Capturing E/M Services in the HOPD
|
|
|
- Sheena Laureen Fowler
- 6 years ago
- Views:
Transcription
1 Capturing E/M Services in the HOPD AAPC Regional Conference Anaheim, CA Linda Martien, COC, CPC, CPMA September 2016
2 Introduction A part of the Federal Balanced Budget Act of 1997 required HCFA (now CMS) to create a new Medicare "Outpatient Prospective Payment System" (OPPS) for hospital outpatient services It was to be separate but similar to the Medicare prospective payment system for hospital inpatients known as "Diagnosis Related Groups" or DRG's. APC's or "Ambulatory Payment Classifications" are the government's method of paying for facility outpatient services for the Medicare program. APC's apply only to hospitals, and have no impact on physician payments under the Medicare Physician Fee Schedule.
3 What is a Hospital Based Clinic? An outpatient department of the hospital just like lab, x-ray, hospital-based clinic. Examples of HBC: IV therapy Clinic, Wound Clinic, Pain Clinic, Ostomy Clinic, Oncology Clinic,, ambulatory outpatient clinic, transfusion clinic, OB, anticoagulation, scheduled visits in the ER Example Hospital-Owned Physician Directed Clinic: Physician does own E&M, hospital uses own criteria for their E&M. Two different sets of criteria; two different E&Ms.
4 Facility vs. Physician E/M Coding Facility coding guidelines are inherently different from professional coding guidelines. Facility coding reflects the volume and intensity of resources utilized by the facility to provide patient care, whereas; Professional codes are determined based on the complexity and intensity of provider performed work and include the cognitive effort expended by the provider. There is no definitive strong correlation between facility and professional coding and thus no rational basis for the application of one set of derived codes, either facility or professional, to the determination of the other on a case-by-case basis.
5 Hospital Owned Physician Directed Challenges Correct claim submission: Physician bills as hospital based and will receive a reduced fee schedule payment as the administrative fees are covered by the facility. Place of service as office (POS 11) receives the full schedule payment in lieu of the reduced payment. This will ensure the full fee schedule is received on one 1500 form claim.
6 The Rules At this point, there is no national standard for hospital assignment of E&M code levels for outpatient services in clinics and the Emergency Department (ED). CMS requires each hospital to establish its own facility billing guidelines. Further, OPPS lists eleven criteria that must be met for facility billing guidelines. (see APC FAQ). Facility billing guidelines should be designed to reasonably relate the intensity of hospital services to the different levels of effort represented by the codes. Coding guidelines should be based on facility resources, should be clear to facilitate accurate payments, should only require documentation that is clinically necessary for patient care, and should not facilitate upcoding or gaming.
7 Understanding the E/M Process E&M = Hospital-based clinic/er visit charge Revenue code 510 CPT Code / /Clinic/Outpatient Dept. Revenue Code 450 CPT Code /ER APC regulations: As long as the services furnished are documented and medically necessary and the facility is following its own system, which reasonably relates intensity of hospital resources to the different levels of HCPC codes, we will assume that it is in compliance with these reporting requirements as they relate to clinic/emergency department visit codes reported on the bill. (Federal Register vol 65, #68, April 7, 2000, Page 18451)
8 Golden Rules HOPD Charge Capture Always, always bill what was done first, i.e., actual procedure: Injection, IV infusion, laceration repair Then evaluate earning the E&M as a separately identifiable service Each visit look for three unique billable services: Nursing procedure/cpt Surgical/interventional procedure/cpt E&M Not always done, but look for them!
9 Evaluate ER & HBC Billing: E&M Nursing Procedures/CPT Interventional/Surgical Procedures/CPT Know what costs are being billed that relate to the above charges Physician Billing: E&M Interventional/Surgical Procedures/CPT E&M levels can be different, but CPT-4 surgical code should be the same
10 What Charges are Covered? Nursing Procedure Nurse doing the injection Risk of giving the injection Cost of routine supplies Separate and identifiable from the E&M? Surgical Procedure Nurse in assistance Set up, clean up Routine supplies Sterilization/tools Overhead of room Separate and identifiable from the E&M?
11 2007 Forward Final Rules CMS offers 11 guiding principles: 1) The coding guidelines should follow the intent of CPT code descriptor in that the guidelines should be designed to reasonably relate the intensity of hospital resources to the different level of effort represented by the codes
12 Guidelines 2) The coding guidelines should be based on hospital facility resources. The guidelines should be not be based on physician resources 3)..should be clear to facilitate accurate payments and be usable for compliance purposes and audits 4) should meet the HIPAA requirements.
13 Guidelines 5) should only require documentation that is clinically necessary for patient care 6) should not facilitate upcoding or gaming 7) should be written or recorded, well documented, and provide the basis for selection of a code 8) should be applied consistently across patients in the clinic or emergency department
14 Guidelines 9) should not change with great frequency 10) should be readily available for fiscal intermediary review 11) should result in coding decision that could be verified by staff & outside auditors
15 Specifics of Current E/M Guidelines Facility and physician levels are not the same. Create facility-specific leveling system. As long as the facility follows it s own guidelines that includes documentation of the E&M elements = compliance. HOLD on any mandated E&M leveling system. Continue to use internal, auditing, resource based system.
16 Understanding the G Codes Type A ERs Paid with newer G codes with each G code having it s own payment. (APC 609, 613, 614, 615, 616, 617/CC) Open 24/7 and staffed as an ER, plus meets licensure issues as a dedicated ER plus EMTALA (pg 335, CMS 1506) --- NOT IMPLEMENTED Type B ERs Paid with newer G codes; included in HBC payment groupers (lesser payment; APC ) Not open 24/7 / meets licensure issues / EMTALA / during previous calendar year, it provides at least 1/3 of all of its outpatient visits for the treatment of emergency medical conditions on an urgent basis without requiring a previously scheduled appointment. (pg 332, CMS 1506) - IMPLEMENTED

17 Facility E/M Level Capture Facilities do not provide any of the three key components in an E/M service So how do you choose an E/M level?
