Zachary Early Learning Center 4400 Rollins Place Zachary, Louisiana 70791
|
|
|
- Adelia Hoover
- 6 years ago
- Views:
Transcription
1 Zachary Early Learning Center 4400 Rollins Place Zachary, Louisiana Pre-Kindergarten Registration Packet Prospective Pre-Kindergarten Students must be 4 years old by September 30, 2012 Requirements for Registration of Pre-K Students: Birth Certificate Social Security Card Immunization Record Four Current Proofs of Residency containing Parent/Legal Guardian s Name and Address Documents must include: Original mortgage or original lease agreement/rental contract on company letterhead Utility bill (City of Zachary gas/water bill) And at least 2 of the following: Entergy or Demco bill Telephone bill Tax Assessor s bill Original, current Medical/Medicare or social security insurance Cable TV/Satellite bill Original Homestead Exemption THERE IS A $50.00 NON-REFUNDABLE SUPPLY FEE DUE AT THE TIME OF REGISTRATION. Tuition will be $ per month. Meal prices for breakfast and lunch are available online. Further questions can be answered at
2 Zachary Community Schools School Registration School Date SID# Teacher Method of Transportation Bus # Student Information Social Security or ID assigned by previous LA District Birth Certificate # Last Name First Name Middle Name Sex Primary Ethnic: (choose one) Grade Generation (Jr., III, etc) 0 White 1 Black 2 Hispanic 3 Asian 4 Native American/Alaskan Native 5 Hawaiian/Pacific Islander Secondary Ethnic: (if applicable) 0 White 1 Black 2 Hispanic 3 Asian 4 Native American/Alaskan Native 5 Hawaiian/Pacific Islander Language spoken at home Language first acquired by student Language most often spoken by student Birth Date Place of Birth Month Day Year Date of Entry to U.S. (if not a natural born citizen) Address Information Physical Address Apt.# Apt. Complex House# City Zip Code Mailing Address City Zip Code Home Telephone (225) Names of Other ZCSB Students living at the student s primary residence
3 Guardian Information Father or Legal Guardian 1 Relationship to Student Title Last Name First Name Apt.# Apt. Complex House# Street City Zip Code Phone Home # Work # Cell # Mother or Legal Guardian 2 Relationship to Student Title Last Name First Name Apt.# Apt. Complex House# Street City Zip Code Phone Home # Work # Cell # Emergency Contact 1 Last Name Phone Medical Information Relationship to Student First Name Address Emergency Contact 2 Relationship to Student Last Name First Name Phone Address Preferred Hospital Physician Telephone Allergies Physical Handicaps Additional Information Please check any special education services your child has ever received Speech Special Education 504 Gifted Talented Other, please list Has this student ever attended school in Zachary Community School System? If yes, where? Elementary aged students: Check all programs attended: Play School Nursery School Pre Kindergarten Kindergarten Headstart Incoming Kindergarteners: Check all programs attended: Home (no Pre-K) Tribal Schools Public School PreK NonPublic PreK Licensed Childcare Head Start Programs Please list the schools with the grades the student has attended School Grade School Grade School Grade School Grade School Grade School Grade My signature attests to the accuracy of the information given on this form under penalty of law.
4 Louisiana Student Residency Questionnaire Form (Form Must Be Included In School Enrollment Packet) Date District/Parish School Name Student Name SSN/ID# Male/Female Date of Birth Address Telephone Number Last School Attended Current Grade Parent/Guardian/Adult Caring for Student Relationship Disclaimer: This questionnaire is intended to address the McKinney-Vento Act. Your child may be eligible for additional educational services through Title I Part A, Title I Part C-Migrant, Individuals with Disabilities Education Act (IDEA) and/or Title X, Part C, Federal McKinney-Vento Assistance Act, 42 U.S.C Eligibility can be determined by completing this questionnaire. It is illegal to knowingly make false statements on this form. If eligible, students are to be immediately enrolled in accordance with Bulletin 741, section Yes No Is the student s address a temporary living arrangement? (Note: If this is a permanent living arrangement or the family owns or rents their home, sign under item 9 and submit form to school personnel.) 2. Yes No Is the temporary living arrangement due to loss of housing or economic hardship? 3. Where is the student currently living? (Check all that apply) In an emergency/transitional shelter. Temporarily with another family because we cannot afford or find affordable housing. With an adult that is not a parent or legal guardian, or alone without an adult. In a vehicle of any kind, trailer park or campground without running water/electricity, abandoned building or substandard housing. Emergency Housing (i.e. FEMA Trailer or FEMA Rental Assistance) In a hotel/motel. Other specific information 4. Yes No Does your child have a disability or receive any special education services? (Check One) 5. Yes No Does your child exhibit any behaviors that may interfere with his or her academic performance? 6. Would you like assistance with uniforms student records school supplies transportation other? (Describe: ) 7. Yes No Migrant - Have you moved at any time during the past three (3) years to seek temporary or seasonal work in agriculture (including poultry processing, dairy, nursery, and timber) or fishing? 8. Yes No Does your child have siblings? Name Grade Name Grade Name Grade Name Grade Name Grade Name Grade 9. The undersigned certifies that the information provided above is accurate. Print Parent/Guardian Name/Adult Caring for Student Signature Date (Area Code) Phone number Street Address City State Zip School Use Only Free or Reduced Price Meals Form submitted/signed Copy Placed in Student s Cumulative Record Homeless Liaison Use Only- Check All That Apply Sheltered Doubled-Up Unsheltered/FEMA Hotel/Motel Unaccompanied youth Yes No Print School Contact Title Signature (required) Date (Revised 3/2010)
5 OFFICE USE ONLY: RETURNING STUDENT NEW ENROLLEE CHANGE OF ADDRESS REQUESTED Complete One Per Student School Year Zachary Community Schools Bus Service Request Form Please NEATLY PRINT or Type All Information Student s Name:. I, (parent/guardian s name), DO ( ) DO NOT ( ) want bus service for my child for the school year. If you DO NOT want bus service for your child, please enter your name and your child s name on the lines above, sign on the signature line below*, and return this form to your child s school. If you DO WANT bus service for your child, please enter ALL requested information on this form and return to your child s school immediately. If a child does not need transportation in the morning or evening because of car pooling or other arrangements, please indicate so by writing no ride in the morning or evening box. Parent/Guardian Signature* Sign Here Today s Date Student s School for : Student s Grade for 2012/13: Parent/Guardian s Name: Physical Home Address (No P.O. Boxes): Town/City, Zip Code: ENTIRE PHYSICAL ADDRESS WHERE CHILD WILL BE PICKED UP IN THE MORNING (NO P.O BOXES): ENTIRE PHYSICAL ADDRESS WHERE CHILD WILL BE DROPPED OFF IN THE EVENING (NO P.O. BOXES): Home Phone Number: Work Phone Number of Mother: Cell #: Work Phone Number of Father: Cell#: Other Emergency Names and Phone Numbers: If your child receives Special Education services, does your child s I.E.P. indicate special transportation services be provided? Yes NO Thanks in Advance for Your Assistance

