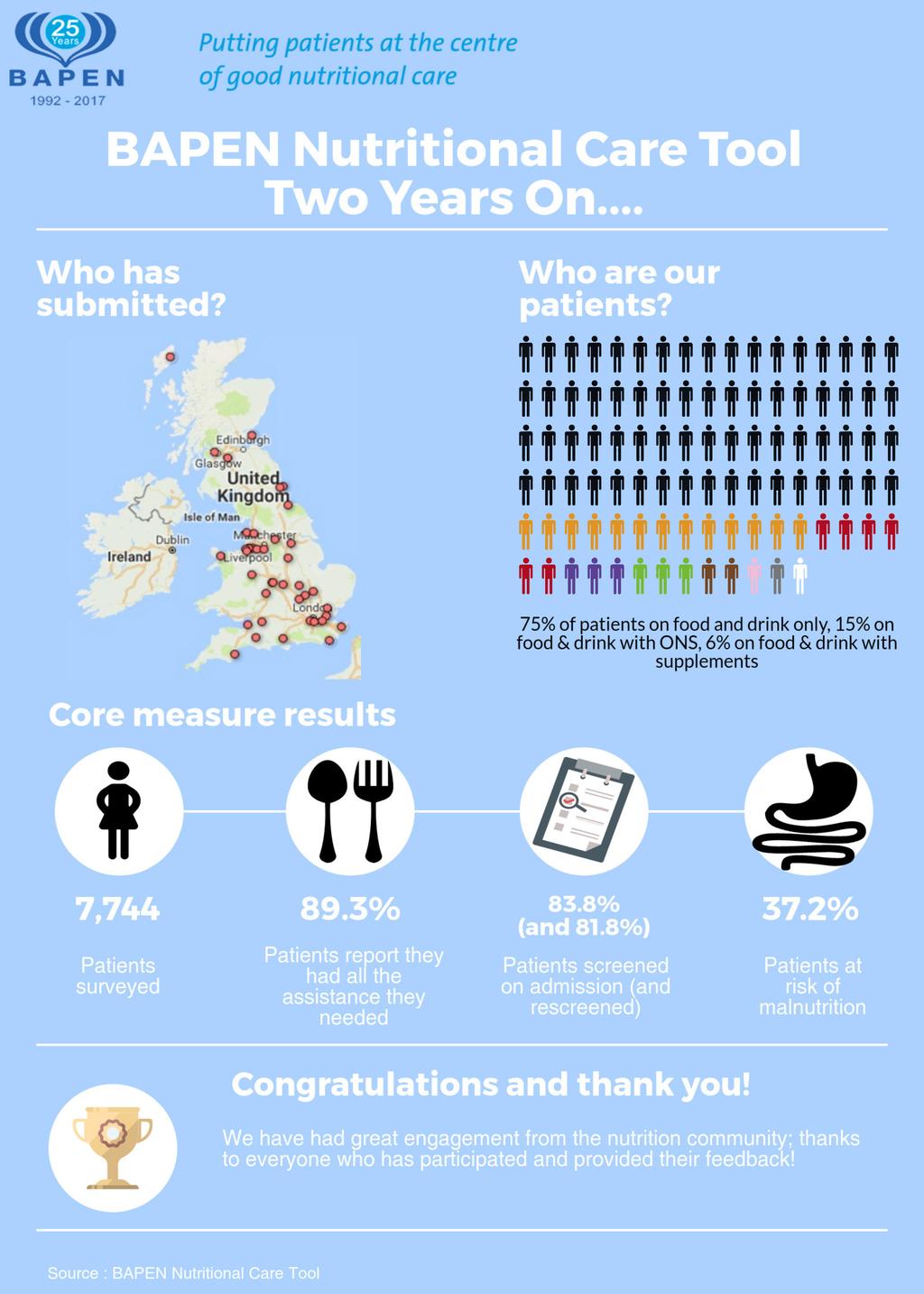
6 Section 2: Executive Summary 1 70 organisations are currently registered to use the BAPEN Nutritional Care tool; all have contributed data at least once since its inception in September The majority of organisations are in the NHS Acute sector, but there is representation from nursing and residential homes, and community organisations. 2 77% of organisations using the BAPEN Nutritional Care Tool reported having a nutrition steering committee and 73% reported having a nutrition support team 3 57% of the organisations employ specialist nutrition nurse(s) with a median number of specialist nurses where in post of 1 whole time equivalent (WTE). There were 2.93 specialist nutrition nurses per 1,000 available beds for all organisations registered to use the tool. 4 The majority of registered organisations provide education and undertake audit in relation to nutritional care % of organisations are undertaking regular audits of nutritional screening, 51.4% undertaking regular audits of nutrition care plans, with only 27.1% tracking nutrition outcomes and 12.7% undertaking regular audits of intentional rounding, where nutrition is included in the intentional rounding tool used. 6 The patient experience questions were answered positively; 89.3% of patients able to answer reported receiving all the food and drink and/or nutritional care they had needed together with all the assistance they had needed to eat and drink % of patients surveyed with the tool had been screened for malnutrition on entry to the care setting. The 16.2% of patients who are [presumably] not screened at entry to the care setting is a clear target area for improvement % of patients surveyed with the tool were re-screened for malnutrition at an appropriate interval % of patients surveyed using the tool were recorded as being at risk of malnutrition either through MUST screening or subjective criteria. This represents a significant proportion of patients surveyed, although it should be remembered that many trusts completing the tool may have focussed on higher risk areas such as care of the elderly wards. 10 Approximately 8% of patients surveyed showed a loss of 5% or more of body weight during their time in the care setting (See section 5 for details regarding the caution required in the interpretation of this finding) % of patients were recorded as receiving only food and drink. Further analysis of the data regarding feeding routes is being undertaken % of patients had objective criteria for the completion of MUST with only 4.6% using subjective criteria of weight recall (3.1%) and weight estimates (1.5%) 6
7 Section 3: Background and Context Measuring Nutritional Care: screening, nutritional care processes, outcomes and patient experience Every provider organisation is required by the Health and Social Act 2008 (Regulated Activities) Regulations 2014 (Regulation 14) to make sure the individuals in care have enough to eat and drink to meet their nutrition and hydration needs and receive the support they need to do so. Individuals must have their nutritional needs assessed and food must be provided to meet those needs. This includes where people are prescribed nutritional supplements and/or parenteral nutrition (Source: CQC website: Despite best efforts of many organisations and individuals, the costs associated with malnutrition, within the UK have continued to rise; (Elia, 2015) a cost likely to continue to increase without a different approach. The personal cost to individuals and their families is also significant, with an increased mortality rate, increased admissions to hospital, increased pressure ulcers, falls and infections and an overall decrease in quality of life. Combating malnutrition in the UK remains a significant challenge requiring a mind-set shift in how we work together to find innovative solutions. Elia, M. (2015) The cost of malnutrition in England and potential cost savings from nutritional interventions; a report on the cost of disease-related malnutrition in England and a budget impact analysis of implementing the NICE clinical guidelines/quality standard on nutritional support in adults. Available from Why is there a need for a new measurement tool with a different approach? Data from the BAPEN led national nutrition screening weeks illustrate the continued high prevalence of malnutrition (24-30% of patients admitted to a UK hospital malnourished or at-risk of malnutrition). Whilst numerous nutrition initiatives (many of them national) such as protected mealtimes and Nutrition Now (Royal College of Nursing), and the publication of numerous standards, including the NICE guidance, have helped to raise the profile of nutrition, the prevalence data indicates more has to be done, not just in hospitals but across a range of care settings, if we are to make a difference in reducing the risk of malnutrition developing and managing it appropriately when present. Purpose and benefits of the BAPEN Nutritional Care Tool Building on the work undertaken during the Nutrition Screening Weeks, which helped create a country-wide picture of the prevalence of malnutrition in the UK, BAPEN developed and tested a web-based Nutritional Care Tool. Whilst the complexities of delivering good nutritional care make measurement fraught with difficulty, we believe that measurement is key to delivering further improvements in the quality of nutritional care. The Nutritional Care Tool was therefore designed to enable organisations to easily monitor the level of screening for malnutrition but to also ease the process for organisations to capture and evaluate the effectiveness of nutritional care provided along with the patient experience. The nutritional care tool utilises quality improvement methodology (i.e. these data are intended to identify improvement opportunities within an organisation, not performance management or research). The tool includes; 7
8 Process measures; screening and care planning Outcome measures weight loss (trackable over time for the duration of admission) Patient experience measures of nutritional care received The Nutritional Care Tool builds on the work previously undertaken by BAPEN and is a unique and valuable addition to BAPEN s toolkit of resources and guidelines, designed to help healthcare professionals in hospitals, care homes and the community prevent malnutrition occurring when possible and treat it properly when it does occur. (For further information on BAPEN s publications and resources are available visit the BAPEN website The BAPEN Nutritional Care Tool overview: The Tool is free to all NHS and social care organisations Completion takes approximately 5 minutes per individual. Key data are instantly available to frontline teams to monitor care and identify areas for improvement. Improvements in nutritional care can be delivered whilst the patient is still in your care. The Tool is completely voluntary so it is up to you how frequently you use it and the scale of use This report presents the first analysis of the data collected since the launch of the tool. Annual update reports will be published at BAPEN conference. 8
9 Section 4: Organisational measures A set of organisational measures has been incorporated into the tool and are completed at the time an organisation registers to use the tool. These measures are: The proportion of registered organisations with a nutrition steering committee The proportion of registered organisations with a nutrition support team The proportion of registered organisations which employ specialist nutrition support nurses The median number of specialist nutrition support nurses employed The number of nutrition support nurses employed per 1,000 overnight beds (using KH03 central return to source number of overnight beds) Proportion of organisations offering education or training in the following areas: Nutritional needs and indications for nutritional support Options for nutrition support Ethical and legal concepts Potential risks and benefits When and where to seek expert advice Proportion of organisations auditing the quality of nutritional care in the following ways: Regular audits of screening Regular audits of nutritional care plans Use of flag and tag facility in NHS Safety Thermometer Tracking of nutritional outcomes Audits of intentional rounding These data form a baseline understanding of how organisations organise themselves to deliver nutritional care and could be gathered again at a later point in time in order to assess whether changes have been made and improvements achieved where necessary. 70 organisations are currently registered to use the BAPEN Nutritional Care tool; all have contributed data at least once since its inception in September The majority of organisations are in the NHS Acute sector, but there is representation from nursing and residential homes, and community organisations. The chart below illustrates the split between different organisation types: Figure 1: Organisational types using the Nutritional Care Tool 9
 are not necessarily well represented within the organisations")
