Moving Healthcare Upstream: Using Quality Improvement to Improve Social Determinants of Health and Clinical Care
|
|
|
- Sharlene Wood
- 6 years ago
- Views:
Transcription
1 Moving Healthcare Upstream: Using Quality Improvement to Improve Social Determinants of Health and Clinical Care Rishi Manchanda MD

2 Social factors contribute up to 60% of premature death Contribution of Social Factors to Premature Mortality Schroeder S. N Engl J Med 2007;357:
3

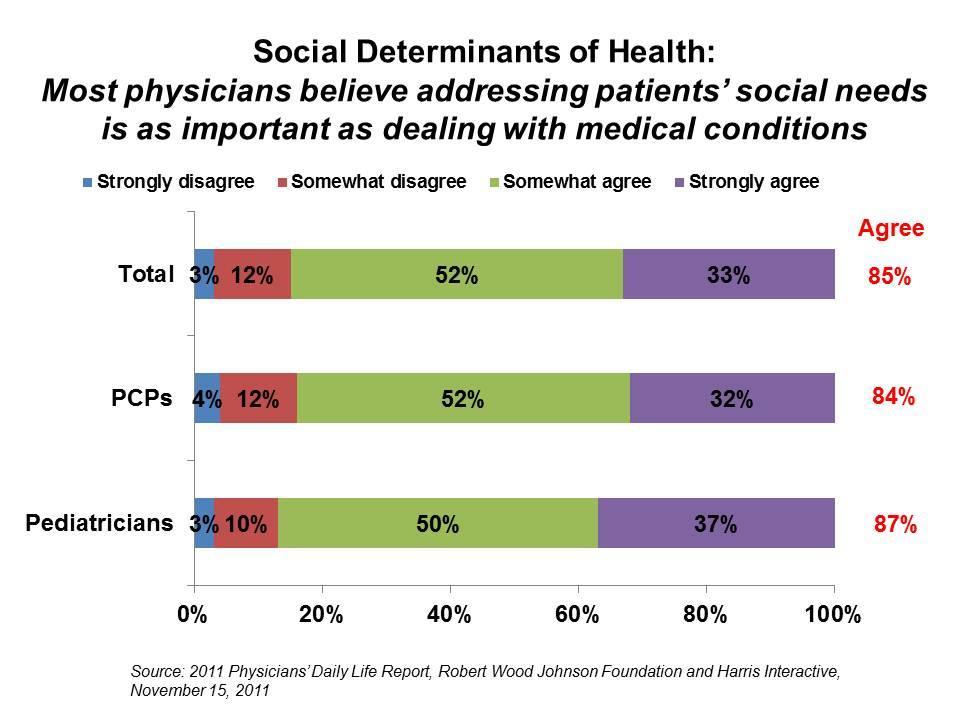
4 Robert Wood Johnson Foundation Health Care s Blind Side December 2011 Propietary/ Confidential

5 How do we move to the NEW way while getting paid for the OLD way? and NEW the while getting paid for a way at same time?

6


7 A workforce model for US healthcare by 2020 By 2020, 25,000 Populationlevel Impact of healthcare 260, ,000
8 Moving Healthcare Upstream HealthBegins.org 1. Mobilize An online network - over 1200 members & growing 2. Equip Upstream Quality Improvement & Practice Redesign Community Health Detailing Campaigns 3. Design Identify Tools and Create Opportunities With partners: Providers, Payers, AMCs, Clinics, Health











9

10 Upstreamists apply common methods to diverse challenges Male youth with high rates of violent injuries Children with Asthma and Allergies due to Substandard Housing Obese children with school absences and depression Young high-risk pregnant women with financial illiteracy Diabetics with frequent hypoglycemiarelated hospitalizations And so on
11 What Makes A Successful Upstreamist? A. Starts with the perfect idea B. Finds a plan that works before running out of resources
12 Quality Improvement in healthcare Late 1990s: Shift from QA to QI Measuring mistakes process redesign Rapid assessment, dynamic implementation, & simpler techniques to measure progress in closing quality gaps Less academic, more results-oriented and lean Core idea = maximize patient value while minimizing waste* 12
13 Volume-based, biomedical views have limited sphere of influence for QI Where does clinical QI focus?
14 How many healthcare Plan-Do-Study-Act cycles (PDSAs) address social factors? Act Plan Study Do
15 PDSAs & QI Tools can be repurposed to address upstream problems Some tools are useful in planning stage Upstreamist Project Canvas Process mapping Pareto Cause and effect diagrams Others help you implement QI project Check lists Others help you study the impact of your QI project Run charts
16 We ll plan an Upstream QI solution for poorly controlled diabetics with food insecurity using the Upstream Project Canvas
17 For this case study, let s focus on food insecurity Food insecurity a household-level economic and social condition of limited or uncertain access to adequate food Hunger is an individual-level physiological condition that may result from food insecurity. One in seven Americans cannot reliably afford food USDA definition Wang EA et al (2013). A Pilot Study Examining Food Insecurity and HIV Risk Behaviors Among Individuals Recently Released From Prison. AIDS Education and Prevention: Vol. 25, No. 2, pp H. K. Seligman, et al Exhaustion of Food Budgets at Month's End and Hospital Admissions for Hypoglycemia," Health Affairs, Jan (1): Weiser SD et al. (2007) Food Insufficiency Is Associated with High-Risk Sexual Behavior among Women in Botswana and Swaziland. PLoS Med 4(10):
18 17 million Food insecure children 91% more likely to be in fair or poor health 31% more likely to require hospitalization Stanford Social Innovation Review, Summer 2012.
19 Upstream impact on Triple Aim Among low-income diabetics, food insecurity linked to 27% increase in hospital admissions at end-of-month vs beginning of month
20 Case Study: FoodRx for at-risk Diabetics - Improve Screening of Food Insecurity by 30% within 1 year - Improve Provider Confidence and Patient Satisfaction by 30% within 12 months - Improve Health Outcomes for Food-Insecure patients by 30% within 12 months
21 Upstream healthcare organizational assessment (Manchanda 2015, in press) Favorable environment (social norms/external incentives/regulations/state contracts/community partners) Perceived value of change among stakeholders Executive sponsorship Integration in clinical services and workflows Integration in sustainable financing structure Scope (Population/Geography and/or Number of SDOH addressed) Program Design Components (including Evaluation and defined Metrics of success) Team Roles/project ownership Dedicated infrastructure (including Information Systems and Human Resources) Continuous Performance/ Quality Improvement processes Total Limited or unclear Moderate Robust
22 An orientation to the canvas
23
24 Upstream QI Project Canvas 1. Identify Patient Population 2. Team formation 3. Analyze Current State (Define Problems and Root Causes) 4. Team Goal (Unique Value Proposition) 5. Develop Upstream QI Solution 6. Identify Key Partners & Roles 7. Identify Channels 8. Key Metrics for Evaluation & Monitoring 9. Financing
25 Guidelines 1. Sketch a canvas in one sitting 3. Think in the present 2. It s okay to leave sections blank 4. This is a tool for engaging clinic staff in upstream action

26 1. Choose Your Population List your target population Reflect on clinic and community interests
27 1. Population Whose needs are you not meeting to achieve the Triple Aim? Assess Clinic priorities: PCMH certification High-utilizer patients No shows Productivity Assess Community priorities: Is the community concerned about a specific set of social or environmental issues? Have you asked?

