Spreading Innovations 2016 Documenting Implementation & Spread of Health Care Innovations in the Safety Ne
|
|
|
- Patience Golden
- 6 years ago
- Views:
Transcription
1 Spreading Innovations 2016 Documenting Implementation & Spread of Health Care Innovations in the Safety Ne Prepared for CCI by White Mountain Research Associates, LLC, Walpole, NH
2 Table of Contents Executive Summary... iii Background... 1 Evaluation Approach... 2 Evaluation Findings... 3 Innovation Metrics Team Highlights... 3 Spread Metrics... 8 Team Challenges Conclusions Page ii October 2016
3 Executive Summary In 2014, the Center for Care Innovations (CCI) launched Round 1 of its Spreading Innovations program. Building on the success of the 2014 program, CCI launched its second round of funding in May Like the first program launched in May 2014, Spreading Innovations 2015 was designed to support the dissemination of current successful innovations but with an eye on readying safety net organizations for a value based payment system and improving timely access to care. Spreading Innovations 2015 is a joint effort of CCI and Blue Shield of California Foundation, with additional funding from Kaiser Permanente. In its Spreading Innovations 2015 program, CCI supported the spread of five types of innovations to improve care access across 16 safety net organizations: (1) telephone visits, (2) video collaboration and instant messaging, (3) patient portal, (4) co- visits, and (5) texting. Two of these five innovations were new to the 2015 program (co- visits and texting). Grantees had the opportunity to visit an innovation host site (with prior experience with the innovation), received one- on- one and group coaching support, received technical assistance on measurement and evaluation, and had access to a peer learning community. Grantees had one year to successfully implement the selected innovation and come up with a plan to sustain their innovation when program funding ended. An external evaluation team (White Mountain Research Associates, LLC) was asked to evaluate the impact of the 2015 program. The evaluation included a combination of coaching around metrics selection and capturing staff/patient feedback, monthly data collection using an Excel workbook, and project milestone updates on innovation implementation. We also documented innovation spread over the course of the implementation process using various measures. Overall, the majority of teams were successful in fully implementing their innovations, despite a number of hurdles reported by teams around software and work flow integration, staff and patient engagement, and other issues. Innovation teams were able to work around these challenges, resulting in successful implementation of the innovations, and in some cases, spread to other departments and/or clinic locations. Although a number of teams had already partially implemented their innovations when the project began, two- thirds of teams transitioned to full implementation and 19% of teams transitioned to spreading their technology by the end of the CCI project period in August Across teams, statistically significant improvements in two of three spread factors people- based factors and innovation- based factors were documented from baseline to the final reporting period. A majority of teams were able to expand their reach at all levels to patients, providers and staff, and other clinics or departments by the end of the project. Virtually all teams had plans to continue spreading the innovation to other clinics and/or departments. Page iii October 2016
4 Background The Center for Care Innovations (CCI) released in May 2015 its second Spreading Innovations request for proposals (RFP). Like the first program release in May 2014, this RFP was designed to support the dissemination of current successful innovations that improve access to care in safety net organizations. Specifically, through its most recent RFP, CCI supported the spread of five types of innovations to improve care access: (1) telephone visits, (2) video collaboration and instant messaging, (3) patient portal, (4) co- visits, and (5) texting. Two of these five innovations were new to the 2015 RFP (co- visits and texting). Grantees received awards ranging from $10,000 to $25,000, depending upon the innovation selected. Grantees had the opportunity to visit an innovation host site (with prior experience with the innovation), and gained access to one- on- one and group coaching support, measurement and evaluation experts, a peer learning community, toolkits, training curriculum, and educational materials. Grantees had one year to successfully implement the selected innovation and come up with a plan to sustain their innovation when program funding ended. Host sites included Shasta Community Health Center (patient portal), Riverside University Health System (telephone visits), West County Health Centers and Petaluma Health Center (video collaboration), and Clinica Family Health Services in Colorado (co- visits). Spreading Innovations 2015 is a joint effort of CCI and Blue Shield of California Foundation, with additional funding from Kaiser Permanente. The following 16 health care delivery systems and clinics were awarded grants through this project: Innovation Type Video Collaboration Texting Solutions Patient Portal Co- Visits Telephone Visits Clinic La Maestra Community Health Centers Monterey County Health Department Martin Luther King, Jr. Outpatient Center OLE Health Native American Health Center Western Sierra Medical Clinic Foothill Community Health Center Golden Valley Health Centers La Clinica de La Raza Serve the People Community Health Center Redwood Coast Medical Services Indian Health Center of Santa Clara Valley Northeast Valley Health Corporation San Mateo Medical Center Multnomah County Health Department (OR) Kern Medical Center Page 1 October 2016
5 Evaluation Approach The evaluation included a combination of quantitative and qualitative data collection. Each team tracked and reported on a quarterly basis metrics on patient volume, efficiency, quality, and satisfaction with care. The evaluator also provided coaching around metrics and data collection. Innovation spread over the course of the implementation process and program successes and challenges faced also were documented. These evaluation activities are summarized below: Innovation Metrics (Quantitative) The evaluation team worked with each site to define a set of tracking measures. Excel workbooks were created for each team so that measures could be tracked and reported on a quarterly basis. The workbook contains self- generating charts, so that teams could track their progress in meeting their measurement goals. Changes in Organizational Capacity for Innovation Spread (Quantitative) The NHS Institute for Innovation and Improvement s Spread and Adoption Tool 1 is a diagnostic tool that is easy to use and allows teams to explore opportunities for growth across three areas of innovation: people- based success factors (e.g., leadership support, incentives for staff), innovation- based success factors (e.g., benefits to organization, easily adapted), and context- based success factors (e.g., infrastructure supports innovation, positive experience with other innovations). The survey was modified to use as a Likert scale in an Excel spreadsheet and administered to each site. Pre/post changes were assessed within and across teams and by innovation type. Project Milestone Updates (Qualitative) Teams provided quarterly project updates and this information was used by CCI staff, the coaches, and evaluator for feedback, as needed. Information collected included stage of innovation implementation, self- reported measure of spread of innovation among providers, patients, departments, and clinics, staff and patient training, challenges faced in areas including patient recruitment, leadership support, provider recruitment, software integration, data collection, marketing, training, HIPAA compliance, legal issues encountered, and staff time and engagement. Technical Assistance The evaluators worked with grantees either directly or through their coach to help them identify the best metrics and measurement strategy for their innovation. Technical assistance needs varied across the grantees, but included feedback on tracking measures, assistance with development of patient and provider/staff feedback surveys, survey sampling strategies, and data analysis and interpretation. Coach Rating of Team Progress Each of the three coaches provided a quarterly team progress rating for each of their clinics. This measure is useful to the internal project team to gauge individual grantee success across projects and has been used successfully for performance improvement initiatives. 1 Healthcare Improvement Scotland (2013). Guide on spread and sustainability. July Page 2 October 2016