18 Building E/M Criteria Working with the care team, brainstorm the detailed services for each main category: Triage/medical screening/emtala (ER only) Assessment Emotional Support Teaching Discharge Planning/Status Interventions (= no CPT-4 code) Remember until mandated system, the E&M is whatever the facility says it is, with nursing s documentation
19 Example Assessment Reassess, vital check, visual acuity, reassess post meds Emotional Support Patient, family, prolonged Teaching Crutch training, infection guidelines, walker, new meds, sling Discharge Status To nursing home, f/u, physician, by ambulance Interventions no CPT Enema, observation postmed, IV attempts, IV more than 2 lines, Admit, rape exam, wound cleansing, ring removal, restraint, rectal exam, 2 nurses, flushes, care coordination Miscellaneous Language barrier, behavior issues, coordination of care, holding/waiting bed; holding/waiting for a ride
20 Example Acuity Resource E/M Assessment Reassessment after meds 10 Repeat vital signs 5 pts Visual Acuity 5 points Teaching Ed requiring demo 20 Ed w/2 or more meds 10 Crutch training 5 Post wound care 20 Sling, ace wrap-minor 5 Emotional Support Discharge Status Interventions Continue brainstorming services, assigning points based on risk, acuity and resource consumption. Each visit, the E&M leveling form is used to determine level of E&M to bill.

21 Completing the E/M Acuity Tool Add points and assign to level based on totals All elements of the E&M must be charted Hint: Explore dating and signing the E&M leveling sheet and making it part of the permanent medical record Match charting to E&M form as much as possible
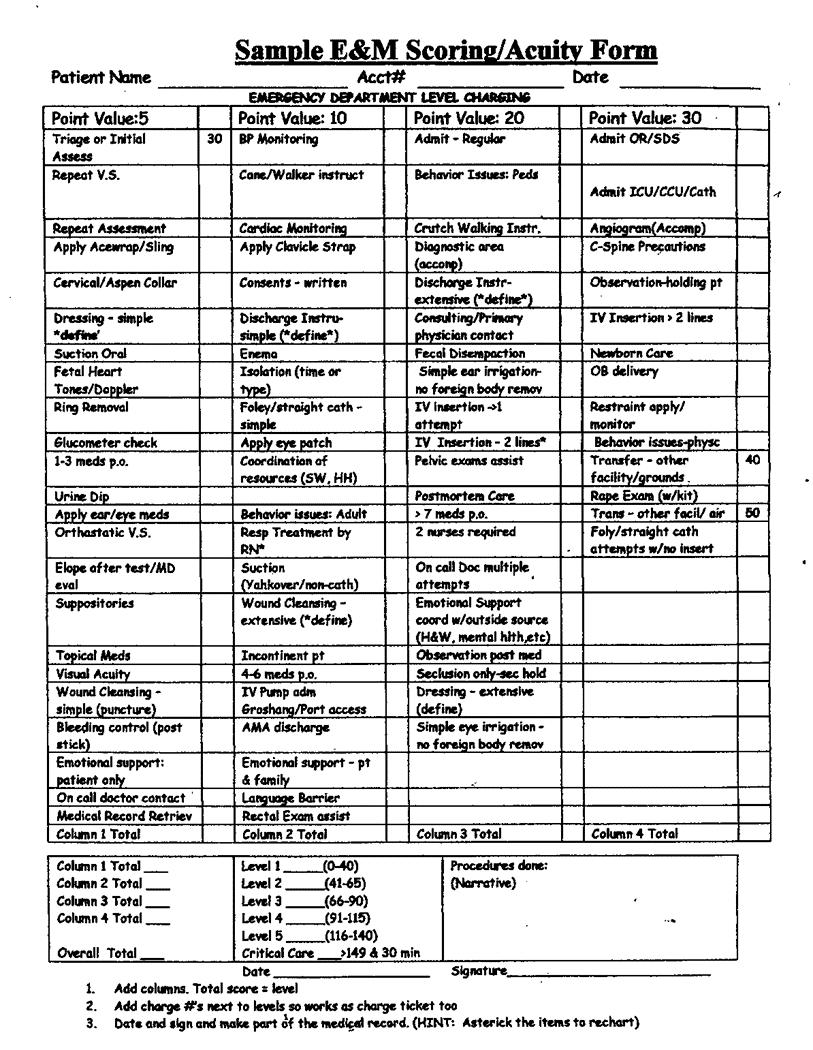
22 Facility ED Leveling Methodology Diagnosis driven Like diagnoses consume like amounts of resources, similar to DRGs Time driven Similar services consume like amounts of resources, similar to APCs Point driven Each service provided is assigned a point value. The total of the points drive the level assigned. Points may NOT be assigned for a service that can be billed separately.
23 Facility ED Leveling Methodology sample Point System 5 POINTS 10 POINTS 15 POINTS 20 POINTS Initial Assessment BP Monitoring Pelvic Exam Admit ICU/CCU Wound Cleanse - simple Apply Clavicle Strap Transport to ICU Apply/Monitor Restraints Topical Meds Foley Cath Sample Enema/Disempaction Cardiac/Thrombolytic Agents Ace Wrap Emotional Support Multiple VS Checks Rape Exam Urine Dip Cardiac Monitoring IV Insertion Multiple IV Infusions Steri-strip Application Accompany to Lab/Rad Newborn Care points ormore or more
24
25 Facility ED Leveling Methodology sample Matrix System CPT Could include interventions from previous levels, plus any of: Minor trauma Receipt of EMS/ambulance patient Heparin/saline lock One (1) nebulizer treatment Preparation for lab test described in CPT Preparation for EKG Preparation for plain x-rays on only one (1) area Prescription medication administed PO Foley catheter; In and Out cath C-spine precautions Fluorescein stain Emesis/Incontinent care Medical condition requiring prescription drug management Fever that responds to antipyretics Headache-hx of, no serial exam Head injury-w/o neurologic symptoms Eye pain Mild dyspnea-not requiring oxygen Prep or assist w/procedures such joint aspiration/injection, simple fracture care Mental Health-anxious, simple treatment Routine psych medical clearance Limited social worker intervention Post morten care Direct admit via ED Discussion of discharge Instructions (moderate complexity)
26 Billing Services in Addition to the E/M Program Memorandum A & A = 25 modifier = separate identifiable services. Golden rule: Always get the CPT-4 procedure code. Earn the E&M as the separate service. Inherent nursing in all procedures/cpt-4 codes ER = Triage = separate identifiable = add E&M Clinic = procedure + unplanned outcome of treatment or other medical condition = E&M Ensure the E&M criteria is well charted in addition to the Procedure Code (separate identifiable E&M)
27
28 Practice Scenario #1 Patient presents to ED with complaints of nausea, vomiting, fever since last night. The patient is otherwise healthy but very distressed, emotional support provided. Initial assessment is completed by the nursing staff, including vital signs, with prolonged emotional support provided. Patient is seen by ED physician who conducts an expanded problem focused history, expanded problem focused exam and medical decision making of low complexity. She orders labs and an abdominal x-ray, all of which are negative. Tigan suppository given for nausea/vomiting. The patient is discharged home with simple instructions to rest, hydrate, and Tylenol for fever, if continues with Rx for Tigan suppositories for the nausea/vomiting. Assessment: flu
29
30 Practice Scenario #1 Initial assessment 30 pts Prolonged support 5 pts Suppository given 5pts Discharge-simple 10 pts TOTAL POINTS 50 PTS E/M LEVEL 99282
31 Practice Scenario #2 A 22-year-old male presents to the ED with right hand pain, after punching another individual during an altercation in a bar. Initial assessment is done and his ring removed due to swelling, using the ring cutter. The patient is clearly inebriated and further injury were undetermined. Patient held in observation until sobered up. C-spine precautions were taken until further evaluations were made. Negative for neuro or spinal injury. He was given Tylenol #3 for pain. X- ray showed a moderately displaced fracture of the 4 th metacarpal. An immobilizing split was applied, as well as a sling. Simple discharge instructions were given. The patient discharged in satisfactory condition. Assessment: right 4 th metacarpal fracture, minimally displaced, reduced with manipulation and splinting.