6 ZACHARY COMMUNITY SCHOOLS SCHOOL NURSE DEPARTMENT Welcome to Zachary Community Schools. We are excited that you have chosen our school system, which is one of the fastest growing, top-rated districts in the state, to educate your child. In order to provide the best care possible for your child while at school, it is important for us to be aware of any medical conditions that might affect them during school hours or any condition that requires medication or possible nursing assistance (e.g. asthma, seizure disorder, diabetes, severe allergies, etc.). If your child does not have any medical issues or does not require any medication at school, we only need your signature on the HIPAA Policy form to be returned to school. If your child has special medical needs, please complete and sign the enclosed forms. In addition, if your child requires medication at school, you may pick up the state mandated medication packet at your child s school or you may download these forms from your child s school s website (click Teacher Pages, then Nurses icon, then Medication Packet ), and complete and return them to school. A parent will have to bring the medication to school to be checked and logged in. Please note that medication of any kind, including over-thecounter medication, may NEVER be sent to school with your child, and MUST be checked in by a parent along with the medication packet completed. Also, please ensure that your child s immunizations are up-to-date and that his/her school has an updated copy. This is required by Louisiana Department of Health and Hospitals and must be on file for your child to attend school. Thank you in advance for your cooperation. We look forward to caring for your child. Zachary Community School Nurses
7 Dear Parent, Attached you will find the Zachary Community School Board HIPAA policy Notice of Use of Personal Health Information. Please sign and return this form, so that we may maintain a record of your having received the information. Failure to return the signed form may result in a delay in servicing your child. Thank you, Zachary Community School Nurses This is to certify that I have received and read a copy of the Notice of Use of Personal Health Information. Parent s Signature Names of children attending Zachary Community Schools and grades/homeroom teachers of each: Name Grade Homeroom Teacher Name Grade Homeroom Teacher Name Grade Homeroom Teacher Name Grade Homeroom Teacher Name Grade Homeroom Teacher If you have any questions, please feel free to contact your child s school. An Equal Opportunity Employer
8 ZACHARY COMMUNITY SCHOOL BOARD NOTICE OF USE OF PERSONAL HEALTH INFORMATION This Notice Describes How Medical Information About Your Child May Be Used and Disclosed and How You Can Get Access To This Information. Please Review It Carefully. We understand that information we collect about your child and their health is personal. Keeping health information of your child private is one our most important responsibilities. We are committed to protecting their health information and following all laws about its use. You have the right to discuss with the system s Privacy Officer your concerns about how their health information is shared. The law says: 1. We must keep their health information from others who do not need it. 2. You may ask us not to share certain health services information. Sometimes, we may not be able to agree to your request. Your child may receive certain services from nurses, therapists, social workers, doctors or other health care related individuals. They may see, use and share your child s health or medical information to determine any plan of treatment, diagnosis, or outcome of information as described in an Individualized Education Program (IEP) or other plan document. This use may cover such health services your child had before now or may have later. We review such health services information and claims to make sure that you get quality services and that all laws about providing and paying for such health services are being followed. We may also use the information to remind you about service or to tell you about treatment alternatives. We also use the information to obtain payments for such services as a result of the Medicaid program. We must submit information that identifies you and your child, your child s diagnosis and the treatment of services provided to your child for reimbursement by Medicaid. We may share your health care information with health plans, insurance companies, or government programs to help get the benefits and so that the School System can be paid or pay for such health care or medical services. In most cases, you may see your child s health information but the request cannot include psychotherapy notes or information gathered for judicial proceedings. There may be legal reasons or safety concerns that may limit the amount of information that you may see. You may ask in writing to receive a copy of your child s health information. We may charge a small amount for copying costs. If you think some of the health information is wrong, you may ask in writing that we correct or add to it. You may ask that the corrected or new information be sent to others who have received your child s health information from us. You may ask us for a list of where we sent the health information. You may ask to have the health information sent to others. You will be asked to sign a separate form, called an authorization form, permitting the health information of your child to go to them. The authorization form tells us what, where and to whom the information must be sent. You can stop or limit the amount of information sent any time by letting us know in writing.
9 Note: A child 18 years old or older can give consent for his or her health information to be kept private from others unless the child signs an authorization form. We follow laws that tell us when we have to share health information of your child even if you do not sign an authorization form. We always report: 1. Contagious diseases, birth defects and cancer; 2. Firearm injuries and other trauma events; 3. Reactions to problems with medicines or defective medical equipment; 4. To the police or other governmental agencies when required by law; 5. When a court orders us to; 6. To the government to review how our programs are working; 7. To a provider or insurance company who needs to know if your child is enrolled in one of our programs; 8. To Worker s Compensation for work related injuries; 9. Birth, death and immunization information; 10. To the federal government when they are investigating something important to protect our country, the President and other government workers; 11. Abuse, neglect and domestic violence, if related to child protection or vulnerable adults; or 12. To parents and other designated by law. We may also share health care information for permitted research purposes, for matters concerning organ donations and for serious threats to public health or safety. This notice is yours. You may ask for a copy at any time. If there are important changes to this notice, you will get a new one within 60 days. If you have any questions about this notice of privacy rights of your child or that such rights have been violated, you can contact: Zachary Community School Board Office (225) telephone 3755 Church Street, Zachary, LA You can also complain to the federal government Secretary of Health and Human Services (HHS) or to the HHS Office of Civil Rights. Your health care services will not be affected by any complaint made to the School Board, Secretary of Health and Human Services or Office of Civil Rights.
