NewYork-Presbyterian/Queens PPS Clinical Integration Strategy
|
|
|
- Rosalind Lyons
- 6 years ago
- Views:
Transcription
1 NewYork-Presbyterian/Queens PPS Clinical Integration Strategy Document Title: NYP/Q PPS Clinical Integration Strategy Version 1.0 Purpose: Approving Committee: This document outlines the needs for a clinically integrated network across PPS partners, highlighting strategies to close identified gaps and risks Clinical Integration Committee Executive Committee Approval Date: October 5, 2016 Page 1
2 Table of Contents OVERVIEW... 4 PPS GOVERNANCE... 4 KEY STAKEHOLDERS... 5 MILESTONES... 6 COMMUNICATIONS & ROLL-OUT PLAN... 6 CLINICAL INTEGRATION STRATEGY... 6 BEST PRACTICES... 6 PRIMARY CARE TRANSFORMATION... 7 PCMH LEVEL 3 CERTIFICATION... 9 Committed DSRIP PCMH Conversion Sites... 9 PPS Implementation Support... 9 CARE TRANSITIONS QUALITY METRICS & REVIEW PROCESS RAPID CYCLE EVALUATION UNIT ROOT CAUSE ANALYSIS POPULATION HEALTH PLATFORM Cureator : Other tools : CLINICALLY INTEGRATED NETWORK TRAINING a.ii Patient Centered Medical Home b.vii INTERACT& 2.b.viii Home Care Collaboration b.i Cardiovascular d.ii Asthma g.ii Palliative Care GOVERNANCE & OPERATIONS APPENDIX ATTACHMENT A: INVENTORY OF PPS APPROVED BEST PRACTICES ATTACHMENT B: CARE MANAGEMENT FRAMEWORK ATTACHMENT C: QUALITY BASED OUTCOMES ATTACHMENT D: BENCHMARKS WITH STATE AND NATIONAL AVERAGE ATTACHMENT E: OVERVIEW OF QUALITY METRICS Page 2
3 ATTACHMENT F: TRAINING SCHEDULE FOR ACP/MOLST/eMOLST ATTACHMENT G: EPEC TRAINING REGISTRATION FORM ATTACHMENT H: EPEC TRAINING SCHEDULE Page 3
4 OVERVIEW The NewYork-Presbyterian/Queens PPS (NYP/Q PPS) is utilizing the DSRIP program to create a clinically integrated system of partners to achieve the triple aim and improve the health of the Medicaid population. The PPS has completed a Clinical Integration Needs Assessment, which guided the creation of the Clinical Integration Strategy. The PPS clinical integration strategy utilizes the concept of primary care to link multiple projects with similar deliverables, quality improvement needs, and engaged partners in order to increase efficiencies and outcomes. The PMO is building a clinical network that is focused to providing the right care, in the right place, at the right time, by the most appropriate healthcare provider. The NYP/Q Clinical Integration Strategy will be the key instrument utilized by the PPS and PMO for project implementation, network development, and organizational development. The strategy includes primary care transformation, PCMH Level 3 Certification, care transition, integrated primary care and behavioral health models, and long-term care, as well as plans for monitoring quality outcomes and performance reporting with the help of integrated technology. PPS GOVERNANCE The NYP/Q PPS leadership team strategically developed the network of partners during the attribution process; the intent was to focus the network to those providers who bring high quality care, have existing relationships with the hospital system, and/or showed interest based on existing strategies which align with PPS deliverables. The network is comprised of both clinical and non-clinical providers across the care continuum that are focused to long-term care, primary care, behavioral health, asthma, cardiovascular, and HIV strategies.. The PPS has established a committee structure within the collaborative contracting model for the DSRIP program, with each clinical committee comprised of representatives from the PPS lead entity, NYP/Q, and PPS partner organizations. These committees research, review, and recommend best practices to the Clinical Integration and Population Health Management committee for review and approval. Each committee is led b a chair and co-chair and the Clinical Integration and Population Health Management Committee is comprised of the chairs from each of the clinical sub-committees in addition to a representative from the PPS RHIO partner, Healthix. The Clinical Integration Strategy aims to identify Page 4
5 best practices and methodologies to create and maintain a clinically integrated system and reduce identified gaps and risks from the Clinical Integration Needs Assessment. KEY STAKEHOLDERS ROLE RESPONSIBILITY Lead Entity (NYP/Q) Establish the strategy & processes for DSRIP network clinical integration PPS Project Maintainstaff focused to clinical integration strategies and Management Office processes Establish reporting policies & expectations Gather data elements & reporting to NYS and partners Monitor use & compliance of partners with policies Data warehousing of partner performance data Ongoing reporting to Clinical Integration & Executive PPS Clinical Integration Committee PPS Executive Committee PPS Network Partnersclinical PPS Network Partnersnon clinical Project Advisory Committee (PAC) Committee Oversight of clinical workgroup integration Approvals of clinical integration processes or strategies Report to the Executive Committee Oversight of the PMO processes Chair accountable to the Lead Entity for ongoing updates Partner to implement the clinical integration strategy specific to the needs of their practice and patient base Identify clinical gaps of patient care needed to improve quality outcomes Communicate with the PMO regarding data & reporting processes Attend workgroup or committee meetings as defined by the PPS Directly communicate with the PMO regarding data & reporting processes Identify risks or concerns regarding the PPS process Attend workgroup or committee meetings as defined by the PPS Receive updates from the PMO regarding the clinical integration strategy or roll-out Provide collaborative feedback pertaining to gaps, industry trends, or lessons learned as it relates to clinical integration Page 5
6 COMMUNICATIONS & ROLL-OUT PLAN The PPS PMO Population Health Manager will take a proactive role in ensuring effective communications on this strategy. The PPS will utilize existing communication sources, sited in the Communications & Engagement Plan, to maximize efforts currently in place. The PMOwill partner with the partners through the clinical sub-committees and site visits to implement the clinical integration strategy. The implementation of the strategy will be managed and monitored utilizing the following tools: Performance Logic Population Health Management Tool (Allscripts / Curerator) Engagement in committee meetings & workgroups Rapid Cycle Evaluation Unit (RCE) The PMO management team will perform continuous outreach to partners for feedback on the process, tools, reports, and data for ongoing updates. CLINICAL INTEGRATION STRATEGY The clinical integration strategy centers on delivering quality based care through utilization of evidence-based guidelines to build a high-value network, leveraging the interdependence across all partner organizations. As healthcare organizations across the care continuum focus to quality metrics and their financial implications, the likelihood of success improves drastically through successful practitioner engagement. Successful clinical integration requires the network to be driven by clinical leadership, clearguidelines, and frequent and effective communication. Clinically integrated systems should choose metrics that span the continuum of care which include focusing on metrics related to care transitions between sites and adopting the same metrics across payors. Additionally, success is contingent upon appropriate investment in infrastructure including systems that connect hospitals and practitioners through patient registries and other electronic systems. A robust infrastructure provides the tools practitioners and hospitals need to monitor quality and cost. The NYP/Q PPS strives to build the robust clinical integration strategy that will address all of the discussed above goals. BEST PRACTICES The PPS clinical sub-committees have adopted best practices based on partner needs and project requirements. The approved best practices, outlined in Attachment A of the Appendix, encompass clinical practices, competency demonstration, and training Page 6
7 programs. The approved best practices have been provided to partners in each project and are available on the PPS website ( The NYP/Q PMO staff have conducted site visits with partners to answered questions and provide clarification and helpful information about best practices, work flows, and project implementation. Feedback received from partners is routinely presented to the Clinical Integration and Population Health Management Committee for further discussion and determination of action as appropriate. As a collaborative contracting model the NYP/Q PPS advocates for partners to adopt these best practices as appropriate at their sites and incentives participation through the funds flow model. PRIMARY CARE TRANSFORMATION TheNYP/Q PPS considers primary care as a building block for transformation within a complex healthcare environment in order to increase network connectivity, maximize quality improvements, and improve patient access. The PPS is based in Queens County, which is a federally designated HPSA area. In order to meet the primary care shortages in the PPS service area, the PPS will utilize the following strategies to address gaps in care: Expanding Primary Care Access at Behavioral Health Sites The collaboration of primary care at behavioral health sites will immediately increase access to patients by providing an additional site of care (right setting) and will build on existing relationships among providers at 9 clinics affecting over 15 primary care providers and 50 behavioral health providers. Integrating Behavioral Health into Primary Care Sites As with the expansion of primary care at behavioral health sites, the increased access of behavioral health visits will allow for patients to seek appropriate care by appropriate providers; therefore, increasing access in primary care provider schedules where the behavioral health patients were historically seen. Implementing Open Access to Primary Care Sites A PCMH Level 3 requirement is to offer open access scheduling to patients seeking care. The PPS has committed to 36 primary care providers achieving this certification by DY3. The implementation will increase access to appointments (same day or future dates), improve no-show rates, and diversify provider schedules in order to maximize clinical time of providers. Page 7
8 Engagement & Inclusion of Non-Physician Clinical Providers Partners will be encouraged to utilize non-physician providers within their scope of practice in order to maximize practice efficiency and allow clinicians to work at the top of scope. This strategy will increase access as well as align patient acuity with provider type for ongoing treatments. Telehealth Program Development Clinical leads will identify potential needs for telehealth programs based on the needs of the patient or providers to ensure access to providers across the continuum of care regardless of geographic location. The telehealth analysis is currently underway to identify population & partner needs, outline partners involved to ensure an effective return on investment, review local and federal regulations, identify capital or operational funding potentials for installation, and plan for sustainability for years outside of the DSRIP program. The PPS is focused to maximizing efforts by engaging specific providers and other PPS s to review existing programs and discuss lessons learned. Connection of Partners to IT Tools (RHIO & Population Health Management Tool) A priority of the PPS is to align providers with RHIO connectivity as well as provide them with IT tools that will help increase connectivity and communication among providers. The RHIO Pilot, which provides funds flow incentives to providers, ensures connectivity, and provides the primary care provider with information about the patient care that will ensure a time effective encounter and clinical planning. Allscripts Care Director (ACD) is the Population Health Management Tool approved for the PPS to create an alert system partnered with a care coordination best practice in order for primary care providers to be well informed of their patient facility-based activity (ED & inpatient). The tools along with care coordination strategies will build on the primary care concepts to result in additional access to those we serve. Conducting Gap Assessment Periodically The PPS is committed to ongoing analysis of our network and community needs and will utilize our governing process inclusive of the PAC committee to complete periodic assessments focused to primary care gaps (patients and providers). According to the studies by the Center for Health Workforce in 2013, Queens borough had significant low number of PCPs, Physician Assistants and Nurse practitioners compared to rest of the other boroughs and counties. The PPS will Page 8
