NOCVA HOSPITAL ENGAGEMENT WEBINAR
|
|
|
- Ethel James
- 6 years ago
- Views:
Transcription



1 NOCVA HOSPITAL ENGAGEMENT WEBINAR Back to the Hospital: A Root Cause Analysis of Surgical Readmissions Henry D. Cremisi, MD, FACP Chairman of Medical Education Novant SPR June 13, 2013

2 How to Participate Today Submit text questions through the Questions box. Use Chat to communicate with organizers Use the Hand Icon to raise your hand, your line will then be unmuted. This session is being recorded and will be made available via the NoCVA Website. The slides from this presentation will be ed to all attendees at the conclusion of the webinar.


3 A Root Cause Analysis of Surgical Readmission Henry D. Cremisi, MD, FACP Chairman of Medical Education Novant SPR
4 Educational Objectives Identify key strategies and tactics for reducing readmissions that can be applied universally Describe actionable strategies for engaging community organizations across the continuum of care Strengthen patient involvement in and understanding of their care Apply effective tools to identify and leverage opportunities for improvement Design an action plan to implement the first tests of change
5 Disclosure Medical Director OPUS IRB Medical Director Morley Research Consortium President Lifescape BioSciences Speakers Bureau Otsuka & Janssen President N4Metrics
6 Studies of Rehospitalizations 90% of rehospitalizations within 30 days appear to be unplanned, the result of clinical deterioration. MedPAC: 75% of readmissions preventable, adding $12 Bn/yr to Medicare spending. Only half of the patients rehospitalized within 30 days had a physician visit before readmission. Unknown if lack of physician visit causes readmissions but poor continuity of care, is a concern for many chronically ill patients. 19% of Medicare discharges are followed by an adverse event within 30 days 2/3 are drug events, the kind most often judged preventable.
7 Optimized Patient Care Processes Knowledge from aggregated health status data Analytics Partners Vendors Patient interface Managing services Scalability Artificial Intelligence- based on multi-objective optimization and multi-criteria decision support
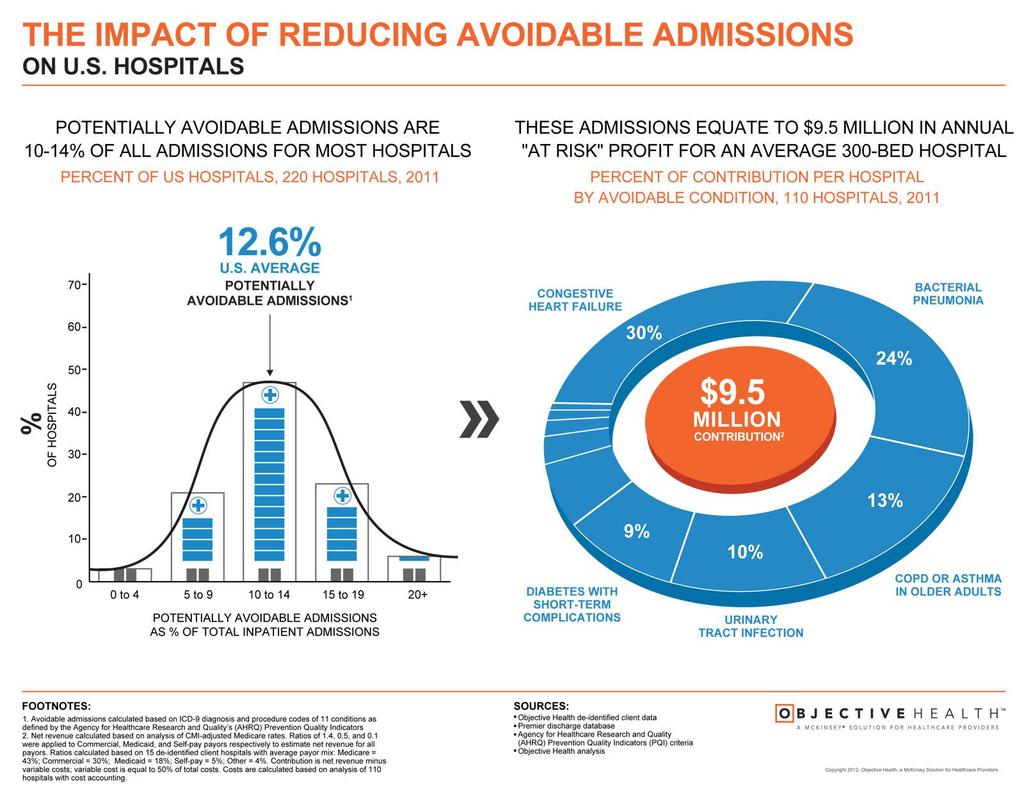
8 Background of the Challenge Kaiser Health News reported that Medicare beneficiaries readmitted to hospitals within 30 days of release account for roughly $17.5 billion a year in additional healthcare expenditures. Beginning FY 2013, hospitals stand to lose up to 1 percent of their Medicare reimbursements for failing to bring readmission rates in line with - or, better yet, under - the expected ratios for that facility, established using a risk adjustment methodology that accounts for differences in patient demographics and comorbidities

9 Post Hospital Syndrome Krumholz NEJM January 2013 An Acquired, Transient Condition of Generalized Risk Comprised of a tremendous amount of physical, emotional, and social stress. Conceptual reframing

10 Post Hospital Syndrome-Implications of Hospitalization Sleep deprivation Disruption of circadian rhythms Nourishment issues Pain and discomfort Baffling array of challenging situations Medications that alter cognition and physical function Deconditioning by bed rest or inactivity
11
12

13 Surgical Readmission Rates

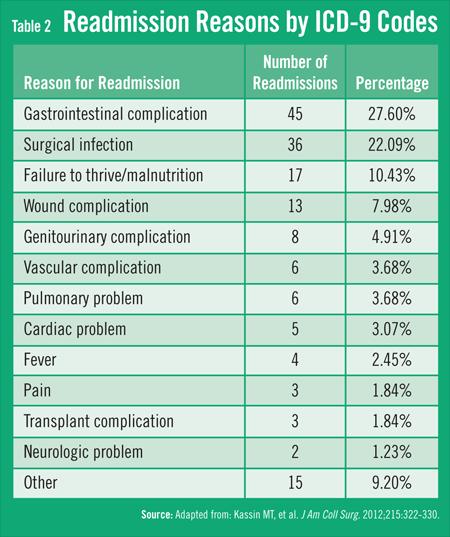
14 Comorbidity Profile of Readmitted Surgical Patients Journal of the American College of Surgeons Volume 215, Issue 3, September 2012, Pages

15 Assessing Risk Of Readmission After General, Vascular, And Thoracic Surgery Using ACS-NSQIP Timothy M Pawlik 1, Donald Lucas* 2, Omar Hyder* 1, Rebecca Dodson* 1, Nita Ahuja* 1, Christopher Wolfgang* 1, Eric Schneider* 1, Michael Choti 1 1 Johns Hopkins, Baltimore, MD; 2 Walter Reed National Military Medical Center, Bethesda, MD
.")
16 Rate of Readmissions by Number of Complications American College of Surgeons 2012Cochran-Armitage trend test demonstrates a significant increasing trend in rate of readmission as more complications occur (p < ).
17
18 Odds Ratio of Surgical Readmission By Age

19
20
21 Modifiable and Non-Modifiable Host- and Procedure-Related Orthopedic SSI Risk Factors Host-specific Modifiable Obesity Current smoking Hematocrit < 36 Elevated preoperative or postoperative serum glucose Nasal carriage of Staphylococcus aureus (as risk factor for Staphylococcus aureus infection) Non Modifiable Diabetes Male gender Rheumatoid arthritis ASA score of 3 or greater Recent weight loss Dependent functional status Disseminated cancer Admission from a healthcare facility
22 Modifiable and Non-Modifiable Host- and Procedure-Related Orthopedic SSI Risk Factors Modifiable Non-Modifiable Procedure Specific Estimated blood loss of > 1 liter* Estimated blood loss of > 1 liter* Longer procedure time* Suboptimal timing of prophylactic antibiotic Longer procedure time* Previous infection at site Spinal procedure via the posterior or the anterior/posterior approach Prolonged wound drainage* Two or more surgical residents participating in procedure Low volume of procedures performed at hospital Prolonged wound drainage* Low volume of procedures performed by surgeon

