Table of Contents Florida Department of Juvenile Justice Daytona Sex Offender Program
|
|
|
- Job Clark
- 6 years ago
- Views:
Transcription
1
2 Table of Contents Transmittal Letter and Addendums Volume 1, Tab 1 Attachment O Cross Reference Table Attachment M and N Addendum 1 and 2 Page Certificate of a Drug-Free Workplace Attachment K Volume 1, Tab 2 Introductory Statement Volume 1, Tab 3 Introductory Statement... 1 Management Capability Volume 1, Tab 4 2.a. Services b. Services in Department Owned or Leased c. Options Staffing Program Services Volume 1, Tab 5 I. General Description II. Youth To Be Served D.1. Admission Requirements and Eligibility D.2. Classification and Grouping of Youth by Needs III. Service Tasks A.1. Care and Custody Services A.2. Case Management A.3. Health Services A.4. Health Education Programming A.5. OSHA Requirements A.6. Mental Health and Substance Abuse Services A.7. Delinquency Programming A.8. Educational Services A.9. Pre-Vocational and Vocational Services A.10. Job Training Placement A.11. Self-Sufficiency Planning A.12. Discharge Policy and Transition Services A.13. Staff Training A.14. Living Environment A.15. Behavioral Management System A.16. Religious/Spiritual Opportunities A.17. Recreational and Leisure Time Activities A.18. Restorative Justice Philosophy and Restorative Programming A.19 Community Involvement Opportunities A.20. Transportation Services IV. Limit of Services V. Staffing/Personnel VI. Service Location VII. Deliverables VIII. Performance Measures RFP R2107
3 Table of Contents Page Exhibits Exhibit 1: Certificate of Fact Exhibit 2: List of Facilities Opened, Transitioned and Acquired by G4S Exhibit 3: Recruitment Process Design Exhibit 4: Behavior Management Level System Exhibit 5: Climate Action Award Nomination Exhibit 6: We connect to YOU DSOP project Exhibit 7: Spirituality Strength License Verifications DSOP DHA- Bonnet G4S Psychiatrist- Amiel G4S VP of Clinical Services- Astringer G4S Contracted renown Licensed Sex Offender Therapist- Cotter G4S Licensed Sex Offender Therapist- Drake G4S Licensed Sex Offender Therapist- McDonald G4S Licensed Sex Offender Therapist- Molyneaux Letters DHA letter Dr. Bonnet Psychiatrist letter- Dr. Amiel Licensed Sex Offender Therapist- Dr. Cotter RFP R2107
4
5
6 Cross Reference Table Attachment O ATTACHMENT O THE COMPLETION OF THIS CROSS REFERENCE TABLE IS A MANDATORY REQUIREMENT SECTION/PART RFP/PROPOSAL CROSS REFERENCE TABLE RFP DOCUMENTATION (TO BE COMPLETED BY DEPARTMENT) LOCATION IN PROPOSAL (TO BE COMPLETED BY PROSPECTIVE PROVIDER) SUBJECT PAGE NUMBERS SECTIONS/PARTS MANDATORY CRITERIA (X FOR YES) GENERAL PROPOSAL RESPONSE REQUIREMENTS PLEASE NOTE: General Proposal Response Requirements that are checked as Mandatory Criteria must be provided by the prospective Provider to be considered responsive to this RFP. Failure to provide the required mandatory documentation will result in a proposal not being evaluated and rejected as non-responsive. Section V. E and Cross Reference Table X Tab 1 Cross Reference Table behind Letter of Section XIX B. Transmittal, Volume I, Tab 1 Section V. B. and Transmittal Letter containing all the information X Tab 1 Transmittal Letter, Volume I, Tab 1 Section XIX A. required by Section XIX. A. Office Name, Address, Telephone Number, Name X Tab 1 Transmittal Letter, Volume I, Tab 1 Section XIX A.1 and Title of Official with authority to bind the Contract. Section XIX A.1 FEID Number X Tab 1 Transmittal Letter, Volume I, Tab 1 Section XIX A.1 DUNS Number X Tab 1 Transmittal Letter, Volume I, Tab 1 Section XIX A.2 Name, Title, Address, Telephone Number of X Transmittal Letter, Volume I, Tab 1 Tab 1 Contract Manager D/B/A Doing Business As with Reason for D/B/A (if X N/A N/A Section XIX A.3 applicable). Statement Provider agrees to all terms and X Tab 1 Transmittal Letter, Volume I, Tab 1 Section XIX A.4 conditions contained in the Request for Proposal for which this proposal is submitted. Statement Provider meets all Terms and X Tab 1 Transmittal Letter, Volume I, Tab 1 Section XIX A.5 Conditions of Attachment A, including not presently debarred, suspended, or proposed for debarment. Section XIX A.6 Section XIX A.7. Section V.C. and Section XIX E. 1. A and b. Statement Provider certifies that neither the prospective Provider nor anyone acting on its behalf has contacted anyone, between the release of the solicitation and due date of this solicitation, any employee or officer of the executive or legislative branch concerning any aspect of this solicitation, except in writing to the procurement officer or as provided in the solicitation documents. Statement Providers certifies that the prospective Provider agrees to be responsible for the reporting of all admissions and releases in the Juvenile Justice Information System (JJIS) within 24 hours of the admission/release and for updating the projected release dates of youth at a minimum of once per week if required by this RFP. Attachment J A completed & signed copy of Attachment J with the proposed annual Contract dollar amount at or below the annual maximum. Contract dollar amount stated in the RFP. X Tab 1 Transmittal Letter, Volume I, Tab 1 X Tab 1 14 X 4 Volume II Transmittal Letter, Volume I, Tab 1 D.1. Admissions Requirement and Eligibility Section V. D. and Section XIX E. 1. c Attachment H Budget X 5-18 Volume II Section XIX E. 2. Supplier Qualifier Report (SQR) Report or X Tab 2 Volume II documentation to determine financial viability Section XIX E. 3 Certified Minority Business (CMBE) Utilization Plan Tab 3 Volume II Section XIX F. Past Performance 1-13 Volume III Section XIX C. Certificate of Drug-Free Workplace Tab 2 Volume I Tab 2 Section XIX D. Technical Proposal Introductory Statement 1 Introductory Statement, Volume I Tab 3 Section XIX D.1. Introduction Statement General Strategy and 1 Introductory Statement, Volume I Tab 3 Methodology RFP R2107
7 Cross Reference Table Attachment O TECHNICAL PROPOSAL RESPONSE (SUGGESTED DOCUMENTATION*) *PLEASE NOTE: Proposer is requested to provide evidence of existing documentation (plans, resumes, charts, etc) as requested in this cross reference table and addressed below. If evidentiary documentation is not currently available, provide evidence of intent or plan to implement and identify as such. This will include proposed plans, schedules, proposed staff contracts, job description etc. Include all relevant information that will assist us in evaluating your proposal. Failure to provide information as requested may result in 0 points being assessed for that portion of the proposal evaluation. If Prospective provider is selected for contract award, the proposed service and all elements thereof will be incorporated by reference into the contract, unless they do not otherwise meet the terms and conditions of this RFP. Category #1: Management Capability 63E F.A.C. and Section XIX. D. 2. a. 63E F.A.C. and Section XIX. D. 2. a. Section XIX, D. 2. b. 63E F.A.C. and Section XIX. D.2.a. 63E F.A.C. and Section XIX. D. 2. a. 63E F.A.C. Attachment I. Section XV and Section XIX D. 2. c. Attachment I, Section XV. and Section XIX D. 2.c. Attachment I, Section XV. and Section XIX D. 2.c. Attachment I, Section III. A.1. Attachment I, Section III. A.1. and Section V. A. Attachment I, Section III. A.1. Describe your company s management capability to manage/control the program. Describe your organizational structure and provide an organizational chart and leadership staff qualifications that indicate sufficient management capability to perform the services required. Describe any issues relevant to providing services in the DJJ owned facility. Describe your corporate oversight and support for the program. Describe Internal quality improvement process utilized to identify problems and improve processes. Provide a copy of training protocols, including specifically a comprehensive training plan to sustain optimum program operations. Category #2: Options Clause Describe the Provider s ability to increase units of service including maximum available beds/slots based on available capacity, or defining what space is available for increasing beds/slots. Describe the plan for recruiting additional staff and provide timeframes for recruitment. Describe capability and flexibility to change restrictiveness level or gender served and add additional services to meet Department needs to treat youth on waiting list. Category #3: Staffing Describe coverage of staff ratios for supervision (Example: 1:8 awake; 1:10 asleep, etc.) as identified in the RFP, specifically addressing issues such as vacancies and absences (relief factor). Provide a Staffing Plan which addresses recruitment of qualified staff and how the provider will sustain staff levels needed. Category #4: Care and Custody Services Submit a plan to provide, at minimum, the following services required by Rule 63E-7: Youth Admission Youth Intake Youth Orientation Quality of Life and Youth Grievance Process Youth Hygiene and Dress Code Facility and Food Services Transfer, Release and Discharge Safety and Security Program Administration 2-11 Considerations Transition Planning Consideration b. Management Capability Services in Department-Owned or Leased 6-8 Consideration Consideration Consideration 5 Considerations 1-4 Staff Training 11 Consideration 1 11 Consideration 2 12 Consideration Consideration 1 and 2 Consideration 3 Coverage for Religious/Spiritual Opportunities Consideration 3 Staffing Plan Consideration 1 Youth Intake/Admission Youth Intake/Admission Orientation Quality of Life/Youth Grievance Procedure Youth Hygiene, Clothing, Dress Code Food Services Transfer, Release and Discharge Safety and Security Program Administration RFP R2107
8 Cross Reference Table Attachment O SECTION/PART SUBJECT MANDATORY CRITERIA (X FOR YES) PAGE NUMBERS SECTIONS/PARTS Attachment I, Section III. A.1. Attachment I, Section III. A.1. Attachment I, Section III. A.1. Attachment I, Section III. A.2. Attachment I, Section III. A.2. Attachment I, Section III. A.2. Attachment I, Section III. A.2. Attachment I, Section II. D.2. Attachment I, Section III. A.2. Attachment I, Section III. A.2. Attachment I, Section III. A.7. Attachment I, Section III. A.7. Attachment I, Section III. A.7. Attachment I, Section III. A.7. Attachment I, Section III. A.7. Describe how you will maintain youth engagement in activities and the treatment process so that at least 80% of youth waking time is devoted to structured therapeutic activity. Describe the tracking system for monitoring youth participation for adherence to structured therapeutic activity schedule. Submit a detailed activity schedule for weekday and weekend activities. Category #5: Case Management Services Describe the assessment process, staffing, etc., of the youth for criminogenic factors. Describe method for completing individualized performance plans developed by a multidisciplinary treatment team in conjunction with youth. Describe motivational interviewing implementation to promote engagement in delinquency intervention. Describe process for ensuring quarterly progress reports are provided to committing court, Department JPO and youth s parents. Describe approach to Identification and grouping of youth within the program according to special characteristics for safety, health and treatment purposes. Describe how the youth will be assessed for progress during delinquency interventions. Describe the capacity to coordinate services, obtain required consent documentation, and communicate with the custodial parent or guardian, the district or circuit liaison, the Department, the courts and other entities. Category #6: Delinquency Programming Provide a copy of the delinquency intervention model or curricula intended to be used and submit implementation plan. Describe the plan to engage and retain the participation of the families of the youth in the program. Describe the overall goals and objectives of the delinquency intervention program. Submit documentation to show that delinquency interventions are evidence-based or promising practices. Describe the process for monitoring delinquency interventions to ensure adherence/fidelity to the original delinquency intervention model s design Consideration 2 Consideration 4 The third principle, second paragraph 18 Consideration Consideration 2 Consideration 4 Consideration 2 Consideration 3 Consideration 1 Consideration 5 Consideration 2 Consideration 5 Consideration 3 A.7.c. Responsivity Factors The fourth principle Motivational Interviewing Pre-service training, specialty services for sex offending population 14.a. Living Environment The third sector A.2.e., Preparing Performance Summary Consideration 4 Consideration 5 D.2. Classification and Grouping of Youth Consideration 1 Discharge/Transition Consideration 6 Consideration 3: Daily, weekly, monthly monitoring Consideration 7 Consideration 6 Consideration 11 Health Care Planning Consideration Delinquency Programming Consideration 2 A.14 Living Environment Consideration 3 40 Consideration Consideration 5 RFP R2107
9 Cross Reference Table Attachment O SECTION/PART SUBJECT MANDATORY CRITERIA (X FOR YES) PAGE NUMBERS SECTIONS/PARTS Attachment I, Section III. A.14. Category #7: Visitation and Family Involvement Describe the plan to ensure youth s on-going communication with family Consideration 1-5 Consideration 2 Orientation Consideration 7 Attachment I, Section III. A.14. and Section III.A.1. Attachment I, Section III. A.14. Attachment I, Section III.A.1. Attachment I, Section III.A.1. Attachment I, Section III. A.8. Attachment I, Section III. A.8. Attachment I, Section III. A.8., Section III. A. 15. Attachment I, Section III. A.9. Attachment I, Section III. A.9. Attachment I, Section III. A.12 Attachment I, Section III. A.12. Attachment I, Section III. A.12. Attachment I, Section III. A.13. Attachment I, Section III. A.13. Describe the mechanisms for soliciting family member input/participation in treatment. Describe the plan for youth to have access to visitors (family). Describe the capacity to provide for comfortable visitation areas. Provide the visitation procedures addressing possible security concerns (escape, contraband, weapons) Category #8: Educational Services Describe the educational services to be provided and the manner of service provision. Describe direct care supervision of youth during school hours. Describe how the educational staff is integrated into the current Behavior Management System. Category #9: Pre-Vocational and Vocational Services Describe coordination of traditional and nontraditional pre-vocational and vocational services with the community resources. Describe the assessment of youth s interest for a specific vocational area. Describe how required vocational training is integrated into treatment goals and planning process. Category #10: Discharge and Transition Services Provide the plan for discharge and transition planning process that considers individual youth needs, characteristics, and risks. Describe how the vendor will work with the community, the JPO, the courts, Department staff, and other partners in their discharge and transition planning. Submit documentation that demonstrates that discharge planning begins at admission. Category #11: Staff Training Describe training necessary for direct care staff to perform their duties. Provide a comprehensive training plan to implement orientation and training programs for all new employees, within thirty (30) days of hire, and on-going staff training to increase knowledge and skills to improve quality of care and training services (outlined in CORE), including specific job responsibilities, care and supervision of youth, first aid, episodic care and CPR as required by Rule 63-7 and the RFP Consideration Consideration Consideration 4 52 Consideration 5 41 Consideration 1 42 Consideration Consideration 3 Consideration 2 A.9.a. Traditional and Non-Traditional Svs Consideration 4 Consideration 1 Accessing Vocational Opportunity 43 Consideration 2 44 Consideration Consideration Consideration A.13 Staff Training & Consideration 1 Consideration 2 Consideration 4 Consideration Consideration 2 RFP R2107
10 Cross Reference Table Attachment O SECTION/PART SUBJECT MANDATORY CRITERIA (X FOR YES) PAGE NUMBERS SECTIONS/PARTS Attachment I, Section III. A.13. and Section III. A. 15. Provide documentation that demonstrates that the principles of cultural competence and trauma informed care to reinforce non-confrontational interaction are incorporated into the comprehensive training plan Consideration 3 Pre-service Training Chart In-service Training Chart Attachment I, Section III. A.3. Attachment I, Section III. A.15. Attachment I, Section III. A.15. Attachment I, Section III. A.15. Attachment I, Section III. A.15. Attachment I, Section III. A.15. Attachment I, Section III. A.15. Attachment I, Section III. A.17. Attachment I, Section III. A.16 and 17. Attachment I, Section III. A. 16 and 17. Attachment I, Section III. A.16. Attachment I, Section III. A.18. Attachment I, Section III. A.18. Attachment I, Section III. A.18. Provide training plan as required in the Health Services Manual (2006). Category #12: Behavioral Management System Describe the behavior management and positive behavior reinforcement system to be utilized and the underlying theory. Describe how the Provider will prepare and plan with youth for crisis prevention. Describe the training plan for staff regarding the Behavior Management System. Describe process for monitoring the staff and youth s daily activities to ensure consistency with the treatment and the behavioral management philosophy. Provide evidence that the Behavioral Management System has a rewards to punishment ratio which exceed the 4 rewards: 1 punishment ratio. Describe how a youth s motivational factors are incorporated in the Behavioral Mgmt System. Category #13: Religious Services and Recreational and Leisure Time Activities Provide methodology for obtaining youth input to ensure recreational activities are meaningful to the youth and encourage positive interaction and participation. Provide a schedule for religious services and recreational and leisure time activities (including weekends). Submit documentation to show that the staffing pattern allows for adequate coverage for religious services and recreational and leisure time activities as offered Consideration 4 Pre-service Training Chart In-service Training Chart A.3.k. Staff Training Consideration 1 55 Consideration Consideration 3 55 Consideration 4 54 Consideration Consideration 1 and 6 57 Consideration 1- Recreational/Leisure Time Activities Describe access to religious services. 56 Consideration 4 Category #14: Restorative Justice Programming Describe plan for providing Impact of Crime training to staff and implementation of an Impact of Crime program. Provide evidence and/or documentation that the program supports the Restorative Justice philosophy. Illustrate the Restorative Justice Programming Plan that creates opportunities for youth to be actively involved, give input, participate indecisions, practice leadership roles, use restorative conflict resolution strategies, and contribute to the community. Consideration 2 A.16.b. Spiritual and leisure activity schedule Consideration 3 Consideration 1 and 2 - Staffing 59 Consideration Consideration Consideration 2 Consideration 3 Consideration 1 A.19 Community Involvement Opportunities A.14.a.8 Community Partnerships RFP R2107
11 Cross Reference Table Attachment O SECTION/PART Attachment I, Section III. A.3. SUBJECT Category #15: Health Services Describe how the vendor will provide the Designated Health Authority (DHA) Services as specified in the Health Services Manual (2006). (Include the proposed physician s CV/resume, letter of intent from the proposed physician, and his/her proposed schedule in the response.) MANDATORY CRITERIA (X FOR YES) PAGE NUMBERS SECTIONS/PARTS A.3. Category 15: Health Services A3.b. Method of On-site Health Services Delivery Consideration 1 Attachment I, Section III. A.3. Attachment I, Section III. A.3. Attachment I, Section III. A.3. Attachment I, Section III. A.3. Attachment I, Section III. A.3. Attachment I, Section III. A.3. Submit plan for comprehensive on-site health services. Describe provision of nursing services including hours and level of staff (ARNP/ RN s/ LPN s/etc.), appropriate coverage for the schedule, as required by the RFP. Submit the protocol for the provision of health services during natural disasters. Describe the linkage to ancillary services to meet a broad range of youth s medical needs and provide/describe, at minimum, the following: Contracts/written agreements for ancillary services Protocols for accessing emergency medical services Protocols for accessing dental care Protocols for accessing eye care Protocols for accessing x-ray and lab services. Provide plan to ensure completion of the physical assessments within the timeframes described in the Health Services Manual (Revised October 2006 with April 2010 Updates). Describe provision of sick call services including, at minimum, the following: Sick call conducted by RN (if by LPN, include protocol for supervision by ARNP or Physician). Provider s written treatment protocols (including complaints, signs/symptoms, criteria of treatment) rendered as described in the Health Services Manual 2006). Frequency for treatment clearly outlined (e.g., x times per as stated in the RFP Scope of Services to be Provided ) Staffing schedule addresses sick call hours Process outlined for youth to obtain health service in the Providers Facility Operating Procedures (FOPs), Health Services Manual Request Forms, etc.). Protocol in place for parental notification of sick call services to a youth. Clearly written sick call documentation requirements. Tracking mechanism for the sick call services performed and related sick call service details Consideration Consideration 3 A.3.b Method of On-site Health Services Delivery 23 Consideration Consideration 5 9. Diagnostic Services 24 Consideration Consideration 7 Program schedule RFP R2107
12 Cross Reference Table Attachment O SECTION/PART SUBJECT MANDATORY CRITERIA (X FOR YES) PAGE NUMBERS SECTIONS/PARTS Attachment I, Section III. A.3. Attachment I, Section III. A.3 Attachment I, Section III. A.3 Attachment I, Section III. A.3 Attachment I, Section III. A.3 Attachment I, Section III. A.3 Attachment I, Section III. A.3 Attachment I, Section III. A.6. Describe provision of Episodic Care, addressing, at minimum, the following: Protocols for emergency drills to address the following emergencies: cardiopulmonary arrest; unconsciousness (youth found down); choking episode; uncontrolled bleeding; seizures; sudden mental status changes; chest pain; shortness of breath; open head injury; fractures or potential fractures, and suicide attempt. Provision of automated external defibrillators (AED s) Protocol for on-site or off-site emergency medical services. Protocol for Protective Action Response (PAR) related medical services. Outline the provision of services for on-going treatment for chronic health conditions which include, at minimum, evaluations at intervals no less than every 3 months. Outline the provision of services for routine immunization in accordance with Center for Disease Control (CDC) recommendations. Describe protocols for transition, addressing at minimum, how the provider plans to coordinate with the aftercare entities regarding medical needs upon the youth s discharge from the DJJ facility. Submit protocol for communicable disease and infection control (in compliance with OSHA s Standard 1910 Subpart I: 29CFR ; 29CFR ; App. A; and 29CFR ) Describe Provider s ability to provide medication administration, including: Description of development, oversight and monitoring of medication policies and practices (including selection, purchasing, storage, distribution, use and safety of medication and related activities). Protocol that ensures oversight by the Designated Health Authority (DHA) and by outside consultations when appropriate. Describe Health Education Programming, including but not limited to: Monthly schedule detailing the health education sessions. Topics covered throughout the youth s length of stay. Category #16: Mental Health and Substance Abuse Services Describe provider s approach to the following: Standardized mental health and substance abuse screening process per Mental Health and Substance Abuse Services Manual (Revised August 2006 with March 2007 and April 2007 Updates): Process to include MAYSI-2 or other mental health/substance abuse screening instruments. Outline the staff responsible for administering the screening instruments. Outline the protocol to be utilized when suicide risk factors are identified. 25 Consideration Consideration 9 26 Consideration Consideration 11 Consideration Consideration Consideration Consideration 14 Program Schedule Consideration 1 Consideration 6 6. Crisis Intervention and Emergency Mental Health and Substance Abuse Care RFP R2107
13 Cross Reference Table Attachment O SECTION/PART SUBJECT MANDATORY CRITERIA (X FOR YES) PAGE NUMBERS SECTIONS/PARTS Attachment I, Section III. A. 6. Describe how the requirements of mental health assessments will be provided: Provide documentation that the assessment will be conducted by mental health/substance abuse licensed professionals. (Include FTE list.) If the proposal indicates that non-licensed staff will perform mental health assessments provide documentation that at least one hour (weekly) face-to-face supervision will be provided by licensed professional. Include protocols to ensure completion of comprehensive mental health evaluations upon 30 days of referral. If completed by a non-licensed staff, include protocol for review and sign off by licensed professional within10 days Consideration 2 SOTS Consideration 4 Designated MH Authority (1.5 hrs supervision) A.6.e. Designated MH Authority ( ) SOTS Consideration 3 Staffing Plan (FTE list) Attachment I, Section III. A.6. Describe how the comprehensive substance abuse evaluations will be conducted in accordance with Rule 65D-30. Specifically address: Provide documentation to evidence that facility is licensed under Chapter 397. OR Provide documentation to evidence that facility staff are licensed under Chapters 397, 458, 459, 490 or 491. Identify how substance abuse evaluations will be conducted within 30 days of referral Consideration 3 Consideration 2 Attachment I, Section III. A.6. Attachment I, Section III. A.6. Describe the youth s access to psychotherapy or professional counseling (i.e., individual, group, or family therapy) as identified in the screening and/or the assessment. Specifically address: Clinical staff qualifications. Schedule for psychotherapy or professional counseling services. Describe the protocol for psychopharmacological therapy and psychopharmacological therapy followup treatment which addresses the following: Provision of medication prescriptions based on individualized assessment of the youth. (Include documentation of rationale including target symptoms in response.) Understanding that medications are required to be administered by licensed personnel with appropriate training. Training to be provided to specific disciplines, including direct care staff (especially side effect monitoring). Obtaining informed consent from the youth s parent or guardian for each medication prescribed prior to its administration. Provision of appropriate laboratory tests as indicated for specific medications and for monitoring of side effects Consideration 4 SOTS Consideration 4 Program Schedule Consideration 5 RFP R2107
14 Cross Reference Table Attachment O SECTION/PART SUBJECT MANDATORY CRITERIA (X FOR YES) PAGE NUMBERS SECTIONS/PARTS Attachment I, Section III. A.6. Describe the procedures for suicide prevention. Specifically address: Incremental levels of suicide precautions and describe how these precautions will be implemented. Examination of the facility s physical features and the program s procedures to identify risks of suicidal behavior. Interventions that are matched to level of risk associated with youth suicidal behavior, based on youth history and clinical assessment Consideration 6 Consideration 7 SOTS Consideration 2 Consideration 1 Pre-Service In-Service Training Consideration 1 Discharge/Transition Youth Intake and Admission Attachment I, Section III. A.6. Describe how the suicide intervention and suicide prevention protocols are established using evidence based and promising practices. 36 Consideration 7 Category #17: Sex Offender Treatment Services Attachment III, A.2. Describe best practices that have been integrated into the selection and availability of treatment program s. Attachment III, A.6. Describe the full array of services and treatment programs (available 7 days a week) designed to meet the needs of individual youth. (Include treatment schedule). Attachment III, A.6. Describe plan for provisions of sex offender treatment services in accordance with the RFP Attachment III, III.A.4, A.5 requirements. Describe the clinical staff to be utilized in the sex offender treatment program, including their qualifications and scheduling SOTS Consideration SOTS Consideration SOTS Consideration 3 Mental Health and Substance Abuse Treatment Planning SOTS Consideration 4 RFP R2107
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33

34
35

36 RFP R2107 Drug-Free Workplace
 G4S programs are rated by QA as Deemed and Two (2) rated Commendable status.")
37 Introductory Statement SIGNIFICANT STRENGTHS G4S management team has more than 200 years combined experience working with DJJ. 100% of G4S sex offender programs hold the highest statewide QA ratings for sex offender programming. Fourteen (14) G4S programs are rated by QA as Deemed and Two (2) rated Commendable status. Six (6) G4S programs hold the highest statewide QA scores. G4S partnership with the Florida DJJ spans more than 14 years. G4S has a proven track record for successfully opening and transitioning complex, multi-level and specialized treatment programs. (G4S) has a significant interest in partnering with the (DJJ) to provide sex offender treatment services at the (DSOP). During the past 14 years, G4S has clearly demonstrated its ability to plan, control and manage juvenile residential facilities effectively, while successfully responding to the sex offender, mental health and substance abuse treatment needs of youth assigned to our programs. G4S looks forward to operating DSOP in a safe and orderly manner, while consistently delivering high quality services to the Department and the youth in our care. We take pride in our experience of providing specialized services, enhancing community partnerships, transitioning programs in a professional manner, and operating numerous low, moderate, high and maximum risk juvenile justice programs. G4S takes pride in conforming to required statutes, administrative rules, and the Department s policies and manuals. This proposal reflects our continuing commitment to provide quality juvenile justice services to youth referred by the Department. In this response, we have proposed services that are fully responsive to RFP specifications and provide protection to the public, create a physically safe and secure environment for youth and staff, and deliver specific mental health and substance abuse treatment services based on individual youth needs. G4S pledges to provide the same comprehensive program of safety, security, education, skills training and transition preparation services as provided in the other programs we operate. This proposal is based on the most current research and incorporates principles of evidence-based treatment supported by research and cognitive approaches specifically developed for youth. These principles and research findings are reflected throughout our description of services. G4S corporate managers offer unrivalled experience in management, treatment and successful operations of residential juvenile facilities. Collectively, G4S corporate officers and managers have more than 200 years of direct juvenile justice experience, and have provided national leadership and expertise in the field of juvenile justice and treatment services. Understanding that no facility or program can successfully provide services or operate in isolation, G4S has successfully built collaborative partnerships with Florida DJJ and local communities that strengthen the services provided and ensure the maximum use of available resources at each of our programs. Our executive officers will continue to be available 24 hours a day to address any operational concerns. Fourteen of G4S Florida programs currently have Deemed Status through the Quality Assurance Review process. Further, 100% of G4S sex offender programs hold the highest ratings of sex offender programming statewide. This demonstrates G4S commitment to fortify and continually improve quality standards and performance objectives. Our programs have received national awards and recognitions and consistently improve recidivism rates. We are committed to providing operations that significantly impact and transform young lives and contribute to long-term public safety. G4S management team has extensive experience in the successful start-up of new secure programs and the smooth transition of services from one provider to another. If awarded this contract, G4S commits to operate DSOP in an organized, safe, secure and orderly manner, while continually looking to enhance services offered. We are proud of our ability to blend and provide safety to the community and provide structured and specialized treatment programming for youth under our care. We believe that our strong corporate management experience, along with the financial and organizational stability of our parent company, enhances our ability to operate and manage DSOP professionally and in compliance with required statutes, guidelines and contract requirements. It is the priority of G4S to follow company policies and procedures and implement best practices to ensure our youth receive quality treatment. RFP R2107 Page 1

38 Management Capability 2.A. CATEGORY 1: MANAGEMENT CAPABILITY SERVICES How well does proposal describe Provider s management capability? COMMITMENT TO FDJJ: G4S is strongly committed to operating programs that significantly and positively impact the lives of youth who are placed in our care. This commitment has been demonstrated in our successful 14 years partnership with the Department of Juvenile Justice (DJJ) in our activation, transition, and operation of low-, moderate-, high-, and maximum-risk programs for males and females needing a variety of specialized treatment services. This has included sex offender treatment, substance abuse services, intensive mental health services, developmental disability services, behavioral health/mental health/substance abuse overlay services, and specialized mental health services. To meet the vision of the Department, G4S staff are actively involved in various DJJ committees in developing innovative ideas to improve policies, standards, manuals and administrative rules to benefit the State and the youth. Likewise, designated G4S staff are members of the Association for the Treatment of Sexual Abusers (ATSA), an international, multi-disciplinary organization that promotes evidence based practice, public policy and community strategies that lead to the effective assessment, treatment and management of individuals who have sexually abused or are at risk to abuse. We have been part of numerous pilot studies with the Department, and currently participate with the National Council on Crime and Delinquency (NCCD) Center for Girls and Young Women on the implementation of SAVVY Sister s model, Department of Juvenile Justice for the Impact of Crime, and Parenting With Love and Limits. Further, we are currently involved in the University of South Florida RFJO empathy research study on personality, emotional and behavioral risk factors with juvenile sex offenders in one of our programs. Our numerous CARF and ACA accreditations show our commitment to excel in professional development, maintain integrity and promote the continuity of care to our youth. Finally, high-scoring results from annual Quality Assurance reviews show our commitment to the Department to deliver quality dayafter-day practice and leadership. 2.A.1.,2.,3. HISTORY OF G4S YOUTH SERVICES: Proudly headquartered in Tampa, Florida, (G4S), is a for-profit, Limited Liability Corporation established in It is a subsidiary of G4S plc, the global leader in security solutions with operations in more than 120 countries on six (6) continents and more than 625,000 employees worldwide (50,000 in North America). Annual revenues for 2010 were over $11.8 billion. G4S is registered to conduct business in the State of Florida under corporate charter number M (copy of our current Certificate of Fact from Florida Department of State is included as Exhibit 1, page 61). G4S ensures that any subcontractors hired will be properly licensed to conduct business in Florida. In April 2009, G4S acquired Sunshine Youth Services, Inc. (SYS), a Florida Juvenile Justice Provider and its six (6) residential programs. G4S specializes in the operation of quality habilitation/rehabilitation programs for juveniles that have been committed by the courts or who are at risk of being committed. To further support our abilities, a table detailing the facilities that G4S has opened (O), transitioned from other providers, either through contract award (C) or emergency procurement (E) and Acquired has been included as List of Facilities G4S Opened, Transitioned and Acquired, Exhibit 2, page 62. The leadership team of G4S Youth Services has more than 135 years of juvenile justice experience, and is highly involved in the planning, developing, and oversight of program operations and services. Led by Jim Hill, CEO/President, the team includes Brian Neupaver, VP of Operations; Karen Astringer, VP of Clinical Services; Peter Plant, Senior VP of Education and Policy Development; Gene Magrini, VP of Administration; Debbie Watts, Director of Business Development; and AJ Swick, Controller. Consideration 1: How well does the proposal describe management and capability to manage/control the program? 2.A.4 MANAGEMENT ABILITY TO PLAN, CONTROL AND MANAGE: G4S has a proven history of planning, controlling and managing juvenile sex offender programs, absorbing troubled programs, transitioning programs from other providers, and starting up new programs, all which have resulted in success. G4S vision to develop the most comprehensive self-measurements of quality of care, safety and security has resulted in modernized methods that directly correlate with our positive outcomes. Currently, G4S manages and supervises 16 contracted programs in Florida, one (1) Juvenile Assessment and Treatment Center in Arkansas and one (1) Juvenile Detention Center in Tennessee, showing strong diversity of management capabilities. Several Florida contracts include more than one (1) program within the contract; therefore, G4S actually operates more 20 programs within the 16 Florida contracts. Throughout the proposal, we will demonstrate our ability to operate high numbers of diverse programs at high quality levels. One of the strengths of G4S lies with executive officers being available 24 hours a day to address operational concerns. The continual expansion of services involves the corporate and leadership teams working together on a daily basis. During the past 14 years, G4S has opened or transitioned treatment, security, and care and custody services in the states of Florida, Arkansas, Tennessee, and Kansas, which allows the ability to implement best practices from numerous states. RFP R2107 Page 2


.")
39 A second strength of G4S is the management ability to consistently self-monitor effectiveness. The best predictor of future behavior is past behavior; therefore, we have full confidence that our abilities to strengthen the DSOP operations will be successful. This is based on the most current Quality Assurance (QA) reports, where G4S has measured its performance against other sex offender programs in the state. Results in the graph to the right show that 100% of G4S sex offender programs hold the highest QA ratings. As of March 24, 2011, 100% of G4S sex offender programs are DEEMED programs, and the only sex offender programs with this status in the state (CJRF moderate-risk, JOCC high- risk, and JOCC maximum-risk sex offender programs). Management Capability Further, in striving to provide the most reputable and highest quality programs for the Department, the four (4) blocks to the left represent DJJ Quality Assurance results as of March 24, Management fosters and encourages an agency culture that emphasizes the importance of integrity and ethical values. This culture is not a choice; it is an expectation. G4S management professional and clinical staff are very knowledgeable of Florida s laws and regulations, DJJ Florida Administrative Codes, Quality Assurance Residential Standards, and DCF/SAMH policies, procedures and standards. Our VP of Education and Policy Development participates on the DJJ workgroups that resulted in the development of every department administrative rule currently in effect. He continues to serve on a variety of other workgroups, such as the current QA Improvement Workgroup, in support of the department s mission and partnership with providers. G4S plans to continue this hands-on partnership with the Department and providers. It will be the mission of G4S to maintain best practices as outlined by the Association for the Treatment of Sexual Abusers (ATSA), an international, multi-disciplinary organization dedicated to enhancing community safety, reducing sexual recidivism, protecting victims and vulnerable populations, transforming the lives of those caught in the web of sexual violence, and illuminating paths to prevent sexual abuse. Through research, education, and shared learning, ATSA promotes evidence based practice, public policy and community strategies that lead to the effective assessment, treatment and management of individuals who have sexually abused or are at risk to abuse. Accreditation will continue to be another driving force, emulating the CARF mission to promote the quality, value, and optimal outcomes of services through a consultative accreditation process that centers on enhancing the lives of the persons served. G4S is accredited with the Commission on Accreditation of Rehabilitation Facilities (CARF) at seven (7) program sites: Hastings Youth Academy, Martin Girls Academy, Polk Halfway House, Columbus Juvenile Residential Facility, Hillsborough Intensive Residential Treatment, Riverside Academy, and Gulf and Lake Academy. Further, G4S believes in the American Corrections Association (ACA) mission to strengthen diversity of leadership, excel in professional development, maintain integrity and ethical behavior on a daily basis, and continue to explore research within the juvenile justice system that promotes the continuity of care. Accreditation at the Okeechobee Juvenile Offender Corrections Center, Avon Park Youth Academy, Arkansas Juvenile Assessment and Treatment Center, and Davidson County Juvenile Detention Center has resulted in recognition of the highest level of G4S exemplary correctional practices. The Okeechobee Juvenile Offender Corrections Center and the Avon Park Youth Academy received first time achievement of 100% (perfect score) performance ratings on all mandatory and non-mandatory standards. To fully understand the idiosyncrasies affiliated with sex offender behavior, concentration will be placed on training. The G4S Hastings Training Academy (HTA) will be the primary location of training. This academy will be the guiding entity to ensure that DSOP staff, in addition to all G4S staff in the area, will receive the highest level of sex offender-specific training. G4S will ensure there is continuity of care across the DSOP community. For additional support, G4S also has the Tampa Training Academy and the Okeechobee Training Academy. The G4S Leadership Academy, G4Stars, and the Management Development Academy are specialized academies to foster leadership development opportunities. Our employees show more self-confidence, independence, compassion and understanding of our youth. Due to the significant levels of trauma, abuse, and victimization endured by our youth, G4S is committed to providing a trauma informed environment that is safe and prevents harm to the youth. The goal is to provide a family environment that many of our youth seek. As part of our approach of training, we will teach on the importance of attitudes and behaviors through the G4S Teachable Points of View: RFP R2107 Page 3