28 1. Identify Priority Population (your early adopters of an upstream approach) using Segmentation Split broad List the characteristics of your population target patient into population segments most to hone likely to use in on service target now. group. List the attributes of your target patient population. What do they do? do? What do they prefer? Where do they live, Where work, learn do or they play? live, work, eat, learn or play?
29 Population Segmentation: Bridges to Health Adapted from: Lynn J, Straube BM, Bell KM, Jencks SF, Kambic RT. Using population segmentation to provide better health care for all: the Bridges to Health model. Milbank Q Jun;85(2): Population Patient and Services 1. Healthy Mr. Smith, a 37-year-old carpenter. Sees PCP for an annual checkup and screenings. Occasional sore throat 2. Maternal and infant health Mrs. Brown, a 26-year-old waitress, normal pregnancy and delivery. newborn gets checkups and immunizations. 3. Acutely ill Mr. Jones, an 18-year-old high school student, broke his femur while playing football. Got surgery, PT. returned to team after 2 months. 4. Chronic conditions, normal function 5. Stable but serious disability 6. Short period of decline before dying 7. Limited reserve and exacerbations 8. Frailty, with or without dementia Mrs. Gomez, a 49-year-old teacher, has hypertension and diabetes, occasionally out of control despite classes. See PCP regularly. Mr. White, a 56-year-old telemarketer, former paratrooper, now quadriplegic from a gunshot wound. lives with his brother, has a paid aide for personal care. Mrs. Black, a 68-year-old realtor, recently dx d with metastatic ovarian carcinoma. losing weight after chemo. accepted hospice services Mr. Simon, a 75-year-old executive, severely limited activity due to emphysema. home oxygen and complex med regimen. Has Caregivers, Frequent use of clinical care Mrs. Evans, an 88-year-old former homemaker, has dementia with incontinence, inability to walk or to communicate verbally, and a serious pressure ulcer. Has family + professional caregivers.
30 Segmentation: Use Triple Aim metrics to Prioritize Population Patient 1. Healthy Mr. Smith, 37, carpenter 2. Maternal and infant health Mrs. Brown, 26, waitress and infant 3. Acutely ill Mr. Jones, 18, student 4. Chronic conditions, normal function 5. Stable but serious disability Mrs. Gomez, 49, teacher Mr. White, 56, telemarketer Outcomes 1- year Good. Occasional sore throat Good. Healthy mom and infant Good. Functional recovery Poor. Poorly controlled diabetes and hypertension Fair. Quadriplegic, ADLs met. Medical Problems (1 year) low cost low-med high, acute high, chronic + acute High, chronic Quality/satisfactio n med high high Low-med med Priority Population for Upstream QI X 6. Short period of decline before dying Mrs. Black, 68, realtor Poor. metastatic ovarian carcinoma. Fatigued, losing weight. High, acute low 7. Limited reserve and exacerbations Mr. Simon, 75, executive Poor. severely limited activity High, acute + chronic Low-med X 8. Frailty, with or without dementia Mrs. Evans, 88, homemaker Fair. dementia with incontinence, High, chronic Mod X Adapted from: Lynn J, Straube BM, Bell KM, Jencks SF, Kambic RT. Using population segmentation to provide better health care for all: the Bridges to Health model. Milbank Q Jun;85(2):
31 Adapted from: Lynn J, Straube BM, Bell KM, Jencks SF, Kambic RT. Using population segmentation to provide better health care for all: the Bridges to Health model. Milbank Q Jun;85(2): Priority Population: What Social Determinants might matter? Population Patient Status 1. Healthy Mr. Smith, 37, carpenter 2. Maternal and infant health Mrs. Brown, 26, waitress and infant Stable. Low cost, high quality Good. Low-med costs, high quality Priority Population Social Determinants Hypotheses 3. Acutely ill Mr. Jones, 18, student Recovery. High, acute costs. High quality 4. Chronic conditions, normal function Mrs. Gomez, 49, teacher Poor. High acute + chronic costs. Low-med quality. Adult diabetics Food insecurity, poverty 5. Stable but serious disability Mr. White, 56, telemarketer Fair. High, chronic costs. Medium quality 6. Short period of decline before dying Mrs. Black, 68, realtor Poor. High, acute costs. Low quality 7. Limited reserve and exacerbations Mr. Simon, 75, executive Poor. High, chronic costs, low-med quality X Food insecurity, poverty, social isolation, substandard housing 8. Frailty, with or without dementia Mrs. Evans, 88, homemaker Fair. High chronic costs, med quality. X Housing insecurity, social isolation, safety
?")
32 2. Team Formation Who needs to be on the team? From healthcare? From community partner(s)? What motivates each team member and what type of power can they leverage?
33 Team member analysis
34 Team Member Organization Role Upstream QI duties Terry Stotts RN Care Manager (Team Captain/Champion) Identify panel of diabetics with recent admissions. Coordinate QI effort. Arran Afflalo LVN Screen for Food Insecurity among diabetics/ chart scrubbing Steve Blake Clinic Social Worker Coordinate Food Resources and Track Referrals Alonzo Gee Food Bank Program Coordinator Accept referrals and coordinate referrals and client assessments Robin Lopez Primary Care Physician/ QI Committee Member Approves standing order to refer food insecure pts; obtains QI Committee resources Dorell Wright CIO Incorporates Food Insecurity in EMR/ Report generation/ QI measures
35 Upstream QI Project Canvas 1. Identify Patient Population 2. Team formation 3. Analyze Current State (Define Problems and Root Causes) 4. Team Goal (Unique Value Proposition) 5. Develop Upstream QI Solution 6. Identify Key Partners & Roles 7. Identify Channels 8. Key Metrics for Evaluation & Monitoring 9. Financing

36 3. Problem List the problems facing your target population. Start with the health problem of interest. Then list upstream causes Proximate Underlying Principal Secondary

