A G E N D A Indicative Timings
|
|
|
- Jemimah Pitts
- 6 years ago
- Views:
Transcription
 2 Jacqui Smith (Enclosure) 4.")
1 Council of Governors Meeting pm on 25 July 2016 Harry Hollier Lecture Theatre, Partnership Learning Centre, Good Hope Hospital A G E N D A Indicative Timings Presenter (minutes) 1. Apologies 1 Jacqui Smith 2. Declarations of Interest - Governors - Directors 3. Minutes of previous meetings May June Jacqui Smith (Enclosure) 2 Jacqui Smith (Enclosure) 4. Matters arising 5 David Burbridge (Enclosure) 5. Chair s Update 5 Jacqui Smith (Enclosure) 6. Chief Executive s Update 5 Julie Moore (Oral) 7. Performance Report 15 Kevin Bolger (Enclosure) 8. Clinical Quality Report 10 David Rosser (Enclosure) 9. Care Quality Report 10 Sam Foster (Enclosure) 10. Finance Report 15 Julian Miller (Enclosure) 11. Compliance and Assurance Report 10 David Burbridge (Enclosure) 12. Any Other Business Previously Advised to the Chair 13. Date of Next Meeting AGM 7 September 2016, Rooms 7 & 8, Education Centre, Heartlands Hospital Light refreshments will be available from 3.30pm David Burbridge Interim Director of Corporate Affairs 28 June 2016
2 COUNCIL OF GOVERNORS REGISTER OF INTERESTS NAME Cllr Mohammed Aikhlaq INTEREST DECLARED Member of Overview & Scrutiny Committee : Health & Social Care DATE DECLARED May 2015 DATE CEASED Arshad Begum Nothing to declare 21 Nov 2011 Kath Bell Nicola Burgess Elaine Coulthard Dr Olivia Craig Carol Doyle Emma Hale Company Secretary - Succeed Services Ltd Assistant Professor of Operations Management, Warwick Business School, Warwick University and honorary contract with HEFT to conduct research. 1. Member of the Conservative Party 2. President of the Friends of Good Hope Hospital Various roles associated with the British Psychological Society Awaiting information Nothing to declare Ron Handsaker 1. Shareholder Santander 2. Director 24/7 Industrial Services UK Ltd Albert Fletcher Director Aquarius (unpaid). A charity that specialises in helping and treating those with drink and/or drug issues. Richard Hughes 1.Chairman Homestart (Tamworth) 2.Chairman Tamworth Credit Union Ltd 3.Director The Pathway Project 4.Director Tamworth Community Advice Network CIC 5.Chairman Tamworth Talking Newspaper Ltd 6.TrusteeChairman The Rawlett Trust 7.Vice Chairman Standards Committee, Tamworth Borough Council 8.Divisional President St John s AmbulancePresident Tamworth and Wilnecote St John s Ambulance. 9.Member Appeal Committee, St Giles Hospice 10.Retired CEO & President Secretary, Tamworth Cooperative Society 11.Mr Hughes son holds a very senior managerial position with Barclays Bank 12.Chairman Tamworth Community Advice Network CIC 13. Independent Member Tamworth Borough Council Nominations Committee 14. Member Conservation Advisory Committee, Tamworth Borough Council 15. President Tamworth Male Voice Choir 16. Treasurer St Andrew s Methodist Church, Tamworth 17. Shareholder BP 21 Nov Jun May May Jun May Oct May Nov 2011 Amended 1 Sep 2013 Amended 2 Sep 2015 Amended 23 Oct Feb Oct Oct Oct Oct Oct Oct Oct Oct Mar Oct Oct Oct May 2016
3 18. Shareholder Santander 19. Trustee Spirit of Tamworth Trust 20. Mr Hughes son is Head of Financial Planning, Mercer 23 Oct 2012 May May 2016 Michael Hutchby Nothing to declare 16 Aug 2013 Sue Hutchings Shareholder in Lloyds TSB 19 Sept 2013 Phillip Johnson Nothing to declare 21 Nov 2011 Michael Kelly Nothing to declare 21 Nov 2011 Attiqa Khan Nothing to declare 16 Aug 2013 Marek Kibilski Nothing to declare 15 June 2015 Andrew Lydon Nothing to declare 16 Aug 2013 Anne McGeever Margaret Meixner Veronica Morgan 1. Registered with Therapy Bank in Worcestershire to provide services to BMI Droitwich Spa Hospital. 2. Unite Professionals Limited (Occupational Therapists) ad hoc employment. Awaiting information 1. Magistrate in criminal and family courts 2. Shareholder in Halifax, Millwall FC and Lloyds TSB 3. Member (patient rep) of West Midlands Breast Expert Advisory Committee 4. Member of West Midlands Cancer patient &public engagement expert advisory group 5. Expert member on Solihull Research Ethics Committee 6. HEFT Employee 12 Sep Apr Jan Jan Jan Jan Jan Jan 2016 Catherine Nothing to declare 13 May 2014 Needham Barry Orriss Member of Project Management Team, Warwick 7 Apr 2016 Medical School, University of Warwick Mark Pearson Member of Green Party 21 Jan 2015 Jean Thomas Nothing to declare 30 Sep 2014 David Treadwell 1. Shareholder - Lloyds TSB 2. Shareholder - STW 3. Shareholder - National Grid Matthew Trotter 1. HEFT Employee 2. Director - Specialist Health Partnership 3. Director - Specialist ENT Care Ltd David Wallis 1. Knowle, Dorridge & Bentley Heath Neighbourhood Plan Ltd Director 2. Prospect (Trade Union) - Member 21 Nov Sep Dec Sept Sept 2015
4 REGISTER OF DIRECTORS and REGISTER OF DIRECTORS INTERESTS VOTING DIRECTORS NAME DATE OF APPOINTMENT INTEREST (if any) DATE OF NOTIFICATION Mr Jonathan Brotherton Nothing to declare DATE OF TERMINATION OF INTEREST Mr Andrew Edwards Couch Perry & Wilkes - in receipt of annuity following business sale until May Voluntary role as a business mentor for the Prince's Trust. Mrs Sam Foster Nothing to declare Prof Jon Glasby Professor / Head of School, University of Birmingham Senior Fellow, NIHR School for Social Care Research Member of Birmingham Health Partners Executive Group 4. Works with Birmingham Safeguarding Children s Board from time to time Ms Hazel Gunter Nothing to declare Mrs Jackie Hendley Director - SC Advisory Services Ltd 2. Director - Smith Cooper - IT Services Ltd 3. Director Smith Cooper Ltd 4. Partner/Member SHH 101 LLP Dr Michael Kinski NED - Infinis Capital Limited (UK) 2. NED - Trireme Holdings Ltd (USA) 3. Senior Independent Director - AWAS Aviation Capital Ltd (Dublin) 4. NED - Lake Woods Holding Pty (Australia) 5. Prof of Business Change Middlesex University. Mrs Karen Kneller CEO of Criminal Cases Review Commission 2. Part time judge Social Entitlement Chamber Fitness to Practise 3. Member for General Dental Council 4. Director (unremunerated) of BRAP, an equalities think tank. Mr Julian Miller Director of Finance (non-voting) University Hospitals Birmingham NHS Foundation Trust Dame Julie Moore Birmingham Systems Ltd 2. Director of Innovating Global Health China Ltd (registered in Hong Kong) 3. Member of Birmingham Business School Advisory Board 4. Court of the University of Birmingham 5. Governor Birmingham City University 6. Non-Executive Director Precision Medicine Catapult (PMC) 7. CEO University Hospitals Birmingham NHS Foundation Trust Dr David Rosser Medical Director University Hospitals Birmingham NHS Foundation Trust Prof Michael Sheppard Chair West Midlands Academic Health Sciences Network Jan Octr 2013
5 2. NED University Hospital Birmingham NHS FT Rt Hon Jacqui Smith Chair The Precious Trust 2. Chair Public Affairs Practice for Westbourne Communications 3. Associate Cumberledge Eden & Partners 4. Associate Global Partners Governance 5. Chair University Hospitals Birmingham NHS Foundation Trust Dec
6 Minutes of a meeting of the Council of Governors of Heart of England NHS Foundation Trust held in the Harry Hollier Lecture Theatre, Partnership Learning Centre, Good Hope Hospital on 11 May 2016 at 4.00pm PRESENT: IN ATTENDANCE: J Smith (Chair) E Coulthard O Craig A Fletcher R Handsaker R Hughes M Hutchby S Hutchings K Bolger J Brotherton A Edwards S Foster J Glasby H Gunter and members of the public. P Johnson M Kelly A Lydon V Morgan J Thomas D Treadwell M Trotter D Wallis A Hudson (Minutes) K Kneller J Miller J Moore D Rosser K Smith (Secretary) APOLOGIES & WELCOME Apologies for Governors had been received from M Aihklaq, A McGeever, M Meixner, B Orriss, Apologies for Directors had been received from J Rao DECLARATIONS OF INTEREST MINUTES The Governors Register of Interests was received. The Directors Register of Interests was noted. 2 March 2016 A Lydon referred to the fourth paragraph on page 9 and questioned the wording; this was amended to.he was told that this would not save money, nor satisfy best practice requirements. Subject to the above amendment the minutes of the meeting held on 2 March 2016 were approved as a true record. 4 April 2016 A Lydon referred to the eighth paragraph page 2; the wording was amended to.. did not fall within the remit of this meeting. E Coulthard referred to the final paragraph on page 5; the final sentence was amended to There had been a 400 charge from Estates for the Good Hope Fete for the installation, by a contractor,
7 P a g e 2 of an electrical supply cable. Subject to the above amendment the minutes of the meeting held on 4 April 2016 were approved as a true record MATTERS ARISING Investigate and report back on statement that Trust was paying 10 and 12 times the going rate for staff through agencies. K Bolger reported that following investigation there was no evidence to support this. There was evidence that some consultants could receive three times above the going rate but this had only occurred at a point where the Trust had been under extreme pressure. The Monitor cap had now been introduced on agency spends however there could still be incidents where paying an enhanced rate may have taken place but only when patient safety might otherwise be compromised Provide (one off) full list of performance indicators. This had been included as an appendix to the Performance Report Provide DTOC information during the last 6 and 12 months and by site. K Bolger reported that the information by site had been provided and he was able to hand out information for the last 12 months by site. He also undertook to report on actual DTOC numbers, not just percentages, going forward Check whether anything more can be done to utilise unoccupied retail units above the Heartlands main reception. K Bolger advised that the Trust was unable to utilise the units without paying rent under the terms of the PFI arrangement Parking item closed Include 4 hour A&E Performance by site in future performance reports this was now being ed to Governors weekly Check when drinking water would be made available in Good Hope Treatment Centre. The equipment had been installed Circulate PwC s presentation. This had been included in the meeting pack Circulate wording for Governors use on social media. K Smith had circulated this by e- mail. A request was received for an update on which fines had been suspended for the new financial year. J Moore advised that one fine had crept back in and an update would be included as part of the Finance report later in the meeting CHAIR S UPDATE The Chair reported that there had been a good response in relation to the advert for the vacant Non-executive Director posts with around 50 applications received; the Council of Governors (CoG) Appointments Committee had met earlier in the week and had identified 15 applicants to proceed to first interviews, following which further shortlisting would take place with final interviews to be held at the beginning of June.