32



33
34 Practice Scenario #2 Initial assessment 30 pts Ring removed 5 pts Oral med given 5pts C-spine prevent 30 pts Discharge-simple 10 pts TOTAL POINTS 80 PTS E/M LEVEL 99284
35 Practice Scenario #3 A Hispanic speaking patient came in to the wound center for her weekly appointment to treat her chronic non-healing ulcer of the plantar aspect of her left foot. Her son was unable to accompany her today so an interpreter was called. Through the interpreter we learned that on her way across the parking lot she tripped and fell, hitting her head, right elbow and right knee on the pavement. After a thorough assessment, the patient was sent to Radiology for x-rays of all three areas. The x-rays proved to be negative for fractures. The abrasions on her forehead, elbow and knee were cleansed, treated with an antibiotic ointment and bandaged. Once this was completed, attention was turned to the ulcer of her left foot. The ulcer was debrided through the subcutaneous level, dressed and bandaged. The patient was urged to continue to offload the affected foot with her boot. She was discharged in satisfactory condition.
36 Practice Scenario #3 A Hispanic speaking patient came in to the wound center for her weekly appointment to treat her chronic non-healing ulcer. Her son was unable to accompany her today so an interpreter was called. Through the interpreter we learned that on her way across the parking lot she tripped and fell, hitting her head, right arm and right knee on the pavement. C-spine precautions were initiated. After a thorough assessment, the patient was sent to Radiology for x-rays of all three areas. The x-rays showed fractures of the both the distal ulna and radius. All others were negative. Social Services were consulted due to the patient being alone and facing surgery. They coordinated with her family. After examination by an Orthopedic surgeon in the wound center the patient was taken to the OR for repair of the fractures. An IV was started. Her superficial abrasions were cleansed, dressed and bandaged prior to her transfer. She was in stable condition.
37
38 Practice Scenario #3 Initial assessment 30 pts Language barrier 10 pts Wound cleansing 5 pts Simple Dressing 5 pts Coordination of res 10 pts IV insertion (1) 20 pts C-spine precautions 30 pts Admit OR 30 pts TOTAL POINTS 140 PTS E/M LEVEL 99285
39 False Claims Reports Lawsuits Involving Hospitals and Health Systems Becker s Hospital Review, July, 2011 Louisville, KY based Norton Healthcare agreed to pay the federal government $782,842 in March to settle allegations that it overbilled Medicare for wound care, infusion and cancer radiation services by adding a separate E&M charge that should have been included in the basic rate. The alleged overbilling, which occurred between Jan Feb 2010 involved outpatient care. The settlement is twice the amount Norton allegedly overbilled. ISSUE: Transmittal A-00-40, A indicates there is inherent nursing in all CPT codes. Therefore, the facility must earn an E&M service when done with a procedure. Unlikely events, other medical conditions being treated, new patient=examples.
40 HOPD E/M Best Practices If no procedure, always look for an E&M ( ) If there is a procedure, the E&M must be earned E&M MUST be a separate, identifiable service Inherent nursing in all procedures (PM A-00-40) Examples of earning E&M in addition to the procedure: Unplanned outcome/event New dx, treatment, meds Other medical conditions Initial treatment
41 Last Thoughts on E/M Charge Capture No separate billable services should be part of the E&M Critical care (99291) - must map to a level 6 through the facility s own system, plus be in compliance with the CPT-4 guidelines, i.e., system failure, etc. If not, move back to 5 TEST and TEST SOME MORE any changes to the E&M leveling system Pull historical utilization, develop bell curve system sorted by like diagnoses. Compare against new proposed leveling system.

42 And Then There Was An Audit Internal self-auditing External assessment Ensure E&M criteria is understood by staff and charted Can the record support the procedure AND the separate identifiable E&M? Note dates of improvement/changes as part of due diligence process
43 Diagnosis Codes (ICD-10-CM) Diagnosis Codes support Medical Necessity! Must match the procedure or service provided Must be sequenced appropriately Must be relevant to the date and type of service Must be consistent with the providers scope of practice
44 Other Providers What happens when a patient sees different doctors who provide the same service on different dates of service? What happens when a patient sees a nonphysician provider (NPP)? What happens when a patient is referred or is a consult? Is there a difference?