10 STATE OF LOUISIANA HEALTH INFORMATION TO BE COMPLETED BY PARENT/LEGAL GUARDIAN EACH SCHOOL YEAR PART 1: PARENT OR LEGAL GUARDIAN TO COMPLETE. Parent/Legal Guardian is encouraged to participate in the development of an Individual Health Care Plan if needed. Use additional sheets, if necessary, for further explanation. Name of School: Grade: Student s Name: Last First M.I. Student s Date of Birth: Sex: M F State or Country of Birth: Student s Mailing Address: City: State: Zip Code: Student s Physical Address: City: State: Zip Code: Name of Mother or Legal Home Phone: Guardian: ( ) Name of Father or Legal Home Phone: Guardian: ( ) Name of child s pediatrician or primary care provider: Work Phone: Cell Phone: Employer: ( ) ( ) Work Phone: Cell Phone: Employer: ( ) ( ) Names of medical specialists or special clinics caring for your child: Parent or Legal Guardian Signature DatePART Please check the type of health insurance your child has: Private Medicaid/LaCHIP None If your child does not have health insurance, would you like information on no cost health insurance? Yes No In case of emergency if parent or legal guardian cannot be reached contact the following: Name Complete Phone Number ( ) My child has a medical, mental, or behavioral condition that may affect his/her school day: No Yes (If yes, please complete Part 2.) PART 2: COMPLETE ALL BOXES THAT APPLY TO YOUR CHILD. Parent/Legal Guardian is responsible for providing the school with any medication and may be responsible for providing the school with any special food or equipment that the student will require during the school day. Check with the school nurse to obtain correct medication and procedure forms. ALLERGIES Allergy Type: Food (list food(s)) Insect sting (list insect(s)) Medication (list medication(s)) Other (list) Reactions: (Date of last occurrence if yes.) Coughing (Date: ) Hives (Date: ) Rash (Date: ) Difficulty breathing (Date: ) Local swelling (Date: ) Wheezing (Date: ) Generalized swelling (Date: ) Nausea (Date: ) Other (Date: ) Currently prescribed medications and treatments: Oral antihistamine(benadryl, etc.) Epi-pen Other ASTHMA Triggers: Environmental (i.e., tobacco, dust, pets, pollen, etc.) (list) Other (list) Does your child experience asthma symptoms with exercise? No Yes Symptoms: Chest tightness, discomfort, or pain Difficulty breathing Coughing Wheezing Other Currently prescribed medications and treatments: Date of last hospitalization related to asthma Date of last emergency room visit related to asthma Does your child have a written asthma management plan? No Yes Is peak flow monitoring used? No Yes Page 1 of 2
11 Name: DOB: DIABETES Currently prescribed medications and treatments: Insulin: Syringe Pen Pump Blood sugar testing Glucagon Oral medication(s) List medication(s) Is special scheduling of lunch or Physical Education required? No Yes SEIZURE DISORDER Type of seizure: Absence (staring, unresponsive) Complex Partial Generalized Tonic-Clonic (Grand Mal/Convulsive) Other (explain) Physical Education Restrictions: No Yes Medication(s): No Yes List medication(s) Date of last seizure Length of seizure OTHER HEALTH CONDITIONS Anemia ADD/ADHD Cancer Cerebral Palsy Chicken Pox Cystic Fibrosis Depression Digestive disorders Emotional/Psychological Juvenile Rheumatoid Arthritis Hemophilia Heart condition Physical disability Sickle Cell Disease Skin disorders Speech problems Other (explain) Physical Education Restrictions: No Yes (explain): Medication(s): No Yes List medication(s) Special procedures required (i.e., catheterization, oxygen, gastrostomy care, tracheostomy care, suctioning): No Yes (explain): Special diet required (i.e., blended, soft, low salt, low fat, liquid supplement): No Yes (explain): Are there anticipated frequent absences or hospitalizations? No Yes (explain): VISION CONDITIONS HEARING CONDITIONS Contacts/glasses Other Hearing aid(s) Other ENVIRONMENTAL ADJUSTMENTS DUE TO A HEALTH CONDITION Special school environmental adjustments of the school environment or schedule: No Yes (explain): (i.e., seizures, limitations in physical activity, periodic breaks for endurance, part-time schedule, building modifications for access) Special school environmental adjustments to classroom or school facilities: No Yes (explain): (i.e., temperature control, refrigeration/medication storage, availability of running water) Special safety considerations: No Yes (explain): (i.e., special precautions in lifting, positioning, special transportation emergency plan, special safety equipment, special techniques for positioning, feeding) Special assistance with activities of daily living: No Yes (explain): (i.e., eating, toileting, walking) PART 3: SCHOOL NURSE TO COMPLETE if parent/legal guardian indicates medical condition. School Nurse Signature Notes: Date RETURN COMPLETED FORM TO SCHOOL NURSE/HEALTH OFFICE AS SOON AS POSSIBLE Page 2 of 2
12 ZACHARY COMMUNITY SCHOOL SYSTEM MEDICAL HISTORY UPDATE FORM To Be Completed By Doctor (This information will be utilized by the school nurse to provide health services to students.) Student s Name DOB Grade School Teacher School Nurse CURRENT DIAGNOSIS & MEDICAL STATUS (additional information may be attached to this form) Recommendations For Student Integration Into The School Setting Activity Restrictions/Limitations Accommodations Nutritional/Dietary Adaptive Physical Education Physical Therapy Occupational Therapy Special Procedures Return to Clinic Physician s Signature Date Print Physician Name Here Office # Address Fax #
13
14
15
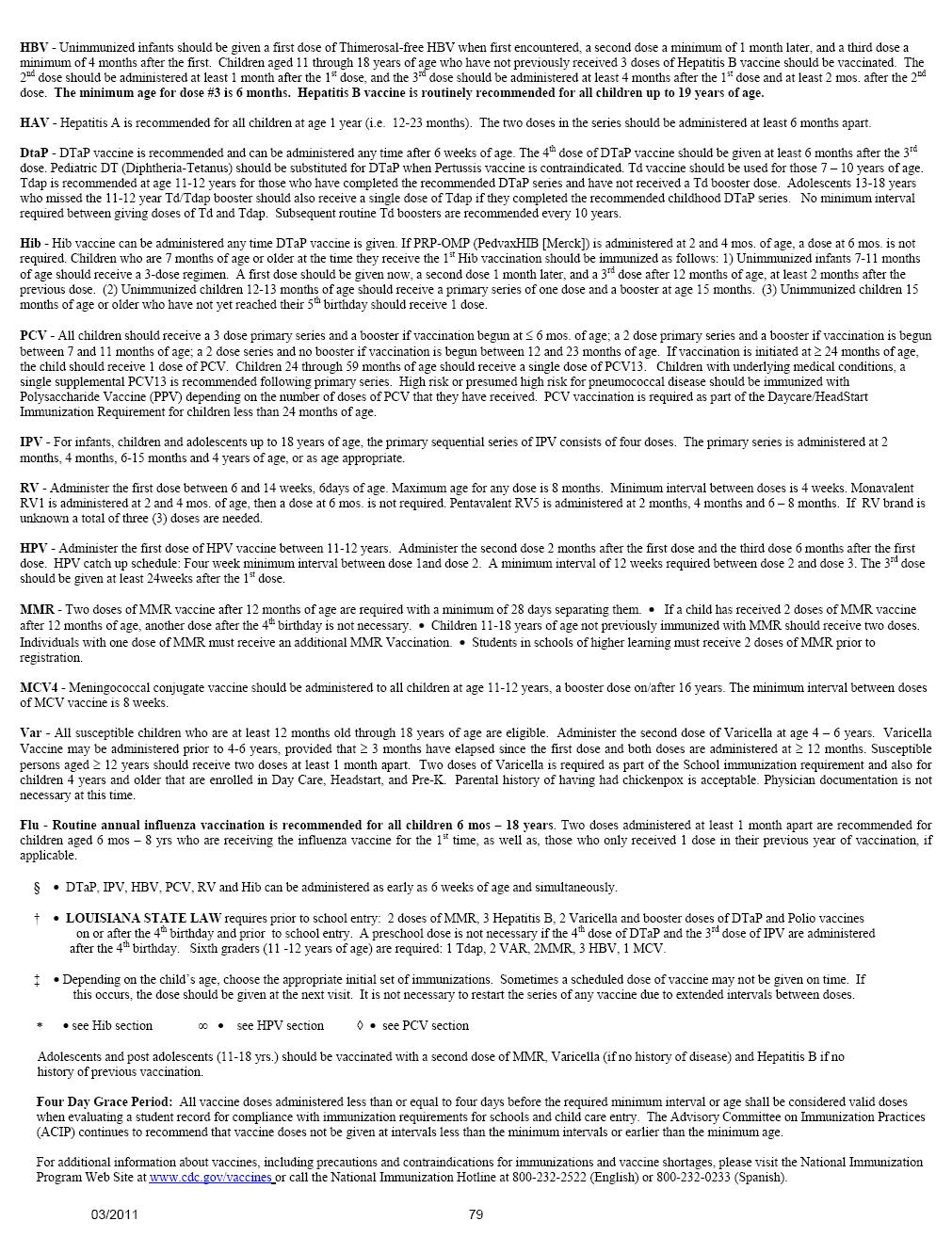
16 LOUISIANA IMMUNIZATION REQUIREMENTS Years of Age, Entering 6 th grade or any other grade One (1) Meningococcal Vaccine (MCV 4) Two (2) doses of Measles, Mumps, Rubella vaccine (MMR) Three (3) doses of Hepatitis B vaccine (HBV) Two (2) doses of Varicella vaccine(var) One (1)dose of Tetanus Diphtheria Acellular Pertussis vaccine (Tdap) 4 Years and older, Entering Kindergarten, Pre K, Daycare or Head Start Booster dose of Poliovirus vaccine (IPV) received on after the 4 th birthday. Two (2) doses of Measles, Mumps, Rubella vaccine (MMR) Three (3) doses of Hepatitis B vaccine (HBV) Two (2) doses of Varicella vaccine (Var) Booster dose of Diphtheria Tetanus Acellular Pertussis vacccine (DtaP)received on after the 4 th birthday Under 4 Years, Entering Pre K, Daycare or Head Start Three (3) doses of Pneumococcal Conjugate vaccine (PCV) for children less than 24 months of age. If a child is less than 24 months of age and has received 4 doses of PCV 7 he/she is to get a single dose of PCV 13 for Daycare and Head Start. Two (2)or (3)Three doses of polio vaccine (IPV) One (1) Or Two (2) doses of Measles, Mumps, Rubella vaccine (MMR) Three doses of Hepatitis B vaccine (HBV) One(1) dose of Varicella Vaccine(Var) Three (3) or Four (4) doses Diphtheria Tetanus Acellular Pertussis vacccine(dtap) Three (3)doses of Haemophilus Influenza Type B vaccine (Hib)
Information Needed for Registration
 Information Needed for Registration Prospective Kindergarten students must be five years old by September 30, 2017. Prospective Pre-Kindergarten students must be four years old by September 30, 2017. All
Information Needed for Registration Prospective Kindergarten students must be five years old by September 30, 2017. Prospective Pre-Kindergarten students must be four years old by September 30, 2017. All
Information Needed for Registration
 Information Needed for Registration Prospective Kindergarten students must be five years old by September 30, 2018. Prospective Pre-Kindergarten students must be four years old by September 30, 2018. All
Information Needed for Registration Prospective Kindergarten students must be five years old by September 30, 2018. Prospective Pre-Kindergarten students must be four years old by September 30, 2018. All
A copy of the birth certificate or proof of birth letter from the hospital. Your support in this matter is greatly appreciated.