8 P a g e 3 The Government mandated Sustainability & Transformation Programme (STP) was designed with the intention of bringing together local healthcare partners and councils for Birmingham and Solihull. However, there was some frustration over the level of central interference within the local group, which had pushed back to maintain local ownership. Progress had been made with the Birmingham & Solihull footprint, resulting in groups being formed including a Leaders and Chairs Group, led by Bob Sleigh, Leader of Solihull Council, a CEO Group and an Executive Leads Group. Former health secretary, Stephen Dorrell, had been appointed to chair the Birmingham & Solihull System Board. The Chair had also held separate meetings with Bob Sleigh and John Clancy (Birmingham City Council) and local MPs, as well as having attended a meeting with representatives from the community to discuss bereavement services. The Chair reported that she had compered Solihull Better Together Awards and was pleased to report that teams from the Trust had been nominated for, and received, awards; she had also attended the Jean Robinson Award celebrations on the Frailty Assessment Unit at Good Hope Hospital. In response to a question from K Bell, the Chair advised that she had met with A Butler, chair of Breast Cancer Support Group, who had agreed to update the Group on the settled actions that included the reinstatement of Gillian Waterhouse to support the Group. The 500 patients in the MDT had not as yet been corresponded with but this was in progress and included a full package of support. In response to a question from A Lydon, J Moore advised that acute trusts had seen very little of the 15m of the Better Care Funding for 2015/16, much of which had been consumed by councils to offset the deficit in their budgets. K Bolger agreed to bring report back setting out how the Better Care Funding had been used (Action: KB). In response to a question from V Morgan, the Chair advised that the areas of focus for the STP were around maternity and paediatrics, social and out of hospital care and future hospitals CHIEF EXECUTIVE S UPDATE J Moore had nothing further to add to the Chair s update PERFORMANCE REPORT K Bolger presented the pre-circulated report that set out the Trust s performance against national indicators and targets, presented by K Bolger. The report covered indicators and targets included in the Monitor Risk Assessment Framework, as well as local priorities and material risks to the Trust s provider licence or governance ratings, finances, reputation or clinical quality resulting from performance against indicators, in order to give an overall view of the position of the Trust and set out the actions for those indicators that were failing to achieve compliance with targets. Monitor Risk Assessment Framework Of the 14 indicators set out in the RAF 12 were on target; the two targets missed were the 4-hour A&E wait target and the in-month C.diff target. March s A&E 4-hour wait performance was 85.1% compared to 85.05% in February and 83% in
9 P a g e 4 March The number of attendances during March was 23,634 compared to 21,786 in March 2015; overall the Trust had seen an average of 60 attendances more per day compared to the same period in There had been no 12 hour trolley breaches. All cancer targets had been met in February, the first time in over a year. The 2 week wait from referral to appointment performance was 97.07% against a target of 93%. The 2 week wait breast cancer referral performance was 95.45% against a target of 93%; this indicator had been met for the second month in a row. The 85% 62-day cancer referral target had been achieved in February with performance at 87.78%. Sustainability was now key. The Trust had met the incomplete 18-week Referral to Treatment Time (RTT) target of 92% for the second consecutive month at 92.01% which was ahead of trajectory. As part of the STP, the Trust had agreed a revised trajectory to deliver sustained performance against this indicator from the end of September There had been 7 cases of C.diff in March against an in month target of 5. This was the fourth month that the Trust had exceeded its target. M Pearson questioned the accuracy or presentation of the A&E attendance data provided at in the report. K Bolger undertook to revise the table for future reports (Action: KB). In response to a question from J Thomas regarding the 15% increase in the number of A&E attendances and whether GPs could provide more cover, K Bolger advised that the Trust was working to identify and reduce A&E attendances across all sites and was developing a pilot scheme in conjunction with CCG s and stakeholders to identify cases that should be handled by GPs; it was hoped that the work would be able to identify the number of patients that should be cared for outside of A&E but the pilot was not due to commence until August. It was noted that despite of the increase in demand, performance was better than the same period in the previous year; all other access targets were also being achieved and that earlier in the day the Board had recognised the contribution of everyone involved and had formally recorded their thanks to all staff for their hard work, particularly around the cancer targets, and their efforts in the face of increased demand. The Council of Governors added its thanks to that of the Board. In response to a question from A Lydon regarding the number of people who do not need to visit A&E but do so because they can t get GP appointments, K Bolger noted that there may well be those with a short length of stay who fall into this category but aren t currently measured. National targets monitored through CCG contract Of the 17 national targets not included in the RAF but included in the CCG contract the Trust had delivered eleven with six behind plan. 6 week diagnostics had improved to 99.31% against the 99% target; this was the second month that the target had been achieved against a significant increase in activity; again sustainability would be key. There had been in an increase of 7% in ambulance attendances compared to January The number of 30 minute breaches was similar to February 2016 but the number of 60 minute breaches had doubled. There had been 2 urgent operations cancelled for the second time in March. Both cancellations
10 P a g e 5 had been in Trauma & Orthopaedics and were due to previous cases overrunning. Both patients had since been treated. There had been no cancelled operations due to the planned doctor s strike and no patients had been cancelled on the day. It was highlighted that the response and performance by medical and nursing staff had been exceptional with A&E 4 hour performance achieving a target of 90% on strike days although there had been an increase in activity for following 2 3 days. The Chair noted the on-going discussions and negotiations around the junior doctor s contract and the implications associated therewith. E Coulthard advised that Good Hope A&E had been almost empty on the days of junior doctors strike and that an influx had been expected in the days thereafter but this had not materialised. The Trust had failed to meet its contractual requirement for VTE assessment for the first time since July with performance at 94.75% against a target of 95%. The main areas of non-compliance related to short stay areas such as AMU. A review of the Trust methodology for measuring this target was being undertaken to ascertain if any changes to the cohort s of patients that could be block risk assessed, could be made; the Trust had begun the work of researching the methodology use to collect information. V Morgan questioned whether the Trust could undertake an audit on A&E attendances, rather than prospective review, K Bolger responded that the Trust had already done so but had very different views from GPs and ED Clinicians and the new review would involve both. Local indicators contract There were a number of contractual maternity screening indicators that the Trust s performance was measured against. As maternity screening indicators were reported a full quarter in arrears, the meeting received the performance against Q3 2015; of the 12 indicators in the contract 5 had not been met. A performance review meeting with the Women s & Children s Division had taken place the previous day and it had been agreed that local indicators and targets required revision. Performance by site would be provided to the next meeting. Breast feeding rates had improved in March to 70.21% compared to February (69.64%) against the 72% target. The Trust had failed to meet the nursing care indicator relating to tissue viability compliance with an overall compliance score of 94% against a target of 95%; the sub-measure that had impacted most on the overall score was the metric to ensure that repositioning frequency is adhered to for 3 days which only achieved 83% against a 90% target. Falls and pressure ulcers would be covered in more detail by S Foster as part of Care Quality Report. Appraisal rates had increased to 81% in April above trajectory but still below the 85% target. Local indicators internal The Trust had 13 workforce indicators of which 8 were not compliant. The March position for the workforce KPI s had shown no significant shift from the February position with continued underperformance in four areas: staff in post versus budget establishment; average time to recruit; voluntary turnover and Trust wide agency spend. Active recruitment continued; 90 nurses were due to start between April and June Recruitment of theatre nurses continued to be a problem area. On a positive note, there had been a reduction in the number of staff leaving but
11 P a g e 6 further focus was required on retention. The Trust was assessing the gap on junior doctor cover. A Lydon questioned where junior doctors wanted to work if they did not want to work in A&E or with GP s. J Moore advised that universities were oversubscribed for medical degrees but a large proportion of students did not qualify and go on to become doctors. The Trust continued to overspend on agency at 7.35% in March, against target of 3%; this had been due to the number of flex beds that remained open. The Trust continued to comply with the Monitor rate caps. Delayed Transfer of Care (DTOC) performance had improved in March to 3.86% from February s position of 4.73%; further work to address this was being undertaken through the financial recovery programme. There had been a downturn in April but a rise across the patch again had once again been seen. Future DTOC reports would include numbers by site. There had been 4 patients who had waited over 100 days for their first definitive cancer treatment; all of which were complex cases. RCAs were being undertaken for those cases in line with national requirements. The Solihull Community Contract was being reviewed to identify areas which the Trust could exploit. The Trust had made its final submission on CQUIN performance and achieved 10.9m, which was above forecast against the target of 13.3m. Targets for 2016/17 were expected to be more achievable due to stronger negotiations. The tables in the appendices had been included following a request at the last Council of Governors meeting for a list of all the targets that the Trust reported on there were around CLINICAL QUALITY REPORT D Rosser presented the new style exception report following the first meeting of the Clinical Quality Monitoring Group (CQMG). Investigations into doctors performance There were currently eleven medical practitioners within the formal review process; nine cases predominantly related to conduct matters and two to capability matters. A robust process was being followed; some investigation were outside of agreed timescale but was normal in such cases. Nominations from each of the Divisions for the case investigation training programme had been received and dates were being finalised. D Rosser explained the acronym SAS as relating to staff and associate specialists. Mortality indicators D Rosser explained that the CUSUM (cumulative summation) Hospital Standardised Mortality Rate (HSMR) methodology looked at deaths over time and required careful interpretation. Any Clinical Classification System (CCS) group that moved to the right of the CUSUM threshold of 5 would trigger a requirement from the CQC for an explanation, such as cardiac dysthymias in the January chart. Coding was very important; multiple coding in patient notes sometimes meant that identifiers were not related to the cause of death. Performance was reported three months in arrears as it
12 P a g e 7 was reliant on national data. The patient case lists for all four CCS groups that exceeded the threshold of 3 had been reviewed by the CQMG and to date no issues had been identified but investigations would continue. Patients admitted with a diagnosis of GI haemorrhage had been the subject of a CQC mortality outlier alert between December 2014 and April 2015, following a run of higher than expected mortality. The Trust had corresponded with the CQC who had advised that they were assured of Trust actions. The interventional radiology scanner at Heartlands had deteriorated to the extent it was no longer suitable for use on large patients. The scanner needed to be rebuilt; this was not ideal as it would need to re-installed in any new interventional radiology facility at some point in the future. Earlier in the day the Board had been informed of an incident, the previous day, involving a patient where the clinician had made a reasoned decision to continue with a procedure where the level of radiation necessary to obtain the desired effect was high and that, subsequently, the Trust had engaged expert advice to assess the level of radiation the patient had been exposed to this would lead to an explanation being given to the patient when the facts were known. Divisions were working on theatre schedules, including the use of the new hybrid theatre, whilst the rebuild took place. Delays could be expected for elective patients. The Queen Elizabeth Hospital was assisting with emergency work as and when required. In response to a question from V Morgan, D Rosser confirmed that the patient concerned had been advised under the duty of candour and expertise had been bought in to look into the case. The Chair reported that the Board had earlier that day asked for a report setting out the cost and impact on patients of the failure of the equipment. J Moore advised that the fundamental problem was the fact that certain equipment should have been replaced a long time ago and until replaced would continue to cause issues for patients and the Board. M Pearson welcomed the Board s openness and the candour of the report. E Coulthard questioned the condition of the two interventional radiology scanners at Good Hope, D Rosser advised these had not been flagged as a particular concern but would require upgrading/ replacement. J Moore reported that the capital budget for 2016/17 was 17-20m with priority being given to scanners, endoscopy and interventional radiology; the total cost required to address these types of issue on the Heartlands site was around 180m. D Rosser explained that HSMR and SHMI data was reported for reputational purposes both of which were below 100 with no cause for concern. It was noted that the data was not a reliable indicator of quality of care within the organisation. The Trust CRAB 30 day surgical mortality ratio continued to show a level below or equal to 1 which gave no cause for concern. Board of Director s unannounced governance visits The planned for March did not take place due to Non-Executive Directors not being able to attend. The most recent visit took place 15 April 2016 to ward 14 (Trauma & Orthopaedics) at GHH. The visit had been very positive and the action plan was currently being finalised and would be shared with the Divisional Management Team. Timely Delivery of Antibiotic Stat Doses D Rosser gave an overview of the project led by A Keogh and the ICT department that had
13 P a g e 8 commenced in June 2013 and was aimed at increasing the timeliness of the administration of antibiotic stat (one off) doses being given to improve outcomes for patients with sepsis. There was clear evidence that first dose of antibiotics from diagnosis, if administered within 60 minutes, massively reduced mortality risk. The project supplied pagers that bleeped to inform nurses that a stat dose had been prescribed and continued to bleep at 15 minute intervals until the stat dose was administered or the time to administer the dose had lapsed. Performance relating to the timely delivery of the dose was measured at Trust, site, ward and administrator level. The bleep system had initially been implemented at Birmingham Heartlands Hospital (BHH) in January 2015 and had since been rolled out across all three hospital sites. Results had shown that HEFT was 75.2% compliant with the one hour target in the last 30 days compared with 72.9% in the last twelve months. The worst performing ward from each site would be invited to the next available Executive Root Cause Analysis (RCA) Care Omissions meeting, along with the best performing ward(s) to review performance and identify improvement actions. In response to a question from V Morgan, D Rosser advised that doctors were not trained to give IV s now and therefore could not administer them during their ward rounds. P Johnson asked whether the Trust bought assets outright or leased equipment; J Miller responded that traditionally the Trust had bought equipment outright but recognised depreciation in the accounts; however given the current lack of capital the Trust was looking at other options. M Pearson noted the detail set out in the reports and that previously the CoG Quality & Risk Committee would have explored the report in more detail; he asked if the CoG could have more detailed reports around for example perinatal mortality rates. D Rosser reassured the meeting that the Clinical Quality Monitoring Group looked at these issues in greater detail and this report was designed to give the Board and the CoG assurance of that process. The Chair reminded the meeting that this was the first time that this information had been presented in this way and that future reports would improve familiarity with the process and hopefully generate greater confidence. Open and Recently Closed Serious Incidents (SIs) The open and recently closed serious incident investigations at the Trust were reviewed; progress would be monitored through the Clinical Quality Monitoring Group and Board Quality Committee. In response to a question from D Wallis, the Chair explained that the Board Assurance Framework and Risk Register sat within the remit of Audit Committee and was reported on to the Board for assurance CARE QUALITY REPORT S Foster referred to the pre-circulated report that summarised the Trust s performance against national quality indicators and targets, including those set out in Monitor s Risk Assessment Framework, and local priorities. The Root Cause Analysis (RCA) Executive Omissions Forum had been running for several months and considered all serious incidents; clinical and operational teams attended as required. A number of incidents had been fully explored and the lessons learned communicated. The Trust had met its C.diff target of 64 for 2015/16 with 61 cases. There had been no cases of post 48 hour MRSA bacteraemia in March. The overall Trust compliance for MRSA screening for March had improved to 86%. The Trust had seen an increased transmission of Serratia marcescens in maternity, S Foster confirmed that the infection caused no harm in babies. Three
14 P a g e 9 wards one at Good Hope and two at Heartlands had been closed during March due to outbreaks of Norovirus. Hand hygiene had continued to be a focus with senior doctors and nursing colleagues very involved resulting in lots of engagement. The Trust had failed to achieve the 2015/16 targets for both grade 2 and grade 3 pressure ulcers with performance for avoidable grade 3 and necrotic pressure ulcers at 51 cases against a target of 29 for the year and for grade 2 ulcers, 190 cases against target of 187 for the year. However, there had been an overall reduction in the total numbers of hospital acquired pressure ulcers year on year. The Trust was continuing the drive to document actions to demonstrate compliance, which would be helped with a steady workforce. The Trust had achieved a 10% reduction in overall falls rates per 1,000 occupied bed days with a year to date position of 6.32 against a target of 6.36 with only two months (January and March 2016) having fallen outside of the trajectory. The Trust was working to reduce the number of falls further with a focus on patients who fell more than once. A new visual report was being piloted by site and ward including ensuring Divisions received all of the relevant information they required. The Trust measured its compliance with safe staffing levels for nursing through a variety of methodologies, including weekly surveillance and submissions of monthly UNIFY returns to NHS England, which compared funded staffing to actual staffing and had identified some hot spots, such as Paediatrics, A&E and Critical Care. In addition, periodic reviews were undertaken of areas of concern, such as the report received by the Board earlier in the day that focused on adult inpatient areas and AMUs/ SAUs across the Trust. Feedback indicated that the current staffing levels on fourteen out of the seventeen areas were at safe levels. There were three areas that required increased staff resource; wards 12, 24 and 26 in Division 3, on the Heartlands site. The additional posts would require an investment of around 263k and would be funded from within existing budgets or through the business case process. Turnover of nursing staff had decreased. A recruitment fair in Dublin had been attended the previous week and an agency had been engaged to recruitment from the wider EU. The current number of vacancies stood at 158 wte (whole time equivalent) across adult wards and AMUs; an improvement of around 30% compared to October There were 34 EU and 20 newly qualified registered nurses awaiting PIN numbers, once in post this would reduce the vacancies by 54 wte. Specialty areas (theatres, paediatrics, critical care and ED) continued to have vacancies and the Trust continued to utilise temporary staff to cover these. The number of complaints closed off continued to increase with 90 closed in March 2016 compared to 40 in December The Trust was now close to having more cases closed in the month than new cases received. Responses to all complaints now went through a quality assurance process that included review by the Chief Executive or Chief Nurse. The themes in the national inpatient staff survey were being investigated. M Kelly, Governor, member of the Patient Community Panel and a PLACE inspector, reported that he was of the opinion that the amount of visits being requested by PCP members was not problematic. The Chair invited T Webster to feedback on a recent PLACE visit; he advised that he had undertaken a visit to Ward 26, at Heartlands and had been very impressed with the environment and staff - he asked that his compliments be passed to the ward staff.