37 Changing Perspective on Root Cause Analysis Upstreamist Comprehensivist Partialist
38 Problem Proximate Cause Hospitalizations due to hypoglycemia among low-income diabetics Hypoglycemia Underlying Cause Underlying Cause of Underlying Cause (Principal) Root Cause Secondary Cause Addressable Cause Food Insecurity Less Feasible to
39 Problem Frequent ER visits due to migraines and URIs Proximate Cause Underlying Cause Underlying Cause of Underlying Cause (Principal) Root Cause Secondary Cause Addressable Cause Less Feasible to Address Cause Viral Infection, Chronic Sinus Congestion, stress, lack of sleep Allergen exposures in damp, moldy, roach-filled apartment Landlord fails to fix water leaks or improve ventilation Outdoor air pollution Damp, moldy housing Air pollution
40 Adapted from: Lynn J, Straube BM, Bell KM, Jencks SF, Kambic RT. Using population segmentation to provide better health care for all: the Bridges to Health model. Milbank Q Jun;85(2): Problems: What Social Determinants might matter? Population Segment Patient Medical Status Priority Sub- Population Social Determinants Hypotheses 4. Chronic conditions, normal function Mrs. Gomez, 49, teacher Poor condition. High acute + chronic costs. Low-med quality. Recent hospitalization due to hypoglycemia Adult diabetics Food insecurity, poverty
41 3. The Problem- Existing Alternatives By target population By your health system By public health & other stakeholders How is the health problem currently addressed? e.g. adult low-income diabetics with hypoglycemia How is the addressable upstream cause of that problem currently addressed? e.g. food insecurity?
42 Upstream QI Project Canvas 1. Identify Patient Population 2. Team formation 3. Analyze Current State (Define Problems and Root Causes) 4. Team Goal (Unique Value Proposition) 5. Develop Upstream QI Solution 6. Identify Key Partners & Roles 7. Identify Channels 8. Key Metrics for Evaluation & Monitoring 9. Financing
43
44 4. Unique Value Proposition A single clear compelling title and message that turns an unaware person into an interested stakeholder. (Team Goal)
45 4. Unique Value Proposition Then UVP into a SMART objective Specific - Measurable - Achievable - Relevant - Time-dated

46 A call to action: FoodRx for At- Risk Diabetics - Improve Screening of Food Insecurity by 30% within 1 year - Improve Provider Confidence and Patient Satisfaction by 30% within 12 months - Improve Outcomes for Food- Insecure patients by 30% within 12 months

47 5. Solution Outline a clinicallyintegrated solution for an addressable upstream cause Identify the level of prevention and scope Does it have major potential? Is it feasible?
48 Choosing a good Upstream intervention Staff involved in choosing & supportive? Already been done? Conflicts? Strategically aligned? Scope narrow? In your control? Do you have adequate resources? Is it an easy win? Metrics easy to obtain? Credit: Mike Haiman MD
49 Upstream Medicine - QI Project Matrix (R. Manchanda 2014) *After identifying an upstream cause of a problem for a specific population, select the level and type of prevention approach for your upstream QI project Primary Prevention Prevent the onset of disease or injury by reducing an upstream risk - via changing risky exposures, behaviors, or by enhancing resistance to the effects of unhealthy exposure Secondary Prevention Halt or slow the progress of disease and/or upstream problem in its earliest stages, via procedures that detect and treat pre-clinical pathology Tertiary Prevention soften the impact caused by a disease and/or upstream problem on a patient s function, longevity, and quality of life Patient-Level How can my clinic detect and reduce an upstream risk among at-risk patients in order to prevent the onset of disease for individual patients? What tools and referrals do we use for these patients? How can my clinic detect and reduce an upstream risk among patients with early stage disease? What screening tools and referrals do we use for these patients? How can my clinic address an upstream problem to improve outcomes among severely ill, high-need and high-cost patients? How we do align our hotspotting, complex care management approaches to reduce upstream problems? Health Care Organization Population-Level How can my clinic prevent the onset of disease for at-risk patients with an approach that leverages internal resources to reduce an upstream risk factor for a clinic population? How can my clinic system use and leverage internal resources to halt or soften the impact of upstream problems for patients with early stage disease? How can my clinic leverage internal resources to soften the impact the impact of an upstream problem for high-cost patients? How do we work with other upstream systems to improve services for high-need patients? General Population-Level How can my clinic system support policy or regulatory changes to reduce upstream risk factors for an at-risk population or community? How can my clinic system support policy or program changes to halt or soften the impact of upstream problems for patients with early stage disease? How can my clinic system support policy or regulatory changes to improve service delivery for high need patients with upstream problem?
50 Upstream QI Solutions Matrix (Example: Diabetes & Food insecurity (R. Manchanda 2014) Patient-Level Health Care Organization Population-Level General Population-Level Primary Prevention Financial literacy, support, & nutrition programs for lowincome families with strong family history of DM Provide on-site Farmers Market, gym, walking trails, or financial counseling for families at risk for DM Advocate for local increase in minimum wage and supports for low-income families, particularly those at risk of DM Secondary Prevention Poverty screening & financial assistance for DM patients atrisk of end-of-month hypoglycemia Subsidize vouchers to local Farmer s Market or hire a financial counselor for lowincome DM patients Change timing and content WIC & school food programs to avoid food insecurity among DM Tertiary Prevention Reduce ED use among high-utilizer severe diabetics using food and income support referrals Coordinate with local banks, collectors, lenders, to reduce debt burden for utilizer diabetics Support legislation/ regulations to provide financial and hotspotter services to severe diabetics

51 Clinical opportunities to leverage upstream interventions and achieve the Triple Aim Community- Centered Health Home Community-Centered Health Home Clinic, public health, policy and community stakeholders coordinate to address upstream social and environmental conditions. Upstream Rxà Engage clinic staff and patients in datadriven advocacy R. Manchanda MD ACOs/ Medical Neighborhood PCMH AICU Accountable Care Organizations (ACOs)/ Medical Neighborhood Clinical neighbors share costs and/or savings to coordinate care for a population. Upstream Rx à Include social service providers in ACOs. Patient-Centered Medical Home (PCMH) Clinic primary care redesign to improve access, continuity, and coordination. Upstream Rxà Use QI framework to integrate upstream data and interventions in redesign Ambulatory Intensive Caring Unit (AICU) Intensive multidisciplinary outpatient care management for complex, high-utilizer patients. Upstream Rxà Use QI framework to integrate upstream data and interventions in redesign Propietary/ Confidential
52 Solution: FoodRx For Diabetics Sources Screen Triage Exam Chart/Cod e Refer Follow-up

53 Social Screening Tools Actionable data? Paper vs EMR-based Self-reported vs staff-assisted Evidence-base Data sharing and tracking Frequency
54 UPSTREAM TOOLS Screen Find Resource Social Screening Tools SAAS Healthify Referral Manage EMR Integration # Community/ Patient Participation Health Leads # Help Steps + + Purple Binder + + Aunt Bertha/ OneDegree + Community Detailing- HB + + HealtheRX + +/- + Enterprise Built County / Other /- +
55 Upstream Risks Screening Tool v1.3 Question Response Scoring GENERAL 1. How is your health in general? [ ] Poor [ ] Not so good [ ] Fair [ ] Good [ ] Very Good +1 for Poor or Not so Good 2. How well do you speak English? Circle one answer: [ ] Not at all [ ] Not well [ ] Well [ ] Very well +1 for Not at all or Not well 3. Do you have concerns about your family s immigration status? YES NO +1 for YES 4. Do you want to register to vote or ever had difficulty registering to vote? YES NO +1 for YES FINANCES 5. Do you ever have problems making ends meet at the end of the month? YES NO +1 for YES
56 6. Key Resources and Partners List internal & external stakeholders & initiatives Do a stakeholder analysis. Is an economic and/or business case helpful?
57 Stakeholder analysis: Key Partners & Resources