23 Surgical Wound Classification Wounds following surgical procedures are classified as superficial incisional, deep incisional, or organ/space, depending upon the tissue or body part involved.
24 Surgical WoundClassification Wound Parameters Clean An uninfected operative wound in which no inflammation is encountered and there is no entry into the respiratory, alimentary, genital, or urinary tract Clean wounds are closed primarily and, if necessary, drained with closed drainage Clean-contaminated Operative wounds in which the respiratory, alimentary, genital, or urinary tracts are entered under controlled conditions and without unusual contamination No evidence of infection is encountered or major break in technique occurs Open- Fresh accidental wounds Operations with major breaks in sterile technique or gross spillage from the gastrointestinal tract Incisions in which acute, non-purulent inflammation is encountered Dirty or infected Old traumatic wounds with retained devitalized tissue Existing clinical infection or perforated viscera is encountered This definition suggests that the organisms causing postoperative infection were present in the operative field prior to the procedure
25 Pathogen Orthopedic surgery Pathogen Orthopedic surgery (N = 963) (N = 963) Coagulase-negative Staphylococcus 173 (15.3) Escherichia coli 34 (3.0) Staphylococcus aureus Enterococcus Species 548 (48.6) Pseudomonas aeruginosa Klebsiella pneumoniae 38 (3.4) 14 (1.2) E. faecalis 57 (5.1) Enterobacter species E. faecium 13 (1.2) Acinetobacter baumannii 37 (3.3) 10 (0.9) Not specified 34 (3.0) Klebsiella oxytoca 5 (0.4) Candida Species Candida albicans 2 (0.2) Total number of pathogenic isolates by surgery type 1,128 Other or not specified 2 (0.2)

26 Percentage of patients who met the criteria of antimicrobial exposure, diagnosis code, readmission, or some combinations of criteria after total hip arthroplasty and total knee arthroplasty. Bolon M K et al. Clin Infect Dis. 2009;48: by the Infectious Diseases Society of America
27 The clinical presentation of infection The clinical presentation of infection is dependent on the properties of the infectious agent (i.e. innate virulence), the nature of host tissue at the site of infection, and the route of infection (locally introduced versus hematogenous spread from a distant site or bloodstream).
28 Diagnosis of SSI related to clean orthopedic surgical procedures Diagnosis of SSI related to clean orthopedic surgical procedures is a complex process, using clinical signs symptoms, laboratory data, and radiologic findings and /or surgeon or medical officer confirmation of diagnosis.

29 The ability of bacteria to flourish is enhanced in; wound hematomas, fresh operative wounds, ischemic wounds, tissue of diabetic patients long-term steroid therapy

30 The Infection Prevention Program An effective infection prevention program for surgery has many components. Implementation of, and consistent adherence to, evidence-based practices to reduce the risk of SSI is key to success. However, it is important to conduct a thorough risk assessment and to collect and analyze surveillance data to drive improvements. Surveillance data can provide measurable results to evaluate the effectiveness of infection prevention interventions.

31 The Risk Assessment A risk assessment is a systematic evaluation for identifying risks in the healthcare setting. Infection Control assessment identifies risks for acquiring or transmitting infections, and includes strategies for prioritizing and mitigating those risks. A risk assessment can be either quantitative or qualitative, and can include both process and outcome measures.
32 Steps for Performing the Risk Assessment: Create the risk assessment team, ensuring input from key support and clinical departments. The team should gather organizational information and set a timeline for assessment. Current literature and past trends should be evaluated. Example: No less than annually Whenever new risks or procedures are identified.

33 Questions to consider: What is the volume of this type of surgery? What are the major procedures performed? What is the frequency of infections in this surgery? What are the major pathogens identified? What is the proportion of multiple drug-resistant organisms? Are there any new procedures performed? What is the frequency of readmissions related to postoperative SSIs in orthopedic surgery?
34 Risk Assessment Type and Template Example: Joan directs an infection prevention program in a mid-size community teaching hospital. She has collected data on total joint replacement surgeries using NHSN for the past two years. Last year, 357 total hip replacements and 240 total knee replacements were performed at her facility. There were seven postoperative hip infections and one knee infection. Of the seven postoperative hip infections, the pathogens isolated were: 5 methicillin-resistant Staphylococcus aureus (MRSA) 1 coagulase-negative Staphylococcus 1 methicillin-sensitive Staphylococcus aureus (MSSA)
35 Quantitative Risk Assessment. SSIs Benchmark Risk Rating High Volume High Risk National Initiative Financial Initiative Hip replacement Relative Risk = High Risk 2 = Moderate Risk 1 = Minimal Risk 0 = No Risk Score 10 or above = High priority Risk rating: Template provided by Shannon Oriola, RN, COHN, CIC, Sharp Metropolitan Medical Center, San Diego, California
36 Using the Tool 1. Benchmark Rates of SSIs in hip replacement surgery are above the NHSN mean, but not by a statistically significant difference. This was considered a moderate risk. Risk score = 2 2. High Risk procedure or activity Patients who develop SSIs may require removal of the prosthesis. Only 88% of patients have antibiotics discontinued within the recommended 24 hours, and there is a high proportion of MRSA in patients who develop an SSI. This was considered high risk. Risk score = 3 3. High Volume Hip replacements are a high-volume procedure in this organization. It is the third highest volume procedure performed, and therefore was identified as a high risk. Risk score = 3 4. Potential Negative Outcome SSIs in hip replacements are associated with increased morbidity, mortality and length of stay. Five patients last year developed deep or organ space infections requiring surgical intervention. Risk score = 3 Guide to the Elimination of Orthopedic Surgical Site Infections National Initiative At the time of the risk assessment, there is not a national initiative associated with outcome measures in orthopedic surgery. Risk score = 0 6. Financial Incentive The cases involved an average of 7-10 days increased length of stay and an excess average cost per case of $ 32,000. Risk score = 3
37 Quantitative Risk Assessment SSIs Benchmark Risk Rating High Volume High Risk National Initiative Financial Initiative Hip replacement Risk rating:14
38 Evaluation Since this procedure is above the 10-point risk priority ranking, it will be part of the annual infection prevention plan. It is important to set goals and expectations as well as strategies for achieving the goals.
39 Comparison of Expertise of the Perioperative Nurse and IP Perioperative Nurse IP Clinical expertise; in-depth knowledge of perioperative clinical needs Knowledge of findings in nursing and perioperative literature A patient care focus: both patient safety and infection prevention Ability to prioritize patient needs, surgeon preferences, costs Representation to achieve consensus within the surgical team A surgical conscience Knowledge of regulations and compliance in perioperative areas identified by the state health department, The Joint Commission, and CMS Clinical expertise on infection risk, control, and prevention Knowledge of findings in infection control and prevention literature Experience of compliance with policies, procedures, and accepted practices A focus on patient and healthcare worker safety; identifying infection safety risks both to patients and staff members, with an emphasis on control and prevention An understanding of compliance with regulations set forth by OSHA, U.S. FDA,and CDC Ability to apply national guidelines in a cost-effective manner A facility conscience
40 Areas/ Topic Current Status Goals Identified Gap Actions Priority SSIs in hip replacements 7 actual Infections versus 3.7 expected (NHSN) SSI rates twice the mean in the first two risk categories 5 of the patients required further surgical intervention Reduce SSIs in hip replacements by at least 30% Improve adherence to discontinuing antibiotics within 24 hours to at least 95% No standard order sets or pathways for discontinuing antibiotics Knowledge deficits by nursing when IV infiltrates or is interrupted during immediate postoperative period MRSA incidence increased from previous year No standard protocols for addressing patients who may be colonized with MRSA preoperativelyno standard perioperative prep procedure No standardized practices for warming patients Incorporate orthopedic prophylactic antibiotic protocols into order sets and pathways Develop MRSA screening program for orthopedic Surgery Engage stakeholders to develop standard prep procedure Incorporate temperature management protocol using active warming, such as forced-air warming, to maintain patient normothermia including prewarming, intraoperative and post-operative HIGH (rates have doubled since last year)
41 Actions Develop MRSA screening program for orthopedic surgery. Engage stakeholders to develop standard prep procedure. Incorporate orthopedic prophylactic antibiotic protocols into order sets and pathways. The above risk assessments use NHSN surveillance criteria. Organizations that do not use NHSN may use overall data collected from surveillance activities. As an alternative, if no surveillance data exists, administrative data may be utilized to assist in case findings. This data cannot be compared to NHSN means, but may be helpful to assist in determining the overall scope of the issues. Likewise, microbiology data may be helpful in determining pathogen frequency and occurrence.


42 Set Goals and Expectations Reduce SSI in total hip replacements by at least 30%. Improve adherence to discontinuing antibiotics within 24 hours to at least 95%.