15 P a g e 10 M Kelly requested that compliments should also be passed to the staff on Ward 12 at Heartlands following a visit he had recently undertaken. S Foster advised that the Trust had held a dump the junk initiative during April and some 5 skips of junk had been disposed of on the Heartlands site alone. In response to a question from P Johnson, J Moore advised that the Outpatients department at Heartlands would be in phase one for capital spend when funding had been secured. In response to a question from V Morgan, J Moore advised that complaints about care tended to come from relatives rather than patients with many of the follow up complaints being a result of the Trust being so slow in responding to the original complaint. Patients and relatives were being encouraged to discuss their concerns before discharge from the hospital, failing which to come in for a meeting. There had been investment in the Safeguarding team in order to ensure that the Trust had responded adequately to the recommendations of the CQC. S Foster referred the Governors to the appendices to her Report, being (1) the National Inpatient Survey 2015, (2) the Ward to Board Assurance Report and (3) the proposed CQUINs for 2016/17. In response to a question from J Thomas, S Foster reported that wards felt that visits were now more coordinated and feedback was being acted upon. The PLACE visits were owned by Patient Experience with feedback to Estates, where applicable. M Kelly reminded the meeting that 12 May was International Nurses Day. S Foster advised that the Trust was celebrating with an event on at Heartlands between noon and 2.00 pm to celebrate and recognise compassionate care across the Trust. Governors were invited to attend NATIONAL STAFF SURVEY RESULTS H Gunter reported that the Trust undertook two compulsory surveys each year, one annually and one quarterly. The National Staff Survey typically went to around 850 staff but the Trust had decided to send it to all staff in both 2014 and The 2015 results had shown an improvement in the overall engagement score at 3.63 compared to 3.53 in The Trust remained in the bottom 20% of Acute Trusts at 97th out of 99 acute trusts nationally; however it was noted that the score was the Trust s highest since It was acknowledged that there remained a huge amount of work to be done in terms of improvement. Out of the 32 key findings, 9 had improved over last year, 2 were worse and 10 were new with no comparators, Divisions and directorates were working on actions plans that would be monitored on a regular basis. Results from the quarterly staff survey undertaken at the end of March 2016 had shown an improvement by 12%, leading to some optimism that things were improving. S Hutchings complimented H Gunter on the layout of the report and went on to refer to the high reported level of staff experiencing physical violence from other staff and questioned whether the response was correct. H Gunter confirmed that this was the correct interpretation of the result and that this was being investigated and would be dealt with separately. In response to a question from D Treadwell, J Moore advised that all members of staff had a responsibility to call the Police or Trust security officers if they believed that they were in a situation
16 P a g e 11 of danger. The Trust had a zero tolerance approach to abusive behaviour and violence FINANCE REPORT J Miller presented the report for the period ending 31 March The Trust had reported an income & expenditure deficit of 3.8m for March, after a net impairment gain of 0.9m, leading to a cumulative deficit of 46.1m for the 2015/16 financial year leading prior to any audit adjustments. The reported position for the year included a 0.9m impairment gain (asset revaluation) realised in month 12 and the previously declared 18.6m benefit from a capital to revenue transfer; the underlying position was a deficit of 4.7m in month 12 and 65.6m for the year. The underlying trend showed some improvement with March being the third consecutive month with a deficit below 5m compared to only two instances in the first nine months of the year. The reported position was in line with the most recent forecast of 66.0m deficit but represented a 55.7m adverse variance against the original plan deficit for the year of 9.9m. The main expenditure variances for the year were medical pay 12.2m adverse that was 0.5m adverse in month versus trend of 1.1m adverse; there had been a slight increase across consultant spend offset by lower spend on junior doctors. Nursing 11.1m adverse where expenditure had been in line with the previous month. Unachieved CIP 27.3m adverse that had included 16.9m relating to prior years. Other expenditure 16.5m adverse, of which the largest item was a bad debt provision against CCG for over-performance invoices. Income was 38.8m above plan with main variances being NHS clinical 23.1m but this had been offset by bad debt. Other income 15.9m had included an 18.6m capital to revenue transfer. Emergency admissions had been 0.1% below plan in March even though A&E attendances had been 3.1% above plan. Elective and day case activity was 10% above plan in month and 3.8% up for the year as a whole. CIP delivery for the current year stood at just under 75% for the year ( 6.1m slippage) and had included 4.4m of run-rate schemes (reducing unfunded expenditure). In total 5.8m of CIP has been delivered non-recurrently (and would need replacement schemes to be identified for 2016/17). Cash had reduced to 31.5m at the end of March, 17.6m below the original plan but 9.2m above the forecast produced at the end of January. The Trust s Financial Sustainability Risk Rating remained at a 1 (the lowest possible rating). The Trust had agreed to set a planned deficit of 13.6m for 2016/17 in line with the control total set by NHSI. The main movements from the outturn deficit of 65.6m to the plan value was reliant upon the key assumptions of 12.7m net cost of inflation less tariff increase, 23.3m from the provider sustainability fund, 15.2m benefit from suspension of fines and penalties. This left a total efficiency challenge of 30.2m broken down as follows, 12.0m of local CIPs (2%), of which 9.2m had been identified as deliverable and 2.8m of further ideas continued to be explored; 7.5m FYE of 2015/16 recovery, 5.5m of new FRP savings with a further stretch target of 5.2m. NHSI had visited the Trust during the previous week to review the plans and had been satisfied with both the quality of the plans and the level of engagement from Divisional teams; the challenge for the Trust was delivering the plans. The Trust had not yet signed a contract with the CCGs; it had also been confirmed that readmissions fines would not be included within the suspension of fines and penalties that had previously been assumed and resulted in the forecast for 2016/17 being 19.0m deficit rather than 13.6m deficit. E Coulthard advised that the A&E weekly performance reports sent to Governors still showed the fines incurred by the Trust, K Bolger advised this would be amended to reflect that with the
17 P a g e 12 exception of readmissions fines had been abolished for 2016/17 (Action: KB) CORPORATE IDENTITY F Alexander delivered a presentation that set out work that had been undertaken with over 1,500 members of staff over the last 15 months to develop and articulate the Trust vision and values. The proposed vision statement was to build healthier lives and proposed values were Caring, Honest, Supportive and Accountable. In order to support these it was proposed that the corporate identity was updated; all the design the work had been undertaken in-house by Medical Illustration. Each of the hospital sites would have its own identity. A task and finish group would be implemented to roll out the branding, that include website rebranding, all new documents would carry the new branding going forward but this would be an incremental introduction to avoid unnecessary cost CoG BUSINESS PLAN 2016/17 K Smith presented the draft CoG Business Plan 2016/17. Further work around the timings for meetings was to be undertaken and would be bought advised to Governors. The plan was approved pro tem ANY OTHER BUSINESS The Chair reminded the meeting that the next meeting of the CoG would be used to explore two or three issues in greater detail and asked for suggestions to be ed to her by Friday 20 May following which, in conjunction with M Trotter and M Pearson, she would determine the items for discussion DATE OF NEXT MEETING The next meeting was scheduled for 6 June 2016, to be held in in the Harry Hollier Lecture Theatre, Partnership Learning Centre, Good Hope Hospital. There being no further business the meeting closed.... Chair
 K Bell E Coulthard O Craig M Hutchby S Hutchings P Johnson M Kelly K Bolger J Brotherton A Edwards S Foster J Glasby H Gunter A Hudson (Minutes) and")
18 Minutes of a meeting of the Council of Governors of Heart of England NHS Foundation Trust held in the Harry Hollier Lecture Theatre, Partnership Learning Centre, Good Hope Hospital on 06 June 2016 at 4.00pm PRESENT: IN ATTENDANCE: J Smith (Chair) K Bell E Coulthard O Craig M Hutchby S Hutchings P Johnson M Kelly K Bolger J Brotherton A Edwards S Foster J Glasby H Gunter A Hudson (Minutes) and members of the public. A Lydon A McGeever V Morgan B Orriss M Pearson J Thomas D Treadwell J Miller J Moore J Rao D Rosser K Smith (Secretary) APOLOGIES & WELCOME Apologies for Governors had been received from A Begum, N Burgess, A Fletcher, E Hale, R Hughes, M Meixner, C Needham, M Trotter and D Wallis. Apologies for Directors had been received from K Kneller. The Chair reminded the meeting that this was the first of new style CoG meetings that would consider two deep dive subjects as suggested by Governors APPOINTMENT OF NON-EXECUTIVE DIRECTORS The Chair began by reminding the Governors that several Non-executive Directors (NEDs) had resigned over the last 10 months and that Jammi Rao had now decided not to stand for re-election at end of his term first three-year of office on 30 June 2016, so there was a clear need to appoint some new NEDs. The process had been taking place over several months with updates on progress reported to CoG meetings and had culminated with final interviews being held during the previous week by an Interview Panel comprising members of the CoG Appointments Committee. The CoG Appointments Committee had made a recommendation for the appointment of three new NEDs: Jackie Hendley, Mike Kinski and Michael Sheppard. D Treadwell commented on the impressive CVs of the candidates and went on to question whether J Hendley, a Chartered Accountant and Tax Adviser, had ever given advice on tax avoidance or
19 P a g e 2 evasion. J Moore advised that all candidates, as part of their screening, had to complete a fit and proper person declaration to satisfy the Trust that they had not done anything illegal or improper. J Thomas advised that she had circulated an that set out her concerns about the limited role that Governors who were not members of the CoG Appointments Committee played in the appointment of NEDs but she now understood that the CoG Appointment Committee had a leading role to play in the process, as determined by the Constitution. However, she felt that membership of CoG committees seemed to be arbitrary, which was disappointing but she did understand the need to identify committee members who were prepared to serve. On balance she recognised that there was a desperate need to proceed to appoint new NEDs and was therefore supportive of the recommendation set out in the pre-circulated paper. A Lydon repeated the concerns that he had expressed previously about the process and was disappointed that Governors had not been able to meet candidates prior to considering the recommendation of the Appointments Committee. He was also concerned about all three candidates relationships with other commercial organisations. In response, the Chair reiterated that the three recommended candidates would be required to complete fit and proper persons declarations as well as declaring any interests. The Chair advised that she would have liked there to be more opportunity for Governors to have met the shortlisted candidates but from a practical perspective this had not be possible. The Chair agreed to look at CoG committee membership following the forthcoming Governor elections. In response to a suggestion from E Coulthard that any Governors who had wanted to sit in on the interviews could have been invited, the Chair advised that the candidates had been subjected to a large Interview Panel and that further additional attendees would not have been appropriate. B Orriss commented that the Governors needed to ensure that the Board was balanced and not overwhelmed by academics, noting that one of the candidates was a Professor from the University of Birmingham as was J Glasby, an existing NED. J Glasby advised that he was a social worker by profession and that M Sheppard was a medic. M Pearson advised that he, along with M Kelly and A McGeever (who were present), were members of the CoG Appointments Committee and noted that whilst the candidates might not fully represent the diversity of the Trust s membership the Board was trying to address this and he believed that the Committee had done a good job under the circumstances and that the CoG should approve the recommendation. M Kelly and A McGeever assured the meeting that the selection of candidates had been subject to a robust process and the candidates had been through rigorous interviews with challenging questions. The Chair put the recommendation to a vote on a show of hands: 13 votes in favour, 1 against. The recommendation was approved.
20 P a g e PERFORMANCE & FINANCIAL POSITION REPORT Performance K Bolger presented the pre-circulated report on the Trust s performance that focussed on Monitor, national and local contract indicators rather than internal indicators and exception summaries had been provided where there was non-compliance with performance for targets and indicators included in Monitor s Risk Assessment Framework, national and contractual targets. Material Risks to Quality Relating to National Targets A&E performance was slightly ahead of STF trajectory (84%) but still behind the national target % of patients left the Emergency Department (ED) within 4 hours in April. Individual site performance in April was: Heartlands 83.26%, Good Hope 89.74% and Solihull 99.11%. There had been no 12 hour trolley waits in April. Activity for April was 21,472 against a planned LDP activity of 21,387 attendances but activity in May had increased significantly triggering further analysis for Trust and CCGs of arrivals that included how patients arrived and from where; initial feedback had suggested that patients were predominantly from within the Trust s catchment area, however there had been an increase in the number of attendees from North Solihull at Heartlands, otherwise attendances were as expected across the region. The Trust had asked CCGs to check their levels of activity. The Trust had achieved all of the national cancer targets in March 2016, which meant that the Q4 performance against all of the Monitor Risk Framework indicators had been achieved for the first time in over 12 months. However, the narrow margin of success meant that this performance remained susceptible to swings. The Trust had achieved the Incomplete Pathways Referral to Treatment (RTT) standard of 92% in April for the third month in a row, achieving 92.27%. There had been no 52 week breaches in the month. However, there were a number of specialities where performance had not been met and had remained static for a number of months; where this was the case confirm and challenge meetings were being held to monitor and support improvement against action plans and trajectories. There had been an increase in the backlog of patients waiting 18 weeks since the Trust had ceased using the private sector providers. The number stood at 1,379 at the end of April. There were clear plans in place to improve the outlying specialities. 6 week diagnostics had delivered 99.22% against a target of 99%, achieving the target for the third consecutive month and the Trust was ahead of trajectory. Gastroscopy continued to be an ongoing issue but plans to increase capacity across the Trust were being explored. C.diff was on target. Two urgent operations had been cancelled for the second time in April, both had been in Trauma. The breaches had been as a result of the lists running out of time due to overbooking and the list starting late, the Theatre Efficiency Group would investigate. Local indicators contract The Trust had met the breast feeding rate in April at 73.1% against a target of 72%; this was the first time this had been met. The process had not change dramatically however the recording of
21 P a g e 4 data had improved. E Coulthard wished to record congratulations to Good Hope for achieving the A&E 4-hour target two weeks previous. In response to a question from A Lydon, K Bolger advised that GP s had undertaken ward rounds and a report was awaited, the Trust had also asked its consultants who had also attended the ward rounds to give a view. On a separate point, K Bolger advised that the contractual requirement on discharge was for a 7 day supply of drugs to be provided not one month s supply. In response to a question from D Treadwell, J Moore advised that CCG boards did have secondary care representation but only from trusts outside of their area. In response to a question from V Morgan, K Bolger reported that closer working with consultants and a multidisciplinary team approach had been happening with encouraging results Finance J Miller presented the report for the period ending 30 April The Trust had agreed a planned deficit of 13.6m for 2016/17. Since the plan had been submitted to Monitor it had been confirmed that emergency readmission penalties of 5.4m would not be included within the national suspension of fines and penalties and would still apply in 2016/17. The Trust had reported an I&E deficit of 2.8m in M1 (April 2016), an adverse variance of 0.5m against the plan of 2.3m deficit, 100k adverse against the revised forecast of 2.7m deficit including the readmissions penalty. As a result the current forecast was a deficit of 19.0m assuming full delivery of 30.2m planned CIP efficiency savings. In response to a question from V Morgan, J Miller confirmed that under Payment by Result (PbR) the Trust received income for increased activity. In response to a question from A McGeever, J Miller advised that Trust was generally charged for any readmissions within 30 days and the total fines for this equated to around 5.3m per annum. M Pearson questioned if the fine was higher or lower than other organisations, K Bolger advised that there were no national figures available and that calculation for the fines had been based on an audit undertaken on the Trust block contract activity in 2013/14 and agreed that that an audit by the operational teams to benchmark against that time would be worthwhile. In response to questions from J Thomas, J Moore advised that (1) the revised financial deficit trajectory had been discussed with NHSi who understood the risks associated with that revision and had confirmed that the Trust would now move from monthly to quarterly reporting, and (2) meetings had been held with the Treasury and the DH to discuss financing for the Trust s capital requirements and that there had been a very strong indication that funding for the Ambulatory Care and Diagnostics centre (ACAD) and a new tower block on the Heartlands site would be forthcoming but this was still to be formally confirmed. Following interest at a recent Governors Breakfast Meeting, the Chair asked S Foster and H Gunter to give an update on the support the Trust gives to nurses recruited from overseas. S Foster explained that the Trust recruited nurses from EU and non-eu countries as well as from Birmingham City University and some from University of Birmingham. Nurses received a pastoral programme of support e.g. help sourcing accommodation, banking, social life advice, 24-hour helpline, as well as reduced night working for the first 3 months. English language support was also provided to those who needed it. A Rate my first year at HEFT survey had recently been conducted.
