Table of Contents. Introduction. Basics. Laws Impacting School Nurses. Chronic Disease Management. IHP s and Emergency Action Plans
|
|
|
- Opal Mills
- 6 years ago
- Views:
Transcription

1
2
3 Table of Contents Introduction Basics Laws Impacting School Nurses Chronic Disease Management IHP s and Emergency Action Plans Medication Administration Screenings Reports INTENT OF THIS MANUAL, HOW TO USE THIS MANUAL DEFINITION OF SCHOOL HEALTH, ROLE OF THE SCHOOL NURSE, DELEGATION, SCHOOL YEAR CALENDAR, STOCKING THE SCHOOL CLINIC FEDERAL LAWS, STATE LAWS AND RULES, LOCAL SCHOOL CORPORATION POLICIES CHRONIC DISEASE OVERVIEW, ASTHMA, DIABETES, SEIZURES, SEVERE ALLERGIES/ANAPHYLAXIS HOW TO DEVELOP, WHEN TO USE MEDICATION STORAGE AND POLICIES, OTHER TYPES OF MEDICATION ADMINISTRATION, SHARPS CONTAINERS, FORMS AND DOCUMENTS HEARING, IMMUNIZATIONS, VISION ABSENTEEISM, EPINEPHRINE ADMINISTRATION, MCT WAIVER REQUEST, SCHOOL CLOSURE CONSIDERATION FORM, SCHOOL HEALTH REPORT Treatment Guidelines Students with Special Needs Procedures Professional Development DIABETES COURSE, EMERGENCY COURSE Training Resources
4 Introduction Intent of this Manual This School Nurse Manual has been developed to provide the school health caregiver with general information, resources and guidelines for meeting the basic healthcare needs of students in Indiana schools. It also serves as a guide to establish a framework for a sound health program as well as delineating the multifaceted role of the school nurse and other personnel providing school health services. These guidelines are not intended to replace the health caregiver s professional judgment or training, or to substitute for school policy or the advice of a healthcare provider. This manual should be used for reference and in collaboration with a school administrator, the student s parents/legal guardians and/or a healthcare provider for questions regarding the care of the student. If a situation appears serious or life-threatening, always follow school policies and procedures regarding notifications or calling for emergency assistance. Indiana History of School Health and the Nurse s Role The historical perspective of nurses practicing in the school setting began in the 1900 s as part of public health nursing. Public health nursing began at Flower Mission in Indianapolis with the hiring of a practical nurse to give care and instruction to families reporting to the city dispensary. In 1921, the American Red Cross and the Tuberculosis Association were instrumental in establishing a Division of Public Health Nursing as a branch of the Indiana State Board of Health. The purpose of this department was to stimulate interest in public health nursing, to standardize public health work throughout the state, to develop a system of state records, and to prepare nurses for working in the public health field. The greatest emphasis was placed on county and rural health nursing. By 1922, there were 242 public health nurses employed in the state. These nurses also worked in schools, mainly to aid in the prevention and control of communicable diseases. The earliest record of nurses being employed in Indiana schools was in 1916, when the Indianapolis City Board of Health employed a staff of 3 nurses. In 1924, a total of 14 nurses were employed by boards of education in the state. Today, the national standard for entry level into practice for professional nurses is the baccalaureate degree in nursing. The Indiana State Nurses Association adopted this standard in 1985 with progression toward implementation ever since. Although it is not mandatory for boards of education to employ school nurses in every building who meet these requirements, IAC states that a school corporation shall employ at least one (1) registered nurse who holds a Bachelor of Science in Nursing and who shall coordinate health services. 1

5 Schools are highly encouraged to have qualified nurses who have the preparation (through education and experience) to work with students, parents, school personnel, and community resources to meet the challenges of today s school children. It is recommended per IAC that a ratio of one registered nurse be employed for every 750 students enrolled in the corporation. The National Association of School Nurses (NASN) Role of the School Nurse position statement serves as a sound resource for supporting the use of registered professional school nurses for providing healthcare in addition to a multitude of additional roles within the school setting. This document can be found in Chapter 2 of this manual. How to Use this Manual The has been created to be a quick, yet informative digital or printed reference for school nurses to use around the state of Indiana. This manual is a compilation of state and federal laws, school health guidelines, sample forms, best practices, and treatment guidelines for various health issues. This manual is intended as a resource guide and is not intended to be a substitute for school policies, comprehensive pediatric or emergency care manuals, the nurse s clinical judgement, the direction or treatment orders from a health care provider, or a student s individual health plan. Every health condition or school emergency situation is unique and requires specific solutions, policies, and protocols. Therefore, the recommendations in this manual are not intended to indicate an exclusive course of treatment or to be applicable in all circumstances. We recommend that you use this manual as a guide for developing local school policies and protocols. This manual is designed to support school nurses in their roles and specifically to provide nurses who work in the school setting with information, guidelines and resources that they can integrate into their current practice and use to deliver care. 2

6 Chapter 1: Basics SECTION 1: DEFINITION OF SCHOOL HEALTH SECTION 2: ROLE OF THE SCHOOL NURSE SECTION 3: DELEGATION SECTION 4: SCHOOL YEAR CALENDAR SECTION 5: STOCKING THE SCHOOL CLINIC 3
7 SECTION 1: Definition of School Health According to The National Academies Press, school health is defined as: A comprehensive school health program is an integrated set of planned, sequential, school-affiliated strategies, activities, and services designed to promote the optimal physical, emotional, social, and educational development of students. The program involves and is supportive of families and is determined by the local community based on community needs, resources, standards, and requirements. It is coordinated by a multidisciplinary team and accountable to the community for program quality and effectiveness. -The National Academies Press, SECTION 2: Role of the School Nurse School nursing has multiple components and the role of the school nurse is a broad one, dependent on many factors, including the school setting (rural, urban, suburban), health needs of the student population, and the availability of specialized instructional student support services and programs. The National Association of School Nurses defines school nursing as a specialized practice of public health nursing that protects and promotes student health, facilitates normal development, and advances academic success. School nurses, grounded in ethical and evidence-based practice, are the leaders that bridge health care and education, provide care coordination, advocate for quality student-centered care, and collaborate to design systems that allow individuals and communities to develop their full potentials (NASN, 2016). "Five Ways a School Nurse Benefits a School" (PDF) "Framework for 21st Century School Nursing Practice" (PDF) NASN- "Role of the School Nurse" Position Statement (PDF) SECTION 3: Delegation INTRODUCTION All students attending public schools must have access to healthcare during the school day and for extracurricular school activities, if necessary, to enable the student to participate fully in school programs pursuant to federal law 1. Indiana law requires school nurses to be registered nurses (RNs). Since some school districts in Indiana do not have full-time school nurses in every building, it is often necessary for school nurses to delegate certain tasks to a licensed practical nurse (LPN) or unlicensed assistive personnel (UAP) so that children with special healthcare needs can attend school and participate in extracurricular activities. Knowing when and how to delegate specific nursing tasks is essential for the school nurse. It is the purpose of this document to provide guidance to registered nurses in the school setting who find it necessary to delegate nursing tasks. Delegation - Part 1: STATE OF INDIANA REGULATIONS Delegation - Part 2: PRINCIPLES OF DELEGATION FOR THE SCHOOL NURSE Delegation - Part 3: DELEGATION TOOLS Delegation - Part 4: REFERENCES 1 Americans with Disabilities Act of 1990 (ADA) (2000), 42 U.S.C Individuals with Disabilities Education Improvement Act (2004), 20 U.S.C et seq. Rehabilitation Act of 1973, 29 U.S.C
8 Delegation - Part 1: State of Indiana Regulations The practice of nursing in Indiana is regulated by Indiana Code Title 25, Article 23 and Indiana Administrative Code Title 848. The provision of healthcare in the school setting is regulated by Indiana Code Title 20, Article 34 and Indiana Administrative Code Title 511, Article 4. Full text of these regulations is available at iga.in.gov. The most relevant provisions are detailed below. DEFINITIONS School Nurse IC As used in this chapter, school nurse refers to an individual who: (1) is employed by a school; (2) is licensed as a registered nurse under IC 25-23; and (3) meets the requirements set forth in 515 IAC School Services: School Nurse 515 IAC The content area school nurse shall appear on the license if the department determines that the applicant: (1) successfully meets the standards for the school services professional and the national standards for school nurse; (2) obtains a bachelor s degree from an approved school of nursing program; (3) obtains a registered nurse s license through the Indiana State Board of Nursing. School Health Services 511 IAC (b) A school corporation shall employ at least one registered nurse who holds a Bachelor of Science in Nursing and who shall coordinate health services. Registered Nurse IC (a) Bears primary responsibility and accountability for nursing practices based on specialized knowledge, judgment, and skill derived from the principles of biological, physical, and behavioral sciences. Registered Nursing IC (b) Registered nursing means performance of services which include, but are not limited to: (1) assessing health conditions; (2) deriving a nursing diagnosis; (3) executing a nursing regimen through the selection, performance, and management of nursing actions based on nursing diagnoses; (4) advocating the provision of healthcare services through collaboration with or referral to other health professionals; (5) executing regimens delegated by a physician with an unlimited license to practice medicine or osteopathic medicine, a licensed dentist, a licensed chiropractor, a licensed optometrist, or a licensed podiatrist; (6) teaching, administering, supervising, delegating, and evaluating nursing practice; (7) delegating tasks which assist in implementing the nursing, medical, or dental regimen; (8) performing acts which are approved by the board or by the board in collaboration with the Medical Licensing Board of Indiana. Licensed Practical Nurse IC Functions at the direction of a registered nurse, physician, dentist, chiropractor, optometrist, or podiatrist in the performance of activities commonly performed by practical nurses and requiring special knowledge or skill. Practical Nursing IC Practical nursing means the performance of services commonly performed by practical nurses, including: 5
9 (1) contributing to the assessment of the health status of individuals or groups; (2) participating in the development and modification of the strategy of care; (3) implementing the appropriate aspects of the strategy of care; (4) maintaining safe and effective nursing care; and (5) participating in the evaluation of responses to the strategy of care. RN STANDARDS OF PRACTICE 848 IAC Responsibility to apply the nursing process Sec. 1. The registered nurse shall do the following: (1) Assess the patient/client in a systematic, organized manner. (2) Formulate a nursing diagnosis based on accessible, communicable, and recorded data which is collected in a systematic and continuous manner. (3) Plan care which includes goals and prioritized nursing approaches or measures derived from the nursing diagnosis. (4) Implement strategies to provide for patient/client participation in health promotion, maintenance, and restoration. (5) Initiate nursing actions to assist the patient/client to maximize his or her health capabilities. (6) Evaluate with the patient/client the status of goal achievement as a basis for reassessment, reordering priorities, new goal setting, and revision of the plan of nursing care. (7) Seek educational resources and create learning experiences to enhance and maintain current knowledge and skills for his or her continuing competence in nursing practice and individual professional growth. 848 IAC Responsibility as a member of the nursing profession Sec. 2. The registered nurse shall do the following: (1) Function within the legal boundaries of nursing practice based on the knowledge of statutes and rules governing nursing. (2) Accept responsibility for individual nursing actions and continued competence. (3) Communicate, collaborate, and function with other members of the health team to provide safe and effective care. (4) Seek education and supervision as necessary when implementing nursing practice techniques. (5) Respect the dignity and rights of the patient/client regardless of socioeconomic status, personal attributes, or nature of health problem. (6) Maintain each patient/client s right to privacy by protecting confidential information unless obligated, by law, to disclose the information. (7) Provide nursing care without discrimination on the basis of diagnosis, age, sex, race, creed, or color. (8) Delegate and supervise only those nursing measures which the nurse knows, or should know, that another person is prepared, qualified, and licensed to perform. (9) Retain professional accountability for nursing care when delegating nursing intervention. (10) Respect and safeguard the property of patient/client, family, significant others, and the employer. (11) Notify, in writing, the appropriate party, which may include: a.) the Office of the Attorney General, Consumer Protection Division; b.) his or her employer or contracting agency; or 6
10 c.) the board; of any unprofessional conduct which may jeopardize the patient/client safety. (12) Participate in the review and evaluation of the quality and effectiveness of nursing care. 848 IAC Unprofessional conduct Sec. 3. Nursing behaviors (acts, knowledge, and practices) failing to meet the minimal standards of acceptable and prevailing nursing practice, which could jeopardize the health, safety, and welfare of the public, shall constitute unprofessional conduct. These behaviors shall include, but are not limited to the following: (1) Using unsafe judgment, technical skills, or inappropriate interpersonal behaviors in providing nursing care. (2) Performing any nursing technique or procedure for which the nurse is unprepared by education or experience. (3) Disregarding a patient/client s dignity, right to privacy, or right to confidentiality. (4) Failing to provide nursing care because of diagnosis, age, sex, race, color, or creed. (5) Abusing a patient/client verbally, physically, emotionally, or sexually. (6) Falsifying, omitting, or destroying documentation of nursing actions on the official patient/client record. (7) Abandoning or knowingly neglecting patients/clients requiring nursing care. (8) Delegating nursing care, functions, tasks, or RN responsibility to others when the nurse knows, or should know, that such delegation is to the detriment of patient safety. (9) Providing one s license/temporary permit to another individual for any reason. (10) Failing to practice nursing in accordance with prevailing nursing standards due to physical or psychological impairment. (11) Diverting prescription drugs for own or another person s use. (12) Misappropriating money or property from a patient/client or employee. (13) Failing to notify, in writing, the appropriate party, which may include: a.) the Office of the Attorney General, Consumer Protection Division; b.) his or her employer or contracting agency; or c.) the board of any unprofessional conduct which may jeopardize patient/client safety. LPN STANDARDS OF PRACTICE 848 IAC Responsibility to apply the nursing process Sec. 1. The licensed practical nurse shall do the following: (1) Know and utilize the nursing process in planning, implementing, and evaluating health services and nursing care to the individual patient or client. (2) Collaborate with other members of the health team in providing for patient/client participation in health promotion, maintenance, and restoration. (3) Seek educational resources and create learning experiences to enhance and maintain current knowledge and skills for his or her continuing competence in nursing practice and individual professional growth. (4) Assess the health status of the patient/client in conjunction with other members of the healthcare team for analysis and identification of health goals. (5) Evaluate with the patient/client the status of goal achievement as a basis for reassessment, reordering of priorities, and new goal setting for contribution to the modification of the plan of nursing care. 7
11 848 IAC Responsibility as a member of the health team Sec. 2. The licensed practical nurse shall do the following: (1) Function within the legal boundaries of practical nursing practice based on the knowledge of statutes and rules governing nursing. (2) Accept responsibility for individual nursing actions and continued competence. (3) Communicate, collaborate, and function with other members of the healthcare team to provide safe and effective care. (4) Seek education and supervision as necessary from registered nurses and/or other members of the healthcare team when implementing nursing techniques or practices. (5) Respect the dignity and rights of the patient/client regardless of socioeconomic status, personal attributes, or nature of health problems. (6) Maintain each patient/client s right to privacy by protecting confidential information unless obligated, by law, to disclose the information. (7) Provide nursing care without discrimination on the basis of diagnosis, age, sex, race, creed, or color. (8) Accept only those delegated nursing measures which he or she knows he or she is prepared, qualified, and licensed to perform. (9) Respect and safeguard the property of patient/client, family, significant others, and the employer. (10) Notify, in writing, the appropriate party which may include: a.) the Office of the Attorney General, Consumer Protection Division; b.) his or her employer or contracting agency; or c.) the board of any unprofessional conduct which may jeopardize the patient/client safety. (11) Participate in the review and evaluation of the quality and effectiveness of nursing care. 848 IAC Unprofessional conduct Sec. 3. Nursing behaviors (acts, knowledge, and practices) failing to meet the minimal standards of acceptable and prevailing licensed practical nursing practices, which could jeopardize the health, safety, and welfare of the public shall constitute unprofessional conduct. These behaviors shall include, but are not limited to the following: (1) Using unsafe judgment, technical skills, or inappropriate interpersonal behaviors in providing nursing care. (2) Performing any nursing technique or procedure for which the nurse is unprepared by education or experience. (3) Disregarding a patient/client s dignity, right to privacy, or right to confidentiality. (4) Failing to provide nursing care because of diagnosis, age, sex, race, color, or creed. (5) Abusing a patient/client verbally, physically, emotionally, or sexually. (6) Falsifying, omitting, or destroying documentation of nursing actions on the official patient/client record. (7) Abandoning or knowingly neglecting patients/clients requiring nursing care. (8) Accepting delegated nursing measures that he or she knows that he or she is not prepared, qualified, or licensed to perform. (9) Providing one s license/temporary permit to another individual for any reason. (10) Failing to practice nursing in accordance with prevailing practical nursing standards due to physical or psychological impairment. (11) Diverting prescription drugs for own or another person s use. 8
12 (12) Misappropriating money or property from a patient/client or employee. (13) Failing to notify, in writing, the appropriate party which may include: a.) the Office of the Attorney General, Consumer Protection Division; b.) his or her employer or contracting agency; or c.) the board of any unprofessional conduct which may jeopardize patient/client safety. VIOLATIONS Indiana Code (a)(8) Powers and duties of board Registered nurses and licensed practical nurses who violate these standards are subject to prosecution by the Indiana State Board of Nursing. Indiana Code Violations; penalty It is a Class B misdemeanor for an unlicensed individual to: (1 ) practice nursing as a registered nurse or licensed practical nurse when unlicensed to do so, or (2) use in connection with the person s name any designation tending to imply that the person is a registered nurse or a licensed practical nurse when unlicensed. MANAGEMENT OF STUDENTS WITH DIABETES IC Requirements of the management and treatment plan for a student with diabetes Sec. 12. (a) A diabetes management and treatment plan must be prepared and implemented for a student with diabetes for use during school hours or at a school-related activity. The plan must be developed by: (1) the licensed healthcare practitioner responsible for the student s diabetes treatment; and (2) the student s parent or legal guardian. (b) A diabetes management and treatment plan must: (1) identify the healthcare services or procedures the student should receive at school; (2) evaluate the student s: (A) ability to manage; and (B) level of understanding of the student s diabetes; and (3) be signed by the student s parent or legal guardian and the licensed healthcare practitioner responsible for the student s diabetes treatment. (c) The parent or legal guardian of a student with diabetes shall submit a copy of the student s diabetes management and treatment plan to the school nurse. The plan must be submitted to and be reviewed by the school nurse: (1) before or at the beginning of a school year; (2) at the time the student enrolls, if the student is enrolled in school after the beginning of the school year; or (3) as soon as practicable following a diagnosis of diabetes for the student. IC Development of the individualized health plan for a student with diabetes Sec. 13. (a) An individualized health plan must be developed for each student with diabetes while the student is at school or participating in a school activity. The school s nurse shall develop a student s individualized health plan in collaboration with: (1) to the extent practicable, the licensed healthcare practitioner responsible for the student s diabetes treatment; 9
13 (2) the school principal; (3) the student s parent or legal guardian; and (4) one (1) or more of the student s teachers. (b) A student s individualized health plan must incorporate the components of the student s diabetes management and treatment plan. IC Use of volunteer health aides Sec. 14. (a) At each school in which a student with diabetes is enrolled, the school principal, after consultation with the school nurse, shall: (1) seek school employees to serve as volunteer health aides; and (2) make efforts to ensure that the school has an adequate number of volunteer health aides to care for students. (b) A volunteer health aide, while providing healthcare services, serves under the supervision and authorization of the principal and the school nurse in accordance with the requirements that apply to the school nurse under IC (c) A volunteer health aide must have access to the school nurse, in person or by telephone, during the hours that the volunteer health aide serves as a volunteer health aide. (d) A school employee may not be subject to any disciplinary action for refusing to serve as a volunteer health aide. The school shall inform school employees that participation as a volunteer health aide is voluntary. A school employee who volunteers as a volunteer health aide may elect to perform only those functions that the school employee: (1) chooses to perform; and (2) is trained to perform in the training program described in Chapter 12 of this manual. Delegation - Part 2: Principles Of Delegation For The School Nurse 2 Delegation is the transfer of responsibility for the performance of a task from one individual to another while retaining accountability for the outcome (ANA, 2010). Through delegation, a registered nurse can direct another individual to do something that that person would not normally be allowed to do (ANA & NCSBN, 2006). The RN retains professional accountability for the overall care of the individual (NASN, 2014). Nursing tasks performed in schools may be delegated solely by the school nurse, who must be a registered nurse. The RN may delegate components of care, but not the nursing process (NASN, 2014). Nursing assessment, planning, evaluation, and judgment cannot be delegated (ANA & NCSBN, 2006). The decision to delegate is based upon professional judgment that the delegatee can safely perform a selected nursing task for a student. Delegation allows school nurses to utilize unlicensed school staff to provide safe and efficient nursing care for individual students or groups of students and provides a mechanism for workload distribution to better utilize the time and skills of each of the members of the school health team (NASN, 2014). Delegation is not appropriate for all students, all nursing tasks, or all school settings (NASN, 2014). Due to individual circumstances or complex medical needs, some nursing tasks can only be performed by an RN or LPN. 2 Adapted from Guide to Delegation for Colorado School Nurses, with the permission of the Colorado Dept. of Education, and from Delegation, The Nurse Practice Act, and School Nursing in Wisconsin (2009) with the permission of the Wisconsin Department of Public Instruction. Who can delegate? Only a registered nurse (RN) can delegate a nursing task. Parents cannot delegate nursing tasks to a teacher or any other unlicensed assistive personnel (UAP) in the school. 10
14 School administrators cannot delegate nursing tasks to a teacher or any other UAP in the school. Licensed practical nurses (LPNs) or UAP cannot delegate nursing tasks. Who are unlicensed assistive personnel (UAP)? Any person who does not have a nursing or medical license, who acts in a complementary role to a registered nurse, and to whom the registered nurse authorizes to perform certain nursing tasks which the unlicensed individual is not otherwise authorized to perform. In a school, UAP may be paraprofessionals, classroom assistants, administrators, teachers, bus monitors or drivers, playground attendants, office staff, or health aides. What is essential information to know about unlicensed assistive personnel (UAP)? UAP cannot train, re-delegate, or ask any other person to perform any nursing task under any circumstance. The use of UAP in schools is a decision made by the school nurse on a case-by-case basis. Persons serving as UAP must do so on a voluntary basis. When can the school nurse delegate? When the task being considered for delegation is within the area of responsibility of the registered nurse. When the task being considered for delegation is within the knowledge, skills, and ability of the registered nurse. When the task being delegated does not require the professional judgment of a registered nurse. When the student s condition is stable and the outcome of the task is predictable. When the nursing task does not inherently involve ongoing assessments, interpretations, or decision making. When the delegatee is deemed competent to perform the task. When ongoing supervision is provided by the registered nurse. What types of nursing acts may be delegated and to whom? There is not a state statute listing nursing tasks that are appropriate for delegation. The decision to delegate a nursing task is based on the registered nurse s assessment of the complexity of the nursing task and care, predictability of the health status of the student, and the educational preparation and demonstrated abilities of the delegatee. Nursing tasks may be delegated when the task does not require assessment and evaluation of the student s health and modifications to the plan of care. The school nurse determines the necessary training required to safely delegate the nursing task. While employers, administrators, and the chart included in these guidelines may suggest which nursing acts should be delegated and/or to whom the delegation may be made, it is the school nurse who must make, and is legally responsible for making, the decision whether, and under what circumstances, the delegation occurs. If the school nurse decides that the delegation may not appropriately or safely take place, then the school nurse should not engage in such delegation. School nurses are encouraged to work with school district administrators to problem solve solutions to the issues of delegation. For further guidance, please refer to the Decision Tree and the Guide to Delegation Chart in Part 3. 11
15 What is involved in delegating nursing tasks? The general steps involved in the process of delegation are: 1. Determine if the delegated nursing task is commensurate with the nurse s education, training, and experience. 2. Determine the appropriateness of the delegation of the nursing task to UAP. 3. Assess the student s health status, environment, and available resources to determine the predictability of the outcomes of the nursing task. 4. Assess UAP willingness and ability to perform the nursing task. 5. Provide training for UAP and document competency level of UAP knowledge and skill. 6. Provide the trained UAP with contact information for the delegating registered nurse, and determine a plan for training supervisory nurse and UAP backups as needed. 7. Supervise and evaluate the ability of UAP to perform the delegated nursing task. 8. Document the student s health status, delegated task, UAP competency and performance of the task, and the evaluation of the outcomes of the nursing task. What is meant by supervision of the delegated nursing task? Inherent in the decision to delegate is the requirement that the school nurse must supervise the delegatee. Supervision means that the RN is available while the task is being performed, to provide direction through direct, written, or verbal communications. If the RN is unable to provide this supervision, the RN is unable to delegate the tasks. The specific amount of time required for supervision will depend upon the abilities of the UAP, training, type, and number of delegated nursing care tasks. It is the nurse s responsibility to safeguard that delegation is not a detriment to patient safety (848 IAC 2-2-3(8)). How often should the registered nurse monitor the delegation of a task? Frequency and extent of monitoring depend on the health status of the student, the complexity of the procedure, and the learning style of the person doing the procedure. For example, administering insulin to a child who has received insulin injections for many years may require less supervision than administering insulin to a child who has recently been diagnosed with type 1 diabetes. As another example, the complexity of the task and the need for monitoring oral medication administration is usually less involved than monitoring for injectable medication. The level of training, experience, and educational preparation of the person assuming the delegation from the nurse will also determine the monitoring needs. The nurse may rescind delegation of the nursing task whenever he/she believes that the student s safety is being compromised or for other reasons according to the judgment of the nurse. Can the nurse delegate and provide supervision in exceptional situations? Exceptional situations include, but are not limited to, activities on campus, off campus, during school hours, and outside of school hours. Delegation and supervision of nursing tasks during exceptional situations shall be determined by the registered nurse in consultation with school administration, and delegation may not be appropriate in some circumstances. The nurse must have adequate time to determine appropriateness of delegation and should consider the following in the decision to delegate: Assessing the student s health status and health needs Establishing a safe plan of care regarding: 12
16 »» Location of activity»» Availability of supplies and equipment»» Availability of parent/guardian during the activity»» Availability of other appropriate healthcare personnel»» Availability of reliable communication modes between the delegating nurse and the UAP, including situations that may occur during 24/7 care What is the difference between training and delegation? Training is the process of providing general health information to others regarding a health skill, condition, injury, medication, or task. When the training becomes specific to a certain child s healthcare needs, medications and/or tasks, then the training by the nurse is part of the process of delegation. The process of delegation includes: instruction regarding the plan of care; administration of medication and/or task; direction, assistance, and observation of those supervised; and evaluation of the effectiveness of the delegated task. For example, a nurse providing instruction to school personnel regarding the effectiveness of administration of rectal diazepam to students who are experiencing ongoing continuous seizure activity would be training. When a nurse provides instruction to school personnel who will be responsible to administer rectal diazepam to a specific student based on the student s IHP, then training becomes part of the delegation process. What is the legal liability for the school nurse? The delegating RN is responsible for the decision to delegate, and the process of delegation, including supervising and evaluating the delegated tasks and could be found liable if harm results from inappropriate actions in those areas. The delegation of nursing tasks to UAP carries legal implications for the delegating RN. However, if the delegating nurse has taken steps to ensure that the task is delegated properly and that appropriate supervision is provided, the risk for legal liability is minimized. The delegatee must follow the steps outlined in the plan of care. The RN must satisfy that all of the criteria for delegation in the Indiana Code and Indiana Administrative Code have been addressed, including responsibility for: determining that the delegation is appropriate; monitoring and evaluating the outcomes for each delegation; documenting the process for training and evaluating the delegatee. What is the procedure for documentation of delegation? 1. Instructions for a delegated task must be specific and broken into specific steps. 2. For complicated tasks, the delegatee must demonstrate each step and the delegatee and the RN should initial when training has occurred for each step. 3. The nursing task can be delegated once the delegatee has demonstrated competence through the training process. 4. A statement, signed and dated by the delegating RN and the delegatee, will document completion of the training. 5. The RN should establish a schedule for the periodic evaluation regarding the continued competence of the delegatee. 6. Errors in carrying out a task must be documented along with the corrective actions taken. 13
17 Can delegation be withdrawn? Delegated tasks must be withdrawn if the registered nurse, who has delegated the task, determines that circumstances have changed in that: the student is less stable and/or the task no longer has a predictable outcome or the delegatee fails, at any time, to demonstrate competence, thus making the safety of task performance questionable. Can all nursing tasks be delegated? All situations must be carefully assessed on a case-by-case basis by the registered nurse for delegation to occur. The following points must be considered: The task must be within the nurse s knowledge, skills, and abilities. The nurse must assess whether the student s health condition is stable relative to the task. The nurse must provide a specific written protocol for the delegated task. The nurse must determine if the delegatee is competent and the task can be safely performed. Can a school nurse refuse to administer a prescribed medication or nursing procedure? Yes, under certain circumstances a school nurse may refuse to provide certain nursing services. A nurse can only accept a medical treatment order delegated by a medical provider for which the nurse is competent to perform, based on the nurse s education, training, or experience. However, the nurse s inability to perform the procedure does not erase the school district s obligation to provide the nursing service for the student to benefit from his/her education. The nurse may have to secure specialized training, or another healthcare professional may need to be employed by the school district to meet the student s healthcare needs. The nurse must refuse to perform a delegated procedure if the nurse suspects that the performance of the task may harm the student. If a nurse believes that a medical directive is not safe or not appropriate, the nurse cannot legally comply with the order. If the nurse complies, the nurse could face disciplinary action. If a nurse refuses to administer a medication or perform a procedure, he/she must notify the prescribing medical provider and parent. What is the difference between assigning and delegating a medication? School administrators and principals have the authority to assign an employee or volunteer to administer prescription and over-the-counter medication. Such assignment must be authorized by the principal in writing. Delegation is a term that is reserved for the relationship between the registered nurse and the individual performing the task. This is a responsibility that is regulated by 848 IAC, Article 2: Standards for the Competent Practice of Registered and Licensed Practical Nursing (listed under RN and LPN Standards of Practice at the beginning of this document). May a parent delegate to a nurse? No, a parent may not delegate to a nurse. Healthcare directions to the school nurse should be in the form of a medical treatment order signed by both a parent/guardian and a healthcare provider with prescriptive authority. 14
18 Five Rights of Delegation 1. Right Task 2. Right Circumstances 3. Right Person 4. Right Communication 5. Right Supervision Delegation - Part 3: Delegation Tools To provide concrete assistance to Indiana school nurses, below are resources to aid in specific delegation decisions and procedures: 1. Delegation Decision Tree Walks through fourteen prerequisites for delegation. Reprinted with the permission of the Washington Department of Health from their Nursing Care Quality Assurance Commission Advisory Opinion 4.0: Registered Nurse Delegation in School Settings. 2. Delegation Task Table Guidance for sixty-one procedures as to what can be delegated by the RN and if so, whether that delegation should be to an LPN or UAP. These are general protocols and each case should be evaluated on an individual basis using the principles above. Adapted from Guide to Delegation for Colorado School Nurses, with the permission of the Colorado Department of Education. The delegatory clause of the Indiana Nurse Practice Act allows registered nurses to determine whether nursing tasks, other than those listed in the Delegation Task Table (Figure 2), can be safely delegated. This can be done only on a case-by-case basis; and assessment, training, on-going supervision, and regular evaluation must be included for each task and each individual. As with all other acts of delegation, a registered nurse must determine the appropriateness of the delegation and provide supervision and follow-up. 3. Skills Checklist for Staff Training Template to document staff training on specific procedures. Reprinted with the permission of the Michigan Department of Education. 4. Medication Administration Checklist Step-by-step guide for delegatee administration of standard medications and emergency medications epinephrine, glucagon, diastat. Reprinted with the permission of the Michigan Department of Education. 5. Training Verification of School Personnel Administering Medication Form to document the delegatee received training in administering medication, verified by the delegating school nurse and the delegatee. Reprinted with the permission of the Michigan Department of Education. 15
19 NCQAC Advisory Opinion 4.0: Registered Nurse Delegation in School Settings School Registered Nurse Delegation Decision Tree YES Does the school RN understand the principles or delegation and the delegation process? NO YES Has the school RN performed a nursing assessment of the student s health care needs? NO YES Does the school or school district policy support delegation of the task? NO YES YES Is the student s condition stable and predictable? Is the delegation of task legally supported? NO NO D O YES YES Is the task within the demonstrated competence of the delegating school RN? Has the appropriate training been provided to the UAP about the task? NO NO N O T YES Does the UAP have demonstrated competence to perform the task? NO D EL YES YES Is the UAP willing and available to perform the task? Can the task be done without requiring nursing judgement? NO NO E G AT YES Can the task be done according to exact, unchanging directions? NO E YES Can the task be done without requiring repeated assessments and complex nursing skills? NO YES Is the school RN able to appropriately supervise performance of the task? NO YES Is the school RN willing to accept the consequences of delegating the task? NO SCHOOL RN MAY DELEGATE * For persons with disabilities, this document is available on request in other formats. To submit a request, call (TDD/TTY 711) 16
20 Delegation Table for Indiana School Nurses W - Within Scope of Practice S - Within Scope with Supervision of RN D - Delegated Tasks with Supervision of RN T - Training with Supervision of RN E - In Emergencies, with Training and 911 Must be Called X - Cannot Perform Y - Yes Practitioner Order Required RN LPN Unlicensed Assistive Personnel Practitioner: Person with legal authority to prescribe or order the treatment RN Scope of Practice: See definitions section above LPN Scope of Practice: See definitions section above UAP: See definitions section above Delegation is determined on a case-by-case basis by the registered nurse 1.0 Activities of Daily Living 1.1 Toileting/Diapering W W T 1.2 Bowel/Bladder Training W W T 1.3 Dental/Oral Hygiene W W T 1.4 Lifting/Positioning/Transfers W W T Depends on student-may need special training 1.5 Oral Feeding Nutritional Assessment W X X Oral Feeding Y* W W T/D* *Need practitioner order if specific food texture or technique is required 1.6 Special Feeding Naso-Gastric Feeding Y W S D* Gastrostomy Feeding Y W S D Jejunostomy Tube Feeding Y W S D Total Parenteral Feeding (intravenous) Gastrostomy Reinsertion to Maintain Stoma Patency Y W X X Y W D* D* *Can be delegated if placement can be determined by an objective measure *Placement instructions should be verified or provided by healthcare provider before use 17
21 W - Within Scope of Practice S - Within Scope with Supervision of RN D - Delegated Tasks with Supervision of RN T - Training with Supervision of RN E - In Emergencies, with Training and 911 Must be Called X - Cannot Perform Y - Yes 2.0 Urinary Catheterization 2.1 Clean Intermittent Catheterization Practitioner order Required RN LPN Y W S D 2.2 Sterile Catheterization Y W S X 2.3 Indwelling Catheter Care (cleanse with soap & water, Y W W D empty bag) 2.4 Bladder Irrigation Y W S X Unlicensed Assistive Personnel Practitioner: Person with legal authority to prescribe or order the treatment RN Scope of Practice: See definitions section above LPN Scope of Practice: See definitions section above UAP: See definitions section above Delegation is determined on a case-by-case basis by the Registered Nurse 3.0 Medical Support Systems 3.1 Ventricular Peritoneal Shunt Monitoring Y W S D 3.2 Mechanical Ventilation Monitoring Y W S X Adjustment of Ventilator Y W S X Ambu Bag W S E 3.3 Oxygen Intermittent/Emergency Y W S D Continuous/Monitoring Y W S D Pulse Oximetry Monitoring Y W S D 3.4 Central Line Port/Catheter Site Monitoring Y W S D 3.5 Dialysis Access Port Monitoring Y W S D 3.6 Subcutaneous Continuous Glucose Monitoring Y W S D 4.0 Medication Administration 4.1 Prescription/Non-Prescription Medications: Oral or Inhaled Y W S D 18
22 W - Within Scope of Practice S - Within Scope with Supervision of RN D - Delegated Tasks with Supervision of RN T - Training with Supervision of RN E - In Emergencies, with Training and 911 Must be Called X - Cannot Perform Y - Yes Practitioner Order Required RN LPN Unlicensed Assistive Personnel Practitioner: Person with legal authority to prescribe or order the treatment RN Scope of Practice: See definitions section above LPN Scope of Practice: See definitions section above UAP: See definitions section above Delegation is determined on a case-by-case basis by the registered nurse 4.2 Insulin Y W S D 4.3 Per Nasogastric Tube Y W S D* *Can be delegated if placement can be determined by an objective measure 4.4 Injectable Epinephrine (EpiPen) Y W S E See notes for E 4.5 Rectal Diazepam (Diastat) Y W S E See notes for E 4.6 Nasal Midazolam (Versed) Y W S E See notes for E 4.7 Glucagon Y W S E See notes for E 4.8 Solu-Cortef (Hydrocortisone) Y W S E See notes for E 4.9 Per Gastrostomy Tube Y W S D Intravenous Medications Y W S* X *LPN needs IV certification 5.0 Ostomies (Colostomy, Ileostomy, and Urostomy) 5.1 Ostomy Care (empty bag, cleanse with soap and water) W S T 5.2 Ostomy Irrigation Y W S X 6.0 Respiratory 6.1 Postural Drainage Y W S D 6.2 Percussion Y W S D 6.3 Suctioning Oral Cavity Suctioning Y W S D Tracheostomy Suctioning Y W S X 6.4 Tracheostomy Tube Replacement Y W S X 6.5 Tracheostomy Care (clean/ dress) Y W S D 19
23 7.0 Screening 7.1 Growth (height/weight) W S T 7.2 Vital Signs W W T W - Within Scope of Practice S - Within Scope with Supervision of RN D - Delegated Tasks with Supervision of RN T - Training with Supervision of RN E - In Emergencies, with Training and 911 Must be Called X - Cannot Perform Y - Yes Practitioner order Required RN LPN 7.3 Hearing W S T 7.4 Vision W S T 7.5 Body Mass Index W S T 8.0 Specimen Collecting/Testing 8.1 Blood Glucose/Ketone Y W S D 8.2 Urine Ketone Y W S D 9.0 Other Healthcare Procedures 9.1 Seizure First Aid/Safety Procedures W S T 9.2 Pressure Lesion/Ulcer Care Y W S D 9.3 Dressing, Sterile Y W S D 9.4 Dressing, Non-sterile W S T 9.5 Vagal Nerve Stimulator Y W S D 10.0 Assessment Skills and Protocol Development 10.1 Healthcare Procedures W X X 10.2 Emergency Protocols W X X 10.3 Individualized Healthcare Plan W X X 10.4 IEP Health Assessments W X X Health Assessments W X X 10.6 Home Bound Services- Health Assessments W X X Unlicensed Assistive Personnel Practitioner: Person with legal authority to prescribe or order the treatment RN Scope of Practice: See definitions section above LPN Scope of Practice: See definitions section above UAP: See definitions section above Delegation is determined on a case-by-case basis by the Registered Nurse Information must be reported to RN promptly for assessment and evaluation 20
24 Skills Checklist for Staff Training Name: Job Title: Date Trained: School Nurse Instructor: Supervision/Evaluation Name and purpose of procedure Preparation for procedure When done Where done Special instructions Supplies Demo Date Return Demo Date Date Date Date Date Date Date Steps to the procedure: Able to state expected student outcomes: Appropriate documentation Appropriate interactions with student (provide examples) Appropriate communication with school nurse (provide examples) 21
25 Medication Administration Checklist Staff Person Trained/Position: Initials: School Nurse/RN: Initials: Standard Medications Dates Procedure Guideline Demonstrate/ Explain or Proficient Return Demonstration Demonstrate/ Explain or Proficient Return Demonstration Demonstrate/ Explain or Proficient Return Demonstration Comments/ School Nurse Initial/Staff Initial, or Non- Applicable Washes hands before and after procedure Gives proper dose of medication at proper time. States 5 Rights Compares labeled medication container with written order Reads label 3 appropriate times Checks student identity with name on label Checks expiration date on label Explains procedure to student if necessary Documents medications given correctly Maintains security of medication area Describes proper actions for medication refusal, field trip, medication error States appropriate times/situations for notification of school nurse Emergency Medications Epinephrine States symptoms of allergic reaction, location of medication and emergency plan Demonstrates with trainer, correct procedure for administration States follow-up procedures Glucagon States symptoms of hypoglycemia, location of medication and emergency plan Demonstrates mixing of medication in syringe Demonstrates proper injection technique using correct site States follow-up procedures Diastat States understanding of when to use this medication, location of medication and emergency plan Demonstrates proper positioning of child, procedure for administering medication States follow-up procedures 22
26 Training Verification of School Personnel Administering Medication Name of School: has received training to administer medications according to our school policy and procedures. He/she has demonstrated knowledge and understanding of the policies and procedures listed above. RN Signature Date I have been instructed in our school's medication policy and administration procedures. I understand that I am to administer medications to students according to these procedures and as delegated to me by the school nurse. I understand that I am to report immediately to the school nurse any new orders, changes in medication orders, changes in a student's health status, and discovery of a medication error. I understand that I may not delegate this task to any other person. School Staff Signature Date 23
27 Delegation - Part 4: References 1. American Nurses Association. (2010). Nursing: Scope and Standards of Practice, 2nd ed. Silver Spring, MD: Nursebooks.org. 2. American Nurses Association & National Council of State Boards of Nursing. (2006). Joint Statement on Delegation. Washington, DC: American Nurses Publishing. 3. American Nurses Association. (2012). Principles for Delegation by Registered Nurses to Unlicensed Assistive Personnel. Silver Spring, MD: Nursebooks.org. 4. National Association of School Nurses. (2014). Nursing Delegation to Unlicensed Assistive Personnel in the School Setting: Principles for Practice. Silver Spring, MD: 5. National Association of School Nurses. (2014). Nursing Delegation to Unlicensed Assistive Personnel in the School Setting: Position Statement. Silver Spring, MD: 6. National Association of School Nurses. (2015). Unlicensed Assistive Personnel: Their Role on the School Health Services Team: Position Statement. PositionPapersandReports/NASNPositionStatementsFullView/tabid/462/ArticleId/116/Unlicensed- Assistive-Personnel-Their-Role-on-the-School-Health-Services-Team-Adopted-January Guide to Delegation for Colorado School Nurses. (2010). Colorado Department of Education, in collaboration with the Colorado Association of School Nurses and Colorado School Nurse Leadership Michigan Department of Education and Michigan Department of Community Health. (2014). Delegation of Nursing Functions to Unlicensed Assistive Personnel in a School Setting. michigan.gov/documents/mde/delegation_of_nursing_functions_to_unlicensed_assistive_ Personnel_In_a_School_Setting_FINAL_6-9-13_450309_7.pdf. 9. Washington Department of Health Nursing Care Quality Assurance Commission Advisory Opinion. (2014). Registered Nurse Delegation in School Settings. Number NCAO Portals/1/ Documents/6000/RegisteredNurseDelegationInSchoolSettings.pdf 10. Wisconsin Department of Public Instruction. (2009). Delegation, The Nurse Practice Act, and School Nursing in Wisconsin, Indiana Code Title 25, Article 23 and Title 20, Article Indiana Administrative Code Title 848 and Title 511, Article 4. SECTION 4: School Year Calendar SCHOOL NURSE MONTHLY CALENDAR OF ACTIVITIES School Year - **This calendar represents an example of a typical school year of school nurse activities. Please note that there will be variations in operations from district to district and that activities will be in a constant state of flux needing periodic attention. It is suggested that this list be read over as a whole and then used as a guide throughout the year August Open clinic stock cabinets and supplies; update voice message for new school year Obtain licensed health care providers orders Meet with parents of students with chronic and special health needs Develop IHP s as needed 24
28 Train all staff bloodborne pathogens and emergency treatment for asthma, diabetes, severe allergies, and seizures Train individual staff as designated in student IHP s Follow school policy regarding Hepatitis B vaccination for staff and obtaining employee health history Organize daily, p.r.n., and emergency medications Check immunizations of new students and follow up on IC from last school year Review health information for all students Distribute first aid bags for staff (gloves/band Aids) Ensure that each school nurse has joined the DOE Learning Connection, knows their password, and is able to access the Files and Bookmarks tab within the School Nurse s Community September Update and complete IHP s for students Send out notes to parents for further clarification of health issues Share student health concerns with appropriate staff with parent permission according to IHP s Send second request for immunizations Send second request for licensed health care provider orders and/or needed medications Document communication that has occured with providers and parents Post on the school website immunization information required by the Indiana State Department of Health Schedule MCT Vision Screening for K or 1 students: with licensed eye professional or submit waiver October Conduct vision screening for students in grades K or 1, 3, 5, and 8; new students and referrals Conduct hearing screening (if done by school nurse) for students in grades 1, 4, 7, and 10 Consider flu clinics for students and/or staff Consider health and safety activities for secondary schools; breast/testicular cancer education (health education classes) and National Red Ribbon Week activities Suggestions for Fall Health and Safety Promotion:» Mosquito-borne illness prevention» Walking or biking safely to school/pedestrian safety» Handwashing» Communicable disease prevention November Conduct vision and hearing screening for those who were absent or need re-screened Send home referral letters for those students that fail a screening Enter screening results into school database 25
29 December January Enter immunizations into school database Enter immunizations into CHIRP for students in grades K, 1, and 6 with parent permission Complete all of the above Check clinic supplies and re-order as needed Complete screening, referrals, and data entry run report Check to see if students with chronic disease (diabetes, life-threatening allergies) are newly enrolled to school or have different second semester teachers and train teachers as needed Review health information for new students Complete all data entry of screening results and immunizations Distribute hand washing and cover your cough reminders for staff and students Obtain password for DOE Online and test entry into system February Consider activities to promote dental health month Consider changes to policies or procedures for next school year Check with Athletic Director regarding sport physicals and school nurse role regarding athletics March April Inventory clinic supplies and assess needs Organize and plan for kindergarten registration Check Learning Connection for any changes regarding immunizations for next school year Consider spring break (sun safety) and prom (underage drinking) prevention education Order clinic supplies Review care plans for next school year and update as needed Prepare for kindergarten registration: make health charts, check immunization status, input information into computer, compile a list of those that are IC, and notify parent Attend conferences for students with special needs Prepare vision, hearing, and immunization data for School Health Report Assist with sport physicals if needed (must be signed by MD/DO after April 1st for next school year s athletic participation) Notify 5th grade and 11th grade students/families about immunization requirements for the upcoming school year by using the following: flyers, website postings, automated calling to incoming 6th and 12th graders over the summer, posting in the school handbook, or including information along with the spring grade cards 26
30 May June Complete computer inputting of screening and immunizations Run computer report in school database and in CHIRP for noncompliance, or those missed Compile a list of those students with IC, ME and RO and notify parents regarding state law and school policy; share list with school administrator Complete School Health Report via DOE Online for vision, hearing, and immunization data Update procedures and/or forms for next school year Print and/or send out health cards/information for next school year Send forms home to parents to complete over summer medical orders, immunizations, and health plan updates Send home medications with students with parent written permission Dispose of needles, sharps, and expired medication Destroy and shred unnecessary documents Complete a transfer sheet for next nurse if applicable Transfer charts to next school or move charts up to next grade level Receive incoming student charts and review Organize and close-up clinic Change voic on phones (message of out of office until return date) Complete School Health Report if not yet submitted Log into CHIRP (password expires after 90 days of non-use) Ensure you have read the End of the Year Newsletter from the Indiana Department of Education regarding new legislative updates or changes to any laws for the upcoming school year SECTION 5: Stocking the School Clinic Recommended School Health Office Equipment: Desk with lockable drawers Various office supplies (clipboards, pens, folders, stapler) Telephone Computer File cabinet: lockable for student health records Chairs: for student waiting area Medication cabinet: double locking Reference materials: first aid manual, medication reference guide, medical dictionary, guide to specialized healthcare procedures Cots 27
31 Screening equipment: audiometer, vision charts Blankets and pillows with disposable or plastic covers Sharps containers Biohazard receptacle and bags Radio: communication Wall mounted soap dispenser Wall mounter paper towel dispenser Trash cans Eye wash station, if possible Clock with second hand Otoscope and ophthalmoscope Flashlight/penlight Gooseneck lamp and/or magnifying lamp Portable stretcher Wheelchair Whistle Refrigerator Toilet facility Privacy Screen Sink with hot and cold water Emergency bag (go to bag) Documentation forms (workman s compensation forms, accident/incident forms) District Emergency Crisis Manual District Health Procedures Manual Recommended Clinic and First Aid Supplies: AED units (with CPR mask, scissors, towel, maintenance cards) Bandages (latex-free, assorted sizes) Compression wraps (assorted widths) Gauze pads (non-stick, assorted sizes) Tape (hypoallergenic, various widths) Basins (emesis, portable wash) Cold packs Cotton tipped applicators Cotton balls CPR masks (pediatric and adult) Ambu bag 28
32 Disinfectant for surfaces Disposable gowns Eye irrigation supplies Eye pads Gloves (latex-free, various sizes) Personal protective equipment (masks, goggles, gloves, disposable gown) Paper or plastic cups (medicine and drinking) Petroleum jelly or other lubricant Plastic bags (large and small, re-sealable) Safety pins Feminine sanitary products Scissors (various sizes and purpose) Sterile wound wash Recording forms (logs, medication sheets, or electronic charting system) Slings and/or triangular bandages Soap for dispenser Assorted splints Tissues Tweezers Tongue blades Stethoscope Blood pressure cuff (adult and pediatric) Thermometer (probe covers if appropriate) Tooth preservation kit Triage cards (red, yellow, green, and black) Optional items - district policy and procedures and licensed health care provider standing written orders are required Stock emergency medication Pulse oximeter Suction equipment Oxygen Nebulizer Glucose monitoring equipment All of the above suggested items are up to the individual schools to determine their need. List borrowed from the Oklahoma State Department of Health: School Nurse Orientation Manual, which has been adapted from the National Association of School Nurses, "School Nursing Practice: An Orientation Manual". 29


33 Five Ways a School Nurse Benefits a School Attendance - School nurses improve attendance through health promotion, disease prevention and disease management. Students with a full-time school nurse have about half the student illness or injuryrelated early releases from school in comparison to a school where no school nurse is present. Academics - Improved attendance means healthy students are in the classroom and ready to learn. School nurses enable better performance, which also contributes to reduced drop-out rates. Time - School nurses save time for principals, teachers and staff. A school nurse in the building saves principals, teachers, and clerical staff a considerable amount of time that they would have spent addressing health concerns of students. A school nurse in the building saves: Principals almost an hour a day Teachers almost 20 minutes a day Clerical staff over 45 minutes a day Staff Wellness - School nurses improve the general health of staff. According to school reports - principals, teachers, and clerical staff are VERY satisfied with having school nurses in their schools for several reasons: Teachers can focus on teaching Office staff spend less time calling parents and sending students home Healthy staff means increased attendance and productivity Accountability - School nurses help schools stay accountable by: Promoting compliance with federal and state law to mitigate lawsuits Advocating for adequate staffing to align with the Healthy People 2020 recommendations of the ratio of one school nurse per 750 well students (1:750) Preparing for emergencies to save lives and property Addressing student mental health concerns to enhance academic achievement School nurses are instrumental in the identification and referral of students to community resources and are often the only health professional that see students on a regular basis. School nurses are responsible for: Significantly decreasing the amount of days missed due to asthma, the leading cause of school absenteeism, accounting for more than 14 million missed days annually Managing students with chronic conditions such as diabetes and seizures to allow them to stay in class Identifying and treating accidents and injuries Counseling students about physical and emotional issues Adapted and used with permission from the Jennings School District, Jennings, MO. 30