9 conduct further analysis on an ongoing basis, which will provide valuable network information on access and quality to address patient and partner needs for future engagements or program developments. PCMH LEVEL 3 CERTIFICATION Committed DSRIP PCMH Conversion Sites The following network providers have committed to the 2.a.ii project for PCMH transformation. The HANYS consulting group has engaged all providers in multiple cohorts to allow for a staged rollout to ensure Level 3 certification by March 31, Practice Name # of Providers ACC (Residency Site) 3 Jackson Heights 4 TLCC (Residency Site) 6 Jose Quiwa 1 Ma Jesus Calagos MD 1 Brightpoint Health (Project Samaritan/HELP/PSI) 3 Community Health Network (FQHC) 14 Advanced Pediatrics PC 3 Total Providers 36 Total Speed & Scale Commitment 36 PPS Implementation Support The NYP/Q PPS contracted with HANYS (Healthcare Association of New York State) to provide implementation services for PCMH certification across the provider network. The consulting group is focused to achieving 2014 Level 3 status for 36 primary care providers inclusive of community-based & institution-based providers. The HANYS team developed a rigorous timeline aligned with PCMH and DSRIP deliverables to meet all expectations and works hand-in-hand with our network providers to achieve deliverables. Along with consultative services, our network providers also have access to the HANYS team to problem-solve PCMH integration needs to ensure a custom approach to clinical integration of this program. HANYS also provides Physician Champion training & engagement opportunities, and staff training based on the needs of the PPS & clinical providers. Page 9
10 Along with the practice transformation support, the NYP/Q PPS built the funds flow model to incentivize primary care transformation inclusive of PCMH transformation and engaged patient activity. The model rewards providers for achieving 2014 Level 3 status as well as provides incentives to partners for meeting engaged patient definitions for all primary care aligned projects. CARE TRANSITIONS According to the Center for Healthcare Strategies, Inc. (CHCS) a Care Management Strategy is a system that applies systems, science, incentives, and information to improve medical practice and assist consumers and their support system to become engaged in a collaborative process designed to manage medical/social/mental health conditions more effectively. The NYP/Q PPS will utilize the Care Management Framework published by CHCS (Attachment B) as a guide to align clinical and operational strategies to ensure effective planning and implementation to build a high value network. The components of the framework include: Identification / Stratification / Prioritization Intervention Evaluation Payment / Financing The clinical integration strategy outlines processes that will support the components of Identification / Stratification / Prioritization, Evaluation, and Payment / Financing and this section will outline concepts associated with Intervention. Utilizing the framework the PPS clinical leadership will be able to connect acute care, PCMH, and post-acute care activities to manage each patient across the continuum of care regardless of location or partner. The key principle is to provide adequate tools and resources to the network and align strategies of quality improvements through engagement, communication, and incentives. The NYP/Q PPS established the DSRIP network based on key needs of patients with existing partners to maximize efforts and build on existing synergies. This principle allows for immediate and increased activities of the network for Information Technology, Performance Reporting, Rapid Cycle Evaluation, and Best Practice Utilization to ensure appropriate care, in the appropriate setting, by the appropriate provider, and with the appropriate tools. Page 10

11 The care management strategy aligns patients with providers and providers with providers regardless of location utilizing tools, resources and programs. Care coordination with connectivity and notifications as well patient access to primary care and behavioral health will allow the PPS to build a system of care management that crosses the continuum of care. The strategy includes: High Risk Patient Identification & Tracking Patient Event Notifications Care Planning Discharge Planning Care Coordination Referral Management Medication Reconciliation Co-Location of Primary Care & Behavioral Health Wellness Screening INTERACT Implementation RHIO Connectivity Electronic Health Record Implementation QUALITY METRICS & REVIEW PROCESS NYP/Q PPS emphasizes a data-driven approach for performance and quality improvement within the clinically integrated system. In order to facilitate the utilization of available data meaningfully and to implement process improvement strategies that will stem from the data trends and analysis, the PMO has taken multiple steps. The PMO team recruited staff, which Page 11
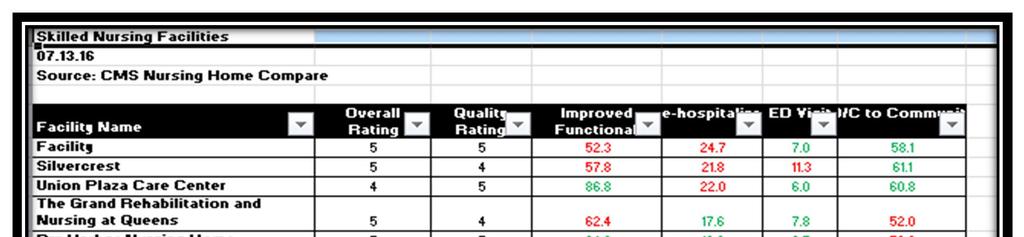
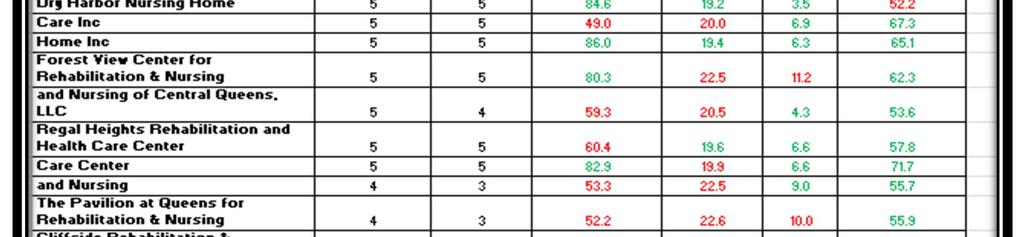
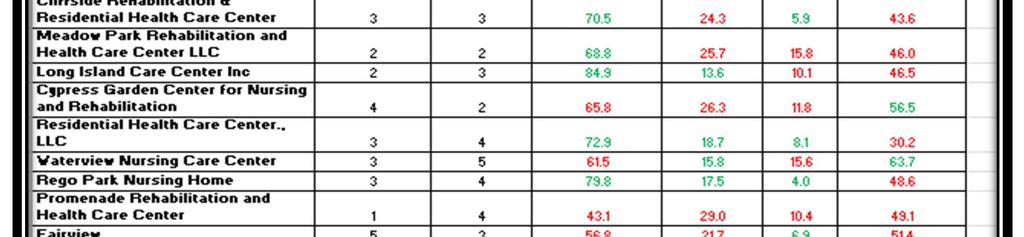
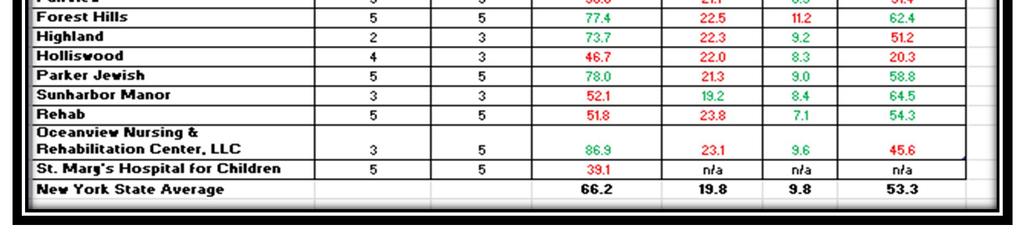
12 includes a data analyst and financial analyst, whose roles, respectively, are to manage the monthly intake of engaged patient information, development of dashboards specific to need of the projects or leaders, partner with the RCE to complete forecasting and risk assessments and to partner with the data analyst to maintain databases, which allow for complete analysis of partners based on outcome data. The Population Health Manager oversees the the quality improvement and performance reporting processes across the PPS and works with the team to identify needs and utilize data to engage partners in the RCE process. Moreover, the PPS produces a quarterly quality based outcome dashboard, Attachment C, for each project sub-committee. The dashboards encompass summaries of quality and metric specific data pulled from MAPP, Salient, and PPS claims data housed on the secure server. Each dashboard is unique to the clinical project and is utilized for further analysis and process improvement planning by the clinical sub-committee. The dashboards also provide tools to the Rapid Cycle Evaluation Unit team to identify trends and risks associated with quality based outcomes. Access to the MAPP released partner based quality data provides the RCE team the ability to complete ongoing quality analytics of partners focused to process improvement efforts, risk identification of providers, partner engagement for best practice utilization, and escalation of concerns to the appropriate governing committees. The performance reporting process tracks partner progress of quality metrics aligned with committed projects. Partners are risk stratified by categories according to the quality outcome expectations of the NYS DOH (improvement over self based on the measurement year). The quality review will focus to ongoing development of our high value network utilizing Salient quality data, project performance data, and engaged patient activity data. The combination of quality data and operational requirements will clearly outline partner expectations in order to develop action plans for continuous network development. The PMO benchmarks quality metrics, Attachment D and Attachment E, for the long-term care partners. Measures include overall rating and quality of services rating of the skilled nursing facilities, improved functional outcome, percentage of short-stay residents who were rehospitalized after a nursing home admission, percentage of short-stay residents who have had an Page 12
13 outpatient emergency department visit, and percentage of short-stay residents who were successfully discharged to the community. The traffic signal scheme of green and red colorcoding is used to identify the partners who are performing on quality measures that are below the state average. The benchmark data is shared with the partners during committee meetings and further discussion is facilitated to improve on measures that most partners are not doing so well across the network. NYS DOH provides reports to the PPS in order to fulfill the requirement of pay-for-reporting and pay-for-performance metrics. o Additional metrics will be completed by an annual chart audit. The audit will be managed by a NYS DOH vendor in order to identify random partners for quality outcome sampling. The PPS will be engaged in the process of chart audits and will receive feedback and results upon completion of the audit. Project Measure Description Measure Type 3.a.i Screening for Clinical Depression and Follow-up Percentage of Medicaid enrollees age 18 and older who were screened for clinical depression using a standardized depression screening tool, and if positive screen, received Hybrid G Codes & Chart Review Information 3.b.i Controlling High Blood Pressure appropriate follow-up care Percentage of Medicaid members years of age who had a diagnosis of hypertension (HTN) and BP effectively controlled during the MY. HEDIS o The PPS PMO RCE will identify additional processes for data reporting & tool utilization for more timely data collection in order to influence process improvement efforts. The timing of performance metrics are aligned with NYS designated measurement years. Description From To Implementation Plan April 1 st March 31 st Distribution Year (DY) Quality Metrics Measurement Year (MY) July 1 st June 30 th The analysis and risk stratification of partners will develop tools needed to influence the additional factor of developing a high value network: establish funds flow criteria to incentivize Page 13