22 P a g e 5 H Gunter added that as part of the recruitment process the Trust held open days, where it undertook interviews, offered jobs and undertook appropriate checks, the Trust then kept in regular contact with candidates up to their start date (e.g. weekly telephone calls). If candidates were waiting for their NMC PIN numbers they were taken on as HCAs until their PINs were confirmed. The Trust also provided 3 month s free accommodation. Turnover of nursing staff had begun to reduce. It was noted, however, that some staff still left because the grass is always greener on the other side but some had returned having realised that this was not necessarily correct. In response to a question from B Orriss, S Foster advised the Trust advertised via Twitter and Facebook as well as on its website when holding open days, advertising in local newspapers was expensive and perceived to be less relevant to today s nurses. In response to a question from M Kelly, S Foster advised that the Trust had a policy and a review group that considered all request to travel home for compassionate leave and supported staff when required DEEP DIVES Incident Reporting Management and Learning from Incidents. D Burbridge and A Keogh delivered a presentation. The Trust followed the national framework for reporting and investigating serious incidents that emphasised the purpose of the investigation was to identify the learning and subsequent actions to minimise the risk of recurrence. A Keogh went on to explore the definitions of: An incident Incident severity A serious incident The level of investigation should be proportionate. The Trust investigation process was explained. Trust incidents were reported to other agencies as appropriate, including the CQC, NHSi, CCGs and the Coroner. Dissemination of learning was crucial and was actioned through multiple channels. The Board had oversight of all serious incidents and the outcome of investigations. The Board Quality Committee.considered rates, numbers, trends, themes and actions. HEFT in numbers. Total number of incident 1,800 per month, 50 a day Patient safety incidents 1,250 per month, 41 a day Severe harm incidents 19 a month, of which 7 were patient SIs The top 5 categories were: Patient fall
23 P a g e 6 Tissue viability Medication Ongoing care, monitoring and review Admissions, transfers and discharge Based on NRLS comparison with 136 other acute trusts HEFT had dropped from just above to just below the 25 th percentile. The Trust s own analysis for Q had indicated improvement in reporting levels, but confirmation was outstanding. The Trust had seen an increase in reported low harm incidents which was favourable as it demonstrated that incident reporting had been made easier and staff were confident that action would be taken. A review of incident reporting had been undertaken in 2015 and it had been identified that the Trust had over 3,000 open incidents following work on the backlog this had now reduced to approximately 200 and would continue to be reduced as part of the business as usual process. D Burbridge explained that the situation would now be kept under regular review to avoid further unacceptable backlogs. In response to a question from M Pearson about to the level of access Governors should have to incident data, the Chair advised that it was more a question of receiving assurance that there were processes in place and that reports to the Board were made on an exceptions basis. D Burbridge advised that assurance that the organisation was learning from incidents was evidenced through dissemination of the learning and managers ensuring that their staff had sight of that learning. Directors were also learning through the RCA forum and Board Unannounced Governance Visits to wards. The Chair advised that an incident reporting culture was key and staff were actively encouraged to report incidents. M Pearson, B Orriss and E Coulthard noted the importance of staff being empowered to report and escalate incidents without fear of the consequences; also that staff should be empowered to say STOP when appropriate Delayed Transfers of Care (DTOCs) J Brotherton and M Ring delivered a presentation on the challenges faced by the Trust. The NHS England s definition of a DTOCs was explored There were three main categories of coding for DTOCs: health, social care and joint health and social care but there many were further sub-divisions. The Trust undertakes weekly and monthly reporting of DTOCs and at April 2016 achieved 4.4% against a 2.2% NHSi target which equates to an average of 54 patients occupying acute beds. Much work had been undertaken over the last 12 months to reduce the number of DTOCs over the three sites and at GHH DTOCs had reduced from 25 patients delayed to 10 at the census date. There were numerous reasons for internal (HEFT) delays 75% of which related to patient/ family
24 P a g e 7 choice and 20% due to health assessment delays. There had been a reduction of around 70 Enhanced Assessment Beds in the local healthcare economy which was exacerbating the position. There was an improvement plan in place for both internal and external delays that included adopting good practice/ learning from the Good Hope experience and UHB, and maintaining pressure on external partners. In response to a question from K Bell, M Ring advised that family or relative choice often meant the family may be going on holiday and wanted the discharge delayed until their return or the rehabilitation home was not their home of choice. The Trust was now increasingly clear with patients, their families and carers on planning to get patients home from the start of the patient pathway. T Webster questioned why Good Hope s performance was so much better than Heartlands; M Ring advised that the main issue was around patient choice, Good Hope was following the correct process NED FEEDBACK J Rao reported that he had become a NED in 2013 and had taken time to reflect that the role was one of providing strategic direction, monitoring performance, managing risk and communication. The strategy for the Trust was inextricably linked to that of the whole NHS as well as bound by technology and would ultimately be determined by the government of the day and the public. Performance measures were not always set by the Board but forced upon the organisation with the consequence that much time was spent discussing measures that were not always the most important. As a NED he had not always been involved in communication with internal and external stakeholders as the Trust, in the main, the Trust had influential chairs and CEOs who had been able to undertake that role. J Rao s main interest had been around risk especially in his role as Chair of the now disbanded Quality and Risk Committee. Healthcare was an inherently risky and unpredictable business. Even when an organisation has the best systems in place ultimately they were dependent upon each member of staff doing everything right and it was a responsibility of the NEDs to ensure that the processes were in place to reduce risk. Every time a clinician recommended treatment there was a cost and a risk of harm and it was hoped that clinicians and patients understood this. It was important that clinicians care and staff were supported; it was the role of the Board and the NEDs to convince staff that they cared. In response to a question from M Pearson, J Rao confirmed that he believed that his role in public health had helped him understand the bigger picture which had helped him in his role as a NED. In response to a question from J Thomas regarding what advice he had for Governors, he said that the Governors were a challenging bunch but should continue to provide challenge to the Board. The Chair on behalf of the Board and Governors thanked J Rao for his presentation and his contribution over the last three years ANY OTHER BUSINESS
25 P a g e 8 K Bell noted the progress with the Paterson breast cancer patients and that the introduction of a telephone helpline had been positively received. There had been an issued where the content of letters had been inaccurate which was being checked DATE OF NEXT MEETING The next meeting was scheduled for 6 July 2016, to be held in in the Education Centre, Birmingham Heartlands Hospital. There being no further business the meeting closed.... Chair
26 Date raised Minute No Action by Completed COUNCIL OF GOVERNORS Matters Arising & Decisions/Recommendations Tracker Detail Due Status 6 Jan Feb Mar Apr May Investigate and report back on statement that the Trust was paying between 10 and 12 times the going rate for staff though agencies Provide DTOC information to B Orriss during the last 6 and 12 months. Provide DTOC information by site, as requested by A Lydon Check whether anything more can be done to utilise unoccupied retail units above Heartlands Main Reception. Check issue regarding (T Webster) parking in disabled spaces on the visitor car park at Heartlands with Governor badge but receiving fine. Check when drinking water will be made available in GHH Treatment Centre Circulate PwC s presentation with minutes Circulate wording for Governors use on social media sites. Report on how local 2015/16 Better Care Fund was utilised. Revise format or data on A&E attendance table (3.1.1) to improve clarity. Revise weekly A&E performance data (circulated by ) to reflect revised position on fines and penalties for 2016/17. KB Mar 16 KB Mar 16 KB Mar 16 KB Mar 16 No evidence to support this - closed Included in Performance Report - closed Provided hand out - closed Not without payment of rent - closed 11 May May May May 16 KB Mar 16 Closed 11 May 16 KB May 16 KS May 16 KS Apr 16 KB Jul 16 KB Jul 16 Drinking water now available - closed Circulated in pack - closed Circulated by - closed 11 May May May 16 KB May 16 Completed May 16
27 HEART OF ENGLAND NHS FOUNDATION TRUST COUNCIL OF GOVERNORS 25 July 2016 Since my last report, the UK has voted to leave the European Union. There may well be some important ramifications for the trust in terms of our ability to recruit from other parts of Europe and the money available to fund the vital research which keeps our NHS at the forefront of medical developments. At the moment, the exact consequences are unclear. However, we already have staff expressing concern about whether they will be able to stay with us and others experiencing unpleasantness from patients and the public. Dame Julie Moore has issued a very strong message of support to our staff and we will continue to be clear with them that we will not accept any abuse, that their job with us is crucial and that we will do all we can to support them. In the longer term we will also be arguing for some of the extra money promised to the NHS in the event of a Brexit I m not very optimistic that promise will be kept. The Sustainability and Transformation Planning process that we outlined at the last Council of Governors continues. The first draft of the Birmingham and Solihull plan has now been submitted. As well as the Chairs and Leaders Group for the STP, I recently attended with representatives from the two councils, CCG and other providers to be grilled by leaders of NHS England, NHS Improvement, CQC, LGA and others. The panel recognised the work which has gone into building relationships across the patch, but also emphasised that there is much work still to be done on the detail of our planning in terms of services and finances before the final submission in September. With Councillor Bob Sleigh, leader of Solihull Council I have commissioned a review into the governance of the ICASS project in Solihull. Whilst there is much good work going on in partnership with the council and CCG in Solihull, it is important to get the structures streamlined and focused on patients rather than meetings. The review has made some important recommendations on this and on how to fit the work within the STP programme. I visited the New Oscott ExtraCare Retirement Village with their Chief Executive, Mick Laverty. This model of keeping older people active and healthy is very effective and we should look to find ways to work together with them more. Rachel Cashman and I attended the Solihull Council Overview and Scrutiny Committee and outlined for the councillors the progress made by the Trust in finances and clinical performance. We were also able to explain the good developments in the Solihull Urgent Care Centre. I am a member of the West Midlands Violence Prevention Network Advisory Board. At the last meeting we received an extremely encouraging presentation on the work to gather injury information from Emergency Departments including at HEFT. This is a first in England and has enabled the police and others to get a much clearer picture of where violence is happening and who is affected. The three new NEDs, Mike Kinski, Jackie Hendley and Michael Sheppard have all started their induction including being allocated times for Board Governance visits to different parts of the Trust.