34 Framework for 21 st Century School Nursing Practice TM STANDARDS OF PRACTICE Community/Public Health STANDARDS OF PRACTICE Care Coordination Students Family and School Community Healthy, Safe, Ready to Learn Quality Improvement Leadership STANDARDS OF PRACTICE Better HealtH. Better learning. tm NASN s Framework for 21st Century School Nursing Practice (the Framework) provides structure and focus for the key principles and components of current day, evidence-based school nursing practice. It is aligned with the Whole School, Whole Community, Whole Child model that calls for a collaborative approach to learning and health (ASCD & CDC, 2014). Central to the Framework is student-centered nursing care that occurs within the context of the students family and school community. Surrounding the students, family, and school community are the non-hierarchical, overlapping key principles of Care Coordination, Leadership, Quality Improvement, and Community/ Public Health. These principles are surrounded by the fifth principle, Standards of Practice, which is foundational for evidence-based, clinically competent, quality care. School nurses daily use the skills outlined in the practice components of each principle to help students be healthy, safe, and ready to learn. Standards of Practice Care Coordination Leadership Quality Improvement Community/ Public Health Clinical Competence Clinical Guidelines Code of Ethics Critical Thinking Evidence-based Practice NASN Position Statements Nurse Practice Acts Scope and Standards of Practice Case Management Chronic Disease Management Collaborative Communication Direct Care Education Interdisciplinary Teams Motivational Interviewing/ Counseling Nursing Delegation Student Care Plans Student-centered Care Student Selfempowerment Transition Planning Advocacy Change Agents Education Reform Funding and Reimbursement Healthcare Reform Lifelong Learner Models of Practice Technology Policy Development and Implementation Professionalism Systems-level Leadership Continuous Quality Improvement Documentation/Data Collection Evaluation Meaningful Health/ Academic Outcomes Performance Appraisal Research Uniform Data Set Access to Care Cultural Competency Disease Prevention Environmental Health Health Education Health Equity Healthy People 2020 Health Promotion Outreach Population-based Care Risk Reduction Screenings/Referral/ Follow-up Social Determinants of Health Surveillance ASCD & CDC. (2014). Whole school whole community whole child: A collaborative approach to learning and health. Retrieved from National Association of School Nurses, Rev. 10/26/15
35 Role of the School Nurse SUMMARY Position Statement It is the position of the National Association of School Nurses that the registered professional school nurse is the leader in the school community to oversee school health policies and programs. The school nurse serves in a pivotal role to provide expertise and oversight for the provision of school health services and promotion of health education. Using clinical knowledge and judgment, the school nurse provides health care to students and staff, performs health screenings and coordinates referrals to the medical home or private healthcare provider. The school nurse serves as a liaison between school personnel, family, community and healthcare providers to advocate for health care and a healthy school environment (American Nurses Association & National Association of School Nurses [ANA & NASN], 2011). HISTORY The practice of school nursing began in the United States on October 1, 1902, when a school nurse was hired to reduce absenteeism by intervening with students and families regarding health care needs related to communicable diseases. After one month of successful nursing interventions in the New York City schools, Lina Rogers, the first school nurse, was able to provide leadership to implement evidence based nursing care across the city. The school nurse s role has expanded greatly from its original focus, the essence and goals of the practice remains the same (Vessey & McGowan, 2006). DESCRIPTION OF THE ISSUE A student s health status is directly related to his or her ability to learn. Children with unmet health needs have a difficult time engaging in the educational process. The school nurse supports student success by providing health care through assessment, intervention, and follow up for all children within the school setting. The school nurse addresses the physical, mental, emotional, and social health needs of students and supports their achievement in the learning process. The school nurse not only provides for the safety and care of students and staff but also addresses the need for integrating health solutions into the education setting. The number of children that have a chronic condition has increased dramatically over the past four decades (Perrin, Bloom, & Gortmaker, 2007). Chronic conditions such as asthma, anaphylaxis, type 1 diabetes, epilepsy, obesity and mental health concerns may impact the student s ability to be in school and ready to learn. The number of students with special health care needs has also increased dramatically over the past decade. Students are coming to school with increasingly complex medical problems, technically intricate medical equipment, and complicated treatments (Robert Wood Johnson Foundation, 2010). The school nurse is a registered professional nurse who has a commitment to lifelong learning. Educational preparation for the school nurse should be at the baccalaureate level, and the school nurse should continue to pursue professional development and continuing nursing education. School nurses typically practice National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland
36 independently and are called upon to assess student health, develop and execute plans for care management, act as first responders, and engage in public health functions such as disease surveillance, immunization compliance, and health promotion. The school nurse is a vital member of the school team that leads change to advance health and collaborates with school staff members, parents and community members to keep students safe at school and healthy to learn. RATIONALE School nursing has multiple components and the role of the school nurse is a broad one, dependent on many factors, including the school setting (rural, urban, suburban), health needs of the student population and the availability of specialized instructional student support services and programs. The National Association of School Nurses defines school nursing as a specialized practice of professional nursing that advances the well being, academic success and lifelong achievement and health of students. To that end, school nurses facilitate normal development and positive student response to interventions; promote health and safety including a healthy environment; intervene with actual and potential health problems; provide case management services; and actively collaborate with others to build student and family capacity for adaptation, self management, self advocacy, and learning (NASN, 2010). School nurses facilitate normal development and positive student response to interventions. The school nurse serves as the health care expert in the school to meet student health needs with an understanding of normal growth and development in children and youth as well as students with special needs. The school nurse develops plans for student care based on the nursing process, which includes assessment, interventions, and identification of outcomes and evaluation of care (Wolfe, 2006). School nurses provide leadership in promoting health and safety, including a healthy environment. The school nurse provides health related education to students and staff in individual and group settings and provides consultation to other school professionals, including food service personnel, physical education teachers, coaches, and counselors. Responsibilities in the provision of a safe and healthy school environment include the school nurse s monitoring of immunizations, managing communicable diseases, assessing the school environment for safety to prevent injury and spearheading infection control measures. The school nurse is also a leader in the development of school safety plans to address bullying, school violence, and the full range of emergencies that may occur at school (Wolfe, 2006). School nurses provide quality health care and intervene with actual and potential health problems. Health care for chronic and acute illness, as well as injuries in the school setting, is a major focus of the role of the school nurse. The school nurse is responsible for medication administration, health care procedures, and the development of health care plans. Students often have multiple needs that should be examined in order for the student to be able to be successful in the classroom, and school nurses often engage in health screenings that include vision, hearing, body mass index, mental health index or other screening procedures (often based on local and state regulations) to address those issues (Wolfe, 2006). School nurses use clinical judgment in providing case management services. The school nurse receives medical orders to guide the health care needed to assist each student to be safe and successful at school. As in other clinical settings, the nurse develops Individualized Healthcare Plans (IHPs) in nursing language to direct nursing care for students as well as Emergency Care Plans (ECPs) written in lay language to guide the response of unlicensed personnel in a health related emergency. National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland
37 Both plans are tailored to the individual needs of a specific student to improve expected care outcomes. The nurse makes decisions related to the appropriate delegation of healthcare tasks as directed by state laws and professional practice guidance (American Nurses Association [ANA]/National Council of State Boards of Nursing [NCSBN], 2006). As medical and information technology advance and change, it is imperative for the school nurse to pursue professional development so the school nurse is able to provide the best possible care for the student population (Wolfe, 2006). School nurses actively collaborate with others to build student and family capacity for adaptation, selfmanagement, self advocacy and learning. Coordinating the linkage between the medical home, family and school is an important aspect of the role of the school nurse. The school nurse has health expertise that is essential to school educational teams, such as the Committee on Special Education, the Individualized Educational Plan (IEP) team and the Section 504 Team so that health related barriers to learning can be reduced for each student. The school nurse can provide families with referral information along with available community resources to improve access to health care. The school nurse can also assist families in obtaining health insurance as needed and can represent the school on community coalitions to advocate for school based health care (Wolfe, 2006). The school nurse may take on additional roles as needed to meet the needs of the school community. Healthy children are successful learners. The school nurse has a multi faceted role within the school setting, one that supports the physical, mental, emotional, and social health of students and their success in the learning process. It is the breadth of nursing activities contained within the role of the school nurse and the unique nonmedical setting that differentiates school nursing from other nursing specialties. REFERENCES American Nurses Association & National Association of School Nurses. (2011). Scope and standards of practice School nursing (2 nd ed.). Silver Spring, MD: Nursesbooks.org. American Nurses Association & National Council of State Boards of Nursing. (2006). Joint statement on delegation. Retrieved from ANA.pdf National Association of School Nurses. (2010). Definition of school nursing. Retrieved from Perrin, J. M., Bloom, S.R., & Gortmaker, S. L. (2007). The increase of childhood chronic conditions in the United States. Journal of the American Medical Association, 297(24), doi: /jama Robert Wood Johnson Foundation. (2010). Unlocking the potential of school nursing: Keeping children healthy, in school, and ready to learn. Retrieved from Vessey, J., & McGowan, K. (2006). A successful public health experiment: School nursing. Pediatric Nursing, 32(3) Wolfe, L. C. (2006). Roles of the school nurse. In J. Selekman (Ed.), School nursing: A comprehensive text. Philadelphia, PA: F.A. Davis Company. National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland
38 Acknowledgement of Authors Connie Board, BSN, RN, NCSN Margo Bushmiaer, MNSc, RN, NCSN Linda Davis Alldritt, MA, BSN, PHN, RN, FNASN, FASHA Nina Fekaris, MS, BSN, RN, NCSN Judith Morgitan, MEd, BSN, RN Kathleen Murphy, DNP, RN, FNP BC Barbara Yow, MEd, BSN, RN, CSN Adopted: 2002 Revised: National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland

39 Chapter 2: Laws Impacting School Nurses SECTION 1: FEDERAL LAWS SECTION 2: STATE LAWS SECTION 3: LOCAL LAWS 36
40 There are many federal and state laws that have an impact on schools. Schools must first follow all federal mandates, then all state mandates, and finally, all school policies that cover topics related to school health (see the flow diagram at the end of this chapter for a more detailed explanation of this process). SECTION 1: Federal Laws Federal laws impacting school health topics fall into the two main categories of confidentiality laws and discrimination laws. The following federal laws will be discussed in the sections below. Confidentiality Laws HIPAA FERPA Discrimination Laws IDEA Section 504 HIPPA The Health Insurance Portability and Accountability Act (HIPAA) addresses the use and disclosure of individuals health information, called protected health information by organizations called covered entities, as well as standards for individuals to understand and control how their health information is used. A major goal of HIPAA is to assure that individuals health information is properly protected while allowing the flow of health information needed to provide and promote high quality healthcare and to protect the public s health and well-being. The HIPAA Privacy Rule governs the release of protected health information by physicians and other healthcare providers [1]. The HIPAA Privacy Rule allows covered healthcare providers to disclose protected health information about students to school nurses, physicians, or other healthcare providers for treatment purposes, without the authorization of the student or student s parent (See 45 CFR ). For example, a student s primary care physician may discuss the student s medication and other healthcare needs with a school nurse who will administer the student s medication and provide care to the student while the student is at school. Generally, the HIPAA Privacy Rule does not apply to public elementary and secondary schools [2]. At the elementary or secondary school level, students immunization and other health records that are maintained by a school district or individual school, including a school-operated health clinic that receives funds under any program administered by the U.S. Department of Education, are education records subject to the Family Educational Rights and Privacy Act (FERPA). FERPA FERPA is a federal law that protects the privacy of students education records (See 20 U.S.C. 1232g; 34 CFR Part 99). FERPA applies to educational agencies and institutions that receive funds under any program administered by the U.S. Department of Education. This includes virtually all public schools and many private schools. [1] Assumes physicians and healthcare providers conduct certain electronic transactions such as processing claims. [2] In most cases, the HIPAA Privacy Rule does not apply an elementary or secondary school because the school either; (1) is not a HIPAA covered entity or (2) is a HIPAA covered entity but maintains health information only on students in records that are by definition education records under FERPA and, therefore is not subject to the HIPAA Privacy Rule. 37
41 Generally, under FERPA, school nurses are not allowed to disclose education records without parent consent. School nurses may disclose educational records without parent consent if the circumstance meets one of the exceptions to FERPA s general consent requirements which include: School officials, including teachers, that the school or district has determined to have "legitimate educational interests." In an emergency "if knowledge of the information is necessary to protect the health or safety of the student or other individuals" (See 34 CFR 99.31(a)(1) and 99.36). Instances of abuse or neglect. Mandatory reporting of communicable diseases classified as immediate or within 24 hours. Information that is required by a school to which the student is transferring. Certain legal situations including subpoenas or investigations of criminal offenses. Parents have a right under FERPA to inspect and review these health and medical records because they are education records under FERPA (See 34 CFR ). In addition, these records may not be shared with third parties without written parental consent unless the disclosure meets one of the exceptions to FERPA s general consent requirement. Thus, under HIPAA, providers may discuss a student s health issues with the school nurse; but the school nurse, under FERPA, must obtain parent permission before discussing the student s health information with the provider. RECOMMENDATIONS To facilitate open communication between schools and providers, parents and/or guardians of students with health conditions are encouraged to sign medical releases for both the school nurse and the provider. Schools should establish policies that address appropriate communication between school staff, parents, and outside entities. Those who oversee the healthcare of children attending school should establish a mechanism for regular and timely communication between all appropriately designated parties. While maintaining the confidentiality of student health information, , text messaging, and phone contact should be easily accessible between these parties. A written individual healthcare plan should be in place for all children who have treatment orders prescribed for actual or potential implementation during the school day or at extracurricular activities. This health plan should be reviewed with all parties on at least an annual basis. Changes to the health plan should be communicated in an expedited manner, whether from caregiver or health provider. Implementation of new medication or treatment orders should commence within one school day of the orders being sent to the school. Feedback from each involved partner (school nurse, parent/guardian, and healthcare provider) should be welcomed and documented in the school and provider health record. 38
42 FREQUENTLY ASKED QUESTIONS REGARDING FERPA 1. What laws and rules regulate confidentiality of health information in public schools? FERPA, HIPAA, and the confidentiality required by one's nursing license all may contribute to the constraints placed on public school nurses. 2. What is FERPA? The Family Educational Rights and Privacy Act is a federal law that outlines who has access to education records. It applies to all schools that receive federal funds from any program administered by the U.S. Department of Education. Complete Law Discussion of the changes that went into effect January of 2009 Summary from the U.S. Department of Education 3. Does FERPA apply to school health records? Yes. Student health records maintained by school employees are considered part of the education record. 4. What about HIPAA? How does that affect school health services? The Health Insurance Portability and Accountability Act is another federal law that dictates how health records are to be handled. A school is subject to HIPAA only if it provides medical care and electronically transmits health information as part of a "covered transaction" (e.g., billing) (45 CFR ). For most schools, HIPAA will only be an issue when you communicate with a student's medical provider. While you are not regulated by HIPAA, almost all medical practitioners you deal with are covered by HIPAA. They cannot disclose protected medical information without authorization except for treatment purposes, payment, and operational purposes. Since "treatment purposes" is one of the exceptions, a practitioner may relay or clarify treatment orders to individuals involved in the treatment of that patient (e.g., school nurse) without obtaining authorization. Some medical offices may not have a thorough understanding of HIPAA. While it is entirely legal for them to clarify treatment plans, etc., without authorization, many offices may still refuse to do so. You might consider sharing the above mentioned summary from the U.S. Department of Health on this matter with the provider. Remember though, that while a practitioner, under HIPAA, can discuss treatment orders with a school nurse without obtaining authorization; the school nurse, under FERPA, must obtain parent consent in order to discuss student health concerns with the practitioner. 5. What is "Directory Information"? FERPA defines "directory information" as information contained in the education records of a student that would not generally be considered harmful or an invasion of privacy, if disclosed. Typically, "directory information" includes information such as name, address, telephone listing, date and place of birth, participation in officially recognized activities and sports, and dates of attendance. A school may disclose "directory information" to third parties without consent if it has given public notice of the types of information which it has designated as "directory information," the parent or eligible student has the right to restrict the disclosure of such information, and the period of time within which a parent or eligible student has to notify the school in writing that he or she does not want any or all of those types of information designated as "directory information has 39
43 been published. The means of notification could include publication in various sources, including a newsletter, in a local newspaper, or in the student handbook. The school could also include the "directory information" notification as part of the general notification of rights under FERPA. The school does not have to notify a parent or eligible student individually (34 CFR 99.37). 6. Since most school health records are covered by FERPA, who can access this information without parental consent? Eligible students and parents of minor students have a right to see their records. (Eligible students are those that are at least 18 or those who are attending a postsecondary institution (34 C.F.R 99.3)). In general, parental consent is required for others to access information in students' health records. Below are some of the circumstances where consent is not required (See 20 USC. 1232g (b)-(j) and 34 C.F.R 99.31). School officials, including teachers, that the school or district has determined to have "legitimate educational interests" (defined below). In an emergency "if knowledge of the information is necessary to protect the health or safety of the student or other individuals" (See 34 C.F.R (a)). Instances of abuse or neglect. Mandatory reporting of communicable diseases (please see below for exceptions). Information that is required by a school to which the student is transferring. Certain legal situations including subpoenas or investigations of criminal offenses. 7. What is "legitimate educational interest"? School officials can have access to only the education records necessary to carry out their job function. "In general, legitimate educational interest refers to the right of certain school officials to access student information and records for the purpose of (a) serving the student; (b) protecting the health, safety, and learning of this student and others; (c) maintaining operations of the school district; (d) obtaining payment for educational programs and services; and (e) other purposes as specified in federal and state law." Source: Schwab NC, Rubin M, Maire JA, Gelfman MHB, Bergren MD, Mazyck D, Hine B. (2005). Protecting and Disclosing Student Health Information: How to Develop School District Policies and Procedures. Kent, OH: American School Health Association. 8. Can a list of students' health issues be distributed to teachers or other staff? A school-wide health concerns distribution list violates FERPA and is not best practice. If school staff members need to be informed of a student's condition, that student requires an ECP (Emergency Care Plan) listing symptoms to be alert for and the required response to those symptoms. It is recommended that parents, as a part of the IHP (Individual Health Plan), participate in deciding who on staff requires identifiable health information for the child's safety. Staff members who are trusted with personally identifiable health information should receive training regarding their responsibility to safeguard that information. Nurses can ensure that confidentiality is respected by revealing only necessary health concerns and only to those individuals whose knowledge may affect the student's health. For example, individuals who have no contact with a particular student have no need to know that student's medical or mental health issues. Using the IHP as the vehicle to determine what information should be shared with specific staff members is not only more discrete but has the additional benefit of delivering more practical information to school employees that generally have limited medical knowledge. The best approach to handling this potential problem is to work with your school administration to draft medical information policies that are consistent with the requirements of both FERPA and the 40
44 Indiana State Board of Nursing. 9. If a school nurse maintains personal notes, are they part of the educational record and thus subject to FERPA? No, but only if all of the following criteria are met: the notes are kept only as a memory aid; they remain in the sole possession of the writer; they are shared with no one except a temporary substitute RN; and they are not used to replace or avoid normal documentation. In general, personal notes are not recommended. Information related to health office visits should be documented in the student's individual record. Source: Schwab NC, Rubin M, Maire JA, Gelfman MHB, Bergren MD, Mazyck D, Hine B. (2005), Protecting and Disclosing Student Health Information: How to Develop School District Policies and Procedures, Kent, OH: American School Health Association. 10. When can schools share health information with other agencies within their state? The Family Policy Compliance Office of the U.S. Department of Education responded to this issue in a letter to University of New Mexico. Abuse or neglect: School employees are required to report suspected abuse or neglect. FERPA does not override that responsibility. Certain reportable diseases: Some communicable diseases require emergent reporting while other diseases represent a less imminent public health threat. For example, the Indiana State Department of Health has a Communicable Disease Rule that states the timeline for reporting certain medical conditions (410 IAC ). If reporting must occur immediately or within 24 hours, the Family Policy Compliance Office of the U.S. Department of Education has determined that indicates "imminent danger." As such, those illnesses may be reported without obtaining consent. The diseases on the 72 Hour List do not pose imminent danger, so school officials must obtain consent before disclosing this information. Concern that a student may hurt self or others: if someone is in imminent danger, no consent is required. De-identified data: It is permissible to share health related data that does not contain information that makes the student's identity readily traceable. For example, the information released applies to at least 10 other students that could fit into the same group. 11. What about immunization records? This issue was discussed by the Family Policy Compliance Office of the U.S. Department of Education in a letter to the Department of Education in Alabama. Based on that response, we offer the following guidance. You can share immunization records with parents or with a school where the student is transferring without obtaining consent. However, before providing immunization records to an outside medical office or state Department of Health, you must get written consent. You can share deidentified data such as total number of students that are up-to-date, total number that require additional immunizations and total number that are exempt without obtaining consent. Please consult your school's attorney if further clarification is needed. 12. What if I am concerned that a student might hurt themselves or someone else but I have no evidence? If the school evaluates the information available at the time and feels that there is an "articulable and significant threat to the health or safety of a student or other individuals, it may disclose information from education records to any person whose knowledge of the information is necessary to protect 41
). 13. Can school personnel talk to a student's healthcare provider without consent?")
45 the health or safety of the student or other individuals." It is not necessary to first collect evidence before contacting those that can intervene to protect the student or others (34 C.F.R (c)). 13. Can school personnel talk to a student's healthcare provider without consent? Generally, schools must have written permission from the parent or eligible student in order to release any information from a student's education record to outside parties, including providers. However, a school nurse may call a student's healthcare provider to clarify facts surrounding a student's condition or treatment plan. The physician's office may relay or clarify treatment orders to individuals involved in the treatment of that patient (e.g. school nurse) without obtaining authorization. The medical office may be hesitant to discuss any details without first getting signed authorization. Remember that both you and the healthcare provider are working in the best interests of the child. Respectful communication should allow both sides to find an acceptable plan so that you can obtain the necessary information. For further guidance regarding FERPA and HIPAA, please click here. 14. One major misconception about FERPA. FERPA does not protect the confidentiality of information in general. FERPA prohibits the improper disclosure of information contained in the education record. FERPA does not apply to one's opinions or observations unless it is entered into the record. However, you must consider that the confidentiality of facts learned in the course of your nursing duties may be required by the virtue of your nursing license. ACKNOWLEDGEMENT This document was developed and adapted with permission from the New Hampshire Department of Education: Confidentiality and School Health Records. Additional Resources National Forum on Education Statistics. (2006). Forum Guide to the Privacy of Student. Information: A Resource for Schools (NFES ). U.S. Department of Education, Washington, DC, National Center for Education Statistics. National Association of School Nurses, Issue Brief - Privacy Standards for Student Health Records,
46 IDEA The Education for All Handicapped Children Act, which is now known as the Individuals with Disabilities Act (IDEA), was first enacted in This legislation was needed to assure that students with disabilities received Free Appropriate Public Education (FAPE) and the related services and support they need to achieve academic success. IDEA was created to help states and school districts meet their legal obligations to educate children with disabilities, and to pay part of the extra expenses of doing so. Part B of IDEA requires school districts to have a multi-disciplinary team to develop an Individualized IEP for each student after an appropriate evaluation and assessment in all areas of suspected disability has been completed. The plan must include information from the multi-disciplinary team, including evaluation results, to decide what special education related services and supplementary aids and services that the student needs to benefit from his/her educational plan. IDEA mandates that special education and related service programming be made available to all children and youth with disabilities who require them. The law also makes available federal funds to help state and local governments establish and maintain special education programs for students with disabilities, as well as provide the related services these students need in order to benefit from special education. As defined by federal law, related services are intended to address the individual needs of students with disabilities, in order that they may benefit from their educational program. The fields, associated with delivering related services that students with disabilities may require to benefit from their special education programs include audiology, occupational therapy, physical therapy, psychological services, medical services for diagnostic or evaluation purposes only, school health services, transportation services, counseling services, social work services, speech-language pathology, parent/ guardian counseling and training, recreation therapy, rehabilitation counseling, and early identification and assessment of disabilities in children. Following identification, the question of whether a disability exists and to what extent it interferes with education must be addressed. This requires a multidisciplinary evaluation. Once the multidisciplinary evaluation is completed, special education eligibility must be established. The eleven categories of special education eligibility are mental retardation, hearing impairment (including deafness), speech or language impairment, visual impairment (including blindness), serious emotional disturbance, physical handicap (including orthopedic) and other health impairment, autism, deaf-blindness, learning disabled, multiple disabilities, and traumatic brain injury. If a student is eligible for special education placement, the multidisciplinary team is responsible for development of an IEP. The decisions on how to provide educational services to a student must be adapted to that student s unique needs and made by a team that includes the student (if appropriate), and the student s parent or legal guardian. The team must address the eligibility criteria, instructional program, placement, and related services to be provided to the student. These programs and services are provided in the least restrictive environment, meaning with non-disabled peers to the greatest extent possible. A comprehensive review of each student s educational progress is mandated every three years. This review serves as the foundation for assessing the student s ongoing eligibility and the need for special education as well as provides information for updating the IEP (Oklahoma 37, 38). For more information, please see: SECTION 504 The Vocational Rehabilitation Act (1973) was the first federal statute to ban discrimination against individuals on the basis of disabilities. It was originally enacted to protect disabled veterans dating back to World War I, 43
47 but was expanded to include all persons with a disability. The revision in 1973 added a section, referred to as Section 504, which prohibits discrimination against qualified persons with disabilities in federally funded programs and activities. Because most schools receive federal assistance of some sort, even if they are private or parochial, they are included in the interpretations of the law. It is a civil rights law addressing nondiscrimination. The Rehabilitation Act defines a person with a disability as someone who (1) has a mental or physical impairment that significantly restricts one or more major life activities; (2) has a record of such impairment; or (3) is regarded as having such impairment. Physical or mental impairment includes (A) any physiological disorder, cosmetic disfigurement or anatomical loss affecting one or more of the following systems: respiratory, including speech; cardiovascular; reproductive; digestive; genitourinary; hematologic and lymphatic; skin; and endocrine or (B) any mental or psychological disorder such as mental retardation, organic brain syndrome, emotional or mental illness and specific learning disabilities (U.S. Department of Education, Code of Federal Regulations Part 104.3). Where IDEA covers only students who are eligible for special education, the Rehabilitation Act covers all students and staff with disabilities, including those with chronic conditions. This is the major difference between IDEA and the Rehabilitation Act. Examples of students who would be covered under Section 504 but not covered under IDEA include those with allergies, inflammatory bowel disease, cystic fibrosis, asthma, obesity, diabetes, and rheumatoid arthritis. The school must first identify students and determine their eligibility under Section 504. The school nurse should be part of the 504 team and be prepared to articulate how the disability affects major life functions and to recommend interventions that may assist the student to be successful in the school environment. The school team must include parents and individuals who are knowledgeable about the student, the disability, and the process to determine both the student s eligibility for accommodations and the accommodations that are necessary (Moses, Gilchrest, & Schwab, 2005). Anyone can make a referral for evaluation of a student s eligibility but the school district must also have reason to believe that the child needs services under Section 504 because of a disability. SECTION 2: State Laws There are many state laws that must be followed in Indiana. There are two types of Indiana Laws Indiana Code passed by state legislators and signed into law by the Governor; and Indiana Administrative Code which are rules passed by a state agency to implement a law. Below is a list of the most commonly referenced school health laws. Please be aware that these laws have the possibility of being changed during each legislative session. Laws can be repealed (deleted), revised (changed), or enacted (added) into the legislative code. At the end of each legislative session (May of each year), the Indiana State Department of Education will send information out to school nurses via the School Nurse Newsletter to all members of the School Nurse Learning Connection regarding any legislative changes that have occurred. School personnel can access the most recent version of any law, or follow a bill as it passes through a legislative session, by visiting the Indiana General Assembly website at Further instructions on how to locate an Indiana law can be found at the end of this section. 44
48 INDIANA LAWS RELATED TO SCHOOL HEALTH Attendance IC : Birth certificate required IC : Certificate of incapacity/illness IC : Attendance IC : Religious objection regarding attendance IC : Reporting above 20% absenteeism 512 IAC 1-2-2: Reporting above 20% absenteeism Child Abuse IC Concussion IC Diabetes IC Hearing IC : Hearing testing, records Immunity IC : Immunity for providing voluntary healthcare IC : Immunity during a disaster IC : School personnel cannot be required to give medications IC : School personnel immunity regarding medication administration IC : School immunity regarding students who self-administer IC : Teacher CPR immunity IC : School nurse CPR immunity IC : School CPR immunity Immunizations IC IC : Religious objection IC : Medical exemption Mandatory Curriculum IC : Bullying prevention IC : Physical activity for elementary students IC : Hygiene IC : Diseases IC : Alcohol, drugs, and tobacco IC : AIDS IC : Sexually transmitted diseases IC : Breast and testicular cancer IC : Organ and blood donor program IC : Student survey and parent consent for participation IC : Meningitis IC : CPR and AED instruction in high school health education curriculum Medications IC : Ability to possess and self-administer 45
49 IC : Describes release of medication to parent IC : Describes lay person giving related to diabetes IC : School personnel cannot be forced to give IC : School personnel immunity regarding medication administration IC : School immunity for students who self-administer 511 IAC : Describes medication administration School Nursing 511 IAC : Describes RN required to provide health services 511 IAC : Recommended ratios of one RN for every 750 students 511 IAC : Defines health services ; defines coordinator 848 IAC (8) and (9): Defines nursing delegation 848 IAC 2-2-3: Defines unprofessional conduct related to improper delegation Stock Epinephrine IC Sudden Cardiac Arrest IC Vision IC : Vision testing, records, and reports IC : Vision, MCT waiver SECTION 3: Local Laws In the United States, the legislative authority given to local governments varies from state to state. Indiana is known as a home rule state where an amendment to our state constitution grants Indiana cities, municipalities, and/or counties the ability to pass laws to govern themselves as they like (as long as state and federal constitutions are obeyed). Thus, in the absence of a federal or state law, Indiana school policies are developed at the local level. School board members are elected to function as members of a governmental body and are the policymakers for their schools. Local school corporations are governed via policies developed and adopted by the school board. Their policies must be in written form with the purpose of determining present and future decisions by school administrators. School corporation policies are to be accessible to board members, administrators, staff members, and members of the community. 46
50 FEDERAL, STATE, AND LOCAL LAWS FLOW CHART Is there a Federal Law to guide your nursing question? Examples: Confidentiality (FERPA, HIPAA) Discrimination (IDEA, 504) If "YES" Follow that guidance If "NO" Is there a State Law to guide your nursing question? Indiana Code (IC ) Examples: Title 16=Health Title 20=Education Title 25= Professions and Occupations or Indiana Administrative Code (IAC) Example: Title 511 =Indiana State Board of Education Agency Examples: Indiana Department of Education Indiana State Department of Health If "YES" Follow that guidance If "NO" Follow your Local School Policies Your School Board Approves Policies Your School Administrators Develop Procedures School Nurse Implements Procedures If NO Local School Policy exists: Use Best Practices and Good Resources to develop your own Procedures Resource Examples: National Association of School Nurses (NASN) Centers for Disease Control (CDC) 47

.")
, A (Article), C (Chapter).")
51 GUIDANCE INSTRUCTIONS FOR LOCATING INDIANA LAWS Step 1: Click on this link: to access the Indiana General Assembly Website Step 2: Know the Indiana Code (IC) numbers to the law you would like to look up (i.e. IC ). Step 3: Go to the right upper side of the computer screen and click on Code Step 4: Enter the Indiana Code Numbers into the appropriate boxes (i.e. T (Title), A (Article), C (Chapter). Step 5: Click Enter and scroll down the until you see the law you were looking for listed below. Step 6: Click on the blue words to see that portion of the law (i.e. the Chapter, Article, or Title) that you would like to view. Note clicking on the Chapter will usually take you to the most specific portion of the law that you would like to see. 48

52 Chapter 3: Chronic Disease Management in Schools SECTION 1: CHRONIC DISEASE OVERVIEW SECTION 2: ASTHMA SECTION 3: SEVERE ALLERGIES/ANAPHYLAXIS SECTION 4: DIABETES SECTION 5: SEIZURES 49
53 SECTION 1: Chronic Disease Overview INTRODUCTION Many children have chronic medical conditions or special healthcare needs. Chronic refers to a health condition that lasts anywhere from three months to a lifetime. Although there are many additional chronic medical conditions and healthcare needs experienced in school-aged children, the most common chronic diseases are considered to be: Asthma Life-Threatening Allergies Diabetes Seizure Disorders The needs of children with chronic medical conditions or special healthcare needs vary as children grow and attain increasing levels of independence. However, school administrators and staff must remain mindful of the fact that these students are in out-of-the-home settings (such as schools) for many hours of the day while their health must be maintained as prescribed by their healthcare provider. This caregiving must be maintained while continuing to provide students with a quality education. To accomplish this mandate for caregiving, it is the position of the National Association of School Nurses (NASN) that students with chronic health conditions should have access to a full-time registered professional school nurse. The NASN encourages school districts to include school nurse positions as school nurses are the health professional who can best plan and implement the complex healthcare needs of students with chronic health conditions. See the complete NASN position paper (PDF) Chronic Health Conditions Managed by School Nurses below for additional information. NASN, Chronic Health Conditions Managed by School Nurses (PDF) SECTION 2: Asthma THE MANAGEMENT OF STUDENTS WITH ASTHMA: What is Asthma? Asthma is a chronic (long-term) disease that causes your airways to become inflamed, swollen, and narrowed, making it hard to breathe. The narrowed passages and increased mucus production can reduce the airflow both to and from the lungs. Wheezing can often be heard as air moves through the narrowed airways. Individuals with asthma may experience repeated episodes of wheezing, chest tightness, and shortness of breath with or without a cough. Asthma is the leading chronic disease in children one in ten American children has asthma. It is also the top reason for missed school days. There is no cure for asthma. The best way to manage asthma is to avoid triggers, take medications to prevent symptoms, and prepare to treat asthma episodes if they occur. Characteristics of Children with Asthma: Asthma can become worse with changes in the weather, infections, and exposure to triggers. Triggers are those things that can make an individual s asthma condition worse. Common triggers include dust mites, animal dander, viral infections, smoke, and cockroaches. Asthma can be experienced occasionally or continuously, as well as mild or severe. 50
54 The symptoms experienced (cough, wheezing, chest tightness, shortness of breath) depend upon the amount of air that moves through the airways. With good asthma care, including student/parent education, asthma can be controlled with minimal symptoms experienced. What are Asthma Emergencies? Consider both these urgent and emergent symptoms when assessing students with asthma. Urgent Signs for Asthma Include: Multiple doses of rescue medication needed during the school day Coughing Breathing using rib and neck muscles (rather than diaphragm) Wheezing Peak flow in the YELLOW ZONE (student must stand for correct method; use best of 3 results) Pulse Oximeter 93%-95% (normal should be %) EMERGENT Signs for Asthma Include: Difficulty walking or talking Fingernails/lips blue or gray Struggling to breath Difficulty talking or walking Symptoms do not improve after second dose of rescue medication Peak Flow in the RED ZONE (student must stand for correct method; use best of 3 results) Pulse Oximeter at 92% or less Notify parents about asthma episodes and symptoms, even when not an emergency, so that they have an opportunity to work with the student s healthcare provider to keep symptoms under good control. Indiana Law Applicable to Care of Students with Asthma: Access this law at Indiana General Assembly: by entering as the Indiana Code or Law Visit the Indiana Department of Education Health Web at: student-services/health/health-laws Synopsis of IC Possession and Self-Administration of Medication Permitted : Students with a chronic disease or medical condition may possess and self-administer medication for the chronic disease or medical condition if the student s parents have annually filed an authorization that included that a physician state the student has a condition for which the physician has prescribed medication, the student has been instructed on how to self-administer, and the condition requires emergency administration. Individual Health Care Plans (IHP) for Asthma: Students with asthma should have an IHP with an Emergency Care Plan written and implemented during both school hours and school-related activities. A sample Asthma Action Plan (found in the forms list below) may 51
55 provide school nurses with a basis for an Emergency Care Plan. School nurses may also use their own local school district forms or those found online. Additional topics to be addressed in a complete IHP, such as field trips, avoidance of triggers, and training of staff, should be incorporated to complete an IHP for students with asthma. (IHP s and Emergency Care Plans are discussed further in Chapter 4 of this manual) Delegating the Care of Students with Asthma: In the absence of a registered nurse (RN) on site for providing student health care, it is necessary to determine the delegation plan of said care to alternate staff members. The Delegation Guidelines for Indiana School Nurses can be found in Chapter 1 of this manual for your reference regarding student healthcare delegation in the absence of a registered nurse. Sample Asthma Forms: Sample Information Form for Parent Asthmatic Students (PDF) Student Readiness Assessment Tool, American Lung Association readiness.html Sample Contract for: Students Carrying Inhalers with Them While at School (PDF) Sample Physician Authorization for Self-Carry Medications (PDF) Sample Asthma Action Plan (PDF) Parent Information Sheet - Children and Adolescents with Asthma: How Can You Help? (PDF) Resources for Managing Students with Asthma: Indiana Department of Education Health Web: School Nurse Learning Connection o Access the Files and Bookmarks Tab o Click on Chronic Conditions Folder o Click on the Asthma Folder Additional Resources Allergy & Asthma Network Mothers of Asthmatics (800) or (703) (link is external) American Academy of Allergy, Asthma & Immunology (800) 822-ASMA or (414) (link is external) American Academy of Pediatrics (800) or (847) (link is external) 52
56 American College of Allergy, Asthma & Immunology (800) or (847) (link is external) American Lung Association For the affiliate nearest you, call (800) LUNG USA (link is external) Asthma and Allergy Foundation of America (800) 7-ASTHMA or (202) (link is external) Centers for Disease Control and Prevention National Center for Chronic Disease Prevention and Health Promotion Division of Adolescent and School Health (800) CDC-INFO NAEPP School Materials National Association of School Nurses (866) National Asthma Control Initiative National Asthma Education and Prevention Program National Heart, Lung and Blood Institute Information Center (301) U.S. Environmental Protection Agency Indoor Environments Division (202) Indoor Air Quality Information Clearinghouse (800)
57 SECTION 3: Severe Allergies/Anaphylaxis THE MANAGEMENT OF STUDENTS WITH LIFE-THREATENING ALLERGIES: What are Life-Threatening Allergies? Life-threatening allergic reactions illicit an anaphylactic response in persons who are exposed to their allergic trigger. Anaphylaxis is a severe, potentially life-threatening allergic reaction. It can occur within seconds or minutes of exposure to an allergen, such as a peanut or the venom from a bee sting. The flood of chemicals released by the immune system during anaphylaxis can cause a person to go into shock, coinciding with a sudden drop in blood pressure and a constriction of the airways that prohibits normal breathing. Common triggers of anaphylaxis include certain foods, some medications, insect venom, and latex. Anaphylaxis requires an immediate injection of epinephrine and prompt transport to the emergency department. If anaphylaxis is not treated immediately, it can lead to unconsciousness or even death. The prevalence of food allergies among children increased 18% during , and allergic reactions to foods have become the most common cause of anaphylaxis in community health settings. Staff who work in schools should develop plans for how they will respond effectively to children with life threatening allergies. Although the number of children with severe allergies in any one school may seem small, allergic reactions can be life-threatening and have far-reaching effects on children and their families, as well as on the schools they attend. Any child with a life-threatening allergy deserves attention and the school should create a plan for preventing an allergic reaction and responding to an allergy emergency. Characteristics of Children with Life-Threatening Allergies: Factors that increase the risk of experiencing a life-threatening reaction include: failure or delay in administering epinephrine, history of asthma, and students aged % of allergic reaction symptoms are first reported to the teacher in the classroom The most common trigger for an anaphylactic reaction is a food item and a reaction most commonly occurs due to a failure to read labels, cross-contamination, and food sharing What are Life-Threatening Emergencies? The following are symptoms indicating a life-threatening anaphylactic reaction when assessing students with severe allergies: Hives or itchy skin Swelling of the throat, lips, or tongue Difficulty breathing or swallowing Nausea or vomiting Anxiety or a sense of impending doom Weakness, loss of consciousness 54
58 Management of Students with Life-Threatening Allergies Includes: Avoidance of triggers Administration of epinephrine Activation of EMS If epinephrine is administered, either the student s own epinephrine or a stock dose of epinephrine provided by the school, please complete the Report of Epinephrine Administration form and fax or the completed form to the Indiana Department of Education. This form can be found on the IDOE Health Web listed below, as well as at the end of this section under Sample Anaphylaxis Forms. Stock Epinephrine Law: IC Access this law at Indiana General Assembly: by entering as the Indiana Code or Law Visit the Indiana Department of Education Health Web at: student-services/health/severe-allergies This law allows schools to stock auto-injectable medication for emergency use. Schools must first have a school policy regarding who can give this medication and under what circumstances. The policy must also include items such as training for school personnel, storage of medication, and proper follow-up once the medication has been administered. The school must also have a written standing order from a licensed healthcare provider. The law allows school nurses and school personnel to administer epinephrine to a student, staff member, or visitor in the school who is demonstrating signs of life-threatening anaphylaxis and the individual does not have epinephrine at the school or the individual s prescription medication is not available. It is the responsibility of the school nurse to determine if this task can be safely delegated following the five rights of delegation. For more information regarding delegation, please refer to the Delegation Guidelines for Indiana School Nurses found in Chapter 1 of this manual. Individual Healthcare Plans (IHP) for Students with Life-Threatening Allergies: It is recommended that every student with a diagnosis of a severe allergy and a medical order for the emergency administration of epinephrine have an IHP with an Emergency Care Plan written by the school nurse and implemented during both school hours and school-related activities. Schools may use the Care of Students with Diabetes Law as a template for managing a chronic disease in the school setting. Please see the Management of Students with Diabetes information found in the section below for additional information. (IHP s and Emergency Care Plans are discussed further in Chapter 4 of this manual) Delegating the Care of Students with Life-Threatening Allergies: In the absence of a registered nurse (RN) on site for providing student healthcare, it is necessary to determine the delegation plan of said care to alternate staff members. The Delegation Guidelines for Indiana School Nurses can be found in Chapter 1 of this manual for your reference regarding student healthcare delegation in the absence of a registered nurse. 55
 NASN Voluntary Guidelines for Managing Food Allergies A Checklist for School Nurses (PDF)")
59 Sample Anaphylaxis Forms: NASN Toolkit Forms (see resource listed below) includes sample IHP, Emergency Action Plan, Presentation for Training Staff, and sample School Policy CDC Voluntary Guidelines for Managing Food Allergies in School and Early Care and Education Programs (see resource listed below) NASN Voluntary Guidelines for Managing Food Allergies A Checklist for School Nurses (PDF) Parent Information Sheet Children and Adolescents with Food Allergies: How Can You Help? (PDF) Report of Epinephrine Administration (PDF) Allergy Self-Carry Form (PDF) Resources for Managing Students with Life-Threatening Allergies: Indiana Department of Education Health Web: School Nurse Learning Connection o Access the Files and Bookmarks Tab o Click on Chronic Conditions Folder o Click on the Severe Allergies Folder Additional Resources National Association of School Nurses Food Allergy and Anaphylaxis Tool Kit Centers for Disease Control and Prevention Voluntary Guidelines for Managing Food Allergies in Schools and Early Care and Education Programs Allergy_Web_508.pdf 56
60 SECTION 4: Diabetes THE MANAGEMENT OF STUDENTS WITH DIABETES: What is Diabetes? Diabetes is a condition that affects the way the body processes food for energy and growth. Most foods that we eat are turned into glucose (sugar) for our bodies to use for energy. Insulin, a hormone made in the pancreas, helps glucose enter into the cells of our bodies. Type I diabetes is a disease in which the immune system destroys the pancreatic cells that make insulin. Genetic and environmental factors are also involved in the development of Type I diabetes. Type I diabetes is most common in children. About 1 in 500 U.S. children have diabetes according to the American Academy of Pediatrics. Type 2 diabetes is a condition in which the pancreas does produce insulin, but the body is unable to use it. Risk factors for Type 2 diabetes include older age, obesity, family history of diabetes, race/ethnicity, physical inactivity and prior history of gestational diabetes. Type 2 diabetes is most often diagnosed in people over the age of 40 but is seen in obese children as well. Characteristics of Children with Diabetes: Symptoms often include: o Excessive thirst o Increased appetite yet weight loss o Frequent urination o Fatigue or lethargy o Incontinence Type 1 diabetes includes the possibility of developing diabetes ketoacidosis (DKA) which is a condition of extreme and dangerous high blood glucose with electrolyte imbalance. In this situation, a child s symptoms may include: o Vomiting o Fruity breathe smell o Labored breathing > unconsciousness > death if untreated Diabetes short-term complications: o Hyperglycemia - blood sugars too high o Hypoglycemia - blood sugars too low Diabetes long-term complications: o Poor wound healing o Early heart disease o Vision problems o High blood pressure o Nerve damage o Kidney failure 57
61 Type 2 diabetes is usually of a slower onset with more gradual onset of symptoms due to high blood sugar levels but sometimes Type 2 diabetes presents with no symptoms. What are Diabetes Emergencies? Consider the following symptoms emergent when assessing students with diabetes: Repeated vomiting Disorientation or unconsciousness Inability to keep food or liquids down while blood sugar is low Lethargy Seizures Care of Students with Diabetes Law: IC Diabetic Law Access this law at Indiana General Assembly: by entering as the Indiana Code or Law Visit the Indiana Department of Education Health Web at: student-services/health/diabetes Synopsis of IC Care of Students with Diabetes This law gives clear guidance for the care of students with diabetes in Indiana schools. The eight sections in this law include the following: Definitions o Licensed Healthcare Provider-has prescriptive authority o School-public, includes charter schools o Volunteer Health Aides-volunteers and completes training Requirements of the plan o Medical and Treatment Plan o Individual Healthcare Plan Development of the plan o Individual Healthcare Plan must be written by RN o Collaborate with parent, practitioner, principal, and teacher o Must incorporate components of both the MMP and IHP Use of volunteer health aides (VHA) o School principal and nurse consult to decide adequate number of VHA s o VHA works under the supervision of the principal and school nurse o VHA must have access to school nurse by either phone or in person o Employee cannot be disciplined for refusing to serve as VHA o Employee can choose only those functions they feel comfortable and trained for 58
62 Diabetes training program Tasks o o o o Annual training for school nurses Training for VHA s Training conducted before start of the school year or before diabetic student attends school Preferably performed by school nurse o VHA can only give care with parent-signed agreement authorizing VHA to assist student and stating VHA is not liable for civil damages o School may not restrict student to any particular school based on VHA Diabetes activities o Must allow student to self-manage if Licensed Healthcare Provider and parent determine student is capable and it is written into the IHP o Must allow student to treat, manage, and carry supplies for use in any area of the school and at any school-related activity o School nurse must have an emergency action plan for those students who self-manage Information sheet o Any transportation and supervisor of the student during off-campus activities must be given an information sheet identifying the student, description of signs and symptoms of emergencies with appropriate response, and contact numbers for emergencies. Individual Healthcare Plans (IHP) for Indiana Students with Diabetes: Students with diabetes must have an IHP with an Emergency Care Plan written and implemented during both school hours and school-related activities. Each of the 8 items outlined in the above law (IC ) must be addressed for each IHP written for students with diabetes. Additionally, the IHP must incorporate all of the medical orders or medical management plan (MMP) written by the student s healthcare provider which could include the following: When to check routine blood sugars Treatments for routine blood sugars Formula for covering lunch blood sugars and carbohydrates consumed Treatments for all non-routine blood sugars Snack coverage (timing and carb/insulin orders) Emergency orders (your emergency action plan) Ability to self-manage Developing an IHP for students with diabetes begins with the MMP which is provided to the school and must be signed by both the healthcare provider and parents/guardians. When developing an IHP, the school should meet with the parents/guardians to discuss additional topics such as: Carbohydrate counting Staff training 59
63 The use of VHA s Contingency planning (times of staffing or schedule changes) Field trips After-school activities Emergency procedures School disaster planning Any format used when developing the IHP for a student is appropriate as long as it remains comprehensive and is student-specific. School nurses should use a format which best fits the needs of the student. Many nurses prefer a narrative format with separate sections addressing each topic of the student s healthcare plan. Another format sometimes used to develop an IHP is a template with sections titled for each part of the IHP. Nurses can then enter student-specific information into each section along with the use of addendums when appropriate. Some Resources for Samples of IHP s Include: Andrews, Robert. (2010). School Nurse Resource Manual: A Guide to Practice. School Health Alert. Arnold, Martha J. (1999). The School Nurse s Source Book of Individualized Healthcare Plans. Sunrise River Press. National Association of School Nurses. (2015). Helping Administer to the Needs of the Student with Diabetes in Schools (H.A.N.D.S.). Silkworth, Cynthia K. (2005). Individualized Healthcare Plans for the School Nurse. Sunrise River Press. (IHP s and Emergency Care Plans are discussed further in Chapter 4 of this manual) Delegating the Care of Students with Diabetes: In the absence of a registered nurse (RN) on site for providing student healthcare, it is necessary to determine the delegation plan of said care to alternate staff members. The Delegation Guidelines for Indiana School Nurses can be found in Chapter 1 of this manual for your reference regarding student healthcare delegation in the absence of a registered nurse. Sample Diabetes Forms: Sample School Nurse Checklist-Diabetes (PDF) Sample School Nurse Intake Interview (PDF) Sample Diabetes Management Supplies (PDF) Riley Information Packet with Cover Letter (PDF) Parent Information Sheet- Children and Adolescents with Diabetes: How Can You Help? (PDF) Resources for Managing Students with Diabetes: American Diabetes Association: The complete ADA Safe at School PowerPoint slides and videos: Diabetes Care Tasks at School: What Key Personnel Need to Know Indiana Department of Education Health Web: 60
64 School Nurse Learning Connection o o o Additional Resources Access the Files and Bookmarks Tab Click on Chronic Conditions Folder Click on the Diabetes Folder National Association of School Nurses: Diabetes in Children DiabetesinChildren National Diabetes Education Program: Helping the Student with Diabetes Succeed: A Guide for School Personnel PublicationDetail.aspx?PubId=97#main National Institute of Diabetes and Digestive and Kidney Diseases Peyton Manning Children s Hospital: Riley Hospital for Children: School Information Forms: SECTION 5: Seizures THE MANAGEMENT OF STUDENTS WITH SEIZURES: What is Epilepsy? (Non-Febrile Seizures) Epilepsy is a neurological condition characterized by recurrent seizures. Seizures are sudden, abnormal episodes that happen because of a problem with brain cell electrical communication. During a seizure, some brain cells send abnormal and exaggerated electrical signals that stop other cells from working properly. Seizures are the most common neurological disorder in children and most are controlled with medication. To be diagnosed with epilepsy, a child must have had at least two seizures that were not caused by another treatable condition (such as fevers) more than 24 hours apart. Many children with seizures have normal intelligence; some have developmental delays. Characteristics of Children with Epilepsy: Various seizure types represent different areas of brain involvement. Most seizures last less than 4-5 minutes. (Always refer to the student s medical management plan for treatment orders regarding seizure duration). Generalized (grand mal) Seizures o The whole brain and body are involved with rhythmic movements o The child may fall and injure themselves during a seizure o The child may lose control of bowel/bladder o Children do not respond to you during a seizure and may be quite sleepy for hours afterward 61
65 Absence (petit mal) Seizures o Look like staring spells or daydreaming o Child will not be aware or alert o The child will not be able to respond to you during the seizure o The child will often not remember the episode afterward o The child may demonstrate eye blinking and lip smacking during the seizure Partial Seizures (can be simple or complex depending on area of the brain involved) Simple Partial o The child may shake one part of the body or see, smell, or hear what is not there o During the seizure, the child is not confused but may be frightened Complex Partial o The child may be confused or experience a distortion of consciousness o The child may behave strangely using unusual words or actions such as lip smacking, hand rubbing, or swallowing o The child is confused and tired after the seizure What are Seizure Emergencies? A generalized seizure lasting longer than 5 minutes (unless otherwise stated in the student s medical management plan) The student experiences repeated seizures without regaining consciousness The student has diabetes The student is injured or has a high fever The student is experiencing a seizure for the first time The student has difficulty breathing The student has a seizure in water The student is pregnant Individual Healthcare Plans (IHP) for Seizures: Students with seizures should have an IHP with an Emergency Care Plan written and implemented during both school hours and school-related activities. Some example care plans are provided by the Epilepsy Foundation Toolkit and are included in the forms list below. Additional topics to be addressed in a complete IHP should be incorporated to complete the plan for students with seizures. School nurses may also use their own local school district forms or those found online. (IHP s and Emergency Care Plans are discussed further in Chapter 4 of this manual) Delegating the Care of Students with Seizures: In the absence of a registered nurse (RN) on site for providing student healthcare, it is necessary to determine the delegation plan of said care to alternate staff members. The Delegation Guidelines for Indiana School Nurses can be found in Chapter 1 of this manual for your reference regarding student healthcare delegation in the absence of a registered nurse. 62
66 Sample Seizures Forms: Epilepsy Foundation of America (see resource listed below) includes a Get Help Toolbox, Sample Seizure Action Plan (PDF) Questionnaire for Parents (PDF) Seizure First Aid Fact Sheet (PDF) CDC Parent Information Sheet - Children and Adolescents with Seizure Disorders: How Can You Help? (PDF) Resources for Managing Students with Seizures: Health Web: School Nurse Learning Connection o Access the Files and Bookmarks Tab o Click on Chronic Conditions Folder o Click on the Seizure Folder Additional Resources American Epilepsy Society: Epilepsy Foundation of America: Epilepsy Foundation of Indiana: National Association of School Nurses: 63
67 Chronic Health Conditions Managed by School Nurses SUMMARY Position Statement It is the position of the National Association of School Nurses that students with chronic health conditions have access to a full time registered professional school nurse (hereinafter referred to as school nurse). School districts should include school nurse positions in their full time instructional support personnel to provide health services for all students, including students with chronic health conditions. The school nurse coordinates and conducts assessment, planning, and implementation of individualized health care plans for safe and effective management of students with health conditions during the school day. The school nurse is both the provider of care and the only person qualified to delegate care to an unlicensed care provider as prescribed in state nurse practice laws and regulations and according to Scope and Standards of School Nurse Practice (National Association of School Nurses [NASN] & American Nurses Association [ANA], 2011). HISTORY The percentage of children and adolescents in the United States with chronic health conditions (CHC) increased from 1.8% in the 1960s to more than 25% in 2007 (Halfon & Newacheck, 2010). There is some difficulty in measuring prevalence due to the lack of a clear definition of chronic health conditions. CHC include both long term physical and mental disorders. It is useful to use a non categorical approach CHC, and for identifying children and adolescents as having special health care needs. These children include those with long term physical, emotional, behavioral, and developmental disorders that require prescription medications and medical or educational services. They also include disorders that affect a child s functional status (Forrest, Bevans, Riley, Crespo, & Louis, 2011). The non categorical approach focuses on needs for service and risk of school failure. Over the past few decades the number of students with CHC in schools has increased for a variety of reasons. Many students who had been confined to therapeutic settings are now being educated in the local school district in the least restrictive environment. Their right of participation is protected by federal law, including the Rehabilitation Act, Section 504 and the Individuals with Disabilities Educational Act [IDEA] of As survival rates associated with chronic conditions in infants and children continue to increase and life expectancy increases, the health care and educational service needs of students will increase. Many children with CHC now are able to attend school and succeed due to critical support services, including those provided by school nurses. The school nurse is a key member of the educational team and is the one who is responsible for planning, implementing, and monitoring the health care plans for students with CHC. DESCRIPTION OF ISSUE The main issues surrounding health management of students with chronic health conditions in schools are as follows: Health care services must be provided for students who qualify for services under IDEA or Section 504 to meet requirements of federal laws. The school nurse has an important role in interpreting a student s health status, in explaining the impairment, and in interpreting medical and other health information in relation to the expanded e standards for eligibility under Section 504 (Zirkel, 2009). Development of individualized health care plans (IHP) is a nursing responsibility and is based on standards of care that are regulated by State Nurse Practice Acts and cannot be delegated to unlicensed individuals (National Council of State Boards of Nursing [NCSBN], 2005). Effective and safe management of chronic health conditions is complex, requires careful planning by a school nurse, and may involve delegation of nursing tasks to both licensed and unlicensed assistive personnel (UAP). A full time school nurse is essential to achieve quality student health services and to meet student health needs. 64
68 Dependable funding is required to ensure quality student health services. RATIONALE Health care needs of students with chronic health conditions are complex and continuous. School nurses assist many children not served by the health care system and work to create access to health care for students and families. Students who may not have been identified as having a chronic condition prior to school entry are identified by school nurses who then coordinate evaluation and intervention services. School nurses assist students in learning to manage chronic illness, increasing seat time in the classroom, decreasing student absenteeism, resulting in cost savings to the school district and an increase in the overall academic success of the student. School nurses are responsible and accountable for the assessment of and planning for safe and effective medical management of students with chronic health conditions. These responsibilities cannot be delegated (NCBSN, 2005). Therefore, it is the position of NASN that school districts should provide a full time school nurse in every school building. NASN recommends school nurse to student ratios based on student populations: 1:750 for students in the general population, 1:225 in the student populations that may require daily professional school nursing services or interventions, 1:125 in student populations with complex health care needs, and 1:1 may be necessary for individual students who require daily and continuous professional nursing services. Additionally, Healthy People 2020 has included an objectiveto increase the proportion of schools that have a fulltime registered school nurse to student of at least 1:750 (USDHHS/CDC, 2010). A full time school nurse is essential for oversight of the staffing plan and for informing school administrators of current staffing needs (Peterson & Wolfe, 2006). REFERENCES Forrest, C. B., Bevans, K. B., Riley, A. W., Crespo, R., & Louis, T. A. (2011).School outcomes for children with special health care needs. Pediatrics, 128, doi: /peds Halfon, N. & Newacheck, P.W. (2010). Evolving notions of childhood chronic illness. JAMA, 303, doi: /jama Individuals with Disabilities Educational Act (IDEA) of 2004, 20 U.S.C. Sec et seq.; 34 C.F.R. Parts 300 et seq. Retrieved from pdf Rehabilitation Act (Section 504): 29. U.S.C, 794; 20 U.S.C. 1405; 34 C.F.R. Part 104. Retrieved from National Association of School Nurses (NASN) and American Nurses Association (ANA). (2011). School nursing: Scope and standards of practice. Silver Spring, MD: Author. National Council of State Boards of Nursing (NCSBN). (2005). Working with others: A position paper. Retrieved from Peterson, B., Wolfe, L. C. (2006). Setting up the school health office. In J. Selekman (Ed.), School nursing: A comprehensive text, (pp ). Philadelphia, PA: F.A. Davis Company. 65
69 U.S. Department of Health and Human Services (USDHHS).Office of Disease Prevention and Health Promotion (CDC).(2010). Healthy people Washington, DC: Author. Available at Zirkel, P. A. (2009). History and expansion of Section 504 student eligibility: Implications for school nurses. Journal of School Nursing, 25, doi: / Acknowledgment of Authors: Judith Morgitan, MEd, BSN, RN Margo Bushmiaer, MNSc, RN, NCSN Marie C. DeSisto, MSM, BSN, NSCN Carolyn Duff, MS, RN, NCSN C. Patrice Lambert, MSN, RN, SNC M. Kathleen Murphy, DNP, RN, FNP BC Sharon Roland, BSN, RN Kendra Selser, MHS, BSN, RN Leah Wyckoff, MS, BSN, RN Kelly White, RN, PhD candidate (SME) Adopted: June 2006 Revised: January 2012 (Formerly titled School Nursing Management of Students with Chronic Health Conditions) This Position Statement replaces the Issue Brief: School Nursing Management of Students with Chronic Health Conditions (adopted 2006) See also National Association of School Nurses. (2010). Position Statement: Caseload Assignments. Available at /ArticleId/7/Caseload Assignments Revised National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland
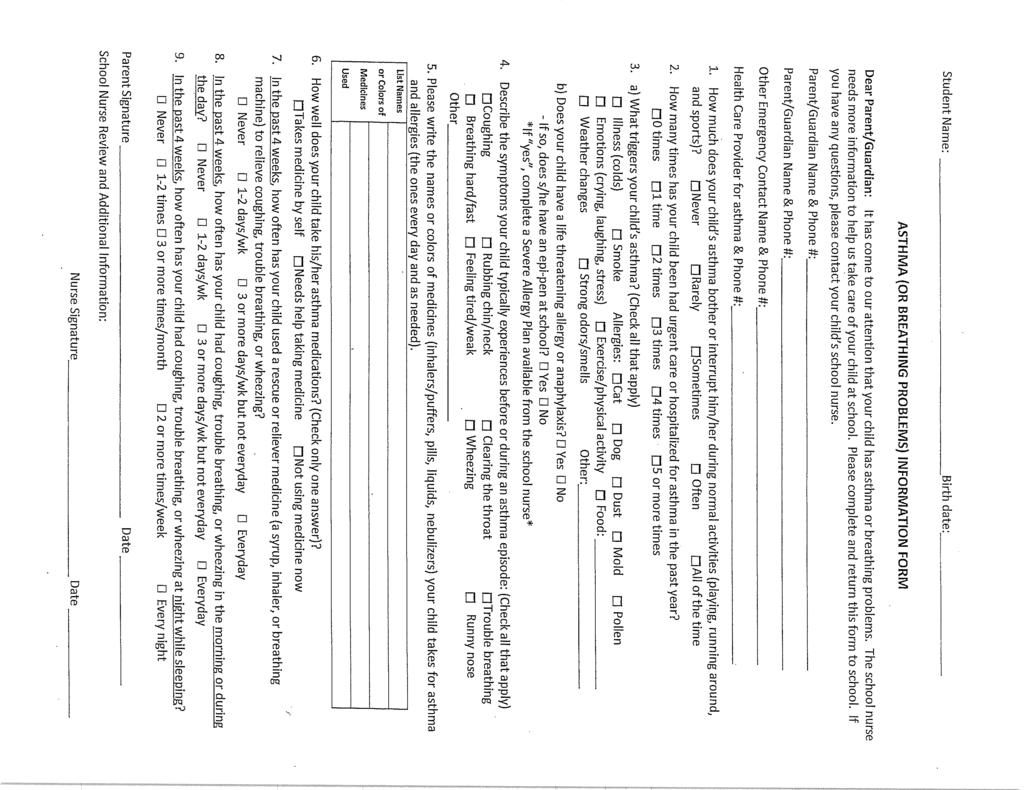
70 67
71 Asthma Self Carry Contract School: Grade: STUDENT : DOB: I plan to keep my rescue inhaler with me at school rather than in the school health office. I agree to use my rescue inhaler in a responsible manner, in accordance with my physician s orders. I will notify the school health office if I am having more difficulty than usual with my asthma. I will not allow any other person to use my inhaler. Student s Signature Date PARENT/GUARDIAN: This contract is in effect for the current school year unless revoked by the physician or the student fails to meet the above safety contingencies. I agree to see that my child carries his/her medication as prescribed, that the device contains medication, and the date is current. It has been recommended to me that a back-up rescue inhaler be provided to the Health Office for emergencies. I will review the status of the student s asthma with the student on a regular basis as agreed in the health care plan. I will provide the school a Health Care Provider signed medication authorization for this medication. Parent s Signature Date Nurse Consultant School The above student has demonstrated correct technique for inhaler use, an understanding of the physician order for time and dosages, and an understanding of the concept of pretreatment with an inhaler prior to exercise. School staff that have the need to know about the student s condition and the need to carry medication have been notified. I will review the medication authorization provided by the parent and signed by the health care provider. Nurse Consultant s Signature Date 68
72 Physician Authorization for Self-Carry Emergency Medication in School I have diagnosed Student Name with Name of chronic disease for which emergency medication may be needed while at school or during school sponsored activities. Name of Medication I have instructed this patient how to safely and appropriately use this medication and I believe that they are capable of using the medication as instructed. I believe that this patient should carry this medication and will use it in a responsible manner, in accordance with my orders and instructions. Physician Name: Physician Signature: Date: Parent Name: Parent Signature: Date: 69
73 ASTHMA MANAGEMENT PLAN & AUTHORIZATION FOR MEDICATION TO BE COMPLETED BY PARENT: Patient s Name Date of Birth School Grade r School r School Fax ( ) Parent/Caregiver Phone (H) Phone (W) Phone (Cell) Emergency Contact Relationship Phone Asthma Care Provider r Office Phone ( ) r Office r Office Fax ( ) (please mark best contact) TO BE COMPLETED BY ASTHMA CARE PROvIDER MONITORING RESCUE (quick-relief) MEDICATION: TREATMENT RED YELLOw GREEN RED ZONE: DANGER SIGNS Very short of breath, or Rescue medicines have not helped, or Cannot do usual activities, or Symptoms are same or get worse after 24 hours in Yellow Zone RED ZONE: EMERGENCY SIGNS Lips and fingernails are blue or gray Trouble walking and talking due to shortness of breath Loss of consciousness YELLOW ZONE: CAUTION Cough, wheeze, chest tightness, or shortness of breath, or Waking at night due to asthma, or Can do some, but not all, usual activities GREEN ZONE: WELL No cough, wheeze, chest tightness, or shortness of breath during the day or night Can do usual activities Give rescue medication: r 2 r 4 r 6 puffs (1 min between puffs) or 1 nebulizer treatment Call parent and/or Asthma Care Provider Call 911 NOW if: 1. Unable to reach medical care provider after arriving in the red zone 2. Child is struggling to breathe and there is no improvement after taking albuterol 3. May repeat rescue medication every 10 minutes if symptoms do not improve, until medical assistance has arrived or you are at the emergency department Continue daily controller medications Give rescue medication: r 2 r 4 r 6 puffs (1 min between puffs) OR 1 nebulizer treatment every 4 hours as needed Wait 10 minutes and recheck symptoms If not better, go to RED ZONE If symptoms improve, may return to class or normal activity, or Parent/School Nurse: If needed, coordinate rescue medications to be given every 4 hours for r 2 r 3 days, if symptoms remain improved If symptoms are not gone after r 2 r 3 days, move to the RED ZONE MEDICATION HOW MUCH WHEN DAILY CONTROLLER MEDICATION HOW MUCH WHEN Before Exercise r Recess r PE/Sports (not to exceed every 4 hours) r Administer medications as instructed above r Student has been instructed in the proper use of all his/her asthma medications, and in my opinion, the student can carry and use his/her inhaler at school r Student needs supervision or assistance to use his/her inhaler medication r Student should NOT carry his/her inhaler while at school r Have student use spacer with inhaler medication ASTHMA CARE PROVIDER SIGNATURE PLEASE PRINT PROVIDER NAME DATE I give permission for the school nurse and any pertinent staff caring for my child to follow this plan, administer medication and care for my child, contact my asthma care provider if necessary and for this form to be faxed/ ed to my child s school or be shared with school staff per FERPA guidelines. I assume full responsibility for providing the school with prescribed medication and delivery/monitoring devices. PARENT SIGNATURE DATE 70 InJAC January 2014 InJAC.org

