Documentation Principles and Their Effect on ICD 10 Coding, Compliance and Risk Management
|
|
|
- Juliana Marsh
- 6 years ago
- Views:
Transcription



1 Documentation Principles and Their Effect on ICD 10 Coding, Compliance and Risk Management Dr Dianne M Baynes RN DC MCSP CPPM Documentation systems based on lots of audits and findings Basics are often the most missing items Training is the foundation Same as Not!!! What are we up against? The KMCU Way Healthcare has been changing for a while The changes are getting more rapid and are hitting closer to home There are now a number of cautionary tales for DCs and team members Ch-Ch-Ch-Ch-Changes 1



2 Chiropractic and the OIG For the first time since May 2010, the Office of Inspector General, of the Dept. of Health and Human Services, has published a report specifically about chiropractic...or rather, one chiropractor in particular. This fellow chiropractor s dire situation represents the current state of risk that most chiropractors are not even aware they face on a daily basis. Is this you? OIG Report Facts Dr. Rick Kuhlman-Georgia and TN 2
3 Doctors AND Assistants in the Cross Hairs Cookie Cutter Protocols Deemed Fraud A Closer Look 3




4 Not Just Medicare! This is PI Medically Unnecessary Definitions 4




5 And so it goes. OIG FY 2012 Report to Congress OIG FY 2013 Report to Congress OIG s Semi-Annual Report to Congress Fall


6 March 2015 State Boards Involved Too Chiropractic and chiropractors being in the cross-hairs stared in Then it started with detailed specifics of what we do wrong. Beginning with Dr Diep in November of 2013 OIG Report Facts OIG Report #2 Then this happened in May of Same issues, same concerns, same lack of Policies and Procedures. Total recoupment: $369,335 for 3 years $737,111 estimated overpayment 6


7 Then this happened in July of Same issues, same concerns, same lack of Policies and Procedures. Total recoupment: $482,867 requested $498,764 estimated overpayment OIG Report #3 And Literally Last Week Audit: Efficiency Check; A systematic check or assessment, especially of the efficiency or effectiveness of an organization or process, typically carried out by an independent assessor 7
 Who s Asking?")

8 Records requests come in all shapes and sizes Sometimes they are a probe Sometimes they are a system Sometimes they are what they are What Does This Mean? Commercial insurance Carrier Personal Injury Carrier or Adjuster Worker s Compensation Carrier or Adjuster Medicare Administrative Contractor (MAC) Who s Asking?? Recovery Audit Contractor (RAC) Comprehensive Error Rate Testing (CERT) Zone Program Integrity Contractor (ZPIC) Program Safeguard Contractor (PSC Why Are They Asking?? Prepayment review of claims always results in an "initial determination'' Post-payment review may result in no change to the initial payment to the provider or may result in a "revised determination" that would require the provider to pay back monies for services determined to be "not reasonable or necessary." Automatic, or non-complex, reviews occur without clinical review of medical documentation submitted by the provider, such as in cases of medically unlikely edits (MUEs) or when there is no timely response to an audit request letter. Complex reviews involve requesting, receiving, and medical review of additional documentation associated with a claim. 8



9 What s Their Motivation? Payment Recovery/Recoupment An overpayment occurs when a provider receives excess payment due to duplicate submission of the same service or claim, payment to the incorrect payee, payment for excluded or medically unnecessary services, or a pattern of furnishing and billing for excessive or noncovered services, as determined in an audit or review. What s Their Motivation? In 2010, President Obama announced the following three goals for cutting improper Medicare payments by 2012: reducing overall payment errors by $50 billion cutting the Medicare fee-for-service error rate in half recovering $2 billion in improper payments They Look For Coding Errors and Patterns Review Outliers Review of high dollar codes-bcbsil SO s Identify Fraud and Abuse This is JOB ONE! What Might Be the Trigger? Overutilization New carrier preexisting condition Unusual codes Unusual errors Billing errors, like lack of Box 14 changing Your number came up 9




10 How This Training Will Protect You! Documentation of Case Management Documentation of Initial Visits ICD-10 Awareness Documentation of Routine Visits Risk Management and Risk Avoidance Compliance Concerns Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements to protect the public Guards against malpractice action Secures appropriate reimbursement Because if it wasn t written down, it didn t happen! Know your Audience Another health care provider Your board A malpractice attorney Third party payer's medical necessity auditor Each has different, but necessary requirements of your documentation 10




11 What Dr. Diep Didn t Know That He Didn t Know! The $708,000 recoupment finding to Medicare: Ignorance of the rules Upcoding charges Billing Medicare inappropriately Poor documentation No Policies and SOP Ignored help when notified of OIG concerns 11



12 The OIG is not out to get us all There is enough low hanging fruit to take care of the federal budget deficit Be aware of the specific errors pointed out in the report OIG Report Facts Problem #1: Stick Out Like a Sore Thumb! So? I m a Full Spine Adjuster! Why It LOOKS Fishy Medical necessity definition dictates that you must prioritize each area of complaint Every visit: S + O (P + ART) for every region treated 2 DX codes for each region Treatment plan for each/short and long term goals 12



13 Problem #2: Did Not Understand The Definitions of Maintenance Care He ONLY billed AT modifier, never ever moving a patient to maintenance care. Even in the details of the rebuttal from his attorney, he also argued that he "never delivered care that was not AT Modifier worthy". Understand the Rules Is All Care Medically Necessary? Who Knows KMC s Favorite? Clinically Appropriate Care Life enhancing Symptom relieving Wellness care Supportive care Maintenance care Medically Necessary Care Yields a significant improvement in clinical findings and patient functionality. 13




14 Maintenance CMS defines Maintenance Therapy as: "Chiropractic maintenance therapy is not considered to be medically reasonable or necessary under the Medicare program, and is therefore not payable. Maintenance therapy is defined as a treatment plan that seeks to prevent disease, promote health, and prolong and enhance the quality of life; or therapy that is performed to maintain or prevent deterioration of a chronic condition. When further clinical improvement cannot reasonably be expected from continuous ongoing care, and the chiropractic treatment becomes supportive rather than corrective in nature, the treatment is then considered maintenance therapy." GA Modifier What s Wrong with this Picture? A Better Way 14




15 Problem #3: Evidently Didn t Understand Episodic Care Episodes of Care The foundation for an episode is contained in the beginning four steps of documentation. There was confusion about what an episode of care is Therefore, the documentation necessary was NOT present Medicare documentation requirements are published. We, as doctors, must know how to diagnose, treat in episodes of care and dismiss patients from active treatment. Have written policies and procedures. Blatant Disregard Any Patients in Your Office in this Circumstance? 15


16 Problem #4: Didn t Understand Requirements and How to Use Software to Meet Them What the OIG Did in This Case Exact OIG Recommendations Extrapolation at Its Finest Refund $708,022 to the Federal Government and Establish adequate policies and procedures to ensure that chiropractic services billed to Medicare are medically necessary, correctly coded, and adequately documented. 16




17 Sure, let me just get my checkbook! They Talked to Patients What Should You Do Now? Don t Learn the Hard Way! The simple steps that could have been taken to avoid this nightmare How expensive was his inaction? $708K back to the government, and probably losing Medicare privileges! Don t let this be YOU! 17




18 A Warning the Should be Heeded The purpose of a compliance program is: To integrate policies and procedures into the physician s practice that are necessary to promote adherence to federal and state laws and statutes and regulations applicable to the delivery of healthcare services. Came out of the sentencing guidelines Affordable Care Act: Mandatory Compliance Plans Coming Soon CMS has NOT finalized the requirements CMS will advance specific proposals at some point in the future Is it Mandatory? Review the 7 Steps of the OIG Compliance Program 18




19 Where to Begin: Set Up Your Manual Step 1- Implement Policies and Procedures Understand the difference between the two Assess what existing policy and procedure is in place that needs attention Step 2- Compliance Officer or Contact Review the role of this person Everyone is responsible for compliance Officer is responsible for overseeing all manner of compliance, but doesn t work alone 19



20 Step 3- Employ Comprehensive Education and Training Training is going to be tracked and documented Webinars, seminars, conventions, and other on the job training should always be recorded when relative to a compliance related issue Step 4- Enforce Disciplinary Standards Review the code of conduct Explain why everyone must commit to compliance Get the Code of Conduct signed after all 7 steps have been reviewed Step 5- Respond Swiftly to Detected Offenses Everyone s eyes and ears must be open and watching at all times Overpayments to Medicare must be within 60 days of the detection Internal processes and audits will assist with the practice finding these occasional missteps Everyone must participate in supporting the compliance officer s efforts Step 6-Internal Audits and Monitoring More internal audits will take place now Four types of audits Documentation E/M Coding Audits Coding Audits EOB Audits Calendar of routine audits will be set 20




21 Step 6-Internal Audits and Monitoring Consider an outside entity to conduct a baseline audit on your behalf Use error rates to determine what is next Coding audits conducted by KMCU as part of PPP or ISP/PhD programs Step 7- Open Lines of Communication Insist on an Open Door Policy Everyone must report things they don t understand or are curious about Create the system that you ll use for reporting Step 7- Open Lines of Communication Install Compliance in Your Office None of this matters if you only talk and don t act Installation of compliance programs can take time Set aside appropriate time to do a little at a time for each of the 7 steps 21