28 Finally I would like to offer my warmest congratulations to those re-elected to the Council of Governors and my commiserations to those who were not successful. At least I understand what it s like to lose an election! Thank you to all the governors for your efforts on behalf of our members and patients. In particular, I would like to offer thanks to Richard Hughes who has taken on the role of Lead Governor and who has come to the end of his term. I am personally grateful to him for his advice and experience and I know that he has worked extremely hard to help lead the Council at a time of considerable turbulence. Thank you. Jacqui Smith 18 July 2016
29 Chief Executive s Update Oral Update
30 HEART OF ENGLAND NHS FOUNDATION TRUST COUNCIL OF GOVERNORS MONDAY 25 JULY 2016 Title: Responsible Director : Contact Performance Indicators Report Kevin Bolger, Interim Deputy CEO - Improvement Purpose The purpose of this report is to provide an overview of performance against a number of key national and local contractual indicators. To provide exception summaries where there are current or future risks to performance for targets and indicators included in Monitor s Risk Assessment Framework, national and contractual targets and indicators. Confidentiality Level & Reason Annual Plan Ref Key Issues Summary: None Affects all strategic aims The Monitor Risk Assessment Framework, A&E 4 hour wait target and the 2 week cancer wait from referral to first appointment were not met. The Trust met the STF trajectories in the current reporting month. Cancer is reported a month in arrears and met the target in May; however June s unvalidated performance shows that the Trust may miss this target in month. An update against the STF trajectories is provided at Appendix 1 Recommendations The Council of Governors is requested to receive the information set out in this report Approved by: Page 1 of 9
31 HEART OF ENGLAND NHS FOUNDATION TRUST COUNCIL OF GOVERNORS MONDAY 25 JULY 2016 PERFORMANCE INDICATORS REPORT 1. Purpose This paper summarises the Trust s performance against national indicators and targets, including those in Monitor s Risk Assessment Framework, as well as local priorities. 2. HEFT Key Performance Indicators The Trust has a suite of Key Performance Indicators that includes national targets set by the Department of Health (DH) and local indicators selected by the Trust as priority areas, some of which are jointly agreed with the Trust s commissioners. This report is intended to give a view of overall performance of the organisation in a concise format and highlight key risks particularly around national and contractual targets. 3. Material Risks Current and future material risks to performance against Monitor and national targets are outlined below. Performance for the latest period for all national targets is shown in the table below: Monitor Targets Indicator Threshold Current Data Period Period actual 18 week RTT - incomplete 92% May 92.46% A&E 4 hour access 95% Jun 88.36% Cancer 2 week 93% May 91.90% Cancer breast - 2 week 93% May 95.48% Cancer 31 days- first treatment 96% May 99.69% Cancer 31 days- subsequent treatment -surgery 94% May % Cancer 31 days - subsequent treatment - drugs 98% May % Cancer 62 day - GP urgent referral 85% May 87.87% Cancer 62 day - national screening 90% May % C.difficile - (all cases) 5 Jun 3 C.difficile - (avoidable cases) 0 Jun 0 Community Data Completeness - RTT information 50% Q % Community Data Completeness - referral information 50% Q % Community Data Completeness -treatment activity information 50% Q % Learning disabilities Declaration made Q4 Yes Page 2 of 9
32 Indicator Other National Targets Threshold Current Data Period Period actual 6 weeks diagnostic test 99% Jun 99.72% Ambulance Handover > 30 minutes >0 May 183 Ambulance Handover > 60 minutes >0 May 2 12 hour Trolley waits A&E 0 Jun 1 52 week waits 0 Jun 0 Cancelled Ops rearranged 28 days 0 Jun 0 Urgent operation cancelled x 2 0 Jun 2 Sleeping Accommodation Breach 0 Jun 10 MRSA 0 Jun 1 VTE risk assessment 95% Jun 98.39% Duty of Candour (2 months in arrears) 0 Apr 0 NHS Number acute 99% Jun 99.63% NHS Number A&E 95% Jun 98.35% 3.1 Monitor Risk Assessment Framework There are 14 indicators currently included in Monitor s Risk Assessment Framework (RAF), 12 were on target in the most recent reporting month. The A&E 4 hour wait target and the 2 week cancer wait from referral to first appointment were not met A&E 4 Hour Waits In June the Trust s performance against the 95% A&E standard was 88.36%. This performance is above than the Strategic Transformation Fund trajectory (STF) which was to achieve 87% in June Cancer Targets (month in arrears) The Trust met all of the Monitor Risk Assessment cancer targets in May, apart from the 2 week urgent referral to first appointment indicator. In May, most specialties achieved the 2ww referral-to-first seen target; the exceptions were Upper GI and Lower GI. The key problem related to a lack of endoscopy capacity resulting from ongoing challenges in recruiting and retaining locum consultants. The endoscopy service was severely impacted during May, resulting in 59 Upper GI breaches and 67 Lower GI breaches. In June, the Cancer Services Team implemented a daily 2ww breach report which tracked the number of breaches by specialty against an Page 3 of 9
33 overall Trust breach threshold. This has ensured a clear focus on 2ww performance throughout the month. Although final validation is still being undertaken, it does look as if the Trust will meet this target in June for both the month and the quarter Current unvalidated performance for the June cancer targets shows a risk to the delivery of the 62 day cancer target in month, primarily due to a high number of breaches in Urology. It does look however as if the Trust will meet the quarter 1 target. June is the first month that the Trust is expected to deliver sustained performance against the STF trajectory, and it is likely that this will be missed Referral to Treatment Time A final validated position against the 92% incomplete 18 week referral to treatment target was not available for the time of this report, with the national reporting deadline date after the submission of papers to the Board. However the current unvalidated position as at 14 July was 92.09%, with ongoing validation usually improving the position. The STF trajectory for June was to achieve 91.52% C.difficile The Trust had 3 cases of post 48-hour c.diff in June against a target of five. The Trust has had 12 cases ytd against a target of 15. Only one of these cases has been deemed avoidable (it was originally reported that 2 of the April cases were avoidable, however this has been revised following further review with clinicians). 3.2 National Targets Monitored Locally Through CCG Contract Of the 13 national targets that are not included in Monitor s Risk Assessment Framework but are included in the CCG contract the Trust is on target for 7 and not delivering against Zero tolerance MRSA In June there was 1 MRSA bacteraemia on Ward 16 at GHH. An RCA is being undertaken in respect of this and will be reported through the Executive RCA Group. The Trust has had 2 MRSA bacteraemias ytd Ambulance Handover - 30 and 60 minutes Performance against the 30 and 60 minute wait targets in June shows that 295 (183 in May) patients waited over 30 minutes and 9 (2 in May) patients waited over 60 minutes (the 60 minutes position is still awaiting final validation, so is likely to improve). Page 4 of 9
34 There has been a significant increase in the number of 30 minute ambulance handover breaches in month, equating to performance of 95.61% ahead of the 95% target set by the CCG for contracting purposes hour trolley waits in A&E There was one 12 hour trolley breach in June on the BHH site, relating to a delay for a patient requiring admission to a mental health bed Mixed Sex Accommodation Breaches There were three occasions in month, when mixed sex accommodation breaches occurred in the Triage Assessment Unit at GHH, the breaches affected 10 patients in total. RCAs are currently being undertaken in respect of these and plans will be put in place to prevent recurrence Urgent Operations cancelled twice There were 2 patients requiring urgent surgery that had their operations cancelled twice. The first was in thoracic surgery, where the patient was cancelled twice due to other emergencies taking priority. The second was a trauma patient who was cancelled due to theatre running out of time, firstly as the list was overbooked and secondly due to a previous case overrunning Both patients have since been treated % patients waiting <6 weeks for 15 key diagnostic tests 4. Local Indicators contract The Trust achieved the 99% diagnostic target in June with performance at 99.72% this is ahead of the STF trajectory of 98.03%. There are 45 local contractual indicators that the Trust s performance is measured against (24 are reported monthly, 18 of these are reported quarterly and three bi-annually). For the monthly and quarterly indicators that required reporting in June, and for which data is available the Trust is non-compliant with three. 4.1 Pressure Ulcer Reduction for avoidable grade 3 pressure ulcers (mia) The Trust had 9 avoidable grade 3 pressure ulcers in May. There is an annual target of less than 41 for this indicator (avg 3 a month). More information is provided in the Care Quality Report 4.2 Tissue viability repositioning frequency. The Trust met the overall tissue viability metric but failed to meet the Compliance with Nursing Care Indicators - Tissue Viability metric (Repositioning frequency Page 5 of 9
35 adhered to 3 days) for the sixth month in a row although performance had improved from 84% in May to 86% in June, against a target of 90%. See Care Quality Report for more detail. 4.3 Delayed Transfers of Care (DTOC) for health and joint delays The Trust has missed this target in month, however there has been a very slight improvement against May (1.95%) with performance at 1.9% in June against a 1.4% target. The Length of Stay Workstream is taking action to improve compliance with this indicator and a sub group has been set up to review the DTOC reporting, to provide assurance that the Trust is reporting correctly against this metric. This work is being undertaken with in collaboration with colleagues from UHB. 4.4 Appraisals The Trust has met the appraisal target of 85% achieving 87.06% in June in line with its trajectory, see table below: Jan Feb Mar Apr May Jun Performance 72% 75.6% 77.7% 81.2% 84.33% 87.06% Revised trajectory 70% 73% 76% 79% 82% 85% 5. Local Indicators - Workforce 5.1 Sickness In June the Trust performance against the sickness target was 4.1% against a target of 4%. 5.2 Staff in post v budget established - Qualified Nurses Of the 3 metrics relating to staff in post v budget establishment only one relating qualified nurses has been missed in month. Further detail on this is provided through the Care Quality Report. 5.3 Time to Hire The target for time to hire is seven weeks and currently the Trust is achieving 9.17 weeks (an improvement on May at 9.68 weeks). Hiring manager time is 5.7 weeks at Trust level against a target of less than three weeks and recruitment time is at 3.47 weeks against a target of less than 4 weeks. Division 5 s performance has improved significantly in month from 14 weeks in May to 9 weeks in June. Page 6 of 9
36 6. Other Contracts The Trust has a number of community contracts, many of the indicators against these contracts are reported quarterly: 6.1 Solihull CCG contract Of the 18 KPIs reported through this contract the Trust is compliant with all but one This failure relates to the percentage of Designated Doctor sessions delivered by the community paediatrician. Performance for Q1 was 84.38% against a target of 85%. This KPI is primarily used as a tool for monitoring delivery of sessions over the year, and any lost time this quarter will be made up in future quarters. 6.2 Solihull Metropolitan Borough Council Contract The Trust has met all 6 of the KPI requirements for quarter Recommendations The Council of Governors is requested to: 10.1 Accept the report on progress made towards achieving performance targets and associated actions and risks. Kevin Bolger Interim Deputy CEO Improvement Page 7 of 9
37 Performance Performance Appendix /17 STF Trajectories at HEFT - June validated unvalidated 62 Day Cancer Trajectory Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 HEFT Performance 89.97% 87.87% 81.80% Trajectory 82.80% 84.90% 85.20% 85.40% 85.50% 85.50% 85.30% 85.50% 85.70% 86.10% 86.20% 86.50% % 95.00% 90.00% 85.00% 80.00% 75.00% 70.00% Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Month HEFT Performance RTT Incomplete pathways Trajectory Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 HEFT Performance 92.27% 92.45% 92.09% Trajectory 91.20% 91.36% 91.52% 91.68% 91.84% 92.00% 92% 92% 92% 92% 92% 92% 93.00% 92.50% 92.00% 91.50% 91.00% 90.50% 90.00% 89.50% 89.00% Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Month HEFT Performance Trajectory Page 8 of 9
38 Performance Performance Diagnostics National Target Trajectory Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 HEFT Performance 99.22% 99.39% 99.7% Trajectory 97.34% 97.68% 98.03% 98.37% 98.71% 99.00% 99% 99% 99% 99% 99% 99% % 99.00% 98.00% 97.00% 96.00% 95.00% 94.00% 93.00% 92.00% 91.00% 90.00% Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Month HEFT Performance Trajectory A&E Trajectory Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 HEFT Performance 87.9% 86.82% 88.36% Trajectory 84.0% 85.5% 87.0% 88.0% 90.0% 91.0% 91.0% 92.0% 91.0% 91.0% 91.5% 92.0% 100.0% 95.0% 90.0% 85.0% 80.0% 75.0% 70.0% Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 Mar-17 Month HEFT Performance Trajectory Page 9 of 9
39 HEART OF ENGLAND NHS Council of Governors 25 th July 2016 Title: Clinical Quality Monitoring Report Presented by: Dr David Rosser, Interim Executive Medical Director To: Council of Governors Prepared by: Amy Fowlie, Project Assistant, Imogen Gray, Interim Head of Quality Development, and Dr Ann Keogh, Director of Medical Safety The Report is being provided for: Decision N Discussion Y Assurance Y Endorsement Y Purpose To provide assurance on clinical quality to the Board of Directors and detail the actions being taken following the Clinical Quality Monitoring Group (CQMG) meetings on 6 th June 2016 and 21 st June Receive and note the contents of this report. Key points/summary: The Council of Governors will receive assurance on: Investigations into Doctors performance currently underway Mortality indicators: CUSUM, SHMI, CRAB and HSMR A mortality review of Other perinatal conditions (224) and Normal Pregnancy and/ or delivery (218) Board of Directors Unannounced Governance Visits Performance for timely delivery of antibiotic stat (one off) doses Assurance Implications: Board Assurance Framework Y/N BAF Risk Reference No. Performance KPIs year to date Y/N Resource/Assurance Implications (e.g. Financial/HR) Information Exempt from Y/N If yes, reason why. Disclosure Identify any Equality & Diversity issues Y/N Which Committees has this paper been to? (e.g. AC, QC, etc.) Board of Directors Page 1 of 7
40 HEART OF ENGLAND NHS Council of Governors 25 th July 2016 CLINICAL QUALITY MONITORING REPORT PRESENTED BY INTERIM EXECUTIVE MEDICAL DIRECTOR 1. Introduction The aim of this paper is to provide assurance of the clinical quality to the Board of Directors, detailing the actions being taken following the two June 2016 CQMG meetings. The Board of Directors is requested to discuss the contents of this report and approve the actions identified. 2. Investigations into Doctors Performance There are currently ten investigations underway into Doctors performance. The investigations relate to four Consultant Grade Doctors and six Specialty and Associate Specialist (SAS) doctors. 3. Mortality CUSUM 3.1 Two CCS (Clinical Classification System) groups had higher than expected deaths in February 2016 but did not breach the mortality thresholds. The groups are Fluid and electrolyte disorders (55) and Pneumonia (except that caused by tuberculosis or sexually transmitted disease) (122). The patient case list for Fluid and electrolyte disorders CCS group was reviewed at the 6 June 2016 CQMG meeting and no concerns or further actions were identified. The patient case list for the Pneumonia (expect that caused by tuberculosis or sexually transmitted disease) CCS group for January 2016 is already being reviewed following the April 2016 CQMG meeting. The purpose of the review is to identify any patients who require a full case note review based on their age, length of stay or diagnosis codes. The outcomes of this review are due to be reported to the next Clinical Quality Monitoring Group in July Please see Figure 1 below. Figure 1: HEFT CUSUM in March 2016 for HSMR CCS Groups Page 2 of 7
, Short gestation; low birth weight; foetal growth retardation (219) and Other non-epithelial cancer of skin (23).")