10 Organisations have varying approaches to delivering nutritional care. The fundamental elements of nutritional care that are recommended in the NICE Guidance (Nutritional Support in Adults; CG 32, 2006) are not necessarily well represented within the organisations currently using the tool. Table 1 provides key statistics for the 70 organisations currently inputting data: Proportion of organisations with a nutrition steering committee 77.1% Proportion of organisations with a nutritional support team 72.9% Proportion of organisations with specialist nutrition nurse(s) 57.1% Median number of specialist nutrition nurses where in post (WTE) 1 Specialist nutrition nurses per 1,000 available beds for all organisations registered to use the BAPEN tool 2.93 Table 1 Organisation of Nutritional Care; key statistics The majority of registered organisations provide education and undertake audit in relation to nutritional care. The charts below illustrate the proportion of organisations taking specific approaches to each of these elements. Figure 2: Proportion of registered organisations offering nutritional care training in specific areas Figure 3: Proportion of organisations auditing the quality of nutritional care 10
11 Section 5: Nutritional Care Core dashboard Patients surveyed using the tool between September 2015 and September 2017: of those able to answer the patient experience questions contained in the tool, the vast majority were able to report positively on their experience of nutritional care, with 89.3% of patients able to answer reported receiving all the food and drink and/or nutritional care they had needed. The proportion of surveyed patients able to answer who had received all assistance they needed to eat and drink was 89.3%. This has remained fairly stable over time (see figure 4 and 5); the SPC charts shown here illustrate a stable process with positive feedback at about the 90% mark in each month for both measures. Points where the control limits are a long way apart indicate months with very small sample sizes (a small number of Trusts are measuring on a monthly rather than quarterly basis), particularly in year two where the majority of respondents collected data on a quarterly basis. Figure 4: Proportion of surveyed patients able to answer who have received all the food and drink and/or nutritional care they have needed Figure 5: Proportion of surveyed patients able to answer who have received all assistance to eat and drink they have needed Screening on entry to the care setting was recorded in the positive for 83.8% of patients surveyed with the tool. Looking at these data over time (figure 6) at first glance looks to be very variable but again this reflects the changing nature of sample sizes over month on month. The variation is within expected boundaries, suggesting that the 16.2% of patients who are presumably not screened at entry to the care setting is a clear target area for improvement. Figure 6: Proportion of surveyed patients screened on entry to the care setting 11
12 Re-screening for malnutrition at an appropriate interval was recorded in the positive for 81.8% of patients surveyed with the tool. This is lower than the initial screening rate and is a key area for improvement; however looking at the data over time (figure 7) shows some suggestion of improvement in the latter parts of 2016 and throughout Although not statistically significant there is a clear change when compared to earlier time periods. Figure 7: Proportion of surveyed patients rescreened at an appropriate interval Just over 37.2% of patients surveyed using the tool were recorded as being at risk of malnutrition either through MUST screening or subjective criteria. This represents a significant proportion of patients surveyed, although it should be remembered that many trusts completing the tool would have focussed on higher risk areas such as care of the elderly wards Figure 8 shows this measure over time which is broadly in control and fairly stable, with the exception of November 2016 which is an astronomical data point. Again, the variability in sample sizes month on month makes interpretation difficult. Figure 8: Proportion of surveyed patients identified as being at risk of malnutrition 12
13 Further analysis of this at risk population provides some insight as to their treatment. Of the 2,700+ patients identified as being at risk of malnutrition, 57% are on food and drink alone, 22% are on food and drink with oral nutritional supplements. The remaining 21% of high risk patients are fed through a variety of other routes (see figure 9 below). Figure 9: Proportion of surveyed patients identified as being at risk of malnutrition by feeding route year Approximately 8% of patients surveyed showed a loss of 5% or more of body weight during their time in the care setting. Trends are reasonably stable, with one or two astronomical data points in months where numbers were very low (in between the quarterly data collection weeks). There is no obvious reason for these extreme data points; the demographics are similar in these months to others. However, caution is required in the interpretation of this measure as only a small number of trusts are tracking weight (this measure is optional). Figure 10: Proportion of surveyed patients who have lost more than 5% of admission weight 13
14 The charts on the previous page illustrate change over time at the national level for core measures. Within this there is significant variation between organisations, primarily driven by volume of patients surveyed. Funnel plots for each of these metrics are shown below in panel 1. One specific organisation is an outlier in terms of the large volume of the patients surveyed, and this makes the plots difficult to read. Truncated plots, excluding this organisation are shown in panel 2. Panel 1 Rate per 1000 surveyed patients able to answer who have received all the food and drink and/ or nutritional care they have needed Rate per 1, Rate per 1000 surveyed patients able to answer who have received all assistance to eat and drink they have needed Rate per 1, Rate per 1000 surveyed patients screened on entry to the care setting Rate per 1, Rate per 1000 surveyed patients rescreened at an appropriate interval Rate per 1, Rate per 1000 surveyed patients identified as being at risk of malnutrition Rate per 1, Rate per 1000 surveyed patients who have lost more than 5% of admission weight Rate per 1, Panel 2 Rate per 1000 surveyed patients able to answer who have received all the food and drink and/ or nutritional care they have needed Rate per 1, Rate per 1000 surveyed patients able to answer who have received all assistance to eat and drink they have needed Rate per 1, Rate per 1000 surveyed patients screened on entry to the care setting Rate per 1, Rate per 1000 surveyed patients rescreened at an appropriate interval Rate per 1, Rate per 1000 surveyed patients identified as being at risk of malnutrition Rate per 1, Rate per 1000 surveyed patients who have lost more than 5% of admission weight Rate per 1,

15 Section 6: Demographics dashboard This dashboard provides a snapshot dashboard providing key demographic information in order to provide context for outcome results This will enable us, over time, to report on the key changing demographics in relation to nutritional care Figure 11: Proportion of surveyed patients by age band and year Figure 12: Proportion of surveyed patients by setting and year 15
16 Figure 13: Proportion of surveyed patients by feeding route and year Figure 14: Proportion of surveyed patients by primary diagnostic area and year 16
17 Section 7: MUST screening dashboard This dashboard provides an overview of the quality and accuracy of the MUST measurement undertaken in the BAPEN Nutritional Care Tool as outlined in Table 2 Proportion of patients where realistic figures for all objective measure can be obtained Proportion of patients where current weight is Recalled Proportion of patients where current weight is Estimated Proportion of patients unable to be weighed due to equipment issues Proportion of patients unable to be weighed due to staffing time Proportion of patients unable to be weighed due to patient choice or illness Proportion of patients where weight loss cannot be calculated due to lack of access to materials to make calculations Proportion of patients where weight loss cannot be calculated due to staffing time Table 2: Overview and accuracy of the MUST measurements undertaken The data for these measures is reported for records where the data item has been completed. If it has been left blank (this is recorded as undefined in the database), then the record is excluded from the numerator and denominator. Thus, with the exception of the first of the following indicators, the denominator is always less than the total number of patients surveyed. This smaller denominator also makes monthly time series analysis virtually untenable as the numbers are so small. Thus, a quarterly analysis is shown as run charts, with data between quarterly collection weeks added to the relevant quarter. Figure 15 17
18 Figure 16 Figure 17 18
19 Figure 18 Figure 19 19
20 Figure 20 Figure 21 20
21 Figure 22 21