14 value. Performance metrics will play a key role in the evolving funds flow model of the NYP/Q PPS. The current model incentivizes engagement, reporting, implementation of project requirements, and patient impact and will include quality based outcome incentives with Phase II of the model. Funds Flow Phase II is anticipated to begin development mid-dy2 dependent on the release of NYS DOH accurate quality data at the network provider level. This will be a task of the PMO Finance team and Finance Committee alongside the Clinical Integration and Population Health Management Committee to align clinical integration quality outcomes and funding. RAPID CYCLE EVALUATION UNIT A Rapid Cycle Evaluation (RCE) Unit will be established in DSRIP DY2 to utilize performance data reported by partners as well as data available in MAPP (Salient) and other tools for quality improvement efforts. A CQI (Continuous Quality Improvement) technique will be established with expectations that align with PPS performance of metrics as well as the timing associated with such metrics. Upon recruitment of the Rapid Cycle Unit team, a focused strategy will be developed to outline the processes associated with the unit. This strategy will outline partners, data sources, process improvement strategies, follow-up methods for improvements, and risks associated by quality based outcomes. National best practices will be utilized to build the strategy & processes for the PPS. ROOT CAUSE ANALYSIS The NYP/Q PPS long-term care project leads have started a root-cause analysis (RCA) exercise with the committee members focused to actual patient outcomes. The blinded patient process is discussed from beginning to end in order to identify areas that the network could have changed processes, tools, or communication channels to avoid an emergency department visit, admission, or re-admission. The exercise is not intended to place blame but to identify process improvement opportunities or gaps in care in order for the long-term care network to improve quality Page 14
15 outcomes. The RCA will continue and will be another tool that is utilized in the Rapid Cycle Evaluation Unit. POPULATION HEALTH PLATFORM Allscripts Care Director: In support of Population Health requirements and to align with the clinical integration assessment needs, the NYP/Q PPS will implement the Allscripts Care Director (ACD) application. As specified by the DOH, the PPS is required to perform population health management by actively using EHRs and other IT platforms to track attributed lives by creating registries. Allscripts Care Director will support population health and performance reporting, through the use of a standardize care plan, Event Notifications, Attribution Plans, Patient Registries, Risk Stratification and Care Coordination. Once fully implemented the Allscripts Care Director System will provide a central location for the management and tracking of all engaged patients. The system will also support performance reporting thorough its ad hoc reporting capabilities. All actively engaged attributed patient will be enrolled into the population health system, where they will be able to be managed and tracked through the various tools such as Event Notifications, Care Plan and Assessment. Implementation of the Population Health System will follow a two-phase roll-out plan. Phase 1 will provision system design to include; Interface builds, Assessments, Care Plans, Patient/Provider Upload, Attribution Plans and Security configuration. Page 15



16 Cureator : In addition to the implementation of the Population Health Management system, Allscripts Care Director, the PPS will also implement Cureatr. This web-based mobile application is used to support data exchange, secure text messaging and clinical event notifications. By leveraging the available tools, providers across the PPS will be able to impact patient outcomes. The main tool within the Cureatr application that will be used to support population health and impact outcomes is the Client event notifications. By leveraging the CENs, providers will be able to close care gaps, improve outcomes and reduce hospitalization. The Cureatr generated clinical event notifications will increase provider awareness and stimulate collaborative decision-making by automatically alerting providers of healthcare events that occur within a defined patient population. Specifically, Cureatr notifies providers about patient care transitions in real-time and Page 16
17 connects them across settings to coordinate care. Once the notification are received, providers using the application can communicate with the appropriate care team members using secure text to exchange necessary patient information and further coordinate care. Providers with a Cureatr account will also be able to receive the alerts on the smart phones or within the desktop app. Integration with this application is supported by certain required resources and tools such as signed data exchange agreements, HIPAA Consents, ADT feeds, and EMR integration along with staff trainings. The PPS plan is to collaborate with the vendor (Cureatr) to engage, integrate, train and provide access to the appropriate downstream partners. Some of the additional steps needed to implement and configure the application include the following: A PPS patient roster indicating all individuals whose care events will be monitored A trigger event, such as registration of a patient to an ED or inpatient service A payload of content to be delivered in a notification message, including patient demographics, encounter site, date and time of trigger event, and potentially additional clinical information A delivery mechanism, such as automated , fax, or EHR message generation; and a recipient, such as a durable provider or care manager who may subsequently impact care delivery and care resource allocation Other tools : The NYP/Q PPS has 4 projects that are specific to the long term care population. An integral requirement of these projects is to improve the mechanisms for advance care planning with this population. As such, the PPS has recommended the following tools for adoption by PPS partners participating in these projects. Each participating partner will have the ability to adopt the ACP tool that is best for their facility and workflows. Page 17
18 Attachment F in Appendix provides the training schedule for ACP/MOLST and emolst. In addition to these tools, the PPS is providing partners with the opportunity to become certified in EPEC (Education in Palliative and End-Of-Life Care). This training will ensure that partners are well versed in both how to use Advance Care Planning tools and how to engage patients and their family members in conversations around this topic. Our commitment is to provide all 16 EPEC modules in order to certify at least one Practitioner at each facility. Each of the modules is clinically driven and completion of all 16 modules will result in EPEC certification. Additionally, CME credits will be provided for each class. Attachment G and H in the Appendix provide the sample of the EPEC Training registration form and the training schedule, respectively. CLINICALLY INTEGRATED NETWORK TRAINING The PPS aims to offer trainings to partners based on their participation in specific projects with the PPS. These trainings will help to form the NYP/Q PPS as a clinically integrated network. In addition to the trainings for specific projects, the PPS is providing trainings on quality improvement initiatives for practitioners and staff. 2.a.ii Patient Centered Medical Home The NYP/Q PPS is working with partners to complete the certification process for Patient Centered Medical Home (PCMH) 2014 Level 3 standards. The PPS has engaged a vendor, HANYS Solutions, to assist partners with the transformation process. Objectives & Target Audience The PPS is working with PCP partners and their office staff on the PCMH transformation process. The PPS committed to having 36 providers obtain the certification and is on track to meet the project requirement by the end of DY3. The goal of the trainings for PCMH is to ensure that the providers and care coordinators have the skills and tools they need to be successful in the PCMH model. Speed & Scale Project Commitment Project 2.a.ii Project Scale Commitment Primary Care Physicians 36 Page 18
19 Learning Objectives and Curricula The PPS is offering two training opportunities specific to the PCMH project. These trainings, in addition to the support provided by HANYS Solutions, will help partners to complete the certification process for PCMH Level standards and fully embrace the shift from a primary care site to a patient centered medical home. Physician Champion Training The PPS hosted a physician champion training for the practices undergoing the PCMH transformation and for those that have completed the transformation but had not yet had champion training. The training focused on: o NCQA s 2014 PCMH Standards o True Practice Transformation o Role of Change Management o Role of HIT o Lessons learned The training session was recorded so that it can be used by practices that were not able to attend or will be undergoing the PCMH transformation process in the future. Care Coordination Training In collaboration with GNYHA, the NYP/Q PPS is hosting an all-day training session for care coordinators in the PPS. Care coordinators and those who will play a coordination role, are invited to participate in the training. The goals of the training are to: o Learn the fundamental, evidence-based concepts for building an effective care coordination process to achieve improved outcomes. o Discuss their roles in the medical home and the medical neighborhood, focusing on coordination opportunities within the primary care practice, as well as across the continuum of care. o Review strategies for implementing care coordination processes within each of the members roles, and develop recommendations for implementing specific elements of team-based care coordination. o Share roles, responsibilities, and best practices within their individual sites. Page 19
20 PPS Milestones The trainings provided by the PPS will help partners to achieve PCMH certification. This will directly impact the PPSs ability to achieve the following milestones: Project 2.a.ii PCMH o Milestone #1 Ensure that all participating PCPs in the PPS meet NCQA 2014 Level 3 PCMH accreditation and/or meet state-determined criteria for Advanced Primary Care Models by the end of DSRIP Year 3. o Milestone #3 Identify care coordinators at each primary care site who are responsible for care connectivity, internally, as well as connectivity to care managers at other primary care practices. o Milestone #7 Ensure that all staff are trained on PCMH or Advanced Primary Care models, including evidence-based preventive and chronic disease management. Project 3.a.i Co-location of Primary Care & Behavioral Health o Milestone #1 Co-locate behavioral health services at primary care practice sites. All participating primary care practices must meet 2014 NCQA level 3 PCMH or Advance Primary Care Model standards by DY 3. Project 3.b.i Cardiovascular o Milestone #3 Ensure that EHR systems used by participating safety net providers meet Meaningful Use and PCMH Level 3 standards and/or APCM by the end of Demonstration Year 3. Financial Sustainability o Milestone #6 Put in place Level 1 VBP arrangement for PCMH/APC care and one other care bundle or subpopulation Competency and Measurements The PPS will use the success of PCMH certification as the measurement for success with these practices. Page 20
21 2.b.vii INTERACT& 2.b.viii Home Care Collaboration Objectives & Target Audience The PPS will provide training to the long-term care providers participating in the INTERACT and home care project. The PPS aims to implement a train-the-trainer model by having the facility champions trained and then having the champions act as the trainers and experts at their own facilities. Speed & Scale Project Commitment Projects 2.b.v & 2.b.vii Project Scale Commitment Primary Care Physicians 97 Non-PCP Practitioners 72 Hospitals 1 Skilled Nursing Facilities 27 All Other 102 SNFs participating in the INTERACT program 27 Learning Objectives and Curricula The PPS will provide training for staff on the INTERACT and INTERACT-like tools that are required for the projects. The PPS will provide an in-person champion training to achieve the goals of a train-the-trainer, or coaching, model for the PPS. Additionally, the PPS will work with partners to ensure that patients, families, and caregivers are educated and engaged in the care planning process. INTERACT & INTERACT-like Tools The PPS will engage a certified INTERACT trainer to provide in person training for the SNF and Home Care INTERACT principles and tools. The learning objectives of the trainings are: 1. Describe the current landscape of health care reform and funding that make the INTERACT an essential QI initiative for post-acute and long-term care organizations 2. Articulate the key strategies that form the foundation of the INTERACT QIP 3. Understand how to optimally utilize INTERACT QIP tools and resources Page 21