45 Modifiers 25 - Appended to the E/M code to indicate a Significant, separately identifiable service by the same physician on the same day of the procedure or other service 51 Multiple procedures, other than E/M services 52 Reduced services 59 (X subsets) Distinct procedural services, independent from other non E/M services performed on the same day. Documentation must support a different session, different procedure or surgery, different site or organ system, separate incision/excision, separate lesion, or separate injury 78 Unplanned return to OR by same surgeon following initial procedure for a related procedure during the post operative period (global period) 79 Unrelated procedure by same physician during the post operative period

46 Modifier Decision Tree
47 Summary Many different and complex factors affect reimbursement Know your codes (and modifiers!) Know the situation Know your policies (NCDs/LCDs) Know your payer (contracts) Hospital specific anomalies and practices
48 Resources ome (previously Highmark) (previously Cigna)


49 Thank You! Contact info:
50 CEU #
Emergency Department Update 2010 Outpatient Payment System
 Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
Emergency Department Update 2010 Outpatient Payment System ED Facility Level Guidelines: Still No National Guidelines Triage Only Services Critical Care Requires CMS Documentation E/M Physician of Payment
8/19/2017. The OIG Report
 This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
This presentation was created by me with the best intentions and believable resources. I however am not a lawyer, doctor or self-proclaimed expert, but I have watched plenty on TV. The information and
11/6/2017. ED Facility Reimbursement: Key 2018 Updates. ED Facility Levels. E/M Level Determination Principles CMS 2008 OPPS Guidance:
 ED Facility Reimbursement: Key 2018 Updates Michael Granovsky, MD, CPC, FACEP President, LogixHealth ED Facility Levels E/M Level Determination Principles CMS 2008 OPPS Guidance: 11 Guiding Principles
ED Facility Reimbursement: Key 2018 Updates Michael Granovsky, MD, CPC, FACEP President, LogixHealth ED Facility Levels E/M Level Determination Principles CMS 2008 OPPS Guidance: 11 Guiding Principles
Deleted Codes. Agenda 1/31/ E/M Codes Deleted Codes New Codes Changed Codes
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
Modifier -25 Significant, Separately Identifiable E/M Service
 Manual: Policy Title: Reimbursement Policy Modifier -25 Significant, Separately Identifiable E/M Service Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM028 Last Updated:
Manual: Policy Title: Reimbursement Policy Modifier -25 Significant, Separately Identifiable E/M Service Section: Modifiers Subsection: None Date of Origin: 1/1/2000 Policy Number: RPM028 Last Updated:
Presented for the AAPC National Conference April 4, 2011
 Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
Presented for the AAPC National Conference April 4, 2011 Penny Osmon, BA, CPC, CPC-I, CHC, PCS Director of Educational Strategies - Wisconsin Medical Society penny.osmon@wismed.org CPT codes, descriptions
February Jean C. Russell, MS, RHIT Richard Cooley, BA, CCS
 February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
February 2013 Jean C. Russell, MS, RHIT jrussell@epochhealth.com Richard Cooley, BA, CCS rcooley@epochhealth.com 518-430-1144 2 2013 E/M Codes Deleted Codes New Codes Changed Codes Agenda Documentation
Using Clinical Criteria for Evaluating Short Stays and Beyond. Georgeann Edford, RN, MBA, CCS-P. The Clinical Face of Medical Necessity
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford, RN, MBA, CCS-P The Clinical Face of Medical Necessity 1 The Documentation Faces of Medical Necessity ç3 Setting the Stage
IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY
 Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
Global Surgery Policy Number GLS03272013RP Approved By UnitedHealthcare Medicare Committee Current Approval Date 04/09/2014 IMPORTANT NOTE ABOUT THIS REIMBURSEMENT POLICY This policy is applicable to UnitedHealthcare
HC 1930 HC 1930 ICD-9-CM III/CPT Coding II
 South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
South Central College HC 1930 HC 1930 ICD-9-CM III/CPT Coding II Course Information Description Total Credits 4.00 Total Hours 80.00 Types of Instruction This course is a continuation of HC 1920, 1925,
Emergency Department Update 2009 Outpatient Payment System
 Emergency Department Update 2009 Outpatient Payment System ED Facility Level Guidelines Critical Care Composite APCs and No Diagnosis Limitations OPPS Facility Conversion Factor Update Hospital Outpatient
Emergency Department Update 2009 Outpatient Payment System ED Facility Level Guidelines Critical Care Composite APCs and No Diagnosis Limitations OPPS Facility Conversion Factor Update Hospital Outpatient
Optima Health Provider Manual
 Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Optima Health Provider Manual Supplemental Information For Ohio Facilities and Ancillaries This supplement of the Optima Health Ohio Provider Manual provides information of specific interest to Participating
Chapter 02 Hospital Based Care
 Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Chapter 02 Hospital Based Care MULTICHOICE 1. The physician sends the patient to the hospital for a radiological examination. The patient returns to the physician's office for follow-up of test results.
Transition Care Management Update: Practical Applications for 2016
 60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
60 th Annual Greenville Postgraduate Seminar: A Primary Care Update Transition Care Management Update: Practical Applications for 206 Nick Ulmer, MD CPC VP Clinical Services and Medical Director of Case
Emergency Department Facility Coding and Billing
 Emergency Department Facility Coding and Billing The Basics of Facility Coding A Historical View of Hospital Coding and Reimbursement for ED Services E/M Visit Level Coding ED Procedure Coding Payment
Emergency Department Facility Coding and Billing The Basics of Facility Coding A Historical View of Hospital Coding and Reimbursement for ED Services E/M Visit Level Coding ED Procedure Coding Payment
Global Days Policy. Approved By 7/12/2017
 Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
Global Days Policy Policy Number 2018R0005A Annual Approval Date 7/12/2017 Approved By Reimbursement Policy Oversight Committee IMPORTANT NOTE ABOUT THIS You are responsible for submission of accurate
Urgent Care Coding. Webinar Subscription Access Expires December 31.
 Urgent Care Coding Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized to access
Urgent Care Coding Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box you utilized to access
Top 10 audio questions
 Top 10 audio questions Question 1 Scenario: A patient is admitted to the ED for acute abdominal pain. The documentation states that he receives the following: Infusion normal saline, 22:30 Zofran IV push,
Top 10 audio questions Question 1 Scenario: A patient is admitted to the ED for acute abdominal pain. The documentation states that he receives the following: Infusion normal saline, 22:30 Zofran IV push,
Chapter 13 Section 2. Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups
 Groups") Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Outpatient Prospective Payment System (OPPS)-Ambulatory Payment Classification (APC) Chapter 13 Section 2 Billing And Coding Of Services Under Ambulatory Payment Classifications (APC) Groups Issue Date:
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice
 Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Mid-Level Providers: What You Need to Know to Use Them Successfully in Your Practice Presented by Sarah Reed, BSE. CPC Senior Managing Consultant Medical Revenue Solutions, LLC AAPC 2016 Disclaimer The
Two Midnight Rule What does it mean for Coders?
 Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
Two Midnight Rule What does it mean for Coders? Heather Greene, MBA, RHIA, CPC, CPMA Vice President, Compliance Services AHIMA Approved ICD-10 CM/PCS Trainer 1 Agenda The Two-Midnight Rule Supportive documentation
GLOBAL DAYS POLICY. Policy Number: SURGERY T0 Effective Date: January 1, 2018
 GLOBAL DAYS POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: SURGERY 011.37 T0 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE LINES OF BUSINESS/PRODUCTS...
GLOBAL DAYS POLICY UnitedHealthcare Oxford Reimbursement Policy Policy Number: SURGERY 011.37 T0 Effective Date: January 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE... 1 APPLICABLE LINES OF BUSINESS/PRODUCTS...
2006 Clinical Coding Workout 5/3/2006 MISSING QUESTIONS Chapter 5, Intermediate Ambulatory Page 1
 Chapter 5, Intermediate Ambulatory Page 1 CPT Modifier Use 5.81. Dr. Raddy, staff radiologist, interprets a chest x-ray that was obtained in the hospital Radiology Department. Dr. Raddy is contracted with
Chapter 5, Intermediate Ambulatory Page 1 CPT Modifier Use 5.81. Dr. Raddy, staff radiologist, interprets a chest x-ray that was obtained in the hospital Radiology Department. Dr. Raddy is contracted with
See the Time chapter for complete instructions regarding how to code using time as the controlling E/M factor.
 2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
2015 EM Survival Guides Chapter 1: Office or Other Outpatient Visit (99201-99215) You should apply 99201-99215 for E/M visits in the office or other outpatient setting. These codes distinguish between
Global Surgery Fact Sheet
 DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Global Surgery Fact Sheet Definition of a Global Surgical Package This fact sheet is designed to provide education on the
OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT
 OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT ALL CHARTING NEEDS TO BE FINISHED AT THE END OF YOUR SHIFT PRIOR TO LEAVING THE ED IF YOU HAVE ANY QUESTIONS, ASK FOR HELP! All of the
OVERVIEW OF ESSENTIAL CHARTING ELEMENTS FOR THE EMERGENCY DEPARTMENT ALL CHARTING NEEDS TO BE FINISHED AT THE END OF YOUR SHIFT PRIOR TO LEAVING THE ED IF YOU HAVE ANY QUESTIONS, ASK FOR HELP! All of the
Care Transition Strategies: The 2013 Transition Care Management Codes
 Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
Care Transition Strategies: The 203 Transition Care Management Codes Sponsored by The Carolinas Center for Medical Excellence (CCME) and The South Carolina Partnership for Health (SC PfH) E. G. Nick Ulmer,
1. Receives report from EMS and/or outlying facility. 5. Adheres to safety and universal precaution guidelines.
 Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Trauma Nurse Specialist 1. Receives report from EMS and/or outlying facility. 2. Reports to trauma room and signs in. 3. Relays reports to trauma team members. 4. Assists with resuscitation readiness:
Coding for the Outpatient Hospital Setting. Webinar Subscription Access Expires December 31.
 Coding for the Outpatient Hospital Setting Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box
Coding for the Outpatient Hospital Setting Questions Answers Webinar Subscription Access Expires December 31. How long can I access the on demand version? You will find that in the same instructions box
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert
 For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
For Vanderbilt Medical Center Carolyn Buppert, NP, JD Law Office of Carolyn Buppert www.buppert.com Describe the services in critical care that nurse practitioners perform that are billable Discuss what
Coding Guidelines for Certain Respiratory Care Services January 2018 (updates in red)
") Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Coding Guidelines for Certain Respiratory Care Services (updates in red) Overview From time to time the AARC receives inquiries about respiratory-related coding and coverage issues through its Help Line
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Amended Date: October 1, Table of Contents
 Amended Date: October 1, Table of Contents") Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
Long Term Care Hospital Clinical Coverage Policy No: 2A-2 Services (LTCH) Table of Contents 1.0 Description of the Procedure, Product, or Service... 1 1.1 Definitions... 1 2.0 Eligibility Requirements...
Using Clinical Criteria for Evaluating Short Stays and Beyond
 Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Using Clinical Criteria for Evaluating Short Stays and Beyond Georgeann Edford I. History A. Social Security Act Medical Necessity and Utilization Review 1. Items or services necessary for the diagnosis
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications
 Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
Presented by: Jodie Edmonds VP Medicaid Revenue Consultant Passport Health Communications Complete and correct coding of claims will become more important, and will have an effect on claim payment. The
ATTENTION PROVIDERS. Billing & Reimbursement Requirements for Observation Services
 EqualityCareNews November 2005 ATTENTION PROVIDERS Provider Bulletin 05-005 Billing & Reimbursement Requirements for Observation Services Effective October 1, 2005, under Outpatient Prospective Payment
EqualityCareNews November 2005 ATTENTION PROVIDERS Provider Bulletin 05-005 Billing & Reimbursement Requirements for Observation Services Effective October 1, 2005, under Outpatient Prospective Payment
2018 Biliary Reimbursement Coding Fact Sheet
 The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
The information contained in this document is provided for informational purposes only and represents no statement, promise, or guarantee by Cordis Corporation concerning levels of reimbursement, payment,
Getting Paid for What You Do! Coding 2010
 Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Getting Paid for What You Do! Coding 20 Children s Mercy Health Network 11/17/09 Richard H. Tuck, MD, FAAP Disclosure I have financial relationships or interests with proprietary entities producing health
Clinic Specific Coding and Reporting Changes for 2017
 January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
January 2017 Jean C. Russell, MS, RHIT jrussell@epochhealth.com 518-369-4986 Richard Cooley, BS, CCS, rcooley@epochhealth.com 518-430-1144 Matthew H. Lawney, MSPT, MBA, CHC mlawney@epochhealth.com 845-642-6462
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Reimbursement for Anticoagulation Services
 Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Journal of Thrombosis and Thrombolysis 12(1), 73 79, 2001. # 2002 Kluwer Academic Publishers, Manufactured in The Netherlands. Reimbursement for Anticoagulation Services Paul W. Radensky McDermott, Will
Critical Care What Makes this so Difficult
 Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Critical Care What Makes this so Difficult Presented by Angela Jordan, CPC Senior Managing Consultant AAPC National Advisory Board, Southwest September 2016 Disclaimer The speaker has no financial relationship
Services That Require Prior Authorization
 Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
Services That Require Prior Authorization Some of the services listed in the Medical Benefits Chart are covered only if your doctor or other network provider gets approval in advance (sometimes called
9/17/2018. Place of Service Type of Service Patient Status
 Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Place of Service Type of Service Patient Status 1 The first factor you must consider in code assingment is the place of service. Office Hospital Emergency Department Nursing Home Type of service is the
Reimbursement guide. IODOSORB/IODOFLEX are Cadexomer Iodine-based products, available in two forms gel or pad.