22 Section 8 Conclusion: Our Ambition The BAPEN Nutritional Care Tool provides a unique opportunity for the Clinical Nutrition Community to collate and publish national level data regarding: the approaches to organising nutritional care at an organisational level with the proportion of Trusts with a nutrition steering committee and nutrition support team in place, with levels of specialist nutrition nurses and; nutritional screening, the quality of nutritional care, patient experience and the tracking of changes in a patient s weight over time If we can work together to ensure each acute trust is registered, this will provide a powerful data set to demonstrate the levels of improvement in leading organisations and the levels of improvement required. Our ambition for the publication of the 2018 report is that ALL acute trusts will register and complete the following four national nutritional care data collection weeks in 2018 Week commencing 12th December 2017 Week commencing 12th March 2018 (Nutrition and Hydration week) Week Commencing 11th June 2018 Week commencing 10th September 2018 On behalf of BAPEN, we would like to thank all the organisations who have participated in the data collection since the launch of the tool. Special thanks to the following organisations who have submitted data for each quarter in at least one of the last two years; the Nutritional Care Tool would not exist without you! Blackpool Teaching Hospitals NHS Foundation Trust Calderdale and Huddersfield NHS Trust Dartford and Gravesham NHS Trust Doncaster and Bassetlaw Hospitals NHS Foundation Trust Kettering General Foundation Trust Northumbria Healthcare NHS Foundation Trust Papworth Hospital NHS Foundation Trust St Helens and Knowsley Teaching Hospitals NHS Trust University Hospital Southampton NHS Foundation Trust Weston Area Health NHS Trust Worcestershire Acute NHS trust Yeovil District Hospital NHS Foundation Trust For further information please visit: 22
23 Appendix Details of the measures contained within the BAPEN Nutritional Care Tool are outlined below. Demographics, organisational and clinical details Organisation The overarching organisation in which the survey is being undertaken (e.g. NHS Trust) Recording organisation name allows data to be analysed to a level at which variations can be identified and ensures appropriate questions appear in the tool (for example, if the organisation is an acute hospital, questions regarding the specialty are included but these are excluded for care homes You do not need to enter your organisation name, this is automatically generated based on your log-in Current ward/team/area The name of the ward, team or area in which or under whose care the survey is being undertaken Improvement and change is most effective when it starts at the front-line of care and goes from the bottom up rather than imposed from the top down. The inclusion of a ward/team/area name allows data collected via the BAPEN Nutritional Care Tool to be analysed at a level that is meaningful to staff working within these groupings, and can potentially be discussed or displayed in patient areas with the same degree of import. Ward/team/area names are set up and linked to your log-in. You may have multiple wards/teams/areas linked to your log-in and will need to ensure that you enter data under the correct ward/team/area. Specialty The main specialty of the ward/team/area that is undertaking the survey Understanding of nutritional care at the specialty level allows identification both of variation between different specialties as well as the ability to identify specific areas within which to target improvement. Select the appropriate specialty from the drop down menu. If the ward or team has more than one specialty area select the specialty where the volume of activity is greatest, or select the mixed specialty option. 23
24 Date of collection The date on which the survey has been carried out The BAPEN Nutritional Care Tool is designed to help track change over time. The date of collection allows this time series analysis to be undertaken. The current date is shown automatically, but can be overwritten if a different date is required. The format should be dd/mm/yyyy; the web tool will not accept dates entered which are not in this format. Admitting ward/team/area The name of the ward, team or area in which or under whose care the patient was first admitted to the care setting. Nutritional screening is primarily initially undertaken on admission (or within 24 hours of admission). In order to track the provision of effective re-screening at appropriate intervals and effective nutritional care throughout the patient s journey within the organisation it is useful to understand where the initial care was provided and to track how many times patients are screened during their admission As for ward/team/area above. Age group The patient s age group Construction Age grouped into 3 groups; 18-64, and 75+ Understanding nutritional processes and outcomes by age can provide important intelligence in deciding where to focus improvement efforts Select appropriate option from drop down menu. Feeding route Construction The route through which the patient receives nutrition Options presented: Oral food & drink, altered textures, food & oral supplements, enteral, parenteral Understanding the route through which patients receive nutrition is critical to assessing whether or not they have received adequate nutritional care and assessment Select all options that apply to the patient from the options presented 24
25 Date of admission to care setting The date on which the patient was admitted to the care setting in which the survey is being carried out The date of admission is used to calculate length of stay (LoS) by subtracting it from the date of collection. The LoS is an important variable in breaking down the data from the BAPEN Nutritional Care Tool to be more meaningful. Select the date from the calendar pop up or type the date into the tool directly. The format should be dd/mm/yyyy; the web tool will not accept dates entered which are not in this format. Setting The type of care setting in which the survey is being undertaken Data from national screening weeks suggests that there are differences in malnutrition rates between different settings. The BAPEN Nutritional Care Tool has been designed, as far as possible, to be applicable across multiple care settings, with exceptions noted above. Recording the setting provides the ability to assess variation between different settings in order to better understand the scope for change in and improvement and identify the differing challenges in each setting. Select the most appropriate setting from a drop down menu Patient diagnosis The primary diagnosis for the patient being surveyed Understanding of nutritional care at the diagnosis level allows identification both of variation between different diagnoses as well as the ability to identify specific areas within which to target improvement. Recording diagnosis and its attendant detail (see below) also allows us to exclude specific cohorts of patients if required. Select the appropriate high level diagnosis from the drop down menu. You will be prompted to enter more detail dependent on your selection. You will only be prompted to enter data for this variable if you have selected Acute Hospital under the setting options. 25
26 Diagnosis detail Diagnosis detail for the patient being surveyed Understanding of nutritional care at the diagnosis level allows identification both of variation between different diagnoses as well as the ability to identify specific areas within which to target improvement. Recording diagnosis and its attendant detail also allows us to exclude specific cohorts of patients if required. Select the appropriate diagnosis detail from the drop down menu. You will be prompted to select detail from a specific list of diagnostic details based on your selections under patient diagnosis. Process details Screening on entry to the care setting The individual was screened with a validated screening tool ( MUST ) on entry to care setting The NICE Guidance (CG32); Nutrition Support in Adults (2006) makes clear recommendations regarding the screening of patients in care settings (e.g. hospital, care homes) and in primary care. By recording the completion of screening on admission to the care setting it is possible to assess compliance to this element of the NICE Guidance / Quality standard. Select yes or no or not applicable from the drop down list Re-screening at an interval appropriate to the care setting The individual was re-screened with a validated screening tool ( MUST ) at the time interval (e.g. weekly, monthly) appropriate to the to care setting The NICE Guidance (CG32); Nutrition Support in Adults (2006) and the MUST screening tool make clear recommendations regarding the re-screening of patients in care settings. By recording the completion of re-screening at intervals appropriate to the care setting it is possible to assess compliance to this element of the NICE Guidance / MUST protocol. Select yes, no or not applicable from the drop down list. If a patient has been in the surveying care setting for less than one week (not the ward/team/ area), the not applicable option should be selected. 26