22 4. Define key strategies for successful INTERACT QIP implementation, including how INTERACT can help meet QAPI requirements 5. Define key strategies for successfully sustaining the INTERACT QIP implementation processes 6. Measure and track organization specific INTERACT QIP implementation processes 7. Measure and track organization specific INTERACT QIP hospitalization and other related outcomes 8. Report and interpret feedback on INTERACT QIP implementation and outcomes to the facility team and leadership 9. Demonstrate an ability to effectively educate facility staff on the INTERACT QIP 10. Understand how to complete the CIC training certification process The PPS will train 2 champions from each partner site; (1) nursing manager and (1) staff manager. Patient, Family, and Caregiver Training To be successful in reducing potentially preventable readmissions, the PPS must engage the community to educate them about the care planning process. The PPS will work with long term care partners to ensure that education for the patient, family, and caregiver is incorporated into the care planning and meetings with the clinicians. The PPS will help partners develop or access educational materials as needed. PPS Milestones INTERACT champion training for the SNF and home care partners will enable the PPS to achieve numerous project milestones. Project 2.b.vii INTERACT o Milestone #4 Educate all staff on care pathways and INTERACT principles o Milestone #6 Create coaching program to facilitate and support implementation o Milestone #7 Educate patient and family/caretakers, to facilitate participation in planning of care Page 22
23 Project 2.b.viii Home Care Collaboration o Milestone #2 Ensure home care staff have knowledge and skills to identify and respond to patient risks for readmission, as well as to support evidence-based medicine and chronic care management. o Milestone #4 Educate all staff on care pathways and INTERACT-like principles o Milestone #6 Create coaching program to facilitate and support implementation o Milestone #7 Educate patient and family/caretakers, to facilitate participation in planning of care Competency and Measurements The PPS will use the DSRIP project metrics and the potentially preventable visit and readmission (PPV and PPR) rates as proxy measures for success with the training and implementation of these milestones. 3.b.i Cardiovascular Objectives & Target Audience The PPS will target partners in the cardiovascular project for training related to the specific 3.b.i milestones. The PPS aims to ensure that the workforce is prepared for the new process of open access blood pressure readings and the utilization of the Million Hearts Campaign. Speed & Scale Project Commitment Project 3.b.i Project Scale Commitment Primary Care Physicians 131 Non-PCP Practitioners 50 Clinics 1 Behavioral Health 1 Pharmacy 2 All Other 100 Page 23
24 Learning Objectives and Curricula The PPS is providing materials related to the Million Hearts Campaign, hypertension diagnosis and medication management, blood pressure check, and tobacco cessation referrals for partners. Million Hearts Campaign The Million Hearts Campaign, provides resources and protocols on hypertension and tobacco-smoking cessation. These protocols have been provided to participating sites for implementation by the clinical director. The PPS will offer an in service, as needed, with partners and participating sites on how to use the tools and protocols for improving patient care. Blood Pressure Competency The PPS has approved the competency checklist for both the manual and automatic blood pressure check. Partners will ensure that the BP competency is incorporated into their annual competency check process and provide copies of the completed certification of competency to the PPS. PPS Milestones The Cardiovascular training on blood pressure competency and the million hearts campaign will help the PPS to accomplish the following milestones: Milestone #9 Ensure that all staff involved in measuring and recording blood pressure are using correct measurement techniques and equipment. Milestone #18 Adopt strategies from the Million Hearts Campaign Competency and Measurements The PPS will request random audits and documentation of the partner blood pressure competency and utilization of the million hearts campaign. The PPS will use these samples as part of the documentation submission process for the IA quarterly reports. Page 24
25 3.d.ii Asthma Objectives & Target Audience The PPS has engaged a CBO partner with expertise in pediatric asthma to create an educational plan for PCPs participating in the project. Additionally, the PPS project has engaged a mental health partner with school-based clinics to aide in addressing the pediatric asthma population while at school. Speed & Scale Project Commitment Project 3.d.ii Project Scale Commitment Primary Care Physicians 13 Non-PCP Practitioners 14 Pharmacy 2 Community Based Organizations 1 All Other 6 Learning Objectives and Curricula The PPS has created a home care flow to identify the entry points into the system for the target patient population and identify the high need areas for provider education. Asthma Education The Asthma Coalition Queens, a CBO partner, is currently in the process of creating an educational program for pediatricians and behavioral health partners to address the pediatric asthma population. This education will include identification of asthma, common prescriptions that can be prescribed at ED presentation, how to use an asthma action plan, and the referral process for home care. PPS Milestones The PPS will achieve the following milestone through the proposed training plan: Milestone #4 Implement training and asthma self-management education services, including basic facts about asthma, proper medication use, identification and avoidance of environmental Page 25

26 exposures that worsen asthma, self-monitoring of asthma symptoms and asthma control, and using written asthma action plans. 3.g.ii Palliative Care Objectives & Target Audience The NYP/Q PPS has implemented a robust training program for partners who currently provide or will be providing this care to patients. The PPS has engaged clinical leadership, social workers, administrators, and providers for the training program. Speed & Scale Project Commitment Project 3.g.ii Project Scale Commitment Primary Care Physicians 98 Non-PCP Practitioners 70 Skilled Nursing Facilities 27 Hospice 6 All Other 99 Learning Objectives and Curricula The PPS has engaged a certified trainer, Dr. Cynthia Pan from NYP/Q, to provide palliative care training. Page 26
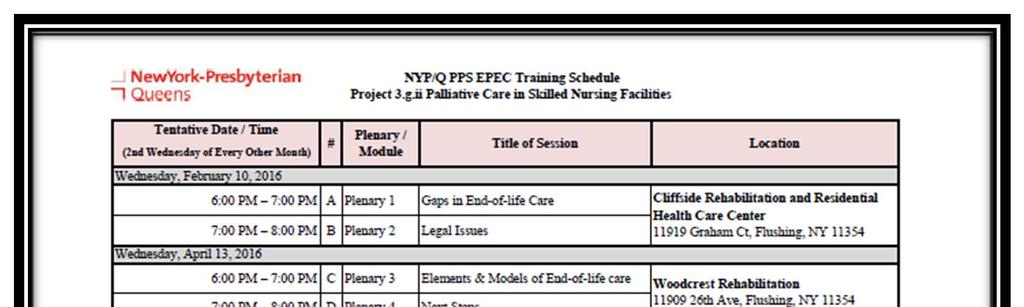
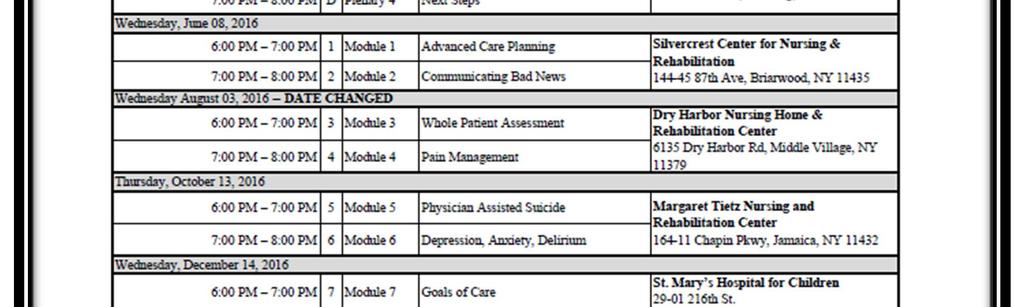
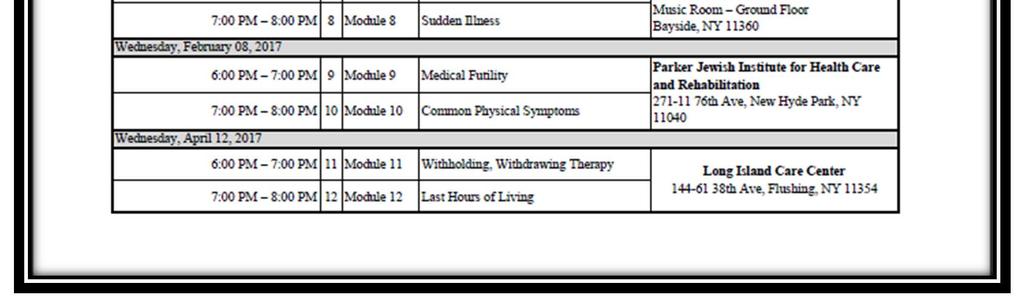
27 Education in Palliative and End-of-Life Care (EPEC) The EPEC training is held bimonthly 1 at different SNF partner sites. Dr. Pan reviews two modules per session, which include the following topics: o Gaps in End-of-Life Care o Legal Issues o Next Steps o Advance Care Planning o Communicating Bad News o Whole Patient Assessment o Pain Management o Elements & Modules in End-of- Life Care o Physician Assisted Suicide o Depression, Anxiety, Delirium o Goals of Care o Sudden Illness o Medical Futility o Common Physical Symptoms o Withholding, Withdrawing Therapy o Last Hours of Living The training incorporates videos, slides, and discussion to create an engaging environment for participants. Providers who attend all 8 sessions (16 modules) will receive EPEC certification in addition to receiving CME credits. Center to Advance Palliative Care (CAPC) The PPS has provided partners with information on joining CAPC for a reduced fee as part of the DSRIP initiatives. CAPC provides educational opportunities and resources specific to palliative care to members. Palliative Care Outcome Score (PCOS) Tool The DOH has implemented a new tool as a mechanism of measuring quality for palliative care for the project. The PPS has begun the process of piloting the tool at a partner site. The pilot kicked-off in August2016 and based on the lessons learned and needs of the partner, the PPS will determine the appropriate next steps for whether a training program is needed for partners. PPS Milestones The PPSs EPEC, CAPC and PCOS tool trainings will be used to complete the following project milestone: Milestone #4 1 EPEC Schedule provided in Appendix Page 27
28 Engage staff in trainings to increase role-appropriate competence in palliative care skills and protocols developed by the PPS. Competency and Measurements The EPEC program required pre- and post-competency exams as part of the training program. These competencies will be used, along with the implementation of all f the project requirements, to determine the success of the training program. Education opportunities from CAPC will include competencies as required by CAPC based on the specific topic and curriculum. The PPS will use the metric for PCOS as a determination on the success of training in addition to feedback from the pilot site. GOVERNANCE & OPERATIONS The Clinical Integration Committee will govern the approval and implementation of the clinical integration strategy. Strategy and updates will be brought to the PPS Executive Committee for review, recommendations, or final approvals. The strategy will be reviewed annually for adjustments based on PPS performance or network needs. The PMO team, Population Health Manager and Data Analytics resources will work with partners monthly to ensure compliance of the strategy and will report compliance issues to the Clinical Integration Committee based on findings. All partner compliance issues will be reported to the Executive Committee quarterly, or more frequently as needed, with an action plan to remedy the issues identified. Page 28
29 APPENDIX ATTACHMENT A: INVENTORY OF PPS APPROVED BEST PRACTICES Project Best Practices / Date Description Tools Approved 2.a.ii - PCMH PCMH Roadmap Timeline & Roadmap for PCMH Transformation 11/30/15 2.a.ii - PCMH PCMH Physician Champion Role & Responsibilities Outlines the role and responsibilities for providers that are the PCMH champion at their site 1/13/16 2.a.ii - PCMH 2.a.ii - PCMH 2.a.ii - PCMH 2.a.ii - PCMH 2.a.ii - PCMH 2.b.v, 2.b.vii, 2.b.viii, 3.g.ii - - LTC Projects 2.b.v Care Transitions 2.b.vii - INTERACT 2.b.vii - INTERACT PCMH Care Coordinator Role & Responsibilities EHR Recommendations PCMH Training Plan & Timeline Open Access Scheduling Pop. Health Management Tool Guideline Advance Care Planning Tools NYS Transition of Care INTERACT Tool INTERACT Facility Champion Outlines the role and responsibilities for care coordinators at PCMH sites Outline resources available to partners who need to implement an EHR and provides an inventory of EHR systems currently used by PPS partners Outline of the training plan and timeline for PCMH sites undergoing transformation 1/13/16 3/31/16 3/31/16 Best practice for open access scheduling at sites 3/31/16 Overview of the best practices for utilizing the PPS provided population health management tool Inventory of approved tools to utilize with patients for advance care planning NYS Requirements of a successful transition of care from hospital to SNF or home care Overview of INTERACT tool and modules for adoption by SNFs Outlines the role and responsibilities for INTERACT champions at participating SNF & home care sites 3.a.i - PC/BH Co-Location Sites Inventory of PPS sites that will be co-locating primary care & behavioral health services 3.a.i - PC/BH Preventative Screening Best Practices - Primary Care & Behavioral Health Tools for preventative care screening including: -PHQ-2 & PHQ-9 -GPCOG -Vaccines -Screening Tests (lipid, colon, cervical etc.) 6/24/16 3/31/16 6/24/16 11/30/15 1/13/16 11/30/15 11/30/15 3.b.i - US Preventative Task Recommendations on Lipid & Hypertension 11/30/15