40 Management Capability Take the high road Be open, non-defensive and admit when you are wrong Be proactive in all you do Be respectful and courteous Be positive and praise what is right Respond to issues without rushing to judgment Do what you say you will do Teach, follow, and protect our systems Go the extra step to help Don t take yourself too seriously G4S understands that planning is a continuous process that causes events to happen. Following the DSOP acquisition, consistent program objectives will be closely monitored by management staff to ensure compliance results in good measure performance outcomes. When improvement is needed, a Fidelity Improvement Plan will be immediately implemented and monitored to ensure improvement objectives are successfully met. The success of DSOP will be contributed to the strong corporate presence extended on a consistent basis, as in all G4S programs. Management is committed to competence and seeks to hire team players with the highest competency abilities to meet the demands of our job descriptions. The different aspects of the program design will be guided by the G4S mission and philosophy that places importance on people. Our philosophy is that juvenile offender services must be focused on reducing re-offense risks and must be delivered within a framework that balances youth services with community needs, public safety and victim rights. G4S recognizes the importance to provide necessary tools to facilitate the professional relationships between G4S, its subcontractors, and stakeholder agencies. Integrity runs throughout the G4S operations and it is our commitment to employ principles that are fundamental to the success of our company. The G4S Core Values (to the right), along with the Company s quality assurance, policies and procedures, will provide the foundation for DSOP. Transition Planning: Due to our extensive experience in transitioning programs, G4S understands the numerous challenges involved and is confident of our ability to provide a smooth transition of the DSOP. We recognize that transitioning the operations and management can elicit stress for everyone involved, and welcome the challenge to provide the stability and support that will be needed. In 1999, G4S assumed the management of Pahokee Youth Development which was considered to be one (1) of the worst facilities in the country. The U.S. Department of Justice was threatening intervention, and local legal advocacy groups were warning of legal action. In 2007, planned and continuous management activity resulted in the program (renamed Sago Palm) achieving Florida Quality Assurance Deemed status. Youth currently in the program will have questions and concerns that will be addressed early in the process. G4S is prepared to dedicate high level, experienced staff, to successfully complete the transition. Upon notice of intent to award, G4S will submit our comprehensive preoperational plan that includes detailed goals for all areas of operations including, but not limited to, employee recruitment, employee retention strategy, training and staff development, food services, safety and security issues, physical plan services, medical services, treatment services, case management services, educational services, accounting services, operational services, management strategies, supply ordering, vendor services, youth meetings, and staff meetings. From the beginning, we will focus on quality and compliance. The written plan will ensure that essential employees are available to provide information and to train current and incoming staff through the Hastings Training Academy. The designated Transition Team for the DSOP will be the following G4S Leaders: Relying on historical process, we anticipate the Department will allow us to proactively access the facility, staff and youth prior to the start date, in order for us to get a head start on the work to be accomplished during the transition. G4S will recruit employees, obtain agreements with sub-contractors, and establish contact with significant partners early on. A comprehensive policy and procedures manual will be developed specific to the sex offender population, based on our exceptional sex offender programming. All of this will be fulfilled under the direct supervision of corporate leaders. RFP R2107 Page 4
41 Management Capability Consideration 2: How well does the proposed organizational structure (as indicated in the organizational chart and leadership staff qualifications) indicate sufficient management capability to perform the services required by the RFP? 2.A.5. DAYTONA SEX OFFENDER PROGRAM ORGANIZATIONAL STRUCTURE AND MANAGEMENT CAPABILITY: G4S approaches every new opportunity with the expectation of obtaining excellence. As a result, our proven track record of providing quality management has resulted in Deemed and Commendable QA ratings. G4S recognizes the quality of service depends on the expertise, dedication, and motivation of the staff involved; therefore, we have designated the following specialized positions to provide a quality level of care for the sex offender population: CEO, Jim Hill, and the Senior Vice President of Education & Policy Development, Peter Plant, will oversee corporate and operational directives, contract compliance, Quality Assurance and Case Management functions. Vice President of Operations, Brian Neupaver will be responsible for operations, business development, strategy implementation and promotion of continuous communications between the program and Corporate Management. Regional Director, Rickie Grant, will work directly with the Facility Administrator in the development/implementation of operating systems. He will report to Corporate levels the DSOP delivery of services and quality of operations. Facility Administrator is expected to have at least a Bachelor s degree from an accredited college, and have at least four (4) years in management of juvenile programming; provide leadership in direct administration, program operations, adherence to contract requirements, budgets, QA and Administrative Rules; and developing relationships with DJJ, community, and family. Assistant Facility Administrator is expected to have at least a Bachelor s degree in business, psychology or nursing; at least six (6) years of experience working with specialized youth, with at least two (2) years supervisory experience; responsible for programming, implementing and monitoring daily operations; staff and program scheduling; financial management; disciplinary procedures; incident reporting; CCC reporting; risk management; behavior management; emergency preparedness; and facility operational procedures. Director of Medical Services will be a licensed RN and will ensure seven (7) days a week medical services; facilitate triages in medical and non-medical situations; provide nurse supervision and training; oversee the daily operations of the medical department. Nurses will be at least LPNs; provide documentation in records; provide health education; provide required parental notifications; provide shift relief and secondary coverage, as needed, to provide the best medical care seven (7) days a week. Shift Managers will have a a high school diploma or GED, two (2) years of direct care experience working with youth, one (1) year of supervisory experience; provide direct supervision to ensure shift-to-shift procedures are followed; staff and campus schedules; incident reporting; volunteer and visitor events; behavior management procedures; safety and security potentials. RFP R2107 Page 5
 who meets requirements to practice juvenile sex offender therapy.")
42 Management Capability Clinical Director of Treatment / Licensed Mental Health Professional / DMHA (licensed pursuant to Chapter 458, 459, 490, or 491, F.S) who meets requirements to practice juvenile sex offender therapy. This person will provide oversight to the mental health professionals delivering onsite sex offender-specific services, mental health, and substance abuse services, ensuring clinicians are qualified to provide services, based on their education, training and experience. The Clinical Director will provide 24/7 emergency on-call coverage. Mental Health Professionals will be Master s degree clinicians, and experienced in working with adolescents with mental health, substance abuse and dual diagnosis needs. Preference will be given for those experienced in working with sex offender youth. Community Coach will have at least a Bachelor s degree in criminology or related field and at least one (1) year experience working with adolescents who have experienced emotional/mental health issues. This coach will serve as the liaison for communication with the Department, committing courts, parents/guardians, and will meet all requirements of case management. Life Planner will have at least a Bachelor s degree in criminology or related field and at least one (1) year experience working with adolescents who have experienced emotional/mental health issues; responsible to provide a seamless connection and transition for the youth and community networks; will implement the G4S Faith and Community Based Delinquency Treatment Initiative Program model. Life Coach will have at least a high school diploma or equivalent and successful completion of a required training program; provide support to enhance the health and well-being of the youth; vocational training, spiritual wellness, constructive leisure activities, wellness planning. Risk Mgr/ QA Specialist is expected to have at least a Bachelor s degree in Human Services or related field; at least five (5) years of direct residential experience; two (2) years in Quality Assurance; G4S Scorecard process and onsite risk management. Staff Development is expected to have a Bachelor s Degree from an accredited college or university in business or human resource management; certified trainer in one of the following: First Aid, CPR, PAR, or Victim of Crime. Physical Plant Manager will have at least a high school diploma or equivalent and successful completion of a required training program; three (3) years of experience in work involving the inspection, repair, and maintenance, of household, office, and buildings, including equipment, appliances, machinery, and furnishings; provide routine and preventative maintanence/repairs. Youth Care Workers will have at least a high school diploma or equivalent and successful completion of a required training program; will manage general conduct and behavior of youth, serve as pro-social role models, provide custodial duties and housekeeping functions, conduct life skills groups, and monitor the daily activities. Administrative Assistant will provide administrative and human resource support needed to maintain consistency and continuity. Master Control will have at least a high school diploma or equivalent and successful completion of a required training program. This position will monitor video surveillance that is not limited to movements, counts, checks, daily campus activity schedule, transportation, and all activity areas; responsible for key control, radio communication; log books. Dietary Manager will possess a certification as a Registered Dietitian by the Commission on Dietetic Registration of the American Dietetic Association, possess a certificate showing satisfactory completion of dietetic technician or dietetic assistant training approved by the American Dietetic Association, or be a graduate from an accredited college with major coursework in the food services area; ensure balanced meals meet requirements and will hold a certificate in food services management. Designated Health Authority will be a Florida Board Certified, licensed physician, trained in Pediatrics, Family Practice or Internal Medicine to provide a minimum of two (2) hours / week contractual medical services and oversight of the health department. Psychiatrist will be a Board Certified in Child and Adolescent Psychiatry or Psychiatry by American Board of Psychiatry and Neurology or has completed a training program in Psychiatry approved by American Board of Psychiatry and Neurology for entrance into its certifying examination; provide a minimum of two (2) hours / week contractual psychiatric services that include, but are not limited to, evaluations, medication management and monitoring, Treatment Team involvement. Psychologist will be licensed under chapter 490, Florida Statutes, and will be contracted as needed. Consideration 3: How well does the proposal clearly identify corporate oversight and support for the program? 2.A. 6. CORPORATE ORGANIZATIONAL STRUCTURE: Through the successful operation and management of juvenile residential facilities, G4S contributes achievements to the exceptional oversight and support from several layers of G4S hierarchy. Our most updated technology allows constant communication between leadership teams, which has proven invaluable to our abilities to achieve our accomplishments. Collectively, G4S officers and management have more than 200 years of direct juvenile justice experience, and have provided national leadership, expertise for many decades in the field of juvenile justice and treatment services. The corporate team has directed state juvenile justice agencies, directed the operations of juvenile and adult corrections and detention facilities, provided alternative education, and coordinated mental health services in large programs. G4S leadership is available 24/7 to address operational issues. RFP R2107 Page 6
43 Management Capability G4S Corporate Organizational Structure Although G4S maintains a large range of corporate professionals, there are specific, designated leaders assigned to provide direct corporate oversight and weekly involvement for the. Our professional team includes: Jim Hill, CEO/President: Mr. Hill joined the executive management team of G4S in April He was the founder and served as the President of Sunshine Youth Services from June 2000 through April Prior to starting Sunshine, Jim was the CEO of Charter Hospital of Tampa Bay and a former Board member of the Tampa Bay Hospital Association. Jim earned his Bachelor s Degree from the University of Florida. Within his role at G4S Youth Services, Mr. Hill ensures the integrity and oversight of the financial systems of the company. Mr. Hill served as President of the Florida Juvenile Justice Association (FJJA) from November 2006 through June 2009 where he was active in the numerous committees working closely with the Department of Juvenile Justice, i.e. Efficiencies, Contract Procurement, Medical and Legislative Affairs. He currently serves on the Executive Board of FJJA as Immediate Past President. Mr. Hill has over 16 years of experience working diligently to improve the interests of the Florida juvenile justice stakeholders consisting of parents, youth, employees and organizations working with the Department of Juvenile Justice. Peter Plant, Senior Vice President of Education and Policy Development: Mr. Plant has over 22 years of experience working with Florida DJJ. In the past two (2) years, Mr. Plant has served on the DJJ Administrative Rule Workgroups for Residential, Quality Assurance, CCC, Training and PAR. He has also served on the DJJ Policy Workgroups for QA Improvements, Contracts and Procurement, Behavior Management, Contract Performance Standards, Administrative Efficiencies, RFP Past Performance Criteria, Common Definitions, PREA Standards and Strategic Plan. Mr. Plant served as a Technical Advisor to the Blueprint Commission and drafting of the Blueprint Bill. He also drafted the legislative language authorizing DJJ to promulgate administrative rules for health care, mental health and substance abuse services, and developmental disabilities services. Mr. Plant has served as the DJJ/FJJA representative on revisions to the DCF Child Abuse Reporting Rule and the FJJA representative on revisions to the AHCA BHOS Rules. Brian Neupaver, Vice President of Operations: Mr. Neupaver has 10 years of experience working with Florida DJJ. He is a graduate of Waynesburg University with a degree in Criminal Justice and is currently a candidate for an Executive MBA Program. As Vice-President of Operations, he is responsible for operations, business development, strategy implementation and promotion of continuous communications RFP R2107 Page 7
 years, he has served in management roles including Chief Operating Officer.")
44 Management Capability between the residential youth facilities and Corporate Management. In a career that reflects positions of increased responsibility within the juvenile system, Mr. Neupaver has been involved in the rehabilitation of youth for the past 13 years. For nine (9) years, he has served in management roles including Chief Operating Officer. He has served on the Board of Directors for the Central Pasco Chamber of Commerce and involves himself in various community projects. Karen Astringer, Vice-President of Clinical Services: Ms. Astringer earned her Master s Degree in Counseling and Psychology, and is a Licensed Mental Health Counselor (L.M.H.C.). She holds membership with the National Board of Certified Counselors (NBCC) and is a Nationally Certified Counselor. She is a Certified Quality Auditor (CQA) through the American Society for Quality. Ms. Astringer's experience over the past 10 years includes a blend of clinical, quality and leadership roles in the mental health field. Her clinical experience includes work with children, adults and families in private practice, and non-profit and community-based programs. This experience includes work with youth in DCF custody and with DJJ involvement, as well as overseeing court-ordered Anger Management Classes. Ms. Astringer served as the Director of Quality Improvement for an agency that held the contract for mental health services at a local detention center. Ms. Astringer has three (3) years of experience as a Quality Auditor with First Health Services Corp, now known as Magellan Medicaid. In this role, she served as one (1) of the primary BHOS program auditors and monitored all of the Medicaid Performance Improvement Plans for the state. Rickie Grant, Regional Director: Mr. Grant has over 30 years of experience in the juvenile justice field, is a Certified Co-Occurring Disorders Professional and a trained Conflict Resolution Mediator. He has a Bachelors Degree in Liberal Arts, with a concentration in Behavioral Science/Psychology from Clarion State College. Mr. Grant has been employed with G4S since He has extensive experience in the regional management and development of therapeutic programming for at risk adolescents in the Juvenile Justice system, has served on a number of County Boards associated with Children, Youth and Family Services, and was an Associate Professor and Internship Supervisor for the University of Pittsburgh School of Social Work Master s Program. Melissa McBride, Director of Corporate Compliance: Ms. McBride has over 18 years of experience working with Florida DJJ and adolescents in residential settings. She has held various positions including Director of Operations, Quality Assurance Director and Executive Director. Ms. McBride holds a Bachelor s Degree in Psychology and has served on DJJ workgroups for policy and Quality Assurance, has served on the Department s R-PACT Implementation Team and is a certified Florida Quality Assurance peer reviewer. Ms. McBride is responsible for risk management systems operations, contract compliance, accreditation and outcomes management. Mary Frances Magan, RN, Director of Health Services: Ms. Magan has 17 years of experience with DJJ and has served on DJJ workgroups for Quality Assurance, the Department s R-PACT Implementation Team and is a trained DJJ Quality Assurance peer reviewer. She has extensive knowledge of the Department s medical standards and has 19 years of experience working as a registered nurse with adolescents in the substance abuse and mental health arena, serving as Director of Nursing for 12 of those years. She provides training in infection control, develops OSHA plans and ensures compliance with health care standards. Bridget Goodrich, Director of Staff Development and Training: Ms. Goodrich has over 22 years of experience. Her educational focus is in Secondary Education and Human Development. Ms. Goodrich possesses an array of certifications that include, but is not limited to Master PAR Instructor, Motivational Interviewing Trainer, Thinking for a Change Train the Trainer, Impact of Crime, Girl Matters, SAVVY Sisters, and Trauma Informed Care Sanctuary Model Trainer. Ms. Goodrich is also a Train the Trainer Instructor for the American Safety and Health Institute. Ms. Goodrich has held various managerial and administrative positions within male and female DJJ residential settings. Consideration 4: How well does the proposal describe the Provider s internal quality improvement process? The quality improvement process is necessary to identify problems and improve processes. G4S maintains an effective risk management system that maintains high levels of quality performance and monitoring. As a result of this system, G4S programs have attained numerous accomplishments as leaders in juvenile justice programming. G4S Youth Services has developed a highly effective three-tiered risk management system that ensures continuous assessment, measurement and management of potential risk. By design, the risk management system includes (1) Operational Management, (2) Fidelity Management and (3) Compliance Management. Each level works collaboratively to ensure adherence to mandated guidelines, meeting contractual obligations, protecting established systems within the program, identification of problem areas, assurance of quality service delivery and achieving superior outcomes. The G4S risk management system employs a coaching philosophy and keeping score which includes on-going evaluation of expected services and service delivery, documentation, observations, fidelity checks and evaluation of overall quality. Quality Improvement will be continuously evaluated through the internal risk management systems via weekly coaching sessions, completion of Facility Systems Review validation reports, daily and monthly management meetings, and development of performance improvement plan initiatives as indicated. G4S employs the specialized Scorecard as an integral component of the risk management system. Scorecards are used at both facility and corporate management levels to validate required processes, verify compliance, and continuously rate the quality of services and documentation within designated areas of the program. 1. Operational Risk Management: Operational risk management components are designed as essential onsite facility based tools and practices used to enhance facility management. Primary operational components are completed at the facility level by department management staff and are managed by the Facility Administrator. RFP R2107 Page 8
45 Management Capability Daily Management Meetings are formal review processes which are conducted daily with key management staff and include review of key facility information, events, preparation for upcoming activities and formal review of incidents, concerns and plans of action for each department. Weekly Department Coaching Sessions are weekly individual supervision sessions facilitated by the Facility Administrator with each department management staff. Coaching sessions are designed as a tool to promote open communication, teaching, accountability and driving opportunities for improvement and department outcomes. Facility Systems Review Scorecards are an integral component of departmental management that G4S has developed. These monthly departmental Scorecards are process validation tools which verify the manager s completion of daily, weekly and monthly responsibilities for the assigned department. Each month department managers are required to validate key management components such as required meeting participation, tracking and completion of key documentation, provision of supervision, service delivery, probationary review status and completion of assigned departmental fidelity checks through Scorecard completion. Each department manager reviews Scorecard progress and outcomes weekly with the Facility Administrator within individual coaching sessions. Through this review process progress is continuously evaluated, opportunities for on-going improvement are explored and objectives are established for quality improvement. Monthly Management Meetings are formally conducted with management staff to review program progress, outcomes and to establish monthly objectives and identification of improvement opportunities. Monthly management meetings are documented and at a minimum include review of essential management information such as: Key Performance Indicator (KPI) data review, Scorecard outcomes and performance improvement needs, review of customer monitoring and audits, critical vacancies and recruitment strategies, labor management, budgetary review, safety and security related issues, departmental reviews as well as concerns and opportunities for improvement. 2. Fidelity Management: Fidelity management components are designed to ensure adherence to mandated guidelines and contractual obligations and to promote quality improvement through self-evaluation, teaching and development of facility staff. Fidelity and Compliance management components are driven by onsite Quality Assurance managers and Regional Compliance staff and include use of Fidelity and Compliance Scorecards, Performance Improvement Plans, Probationary Review Status and Risk Management meetings that are used to review data, discuss trends, patterns, progress and opportunities for improvement. Fidelity and Compliance Scorecard, completed monthly, is a facility review process which is designed to evaluate the program s performance related to contractual compliance, adherence to mandated guidelines and includes a quality rating score for services delivered and associated documentation. The Fidelity and Compliance Scorecard includes monthly evaluation of key areas to include at a minimum: operations, safety and security, case management, health services, training and clinical services. As a part of the Scorecard process, the onsite Quality Assurance manager completes a thorough review of documentation, completes observations and verification activities, and conducts formal fidelity checks for assigned services. Additionally, the Scorecard includes completion and trending of youth and staff surveys and identification of follow up needs when indicated. Review and Scoring Activities includes Scorecard outcome review processes that are conducted at program, regional and corporate levels as a method of continuous monitoring and review of the program s service delivery, quality and evaluation of outcomes, trends and to ensure on-going quality improvement. Facility Risk Management Meeting (Program Level Scorecard Review) is a monthly operational risk management meeting conducted to review the program s performance on the facility-based Scorecard. Department managers and facility staff are provided Scorecard outcome information which includes review of progress, ratings as well as identification of opportunities for improvement. Meetings are used as a forum to recognize best practices, review areas in need of improvement, and to teach and mentor department management staff in areas of quality improvement. Performance Improvement Plans are an integral component of the Scorecard process. G4S has implemented requirements for development of formalized Performance Improvement Plans for any area rated below acceptable standards within the monthly Scorecard process. Performance Improvement Plans are used as a proactive management intervention designed to immediately address identification of any potential risk, continuously ensure compliance and promote quality improvement efforts. Performance Improvement Plans are developed by the onsite Quality Assurance Manager in collaboration with the Facility Administrator and submitted to Regional Director and Regional Compliance staff for review and assurance of improvement actions. Probationary Review Status is a proactive management tool designed to assist in effective management of risk that is completed through individualized coaching, training and verification activities. G4S Youth Services recognizes the importance of increased support, training and supervision for all newly hired staff and staff who have been identified with a specific need. Probationary Review Status includes individual weekly meetings with the assigned staff and review of the staff s key documentation to verify understanding, to provide support and offer additional individualized training based upon the identified need. 3. Compliance Management: Compliance management components are designed to continuously evaluate and assess system management, assess data, trends and opportunities for improvement, build internal capacities and drive successful outcomes. Compliance management activities are conducted by Regional and Corporate level leadership staff and include: Monthly Scoring Meetings, Regional Leadership Meetings, Regional Verification Activities, Key Performance Indicator (KPI) review and reporting, Monthly Specialty Services Meetings and completion of Weekly Regional Reporting. RFP R2107 Page 9
46 Management Capability Monthly Scoring Meetings are conducted by Regional Compliance Managers with all assigned Quality Assurance staff. Monthly scoring meetings are a cumulative review reporting process that outlines in detail the findings of each Scorecard indicator for each assigned program within the region. Within the scoring process, facility data, trends and outcomes are addressed. The meeting is used as a forum for regional review of the programs progress, risk and on-going needs. Scoring meeting forums are also used as individualized training sessions for the quality assurance managers and to validate consistency and fidelity of Scorecard practices within the region. Key Performance Indicator Review and Reporting (KPI) data is collected and reported by each facility on a monthly basis. KPI data is compiled for all programs within the organization and formal report is generated and reviewed at program, regional and corporate management levels each month. Regional Verification Review activities are conducted by senior compliance management staff to ensure on-going system fidelity within the programs. The primary objective of regional review activities is to validate system integrity and to ensure that we effectively Teach, Follow and Protect our established systems. Regional Verification Reviews are conducted at routine intervals across the organization and are prioritized based upon identified risks. Corporate leadership team members actively participate in region verification review activities. Regional Leadership Meetings occur once per month with the VP of Operations, VP of Clinical Services, Director of Medical Services, and Director of Corporate Compliance meet with each Regional Director and Regional Compliance Manager to review individual program status and performance. Meetings include a thorough review of each facility s individualized Scorecard outcomes, regional verification monitoring reports, KPI data, FTE utilization and financial performance. Through meeting processes, executive leadership reviews performance and evaluates areas requiring immediate intervention ensuring a concise plan is developed and implemented when indicated. Following the meeting, the VP of Operations meets with each Regional Director weekly to discuss progress toward plan and assess if modifications are necessary to accomplish the intended goal. Monthly Specialty Services Meetings are formal meetings conducted monthly that are facilitated by corporate leadership for the areas of Health and Clinical services. Teleconference meetings are conducted company-wide and include all specialty services department managers and compliance management staff. The meetings provide corporate level supervision and a forum to share pertinent medical and clinical information amongst the G4S programs. Meetings include discussion of relevant policy or form changes, procedural review and changes, review of memos/bulletins and relevant information from our customers, identification and review of current trends and improvement needs. The meeting also provides an open forum to problem solve and share best practices. Consideration 5: How well does the proposal describe the Provider s training protocols, including specifically a comprehensive training plan to sustain optimum program operations? G4S understands staff training is critical to the quality of services and operations, and is directly related to a healthy program. To ensure all DSOP employees receive the most comprehensive pre-service and in-service training, DSOP employees will receive training through our: The Hastings Training Academy (HTA) is under the supervision of our full-time Staff Development Director and our full-time Staff Development Manager. Staff Training, cultural competence and trauma informed care training will be delivered to teach staff how to effectively work with sex offenders, to include youth who have been abused and victimized, while ensuring there is a trauma informed culture throughout the DSOP community. New Hire training classes will be provided every two (2) weeks if needed to meet the needs of the DSOP. All new employees will be provided 138 hours of pre-service training within the first 30 days of hire, which exceeds RFP requirements. New management staff will be required to go through the 138 hours of pre-service, in addition to attending the 20 Hour Management Development Academy, which exceeds RFP requirements. Further, the Facility Administrator and the Assistant Facility Administrator will be PAR certified, which exceeds RFP requirements. In-service training will be a minimum of 32 hours a year, with management staff receiving at least 40 hours of annual training, all which exceeds RFP requirements. Training will follow the format for evidence-based standards, including the use of pre- and post-tests and clearly defined goals and objectives. Both internal and external fidelity monitoring processes will ensure delivery of the training curricula design. G4S has invested many hours in producing numerous highly qualified trainers to be utilized at the Hastings Training Academy. With over 32 years of combined training and juvenile justice experience, the G4S trainers will ensure the delivery of a comprehensive training plan at the highest standards. The G4S cadre of qualified and certified staff trainers consists of master trainers and facilitators for Impact of Crime; Motivational Interviewing; CPR, First Aid, and AED; Thinking For a Change (T4C); R-PACT; Performance Plan; PAR, ARISE, Trauma Informed Care; Sanctuary Model; and Conflict Resolution-Peace Keeping (further described in training, page 47). To ensure that each newly hired employee receives training that is detailed and specific, the DSOP will use a job-specific training plan that will guide and monitor each employee s training, while allowing the program to test the competencies of the employee post-training. Additionally, each employee will be paired with a trained staff member during week three (3) of employee orientation. Veteran employees will teach, mentor and coach new employees through their 90-day probationary period. Job specific training hours vary according to each position; however, the minimum number of hours devoted to job-specific training will be 24. Each employee will be fully evaluated within his or her initial 90 days on the job for competency, and application of training, and the skills needed to perform. On an annual basis, a Training Needs Assessment is conducted, followed by the development of a Staff Development Plan. This is done for all full-time, part-time and volunteer positions, to continually measure and strengthen skills. Further, all G4S employees have access to both the Harvard Manager Mentor Performance Support RFP R2107 Page 10
47 Management Capability Tool and the ISO 9001 certified G4S Secure Solutions Training Institute programs which provide many opportunities for career development. To ensure compliance to G4S training regimen, the Training Manager maintains a comprehensive tracker that monitors all staff trainings and ensures the Department s LMS/CORE system is current. The Facility Administrator maintains monthly communication with the Training Manager to ensure all staff are efficiently trained to meet requirements and work effectively with our youth. In addition to the G4S Hastings Training Academy, G4S provides three (3) additional specialized training academies as part of our mission to enhance professional development opportunities for employees. 2.b. MANAGEMENT CAPABILITY DEPARTMENT-OWNED OR LEASED G4S will operate the DSOP in the state-owned building located in DJJ Northeast Region, Circuit 7 at 1386 Indian Lake Road, Daytona Beach, Florida G4S believes that proper maintenance of facility, grounds and equipment is essential to program integrity, security and the safety of youth, staff, volunteers, visitors and the community. We consider ourselves custodians of any property entrusted to us by a government agency and have unequivocally maintained physical property in better condition than when we originally received use of the property. During our partnership with the Department, we have worked successfully with DJJ staff, DJJ regional staff and DJJ facility services staff to resolve physical plant matters at facilities we operate. To ensure the facilities and grounds are properly maintained, a Physical Plant Manager will be on-call 24/7 and will be responsible for activities related to maintaining the physical plant, equipment and physical environment. A comprehensive preventive maintenance (PM) system will be in place that includes all mechanical equipment, HVAC equipment, emergency generators, electronic controls, fire alarm system, locks and locking controls, and exceeds manufacturer s suggested PM schedule for covered equipment. The content will additionally cover a manual detailing all policies, procedures, protocols, including factory specifications, where applicable; inventory including equipment, furnishings, major mechanical, electrical, plumbing and other systems; staff assignments clearly delineating areas of responsibility and accountability; checklist detailing every aspect of PM for the equipment in the facility; spare parts inventory including onhand and adequate supply of parts and other routinely needed items. Daily random safety and security inspections will be made by the Physical Plant Manager and the management staff to identify potential problems and/or maintenance issues before they infringe on the integrity of the operation. The Physical Plant Manager and Facility Administrator will be responsible for implementation, maintenance and review of the day-today work order system. G4S will contract for services that require specific expertise or qualifications, such as fire safety testing, refuse, pest control and some grounds maintenance. G4S will comply with all inspections, insurances, health and fire authorities, and occupational licensing requirements. All equipment will be inventoried and maintained according to Departmental policy and procedures and service agreements. Further, G4S will ensure all buildings and grounds, equipment, and furnishings are maintained in a manner that provides a safe, sanitary, and comfortable environment for youth, visitors, and employees. 2.C. CATEGORY 2: MANAGEMENT CAPABILITY OPTIONS How well does the proposal document the ability to fulfill the obligations of the Options Clause stated in the Standard Contract and described in the RFP? Consideration 1: How well does the proposal identify the Provider s ability to increase units of service including maximum available beds/slots based on capacity? In the past two (2) years, G4S has demonstrated the capability to respond to the Department s changing needs, as evidenced by adding 16 intensive mental health beds at Orange Youth Academy, transporting 10 youth from Red Road to Avon Park Youth Academy, operationalizing 16 beds at Pasco Girls Academy in two (2) days, and operationalizing 16 beds at Okeechobee Girls Academy in one (1) day. If increased units of service and available beds/slots were requested, G4S would evaluate the request and work with the Department to develop a plan to increase living space at the program. G4S is fully prepared to accept a 50% increase in the units of services described in the RFP, and is confident of our ability to provide a plan to the Department that includes, but not limited to, FTE analysis, staffing resources, safety and security issues, reconfiguration of housing design and program model if applicable, and budget revisions. If awarded the contract, G4S is prepared to further discuss with the Department the opportunity to utilize the additional building (not part of this RFP) to increase units of service and integrate creative youth opportunities. Consideration 2: How well does the proposal describe a plan and the ability to recruit additional staff, define its staffing needs and provide timeframes for recruitment? If the Department exercises the option to increase bed/slots, G4S will ensure staffing ratios are maintained. This will be accomplished through utilization of our proven staffing analysis process and implementation of our recruitment strategy. Not only can G4S commit to continuing to meet the Department needs regarding staffing in the event of bed increase, it will also commit to doing so in the timeframe needed. Our quick turn-around commitment has been evidenced by recent RFI responses for both Okeechobee Girls Academy and Pasco Girls Academy, where over 20 vacancies were filled and staff appropriately trained at each site within 30 days. One of G4S strengths is our leadership capability to expedite a comprehensive plan of strategy and implementation pertinent to the needs of the youth and operations of the program. We have the experience and financial capability to put systems and staff into place to meet needs of the Department. G4S uses multiple-pronged recruitment strategy. This strategy includes: promoting from within our organization; accessing our large pool of PRN and part-time (over 170 employees) staff to migrate to full-time status or to utilize on a temporary basis until full-time staff are fully trained; utilizing staff from our current operating facilities that are close to the DSOP area; and quickly identifying qualified candidates from our large pool of external applicants which are constantly recruited through our internet and print media outlets including: Jobing.com, Careerbuilder.com, The Daytona Beach News Journal, the Orlando Sentinel, in addition to other applicable resources. DSOP will actively utilize the Florida Ready-To-Work, Employ Florida, Florida Workforce Solutions referral programs. Preference will be given to those presenting as the most qualified candidates to work with the DSOP youth (recruitment process design, Exhibit 3, page 63). RFP R2107 Page 11
48 Management Capability Consideration 3: How well does the proposal identify the capability and flexibility to change restrictiveness level or gender served and add additional services to meet Department needs to treat youth on the waiting list? For 14 years, G4S has successfully partnered with the Department to provide specialized mental health and medical services at varying levels of intensity to a diverse population of youth with a full range of criminogenic risk/needs. G4S is diverse in the populations served within the 21 current programs. These include, but are not limited to, youth with mild to severe mental health, substance abuse, dual diagnosis, sex offenses, general delinquency and developmental needs and impairments in level of functioning. G4S has extensive experience providing gender-responsive services to both boys and girls classified as low, moderate, high and maximum risk offenders. Our vast experience with the population, depth in seasoned treatment professionals and ability to design effective programming uniquely qualifies G4S to respond to contract service changes. Demonstrating capability and flexibility, G4S has worked closely with the Department to change contract services and meet the needs of youth on the waiting list as follows: Gender Served: In 1999, Hastings Youth Academy was originally designated to serve moderate and high-risk girls and moderaterisk boys. The contract was changed to serve only boys. Restrictiveness Level: In 2000, the contract for Hastings Youth Academy was amended to add 25 high-risk males. Additional Services: Later in 2000, the contract for Hastings was amended again to include youth with Behavioral Health Overlay Service needs. In 2007, the contract was amended again to add 39 Specialized Mental Health moderate risk and 25 Intensive Mental Health moderate risk beds replacing the 64 high-risk beds. In conjunction with the legislative budget proviso language, the Department reduced the bed capacity at Hastings from 184 to 165. CATEGORY 3: Staffing: How well does the Provider s proposed plan for its staffing levels demonstrate that it employs a sufficient number of trained staff to perform the duties and responsibilities outlined in this RFP? Consideration 1: How well does the proposal clearly outline required coverage of staff ratios for supervision as identified in the RFP, specifically addressing issues such as vacancies and absences? The DSOP staffing plan will provide 24 hours awake supervision every day of the year and will maintain appropriate levels of staff as per the Staffing Plan below. DSOP will provide supervision ratios of 1:6 during awake hours and 1:10 during sleep hours. Five (5) days of the week, G4S will employ a specialized Life Coach who will provide direct supervision of youth, maintaining ratios of 1:5, which exceeds RFP requirements. Due to being a high-risk program, it will not be common practice for youth to go off campus. The plan will provide adequate staff to actively supervise the youth, tend to the everyday needs and immediately respond to emergencies, while maintaining safety and security within the program. A shift relief factor of 1.67 has been incorporated into the plan for direct care that provides for vacations, holidays, and sick time. The Facility Administrator will post schedules in advance that ensure adequate staffing and coverage of program needs. Additionally, a holdover system and reserve workforce of trained personnel will be employed to cover staff absences and vacancies, ensuring that staffing ratios are continuously maintained with trained and experienced personnel. G4S will use a structured system for staff to make advance requests for time off. In the event of an emergency, G4S has additional staff available within close proximity to provide back-up coverage. Further, staff recruitment is an on-going HR function to maintain a viable applicant pool for vacancies. The specialized staffing plan will be as follows: STAFFING PLAN FOR DAYTONA SEX OFFENDER PROGRAM EQUIVALENT # OF TYPE OF STAFF YOUTH TO STAFF FACILITY RESPONSIBILITY WEEKLY HOURS FTE S RATIO Facility Administrator to 30 Overall facility oversight and management. 40 hours per week Assistant Facility Administrator to 30 Oversight of behavioral and safety issues. 40 hours per week Direct Care & Mgmt Supervision Implementation of program schedule, behavior 40 hours per week per management and security FTE Days Evenings Nights to 6 1 to 6 1 to 10 Community Coach to 20 Performance planning, external communication 40 hours per week Life Planner to 10 Transition and support linkages to home community 40 hours per week Life Coach to 30 Physical, vocational, spiritual wellness; special projects 40 hours per week Clinical Director of Treatment 1.0 n/a Administrative oversight of all services related to sex 40 hours per week offender, mental health, substance abuse treatment Mental Health Professional to 10 Implementation of SO, MH, SA services 40 hours per week Director of Medical Services 1.0 n/a Implementation of sick call and medical component 40 hrs/week minimum Nurses (LPN) 2 part time 1.0 n/a Provide shift relief and secondary coverage 20 hrs/wk per FTE Physical Plant Manager 1.0 n/a Physical plant repairs 40 hours per week Administrative Assistant 1.0 n/a Administrative tasks, human resources support 40 hours per week Risk Mgr/QA Specialist.5 n/a Fidelity of scorecard process and risk mgmt. system 20 hours per week Staff Development.10 n/a To meet staff and training needs 4 hours per week Dietary Manager 1.0 n/a Oversee daily operation of the food service department 40 hours per week Master Control 2.95 n/a Monitors security camera for 10 hours per day 40 hrs/wk per FTE Total RFP R2107 Page 12
49 Management Capability Consideration 2: How well does the proposal address an appropriate relief factor that ensures required staff coverage? G4S provides awake supervision and staffing 24 hours a day, 365 days a year, to youth in a physically, emotionally, safe and secure environment. DSOP will provide supervision ratios of 1:6 during awake hours and 1:10 during sleep hours. Five (5) days of the week, G4S will employ a specialized Life Coach who will provide direct supervision of youth, maintaining ratios of 1:5, which exceeds RFP requirements. In addition, DSOP will deploy clinical, case management and administrative staff who will be regularly scheduled to work weekends and holidays. Staffing levels provide active supervision of youth, suitable and timely response to the youth s everyday needs and immediate response to emergencies. The staffing pattern includes a shift relief factor (SRF) of 1.67 FTE to provide for staff coverage, supervision and programs during weekends, holidays, vacations, training and other employee absences. The number of hours is based on G4S leave policies and history at other company programs, as follows: HOURS CALCULATION HOURS PER YEAR Total work hours/year 8 hours x days 2,922 Total rest hours/year 16 hours x weeks -835 Company holidays/year (8 days) 8 hours x 8 days -64 Average other leave/civil/military 12 hours -12 Average paid time off 4.5 hours x 26 pay periods -117 Average training -129 Average staff meetings 2 hours x 12 months -24 Available Work Hours 1,741 SRF: 8hr/7 day per week post 2,922 hrs/1,741 hrs 1.67 FTE Consideration 3: How well does the proposal s staffing plan address the requirements of recruitment of qualified staff and sustain the level needed? G4S has designed and implemented hiring policies to identify, recruit and hire a qualified diverse employee group that embodies our corporate values. To consistently maintain the staffing levels required for ratios and staffing plan compliance, G4S maintains a multi-pronged recruitment and retention strategy within the Human Resources Department. The G4S recruitment process diagram has been included as Exhibit 3, page 63. The recruitment strategy will include a comprehensive network of internet and print media outlets including: Jobing.com, Careerbuilder.com, Daytona Beach News Journal, Orlando Sentinel, in addition to other applicable resources. DSOP will actively utilize the Florida Ready-To-Work, Employ Florida, Florida Workforce Solutions referral programs. Preference will be given to those presenting as the most qualified candidates to work with DSOP youth. Plan for Pre-Screening for Suitability and Hiring: G4S has continuously improved its applicant screening activities by utilizing a candidate vetting system that pre-screens for suitability within our industry and establishes employment eligibility. Careful scrutiny of criminal checks, personal and professional references, education verification and school accreditation has proven vital for pre-screening applicants that are an appropriate match for the position and the youth population served. In addition, the G4S Human Resource Team ensures compliance with requirements of the Florida Drug-Free Workplace. To expedite hiring, the Human Resources Department maintains a tracking system that allows job offers to be made the same day as background clearance by the DJJ Background Screening office. Further, HR will maintain an active list of both PRN and part-time employees, which will not only supplement our full-time workforce on an as-needed basis, but in many instances, will be a source to fill full-time vacancies with a fully trained employee. Through our retention strategy, G4S has consistently improved performance in employee turnover and employee stability. This has been achieved through the numerous positive incentives offered by G4S: G4Stars program, where emphasis is placed on growing and developing internal talent; employee referral incentive program that rewards employees when they refer qualified applicants who join the team and are successful; Employee Development and Succession Planning to increase competencies and career progression; Employee Engagement Surveys; Employee Newsletters; Employee Recognition Program; Employee Problem Solving process to address employee relation matters directly; Formal Performance Appraisal process based on defined job expectations after 90 day probation and annually for all employees; Management Formal Performance Appraisal, where management undergoes a 360 degree appraisal process to ensure work quality. DSOP will implement a morale committee who will plan events to motivate staff and enhance the overall program. To attract and retain talent within G4S, a total compensation package will be offered that includes competitive base pay and a performance based pay system; Health and Dental Insurance, Long-term Disability, Life, Accidental Death and Dismemberment Insurance; 401(k) plan; comprehensive Employee Handbook with defined employment practices and policies to cover work hours, staff benefits, promotions, increases; non-tolerance of harassment or discrimination; strict adherence to G4S Standards of Conduct defining expectations against drugs and alcohol, nepotism, fraternization and other unacceptable conduct with consequences; EEOC compliant employment decisions that align with G4S Affirmative Action Plan. G4S will utilize a weekly FTE monitoring strategy to ensure that proper staff ratios are maintained and will track staffing patterns through the Position Control system. The holdover system will require specific staff to remain on shift in the event of staff shortage. Further, an overtime roster of contact information for staff authorized for overtime will be available for management staff to use for additional backup needs. The Facility Administrator will be authority to grant approvals for personal time or leave, which will be required in advance. All staff will meet specific requirements (e.g., years of experience, training, academic credentials) to qualify for their positions. Staff training will be comprehensive and appropriate to the services offered, and exceed the Department s requirements and regulations. RFP R2107 Page 13
50 Program Services GENERAL DESCRIPTION G4S is committed to achieving positive results for youth and excellent outcomes for the programs that we operate and will continue that same commitment and dedication if selected to operate the located in DJJ Northeast Region, Circuit 7, at 1386 Indian Lake Road, Daytona, Florida Specialized sex offender treatment and customary program services will be provided to 30 high-risk males between the ages 13-18, who are adjudicated delinquent and committed to the Department after being assessed and classified. Exceptions to the age can only be made to with the approval of the Chief of Commitment. The anticipated length of stay for each youth is months. G4S agrees to work with the Department in accomplishing the major program goals, including: focusing on treatment and provisions of high-quality care; providing an environment that fosters healthy social, emotional, intellectual, and physical development; delivering comprehensive on-site medical services to meet the specialized health needs of the youth; maintaining adequate staffing to provide a safe, secure and therapeutic environment; creating and maintaining good working relationships with relevant community agencies; and providing quality and effective education that meets individual needs of each youth. II. YOUTH TO BE SERVED G4S looks forward to providing treatment and security services to 30 boys who have been committed to the Department after being assessed and classified as a high-risk to public safety. Youth served at DSOP will be between the ages of 13 to 18 and have a documented need for sex offender treatment services. As discussed throughout this proposal, G4S has substantial experience serving youth needing specialized sex offender treatment and will use that experience to design, develop, implement and operate successful programming at DSOP. G4S understands that Regional Department Commitment Management Offices throughout Florida will decide placements of youth in the program, placements are considered final and binding on all parties, and the Department may grant exceptions on a case-by-case basis. D.1. ADMISSION REQUIREMENTS AND ELIGIBILITY: G4S understands that a properly designed admission, intake and classification process is essential to ensuring that the most effective delivery of treatment is available to meet the needs of the youth, facilitate the safety of all youth, staff and the public, and reduce escapes. The designated intake staff will consist of the case manager, counselors, and nurse who will all be trained in Motivational Interviewing (MI) techniques, and the admission policies established by the Department. Only male youth between the ages of 13 to 18 referred from the Department will be accepted. Should G4S disagree with the placement of a particular youth, the youth will be accepted and the Department Commitment Manager will be notified. Recognizing the need for scheduling flexibility, G4S will coordinate admissions with the Department and agrees to provide admission services in the evenings, on weekends and during regular business hours, Monday through Friday, 8:00 am to 5:00 pm. Admissions will be coordinated in advance with the Department Commitment Manager and the Department Juvenile Probation Officer. A program orientation will be provided to all youth in accordance with Florida Administrative Code Rule 63E that includes, but is not limited to, the behavior management system, property inventory, program rules, services available, program goals, youth rights, grievance procedure, rules governing conduct, potential disciplinary action and length of stay. G4S will not accept placement of youth other than those placed by the Department nor share any physical plant or program activities with youth not committed by the Department. D.2. CLASSIFICATION AND GROUPING OF YOUTH BY NEEDS: DSOP will use a comprehensive classification system that promotes safety and security, and delivers effective treatment services based upon risk factors and individualized needs. Newly admitted youth will be assessed and classified by the Treatment Team to ensure appropriate assignment to an individual sleeping room, treatment services and level of supervision that best meets the individual needs of the youth. The case manager, Master s level counselors and licensed nurse will complete numerous admission classification screening assessments, which will exceed RFP requirements. Immediately following intake and screening, a formal classification meeting will be conducted with the youth, case manager, mental health counselor, nurse, and representatives from the living unit and administration. Classification information will be pertinent in room assignment and identifying potential alerts. Re-classification will occur minimally at every Treatment Team review or at any time based upon youth need. Detailed classification process is further discussed in the case management (comprehensive risk classification process) section. III. SERVICE TASKS A.1. CATEGORY 4: CARE AND CUSTODY SERVICES: required by the RFP and Rule 63E-7? How well does proposal provide for care and custody services as Consideration 1: How well does the Provider s proposal describe its ability to provide services required by Rule 63E-7? A.1.a. G4S will provide supervision and staffing 24 hours a day, 365 days a year in a physically and emotionally safe and secure environment at ratios of 1:6 during awake hours and 1:10 during sleep hours. Five (5) days of the week, G4S will employ a specialized Life Coach who will provide direct supervision of youth, maintaining ratios of 1:5, which exceeds RFP requirements. Off-site activity will not typically occur due to the youth being high-risk. G4S proudly integrates specific treatment activities as a significant element of programming that integrates the restorative justice philosophy and the behavior management system designed to ensure protection of youth, staff, visitors and the public. Youth Intake and Admission: Intake will be conducted by the community coach, mental health professional, and nurse who are trained in the use of Motivational Interviewing (MI) techniques to assess initial needs, while providing support for the youth s positive adjustment. DSOP will use a comprehensive screening and assessment process that is in accordance with Rule 63E-7, F.A.C., the Health Services Manual (Revised October 2006 with April 2010 Updates) and the Mental Health and Substance Abuse Services Manual (Approved August 2006 with March 2007 and April 2007 Updates). This screening and assessment process, which exceeds RFP requirements, will be used to identify the youth s RFP R2107 Page 14
51 Program Services treatment needs and make referrals for appropriate services. All admissions and releases to the program will be reported in the JJIS Bed Management System within 24 hours of admission or release. Projected release dates of youth will be updated in JJIS by the Facility Administrator at least weekly and reconciled with the Program Monitor on a monthly basis. Admission and intake processes will begin at the time of the youth s arrival to the program. Prior to a youth s arrival, the Treatment Team will conduct a pre-admission review of the youth s Electronic Commitment Packet (ECP) to prepare for the youth s arrival and determine any special needs, as applicable, including availability of bi-lingual staff and materials. The youth will be brought to the facility, provided with preliminary program information, and introduced to key staff. Each newly admitted youth will be strip searched to ensure that contraband is not introduced into the program. G4S understands that youth admitted to DSOP may be boys who have experienced significant trauma. All searches will be conducted in a private room by two (2) male staff members who have been properly trained and will maintain a professional demeanor throughout the process. Physical health screenings will be initiated for all new admissions immediately following the initial strip search. A Facility Entry Physical Health Screening will be completed by a licensed health care staff to identify potential health concerns that may need immediate action and/or referral for further assessment by health care staff. HIV Risk Assessments, STD screenings and oral assessments will also be completed on all new admissions. Additionally, a Master s level mental health professional will complete the initial sex offender, mental health and substance abuse screenings and assessments. Screenings will be completed using various instruments, reviews of records and interview processes. The initial mental health and substance abuse comprehensive admission screening process will include, but not be limited to, administration of the Massachusetts Youth Screening Instrument-Second Version (MAYSI-2) by the community coach. A referral will be made to the Master s degree mental health professional in the screening indicates further need of evaluation. The Vulnerability to Victimization of Sexually Aggressive Behavior (VSAB) conducted by the mental health professional. The mental health professional will conduct a records review of history, and then administer ERASOR (a structured clinical interview based on empirical research). A licensed mental health professional will review and sign pertinent assessments. The initial screening presence of any acute or chronic health and/or mental health or substance abuse disorders will be integrated into the admission classification and formal assessment processes and shared with the Treatment Team to assist in the determination of need, risk and follow up as indicated. Notifications will be made through summaries, admission classification review, alert system notification and formal needs assessment meetings. The community coach will make phone contact with the youth s parent/guardian and JPO to notify of the youth s safe arrival, and provide key contact information and invitation to participate in their child s Treatment Team. Diligent efforts will be made to ensure families are well informed of program expectations as well as youth progress and opportunities to participate within the youth s treatment program. Written notifications to the parent/guardian, committing court and JPO will also be initiated by the community coach on the date of admission. Orientation: As part of G4S mission to integrate the family into our boys treatment, DSOP will extend an invitation to the parent prior to the youth s arrival. Parent/guardians will be invited to go through the orientation process with the youth on his day of arrival to the program. This will help the youth and families get acclimated to DSOP. The orientation process begins with review and explanation of the program philosophy and goals, emergency building evacuation procedures and routes, fire drill procedures, policy on contraband, daily program schedule, dress code and hygiene practices, resident rights and grievance procedure, abuse and CCC reporting numbers, program services, confidentiality and parent/guardian access to information, participation in Treatment Team, procedures to access medical, mental health and substance abuse services, performance planning and development of goals, visitation schedule and policies, telephone procedures, mail procedures, policies for community access, program rules governing resident conduct, program search policy, anticipated length of stay and expectations and rules for recreation and leisure time activities. Each youth will be provided a Student Handbook which explains the program rules, policies, access to services, safety and security procedures, consequences for rule violations, performance planning and release procedures. The case manager will review the youth handbook and daily schedule with the youth. Parent/guardians will be provided a Parent Handbook that explains the program rules, terminology, key contacts, parental involvement and participation within the treatment process, as well as relevant policies and procedures. If needed, bi-lingual staff and program materials will be provided to the youth and parents in their primary language. In the event a parent/guardian is not able to personally attend orientation, he/she will be mailed a welcome package that includes the parent handbook, program orientation activities, written notifications, offering of a program tour, and provided a map to the facility. As part of youth support, each youth is assigned a peer mentor to assist with basic understanding, review and program integration. Quality of Life and Youth Grievance Procedures: G4S is committed to developing, implementing and managing services based on the highest ethical and performance standards to ensure a desirable quality environment for youth and staff. By maintaining high standards, staff and youth are more likely to contribute to achieving the goals of the intentional therapeutic community in a genuine manner, the safety of staff and youth is greatly enhanced, and an environment conducive to effective programming is established. Among the essential quality of life issues that the program acknowledges are youth rights and a grievance system; religious services; access to mail, telephone and visitation; and unimpeded access to self-report abuse or neglect. All youth will have ready access to an established, published grievance system with guarantees against reprisals. The system is available to all youth and serves as an administrative means for the expression and resolution of youth's problems and concerns. All grievances are reviewed daily by facility management, weekly by corporate personnel and responded to within 24 hours. Grievances not resolved at the first level will progress through a system of formal resolution, which allows for investigations and at least one (1) level of appeal. The Facility Administrator/designee and program Management Team will review all grievances on a weekly basis for patterns and trends, thus exceeding RFP requirements and the Florida Administrative Code 63E (15). Youth Hygiene, Clothing and Dress Code: In accordance with Departmental policy and procedure and Florida Administrative Rule 63E (5) (b) 1, staff and youth will be easily recognizable by attire. The employee uniform dress code will be professional in appearance and RFP R2107 Page 15
52 Program Services strictly enforced. During intake, youth will be issued facility clothing that is climate-appropriate, clean, in good repair and fits properly. The clothing supply will exceed requirements so immediate replacement may occur when necessary. At DSOP, youth will be uniformly attired for easy identification to enhance security, treatment and programming systems. This will include a comprehensive alert system. To maintain good personal hygiene, youth will be provided personal care articles (e.g., toothpaste, toothbrush, soap, comb, toilet paper and deodorant), required to shower daily unless medically contraindicated and must keep their fingernails clean and clipped. Shaving equipment will be available and utilized under strict staff supervision. Youth will be encouraged and permitted to brush their teeth in the morning when they wake up and prior to going to bed. Youth will be allowed to shampoo their hair each day and prompted to groom themselves after strenuous activity and prior to meals, court, visitation, etc. Instruction in personal hygiene and general sanitation habits will be part of the youth s healthy living program that will be developed under the supervision and approval of the Designated Health Authority and discussed later in this proposal in Section A.4 Health Education Programming. Youth will receive clean bed linens at least once weekly, towels at least daily and clean blankets as appropriate to the season and in accordance with Rule 63E-7.007(4), FAC. Food Services: DSOP will consider contracting with an external provider to deliver meals that are nutritious and well balanced, served at the proper temperature, presented in a caring manner and in a pleasant atmosphere. Meals will meet or exceed dietary standards required under the U.S. Department of Agriculture s National School Lunch Program, Florida Administrative Code Rule 63E-7.008, and other state and local health/ food services rules and regulations. A licensed dietician will review and approve the menus in accordance with chapter 468, Florida Statutes, with the approved menu being posted in conspicuous places. Each day, youth will receive three (3) meals and a nutritious evening snack. All meals will be served at reasonable times with no more than 14 hours between the evening meal and breakfast. Special arrangements will be made to provide youth with meals when events outside their control prevent them from eating at normal meal times (e.g., court appearances, admissions). Quality food service is essential to the care, treatment and custody of youth at the facility and youth participate more fully in the total program when they are satisfied with the food. Additionally, youth will participate in the development of menu planning. Staff will be encouraged to eat the same meals as the youth, providing the staff an opportunity to interact, model and reinforce positive social skill development to the youth. During mealtime, staff will serve as role models for proper mealtime etiquette and behavior in accordance with a holistic Restorative Justice Philosophy. Youth will not be permitted to trade or give away food, and food will never be withheld as punishment. The menu will not be modified as a result of behavior. Youth preferences, nutritional needs, and the flavor, texture, temperature, appearance and palatability of the food will be considered by Facility Administration. Special diets will be provided for youth with medical needs as prescribed by the treating physician or dentist, and provisions will be made to meet religious dietary requirements. All special diet prescriptions will be in writing and rewritten monthly. In addition to regularly scheduled meals, the program will provide special event meals such as weekly incentives, Father s Day and Mother s Day Celebrations, and family fun days. Transfer, Release and Discharge: Discharge planning will begin at the time of admission to the program. At the time of entrance to the program, the youth will be provided an orientation that clearly explains the expectations, program rules and behavior management system. The youth will be explained the level that must achieved in order to receive a discharge staffing, expected discussion during discharge staffing, and expectations of release requirements. The youth will be encouraged to read his handbook and to earn opportunities to progress at DSOP. Transfer requests will be made only as the last resort, and only under the following conditions: new law violation; all efforts have been exhausted to modify non-compliant behavior; gang affiliation/involvement blocks ability to progress in treatment; protection of the public; incapacity to meet changing treatment needs; impending program closure or reduction in bed capacity. The youth will progress through the DSOP level system in order to be scheduled for discharge. All discharge processes of Administrative Rule 64E.7012 will be followed to ensure that transportation plans are in place. DSOP will obtain written approval from the Department prior to any youth s transfer, release or discharge. Transfer, release and discharge policies and procedures that comply with the Department s current procedures, including the sexually violent predator requirements, will be developed and implemented as stated in A.12. Discharge Policy and Transition Services. Safety and Security: G4S is committed to providing a safe and secure environment at DSOP through strong systems of security and control as a foundation for the provision of proper youth care and treatment. We will use a combination of staff to youth supervision (1:6 awake hours, 1:10 sleep hours), accountability and clearly defined written policies and procedures to promote safe and orderly operations for the public, our youth, staff, visitors and the community. However, during five (5) days of the week, G4S will employ a specialized Life Coach who will provide direct supervision of youth and reduce ratios to 1:5, exceeding RFP requirements. All staff will be thoroughly trained in Safety and Security topics during documented pre-service and additional in-service training. Written policies and procedures for safety and security will include at a minimum: a system of formal, random physical and emergency counts; youth movement in an orderly and structured manner under direct staff supervision; use of radios for communication and staff training for radio protocol; maintenance of permanent logbook for accounts of all routine and emergency situations; contraband control, searches, and documentation; control of facility keys through chit based system key assignments; control of all tools by locked cabinets and logs; and a system of securing vehicles when not in use. Master control staff and management staff will monitor the safety and security via the Department s 24 cameras to maximize visibility. The maintenance of the facility and its equipment are key elements of operational integrity, security, and the safety and protection of youth, staff, volunteers, visitors and the community. Facilities and grounds at DSOP will be maintained to ensure a safe, sanitary and comfortable environment for youth, staff, visitors and subcontracted personnel. Loss control audits by our insurance carrier and state inspections occur annually and any needed corrections will be addressed expeditiously. Systems will be monitored internally through Safety Committee meetings and fidelity checks, weekly inspections and consultation with the insurance carrier. RFP R2107 Page 16
53 Program Services The use of flammable, toxic and caustic materials requires special safety precautions and attention. At no time will youth be permitted to use any flammable, toxic and/or caustic materials such as lye, insecticide or antifreeze. All such materials will be stored in secure areas inaccessible to youth and carefully labeled, controlled, regularly inventoried and distributed only for use by staff. Noncombustible receptacles will be placed at accessible locations throughout the facility for combustible refuse. Special containers will be provided for flammable liquids and rags used with such liquids. As required by OSHA, Material Safety Data Sheets will be appropriately available for all employees and Hazardous Communication Training will take place at hire and on an annual basis thereafter.g4s strives to follow safety and security measures through compliance with local fire and health authorities. Fire and emergency protection and disaster assistance will be clearly detailed, reviewed and approved in the COOP Plan, which will be updated annually. Fire prevention regulations and practices will include unscheduled fire, hurricane and tornado drills, which are fully documented; maintaining fire protection equipment at appropriate locations throughout the facility; maintaining cooperative agreements with the local Fire Department under the approval of the Fire Marshall; implementing and documenting weekly, monthly and quarterly fire inspections and equipment testing. G4S has substantial experience in disaster preparedness. In 2004, G4S Youth Services successfully implemented COOP procedures during four (4) major hurricanes without incident. To strengthen the condition of the DSOP, G4S has established a schedule of repairs and enhancements to be approved by the Department, tentatively as follows: floors refinished: Q3 2011; sod replacement: Q3 2011; roof repair: Q4 2011; pressure wash main building exterior: Q1 2012; paint main building exterior: Q-1 and Q ; replace ceilings beginning Q2 2012; refurbish tool room and repair maintenance building: Q Program Administration: On a daily basis, DSOP will function with oversight of the Facility Administrator, in accordance with Florida Administrative Code 63E-7.016, Program Administration. This will include, but not be limited to, daily operations relating to staff professionalism, code of conduct, reporting to the Central Communications Center, incident reporting, monitoring and reporting of Protective Action Responses (PAR) incidents, updating the Department s JJIS, and enhancing collaborative community partnerships. The Facility Administrator will create an environment at DSOP that enhances staff awareness, reinforces pro-social skill development, and creates a positive peer culture community, which leads to the foundation of a safe and secure environment for youth and staff. Consideration 2: How well does the proposal explain how the Provider will maintain youth engagement in activities and the treatment process so that at least 80% of their waking time is devoted to structured therapeutic activity as required by the RFP? A.1.C. STRUCTURED ACTIVITY: DSOP will carefully plan activities designed to maximize the probability that youth learn appropriate and pro-social behavior through regular practice and consistent modeling by all staff. All youth will have basic requirements they must meet (e.g., hygiene, chores, treatment, recreation, homework, religious/spiritual opportunities and community service) that are a part of the daily routine of activities. The routine will require accountability for decisions made every day. G4S recognizes that education is an extremely important component of the youth s rehabilitation process and will include structured time in the schedule for youth to complete and seek needed help with homework. DSOP will carefully plan a schedule that is comprehensive, gender-specific, and structured in activities in over 94% of awake hours, seven (7) days a week, which exceeds RFP requirements. A sample is as follows: Time Weekday Time Weekend 6:00a Wake-up / Room preparation 7:30-7:45a Wake-up / Room preparation 6:30-7:00a Breakfast 7:45-8:00a Personal Hygiene / Sick call / Meds 7:00-7:30a Hygiene / Maintenance of Living / Meds 8:00-8:30a Breakfast 7:30-7:45a Performance Goals Review 8:30-9:30a Pathways group (Sat); Relapse Prevention Group (Sun) Health Education (Sat) 7:45-11:10a School 9:30-10:30a Sex Offense-Specific Specific Group (Sat) Sex Offense-Specific Relapse Prevention Group (Sun) Health Education (1 time/month Sat) 11:10-11:40a Lunch / Hygiene / Sick Call 10:30-11:30a Pathways group (Sat) Relapse Prevention Group (Sun) 11:40-12:25p Just Read 11:30-12:15p Outdoor Activities Impact of Crime 12:25-2:05p School 12:15-12:45p Lunch / Hygiene / Visitation Prep 2:05-2:15p Group preparation / Restroom Break 12:45-1:45p Visitation / Educational TV / Movies / Board Games 2:15-3:15p Sex Offense-Specific Healthy Sexuality Group (Mon) Sex Offense-Specific Treatment Group (Tues-Thurs) Sex Offense-Specific Trauma Group (Fri) 1:45-2:45p Arts Programming 3:15-4:15p Community Meeting 2:45-3:45p Team Building Activity Conflict Resolution (Mon) Awards Assembly (Wed) 4:15-4:45p Personal Hygiene / Leisure Awareness 3:45-4:45p T4C Group 4:45-5:45p Homework (school) 4:45-5:45 Recreation 5:45-6:15p Dinner 5:45-6:15p Dinner 6:15-7:15p Recreation 6:15-7:15 Special Events / Spirituality (Sun) 7:15-7:30p Snack / Meds / Spirituality (Tues and Thurs, 7-8p) 7:15-7:30p Snack / Meds 7:30-8:45p Showers 7:30-8:45p Showers 8:45-9:30p Privilege Time / Phase Assignment / Community Cleanup 8:45-9:30p Privilege Time / Phase Assignment / Community Cleanup 9:30p Lights out 9:30p Lights out RFP R2107 Page 17
54 Program Services Consideration 4: How well does the proposal support the successful implementation of the schedule (i.e. are there enough trained staff, staff training support, appropriate number/level of staff planned into the schedule? Does it outline a realistic schedule for youth? DSOP will provide 24-hours awake supervision every day of the year and ensures appropriate levels of staff are available at ratios of the following: 1:6 during awake hours and 1:10 during sleep hours. Five (5) days of the week, G4S will employ a specialized Life Coach who will provide direct supervision of youth, maintaining ratios of 1:5, which exceeds RFP requirements. The Facility Administrator will post advanced schedules to provide adequate staffing coverage. Preparation of the staff schedule will consider all activities throughout the week that includes, but is not limited to transports, staff training and other events to follow the 94% of structured activities during awake hours. During on-campus family day activities, staffing ratios will be increased to accommodate the activity. These staffing ratios will provide appropriate supervision, suitable and timely response to the youth s everyday needs, safety and security issues as they arise, and immediate response to emergencies. As earlier identified, G4S will provide a comprehensive staffing expectation that will include a shift relief factor (SRF) of 1.67 to provide for staff coverage, supervision and programs during weekends, holiday, training and other employee absences. The Facility Administrator/designee will have the authority to modify the staff schedule to approve leave time and ensure staff ratios are being met. Additionally, DSOP will utilize part-time staff to enhance ratios and quality of care to youth. The part-time employees will receive the same 138 hours of training as full-time employees and are expected to attend all mandatory staff meetings. DSOP will maintain a holdover roster for those required to remain on shift, and an overtime roster that includes the names and phone numbers of those available for overtime shifts. Further, DSOP counselors and other non-direct care staff will be PAR trained and will provide supervision team support in the event of immediate necessity. This will provide back-up systems to ensure that additional staffing resources are available in the event of a vacancy or an emergency. Regular Treatment Team meetings will be held with the youth to evaluate participation in planned structured activities. Consideration 3: How well does the proposal describe a tracking system for monitoring youth participation for adherence to a structured therapeutic activity schedule? G4S will maintain a comprehensive tracking system that has proven to yield compliance to activities designed to meet the educational and behavioral treatment needs of the youth. Adherence to youth structured activities will include specific checks and balances, mentioned below, to ensure that structured activities occupy over 94% of the awake hours, seven (7) days per week. The Assistant Facility Administrator will have the ultimate responsibility for ensuring the schedule is followed throughout the day. The DSOP activity schedule will be posted throughout the facility, given to each youth during orientation, and provided to the parents as part of the admission process. Staff will be trained to proactively engage the youth in all scheduled therapeutic activities. The G4S comprehensive tracking techniques to ensure DSOP s adherence to the schedules will be as follows: Daily Monitoring Shift Reports, completed by supervisors and staff, then reviewed each morning by the FA and AFA during management meetings Behavior Cards, reviewed daily by the case manager and AFA Activity Tracking System reviewed by direct care, with notification to the Clinical Director if there is a breech in schedule events Group Check Sheet signed by the youth, reviewed by the Clinical Director and communicated to the Facility Administrator to ensure youth receive daily therapeutic services and psychosocial activities Daily Points incorporate the allocation of daily points that are earned based upon the youth s performance and adherence to scheduled activities. The total points are evaluated by the Facility Administrator weekly then sent to the Treatment Team and parents for review. Monitoring effectiveness of services is done by the Clinical Director, with follow-up communication to the management team during daily management meeting Weekly Monitoring Trends are reviewed during weekly management meeting to improve services / interventions Compliance of daily schedules is reviewed by the Quality Assurance Specialist and relayed to the Compliance Manager Group Monitoring by the Clinical Director to ensure adherence to schedule, and quality of services Review of above by corporate support personnel Monthly Monitoring Adherence to activity schedule, points, progress, and adherence is reviewed by the multidisciplinary Treatment Team during formal monthly staffing to determine how the youth is responding to treatment Adherence to activity schedule is monitored and evaluated by the Quality Assurance Manager as part of the Scorecard process and reviewed in the monthly facility verification and regional meetings. Monthly Facility Systems Review Sheet is completed by the Facility Department Director to keep score of compliance A.2. CATEGORY 5: CASE MANAGEMENT How well does the proposal describe Case Management services required by RFP? Consideration 7: How well does the proposal outline the Provider s capacity to coordinate services, obtain required consent documentation, communicate with the custodial parent or guardian, the district or circuit liaison, the Department, the courts, etc? A.2.a. COORDINATION OF CASE MANAGEMENT SERVICES: Case coordination will be a collaborative effort between the program s Treatment Team, JPO, parent/guardian and other agencies and community resources involved in the youth s care. The program will employ a community coach who will serve as the liaison for communication with the Department, committing courts, parents/guardians and other agencies and will be responsible for coordinating services and obtaining required consent. Upon admission, the community coach will review the youth s Electronic Commitment Packet (ECP) to ensure all documentation is available. This will include, but not be limited to, confirming the Authority for Evaluation and Treatment (AET) is signed within the requirements of 63E (3)(a)(1-9) Treatment Services. The community coach will RFP R2107 Page 18
55 Program Services be responsible for establishing community relationships, which are conducive to strengthening competency development. Additionally, the DSOP will be responsible for providing a comprehensive system of case management that facilitates the scheduled and documented transition of cases from referral and admission through transition and discharge. During the last stages of the program, the DSOP s life planner (further mention in the Discharge Policy and Transition section) will implement the Faith and Community Based Delinquency Treatment Initiative Program model. This will include establishing relationships with the youth s home community, as a means of strengthening transitions needs, while maintaining consistent communication with the parent/guardian, court, Department, and other entities involved. Consideration 1: How well does the proposal describe the Provider s assessment process, staffing, etc., of the youth for criminogenic factors? The DSOP assessment process will be the initial stage of treatment and performance planning for sex offender, mental health and substance abuse services and the beginning of formal discharge planning for each youth admitted to the program. The design of assessing needs will identify strengths, weaknesses, opportunities, and threats to each youth s behavior through a detailed history of the youth s family, health, sexual aggression, delinquency history, prior treatment experiences, academic performance, drug/alcohol use and developmental problems. Risk factors, strengths and protective factors will be closely reviewed in preparation for performance planning. The youth s antisocial behavior will be confronted and he learns to build strengths in order to protect from reverting back to antisocial behavior. DSOP will maintain a comprehensive multi-disciplinary needs assessment process conducted by multiple experienced personnel to thoroughly assess each youth, with follow-up phone contact with the parent and Juvenile Probation Officer (JPO). The community coach will administer the Massachusetts Youth Screening Instrument-Second Version (MAYSI-2), screen for past gang relations, and conduct a review of historical documents (Commitment Positive Achievement Change Tool (C-PACT), Pre-Dispositional Report (PDR), DJJ Comprehensive Evaluation, DJJ Face Sheet, sexual evaluations, and any other additional evaluations/assessments in the youth s history). In the event of gang affiliation, the information will be documented, shared with Treatment Team members, entered in the facility alert system, and notifications made with appropriate law enforcement. The mental health professional will administer the Vulnerability to Victimization of Sexually Aggressive Behavior (VSAB), the Assessment of Suicide Risk, clinical review of historical documentation, in addition to the "ERASOR" (a structured clinical interview based on empirical research). Results will provide a baseline measure of the youth s present strengths, needs, psychopathology and recidivism risk. In the event the MAYSI-2 refers for follow-up for mental/emotional disturbance or distress, the Facility Administrator and the licensed mental health professional will be immediately notified. The mental health professional will further screen using a tool pertinent to the need including, but not limited to, Beck Depression Inventory, State Trait Anger Expression Inventory, Trauma Symptom Checklist, SASSI, and Reynolds Children Manifest Anxiety Scale. A Psychiatric Evaluation will be conducted by a licensed/board certified child and adolescent psychiatrist. An educational assessment will be conducted by educational staff. The Facility Entry Physical Health Screen will be completed by a licensed medical staff. A new Comprehensive Physical Health Assessment will be conducted by a physician or other qualified medical professional on all youth. The community coach will contact with the parent/guardian and JPO to elicit risk and needs that will be staffed with the Treatment Team and included in the risk classification process below. Consideration 5: How well does the proposal describe how the Provider will identify and group youth within the program according to special characteristics for safety, health and treatment purposes, as specified and required by the RFP? G4S will implement a comprehensive risk classification process to identify and group youth, based upon consideration of safety and security, sexual aggression and history, health, special characteristics and individualized treatment needs. The classification process will be conducted by the youth s Treatment Team who will consider the age, sex, height, weight, physical size, maturity level, special needs, medical or mental health risk factors, gang affiliation, physical and/or sexual violence potential, suicide risk, escape risk and safety and security risks. The classification process will include pre-admission screening of each youth s Electronic Commitment Packet by Treatment Team members. Intake and screening will be conducted by licensed and unlicensed medical, mental health, and case management staff noted above to determine immediate mental health, substance abuse, potential acute, chronic or emergency health conditions that require immediate evaluation and treatment. Then, following intake and screening processes noted above and prior to youth s transition into general population, a formal admission classification meeting will be conducted with the youth and the multidisciplinary Treatment Team. The purpose of the meeting will be to review the findings of the records reviews, screenings, assessments and interview processes and to determine room and staff assignments, identification of physically and/or sexually aggressive youth and placement on alerts, identify any medical issues, acute or chronic substance abuse and mental health disorders, presence of withdrawal symptoms, gang affiliation, safety or security issues, or any other pertinent concerns, etc. Each youth will be assigned a single room. The classification information will be documented on the admission classification form and shared with staff as appropriate through documentation within the facility logbook, shift change briefings and on the alert communication board. Alerts will be entered into the JJIS system. All youth will be placed on Security Alert at admission for a limited time to allow adjustment to the program. Youth placed on Precautionary Observation or Mental Health Alert Status will wear a color-coded uniform to increase visibility and supervision. Youth with documented gang-related activity will be referred to the Gang Liaison. Reclassification will occur at every Treatment Team review and at any time, based upon need. Consideration 2: How well does the proposal describe how the Provider will complete individualized performance plans developed by a multidisciplinary Treatment Team in conjunction with youth? A.2.b. DEVELOPMENT OF DELINQUENCY PERFORMANCE PLANS: Following the initial assessment of the youth, all risk factors will be presented to the multi-disciplinary Treatment Team meeting for collaboration of performance planning. Input for the planning will be encouraged from the youth, parent/guardian, mental health professional, community coach, clinical director, program management, educator, psychiatrist, program specialist, DCF (if applicable), and JPO (or conditional release counselor). Assessment of risk for re-offending will be incorporated in treatment RFP R2107 Page 19
56 Program Services planning and monitored throughout the youth s stay, with administrations at pre-treatment (first phase) and post-treatment (last phase). The community coach, life planner, and mental health professionals will be trained to implement the Residential Positive Achievement Change Tool (R-PACT) in order to identify criminogenic risk and protective factors, and to prioritize the youth s criminogenic needs. To maximize communication and motivation with the youth, the DSOP will use Motivational Interviewing readiness ruler to assess the youth s readiness to engage in delinquency interventions from the Stages of Change perspective. This comprehensive initial assessment process will address any resulting information that is applicable to the criminogenic risk and needs assessment, and will be documented on the Youth Needs Assessment Summary (YNAS) within 21 days, which exceeds RFP requirements. The youth s risk factors, strengths and protective factors will be inclusive of the delinquency Performance Plan development. The Treatment Team will recommend the development of goals and interventions for the performance plan, based upon ranked domains prioritized within the R-PACT and the needs assessment process. The youth and community coach will develop individualized goals based upon the top three (3) dynamic criminogenic needs and three (3) protective factors. The goals will identify a target date for completion, the youth s responsibility to complete the goal and the program s responsibility to encourage the youth to complete the goal. The performance plan will be completed within 25 days of the youth s admission to the program, which exceeds RFP requirements. To facilitate the youth s rehabilitation and promote public safety, the Treatment Team will revise the youth s performance plan based upon the youth s formal progress reviews, R-PACT reassessment results, demonstrated progress towards goal completion, or newly acquired or revealed information. Goals will be developed to facilitate the youth s successful reintegration into the community upon release from the program and include delinquency interventions with measurable outcomes that decrease criminogenic risk factors; delinquency interventions that promote strengths, skills, and supports to reduce the likelihood of reoffending; target court-ordered sanctions that can be reasonably initiated or completed while the youth is in the program; and identify transition activities targeted for the last 60 days of the youth s anticipated stay in the program. Consideration 3: How well does the proposal detail how Motivational Interviewing is implemented by the Provider to promote engagement in delinquency intervention? A.2.c. EMPLOYING MOTIVATIONAL INTERVIEWING TECHNIQUES: Motivational Interviewing (MI) is a key element in the engagement of youth in delinquency intervention services. Research shows that behavioral change occurs most frequently when the motivation for change comes from within the individual rather than externally. To enhance internal motivation and promote engagement in delinquency intervention services, 100% of DSOP staff will be trained to use MI technique, which exceeds RFP requirements. G4S will employ Dr. Deena Green, Ph.D. and Bridget Goodrich who are state-recognized MI Trainers to conduct MI pre-service and in-service training for program staff. All direct care staff will receive eight (8) hours of MI training during pre-service. The facility administrator, assistant facility administrator, community coach, life planner, clinical director, mental health professionals and delinquency intervention facilitators will complete the 16-hour MI certification training required to administer the R-PACT. Staff will use MI skills daily while interacting with the youth, implementing the behavior management system, conducting needs assessments, mental health evaluations and R-PACT assessments, developing performance/ treatment plans, conducting bi-weekly and formal performance reviews and facilitating delinquency services. In addition, the youth s stage of change will be assessed by the Treatment Team at admission, classification, assessment, bi-weekly and monthly performance reviews, transition conference, and exit conference, utilizing the Readiness Ruler/Readiness to Change questionnaire. The trans-theoretical model of change will identify appropriate motivational strategies to use depending upon the youth s stage of change. The stages of change will be predicated upon the premise that change follows a pattern of predictable stages; change is a dynamic continuum; and services need to meet the youth where they are at on the continuum. In developing the performance plan, the community coach will use the level of risk as defined by the R-PACT to govern the nature, intensity and duration of delinquency interventions, the identified criminogenic needs to target interventions and MI techniques, coupled with youth s stage of change to engage youth in delinquency intervention services. Consideration 6: How well does proposal describe how Provider will assess youth for progress during delinquency interventions? A.2.d. ON-GOING REVIEW OF PERFORMANCE PROGRESS: DSOP will provide consistent review of performance progress through daily group notes, observations, logbook documentation, positive and negative write-ups, daily management meeting and radio communication. The licensed mental health professional will review the documentation daily and immediately discusses any behavioral concerns with the Program Administrator/designee. On a bi-weekly basis, the youth s performance progress, performance goals, positive and negative behavior, physical interventions, R-PACT reassessments and treatment progress will be reviewed during Treatment Team. Such reviews will require at least one (1) formal meeting each month where the collaborative review is facilitated by the community coach and include the Treatment Team, youth, parent/guardian, JPO and other members involved in the youth s care. The youth will be encouraged to present 70% of the discussion and the Treatment Team 30% of the discussion, which exceeds RFP requirements. The performance plan will be the benchmark used by the Treatment Team to measure the youth s progress or lack of progress during delinquency interventions. The R-PACT reassessment will determine changes in risks and needs, so that updated information is available for the 90-day Performance Summary. Any additional updates will be completed when deemed necessary by the Treatment Team, with all documentation being maintained in the case management record. A.2.e. PREPARING PERFORMANCE SUMMARIES: Formal written notifications of progress will be documented through performance summaries and sent to the committing court, JPO, parent/guardian and other pertinent parties every 90 days, beginning 90 days from the signing of the youth s RFP R2107 Page 20
57 Program Services performance plan, or at shorter intervals when requested by the committing court. Youth will be assessed for delinquency intervention progress, using specifically designed instruments such as the T4C Structured Assessment and Youth Structured Self-Assessment. The Treatment Team will prepare a Performance Summary prior to the youth s release, discharge or transfer from the program. The Performance Summary will address the youth s status on each performance plan goal, overall treatment progress, academic status including behavior in school, behavior including level of motivation and readiness for change, interactions with peers and staff, initial and overall behavior adjustment, significant positive and negative incidents or events, and justification for a request for release, discharge or transfer, if applicable. The staff preparing the Performance Summary, the Treatment Team leader, the Facility Administrator or designee, and the youth review, will sign and date the report. Youth will be given the opportunity to write personal comments in the summary with assistance provided, if requested. Copies of the Performance Summary will be distributed within five (5) working days of signing the plan to the committing court, the youth, JPO or Aftercare Provider and parent/guardian, which exceeds RFP requirements and Rule 63E-7.010(9)(b)(2), F.A.C. Consideration 4: How well does the proposal outline the Provider s process for ensuring quarterly progress reports are provided to the committing court, Department JPO and youth s parents? A.2.f. PROVISION OF QUARTERLY PROGRESS REPORTS AND ADHERING TO DEPARTMENTAL TIMEFRAMES: DSOP will use tracking systems, weekly coaching sessions, Facility System Review tools, satisfaction surveys, and risk management processes to ensure that timely completion of documentation is provided to the committing court, Department JPO and youth s parents, which exceeds RFP requirements. As a part of the on-site risk management system, internal trackers will be in place to monitor and target key documentation requirements, as per F.A.C. 63E , Residential Case Management Services. Progress reports will be included on the facility tracker in accordance with quarterly reporting requirements, or at earlier intervals as requested by the court. The Facility Administrator and community coach will use the internal tracker to target upcoming due dates for documentation submission. Additionally, the community coach will maintain a Facility System Review Tool which validates daily review of due dates for key documentation. On a weekly basis, the Facility Administrator will conduct a coaching (supervision) session with the community coach and review the Facility System Review tool and completed documentation. The Facility Administrator will formally review each document and sign off as the reviewer. Formal transmittal letters will accompany each performance summary as a part of the review process. Corporate Quality Assurance staff will monitor facility trackers and complete verification activities to ensure that the program consistently meets requirements. Additionally, the corporate office will send periodic satisfaction surveys to the parents validating required reporting practices. Finally, the DSOP will establish and implement a tracking system to ensure that any case of a youth who is screened by the department as potentially eligible for involuntary commitment as a sexually violent predator (SVP) will be managed as follows: Not less than 240 days prior to the anticipated release of a youth who is potentially SVP eligible, DSOP will notify the JPO of the anticipated release. The program will identify the youth s potential SVP eligibility as part of the initial assessment documentation and the youth s performance plan. The program will include transition activities on the youth s performance plan that facilitate determination of the youth s SVP eligibility status. When planning the youth s release pursuant to paragraph 63E-7.012(2)(b), F.A.C., the program will assist the DCF multidisciplinary team and the State Attorney by providing additional information requested or by accommodating their request to interview the youth (Rulemaking Authority FS. Law Implemented (3)(a) FS. History New , Amended , , Amended ). A.3. CATEGORY 15: HEALTH SERVICES How well does proposal meet requirements identified in Health Services Manual (2006)? The provision of health care services at DSOP is available seven (7) days a week. The Medical Department is fully equipped to provide routine care inside the facility. G4S recognizes there are unique health care delivery requirements associated with a juvenile environment and has tailored the medical program to DJJ specifications. Dr. Dianne Rechtine, MD, FAAFP, CCHP-A, our correctional Health Care Consultant, provides expert consultation for the Medical Department and/or special medical needs youth. Basic, primary medical care will be provided by a Florida Board-Certified and licensed physician. Health care staff will be responsible for serving as the liaison between the facility and local health services. G4S also employs a full-time Corporate Director of Health Services (DHS), Mary Frances Magan, RN, to provide on-going training and support to health care medical staff. All DSOP medical staff will be properly trained in pediatric and adolescent healthcare and licensed in accordance with Florida Statutes. Consideration 2: How well does the proposal describe the provision of comprehensive on-site health services? A.3.a. COMPREHENSIVE ON-SITE MEDICAL SERVICES: Comprehensive on-site medical services will be provided seven (7) days a week by licensed healthcare staff to address the health needs and promote the growth and development of adolescent boys. These will include, at a minimum, primary and preventative care, sick call and episodic care, and management of acute and chronic medical issues and follow-up. These services will be provided by skilled licensed medical staff who are thorough in assessment and observations. Services that will be provided and exceed RFP requirements will include, but not limited to the list below: Assessment of Tuberculosis status and Tuberculosis Skin Testing as required; Screening of all boys for Sexually Transmitted Diseases and applicable testing; HIV risk assessment of all boys and applicable testing.; Assessments of immunization status and subsequent inoculations as required; Dental screening with a referral for all youth to a local dentist at the Volusia County Health Department; RFP R2107 Page 21
58 New comprehensive physical assessments for all youth within seven days of admission; Eye examinations with a referral for all youth by a certified Optometrist; Lab and Diagnostic Services. Program Services A.3.b. METHOD OF ON-SITE HEALTH SERVICES DELIVERY: G4S is committed to providing the highest level of quality medical services in accordance with the Department s Health Services Manual (Revised October 2006 with April 2010 Updates), under the direction of the DHA. The figure below outlines the level of medical services to ensure that observation, assessments, and appropriate services are available. Position Qualifications Responsibilities Hrs / Week G4S Health Care Previous Medical Director for several Develop and oversee the G4S Medication Formulary Consultant major correctional facilities; Clinical Assist with development of policies, procedures and protocols As Needed On-Call 24/7 Diane Rechtine MD, Assistant Professor at NOVA Provide on-site and/or telephonic physician-to-physician consultations FAAFP, CCHP-A Southeastern University; FAAFP; CCHP-A Designated Health Authority Contracted Psychiatrist G4S Director of Health Services Mary Frances Magan RN Florida Board Certified and licensed physician (MD), trained in Pediatrics, Family Practice or Internal Medicine, to serve as the Designated Health Authority (DHA) Board Certified in Child and Adolescent Psychiatry or Psychiatry by American Board of Psychiatry and Neurology or has completed a training program in Psychiatry (approved by American Board of Psychiatry and Neurology for entrance into its certifying examination) Develop medical/nursing protocols; supervise all program physical health services and healthcare staff, and provide final clinical judgments Review and revise Facility Health Operating Procedures in concert with FA Provide on-site supervision and practices, emergency situation response and 24/7 on-call services Conduct comp. physical assessments and periodic evaluations Provide primary care and medication management Conduct psychiatric evaluations, provide diagnoses and treatment planning Provide emergency situation response; 24/7 on-call services Provide pharmacologic management of all youth on psychotropic medication Attend staffing/consultation as needed RN Develop policies, procedures and protocols in conjunction with G4S Medical Consultant and DHA Provide regular on-site fidelity reviews of practices in health care Ensure compliance of DJJ health care standards and contract Provide oversight and support of RN/LPNs Director of Nursing RN Overall responsibility for nursing services/dha Communication Schedule and monitor emergency health-related drills Participate in Facility Management team activities Provide admission nursing assessments, sick call care, episodic care and medication administration Coordinate continuity of care and needed follow up care Provide health education Coordinate health care services during off site evacuations Prepare required DJJ reports Monitor Medication Administration Records Maintain alert system Consult on all Infection Control matters Nurses LPN Communication with DHA as applicable (ex: acute/chronic concerns, etc) Provide admission nursing assessments, sick call care, episodic care and medication administration Provide documentation in Individual Health Care Record Provide health education Provide required parental notifications Maintain Individual Health Care Records At least 2 hrs/wk On-Call 24/7 2 hrs/wk On-Call 24/7 As Needed On-Call 24/7 40 hrs/wk On-Call 24/7 40 hrs/wk (20 hrs/wk each) G4S will maintain agreements with providers for consultation or treatment when resources are not available on-site or when the youth needs specialized care that can only be provided off-site. Section A.3.e.6. below further addresses current contracting arrangements that will be made available upon request. A.3.c. OPERATING PROCEDURES: To facilitate operation of an effective system of health care, facility operating procedures and health care protocols will be developed by the Director of Health Services in consultation with the DHA and Dr. Rechtine. All Facility Operating Procedures and Health Care Protocols will be approved by the DHA, reviewed annually and updated as needed. All health care providers and subcontractors will undergo employment background screening as indicated by law. A.3.d. EMERGENCIES: Medical emergencies and accidents can occur anytime at the program. To enable a quick and efficient response to emergencies, policies and procedures will be developed and practiced on a regular basis. All staff having direct contact with youth will be trained in Automated External Defibrillator (AED) operation, CPR and Emergency First Aid. In addition, all staff or volunteers having direct contact with youth will be trained to call 911 for a medical emergency requiring urgent medical attention. Posters will be placed throughout the facility in visible areas detailing these procedures. First aid kits, AED s, knife-for-life and wire cutters will be located in designated locations. A.3.e. SERVICE AGREEMENTS: The following health care components will be established and maintained to ensure the provision of necessary and appropriate health care discussed throughout this Health Services Section. RFP R2107 Page 22
59 Program Services Consideration 1: How well does the proposal describe the provision of the Designated Health Authority (DHA) Services as Specified in the Health Services Manual (2006)? (Review the proposed physician's CV/resume, letter of intent from the proposed physician, and his/her proposed schedule.) 1. Designated Health Authority: To ensure quality healthcare services continue in a consistent manner, Dr. Ramin Bonnet, current DHA of the, has provided a letter of interest to remain as the interim DHA, (see Letter tab section). A formal written contract will be established with a Florida Board-Certified and licensed physician, (MD or DO) trained in Pediatrics, Family Practice or Internal Medicine, and experienced in adolescent boys health, in accordance with the Department s Health Services Manual (Revised October 2006 with April 2010 Updates). The contract will clearly define the roles and functions of the DHA and will be provided to the Department. The DHA will provide oversight of the program s health and medical care to youth and be responsible for the overall clinical direction, policies and protocols for the medical services provided, including supervision of all medical personnel. The contract will include services provided and frequency, extent of available emergency and on-call services, and specification of other duties. Final clinical judgments will rest with the DHA who will be on-site at least two (2) hours per week or more as the clinical needs of the population may dictate. The DHA will perform all necessary comprehensive physical assessments, periodic evaluation, chronic care services, medication management, sick call referrals, coordination of specialty off-site medical services and other services as outlined in the manual. If clinical responsibilities are delegated to an Advanced Registered Nurse Practitioner (ARNP), the physician will remain the DHA but will have an assignment written, formulized and specified in the current and valid collaborative practice protocol between the ARNP and the DHA. This responsibility will not be delegated to lesser-trained health care providers. Consideration 3: How well does the proposal outline the provision of nursing services including hours and level of staff (ARNP/ RN's/ LPN's/ etc.), appropriate coverage for the schedule as required by the RFP? 2. Nursing Services: On-site nursing coverage will be provided by Florida Licensed Registered Nurses (RNs) and Licensed Practical Nurses (LPNs). DSOP will provide up to 80 hours a week of on-site health care staff, which exceeds RFP requirements. G4S full-time Corporate Director of Health Services, Mary Frances Magan, RN, will provide on-going fidelity health care reviews, training and support to all health care medical staff. The following sample table shows health care coverage that will be provided seven (7) days a week, which will allow opportunity for flexibility on the weekend for health education training to be conducted by a licensed nurse: Sunday Monday Tuesday Wednesday Thursday Friday Saturday #1 LPN: 10 hrs RN: 8 hrs RN: 8 hrs RN: 8 hrs RN: 8 hrs RN: 8 hrs #2 LPN: 10 hrs #1 LPN: 10 hrs #2 LPN: 10 hrs 3. On Call Services: The contracted DHA and Psychiatrist will be available by telephone for medical and mental health emergencies, and consultations 24 hours a day, seven (7) days a week. Emergency contact numbers will be posted in the medical clinic. 4. Vacations and Absences: G4S will ensure that uninterrupted physician and nursing services are provided in the event of absences by authorizing overtime hours for available staff and having part-time medical staff on-call as needed. The DHA will be contractually responsible to provide another MD, DO or ARNP for vacation coverage. As a secondary back up, G4S will maintain a service agreement with an ARNP and nursing agency to provide coverage in the event of an unexpected absence or vacation coverage. Consideration 4: How well does the proposal outline its protocol for the provision of health services during natural disasters? 5. Disaster Preparedness: DSOP will maintain a Comprehensive Disaster Preparedness Plan (COOP), which addresses a variety of disasters. G4S has substantial experience in disaster preparedness. In 2004, G4S successfully implemented COOP procedures during four (4) major hurricanes, which resulted in the resumption of normal operations without incident. G4S partners with DJJ and Pinellas County Department of Emergency Management and other Disaster Preparedness entities to identify evacuation sites that will provide both security and safety for youth and the employees during emergencies. The disaster plan will include basic medical staff coverage with attention to medications (via a contracted pharmacy), first aid supplies, medical documentation portability, and on-going treatment needs (respiratory treatments, etc.). Hospitals will be those closest to the primary and secondary evacuation site(s), and arrangements will be made in advance for any emergency medical needs during a disaster, along with associated security needs. All program staff at DSOP will be trained in Disaster Preparedness during new orientation at the Corporate Training Academy with updates annually. Consideration 5: How well does proposal outline linkage to ancillary services to meet a broad range of youth's medical needs addressing, at minimum: a) Contracts/written agreements for ancillary services; b) Protocols for accessing emergency medical services; c) Protocols for accessing dental; d) Protocols for accessing eye care; e) Protocols for accessing x-ray and lab services. 6. Ancillary Service Agreements: DSOP will establish and maintain written agreements with providers for consultation and/or treatment when resources are not available on-site or when youth need intensive, specialized medical care that can only be provided off-site. Medical and dental emergencies and accidents can occur any time at the program. To enable a quick and efficient response to emergencies, policies, procedures and protocols will be practiced on a regular basis at DSOP. All staff having direct contact with youth will be trained in Automated External Defibrillator (AED) operation, CPR and Emergency First Aid, which exceeds RFP requirements. In addition, all staff or volunteers having direct contact with youth will be trained to call 911 for a medical emergency requiring urgent medical attention. Additionally, policies, procedures and protocols will be developed to access dental care, eye care x-ray and lab services through a RFP R2107 Page 23
60 Program Services Physician, ARNP or PA order or referral. A copy of each service agreement will be kept on file in the facility. The following agreements will be pursued to ensure quality health, mental, dental, pharmaceutical, vision and support services provide treatment for our youth: Hospital Pharmacy Mental Health Emergency Consulting Pharmacist Designated Health Authority Laboratory and Diagnostic Services Psychiatrist Eye Care (Optometrist) Dental Bio-Hazard Waste Removal X-Rays & EKG s Volusia Co. Health Department (HIV Education/ & HIV Testing) Consideration 6: How well does the proposal describe its plan or process to ensure completion of the physical assessments within the timeframes described in the Health Services Manual (2006)? A.3.f. GENDER-RESPONSIVE SERVICES: G4S will provide the following necessary and gender responsive health care services to DSOP youth. 1. Screening and Evaluation: All youth entering DSOP will receive gender responsive routine screenings and evaluations for health related conditions as required by the Department. Health care services will be performed by appropriately licensed and trained personnel who meet statutory and regulatory standards of care in accordance with the Department s Health Services Manual (revised October 2006 with April 2010 Updates). The Facility Entry Physical Health Screening will be completed by medical staff at the time of the youth s admission to the program and the DHA will immediately be notified of any youth admitted with specific conditions as required by DJJ. This screening process will not take the place of the required medical evaluations completed upon admission, but include at a minimum: Health Related History Thorough assessment of all body systems and an assessment of nutritional status, growth and development Implement Body Mass Index Protocol designed by the DHA specifically for adolescents Screening for Sexually Transmitted Diseases for all youth HIV Risk Assessment for all youth Assessment for chronic conditions and medical concerns requiring immediate medical attention Assessment of tuberculosis status Assessment of immunization status and subsequent inoculations as required Assessment of dental health with a referral to the dentist as necessary; vision and hearing screening If applicable (youth currently under the influence of drugs or alcohol at admission), the health care staff will initiate a Detoxification Assessment. If a youth is identified as demonstrating signs or symptoms of detoxification, the nurse will identify this information on the assessment, then contact the DHA for notification and further instructions for the youth s health care needs. The DHA will evaluate the needs of the youth and may prescribe medication or will make a referral to Halifax Health Center, if indicated. DHA notification for new admissions and orders obtained, as applicable (i.e. routine standing orders, medication continuance, etc). 2. Comprehensive Physical Assessments: Youth entering the facility will receive a gender responsive Comprehensive Physical Assessment (CPA) completed within seven (7) calendar days of admission, regardless if one (1) had been completed within the year or not, and annually thereafter regardless of their assigned medical grade, which exceeds the RFP requirements. This Comprehensive Physical Assessment will be performed by the Designated Health Authority/designee to establish a clinical database for each youth and includes, at a minimum, the following: Review of the Health Related History Palpitation of thyroid as male adolescents are more prone to thyroid issues Physical health history and assessment of all body systems for acute, chronic, functional medical and dental problems (if any) Tanner Level is a physical assessment of genitals to gauge and assess for abnormalities Gynecomastia examination of male breasts as breast enlargement is common for this age group along with breast lumps Investigation of any current complaints Assessment of nutritional status/bmi Assessment of growth and development Physical activity restrictions, if applicable Assignment of Medical Grade Laboratory or diagnostic testing; when clinically indicated Determination of the need for additional evaluations if necessary The program will established a community partnership with Volusia County Health Department to provide HIV testing/education Consideration 7: How well does the proposal describe the provision of Sick Call Services....? 3. Sick Call Care: In accordance with the Health Services Manual (revised October 2006 with April 2010 Updates), Treatment Protocols will be developed by the DHS through consultation with the DHA and Dr. Dianne Rechtine MD (G4S Medical Consultant). The DHA will review and approve all Treatment Protocols. The sick call process will be available to all youth at DSOP seven (7) days a week, exceeding RFP requirements. Sick call care services will be available to all youth to provide care in response to complaints which are non-emergent in nature, typically minor and which can safely wait until the next scheduled sick call without worsening or causing significant pain and/or discomfort or deterioration in the youth s status. The dental sick call will be incorporated into the sick call policy. If a youth is experiencing a dental emergency, RFP R2107 Page 24
61 Program Services they should report this to any staff immediately, rather than waiting for the regularly scheduled sick call process. Staff will be available to escort youth to sick call in a timely and expeditious manner if needed. Once the youth has been seen, the sick call form will document any treatment given, any referral to appropriate health care provider if needed, e.g. MD, DDS, etc. and placed in the youth s medical file. The Sick Call Index and Sick Call/Referral Log will be completed and placed on the daily shift report at the end of the day to track sick call requests and treatment. If a youth submits sick call for the same issue three (3) times in a two-week period, the youth will be referred to the DHA for evaluation and the parent/guardian notified. Procedures will be developed for off-site referral when the complaint warrants evaluation beyond the scope of on-site personnel. Sick Call Request forms will be readily available for all youth to utilize 24/7. For easy access, sick call request forms and confidential boxes will be located on each unit. Medical services will be captured in the DSOP facility operating procedures, signed and approved by the DHA and Facility Administrator. All required DJJ health forms will be utilized by DSOP. Program staff are trained on the sick call process during their orientation period and taught how to respond to youth health or medical complaints in a professional manner. When on-site, health care staff will be expected to review sick call requests within two (2) hours, which exceeds RFP requirements. When a health care staff is not on-site, all sick requests are turned into the Shift Manager/designee for review within (2) hours, which exceeds the requirements. The Shift Manager/designee determines when a sick call request requires immediate attention; if the Shift Manager/designee cannot determine the needs of the youth; the healthcare staff is notified and consulted via telephone to determine if the sick call requires immediate attention and/or for instructions. Any youth complaining of severe pain (including dental) which a staff member is unfamiliar and cannot determine the severity, will be treated as emergencies and require immediate referrals to a licensed health care professional. If health care staff is not on-site, emergency medical services will be obtained at the Halifax Health Center. If the symptoms appear life threatening, staff is required to call and then notify the manager on duty and the healthcare provider on call. If youth presents to a nonlicensed staff with regard to medical issues which are not life threatening, the staff will instruct the youth to complete a sick call request in order to be evaluated by the health care staff during the regularly scheduled sick call clinic. The Shift Manager/designee can treat youth for minor complaints outside of sick call utilizing the approved over-the-counter medication(s) in accordance with the Health Services Manual (2006). Consideration 8: How well does the proposal describe its provision of Episodic Care,......? 4. Episodic Care: DSOP will provide care in response to unexpected illnesses, accidents or conditions of a nature that require immediate attention or professional assessment to determine severity. The Director of Health Services will provide an annual medical drills calendar outlining (3) three drills each month to be conducted by the DSOP health care staff, which exceeds RFP requirements. These drills will include, but not be limited to: cardiopulmonary arrest, unconsciousness, choking, bleeding, seizures, dental trauma, first aid, sudden mental status changes, chest pain, shortness of breath, open head injury, fractures or potential fractures and suicide attempt. The DSOP health care staff and management will plan these drills and maintain related records. The Facility Administrator and health care staff facilitating the drills will critique the effectiveness of the drill and determine if further training is deemed necessary. The DSOP staff will conduct daily inspections of the facility, which include the first aid kits. Any kits that are found to be open will be immediately brought to the health care staff to be refilled and sealed. The health care staff will perform, at a minimum, weekly inspections of the first aid kits. One (1) Automated External Defibrillators (AED), Knife-for Life, wire cutters, needle nose pliers, window punch and first aid kits will be stored in appropriate locations determined by the DHA and Facility Administrator. The AED will be located in a central location available to all staff for emergency use and all emergency equipment will be routinely inspected by the health care staff to ensure the equipment is in proper working order. G4S will provide pre-service training by a certified instructor to all new employees in the areas of Basic First Aid, Cardiopulmonary Resuscitation (CPR) with Automated External Defibrillator (AED) training, and as needed to keep their certifications valid. All staff will be trained to recognize the difference between minor complaints, emergencies, sick call complaint, or simple need for on-site first aid care not requiring a higher level of medical care. Upon contract award, G4S will pursue an agreement with the Halifax Health Medical Center for off-site medical and mental health emergencies, due to the close proximity to DSOP and the ability to have a youth at the emergency room within approximately 12 minutes. DSOP will provide nursing coverage 7 days a week, which exceeds RFP requirements. Further, medical staff will provide emergency on-call coverage 24 hours a day, 7 days per week. PAR: DSOP will maintain written protocols in place and comply with Protective Action Response (PAR) protocol as per Florida Administrative Code Rule 63H as it relates to episodic care. After a PAR occurrence, a post-par interview with the youth will be conducted immediately assuming the youth is under control, and will not exceed 30 minutes to determine if there are any physical injuries, complaints, shortness of breath or other distresses that require a medical review. If a medical review is necessary, it will be conducted by an RN or LPN on-site. All findings, descriptions of injuries or complications and medical treatment provided, if any, will be documented in the youth s individual health record. Consideration 9: How well does the proposal outline the provision of services for ongoing treatment for chronic health conditions which include, at minimum, evaluations at intervals no less than every 3 months? 5. Acute and Chronic Conditions: The frequency of the periodic evaluation will be determined by the youth s condition, clinical needs and clinically appropriate medical standards. For all youth who have a chronic condition or communicable disease and are receiving prescription medications, excluding anti-tuberculosis medications and psychotropic medications, a periodic evaluation will be conducted at least every two (2) months by a MD, DO, PA or ARNP, exceeding the RFP requirements. In case of condition for which more frequent monitoring is required (e.g. monitoring for side effects to anti-tuberculosis medication, follow-up after initiation of antiretroviral medications, adjustment of insulin dosage or for monitoring of responses to psychotropic medications) the periodic evaluation will be conducted at a frequency which is accordance with acceptable standards and practice, but will not exceed two (2) months, which exceeds RFP requirements. Periodic evaluations will also be conducted prior to the renewal or change of medication(s). RFP R2107 Page 25
62 Program Services DSOP healthcare staff utilizes a Medical Services Tracking system to document the list of youth with chronic medical conditions and to track and schedule youth at the appropriate intervals for required follow up/periodic evaluations. Additionally, the Director of Health Services and/or Risk Manager perform regular chart audits and system audits to determine if youth s health care needs are met in the required timeframes. If lapses are identified, the Director of Health Services re-evaluates the systems and implements a corrective action plan to correct the identified deficiencies. If conducted on-site, these periodic evaluations are documented on the Physician Progress Note Form in SOAP format, which include the documentation of a change in the youth s Medical Grade (if applicable). All new orders are documented by the Physician on the Physician s Order Form. If conducted off-site, these evaluations are recorded on the DJJ Summary of Off-Site Care Form, reviewed by the Designated Health Authority and filed in the youth s Individual Health Care Record. Additionally, the healthcare staff will follow any written instructions/laboratory testing provided by the credentialed Physician, PA or ARNP to sufficiently monitor the youth s identified chronic health condition. All orders are reviewed by the healthcare staff to ensure orders/testing are received/conducted. All specialty consultations are tracked by the healthcare staff to ensure the youth s appointment is scheduled and conducted. A Parental Notification of Health Related Care Form (general and/or medication) is sent to the parent/guardian whenever there is a significant change in the youth s condition, change in medication and/or new medication(s) via regular mail. Consideration 10: How well does the proposal outline the provision of services for routine immunization in accordance with Center for Disease Control (CDC) recommendations? 6. Immunizations: DSOP health care staff will receive the youth s Immunization Record upon admission, or contact the Juvenile Probation Officer, School or Parent/Guardian to assist with efforts to acquire such documentation. A review for needed immunizations will be conducted to determine if the youth has received all appropriate immunizations. DSOP health care staff will determine if any additional immunizations are required based on CDC immunization guidelines, and document them on the chronological progress notes. Immunizations will be completed within 30 days of admission into the program. The DSOP health care staff will then notify and obtain consent from the youth s parent/guardian for any needed immunizations in accordance with the Health Services Manual (revised October 2006 with April 2010 Updates). After receiving an order from the Designated Health Authority, the health care staff will administer the necessary vaccines. DSOP will participate in the Florida Vaccine for Children s Program (VFC) and obtain necessary vaccinations through VFC. DSOP will enroll in the Department of Health (DOH) Florida Shots Program to have access to immunization records, input new immunization data, or initiate a patient record in this confidential electronic DOH vaccine registry. In addition, G4S will establish a partnership with the Department of Health Florida Shots Program to secure annual Influenza Vaccines for youth. Consideration 11: How well does the proposal describe its protocols for transition, addressing at minimum, how the Provider plans to coordinate with the aftercare entities regarding medical needs upon the youth's discharge from the DJJ facility? 7. Transitional Health Care Planning: DSOP s transitional health care planning will begin within days prior to the youth s anticipated release to the community. Health care staff will communicate information about pending health related issues and when applicable facilitate linkages or scheduling appointments with community providers. The planning will involve the youth s parent or guardian (in person or telephonically), the Juvenile Probation Officer (JPO), the facility s case manager and health care staff. All efforts to facilitate linkages and schedule appointments will be documented in the Individual Health Care Record. If the youth is released to the community under continuing supervision of DJJ, the health care staff will attend the youth s exit conference to review the need for any upcoming appointments and/or any unresolved health-related needs, and ensure the parent/guardian and JPO are informed. The health care staff will provide a summary of healthrelated needs (pending scheduled appointments, the need for medication, information about community resources and the links) which will be included in the youth s exit conference and on the required DJJ Health Discharge Summary/Transitional Plan form. A copy of the Discharge Summary/Transitional Plan will be given to the parent/guardian, JPO and the original remains filed in the Individual Health Care Record. DSOP will provide the parent/guardian with the youth s current medication(s) and a 30-day prescription for psychotropic medication(s), which exceeds RFP requirement. Any statutorily protected health information will be reviewed with the youth, unless consent has been given to release the information to the parent/guardian. The health care staff will document any transitional planning provided to the youth in the individual Health Care Record. The disposition of the Individual Health Care Record is accomplished by affixing the record to the case management file and stored in compliance with Department policy and state retention law and rule. Consideration 12: How well does the proposal's protocol for communicable disease and infection control comply with OSHA's Standard 1910 Subpart I: 29CFR ; 29CFR ; App. A; and 29CFR ? 8. Infection Control Measures: DSOP will maintain a site specific Exposure Control Plan. The exposure and infection control program will follow guidelines and recommendations of the Center for Disease Control and Prevention (CDC), Occupational Safety and Health Administration and State and Federal Standards recommendations related to infection control, including, but not limited to the Occupational Exposure to Blood borne Pathogens Compliance Manual, OSHA Rule 29 CFR Part and guidelines from the CDC for testing, decontamination, sterilization and proper disposal of sharps and bio-hazardous wastes. Personal Protective Equipment, such as specialized clothing or equipment, will be worn by an employee for protection against a hazard material and is readily available. DSOP will maintain a contract for the removal of biomedical waste. Exposure and infection control matters will be regularly included as agenda items in administrative meetings and continuous program planning and evaluation meetings. G4S employs Kathleen Bingham, Med, RN, CNA-BC, LHCRM, a licensed health care risk manager, who is consulted for all infection controls matters. The health care staff will complete and file all reports regarding infectious diseases consistent with local, state and federal laws and regulations. Annual statistics will be maintained monthly of infectious diseases by category. Youth with communicable diseases will be isolated, as clinically indicated. All youth admitted to the facility will be screened by the facility health care staff. During the initial evaluation, the youth will be screened via facility entry physical health screening for symptoms of Tuberculosis. If the youth has RFP R2107 Page 26
63 Program Services been tested in the last year and exhibits no signs and/or symptoms of Tuberculosis, he will not be re-tested. All other youth will receive a Tuberculin Skin Test unless contraindicated by the DHA. In addition, DSOP will establish a partnership with the Department of Health Florida Shots Program to secure annual influenza vaccine for youth. 9. Diagnostic Services: DSOP will provide lab and diagnostic services that includes blood work, X-rays, EKGs and ultrasounds. Timely follow up of results and interpretations, in addition to appropriate referrals for specialized medical services will be completed. Consideration 13: How well does the proposal describe its ability to provide medication administration? A.3.g. MEDICATION ADMINISTRATION: Medication administration protocols will ensure oversight by the DHA and by outside consultation when deemed necessary, as described below. All new or existing prescription medications will be the responsibility of DSOP. Prescription medication will be filled immediately or no more than 12 hours after originally written and procured within 24 hours. If the contracted pharmaceutical vendor cannot provide medication in a timely manner, a local pharmacy (Wal-Mart Pharmacy or CVS Pharmacy) will be used. Parents/guardians will receive notification, and additional consent if needed, as required by the Health Services Manual (revised October 2006 with April 2010 Updates). Medication Management: Prescription medication at G4S is administered per direction of the DHA pursuant to Physician, PA or ARNP order, and/or Dentist order or per instruction on a youth s current prescription container with a current patient specific label. An order may be written directly in the Individual Health Care Record (IHCR) by a properly credentialed MD, DO, PA or ARNP. If off-site care is rendered, an order may be written on the Summary of Off-Site Care Form by a properly credentialed MD, DO, ARNP, PA or Dentist, accompanied by a written prescription. The written prescription is copied and placed in the youth s IHCR prior to filling at the pharmacy. A youth may arrive with a current prescription; if the medication(s) are administered from a current individual prescription container/bubble pack with a current patient-specific label. All prescribed medications (including insulin) are ordered in a timely manner with no lapses occurring between ordering and administering. All prescribed nonpsychotropic medications for chronic conditions are integrated into the youth s medical treatment plan via the physician progress notes, treatment orders and medication orders by the DHA through the periodic evaluation process. The licensed health care staff is primarily responsible for medication administration. The nursing staff performs medication administration, documentation of the administration, and maintains strict accountability and inventory of all medications. Healthcare staff will be available on-site and administer the bulk of medications. During hours when no nurse is on-site and ordered doses of medication are required to be taken by the youth, trained staff will monitor the self-administration of medication. Training of applicable staff in medication observation and documentation is completed by the RN, utilizing a curriculum developed by the Director of Health Services and approved by the DHA. All training is documented in the applicable employee training files. If audits of medication records reveal error patterns, retraining will take place until competency is achieved. All trained staff will follow the restricted key control procedure to ensure security. The nurse is responsible for maintaining the inventory of required medications, and for following procedures to maintain accountability for controlled substances. Medication Administration Documentation: The five (5) rights, which was recognized by DJJ as a best practice, will be utilized for medication administration: Right Youth (photo with MAR), Right Medication(s) (verify physician order, MAR and prescription label), Right Route (verify prescription bottle and MAR), Right Dosage (verify prescription bottle to MAR) and Right Time (medication to be administered within one (1) hour of scheduled time). The health care staff will be responsible for transcribing all written/telephone orders to the youth s individual MAR. The administration of each dosage of all medications (including OTC s) to a youth will be documented on the youth s individual monthly MAR, which will be generated by contracted Pharmacy in compliance with the Health Services Manual (revised October 2006 with April 2010 Updates). In the event a health care staff makes a medication error, he/she will notify the DHA/prescriber for instructions/orders and complete a medication error report noting the error, which meets all the requirements outlined in the DJJ Health Service Manual (revised October 2006 with April 2010 Updates). The DHA and the Facility Administrator will review medication error reports every two (2) weeks (as applicable) to identify trends and institute a corrective action in the medication management system. A.3.h. REPORTS: G4S will implement and maintain an organized, consistent and accurate system of medical statistics in order to provide the Department with a Monthly Health Services Report as specified by the Department s Health Services Manual (revised October 2006 with April 2010 Updates). This report will be submitted as required and information reported on both youth health characteristics and services provided. At a minimum, it will indicate the number of youth receiving health care services by category of care and nature of complaint, along with other pertinent information, e.g., referrals to a specialist, emergency transfers, hospitalizations, medications, etc. G4S will also compile key performance indicators that include medical statistics. G4S understands this information will be used to identify trends and manage risks. G4S will advise the Department s Office of Health Services when a youth has been involuntarily committed to a Crisis Stabilization Unit (Baker Acted) two (2) times within a seven (7) day period or three (3) times within a 30-day period. Additionally, we realize that our medical personnel may also contact the Office of Health Services if there is a medical or mental health concern or dispute. A.3.i. BIO-HAZARDOUS MATERIALS: Staff will be trained in the proper methods of handling, storage and disposal of hazardous waste, sharp containers and contaminated medical waste in accordance with OSHA, federal regulations and DJJ policy. Sharps, needles and syringes will be placed in sharp containers. DSOP will maintain a contract for the removal of biomedical waste. A.3.j. MEDICAL SUPPLIES: G4S will provide necessary medical equipment, products, supplies and materials needed for provision of medical care to the youth. RFP R2107 Page 27
64 Program Services A.3.k. STAFF TRAINING: G4S believes that professionalism in practice is enhanced by continuously updating knowledge and skills. Pre-service, in-service and continuing education training for all staff will be heavily emphasized and geared specifically to health care delivery in a correctional setting. Training will comply with the Health Services Manual (revised October 2006 with April 2010 Updates) and include, but not be limited to, the following health-related topics: First Aid and CPR Use of 911 for emergencies Control of Infectious Diseases (Site Specific Exposure Plan) Common health issues Use of Knife-for-Life/Suicide Prevention Use of AED device Principles of safe and effective pharmacology/dispensing of Universal precautions and Blood Borne Pathogens training to medication (applicable staff) meet Federal Rule CFR (OSHA Standard) Side effects of medication PAR; as applicable Sick Call /Med pass Emergency evacuation procedures for youth on medical alert Facility Entry Physical Health Screening form and process Physical development of youth Additional training topics will reflect the particular educational needs of staff and be identified on an on-going basis through the Quality Improvement Program. An annual roster will be maintained of all employee names, the training provided, signatures, dates, and number of hours attended. Copies of these training rosters will be kept in individual employee training files and available for Department review. A.3.l. MEDICAID: Youth at are classified as high-risk and are not eligible for Medicaid services while in the program. Therefore, DSOP will make every effort to have medical or dental expenses paid for with the assistance of the youth s parents or guardians to access to their personal insurance company, if a third party health insurance exists. A.3.m. ROUTINE COSTS: G4S understands the Department is not responsible or liable for the costs of routine and necessary medical, dental or behavioral health care beyond the limits identified under the terms and conditions of this contract. A.3.n. NON-ROUTINE HEALTH SERVICES: G4S understands that it is responsible for the cost of routine health care and has included these costs in the proposal budget. For any non-routine health care needed that will exceed $5, per youth per incident, prior approval will be obtained from the Department unless it is an emergency. If emergency services are required, the Contract Manager will be notified as soon as possible following the incident. Every effort will be made to have medical or dental expenses paid for with the assistance of the youth s parents or guardians access to their personal insurance company, if a third party health insurance exists. The Department will be responsible for non-routine costs that exceed $5, per youth, per incident and will be invoiced by G4S, less any costs recouped from other sources. A.4. HEALTH EDUCATION PROGRAMMING Consideration 14: How well does the proposal describe its provision of Health Education Programming? Health education gives youth the knowledge and life skills to be successful in setting personal health goals, resolving conflicts, solving complex problems and communicating effectively. For adolescents to become health literate, they must be taught how to make healthy choices and avoid the behaviors that can harm their well-being and overall health. G4S will provide youth at DSOP with a Comprehensive Health Education Program that is developmentally appropriate for adolescent males, beginning in orientation and continuing throughout their stay in the program. Each month, the staff nurse will prepare an individual health topic that rotates so each youth receives the benefit of all topics during their stay. All health education will be documented on the Health Education Record and maintained in the youth s individual health care record. Health education information will be reinforced during life skill training and healthy living activities and include, but not be limited to: Emotional, physiological, physical development Smoking effects and cessation; tobacco use products of adolescent boys Dental hygiene and preventative dental care Prevention of accidents Basic personal hygiene Eating disorders Immunizations Body image Infection control: hand washing, understanding Hepatitis and TB Self-esteem Prevention of sexual and other physical violence Transitional health care planning for chronic health (applicable youth) Nutrition Seat belt usage Physical fitness Alcohol and drug related problems Self-examinations: testicular and breast HIV/AIDS infection Sexually transmitted diseases and prevention of STDs Family Planning: pregnancy prevention, parenting skills (where applicable) To further health education and needs, DSOP will establish a Health/Mental Health DVD Library where youth may request the specific educational DVD of choice. This library will also be used by health/mental health and counseling staff for individual and group counseling with youth. The DSOP health care staff commits to providing health education as needed to maximize each individual youth s awareness, demonstrating the program s dedication to providing health education to promote physical and mental wellness. In addition, the program will make all efforts to establish a community partnership with Volusia County Health Department to provide health education and HIV testing to ensure the quality of care for the DSOP boys. RFP R2107 Page 28