58 7. Channels How will you reach your target population? Clinic Community

59 8. Key Metrics List key numbers that will tell you how well your upstream QI intervention is working. Identify Process And Outcome Measures Screen Triage Exam Chart/Code Refer Follow-up Quick Pass: Do a AARRR! Acquisition Activation Referral Retention Results
60 8. Key Metrics Acquisition Activation Referral Patients come to project through multiple channels Patients screen positive and are triaged Patients referred to partners Retention Results Patients remain engaged in project Patient receive benefits individual health, clinic & community benefits
61 9. Financial Let stakeholder analysis inform need for economic and/or business case Economic Case Patient/Population Benefits Health Impact among Target Population Health Impact among social network of Target Population Economic Impact on Target Population Business Case Organization Benefits Costs Avoided for Organization Revenue Added to Organization Value Created for Patients
62 Budget Basics: Breakeven Analysis Determines when you will be able to cover project expenses and (maybe) generate revenue. To calculate the Breakeven # of patients (BEP): BEP = Total Fixed Costs (Avg Revenue/pt) (Avg. Variable Cost/ pt) e.g. $10000 / ($110/pt) ($10/pt) = 100 pts BEP
63 With upstream quality improvement, providers can create systems that work better Provider confidence to address housing & other social needs (v1.0) Baseline After
64 To improve social determinants, it is necessary, but not sufficient, to engage and transform health care We can't get health care as a right without addressing social determinants We can t get health care right without addressing social determinants of health
Is your clinic upstream ready?
 Is your clinic upstream ready? Are you happy? Rishi Manchanda MD MPH @RishiManchanda Burned Out 37.5% 1 Patient Experience Hope Satisfaction Trust Outcomes Effective interventions Prevent illness Advance
Is your clinic upstream ready? Are you happy? Rishi Manchanda MD MPH @RishiManchanda Burned Out 37.5% 1 Patient Experience Hope Satisfaction Trust Outcomes Effective interventions Prevent illness Advance
Health System Leadership to Address Population Health & Reducing Disparities
 Health System Leadership to Address Population Health & Reducing Disparities Andrew Shin, JD, MPH Chief Operating Officer Health Research & Educational Trust American Hospital Association 1 Changes in
Health System Leadership to Address Population Health & Reducing Disparities Andrew Shin, JD, MPH Chief Operating Officer Health Research & Educational Trust American Hospital Association 1 Changes in
Moving upstream to achieve the Quadruple Aim
 Moving upstream to achieve the Quadruple Aim Rishi Manchanda MD MPH @RishiManchanda Objectives Describe the importance of upstream social determinants to the Quadruple Aim Describe how QI and practice
Moving upstream to achieve the Quadruple Aim Rishi Manchanda MD MPH @RishiManchanda Objectives Describe the importance of upstream social determinants to the Quadruple Aim Describe how QI and practice
Executing on Population Health Project for A Community. Objectives
 D9/E9 These presenters have nothing to disclose Executing on Population Health Project for A Community Objectives Explain a framework for working on population health projects in a community Share examples
D9/E9 These presenters have nothing to disclose Executing on Population Health Project for A Community Objectives Explain a framework for working on population health projects in a community Share examples
Using Data for Proactive Patient Population Management
 Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Using Data for Proactive Patient Population Management Kate Lichtenberg, DO, MPH, FAAFP October 16, 2013 Topics Review population based care Understand the use of registries Harnessing the power of EHRs
Strategy Guide Specialty Care Practice Assessment
 Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Practice Transformation Network Strategy Guide Specialty Care Practice Assessment 1/20/2017 1 Strategy Guide: Specialty Care PAT 2.2 Contents: Demographics Tab: 3 Question 1: Aims... 3 Question 2: Aims...
Population Health or Single-payer The future is in our hands. Robert J. Margolis, MD
 Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Population Health or Single-payer The future is in our hands Robert J. Margolis, MD Today s problems Interim steps Population health Alternatives Conclusions Outline $3,000,000,000,000 $1,000,000,000,000
Achieving Health Equity After the ACA: Implications for cost, quality and access
 Achieving Health Equity After the ACA: Implications for cost, quality and access Michelle Cabrera, Research Director SEIU State Council April 23, 2015 SEIU California 700,000 Members Majority people of
Achieving Health Equity After the ACA: Implications for cost, quality and access Michelle Cabrera, Research Director SEIU State Council April 23, 2015 SEIU California 700,000 Members Majority people of
From Reactive to Proactive: Creating a Population Management Platform
 Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
Session D9 / E9 From Reactive to Proactive: Creating a Population Management Platform Richard Gitomer, MD Director, Brigham and Women s Primary Care Center of Excellence Vice Chair, Primary Care, Dept.
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
7/7/17. Value and Quality in Health Care. Kevin Shah, MD MBA. Overview of Quality. Define. Measure. Improve
 Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Value and Quality in Health Care Kevin Shah, MD MBA 1 Overview of Quality Define Measure 2 1 Define Health care reform is transitioning financing from volume to value based reimbursement Today Fee for
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery
 Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Breaking Down Silos of Care: Integration of Social Support Services with Health Care Delivery Betty Shephard Lead VP, Care Management HealthCare Partners National Health Policy Forum October 19, 2012 HCP
Improving Clinical Flow ECHO Collaborative Change Package
 Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Primary Drivers (driver diagram) Change Concepts Change Ideas Examples, Tips, and Resources Engaged Leadership Develop culture for transformation Use walk-arounds and attendance at team meetings to talk
Draft. Public Health Strategic Plan. Douglas County, Oregon
 Public Health Strategic Plan Douglas County, Oregon Douglas County 2014 Letter from the Director Dear Colleagues It is with great enthusiasm that I present the Public Health Strategic Plan for 2014-2015.
Public Health Strategic Plan Douglas County, Oregon Douglas County 2014 Letter from the Director Dear Colleagues It is with great enthusiasm that I present the Public Health Strategic Plan for 2014-2015.
Primary Care Workforce and Training of Future Leaders in Underserved Populations
 Hanna Yoon MD Association of Clinicians for the Underserved Community Health Leadership Development Fellow, Georgetown University SOM Unity Healthcare, Family Medicine Primary Care Workforce and Training
Hanna Yoon MD Association of Clinicians for the Underserved Community Health Leadership Development Fellow, Georgetown University SOM Unity Healthcare, Family Medicine Primary Care Workforce and Training
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Stanford Coordinated Care
 Stanford Coordinated Care Support the patients, manage their care Ann Lindsay MD Alan Glaseroff MD IHI Innovation Network Webinar April 12, 2013 Where s the Leverage on Trend? Registries Gaps in Care Planned
Stanford Coordinated Care Support the patients, manage their care Ann Lindsay MD Alan Glaseroff MD IHI Innovation Network Webinar April 12, 2013 Where s the Leverage on Trend? Registries Gaps in Care Planned