30 Project Best Practices / Tools Description Cardiovascular Force Screening Best Practices 3.b.i - Million Hearts Best practice for cardiovascular including Cardiovascular Campaign hypertension diagnosis workflow 3.b.i - BP Competency Outline of requirement for competency on blood Cardiovascular Forms pressure screening and forms for documentation 3.b.i - Medication Best practice for prescribing single pill or fixed Cardiovascular Management dose combination medication for hypertension 3.b.i - Blood Pressure Self- Best practice from Million Hearts Campaign for Cardiovascular Management patient self-management for blood pressure 3.b.i 5 A s of Tobacco Best practice for smoking cessation using the 5 Cardiovascular Cessation A s and NYS quitline 3.d.ii Clinical Flow Asthma 3.d.ii Asthma 3.g.ii Palliative Care 3.g.ii Palliative Care 3.g.ii Palliative Care Diagram Asthma Best Practices Provider & Community Recourses Date Approved 3/31/16 3/31/16 6/24/16 6/24/16 6/24/16 Process flow for referrals for pediatric asthma 4/13/16 Asthma best practices including home assessments, surveys, school programs and checklists Inventory of resources available to PPS partners specific to palliative care 4/13/16 3/31/16 EPEC Training Best practice training program for partners 6/24/16 MOLST / emolst Best practice for utilizing the MOSLT forms for partners with an emphasis on using the electronic version (emolst) 6/24/16 Page 30


31 ATTACHMENT B: CARE MANAGEMENT FRAMEWORK Page 31


32 ATTACHMENT C: QUALITY BASED OUTCOMES Page 32
33 ATTACHMENT D: BENCHMARKS WITH STATE AND NATIONAL AVERAGE Page 33
34 ATTACHMENT E: OVERVIEW OF QUALITY METRICS Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 2.a.ii Increase certification of primary care practitioners with PCMH certification and/or Advanced Primary Care Models (as developed under the NYS Health Innovation Plan (SHIP)) Adult Access to Preventive or Ambulatory Care - 20 to 44 years Adult Access to Preventive or Ambulatory Care - 45 to 64 years Adult Access to Preventive or Ambulatory Care - 65 and older CAHPS Measures - Care Coordination with provider up-to-date about care received from other providers Children's Access to Primary Care - 12 to 19 years Children's Access to Primary Care - 12 to 24 Months Children's Access to Primary Care - 25 months to 6 years Children's Access to Primary Care - 7 to 11 years Getting Timely Appointments, Care and information (Q6, 8, 10, and 12) H-CAHPS - Care Transition Metrics (Q23, 24, and 25) Helpful, Courteous, and Respectful Office
35 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Staff (Q24 and 25) Medicaid Spending on ER and Inpatient Services +/ Medicaid spending on Primary Care and community based behavioral health care PDI 90 - Composite of all measures +/ Percent of eligible providers meeting Meaningful Use criteria who conduct bidirectional exchange with qualified entities (RHIOs) Percent of eligible providers meeting Meaningful Use criteria who have participating agreements with qualified entities (RHIOs) Percent of PCP meeting PCMH (NCQA) or Advance Primary Care (SHIP) standards Potentially Avoidable Emergency Room Visits +/ Potentially Avoidable Readmissions +/ PQI 90 - Composite of all measures +/ Primary Care - Length of Relationship - Q Primary Care - Usual Source of Care - Q b.v Care transitions intervention for skilled nursing facility (SNF) residents Adult Access to Preventive or Ambulatory Care - 20 to 44 years Adult Access to Preventive or Ambulatory Care - 45 to 64 years Page 35
36 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Adult Access to Preventive or Ambulatory Care - 65 and older CAHPS Measures - Care Coordination with provider up-to-date about care received from other providers Children's Access to Primary Care - 12 to 19 years Children's Access to Primary Care - 12 to 24 Months Children's Access to Primary Care - 25 months to 6 years Children's Access to Primary Care - 7 to 11 years Getting Timely Appointments, Care and information (Q6, 8, 10, and 12) H-CAHPS - Care Transition Metrics (Q23, 24, and 25) Helpful, Courteous, and Respectful Office Staff (Q24 and 25) Medicaid Spending on ER and Inpatient Services +/ Medicaid spending on Primary Care and community based behavioral health care PDI 90 - Composite of all measures +/ Percent of eligible providers meeting Meaningful Use criteria who conduct bidirectional exchange with qualified entities (RHIOs) Page 36
37 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Percent of eligible providers meeting Meaningful Use criteria who have participating agreements with qualified entities (RHIOs) Percent of PCP meeting PCMH (NCQA) or Advance Primary Care (SHIP) standards Potentially Avoidable Emergency Room Visits +/ Potentially Avoidable Readmissions +/ PQI 90 - Composite of all measures +/ Primary Care - Length of Relationship - Q Primary Care - Usual Source of Care - Q b.vii Implementing the INTERACT project (inpatient transfer avoidance program for SNF) Adult Access to Preventive or Ambulatory Care - 20 to 44 years Adult Access to Preventive or Ambulatory Care - 45 to 64 years Adult Access to Preventive or Ambulatory Care - 65 and older CAHPS Measures - Care Coordination with provider up-to-date about care received from other providers Children's Access to Primary Care - 12 to 19 years Children's Access to Primary Care - 12 to 24 Months Page 37
38 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Children's Access to Primary Care - 25 months to 6 years Children's Access to Primary Care - 7 to 11 years Getting Timely Appointments, Care and information (Q6, 8, 10, and 12) H-CAHPS - Care Transition Metrics (Q23, 24, and 25) Helpful, Courteous, and Respectful Office Staff (Q24 and 25) Medicaid Spending on ER and Inpatient Services +/ Medicaid spending on Primary Care and community based behavioral health care PDI 90 - Composite of all measures +/ Percent of eligible providers meeting Meaningful Use criteria who conduct bidirectional exchange with qualified entities (RHIOs) Percent of eligible providers meeting Meaningful Use criteria who have participating agreements with qualified entities (RHIOs) Percent of PCP meeting PCMH (NCQA) or Advance Primary Care (SHIP) standards Potentially Avoidable Emergency Room Visits +/ Potentially Avoidable Readmissions +/ PQI 90 - Composite of all measures +/ Primary Care - Length of Relationship Page 38
39 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Q3 Primary Care - Usual Source of Care - Q b.viii Hospital-Home Care Collaboration Solutions Adult Access to Preventive or Ambulatory Care - 20 to 44 years Adult Access to Preventive or Ambulatory Care - 45 to 64 years Adult Access to Preventive or Ambulatory Care - 65 and older CAHPS Measures - Care Coordination with provider up-to-date about care received from other providers Children's Access to Primary Care - 12 to 19 years Children's Access to Primary Care - 12 to 24 Months Children's Access to Primary Care - 25 months to 6 years Children's Access to Primary Care - 7 to 11 years Getting Timely Appointments, Care and information (Q6, 8, 10, and 12) H-CAHPS - Care Transition Metrics (Q23, 24, and 25) Helpful, Courteous, and Respectful Office Staff (Q24 and 25) Medicaid Spending on ER and Inpatient Services +/ Page 39
40 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Medicaid spending on Primary Care and community based behavioral health care PDI 90 - Composite of all measures +/ Percent of eligible providers meeting Meaningful Use criteria who conduct bidirectional exchange with qualified entities (RHIOs) Percent of eligible providers meeting Meaningful Use criteria who have participating agreements with qualified entities (RHIOs) Percent of PCP meeting PCMH (NCQA) or Advance Primary Care (SHIP) standards Potentially Avoidable Emergency Room Visits +/ Potentially Avoidable Readmissions +/ PQI 90 - Composite of all measures +/ Primary Care - Length of Relationship - Q Primary Care - Usual Source of Care - Q a.i Integration of primary care and behavioral health services Adherence to Antipsychotic Medications for People with Schizophrenia Antidepressant Medication Management - Effective Acute Phase Treatment Antidepressant Medication Management - Effective Continuation Phase Treatment Page 40
41 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Cardiovascular Monitoring for People with Cardiovascular Disease and Schizophrenia Diabetes Monitoring for People with Diabetes and Schizophrenia Diabetes Screening for People with Schizophrenia or Bipolar Disease who are Using Antipsychotic Medication Engagement of Alcohol and Other Drug Dependence Treatment (Initiation and 2 visits within 44 days) Follow-up after hospitalization for Mental Illness - within 30 days Follow-up after hospitalization for Mental Illness - within 7 days Follow-up care for Children Prescribed ADHD Medications - Continuation Phase Follow-up care for Children Prescribed ADHD Medications - Initiation Phase Initiation of Alcohol and Other Drug Dependence Treatment (1 visit within 14 days) Potentially Preventable Emergency Department Visits (for persons with BH diagnosis) +/ Screening for Clinical Depression and Follow-Up Plan b.i Evidence-based strategies for disease management in high risk/affected Page 41
42 Measure populations (adult only) Baseline for MY2 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Aspirin Use Discussion of Risks and Benefits of Aspirin Use Flu Shots for Adults Ages Health Literacy - Describing How to Follow Instructions Health Literacy - Explained What To Do If Illness Got Worse Health Literacy - Instructions Easy to Understand Medical Assistance with Smoking and Tobacco Use Cessation - Advised to Quit Medical Assistance with Smoking and Tobacco Use Cessation - Discussed Cessation Medication Medical Assistance with Smoking and Tobacco Use Cessation - Discussed Cessation Strategies Prevention Quality Indicator # 13 (Angina without procedure) +/ Prevention Quality Indicator # 7 (HTN) +/ d.ii Expansion of asthma home-based selfmanagement program Asthma Medication Ratio (5-64 Years) Medication Management for People with Asthma (5-64 Years) - 50% of Treatment Days Covered Page 42
43 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Measure Baseline for MY2 Medication Management for People with Asthma (5-64 Years) - 75% of Treatment Days Covered Pediatric Quality Indicator # 14 Pediatric Asthma +/ Prevention Quality Indicator # 15 Younger Adult Asthma +/ c.ii Increase early access to, and retention in, HIV care Age-adjusted percentage of adults who have a regular health care provider - Aged 18+ years 76.8 Age-adjusted preventable hospitalizations rate per 10,000 - Aged 18+ years Age-adjusted preventable hospitalizations rate per 10,000 - Aged 18+ years - Ratio of Black non-hispanics to White non- Hispanics 1.67 Age-adjusted preventable hospitalizations rate per 10,000 - Aged 18+ years - Ratio of Hispanics to White non-hispanics 0.97 Chlamydia case rate per 100,000 women - Aged years Newly diagnosed HIV case rate per 100, Newly diagnosed HIV case rate per 100,000 - Difference in rates (Black and White) of new HIV diagnoses 27.6 Newly diagnosed HIV case rate per 100,000 - Difference in rates (Hispanic 23.8 Page 43