 Attention Parents We are required by the Commonwealth of Virginia to secure, before the child may attend, and maintain, while in our care, a current file containing specific information regarding the health
Attention Parents We are required by the Commonwealth of Virginia to secure, before the child may attend, and maintain, while in our care, a current file containing specific information regarding the health
Kenilworth Public Schools Harding Elementary School 426 Boulevard Kenilworth, New Jersey
 Assistant Dear Parent/Guardian: Harding Elementary School Kathleen Murphy Principal Ronald Bubnowski Assistant Principal Attached, please find the Kindergarten registration packet for the Kenilworth School
Assistant Dear Parent/Guardian: Harding Elementary School Kathleen Murphy Principal Ronald Bubnowski Assistant Principal Attached, please find the Kindergarten registration packet for the Kenilworth School
RETURNING Student Information Update
 Today s Date: RETURNING Student Information Update OFFICE USE ONLY School # Student # Grade Level Teacher Student Legal Name (first, middle, last) Suffix (Jr., Sr., II, lii, IV, V) Student Date of Birth
Today s Date: RETURNING Student Information Update OFFICE USE ONLY School # Student # Grade Level Teacher Student Legal Name (first, middle, last) Suffix (Jr., Sr., II, lii, IV, V) Student Date of Birth
ALFRED ALINGU, MD INTERNAL MEDICINE
 Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Name Date of Birth Social Security Number Marital Status Address City State Zip Code Home Phone Cell Phone E-mail Address Pharmacy Name Pharmacy Phone Number Emergency Contact Phone Number Relationship
Student s Name; Date: Identification and Emergency Information. Child s Preadmission Health History Parent s Report
 FOURSQUARE CHRISTIAN EARLY LEARNING CENTER ENROLLMENT CHECKLIST 2017-2018 Student s Name; Date: Appointment with Administrator/Director (mandatory before starting school) Student & Family Information Identification
FOURSQUARE CHRISTIAN EARLY LEARNING CENTER ENROLLMENT CHECKLIST 2017-2018 Student s Name; Date: Appointment with Administrator/Director (mandatory before starting school) Student & Family Information Identification
Health Clinic Policies:
 Health Clinic Policies: Burris has one full time nurse on duty daily. The health of your student is our concern. Habits are formed in early childhood. These habits are important to growth, health, happiness
Health Clinic Policies: Burris has one full time nurse on duty daily. The health of your student is our concern. Habits are formed in early childhood. These habits are important to growth, health, happiness
Home Address: City/State (if other than D.C.) Other. Glasses Referred
 Other. Glasses Referred") DISTRICT OF COLUMBIA UNIVERSAL HEALTH CERTIFICATE Part 1: Child s Personal Information Parent/Guardian: Please complete Part 1 clearly and completely & sign Part 5 below. Child s Last Name: Child s First
DISTRICT OF COLUMBIA UNIVERSAL HEALTH CERTIFICATE Part 1: Child s Personal Information Parent/Guardian: Please complete Part 1 clearly and completely & sign Part 5 below. Child s Last Name: Child s First
Greetings! Sincerely, St. Margaret s School Health Center
 Greetings! We are excited to have your child join us at St. Margaret s School and want to do all we can to ensure your arrival to campus goes smoothly. The following outlines the information and medical
Greetings! We are excited to have your child join us at St. Margaret s School and want to do all we can to ensure your arrival to campus goes smoothly. The following outlines the information and medical
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE Phone: Fax:
 School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
School-Based Health Center William Penn High School 713 E. Basin Road New Castle, DE 19720 Phone: 324 5740 Fax: 324 5745 Dear Parents/Guardians: The William Penn School Based Health Center (SBHC) is a
COUNSELOR IN TRAINING PROGRAM FARM CAMP AT THE FARM INSTITUTE
 COUNSELOR IN TRAINING PROGRAM FARM CAMP AT THE FARM INSTITUTE Counselor In Training Program Overview Farm Camp at TFI provides the opportunity for teens to gain valuable job experience working with children
COUNSELOR IN TRAINING PROGRAM FARM CAMP AT THE FARM INSTITUTE Counselor In Training Program Overview Farm Camp at TFI provides the opportunity for teens to gain valuable job experience working with children
HIGHLAND MEDICAL INFORMATION FORM
 HIGHLAND MEDICAL INFORMATION FORM TODAY S DATE: SESSION NAME SESSION DATE Having adequate information about your child is crucial to our ability to provide a supportive environment. We rely on you to tell
HIGHLAND MEDICAL INFORMATION FORM TODAY S DATE: SESSION NAME SESSION DATE Having adequate information about your child is crucial to our ability to provide a supportive environment. We rely on you to tell
School Based Oral Health Services
 Seal a Smile Oral Health Program A project of Whitney M. Young Jr. Health Services and the Healthy Capital District Initiative School Based Oral Health Services Oral health classroom education Dental screenings
Seal a Smile Oral Health Program A project of Whitney M. Young Jr. Health Services and the Healthy Capital District Initiative School Based Oral Health Services Oral health classroom education Dental screenings
New Kent County Public Schools DR. DAVID A. MYERS, SUPERINTENDENT POST OFFICE BOX 110 NEW KENT, VIRGINIA (804)
") Dear Parent/Guardian: We welcome you and your child to the New Kent County Public School System. In order to make the transition smoother, we would appreciate your cooperation by completing the attached
Dear Parent/Guardian: We welcome you and your child to the New Kent County Public School System. In order to make the transition smoother, we would appreciate your cooperation by completing the attached
School Based Health Consent for Services Grace Community Health Center, Inc.
 School Based Health Consent for Services Grace Community Health Center, Inc. Please read carefully: In order for us to see your child in school based clinics, all pages of this form must be completed by
School Based Health Consent for Services Grace Community Health Center, Inc. Please read carefully: In order for us to see your child in school based clinics, all pages of this form must be completed by
Welcome Letter- Orchard School Clinic
 Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
Welcome Letter- Orchard School Clinic Dear Parent or Guardian: Orchard School Clinic is a school-based location of RiverStone Health Clinic. This is a collaborative effort between RiverStone Health, Billings
MONTAGUE SCHOOL. 1 st 7 th Grade Registration Packet
 MONTAGUE SCHOOL 2015 2016 1 st 7 th Grade Registration Packet Janice L. Hodge Chief School Administrator/Principal Donna Pinzone Administrative Assistant MONTAGUE TOWNSHIP SCHOOL DISTRICT 475 Route 206
MONTAGUE SCHOOL 2015 2016 1 st 7 th Grade Registration Packet Janice L. Hodge Chief School Administrator/Principal Donna Pinzone Administrative Assistant MONTAGUE TOWNSHIP SCHOOL DISTRICT 475 Route 206
Camper Health Form Camp Y-Owasco
 Camper Health Form Camp Y-Owasco Health History Forms must be filled out by a parent/guardian. Please complete all pages. Incomplete or unsigned forms will be returned to you. Please return the completed
Camper Health Form Camp Y-Owasco Health History Forms must be filled out by a parent/guardian. Please complete all pages. Incomplete or unsigned forms will be returned to you. Please return the completed
ZooCrew Registration Packet Summer ZooCrew
 Summer ZooCrew Check the weeks you would like to sign your child(ren) up for ZooCrew: 4 & 5 year olds* Week of 7/18 In My Backyard Week of 8/1 Once Upon a Story Week of 8/15 Where the Wild Things Are 6
Summer ZooCrew Check the weeks you would like to sign your child(ren) up for ZooCrew: 4 & 5 year olds* Week of 7/18 In My Backyard Week of 8/1 Once Upon a Story Week of 8/15 Where the Wild Things Are 6
Health Record Health Services 1025 North Broadway, K-254 Milwaukee, Wisconsin Phone: Fax:
 For office use only: Jenzabar: / / MM DD YY (Initial) Revision date: 7/10/17 Health Record Health Services 1025 North Broadway, K-254 Milwaukee, Wisconsin 53202 Phone: 414-277-7333 Fax: 414-277-2897 Student
For office use only: Jenzabar: / / MM DD YY (Initial) Revision date: 7/10/17 Health Record Health Services 1025 North Broadway, K-254 Milwaukee, Wisconsin 53202 Phone: 414-277-7333 Fax: 414-277-2897 Student
Practice Limited to Infants, Children, & Adolescents
 Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
Practice Limited to Infants, Children, & Adolescents 9290 SE Sunnybrook Blvd., #200, Clackamas, OR 97015 (503) 659-1694 5050 NE Hoyt St., #B55, Portland, Oregon 97213 (503) 233-5393 16144 SE Happy Valley
BOSTON COLLEGE BOYS BASKETBALL CAMP
 BOSTON COLLEGE BOYS BASKETBALL CAMP 2015 APPLICATION Conte Forum 224 Camp phone: 617-552-3003 Dan McDermott, Director Chestnut Hill, MA 02467 MBB Office: 617-552-3006 Evan Librizzi, Assistant Director
BOSTON COLLEGE BOYS BASKETBALL CAMP 2015 APPLICATION Conte Forum 224 Camp phone: 617-552-3003 Dan McDermott, Director Chestnut Hill, MA 02467 MBB Office: 617-552-3006 Evan Librizzi, Assistant Director
AGE Is the student age 18 or older? (If YES, please skip to signature section below) p YES p NO
 p YES p NO") New York Summer music FeStivaL PERMISSION FORM This form must be emailed or faxed to NYSMF before your arrival. StudentName _ Festival Year AGE Is the student age 18 or older? (If YES, please skip to signature
New York Summer music FeStivaL PERMISSION FORM This form must be emailed or faxed to NYSMF before your arrival. StudentName _ Festival Year AGE Is the student age 18 or older? (If YES, please skip to signature
Columbia Medical Practice- Pediatrics Ken Klebanow M.D. and Associates
 HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
HOWARD COUNTY HEALTH DEPARTMENT SCHOOL-BASED WELLNESS CENTERS PROGRAM TELEMEDICINE SERVICES A partnership between the Howard County Health Department and the Howard County Public School System What is
APPLICATION PACK BURJ DAYCARE NURSERY
 APPLICATION PACK BURJ DAYCARE NURSERY Child s Name: This application form must be fully completed and the necessary documents provided before a child can start at nursery. Child s Details Child s name:
APPLICATION PACK BURJ DAYCARE NURSERY Child s Name: This application form must be fully completed and the necessary documents provided before a child can start at nursery. Child s Details Child s name:
MOODY BIBLE INSTITUTE HEALTH SERVICE DEPARTMENT
 HEALTH SERVICE DEPARTMENT Welcome to Moody! Congratulations on your acceptance to the Moody Bible Institute! Health Service is available to assist you with health concerns you may have as a student here
HEALTH SERVICE DEPARTMENT Welcome to Moody! Congratulations on your acceptance to the Moody Bible Institute! Health Service is available to assist you with health concerns you may have as a student here
2017 Medi-Slim Weight Loss Patient Information Form
 Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
Medi-Slim Weight Loss Patient Information Form Patient Name (Last) (First) (MI) Name you prefer to be called: Patient Address: City:_ State Zip Phone number you would prefer us to use: May we email you?