43 NHSN Surgical Methodology is: Active Patient-based Prospective Retrospective Priority-directed Risk-adjusted, incidence rates
44 Methods utilized by facilities include: 1. Line lists of patients undergoing surgical procedures who are sent to respective surgeons and returned on a regular basis (usually monthly) 2. Follow-up phone calls to patients 3. Outpatient culture reports 4. Readmission data to hospital or to another hospital 5. Self reporting by surgeons 6. Outpatient reports of antibiotic usage data
45 Methods to increase compliance to antibiotic prophylaxis: 1. Provide visual reminders, checklists, and antibiotic prophylaxis as part of the time out. A study by Wax et al. demonstrated very high rates of compliance when a visual electronic interactive reminder was added to the anesthesia electronic record. 2. Incorporate documentation of prophylaxis into electronic documentation forced field functions. 3. Incorporate antibiotic selection and duration into order sets and pathways. 4. Provide feedback to care providers, on both an individual and overall aggregate level.

46 Nasal Decolonization Mupirocin 2% ointment Apply inside each nostril twice daily for 7 days, using a cotton tipped swab. No need to put deep into the nose. One Rx enough for all. Duration: 7 days

47 Hair Removal Preoperative shaving of the surgical site the night before an operation is associated with a significantly higher SSI risk than other methods of hair removal or no hair removal at all.62 The increased SSI risk associated with shaving has been attributed to microscopic cuts in the skin that provide a portal of entry for bacteria and a focusfor bacterial multiplication. The hair removal methodology should be reviewed with the perioperative staff. The timing of the hair removal and the removal with the use of clippers versus razors are important processes. If hair is removed, it should be as close to the incision as possible. One of the most effective strategies is to remove razors from the OR. In many cases, no hair removal is needed. However, the decision to remove surgical site hair should include consideration of the potential for access to the surgical site and the field of view. Female patients who are undergoing knee replacements, hip replacements or other lower leg surgeries should be instructed not to shave their legs prior to surgery for the reason described above.
48 Examples of Feedback: September 5, 2012, M.D. Anesthesiology Service Medical Group 3626 Ruffin Road Charlotte, NC Dear Dr., The Medical Executive Committee has requested that the Infection Prevention Department monitor the administration of preoperative prophylactic antibiotics for total hip/knee arthroplasty procedures and provide feedback to surgeons and anesthesiologists should our department identify missed opportunities for the optimal use of prophylactic antibiotics. Enclosed is a copy of the Anesthesia Record (MR# ) and Visit #( ) that documents the administration of cefazolin 2 grams at 0804 with the operative procedure start time of 0851 and completed at Generally, if an operative procedure exceeds the half-life of the antibiotic, then a repeat dose is given. The half live of cefazolin is 3-4 hours; therefore, a repeat dose before 1204 would have been ideal. It is the time that the antibiotic is initially given and not the incision time that determines when the antibiotic is redosed. Thank you for your attention to this matter. We appreciate your efforts to further minimize the risk of post-operative surgical site infections. Sincerely, Hospital Epidemiologist
49 Perioperative Normothermia Perioperative hypothermia is physiologically stressful because it elevates blood pressure, heart rate and plasma catecholamineconcentration, which may increase the risk of cardiac complications, bleeding, wound infection, and postanesthesia care unit stay. Studies of the impact of hypothermia on the incidence of wound infection have shown that the hypothermic patient is at an appreciably greater risk for wound infection than a normothermic patient. Studies of the impact of hypothermia on the incidence of wound infection have shown that the hypothermic patient is at an appreciably greater risk for wound infection than a normothermic patient. Intraoperative hypothermia triggers thermoregulatory vasoconstriction, decreasing the partial pressure of oxygen in the tissues, thereby lowering resistance to infection. A reduction in core temperature of 1.9 C has been shown to triple the incidence of surgical wound infections after colon resection and to increase length of hospital stays.
50 Bone Cement When antibiotics were added to the cement, they were found to elute into involved tissue area, thus aiding in the eradication of an infection.111 Antibiotic laden cement (ABLC) was released for commercial distribution in the United States in May 2003, specifically for the treatment and reimplantation of infected arthroplasties. In Europe, Australia and likely other settings, ABLC has been available for many years. The indications and scientific evidence for its use have expanded to primary arthroplasty; however, the use of ABLC for this purpose remains controversial in the United States. Since its release, a variety of cements, cement preparation methods, antibiotics, and doses have been used with varying outcomes. It is important for the OR team to keep in mind that that the current principles of bone cement preparation do not apply in the treatment of infection. Although the addition of more than 2 g of antibiotic per 40 g of cement reduces the antibiotic s mechanical strength, this is irrelevant to the treatment of infection. Vacuum mixing decreases the cement s porosity, thereby reducing elution of the antibiotic; for this reason, vacuum mixing is contraindicated. Homogeneous, commercial mixing of the antibiotic in cement results in better mechanical strength, but potentially less elution. Using what is considered to be a traditionally poor mixing technique, i.e., whipping of the mixture, may actually improve elution. Hand mixing, without fully crushing the antibiotic crystals, may also improve elution. Normally, cement is used only in powder form because the liquid reduces mechanical strength.
51
52
53

54 Medicare Readmissions Update enewsletter
55

56 How Do We Pull It All Together?
57
, and correct application?")
58 Evaluation of Process Measures: Are antibiotic prophylaxis criteria, including preoperative timing, antibiotic selection and postoperative duration, part of standing orders and pathways? Are there standardized procedures for preoperative preparation of the skin that specify the appropriate antiseptic agent(s), and correct application? Do patients and families receive instructions as to their preoperative, perioperative and postdischarge roles in prevention of SSIs? Do healthcare workers and licensed independent practitioners receive education upon hire and annually related to prevention of SSIs?

59 Targeting Zero As healthcare has attempted to move from silos of care driven by specialized groups to collaborative groups and integrated systems, it is imperative that both processes and products are designed and implemented in the most effective and efficient manner to achieve desired outcomes. Central to this theme is the philosophy of targeting zero. Targeting Zero is the philosophy that every healthcare institution should be working toward a goal of zero HAIs. While not all HAIs are preventable, APIC believes that all organizations should set the aspirational goal of elimination and strive for zero infections. Every HAI impacts the life of a patient and a family, and even one HAI should be considered too many.
60
61
62 Summary of Key Points Key Point Vertical, Unidirectional Flow at low velocity over the OR table Body Evacuation Suits Surgical Hand Antisepsis Recommendation A minimum of 20 air changes/hour Generally recommended for total joint arthroplasty Use either an antimicrobial surgical scrub agent or an alcohol-based surgical hand rub with documented cumulative and persistent activity. Use of alcohol product immediately reduces resident flora by 95% and continues to act for hours Hair Removal Hair removal: either no hair removal or removal with clippers immediately before surgery; razors are not appropriate and are associated with an SSI rate of 3.1%-20%
63 Summary of Key Points Key Point Skin Prep. Drains Antibiotic Cement Traffic Control Maintenance of Body Temperature Recommendation Preoperative skin cleansing ( CHG) Surgical prep Use a dual agent with alcohol and active ingredient ( CHG, iodine povacrylex, povodine iodine) Allow prep to dry completely Avoid pooling of the prep Controlled studies show no benefit Meta-analysis: shows increased transfusions and no benefit in total knee or hip Norwegian Arthroplasty Register 2006: evidence of effectiveness; now widely used in primary surgery in Europe FDA-approved in the U.S. for revision surgery Multiple studies support limiting the number of and movement of OR personnel Active warming of patients whose core temperature is at or below 36 degrees C
64 Summary of Key Points Key Point Universal Protocol/Time-Out Recommendation Identify all items required for the procedure: relevant documentation labeled diagnostic and radiology test results are properly displayed any required blood products, implants, devices, and/or special equipment for the procedure; match the items to the patient in the procedure area use a standardized list to confirm availability Agree on the: correct patient identity correct site (site is marked and visible) procedure to be done Confirm sterility indicators Identify and address any equipment issues or concerns Document the time-out

65 Critical Analysis

66 Cause Mapping

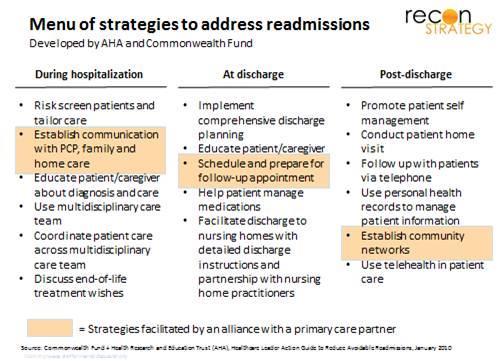
67 Reducing Readmissions Implement an integrated approach to post-discharge care Postdischarge care for seniors is most effective when integrated among various experts, including trained medical staff, family members who best know the senior who can offer moral and social support, and professional in-home caregivers to employ expert knowledge and experience. "The United Kingdom recently established an integrated care pilot program for seniors with the results of the program suggesting that well-managed integrated care can reduce the number of hospital readmissions among elderly patients by 20 percent,