22 Risk #1 Risk #2 Risk #3 22
23 Risk #4 Opportunity #1 Opportunity #2 Opportunity #3 23



24 Opportunity #4 Basics of Documentation Good Documentation Tells a Story Implement the Basics Basic documentation principles Proper use of abbreviations Addressing legibility Authentication of signatures Records management Managing the day-today flow of your patient records 24




25 The Marks of Bad Documentation Pencil/whiteout/erasures Illegible documents Non-standard abbreviations No date/no signature Blank spaces No identifying patient information (each page/side of page) Consents not documented Use blue or black ink Never use correction fluid or erase Correct errors by putting one line through it, make your correction, and initial and date the change Legibility Use Standard Abbreviations All abbreviations should be standard The easier your charts are to read, the better they will perform under scrutiny Supply a legend or key if you use non-standard abbreviations for any reason 25
 Don t add signature later Must be legal signature Signature must be authenticated Parent or Guardian Signature Everyone in office is a point of contact to recognize abuse")

26 Signature and Authentication Consent to Treat a Minor Must be provider of service Handwritten or electronic Must be legible Shared services must bear all signatures Policy in place to ensure timely signatures (48 to 72 hours) Don t add signature later Must be legal signature Signature must be authenticated Parent or Guardian Signature Everyone in office is a point of contact to recognize abuse or neglect (legally must report) A parent has the right to obtain a child's health information except when: State law does not require parental consent Separate guardian is appointed by the courts When the parent agrees to confidentiality When the provider suspects abuse or neglect Informed Consent NCQA Guidelines for Documentation Prior to treating a patient, the doctor must provide adequate information regarding the possible risks and benefits of and possible alternatives to a particular procedure Doctors must properly and clearly communicate with their patients If care or outcomes are called into question, documentation of this consent is vital Organization Patient identification Personal/Biographical data Provider identification Entry date Legibility Problem list Allergies Past medical history Smoking/Alcohol/Substance abuse Physical exam History and physical Working diagnosis Plan/Treatment Patient Education/Instructions Consults/X-ray/Lab/Imaging reports/referral records Follow up/return visits Medical care services/consults Immunization records Preventative services Advanced directives 26




27 Records Protection & Destruction There are national and local regulations to be followed as the custodian of record HIPAA-required protection of records How long to keep? 6 years HIPAA 10 years Medicare Advantage Forever per malpractice carrier Case Management Driven Documentation 27



28 Subjective?? NOT! What About This One? Daily Subjective? Objective?? Really? 28




29 Can You Tell What s Up? Assessment?? Guarded? Or This One? Medical Review Policies Aetna BCBS 29




30 Medicare Guidelines Our First Name is Doctor We are responsible for the welfare of our patients. Our primary job is to effectively document and manage the patient s episodic cases Our goal is to resolve their functional deficits. You Need Clarity FIRST Your patients must understand that their active treatment has a beginning, middle, and end, from the onset of care. If you are not clear on the definition of an episode of care, you will not explain this clearly 30


31 Let Them Know What to Expect Episodes of Care Teach your patient to be observant about their functional performance Let them know that will help you document their progress clearly and easily for their Insurance company Medicare Documentation Guidelines Initial Visit History Description of Present Illness Physical Exam Diagnosis Treatment Plan Date of initial treatment Subsequent Visits History Review of chief complaint Physical Exam Document daily treatment Progress related to treatment goals/plan 31

32 Impeccable Initial Visit/Episode Documentation Episodes of Care The Foundational Visit of the Episode Documentation LOOKS Different E/M visits should and will look different from daily visit notes The components are different The intent is different Initial visit documentation has a job to do 32







33 New Patient? New Condition? New Episode? These should be handled the same From a documentation point of view, they ARE the same Known as the E/M visit Treat if you wish, but THIS material must be covered History Exam INPUT E/M Visit Clinical Decision Making OUTPUT Let s Be Crystal Clear! Ever Want To Say This to a Patient? E/M services can be initial or established patient If a NEW patient, haven t been seen EVER or within THREE years Everyone else is an ESTABLISHED patient 33



34 You Be the Judge Easy to Follow? Initial Visit History 34



35 Initial Visit Examination Exam Helps Dr. Jeff Miller Start Your Examination with Outcomes Assessment Tools Visual Analog Scale Revised Oswestry Pain Drawings Roland-Morris Disability Neck Pain Disability Index Headache Disability Index Bournemouth Functional Rating Index 35
36 X-ray Policy To x-ray or not x-ray that is the question. Imaging and diagnostic testing are for documentation not education. There should never be a blanket x-ray policy in any office. Proper documentation is key in diagnostic imaging: you must have a solid rationale, and a report showing clinical outcome, otherwise the test is not considered medically necessary. X-ray Report Documenting X-ray Necessity Your documentation holds the key: Clinical indicators that make taking films an obvious choice Write your orders for the need for radiographic follow up in your documentation Remember to write the x-ray report Clinical Decision Making 36
37 The Assessment/Day 1.5 NP, New Condition, New Episode: requires the DX and TX plan to be completed as part of the foundational episode The DX and TX Plan will set the tone for all treatment Diagnosis Hierarchy Position 1 Nerve Position 2 Bone/Joint/Disc Position 3 & 4 Muscle/Disc/Other Position 3 & 4 Extremity/Catchall/Other You ve Already Decided You have likely already decided what you think is the best recipe Make it easy to recreate when it is time to create a written treatment plan Create your written standards for care 37

 Procedures (list) Cervical pillow Ice pack Biofreeze Nutrition pain pack Home traction unit Rehab equipment")

38 Codify it Now 26 Adjustments 8 Ext Adjustments 5 Ultrasound 4 EMS 23 Therapeutic Exercise 3 Re-exams The first step is to codify your preferences: mild through severe conditions, include length of treatment number of visits and which modalities and procedures may be utilized. Adjustments Modalities (list) Procedures (list) Cervical pillow Ice pack Biofreeze Nutrition pain pack Home traction unit Rehab equipment Cervical collar Tens unit Etc. Reverse Protocols Adjustments Modalities (list) Procedures (list) Cervical pillow Ice pack Biofreeze Nutrition pain pack Home traction unit Rehab equipment Cervical collar Tens unit Reverse Protocols Frequency and duration Treatment goals for each region/treatment to include long term goal An evaluation of treatment effectiveness measurement Date of the plan Meet the Requirements 38




39 CCGPP Prognostic Factors Older age History of prior episodes Severity of initial episode of injury Number of exacerbations Duration of current episode longer than 1 month Psycho-social factors CCGPP Prognostic Factors Pre-existing pathology Nature of employment Waiting more than 7 days to seek treatment Congenital Anomalies Patient compliance 39




40 EHR TX Plan Sample Let s Grade This One! Better? 40




41 You Did It!--Initial Visit Mastery Whether brand NP or existing patient with new condition, the components are the same Start the episode correctly and you ll end it perfectly A little time invested now, saves hours later! Find Your Way to the Codes 41




42 What Have YOU Done So Far? Got a Book?? Begin testing claims CMS has a process Check with each additional carrier When do they accept testing? Testing Anyone? Who s In Charge? Have you selected an ICD-10 project manager? Someone must coordinate and ensure all the steps get done What gets measured gets managed! 42


43 GEMS Code Map 43

 Some pointing based")


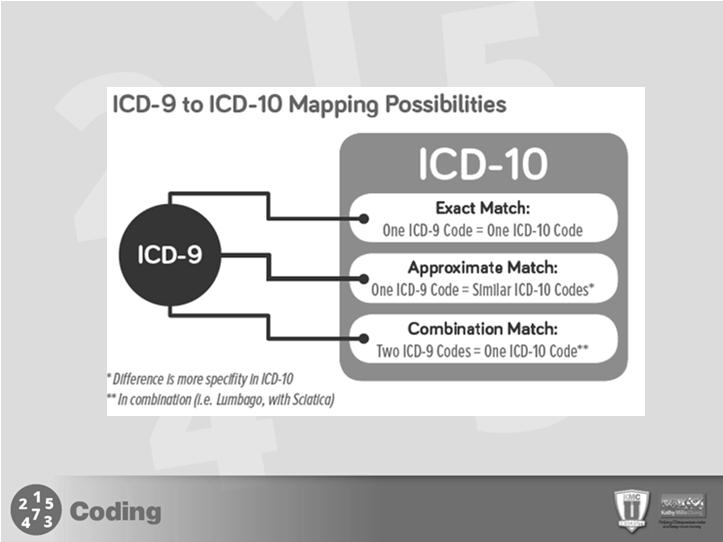
44 Can We Just Crosswalk from ICD-9? General Equivalence Mappings (GEMs) Some pointing based on the initial set up Three possible ways to define subluxation: M99.01, M99.11, or S13.11 Now we know Conversion Tools Conversion Tools 44




45 Medicare s GEM Guide Action Step: Write down your most commonly used codes Mapping Made Easy! 45

46 How are ICD-9 and ICD-10 Different? ICD-10 For Example ICD-10-CM code for chronic gout due to renal impairment, left shoulder, without tophus. ICD-9 ICD-10 Coding and Documentation Site Laterality 5 th or 6 th digit - Sciatica Left M54.31 Right M54.32 Episodes of care 7 th digit A D S Injuries Why the 7 th Digit? Most categories in chapter 19 have seventh character extensions Required for each applicable code, and most categories have three extensions A, Initial encounter D, Subsequent encounter S, Sequela 46