Patient Centered Medical Home 2011 Standards
 PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
PCMH Standard 6 1 Patient Centered Medical Home 2011 Standards 2 Today s Agenda PCMH 6 PCMH 6 PCMH 6 Elements A-B Elements C-E Elements F-G Standard 6 A MEASURE PERFORMANCE PCMH 6A Measure Performance
Back-Up Care Advantage Program Registration Materials
 Registration Materials Dear Parent, Welcome to the Back-Up Care Advantage Program! An important part of preparing for a day of back-up care is ensuring that your care provider will have the information
Registration Materials Dear Parent, Welcome to the Back-Up Care Advantage Program! An important part of preparing for a day of back-up care is ensuring that your care provider will have the information
To be completed by healthcare provider
 Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
Allergy and Anaphylaxis Action Plan and Medication Orders Student s Name: D.O.B. Grade: School: Teacher: ALLERGY TO: Place child s photo here To be completed by healthcare provider History: Asthma: YES
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS
 NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
NURSING STUDENT HEALTH & IMMUNIZATION RECORDS *********************************** COMPLETE THE ATTACHED HEALTH PACKET AND SUBMIT TO THE NURSING DEPARTMENT NO LATER THAN THE ASN ORIENTATION. **************************************
Wabash Student Health Center
 Wabash Student Health Center Information and Instructions for Completing the Student Health Record Dear Incoming Wabash Student: Welcome to Wabash College! In order to make your experience at Wabash a
Wabash Student Health Center Information and Instructions for Completing the Student Health Record Dear Incoming Wabash Student: Welcome to Wabash College! In order to make your experience at Wabash a
Ambassador Program Application Packet
 Ambassador Program Application Packet Thank you for your interest in becoming an Ambassador at Centinela Hospital Medical Center. Please complete the attached forms and then contact the Centinela Hospital
Ambassador Program Application Packet Thank you for your interest in becoming an Ambassador at Centinela Hospital Medical Center. Please complete the attached forms and then contact the Centinela Hospital
REGISTRATION REQUIREMENTS
 IRVINGTON PUBLIC SCHOOLS REGISTRATION REQUIREMENTS INFORMATION ACCEPTED (2 Forms Required): Current: 1. PSE&G Bill 2. Homeowner s Tax Bill 3. Mortgage Statement 4. Department of Labor (Unemployment) 5.
IRVINGTON PUBLIC SCHOOLS REGISTRATION REQUIREMENTS INFORMATION ACCEPTED (2 Forms Required): Current: 1. PSE&G Bill 2. Homeowner s Tax Bill 3. Mortgage Statement 4. Department of Labor (Unemployment) 5.
MANDATORY HEALTH FORMS
 MANDATORY HEALTH FORMS All forms must be completed prior to enrollment Contact Information: School Nurse: nurse@grandriver.org Admissions: admissions@grandriver.org Checklist of Required Forms & Items:
MANDATORY HEALTH FORMS All forms must be completed prior to enrollment Contact Information: School Nurse: nurse@grandriver.org Admissions: admissions@grandriver.org Checklist of Required Forms & Items:
Hampton Roads Regional Schools Life-Threatening Allergy Management Protocol Forms
 Newport News Public Schools Hampton Roads Regional Schools Life-Threatening Allergy Management Protocol Forms Developed by the Hampton Roads School Nurse Managers Parents/Guardians: Please complete Life
Newport News Public Schools Hampton Roads Regional Schools Life-Threatening Allergy Management Protocol Forms Developed by the Hampton Roads School Nurse Managers Parents/Guardians: Please complete Life
RSU 25 ADULT AND COMMUNITY EDUCATION Create Your Path to Success
 Application/1 To: From: Re: CCMA Applicants RSU 25 Adult and Community Education Certified Clinical Medical Assistant Program Packet Enclosed is our CCMA packet. Please read this information carefully,
Application/1 To: From: Re: CCMA Applicants RSU 25 Adult and Community Education Certified Clinical Medical Assistant Program Packet Enclosed is our CCMA packet. Please read this information carefully,
KANSAS PACKET INSTRUCTIONS
 KANSAS PACKET ALL LOCATIONS EXCEPT HIGHLANDS AND SANTA FE TRAIL All of our programs are licensed by the Kansas Department of Health and Environment. This is a set of documents which is required by state
KANSAS PACKET ALL LOCATIONS EXCEPT HIGHLANDS AND SANTA FE TRAIL All of our programs are licensed by the Kansas Department of Health and Environment. This is a set of documents which is required by state
CAMP WASTAHI MEDICAL FORM DUE ON OR BEFORE JULY 1, 2018
 1 CAMP WASTAHI MEDICAL FORM DUE ON OR BEFORE JULY 1, 2018 CHECK LIST & INSTRUCTIONS FOR COMPLETING THIS FORM: This Medical Form is required EACH YEAR for every participant of Camp Wastahi. As a requirement
1 CAMP WASTAHI MEDICAL FORM DUE ON OR BEFORE JULY 1, 2018 CHECK LIST & INSTRUCTIONS FOR COMPLETING THIS FORM: This Medical Form is required EACH YEAR for every participant of Camp Wastahi. As a requirement
Welcome to St. Bonaventure University. We are glad you re here!