68 A Call to Action Provide clear discharge instructions One of the key factors of hospital readmission among seniors is a misunderstanding of the discharge instructions. It happens frequently: an elderly patient leaves the hospital with a stack of complicated paperwork, dozens of medications that all have different timeframes in which they need to be taken and limited instructions on how to manage it all. "To resolve this issue, the discharge planning staff should provide clear, straightforward postdischarge instructions that are easy for nonmedical experts to understand, "The staff should closely review them with the senior, the senior's family members, and the in-home care professionals before discharge. It is also important that the planning staff help the senior's caregivers understand what various signs and symptoms might mean during the recovery process. Finally, there should be a designated hospital contact that works with the senior's integrated team to answer questions and monitor the senior's postdischarge progress.
69 Action Plan Continue to adjust the post-discharge plan "Individualized, tailored care is essential to ensuring a successful recovery, and the post-discharge plan should be monitored and adjusted based upon the daily needs of the senior over time," Huber said. The hospital contact in charge of the post-discharge should work closely with both the family and the professional caregivers of the elderly patient to monitor progress, keep records and modify the plan of care to meet variations in need. This may start with intensive care and then move to less-intensive care as the senior recovers. It may also include increasing support if a senior's health begins to decline over time.
70 Technology Assists Easily accessible bioinformatics would allow providers to easily determine whether a patient has a high, moderate, or low risk of readmission. This information would be shared with a multidisciplinary transitional team responsible for developing a plan of care based on that patient s specific needs. Educating the patient about post treatment procedures and preventative measures are integral in reducing the number of hospital readmissions. For example, bedside tablets would allow nurses to give and send interactive instructions quickly. Mobile Apps allow for the seamless communication between the providers. These apps also allow patients to store information like appointment times in a central location. Systems for mobile communication and medication adherence reminders given prior to being discharged from the hospital can ensure that providers are aware of any problems prior to the escalation of any post treatment complications Telehealth conferencing allows experts to supplement remote monitoring and benefit patients at high risk of readmission
71 Future Trends Although the use of antimicrobial sutures is not a routine practice, the benefits are becoming increasingly apparent. Recent evidence-based clinical studies have demonstrated both the clinical and economic benefit of this technology. Future studies may prove useful. Likewise, advances in antimicrobial coatings for products such as implants, instruments, equipment and the environment may provide additional support to reach the goal of zero SSIs. The practice of prescreening selected patients for MRSA prior to surgery is controversial. However, future trends could incorporate this as a recommended practice, as part of a comprehensive program to eliminate SSIs in orthopedic surgery, especially in cases involving an implantable device. Future trends in preoperative preparation will likely include standardized protocols for preoperative showers and state-of-the-art skin cleansing, which will become the recommended standard of practice. Innovative techniques for postoperative care, including optimaldressing materials and techniques, will most likely become the standard of care.

72 High Risk Post Discharge Clinic Offers a comprehensive line of intravenous therapies ranging from chemotherapy to blood transfusions and antibiotic infusion therapies. Provides a private, comfortable setting for our patients. Staffed with highly experienced registered nurses trained in intravenous therapy

73 LESSONS LEARNED In today s surgical practice environment, challenged by newly recognized pathogens and well-known pathogens that have become resistant to current therapeutic modalities, all members of the healthcare team must remain aware of the impact of HAIs in surgical patients and must implement evidence based prevention strategies to reduce the incidence of HAIs. Given the associated unnecessary morbidity and mortality that could be prevented, the suffering that could be eliminated, and the money that could be saved, no healthcare organization can risk ignoring the benefits of effective strategies aimed at preventing HAIs. Effective teamwork and communication among all members of the surgical team is an important factor in improving patient outcomes. Various tools and checklists, which can be customized by the facility, have been developed to assist in preventing SSIs in surgical patients. Perioperative personnel and IPs are in a unique position to provide leadership in improving the quality and safety of patient care; by forming an alliance, they can be effective change agents in product evaluation and selection, thereby promoting positive patient outcomes.
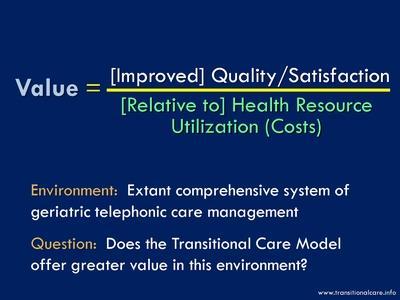
74 Generating Value