65 Program Services A.5. OSHA REQUIREMENTS A.5.a. G4S will maintain and annually update a comprehensive OSHA education and prevention program including: 1. A written exposure control plan to minimize or eliminate employee exposure to blood borne pathogens. The plan is site-specific in accordance with OSHA s Occupational Exposure to Blood borne Pathogens Final Rule (29 CFR Part ), is reviewed annually and updated when necessary. The Exposure Control Plan complies with incident reporting requirements mandated by the 1992 OSHA blood borne pathogen standard. 2. Standard precaution training for all staff and observance of all elements of the exposure control plan including the use of standard precautions and personal protective clothing. 3. Post-exposure management that follows the CDC s U.S. Public Health Service Guidelines for the management of occupational exposures to HBV, HCV and HIV and recommendations for post exposure prophylaxis. This includes post-exposure evaluation, medication, monitoring for major and minor signs of disease, and maintenance of post exposure records as required by OSHA. 4. The provision of Hepatitis B immunizations for all staff. The Hepatitis B vaccination series is available to all employees that have occupational exposure. Post-exposure evaluation and follow-up are provided to any employee that experiences an exposure incident. The vaccine, medical evaluations and follow-up are available at no cost to the employee. Employees that decline vaccinations sign a declination form. They may request and obtain the vaccination series at a later date at no cost. A.5.b. G4S will provide Oral Swab Collection for DNA testing that is consistent with Rule 63E7.003(7), Florida Administrative Code and Departmental policy and procedure. We will also ensure that the requirement for imprinting the juvenile s left and right thumbprints is completed and the prints attached to the FDLE request for DNA testing. A.6. MENTAL HEALTH AND SUBSTANCE ABUSE SERVICES How well does the proposal meet the requirements described in the Mental Health and Substance Abuse Services Manual (2006 including, 2007 revisions)? (CATEGORY 16) SEX OFFENDER TREATMENT SERVICES How well does the proposal describe a plan for provision of sex offender treatment services as described in the RFP? (CATEGORY 17) A.6.a. MENTAL HEALTH AND SUBSTANCE ABUSE SERVICES: G4S currently operates successful moderate-, high-, and maximum-risk juvenile sex offender treatment programs at the Columbus Juvenile Residential Facility and the Okeechobee Juvenile Offender Corrections Center. Upon contract award to G4S, the program will provide sex offender treatment services at the Daytona Sex Offender Program (DSOP) to include, but not limited to, comprehensive sex offender assessments and evaluations, sex offender therapy services and individualized sex offender treatment planning. Further, DSOP will implement coordinated and comprehensive mental health and substance abuse services designed to meet the youth s individualized needs. Such intensive services will be in accordance with the Department s Mental Health and Substance Abuse Services Manual (Revised August 2006, with March 2007 and April 2007 Updates), applicable provisions of the Department s Health Services Manual (Revised October 2006 with April 2010 updates) including, but not limited to, Chapter 12, and applicable Department rules. These will be described in the next several pages of this mental health and substance abuse services section. Services shall be provided to 30 high-risk males, ages 13-18, as determined by the Department as meeting the eligibility criteria for Sex Offender Treatment Services. SOTS Consideration 3: How well does the proposal described provisions meet the required sex offender treatment services? DSOP will provide a therapeutic environment that has a sex offender-specific treatment culture throughout all components of the program. It will be individualized in sex offender-specific services to meet the special needs of the youth, staffing patterns for continuity of safety, security, and support, and provide 24-hour response capability with access to an acute care setting and emergency management services. Due to sex offender-specific treatment services encompassing the whole continuum of services we will provide, G4S will present our sex offenderspecific design over the next several pages that is multifaceted and incorporates daily consistency in all areas of treatment. Evidence of the design s effectiveness is demonstrated in Exceptional Quality Assurance ratings in our moderate-, high-, and maximum-risk sexual offender programs, in addition to measurable reduced recidivism. Therefore, we are not promoting a design that we think can work; rather, we are promoting a design that we know will work. At a minimum, the offender treatment services by the Master s degree mental health professional will include the following minimum components, with in-depth description over the next several pages: Comp sex offender-specific evaluations Suicide/Crisis intervention svs Victim clarification and family reunification Comp mental health/substance abuse Psychiatric services Ongoing and consistent staff training evaluations Individual, group, family therapy Evidenced based services Individualized sex offender treatment planning Trauma and grief treatment 24-hour response capability Consideration 1: How well does the proposal address the screening requirements? 1. Mental Health and Substance Abuse Intake and Screening: Mental health and substance abuse screening will be conducted on all youth at admission or when they re-enter the program after being on inactive status. The purpose of screening will be to identify the youth s mental RFP R2107 Page 29
66 Program Services health and substance abuse risk factors to determine if further evaluation or immediate attention is needed. The screening process will include a review of the youth s prior documented history, administration of current screening tools, conducting of interviews, and assignment of the primary counselor to identify needs or risk factors for: Mental health inpatient or outpatient treatment Significant trauma history Substance abuse inpatient or outpatient treatment Drug/alcohol use or drug/alcohol possession Self-injurious behaviors, i.e. head banging, intentional self-injury Emotional instability: depression, anxiety, mood, rage Suicide attempt, suicide behaviors or suicide risk Psychotropic medication treatment Emergency room evals for mental health/substance related needs History of mental illness in family Youth eligible for sex offender treatment services generally will have a diagnosed DSM-IV-TR Sexual Disorder and/or diagnosis of Sexual Abuse of a Child where the focus of attention will be on the perpetrator of the abuse. DSM-IV-TR diagnoses will include, but are not limited to, Pedophilia, Frotteurism, Voyeurism, and Sexual Abuse of Child. Admission criteria for youth will include: A documented need for sexual offender treatment based upon a psychosexual assessment; An adjudicated sex offense; DSM-IV-TR GAF or CGAS typically between 30 and 50; A documented need for an intensive level of sex offender treatment services; Possibility of co-occurring mental health diagnoses and needs; Possibility of co-occurring diagnosed substance-related disorder; Complex risk factors such as deviant sexual arousal or interests, predatory behaviors, and risk of victimizing others. Immediately following admission, there will be a records review by the case manager and the Master s degree mental health professional that includes the Pre-disposition Release (PDR), C-PACT, Face Sheet, and all past evaluations or documentation of mental health, sexual, and substance abuse issues. Administration of the MAYSI-2 will be conducted by the Bachelor s degree community coach, who has successfully completed the Department s training entitled, Using the MAYSI-2 to Screen for Mental Health and Substance Abuse Problems. The MAYSI-2 will be administered in a private and confidential manner to all admitted youth, minimizing the new youth s anxiety to the program. In the event the MAYSI-2 identifies potential indication of a mental health, substance abuse or suicide concern, the case manager will check the applicable box on the form, refer the youth for further evaluation and immediately notify the counselor and the Licensed Director of Clinical Services. A specific tool to further assess the concern will include one (1) or more of the following: Beck Depression Inventory, State Trait Anger Expression Inventory, Trauma Symptom Checklist, SASSI, and Reynolds Children Manifest Anxiety Scale. Regardless if a youth presents no initial suicide indications on the MAYSI screening tool, he will be screened by a Master s degree mental health professional for potential suicide via the Assessment of Suicide Risk (ASR). This will be reviewed and signed by a licensed clinician within 24 hours of referral. Given the high number of incidences of suicidal behavior of youth admitted in juvenile facilities, any youth with suicide risk factors will be immediately referred for an ASR or emergency mental health services. When a youth is identified as a suicide risk, following the screening by the Master s degree clinician, the counselor will notify the Facility Administrator/designee and the Licensed Mental Health Professional to approve placement on Suicide Precautions. The DSOP will follow the alert system procedures where information is entered into the JJIS, and notifications are made to staff, parent/guardian and JPO. In addition to the MAYSI-2 and the suicide screening, the mental health professional will administer the "ERASOR" (a structured clinical interview based on empirical research). Results will provide a baseline measure of the youth s present strengths, needs, psychopathology and recidivism risk. The mental health professional will further screen for Vulnerability to Victimization and Sexually Aggressive Behavior (VSAB), with results from all screening being discussed in a meeting of Treatment Team members, as a collaborated effort to ensure that potentially critical areas are addressed. Consideration 2: How well are the requirements of mental health assessments clearly outlined? 2. Comprehensive Mental Health and Substance Abuse Evaluations or Updated Evaluations: The DSOP will employ a Licensed Mental Health Professional who will perform mental health and substance abuse services and has experience in behavioral health services delivery and management. The Licensed Mental Health Professional will be a psychiatrist licensed under Chapter 458 or 459, F.S. (board certified in Child and Adolescent Psychiatry or Psychiatry by the American Board of Psychiatry and Neurology or has completed a training program in Psychiatry approved by the American Board of Psychiatry and Neurology for entrance into its certifying examination), psychologist licensed under Chapter 490, F.S., or mental health counselor, clinical social worker or marriage and family therapy licensed under Chapter 491, F.S. All Comprehensive Mental Health and Substance Abuse Evaluations and Updated Evaluations will be sex offender-specific, and will be conducted by, or under the direct supervision of the Licensed Mental Health Professional. In the event a psychological evaluation is needed, G4S will elicit consultation services by a psychologist who is experienced in working with this population. Every youth will receive a psychosexual evaluation to determine individualized sexual offender treatment services and appropriate sequencing of treatment interventions and the materials and curricula that will be used, based upon the assessed needs of the youth. The evaluation will include assessment of level of psychopathology, anger and responsibility; developmental, social, educational and sexual history; religious beliefs; ability to empathize; awareness of cognitive distortions and sexual arousal patterns; and history of trauma and any previous victimization. G4S does not support or implement the use of intrusive assessment measures, such as penile plethysmography. The psychosexual evaluation will be integrated into the Comprehensive Mental Health and Substance Abuse Evaluation. When there is indication that a youth poses a risk to self or others, the RFP R2107 Page 30
67 Program Services evaluation will be expedited. The numerous screenings, assessments, and evaluations for integration into the Comprehensive Mental Health and Substance Abuse Evaluation will include, but not limited to: MAYSI-2, identifying immediate mental health, substance abuse and suicidal concerns; Vulnerability to Victimization and Sexually Aggressive Behavior (VSAB), identifying vulnerability to physical/sexual victimization and sexual aggression; Assessment of Suicide Risk (ASR), assessing past and current potential for self-harm; Interviews with youth, parent/guardian, and other professionals for developmental and historical information; Psychosexual evaluation, gathering of historical and present sexual history; ERASOR (a structured clinical interview based on empirical research) or the J-SOAP (an actuarially based risk assessment instrument for juvenile sex offenders), providing a baseline measure of strengths, needs, psychopathology and recidivism risks Beck Depression Inventory, State Trait Anger Expression Inventory, Trauma Symptom Checklist, SASSI, and Reynolds Children Manifest Anxiety Scale, as follow up to MAYSI referrals; Psychiatric Evaluation, comprehensive diagnostic evaluation that guides treatment plan formulation; Residential Positive Achievement Change Tool (R-PACT), identifying risk and protective factors; Records review, identifying historical mental health, substance abuse, suicide areas The purpose of the comprehensive evaluation will be to evaluate DSM-IV-TR diagnosis, risks and functional status issues identified in screening, guide treatment decisions and determine service levels needed to address the youth s risk, needs and problems. The aforementioned documents will then be incorporated into the comprehensive mental health and substance abuse evaluation to guide treatment. The Comprehensive Mental Health and Substance Abuse Evaluation will be completed within 21 days of admission or referral, which exceeds RFP requirements. The Licensed Mental Health Professional will review, sign as Reviewer and date the evaluation within five (5) days of the completion of the evaluation, which exceeds RFP requirements. To ensure the timely completion of comprehensive evaluations, the Clinical Director will monitor progress via daily tracker, review of deadlines at daily Management Meetings, review of deadlines during weekly coaching sessions with the Facility Administrator, review of deadlines with the mental health professional during weekly clinical supervision sessions, and submit a weekly verification report to the QA Manager, documenting the completion of evaluations. Progressive disciplinary measures will be initiated when deadlines are not met. Further, the Clinical Director will provide 1.5 hrs/wk of clinical supervision. Consideration 3: How well does the proposal describe how the comprehensive substance abuse evaluations will be conducted in accordance with Rule 65D-30? Comprehensive substance abuse evaluation services will be in accordance with the licensure requirements in Rule 65D (15), Florida Administrative Code. DSOP will obtain a probationary license issued by the DCF-SAMH Program Office to provide Outpatient substance abuse treatment services under Chapter 397, F.S. Until the facility is licensed under Chapter 397, F.S., the program will provide substance abuse services by a licensed qualified professional licensed under Chapter 458, 459, 490, or 491, F.S. Mental Health and Substance Abuse Treatment Planning: Once all assessments and evaluations are completed, the multidisciplinary Treatment Team members will meet with the youth, his JPO and family, as available, to discuss the findings and to prioritize needs for the development of the individualized sex offender treatment plan. Special consideration will be given to the youth s stage of development, gender, culture, family issues, mental health, substance abuse and sex offender treatment needs. The prioritized needs will form the basis for the development of the youth s treatment plan and will include objectives, responsibilities and targeted timeframes. The facility will provide individualized sex offender treatment planning and interventions that target anti-social behaviors. Recommendations will be included in the treatment plan for individualized clinical services for individual and group therapy, and family counseling, and treatment models such as the Pathways Treatment Curriculum, Steps of Progress intervention modules, and Relapse Prevention Workbook. The plan for services will be developed with the input of the psychiatrist, youth, counselor, family, and other Treatment Team members within 25 days of admission or initiation of treatment, which exceeds RFP requirements. The Licensed Mental Health Professional will review, date and sign as reviewer within five (5) days of the plan s completion, which exceeds RFP requirements. In the event parents are uninvolved in the development, at least three (3) documented efforts will be made to obtain signatures. As needs change, modifications of services will be made to maintain consistency in treatment and care, and continually reiterate efforts to keep the youth on a track of progress. Every 30 days, the Treatment Team will review the youth s progress as it relates to goals and objectives and determine whether modifications to the plan are necessary. Our continuous efforts to decrease future sexual aggressive or criminal acts and increase community safety lies with expectation for youth to: Demonstrate an increase in knowledge of the effects of sexual abuse and trauma; Develop a system of internal motivation for change and prevention of further sexually abusive acts; Learn new coping skills to deal with stress and anxiety; Show a decrease in criminal thinking and cognitive distortions; Demonstrate an increase in ability to engage in healthy interpersonal relationships, social competencies and confidence; Show an increase in assertive behaviors and ability to self-regulate negative emotions; Show an increase in empathy for the victims of past abusive acts; Show an increase in attitudes and values consistent with healthy masculinity; Develop a comprehensive relapse prevention plan and share with family members. RFP R2107 Page 31
68 Program Services Treatment Team assessments, services, and performance planning will assist the youth in five (5) basic core treatment areas. These include youth acceptance, correction of cognitive distortions, victim awareness, familial education, and relapse prevention. Youth Acceptance: The first stage of therapy assists the youth with gaining an acceptance of sexual offending behavior. Minimizing, denial, and blaming will be defensive mechanisms that are addressed. Education regarding the offense cycle assists the identification of factors leading to deviant sexual arousal. Correction of Cognitive Distortions: This treatment focus is the core of clinical interventions. The treatment team assists the youth with empathy training, clarification of values, abusive vs. non-abusive behavior, healthy mood management, impulse control, reducing deviant sexual arousal, and social skills training. Victim Awareness: The research of Barbaree and Corterni (1993) suggests that juvenile sex offenders begin the therapeutic process to relapse prevention once they begin to empathize with their victim or victims. Treatment modalities through the clinical department and social skills address victim awareness. This is also a significant part of the restorative justice programming. Familial Education: Familial education and planning comprises a large part of the therapeutic interventions. Families that provide support and are educated will assist with reducing recidivism. Family members are provided with information on relapse prevention and cognitive distortions. Family therapy is provided to address familial system issues that correlate with the youth s behavior. The identified community case manager also works with the family system to assist with release planning. Relapse Prevention: Relapse prevention planning starts with the juvenile s initial assessment at the time of entry into the juvenile program. Knowing the juvenile s intended placement after discharge from the residential program and assisting with continuity of care are essential components to the juvenile s long-term community adjustment. Discharge planning consists of three (3) primary components: 1) Relapse Prevention Plan, 2) Safety Plan, and 3) Aftercare service linkages to community providers. During the course of treatment, each juvenile will develop a Relapse Prevention Plan that clearly identifies sexual abuse history, situations in daily lifestyle that presents a risk, who would be the next most likely victim, warning signs to notice, and what he and his support system can do to intervene potential backsliding behavior. The Relapse Prevention Plan is a formal document that will be developed by each juvenile and modified as he processes through treatment. The Safety Plan is a formal document that will be developed by the therapist with the juvenile and his family, in both the family therapy session and group therapy sessions. This plan will establish boundaries in the home setting and roles and responsibilities of each family member once the juvenile is returned to the home setting. SOTS Consideration 4: How well does the proposal describe the clinical staff to be utilized in the sex offender treatment program, including their qualifications and scheduling? G4S strongly supports the position that individuals providing treatment for sexual offenders in a residential setting must be personally and professionally qualified (Association for the Treatment of Sexual Abusers, 1997a; National Adolescent Perpetrator Network, [NAPN] 1993). Personal qualifications include being emotionally healthy, having the ability to monitor internal states, having respect for oneself and others, using good listening skills, and having the ability to empathize. Professional qualifications include relevant education, training, and experience. Treatment providers should receive appropriate training before they begin their work and thereafter on a continuing basis. Working with juveniles who have sexually offended is a challenging job, particularly in a residential setting. As NAPN (1993) observed, Systems must be aware of potential emotional/ psychological impacts on providers and take steps to protect against or counter negative effects (p.46). Staff will be encouraged to meet on a weekly basis to discuss cases and provide emotional support for each other. G4S commits to providing on-going training for understanding juvenile sex offenders and treatment necessary to ensure a safe and therapeutic environment. Experienced Juvenile Sex Offender Therapists: G4S currently employs Robert (Ruben) Drake M.A., L.M.H.C. and contracts with Dr. Leo Cotter, LMHC, both who meet requirements to practice juvenile sex offender therapy under Section , F.S., and Rule 64B F.A.C. Further, both have been instrumental in the successful results of G4S current moderate-, high-, and maximum-risk sex offender programs, as evidenced by low recidivism rates, Exceptional Quality Assurance scores, CARF reviews, and ACA reviews. It is G4S intention to utilize the skills of Dr. Cotter (see Letters Tab for his interest) and Rubin Drake at the DSOP (see License Verification Tab). Leo Cotter, Ph.D., LMHC (##MH46) is a licensed Mental Health Counselor under Chapter 491, Florida Statutes. Dr. Cotter has over 20 years of experience working in the field of Sexual Offending Treatment, and has worked for the Department of Corrections and Department of Children and Families. Dr. Cotter is the founder, past-president, and current board member of the Florida Association for the Treatment of Sexual Abusers. He has provided national, statewide and local training seminars in the area of sexual offending evaluation and treatment. Dr. Cotter was an Assistant Professor at the University of South Florida and provided training, consultation and research in the area of forensic psychology. Dr. Cotter has conducted and published a vast amount of research related to sexual deviancy. A few publications include: Levenson, J.S., Macgowan, M.J., Morin, J.W., Cotter, L.P. (2009). Perceptions of Sex Offenders About Treatment. Sexual Abuse: A Journal of Research and Treatment, 21, Levenson, J.S. and Cotter, L.P. (2005). The Impact of Megan s Law on Sex Offender Reintegration. Journal of Contemporary Criminal Justice, 21(1), Levenson, J.S. and Cotter, L.P. (2005). The Impact of Sex Offender Residence Restrictions: 1,000 Feet from Danger or One Step from Absurd? International Journal of Offender Therapy and Comparative Criminology. Cotter, L. Morin, J. and Levenson, J. New Directories in the Management of Sexual Offenders. Position statements produced by the Florida Association for the Treatment of Sexual Abusers, Cotter, L., and Kuehnle, K., Sexual Abuse Within The Family. Book chapter from current Perspectives in Psychological, Legal and ethical Issues. Jessica Kingsley Publishers, RFP R2107 Page 32
69 Program Services Robert Ruben Drake, LMHC, NCC, CAP, SAP (#MH 7324) is currently the Director of Clinical Services at our 50-bed moderate-risk Columbus Juvenile Residential Facility. He is qualified as a Juvenile Sex Offender Therapist under Chapter , Florida Statutes and is a Licensed Mental Health Counselor, a Nationally Certified Counselor, a Certified Addiction Professional, and a Substance Abuse Professional. Ruben currently serves as a board member of the Association for the Treatment of Sexual Abusers (ATSA) and is former board member of the Florida Association for the Treatment of Sexual Abusers (FATSA). He has authored articles for the international newsletter for ATSA (The Forum) and a column for the Florida Forum (FATSA) newsletter titled, The Therapist s Tool Box, which offers information to help therapists working in the field of sexual abuse. Ruben has experience treating both adult and juvenile sex offenders and has facilitated sexual offender specific treatment for adults and juveniles in outpatient treatment, as well as juveniles in residential treatment. He has served on the Florida Governor s Task Force on Juvenile Sex Offenders and their Victims. He has trained with Albert Ellis Ph.D.; the founder of Rational Emotive Behavior Therapy, and is an Associate Fellow of the Albert Ellis Institute (REBT). Further, Rubin is qualified as a supervisor for Rational Emotive Behavior Therapy (REBT) training. He has also received beginning and advanced training in Motivational Interviewing with Steven Andrews, a Motivational Interviewing Network Trainer (MINT). Mr. Drake has presented at conferences such as the Sexual Abuse Intervention Network and the Florida Association for the Treatment of Sexual Abuser. He has provided training for the Polk County DJJ probation officers and treatment providers, and lectured on professional court testimony at USF. Mr. Drake provides G4S training on Rational Emotive Behavior Therapy, Motivational Interviewing, Trauma Informed Care, and specialty trainings such as emotional and sexual behavior problems. Mental Health and Substance Abuse Clinical Staff Designated Mental Health Authority (DMHA): The Licensed Mental Health Professional will be a psychiatrist licensed under Chapter 458 or 459, F.S., a psychologist licensed under Chapter 490, F.S., a mental health counselor, clinical social worker or marriage and family therapy licensed under Chapter 491, F.S., or a psychiatric nurse as defined in Chapter (23), F.S. The Licensed Mental Health Professional/DMHA will work under, and in concert with, the Designated Health Authority (DHA). There will be a direct line of communication between the DHA and DMHA that is relayed to licensed and non-licensed professionals. The DMHA will provide to counselors/therapists at least 1.5 hours per week of direct supervision, which exceeds RFP requirements, to include directions, instructions, and recommendations of services provided by the counselor. G4S VP of clinical services will provide interim services if needed (see License Verification Tab). Juvenile Sex Offender Therapist/Clinical Director: DSOP will employ a full-time Juvenile Sexual Offender Therapist under Chapter or , Florida Statutes who meets the qualifications set forth by the Board of Psychology and Rule 64B F.A.C., to practice juvenile sex offender therapy or a person licensed under Chapter 491 who meets the qualifications set forth by the Board of Clinical Social Work, Marriage and Family Therapy and Mental Health Counseling and Rule 64B F.A.C., to practice juvenile sex offender therapy. This position will be on-site at least five (5) days a week, 40 hours per week, and will be responsible for supervision of sex offender treatment services. The Clinical Director will ensure the clinical counselors perform services that they are qualified to provide, based on their education, training and experience. The Clinical Director will provide emergency on-call coverage 24 hours, 7 days/wk. G4S has three (3) licensed sex offender therapists available to provide support to the DSOP if interim experience is needed (see License Verification Tab). Clinical Counselors: DSOP will employ three (3) therapists (licensed or unlicensed) with a master s degree from an accredited university or college in the field of counseling, social work, psychology, or related human services field. Each therapist will maintain a caseload not to exceed 10 youth. The therapists will work under the direct supervision of a Licensed Mental Health Professional, and will be scheduled to provide daily counseling services to DSOP seven (7) days a week, 40 hours per week, and emergency on-call coverage 24 hours, 7 days/wk. Psychiatrist: DSOP will contract with a Licensed Psychiatrist (a physician licensed under Chapter 458 or 459, F.S., Board certified in Child and Adolescent Psychiatry or Psychiatry by the American Board of Psychiatry and Neurology or has completed a training program in Psychiatry approved by the American Board of Psychiatry and Neurology for entrance into its certifying examination. The Psychiatrist will be on-site weekly for consultation, medication management and to participate in treatment planning for youth receiving psychotropic medication, which exceeds RFP requirements. Further, the Psychiatrist will be available 24 hours/day, 7 days per week, for consultation and crisis services. During the interim, Dr. Amiel has agreed to provide psychiatric services (see Letter and License Verification Tabs). Psychologist: A licensed psychologist under chapter 490, Florida Statutes, will be available as needed. Consideration 4: How well does the proposal describe the youth s access to psychotherapy or professional counseling? SOTS Consideration 2: How well does the Provider describe a full array of services and treatment programs available 7 days a week? 3. Psychotherapy or Professional Counseling Services: DSOP will have the capacity to provide psychiatric services, psychopharmacological therapy and 24-hour crisis services, as well as mental health and substance abuse treatment services for juvenile sex offenders who have co-occurring mental health and substance-related disorders. When deemed necessary, the DSOP will contract with a psychologist to provide service as needed. All youth will have access to professional mental health and substance abuse treatment services including individual, group or family therapy seven (7) days a week, which exceeds RFP requirements, as a result of thorough screening and assessing and as prescribed in their individualized treatment plans. Individualized sex offense-specific treatment will be performed by Master s degree counselors. Staff, parents, JPOs and educators will have the ability to refer youth, in addition to the youth being able to self-refer for counseling services. All youth will receive daily therapeutic activities seven (7) days per week. Individual, family and group therapy, psychosocial skills training and behavior therapy will be provided by, or under the direct supervision of the Clinical Director. Individual Therapy: The DSOP clinicians will provide individualized sex offense-specific therapy one (1) day each week. Sessions will be available seven (7) days a week, which exceeds RFP requirements. Victims of trauma will benefit from individual therapy as it allows disclosure of trauma, the safe expression of related feelings and the re-establishment of a trusting relationship with one other RFP R2107 Page 33
70 Program Services person. Clients are provided instruction and treatment based upon research and evidence of efficacy. Most survivors of traumatic experiences and traumatic grief require individual services to address issues that the youth is uncomfortable disclosing to other peers in their treatment groups. Family Therapy: G4S considers sex offense-specific family therapy, in addition to family involvement, as mandatory components in the youth s treatment program. The success of a youth is largely influenced by the on-going support and supervision received from the family. The program will provide numerous avenues of family involvement (described on pages 49-52) where families will be invited to attend additional family therapy sessions while on campus. Family therapy will be conducted in-person or telephonically by a mental health counselor with a youth and designated family members as frequently as required by the youth, but at least one (1) time per month. Family contacts may be increased to address treatment needs such as family reunification, relapse prevention planning, and/or family safety planning. Family therapy will be provided during the day, evenings, weekends and holidays, with the program maintaining flexibility in scheduling family therapy seven (7) days a week to meet the needs of the family. Further, the program will use victim clarification for those family members who are actually a victim and reside in the household. Such victims will attend outside counseling, with constant communication between the victim s counselor and the DSOP counselor. Prior to the youth s discharge, the victim and the outside counselor will be integrated into family therapy at DSOP for intensive therapy. Prior to being discharge, the youth and his parent/guardian will participate in family reunification services, a Family Safety Plan and a Relapse Prevention Plan (more thoroughly mentioned in Transition/Discharge section, page 46). Group Therapy: Group therapy will be conducted by a Master s degree mental health professional seven (7) days a week, and is shown on the schedule on page 17. Group therapy is provided every day in a format with 6-10 juveniles per group. Groups are a minimum 60 minutes in length. The focus of group counseling will be to obtain relief from distressing symptoms, modify behaviors, and acquire new skills that generalize from the group, to the residential community, then to the home environment. When a youth has demonstrated an ability and willingness to attend trauma treatment groups, they can then process their experiences with their peers. Abuse process groups provide a safe and supportive environment that promotes healing by allowing survivors of abuse to disclose and process traumatic issues without fear of judgment. It is intended that the youth gain the strength and insight to examine and integrate their past experiences into their life histories. Youth learn effective methods of coping and self-empowerment by identifying and distinguishing unhealthy defense mechanisms and faulty belief systems. Youth gain a sense of interdependency, displaying healthy emotional and physical boundaries with an ability to engage in mutually rewarding relationships. It is intended that the youth will gain the strength and insight to examine and integrate their past experiences into life histories, and therefore able to exhibit healthy moods and behaviors. For substance abuse groups, youth will be taught the Stages of Change model and the treatment is conducted using Motivational Interviewing as its treatment modality. Educational groups: Education groups will be facilitated to provide a basic understanding of the dynamics of abuse and victimization. Youth will learn about the cycle of abuse and violence with an ability to identify the psychological impact and behavioral manifestations of traumatic experiences. He will learn how the experience of traumatic sexualization impacts sexuality in developmentally inappropriate ways and affects interpersonal growth. This arena addresses issues of stigmatization, betrayal, and powerlessness. Youth will address cognitive distortions, alterations of social functioning and posttraumatic stress symptomology. Behavior Therapy/modification activities: As part of the numerous individualized sex offense-specific treatment services that DSOP will provide, behavior modification activities will be individualized specific to the youth, then delivered through therapy by qualified professionals. Treatment will focus on learning more acceptable and adaptable forms of behavior. Consideration 5: How well does the proposal describe a coherent, complete and responsible protocol for psychopharmacological therapy and psychopharmacological therapy follow-up treatment? 4. Psychiatric Services, Psychopharmacological Therapy and Follow-Up Treatment: The prescription and monitoring of psychotropic medication will be conducted and monitored by the program s Licensed Psychiatrist, in accordance with the standards set forth by the American Academy of Child and Adolescent Psychiatry and American Academy of Pediatrics, and Florida law, Departmental policies and standards and the commonly accepted practices of the psychiatric community. The psychiatrist will have the ultimate responsibility for the prescription and monitoring of psychotropic medications, the management and supervision of psychotropic medication services, and the rendering of psychiatric services. The program psychiatrist will be a licensed and board certified psychiatrist in the State of Florida. The psychiatrist will be on-site weekly, which exceeds RFP requirements, available 24 hours a day for consultation, and will participate in the treatment planning for any youth receiving psychotropic medication. All clinical and direct care staff will be required to be knowledgeable of possible side effects as presented during pre-service and in-service training that addresses common side effects. The psychiatrist will develop and authorize the procedures for administering of medication and pharmacological management. Individualized Assessment for Medication: Nursing staff will ensure that an original, current and valid Authority for Evaluation and Treatment (AET) is present in the youth s individual health care record. Youth receiving psychotropic medications prior to admission will continue to be administered medication until the psychiatrist conducts the initial diagnostic psychiatric interview within 14 days of facility admission. Any adjustment or change in the youth s pre-admission psychotropic medication regimen will be based upon a written order from the psychiatrist. Any youth who later presents with serious mental health symptoms will be referred to the psychiatrist for an initial diagnostic psychiatric interview within 14 days of referral. The psychiatrist will document the initial diagnostic psychiatric interview on the Clinical Psychotropic Progress Note (CPPN) that will include targeted symptoms and rationale for the prescription of medication. When the initial psychiatric diagnostic interview results in the prescription of psychotropic medications or changes to a youth s existing psychotropic medication regimen, the psychiatrist will complete page three (3) of the CPPN. All youth currently receiving psychotropic medications at the time of admission or RFP R2107 Page 34
71 Program Services prescribed psychotropic medication subsequent to admission will receive an in-depth psychiatric evaluation or updated psychiatric evaluation within 14 days of admission (for youth currently receiving psychotropic medications at the time of admission) or within 30 days of the initial prescription of psychotropic medication (for youth prescribed psychotropic medication subsequent to admission). The psychiatrist will document the psychiatric evaluation on the CPPN that includes targeted symptoms/rationale for the prescription of medication. If the psychiatric evaluation results in the prescription of psychotropic medications/changes to a youth s existing psychotropic medication regimen, the psychiatrist will complete page three (3) of the CPPN. Administration of Medications: Designated nursing staff will administer medications to the youth. In the absence of nursing staff, designated trained program staff will facilitate the delivery of medications so that the youth can actively perform self-administration of oral prescription medications. Medical staff and program staff will document the administration (or youth self-administration) of each dosage of psychotropic medication on the Medication Administration Record (MAR). Psychotropic Medication Monitoring/Review: Medication monitoring/review will include evaluating and monitoring medication side effects and the need for continuing or changing the medication regimen. At a minimum, follow-up medication monitoring/review will be provided by the psychiatrist every 30 days in accordance with Departmental policies and standards. Side Effects Training and Monitoring: Medication monitoring will be a shared responsibility between the psychiatrist, youth, parent/guardian and program staff. The program staff and the youth s Treatment Team will be required to know the common side effects of psychotropic medications. Pre-service and in-service training will be provided to all staff that addresses: Allergic reaction (difficulty breathing, swelling of lips/face/tongue, rash or fever) Change in level of alertness (excessive sleepiness, insomnia or confusion) Eating problems (nausea, vomiting, weight gain or loss) Change in heartbeat (slow, fast, irregular) Change in blood pressure (high or low) Fainting or dizziness (especially with change in position such as standing) Abnormal posture, body or muscle movements or gait Yellowing of eyes or skin Unusual bruising or bleeding Abnormal, involuntary movement of the face, eyes, mouth, tongue or trunk (tardive dyskinesia) Parent/Guardian Informed Consent: Parent/guardian notification and informed consent will always be obtained when a psychotropic medication is initially prescribed, discontinued and/or a significant dosage adjustment is made. When a youth is prescribed any new psychotropic medication, a copy of the third page of the CPPN will be sent via certified mail to the parent/guardian at the address on record after completion by the psychiatrist. A cover letter accompanied by the Acknowledgement of Receipt of CPPN Form will be sent to the parent/guardian along with the third page of the CPPN. Telephone consent, preferably but not mandatorily by the psychiatrist will be attempted and include a discussion of the information contained on page 3 of the CPPN. Whenever a new medication is prescribed, a medication is discontinued, or the dosage is significantly changed, a copy of the third page of the completed CPPN will be sent to the parent/guardian to provide consistent, updated information regarding the youth s progress and/or recommendations for changes in medications. For psychotropic medication purposes only, a copy of the third page of the CPPN will replace the standardized Department form entitled Parental Notification. Parent notification and informed consent will always be obtained and the Parental Notification/CPPN/AOR process will be followed when the parent/guardian has informed the Department that they desire notification of any change; the youth has been receiving the same total dosage of a medication for 90 days or more and the psychiatrist believes that a change in the total daily dosage is warranted; or the dosage change results in a total daily dosage, which exceeds the normal range. Laboratory Tests: The psychiatrist will prescribe psychotropic medications, as appropriate, which addresses the youth s specific diagnoses and target symptoms. When psychotropic medications are prescribed, the psychiatrist will monitor target symptoms, order laboratory tests required by the prescribed medication, including serum drug levels to ensure a safe and therapeutic range, review laboratory results within 72 hours of notification of results via an electronically transmitted or faxed copy when off-site, assist with parental/guardian notification and document medication management services. The psychiatrist will conduct a thorough re-assessment for non-response to psychotropic medications after six (6) weeks of treatment if a youth does not show a positive response. Reassessment may include checking blood levels in medications with known therapeutic levels. The psychiatrist will conduct monthly screening, or more often as ordered, for tardive dyskinesia (TD). Consideration 6: How well does the proposal describe its procedures for suicide prevention? 5. Suicide Prevention Services: DSOP will implement a comprehensive Suicide Prevention Plan that details the elements required in the Mental Health and Substance Abuse Manual (2006, including 2007 revisions). Suicide risk screening will be conducted on all youth admitted to the program using the MAYSI-2, and if there is a hit on the suicide section, the clinician will immediately be notified. However, regardless of the MAYSI, 100% of youth will be given the Assessment of Suicide Risk (ASR) by the Master s degree mental health professional at admission. Suicide Precautions: Precautionary Observation (PO) is the method of Suicide Precaution that will be used at the program for supervising, observing, monitoring and housing youth who have been identified as having suicide risk factors or as a potential suicide risk. The Suicide RFP R2107 Page 35
72 Program Services Prevention Plan will require that specific action be taken to protect the at risk youth from potential self-injury or suicide. Any youth exhibiting suicide risk behaviors will be placed on PO at least Constant Supervision until an ASR is conducted. While on PO, youth will not be locked behind a closed door or limited or restricted to a sleeping room. PO will not be used for youth who present an imminent threat of suicide. These youth will be referred for emergency care. Identification of At Risk Youth: All staff will be made aware of the necessity to immediately document and report any observations, signs, symptoms or risk factors to the Facility Administrator/designee that may indicate potential for suicide such as the youth s statements/behavior suggesting current suicide thoughts, suicide threats/plan; the youth s statements/behavior suggesting serious depression, withdrawal, and/or hopelessness; the youth s statements/behavior suggesting thoughts of death and/or thoughts of harming self, or the youth has a recent history of attempting suicide, self-mutilation or self-injury. Supervision Requirements: A youth placed on PO will be maintained on one-to-one supervision or constant supervision at all times. Staff observations of youth will be documented on the Suicide Precautions Observation Log at 30-minute intervals. One-to-One Supervision: Refers to constant sight and sound supervision of one (1) youth by one (1) staff member who remains within five (5) feet of the youth at all times, including when the youth uses the shower/toilet. Constant Supervision: Refers to constant sight and sound supervision of a youth by a staff member at all times, including when the youth uses the shower or toilet. Close Supervision: Upon removal from PO; requires supervision of youth behind a closed door; 5-minute intervals. Designated Safe Housing/Observation Areas: To ensure the safety of youth placed on PO, the Facility Administrator or designee will identify in writing on the Suicide Precautions Observation Log, the specific safe housing/observation areas of the facility and activities in which the youth is allowed to participate. The designated safe housing/observation areas, typically the day room areas and unit hallways, will be regularly inspected by the shift manager to ensure that the area is safe and secure. The daily safety/security checks of the facility will be documented in the master log and on the Suicide Precautions Observation Log. The designated safe housing/observation areas will be in close proximity to and immediately accessible by the direct care staff providing supervision. The area will be open and structurally designed to eliminate devices or materials that might aid in self-harm. Interventions Matched to Level of Suicide Risk: At risk youth will be matched to interventions based on their level of suicide risk factors as determined by the Assessment of Suicide Risk as shown below: Suicide Risk Level Method Level of Supervision Interventions Minimum no recent/current suicidal thoughts or risk behaviors; no recent/current desire to die/harm self; denies plan to harm self Moderate - youth indicates recent or current non-specific thoughts of death; recently feels he would be better off dead; recently wants to hurt himself; had a detailed plan in the past but not at present, has an unclear plan, lethality cannot be determined High youth has engaged in recent or current self-injurious behaviors requiring emergency medical attention, recently or currently wants to die/has lost will to live, has current specific plan for self-injury or suicide, plan-if carried out would be lethal None Standard Supervision Administer Assessment of Suicide Risk Confer with Facility Administrator/designee and Clinical Director Consult with Treatment Team & Direct Care Staff Provide daily supportive counseling Continue provision of interventions outlined in treatment plan Precautionary Observation Precautionary Observation Constant Supervision (Initiate Emergency Mental Health Services, if applicable) (Assess for involuntary hospitalization, if indicated) One-to-One Supervision Includes above Amend Treatment Plan to address suicidal/self-injuring behaviors Develop safety plan and build upon strengths/goals/future focus Teach problem solving, conflict resolution & stress management skills Address underlying mental health issues, i.e., depression, trauma Involve family and engage support network inside/outside program Make necessary notifications to family/jpo Refer for psychiatric evaluation and consult with doctor Provide daily crisis intervention counseling Includes all above Initiate Emergency Mental Health Services Assess for involuntary hospitalization, Baker Act Assign necessary number of staff to ensure youth s safety Contact local Police or Sherriff s Office for transportation Provide off-site staff supervision Coordinate mental health and medical care upon youth s return Plan with direct care staff responsible for supervising youth Consideration 7: How well does the proposal document that the Provider s suicide intervention and suicide prevention protocols are established using evidence-based or promising practices? Suicide Intervention and Suicide Prevention Protocols: Trauma recovery will be composed of three (3) main components which include individual services, education groups, and abuse process groups. As part of their job description, the licensed clinical director will oversee the trauma and grief treatment component, and the assigned primary mental health professionals will conduct individual and group sessions. The trauma recovery program is based on the Trauma Focused Cognitive Behavior Therapy and Traumatic Grief Focused Cognitive Behavior Therapy (TF-CBT and TG-CBT) developed by Cohen, Mannarino, and Deblinger, and is recommended by DJJ Health Services for evidence-based treatment for adolescents with successful outcome studies related to depressive symptoms and self-injuring behaviors. RFP R2107 Page 36