 Welcome to. We are glad you re here! The staff of the Center for Student Wellness in Doyle Hall welcomes you to the next step of your life: COLLEGE! We want to make sure you have the best experience possible
Welcome to. We are glad you re here! The staff of the Center for Student Wellness in Doyle Hall welcomes you to the next step of your life: COLLEGE! We want to make sure you have the best experience possible
VETERINARY & BIOMEDICAL SCIENCES SUMMER CAMP-2018 REGISTRATION FORM
 1 VETERINARY & BIOMEDICAL SCIENCES SUMMER CAMP-2018 REGISTRATION FORM When: Residential camp: June 24 (Sunday)-June 29 (Friday), 2018 Commuters: June 25 (Monday)-June 29, 2018 In order to get personal
1 VETERINARY & BIOMEDICAL SCIENCES SUMMER CAMP-2018 REGISTRATION FORM When: Residential camp: June 24 (Sunday)-June 29 (Friday), 2018 Commuters: June 25 (Monday)-June 29, 2018 In order to get personal
Fulcrum Orthopaedics Patient Registration Packet
 Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
Fulcrum Orthopaedics Patient Registration Packet 2 Patient Information Form 8 Consent for Use and Disclosure of Information 9 Authorization for Use and Disclosure of Protected Health Information 10 Notice
*** Program Guidelines ***
 *** Program Guidelines *** *The Junior Volunteer program has a limited number of available positions. Placement decisions will be based upon first come, first serve. Volunteers must be at least 15 years
*** Program Guidelines *** *The Junior Volunteer program has a limited number of available positions. Placement decisions will be based upon first come, first serve. Volunteers must be at least 15 years
Additionally, the parent or legal guardian must provide the following documents upon registration of a new student:
 Montgomery County Public Schools requires several documents upon registration of a new student. Below is a list of documents which may be downloaded and reviewed and/or completed by the parent or legal
Montgomery County Public Schools requires several documents upon registration of a new student. Below is a list of documents which may be downloaded and reviewed and/or completed by the parent or legal
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip
 PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
PATIENT INFORMATION Name: Date of Birth Address: City: State: Zip Primary Phone ( ) Secondary Phone ( ) Other Phone ( ) SS# - - Race Ethnicity Email address Preferred language Marital Status Minor Single
Pediatric New Patient Form
 Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
Pediatric New Patient Form Internal Medicine & Pediatrics Patient Information Today's Date: Legal Name: Gender: M / F Date of Birth: Age: Race : Ethnicity: E-mail Address: Other: Home Address: Primary
FROM THE DESK OF THE SCHOOL NURSE School Year
 FROM THE DESK OF THE SCHOOL NURSE School Year 2016-2107 Dear Parents, Our goal is to provide for the health and well being of your child while s/he is attending school. Please read this letter carefully,
FROM THE DESK OF THE SCHOOL NURSE School Year 2016-2107 Dear Parents, Our goal is to provide for the health and well being of your child while s/he is attending school. Please read this letter carefully,
Food / Insect Allergy Action Plan
 Food / Insect Allergy Action Plan 2017-2018 Student s Name: of Birth: Teacher Allergy to: Asthmatic: Yes* No Grade *Higher risk for severe reaction Step 1: Treatment Symptoms Give Checked Medication**
Food / Insect Allergy Action Plan 2017-2018 Student s Name: of Birth: Teacher Allergy to: Asthmatic: Yes* No Grade *Higher risk for severe reaction Step 1: Treatment Symptoms Give Checked Medication**
Extended Day Registration Packet
 St. Benedicts School Extended Day Registration Packet 2014 2015 School Year 4811 Wallingford Avenue North Seattle, Washington 98103 206-518.6009 l.wescott@stbens.net A Registration Packet Contents The
St. Benedicts School Extended Day Registration Packet 2014 2015 School Year 4811 Wallingford Avenue North Seattle, Washington 98103 206-518.6009 l.wescott@stbens.net A Registration Packet Contents The
CENTRAL JERSEY COLLEGE PREP
 CENTRAL JERSEY COLLEGE PREP CHARTER SCHOOL Dear Parents/Guardians, Congratulations and welcome to the Central Jersey College Prep Charter School. We will do our best to help you with the enrollment process.
CENTRAL JERSEY COLLEGE PREP CHARTER SCHOOL Dear Parents/Guardians, Congratulations and welcome to the Central Jersey College Prep Charter School. We will do our best to help you with the enrollment process.
Naturopathic Wellness Center
 Naturopathic Wellness Center Ashley G. Lewin, N.D. Erica Waters, ND Mychael Seubert, ND Pediatric Intake Birth to 3 years Name Sex Date of Birth / / Age Parent(s)/Guardian(s) Address City/State/Zip Telephone
Naturopathic Wellness Center Ashley G. Lewin, N.D. Erica Waters, ND Mychael Seubert, ND Pediatric Intake Birth to 3 years Name Sex Date of Birth / / Age Parent(s)/Guardian(s) Address City/State/Zip Telephone
Patient s Full Name DOB Age. Patient s SSN Sex: Male Female Preferred Language. Place of Birth: City State Country
 Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Hoover Hearing Clinic A division of Hoover ENT Hoover, Alabama 35244 205-733-9694 Tel PATIENT INFORMATION ACCOUNT # DATE MD NEW UPDATE Patient s Full Name DOB Age Patient s SSN Sex: Male Female Preferred
Patient Information. Date of Birth Sex Marital Status / / Male Female Single Married Other. Address
 Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
Patient Information Patient Information Date of Birth Sex Marital Status Male Female Single Married Other Social Security Number - - Why We Ask for Race and Ethnicity Patient Goes By: Email Address In
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D KLONDIKE RD SW SUITE 205 CONYERS, GA TELEPHONE FAX
 PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
PEDIATRIC CENTER FOR WELLNESS, P.C. CRYSTAL B. HOOD, M.D. 1506 KLONDIKE RD SW SUITE 205 CONYERS, GA 30094 678-750-4000 TELEPHONE 678-750-4005 FAX www.pcfwellness.com Dear Family, We are excited to welcome
LONE STAR COLLEGE-TOMBALL DOCUMENTATION OF REQUIRED IMMUNIZATIONS Please Print
 LONE STAR COLLEGE-TOMBALL DOCUMENTATION OF REQUIRED IMMUNIZATIONS Please Print Name: (Last) (First) (MI) of Birth ID# Enrollment All students enrolled in health related courses who have or will have any
LONE STAR COLLEGE-TOMBALL DOCUMENTATION OF REQUIRED IMMUNIZATIONS Please Print Name: (Last) (First) (MI) of Birth ID# Enrollment All students enrolled in health related courses who have or will have any
TOS Health Questionnaire
 Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
Name Referring Physician Main Reason for Medical Evaluation of Injury/Length of symptoms: Is this a work related problem? Y N Are you right or left handed? Occupation What treatment have you received for
Department of State Academic Exchanges Participant Medical History and Examination Form
 Department of State Academic Exchanges Participant Medical History and Examination Form Having been selected to participate in a U.S. Department of State educational exchange program, you are required
Department of State Academic Exchanges Participant Medical History and Examination Form Having been selected to participate in a U.S. Department of State educational exchange program, you are required
Pediatric New Patient Intake Form
 Name: DOB: Page 1 of 5 Pediatric New Patient Intake Form Patient Information Last Name: First Name: DOB: Home Mobile Preferred (circle) : Home / Cell Email: Gender: Primary Pediatrician: Pediatrician Address:
Name: DOB: Page 1 of 5 Pediatric New Patient Intake Form Patient Information Last Name: First Name: DOB: Home Mobile Preferred (circle) : Home / Cell Email: Gender: Primary Pediatrician: Pediatrician Address:
Dodge. County. Schools
 Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
Welcome to the Dodge School Based Health Clinic. Dodge Board of Education and Dodge Connection-Communities In of Dodge, Inc. are continuing to move forward with our goal of serving the children and families
12 King Philip Rd. Sudbury, MA (585)
") Dear Parents, In order to get started with speech therapy services including screening, evaluation, and treatment, we ask that you submit the following registration paperwork to Sudbury Speech and Language
Dear Parents, In order to get started with speech therapy services including screening, evaluation, and treatment, we ask that you submit the following registration paperwork to Sudbury Speech and Language
DEPN AND GRADUATE NURSING MANDATORIES INFORMATION
 DEPN AND GRADUATE NURSING MANDATORIES INFORMATION INITIAL MANDATORIES DUE AUGUST 15, 2018 Pre Clinical Mandatories Form If you have a first time positive PPD, include a radiology report If you have a history
DEPN AND GRADUATE NURSING MANDATORIES INFORMATION INITIAL MANDATORIES DUE AUGUST 15, 2018 Pre Clinical Mandatories Form If you have a first time positive PPD, include a radiology report If you have a history
(Please Print) PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )
 PATIENT INFORMATION. Sex: Male Female Home phone no: ( ) City: State: Zip: Cell phone no: ( ) Occupation: Employer: Work phone no: ( )") (Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
(Please Print) Today s date: Primary Care Physician: PATIENT INFORMATION First name: Middle: Last: Former name: Marital Status: Single Married Divorced Widowed Street address: Birthdate: SSN: Email Address:
MOORE COUNTY. 4-H Enrollment Form. Name of 4-H Club/Group: Year: Jan 2018 Dec 2018 Member Name: First Middle Last