75 Take Ownership



76 Teamwork


77 Winning..

78 Questions?
Surgical Site Infection Prevention: Guidelines, Recommendations and Best Practice
 Surgical Site Infection Prevention: Guidelines, Recommendations and Best Practice Linda Goss BS, MSN, APN-BC, CIC, COHN-S Director, Infection Prevention and Control and Vascular Access Specialist Team
Surgical Site Infection Prevention: Guidelines, Recommendations and Best Practice Linda Goss BS, MSN, APN-BC, CIC, COHN-S Director, Infection Prevention and Control and Vascular Access Specialist Team
Canadian Surgical Site Infection Prevention Audit Month
 Canadian Surgical Site Infection Prevention Audit Month February 2016 CONTENTS KEY FACTS...3 SSI PREVENTION AUDIT RESULTS...3 BACKGROUND...4 METHODOLOGY...4 Data Scores... 5 How to Interpret the Indicator
Canadian Surgical Site Infection Prevention Audit Month February 2016 CONTENTS KEY FACTS...3 SSI PREVENTION AUDIT RESULTS...3 BACKGROUND...4 METHODOLOGY...4 Data Scores... 5 How to Interpret the Indicator
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative
 Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
Oscar Guillamondegui, MD, MPH, FACS Associate Professor of Surgery Tennessee Surgical Quality Collaborative NSQIP 2014 A Collaborative that has Reduced Surgical Site Infections Tennessee Surgical Quality
Health Care Associated Infections in 2017 Acute Care Hospitals
 Health Care Associated Infections in 2017 Acute Care Hospitals Christina Brandeburg, MPH Epidemiologist Katherine T. Fillo, Ph.D, RN-BC Director of Clinical Quality Improvement Eileen McHale, RN, BSN Healthcare
Health Care Associated Infections in 2017 Acute Care Hospitals Christina Brandeburg, MPH Epidemiologist Katherine T. Fillo, Ph.D, RN-BC Director of Clinical Quality Improvement Eileen McHale, RN, BSN Healthcare
Health Care Associated Infections in 2015 Acute Care Hospitals
 Health Care Associated Infections in 2015 Acute Care Hospitals Alfred DeMaria, M.D. State Epidemiologist Bureau of Infectious Disease and Laboratory Sciences Katherine T. Fillo, Ph.D, RN-BC Quality Improvement
Health Care Associated Infections in 2015 Acute Care Hospitals Alfred DeMaria, M.D. State Epidemiologist Bureau of Infectious Disease and Laboratory Sciences Katherine T. Fillo, Ph.D, RN-BC Quality Improvement
HOSPITAL EPIDEMIOLOGY AND INFECTION CONTROL: SURGICAL SITE INFECTION REPORTING TO CALIFORNIA DEPARTMENT OF PUBLIC HEALTH
 Office of Origin: Department of Hospital Epidemiology and Infection Control (HEIC) I. PURPOSE To comply with reporting cases of surgical site infection as required by Sections 1255.8 and 1288.55 the California
Office of Origin: Department of Hospital Epidemiology and Infection Control (HEIC) I. PURPOSE To comply with reporting cases of surgical site infection as required by Sections 1255.8 and 1288.55 the California
Recommendation II. Recommendation I. Who s on Your Team? Recommendation III
 Infection Prevention In the Surgical Suite Janie Kinsey, RN, CASC Administrator, St. Luke s South Surgery Center President, Kansas Association of Ambulatory Surgery Centers Objectives Recommendation I
Infection Prevention In the Surgical Suite Janie Kinsey, RN, CASC Administrator, St. Luke s South Surgery Center President, Kansas Association of Ambulatory Surgery Centers Objectives Recommendation I
Nosocomial Infection in a Teaching Hospital in Thailand
 Nosocomial Infection in a Teaching Hospital in Thailand Somsak Lolekha, M.D., Ph.D.,* Banchong Ratanaubol R.N.** and Pranom Manu R.N.** (*Department of Pediatrics; **Department of Nursing, Faculty of Medicine
Nosocomial Infection in a Teaching Hospital in Thailand Somsak Lolekha, M.D., Ph.D.,* Banchong Ratanaubol R.N.** and Pranom Manu R.N.** (*Department of Pediatrics; **Department of Nursing, Faculty of Medicine
Healthcare-Associated Infections
 Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
Healthcare-Associated Infections A healthcare crisis requiring European leadership Healthcare-associated infections (HAIs - also referred to as nosocomial infections) are defined as an infection occurring
2014 Partnership in Prevention Award. November 21, :00-1:00PM EST. Introduction
 2014 Partnership in Prevention Award November 21, 2014 12:00-1:00PM EST Introduction Don Wright, MD, MPH Deputy Assistant Secretary for Health (Disease Prevention and Health Promotion) U.S. Department
2014 Partnership in Prevention Award November 21, 2014 12:00-1:00PM EST Introduction Don Wright, MD, MPH Deputy Assistant Secretary for Health (Disease Prevention and Health Promotion) U.S. Department
National Priorities for Improvement:
 National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
National Priorities for Improvement: Standardization of Performance Measures, Data Collection, and Analysis Dale W. Bratzler, DO, MPH Principal Clinical Coordinator Oklahoma Foundation Contracting for
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION
 NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
NOSOCOMIAL INFECTION : NURSES ROLE IN MINIMIZING TRANSMISSION DR AHMAD SHALTUT OTHMAN JAB ANESTESIOLOGI & RAWATAN RAPI HOSP SULTANAH BAHIYAH ALOR SETAR, KEDAH Nosocomial infection Nosocomial or hospital
Prevention of Orthopaedic Surgical Site Infections in the Perioperative Setting. Disclosures. Objectives
 Prevention of Orthopaedic Surgical Site Infections in the Perioperative Setting Mary Atkinson Smith, DNP, FNP-BC, ONP-C, RNFA, CNOR & W. Todd Smith, MD, FAAOS Disclosures We hereby certify that, to the
Prevention of Orthopaedic Surgical Site Infections in the Perioperative Setting Mary Atkinson Smith, DNP, FNP-BC, ONP-C, RNFA, CNOR & W. Todd Smith, MD, FAAOS Disclosures We hereby certify that, to the
Strategy/Driver Prevention Strategies Action Strategies
 I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
I. Hospital executive leadership commitment to prevention of surgical site infections 1. Establish Surgical Site Infection prevention as a strategic priority 2. Develop and implement business/strategic
FY 2014 Inpatient Prospective Payment System Proposed Rule
 FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
FY 2014 Inpatient Prospective Payment System Proposed Rule Summary of Provisions Potentially Impacting EPs On April 26, 2013, the Centers for Medicare and Medicaid Services (CMS) released its Fiscal Year
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.
 Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W.") Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Using the Trauma Quality Improvement Program (TQIP) Metrics Data to Change Clinical Practice Abigail R. Blackmore, MSN, RN Pamela W. Bourg, PhD, RN, TCRN, FAEN Learning Objectives Explain the importance
Infection Prevention and Control
 Infection Prevention and Control Infection Control in the Healthcare Setting Chain of Infection Hand Hygiene Hospital Acquired Infections Isolation Exposures Tuberculosis Chain of Infection Most Common
Infection Prevention and Control Infection Control in the Healthcare Setting Chain of Infection Hand Hygiene Hospital Acquired Infections Isolation Exposures Tuberculosis Chain of Infection Most Common
2.0. The lowdown on SSIs. I just love to hang out in a fresh incision.
 FAQs about SSIs According to the CDC, surgical site infections, or SSIs, can increase a patient s hospital stay by an average of 7 days an entire week! What can you do to reduce the incidence of SSIs in
FAQs about SSIs According to the CDC, surgical site infections, or SSIs, can increase a patient s hospital stay by an average of 7 days an entire week! What can you do to reduce the incidence of SSIs in
Medicare Value Based Purchasing August 14, 2012
 Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
Medicare Value Based Purchasing August 14, 2012 Wes Champion Senior Vice President Premier Performance Partners Copyright 2012 PREMIER INC, ALL RIGHTS RESERVED Premier is the nation s largest healthcare
How to Add an Annual Facility Survey
 Add an Annual Facility Survey https://nhsn.cdc.gov/nhsndemo/help/patient_safety_component/how_to/add_an_annual... Page 1 of 1 10/9/2017 Show Patient Safety Component > How To > Facility > Add an Annual
Add an Annual Facility Survey https://nhsn.cdc.gov/nhsndemo/help/patient_safety_component/how_to/add_an_annual... Page 1 of 1 10/9/2017 Show Patient Safety Component > How To > Facility > Add an Annual
BUGS BE GONE: Reducing HAIs and Streamlining Care!
 BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
BUGS BE GONE: Reducing HAIs and Streamlining Care! SUSAN WHITNEY, RN, PCCN, MM, BME FLORIDA HOSPITAL ORLANDO, FL SUWHIT@AOL.COM LEARNING OUTCOMES 1. Describe HAI s and the impact disposable ECG leads have
The dawn of hospital pay for quality has arrived. Hospitals have been reporting
 Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Value-based purchasing SCIP measures to weigh in Medicare pay starting in 2013 The dawn of hospital pay for quality has arrived. Hospitals have been reporting Surgical Care Improvement Project (SCIP) measures
Actionable Patient Safety Solution (APSS) #2C: SURGICAL SITE INFECTIONS (SSI)
 #2C: SURGICAL SITE INFECTIONS (SSI)") Actionable Patient Safety Solution (APSS) #2C: SURGICAL SITE INFECTIONS (SSI) Executive Summary Checklist In order to establish a program to reduce surgical site infections (SSIs) the following implementation
Actionable Patient Safety Solution (APSS) #2C: SURGICAL SITE INFECTIONS (SSI) Executive Summary Checklist In order to establish a program to reduce surgical site infections (SSIs) the following implementation
Translating recommendations into practice for surgical site infection prevention. Claire Kilpatrick IPC Global Unit SDS, HIS, WHO HQ
 Translating recommendations into practice for surgical site infection prevention Claire Kilpatrick IPC Global Unit SDS, HIS, WHO HQ XXVIII e Congrès National de la Société Française d Hygiène Hospitalière
Translating recommendations into practice for surgical site infection prevention Claire Kilpatrick IPC Global Unit SDS, HIS, WHO HQ XXVIII e Congrès National de la Société Française d Hygiène Hospitalière