Best Management Practices In Integrated Behavioral Health/Primary Care Programs
 Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Best Management Practices In Integrated Behavioral Health/Primary Care Programs The 2017 OPEN MINDS Strategy & Innovation Institute Wednesday, June 7, 2017 2:00pm 3:15pm Steve Ramsland, Ed.D., Senior Associate,
Population Health: The Role of the DNP. Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare
 Population Health: The Role of the DNP Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare TOPICS in Population Health Definitions Hopkins Conceptual Model Interventions Relationship
Population Health: The Role of the DNP Linda Dunbar, PhD, RN Vice President, Population Health Johns Hopkins HealthCare TOPICS in Population Health Definitions Hopkins Conceptual Model Interventions Relationship
Maximizing the Power of Your Data. Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker
 Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Maximizing the Power of Your Data Peggy Connorton, MS, LNFA AHCA Director, Quality and LTC Trend Tracker Objectives Explore selected LTC Trend Tracker reports & features including: re-hospitalization,
Transforming Health and Health Care Through Nurses in Tennessee
 Transforming Health and Health Care Through Nurses in Tennessee Nursing Leadership Workshop I: Building a Culture of Health in Tennessee Carole R. Myers, PhD, RN Nursing Lead-Tennessee Action Coalition
Transforming Health and Health Care Through Nurses in Tennessee Nursing Leadership Workshop I: Building a Culture of Health in Tennessee Carole R. Myers, PhD, RN Nursing Lead-Tennessee Action Coalition
Working Cities Challenge Learning Community
 Working Cities Challenge Learning Community Lifting People and Places Out of Poverty: Strategies for Linking Human Capital and Neighborhood Development Robert Kahn, MD MPH Associate Chair for Community
Working Cities Challenge Learning Community Lifting People and Places Out of Poverty: Strategies for Linking Human Capital and Neighborhood Development Robert Kahn, MD MPH Associate Chair for Community
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement?
 Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Roadmap to accountable care: The chicken or the egg technology investment or clinical process improvement? August 29, 2012 Meet the Presenters Michael Griffis CIO Innovative Practices Tucson, AZ Beth Hartquist,
Examples of Measure Selection Criteria From Six Different Programs
 Examples of Measure Selection Criteria From Six Different Programs NQF Criteria to Assess Measures for Endorsement 1. Important to measure and report to keep focus on priority areas, where the evidence
Examples of Measure Selection Criteria From Six Different Programs NQF Criteria to Assess Measures for Endorsement 1. Important to measure and report to keep focus on priority areas, where the evidence
Enhancing Specialty and Primary Care Communication May 2016
 Enhancing Specialty and Primary Care Communication May 2016 ACO Announcements Reminders: ACO Notifications PECOS-Maintain active enrollment 2016 Patient Prospective Lists Upcoming provider meetings: Annual
Enhancing Specialty and Primary Care Communication May 2016 ACO Announcements Reminders: ACO Notifications PECOS-Maintain active enrollment 2016 Patient Prospective Lists Upcoming provider meetings: Annual
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016
 Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Building Evidence-based Clinical Standards into Care Delivery March 2, 2016 Charles G. Macias MD, MPH Chief Clinical Systems Integration Officer, Texas Children's Associate Professor of Pediatrics, Section
Community Health Needs Assessment Implementation Strategy Adopted by St. Vincent Charity Medical Center Board of Directors on April 5, 2017
 St. Vincent Charity Medical Center Community Health Needs Assessment Implementation Strategy Adopted by St. Vincent Charity Medical Center Board of Directors on April 5, 2017 Introduction In 2016, St.
St. Vincent Charity Medical Center Community Health Needs Assessment Implementation Strategy Adopted by St. Vincent Charity Medical Center Board of Directors on April 5, 2017 Introduction In 2016, St.
Understanding Patient Choice Insights Patient Choice Insights Network
 Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
Quality health plans & benefits Healthier living Financial well-being Intelligent solutions Understanding Patient Choice Insights Patient Choice Insights Network SM www.aetna.com Helping consumers gain
11/7/2016. Objectives. Patient-Centered Medical Home
 Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Team-Based Care November 10, 2016 Objectives Overview of Patient-Centered Medical Home (PCMH) Recognition Overview of PCMH Team-Based Care Discuss examples of practice teams in Montana health centers Source:
Patient Centered Medical Home: Transforming Primary Care in Massachusetts
 Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
Patient Centered Medical Home: Transforming Primary Care in Massachusetts Judith Steinberg, MD, MPH Deputy Chief Medical Officer Commonwealth Medicine UMass Medical School Agenda Overview of Patient Centered
MATCHING ASSETS TO COMMUNITY HEALTH 2018 GRANT PROGRAMS REQUEST FOR PROPOSALS
 MATCHING ASSETS TO COMMUNITY HEALTH 2018 GRANT PROGRAMS REQUEST FOR PROPOSALS Table of contents Our focus on communities MATCH programs Increasing access to and consumption of nutritious foods Promoting
MATCHING ASSETS TO COMMUNITY HEALTH 2018 GRANT PROGRAMS REQUEST FOR PROPOSALS Table of contents Our focus on communities MATCH programs Increasing access to and consumption of nutritious foods Promoting
The New York State Value-Based Payment (VBP) Roadmap. Primary Care Providers March 27, 2018
 Roadmap. Primary Care Providers March 27, 2018") The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
The New York State Value-Based Payment (VBP) Roadmap Primary Care Providers March 27, 2018 1 Housekeeping All lines have been muted To ask a question at any time, use the Chat feature in WebEx We will
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment
 Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Next Generation Physician Compensation Design in a Schizophrenic Payer Environment Presented to: 2015 Spring Managed Care Forum Friday, April 24, 2015 Today s agenda Setting the Stage Why are we Here?
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks
 Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
Healthcare Financial Management Association October 13 th, 2016 Introduction to Accountable Care Organizations and Clinically Integrated Networks Agenda Define ACO, CIN, and Coordinated Care Review ACO/CIN
NEW MODELS OF CARE AND THE PREVENTION AGENDA: AN INTEGRAL PARTNERSHIP CHAIR: ROB WEBSTER, CHIEF EXECUTIVE, NHS CONFEDERATION
 NEW MODELS OF CARE AND THE PREVENTION AGENDA: AN INTEGRAL PARTNERSHIP CHAIR: ROB WEBSTER, CHIEF EXECUTIVE, NHS CONFEDERATION 10.10am 10.30pm 11.15am 12.00pm 12.45pm 1.30pm 2.15pm 2.45pm 3.30pm Interview
NEW MODELS OF CARE AND THE PREVENTION AGENDA: AN INTEGRAL PARTNERSHIP CHAIR: ROB WEBSTER, CHIEF EXECUTIVE, NHS CONFEDERATION 10.10am 10.30pm 11.15am 12.00pm 12.45pm 1.30pm 2.15pm 2.45pm 3.30pm Interview
PPS Performance and Outcome Measures: Additional Resources
 PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
PPS Performance and Outcome Measures: PPS Performance and Outcome Measures: This document includes supplemental resources to the content on PPS Performance and Outcome Measures presented at the December
2/21/2018. Chronic Conditions Health and Productivity Specialty Medications. Behavioral Health
 Employee Health, Engagement and Productivity: Moving Beyond the Traditional Approach Sarah Smith Senior Consultant, Lockton Health Risk Solutions Hot topics in population health management Behavioral Health