44 Measure and White) of new HIV diagnoses Baseline for MY2 Increase Flag MY2 Annual Improvement Target MY2 High Performance Target Change needed to meet MY 2 Target Statewide Performance Goal Percentage of adults with health insurance - Aged years 76.4 Percentage of premature death (before age 65 years) 23.9 Percentage of premature death (before age 65 years) - Ratio of Black non- Hispanics to White non-hispanics 2.04 Percentage of premature death (before age 65 years) - Ratio of Hispanics to White non-hispanics 2.15 Primary and secondary syphilis case rate per 100,000 females 0.5 Primary and secondary syphilis case rate per 100,000 males 15.7 Domain 1 Measure Health Home assigned/referred members in outreach or engagement Health Home engaged members with a care plan during the measurement year Health Home members who were in outreach/engagement who were engaged during the measurement year Page 44



45 ATTACHMENT F: TRAINING SCHEDULE FOR ACP/MOLST/eMOLST
46 ATTACHMENT G: EPEC TRAINING SCHEDULE Page 46
47 Page 47
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER
 PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
PERFORMANCE REPORTING & IMPROVEMENT A GLIMPSE AT THE SCC S PERFORMANCE MEASURES & DASHBOARDS AND ONLINE LEARNING CENTER Presented by: Kevin Bozza, MPA, FACHE, CPHQ, RHIT Sr. Director, Network Development
# Topic Responsible Person Document
 NYPQ DSRIP PPS PCMH Committee Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: September 5, 2017 Conference Line: 877-594-8353 Code: 79706143# Location:
NYPQ DSRIP PPS PCMH Committee Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: September 5, 2017 Conference Line: 877-594-8353 Code: 79706143# Location:
Performing Provider System (PPS) CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK
 CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK") Performing Provider System (PPS) Westchester Medical Center Health Network CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK 7 SKYLINE DRIVE, SUITE 385 HAWTHORNE, NY 10532 914.326.4200
Performing Provider System (PPS) Westchester Medical Center Health Network CENTER for REGIONAL HEALTHCARE INNOVATION A MEMBER OF THE WMCHEALTH NETWORK 7 SKYLINE DRIVE, SUITE 385 HAWTHORNE, NY 10532 914.326.4200
Exhibit A.11.DY3. DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements
 Requirements") Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
Exhibit A.11.DY3 DSRIP Year 3 Extra Large Primary Care Provider ( PCP ) Requirements 1. Generally. This Exhibit contains the requirements and substantiations associated with each of the metrics required
CLINICAL INTEGRATION STRATEGY
 CLINICAL INTEGRATION STRATEGY ABSTRACT The Suffolk Care Collaborative Clinical Integration Strategy focuses on the ability to coordinate care across the continuum through clinically interoperable systems.
CLINICAL INTEGRATION STRATEGY ABSTRACT The Suffolk Care Collaborative Clinical Integration Strategy focuses on the ability to coordinate care across the continuum through clinically interoperable systems.
# Topic Responsible Person Document
 Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: August 1, 2017 Conference Line: 877-594-8353 Code: 79706143# Location: Meeting Purpose: NYPQ 56-45
Meeting Title: Facilitator(s): NYPQ DSRIP PCMH Project M. D Urso/ M. Cartmell Meeting Date: Meeting Time: August 1, 2017 Conference Line: 877-594-8353 Code: 79706143# Location: Meeting Purpose: NYPQ 56-45
Delivery System Reform Incentive Payment (DSRIP)
") Delivery System Reform Incentive Payment (DSRIP) Community Advisory Committee Meeting April 15, 2015 Maureen Buglino, RN, MPH Vice President for Community Medicine & Emergency Medicine What is DSRIP? Main
Delivery System Reform Incentive Payment (DSRIP) Community Advisory Committee Meeting April 15, 2015 Maureen Buglino, RN, MPH Vice President for Community Medicine & Emergency Medicine What is DSRIP? Main
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
MPA Reference Guide. Millennium Collaborative Care
 Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Millennium Collaborative Care 1. MPA... 3 2. Provider Types... 3 2.1. Primary Care Practices... 3 2.2. Pediatric Practices... 9 2.3. Behavioral Health... 12 2.4. Acute Care... 18 2.5. Post-Acute Care...
Medicaid Payment Reform at Scale: The New York State Roadmap
 Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Medicaid Payment Reform at Scale: The New York State Roadmap ASTHO Technical Assistance Call June 22 nd 2015 Greg Allen Policy Director New York State Medicaid Overview Background and Brief History Delivery
Meeting Title. Facilitator. Conference Line
 DSRIP Meeting Agenda Date and Time Location 3/21/17, 10-11am Heart Center Room 4, GoTo meeting Meeting Title Facilitator NYP PPS IT/Data Governance Committee Gil Kuperman, Alvin Lin Go to Meeting https://global.gotomeeting.com/join
DSRIP Meeting Agenda Date and Time Location 3/21/17, 10-11am Heart Center Room 4, GoTo meeting Meeting Title Facilitator NYP PPS IT/Data Governance Committee Gil Kuperman, Alvin Lin Go to Meeting https://global.gotomeeting.com/join
I. Welcome M. Buglino. II. Review & Approve Minutes of Previous Meeting Action Item M. Buglino
 EXECUTIVE COMMITTEE MEMBERS: NYP Queens DSRIP Executive Committee Meeting Thursday June 22, 2017-4:00p.m. 5:00p.m. Call in# 866-692-4538; Passcode: 26098085# Maureen Buglino (Chair) - NewYork-Presbyterian
EXECUTIVE COMMITTEE MEMBERS: NYP Queens DSRIP Executive Committee Meeting Thursday June 22, 2017-4:00p.m. 5:00p.m. Call in# 866-692-4538; Passcode: 26098085# Maureen Buglino (Chair) - NewYork-Presbyterian
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Revised DSRIP Actively Engaged: Project Specific Definitions and Clarifying Information. As of October 28, 2015
 Revised DSRIP Actively Engaged: Project Specific Definitions and Clarifying Information As of October 28, 2015 10/28/2015 2 General Guidance regarding Domain 1 Active Engagement The Independent Assessor
Revised DSRIP Actively Engaged: Project Specific Definitions and Clarifying Information As of October 28, 2015 10/28/2015 2 General Guidance regarding Domain 1 Active Engagement The Independent Assessor
New York State s Ambitious DSRIP Program
 New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
New York State s Ambitious DSRIP Program A Case Study Speaker: Denise Soffel, Ph.D., Principal May 28, 2015 Information Services Webinar HealthManagement.com HealthManagement.com HealthManagement.com HealthManagement.com
NYS Value Based Payments (VBP):
:") NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
NYS Value Based Payments (VBP): Provider Associations, Community Based Organizations, and Consumer Advocates Town Hall Meeting Jason Helgerson NYS Medicaid Director December 16, 2016 2 Today s Agenda Agenda
2.b.iii ED Care Triage for At-Risk Populations
 2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
2.b.iii ED Care Triage for At-Risk Populations Project Objective: To develop an evidence-based care coordination and transitional care program that will assist patients to link with a primary care physician/practitioner,
Domain 1 Patient Engagement Speed Data Reports & Schedule
 Domain 1 Patient Engagement Speed Data Reports & Schedule Suffolk Care Collaborative (SCC) Suffolk County Performing Provider System (PPS) Delivery System Reform Incentive Payment (DSRIP) Program 2 PRESENTATION
Domain 1 Patient Engagement Speed Data Reports & Schedule Suffolk Care Collaborative (SCC) Suffolk County Performing Provider System (PPS) Delivery System Reform Incentive Payment (DSRIP) Program 2 PRESENTATION
Adopting a Care Coordination Strategy
 Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Adopting a Care Coordination Strategy Authors: Henna Zaidi, Manager, and Catherine Castillo, Senior Consultant Current state of health care The traditional approach to health care delivery is quickly becoming
Albany Medical Center. AMCH PPS Clinical & Quality Affairs Committee
 Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Tara Foster, MS, RN Mingie Kang, MPH Mark Quail, MEd Brendon Smith, PhD Susan Kopp MBA, BSN, RN January
Albany Medical Center AMCH PPS Clinical & Quality Affairs Committee Kallanna Manjunath MD, FAAP, CPE Tara Foster, MS, RN Mingie Kang, MPH Mark Quail, MEd Brendon Smith, PhD Susan Kopp MBA, BSN, RN January
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request
 DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
DSRIP Demonstration Year 1, Quarter 1-2 Domain 1 Patient Engagement Data Request Webinar: Monday, October 5, 2015 Time: 1:30pm-3:00pm Presented by Suffolk Care Collaborative (SCC) Suffolk County Performing
10/31/2016. Primary Care Plan. DY2 - Revised
 10/31/2016 Primary Care Plan DY2 - Revised Table of Contents CONTENTS Executive Summary... 2 Fundamental 1: Assessment of current primary care capacity, performance and needs, and a plan for addressing
10/31/2016 Primary Care Plan DY2 - Revised Table of Contents CONTENTS Executive Summary... 2 Fundamental 1: Assessment of current primary care capacity, performance and needs, and a plan for addressing
Using population health management tools to improve quality
 Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
Using population health management tools to improve quality Jessica Diamond, MPA, CPHQ Chief Population Health Officer CHCANYS Statewide Conference and Clinical Forum Sunday, October 18, 2015 Introduction
New York State Department of Health Innovation Initiatives
 New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
New York State Department of Health Innovation Initiatives HCA Quality & Technology Symposium November 16 th, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety
Patient-Centered Medical Home Assessment & Roadmap
 11/30/2016 Patient-Centered Medical Home Assessment & Roadmap Population Health Management Workstream Milestone 1 Table of Contents 1) Executive Summary 2) Overview of Primary Care Providers 3) PCMH Timeline
11/30/2016 Patient-Centered Medical Home Assessment & Roadmap Population Health Management Workstream Milestone 1 Table of Contents 1) Executive Summary 2) Overview of Primary Care Providers 3) PCMH Timeline
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Reducing Hospital Admissions Through the Use of IT. Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods
 Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
Reducing Hospital Admissions Through the Use of IT Steven Milligan MD Medical Director of ACO Management Colorado Health Neighborhoods Conflict of Interest Steven Milligan, MD Has no real or apparent conflicts
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017
 Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
Primary Care Redesign: Perspective from the New York State Department of Health October 3, 2017 Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NYSDOH Marcus.Friedrich@Health.NY.Gov
Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers. LeadingAge New York Webinar
 Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers LeadingAge New York Webinar November 10, 2014 Tracy E. Miller, Esq. Health Care Group Bond, Schoeneck & King, PLLC Delivery