47 A vs. D Placeholder x character Placeholder character x in positions 4, 5, and/or 6 in certain codes to allow for future expansion. So sayeth ACA, Chiro Code, and KMC University 7 th Characters The 7 th character must always be the 7 th character in the data field. If a code that requires a 7 th character is not 6 characters, a placeholder x must be used to fill in the empty characters This information in NOT final Clarity will come as we inch closer to implementation or after implementation Follow Medicare guidance using A Stay Tuned! Key Takeaways So What is Excludes 1 or Excludes 2? Similar to Correct Coding Initiative Edits for CPT Codes Dictates when certain codes can be used together and when not The explanation will be helpful in the long run 47


48 Remember the CCI Edits? Excludes 1 - is used when two conditions cannot occur together or NOT CODED HERE! Mutually exclusive codes; two conditions that cannot be reported together (A condition may be acquired OR congenital but not both!) Remember the CCI Edits? Excludes 2 Indicates NOT INCLUDED HERE. Although the excluded condition is not part of condition, it is excluded from, a patient may have both conditions at the same time. The excluded code and the code above the excludes can be used together if the documentation supports them. Read the Instructions! Read the Instructions! 48

 Subcategories 4 th or 5 th characters (etiology, location, etc.")
49 Chapter 13-Diseases of the Musculoskeletal System and Soft Tissue But Wait! There s More! Our Wheelhouse M-00 through M-99 series Tabular list layout Confirm with Tabular List! Chapter 21 of them from A to Z (body system or condition) Block Ranges of categories (related conditions) Categories 3 characters (more specific condition) Subcategories 4 th or 5 th characters (etiology, location, etc.) Codes 6 th or 7 th characters (laterality, encounter, etc.)

 One-to-Five Mapping ICD-10 M54.14, M54.15, M54.")
50 Confirmation Required One-to-one Mapping Cervicalgia M54.2 Cervicalgia Thoracic or lumbosacral neuritis (radicular syndrome of the lower limbs) One-to-Five Mapping ICD-10 M54.14, M54.15, M54.16, M54.17, M54.18 Radiculopathy Deconditioning Syndrome 50





51 Combination Mapping Sciatica M54.30 Sciatica, unspecified side M54.31 Sciatica, right side M54.32 Sciatica, left side OR M54.40 Sciatica with lumbago, unspecified M54.41 Sciatica with lumbago, right side M54.42 Sciatica with lumbago, left side Talk About Detail! Take Cervical Sprain Could be S13.4xxA Could be S13.8xxA Much more detail is possible in ICD-10 Item one: sprain of ligaments of the cervical spine Item two: sprain of joints and ligaments of other parts of the neck An Example of 7 th Digit Unspecified Use Sparingly 51
 Never sequenced first Provide data about the cause,")
52 E Codes in ICD-9 Expanded External Cause Codes Do you use them? E844.8 Sucked up into a jet without damage to the airplane; ground crew V Y Codes Chapter 20: Guidelines for external causes of morbidity (V00-Y99) Never sequenced first Provide data about the cause, intent, place, activity, or status of the accident or patient No national requirement to use these codes, but voluntary reporting is encouraged Y92 Place of occurrence should be listed after other codes, used only once an initial encounter, in conjunction with Y93 Y93 Activity code should be used only once, at initial encounter V, W, X, Y Codes For Fun Bus Occupant V79.9 (collision with) Animal in traffic being ridden Bus Occupant V70.3 (collision with) animal, non-traffic Bus Occupant V70.4 (collision with) animal, while boarding or alighting Quick but Quality Routine Visit Documentation 52



53 Error Rate Information Insufficient documentation is a known issue in the chiropractic profession Failure to provide any documentation to auditors represents nearly 50% of the poor scores 53

 O = ART (DC s assessment per area) A = Doctor")
54 Medicare Documentation Guidelines What Does PART Mean, Anyway? Initial Visit History Description of Present Illness Physical Exam Diagnosis Treatment Plan Date of initial treatment Subsequent Visits History Review of chief complaint Physical Exam Document daily treatment Progress related to treatment goals/plan Example of PART Documentation Lumbar Subluxation PART example S = P (Patient s assessment per area) O = ART (DC s assessment per area) A = Doctor s Assessment (How and Why) P = Plan for today (what was done) Get Right To It 54





55 Best Practices for Gathering Functional Self-Assessment First, train them that it is their job to be observant about their functional deficits Help them understand that measurable information helps you to assist them in faster improvement Master Internal Systems that can Streamline this Process Team member driven documentation They gather relevant data You review out of sight of the patient then You lead the conversation Save as much as an hour a day Day to Day Visits-Part One Day to Day Visits Part Two 55



56 Ancillary Documentation Best Practices for Defining your Doctor s Assessment Remember it is all about Function, Function, FUNCTION Identify HOW the patient has improved Identify WHY they need continued care That is Medical Necessity by definition! 56




57 Maintenance Preventative or maintenance care defined as care to reduce the incidence or prevalence of illness, impairment, and risk factors and to promote optimal function. 57





58 Episodes of Care Maintenance Wellness Prevent disease Promote health Prolong/enhance the quality of life Supportive Maintain or prevent deterioration of a chronic condition 58
59 Anti-Trust Statement Compliant Financial Plans and Payment Plans Please be advised that any discussion which leads to an agreement as to price among competitors is a per se violation of the Sherman Act. Providers gathered in any setting must always exercise caution to avoid discussions or exchanges of information with their competitors on prices or pricing at meetings since such discussions or information exchanges may give rise to inferences of agreement. Any agreement not to compete among business firms is also a per se violation of the antitrust laws. Thus, no discussion of division of territories or customers, or limitation on nature of business, should be held at any function. Joint refusals to deal (boycotts), including discussions of blacklists, are likewise unlawful per se, and no discussions related to these practices are permitted. Discussion of fees by KMC University or examples used are for instructional purposes only should not be considered as a recommendation for any provider or group of providers. Meet Mrs. Jones Definitions 1. Dual Fee Schedules 2. Improper Time of Service Discounts Improper Collection Policies 3. Inducement Violations 4. False Claims Act Violations 5. Anti-kickback Statue Violations 59



![law] No more than $10 per item or $50 in the aggregate annually Even one free examination, x-ray, or therapy is a](/docs-images/79/79260689/images/60-3.jpg "risk 4.")
60 1. Avoid Dual Fee Schedules Charging more to insurance companies than you do to cash patients Considered illegal in many states Misrepresents charges to carriers False Claims Act violation May violate provider agreements Triggers investigations Florida Geico 2. Time of Service Discounts Discount based on bookkeeping savings May or may not be defined Often not defensible or unreasonable May not be permissible on Federally insured patients 3. Inducement Violations Per the OIG: incentives that are only nominal in value are NOT prohibited by [inducement law] No more than $10 per item or $50 in the aggregate annually Even one free examination, x-ray, or therapy is a risk 4. False Claims Act Violations Establishes liability when any person or entity improperly receives from or avoids payment to the Feds Prohibits knowingly presenting or causing to be presented, a false claim for payment or approval 60




61 4. False Claims Act Violations Prohibits knowingly presenting or causing to be presented, a false claim for payment or approval Examples: Waiving deductibles or co-payments and not reporting to carriers Up-coding for higher reimbursements Down-coding based on payer type Do Not Take This Lightly! 61

 and transfers of items or services for free or for other than fair")
62 Or This! 5. Anti-Kickback Violations A person who offers or transfers to a Medicare or Medicaid beneficiary any remuneration that the person knows or should know is likely to influence the beneficiary s selection of a particular provider, practitioner, or supplier of Medicare or Medicaid payable items or services may be liable for civil money penalties (CMPs) of up to $10,000 for each wrongful act. The statute defines remuneration to include, without limitation, waivers of copayments and deductible amounts (or parts thereof) and transfers of items or services for free or for other than fair market value. Why Worry? Who Cares What We Charge? Here s Who Cares! When insurance companies, state and federal payers are involved, there are state and federal regulations. If violated, carry serious risks, fines and penalties. Be very careful we have never been under more scrutiny 62
.")
 probation for two years, pay $10,000 in fines and reimburse the Board for its costs not to exceed $5,000. Why You Should Care!")
63 Here s Who Cares? State Board Actions DISCIPLINARY ACTION UPDATE Effective May 20, 2006, an Agreed Settlement of Disciplinary Action was entered into by Dr. X and the CPBN for violations of unprofessional conduct (NRS (10). The charges included failure to collect proper co-payment amounts, waiving deductibles and, by office policy, having a dual fee schedule, i.e., cash vs. insurance (NAC ) probation for two years, pay $10,000 in fines and reimburse the Board for its costs not to exceed $5,000. Why You Should Care! 2005: OIG study shows 67% of claims were fraudulent 2008: OIG proudly proclaims that for every $1 spent, they recouped $17 RAC Audits Probe Audits 2012: OIG Work Plan includes chiropractic again Their investigations = recoupment= BIG BUCKS $1.00 nets $7.70 State Rules & Regulations Time of Service Discount Percentages are permitted in some states. Not always defined! OIG indicates 5-15% per 2009 opinion. PIP law (FL) prohibits charging more to PI patients than other patients. NOTICE: STATE LAW DOES NOT SUPERCEDE FEDERAL REGULATIONS AGAINST GIFTS &INDUCEMENTS AND CHARGING LESS THAN FAIR MARKET VALUE! Actual Fees are in line with R/C and Fair Market Value Discounts for cash paying patients are legal Hardship agreements are in place and utilized Financial policy is solid and clearly explained Let s Fix This Mess! 63