Employee Health, Engagement and Productivity: Moving Beyond the Traditional Approach Sarah Smith Senior Consultant, Lockton Health Risk Solutions Hot topics in population health management Behavioral Health
Implementation Strategy Addressing Identified Community Health Needs
 2014-2017 Implementation Strategy Addressing Identified Community Health Needs Response to Schedule H Form 990 Table of Contents Page Overview of the Patient Protection and Affordable Care Act 3 Defined
2014-2017 Implementation Strategy Addressing Identified Community Health Needs Response to Schedule H Form 990 Table of Contents Page Overview of the Patient Protection and Affordable Care Act 3 Defined
From the Desk of the Medical Director Using Phone Triage to Meet Timely Access Regulations
 MD Health Plan of San Mateo Provider Newsletter Fall 2010 healthmatters From the Desk of the Medical Director Using Phone Triage to Meet Timely Access Regulations In our spring newsletter, we informed
MD Health Plan of San Mateo Provider Newsletter Fall 2010 healthmatters From the Desk of the Medical Director Using Phone Triage to Meet Timely Access Regulations In our spring newsletter, we informed
Providence Hood River Memorial Hospital 2010 Community Assets and Needs Assessment Report
 Providence Hood River Memorial Hospital 2010 Community Assets and Needs Assessment Report Produced by Lauren M. Fein, M.P.H. How the study was conducted Every three years, Providence Hood River Memorial
Providence Hood River Memorial Hospital 2010 Community Assets and Needs Assessment Report Produced by Lauren M. Fein, M.P.H. How the study was conducted Every three years, Providence Hood River Memorial
How BC s Health System Matrix Project Met the Challenges of Health Data
 Big Data: Privacy, Governance and Data Linkage in Health Information How BC s Health System Matrix Project Met the Challenges of Health Data Martha Burd, Health System Planning and Innovation Division
Big Data: Privacy, Governance and Data Linkage in Health Information How BC s Health System Matrix Project Met the Challenges of Health Data Martha Burd, Health System Planning and Innovation Division
ACOs: Transforming Systems with New Payment Models & Community Integration
 ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
ACOs: Transforming Systems with New Payment Models & Community Integration Sunnah Kim PNP (Moderator), American Academy of Pediatrics Herbert Druilhet, RN, DNP, FNP-BC Lafayette General Medical Doctors
Predicting 30-day Readmissions is THRILing
 2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
2016 CLINICAL INFORMATICS SYMPOSIUM - CONNECTING CARE THROUGH TECHNOLOGY - Predicting 30-day Readmissions is THRILing OUT OF AN OLD MODEL COMES A NEW Texas Health Resources 25 hospitals in North Texas
SNF REHOSPITALIZATIONS
 SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
SNF REHOSPITALIZATIONS David Gifford MD MPH SVP Quality & Regulatory Affairs National Readmission Summit Arlington VA Dec 6 th, 2013 Use of Long Term Care Services 19% 4 35% 2 20% 1 23% 1 20% 3 1. Mor
Measurement Strategy Overview
 Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome
Mobile Integrated Healthcare Program 911 Nurse Triage Measurement Strategy Overview Aim A clearly articulated goal statement that describes how much improvement by when and links all the specific outcome
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans
 Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Alberta Breathes: Proposed Standards for Respiratory Health of Albertans The concept of Alberta Breathes and these standards was developed in consultation with over 150 health professionals and stakeholders
Introducing Social Determinants of Health. Michigan Osteopathic Association 119 th Annual Spring Scientific Convention May 18, 2018
 Introducing Social Determinants of Health Michigan Osteopathic Association 119 th Annual Spring Scientific Convention May 18, 2018 Learning Objectives v Define Social Determinants of Health v List three
Introducing Social Determinants of Health Michigan Osteopathic Association 119 th Annual Spring Scientific Convention May 18, 2018 Learning Objectives v Define Social Determinants of Health v List three
February February
 February 2 2016 February PCMH TRANSFORMATION PCMH KEY COMPONENTS* Personal Clinician: first contact, continuous, comprehensive, care team Whole Person Orientation: all patient health care needs, all stages
February 2 2016 February PCMH TRANSFORMATION PCMH KEY COMPONENTS* Personal Clinician: first contact, continuous, comprehensive, care team Whole Person Orientation: all patient health care needs, all stages
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination
 Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
Attaining the True Patient-Center in the PCMH Through Health Coaching and Office-Based Care Coordination Heartland Rural Physician Alliance Annual Conference IV May 8, 2015 William Appelgate, PhD, CPC
The Physician s Perspective
 The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
The Physician s Perspective How the Changing Role of the PCP is Leading Healthcare Reform May 22, 2015 Carman A. Ciervo, DO Chief Physician Executive Our Vision To transform the healthcare To transform
Executive Summary November 2008
 November 2008 Purpose of the Study This study analyzes short-term risks and provides recommendations on longer-term policy opportunities for the Marin County healthcare delivery system in general as well
November 2008 Purpose of the Study This study analyzes short-term risks and provides recommendations on longer-term policy opportunities for the Marin County healthcare delivery system in general as well
PCMH 2014 Record Review Workbook (RRWB)
") PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
PCMH 2014 Record Review Workbook (RRWB) Purpose of the Record Review Workbook (RRWB) There are three elements in PCMH 2014 that require an accurate estimate of the percentage of patients for whom practices
Connected Care Partners
 Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Connected Care Partners Our Discussion Today Introducing the Connected Care Partners CIN What is a Clinically Integrated Network (CIN) and why is the time right to join the Connected Care Partners CIN?
Physician Alignment Strategies and Options. June 1, 2011
 Physician Alignment Strategies and Options June 1, 2011 1 Today s Discussion Review physician-hospital alignment objectives Understand the changing paradigm Evaluate alignment strategies for a new delivery
Physician Alignment Strategies and Options June 1, 2011 1 Today s Discussion Review physician-hospital alignment objectives Understand the changing paradigm Evaluate alignment strategies for a new delivery
FOOD INSECURITY, FOOD BANKS, & HEALTH CARE: A JOURNEY HILARY SELIGMAN MD MAS
 FOOD INSECURITY, FOOD BANKS, & HEALTH CARE: A JOURNEY HILARY SELIGMAN MD MAS Triple Aim of Health Care Lower Costs Triple Aim Better care for the whole population at the lowest cost Improve Patient Care
FOOD INSECURITY, FOOD BANKS, & HEALTH CARE: A JOURNEY HILARY SELIGMAN MD MAS Triple Aim of Health Care Lower Costs Triple Aim Better care for the whole population at the lowest cost Improve Patient Care
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost
 Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Measuring High Performers and Assessing Readiness to Change Looking Beyond the Lamppost Mathematica Policy Research Washington, DC November 19, 2014 Moderator Timothy Lake Director of Health Research,
Linking Social Support with Pillar 2/ Universal Health Coverage component of the End TB strategy
 Linking Social Support with Pillar 2/ Universal Health Coverage component of the End TB strategy October 26, 2016 Samson Haumba www.urc-chs.com Presentation outline Goal of TB care and Control Introduction