 Reimbursement guide IODOSORB/IODOFLEX are Cadexomer Iodine-based products, available in two forms gel or pad. IODOSORB/IODOFLEX remove barriers to healing by its dual action antimicrobial and desloughing
Reimbursement guide IODOSORB/IODOFLEX are Cadexomer Iodine-based products, available in two forms gel or pad. IODOSORB/IODOFLEX remove barriers to healing by its dual action antimicrobial and desloughing
Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1
 Services 1") GE Healthcare Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
GE Healthcare Reimbursement Information for Contrast Enhanced Spectral Mammography (CESM) Services 1 May 2018 www.gehealthcare.com/reimbursement This advisory addresses Medicare coding, coverage and payment
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
July 2011 Quarterly CMS OCCB Q&As
 July 2011 Quarterly CMS OCCB Q&As Category 1 - Applicability Face-to-Face Question 1: If the F2F does not occur within 30 days, but it does occur, for example, on the 35th day, does the agency have to
July 2011 Quarterly CMS OCCB Q&As Category 1 - Applicability Face-to-Face Question 1: If the F2F does not occur within 30 days, but it does occur, for example, on the 35th day, does the agency have to
The ASA defines anesthesiology as the practice of medicine dealing with but not limited to:
 1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
1570 Midway Pl. Menasha, WI 54952 920-720-1300 Procedure 1205- Anesthesia Lines of Business: All Purpose: This guideline describes Network Health s reimbursement of anesthesia services. Procedure: Anesthesia
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I
 Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Medicare Part A SNF Payment System Reform: Introduction to Resident Classification System - I Introduction to the Resident Classification System - I Concepts Structure Implications RCS is NOT the Unified
Preventive and Sick Visits Same Day. Objectives
 Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Preventive and Sick Visits Same Day Brenda Chidester-Palmer CPC, CPC-I, CEMC, CCS-P AAPC National Conference June 8, 2010 Nashville, Tennessee Objectives Preventive visit definition Services included in
Global Surgery Package
 Private Property of Florida Blue. This payment policy is Copyright 2017 Florida Blue. All Rights Reserved. You may not copy or use this document or disclose its contents without the express written permission
Private Property of Florida Blue. This payment policy is Copyright 2017 Florida Blue. All Rights Reserved. You may not copy or use this document or disclose its contents without the express written permission
2. During an emergency room visit, Sally was diagnosed with pneumonia. She was admitted to the hospital observation unit and treated with 500 mg of
 1. A patient received a 12 sq. cm. dermal tissue substitute of human origin, dermagraft. This treatment was completed due to a burn on the abdomen. How would you report the supply? a. Q4107x12 b. Q4105
1. A patient received a 12 sq. cm. dermal tissue substitute of human origin, dermagraft. This treatment was completed due to a burn on the abdomen. How would you report the supply? a. Q4107x12 b. Q4105
See the Time chapter for complete instructions on how to code using time as the controlling factor when selecting an E/M code.
 2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
2015 EM Survival Guides Chapter 4: Initial Hospital Care (99221-99223) You should select the appropriate-level initial hospital care code (99221-99223) using the key E/M criteria of history, examination
Coding, Corroboration, and Compliance How to assure the 3 C s are met
 Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
Coding, Corroboration, and Compliance How to assure the 3 C s are met Sue Roehl, RHIT, CCS sroehl@eidebailly.com 701-476-8770 OIG 1996 - $23.2 Billion errors Figure 1 Insufficient/No documentation 46.76%
6/14/2017. Evaluation and Management Coding. Jeffrey D. Lehrman, DPM, FASPS, MAPWCA
 Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
Evaluation and Management Coding Jeffrey D. Lehrman, DPM, FASPS, MAPWCA APMA Coding Committee APMA MACRA Task Force Expert Panelist, Codingline Fellow, American Academy of Podiatric Practice Management
NP Discharge & Admission: Legislative Authority
 The Canadian Nurses Protective Society Admission & Discharge: Professional Liability Considerations Chantal Léonard, CEO, CNPS OHA Conference, March 29, 2012 NP Discharge & Admission: Legislative Authority
The Canadian Nurses Protective Society Admission & Discharge: Professional Liability Considerations Chantal Léonard, CEO, CNPS OHA Conference, March 29, 2012 NP Discharge & Admission: Legislative Authority
Chapter 9 Section 1. Ambulatory Surgical Center (ASC) Reimbursement
 Reimbursement") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Issue Date: August 26, 1985 Authority: 32 CFR 199.14(d) Copyright: CPT only 2006 American Medical Association (or such other date of publication of
Developing an ED Facility Charge Calculator March 3, :00pm
 Developing an ED Facility Charge Calculator March 3, 2016 4:00pm Neal Kothe, The Ohio State University Wexner Medical Center Carol Gray, The Ohio State University Wexner Medical Center Conflict of Interest
Developing an ED Facility Charge Calculator March 3, 2016 4:00pm Neal Kothe, The Ohio State University Wexner Medical Center Carol Gray, The Ohio State University Wexner Medical Center Conflict of Interest
Shared and Incident To Billing of E/M Services in Radiation Oncology Updated November 2017
 ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
ASTRO Guidance on Shared and Incident To Billing of Evaluation and Management Services in Radiation Oncology The Centers for Medicare and Medicaid Services (CMS) establishes Medicare policy for the payment
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: skilled_nursing_services 07/2001 2/2018 2/2019 2/2018 Description of Procedure or Service Skilled Nursing
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: skilled_nursing_services 07/2001 2/2018 2/2019 2/2018 Description of Procedure or Service Skilled Nursing
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011
 PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
PECULIARITIES OF BILLING AND CODING IN LTC OCTOBER 14, 2011 PRESENTED BY ALVA S. BAKER, MD, CMD Maine Medical Directors Association Faculty Disclosures: Dr. Baker has disclosed that he has no relevant
ABOUT THE CONE HEALTH NETWORK OF SERVICES
 THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
THE MOSES H. CONE MEMORIAL HOSPITAL (536 beds) Critical Care Services All system ICU patients are monitored with the help an electronic ICU monitoring system (VISICU ). Emergency Services Medical Intensive
Evaluation and Management Services
 Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Evaluation and Management Services Print 1. If a physician sees a patient in the morning and again in the afternoon for a new or worsened condition, do we report modifier 25 for the second visit? 2. When
Acromioclavicular Joint Billing
 Acromioclavicular Joint Billing October 27, 2016 When our physician performs an injection into the acromioclavicular (AC) joint of a patient in the office, can we bill 20610 for a large joint arthrocentesis?