 4-H Enrollment Form Name of 4-H Club/Group: Year: Jan 2018 Dec 2018 Member Name: First Middle Last Address: Phone:( ) Email: County: Gender*: Male Female Date of Birth: Grade: School Attending: If re-enrolling
4-H Enrollment Form Name of 4-H Club/Group: Year: Jan 2018 Dec 2018 Member Name: First Middle Last Address: Phone:( ) Email: County: Gender*: Male Female Date of Birth: Grade: School Attending: If re-enrolling
School Based Health Services Consent Form
 MRN: PCP: Teacher: Grade: School Based Health Services Consent Form Before your child sees a provider, we are asking you to authorize medical and/ or dental treatment. We will work with you to improve
MRN: PCP: Teacher: Grade: School Based Health Services Consent Form Before your child sees a provider, we are asking you to authorize medical and/ or dental treatment. We will work with you to improve
Adventure Club. Before and After School Care Enrollment Packet. Before and After School Care Mission:
 Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
Adventure Club Before and After School Care Enrollment Packet Before and After School Care Mission: Our before and after school care is designed to provide children with a safe, loving and exciting environment
Total Grace Achievers Academy Summer Camp Enrollment Application. Where kids can experience Life and Learn to Achieve
 Total Grace Achievers Academy Summer Camp Enrollment Application Where kids can experience Life and Learn to Achieve Student Information Child s Name DOB Age Grade School: Street Address City State Zip
Total Grace Achievers Academy Summer Camp Enrollment Application Where kids can experience Life and Learn to Achieve Student Information Child s Name DOB Age Grade School: Street Address City State Zip
REGISTRATION FORM. Parent Name Relationship to child. Address (if different) . Place of employment Hours - Work phone
 . Place of employment Hours - Work phone") REGISTRATION FORM FUN FITNESS CAMP All forms can be filled electronically. Please complete forms and submit with original signature and registration fee. Child s name Age Sex Address State City Zip Date
REGISTRATION FORM FUN FITNESS CAMP All forms can be filled electronically. Please complete forms and submit with original signature and registration fee. Child s name Age Sex Address State City Zip Date
School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE Phone: Fax:
 Dear Parents/Guardians: School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE 19807 Phone: 651-2100 Fax: 651-2111 The Wilmington Charter/Cab Calloway
Dear Parents/Guardians: School-Based Health Center Wilmington Charter/Cab Calloway High Schools 100 N. Dupont Road Wilmington, DE 19807 Phone: 651-2100 Fax: 651-2111 The Wilmington Charter/Cab Calloway
Hope Academy of Public Service GENERAL STUDENT INFORMATION
 Hope Academy of Public Service GENERAL STUDENT INFORMATION First Name: Middle Name: Last Name: SSN: Current Grade: Birth date: Age: Gender: M or F Ethnicity (check one): Primary Race (check only one):
Hope Academy of Public Service GENERAL STUDENT INFORMATION First Name: Middle Name: Last Name: SSN: Current Grade: Birth date: Age: Gender: M or F Ethnicity (check one): Primary Race (check only one):
MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM
 Entry : Homeroom Teacher: NEW STUDENT ENROLLMENT ONLY MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
Entry : Homeroom Teacher: NEW STUDENT ENROLLMENT ONLY MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
2201 Murphy Avenue, Suite 307 Nashville, TN Phone Fax Date. Patient s Full Name
 Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
Patient Information 2201 Murphy Avenue, Suite 307 Nashville, TN 37203 Phone 615-401- 9454 Fax 615-873- 1934 www.robbinsplasticsurgery.com Date Patient s Full Name Last First M.I. Preferred Name (if different
If you would like to volunteer in the Gift Shop as part of the Hospital Auxiliary, please call for additional information.
 Dear Prospective Volunteer. Thank you for your interest in the volunteer program at Robert Wood Johnson University Hospital Rahway. We are happy to know that you are considering becoming a part of the
Dear Prospective Volunteer. Thank you for your interest in the volunteer program at Robert Wood Johnson University Hospital Rahway. We are happy to know that you are considering becoming a part of the
Date: PATIENT REGISTRATION Chart # PLEASE PRINT FILL OUT ALL AREAS PATIENT INFORMATION CHILD S NAME BIRTHDATE SSN SEX CELL PHONE# (14 YRS & OLDER)
") PEDIATRIC ASSOCIATES OF MADISON 21 Hughes Rd., Suite 2 Madison, Alabama 35758 256-772-2037 Fax 256-772-9523 www.pedsofmadison.com Tonya T. Zbell, M.D. Robbie F. Dudley, M.D. Charlotte M. Meadows, M.D.
PEDIATRIC ASSOCIATES OF MADISON 21 Hughes Rd., Suite 2 Madison, Alabama 35758 256-772-2037 Fax 256-772-9523 www.pedsofmadison.com Tonya T. Zbell, M.D. Robbie F. Dudley, M.D. Charlotte M. Meadows, M.D.
VOLUNTEER APPLICATION
 Please return to: Mount Nittany Medical Center Volunteer Services Department 1800 East Park Avenue State College, PA 16803 814.234.6170 VOLUNTEER APPLICATION Application Date Assignment Interview Date!
Please return to: Mount Nittany Medical Center Volunteer Services Department 1800 East Park Avenue State College, PA 16803 814.234.6170 VOLUNTEER APPLICATION Application Date Assignment Interview Date!
2018 Summer Camp Registration
 018 Summer Camp Registration Maple Branch Kinder Camp Ages 3-5 P: (69) 345-96 x 167 E: childcare@kzooymca.org F: (69) 34-4088 Child s Name: Birth date: Male/Female: Age Today s Date: (child must be fully
018 Summer Camp Registration Maple Branch Kinder Camp Ages 3-5 P: (69) 345-96 x 167 E: childcare@kzooymca.org F: (69) 34-4088 Child s Name: Birth date: Male/Female: Age Today s Date: (child must be fully
Hello and Welcome! I truly look forward to working with you and your child on the journey towards optimal health. Warmly, Amanda H.
 Hello and Welcome! Attached you will find pediatric intake forms. Before your child s scheduled appointment, please fill out the forms as thoroughly as possible. I know your time is valuable and by bringing
Hello and Welcome! Attached you will find pediatric intake forms. Before your child s scheduled appointment, please fill out the forms as thoroughly as possible. I know your time is valuable and by bringing
Sick Kids' Family Journal
 Sick Kids' Family Journal Working together sharing all that we know This Journal belongs to 2000 555 University Avenue, Toronto, ON, Canada M5G 1X8 How to Use Your Sick Kids Family Journal What is the
Sick Kids' Family Journal Working together sharing all that we know This Journal belongs to 2000 555 University Avenue, Toronto, ON, Canada M5G 1X8 How to Use Your Sick Kids Family Journal What is the
MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM
 NEW STUDENT ENROLLMENT ONLY Entry : Homeroom Teacher: MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
NEW STUDENT ENROLLMENT ONLY Entry : Homeroom Teacher: MONTGOMERY COUNTY SCHOOLS STUDENT INFORMATION FORM Student s Legal Name: Last First Middle Suffix Social Security Number: / / of Birth: Birthplace:
SUMMER CAMP REGISTRATION
 SUMMER CAMP REGISTRATION 018 Please fill out both sides completely and return to: Grand Traverse Bay YMCA 3000 Racquet Club Drive, Traverse City, MI 49684 31-933-96 Fax 31-947-0651 Camper Information:
SUMMER CAMP REGISTRATION 018 Please fill out both sides completely and return to: Grand Traverse Bay YMCA 3000 Racquet Club Drive, Traverse City, MI 49684 31-933-96 Fax 31-947-0651 Camper Information:
PRE-K ENROLLMENT APPLICATION
 Student Name First Middle Last Date of Birth PRE-K ENROLLMENT APPLICATION 2017-18 Early Childhood Program Fill out this application if your student is applying to an Early Childhood School. Required Documents
Student Name First Middle Last Date of Birth PRE-K ENROLLMENT APPLICATION 2017-18 Early Childhood Program Fill out this application if your student is applying to an Early Childhood School. Required Documents
Pediatrics How-to Guide for TRICARE Beneficiaries. Readiness Better Care Trusted Care, Anywhere Best Value Better Health
 Pediatrics How-to Guide for TRICARE Beneficiaries Pediatric Clinic Operations How to Set Up an Appointment Appointment Line 722-1802 (0700-1630) Call early for same day appointment! 1. The Appointment
Pediatrics How-to Guide for TRICARE Beneficiaries Pediatric Clinic Operations How to Set Up an Appointment Appointment Line 722-1802 (0700-1630) Call early for same day appointment! 1. The Appointment
MEDICAL LABORATORY SCIENCE MANDATORIES INFORMATION
 MEDICAL LABORATORY SCIENCE MANDATORIES INFORMATION FIRST YEAR MANDATORIES HIPAA/OSHA Training You will complete your training through the Evolve e Learning Solutions website. You will receive an email
MEDICAL LABORATORY SCIENCE MANDATORIES INFORMATION FIRST YEAR MANDATORIES HIPAA/OSHA Training You will complete your training through the Evolve e Learning Solutions website. You will receive an email
Health & Safety Packet for Incoming Students
 Health Occupations Division 707-256-7600 Health & Safety Packet for Incoming Students This packet has been designed to help Health Occupations students comply with CPR and health/physical documentation
Health Occupations Division 707-256-7600 Health & Safety Packet for Incoming Students This packet has been designed to help Health Occupations students comply with CPR and health/physical documentation
Camp JRA will be held at Camp Victory in Millville, PA, from July 19-24, Counselors are required to attend staff orientation on July 18 th.