74 Children and Adolescents with Asthma How Can You Help? IDEAS FOR PARENTS Asthma is a disease that affects airways in the lungs and is one of the most common long-term diseases. Asthma may cause wheezing, breathlessness, chest tightness, or coughing at night or early in the morning. An asthma episode can happen when a person is exposed to asthma triggers, such as tobacco smoke, mold, dust mites, cockroaches, pets, fragrances, and exercise. 1 Colds and flu can also cause asthma symptoms to worsen. Asthma symptoms can be controlled by avoiding triggers and using medications prescribed by a health care provider, if needed. Asthma that is not well controlled may lead to emergency room visits, and possibly being admitted to the hospital. It is the leading cause of days missed at school. 2 Schools can support students with asthma by working with families and medical providers to help manage asthma care at school. Healthy students are more likely to have better attendance, grades, and test scores. 3 Knowing the answers to the following questions can help you support your child s school to address asthma. If you don t know the answers to these questions, check out the school handbook or school website, attend a school wellness meeting or Parent- Teacher Association (PTA) meeting, or simply ask your child s teacher. What s Happening at School? 1. Is there a full-time registered nurse in the school building at all times, or a school-based health center to help children with chronic medical conditions or emergencies? 2. How does the school identify and share information about students with asthma? 3. Does the school require that each student with asthma have a current Asthma Action Plan on file? 4 4. Does the school allow students to carry their own medication, such as an inhaler, at school? 5. What are the school protocols if a student is having asthma symptoms at school, on the school bus, on a field trip, or in cases of emergency or lockdown? 6. Are other school staff, such as teachers, bus drivers, and food services staff, trained to recognize and respond to a student that may be having asthma symptoms? 7. What is the policy for student participation in physical activity (e.g., recess or classroom activity breaks) or physical education at school if he or she has asthma? 8. Is there a bullying prevention policy in the school or district that discourages bullying or encourages awareness or anti-stigma of students with medical conditions? 9. Does the school or district have an indoor air quality management program to improve the school environment and reduce exposure to asthma triggers? 71


75 Ideas for Parents You can be involved in your child s school by attending meetings, workshops, or training events offered by the school; communicating with school staff and other parents; volunteering for school events or in your child s classroom; reinforcing healthy messages and practices your child learns at school; helping make decisions about health in the school; and being part of community activities supported by the school. Here are some specific ideas for how you can support your child s school in addressing asthma. Advocate for a full-time registered nurse in school. Have an ongoing conversation with your child to discuss their asthma triggers, their feelings about having asthma, and if they feel safe and supported at school. 5 Work with your child s health care provider to provide an Asthma Action Plan for the school and for the timely completion of required school forms. Encourage communication between school health services and your child s health care provider. Make sure that the school has your child s emergency asthma medication so that asthma symptoms can be managed at school. Keep your emergency contact information up-todate with the teacher and school nurse. Communicate with your child s teachers, counselors, and school health services staff about your child s asthma triggers and any concerns about coping while at school. Join groups, such as the PTA, school wellness committee, or school health advisory council, that address the needs of a supportive and healthy school environment. 6 Share research-based websites or written materials about asthma with teachers, nurses, and administrators, when possible, e.g., cdc.gov/healthyschools/asthma/index.htm. Advocate for asthma-friendly school policies. Check out additional resources for parents related to the school nutrition environment and services, physical education and physical activity, and managing chronic health conditions at REFERENCES 1. Centers for Disease Control and Prevention. Asthma Prevalence in the United States Accessed November 19, Centers for Disease Control and Prevention. Asthma and Schools. Accessed August 5, Centers for Disease Control and Prevention. Health and Academic Achievement. Atlanta: US Dept of Health and Human Services; American Lung Association. Creating an Asthma Action Plan. create-an-asthma-management-plan.html. Accessed November 19, Centers for Disease Control and Prevention. School Connectedness: Strategies for Increasing Protective Factors among Youth. Atlanta: US Dept of Health and Human Services; Centers for Disease Control and Prevention. Parent Engagement: Strategies for Involving Parents in School Health. Atlanta: US Dept of Health and Human Services; CS B
 provide valuable information to assist school nurses in developing or enhancing a comprehensive food allergy management program for the school community.")

76 Voluntary Guidelines for Managing Food Allergies in Schools and Early Care and Education Programs A Checklist for School Nurses The Voluntary Guidelines from the Centers for Disease Control and Prevention (CDC) provide valuable information to assist school nurses in developing or enhancing a comprehensive food allergy management program for the school community. The checklist below provides an overview of how to use this document and provide leadership in your individual practice of school nursing. Review the signs and symptoms of an allergic reaction to food Pages Be prepared to share signs and symptoms with all faculty and staff Go over risk factors for anaphylaxis and fatal food allergy reactions Review treatment and use of epinephrine Follow the three essential first steps to manage food allergies in school Pages Use a coordinated approach that is based on effective partnerships Provide clear leadership to guide planning and ensure implementation of food allergy management plans and practices Develop and implement a comprehensive plan for managing food allergies Identify priorities for managing food allergies Pages Ensure the daily management of food allergies for individual children Prepare for food allergy emergencies Provide professional development on food allergies for staff Educate children and family members about food allergies Create and maintain a healthy and safe educational environment Assess your school district s food allergy management program using the Food Allergy Management and Prevention Plan (FAMPP) Checklist Page 44 Review and disseminate the Actions for School Boards and District Staff Pages Include school board members, school district superintendent, health services director, student support services director and district food service director Review and disseminate the Actions for School Administrators and Staff Pages Include school administrator, registered school nurses, school doctors, health assistants, health aides or other unlicensed personnel, classroom teachers, school food service managers and staff, school counselors and other mental health services staff, bus drivers and school transportation staff and facilities maintenance staff Familiarize yourself with federal laws and regulations Pages Know the requirements of Section 504 of the Rehabilitation Act, Child Nutrition Programs, Individuals with Disabilities Education Act, Family Educational Rights and Privacy Act Be able to identify and refer families to food allergy resources Pages Sources include federal resources, federal laws, national non-governmental resources Consider providing a glossary of abbreviations and acronyms National Association of School Nurses May

77 Children and Adolescents with Food Allergies How Can You Help? IDEAS FOR PARENTS Food allergies are a growing concern for many people and affect about 1 of 25 school-aged children. 1 Among those with food allergies, 1 of 5 will have an allergic reaction while at school. Anaphylaxis is a severe allergic reaction that has rapid onset and may cause death, and 1 of 4 students who have a severe and potentially life-threatening reaction at school have no previous known food allergy. 1 Schools should have a food allergy management and prevention plan to help support the needs of students with allergies. They should also teach staff members, as well as students and family members, about food allergies. This can create and maintain a healthy, safe, and inclusive educational environment. Knowing the answers to the following questions can help you support your child s school to address food allergies. If you don t know the answers to these questions, check out the school handbook or school website, attend a school wellness meeting or Parent-Teacher Association (PTA) meeting, or simply ask your child s teacher. What s Happening at School? 1. Is there a full-time registered nurse in the school building at all times or a school-based health center to help children with chronic medical conditions or emergencies? 2. How does the school identify and share information about students with food allergies? 3. Is the school aware of the CDC Voluntary Guidelines for Managing Food Allergies in Schools and Early Care and Education Programs? 4. Is it required that each student with food allergies have an individualized health plan or emergency care plan on file? 2 Has the child been evaluated for a Section 504 Plan, if appropriate? 5. Are students allowed to carry their medication (such as emergency epinephrine) at school? 6. Does the school or district have stock epinephrine that can be used for any student having a life threatening allergic reaction, and are nurses, teachers, and other staff appropriately trained to administer it? 3 7. What are school or district protocols for students suspected of having an allergic reaction at school, on the school bus, on a field trip, or in cases of emergency or lockdown? 8. Are other school staff, such as teachers, bus drivers, and food services staff, trained to recognize and respond to a student who may be having an allergic reaction? 9. What practices are used to safely prepare and serve foods to students with food allergies within the cafeteria, classroom, school parties, and other school events? 10. Is food sharing among students allowed? Is the student with food allergies protected during classroom parties and activities involving food without having to be isolated from the activity? 11. Is there a bullying prevention policy in the school or district that discourages bullying or encourages awareness or anti-stigma of students with medical conditions? 74


78 Ideas for Parents You can be involved in your child s school by attending meetings, workshops, or training events offered by the school; communicating with school staff and other parents; volunteering for school events or in your child s classroom; reinforcing healthy messages and practices your child learns at school; helping make decisions about health in the school; and being part of community activities supported by the school. Here are some specific ideas for how you can support your child s school in addressing food allergies. Have an ongoing conversation with your child to discuss their food allergies, their feelings about having food allergies, and if they feel safe and supported at school. 4 Work with your child s health care provider to establish a current emergency care plan and for timely completion of required school forms. 3 Encourage communication between school health services and your child s health care provider. Provide emergency medication to the school nurse or other school health official. Ensure that there is a current individualized health care plan, and assist with setting goals. 2 Communicate with your child s teachers, counselors, and school health services staff about your child s food allergies and how they are coping while at school. Work with teachers and other staff to identify non-food rewards for your child, thereby reducing exposure to allergens. Talk with school nutrition services about your child s allergies and advanced menu viewing. Volunteer with your child, or get involved at school health events to educate staff and other families about food allergies. Inquire about the student health education curriculum. Join a group, such as the PTA, school wellness committee, or school health advisory council, that addresses the needs of a supportive and healthy school environment. 5 Share research-based websites or written materials about food allergies with teachers, nurses, and administrators, when possible, (e.g., gov/healthyyouth/foodallergies/index.htm). Check out additional resources for parents related to the school nutrition environment and services, physical education and physical activity, and managing chronic health conditions at REFERENCES 1. Centers for Disease Control and Prevention. Voluntary Guidelines for Managing Food Allergies in Schools and Early Care and Education Programs. Washington, DC: US Dept of Health and Human Services; National Association of School Nurses. Individualized Healthcare Plans: The Role of the School Nurse; Individualized-Healthcare-Plans-The-Role-of-the-School-Nurse-Revised-January Accessed August 6, National Association of School Nurses. Position Statement. Allergy/Anaphylaxis Management in the School Setting; Allergy-Anaphylaxis-Management-in-the-School-Setting-Revised-June Accessed August 5, Centers for Disease Control and Prevention. School Connectedness: Strategies for Increasing Protective Factors among Youth. Atlanta: US Dept of Health and Human Services; Centers for Disease Control and Prevention. Parent Engagement: Strategies for Involving Parents in School Health. Atlanta: US Dept of Health and Human Services; 2012 CS B
79 Report of Epinephrine Administration Indiana Department of Education Please Print this 2 Page Form, Complete, and or Fax this Form to: Jolene Bracale at jbracale@doe.in.gov or Fax School District: Name of School: 2. Age: Type of Person: Student Staff Visitor Gender: M F 3. History of allergy: Yes No Unknown If known, specify type of allergy: 4. If yes, was allergy action plan available? Yes No Don t Know Previous epinephrine use: Yes No Don t Know 5. Date/Time of occurrence: Vital signs: BP / Temp Pulse Respiration 6. If known, specify trigger that precipitated this allergic episode: Food Insect Sting Exercise Medication Latex Other Unknown If food was a trigger, please specify which food Please check: Ingested Touched Inhaled Other specify 7. Did reaction begin prior to school? Yes No Don t Know 8. Location where symptoms developed: Classroom Cafeteria Health Office Playground Bus Other specify 9. How did exposure occur? 10. Symptoms: (Check all that apply) Respiratory GI Skin Cardiac/Vascular Other Cough Abdominal discomfort Angioedema Chest discomfort Diaphoresis Difficulty breathing Diarrhea Flushing Cyanosis Irritability Hoarse voice Difficulty swallowing General pruritis Dizziness Loss of consciousness Nasal congestion/rhinorrhea Oral Pruritis General rash Faint/Weak pulse Metallic taste Swollen (throat, tongue) Nausea Hives Headache Red eyes Shortness of Breath Vomiting Lip swelling Hypotension Sneezing Stridor Localized rash Tachycardia Uterine cramping Tightness (chest, throat) Pale Wheezing 11. Location where epinephrine administered: Health Office Other specify 12. Location of epinephrine storage: Health Office Other specify 13. Epinephrine administered by: RN Self Other specify 14. The epinephrine was: the student s own epinephrine provided by the parent stock epinephrine provided by the school 15. Time elapsed between communication of symptoms and administration of epinephrine: minutes 16. Individual Health Care Plan (IHCP) in place? Yes No Don t know 17. Was a second dose of epinephrine required? Yes No Don t know Rev. 8/2015 Please complete s one and two. 761
80 Report of Epinephrine Administration Indiana Department of Education 18. Transferred to ER: Yes No Don t know 19. Staff/student/visitor outcome: _ 20. Other Comments: 21. Form completed by: (please print) Date: Title: RN LPN MA Other specify: Phone number: ( ) - Ext.: City: County: Rev. 8/2015 Please complete s one and two. 772
81 Allergy Self Carry Contract School: Grade: STUDENT : DOB: I plan to keep my Epi-pen with me at school rather than in the school health office. I agree to use my Epi-pen in a responsible manner, in accordance with my physician s orders. I will notify the school health office immediately if my Epi-pen has been used. I will not allow any other person to use my Epi-pen. Student s Signature Date PARENT/GUARDIAN: This contract is in effect for the current school year unless revoked by the physician or the student fails to meet the above safety contingencies. I agree to see that my child carries his/her medication as prescribed, that the device contains medication, and that the medication has not expired. It has been recommended to me that a back-up Epi-pen be provided to the Health Office for emergencies. I will review the status of the student s allergy with the student on a regular basis as agreed in the health care plan. I will provide the school a signed medication authorization for this medication. Guardian s Signature Date Nurse Consultant School The above student has demonstrated correct technique for Epi-pen use, an understanding of the physician order for emergency use of the Epi-pen. School staff that have the need to know about the student s condition and the need to carry medication have been notified. I will review the medication authorization provided by the parent and signed by the parent and health care provider. Nurse Consultant s Signature Date 78
82 SCHOOL NURSE CHECKLIST Assessment: 1. Complete School Nurse Intake Form (can be done by phone or in person) this can be updated annually or as needed. 2. Meet with family and student (if available) prior to start of school or at the time of diagnosis if school year is already in progress 3. Parents should bring to the meeting the Health Care Provider Orders (MMP) signed by the provider and the parents 4. Healthcare Provider Orders should be available to the School Nurse prior to the start of school or return to school for newly diagnosed student. 5. Review Healthcare Provider Orders and student schedule with parents. Individualized Health Plans 1. School Nurse to develop an Individualized Health Plan and appropriate addendums. 2. Assess student s ability to do diabetes self-management tasks at school with parents.the Diabetes Healthcare Provider must indicate ability level on the MMP. 3. Review the IHP with the parent and obtain parent/guardian written consent to allow communication with the health care provider. IHP parental signature indicates receiving plan, no Health Care Provider s signature required. 4. The Individualized Health Plan (IHP) and Addendums are designed for the school nurse and unlicensed assistive personal providing delegated student health care. 5. Parents should provide any updated Provider order s and the School Nurse will update the IHPs as needed. Training and Delegation 1. The School Nurse and/or School Health Services will provide the appropriate level of diabetes management training to school staff. 2. The tiered training model has three levels of training for school personnel, which is based upon the staff member s level of responsibility. Tier 2 & 3 training builds on the previous training s knowledge. Tier 1 For all school personnel Tier 2 For school personnel that have responsibility for the student during the school day (classroom, physical education, music, and art teachers and other personnel such as lunchroom staff, coaches, and bus drivers) Tier 3 For school staff personnel that are designated as the trained diabetes unlicensed assistive personnel (UAP) to perform or assist the student in diabetes care tasks. 3. Meet with building principal to determine staff that will be trained and delegated in student s diabetes care. 4. Collaborate with staff that has been identified to assist students with diabetes. 5. Determine if delegation is appropriate and if identified staff is capable of assisting student to carry out the Individualized Health Plan. 6. The Health Plan should be kept in the clinic accessible to trained diabetes personnel for reference 7. Diabetes overview and training should be given to classroom teacher and other staff as indicated. 8. Relevant information and training should be distributed to staff, to include but not limited to: Clinic aide Classroom teacher 79
83 Specials teachers Bus driver Cafeteria Classroom/recess aides 9. Instruct teachers to have a plan in place to notify substitute teachers regarding identification of the student with diabetes, and the day-to-day and emergency needs of the student. Communication 1. Identify how substitute teachers are informed of student s health conditions. 2. Provide information on student with diabetes including recognition and response to hypo/hyperglycemia and classroom management for substitute teachers. 3. Provide communication plan for communicating daily or weekly medical care, needed supplies or concerns with the parent. Ongoing Supervision and Training 1. School Nurse should routinely monitor student s blood glucose levels and insulin management. 2. School Nurse should provide ongoing assessment and supervision of trained ULPs, staff,. 3. School Nurse should document assessment and supervision of delegated tasks by ULPs. 4. School Nurse should provide feedback to trained ULPs, staff, providers, and parents as needed. 5. School Nurse should provide ongoing assessment of the dependent student s self-care skills. The school nurse should provide education to the student and encourage as age-appropriate self-care skills. 6. Parents should provide any updated Provider order s and the School Nurse will update the IHPs as needed. Field Trips, Out-of-State, Overnight Trips 1. School Staff should include the School Nurse in planning of field trips and overnight trips. 2. The school nurse will need ample time to prepare (e.g. training and delegation) staff for trips. 3. It is the responsibility of the school district to provide for the diabetes care of students going on such fieldtrips. The parent does not have to be in attendance for the student to participate. School nurses should check their school district field trip policies for additional guidance. Before and After School Activities & Programs 1. Parents are responsible for notifying the school nurse of their student s participation in before and after school-sponsored activities and programs. 2. The staff of the Before and After School Activities and programs will need to be trained in diabetes care by the parent or a qualified employee of that program. Adapted and used with permission by the Colorado Department of Education 80
84 School Nurse SCHOOL INTAKE INTERVIEW - DIABETES Student Date of Birth School Grade Homeroom Teacher Parent(s)/Guardian(s) Phone (H) (W) (Other) Emergency contact (other than Phone parent/guardian) Physician Name Office Phone Fax Diabetes Nurse Educator s Name Office Phone Medical release of information signed? Yes No Mode of transportation to and from school? Bus driver notified of diabetes? Yes No Does child participate in after school activities? Yes No Before Or after Care? Explain Adult leader notified of diabetes? Yes No Field trip recommendations: Blood Sugar Monitoring: Test will be performed in (location). Needs assistance with testing? Yes No Explain Required test times Call parent if blood sugar is below Or above Staff to record values and report to parents daily weekly Comments: Continuous Glucose Monitoring: Model: Alarm parameters: Meds: Insulin: Can child give own injections? Yes No Explain Order for insulin on file? Yes No Time(s) insulin to be administered at school: Type/Dosages: Form of administration: (Injection, Pen, Pump) Oral medications: Type Times Dose Comments: Diet: Assigned student lunch time(s)? Is child following a prescribed meal plan? Yes No Assistance required? Yes No Explain Snack Time(s)? Assistance required? Yes No Explain Snack will be eaten in (location) Snacks will be stored in (location) Recommended snacks Parent wishes to be notified in advance of class parties? Yes No Child may partake in class treats? Yes No Explain Comments: Physical Education: Scheduled at: Is snack necessary before physical education? Yes Does child participate in after school sports? Yes P.E. Teacher/Coach aware of child s diabetes? Yes Comments: No No No Adapted and used with permission by the Colorado Department of Education 81
85 Diabetes Management Supplies Student: DOB: Date of Plan: Supplies to be Provided by Parent/Guardian: Parents/Guardian and student are responsible for maintaining necessary supplies, snacks, blood glucose meter, medications and other equipment. General Supplies: Insulin Supply (Pen, Vial) Needed Provided Not Needed Insulin Syringes/needles Needed Provided Not Needed Oral Medication Needed Provided Not Needed Blood glucose meter and glucose strips Needed Provided Not Needed Lancets with lancing device Needed Provided Not Needed Blood ketone monitor/strips Needed Provided Not Needed Urine ketone strips Needed Provided Not Needed Antibacterial skin cleaner or alcohol wipes Needed Provided Not Needed Fast Acting Sugar: (e.g. Glucose tabs, juice, Smartees) Needed Provided Not Needed Glucose Gel/Cake Mate Needed Provided Not Needed Carbohydrate/Protein snack Needed Provided Not Needed Glucagon Emergency Kit Needed Provided Not Needed Other: Pump Supplies: Insulin Pump Needed Provided Not Needed Insulin Pump Batteries Needed Provided Not Needed Insulin Pump Cartridge Needed Provided Not Needed Infusion Set Needed Provided Not Needed Quick-seter/Sof-sert/Sil-serter Needed Provided Not Needed Dressings/tape Needed Provided Not Needed Manufacturer Instructions Needed Provided Not Needed Batteries Needed Provided Not Needed Other Pods for OMNI POD Manufacturer Instructions Needed Provided Not Needed Continuous Glucose Monitor Needed Provided Not Needed Needed Provided Not Needed Disaster Supplies: Parents determination (insulin/supplies for 72 hours) Needed Provided Not Needed Supplies Location: Location of hypoglycemia supplies: Location of other supplies & equipment: Student Self Carries/Supplies are kept: Supplies provided for: Extracurricular Activities Before and After School Programs Other: Notification of needed supplies to Parents/Guardians by: Telephone Text Note home Parent: Parent Signature: Date: School Nurse: School Nurse Signature: Date: Adapted and used with permission from the Colorado Department of Colorado 82

86 This informational packet from Riley Hospital for parents and schools is an example of an instructional tool intended to begin the process of taking care of students with diabetes while in school. 83
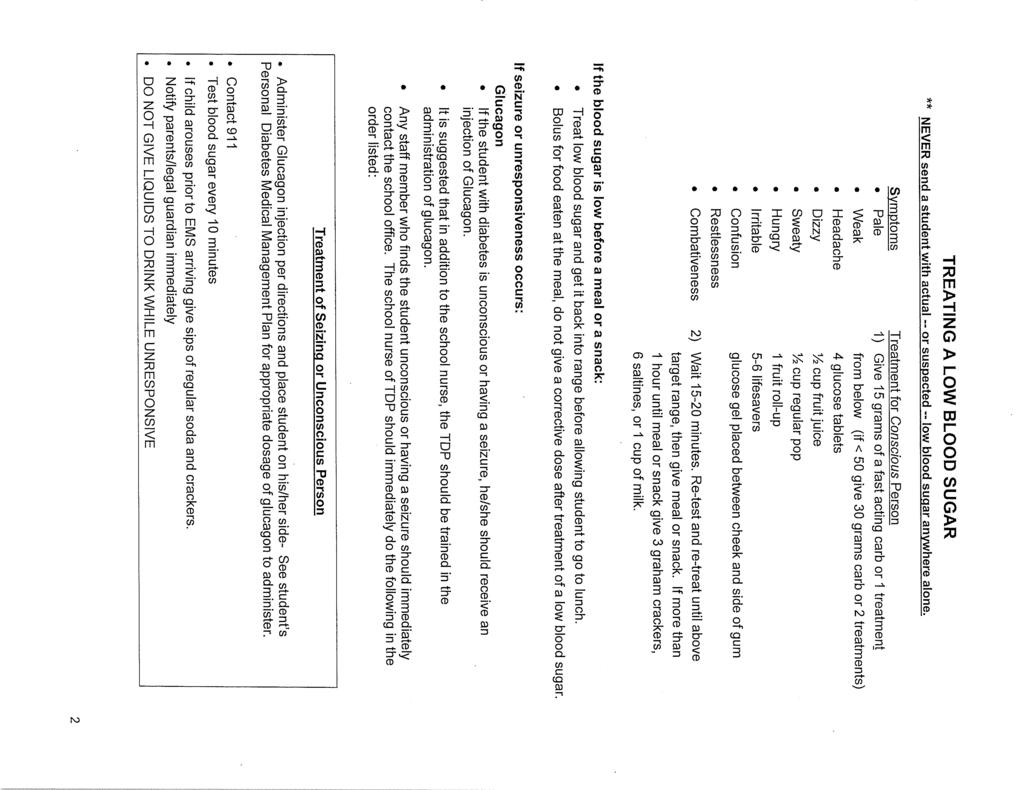
87 84
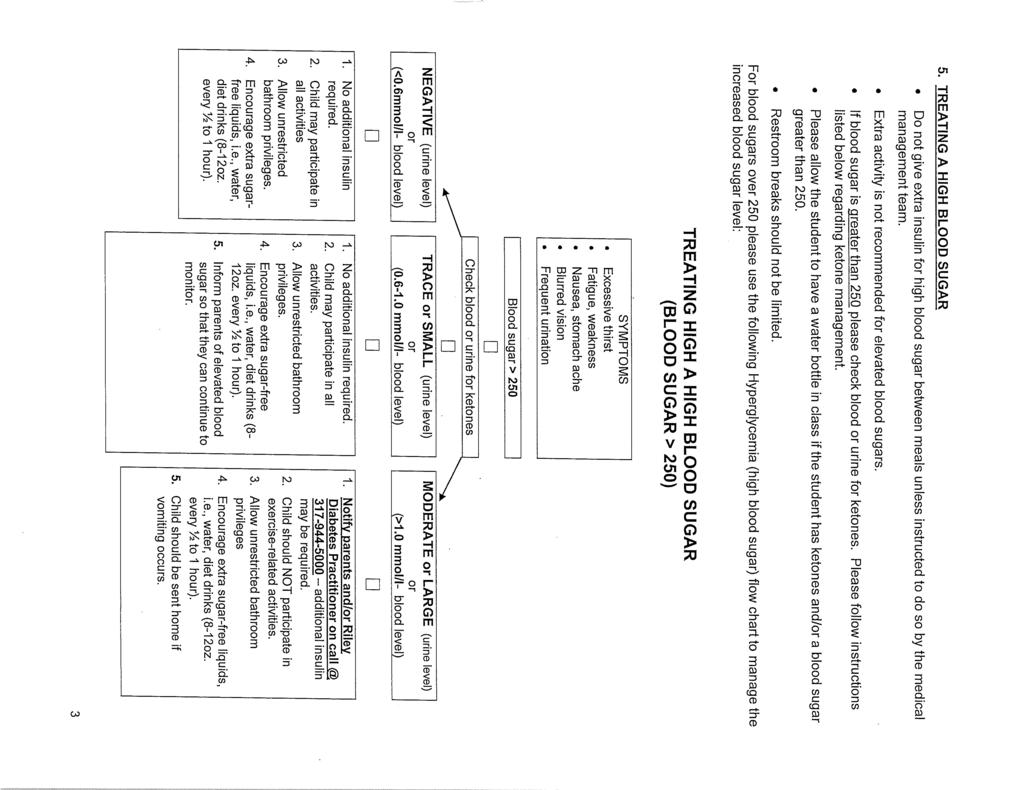
88 85
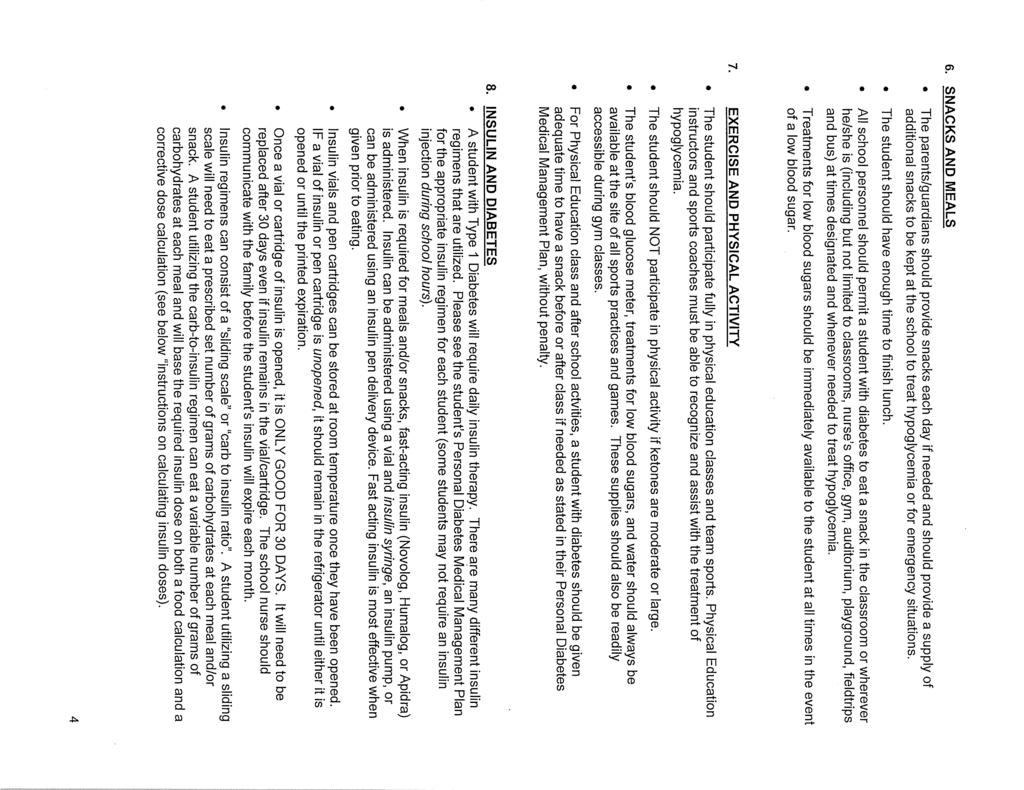
89 86
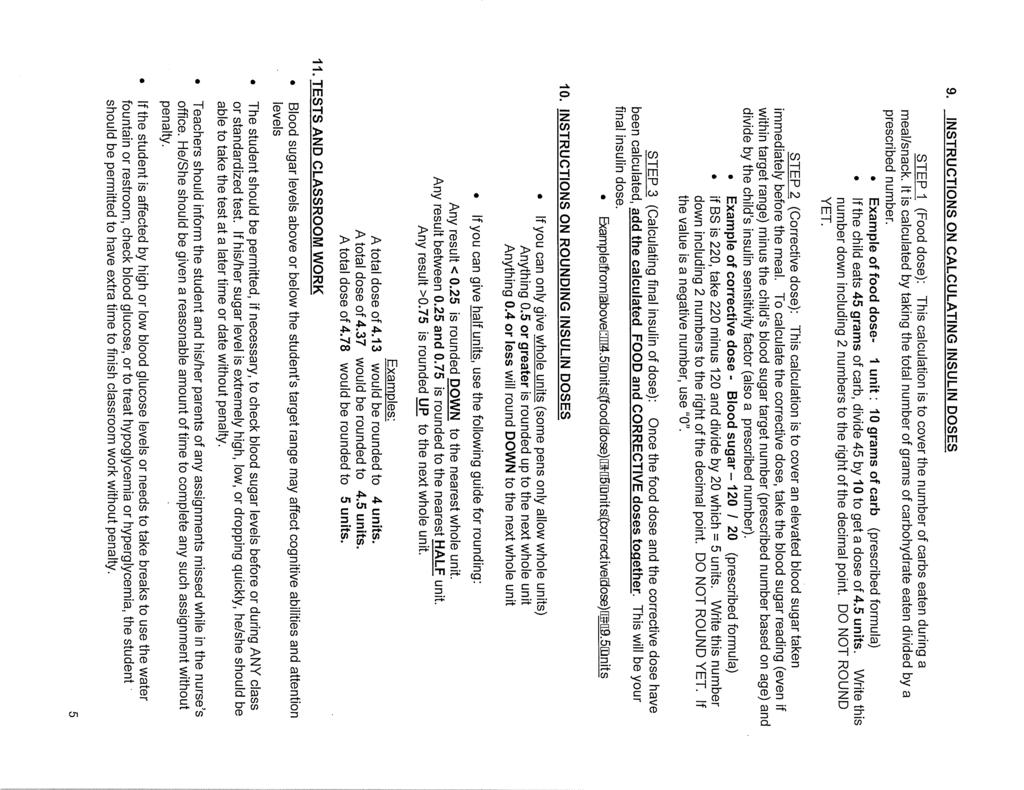
90 87
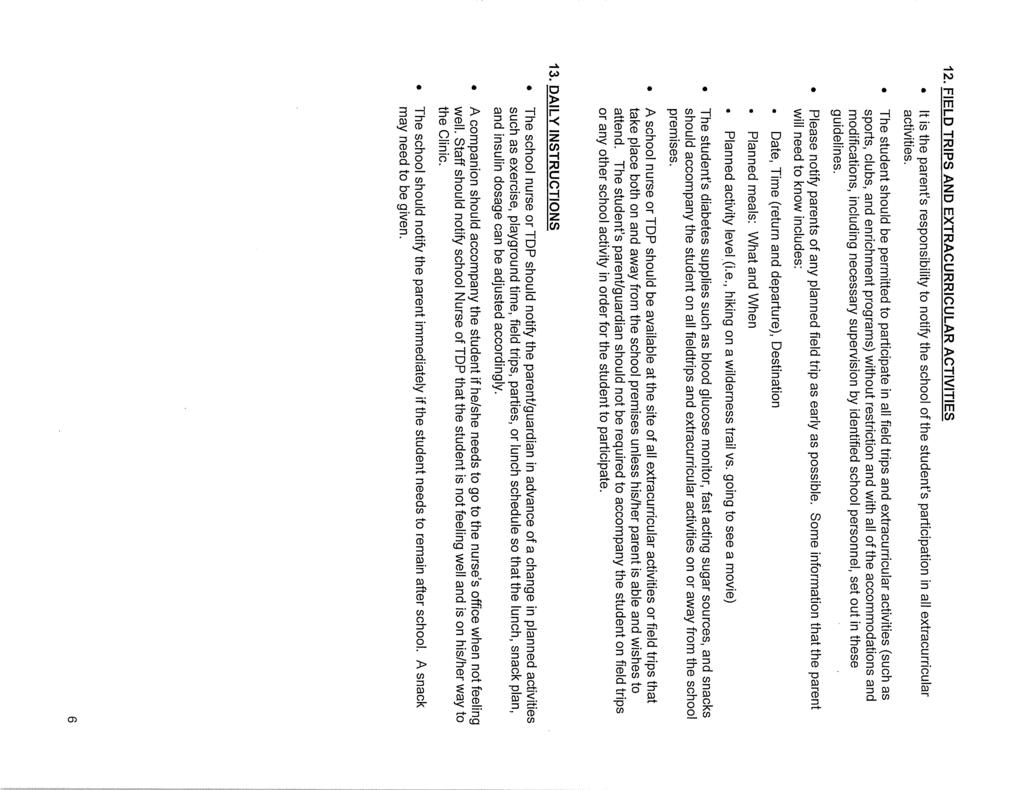
91 88
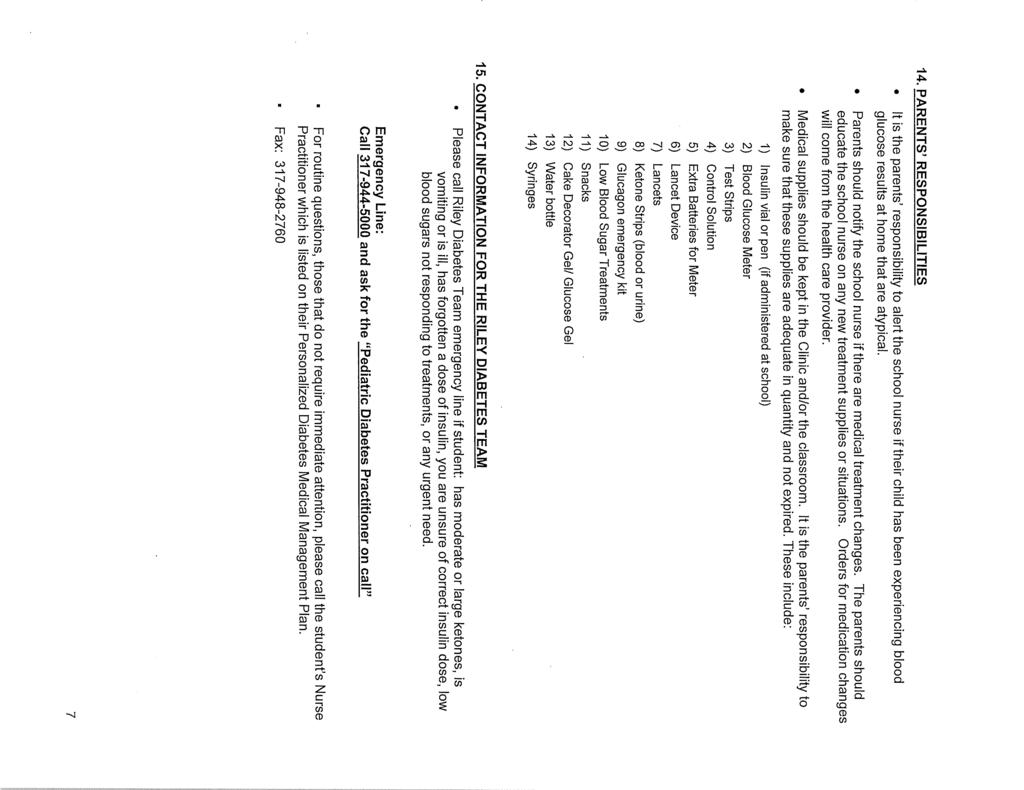
92 89
93 90

94 Children and Adolescents with Diabetes How Can You Help? IDEAS FOR PARENTS Diabetes (Types 1 and 2) is a serious disease that may affect children in the United States. 1 Diabetes can result in a buildup of sugar or glucose, which is the body s main source of fuel in the blood, and over time can cause damage to the eyes, kidneys, heart, nerves, and blood vessels. Persons with diabetes may require careful daily monitoring and management of blood glucose levels to prevent serious complications. Students who have diabetes need appropriate care in the school setting for their safety, well-being, and school performance. 2,3 Having abnormally high (hyperglycemia) or low glucose (hypoglycemia) levels can be life-threatening and require immediate attention by qualified health professionals. Schools should work with parents and health care providers to ensure a safe learning environment in which students with diabetes can fully participate in the school experience, while having their health needs met. Knowing the answers to the following questions can help you support your child s school to address diabetes. If you don t know the answers to these questions, check out the school handbook or school website, attend a school wellness meeting or Parent-Teacher Association (PTA) meeting, or simply ask your child s teacher. What s Happening at School? 1. Are there School Health Services, including a full-time registered nurse, in the school building at all times to help students with chronic medical conditions or with emergencies? 2. How does the school identify and share information about those students who have diabetes? 3. Is it required that each student with diabetes have a school diabetes medical management or emergency management plan? 3 4. What are school policies for self-medication administration? Does the school allow students to carry their own medication, such as oral medicine or insulin, snacks, and glucose monitoring supplies at school? Can the student with diabetes test his or her glucose in school? 5. Does the cafeteria provide information about the nutritional content of meals, including carbohydrates, for diabetic students? If so, where can this information be found? 6. What are the school protocols for managing diabetes at school, on the school bus, on a field trip, or in cases of emergency or lockdown? 7. Are other school staff, such as teachers, bus drivers, and food services staff, trained to recognize and respond to hypoglycemia (low blood sugar) and hyperglycemia (high blood sugar)? 8. What is the policy for student participation in physical activity (e.g., recess or classroom activity breaks) or physical education at school if he or she has diabetes? 9. Is there a bullying prevention policy in the school or district that discourages bullying or encourages awareness or anti-stigma of students with medical conditions? 91