Preparing for DSRIP: Legal and Strategic Issues for Long-Term Care Providers LeadingAge New York Webinar November 10, 2014 Tracy E. Miller, Esq. Health Care Group Bond, Schoeneck & King, PLLC Delivery
Russell B Leftwich, MD
 Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Russell B Leftwich, MD Chief Medical Informatics Officer Office of ehealth Initiatives, State of Tennessee 1 Eligible providers and hospitals can receive incentives for meaningful use of certified EHR
Moving into DSRIP Year 4 What Do We Need To Do. Peggy Chan DSRIP Program Director
 Moving into DSRIP Year 4 What Do We Need To Do Peggy Chan DSRIP Program Director 2 DSRIP Implementation Timeline and Key Benchmarks We are here Focus on Infrastructure Development/System Design Focus on
Moving into DSRIP Year 4 What Do We Need To Do Peggy Chan DSRIP Program Director 2 DSRIP Implementation Timeline and Key Benchmarks We are here Focus on Infrastructure Development/System Design Focus on
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
HHSC Value-Based Purchasing Roadmap Texas Policy Summit
 HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
HHSC Value-Based Purchasing Roadmap Texas Policy Summit Andy Vasquez, Deputy Associate Commissioner MCS, Quality & Program Improvement Section October 19, 2017 1 HHSC Value-Based Purchasing Roadmap Topics
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
QUALITY IMPROVEMENT. Molina Healthcare has defined the following goals for the QI Program:
 QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
QUALITY IMPROVEMENT Molina Healthcare maintains an active Quality Improvement (QI) Program. The QI program provides structure and key processes to carry out our ongoing commitment to improvement of care
DRAFT Complex and Chronic Care Improvement Program Template. (Not approved by CMS subject to continuing review process)
") DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
DRAFT Complex and Chronic Care Improvement Program Template Performance Year 2017 (Not approved by CMS subject to continuing review process) 1 Page A. Introduction The Complex and Chronic Care Improvement
POPULATION HEALTH PLAYBOOK. Mark Wendling, MD Executive Director LVPHO/Valley Preferred 1
 POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
POPULATION HEALTH PLAYBOOK Mark Wendling, MD Executive Director LVPHO/Valley Preferred www.populytics.com 1 Today s Agenda Outline LVHN, LVPHO and Populytics Overview Population Health Approach Population
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
A. PCMH Service Site: 1. Co-locate behavioral health services at primary care practice sites. All participating primary
 Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Domain 3 Projects 3.a.i Integration of Primary Care and Behavioral Health Services Project Objective: Integration of mental health and substance abuse with primary care services to ensure coordination
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
The Heart and Vascular Disease Management Program
 Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Element A: Program Content The Heart and Vascular Disease Management Program GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to
Montefiore Hudson Valley Collaborative
 Montefiore Hudson Valley Collaborative DSRIP Application As submitted to New York State Department of Health on December 22, 2014 Succinctly explain the identified goals and objectives of the PPS, and
Montefiore Hudson Valley Collaborative DSRIP Application As submitted to New York State Department of Health on December 22, 2014 Succinctly explain the identified goals and objectives of the PPS, and
Jumpstarting population health management
 Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Jumpstarting population health management Issue Brief April 2016 kpmg.com Table of contents Taking small, tangible steps towards PHM for scalable achievements 2 The power of PHM: Five steps 3 Case study
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2016 This document is a guide to the 2016 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Using Healthix to Support DSRIP: Opportunities and Challenges. February 25, 2016
 Using Healthix to Support DSRIP: Opportunities and Challenges February 25, 2016 Contents 1. Community Care of Brooklyn Overview (2 5) 2. Healthix Enablement of CCB IT Strategy (6-13) 3. Challenges (slide
Using Healthix to Support DSRIP: Opportunities and Challenges February 25, 2016 Contents 1. Community Care of Brooklyn Overview (2 5) 2. Healthix Enablement of CCB IT Strategy (6-13) 3. Challenges (slide
Accountable Care and the Laboratory Value Proposition. Les Duncan Director of Operations Highmark Health - Home and Community Services
 Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Accountable Care and the Laboratory Value Proposition Les Duncan Director of Operations Highmark Health - Home and Community Services Agenda The Goals and Status of Delivery System Reform and Alternative
Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet
 Cohort 3 Request for Application (RFA) Packet") Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet 1 P age REQUEST FOR APPLICATION (RFA) TIMELINE OVERVIEW For questions related to the Cohort 3 SIM Practice Request for
Colorado State Innovation Model (SIM) Cohort 3 Request for Application (RFA) Packet 1 P age REQUEST FOR APPLICATION (RFA) TIMELINE OVERVIEW For questions related to the Cohort 3 SIM Practice Request for
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way
 The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
The Long and Winding Road-map: From Waiver Services to VBP and Other Stops Along the Way Mental Health Association in New York State, Inc. Annual Meeting Gregory Allen, MSW Director Division of Program
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
NYP-Led Performing Provider System PAC Kickoff Meeting MINUTES October 21, 2014
 NYP-Led Performing Provider System PAC Kickoff Meeting MINUTES October 21, 2014 Present: D. Johansson-ACMH, L. Capitelli-NY Psychiatric Institute, K. Meyer-Community Healthcare Network, E. Eng-ArchCare,
NYP-Led Performing Provider System PAC Kickoff Meeting MINUTES October 21, 2014 Present: D. Johansson-ACMH, L. Capitelli-NY Psychiatric Institute, K. Meyer-Community Healthcare Network, E. Eng-ArchCare,
Requirements Document for the Blue Quality Physician Program sm Criteria Effective 08/03/2015
 All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
All practices must reapply to the BQPP every 18 months Criteria Definition Validation Source(s) 7 Practice Elements 3 Provider Elements Practice level points: 1. PCMH/PPC/PCSP Recognition *Mandatory 2.
DSRIP 2017: Lessons Learned and Paving the Way for Success
 DSRIP 2017: Lessons Learned and Paving the Way for Success Greg Allen, MSW (Moderator) Director, Division of Program Development and Management Office of Health Insurance Programs, New York State Department
DSRIP 2017: Lessons Learned and Paving the Way for Success Greg Allen, MSW (Moderator) Director, Division of Program Development and Management Office of Health Insurance Programs, New York State Department
Michigan s Vision for Health Information Technology and Exchange
 Michigan s Vision for Health Information Technology and Exchange Health information exchange or HIE is the mobilization of health care information electronically across organizations within a region, community
Michigan s Vision for Health Information Technology and Exchange Health information exchange or HIE is the mobilization of health care information electronically across organizations within a region, community
The Michigan Primary Care Transformation (MiPCT) Project. PGIP Meeting Update March 09, 2012
 Project. PGIP Meeting Update March 09, 2012") The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
The Michigan Primary Care Transformation (MiPCT) Project PGIP Meeting Update March 09, 2012 2 Agenda MiPCT March Launch meetings Care Management Update Performance Incentive Six Month Metrics MiPCT Quarterly
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community. Stewards of Change June 11, 2013
 An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
An Emerging Rural ACO: Chautauqua Region s Transitioning Medical Neighborhood/ Accountable Care Community Stewards of Change June 11, 2013 Chautauqua County, New York Population: 130,000+ Northern tip
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Deriving Value from a Health Information Exchange. HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017
 Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
Deriving Value from a Health Information Exchange HIMSS17 DA-CH Community Conference Healthix I New York I February 20, 2017 About Healthix About Healthix Hundreds of healthcare organizations at more than
Central New York Care Collaborative (CNYCC) Oneida County Health Coalition Meeting June 30, 2016
 Oneida County Health Coalition Meeting June 30, 2016") Central New York Care Collaborative (CNYCC) Oneida County Health Coalition Meeting June 30, 2016 Agenda 1. Overview of the NYS DSRIP Program 2. History of Performing Provider Systems in Central New York
Central New York Care Collaborative (CNYCC) Oneida County Health Coalition Meeting June 30, 2016 Agenda 1. Overview of the NYS DSRIP Program 2. History of Performing Provider Systems in Central New York
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Draft Covered California Delivery Reform Contract Provisions Comments Welcome and Encouraged
 TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
TO: FROM: RE: State Based Marketplaces State Medicaid Directors Delivery Reform/Value Promoting Colleagues Peter V. Lee, Executive Director Draft Covered California Delivery Reform Contract Provisions
About the National Standards for CYSHCN
 National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
National Standards for Systems of Care for Children and Youth with Special Health Care Needs: Crosswalk to National Committee for Quality Assurance Primary Care Medical Home Recognition Standards Kate
Improving Effectiveness in the PCMH. Shawn Stinson, MD FACP
 Improving Effectiveness in the PCMH Shawn Stinson, MD FACP 1 Overview Introduction to BCBSSC PCMH program Must haves for successful outcomes in a primary care practice Agreement on evidence based practices
Improving Effectiveness in the PCMH Shawn Stinson, MD FACP 1 Overview Introduction to BCBSSC PCMH program Must haves for successful outcomes in a primary care practice Agreement on evidence based practices
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology
 Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Challenges and Opportunities for Improving Health and Healthcare in Ohio through Technology Ohio Health IT Advocacy Day Craig Brammer, CEO cbrammer@healthbridge.org @CraigABrammer Challenge #1: Information
Expanding Your Pharmacist Team
 CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
CALIFORNIA QUALITY COLLABORATIVE CHANGE PACKAGE Expanding Your Pharmacist Team Improving Medication Adherence and Beyond August 2017 TABLE OF CONTENTS Introduction and Purpose 1 The CQC Approach to Addressing
Task for Partner PCMH Standard APC Requirement TCPI Milestone
 Page 2/ Question 1 2aiM4D1* 2aiiiM3D1* Submit last page of signed participation agreement with HealthLinkNY or other Qualified Entity (QE). Standard 5B - Referral Tracking and Follow-up 5.B.7. Has the
Page 2/ Question 1 2aiM4D1* 2aiiiM3D1* Submit last page of signed participation agreement with HealthLinkNY or other Qualified Entity (QE). Standard 5B - Referral Tracking and Follow-up 5.B.7. Has the
NYP/Q DSRIP PPS Asthma Committee. H. Jabbar, MD C. Guglielmo. Meeting Purpose: DSRIP Project Implementation Committee meeting.