27 Documented nutritional care plan Individuals found to be at risk on last nutritional screening have a documented nutrition care plan appropriate to the organisation and setting The MUST screening tool makes clear recommendations regarding the development and implementation of an individualised nutritional care plan for patients found to be at risk of malnutrition. By recording the documented nutritional care plan it is possible to begin to assess implementation of improved nutritional care. However, we are very aware of the ease of ticking a box and we ask that on completing this question, the care plan is appropriately reviewed. Select yes or no or not applicable from the drop down list Nutritional care plan being followed An appropriate nutrition care plan is being followed or has been offered to the individual We know from audits of nutritional care that screening and care planning is often completed/ documented but not then implemented. We fully appreciate the complexities of this question but it is an attempt to determine to what extent the nutritional care plans are implemented. By recording the implementation of the nutritional care plan it is possible to begin to assess improvements in the nutritional care delivered. As above, we are very aware of the ease of ticking a box to indicate that the care is being delivered (when it may be variable) and we ask that on completing this question, the care plan and food and fluid record charts are appropriately reviewed. Select no, some elements, most elements, yes or not applicable Outcome details Current weight Patient s weight in kilograms recorded at time of survey Weight is considered a reasonable and easily measured outcome measure when considering the quality of nutritional care, though has significant limitations which must be noted. Combined with current height this allows calculation of Body Mass Index (BMI) which is a critical element in calculating the MUST score for the patient. For more detail see: MUST Explanatory Booklet Record patient s weight as a whole number. If no weight is available enter N/A. 27
28 Estimation of current weight Indication of how current weight (at time of survey) has been recorded Weight is a critical factor in assessing for risk of malnutrition and it is important to understand the accuracy and quality of the measurements taken. For more detail see: MUST Explanatory Booklet Select Recalled,, Estimated, Calculated from subjective criteria, Actual weight, Patient weighed at time of survey Unplanned weight loss in past 3-6 months Unplanned patient weight loss recorded in the most recent 3-6 months in kilograms Weight loss is considered a reasonable and easily measured outcome measure when considering the quality of nutritional care, though has significant limitations which must be noted. Unplanned weight loss is a critical element in calculating the MUST score for the patient. For more detail see: MUST Explanatory Booklet Record patient s weight in kilograms. If no weight is available enter N/A. Estimation of weight loss in past 3-6 months Indication of how unplanned weight loss in past 3-6 months has been recorded Weight is a critical factor in assessing for risk of malnutrition and it is important to understand the accuracy and quality of the measurements taken. Using this measure alongside the current weight enables calculation and categorisation of weight loss to help take into account fluctuations of weight due to causes other than poor nutrition or poor nutritional care. For more detail see: MUST Explanatory Booklet Select Recalled, Estimated, Calculated from subjective criteria, Actual weight, Patient weighed at time of survey Patient s height Patient s current height in metres Combined with current weight this allows calculation of Body Mass Index (BMI) which is a critical element in calculating the MUST score for the patient. For more detail see: MUST Explanatory Booklet Record patient s height in metres. If no height is available enter N/A. 28
29 Estimation of current height Indication of how current height (at time of survey) has been recorded Height is a critical factor in calculating BMI and thus assessing for risk of malnutrition and it is important to understand the accuracy and quality of the measurements taken. For more detail see: MUST Explanatory Booklet Select Recalled,, Estimated, Calculated from subjective criteria, Actual height, Patient measured at time of survey Impact of acute illness Has the patient been acutely ill AND has there been, or likely to be, no nutritional intake for more than 5 days If the subject is currently affected by an acute patho-physiological or psychological condition, and there has been no nutritional intake or likelihood of no intake for more than 5 days, they are likely to be at nutritional risk. Such patients include those who are critically ill, those who have swallowing difficulties (e.g. after stroke), or head injuries or are undergoing gastrointestinal surgery. This consideration of the impact of acute disease is a critical element in calculating the MUST score for the patient. For more detail see: MUST Explanatory Booklet Select Yes or No MUST score on admission Construction (if applicable) The MUST score that has been recorded on admission to the care setting Score as per the MUST screening tool. For more details see: MUST toolkit MUST is the dominant screening tool for adults in care, with some specialty exclusions which have specialist screening tool (e.g. renal, liver and paediatric specialties). The risk of malnutrition is, in this context, considered the most effective and reliable measure indicating the need for nutritional care. The initial risk assessment on entry to the care setting provides a baseline from which to assess change in nutritional status, which is assumed to be directly linked to the quality of nutritional care, although it is appreciated that this is multifactorial. Select the appropriate option from the drop down menu; if the patient has not been screened before due to recent admission, select This is patient s first screen. If the patient has not been screened or the score is not documented or known select Not known/done. Otherwise select the relevant score for the patient on the scale of 0 to 6. The score entered should be that which was first recorded on entry to the care setting, as opposed to the specific ward or team undertaking the survey (i.e. the admitting ward). 29
30 Patient experience: receiving food drink or nutritional care needed Has the patient received all the food and drink and/or nutritional care they have needed The experience of the patient is crucial in ensuring that all services are delivered effectively and in a truly patient centered way. Whilst the measurement of patient experience of nutritional care is a relatively untested area, and fraught with complexity, the inclusion of experiential questions will help to ensure that the patient plays a crucial part in the assessment and improvement of nutritional care. Select the appropriate option from the drop down menu, Yes, Yes to some extent or No. Is is very important that this question is asked of the patient and their views recorded. If the patient is unable to answer for any reason, or it is not felt clinically appropriate to ask the question at that time, a carer or relative may be asked if present. If this is not possible select the option Patient unable to answer. Patient experience: receiving help to eat and drink Has the patient received assistance to eat and drink if required The experience of the patient is crucial in ensuring that all services are delivered effectively and in a truly patient centered way. Whilst the measurement of patient experience of nutritional care is a relatively untested area, and fraught with complexity, the inclusion of experiential questions will help to ensure that the patient plays a crucial part in the assessment and improvement of nutritional care. Select the appropriate option from the drop down menu, Yes, Yes to some extent, No or Not applicable (I haven t needed any help). It is very important that this question is asked of the patient and their views recorded. If the patient is unable to answer for any reason, or it is not felt clinically appropriate to ask the question at that time, a carer or relative may be asked if present. If this is not possible select the option Patient unable to answer. Patient experience: receiving help to eat and drink, additional information If the patient did not feel they received the assistance to eat and drink they required, record the reasons for this The experience of the patient is crucial in ensuring that all services are delivered effectively and in a truly patient centered way. Whilst the measurement of patient experience of nutritional care is a relatively untested area, and fraught with complexity, the inclusion of experiential questions will help to ensure that the patient plays a crucial part in the assessment and improvement of nutritional care. This additional information will provide insight into issues that may affect the ability of services to assist patients in accessing nutrition. Free text question; enter details up to 100 characters describing the reason why the patient was not able to received assistance to eat and/or drink. 30
31 2018 Data Collection Weeks The four national nutritional care data collection weeks in 2018 are: Week commencing 12th December 2017 Week commencing 12th March 2018 (Nutrition and Hydration week) Week Commencing 11th June 2018 Week commencing 10th September 2018 Register to take part:
32 BAPEN 2017 ISBN
National Update on Malnutrition
 National Update on Malnutrition Dr Trevor Smith Consultant Gastroenterologist University Hospital Southampton BAPEN Executive Officer Chair, British Artificial Nutrition Survey British Association for