95 Ideas for Parents You can be involved in your child s school by attending meetings, workshops, or training events offered by the school; communicating with school staff and other parents; volunteering for school events or in your child s classroom; reinforcing healthy messages and practices your child learns at school; helping make decisions about health in the school; and being part of community activities supported by the school. Here are some specific ideas for how you can support your child s school in addressing diabetes. Advocate for a full-time registered nurse in school. Have an ongoing conversation with your child to discuss their diabetes, their feelings about having diabetes, and if they feel safe and supported at school. 5 Work with your child s health care provider to establish a school diabetes medical management plan and the timely completion of required school forms. 3 Encourage communication between school health services and your child s health care provider. Provide medication, monitoring supplies, and snacks to the registered nurse or other school health official. Ensure that there is a current individualized health care plan, and assist with setting goals. 4 Keep your emergency contact information up-to-date with the teacher, school secretary, and registered nurse. Communicate with your child s teachers, counselors, school health services, and food services staff about your child s diabetes and any concerns about how they cope while at school. Volunteer with your child, or get involved at school health events to educate staff and other families about diabetes. Join a group, such as the PTA, school wellness committee, or school health advisory council, that addresses the needs of a supportive and healthy school environment. 6 Share research-based websites or written materials about diabetes with teachers, nurses, and administrators, when possible, (e.g., gov/features/diabetesinschool). Check out additional resources for parents related to the school nutrition environment and services, physical education and physical activity, and managing chronic health conditions at REFERENCES 1. Centers for Disease Control and Prevention. Basics About Diabetes. Accessed November 19, American Diabetes Association. Diabetes care in the school and daycare setting. Diabetes Care. 2008;31 Suppl 1:S National Association of School Nurses. Position Statement. Diabetes Management in the School Setting; PolicyAdvocacy/PositionPapersandReports/NASNPositionStatementsFullView/tabid/462/ArticleId/22/Diabetes-Management-inthe-School-Setting-Adopted-January Accessed August 6th, National Association of School Nurses. Individualized Healthcare Plans: The Role of the School Nurse; PolicyAdvocacy/PositionPapersandReports/NASNPositionStatementsFullView/tabid/462/ArticleId/32/Individualized-Healthcare-Plans-The-Role-ofthe-School-Nurse-Revised-January Accessed August 6th, Centers for Disease Control and Prevention. School Connectedness: Strategies for Increasing Protective Factors among Youth. Atlanta: US Dept of Health 92 and Human Services; Centers for Disease Control and Prevention. Parent Engagement: Strategies for Involving Parents in School Health. Atlanta: US Dept of Health and Human Services; CS B
96 Seizure Action Plan Effective Date This student is being treated for a seizure disorder. The information below should assist you if a seizure occurs during school hours. Student s Name Date of Birth Parent/Guardian Phone Cell Other Emergency Contact Phone Cell Treating Physician Phone Significant Medical History Seizure Information Seizure Type Length Frequency Description Seizure triggers or warning signs: Student s response after a seizure: Basic First Aid: Care & Comfort Please describe basic first aid procedures: Does student need to leave the classroom after a seizure? Yes No If YES, describe process for returning student to classroom: Emergency Response A seizure emergency for this student is defined as: Seizure Emergency Protocol (Check all that apply and clarify below) Contact school nurse at Call 911 for transport to Notify parent or emergency contact Administer emergency medications as indicated below Notify doctor Other Treatment Protocol During School Hours (include daily and emergency medications) Basic Seizure First Aid Stay calm & track time Keep child safe Do not restrain Do not put anything in mouth Stay with child until fully conscious Record seizure in log For tonic-clonic seizure: Protect head Keep airway open/watch breathing Turn child on side A seizure is generally considered an emergency when: Convulsive (tonic-clonic) seizure lasts longer than 5 minutes Student has repeated seizures without regaining consciousness Student is injured or has diabetes Student has a first-time seizure Student has breathing difficulties Student has a seizure in water Emerg. Dosage & Med. Medication Time of Day Given Common Side Effects & Special Instructions Does student have a Vagus Nerve Stimulator? Yes No If YES, describe magnet use: Special Considerations and Precautions (regarding school activities, sports, trips, etc.) Describe any special considerations or precautions: Physician Signature Date Parent/Guardian Signature Date DPC772 Copyright 2008 Epilepsy Foundation of America, Inc. 93
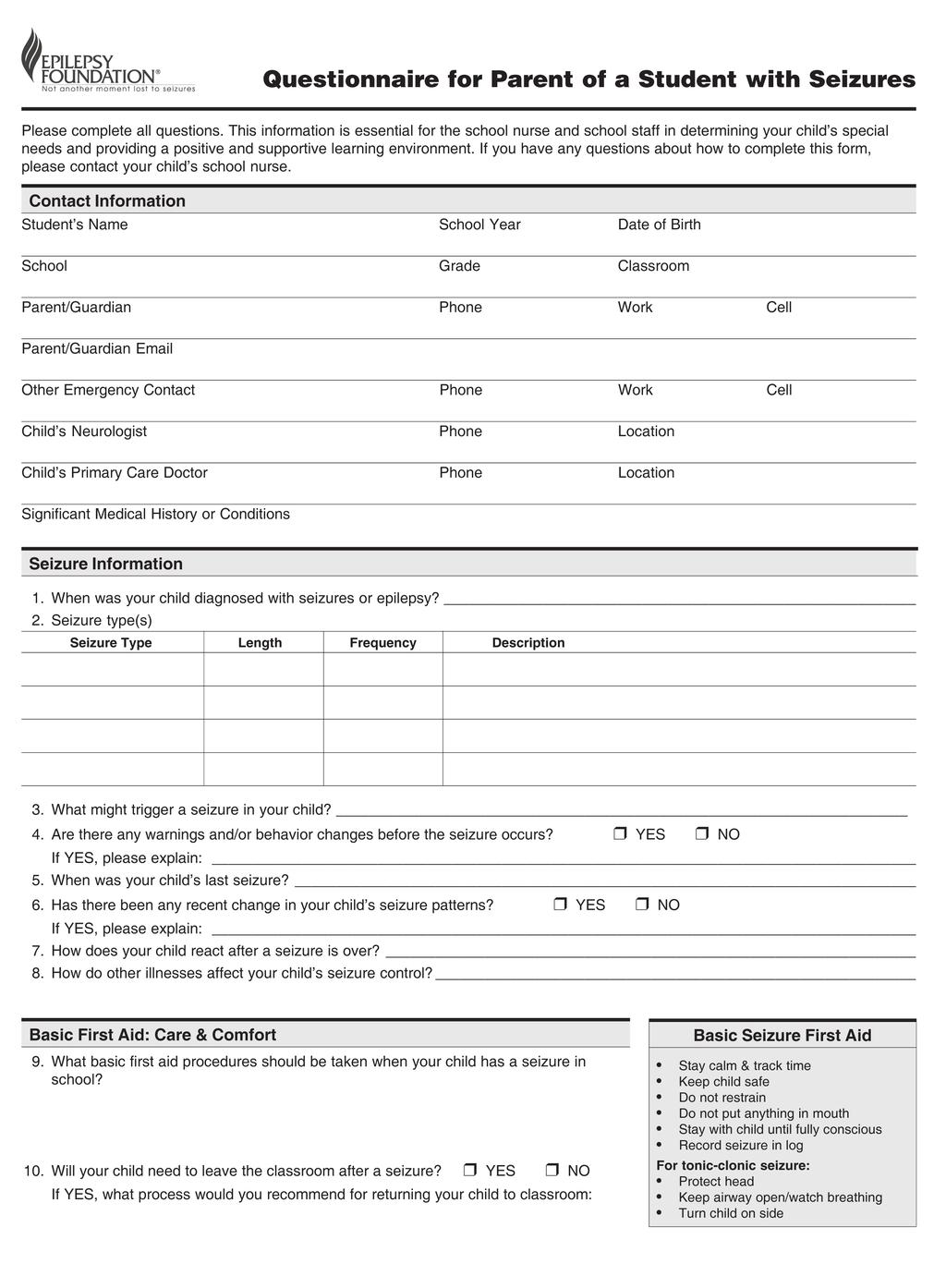
97 94
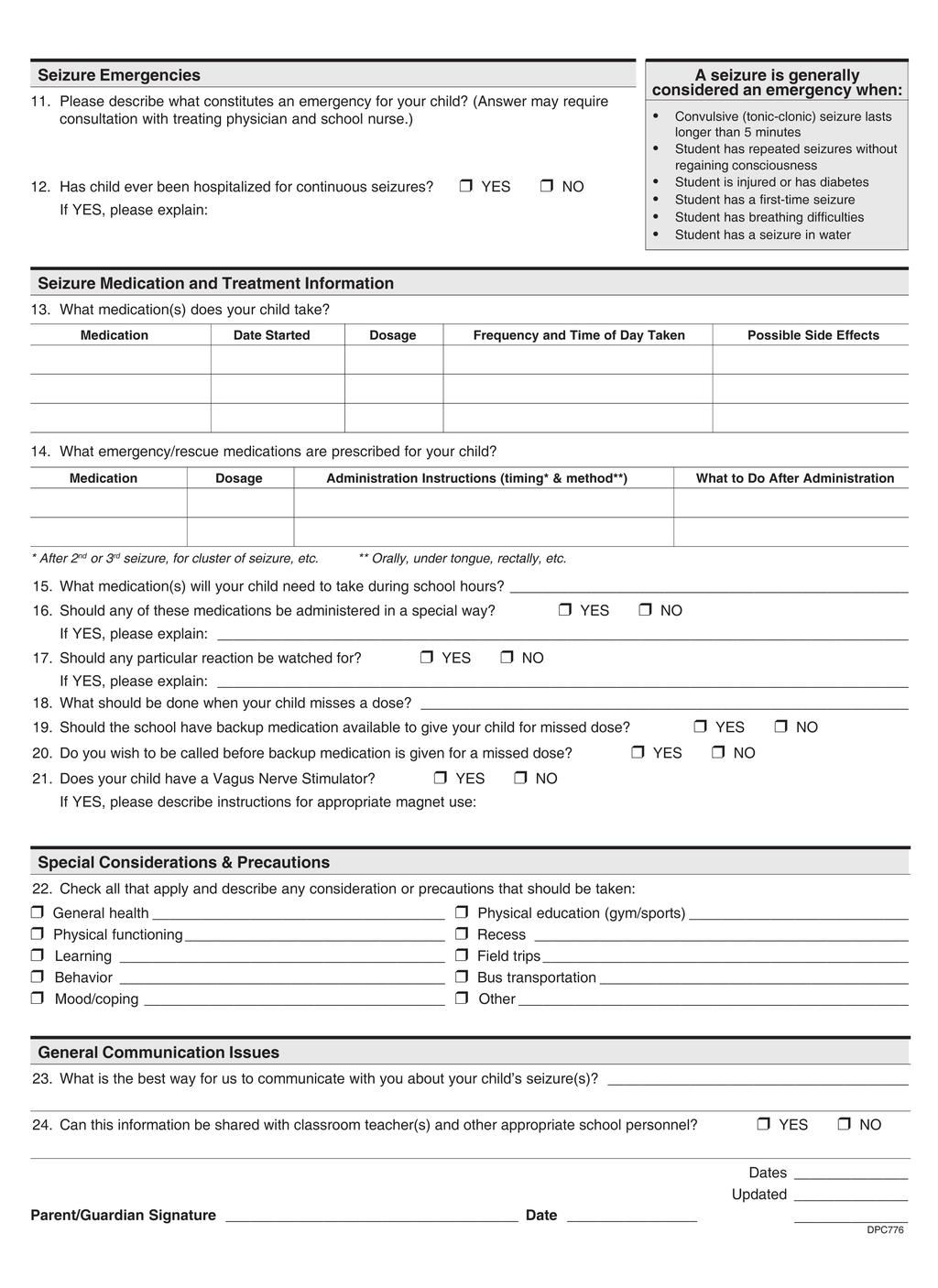
98 95
99 96

100 Children and Adolescents with Seizure Disorders How Can You Help? IDEAS FOR PARENTS Seizure disorders occur when a disturbance in the brain produces changes in awareness or sensation, involuntary body movements, or changes in behavior lasting from a few seconds to a few minutes. Seizure disorders are the 4th most common nervous system problem and can lead to learning problems that require special help or accommodations. 1 A seizure disorder affects people differently depending on age, types of seizures, response to treatment, and whether the person has other health issues. For some, seizures are easily controlled with medicine and eventually outgrown. For others, a seizure disorder can create difficult challenges throughout their lives. 2 School health services can identify students with seizure disorders and work with parents and health care providers to meet both urgent and nonurgent needs during the school day by developing an individualized health care plan. 3 Knowing the answers to the following questions can help you support your child s school to address seizure disorders. If you don t know the answers to these questions, check out the school handbook or school website, attend a school wellness meeting or Parent- Teacher Association (PTA) meeting, or simply ask your child s teacher. What s Happening at School? 1. Is there a full-time registered nurse in the school building at all times or a school-based health center to help students with chronic medical conditions or with emergencies? 2. How does the school identify and share information about which students have seizure disorders? 3. Does the school require that each student with a seizure disorder have a school seizure action plan? 4. Does the school allow students to carry their own medication at school? 5. What are the school protocols if a student is having a seizure at school, during after-school activities, on the school bus, on a field trip, or in cases of emergency or lockdown? 6. Are other school staff, such as teachers, bus drivers, and food services staff, trained to recognize and respond to a student that may be having a seizure? 7. What is the policy for student participation in physical activity (e.g., recess or classroom activity breaks) or physical education at school if he or she has a diagnosis of seizure disorder? 8. Is there a bullying prevention policy in the school or district that discourages bullying or encourages awareness or anti-stigma of students with medical conditions? 97


101 Ideas for Parents You can be involved in your child s school by attending meetings, workshops, or training events offered by the school; communicating with school staff and other parents; volunteering for school events or in your child s classroom; reinforcing healthy messages and practices your child learns at school; helping make decisions about health in the school; and being part of community activities supported by the school. Here are some specific ideas for how you can support your child s school in addressing seizure disorders. Have an ongoing conversation with your child to discuss their seizures, their feelings about having a seizure disorder, and if they feel safe and supported at school. 4 Work with your child s health care provider to coordinate care with school health services by establishing a school seizure action plan and the timely completion of required school forms. Encourage communication between school health services and your child s health care provider. Provide emergency medication to the school nurse or other school health official. Ensure that there is a current individualized health care plan, and assist with setting goals. 3 Keep your emergency contact information up-todate with the teacher and school nurse. Communicate with your child s teachers, counselors, and school health services staff regarding your child s seizures and how they are coping while at school. Volunteer with your child, or partner with an advocacy organization (e.g., Epilepsy Foundation) to help provide leadership at school health events, and to educate staff and other families about seizure disorders. Join a group, such as the PTA, school wellness council, or school health advisory council, that addresses the needs of a supportive and healthy school environment. 5 Share research-based websites or written materials about seizure disorders with teachers, nurses, and administrators, when possible, (e.g., cdc.gov/epilepsy/index.html). Check out additional resources for parents related to the school nutrition environment and services, physical education and physical activity, and managing chronic health conditions at REFERENCES 1. Hirtz D, Thurman DJ, Gwinn-Hardy K, Mohamed M, et al. How common are the common neurologic disorders? Neurology. 2007;68(5): National Epilepsy Foundation. Epilepsy & My Child Toolkit: A Resource for Parents with a Newly Diagnosed Child; Accessed August 5, National Association of School Nurses. Individualized Healthcare Plans: The Role of the School Nurse; PolicyAdvocacy/PositionPapersandReports/NASNPositionStatementsFullView/tabid/462/ArticleId/32/Individualized-Healthcare- Plans-The-Role-of-the-School-Nurse-Revised-January Accessed August 6, Centers for Disease Control and Prevention. School Connectedness: Strategies for Increasing Protective Factors among Youth. Atlanta: US Dept of Health and Human Services; Centers for Disease Control and Prevention. Parent Engagement: Strategies for Involving Parents in School Health. Atlanta: US Dept of Health and Human Services; CS B
 as well as those who have a health diagnosis which requires care during the school day and during school-related activities,")
102 Chapter 4: IHPs and Emergency Action Plans Introduction School corporations must provide and manage healthcare services for every enrolled student. Students who require chronic disease management (discussed in Chapter 4) as well as those who have a health diagnosis which requires care during the school day and during school-related activities, should have an individual healthcare plan (IHP) written and in place to ensure that needed healthcare services are received. The IHP can be a stand-alone document or be incorporated into a 504 plan or IEP when appropriate. The IHP is developed from information provided by the families and the healthcare provider and is tailored to the school environment. The IHP should include provisions for after-school activities, extracurricular activities, and field trips. It also includes provisions for self-care in students who are able with parent, nurse, and physician input and permission. The IHP is written by a school/school district RN who manages student healthcare in the school setting. Evaluation of the IHP should occur at least annually-but also at any time there is evidence that the interventions are ineffective or no longer needed. SECTION 1: HOW TO DEVELOP IHP s SECTION 2: WHEN TO USE IHP s SECTION 3: EMERGENCY ACTION PLANS 99
103 SECTION 1: How To Develop IHP s To begin the process of developing an IHP, the RN can use the Individualized Healthcare Plan Process: INDIVIDUALIZED HEALTHCARE PLAN PROCESS IDENTIFYING How are students with healthcare needs identified in your school? NOTIFYING THE SCHOOL NURSE How and when is the school nurse notified of these students? Consider any student with special healthcare needs and chronic conditions DEVELOPING AN INDIVIDUALIZED HEALTHCARE PLAN Which students need an IHP and how do I create one? ASSESSING STUDENT S HEALTH CONDITION 1. What is the student s ability to self-manage? 2. What plan was in place for this student last year and was it effective? CREATING THE INDIVIDUALIZED HEALTHCARE PLAN 1. Do you have healthcare orders for the medical interventions? (The beginning of IHP s) 2. Are those orders signed by both the provider and the student s parents? 3. Did the parent give permission to share the information with pertinent staff and permission to discuss treatment orders and questions with the provider? 3. Have you reviewed your school policies regarding students with chronic health conditions? 4. Have you completed your student assessment? 5. Gather all of these pieces together and write an IHP addressing each topic (below) SHARING THE INDIVIDUALIZED HEALTHCARE PLAN Has the parent/guardian recieved a copy of the plan? IMPLEMENTING THE HEALTHCARE PLAN What do I do next, now that I have a written plan? Distribution of Healthcare Plan Staff/Student Training Delegation of Nursing Tasks EVALUATING AND OUTCOMES Is this plan working? Do I have measurable outcomes? Adapted and used with permission by the Colorado Department of Education 100
104 PURPOSE OF THE IHP: The purpose of the IHP is to provide a road map or plan for anyone charged with the healthcare of students during the school day as well as during school-related activities. The IHP also provides: Continuity of care both among caregivers within one school as well as from school to school Documentation of healthcare required and provided Legal protection for those providing healthcare according to the plan A standard of nursing practice Definition of the nursing care required Direction for delegated nursing care IHP s should be written for students who: Have a health diagnosis requiring nursing care during school Have medical, procedure, or treatment orders not addressed in school policy/procedures Have emergency medical orders for medications or procedures should they be needed Have medical orders that would require delegation of nursing care to a non-rn Would require special consideration if presenting with symptoms Those who do not require an IHP: Example: Students taking daily medications. Follow your school policy and procedures regarding daily medications. o You DO need to document any training done o You DO need to document all medications administered IHP s should include the following sections: Student demographics Contact information for families including doctors and medical specialists Medical diagnosis Symptoms of concern Allergies and/or triggers to avoid Diet, activity, or environmental modifications Schedule of daily care Contingency planning (who gives healthcare in the event of nurse or VHA s absence?) Field trip considerations and plans Extracurricular events planning Transportation planning Supplies needed for daily and/or emergency healthcare Communication plan (daily event communication, needed supplies as well as emergency contact information) 101
105 Signatures o o RN who wrote the IHP Signature of parent; indicating that they have received a copy of the plan and acknowledgement that they understand the date the plan will go into effect Note: If parent refuses or fails to sign the IHP, document all communications and efforts to obtain their signature. Suggestions/Reminders for Writing an IHP: Every IHP is different o Use a format that is comfortable for you: You may prefer a narrative format or a template with appropriate addendums, as long as each of the sections listed above are included o IHP s are student specific-therefore no one size fits all Some will be simple but others will be more detailed Use our Indiana law: The Care of Students with Diabetes (IC ) as a guide for IHP writing as this law is very detailed regarding IHP development There are two plans described in the diabetic law: 1. Management and Treatment Plan written by the healthcare provider o Also called physician orders or medical management plan o Treatment orders using their forms adapted to school forms OR have them complete school forms o Apply to school hours and school-related activities o Routine medication or treatment orders o Emergency orders o Developed and signed by parent and licensed healthcare provider o Submitted to the school RN 2. IHP-written by an RN incorporating the medical orders Hold an initial discussion with the parent and ask for the orders from the healthcare provider o Important time to set the tone for working together with the parents o Listen and instill confidence o Ask about the child, history of the disease and what has worked well in the past, what is their current self-care ability, what things worry the parents o Share with parents how you are looking forward to working with them Draft IHP o Gather all information from parent, medical orders, school policy, and any past IHP s o Check student s schedule including lunch, PE, recess, and location of their locker o Develop the daily plan based on all of the above Parent meeting after IHP has been drafted o Time to review the drafted IHP o Discuss treatment orders, transportation, use of unlicensed assistive personnel (UAP) and their training, contingency planning should nurse be absent, field trips, emergency procedures, agree on a communication system 102

106 o Discuss any changes parents request The IHP represents a legal standard you will be held to-so whatever you write into the plan must be done Do not agree to requests which cannot be accomplished. Discuss and negotiate those requests before finalizing the IHP. Be sure to update the IHP after visits to the healthcare provider or hospitalizations which result in changes to the daily healthcare of the student while at school SECTION 2: When To Use STAFF TRAINING Parent permission is required before you share health information with school personnel and should be included in the IHP such as: I give permission for the school nurse and any pertinent staff caring for my child to follow this plan, administer medication and care for my child, contact my licensed healthcare provider if necessary, and for this healthcare information to be shared with pertinent school staff per FERPA guidelines. I assume full responsibility for providing the school with prescribed medication and delivery/monitoring devices. Levels of staff training o Level 1= All staff-general information including the basics of emergency care o Level 2= Staff with frequent contact with the student (teachers, coaches, bus driver, office staff, UAP s) o Level 3= Staff assigned to give direct student care (nurse and/or delegated staff, VHA s) Information sheets- Individuals who transport the student and/or supervise the student during activities off campus should be provided with individual student information sheets (instead of the entire IHP) which include the following information: Identification of the student with IHP Diagnosis Description of the signs and symptoms of emergencies Appropriate emergency response Contact information, emergency contacts SECTION 3: Emergency Action Plans Emergency action plans should not be confused with individual healthcare plans (IHP s) as they do not outline the daily healthcare requirements and plans put into place in order to adequately care for a student while in school or at any school-related activities. IHP s are put into place in hopes of avoiding health emergencies. Emergency action plans are directions to follow in the event of a health emergency. They almost always include 103
107 emergency medicine or treatment orders and parameters from a licensed healthcare provider to be put into action at times of a medical emergency. Emergency action plans should always be included as an addendum to the IHP but do not replace any IHP. Examples of an emergency action plan scenario: Physician orders for a specific student experiencing hyperglycemia or hypoglycemia: At what blood sugar level to treat, how to treat, how to monitor thereafter Physician orders for a specific student experiencing anaphylaxis: What is considered an anaphylaxis event for that individual, how to treat the emergency, and what actions should be put into place after emergency treatment Physician orders for a student s use of their prescribed rescue inhaler What action to follow in the event poor results are experienced by the individual after using their rescue inhaler; how to monitor those results o Physician direction and possible medication orders for an individual experiencing a seizure emergency When to seek emergency assistance, how to keep that individual safe and how to monitor them Individual healthcare plan resource document: NASN, Individualized Healthcare Plans: The Role of the School Nurse (PDF) Some resources for samples of IHP s include: Andrews, Robert. (2010). School Nurse Resource Manual: A Guide to Practice. School Health Alert. Arnold, Martha J. (1999). The School Nurse s Source Book of Individualized Healthcare Plans. Sunrise River Press. National Association of School Nurses. (2015). Helping Administer to the Needs of the Student with Diabetes in Schools (H.A.N.D.S.) Silkworth, Cynthia K. (2005). Individualized Healthcare Plans for the School Nurse. Sunrise River Press. 104
108 Individualized Healthcare Plans: The Role of the School Nurse SUMMARY Position Statement It is the position of the National Association of School Nurses (NASN) that the registered professional school nurse (hereinafter referred to as school nurse), in collaboration with the student, family and healthcare providers, shall meet nursing regulatory requirements and professional standards by developing an Individualized Healthcare Plan (IHP) for students whose healthcare needs affect or have the potential to affect safe and optimal school attendance and academic performance. Because health conditions can be complex and unfamiliar to school staff and the student s requirement for nursing care can be frequent and sometimes emergent, accurate and adequate documentation of chronic medical conditions and individual needs is critical (Lyon, 2012). Development of IHPs is a nursing responsibility, based on standards of care regulated by state nurse practice acts and cannot be delegated to unlicensed individuals (National Council of State Boards of Nursing [NCSBN], 2005). It is the responsibility of the school nurse to implement and evaluate the IHP at least yearly and as changes in health status occur to determine the need for revision and evidence of desired student outcomes. BACKGROUND The IHP is a document based on the nursing process. Since emerging in the 1970s, the nursing process is the cornerstone of nursing practice, using a scientific approach in the identification and solution of health problems in nursing practice (Hermann, 2005). The American Nurses Association (ANA) and NASN define the nursing process as a circular, continuous and dynamic critical thinking process comprised of six steps and that is client centered, interpersonal, collaborative, and universally applicable (American Nurses Association [ANA] & NASN, 2011, p. 76). Documentation of these steps for individual students who have healthcare issues results in the development of an IHP, a variation of the nursing care plan. The term IHP refers to all care plans developed by the school nurse, especially those for students who require complex health services on a daily basis or have an illness that could result in a health crisis. These students may also have an Individualized Education Plan (IEP), a 504 Student Accommodation Plan to ensure school nursing services and access to the learning environment, or an Emergency Care Plan (ECP) for staff caring for these students (Hermann, 2005). RATIONALE Development of the IHP by the school nurse provides a framework for meeting clinical and administrative needs: Demonstrates Standard of School Nursing Practice Development and implementation of the IHP is documentation of professional performance in accordance with standards of school nursing practice, the professional expectations that guide the practice of school nursing (ANA & NASN, 2011). The Standards of School Nursing Practice are authoritative statements of the duties that school nurses, regardless of role, population, or specialty within school nursing are expected to competently perform (ANA & NASN 2011, p. 4). These standards describe a competent level of nursing care as demonstrated by the critical thinking model known as the nursing process (ANA & NASN, 2011, p. 12). Documents the Nursing Process Creation of the IHP incorporates and documents the nursing process in student care in accordance with state nurse practice acts. The nursing process provides a framework for the nurse s responsibility and accountability. The RN may delegate components of care but does not delegate the nursing process itself. The practice pervasive 105
109 functions of assessment, planning, evaluation and nursing judgment cannot be delegated (ANA & NCSBN, 2005, p.2). School Nursing: Scope and Standards of Practice (ANA & NASN, 2011) outlines how implementation of each step of the nursing process strengthens and facilitates educational outcomes for students. These steps parallel components of a well developed IHP. Standard 1. Assessment: The school nurse collects comprehensive data pertinent to the healthcare consumer s health and/or situation. Standard 2. Nursing Diagnosis: The school nurse analyzes the assessment data to determine the diagnoses or issues. Standard 3. Outcome Identification: The school nurse identifies expected outcomes for a plan individualized to the healthcare consumer or the situation. Standard 4. Planning: The school nurse develops a plan that prescribes strategies and alternatives to attain expected outcomes. Standard 5. Implementation: The school nurse implements the identified plan. Standard 6. Evaluation: The school nurse evaluates progress toward attainment of outcomes. Provides Legal Documentation A school nurse plans safe care for students and demonstrates an appropriate standard of professional care when the IHP is used as the foundation for student health interventions. Judicious use of the IHP as a vehicle to ensure safe nursing services and continuity of care for students with special (health) needs is a standard of care against which a school nurse s conduct can be judged in a legal proceeding (Hootman, Schwab, Gelfman, Gregory, & Pohlman, 2005, p. 190). Along with applicable laws including state nurse practice acts, expert testimony, organizational policies and procedures, the standard of care is a significant factor used by courts in professional liability cases (Pohlman, 2005). Clarifies Clinical Practice The IHP s clinical purposes include clarifying and consolidating meaningful health information, establishing the priority set of nursing diagnoses for a student, providing communication to direct the nursing care of a student, documenting nursing practice, ensuring consistency and continuity of care as students move within and outside school districts, directing specific interventions, identifying (safe and appropriate) delegation of care, and providing methods to review and evaluate nursing goals and student outcomes (Hermann, 2005). It is important to note that student centered outcomes are developed early in the IHP process to guide interventions and provide a basis for evaluation to take place. The IHP is the document that combines all of the student s healthcare needs into one document for management in the school setting (Zimmerman, 2013). Provides Administrative Information The IHP serves administrative purposes, which include defining the focus of nursing; validating the nurse s role in the school; facilitating management of health conditions to optimize learning; differentiating accountability of the nurse from others in the school; providing criteria for reviewing and evaluating care (quality assurance); providing data for statistical reports, research, third party reimbursement and legal evidence; and creating a safer process for delegation of care in the school setting (Hermann, 2005). Serves as the Foundation for Health Portion of Other Educational Plans and Emergency Plans The IHP provides the health information and activities that can be incorporated into the health portion of other school educational plans to foster student academic success and to meet state and federal laws and regulations. These include the Individualized Education Plan (IEP) in accordance with the Individuals with Disabilities Education 106
110 Improvement Act (P.L , 2004) and a 504/ADA plan in accordance with Section 504 of the Rehabilitation Act (P.L , 1992) and the Americans with Disabilities Act (P.L , 2008). The student Emergency Care Plan (ECP) is an emergency plan developed by the registered professional school nurse and is based on the IHP or is sometimes used instead of an IHP. The ECP is written in clear action steps using succinct terminology that can be understood by school faculty and staff who are charged with recognizing a health crisis and intervening appropriately (Zimmerman, 2013). The ECP is distributed to these individuals with the expectation that the information will be treated with confidentiality. The names of the individuals who have a copy of the ECP should be listed at the bottom (Zimmerman, 2013). CONCLUSION It is the responsibility of the registered professional school nurse to develop an IHP and ECP for students with healthcare needs that affect or have the potential to affect safe and optimal school attendance and academic performance. The IHP is developed by the school nurse using the nursing process in collaboration with the student, family and healthcare providers. The school nurse utilizes the IHP to provide care coordination, to facilitate the management of the student s health condition in the school setting, to inform school educational plans, and to promote academic success. The ECP, written by the school nurse, is for support staff with an individual plan for emergency care for the student. These plans are kept confidential yet accessible to appropriate staff. REFERENCES American Nurses Association & National Association of School Nurses. (2011). School nursing: Scope and standards of practice (2nd ed.). Silver Spring MD: Nursesbooks.org. American Nurses Association & National Council of State Boards of Nursing. (2005). Joint statement on delegation. Retrieved from ANA.pdf Americans with Disabilities Act of 1990 as Amended. (2008). Publ Law Hermann, D. (2005). Individualized healthcare plans. In C. Silkworth, M. Arnold, J., Harrigan, & D. Zaiger, (Eds.), Individualized healthcare plans for the school nurse: Concepts, framework, issues and applications for school nursing practice (pp. 1 4). North Branch, MN: Sunrise River Press. Hootman, J., Schwab, N.C., Gelfman, M.H.B., Gregory, E.K. & Pohlman, K. J. (2005). School nursing practice: Clinical performance issues. In N. C. Schwab, & M. H. B. Gelfman, (Eds.), Legal issues in school health services (pp ). North Branch, MN: Sunrise River Press. Individuals with Disabilities Education Act. (2004). 20 U.S.C. 1400, 602 (26) [Definitions]. Code Federal Regulations (CFR), part 300. Lyon, L. (2012). School assessment form for students with special health care needs. NASN School Nurse, 27 (6), 288. doi: / X National Council of State Boards of Nursing (NCSBN). (2005). Working with others: A position paper. Retrieved from Pohlman, K. J. (2005). Legal framework and financial accountability for school nursing practice. In N. C. Schwab, & M. H. B. Gelfman, (Eds.), Legal issues in school health services (pp ). North Branch, MN: Sunrise River Press. 107
111 Section 504 of Rehabilitation Act of 1973 (P.L U.S.C.A 794; 34 C.F. R., Part 104). U.S. Department of Labor. Zimmerman, B. (2013). Student health and education plans. In J. Selekman (Ed.), School nursing: A comprehensive text, 2nd ed.(pp ). Philadelphia, PA: FA Davis Company. Acknowledgment of Authors: Bernadette Moran McDowell, MEd, BSN, RN Sue A. Buswell, MSN, RN, NCSN Cheryl Mattern, MEd, BSN, RN Georgene Westendorf, MPH, BSN, RN, NCSN, CHES Sandra Clark, ADN, RN Acknowledgment of 2013 Authors: Janet Bryner, BSN, RN, NCSN Sue A. Buswell, MSN, RN, NCSN Sandra Clark, ADN, RN Cheryl Mattern, MEd, BSN Bernadette Moran McDowell, MEd, BSN, RN Georgene Westendorf, MPH, BSN, RN, NCSN, CHES Susan Will, MPH, BS, RN, NCSN, FNASN Adopted: June, 1998 Revised: November 2003, March 2008, June 2008, June 2013, January 2015 Suggested citation: National Association of School Nurses. (2015). Individualized healthcare plans: The role of the school nurse (Position Statement). Silver Spring, MD: Author. All position statements from the National Association of School Nurses will automatically expire five years after publication unless reaffirmed, revised, or retired at or before that time. National Association of School Nurses 1100 Wayne Ave. Suite 925 Silver Spring, MD


112 Chapter 5: Medication Administration SECTION 1: MEDICATION STORAGE AND POLICIES SECTION 2: OTHER TYPES OF MEDICATION ADMINISTRATION SECTION 3: SHARPS CONTAINERS SECTION 4: FORMS AND DOCUMENTS 109
113 SECTION 1: Medication Storage and Policies MEDICATION STORAGE AND ADMINISTRATION School districts are required to have policies related to student medication administration based on established state regulations and guidelines. The goal of medication administration is to provide a safe means of effectively administering medication to students, enabling them to remain in school. Parents must be notified of their responsibility to provide the medication and the information stated in the school s medication policy. Policy and procedure recommendations include the following: Medications should be in their original containers labeled with the student s name, name of the drug, drug dosage, route of administration, directions or interval for the drug to be given, name of the licensed healthcare provider prescribing the medication, and expiration date. An accompanying order from the primary care physician, as well as signed permission from the parent or guardian should be in the student s health record. The prescription should be renewed annually with updated orders provided to the school nurse. Medication Storage: All student medications should be in a locked cabinet or locked drawer. Medication cabinets should be securely mounted to a solid surface. It is preferable to have a solid door on the cabinet instead of glass. These designated locked areas should be accessible to only those persons authorized to administer medications. Only those persons responsible for administering medication and the school administrator should have access to the keys and knowledge of key location. At the end of each school day, the keys should be secured as to avoid falling into unauthorized hands. o o Emergency Medication Storage: Emergency medications should be stored in a secure area inaccessible to children. The medication must be unlocked and immediately available to school personnel at all times when students are present. Controlled Substance Storage: Controlled substances should be stored separately from other medications in a secure, substantially constructed, locked metal or wood cabinet or drawer. Controlled substances should be kept under single lock (locked cabinet) when students are present and under double lock (locked office and locked cabinet) at all other times. All controlled substance medications should be counted and recorded upon receipt from the parent/guardian. This medication should be recounted on a regular basis and this count reconciled with the medication administration log/record. If medications are found to be missing or if there is suspicion of tampering, local law enforcement should be contacted to assist with an investigation. If refrigerators are used to store medication, the temperature of the refrigerator should be monitored. If over-the-counter stock medications are kept in the health office to be administered as needed to students (i.e. ibuprofen, acetaminophen), these would be considered stock medications and healthcare provider orders, as well as parent permission are needed in order to administer these medications to students. The administration of herbs, homeopathic medicines, vitamins, cultural treatments, salves, nutritional supplements and other over-the-counter medications must follow the district medication policy. The school nurse has the responsibility to know both the actions and potential negative side effects of any medication. If this information is not available in standard healthcare resources, the school nurse may refuse to administer the substance unless 110
114 accompanied by a physician s order and information about the medication (Taras et al., 2004). Many districts do not allow students to bring non-prescribed medication to school or allow students to carry their own prescription medications. When these types of situations occur, the school nurse must follow district policy for medication administration. SECTION 2: Other Types of Medication Administration RESCUE MEDICATIONS Rescue medications are those medications that are required to be administered during a life-threatening situation. Examples of these medications include epinephrine, glucagon, albuterol, rectal diazepam or versed, and naloxone. Emergency situations are episodic and cannot be planned. DELEGATION All medications administered must be documented, including those administered by delegated staff. It is the responsibility of the registered school nurse to determine whether delegation can occur and under what circumstances. 511 IAC requires school corporations to employ at least one registered nurse with a Bachelor s of Science in Nursing to coordinate health services. Inherent in this responsibility to coordinate health services is the responsibility for the registered school nurse to delegate health services when appropriate. Those delegated with the task of administering medications to students should have training in the following: how to keep the medication locked and secured until needed and how to document administration (i.e., the name of the child, how many pills were given, time of administration, name of the person who administered the medication). If a dosage is missed, information is needed as to why it was missed and this information must be reported to the supervising registered school nurse. Safeguards must be in place to prevent medication errors. Students should be asked to identify themselves and their picture should be available to the person administering the medication to compare for accuracy (The Center for Health and Health Care in Schools, 2004). For more information regarding delegation, see Chapter 1 of this manual. Staff Administration of Diabetes Medication: Code (2007) allows school nurses to administer glucagon, insulin, or other emergency treatments prescribed by a licensed healthcare practitioner to diabetic students with an individual health plan and diabetes management plan. It also allows for staff members to serve as voluntary health aides after receiving diabetes training, including testing and the administration of medication. A volunteer health aide may perform the tasks necessary to assist a student in carrying out his or her individualized health plan, in compliance with the training guidelines provided in Code (2007). This includes the administration of glucagon, insulin, or other emergency treatments. A volunteer health aide may act to assist a student only if the parent or guardian signs an agreement that authorizes the volunteer aide to assist the student, and states an understanding that the aide is not liable for civil damages for assisting in the student s care. See Chapter 3 of this manual for further information regarding care of the student with diabetes. SELF-ADMINISTRATION OF MEDICATIONS FOR STUDENTS Some school districts allow students to carry and self-administer select medications, especially those for treatment of asthma, severe allergies, and diabetes. School policies must be written with guidelines for selfadministration of medication. The student must be able to demonstrate responsibility and proper care and administration of medication, and the school nurse should provide periodic monitoring and education to ensure skills are maintained (American Academy of Pediatrics, 2009). The same guidelines for authorization 111
115 from the primary care provider and parental/guardian permission must still be followed. Furthermore, the school nurse may need to educate staff in order to assist the student in emergency situations. Self-Administration of Emergency Medication: Code (2005) permits students with a chronic disease or medical condition to possess and self-administer emergency medication for the chronic disease or medical condition upon the written request of a parent or guardian. The physician must also state in writing that the student has a chronic disease or medical condition for which the physician has prescribed the medication, the student has been instructed on how to administer the medication, and the nature of the disease or medication condition requires emergency administration of medication. Code (2001) declares a school or school board not liable for civil damages as a result of a student s self-administration of medication. Self-Administration of Diabetes Medication: Code (2007) allows a student to attend to the management and care of their diabetes, once the student has been evaluated and determined to be capable of doing so, as reflected in their individual health plan and diabetes management and treatment plan. This includes the administration of insulin and possession of relevant supplies in any area of the school or school grounds, or at any school-related activity. SECTION 3: Sharps Containers DISPOSAL OF NEEDLES SHARPS CONTAINERS School health offices should have sharps containers and policies for medical waste. Needles should be discarded in an approved hard plastic container with a biohazard label. The school nurse is responsible for making arrangements with the custodial staff, district, and an appropriate local or state agency to have the containers disposed of according to federal and state guidelines. For more information regarding the proper disposal of medications, please see the Indiana Department of Environmental Management s Disposal of Unused Medication in Schools document in Section 4. FIELD TRIPS If schools have scheduled field trips, it is the school s responsibility to provide necessary accommodations so that all students can attend. Some students may need assistance with medication administration during the trip. To accommodate for these needs, the school can request parental participation; however, if a parent is unable to attend, the school must provide either a nurse or trained delegate to safely administer any needed medication or treatments. Further guidance regarding delegation can be found in Chapter 1 of this manual. SECTION 4: Forms and Documents Sample Staff Medication Administration Checklist (PDF) Sample Training Verification of School Personnel-Administering Medication (PDF) Disposal of Unused Medication in Schools Indiana Department of Environmental Management (PDF) Medication Administration in the School Setting NASN Position Paper (PDF) Medication Storage Guidelines Indiana Department of Education (PDF) 112
116 Medication Administration Checklist Staff person trained/position: Initials: School Nurse/RN: Initials: Standard medications Dates Procedure Guideline Demonstrate/ Demonstrate/ Demonstrate/ Comments/ Explain or Proficient Return Demonstration Explain or Proficient Return Demonstration Explain or Proficient Return Demonstration School Nurse initial/staff initial, or nonapplicable Washes hands before and after procedure Gives proper dose of medication at proper time. States 5 Rights Compares labeled medication container with written order Reads label 3 appropriate times Checks student identity with name on label Checks expiration date on label Explains procedure to student if necessary Documents medications given correctly Maintains security of medication area Describes proper actions for medication refusal, field trip, medication error States appropriate times/situations for notification of school nurse Emergency medications Epinephrine States symptoms of allergic reaction, location of medication and emergency plan Demonstrates with trainer, correct procedure for administration States follow-up procedures Glucagon States symptoms of hypoglycemia, location of medication and emergency plan 113
117 Demonstrates mixing of medication in syringe Demonstrates proper injection technique using correct site States follow-up procedures Diastat States understanding of when to use this medication, location of medication and emergency plan Demonstrates proper positioning of child, procedure for administering medication States follow-up procedures 114
118 Training Verification of School Personnel Administering Medication Name of School: has received training to administer medications according to our school policy and procedures. He/she has demonstrated knowledge and understanding of the policies and procedures listed above. RN Signature Date I have been instructed in our school's medication policy and administration procedures. I understand that I am to administer medications to students according to these procedures and as delegated to me by the school nurse. I understand that I am to report immediately to the school nurse any new orders, changes in medication orders, changes in a student's health status, and discovery of a medication error. I understand that I may not delegate this task to any other person. School Staff Signature Date 115

119 FACT SHEET INDIANA DEPARTMENT OF ENVIRONMENTAL MANAGEMENT Disposal of Unused Medication in Schools Community and Environmental Health Program Office of Program Support (317) (800) N. Senate Ave., Indianapolis, IN Introduction: The Indiana Prescription Drug Abuse Prevention Task Force (Task Force) is working to fight prescription drug misuse and diversion in Indiana. In addition to preventing medicine theft, prescription drug abuse, accidental poisoning, and identity theft, proper disposal of medicines also prevents adverse environmental impacts. Pharmacists, educators, health care providers, and waste managers are working to promote safe disposal. As a member of the Task Force, the Indiana Department of Environmental Management (IDEM) is helping to spread the word about alternatives. This fact sheet discusses procedures for schools. Disposal Options: Preferred disposal methods vary based on the given medication(s). School Nurses who are in possession of leftover and unclaimed medications should seek assistance from the school-based law enforcement officer (such as the School Resource Officer), and the school contact for waste disposal. Controlled Substances Under U.S. Drug Enforcement Administration (DEA) regulations, it is illegal to transport controlled substances or give them to anyone other than a police officer or a person who is under law enforcement supervision. The School Nurse should work directly with the School Resource Officer, who will be able to take proper steps to ensure the lawful transportation and disposal of the substances. The DEA website provides a list of controlled substances at Hazardous Waste The U.S. Environmental Protection Agency s (U.S. EPA s) Hazardous Waste Pharmaceuticals Wiki site, at contains information to help healthcare professionals and stakeholders determine whether the pharmaceuticals they discard meet the Resource Conservation and Recovery Act (RCRA) definition of hazardous wastes. Some pharmaceutical waste may need to be managed under federal hazardous waste regulations overseen by U.S. EPA. Inform the school s waste management staff for guidance prior to disposal of hazardous waste. Guidance will vary depending on the amount of total hazardous waste managed by the school (including hazardous waste generated by science labs, art classrooms, etc.). IDEM s Compliance and Technical Assistance staff is available upon request, at (toll free) or (317) , to provide free, confidential technical and compliance assistance on hazardous waste management. For All Other Pharmaceutical Waste Local household hazardous waste collection programs, police departments, and pharmacies may accept unwanted medications which are not controlled substances from schools. Some pharmacies sell postage-paid envelopes for the public to mail in non-controlled substances for disposal. A listing of local programs and pharmacies that provide assistance with non-controlled medications is available at Contact your School Resource Officer or local police department to coordinate the transportation of unwanted medications for proper disposal at a collection site. IDEM Fact Sheet DIOPS Disposal of Unused Medication in Schools 1 of 2 116



120 When Collection Opportunities Are Not Available If no collection programs are available in your community, you may need to dispose of the medication. For medication that is NOT a controlled substance and not required to be managed as a hazardous waste, common steps for disposal include rendering the medicine unusable (place liquids in a sorbent such as flour, sawdust or kitty litter or dissolve tablets or capsules in the original container with water and sorbent). Different types of medicine should never be mixed because dangerous chemical reactions may occur. All personal information on prescription bottles should be blacked out to prevent identity theft. Containers should be resealed with lids and/or placed in a heavy-duty sealed bag to keep medications from leaking. Medicine should not be flushed down the sink or drain unless accompanying product information instructs that it is safe to do so. Of course, medicine should not be given or sold to family and friends. Contact your School Resource Officer or local police/sheriff department to coordinate transportation immediately to a safe disposal location such as a solid waste facility. Disposal of medicine in the trash dumpster on school grounds is not advisable unless the dumpster is locked and tamper-proof. Waste Minimization: Schools can minimize waste they must manage by putting measures in place to give medicine back to the family. It may be helpful to remind parents and guardians to retrieve their children s medicines at the end of the school year or when a student withdraws. Having procedures for documenting disposal activities may also help ensure the safe and lawful management of leftover medicines. Sharps: The improper or careless disposal of needles, syringes, and lancets, also called sharps, is a risk to sanitation and sewage treatment workers, janitors and housekeepers, and curious children. Many solid waste management districts, health departments and communities offer safe disposal options for sharps users. If your school needs help with a sharps collection program, you can find a list of local collection programs and links to Indiana Department of Health and U.S. EPA publications on the IDEM website at More Information: For the Indiana Prescription Drug Abuse Task Force, including Take Back programs for unused controlled substances and links to Task Force partner sites and national experts, visit For a list of controlled substances, visit DEA s website at For regulations for the disposal of unwanted controlled substances, visit DEA s website at The DEA Registration Service Center can be reached at For information to help healthcare professionals and stakeholders determine whether the pharmaceuticals they discard meet the Resource Conservation and Recovery Act (RCRA) definition of hazardous wastes, visit U.S. EPA s Hazardous Waste Pharmaceuticals Wiki site, at For some examples of policies and procedures aimed at minimizing waste, visit the New Mexico School Health Manual at and the Medication Disposal Form used by the Glendale-River Hills School District at students. (Policies adopted by Indiana schools should be consistent with applicable Indiana regulations.) For local household hazardous waste and medicine collection programs for residents, visit IDEM s Recycle Indiana website at or contact IDEM s Office of Pollution Prevention and Technical Assistance, at (toll free) or (317) IDEM Fact Sheet DIOPS Disposal of Unused Medication in Schools 2 of 2 117
.")
121 Medication Administration in the School Setting SUMMARY Position Statement It is the position of the National Association of School Nurses (NASN) that school districts develop written medication administration policies and procedures that focus on safe and efficient medication administration at school by a registered professional school nurse (hereinafter referred to as school nurse). Policies should include prescription and non prescription medications, and address alternative, emergency, research medication, controlled substances, and medication doses that exceed manufacturer's guidelines. These policies shall be consistent with federal and state laws, nursing practice standards and established safe practices in accordance with evidence based information. The Individuals with Disabilities Education Act, and Section 504, mandate schools receiving federal funding to provide required related service, including medication administration (O Dell, O Hara, Kiel, & McCullough, 2007). HISTORY Medication administration to students is one of the most common health related activities performed in school. Historically, administering medication within the school setting has been a school nurse responsibility. As more chronically ill, medically stable children enter the school system each year, awareness of the factors that can promote and support their academic success increases, including the need for medications that enhance the student s overall health or stabilize their chronic condition. DESCRIPTION OF ISSUE There has been a dramatic increase in the range of medications used in schools, making the medication administration process in school more complex, not less (McCarthy, Kelly, Johnson, Roman, & Zimmerman, 2006). Medication non adherence at school has been linked to a variety of poor educational, social/emotional and physical outcomes. In addition, non adherence to medication treatment regimes can lead to an array of educational, behavioral, and academic consequences for a child with chronic health conditions (Clay, Farris, McCarthy, Kelly, & Howard, 2008). Policies regarding administration or carrying of any medication or product should be applied consistently with all students. The school nurse should assess each request for administration or student self administration of any medication based on school district medication policies. The school nurse can administer medication safely and effectively while adhering to the following set of guidelines that include: Adherence to school district specific medication handling and administration procedures/policies, national school nurse standards of practice, state nurse practice acts and state laws governing these practices. The administration of a specific medication is in accordance with existing State Board of Nursing rules and regulations, school district policies, school nursing protocols or standing orders. District policies must address how over the counter (OTC) medications are received, stored, and labeled. Procedures must be established and periodically reviewed for receiving, storing, administering, clarifying prescriptive orders, determining the prescribed dosage is within the safe dose range for the child s age and weight and accounting for all medications held or administered in the school setting. District policies must require parental consent for exchange of information between the school nurse and prescriber for clarification of administration and report of response to medication and adverse effects. National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland
122 Student confidentiality is maintained in all written and verbal communications, in accordance with FERPA regulations. Specific issues and procedures are addressed on a district by district basis including medication errors, missed doses, transportation concerns and monitoring unlicensed assistive personnel (UAP) administration. Medication administration policies and procedures should also address the following: Delegation In some states, medication administration can be delegated to licensed practical nurses and UAP. Delegation by nurses is defined by the American Nurses Association (ANA) as transferring the responsibility of performing a nursing activity to another person while retaining accountability for the outcome (ANA/NCSBN, 2006; National Association of State School Nurse Consultants [NASSNC], 2010). Nurses remain accountable to: o State laws, rules, and regulations; o Employer/agency regulations, and o Standards of professional school nursing practice, including those pertaining to delegation. The decision to delegate is a serious responsibility that the school nurse determines on a case by case basis based on the needs and condition of the student, stability and acuity of the student s condition, potential for harm, complexity of the task, and predictability of the outcome (ANA, 2005). Prior to medication administration, a student assessment is completed by the school nurse. This assessment will guide the school nurse in determining if the task can be delegated and what level of training and supervision is required for safe delegation for this specific student and assignment (Gursky & Ryser, 2007). In most circumstances, a UAP is an ancillary health office staff member (health assistant/aide) who is trained in basic first aid, selected medical procedures as indicated by the needs of the school and the students served, in addition to the district health office clerical and confidentiality procedures (AAP, 2009). An audit completed by Canham, et al. (2007), highlights the importance of training in medication administration by stating that training is not a once a year event, but a process that is needed to ensure and sustain the safe and accurate administration of medication. Alternative Medication The National Center for Complementary and Alternative Medicine (NCCAM) defines Complimentary and Alternative Medicine (CAM) as group of diverse medical and health care systems, practices, and products that are not generally considered part of conventional medicine. (NCCAM, 2011). Medication administration policies should reflect local and state policies related to the administration of alternative medications and treatments. Controlled Substances Pharmaceutical controlled substances are drugs that have a legitimate medical purpose, coupled with a potential for abuse and psychological and physical dependence. They include opiates, stimulants, depressants, hallucinogens, and anabolic steroids. The safe and effective use of controlled substances by students at school has increased dramatically because of their accepted use in treatment of illness and disability enabling many sick and disabled children to attend school. Emergency Medication Immediate access to emergency medication is a high priority and is crucial to the effectiveness of these life saving interventions (AAP, 2009). The administration of emergency medications, like all medications, is regulated by state laws and guidelines as well as local school district policies and protocols. Students with medical orders for life saving medications should have a nursing assessment, and an Emergency Care Plan, developed by the school nurse. National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland
123 RATIONALE Research Medication Medication prescriptions for children that do not fall within the established United States Food and Drug Administration (FDA) guidelines for pediatric use and/or dosing may fall into two categories: off label medication and experimental medications. Off label medications are those FDA approved medications prescribed for non approved indications in children. Pediatric experimental or investigational drugs are those medications currently involved in clinical trials. These medications are undergoing formal study to determine the efficacy and safety of pediatric dosing, but they do not have FDA approval. Medication administration policies should address the specific requirements for administering research medication in school, including providing the school nurse with information regarding the protocol or a study summary from the research organization, signed parental permission, reporting requirements, and any follow up nursing actions to be taken. School nurses are in a position to influence the development and use of school medication policies. They are a valuable resource and should be utilized in the development of school district policies/procedures and consult on the creation of legislative policies relating to medication administration in the school setting (Canham et al., 2007). The school nurse is often the sole healthcare provider in the school setting, providing an expertise in health related care for students. A school nurse is the professional that has the knowledge and skills required for delivery of medication, the clinical knowledge and understanding of the student s health and the responsibility to protect the health and safety of students (AAP, 2009). REFERENCES American Academy of Pediatrics. (2009). Policy statement guidance for the administration of medication in school. Pediatrics 124, American Nurses Association / National Council of State Boards of Nursing (ANA/NCSBN). (2006). Joint statement on delegation. Retrieved from American Nurses Association (ANA). (2005). Principles of delegation. Silver Springs, MD: Author. Canham, D.L., Bauer, L., Concepcion, M., Luong, J., Peters, J., & Wilde, C. (2007). An audit of medication administration: A glimpse into school health offices. Journal of School Nursing, 23, doi: / Clay, D., Farris, K., McCarthy, A.M., Kelly, M.W., Howard, R. (2008). Family perceptions of medication administration at school: errors, risk factors and consequences. Journal of School Nursing, 24, doi: / Gursky, B. S., & Ryser, B. J., (2007). A training program for unlicensed assistive personnel. Journal of School Nursing, 23, doi: / McCarthy, A.M., Kelly, M., Johnson, S., Roman, J., & Zimmerman, M.B. (2006). Changes in medications administered in schools. Journal of School Nursing, 22, doi: / National Association of State School Nurse Consultants (NASSNC). (2010). Position statement: Delegation of school health services. Retrieved from: National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland
124 National Center for Complementary and Alternative Medicine. (2011, March). What is complementary and alternative medicine? Retrieved from Odell, C., O Hara, K., Kiel, S., & McCullough, K. (2007). Emergency management of seizures in the school setting. Journal of School Nursing, 23, doi: / Wilt, L. & Foley, M. (2011). Delegation of glucagon in the school setting: A comparison of state legislation. Journal of School Nursing. Pub ahead of print. doi: / Acknowledgment of Authors: Susan Zacharski, MEd, BSN, RN Carole A. Kain, PhD, ARNP, PNP BC Robin Fleming, PhD, RN, CNS Deborah Pontius, MSN, RN, NCSN Adopted: 1993 Revised: September 1997 Revised: June 2003 Revised: June 2011 Amended: January 2012 This document combines and replaces the following Position Statements: Alternative Medication in the School Setting (Adopted: June 2001; Revised: June 2006) Controlled Substances in the School Setting (Adopted: November 2001) Rectal Medication for Seizures, The Role of the School Nurse Caring for Students Requiring (Adopted: November 2003) Research Medications in the School Setting (Adopted; June 2001) Resources for supporting information: NASN s Position Statement on Delegation, 2010 and AAP Clinical Guidelines for Medication Administration, 2009 Non Patient Specific Epinephrine, National Association of School Nurses 8484 Georgia Avenue Suite 420 Silver Spring, Maryland