73 Program Services 6. Crisis Intervention and Emergency Mental Health and Substance Abuse Care: DSOP will implement a comprehensive and detailed Crisis Intervention and Emergency Mental Health and Substance Abuse Care Plan. The plan will call for the provision of crisis intervention utilizing the least restrictive methods possible to help a youth de-escalate while protecting the personal safety of the youth and others and maintaining program control and safety. Low-level crisis intervention is typically provided by direct care and supervisory staff using PAR verbal de-escalation skills, processing with the youth or removing the youth from a potentially volatile situation. Physical intervention is only used as a last resort and only after the youth has failed to respond to verbal intervention. All physical interventions are utilized in accordance with Rule 63H Protective Action Response (PAR). The plan will detail the procedures to implement Mental Health Alert status for youth identified as having acute emotional or behavioral problems that may pose a safety/security risk, following the assessment by the mental health professional. A 24- hour response capability will be provided by the Clinical Director, and an on-call schedule is utilized with clinicians. The program psychiatrist will provide 24-hour response capability. The program will pursue a written agreement with the Halifax Health Medical Center for acute care and mental health and substance abuse emergency management services. The hospital is approximately 7.4 miles from the DSOP, and within 12 minutes. A.6.b. EVIDENCE-BASED MENTAL HEALTH AND SUBSTANCE ABUSE SERVICES: G4S will implement evidence-based or promising mental health and substance abuse practices to include the following: Use of validated and reliable instruments to assess risk/needs (PACT and R-PACT) and other standardized assessment instruments; development of individualized performance and treatment plans based on risk, need and responsivity factors; enhancement of youth s intrinsic motivation using Motivational Interviewing techniques and Stages of Change strategies to promote healthy mood and behavior regulation; application of cognitive behavioral treatment methods that teach skills, promote practice through role play and reinforced by all staff; integration of treatment throughout commitment/sanction process; utilization of a behavior management system with increased positive reinforcement to promote behavior change; active recruitment and engagement of pro-social supports from the youth s community including peer mentoring, non-denominational religious/volunteer activities and family involvement; routine assessment and measurement of youth change in cognitive and skills development; and use of constructive feedback re: youth change through measures of accountability and fidelity. A.6.c. EVIDENCE-BASED MENTAL HEALTH AND SUBSTANCE ABUSE TREATMENT: While cognitive behavioral interventions have been shown to be effective with adult sex offenders, treatment for juvenile sexual aggressors needs to be tailored further to meet the individual developmental stage and intellectual ability of the youth. Research indicates that adolescents who commit sexual offenses show broad deficits in a variety of social and coping skills. They often exhibit patterns of distorted thinking and perception that can lead to sexually aggressive behavior. They are frequently diagnosed with co-morbid conditions such as Attention Deficit Disorder (ADD), Post Traumatic Stress Disorder (PTSD) and major affective disorders. Interventions, therefore, will address underlying mental health issues that may interfere with effective sex offender treatment. G4S recognizes that adolescent sex offenders are a heterogeneous group differing in a variety of dimensions (Juveniles Who Sexually Offend, OJJDP 2001). Therefore, treatment materials will be designed in modular form to allow for individualization based on needs. G4S will incorporate Cognitive Behavioral Therapy (CBT) as the core approach that utilizes a relapse prevention model in working with sex offenders. This has been outlined by The American Association for the Treatment of Sexual Abusers (ASTA) as the evidenced based course of treatment. Cognitive behavioral treatment assists youth in changing their attitudes and reducing negative emotional states, which often motivate juveniles to act out sexually. In addition, G4S will incorporate the Rational Emotive Behavior Therapy (REBT) that falls under the CBT heading, and recommended for sex offenders irrational thinking. To help our adolescents and their parents overcome the negative effects of violence or traumatic life events, the Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) and Traumatic Grief Focused Cognitive Behavior Therapy, mentioned above, are listed on OJJDP as exemplary Model programs and will be available for the DSOP youth. SOTS Consideration 1: How well does the proposal describe that best practices have been integrated into the selection and availability of treatment programs? While juvenile sexual offenders share many characteristics with other adolescents who commit crimes, they have a variety of unique needs that must be addressed in the therapeutic milieu, in order to enhance their psychological well-being and facilitate their safe integration back into the family and community. G4S has become part of the cutting edge of new models and techniques. In collaboration with renown sex therapists, Leo Cotter, Ph.D, L.M.H.C. and Ruben Drake, L.M.H.C., NCC, CAP, SAP, G4S will amalgamate its successful sex offender model that has been described as best practice and which has shown positive outcomes in our sex offender programs. This is a cognitive-behavioral treatment program hereafter referred to as the Pathways Treatment Curriculum and Steps of Progress for Adolescent Male Sex Offenders. The Pathways Treatment Curriculum (Timothy J. Kahn) is a model of standard and accepted practices in the field of adolescent sexual offending treatment, and is often used as the primary treatment curriculum. G4S has found better outcomes when using the Pathways in conjunction with The Steps of Progress Sex Offender-specific Curriculum. This curriculum was developed by Leo Cotter, Ph.D., LMHC, with revisions to include more Rational Emotive Behavior Therapy by Robert Whitford, Ed.S., LMHC, with further revisions made to include relapse prevention planning and safety planning objectives by Robert (Ruben) Drake, LMHC, NCC, CAP, SAP. This elaborate sex offender model incorporates process groups, work groups, trauma groups, healthy sexuality work groups, relapse prevention work groups, and individual counseling work. The DSOP will require residents to complete the Pathways curriculum in the first 11 weeks of treatment, with the Steps of Progress being implemented throughout the program. The Pathways curriculum addresses the treatment process, accepting responsibility for behaviors, victim empathy, understanding precursors and influences that allowed deviant sexual behavior, behavior cycles, thinking errors, relapse prevention planning, victim clarification and family reunification. Another strong curriculum to be used is the Group Treatment for Substance Abuse: A Stages-of-Change Therapy Manual (Velasquez, Maurer, Crouch, DiClemente). This is a RFP R2107 Page 37