 Dear Prospective Counselor, Thank you for your interest in being a Camp JRA (Juveniles Reaching Achievement) counselor. We are excited to be planning for a fun-filled week for our campers in 2015. Camp
Dear Prospective Counselor, Thank you for your interest in being a Camp JRA (Juveniles Reaching Achievement) counselor. We are excited to be planning for a fun-filled week for our campers in 2015. Camp
PAYMENT IS REQUIRED AT THE TIME SERVICES ARE RENDERED. THANK YOU!
 PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
PATIENT INFORMATION FORM PATIENT DATA: - - PATIENT NAME (LAST, FIRST, MIDDLE) SOCIAL SECURITY # SEX ( ) - ( ) - ADDRESS HOME PHONE NUMBER MOBILE PHONE NUMBER CITY STATE ZIP CODE OCCUPATION / / DATE OF
Broomall Patients ONLY may send forms via to:
 Thank you for choosing Children s Dentistry! To expedite your check in, please complete the forms in this packet and bring with you to your appointment. You may also FAX these forms to the office where
Thank you for choosing Children s Dentistry! To expedite your check in, please complete the forms in this packet and bring with you to your appointment. You may also FAX these forms to the office where
Health History and Examination Form for Children, Youth and Adults Attending Camps
 Health History and Examination Form for Children, Youth and Adults Attending Camps Suggested for resident camp use. Developed and approved by American Camping Association American Academy of Pediatrics
Health History and Examination Form for Children, Youth and Adults Attending Camps Suggested for resident camp use. Developed and approved by American Camping Association American Academy of Pediatrics
Pediatric Patient History
 Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Pediatric Patient History Childs Name: Today s Date: Primary Doctor: Date of Birth: Age: Reason for visit: List all chronic medical problems: List all medication dosages and frequency taken (including
Palmetto Health Tuomey Student Volunteer Application Application to be completed by the student, NOT the parent. Full Name: Phone: (
 1 Palmetto Health Tuomey Student Volunteer Application Application to be completed by the student, NOT the parent. Full Name: Phone: ( ) Email address: Cell Phone: ( ) Address: City: Zip: Social Security
1 Palmetto Health Tuomey Student Volunteer Application Application to be completed by the student, NOT the parent. Full Name: Phone: ( ) Email address: Cell Phone: ( ) Address: City: Zip: Social Security
EMERGENCY CONTACT INFORMATION LIST ALL OTHER ADULTS YOU AUTHORIZE CONNECT STAFF TO RELEASE YOUR CHILD TO:
 AFTER SCHOOL PROGRAM Fall Spring CHILD PERSONAL DATA SHEET Child s DOB Home Address City State Zip Gender School Enrolled in: : Employer Email : Employer Email Work APP Requested Work APP Requested EMERGENCY
AFTER SCHOOL PROGRAM Fall Spring CHILD PERSONAL DATA SHEET Child s DOB Home Address City State Zip Gender School Enrolled in: : Employer Email : Employer Email Work APP Requested Work APP Requested EMERGENCY
Opening Day for the School Year. Tuesday, August 15, 2017 for all schools in. Lompoc Unified School District
 Opening Day for the 2017-2018 School Year Tuesday, August 15, 2017 for all schools in Lompoc Unified School District GENERAL REGISTRATION INFORMATION ALL STUDENTS - GRADES K-12 PARENTS OR GUARDIANS MUST
Opening Day for the 2017-2018 School Year Tuesday, August 15, 2017 for all schools in Lompoc Unified School District GENERAL REGISTRATION INFORMATION ALL STUDENTS - GRADES K-12 PARENTS OR GUARDIANS MUST
NEW PATIENT INFORMATION: ADULT
 NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
NEW PATIENT INFORMATION: ADULT Patient Last Name: Patient First Name: Patient Middle Name: DOB: Sex: M F SSN: Address: City: Zip: Home Phone: Cell Phone: Email: EMERGENCY CONTACT INFORMATION Last Name:
MAIN STREET MEDICAL NEW PATIENT QUESTIONNAIRE
 NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
NEW PATIENT QUESTIONNAIRE Patient Name: Date: Date of Birth: SSN: Male Female Guarantor Name: SSN: DOB: Home Phone: Cell Phone: Street Address: Apt#: City: State: Zip: Billing Address (if different): Email
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease
 Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
Allergy Consultants, P.A. Visit Date: Specialist in Pediatric and Adult Allergy, Asthma, and Sinus Disease Arthur Fost, M.D. David Fost, M.D. Satya Narisety, M.D. Anthony J. Piccolo, PA-C Patient s Name
2.. The two persons trained shall be regular members of the school staff, which ensures at least one of the two being present during school hours.
 STUDENTS August 30, 2012 STUDENTS Health Services Allergic Reactions When a student s physician prescribes emergency allergy injections and related medication (Epinephrine, EpiPen, EpiPen Jr.), and there
STUDENTS August 30, 2012 STUDENTS Health Services Allergic Reactions When a student s physician prescribes emergency allergy injections and related medication (Epinephrine, EpiPen, EpiPen Jr.), and there
Homestay Agreement Please read this thoroughly
 Homestay Agreement Please read this thoroughly To treat the Host s home as you would your own home, with respect and courtesy If you have permission to share the house with a student of the same nationality,
Homestay Agreement Please read this thoroughly To treat the Host s home as you would your own home, with respect and courtesy If you have permission to share the house with a student of the same nationality,
Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM
 Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM TO THE PHYSICIAN: Southwestern College requires a physical examination for students enrolling in the Nursing and Health
Southwestern College Nursing & Health Occupations Programs MEDICAL EXAMINATION FORM TO THE PHYSICIAN: Southwestern College requires a physical examination for students enrolling in the Nursing and Health
Oregon State University School of Biological and Population Health Sciences KIN 344: Pre-Therapy/Allied Health Practicum.
 KIN 344: Pre-Therapy/Allied Health Practicum Checklist Obtain application packet and read all enclosed information Complete the Application Form Complete the Immunization Form Attach copies of medical
KIN 344: Pre-Therapy/Allied Health Practicum Checklist Obtain application packet and read all enclosed information Complete the Application Form Complete the Immunization Form Attach copies of medical
ADMISSION INFORMATION
 Texas Dept of Family and Protective Services ADMISSION INFORMATION Form 2935 Aug 2010 / Pg 1 of 3 Operation Name The Stepping Stone Director s Name Ashley Stock Child s Full Name Child s of Birth Child
Texas Dept of Family and Protective Services ADMISSION INFORMATION Form 2935 Aug 2010 / Pg 1 of 3 Operation Name The Stepping Stone Director s Name Ashley Stock Child s Full Name Child s of Birth Child