125 SUBJECT: Medication Storage Guidelines It is the recommendation of the IDOE that each local school board or authority in charge of an accredited nonpublic school adopt policies for medication administration, storage and recording. Procedures for medication administration (when not included in the school s policy) must be developed for: Administration of Medication to Students in School Self-Administration and Possession of Medications School Staff Training Storage and Access to Medications in School Record-Keeping Related to Medications in School Addressing Medication Errors It is important to include in school medication procedures the following storage safety procedures: All medications should be locked and stored in drawers or cabinets for that purpose. These designate locked areas should be accessible to only those persons authorized to administer medications. The person(s) responsible for administering medication and the school administrator should have access to the keys and be the only people with knowledge of the keys location. The keys shall be in a monitored area at all times where school personnel can ensure the security of the keys. At the end of each school day, the keys will be secured to proved assurance that they will not fall into unauthorized hands. Indiana Department of Education Indiana State Capitol 200 W Washington Street, Room 225 Indianapolis, IN doe.in.gov 122
126 Emergency medications should be stored in a secure area inaccessible to children. The medication must be unlocked and immediately available to school personnel at all times students are present. In the case of controlled substances, they are to be stored separately from other medications in a secure, substantially constructed, locked metal or wood cabinet or drawer. A list of controlled substances can be found at the following link: Controlled substances are to be kept under single lock (locked cabinet) when students are present and under double lock (locked office and locked cabinet) at all other times. All controlled-substance medications will be counted and recorded upon receipt from the parent/guardian. This medication shall be recounted on a regular basis and this count reconciled with the medication administration log/record. If medications are found to be missing or if there is suspicion of tampering, local law enforcement should be contacted to assist with an investigation. 123

127 Chapter 6: Screenings SECTION 1: HEARING SECTION 2: IMMUNIZATIONS SECTION 3: VISION 124
128 SECTION 1: Hearing INDIANA DEPARTMENT OF EDUCATION HEARING SCREENING GUIDELINES THE FOLLOWING GUIDELINES ARE BASED ON INDIANA CODE Sec. 14 (a) The governing body of each school corporation shall annually conduct an audiometer test or a similar test to determine the hearing efficiency of the following students: (1) Students in grade 1, grade 4, grade 7 and grade 10. (2) A student who has transferred into the school corporation. (3) A student who is suspected of having hearing defects. (b) A governing body may appoint the technicians and assistants necessary to perform the testing required under this section. (c) Records of all tests shall be made and continuously maintained by the school corporation to provide information that may assist in diagnosing and treating any student s auditory abnormality. However, diagnosis and treatment shall be performed only on recommendation of an Indiana physician who has examined the student. (d) The governing body may adopt rules for the administration of this section. Purpose of the hearing screening program is to identify students at risk for hearing difficulties that may adversely affect their health or school performance. A well-balanced program will include screening, rescreening, and follow-up for failures. Hearing - Part 1: PERSONNEL Hearing - Part 2: EQUIPMENT Hearing - Part 3: AUDIOMETER CALIBRATIONS Hearing - Part 4: HEARING SCREENING ADMINISTRATION Hearing - Part 5: HEARING SCREENING PROCEDURE Hearing - Part 6: SCREENING FOLLOW-UP PROCEDURES Hearing - Part 7: RECORDS AND REPORTS Hearing - Part 8: EDUCATIONAL NEEDS Hearing - Part 1: PERSONNEL A. Each school should designate an audiologist, speech language pathologist (SLP), or school nurse to oversee the hearing screening program. B. Responsibilities of Screening Personnel: 1. Organizes, coordinates, and implements a systematic program for conducting the hearing screening in the school. 2. Keeps and maintains records, initiates referrals, coordinates follow-up (tracking/monitoring) procedures, and prepares/submits electronic reports to the Indiana Department of Education. 125
129 3. Reports screening results to school personnel and parents. 4. Knowledgeable in testing technique and assures that all hearing screening personnel involved are properly trained. Hearing - Part 2: EQUIPMENT A. Audiometer 1. Each audiometer should be calibrated annually with the date of calibration posted on the device. 2. Handle carefully when transporting place on a solid surface and avoid jolts to keep the audiometer in calibration. 3. Avoid extreme heat or cold do not store in your vehicle. D. Table E. Two chairs F. Pens for recording G. Class lists H. Alcohol-free antiseptic wipes I. Sign noting Testing in Progress Quiet Please Hearing - Part 3: AUDIOMETER CALIBRATIONS A. Equipment Standards: 1. All audiometric testing equipment shall meet specifications set forth in ANSI S : Specifications for Audiometers. 2. Listening Check: Before each use, perform biological check (putting on the earphones and verifying that the tones can be heard at all frequencies at a 20dB level). If there is any indication that the equipment is not working properly, the audiometer should not be used until re-calibrated. B. Minimum Annual Calibration: 1. Calibration and any necessary repairs shall be made at least annually. 2. The person or company performing the calibration shall be required to furnish data which specify: a. How closely the equipment meets the specifications. b. Documentation of calibration date and record of any repairs performed. c. The school corporation shall maintain a continuing record of such calibration and repair and keep the latest calibration certificate on file. It is also recommended that the date of the most recent calibration be noted on each piece of equipment. C. Minimum Test Specifications: 1. The test environment for both screening and re-screening shall be sufficiently quiet to allow determination of at least a 20 db hearing threshold level at each of the test frequencies. 126
130 Hearing - Part 4: HEARING SCREENING ADMINISTRATION A. Students to be screened: 1. It is mandated that hearing screening be administered to all students in grades 1, 4, 7, and 10 (kindergarten is strongly recommended). 2. All students newly enrolled in the school system unless there is proof of a current hearing screening. a. All students who were referred the previous year should be re-screened unless there is documentation of normal hearing. b. All students who missed the original screening date should be screened within 60 days (usually completed at re-screening date). c. All students specifically referred due to suspicion of hearing difficulty. d. Preschoolers should be screened as needed, requested, or when they have conditions that place them at risk for hearing concerns. B. Students not to be screened or other factors to consider: 1. Any student that has written documentation by an audiologist or physician stating a known hearing loss in both ears does not need to be screened. If a student has a unilateral hearing loss (loss only in one ear), the non-affected ear should be screened. Appropriate school personnel must be notified of this child with hearing loss. 2. No student should be required to submit to hearing screening testing if written objection by the parent/guardian is submitted to the proper school authority. 3. Any student that is unable to be screened with traditional methods should be referred for follow-up testing. C. Preparation for screening: 1. Completed by personnel designated in Part 1 a. Schedule hearing screening program with school principal and personnel early in the school year. Re-screening date is set at least two weeks later. Inform staff of upcoming screening of grades 1, 4, 7, 10 (kindergarten recommended/preschoolers as needed). b. Have school personnel send names of students suspected of hearing difficulties in nonmandated grade level testing (see example of hearing screening worksheet). c. Arrange for a quiet room in the school away from locker areas, music rooms, cafeteria, noisy equipment, etc. d. Arrange for testing personnel and volunteers. e. Inform staff of your screening schedule. f. The school principal is responsible for notifying families regarding the hearing screening. Parents are responsible for notifying the school in writing if their child has an exemption, such as religious beliefs. g. Secure daily class schedule for use by individuals conducting the hearing screening testing. 127
131 h. Assume guidance and responsibility for completed screening situation including technical skill, statistical reporting, and recording. Hearing - Part 5: HEARING SCREENING PROCEDURE A. Visually inspect ears for abnormalities or drainage (automatic failure for drainage). Do not place headset on draining ears. B. Place headset on child (red for right/blue for left). C. Place the headset directly over the ears. D. Hearing screening is completed at 20dBHL. E. Present tone at 1000Hz, 2000Hz, and 4000Hz in the right ear then repeat for the left ear. Pure tone screening 1000Hz 2000Hz 4000Hz Right ear 20dB 20dB 20dB Left ear 20dB 20dB 20dB No response at any frequency in either ear constitutes a failure. F. Document those students that were tested and those that failed the initial hearing screening (see hearing screening worksheet example in appendix). G. Re-screening 1. If screening is done by trained support personnel, re-screening should be done by nurse, speech/ language pathologist, or audiologist. 2. All failures should be re-screened two weeks after original screening, using the same frequencies, levels, and failure criterion. Hearing - Part 6: SCREENING FOLLOW-UP PROCEDURES (A comprehensive follow-up plan is the most important component of the screening process) A. Parents/Guardians will be notified of a failure on the hearing re-screening and to contact their healthcare provider about the results. 1. Within a reasonable time, parents shall be provided with notification that their child failed a hearing screening test and referred to an audiologist or appropriate physician. A referral response form (see example), which is to be completed by the appropriate examiner (doctor or audiologist), should be returned to the speech/language pathologist, audiologist, and/or school nurse. IC (c) However diagnosis and treatment shall be performed only on the recommendation of an Indiana physician who has examined the student. 2. If no documentation is received from the parents/guardians, the child will be re-screened the following school year. 128
132 B. Documentation of the hearing screening results should be placed in the student s school record. Hearing - Part 7: RECORDS AND REPORTS A. A complete and continuing record of all audiometric tests and related recommendation for followup and rehabilitation shall be maintained by the school corporation. It is recommended the speech/ language pathologist, audiologist, or school nurse include the results as part of each student s record. 1. Each student s health record shall clearly indicate: a. The date of the hearing screening. b. The results of the screening for each ear, either ear passed or failed on each test given. c. Any pertinent referral and follow-up comments should be recorded. 2. School hearing screening reports should be made available to appropriate school personnel: a. Student s record of hearing screening results should be part of the student s permanent file according to school policy. b. A record of the school s hearing screening results shall be kept by the school nurse or speech language pathologist. c. Yearly reports shall be filed with the Indiana Department of Education, as part of the accreditation reporting by completing the School Health Report. d. Complete hearing records should accompany transferring students according to school policy. e. Hearing screening records should be kept for a minimum of 5 years or in accordance with the school s health record policy. Hearing - Part 8: EDUCATIONAL NEEDS A. It is the responsibility of the speech/language pathologist, audiologist, or school nurse to inform the appropriate personnel of hearing screening failures. B. If the hearing loss is documented per a health care provider s follow-up form, the results will be shared with the administrator of the building. C. If the referral response form or other documentation is not received from the parent or provider, the student should be re-screened. If student continues to fail, consider the educational impact and notify the appropriate school personnel. D. If parent response is not received by the end of the school year, the child should be re-screened the following school year. Please note: If a student cannot be screened by following these guidelines, the school-appointed designee (audiologist, speech language pathologist or school nurse) should be notified. This may include children who are frightened or crying, children with a developmental delay, or children with a language barrier. The school designee should follow up with parents to see if previous testing has ruled out a hearing loss or if further testing is warranted. 129

133 The school-appointed designee should make sure the student s records are documented regarding the status of the student s hearing. If a hearing loss is documented, the results should be shared with the administrator of the student s building. Hearing Screening Sample Forms and Documents: Sample Referral Response Form (PDF) Sample Hearing Screening Worksheet (PDF) Sample Hearing Screening Results (PDF) SECTION 2: Immunizations THE FOLLOWING GUIDELINES ARE BASED ON INDIANA CODE : IMMUNIZATIONS IC Keeping immunization records; student transfer (a) Each school shall keep an immunization record of the school s students according to procedures prescribed by the state department of health. (b) Whenever a student transfers to another school, the school from which the student is transferring may furnish, not later than twenty (20) days after the transfer, a copy of the student s immunization record to the school to which the student is transferring. (c) Whenever a student enrolls in a state educational institution, the school from which the student graduated may furnish a copy of the student s immunization record to the state educational institution. If the student is enrolled in a state educational institution while still attending a secondary level school, the secondary level school that the student is attending may furnish a copy of the student s immunization record to the state educational institution. IC Required immunizations; immunization calendar; rules (a) Every child residing in Indiana who is enrolled in an accredited elementary school or high school shall be immunized as determined by the state department of health against: diphtheria; pertussis (whooping cough); tetanus; measles; rubella; poliomyelitis; mumps; varicella; hepatitis A; hepatitis B; and meningitis. 130
134 (b) The state department of health may expand or otherwise modify the list of communicable diseases that require documentation of immunity as medical information becomes available that would warrant the expansion or modification in the interest of public health. (c) Before November 30 of each year, the state department of health shall publish a two (2) year calendar of immunization requirements and recommendations. The calendar must include: (1) the immunization requirements for the following school year; and (2) recommendations for immunization requirements for the year subsequent to the following school year. (d) The publishing time frame for the calendar described in subsection (c) does not apply in the event of an emergency as determined by the state health commissioner. (e) The state department of health shall adopt rules under IC specifying the: required immunizations; child s age for administering each vaccine; adequately immunizing doses; and method of documentation of proof of immunity. IC Notification; provision of information to parents (a) Each school shall notify each parent of a student who enrolls in the school of the requirement that the student must be immunized and that the immunization is required for the student s continued enrollment, attendance, or residence at the school unless: (1) the parent or student provides the appropriate documentation of immunity; or (2) IC or IC applies. (b) A school that enrolls grade 6 students shall provide each parent of a student who is entering grade 6 with information prescribed by the state department of health under subsection (c) concerning the link between cancer and the human papillomavirus (HPV) infection and that an immunization against the human papillomavirus (HPV) infection is available. (c) The state department of health shall provide a school described in subsection (b) with the information concerning cancer and the human papillomavirus (HPV) infection required in subsection (b). The information must include the following: (1) The latest scientific information on the immunization against the human papillomavirus (HPV) infection and the immunization s effectiveness against causes of cancer. (2) That a pap smear is still critical for the detection of precancerous changes in the cervix to allow for treatment before cervical cancer develops. (3) Information concerning the means in which the human papillomavirus (HPV) infection is contracted. (4) A statement that any questions or concerns concerning immunizing the child against human papillomavirus (HPV) could be answered by contacting a health care provider. (d) The state department of health shall provide the department of education with material concerning immunizations and immunization preventable diseases for distribution to parents and guardians. The department of education shall provide these materials to schools to be provided to students parents and guardians. These materials may be distributed by a school by posting the required information on the school s internet web site. IC Presenting student for immunization; entering information into immunization data registry (a) The parent of any student who has not received the immunizations required under this chapter shall present the student to a health care provider authorized to administer the immunizations. (b) The health care provider who administers the required immunizations to a student or the health 131
135 care provider s designee shall enter the immunization information into the state immunization data registry in accordance with IC IC Statement of immunization history; waiver; rules (a) Each school shall require the parent of a student who has enrolled in the school to furnish, not later than the first day of school attendance, proof of the student s immunization status, either as a written document from the health care provider who administered the immunization or documentation provided from the state immunization data registry. (b) The statement must show, except for a student to whom IC or IC applies, that the student has been immunized as required under section 2 of this chapter. The statement must include the student s date of birth and the date of each immunization. (c) A student may not be permitted to attend school beyond the first day of school without furnishing the documentation described in subsections (a) and (b) unless: (1) the school gives the parent of the student a waiver; or (2) the local health department or a health care provider determines that the student s immunization schedule has been delayed due to extreme circumstances and that the required immunizations will not be completed before the first day of school. The waiver referred to in subdivision (1) may not be granted for a period that exceeds twenty (20) school days. If subdivision (2) applies, the parent of the student shall furnish the written statement and a schedule, approved by a health care provider who is authorized to administer the immunizations or the local health department, for the completion of the remainder of the immunizations. (d) The state department of health may commence an action against a school under IC or IC for the issuance of an order of compliance for failure to enforce this section. (e) Neither a religious objection under IC nor an exception for the student s health under IC relieves a parent from the reporting requirements under this section. (f) The state department of health shall adopt rules under IC to implement this section. IC Collection of immunization data; onsite review or examination (a) The state department of health shall collect immunization data on school age children using the state immunization data registry. Each school corporation shall ensure that all applicable immunization information is complete in the state immunization data registry not later than the first Friday in February each year. The state department of health shall use the data to create aggregate reports. (b) The state department of health and the local health department shall, for good cause shown that there exists a substantial threat to the health and safety of a student or the school community, be able to validate immunization reports by onsite reviews or examinations of nonidentifying immunization record data. This section does not independently authorize the state department of health, a local department of health, or an agent of the state department of health or local department of health to have access to identifying medical or academic record data of individual students attending nonaccredited nonpublic schools. (c) The state department of health has exclusive power to adopt rules for the administration of this section. Immunizations - Part 1: PERSONNEL Immunizations - Part 2: IMMUNIZATION VERIFICATION PROCEDURE Immunizations - Part 3: IMMUNIZATION FOLLOW-UP PROCEDURES, RECORDS AND REPORTS, EDUCATIONAL NEEDS, AND SAMPLE FORMS 132
136 Immunizations - Part 1: PERSONNEL A. Each school should designate a person, trained in reviewing the immunization record for accuracy and preferably a school nurse, to oversee the immunization verification program. B. Responsibilities of designated personnel 1. Organizes, coordinates, and implements a systematic program for reviewing the immunization records of all enrolled students. 2. Knowledgeable in reviewing the immunization record for accuracy, and obtains a password for CHIRP and for DOE Online. 3. Keeps and maintains records, initiates referrals for those who are incomplete, develops follow-up (tracking/second notice) procedures, and prepares/submits the School Health Report to the Indiana Department of Education. 4. Reports incomplete or invalid immunization records to parents and school administrator. Immunizations - Part 2: IMMUNIZATION VERIFICATION PROCEDURE 1. Print and review the most current versions of the school immunization requirements, the sample letters and the FAQ documents posted on the Indiana State Department of Health CHIRP Web and/or the Indiana Department of Education Health Immunization Web. 2. Review all student records, concentrating on newly enrolled students and students in grades requiring additional immunizations, for completeness. 3. If an immunization record is found to be incomplete or contains invalid immunization dates, the parent or guardian should be notified. 4. Review all student records, in all grades, for completeness. 5. Create a list of those students who are incomplete, have a religious objection, or a medical exemption for a particular immunization. 6. Submit a copy of those students who are incomplete to the building administrator. 7. Maintain records, offer suggestions to parents/guardians for immunization sites (providers, pharmacists, local health department), and initiate follow-up and tracking procedures for those students who do not meet the minimum requirements. Immunizations - Part 3: IMMUNIZATION FOLLOW-UP PROCEDURES, RECORDS AND REPORTS, EDUCATIONAL NEEDS, AND SAMPLE FORMS More specific information regarding all of these items can be found on the CHIRP Website or the IDOE Health Immunization Website. 1. CHIRP Website for school nurses can be found by clicking here. 2. IDOE Health Immunization Website can be found by clicking here. 133
 and fourteen inches for near vision")
137 SECTION 3: Vision INDIANA DEPARTMENT OF EDUCATION VISION SCREENING GUIDELINES THE FOLLOWING GUIDELINES ARE BASED ON INDIANA CODE Vision screening means the testing of visual acuity to determine a student s ability to see at various distances either ten or twenty feet for distance vision (depending on the calibration of the chart being used) and fourteen inches for near vision using the Snellen Chart, Sloan Letters, HOTV, or LEA Symbol Optotypes. The governing body of each school corporation shall annually conduct a visual acuity test to determine the visual acuity for both far and near vision of the following students enrolling in or transferring into: (1) Either kindergarten or grade 1 (2) Grade 3 (3) Grade 5 (4) Grade 8 (5) Any student who is suspected of having a visual defect. Additionally, schools with students in grades K or 1 st, must also conduct a Modified Clinical Technique (MCT), vision screening that is performed by a licensed ophthalmologist or optometrist unless a waiver has been granted by the Indiana Department of Education. If an MCT waiver has been granted, schools are still responsible for conducting the visual acuity testing for near and far vision for students in either grades K or 1 st. A waiver is required for each individual school as corporation wide waivers are not allowed. A student who is unable to read with each eye the 20/30 line of the Snellen Chart or the 20/32 line of the Sloan Letters, HOTV, or LEA Symbol Optotypes shall be recommended for further examination by a licensed eye professional. A student must also be referred if they fail the MCT portion of the eye exam. The licensed provider who performs the MCT will indicate whether a student has passed or failed. Records of all tests shall be made and continuously maintained by the school corporation to provide information useful in protecting, promoting, and maintaining the health of students. Each school corporation shall annually provide information to the Indiana Department of Education regarding the vision screening results for each school within the school corporation by completing the School Health Report. The purpose of a vision screening program is to identify students at risk for visual difficulties that may adversely affect their health or school performance. A well-balanced program will include screening, referral, and follow-up for failures. 134
138 Vision - Part 1: PERSONNEL Vision - Part 2: EQUIPMENT Vision - Part 3: VISION SCREENING ADMINISTRATION Vision - Part 4: VISION SCREENING PROCEDURE Vision - Part 5: SCREENING FOLLOW-UP PROCEDURES Vision - Part 6: RECORDS AND REPORTS Vision - Part 7: EDUCATIONAL NEEDS Vision - Part 1: PERSONNEL A. Each school should designate a school nurse to oversee the vision screening program. B. Responsibilities of screening personnel: 1. Organizes, coordinates, and implements a systematic program for conducting the vision screening in the school. 2. Keeps and maintains records, initiates referrals, develops follow-up (tracking/monitoring) procedures, and prepares/submits the School Health Report (electronic report) to the IDOE. 3. Reports screening results to school personnel and parents. 4. Becomes knowledgeable regarding vision testing technique and assures that all vision screening personnel involved are properly trained. Vision - Part 2: EQUIPMENT A. Charts 1. The Snellen Chart 2. Sloan Letters Chart 3. HOTV Chart 4. LEA Symbols Optotypes Chart 5. Near Vision Card NOTE: As new technology advances are made, it is possible new methods of vision screening may provide more efficient and accurate results. If you are considering using technology and/or other methods not specifically outlined in I.C and 13, you should seek the advice and endorsement of your school physician or a local ophthalmologist before proceeding. 6. Pens for recording 7. Class list 8. Sign noting Testing in Progress Quiet Please 135
139 9. Eye cover (occluder or other method for covering an eye) 10. Lamp Vision - Part 3: VISION SCREENING ADMINISTRATION A. Students to be screened: 1. It is mandated that vision screening be administered to all students in kindergarten or grade 1, and students in grades 3, 5, and All students enrolling in or transferring into any of the grades listed in (1) unless there is proof of a current vision screening. 3. Any student specifically referred due to suspicion of vision difficulty. B. Students not to be screened: 1. Any student that has written documentation by an optometrist, ophthalmologist, or physician stating a known vision loss in both eyes does not need to be screened. If a student has a permanent unilateral vision loss (loss only in one eye), the non-affected eye should be screened. Appropriate school personnel must be notified of this child with vision loss. 2. No student should be required to submit to vision screening testing if written objection by the parent/guardian is submitted to the proper school authority. 3. Any student that is unable to be screened with traditional methods should be referred for follow-up testing. C. Other factors to consider: 1. All students who missed the original screening date should be screened within 60 days (usually completed at the rescreening date). 2. All students who were referred the previous year should be re-screened if documentation from a licensed eye professional is not on file with the school. D. Preparation for screening: 1. Completed by personnel designated in Part 1 a. Schedule vision screening program with school principal and personnel early in the school year. Inform staff and parents of upcoming screening for students in grades kindergarten or 1 st, and grades 3, 5, and 8. b. Have school personnel send names of students suspected of vision difficulties in non-mandated grade level to the testing personnel. c. Arrange for a quiet room in the school away from locker areas, music rooms, cafeteria, noisy equipment, etc. d. Arrange for testing personnel and volunteers. e. Inform staff of your screening schedule. f. The school must notify families regarding the vision screening. Parents are responsible for notifying the school in writing if their child has an exemption, such as religious beliefs. 136
140 g. Secure daily class schedule for use by individuals conducting the vision screening testing. Vision - Part 4: VISION SCREENING PROCEDURE A. Grades: kindergarten or 1 st grade, 3 rd, 5 th, and 8 th grades, and those suspected of having a visual deficit (referral). B. Equipment: Choice of charts: 1. The Snellen Chart 2. Sloan Letters 3. HOTV or LEA Symbol Optotypes (these two charts should be used only for those children under the age of 7 or in cases where the child may not know their letters or cannot respond to a letter chart) 4. Near Vision Card Use at a distance of either ten (10) or twenty (20) feet for distance vision, depending on the calibration of the chart being used, and a distance of fourteen (14) inches for near vision. Note: Self-illuminated charts are preferred over non-illuminated because self-illuminated equipment avoids yellowing, shadows are minimized, and the letters are well contrasted. However, clean, white wall charts with clear contrast between the letters and the background are also acceptable. C. Procedure: 1. The room should be darkened, with no natural lighting, if self-illuminating charts are used. If nonilluminating charts are used, the room should be well-lit, preferably with subdued ambient room lighting and maximum natural lighting (sunlight). All glare must be eliminated from the chart. 2. If a child wears glasses or contact lenses, testing should be conducted with the prescription on. If they are supposed to wear glasses or contact lenses and the student does not have them on, a note should be made on the recording form. 3. Mount the wall chart at the child s eye level. Adjust the chart height for the size of the person being screened. A suggestion is to place Velcro on the wall and move the chart as needed. 4. Mark off 10 or 20 feet, whichever is appropriate for the chart. The line may be marked with masking tape or paper, so that the child will be the required distance from the chart. 5. Ask the child to position toes on the line or other floor marking. Do not allow the child to lean the torso or head forward. 6. Occlude left eye with an occluder, an index card, or disposable cup (ensuring that the student is not peeking with the covered eye) and test the right eye. Then reverse the procedure and test the left eye. Be consistent in testing the right eye first to avoid recording errors. 7. Instruct students to keep both eyes open and read the selected letter or line of letters with the uncovered eye. Point to the letters below the line or symbol. A paper cut out or pointer may be used to isolate a line of letters. 137
141 8. When testing, start with at least a 20/50 line on the Snellen Chart and move down to the 20/20 line. If the student is unable to read the 20/50 line, move upward. 9. Record the results - record the line number for the last line read correctly with each eye. 10. Refer all failures to the registered school nurse for re-screening (re-screening is not necessary if a registered school nurse has done the initial screening). 11. For younger children: use the Tumbling E, HOTV, or LEA Symbols. These charts should not be used on children older than 7, if they know their letters and can respond to a letter chart. D. Standards: The following standards apply for a vision screening in kindergarten or 1 st, 3 rd, 5 th, and 8 th : Table 1. Indiana Standards Grade Line Chart Either kindergarten or 1 st 20/30 = pass Snellen Chart Either kindergarten or 1 st 20/32 = pass Sloan Letters, HOTV, or LEA Symbol Optotypes 3 rd, 5 th, and 8 th, or suspected of having a visual defect 20/30 = pass Snellen Chart Any student that is unable to read these standards with each eye will be recommended for further examination based on the recommendation of the individual performing the screening. E. Referral Criteria: For any students screened in grades K-12, each eye must meet the above criteria. Students must read as least half of the letters on row 20/30 or 20/32 correctly in order to pass. If students read less than half of the letters on row 20/30 or 20/32 correctly, they should be referred. For students in grades K or 1, a referral must also be made if the student fails the MCT portion of the vision screening. Even if the student is able to read at a level of 20/30 or 20/32, but fails the MCT portion, this student should be referred to an eye professional. F. Suggestions and Tips: 1. Show the child what is expected to be done: a. Students should be encouraged to read down the chart as far as possible; making a guess is allowed. Tell the student try and do your best and read as much of the chart as you can. b. The student may point to a wooden block E, the letters H, O, V, T, or symbols to identify what is seen on the chart. c. Demonstrate how to occlude the eye. d. Test from the top of the chart (large letters or symbols first) down toward the bottom (smaller letters or symbols). 138
142 e. Do not allow students to squint during the test. f. Present letters or symbols in reverse or inconsistent order between students. g. Do not allow children to stand directly behind the child performing the visual acuity test. h. Familiarize younger children with the letters or symbols prior to the screening. i. If using Tumbling E s instruct the student by saying: This is an E - see which way the legs of the E are pointing. With younger children, have them use their arms to show which way the E is pointing. Be sure the young child understands the E game and can show you which direction the E is pointing. It may be helpful to ask teachers to practice with students in the classroom before screening day. j. Vision is recorded as a fraction. The top number (numerator) recorded refers to the number of feet from the eye chart, and the lower number (denominator) refers to the line on the chart the student is able to read. G. Near Vision Cards are used to assess near visual acuity 1. Grades: Students in kindergarten or grade 1, 3, 5, and 8 as well as students enrolling or transferring into these grades. 2. Equipment: Near Vision Cards with Lea Symbols or Sloan Letters, occluders. 3. Procedure: Conduct the vision screening test with glasses if the student is wearing glasses. a. Mount or hold the card at the appropriate distance from the face at eye level. b. Test in a room that is well-lit. As the card is presented make sure it is free from shadows, glare, and yellowing. c. Do not allow the child to lean the head or torso forward. d. Occlude the left eye with the occluder, an index card, or cone shaped cup and test the right eye. Then reverse the procedure and test the left eye. e. Direct the child s eye to the 20/70 line on the card/chart and move down the card. f. Ask the child to name or read the letter or symbol on each line as directed. The criteria for referral and results outcome are listed in Table 1 above. g. If the near card is calibrated for 16 inches, (as most are), the child still needs to read at least half of the 20/30 or 20/32 line to pass. Vision - Part 5: SCREENING FOLLOW-UP PROCEDURES A. Parents/Guardians must be notified of a failure on the vision screening and instructed to contact a licensed eye professional or their healthcare provider about the results. 1. A Referral Response Form (see example), which is to be completed by the appropriate health professional, should be returned to the school nurse. 2. If no documentation is received from the parents/guardians, the child must be re-screened the following school year. B. Documentation of the vision screening results should be placed in the student s school record. C. Documentation of the vision screening must be maintained by each school. 1. Records of all tests must be made and continuously maintained by the school corporation to provide information useful in protecting, promoting, and maintaining the health of students. 139
143 2. The school corporation s governing body and the superintendent must annually receive information concerning the vision tests conducted. Testing information should include the number of students tested per grade; the number of students by grade who were tested using the modified clinical technique; the number of students by grade who were tested using vision screenings; the number of students tested by grade who passed or failed the testing; the number of students tested by grade who were referred for further testing; and the name of the individual or departments that supervised the testing. 3. Each school corporation shall annually provide to the Indiana Department of Education, for each school within the school corporation, information concerning the tests conducted. Testing information must be submitted via the School Health Report and should include the information listed above in item 2, as well as those schools applying for an MCT waiver, the total number of students eligible for testing and the total number of students tested. Vision - Part 6: RECORDS AND REPORTS A. A complete and continuing record of all vision tests shall be maintained by the school corporation. It is recommended that the school nurse include the results as part of each student s record. 1. Each student s health record shall clearly indicate: a. The date of the vision screening. b. The results of the screening for each eye, either eye passed or failed on each test given. c. Any pertinent referral and follow-up comments should be recorded. 2. School vision screening reports should be made available to appropriate school personnel: a. A record of the student s vision screening results should be part of the student s permanent file according to school policy. b. A record of the school s vision screening results should also be kept by the school nurse. c. Yearly reports shall be filed with the Indiana Department of Education, as part of the accreditation reporting process, by completing the School Health Report for each individual school. d. Complete vision records should accompany transferring students according to school policy. e. Vision screening records should be kept for the length of the student s enrollment. Vision - Part 7: EDUCATIONAL NEEDS A. It is the responsibility of the school nurse to inform the appropriate school personnel of vision screening failures. B. If parent response is not received by the end of the school year, the child should be re-screened the following school year. Note: If a student cannot be screened by following these guidelines, the school-appointed designee (optometrist, ophthalmologist, or school nurse) should be notified. This may include children who are frightened or crying, children with a developmental delay, or children with a language barrier. The school designee must follow up with parents to share any vision results obtained by the school and to see if previous testing has ruled out a vision loss or if further testing is warranted. The school appointed designee must ensure the student s records are documented regarding the status 140
144 of the student s vision. If a vision loss is documented, the results should be shared with appropriate school personnel. Vision Screening Sample Forms and Documents: Sample Vision Screening Referral Letter (PDF) Sample Referral Response Form (PDF) Glossary (PDF) Vision Screening Resources: 141
145 REFERRAL RESPONSE FORM Dear Parent: Your child did not pass his/her hearing screening. The hearing screening results are shown in the middle of this form. There are many reasons that a child can fail a hearing screening, such as temporary fluid in the ear, impacted ear wax or an actual hearing loss. Because your child did not pass this screening, it is recommended that you seek a medical evaluation with your child s physician. Please have your child s physician fill out the bottom of this form. Then please return it to your child s school. IC (c) However diagnosis and treatment shall be performed only on the recommendation of an Indiana physician who has examined the student. Thank you for your cooperation. Tested by Date Tested: HEARING SCREENING RESULTS Student s Name: Birthdate: School: Grade: # of referrals made to date: KEY: Right Left P PASS 1000Hz 2000Hz 4000Hz 1000Hz 2000Hz 4000Hz F FAIL (No response at any frequency at 20dBHL in either ear constitutes a failure) Dear Physician: Your diagnosis and prognosis of this case will help determine if remedial measures are necessary for this student from an educational standpoint. PHYSICIAN S RESULTS Ears: Right Left Diagnosis/Treatment: Prognosis: Date Seen: Physician: M.D. 142
146 Hearing Screening Worksheet Example SCHOOL: TEACHER: GRADE(S): DATE: STUDENT Audiometer (1 st screening) P=Pass Circle frequency F=Fail missed below. Re-screening P=Pass F=Fail Comments P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P F R: P F L: P P P P P P P P P P P P P P P P P P P P F F F F F F F F F F F F F F F F F F F F 143
147 HEARING SCREENING RESULTS (Example) Dear Parents/Guardian, As part of the school program, your child s hearing has been screened. The results revealed that your child passed the hearing screening at this time (so no further hearing testing is needed). If you would like further information or if you think your child needs another hearing screening at any time during the school year, please contact me at your child s school. Date Speech-Language Pathologist/School Nurse 144
148 Children s Vision Screening Program Referral Letter Child s Name: Date: Parent/Guardian, A recent vision screening indicates that our child may be experiencing some vision difficulty. Although these results are not a diagnosis and do not necessarily mean that glasses or treatment is needed, we urge you to make an appointment and take your child to an eye doctor of your choice to determine if there is a vision problem. Your child s vision screening indicated the following: o Child did not pass the distance vision test: Right: 20/ Left: 20/ o There was a two-line difference between the eyes: Right: 20/ Left: 20/ o A sign or symptom of a problem was observed: o Child did not pass the near vision test: Binocular: 20/ Please give this form to the eye care professional when you take your child for an examination so they understand the reason for referral. If you have any questions or concerns regarding this vision referral, please contact me at the number below. School Nurse/ Screener Telephone Number 145
149 Referral Response Form Attending Doctor: This child s vision was recently screened at school and a professional eye examination was recommended based on the results of the screening. Please complete this report form and ask that it be returned to the school nurse or school vision screener listed below. Child s Name: Date of Examination: Diagnosis: o Amblyopia o Muscle Imbalance (specify) o Refractive Error: Myopia Hyperopia Astigmatism o Other (Specify) o No Problem Detected Treatment: o Glasses Prescribed: Yes N0 Full-Time Part-Time Comments: o Other (Specify) o Follow-Up Care Recommended Examiner s Name: Phone Number: 146
150 APPENDIX A: GLOSSARY Alternate cover test - A traditional measure of ocular alignment in which first one eye and then the other is occluded in rapid succession: the occluded eye is observed for movement when the cover is removed, and the unoccluded eye is observed for movement while the other eye is under cover. The alternate cover test will detect both heterophoria and heterotropia and is the only measure of heterophoria possible in the school setting. Amblyopia - An ocular condition in an otherwise healthy eye, in which there is an abnormality of corticol response in the occipital lobe of the brain due to insufficient or inadequate stimulation of the fovea, neural pathway, and cortex that may result in unilateral vision loss if untreated. Astigmatism - A refractive error of the eye in which, with accommodation suspended, the refracting power of the eye is not uniform in all directions such as that incoming rays of light in a single eye do not come together to focus at a single point, but rather are focused at two or more points that usually results in blurred or partially blurred vision. Binocularity - The characteristic of the eyes when binocular vision is intact. Used interchangeably with binocular vision and requires both ocular alignment and stereoacuity. Color vision deficiency - A diminution or lessening of one of the three pigments in the color-sensitive cones of the retina that usually results in difficulty with saturation and brightness of colors rather than color or hue. Conjunctivitis - An inflammation of the palpebral conjunctiva, the lining of the upper and lower eyelids, and occasionally the bulbar conjunctiva, the layer of the conjunctiva over the sclera. Convergence/convergence reflex - The result of action of the extraocular muscles turning the eyes inward or medially-nasally to focus on an object near at hand; together with accommodation, one of two essential components of near vision. Denominator - The number below the bar in the Sloan notation. The denominator indicates the smallest line on an acuity chart (near or distance) successfully read by an examinee, or the distance from the chart or focal object for successful reading of the optotypes by an individual with no refractive error. Diplopia - Double vision or the perception of two images, one by each fovea, experienced when the eyes are intentionally crossed or out of alignment due to imbalance of the extraocular muscles. Distance vision - The ability of the eye to see images clearly at a distance (often a great distance). The inability to see a distant object clearly is called myopia. Esophoria - A type of heterophoria in which the eye deviates inward or nasally when covered, that is, when fusion is suspended. Esotropia - A type of strabismus in which one or both eyes deviate inward toward the nose from a parallel axis of vision. Also called convergent strabismus. 147
151 Exophoria - A type of heterophoria in which the eye deviates outward or laterally when covered, that is, when fusion is suspended. Exotropia - A type of strabismus in which one or both eyes deviate outward away from the nose from a parallel axis of vision. Also called divergent strabismus. Fovea - The area of the retina made up entirely of cones at the center of the macula, responsible for the very keenest vision. Fusion The union of two single images, one from each eye, into a single three-dimensional image within the occipital cortex. Heterophoria - A latent alignment disorder in which the eyes are not parallel during monocular vision, that is, when only one eye is seeing and binocularity and fusion are disrupted. Also referred to as phoria. Heterotropia - A manifest alignment disorder, or strabismus, in which one or both eyes deviate from parallelism when attempting to focus on a target while both eyes are open. Also referred to as tropia. Hypermetropia - A refractive error in which the light rays from an incoming visual image have not converged by the time they reach the retina. Used interchangeably with the term hyperopia. (Formerly called farsightedness, a sometimes confusing term no longer used.) Hyperopia - A refractive error in which the light rays from an incoming visual image have not converged by the time they reach the retina. Used interchangeably with the term hypermetropia. (Formerly called farsightedness, a sometimes confusing term no longer used.) Hypophoria - A type of heterophoria in which the eye deviates downward, when covered, while fusion is suspended. Hypotropia - A type of strabismus in which one or both eyes deviate downward from a parallel axis of vision. Legal blindness - Best-corrected central vision of 20/200 or less, and peripheral vision of 20 degrees or less. Myopia - The most common of the refractive errors in which light rays from an incoming visual image converge before they reach the retina, or preretinally. (Formerly called nearsightedness, a confusing term no longer used.) Near vision - The ability of the human eye to see objects with clarity at close range, also termed near point acuity or near acuity. Optimal near vision requires both accommodation and convergence. Numerator - The number above the bar in the Sloan notation. The numerator indicates the distance the examinee is away from the chart. Nystagmus - An involuntary, jerky movement of one or both eyes suggestive of primary ocular or systemic disease. 148
152 Occluder - An object that temporarily obstructs vision during vision screening or testing, preventing an eye from visualizing a focal target. Ocular alignment - A positioning of both eyes by the extraocular muscles so they are targeting the same focal object simultaneously with the result that two images, one from each eye, fall on the respective foveae. The eyes are said to be orthotropic or parallel. Ocular motility - The ability of the eyes to move together smoothly and fluidly, in all directions, at will. Ocular tracking - The movement of the eyes together, at will, following a target in any direction. Also termed tracking. Optotype - A focal image or target, very often letters or symbols on a chart, placed before the examinee s eyes and used to discern visual functioning. Plus lens - A convex lens used in the diagnosis and treatment of hyperopia, which refracts light when placed in front of the eye. Pseudoisochromatic plates - A test of color vision that is a saturation test and a measure of the purity of color, which works by detecting false perception of color. Sensitivity - The ability of a screening test to correctly identify those who actually have a disease, health problem, or condition. Serif The short lines stemming from and at any angle to the upper and lower ends of a letter. Sloan letters chart - A vision acuity chart named after ophthalmologist, Dr. Louise Sloan, composed of ten letters of the Roman alphabet intentionally selected, placed, and ordered on the chart. Sloan letters are sans (without) serif and employ uniform fonts in all charts, and for this reason are now the preferred charts. Snellen chart - The most common and well known of the vision acuity charts, named after its nineteenth century developer, Dr. Hermann Snellen. A modern version presents nine letters of the Roman alphabet in a font with serifs. Many charts in use are erroneously called Snellen charts. Snellen charts are no longer recommended because of the confusion with the discrimination of the serifs on the letters. (See Sloan chart) Specificity - The ability of a test to correctly identify all those who do not have a disease, health problem or condition. Stereopsis - Depth perception or three-dimensionality possible only when both eyes are in alignment and perceive the same image clearly. Strabismus - A manifest deviation of one or both eyes from the visual axis of the other so they are not simultaneously directed to the same object. Also referred to as heterotropia or tropia. Visual acuity - The state, condition, or effectiveness of central vision 149
153 Vision Testing of Young Children and Children with Special Needs Young children and children with special needs require particular screening attention. They may have short attention spans, limited verbal expression and language skill, processing delays or difficulties, and possible fear of new situations and unfamiliar adults. When planning, organizing, and implementing a vision screening program for children in need of special care follow the recommendations and procedures for a regular testing. Vision testing of young children with special needs should be conducted by using methods and equipment suitable for the child s developmental abilities. The following charts are listed in the order of ascending cognitive order: All symbol charts HOTV Tumbling or Illiterate E Number charts Letter charts Prescreening activities may include the following: If using the Tumbling E, use an E shaped paper cut out to teach the positions of up, down, right, and left positions in the classroom. Ask the students to state the direction in which the legs are pointing. If using the HOTV or symbols, make up a card with enlarged images of those letters so that the student can point to the symbol they see, if verbal skills are limited. Have the parent/guardian and the teacher fill out the ABC Checklist. It may be appropriate to set aside a time and setting away from the mass school screening so more time and attention can be provided to the student. The McDowell Vision Screening Kit is a tool that can be used for testing very young or severely disabled students. This kit provides a functional assessment of distance, near, and color vision, and ocular alignment and ocular motility. Implementation procedures, such as planning, referral, recording, and follow-up, for young children and special education students are done in the same manner as the regular vision test procedures outlined in these guidelines. Vision recording or documentation on the Individual Education Plan (IEP). Record the vision tests in lay terms; i.e. distance, near, color, etc. Record actual numerical results when appropriate; i.e. right 20/20, left 20/80. Record date of the testing. Describe any barriers to testing or delays in acquiring a professional eye examination. Include any special vision recommendations for visual accommodations in the classroom setting. 150

154 Chapter 7: Reports SECTION 1: ABSENTEEISM SECTION 2: EPINEPHRINE ADMINSTRATION SECTION 3: MCT WAIVER REQUEST SECTION 4: SCHOOL CLOSURE CONSIDERATION FORM SECTION 5: SCHOOL HEALTH REPORT 151
155 All of the required reports, along with links and instructions, can be found on the DOE Health Web at the following web address: SECTION 1: ABSENTEEISM ABSENTEE RATE OF 20% OR GREATER If your school reaches an absentee rate of 20% or more, please complete the Absentee Report which can be found by clicking here. Per 512 IAC 1-2-1, public and accredited nonpublic schools are required to develop a local attendance system for reporting symptoms and health outbreaks. The school nurse is required to report any known or suspected reason for the excessive rate of absenteeism directly to the superintendent or designated administrator. Per 512 IAC 1-2-2, public and accredited nonpublic schools are required to report to the local health department and the state attendance officer the percentage of student absences when the percentage of students absent from a school is equal to or greater than 20% of the enrolled students. Reports are not required on days immediately before or after a school vacation day or a scheduled instructional day that is canceled due to any weather-related emergency. Schools are to complete this report on any individual school that reaches the 20% absenteeism threshold and is not dependent on the entire school corporation reaching this threshold. SECTION 2: EPINEPHRINE ADMINSTRATION If your school administers epinephrine during the school day, please complete the Report of Epinephrine Administration. Please complete the report if any epinephrine is given person s prescribed or stock; given to staff, student or visitor; given by the nurse, school personnel or self-administered. To access the report, please click here. SECTION 3: MCT WAIVER REQUEST IC allows for schools to request a waiver for the MCT portion of the vision screening exam for students in grades K or 1 before November 1 of each school year. A waiver request must be made on an annual basis. Schools are required to complete the vision acuity (near and far) vision screening for all students in grades K or 1, 3, 5, and 8. However, if a school is not able to complete the MCT Vision Requirement for students in grades K or 1, a waiver for the MCT requirement only is available by clicking here. SECTION 4: SCHOOL CLOSURE CONSIDERATION FORM Schools are required to have 180 days of school instruction. Per IC , waivers to the 180 day requirement can be made by the Indiana Department of Education for extraordinary circumstances. If time allows, please complete one form for each building in your corporation before you make the decision to close a building. Your form will automatically be sent to the IDOE Director of School Accreditation and to IDOE Program Coordinator for Student Health Services. To complete the form, please click here. SECTION 5: SCHOOL HEALTH REPORT The School Health report collects data regarding the results of vision screening, hearing screening, and immunization verification. It is mandatory for all schools that are accredited by the Indiana Department of Education. Reports must be completed per individual school at the building level and cannot be combined into a corporation level report. In order to complete the report, a password for the DOE Online System is required. Please ensure that you have a password if you will be the person entering the data into the report. The report will be open for schools to submit their data from March 1 to June 15. For instructions on completing the report, please click here. 152

156 Chapter 8: Treatment Guidelines Abdominal Pain Anaphylaxis Asthma Bites and Stings Bleeding Blisters Bruises Burns Burn Assessment Chest Pain Chest Trauma Cold-Related Injuries Dermatitis Dental Injuries Dental, Oral, and Maxillofacial Emergencies Diabetic Emergencies Ear Emergencies Eye Emergencies Foreign Body Airway Obstruction Headaches Head/Spinal Cord Trauma Heat-Related Injuries Impaled Objects Increased Intracranial Pressure in a Student with VP Shunt Lacerations/Abrasions Musculoskeletal Injuries Interventions for Musculoskeletal Injuries Near-Drowning/Submersion Normal Vital Signs Nose Emergencies Overdose Poisoning/Toxic Exposure Scrotal Injury Seizures Shock Indicators of Hypoperfusion Pediatric Vital Signs by Age Splinters Sprains Syncope/Unconsciousness Ticks 153
157 ABDOMINAL PAIN ASSESSMENT KEY ASSESSMENT POINTS FOR ABDOMINAL PAIN Focused abdominal assessment Time of last bowel movement Urinary symptoms Events preceding episode, including trauma Menstrual history and possibility of pregnancy History/pattern of previous occurrences DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT Capillary refill time exceeds 2 Stable vital signs with: Stable vital signs with: seconds Moderate abdominal pain or Mild or intermittent abdominal Change in mental status or dysuria pain/cramps level of consciousness (LOC) Nausea/vomiting or significant Onset related to menses Decreased or absent bowel diarrhea sounds Significant pain with fever Abdominal/GU trauma Mucus or frank blood in stool; Abdominal distention, rigidity, or tarry stools guarding Abnormal vaginal bleeding or Bluish discoloration of flank or discharge without pregnancy periumbilical area (Grey Turner sign) Severe abdominal pain Imminent childbirth Pregnant with vaginal bleeding INTERVENTIONS Activate EMS Support C-ABCDE Place student supine Give nothing by mouth Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up INTERVENTIONS Determine need for EMS Observe student closely Give nothing by mouth Contact parent/guardian to transport student to medical care or home Follow-up INTERVENTIONS If recurrent abdominal pain (RAP) has been diagnosed, allow student to rest in health office Observe student Contact parent/guardian Return student to class or send home as indicated Refer to medical care or school support services as indicated for frequent complaints Follow-up as needed or per policy 154
158 ANAPHYLAXIS Respiratory assessment Focused assessment of skin findings ASSESSMENT KEY ASSESSMENT POINTS FOR ANAPHYLAXIS History of systemic allergic reaction History of food allergy Events preceding reaction, such as a bite/sting DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT S/S of cardiopulmonary compromise Airway compromise Change in mental status or LOC Cyanosis at mouth and lips S/S of severe respiratory distress (wheezing, dyspnea) Signs of shock/hypotension History of anaphylaxis Edema of face, lips, eyes, or tongue Generalized hives involving large area Diaphoresis Complains of (C/o) tightness in throat or chest C/o apprehension and/or weakness INTERVENTIONS Activate EMS Support C-ABCDE Administer prescribed autoinjectable epinephrine if available Repeat autoinjectable epinephrine in 10 min if no response Initiate CPR if necessary For severe respiratory distress, administer prescribed bronchodilator Consult IHP/ECP Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT S/S of mild systemic reaction; e.g., localized hives, abdominal cramps, nausea, or vomiting Edema of extremities Persistent coughing Tingling, itching of face, ears, or nose History of allergy INTERVENTIONS Determine need for EMS Consult IHP/ECP Observe student closely Administer prescribed autoinjectable epinephrine if available and activate EMS Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Local reaction only Responsive to medications Nasal congestion Persistent sneezing INTERVENTIONS Consult IHP/ECP Apply cold pack to site Observe student Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy 155
159 ASTHMA ASSESSMENT KEY ASSESSMENT POINTS FOR ACUTE ASTHMA ATTACKS Airway inspection to rule out (R/O) obstruction due to infection or foreign body aspiration Respiratory assessment Skin assessment IMMEDIATE INTERVENTIONS Even before you determine triage category, perform the following actions as indicated: Help student into a position of comfort Perform peak flow assessment if possible Note: Obtain peak expiratory flow reading before administering bronchodilator and again 20 minutes later (or per ECP orders) Administer prescribed bronchodilator or other medication as directed Note: Use spacer or holding chamber with MDI/nebulizer, if available DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT S/S of severe asthma URGENT S/S of moderate asthma NON-URGENT S/S of mild asthma Cannot tolerate normal activity Symptoms respond to No improvement within bronchodilator minutes of bronchodilator Student is able to maintain administration normal level of activity Bronchodilator unavailable INTERVENTIONS Support C-ABCDE Prepare to ventilate if necessary Activate EMS if S/S are not relieved by medication or if medication is not available Administer high-flow O 2 if available Repeat prescribed bronchodilator/other medications Directly/continuously observe student Consult IHP/ECP Contact parent/guardian Notify school administrator Follow-up INTERVENTIONS Determine need for EMS Administer high-flow O 2 if available Repeat prescribed bronchodilator/other medications Consult IHP/ECP Directly/continuously observe student Contact parent/guardian to transport student to medical care or home Follow-up INTERVENTIONS Repeat prescribed bronchodilator/other medications Consult IHP/ECP Monitor student Contact parent/guardian Return student to class or send home as indicated Assess need for parent/ guardian student asthma education Follow-up as needed or per policy 156
160 BITES AND STINGS Time bite/sting occurred Location of bite/sting on body Type of bite/sting Number of bites/stings Intensity of pain ASSESSMENT KEY ASSESSMENT POINTS FOR BITES AND STINGS Previous exposure/allergic/anaphylactic reaction to same type of bite/ sting Wound characteristics (erythema, edema, ecchymosis, drainage, and size/depth) Inspection for foreign body (stinger, tooth, or tick) DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT S/S of anaphylaxis or history of anaphylactic reaction (see Anaphylaxis protocol) S/S of respiratory distress Hypotension Cardiac arrest Loss of consciousness Known exposure to toxin (see Poison Control protocol) Severe pain INTERVENTIONS Activate EMS Support C-ABCDE Perform CPR as appropriate Administer IM epinephrine as per ECP Directly/continuously observe student Report animal bites to appropriate local official Contact poison control center (PCC) as appropriate ( ) a Contact parent/guardian Notify school administrator Follow-up S/S of mild systemic reaction with wheezing, progressive pain/edema but normal vital signs (see Anaphylaxis protocol) Deep puncture wounds Moderate pain Lacerations that require sutures (see Lacerations/Abrasions protocol) Nausea/vomiting Human bite with broken skin INTERVENTIONS Determine need for EMS Wash lacerations with soap and water; irrigate as indicated Observe student closely Report animal bites to appropriate local official Refer all incidents involving human bites to ED Contact PCC as appropriate ( ) a Contact parent/guardian to transport to medical care or home Follow-up Mild localized allergic reaction without systemic/respiratory S/S Mild pain Mild pruritus Stinger/tick present INTERVENTIONS Stinger Remove stinger by scraping with stiff cardboard/credit card; do not squeeze Apply cold pack Observe student for 20 minutes before returning to class Tick Grasp tick with fine-point tweezers or gloved fingertips as close to skin as possible Pull upward with steady, even pressure Wash bite area and hands with soap and water In All Cases Observe student Contact parent/guardian Contact PCC as appropriate ( ) a Return student to class or send home as indicated Follow-up as needed or per policy 157
161 First Aid Don ts Do not apply a tourniquet for bites or stings because it can lead to ischemia. Use of tourniquets is limited to uncontrolled hemorrhage. Do not incise wound or apply suction; these methods are ineffective and potentially dangerous. a To contact the Poison Control Center ( ): identify yourself as a healthcare professional and provide your name and phone number; student s name, age, weight, and vital signs; insect or animal involved (if known); time, route, and duration of exposure; abnormal S/S; first aid and immediate interventions rendered. POISON CONTROL Refer student for tetanus booster if it has been 5 years or more since the last vaccination. Tetanus booster is recommended every 10 years. 158
162 BLEEDING Large lacerations without severe bleeding: Control bleeding by placing a sterile/clean covering over wound and applying firm pressure. Apply roller bandage snugly over sterile dressing. If bandage has been applied to an extremity, check distal extremities (fingers or toes) for warmth, color, and feeling. Notify parents and recommend evaluation by primary healthcare provider. If bleeding doesn t stop Apply additional dressings. DO NOT remove original dressing. If no broken bones are suspected, elevate the injured area above the level of the heart. If bleeding is still not controlled, put pressure against artery pressure point (nearest artery between wound and heart). Request immediate emergency medical services. Notify parent. 159