74 Program Services 29-session treatment program, based on the research-supported transtheoretical model of behavior change and simulates the stages of change in all stages of recovery. G4S will utilize cognitive restructuring as continual affirmation of where the youth sees himself in each stage. Another best practice will be to continue membership with the Association for the Treatment of Sexual Abusers (ATSA). This international, multi-disciplinary organization is dedicated to enhancing community safety, reducing sexual recidivism, protecting victims and vulnerable populations, transforming the lives of those caught in the web of sexual violence, and illuminating paths to prevent sexual abuse. Through research, education, and shared learning, ATSA promotes evidence based practice, public policy and community strategies that lead to the effective assessment, treatment and management of individuals who have sexually abused or are at risk to abuse. It is through this affiliation that has strengthened G4S concepts and outcomes with our sexual offender moderate-, high-, and maximum-risk populations. A third area of best practice is to provide consistent effective sex offender treatment training, in order to keep clinicians abreast of the newest treatment and interventions. G4S will offer training at the Hastings Training Academy or on-site DSOP as new research and best practices are identified. Further, it will be an interest to pursue CEU sex offender training, in order to bring national sex offender trainers to G4S. A.6.d. CULTURAL AND ETHNIC BACKGROUND AND OTHER TREATMENT CONSIDERATIONS: Cultural and ethnic background and gender will be considered in all aspects of the sex offender-specific, mental health and substance abuse treatment services. Treatment will be based on the youth s individualized needs. When co-existing mental health and substance-related disorders exist, integrated treatment addressing cooccurring mental health disorders and substance-related disorders will be provided. A.6.e. DESIGNATED MENTAL HEALTH AUTHORITY will provide oversight to the clinical staff delivering on-site mental health and substance abuse services, and is on call 24 hours a day, seven (7) days week for any immediate needs the youth may have. There will be clear organizational lines of authority and communication between the DMHA and the mental health counselors delivering services. This licensed clinician will be licensed pursuant to Chapter 458, 459, 490, or 491, F.S, and will be on-site at least 40 hours, five (5) days a week, and on-call 24 hours a day, seven (7) days week. Further, the DMHA will provide to counselors/therapists at least 1.5 hours per week of direct supervision, which exceeds RFP requirements, to include directions, instructions, and recommendations of services provided by the counselor. It will be the responsibility to ensure quality, coordination and implementation of services. This includes understanding the symptoms of functional impairment associated with sex offenders and having experience in dealing with victims of physical/sexual abuse or neglect. Further, the Licensed Mental Health Professional will develop and maintain working relationships with local mental health and substance abuse agencies as referrals for services. A.7. CATEGORY 6: DELINQUENCY PROGRAMMING How well does proposal describe a detailed plan for implementing an effective delinquency program? Consideration 1: How well does the proposal describe the delinquency intervention model or curricula intended to be used? A.7.a DELINQUENCY INTERVENTION MODEL: Through years of trouble-shooting, strengthening assessment tools, researching, participating in workshops, presenting evidence to therapists working in the field of sexual abuse, and serving on task force boards, G4S has become part of the cutting edge of new models and techniques. G4S provides the tools to influence risk factors associated with accepting responsibility for behaviors, victim empathy, understanding precursors and influences that allowed deviant sexual behavior, behavior cycles, thinking errors, relapse prevention planning, victim clarification and family reunification. G4S has developed an effective SPECIFIC DELINQUENCY INTERVENTION MODEL that is comprehensive, detailed, and encompasses evidence based practices found to be successful in corrections. In order for G4S to reach our SPECIFIC results of having a specialized program of effective counseling interventions by all levels of staff to directly affect the family, individual, and the community, we will follow the eight (8) Principles of Effective Correctional Intervention, which are components of the Justice Research Center (JRC) What Works Principles that is supported by the National Institute of Corrections (NIC) for evidenced based correctional practices. These eight (8) principles have been implemented with offenders in programs and communities. Due to proven effectiveness, G4S will implement each principle into our delinquency intervention model as best practice to reshape thinking and behavior. We are confident our design will result in successful data at the DSOP, and teach prosocial skills needed to strengthen family and community relationships. If done effectively, the youth has greater opportunity to decrease recidivism; therefore, it is our intention to provide those opportunities. The following several pages will describe our model and plan to provide high quality sex offender-specific delinquency intervention and treatment, following evidenced based correctional practices. Consideration 3: How well does the proposal describe the goals and objectives of the delinquency intervention program? Consistent with the Restorative Justice philosophy and G4S mission, the goal will be to use evidence based tools and systems that accurately access RFP R2107 Page 38
75 Program Services needs, enhance motivation, provide evidence based interventions, effectively train youth and staff on evidence based cognitive behavioral models, increase positive reinforcement to at least 8:1 positive to negative reinforcers, increase community involvement to strengthen support systems, follow fidelity measurement of our practices, then provide measurement feedback to youth and staff. The objectives will be to use evidence based delinquency interventions to prevent further criminal and antisocial behavior, reduce recidivism, and reduce criminogenic risk factors that are the major causes of criminal behavior. As a result, the youth will have lower recidivism, higher rates of success, and the community will be safer. G4S will re-socialize the youth, increase a sense of accountability, strengthen cognitive reasoning and behavioral competencies, and empower youth to live responsibly in society. Diligence will be placed to accurately identify criminogenic needs, provide for physical and mental well-being, strengthen education and life skills, strengthen family involvement, and teach parenting skills where applicable. A.7.b. CRIMINOGENIC NEEDS AND PROTECTIVE FACTORS: The first principle will efficiently assess risk and needs, using the Department s evidence-based Positive Achievement Change Tool (PACT). Pre-commitment will include the completion of the C-PACT, which will be reviewed at admission to identify and prioritize the youth s criminogenic risk/needs and protective factors. The R-PACT will further match criminogenic needs to interventions with the goal of reducing risk factors associated with re-offending and strengthening protective factors associated with resilience and pro-social behavior. A.7.c. RESPONSIVITY FACTORS: The second principle will enhance motivation of the youth, taking into consideration factors that can block his ability to respond to treatment, such as age, intelligence, mental health, learning styles, temperament, and other relevant characteristics. Evidence based motivational interviewing will be used as a delinquency intervention by the Treatment Team, due to higher probability of youth responding to motivation rather than persuasion to change. Furthermore, the program will provide a variety of positive and challenging learning experiences that are designed to increase the youth s pro-social skills, social responsibility and awareness of the impact of one s behavior on others. For lower functioning youth, G4S will tailor interventions to assist the youth with gaining greater awareness through individualizing treatment and delinquency interventions to meet his developmental needs. Delinquency interventions will be delivered in a culturally competent manner, and include the use of active learning through demonstration, role-play and rehearsal, modeling of pro-social behaviors, guiding and re-directing toward pro-social and positive choices, and engaging him in constructive dialogue to resolve conflict. The third principle will target interventions that are evidenced based and conducive to the sex offenders. G4S will follow evidence that shows recidivism reduction of 31% by targeting at least four (4) to six (6) criminogenic needs (Gendreau, Franch, Taylor, 2002). Within this targeting intervention principle, G4S will further integrate five (5) sub-principles that are validated as effective evidence based correctional practices: 1) risk principle- G4S will ensure supervision meets requirements, and with the assistance of the specialized Life Coach during five (5) days of the week, supervision will exceed requirements. Further, G4S will implement evidence based treatment for high- risk sex offenders to reduce their risk of re-offending; 2) need principle- G4S will provide services according to the youth s deficits that are not limited to sex offender-specific training, social skills, thinking errors, vocational training, misuse of leisure time, drug and alcohol abuse. The Life Coach will be an integral part of specialized, hands-on vocational training, health and wellness planning, connecting with constructive leisure alternatives available in the youth s home community, broadening personal interests and reinforcing skills; 3) treatment principle- G4S will implement cognitive/behavioral strategies that includes structured social skills teaching and positive reinforcement of pro-social behaviors and attitudes; interventions that target attitudes, appropriate sexual behavior, values, substance abuse, anger, anti-social peers, and other factors that are responsible for criminal behavior; and family based interventions where we will train families on behavioral techniques to strengthen relationships. It is critical with sex offender populations to consistently confront irrational thinking to enact more rational thinking that can be measured to show progress toward pro-social skills; 4) responsivity principle- G4S will match the therapist with the learning and personality style of the youth to increase personal strengths and decrease limitations. Further, treatment and delinquency interventions will meet the youth s cognitive abilities; and 5) fidelity principle- G4S will implement its comprehensive fidelity monitoring design that has resulted in significantly high QA ratings in over 94% of our FDJJ programs, and Deemed results in 100% of our FDJJ sex offender programs. Our fidelity control is detailed below in A.7.e. Fidelity to Original Design. The Treatment Team will develop the performance plan that prioritize and individualize the type, intensity, frequency and duration of services based upon the youth s risk and needs. Efficacy studies (Gendreau and Goggin (1995) have shown that high-risk offenders should spend 40%-70% in highly structured activities; however, G4S will maintain at least 94% structured activities. Youth with higher risk levels will receive more cognitive-behavioral services at a greater intensity and frequency for a longer period of time. Youth with a lower level of risk will receive fewer services for a shorter timeframe. G4S will not use a one size fits all philosophy and all youth will not receive the same delinquency intervention services. For example, youth with poor impulse control and anger management problems will receive delinquency intervention services targeted at social skills training, problem solving, moral reasoning and decision-making. However, those with greater ability to self-regulate their emotions/behaviors will not participate in the same activities. Likewise, those with identified substance abuse needs will receive substance abuse groups. G4S is confident that providing continuity in structure, treatment, and accountability, there will be more probability of changing the behavior of the DSOP youth, while reaching the ultimate goal of reducing recidivism and victimization. Consideration 2: How well does proposal explain how Provider will engage and retain the participation of the families of the youth in the program? DSOP will provide a range of activities available to youth and families designed to promote family reunification, described in detail on pages Visitation opportunities will be provided on Saturday and Sunday, quarterly Family Fun Days, and special holiday events that promote family communication and reunification. Significant importance will be placed with participation of the family in family therapy, RFP R2107 Page 39
76 Program Services relapse prevention planning, safety planning, and aftercare service linkages, all significant elements in working with sex offenders. G4S programs have a history of successfully engaging parent/guardians as evidence by superior ratings for parental involvement in QA reviews, large numbers of returned parental satisfaction surveys with exemplary ratings and feedback, significant turnout and participation in all scheduled family days and special events, as well as documented participation in Treatment Team meetings and family therapy services. The fourth principle will ensure skills training will effectively train all staff responsible for implementing evidenced based cognitive behavior strategies. Training will be conducted on-site or at the Hastings Training Academy. G4S Certified instructors will be responsible for ensuring thorough training on T4C, LifeSkills, Impact of Crime, and Motivational Interviewing delinquency interventions. As part of the competencybased training, certified trainers will co-facilitate the delinquency curriculum with trained facilitators, and then will provide on-the-job coaching to give feedback to each facilitator s strengths and weaknesses. This will ensure trainers have the appropriate knowledge and skills to effectively facilitate the curriculum. As for the DSOP youth, they will be taught new thinking and behavior responses via CB strategies. The fifth principle will increase positive reinforcement, following an 8:1 positive to negative reinforcement, exceeding recommended 4:1. The sixth principle will engage community support in the Daytona community. The Life Planner will refer offenders to aftercare programs as additional support and oversight of sex offenders, once they are discharged. Also, the Life Planner will connect and engage the youth s home community to establish relationships and support for the youth once he returns home. Consideration 4: How well does the proposal explain how the interventions employed are considered to be an evidence-based or promising practice? A.7.d. EVIDENCE-BASED OR PROMISING PRACTICE: As defined in Rule 63E-7.002, F.A.C, the delinquency interventions employed at the DSOP will be evidence-based practice, promising practice or a practice with demonstrated effectiveness under the social learning approaches, cognitive behavioral approaches and family therapy. Cognitive-Behavioral Therapy (CBT) is recognized by the Office of Juvenile Justice Delinquency Prevention (OJDDP) as an evidence-based practice, and will be intertwined in the numerous intervention styles to help identify and change dysfunctional beliefs, thoughts and patterns of behavior that contribute to problems. Studies have shown the following evidenced based or promising cognitive/behavioral interventions have reduced recidivism and will be integrated into the DSOP plan: Thinking for a Change (T4C) was developed by the National Institute of Corrections (NIC) and is identified as an evidence-based practice in the Department s 2010 Sourcebook of Delinquency Interventions. The goal of T4C is to effect change in thinking so behavior is positively impacted. Youth are expected to demonstrate proficiency in goal attainment by demonstrating the ability to learn cognitive restructuring techniques, develop problem-solving skills and enhance basic and critical social skills, all which are components of the model. T4C will be facilitated by trained staff, under the supervision and fidelity checks of Dr. Deena Green and Bridget Goodrich, both state recognized facilitator certification trainers for Thinking for a Change. Life Skills Training (LST) is listed in the Department s 2010 Sourcebook of Delinquency Interventions as evidence based practice. Life Skills is a research-validated substance abuse prevention program proven to reduce the risks of alcohol, tobacco, drug abuse, and violence by targeting the major social and psychological factors that promote the initiation of substance use and other risky behaviors. This program will provide DSOP youth with the confidence and skills necessary to handle challenges. Motivational Interviewing (MI) is listed as an evidence-based, goal-directed and client-centered interactional style in SAMHSA s National Registry of Evidence-based Programs and Practices. The goal is to create tension in the youth to motivate him to rely on his inner self to resolve tension through pro-social ways, rather than relying on external control. This elicits behavioral change by helping youth to explore and resolve ambivalence. MI is facilitated by trained staff, under the supervision and fidelity checks of Dr. Deena Green and Bridget Goodrich, both state recognized facilitator certification trainers for Motivational Interviewing. Trained staff will use MI techniques daily to examine and resolve ambivalence and to motivate the youth to progress through the stages of change. Impact of Crime: Addressing the Harm to Victims and the Community (IOC) is listed in the Department s 2010 Sourcebook as a practice with demonstrated effectiveness that helps offenders understand the harm they have created and assists them in taking personal accountability for their actions. IOC is facilitated by trained staff, and youth attend IOC classes weekly. The goal is to increase the youth s awareness of and empathy for crime victims and survivors, and increase the youth s personal accountability for his criminal actions and harm to others. Consideration 5: How well does proposal explain how delinquency interventions will be monitored to ensure fidelity to original delinquency intervention model s design? A.7.e. FIDELITY TO ORIGINAL DESIGN: The seventh principle will measure practices and services to ensure we are providing quality control and program fidelity. An Ohio Department of Corrections study showed that programs with high integrity reduced recidivism by 22% (Latessa and Lowenkamp, 2006). G4S will deploy operational staff 24/7 to ensure the master schedule is followed in accordance to the schedule. Certified trainers will observe facilitators delivering the delinquency curriculum to ensure fidelity to design. Additionally, coaching sessions will be conducted as needed to strengthen the presentation. The licensed mental health professional will be responsible for observing the facilitation of delinquency interventions and conducting fidelity checks with standardized checklists designed for each curriculum. The licensed mental health professional will conduct weekly supervision with the staff that facilitates the delinquency curriculum and provides instruction and support on group skills, behavior management and fidelity to curriculum design. As part of the monthly risk management system review, the facility Risk Manager/QA Specialist will conduct verification checks on the delivery, quality and fidelity of delinquency intervention curriculum. RFP R2107 Page 40

77 Program Services Delinquency intervention services will be discussed and reviewed at the daily management meetings, bi-weekly Treatment Team staffing, weekly coaching sessions with the Facility Administrator, weekly supervision sessions with the licensed mental health professional and monthly risk management verification reviews. Fidelity to the design will include three (3) levels of company involvement, which are the program, regional, and corporate levels. On a consistent basis, multi-level leaders will collaboratively discuss the fidelity of delinquency design to reduce future recidivism, re-socialize youth, increase a sense of accountability through development of pro-social skills, improve cognitive reasoning and behavioral competencies, and empower youth to live responsibly. The eighth principal will provide our measurement feedback to staff and youth to build accountability, maintain integrity, and improve outcomes. G4S will reward youth s positive behavior and provide positive feedback to staff delivering effective programming. G4S intends to link effective practices with resources so there is a continual flow of consistency between needs, interventions and support. A.8. CATEGORY 8: Educational Services How well does proposal specify educational services/coordination with local school board? Consideration 1: How well does proposal specify the educational services to be provided? A.8.a. COORDINATION OF EDUCATIONAL SERVICES: The education program at the DSOP is currently provided by the Volusia County School District, operating under a Cooperative Agreement with the FDJJ that was most recently renewed in July Upon being awarded the contract, we will approach the District to determine whether it wishes to continue operating the school at the program or enter into a contract with G4S to operate the school, as provided for under Section , F.S. We will inform the District that G4S currently operates nine (9) schools in nine (9) FDJJ residential commitment programs under contract with five (5) local school districts. G4S has the expertise to operate the school program at the DSOP, but understands that it is the District s choice whether to operate the program or contract for its operation. We also understand that the District-operated school at DSOP has been awarded Exemplary Program status by JJEEP and may wish to continue operating the school. A.8.b. COOPERATIVE AGREEMENT: If awarded this contract, G4S will comply with the Cooperative Agreement between the School District and the FDJJ. If contracted to operate the education program, G4S will enter into a Memorandum of Understanding and Agreement with the District that will mirror the District/FDJJ Agreement requirements and responsibilities. This will include ensuring that the education program is fully integrated into the operational components of the DSOP program, including treatment, interventions, and behavior management. Importantly, the youth s IEP or IAP is fully integrated into his DJJ Individual Performance Plan. Working cooperatively, we will ensure that the youth s individualized goal of obtaining a high school diploma or GED, as age appropriate, is achieved. Education services will be integrated into the overall living environment and the program s behavioral motivation program. We will work collaboratively with school personnel to build a daily schedule that provides the required instructional time and structured study hours for homework and out of class assignments. In addition, we will work as a team with the school district to provide: a learning environment where each student is treated with respect educational academic and vocational services that are in accordance with Florida Standards core courses that reflect instructional requirements to ensure earned credits and grades are carried over to the public school curricula and learning objectives that are individualized for the needs of each student with courses that are open entry/exit, competency based and result in progress toward measurable objectives approved textbooks, assessments and educational software education services for youth not in general population a records system that documents the performance and achievement of each student, ensures youth rights to privacy, and complies with DJJ and DOE regulations and requirements of the Federal Education Rights and Privacy Act compliance with all reporting requirements of the DJJ and the DOE to ensure access to state and federal funds and preparation for the JJEEP Quality Assurance review process (if continued by Legislative action). a school day that provides the required minutes of educational courses, including those courses which can be modified to fit both the education and the rehabilitative mission, for all grades Consideration 3: How well does proposal describe how the Provider will integrate the educational staff into the current BMS? A.8.c. COLLABORATION: We have experience in working under agreements with School Districts and will continue to comply with the Interagency Agreement between the FDJJ and the Volusia County School Board, as specified by section , F.S. Collaborative relationships with local School Districts has consistently presented a seamless transition for the youth. At the FDJJ programs we operate, we have built an effective partnership with the local School District by: meeting regularly with school district personnel, both those assigned to the program, as well as the central office including school district staff as part of the management team for planning and monitoring encouraging school personnel s participation in Treatment Team meetings establishing adaptive school performance as a primary task of the youth s daily schedule opening all staff training sessions to teaching staff coordinating assemblies, parent days, etc. to support education and program goals ensuring background screening and supervision scheduling RFP R2107 Page 41
78 Program Services Most importantly, we have found that frequent discussions and meetings to ensure there are no conflicts in program and bell schedules, school holidays, and program activities are critical to success. Of equal importance, and further mentioned below, is the development of and daily adherence to a joint behavior management plan that includes consistent reinforcers and logical consequences. There will be one (1) behavior management system at DSOP that will be used throughout the day, including school. G4S will utilize a behavior management and positive behavior reinforcement system that is grounded upon the principles of Social Learning Theory. G4S operations and education staff participate in routine joint trainings that emphasize this behavior management system that forms the foundation of the common discipline plan. These joint trainings, as well as joint administrative and Treatment Team meetings, continually emphasize the critical element of the common plan that teachers and youth care workers are a team both inside and outside of the classroom. The program s behavior management system will form the foundation of the common discipline plan and other significant issues related to the safety and security of the youth, staff, educators and program. This system, as well as joint administrative and Treatment Team meetings, will continually emphasize the critical element of the common plan that the teacher and the youth care worker are a team inside and outside of the classroom. G4S deploys a best practice in which the Facility Administrator and the Lead Teacher have daily conversations followed up by a weekly report that includes a summary of the preceding week s activities, issues, concerns and achievements. The Facility Administrator and the Lead Teacher speak daily in an effort to make the educational experience as meaningful as possible for students to include programming, scheduling, most convenient time for school, annual calendar, cooperative efforts in grant writing, behavior issues, determining how Title I grants can improve the learning environment in the school, and to be open to new ideas to expand career opportunities through speakers from the community. Teachers will attend monthly treatment team meetings and bring information relating to academic performance and progress toward attainment of academic goals, as well as information related to classroom behavior. A.8.d. ACCESS TO READING MATERIALS: Reading materials will be provided to youth outside of the educational program with appropriately approved newspapers, magazines and books. We will use the Florida Just Read program that incorporates the academic program with the youths living units, and maintain a diverse media center. For special holidays, we will periodically hold contests, i.e. an essay or poster contest that requires reading and research outside the classroom. Youth care workers will be encouraged to promote reading and other educational pursuits for youth during non-school hours. A.8.e. TRANSITION PLANNING: G4S believes that transition of the youth back to his home or future community is the most critical process in ensuring a successful and law-abiding integration. The program and school must work cooperatively to ensure a smooth and effective transition of each youth back to his home community or next placement. FDJJ s Administrative Rule 63E-7 and FDOE s Administrative Rule 6A (5) are very specific regarding the procedures that must take place in transition planning. The Case Manager will notify school personnel of transition meetings. School personnel will attend and provide information to case managers, JPO s, after care providers, and other involved parties (including DCF) as to where the student will be attending school after leaving DSOP and how the student is to re-enter the local school district, who he is to see, where he is to go, what the parent should bring, and other useful information. The school personnel, in cooperation with the Case Manager, will forward an exit portfolio to the youth s receiving school district transition contact one (1) week prior to student s release, to include withdrawal grades, transcripts, commendations, work and project samples, IAPs, IEPs, 504 plans and ESL plans. Consideration 2: How well does the proposal detail direct care supervision of youth during school hours? A.8.f. STAFF ASSIGNMENT: In a DJJ Monitoring Summary dated March 5, 2010, the following observations were made, Appropriate staff to youth ratios were observed throughout the monitoring visit. A staff member remained in each classroom to assist the teachers with behavior management and provided assistance to the youth. The staff interacted in a calm and professional manner that fostered positive mentoring relationships. Youth were redirected when acting inappropriately and were praised for their accomplishments. G4S takes seriously its role and responsibility in the classroom, regardless of whether the education program is provided by the School District or G4S. Youth care staff will be assigned to classrooms to provide care, custody and supervision and respond to the everyday needs of the youth. In all of our programs, we have been very successful in training youth care workers to become a member of the classroom team where they provide proper supervision and control in the classroom and assist with the education process. Youth care workers who are involved in the educational process, under the direction of the teacher, have proven that they provide better supervision than if their only assignment is to supervise and control the youth. G4S staff and School District staff are most effective when they participate in joint trainings that emphasize the behavior management and motivation system mutually agreed to by G4S and the School District. Youth who are disruptive in the classroom will be immediately removed and counseled by the youth care worker, regarding their behavior. When the youth accepts accountability for his behavior and commits to remaining orderly, he will be allowed by the teacher to return to the classroom. Either the teacher or the youth care worker can prompt a youth, award a reinforcer for good behavior, or sanction a negative behavior. A.9. CATEGORY 9: PRE-VOCATIONAL AND VOCATIONAL SERVICES How well does the proposal describe the traditional and nontraditional pre-vocational and vocational services to be provided and the manner in which the services will be provided? Consideration 1: How well does the proposal describe how the Provider will coordinate the traditional and nontraditional prevocational and vocational services with the community resources? A.9.a. TRADITIONAL AND NON-TRADITIONAL SERVICES: Since 1997, G4S has successfully provided youth of all ages in FDJJ programs with traditional and non-traditional pre-vocational work services. To ensure that traditional and non-traditional pre-vocational and vocational services are provided, G4S will work cooperatively with Volusia School District personnel to provide pre-vocational services to youth at the facility. The pre-vocational services are closely linked to the academic portion of RFP R2107 Page 42
79 Program Services the program and to life skills training. Our goal for vocational training will be to develop age appropriate skills, discover career interests and aptitudes, identify and then build upon the strengths of the youth. We will expose the youth to various careers by sponsoring Career Days where guest speakers inform the youth about various vocations and support instruction and enhancement activities that expose youth to a variety of cultures and occupations. Potential vocational opportunities for high-risk youth are further discussed below. Consideration 2: How well does the proposal describe how the Provider will assess youth's interest for a specific vocational area? How well is this training integrated into treatment goals and planning? Youth will also take the CHOICES career interest survey. This information on career interests will be forwarded to Case Managers for inclusion in the youth s DJJ Performance Plan. We will also forward these data to teachers in the school who use the CHOICES assessment in development of lesson plans to promote student interest and enrichment. G4S will contribute to this assessment by including the information obtained during the admission intake assessment process, where the youth is asked to state his career and employment goals. G4S community coach and teachers will meet monthly at Treatment Team meetings to assess progress with each youth s vocational goals and make revisions, as needed, to ensure each youth s success in attaining those goals prior to release from the program. The behavior management system will be integrated into vocational training, establishing the importance of behavior and decision-making. Workforce Florida Inc. has identified a number of barriers youth, such as those placed at DSOP, have in seeking and holding gainful employment. Interestingly, the lack of hard skills needed for a particular job or trade are not considered a barrier. Employers consistently state that they will provide the requisite training needed. What employers state they need in a prospective employee is the ability to read, write, and compute at grade level. The foundation of an effective pre-vocational/vocational program for youth is a quality education program that emphasizes the attainment of reading, writing, and math skills. Employers also state that they need employees who have attained industry-recognized workplace certifications. These include Microsoft Office, Adobe, OSHA, WorkKeys, and Ready to Work. G4S offers these certification programs in the FDJJ programs it currently operates and will do so at DSOP. During FY , G4S awarded 635 Vocational Occupation Completion Points and 129 Ready to Work Certifications, among others. A.9.b. ACCESSING VOCATIONAL OPPORTUNITIES: G4S has been successful in securing additional grant funding for enhancing the vocational opportunities we provide at the programs we operate. In the school year, seven (7) DJJ programs received Carl D. Perkins grants totaling $450,000. Three (3) of those grants were won by G4S programs Avon Park Youth Academy, Hastings Youth Academy, and Okeechobee Juvenile Offender Correctional Center totaling $169,064. We continue to work with many of the 24 Regional Workforce Boards to develop opportunities for funding services for the youth we serve; however, it should be recognized that, according to Terri Eggers, during the previous school year only 559 DJJ students, a very small number of the total, received services from regional Workforce Boards or Workforce Florida. A major barrier is that many of the youth in our programs do not reside within the geographical boundaries of the local Board. Recently, the FDJJ Office of Education initiated a meeting with our Polk Halfway House program and other community partners to enhance the employability of court-ordered youth. This partnership is intending to mirror the federal Shared Youth Vision and state level Strengthening Youth Partnerships initiated by Workforce Florida, Inc. with the support of the Agency for Workforce Innovation and the Department of Juvenile Justice. Our PHH program volunteered to be the coordination site for these services in partnership with PACE Center for Girls Orlando; Orlando Marine Institute; HBI Project Craft Orlando; Orlando Marine Institute; Workforce Central Florida; Polk County School Board; SEDNET Polk County Public Schools, Employ Florida Banner Center for Construction (BCC); Florida Ready to Work; and Department of Children and Families. We anticipate participating in much the same activity in Volusia County, if the opportunity arises. Post release employment has been found to significantly reduce recidivism; therefore, G4S will utilize our Life Planner to provide hands-on vocational training to the DSOP youth, and where possible, provide industry recognized certifications. We will implement our job connections as part of our We Connect to YOU model (further described in Exhibit 6, pages 67-68) where G4S will provide training to youth to meet Florida s workforce needs. It will be our goal to implement new vocational trainings each year. For example, we will consider the feasibility of a Digital Printing lab the first year, which will provide hard skills vocational training. Adobe Photoshop and Microsoft office will for further explored as components of the digital printing skills development. The second year, we will consider implementing the horticultural program, third year implementing the culinary project, and so on. Our research has found there are several areas of job demand in Florida that includes, but not limited to, opportunities in printing, horticulture, food services, career and technical instruction in Business Education, flooring installation, heating and cooling systems, and carpentry and painting. For this reason, G4S will evaluate best job placement opportunities when considering the vocational hands-on training for our youth that will be in addition to vocational requirements of the RFP. It is G4S intention to provide a turn-key opportunity for youth that includes training, interviewing, and job placement prior to release from the program. A.10. JOB TRAINING PLACEMENT: Youth with special Mental Health needs are particularly vulnerable in the workforce and need special help in job training and job placements. We are aware of these special needs and place emphasis on preparing eligible youth for transition to work upon return to the community. Training in job and employability skills will be provided as delinquency interventions, and include courses in industry-recognized workplace skills and certifications, life choices, key skills, workplace essentials, and entrepreneurial principles. Development of a solid work ethic and reinforcement of training curricula are strengthened through skill development groups provided by staff. Employment skills lessons, including Networking, Jobs & Money and Ready, Set, Work, will be included in the Arise Foundation curricula. The Life Planner will work with each youth's JPO and conditional release provider, as applicable, to connect youth to their communities for job placement, continued education and/or vocational training, and other support services and resources. These activities include ensuring the youth has the contact information for his local community s One Stop Center. G4S is fortunate to have an extensive network of working relationships with employers and community support agencies throughout Florida. This network and contact data will be readily accessible to program staff, serving as a valuable resource in their work with the youth during transition planning. Youth with employability as one (1) of their transition goals will be provided, at the time of release, a portfolio that includes a plan for continuation of education and/or employment when RFP R2107 Page 43
80 Program Services they return to the community; a sample completed employment application; a resume summarizing education, work experience and/or career training; an appointment with their local One Stop Center; appropriate identification documents; and, all workplace certifications awarded. A.11. SELF-SUFFICIENCY PLANNING Self-sufficiency planning for youth will be an integral component of the case management and transition processes. Self-sufficiency planning will include monitoring the youth s progress in demonstrating restorative justice traits and identifying the community network that will assist, support and mentor the youth upon his return. Planning will begin upon the youth s arrival and require the participation and feedback of all involved parties. During intake and admission and throughout the youth s stay, the specific assistance each youth needs for self-sufficiency will be monitored. Some youth will return to a home that can provide assistance in community transition and reintegration including mental health and substance abuse counseling, while other youth will return to families that can provide only limited adaptive help. The specific assistance anticipated to successfully reintegrate the youth will be regularly reviewed at bi-weekly and monthly reviews by the Treatment Team with involved parties. Adjustments to self-sufficiency plans will be based on the youth s Performance Plan progress and any changes identified in community support systems and individuals. The Treatment Team will also work in conjunction with the DCF case worker for those youth who are in DCF custody or with other community providers to assist youth in obtaining independent living arrangements for those situations where age and family circumstances indicate that independence and self-sufficiency are more realistic goals. A.12. CATEGORY 10: DISCHARGE POLICY AND TRANSITION SERVICES How well does the proposal describe a detailed and feasible discharge and transition plan for ensuring that youth are discharge-ready prior to release? Consideration 1: How well does the discharge and transition plan consider individual needs, characteristics and risks? Upon admission, the Bachelor s degree community coach will screen the youth for risks that include age, sex, height, weight, physical size, maturity level, special needs, medical or mental health risk factors, gang affiliation, physical and/or sexual violence potential, sexual history, suicide risk, escape risk and safety. Further, he will be screened for mental health and substance abuse needs that include mental health inpatient or outpatient treatment, substance abuse inpatient or outpatient treatment, emergency room evaluations for mental health and substance-related issues, suicide attempt, suicide behaviors or suicide risk, self-injurious behaviors such as head banging, intentional selfinjury, psychotropic medication treatment, drug/alcohol use and drug/alcohol possession, emotional instability such as depression, anxiety, mood swings or violent rage, and significant trauma history. Room assignment will then be discussed with the Treatment Team during the formal admission classification meeting. Once the risks and needs are identified, G4S will focus on responsivity factors that may enhance or impede the youth s progress. These include, but are not limited to, age, intelligence, mental health and motivation. While in the program, the youth s unique characteristics, needs, strengths, interests and abilities will be addressed through treatment and performance objectives and services. These will include a variety of positive and challenging learning experiences that are designed to increase the youth s pro-social skills, social responsibility and awareness of the impact of one s behavior on others. Throughout the youth s stay at DSOP, he will be re-assessed with the Residential Positive Achievement Change Tool (R-PACT) to identify his progress in reducing risk factors associated with re-offending, while strengthening protective factors associated with resilience and pro-social behavior. Further, new needs will be continually sought as a means to diminish problem areas as quickly as possible that may hinder future success. As the youth progresses in the program, he will achieve ability to pursue Discharge staffing (further mentioned below). Once this occurs, the DSOP will follow with a detailed Transition Plan. This plan will be a document that carefully considers the youth s individual needs, characteristics and risks in the planning for a successful community reintegration. The Transition Plan will incorporate the results from the Exit R-PACT, which details the youth s criminogenic risk and needs. The Transition Plan will include recommendations addressing the youth s ongoing medical, mental health, substance abuse, psychiatric and psychotropic medication needs. Educational, vocational and employment needs, medical issues, recreation and leisure activities, and individual and social supports will be addressed in the Transition Plan. The Transition Plan will be designed as an on-going fluid document that prompts required practices and timeline schedules to promote compliance. The document will include anticipated date of release and relevant changes as applicable, required documentation timeline prompts for release related documentation such as the PRN, Release Summary, parental travel arrangements, exit conference, victim notification as applicable, commitment management notification, as well as supervisory review to ensure compliance and active addressing of any follow up needs. G4S understands the crucial need to obtain resources for the youth, once he returns to the community. This may be accomplished in several ways. First, all youth in DJJ programs are eligible to receive assistance from the Florida Juvenile Justice Foundation which provides cash awards (up to $1,500) that may be used for tuition, transportation, education, employability assistance, special tools, clothing and equipment that may be needed to obtain employment, licenses, birth certificates, and virtually any other resource that may be needed. Program staff will assist the youth in completing the application and monitoring/tracking its progress. Second, for those youth in DCF care, program staff assist the youth in filing a petition under s (2) to request that the court either extend or reinstate DCF jurisdiction until their 19 th birthday. The purpose of this process is to allow the youth to seek various independent living benefits, such as housing and education. Third, certain youth served by more than one (1) state agency may be referred to the appropriate DJJ Circuit Coordinator to implement the provisions of the Interagency Agreement between DJJ and various other state agencies that can assist these youth with permanency and transition planning. Consideration 3: How well does the proposal demonstrate that discharge planning begins at admission? Transition and release planning will be an on-going evaluation and planning process that begins at the time of the youth s admission to the program. The specialized community coach will begin establishing discharge planning needs immediately upon the assessment process, which will be reviewed by the Treatment Team. This will include the needs, characteristics, and needs to be addressed during the stay at the DSOP, in addition to post-commitment. Criteria for discharge will be developed during the preparation of the performance and treatment RFP R2107 Page 44
81 Program Services planning, and will be fully discussed with the treatment team and communicated to the JPO, aftercare provider, family and other agencies to establish appropriate aftercare linkage for the youth. The transition process will be continuously re-evaluated to consider youth risks, protective factors and on-going needs upon release from the program. Anticipated release date, discharge criteria and initial transition objectives will be included as a part of the initial performance planning development process, completed within 21 days of the youth s admission to the program, which exceeds RFP requirements. Release planning will be a collaborative effort with the community coach, youth, parent/guardian, JPO, committing court, post-residential services counselor, additional Treatment Team members, and other external professionals involved in the youth s care as applicable. Members will be included in all planning efforts, from the time of the youth s admission, to ensure proactive planning and effective coordination of care needs to ensure the youth s successful transition. Each youth s anticipated release date will be determined within the initial performance plan development. The community coach will facilitate a monthly review of the youth s progress and anticipated release date within monthly formal progress review meetings held with the Treatment Team, youth, parent/guardian, JPO and external professionals involved. A youth s length of stay will be a collaborative progress-based determination effort, never as a form of punishment. Consideration 2: How well does the Provider s proposal describe their discharge and transition plans and how the vendor will work with the community, the JPO, the courts, Department staff and other partners in their discharge and transition planning? G4S Advantage: G4S Columbus sex offender program has developed and piloted its own Faith and Community Based Delinquency Treatment Initiative Program model. Due to its resulting success in lowered recidivism and higher community success rates, G4S will implement best practices at the DSOP. It will be in the concluding stages of the youth s program where the specialized life planner will assume the caseload from the community coach and implement the aforesaid mentioned model. The life planner will provide a seamless connection and transition of a youth to his community networks. The role is crucial in safeguarding that a continuum of care design is closely followed. First, the life planner will familiarize himself/herself with all risk and protective factors identified at admission by the community coach and youth. Risk assessment findings, as well as program and treatment progress, will be used to determine individual readiness for the community reintegration component of the program. Throughout the youth s stay at DSOP, the community coach and life planner will work closely with the JPO, courts, Department and other external providers to provide progress updates, address planning needs, and establish appropriate postrelease resources and linkages to ensure the youth s successful transition to community living. As part of the behavior management system, the youth will meet regularly with the life planner and counselor to work on transitional needs and planning. Further, the youth, life planner and counselor will collaboratively work to finalize and review his relapse prevention plan, court ordered sanctions and to complete and/or process any release related assignments such as restorative justice activities. The Treatment Team will recommend youth readiness for transition at a minimum of 60 days prior to the anticipated release date, unless otherwise indicated. The life planner will notify the Treatment Team of the scheduled, formal transition conference that will address medical, mental health, sex offender-specific, and other areas for postcommitment needs. A notification letter will be sent to the JPO, post-residential services counselor, if different than the JPO, the youth s parent or guardian, the waiver support coordinator if the youth is an identified client of APD, a Division of Vocational Rehabilitation representative if the youth has a disability as evidenced on his or her Individual Education Plan (IEP), and if applicable, the DCF counselor, and other agencies involved in the youth s care, inviting them to participate in the transition conference, advising of the anticipated release date. The DSOP will encourage invitees participation through advanced notifications and reasonable accommodations. However, when arrangements cannot be made for their participation in the transition conference, the intervention and treatment team leader shall request their input and offer an opportunity for them to provide it prior to the conference. During the transition conference, participants will review transition activities on the youth s performance plan and identify additional activities as needed. A thorough review of the youth s history, treatment progress and determination of on-going and/or follow up needs will be conducted. The intervention and treatment team leader shall obtain conference attendees dated signatures, representing their acknowledgement of the transition activities and accountability for their completion pursuant to the youth s performance plan. In follow-up to the conference, if anyone not in attendance is identified as having responsibility for completing a transition activity, the intervention and treatment team leader shall send a copy of the plan and request its return with a dated signature. In this case, an original signature is not necessary. Electronic transmittal of the plan to the youth s JPO and, if applicable, the DCF counselor is acceptable. If transmitted electronically, a return acknowledging receipt and review suffices and shall be printed and filed with the youth s plan (63E-7.010, F.A.C.). As notification of intent to release or discharge a youth, the life planner will send the original, signed release Performance Summary together with the Pre-Release Notification and Acknowledgement form (PRN) to the JPO at least 45 days prior to the youth s release. In the case of a sex offender who is not SVP eligible, documentation will be sent at least 90 days prior to the youth s planned release date to the committing court. Copies will be sent to the parent/guardian and post-conditional release provider as applicable. The life planner will initiate specialized activities that follow the Faith and Community Based Delinquency Treatment Initiative Program model. Focus will be placed on establishing relationships with the youth s home community to strengthen support when he returns, hold him accountable for his behavior, give back to society for the harm he has caused, and initiate the resources necessary for the youth s return: Targeted community group connection: The youth will be assigned at least one (1) specific project that will be meaningful for youth and community. The selected project will require the youth s planning, personal hands-on development and construction, and consistent communication between youth and hone community to share ideas and discuss progress. This will set the stage of connection between the youth and community with expectation he can continue his community responsibility upon returning home. Spiritual health: As follow-up to the program s Chaplaincy Program, the life planner will establish or strengthen spiritual connections in the youth s community. If deemed necessary, the life planner will make face-to-face contact with the community entities to bridge the gap and ensure support is in place for the youth prior to discharge. RFP R2107 Page 45
82 Program Services Family Reunification: The life planner will ensure families are actively engaged in different aspects of services and activities that targets strengthening the family relationship. Family Support: The life planner will maintain a strong relationship with the Food Bank, which will be utilized to provide food to the youth s families in time of crisis. Job Connections and Workforce: In the event DSOP is able to implement a culinary program, youth will attend food services classes and receive a food certificate. The life planner will set up orientation and application processes, and make contact with restaurants in the youth s community to set up an interview. The goal is to have job placement upon discharge from the program. Further, the life planner will work closely with Workforce to provide training and placement in jobs in the home community. CARF reviewer s remarks about the G4S Columbus sex offender facility: Program goes above and beyond to find appropriate community resources for the youth and community at large including helping a child find a college and utilizing specialty programming. Dress for success: The life planner will connect with community resources to outfit the youth for interviews, applications, and appointments to prepare for a professional future career. Home Assessment: The life planner will assess the home, environment, school, transportation, post commitment needs, in addition to any additional needs identified during the visit. Results will be forwarded to the JPO, court, and aftercare provider. Safety Plan: A home assessment will be conducted by the life planner, in concert with the youth s parent/guardian. This will identify risks to a youth s timely and effective return, and ensure that everyone feels safe. If security is needed in the home, the life planner will connect with an alarm company to refer the need for an alarm on the youth s window or door. Relapse Prevention Plan: The plan identifies sexual abuse history, daily risk situations, potential victim, warning signs and interventions to prevent potential backsliding behavior. Vocational Rehabilitation: The life planner will ensure an assessment is completed for those applicable youth showing mental disabilities. The life planner will connect the youth to Voc Rehab up to six (6) months prior to release to begin application and pursue post commitment placement. College: Applicable DCF/Foster Care youth will be pressed for GED/High School Diplomas, then will be given opportunities to attend community college following discharge from the program. The life planner will pursue grants that cover a 2-year college or 18- month vocational school. The life planner will participate with the college application process and the college orientation. A final risk assessment (post-treatment risk assessment) will be performed prior to the youth's departure from the program. Results will be communicated to the aftercare provider to ensure a "seamless" transition to outpatient treatment. Final treatment summaries will address the youth s likelihood of re-offending and recommendations for further services. A formal exit conference will be conducted not less than 14 days prior to the youth s anticipated release. Notification and invitation letters will be sent out prior to the meeting to the youth s Juvenile Probation Officer and/or post-residential services counselor, the youth s parent or guardian, and other pertinent parties. The exit conference will be used to review the status of transition activities established at the transition conference and to finalize plans for the youth s release. Those in attendance will be the Treatment Team, youth, parent/guardian, post-residential services counselor, education and other external agencies. Prior to the 14-day exit conference, the lead teacher will contact the receiving district to advise them of the student s return and to seek information needed for re-entry. An exit portfolio will be forwarded to the receiving district contact seven (7) days prior to the student s release to include withdrawal grades, certificates or GED, transcripts, etc. In cases where Victim Notification is required, the life planner will mail a letter to the Victim, the returning school and local law enforcement at least 10 days prior to the youth s release, advising the parties of the release date. Further, educational staff and vocational staff will be notified to allow time for post-testing, in addition to all parties or entities requiring notification pursuant to Section , F.S. Within 24 hours of any release (or on the first regular workday of the following week when the youth is released on a holiday, a weekend or Friday afternoon), the life planner will update the JJIS Bed Management System, which includes a digitized photograph. Prior to updating the JJIS system, staff will ensure entry of the Exit R-PACT information on the released youth. Within five (5) days following release of the youth, the life planner will ensure that all required documentation is forwarded to the post-residential services provider or designated party as applicable. The program will not release any youth who is potentially SVP eligible and subject to the provisions of chapter 394, F.S., until the Sexual Predator Unit at DCF has determined eligibility and the JPO has given DSOP direction to proceed, following receiving the residential notification checklist, performance plan, performance summary, physical health summary, and a psychiatric report. If it is determined by DCF the youth is not subject to civil commitment as a SVP pursuant to Chapter 394, F.S., the DSOP will comply with provisions set forth in 63E (2)(a), F.A.C. The DSOP will maintain internal quality assurance methods to ensure identification and monitoring of time sensitive documentation, requests and meetings. The program will utilize a discharge chronological note which is a working document used to prompt and provide validation for required and completed transition, meetings and documentation. As a part of the G4S Risk Management system, transition activities will be continuously evaluated to ensure timeline adherence, quality of documentation and services delivered. All transition activities, including notifications and exit conferences will be completed in accordance with timeframes specified by the Administrative Rule. A.13. CATEGORY 11: STAFF TRAINING How well does the proposal describe a staff training plan as required by the RFP? G4S has continually shown a commitment to ensuring effective training for all of our employees. Our success at DSOP will be based largely on the foundation established by the quality of the training provided during the orientation phase for new hire staff and the in-service training for veteran staff. G4S programs have consistently exceeded the QA standards in both pre-service and in-service staff training as evidenced by achieving Superior QA ratings. RFP R2107 Page 46
83 Program Services Consideration 1: How well does Provider s proposal demonstrate an understanding of training necessary for direct care staff to perform their duties? G4S understands that success in Juvenile treatment is directly related to how well we train and manage our direct care staff. G4S has demonstrated consistent success at using proven methods that achieve desirable outcomes in these areas. G4S has established the G4S Hastings Training Academy (HTA) to ensure that each staff member is fully-trained on effectively working with juveniles. This academy is the guiding entity to ensure that DSOP, in addition to all G4S staff in the area, receives the highest level of quality training. Under the direction of a Staff Development Coordinator, the HTA conducts all pre-service and in-service training. The HTA Staff Development Coordinator reports directly to G4S Director of Staff Development. To ensure that each newly hired direct care employee receives training that is detailed and specific, the DSOP will use a job-specific training plan. This plan will be designed to guide and monitor the training that each employee receives, while allowing the program to test the competencies of the employee post-training. Additionally, each direct care employee at DSOP will be paired up with a trained staff member during week three (3) of employee orientation. Veteran employees will teach, mentor, and coach new employees through their 90-day probationary period. Job specific training hours will vary according to each position; however, the minimum number of hours devoted to jobspecific training for direct care staff will be 24. Each employee will be fully evaluated within their initial 90 days on the job for competency, and application of training, and the skills needed to perform the functions of a Youth Care Worker. On an annual basis, a Training Needs Assessment will be conducted, followed by the development of a Staff Development Plan. This will be done for all full-time, part-time and volunteer positions to continually measure and strengthen skills. All pre-service training will be provided within the first 30 days of hire and follow the format for evidence-based standards, including the use of pre- and post-tests and clearly defined goals and objectives. The training modules will be cognitive behavioral in structure, which means they are experiential and require active demonstration of skills learned. In addition, an extensive on-the-job training (OJT) plan will be implemented for specific work-related responsibilities (i.e. youth care worker) to ensure the transfer of training from the classroom setting to the field of operations within the facility. All training, instructor-led, along with OJT supervision will be provided by trainers that are highly qualified for the area of discipline. Both internal and external fidelity monitoring processes will be established to ensure delivery of the training curricula as designed. All training modules have been developed in accordance with Departmental standards, Chapter 65D-30 Licensure Standards for Substance Abuse Services and CARF Accreditation compliance. All DSOP training plans will be submitted and approved by the Department. New Hire training classes are provided every two (2) weeks. The Staff Trainer will be responsible for developing and maintaining the preservice and annual training program schedule for all staff including maintenance of all records. All annual training plans will be individualized and developed according to department requirements and designed for ease of use and understanding. A Training Calendar will be developed by the DSOP Training Coordinator and provide, at a minimum: New Hire Training (Monthly) First Aid, CPR and AED Recertification Job Specific/ Site Specific Training Motivational Interviewing 16 hour Certification (Bi-monthly) Annual Instructional Training Thinking for a Change Facilitation Certification (Quarterly) Annual Protective Action Response Updates Restorative Justice/Impact of Crime Facilitation (Quarterly) To ensure compliance to G4S training regimen, the Training Coordinator will maintain a comprehensive tracker that monitors all staff trainings and ensures the Department s LMS/CORE system is current. The Facility Administrator will maintain monthly communication with the Training Coordinator to ensure that all training requirements are met and staffs are being efficiently trained to provide quality care. Consideration 2: How well does the proposal describe a comprehensive training plan to implement orientation and training programs for all new employees, within thirty (30) days of hire, and ongoing staff training to increase knowledge and skills to improve quality of care and training services (outlined in CORE), including specific job responsibilities, care and supervision of youth, first aid, episodic care and CPR as required by Rule 63-7 and the RFP? The G4S Hastings Training Academy, mentioned above, will be responsible for implementing standardized orientation and pre-service training for all new employees within thirty (30) days of hire. The goals of the Training Academy will be to increase the knowledge and skills of new and veteran staff, while continually improving the quality of care provided to the youth we serve. All full and part-time direct care staff will be trained in accordance with Rule 63-H, Florida Administrative Code, including PAR certification by DJJ approved PAR Instructors and overseen for fidelity by Master PAR Instructors. Further, First Aid, Cardiopulmonary Resuscitation and A.E.D. training will be provided by certified trainers. In order to reach those goals, G4S has invested many hours in producing numerous highly qualified trainers for the Hastings Training Academy. With over 32 years of combined training and juvenile justice experience, the G4S trainers will be responsible for ensuring the delivery of a comprehensive training plan and training services as outlined in CORE and required by Rule 63-H and the RFP. To ensure that all training is maintained to the highest standard and can be sustained when staff turnover occurs, G4S has a cadre of certified staff trainers for following Department approved curricula and programming: Impact of Crime Train-the-Trainer Thinking For a Change Facilitator ARISE Life Skills Instructor Impact of Crime Facilitator R-PACT Basic Trainer Trauma Informed Care Motivational Interviewing Training R-PACT Booster Trainer Sanctuary Model Trainer 1 st Aid/CPR, AED Instructor Performance Plan Trainer Conflict Resolution-Peace Keeping Facilitator Thinking For a Change Trainer Master PAR Instructor ARISE Life Skills Instructor RFP R2107 Page 47
84 Program Services PRE-SERVICE TRAINING DURATION PRE-SERVICE TRAINING DURATION Intro To DJJ/G4S DJJ Mission Program Mission, Goals, Service 2 hours Cultural Competence and Trauma Informed Care: Adolescent behavior of boys Risk factors and triggers relating to the youth with history of victimization; PTDS; Exploitation; Domestic Violence; Trauma; Sanctuary Model Professionalism & Sexual Harassment 3 hours Human and Cultural Diversity 8 hours Confidentiality, HIPAA and HIV/Aids 2.5 hours Motivational Interviewing and Communication Skills Ethics within the correctional environment; maintenance of 1 hour documents and recorded material relating to security Child Abuse, Youth Rights, Grievances 1 hour Protective Action Response 40 hours Gang Awareness 1 hour Infection Control 2 hours Mental Health and Substance Abuse 2 hours Fire Safety and Awareness Emotional and Behavioral Development of Children and adolescents; Immediate access to emergency medical, 1 hour mental health, and substance abuse services Restorative Justice 2 hours Emergency Procedures and Tool Management 2 hours Suicide Prevention and Precautions 6 hours Youth Supervision, Safety and Security Risk factors and triggers relating to homicidal risk 2 hours and homicidal prevention First Aid, CPR and AED 6.5 hours Behavior Management and Modification 2 hours Program s Treatment Model Medical/Health Services 2 hours Job Specific Duties 24 hours (List of trainings noted under consideration 4 below) Includes PACT and R-PACT Positive Reinforcement / Effective Principles of Intervention 1 hour Staff Stress Management 1 hour Risk factors for delinquency and their treatment Specialty Services for Sex Offending Population 8 hours Specialty Services 2 hours Rational Emotive Behavior Therapy and Motivational Interviewing approaches to promote healthy mood and behavior regulation, Trauma and grief treatment utilizing the Trauma Focused Cognitive Behavior Therapy (TF-CBT) and Traumatic Grief CBT modality as recommended by Dr. Turner, five basic core treatment areas. These include youth acceptance, correction of cognitive distortions, victim awareness, familial education, and relapse prevention. TOTAL PRE-SERVICE HOURS 138 Hours Important G4S Advantages: Specialized Training: Specific DSOP employees administering the Facility Entry Physical Health Screening Form or the Massachusetts Youth Screening Instrument-Second Edition (MAYSI-2) screening will be trained prior to using the tools and techniques with the youth. Staff that is expected to be part of monitoring the self-administration of mediations will be trained for medication observation and administration by a licensed health care professional. Specialized training will be offered for employees who perform specific functions in mental health/substance abuse or sex offense treatment, case management, medical, security issues or other specialized duties. This specialized training is not included in the above pre-service table. Management Training: All new management staff will receive, at a minimum, 158 hours of training. This will include the 138 hours of pre-service shown on the training list above in addition to attending the 20 Hour Management Development Academy. This exceeds RFP requirements. The management academy will include training in the following areas: Leadership, Accountability, Red Flags, Communication Skills, Creating a Trauma Informed Culture, Medication Administration and Risk Management. Training will be conducted by corporate staff that are highly experienced, qualified and well versed in their respective area. Further, the Facility Administrator, Assistant Facility Administrator and security coordinator will be PAR certified, which exceeds RFP requirements. Consideration 4: How well does the proposal describe providing the training as required in the Health Services Manual (2006)? Medical / Health Services Training: All staff will be trained and certified through the American Safety and Health Institute in First Aid, C.P.R and A.E.D within their first week of employment and are updated annually or as required. In addition, all staff will receive Medical/ Health Services training listed in pre-service and in-service training, and include: 16 hours Hand washing techniques according to CDC guidelines Biohazard waste Standard precautions Medication pass Prevention and transmission of communicable diseases Medical Alerts Common health issues with adolescents On-site doctor visits Site specific infection control Urine collections Updated health issues, Vaccinations Medical emergencies and access Sick call requirements and procedures First Aid, CPR and A.E.D. kits Universal precautions/ blood borne paths (CFR OSHA) Documentation requirements for Non-Licensed health professionals Exposure plan/control of Infectious Diseases Common side effects for youth on medications Emergency evaluation procedures for youth with medical alert Physical development / common health issues of adolescent youth RFP R2107 Page 48
85 Program Services Principles of safe/effective pharmacology/dispensing of medications Use of Knife-for-Life / First Aid Kit Site Specific Infection Control Plan IN-SERVICE TRAINING DURATION IN-SERVICE TRAINING DURATION Professionalism and Ethics 3 hours PAR-Recertification 8 hours Suicide Prevention 6 hours Site Specific Infection Control Plan 1 hour Communication Skills / Conflict Resolution 1 hour Supervision, Safety and Security 1 hour Stress Management 1 hour Balanced and Restorative Justice 1 hour Cultural Diversity 1 hour Sexual Harassment 1 hour Fire Safety and Emergency Procedures 2 hours Gang Awareness 1 hour Medical/Health Services (see consideration 4 for list) 1 hour Confidentiality, HIPAA and HIV/Aids 2 hours Trauma-Informed Care and Cultural Competence 1 hour Gender Responsive / Sex Offending 1 hour TOTAL IN-SERVICE HOURS 32 hours Important G4S Advantages: All staff will receive, at a minimum, 32 hours of annual in-service training, which exceeds RFP requirements. CPR/First Aid renewal is every two (2) years; when due, the employee will attend four (4) additional hours to renew certification. Management: All management staff will receive, at a minimum, 40 hours of training per year, which exceeds RFP requirements. This training will include eight (8) hours of supervisory training in the areas of management, leadership, personal accountability, employee relations, communication skills or fiscal training. In addition, the Facility Administrator, Assistant Facility Administrator and security personnel will be PAR re-certified, although not anticipating being part of the ratio, which exceeds the RFP requirements. Specialty Training: All clinical personnel will receive 10-hours of Trauma Focused-Cognitive Behavioral Therapy Consideration 3: How well does the training plan incorporate the principles of cultural competence and trauma informed care to reinforce non-confrontational interaction? Cultural Competence and Trauma Informed Care: DSOP will provide training on cultural diversity and trauma informed care to all staff during pre-service and in-serving training. The goal of G4S will be to teach staff how to effectively work with youth who have been abused and victimized. The Andrus Center s Trauma Informed Care, Sanctuary Model curriculum, was developed by Dr. Sandra L. Bloom, MD., with whom G4S maintains a strong relationship. In partnership, the Andrus Center has provided consultations, training and assistance in creating a Trauma Informed culture in G4S programs. Further, the Andrus Center has assisted G4S with the Trauma Informed training curriculum development, which teaches the effects of trauma and reinforces non-physical interactions. G4S is proud to present this sensitive, yet comprehensive and dynamic, training that deals with cultural competence and trauma informed care. The goal of G4S is to provide appropriate strategies for working with youth to avoid challenging behavior and possible re-victimization. All staff will be trained in a specific module for increasing verbal skills and utilizing non-aggressive interventions that incorporates Motivational Interviewing and Choice Language techniques. All staff will be trained for management skill techniques to efficiently work with sex offenders with potential mental health, substance abuse, behavioral health and medication symptoms. The modules are designed to be interactive, rather than didactic, to ensure that staff practices the skills that are being taught, and can demonstrate understanding and mastery of those competencies. This has been shown to be a best practice used by G4S. To further enhance skills of clinical personnel, counselors will be required to complete 10 hours of on-line Trauma Focused-Cognitive Behavioral Therapy through the Medical University of South Carolina, which exceeds RFP requirements. A.14. Category 7: LIVING ENVIRONMENT How well does the provider present a comprehensive, coherent and appropriate strategy for involving and interacting with a youth s family? 14.a. LIVING ENVIRONMENT: DSOP will be committed to protecting the youth s physical and emotional safety by teaching and enforcing the use of effective pro-social communication, staff role modeling skills, incorporating community partnerships and providing effective security systems. Youth will have the opportunity to emulate staff s interactions, while learning productive and positive ways to deal with issues. Adequate staffing levels will be followed, and staff will be trained to reinforce firm, fair and consistent treatment to all youth. Motivational interviewing techniques will be used to strengthen the youth s relationship to his family or guardian. Regardless of experiences, youth have need to feel a sense of belonging to a family environment, which G4S will provide. We have designed the We connect to YOU project (to the right) to teach youth that it takes many types of external connections to discover one s internal sense of wholeness. This design allows youth to find true happiness and success through connections of: parent/guardian, spiritual, health, cultural, peer, community, and jobs (see full design and description on pages 67-68). Consideration 1: How well does the Provider provide ongoing and direct avenues of communication to the family members? Youth at DSOP will be expected to participate in campus-wide events that support a positive living environment. G4S recognizes that one (1) of the main contributors to youth success is the positive support and involvement of the family. Therefore, the inclusion of family participation will be continually encouraged to blend campus activities that enhance progress and relationships. In order to motivate parents/guardians, the DSOP will consistently promote family engagement in daily activities, treatment and progress. First, this will be accomplished through a multitude of established communication sources consisting of, but not limited to: RFP R2107 Page 49
86 Program Services Admission notification contact calls Administering weekly, monthly, quarterly family surveys Mailing Parent Handbook and admission letter Bi-annual family conference Weekly telephone contacts by the case manager Providing accessibility to communicate via Weekly telephone calls by the youth Family orientations facility tour Counselor interviews, consultations, phone contacts Invitation to attend/provide input at transitional activities Mailing of the youth s weekly behavior evaluation sheets Mailing invitation and calendar for formal progress reviews Mailing of a DSOP facts sheet Mailing of performance summaries that document progress Next, G4S will engage families in special campus activities where families can be part of youth learning the importance of giving back to others in need. These will include at a minimum, participation with volunteers, guest speakers, teen musical group presentations, advisory board members, tutors, victim rights groups, faith based groups, and guest speakers as part of valuable, restorative justice projects to benefit families and the community. A.14.a.1. Input from Youth: Communication will begin within the DSOP community and then extended to family involvement. Youth at DSOP will be encouraged to provide input on rules governing community living, program design, and evaluation in various ways: Youth will participate in weekly community (house) meetings with Treatment Team members. This forum will be designed to discuss agenda items that include facility programming and living community specific issues. Information will then be forwarded to the management team for discussion with the youth. The program will have a bi-weekly Youth Advisory Board chosen by the administrative team. Board members will be expected to meet certain behavioral and performance criteria, assist in problem solving and decision-making, planning, teamwork, and report the information back to their living unit through house meetings and informal conversations. Youth will participate in monthly surveys that directly affect their program as a community such as food service, treatment, case management, education, medical, etc. The results will be used to identify trends and make changes. Youth will be given the opportunity to learn and practice leadership skills, presentation skills and openly address complaints or observations of their peers. DSOP will support mentoring programs and activities that promote the pro-social expected norms. A.14.a.2. Communication and listening: It has been the G4S experience that open communication lines contribute significantly to a safer and more secure environment, as subtle changes in youth attitudes and behaviors are noticed more quickly. In building a strong program, all members of the DSOP community will effectively communicate with each other that will be also integrated into family relationships. All management staff at DSOP will adhere to an open door policy for staff and youth to communicate through informally requested closed or open meetings. This will allow direct communication in a positive atmosphere. In addition, surveys and youth advisory board meetings will allow youth on-going communication of ideas and feedback to better serve the program. DSOP will hold daily, weekly, and monthly staff meetings to evaluate services, operational procedures, and discuss future plans. Consideration 2: How well does the Provider include specific mechanisms for soliciting input from the family members? A.14.a.3. Relationships: The DSOP will provide opportunities for youth to build relationships of trust and interdependence with families, peers, staff and volunteers. In order to accomplish this, mechanisms will encourage family input and participation. DSOP will maintain resources that promote internal, healthy growth. First, the DSOP will use established mechanisms where opportunities are available for families to give input. These will include contact with families during orientation, assessments, treatment and performance plan development, treatment team, visitations, weekly calls to parents by case manager and/or case manager, family therapy session, satisfaction surveys, invitation for youth birthday celebrations or other special activities that celebrate the youth s success. Next, the DSOP will target support systems that will be integrated into the youth s activities to build trust. Families will be encouraged to partake in the activities, or to give input on the activities and progress made by the youth. The DSOP Chaplaincy Program will be established where volunteer clergy from the community will be matched to each youth s personal faith. This clergy will have unimpeded access to the campus, and will be integrated into the relationship of the family, if both youth and family are willing. Also, the Chaplaincy Program will be utilized as the best practice, where the matched clergy is notified in the event of a crisis with the youth. Further, the DSOP will offer spirituality events several times a week on a volunteer basis. If parental input identifies the request for personal involvement in the spiritual activity, the DSOP will make every effort to accommodate. Life Skills will be implemented to strengthen and build relationships, and family input will be sought to confirm the progress being made. Family visitation will work on strengthening communication and trust. DSOP staff will serve as role models to teach youth the importance of respect, and the program will hold special activities on a quarterly basis that includes the participation of family members. G4S will strive to provide more than 70 opportunities per month for parents to provide input. A.14.a.4. Cultural diversity and identification: In order to fully strengthen the youth and his family cohesiveness, G4S is committed to reflecting the context of individual, cultural and ethnic variables. This will include our We connect to YOU design (Exhibit 6, pages 67-68), where G4S will integrate cultural connection in all treatment and service intervention systems. This commitment goes beyond simple sensitivity to cultural issues, and incorporates staff training, involvement of the family, care-giver and community, and ensuring that assessments and evaluations are not influenced by cultural or other bias. A variety of cultural activities will be held on a quarterly basis to familiarize youth with cultures different than their own, and youth and families will be encouraged to discuss potential cultural bias. RFP R2107 Page 50
87 Program Services A.14.a.5. Positive identity, self-esteem, self-respect and respect for others: Respect is one of the hallmarks of the program and will be a basic rule of conduct that all staff and youth are trained to model. Self-esteem and self-respect will be enhanced by the visual display of youth s work and recognition of their efforts and achievements during formal events including graduation and award ceremonies. Parental input will be encouraged as a means of providing positive reinforcement to youth and as suggestions to further encourage youth talents. A.14.a.6. Opportunities to create positive changes to benefit youth: Many of the positive change opportunities G4S will provide for youth will occur in treatment groups, recreational activities, dining, hygiene, educational forums and in normal daily conversation with staff. All youth will be required to meet the following expectations in order to be rewarded for positive behaviors: 1) follow program rules, 2) have no education disruptions, 3) facilitate Daily Reflection Groups; and 4) participate in groups. Families will have opportunity to experience the growth and maturity of their youth. Daily reinforcers will be consistently provided throughout the day to encourage good decisions. A.14.a.7. Reasonable opportunities for visitation, correspondence and telephone access: Consideration 3: How well does the Provider include provisions to allow youth to have access to visitors (family)? Visitation: G4S recognizes the need for flexibility in scheduling visitation with families so that family connections are strengthened and maintained. An authorized visitation list will be developed for the youth upon admission to the facility, and only authorized visitors will be allowed on campus. Each youth will be given the opportunity to visit with approved visitors on Saturday and Sunday; however, unlimited visits by attorneys or legal representatives, juvenile probation officer, and the Department of Children and Families, Family Services Workers will be permitted. The mental health professional will be available during visitation hours for scheduled and unscheduled family sessions and interactions scheduled to accommodate family s needs. Through requests to the Facility Administrator or designee, flexible and extended visiting hours will be provided for for visitors who are unable to visit at regular times. All visitation rules will be explained to the youth and family during orientation and included in both the Resident and Parent Handbooks. In addition to regular weekly visitation opportunities, the program will provide a range of varying activities available to youth and families that will be designed to promote family reunification. Every three (3) months, the program will host a Family Fun Day event that is open to parents/guardians, siblings and grandparents. Family therapy services will be available to all youth and families at DSOP with family therapy sessions offered as often as needed. These provisions for family visitation access will include special and scheduled weekly visitation, weekly telephone calls, family therapy sessions, written correspondence, communication, and the possible implementation of internet webbased visitation or therapy. Strong family and community connections increase the probability of success for a youth after release. Correspondence: Youth admitted to DSOP will be provided postage, envelopes, paper and writing implements for a minimum of two (2) letters per week to all approved persons. The amount of mail a youth may receive will be unlimited, unless there is clear and convincing evidence to justify a specific limitation. Mail will be delivered and sent out at least once per day Monday through Friday, excluding holidays. All incoming letters and packages will be opened and inspected for contraband in accordance with the Florida DJJ administrative rule. Youth will be allowed to send uncensored, unopened mail to the court, attorney and DJJ officials. Telephone: Telephone contact will be an effective tool for reducing a youth s tension and anxiety in the program. Upon admission, the telephone correspondence process will be discussed with the youth and his parent to identify who the youth may contact. A Resident Handbook and a Parent Handbook will be issued for further reference of processes. DSOP will provide, at a minimum, one (1) 10-minute telephone call per week to each parent/guardian, with the opportunity to earn two (2), twenty-minute telephone calls in accordance with the BMS. Additionally, an extra call will be permitted on holidays as a support to the youth. If the parent or guardian is unavailable, a message will be left to encourage a call back. Telephone calls will be private and will not be restricted unless they present an adverse disruption to treatment or security. Staff will maintain a record of all telephone calls in a logbook that verifies pertinent information. Consideration 4: How well does the proposal describe its capacity to provide for comfortable visitation areas? DSOP will make every effort to assist the youth in maintaining and strengthening positive family and community ties in an environment that unobtrusively monitors and controls movement of visitors within the program. Visitation will be supervised by staff that provides privacy for appropriate, contact visits. The DSOP will provide different locations for visitation, depending on the weather conditions. The primary location will be the facility s dining hall, due to the large, comfortable area equipped with ample couches, tables and chairs. G4S will implement its color connection scheme and theme (further discussed on the next page) as a best practice of correlating mood, color, and theme in our sex offender programs. The relaxed area will be neatly painted, color coordinated, and well lit to provide a calming and interactive environment. Walls will provide gender specific artwork representative of healthy male role models and themes. Positive Art of Hip Hop projects will display inspirational messages referencing truth about harm from drugs, alcohol, and crime. In the event a backup area is needed, DSOP may use the activity group room, which will also follow the color connection scheme and theme. Refreshments will be available. When weather permits, the DSOP will utilize the outdoor pavilion area that gives families opportunity to talk, play games and interact with each other. To strengthen communication and elicit family participation, the DSOP will use a family informational board (pictured on the right) in the visitation area that will contain posters and announcements describing upcoming facility events. In addition, this board will provide information relating to treatment issues, medical issues, restorative justice projects, incentive and reward programs, on-site and off-site activities, and Treatment Team schedules. On occasion, the RFP R2107 Page 51