6 Evaluation Findings Innovation Metrics Team Highlights Overall, teams were successful in launching their innovations, despite a number of hurdles reported by teams around software and work flow integration, staff and patient engagement, and other issues. In many cases, innovation teams were able to work around these challenges, resulting in successful implementation of the innovations, and in some cases, spread to other clinic locations. Sites collected monthly data on measures that fell broadly into four categories: patient volume, efficiency, quality measures, and patient/provider satisfaction with care. Teams were most successful at capturing patient volume, as well as staff and patient feedback/satisfaction measures. We provide below a summary of these findings for each innovation type by team. Video Collaboration La Maestra Community Health Centers implemented video collaboration and recruited patients with chronic conditions for medication management by a pharmacist via video conference. Patients were referred through a warm- handoff from the medical assistant to a pharmacy technician. Offered initially to patients with chronic conditions at their National City clinic, the team broadened the scope to specialty needs, such as ENT patients because of high no- show rates among patients with chronic conditions (upwards of 86% no show rates). The team also experienced high no- show rates with its ENT patients due to lack of transportation, inconvenient hours, and language barriers. The team subsequently expanded video collaboration to its El Cajon site for chronic condition patients, where no- show rates are relatively lower. Over time, the team was able to significantly reduce the no- show rate for ENT patients from 50% to 13%. Texting Solutions Monterey County Clinic Services Bureau implemented Care Message at seven of its clinics by providing text message reminders to its patients. The team currently has about 4,700 patients who receive appointment reminders through text messaging, representing 20% of their appointment reminders. The team estimates that manual confirmation work time has been reduced by 70%. The text messaging software is not integrated with the EMR, but the implementation team is working with OCHIN and Care Message to develop a bidirectional interface. Martin Luther King, Jr. Outpatient Center, Los Angeles County, Department of Health Services experiences a no- show rate of about 20% and nursing staff have to do reminder calls every day. Through a needs assessment, staff determined that 84% of patients were receptive to text message reminders. The team piloted Twilio text messaging software at their patient- centered medical home, where no- show rates range from 25-30%. Although data are still preliminary, early results indicate a decrease in no- show rates. The team was able to initiate a new communication bridge for patient outreach, integrate their EHR data with SMS technology, generate a prospective appointment scheduling reminder report, and open an additional data collection pathway for patient behavioral analysis. Page 3 October 2016
7 OLE Health implemented texting reminders using ecwmessenger with over 200 patients at their St. Helena Health Center. Early in its implementation, the team surveyed patients to gain feedback on using the text messaging software. In general, patient feedback was positive, but they did offer useful feedback to improve the content of the reminders. For example, some patients were not sure how to confirm or cancel their appointments while others provided feedback on the timing of the reminder (e.g., day of or day before appointment) and how to make the message sound friendlier. As the team moves forward with its launch of the reminder system, they are working with their compliance officer to be sure their work flows are in compliance with ecwmessenger and are continuing to explore ways to mass enable their patients. OLE Health s Early Feedback from Patients I wasn t sure how to answer it because it didn t give me an option to confirm or cancel by replying with a number. It should be a day before [my appointment]. If I have questions, I have to call back. I didn t know how to respond to confirm; it s in English and confusing. Patient Portal Native American Health Center faced initial challenges with portal implementation, ranging from software integration and upgrade issues to buy- in from staff and providers. However, despite these challenges, the team was successful in launching the portal and fully implementing it at its school- based clinics. By the end of the project, the team had 132 patients enrolled in the portal, developed work flows and trained staff members on portal use, and created a marketing brochure for its members on how to use the portal. The team plans to continue staff training and support, integrate telephone support for its members, and increase enrollment numbers. Western Sierra Medical Clinic successfully enrolled over 3,600 members into its My Health Gateway patient portal. The team also developed a rigorous training protocol to use the portal to ensure buy- in from staff and clinicians. Every clinician and staff member has been through multiple trainings in group settings and each has received one- on- one training for their respective scope. Use of the portal is also reviewed in onboarding for new staff and clinicians. Over the course of the project, the team also documented a decrease in call volume from about 11,500 calls in September 2015 to about 7,900 calls in July Foothill Community Health Center successfully launched its Health Connect patient portal at three locations: Foothill Family Health Center, Monterey Plaza Clinic, and Gilroy Health clinic. The team has reported that patients are actively using secure messaging with providers and staff and other portal functionalities like appointment reminders and confirmations and lab views. The implementation team also reported a reduction in phone calls to the clinics requesting patient medical records. As implementation of the portal moves forward, the team is working with its vendor to make the portal available in Spanish by the end of the year. Finally, the implementation team is exploring the use of patient kiosks at the front desks of its three clinics to help streamline front desk operations. Golden Valley Health Centers targeted their Senior Health and Wellness Center and Women s Health Clinic. The team faced a number of challenges around portal implementation, including unengaged staff, lack of leadership support, staff turnover, and inability to engage patients in using the portal. By the end Page 4 October 2016
8 of the project, the implementation team was able to break down many of these barriers. Staff competition and incentives were successfully used to boost patient enrollment in the portal, and the team reported that about 30 patients a month receiving tokens prior to the pilot, while during the pilot the average increased to about 315 patients a month. Bolstered by these successes, the portal team continues to explore strategies to boost patient enrollment and patient use of the portal. The implementation team also plans to expand use of the portal at other clinic locations, release other portal functions like the appointment feature, and encourage self- enrollment by patients into the portal. La Clinica de La Raza was able to rejuvenate the launch of its patient portal at 11 new clinics across Solano, Contra Costa, and Alameda Counties since the start of the CCI project, despite competing challenges, such as an EHR rollout. The implementation team began accepting patient- initiated enrollment and created their own portal dashboard that they could use as a springboard for their own internal analytics. While the team continues to face slow patient enrollment into the portal and low use, it has learned that while an initial spike in enrollment is typical early in the implementation process, to sustain a boost in enrollment numbers, monthly feedback on enrollment numbers to the clinics is critical. The team also learned that exploring new features of the portal while simultaneously rolling it out to new clinics was not wise; they faced technical challenges with different testing environments with the portal. The implementation team plans to continue rolling out the portal to all remaining Alameda clinics in the first quarter of Co-Visits Serve the People Community Health Center in Santa Ana serves primarily a Latino population of adult insured. The team implemented nurse co- visits with the goals of improving patient access to care, improving team- based care, and giving patients more choice in when they are seen. Since implementing co- visits, the care team experienced a number of positive changes around patient access. When the project rolled out in January 2016, the provider saw an average of 2.3 patients per hour and by June 2016, provider productivity rate increased to 3.0 patients per hour. By adding a nurse to the care team, the care team was able to add 2 patients per provider per day and create a total of 6 new slots for co- visits per day. Another success has been an increase in their patient show rate: the initial show rate was 69% and this increased to 77% by June The team also documented a decrease in cycle time from an average of 66 minutes in February 2016 to 52 minutes in May 2016, saving patients an average of 16 minutes per visit. To take advantage of their new EHR, the team is tailoring a template that is appropriate for the expanded functions of the nurse in the co- visit. The care team is also developing a planned visit template to be used by the whole care team, similar to a dashboard which provides a history at a glance of the patient s conditions, medications, and treatment plan. The implementation team believes the co- visit model is financially sustainable; the addition of the RN to the team adds 6 more billable visits per day, which adds about 120 extra billable visits on top of their regularly scheduled patients. Based on these successes, the implementation team is planning on spreading nurse co- visits to the rest of their care teams, expanding the list of co- visit types, and is moving to complete two co- visits per provider per day. Redwood Coast Medical Services is a community health clinic in a frontier area. The care team initially considered implementing the nurse co- visit model with chronic care patients, but given their focus on acute cases and a very busy and robust Urgent Care department, the care team decided to implement co- visits with Urgent Care. Urgent care is staffed by two physician assistants and four registered nurses. Since implementing the co- visit model, the care team has demonstrated an increase in provider and Page 5 October 2016