Linking Social Support with Pillar 2/ Universal Health Coverage component of the End TB strategy October 26, 2016 Samson Haumba www.urc-chs.com Presentation outline Goal of TB care and Control Introduction
PCC Resources For PCMH
 PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
PCC Resources For PCMH Tim Proctor Users Conference 2015 Goals and Takeaways Introduction to NCQA's 2014 PCMH. What is it? Why get recognition? Show how PCC functionality and reports can be used for PCMH
Pursuing the Triple Aim: CareOregon
 Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Pursuing the Triple Aim: CareOregon The Triple Aim: An Introduction The Institute for Healthcare Improvement (IHI) launched the Triple Aim initiative in September 2007 to develop new models of care that
Patient Centered Medical Home The next generation in patient care
 Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Patient Centered Medical Home The next generation in patient care Provider Training Module I OBJECTIVE To explain... What Patient Centered Medical Home is How it works Why it s important Where to begin
Kentucky Rural Health Summit June 8, 2018
 Kentucky Rural Health Summit June 8, 2018 Kentucky Health Program Overview Kentucky HEALTH is the Commonwealth s new program for certain low-income adults and their families. The program gets its name
Kentucky Rural Health Summit June 8, 2018 Kentucky Health Program Overview Kentucky HEALTH is the Commonwealth s new program for certain low-income adults and their families. The program gets its name
Table of Contents. Bellin Health Lessons from a Successful Medicare Pioneer ACO
 Bellin Health Lessons from a Successful Medicare Pioneer ACO March 31, 2016 Table of Contents I. We Are Doing Some Good Things Rating Agency Actions II. Who We Are Bellin Health s Platform Organizational
Bellin Health Lessons from a Successful Medicare Pioneer ACO March 31, 2016 Table of Contents I. We Are Doing Some Good Things Rating Agency Actions II. Who We Are Bellin Health s Platform Organizational
Community Needs Assessment. Swedish/Ballard September 2013
 Community Needs Assessment Swedish/Ballard September 2013 Why Do This? Health Care Reform Act requirement Support our mission to give back to community while targeting its specific health needs Strategically
Community Needs Assessment Swedish/Ballard September 2013 Why Do This? Health Care Reform Act requirement Support our mission to give back to community while targeting its specific health needs Strategically
Community Health Improvement Plan
 Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
Community Health Improvement Plan Methodist Le Bonheur Germantown Hospital Methodist Le Bonheur Healthcare (MLH) is an integrated, not-for-profit healthcare delivery system based in Memphis, Tennessee,
IS YOUR QAPI COP READY?
 IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
IS YOUR QAPI COP READY? Lisa Meadows/MSW Clinical Compliance Educator Accreditation Commission for Health Care OBJECTIVES Review the CMS requirements for the Medicare Condition of Participation: Quality
Evolving Roles of Pharmacists: Integrating Medication Management Services
 Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
Evolving Roles of Pharmacists: Integrating Management Services Marie Smith, PharmD, FNAP Palmer Professor and Assistant Dean, Practice and Policy Partnerships UCONN School of Pharmacy (marie.smith@uconn.edu)
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE
 COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
COLLABORATIVE PRACTICE SUCCESSES IN PRIMARY CARE KPhA Annual Meeting September 7, 2014 Tiffany R. Shin, PharmD, BCACP Lyndsey N. Hogg, PharmD, BCACP Objectives Describe basic concepts of collaborative
Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011
 Accountable Care: Health System View CHC Best Practices Forum Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011 Who we are Southeastern New Jersey s largest health system
Accountable Care: Health System View CHC Best Practices Forum Katherine Schneider, MD, MPhil Senior Vice President, Health Engagement July 29, 2011 Who we are Southeastern New Jersey s largest health system
2015 DUPLIN COUNTY SOTCH REPORT
 2015 DUPLIN COUNTY SOTCH REPORT Reported March 2016 State of the County Health Report The State of the County Health Report provides a review of the current county health statistics and compares them to
2015 DUPLIN COUNTY SOTCH REPORT Reported March 2016 State of the County Health Report The State of the County Health Report provides a review of the current county health statistics and compares them to
Community Mental Health and Care integration. Zandrea Ware and Ricardo Fraga
 Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
Community Mental Health and Care integration Zandrea Ware and Ricardo Fraga One in Five Approximately 1 in 5 adults in the U.S. 43.8 million, or 18.5% experiences mental illness in their lifetime. Community
DRAFT OCFSN VEGGIE RX STRATEGIC PLAN - July 2018
 THE ISSUE - OUR HEALTH DRAFT OCFSN VEGGIE RX STRATEGIC PLAN - July 2018 The question of diet has been elevated from a personal issue to a public health crisis. In 1990, the Centers for Disease Control
THE ISSUE - OUR HEALTH DRAFT OCFSN VEGGIE RX STRATEGIC PLAN - July 2018 The question of diet has been elevated from a personal issue to a public health crisis. In 1990, the Centers for Disease Control
Overcoming Psycho-Social Hurdles to Transitional Care
 Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
Overcoming Psycho-Social Hurdles to Transitional Care Matt Eisenhower Director, Community Health Development Peter Rice, M.D. Medical Director Overcoming Psycho-Social Hurdles to Transitional Care This
WHY WHAT RISK STRATIFICATION. Risk Stratification? POPULATION HEALTH MANAGEMENT. is Risk-Stratification? HEALTH CENTER
 1 WHY Risk Stratification? Risk stratification enables providers to identify the right level of care and services for distinct subgroups of patients. It is the process of assigning a risk status to a patient
1 WHY Risk Stratification? Risk stratification enables providers to identify the right level of care and services for distinct subgroups of patients. It is the process of assigning a risk status to a patient
Caregiving: Health Effects, Treatments, and Future Directions
 Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
Caregiving: Health Effects, Treatments, and Future Directions Richard Schulz, PhD Distinguished Service Professor of Psychiatry and Director, University Center for Social and Urban Research University
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016
 ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
ACHIEVING THE TRIPLE AIM THROUGH LARGE SCALE IMPROVEMENT EFFORTS JASON FOLTZ, D.O. TEACHERS OF QUALITY ACADEMY QI SYMPOSIUM MARCH 2, 2016 OVERVIEW: WHAT, WHO, HOW? What: How do you move a large multi-specialty
Standards of Practice for Professional Ambulatory Care Nursing... 17
 Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
Table of Contents Scope and Standards Revision Team..................................................... 2 Introduction......................................................................... 5 Overview
NEW MEXICO ACTION COALITION
 1 NEW MEXICO ACTION COALITION The New Mexico Action Coalition strives to provide strategic direction through community collaboration and grassroots efforts with key stakeholders to transform the health
1 NEW MEXICO ACTION COALITION The New Mexico Action Coalition strives to provide strategic direction through community collaboration and grassroots efforts with key stakeholders to transform the health
Quality Improvement in Neonatology. July 27, 2013
 Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
Quality Improvement in Neonatology July 27, 2013 Disclosure Nothing to disclose Nothing off label No commercial products No financial affiliation Objectives Key components of Quality Improvement work Advances