88 Program Services DSOP will schedule special performances during visitation, where youth can choose different types of art for self-expressing messages of accountability, hope, and change. G4S will continually encourage youth to communicate through verbal and non-verbal channels that allows for messages to be delivered. This will not be limited to Hip Hop break dancing, drums, music, and stage performances. Consideration 5: How well does the visitation procedure address possible security concerns (escape, contraband, weapons, etc)? DSOP will maintain visitation safety and security procedures to ensure youth, staff and all visitors remain safe. In order to ensure that all families are familiar with the visitation rules, each parent will receive a formal orientation letter from the Facility Administrator at admission that includes the visitation rules. In addition, the Facility Administrator will send a formal letter to parents and guardians prior to each special event to encourage attendance. G4S recognizes that visitation and special events can become disruptive to the regular daily schedule and can become an opportunity for a youth to contemplate absconding from the program. The shift manager will identify staff member(s) to supervise visitation, monitor the location of the families and the positioning of staff, and follow all procedures to ensure the campus is safe and secure, while maintaining ratio. All approved visitors 14 years of age and older will be required to present a picture ID. No bags, food, money or gifts will be allowed in the visitation area without prior authorization from the Facility Administrator. Searches of the visitation area will be conducted before and after each visitation for contraband, weapons, escapes or other safety/security issues. Youth will be frisk-searched after each visitation is completed. Program rules, including dress code, will be explained to visitors and all visitors will be wanded and frisk-searched by a same sex staff member. Any visitor who refuses a proper search will be denied access. Any contraband discovered will be immediately confiscated, delivered to the management staff on duty and documented with required processes being followed. In the event that illegal contraband or weapon is found, or if a disruption ensues with visitors, Law Enforcement will be notified. A.14.a.8. Use of Trained Volunteers, Mentors and Others: Community Partnerships and Participation: G4S will follow the principle of engaging on-going natural support in communities, which is an Evidence-Based Principle of Effective Interventions and follows the Restorative Justice philosophy. Mentors will be established in the residential community of DSOP, the Daytona community, and the home community where the youth will return. Local victim service providers, community volunteers, and G4S advocates in other programs will be utilized as mentors at DSOP to provide opportunity healthy support systems (further community opportunities, page 59). A.15 CATEGORY 12: BEHAVIORAL MANAGEMENT SYSTEM How well does the proposal describe the Behavior Management System to be implemented? Consideration 1: How well does the proposal describe the behavioral management system, a positive behavior reinforcement system, and the underlying theory? Consideration 6: How well does the proposal describe the youth s motivational factors, determined via assessment, are taken into consideration when the Behavioral Management System (especially in regard to rewards and punishments for the youth), is established? A.15.a. BEHAVIORAL MANAGEMENT SYSTEM: The population at the DSOP is comprised of a unique sex offender population; therefore, G4S will tie the behavior management system to its distinctive 3-sector approach to attain premier benefit to a population whose reputation shows it is the most difficult to change. This will be through stimulation of: 1) color connections, 2) cortisol levels, and 3) positive and negative reinforcement. G4S prides itself on the most recent research where specific factor(s) influence and result in an effect, or does not show an effect but is believed to have an effect. The first sector of the behavior management plan will induce mood as a result of color connection. This color connection scheme and theme plan will utilize colors throughout the environment that include those in the upper half of the mood chart (pictured to the right). These are expected to create more relaxed environments that reduce stress, anxiety, and tension. As a result, our residence will be able to maximize learning that is often blocked by anger and maladaptive behavior. Throughout the facility, G4S will implement visuals that follow primary and secondary colors of blue, green, and yellow. These will not be limited to verdigris to celadon (euclase), teal to cyan (aquamarine), cobalt blue to sky blue (sapphire), green aurora to cat eye green (chrysolite), jade green to light green (emerald), violet-blue to lavenflower (lilite/lapis), magenta to blush (rose quartz), and purple green to indigo green (chrysocolla). A second factor significant to color is the actual theme / message that will be transmitted through color, either in covert or overt manners, as continual reinforcers to encourage positive behavior. The outcome is expected to increase sensitivity, relaxation, stimulation, acceptance, inquisitiveness, harmony, tranquility, reflection, perception, and involvement. The second sector of the behavior management plan will be to integrate the life coach s wellness plan that will include distinct types of exercise that are expected to result in healthier cortisol levels. Physical and mental wellness will allow the youth stronger ability to think constructively, rather than pathologically. Research has found that salivary cortisol levels were strongly and inversely related to aggressive conduct disorder, peer aggression and oppositional defiant disorder. It is believed that male youth with lower levels may not be as afraid of retribution (University of Chicago Medical Center, 2000). Further, cortisol elevations are one (1) mechanism through which stress affects learning and memory (Abercrombie, Kalin, Thurow, Rosenkranz, and Davidson, University of Wisconsin, 2003). In the short term, high levels of cortisol help the body respond to stress; however, in the long term, high levels of cortisol are linked to a range of physical and mental health problems (Ruttle, Science Daily, February 10, 2011). Further, high levels of cortisol increase blood pressure and blood sugar, weaken the immune response and can ultimately lead to inflammation and damage of the organs. Sleep problems, weight gain, and impulsive behavior are common issues often shared by our sex offenders. RFP R2107 Page 52
89 Program Services The third sector will be to implement a behavior management system (BMS) that is responsive to the unique needs, characteristics and motivations of the youth. It will foster accountability for behavior and compliance with the rules and expectations of the residential community. The BMS will be based on social learning theory and operant conditioning research and incorporates the Stages of Change and Motivational Interviewing techniques. DSOP will use an award system which research has shown to be effective. The goals of the BMS will be to develop the youth s self-monitoring and self-regulation skills, improve emotional and behavioral functioning, address and eliminate criminogenic behaviors/needs, and promote pro-social behavior and competencies that encourage self-growth and law-abiding behavior. Behavior modification will be accomplished through the provision of positive reinforcement (award of points and privileges). This will utilize reinforcers that motivate youth when specific behavior change is achieved or goals are accomplished. There is application of negative punishment (removal of privileges) to modify or extinguish maladaptive behavior. Rewards and punishments will be assessed and individualized, based upon the youth s motivational factors and stage of change. Rewards will be both tangible and intangible and administered at scheduled, intermittent, and random intervals. Rewards will not be provided when not earned. Punishers will be related, logical consequences to encourage youth to meet expectations for appropriate behavior. In most cases, consequences will be tied to the youth s level system and/or Performance or Treatment Plan, and will incorporate the principles of restorative justice. The BMS will not be used to increase a youth s length of stay in the program or to deny basic rights or services. Use of group discipline, allowing youth to sanction other youth, and using disciplinary confinement will be prohibited. Further, G4S will implement our We connect to YOU design (Exhibit 6, pages 67-68) into the BMS, where youth can earn the privilege of being part of job connection training and activities, based on leadership behavior that will extend into community jobs once discharging from the program. Upon program admission, each youth will receive a Resident Handbook that clearly describes the BMS and includes the program rules, expectations and consequences for both positive and negative behaviors. Youth will earn points/credits each day for complying with scheduled activities, participating in mental health groups and delinquency intervention activities, maintaining a positive attitude, following the rules, and developing positive relationships with staff and other youth. The performance points will be applied weekly toward the youth s stage advancement and opportunity into job connection. Staff will consistently award extra reinforcers when exemplary behaviors exceed minimum compliance standards. All youth will be given phase packets at the beginning of each level that detail the progression requirements to the next level, rewards for pro-social behavior and punishers for misbehavior. The phase packets will contain readings and assignments at each stage of change, with Motivational Interviewing techniques being used to elicit self-motivational statements from the youth. At the end of each week, evaluation sheets will be calculated and level points/credits awarded for the required areas of compliance, and posted on the hall. During community group, the Facility Administrator or designee will review the weekly evaluation sheets, total cumulated points for each youth and publicly recognize the individual progress from the previous week. The youth will personally review progress at bi-weekly Treatment Team meetings, with information being mailed to parents/guardians and discussed via phone with the case manager weekly. The program will use a four (4) stage system with graduated responsibilities and privileges and incentives to motivate toward improving performance. These will include initial phase, historical phase, integration phase, and transition phase. The system will provide positive reinforcement and recognition for accomplishments and positive behaviors. The following diagram represents a sample of the first stage, which is Initial Phase. Additional detailed description of DSOP s behavior management phase system is shown as Exhibit 4, beginning on page 64. Level Name How to Advance Privileges Phase 1 INITIAL PHASE Phase one is designed to allow you to take responsibility for your actions and offense, and decrease your level of denial As a resident, you will be required to gain a greater understanding of victim awareness and the impact of crime. You will learn the rules and regulations of the program and demonstrate verbally and physically your understanding. You will comply with all aspects of the assessment and treatment planning to include educational testing. You will identify methods and timelines to achieve treatment plan and performance plan objectives and goals You will not exhibit physical aggression toward staff or peers. You will participate positively in group and individual therapy. You must develop and write out your group introduction and demonstrate the ability to begin group with your group introduction. You must have your hair cut with a two guard You must earn designated daily points and tokens Required assignment: You must write out your commitment phase and share it with the community and treatment team. Victim Awareness requirements to phase up: To be able to identify the stake holders: (Victim, Offender & Community) To be able to identify the four harms: (Physical, Financial, Social & Psychological) To identify the stinkin thinkin (Rationalizing, denial, minimizing and victim blaming) Restorative Justice A way of looking at crime by focusing on the harm created by the offender when a crime occurs; primary victims; secondary victims To attend all victim impact groups. One 15 min. weekly phone call Mail privileges Socialization during meal times Recreational time Decorate your room with pictures, drawings, etc. in your designated area. (Please note that all property that is displayed in the designated area must first be approved by the Assistant Facility Administrator with the approved hole punch). Integrating climate action into the behavioral management system: Over the last several months, G4S youth and staff have implemented projects that dramatically effect changes in conservation. As a result, our accomplishment involved 490 G4S-DJJ youth who earned RFP R2107 Page 53
90 Program Services opportunities to participate in successful events such as the Avon Park Youth Academy solar water heater project, re-roofing resident duplexes, recycling projects, preventative a/c maintenance project, light efficiency project; Hastings Youth Academy Greenhouse project; the Okeechobee Juvenile Offender Correction Center solar lights and panels project, motion detector/light control project, garden project, computer project; and the Davidson County Juvenile Detention Center Going Green Art Project (Exhibit 5, page 66). If awarded the DSOP contract, the DSOP will be expected to participate in projects that positively impact conservation. Consideration 5: How well does the proposal s description of the BMS ensure rewards to punishment shall exceed 4 rewards: 1 punishment ratio? The Behavior Management System will feature a small number of reasonable program expectations that will be based primarily upon the physical and emotional safety and respect for the youth and property of others within the residential community. Consequences for both positive and negative behaviors are clearly articulated in the Resident Handbook, assessed and individualized based on the youth s motivational factors and discussed with the youth during the orientation process, community meetings and informal and monthly Treatment Team meetings. G4S successful sex offender programming experience will exceed RFP requirements for the Department s suggested 4:1 reinforcement ratios. Rather, G4S will follow its experience of providing consistent, positive reinforcement from all levels of staff throughout the day, using an 8:1 ratio of positive rewards to negative consequences. The following list of positive reinforcements has won Best Practice awards and will be utilized by DSOP: Pro-social Behaviors and Positive Reinforcement Examples Pro-Social Behaviors Daily Reinforcers Weekly Reinforcers Monthly Reinforcers Comply with scheduled activities Participate in mental health groups Participate in delinquency services Maintaining a positive attitude Develop positive relationships with staff Develop positive relationships with youth Work on performance/treatment plan Exemplify a Pillar of Character Follow directions without prompts Encourage a peer to follow directions Engage in positive conversations Participate in school Maintain hygiene, dress code, clean room Comply with schedule Follow bedtime rules without prompts Walk away from a verbal altercation Walk away from a physical altercation Offer positive advice to other peers Help other peers with schoolwork Demonstrate leadership Maintain line movement Display appropriate manners Redirect other peers from teasing/bullying Praise and complement others Verbal praise Smiles Thumbs Up Pat on back Certificates Announcements Stars Stickers Unit jobs Points/Tokens Level Privileges Earn Your Day Special Activity Extra letter writing materials Photographs Morning Expectations Groups Evening Reflections Groups Special activities Extra recreation time Extra phone call Later bed time Extra time in game room Burger Bingo Arts and Crafts Music and Poetry Events Clean Room Awards Trivia Contests Spelling B s Points / token Level Privileges Community Meetings Informal Progress Review Special Visitation Weekly Incentive Party Pizza and Wings McDonalds Family Feud Video Game Night Chinese Food Night Bar-b-ques Fish Frys Resident Council Leadership Club Platinum Breakfast Hall of the Month Party Cultural Meal for Facility Special Activity Day Unit Birthday Party Facility Activity Theme Day Points/Tokens Level Advancement Monthly Treatment Team Meeting A.15.b. BEHAVIORAL ACCOUNTABILITY WITHIN THE RESIDENTIAL COMMUNITY: In compliance with Rule 63E-7.009, F.A.C., the BMS fosters accountability for behavior and compliance within the residential community s rules and expectations. Youth will not be violated for an event that is a potential crisis resulting in subsequent placement on Precautionary Observation or Mental Health Status. Infractions are designed to model society s rules and the residential community will be expected to provide an environment free of victimization and maladaptive behavior. The Treatment Team will determine the youth s consequences for violations of community rules, taking into account the youth s motivational factors determined by assessment and the severity of the infraction. Using Restorative Justice principles, consequences will be intended to address the harm caused to victim(s) and other community members, and provide opportunity for reparations to the victim(s) and community. Any violations that relate to the youth s criminal behaviors may indicate the need for a revision to the Performance Plan. Major violations will be considered to be more serious violations of the community rules and result in emergency Treatment Team meetings with the youth, parent/guardian, JPO and other involved persons to process the incident, identify consequences, and modify the Performance/Treatment Plan as deemed necessary. Following are examples of major violations: Major Violations Bedtime Non-Compliance Gang related behavior, activity or drawings Boundary Violation Physical Altercation or threats Tattooing, Destruction of Property Possession of Major Contraband Racial / Gender-Biased Comments Disruption of any Activity Positive Home Pass Drug Screen Stealing or forgery Dismissal from Group Arguing with Staff Lying Talking During Med Pass Lewd and Lascivious Behavior Breach of Confidentiality Out of Area Consideration 3: How well does the proposal describe a training plan for staff regarding the Behavior Management System? A.15.c.d.e. TRAINING PLAN: G4S has developed a comprehensive pre-service training module for all staff on the implementation of the behavior management system. In accordance with Rule 63H, F.A.C., this two (2) hour module will be provided to all staff, subcontractors, educators, and volunteers, during the first week of the training cycle for new employees. It will include an introduction to the principles and philosophical RFP R2107 Page 54
91 Program Services orientation of the behavior management system, the use of rewards and consequences, verbal crisis intervention and de-escalation skills and the use of safety plans. Continuous training on the behavior management system will be provided to all staff, on a monthly basis, during campus-wide and departmental meetings. Additionally, DSOP will work collaboratively with the Volusia County School Board to provide joint training sessions to the educational and program staff on the DSOP s behavior management system that will include, but not be limited to, classroom management, implementation and enforcement of the common discipline plan. Consideration 2: How well does the proposal explain how the Provider will prepare and plan with the youth for crisis prevention, as part of the BMS? Crisis Prevention Preparation: DSOP will follow a crisis prevention / intervention plan that prepares both the youth and staff for situations that can evolve into a crisis. The Crisis Plan will focus on recognizing the signs of potential crisis, responding quickly and regrouping the focus. Quality monitoring of the crisis prevention as part of the behavior management system will ensure that youth are not given consequences because of a potential crisis event; rather, staff understand the reasons for the youth s crises and make a referral to Master s degree clinicians for further crisis assessment. The assessment will be reviewed and signed by the licensed mental health professional. The plan for crisis prevention will be to thoroughly train staff and youth on prevention strategies and intervention techniques. DSOP will prepare the staff for crisis prevention through training in the following areas: learning how to de-escalate negative situations and disruptive behaviors without using physical techniques; understanding the reasons for the youth s crisis; 3-hour Trauma Informed Care; 10-hour Trauma-Focused Cognitive Behavioral Therapy Training course (for mental health counselors); understanding the Crisis Response Plan; learning how to conduct community meetings that address and resolve problems without reaching the level of crisis; understanding the Safety Plan for youth; and learning how to help youth recognize precipitating events. Annual in-service training will further train staff how to respond effectively to a youth in crisis and understand the role that trauma history plays in triggering a crisis. DSOP will prepare youth for crisis prevention through the following measures: Conduct risk assessments to identify youth with histories of trauma, violence and/or behavior management issues Conduct mental health crisis assessments of youth when indicated Employ crisis intervention techniques to resolve acute emotional or behavioral problems Help youth to identify precipitating events, learn how to alleviate distressing symptoms and regain normal functioning Implement mental health alert status placing the youth on One-to-One or Constant Supervision when indicated Develop safety plans for youth with identified trauma, violence and/or behavior issues and include the youth s triggers, high-risk situations, coping skills and staff support strategies Incorporate Safety Plans into the youth s treatment plan and aftercare plan and update as needed Provide copies of the Safety Plan to the youth and assigned staff for use when needed and share plan with parent/guardian Develop a Behavior Management Plan for youth with severe chronic internalized/externalized behavior problems Utilize effective treatments of Trauma-Focused Cognitive Behavioral Therapy and the Adolescent Coping with Depression Course Conduct community meetings to address and resolve problems within the residential community Research shows that many juvenile offenders have been exposed to traumatic events, either as victims or witnesses, resulting in many youth developing Post-Traumatic Stress Disorder (PTSD) or trauma-related symptoms. The goal at DSOP will be to maintain a safe and non-violent environment. To achieve a safe and healthy residential community, G4S will cultivate a trauma-informed culture that is sensitive to and meets the needs of the youth and staff. At the first signs of a potential crisis, the youth will be encouraged to use the conference request process, which is an informal process of encouraging the youth to communicate feelings and thoughts. G4S will employ the most effective, least restrictive, and safest techniques for the modification of maladaptive behaviors. As additional support to the youth in crisis, DSOP will activate the voluntary Chaplaincy Program. This will immediately notify the youth s designated spiritual clergy and access to the youth will be granted. G4S will operate its residential community on the principles that residents are considered the most powerful influence in helping each other during times of stress and crisis. Youth will be encouraged to lean on each other as a support system and peacefully resolve conflict. Consideration 4: How well does the proposal describe how the Provider will monitor the staff and youth s daily activities to ensure consistency with the treatment and the behavioral management philosophy? Fidelity Monitoring: G4S operates effective behavior management systems that have resulted in numerous programs receiving excellent scores for DJJ QA reviews. The Facility Administrator at DSOP will serve as the Youth Advocate and oversee the BMS. The daily activities of staff and youth will be carefully monitored to ensure consistency with the treatment and behavioral management philosophy of the program. Daily management meetings will review and discuss program events and issues, CCC reports, PAR reports, shift reports, occurrence reports, grievances, and Let s Talk forms. The Assistant Facility Administrator/designee will conduct reviews and observations of the direct care staff providing care and custody services. The Assistant Facility Administrator or designee will conduct daily checks of the Master Control Schedule for scheduled activities and groups. Key management staff will conduct daily facility inspections to observe the treatment of youth. The Facility Administrator and management team will maintain close communication with the youth at weekly community meetings, bi-weekly performance reviews, monthly Treatment Team meetings, Youth Advisory Board meetings and Resident Council meetings. The management team will review BMS data. The licensed mental health professional will observe the provision of clinical and delinquency intervention services and conduct weekly clinical supervision with the mental health counselors and delinquency intervention facilitators. The management team will facilitate the monthly Scorecard process, mock QA audit and comprehensive reviews of management, operations, mental health, medical and case management practices, processes and services, sample chart reviews, and youth and staff interviews and surveys. The management team will conduct monthly campus-wide meetings for all staff members and teachers to disseminate information related to the BMS. RFP R2107 Page 55
92 Program Services A.16. CATEGORY 13: RELIGIOUS/SPIRITUAL OPPORTUNITIES How well does the proposal define a plan for access to Religious Services and Recreational and Leisure Time Activities, as required by the RFP? Consideration 4: How well does the proposal describe access to religious services? A.16.a. Spiritual Opportunities: G4S has uniqueness in its partnerships with community ministries to provide powerful spiritual and emotional support to our youth. G4S has established a relationship and commitment from Rev. John Ferro to continue his relationship with the. Rev. John has been affiliated with the program for several years and has been instrumental in recruiting faith based providers (see Exhibit 7, beginning on page 69). Rev. John is supportive of bringing community college teams with the Campus Crusade for Christ to mentor to the youth a couple of times a year. Further, Rev. John has proactively offered to provide faith-based volunteers to exceed the current availabilities. The DSOP will have an identified spiritual coordinator who will work in concert with youth and community ministries to provide diverse spiritual activities at the program. Spirituality opportunities will be offered, at a minimum, at least three (3) times a week through numerous projects that not only connect youth to peers and staff, but encourage connections to the surrounding communities. Limitations will apply only when the activity threatens the safety of the youth and/or others, or disrupts order in the facility. The purpose of our strong religious / spiritual program at DSOP will be to offer culturally neutral values that enhance human growth and offer perspectives that look beyond cultural materialism. Youth will be encouraged to explore their spiritual resources for growth and change. Religious activities will be consistent with religious beliefs and will include access to publications, congregate worship services, counseling, fellowship meetings, study classes, mentoring, life skills training and adherence to dietary requirements. The DSOP will establish the Volunteer Chaplaincy Program, which will allow each youth to be matched up with clergy of his personal faith. If requested by the youth, the clergy will be called during a significant crisis, as an additional support system and as a best practice. This partnership will tie together the dynamic relationship of DSOP youth with community spirituality teams. Further, the DSOP life planner will connect the youth to his home community faith group during the last phase so that relationships are established and can continue once he returns home. The home church will be invited to visit the youth while in the program, and encouraged to be part of the development of the youth s spiritual plan that he will follow post commitment. The goal will be to bridge the transition process from the program to the youth s community, with local chaplains offering pastoral care, support, and counseling to the youth and his family. Consideration 2: How well does proposal describe schedule for religious services and recreational and leisure time activities (including weekends)? A.16.b. As part of our We connect to YOU design (Exhibit 6, pages 67-68), G4S will integrate the many connections we believe are part of the helping the youth to become whole. Parent-guardian connection will take place on Saturday and Sunday, spiritual connections at least three (3) times a week, health connection, cultural connection, and peer connection five (5) days a week during leisure awareness, and community awareness during monthly scheduled events as needed for community volunteers. G4S will encourage youth to address their personal spiritual health and inner strength through weekly volunteer mentoring, cultural activity days, cultural food days, and cultural art and music projects. G4S is committed to providing services, programs and intervention systems that encourage youth to be strong, centered and at peace within the context of individual, local and regional cultural and ethnic variables. We will promote spiritual and character-building practices that include time for personal reflection, cultural traditions, rituals and discussions about life, guidance values, morals and ethics. All youth will be permitted to participate in religious services and programs on a voluntary basis. Adequate time will be built into the schedule to allow youth to take advantage of religious services, activities and personal reflection. The program will maintain safety and security during spirituality and leisure activities by maintaining, at a minimum, 1:6 staff to youth ratio. The following is a sample schedule of DSOP structured spiritual and leisure activities: Time Weekday Time Weekend 6:30-7:00a Breakfast 8:00-8:30a Breakfast 11:10-11:40a Lunch 11:30-12:15p Outdoor Activities 4:15-4:45p Leisure Awareness 12:15-12:45p Lunch 5:45-6:15p Dinner 12:45-1:45p Visitation / Educational TV / Movies / Board Games 6:15-7:15p Recreation 1:45-2:45p Arts Programming 7:00-8:00p Spirituality (Tues and Thurs, 7:00-8:00p) 2:45-3:45p Team Building Activity 7:30-8:45p Privilege Time 4:45-5:45 Recreation 5:45-6:15p Dinner 6:15-7:30p Special Events / Snacks / Spirituality (Sunday) 8:45-9:30p Privilege Time Consideration 3: How well does the proposal s staffing pattern allow for adequate coverage for religious services and recreational and leisure time activities as offered? To maintain safe and secure program operations, G4S recognizes the need for adequate staffing in all activities, including religious/spirituality, recreational and leisure time activities. When activities involve youth to be separated from the population, DSOP will continue to maintain 1:6 ratio to ensure staff are placed in the visitor area for safety and security. Off campus activities maintain 1:4 staff to youth ratio, which exceeds RFP requirements. In addition, DSOP will deploy clinical, case management, administrative, and supervisory staff that are regularly scheduled to work weekends and holidays. Staffing levels will provide active supervision of youth, suitable and timely response to the youth s everyday needs and immediate response to emergencies. The staffing pattern will include a shift relief factor (SRF) of 1.67 FTEs to provide for staff coverage and supervision during weekends, holidays, vacations, training, and absences. RFP R2107 Page 56