 NYP/Q DSRIP PPS Asthma Committee Meeting Title: NYP Queens DSRIP Asthma Home Based Care Meeting Date: September 13 th, 2017 Facilitator(s): C. Guglielmo Meeting Time: 1:00 pm-2:00 pm Location: NYP Queens
NYP/Q DSRIP PPS Asthma Committee Meeting Title: NYP Queens DSRIP Asthma Home Based Care Meeting Date: September 13 th, 2017 Facilitator(s): C. Guglielmo Meeting Time: 1:00 pm-2:00 pm Location: NYP Queens
Community Needs Assessment for Albany Medical PPS Stage 1 Summary Results. HCDI Assessment Team 9/29/14
 Community Needs Assessment for Albany Medical PPS Stage 1 Summary Results 1 HCDI Assessment Team 9/29/14 HCDI Assessment Team Healthy Capital District Initiative Project Management Kevin Jobin-Davis, Executive
Community Needs Assessment for Albany Medical PPS Stage 1 Summary Results 1 HCDI Assessment Team 9/29/14 HCDI Assessment Team Healthy Capital District Initiative Project Management Kevin Jobin-Davis, Executive
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY
 Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
Appendix 4 CMS Stage 1 Meaningful Use Requirements Summary Tables 4-1 APPENDIX 4 CMS STAGE 1 MEANINGFUL USE REQUIREMENTS SUMMARY 1. Use CPOE (computerized physician order entry) for medication orders directly
NYS DSRIP Overview. Todd Ellis, DHA Corey M. Zeigler, MBA, CHCIO. November 2016
 NYS DSRIP Overview Todd Ellis, DHA Corey M. Zeigler, MBA, CHCIO November 2016 DSRIP: A Mechanism to Transform Medicaid Delivery Delivery System Reform Incentive Payment (DSRIP) programs are a key mechanism
NYS DSRIP Overview Todd Ellis, DHA Corey M. Zeigler, MBA, CHCIO November 2016 DSRIP: A Mechanism to Transform Medicaid Delivery Delivery System Reform Incentive Payment (DSRIP) programs are a key mechanism
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Quality Measurement at the Interface of Health Care and Population Health
 1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
1 Institute of Medicine Committee on Quality Measures Healthy People Leading Health Indicators December 10, 2012 Quality Measurement at the Interface of Health Care and Population Health Shari M. Ling,
Presentation Objectives
 At Home: Comprehensive Care of the Frail Elderly Ramiro Jervis, MD Asantewaa Poku, MPH Kristofer Smith, MD, MPP December 10, 2013 1 Presentation Objectives Develop, both culturally and operationally, an
At Home: Comprehensive Care of the Frail Elderly Ramiro Jervis, MD Asantewaa Poku, MPH Kristofer Smith, MD, MPP December 10, 2013 1 Presentation Objectives Develop, both culturally and operationally, an
APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS
 Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Appendix 2 NCQA PCMH 2011 and CMS Stage 1 Meaningful Use Requirements 2-1 APPENDIX 2 NCQA PCMH 2011 AND CMS STAGE 1 MEANINGFUL USE REQUIREMENTS CMS Meaningful Use Requirements* All Providers Must Meet
Payer s Perspective on Clinical Pathways and Value-based Care
 Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Payer s Perspective on Clinical Pathways and Value-based Care Faculty Stephen Perkins, MD Chief Medical Officer Commercial & Medicare Services UPMC Health Plan Pittsburgh, Pennsylvania perkinss@upmc.edu
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State
 Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
Practice Transformation Alignment: NYS PCMH Marcus Friedrich, MD, MBA, FACP Chief Medical Officer Office of Quality and Patient Safety NY State Department of Health Marcus.Friedrich@health.ny.gov 2 Primary
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions
 2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
2.b.iv Care Transitions Intervention Model to Reduce 30-day Readmissions for Chronic Health Conditions Project Objective: To provide a 30-day supported transition period after a hospitalization to ensure
DY3 PP1 Contracting Webinar. Mount Sinai PPS (DSRIP) August 2017
 August 2017") DY3 PP1 Contracting Webinar Mount Sinai PPS (DSRIP) August 2017 Introductions Nina Bastian Associate Director, Operations Mount Sinai Ashley Fitch Senior Project Manager Mount Sinai Jocelyn Levine Data
DY3 PP1 Contracting Webinar Mount Sinai PPS (DSRIP) August 2017 Introductions Nina Bastian Associate Director, Operations Mount Sinai Ashley Fitch Senior Project Manager Mount Sinai Jocelyn Levine Data
Planning a Course to Population Health Management
 Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Planning a Course to Population Health Management A Complimentary Webinar From healthsystemcio.com Your Line Will Be Silent Until Our Event Begins at 12:00 ET Thank You! Slide Deck: http://goo.gl/1w119j
Introducing AmeriHealth Caritas Iowa
 Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
Introducing AmeriHealth Caritas Iowa A presentation for Iowa providers. CPC; Q215 Iowa V1 Who We Are Who We Serve Agenda Our Mission AmeriHealth Caritas Iowa Why Partner With Us? Questions 2 2 Who We Are
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation
 A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
A Practical Approach Toward Accountable Care and Risk-Based Contracting: Design to Implementation Daniel J. Marino, President/CEO, Health Directions Asad Zaman, MD June 19, 2013 Session Objectives Establish
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
Telecare Services 7/19/2017
 Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Telecare Services 7/19/2017 Rebecca Sienko, RN Manager, Nurse Care Line 15,000 Employees 1,900 MDs/APCs 15 Hospitals 17 Clinics 7 Long Term Care Facilities 2 Assisted Living 4 Independent Living 5 Ambulance
Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs
 TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
TECHNICAL ASSISTANCE TOOL September 2014 Quality Measurement Approaches of State Medicaid Accountable Care Organization Programs S tates interested in using an accountable care organization (ACO) model
The Drive Towards Value Based Care
 The Drive Towards Value Based Care Thursday, March 3, 2016 Michael Aratow, MD, FACEP Chief Medical Information Officer, San Mateo Medical Center Gaurav Nagrath, MBA, Sr. Strategist, Population Health Research
The Drive Towards Value Based Care Thursday, March 3, 2016 Michael Aratow, MD, FACEP Chief Medical Information Officer, San Mateo Medical Center Gaurav Nagrath, MBA, Sr. Strategist, Population Health Research
Meeting Title. Facilitator. Conference Line. Corporation)
") DSRIP Meeting Agenda 5/29/15 NYP PPS Date and Time Meeting Title Committee Location 45 Wadsworth Street, 9 th Floor Facilitator Dr. Emilio Carrillo Go to Meeting https://global.gotomeeting.com/ join/158738573
DSRIP Meeting Agenda 5/29/15 NYP PPS Date and Time Meeting Title Committee Location 45 Wadsworth Street, 9 th Floor Facilitator Dr. Emilio Carrillo Go to Meeting https://global.gotomeeting.com/ join/158738573
Integrating Public Health and Social Services with Delivery System Reform
 Integrating Public Health and Social Services with Delivery System Reform New York State Department of Health Office of Health Insurance Programs Greg, Policy Director October 2015 1 Agenda 1. DSRIP &
Integrating Public Health and Social Services with Delivery System Reform New York State Department of Health Office of Health Insurance Programs Greg, Policy Director October 2015 1 Agenda 1. DSRIP &
Using Data for Quality Improvement in a Clinical Setting. Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center
 Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Using Data for Quality Improvement in a Clinical Setting Wadia Wade Hanna MD, MPH Technical Assistance Consultant Georgia Health Policy Center Dr. W. Hanna, PLS, November 2015 Quality An organizational
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers
 Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Implementing Medicaid Value-Based Purchasing Initiatives with Federally Qualified Health Centers Beth Waldman, JD, MPH June 14, 2016 Presentation Overview 1. Brief overview of payment reform strategies
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Informatics, PCMHs and ACOs: A Brave New World
 Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
Informatics, PCMHs and ACOs: A Brave New World R. Clark Campbell, MSN, RN-BC, CPHIMS, FHIMSS Kathleen Kimmel, RN, BSN, MHA, CPHIMS, FHIMSS Engagement Executive with Health Catalyst Objectives - Define
QUALITY IMPROVEMENT PROGRAM
 QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
QUALITY IMPROVEMENT PROGRAM EmblemHealth s mission is to create healthier futures for our customers and communities. We will do this by providing members with a broad range of benefits and conscientious
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual
 Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Arkansas Blue Cross and Blue Shield Patient Centered Medical Home Provider Manual 2017 This document is a guide to the 2017 Arkansas Blue Cross and Blue Shield Patient-Centered Medical Home program (Arkansas
Maryland s Integrated Care Network. Heading into Year Three
 Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain
Maryland s Integrated Care Network Heading into Year Three Facilitator David Finney Chief of Staff, CRISP Partner, Leap Orbit Learning Objectives At the end of this session, you will be able to Explain