The Impact of Healthcare-associated Infections in Pennsylvania 2010
 The Impact Healthcare-associated Infections in Pennsylvania 2010 Pennsylvania Health Care Cost Containment Council February 2012 About PHC4 The Pennsylvania Health Care Cost Containment Council (PHC4)
The Impact Healthcare-associated Infections in Pennsylvania 2010 Pennsylvania Health Care Cost Containment Council February 2012 About PHC4 The Pennsylvania Health Care Cost Containment Council (PHC4)
NoCVA SSI/VTE Safe Surgery Collaborative
 NoCVA SSI/VTE Safe Surgery Collaborative Orientation Webinar #3 Measures and Data Collection July 19, 2012 Presented by: Jan Mangun, MT(ASCP), MSA, CPHRM Executive Director, Quality and Patient Safety
NoCVA SSI/VTE Safe Surgery Collaborative Orientation Webinar #3 Measures and Data Collection July 19, 2012 Presented by: Jan Mangun, MT(ASCP), MSA, CPHRM Executive Director, Quality and Patient Safety
Improving Hospital Performance Through Clinical Integration
 white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
white paper Improving Hospital Performance Through Clinical Integration Rohit Uppal, MD President of Acute Hospital Medicine, TeamHealth In the typical hospital, most clinical service lines operate as
Provincial Surveillance
 Provincial Surveillance Provincial Surveillance 2011/12 Launched first provincial surveillance protocols Establishment of provincial data entry & start of formal surveillance reports Partnership with AB
Provincial Surveillance Provincial Surveillance 2011/12 Launched first provincial surveillance protocols Establishment of provincial data entry & start of formal surveillance reports Partnership with AB
Welcome and Instructions
 Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Welcome and Instructions For audio, join by telephone at 877-594-8353, participant code 56350822# Your line is OPEN. Please do not use the hold feature on your phone but do mute your line by dialing *6.
Total Joint Partnership Program Identifies Areas to Improve Care and Decrease Costs Joseph Tomaro, PhD
 WHITE PAPER Accelero Health Partners, 2013 Total Joint Partnership Program Identifies Areas to Improve Care and Decrease Costs Joseph Tomaro, PhD ABSTRACT The volume of total hip and knee replacements
WHITE PAPER Accelero Health Partners, 2013 Total Joint Partnership Program Identifies Areas to Improve Care and Decrease Costs Joseph Tomaro, PhD ABSTRACT The volume of total hip and knee replacements
Clinical Standardization
 Clinical Standardization Joe Sharma, MD, FACS, FACE Associate Professor of Surgery Director, of Endocrine Surgery Chief Quality Officer Emory University School of Medicine Disclosures Engineer US Navy
Clinical Standardization Joe Sharma, MD, FACS, FACE Associate Professor of Surgery Director, of Endocrine Surgery Chief Quality Officer Emory University School of Medicine Disclosures Engineer US Navy
METICILLIN RESISTANT STAPHYLOCOCCUS AUREUS (M.R.S.A.) DECOLONISATION GUIDANCE PRIMARY CARE. Purpose of Issue/Description of Change
 DECOLONISATION GUIDANCE PRIMARY CARE. Purpose of Issue/Description of Change") METICILLIN RESISTANT STAPHYLOCOCCUS AUREUS (M.R.S.A.) DECOLONISATION GUIDANCE PRIMARY CARE First Issued by/date Issue Version Purpose of Issue/Description of Change Planned Review Date 10/2008 1 Guidance
METICILLIN RESISTANT STAPHYLOCOCCUS AUREUS (M.R.S.A.) DECOLONISATION GUIDANCE PRIMARY CARE First Issued by/date Issue Version Purpose of Issue/Description of Change Planned Review Date 10/2008 1 Guidance
Minnesota Statewide Quality Reporting and Measurement System: APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654
 Minnesota Statewide Quality Reporting and Measurement System: APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 DECEMBER 2017 APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 Minnesota
Minnesota Statewide Quality Reporting and Measurement System: APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 DECEMBER 2017 APPENDICES TO MINNESOTA ADMINISTRATIVE RULES, CHAPTER 4654 Minnesota
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Effect of Colon Bundle Implementation in a Community Hospital. Michael Barringer, MD, FACS CHS Cleveland
 Effect of Colon Bundle Implementation in a Community Hospital Michael Barringer, MD, FACS CHS Cleveland Doug Hobson, MD, Surgeon Champion Mike Barringer, MD, Surgeon Champion No Disclosures Except for
Effect of Colon Bundle Implementation in a Community Hospital Michael Barringer, MD, FACS CHS Cleveland Doug Hobson, MD, Surgeon Champion Mike Barringer, MD, Surgeon Champion No Disclosures Except for
HOSPITAL QUALITY MEASURES. Overview of QM s
 HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
HOSPITAL QUALITY MEASURES Overview of QM s QUALITY MEASURES FOR HOSPITALS The overall rating defined by Hospital Compare summarizes up to 57 quality measures reflecting common conditions that hospitals
Healthcare- Associated Infections in North Carolina
 2018 Healthcare- Associated Infections in North Carolina Reference Document Revised June 2018 NC Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program NC Department of Health
2018 Healthcare- Associated Infections in North Carolina Reference Document Revised June 2018 NC Surveillance for Healthcare-Associated and Resistant Pathogens Patient Safety Program NC Department of Health
Combined SSI Bundles and ERAS in Colorectal Surgeries
 Combined SSI Bundles and ERAS in Colorectal Surgeries Joy Lanfranchi BSN, RN, CNOR, CMLSO Richard Bollin Jr. M.D. Kevin Kinzinger M.D. MBA, FACS, FASCRS Joanne Bonnot MSN, RN, BBA, NE-BC Claudia Skinner
Combined SSI Bundles and ERAS in Colorectal Surgeries Joy Lanfranchi BSN, RN, CNOR, CMLSO Richard Bollin Jr. M.D. Kevin Kinzinger M.D. MBA, FACS, FASCRS Joanne Bonnot MSN, RN, BBA, NE-BC Claudia Skinner
HealthStream Ambulatory Regulatory Course Descriptions
 This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
This course covers three related aspects of medical care. All three are critical for the safety of patients. Avoiding Errors: Communication, Identification, and Verification These three critical issues
Consumers Union/Safe Patient Project Page 1 of 7
 Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
Improving Hospital and Patient Safety: An overview of recently passed legislation and requirements towards improving the safety of California s hospital patients June 2009 Background Since 2006 several
EP20EO Clinical nurses are involved in the review, action planning, and evaluation of patient safety data at the unit level.
 Exemplary Professional Practice CULTURE OF SAFETY EP20EO Clinical nurses are involved in the review, action planning, and evaluation of patient safety data at the unit level. Example B: Provide one example,
Exemplary Professional Practice CULTURE OF SAFETY EP20EO Clinical nurses are involved in the review, action planning, and evaluation of patient safety data at the unit level. Example B: Provide one example,
Healthcare Acquired Infections
 Healthcare Acquired Infections Emerging Trends in Hospital Administration 9 th & 10 th May 2014 Prof. Hannah Priya HICC In charge What is healthcare acquired infection? An infection occurring in a patient
Healthcare Acquired Infections Emerging Trends in Hospital Administration 9 th & 10 th May 2014 Prof. Hannah Priya HICC In charge What is healthcare acquired infection? An infection occurring in a patient
CMS Quality Program- Outcome Measures. Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018
 CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
CMS Quality Program- Outcome Measures Kathy Wonderly RN, MSEd, CPHQ Consultant Developed: December 2015 Revised: January 2018 Philosophy The Centers for Medicare and Medicaid Services (CMS) is changing
IHI Expedition. Expedition Coordinator 12/18/2013
 Thursday, December 19, 2013 These presenters have nothing to disclose IHI Expedition Improving Safety and Reliability for Surgical Procedures Session 3 Deborah Yokoe, MD, MPH Kathy Duncan, RN Expedition
Thursday, December 19, 2013 These presenters have nothing to disclose IHI Expedition Improving Safety and Reliability for Surgical Procedures Session 3 Deborah Yokoe, MD, MPH Kathy Duncan, RN Expedition
2010 PQRI REPORTING OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY
 Measure #193: Perioperative Temperature Management 2010 PQRI REPTING OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients, regardless of age, undergoing surgical or therapeutic
Measure #193: Perioperative Temperature Management 2010 PQRI REPTING OPTIONS F INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage of patients, regardless of age, undergoing surgical or therapeutic
Joint Commission NPSG 7: 2011 Update and 2012 Preview
 Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Joint Commission NPSG 7: 2011 Update and 2012 Preview Pharmacy OneSource Webinar June 1, 2011 Louise M. Kuhny, RN, MPH, MBA, CIC The Joint Commission Objectives Upon completion of this program, participants
Reducing Surgical Site Infections in Colon Surgery Patients
 Reducing Surgical Site Infections in Colon Surgery Patients Mercy Health St. Elizabeth Boardman Hospital A Catholic healthcare ministry serving Ohio and Kentucky Mercy Health St. Elizabeth Boardman Hospital
Reducing Surgical Site Infections in Colon Surgery Patients Mercy Health St. Elizabeth Boardman Hospital A Catholic healthcare ministry serving Ohio and Kentucky Mercy Health St. Elizabeth Boardman Hospital
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children
 Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Scrubbing down on Surgical Site Infections: Decreasing the incidence of surgical site infections in children Tiffany Trenda, DO PGY2, Jessie Allen, DO PGY2, Elizabeth Mack, MD MS, Chris Hydorn, MD, Lori
Clinical Intervention Overview: Objectives
 AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