National Update on Malnutrition Dr Trevor Smith Consultant Gastroenterologist University Hospital Southampton BAPEN Executive Officer Chair, British Artificial Nutrition Survey British Association for
NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN)
") NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN) HOSPITALS, CARE HOMES AND MENTAL HEALTH UNITS NUTRITION
NUTRITION SCREENING SURVEY IN THE UK AND REPUBLIC OF IRELAND IN 2010 A Report by the British Association for Parenteral and Enteral Nutrition (BAPEN) HOSPITALS, CARE HOMES AND MENTAL HEALTH UNITS NUTRITION
NUTRITION SCREENING SURVEYS IN HOSPITALS IN NORTHERN IRELAND,
 NUTRITION SCREENING SURVEYS IN HOSPITALS IN NORTHERN IRELAND, 2007-2011 A report based on the amalgamated data from the four Nutrition Screening Week surveys undertaken by BAPEN in 2007, 2008, 2010 and
NUTRITION SCREENING SURVEYS IN HOSPITALS IN NORTHERN IRELAND, 2007-2011 A report based on the amalgamated data from the four Nutrition Screening Week surveys undertaken by BAPEN in 2007, 2008, 2010 and
Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
 APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
APPENDIX 5 BOARD OF DIRECTORS 18 JUNE 2014 Report to: Report from: Subject: Board of Directors Associate Director of Patient Safety and Quality on behalf of the Director of Nursing and Clinical Governance
Scottish Hospital Standardised Mortality Ratio (HSMR)
") ` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
` 2016 Scottish Hospital Standardised Mortality Ratio (HSMR) Methodology & Specification Document Page 1 of 14 Document Control Version 0.1 Date Issued July 2016 Author(s) Quality Indicators Team Comments
Malnutrition Matters. Meeting Quality Standards in Nutritional Care
 A Toolkit for Commissioners and Providers in England Malnutrition Matters Meeting Quality Standards in Nutritional Care Ailsa Brotherton, Nicola Simmonds and Mike Stroud on behalf of the BAPEN Quality
A Toolkit for Commissioners and Providers in England Malnutrition Matters Meeting Quality Standards in Nutritional Care Ailsa Brotherton, Nicola Simmonds and Mike Stroud on behalf of the BAPEN Quality
MALNUTRITION UNIVERSAL SCREEING TOOL (MUST) MUST IS A MUST FOR ALL PATIENTS
 MUST IS A MUST FOR ALL PATIENTS") MALNUTRITION UNIVERSAL SCREEING TOOL (MUST) MUST IS A MUST FOR ALL PATIENTS Eimear Digan Senior Dietitian, Tallaght Hospital Groups at Risk of Pressure Ulcers Critically ill. Neurologically compromised
MALNUTRITION UNIVERSAL SCREEING TOOL (MUST) MUST IS A MUST FOR ALL PATIENTS Eimear Digan Senior Dietitian, Tallaght Hospital Groups at Risk of Pressure Ulcers Critically ill. Neurologically compromised
Reducing emergency admissions
 A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
A picture of the National Audit Office logo Report by the Comptroller and Auditor General Department of Health & Social Care NHS England Reducing emergency admissions HC 833 SESSION 2017 2019 2 MARCH 2018
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013
 TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
TRUST BOARD SAFETY AND QUALITY MONTHLY REPORT SEPTEMBER 2013 1. EXECUTIVE SUMMARY As reported to the Board last month, the reporting on safety and quality to the Trust Board has changed. Each month a summary
Clinical. Food, Fluid and Nutritional Care Policy (Adults)
") Clinical Food, Fluid and Nutritional Care Policy (Adults) SECTION 6: DECISION MAKING IN THE MANAGEMENT OF ADULT PATIENTS WITH DYSPHAGIA Policy Manager Joyce Thompson Policy Group Food Fluid & Nutritional
Clinical Food, Fluid and Nutritional Care Policy (Adults) SECTION 6: DECISION MAKING IN THE MANAGEMENT OF ADULT PATIENTS WITH DYSPHAGIA Policy Manager Joyce Thompson Policy Group Food Fluid & Nutritional
#NeuroDis
 Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
Each and Every Need A review of the quality of care provided to patients aged 0-25 years old with chronic neurodisability, using the cerebral palsies as examples of chronic neurodisabling conditions Recommendations
NHS Greater Glasgow and Clyde Equality Impact Assessment Tool For Frontline Patient Services
 NHS Greater Glasgow and Clyde Equality Impact Assessment Tool For Frontline Patient Services It is essential to follow the EQIA Guidance in completing this form Name of Current Service/Service Development/Service
NHS Greater Glasgow and Clyde Equality Impact Assessment Tool For Frontline Patient Services It is essential to follow the EQIA Guidance in completing this form Name of Current Service/Service Development/Service
Frequently Asked Questions (FAQ) Updated September 2007
 Updated September 2007") Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Frequently Asked Questions (FAQ) Updated September 2007 This document answers the most frequently asked questions posed by participating organizations since the first HSMR reports were sent. The questions
Mind the Hunger Gap Case Studies
 Mind the Hunger Gap Case Studies Team Alpha Queen Elizabeth Hospital, London As part of London s Queen Elizabeth Hospital s long-standing battle against malnutrition in the acute setting, they put together
Mind the Hunger Gap Case Studies Team Alpha Queen Elizabeth Hospital, London As part of London s Queen Elizabeth Hospital s long-standing battle against malnutrition in the acute setting, they put together
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Enhancing nutritional care
 Enhancing nutritional care Supported by Enhancing nutritional care The RCN launched Nutrition Now in 2007 to help raise standards of nutrition and hydration in hospitals and the community and raise awareness
Enhancing nutritional care Supported by Enhancing nutritional care The RCN launched Nutrition Now in 2007 to help raise standards of nutrition and hydration in hospitals and the community and raise awareness
MQii Malnutrition Knowledge and Awareness Test
 MQii Malnutrition Knowledge and Awareness Test This test intends to assess hospital staff members knowledge of the impact of malnutrition and importance of optimal malnutrition care practices, specifically
MQii Malnutrition Knowledge and Awareness Test This test intends to assess hospital staff members knowledge of the impact of malnutrition and importance of optimal malnutrition care practices, specifically
NHS Grampian. Intensive Psychiatric Care Units
 NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
NHS Grampian Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance
Primary Care Workforce Survey Scotland 2017
 Primary Care Workforce Survey Scotland 2017 A Survey of Scottish General Practices and General Practice Out of Hours Services Publication date 06 March 2018 An Official Statistics publication for Scotland
Primary Care Workforce Survey Scotland 2017 A Survey of Scottish General Practices and General Practice Out of Hours Services Publication date 06 March 2018 An Official Statistics publication for Scotland
Community Care Statistics : Referrals, Assessments and Packages of Care for Adults, England
 Community Care Statistics 2006-07: Referrals, Assessments and Packages of Care for Adults, England 1 Report of the 2006-07 RAP Collection England, 1 April 2006 to 31 March 2007 Editor: Associate Editors:
Community Care Statistics 2006-07: Referrals, Assessments and Packages of Care for Adults, England 1 Report of the 2006-07 RAP Collection England, 1 April 2006 to 31 March 2007 Editor: Associate Editors:
Policy on Learning from Deaths
 Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
Trust Policy Policy on Learning from Deaths Key Points Mortality review is an important part of our Safety and Quality Improvement Process. All patients who die in our trust have a review of their care.
NUTRITION SCREENING SURVEY IN THE UK IN 2007
 NUTRITION SCREENING SURVEY IN THE UK IN 2007 A Report by BAPEN British Association for Parenteral and Enteral Nutrition Nutrition Screening Survey and Audit of Adults on Admission to Hospitals, Care Homes
NUTRITION SCREENING SURVEY IN THE UK IN 2007 A Report by BAPEN British Association for Parenteral and Enteral Nutrition Nutrition Screening Survey and Audit of Adults on Admission to Hospitals, Care Homes
Physiotherapy outpatient services survey 2012
 14 Bedford Row, London WC1R 4ED Tel +44 (0)20 7306 6666 Web www.csp.org.uk Physiotherapy outpatient services survey 2012 reference PD103 issuing function Practice and Development date of issue March 2013
14 Bedford Row, London WC1R 4ED Tel +44 (0)20 7306 6666 Web www.csp.org.uk Physiotherapy outpatient services survey 2012 reference PD103 issuing function Practice and Development date of issue March 2013
Commissioning for quality and innovation (CQUIN): 2014/15 guidance. February 2014
: 2014/15 guidance. February 2014") Commissioning for quality and innovation (CQUIN): 2014/15 guidance February 2014 1 NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning
Commissioning for quality and innovation (CQUIN): 2014/15 guidance February 2014 1 NHS England INFORMATION READER BOX Directorate Medical Operations Patients and Information Nursing Policy Commissioning
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Same day emergency care: clinical definition, patient selection and metrics
 Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
Ambulatory emergency care guide Same day emergency care: clinical definition, patient selection and metrics Published by NHS Improvement and the Ambulatory Emergency Care Network June 2018 Contents 1.
THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER
 Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
Agenda item A5(vi) THE NEWCASTLE UPON TYNE HOSPITALS NHS FOUNDATION TRUST NHS SAFETY THERMOMETER EXECUTIVE SUMMARY The NHS Safety Thermometer is a point of care survey, which is a local improvement tool
NHS Dental Services Quarterly Vital Signs Reports
 NHS Dental Services Quarterly Vital Signs Reports Dental Services Gateway ref: NHSBSA/DSD/0008 Introduction The NHS Dental Services (NHS DS) has been working closely with the Department of Health (DH)
NHS Dental Services Quarterly Vital Signs Reports Dental Services Gateway ref: NHSBSA/DSD/0008 Introduction The NHS Dental Services (NHS DS) has been working closely with the Department of Health (DH)
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST National Inpatient Survey Report July 2011
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST 2010 National Inpatient Survey Report July 2011 Report to: Trust Board - 2 nd August 2011 Report from: Sponsoring Executive: Aim of Report: Joanne Dimmock, Head
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST 2010 National Inpatient Survey Report July 2011 Report to: Trust Board - 2 nd August 2011 Report from: Sponsoring Executive: Aim of Report: Joanne Dimmock, Head
RBCH Actions to meet CQC Essential Standards
 RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
RBCH Actions to meet CQC Essential Standards REGULATION 17 How the regulation was not being met Patients, their relatives, and staff told us about incidents where people had not been treated with dignity
NHS Safety Thermometer CQUIN 2014/15. Frequently Asked Questions
 NHS Safety Thermometer CQUIN 2014/15 Frequently Asked Questions This document is designed to support commissioners and providers in using the CQUIN, the CQUIN guidance and supporting resources. Page references
NHS Safety Thermometer CQUIN 2014/15 Frequently Asked Questions This document is designed to support commissioners and providers in using the CQUIN, the CQUIN guidance and supporting resources. Page references
UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose
 Nephron 2018;139(suppl1):287 292 DOI: 10.1159/000490970 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose 1. Executive summary
Nephron 2018;139(suppl1):287 292 DOI: 10.1159/000490970 Published online: July 11, 2018 UK Renal Registry 20th Annual Report: Appendix A The UK Renal Registry Statement of Purpose 1. Executive summary
The size and structure of the adult social care sector and workforce in England, 2014
 The size and structure of the adult social care sector and workforce in England, 2014 September 2014 Acknowledgements We are grateful to many people who have contributed to this report. Particular thanks
The size and structure of the adult social care sector and workforce in England, 2014 September 2014 Acknowledgements We are grateful to many people who have contributed to this report. Particular thanks
Delivering surgical services: options for maximising resources
 Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Delivering surgical services: options for maximising resources THE ROYAL COLLEGE OF SURGEONS OF ENGLAND March 2007 2 OPTIONS FOR MAXIMISING RESOURCES The Royal College of Surgeons of England Introduction
Document Details Clinical Audit Policy
 Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Title Document Details Clinical Audit Policy Trust Ref No 1538-31104 Main points this document covers This policy details the responsibilities and processes associated with the Clinical Audit process within
Safe staffing for nursing in adult inpatient wards in acute hospitals
 NICE guidelines Safe staffing for nursing in adult inpatient wards in acute hospitals Example scenario to illustrate the process of setting ward nursing staff requirements Published: July 2014 www.nice.org.uk/guidance/sg1
NICE guidelines Safe staffing for nursing in adult inpatient wards in acute hospitals Example scenario to illustrate the process of setting ward nursing staff requirements Published: July 2014 www.nice.org.uk/guidance/sg1
The Royal Wolverhampton Hospitals NHS Trust
 The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
The Royal Wolverhampton Hospitals NHS Trust Trust Board Report Meeting Date: 24 October 2011 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public
APPENDIX 1 An Appetite to Improve
 APPENDIX 1 An Appetite to Improve A Delivery Plan for Food and Fluid 2017 to 2020 Contents Foreword 3 Introduction 4 Strategic Aims/ Objectives 6 Strategic Context 7 Strategic Drivers 8 Primary and Secondary
APPENDIX 1 An Appetite to Improve A Delivery Plan for Food and Fluid 2017 to 2020 Contents Foreword 3 Introduction 4 Strategic Aims/ Objectives 6 Strategic Context 7 Strategic Drivers 8 Primary and Secondary
Reference costs 2016/17: highlights, analysis and introduction to the data
 Reference s 2016/17: highlights, analysis and introduction to the data November 2017 We support providers to give patients safe, high quality, compassionate care within local health systems that are financially
Reference s 2016/17: highlights, analysis and introduction to the data November 2017 We support providers to give patients safe, high quality, compassionate care within local health systems that are financially
National clinical audit of inpatient care for adults with ulcerative colitis
 National clinical audit of inpatient care for adults with ulcerative colitis UK inflammatory bowel disease (IBD) audit Executive summary report June 2014 Prepared by the Clinical Effectiveness and Evaluation
National clinical audit of inpatient care for adults with ulcerative colitis UK inflammatory bowel disease (IBD) audit Executive summary report June 2014 Prepared by the Clinical Effectiveness and Evaluation
A. Commissioning for Quality and Innovation (CQUIN)
") A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
A. Commissioning for Quality and Innovation (CQUIN) CQUIN Table 1: Summary of goals Total fund available: 3,039,000 (estimated, based on 2015/16 baseline) Goal Number 1 2 3 4 5 Goal Name Description of
Protected Mealtimes Policy
 Protected Mealtimes Policy DRAFT 7 [Jan 2012] SG Approved by: On: Review date: Directorate responsible for review: Policy Number: To be read in conjunction with the following policies: Food Safety Policy
Protected Mealtimes Policy DRAFT 7 [Jan 2012] SG Approved by: On: Review date: Directorate responsible for review: Policy Number: To be read in conjunction with the following policies: Food Safety Policy
Diagnostic Waiting Times
 Publication Report Diagnostic Waiting Times Monthly Data to 30 June 2014 Publication date 26 August 2014 A National Statistics Publication for Scotland Contents Introduction... 2 Key points... 3 Results
Publication Report Diagnostic Waiting Times Monthly Data to 30 June 2014 Publication date 26 August 2014 A National Statistics Publication for Scotland Contents Introduction... 2 Key points... 3 Results
Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification
 Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification Healthwatch Sunderland October 2014 Elderly People are not always thoroughly assessed in hospital. This
Report on Call for Evidence: Elderly Hospital Care, Hospital Discharge & Dementia Identification Healthwatch Sunderland October 2014 Elderly People are not always thoroughly assessed in hospital. This
MORTALITY REVIEW POLICY
 MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
MORTALITY REVIEW POLICY Version 1.3 Version Date July 2017 Policy Owner Medical Director Author Associate Director of Patient Safety & Quality First approval or date last reviewed July 2017 Staff/Groups
The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance
 Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
Briefing October 2017 The non-executive director s guide to NHS data Part one: Hospital activity, data sets and performance Key points As a non-executive director, it is important to understand how data
The PCT Guide to Applying the 10 High Impact Changes
 The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
The PCT Guide to Applying the 10 High Impact Changes This Guide has been produced by the NHS Modernisation Agency. For further information on the Agency or the 10 High Impact Changes please visit www.modern.nhs.uk
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 30 June 2016 Publication date 30 August 2016 A National Statistics Publication for Scotland
Commissioning for Quality & Innovation (CQUIN)
") Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Commissioning for Quality & Innovation () The following suite of s are goals relating to improvements in the quality of patient care which the Trust has agreed with commissioners (with the exception of
Emergency admissions to hospital: managing the demand
 Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Report by the Comptroller and Auditor General Department of Health Emergency admissions to hospital: managing the demand HC 739 SESSION 2013-14 31 OCTOBER 2013 4 Key facts Emergency admissions to hospital:
Mental Health Crisis Pathway Analysis
 Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Mental Health Crisis Pathway Analysis Contents Data sources Executive summary Mental health benchmarking project (Provider) Access Referrals Caseload Activity Workforce Finance Quality Urgent care benchmarking
Specialist mental health services
 How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
How CQC regulates: Specialist mental health services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We make
Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation
 Health Informatics Unit Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation April 2011 Funded by: Acknowledgements This project was funded by the Academy of
Health Informatics Unit Evidence on the quality of medical note keeping: Guidance for use at appraisal and revalidation April 2011 Funded by: Acknowledgements This project was funded by the Academy of
Overview. Dr Stephen Gulliford & AKI Specialist Nurse Suzanne Wilson Page 1
 Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Improving Patient Safety and Reducing Harm through the Development of an Acute Kidney Injury Specialist Service at Wrightington, Wigan and Leigh NHS Foundation Trust Overview Acute Kidney Injury (AKI)
Key facts and trends in acute care
 Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
Factsheet November 2015 Key facts and trends in acute care Introduction Welcome to our factsheet giving an overview of major trends and challenges facing the acute sector. The information has been compiled
Food, Fluid and Nutritional Care in Hospitals
 National Overview ~ April 2010 Food, Fluid and Nutritional Care in Hospitals NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance assessment
National Overview ~ April 2010 Food, Fluid and Nutritional Care in Hospitals NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We have assessed the performance assessment
17. Dementia: John s Campaign
 17. Dementia: John s Campaign name weighting (% of CQUIN scheme available) Description of indicator Numerator Implementing a policy on welcoming carers and family members of people with dementia according
17. Dementia: John s Campaign name weighting (% of CQUIN scheme available) Description of indicator Numerator Implementing a policy on welcoming carers and family members of people with dementia according
Our next phase of regulation A more targeted, responsive and collaborative approach
 Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Consultation Our next phase of regulation A more targeted, responsive and collaborative approach Cross-sector and NHS trusts December 2016 Contents Foreword...3 Introduction...4 1. Regulating new models
Intensive Psychiatric Care Units
 NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
NHS Highland Argyll & Bute Hospital, Lochgilphead Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity.