9 patient satisfaction. Between April and July 2016, the care team implemented 476 co- visits. The care team notes that an unanticipated but welcome outcome of the co- visit model is an increase in staff empowerment and confidence in bringing patients in soon after arrival and initiating the visit resulting in reduced wait times and happier patients. Although one of the Urgent Care providers has not fully adopted co- visits, the staff has contributed greatly to a reduction in the wait time for patients for this department. One of the RNs that regularly rotates in Urgent Care has the technical capability to help create templates for standing order visits that will help lay the groundwork for initiating co- visits in the Primary Care setting. Telephone Visits Indian Health Center of Santa Clara Valley began piloting telephone visits with one medical provider in January The provider scheduled phone visits on Mondays and Fridays for two hours each day. The team originally targeted patients with hypertension but then decided to expand to all patients who may benefit from the telephone visits. Eligibility staff was included in the pilot to increase phone coverage. With about 400 newly assigned patients, the team decided to do patient intakes over the phone instead of through clinic- based appointments. This proved to be a success, and as a result the telephone visits were expanded to include Health Educators and RN Case Managers. Health Educators frequently do breast health questionnaires before the PCP visits, so the care teams utilized the same script and started doing the breast health assessments over the phone. The care team determined that a breast exam clinic visit did not need to be scheduled and they could directly order their mammograms. As a result, this opened up more slots in the providers schedules, which could be used for other patient care encounters. Based on these early successes, the team expanded telephone visits to a second medical provider by the end of February Although the team lost one of the two primary care providers, the project includes one medical provider, four Eligibility staff, and the Clinic Support team (Women s Health and Health Education). During the course of the project, the mammography rate increased from 55% to 60%, the number of patient walk- ins decreased by 60% following the new phone- based eligibility intake protocol, and health education productivity increased from 55% to 78%. Northeast Valley Health Corporation s care team experimented with different approaches to conducting telephone visits, including documenting unscheduled (i.e., documenting current experiences with both outgoing and incoming, unscheduled calls to patients) and scheduled visits, and including either care team members (i.e., non- providers) or providers. Unscheduled calls were implemented by a variety of care team members at Pacoima as well as San Fernando and Valencia Health Centers to provide chronic disease management and follow- up to health education and self- management goals. Between the first and second quarters of 2016, care team members increased their unscheduled calls from 32 to 720. Although the team is early in the process with conducting scheduled telephone visits, there are currently 18 providers and 35 care team members conducting telephone visits. The CCI project gave the care team an opportunity to develop a system to quantify telephone visits and the amount of time spent on these visits. As the team moves to payment reform and alternative encounters, this project is an important step in that direction and has raised awareness of the financial impact of utilizing telephone- based vs. in- person patient encounters. San Mateo Medical Center began conducting telephone visits in two clinics: Daly City and Coastside Clinic. With this as their starting point, the implementation team has been quite successful in spreading this innovation across sites. Since September 2015, staff has conducted about 1,000 telephone visits across five primary care clinics and one specialty clinic. Telephone visits have been adopted by 15 Page 6 October 2016
10 providers and nine nursing staff. One of the major goals of the project was to improve access to care for patients. Although the team has been unable at this point to improve time to third next available appointment (TNAA), average TNAA is still below the team s goal of less than 10 days. Another goal was to improve their patient satisfaction scores around likelihood to recommend. The team was able to improve this score over the course of the project at their Coastside Clinic. In addition to documenting patient volume metrics, major diagnoses treated and efficiency, the implementation team also recognized the importance of coding and submitting telehealth encounters correctly, so staff received training and refresher training. Over the course of the project, the team improved the percentage of encounters that were coded correctly from 56% in September 2015 to 93% in June Multnomah County Health Department s goals for its televisit program were to increase patient access from 20 to 24 patient touches per day and improve patient and provider satisfaction. The implementation team was cautious with their rollout and piloted televisits with just one provider from December 2015 through May Over time, the implementation team received much feedback from their providers and patients, and now 100% of their patients prefer a phone visit when appropriate. Interestingly, the care team found that over time, some patients thought that they no longer had an option for either an office visit or a televisit, so they had to clearly communicate and remind patients that they still had options for the type of appointment they wished. The implementation team developed a tool kit and work flows, and continues to provide elbow visits to enhance and refresh their training with providers. Starting in September/October 2016, the team plans to expand their services to include nurse visits and behavioral health provider visits. Kern Medical Center launched their televisits pilot with two providers from their Pediatrics Department. Providers began by blocking off one hour per week for phone consults. During the initial launch of their phone consults, the implementation team was faced with numerous technological setbacks and had to develop workarounds for these issues. One of the greatest obstacles that the team continues to face is with software integration; the clinic uses several different platforms for scheduling and billing that do not communicate well with each other and also uses an older EMR system. This has impacted the pre- registration and registration process; the process is time consuming and information must be entered into multiple interfaces before the physician is to be able to generate a phone visit note in the EMR. Because of this, the care team has only been able to make cold calls for patient phone visits. While the team was able to develop workarounds for these technology issues, they are still not at the point yet where the two pilot providers feel comfortable with expanding the types of phone visits and have limited communication to patients to lab and radiology results. Despite these setbacks, the two providers are staying within their goals of conducting 48 phone visits per month. Page 7 October 2016

 Designing (design project solution from a technical and operational perspective) Piloting (test innovation/solution with a limited number of providers, staff, patients;")
11 Spread Metrics In addition to documenting changes in patient volume, efficiency, and quality measures, we also were interested in tracking the extent to which the sites were successful in launching, implementing, and spreading their innovations over the course of the project. During each of the three reporting periods, we tracked stage of implementation for each team using the following stages: Planning (define scope and approach, determine resources needed, and create a high- level plan for project) Designing (design project solution from a technical and operational perspective) Piloting (test innovation/solution with a limited number of providers, staff, patients; develop work flow plan) Pre- implementation (create and execute training plan, develop go- live plan, refine and execute work flow plan) Partial implementation (Go- Live, initial rollout of innovation to some providers and patients) Full implementation (rollout complete at site/clinic, continue training, monitoring) Spread technology/innovation to other sites/clinics within organization The area chart above illustrates the progression of teams moving from planning and designing through full implementation and spread. Although a number of teams were already in partial implementation when the project began, 63% of teams transitioned to full implementation and 19% of teams transitioned to spreading their technology by the end of the CCI project period. The number of teams transitioning into higher stages of implementation improved significantly across the three reporting periods (Friedman test; χ 2 (2, N=16) = 25.1, p<.001)(see table below). Page 8 October 2016


12 Reporting Period Clinic Sep- Dec '15 Jan- Mar '16 Apr- Jul '16 Foothill Community Health Center Pre- Implementation Full Implementation Spread Golden Valley Health Centers Partial Implementation Partial Implementation Full Implementation Indian Health Center of Santa Clara Valley Designing Partial Implementation Partial Implementation Kern Medical Center Pre- Implementation Partial Implementation Partial Implementation La Clinica de La Raza Inc Partial Implementation Partial Implementation Partial Implementation LA County Department of Health Services Designing Piloting Full Implementation La Maestra Family Clinic Designing Partial Implementation Full Implementation Monterey County Health Dept. Designing Partial Implementation Full Implementation Multnomah County Health Dept. Partial Implementation Partial Implementation Full Implementation Native American Health Center Partial Implementation Partial Implementation Full Implementation Northeast Valley Health Corp. Pre- Implementation Partial Implementation Full Implementation OLE Health Pre- Implementation Piloting Full Implementation Redwood Coast Medical Services Designing Piloting Full Implementation San Mateo Medical Center Partial Implementation Spread Spread Serve the People Planning Partial Implementation Full Implementation Western Sierra Medical Clinic Partial Implementation Full Implementation Spread In addition, a majority of teams were able to expand their reach to patients, providers and staff, and other clinics or departments by the end of the project (see figure below). Virtually all teams had plans to continue spreading the innovation to other clinics and/or departments. Page 9 October 2016