AHRQ Safety Program for Long-term Care: HAIs/CAUTI Clinical Intervention Overview: Preventing Infections to Enhance Resident Safety Cohort 5 Learning Session #1 Steven J. Schweon RN, CIC APIC Infection
Research from the Health Protection Agency
 Changing wound care protocols to reduce postoperative caesarean section infection and readmission KEY WORDS Caesarean section Infection Diabetes Obesity PICO Opsite Post-Op Visible Due to concern centring
Changing wound care protocols to reduce postoperative caesarean section infection and readmission KEY WORDS Caesarean section Infection Diabetes Obesity PICO Opsite Post-Op Visible Due to concern centring
10/18/2010. Disclosure. Learning Objectives. Components of an Effective Infection Control Program
 Components of an Effective Infection Control Program Mary Kundus RN, BSN, CIC, MPH 3M Technical Service, Infection Prevention Division Disclosure Mary Kundus is a 3M Employee Supervisor, Technical Service
Components of an Effective Infection Control Program Mary Kundus RN, BSN, CIC, MPH 3M Technical Service, Infection Prevention Division Disclosure Mary Kundus is a 3M Employee Supervisor, Technical Service
Lightning Overview: Infection Control
 Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Lightning Overview: Infection Control Gary Preston, PhD, CIC, FSHEA Terry Caton, CIC Carla Ward, CIC 2012 Healthcare Management Alternatives, Inc. Objectives At the end of this module you will know: How
Internal Medicine Curriculum Infectious Diseases Rotation
 Contact Person: Dr. Stephen Hawkins Internal Medicine Curriculum Infectious Diseases Rotation Educational Purpose The infectious disease rotation is a required rotation primarily available for PGY, 2 and
Contact Person: Dr. Stephen Hawkins Internal Medicine Curriculum Infectious Diseases Rotation Educational Purpose The infectious disease rotation is a required rotation primarily available for PGY, 2 and
(202) or CMS Proposals to Improve Quality of Care during Hospital Inpatient Stays
 or CMS Proposals to Improve Quality of Care during Hospital Inpatient Stays") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE April 30, 2014 Contact: CMS Media
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE April 30, 2014 Contact: CMS Media
Objectives 2/23/2011. Crossing Paths Intersection of Risk Adjustment and Coding
 Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Crossing Paths Intersection of Risk Adjustment and Coding 1 Objectives Define an outcome Define risk adjustment Describe risk adjustment measurement Discuss interactive scenarios 2 What is an Outcome?
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals
 Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
Kristi Felix RN, BSN, CRRN, CIC, FAPIC Infection Prevention Coordinator Madonna Rehabilitation Hospitals Resident safety-priority for staff and for CMS Providing care in a homelike environment but still
The How to Guide for Reducing Surgical Complications
 The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
The How to Guide for Reducing Surgical Complications Post operative wound (surgical site) infections Maintaining perioperative normothermia Main contacts for Reducing Surgical Complications Campaign Director:
The Patient Protection and Affordable Care Act of 2010
 INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
INVITED COMMENTARY Laying a Foundation for Success in the Medicare Hospital Value-Based Purchasing Program Steve Lawler, Brian Floyd The Centers for Medicare & Medicaid Services (CMS) is seeking to transform
ENVIRONMENT Preoperative evaluation clinic. Preoperative evaluation clinic. Preoperative evaluation clinic. clinic. clinic. Preoperative evaluation
 Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Goals and Objectives, Preoperative Evaluation Clinic Rotation, CA-1 and CA-2 year UCSD DEPARTMENT OF ANESTHESIOLOGY PREOPERATIVE EVALUATION CLINIC ROTATION GOALS AND OBJECTIVES, CA-1 and CA-2 YEAR PATIENT
Risk Assessment. Developing an Infection Prevention plan
 Risk Assessment Developing an Infection Prevention plan Success Depends on Preparation and Planning OBJECTIVES: Identify at risk services, populations, and procedures at your hospital Construct an IC Risk
Risk Assessment Developing an Infection Prevention plan Success Depends on Preparation and Planning OBJECTIVES: Identify at risk services, populations, and procedures at your hospital Construct an IC Risk
Infection Prevention & Control Orientation for Housestaff Welcome to Shands at UF!
 Infection Prevention & Control Orientation for Housestaff 2011 Welcome to Shands at UF! Hot Topics: Prevention Initiatives National Patient Safety Goal 07: Prevent Healthcare Associated Infections Prevent
Infection Prevention & Control Orientation for Housestaff 2011 Welcome to Shands at UF! Hot Topics: Prevention Initiatives National Patient Safety Goal 07: Prevent Healthcare Associated Infections Prevent
HOSPITAL ACQUIRED COMPLICATIONS. Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program
 HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
HOSPITAL ACQUIRED COMPLICATIONS Shruti Scott, DO, MPH Department of Medicine UCI Hospitalist Program HOSPITAL ACQUIRED COMPLICATIONS (HACS) A medical condition or complication that a patient develops during
August 1, 2012 (202) CMS makes changes to improve quality of care during hospital inpatient stays
 CMS makes changes to improve quality of care during hospital inpatient stays") DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Medicare & Medicaid Services Room 352-G 200 Independence Avenue, SW Washington, DC 20201 FACT SHEET FOR IMMEDIATE RELEASE Contact: CMS Media Relations
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services
 Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
Clinical Documentation: Beyond The Financials Cheryll A. Rogers, RHIA, CDIP, CCDS, CCS Senior Inpatient Consultant 3M HIS Consulting Services Clinical Documentation: Beyond The Financials Key Points of
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence
 Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
Risk Factor Analysis for Postoperative Unplanned Intubation and Ventilator Dependence Adam P. Johnson MD, MPH, Anisha Kshetrapal MD, Harold Hsu MD, Randi Altmark RN, BSN, Herbert E Cohn MD, FACS, Scott
Patient Safety Course Descriptions
 Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Adverse Events Antibiotic Resistance This course will teach you how to deal with adverse events at your facility. You will learn: What incidents are, and how to respond to them. What sentinel events are,
Care Redesign: An Essential Feature of Bundled Payment
 Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
Issue Brief No. 11 September 2013 Care Redesign: An Essential Feature of Bundled Payment Jett Stansbury Director, New Payment Strategies, Integrated Healthcare Association Gabrielle White, RN, CASC Executive
Physician Executive Council. Using the Perioperative Surgical Home to Improve Joint Replacement
 Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
Physician Executive Council Using the Perioperative Surgical Home to Improve Joint Replacement 9 Today s Presenters Julie Riley Physician Executive Council Senior Consultant 202-266-5628 RileyJu@advisory.com
Reducing Infections and Improving Engagement St. Luke's Nephrology Associates. Contact Information: Robert Gayner, M.D., FASN
 BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
BEST PRACTICES Vascular Access and CLABSI Reduction Reducing Infections and Improving Engagement St. Luke's Nephrology Associates Contact Information: Robert Gayner, M.D., FASN St. Luke's Nephrology Associates
Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health
 Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health Mary McGoldrick, MS, RN, CRNI Home Care and Hospice Consultant Saint Simons Island, GA Nothing to Disclose
Infection Prevention and Control: How to Meet the Conditions of Participation for Home Health Mary McGoldrick, MS, RN, CRNI Home Care and Hospice Consultant Saint Simons Island, GA Nothing to Disclose
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient)
") Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
Patient Experience of Care Survey Results Hospital Consumer Assessment of Healthcare Providers and Systems (Inpatient) HCAHPS QUESTION DESCRIPTION (April 2016 - March 2017) Patients who reported that their
State of California Health and Human Services Agency California Department of Public Health
 State of California Health and Human Services Agency California Department of Public Health MARK B HORTON, MD, MSPH Director ARNOLD SCHWARZENEGGER Governor AFL 10-07 TO: General Acute Care Hospitals SUBJECT:
State of California Health and Human Services Agency California Department of Public Health MARK B HORTON, MD, MSPH Director ARNOLD SCHWARZENEGGER Governor AFL 10-07 TO: General Acute Care Hospitals SUBJECT:
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES. James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP
 CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
CMS TRANSPLANT PROGRAM QUALITY WEBINAR SERIES Comprehensive Program and 5 Key Aspects James Ballard, MBA, CPHQ, CPPS, HACP Eileen Willey, MSN, BSN, RN, CPHQ, HACP QAPI Specialist/ Quality Surveyor Educators
June 27, Dear Ms. Tavenner:
 1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 27, 2014 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
1275 K Street, NW, Suite 1000 Washington, DC 20005-4006 Phone: 202/789-1890 Fax: 202/789-1899 apicinfo@apic.org www.apic.org June 27, 2014 Ms. Marilyn Tavenner Administrator Centers for Medicare & Medicaid
AMERICAN COLLEGE OF SURGEONS Inspiring Quality: Highest Standards, Better Outcomes
 AMERICAN COLLEGE OF SURGEONS Inspiring Quality: Highest Standards, Better Outcomes SSI Measure Harmonization ACS NSQIP and CDC NHSN Bruce Lee Hall, MD, PhD, MBA, FACS 2012 ACS NSQIP National Conference
AMERICAN COLLEGE OF SURGEONS Inspiring Quality: Highest Standards, Better Outcomes SSI Measure Harmonization ACS NSQIP and CDC NHSN Bruce Lee Hall, MD, PhD, MBA, FACS 2012 ACS NSQIP National Conference