Intensive Psychiatric Care Units
 NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
NHS Lothian St John s Hospital, Livingston Intensive Psychiatric Care Units Service Profile Exercise ~ November 2009 NHS Quality Improvement Scotland (NHS QIS) is committed to equality and diversity. We
Vision 3. The Strategy 6. Contracts 12. Governance and Reporting 12. Conclusion 14. BCCG 2020 Strategy 15
 Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Bedfordshire Clinical Commissioning Group Quality Strategy 2014-2016 Contents SECTION 1: Vision 3 1.1 Vision for Quality 3 1.2 What is Quality? 3 1.3 The NHS Outcomes Framework 3 1.4 Other National Drivers
Surgical Variance Report General Surgery
 Surgical Variance Report General Surgery Table of Contents Introduction to Surgical Variance Report: General Surgery 1 Foreword 2 Data used in this report 3 Indicators measured in this report 4 Laparoscopic
Surgical Variance Report General Surgery Table of Contents Introduction to Surgical Variance Report: General Surgery 1 Foreword 2 Data used in this report 3 Indicators measured in this report 4 Laparoscopic
Aneurin Bevan University Health Board Clinical Record Keeping Policy
 N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
N.B. Staff should be discouraged from printing this document. This is to avoid the risk of out of date printed versions of the document. The Intranet should be referred to for the current version of the
Annual Complaints Report 2014/15
 Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Annual Complaints Report 2014/15 1.0 Introduction This report provides information in regard to complaints and concerns received by The Rotherham NHS Foundation Trust between 01/04/2014 and 31/03/2015.
Fleet and Marine Corps Health Risk Assessment, 02 January December 31, 2015
 Fleet and Marine Corps Health Risk Assessment, 02 January December 31, 2015 Executive Summary The Fleet and Marine Corps Health Risk Appraisal is a 22-question anonymous self-assessment of the most common
Fleet and Marine Corps Health Risk Assessment, 02 January December 31, 2015 Executive Summary The Fleet and Marine Corps Health Risk Appraisal is a 22-question anonymous self-assessment of the most common
The new CQC approach to hospital inspection. Ann Ford Head of Hospital Inspection (North West) June 2014
 June 2014") The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
The new CQC approach to hospital inspection Ann Ford Head of Hospital Inspection (North West) June 2014 1 Our purpose and role Our purpose We make sure health and social care services provide people with
A pilot study examining nutrition and cancer patients: factors influencing oncology patients receiving nutrition in an acute cancer unit.
 A pilot study examining nutrition and cancer patients: factors influencing oncology patients receiving nutrition in an acute cancer unit. WARNOCK, C., TOD, A., KIRSHBAUM, M., POWELL, C. and SHARMAN, D.
A pilot study examining nutrition and cancer patients: factors influencing oncology patients receiving nutrition in an acute cancer unit. WARNOCK, C., TOD, A., KIRSHBAUM, M., POWELL, C. and SHARMAN, D.
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011)
") NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
NHS LANARKSHIRE QUALITY DASHBOARD Board Report June 2011 (Data available as at end April 2011) INTRODUCTION This paper provides a monthly quality dashboard for NHS Lanarkshire. This is in line with the
Learning from Deaths Framework Policy
 Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Learning from Deaths Framework Policy Profile Version: 1.0 Author: Dr Nigel Kennea, Associate Medical Director (Mortality) Executive/Divisional sponsor: Medical Director Applies to: All staff Date issued:
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum. May 2015 avalere.com
 Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Malnutrition Quality Improvement Opportunities for the District Hospital Leadership Forum May 2015 avalere.com Malnutrition Has a Significant Impact on Patient Outcomes MALNUTRITION IS ASSOCIATED WITH
Delayed Transfers of Care Statistics for England 2016/17
 Delayed Transfers of Care Statistics for England 2016/17 Delayed Transfers of Care Statistics for England 2016/17 Version number: 1.0 First published: 9 th June 2017 Prepared by: Operational Information
Delayed Transfers of Care Statistics for England 2016/17 Delayed Transfers of Care Statistics for England 2016/17 Version number: 1.0 First published: 9 th June 2017 Prepared by: Operational Information
Numerator. Denominator Rationale for inclusion
 Goal number Goal name Indicator number Indicator name Goal weighting (% of CQUIN scheme Indicator weighting (% of goal Description of indicator Numerator Denominator Rationale for inclusion Data source
Goal number Goal name Indicator number Indicator name Goal weighting (% of CQUIN scheme Indicator weighting (% of goal Description of indicator Numerator Denominator Rationale for inclusion Data source
102/14(ii) Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review
 Bridgewater Board Date. Thursday 5 June Agenda item. Safe Staffing April 2014 Review") Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Bridgewater Board Date Thursday 5 June 2014 Agenda item 102/14(ii) Title Safe Staffing April 2014 Review Sponsoring Director Authors Presented by Purpose Dorian Williams, Executive Nurse/Director of Governance
Exploring the cost of care at the end of life
 1 Chris Newdick and Judith Smith, November 2010 Exploring the cost of care at the end of life Research report Theo Georghiou and Martin Bardsley September 2014 The quality of care received by people at
1 Chris Newdick and Judith Smith, November 2010 Exploring the cost of care at the end of life Research report Theo Georghiou and Martin Bardsley September 2014 The quality of care received by people at
NHS Sickness Absence Rates. January 2016 to March 2016 and Annual Summary to
 NHS Sickness Absence Rates January 2016 to March 2016 and Annual Summary 2009-10 to 2015-16 Published 26 July 2016 We are the trusted national provider of high-quality information, data and IT systems
NHS Sickness Absence Rates January 2016 to March 2016 and Annual Summary 2009-10 to 2015-16 Published 26 July 2016 We are the trusted national provider of high-quality information, data and IT systems
NHS and independent ambulance services
 How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
How CQC regulates: NHS and independent ambulance services Provider handbook March 2015 The Care Quality Commission is the independent regulator of health and adult social care in England. Our purpose We
(NAME OF AGENCY) Procedures Manual
 Procedures Manual") (NAME OF AGENCY) Procedures Manual Title: ASSISTING SERVICE USERS WITH EATING AND DRINKING (KLOE) 1.0 Scope 1.1 Assistance for Service Users with eating and drinking. 2.0 Aims and Values 2.1 To ensure
(NAME OF AGENCY) Procedures Manual Title: ASSISTING SERVICE USERS WITH EATING AND DRINKING (KLOE) 1.0 Scope 1.1 Assistance for Service Users with eating and drinking. 2.0 Aims and Values 2.1 To ensure
Greater Manchester Neuro-Rehabilitation Services information for patients and carers
 THIS BOOKLET IS BEING TRIALLED Greater Manchester Neuro-Rehabilitation Services information for patients and carers Greater Manchester Neuro-Rehabilitation Services gmnrodn@srft.nhs.uk All Rights Reserved
THIS BOOKLET IS BEING TRIALLED Greater Manchester Neuro-Rehabilitation Services information for patients and carers Greater Manchester Neuro-Rehabilitation Services gmnrodn@srft.nhs.uk All Rights Reserved
Inpatient, Day case and Outpatient Stage of Treatment Waiting Times
 Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 31 December 2016 Publication date 28 February 2017 A National Statistics Publication
Publication Report Inpatient, Day case and Outpatient Stage of Treatment Waiting Times Monthly and quarterly data to 31 December 2016 Publication date 28 February 2017 A National Statistics Publication
Control: Lost in Translation Workshop Report Nov 07 Final
 Workshop Report Reviewing the Role of the Discharge Liaison Nurse in Wales Document Information Cover Reference: Lost in Translation was the title of the workshop at which the review was undertaken and