64 Actual Fees are Correct Based on costs to deliver services Considers existing reimbursement data and allowable third party fees Are updated annually Should be compared to regional averages by CODE not physician Decide If You Want to Discount Use federal prompt pay discount guidelines for hardship policy Never discount on copay or deductible for insurance patients Never make side deals with the patient Remember, charge correctly, bill correctly, then COLLECT according to your policy Easiest Fix: join a DMPO You Are Likely Already Discounting When a patient that has insurance enters your office for care they are bringing another person to the relationship Initial Visit Exam: $120 X-Rays: $130 CMT: $ : $35 Total: $350 Routine Visit CMT $ : $ : $ : $35 Total: $185 Initial Visit Exam: $95 X-Rays: $75 CMT: $ : $15 Total: $ : $ : $ : $42.75 Routine Visit CMT $ : $ : $ : $15 Total: $95 100%Poverty: 75%Discount 125%Poverty: 50%Discount 150%Poverty: 25%Discount 64
65 Discounting and dual fees for cash patients can also put you at risk with your Provider Agreements as well, like those with BCBS, UHC, Aetna, etc. Many agreements have specific clauses that restricts this activity. Reference : Kennedy vs. Cigna Kennedy v. CIGNA, 924 F.2d 698 (7th Cir.) Cases on Waiver Feiler v. New Jersey Dental Assn, 467 A.2d 276 (N.J. Super Ct.) Plan sued provider after discovering he was waiving patient responsibility obligations. Plan argued provision in member s policy applied, which provided no payment would be made for charges which member was not legally obligated to pay. Court agreed with plan. If provider wanted to receive payment under plan, he must collect co-payments. Suit by state dental association against dentist for fraudulent billing practices. Court found dentist lied to payors when he submitted charge of $100 and only intended to collect $80 from payor and waive patient responsibility. Court ordered dentist to disclose waiver practice to all payors so they could make correct payments based on actual charges. Initial Visit Exam: $120 X-Rays: $130 CMT: $ : $35 Total: $350 Routine Visit CMT $ : $ : $ : $35 Total: $185 Initial Visit Capped Fee: $150 Or 20% Discount Modalities: $10 Procedures: $20 Routine Visit Capped Fee: $65 Or 20% Discount Re-Exams: $25 Each Film: $15 100%Poverty: 75%Discount 125%Poverty: 50%Discount 150%Poverty: 25%Discount 65




66 How Do We Join? What About Professional Courtesy? Review the Fact Sheet Who do you offer courtesy to? Staff? Other DCs? What about when insurance is involved? Write your policy Clear Understanding of Hardship and Discounted Fees Your hardship agreement can co-exist with other fee schedules. You must set the standard up front, have qualifying factors, and verify eligibility. Utilize a standardized form and system What may NOT be financial hardship? No insurance High deductible I don t wanna pay that much My other doctor didn t charge my copays Pulse and a spine Mistakes and Blunders 66