13 We also asked the innovation project team leader at each site to complete a Spread and Adoption Tool at baseline and then again at the end of the project. Change in organizational capacity for innovation spread was measured using the NHS Institute for Innovation and Improvement s Spread and Adoption Tool. As described earlier in this report, the Spread and Adoption Tool is a diagnostic tool that allows teams to explore opportunities for growth across three areas of innovation: people- based success factors, innovation- based success factors, and context- based success factors. Pre/post changes were assessed within and across teams and by innovation type. Additionally, to supplement the innovation scores, we asked each of the three coaches to score each their teams periodically, based on team progress in implementing their innovations using the following rating scale: Coach Rating Scale 1.0 = nonstarter; no report 1.5 = beginning activities 2.0 = activity and clear goals set; no changers 2.5 = began testing; no measurable progress 3.0 = testing; initial measurable progress 3.5 = testing multiple changes; measurable progress made 4.0 = innovation has been implemented with clear changes in structure and care processes 4.5 = innovation is institutionalized with plan for spread to other parts of organization 5.0 = innovation has been successfully spread across organization with sustainable business model Across teams, statistically significant improvements in people factors and innovation factors were documented from baseline to the final reporting period, but not for contextual factors (see figure below). Page 10 October 2016




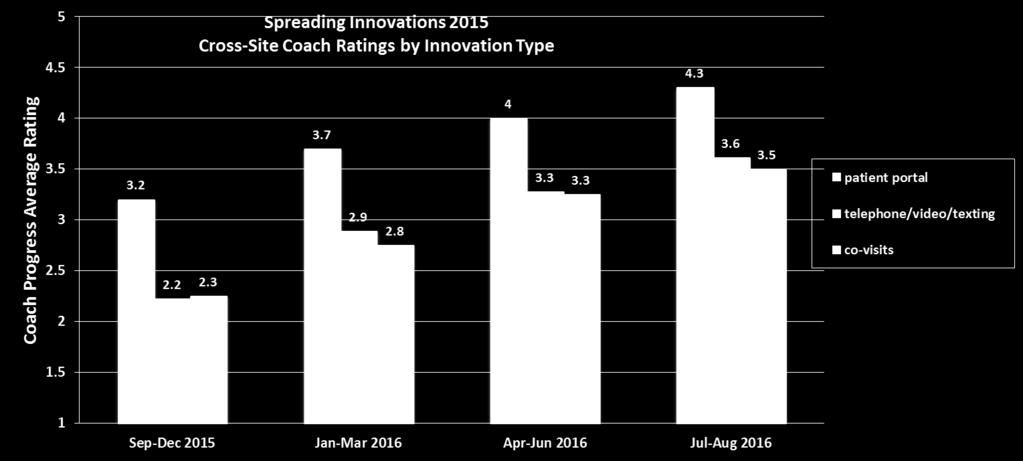
14 In addition, across innovation types, with the exception of contextual factors for patient portal grantees, improvements across all factors were documented from baseline to the final reporting period. In general, scores at the end of the project period were the highest for sites implementing co- visits and phone, video, or texting innovations (see figure below). Finally, we summarized the coach ratings for teams in the two charts below. As illustrated in the charts, all coaches reported improvements in each team s progress with implementing their solutions; this was true across teams as well as across innovation types, reflecting the teams ratings of progress with implementation and spread shown above. Note: Average score shown along with high and low scores Page 11 October 2016

15 Page 12 October 2016


16 Team Challenges Teams were asked to document the challenges to implementing their innovations over the course of the reporting period; we asked teams to summarize these challenges midcourse and then again at the end of the CCI project reporting period. At the project midpoint, all but one site reported some type of challenge associated with implementation of the innovation, and by the end of the project, all but two teams reported some type of implementation challenge. However, across all teams 46 total challenges were identified at midcourse compared to 36 by the end of the project. The pie charts below illustrate the types of the challenges faced by the teams, as well as their most commonly reported challenges. In general, although the teams were able to overcome a number of these challenges by the final reporting period, the teams still face these issues but many have developed workarounds for them or are working on ways to address these barriers. The top three challenges across all innovation types identified at program midcourse included staff and provider time/engagement, work flow integration, and data collection, while at the end of the project, software integration (except for co- visits) was the biggest challenge followed by staff and provider time/engagement and work flow integration. We also explored differences in top challenges identified by type of innovation implemented at midcourse and during the final reporting period. Regardless of innovation type, teams experienced these challenges to varying degrees. However, by end of project, the biggest challenges that persisted included software integration (except for co- visits) and data collection. Work flow integration appeared to be more of a challenge for teams that implemented texting, video visits, or televisits, as teams had to develop workarounds and new work flows for software incompatibility issues, until the issues were resolved. Page 13 October 2016
17 Conclusions While teams were in varying stages of innovation implementation at the beginning of the program, the majority of teams were successful in fully implementing their innovations by the end of the project. Teams experienced a number of barriers to innovation implementation to varying degrees over the course of implementation; the top three challenges across all innovation types identified at the end of the project included software integration (except obviously for co- visits), staff and provider time/engagement and work flow integration. Innovation teams were able to work around these challenges, resulting in successful implementation of the innovations, and in some cases, spread to other departments and/or clinic locations. Two- thirds of teams transitioned to full implementation and 19% of teams transitioned to spreading their technology by the end of the CCI project period in August Across teams, statistically significant improvements in two of three spread factors people factors and innovation factors, but not contextual factors were documented from baseline to the final reporting period. A majority of teams were able to expand their reach at all levels to patients, providers and staff, and other clinics or departments by the end of the project. Virtually all teams had plans to continue spreading the innovation to other clinics and/or departments. Page 14 October 2016
POPULATION HEALTH LEARNING NETWORK 1
 In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
In partnership with the California Health Care Foundation (CHCF) and the Blue Shield of California Foundation (BSCF), the Center for Care Innovations (CCI) is launching a Population Heath Learning Network
1 Title Improving Wellness and Care Management with an Electronic Health Record System
 HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
HIMSS Stories of Success! Graybill Medical Group 1 Title Improving Wellness and Care Management with an Electronic Health Record System 2 Background Knowledge It is widely understood that providers wellness
SACRAMENTO COUNTY: DATA NOTEBOOK 2014 MENTAL HEALTH BOARDS AND COMMISSIONS FOR CALIFORNIA
 SACRAMENTO COUNTY: DATA NOTEBOOK 2014 FOR CALIFORNIA MENTAL HEALTH BOARDS AND COMMISSIONS Prepared by California Mental Health Planning Council, in collaboration with: California Association of Mental
SACRAMENTO COUNTY: DATA NOTEBOOK 2014 FOR CALIFORNIA MENTAL HEALTH BOARDS AND COMMISSIONS Prepared by California Mental Health Planning Council, in collaboration with: California Association of Mental
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA)
") The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
The 10 Building Blocks of Primary Care Building Blocks of Primary Care Assessment (BBPCA) Background and Description The Building Blocks of Primary Care Assessment is designed to assess the organizational
Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit
 Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit Presented by: Julie Murchinson, Manatt Health Solutions Jonah Frohlich, California HealthCare Foundation
Creating Quality Improvement and Incentive Platforms in the Safety Net 2009 Pay for Performance Summit Presented by: Julie Murchinson, Manatt Health Solutions Jonah Frohlich, California HealthCare Foundation
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure
 Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
Move the Needle on Difficult Quality Measures: How Health Plans Can Control High Blood Pressure A Centauri Health Solutions Sm White Paper By melanie Richey 2016 by Centauri Health Solutions, Inc. All
Electronic Physician Documentation: Increased Satisfaction
 Electronic Physician Documentation: Increased Satisfaction Session 222, February 23, 2017 Robert (Bob) Diamond, Sr. Vice President / CIO, Health Quest Kshitij (Tij) Saxena, MD, CMIO, Health Quest 1 Speaker
Electronic Physician Documentation: Increased Satisfaction Session 222, February 23, 2017 Robert (Bob) Diamond, Sr. Vice President / CIO, Health Quest Kshitij (Tij) Saxena, MD, CMIO, Health Quest 1 Speaker
Visit to download this and other modules and to access dozens of helpful tools and resources.
 This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
This is the third module of Coach Medical Home a six-module curriculum designed for practice facilitators who are coaching primary care practices around patient-centered medical home (PCMH) transformation.
Pathways to Diabetes Prevention
 Pathways to Diabetes Prevention How Colorado Organizations are Creating Healthcare Referral Systems that Work Introduction It is estimated that 35% of Colorado adults and half of all adults aged 65 years
Pathways to Diabetes Prevention How Colorado Organizations are Creating Healthcare Referral Systems that Work Introduction It is estimated that 35% of Colorado adults and half of all adults aged 65 years
CPC+ CHANGE PACKAGE January 2017
 CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
CPC+ CHANGE PACKAGE January 2017 Table of Contents CPC+ DRIVER DIAGRAM... 3 CPC+ CHANGE PACKAGE... 4 DRIVER 1: Five Comprehensive Primary Care Functions... 4 FUNCTION 1: Access and Continuity... 4 FUNCTION
Driving the value of health care through integration. Kaiser Permanente All Rights Reserved.
 Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Driving the value of health care through integration February 13, 2012 Kaiser Permanente 2010-2011. All Rights Reserved. 1 Today s agenda How Kaiser Permanente is transforming care How we re updating our
Driving Patient Engagement through Mobile Care Management
 Driving Patient Engagement through Mobile Care Management Session #97, February 21, 2017 Susan Beaton, Senior Director of Provider Services and Care Management, Blue Cross Blue Shield of Nebraska Jacob
Driving Patient Engagement through Mobile Care Management Session #97, February 21, 2017 Susan Beaton, Senior Director of Provider Services and Care Management, Blue Cross Blue Shield of Nebraska Jacob
Supplemental materials for:
 Supplemental materials for: Krist AH, Woolf SH, Bello GA, et al. Engaging primary care patients to use a patient-centered personal health record. Ann Fam Med. 2014;12(5):418-426. ONLINE APPENDIX. Impact
Supplemental materials for: Krist AH, Woolf SH, Bello GA, et al. Engaging primary care patients to use a patient-centered personal health record. Ann Fam Med. 2014;12(5):418-426. ONLINE APPENDIX. Impact
Adopting Accountable Care An Implementation Guide for Physician Practices
 Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Adopting Accountable Care An Implementation Guide for Physician Practices EXECUTIVE SUMMARY November 2014 A resource developed by the ACO Learning Network www.acolearningnetwork.org Executive Summary Our
Core Item: Clinical Outcomes/Value
 Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Cover Page Core Item: Clinical Outcomes/Value Name of Applicant Organization: Fremont Family Care Organization s Address: 2540 N Healthy Way, Fremont, NE 68025 Submitter s Name: Elizabeth Belmont Submitter
Chat with a Doctor: On-Demand, Asynchronous Physician Advice
 Chat with a Doctor: On-Demand, Asynchronous Physician Advice Session 189: March 7, 2018 Ari Melmed, MD, FACEP Assistant Regional Director for Telehealth, Colorado Permanente Medical Group 1 Conflict of
Chat with a Doctor: On-Demand, Asynchronous Physician Advice Session 189: March 7, 2018 Ari Melmed, MD, FACEP Assistant Regional Director for Telehealth, Colorado Permanente Medical Group 1 Conflict of
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP)
") BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
BUILDING BLOCKS OF PRIMARY CARE ASSESSMENT FOR TRANSFORMING TEACHING PRACTICES (BBPCA-TTP) DIRECTIONS FOR COMPLETING THE SURVEY This survey is designed to assess the organizational change of a primary
Asthma Disease Management Program
 Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Asthma Disease Management Program A: Program Content GHC-SCW is committed to helping members, and their practitioners, manage chronic illness by providing tools and resources to empower members to self-manage
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws.
 Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
Disclaimer This webinar may be recorded. This webinar presents a sampling of best practices and overviews, generalities, and some laws. This should not be used as legal advice. Itentive recognizes that
COMPARING FULL SERVICE CALIFORNIA HMO ENROLLMENT FOR MARCH 31, 2014 AND MARCH 31, 2015 (see Notes, pg 8)
") COMPARING FULL SERVICE CALIFORNIA HMO ENROLLMENT FOR MARCH 31, 2014 AND MARCH 31, 2015 (see Notes, pg 8) ALL HMO PRODUCT LINES ENROLLMENT HMO Plans 2014 HMO Plans 2015 Difference Percent Chg Commercial
COMPARING FULL SERVICE CALIFORNIA HMO ENROLLMENT FOR MARCH 31, 2014 AND MARCH 31, 2015 (see Notes, pg 8) ALL HMO PRODUCT LINES ENROLLMENT HMO Plans 2014 HMO Plans 2015 Difference Percent Chg Commercial
REDUCING HEALTH DISPARITIES AT CALIFORNIA S PUBLIC HEALTH CARE SYSTEMS THROUGH THE MEDI-CAL 2020 WAIVER S PRIME PROGRAM May 2018
 1 CALIFORNIA ASSOCIATION of PUBLIC HOSPITALS AND HEALTH SYSTEMS REDUCING HEALTH DISPARITIES AT CALIFORNIA S PUBLIC HEALTH CARE SYSTEMS THROUGH THE MEDI-CAL 2020 WAIVER S PRIME PROGRAM May 2018 INTRODUCTION
1 CALIFORNIA ASSOCIATION of PUBLIC HOSPITALS AND HEALTH SYSTEMS REDUCING HEALTH DISPARITIES AT CALIFORNIA S PUBLIC HEALTH CARE SYSTEMS THROUGH THE MEDI-CAL 2020 WAIVER S PRIME PROGRAM May 2018 INTRODUCTION
Advocate Health Care. PURPOSE: Describe briefly the overall purpose of this position, i.e., Why does it exist?
 http://corp2371.ahc-ad.advocatehealth.com/jobdescriptions/printpreview.aspx?jdid=40442 4/24/2012 Advocate Health Care Title: Practice Operations Coach PURPOSE: Describe briefly the overall purpose of this
http://corp2371.ahc-ad.advocatehealth.com/jobdescriptions/printpreview.aspx?jdid=40442 4/24/2012 Advocate Health Care Title: Practice Operations Coach PURPOSE: Describe briefly the overall purpose of this
Telehealth: Overcoming the challenges of implementing innovative health care solutions
 Telehealth: Overcoming the challenges of implementing innovative health care solutions NRTRC 5 TH ANNUAL CONFERENCE MARCH 22, 2016 ROKI CHAUHAN, MD, FAAFP Disclaimer 2 The material presented here is being
Telehealth: Overcoming the challenges of implementing innovative health care solutions NRTRC 5 TH ANNUAL CONFERENCE MARCH 22, 2016 ROKI CHAUHAN, MD, FAAFP Disclaimer 2 The material presented here is being
Appendix 1. Immediate Postpartum Long-Acting Reversible Contraception (LARC)
") Appendix 1. Immediate Postpartum Long-Acting Reversible Contraception (LARC) Program Implementation Guide: Exploration Stage Implementation Guide Overview Each stage of the implementation guide is organized
Appendix 1. Immediate Postpartum Long-Acting Reversible Contraception (LARC) Program Implementation Guide: Exploration Stage Implementation Guide Overview Each stage of the implementation guide is organized
Part 2: PCMH 2014 Standards
 Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
Part 2: PCMH 2014 Standards Heather Russo, CCE PCMH Consultant September 15, 2015 Advancing Healthcare Improving Health For Practices Recognized at Level 2 or Level 3 under the 2011 Standards Your Guide
TELEHEALTH FOR HEALTH SYSTEMS: GUIDE TO BEST PRACTICES
 TELEHEALTH FOR HEALTH SYSTEMS: GUIDE TO BEST PRACTICES Overview Telemedicine delivers care that s convenient and cost effective letting physicians and patients avoid unnecessary travel and wait time. Health
TELEHEALTH FOR HEALTH SYSTEMS: GUIDE TO BEST PRACTICES Overview Telemedicine delivers care that s convenient and cost effective letting physicians and patients avoid unnecessary travel and wait time. Health
econsultation Technical Assistance Webinar #1: Background, Conceptual Framework and Early Successes SEPTEMBER 9, 2015 WEBINAR #1
 econsultation Technical Assistance Webinar #1: Background, Conceptual Framework and Early Successes SEPTEMBER 9, 2015 WEBINAR #1 Agenda 1 2 3 Introductions of grantees Overview of program and foundation
econsultation Technical Assistance Webinar #1: Background, Conceptual Framework and Early Successes SEPTEMBER 9, 2015 WEBINAR #1 Agenda 1 2 3 Introductions of grantees Overview of program and foundation
Beau Hennemann IHSS Program Manager
 Beau Hennemann IHSS Program Manager Consumer, Family and Caregiver Forum February 1, 2013 L.A. Care is the nation s largest public health plan, with more than 1 million members. L.A. Care is governed by
Beau Hennemann IHSS Program Manager Consumer, Family and Caregiver Forum February 1, 2013 L.A. Care is the nation s largest public health plan, with more than 1 million members. L.A. Care is governed by
HEALTHY FAMILIES PROGRAM TRANSITION TO MEDI-CAL
 HEALTHY FAMILIES PROGRAM TRANSITION TO MEDI-CAL NETWORK ADEQUACY ASSESSMENT REPORT PHASE 1 November 1, 2012 Submitted by the California Department of Managed Health Care in Fulfillment of the Requirements
HEALTHY FAMILIES PROGRAM TRANSITION TO MEDI-CAL NETWORK ADEQUACY ASSESSMENT REPORT PHASE 1 November 1, 2012 Submitted by the California Department of Managed Health Care in Fulfillment of the Requirements
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability
 for Hypertension Patients: Driving Value and Sustainability") Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Comprehensive Medication Management (CMM) for Hypertension Patients: Driving Value and Sustainability Steven W. Chen PharmD, FASHP, FCSHP, FNAP Associate Dean for Clinical Affairs chens@usc.edu, 323-206-0427
Introduction Overview of the Specialty Care Initiative Overview of the Case Study
 Introduction Overview of the Specialty Care Initiative The Specialty Care Initiative (SCI) supported community coalitions in developing and implementing strategies to address specialty care demand and
Introduction Overview of the Specialty Care Initiative The Specialty Care Initiative (SCI) supported community coalitions in developing and implementing strategies to address specialty care demand and
Integrated Behavioral Health Project Phase III Project Description
 Integrated Behavioral Health Project Phase III Project For Phase III, the Integrated Behavioral Health Project has selected seven grantees to advance the base of knowledge concerning integrated care in
Integrated Behavioral Health Project Phase III Project For Phase III, the Integrated Behavioral Health Project has selected seven grantees to advance the base of knowledge concerning integrated care in
Team Care Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc.