93 Program Services A.17. RECREATIONAL AND LEISURE TIME ACTIVITIES Consideration 1: How well does proposal describe youth input to ensure activities are meaningful and encourage positive interaction/ participation? G4S commits to establishing a Therapeutic Community within the residential setting. The Therapeutic Community can be an invaluable tool in helping adolescents develop into responsible young adults and mirrors external community norms and expectations, with the purpose of making a more fluid transition for the youth into the real world. Therefore, all areas of the youth s academic, social and personal behavior will be related to sex offense specific issues. For example, if a youth depersonalizes or is disrespectful to female staff, this behavior will be treated as a "lapse" or "relapse. By linking day-to-day behavior to prior sexual offenses, youth will learn to identify high-risk situations and practice new coping skills for use after release. Recreational policy at the program will take into consideration the unique needs of the population while ensuring prevention of inappropriate touching. Contraband lists will be individually tailored to each youth s treatment plan to control material that may stimulate deviant fantasies. G4S places importance on youth being part of the discussion and planning of recreational activities, leisure time activities and spiritual activities of their faith. To maximize opportunities to receive input, G4S will hold weekly community meetings, monthly Treatment Team meetings, Youth Advisory Board meetings, conference request, youth surveys, shift report, and daily interactions with staff as occasions. Youth surveys will be periodically collected to elicit suggestions to enhance activities. DSOP will provide daily activities that are challenging, educational and constructive with special attention given to free time activities of youth. The program will include activities that contribute to the health, social skills development and mental health treatment services. Research indicates that many offenders return to the community with good skills, but quickly fall back to their old (and often delinquent) habits. In following the 3-sector behavior management plan (discussed on pages 52-53), the DSOP life coach will set up a wellness plan to include distinct types of exercise that are expected to result in healthier cortisol levels. Physical and mental wellness will allow stronger abilities to think constructively than pathological. Balancing healthy cortisol levels is expected to strengthen sleep and better manage weight control and impulsive behavior of our sex offenders. Further, the life coach will ensure daily schedules include physically challenging activities that teach healthy ways of maintaining physical well-being, in addition to alternative, pro-social ways of spending leisure time. Leisure games, activities and large muscle activities, both indoor and outdoor, will reflect youth interests, ages, and emotional, mental or physical abilities. The large outside activity area of DSOP will allow for a multitude of activities that will not be limited to, basketball, ball tossing, kickball, dodge ball, relay racing, and volleyball. If youth cannot go outside, they will be engaged in aerobic activities, video exercising, and calisthenics, unless medically prohibited. These experiential activities will facilitate growth and personal achievement, and follow the Restorative Justice principles of accountability, competency development, community partnerships, and maintaining a safe environment. A monthly activity calendar will be posted at the facility to motivate youth participation in special activities, such as debates, cultural events, DJJ Youth Success Week, talent shows and olympic games. To provide non-competitive events as alternatives during leisure time, G4S will offer art, music, poetry, drama, chess, checkers and reading. These will provide constructive outlets to develop self-control, heighten sensitivity towards victims, strengthen reading and writing skills, and alter patterns of delinquent behavior. Activities will embrace the Florida Just Read program to continually reinforce reading. As part of our We connect to YOU design (Exhibit 6, pages 67-68), G4S will integrate parent-guardian connection, health connection, cultural connection, community connection and peer connection goals during recreational and leisure time, in addition to scheduled times that provide the greatest benefit to the youth. We believe that constantly providing support connections as our vision of helping the youth become whole. A.18 CATEGORY 14: RESTORATIVE JUSTICE PHILOSOPHY AND RESTORATIVE PROGRAMMING How well does the proposal describe a plan to provide Restorative Justice Programming? Consideration 2: How well does the proposal document that the program supports the Restorative Justice philosophy? A.18.a. BALANCED AND RESTORATIVE JUSTICE MODEL: G4S has incorporated the principles of balanced and restorative justice from the Guide for Implementing the Balanced and Restorative Justice Model (OJJDP, December 1998) in our mission. DSOP will operationally reflect the restorative justice philosophy of repairing harm to people caused by crime. G4S will focus on restorative instruction and activities designed to assist youth in accepting responsibility for harm caused through past criminal actions, while challenging to recognize and modify their irresponsible thinking. Youth will be taught about the impact that crime has had on their victims, families and communities. G4S will integrate restorative justice into its behavioral management system that will have requirements the youth must complete before being awarded a phase up. This can be further reviewed in the detailed phase description in Exhibit 4, page 64. As part of reinforcement, the DSOP will expose youth to victim speakers and victim impact statements, in person, videotaped or audiotaped. Staff will engage youth in follow-up activities to process reactions to each victim s account of how crime affected his/her life. Restitution activities and community service opportunities will be provided as a means of giving back to the community for the damage the youth has caused. Once the youth enters his last 60 days of the program, he and his life planner will select a targeted community group in the youth s home community who will be the recipient of at least one (1) project the youth will contribute. The selected project will require the youth s planning, personal hands-on construction, development, and completing, in addition to maintaining consistent communication between the youth and the community group leader to share ideas and discuss his progress. This will set the stage of connection between the youth and community with expectation the youth can continue his community responsibility upon returning home. RFP R2107 Page 57
94 Program Services A.18.a.1. ACCOUNTABILITY: The most notable difference between a restorative justice model and a more traditional retributive and rehabilitative model is restorative justice s emphasis on offender accountability and reparation to the victims and communities. In restorative justice, the offender s obligation to make amends requires an understanding of the basic values that define our rights and responsibilities in a democratic society. Offender accountability, including understanding the harm to victims and the community, and making reparations, will be stressed throughout the youth s stay in the program. Beginning the first day in the program, one (1) of the fundamental intervention goals will be to hold each youth accountable for behavior, while strengthening acceptance for actions and decisions via the behavioral management system. Through the services provided, G4S ensures that a specialized psychotherapeutic intervention system is created to address offending, community linkage, and reduction of risk factors. The program will consist of treatment approaches found through research to be effective in addressing the specific needs of this juvenile population. The program will focus on: 1. Holding the juvenile sex offender accountable for behavior and the harm caused to their victims and the community; 2. Protecting the public by reducing the probability of future deviant sexual and criminal behavior by establishing discharge planning that will help ensure a successful reintegration back into the community; 3. Providing juvenile sex offender competency based treatment focused on developing awareness of deviant sexual impulses and criminal behaviors, while acquisitioning specific skills to deal with future impulses; 4. Establish inter-agency contacts to provide continuity of care upon release. A.18.a.2. PROTECTION OF THE PUBLIC: Supervision and structure will be critical to operational success and achieved by the delivery of specific, organized daily practices that protect the public, ensure the safety of youth, staff and visitors, comply with professional standards and are lawful, constitutional, fair and just. DSOP will maintain written policies and procedures for safety, security and control, which will be reviewed annually, to remain current and appropriate to changing conditions of care. A facility-specific operating manual, containing all safety/control procedures, will serve as the basis for staff training and supervision. The DSOP will invite victims of crime to share stories of the harm that delinquency behavior has caused. In return, DSOP will seek opportunities to share what delinquent thinking has caused the youth and others. A.18.a.3. OPPORTUNITIES FOR COMPETENCY DEVELOPMENT: DSOP will develop competencies to enhance the youth s successful return to the community. Competency development curricula and the behavior incentive system will strengthen the ability to function in society in a meaningful, adaptive way; develop skills and become stronger in character and empathy; demonstrate empathy and remorse; practice how to lead, belong, mentor, contribute and make meaningful choices; connect to the community; and understand positive contribution. A.18.a.4. PARTNERS WITH COMMUNITY STAKEHOLDERS: Community participation and knowledge of the program s goals will be addressed through our involved Community Advisory Board and an active volunteer program. Community activity planning may include visiting the local homeless shelter, conducting car washes to raise money for needy families, and participating in community projects, activities and services. Additionally, youth will participate in writing essays to victims about being a victim and preparing posters for Victim Rights Week. These activities will provide youth opportunities to see and experience the benefits of active community involvement. Consideration 3: How well does proposal s described Restorative Justice Programming plan create opportunities for youth to be actively involved, give input, participate in decisions, practice leadership roles, use restorative conflict resolution strategies, and contribute to the community? A.18.b. RESTORATIVE CULTURE: G4S will follow the We Connect to You design (described in Exhibit 6, pages 67-68) to incorporate the importance of community connection as one (1) of seven (7) connections to becoming whole. We will maintain an environmental culture that promotes and reinforces community values by giving youth opportunities to assume the responsibilities and experience the benefits of being part of a community. The program will create many opportunities for the youth to be actively involved, give input, participate in decisions, practice leadership roles, use restorative conflict resolution skills and contribute to the community. DSOP will maintain a Youth Advisory Board that provides a formal process for constructive input, identifying systemic issues impacting the residential community and making recommendations for resolution. The DSOP will establish weekly resolution groups that encourage youth to take leadership roles in identifying and resolving issues of the community. Youth will be part of planning special community project events that benefit the DSOP community and give back to targeted populations in the Daytona community. The program s residential community will promote each youth s personal accountability for actions and how they impact others; community safety through peaceful conflict resolution and youth learning to manage their behavior; competency development through opportunities to practice skills for responsible community living; youth s active participation through opportunities to make choices, assume meaningful roles, and give input into the rules and operation of the residential community. A.18.c. COMPETENCY DEVELOPMENT: Competency development curricula, discussed in the Opportunities section above, will further strengthen each youth s ability to better function in society, develop skills, become stronger in character, become more connected to the community and practice opportunities to lead, belong, mentor, contribute and make meaningful choices. These competency development skills will be taught using the SkillsStreaming program, which offers over 200 lessons on specific competency development skills that the youth may use in the community. Examples are lessons on manners, proper speech, proper dress, employment interviewing, independent living finances, cooking and many more. Through skills training and the DSOP community support, youth will develop character, become leaders and mentors and learn how to make good choices. RFP R2107 Page 58
95 Program Services Consideration 1: How well does proposal describe plan for providing Impact of Crime training to staff & implementation of Impact of Crime program? A.18.d. IMPACT OF CRIME INSTRUCTION: DSOP will maintain a designated Restorative Justice Coordinator, who will be trained in the Department s Impact of Crime on Victims (IOC) curriculum. The Restorative Justice Coordinator will schedule the provision of IOC instruction by trained staff and the implementation of restorative activities and projects within the facility and the local community. The IOC instruction will be provided weekly to the youth, using the Department s curriculum. This curriculum will provide structure and direction in assisting youth in accepting responsibility for the harm they have caused their victims, families, and community; increasing ability to empathize with victims through education on the impact of crime; providing a safe forum where victims may share their experiences with the youth; guiding youth in activities for victims, family, and community restoration; holding youth accountable to apologize to victims and/or participate in victim-offender mediation. The goal of DSOP will be to instill a sense of responsibility and need for community belonging. All staff will receive two (2) hours of pre-service instruction on the Restorative Justice principles, philosophy and practices, which exceeds RFP requirements. Further, all staff will receive training on an annual basis. G4S has Department recognized and certified Impact of Crime trainers who will provide the IOC Train-the- Trainer training on a quarterly basis. Staff will be encouraged to participate in activities that are based on the principles of restorative justice. Such on-campus and off-campus participation will continually reinforce the need to decrease desire to take from others; instead, strengthen basic values to give back. The Restorative Justice principles and philosophy will be incorporated into the behavior management system. All youth will be required to write a letter of apology, know all their crimes and demonstrate an understanding of the impact of their crime on the victims in order to graduate from the program. A.18.e. As discussed throughout the proposal, all aspects of the DSOP program will reflect the restorative justice philosophy including case planning, competency development, meaningful community service, restitution, conflict resolution, victim and community involvement. A.19. COMMUNITY INVOLVEMENT OPPORTUNITIES G4S believes in giving back to the community as part of its adherence to BARJ principles of reparation and accountability. DSOP will maintain effective community relationships that allow the youth many opportunities to improve and use social and life skills, enhance a sense of empathy and ability to give-back, and increase pro-social experiences and activities. G4S will follow the principle of engaging on-going natural support in communities, which is an Evidence-Based Principle of Effective Interventions. G4S understands there are three (3) community components that play a role in supporting the youth s growth: 1) the community where the youth will live upon release from the program, 2) the DSOP community, and 3) the community in which the facility is located. The DSOP will utilize all of these to provide wrap-around services for the youth s successful rehabilitation and transition upon release. DSOP will work with local community partners through our Community Advisory Board (CAB) to develop partnerships and linkages to serve our residential and surrounding communities. The CAB will help coordinate community projects with entities such as the Salvation Army, Hope Center, Council on Aging, community food banks, humane society, state and local parks, veterans groups, homeless shelters and special projects for targeted populations. Mentoring services, local victim service providers, and advocates connected to other G4S programs will be integrated. These groups have been invaluable resources to suggest ways youth can make reparations on-site, recommend local victim awareness resources and present ideas regarding victim involvement. All of these opportunities will provide the staff and youth with technical assistance and opportunities that foster the goals of the treatment program. The group will serve as a strong link to the business community, law enforcement, social service agencies, the media, legal services, local government, victim services youth and other key groups and organizations. Further, the DSOP will maintain an active volunteer program where mentoring services will be available to our youth. It is the goal of G4S to provide opportunity to see and experience the benefits of active involvement, while giving back to the local communities that make significant contributions to the program. A.20. TRANSPORTATION SERVICES G4S Youth Services understands and accepts responsibility for providing transportation services for program related purposes to youth in the program, including but not limited to transportation of new admissions from the detention center, medical/dental/counseling appointments, emergency transportation, within region, facility-to-facility transportation of administrative transfers, counseling appointments with community agencies, community service projects, transportation to and from home visits (if applicable), and releases and discharges (if within 75 miles from the program). G4S will ensure compliance with the recently updated mileage requirement for transportation of youth upon release, working with the JPO to ensure a timely discharge and drop-off point. Only staff that have valid driver s licenses and successfully complete the appropriate and required vehicle training are authorized to provide transportation. Whenever youth are transported, a secure vehicle will be used and the appropriate staff-to-youth ratio will be exceeded. Departmental requirements regarding searches and the use of restraints for transportation will be followed. At no time will youth be left unsupervised in a vehicle or permitted to drive. During transportation, youth and staff will be required to wear seatbelts, and horseplay is prohibited. When facility vehicles are not in use, they will be locked and the keys placed in the facility's secure lock box provided for key storage. IV. LIMIT OF SERVICES: DSOP will provide mental health and substance abuse services in accordance with the Department s Mental Health and Substance Abuse Services Manual (approved August 2006 with March 2007 and April 2007 updates). Youth in the program will have access to necessary and appropriate mental health and substance abuse services, both on-site and off-site, provided by qualified mental health and substance abuse professionals or service provider(s) licensed in accordance with chapter 394, Florida Statutes, and/or chapter 397, Florida Statutes, and as specified in Rule 65D (15), Florida Administrative Code. See Section A.6. of this proposal for detail discussion of treatment services. RFP R2107 Page 59
96 Program Services V. STAFFING/PERSONNEL: G4S agrees that all personnel and subcontractors provided under this Contract will maintain all necessary, required and appropriate licenses, protocols and certifications required by local, state or federal agencies for services to be performed or for the position held. G4S will provide the Department s Contract Manager with copies of all current and renewed licenses or certificates when selected for contract award. As discussed throughout the proposal, G4S looks forward to providing care and custody to DSOP youth. During all hours of program operation or service, we will provide: Twenty-four (24) hours awake supervision every day of the year; appropriate levels of staff (1:6 awake hours, 1:10 sleep hours, 1:4 for off-site activities) to provide immediate response to emergencies, active supervision of the youth, and suitable and timely response to the everyday needs of youth while maintaining safety and security within the program. Five (5) days of the week, G4S will employ a specialized Life Coach who will provide direct supervision of youth, maintaining ratios of 1:5, which exceeds RFP requirements. For all Health Services, Sex Offender, Mental Health and Substance Abuse treatment providers, G4S agrees to comply with all professional qualifications, applicable rules, statutes and licensing standards as stated in the RFP, pursuant to applicable law in the State of Florida. Licenses and certifications will be available to the Department on-site or upon request prior to the execution of a new contract. G4S understands the Facility Administrator, Nursing Staff, MD/Designated Health Authority, and the Designated Mental Health Authority/DMHA/Licensed Mental Health Professional are essential for successful program compliance. If personnel in any of these positions resign, are removed, substituted or changed in status, DSOP will provide the Contract Monitor a detailed written report within 48 hours, explaining the action taken, the plan to ensure contractual services will continue, a timeline for the position to be permanently filled, and will work with the Department to evaluate the vacancy impact. VI. SERVICE LOCATION: Services for DSOP will be provided in the Department owned or leased building in Circuit 7, Northeast Residential Region located at 1386 Indian Lake Road, Daytona Beach, Florida G4S has successfully operated similar programs for DJJ and would welcome the opportunity to provide evidence-based treatment services to 30 high-risk males needing specialized Sex Offender Treatment Services, between the ages of 13 to 18, 24 hours per day, seven (7) days per week. G4S understands and agrees to comply with all the requirements as listed in this section of the RFP. VII. DELIVERABLES: G4S understands and agrees to the definition of filled, unfilled and available beds as described in this section of the RFP. Detailed invoices will be submitted monthly in a timely and accurate manner that will allow a proper pre-audit and post-audit by the Department. Mental Health Overlay Services (IMH) reimbursement will be requested for each day a youth receives treatment services provided by a licensed mental health professional or a non-licensed mental health clinical staff person working under the direct supervision of a licensed mental health professional as defined in the DJJ Mental Health and Substance Abuse manual and in accordance with Exhibit II of this RFP. All treatment will be documented in the youth s official health care record. G4S will comply with reporting requirements and due dates established by the Department and detailed in the RFP. We understand that non-compliance of the requirements of this contract, including submittal of information that is due, may result in payments being withheld until compliance. VIII. PERFORMANCE MEASURES: G4S has developed a system that measures and captures performance data on each youth in accordance with objectives and requirements of the contract, while maintaining the provision of services as outlined in this proposal. G4S will ensure that all required data is collected, maintained and reported in accordance with Departmental policy, procedures and standards. G4S has a management information system that will be implemented at DSOP to maintain data on youth progress and demographics and a multilayered tracking procedure to ensure rate of service delivery. Treatment data collection will incorporate multi-disciplinary and interactive methods/tools to collect relative qualitative/quantitative performance information. Performance based budgeting data elements will be accurately entered into the Department s JJIS website in a timely manner. As in our other Florida programs, we will comply with current reporting requirements that pertain to PB2 Measures, including the reporting of incidents to the Central Communications Center. G4S is familiar with Departmental review of program content, components and duration through outcome evaluations, recidivism studies and other program assessments, and agrees that program data requested will be provided to assist in conducting evaluations, studies/assessments of programs and service delivery. To document DSOP s level of services and programming, we will implement an organized system of research and evaluation that will include on-going data collection, storage, retrieval, reporting and review. The Department s PB2 data will be included in this process. The system will include research design and methodologies for both process evaluation and outcome evaluation. G4S is familiar with program and performance data that is requested by the Department to conduct evaluations, studies or assessments of program and program service delivery. G4S has developed and will implement an internal electronic database that calculates and tracks required reporting benchmarks to aid in the compilation of data needed. Monthly internal reports will be produced and reviewed to allow for adjustment in any areas where quality improvement is needed. G4S also understands that program outcome evaluation, recidivism studies and other program assessments may be used in rating the program for its future funding. This will also be used for long-term program planning, performancebased budgeting and legislative budget requests. G4S has participated in many DJJ pre-operational reviews and is fully experienced in the process. If awarded this contract, G4S will work with the Department and follow a Pre-Operational Review that includes employee recruitment, employee retention strategy, training and staff development, food services, safety and security, physical plan services, medical services, treatment services, case management services, educational services, accounting services, operational services, and vendor services. Focus will target quality and compliance. RFP R2107 Page 60

97 Exhibits Exhibit 1: Florida Certificate of Fact RFP R2107 Page 61
98 Exhibits Exhibit 2: List of G4S Facilities G4S Opened, Transitioned and Acquired The table below details the facilities that G4S has opened (O), transitioned from other providers, either through contract award (C) or emergency procurement (E) or acquired (A). We have listed the program name, if applicable, population, youth level of risk and specialized services provided. ST Program Name Population Risk Specialized Services FL Avon Park Youth Academy O 165 males Moderate BHOS FL Avon Park and Street Smart Transition Program - program closed 1/31/08 due to legislative budget cuts. O Originally 200, changed to 70 Transition program; changed to Conditional Release Program FL Columbus Juvenile Residential Facility A 50 males Moderate Sex Offender FL Cypress Creek Juvenile Offender Correctional Center C 39 males 57 males High Max MHOS, RSAT FL Dade Juvenile Residential Facility O 56 males Moderate Intensive Mental Health, Dual Diagnosis FL Gulf and Lake Academy A 29 males and 46 females Moderate Intensive MH, Medical, Borderline, Developmental Disability FL Hastings Youth Academy O 165 males Moderate BHOS, Specialized Mental FL Hillsborough Intensive Residential Treatment Facility FL Marion Youth Development Center -- transitioned to new provider. Health, Intensive Mental Health A 25 males High MHOS O 104 males High FL Martin Girls Academy A 30 females High Intensive Mental Health FL Okeechobee Girls Academy O 24 females Low, Moderate FL Okeechobee Juvenile Offender Correction Center C 64 males High 32 males Maximum FL Okeechobee Youth Development Center and C 143 males High Intensive Halfway House 30 males Moderate MHOS Sex Offender MHOS BHOS FL Orange Youth Academy and O 48 males High MHOS, Intensive Mental Health Orlando Intensive Youth Academy 16 males Moderate FL Palmetto Youth Academy O 48 males High RSAT FL Pasco Girls Academy O 24 females Low, MHOS Moderate FL Polk Halfway House A 24 males Moderate MHOS FL Polk Juvenile Correctional Facility -- closed the facility by 01/31/08 as directed by the 2007 legislature. C 240 males High MHOS FL Riverside Academy A 165 males Moderate RSAT FL Sago Palm Academy closed the facility by 06/30/08 as directed by the 2007 legislature. FL Southwest Regional Juvenile Detention Center -- transitioned back to the state. FL The Achievement Center - opted not to exercise renewal because of budget cuts to education funding; closed program. AR Arkansas Juvenile Assessment and Treatment Center E 252 males High Sex Offender, RSAT, MHOS, Developmentally Disabled C O E 65 male and female youth 30 males and female youth 143 males and females All levels Detention Center Alternative Education Sex Offender, Substance Abuse, Girls Specific Programming KS Atchison Youth Residential Center closed O 54 males Sex Offender Transition 12/18/09 due to budget cuts. TN Davidson County Juvenile Detention Center C 64 males and females Detention Center RFP R2107 Page 62

99 Exhibits Exhibit 3: Recruitment Process RFP R2107 Page 63
100 Exhibit 4: Sample DSOP Behavior Management Level System Exhibits Level Name How to Advance Privileges Phase 1 INITIAL PHASE Phase one is designed to allow you to take responsibility for your actions and offense, and decrease your level of denial You will learn the rules and regulations of the program and demonstrate verbally and physically your understanding. You will comply with all aspects of the assessment and treatment planning to include educational testing. You will identify methods and timelines to achieve treatment plan and performance plan objectives and goals You will not exhibit physical aggression toward staff or peers. You will participate positively in group and individual therapy. You must develop and write out your group introduction and demonstrate the ability to begin group with your group introduction. You must have your hair cut with a two guard You must earn designated daily points and tokens Required assignment: You must write out your commitment phase and share it with the community and treatment team. One 15 min. weekly phone call Mail privileges Socialization during meal times Recreational time Decorate your room with pictures, drawings, etc. in your designated area. (Please note that all property that is displayed in the designated area must first be approved by the Assistant Facility Administrator with the approved hole punch). As a resident, you will be required to gain a greater understanding of victim awareness and the impact of crime. Phase 2 HISTORICAL PHASE Phase two is designed for you to reflect on your history and identify how it may relate to your offense. During this phase you will identify your triggers, cognitive distortions, beliefs, morals, family experiences, social experiences, violent experiences, and sexual experiences. Victim Awareness requirements to phase up: To be able to identify the stake holders: (Victim, Offender & Community) To be able to identify the four harms: (Physical, Financial, Social & Psychological) To identify the stinkin thinkin (Rationalizing, denial, minimizing and victim blaming) To be able to define the following: Restorative Justice A way of looking at crime by focusing on the harm created by the offender when a crime occurs. Instead of just considering the offender, criminal charges and punishment it looks for ways to heal those hurt by the crime. Restorative justice values the offender s responsibility in repairing the harm they created when they commit a crime. It also values the victim s point of view. Primary Victims Those individuals who are directly harmed by the crime. Secondary Victims The family members and friends of victims, or neighbors who are also greatly harmed by crime. Victim Impact The harm caused to a victim, their families, or the community because of criminal action. To attend all groups. Meet all requirements for phase one. Follow all rules and staff directives. Display honesty Demonstrate respectful and positive interactions with peers and staff. Demonstrate an understanding or purpose of medication management and cooperate with medication regimen (if applicable). Positively participate in groups, classes, and unit activities. Complete life story and discuss in individual and group therapy. Identification of themes, values, and messages that define you. Recognize victimization issues. Identify triggers. You must have your hair cut with a two guard. You must earn designated daily points and tokens Required assignment: Upon completion of your life story, you must present this in writing to your process group. Victim Awareness requirements to phase up: To be able to identify stinkin thinkin and apply how it is harmful. To be able to identify and explain the impact of the four harms and how it effects the victim. To accept that they have a victim and have caused harm. To attend all groups. To provide feedback in groups. All privileges from phase one One 15 min. phone call and one 10 min. phone call per week Use of board games during leisure time Permitted to use own bed covers and pillow RFP R2107 Page 64
101 Exhibits Level Name How to Advance Privileges Phase 3 INTEGRATION PHASE Phase three is the bringing together of all parts of the self. During this phase you will develop an understanding of the emotional and cognitive elements of deviant behavior. You will be asked to look inside of yourself and examine your triggers that led to you offending. You will develop and relate concepts of guilt, shame, empathy, victim awareness, responsibility, and appropriate family relationships. Meet all requirements from phase two. Demonstrate leadership. Understand the concepts of remorse and empathy by acknowledging consequences to victims. Participate actively in family therapy with emphasis on accountability and boundaries. Explain the generic cycle of abuse. Develop a personalized cycle of abuse/links in the offense chain. You must have your hair cut with a two guard. You must earn designated daily points and tokens Required assignment: You must present in writing, your complete personalized cycle of abuse in process groups and in individual therapy. Victim Awareness requirements to phase up: To be able to confront when others are applying stinkin thinkin. To be able to identify the four harms that they have caused their victim. To identify at least two ways that they can begin to make amends with family for the harm that they caused by committing the crime. To identify at least two ways that they can begin to make amends with their victim. To identify at least two ways that they can begin to make amends with their community. To identify and implement restorative justice within the program. All privileges from phase two One 15 min. phone call and two 10 min. weekly phone calls Participate in vocational programming Attend game room Radio privileges Extended bed time Weekend movie Become a peer mentor Phase 4 TRANSITION PHASE Phase four is the time to pull together all elements of treatment and incorporate them into your relapse prevention/safety plan. During this phase, you will develop a comprehensive plan that includes social skills, recreation, spiritual, employment, academic, family, and internal and external management plans that will assist you in future success. Meet all requirements for phase three. Show initiative by promoting individual thought and activity. Understand and communicate thoughts, feelings, and needs. Positively give and receive constructive criticism and feedback. Participate in healthy sexuality group Write appropriate sexual fantasy. Demonstrate remorse and empathy and victim awareness by writing victim s eyes and clarification. Report to community on reality and difficulties of maintaining relapse prevention on off campus outings or home pass. Maintain leadership position. Be consistent in all aspects of treatment. Demonstrate self- management and responsibility. Develop and complete your relapse prevention/ safety plan. You must earn designated daily points and tokens Required assignment: You must present in writing your relapse prevention/ safety plan in process groups and in individual therapy. All privileges from phase three One 15 min. phone call and three 10 min. weekly phone calls Ability to participate in competitive/contact rec. activities Attend community outings Attend home pass (within days remaining in the program) Wear personal clothing Order from special menu during lunch Order out privileges while on an outing Have your hair cut up to a four guard RFP R2107 Page 65
102 Exhibit 5: Climate Action Award Nomination Exhibits G4S Climate Action Over the several months, Youth Services challenged 490 youth, in addition to program staff, to plan projects that dramatically effect changes in conservation. As a result, the success far exceeded the expectations: The Avon Park Youth Academy (APYA) in Avon Park, Florida, houses 165 moderate-risk DJJ male youth, ages As part of the conservation projects at APYA, several initiatives have been successfully introduced over the last few months. The solar water heater project is funded through on-going two (2) year cumulative $45,000 Perkins grants. Currently, there are three instructors and over 30 vocational students participating in the installation of five (5) solar heaters that are both off-grid and ongrid. A second project was the reroofing of three resident duplexes to install light colored shingles for energy reductions. Vocational instructors and approximately 20 youth have participated in this on-going project. A third project is the recycling of food wastes from the dining hall. Waste food is picked up weekly by "Swell Sweet Dreams" and transported to a farm to feed the animals, rather than disposing the food at the land fill. A fourth conservation project is the on-going, consistent preventative maintenance on all air conditioners that includes changing a/c filters and cleaning grills. The APYA maintenance department has further instituted a systematic monitoring of lights in different locations for maximum efficiency. A fifth effort is the ongoing recycling of paper, plastic, cardboard, oil and grease into the recycling bins placed in targeted locations. All facility departments and students recycle daily newspapers and other paper products. Furthermore, all facilities at the Air Force Range, where the Avon Park Youth Academy is located, are invited and encouraged to use the APYA recycle bins. The Hastings Youth Academy (HYA) in Hastings, Florida, houses 165 moderate-risk DJJ male youth, ages The Greenhouse Project was implemented as HYA s conservation project through $10,000 Perkins grant funds, and is associated with the school's horticulture class which enrolls 40 students. The concept utilizes solar panels to heat and light the greenhouse that grows organic foods such as watermelon and tomatoes, in addition to landscaping plants for facility projects. The Okeechobee Juvenile Offender Correction Center (OJOCC) / Tantie School in Okeechobee, Florida, houses 96 high and maximum- risk DJJ male youth. To date, OJOCC/Tantie School has received $150,000 for the Going green projects, through two (2) Perkins grants over the past two (2) years. With the funding, the Tantie School has taken on conservation projects that included the purchase solar lights for its Building Construction Shop-port, which is where all of the hands on classes are held. The lights have solar panels installed on top of the building which emits power and allows motion detectors to automatically turn off lights when the building is empty. Further, the purchase of solar insulation, weatherization materials, and six (6) portable air conditioners have been part of the project to reduce energy costs. Three (3) ground tillers were purchased for youth construction projects and the growing of nutritional vegetables for the students and vegetation for the campus. Finally, projectors, white boards, document cameras, and LED TVs have been placed in all classrooms for more efficient technology and reduction of paper usage and power. Each of the 92 students at the school has been funded to be provided a Dell computer that is environmentally friendly, uses less power, set to idle in minimal power mode, and when recycled, they are environmentally friendly. In addition, each educational staff has a green lap top that uses less power and is environmentally friendly. The Davidson County Juvenile Detention Center based in Nashville, Tennessee, is a secure juvenile detention center that provides services to 64 male and female youth detained by the Davidson County Juvenile Court Davidson. As a special conservation goal, 38 students participated in the "Going Green Art Project". Students drew representations of ideas that could help the facility use less traditional energy. The art ideas included the installation of solar panels to reduce the electric bill, unplugging cell phone and walkie-talkie chargers when not in use; replacing incandescent light bulbs with more energy efficient light bulbs, and several other innovative energy reduction ideas. Student art work was posted throughout the facility to encourage and motivate all staff to make efforts to conserve our environment. RFP R2107 Page 66



103 Exhibit 6: We Connect to YOU DSOP Project We have designed the We connect to YOU project to teach youth that it takes many types of external connections to discover one s internal sense of wholeness. With internal awareness of self, one has the opportunity to find true happiness and success, while leaving old behavior and thinking in the past. Exhibits PARENT-GUARDIAN CONNECTION We embrace a family environment. On a bi-monthly basis, DSOP will offer a workshop for parents, youth and staff to work together on themed projects to reinforce the importance of family. We emphasize our vision that success of a youth is largely influenced by on-going support received from family. Parent Connection will teach families how to identify problems, communicate healthy resolution, and develop relationships. Parents will be integrated into the program from orientation to discharge. SPIRITUAL CONNECTION We embrace spiritual freedom. At least 3 times a week, community volunteers will provide faith opportunities to the program. It will be our goal for community faith based volunteers to work side-by-side with our youth each month on special projects that identify a theme, goal and objective for spiritual wellness. On a quarterly basis, it will be our goal to have peers from colleges and schools provide oncampus special presentations so our youth can see how faith and healthy relationships go hand-in-hand. HEALTH CONNECTION We embrace maintaining a healthy body to have a healthy mind. Our health and fitness lab will allow the Life Coach and the youth to develop a personal wellness plan for maintaining quality health. It will be our goal to implement a workout station, where donated exercise equipment will be integrated into the behavior management system and the wellness plan. CULTURAL CONNECTION We embrace the many cultures of the world. On a quarterly basis, youth will participate in cultural activities that honor different cultures of the world. Projects will be on display for parents/guardians and visitors and, if performances are integrated, they will be presented to family and visitors during visitation or special events. PEER CONNECTION We embrace pro-social friendships. Youth leaders will be matched to new youth to teach skills of leadership, accountability, trust, responsibility, and respect. This self-esteem building relationship will be maintained throughout the program, and then passed to the next in-coming peers. COMMUNITY CONNECTION We embrace society s professionals who have expertise and knowledge. It will be our goal to provide a community speaker once a month to present motivation and guidance to our youth. Community partnerships are vital in providing on-going natural support to our youth. RFP R2107 Page 67





104 Exhibits JOB CONNECTION We embrace job skills that are conducive to the job market in Florida. This allows youth greater opportunities to find jobs that will bring success and build strong resumes. Given that post-release employment has been found to significantly reduce recidivism, job connection incorporates specialized vocational services that translate into job skills that ultimately increase public safety. We believe in short term training for long term careers. One of our model programs is the Avon Park Youth Academy, which has achieved Exemplary School status as defined by the Florida Department of Education and serves as a model demonstration site for the state. G4S received an award by The International Corrections and Prisons Association for Management and Staff Training for Overcoming Barriers to Employment for Juvenile Offenders-Avon Park. Avon Park has since been recognized as one of the premier juvenile justice facilities in the nation. Given that post-release employment has been found to significantly reduce recidivism, G4S has a strong commitment to providing premier career and vocational programming that leads to industry recognized certifications. Digital Printing G4S will explore feasibilities of setting up an entrepreneurial program with a digital print lab where youth will receive digital publishing training that open opportunities to find jobs at printing companies, newspaper companies, advertising companies, Kinko s, FedEx Copy Centers, Target Copy Center, or UPS. Further, we are interested in providing our printing services to the community at nominal fees that are lower in costs, quicker response of orders, and strengthen our community relationships. This is a win-win situation for the community as printing services may include items such as newsletters, flyers, business cards, brochures, invitations, and awards. Students in the digital print lab program may be able to work toward their industry certification for Visual Communication with Adobe Photoshop. This industry recognized certification was developed to validate entry-level skills in communication corresponding to Adobe Photoshop software. Students in the digital print lab may receive credit in Desktop Publishing Horticulture Culinary/Food Service G4S has successfully launched horticulture programs in our sex offender programs that teach the skills of landscaping design and beauty. Youth will learn the importance and skills of growing vegetables to provide food for the campus and for special projects that benefit the community. Further, it will be the intention to teach youth how to build a business in horticulture, through growing plants, marketing plants to the community, and setting up checks and balances systems to operate a successful business. G4S will consider establishing a scholarship account to be used from proceeds of plant sales that will be given to a youth as an educational scholarship. Culinary or food service programs are one of G4S many strengths. Food service is a high demand in Florida, and we often establish food service jobs for our youth in his home community prior to discharge from our programs. If culinary arts is the vocational program selected to be implement at DSOP, our culinary arts program will pursue teaching basic food preparation, safety, sanitation, storage, service and culinary arts career pathways. Lessons and activities will support an appropriate internship based program. Students would also have the opportunity to earn the ServSafe Food Protection Manager Certification which is nationally recognized and accredited by the National Restaurant Association. Additional Career Areas for Further Exploration G4S will continuously explore vocational training that yields the best opportunities for job placement. Examples of job areas to be further evaluated are: career and technical instruction in Business Education; flooring installation; heating and cooling systems; carpentry and painting. RFP R2107 Page 68
105 Exhibits Exhibit 7: Spirituality Strength Ministry Experience From 2010 to present Rev. John A. Ferro Volunteer for Volusia County Juvenile Program and Volusia County Division of Corrections Currently employed full-time as the Social Service Coordinator at the RAP juvenile substance abuse program at SMA Behavioral in Daytona Beach, Fl. From: 8/1996 to 2/2010 From: 8/1991 to 12/1994 DUNAMIS Community & Outreach Ministries, Inc. Cassadaga, Florida Pastor: Teaching, Pastoral Counseling, Outreach, Music, Management and Chaplaincy Department of Juvenile Justice: Participation and coordination of Faith-based Services, Bible Studies, Pastoral Counseling; Coordination of Faith-based Volunteers, Groups, and Special Ministry Presentations at Volusia County s Regional Juvenile Detention Center, SMA Behavioral Adolescent Center, PACE Center for Girls, Three Springs/Sequel male sex offender facility and Volusia House Boys Program. Work with troubled youth began in 1988 at the Juvenile Detention Center in Bartow, Florida Volusia County Division of Corrections: Conducting four Bible Studies per week. Faith-based Substance Abuse Recovery Meetings for men and women. Needs assessments and recommendations, Pastoral Counseling. Coordination of Faith-based group volunteers and area clergy. Cross Road Ministries, Inc. /Teen Challenge Daytona Beach, Florida Pastor/Director: Teaching, Pastoral Counseling, Street & Neighborhood outreach and intervention, Music and Chaplaincy. During its four years, Cross Road Ministry merged with Youth for Christ and later became a Teen Challenge Church/Crisis Intervention Center serving up to approximately 50 homeless and run-away youth per day with food, clothing, short-term housing, recreation, rehabilitation referrals and pastoral counseling. Although my first involvement with incarcerated youth began in 1988 at the Bartow Juvenile Detention Center, it was while at Cross Road Ministries I became involved with juvenile and adult correctional facilities in Volusia County on a regular basis. Judicial Reviews, assessments and recommendations assisting Judges, State Attorney s Office, Department of Juvenile Justice, parents and children. Department of Juvenile Justice Faith, Girls and Mentoring Initiatives. From: 1989 to 1990 Lighthouse Rescue Mission Scheduled Ministry for adult homeless clients AWARDS AND ACCOMPLISHMENTS Lakeland, Florida 2009 Commissioned by Governor Charlie Crist, of Florida as a Member of the Juvenile Justice and Delinquency Prevention State Advisory Group [SAG] and currently serving as Vice-Chair- Finance Committee Volusia County Juvenile Justice Council Volunteer of the Year for outstanding service & contributions to the youth of Volusia County at the Juvenile Detention Center 2002 Volusia County Division of Corrections ~ Special Recognition Award for Dedication, Commitment, and Service United Way ~Outstanding Volunteer of the Year Award Runner-Up Civic Group category as Founder of the Department of Juvenile Justice District 12 Faith Initiative: P.R.A.Y. - Partners Reaching Area Youth Volusia County Chapter of United Nations Association U.S.A. ~ Award for Outstanding Volunteer Service Points of Light Foundation, the Corporation for National Service and the Knights of Columbus and Recognized by the President of the United States ~ Daily Points of Light Award as: Founder of PRAY [Partners Reaching Area Youth] Department of Juvenile Justice Faith Initiative 2000 Department of Juvenile Justice District 12~ Volunteer of the Year for their Initiatives and Volunteer Programs Three Springs Program ~ Volunteer of the Year 1999 Department of Juvenile Justice District 12 ~ Volunteer of the Year 1998 Department of Juvenile Justice District 12 ~ Volunteer of the Year for Residential Services RFP R2107 Page 69
106 License Verifications DSOP DHA- Bonnet G4S Psychiatrist- Amiel G4S VP of Clinical Services- Astringer G4S Contracted Licensed Sex Offender Therapist, Researcher, Author - Cotter G4S Licensed Sex Offender Therapist- Drake G4S Licensed Sex Offender Therapist- McDonald G4S Licensed Sex Offender Therapist- Molyneaux License Verifications
107 License Verifications
108 License Verifications
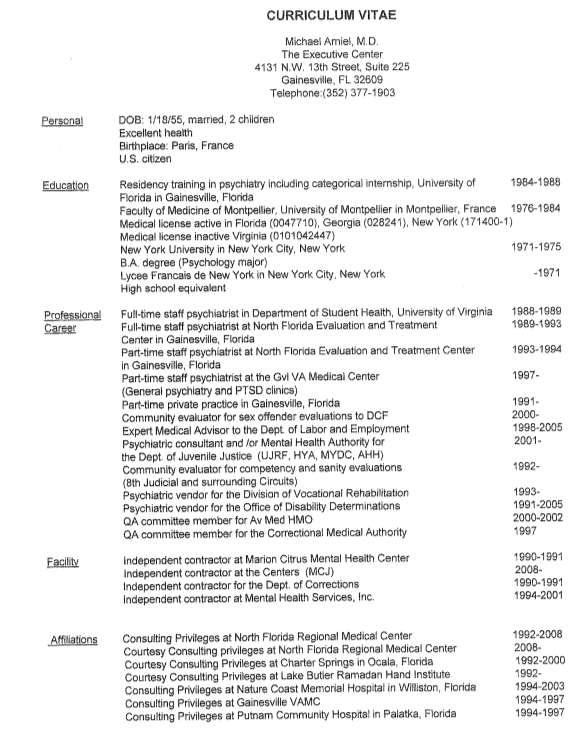
109 License Verifications

110 License Verifications
111 License Verifications
112 License Verifications
113 License Verifications
114 License Verifications
115 Letters DHA letter Dr. Bonnet Psychiatrist letter- Dr. Amiel Licensed Sex Offender Therapist- Dr. Cotter Letters
116
117
118
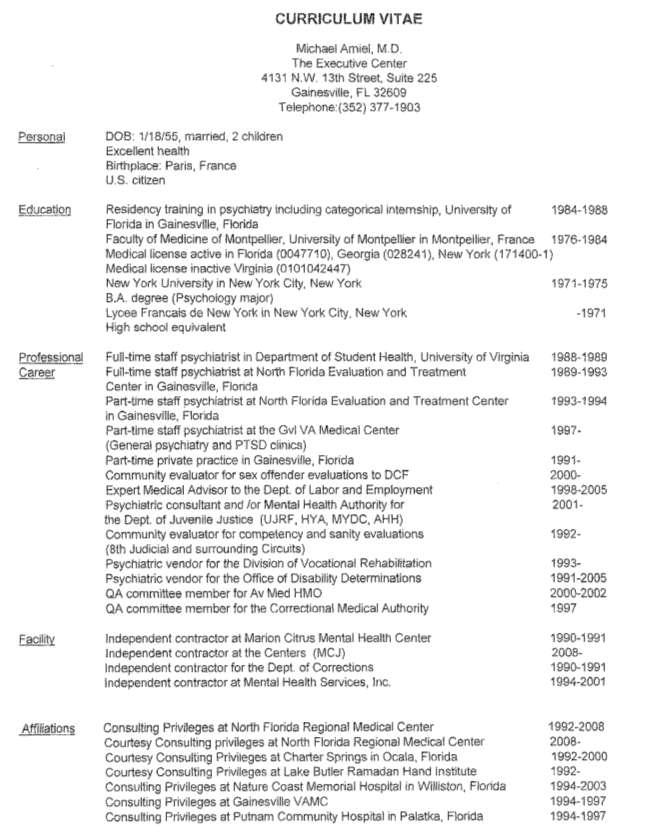
119
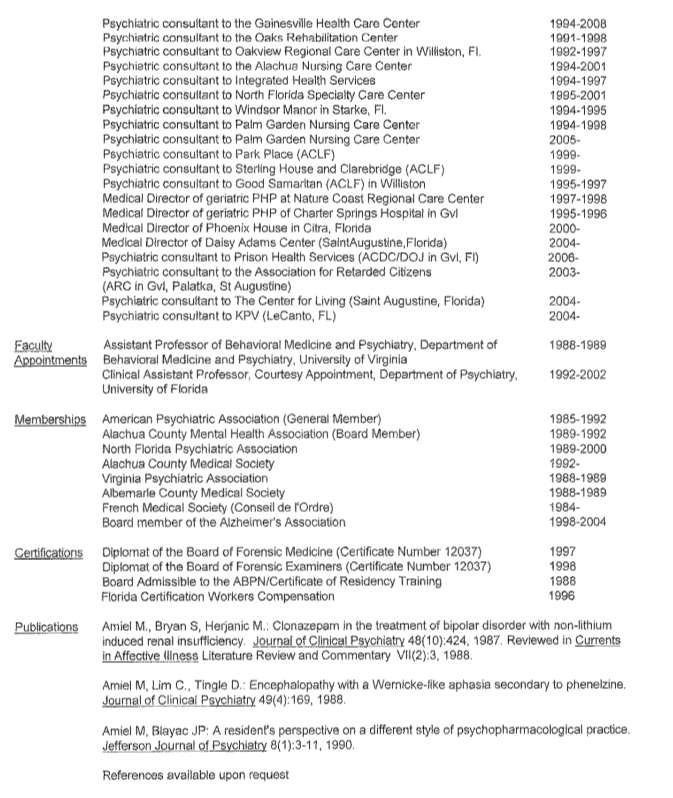
120
121
122
123 Volume II Financial Proposal TABLE OF CONTENTS Financial Proposal Volume II, Tab 1 Cost Pricing Approach... 1 Cost Sheet Attachment J... 4 Consultant Cost Attachment H Operating Capital Outlay Attachment H Personnel Detail Attachment H Expenditures Attachment H Expenditures Attachment H Expenditures Attachment H Service Expenditures Attachment H Budget Summary H Staffing Plan...19 Supplier Evaluation Report (SQR) Volume II, Tab 2 Certified Minority Business (CMBE) Utilization Plan Volume II, Tab 3 Page Response to RFP R2107
124 Introduction Cost Pricing Approach s (G4S) cost pricing proposal for the operation of the 30 bed juvenile program known as (DSOP), provides a budget for operation and programming of the 24 hour, seven (7) days per week juvenile residential program for high risk youth boys between the ages of 13 to 18. A number of variables have been considered and assumptions made in the development of this cost pricing proposal. The budgeting methodology and assumptions used are outlined below. Methodology and Assumptions - General The budget for this residential program includes costs to provide 30 high risk beds for boys between the ages of 13 and 18 who are committed to the Department and in need of Sex Offender Treatment Services. This program provides custody, treatment and supervision to youth 24 hours per day, seven (7) days per week utilizing evidence-based or promising treatment and practices within a framework based upon restorative justice philosophies, principles and practices. G4S used all information available to proposers at the time of the bid for the cost pricing proposal development. All costs are estimates and subject to negotiation. Many of the cost estimates used in the pricing proposal were based on cost data from the operations of the Company s other Florida residential facilities (Polk Halfway House, a 24 bed moderate risk program for boys, Okeechobee Girls Academy, a 24 bed low/moderate risk program for girls; Pasco Girls Academy, a 24 bed low/moderate risk program for girls, Dade Juvenile Residential Facility, a 56 bed moderate risk program, and Martin Girls Academy, a 30 bed high risk program for females). We are experienced in providing these types of services in the state of Florida and believe that the budget is realistic, reasonable and complete. G4S strives to use the lowest price as ascertained from catalog pricing and local quotes for purchasing. The Company prefers to support minority vendors and the local economy by purchasing through local vendors whenever possible, i.e., whenever the local value closely approximates the value that could be obtained from a non-minority vendor or a vendor outside the local area. Value for the purposes of this discussion considers quality, price, availability, speed of delivery, and, if applicable, any warranties or guarantees. The budget does not include any expenses associated with the operation of the school. Youth at DSOP are currently provided education directly by the District School Board of Volusia County. Normally, the price proposal for the renewal period includes an estimated Consumer Price Index Increase-All Urban Consumers on materials and other direct costs. We have not included this increase in future years, as the annual maximum contract dollar amount limit does not allow for a budget increase based on our Year One budget figures. The Company has ample financing available to pay initial costs and to finance accounts receivable for new contracts through a line of credit agreement with its parent company, G4S plc. G4S plc is listed on the London stock exchange and had revenues of over $11.8 billion for its last fiscal year ended December 31, Through successful program management and completed start-ups and transitions of programs in Florida, G4S has developed and refined a comprehensive system of materials procurement and logistics that will continue to ensure a fully stocked and equipped facility. Response to RFP R2107 Page 1
125 Cost Pricing Approach Methodology and Assumptions Expenditures and Services DSOP is located in a Department owned building located in DJJ Northeast Region, Circuit 7, at 1386 Indian Lake Road, Daytona, Florida Costs for repair and maintenance, supplies and services were based on similar operations taking into consideration the age and condition of the facility. G4S has budgeted $51,000 for repairs and enhancements that will be made during the first fiscal year at DSOP with DJJ approval and amortized over the life of the contract. Tentative enhancements anticipated are: floors refinished: Q3 2011; sod replacement: Q3 2011; roof repair: Q4 2011; pressure wash main building exterior: Q1 2012; paint main building exterior: Q-1 and Q ; replace ceilings beginning Q2 2012; and refurbish tool room and repair maintenance building: Q G4S has incorporated the costs for a single medical incident with a limit of $5,000. Outside medical costs were budgeted based on our prior experience at other facilities that we operate in Florida. Insurance costs were based on estimates received from AON, our insurance broker, based on information supplied during the bidding process. The insurances included in the cost proposal are general/professional liability, vehicle insurance, and workmen s compensation. The facility will also be covered under G4S umbrella policy and crime insurance policy. Methodology and Assumptions Personnel Costs Staffing and related personnel costs account for 75% of the direct costs associated with this contract. The Staffing Pattern provides information on planned staffing by shift, by department, the staff to resident ratios and the Shift Relief Factor applied to each position. The Shift Relief Factor is based on the Company s leave and training policies. Salaries are based on data collected for the current job market in Volusia County, Florida. Background checks will be conducted on all new staff, volunteers and interns. Filled Bed Rate Per Diem Description of Service Per Diem # of Youth Served Annual Contract Amount Program Operations $ $1,788, Unfilled Bed Rate Per Diem Description of Service Unfilled Per Diem Program Operations $ Response to RFP R2107 Page 2
126 Summary Cost Pricing Approach Based on the above, we have calculated a total cost per year to be a maximum of $1,788, The total cost meets the limit imposed by the RFP. Response to RFP R2107 Page 3

127 Cost Pricing Approach Response to RFP R2107 Page 4
128 Cost Pricing Approach Response to RFP R2107 Page 5
129 Cost Pricing Approach Response to RFP R2107 Page 6

130 Cost Pricing Approach Response to RFP R2107 Page 7
131 Cost Pricing Approach Response to RFP R2107 Page 8
132 Cost Pricing Approach Response to RFP R2107 Page 9
133 Cost Pricing Approach Response to RFP R2107 Page 10
134 Cost Pricing Approach Response to RFP R2107 Page 11
135 Cost Pricing Approach Response to RFP R2107 Page 12
136 Cost Pricing Approach Response to RFP R2107 Page 13
137 Cost Pricing Approach Response to RFP R2107 Page 14
138 Cost Pricing Approach Response to RFP R2107 Page 15
139 Cost Pricing Approach Response to RFP R2107 Page 16
140 Cost Pricing Approach Response to RFP R2107 Page 17
141 Cost Pricing Approach Response to RFP R2107 Page 18
142 Staffing Plan Staffing Plan for EQUIVALENT # OF TYPE OF STAFF YOUTH TO STAFF FACILITY RESPONSIBILITY WEEKLY HOURS FTE S RATIO Facility Administrator to 30 Overall facility oversight and management. 40 hours per week Assistant Facility Administrator to 30 Oversight of behavioral and safety issues. 40 hours per week Direct Care & Mgmt Supervision Implementation of program schedule, behavior 40 hours per week per management and security FTE Days Evenings Nights to 6 1 to 6 1 to 10 Community Coach to 20 Performance planning, external communication 40 hours per week Life Planner to 10 Transition and support linkages to home community 40 hours per week Life Coach to 30 Physical, vocational, spiritual wellness; special projects 40 hours per week Clinical Director of Treatment 1.0 n/a Administrative oversight of all services related to sex 40 hours per week offender, mental health, substance abuse treatment Mental Health Professional to 10 Implementation of SO, MH, SA services 40 hours per week Director of Medical Services 1.0 n/a Implementation of sick call and medical component 40 hrs/week minimum Nurses (LPN) 2 part time 1.0 n/a Provide shift relief and secondary coverage 20 hrs/wk per FTE Physical Plant Manager 1.0 n/a Physical plant repairs 40 hours per week Administrative Assistant 1.0 n/a Administrative tasks, human resources support 40 hours per week Risk Mgr/QA Specialist.5 n/a Fidelity of scorecard process and risk mgmt. system 20 hours per week Staff Development.10 n/a To meet staff and training needs 4 hours per week Dietary Manager 1.0 n/a Oversee daily operation of the food service department 40 hours per week Master Control 2.95 n/a Monitors security camera for 10 hours per day 40 hrs/wk per FTE Total Response to RFP R2107 Page 19