Acromioclavicular Joint Billing October 27, 2016 When our physician performs an injection into the acromioclavicular (AC) joint of a patient in the office, can we bill 20610 for a large joint arthrocentesis?
E/M Auditing: History is the Key
 E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
E/M Auditing: History is the Key By Brandi Tadlock CPC, CPC-P, CPMA, CPCO CPC, CPMA, CEMC, CPC-H, CPC-I SUMMARY Review the history component in your E/M documentation to make sure it tells the patient
Objectives. Emergency Medicine Risk Factors
 The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
The Uniqueness of Emergency Medicine Risk Management W. Peter Vellman, MD, FACEP Serio Physician Management, LLC Littleton, CO Objectives Recognize key areas impacting the provision of emergency medical
EM Coding Newsletter & Advisory Critical Care Update
 EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
EM Coding Newsletter & Advisory Critical Care Update Keep Your Critical Care Up With The Times Critical Care Case Scenarios Frequently Asked Questions Keep Your Critical Care Up With The Times In the last
Modifiers 58, 78, and 79 Staged, Related, and Unrelated Procedures
 Manual: Policy Title: Reimbursement Policy Modifiers 58, 78, and 79 Staged, Related, and Unrelated Procedures Section: Modifiers Subsection: None Date of Origin: 9/22/2004 Policy Number: RPM010 Last Updated:
Manual: Policy Title: Reimbursement Policy Modifiers 58, 78, and 79 Staged, Related, and Unrelated Procedures Section: Modifiers Subsection: None Date of Origin: 9/22/2004 Policy Number: RPM010 Last Updated:
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Coding and Billing for Lifestyle Medicine
 Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
Coding and Billing for Lifestyle Medicine Presented to Tools for Healthy Change June 21, 2014 Agenda Understanding Documentation Guidelines and key components of E/M Services History, Exam, Medical Decision
EMTALA. Mark Reiter MD MBA FAAEM
 EMTALA Mark Reiter MD MBA FAAEM Residency Director, U. Tennessee Murfreesboro/Nashville Past President, American Academy of Emergency Medicine CEO, Emergency Excellence Objective To educate on EMTALA using
EMTALA Mark Reiter MD MBA FAAEM Residency Director, U. Tennessee Murfreesboro/Nashville Past President, American Academy of Emergency Medicine CEO, Emergency Excellence Objective To educate on EMTALA using
KANSAS MEDICAL ASSISTANCE PROGRAM. Fee-for-Service Provider Manual. Podiatry
 Fee-for-Service Provider Manual Podiatry Updated 03.2014 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim..................
Fee-for-Service Provider Manual Podiatry Updated 03.2014 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim..................
Disclosure of Proprietary Interest
 HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
HomeTown Health HCCS Hospital Consortium Project: Track 3- Clinical Documentation: Strategies for Sharpening Focus Jenan Custer RHIT, CCS, CPC, CDIP AHIMA Approved ICD-10-CM/PCS Trainer Director of Coding
Programming a Spinal Cord Neurostimulator
 Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
Programming a Spinal Cord Neurostimulator August 10, 2017 My surgeon wants to bill 95972 for programming along with placement of a spinal neurostimulator. Isn t the programming inclusive to the surgical
KANSAS MEDICAL ASSISTANCE PROGRAM. Provider Manual. Podiatry
 Provider Manual Podiatry Updated 07/2012 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim.................. 7-1 7010 Podiatry
Provider Manual Podiatry Updated 07/2012 PART II Introduction Section BILLING INSTRUCTIONS Page 7000 Podiatry Billing Instructions.................. 7-1 Submission of Claim.................. 7-1 7010 Podiatry
Observation Coding and Billing Compliance Montana Hospital Association
 Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Observation Coding and Billing Compliance Montana Hospital Association Sue Roehl, RHIT, CCS sroehl@eidebaill.com 701-476-8770 IP versus Observation considerations Severity of patient s signs and symptoms
Emergency Department
 Emergency Department Elizabeth Lowry, Director, Internal Audit Darlene FitzPatrick, Director, Internal Audit Bon Secours Health System, Inc. ED: Performing a Value-Added Audit Understanding the structure
Emergency Department Elizabeth Lowry, Director, Internal Audit Darlene FitzPatrick, Director, Internal Audit Bon Secours Health System, Inc. ED: Performing a Value-Added Audit Understanding the structure
2015 Summary of Benefits
 2015 Summary of Benefits Health Net Cal MediConnect Plan (Medicare-Medicaid Plan) Los Angeles County, CA H3237_2015_0291 CMS Accepted 09082014 Health Net Cal MediConnect Summary of Benefits! This is a
2015 Summary of Benefits Health Net Cal MediConnect Plan (Medicare-Medicaid Plan) Los Angeles County, CA H3237_2015_0291 CMS Accepted 09082014 Health Net Cal MediConnect Summary of Benefits! This is a
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair
 William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
William J. Ennis D.O.,MBA University of Illinois at Chicago Professor Clinical Surgery, Chief Section wound healing and tissue repair What are the revenue streams What are the expenses How does the hospital
Empire BlueCross BlueShield Professional Reimbursement Policy
 Subject: Global Surgery NY Policy: 0012 Effective: 02/01/2014 05/31/2014 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
Subject: Global Surgery NY Policy: 0012 Effective: 02/01/2014 05/31/2014 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
today! Visit or call 800/
 The bestselling Certified Coder Boot Camp is now available online! Register today! Visit www.hcprobootcamps.com or call 800/750-0584. Register 30 days in advance and save $200! Call HCPro at 800/750-0584
The bestselling Certified Coder Boot Camp is now available online! Register today! Visit www.hcprobootcamps.com or call 800/750-0584. Register 30 days in advance and save $200! Call HCPro at 800/750-0584
Title: ED Management of Trauma Patient Protocol
 Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