 2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
2008 Best Practices in Managing Hypertension Learning Collaborative Sponsored by AMGA and Daiichi Sankyo, Inc. November 12-14, 2008, Scottsdale, AZ Great Falls Clinic, LLP Great Falls, Montana Team Care
Patient Care: Case Study in EHR Implementation. With Help From Monkeys, Mice, and Penguins. Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007
 Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Using Information Technology to Drive Patient Care: Case Study in EHR Implementation With Help From Monkeys, Mice, and Penguins Tom Goodwin, MHA MIT Medical Cambridge, MA March 2007 MIT Medical Staff 122
Medical Home Renovations: A Patient-centered Medical Home Case Study
 Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Medical Home Renovations: A Patient-centered Medical Home Case Study Robert Reid MD PhD, Group Health Research Institute Annual Snively Lecture, University of California Davis January 18, 2011 Medical
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care. Barbara Craig, Midas+ SaaS Advisor
 Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
Using Facets of Midas+ Hospital Case Management to Support Transitions of Care Barbara Craig, Midas+ SaaS Advisor What does Transitional Care Include? Transitional Care is the smooth conversion of a patient
DHCS Update: Major Initiatives and Strategies Towards Standardization
 DHCS Update: Major Initiatives and Strategies Towards Standardization Javier Portela, Division Chief Managed Care Operations Department of Health Care Services ICE 2016 Annual Conference December 2016
DHCS Update: Major Initiatives and Strategies Towards Standardization Javier Portela, Division Chief Managed Care Operations Department of Health Care Services ICE 2016 Annual Conference December 2016
Request for Proposals
 Request for Proposals External Program Office for the California Improvement Network Proposals due July 14, 2017, noon PDT Grant recipient announced August 1, 2017 Onboarding and planning period August
Request for Proposals External Program Office for the California Improvement Network Proposals due July 14, 2017, noon PDT Grant recipient announced August 1, 2017 Onboarding and planning period August
California ED Diversion Project Evaluation Final Report
 California ED Diversion Project Evaluation Final Report February 2009 Edward M. Castillo, Ph.D., MPH Gary M. Vilke, M.D. Theodore C. Chan, M.D. University of California, San Diego Department of Emergency
California ED Diversion Project Evaluation Final Report February 2009 Edward M. Castillo, Ph.D., MPH Gary M. Vilke, M.D. Theodore C. Chan, M.D. University of California, San Diego Department of Emergency
Sutter Health. Steven Lane, MD, MPH, FAAFP Sutter EHR Ambulatory Physician Director
 Interoperability @ Sutter Health Steven Lane, MD, MPH, FAAFP Sutter EHR Ambulatory Physician Director Main Points Secure health information exchange is happening in Northern California Sutter Health utilizes
Interoperability @ Sutter Health Steven Lane, MD, MPH, FAAFP Sutter EHR Ambulatory Physician Director Main Points Secure health information exchange is happening in Northern California Sutter Health utilizes
California County Customer Service Centers Survey of Current Human Service Operations July 2012
 California County Customer Service Centers Survey of Current Human Service Operations July 2012 I. Introduction Early this spring, the County Welfare Directors Association of California (CWDA) worked with
California County Customer Service Centers Survey of Current Human Service Operations July 2012 I. Introduction Early this spring, the County Welfare Directors Association of California (CWDA) worked with
Executive Summary: Davies Ambulatory Award Community Health Organization (CHO)
") Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
Davies Ambulatory Award Community Health Organization (CHO) Name of Applicant Organization: Community Health Centers, Inc. Organization s Address: 110 S. Woodland St. Winter Garden, Florida 34787 Submitter
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH
 IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
IMPROVING TRANSITIONS OF CARE IN POPULATION HEALTH TABLE OF CONTENTS 1. The Transitions Challenge 2. Impact of Care Transitions 3. Patient Insights from Project Boost 4. Identifying Patients 5. Improving
Department of Health Care Services
 State of California Department of Health Care Services Streamlining the Cal MediConnect Voluntary Enrollment Experience April 2016 This is one of three documents released by the Department of Health Care
State of California Department of Health Care Services Streamlining the Cal MediConnect Voluntary Enrollment Experience April 2016 This is one of three documents released by the Department of Health Care
Kern County s Health Care Coverage Initiative Network Structure: Interim Findings
 Kern County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The Health Care Coverage Initiative (HCCI) program in Kern County is known as the Kern Medical Center Health
Kern County s Health Care Coverage Initiative Network Structure: Interim Findings Introduction The Health Care Coverage Initiative (HCCI) program in Kern County is known as the Kern Medical Center Health
Transforming Healthcare Delivery, the Challenges for Behavioral Health
 Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
Transforming Healthcare Delivery, the Challenges for Behavioral Health Presented by: M.T.M. Services, LLC P. O. Box 1027, Holly Springs, NC 27540 Phone: 919-434-3709 Fax: 919-773-8141 E-mail: mtmserve@aol.com
New Approaches in a Shifting Health Care Environment: Case Studies from CA's Title X Family Planning Network
 New Approaches in a Shifting Health Care Environment: Case Studies from CA's Title X Family Planning Network California Family Health Council 2016 1 New Approaches in a Shifting Health Care Environment:
New Approaches in a Shifting Health Care Environment: Case Studies from CA's Title X Family Planning Network California Family Health Council 2016 1 New Approaches in a Shifting Health Care Environment:
Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
 Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Organization: Solution Title: Calvert Memorial Hospital Calvert CARES: Collaborative Activation of Resources and Empowerment Services Building Programs to Fit Patients vs. Bending Patients to Fit Programs
Program Overview
 2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
2015-2016 Program Overview 04HQ1421 R03/16 Blue Cross and Blue Shield of Louisiana is an independent licensee of the Blue Cross and Blue Shield Association and incorporated as Louisiana Health Service
Preparing California s Community-Based Organizations to Partner with the Health Care Sector by Building Business Acumen:
 Preparing California s Community-Based Organizations to Partner with the Health Care Sector by Building Business Acumen: Case Studies from the First Cohort of Linkage Lab Grantees August 2015 Authors:
Preparing California s Community-Based Organizations to Partner with the Health Care Sector by Building Business Acumen: Case Studies from the First Cohort of Linkage Lab Grantees August 2015 Authors:
Colorado Medical-Dental Integration Project (CO MDI)
") Colorado Medical-Dental Integration Project (CO MDI) Allison Cusick, MPA, CHES National Oral Health Conference April 2016 Colorado Medical-Dental Integration CO MDI Five-Year Initiative Launched in 2014
Colorado Medical-Dental Integration Project (CO MDI) Allison Cusick, MPA, CHES National Oral Health Conference April 2016 Colorado Medical-Dental Integration CO MDI Five-Year Initiative Launched in 2014
Grove Medical Associates, P.C. A Case Study in Continuous Quality Improvement
 CASE STUDY The Organization Privately owned internal medicine practice 5 physicians, 1 location 9,000+ active patients The Challenge Find an Electronic Medical Record solution that would track continuous
CASE STUDY The Organization Privately owned internal medicine practice 5 physicians, 1 location 9,000+ active patients The Challenge Find an Electronic Medical Record solution that would track continuous
Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience
 University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
University of Michigan Health System Program and Operations Analysis Neurosurgery Clinic Analysis: Increasing Patient Throughput and Enhancing Patient Experience Final Report To: Stephen Napolitan, Assistant
Project Report Health Information Exchange Readiness Assessment/Survey
 Prepared for California Emergency Medical Services Authority Project Report Health Information Exchange Readiness Assessment/Survey RFO#: EMS-1324 Submission Date: December 13, 2013 Submitted by: Lumetra
Prepared for California Emergency Medical Services Authority Project Report Health Information Exchange Readiness Assessment/Survey RFO#: EMS-1324 Submission Date: December 13, 2013 Submitted by: Lumetra
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING
 Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING") Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
Generations Advantage Focus DC (HMO SNP) Diabetes Care Special Needs Plan GENERAL MODEL OF CARE (MOC) TRAINING Through this training you will learn: What is a SNP? What is Martin s Point Generations Advantage
IMPACT OF RN HYPERTENSION PROTOCOL
 1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
1 IMPACT OF RN HYPERTENSION PROTOCOL Joyce Cheung, RN, Marie Kuzmack, RN Orange County Hypertension Team Kaiser Permanente, Orange County Joyce.m.cheung@kp.org and marie-aline.z.kuzmack@kp.org Cell phone:
Whole Person Care Pilots & the Health Home Program
 Whole Person Care Pilots & the Health Home Program Molly Brassil, MSW Director of Behavioral Health Integration, Harbage Consulting December 13, 2016 Presentation Overview Delivery System Reform in California
Whole Person Care Pilots & the Health Home Program Molly Brassil, MSW Director of Behavioral Health Integration, Harbage Consulting December 13, 2016 Presentation Overview Delivery System Reform in California
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care
 Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Kaiser Permanente: Integration, Innovation, and Transformation in Health Care March 2018 Karin Cooke, MBA, Director, Kaiser Permanente International Karin.C.Cooke@kp.org kp.org/international Copyright
Lessons Learned from the Dual Eligibles Demonstrations. Real-Life Takeaways from California and Other States
 Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
Lessons Learned from the Dual Eligibles Demonstrations 1 May 28, 2015 Real-Life Takeaways from California and Other States Introductions Toby Douglas Consultant, MAXIMUS Former Director of California Department
Introduction. Summary of Approved WPC Pilots
 The California Whole Person Care Pilot Program: County Partnerships to Improve the Health of Medi-Cal Beneficiaries Prepared by Lucy Pagel, Tanya Schwartz and Jennifer Ryan with support from The California
The California Whole Person Care Pilot Program: County Partnerships to Improve the Health of Medi-Cal Beneficiaries Prepared by Lucy Pagel, Tanya Schwartz and Jennifer Ryan with support from The California
DMC-ODS. System Transformation. Presented at DHCS 2017 Annual Conference. Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW
 DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
DMC-ODS System Transformation Presented at DHCS 2017 Annual Conference Elizabeth Stanley-Salazar, MPH Doug Bond Lisa Garcia, LCSW Objectives Understand managed care principles applied to DMC-ODS Waiver
Project Update. November 2017
 Project Update November 2017 CWDS / Child Welfare Digital Services Digital Services & Support CWDS Web (Development) CWDS Technology Platform (Development) CWDS Infrastructure (Development) Digital Services
Project Update November 2017 CWDS / Child Welfare Digital Services Digital Services & Support CWDS Web (Development) CWDS Technology Platform (Development) CWDS Infrastructure (Development) Digital Services
Fostering Effective Integration of Behavioral Health and Primary Care in Massachusetts Guidelines. Program Overview and Goal.
 Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
Blue Cross Blue Shield of Massachusetts Foundation Fostering Effective Integration of Behavioral Health and Primary Care 2015-2018 Funding Request Overview Summary Access to behavioral health care services
HEALTH PLANS FOR PARTICIPANTS
 Kern County 2018 Retiree HEALTH PLANS FOR PARTICIPANTS OVER AGE 65 (Must have BOTH Medicare Parts A & B) For current participating physician information, please contact each plan directly. This summary
Kern County 2018 Retiree HEALTH PLANS FOR PARTICIPANTS OVER AGE 65 (Must have BOTH Medicare Parts A & B) For current participating physician information, please contact each plan directly. This summary
Coastal Medical, Inc.
 A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
A Culture of Collaboration The Organization Physician-owned group Currently 19 offices across the state of Rhode Island and growing 85 physicians, 101 care providers The Challenge Implement a single, unified
Community Leadership Project Request for Proposals August 31, 2012
 Community Leadership Project Request for Proposals August 31, 2012 We are pleased to invite proposals for a second phase of the Community Leadership Project, a funding partnership between the Packard,
Community Leadership Project Request for Proposals August 31, 2012 We are pleased to invite proposals for a second phase of the Community Leadership Project, a funding partnership between the Packard,
Understanding the Initiative Landscape in Medi-Cal. IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager
 Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Understanding the Initiative Landscape in Medi-Cal IHA Stakeholder Meeting September 23, 2016 Sarah Lally, Project Manager Agenda Welcome / Introduction Sarah Lally, Project Manager Inland Empire Health
Using Federal Funds to Engage Agencies to Address Job Placement
 Using Federal Funds to Engage Agencies to Address Job Placement Presented by: Cynthia D. Banks, Director Community and Senior Services and Dr. Steven J. Golightly, Director Child Support Services Department
Using Federal Funds to Engage Agencies to Address Job Placement Presented by: Cynthia D. Banks, Director Community and Senior Services and Dr. Steven J. Golightly, Director Child Support Services Department
FACT SHEET Low Income Assistance: Cal MediConnect(E-004) p. 1 of 6
 p. 1 of 6") FACT SHEET Low Income Assistance: Cal MediConnect(E-004) p. 1 of 6 Low Income Assistance: Cal MediConnect What is Cal MediConnect? California is 1 of 15 states that has signed a Memorandum of Understanding
FACT SHEET Low Income Assistance: Cal MediConnect(E-004) p. 1 of 6 Low Income Assistance: Cal MediConnect What is Cal MediConnect? California is 1 of 15 states that has signed a Memorandum of Understanding
HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT SEPTEMBER 2011 MELBOURNE, AUSTRALIA
 HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT 20 22 SEPTEMBER 2011 MELBOURNE, AUSTRALIA Public-Private Partnership (PPP) Projects as Cornerstones of ehr Development in Hong Kong Dr CHOY Khai Meng Chief
HIMSS ASIAPAC 11 CONFERENCE & LEADERSHIP SUMMIT 20 22 SEPTEMBER 2011 MELBOURNE, AUSTRALIA Public-Private Partnership (PPP) Projects as Cornerstones of ehr Development in Hong Kong Dr CHOY Khai Meng Chief
[Evelyn will get back to us this evening with her changes.]
![[Evelyn will get back to us this evening with her changes.]](/thumbs/83/88705724.jpg "[Evelyn will get back to us this evening with her changes.]") Page 1 of 10 Introduction Hello, my name is Mary Burke, RN. I have more than 20 years of experience as a nurse; primarily in outpatient and clinic settings. I m now at the University of Iowa Hospitals
Page 1 of 10 Introduction Hello, my name is Mary Burke, RN. I have more than 20 years of experience as a nurse; primarily in outpatient and clinic settings. I m now at the University of Iowa Hospitals
All ACO materials are available at What are my network and plan design options?
 ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
ACO Toolkit: A Roadmap for Employers What is an ACO? Is an ACO strategy right for my company? Which ACOs are ready? All ACO materials are available at www.businessgrouphealth.org What are my network and
Patient Payment Check-Up
 Patient Payment Check-Up SURVEY REPORT 2017 Attitudes and behavior among those billing for healthcare and those paying for it CONDUCTED BY 2017 Patient Payment Check-Up Report 1 Patient demand is ahead
Patient Payment Check-Up SURVEY REPORT 2017 Attitudes and behavior among those billing for healthcare and those paying for it CONDUCTED BY 2017 Patient Payment Check-Up Report 1 Patient demand is ahead
Core Item: Hospital. Cover Page. Admissions and Readmissions. Executive Summary
 Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Cover Page Core Item: Hospital Admissions and Readmissions Name of Applicant Organization: Horizon Family Medical Group Organization s Address: 4 Coates Drive, Goshen NY 10924 Submitter s Name: Rinku Singh
Developing and Operationalizing a Telehealth Strategy. Cone Health s Story \370127(pptx)-E2 DD
-E2 DD") Developing and Operationalizing a Telehealth Strategy Cone Health s Story 0 At the conclusion of this presentation, attendees should have developed a comfortable understanding of the following: Learning
Developing and Operationalizing a Telehealth Strategy Cone Health s Story 0 At the conclusion of this presentation, attendees should have developed a comfortable understanding of the following: Learning
HPV Vaccination Quality Improvement: Physician Perspective
 HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
HPV Vaccination Quality Improvement: Physician Perspective Discussion of efforts to raise HPV vaccine coverage using quality improvement from a physician s perspective Alix Casler, M.D., F.A.A.P. Chief
2017 HIMSS DAVIES APPLICANT
 2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
2017 HIMSS DAVIES APPLICANT Introduction of NOMS Team Members Melissa Thomas IT Project Director Joshua Frederick, CPA, MT Chief Executive Officer Jennifer Hohman, MD Executive Vice President, NOMS Healthcare
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year
 A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
A Bigger Bang Patient Portal Strategy: How we activated 100K patients in our First Year Saturday March 25 th, 2017 Lindsay Altimare, MPA Director, LVPG Operations Lehigh Valley Health Network Michael Sheinberg,
Technology Fundamentals for Realizing ACO Success
 Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
Technology Fundamentals for Realizing ACO Success Introduction The accountable care organization (ACO) concept, an integral piece of the government s current health reform agenda, aims to create a health
PCSP 2016 PCMH 2014 Crosswalk
 - Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
- Crosswalk 1 Crosswalk The table compares NCQA s Patient-Centered Specialty Practice (PCSP) 2016 standards with NCQA s Patient-Centered Medical Home (PCMH) 2014 standards. The column on the right identifies
3 Ways to Increase Patient Visits
 3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
3 Ways to Increase Patient Visits 3 Ways to Increase Patient Visits www.kareo.com kareo.com Table of Contents Introduction 03 Create an Effective Recall/Recare Program 04 Build and Manage Your Online Presence
National Council for Behavioral Health. Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community
 National Council for Behavioral Health Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community Request for Applications INTRODUCTION The National Council for Behavioral Health
National Council for Behavioral Health Trauma-informed Primary Care: Fostering Resilience and Recovery Learning Community Request for Applications INTRODUCTION The National Council for Behavioral Health
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA
 Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
Community Care Coordination Cross Continuum Care IHC Medical Home Conference September 5, 2012 Des Moines IA Peg Bradke, RN, MA Director of Heart Care Services St. Luke s Hospital, Cedar Rapids, IA Session
FOR IMMEDIATE RELEASE April 17, Media Line Contacts: Covered California (916)
") FOR IMMEDIATE RELEASE April 17, 2014 Media Line Contacts: Covered California (916) 205-8403 California Department of Health Care Services (916) 440-7660 COVERED CALIFORNIA S HISTORIC FIRST OPEN ENROLLMENT
FOR IMMEDIATE RELEASE April 17, 2014 Media Line Contacts: Covered California (916) 205-8403 California Department of Health Care Services (916) 440-7660 COVERED CALIFORNIA S HISTORIC FIRST OPEN ENROLLMENT
Strengthening Primary Care for Patients:
 Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
Strengthening Primary Care for Patients: Geisinger Health Plan Danville, Pa. Background Geisinger Health Plan (GHP) is a nonprofit health maintenance organization serving the health care needs of more
PCMH 2014 Standards and Guidelines
 PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
PCMH 2014 Standards and Guidelines 28 NCQA Patient-Centered Medical Home (PCMH) 2014 April 13, 2015 PCMH 1: Patient-Centered Access 29 PCMH 1: Patient-Centered Access 10.00 points provides access to team-based
Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:
 Tier One Milestone (STC-61) Application for Enhancement Projects. Submitted by:") 2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
2012-2013 Low Income Pool (LIP) Tier One Milestone (STC-61) Application for Enhancement Projects Submitted by: Florida Health Sciences Center, Inc. d/b/a Tampa General Hospital July 31, 2012 1 1. Applicant:
Annual Reporting Requirements for PCMH Recognition Overview & Table Reporting Period: 4/3/ /31/2018
 Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
Annual Reporting s for PCMH Recognition Overview & Table Reporting Period: 4/3/2017 12/31/2018 Redesign Goals NCQA redesigned its PCMH Recognition program in April 2017 for practices to maintain an ongoing
ACOs: California Style
 ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
ACOs: California Style ACO Congress John E. Jenrette, M.D. Chief Executive Officer Sharp Community Medical Group November 2, 2011 California Style California Style A CO California Style California Style
UTILIZING HEALTH CLINICS TO MANAGE AND REDUCE HEALTHCARE COSTS
 UTILIZING HEALTH CLINICS TO MANAGE AND REDUCE HEALTHCARE COSTS PRESENTED BY: Mardi Burns, CHC Senior Vice President, Senior Benefits Consultant Al Jaeger, CEBS Senior Vice President, Senior Benefits Consultant
UTILIZING HEALTH CLINICS TO MANAGE AND REDUCE HEALTHCARE COSTS PRESENTED BY: Mardi Burns, CHC Senior Vice President, Senior Benefits Consultant Al Jaeger, CEBS Senior Vice President, Senior Benefits Consultant
Performance Incentives in the Southern California Permanente Medical Group (SCPMG):
:") Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
Performance Incentives in the Southern California Permanente Medical Group (SCPMG): 1994-2007 Joel D. Hyatt, MD Assistant Medical Director Southern California Permanente Medical Group joel.d.hyatt@kp.org
Medi-Cal Managed Care: Continuity of Care
 California s Protection & Advocacy System Toll-Free (800) 776-5746 Medi-Cal Managed Care: Continuity of Care February 2017, Pub #5545.01 If you have regular Medi-Cal 1 and you are now being told that you
California s Protection & Advocacy System Toll-Free (800) 776-5746 Medi-Cal Managed Care: Continuity of Care February 2017, Pub #5545.01 If you have regular Medi-Cal 1 and you are now being told that you
KPMG Digital Health Pulse April 2017
 KPMG Digital Health Pulse 2017 April 2017 Research purpose and design To identify key perceptions about the pace of digital health adoption and key challenges to implementing virtual care programs at hospitals
KPMG Digital Health Pulse 2017 April 2017 Research purpose and design To identify key perceptions about the pace of digital health adoption and key challenges to implementing virtual care programs at hospitals
Table of Contents. Table of Contents
 Table of Contents Table of Contents Table of Contents... 1 Acknowledgements... 4 Definitions and Abbreviations... 5 Executive Summary... 6 1.0 Background Information... 8 Introduction... 8 Overview of
Table of Contents Table of Contents Table of Contents... 1 Acknowledgements... 4 Definitions and Abbreviations... 5 Executive Summary... 6 1.0 Background Information... 8 Introduction... 8 Overview of
Outreach & Sales Division Business Development Unit Introduction to the Outreach & Sales Division Field Team Webinar
 Outreach & Sales Division Business Development Unit Introduction to the Outreach & Sales Division Field Team Webinar Tuesday, August 18, 2015 11am to 12noon Webinar Housekeeping Webinar link: http://hbex.coveredca.com/stakeholders/webinar/
Outreach & Sales Division Business Development Unit Introduction to the Outreach & Sales Division Field Team Webinar Tuesday, August 18, 2015 11am to 12noon Webinar Housekeeping Webinar link: http://hbex.coveredca.com/stakeholders/webinar/
SC Telehealth All 2017
 SC Telehealth Alliance QUARTERLY REPORT 2017 QUARTER THREE PAGE 1 Executive Summary In the third quarter of 2017, the South Carolina Telehealth Alliance (SCTA) continued its work executing the tactics
SC Telehealth Alliance QUARTERLY REPORT 2017 QUARTER THREE PAGE 1 Executive Summary In the third quarter of 2017, the South Carolina Telehealth Alliance (SCTA) continued its work executing the tactics
Virtual Care Solutions Moving Care from the Hospital to the Home
 Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
Virtual Care Solutions Moving Care from the Hospital to the Home Access Strategy Revenue Strategy Primary Care Strategy Building onto existing infrastructure to move to the next paradigm of healthcare
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013
 State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
State Medicaid Directors Driving Innovation: Continuous Quality Improvement February 25, 2013 The National Association of Medicaid Directors (NAMD) is engaging states in shared learning on how Medicaid
BCBSM Physician Group Incentive Program
 BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
BCBSM Physician Group Incentive Program Organized Systems of Care Initiatives Interpretive Guidelines 2012-2013 V. 4.0 Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS
 CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies
CROSSWALK: CHANGE CONCEPTS FOR PRACTICE TRANSFORMATION AND 2014 NCQA PCMH TM RECOGNITION STANDARDS 1a. Provide visible and sustained leadership to lead overall cultural change as well as specific strategies