163 BLISTERS Do not break blister. Wash area. Cover with sterile dressing. If blister breaks, treat as open wound and keep covered with sterile dressing and observe for signs of infection. 160

164 BRUISES Apply ice pack for approximately 20 minutes. Elevate injured part. If bruise is swollen and painful, notify parent. 161
165 BURNS Scene safety (e.g., live electrical wire) Burn characteristics (see next ) Duration of contact with burn source SYSTEMATIC ASSESSMENT KEY ASSESSMENT POINTS FOR BURN INJURIES Student s age, weight, and general health status Associated injuries Pediatric Glasgow Coma Scale (PGCS) score IMMEDIATE INTERVENTIONS Even before you determine triage category, perform the following actions as indicated: Remove student from burn source (e.g., heat/electricity) Remove jewelry, rings, and constricting clothing (if possible) Do not remove clothing that has adhered to skin! Begin irrigation of chemical burns with cool water Cool thermal burns if less than 20% body surface area (BSA) is involved NOTE: Protect student from hypothermia; only immerse superficial or partial-thickness burns less than 5% BSA 162
166 DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT Apnea or pulseless Full-thickness burn (tough, brownish surface) Deep partial-thickness burn (charred/white) Burns involving face, hands, feet, eyes, ears, or genitalia (see Eye or Ear Emergencies protocols) Electrical burns S/S of inhalation injury (singed nasal hair or carbonaceous sputum) or other complicating injuries Altered level of consciousness (LOC) Respiratory distress (see Respiratory Distress protocol) Suspected child maltreatment (see Child Maltreatment protocol after providing burn care) Severe pain Interventions Activate EMS Support C-ABCDE Electrical burns Safely remove student from burn source Initiate CPR as needed/have AED ready Inspect for entrance and exit wounds Chemical burns Continue copious irrigation of chemical burns with tepid running water for at least 20 minutes Consider contacting PCC ( ) Send burn agent and MSDS/SDS to ED with student Do not apply cold packs Thermal burns Cover with dry, sterile dressings or clean sheet In all cases Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up Superficial partialthickness burn without complicating factors Moderate pain Erythema/edema, wet/ oozing blisters Too large to cover with adhesive bandage Signs of associated infection INTERVENTIONS Determine need for EMS Flush copiously with tepid running water If unable to immerse, apply clean, wet, cool cloth Do not apply cold packs Do not break blisters Bandage loosely Observe student closely Contact parent/guardian to transport student to medical care or home Follow-up Superficial burn (e.g., sunburn) Minor erythema Local, mild pain Student is alert INTERVENTIONS Immerse area in tepid water 2 5 minutes Apply tepid cloths Bandage loosely Observe student Contact parent/ guardian Return student to class or send home as indicated Follow-up as needed or per policy 163


 as a reference; this is approximately equal to 1% of the student s total body")
167 BURN ASSESSMENT The depth, extent, and location of a burn provide a consistent basis for conveying information about a burn injury to EMS and other healthcare providers. The following parameters are used to describe depth: A superficial burn involves only the epidermis. It is characterized by erythema and local pain. A superficial partial-thickness burn involves both the epidermis and the corium. This type of burn generally produces erythema and blisters. A deep partial-thickness burn may appear white and dry, with locally reduced sensitivity to touch and pain. A full-thickness burn has a tough, brownish surface and a hard eschar. The area will be locally insensitive to touch or pain. This type of burn will not heal without intervention. Extent is described as a percentage of the body surface area (% BSA). A quick way to determine % BSA for small or irregular burns is to use the student s hand (including the palm and fingers) as a reference; this is approximately equal to 1% of the student s total body surface area. The figure on the left illustrates % BSA by anatomical area for an infant, child, and adult; the figure on the right illustrates the palm-andhand method of estimating % BSA based on the child s hand size. % BSA BY ANATOMICAL AREA PALM-AND-HAND CALCULATION a a INCLUDE CHILD S FINGERS 164
168 CHEST PAIN ASSESSMENT KEY ASSESSMENT POINTS FOR CHEST PAIN Consider etiology Cardiac Respiratory Musculoskeletal Trauma Psychosocial stress DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT Severe chest pain Bradycardia/tachycardia Cyanosis of lips and nail beds Decreased LOC Palpitations Dyspnea Peripheral pulses weak/thready/ absent Diaphoresis; clammy, cool skin Restlessness Hypotension Nausea Weakness Capillary refill exceeds 2 seconds INTERVENTIONS Activate EMS Support C-ABCDE Have AED readily available Maintain position of comfort Directly/continuously observe student Reassess vital signs every 5 minutes Contact parent/guardian Notify school administrator Follow-up Moderate, persistent chest pain Anxiety Stable vital signs No history of:»» Recent chest trauma»» Recent asthma attack»» Loss of consciousness INTERVENTIONS Support C-ABCDE Determine need for EMS Maintain position of comfort Observe student closely Reassess vital signs Contact parent/guardian to transport student to medical care or home Follow-up Mild chest pain Normal vital signs No history of:»» Recent chest trauma»» Recent asthma attack»» Loss of consciousness INTERVENTIONS Support C-ABCDE Maintain position of comfort Monitor closely Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy 165
169 CHEST TRAUMA ASSESSMENT Stabilize c-spine if head/spinal injury is suspected! KEY ASSESSMENT POINTS FOR CHEST TRAUMA Respiratory assessment Chest wall inspection for symmetry, wounds, and/or ecchymoses IMMEDIATE INTERVENTIONS Even before you determine triage category, perform the following actions as indicated: If student is apneic, perform rescue breathing using mouth-to-mask If student is pulseless, initiate CPR; apply AED Apply clean, non-porous dressing to open chest wounds (if S/S of tension pneumothorax develop, open the dressing) Apply direct pressure for profuse hemorrhage DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT S/S of respiratory distress Open chest wound Crush injury Uncontrollable hemorrhage Muffled heart sounds Paradoxical or asymmetrical chest wall movement S/S of shock S/S of tension pneumothorax or cardiac tamponade:»» Apprehension»» Rapid/shallow respiration»» Painful respiration»» Jugular vein distension»» Cyanosis»» Hypotension (late/ominous sign) INTERVENTIONS Activate EMS Support C-ABCDE Maintain spinal stabilization Cover open chest wounds (occlude on three sides only) Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up Closed chest injury without respiratory distress S/S of closed rib fracture (shallow/painful but unimpaired respiration) INTERVENTIONS Support C-ABCDE Determine need for EMS Monitor respiratory/ cardiac status Observe student closely Contact parent/ guardian to transport student to medical care or home Follow-up Stable vital signs Ecchymoses No S/S of rib fracture INTERVENTIONS Apply cold packs as appropriate Observe student Contact parent/ guardian Return student to class or send home as indicated Follow-up as needed or per policy NOTE: Pneumothorax/cardiac tamponade may develop slowly during a hour period following chest trauma; reassessment is crucial. A pneumothorax should be considered emergent; a tension pneumothorax may form if left untreated. Signs/symptoms (S/S) of pneumothorax include tachypnea, tachycardia, unequal chest expansion, and unilateral absent or diminished breath sounds. 166
170 COLD-RELATED INJURIES GENERAL GUIDELINES Hypothermia: rewarm slowly Frostbite: rewarm quickly Do not rub affected area Use warm water to rewarm; never use hot water to rewarm Educate students regarding susceptibility to hypothermic injury and need for precautions FROSTBITE CATEGORIES Frostnip Blanched, white skin that is cold to touch Superficial frostbite Firm, waxy skin with softer tissue underneath Blisters develop in hours Deep frostbite Mottled or gray-blue skin that is firm to touch Severity not apparent until frostbitten area is rewarmed Sensory: cold; pruritus or paresthesia Necrosis develops over time ASSESSMENT KEY ASSESSMENT POINTS FOR COLD-RELATED INJURIES Skin assessment Duration of exposure Events preceding episode Focused physical examination of extremities DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Altered LOC Cyanosis Slow/shallow respiration Weak, thready pulses, no pulses, or bradycardia Hypotension Extremities edematous and discolored No shivering (severe hypothermia) Slurred speech Abnormally low body temperature S/S of deep frostbite INTERVENTIONS Activate EMS Remove student s wet clothing Keep student warm and completely covered Assess vital signs for 1 full minute If pulseless, initiate CPR Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT Normal LOC or drowsy Shivering (mild hypothermia) S/S of superficial frostbite or frostnip INTERVENTIONS Remove wet clothing and keep student warm Determine need for EMS Observe student closely If alert, give sips of warm liquid Warm area with warm water Reinforce need for precautions when exposed to cold Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Alert Slight shivering Exposed skin feels cold No signs of frostbite or frostnip INTERVENTIONS Remove wet clothing and replace with dry coverings If student is alert, give sips of warm liquid Warm cold skin with warm water Observe student Reinforce need for precautions when exposed to cold Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy 167
171 DERMATITIS Contact Dermatitis (i.e. Poison Ivy, Poison Oak, Poison Sumac) Wash area with soap and water. If reaction is mild, apply cool compress. If reaction is severe (covers large portion of body or the face, especially near the eyes), contact parent and recommend evaluation by primary healthcare provider. 168

172 DENTAL INJURIES Broken or Displaced Teeth Try to clean the soil, blood, and other debris from the injured area with a sterile gauze or cotton swab and warm water. Apply a cold compress in the cheek next to the injured tooth to reduce swelling. If possible, gently move the displaced tooth or teeth into their correct position. If the tooth has been pushed up into the socket or gum by the blow, do not attempt to pull it out into position. If the broken tooth has created a sharp edge, it may be covered with paraffin (wax) to prevent tissue lacerations. If the chip or fractured part can be located, place in saline, milk, or water and take to dentist. Notify parent and recommend immediate dental care. For students with braces, it is recommended to have dental wax available and notify parent if any wires break. 169
173 DENTAL, ORAL, AND MAXILLOFACIAL EMERGENCIES NOTE Refer student for tetanus booster if it has been 5 years or more since the last vaccination. Tetanus booster is recommended every 10 years. ASSESSMENT Stabilize c-spine if head/spinal injury is suspected! KEY ASSESSMENT POINTS FOR DENTAL, ORAL, AND MAXILLOFACIAL EMERGENCIES Inspect teeth Assess ability to open and close mouth Assess facial bones, including mandible IMMEDIATE INTERVENTIONS Even before you determine triage category, ensure the adequacy of the student s airway. DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT Airway compromise Change in mental status or LOC Excessive bleeding Suspected fracture of mandible or other facial bones (see Trauma protocol as indicated) INTERVENTIONS Activate EMS Maintain c-spine stabilization Support C-ABCDE Treat hemorrhage with direct pressure Apply cold packs to reduce pain/edema For suspected mandible fracture only, stabilize jaw by wrapping cravat around the point of the chin and securing it on top of the head; avoiding pressure on the neck Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up Displacement of multiple teeth Avulsion of permanent tooth a Major chip/fracture of permanent tooth Broken orthodontic appliance Severe toothache INTERVENTIONS If possible, save large tooth chips; cover jagged edge of tooth with gauze For wire protruding from appliance, gently attempt to bend away from oral tissue; if unsuccessful, cover end with gauze or dental wax (do not remove embedded wire) Observe student closely Contact parent/guardian to transport student to dental care or home Follow-up a Avulsion of permanent tooth Note: Replantation is most likely to succeed if attempted within 60 minutes. Activate EMS or transport immediately to dentist Handle the tooth by the crown, not the root If the tooth is dirty, gently rinse in milk or water Caries Exfoliation of primary tooth Eruption of permanent tooth Bleeding gums Minor chip/fracture of tooth INTERVENTIONS For minor tooth chip, have student rinse mouth with warm salt water Apply cold compress to edematous areas Observe student Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy Gently replace tooth in socket (do not use force) only if student is alert and able to cooperate; instruct student to keep pressure on tooth by biting gently on clean gauze If unable to replace tooth in socket, place the tooth in a protective container filled with ph-balanced solution for transport with student to the ED or dental specialist; if this solution is not available, use cold milk or water 170
174 DIABETIC EMERGENCIES ASSESSMENT KEY ASSESSMENT POINTS FOR DIABETIC EMERGENCIES Respiratory assessment Skin assessment Last insulin dose/type of insulin used and delivery route Last meal/carbohydrate intake Precipitating factors (exercise, change in eating habits/diet, stress, missed insulin dose, or illness) Current blood glucose level DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Severe hypoglycemia Glucose less than 60 mg/dl with loss of consciousness or seizures (see Seizures protocol) Severe hyperglycemia/diabetic ketoacidosis (DKA) Glucose exceeds 250 mg/dl with at least one of the following: Moderate to severe dehydration Abdominal pain/tenderness Kussmaul respiration and/or fruity breath odor Tachycardia Cool extremities Altered LOC (lethargic to comatose) INTERVENTIONS Activate EMS Support C-ABCDE Directly/continuously observe student Place in left lateral recovery position to prevent aspiration Consult IHP/ECP Hypoglycemia Administer 1 mg glucagon IM/SQ if available per ECP (place student in recovery position because glucagon may precipitate vomiting) Severe hyperglycemia Administer insulin per ECP Diabetic ketoacidosis Prepare for immediate transport Give nothing by mouth In all cases Contact parent/guardian Notify school administrator Determine need for diabetes education (parent/ guardian, student, and school personnel) Follow-up URGENT S/S of moderate hypoglycemia; glucose less than 60 mg/dl, student awake and responsive S/S of moderate hyperglycemia; glucose mg/dl; student awake and responsive with mild abdominal pain/tenderness, nausea, headache, tachycardia, and/or fruity breath odor INTERVENTIONS Support C-ABCDE Determine need for EMS Monitor student closely Consult IHP/ECP Hypoglycemia Give glucose tablets/instant glucose equivalent to 15 grams carbohydrates, or 4 oz regular soda or juice (orange/apple), followed by snack/next meal As indicated, give extra snack (e.g., two peanut butter crackers or one-half sandwich and 8 oz milk) Hyperglycemia Administer insulin per ECP Increase intake of water Test for ketonuria In all cases Contact parent/guardian to transport student to medical care or home Determine need for diabetes education (parent/guardian, student, and school personnel) Follow-up NON-URGENT S/S of mild hypoglycemia; glucose mg/dl, student awake and alert S/S of mild hyperglycemia; glucose mg/dl, student awake and alert INTERVENTIONS Consult IHP/ECP Mild hypoglycemia Give glucose tablets/instant glucose equivalent to 15 grams carbohydrates, or 4 oz regular soda or juice (orange/apple), followed by snack/next meal As indicated, give extra snack (e.g., two peanut butter crackers or onehalf sandwich and 8 oz milk) Recheck glucose in 15 min; if no improvement, repeat treatment If improvement is noted, return student to class or send home as indicated Instruct student to refrain from tasks requiring intense concentration or exertion for 1 hour Mild hyperglycemia Administer insulin per ECP Increase intake of water Return student to class or send home as indicated In all cases Contact parent/guardian as needed or per policy Determine need for diabetes education (parent/guardian, student, and school personnel) Follow-up as needed or per policy 171
175 WHAT TO DO WITH A STUDENT WHO HAS A BLOOD SUGAR LEVEL OF >250 BUT MINIMAL SYMPTOMS: Follow IHP Notify parent and physician. Push fluids (water) and possibly insulin coverage if physician directs. CHECKING KETONES: Ketones are checked when the blood glucose level is greater than 250 or 300 mg/dl, or when the student is experiencing nausea or vomiting as per the DMMP (diabetes medical management plan). Both urine and blood can be checked for ketones. Urine ketone monitoring can be done using a test strip that is dipped into the urine. The bottle of strips should be dated when opened and discarded in 6 months. Individual foil-wrapped strips are available and preferred. The color change of the test strip, after exactly 15 seconds, indicates the level of ketones. The presence of ketones may indicate a failure of the insulin pump. Additional insulin is often required and fluid replacement (water or noncaloric fluids) is important. A student should not participate in any physical activities, such as gym class, if ketones are present because this may increase the blood glucose and worsen the ketosis (Diabetes Research in Children Network [DirecNet], 2006). If ketones are present, the parent/guardian should be notified and the plan for the management of ketones and/or illness should be initiated as per the DMMP. (NASN Manual pg. 888) 172
176 EAR EMERGENCIES ASSESSMENT Stabilize c-spine if head/spinal injury is suspected! KEY ASSESSMENT POINTS FOR EAR EMERGENCIES Skin assessment for wounds, blisters, erythema, edema, hematomas, or bleeding Focused physical assessment (external/otoscopic) Hearing evaluation IMMEDIATE INTERVENTIONS Even before you determine triage category, perform the following actions as indicated: Control bleeding Apply appropriate dressing DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Change in mental status or LOC Laceration/avulsion/ hematoma of external ear with uncontrollable bleeding (see Head/Spinal Cord protocol as indicated) Burn or direct thermal injury Acute hearing loss INTERVENTIONS Activate EMS Maintain spinal stabilization if applicable Support C-ABCDE Directly/continuously observe student Maintain position of comfort Keep student calm Contact parent/guardian Notify school administrator Follow-up URGENT Foreign body in ear Mild hematoma Abrasions/minor lacerations of external ear (see Lacerations/ Abrasions protocol) INTERVENTIONS Determine need for EMS Foreign body Do not attempt to remove unless object is visible and can be gripped with forceps or fingers If object is a live insect, instill 1 2 drops of mineral oil In all cases:»» Closely monitor student»» Contact parent/guardian to transport student to medical care or home»» Maintain position of comfort»» Observe student»» Follow-up as needed or per policy NON-URGENT Mild earache without drainage Associated low-grade fever INTERVENTIONS Send student home if pain is persistent or accompanied by fever Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy NOTE Refer student for tetanus booster if it has been 5 years or more since the last vaccination. Tetanus booster is recommended every 10 years. There is a high risk for long-term complications with injury to the ear. Always refer the student for evaluation by a healthcare practitioner. 173
177 EYE EMERGENCIES ASSESSMENT Stabilize c-spine if spinal injury is suspected! KEY ASSESSMENT POINTS FOR EYE EMERGENCIES Events leading up to injury (e.g., chemical exposure or other burn) AS TOLERATED, focused physical examination of the eye/vision assessment for Visible wounds, drainage, or foreign body Extraocular movement PERRL Visual acuity IMMEDIATE INTERVENTIONS For chemical burns involving the eye, IMMEDIATELY activate EMS, then ensure scene safety and begin flushing the eye copiously with saline, eyewash solution, or water. DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Change in mental status or LOC Penetrating injury Chemical/thermal burn Unequal/irregular pupils Blunt injury (see Head/Spinal Cord protocol) Embedded foreign body Hyphema (haze or blood in iris) Reduced visual acuity/loss of vision INTERVENTIONS Maintain c-spine stabilization as applicable Support C-ABCDE Activate EMS Protect eye from further injury Chemical burns Continue irrigation while awaiting EMS Send copy of MSDS/SDS to ED Penetrating injuries Stabilize object with gauze pads Tape disposable drinking cup over dressing (do not allow it to contact object) Thermal burns Do not inspect eyes Apply loose, moist dressing Radiation burns (From arc welder, sunlight, or sun lamp) Cover with eye patch In all cases Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT Blunt trauma without vision changes S/S extraocular muscle entrapment Suspected corneal abrasion Laceration of lid Blurry/impaired vision Diplopia Eye pain/guarding Sensation of foreign body that persists for more than 1 hour Bilateral periorbital ecchymoses (raccoon eyes) INTERVENTIONS Determine need for EMS If no evidence of injury, apply cool compress for 20 minutes Instruct student not to move rapidly, bend over, or cough Observe student closely Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Superficial foreign body Subconjunctival hemorrhage (may result from violent coughing or vomiting) Minor periorbital lacerations Minor periorbital ecchymoses INTERVENTIONS Foreign body If foreign body is visible in sac of lower lid, remove with cotton-tipped applicator If removal is unsuccessful after two attempts, or if foreign body is located elsewhere, flush eye with saline, eyewash solution, or water In all cases Observe student Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy 174
178 FOREIGN BODY AIRWAY OBSTRUCTION ASSESSMENT KEY ASSESSMENT POINTS FOR FOREIGN BODY AIRWAY OBSTRUCTION Evaluation of airway/respiratory status Suddenness of onset Events leading up to incident (e.g., witnessed ingestion/aspiration of small object, toy, or food) Note: Fever or S/S of respiratory illness decreases the likelihood of foreign body etiology. DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Severe airway obstruction Choking, silent cough, or Unable to cough, speak, or make any sound Apnea Pallor or cyanosis Loss of consciousness INTERVENTIONS Severe obstruction Begin AHA airway clearing maneuvers (see next for detailed procedure) In infants younger than 1 year, apply five back blows/slaps and five chest thrusts In children older than 1 year, perform abdominal thrusts (Heimlich maneuver) Continue until either the object is expelled or the infant or child becomes unresponsive Begin CPR, checking inside the mouth before each series of rescue breaths to see whether the object is visible and can be removed Note: Do not attempt blind finger sweeps! Foreign body may be pushed further into the airway, exacerbating obstruction Activate EMS if efforts are unsuccessful after 1 minute Contact parent/guardian Notify school administrator Follow-up URGENT Mild airway obstruction History of aspiration Fast breathing Intermittent wheezing or stridor Gagging, choking, or coughing Pink skin color Mild to moderate dyspnea INTERVENTIONS Encourage forceful cough Do not interfere in any other way Monitor for worsening distress, ineffective cough, inspiratory wheezing, labored breathing, or tachycardia If signs of severe obstruction develop, triage as emergent and begin AHA airway clearing maneuvers (see next ) If student s efforts clear the obstruction, contact parent/ guardian to transport student to medical care or home Notify school administrator Provide psychological support Follow-up NON-URGENT Witnessed ingestion/ aspiration Student clears obstruction by coughing No S/S of continued obstruction INTERVENTIONS Observe student at frequent intervals throughout day Contact parent/guardian Provide psychological support Return student to class or send home as indicated NOTE: If student continues to cough the next day, suspect retained bronchial foreign body, bronchitis, or pneumonia Follow-up as needed or per policy 175
179 HEADACHES Mental status/neurological assessment Past health history of headaches or recent head injury ASSESSMENT KEY ASSESSMENT POINTS FOR HEADACHES Events leading up to onset, such as stress, exposure to a known trigger, and/or aura Focused physical assessment for neck stiffness Assessment for visual disturbances (see Eye Emergencies protocol) DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Change in mental status or LOC Acute neurological deficit Seizure activity (see Seizures protocol) Severe headache (e.g., c/o worst headache of my life ) Stiff neck with fever Recent head injury Hypertension INTERVENTIONS Activate EMS Support C-ABCDE Consult IHP/ECP Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT Moderate headache with vomiting History of aura Exposure to known trigger Blurred vision, dizziness, or photophobia No neurological deficit History of migraines INTERVENTIONS Determine need for EMS Provide rest in quiet, darkened room Consult IHP/ECP Administer medication per IHP/ ECP Observe student closely Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Generalized mild headache S/S of upper respiratory infection (URI) S/S of sinus infection INTERVENTIONS Allow student to rest Consult IHP/ECP Administer medication per IHP/ECP Observe student Reassess Educate about avoiding triggers Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy 176
180 HEAD/SPINAL CORD TRAUMA ASSESSMENT Stabilize c-spine DO NOT move student! KEY ASSESSMENT POINTS FOR HEAD/SPINAL CORD TRAUMA Mental status/neurological assessment Events leading up to injury Mechanism of injury Assessment for visual disturbances (see Eye Emergencies protocol) DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT Change in mental status or LOC (including drowsiness or lethargy) Abnormal behavior/loss of normal abilities Seizure activity (see Seizures protocol) Loss of/decreased movement or sensation in extremities Blood/cerebrospinal fluid (CSF) discharge from nose/ears Significant trauma to head/ neck or high-risk mechanism of injury Evidence of depressed skull fracture Paresthesia INTERVENTIONS Activate EMS Support C-ABCDE while maintaining c-spine stabilization Apply direct pressure to bleeding except over depressed skull injury Keep student warm Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up Brief period of confusion/ amnesia Neck pain Dizziness Blurred vision/diplopia Headache Nausea/vomiting Laceration requiring sutures (see Lacerations/Abrasions protocol) INTERVENTIONS Support C-ABCDE Determine need for EMS Maintain c-spine stabilization Control bleeding with direct pressure Apply cold packs to swollen areas Keep student warm Observe student closely Contact parent/guardian to transport student to medical care or home Follow-up Alert Minor abrasions, lacerations, or edema INTERVENTIONS Apply cold packs as indicated Observe student closely Reassess after minutes Contact parent/guardian Return student to class or send home as indicated Advise parent/guardian, teachers, and coaches of injury and emphasize the need for observation during next hours; seek medical care if the student exhibits any of the following:»» Dizziness»» Headache»» Nausea»» Photophobia»» Diplopia»» Irritability»» Poor concentration»» Decline in academic ability»» Personality changes Follow-up as needed or per policy 177
181 HEAT-RELATED INJURIES ASSESSMENT KEY ASSESSMENT POINTS FOR HEAT-RELATED INJURIES Skin assessment (e.g., color, temperature, moisture, and other related skin findings) DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT S/S of heat stroke Hyperthermia (temperature exceeding 104 F/40 C) Confusion/diminished LOC Hot/dry/red skin Tachycardia/weak peripheral pulses Syncope Ataxia Seizure activity (see Seizures protocol) INTERVENTIONS Heat stroke is a life-threatening emergency! Activate EMS Support C-ABCDE Immediately remove from heat to a cool environment Immediately initiate cooling measures:»» Loosen clothing»» Apply cool, wet towels to neck, groin, and axillae»» Sponge with cool compresses»» Fan student Place in left lateral recovery position in case of vomiting Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT Disoriented Mild tachycardia S/S of heat exhaustion Cool, moist, and pale skin Dilated pupils Mild to moderate headache Nausea/vomiting Muscle cramps Weakness or dizziness Normothermic to mildly hyperthermic (temperature less than 101 F/38.3 C) Diaphoresis INTERVENTIONS Determine need for EMS Observe continuously Allow to rest in cool environment Loosen clothing Apply cool, wet towels Fan student In the absence of vomiting, encourage fluid replacement with water or a diluted electrolyte-replacement drink as permitted by applicable protocols Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Mild cramping of calves, thighs, or shoulders Normothermic Awake and alert INTERVENTIONS Allow to rest in cool environment Loosen clothing Observe student Encourage fluid replacement with water or a diluted electrolyte-replacement drink as permitted by applicable protocols Educate student about maintaining adequate hydration during higher-risk activities Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy 178
182 IMPALED OBJECTS Never remove an impaled object; immobilize object in place. Control bleeding by pressure dressing. If eye is site of injury, protect impaled object with paper cup and cover both eyes. Request immediate emergency medical services. Notify parent. 179
183 INCREASED INTRACRANIAL PRESSURE IN A STUDENT WITH A VP SHUNT ASSESSMENT KEY ASSESSMENT POINTS FOR STUDENTS WITH VP SHUNTS Facial symmetry Gag reflex Pupil size/reactivity Extraocular eye movements Neurological function Pediatric Glasgow Coma Scale (PGCS) score Symmetry of function/strength, posture, gait, balance, and spontaneous movement DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Change in mental status or LOC Lethargy Acute neurological deficit Inability to look up/roll eyes upward New onset eye deviation Seizure (see Seizures protocol) INTERVENTIONS Activate EMS Support C-ABCDE Consult IHP/ECP Directly/continuously observe student Contact physician for instructions Contact parent/guardian Notify school administrator Follow-up URGENT Early S/S of shunt dysfunction:»» Headache»» Irritability»» Vomiting»» Decreased appetite»» Change in personality»» Loss of existing skills or abilities»» Swelling/erythema along shunt path»» Seizures»» Loss of balance S/S of shunt tract infection INTERVENTIONS Support C-ABCDE Determine need for EMS Place student supine Elevate head Allow student to rest Reduce environmental stimuli Consult IHP/ECP Observe student closely Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Mild headache without other S/S of shunt dysfunction Normal neurological assessment and PGCS score INTERVENTIONS Consult IHP/ECP Allow student to rest, and then reassess Contact parent/guardian Return student to class or send home as indicated Reassess every 2 hours if student remains at school Follow-up as needed or per policy 180
184 LACERATIONS Apply direct pressure to the bleeding area with a sterile 2x2 gauze square for minutes. If swelling is present, apply a cold compress. If not severe: o Clean with soap and water. o Cover with sterile dressing. If the cut is deep or dirty: o Clean with soap and water. o Cover with sterile dressing. Notify parent and recommend evaluation for deep cleaning, sutures, and/or tetanus toxoid booster by primary healthcare provider. 181
185 LACERATIONS/ABRASIONS ASSESSMENT KEY ASSESSMENT POINTS FOR LACERATIONS AND ABRASIONS Inspection of wound Neurovascular assessment distal to injury: - Pain, pulse, pallor, paresthesia, paralysis, and poikilothermia (6 Ps mnemonic) - Capillary refill - Edema - Skin temperature DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Absent distal pulses Significant blood loss Crush injury Amputation (see Trauma protocol) Penetrating wound Capillary refill exceeds 2 seconds Altered LOC S/S of respiratory distress INTERVENTIONS Control hemorrhage Activate EMS Support C-ABCDE Elevate/immobilize extremity Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT Stable vital signs Pulses present distal to injury Significantly contaminated lacerations Facial lacerations Puncture wounds of foot Wounds requiring sutures Controllable bleeding INTERVENTIONS Support C-ABCDE Determine need for EMS Control bleeding with direct pressure Observe student closely Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Stable vital signs Superficial abrasion, scrape, or wound Small splinter or foreign body INTERVENTIONS Remove splinter or foreign body Cleanse wounds using aseptic technique (see below) Bandage wounds Observe student Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy 182
186 General wound care/aseptic cleansing Clean wounds thoroughly with soap Rub abrasions gently with 4 4 gauze to remove debris and crusts Rinse copiously with water Bandage abrasions loosely using nonadherent gauze to allow air circulation Apply butterfly bandage to lacerations after bleeding has been controlled Due to high risk of infection, all deep puncture wounds of the foot must be referred to a physician. How to control bleeding Controlling bleeding is a priority that initially involves direct pressure. Activate EMS for severe injuries that result in hemorrhage. Apply dressing and direct manual pressure to any hemorrhage Elevate area if possible Do not remove dressing; reinforce with additional gauze if needed Apply tourniquet or hemostatic dressing for hemorrhage not controlled by the above measures, if available and allowed by policy/protocol Note Refer student for tetanus booster if it has been 5 years or more since the last vaccination. Tetanus booster is recommended every 10 years. 183
187 MUSCULOSKELETAL INJURIES ASSESSMENT Stabilize c-spine if head/spinal injury is suspected! KEY ASSESSMENT POINTS FOR MUSCULOSKELETAL INJURIES Focused physical examination of affected area: Bilateral symmetry Range of motion (ROM)/strength Visual inspection for abnormalities Neurovascular status distal to injury: Pain, pulse, pallor, paresthesia, paralysis, and poikilothermia (6 Ps) Edema Capillary refill time Skin temperature IMMEDIATE INTERVENTIONS Even before you determine triage category, immobilize and support the affected area proximal and distal to the injury! DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Open fracture Amputation (see Trauma protocol) Degloving injury Neurovascular compromise Severe edema/deformity at joint or extremity Joint deviation Suspected femoral fracture INTERVENTIONS Activate EMS Support C-ABCDE Instruct student to avoid weightbearing/movement of injured area Immobilize and position suspected fractures/dislocations (see next ) Reassess neurovascular status distal to injury every 5 10 minutes Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT Stable vital signs Moderate deformity/discoloration without open wound Moderate edema at joint or extremity Moderate pain/guarding Normal neurovascular findings INTERVENTIONS Support C-ABCDE Determine need for EMS Immobilize and position suspected fracture/dislocation (see next ) Elevate extremity Apply cold packs Observe student closely Reassess neurovascular status distal to injury every 5 10 minutes Contact parent/guardian to transport student to medical care or home Follow-up NON-URGENT Normal vital signs No deformity Mild soft tissue edema Mild pain/point tenderness Able to bear weight Normal neurovascular findings INTERVENTIONS Apply cold pack Elevate area Observe student Contact parent/ guardian Return student to class or send home as indicated Follow-up as needed or per policy 184






188 INTERVENTIONS FOR MUSCULOSKELETAL INJURIES MANUAL CERVICAL SPINE STABILIZATION Position student supine Place both hands along lateral aspect of student s head Position the head so that the neck is in neutral alignment with the spine Continue to support the head to maintain neutral cervical alignment Correct method of simultaneous cervical spine stabilization during airway opening in the child with multiple injuries. IMMOBILIZATION/POSITIONING OF FRACTURES AND DISLOCATIONS Area/Injury Upper extremity Clavicular injury/shoulder dislocation Angulation with unimpaired circulation Angulation with absent distal pulse and/or cyanosis Treatment Apply sling/triangular bandage Swathe if additional immobilization is indicated Apply sling/triangular bandage Swathe if additional immobilization is indicated Immobilize as presented Do not move extremity Return extremity to proper physiological position Apply gentle traction until pulse is restored Splint or immobilize injured area and joints proximal and distal to injury Reassess pulses every 5 10 minutes SLING-AND-SWATHE IMMOBILIZATION Place the arm across the chest and position as shown. Bring the bandage over the arm and behind the neck. Adjust the length as necessary and tie the ends. The arm should be well supported and relieve pressure on the shoulder. Place the knot so that it lies over the shoulder rather than against the cervical spine. Placing a pad under the knot will enhance comfort. Secure the sling at the elbow with a safety pin or knot to create a pocket in which the elbow rests securely. Reassess neurovascular integrity. If further immobilization is needed to secure the extremity and a second bandage is available, swathe the arm as permitted by applicable protocols. Lay the second bandage flat, and then fold it several times lengthwise. Use the folded bandage to swathe the injured arm against the chest wall, which immobilizes the injured extremity. 185
189 NEAR-DROWNING/SUBMERSION CAUTION Ensure scene safety! Never attempt a water rescue unless you are trained to do so. ASSESSMENT KEY ASSESSMENT POINTS FOR SUBMERSION INJURIES Skin assessment Inspection for associated injuries Duration of exposure KEY FINDINGS Dyspnea, crackles, rhonchi, Altered LOC wheezing, or apnea Fixed, dilated pupils Bradycardia or asystole Hypothermia and cool skin Cyanosis or pallor DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS The triage category for ALL instances of near-drowning is EMERGENT! INTERVENTIONS Activate EMS EMS transport to ED for evaluation is REQUIRED in all cases of near-drowning! If still in water Do not remove student without assistance Keep student afloat face-up Support head and neck in neutral alignment with spine Open airway using the jaw-thrust technique and support ventilation When adequate assistance is available, place student supine on backboard or other rigid support for removal from water If out of water Support C-ABCDE (use jaw-thrust technique if spinal injury is suspected) Assess Pediatric Glasgow Coma Scale score Cover student and maintain warmth to prevent hypothermia In all cases Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up 186
190 Normal Vital Signs Pediatric Vital Signs by Age Age RR HR BP Neonate (birth-30 days) Infant (1-12 months) Toddler (1-3 years) Preschooler (3-5 years) School-aged (5-12 years) Adolescent (12 years and older)
191 NOSE EMERGENCIES ASSESSMENT Stabilize c-spine if head/spinal injury is suspected! KEY ASSESSMENT POINTS FOR EMERGENCIES INVOLVING THE NOSE Airway status Mechanism of injury/events preceding episode Physical assessment/ inspection for abnormalities, bleeding, and drainage IMMEDIATE INTERVENTIONS Even before you determine triage category, begin to control bleeding with pressure. DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT Suspected nasal fracture with potential head/neck injury (see Head/Spinal Cord protocol) Change in mental status or LOC Airway compromise Cerebrospinal fluid (CSF) drainage INTERVENTIONS Activate EMS Maintain spinal stabilization as applicable Support C-ABCDE Directly/continuously observe student Keep student calm Contact parent/ guardian Notify school administrator Follow-up Suspected nasal fracture, but no possibility of head/ neck injury Tenderness on palpation Epistaxis not controlled after 10 minutes Moderate periorbital edema INTERVENTIONS Determine need for EMS Prolonged epistaxis Have student blow their nose to remove clots Pinch nostrils closed and apply pressure for 10 minutes while student leans forward If epistaxis continues, consider activating EMS Suspected nasal fracture Apply cold packs See Lacerations/Abrasions protocol for treatment of associated wounds In all cases Observe student closely Contact parent/guardian to transport student to medical care or home Follow-up Foreign body Controllable epistaxis S/S of acute sinusitis:»» Pain/pressure over sinus areas»» Throbbing»» Headache, malaise, fever»» Mucopurulent secretions»» Mild periorbital edema INTERVENTIONS Epistaxis Have student blow their nose to remove clots Pinch nostrils closed and apply pressure for 10 minutes Foreign body Have student blow nose while occluding unobstructed nostril Attempt removal only if object is visible and can be grasped with forceps or fingers During extraction, occlude nostril superior to object so that it cannot be pushed further in If object cannot be removed, reclassify as urgent In all cases Observe student Contact parent/guardian for referral to primary care physician Return student to class or send home as indicated Follow-up as needed or per policy 188
192 Overdose If assessment findings suggest a toxic ingestion and you do not know what substance is involved, it may be helpful to look for signs of identifiable toxic syndromes (toxidromes). Toxidromes involve a recognizable group of signs and symptoms that tend to occur consistently with particular toxins. The following table describes the four major toxidromes and provides mnemonics that can help you remember the associated findings. Examples of substances that can cause each toxidrome are included. T ox i d r o m e s Toxidrome Clinical Findings Causative Substances Opioid Sympathomimetic Anticholinergic Listed phrases may help you recall clinical findings Constricted pupils CNS depression Respiratory depression Hypertension Tachycardia Hyperthermia Diaphoresis Dilated pupils Hyperthermia (hot as a hare) Flushed skin (red as a beet) Hypertension, dry skin (dry as a bone) Delirium (mad as a hatter) Dilated pupils (blind as a bat) Urinary retention (full as a flask) Tachycardia Absent bowel sounds Heroin Codeine Fentanyl Methadone Epinephrine OTC diet aids containing caffeine Amphetamines Oral decongestants (e.g., pseudoephedrine) Bronchodilators Antihistamines GI antispasmodics Certain toxic plants (e.g., jimson weed, deadly nightshade, atropine) Tricyclic antidepressants Diarrhea Urination Miosis, muscle fasciculations Organophosphate and Bradycardia, bronchorrhea Cholinergic carbamate insecticides Emesis Physostigmine Lacrimation Salivation, sweating Weakness CNS, central nervous system; OTC, over-the-counter; GI, gastrointestinal 189
193 POISONING Ingested (Poison Control Center # ) Identify suspected poison, how much was taken, and when it was taken. Call Poison Control immediately and follow instructions provided. Request immediate emergency medical services, if recommended by Poison Control Center. Send the suspected poison and vomitus (in container) with the person to the hospital emergency room. DO NOT give the person anything to drink unless directed to do so by the Poison Control Center or medical professional. POISON CONTROL
194 POISON CONTROL Assess/ensure scene safety (notify school administrator as indicated to activate hazmat protocols) Respiratory assessment Skin assessment LOC/neurological assessment, including PERRL Type/amount of substance (get container if available) Time/route of exposure (dermal, ocular, inhalation, or ingestion) ASSESSMENT KEY ASSESSMENT POINTS FOR TOXIC EXPOSURES Location where exposure occurred Subsequent S/S; respiratory status, LOC, and emesis Ability to recall event, including injuries incurred Underlying health problems (SAMPLE history) Focused physical assessment, including injury and/or odors Other students involved DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Respiratory arrest Seizures (see Seizures protocol) Loss of consciousness Dyspnea or severe respiratory distress Signs of shock/hypotension INTERVENTIONS Activate EMS Support C-ABCDE Initiate CPR as necessary Contact PCC a Refer for medical care as recommended by PCC Send material safety data sheet/ safety data sheet (MSDS/SDS) and substance (if possible) to ED with student Contact parent/guardian Notify school administrator Follow-up Refer to Toxidromes table (see next ) URGENT Unusual behavior History of emesis Minor abnormal findings INTERVENTIONS Determine need for EMS Contact PCC a Refer for medical care as recommended by PCC Consult MSDS/SDS Contact parent/guardian to transport student to medical care or home Notify school administrator Follow-up NON-URGENT Asymptomatic Stable vital signs INTERVENTIONS Observe student Consult MSDS/SDS Contact PCC a Refer for medical care as recommended by PCC Provide supportive care as indicated Contact parent/guardian Return student to class or send home as indicated Notify school administrator Follow-up as needed or per policy NOTE a When calling the Poison Control Center ( ), identify yourself as a healthcare professional and provide the following information: your name and phone number; student s name, age, weight, and vital signs; substance involved (if known); amount, time, route, and duration of exposure; abnormal signs and symptoms (S/S); first aid and immediate interventions rendered. 191
195 SCROTAL INJURY Provide privacy while determining extent of injury (a chaperone should be present during the assessment by the school nurse). Position ice pack so it elevates to the scrotum. Apply ice for 10 minutes. If symptoms (bleeding, redness, or pain more than 30 minutes) persist, refer for evaluation by primary healthcare provider (in the absence of external bleeding, internal bleeding may occur). Notify parent. 192
196 SEIZURES ASSESSMENT Stabilize c-spine if head/spinal injury is suspected! Open airway as necessary using the jaw-thrust maneuver. KEY ASSESSMENT POINTS FOR SEIZURES Past health history; particularly note: Events preceding episode, particularly head - Epilepsy injury - Syncope Indicators of drug overdose, meningitis, or hypoglycemia (see Substance Abuse and - Diabetes Diabetic Emergencies protocols) IMMEDIATE INTERVENTIONS During an active seizure, perform the following actions before you proceed with triage: Do not put anything in student s mouth do not restrict movement in any way Provide privacy Protect student from injury DETERMINE TRIAGE CATEGORY AND ADDITIONAL INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT URGENT NON-URGENT First-time seizure/no known history of seizures History of seizures and medication noncompliance with no recent seizures Seizure/series of seizures that persist for more than 5 minutes Associated respiratory compromise Associated head injury or trauma INTERVENTIONS Activate EMS Support C-ABCDE Consult IHP/ECP Directly/continuously observe student Provide psychological support Document time, characteristics, and duration of seizure Contact parent/guardian Notify school administrator Follow-up Atypical seizure in student with history of seizures INTERVENTIONS Support C-ABCDE Determine need for EMS Consult IHP/ECP Check glucose if possible Allow to rest in left lateral recovery position Provide psychological support Observe student closely Document characteristics and duration of seizure Contact parent/guardian to transport student to medical care or home Follow-up Typical seizure in student with baseline history of frequent seizures INTERVENTIONS Consult IHP/ECP Check blood glucose if possible Allow to rest in left lateral recovery position during postictal phase Provide psychological support Observe student Document characteristics and duration of seizure Contact parent/guardian as per policy Return student to class or send home as indicated For persistent drowsiness, notify parent/guardian to transport student home Follow-up as needed or per policy 193
197 SHOCK Restlessness or irritability, altered consciousness, pale, cool, moist skin, rapid breathing, rapid pulse Have person lie down. Control any external bleeding. Elevate legs approximately 12 inches EXCEPT when head, neck, or back injuries are suspected, or there is a possibility of broken bones involving the lower extremities, or if the elevation causes pain or respiratory distress. Cover person to maintain normal body temperature. Blood pressure and pulse checked by school nurse. Do not give fluids or anything to eat. Request immediate emergency medical services. Indicators of Hypoperfusion Sign Tachycardia Increased breathing rate Decreased level of consciousness Central pallor or cyanosis with cool skin Weak, thready, or absent peripheral pulses Delayed capillary refill time Bradycardia Hypotension Comment Early sign Early sign Worsening sign Worsening sign Deteriorating condition Deteriorating condition Late sign Late sign Pediatric Vital Signs by Age Age RR HR BP Neonate (birth-30 days) Infant (1-12 months) Toddler (1-3 years) Preschooler (3-5 years) School-aged (5-12 years) Adolescent (12 years and older)
198 SPLINTERS Wash area with soap and water. If easily accessible, protruding minor splinters may be removed. Use disinfected splinter forceps/tweezers to remove splinter. Wash area a second time and cover with a sterile dressing. If splinter imbedded, wash area, cover with sterile dressing. Notify parent and recommend evaluation by primary healthcare provider. 195

199 SPRAINS Rest injured part if ankle or knee, do not allow to walk. Apply ice pack for 20 minutes. Elevate injured part. If fracture suspected, immobilize injured part. Notify parent and recommend evaluation by primary healthcare provider. National Association of School Nurses Manual suggests: (pg 664) Rest of the injured area for 48 hours Ice placed on the injured area for 20 minutes at a time, 4 to 8 times per day Compression with elastic bandages, splints, or special appliances Check CSMs (circulation, sensation, and movement) every 15 minutes twice (x2) to make sure it is not too tight. Elevation of the injured body part 196
200 SYNCOPE/UNCONSCIOUSNESS ASSESSMENT Stabilize c-spine if head/spinal injury is suspected! Mental status/neurological assessment Psychosocial history Past health history/current menstrual status KEY ASSESSMENT POINTS FOR SYNCOPE Medications taken Events leading up to episode, including activities and weather conditions Last food/drink taken DETERMINE TRIAGE CATEGORY AND APPROPRIATE INTERVENTIONS Determine triage category and activate EMS AS SOON AS the need becomes apparent! EMERGENT Acute change from baseline mental status/loc Irregular pulse Acute neurological deficit Head injury/headache with altered LOC or vomiting Severe headache with altered LOC Head injury/history of anemia, hemophilia, or other coagulopathy Associated seizure activity (see Seizures protocol) INTERVENTIONS Activate EMS Maintain c-spine stabilization as applicable Support C-ABCDE Directly/continuously observe student Contact parent/guardian Notify school administrator Follow-up URGENT Possible ventriculoperitoneal (VP) shunt dysfunction S/S of moderate hypoglycemia Signs of dehydration Severe headache without altered LOC Persistent or severe dizziness Exercise-induced syncope (possible cardiac etiology) Possible medication reaction without emergent findings History of substance abuse or eating disorder INTERVENTIONS Support C-ABCDE as indicated Determine need for EMS Contact parent/guardian to transport student to medical care or home Closely observe student Follow-up NON-URGENT Hyperventilation Vasovagal reaction to anxiety/ pain or other known trigger Exposure to ambient heat Evidence of carotid sinus reaction (e.g., subsequent to neck hold by classmate) No associated injuries INTERVENTIONS Place student supine Allow student to wake spontaneously For hyperventilation, encourage student to relax Observe student Contact parent/guardian Return student to class or send home as indicated Follow-up as needed or per policy See the following protocols as appropriate: Diabetic Emergencies Increased intracranial pressure (ICP) in a Student With a VP Shunt Head/Spinal Cord Trauma Seizures Heat-Related Injuries Trauma Hemophilia 197
201 TICKS Grasp with fine-tipped tweezers as close to skin surface as possible and slowly pull upward. Do not use fingernail polish, alcohol, hot matches, or prick with a pin. After tick removal, clean the area thoroughly and cover with a sterile dressing. Save the tick in a sealed plastic bag for further evaluation by the health department (parents take tick to health department). Notify parent of tick removal. If tick was on the body for a prolonged time (24-48 hours), the student may need additional treatment with an antibiotic. If removal of tick is incomplete or unsuccessful, recommend evaluation by primary healthcare provider. Recheck bite within 3-7 days. 198