Workshop Report Reviewing the Role of the Discharge Liaison Nurse in Wales Document Information Cover Reference: Lost in Translation was the title of the workshop at which the review was undertaken and
Methods: Commissioning through Evaluation
 Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Methods: Commissioning through Evaluation NHS England INFORMATION READER BOX Directorate Medical Operations and Information Specialised Commissioning Nursing Trans. & Corp. Ops. Commissioning Strategy
Delivering the Five Year Forward View. through Business Intelligence
 Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
Delivering the Five Year Forward View through Business Intelligence Introduction The market for analytics has matured significantly in the past five years and, although the health sector in the UK has
Quality Management Building Blocks
 Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
Quality Management Building Blocks Quality Management A way of doing business that ensures continuous improvement of products and services to achieve better performance. (General Definition) Quality Management
NHMC. Homecare Medicines Services: National Homecare Medicines Committee. History
 NHMC National Homecare Medicines Committee Homecare Medicines Services: History Version Date Reason for change Person responsible for change V1 12/06/2018 New NHMC RPS Handbook for Homecare Services -
NHMC National Homecare Medicines Committee Homecare Medicines Services: History Version Date Reason for change Person responsible for change V1 12/06/2018 New NHMC RPS Handbook for Homecare Services -
The size and structure
 The size and structure of the adult social care sector and workforce in England, 2017 Acknowledgements Skills for Care is grateful to the many people who have contributed to this report. Particular thanks
The size and structure of the adult social care sector and workforce in England, 2017 Acknowledgements Skills for Care is grateful to the many people who have contributed to this report. Particular thanks
Mental Capacity Act (2005) Deprivation of Liberty Safeguards (England)
 Deprivation of Liberty Safeguards (England)") Mental Capacity Act (2005) Deprivation of Liberty Safeguards (England) England 2016/17 National Statistics Published 1 November 2017 This official statistics report provides the findings from the Mental
Mental Capacity Act (2005) Deprivation of Liberty Safeguards (England) England 2016/17 National Statistics Published 1 November 2017 This official statistics report provides the findings from the Mental
Solent. NHS Trust. Patient Experience Strategy Ensuring patients are at the forefront of all we do
 Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
Solent NHS Trust Patient Experience Strategy 2015-2018 Ensuring patients are at the forefront of all we do Executive Summary Your experience of our services matters to us. This strategy provides national
NHS patient survey programme. CQC s response. to the 2015 survey of women s experiences of maternity care. January 2016
 NHS patient survey programme CQC s response to the 2015 survey of women s experiences of maternity care January 2016 Contents Summary...3 Interpreting the results...4 Key findings...5 What the survey tells
NHS patient survey programme CQC s response to the 2015 survey of women s experiences of maternity care January 2016 Contents Summary...3 Interpreting the results...4 Key findings...5 What the survey tells
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Care Quality Commission (CQC) Inspection Briefing
 Inspection Briefing") Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
Care Quality Commission (CQC) Inspection Briefing The CQC exists to make sure hospitals, care homes, dental and GP surgeries, and all other care services in England provide people with safe, effective,
EMERGENCY CARE DISCHARGE SUMMARY
 EMERGENCY CARE DISCHARGE SUMMARY IMPLEMENTATION GUIDANCE JUNE 2017 Guidance for implementation This section sets out issues identified during the project which relate to implementation of the headings.
EMERGENCY CARE DISCHARGE SUMMARY IMPLEMENTATION GUIDANCE JUNE 2017 Guidance for implementation This section sets out issues identified during the project which relate to implementation of the headings.
PATIENT MEALTIMES RED TRAY POLICY
 PATIENT MEALTIMES RED TRAY POLICY Policy Title: Executive Summary: To improve the nutritional intake of patients by providing help and/or extra time to eat, by identifying a patient and providing specially
PATIENT MEALTIMES RED TRAY POLICY Policy Title: Executive Summary: To improve the nutritional intake of patients by providing help and/or extra time to eat, by identifying a patient and providing specially
The adult social care sector and workforce in. Yorkshire and The Humber
 The adult social care sector and workforce in Yorkshire and The Humber 2015 Published by Skills for Care, West Gate, 6 Grace Street, Leeds LS1 2RP www.skillsforcare.org.uk Skills for Care 2016 Copies of
The adult social care sector and workforce in Yorkshire and The Humber 2015 Published by Skills for Care, West Gate, 6 Grace Street, Leeds LS1 2RP www.skillsforcare.org.uk Skills for Care 2016 Copies of
Guidance notes to accompany VTE risk assessment data collection
 Guidance notes to accompany VTE risk assessment data collection April 2015 1 NHS England INFORMATION READER BOX Directorate Medical Nursing Finance Commissioning Operations Patients and Information Human
Guidance notes to accompany VTE risk assessment data collection April 2015 1 NHS England INFORMATION READER BOX Directorate Medical Nursing Finance Commissioning Operations Patients and Information Human
Changes to Inpatient Disability Services in Clyde
 Changes to Inpatient Disability Services in Clyde Your chance to comment on the proposals This document explains proposed new arrangements for providing specialist inpatient physical disability services,
Changes to Inpatient Disability Services in Clyde Your chance to comment on the proposals This document explains proposed new arrangements for providing specialist inpatient physical disability services,
Appendix 10a SBAR REPORT MARCH 2010 FREE TO LEAD FREE TO CARE, EMPOWERING WARD SISTER / CHARGE NURSE SITUATION
 SBAR REPORT MARCH 2010 FREE TO LEAD FREE TO CARE, EMPOWERING WARD SISTER / CHARGE NURSE SITUATION The purpose of this report is to inform the Board members of the current position and progress of Cwm Taf
SBAR REPORT MARCH 2010 FREE TO LEAD FREE TO CARE, EMPOWERING WARD SISTER / CHARGE NURSE SITUATION The purpose of this report is to inform the Board members of the current position and progress of Cwm Taf
My Discharge a proactive case management for discharging patients with dementia
 Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
Shine 2013 final report Project title My Discharge a proactive case management for discharging patients with dementia Organisation name Royal Free London NHS foundation rust Project completion: March 2014
The size and structure
 The size and structure of the adult social care sector and workforce in England, 2018 Acknowledgements Skills for Care is grateful to the many people who have contributed to this report. Particular thanks
The size and structure of the adult social care sector and workforce in England, 2018 Acknowledgements Skills for Care is grateful to the many people who have contributed to this report. Particular thanks
National Health Promotion in Hospitals Audit
 National Health Promotion in Hospitals Audit Acute & Specialist Trusts Final Report 2012 www.nhphaudit.org This report was compiled and written by: Mr Steven Knuckey, NHPHA Lead Ms Katherine Lewis, NHPHA
National Health Promotion in Hospitals Audit Acute & Specialist Trusts Final Report 2012 www.nhphaudit.org This report was compiled and written by: Mr Steven Knuckey, NHPHA Lead Ms Katherine Lewis, NHPHA
National Patient Experience Survey UL Hospitals, Nenagh.
 National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families
National Patient Experience Survey 2017 UL Hospitals, Nenagh /NPESurvey @NPESurvey Thank you! Thank you to the people who participated in the National Patient Experience Survey 2017, and to their families