C. difficile Infection and C. difficile Lab ID Reporting in NHSN
 C. difficile Infection and C. difficile Lab ID Reporting in NHSN MARY ANDRUS, BA, RN, CIC Infection Preventionist Consultant Learning Objectives Review the structure and of the MDRO/CDAD Module within
C. difficile Infection and C. difficile Lab ID Reporting in NHSN MARY ANDRUS, BA, RN, CIC Infection Preventionist Consultant Learning Objectives Review the structure and of the MDRO/CDAD Module within
General information. Hospital type : Acute Care Hospitals. Provides emergency services : Yes. electronically between visits : Yes
 General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
General information 80 JESSE HILL, JR DRIVE SE ATLANTA, GA 30303 (404) 616 45 Overall rating : 1 out of 5 stars Learn more about the overall ratings General information Hospital type : Acute Care Hospitals
Skin and Nasal Decolonization for Adult
 01.30.02 Skin and Nasal Decolonization for Adult Purpose A. Patient Population Included: B. Process for Obtaining and Processing Specimen C. Procedure for Notification of MRSA/MSSA Positive Samples To
01.30.02 Skin and Nasal Decolonization for Adult Purpose A. Patient Population Included: B. Process for Obtaining and Processing Specimen C. Procedure for Notification of MRSA/MSSA Positive Samples To
Organization: MedStar Franklin Square Medical Center Solution Title: Reduction of Peripheral Vascular Bypass Infections in the Vascular Operating
 Organization: MedStar Franklin Square Medical Center Solution Title: Reduction of Peripheral Vascular Bypass Infections in the Vascular Operating Room Project Description: The purpose of this project is
Organization: MedStar Franklin Square Medical Center Solution Title: Reduction of Peripheral Vascular Bypass Infections in the Vascular Operating Room Project Description: The purpose of this project is
SURGICAL SAFETY CHECKLIST
 SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
SURGICAL SAFETY CHECKLIST WHY: INFORMATION, RATIONALE, AND FAQ May 2009 Building a safer health system INFORMATION, RATIONALE, AND FAQ May 2009 - Version 1.0 The aim of this document is to provide information
Which Elements in a Wound Infection Prevention Process are Important? Aaron Chen, BS, Sebastian Perez, MSPH, John Sweeney, MD, Joe Sharma, MD
 Which Elements in a Wound Infection Prevention Process are Important? Aaron Chen, BS, Sebastian Perez, MSPH, John Sweeney, MD, Joe Sharma, MD Disclosure Slide No COI and no disclosures. SSI Surgical Site
Which Elements in a Wound Infection Prevention Process are Important? Aaron Chen, BS, Sebastian Perez, MSPH, John Sweeney, MD, Joe Sharma, MD Disclosure Slide No COI and no disclosures. SSI Surgical Site
Hospital Acquired Conditions. Tracy Blair MSN, RN
 Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
Hospital Acquired Conditions Tracy Blair MSN, RN A hospitalacquired infection (HAI), also known as a nosocomial infection, is an infection that is acquired in a hospital or other health care facility Hospital
SCORING METHODOLOGY APRIL 2014
 SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
SCORING METHODOLOGY APRIL 2014 HOSPITAL SAFETY SCORE Contents What is the Hospital Safety Score?... 4 Who is The Leapfrog Group?... 4 Eligible and Excluded Hospitals... 4 Scoring Methodology... 5 Measures...
GENERAL PROGRAM GOALS AND OBJECTIVES
 BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
BENJAMIN ATWATER RESIDENCY TRAINING PROGRAM DIRECTOR UCSD MEDICAL CENTER DEPARTMENT OF ANESTHESIOLOGY 200 WEST ARBOR DRIVE SAN DIEGO, CA 92103-8770 PHONE: (619) 543-5297 FAX: (619) 543-6476 Resident Orientation
SURGICAL SITE INFECTION AT KILIMANJARO CHRISTIAN MEDICAL CENTER, TANZANIA
 SURGICAL SITE INFECTION AT KILIMANJARO CHRISTIAN MEDICAL CENTER, TANZANIA By Hanne-Merete Eriksen Thesis submitted to the International Health Department, University of Oslo as a partial fulfillment of
SURGICAL SITE INFECTION AT KILIMANJARO CHRISTIAN MEDICAL CENTER, TANZANIA By Hanne-Merete Eriksen Thesis submitted to the International Health Department, University of Oslo as a partial fulfillment of
Mohamad Fakih, MD, MPH
 Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
Ensuring Sustainability for CAUTI Prevention Efforts Mohamad Fakih, MD, MPH Professor of Medicine, Wayne State University School of Medicine St John Hospital and Medical Center Detroit, MI So we often
A Program for Surveillance of Hospital-Acquired Infections in a General Hospital: A Two-Year Experience
 REVIEWS OF INFECTIOUS DISEASES. VOL. 3, NO.4. JULY-AUGUST 1981 1981 by The University of Chicago. All rights reserved. 0162-0886/81/0304-Q004$02.00 A Program for Surveillance of Hospital-Acquired Infections
REVIEWS OF INFECTIOUS DISEASES. VOL. 3, NO.4. JULY-AUGUST 1981 1981 by The University of Chicago. All rights reserved. 0162-0886/81/0304-Q004$02.00 A Program for Surveillance of Hospital-Acquired Infections
CNA SEPSIS EDUCATION 2017
 CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
CNA SEPSIS EDUCATION 2017 WHAT CAUSES SEPSIS? Sepsis occurs when the body has a severe immune response to an infection Anyone who has an infection is at risk for developing sepsis Sepsis occurs when the
3/14/2014. Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking. Objectives. Background Information
 Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Preventing Rehospitalizations How to Change Your When in Doubt, Send em Out Way of Thinking Jennifer Moore, RN Content Developer Objectives Describe two reasons why returns to the hospital are not desirable
Perioperative Surgical Home
 None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
None Disclosures Debnath Chatterjee, M.D. Associate Professor of Anesthesiology CRASH 2015 - Vail, Colorado 2 Learning Objectives What is the PSH model? Describe the concept of the Perioperative Surgical
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3)
") Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
Beth Israel Deaconess Medical Center Department of Anesthesia, Critical Care, and Pain Medicine Rotation: Post Anesthesia Care Unit (CA-1, CA-2, CA-3) Goals GOALS AND OBJECTIVES To analyze and interpret
SSI surveillance: Whats new, what s next and what is over the horizon. Glossary of terms
 SSI surveillance: Whats new, what s next and what is over the horizon Professor of Medicine, Pathology and Epidemiology Johns Hopkins University Senior Epidemiologist Johns Hopkins Healthsystem Tperl@jhmi.edu
SSI surveillance: Whats new, what s next and what is over the horizon Professor of Medicine, Pathology and Epidemiology Johns Hopkins University Senior Epidemiologist Johns Hopkins Healthsystem Tperl@jhmi.edu
PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation
 PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation Rowena Chona O. Sano, MSN, RN, CNL, CPHQ Memorial Hermann Greater Heights Hospital Houston, TX Nothing
PREVENTION OF POSTOPERATIVE PULMONARY COMPLICATIONS: Reducing Postoperative Mechanical Ventilation Rowena Chona O. Sano, MSN, RN, CNL, CPHQ Memorial Hermann Greater Heights Hospital Houston, TX Nothing
Prevention and control of healthcare-associated infections
 Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Prevention and control of healthcare-associated infections Quality improvement guide Issued: November 2011 NICE public health guidance 36 guidance.nice.org.uk/ph36 NHS Evidence has accredited the process
Actionable Patient Safety Solution (APSS) #2C: SURGICAL SITE INFECTIONS (SSI)
 #2C: SURGICAL SITE INFECTIONS (SSI)") Actionable Patient Safety Solution (APSS) #2C: SURGICAL SITE INFECTIONS (SSI) Endorsed by: The trademarks listed above are used with permission of the respective owners. Executive Summary Checklist Postoperative
Actionable Patient Safety Solution (APSS) #2C: SURGICAL SITE INFECTIONS (SSI) Endorsed by: The trademarks listed above are used with permission of the respective owners. Executive Summary Checklist Postoperative
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY. Dr. Paul Vercruysse M.D. Belgium
 ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
ROLE OF THE ANESTHETIST IN ORGANIZING AMBULATORY SURGERY Dr. Paul Vercruysse M.D. Belgium DISCLOSURES - Conflicts of interest? I am an anesthesiologist... TRADITIONAL ROLE OF THE ANESTHESIOLOGIST EVOLVING
Nursing Home Pearls or
 Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
Nursing Home Pearls or How to Enjoy Practicing in Skilled Nursing Facilities Lowell C. Dale, MD November 11, 2016 2016 MFMER slide-1 DISCLOSURE Relevant Financial Relationship Medical Director Golden Living
QUALITY NET REPORTING
 5/18/15% A webinar series that keeps you in the know Brought to you by Progressive QUALITY NET REPORTING Sarah Martin, MBA, RN, CASC Progressive Huddle May 18, 2015 ASCQR ASC Quality Reporting started
5/18/15% A webinar series that keeps you in the know Brought to you by Progressive QUALITY NET REPORTING Sarah Martin, MBA, RN, CASC Progressive Huddle May 18, 2015 ASCQR ASC Quality Reporting started
Staphylococcus aureus bacteraemia in Australian public hospitals Australian hospital statistics
 Staphylococcus aureus bacteraemia in Australian public hospitals 2013 14 Australian hospital statistics Staphylococcus aureus bacteraemia (SAB) in Australian public hospitals 2013 14 SAB is a serious bloodstream
Staphylococcus aureus bacteraemia in Australian public hospitals 2013 14 Australian hospital statistics Staphylococcus aureus bacteraemia (SAB) in Australian public hospitals 2013 14 SAB is a serious bloodstream
CMS and NHSN: What s New for Infection Preventionists in 2013
 CMS and NHSN: What s New for Infection Preventionists in 2013 Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the current status of
CMS and NHSN: What s New for Infection Preventionists in 2013 Joan Hebden RN, MS, CIC Clinical Program Manager Sentri7 Wolters Kluwer Health - Clinical Solutions Objectives Define the current status of