41 HEART OF ENGLAND NHS Council of Governors 25 th July Three CCS groups had higher than expected deaths in March 2016 but have not breached the mortality thresholds. The groups are Inflammatory conditions of male genital organs (165), Short gestation; low birth weight; foetal growth retardation (219) and Other non-epithelial cancer of skin (23). The patient case lists for these groups were reviewed at the CQMG meeting on 21 st June 2016 and no further concerns were identified. 3.3 The Trust s overall mortality rate as measured by the CUSUM is within the acceptable limits. Please see Figure 2 below. Figure 2: HEFT CUSUM in February 2016 at Trust level Page 3 of 7
42 HEART OF ENGLAND NHS Council of Governors 25 th July Mortality SHMI (Summary Hospital-Level Mortality Indicator) The Trust s SHMI performance from April 2015 to February 2016 is The Trust has had 3,954 deaths compared with 4,216 expected. The Trust is within the acceptable limits as shown in Figure 3 below. Figure 3: HEFT SHMI (April 2015 to February 2016) 5. Mortality HSMR (Hospital Standardised Mortality Radio) The Trust s HSMR in 2015/16 (April-March) is which is slightly lower than expected. The Trust had 2,799 deaths compared with 2,825 expected (see Figure 4 below). Page 4 of 7
43 HEART OF ENGLAND NHS Council of Governors 25 th July 2016 Figure 4: HEFT HSMR 6. CRAB (Copeland Risk Adjusted Barometer) surgical 30 day risk adjusted mortality ratio to April The Trust s CRAB 30 day surgical mortality O/E (outcome versus expected) ratio has stabilised following a rise and has returned to a level below or equal to the average of 1 (see Figure 5 below). Figure 5: CRAB 30 day surgical mortality O/E ratio. Page 5 of 7
44 HEART OF ENGLAND NHS Council of Governors 25 th July Mortality Review of Other perinatal conditions (224) and Normal Pregnancy and/ or delivery (218) (reported June 6 th ) 7.1 A mortality review of Other perinatal conditions (224) and Normal Pregnancy and/ or delivery (218) has been provided to the CQMG. The CCS groups triggered and/or were approaching the trigger line in the January 2016 mortality CUSUM. 7.2 Several learning and action points have been identified and implemented by Division 2 Women s and Children s following mortality review. The Division will review current compliance with GROW training which will become mandatory. The Royal College of Obstetricians and Gynaecologists guideline states that in cases of late stage identification of FGR, labour should be induced at 37 weeks; this guideline will now be implemented at HEFT. The Division is also working towards ensuring that a Consultant is consistently available in clinic. 8. Board of Directors Unannounced Governance Visits The programme of monthly Board of Directors Unannounced Governance Visits involving Non-Executive Directors and other Directors commenced in December The most recent visit took place 20 th May 2016 and was to ward 24 (Respiratory Medicine) at Birmingham Heartlands Hospital (BHH). The visit was positive and the action points were predominantly concerned with environmental factors which have been shared with the Divisional Management Team. 9. Timely Delivery of Antibiotic Stat (One-off) Doses The information contained in the report was correct as of 6 th June HEFT was 74.8% compliant with the one hour target from prescription to administration of the antibiotic stat dose in the last 30 days compared with 73.2% in the last twelve months. The antibiotic stat doses dashboard is currently being rolled out across the Page 6 of 7
45 HEART OF ENGLAND NHS Council of Governors 25 th July 2016 Trust following the successful pilot at Solihull Acute Medical Unit (AMU), which achieved 89% compliance with 196 doses administered in the month to June 6 th. 10. Recommendations The Board of Directors is asked to: Discuss the contents of this report and approve the actions identified. Dr David Rosser Interim Executive Medical Director Page 7 of 7
46 HEART OF ENGLAND NHS FOUNDATION TRUST COUNCIL OF GOVERNORS MONDAY 25 TH JULY 2016 Title: Care Quality Report From: Sam Foster - Chief Nurse The Report is being provided for: To Council of Governors Decision N Discussion N Assurance Y Endorsement Y Purpose: The purpose of this report is to provide an overview of performance against a number of key national and local contract indicators, and to provide exception summaries where there are current or future risks for targets and indicators. Key Points/Summary: 1. Infection Control 1.1 Clostridium Difficile There were four cases of post 48 hour toxin positive Clostridium difficile in May A post infection review carried out in conjunction with the CCG established that all of the cases were unavoidable. Division 3 had one case on Ward 10 GHH, division four had one case on Rowan Ward BHH, and division 5 had two cases - one on ward 8 BHH and one on ward 5 BHH. There were three cases of post 48 hour toxin positive Clostridium difficile in June A post infection review carried out in conjunction with the CCG established that all of the cases were unavoidable. Division 4 had two cases - one on ward 20A SH and one on ward 3 BHH, division 5 had one case on ward 10 BHH. 1.2 MRSA Bacteraemia There was one unavoidable Trust attributable post 48 hour MRSA bacteraemia in May 2016 on ward 22 HDU / ITU at GHH. There was one Trust attributable MRSA bacteraemia in June 2016 on ward 16 at GHH. The full post infeciton review is yet to be completed. 1.3 Unannounced Inspection - CPE An unannounced inspection visit was conducted on 28 th June 2016 at Birmingham Heartlands Hospital on wards 9 and 12 by Infection Prevention team Birmingham Cross City Commissioners.
47 2. Tissue Viability During the visit the Team assessed: - Compliance with the CPE Action Plan. - Infection Prevention Standards. - Hand hygiene compliance. - Peripheral Venous Cannula scores. - Isolation. Findings/Recommendations: - The Matrons and staff at Heartlands were very receptive, open and honest, and communication and knowledge of CPE appeared good within the wards visited. - The Trust to continue with the trust wide Hand Hygiene programme and PPE policy and decontaminate hands in line with 5 moments. - VIP scores to be completed for all patients with a cannula in line with IV policy. - Continue staff education programme for CPE. - Review cleaning programme for frequently used items such as observations trollies. There has been a decrease in the incidence of avoidable hospital acquired Grade 3 pressure ulcers June 2016 with a total of 4 reported across Divisions 3, 4 and 5 on a mix of wards. Compliance against the total number of hospital acquired Grade 2 pressure ulcers remains static at 14 in month this means that the organisation is currently below trajectory. Adherence to the frequency of repositioning has improved and is at 86%, this is the highest score reported since December The actions taken relate to individual accountabilty, revision of divisional RCA forums, and the introduction of a quarterly Trust wide RCA forum to monitor improvement in performance. ulcers. Viability Steering Group meeting. 3. UNIFY Staffing 3.1 Division One ITU GHH and ITU BHH patient acuity fluctuates and therefore staffing is adjusted accordingly. Staffing levels are compliant with the national guidance for staffing in level 2 and level 3 units. 3.2 Division Three HASU BHH is staffed safely according to patient acuity. Ward 17 Solihull shortfalls noted but reported as safe by Matron and Associate Head Nurse. 3.3 Division Five Ward 4 HDU patient acuity fluctuates and therefore staffing is adjusted accordingly. Staffing levels are compliant with the national guidance for staffing in level 2 units. Ward 14 Sol reduces in patient numbers over the weekend or closes from Saturday afternoon through to Monday morning. Ward consistently staffed safely for patient numbers
48 4. Nursing & Midwifery Staffing 4.1 Nursing Vacancies There are WTE qualified vacancies across the Trust with 159 planned starters between July and October This is a positive position for the Trust of these vacancies are across base wards and AMUs (a 32% reduction in qualified vacancies across these areas when compared with June 2015 when the vacancy rate was 200). Recruitment campaigns continue on a monthly basis via the Saturday recruitment days and twice monthly via Skype for our EU nurse interviews. In addition to this specialities run their own adverts and recruitment events. There is a planned recruitment trip to Romania in August 2016 with an estimated 40 interviews, these will be a mixture of nurses that have already submitted their NMC application for their PIN number and those that require IELTS level 7 before the NMC registration process can begin. 4.2 Care Hours per Patient Day This is a new measure of nurse to patient ratios and measures the average care hours available to each patient in a clinical area. This is a crude measure as it takes the number of actual hours available from qualified and HCA staff and divides this by the number of patients, giving the average care hours available for each patient each day. There are no national plans to benchmark this data. The trust data will be reviewed at ward level along with quality outcome data to inform planned staffing levels. We are currently rolling our Safe Care a function of our e-rostering system which will enable live data capture of acuity and dependency twice a day. 4.3 erostering KPIs There are four key e- Rostering KPIs that we have selected as a measure of roster efficiency as recommended in the Carter report: Unfilled Duties: The percentage of planned duties that were left unfilled for June was 12.9% which remains below the Trust target of <30% Additional Duties The number of duties that were rostered in addition to those planned was 2595 across the whole trust which is a decrease from May (2953) Unavailability The percentage of staff unavailable or on leave remains static at 28.4% Temporary Staffing The proportion of duties that were filled by bank and agency staff for June was 18.5% which is a slight reduction from May and remains below the Trust target of <20%.
49 5. Complaints The numbers of formal complaints has reduced from of 434 in February to 355 complaints at the end of June. The numbers of complaints closed in month in the period March - June 2016 (374 closed complaints) is 73% higher than the four month period immediately before (November February 2016, 216 closed complaints). The backlog continues to be an area of priority along with adhering to strict quality standards for all complaint responses. The 30 day closure rate was 11% in May, this increased to 15%% in June. Whilst the backlog of complaints is being addressed. All divisions will agree their divisional complaints officer a trajectory of improvement to achieve 85% in the next six to nine months. A complaints seminar will take place in July to share good practice and explore processes and areas for improvement. This will be facilitated by University Hospitals Birmingham. 6. Friends & Family Test (FFT) A review of themes evident in FFT and complaints is currently being undertaken by the patient services department. This will be shared with Divisions and agreed projects will be implemented in collaboration with the divisions to enhance patient experience across the Trust. The newly formed senior nurse patient and staff experience group will be supporting these projects going forward. A patient experience group has been formed for ED supported by the Head Nurse for Division 3 and the Head Nurse for Patient Experience. The aim of the group is to improved patient experience and increase FFT responses and recommendations at GHH and BHH and AMU at Solihull. 7. Nursing Financial Recovery Programme Schemes 7.1 Associate Nurse Role (AN) Health Education England (HEE) have invited health and care employers across STP footprints and education providers to apply to become test site partnerships and be part of an innovative programme across England to test and establish the new nursing support role - the Nursing Associate. The role will be introduced across the chosen test sites from December/January 2016/2017. HEFT are leading a joint application across Birmingham and Solihull STP to become a test site for the Nursing Associate role, enabling multiple partnership working and the testing of the role in multiple areas across the STP health economy. 7.2 Advanced Clinical Practitioner (ACP) On behalf of a wide group of Trusts, HEFT is leading the scoping the opportunity to develop an accredited a higher level apprenticeship to ensure that we are at the forefront to enable best use of the levy changes which will go live next year. This will support the Trust plan to extend and advance the skills of our non-medical staff to deliver care and release our medical staff to deliver the most technical care.
50 Recommendation(s): The Council of Governors is asked to receive the information set out in this report. Assurance Implications: Board Assurance Framework Y/N BAF Risk Reference No. Performance KPIs year to date Information Exempt from Disclosure Y/N Y/N Identify any Equality & Diversity issues Resource/Assurance (e.g. Financial/HR) If yes, reason why. Implications Y/N Which Committees has this paper been to? (e.g. AC, QC, etc.) Board of Directors
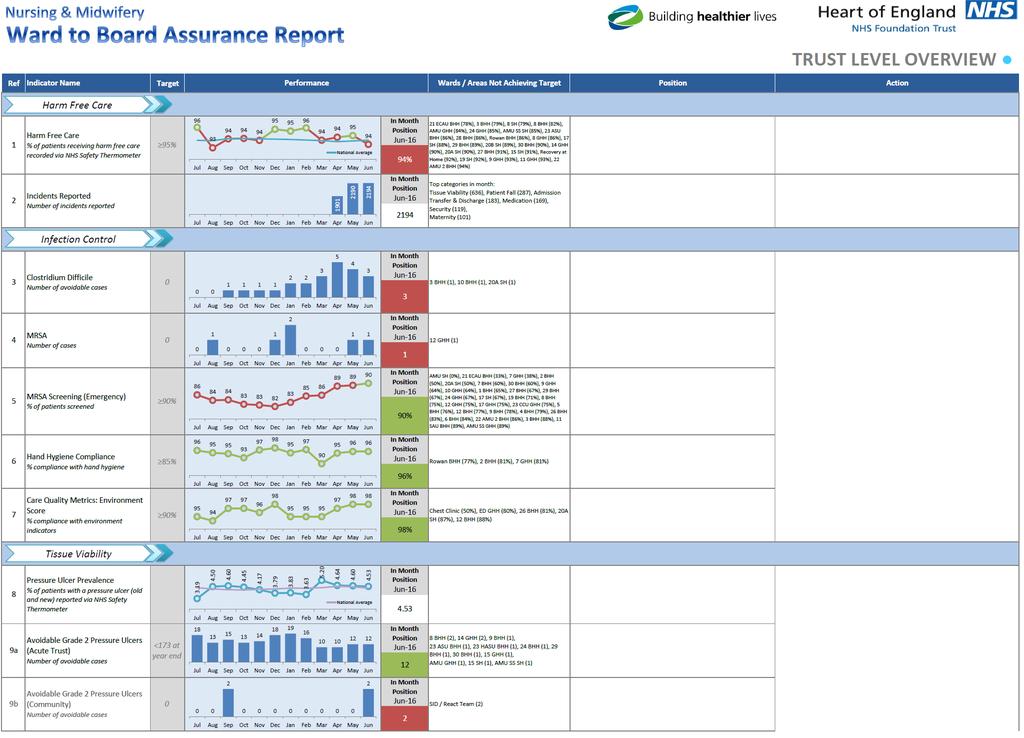
51
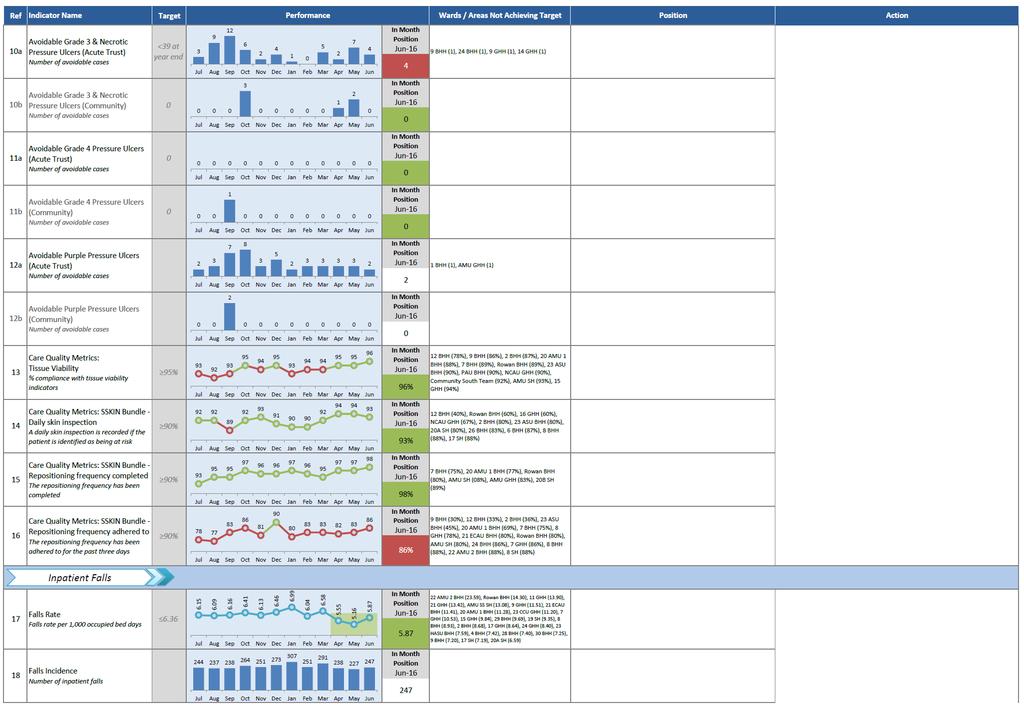
52

53

54
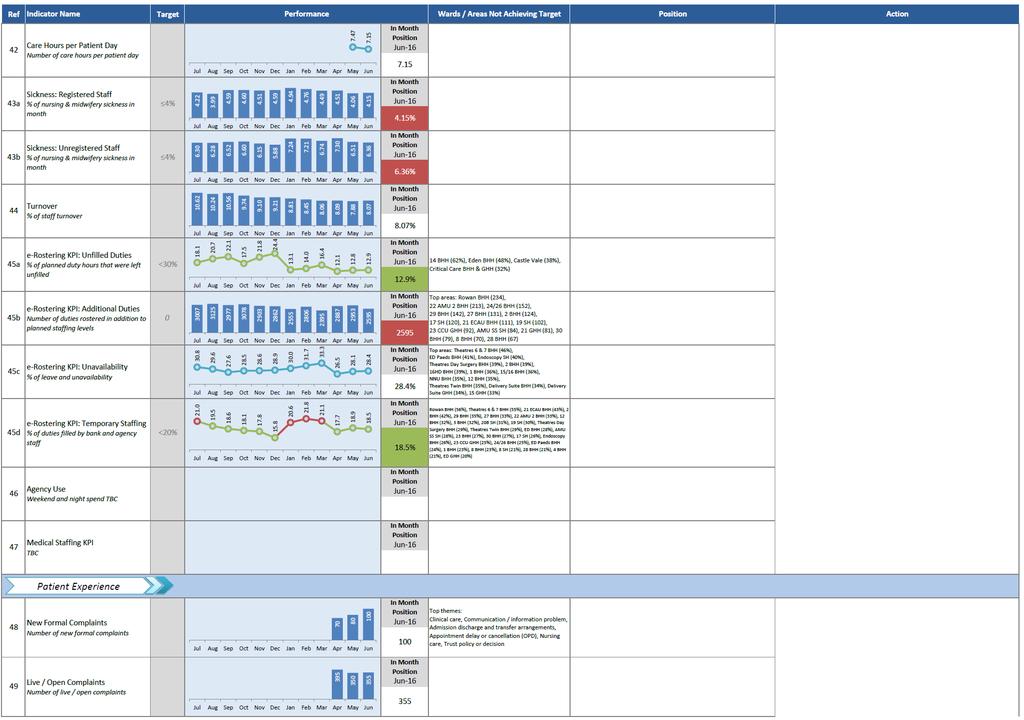
55

56
Integrated Performance Report
 Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report M06 September 2014 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An
Integrated Performance Report August 2017
 Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report Contents Section Page High Level Dashboard Balanced scorecard 3 Domain Scorecards and Director Commentaries Operational Performance 4 Quality and Patient Safety 9 Workforce
Integrated Performance Report
 Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M12 March 2015 Presented by: Paul Bostock (Chief Operating Officer) Des Holden (Medical Director) Fiona Alsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
RTT Recovery Planning and Trajectory Development: A Cambridge Tale
 RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
RTT Recovery Planning and Trajectory Development: A Cambridge Tale Linda Clarke Head of Operational Performance Addenbrooke s Hospital I Rosie Hospital Apr 2014 May 2014 Jun 2014 Jul 2014 Aug 2014 Sep
NHS performance statistics
 NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 14 th December 217 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May Regular report to Trust Board
 SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
SOUTHAMPTON UNIVERSITY HOSPITALS NHS TRUST Trust Key Performance Indicators May 20 Report to: Trust Board July 20 Report from: Sponsoring Executive: Aim of Report/Principle Topic: Review History to date:
WEST HAMPSHIRE PERFORMANCE REPORT. Based on performance data available as at 11 th January 2018
 WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
WEST HAMPSHIRE PERFORMANCE REPORT Based on performance data available as at 11 th January 2018 1 CCG Quality and Performance Executive Summary Introduction: The purpose of this report is to provide an
Council of Governors
 Council Governors 17 4.00pm St Johns Hotel, Warwick Road, Solihull Interests Minutes s Council Governors 1. Welcome 2. 3. s Interest (Enclosure) 4. Minutes meeting held on 20 January 2014 (Enclosure) 5.