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together
 Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Saint Francis Care and Cigna CAC Meeting the Triple Aim Together Christopher M. Dadlez, President and CEO Saint Francis Care Jess Kupec, President and CEO Saint Francis HealthCare Partners 22 nd Annual
Integration of Behavioral Health & Primary Care in a Homeless FQHC
 Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
Integration of Behavioral Health & Primary Care in a Homeless FQHC AtlantiCare Health Services Mission Health Care May 2012 Bridgette Richardson, LCSW Executive Director, AtlantiCare Health Services, Mission
3/30/2015. Objectives. Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1
 Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Cooking Up a QAPI: Recipe for Success Under the new COPs Part 1 Catherine Gill, MS, PT, MHA Director, North Kansas City Hospital Home Health Teresa Northcutt, BSN, RN, COS-C, HCS-D Consultant Objectives
Clinical Operations. Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012
 Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Clinical Operations Kelvin A. Baggett, M.D., M.P.H., M.B.A. SVP, Clinical Operations & Chief Medical Officer December 10, 2012 Forward-looking Statements Certain statements contained in this presentation
Population Health: Physician Perspective. Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015
 Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
Population Health: Physician Perspective Kallanna Manjunath MD, FAAP, CPE Medical Director AMCH DSRIP September 24, 2015 Population Health: Physician Perspective Presentation objectives: Brief Bio Population
2015 Annual Convention
 2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
2015 Annual Convention Date: Tuesday, October 13, 2015 Time: 8:00 am 9:30 am Location: Gaylord National Harbor Resort and Convention Center, National Harbor 10 Title: Activity Type: Speaker: Opportunities
Building & Strengthening Patient Centered Medical Homes in the Safety Net
 Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Blue Shield of California Foundation County Coverage Expansion Planning Workshop #2 Building & Strengthening Patient Centered Medical Homes in the Safety Net July 8, 2011 Presented by: Kathryn Phillips,
Community Health Plan. (Implementation Strategies)
") 2017-2019 Community Health Plan (Implementation Strategies) May 15, 2017 Community Health Needs Assessment Process Winter Park Memorial Hospital A Florida Hospital (the Hospital) conducted a Community
2017-2019 Community Health Plan (Implementation Strategies) May 15, 2017 Community Health Needs Assessment Process Winter Park Memorial Hospital A Florida Hospital (the Hospital) conducted a Community
2012 Community Health Needs Assessment
 2012 Community Health Needs Assessment University Hospitals (UH) long-standing commitment to the community spans more than 145 years. This commitment has grown and evolved through significant thought and
2012 Community Health Needs Assessment University Hospitals (UH) long-standing commitment to the community spans more than 145 years. This commitment has grown and evolved through significant thought and
Rethinking the model of primary care. Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine
 Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Rethinking the model of primary care Tom Bodenheimer MD Center for Excellence in Primary Care UCSF Department of Family and Community Medicine Why should primary care be the foundation for any healthcare
Professional Drivers Health Network. What?
 Professional Drivers Health Network What? An Integrated Occupational Health Program The definition - the ability of a worker to function at an optimum level of well-being at a worksite as reflected in
Professional Drivers Health Network What? An Integrated Occupational Health Program The definition - the ability of a worker to function at an optimum level of well-being at a worksite as reflected in
Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente
 Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente Association for Community Health Improvement (ACHI) 2015 Conference What We
Leveraging the Community Health Needs Assessment Process to Improve Population Health: Lessons Learned from Kaiser Permanente Association for Community Health Improvement (ACHI) 2015 Conference What We
Social Determinants of Health and Medicaid Payment Reform
 Social Determinants of Health and Medicaid Payment Reform Community Integration Leadership Institute June 2, 2016 Kate Breslin, President and CEO www.scaany.org www.scaany.org Schuyler Center 2 Shaping
Social Determinants of Health and Medicaid Payment Reform Community Integration Leadership Institute June 2, 2016 Kate Breslin, President and CEO www.scaany.org www.scaany.org Schuyler Center 2 Shaping
WHAT IT FEELS LIKE
 PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
PCMH and PCSP WHAT IT FEELS LIKE Presentation Outline Goals of the Patient Centered Medical Home and the Patient Centered Specialty Practice Identifying the Joint Principles Recognition Programs Standards
Good practice in the field of Health Promotion and Primary Prevention
 Good practice in the field of Promotion and Primary Prevention Dr. Mohamed Bin Hamad Al Thani Med Cairo February 28 th March 1 st, 2017 - Cairo - Egypt 1 Definitions Promotion Optimal Life Style Change
Good practice in the field of Promotion and Primary Prevention Dr. Mohamed Bin Hamad Al Thani Med Cairo February 28 th March 1 st, 2017 - Cairo - Egypt 1 Definitions Promotion Optimal Life Style Change
ROOTS Program. Webinar: Using Data to Drive SDOH Priorities: Lessons Learned from Cincinnati Children s Hospital November 16, 2017
 ROOTS Program Webinar: Using Data to Drive SDOH Priorities: Lessons Learned from Cincinnati Children s Hospital November 16, 2017 Webinar Reminders 1. Everyone is unmuted. Press *6 to mute yourself and
ROOTS Program Webinar: Using Data to Drive SDOH Priorities: Lessons Learned from Cincinnati Children s Hospital November 16, 2017 Webinar Reminders 1. Everyone is unmuted. Press *6 to mute yourself and
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM. Bluebonnet Trails Community Services
 TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
TEXAS HEALTHCARE TRANSFORMATION & QUALITY IMPROVEMENT PROGRAM Regional Healthcare Partnership Region 4 Bluebonnet Trails Community Services Delivery System Reform Incentive Payment (DSRIP) Projects Category
WellCare of Kentucky s Quest for Quality
 WellCare of Kentucky s Quest for Quality WellCare of Kentucky Offices Lexington Office 859-264-5100 Louisville Office 502-253-5100 Ashland Office 606-327-6200 Owensboro Office 270-688-7000 Hazard Office
WellCare of Kentucky s Quest for Quality WellCare of Kentucky Offices Lexington Office 859-264-5100 Louisville Office 502-253-5100 Ashland Office 606-327-6200 Owensboro Office 270-688-7000 Hazard Office
Building the Universal Roadmap to Population Health Management
 Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
Building the Universal Roadmap to Population Health Management Executive Webinar January 21, 2016 Karen Handmaker, MPP, PCMH CCE IBM Watson Health House Keeping 1. Using the control panel Use the control
FINDING ANSWERS: A ROADMAP TO REDUCE RACIAL AND ETHNIC HEALTH DISPARITIES IN HEALTH CARE
 FINDING ANSWERS: A ROADMAP TO REDUCE RACIAL AND ETHNIC HEALTH DISPARITIES IN HEALTH CARE Addressing Health Disparities and Advancing Health Equity February 28, 2017 Angela Dawson, MS, MRC, LPC Executive
FINDING ANSWERS: A ROADMAP TO REDUCE RACIAL AND ETHNIC HEALTH DISPARITIES IN HEALTH CARE Addressing Health Disparities and Advancing Health Equity February 28, 2017 Angela Dawson, MS, MRC, LPC Executive