67 Co-Pay or Deductible Waivers for Hardship-(Fact Sheet) The waiver is not offered as part of any advertisement or solicitation; Waivers are not routinely offered to patients; The waiver occurs after determining in good faith that the individual is in financial need; The waiver occurs after reasonable collection efforts have failed Financial Hardship Form Need Help? 67
Getting Started with OIG Compliance
 Getting Started with OIG Compliance Kathy Mills Chang, MCS-P CCPC Do You Feel Like This? Or This? Does Your Business Deserve the Same Focus Your Patients Do? How This Training Will Protect You! Stay within
Getting Started with OIG Compliance Kathy Mills Chang, MCS-P CCPC Do You Feel Like This? Or This? Does Your Business Deserve the Same Focus Your Patients Do? How This Training Will Protect You! Stay within
Under the Magnifying Glass
 5 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
5 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
Certified Ophthalmic Executive (COE) Review Day
 Review Day") Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Certified Ophthalmic Executive (COE) Review Day Compliance Plan & Chart Audits Financial Disclosure The instructor acknowledges a financial interest in the subject matter of this presentation. Presented
Under the Magnifying Glass
 5 6 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
5 6 Most Common Documentation Mistakes And What to Do About Them Kathy Mills Chang, MCS-P, CCPC KMC University Why Is Documentation So Important? Ensures quality patient care Meets licensure requirements
Stark, False Claims and Anti- Kickback Laws: Easy Ways to Stay Compliant with the Big Three in Healthcare
 Stark, False Claims and Anti- Kickback Laws: Easy Ways to Stay Compliant with the Big Three in Healthcare In health care, we are blessed with an abundance of rules, policies, standards and laws. In Health
Stark, False Claims and Anti- Kickback Laws: Easy Ways to Stay Compliant with the Big Three in Healthcare In health care, we are blessed with an abundance of rules, policies, standards and laws. In Health
A Day in the Life of a Compliance Officer
 A Day in the Life of a Compliance Officer (for small physician practices) Mina Sellami, MBA, PMP, JD MedProv, LLC Julia Konovalov Medical Business Partners September 29, 2016 Agenda Government Regulations
A Day in the Life of a Compliance Officer (for small physician practices) Mina Sellami, MBA, PMP, JD MedProv, LLC Julia Konovalov Medical Business Partners September 29, 2016 Agenda Government Regulations
BILLING COMPLIANCE HANDBOOK
 BILLING COMPLIANCE HANDBOOK Southeastern Pathology Associates Original: August 8, 2010 Revised: September 12, 2011 Reaffirmed: April 18, 2012 Reaffirmed: March 26, 2013 Reaffirmed: May 12, 2015 Reaffirmed:
BILLING COMPLIANCE HANDBOOK Southeastern Pathology Associates Original: August 8, 2010 Revised: September 12, 2011 Reaffirmed: April 18, 2012 Reaffirmed: March 26, 2013 Reaffirmed: May 12, 2015 Reaffirmed:
Recover Health Training. Corporate Compliance Plan Code of Conduct Fraud & Abuse
 Recover Health Training Corporate Compliance Plan Code of Conduct Fraud & Abuse 1 The Course Objectives When you complete this course you will be able to: Understand Recover Health s reasons for implementing
Recover Health Training Corporate Compliance Plan Code of Conduct Fraud & Abuse 1 The Course Objectives When you complete this course you will be able to: Understand Recover Health s reasons for implementing
Assessment. SMP Foundations Training Kit. Table of Contents
 SMP Foundations Training Kit Assessment Table of Contents Participant Assessment Questions and Answer Form Assessment Questions... 10 Pages Answer Form... 2 Pages Trainer s Resources Answer Key... 2 Pages
SMP Foundations Training Kit Assessment Table of Contents Participant Assessment Questions and Answer Form Assessment Questions... 10 Pages Answer Form... 2 Pages Trainer s Resources Answer Key... 2 Pages
Compliance Program Updated August 2017
 Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
Compliance Program Updated August 2017 Table of Contents Section I. Purpose of the Compliance Program... 3 Section II. Elements of an Effective Compliance Program... 4 A. Written Policies and Procedures...
AVOIDING HEALTHCARE FRAUD AND ABUSE; Responsibility, Protection, Prevention
 AVOIDING HEALTHCARE FRAUD AND ABUSE; Responsibility, Protection, Prevention Presented by: www.thehealthlawfirm.com Copyright 2017. George F. Indest III. All rights reserved. George F. Indest III, J.D.,
AVOIDING HEALTHCARE FRAUD AND ABUSE; Responsibility, Protection, Prevention Presented by: www.thehealthlawfirm.com Copyright 2017. George F. Indest III. All rights reserved. George F. Indest III, J.D.,
Responding to Today s Health Care Regulatory Environment
 Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
Responding to Today s Health Care Regulatory Environment St. Joseph s Health Michael R. Holper SVP, Compliance and Audit Services October 26, 2016 2014 Trinity Health. All Rights Reserved. 1 We operate
HealthStream Regulatory Script. Corporate Compliance: A Proactive Stance. Version: [February 2007]
![HealthStream Regulatory Script. Corporate Compliance: A Proactive Stance. Version: [February 2007]](/thumbs/80/80691517.jpg "HealthStream Regulatory Script. Corporate Compliance: A Proactive Stance. Version: [February 2007]") HealthStream Regulatory Script Corporate Compliance: A Proactive Stance Version: [February 2007] Lesson 1: Introduction Lesson 2: Importance of Compliance & Compliance Programs Lesson 3: Laws and Regulations
HealthStream Regulatory Script Corporate Compliance: A Proactive Stance Version: [February 2007] Lesson 1: Introduction Lesson 2: Importance of Compliance & Compliance Programs Lesson 3: Laws and Regulations
CRCE Exam Study Manual Update for 2017
 CRCE Exam Study Manual Update for 2017 This document reflects updates made to the instructional content from the Certified Revenue Cycle Executive (CRCE-I, CRCE-P) Exam Study Manual - 2016 to the 2017
CRCE Exam Study Manual Update for 2017 This document reflects updates made to the instructional content from the Certified Revenue Cycle Executive (CRCE-I, CRCE-P) Exam Study Manual - 2016 to the 2017
Medicare Fraud & Abuse: Prevention, Detection, and Reporting ICN
 Medicare Fraud & Abuse: Prevention, Detection, and Reporting ICN 908103 1 Disclaimers This presentation was current at the time it was published or uploaded onto the web. Medicare policy changes frequently
Medicare Fraud & Abuse: Prevention, Detection, and Reporting ICN 908103 1 Disclaimers This presentation was current at the time it was published or uploaded onto the web. Medicare policy changes frequently
Compliance Considerations for Clinical Laboratories
 Compliance Considerations for Clinical Laboratories Elizabeth Sullivan, Esq. McDonald Hopkins, LLC 600 Superior Ave., E, Suite 2100 Cleveland, Ohio 44114 P: 216.348.5401 / F: 216.348.5474 esullivan@mcdonaldhopkins.com
Compliance Considerations for Clinical Laboratories Elizabeth Sullivan, Esq. McDonald Hopkins, LLC 600 Superior Ave., E, Suite 2100 Cleveland, Ohio 44114 P: 216.348.5401 / F: 216.348.5474 esullivan@mcdonaldhopkins.com
6/25/2013. Knowledge and Education. Objectives ZPIC, RAC and MAC Audits. After attending this presentation, the attendees will be able to :
 Objectives ZPIC, RAC and MAC Audits Approach After attending this presentation, the attendees will be able to : 1. Understand the different types of audits related to reimbursement: ZPIC, RAC, and MAC
Objectives ZPIC, RAC and MAC Audits Approach After attending this presentation, the attendees will be able to : 1. Understand the different types of audits related to reimbursement: ZPIC, RAC, and MAC
PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE COMPLIANCE AND ETHICS PROGRAM MANUAL
 PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE COMPLIANCE AND ETHICS PROGRAM MANUAL I. COMPLIANCE AND ETHICS PROGRAM BACKGROUND Philadelphia College of Osteopathic Medicine (PCOM) is committed to upholding
PHILADELPHIA COLLEGE OF OSTEOPATHIC MEDICINE COMPLIANCE AND ETHICS PROGRAM MANUAL I. COMPLIANCE AND ETHICS PROGRAM BACKGROUND Philadelphia College of Osteopathic Medicine (PCOM) is committed to upholding
CORPORATE COMPLIANCE POLICY AUDIT & CROSSWALK WHERE ADDRESSED
 QUALITY OF CARE Sufficient Staffing Inadequate staffing levels or insufficiently trained (inadequate clinical expertise) or insufficiently supervised staff providing medical, nursing, and related services
QUALITY OF CARE Sufficient Staffing Inadequate staffing levels or insufficiently trained (inadequate clinical expertise) or insufficiently supervised staff providing medical, nursing, and related services
SNF Compliance: What s at Stake?
 SNF Compliance: What s at Stake? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Elisa Bovee, MS OTR/L Vice President of Operations About Elisa Elisa
SNF Compliance: What s at Stake? HARMONY UNIVERSITY The Provider Unit of Harmony Healthcare International, Inc. (HHI) Presented by: Elisa Bovee, MS OTR/L Vice President of Operations About Elisa Elisa
Topics. Overview of the Medicare Recovery Audit Contractor (RAC) Understanding Medicaid Integrity Contractor
 Understanding Medicaid Integrity Contractor") RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
RACS, ZPICS & MICS John Falcetano, CHC-F, CCEP-F, CHPC, CHRC, CIA Chief Audit and Compliance Officer University Health Systems of Eastern Carolina jfalceta@uhseast.com Topics Overview of the Medicare Recovery
A Review of Current EMTALA and Florida Law
 A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
A Review of Current EMTALA and Florida Law South Carolina Hospital Fined $1.28 Million for EMTALA violations Doctor fined $40,000 for not showing up at Emergency Room Chicago Hospital and Docs settle EMTALA
Compliance Program And Code of Conduct. United Regional Health Care System
 Compliance Program And Code of Conduct United Regional Health Care System TABLE OF CONTENTS Page MESSAGE FROM OUR PRESIDENT... 1 COMPLIANCE PROGRAM... 2 Program Structure...2 Management s Responsibilities
Compliance Program And Code of Conduct United Regional Health Care System TABLE OF CONTENTS Page MESSAGE FROM OUR PRESIDENT... 1 COMPLIANCE PROGRAM... 2 Program Structure...2 Management s Responsibilities
Compliance Plan. Table of Contents. Introduction... 3
 Compliance Plan Compliance Plan Table of Contents Introduction... 3 Administrative Structure... 4 A. CorporateCompliance Officer... 4 B. Compliance Committee... 5 C. Hospital Compliance Officer Communications...
Compliance Plan Compliance Plan Table of Contents Introduction... 3 Administrative Structure... 4 A. CorporateCompliance Officer... 4 B. Compliance Committee... 5 C. Hospital Compliance Officer Communications...
2013 AHLA Physicians and Physicians Organization Law Institute. Presented by Judd Harwood & Lori Foley. Agenda
 BUYER BEWARE! THE VALUE OF DUE DILIGENCE IN HOSPITAL-PHYSICIAN TRANSACTIONS 2013 AHLA Physicians and Physicians Organization Law Institute Presented by Judd Harwood & Lori Foley Agenda I. Opening Remarks
BUYER BEWARE! THE VALUE OF DUE DILIGENCE IN HOSPITAL-PHYSICIAN TRANSACTIONS 2013 AHLA Physicians and Physicians Organization Law Institute Presented by Judd Harwood & Lori Foley Agenda I. Opening Remarks
4/20/2015. NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals. Today s Objectives. Background
 NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
NE Home Care & Hospice Conference: Strategic Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Consulting Services Pamela Meliso, JD, MPH Director of Consulting Services Today
Managing Towards Compliance
 Managing Towards Compliance Presented by Bruce Rappoport, MD, CPC, CPCO AAPC National Conference April 14, 2014 Disclaimer This presentation is designed to provide educational information in regard to
Managing Towards Compliance Presented by Bruce Rappoport, MD, CPC, CPCO AAPC National Conference April 14, 2014 Disclaimer This presentation is designed to provide educational information in regard to
Addressing Documentation Insufficiencies
 Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
Objectives Addressing Documentation Insufficiencies ICAHN June 9,2015 Glenn Krauss, BBA, RHIA, CCS, FCS, PCS,CCS-P, CPUR, C-CDI, CCDS, C- DAM Understand and appreciate physician frustrations with the EHR
OIG Risk Areas: Anti- Supplementation; Therapy Services, Physicial Self-Referral & Hospice
 OIG Risk Areas: Anti- Supplementation; Therapy Services, Physicial Self-Referral & Hospice Presented by: Ken Burgess, Esq. Paul Pitts, Esq. Suzie Berregaard, Esq. Where We ve Been & Today s Topics Review
OIG Risk Areas: Anti- Supplementation; Therapy Services, Physicial Self-Referral & Hospice Presented by: Ken Burgess, Esq. Paul Pitts, Esq. Suzie Berregaard, Esq. Where We ve Been & Today s Topics Review
CCT Exam Study Manual Update for 2018
 CCT Exam Study Manual Update for 2018 This document reflects updates made to the instructional content from the CCT Exam Study Manual 2017 to the 2018 version of the manual. This does not include updates
CCT Exam Study Manual Update for 2018 This document reflects updates made to the instructional content from the CCT Exam Study Manual 2017 to the 2018 version of the manual. This does not include updates
WOW! Kathy s. Words of Wisdom. The Compliance Corner. In this issue: December 2013 Theme: Collections. Kathy s Opening Message. The Compliance Corner
 Kathy s WOW! Words of Wisdom December 2013 Theme: Collections In this issue: Kathy s Opening Message The Compliance Corner KMC University s Q&As Upcoming AnswerCall and Live Webinar Information ICD-10
Kathy s WOW! Words of Wisdom December 2013 Theme: Collections In this issue: Kathy s Opening Message The Compliance Corner KMC University s Q&As Upcoming AnswerCall and Live Webinar Information ICD-10
San Francisco Department of Public Health
 San Francisco Department of Public Health Barbara A. Garcia, MPA Director of Health City and County of San Francisco Edwin M. Lee, Mayor San Francisco Department of Public Health Policy & Procedure Detail*
San Francisco Department of Public Health Barbara A. Garcia, MPA Director of Health City and County of San Francisco Edwin M. Lee, Mayor San Francisco Department of Public Health Policy & Procedure Detail*
Chiropractic Record Keeping
 Chiropractic Record Keeping (DeskBook Chapter 4.1) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science, Accounting
Chiropractic Record Keeping (DeskBook Chapter 4.1) Presented by Evan M. Gwilliam, DC MBA BS CPC CCPC NCICS CCCPC CPC-I MCS-P CPMA Vice President 1 Dr. Evan Gwilliam Education Bachelor s of Science, Accounting
Informed Consent for Chiropractic Care
 Informed Consent for Chiropractic Care When a patient seeks chiropractic health care and we accept a patient for such care, it is essential for both of us to be working toward the same objective. This
Informed Consent for Chiropractic Care When a patient seeks chiropractic health care and we accept a patient for such care, it is essential for both of us to be working toward the same objective. This
PROPOSED REGULATION OF THE CHIROPRACTIC PHYSICIANS BOARD OF NEVADA. LCB File No. R October 3, 2005
 PROPOSED REGULATION OF THE CHIROPRACTIC PHYSICIANS BOARD OF NEVADA LCB File No. R140-05 October 3, 2005 EXPLANATION Matter in italics is new; matter in brackets [omitted material] is material to be omitted.
PROPOSED REGULATION OF THE CHIROPRACTIC PHYSICIANS BOARD OF NEVADA LCB File No. R140-05 October 3, 2005 EXPLANATION Matter in italics is new; matter in brackets [omitted material] is material to be omitted.
UNIVERSITY OF ROCHESTER MEDICAL CENTER BILLING COMPLIANCE PLAN
 UNIVERSITY OF ROCHESTER MEDICAL CENTER BILLING COMPLIANCE PLAN Revised December 31, 1998 INTRODUCTION This plan is an integral part of the University s ongoing efforts to achieve compliance with federal
UNIVERSITY OF ROCHESTER MEDICAL CENTER BILLING COMPLIANCE PLAN Revised December 31, 1998 INTRODUCTION This plan is an integral part of the University s ongoing efforts to achieve compliance with federal
601-Audit Plan for Medicare s Shared Visit Rule
 601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
601-Audit Plan for Medicare s Shared Visit Rule Elin Baklid-Kunz, MBA, CPC, CCS Health Care Compliance Association 6500 Barrie Road, Suite 250, Minneapolis, MN 55435 888-580-8373 www.hcca-info.org Presentation
THE MONTEFIORE ACO CODE OF CONDUCT
 THE MONTEFIORE ACO CODE OF CONDUCT 2017 Approved by the Board of Directors on March 10, 2017 Our Commitment to Compliance As a central part of its Compliance Program, the Bronx Accountable Healthcare Network
THE MONTEFIORE ACO CODE OF CONDUCT 2017 Approved by the Board of Directors on March 10, 2017 Our Commitment to Compliance As a central part of its Compliance Program, the Bronx Accountable Healthcare Network
Compliance Program Code of Conduct
 City and County of San Francisco Department of Public Health Compliance Program Code of Conduct Purpose of our Code of Conduct The Department of Public Health of the City and County of San Francisco is
City and County of San Francisco Department of Public Health Compliance Program Code of Conduct Purpose of our Code of Conduct The Department of Public Health of the City and County of San Francisco is
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT
 CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
CONTRACT YEAR 2011 MEDICARE ADVANTAGE PRIVATE FEE-FOR-SERVICE PLAN MODEL TERMS AND CONDITIONS OF PAYMENT Table of Contents 1. Introduction 2. When a provider is deemed to accept Flexi Blue PFFS terms and
TOP Education s 2018 Synergy Conference
 TOP Education s 2018 Synergy Conference Medicare Active to Maintenance 1 CEU Presented By: Mark A. Davini, DC, DABCN Please scan IN at the start of class Please scan OUT at the end of class You must attend
TOP Education s 2018 Synergy Conference Medicare Active to Maintenance 1 CEU Presented By: Mark A. Davini, DC, DABCN Please scan IN at the start of class Please scan OUT at the end of class You must attend
What s New with the NYS OMIG Audit Process. NYSHFA Nurse Leadership Conference April 23, Disclosure
 What s New with the NYS OMIG Audit Process NYSHFA Nurse Leadership Conference April 23, 2015 Disclosure Information contained in this program has been collected and collated by Zimmet Healthcare Services
What s New with the NYS OMIG Audit Process NYSHFA Nurse Leadership Conference April 23, 2015 Disclosure Information contained in this program has been collected and collated by Zimmet Healthcare Services
Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training 2015
 Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training 2015 Overview This Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training for first-tier, downstream and related
Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training 2015 Overview This Medicare Advantage and Part D Fraud, Waste and Abuse Compliance Training for first-tier, downstream and related
UCLA HEALTH SYSTEM CODE OF CONDUCT
 UCLA HEALTH SYSTEM CODE OF CONDUCT STANDARD 1 - QUALITY OF CARE The University s health centers and health systems will provide quality health care that is appropriate, medically necessary, and efficient.
UCLA HEALTH SYSTEM CODE OF CONDUCT STANDARD 1 - QUALITY OF CARE The University s health centers and health systems will provide quality health care that is appropriate, medically necessary, and efficient.
STANDARDS OF CONDUCT SCH
 STANDARDS OF CONDUCT SCH01242018 2018 LETTER FROM THE CEO Welcome, Thank you for choosing St. Croix Hospice. The care you provide impacts our patients, families, caregivers, and countless others every
STANDARDS OF CONDUCT SCH01242018 2018 LETTER FROM THE CEO Welcome, Thank you for choosing St. Croix Hospice. The care you provide impacts our patients, families, caregivers, and countless others every
Hospice House Network Inpatient Conference
 Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
Hospice House Network Inpatient t Conference Trends & Recent Developments in Hospice General Inpatient Care Policy and Enforcement June 7, 2013 1 www.morganlewis.com Presented by Howard J. Young, Esq.
This Material is Copyright Protected
 ICD-10 Utilization in the NEW World With Mario Fucinari DC, CCSP, CPCO, MCS-P, MCS-I Presented by NCMIC The information contained in these notes is for educational purposes and is not intended to be and
ICD-10 Utilization in the NEW World With Mario Fucinari DC, CCSP, CPCO, MCS-P, MCS-I Presented by NCMIC The information contained in these notes is for educational purposes and is not intended to be and
Our Services Include. Our Credentials
 is a healthcare consulting and education firm providing services such as: IRO services, practice management and assessment services, A/R management and oversight, new practice set up that includes lease
is a healthcare consulting and education firm providing services such as: IRO services, practice management and assessment services, A/R management and oversight, new practice set up that includes lease
CDx ANNUAL PHYSICIAN CLIENT NOTICE
 CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
CDx ANNUAL PHYSICIAN CLIENT NOTICE - 2018 CDX Diagnostics is providing this annual notice in accordance with the recommendations made by the Office of Inspector General (OIG) as part of our CDx Compliance
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals
 NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
NE Home Care Conference: Effective & Efficient Preparation for Medicare Audits & Appeals Cheryl Leslie, RN, MPH Director of Home Care & Hospice Services Pamela Meliso, JD, MPH Director of Consulting &
Compliance Program, Code of Conduct, and HIPAA
 Compliance Program, Code of Conduct, and HIPAA Agenda Introduction to Compliance The Compliance Program Code of Conduct Reporting Concerns HIPAA Why have a Compliance Program Procedures to follow applicable
Compliance Program, Code of Conduct, and HIPAA Agenda Introduction to Compliance The Compliance Program Code of Conduct Reporting Concerns HIPAA Why have a Compliance Program Procedures to follow applicable
General Documentation Compliance. Review for Provider Reappointment
 U N C U H N E C A L H T E H A L C T A H R E C A S R Y E S T E M General Documentation Compliance Review for Provider Reappointment May 2018 Objectives 1 2 Review the principles of compliant billing and
U N C U H N E C A L H T E H A L C T A H R E C A S R Y E S T E M General Documentation Compliance Review for Provider Reappointment May 2018 Objectives 1 2 Review the principles of compliant billing and
Medicare Advantage and Part D Compliance Training. 42 CFR Parts and
 Medicare Advantage and Part D Compliance Training 42 CFR Parts 422.503 and 423.504 Background > As a Medicare Advantage (MA) and Part D (PDP) Plan Sponsor ( Sponsor ), Blue Cross and Blue Shield Northern
Medicare Advantage and Part D Compliance Training 42 CFR Parts 422.503 and 423.504 Background > As a Medicare Advantage (MA) and Part D (PDP) Plan Sponsor ( Sponsor ), Blue Cross and Blue Shield Northern
Code of Conduct. at Stamford Hospital
 Code of Conduct at Stamford Hospital As a Planetree hospital, we are committed to personalizing, humanizing and demystifying the healthcare experience for patients and their families. Our approach is holistic
Code of Conduct at Stamford Hospital As a Planetree hospital, we are committed to personalizing, humanizing and demystifying the healthcare experience for patients and their families. Our approach is holistic
Preventing Fraud and Abuse in Health Care
 Preventing Fraud and Abuse in Health Care Corporate Compliance what is it? Corporate Compliance is about the effort to fight healthcare fraud and abuse by making it a state and federal criminal offense
Preventing Fraud and Abuse in Health Care Corporate Compliance what is it? Corporate Compliance is about the effort to fight healthcare fraud and abuse by making it a state and federal criminal offense
April, 2007 QUESTIONABLE PRACTICES BY HOSPICES AND NURSING HOMES UNDER HEALTH CARE FRAUD AND ABUSE RULES
 HOSPICE AND PALLIATIVE CARE PRACTICE GROUP: Mary H. Michal, Chair Linda Dawson Meg S.L. Pekarske Matthew K. McManus LONG TERM CARE AND SENIOR HOUSING PRACTICE GROUP: Robert J. Heath, Chair Burton A. Wagner
HOSPICE AND PALLIATIVE CARE PRACTICE GROUP: Mary H. Michal, Chair Linda Dawson Meg S.L. Pekarske Matthew K. McManus LONG TERM CARE AND SENIOR HOUSING PRACTICE GROUP: Robert J. Heath, Chair Burton A. Wagner
1/21/2011. Cindy C. Parman, CPC, CPC H Coding Strategies, Inc.
 Cindy C. Parman, CPC, CPC H Coding Strategies, Inc. www.codingstrategies.com The format and/or content of this presentation is copyright 2011 by Coding Strategies, Inc. (CSI), Powder Springs, GA. This
Cindy C. Parman, CPC, CPC H Coding Strategies, Inc. www.codingstrategies.com The format and/or content of this presentation is copyright 2011 by Coding Strategies, Inc. (CSI), Powder Springs, GA. This
One Year Later THE IMPACT OF HEALTH CARE REFORM on Health Care Provider Audits and Compliance Programs
 24 Health Care Law One Year Later THE IMPACT OF HEALTH CARE REFORM on Health Care Provider Audits and Compliance Programs By Andrew B. Wachler, Jennifer Colagiovanni, and Christopher J. Laney FAST FACTS:
24 Health Care Law One Year Later THE IMPACT OF HEALTH CARE REFORM on Health Care Provider Audits and Compliance Programs By Andrew B. Wachler, Jennifer Colagiovanni, and Christopher J. Laney FAST FACTS:
9/25/2012 AGENDA. Set the Stage Monitoring versus Audit Identifying Risk Strategies related to an audit plan Corrective Action Plans Examples
 The Art and Science of Designing a Physician Practice Audit : Unique Techniques Lori Laubach, Partner MOSS ADAMS LLP 1 AGENDA Set the Stage Monitoring versus Audit Identifying Risk Strategies related to
The Art and Science of Designing a Physician Practice Audit : Unique Techniques Lori Laubach, Partner MOSS ADAMS LLP 1 AGENDA Set the Stage Monitoring versus Audit Identifying Risk Strategies related to
Compliant Documentation for Coding and Billing. Caren Swartz CPC,CPMA,CPC-H,CPC-I
 Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
Compliant Documentation for Coding and Billing Caren Swartz CPC,CPMA,CPC-H,CPC-I caren@practiceintegrity.com Disclaimer Information contained in this text is based on CPT, ICD-9-CM and HCPCS rules and
INFORMATION ABOUT YOUR OXFORD COVERAGE REIMBURSEMENT PART I OXFORD HEALTH PLANS OXFORD HEALTH PLANS (NJ), INC.
, INC.") OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
OXFORD HEALTH PLANS (NJ), INC. INFORMATION ABOUT YOUR OXFORD COVERAGE PART I REIMBURSEMENT Overview of Provider Reimbursement Methodologies Generally, Oxford pays Network Providers on a fee-for-service
OIG Hospice Risk Areas With Footnotes
 Moreover, the compliance programs should address the ramifications of failing to cease and correct any conduct criticized in a Special Fraud Alert, if applicable to hospices, or to take reasonable action
Moreover, the compliance programs should address the ramifications of failing to cease and correct any conduct criticized in a Special Fraud Alert, if applicable to hospices, or to take reasonable action
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care
 Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
Becoming a Champion of Physician and Hospital Alignment: Focusing on Length of Stay, Discipline and Standards of Care Marc Tucker, DO Senior Director Audit, Compliance & Education AHA Solutions, Inc.,
3/16/2016. Swapping, Kickbacks, Fair Market Value: Risks for a Post-Acute Provider. AKS designed to prevent improper referrals, which can lead to:
 Swapping, Kickbacks, Fair Market Value: Risks for a Post-Acute Provider Alan Schabes, Partner Benesch, Friedlander, Coplan & Aronoff LLP Shannon Drake, VP, Associate General Counsel Kindred at Home Amanda
Swapping, Kickbacks, Fair Market Value: Risks for a Post-Acute Provider Alan Schabes, Partner Benesch, Friedlander, Coplan & Aronoff LLP Shannon Drake, VP, Associate General Counsel Kindred at Home Amanda
The Business of Medicine
 The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
The Business of Medicine Coding as a profession Objectives How the coder fits in Hospital vs. physician services Hierarchy of providers Reimbursement aspects Payers Medical necessity ABN 1 Regulations
Learning Objectives. The EMTALA Framework. EMTALA Update: Challenges in Community and Specialty Hospitals. Originally known as Anti-Dumping Law
 EMTALA Update: Challenges in Community and Specialty Hospitals Presented by Jan Corcoran, RN, BS, CEN Divisional Director of Clinical Services Learning Objectives 1) Describe the definition and history
EMTALA Update: Challenges in Community and Specialty Hospitals Presented by Jan Corcoran, RN, BS, CEN Divisional Director of Clinical Services Learning Objectives 1) Describe the definition and history
Swapping, Kickbacks, Fair Market Value: Risks for a Post-Acute Provider
 Swapping, Kickbacks, Fair Market Value: Risks for a Post-Acute Provider Alan Schabes, Partner Benesch, Friedlander, Coplan & Aronoff LLP Shannon Drake, VP, Associate General Counsel Kindred at Home Amanda
Swapping, Kickbacks, Fair Market Value: Risks for a Post-Acute Provider Alan Schabes, Partner Benesch, Friedlander, Coplan & Aronoff LLP Shannon Drake, VP, Associate General Counsel Kindred at Home Amanda
Cloning and Other Compliance Risks in Electronic Medical Records
 Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Cloning and Other Compliance Risks in Electronic Medical Records Lori Laubach, Partner, Moss Adams LLP Catherine Wakefield, Vice President, Corporate Compliance and Internal Audit, MultiCare 1 AGENDA Basic
Alignment. Alignment Healthcare
 Alignment CODE OF CONDUCT Alignment Healthcare Our commitment to ethical conduct and compliance depends on all Alignment Healthcare personnel. If you find yourself in an ethical dilemma or suspect inappropriate
Alignment CODE OF CONDUCT Alignment Healthcare Our commitment to ethical conduct and compliance depends on all Alignment Healthcare personnel. If you find yourself in an ethical dilemma or suspect inappropriate
RUTGERS BIOMEDICAL AND HEALTH SCIENCES CODE OF CON DU CT
 RUTGERS BIOMEDICAL AND HEALTH SCIENCES CODE OF CONDUCT PREAMBLE On August 22, 2012, Governor Chris Christie signed legislation into law known as the New Jersey Medical and Health Sciences Education Restructuring
RUTGERS BIOMEDICAL AND HEALTH SCIENCES CODE OF CONDUCT PREAMBLE On August 22, 2012, Governor Chris Christie signed legislation into law known as the New Jersey Medical and Health Sciences Education Restructuring
Annual Leadership Institute August 25, Triple Check: A Process for Preventing False Claims
 Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
Annual Leadership Institute August 25, 2016 Triple Check: A Process for Preventing False Claims 1 Your presenter today is: Sophie A. Campbell, MSN, RN, CRRN, RAC-CT, CNDLTC Director, Clinical Advisory
The Intersection of Compliance and Quality Health Care Compliance Association North Central Regional Annual Conference
 The Intersection of Compliance and Quality Health Care Compliance Association North Central Regional Annual Conference October 1, 2010 Mark J. Swearingen, Esq. Hall, Render, Killian, Heath & Lyman One
The Intersection of Compliance and Quality Health Care Compliance Association North Central Regional Annual Conference October 1, 2010 Mark J. Swearingen, Esq. Hall, Render, Killian, Heath & Lyman One
Welcome to the beginning of optimal health!
 Welcome to the beginning of optimal health! would like to thank you for choosing us to partner with you as you embark on your journey towards optimal health! We ve developed this guide to help you prepare
Welcome to the beginning of optimal health! would like to thank you for choosing us to partner with you as you embark on your journey towards optimal health! We ve developed this guide to help you prepare
Medicare Chiropractic Documentation Guidelines
 Medicare Chiropractic Documentation Guidelines Subsequent Visits Correct documentation is the key to passing a Medicare Chiropractic audit. This tutorial goes through the documentation guidelines stepby-step
Medicare Chiropractic Documentation Guidelines Subsequent Visits Correct documentation is the key to passing a Medicare Chiropractic audit. This tutorial goes through the documentation guidelines stepby-step
Diane Meyer, CHC (650) Agenda
 Agenda") The Road Ahead and How to Navigate It Kevin D. Lyles, Esq. kdlyles@jonesday.com (614) 281-3821 Diane Meyer, CHC DMeyer@stanfordmed.org (650) 724-2572 Frank E. Sheeder, Esq. fesheeder@jonesday.com (214)
The Road Ahead and How to Navigate It Kevin D. Lyles, Esq. kdlyles@jonesday.com (614) 281-3821 Diane Meyer, CHC DMeyer@stanfordmed.org (650) 724-2572 Frank E. Sheeder, Esq. fesheeder@jonesday.com (214)
Risk Management including Documentation
 Risk Management including Documentation Stephen M. Perle, DC, MS Professor of Clinical Sciences University of Bridgeport College of Chiropractic No competing interests No association with providers of
Risk Management including Documentation Stephen M. Perle, DC, MS Professor of Clinical Sciences University of Bridgeport College of Chiropractic No competing interests No association with providers of
Are they coming to get you! Todd Thomas, CCS-P
 Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
Are they coming to get you! Todd Thomas, CCS-P Who is coming for you? Medicare Administrative Contractors (MACs) Recovery Audit Contractors (RACs) Medicaid Recovery Audit Contractors (MACs) Comprehensive
DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL
 DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL Washington, D.C. 20201 The Office of Inspector General (OIG) for the U.S. Department of Health & Human Services has created the educational
DEPARTMENT OF HEALTH & HUMAN SERVICES OFFICE OF INSPECTOR GENERAL Washington, D.C. 20201 The Office of Inspector General (OIG) for the U.S. Department of Health & Human Services has created the educational
1.Cultural & Linguistic Competence. 2.Model of Care for Special Needs Patients. 3.Combating Medicare Fraud, Waste and Abuse. Revised January 2017
 Corporate Compliance Training: 1.Cultural & Linguistic Competence 2.Model of Care for Special Needs Patients 3.Combating Medicare Fraud, Waste and Abuse Revised January 2017 1 This training presentation
Corporate Compliance Training: 1.Cultural & Linguistic Competence 2.Model of Care for Special Needs Patients 3.Combating Medicare Fraud, Waste and Abuse Revised January 2017 1 This training presentation
Managed Care Fraud: Enforcement and Compliance HCCA Compliance Institute March 28, 2017
 Managed Care Fraud: Enforcement and Compliance HCCA Compliance Institute March 28, 2017 Pamela Coyle Brecht, Partner Pietragallo Gordon Alfano Bosick & Raspanti, LLP Risk Area: False Data and/or Certifications
Managed Care Fraud: Enforcement and Compliance HCCA Compliance Institute March 28, 2017 Pamela Coyle Brecht, Partner Pietragallo Gordon Alfano Bosick & Raspanti, LLP Risk Area: False Data and/or Certifications
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN. Post Acute Provider Specific Sections from OIG Work Plans
 HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
HCCA South Central Regional Annual Conference November 21, 2014 Nashville, TN Kelly Priegnitz # Chris Puri # Kim Looney Post Acute Provider Specific Sections from 2012-2015 OIG Work Plans I. NURSING HOMES
CAH SWING BED BILLING, CODING AND DOCUMENTATION. Lisa Pando, Sr. Consultant GPS Healthcare Consultants
 CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
CAH SWING BED BILLING, CODING AND Lisa Pando, Sr. Consultant GPS Healthcare Consultants Learning Objectives: 1. Review Medical Necessity documentation specific to swing bed patients 2. Reasons to use the
State Medicaid Recovery Audit Contractor (RAC) Program
 Program") State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
State Medicaid Recovery Audit Contractor (RAC) Program Section 6411 of the Patient Protection and Affordable Care Act 2010 (ACA) requires by December 31, 2010 each state Medicaid program to contract with
Physician Practices Reimbursement, Risk, and Recommendations
 Physician Practices Reimbursement, Risk, and Recommendations Alice V. Cudlipp, Senior Consultant.1 M. H. West & Co., Inc In July of 1997, the US Department of Health and Human Services' ("HHS") Office
Physician Practices Reimbursement, Risk, and Recommendations Alice V. Cudlipp, Senior Consultant.1 M. H. West & Co., Inc In July of 1997, the US Department of Health and Human Services' ("HHS") Office
CMS Observation vs. Inpatient Admission Big Impacts of January Changes
 CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
CMS Observation vs. Inpatient Admission Big Impacts of January Changes Linda Corley, BS, MBA, CPC Vice President Compliance and Quality Assurance 706 577-2256 Cellular 800 882-1325 Ext. 2028 Office Agenda
Medicare Preventive Services
 Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
Medicare Preventive Services Presented by Part B Provider Outreach & Education December 16, 2015 Event Instructions Today s event is a teleconference Slides will not be advanced during the presentation
STATEMENT OF THE ACP-ASIM WORKING GROUP EVALUATION AND MANAGEMENT (E/M) DOCUMENTATION GUIDELINES. March 19, 1998
 DOCUMENTATION GUIDELINES. March 19, 1998") STATEMENT OF THE ACP-ASIM WORKING GROUP ON EVALUATION AND MANAGEMENT (E/M) DOCUMENTATION GUIDELINES March 19, 1998 PURPOSE The purpose of the statement is to: (1) describe the issues surrounding the evaluation
STATEMENT OF THE ACP-ASIM WORKING GROUP ON EVALUATION AND MANAGEMENT (E/M) DOCUMENTATION GUIDELINES March 19, 1998 PURPOSE The purpose of the statement is to: (1) describe the issues surrounding the evaluation
General Information. Overview. Purpose. Table of Contents
 Blue Cross and Blue Shield of Georgia, Inc. and Blue Cross Blue Shield Healthcare Plan of Georgia, Inc.engage Inovalonto conduct outreach efforts for ouraca individual and small group on and off exchange
Blue Cross and Blue Shield of Georgia, Inc. and Blue Cross Blue Shield Healthcare Plan of Georgia, Inc.engage Inovalonto conduct outreach efforts for ouraca individual and small group on and off exchange
AHLA. O. Stark and Reimbursement: A Deeper Dive to Debunk the Myths. Alice G. Gosfield Alice G. Gosfield & Associates PC Philadelphia, PA
 AHLA O. Stark and Reimbursement: A Deeper Dive to Debunk the Myths Alice G. Gosfield Alice G. Gosfield & Associates PC Philadelphia, PA Fraud and Compliance Forum October 6-7, 2014 Alice G. Gosfield American
AHLA O. Stark and Reimbursement: A Deeper Dive to Debunk the Myths Alice G. Gosfield Alice G. Gosfield & Associates PC Philadelphia, PA Fraud and Compliance Forum October 6-7, 2014 Alice G. Gosfield American
COMPLIANCE PLAN PRACTICE NAME
 COMPLIANCE PLAN PRACTICE NAME Table of Contents Article 1: Introduction A. Commitment to Compliance B. Overall Coordination C. Goal and Scope D. Purpose Article 2: Compliance Activities Overall Coordination
COMPLIANCE PLAN PRACTICE NAME Table of Contents Article 1: Introduction A. Commitment to Compliance B. Overall Coordination C. Goal and Scope D. Purpose Article 2: Compliance Activities Overall Coordination
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL
 Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Payment Policy: High Complexity Medical Decision-Making Reference Number: CC.PP.051 Product Types: ALL Effective Date: 6/2017 Last Review Date: See Important Reminder at the end of this policy for important
Pharmacies Medicare Part D Training Obligations and Medicare Training Resources
 Pharmacies Medicare Part D raining Obligations and Medicare raining Resources. Your obligation - MS regulations require that all pharmacies contracted with Medicare Part D Plan Sponsors, such as the Medco
Pharmacies Medicare Part D raining Obligations and Medicare raining Resources. Your obligation - MS regulations require that all pharmacies contracted with Medicare Part D Plan Sponsors, such as the Medco
Hospice Program Integrity Recommendations
 Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
Hospice Program Integrity Recommendations Projected increases in the elderly population and the number of Medicare beneficiaries will likely result in continued growth in utilization of hospice services.
CHAPTER 1. Documentation is a vital part of nursing practice.
 CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
CHAPTER 1 PURPOSE OF DOCUMENTATION CHAPTER OBJECTIVE After completing this chapter, the reader will be able to identify the importance and purpose of complete documentation in the medical record. LEARNING
Keeping Your Compliance Program in Pace with Rapidly Expanding TeleHealth Services
 Keeping Your Compliance Program in Pace with Rapidly Expanding TeleHealth Services In April 1924, an imaginative cover for the magazine Radio News foreshadowed telemedicine in its depiction of a "radio
Keeping Your Compliance Program in Pace with Rapidly Expanding TeleHealth Services In April 1924, an imaginative cover for the magazine Radio News foreshadowed telemedicine in its depiction of a "radio
THE 6 MUST-HAVE DOCUMENTS FOR AN EFFECTIVE MEDICAID/MEDICARE ELIGIBILITY PROGRAM
 THE 6 MUST-HAVE DOCUMENTS FOR AN EFFECTIVE MEDICAID/MEDICARE ELIGIBILITY PROGRAM WHO WE ARE founded in 2004 work in over 44 states 23 staff attorneys and 30+ national contract attorneys Now representing
THE 6 MUST-HAVE DOCUMENTS FOR AN EFFECTIVE MEDICAID/MEDICARE ELIGIBILITY PROGRAM WHO WE ARE founded in 2004 work in over 44 states 23 staff attorneys and 30+ national contract attorneys Now representing
Welcome to the beginning of optimal health!
 Welcome to the beginning of optimal health! would like to thank you for choosing us to partner with you as you embark on your journey towards optimal health! We ve developed this guide to help you prepare
Welcome to the beginning of optimal health! would like to thank you for choosing us to partner with you as you embark on your journey towards optimal health! We ve developed this guide to help you prepare
What To Do When An Audit Letter Comes
 What To Do When An Audit Letter Comes Sarah Reed BSE,CPC,CPC-I AAPC Fellow 2 The speaker has no financial relationship to any products or services referenced in this program. This program is intended to
What To Do When An Audit Letter Comes Sarah Reed BSE,CPC,CPC-I AAPC Fellow 2 The speaker has no financial relationship to any products or services referenced in this program. This program is intended to
Medicare s Electronic Health Records Incentive Program- Overview
 HCCA Upper Northeast Regional Conference Meaningful Use Best Compliance Practices May 17, 2013 Lourdes Martinez, Esq. lmartinez@garfunkelwild.com 111 Great Neck Road Great Neck, NY 11021 (516) 393-2200
HCCA Upper Northeast Regional Conference Meaningful Use Best Compliance Practices May 17, 2013 Lourdes Martinez, Esq. lmartinez@garfunkelwild.com 111 Great Neck Road Great Neck, NY 11021 (516) 393-2200
9/17/2018. Critical to Practices
 Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending
Critical to Practices Provides: Reviewing quality of care provided to patients. Education to providers on documentation guidelines. Ensuring all services are supported, and revenue captured. Defending