Council Governors 17 4.00pm St Johns Hotel, Warwick Road, Solihull Interests Minutes s Council Governors 1. Welcome 2. 3. s Interest (Enclosure) 4. Minutes meeting held on 20 January 2014 (Enclosure) 5.
21 March NHS Providers ON THE DAY BRIEFING Page 1
 21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
21 March 2018 NHS Providers ON THE DAY BRIEFING Page 1 2016-17 (Revised) 2017-18 (Revised) 2018-19 2019-20 (Indicative budget) 2020-21 (Indicative budget) Total revenue budget ( m) 106,528 110,002 114,269
Strategic KPI Report Performance to December 2017
 Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
Strategic KPI Report Performance to December 2017 Trust Board 25 th January 2018 Strategic KPI summary SROs: All Directors Objective KPI SRO Target Apr May Jun Jul Aug Sep Oct Nov Success Is Deliver A
NHS performance statistics
 NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS performance statistics Published: 8 th February 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
Mortality Report Learning from Deaths. Quarter
 Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Mortality Report Learning from Deaths Quarter 3 2017 Introduction In December 2016 the CQC report Learning, Candour and accountability: A review of the way NHS Trusts review and investigate the deaths
Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018
 Produced in February 2018") 6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
6b Integrated Performance Report Executive Summary (for NHS Fife Board Meeting) Produced in February 2018 2 Contents Integrated Performance Report: Executive Summary 5 Clinical Governance: Chair and Committee
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care.
 Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Learning from Deaths Policy A Framework for Identifying, Reporting, Investigating and Learning from Deaths in Care. Associated Policies Being Open and Duty of Candour policy CG10 Clinical incident / near-miss
Performance and Delivery/ Chief Nurse
 Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
Governing Body 26th May 2017 Quality and Performance Report 22nd May 2017 Author: Other contributors: Executive Lead Audience Eileen Clark - Acting Director of Clinical Performance and Delivery/ Chief
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Meeting Date: 3 th June 214 Trust Board Report Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Paper 12 Ayrshire and Arran NHS Board Monday 9 October 2017 Planned Care Performance Report Author: Fraser Doris, Performance Information Analyst Sponsoring Director: Liz Moore, Director for Acute Services
Section 1 - Key Performance Indicators
 Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Clinical Quality Report Month 6 2016/17 period ending 30th September 2016 Section 1 - Key Performance Indicators 1.1 NHS Improvement; Risk Assessment Framework Clostridium difficile Indicator M6 2 YTD
Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee
 EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
EPB53/825 Title of Report: Prepared By: Sponsor: Action Required: Integrated Performance Committee Assurance Reports, January 2016 and December 2015 Crishni Waring, Chair, IPC Committee Gale Hart, Director
NHS Performance Statistics
 NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS Performance Statistics Published: 8 th March 218 Geography: England Official Statistics This monthly release aims to provide users with an overview of NHS performance statistics in key areas. Official
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER C Hickson, Head of Management Accounts
 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING FINANCIAL POSITION AS AT 30TH NOVEMBER 2013 Date of the meeting 15/01/2014 Author Sponsoring GB member Purpose of report Recommendation Resource
EXECUTIVE SUMMARY REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY Anne Gibbs, Director of Strategy & Planning
 EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
EXECUTIVE SUMMARY D REPORT TO THE BOARD OF DIRECTORS HELD ON 22 MAY 2018 Subject Supporting TEG Member Author Status 1 A review of progress against Corporate Objectives 2017/18 and planned Corporate Objectives
BSUH INTEGRATED PERFORMANCE REPORT. 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain
 Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well Led Domain") BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
BSUH INTEGRATED PERFORMANCE REPORT 1) Responsive Domain 2) Safe Domain 3) Effective Domain 4) Caring Domain 5) Well ed Domain RESPONSIVE DOMAIN RESPONSIVE DOMAIN Metric Defined by Standard Apr-16 May-16
Newham Borough Summary report
 Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
Newham Borough Summary report March 2013 Prepared on 18/03/13 by Commissioning Support team Finance and Activity Millions Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Newham Headlines March 2013 Feb-12 Apr-12 Jun-12
BOARD OF DIRECTORS. Minutes of the Meeting of 29 March 2018 Lecture Theatre 2, Education Centre QEMC
 BOARD OF DIRECTORS Minutes of the Meeting of 29 March 2018 Lecture Theatre 2, Education Centre QEMC Present: In Attendance: Observers: Rt Hon Jacqui Smith, Chair Dame Julie Moore, Chief Executive Officer
BOARD OF DIRECTORS Minutes of the Meeting of 29 March 2018 Lecture Theatre 2, Education Centre QEMC Present: In Attendance: Observers: Rt Hon Jacqui Smith, Chair Dame Julie Moore, Chief Executive Officer
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Queen Elizabeth Medical Centre Edgbaston, Birmingham, B15 2TH
Newham Borough Summary report
 Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Newham Borough Summary report April 2013 Prepared on 17/04/13 by Commissioning Support team Apr-11 Jun-11 Aug-11 Oct-11 Dec-11 Feb-12 Apr-12 Jun-12 Aug-12 Oct-12 Dec-12 Feb-13 GREE N Finance and Activity
Quality Accounts: Corroborative Statements from Commissioning Groups. Nottingham NHS Treatment Centre - Corroborative Statement
 Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
Quality Accounts: Corroborative Statements from Commissioning Groups Quality Accounts are annual reports to the public from providers of NHS healthcare about the quality of services they deliver. The primary
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY
 MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
MERTON CLINICAL COMMISSIONING GROUP GOVERNING BODY Date of Meeting: 23 rd March 2017 Agenda No: 9.3 Attachment: 15 Title of Document: CCG Governing Body Assurance Report & Scorecards: Month 9 Quality &
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 2018
 Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Learning from Patient Deaths: Update on Implementation and Reporting of Data: 5 th January 218 Purpose The purpose of this paper is to update the Trust Board on progress with implementing the mandatory
Ayrshire and Arran NHS Board
 Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
Paper 12 Ayrshire and Arran NHS Board Monday 26 March 2018 Financial Management Report for the 11 months to 28 February 2018 Author: Bob Brown, Assistant Director of Finance Governance and Shared Services
Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk
 Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Norfolk Health Overview and Scrutiny Committee 7 December 2017 Item no 6 Norfolk and Suffolk NHS Foundation Trust mental health services in Norfolk Suggested approach by Maureen Orr, Democratic Support
Nottingham University Hospitals Emergency Department Quality Issues Related to Performance
 RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
RCCG/GB/14/123 Nottingham University Hospitals Emergency Department Quality Issues Related to Performance Introduction NUH have failed to meet the 95% 4 hour wait standard for a number of consecutive months.
The Royal Wolverhampton NHS Trust
 The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
The Royal Wolverhampton NHS Trust Trust Board Report Meeting Date: 24 June 2013 Title: Executive Summary: Action Requested: Report of: Author: Contact Details: Resource Implications: Public or Private:
Quality Improvement Scorecard December 2017
 Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Mortality: HSMR Performance improved in August Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR (weekend)
Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations
 No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
No. Domain CQC Recommendation Lead Operational Lead Current Status 1 Appendix A: University Hospitals Birmingham NHS Foundation Trust Draft Action Plan in Response to CQC Recommendations Wording in long
Summary two year operating plan 2017/18
 One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
One Trust - serving our local communities Summary two year operating plan 2017/18 & 2018/19 www.lewishamandgreenwich.nhs.uk Summary two year operating plan: 2017/18 and 2018/19 1. Introduction This summary
2017/18 Trust Balanced Scorecard
 ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
ITEM 8b ENC 9 2017/18 Trust Balanced Scorecard Author: Performance Management Team March 2017 The purpose of this paper is to provide an update on the development of the 2017/18 Balanced Scorecard for
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP
 COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
COVENTRY AND RUGBY CLINICAL COMMISSIONING GROUP Report To: Governing Body 11 September 2013 Report From: Title of Report: Purpose of the Report: Jacqueline Barnes, Executive Nurse The Nursing and Quality
FT Keogh Plans. Medway NHS Foundation Trust
 FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
FT Keogh Plans Medway NHS Foundation Trust July 2014 KEY Delivered On Track to deliver Some issues narrative disclosure Not on track to deliver Medway - Our improvement plan & our progress What are we
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST CHIEF EXECUTIVE S REPORT. BOARD OF DIRECTORS 21 st March 2012
 SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
SHEFFIELD TEACHING HOSPITALS NHS FOUNDATION TRUST I CHIEF EXECUTIVE S REPORT BOARD OF DIRECTORS 21 st 212 1. PERFORMANCE In overall terms, the Trust continues to perform well against both regulatory and
WAITING TIMES 1. PURPOSE
 Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
Agenda Item Meeting of Lanarkshire NHS Board 28 April 2010 Lanarkshire NHS board 14 Beckford Street Hamilton ML3 0TA Telephone 01698 281313 Fax 01698 423134 www.nhslanarkshire.org.uk WAITING TIMES 1. PURPOSE
Quality Improvement Scorecard June 2017
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance remained below target in February. Mortality: HSMR (weekday) vs.
Hard Truths Public Board 29th September, 2016
 Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Hard Truths Public Board 29th September, 2016 Presented for: Presented by: Author Previous Committees Governance Professor Suzanne Hinchliffe CBE, Chief Nurse/Deputy Chief Executive Heather McClelland
Quality & Performance Report. Public Board
 Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
Agenda Item 12.1 Quality & Performance Report Public Board 27 th November 2014 Presented for: Presented by: Author: Previous Committees: Governance Professor Suzanne Hinchliffe CBE Chief Nurse / Interim
2017/ /19. Summary Operational Plan
 2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
2017/18 2018/19 Summary Operational Plan Introduction This is the summary Operational Plan for Central Manchester University Hospitals NHS Foundation Trust (CMFT) for 2017/18 2018/19. It sets out how we
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014
 Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
Prime Contractor Model King s Fund Nick Boyle Consultant Surgeon 27 March 2014 Current Referral Route options - Information 1. Horizon Health Choices Horizon Musculoskeletal Triage & Treatment Chronic
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs
 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPs December 2012 SUPPORTING PLANNING 2013/14 FOR CLINICAL COMMISSIONING GROUPS First published: 21 December 2012 2 Contents 1. INTRODUCTION...
Organisational systems Quality outcomes Patient flows & pathways Strategic response to activity
 Operational Plan 2017 2019 1 1. Introduction This narrative supports the finance, activity and workforce return elements of University Hospitals Birmingham NHS Foundation Trust s Operational Plan for 2017-19.
Operational Plan 2017 2019 1 1. Introduction This narrative supports the finance, activity and workforce return elements of University Hospitals Birmingham NHS Foundation Trust s Operational Plan for 2017-19.
Item E1 - Bart s Health Quality Indicators
 Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Item E1 - Bart s Health Quality Indicators 1.0 Purpose 1.1 The purpose of this report is to provide the CCG Board with an update on quality matters across pertaining to our main local Provider organisations.