Title: ED Management of Trauma Patient Protocol Document Category: Clinical Document Type: Protocol Department/Committee Owner: Emergency Department Original Date: August 2009 Approver(s) last review:
DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI
 DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI triage, both in terms of levels and context in which they
DMAT Intermediate Triage Lecture Notes Keith Conover, M.D., FACEP 1.0 7/11/14 Objectives: Describe the differences between START triage and ESI triage, both in terms of levels and context in which they
Outpatient Hospital Facilities
 Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Outpatient Hospital Facilities Chapter 6 Chapter Outline Introduce students to 1. Different outpatient facilities 2. Different departments involved in the reimbursement process 3. The Chargemaster 4. Terminology
Evaluation and Management of Emergency Department Coding
 In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
In the event of conflict between a Clinical Payment and Coding Policy and any plan document under which a member is entitled to Covered Services, the plan document will govern. Plan documents include,
HealthPartners Freedom Plan (Cost) 2011 Medical Summary of Benefits Wisconsin
 2011 Medical Summary of Benefits Wisconsin") HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
HealthPartners Freedom Plan 2011 Medical Summary of Benefits Wisconsin HealthPartners Wisconsin Freedom Plan I HealthPartners Wisconsin Freedom Plan II 420421 (10/10) H2462_SB WI_151 CMS Approved 10/5/10
Medical Coding Best Practices for Emergency Departments
 1 Medical Coding Best Practices for Emergency Departments Medical Coding Best Practices for Emergency Departments 1 2 Medical Coding Best Practices for Emergency Departments Summary Delivering quality
1 Medical Coding Best Practices for Emergency Departments Medical Coding Best Practices for Emergency Departments 1 2 Medical Coding Best Practices for Emergency Departments Summary Delivering quality
2/28/2017 NO DISCLOSURES. K 1/Partner
 NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
NO DISCLOSURES LaMon Norton NP Participant will recognize origin & role of Relative Value Unit (RVU) in coding and reimbursement. Participant will be able to link documentation points to coding and RVU
TRICARE Reimbursement Manual M, February 1, 2008 Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1
 Chapter 9 Section 1") Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Ambulatory Surgical Center (ASC) Reimbursement Prior To Implementation Of Outpatient Prospective Payment (OPPS), And Thereafter, Freestanding ASCs,
Ambulatory Surgery Centers (ASCs) Chapter 9 Section 1 Ambulatory Surgical Center (ASC) Reimbursement Prior To Implementation Of Outpatient Prospective Payment (OPPS), And Thereafter, Freestanding ASCs,
Summary of benefits Health Net. seniority plus green. Benefits effective January 1, 2009 H0562 Medicare Advantage HMO
 2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
2009 Health Net Summary of benefits Los Angeles, Orange, Riverside and San Bernardino counties s effective January 1, 2009 H0562 Medicare Advantage HMO Material ID H0562-09-0041 CMS Approval 9/08 Section
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Cigna Medical Coverage Policy Subject Observation Care Table of Contents Coverage Policy... 1 General Background... 2 Coding/Billing Information... 4 References... 5 Effective Date... 10/15/2014 Next Review
Global Period for Surgery. Is it billable?
 Global Period for Surgery. Is it billable? August 10, 2017 Question: My patient presented to the ED with an infection at the incision site from a surgery that I did 4 weeks ago. It has a 90 day global.
Global Period for Surgery. Is it billable? August 10, 2017 Question: My patient presented to the ED with an infection at the incision site from a surgery that I did 4 weeks ago. It has a 90 day global.
CHARGE CAPTURE. LEE TINSLEY RN NORTHWEST HEALTHCARE CONSULTING UR Nurse, Infection Control Officer, Compliance Officer Lake Chelan Community Hospital
 CHARGE CAPTURE LEE TINSLEY RN NORTHWEST HEALTHCARE CONSULTING UR Nurse, Infection Control Officer, Compliance Officer Lake Chelan Community Hospital PRESENTATION OF THREE ELEMENTS Audit process. ER billing.
CHARGE CAPTURE LEE TINSLEY RN NORTHWEST HEALTHCARE CONSULTING UR Nurse, Infection Control Officer, Compliance Officer Lake Chelan Community Hospital PRESENTATION OF THREE ELEMENTS Audit process. ER billing.
Anthem Blue Cross and Blue Shield Commercial Professional Reimbursement Policy
 Subject: Global Surgery IN, KY, MO, OH, WI Policy: 0012 Effective: 01/01/2018 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
Subject: Global Surgery IN, KY, MO, OH, WI Policy: 0012 Effective: 01/01/2018 Coverage is subject to the terms, conditions, and limitations of an individual member s programs or products and policy criteria
CAH PREPARATION ON-SITE VISIT
 CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
CAH PREPARATION ON-SITE VISIT Illinois Department of Public Health, Center for Rural Health This day is yours and can be flexible to the timetable of hospital staff. An additional visit can also be arranged
Observations of Off Unit Clinical Experiences for Students
 Observations of Off Unit Clinical Experiences for Students This reference has been assembled to assist school of nursing instructors in pursuing appropriate patient experiences and observations for their
Observations of Off Unit Clinical Experiences for Students This reference has been assembled to assist school of nursing instructors in pursuing appropriate patient experiences and observations for their
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule. Grace Wilson, RHIA
 Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Calculating E&M codes & 2018 Medicare Physician Fee Schedule Proposed Rule Grace Wilson, RHIA Objectives 2018 Medicare Physician Fee Schedule E/M Coding Overview Documentation Examples Proposed Documentation
Evaluation and Management
 Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by
Evaluation and Management CPT CPT copyright 2011 American Medical Association. All rights reserved. Fee schedules, relative value units, conversion factors and/or related components are not assigned by