202 Chapter 9: Students with Special Needs 199
203 Resource Sites for Information Searches: AUTISM: CHILD ABUSE: IC Duty to Report Child Abuse or Neglect IC Duty to make report Sec.1. In addition to any other duty to report arising under this article, an individual who has reason to believe that a child is a victim of child abuse or neglect shall make a report as required by this article. (As added by P.L , SEC. 16.) IC Notification of individual in charge of institution, school, facility, or agency; report Sec. 2 (a) If an individual is required to make a report under this article in the individual s capacity as a member of the staff of a medical or other public or private institution, school, facility, or agency, the individual shall immediately notify the individual in charge of the institution, school, facility, or agency or the designated agent of the individual in charge of the institution, school, facility, or agency. (b) An individual notified under subsection (a) shall report or cause a report to be made. (As added by P.L , SEC. 16.) IC Effect of compliance on individual s own duty to report. Sec. 3 This chapter does not relieve an individual of the obligation to report on the individual s own behalf, unless a report has already been made to the best of the individual s belief. (As added by P.L , SEC.16.) IC Sec. 4. A person who has a duty under this chapter to report that a child may be a victim of child abuse or neglect shall immediately make an oral report to: (1) the department; or (2) the local law enforcement agency. (As added by P.L , SEC.16. Amended by P.L , SEC.107.) Additional Resources tabid/462/smid/824/articleid/639/default.aspx 200
204 CONCUSSIONS: Indiana Law (IC ) deals with the management of concussions for student athletes. Since this law was enacted in 2012, it has undergone almost yearly revisions. Below is a synopsis of the history of this law: 2012 o o 2013 o 2014 o o 2015 o 2016 o o o Required that high school students and their parents be given information sheets regarding the risks of concussions and that each sign an acknowledgement form Required that high school student athletes with a suspected concussion be removed from play and could not return to play until he/she received written clearance from a healthcare provider trained in the evaluation and management of concussions No changes Added a requirement that football coaches take a certification course regarding concussions, heat exhaustion, proper technique, and equipment fitting Required that high school student athletes with a suspected concussion be removed from play and were not allowed to return to play until at least 24 hours had passed Clarified that the football certification course applied to coaches of student athletes under the age of 20, but only those students who were in grades 1-12 Expanded the law to include, not only high school students, but also students in grades 5-8 regarding the information sheets and the return to play protocols Clarified that the law was mandatory for interscholastic sports and cheerleading, but although recommended, was optional for other sports such as club and intramural sports Requires coaches of all other interscholastic sports (excluding football) to take a concussion certification course beginning June 30, 2017 For the most up to date information, please refer to the following website which contains information regarding the law, guidance materials, sample forms and a list of the approved courses: in.gov/student-services/health/concussion-and-sudden-cardiac-arrest. DNR ORDERS: tabid/462/articleid/640/do-not-attempt-resuscitation-dnar-the-role-of-the-school-nurse-adopted- January-2014 EATING DISORDERS: 201
205 FAMILY CRISIS: Death Divorce Unemployment HOMELESS STUDENTS: MENTAL HEALTH ISSUES: tabid/462/articleid/36/mental-health-of-students-revised-june-2013 NON-VERBAL STUDENTS: PREGNANT STUDENTS: SPECIAL EDUCATION STUDENTS: SUBSTANCE ABUSE:
206 SUDDEN CARDIAC ARREST: Beginning July of 2015, Indiana passed a law (IC ) regarding the education of student athletes and their parents on the symptoms of sudden cardiac arrest and the removal of play for student athletes suspected of having symptoms of sudden cardiac arrest. The law states the following: Requires schools to distribute information sheets to student athletes and parents regarding the signs and symptoms of sudden cardiac arrest Requires that student athletes and their parents sign an acknowledgement form Requires that student athletes (under the age of 18) be removed from play, the parent must be notified and the student athlete cannot return to play until verbal permission from the parent has been obtained Requires that parent verbal permission be replaced with written permission from the parent within 24 hours For the most up to date information, please refer to the following website: This website has a link to the law, guidance materials in the form of a FAQ document, sample information sheets, sample acknowledgement form, and sample return to play forms. SUICIDE:
 Lifting Oxygen PICC Line Care (Central Line Care) Tracheostomy Care/Suctioning")
207 Chapter 10: Procedures Catheterizations Colostomy Care - Ostomy Management and Care Gastronomy Care/Feeding Tube (Enteral Tube Feeding) Lifting Oxygen PICC Line Care (Central Line Care) Tracheostomy Care/Suctioning 204
208 The following is a list of procedures commonly seen in the school setting. These are general guidelines and are not intended to take the place of individual provider orders for a specific student. CATHETERIZATIONS Catheterization: Clean Intermittent DEFINITION Clean intermittent catheterization is done with or for students who are either unable to completely empty their bladders or unable to void independently (AUA Foundation, 2011). PURPOSE 1. To allow students to completely empty their bladders on a periodic basis to prevent urinary tract infection or bladder leakage. 2. To assist students who do not have bladder control to empty their bladders on a periodic basis to prevent leakage. 3. The ultimate goal is for the student (if able physically and cognitively) to become independent in this procedure. EQUIPMENT -- Gloves -- Clean or sterile straight catheter -- Disposable wipes or soap and water -- Urinal or receptacle for urine (if procedure is not performed on the toilet) -- Water-based lubricant -- Disposable towel or Chux to place under the student if procedure is done on a cot PROCEDURE Male Catheterization 1. Wash hands. 2. Apply gloves. 3. Grasp sides of penis below the glans. 4. Clean the tip of the penis and urethra. 5. Retract foreskin if uncircumcised. 6. Gently stretch the penis upward. 7. Generously lubricate the catheter. 8. Have student take a deep breath. 9. Slowly insert the catheter until urine begins to flow and then about an inch more. 10. If you meet resistance before urine flows, have the student take another deep breath and continue with insertion (resistance in male catheterization is normal at about the level of the prostate). 11. If resistance continues or the student experiences pain, stop insertion. Never force the catheter. 12. When urine flow has stopped, pinch the catheter and remove it slowly when urine flow has stopped. 13. Measure urine per student s order. 14. Discard bodily fluids and catheter per infection control procedures and school district policy. 205
209 15. Remove gloves. 16. Wash hands. (American Academy of Pediatrics, Healthy Children, 2012). Female Catheterization 1. Wash hands. 2. Apply gloves. 3. Prepare equipment: Using clean techniques, open the urine catheterization package and lubricating jelly. 4. Place within easy reach. 5. Prepare the student. 6. Expose the urethral opening. 7. Clean the vulva and urethral opening from front to back, starting over the urethral meatus, then each side. 8. Continue to keep one hand in place, exposing the urethral opening. 9. Generously lubricate catheter. 10. Separate the labia minora to clearly see the urinary meatus. 11. Have the student take a deep breath. 12. Slowly insert the catheter until urine begins to flow, then advance about an inch more. 13. Pinch the catheter and remove it slowly when urine flow has stopped. 14. Measure urine per student s order. 15. Discard bodily fluids and catheter per infection control procedures and school district policy. 16. Remove gloves. 17. Wash hands. (American Academy of Pediatrics, Healthy Children, 2012). DELEGATION RECOMMENDATIONS This procedure may be performed by a school nurse (RN) or delegated to an appropriately trained staff member. Delegation is the transfer of the responsibility for the performance of a task from one individual to another while retaining accountability for the outcome. Delegation can only occur after the school nurse (RN) has utilized the fundamentals of the delegation process which includes assessment, supervision, accessibility, communication, feedback, and evaluation. An individual health plan is required for each student requiring medical procedures during the school day. More information regarding the delegation process can be found in Chapter 1 of this manual. SELECT NURSING CONSIDERATIONS -- Assess area for redness, breakdown, swelling, or discharge. -- Note change in urine color, clarity, or odor; report signs and symptoms of urinary tract infection. -- Never use non-water-soluble lubricant. -- Some students will use a new catheter each time, others will need to wash and reuse catheters. -- Follow healthcare provider s orders (such as frequency; strict measuring of output). 206
210 REFERENCES AUA Foundation. (2011). Bladder augmentation. Retrieved January 3, 2012, from Centers for Disease Control and Prevention. (2009). Guideline for Prevention of Catheter-Associated Urinary Tract Infections. Retrieved January 14, 2012, from evidencereview.html. American Academy of Pediatrics. (2012). Clean Intermittent Catheterization. Healthy Children. Catheterization.aspx. RESOURCES Centers for Disease Control and Prevention. (2009). Guideline for Prevention of Catheterassociated Urinary Tract Infections. Retrieved January 14, 2012, from cauti/008evidencereview.html. Bray, L., and Sanders, C. (2007). Teaching children and young people intermittent self-catheterization. Urologic Nursing, 27, 203-9, 242. Infectious Disease Association of America, American Hospital Association, Centers for Disease Control and Prevention, (n.d.). FAQs about catheter associated urinary tract infection. Retrieved January 14, 2012, from Catheterization Care: Indwelling DEFINITION An indwelling catheter is inserting into the bladder to provide urinary drainage over a period of time from hours to weeks. It is attached to a closed drainage system that must be emptied periodically (AUA Foundation, 2011). PURPOSE To empty the bladder of urine as it accumulates; to minimize residual urine; to decrease incidence of bladder infection; to control incontinence. EQUIPMENT -- Gloves -- Disposable washcloth -- Soap and water -- Graduated drainage container PROCEDURE In general, other than emptying the drainage bag into a container and measuring the output, the only care required for an indwelling catheter in school would be if the student were toileted for a bowel movement, the area around the urinary meatus would have to be cleansed if contaminated with feces. DELEGATION RECOMMENDATIONS This procedure may be performed by a school nurse (RN) or delegated to an appropriately trained staff member. Delegation is the transfer of the responsibility for the performance of a task from one individual to another while retaining accountability for the outcome. Delegation can only occur after the school nurse (RN) has utilized the fundamentals of the delegation process which includes 207
211 assessment, supervision, accessibility, communication, feedback, and evaluation. An individual health plan is required for each student requiring medical procedures during the school day. More information regarding the delegation process can be found in Chapter 1 of this manual. SELECT NURSING CONSIDERATIONS Most students with an indwelling catheter will not require care of it during the school day; however, the school nurse must be notified if there is evidence of infection; pain; skin breakdown; displacement or obstruction of the catheter; bleeding; or change in urine consistency, color, or odor. REFERENCES AUA Foundation. (2011). Managing bladder dysfunction with products and devices. Retrieved January 3, 2012, from Centers for Disease Control and Prevention. (2010). Catheter-associated urinary tract infections. Retrieved January 14, 2012, from Catheterization: Reinsertion of Indwelling Urinary Catheter DEFINITION Replacement of a dislodged indwelling urinary catheter. An indwelling urinary catheter is inserted into the bladder to provide urinary drainage over a period from hours to weeks. It is attached to a closed drainage system that must be emptied periodically (AUA Foundation, 2011). PURPOSE To maintain patency of the indwelling urinary catheter and to ensure emptying of the bladder of urine as it accumulates in order to: minimize residual urine; decrease incidence of bladder infection; and to control incontinence. DELEGATION RECOMMENDATIONS This procedure may be performed by a school nurse (RN) or delegated to an appropriately trained staff member. Delegation is the transfer of the responsibility for the performance of a task from one individual to another while retaining accountability for the outcome. Delegation can only occur after the school nurse (RN) has utilized the fundamentals of the delegation process which includes assessment, supervision, accessibility, communication, feedback, and evaluation. An individual health plan is required for each student requiring medical procedures during the school day. More information regarding the delegation process can be found in Chapter 1 of this manual. SELECT NURSING CONSIDERATIONS In particular circumstances, nursing assessment may indicate that reinsertion of the catheter requires physician evaluation, such as when displacement is traumatic (i.e., frank bleeding or swelling is present), or when reinsertion is difficult. It is recommended that the same size catheter be reinserted or as close a size as possible. If reinsertion is difficult or the decision is made not to replace the catheter, make sure the student is diapered or protected from soiling himself or herself or his or her clothing. REFERENCES 208
212 COLOSTOMY CARE OSTOMY MANAGEMENT AND CARE DEFINITION An ostomy is a surgically created opening through the skin to the intestine or urinary tract to provide for elimination of bodily wastes. Urinary stomas and colostomies usually drain into a bag (National Library of Medicine, 2011). PURPOSE To maintain continence; to keep the stoma and the surrounding skin in good condition; to encourage self-care as much as developmentally and physically possible; to facilitate acceptance of the student in school; to replace a bag that is leaking. EQUIPMENT -- Gloves -- Scissors -- Stoma wafer -- Disposable washcloth -- Gauze -- Ostomy bag -- Skin protectant or barrier PROCEDURE Management (emptying bag) 1. Empty or assist student to empty contents of bag into toilet. 2. Inspect skin around stomas for redness, rash, blistering, lesions, or bleeding and notify parent if observed. 3. Notify parent if there is any redness, rash, blistering, lesions, or bleeding. 4. Remind students to wash hands when procedure is completed. Care (changing appliance) 1. Carefully remove the used bag and skin barrier by pushing the skin away from the bag, instead of pulling the bag off the skin. 2. Inspect skin for redness, rash, blistering, lesions, or bleeding and notify parent if observed 3. Cut skin barrier to fit stoma. 4. Pat stoma dry with disposable washcloth, cover the stoma with moistened gauze while awaiting placement of bag. 5. Pat skin dry with disposable washcloth. 6. Apply skin protectant or barrier to skin around stoma. 7. Peel off backing from adhesive. 8. Center the new bag directly over the stoma. 9. Firmly press the bag to the skin barrier so there are no leaks or wrinkles. 10. Remind students to wash hands when procedure is completed. DELEGATION RECOMMENDATIONS 209
213 This procedure may be performed by a school nurse (RN) or delegated to an appropriately trained staff member. Delegation is the transfer of the responsibility for the performance of a task from one individual to another while retaining accountability for the outcome. Delegation can only occur after the school nurse (RN) has utilized the fundamentals of the delegation process which includes assessment, supervision, accessibility, communication, feedback, and evaluation. An individual health plan is required for each student requiring medical procedures during the school day. More information regarding the delegation process can be found in Chapter 1 of this manual. SELECT NURSING CONSIDERATIONS - Healthcare provider order and parent/guardian authorization is required. - Consider the developmental and physical limitations of student. - If the school nurse (RN) is unfamiliar with the procedure, training, and consultation for the school nurse (RN) may be provided by an ostomy-care nurse specialist. - Contact parent if irritation at or around the stoma, skin breakdown, increased or decreased ostomy output, vomiting, or pain is noted. REFERENCE National Library of Medicine. (2011). Ostomy. Retrieved January 19, 2012, from nlm.nih govmedlineplus/ostomy.html. GASTRONOMY CARE/FEEDING TUBE (Enteral Tube Feeding) DEFINITIONS Delivering a liquid nutrient formula directly to the stomach, duodenum, or jejunum. - Enteral nutrition: nutrition administered in the gastrointestinal tract. - Tube feeding: enteral nutrition delivered via a tube, catheter, or stoma. - Stoma: a stoma is a surgical bypass of a natural conduit. - Gastrostomy: a stoma that bypasses the upper digestive tract and directly enters the stomach. - Jejunostomy: surgical creation of an opening to the middle portion of the small intestine (jejunum), through the abdominal wall. (American Society for Parenteral and Enteral Nutrition, 2011). METHODS Bolus feeding is the administration of liquid into a feeding tube using gravity to determine the rate the liquid passes through the tube. The liquid is either poured into a 60 cc syringe or a tube-feeding bag and held (or hung) at a height above the stomach that allows for the most desirable and tolerated rate of administration, typically over minutes. Pushing the liquid in with the syringe is sometimes used to augment a bolus feeding (Altman GB, ed., 2003). Tube feeding pump is a mechanical device that uses a matching tube-feeding bag and tubing. A set rate to administer a set volume over a specific period of time is programmed into the pump. Pumps vary in size and battery power potential. Tube feedings using pumps can be continuous (i.e., 30 cc/hr.) or intermittent (i.e., 240 cc/hr.). Types of Feeding Tubes Feeding tubes are named using an abbreviation system that indicates the point where it enters the body and the point where it ends (and the liquid is infused). 210
214 1. NGT (Nasogastric Tube): These can either be inserted for each feeding or remain in place for a set period of time. 2. GT (Gastrostomy Tube): These are surgically inserted though the stomach wall, leaving one end accessible on the abdomen and the other in the stomach. The most common types used in children is the low-profile brand Mic-Key (also referred to as a button ). An extension tube is connected and locks in place when used for feedings, hydration, and medication. When not in use, this device caps off to remain relatively flush with the abdominal wall. 3. G-JT (Gastrojejunostomy Tube): Also surgically inserted through the stomach wall, entering the stomach, passing through the pylorus, and ending in the jejunal segment of the small intestines. These tubes are generally indicated for children who cannot tolerate food in their stomach. They may have a lumen that ends in the stomach and another lumen that ends in the jejunum, so the nurse needs to be clear if one lumen is for medication and the other is for feeding (it is helpful to label the two lumens). 4. JT (Jejunostomy Tube): Similar to the GT, except it is surgically inserted through the abdominal wall directly into the jejunal section of the small intestine (Rosewell Park Cancer Insitute, n.d.). PURPOSE To provide a safe method of feeding a student who cannot tolerate oral feeding or requires supplementation to oral feeding in order to ensure adequate nutritional intake. Also, to provide continuity with the healthcare plans that students follow at home. EQUIPMENT Per provider s order and individual healthcare plan. PROCEDURE Tube Feeding 1. Prepare formula or liquid to be administered (normally room temperature). 2. Ensure feeding tube is intact and in the correct anatomical position. 3. Prime the feeding tube to minimize the amount of excess enteral air. 4. Clamp or pinch-off feeding tube prior to opening to air (to avoid reflux of gastric contents out of tube). 5. Attach syringe and administer fluids. 6. Unclamp feeding tube. 7. Administer feeding as directed. 8. When feeding is complete, flush tube with prescribed amount of water. 9. Cap or disconnect tube as indicated. Medication Administration 1. Prepare medication prescribed. 2. If administering a pill or capsule, ensure that solid particles are adequately dissolved or mixed in water. 3. Clamp or pinch-off feeding tube prior to opening to air (to avoid reflux of gastric contents out of tube). 4. Attach syringe and administer medication. 5. Clamp or pinch-off feeding tube prior to disconnecting syringe in order to avoid reflux (and loss) of medication back out of the tube. 6. Flush with sufficient water to ensure that no medication is left in tube. 211
215 7. If administering medication immediately before tube feeding, tube feeding may be used to flush through the medication. DELEGATION RECOMMENDATIONS This procedure may be performed by a school nurse (RN) or delegated to an appropriately trained staff member. Delegation is the transfer of the responsibility for the performance of a task from one individual to another while retaining accountability for the outcome. Delegation can only occur after the school nurse (RN) has utilized the fundamentals of the delegation process which includes assessment, supervision, accessibility, communication, feedback, and evaluation. An individual health plan is required for each student requiring medical procedures during the school day. More information regarding the delegation process can be found in Chapter 1 of this manual. SELECT NURSING CONSIDERATIONS 1. Tube feedings in school require a procedure authorization order and plan signed by a prescribing healthcare provider and parent/guardian, including: the type of formula; amount; infusion type and rate; frequency of administration; and amount of water used to flush the tube. 2. The most significant risk with tube feedings is aspiration of liquid nutrition into the lungs. 3. Keys to preventing aspiration include: a. Ensuring tube placement is appropriate. b. Proper positioning. c. Monitoring during feedings: Stop feeding immediately for gagging, vomiting, coughing, change in skin color, or difficulty breathing. An immediate nursing assessment would then be indicated. 4. Additional considerations include: a. Any specific method for securing a feeding tube. b. Storage and preparation of the formula. c. Caring for the insertion site: Rashes tend to occur as a result of leaking around a GT stoma site. Management may include using a barrier ointment and frequent dry dressing application. Granulation tissue usually forms as a result of excess friction between the tube and the stoma site. Daily monitoring of the insertion site to ensure healthy skin integrity at the insertion site is essential. 5. Mic-Key tube considerations: a. Mic-Key tubes should be level with the skin, able to rotate 360 degrees, and use a water-filled balloon in the stomach side of the stoma to maintain it in place. b. The balloon is usually filled with 5 cc of sterile or distilled water and should routinely be checked once a week (at home), and more often if it appears loose or leaking (Kimberley Clarke, 2010). c. A balloon that is leaking and unable to hold water is an indication for Mic-Key tube replacement. d. A spare Mic-Key could be maintained at school, and if provider orders and instructions have been sent to the school, the nurse could be trained in inserting a new one if it falls out: 212
216 Prompt reinsertion of a Mic-Key tube is vital to maintain the opening of the stoma site. If the nurse is unable to reinsert the Mic-Key, prompt medical attention is indicated. Reinsertion procedures should be outlined in the IHP. 6. NGT insertion in school is a relatively unique procedure that goes beyond the scope of this manual. Specific procedures and training needs for the school nurse should be obtained on a case-by-case basis. Once an NGT is properly inserted, the procedural steps listed above for feeding and medications can be applied. 7. Medication and nutrition administered into the jejunum require careful consideration since bypassing the stomach can affect absorption rates and tolerance. ADDITIONAL RESOURCES Enteral Nutrition - MIC-KEY Care and Use Guide - English.pdf Jejunostomy Tube Feeding - REFERENCES Altman GB, ed. (2003). Feeding and medicating via a gastrostomy tube. Delmar s Fundamental and Advanced Nursing Skills, 2nd Ed. Albany, NY: Delmar Thomson Learning: gov/medlineplus/ency/patientinstructions/ htm. American Society for Parenteral and Enteral Nutrition. (2011). What is enteral nutrition? Retrieved January 17, 2012, from Bankhead R., Boullata J., Brantley S., Corkins M., Guenter P., Krenitsky J., Lyman B., Metheny N.A., Mueller C., Robbins S., Wessel J.(2009). Enteral nutrition administration. In: A.S.P.E.N. Enteral nutrition practice recommendations. JPEN Journal of Parenteral and Enteral Nutrition; 33, Retrieved June 20, 2016, from Bowden, V.R., and Greenberg, C.S. (2008). Pediatric Nursing Procedures, 2nd Ed. Philadelphia, PA: Lippincott Williams and Wilkins. Guenter, P. and Silkroski, M. (2001). Tube feeding: practical guidelines and nursing protocols. Gaitherberg, MD: Aspen Publications, Inc. Kimberley Clarke. (2010). MIC-KEY care and usage guide. Retrieved January 19, 2012, from National Institutes of Health. (2014). Medline Plus. Gastronomy feeding tube bolus. Retrieved May 16, 2016, from Rosewell Park Cancer Institute. (n.d.). Jejunostomy tube. Retrieved January 17, 2012, from Wilson, D. and Hockenberry, MJ. (2007). Wong s clinical manual of pediatric nursing, 7th Ed. Denver, CO: CV Mosby. 213
217 LIFTING Guidelines for Lifting Students Who are Non-ambulatory Only trained employees may lift a student. Training procedures are dictated by the individual needs of the student as noted in their IEP and/or by a healthcare provider s order. Generally, OTs and PTs can assist with training specific to the student. Universal Do s and Don ts of Lifting* - Do lock the wheelchair brakes whenever moving the student in or out of the wheelchair. - Do tell the student what you are going to do. - Do wear non-skid, low-heeled footwear, both staff members and student. Flip flops and/or other sandal type shoes are NOT appropriate. - Do keep feet apart for a wide base of support. - Do remember to unfasten all seat belts and harnesses. - Do bend at the hips and knees. - Do not bend forward at the hips while standing with the knees straight. - Any student who weighs over 40 lbs. requires an approved two-person lift procedure. Items to Consider When Lifting a Student - Staff must never attempt a lift from two sides or by grasping clothing instead of a student s legs or trunk. - Staff must never carry a student more than 5 feet. Rather staff should move chair, wheelchair, or equipment to the student. - Any other lifting procedure (mobility or behavior related) requires additional training from a therapist, nurse, behavioral consultant, or resource consultant. - Staff is not to lift or carry a student in his/her wheelchair. - Staff is trained and reminded to always use good body mechanics when lifting or carrying students. Good Body Mechanics - Do not bend forward. Keep back flat or arched inward. - Maintain a firm base of support by keeping your legs apart, with one foot forward when possible. - Bend at the knees and hips. Lift with your legs-let your legs do the work. - Hold students or objects close to your trunk. - Turn by moving your feet instead of twisting your back. - Dress appropriately-wear flat heeled shoes and clothes for freedom of movement. Procedure Description Two Person Lift - 1st individual lifts the upper half of the student s body from behind. - 2nd individual lifts the lower half of the student s body (thigh level) from in front or from the side. Procedure Description Floor to Wheelchair Two Person Lift* 1. The student is in a sitting position on the floor. The wheelchair is placed parallel to the student. The brakes are locked and the footrests are moved out of the way. The seat belt is unfastened and is hanging at the side of the chair, not in the seat. 214
218 2. The taller person squats behind the student, reaches under the student s arms and holds the student s forearms, which have been crossed, over his/her chest. Avoid injury to the child by lifting under the arms. 3. The other person squats beside the student and supports the child s legs, placing one hand under the thighs and the other hand under the lower legs, and flexes the legs in an approximation of the sitting position. 4. At the count of three, lifting the student slowly, staff stand erect using leg muscles, not back muscles (this avoids back injury to staff). The person supporting the student s legs will likely find holding the legs under the knees easiest. 5. Staff position the student over the seat and lower slowly until the student is seated on the chair. Staff position the student properly in the chair and replace the seat belt and other positioning harnesses/hardware. Note: the student s healthcare provider may give special instructions. Procedure Description Wheelchair to Bed/Table Two Person Lift* 1. Place the wheelchair parallel to the bed or table. The taller person stands behind the wheelchair, reaches under the student s arms and holds the student s forearms, which have been crossed over the chest. 2. The other person squats close to the student and places one hand high under the thighs while placing the other hand under the calves. 3. At the count of three, both persons slowly lift the student straight upward. 4. Both persons bring the student over the bed/table and lower slowly until the student is resting upon it. Note: the student s healthcare provider may give special instructions. (*)From Guidelines for the Health Care Management of School Children with Special Needs, Indiana Department of Education, Division of Special Education, Wheelchair Safety Procedures Students in wheelchairs must have their seat belts secured at all times at school and during school activities or functions. Only authorized staff should push students in wheelchairs. It is not advisable for other students to push wheelchairs except under direct staff supervision (e.g. emergencies). ONLY the wheelchair owner shall propel, ride, or sit in a student s wheelchair (whether manual or power). Taken from: South Bend Community School Corporation Special Education Services Guidelines for Lifting ( 215
219 OXYGEN DEFINITIONS Oxygen administration refers to a supplemental source of oxygen above the normal 21 percent oxygen concentration found in room air. Continuous oxygen: the student has a treatment order to be on a continuous source of supplemental oxygen that needs to be maintained throughout the school day and during transportation to and from school. Intermittent oxygen: the student has a treatment order to use a prescribed amount of PRN oxygen based on objective clinical assessment data (increased respiratory rate or increased respiratory effort). Emergency oxygen: requires a standing healthcare provider order to administer oxygen to any student under emergency medical situations (such as seizure activity or acute respiratory distress). PURPOSE Oxygen administration in school is indicated to treat either acute or chronic hypoxia as prescribed by a treatment procedure authorization. METHODS Nasal Cannula: Plastic tube that connects on one end to an oxygen source (tank) with the other end having two short prongs that each fit into the nostrils. Generally indicated as an option for planned use of continuous or intermittent oxygen. Mask: A plastic facemask with tubing connected to an oxygen source. The two main sizes of oxygen masks are pediatric and adult. They are generally indicated for emergency situations. Tracheostomy Mask: A plastic mask designed to fit over a tracheostomy cannula and secured by an elastic strap around the neck (over the tracheostomy ties). This may be indicated for planned use of continuous or intermittent oxygen. Mechanical Ventilation: A variety of portable mechanical ventilation devices may be used for children who attend school. They are attached to the student via a tracheostomy and may or may not involve the routine delivery of supplemental oxygen. Ambu Bag (Manual Resuscitation): In case of extreme medical emergency (i.e., severe oxygen desaturation, impending respiratory failure, or respiratory or cardiac arrest), oxygen can be delivered at full flow (>10 L/min.) with an Ambu Bag using an appropriately sized sealed face mask or fitted directly onto a tracheostomy cannula. For schools to stock and administer oxygen, a healthcare provider s standing order and a school policy must be in place. EQUIPMENT Per healthcare provider s order and IHP. PROCEDURE OXYGEN TANKS 1. Require a regulator that has: a. A valve to turn the oxygen source on and off. b. A flow meter to measure and adjust the flow of oxygen. c. A pressure gauge to determine the amount of oxygen remaining in the tank. 216
220 2. Open the tank by turning the valve at the top counterclockwise until the needle on the pressure gauge moves. 3. Set the flow meter to the prescribed rate (liters/minute) by turning the dial to the number or until the ball rises to the correct level on the scale. 4. If using a nasal cannula: a. Place prongs into nose so they follow the curve of the nostrils. b. Secure around back of ears. c. Adjust below the chin. 5. If using a face mask: a. Place mask over nose and mouth. b. Secure with elastic strap around the head and above the ears. c. The mask needs to fit comfortably, but firmly against the face: Any space between the mask and face dilutes the intended concentration of oxygen. For students unable to tolerate the elastic strap around their head, the mask can be held against the face without the strap (only appropriate for a limited period of time). 6. If using a tracheostomy mask: a. Follow the same procedure as a facemask, except cover the tracheostomy cannula with the mask and secure it around the neck. 7. If using an Ambu Bag: a. Turn oxygen flow rate > 10 L/min. b. Administer by either face mask or tracheostomy connection: Either option requires a tight seal to the airway. Rate and force of manual resuscitation breaths is determined by CPR-certified personnel. 8. To close the tank: a. Disconnect oxygen from the student. b. Turn valve clockwise until it cannot go any further. The flow meter should steadily decrease to zero, indicating that no oxygen is flowing (or leaking) from the tank (referred to as bleeding the tank off ). c. Turn the flow meter dial to zero. 9. Tank needs to be stored in a secured upright position to prevent it from falling or tipping over. 10. Storage area for oxygen tank must be free of petroleum products. DELEGATION RECOMMENDATIONS This procedure may be performed by a school nurse (RN) or delegated to an appropriately trained staff member. Delegation is the transfer of the responsibility for the performance of a task from one individual to another while retaining accountability for the outcome. Delegation can only occur after the school nurse (RN) has utilized the fundamentals of the delegation process which includes assessment, supervision, accessibility, communication, feedback, and evaluation. An individual health plan is required for each student requiring medical procedures during the school day. More information regarding the delegation process can be found in Chapter 1 of this manual. 217
221 SELECT NURSING CONSIDERATIONS 1. Oxygen may be drying to the airway mucosa. Humidification systems are often indicated with long-term or continuous use. 2. Skin assessments around tubing or elastic straps are indicated. 3. The presence of any source of supplemental oxygen must be designated per Oxygen in Use signs which should be posted at the entrance of all building sections, classrooms, or nursing offices. 4. Notify the fire department of oxygen use in school. 5. School custodian should know of oxygen location, safety, and fire department recommendations. 6. Oxygen supply vendor-contact information should be kept readily available and included in the IHP. 7. Any oxygen tank that is heard hissing or noted to be leaking needs to be replaced promptly. 8. Checking monthly to ensure that tanks have an adequate supply to use in an emergency situation is a reasonable option. 9. Emergency ( stock ) high-pressure oxygen tanks should not lose oxygen if they are not being used or if they were turned off properly. 10. Tanks noted to be less than half-full or expired should be refilled or replaced. 11. For students on long-term or PRN oxygen, backup oxygen source should be part of the IHP. Oxygen Safety Guidelines General safety guidelines No open flames, heaters, radiators near oxygen. No oil, grease, flammable material near oxygen. Do not cover the oxygen cylinder. Use only the flow meter setting as prescribed. Always check to make sure oxygen is coming out of the tube or mask. If oxygen is not felt : -- Check tubing fit. -- Check flow control knob to make sure it is directly on the oxygen setting. -- Check to make sure the oxygen unit is not empty. -- Check to make sure the cannula/tubing is not dirty or faulty- replace it if it is. Safety with liquid oxygen Liquid oxygen is chilled to 300 degrees. If you touch a frosted part, you might get a skin burn. If so, flush with cool water, and call the doctor. 218
222 Keep liquid oxygen upright at all times. It can spill if it falls on its side. If that occurs, open doors and windows to vent, call the school nurse. Indiana Law Applicable for Transportation of Students Using Oxygen 575 IAC Special requirements Authority: IC Affected: IC Sec. 11. (a) Any passenger seat that has a child safety seat or restraint system attached to it must: (1) have a reinforced frame; and (2) meet the requirements of FMVSS 208, 209, and 210. (b) The seat behind a seat that has a child restraint system that is secured using a portable seat mount (for example, cam wrap belt used for a safety vest, Star seat, ProTech seat) must be kept empty or occupied by a child who is also in a child safety restraint system. (c) All child safety seats or restraint systems used in a school bus must be secured to a bus seat in a manner prescribed and approved by the manufacturer and must meet safety specifications as follows: (1) A child below the grade of kindergarten must be transported in a child safety restraint system that meets all applicable Federal Motor Vehicle Safety Standards beginning January 1, (2) For any child below the grade of kindergarten, the use of a lap belt alone is not appropriate. (d) Lap boards attached to wheelchairs or to adaptive equipment shall be removed and secured separately during transport. (e) All respiratory related equipment, such as oxygen, aspirators, and ventilators, must be securely mounted or fastened to a wheelchair, bus seat, bus floor, or to the bus wall below the window line during transit. (f) Tanks of compressed oxygen transported in a school bus may be no larger than twenty-two (22) cubic feet. (g) Any liquid oxygen container transported in a school bus may be no larger than thirty-eight (38) cubic feet. (h) Oxygen tanks must have valves and regulators that are protected against breakage. Tanks must be secured to avoid exposure to intense heat, flames, sparks, or friction. (i) A bus transporting any oxygen container must display a warning statement formatted in blockstyle letters not less than two (2) inches and not more than four (4) inches in height and in a color that contrasts with the color of its background that reads OXYGEN IN USE. The statement may be formatted in decal, paint, or magnetic material and be located: (1) in the service door entrance on the face of the riser; (2) on the underneath side of a wheelchair platform; and (3) on the ceiling above the window section of a passenger s seating position. (State School Bus Committee; 575 IAC ; filed May 24, 1990, 4:20 p.m.: 13 IR 1859; filed May 21, 1992, 5:00 p.m.: 15 IR 2222; readopted filed Oct 10, 2001, 3:37 p.m.: 25 IR 938; readopted filed Jun 19, 2007, 10:10 a.m.: IR RFA; errata filed Jul 6, 2007, 10:04 a.m.: IR ACA; readopted filed Nov 12, 2013, 11:21 a.m.: IR RFA; filed Aug 15, 2014, 10:20 a.m.: IR FRA; errata filed Sep 18, 2014, 10:40 a.m.: I 219
223 REFERENCE Bowden, V.R., and Greenberg, C.S. (2008). Pediatric Nursing Procedures, 2 nd edition. Philadelphia, PA: Lippincott Williams and Wilkins. PICC LINE CARE (Peripherally Inserted Central Catheter) DEFINITION A central line is a catheter most frequently placed through the chest wall into the right atrial chamber of the heart or a large central blood vessel. Central lines are placed internally (implanted), such as portacaths, or externally such as Hickman catheters. In school, central line care should be limited to ensuring that the dressing is occlusive and intact when applicable, intervening in an emergency, or care required to access the line for medication administration or nutrient administration. This procedure may include dressing reinforcement and/or heparin or saline flush. PURPOSE Long-term access to the circulatory system for medications, fluids, and nutrients. EQUIPMENT -- Gloves -- Antiseptic wipes/swabs -- Heparin or saline if ordered -- Appropriate size needle and syringe -- Sterile gauze -- Tape -- An emergency kit containing wipes, injection cap, heparin flushing supplies, dressing change supplies, and an extra clamp should be available at all times PROCEDURE General guidelines for flushing or administering medications through a central line 1. Clean the injection cap for 30 seconds using an appropriate (chlorhexidine, povidone iodine, alcohol) wipe; allow to air dry. 2. Using the appropriate flush solution or medication, draw up the solution as ordered. 3. Inject the flush or medication. 4. Flush line if ordered following administration of medication (Mannheim, J.K., 2010). General guidelines for changing cap on central line 1. Set up a clean work surface. 2. Gather all the supplies. 3. Wash your hands for 15 seconds with liquid antibacterial soap. Dry your hands thoroughly using paper towels. 4. Make sure that the central venous catheter (CVC) lumens are clamped. 5. Remove the new cap from its package. 6. Loosen, but do not remove, the cover on the end of the new cap. 7. While holding onto the lumen of the CVC with one hand, use the other hand to: a. Remove the old cap and set it aside. 220
224 b. Remove the cover from the new cap. c. Screw the new cap onto the open end of the lumen. This requires doing a lot with only one hand, but it is important to hold onto the lumen of the CVC to keep it from hanging free and touching anything. d. Repeat these steps for each of the lumens. e. Follow your routine to change caps in the same order as flushing. Note: Specific provider orders must be followed for each student, including orders regarding accidental removal of line or any restrictions needed for student safety. DELEGATION RECOMMENDATIONS Must be performed by a trained registered nurse. SELECT NURSING CONSIDERATIONS Flushing or administering medications via a central line requires specialized nursing education. Contact an area hospital or other healthcare groups for training, as necessary. School nurses may need to provide central line care if a student is experiencing symptoms of infection, the catheter is dislodged, or if a student is experiencing shortness of breath or chest pain. Monitoring and ongoing assessments of the central line dressing and site are essential nursing care in a school environment. ADDITIONAL RESOURCE PICC Line Care - V6TLraLGpj8 REFERENCE Mannheim, J.K. (2010). Central venous catheter - flushing. Retrieved January 14, 2012, from TRACHEOSTOMY CARE/SUCTIONING DEFINITIONS Tracheostomy is a surgical opening creating a stoma through the neck into the trachea where a tracheostomy tube can be inserted. Tracheostomy ( trach ) tube is a plastic (most common) or metal tube inserted through the tracheostomy stoma that provides a fixed airway to accommodate breathing while bypassing the upper airway. This tube can be used with or without mechanical ventilation or supplemental oxygen, but generally requires at least some means of humidification. There are a variety of tracheostomy tube brands; the most common are Shiley and Bivona. Most pediatric trach tubes consist of a single cannula. If the tube has two cannulas, the inner cannula can be removed for cleaning while the outer cannula stays in place. Obturator is a small plastic device used as a guide during the insertion of the tracheostomy tube. Ambu bag (manual ventilation bag) is a device used to manually instill air into the airway. A universal 15 mm adaptor allows it to fit directly onto the trach tube so that each squeeze of the bag correlates 221
225 with a breath. A facemask can also be fitted onto the bag to instill air via the mouth in the event that the tracheostomy tube is occluded or not functioning. Decannulization is the intentional or accidental removal of the trach tube out of the trachea. Passy-Muir Valve is a one-way valve that fits directly onto a trach tube, allowing air to be inspired through the trach tube, and forcing the exhaled air through the vocal cords and out of the mouth to facilitate vocalization and speech. PURPOSE There are two broad medical indications for a tracheostomy: 1. An acquired or congenital anatomic defect in the upper airway. 2. An inability to maintain adequate respiratory function due to chronic intrapulmonary or extrapulmonary (neuromuscular or metabolic) disease. Nurses must understand the underlying etiology of the need for each student who has a tracheostomy. A student with a tracheostomy is at risk for life-threatening complications that can be avoided with accurate physical assessment and diligent care of the airway. Proper care of a tracheostomy includes adequate skin care around the stoma and ensures the maintenance of the student s airway. EQUIPMENT The essential equipment to be kept with the student at all times is as follows: - Gloves - Portable oxygen with appropriate sized Ambu bag - Appropriate size Ambu bag facemask (for emergencies when unable to reinsert a new tracheostomy tube) - Portable suction machine that can operate with battery or electricity - Sterile suction catheters - Sterile saline vials - Water-based lubricant - Two spare tracheostomy tubes one the size the student currently uses and one that is a size smaller in the event that the tube needs to be changed and there is difficulty passing it through the stoma - Spare tracheostomy ties - Blunt scissors - Personal protective equipment to be used for all tracheostomy procedures - Emergency phone numbers - Pulse oximeter may be optional if student is not on oxygen or mechanical ventilation It is recommended that this equipment be stored together in an emergency travel bag that is easily transported with the student during transportation and the entire school day. Additional equipment may be indicated per the IHP. PROCEDURES Stoma and Skin Care 1. The frequency of stoma care and the care of the surrounding skin is based on the individual 222
226 student s current skin condition and associated factors, such as the amount of secretions and the degree of skin folds around the neck. 2. Ensure all essential equipment or travel bag is within reach prior to initiating stoma and skin care. 3. Use gauze sponges and cotton-tipped swabs with water or a diluted peroxide solution per IHP: a. Cleanse outer portion of tracheostomy tube and surrounding skin going from using wet to dry sponges or swabs. b. Minimize direct moisture to the tracheostomy ties. c. Drying the skin is vital to maintaining skin integrity. Changing tracheostomy ties 1. The two most common forms of tracheostomy ties are a soft-padded tie with Velcro tabs (most common) or a simple thin cloth or twill tie that requires tying to secure. 2. Changing tracheostomy ties in the school setting is usually not done on a routine basis, rather it is an, as-needed (PRN) procedure based on the integrity of the ties, the skin, or as part of an emergency tracheostomy change. 3. Two people should be present during the procedure in the event of accidental decannulization. 4. A shoulder roll is recommended to assist with the visualization and access to the tracheostomy site. 5. Remove the old ties while holding the tracheostomy tube in place: a. Use caution not to occlude the tracheostomy tube. b. Removal of cloth ties requires the use of a blunt scissor. c. Removal of Velcro tab ties is done by detaching each end of the tie. 6. Skin care is performed as indicated. 7. Maintaining the tracheostomy tube in place is always the priority: a. Insert one end of the tie through the slit opening on the side of the tracheostomy tube. b. Bring the other end of the tie around the back of the neck. c. Repeat with the other end of the tie through the slit opening on the other side of the tracheostomy tube. d. Velcro tabs are fastened back on themselves. e. Cloth ties are secured using a single square knot on the side or back of the neck. f. The ties should allow enough space for fingers between it and the neck. 8. If a split gauze is used around the stoma, replace it now with a clean one. 9. Re-assess the student s respiratory status to ensure that the tracheostomy tube remained in place and patent during procedure. Cleaning an Inner Cannula 1. Remove the inner cannula as indicated per manufacturer s instructions. 2. The inner cannula is generally cleansed with a half-strength hydrogen peroxide solution using pipe cleaners to remove any dried secretions from inside the cannula. 3. Thoroughly rinse the cannula with sterile water and dry. 4. Reinsert the inner cannula by turning it 90 degrees from its usual position, introduce the tip into the outer cannula, slowly rotating it back 90 degrees to its final position. 5. Lock the cannula in place per manufacturer s instructions. 223
227 Tracheostomy Tube Suctioning Suctioning is performed based on clinical assessment with consideration of individual student factors and considerations. Many students can cough out their secretions through their tracheostomy tubes without the need for suctioning (this maneuver is synonymous with blowing their nose ). 1. As with all invasive procedures, carefully consider an appropriate and safe location based on degree of urgency and physical design of the school, student s classroom, and the health office. 2. Confirm that respiratory assessment requires the suctioning procedure. 3. Emergency travel bag (essential equipment listed above) must be present before suctioning. 4. Ensure the suction machine has the appropriate level of subatmospheric pressure: a. Standard maximal pressure for children ranges from mm Hg. b. Maximal pressure may be determined by turning on suction and occluding extension tubing by folding it in half. Pressure reading on the gauge when the tubing is completely occluded is the maximal suction pressure. 5. The option of using a sterile catheter should be determined per treatment procedure authorization and IHP. 6. Positioning of the student is based on the clinical situation: a. Students in wheelchairs or other supportive seating devices can remain sitting upright or reclined up to, but not exceeding, semi-fowlers of 45 degrees. b. Students who are lying either on the floor or health office couch should be turned on their side (this position may be commonly associated with a student experiencing a seizure who may require supplemental oxygen and/or suctioning). 7. The respiratory assessment should be an ongoing process to determine: a. How well the student is tolerating the procedure. b. The amount of time and suction attempts that are clinically indicated. 8. Determine the length of catheter insertion: a. It should be limited to just beyond the distal end of the tracheostomy tube. b. Deep suctioning up to or beyond the tracheal carina (point of bronchial bifurcation and tissue resistance) should not be indicated in a school setting, as it may cause epithelial damage. 9. Hold the suction catheter at the point of maximal insertion length. 10. Lubricate the catheter with normal saline. 11. The use of normal saline to lavage the tracheostomy tube is based on the IHP and, if indicated, to assist with the removal of thick secretions, should be used judiciously. 12. Remove tracheostomy mask or ventilator connection and promptly insert catheter while gently rotating within the cannula. Do not apply suction during catheter insertion. 13. At point of maximal insertion, apply suction while gently rotating the catheter out of the cannula. a. Tracheal suction should not exceed five seconds. b. If secretions are visible at the onset of suctioning, an initial shallow pass may be appropriate before proceeding further down the cannula. 14. Rinse the catheter and repeat as indicated based on the clinical assessment and treatment 224
228 order. 15. Provide hyperventilation with Ambu bag, if indicated. 16. Rinse suction catheter and extension tubing. (Ireton, J., 2007; Cincinnati Children s Hospital, 2009) Tracheostomy Tube Change The changing of a tracheostomy tube in the school setting should be considered an emergency situation based on clinical assessment and the student s history. Any concern that the situation is potentially life-threatening requires the activation of the EMS/911 system while the procedure is being performed. If there are complications during the procedure, the nurse must have an understanding of the student s underlying need for the tracheostomy and ability to breathe without one. The nurse must be prepared to take control of the situation by acting swiftly, calmly, and clearly. The two most common emergency scenarios are: Accidental decannulization Tracheostomy tube obstruction unrelieved by reasonable suction attempts. Obstruction can be caused by thick secretions/mucus plugging, foreign body, or airway granuloma tissue. Airway granuloma tissue can persist to obstruct a new tracheostomy tube, resulting in the highest degree of medical emergency. 1. Ensure the emergency travel bag is present. 2. Ensure the presence of another responsible adult, preferably another nurse if available. 3. If not already done, attach Ambu bag to oxygen with gauge set at > 10 L/min. 4. If able, position the student supine on the floor with a shoulder roll to gently hyperextend the neck. 5. Open the new tracheostomy tube that is the same size as is currently in the student. Have the size smaller new tracheostomy tube readily available if needed. Taking care to not touch the curved part of the tracheostomy tube: a. be sure the obturator is in the tube; b. attach one end of the tracheostomy tie to a slot on the side of the tracheostomy tube; c. lubricate the distal end of the new tracheostomy tube with water-based lubricant; and d. return it to the clean package that it was sealed in. 6. Remove or cut old tracheostomy ties. 7. If possible, have assistant hold old tracheostomy tube in place: a. most students will not have cuffed tracheostomy tubes (with a balloon); and b. if this student does, deflate the cuff at this time per manufacturer s instructions. 8. With one hand remove the old tracheostomy tube and set it out of the way. 9. Gently and quickly insert the new tracheostomy tube, pushing back and then down, in an arching motion: a. if unable to insert the new tracheostomy tube, attempt the same procedure using the new tracheostomy that is one size smaller; and b. if still unable to insert a new tracheostomy tube, use the Ambu bag with facemask as indicated to maintain a stable airway while awaiting the emergency 225
229 medical system (EMS). 10. Once inserted, immediately remove the obturator (if used). 11. Have assistant continue to hold new tracheostomy in place. 12. Since this procedure done in school would most likely be an emergency situation, provide the student with manual breaths using the Ambu Bag and oxygen while auscultating the lungs to confirm adequate and symmetrical air movement. 13. Continue the respiratory assessment, using pulse oximetry if available to confirm a return to the student s baseline status. 14. Secure the new tracheostomy tube in place by fastening the tracheostomy ties. 15. If this is a cuffed tracheostomy tube, inflate at this time per manufacturer s instructions. 16. Position the student comfortably and observe to ensure he or she remains stable on their baseline level of supplemental or ventilator support (if any). 17. If EMS was activated, the RN in charge can determine, in collaboration with the family and healthcare provider if necessary, if transportation to the local emergency room is still indicated. 18. Regardless of outcome, notify family and medical provider that student required a tracheostomy change procedure. (Cincinnati Children s Hospital, 2011) DELEGATION RECOMMENDATIONS This procedure may be performed by a school nurse (RN) or delegated to an appropriately trained staff member. Delegation is the transfer of the responsibility for the performance of a task from one individual to another while retaining accountability for the outcome. Delegation can only occur after the school nurse (RN) has utilized the fundamentals of the delegation process which includes assessment, supervision, accessibility, communication, feedback, and evaluation. An individual health plan is required for each student requiring medical procedures during the school day. More information regarding the delegation process can be found in Chapter 1 of this manual. SELECT NURSING CONSIDERATIONS -- Maintaining adequate hydration is essential to minimize thick and crusting secretions. -- Do not permit the use of powders, aerosols, or any small airborne particles around the student, especially if the tracheostomy tube is not covered with a ventilator, filter, or Passy-Muir valve. -- If foreign material is aspirated into the tracheostomy tube, attempt to suction prior to giving breaths with an Ambu bag. -- Potential complications related to suctioning are bronchospasm and bleeding, which generally occur as a result of excessive suctioning or insertion of catheter past the distal end of the tracheostomy tube. -- Comprehensive oral hygiene is required for a student with a tracheostomy. -- Water activities must be carefully considered and supervised. -- The emergency travel bag should be inspected daily to ensure all used essential supplies have been replaced and are present. -- Gauze used around the tracheostomy tube should be pre-split, not cut, to prevent threads from entering the airway. ADDITIONAL RESOURCE Tracheal Suction Guidelines
230 REFERENCES Bowden, V.R., and Greenberg, C.S. (2008). Pediatric Nursing Procedures, 2nd edition. Philadelphia, PA: Lippincott Williams and Wilkins. Cincinnati Children s Hospital. (2009). Suctioning. Retrieved January 19, 2012, from cincinnatichildrens.org/workarea/linkit.aspx?linkidentifier=id&itemid=88058&libid= Cincinnati Children s Hospital. (2011). Basic Pediatric Tracheostomy Care. Retrieved January 19, 2012, from 57&libID=87745 Connecticut State Department of Education. (n.d.) Clinical Procedure Guidelines for Connecticut School Nurses. Retrieved May 15, 2016, from clinical_guidelines/clinical_guidelines.pdf Ireton, J. (2007). Tracheostomy suction: A protocol for practice. Pediatric Nursing, 19(10), Passy-Muir Inc. (2003). Passy-Muir Tracheostomy and Ventilator Speaking Valve Resource Guide. Retrieved May 15, 2016, from resource_guide.pdf 227


231 Chapter 11: Professional Development SECTION 1: DIABETES COURSE MODULE SECTION 2: EMERGENCY COURSE MOODLE 228
232 The Indiana Department of Education offers various school personnel a resource for online courses applicable to their training and educational needs. This site is password protected requiring a one-time account set-up and the chosen password which are used for all courses attended thereafter. Additional courses are added to site as they are developed and announced via the Indiana Department of Education s Learning Connection. Courses developed by the Indiana Department of Education for school personnel are located on the Moodle website located at: One may navigate to courses for school nurses via the Indiana Department of Education Health Services located at: and select Online Courses for School Nurses. Login and course directions are found on this. School Nurse Courses developed by the Indiana Department of Education: Care of Students with Diabetes EMSC School Nurse Emergency Care Course SECTION 1: DIABETES COURSE MODULE Step-by step instructions for course participation are presented at the start of this course. The enrollment key for this course is: diabetes 2000 The Indiana Department of Education, in conjunction with diabetes experts, has developed this online training course for school nurses to assist in the care of students with diabetes. The course contains 9 different modules. These modules consist of the following topics: 1. Indiana Code : Understanding the Law and IHP s 2. Nutrition in the School Setting 3. Helping Your Students Make Better Food Choices 4. Meters and Pen Overview 5. Pumps in the School Setting 6. Managing Hyperglycemia and Hypoglycemia 7. Scenarios in the School Setting 8. Care of Student with Diabetes Three Quizzes 9. Additional Training Resources At the end of this course, there are three quizzes to substantiate competency. Each quiz counts towards one s final grade. The quizzes are 10 questions each and are divided into three topics. These topics include: The Diabetic Law and IHP s, Out of Range and Emergency Care, and Daily Management and Care. In order to successfully complete and receive credit and a professional growth certificate for this course, one must achieve a 100% mastery on all quizzes. These quizzes may be taken as many times as needed and each time that one logs in to take a quiz, random questions in a random order are generated. 229
233 For an additional update regarding current technology and new diabetes trends, please see the DOE Health Web for the link to the webinar entitled Care of Student with Diabetes Updates, Fall of By successfully completing the original diabetes course at least once, as well watching the above webinar outlining updates in the care of students with diabetes, school nurses (RN s) have met the requirements of Indiana Code This combined program serves as the minimum requirement of the law and school nurses are encouraged to seek further education as they feel appropriate. SECTION 2: EMERGENCY COURSE MOODLE EMSC School Nurse Emergency Care Course Step-by step instructions for course participation are presented at the start of this course. The enrollment key for this course is: emergency 2015 The Indiana Department of Education, in conjunction with the Indiana Emergency Medical Services for Children, has developed this training course to assist school nurses in their preparedness for possible health emergencies. This course is designed to pair the online training modules with a hands-on full day of trainee participation which focuses on learned and practiced skills with attending professionals. This live training is designed to support the content of the online module training. The course contains 8 online modules consisting of the following topics: 1. The School Nurse Role in Emergency Care 2. Legal Issues in Nursing 3. Assessment and Triage 4. Medical Emergencies 5. Abdominal and Genitourinary Emergencies 6. EENT and Dental Emergencies 7. Emergencies Involving Mental or Behavioral Health 8. School Emergency Response and Crisis Management After viewing all of the training modules, a comprehensive test consisting of 24 total questions is presented to the trainee to substantiate competency. A passing score of at least 90% is required in order for successful completion of the online portion of this course. Unlimited attempts at passing these quizzes are offered to the trainee with random questions in random order presented with each attempt. After a passing score has been registered at the DOE, a certificate of completion is sent to the trainee awarding professional growth points and registration information for the hands-on participation portion of this course. Upon completion of the hands-on training day, the trainee will receive another certificate of completion awarding additional professional growth points from the Indiana Department of Education. 230