Governing Body meeting on 13th September 2018
 Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Governing Body meeting on 13th September 2018 Report from the Chair of the Integrated Governance Committee (IGC) Date of Meetings Reported: 9 th August 2018 Key achievements Author: Martin Wilkinson, Chair
Board of Director s Meeting
 Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Board of Director s Meeting Meeting Date: 15 November 212 Agenda item: 6.1 Title: Purpose: Summary: Recommendation: Author: Presented by: QUALITY AND PATIENT SAFETY ASSURANCE COMMITTEE To provide an exception
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 25 th February 2009 at 2.00 pm in Rooms 2 and 3 at Hertford County Hospital DRAFT Present:
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 25 th February 2009 at 2.00 pm in Rooms 2 and 3 at Hertford County Hospital DRAFT Present:
Operational Focus: Performance
 Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Operational Focus: Performance Sandra Iskander Changes for 2015/16 Change of focus of 18-weeks and A&E 4-hour wait targets as recommended by Sir Bruce Keogh, Medical Director, NHS England. 18-weeks to
Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality and Safety
 Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Minutes (confirmed) Subject Quality Committee Date 4 April 2017 Time 10.00am 12.30pm Venue Goodwood Room Chair Alison Lewis-Smith Members Position Voting Rights Alison Lewis-Smith Chair, Lay member, Quality
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board. Audit year: Issued: October 2015 Document reference: 491A2015
 Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Review of Follow-up Outpatient Appointments Hywel Dda University Health Board Audit year: 2014-15 Issued: October 2015 Document reference: 491A2015 Status of report This document has been prepared as part
Performance and Quality Report Sean Morgan Director of Performance and Delivery Mary Hopper Director of Quality Dino Pardhanani, Clinical Director
 Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Sutton CCG Clinical Commissioning Group Governing Body Date Thursday, 06 September 2018 Document Title Lead Director (Name and Role) Clinical Sponsor (Name and Role) Performance and Quality Report Sean
Staffordshire and Stoke on Trent Partnership NHS Trust. Operational Plan
 Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Staffordshire and Stoke on Trent Partnership NHS Trust Operational Plan 2016-17 Contents Introducing Staffordshire and Stoke on Trent Partnership NHS Trust... 3 The vision of the health and care system...
Report of the Care Quality Commission. May 2017
 Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
Report of the Care Quality Commission May 2017 1. Purpose 1.1 The purpose of this report is to formally confirm the findings of the Care Quality Commission (CQC) following its inspection in October 2016;
EDS 2. Making sure that everyone counts Initial Self-Assessment
 EDS 2 Making sure that everyone counts Initial Self-Assessment Equality Delivery System for the NHS EDS2 Summary Report Implementation of the Equality Delivery System EDS2 is a requirement on both NHS
EDS 2 Making sure that everyone counts Initial Self-Assessment Equality Delivery System for the NHS EDS2 Summary Report Implementation of the Equality Delivery System EDS2 is a requirement on both NHS
Trust Board Meeting: Wednesday 13 May 2015 TB
 Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
Trust Board Meeting: Wednesday 13 May 2015 Title Update on Quality Governance Framework Status History For information, discussion and decision This paper has been presented to Quality Committee in April
BOLTON NHS FOUNDATION TRUST. expansion and upgrade of women s and children s units was completed in 2011.
 September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
September 2013 BOLTON NHS FOUNDATION TRUST Strategic Direction 2013/14 2018/19 A SUMMARY Introduction Bolton NHS Foundation Trust was formed in 2011 when hospital services merged with the community services
Status: Information Discussion Assurance Approval. Claire Gorzanski, Head of Clinical Effectiveness
 Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Report to: Trust Board Agenda item: Date of Meeting: 2 October 2017 SFT3934 Report Title: Annual quality governance report 2016-2017 Status: Information Discussion Assurance Approval X Prepared by: Executive
Quality Improvement Scorecard March 2018
 Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Mortality: HSMR Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Performance further improved in October. November data not yet available. Mortality:
Quality Improvement Scorecard November 2017
 Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Mortality: HSMR Performance remained below target in July Nat NB: Each month is a 12 month rolling value. I.e. Mar-16 reports the monthly average of Apr-15 to Mar-16. Mortality: HSMR (weekday) vs. HSMR
Integrated Performance Report
 Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Integrated Performance Report M04 July 2016 Presented by: Angela Stevenson (Chief Operating Officer) Des Holden (Medical Director) Fiona Allsop (Chief Nurse) Paul Simpson (Chief Financial Officer) An Associated
Trust Key Performance Indicators
 Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
Monthly - February 2007 Patient Experience Length of Stay - Overall A Mortality Rate G Cancelled Operations R Elective A Peri-operative Mortality Rate Cancelled Operations (28 day reschedule) A Non-elective
Balanced Scorecard. Paper 5.2. TRUST BOARD 24 th September 2015 TITLE EXECUTIVE SUMMARY
 TRUST BOARD 24 th September 2015 TITLE EXECUTIVE SUMMARY Balanced Scorecard The Trust reported an in-month deficit of 0.7m against a deficit budget of 0.6m, resulting in a year to date surplus to 0.2m
TRUST BOARD 24 th September 2015 TITLE EXECUTIVE SUMMARY Balanced Scorecard The Trust reported an in-month deficit of 0.7m against a deficit budget of 0.6m, resulting in a year to date surplus to 0.2m
November NHS Rushcliffe CCG Assurance Framework
 November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
November 2015 NHS Rushcliffe CCG Assurance Framework ASSURANCE FRAMEWORK SUMMARY No. Lead & Sub Committee Date placed on Assurance Framework narrative Residual rating score L I rating in 19 March 2015
Improve, Inspire, Innovate Quality Improvement Plan
 Improve, Inspire, Innovate Quality Improvement Plan 1 QIP Final version 20170706 Contents Background & Summary Page 3 Who is Responsible? Page 4 How will we communicate our progress to you? Page 4 Chair
Improve, Inspire, Innovate Quality Improvement Plan 1 QIP Final version 20170706 Contents Background & Summary Page 3 Who is Responsible? Page 4 How will we communicate our progress to you? Page 4 Chair
Quality, Safety & Experience (QSE) Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph
 Committee. Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph") 1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
1 Minutes QSE Public 29.3.17 V1.0 Present: Quality, Safety & Experience (QSE) Committee Minutes of the Meeting Held on Wednesday 29 th March 2017 in the Boardroom, Carlton Court, St Asaph Mrs Margaret
RTT Assurance Paper. 1. Introduction. 2. Background. 3. Waiting List Management for Elective Care. a. Planning
 RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
RTT Assurance Paper 1. Introduction The purpose of this paper is to provide assurance to Trust Board in relation to the robust management of waiting lists and timely delivery of elective patient care within
Overall rating for this trust Good. Inspection report. Ratings. Are services safe? Requires improvement. Are services effective?
 Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Barnsley Hospital NHS Foundation Trust Inspection report Gawber Road Barnsley South Yorkshire S75 2EP Tel: 01226 730000 www.barnsleyhospital.nhs.uk Date of inspection visit: 17 to 19 October, 15 to 17
Business Case Authorisation Cover Sheet
 Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Business Case Authorisation Cover Sheet Section A Business Case Details Business Case Title: Directorate: Division: Sponsor Name Consultant in Anaesthesia and Pain Medicine Medicine and Rehabilitation
Strategic Risk Report 12 September 2016
 Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
Strategic Report September 20 Haringey CCG Register Introduction The Strategic Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group s control over
BOARD PAPER - NHS ENGLAND
 BOARD PAPER - NHS ENGLAND Title: Chief Executive s report By: Simon Stevens, CEO Purpose of paper: Update on the work of the Chief Executive over the last month Information on a number of NHS England priorities
BOARD PAPER - NHS ENGLAND Title: Chief Executive s report By: Simon Stevens, CEO Purpose of paper: Update on the work of the Chief Executive over the last month Information on a number of NHS England priorities
Supporting all NHS Trusts to achieve NHS Foundation Trust status by April Ipswich Hospital NHS Trust NHS East of England Department of Health
 TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
TFA document Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014 Tripartite Formal Agreement between: Ipswich Hospital NHS Trust NHS East of England Department of Health Introduction
Delivering Improvement in Practice
 v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
v Delivering Improvement in Practice NHS Providers Governance Conference 7 July 2016 Sir Mike Aaronson Chairman, Frimley Health NHS Foundation Trust 2006-2016 Frimley Health FT Comprises: Frimley Park
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12. Date of Meeting: 23 rd March 2018 TITLE OF REPORT:
 NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
NHS BOLTON CLINICAL COMMISSIONING GROUP Public Board Meeting AGENDA ITEM NO: 12 Date of Meeting: 23 rd March 2018 TITLE OF REPORT: AUTHOR: PRESENTED BY: PURPOSE OF PAPER: (Linking to Strategic Objectives)
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017
 Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
Standardising Acute and Specialised Care Theme 3 Governance and Approach to Hospital Based Services Strategy Overview 28 th July 2017 Background Theme 3 builds upon previous key strategic commissioning
INTEGRATED PERFORMANCE REPORT. BOARD OF DIRECTORS 20 September 2017
 INTEGRATED PERFORMANCE REPORT BOARD OF DIRECTORS 20 September 2017 1 S Section Page Executive Summary 4 Trust Performance Overview 7 Trust Performance Report by Exception 9 MSSA Bacteraemia - Actual numbers
INTEGRATED PERFORMANCE REPORT BOARD OF DIRECTORS 20 September 2017 1 S Section Page Executive Summary 4 Trust Performance Overview 7 Trust Performance Report by Exception 9 MSSA Bacteraemia - Actual numbers
NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT
 9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
9.6 NHS DORSET CLINICAL COMMISSIONING GROUP GOVERNING BODY MEETING ADULT AND CHILDREN CONTINUING HEALTHCARE ANNUAL REPORT Date of the meeting 18/07/2018 Author Sponsoring Board member Purpose of Report
ESHT Our ambition to be outstanding by 2020
 ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
ESHT 2020 Our ambition to be outstanding by 2020 June 2018 1 Contents Page 3 Page 4 Page 6 Page 8 Background 2017/18 progress Vision, values and objectives CQC ratings Page 10 What we will have achieved
Newham Borough Summary report
 Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Newham Borough Summary report Item K1 September 2013 Prepared on 30/09/2013 by Support team GREEN Finance and Activity Millions AMBER RED Headlines M5 Financial position M4 activity data The QIPP net savings
Learning from Deaths Policy
 Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy Version: 3 Approved by: Board of Directors Date Approved: October 2017 Lead Manager: Associate Medical Director for Patient Safety and Clinical Risk Responsible Director: Medical
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE
 Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
Learning from Deaths Policy LISTEN LEARN ACT TO IMPROVE EQUALITY IMPACT The Trust strives to ensure equality and opportunity for all, both as a major employer and as a provider of health care. This policy
ENCLOSURE: J. Date of Trust Board 29 February Pressure Ulcer Clinical Improvement Programme. Purpose of Report
 ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
ENCLOSURE: J Date of Trust Board 29 February 2012 Title of Report Purpose of Report Abstract Pressure Ulcer Clinical Improvement Programme This paper provides a progress report on our work in support of
Urgent Care Short Term Actions to Improve Performance
 To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
To: Trust Board From: Chief Operating Officer Date: March 2017 Healthcare standard Title: Urgent Care Short Term Actions to Improve Performance Author/Responsible Director: Michael Woods / Andrew Prydderch
Welcome, Apologies for Absence and Declaration of Board Members Interest
 DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
DRAFT Minutes of the of the Royal Cornwall Hospitals NHS Trust held on Thursday 30 March 2017 11.00 13.00 in the Knowledge Spa, Royal Cornwall Hospital Present: Mr Jim McKenna Ms Kathy Byrne Ms Catrin
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT
 NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
NHS DUMFRIES AND GALLOWAY ANNUAL REVIEW 2015/16 SELF ASSESSMENT Chapter 1 Introduction This self assessment sets out the performance of NHS Dumfries and Galloway for the year April 2015 to March 2016.
Appendix 1 MORTALITY GOVERNANCE POLICY
 Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Appendix 1 MORTALITY GOVERNANCE POLICY 1 Policy Title: Executive Summary: Mortality Governance Policy For many people death under the care of the NHS is an inevitable outcome and they experience excellent
Debbie Edwards Interim Deputy Director of Nursing Gail Naylor- Executive Director of Nursing & Midwifery. Safety & Quality Committee
 Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
Report to Trust Board of Directors Date of Meeting: 29 July 2014 Enclosure Number: 7 Title of Report: Author: Executive Lead: Responsible Sub- Committee (if appropriate): Executive Summary: Ward Accreditation
National Waiting List Management Protocol
 National Waiting List Management Protocol A standardised approach to managing scheduled care treatment for in-patient, day case and planned procedures January 2014 an ciste náisiúnta um cheannach cóireála
National Waiting List Management Protocol A standardised approach to managing scheduled care treatment for in-patient, day case and planned procedures January 2014 an ciste náisiúnta um cheannach cóireála
EAST AND NORTH HERTFORDSHIRE NHS TRUST
 Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Agenda item: 5 EAST AND NORTH HERTFORDSHIRE NHS TRUST Minutes of the Trust Board meeting held in public on Wednesday 24 July 2013 at 2pm in the Post Graduate Centre, QEII Hospital. Present: Mr Ian Morfett
Waiting Times Report Strategic. Thematic Goals
 Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
Strategic Improved Quality of Care Transformation - Prevention & Wellbeing Thematic Goals Waiting Times Report 2016-17 Transformation through Integration Improved Access to Services Improved Value This
Quality Framework Healthier, Happier, Longer
 Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
Quality Framework 2015-2016 Healthier, Happier, Longer Telford & Wrekin Clinical Commissioning Group (CCG) makes quality everyone s business. Our working processes are designed to ensure we all have the
OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING
 22 September Month 2016 2017-2019 OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING Today the national bodies NHS England (NHSE) and NHS Improvement (NHSI) have published their planning
22 September Month 2016 2017-2019 OPERATIONAL PLANNING & CONTRACTING PLANNING GUIDANCE ON THE DAY BRIEFING Today the national bodies NHS England (NHSE) and NHS Improvement (NHSI) have published their planning
Sponsoring director: Purpose: Decision Assurance For information Disclosable X Non-disclosable
 TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
TRUST BOARD (Public session) 23 MAY 2018 AGENDA ITEM 10 Report title: Thematic Review of Serious Incidents Report author(s): T Nicholls Acting Director of Clinical Quality & Improvement Sponsoring director:
We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards.
 Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Wellesley Hospital Eastern Avenue, Southend-on-Sea, SS2
Inspection Report We are the regulator: Our job is to check whether hospitals, care homes and care services are meeting essential standards. Spire Wellesley Hospital Eastern Avenue, Southend-on-Sea, SS2
July (Month 4) Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval
 Integrated Performance Report. John Grinnell, Director of Finance. Executive Directors. For Information For Discussion For Approval") BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature
BOARD OF DIRECTORS Subject/Title July (Month 4) Integrated Performance Report Executive Responsible Paper prepared by (if different from above) John Grinnell, Director of Finance Executive Directors Nature