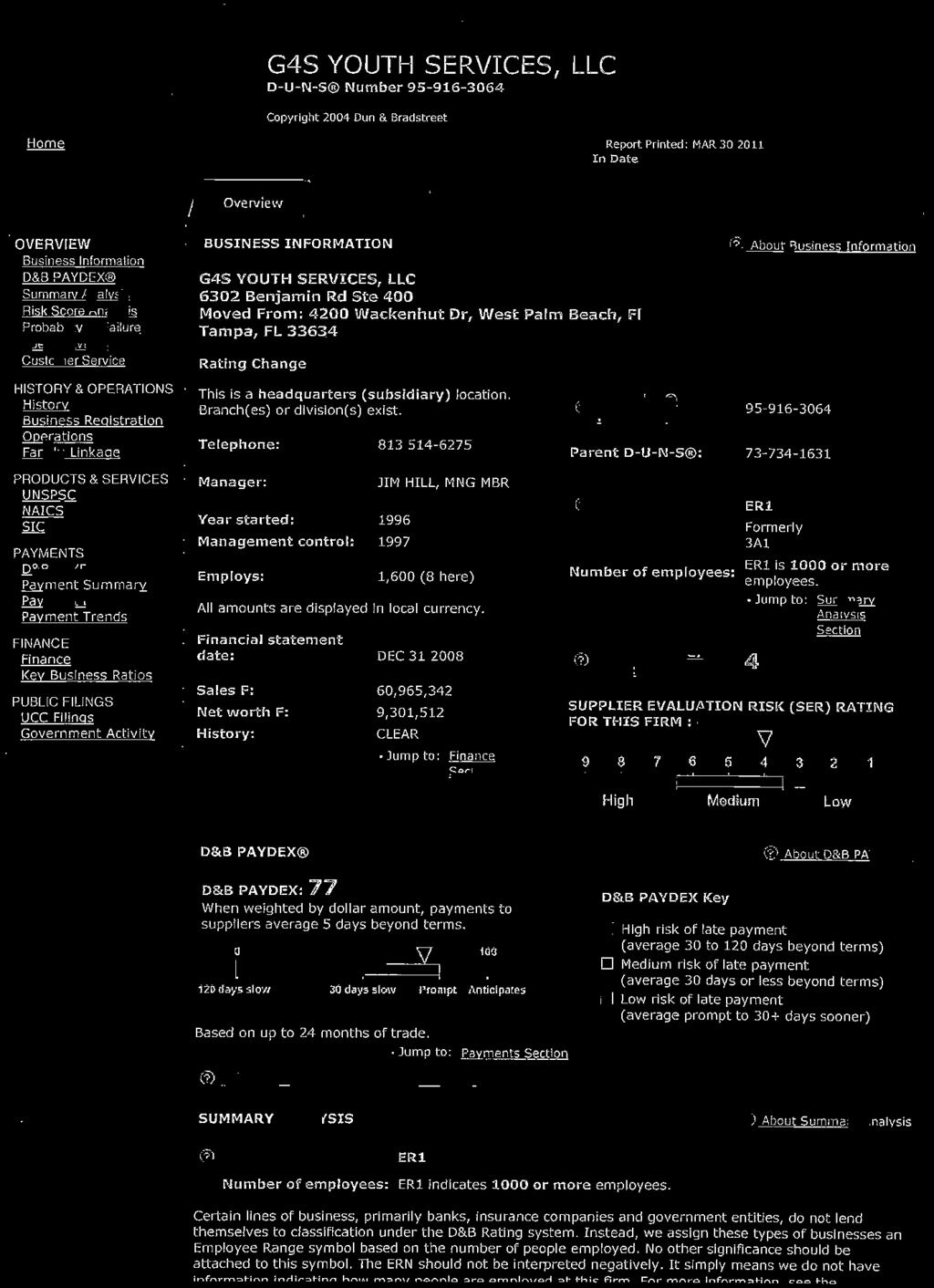
143
144
145
146
147 30 Bed High Risk Program RFP #R2107 Attachment H-3 Personnel Detail (1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) Position Fringe Benefits Annual % of Year Total No. Name Salary Retire FICA/ Health Life Other Total Salary on Con- Salary on Medicare Ins Ins w/benefits tract Contract Management/Support 1.00 Facility Administrator 4, , % 64, Administrative Assistant/HR 2, , % 31, Risk Manager/QA Specialist 1, , % 18, Staff Development , % 4, % % % Totals - Management/Support 8, , , ,572 Programs 1.00 Clinical Director of Treatment 4, , % 61, Mental Health Professionals 9, , , % 130, Life Coach 2, , % 35, Community Coach 2, , % 34, Life Planner 2, , % 36, % % % Totals - Programs 20, ,578 1, , , % 299,198 Food Service 1.00 Dietary Manager 2, , % 30, % % Totals - Food Service 2, , % 30,154 Health Care 1.00 Director of Medical Services 4, , % 58, Licensed Practical Nurses (2 Part-Time) 3, , % 46, % Totals - Health Care 7, , , % 104,695 Security/Supervision 1.00 Assistant Facility Administrator 2, , % 42, Shift Managers 12, , , , % 179, Youth Care Worker I 14, ,118 1, , , % 223, Youth Care Worker II 15, ,171 1, , , % 232, Master Control 4, ,386 75, % 75, % Totals - Custody/Security 49, ,814 6, ,532 12, , % 753,997 G4S Youth Services Response to RFP #R2107 Page 7
148 Attachment H-3 Personnel Detail (1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) Position Fringe Benefits Annual % of Year Total No. Name Salary Retire FICA/ Health Life Other Total Salary on Con- Salary on Medicare Ins Ins w/benefits tract Contract Sanitation/Maintenance Services 1.00 Physical Plant Manager 2, , % 34, Totals- Physical Plant 2, , % 34, Totals - Direct Labor 90, ,909 9, ,250 41,635 1,341,276 1,341,276 Budget for each future contract year 1,341,276 NOTES: Column 8 represents costs for federal and state unemployment (3.5%) and workers' compensation. G4S Youth Services Response to RFP #R2107 Page 8
149
150 Table of Contents TABLE OF CONTENTS Page Attachment C Part 1 Data Sheet... 1 Part III: Evaluation Questionnaire for Professional Accreditation... 3 Copies of Certificates and Quality Assurance Reports Hillsborough Intensive Residential Treatment Program... 4 Martin Girls Academy... 6 Columbus Juvenile Residential Facility... 8 Letters of Good Standing CARF Response to RFP R2107
151 Volume III - Past Performance Attachment C Part I RFP/CONTRACT #R2107 Data Sheet: Past Performance of Residential Commitment Programs Vendor: RFP Number: R2107 Date RFP Issued: 02/03/2011 Program Name 1 Contract Number 2 Program Level 3 Program Operation Begin Date 4 Program Operation End Date 5 Most Recent QA Performance Percentage Score 6 Most Recent QA Compliance Percentage Score 7 (if evaluated prior to 2007) Failure to Report 8 Escapes 9 Total Releases 10 Successful Completions during FY Contract Cure Notice (initiated after 7/1/08) 12 QA Deemed Status 13 Avon Park Youth Academy J7G01 Mod 07/01/98 06/30/13 83 N/A N/A *Columbus Juvenile Residential R2087 Mod 04/15/09 12/31/12 88 N/A 0 0 N/A N/A N/A Yes Cypress Creek Correctional Center R2078 High 07/01/03 08/31/12 88 N/A N/A Yes Cypress Creek Correctional Center R2078 Max 07/01/03 08/31/12 88 N/A N/A Dade Juvenile Residential Facility R2028 Mod 12/01/06 11/30/12 84 N/A N/A Yes *Gulf & Lake Academy F7G02 Mod 07/01/04 01/31/16 85 N/A 0 0 N/A N/A N/A Yes Hastings Youth Academy R2059 Mod 06/01/99 12/31/11 84 N/A N/A Yes Hastings Youth Academy R2059 High 06/01/99 12/31/11 84 N/A 0 0 ** 18 ** 18 N/A Hastings Youth Specialized &IMH R2059 Mod 06/01/99 12/31/11 84 N/A N/A *Hillsborough IRT M8G02 High 04/15/09 09/14/11 90 N/A 0 0 N/A N/A N/A Yes *Martin Girls Academy R2050 High 04/15/09 07/24/11 89 N/A 0 0 N/A N/A N/A Yes Okeechobee Girls Academy R2091 Low/Mod 02/17/10 02/16/16 N/A N/A 0 0 N/A N/A N/A Okeechobee JOCC R2075 High 03/01/03 12/31/12 86 N/A N/A Yes Okeechobee JOCC R2075 Max 03/01/03 12/31/12 86 N/A N/A Okeechobee Youth Development R2069 High 07/01/09 06/30/12 80 N/A 0 0 N/A N/A N/A Okeechobee IHH R2069 Mod 07/01/09 06/30/12 78 N/A 0 0 N/A N/A N/A Orange Youth Academy R2060 High 01/01/08 10/22/11 88 N/A N/A Yes Orlando Intensive Youth Academy R2060 Mod 09/15/09 10/22/11 88 N/A 0 0 N/A N/A N/A Palmetto Youth Academy R2062 High 03/01/08 09/22/11 83 N/A N/A Pasco Girls Academy R2092 Low/Mod 02/01/10 01/31/16 88 N/A 0 0 N/A N/A N/A *Polk Halfway House J6G01 Mod 10/01/03 09/30/13 86 N/A 0 1 N/A N/A N/A Yes *Riverside Academy R2035 Mod 04/15/09 06/30/13 85 N/A 0 0 N/A N/A N/A Yes Department Use Only * Contracts for these programs were assumed when G4S purchased Sunshine Youth Services on April 15, There was no past performance activity from the date acquired to the date of RFP release. ** Used 2010 CAR numbers for this report. Per DJJ, Hasting Youth Academy high risk numbers on CAR are incorrect; on 09/01/07 the program was closed and 26 high risk youth were transferred to other high risk programs; 5 were transferred to a lower risk; 1 transferred early and 18 completed the program. The numbers should be 18 releases and 18 successful completions. Response to RFP R2107 Page 1
152 Volume III - Past Performance As found in the program contract. This information is only to aid the Department in identifying the program name. During the past year from the date of RFP issuance, the restrictiveness level for the majority of the time the Vendor operated the program. First date Vendor operated the program. Last date Vendor operated the program or, if the current Provider, the date the contract will expire. NOTE: If the program was evaluated prior to 2007, place scores in both columns. If program evaluated in 2007 or later, place score in Performance percentage column and NA in Compliance column. Most recent Quality Assurance Performance percentage score published on or before the date of the RFP. Most recent Quality Assurance Compliance percentage score published on or before the date of the RFP (if program was evaluated prior to 2007). The number of failure to report reportable incidents in accordance with policy FDJJ-8000 during the past year from the date of RFP issuance. The number of incidents of escape during the past year from the date of RFP issuance. Escapes are defined using criteria of the FDJJ Office of the Inspector General (FDJJ-8000). The number of youth released from the program during FY as documented in the Residential Release and Completion Report. This data may be found at The number of youth completing the program during FY as documented in the Residential Release and Completion Report. This number is multiplied by 2. This data may be found at 20 point deduction for Provider s receiving a Cure Notice after 7/1/08, and are successful in completion and compliance within the initial time period established in the notice; 40 point deduction for providers receiving a Cure Notice after 7/1/08, and are successful in completion and compliance after one or more extensions of the deadline established in the notice. 10 points for each program holding Deemed Status as defined in FDJJ at the date of RFP issuance, up to 20 points maximum. Response to RFP R2107 Page 2
153 Volume III - Past Performance PART III: Evaluation Questionnaire for Accreditation in the United States Does the prospective Provider currently operate or perform residential commitment juvenile justice program (accredited entity ) in the United States which is being offered as a part of its RFP proposal, AND is that accredited entity in good standing and without restrictions by: (1) American Correctional Association (ACA); (2) Commission on Accreditation of Rehabilitation Facilities (CARF); (3) Council on Accreditation (COA); or (4) Joint Commission (Formerly JCAHCO) Prospective Provider Check one: Yes No If No is checked above, the prospective Provider will be awarded zero (0) points for this section. If Yes is checked above, the prospective Provider will provide all of the information and documentation listed below for EACH accredited entity, to be evaluated for the points for this section. 1. Must provide the name of the prospective Provider s organization; Shown on Certificate 2. Must provide the name of the accredited entity; Shown on Certificate 3. If the accredited entity name is different than the name on the prospective Not applicable Provider s proposal, must provide documentation that both entities are part of the same organizational structure. (If not applicable, just state not applicable ); 4. Must provide the name of the accreditation organization, AND the accreditation Shown on Certificate organization must be one of the following: American Correctional Association (ACA), Commission on Accreditation of Rehabilitation Facilities (CARF), Council on Accreditation (COA), or Joint Commission (Formerly JCAHO); 5. Must provide documentation that evidences the accreditation award for each accredited entity; The following are acceptable forms of documentation as evidence of accreditation: a. An official letter(s) of the accreditation decision; b. An official accreditation report(s); c. A copy of the original accreditation certificate(s); or Copies on following pages d. An notification from COA if within seven (7) days of accreditation decision by COA. 6. Must provide documentation that establishes the accredited entity as a residential commitment juvenile justice program; See copies of QA Reports following certificates 7. Must provide documentation that establishes the residential commitment juvenile justice program as an included component of its accreditation award; See copies of QA Reports following certificates 8. Must provide documentation that establishes the accredited entity is physically See copies of QA Reports located in the United States; 9. Must provide documentation that establishes that the prospective Provider operated the accredited entity when the accreditation certification was awarded; 10. Must provide documentation that establishes that the accreditation period is valid at least through the start date of the contract that results from this RFP; AND 11. Must provide documentation that establishes that the accreditation certificate is in good standing and without restrictions. following certificates See copies of QA Reports following certificates See dates on copies of certificates See copy of letter from CARF on Page 10. Points Response to RFP R2107 Page 3
154 Volume III - Past Performance (A) The name of the Prospective Provider organization as stated on the proposal: (B) Name of Accredited Entity #1 (submitted for consideration for points in this section): Hillsborough Intensive Residential Treatment Program 10 Response to RFP R2107 Page 4


155 Volume III - Past Performance Hillsborough Intensive Residential Treatment Program Quality Assurance Review Response to RFP R2107 Page 5
156 Volume III - Past Performance (A) (B) The name of the Prospective Provider organization as stated on the proposal: Name of Accredited Entity #1 (submitted for consideration for points in this section): Points Martin Girls Academy 10 Response to RFP R2107 Page 6

157 Volume III - Past Performance Martin Girls Academy Quality Assurance Review Response to RFP R2107 Page 7
158 Volume III - Past Performance (A) (B) The name of the Prospective Provider organization as stated on the proposal: Name of Accredited Entity #1 (submitted for consideration for points in this section): Points Columbus Juvenile Residential Facility 10 Response to RFP R2107 Page 8

159 Volume III - Past Performance Columbus Juvenile Residential Facility Quality Assurance Reviews Response to RFP R2107 Page 9
VOLUME I TECHNICAL PROPOSAL
 VOLUME I TECHNICAL PROPOSAL TABLE OF CONTENTS Page Transmittal Letter and Addendums (#1 & #2 #3 #4 #5 & #6) Volume 1, Tab 1 Attachment O Cross Reference Table Attachment M and N Addendums Site Visit Sign-in
VOLUME I TECHNICAL PROPOSAL TABLE OF CONTENTS Page Transmittal Letter and Addendums (#1 & #2 #3 #4 #5 & #6) Volume 1, Tab 1 Attachment O Cross Reference Table Attachment M and N Addendums Site Visit Sign-in
REQUEST FOR PROPOSALS (RFP) ADDENDUM. Date: February 6, 2014 ADDENDUM: #1 DMS CLASS CODE:
 ADDENDUM. Date: February 6, 2014 ADDENDUM: #1 DMS CLASS CODE:") REQUEST FOR PROPOSALS (RFP) ADDENDUM Date: February 6, 2014 ADDENDUM: #1 DMS CLASS CODE: 913-180 RFP#: 10164 TITLE: Detention Screening, Intake Services at the Broward County Juvenile Assessment Center
REQUEST FOR PROPOSALS (RFP) ADDENDUM Date: February 6, 2014 ADDENDUM: #1 DMS CLASS CODE: 913-180 RFP#: 10164 TITLE: Detention Screening, Intake Services at the Broward County Juvenile Assessment Center
BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Redirection Service - Circuit 7 The Chrysalis Center, Inc.
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Redirection Service - Circuit 7 The Chrysalis Center, Inc.
BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Redirection Service - Circuit 10 The Chrysalis Center,
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Redirection Service - Circuit 10 The Chrysalis Center,
CHILDREN'S MENTAL HEALTH ACT
 40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
40 MINNESOTA STATUTES 2013 245.487 CHILDREN'S MENTAL HEALTH ACT 245.487 CITATION; DECLARATION OF POLICY; MISSION. Subdivision 1. Citation. Sections 245.487 to 245.4889 may be cited as the "Minnesota Comprehensive
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Project Connect Twin Oaks Juvenile Development Corporation
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Project Connect Twin Oaks Juvenile Development Corporation
FLORIDA DEPARTMENT OF JUVENILE JUSTICE PROCEDURE
 SECTION: FLORIDA DEPARTMENT OF JUVENILE JUSTICE PROCEDURE Title: Employee Training Procedures Related Policy: FDJJ 1520 I. DEFINITIONS Administrator One whose primary responsibility is to oversee the daily
SECTION: FLORIDA DEPARTMENT OF JUVENILE JUSTICE PROCEDURE Title: Employee Training Procedures Related Policy: FDJJ 1520 I. DEFINITIONS Administrator One whose primary responsibility is to oversee the daily
INVITATION TO NEGOTIATE (ITN) ADDENDUM #1. July 21, 2017
 ADDENDUM #1. July 21, 2017") INVITATION TO NEGOTIATE (ITN) ADDENDUM #1 July 21, 2017 ITN Number: 10511 ITN Services: The Department seeks replies from qualified non-profit, for profit and government entities to serve as the single
INVITATION TO NEGOTIATE (ITN) ADDENDUM #1 July 21, 2017 ITN Number: 10511 ITN Services: The Department seeks replies from qualified non-profit, for profit and government entities to serve as the single
DATA SOURCES AND METHODS
 DATA SOURCES AND METHODS In August 2006, the Department of Juvenile Justice s (DJJ) Quality Assurance, Technical Assistance and Research and Planning units were assigned to the Office of Program Accountability.
DATA SOURCES AND METHODS In August 2006, the Department of Juvenile Justice s (DJJ) Quality Assurance, Technical Assistance and Research and Planning units were assigned to the Office of Program Accountability.
SOLICITATION CONFERENCE CALL AGENDA
 SOLICITATION CONFERENCE CALL AGENDA INVITATION TO NEGOTIATE (ITN) #10573 DESIGN, DEVELOP, IMPLEMENT & OPERATE A FACILITY BASED DAY TREATMENT (FBDT) PROGRAM IN FLORIDA Thursday, May 3, 2018 @ 10:00 a.m.
SOLICITATION CONFERENCE CALL AGENDA INVITATION TO NEGOTIATE (ITN) #10573 DESIGN, DEVELOP, IMPLEMENT & OPERATE A FACILITY BASED DAY TREATMENT (FBDT) PROGRAM IN FLORIDA Thursday, May 3, 2018 @ 10:00 a.m.
RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES
 RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES CHAPTER 0940-5-41 MINIMUM PROGRAM REQUIREMENTS FOR ALCOHOL AND DRUG HALFWAY HOUSE TREATMENT FACILITIES TABLE OF CONTENTS
RULES OF THE TENNESSEE DEPARTMENT OF MENTAL HEALTH AND DEVELOPMENTAL DISABILITIES CHAPTER 0940-5-41 MINIMUM PROGRAM REQUIREMENTS FOR ALCOHOL AND DRUG HALFWAY HOUSE TREATMENT FACILITIES TABLE OF CONTENTS
Available at: urces/purchasingforms 2
 Date: March 1, 2017 Solicitation #: 10476 Subject: The Department of Juvenile Justice currently contracts for operation of the Columbus Juvenile Residential Facility program, a fifty (50) bed nonsecure
Date: March 1, 2017 Solicitation #: 10476 Subject: The Department of Juvenile Justice currently contracts for operation of the Columbus Juvenile Residential Facility program, a fifty (50) bed nonsecure
LOUISIANA MEDICAID PROGRAM ISSUED: 06/09/17 REPLACED: CHAPTER 2: BEHAVIORAL HEALTH SERVICES SECTION 2.2: OUTPATIENT SERVICES PAGE(S) 8
 8") Licensed Practitioner Outpatient Therapy includes: Individual; Family; Group; Outpatient psychotherapy; Mental health assessment; Evaluation; Testing; Medication management; Psychiatric evaluation; Medication
Licensed Practitioner Outpatient Therapy includes: Individual; Family; Group; Outpatient psychotherapy; Mental health assessment; Evaluation; Testing; Medication management; Psychiatric evaluation; Medication
BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 18 Department of Juvenile
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 18 Department of Juvenile
CHAPTER 63D-9 ASSESSMENT
 CHAPTER 63D-9 ASSESSMENT 63D-9.001 Purpose and Scope 63D-9.002 Detention Screening 63D-9.003 Intake Services 63D-9.004 Risk and Needs Assessment 63D-9.005 Comprehensive Assessment 63D-9.006 Comprehensive
CHAPTER 63D-9 ASSESSMENT 63D-9.001 Purpose and Scope 63D-9.002 Detention Screening 63D-9.003 Intake Services 63D-9.004 Risk and Needs Assessment 63D-9.005 Comprehensive Assessment 63D-9.006 Comprehensive
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services.
 907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
907 KAR 15:080. Coverage provisions and requirements regarding outpatient chemical dependency treatment center services. RELATES TO: KRS 205.520, 42 U.S.C. 1396a(a)(10)(B), 1396a(a)(23) STATUTORY AUTHORITY:
INVITATION TO NEGOTIATE (ITN) ADDENDUM #1. May 8, 2018
 ADDENDUM #1. May 8, 2018") INVITATION TO NEGOTIATE (ITN) ADDENDUM #1 May 8, 2018 ITN Number: 10573 ITN Services: The Department of Juvenile Justice (Department or DJJ) is issuing this ITN to obtain replies and further negotiate
INVITATION TO NEGOTIATE (ITN) ADDENDUM #1 May 8, 2018 ITN Number: 10573 ITN Services: The Department of Juvenile Justice (Department or DJJ) is issuing this ITN to obtain replies and further negotiate
APPROVED: Early Release: Release before the minimum length of stay.
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Users { } Administration {x} Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 17: ADMISSION AND RELEASE Subject: RELEASE
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Users { } Administration {x} Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 17: ADMISSION AND RELEASE Subject: RELEASE
GEORGIA DEPARTMENT OF JUVENILE JUSTICE I. POLICY:
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities Chapter 12: BEHAVIORAL HEALTH SERVICES Subject: MENTAL HEALTH ASSESSMENT
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities Chapter 12: BEHAVIORAL HEALTH SERVICES Subject: MENTAL HEALTH ASSESSMENT
Clinical Utilization Management Guideline
 Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Clinical Utilization Management Guideline Subject: Therapeutic Behavioral On-Site Services for Recipients Under the Age of 21 Years Status: New Current Effective Date: January 2018 Description Last Review
Covered Service Codes and Definitions
 Covered Service Codes and Definitions [01] Assessment Assessment services include the systematic collection and integrated review of individualspecific data, such as examinations and evaluations. This
Covered Service Codes and Definitions [01] Assessment Assessment services include the systematic collection and integrated review of individualspecific data, such as examinations and evaluations. This
BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 20 Department of Juvenile
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 20 Department of Juvenile
Standardized Program Evaluation Protocol [SPEP] Report
![Standardized Program Evaluation Protocol [SPEP] Report](/thumbs/81/83184960.jpg "Standardized Program Evaluation Protocol [SPEP] Report") Standardized Program Evaluation Protocol [SPEP] Report Hillsborough Girls Academy G4S Youth Services, LLC (Contract Provider) 9502 East Columbus Drive Tampa, Florida 33619 Primary Service: Female Healthy
Standardized Program Evaluation Protocol [SPEP] Report Hillsborough Girls Academy G4S Youth Services, LLC (Contract Provider) 9502 East Columbus Drive Tampa, Florida 33619 Primary Service: Female Healthy
CHAPTER 24 ACCREDITATION OF PROVIDERS OF SERVICES TO PERSONS WITH MENTAL ILLNESS, MENTAL RETARDATION, AND DEVELOPMENTAL DISABILITIES PREAMBLE
 Human Services[441] Ch 24, p.1 CHAPTER 24 ACCREDITATION OF PROVIDERS OF SERVICES TO PERSONS WITH MENTAL ILLNESS, MENTAL RETARDATION, AND DEVELOPMENTAL DISABILITIES PREAMBLE The mental health, mental retardation,
Human Services[441] Ch 24, p.1 CHAPTER 24 ACCREDITATION OF PROVIDERS OF SERVICES TO PERSONS WITH MENTAL ILLNESS, MENTAL RETARDATION, AND DEVELOPMENTAL DISABILITIES PREAMBLE The mental health, mental retardation,
MQI Standards for Probation and Community Intervention Programs
 Standard 1. Management Accountability MQI Standards for Probation and Community Intervention Programs Standard 1: Management Accountability 1.01 Initial Background Screening* 1-2 1.02 Five-Year Rescreening
Standard 1. Management Accountability MQI Standards for Probation and Community Intervention Programs Standard 1: Management Accountability 1.01 Initial Background Screening* 1-2 1.02 Five-Year Rescreening
256B.0943 CHILDREN'S THERAPEUTIC SERVICES AND SUPPORTS.
 1 MINNESOTA STATUTES 2016 256B.0943 256B.0943 CHILDREN'S THERAPEUTIC SERVICES AND SUPPORTS. Subdivision 1. Definitions. For purposes of this section, the following terms have the meanings given them. (a)
1 MINNESOTA STATUTES 2016 256B.0943 256B.0943 CHILDREN'S THERAPEUTIC SERVICES AND SUPPORTS. Subdivision 1. Definitions. For purposes of this section, the following terms have the meanings given them. (a)
Levels of Observation: The frequency of youth supervision.
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Transmittal # 17-17 Policy # 12.21 Applicability: {x} All DJJ Staff { } Administration { } Community Services { } Secure Facilities (RYDCs and YDCs) Chapter 12: BEHAVIORAL
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Transmittal # 17-17 Policy # 12.21 Applicability: {x} All DJJ Staff { } Administration { } Community Services { } Secure Facilities (RYDCs and YDCs) Chapter 12: BEHAVIORAL
ARIZONA DEPARTMENT OF CORRECTIONS
 ARIZONA DEPARTMENT OF CORRECTIONS FIVE-YEAR STRATEGIC PLAN FY 2012 to FY 2016 Charles L. Ryan Director TABLE OF CONTENTS Executive Summary... i Strategic Plan.. 1 Agency Vision 1 Agency Mission 1 Agency
ARIZONA DEPARTMENT OF CORRECTIONS FIVE-YEAR STRATEGIC PLAN FY 2012 to FY 2016 Charles L. Ryan Director TABLE OF CONTENTS Executive Summary... i Strategic Plan.. 1 Agency Vision 1 Agency Mission 1 Agency
Florida Medicaid. Statewide Inpatient Psychiatric Program Coverage Policy
 Florida Medicaid Statewide Inpatient Psychiatric Program Coverage Policy Agency for Health Care Administration December 2015 Table of Contents 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority...
Florida Medicaid Statewide Inpatient Psychiatric Program Coverage Policy Agency for Health Care Administration December 2015 Table of Contents 1.0 Introduction... 1 1.1 Description... 1 1.2 Legal Authority...
BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Youth and Family Alternatives - George W. Harris The Florida Network of
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Youth and Family Alternatives - George W. Harris The Florida Network of
Mental Health Services In the Detention Center Project~ Request For Proposal (RFP)
") Mental Health Services In the Detention Center Request For Proposal (RFP) Release Date: February 6, Submission Due Date: March 2, Overview: The mission of Cuyahoga County s Juvenile Court is to administer
Mental Health Services In the Detention Center Request For Proposal (RFP) Release Date: February 6, Submission Due Date: March 2, Overview: The mission of Cuyahoga County s Juvenile Court is to administer
OUTPATIENT SERVICES. Components of Service
 OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
OUTPATIENT SERVICES Providers contracted for this level of care or service are expected to comply with all requirements of these service-specific performance specifications. Additionally, providers contracted
BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR
 STATE OF FLORIDA DEPARTMENT OF JUVENILE JUSTICE BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Duval Halfway House Department of Juvenile Justice (State-Operated) 7500 Ricker Road Jacksonville, Florida
STATE OF FLORIDA DEPARTMENT OF JUVENILE JUSTICE BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Duval Halfway House Department of Juvenile Justice (State-Operated) 7500 Ricker Road Jacksonville, Florida
BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Rainwater Center for Girls Crosswinds Youth Services, Inc. (Contract Provider)
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Rainwater Center for Girls Crosswinds Youth Services, Inc. (Contract Provider)
BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 8 Department of Juvenile
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 8 Department of Juvenile
RELEVANT STATE STANDARDS OF CARE AND SERVICES AND PROCESSES TO ENSURE STANDARDS ARE MET 1
 Appendix D RELEVANT STATE STANDARDS OF CARE AND SERVICES AND PROCESSES TO ENSURE STANDARDS ARE MET 1 I. STATE STANDARDS OF CARE AND SERVICES Excerpts From RSA 171-A 171-A:1 Purpose and Policy. The purpose
Appendix D RELEVANT STATE STANDARDS OF CARE AND SERVICES AND PROCESSES TO ENSURE STANDARDS ARE MET 1 I. STATE STANDARDS OF CARE AND SERVICES Excerpts From RSA 171-A 171-A:1 Purpose and Policy. The purpose
Deputy Probation Officer I/II
 Santa Cruz County Probation September 2013 Duty Statement page 1 Deputy Probation Officer I/II 1. Conduct dispositional or pre-sentence investigations of adults and juveniles by interviewing offenders,
Santa Cruz County Probation September 2013 Duty Statement page 1 Deputy Probation Officer I/II 1. Conduct dispositional or pre-sentence investigations of adults and juveniles by interviewing offenders,
CHAPTER 63N-1 SERVICE DELIVERY
 CHAPTER 63N-1 SERVICE DELIVERY 63N-1.001 63N-1.002 63N-1.0031 63N-1.0032 63N-1.0033 63N-1.0034 63N-1.0035 63N-1.0036 63N-1.004 63N-1.0041 63N-1.0042 63N-1.0051 63N-1.0052 63N-1.0053 63N-1.0054 63N-1.0055
CHAPTER 63N-1 SERVICE DELIVERY 63N-1.001 63N-1.002 63N-1.0031 63N-1.0032 63N-1.0033 63N-1.0034 63N-1.0035 63N-1.0036 63N-1.004 63N-1.0041 63N-1.0042 63N-1.0051 63N-1.0052 63N-1.0053 63N-1.0054 63N-1.0055
BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR White Foundation IDDS - Circuit 1 Henry and Rilla White Youth Foundation,
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR White Foundation IDDS - Circuit 1 Henry and Rilla White Youth Foundation,
FLORIDA DEPARTMENT OF JUVENILE JUSTICE PROCEDURE
 PROCEDURE Title: Medicaid Policy/Child in Care Procedures Related Policy: FDJJ 9325 I. DEFINITIONS Agency for Health Care Administration (AHCA)- State agency that administers the Medicaid program, grants
PROCEDURE Title: Medicaid Policy/Child in Care Procedures Related Policy: FDJJ 9325 I. DEFINITIONS Agency for Health Care Administration (AHCA)- State agency that administers the Medicaid program, grants
BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Lutheran Services Florida - HOPE House The Florida Network of Youth and
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Lutheran Services Florida - HOPE House The Florida Network of Youth and
POLICY AND PROCEDURE CHECKLIST ODYS Policy and Procedure
 Case 2:04-cv-01206-ALM-TPK Document 120-2 Filed 05/22/2009 Page 1 of 11 POLICY AND PROCEDURE CHECKLIST ODYS Policy and Procedure Black indicates policies reviewed and revised as needed Blue indicates policy
Case 2:04-cv-01206-ALM-TPK Document 120-2 Filed 05/22/2009 Page 1 of 11 POLICY AND PROCEDURE CHECKLIST ODYS Policy and Procedure Black indicates policies reviewed and revised as needed Blue indicates policy
Agency for Health Care Administration
 Page 1 of 24 ST - Q0000 - Initial Comments Title Initial Comments Statute or Rule Type Memo Tag These guidelines are meant solely to provide guidance to surveyors in the survey process. ST - Q0100 - License
Page 1 of 24 ST - Q0000 - Initial Comments Title Initial Comments Statute or Rule Type Memo Tag These guidelines are meant solely to provide guidance to surveyors in the survey process. ST - Q0100 - License
BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Kissimmee Juvenile SOP Correctional Facility Sequel Youth and Family Services
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Kissimmee Juvenile SOP Correctional Facility Sequel Youth and Family Services
BERKELEY COMMUNITY MENTAL HEALTH CENTER (BCMHC) OUTPATIENT PROGRAM PLAN 2017
 OUTPATIENT PROGRAM PLAN 2017") BERKELEY COMMUNITY MENTAL HEALTH CENTER (BCMHC) OUTPATIENT PROGRAM PLAN 2017 REVIEWED AND UPDATED NOVEMBER 2017 OUR MISSION PHILOSOPHY The staff of the Berkeley Community Mental Health Center, in partnership
BERKELEY COMMUNITY MENTAL HEALTH CENTER (BCMHC) OUTPATIENT PROGRAM PLAN 2017 REVIEWED AND UPDATED NOVEMBER 2017 OUR MISSION PHILOSOPHY The staff of the Berkeley Community Mental Health Center, in partnership
Quality Improvement Standards for Probation and Community Intervention Programs
 for Programs Promoting continuous improvement and accountability in juvenile justice programs and services QI Standards for Probation and Community Intervention Programs Standard 1: Management Accountability
for Programs Promoting continuous improvement and accountability in juvenile justice programs and services QI Standards for Probation and Community Intervention Programs Standard 1: Management Accountability
REQUEST FOR PROPOSALS:
 REQUEST FOR PROPOSALS: Behavioral Health Care in the Baltimore City Juvenile Justice Center Release Date: February 6, 2018 Pre-Proposal Conference: February 26, 2018 Proposal Due: March 19, 2018 Anticipated
REQUEST FOR PROPOSALS: Behavioral Health Care in the Baltimore City Juvenile Justice Center Release Date: February 6, 2018 Pre-Proposal Conference: February 26, 2018 Proposal Due: March 19, 2018 Anticipated
POSITION: DATE WRITTEN: DEPARTMENT:
 POSITION: Youth Development Specialist, Full-Time DATE WRITTEN: BB DEPARTMENT: Court Administration, Juvenile Detention REVIEWED BY: DH REPORTS TO Assistant Superintendent Lead Assistant Superintendent
POSITION: Youth Development Specialist, Full-Time DATE WRITTEN: BB DEPARTMENT: Court Administration, Juvenile Detention REVIEWED BY: DH REPORTS TO Assistant Superintendent Lead Assistant Superintendent
Specialized Therapeutic Foster Care and Therapeutic Group Home (Florida)
") Care1st Health Plan Arizona, Inc. Easy Choice Health Plan Harmony Health Plan of Illinois Missouri Care Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona OneCare (Care1st Health
Care1st Health Plan Arizona, Inc. Easy Choice Health Plan Harmony Health Plan of Illinois Missouri Care Ohana Health Plan, a plan offered by WellCare Health Insurance of Arizona OneCare (Care1st Health
Program Description / Disclosure Statement for CWC s Acquired Brain Injury Services 2017
 Program Description / Disclosure Statement for CWC s Acquired Brain Injury Services 2017 Three 24/7 Residential homes: The Charlotte White Center's Level III Residential Housing Programs for Individuals
Program Description / Disclosure Statement for CWC s Acquired Brain Injury Services 2017 Three 24/7 Residential homes: The Charlotte White Center's Level III Residential Housing Programs for Individuals
CRISIS STABILIZATION (Children and Adolescents)
") CRISIS STABILIZATION (Children and Adolescents) Providers contracted for this level of care or service will be expected to comply with all requirements of these service-specific performance specifications.
CRISIS STABILIZATION (Children and Adolescents) Providers contracted for this level of care or service will be expected to comply with all requirements of these service-specific performance specifications.
UnitedHealthcare Guideline
 UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
UnitedHealthcare Guideline TITLE: CRS BEHAVIORAL HEALTH HOME CARE TRAINING TO HOME CARE CLIENT (HCTC) PRACTICE GUIDELINES EFFECTIVE DATE: 1/1/2017 PAGE 1 of 14 GUIDELINE STATEMENT This guideline outlines
Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria. Effective August 1, 2014
 Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria Effective August 1, 2014 1 Table of Contents Florida Medicaid Handbook... 3 Clinical Practice Guidelines... 3 Description
Statewide Inpatient Psychiatric Programs Admission Process and Level of Care Criteria Effective August 1, 2014 1 Table of Contents Florida Medicaid Handbook... 3 Clinical Practice Guidelines... 3 Description
INTEGRATED CASE MANAGEMENT ANNEX A
 INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
INTEGRATED CASE MANAGEMENT ANNEX A NAME OF AGENCY: CONTRACT NUMBER: CONTRACT TERM: TO BUDGET MATRIX CODE: 32 This Annex A specifies the Integrated Case Management services that the Provider Agency is authorized
I. POLICY: DEFINITIONS:
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs & YDCs) Transmittal # 12-04 Policy # 18.11 Related Standards
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs & YDCs) Transmittal # 12-04 Policy # 18.11 Related Standards
C I N S / F I N S C h i l d r e n / F a m i l i e s I n N e e d o f S e r v i c e s S T A N D A R D S
 C I N S / F I N S C h i l d r e n / F a m i l i e s I n N e e d o f S e r v i c e s S T A N D A R D S Bureau of Quality Improvement Introduction The quality improvement process was developed pursuant to
C I N S / F I N S C h i l d r e n / F a m i l i e s I n N e e d o f S e r v i c e s S T A N D A R D S Bureau of Quality Improvement Introduction The quality improvement process was developed pursuant to
Non-Time Limited Supportive Housing Program for Youth Request for Proposals for Supportive Housing Providers (RFP)
") Non-Time Limited Supportive Housing Program for Youth Request for Proposals for Supportive Housing Providers (RFP) A collaborative program between the Ohio Department of Youth Services and CSH I PROJECT
Non-Time Limited Supportive Housing Program for Youth Request for Proposals for Supportive Housing Providers (RFP) A collaborative program between the Ohio Department of Youth Services and CSH I PROJECT
BUPERSINST B BUPERS-00D 22 Nov 2016 BUPERS INSTRUCTION B. From: Chief of Naval Personnel. Subj: THE MILITARY MODEL OF NAVY CORRECTIONS
 BUPERS-00D BUPERS INSTRUCTION 1640.21B From: Chief of Naval Personnel Subj: THE MILITARY MODEL OF NAVY CORRECTIONS Ref: (a) 10 U.S.C. 951 (b) SECNAVINST 1640.9C (c) BUPERSINST 1640.22 (d) Manual for Courts-Martial
BUPERS-00D BUPERS INSTRUCTION 1640.21B From: Chief of Naval Personnel Subj: THE MILITARY MODEL OF NAVY CORRECTIONS Ref: (a) 10 U.S.C. 951 (b) SECNAVINST 1640.9C (c) BUPERSINST 1640.22 (d) Manual for Courts-Martial
I. POLICY: DEFINITIONS:
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff {x} Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Transmittal # 18-1 Policy # 12.1 Related Standards
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff {x} Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Transmittal # 18-1 Policy # 12.1 Related Standards
907 KAR 10:014. Outpatient hospital service coverage provisions and requirements.
 907 KAR 10:014. Outpatient hospital service coverage provisions and requirements. RELATES TO: KRS 205.520, 42 C.F.R. 447.53 STATUTORY AUTHORITY: KRS 194A.030(2), 194A.050(1), 205.520(3), 205.560, 205.6310,
907 KAR 10:014. Outpatient hospital service coverage provisions and requirements. RELATES TO: KRS 205.520, 42 C.F.R. 447.53 STATUTORY AUTHORITY: KRS 194A.030(2), 194A.050(1), 205.520(3), 205.560, 205.6310,
Welcome Package. Information for Families
 Welcome Package Information for Families 35 Blackmarsh Rd. St. John s, NL A1E 1S4 Phone: 709-733-2273 Fax: 709-757-3551 Email: info@blueskyfamilycare.com Welcome to Blue sky Residential Care Blue sky is
Welcome Package Information for Families 35 Blackmarsh Rd. St. John s, NL A1E 1S4 Phone: 709-733-2273 Fax: 709-757-3551 Email: info@blueskyfamilycare.com Welcome to Blue sky Residential Care Blue sky is
Standardized Program Evaluation Protocol [SPEP] Report
![Standardized Program Evaluation Protocol [SPEP] Report](/thumbs/85/91550053.jpg "Standardized Program Evaluation Protocol [SPEP] Report") Standardized Program Evaluation Protocol [SPEP] Report Okeechobee Intensive Halfway House TrueCore Behavioral Solutions, LLC (Contract Provider) 800 North East 72 nd Circle Okeechobee, Florida 34972 Primary
Standardized Program Evaluation Protocol [SPEP] Report Okeechobee Intensive Halfway House TrueCore Behavioral Solutions, LLC (Contract Provider) 800 North East 72 nd Circle Okeechobee, Florida 34972 Primary
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS TARGETED CASE MANAGEMENT Provider will comply with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
GEORGIA DEPARTMENT OF JUVENILE JUSTICE I. POLICY:
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 12: BEHAVIORAL HEALTH SERVICES Subject:
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 12: BEHAVIORAL HEALTH SERVICES Subject:
Assertive Community Treatment (ACT)
") Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
Assertive Community Treatment (ACT) Assertive Community Treatment (ACT) services are therapeutic interventions that address the functional problems of individuals who have the most complex and/or pervasive
DEPARTMENT OF CHILDREN AND FAMILIES DIVISION OF CHILD BEHAVIORAL HEALTH SERVICES
 DEPARTMENT OF CHILDREN AND FAMILIES DIVISION OF CHILD BEHAVIORAL HEALTH SERVICES Effective Date: May 1, 2008 DCBHS Policy #4 Date Issued: April 11, 2008 I. TITLE Admissions to Out-of-Home Treatment Settings
DEPARTMENT OF CHILDREN AND FAMILIES DIVISION OF CHILD BEHAVIORAL HEALTH SERVICES Effective Date: May 1, 2008 DCBHS Policy #4 Date Issued: April 11, 2008 I. TITLE Admissions to Out-of-Home Treatment Settings
GEORGIA DEPARTMENT OF JUVENILE JUSTICE I. POLICY:
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 12: BEHAVIORAL HEALTH SERVICES Subject:
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Chapter 12: BEHAVIORAL HEALTH SERVICES Subject:
BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Polk Halfway House G4S Youth Services, LLC. (Contract Provider)
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR Polk Halfway House G4S Youth Services, LLC. (Contract Provider)
BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 3 Department of Juvenile
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY IMPROVEMENT PROGRAM REPORT FOR Probation and Community Intervention - Circuit 3 Department of Juvenile
GUIDELINES FOR SCORING INDIVIDUAL RECORDS. Y = Meets Standard N = Does Not Meet Standard. N/A = Not Applicable
 QUALITY OF DOCUMENTATION IOP GUIDELINES FOR SCORING INDIVIDUAL RECORDS Y = Meets Standard N = Does Not Meet Standard N/A = Not Applicable GUIDELINES FOR DETERMINING PROGRAM COMPLIANCE WITH STANDARDS Programs
QUALITY OF DOCUMENTATION IOP GUIDELINES FOR SCORING INDIVIDUAL RECORDS Y = Meets Standard N = Does Not Meet Standard N/A = Not Applicable GUIDELINES FOR DETERMINING PROGRAM COMPLIANCE WITH STANDARDS Programs
DEPARTMENT OF HUMAN SERVICES DIVISION OF MENTAL HEALTH & ADDICTION SERVICES
 DEPARTMENT OF HUMAN SERVICES DIVISION OF MENTAL HEALTH & ADDICTION SERVICES ADDENDUM to Attachment 3.1-A Page 13(d).10 Service Description Community Support Services consist of mental health rehabilitation
DEPARTMENT OF HUMAN SERVICES DIVISION OF MENTAL HEALTH & ADDICTION SERVICES ADDENDUM to Attachment 3.1-A Page 13(d).10 Service Description Community Support Services consist of mental health rehabilitation
BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR University Area Community Development Corporation, Inc.
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR University Area Community Development Corporation, Inc.
Defining the Nathaniel ACT ATI Program
 Nathaniel ACT ATI Program: ACT or FACT? Over the past 10 years, the Center for Alternative Sentencing and Employment Services (CASES) has received national recognition for the Nathaniel Project 1. Initially
Nathaniel ACT ATI Program: ACT or FACT? Over the past 10 years, the Center for Alternative Sentencing and Employment Services (CASES) has received national recognition for the Nathaniel Project 1. Initially
LAKESHORE REGIONAL ENTITY Clubhouse Psychosocial Rehabilitation Programs
 Attachment A LAKESHORE REGIONAL ENTITY This service must be provided consistent with requirements outlined in the MDHHS Medicaid Provider Manual as updated. The manual is available at: http://www.mdch.state.mi.us/dch-medicaid/manuals/medicaidprovidermanual.pdf
Attachment A LAKESHORE REGIONAL ENTITY This service must be provided consistent with requirements outlined in the MDHHS Medicaid Provider Manual as updated. The manual is available at: http://www.mdch.state.mi.us/dch-medicaid/manuals/medicaidprovidermanual.pdf
Provider Certification Standards Adult Day Care
 Provider Certification Standards Adult Day Care December 2015 1 Definitions: Activities of Daily Living (ADL s)- Includes but is not limited to the following personal care activities: bathing, dressing,
Provider Certification Standards Adult Day Care December 2015 1 Definitions: Activities of Daily Living (ADL s)- Includes but is not limited to the following personal care activities: bathing, dressing,
BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR West Florida Wilderness Institute AMIkids, Inc. (Contract Provider) 1912
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR West Florida Wilderness Institute AMIkids, Inc. (Contract Provider) 1912
(b) The goals of in-home community based services are to: (1) Ensure the safety of children, families, and communities;
 The goals of in-home community based services are to: (1) Ensure the safety of children, families, and communities;") PART He-C 6339 CERTIFICATION FOR PAYMENT STANDARDS FOR COMMUNITY-BASED IN HOME SERVICE PROVIDERS: CHILD HEALTH SUPPORT, HOME BASED THERAPEUTIC, THERAPEUTIC DAY TREATMENT, ADOLESCENT COMMUNITY THERAPEUTIC
PART He-C 6339 CERTIFICATION FOR PAYMENT STANDARDS FOR COMMUNITY-BASED IN HOME SERVICE PROVIDERS: CHILD HEALTH SUPPORT, HOME BASED THERAPEUTIC, THERAPEUTIC DAY TREATMENT, ADOLESCENT COMMUNITY THERAPEUTIC
APPROVED: Low: Youth has a below average likelihood of being involved in a subsequent incident while in the facility.
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Transmittal # 17-2 Policy # 17.3 Related Standards
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: { } All DJJ Staff { } Administration { } Community Services {x} Secure Facilities (RYDCs and YDCs) Transmittal # 17-2 Policy # 17.3 Related Standards
COUNTY OF SANTA CLARA PUBLIC SAFETY REALIGNMENT PROGRAM MONTHLY STATUS REPORT
 COUNTY OF SANTA CLARA PUBLIC SAFETY REALIGNMENT PROGRAM MONTHLY STATUS REPORT October 1, 2011 November 1, 2011 PROBATION DEPARTMENT: The Probation Department received an initial combined allocation of
COUNTY OF SANTA CLARA PUBLIC SAFETY REALIGNMENT PROGRAM MONTHLY STATUS REPORT October 1, 2011 November 1, 2011 PROBATION DEPARTMENT: The Probation Department received an initial combined allocation of
Rule 132 Training. for Community Mental Health Providers
 Rule 132 Training for Community Mental Health Providers October 2013 Goals for training Understand purpose and vision of Rule 132 Understand Rule 132 requirements Understand the appropriate application
Rule 132 Training for Community Mental Health Providers October 2013 Goals for training Understand purpose and vision of Rule 132 Understand Rule 132 requirements Understand the appropriate application
COWLITZ COUNTY REQUEST FOR PROPOSALS INMATE HELATH CARE # Issued September 13th, 2017 ADDENDUM #2. Issued: October 6th 2017
 COWLITZ COUNTY REQUEST FOR PROPOSALS INMATE HELATH CARE #09-2017 Issued September 13th, 2017 ADDENDUM #2 Issued: October 6th 2017 1 Vendor submitted questions; 1. Do you expect your inmate population to
COWLITZ COUNTY REQUEST FOR PROPOSALS INMATE HELATH CARE #09-2017 Issued September 13th, 2017 ADDENDUM #2 Issued: October 6th 2017 1 Vendor submitted questions; 1. Do you expect your inmate population to
BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR
 STATE OF FLORIDA DEPARTMENT OF JUVENILE JUSTICE BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Sarasota YMCA Shelter Sarasota Family YMCA Inc. (Contract Provider) 1106 Briggs Avenue Sarasota, Florida 34234-8140
STATE OF FLORIDA DEPARTMENT OF JUVENILE JUSTICE BUREAU OF QUALITY ASSURANCE PROGRAM REPORT FOR Sarasota YMCA Shelter Sarasota Family YMCA Inc. (Contract Provider) 1106 Briggs Avenue Sarasota, Florida 34234-8140
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS HOME-BASED SERVICES
 NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS HOME-BASED SERVICES Provider will be in compliance with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
NETWORK180 PROVIDER MANUAL SECTION 1: SERVICE REQUIREMENTS HOME-BASED SERVICES Provider will be in compliance with regulations and requirements as outlined in the Michigan Medicaid Provider Manual, Behavioral
Respite Care DEFINITION
 DEFINITION Respite Care programs provide temporary relief to caregivers with responsibility for the care and supervision of adults or children who: have physical, emotional, developmental, cognitive, behavioural,
DEFINITION Respite Care programs provide temporary relief to caregivers with responsibility for the care and supervision of adults or children who: have physical, emotional, developmental, cognitive, behavioural,
Sacramento County Community Corrections Partnership
 Sacramento County Community Corrections Partnership AB 109 Mental Health & Substance Abuse Work Group Proposal Mental Health & Alcohol / Drug Service Gaps: County Jail Prison ( N3 ), Parole, and Flash
Sacramento County Community Corrections Partnership AB 109 Mental Health & Substance Abuse Work Group Proposal Mental Health & Alcohol / Drug Service Gaps: County Jail Prison ( N3 ), Parole, and Flash
Behavior Rehabilitation Services (BRS)
") Behavior Rehabilitation Services (BRS) Oregon Administrative Rules Guide Oregon Health Authority Division of Medical Assistance Programs Oregon Department of Human Services Child Welfare Program Oregon
Behavior Rehabilitation Services (BRS) Oregon Administrative Rules Guide Oregon Health Authority Division of Medical Assistance Programs Oregon Department of Human Services Child Welfare Program Oregon
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: {x} All DJJ Staff {x} Administration {x} Community Services {x} Secure Facilities I.
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: {x} All DJJ Staff {x} Administration {x} Community Services {x} Secure Facilities Chapter 1: ADMINISTRATION Subject: CITIZEN AND VOLUNTEER INVOLVEMENT
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: {x} All DJJ Staff {x} Administration {x} Community Services {x} Secure Facilities Chapter 1: ADMINISTRATION Subject: CITIZEN AND VOLUNTEER INVOLVEMENT
VIVIAN ALVAREZ, Ph.D.
 VIVIAN ALVAREZ, Ph.D. OFFICE: 12304 Santa Monica Blvd., Suite 210, Los Angeles, CA 90025 Telephone: (310) 473-1210; Cellular: (310) 387-0602 e-mail: valvarezphd@gmail.com BIRTH DATE: June 9, 1958 CITIZENSHIP:
VIVIAN ALVAREZ, Ph.D. OFFICE: 12304 Santa Monica Blvd., Suite 210, Los Angeles, CA 90025 Telephone: (310) 473-1210; Cellular: (310) 387-0602 e-mail: valvarezphd@gmail.com BIRTH DATE: June 9, 1958 CITIZENSHIP:
BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR
 S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR JDAP Circuit 12 Bay Area Youth Services (Contract Provider)
S T A T E O F F L O R I D A D E P A R T M E N T O F J U V E N I L E J U S T I C E BUREAU OF MONITORING AND QUALITY IMPROVEMENT PROGRAM REPORT FOR JDAP Circuit 12 Bay Area Youth Services (Contract Provider)
NO TALLAHASSEE, July 17, Mental Health/Substance Abuse
 CFOP 155-18 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 155-18 TALLAHASSEE, July 17, 2017 Mental Health/Substance Abuse GUIDELINES FOR CONDITIONAL RELEASE PLANNING FOR
CFOP 155-18 STATE OF FLORIDA DEPARTMENT OF CF OPERATING PROCEDURE CHILDREN AND FAMILIES NO. 155-18 TALLAHASSEE, July 17, 2017 Mental Health/Substance Abuse GUIDELINES FOR CONDITIONAL RELEASE PLANNING FOR
I. General Instructions
 Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
Contra Costa Behavioral Health Services Request for Proposals (RFP) Outpatient Mental Health Services September 30, 2015 I. General Instructions Contra Costa Behavioral Health Services (CCBHS, or the County)
Department of Juvenile Justice Guidance Document COMPLIANCE MANUAL 6VAC REGULATION GOVERNING JUVENILE SECURE DETENTION CENTERS
 COMPLIANCE MANUAL 6VAC35-101 REGULATION GOVERNING JUVENILE SECURE DETENTION CENTERS This document shall serve as the compliance manual for the Regulation Governing Juvenile Secure Detention Centers 6VAC35-101)
COMPLIANCE MANUAL 6VAC35-101 REGULATION GOVERNING JUVENILE SECURE DETENTION CENTERS This document shall serve as the compliance manual for the Regulation Governing Juvenile Secure Detention Centers 6VAC35-101)
HUMAN SERVICES. What can I do with this major?
 AREAS HUMAN SERVICES What can I do with this major? EMPLOYERS DESCRIPTIONS/STRATEGIES SOCIAL SERVICES Administration and Planning Program Evaluation Volunteer Coordination Prevention Public welfare agencies
AREAS HUMAN SERVICES What can I do with this major? EMPLOYERS DESCRIPTIONS/STRATEGIES SOCIAL SERVICES Administration and Planning Program Evaluation Volunteer Coordination Prevention Public welfare agencies
Voluntary Services as Alternative to Involuntary Detention under LPS Act
 California s Protection & Advocacy System Toll-Free (800) 776-5746 Voluntary Services as Alternative to Involuntary Detention under LPS Act March 2010, Pub #5487.01 This memo outlines often overlooked
California s Protection & Advocacy System Toll-Free (800) 776-5746 Voluntary Services as Alternative to Involuntary Detention under LPS Act March 2010, Pub #5487.01 This memo outlines often overlooked
PREA AUDIT: AUDITOR S SUMMARY REPORT 1 COMMUNITY CONFINEMENT FACILITIES
 PREA AUDIT: AUDITOR S SUMMARY REPORT COMMUNITY CONFINEMENT FACILITIES Name of facility: OhioLink-Lima Physical address: 517 S. Main Street, Lima, Ohio 45801 Date report submitted: Auditor Information Address:
PREA AUDIT: AUDITOR S SUMMARY REPORT COMMUNITY CONFINEMENT FACILITIES Name of facility: OhioLink-Lima Physical address: 517 S. Main Street, Lima, Ohio 45801 Date report submitted: Auditor Information Address:
UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009)
") UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009) The UCare Model of Care for Mental Health Targeted Case Management is designed to provide care for the child member and their families and adult members,
UCARE MODEL OF CARE SUMMARY FOR MH-TCM (February 2009) The UCare Model of Care for Mental Health Targeted Case Management is designed to provide care for the child member and their families and adult members,
Acute Crisis Units. Shelly Rhodes, Provider Relations Manager
 Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Acute Crisis Units Shelly Rhodes, Provider Relations Manager Shelly.Rhodes@beaconhealthoptions.com Training Agenda Agenda: Transition and Certification Coverage of Services Service Code Definition Documentation
Personal Support Worker
 PROGRAM OBJECTIVES The Personal Support Worker program prepares students to deliver appropriate short or longterm care assistance and support services in either a long-term care facility, acute care facility,
PROGRAM OBJECTIVES The Personal Support Worker program prepares students to deliver appropriate short or longterm care assistance and support services in either a long-term care facility, acute care facility,
Florida Minority Business Enterprise (MBE) Utilization Report
 Utilization Report") October 10, 2012 ITB# D2056 Bidder: Subject: DJJ ITB# D2056 This is an Invitation to Bid (ITB) for Medical Services to youth in custody at the Hillsborough Regional Juvenile Detention Center located in
October 10, 2012 ITB# D2056 Bidder: Subject: DJJ ITB# D2056 This is an Invitation to Bid (ITB) for Medical Services to youth in custody at the Hillsborough Regional Juvenile Detention Center located in
Request for Proposals for Transitional Living Centers
 Request for Proposals for Transitional Living Centers I. Introduction: Central Iowa Community Services (CICS) is announcing this Request for Proposals (RFP) for the following counties: Boone, Franklin,
Request for Proposals for Transitional Living Centers I. Introduction: Central Iowa Community Services (CICS) is announcing this Request for Proposals (RFP) for the following counties: Boone, Franklin,