234 Chapter 12: Training School Nurses are often asked to train school staff on important health topics during the school year. Two of the most frequent topics include: Hand Washing Hand Washing Links: Universal Precautions and Blood-Borne Pathogens Blood-Borne Pathogens/ Universal Precautions Links: Other Training for Volunteer Health Aides Regarding the Care of Students with Diabetes: 231
235 Chapter 13: Resources Centers for Disease Control and Prevention (CDC) Covering Kids and Families of Indiana (CKF) Children and Hoosier Immunization Registry Program (CHIRP) Communicable Disease Reference Guide for Schools 2015 Edition (IDOH) July28_2015docx--ppedits.pdf Indiana Department of Education (IDOE) IDOE Crucial Websites for School Nurses (pdf) Indiana Department of Education- School Health Page (IDOE) Indiana Department of Health (IDOH) Indiana Association of School Nurses (ISAN) Learning Connection (IDOE) Instructions for joining the Learning Connection: Instructions for Joining the Learning Connection (pdf) National Association of School Nurses (NASN) Student Records Retention Schedule-Indiana Student Assistance Sites and Clinics -Learning Connection (IDOE) Log In> Contacts and Communities> My Communities> School Nurses> Files and Bookmarks> Resources>State Resource List, Statewide Resource list 232
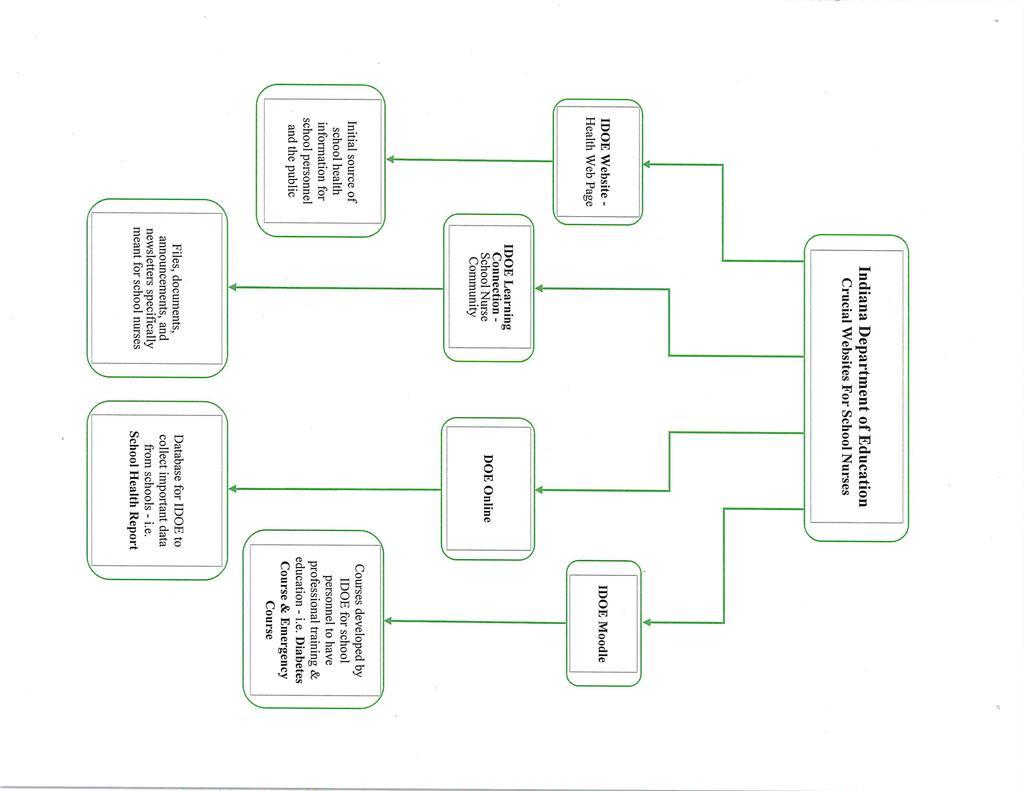
236 233

237 Instructions, Tips & FAQs How to Log Into the Learning Connection and Register 1. Log into 2. Select Educators tab 3. Click Learning Connection 4. Click on Register box in the upper right hand corner of 5. User Type Page a. Click Educator b. Click No registration code c. Click Continue 6. User Information Page: Enter Information About Yourself a. Complete all fields (*SPN-may leave blank) b. Click Register c. FAQs: o Q: Do I need a *SPN to register on the Learning Connection A: No, you may leave this space blank (otherwise, check with school s IT department) o Q: Why do I need to provide my D.O.B. and the last 4 digits of my social security number A: This information is only used to match you in the Learning Connection s system 7. A confirmation will be sent to your Inbox. When received, click on the link to verify your account 8. Read and Complete Confirm -Accept Terms of Agreement 9. Learning Connection: Welcome a. Enter Username and Password b. Click Log In 10. You re now a member of the Learning Connection...you re almost done! Important: How to Join the IDOE School Nurse Community (p.2) 234
Guidance on Delegation for Colorado School Nurses & Child Care Consultants
 School district s responsibility for the student with special health needs All students attending public schools must have access to health care during the school day and for extracurricular school activities,
School district s responsibility for the student with special health needs All students attending public schools must have access to health care during the school day and for extracurricular school activities,
CHAPTER 13 RULES AND REGULATIONS REGARDING THE DELEGATION OF NURSING TASKS
 CHAPTER 13 RULES AND REGULATIONS REGARDING THE DELEGATION OF NURSING TASKS 1. STATEMENT AND BASIS OF PURPOSE The rules contained in this Chapter are adopted pursuant to authority granted the Board by section
CHAPTER 13 RULES AND REGULATIONS REGARDING THE DELEGATION OF NURSING TASKS 1. STATEMENT AND BASIS OF PURPOSE The rules contained in this Chapter are adopted pursuant to authority granted the Board by section
AN OVERVIEW OF THE NEWLY REVISED GUIDELINES FOR MEDICATION ADMINISTRATION IN KANSAS SCHOOLS, JUNE 2017
 AN OVERVIEW OF THE NEWLY REVISED GUIDELINES FOR MEDICATION ADMINISTRATION IN KANSAS SCHOOLS, JUNE 2017 A COLLABORATIVE EFFORT OF LICENSED PROFESSIONAL REGISTERED NURSES FROM SCHOOL DISTRICTS AND PUBLIC
AN OVERVIEW OF THE NEWLY REVISED GUIDELINES FOR MEDICATION ADMINISTRATION IN KANSAS SCHOOLS, JUNE 2017 A COLLABORATIVE EFFORT OF LICENSED PROFESSIONAL REGISTERED NURSES FROM SCHOOL DISTRICTS AND PUBLIC
CHAPTER 3 SCOPE AND STANDARDS OF NURSING PRACTICE AND CNA ROLE. Statement of Purpose. These Board Rules are adopted to implement the
 CHAPTER 3 SCOPE AND STANDARDS OF NURSING PRACTICE AND CNA ROLE. Section 1. Board s authority to: Statement of Purpose. These Board Rules are adopted to implement the the CNA; Regulate the scope and practice
CHAPTER 3 SCOPE AND STANDARDS OF NURSING PRACTICE AND CNA ROLE. Section 1. Board s authority to: Statement of Purpose. These Board Rules are adopted to implement the the CNA; Regulate the scope and practice
Students with Special Health Care Needs Medically Fragile Children
 Students with Special Health Care Needs Medically Fragile Children A. Regulations As used in this chapter unless the context requires otherwise: 1) Children with disabilities means those school-age children
Students with Special Health Care Needs Medically Fragile Children A. Regulations As used in this chapter unless the context requires otherwise: 1) Children with disabilities means those school-age children
ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS
 Nursing Chapter 610-X-7 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS 610-X-7-.01 610-X-7-.02 610-X-7-.03 610-X-7-.04 610-X-7-.05
Nursing Chapter 610-X-7 ALABAMA BOARD OF NURSING ADMINISTRATIVE CODE CHAPTER 610-X-7 STANDARDS OF NURSING PRACTICE; SPECIFIC SETTINGS TABLE OF CONTENTS 610-X-7-.01 610-X-7-.02 610-X-7-.03 610-X-7-.04 610-X-7-.05
Students Controlled drugs means those drugs as defined in Conn. Gen. Stat. Section 21a-240.
 Students 5143 ADMINISTRATION OF STUDENT MEDICATIONS IN THE SCHOOLS A. Definitions Administration of medication means any one of the following activities: handling, storing, preparing or pouring of medication;
Students 5143 ADMINISTRATION OF STUDENT MEDICATIONS IN THE SCHOOLS A. Definitions Administration of medication means any one of the following activities: handling, storing, preparing or pouring of medication;
Ohio Nurse Practice Act (1 Hour) Standards of Safe Nursing Practice
 Standards of Safe Nursing Practice") Continuing Education (CEU) course for healthcare professionals. View the course online at wildirismedicaleducation.com for accreditation/approval information, course availability and other details, and
Continuing Education (CEU) course for healthcare professionals. View the course online at wildirismedicaleducation.com for accreditation/approval information, course availability and other details, and
Advisory Opinion 52 1
 ADVISORY OPINION # 52 Formulated: May 19, 2006 Revised: May 2013 Reviewed: July 2007 Question: Is it within the role and scope of a registered nurse (RN) or licensed practical nurse (LPN) practicing in
ADVISORY OPINION # 52 Formulated: May 19, 2006 Revised: May 2013 Reviewed: July 2007 Question: Is it within the role and scope of a registered nurse (RN) or licensed practical nurse (LPN) practicing in
"Diabetes management and treatment plan" defined.
 Indiana Statutes Title 20 Education Article 34 Student Health And Safety Measures Chapter 5 Care of Students With Diabetes Burns Ind. Code Ann. 20-34-5 (2008) 20-34-5-1. "Diabetes management and treatment
Indiana Statutes Title 20 Education Article 34 Student Health And Safety Measures Chapter 5 Care of Students With Diabetes Burns Ind. Code Ann. 20-34-5 (2008) 20-34-5-1. "Diabetes management and treatment
Role of the School Nurse: Did you know?
 Role of the School Nurse: Did you know? Sherry Marbury, RN, MSN, CCRC State School Nurse Consultant Alabama Department of Education 50 North Ripley Street, GPB 5227 Montgomery, AL 36130-2101 Phone: 334-242-8174
Role of the School Nurse: Did you know? Sherry Marbury, RN, MSN, CCRC State School Nurse Consultant Alabama Department of Education 50 North Ripley Street, GPB 5227 Montgomery, AL 36130-2101 Phone: 334-242-8174
Delegation in Assisted Living. Prepared for: Wisconsin Health Care Association
 Delegation in Assisted Living Prepared for: Wisconsin Health Care Association Summary and Objectives Those who manage people and tasks cannot manage everything themselves. Because of the pressure to reduce
Delegation in Assisted Living Prepared for: Wisconsin Health Care Association Summary and Objectives Those who manage people and tasks cannot manage everything themselves. Because of the pressure to reduce
Guidelines on Medication Administration for School Personnel
 2017 Guidelines on Medication Administration for School Personnel ACKNOWLEDGMENTS Utah Department of Health Environment, Policy, and Improved Clinical Care (EPICC) Utah School Nurse Consultant Elizabeth
2017 Guidelines on Medication Administration for School Personnel ACKNOWLEDGMENTS Utah Department of Health Environment, Policy, and Improved Clinical Care (EPICC) Utah School Nurse Consultant Elizabeth
2. Short term prescription medication and drugs (administered for less than two weeks):
:") Medication Administration Procedure This is a companion document with Policy # 516 Student Medication To access the policy: click on Policies (under the District Information heading) The Licensed School
Medication Administration Procedure This is a companion document with Policy # 516 Student Medication To access the policy: click on Policies (under the District Information heading) The Licensed School
ASSISTING STUDENTS WITH MEDICATIONS AND THEIR HEALTHCARE NEEDS
 Administrative Rule ASSISTING STUDENTS WITH MEDICATIONS AND THEIR HEALTHCARE NEEDS Code JLCD-R Issued 10/07 The needs of children who require medication during school hours to maintain and support presence
Administrative Rule ASSISTING STUDENTS WITH MEDICATIONS AND THEIR HEALTHCARE NEEDS Code JLCD-R Issued 10/07 The needs of children who require medication during school hours to maintain and support presence
Policy Title: Administration of Medication by School Personnel Policy No:
 Policy Title: Administration of Medication by School Personnel Policy No: 504.14 The Board of Trustees recognizes that students attending schools in St. Maries Joint School District No. 41 may be required
Policy Title: Administration of Medication by School Personnel Policy No: 504.14 The Board of Trustees recognizes that students attending schools in St. Maries Joint School District No. 41 may be required
Wyoming State Board of Nursing
 Wyoming State Board of Nursing CNAII Training and Competency Evaluation Course Curriculum OVERALL OBJECTIVE: For the Wyoming State Board of Nursing to establish curriculum standards for Level II Certified
Wyoming State Board of Nursing CNAII Training and Competency Evaluation Course Curriculum OVERALL OBJECTIVE: For the Wyoming State Board of Nursing to establish curriculum standards for Level II Certified
TENNESSEE CODE ANNOTATED 2008 by The State of Tennessee Title 49 Education Chapter 5 Personnel Part 4 --Employment and Assignment of Personnel
 TENNESSEE CODE ANNOTATED 2008 by The State of Tennessee Title 49 Education Chapter 5 Personnel Part 4 --Employment and Assignment of Personnel Tenn. Code Ann. 49-5-415 (2008) 49-5-415. Assistance in self-administration
TENNESSEE CODE ANNOTATED 2008 by The State of Tennessee Title 49 Education Chapter 5 Personnel Part 4 --Employment and Assignment of Personnel Tenn. Code Ann. 49-5-415 (2008) 49-5-415. Assistance in self-administration
STUDENTS Any school employee authorized in writing by the school administrator or school principal:
 Fremont School District No. 215 STUDENTS 3510 Student Medicines Assistance in Self Administration of Medicines to Students Any school employee authorized in writing by the school administrator or school
Fremont School District No. 215 STUDENTS 3510 Student Medicines Assistance in Self Administration of Medicines to Students Any school employee authorized in writing by the school administrator or school
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SKILLED NURSING SERVICES
 DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
DEMONSTRATED NEED FOR SKILLED CARE FOR MEDICARE PATIENTS: SCOPE: All Ascension At Home, LLC colleagues. For purposes of this policy, all references to colleague or colleagues include temporary, part-time
SUBJECT: Policy for Administration of Medications Permitting the Delegation of Nursing Tasks and the Giving or Applying of Medications.
 Carroll County Board of MRDD Policy Reference: Administration of Medications Permitting the Delegation of Nursing Tasks and the Giving or Applying of Medications Ohio Administration Code Reference: OAC
Carroll County Board of MRDD Policy Reference: Administration of Medications Permitting the Delegation of Nursing Tasks and the Giving or Applying of Medications Ohio Administration Code Reference: OAC
4.35 STUDENT MEDICATIONS
 4.35 STUDENT MEDICATIONS General Authority of School Nurses Regarding Student Medications School nurses are not permitted to diagnose medical conditions or prescribe medications, including over-thecounter
4.35 STUDENT MEDICATIONS General Authority of School Nurses Regarding Student Medications School nurses are not permitted to diagnose medical conditions or prescribe medications, including over-thecounter
STUDENTS 3416 page 1 of 4 Administering Medicines to Students
 0 1 0 1 Livingston School District STUDENTS page 1 of Administering Medicines to Students Medication means prescribed drugs and medical devices that are controlled by the U.S. Food and Drug Administration
0 1 0 1 Livingston School District STUDENTS page 1 of Administering Medicines to Students Medication means prescribed drugs and medical devices that are controlled by the U.S. Food and Drug Administration
The nurse delegating the activity is directly responsible for the nursing care given to the patient, and the final decision as to what nursing
 5.1 Detail how the state Nurse Practice Act, other regulatory stipulations (e.g., Staffing ratios mandated in California), and professional standards influence the care delivery model(s). At Massachusetts
5.1 Detail how the state Nurse Practice Act, other regulatory stipulations (e.g., Staffing ratios mandated in California), and professional standards influence the care delivery model(s). At Massachusetts
Based on the comprehensive assessment of a resident, the facility must ensure that:
 7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
7. QUALITY OF CARE Each resident must receive, and the facility must provide, the necessary care and services to attain or maintain the highest practicable physical, mental and psychosocial wellbeing,
Adopted: August 26, 2002 MSBA/MASA Model Policy 516 Orig Revised: February 26, 2018 Rev STUDENT MEDICATION
 Adopted: August 26, 2002 MSBA/MASA Model Policy 516 Orig. 1995 Revised: February 26, 2018 Rev. 2001 516 STUDENT MEDICATION [Note: The necessary provisions for complying with Minn. Stat. 121A.22, Administration
Adopted: August 26, 2002 MSBA/MASA Model Policy 516 Orig. 1995 Revised: February 26, 2018 Rev. 2001 516 STUDENT MEDICATION [Note: The necessary provisions for complying with Minn. Stat. 121A.22, Administration
Skills/Experience Checklist Home Health Registered Nurse
 This form is a self-assessment of your current skills and abilities. This form is also used to document skill demonstration. EMPLOYEE PROFILE Last Name First Name Middle Initial Employee Number Direct
This form is a self-assessment of your current skills and abilities. This form is also used to document skill demonstration. EMPLOYEE PROFILE Last Name First Name Middle Initial Employee Number Direct
NEBO SCHOOL DISTRICT BOARD OF EDUCATION POLICIES AND PROCEDURES
 NEBO SCHOOL DISTRICT BOARD OF EDUCATION POLICIES AND PROCEDURES J - Students Administering Medication to Students JHCD DATED: August 8, 2018 SECTION: POLICY TITLE: FILE NO.: TABLE OF CONTENTS 1. PURPOSE
NEBO SCHOOL DISTRICT BOARD OF EDUCATION POLICIES AND PROCEDURES J - Students Administering Medication to Students JHCD DATED: August 8, 2018 SECTION: POLICY TITLE: FILE NO.: TABLE OF CONTENTS 1. PURPOSE
Medication Administration
 Delegating Medication Administration to Licensed Nursing Assistants Gina Balkus HCANH Private Duty Directors Meeting March 8, 2017 HB 484 Expanded the Scope of Practice for LNAs in New Hampshire HB 484,
Delegating Medication Administration to Licensed Nursing Assistants Gina Balkus HCANH Private Duty Directors Meeting March 8, 2017 HB 484 Expanded the Scope of Practice for LNAs in New Hampshire HB 484,
Adopted: MSBA/MASA Model Policy 516 Orig Revised: Brd. Approved Rev. 2013
 Adopted: MSBA/MASA Model Policy 516 Orig. 1995 Revised: Brd. Approved 3.13.14 Rev. 2013 516 STUDENT MEDICATION [Note: The necessary provisions for complying with Minn. Stat. 121A.22, Administration of
Adopted: MSBA/MASA Model Policy 516 Orig. 1995 Revised: Brd. Approved 3.13.14 Rev. 2013 516 STUDENT MEDICATION [Note: The necessary provisions for complying with Minn. Stat. 121A.22, Administration of
RULES AND REGULATIONS OF THE MAINE STATE BOARD OF NURSING CHAPTER 4
 RULES AND REGULATIONS OF THE MAINE STATE BOARD OF NURSING CHAPTER 4 AS AMENDED 2015 The RULES AND REGULATIONS OF THE MAINE STATE BOARD OF NURSING are adopted and amended as authorized by Title 32, Maine
RULES AND REGULATIONS OF THE MAINE STATE BOARD OF NURSING CHAPTER 4 AS AMENDED 2015 The RULES AND REGULATIONS OF THE MAINE STATE BOARD OF NURSING are adopted and amended as authorized by Title 32, Maine
E: Nursing Practice. Alberta Licensed Practical Nurses Competency Profile 51
 E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
E: Nursing Practice Alberta Licensed Practical Nurses Competency Profile 51 Competency: E-1 Critical Thinking E-1-1 E-1-2 E-1-3 Demonstrate knowledge and ability to apply critical thinking concepts throughout
MIAMI DADE COLLEGE MEDICAL CAMPUS BENJAMIN LEON SCHOOL OF NURSING RN-BSN PROGRAM MANUAL OF CLINICAL PERFORMANCE
 MIAMI DADE COLLEGE MEDICAL CAMPUS BENJAMIN LEON SCHOOL OF NURSING RN-BSN PROGRAM MANUAL OF CLINICAL PERFORMANCE 1 INTRODUCTION Welcome to Miami Dade College Bachelor of Science in Nursing Program. The
MIAMI DADE COLLEGE MEDICAL CAMPUS BENJAMIN LEON SCHOOL OF NURSING RN-BSN PROGRAM MANUAL OF CLINICAL PERFORMANCE 1 INTRODUCTION Welcome to Miami Dade College Bachelor of Science in Nursing Program. The
1.1 To provide guidelines for medication administration to students while at school.
 Windsor-Essex Catholic District School Board NUMBER: Pr ST: 11 Section: Students PROCEDURE Pr ST: 11 Student Health Support (Including Medication Administration at School) EFFECTIVE: Oct. 26, 1999 AMENDED:
Windsor-Essex Catholic District School Board NUMBER: Pr ST: 11 Section: Students PROCEDURE Pr ST: 11 Student Health Support (Including Medication Administration at School) EFFECTIVE: Oct. 26, 1999 AMENDED:
DATE ISSUED: 10/2/ of 5 UPDATE 103 FFAF(LEGAL)-P
-P") Diabetes Management and Treatment Plan Required Elements Submission to School Individualized Health Plan Independent Monitoring and Treatment The parent or guardian of a student who will seek care for
Diabetes Management and Treatment Plan Required Elements Submission to School Individualized Health Plan Independent Monitoring and Treatment The parent or guardian of a student who will seek care for
ASSISTING STUDENTS WITH MEDICATIONS
 Administrative Rule ASSISTING STUDENTS WITH Code JLCD-R Issued DRAFT/17 The needs of children who require medication during school hours to maintain and support their presence in school will be met in
Administrative Rule ASSISTING STUDENTS WITH Code JLCD-R Issued DRAFT/17 The needs of children who require medication during school hours to maintain and support their presence in school will be met in
ADMINISTRATIVE PROCEDURES
 Batch #4, Redline Edits SHELTON SCHOOL DISTRICT ADMINISTRATIVE PROCEDURES Policy No. 3416P Series 3000 (Students) Page 1 of 8 PROCEDURE - MEDICATION AT SCHOOL Under normal circumstances prescribed or oral
Batch #4, Redline Edits SHELTON SCHOOL DISTRICT ADMINISTRATIVE PROCEDURES Policy No. 3416P Series 3000 (Students) Page 1 of 8 PROCEDURE - MEDICATION AT SCHOOL Under normal circumstances prescribed or oral
ADMINISTRATION OF MEDICATION BY DELEGATION
 ADMINISTRATION OF MEDICATION BY DELEGATION ROLE AND RESPONSIBILITY OF THE TEACHER TRAINING MANUAL Medication Training Manual Final 10-2-17 Page 1 of 17 MEDICATION ADMINISTRATION TRAINING OBJECTIVES UPON
ADMINISTRATION OF MEDICATION BY DELEGATION ROLE AND RESPONSIBILITY OF THE TEACHER TRAINING MANUAL Medication Training Manual Final 10-2-17 Page 1 of 17 MEDICATION ADMINISTRATION TRAINING OBJECTIVES UPON
Nursing Services for the Individual Options Waiver. Donna Patterson, RN Medicaid Development and Administration
 Nursing Services for the Individual Options Waiver Donna Patterson, RN Medicaid Development and Administration Waiver Nursing Services Services provided to an individual that require the skill of an RN
Nursing Services for the Individual Options Waiver Donna Patterson, RN Medicaid Development and Administration Waiver Nursing Services Services provided to an individual that require the skill of an RN
ASSISTING STUDENTS WITH MEDICATIONS
 Administrative Rule ASSISTING STUDENTS WITH Code JLCD-R Issued 10/06 The needs of children who require medication during school hours to maintain and support their presence in school will be met in a safe
Administrative Rule ASSISTING STUDENTS WITH Code JLCD-R Issued 10/06 The needs of children who require medication during school hours to maintain and support their presence in school will be met in a safe
RN Delegation ALF & RCF
 RN Delegation ALF & RCF Raeann J Voorhies RN, MBA, AL-C & Heather Madden RN, AL-C VOORHIES AND ASSOCIATES SENIOR LIVING MANAGEMENT AND CONSULTING OUTLINE Definitions- Delegation Definition- Unlicensed
RN Delegation ALF & RCF Raeann J Voorhies RN, MBA, AL-C & Heather Madden RN, AL-C VOORHIES AND ASSOCIATES SENIOR LIVING MANAGEMENT AND CONSULTING OUTLINE Definitions- Delegation Definition- Unlicensed
2. Unlicensed assistive personnel: any personnel to whom nursing tasks are delegated and who work in settings with structured nursing organizations.
 XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
XVIII. A. General Information: The judgments that you make in about coordinating and facilitating client care situations have to be based on knowledge. You MUST know your content, and then you can move
Staff Model for the Delivery of School Health Services
 Staff Model for the Delivery of School Health Services Washington State Nursing Care Quality Assurance Commission Washington State Office of Superintendent of Public Instruction Dr. Terry Bergeson State
Staff Model for the Delivery of School Health Services Washington State Nursing Care Quality Assurance Commission Washington State Office of Superintendent of Public Instruction Dr. Terry Bergeson State
Subject: Skilled Nursing Facilities (Page 1 of 6)
") Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Subject: Skilled Nursing Facilities (Page 1 of 6) Objective: I. To ensure that Tuality Health Alliance (THA) and delegated Providence Health Plan Medicare members are appropriately placed in skilled nursing
Policy/Program Memorandum No. 161
 Ministry of Education Policy/Program No. 161 Date of Issue: February 28, 2018 Effective: September 1, 2018 Subject: Application: SUPPORTING CHILDREN AND STUDENTS WITH PREVALENT MEDICAL CONDITIONS (ANAPHYLAXIS,
Ministry of Education Policy/Program No. 161 Date of Issue: February 28, 2018 Effective: September 1, 2018 Subject: Application: SUPPORTING CHILDREN AND STUDENTS WITH PREVALENT MEDICAL CONDITIONS (ANAPHYLAXIS,
Clinical Transition Practicum Packet General Information Policies and Procedures Preceptor and Nursing Student Forms
 Clinical Transition Practicum Packet General Information Policies and Procedures Preceptor and Nursing Student Forms Fall 2014 1 Description The McLennan Community College Clinical Transition Practicum
Clinical Transition Practicum Packet General Information Policies and Procedures Preceptor and Nursing Student Forms Fall 2014 1 Description The McLennan Community College Clinical Transition Practicum
CHAPTER 7 CERTIFIED NURSING ASSISTANTS
 CHAPTER 7 CERTIFIED NURSING ASSISTANTS Section 1. Authority (a) These rules and regulations are promulgated by the Wyoming State Board of Nursing pursuant to its authority under W.S. 33-21-119 thru 33-21-156
CHAPTER 7 CERTIFIED NURSING ASSISTANTS Section 1. Authority (a) These rules and regulations are promulgated by the Wyoming State Board of Nursing pursuant to its authority under W.S. 33-21-119 thru 33-21-156
5. returning the medication container to proper secured storage; and
 111-8-63-.20 Medications. (1) Self-Administration of Medications. Residents who have the cognitive and functional capacities to engage in the self-administration of medications safely and independently
111-8-63-.20 Medications. (1) Self-Administration of Medications. Residents who have the cognitive and functional capacities to engage in the self-administration of medications safely and independently
Standards for Community-Based Care Registered Nurse Delegation
 Division 47 Standards for Community-Based Care Registered Nurse Delegation 851-047-0000 Rule Summary, Statement of Purpose and Intent These rules provide standards and guidance for nurses to delegate specific
Division 47 Standards for Community-Based Care Registered Nurse Delegation 851-047-0000 Rule Summary, Statement of Purpose and Intent These rules provide standards and guidance for nurses to delegate specific
a. Principles of administration including budgeting, accounting, records management, organization, personnel, and business management.
 DEPARTMENT OR REGULATORY AGENCIES State Board of Examiners of Nursing Home Administrators RULES AND REGULATIONS FOR NURSING HOME ADMINISTRATORS 3 CCR 717-1 RULE 1. LICENSING EXAMINATION 1. All applicants
DEPARTMENT OR REGULATORY AGENCIES State Board of Examiners of Nursing Home Administrators RULES AND REGULATIONS FOR NURSING HOME ADMINISTRATORS 3 CCR 717-1 RULE 1. LICENSING EXAMINATION 1. All applicants
DATE ISSUED: 9/30/ of 7 UPDATE 103 FFAC(LEGAL)-P
-P") CONSENT TO FORM OF CONSENT MINOR S CONSENT TO TREATMENT The school in which a minor student is enrolled may consent to medical, dental, psychological, and surgical treatment of that student, provided all
CONSENT TO FORM OF CONSENT MINOR S CONSENT TO TREATMENT The school in which a minor student is enrolled may consent to medical, dental, psychological, and surgical treatment of that student, provided all
PATIENT RIGHTS TO ACCESS PERSONAL MEDICAL RECORDS California Health & Safety Code Section
 PATIENT RIGHTS TO ACCESS PERSONAL MEDICAL RECORDS California Health & Safety Code Section 123100-123149. 123100. The Legislature finds and declares that every person having ultimate responsibility for
PATIENT RIGHTS TO ACCESS PERSONAL MEDICAL RECORDS California Health & Safety Code Section 123100-123149. 123100. The Legislature finds and declares that every person having ultimate responsibility for
Kechi Iheduru-Anderson DNP-c, MSN, RN, CWCN. December 2013
 Kechi Iheduru-Anderson DNP-c, MSN, RN, CWCN. December 2013 As a nurse in the united states you will encounter a variety of different types of caregivers. You may work with unlicensed assistive personnel
Kechi Iheduru-Anderson DNP-c, MSN, RN, CWCN. December 2013 As a nurse in the united states you will encounter a variety of different types of caregivers. You may work with unlicensed assistive personnel
Corporate Medical Policy
 Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: skilled_nursing_services 07/2001 2/2018 2/2019 2/2018 Description of Procedure or Service Skilled Nursing
Corporate Medical Policy File Name: Origination: Last CAP Review: Next CAP Review: Last Review: skilled_nursing_services 07/2001 2/2018 2/2019 2/2018 Description of Procedure or Service Skilled Nursing
POLICY TITLE: Administering Medications POLICY NO: 561 PAGE 1 of 5 MEDICATIONS
 POLICY TITLE: Administering Medications POLICY NO: 561 PAGE 1 of 5 MEDICATIONS The Board of Trustees of the Mountain Home School District recognizes that students attending the schools in this district
POLICY TITLE: Administering Medications POLICY NO: 561 PAGE 1 of 5 MEDICATIONS The Board of Trustees of the Mountain Home School District recognizes that students attending the schools in this district
Patient s Bill of Rights (Revised April 2012)
") Patient s Bill of Rights (Revised April 2012) TIRR Memorial Hermann recognizes the rights of human beings for independence of expression, decision, and action and will protect these rights of all patients,
Patient s Bill of Rights (Revised April 2012) TIRR Memorial Hermann recognizes the rights of human beings for independence of expression, decision, and action and will protect these rights of all patients,
Mandatory Reporting: Child Abuse and Neglect in Indian Country
 Mandatory Reporting: Child Abuse and Neglect in Indian Country Mandatory reporting requires that anyone with knowledge that a minor/child is being harmed or may be harmed must inform the legal authorities.
Mandatory Reporting: Child Abuse and Neglect in Indian Country Mandatory reporting requires that anyone with knowledge that a minor/child is being harmed or may be harmed must inform the legal authorities.
Omak School District Administrative Procedure Page 1 of 6
 Administrative Procedure Page 1 of 6 STUDENTS Parent Designated Adult for Diabetic Student ACCOMMODATING STUDENTS WITH DIABETES If parents choose they may designate an adult through proper legal procedures
Administrative Procedure Page 1 of 6 STUDENTS Parent Designated Adult for Diabetic Student ACCOMMODATING STUDENTS WITH DIABETES If parents choose they may designate an adult through proper legal procedures
The First National Survey of Medication Aides
 The First National Survey of Medication Aides Jill Budden, PhD May 24, 2012 Background Goal to provide insights into Med Aide: Work setting Training Supervision Work role Help regulators make decisions
The First National Survey of Medication Aides Jill Budden, PhD May 24, 2012 Background Goal to provide insights into Med Aide: Work setting Training Supervision Work role Help regulators make decisions
Certified Advanced Alcohol & Drug Counselor (CAADC) Appendix B. Code of Ethical Standards
 Appendix B. Code of Ethical Standards") Certified Advanced Alcohol & Drug Counselor (CAADC) Appendix B Code of Ethical Standards Michigan Certification Board for Addiction Professionals Certified Advanced Alcohol & Drug Counselor (CAADC) Code
Certified Advanced Alcohol & Drug Counselor (CAADC) Appendix B Code of Ethical Standards Michigan Certification Board for Addiction Professionals Certified Advanced Alcohol & Drug Counselor (CAADC) Code
PERSONAL CARE WORKER (PCW) - Job Description
 - Job Description") PERSONAL CARE WORKER (PCW) - Job Description Definition Provides unskilled personal care and household services for stable, maintenance clients in their homes in compliance with a service plan. Level of
PERSONAL CARE WORKER (PCW) - Job Description Definition Provides unskilled personal care and household services for stable, maintenance clients in their homes in compliance with a service plan. Level of
Frequently Asked Questions about Individual Health Care Plans
 Frequently Asked Questions about Individual Health Care Plans Based on the Requirements of Section 59-63-80 of the South Carolina Code of Laws Office of Nutrition Programs South Carolina Department of
Frequently Asked Questions about Individual Health Care Plans Based on the Requirements of Section 59-63-80 of the South Carolina Code of Laws Office of Nutrition Programs South Carolina Department of
1. To comply with state and federal laws that protect children with severe food allergies, including but not limited to:
 Plano Independent School District Health Services Food Allergy Management Plan Purpose The Plano Independent School District (Plano ISD) Health Services Food Allergy Management Plan will enable all staff
Plano Independent School District Health Services Food Allergy Management Plan Purpose The Plano Independent School District (Plano ISD) Health Services Food Allergy Management Plan will enable all staff
COLORADO MEDICAL BOARD RULES
 RULE 800 3 CCR 713-30 RULES REGARDING THE DELEGATION AND SUPERVISION OF MEDICAL SERVICES TO UNLICENSED PERSONS PURSUANT TO SECTION 12-36-106(3)(l), C.R.S. INTRODUCTION Basis. The general authority for
RULE 800 3 CCR 713-30 RULES REGARDING THE DELEGATION AND SUPERVISION OF MEDICAL SERVICES TO UNLICENSED PERSONS PURSUANT TO SECTION 12-36-106(3)(l), C.R.S. INTRODUCTION Basis. The general authority for
RULES DEFINING COMPONENTS OF PRACTICE FOR THE REGISTERED NURSE
 RULES DEFINING COMPONENTS OF PRACTICE FOR THE REGISTERED NURSE Rules which further define the Nursing Practice Act have been established by the Board of Nursing. These rules are considered law and provide
RULES DEFINING COMPONENTS OF PRACTICE FOR THE REGISTERED NURSE Rules which further define the Nursing Practice Act have been established by the Board of Nursing. These rules are considered law and provide
RULES FOR STUDENT POSSESSION AND ADMINISTRATION OF ASTHMA, ALLERGY AND ANAPHYLAXIS MANAGEMENT MEDICATIONS OR OTHER PRESCRIPTION MEDICATIONS
 DEPARTMENT OF EDUCATION Colorado State Board of Education RULES FOR STUDENT POSSESSION AND ADMINISTRATION OF ASTHMA, ALLERGY AND ANAPHYLAXIS MANAGEMENT MEDICATIONS OR OTHER PRESCRIPTION MEDICATIONS 1 CCR
DEPARTMENT OF EDUCATION Colorado State Board of Education RULES FOR STUDENT POSSESSION AND ADMINISTRATION OF ASTHMA, ALLERGY AND ANAPHYLAXIS MANAGEMENT MEDICATIONS OR OTHER PRESCRIPTION MEDICATIONS 1 CCR
SECTION A CLARK COUNTY SCHOOL DISTRICT HEALTH SERVICES PROGRAM
 SECTION A CLARK COUNTY SCHOOL DISTRICT HEALTH SERVICES PROGRAM ORGANIZATION, INTERDISCIPLINARY RELATIONSHIPS, JOB RESPONSIBILITIES, AND SPECIAL ASSIGNMENTS SECTION A CONTENTS SECTION A - ORGANIZATION,
SECTION A CLARK COUNTY SCHOOL DISTRICT HEALTH SERVICES PROGRAM ORGANIZATION, INTERDISCIPLINARY RELATIONSHIPS, JOB RESPONSIBILITIES, AND SPECIAL ASSIGNMENTS SECTION A CONTENTS SECTION A - ORGANIZATION,
Effective Date: September, 2007 Revision Date: May 9, FASA Handbook - Chapter 4 MEDICATION
 FASA Handbook - Chapter 4 MEDICATION Purpose: To create a uniform policy to promote continuity in the Clark County School District (CCSD) Health Services department regarding Medication Administration
FASA Handbook - Chapter 4 MEDICATION Purpose: To create a uniform policy to promote continuity in the Clark County School District (CCSD) Health Services department regarding Medication Administration
PART 226 SPECIAL EDUCATION SUBPART A: GENERAL
 TITLE 23: EDUCATION AND CULTURAL RESOURCES SUBTITLE A: EDUCATION CHAPTER I: STATE BOARD OF EDUCATION SUBCHAPTER f: INSTRUCTION FOR SPECIFIC STUDENT POPULATIONS PART 226 SPECIAL EDUCATION SUBPART A: GENERAL
TITLE 23: EDUCATION AND CULTURAL RESOURCES SUBTITLE A: EDUCATION CHAPTER I: STATE BOARD OF EDUCATION SUBCHAPTER f: INSTRUCTION FOR SPECIFIC STUDENT POPULATIONS PART 226 SPECIAL EDUCATION SUBPART A: GENERAL
Best Practices Tip! Do you have a system in place to obtain annual physician orders for APC services authorized by the State? You should be sure there
 The Recipe for APC Best Practices Objectives Review the Basic Regulations regarding Advanced Personal Care, i.e. hiring, training, and supervision. Discuss Effective APC Training Protocols. Identify Best
The Recipe for APC Best Practices Objectives Review the Basic Regulations regarding Advanced Personal Care, i.e. hiring, training, and supervision. Discuss Effective APC Training Protocols. Identify Best
Code of Ethics Guidance Document for the Respiratory Care Practitioner
 Code of Ethics Guidance Document for the Respiratory Care Practitioner Preamble The Code of Ethics for the Respiratory Care Practitioner (Code of Ethics) delineates the ethical obligations of all Respiratory
Code of Ethics Guidance Document for the Respiratory Care Practitioner Preamble The Code of Ethics for the Respiratory Care Practitioner (Code of Ethics) delineates the ethical obligations of all Respiratory
HIV, HBV, and HCV prevention program; purpose and scope.
 Health Care Worker Law: MINNESOTA STATUTES 2002 EXAMINING AND LICENSING BOARDS 214.17 HIV, HBV, and HCV prevention program; purpose and scope. Sections 214.17 to 214.25 are intended to promote the health
Health Care Worker Law: MINNESOTA STATUTES 2002 EXAMINING AND LICENSING BOARDS 214.17 HIV, HBV, and HCV prevention program; purpose and scope. Sections 214.17 to 214.25 are intended to promote the health
PERFORMANCE OF NURSING TASKS BY SUPPORT WORKERS IN COMMUNITY SETTINGS
 2003 PERFORMANCE OF NURSING TASKS BY SUPPORT WORKERS IN COMMUNITY SETTINGS This Interpretive Document was approved by ARNNL Council in 2003 and replaces Delegation of Nursing Tasks and Procedures to Support
2003 PERFORMANCE OF NURSING TASKS BY SUPPORT WORKERS IN COMMUNITY SETTINGS This Interpretive Document was approved by ARNNL Council in 2003 and replaces Delegation of Nursing Tasks and Procedures to Support
Medical Review Criteria Skilled Nursing Facility & Subacute Care
 Medical Review Criteria Skilled Nursing Facility & Care Subject: Skilled Nursing Facility and Care Background: Skilled nursing facilities () provide facility-based skilled nursing care and related services
Medical Review Criteria Skilled Nursing Facility & Care Subject: Skilled Nursing Facility and Care Background: Skilled nursing facilities () provide facility-based skilled nursing care and related services
Frequently Asked Questions
 450 Simmons Way #700, Kaysville, UT 84037 (801) 547-9947 unar@davistech.edu www.utahcna.com Frequently Asked Questions UNAR stands for the Utah Nursing Assistant Registry, the agency in charge of the registry
450 Simmons Way #700, Kaysville, UT 84037 (801) 547-9947 unar@davistech.edu www.utahcna.com Frequently Asked Questions UNAR stands for the Utah Nursing Assistant Registry, the agency in charge of the registry
Developmental Disabilities Supports Division (DDSD) Supersedes: New Policy. Policy Title: Medication Assessment and Delivery Policy
 Supersedes: New Policy. Policy Title: Medication Assessment and Delivery Policy") Department of Health Developmental Disabilities Supports Division (DDSD) Policy Title: Medication Assessment and Delivery Policy Policy Number: M-001 Supersedes: New Policy Effective Date: November 1,
Department of Health Developmental Disabilities Supports Division (DDSD) Policy Title: Medication Assessment and Delivery Policy Policy Number: M-001 Supersedes: New Policy Effective Date: November 1,
Skilled skin care should be provided by an agency licensed to provide home health
 8.5.D. LIMITATIONS OF PERSONAL CARE In order to delineate the types of services that can be provided by a personal care worker, the following are examples of limitations where skilled home healthcare would
8.5.D. LIMITATIONS OF PERSONAL CARE In order to delineate the types of services that can be provided by a personal care worker, the following are examples of limitations where skilled home healthcare would
Amerigroup Community Care Enrollee/Caregiver Training Checklist
 https://providers.amerigroup.com Amerigroup Community Care Enrollee/Caregiver Training Checklist Include this completed and signed form with each prior authorization requests for initial, revised, or subsequent
https://providers.amerigroup.com Amerigroup Community Care Enrollee/Caregiver Training Checklist Include this completed and signed form with each prior authorization requests for initial, revised, or subsequent
Medication Administration Skill Checklist (to be accompanied by daily medication log for applicable students) 1 page
 1 page") See the following pages for exhibits relating to medical treatment: Exhibit A: Exhibit B: Exhibit C: Exhibit D: Exhibit E: Medication Administration Request Form and Guidelines for Administration of Medication
See the following pages for exhibits relating to medical treatment: Exhibit A: Exhibit B: Exhibit C: Exhibit D: Exhibit E: Medication Administration Request Form and Guidelines for Administration of Medication
Guidance: Personal Care Assistance Service Agreement Fields
 Guidance: Personal Care Assistance Service Agreement Fields As of December 30, 2015 Purpose The purpose of this document is to help lead agencies understand the data that is automatically populated from
Guidance: Personal Care Assistance Service Agreement Fields As of December 30, 2015 Purpose The purpose of this document is to help lead agencies understand the data that is automatically populated from
Policy for use of the Royal Marsden Manual of Clinical Nursing Procedures (9th Edition)
") Policy for use of the Royal Marsden Manual of Clinical Nursing Procedures (9th Edition) Document Summary This Policy defines the clinical procedures for all Clinical staff (including temporary staff, contracted
Policy for use of the Royal Marsden Manual of Clinical Nursing Procedures (9th Edition) Document Summary This Policy defines the clinical procedures for all Clinical staff (including temporary staff, contracted
ICD 9/DSM 4/Other Axis Description Diagnosis Date Diagnosed By. Allergies: Yes No List Allergies and known reactions to medications, food, other:
 Medication Administration Assessment Tool Profile Information Individual Name * : Provider/Program Name: Create Date * : Entered By * : Title: Birth Date: Age: Check all services that apply: Independent
Medication Administration Assessment Tool Profile Information Individual Name * : Provider/Program Name: Create Date * : Entered By * : Title: Birth Date: Age: Check all services that apply: Independent
Medicine and Supporting Pupils at School with Medical Conditions Policy
 Medicine and Supporting Pupils at School with Medical Conditions Policy This Policy is founded within our School ethos which provides a caring, friendly and safe environment for all members of our community.
Medicine and Supporting Pupils at School with Medical Conditions Policy This Policy is founded within our School ethos which provides a caring, friendly and safe environment for all members of our community.
ADMINISTRATION OF MEDICATION PROCEDURE
 1302.47 Safety practices. ADMINISTRATION OF MEDICATION PROCEDURE b) A program must develop and implement a system of management, including ongoing training, oversight, correction and continuous improvement
1302.47 Safety practices. ADMINISTRATION OF MEDICATION PROCEDURE b) A program must develop and implement a system of management, including ongoing training, oversight, correction and continuous improvement
May 2015 Assistive Devices Program Ministry of Health and Long-Term Care
 Grants Policy and Administration Manual Assistive Devices Program Ministry of Health and Long-Term Care Table of Amendments This page will list all substantive changes to policies and procedures listed
Grants Policy and Administration Manual Assistive Devices Program Ministry of Health and Long-Term Care Table of Amendments This page will list all substantive changes to policies and procedures listed
The California End of Life Option Act (Patient s Request for Medical Aid-in-Dying)
") Office of Origin: I. PURPOSE II. III. A. The California authorizes medical aid in dying and allows an adult patient with capacity, who has been diagnosed with a terminal disease with a life expectancy
Office of Origin: I. PURPOSE II. III. A. The California authorizes medical aid in dying and allows an adult patient with capacity, who has been diagnosed with a terminal disease with a life expectancy
ST PAUL S CATHOLIC PRIMARY SCHOOL AND NURSERY. Supporting Pupils with Medical Conditions Policy
 ST PAUL S CATHOLIC PRIMARY SCHOOL AND NURSERY Supporting Pupils with Medical Conditions Policy Our Mission Statement Do everything with love. (St Paul s first letter to the Corinthians 16:14) This means
ST PAUL S CATHOLIC PRIMARY SCHOOL AND NURSERY Supporting Pupils with Medical Conditions Policy Our Mission Statement Do everything with love. (St Paul s first letter to the Corinthians 16:14) This means
Course Outline and Assignments
 Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
Course Outline and Assignments WEEK ONE 10-16-12 Instructional In Class-Learning to be completed prior to class 10-17-12 Total Hours Assessment 1. proper hand washing techniques 2. donning and removing
RIVER EDGE BOARD OF EDUCATION FILE CODE: 5141 River Edge, NJ 07661
 RIVER EDGE BOARD OF EDUCATION FILE CODE: 5141 River Edge, NJ 07661 Policy HEALTH The board of education believes that good health is vital to successful learning. In order to help district pupils achieve
RIVER EDGE BOARD OF EDUCATION FILE CODE: 5141 River Edge, NJ 07661 Policy HEALTH The board of education believes that good health is vital to successful learning. In order to help district pupils achieve
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND MENTAL RETARDATION
 RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND MENTAL RETARDATION CHAPTER 0940-5-30 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL HEALTH INTENSIVE DAY TREATMENT PROGRAM FOR TABLE OF CONTENTS 0940-5-30-.01
RULES OF TENNESSEE DEPARTMENT OF MENTAL HEALTH AND MENTAL RETARDATION CHAPTER 0940-5-30 MINIMUM PROGRAM REQUIREMENTS FOR MENTAL HEALTH INTENSIVE DAY TREATMENT PROGRAM FOR TABLE OF CONTENTS 0940-5-30-.01
During pre-briefing, you will be assigned one of these roles according to the description below to participate in the simulation as a nurse.
 Student Instructions for Standardized Simulation NR 452 Eric Chilton PURPOSE The following information is to be used in guiding your preparation and participation in the scenario for this course. This
Student Instructions for Standardized Simulation NR 452 Eric Chilton PURPOSE The following information is to be used in guiding your preparation and participation in the scenario for this course. This
McMinnville School District #40
 McMinnville School District #40 Code: JHCD/JHCDA-AR Adopted: 1/08 Revised/Readopted: 8/10; 2/14; 2/15 Orig. Code: JHCD/JHCDA-AR Prescription/Nonprescription Medication Students may, subject to the provisions
McMinnville School District #40 Code: JHCD/JHCDA-AR Adopted: 1/08 Revised/Readopted: 8/10; 2/14; 2/15 Orig. Code: JHCD/JHCDA-AR Prescription/Nonprescription Medication Students may, subject to the provisions
NEW JERSEY. Downloaded January 2011
 NEW JERSEY Downloaded January 2011 SUBCHAPTER 25. MANDATORY NURSE STAFFING 8:39 25.1 Mandatory policies and procedures for nurse staffing (a) There shall be a full time director of nursing or nursing administrator
NEW JERSEY Downloaded January 2011 SUBCHAPTER 25. MANDATORY NURSE STAFFING 8:39 25.1 Mandatory policies and procedures for nurse staffing (a) There shall be a full time director of nursing or nursing administrator
South Carolina Radiation Quality Standards Association Code of Ethics
 South Carolina Radiation Quality Standards Association Code of Ethics 1. Introduction a. Code of ethics. These rules of conduct constitute the code of ethics as required by the Code of Laws of South Carolina.
South Carolina Radiation Quality Standards Association Code of Ethics 1. Introduction a. Code of ethics. These rules of conduct constitute the code of ethics as required by the Code of Laws of South Carolina.
60 Memorial Medical Parkway Palm Coast, Florida 32164
 POLICY & PROCEDURES TITLE: Privileges of Student Nurses and Student Nursing Assistants POLICY # EDU 001 POLICY CATEGORY: Administrative / Education Origination Date: 12/2008 Last Review/Revision Date:
POLICY & PROCEDURES TITLE: Privileges of Student Nurses and Student Nursing Assistants POLICY # EDU 001 POLICY CATEGORY: Administrative / Education Origination Date: 12/2008 Last Review/Revision Date:
5. Personal Care Services
 5. Personal Care Services Chapter IV - Services to Children A. Overview A child who requires personal care services is a child with a chronic medical condition or with medical needs requiring specialized
5. Personal Care Services Chapter IV - Services to Children A. Overview A child who requires personal care services is a child with a chronic medical condition or with medical needs requiring specialized
RULES OF TENNESSEE BOARD OF NURSING CHAPTER MEDICATION AIDES TABLE OF CONTENTS
 RULES OF TENNESSEE BOARD OF NURSING CHAPTER 1000-05 MEDICATION AIDES TABLE OF CONTENTS 1000-05-.01 Purpose 1000-05-.07 Training Programs 1000-05-.02 Definitions 1000-05-.08 Peer Assistance Program 1000-05-.03
RULES OF TENNESSEE BOARD OF NURSING CHAPTER 1000-05 MEDICATION AIDES TABLE OF CONTENTS 1000-05-.01 Purpose 1000-05-.07 Training Programs 1000-05-.02 Definitions 1000-05-.08 Peer Assistance Program 1000-05-.03
Medication Management Policy and Procedures
 POLICY STATEMENT This policy establishes guidelines for ensuring safe and correct management of client medications in accordance with legislative and regulatory requirements and professional practice competency
POLICY STATEMENT This policy establishes guidelines for ensuring safe and correct management of client medications in accordance with legislative and regulatory requirements and professional practice competency
MEDICATION AIDE EDUCATION & ROLE IN LONG TERM CARE/SKILLED NURSING FACILITIES VS ADULT CARE SETTINGS POSITION STATEMENT
 FACILITIES VS ADULT CARE SETTINGS A Position Statement is not a regulation of the NC Board of Nursing and does not carry the force and effect of law and rules. A Position Statement is not an interpretation,
FACILITIES VS ADULT CARE SETTINGS A Position Statement is not a regulation of the NC Board of Nursing and does not carry the force and effect of law and rules. A Position Statement is not an interpretation,
ITT Technical Institute. NU260 Maternal Child Nursing SYLLABUS
 ITT Technical Institute NU260 Maternal Child Nursing SYLLABUS Credit hours: 8 Contact/Instructional hours: 160 (40 Theory Hours, 120 Clinical Hours) Prerequisite(s) and/or Corequisite(s): Prerequisites:
ITT Technical Institute NU260 Maternal Child Nursing SYLLABUS Credit hours: 8 Contact/Instructional hours: 160 (40 Theory Hours, 120 Clinical Hours) Prerequisite(s) and/or Corequisite(s): Prerequisites: